Challenges for molecular profiling of chronic fatigue syndrome
8
Author Proof 10.2217/14622416.7.2.xxx © 2006 Future Medicine Ltd ISSN 1462-2416 Pharmacogenomics (2006) 7(2), xxx–xxx 1 R EVIEW Challenges for molecular profiling of chronic fatigue syndrome Suzanne D Vernon 1† , Toni Whistler 2 , Eric Aslakson 3 , Mangalathu Rajeevan 4 & William C Reeves 5 † Author for correspondence 1 Center for Infectious Diseases, Division of Viral and Rickettsial Diseases, National, Centers for Disease Control and Prevention, Atlanta GA, 30333, USA E-mail: [email protected] 2 E-mail: [email protected] 3 E-mail: [email protected] 4 E-mail: [email protected] 5 E-mail: [email protected] Keywords: keyword, keyword, keyword, keyword, keyword, keyword, keyword Successful utilization of genomics data to identify pharmacological targets for complex illnesses such as chronic fatigue syndrome (CFS) will require systematic integration of epidemiological, clinical, and laboratory data. Sound epidemiolog- ical and clinical data is necessary to obtain infor- mation to calculate the associations and magnitude of risk from laboratory measurements. Population-based studies have clearly docu- mented the medical and public health problem CFS poses. Between 400,000–900,000 adults in the USA suffer from the illness [1,2]; most have been ill for at least 5 years [2]; they are function- ally impaired to a similar extent as persons with multiple sclerosis and heart disease [3]; a quarter of them are unemployed or receiving disability allowance; and, the average family in whom a member has CFS foregoes US$20,000 annually in lost earnings and wages (half the median US household income) [4]. As no characteristic phys- ical signs or diagnostic laboratory abnormalities herald CFS, diagnosis depends on the evaluation of self-reported symptoms and ruling out medi- cal or psychiatric conditions that could explain the illness. There is no specific treatment, so management aims to relieve symptoms. Progno- sis is poor as only one third of primary care CFS patients improve by 1 year and, of those referred to secondary care, less than 10% return to pre- morbid functioning [5,6]. As a result of this, med- ical management of CFS is extraordinarily difficult and time consuming; one report docu- mented that CFS patients undergo an average of 13 primary care and five referral care visits [7]. CFS consists of incapacitating, persistent or relapsing fatigue of at least 6-months duration that is not relieved by rest and is accompanied by a characteristic (but nonspecific) symptom com- plex, which includes unusual postexertional malaise, unrefreshing sleep, impaired mem- ory/concentration, headache, muscle pain, joint pain, sore throat and tender lymph nodes [8]. Studies have consistently identified several risk factors for CFS, in particular, age, female sex, physical and emotional stressors, and certain personality and behavioral traits [9]. This understanding of the epidemiology of CFS has not been paralleled by achievements elu- cidating its pathophysiology or etiology. Despite more than 3000 peer-reviewed scientific publica- tions, no characteristic laboratory marker for CFS has been consistently identified. Research has instead demonstrated what CFS is not attrib- uted to – a muscle disorder, a retroviral infection, an autoimmune disease, or a psychiatric disorder [10,11]. Alterations in the immune system and hypothalamic–pituitary–adrenal (HPA) axis function have been well documented, however it is still unclear whether these alterations are primary or secondary factors in CFS [12]. There are at least three reasons why biomarker discovery and the elucidation of CFS pathophysi- ology has proved challenging. First is the fact that CFS is a diagnosis of exclusion, defined by self- reported symptoms. Recently an International CFS Study Group [13] recommended the use of standardized instruments to objectively measure the major domains of the illness, specifically:
Transcript of Challenges for molecular profiling of chronic fatigue syndrome

REVIEW
Challenges for molecular profiling of chronic fatigue syndrome
Suzanne D Vernon1†, Toni Whistler2, Eric Aslakson3, Mangalathu Rajeevan4 & William C Reeves5
†Author for correspondence1Center for Infectious Diseases, Division of Viral and Rickettsial Diseases, National, Centers for Disease Control and Prevention, Atlanta GA, 30333, USAE-mail: [email protected]: [email protected]: [email protected]: [email protected]: [email protected]
A
Keywords: keyword, keyword, keyword, keyword, keyword, keyword, keyword10.2217/14622416.7.2.xxx © 2
of
uthor ProSuccessful utilization of genomics data to identify
pharmacological targets for complex illnessessuch as chronic fatigue syndrome (CFS) willrequire systematic integration of epidemiological,clinical, and laboratory data. Sound epidemiolog-ical and clinical data is necessary to obtain infor-mation to calculate the associations andmagnitude of risk from laboratory measurements.
Population-based studies have clearly docu-mented the medical and public health problemCFS poses. Between 400,000–900,000 adults inthe USA suffer from the illness [1,2]; most havebeen ill for at least 5 years [2]; they are function-ally impaired to a similar extent as persons withmultiple sclerosis and heart disease [3]; a quarterof them are unemployed or receiving disabilityallowance; and, the average family in whom amember has CFS foregoes US$20,000 annuallyin lost earnings and wages (half the median UShousehold income) [4]. As no characteristic phys-ical signs or diagnostic laboratory abnormalitiesherald CFS, diagnosis depends on the evaluationof self-reported symptoms and ruling out medi-cal or psychiatric conditions that could explainthe illness. There is no specific treatment, somanagement aims to relieve symptoms. Progno-sis is poor as only one third of primary care CFSpatients improve by 1 year and, of those referredto secondary care, less than 10% return to pre-morbid functioning [5,6]. As a result of this, med-ical management of CFS is extraordinarilydifficult and time consuming; one report docu-mented that CFS patients undergo an average of13 primary care and five referral care visits [7].
CFS consists of incapacitating, persistent orrelapsing fatigue of at least 6-months durationthat is not relieved by rest and is accompanied bya characteristic (but nonspecific) symptom com-plex, which includes unusual postexertionalmalaise, unrefreshing sleep, impaired mem-ory/concentration, headache, muscle pain, jointpain, sore throat and tender lymph nodes [8].Studies have consistently identified several riskfactors for CFS, in particular, age, female sex,physical and emotional stressors, and certainpersonality and behavioral traits [9].
This understanding of the epidemiology ofCFS has not been paralleled by achievements elu-cidating its pathophysiology or etiology. Despitemore than 3000 peer-reviewed scientific publica-tions, no characteristic laboratory marker forCFS has been consistently identified. Researchhas instead demonstrated what CFS is not attrib-uted to – a muscle disorder, a retroviral infection,an autoimmune disease, or a psychiatric disorder[10,11]. Alterations in the immune system andhypothalamic–pituitary–adrenal (HPA) axisfunction have been well documented, however itis still unclear whether these alterations areprimary or secondary factors in CFS [12].
There are at least three reasons why biomarkerdiscovery and the elucidation of CFS pathophysi-ology has proved challenging. First is the fact thatCFS is a diagnosis of exclusion, defined by self-reported symptoms. Recently an InternationalCFS Study Group [13] recommended the use ofstandardized instruments to objectively measurethe major domains of the illness, specifically:
006 Future Medicine Ltd ISSN 1462-2416 Pharmacogenomics (2006) 7(2), xxx–xxx 1

REVIEW – Vernon, Whistler, Aslakson, Rajeevan & Reeves
2
Author Pro
of
• The Medical Outcomes Survey Short Form-36 (SF-36), to measure functional impair-ment [14]
• A comprehensive instrument like the multidi-mensional fatigue inventory (MFI) [15] toevaluate dimensions of fatigue
• The Centers for Disease Control (CDC)Symptom Inventory to document the occur-rence, duration and severity of the symptomcomplex [16]
These standardized measures can be used toidentify (and stratify) patients with CFS basedon the extent of their disability, the duration andseverity of fatigue and the duration and severityof their symptoms [17].
The second reason why biomarker discoveryand the elucidation of CFS pathphysiology hasproved challenging involves study design and thestudy subjects themselves. Numerous, elegantpopulation-based studies have been conductedin order to estimate the prevalence of CFS[1,2,18–23]. The next step is to enroll subjects,identified in these population-based studies, intothose aimed at biomarker discovery. However,because of the high cost and challenging logisticsinvolved in enrolling individuals identified inpopulation-based studies for subsequent biomar-ker studies, many investigators rely on studyingcase and control subjects that are convenient.These types of convenience samples lead to diffi-culties in determining associations, relating riskback to the general population and replicatingthe findings. In addition, studies of patientsidentified from clinics suffer from referral bias,which cannot be measured and is likely to bequite large for illnesses such as CFS. For exam-ple, only half of individuals identified to sufferfrom CFS in the general population of Chicago(IL, USA) had consulted a physician for their ill-ness [1] and only 16% of people with CFS identi-fied in the general population of Wichita (KS,USA) had been diagnosed and treated for CFSby a physician [2].
The third reason is that CFS is an illness withalterations in complex bodywide systems ofhomeostasis. New, high-throughput technologyexists to detect and characterize every genetic pol-ymorphism, gene transcript and protein, but isthis sufficient to enable the discovery of biomark-ers for detection and surveillance, risk assessment,and therapeutic intervention of CFS? If thesetechnological advances are coupled with a soundstudy design and integrated along with carefuland appropriate epidemiological and clinical
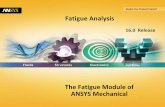
measurements, optimal sample collection andpowerful computational tools, then sensitive andspecific biomarkers can be identified (Figure 1).
Objectively measured and empirically evalu-ated biomarkers, at the least, identify uniquegroups of people and serve as indicators of nor-mal vs. abnormal biological processes [24].Biomarkers can be used to stratify and diagnosepatient populations and may serve as indicatorsof drug efficacy or toxicity. The most pressingneed for the CFS research community isbiomarkers that can be used to objectively iden-tify and stratify CFS cases in order to customizeintervention. The following sections describesome of the successes and challenges of molecu-lar profiling in the discovery of biomarkers forthe diagnosis, therapeutic intervention andultimately prevention of CFS.
Molecular profiling of chronic fatigue syndromeThe 21st Century postgenomic era offers greatpromise to relieve the tremendous personal,social and economic burden of CFS by providinglaboratory tools to identify specific biomarkersfor CFS, characterize its pathogenesis and ulti-mately the therapeutic intervention required.Sophisticated laboratory methods for profilingthe entire transcriptome, proteome and genomeare widely available. Any biological sample withsufficient DNA can be used for the identificationof genetic polymorphisms. The blood is a practi-cal sample for proteomics as it contains proteinsfrom physiological processes occurring through-out the body [25]. However, selecting the mostappropriate biologic sample for transcriptomeprofiling is less straightforward.
The challenge for gene expression profiling ofCFS is that both central and peripheral pertur-bations contribute to the illness state. Profilingthe activity of the genome in people with CFS isfurther complicated by the lack of a known, oraccessible, anatomic lesion. To date, the pub-lished high-density gene expression studies onCFS have relied on the peripheral blood to pro-vide clues of CFS pathophysiology and identifybiomarkers [26–30]. Transcriptome profiling ofperipheral blood cells is a reasonable startegy ascells travel throughout the body, including toand from the CNS [31], helping to maintainhomeostasis or potentially causing immune-mediated pathology. By measuring the activityof peripheral blood cell genes, it is anticipatedthat CFS biomarkers and pathophysiology willbe revealed.
Pharmacogenomics (2006) 7(2)

A
www.futuremedicine.com
Challenges for molecular profiling of chronic fatigue syndrome – REVIEW
uthor Pro
of
Gene expression in chronic fatigue syndromeThe remarkable lack of variability in peripheralblood gene expression within healthy age andsex-matched populations provides an importantgauge of health [32,33], and serves as a baselinefor measuring peripheral blood changes associ-ated with illness. There are several exampleswhere peripheral blood has been used forbiomarker and pattern discovery, when there isno known or accessible lesion including autoim-mune diseases that affect the CNS [34], neuro-logical injury [35], post-traumatic stress disorder[36] and CFS [26–30]. As most of these disordersare centrally mediated, the fact that peripheralblood gene expression studies have been success-ful is likely attributed to the bi-directional com-munication between the brain and theperiphery, as leukocytes routinely traffic acrossthe blood–brain barrier for immune surveillance[31]. Soluble molecules of the immune, endo-crine, and nervous systems are the primarymolecular signals between the brain and thebody and the authors have demonstrated thatapproximately 65% of the 1600 genes thatmediate neuroendocrine and immune processesare expressed in peripheral blood cells [37]. Deci-phering these peripheral signatures could pro-vide key insight into centrally mediatedsymptoms that characterize CFS.
Expression profiling studies of CFS have iden-tified differentially expressed genes implicated inpathways that disrupt normal immune functionof peripheral mononuclear blood cells [26–30]. Allhave identified differentially expressed genes thatdistinguished individuals with CFS from nor-mal, nonfatigued controls. However, only onestudy, by Kaushik and colleagues, validated theexpression of nearly half of the differentiallyexpressed genes identified using microarrays [26].Validated differential expression included genesinvolved in the transcription of mRNA, process-ing of pre-mRNA, translation, mitochondrialdysfunction and apoptosis [26]. A recent analysisof gene expression in patients suffering fromCFS following infection with Epstein Barr virusidentified differentially expressed genes involvedin transcription, apoptosis and mitochondrialfunctions [38]. Even though the study by Kaushikand colleagues [26] is the only one to validate dif-ferentially expressed genes using real time-polymerase chain reaction (RT-PCR), reproduc-ing the same results across studies is also thoughtof as validation. For example, the differentiallyexpressed genes reported in all microarray papersmap to the same biological pathways as validatedby Kaushik and colleagues [26]. Research report-ing differences between cytokine responses andcell surface markers in sudden versus gradualCFS patients [39] corroborated the observation
Figure 1. The prevention and control of CFS will require accurate diagnosis and an improved understanding of the pathophysiology of CFS.
Discovering biomarkers can help on both of these fronts. However, complex illnesses such as CFS pose additional challenges requiring the collection and integration of comprehensive information that help to characterize the epidemiological, clinical and molecular aspects of the illness.CFS: Chronic fatigue syndrome.
Genomics
Proteomics
Genetics
Clinical
Epidemiology
Bioinformatics andinformation management
Analysis tools,data integration,computational biology
Cell and systemmodeling
Networks andpathways
Diagnosticmarker
Therapeuticintervention
Prevention
Informationgathering anddescription
Information management
Informationinterpretation andconclusion
Implementation
3

REVIEW – Vernon, Whistler, Aslakson, Rajeevan & Reeves
4
Author Pro
of
that CFS patients reporting sudden or gradualonset of illness had different peripheral bloodgene expression patterns [40].
Two studies using a comprehensive geneexpression profiling method, called differentialdisplay PCR, found unique gene expressionmarkers between CFS cases and controls.Despite the fact that these two studies wereconducted on peripheral blood samples fromgeographically distinct CFS subjects, bothfound differentially expressed genes implicat-ing immune system dysfunction and, moreimportantly, both discovered the upregulationof genes in the cathepsin family in CFSpatients [28,29].
The factors most likely to be responsible fordifferences observed in gene expression find-ings are differences in sample collection,processing and microarray platforms. Reliableand reproducible results are linked to the qual-ity of the biological sample [41]. In addition,sample quality is one of the factors that con-tributes to the lack of conformity when com-paring results from various microarrayplatforms [42]. Peripheral blood is an ideal sam-ple for molecular profiling in population-basedepidemiology studies as it is relatively noninva-sive and collection tubes have been optimizedfor maximizing viable cell recovery and mini-mizing ex vivo affects [43]. The BD Vacutainer®
CPT™ Cell Preparation Tube (BD, NJ, USA)allows the collection of viable lymphocyte andmononuclear cells while minimizing the timeto storage. This blood sample collection strat-egy allows the use of the sample in multipletypes of assays, such as plasma for protein anal-ysis, viable cells for functional assays, and cellsfrom which RNA and DNA can be extractedfor genomic studies. It should be emphasizedthat it is essential that all samples are preparedand handled in the same way to minimize theex vivo cell stimulation and minimize altera-tions in gene expression. Recent developmentof the PAXgene™ (QIAGEN, Hilden, Ger-many) Blood RNA system [101] simplifies theblood handling process and immediately stabi-lizes the expression patterns. It should be notedthat, since this collection system was designedspecifically for gene expression assays, addi-tional blood samples should be collected forother non-RNA assays. Standardization of thesample collection and processing, in additionto improved gene annotation, will help toimprove the likelihood of discovering the samedifferentially expressed genes.
Genetics & proteomicsCFS is not the result of a single behavior, expo-sure or mutation, arising from the combinedaction of many genes, environmental factors andrisk conferring behaviors. The contribution ofgenetic factors in the initiation and progressionof CFS has been explored and CFS may beinherited [44,45]. Several twin studies suggest CFShas a moderate genetic risk, which is independ-ent of psychiatric disorders [45–48]. More recently,genetic predisposition to CFS was related tosequence variations in specific genes involved inneurotransmission. A novel complete loss offunction mutation of the corticosteroid-bindingglobin gene was associated with chronic fatiguein a study conducted with a 39 member Ital-ian–Australian family [49]. Human serotonintransporter gene (5-HT) expression is regulatedby a common polymorphism in its upstream reg-ulatory region (5-HTTLPR). The polymorphismconsists of a 44 bp insertion or deletion involv-ing repeat elements resulting in short (S) andlong (L) allelic forms of the repeats. While a sig-nificant increase of the L allelic variant wasfound in CFS patients compared with controls,individuals with one or two copies of the S alleleof the 5-HTTLR exhibited more diagnosabledepression in relation to stressful life events[50–52]. Among three metabolic genes tested (ade-nosine monophosphate deaminase 1 [AMPD1],carnitine palmitolyltransferase II [CPT2], andangiotensin I converting enzyme [ACE])increased risk for CFS among Gulf war veteranswas associated with alterations in the inser-tion/deletion (I/D) polymorphism of the ACEgene [53]. A significant association with multiplepolymorphisms and haplotypes of the glucocor-ticoid receptor and a moderate association with amissense mutation in the monoamine oxidasegene have been identified in CFS subjects from apopulation-based study [54]. Although limited,these data from candidate gene studies suggest agenetic vulnerability in nervous and immunefunction genes in CFS.
Differential gene expression and sequence var-iations result in potential alterations in proteinstructure and protein levels. Here again, theperipheral blood serves as an ideal surrogate tosurvey protein profiles as serum contains pro-teins from every organ [25]. Surface-enhancedlaser desorption/ionization time of flight(SELDI-TOF) is a new, high-throughput massspectroscopy technique that defines protein pro-files in biological samples. This technique hasbeen used successfully to identify serum biomar-
Pharmacogenomics (2006) 7(2)

A
www.futuremedicine.com
Challenges for molecular profiling of chronic fatigue syndrome – REVIEW
uthor Pro
of
kers in ovarian and prostate cancer patients[55,56]. One recent study used SELDI-TOF tosuccessfully identify serum biomarkers in chil-dren with systemic-onset juvenile idiopathicarthritis following conventional therapy [57].
Recently, quadropole time-of-flight mass spec-troscopy has been used to profile proteins in thecerebral spinal fluid from patients suffering fromCFS, Persian Gulf War Illness and normal con-trols [58]. A constellation of proteins was commonbetween the two illnesses and distinct from nor-mal cerebral spinal fluid. This common proteinpattern supports that idea that no individualmolecular profile, be it genomic, genetic or pro-teomic, will be sufficient to distinguish CFS fromother chronic, medically undefined illnesses.Currently, there are no published studies apply-ing mass spectroscopy methods to plasma orserum. It is likely that the plasma proteome willreveal proteins that distinguish between CFScases and controls. Once identified, these pro-teins should be subjected to rigorous characteri-zation so their diagnostic utility can be exploredfurther and protein information can be inte-grated with genetic and gene expression data.
Data analysisSince CFS is not the result of a single mutationor environmental factor, a few differentiallyexpressed genes, or a characteristic protein pro-file, it is essential to collect all possible data inorder to explore specific hypotheses and identifypreviously unanticipated associations. To date,the majority of CFS research has been hypothesisdriven, for example, examining perturbations ofimmune cell and HPA axis function. Theremarkable lack of significant findings is, in part,due to the complexity and heterogeneity of CFS,however, it is also due to the lack of explorationof the data using powerful data miningapproaches that are more likely to help definehypotheses by examining unusual data connec-tions and correspondences. In this postgenomicera, data mining methods should be comple-mented with traditional biostatistical approachesand in conjunction with information that helpsto explain the relationships between genomicinformation and phenomena at biochemical,physiological and behavioral levels.
There are many advanced methods for gener-ating data that describe the disease state of anindividual. For example, high-throughputgenomic, proteomic and imaging data collectionhas resulted in a wealth of information that mustbe associated with clinical and epidemiological
data from each individual and integrated withthe study population as a whole. Often, the datatypes are quite different and need to be acquiredand stored in ways that are conducive for inte-gration and analysis using both traditional statis-tical tools and innovative data mining methods.This poses technical and logistical challenges,such as managing millions of data points andhundreds of files generated for each individual,in addition to keeping the data secure, backed upand stored in the most efficient manner.
Properly constructed databases with self-describing metadata allow easy integration withvarious open source and proprietary tools andprovide the means for effective biomarker dis-covery. For the authors’ studies, the data isassembled in a star schema where CFS subjectsare linked with all the available data gathered forthose subjects. Recently, the authors haveemployed knowledge discovery in data mining(KDD) methodology as this is effective for theanalyzing of large clinical databases. The mostimportant aspect of any data analysis process,including KDD, is the preprocessing step. Here,data cleaning and handling of missing values isparamount, since the validity of the results willdepend on the quality of the input data [58].Once datasets are ready, standard statistical anal-ysis can be augmented with KDD techniques,including construct classifiers, principal compo-nents analysis, neural network pattern recogni-tion discovery methods, hidden Markov models,genetic algorithms and support vector machinetechniques to search for previously hidden rela-tionships.
Key to investigating complex illnesses such asCFS, is the reduction of data complexity whileretaining as much biological information ofpotential importance to CFS as possible.
The use of both biostatistical and data miningmethods will yield testable hypotheses that willlead to effective therapeutic intervention andultimately the prevention of CFS.
OutlookCurrently, CFS is defined by self-reportedsymptoms and can serve as the research modelfor many medically unexplained fatiguing ill-nesses that comprise up to 80% of physician vis-its. The postgenomic era has given rise to bothhigh-throughput molecular and computationaltechnologies that will allow the identification ofan objective diagnostic marker and the elucida-tion of CFS pathophysiology. It is now generallyaccepted that CFS is a heterogeneous illness
5

REVIEW – Vernon, Whistler, Aslakson, Rajeevan & Reeves
6
uthor Pro
of making it critically important to define this het-erogeneity at both a clinical and molecular level.This will require accurate assessment and meas-urement of all the systems that are perturbedand the collection of information that can eluci-date risk factors. There are multiple system fail-ures in patients with CFS. This complexitydemands that CFS is studied using a multidisci-plinary approach in order to diagnose CFS andidentify effective therapeutic interventions.Research should include individuals identifiedfrom the population and studied longitudinally.As the severity of the illness varies over time,biomarker discovery and pathophysiology stud-ies should include a challenge with the intentionof synchronizing research subjects. For gene
expression markers, time series samples shouldbe acquired to better define altered pathways.Genomic data should be integrated with geneticand proteomic data in order to increase the like-lihood of defining the extent of the heterogene-ity of CFS and the underlying pathophysiology.Empirically defining the heterogeneity of CFSusing epidemiological, clinical and molecularmeasurements will result in effective and cus-tomized therapeutic interventions and,ultimately, control of CFS.
DisclosureThe findings and conclusions in this report are those of the
authors and do not necessarily represent the views of thefunding agency.
Highlights
• There are 400,000–900,000 adults suffering from chronic fatigue syndrome (CFS) in the USA and, as sufferers, are functionally impaired to a similar extent as patients with multiple sclerosis and heart disease.
• The average family in whom a member has CFS foregoes US$20,000 annually in lost earnings and wages, half the median household income in the USA.
• There have been significant achievements in understanding the epidemiology of CFS. However, this success has not been paralleled by achievements elucidating its pathophysiology or etiology. The postgenomic era offers promise to relieve the tremendous personal, social and economic burden of CFS.
• Technological advances must be coupled with a sound study design and integrated along with careful and appropriate epidemiological and clinical measurements, optimal sample collection, and powerful computational tools for effective biomarker discovery in CFS.
• As there is no known lesion in CFS, the peripheral blood is an ideal sample for molecular profiling both central and peripheral affects that occur in this illness.
• Gene expression profiling using microarray technology and differential display polymerase chain reaction have identified differentially expressed genes, implicating pathways that disrupt the normal immune function of peripheral mononuclear blood cells.
• Single nucleotide polymorphisms from several candidate gene studies suggest a genetic vulnerability in nervous and immune function genes in individuals suffering from CFS.
• The peripheral blood serves as an ideal surrogate to survey protein profiles as serum contains proteins from every organ.
• Data mining methods are essential for investigating complex illnesses since these approaches are effective for the analysis of large databases containing disparate information.
ABibliographyPapers of special note have been highlighted as either of interest (•) or of considerable interest (••) to readers.1. Jason LA, Richman JA, Rademaker AW
et al.: A community-based study of chronic fatigue syndrome. Arch. Intern. Med. 159, 2129–2137 (1999).
2. Reyes M, Nisenbaum R, Hoaglin DC et al.: Prevalence and incidence of chronic fatigue syndrome in Wichita, Kansas. Arch. Intern. Med. 163, 1530–1536 (2003).
3. Solomon L, Nisenbaum R, Reyes M, Papanicolaou DA, Reeves WC: Functional status of persons with chronic fatigue syndrome in the Wichita, Kansas,
population. Health Qual. Life Outcomes1, 48 (2003).
4. Reynolds KJ, Vernon SD, Bouchery E, Reeves WC: The economic impact of chronic fatigue syndrome. Cost Eff. Resour. Alloc. 2, 4 (2004).
• One of the only recent economic impact papers to be conducted on a population-based sample that clearly documents the costs due to lost productivity per year from chronic fatigue syndrome (CFS).
5. Wessely SC, Hotopf M, Sharpe M: Chronic fatigue and its syndromes. Oxford University Press, USA (1998).
6. Joyce J, Hotopf M, Wessely SC: The prognosis of chronic fatigue and chronic
fatigue syndrome: a systematic review. QJM 90(3), 223–233 (1997).
7. Lloyd A, Pender H: The economic impact of chronic fatigue syndrome. Med. J. Australia 157, 599–601 (1992).
8. Fukuda K, Straus SE, Hickie I, Sharpe MC, Dobbins JG, Komaroff A: The chronic fatigue syndrome: a comprehensive approach to its definition and study. Ann. Intern. Med. 121, 953–959 (1994).
9. Ranjith G: Epidemiology of chronic fatigue syndrome. Occup. Med. (Lond.) 55, 13–19 (2005).
•• Recent and thorough review summarizing the epidemiology of CFS.
Pharmacogenomics (2006) 7(2)

Challenges for molecular profiling of chronic fatigue syndrome – REVIEW
Author Pro
of
10. Afari N, Buchwald D: Chronic fatigue syndrome: a review. Am. J. Psychiatry. 160, 221–236 (2003).
11. Reid S, Chalder T, Cleare A, Hotopf M, Wessely SC: Chronic fatigue syndrome. Clin. Evid. 12, 1578–1593 (2004).
12. Cleare AJ: The HPA axis and the genesis of chronic fatigue syndrome. Trends Endocrinol. Metab. 15, 55–59 (2004).
13. Reeves WC, Lloyd A, Vernon SD et al.: The chronic fatigue syndrome research case definition: lessons learned 1994–2002. BMC Health Serv. Res. 3, 25 (2003).
14. Ware JE, Sherbourne CD: The MOS 36-item short form health survey (SF-36): conceptual framework and item selection. Med. Care. 30, 473–483 (1992).
15. Smets EM, Garssen BJ, Bonke B, DeHaes JC: The multidimensional fatigue inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom. Res. 39, 315–325 (1995).
16. Wagner D, Nisenbaum R, Heim C, Jones JF, Unger ER, Reeves WC: Psychometric properties of the CDC symptom inventory for the assessment of chronic fatigue syndrome. Popul. Health Metr. 3, 8 (2005).
17. Reeves WC, Wagner D, Nisenbaum R, et al.: Chronic fatigue syndrome: a clinically empirical approach to its definition and study. BMC Med. 3, 9 (2005).
18. Sullivan PF, Pedersen NL, Jacks A, Evengard B: Chronic fatigue in a population sample: definitions and heterogeneity. Psychol. Med. 35(9), 1337–1348 (2005).
19. Huibers MJ, Kant IJ, Knottnerus JA, Bleijenberg G, Swaen GM, Kasl SV: Development of the chronic fatigue syndrome in severely fatigued employees: predictors of outcome in the Maastricht cohort study. J. Epidemiol. Community Health 58, 877–882 (2004).
20. Farmer A, Fowler T, Scourfield J, Thapar A: Prevalence of chronic disabling fatigue in children and adolescents. Br. J. Psychiatry. 184, 477–481 (2004).
21. Bierl C, Nisenbaum R, Hoaglin DC et al.: Regional distribution of fatiguing illnesses in the United States: a pilot study. Popul. Health Metr. 2, 1 (2004).
22. Hatcher S, House A: Life events, difficulties and dilemmas in the onset of chronic fatigue syndrome: a case-control study. Psychol. Med. 33, 1185–1192 (2003).
23. Skapinakis P, Lewis G, Meltzer H: Clarifying the relationship between unexplained chronic fatigue and psychiatric morbidity: results from a community survey in Great Britain. Int. Rev. Psychiatry. 15, 57–64 (2003).
24. Rolan P, Atkinson AJ Jr, Lesko LJ: Use of biomarkers from drug discovery through clinical practice: report of the Ninth European Federation of Pharmaceutical Sciences Conference on Optimizing Drug Development. Clin. Pharmacol. Ther. 73, 284–291 (2003).
25. Liotta LA, Ferrari M, Petricoin E: Clinical proteomics: written in blood. Nature 425, 905 (2003).
26. Kaushik N, Fear D, Richards SC et al.: Gene expression in peripheral blood mononuclear cells from patients with chronic fatigue syndrome. J. Clin. Pathol. 58, 826–832 (2005).
27. Whistler T, Jones JF, Unger ER, Vernon SD: Exercise responsive genes measured in peripheral blood of women with chronic fatigue syndrome and matched control subjects. BMC Physiol. 5, 5 (2005).
28. Steinau M, Unger ER, Vernon SD, Jones JF, Rajeevan MS: Differential-display PCR of peripheral blood for biomarker discovery in chronic fatigue syndrome. J. Mol. Med. 82, 750–755 (2004).
29. Powell R, Ren J, Lewith G, Barclay W, Holgate S, Almond J: Identification of novel expressed sequences, upregulated in the leucocytes of chronic fatigue syndrome patients. Clin. Exp. Allergy. 33, 1450–1456 (2003).
30. Vernon SD, Unger ER, Dimulescu IM, Rajeevan M, Reeves WC: Utility of the blood for gene expression profiling and biomarker discovery in chronic fatigue syndrome. Dis. Markers 18, 193–199 (2002).
31. Hickey WF: Basic principles of immunological surveillance of the normal central nervous system. Glia 36, 118–124 (2001).
32. Campbell C, Vernon SD, Karem KL, Nisenbaum R, Unger ER: Assessment of normal variability in peripheral blood gene expression. Dis. Markers 18, 201–206 (2002).
33. Whitney AR, Diehn M, Popper SJ et al.: Individuality and variation in gene expression patterns in human blood. Proc. Natl Acad. Sci. USA 100, 1896–1901 (2003).
34. Lock CB, Heller RA: Gene microarray analysis of multiple sclerosis lesions. Trends Mol. Med. 9, 535–541 (2003).
35. Tang Y, Nee AC, Lu A, Ran R, Sharp FR: Blood genomic expression profile for neuronal injury. J. Cereb. Blood Flow Metab. 23, 310–319 (2003).
36. Segman RH, Shefi N, Goltser-Dubner T, Friedman N, Kaminski N, Shalev AY:
Peripheral blood mononuclear cell gene expression profiles identify emergent post-traumatic stress disorder among trauma survivors. Mol. Psychiatry 10, 500–513 (2005).
•• Clearly demonstrates the utility of gene expression profiling of the peripheral blood for classifying people with psychiatric illness and characterizing perturbed peripheral pathways.
37. Nicholson AC, Unger ER, Rajeevan M, Ojaniemi H, Vernon SD: Exploration of neuroendocrine and immune gene expression in peripheral blood mononuclear cells. Brain Res. Mol. Brain Res. 129, 193–197 (2004).
•• Demonstrates the potential for using the peripheral blood to explain central nervous system functions.
38. Vernon SD, Whistler T, Cameron B, Hickie IB, Reeves WC, Lloyd A: Preliminary evidence of mitochondrial dysfunction associated with post-infective fatigue after acute infection with Epstein Barr Virus. BMC Infectious Diseases 6, 15 (2006).
39. Mawle AC, Nisenbaum R, Dobbins JG et al.: Immune responses associated with chronic fatigue syndrome: a case-control study. J. Infect. Dis. 175, 136–141 (1997).
40. Whistler T, Unger ER, Nisenbaum R, Vernon SD: Integration of gene expression, clinical, and epidemiologic data to characterize chronic fatigue syndrome. J. Transl. Med. 1, 10 (2003).
41. Ojaniemi H, Evengard B, Lee DR, Unger ER, Vernon SD: Impact of RNA extraction from limited samples on microarray results. Biotechniques 35, 968–973 (2003).
42. Irizarry RA, Warren D, Spencer F et al.: Multiple-laboratory comparison of microarray platforms. Nature Methods 2, 345–350 (2005).
43. Baechler EC, Batliwalla FM, Karypis G et al.: Expression levels for many genes in human peripheral blood cells are highly sensitive to ex vivo incubation. Genes Immun. 5, 347–353 (2004).
• Emphasizes the importance of sample handling and preparation when using genomic technologies.
44. Walsh CM, Zainal NZ, Middleton SJ, Paykel ES: A family history study of chronic fatigue syndrome. Psychiatr. Genet. 11, 123–128 (2001).
45. Hickie I, Kirk K, Martin N: Unique genetic and environmental determinants of prolonged fatigue: a twin study. Psychol Med. 29, 259–268 (1999).
www.futuremedicine.com 7

REVIEW – Vernon, Whistler, Aslakson, Rajeevan & Reeves
Author Pro
of
46. Hickie I, Bennett B, Lloyd A, Heath A, Martin N: Complex genetic and environmental relationships between psychological distress, fatigue and immune functioning: a twin study. Psychol Med 29, 269–277 (1999).
47. Farmer A, Scourfield J, Martin N, Cardno A, McGuffin P. Is disabling fatigue in childhood influenced by genes? Psychol Med. 29, 279–282 (1999).
48. Buchwald D, Herrell R, Ashton S et al.: A twin study of chronic fatigue. Psychosom. Med. 63, 936–943 (2001).
49. Torpy DJ, Bachmann AW, Grice JE et al.: Familial corticosteroid-binding globulin deficiency due to a novel null mutation: association with fatigue and relative hypotension. J. Clin. Endocrinol. Metab. 86, 3692–3700 (2001).
50. Lesch KP, Bengel D, Heils A et al.: Association of anxiety-related traits with a polymorphism in the serotonin transporter gene regulatory region. Science 274, 1527–1531 (1996).
51. Narita M, Nishigami N, Narita N et al.: Association between serotonin transporter
gene polymorphism and chronic fatigue syndrome. Biochem. Biophys. Res. Commun. 311, 264–266 (2003).
52. Caspi A, Sugden K, Moffitt TE et al.: Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science 301, 386–389 (2003).
53. Vladutiu GD, Natelson BH: Association of medically unexplained fatigue with ACE insertion/deletion polymorphism in Gulf War veterans. Muscle Nerve 30, 38–43 (2004).
54. Rajeevan MS, Smith AK, Dimulescu I, Vernon SD, Heim C, Reeves WC: Association of polymorphisms and haplotypes in the glucocorticoid receptor with chronic fatigue syndrome. American Society for Human Genetics 55th Annual meeting, Salt Lake city, Utah, USA (2005).
55. Moshkovskii SA, Serebryakova MV, Kuteykin-Teplyakov KB et al.: Ovarian cancer marker of 11.7 kDa detected by proteomics is a serum amyloid A1. Proteomics 5, 3790–3797 (2005).
56. Malik G, Ward MD, Gupta SK et al.: Serum levels of an isoform of apolipoprotein A-II as
a potential marker for prostate cancer. Clin. Cancer Res. 11, 1073–1085 (2005).
57. Miyamae T, Malehorn DE, Lemster B, et al.: Serum protein profile in systemic-onset juvenile idiopathic arthritis differentiates response versus nonresponse to therapy. Arthritis Res. Ther. 7, R746–R755 (2005).
58. Baraniuk JN, Casado B, Maibach H, Clauw DJ, Pannell LK, Hess SS: A chronic fatigue syndrome – related proteome in human cerebrospinal fluid. BMC Neurol. 5, 22 (2005).
59. Duhamel A, Nuttens MC, Devos P, Picavet M, Beuscart R: A preprocessing method for improving data mining techniques. Application to a large medical diabetes database. Stud. Health Technol. Inform. 95, 269–274 (2003).
Website101. PAXgene™ Blood RNA System webpage.
www.preanalytix.com/RNA.asp
8 Pharmacogenomics (2006) 7(2)