
Polarized Signaling Endosomes Coordinate BDNF-Induced Chemotaxis of Cerebellar Precursors

CEREBELLAR HEMANGIOBLASTOMA: HISTOGENESIS OF STROMA CELLS JUNICHIRO KAWAMURA, MD,* JULIO H. GARCIA, M D , ~
AND YOSHINARI KAMI JYO, MD*
Light and electron microscopic features of a Cerebellar hemangiohlastoma were evaluated with special emphasis on the matter of the origin of intersti- tial (stroma) cells. Many of the capillary components were of embryonal type, and the stroma cells shared several morphological features with them. It was concluded that the stroma cells originate from vasoformative ele- ments (endothelium and pericytes) and that the endothelial cells are active components of the neoplasm. No convincing morphological counterpart for the erythropoietic activity of this neoplasm was uncovered. Structures identi- cal to ciliary rootlets were identified in many endothelial cells.
HE HISTOGENESIS OF THE STROMA (INTER- T stitial) cells of cerebellar hemangioblas- toma is unsettled.28 Such cells have been thought to originate from microglia,’* “neuro- epithelial” cells,26 reticuloendothelial sys- tem,7.19,27 pia mater,28 or vasoformative cells.2~51s825332.37 Special staining methods have ruled out the inicroglial and neurologlial ori- gins of stroma cells; for similar reasons, these are felt not to be ordinary macrophages.28 Few electron microscopic reports have at- tempted to identify the various components of cerebellar hemangiobla~torna,~~7.R and re- cent views are confined to the following possi- ble origins for the stroma cell: reticuloendo- thelial system, pia mater, and “vasoformative” cells, e.g., pericytes or endothelial cells.
This report deals with the light and elec- tron microscopic examination of a cerebellar hemangioblastoma, removed from a 1 2-year- old patient afflicted with trunkal ataxia, reti- nal angiomata, and erythrocytosis. A histologi- cally similar neoplasm had been removed from the posterior fossa of his father, who died at age 36.
From the Departments of Neurology and Pathology, University of Maryland School of Medicine, Baltimore, Md .
Supported by USPHS Grants NS 06779 and NS 08 261.
Presented in part, at the 48th Annual Meeting of the American Association of Neuropathologists, Chi- cago, Ill., 1972.
Assistant Professor of Neurology. t Head, Division of Neuropathology. t Instructor, Neuropathology. Address for reprints: J. H. Garcia, MD, 31 South
Creme, Baltimore, Md. 21201. The authors acknowledge the secretarial help of Miss
Pamela Cook and MIS. Dehra Haines. Received for publication December 15, 1972.
CASE REPORT The patient, a 12-year-old Negro boy, was
well until November 1950, when he began walking unsteadily and writing poorly. He be- came “lazy,” even drowsy, and his perform- ance at school deteriorated. He started com- plaining of headaches without nausea and vomiting; drowsiness became persistent and progressive. On August 2, 1971, he was admit- ted to University of Maryland Hospital.
The previous history was unremarkable, eK- cept for a minor head injury in 1965. Three siblings were alive and well; one died 5 days after premature birth. T h e patient’s fa- ther had a right-sided cerebellopontine-angle tumor removed at the Medical College of Vir- ginia Hospital in 1964. The histologic diagnc- sis was hemangioblastoma. The patient’s father died of recurrent tumor on May Zfi, 1971, and results of the postmorten examina- tion were not available a t this writing.
Physical examination on admission was nor- mal. Patient was alert, and no bruits were heard over head and neck; cranial nerve func- tion wa4 intact but there was early bilateral papilledema and symmetrical horizontal nys- tagmus on lateral gaze. Muscle tone was nor- mal, and there was no weakness of the extrem- ities. Deep tendon reflexes were brisk and equal. Pathologic reflexes were not elicitable. He walked on a broad base and was unable 1 0 walk on tandem position. Romberg sign was negative. Performance of finger-to-nose and heel-to-knee tests was normal, but hands de K- terity was impaired. Sensory examination was normal for all modalities.
Ophthalmologic examination, on August 16, 197 1, revealed visual acuity of 20/25 bilat- erally, hyperemic discs with early papilledema, and a large retinal “angioma” in the right eye. Ocular dysmetria was also noted.
1528

No. 6 CEREBELLAR HEMANGIOBLASTOMA - Kauramura et al. 1529
Laboratory studies: Urinalyses were normal. Blood cell counts at repeated intervals showed hemoglobin levels of 20.0, 18.7, and 18.6 g, he- matocrit of 63, 47, and 58Iy0, red blood cell counts of 8.50 and 7.86 million, and white cell counts of 5,100 and 4,300 with normal differ- ential. Platelet counts were normal. Chest x- rays were normal, and skull films disclosed separated cranial sutures. EKG showed ques- tionable left ventricular hypertrophy, but no evidence of cardiac disease was demonstrated. Brain and liver scans, as well as intravenous pyelogram, were normal. Titers of urinary ery- thropoietin measured with radioactive iron were within normal range.
Hospital course: A right retrograde brachial arteriogram, on August 6, 1971, revealed a large “A-V malformation” of the posterior fossa and severe hydrocephalus. A craniotomy, 5 days later, disclosed a highly vascular neo- plasm in the midline of the cerebellum. The inferior part of the vermis was replaced by neoplasm; the tumor capsule protruded below the tonsils and extended into the fourth ven- tricle. The left posterior inferior cerebellar ar- tery was clipped, but the superior cerebellar artery, another main feeder to the neoplasm, was left intact. One third to one half of the tumor was removed.
Ten days after surgery, blood hemoglobin was 15.5 g, hematocrit 46%, red blood cell counts 6.07 million, and white cell coiints 10,400 with shift to the left. A second axil- lary retrograde arteriogram revealed residual tumor, which was mainly fed from the supe- rior cerebellar artery. Because of persistent and severe hydrocephalus a ventricu- loauricular shunt was performed on Septem- ber 1, 1971. A week later, radiation therapy to the posterior fossa was started and the patient was discharged in October 1971.
On January 10, 1972, he was admitted to ophthalmology for treatment of his retinal an- gioma. At this time, he complained of inter- mittent nausea and vomiting; diplopia and broad-based gait were also noted. Large reti- nal angiomata were seen bilaterally. These were frozen with cryosurgical technique. On January 13, 1972, hemoglobin was 17.9 g, he- matocrit 557”, red blood cell counts 7.71 mil- lion, and white cell counts 4,500. He was dis- charged on January 19, 1972, to be followed at the outpatient clinic.
MATERIALS AND METHODS
Fragments of tissue were obtained at the time of surgery for microscopic evaluation. A portion of these specimens was promptly im- mersed in 10% formaldehyde solution and others in 6.25% glutaraldehyde with 0.1 M so-
dium cacodylate buffer at pH 7.28. The for- mer were processed for paraffin embedding and stained with hematoxylin-eosin, Masson’s trichrome method, Wilder’s method for retica- lin fibers, and phosphotungstic acid hematoxy- lin. Unembedded, frozen sections were stained with oil-red 0. Glutaraldehyde-fixed material was minced and maintained in the fixing solu- tion for 4 hours. The fragments were then placed overnight in a solution of 0.1 M caco- dylate buffer (pH 7.28) and post-fixed in 1.0% osmium tetroxide in cacodylate buffer for 90 min. Dehydration in methanol was followed by propylene oxide. Tissues were embedded in Epon 812. One-micron thick sections were stained with toluidine blue and were exam- ined by light microscopy. Thin sections were cut with a diamond knife in a Porter-Blum uI- tramicrotome and were stained with Watson’s uranyl acetate and Reynold’s lead citrate. These were examined and photographed in a Philips EM 200 electron microscope.
RESULTS Light Microscopy
The vascular portion of the neoplasm was made up of numerous channels containing abundant red blood cells (Fig. 1); these chan- nels were surrounded by a few “reticulin fibers.” Numerous, large interstitial cells dis- played a foamy, clear cytoplasm which stained intensively with oil-red 0 and toluidine blue (Figs. 2, 3); with the latter staining method, it was also possible to identify occasional me- tachromatic granules within mast cells. A small A-V malformation could also be seen in the cerebellar cortex but outside of the main neoplasm.
Electron Microscopy The neoplasm was characterized by numer-
ous vascular channels closely associated with “dark” and “clear” cells in the interstices. There were four major types of cellular ele- ments: endothelial cells, pericytes, stroma cells, and occasional mast cells (Fig. 4).
Vascul& channels: Most were lined by mon- olayers of endothelial cells separated from per- icytes and stroma cells by well-formed basal lamina. These vessels were largely capillary; some of the large vessels showed adventitia, in- ternal elastic lamina, and smooth muscle cells. Larger vessels showed irregular luminal con- tours, filled with presumed red blood cells and relatively electron-dense material (Fig. 5) .
1530 CANCER June 1973 Vol. 31
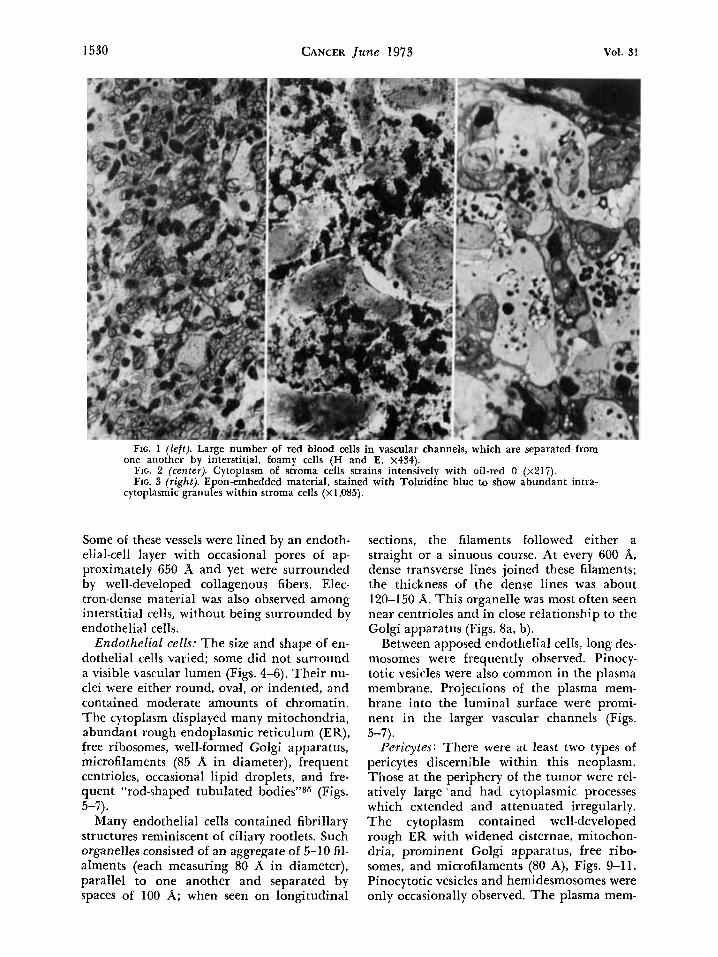
Frc. 1 (left). Large number of red blood cells in vascular channels, which are separated from
FIG. 2 (center). Cytoplasm of stroma cells strains intensively with oil-red 0 (x217). FIG. 3 (right). Epon-embedded material, stained with Toluidine blue to show abundant intra-
one another by interstitial, foamy cells (H and E, x434).
cytoplasmic granules within stroma cells (~1 ,085) .
Some of these vessels were lined by an endoth- elial-cell layer with occasional pores of ap- proximately 650 A and yet were surrounded by well-developed collagenous fibers. Elec- tron-dense material was also observed among interstitial cells, without being surrounded by endothelial cells.
Endothelial cells: The size and shape of en- dothelial cells varied; some did not surround a visible vascular lumen (Figs. 4-6). Their nu- clei were either round, oval, or indented, and contained moderate amounts of chromatin. The cytoplasm displayed many mitochondria, abundant rough endoplasmic reticulum (ER), free ribosomes, well-formed Golgi apparatus, microfilaments (85 A in diameter), frequent centrioles, occasional lipid droplets, and fre- quent “rod-shaped tubulated bodies”35 (Figs.
Many endothelial cells contained fibrillary structures reminiscent of ciliary rootlets. Such organelles consisted of an aggregate of 5-10 fil- alments (each measuring 80 A in diameter), parallel to one another and separated by spaces of 100 A; when seen on longitudinal
5-7).
sections, the filaments followed either a straight or a sinuous course. At every 600 A, dense transverse lines joined these filaments; the thickness of the dense lines was about 120-150 A. This organelle was most often seen near centrioles and in close relationship to the Golgi apparatus (Figs. 8a, b).
Between apposed endothelial cells, long des- mosomes were frequently observed. Pinocy- totic vesicles were also common in the plasma membrane. Projections of the plasma mem- brane into the luminal surface were promi- nent in the larger vascular channels (Figs.
Pericytes: There were at least two types o f pericytes discernible within this neoplasm. Those at the periphery of the tumor were rel- atively large ’ and had cytoplasmic processes which extended and attenuated irregularly. The cytoplasm contained well-developed rough ER with widened cisternae, mitochon- dria, prominent Golgi apparatus, free ribo- somes, and microfilaments (80 A), Figs. 9-1 1. Pinocytotic vesicles and hemidesmosomes were only occasionally observed. The plasma mem-
5-7).

No. 6 CEREBELLAR HEMANGIOBLASTOMA - Kawamura et al.
FIG. 4. Representative field of the neoplasm showing “dark” and “light” cells. A well-formed capillary can be seen at the bottom. Immediately above, there is a group of endothelial cells without visible lumen, but completely surrounded by basal lamina. Numerous lipid droplets can be seen within some of the stroma cells ( ~ 3 , 7 7 0 ) .
1531

1532 CANCER June 1973 Vol. 31
FIG. 5a (left). Endothelial cell lining a large vascular channel which contains abundant elec- tron-dense material. This material appears continuous with intracytoplasmic “dense boaies.” Ex- tensive finger-like processes project into the lumen (X 12,OOO).
FIG. 5b (right). Group of endothelial cells without visible lumen. Note desmosomal contacts, pinocytotic vesicles, and cytoplasmic “rod-shaped tubulated bodies” (~20,000).
brane was surrounded by thick basal lamina which was in contact with abundant collagen fibers. Nuclei were usually round, smooth, and less lobulated than those in the second type of pericyte (Fig. 10).
Pericytes in the center of the neoplasm were “dark,” and clearly discernible from stroma cells. They were surrounded by basal lamina and were closely associated with endothelial cells. Their nuclei were irregular and lobu- lated. The cytoplasm contained mitochondria, microfilaments, free ribosomes, prominent Golgi apparatus, and occasional lipid drop- lets; ER cisternae were scarce (Fig. 10). Some pericytes were not easily differentiated from endothelial cells, since a few of them had rela- tively “dark” cytoplasm, containing abundant free ribosomes and microfilaments, as well as lobulated nuclei.
Those pericytes seen in the surrounding, gliotic, non-neoplastic tissue contained, in ad- dition, dense cytoplasmic bodies of various
sizes enveloped by double membrane (Fig.
Stroma ceZZs : Many of these “clear” intersti- tial (pseudoxanthomatous) cells contained lipid droplets (Fig. 12). The size of each cell was comparatively large and nuclei weire round, oval, or lobulated. The basement menn- brane surrounding the stroma cell was thin and irregular; it appeared closely associated with collagenous fibers. The basal lamina was frequently absent between apposed strorria cells. ,Centrioles were also occasionally seen in this type of cell. Pinocytotic vesicles were eas- ily identified in most stroma cells.
A second type of stroma cell contained abundant microfilaments (85 A), rough and smooth ER but few lipid droplets (Fig. 13). Within other types of stroma cells microfila- ments were almost totally replaced by coarse granules each measuring approximately 230 A in diameter; in these, the smooth ER formed prominent whorls which occasionally con-
11).

FIG. 6 (top). Endothelial cell with prominent rough ER. Note centriole, adjoining root- let, and several tubular bodies (~26,500). FIG. 7 (bottom). Endothelial cell showing numerous tubular bodies in cross section. The bodies contain many hollow cylinders and are enveloped by a continuous membrane (~43,000).

1534 CANCER June 1973 Vol. 31
tained lipid droplets (Fig. 14). Microfilaments in stroma cells were arranged more loosely, ir- regularly, and were more attenuated than those seen in astroglia (Fig. 15).
Mast cells: These were only occasionally ob- served in this case (Fig. 16). They were rela- tively small, appeared isolated, and were rarely seen outside of the neoplasm. Their nu- clei were round and contained moderate amounts of chromatin granules scattered un- evenly. The cytoplasm contained mitochon- dria, Golgi apparatus, free ribosomes, granu- lar ER, microfilaments, lipid droplets, and
most characteristically, “free cytoplasmic ag- gregates of electron-dense material”6 contain- ing variegated profiles. These were whorls, spi- rals, or concentric lamellar bodies with or without electron-dense material in between. Those containing electron-dense profiles were surrounded by membranous structures, which at low magnification resembled “dense bod- ies.’’ The plasma membrane of mast cells was markedly attenuated and invaginated, and ap- peared to be surrounded by thin basal lamina. Mast cells did not appear to form an integral component of the neoplasm.
FIG. 8a (top). Endothelial cell showing “fibrillary” rootlet in longitudinal section, adjacent to the Gold apparatus. Transverse and longitudinal sections of microtubular bodies are also seen
FIG. 8b (bottom). Close-up view of rootlet (~142,600). (~39,000) .

No. 6 CEREBELLAR HEMANGIOBLASTOMA Kawamura et al. 1535
FIG. 9 ( lef t ) . Pericyte from periphery of neoplasm showing spherical nucleus, prominent nu- cleolus, Golgi apparatus, and abundant ER cisternae; note several mitochondria and complete encircling of cell by basal lamina (~9,100).
FIG. 10 (center). Centrally located pericyte with lobulated nucleus, scarce ER cisternae, and abundant free ribsosomes; microfilaments are more numerous than in previously described cell type (~9,800).
FIG. 11 (right). Double membrane-bound “dense bodies” of various sizes in cytoplasm of pericyte. Note similarities with fibroblastic cells (~24,000).
DISCUSSION The familial occurrence of cerebellar
hemangioblastoma is and its low incidence in childhood is well-docu- mented.22q28s31 Clinically, patients with cere- bellar hemangioblastoma often show erythro- cytosis17131.3* which disappears, in more than 50% of the cases, after the complete extirpa- tion of the neoplasm.6~~~13
The present case is characterized by the early onset of symptoms (12 years of age), the paternal history of a similar tumor, erythrocy- tosis, and bilateral retinal angiomata. Histo- logically, the neoplasm consisted of a solid he- mangioblastoma combined with A-V malfor- mation and fibrillary astrocytoma. The latter finding (i.e., the coexistence of glioma and he- mangioblastoma) is to be discussed in a sepa- rate communication. Ultrastructural evalua- tion of this patient’s cerebellar hemangioblas- toma demonstrated numerous vascular chan- nels, proliferated primitive endothelial cells, with or without visible lumen, pericytes, mast cells, and pseudoxanthomatous interstitial cells.
There are but few published electron micro- scopic studies on cerebellar hemangioblas- toma.6~7.8 Cancilla and Zimmerman6 stated
that the two most common types of cells in this neoplasm were those lining the vascular channels and those in the extravascular space. Both types contained numerous mitochondria, microfilaments (70 A in diameter), and mark- edly dilated smooth ER with accumulations of a granular electron-dense material in the cis- ternae. The close similarity between these two types of cells, particularly with respect to intra- cytoplasmic filamentous structures, led these authors to conclude that the tumor was com- posed of a single cell type which originated from endothelium.
Castaigne et a1.7 consider that the evidence presented by the previous workers did not allow identification of the stroma cells as orig- inating from capillary endothelium. The he- mangioblastomas examined ultrastructurally by Castaigne et al. showed endothelium of normal appearance. Although they were una- ble to reach a definite conclusion on the na- ture of the stroma cells, these authors ex- cluded their origin from glial cells, pia mater, endothelial cells, or pericytes. They concluded that stroma cells were more akin to reticular cells, mainly because of the presence of extra- cellular reticulin fibers and intracytoplasmic lipid droplets. They interpreted the latter fin-

1536 CANCER June 1973
FIG. 12 (top). This is the most typical variety of stroma cell showing, in addition to lipid droplets, few microfilaments (~7,450). FIG. 13 (bottom). Adjoining processes of stroma cells; note desmosomal contacts and concentric arrangement of microfilaments (~15,500).
Vol. 31

FIG. 14 (top). Stroma cell from periphery of hemangioblastoma; whorl-like arrangement of smooth ER and notching of plasma membrane are evident. Evenly distributed granules in the cytoplasm (average diameter 230A) are felt to represent disintegrating filaments (~17 ,500) . FIG. 15 (bottom). Transitional-type of stroma cell surrounded by glial processes. The structural differences between glial and stroma-cell filaments are apparent. Three different areas are seen in this cell-to the left, prominent ER and coarse granules: lipid droplets occupy the mid-portion, and numerous filaments with fragmented ER are seen at right (~5,700).

1538 CANCER June 1973 Vol. 31
FIG. 16. Mast cell in cerebellar hemangioblastoma; cytoplasmic dense bodies and interdigi- tating plasma membrane are typical (~15,000).
ing as evidence of phagocytosis,7 but it is known that endothelial cells and pericytes are also capable of phagocytosis, as demonstrated in experimental xanthoma.23 Furthermore, it is conceivable that lipid droplets represent an endogenous product of the cell. Precollagen- ous or primitive elastic fibers, which are often referred to as “reticulin fibers” by light microscopy,l* are commonly associated with active pericytes in wound healing10 and are not a specific product of reticular cells.
Microfilaments in the cytoplasm of stroma cells are one of their most constant features. Russell and Rubinstein refer to one of the il- lustrations published by Castaigne et al. in which abundant intracytoplasmic microfila- ments formed a whorl, and mention that a similar feature is present in meningiomas28 adding that the stromal cells lacked the inter- digitations of the plasmalemma and the sur- face specializations that are characteristic of most meningiomas. The elongated and undu- lated processes of the plasma membrane char-
acteristic of meningiomasls were not observed in our case.
Cervos-Navarro divided stroma cells into four types according to variations in their in- tracytoplasmic organelles (including the num- ber of cytofilaments), and concluded tlhat stroma cell originate in vasoformative ele- ments.8 In our opinion, the presence of abundant microfilaments is not crucial for the identification of stroma cells; it is possible that the interstitial cells free of prominent imi- crofilaments could merely represent one of the evolutionary stages of this cell type.
Stroma cells containing lipid droplets and located in the center of the tumor showed fre- quent pinocytotic vesicles in the plasma mem- brane which was surrounded by thin, irregu- lar basal lamina, closely associated with pre- collagenous fibers. In contrast, those with abundant, coarse granules (Fig. 14) appeared at the periphery of the neoplasm and Idis- played irregular, shallow notches of the plasma membrane. The latter was surrounded

No. 6 CEREBELLAR HEMANGIOBLASTOMA * Kawamura et al. 1539
by thick basal lamina with abundant precolla- genous material. The morphological differ- ences described among stroma cells might rep- resent different stages of their metabolic cycle.
A close morphological similarity between the stroma cells and the vasoformative cells was noted in this case. Some of the stroma cells were reminiscent of either pericytes (with surrounding basal lamina, irregularly shaped nucleus, abundant microfilaments, and free ri- bosomes) or neoplastic endothelial cells (with prominent microfilaments, fragmented rough ER, free ribosomes, and well-developed Golgi apparatus). Lipid droplets were occasionally observed in pericytes. The stroma cells with abundant microfilaments and fragmented rough ER also resembled the poorly differen- tiated subendothelial cells found in the inti- ma1 cushion of aorta; such subendothelial cells are considered to be primitive smooth muscle cells.15 T h e electron-dense material, presumed by us to be primitive blood plasma, was sometimes seen surrounded solely by stroma cells. In light microscopy, this feature was presented as evidence of the endothelial origin of stroma cells.37 Other histologic stud- ies have also pointed to the transitional fea- tures noted in the morphology of endothelial and stroma cells.36
The previously listed findings strongly sug- gest that the stroma cells of cerebellar heman- gioblastoma originate from vasoformative ele- ments.
Whether the endothelial cells of heman- gioblastoma secrete erythropoietin or its pre- cursors is still uncertain. More than coinciden- tal association of erythrocytosis with heman- gioblastoma has led many authors to postulate that some cells of this neoplasm may secrete an erythropoietic material.6~9~13.34 A recent ul- trastructural study of multiple supratento- rial hemangioblastoma illustrated “secretory” granules within some “tumor” cells.14 In the present study, membrane-bound electron-dense material was observed in some pericytes lo- cated within the perineoplastic, gliotic tissue (Fig. 11). Furthermore, seemingly “dense” bodies in neoplastic endothelial cells were in
reality “rod-shaped tubulated bodies” when viewed at higher magnification (Figs. 5b, 7). These organelles are commonly observed in the endothelium of small arteries, arterioles, and arterial capillaries of several organs, par- ticularly in the lung of both animals and man.35
Endothelial “dense bodies,” such as seen in Fig. 5a, have an electron density similar to that shown by the intraluminal material and by the intercellular substance shown in Figs. 4 and 8a. These observations suggest that such material could be secreted into the capillary lumen from the endothelial cells, as was sug- gested in studies of embryogenesis of human cerebral blood vesse1s.m Thus, in the present study, the existence of endothelial “secretory” granules could not be confirmed.
It has been postulated that the blood vessels in hemangioblastoma are formed from angio- blastic anlage much in the same manner as in embryonic brains.9J1116J2 Another view is that the capillary formation in this neoplasm is similar to the process prevailing in granula- tion tissues, e.g., neoplastic vessels are formed from prexisting capillaries.= As shown above, pericytes at the periphery of the neoplasm in- deed resemble those described in wound heal- ing;lO this might suggest that such pericytes were part of a reactive, non-neoplastic process; nevertheless, the possibility of their neoplastic nature cannot be completely ruled out.
The fibrillary structure of endothelial cells (Figs. 6a, 8a, b) appears identical to the root- let of cilium30 as recently illustrated by Ander- son in the epithelial cells of the oviduct.1 The existence of cilia in nonepithelial cells (e.g., neurons and astrocytes) is well documented.24
The frequent presence of centrioles and cil- iary rootlets in many endothelial cells makes them different from adult normal endothe- lium and suggests that these endothelial cells form a major part of the neoplasm.
On the basis of our observations, it is con- cluded that the predominant cell in this neo- plasm is a “primitive” vasoformative element, and therefore i t is justified to retain the desig- nation of hemangioblastoma.
REFERENCES
1 . Anderson, R . G. W.: The three-dimensional struc- ture of the basal body from the rhesus monkey ovi- duct. J . CeZZ BioZ. 54246-265, 1972.
2. Bailey, 0. T., and Ford, R.: Sclerosing hemangio-
mas of the central nervous system. Progressive tissue changes in hemangioblastomas of the brain and in so-called angioblastic meningiomas. Am. J . Pulhol. 18: 1-27, 1942.

1540 CANCER June 1973 Vol. 31
3. Bauer, K. Fr., and Vester, G . : Das elektronen- mikroskopische Bild der Hirnkapillaren menschlicher Feten. Fortschr. Neurol. Psychiatr. 38:369-318, 1970.
4. Bonebrake, R. A,, and Siqueira, E. B.: The familial occurrence of solitary hemangioblastoma of the cere- bellum. Neurology 14:733-743, 1964.
5. Cancilla, P. A,, and Zimmerman, H. M.: The fine structure of a cerebellar hemangioblastoma. J. Neuro- pathol. Exp. Neurol. 24:621-628, 1965.
6. Carpenter, G., Schwartz, H., and Walker, A. E.: Neurogenic polycythemia. Ann. Intern. Med. 19:47& 481, 1943.
7. Castaigne, P., David, M., Pertuiset, B., Escourolle, R., and Poirier, J.: L’ultrastructure des hemangio- blastomes du systeme nerveux central. Rev. Neurol. (Paris) 118:5-26, 1968.
8. Cervos-Navarro, J.: Elektronmikroskopie der He- mangioblastome des ZNS und der angioblastishen Meningiome. Acta Neuropathol. (Berl.) 19: 184-207, 1971.
9. Cramer, F., and Kimsey, W.: The cerebellar hemangioblastoma: Review of fifty-three cases, with special reference to cerebellar cysts and the association of polycythemia. Arch. Neurol. 67:237-252, 1952.
10. Crocker, D. J., Murad, T. M., and Geer, J . C.: Role of the pericyte in wound healing. An ultrastruc- tural study. Exp. Mot. Pathol. 13:51-65, 1970.
1 1 . Cushing, H., and Bailey, P.: Tumors arising from the blood-vessels of the brain. Angiomatous malforma- tions and hemangioblastomas. Springfield, Ill. Charles C Thomas, Publisher, 1928.
12. Harkin, J . C., and Reed, R. J.: In Tumors of Peripheral Nervous System. Washington, D. C., Armed Forces Institute of Pathology, 1969; p. 17.
13. Hennessy, T. G., Stern, W. E., and Herrick, E. S.: Cerebellar hemangioblastoma: Erythropoietic activity by radioiron assay. J. Nucl. Med. 8:601-606, 1967.
14. Ishwar, S., Taniguchi, R. M., and Vogel, F. S.: Multiple supratentorial hemangioblastomas. Case study and ultrastructural characteristics. J. Neurosurg. 35: 396-405, 1971.
15. Lee, K. T., Lee, K . J.. Lee, S. K., Imai, H., and O’Neal, R. M.: Poorly differentiated subendothelial cells in swine aortas. Exp. Mol. Pathol. 13:118-129,
1970. 16. Lindau, A.: Studien uber Kleinhirncysten. Bau,
Pathogenese und Beziehungen zur Angiomatosis retinae. A d a . Pathot. Microbiol. Scand. Suppl. I, 1926.
17. - : Discussion on vascular tumors of the brain and spinal cord. Proc. R . SOC. Med. 24:363-370, 1931.
18. Lozano, R., and Costeio, I: Ein Tumor des ver- langerten Ruckenmarks. Dtsch. Z. Chir. 198:27&276, 1926.
19. McGovern, V. J., and Wyke, B. D.: Haemangio- xanthoma of the brain: A study of eight cases of
so-called “pseudoxanthomatous” haemangioblastoma. Med. J. Aust. 1:397402, 1948.
20. Napolitano, L., Kyle, R., and Fisher, E. R.: Ultra- structure of meningiomas and the derivation and na- ture of their cellular components. Cancer 17:233-241, 1963.
21. Norlen, G.: Familial occurrence of cerebellar angioma. Acta Chir. Scand. 85: 198-202, 1941.
22. Olivecrona, H.: Cerebellar angioreticulomas. J . Neurosurg. 9:317-330, 1952.
23. Parker, F., and Odland, G. F.: Experimental xanthoma. A correlative biochemical, histologic, histo- chemical, and electron microscopic study. Am. J.
24. Peters, A., Palay, S. L., and Webster, H. de F.: In The Fine Structure of the Nervous System. New York, Harper and Row, 1970; pp. 26-30, 108, 114.
25. Ramsay, H. J.: Fine structure of hemangioperi- cytoma and hemangioendothelioma. Cancer 19:20805- 2018, 1966.
26. Roussy. G., Lhermitte, J., and Cornil, L.: Essai de classification des tumerus ctrtbrales. Ann. Anat. Pathol. (Paris) 1:333-382, 1924.
27. Roussy, G., and Oberling. C.: Les tumeurs angio- mateus des centres nerveux. Presse Med. 38:179-185, 1930.
28. Russell, D. S., and Rubinstein, L. J.: In Pathology of Tumors of the Nervous System. Baltimore, Williams & Wilkins Co., 1971; pp, 63, 85-91.
29. Sabin, F. R.: Preliminary note on the differentia- tion of angioblasts and the method by which they produce blood-vessels, blood plasma and red blood-cells as seen in the living chick. Anat. Rec. 13:199-304, I!H7.
30. Satir, P.: Cilia Sci. A m . 204:108-116, 1961. 31. Silver, M. L.. and Hennigar, G.: Cerebellar he-
mangioma (hemangioblastoma). A clinicopathological review of 40 cases. J . Neurosurg. 9484-494, 1952.
32. Stein A. A., Schilp, A. O., and Whitfield, R. D.: The histogenesis of hemangioblastoma of the brain: A review of twenty-one cases. J. Neurosurg. 17:751- 761, 1960.
33. Stout, A. P.: Hemangio-endothelioma-A tumor of blood vessels featuring vascular endothelial cells. Ann. Surg. 118:445464, 1943. 34. Waldmann, T. A.. Levin, E. H., and Baldwin, M.: The association of polycythemia with a cerebellar he- mangioblastoma. A m . J. Med. 31:318-324, 1961.
35. Weihel, E. R.. and Palade, G. E.: New cytoplasmic components in arterial endothelia. J. Cell Biol. 23:101- 112, 1964.
36. Zeitlin, H.: Hemangioblastomas of the meninges and their relation to Lindau’s disease. J. Neuropathol. Exp. Neurol. 1: 14-23, 1942.
37. Zimmerman, H. M.: Vascular tumors of the brain. Clin. Neurosurg. 9:245-276, 1963.
Pathol. 53:537-565, 1968.
Copyright © 2022 FDOKUMEN




















