Efficacy of cognitive behavioral therapy for chronic fatigue syndrome: A meta-analysis

10.1192/bjp.168.1.121Access the most recent version at doi: 1996 168: 121-126 The British Journal of Psychiatry
R Euga, T Chalder, A Deale and S Wessely
primary and tertiary careA comparison of the characteristics of chronic fatigue syndrome in
References
http://bjp.rcpsych.org/cgi/content/abstract/168/1/121#otherarticlesArticle cited in:
permissionsReprints/
[email protected] To obtain reprints or permission to reproduce material from this paper, please write
to this article atYou can respond http://bjp.rcpsych.org/cgi/eletter-submit/168/1/121
serviceEmail alerting
click heretop right corner of the article or Receive free email alerts when new articles cite this article - sign up in the box at the
fromDownloaded
The Royal College of PsychiatristsPublished by on July 15, 2011 bjp.rcpsych.org
http://bjp.rcpsych.org/subscriptions/ go to: The British Journal of PsychiatryTo subscribe to

British Journal of Psychiatry (1996), 168, 121-126
A Comparison of the Characteristics of Chronic Fatigue Syndromein Primary and Tertiary Care
R. EUBA,T. CHALDER,A. DEALEand S. WESSELY
Background. To evaluate the characteristics of Chronic Fatigue Syndrome (CFS) in primaryand tertiarycare.Method. A comparison of subjects fulfilling criteria for CFS seen in primary care and in a hospitalunit specialising in CFS. Subjects were 33 adults fulfilling criteria for CFS, identified as partof a prospective cohort study in primarycare, compared to 79 adults fulfillingthe same criteriareferred for treatment to a specialist CFS clinic.Results. Hospital cases were more likelyto belong to upper socio-economic groups, and tohave physicalillnessattributions. They had higherlevelsof fatigue and more somatic symptoms,and were more impairedfunctionally, but had less overt psychological morbidity. Women wereover-represented in both primary care and hospital groups. Nearly half of those referred toa specialist clinic did not fulfil operational criteria for CFS.Conclusion. The high rates of psychiatric morbidity and female excess that characterise CFSin specialist settings are not due to selection bias. On the other hand higher social class andphysical illness attributions may be the result of selection bias and not intrinsic to CFS.
The ChronicFatigueSyndrome(CFS)continuesto beregarded as a controversial condition, particularly withregards to competing claims concerning aetiology andtreatment. There is little disagreement about whatconstitutes the classic clinical presentation of thissyndrome, and the usual demographic features of thesufferers. Many studies report that CFS sufferers aremore likely to be women, to belong to higher socialclasses (with a particular over-representation ofprofessionals), to be very impaired functionally, havehigh levelsof psychological distress, hold characteristicillness beliefs, and have a poor prognosis (Wessely &Powell, 1989; Dowsett et al, 1990; Buchwald &Komaroff, 1991;Sharpeet a!, 1992;Wilson et a!,1994). All these observations come from studies ofspecialistclinics,where patients frequently have alreadyreceived a diagnosis of CFS prior to their referral.Although aetiological claims have been made on thebasis of some of these observations, all could be theresult of selection or referral bias. If so, thecharacteristics of the syndrome would differ betweenprimary and tertiary care. We now report a comparisonbetween a group of patients referred to a clinicspecialisingin CFS, and another group of subjects seenin primary care. Both groups fulfilled criteria for CFS(Sharp eta!, 1991) (‘Oxfordcriteria'), but were notnecessarily seeking help under that label.
Selection of cases
cohort study of 1199 subjects presenting to GPs withclinically diagnosed viral infections, compared to1177 attending for other reasons. The prevalence ofchronic fatigue and CFS was determined six monthslater in the 1985 subjects in both cohorts who weresuccessfullyfollowedup (84%). The main findingof the study was that no differences emerged in theprevalence of chronic fatigue and CFS between thosewith, and without, initial viral infections (Wesselyet a!, 1995). In this paper we have thus joined thetwo groups.
Hospital cases: The hospital chronically fatiguedcases were patients who had been referred to a CFSclinic at an inner London teaching hospital. Thisclinic receives referrals largely from local GPs andphysicians, and specialises in research andmanagement of CFS. The senior author (SW) carriedout the majority of the assessments.
All those included in this study fulfilled the samecriteria for CFS (Sharpe et a!, 1991). There was no
differenceto the pattern of resultsif the samecomparisonswererepeatedusingthe latestcriteriaproposed by the Centers for Disease Control (Fukadaet a!, 1994).
Measures
A variety of outcome measures were used during thecohort study. Those relevant to the current studywere: the Fatigue Questionnaire (Chalder et a!,1993)—this also includes a question on selfattribution of fatigue; the 12-item General HealthQuestionnaire (GHQ-12; Goldberg, 1972). The
Method
Primary care cases: Cases of CFS in primary carewere identified at the fmal stage of a prospective
121

Group nMean age(years)% Female% Married
or cohabiting%
Socialclass1Community
33Hospital
7936.4
(33.7-39.1)35
(32.5-37.4)81.8
(27)(67-94)
68.4 (54)(58-78)71.9
(23)(52-84)50 (39)(39-61)3%
(1)(—2-8)
35.9 (28)(25-47)95%
Cl shown in brackets
122 EUBA ET AL
conservative cut-off of 3/4 was used to determinepsychiatric caseness; the Medical Outcomes StudyHealth Survey Questionnaire (20—itemMOS ShortForm; Ware et a!, 1992) was used to assess functionalimpairment. Although functional impairment is adimensional measure, it was necessary to choose acut-off to fulfil operational criteria for CFS, thelatest of which defines functional impairment as‘¿�substantial'without further elaboration. Wearbitrarily defined impairment as present when asubject answered positively to being limited for sixmonths or more on any one of the following fourquestions asked in the MOS Short Form: beingimpaired on either moderate activities, walkinguphill, walking 100 yards, or needing simple aids todaily living; and the Somatic Symptom Check List,which contains 32 somatic symptoms, modified fromthe Somatic Discomfort Questionnaire (Wittenborn& Buhler, 1979).
Most of these measures have been previously usedin hospital based studies of CFS (Wessely & Powell,1989; Butler et a!, 1991). Information regarding pastpsychiatric history and past use of psychotropicdrugs was obtained from the subjects themselves, aswell as the GPs clinical notes. Social class wasassessed using the Registrar General's classification(OPCS, 1970).
Statistics
The Student's 1-test (2-tail probability) was used forparametric comparisons, and the Mann—WhitneyU-test and x2 for non-parametric analyses. Oddsratios were calculated with 95% confidence intervals.
Results
We identified 214 subjects with chronic fatiguein the primary care cohort. Of these only 33subjects fulfilled criteria for CFS (i.e. were knownto have continuous fatigue at the start and finish ofthe six-month follow-up study, and to fulfil theappropriate criteria regarding severity, othersymptoms and functional impairment). Full detailsof the epidemiology and nature of chronic fatigueand CFS in this primary care sample are reportedelsewhere.
To recruit hospital cases of CFS, 142 patients werescreened in the clinic. Sixty-three were excluded; 35(25%) did not meet the positive criteria for CFS(usually failing to fulfil the functional impairmentcriteria, or not having fatigue as the principalcomplaint); 28 (20°lo)satisfied criteria for diagnosesincompatible with CFS, such as somatisationdisorder (8 cases), asthenic personality disorder
(2 cases excluded because of life-long fatigue),substance abuse (2 cases) or other primary physicaland/or psychiatric diagnoses. Thus 79 (56°lo)casesfulfilled criteria for CFS. Most of the data used inthis comparison includes all those fulfilling criteriafor CFS seen in the clinic. However, 12 were toodisabled for out-patient treatment (5). This groupdid not complete all the questionnaire measures, andare treated as missing for those comparisons. Thisapplies to the GHQ (13°lo),MOS Short Form (13%),somatic symptom questionnaire (13%), and fatiguequestionnaire (ll°lo).
Demography
The proportion of women in the Primary care sampleexceeded that of the hospital group, but thedifference was not statistically significant (Table 1).There was no difference in age between the groups.Primary cases were more likely to be married or cohabiting than hospital cases (Table 1) (oddsratio=2.5, 95°loCI: 1.0—6.2,x@P<0.05). Hospitalcases were substantially more likely to belong tosocial class 1 (Table 1) (odds ratio = 17.9, 95% CI:2.3—138.2),or to social class 1 and 2 combined (oddsratio=2.8, 95% CI: 1.2—6.7, x@P<0.05).
Fatigue and myalgia
The total fatigue score was significantly higher forhospital than for primary care cases (Table 2)(1 = 2.63, d.f. = 92, P< 0.05). Hospital cases scoredhigher on both the mental and the physical sectionsof the Fatigue Questionnaire.
Myalgia at rest and after exercise did not differbetween the groups: 76.1% (n = 51) of the hospitaland 63.6% (n = 21) of the primary care groupcomplained of muscle pain at rest (odds ratio = 1.8,959 CI: 0.7—4.5).Post-exertional muscle pain wasreported in 85.1 010(n = 57) in the hospital and 81 .8°lo(n = 27) in the primary caregroup (odds ratio = 1.2,95% CI: 0.4—3.8).Duration of fatigue did not differbetween hospital and primary care cases (Table 2).
Table 1Comparison of demographic data
Group nMean fatiguescore (Likert)Mean
GHQscore (Ukert)PsychologicalattributionMean
durationoffatigueSomatic
symptomsmeanscore(weeks)Community
3334(32-35.9)34.7 (31.9-37.5)58.6%
(17)(41-77%)161 (81-241)11.9(9.9—13.8)Hospital
7936.9(35.8-38)30.6 (28.9—32.4)6.5%
(5)(0-1 1%)224 (171-277)14.7(13.3-16.6)Group
nPreviouspsychiatric
diagnosisWorkfunctioningmeanscoreSocial
functioningmeanscorePhysical
functioningmeanscoreDo
not drink orreducedalcoholCommunity
3374.2% (23)(58-89%)28.9 (14.2-43.5)43 (30.9-55)10.5 (9.5-1 1.5)62.1%
(18&(44-79%)Hospital
7921.1% (15)(12-30%)9 (4.5—13.4)31.9 (27.1-36.7)9.5 (8.9-10.2)90.9%
(50)(83-99%)95%
confidence intervels in brackets.
GeneralHealth
itemsCommunityHospitalOdds
ratioC_
Hospital@2(@)Not
beingabletoconcentrate78.8%79.7%NSNSLost
sleepover37.5%29%NSNSworryNotplayinga
@ pert51.5%59.4%NSNSNotcapebleof
—¿�57.8%53.8%NSNSFeltconstantly
understrein84.8%55.1%4.51.5-13.2P<0.01Couldn't80.8%48.4%NSNSovercome
difficultiesPlot
ableto—¿�d
84.8%79.7%NSNSNot
ableto faceuptoproblems66.7%37.7%3.31.3—7.9P<0.01Feel•mg
unhappyand depressed75%44.9%3.61.4-9.3P<0.01Losing
[email protected]%43.5%2.9
1.2-7.2P<O.05Thinking
of—¿�asa
worthWu42.4%29%NSNSpersonNot
[email protected]%43.5%2.8
1.0-8.1P<0.05
123CHARACTERISTICSOF CFS IN PRIMARY AND TERTIARY CARE
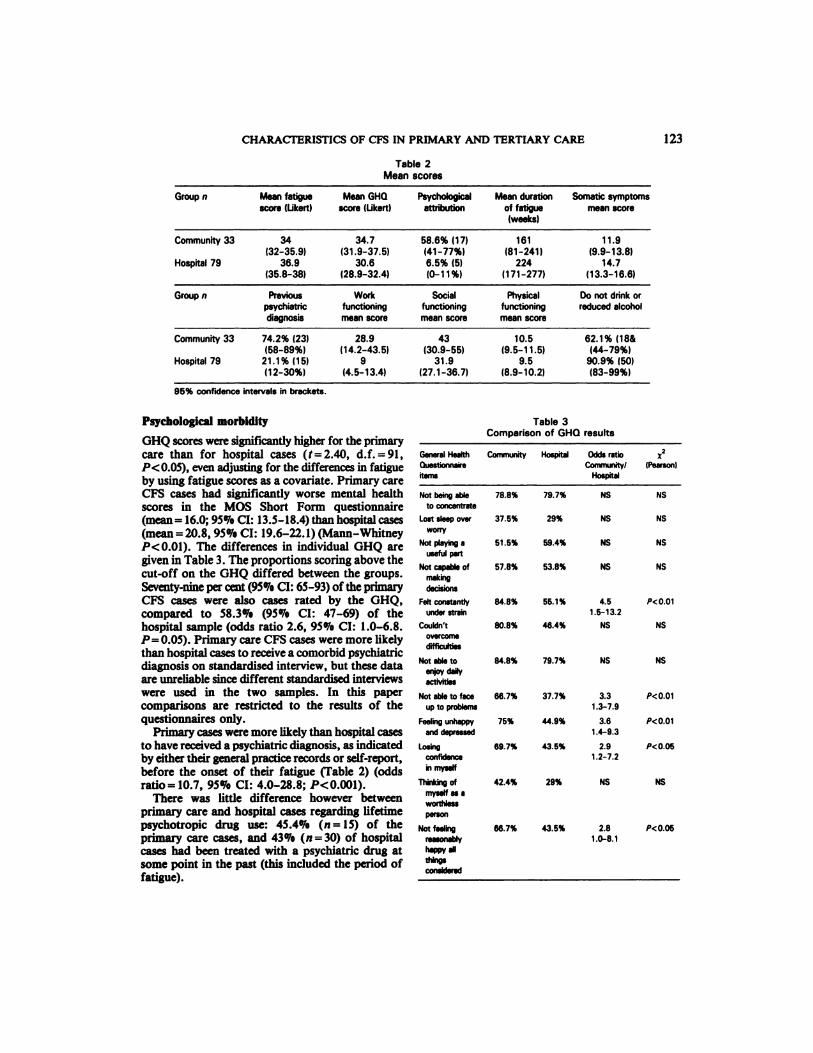
Table2Mean scores
Table3Comparison of GHQresults
Psychological morbidity
GHQ scores were significantly higher for the primarycare than for hospital cases (t=2.40, d.f. =91,P<0.05), even adjustingfor the differencesin fatigueby using fatigue scores as a covariate. Primary careCFS cases had significantly worse mental healthscores in the MOS Short Form questionnaire(mean= 16.0; 95¾CI: 13.5—18.4)thanhospital cases(mean=20.8, 95¾CI: 19.6—22.1)(Mann—WhitneyP<0.01). The differences in individual GHQ aregiven in Table 3. The proportions scoring above thecut-off on the GHQ differed between the groups.Seventy-nine per cent (95% CI: 65-93) of the primaryCFS cases were also cases rated by the GHQ,compared to 58.3°!. (95°loCI: 47—69)of thehospital sample (odds ratio 2.6, 95% CI: 1.0—6.8.P= 0.05). Primary care CFS cases were more likelythan hospital cases to receive a comorbid psychiatricdiagnosis on standardised interview, but these dataare unreliable since different standardised interviewswere used in the two samples. In this papercomparisons are restricted to the results of thequestionnaires only.
Primary cases were more likely than hospital casesto have received a psychiatricdiagnosis, as indicatedby eithertheir general practicerecordsor self-report,before the onset of their fatigue (Table 2) (oddsratio= 10.7, 95°loCI: 4.0—28.8;P<0.001).
There was little difference however betweenprimary care and hospital cases regarding lifetimepsychotropic drug use: 45.4°lo(n = 15) of theprimary care cases, and 43¾(n=30) of hospitalcases had been treated with a psychiatric drug atsome point in the past (this included the period offatigue).

SomaticsymptomsHospital
Community(n =79) (n =33)Odds
ratiox2(Pearson)Chest
pain32.9% (23) 6.1% (2)7.5(1.6-34.4)<0.01Stiffness81.4%
(57) 60.6% (20)2.8(1.1—7.1)P<O.05Tingling
infingers or46.4%
(32) 24.2% (8)2.7(1.1—6.8)P<O.05armsLight
headedness71.4%(50) 45.5% (15)3.0
(1.2—7.1)P<O.05Increased
sensitivityto noise66.7%
(46) 42.4% (14)2.7(1.1—6.3)P<O.05
124 EUBA ET AL
Alcohol consumption
Hospital and primary care cases were equally likelyto report that they drank alcohol, but a largerproportion of hospital cases either did not drink, orhad reduced their alcohol intake, (Table 2) (oddsratio=6.l, 95°loCI: 1.8—20.0;Pcz0.0l).
Self-help group
More hospital (n = 26, 33°lo)than primary carecases (n = 3, lO.3°lo)belonged to one or more MEself-help groups (odds ratio = 4.1, 95% CI: 1.1—15.0;P< 0.05). Members and non-members of a self-helpassociation did not differ in terms of fatigue scores,health perception, functional impairment, or numberof somatic symptoms, but GHQ scores weresignificantly lower than those of the non-members(mean Likert score for members: 28.1, 9501oCI;24.7—31.5;non-members: 32.5, 9501oCI: 30.8—34.1;I = 2.546, d.f. = 87, P< 0.05). Non-members weremore likely to have received a previous psychiatricdiagnosis (odds ratio 3.7, 95°loCI: 1.4—9.7).
Discussion
The purpose of this study was to identify which ofthe many characteristics of CFS seen in specialistclinics were intrinsic to the condition, and whichmight be the result of selection/referral bias.
Gender
Women wereover-representedin the hospital sample,but, contrary to our expectation, this did notrepresent an excess over primary care. Instead, therewas a non-significant trend for females to be lesslikely to attend the specialist setting. This wasunexpected, since we reported in the communitystudy that preceded this cohort study a trend towardsan increase in the proportion of females as morestringent categories of Chronic Fatigue and CFS arecreated (Pawlikowska et a!, 1994). That women wereover-represented at all stages of the study is largelyaccounted for by the fact that women overall presentmore frequently to their GP than men. Gender itselfis only a weak risk factor for CFS.
There are several possible explanations for thisresult. First, doctors may be less willing to referwomen with fatigue to the specialist clinic (oralternatively more willing to refer men). A recent studyoffatigueinFrenchgeneralpracticehasshown thatwhile women reported more fatigue than men, doctorswere less likely to diagnose fatigue conditions andmore likely to invoke the psychological construct of
Functional scores and somatic symptoms
Health perception, as measured by the MOS ShortForm, was worse in the hospital than in the primarycare cases (Mann-Whitney P< 0.0001). Primary carecases were less likely to be impaired in terms of work(‘Rolefunctioning') than hospital cases (MannWhitney P< 0.05) (Table 2). Primary care cases hadbetter physical and social functioning scores thanhospital cases (MOS), but these differences did notreach statistical significance. Bodily pain (MOS ShortForm) was similar for both hospital and primary caregroups.
Hospital cases had more somatic symptoms thanprimary cases (Table 2) (Mann—WhitneyP< 0.05).Individual symptom differences are shown inTable 4.
Fatigue attribution
Replies regarding perceived causes for the fatiguewere classified as psychological, physical, mixed orunknown. Fifty-nine per cent of the primary care,but only 7% of the hospital thought their illnessmight be due to psychological or psychosocial causes.Alternatively 33% of the primary care cases thoughtit was physical, compared to 56°loof the hospitalcases. Contrasting psychological with the rest,primary care cases were substantially more likely togive a psychological or psychosocial attribution totheir fatigue than hospital cases (odds ratio = 20.4;95°lo CI: 6.3—65.7) (Table 2). l2°lo of the primarycare,but94°loof thehospitalcasesusedthetermsMyalgiaEncephalomyelitis(ME),PostviralFatigueSyndrome (PVFS) or CFS to describe their illness(althoughthiswas not synonymous witha solelyphysical attribution of symptoms).
Table 4Differences in somatic symptoms

125CHARACTERISTICS OF CFS IN PRIMARY AND TERTIARY CARE
depression in fatigued women than men (Fuhrer &Wessely, 1995). It is also possible that gender itselfdirectly influences the desire for referral - we foundthat although women with CFS had worse physicalfunctioning than men, it was the men who had theworst perception of their health, a fmding also notedin an American study (Buchwald et a!, 1994).
Psychological morbidity
Hospital cases report less psychological distressthan primary care cases, as judged by the scores onboth the GHQ and the Mental Health section of theMOS Short Form, despite the fact that hospital caseshad more severe levels of fatigue. Given that severityof fatigue is associated with increased psychologicalmorbidity (Pawlikowska et a!, 1994), this reversalof the expected pattern is surprising. Furthermore,since self-ratings of functional impairment, togetherwith measures of fatigue and somatic distress, wereall worse in the hospital cases (who had also beenill for slightly longer), one would again predict thatpsychological health would be worse.
Thereare a numberof possible explanations. First,this may be partly artefactual related to the exclusionof categories such as somatisation disorder, whichis common in specialist clinics but very rare in thecommunity (no cases were found in the primary caresample). Second, prior psychiatric diagnosis, morecommon in the primary care cases, could deter a OPfrom referring the case to a CFS specialist clinic,choosing instead to identify the problem as a reoccurrence of the previous diagnosis. Given identicalcase vignettes, GPs were more likely to refer thosewith a self diagnosis of ME to hospital (Scott eta!,1995). Third, a reluctance to endorse psychiatricsymptoms may be relevant. Primary care cases weremost likely to make psychosocial attributions fortheir symptoms, as noted elsewhere (McDonald eta!, 1993), whereas nearly all the hospital casessaid their problem was ME or a related condition.This marked difference in self-diagnosis is oneof the principal differences between the primarycare and hospital samples. Looking at the individualGHQ items endorsed, it appears that the differencesbetween primary care and hospital samples are morein the obviously psychological flavoured responses(feeling unhappy, loosing confidence, being understrain), and less in more neutral concepts suchas inability to concentrate, unable to make decisionsand not enjoying daily activities. However, thesedifferences are not based on any apriori hypotheses,and would need independent replication.
Comparisons of primary care and hospital sampleshave been made in other conditions with possible
relevance to CFS. In irritablebowel syndrome (IBS)studies have suggested that the excess ofpsychological morbidity in lBS subjects attendinggastroenterology clinics is not found in thecommunity, and may reflect the effect ofpsychological distress on illness behaviour, ratherthan an intrinsicfeature of the condition (Whiteheadet a!, 1988). Our findings in CFS contradictthis model. Although there is no doubt thatCFS seen in a hospital setting is associated withrates of psychiatric disorder in excess of thoseassociated with other chronic physical conditions(Wessely & Powell, 1989; Katon et a!, 1991;Wood et a!, 1991), these rates are comparable tothose reported for chronic fatigue (McDonald et a!,1993) and CFS in primary care. Indeed, there is asuggestion in this study that the association may bestronger in primary than in specialist care. Thus thepreviously reported excess of psychiatric disorder inspecialised settings cannot be attributed to illnessbehaviour or selection bias alone.
Social class
We confirmed the considerable excess of socialclass 1 among the hospital cases This did representa considerable difference from primary care. It hasbeen postulated that the lifestyle of professionalsrenders this section of society more vulnerable todeveloping CFS (Dowsett et a!, 1990). Our fmdingssuggest that the social class bias found in specialistcare is more likely to reflect alternative factors, suchas the social meaning of physical and psychiatricillness, the relationshipbetween this and social class,and access to specialist care.
Prognosis
Two recent studies have reported a poor outcomefor CFS seen in specialistsettings (Sharpeeta!, 1992;Wilson et a!, 1994). In both studies poor outcomewas independently associated with the strength ofphysicalattributionsand currentemotional disorder,while the latteralso found that membershipof a selfhelp organisationand avoiding alcohol also predictedpoor outcome. We report that hospital cases aremore likely to have physical beliefs about theirillness, to be membersof a self-help organisationandto avoid alcohol, but were no more likely to havecurrent emotional disorder. It will therefore beinstructive to compare the longer-term outcomes ofthe two groups in order to determine which of thesefactors is the most important association of poorprognosis.

126
Acknowledgements
DowsErr, E. , RAMSAY,A. , MCCARTNEY,R., et a! (1990) Myalgicencephalomyelitis —¿�a persistent enteroviral infection?Postgraduate Medical Journal, 66, 526—530.
FUHRER, R. & WESSELY, S. (1995) Fatigue in French Primary Care.Psychological Medicine, in press.
FUKADA, K., SrR'@us, S., Hiciua, I., et a! (1994) The chronic fatigue
syndrome: a comparative approach to its definition and study.Annals of Internal Medicine, 121, 953—959.
GOLDBERG, D. (1972) The Detection of a Psychiatric Illness by
Questionnaire. London: Oxford University Press.KATON, W., BUCHwALD, D. , SIMoN, G., et a! (1991) Psychiatric
illness in patients with chronic fatigue and rheumatoid. Journalof Genera! Internal Medicine, 6, 277—285.
MCDONALD,E., DAVID,A., PELosI,A., eta!(1993)Chronicfatigueingeneral practice attenders. Psychological Medicine, 23, 987-998.
OFFICE OF PopuwioN Car-isusas @mSuaviws (1970) C!ass@fication of
Occupations. London: OPUS.PAwLIKowsic@,T., CHALDER,T., Hutscii, S., et a! (1994) A
population based study of fatigue and psychological distress.British Medical Journal, 308, 743-746.
Sco@rr, S., DEARY, I. & Pausi, A. (1995) General practitioners'attitude to patients with a self-diagnosis of myalgicencephalomyeitis. British Medico! Journal, 310, 508.
SHARPE, M., ARCHARD,L., BANATVALA,J., et a! (1991) Chronicfatigue syndrome: guidelines for research. Journal of the RoyalSociety ofMedicine, 84, 118—121.
, HAWTON,K.,SEAGROATr,V.,eta!(1992)Follow-upofpatients with fatigue presenting to an infectious diseases clinic.British Medical Journal, 302, 347-352.
WARE, J., SmRaouas@, C. & DAVIES,A. (1992) Developing andtesting the MOS 20-Item Short-Form Health Survey: A generalpopulation application. In Measuring Functioning and Well-Being:The Medical Outcomes Study Approach (eds A. Stewart & J.Ware), pp. 277-290. Durham: Duke University Press.
WESSELY,S. & Poww, R. (1989) Fatigue syndromes: a comparisonof chronic ‘¿�postviral'fatigue with neuromuscular and affectivedisorder. Journal of Neurology, Neurosurgery and Psychiatry, 52,940-948.
CHALDER, T., HIRSCH, S., et a! (1995) Post InfectiousFatigue: A prospective study in primary care. Lancet, 345,1333—1338.
WHrrEHEAD, W., Bossuu@, L., ZONDERMAN,A., et a! (1988)Symptoms of psychologicaldistress associated with irritable bowelsyndrome: comparison of community and medical clinicalsamples.Gastroentero!ogy, 95, 709-714.
WILSON,A., HICIUE, I., LLOYD,A., et a! (1994) Longitudinal studyof the outcome of chronic fatigue syndrome. British MedicalJournal, 308, 756-760.
WIi-ra1@mo@,J. & BUHLER,R. (1979) Somatic discomforts amongdepressed women. Archives of Genera! Psychiatry, 36, 465-471.
Wooo, G., BENTALL, R., GOPFERT, M., et a! (1991)A comparative
psychiatric assessment of patients with chronic fatigue syndromeand muscle disease. Psychological Medicine, 21, 619-628.
Clinical implications. CFS sufferers seen in primarycare show no social
class bias —¿�the stereotype of ‘¿�‘¿�Yuppieflu' ‘¿�is anartefact of referral bias
. A firmbelief in a physical attributionof symptomsthat characterises CFS patients in specialistsettings is not found in primary care
•¿�There is an excess of psychological morbidityassociatedwithCFS ineithersetting
•¿�A substantialnumberofpatientsarebeingreferredtospecialistwho do notfulfilcriteriaforCFS
Limitations•¿�Only 33 cases of CFS were identified in the
primary care sample•¿�More complex measuresof attributionalstyle
should be used in future studies
R. Euba, MRCPsych,T. Chalder, MSc,A. Deale, MSc,S. Wessely, MD,Academic Departmentof PsychologicalMedicine, King's College School of Medicine and Dentistry, and Institute of Psychiatry
Correspondence: Dr Simon Wessely, Department of Psychological Medicine, King's College School of Medicine and Dentistry,Denmark Hill, London SE5 9RS
(First received 12 May 1995, final revision 20 July 1995, accepted 24 July 1995)
EUBA ET AL
The primary care component of this study was funded by theLinbury Trust. The hospital component was funded by the SouthEast Thames Regional Health Authority. R. Euba was supportedby the Priory Hospital Group. We thank the five General Practicesthat took part in the community study: Jenner Health Centre,London SE23; The Hurley Clinic, London SEll; The YateleyMedical Centre, Yateley, Surrey; The Rosemary Medical Centre,Poole, Dorset, and the Mendip Country Practice, Somerset. Wealso thank the seven Research Nurses who collected the communitydata: Melanie Brown, Julie Dennison, Sue Fox, Brenda Hinton,Vivien Hobbs, Margerie Peers and Dawn Baker.
References
BUCHWALD, D. & KOMAROFF, A. (1991) Review of laboratoryfindings for patients with chronic fatigue syndrome. Review ofInfectious Diseases, 13(suppl. 1), 12—18.
PEARLMAN, T., KITH, P., et al (1994) Gender differencesin patients with chronic fatigue syndrome. Journal of the GeneralInternal Medicine, 9, 397—401.
BUTLER, S., CHALDER, T., RON, M., et a! (1991) Cognitive
behaviour therapy in chronic fatigue syndrome. Journalof Neurology, Neurosurgery and Psychiatry, 54, 153—158.
CHALDER, T., BERELOWITZ, G., PAWLHCOWSKA, T., et a! (1993)Development of a Fatigue Scale. Journal of PsychosomaticResearch, 37, 147—153.
Copyright © 2022 FDOKUMEN