Targeted Anticytokine Therapy in Patients With Chronic Heart Failure: Results of the Randomized...
10
Targeted Anticytokine Therapy in Patients With Chronic Heart Failure Results of the Randomized Etanercept Worldwide Evaluation (RENEWAL) Douglas L. Mann, MD; John J.V. McMurray, MD, FRCP, FESC; Milton Packer, MD; Karl Swedberg, MD, PhD, FESC; Jeffrey S. Borer, MD; Wilson S. Colucci, MD; Jacques Djian, MD, FESC; Helmut Drexler, MD; Arthur Feldman, MD, PhD; Lars Kober, MD; Henry Krum, MD, PhD, FRACP; Peter Liu, MD; Markku Nieminen, MD, PhD; Luigi Tavazzi, MD; Dirk Jan van Veldhuisen, MD, PhD; Anders Waldenstrom, MD, PhD; Marshelle Warren, MD; Arne Westheim, MD; Faiez Zannad, MD, PhD; Thomas Fleming, PhD Background—Studies in experimental models and preliminary clinical experience suggested a possible therapeutic role for the soluble tumor necrosis factor antagonist etanercept in heart failure. Methods and Results—Patients with New York Heart Association class II to IV chronic heart failure and a left ventricular ejection fraction 0.30 were enrolled in 2 clinical trials that differed only in the doses of etanercept used. In RECOVER, patients received placebo (n373) or subcutaneous etanercept in doses of 25 mg every week (n375) or 25 mg twice per week (n375). In RENAISSANCE, patients received placebo (n309), etanercept 25 mg twice per week (n308), or etanercept 25 mg 3 times per week (n308). The primary end point of each individual trial was clinical status at 24 weeks. Analysis of the effect of the 2 higher doses of etanercept on the combined outcome of death or hospitalization due to chronic heart failure from the 2 studies was also planned (RENEWAL). On the basis of prespecified stopping rules, both trials were terminated prematurely owing to lack of benefit. Etanercept had no effect on clinical status in RENAISSANCE (P0.17) or RECOVER (P0.34) and had no effect on the death or chronic heart failure hospitalization end point in RENEWAL (etanercept to placebo relative risk1.1, 95% CI 0.91 to 1.33, P0.33). Conclusions—The results of RENEWAL rule out a clinically relevant benefit of etanercept on the rate of death or hospitalization due to chronic heart failure. (Circulation. 2004;109:1594-1602.) Key Words: heart failure tumor necrosis factor etanercept cytokines T he finding of elevated levels of tumor necrosis factor (TNF) in patients with chronic heart failure (CHF) suggested that inflammatory mediators might play a role in the pathophysiology of this syndrome. 1,2 This hypothesis was strengthened by the finding that exogenous administration and transgenic overexpression of proinflammatory cytokines could mimic many aspects of the heart failure phenotype, including left ventricular remodeling and reduced survival, in experimental animals. 3–5 Etanercept is a recombinant human TNF receptor that binds to soluble (circulating) TNF and functionally inacti- vates TNF by preventing it from binding to its receptors on Received December 20, 2003; revision received January 26, 2004; accepted January 26, 2004. From the Winters Center for Heart Failure Research (D.L.M.), Baylor College of Medicine and the Houston VA, Houston, Tex; Department of Cardiology, Western Infirmary (J.J.V.M.), Glasgow, United Kingdom; Department of Medicine, University of Texas Dallas Southwestern Medical Center (M.P.), Dallas, Tex; Department of Medicine, Sahlgrenska University Hospital/Östra (K.S.), Göteborg, Sweden; Division of Cardiovascular Pathophysiology, Weill Medical College of Cornell University (J.S.B.), New York, NY; Division of Cardiology, Boston Medical Center (W.S.C.), Boston, Mass; Wyeth Research (J.D.), Paris, France; Medizinische Hochschule (H.D.), Hannover, Germany; Division of Cardiology, University of Pittsburgh Medical Center (A.F.), Pittsburgh, Pa; Gentofte Hospital/University of Copenhagen (L.K.), Department of Cardiology, Niels Andersens Vej, Denmark; Clinical Pharmacology Unit, Alfred Hospital (H.K.), Prahran, Victoria, Australia; The Toronto Hospital (P.L.), Cardiology Research, Toronto, Ontario, Canada; Division of Cardiology, Helsinki University Central Hospital (M.N.), Haartmaninkatu, Helsinki, Finland; Divisione di Cardiologia, Policlinico San Matteo-IRCCS (L.T.), Pavia, Italy; Academisch Ziekenhuis Groningen (D.J.v.V.), Cardio Research, GZ Groningen, The Netherlands; Department of Medicine, Umea University Hospital (A.W.), Umea, Sweden; Amgen Inc (M.W.), Thousand Oaks, Calif; Medicinsk Klinikk (A.W.), Hjertemedisinsk Avd, Ullevål Sykehus, Oslo, Norway; Centre d’Investigation Clinique (F.Z.), Hopital Jeanne d’Arc, Dommartin Les Toul Cedex, France; and Department of Biostatistics (T.F.), University of Washington, Seattle, Wash. Guest Editor for this article was Marvin Konstam, MD, Tufts–New England Medical Center, Boston, Mass. This article originally appeared Online on March 15, 2004 (Circulation. 2004;109:r76 –r84). Correspondence to Douglas L Mann, MD, Winters Center for Heart Failure Research, MS 524, 6565 Fannin, Houston, TX 77030. E-mail [email protected] © 2004 American Heart Association, Inc. Circulation is available at http://www.circulationaha.org DOI: 10.1161/01.CIR.0000124490.27666.B2 1594 Clinical Investigation and Reports by guest on February 29, 2016 http://circ.ahajournals.org/ Downloaded from
Transcript of Targeted Anticytokine Therapy in Patients With Chronic Heart Failure: Results of the Randomized...

Targeted Anticytokine Therapy in Patients WithChronic Heart Failure
Results of the Randomized Etanercept WorldwideEvaluation (RENEWAL)
Douglas L. Mann, MD; John J.V. McMurray, MD, FRCP, FESC; Milton Packer, MD;Karl Swedberg, MD, PhD, FESC; Jeffrey S. Borer, MD; Wilson S. Colucci, MD;
Jacques Djian, MD, FESC; Helmut Drexler, MD; Arthur Feldman, MD, PhD; Lars Kober, MD;Henry Krum, MD, PhD, FRACP; Peter Liu, MD; Markku Nieminen, MD, PhD; Luigi Tavazzi, MD;
Dirk Jan van Veldhuisen, MD, PhD; Anders Waldenstrom, MD, PhD; Marshelle Warren, MD;Arne Westheim, MD; Faiez Zannad, MD, PhD; Thomas Fleming, PhD
Background—Studies in experimental models and preliminary clinical experience suggested a possible therapeutic role forthe soluble tumor necrosis factor antagonist etanercept in heart failure.
Methods and Results—Patients with New York Heart Association class II to IV chronic heart failure and a left ventricularejection fraction �0.30 were enrolled in 2 clinical trials that differed only in the doses of etanercept used. In RECOVER,patients received placebo (n�373) or subcutaneous etanercept in doses of 25 mg every week (n�375) or 25 mg twiceper week (n�375). In RENAISSANCE, patients received placebo (n�309), etanercept 25 mg twice per week (n�308),or etanercept 25 mg 3 times per week (n�308). The primary end point of each individual trial was clinical status at 24weeks. Analysis of the effect of the 2 higher doses of etanercept on the combined outcome of death or hospitalizationdue to chronic heart failure from the 2 studies was also planned (RENEWAL). On the basis of prespecified stoppingrules, both trials were terminated prematurely owing to lack of benefit. Etanercept had no effect on clinical status inRENAISSANCE (P�0.17) or RECOVER (P�0.34) and had no effect on the death or chronic heart failurehospitalization end point in RENEWAL (etanercept to placebo relative risk�1.1, 95% CI 0.91 to 1.33, P�0.33).
Conclusions—The results of RENEWAL rule out a clinically relevant benefit of etanercept on the rate of death orhospitalization due to chronic heart failure. (Circulation. 2004;109:1594-1602.)
Key Words: heart failure � tumor necrosis factor � etanercept � cytokines
The finding of elevated levels of tumor necrosis factor(TNF) in patients with chronic heart failure (CHF)
suggested that inflammatory mediators might play a role inthe pathophysiology of this syndrome.1,2 This hypothesis wasstrengthened by the finding that exogenous administrationand transgenic overexpression of proinflammatory cytokines
could mimic many aspects of the heart failure phenotype,including left ventricular remodeling and reduced survival, inexperimental animals.3–5
Etanercept is a recombinant human TNF receptor thatbinds to soluble (circulating) TNF and functionally inacti-vates TNF by preventing it from binding to its receptors on
Received December 20, 2003; revision received January 26, 2004; accepted January 26, 2004.From the Winters Center for Heart Failure Research (D.L.M.), Baylor College of Medicine and the Houston VA, Houston, Tex; Department of
Cardiology, Western Infirmary (J.J.V.M.), Glasgow, United Kingdom; Department of Medicine, University of Texas Dallas Southwestern Medical Center(M.P.), Dallas, Tex; Department of Medicine, Sahlgrenska University Hospital/Östra (K.S.), Göteborg, Sweden; Division of CardiovascularPathophysiology, Weill Medical College of Cornell University (J.S.B.), New York, NY; Division of Cardiology, Boston Medical Center (W.S.C.), Boston,Mass; Wyeth Research (J.D.), Paris, France; Medizinische Hochschule (H.D.), Hannover, Germany; Division of Cardiology, University of PittsburghMedical Center (A.F.), Pittsburgh, Pa; Gentofte Hospital/University of Copenhagen (L.K.), Department of Cardiology, Niels Andersens Vej, Denmark;Clinical Pharmacology Unit, Alfred Hospital (H.K.), Prahran, Victoria, Australia; The Toronto Hospital (P.L.), Cardiology Research, Toronto, Ontario,Canada; Division of Cardiology, Helsinki University Central Hospital (M.N.), Haartmaninkatu, Helsinki, Finland; Divisione di Cardiologia, PoliclinicoSan Matteo-IRCCS (L.T.), Pavia, Italy; Academisch Ziekenhuis Groningen (D.J.v.V.), Cardio Research, GZ Groningen, The Netherlands; Departmentof Medicine, Umea University Hospital (A.W.), Umea, Sweden; Amgen Inc (M.W.), Thousand Oaks, Calif; Medicinsk Klinikk (A.W.), HjertemedisinskAvd, Ullevål Sykehus, Oslo, Norway; Centre d’Investigation Clinique (F.Z.), Hopital Jeanne d’Arc, Dommartin Les Toul Cedex, France; and Departmentof Biostatistics (T.F.), University of Washington, Seattle, Wash.
Guest Editor for this article was Marvin Konstam, MD, Tufts–New England Medical Center, Boston, Mass.This article originally appeared Online on March 15, 2004 (Circulation. 2004;109:r76–r84).Correspondence to Douglas L Mann, MD, Winters Center for Heart Failure Research, MS 524, 6565 Fannin, Houston, TX 77030. E-mail
[email protected]© 2004 American Heart Association, Inc.
Circulation is available at http://www.circulationaha.org DOI: 10.1161/01.CIR.0000124490.27666.B2
1594
Clinical Investigation and Reports
by guest on February 29, 2016http://circ.ahajournals.org/Downloaded from

cell surface membranes. Thus far, treatment with etanercepthas resulted in clinical improvements in patients with rheu-matoid arthritis, ankylosing spondylitis, and psoriasis.6–8
Preclinical studies showed that etanercept reversed some ofthe deleterious effects of TNF in vitro and in vivo.3,9
Moreover, phase I safety studies showed that a single intra-venous infusion of etanercept was safe and well tolerated andled to an improvement in the functional status of heart failurepatients.10 In a subsequent study, biweekly injections ofetanercept for 3 months resulted in a significant increase inleft ventricular ejection fraction and a significant decrease inleft ventricular volumes.11 On the basis of the preclinical andclinical studies, 2 multicenter clinical trials were designed totest the effect of etanercept on patient functional status andmorbidity/mortality.
MethodsStudy DesignTwo similar double-blind, randomized, placebo-controlled multi-center clinical trials were conducted, 1 in Europe, Israel, Australia,and New Zealand, known as Research into Etanercept CytOkineantagonism in VEntriculaR dysfunction (RECOVER), and the other
in North America, known as Randomized Etanercept North AmerI-can Strategy to Study AntagoNism of CytokinEs (RENAISSANCE).The trials differed, importantly, only in the doses of etanercept used.In RECOVER, the patients were randomized on a 1:1:1 basis toplacebo or etanercept 25 mg SC once weekly (QW) or twice weekly(BIW), whereas in RENAISSANCE, patients were randomized toplacebo or etanercept 25 mg BIW or 25 mg 3 times weekly (TIW).
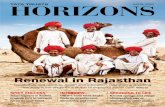
Figure 1. Study design of RECOVER and RENAISSANCE trials andRENEWAL analysis, which used pooled data from RECOVER (etaner-cept BIW) and RENAISSANCE (etanercept BIW and TIW) trials.
TABLE 1. Baseline Demographics and Characteristics for RECOVER and RENAISSANCE
RECOVER RENAISSANCE
Placebo(n�373)
Etanercept25 mg QW(n�375)
Etanercept25 mg BIW
(n�375)Placebo(n�309)
Etanercept25 mg BIW
(n�308)
Etanercept25 mg TIW
(n�308)
Mean (SD) age, y 64.6 (10.8) 64.8 (10.3) 64.1 (10.4) 62.6 (11.9) 61.8 (12.1) 62.4 (11.0)
Mean (SD) LVEF 24 (5) 24 (5) 24 (5) 22 (6) 22 (5) 22 (6)
Mean (SD) SBP, mm Hg 122 (18) 122 (18) 122 (18) 110 (16) 110 (17) 108 (16)
Mean (SD) DBP, mm Hg 75 (10) 75 (10) 74 (11) 68 (10) 67 (11) 66 (10)
Mean (SD) heart rate, bpm 74 (12) 74 (12) 74 (12) 74 (12) 74 (11) 74 (11)
White 99 99 99 82 85 83
Nonwhite �1 �1 �1 18 15 17
Male 75 77 81 77 77 81
Ischemic etiology 60 62 61 60 63 62
NYHA class
II 28 27 27 23 23 24
IIIA 43 45 45 47 47 47
IIIB 25 25 24 26 25 24
IV 3 3 3 4 5 5
Comorbidity
Hypertension 46 45 43 49 60 56
Diabetes mellitus 36 34 36 34 41 37
Medical treatment
Digoxin/digitalis 53 56 53 81 81 83
ACE inhibitor 85 83 87 82 77 79
ARB 13 14 12 16 23 19
�-Blocker 64 62 62 63 59 59
K-sparing diuretic 37 44 44 34 37 32
Any diuretic 99 99 99 99 98 100
LVEF indicates left ventricular ejection fraction; SBP, systolic blood pressure; DBP, diastolic blood pressure; and ARB,angiotensin-receptor blocker.
Values are percentages except where otherwise noted.
Mann et al Targeted Anticytokine Therapy in Chronic HF 1595
by guest on February 29, 2016http://circ.ahajournals.org/Downloaded from

The intent was for each trial to enroll 900 patients (Figure 1). Theprimary end point in RENAISSANCE and RECOVER was a changein clinical status from baseline to 24 weeks. This end point is basedon a composite score, wherein patients are considered improved,worsened, or unchanged on the basis of death, CHF hospitalization,New York Heart Association (NYHA) class, and patient globalassessment, as detailed previously.12
A prespecified analysis of the effect of etanercept on longer-termmorbidity/mortality was also planned. This analysis, which wasreferred to as the Randomized EtaNErcept Worldwide evALuation(RENEWAL), combined the BIW treatment arm of RECOVER withthe BIW and TIW arms of RENAISSANCE and compared thesewith the pooled placebo arms from both studies, with an anticipatedtotal of 1500 patients. The primary end point of RENEWAL was thecomposite of death (of all causes) or hospitalization for or with CHF.The RENEWAL analysis was event driven (see statistical analysis).Secondary end points included all-cause mortality and the totalnumber of hospitalizations and emergency room visits for or withworsening CHF, as well as, at 24 weeks, change in NYHA class,patient global assessment, and quality of life.
PatientsThe main inclusion criteria were age 18 to 85 years; NYHA class IIto IV; ischemic or nonischemic etiology; left ventricular ejectionfraction �0.30; stable doses of diuretic, ACE inhibitor (unless not
tolerated), and �-blocker and/or spironolactone (if taking) for �3months; and 6-minute walk distance of �375 m (or �425 m ifhospitalized for CHF within previous 6 months). The main exclusioncriteria were severe infection within 1 month, surgically correctablecauses of heart failure, other serious illness, acute myocardialinfarction or hospitalization (3 months), and recent (3 months) orplanned surgery/coronary revascularization. The studies receivedethics approval in all participating centers, and all patients gavewritten informed consent.
Statistical AnalysesIn RECOVER and RENAISSANCE, the clinical composite scorewas analyzed with a Cochran-Mantel-Haenszel test. The statisticalassumptions in RECOVER were that in the placebo group, 40% ofthe patients would be worse, 42% would remain unchanged, and18% would be improved, and in the treatment group (QW and BIWetanercept), 28% of the patients would be worse, 42% would remainunchanged, and 30% would be improved. There was 90% power forthe primary hypothesis test of 25 mg BIW versus placebo and 81%power for the conditional primary hypothesis test of 25 mg QWversus placebo, both tested at the 2-sided 0.04 level. The statisticalassumptions in RENAISSANCE were that in the placebo group,25% of the patients would be worse, 55% would remain unchanged,and 20% would be improved, and in the treatment group (BIW andTIW etanercept), 17% of the patients would be worse, 53% wouldremain unchanged, and 30% would be improved. There was 84%power for each comparison of an etanercept treatment arm to placebowhen controlling the overall type I error rate at 0.04. In theRENEWAL trial, using a stratified log-rank analysis, 389 eventswould provide 90% power for a 2-sided 0.01 level test to detect a32.4% relative reduction in risk for this end point, when thecombined BIW and TIW etanercept treatment arms were comparedwith placebo. To control the overall type I error rate within eachstudy at 0.05, analyses of the clinical status composite wereconducted at the 2-sided 0.04 level, and the combined analysis ofall-cause mortality or CHF hospitalization was conducted at the2-sided 0.01 level. The log-rank statistic for the RENEWAL analysiswas stratified by study, baseline �-blocker status, and NYHAfunctional class.
Safety Monitoring and Stopping GuidelinesA single independent Data Monitoring Committee (DMC) monitoredboth RENAISSANCE and RECOVER. The DMC could recommendmodifications to the protocols to enhance patient safety or quality oftrial conduct. Early termination of the studies could be recommendedif there was strong evidence that etanercept would show no benefitat the end of the study for the clinical composite end point. Suchevidence was defined as having sufficiently unfavorable interimresults in the 4 pairwise comparisons with placebo (by comparison of
Figure 2. Analysis of clinical status composite score forRECOVER and RENAISSANCE trials in placebo and etanerceptgroups (number of patients who had completed planned24-week treatment when these trials were stopped).
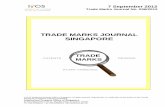
Figure 3. Kaplan-Meier analysis of time to death orheart failure hospitalizations in placebo and etaner-cept group (BIW and TIW) in RENEWAL analysis.
1596 Circulation April 6, 2004
by guest on February 29, 2016http://circ.ahajournals.org/Downloaded from

each of the 2 dose groups with placebo in both RECOVER andRENAISSANCE) that the conditional probability for achieving apositive effect on the clinical composite end point (if one continuedto assume the protocol-specified targeted level of benefit) was �0.25for each of these 4 pairwise comparisons. Early termination couldalso be recommended by the DMC for conclusive interim results onthe morbidity/mortality end point in RENEWAL, either becauseinterim data for the combined end point of mortality and hospital-ization for heart failure would be sufficiently unfavorable as to ruleout a 10% reduction in relative risk or because interim data forall-cause mortality would be sufficiently favorable as to establishbenefit, where both of these assessments would be guided by use ofthe O’Brien-Fleming monitoring boundary.
ResultsPatients EnrolledBetween June 1999 and December 2000, a total of 1123patients from 194 centers were enrolled in RECOVER. InRENAISSANCE, 925 patients from 105 centers were ran-domized between March 1999 and January 2001. The base-line characteristics of the patients are summarized in Table 1.The placebo and etanercept groups in each study weregenerally well matched, although there were imbalancesbetween treatment groups for diabetes in both studies. Therewas also an imbalance in the number of patients with a history
Figure 4. Kaplan-Meier analysis of time to death inplacebo and etanercept group (BIW and TIW) inRENEWAL analysis.
TABLE 2. Main Outcomes in RECOVER, RENAISSANCE, and RENEWAL
RECOVER
Placebo(n�373)
25 mgEtanercept QW
(n�375)RR*
(95% CI) P†
25 mgEtanercept BIW
(n�375)RR*
(95% CI) P†
Death or CHFhospitalization
66 68 1.01 (0.72–1.41) 0.97 60 0.87 (0.61–1.24) 0.45
Death 33 22 0.68 (0.39–1.17) 0.16 27 0.83 (0.50–1.39) 0.47
RENAISSANCE
Placebo(n�309)
25 mgEtanercept BIW
(n�308)RR*
(95% CI) P†
25 mgEtanercept TIW
(n�308)RR*
(95% CI) P†
Death or CHFhospitalization
100 112 1.21 (0.92–1.58) 0.17 116 1.23 (0.94–1.61) 0.13
Death 44 55 1.27 (0.85–1.89) 0.24 61 1.37 (0.93–2.02) 0.12
RENEWAL
Placebo(n�682)
25 mgEtanercept BIW
(n�683)RR*
(95% CI) P†
25 mgEtanercept BIW�TIW
(n�991)RR*
(95% CI) P†
Death or CHFhospitalization
166 172 1.08 (0.87–1.33) 0.51 288 1.10 (0.91–1.33) 0.33
Death 77 82 1.07 (0.78–1.46) 0.67 143 1.13 (0.86–1.50) 0.39
*RR for active vs placebo group.†P values for Cox regression analysis with point estimate for RRs plus 95% CIs. The model includes terms for the study, NYHA
functional classification, and baseline use of �-blockers. P values for the Cox regression, etc, as already written plus key.
Mann et al Targeted Anticytokine Therapy in Chronic HF 1597
by guest on February 29, 2016http://circ.ahajournals.org/Downloaded from

of hypertension, which was lower in the group inRENAISSANCE.
Early Termination of StudiesOn March 22, 2001, the DMC recommended termination ofboth studies because the prespecified criteria for stopping dueto lack of benefit were met in the RECOVER and RENAIS-SANCE studies and the RENEWAL analysis. The mediantime from randomization to the last visit was 5.7 months inRECOVER and 12.9 months in RENAISSANCE. At the timethe studies were closed, 37% and 73% of the patients inRECOVER and RENAISSANCE, respectively, had com-pleted the 24-week evaluation. One percent or less of anytreatment group of RECOVER or RENAISSANCE was lostto follow-up for assessment of vital status, and 0.4% and0.9% of patients withdrew consent for evaluation of clinicalstatus in RECOVER and RENAISSANCE, respectively.
Primary End Point in RENAISSANCEand RECOVERFigure 2 shows that there were not significant differencesbetween placebo and etanercept with respect to change in theclinical composite score from baseline to 24 weeks (or the lastevaluated visit before study stoppage) in either RECOVER(P�0.34 overall; P�0.76 QW; P�0.27 BIW) or RENAIS-SANCE (P�0.17 overall; P�0.07 BIW; P�0.17 TIW). InRENAISSANCE, there was a higher proportion (29%,P�0.046) of patients given etanercept 25 mg BIW thanplacebo patients (20%) in the “worsened” category at 24weeks; however, this difference was not observed inRECOVER.
Outcome of Death or CHF Hospitalizationin RENEWALFor the death and CHF hospitalization end point, the log-rankanalysis was stratified by trial, baseline NYHA class, and�-blocker use and included 682 placebo patients (309 fromRENAISSANCE and 373 from RECOVER) and the 991etanercept patients (375 BIW patients from RECOVER and308 BIW and 308 TIW patients from RENAISSANCE). InRENAISSANCE, there were 100 events in 309 patients in theplacebo group and 228 events in 616 patients in the combinedetanercept groups; in RECOVER, there were 66 events in 373
patients in the placebo group and 60 events in 375 patients inthe BIW etanercept group. These data yielded an estimatedetanercept-to-placebo relative risk of 1.1 (95% CI 0.91 to1.33; P�0.33; Figure 3). Hence, the results were sufficientlyunfavorable as to exclude a 10% reduction in the rate of deathor CHF hospitalization with etanercept.
Secondary Outcomes in RENEWALWith regard to overall mortality, in RENAISSANCE, therewere 44 deaths in 309 patients in the placebo group and 116deaths in 616 patients in the combined etanercept groups; inRECOVER, there were 33 deaths in 373 patients in theplacebo group and 27 deaths in 375 patients in the BIWetanercept group. These data yielded an estimated etanercept-to-placebo relative risk of 1.13 (95% CI 0.86 to 1.50;P�0.39; Figure 4). There were no significant differences inany of the other secondary outcomes.
RENEWAL Subgroup AnalysesFigure 5 summarizes the RENEWAL subgroup analyses.Overall, there were no significant differences between treat-ments for any of the subgroups.
Adverse Events and SafetyTable 3 summarizes the incidence of adverse events thatoccurred in both trials. Adverse events that occurred in morethan 10% of patients overall in the RENAISSANCE trialwere upper respiratory tract infections, dizziness, injection-site reaction, pain, diarrhea, chest pain, bronchitis, headache,flu syndrome, constipation, and cough. Of these events,injection-site reaction, bronchitis, and constipation occurredstatistically significantly (P�0.05) more frequently in pa-tients receiving etanercept than in those given placebo. In theRECOVER trial, adverse events that occurred in more than5% of patients were upper respiratory infection, injection-sitereaction, bronchitis, dizziness, pneumonia, chest pain, ab-dominal pain, angina pectoris, flu syndrome, increasedcough, and dyspnea; there were no statistically significantdifferences (P�0.10) among the 3 treatment groups for theseevents.
Table 4 summarizes the incidence of serious and nonseri-ous infections in both trials and shows a trend (P�0.067)toward more infections, overall, in the etanercept-treated
Figure 5. Etanercept:placebo hazardratios (squares) and 95 CIs of effect oftreatment on combined risk of all-causemortality or hospitalization for heart fail-ure in RENEWAL analysis. BMI indicatesbody mass index; LVEF, left ventricularejection fraction.
1598 Circulation April 6, 2004
by guest on February 29, 2016http://circ.ahajournals.org/Downloaded from

patients in RECOVER, although this was not observed inRENAISSANCE. There was not an increase in seriousinfections in either study.
DiscussionThe clinical trials reported here did not demonstrate a benefitof etanercept in patients with heart failure despite the wealthof preclinical and preliminary clinical data suggesting atherapeutic role for TNF antagonism in this condition. Al-though the reasons for this lack of benefit of etanercept are
not known, there are several possible explanations. Onepossibility is that proinflammatory cytokines do not play adeleterious role in the pathophysiology of CHF. A secondpossibility is that the doses of etanercept that we used werenot sufficient to neutralize circulating and/or myocardialtissue levels of TNF. A third possibility is that the targetedapproach that was taken was not sufficient to disrupt thenetwork of inflammatory mediators (eg, interleukin-1�,interleukin-6, and nitric oxide) that are activated in heartfailure.13 Targeted anticytokine treatment with etanercept hasbeen beneficial in some (eg, rheumatoid arthritis, ankylosingspondylitis, and psoriasis6–8) but not all (eg, Crohn’s diseaseand systemic sepsis14,15) conditions in which TNF is thoughtto play an important pathophysiological role. It is not possibleto definitively address these latter 2 possibilities becauseneither circulating levels of inflammatory mediators normeasures of TNF bioactivity were analyzed systematically inRECOVER and RENAISSANCE. A fourth possibility is thatthe short-term benefits of etanercept observed in the earliersmall phase I studies in CHF were offset in the long term bythe ability of etanercept to stabilize biologically active (ho-motrimeric) TNF, thereby acting as an TNF agonist.16 Theobservation that there was a higher proportion of patients inthe worsened category in RENAISSANCE, in which patientswere exposed to etanercept for the longest time, is consistentwith this point of view. A final consideration suggested byexperimental studies is that physiological levels of TNF arenecessary for cardiovascular homeostasis.17,18 Accordingly,sustained lowering of TNF may have contributed to thehigher proportion of patients in the worsened category be-cause of loss of the beneficial aspects of cytokine signaling.
The results of the present study need to be discussed inlight of the recently reported ATTACH (Anti-TNF-� inCongestive Heart Failure) trial,19 a smaller study of 150patients that used a chimeric anti-TNF antibody that exertsanti-inflammatory effects by binding to and neutralizingcirculating TNF, as well as lysing TNF-expressing cellsthrough complement fixation. In ATTACH, there was asignificant increase in death and heart failure hospitalizationat 28 weeks in the patients who received infliximab 10 mg/kg.Although we cannot discount the possibility that the worsen-ing heart failure observed in the ATTACH trial and thesuggestion of worsening heart failure outcome seen in theRENAISSANCE trial both may have been related to exces-sive TNF antagonism or loss of the beneficial aspects ofcytokine signaling, there are other possible explanations,including “TNF rebound”20 and complement fixation, thatmay have contributed to worsening heart failure outcomes inthe ATTACH trial. However, precise mechanistic explana-tions for the differences in outcomes in the ATTACH andRENEWAL trials are not known, and the above suggestionsare speculative.
A potential concern with etanercept was increased suscep-tibility to infection or decreased resistance to infection.Although there was a trend toward increased infections inpatients in RECOVER, this was not observed in RENAIS-SANCE, wherein the patients were treated for longer periodsof time. Moreover, there was no significant increase inserious infections in either trial (Table 4). Of note, no
TABLE 3. Adverse Events Reported by >5% of Patients inRECOVER and RENAISSANCE
RECOVER (n�1123)
Placebo(n�373)
EtanerceptQW
(n�375)
EtanerceptBIW
(n�375)
Upper respiratory infection 45 (12.1) 58 (15.5) 44 (11.7)
Pneumonia 24 (6.4) 15 (4.0) 24 (6.4)
Flu syndrome 16 (4.3) 19 (5.1) 22 (5.9)
Injection-site reaction 28 (7.5) 44 (11.7) 42 (11.2)
Anemia 5 (1.3) 5 (1.3) 5 (1.3)
Chest pain 20 (5.4) 21 (5.6) 18 (4.8)
Abdominal pain 24 (6.4) 17 (4.5) 17 (4.5)
Angina pectoris 20 (5.4) 20 (5.3) 18 (4.8)
Dizziness 22 (5.9) 20 (5.3) 22 (5.9)
Cough increased 20 (5.4) 17 (4.5) 18 (4.8)
Dyspnea 12 (3.2) 24 (6.4) 15 (4.0)
Hyperkalemia 3 (0.8) 3 (0.8) 3 (0.8)
Constipation 3 (0.8) 10 (2.7) 7 (1.9)
Bronchitis 30 (8.0) 35 (9.3) 26 (6.9)
RENAISSANCE (n�925)*
MPlacebo(n�307)
EtanerceptBIW
(n�305)
EtanerceptTIW
(n�307)
Upper respiratory infection 80 (26) 86 (28) 93 (30)
Diarrhea 49 (16) 52 (17) 57 (19)
Headache 36 (12) 45 (15) 35 (11)
Flu syndrome 37 (12) 37 (12) 38 (12)
Injection-site reaction† 16 (5) 55 (18) 62 (20)
Anemia† 8 (3) 23 (8) 17 (6)
Chest pain 37 (12) 42 (14) 56 (18)
Abdominal pain 24 (8) 25 (8) 29 (9)
Angina pectoris 20 (7) 17 (6) 10 (3)
Dizziness 52 (17) 62 (20) 71 (23)
Cough increased 28 (9) 37 (12) 27 (9)
Dyspnea 13 (4) 21 (7) 16 (5)
Hyperkalemia† 8 (3) 20 (7) 19 (6)
Constipation† 21 (7) 41 (13) 30 (10)
Bronchitis† 34 (11) 46 (15) 52 (17)
Values are n (%).*n�919 owing to 6 patients who were randomized but did not receive study
drug.†P�0.05, Fisher’s exact test combined etanercept vs placebo.
Mann et al Targeted Anticytokine Therapy in Chronic HF 1599
by guest on February 29, 2016http://circ.ahajournals.org/Downloaded from

significant increase in infections has been seen in randomizedcontrolled trials with etanercept in patients with rheumatoidarthritis and psoriasis. Adverse events that were observedmore frequently and that were statistically significant oc-curred only in the treatment arm of RENAISSANCE andincluded injection-site reaction, bronchitis, and constipation.
In conclusion, the results of RENEWAL were sufficientlyunfavorable as to rule out a clinically relevant benefit oftargeted anticytokine therapy with the soluble TNF antagonistetanercept on the rate of death or CHF hospitalization inCHF. Although one interpretation of the disappointing resultsof the recent clinical trials with targeted anticytokine therapyin heart failure is that inflammatory mediators are not viabletargets in heart failure, a countervailing point of view is thatwe simply have not targeted proinflammatory mediators withagents that can be used safely in the context of heart failure,21
or alternatively, that targeting a single component of theinflammatory cascade is not sufficient in a disease as com-plex as heart failure. Moreover, these studies do not excludethe possibility that there exists a select group of patients inwhom TNF antagonism may be beneficial. Whether broader-spectrum anti-inflammatory strategies (eg, statins, immuno-adsorption, or immune modulation therapy) will have anyadded value in heart failure is currently being addressed inongoing clinical trials.
AppendixCommittees
RENEWAL Steering CommitteeK. Swedberg (Co-Chair), M. Packer (Co-Chair), J. McMurray, D.Mann, M. Warren (Amgen Corporation representative), and B. Riggs(Wyeth Research representative).
RECOVER Steering CommitteeJ. McMurray (Chair), N. Andersens, J. Djian (Wyeth Researchrepresentative), L. Kober, H. Krum, K. Swedberg, A. Waldenstrom,F. Zannad, H. Drexler, L. Tavazzi, M. Nieminen, D. Jan vanVeldhuisen, and A. Westheim.
RENAISSANCE Steering CommitteeD. Mann (Chair), J. Borer, W. Colucci, A. Feldman, P. Liu, M.Packer, and M. Warren (Amgen Corporation representative).
End-Points CommitteeJ. Cleland (Chair), A.B. Miller, C. O’Connor, C. Torp-Pedersen, P.Carson, M. Komajda, J. Sackner-Bernstein, A. Gavazzi, J. Djian, andM. Warren (Amgen Corporation representative).
Data Monitoring and Safety BoardB. Massie (Chair), J. Djian (Wyeth Research representative), G.Francis, S. Gabriel, D. Julian, J. Kjekshus, A. Leizorovicz, A.M.Tonkin, and M. Warren (Amgen Corporation representative).
Biostatistical GroupThomas Fleming (University of Washington), David Kerr (AXIOResearch Corporation), Ruth McBride (AXIO Research Corpora-tion), Ron Pedersen (Wyeth Research), and Jim Whitmore (Amgen).
Principal Investigators
RECOVER InvestigatorsGreger Ahlberg (Falun, Sweden), Maria Cecila Albanese (Udine,Italy), Jan Aldershvilé (København Ö, Denmark), Eduardo Alegria(Pamplona, Spain), Vera Ambrovicova (Levice, Slovakia), JohnVincent Amerena (Geelong, Victoria, Australia), Bert Andersson(Göteborg, Sweden), Ruta Babarskiene (Kaunas, Lithuania), NoëlBaille (Metz Cedex, France), Stellan Bandh (Västerås, Sweden),Robert Barraine (Poitiers Cedex, France), Jens Berning (Aalborg,Denmark), Jose Ramón Berrazueta (Santander, Spain), EgidijusBerukstis (Vilnius, Lithuania), Kurt Boman (Skellefteå, Sweden),Jean Bour (St. Avold Cedex, France), Angelo Branzi (Bologna,Italy), Jordi Bruguera (Barcelona, Spain), Manuel Oliveira Carrageta(Almada, Portugal), Avraham Caspi (Rehovot, Israel), AntoniaoAmaro Cendon (A Coruna, Spain), Zukai Chati (Essey Les Nancy,France), J.H. Cornel (Alkmaar, The Netherlands), David Cross(Auchenflower, Queensland, Australia), Arturo Fernandez Cruz(Madrid, Spain), Saenz Cusi (Barcelona, Spain), Morten GundtvigDahle (Lillehammer Fylkessykehus, Norway), Ulf Dahlstrom(Linköping, Sweden), Thomas Drawin (Saint Dié, France), HelmutDrexler (Hannover, Germany), Andrzej Dubinski (Walbrzych, Po-land), Kennet Egstrup (Svendborg, Denmark), Jerónimo Farre (Ma-drid, Spain), Roberto Ferrari (Ferrara, Italy), Charles Mark Francis(Kircaldy, United Kingdom), A. Galbraith (Chermside, Queensland,Australia), Michel Galinier (Toulouse Cedex, France), EnriqueGalve (Barcelona, Spain), Pantaleo Giannuzzi (Veruno [Novara],Italy), M. Goethals (Aalst, Belgium), Jacek Gorski (Gdynia, Poland),Robert Greenbaum (Middlesex, United Kingdom), Peter H. Groves(Cardiff, United Kingdom), Markus Haass (Heidelberg, Germany),Torben Helge Haghfelt (Odense C, Denmark), Henryk Halaczk-iewicz (Starachowice, Poland), Angus Hamer (Box Hill, Victoria,Australia), Silvija Hansone (Riga LV, Latvia), Ilona Hegyi (Vasvari,Hungary), Per Hildebrandt (Frederiksberg, Denmark), Christer Hö-glund (Stockholm, Sweden), Laurence Howes (Kogarah, New SouthWales, Australia), I. Hudson (Leicester, United Kingdom), MattiHuttunen (Savonlinna, Finland), Bruce Jackson (Epping, Victoria,Australia), Ashok Jacob (Livingstone, United Kingdom), JytteJensen (Glostrup, Denmark), Janis Jirgensons (Riga LV, Latvia),Christopher Jones (Glamorgan, United Kingdom), H.H. Kadr (Essex,United Kingdom), Thomas Kahan (Danderyd, Sweden), Pál Kárpáti(Budapest, Nygyvarad, Hungary), Julius Kasper (Bratislava, Slova-kia), Per Katzman (Helsingborg, Sweden), Elsadig Kazzam (Eskil-stuna, Sweden), Anne M. Keogh (DarlingHurst, New South Wales,Australia), Khalife Khalife (Metz Cedex, France), Kai Kiilavuori(Espoo, Finland), Lars Køber (Hellerup, Denmark), Jaspal S. Kooner(Southall, Middlesex, United Kingdom), Jerzy Korewicki(Warszawa, Poland), R. Körfer (Bad Oeynhausen, Germany), J.A.Kragten (Heerlen, The Netherlands), Thomas Kronvall (Örebro,Sweden), Henry Krum (Prahran, Victoria, Australia), MariaKrzeminska-Pakula (Lodz, Poland), Krzysztof Kuc (Zielona Gora,Poland), Gyula Kurta (Berettyoujfalu, Orban, Hungary), Jean MarcLablanche (Lille Cedex, France), Finn Landgren (Kalmar, Sweden),Geoffrey Lane (Fremantle, West Australia, Australia), Aleksandras
TABLE 4. Incidence of Infections in RECOVER and RENAISSANCE
RECOVER
P
RENAISSANCE
PPlaceboEtanercept25 mg QW
Etanercept25 mg BIW Placebo
Etanercept25 mg BIW
Etanercept25 mg TIW
Any infection 33 39 40 0.067 65 68 66 0.824
Severe or life-threateninginfection
3 4 5 0.373 10 9 7 0.539
Values are percentages. Data were analyzed with Fisher’s exact test.
1600 Circulation April 6, 2004
by guest on February 29, 2016http://circ.ahajournals.org/Downloaded from

Laucevicius (Vilnius, Lithuania), Ronald Lehman (Ashford, SouthAustralia, Australia), Hanna Lewandowska-Stanek (Lublin, Poland),A.H. Liem (Goes, The Netherlands), Kjell Lindberg (Södertälje,Sweden), W.A. Littler (Birmingham, United Kingdom), Per Löfdahl(Helsingborg, Sweden), Jyri Lommi (Helsinki, Finland), ChaimLotan (Jerusalem, Israel), Bernhard Mox (Greifswald, Germany),Eva Mandysová (Prague, Czech Republic), Nicolas Manito (Barce-lona, Spain), Alon Marmor (Safed, Israel), Ignacio Rada Martinez(Madrid, Spain), W.J. McKenna (London, United Kingdom), JamesMcLay (Aberdeen, United Kingdom), John McMurray (Glasgow,United Kingdom), Garry McVeigh (Belfast, United Kingdom), H.R.Michels (Eindhoven, The Netherlands), Karol Micko (Lucenec,Slovakia), Pawel Miekus (Gdynia, Poland), Modesto Garcia Moll(Barcelona, Spain), David Murdoch (Glasgow, United Kingdom),Eivind S.P. Myhre (Tromso, Norway), Lajos Nagy (Szabo Miklos,Hungary), P.R. Nierop (Rotterdam, The Netherlands), Jan ErikNordrehaug (Bergen, Norway), Ole Nyvad (Holstebro, Denmark),Gerry O’Driscoll (Perth, West Australia, Australia), Keith Oldroyd(East Kilbride, United Kingdom), Jean Pierre Ollivier (Paris,France), Muhamad Omary (Nazareth, Israel), Stein Örn (Stavanger,Norway), Karl Josef Osterziel (Berlin, Germany), Adam Ostrzycki(Warszawa, Poland), Dwain Owensby (Wollongong, Australia),Richard Pacher (Vienna, Austria), Carmine de Pasquale (BedfordPark, South Australia, Australia), Terje Rolf Pedersen (Oslo, Nor-way), Keijo Peuhkurinen (Kuopio, Finland), Marek Piepiorka (We-jherowo, Poland), J. Pohl (Leicester, United Kingdom), Lech Polon-ski (Zabrze, Poland), Piotr Ponikowski (Wroclaw, Poland), J.L.Posma (Groningen, The Netherlands), István Préda (Budapest, Hun-gary), Grzegorz Pulkowski (Bydgoszcz, Poland), John Purvis (Lon-donderry, United Kingdom), Søren Lind Rasmussen (Hvidovre,Denmark), Irena Rawczynska-Englert (Warszawa, Poland), Leo-nardo Reisin (Ashkelon, Israel), Jerzy Rekosz (Warszawa, Poland),Arthur Richards (Christchurch, New Zealand), Martin Risenfors(Mölndal, Sweden), Paolo Rizzon (Bari, Italy), David Roberts(Blackpool, United Kingdom), Enrique Rodriguez (Vizcaya, Spain),Eulalia Roig (Barcelona, Spain), Aldár Rónaszéki (Also erdosor,Hungary), Witold Ruzyllo (Warszawa, Poland), Markku Saksa(Hämeenlinna, Finland), Bassem Samad (Stockholm, Sweden),Maria Schaufelberger (Göteborg, Sweden), Peter M. Schofield(Cambridge, United Kingdom), H.P. Schultheiss (Berlin, Germany),Bernhard Schwaab (Homburg/Saar, Germany), Norman Sharpe(Auckland, New Zealand), Gianfranco Sinagra (Trieste, Italy), An-drew Sindone (Concord, Australia), Bhuwan Singh (Launceston,Australia), Wladyslaw Sinkiewicz (Bydgoszcz, Poland), Jana Siro-tiakova (Nitra, Slovakia), Knud Skagen (Herlev, Denmark), JanisSkards (Riga, Latvia), Marcela Skvarilová (Olomouc, Czech Repub-lic), Miroslav Slanina (Presov, Slovakia), David Ian Slovick(Westcliffe-on-Sea, Essex, United Kingdom), Anton Smalcelj(Zagreb, Croatia), Ian Squire (Leicester, United Kingdom), VerenaStangl (Berlin, Germany), Martin Studencan (Kosice, Slovakia),Torbjörn Sundelin (Sundsvall, Sweden), Wieslaw Supinski (GorzowWlkp, Poland), John Swan (Manchester, United Kingdom), StephenSylivris (Noble Park, Australia), Christer Sylvén (Stockholm, Swe-den), Lip-Bun Tan (Leeds, United Kingdom), Luigi Tavazzi (Pavia,Italy), József Tenczer (Budapest, Hungary), Eduardo de Teresa(Malaga, Spain), Sandor Timar (Kescskemet, Hungary), RobertoTramarin (Pavia, Italy), Bruno Trimarco (Napoli, Italy), Marek Ujda(Stalowa Wola, Poland), Göran Ulvenstam (Göteborg, Sweden), PerUrdahl (Skien, Norway), Paavo Uusimaa (Oulu, Finland), Vin-centeValle (Barcelona, Spain), P.H. van der Burgh (Enschide, TheNetherlands), D.J. van Veldhuisen (Groningen, The Netherlands),Juraj Vancík (Kosice-Saca, Slovakia), G.J.E. Verdel (Haarlem, TheNetherlands), Zvi Vered (Beer Yaacov, Israel), Margus Viigimaa(Tartu, Estonia), Jonathon Waites (Coffs Harbor, New South Wales,Australia), Anders Waldenström (Umea, Sweden), Jean Mark Wein-stein (Beer-Sheva, Israel), Peter L. Weissberg (Cambridge, UnitedKingdom), Arne Westheim (Oslo, Norway), B. Gerhard Wikström(Uppsala, Sweden), A.J.A.M. Withagen (Delft, The Netherlands),Dariusz Wojciechowski (Warszawa, Poland), Faiez Zannad (Dom-martin Les Toul Cedex, France), and Reuven Zimlichman (Holon,Israel).
RENAISSANCE InvestigatorsJonathan Abrams (Albuquerque, NM), Kirkwood Adams (ChapelHill, NC), Inder Anand (Minneapolis, Minn),
J. Malcolm Arnold (London, ON, Canada), Deborah Ascheim(New York, NY), Alan Bank (St. Paul, Minn), Raye Lynn Bellinger(Sacramento, Calif), James Bergin (Charlottesville, Va), VictoriaBernstein (Vancouver, BC, Canada), Girish Bhaskar (Lake City,Fla), Philip Binkley (Columbus, Ohio), John Boehmer (Hershey, Pa),Robert Bourge (Birmingham, Ala), Doug Chapman (Omaha, Neb),Barry Clemson (Peoria, Ill), Maria Costanzo (Chicago, Ill), BarbaraCzerska (Detroit, Mich), Richard Davies (Ottawa, ON, Canada),Teresa DeMarco (San Francisco, Calif), Vincent DeQuattro (LosAngeles, Calif), Thomas DiSalvo (Boston, Mass), Eric Eichhorn(Dallas, Tex), Howard Eisen (Philadelphia, Pa), R. Douglas Ensley(Tulsa, Okla), Arthur Feldman (Pittsburgh, Pa), Daniel Fishbein(Seattle, Wash),
Michael Fowler (Stanford, Calif), Jalal Ghali (Shreveport, La),Mihai Gheorghiade (Chicago, Ill), E. Gilbert (Salt Lake City, Utah),Thomas Giles (New Orleans, La), Michael Givertz (Boston, Mass),Stephen Gottlieb (Baltimore, Md), Barry Greenberg (San Diego,Calif), Stephen Halpern (Santa Rosa, Calif), Joshua Hare (Baltimore,Md), Grady Hendrix (Charleston, SC), Ray Hershberger (Portland,Ore), Michael Higginbotham (Durham, NC), James Hill (Gaines-ville, Fla), Clare Hochreiter (New York, NY), Debra Issac (Calgary,Alberta, Canada), Mariell Jessup (Philadelphia, Pa), Jill Kalman(New York, NY), Ronald Karlsberg (Beverly Hills, Calif), MarcKates (Phoenix, Ariz), Andrew Keller (Fairfax, Va), Dean Kereiakes(Cincinnati, Ohio), Marc Klapholz (New York, NY), Michael Koren(Jacksonville, Fla), Greg Koshkarian (Tucson, Ariz), Steven Krueger(Lincoln, Neb), Marrick Kukin (New York, NY), Robin Kuritzky(Vancouver, British Columbia, Canada), Charles Lanzarotti (Mil-waukee, Wis), Joseph Lash (Louisville, Ky), Richard Lee (Scotts-dale, Ariz), Wayne Leimbach (Tulsa, Okla), Thierry LeJemtel(Bronx, NY), T. Barry Levine (Farmington Hills, Mich), Chang-sengLiang (Rochester, NY), Peter Liu (Toronto, Ontario, Canada), IrvingLoh (Thousand Oaks, Calif), Alan Maisel (San Diego Calif),Douglas Mann (Houston, Tex), Frank McGrew (Memphis, Tenn),Robert McKelvie (Hamilton, Ontario, Canada), Edward McMillan(Charlotte, NC), Alan Miller (Jacksonville, Fla), Leslie Miller(Minneapolis, Minn), Gordon Moe (Toronto, Ontario, Canada), SyedMohiuddin (Omaha, Neb), David Murray (San Antonio, Tex), ImranNiazi (Elkhorn, Wis), John Nicklas (Ann Arbor, Mich), JosephO’Bryan (Ft. Myers, Fla), Ronald Oren (Iowa City, Iowa), RobertPalac (Lebanon, NH), Gregory Pennock (Tucson, Ariz), CharlesPorter (Kansas City, Mo), Steven Promisloff (Hillsboro, Ore),Normand Racine (Montreal, Quebec, Canada), Hillel Ribner (New-ark, NJ), Jonathan Sackner-Bernstein (New York, NY), JohnSchmedtje (Roanoke, Va), Douglas Schocken (Tampa Fla), MarcSilver (Oak Lawn, Ill), Eugene Smith (Little Rock, Ark), AndrewSmith (Atlanta, Ga), Maureen Smithers (Colorado Springs, Colo),David Stagaman (Spokane, Wash), Allan Stahl (Las Vegas, Nev),Alan Steljes (Las Vegas, Nev), John Strobeck (Hawthorne, NJ),James Tam (Winnipeg, Manitoba, Canada), John Teerlink (SanFrancisco, Calif), Udho Thadani (Oklahoma City, Okla), RobertTobar (Vero Beach, Fla), Guillermo Torre (Houston, Tex), CondonVander Ark (Madison, Wis), Lynne Wagoner (Cincinnati, Ohio),John Wilson (Nashville Tenn), Richard Wright (Santa Monica,Calif), Clyde Yancy Jr (Dallas, Tex), and James Young (ClevelandOhio).
AcknowledgmentsThe RENAISSANCE and RECOVER trials were funded by AmgenInc (Amgen Corporation), Thousand Oaks, Calif, and Wyeth Re-search, Collegeville, Pa. The authors would like to thank thefollowing individuals for assistance with preparation of the manu-script: Ann Dugan, Margaret Summersgill, and Jim Whitmore(Amgen) and Evan Loh, Debra Marshall, Maureen Murphy, RonPedersen, Scott Saunders, and Donna Simcoe (Wyeth Research)
Mann et al Targeted Anticytokine Therapy in Chronic HF 1601
by guest on February 29, 2016http://circ.ahajournals.org/Downloaded from

References1. Levine B, Kalman J, Mayer L, et al. Elevated circulating levels of tumor
necrosis factor in severe chronic heart failure. N Engl J Med. 1990;223:236–241.
2. McMurray J, Abdullah I, Dargie HJ, et al. Increased concentrations oftumour necrosis factor in “cachectic” patients with severe chronic heartfailure. Br Heart J. 1991;66:356–358.
3. Bozkurt B, Kribbs S, Clubb FJ Jr, et al. Pathophysiologically relevantconcentrations of tumor necrosis factor-� promote progressive left ven-tricular dysfunction and remodeling in rats. Circulation. 1998;97:1382–1391.
4. Kubota T, McTiernan CF, Frye CS, et al. Dilated cardiomyopathy intransgenic mice with cardiac specific overexpression of tumor necrosisfactor-alpha. Circ Res. 1997;81:627–635.
5. Sivasubramanian N, Coker ML, Kurrelmeyer K, et al. Left ventricularremodeling in transgenic mice with cardiac restricted overexpression oftumor necrosis factor. Circulation. 2001;2001:826–831.
6. Weinblatt ME, Kremer JM, Bankhurst AD, et al. A trial of etanercept, arecombinant tumor necrosis factor receptor:Fc fusion protein, in patientswith rheumatoid arthritis receiving methotrexate. N Engl J Med. 1999;340:253–259.
7. Gorman JD, Sack KE, Davis JC Jr. Treatment of ankylosing spondylitisby inhibition of tumor necrosis factor alpha. N Engl J Med. 2002;346:1349–1356.
8. Mease PJ, Goffe BS, Metz J, et al. Etanercept in the treatment of psoriaticarthritis and psoriasis: a randomised trial. Lancet. 2000;356:385–390.
9. Kapadia S, Torre-Amione G, Yokoyama T, et al. Soluble tumor necrosisfactor binding proteins modulate the negative inotropic effects of TNF-�in vitro. Am J Physiol. 1995;37:H517–H525.
10. Deswal A, Bozkurt B, Seta Y, et al. A phase I trial of tumor necrosisfactor receptor (p75) fusion protein (TNFR:Fc) in patients with advancedheart failure. Circulation. 1999;99:3224–3226.
11. Bozkurt B, Torre-Amione G, Warren MS, et al. Results of targetedant-tumor necrosis factor therapy with etanercept (ENBREL) in patientswith advanced heart failure. Circulation. 2001;103:1044–1047.
12. Packer M. Proposal for a new clinical end point to evaluate the efficacyof drugs and devices in the treatment of chronic heart failure. J Card Fail.2001;7:176–182.
13. Aukrust P, Ueland T, Lien E, et al. Cytokine network in congestive heartfailure secondary to ischemic or idiopathic dilated cardiomyopathy. Am JCardiol. 1999;83:376–382.
14. Sandborn WJ, Hanauer SB, Katz S, et al. Etanercept for active Crohn’sdisease: a randomized, double-blind, placebo-controlled trial. Gastroen-terology. 2001;121:1088–1094.
15. Fisher CJ Jr, Agosti JM, Opal SM, et al. Treatment of septic shock withthe tumor necrosis factor receptor:Fc fusion protein. N Engl J Med.1996;334:1697–1702.
16. Evans TJ, Moyes D, Carpenter A, et al. Protective effect of 55- but not75-kD soluble tumor necrosis factor receptor-immunoglobulin G fusionproteins in an animal model of gram- negative sepsis. J Exp Med.1994;180:2173–2179.
17. Kurrelmeyer K, Michael L, Baumgarten G, et al. Endogenous myocardialtumor necrosis factor protects the adult cardiac myocyte against ische-mic-induced apoptosis in a murine model of acute myocardial infarction.Proc Natl Acad Sci U S A. 2000;290:5456–5461.
18. Sack MN, Smith RM, Opie LH. Tumor necrosis factor in myocardialhypertrophy and ischaemia: an anti- apoptotic perspective. CardiovascRes. 2000;45:688–695.
19. Chung ES, Packer M, Lo KH, et al, for the Anti-TNF Therapy AgainstCongestive Heart Failure Investigators. Randomized, double-blind,placebo-controlled, pilot trial of infliximab, a chimeric monoclonalantibody to tumor necrosis factor-alpha, in patients with moderate-to-severe heart failure: results of the anti-TNF Therapy Against CongestiveHeart Failure (ATTACH) trial. Circulation. 2003;107:3133–3140.
20. Clark MA, Plank LD, Connolly AB, et al. Effect of a chimeric antibodyto tumor necrosis factor-alpha on cytokine and physiologic responses inpatients with severe sepsis: a randomized, clinical trial. Crit Care Med.1998;26:1650–1659.
21. Kwon HJ, Cote TR, Cuffe MS, et al. Case reports of heart failure aftertherapy with a tumor necrosis factor antagonist. Ann Intern Med. 2003;138:807–811.
1602 Circulation April 6, 2004
by guest on February 29, 2016http://circ.ahajournals.org/Downloaded from

Marshelle Warren, Arne Westheim, Faiez Zannad and Thomas FlemingPeter Liu, Markku Nieminen, Luigi Tavazzi, Dirk Jan van Veldhuisen, Anders Waldenstrom,
Wilson S. Colucci, Jacques Djian, Helmut Drexler, Arthur Feldman, Lars Kober, Henry Krum, Douglas L. Mann, John J.V. McMurray, Milton Packer, Karl Swedberg, Jeffrey S. Borer,
Randomized Etanercept Worldwide Evaluation (RENEWAL)Targeted Anticytokine Therapy in Patients With Chronic Heart Failure: Results of the
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2004 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.0000124490.27666.B2
2004;109:1594-1602; originally published online March 15, 2004;Circulation.
http://circ.ahajournals.org/content/109/13/1594World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on February 29, 2016http://circ.ahajournals.org/Downloaded from