Cancer risk diversity in non-western migrants to Europe: An overview of the literature
13
Cancer risk diversity in non-western migrants to Europe: An overview of the literature Melina Arnold a,b, * , Oliver Razum a , Jan-Willem Coebergh b,c a Department of Epidemiology and International Public Health, Bielefeld University, Germany b Department of Public Health, Erasmus Medical Centre Rotterdam, The Netherlands c Comprehensive Cancer Centre South, Eindhoven Cancer Registry (IKZ), The Netherlands ARTICLE INFO Article history: Received 4 January 2010 Received in revised form 11 May 2010 Accepted 29 July 2010 Keywords: Migrants Cancer Inequalities Health transition Europe Review literature ABSTRACT Background: Cancer risk varies geographically and across ethnic groups that can be moni- tored in cancer control to respond to observed trends as well as ensure appropriate health care. The study of cancer risk in immigrant populations has great potential to contribute new insights into aetiology, diagnosis and treatment of cancer. Disparities in cancer risk patterns between immigrant and autochthonous populations have been reported many times, but up to now studies have been heterogeneous and may be discordant in their find- ings. The aim of this overview was to compile and compare studies on cancer occurrence in migrant populations from non-western countries residing in Western Europe in order to reflect current knowledge in this field and to appeal for further research and culturally sen- sitive prevention strategies. Methods: We included 37 studies published in the English language between 1990 and April 2010 focussing on cancer in adult migrants from non-western countries, living in the industrialised countries of the European Union. Migrants were defined based on their coun- try of birth, ethnicity and name-based approaches. We conducted a between-country com- parison of age-adjusted cancer incidence and mortality in immigrant populations with those in autochthonous populations. Findings: Across the board migrants from non-western countries showed a more favourable all-cancer morbidity and mortality compared with native populations of European host countries, but with considerable site-specific risk diversity: Migrants from non-western countries were more prone to cancers that are related to infections experienced in early life, such as liver, cervical and stomach cancer. In contrast, migrants of non-western origin were less likely to suffer from cancers related to a western lifestyle, e.g. colorectal, breast and prostate cancer. Discussion: Confirming the great cancer risk diversity in non-western migrants in and between different European countries, this overview reaffirms the importance of exposures experienced during life course (before, during and after migration) for carcinogenesis. Cul- turally sensitive cancer prevention programmes should focus on individual risk patterns and specific health care needs. Therefore, continuously changing environments and subse- quently changing risks in both migrant and autochthonous populations need to be observed carefully in the future. Ó 2010 Elsevier Ltd. All rights reserved. 0959-8049/$ - see front matter Ó 2010 Elsevier Ltd. All rights reserved. doi:10.1016/j.ejca.2010.07.050 * Corresponding author: Address: Bielefeld University, School of Public Health, Department of Epidemiology and International Public Health, University of Bielefeld, P.O. 10 01 31, D-33501 Bielefeld, Germany. Tel.: +49 (0)521 106 2539; fax: +49 (0)521 106 6465. E-mail address: [email protected] (M. Arnold). EUROPEAN JOURNAL OF CANCER 46 (2010) 2647 – 2659 available at www.sciencedirect.com journal homepage: www.ejconline.com
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Cancer risk diversity in non-western migrants to Europe: An overview of the literature
E U R O P E A N J O U R N A L O F C A N C E R 4 6 ( 2 0 1 0 ) 2 6 4 7 – 2 6 5 9
. sc iencedi rec t . com
ava i lab le a t wwwjournal homepage: www.ejconl ine.com
Cancer risk diversity in non-western migrants to Europe: Anoverview of the literature
Melina Arnold a,b,*, Oliver Razum a, Jan-Willem Coebergh b,c
a Department of Epidemiology and International Public Health, Bielefeld University, Germanyb Department of Public Health, Erasmus Medical Centre Rotterdam, The Netherlandsc Comprehensive Cancer Centre South, Eindhoven Cancer Registry (IKZ), The Netherlands
A R T I C L E I N F O
Article history:
Received 4 January 2010
Received in revised form 11 May
2010
Accepted 29 July 2010
Keywords:
Migrants
Cancer
Inequalities
Health transition
Europe
Review literature
0959-8049/$ - see front matter � 2010 Elsevidoi:10.1016/j.ejca.2010.07.050
* Corresponding author: Address: Bielefeld UHealth, University of Bielefeld, P.O. 10 01 31,
E-mail address: melina.arnold@uni-bielef
A B S T R A C T
Background: Cancer risk varies geographically and across ethnic groups that can be moni-
tored in cancer control to respond to observed trends as well as ensure appropriate health
care. The study of cancer risk in immigrant populations has great potential to contribute
new insights into aetiology, diagnosis and treatment of cancer. Disparities in cancer risk
patterns between immigrant and autochthonous populations have been reported many
times, but up to now studies have been heterogeneous and may be discordant in their find-
ings. The aim of this overview was to compile and compare studies on cancer occurrence in
migrant populations from non-western countries residing in Western Europe in order to
reflect current knowledge in this field and to appeal for further research and culturally sen-
sitive prevention strategies.
Methods: We included 37 studies published in the English language between 1990 and April
2010 focussing on cancer in adult migrants from non-western countries, living in the
industrialised countries of the European Union. Migrants were defined based on their coun-
try of birth, ethnicity and name-based approaches. We conducted a between-country com-
parison of age-adjusted cancer incidence and mortality in immigrant populations with
those in autochthonous populations.
Findings: Across the board migrants from non-western countries showed a more favourable
all-cancer morbidity and mortality compared with native populations of European host
countries, but with considerable site-specific risk diversity: Migrants from non-western
countries were more prone to cancers that are related to infections experienced in early
life, such as liver, cervical and stomach cancer. In contrast, migrants of non-western origin
were less likely to suffer from cancers related to a western lifestyle, e.g. colorectal, breast
and prostate cancer.
Discussion: Confirming the great cancer risk diversity in non-western migrants in and
between different European countries, this overview reaffirms the importance of exposures
experienced during life course (before, during and after migration) for carcinogenesis. Cul-
turally sensitive cancer prevention programmes should focus on individual risk patterns
and specific health care needs. Therefore, continuously changing environments and subse-
quently changing risks in both migrant and autochthonous populations need to be
observed carefully in the future.
� 2010 Elsevier Ltd. All rights reserved.
er Ltd. All rights reserved.
niversity, School of Public Health, Department of Epidemiology and International PublicD-33501 Bielefeld, Germany. Tel.: +49 (0)521 106 2539; fax: +49 (0)521 106 6465.eld.de (M. Arnold).

2648 E U R O P E A N J O U R N A L O F C A N C E R 4 6 ( 2 0 1 0 ) 2 6 4 7 – 2 6 5 9
1. Backgroundsults from studies conducted all over Europe dealing with
Studies on cancer risk in migrant populations have recently
gained increased recognition, but still have rather heteroge-
neous study populations and methods applied. However, in-
sights into risk diversity deduced from such studies
contribute to our understanding of carcinogenesis and might
help answer unclear aetiology questions.
Migration has become an important phenomenon in Wes-
tern Europe in terms of population changes and the composi-
tion of society during the past decades. In 2005, Western and
Central Europe hosted 44.1 million migrants, defined as for-
eign-born persons.1 Many of them originate from non-wes-
tern countries, seeking social security, employment
opportunities and a better future.
European societies characterised by an increasing degree
of heterogeneity pose major challenges to health care sys-
tems and policies. Evidence-based research is therefore a pre-
requisite for appropriate and individual health care of high
quality and effectiveness as well as the implementation of
culturally sensitive measures of prevention.2,3
Health is closely related to global movements. The transi-
tion of disease and risk patterns over time and across coun-
tries have been the scope of many epidemiological research
questions. Accordingly, infectious diseases become less
important as populations advance in terms of westernisation
and the role of chronic health conditions, such as cancer and
cardio-vascular diseases, becomes predominant.4
Hence, migrants from non-western countries are equipped
with a unique constellation of risk factors that are deter-
mined by exposure and disease patterns experienced in both
their home as well as their host country.5,6 This sudden
change in the stage of epidemiological transition as well as
environmental determinants has a major impact on an indi-
vidual’s lifetime disease risk.
Many theories have been developed to explain differences
in mortality and morbidity between migrants and the popula-
tion of their host and home countries, respectively, one of them
being the healthy migrant effect. Thus, migrants are subject to
selection processes that initially underlie good physical and
mental health. Those health advantages after migration are
thought likely to disappear with advancing duration of resi-
dence and generations. As suggested in some studies, no evi-
dence of quickly diminishing health advantages could be
observed, challenging this concept and allowing room for other
explanations.7 Nonetheless, the change in risk patterns over
time is of special interest in epidemiological research.
Multi-causality and geographical variation make cancer in
migrant populations highly suitable for research, especially
in cancers whose main causes are still not attributable to either
environmental (‘nurturecomponents’) orgenetic (‘nature com-
ponents’) risk factors.8 In this context, the individual life course
and particularly early life experiences (as the first step in carci-
nogenesis) have a great impact and play a major role in the
effects of exposure and their association with cancer risks.9,10
Investigating the occurrence of cancer in migrant popula-
tions may allow for a better understanding of cancer aetiology
and of biological factors that can be integrated into preven-
tion and treatment programmes.
The purpose of this article is to compile and compare re-
cancer in non-western migrant populations. The resulting
overview can serve as a guide, reflecting the present state of
knowledge in this field, and as an appeal for further research
and prevention.
2. Methods
2.1. Inclusion criteria of studies
We included studies focussing mainly or partly on cancer
incidence and mortality in adult migrants from non-western
countries, living in the industrialised countries of the Euro-
pean Union, published in English between 1990 and April
2010. Studies were identified by searching pubmed and other
established scientific databases in combination with the fol-
lowing keywords: cancer + ethnicity/ethnic minority/(im)mi-
grant(s)/foreign(ers)/country of birth. A further inclusion
criterion was a comparison of the migrant population with
the native population of the country of the study (no studies
conducted within migrant populations).
2.2. Study descriptions
We identified 37 studies conducted in the following seven
countries: Denmark (3), France (4), Germany (6), Spain (1),
Sweden (7), The Netherlands (5) and the United Kingdom
(11). In 51% of the studies (19/37) incidence data were ana-
lysed, in 41% (15/37) mortality data and in 8% (3/37) both.
All studies were based on the retrospective cohort design.
Owing to the heterogeneous measures of association ap-
plied in the studies, we described tendencies instead of com-
bined rate ratios (RRs) or odds ratios (ORs) to indicate
differences in risks as follows: significantly elevated, elevated,
no difference, decreased and significantly decreased. Age-
adjustment procedures had been carried out in all the studies
included. Other covariables are listed in Table 1.
In general 70% of the studies (26/37) involved all-cancer
comparisons and 24% of the studies (9/37) focused on only
one specific cancer site. The most commonly investigated
sites were breast (28 studies) and lung cancer (26 studies) as
well as stomach and colorectal cancer (24 studies each).
2.3. Defining the migrant status, generations involvedand pooling of migrant origins
The indicator for defining the migrant population under study
ranged from country of birth (of the patient or in combination
with the parental country of birth) in 73% (27/37), name-based
approaches in 14% (5/37), (self-assigned) ethnicity in 11% (4/
37) and a combination in one study.
The applied indicator or proxy for ethnicity is highly
dependent on the availability and completeness of potential
variables in the particular host country. However, country of
birth is the most widely used and accepted proxy although
it has some validity limitations with regard to cultural and
ethnic identity.11
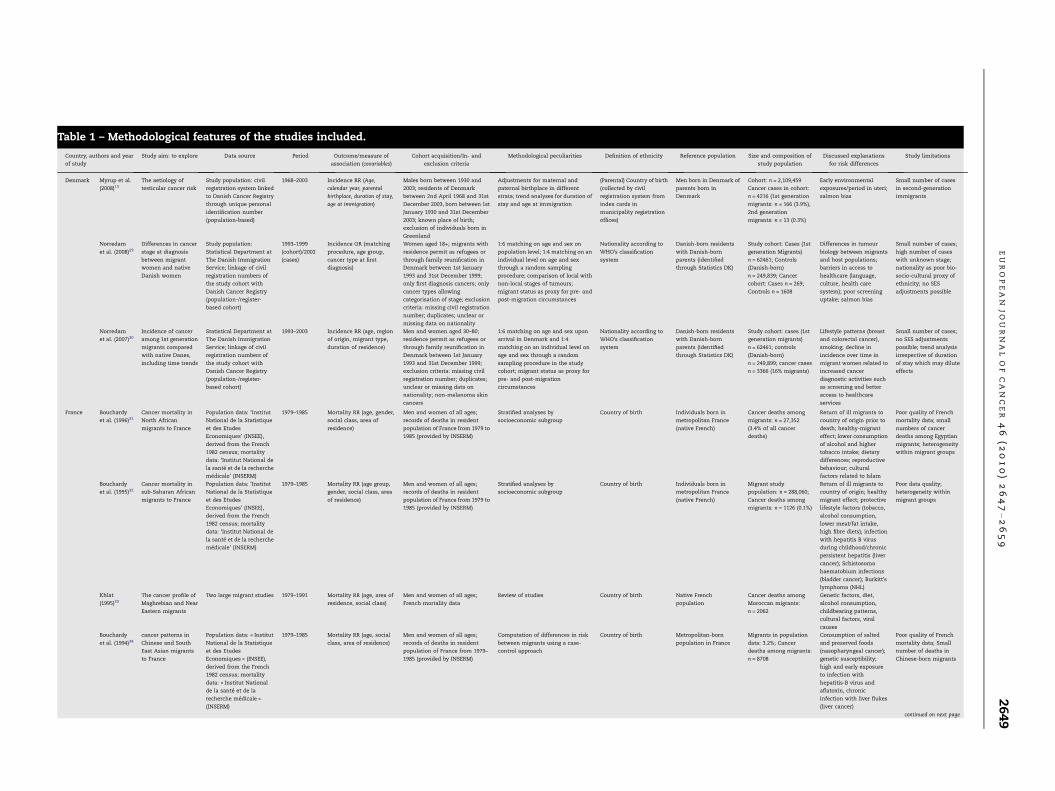
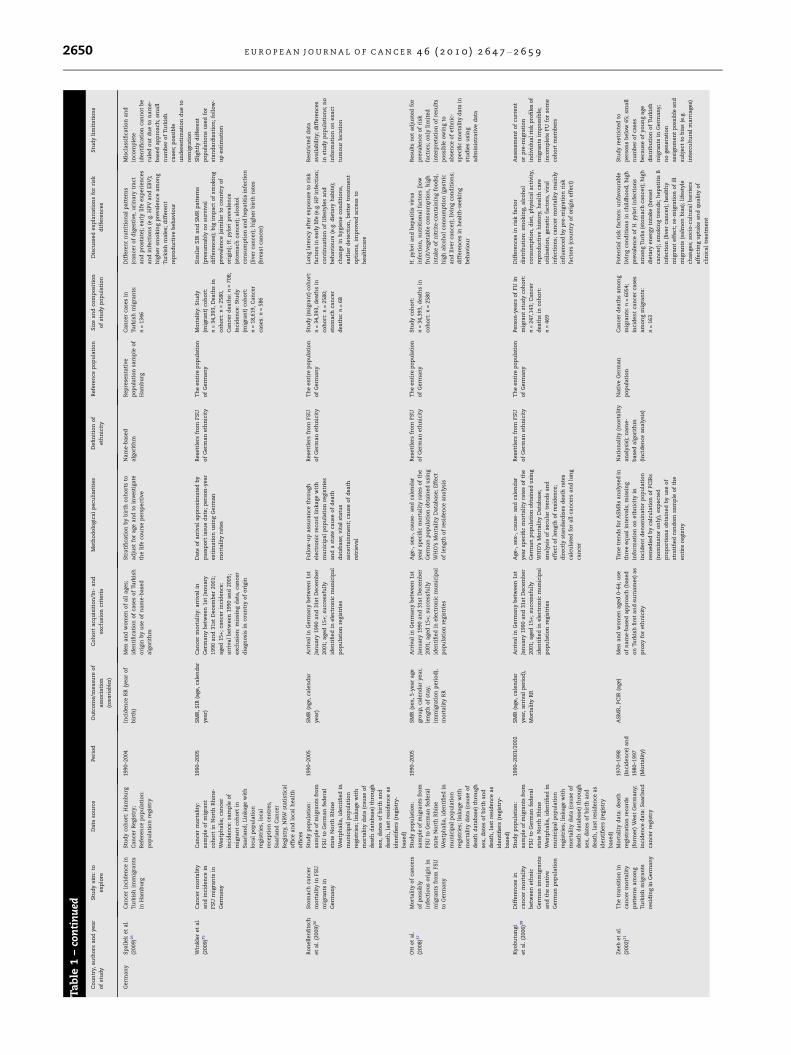
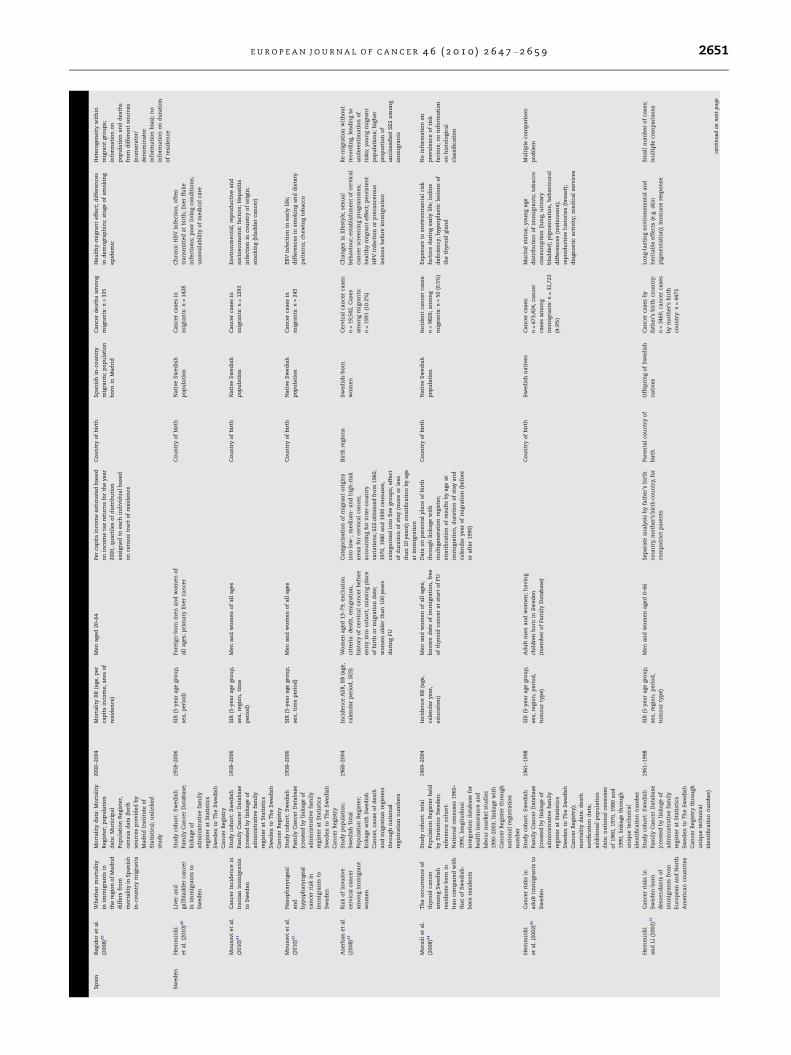
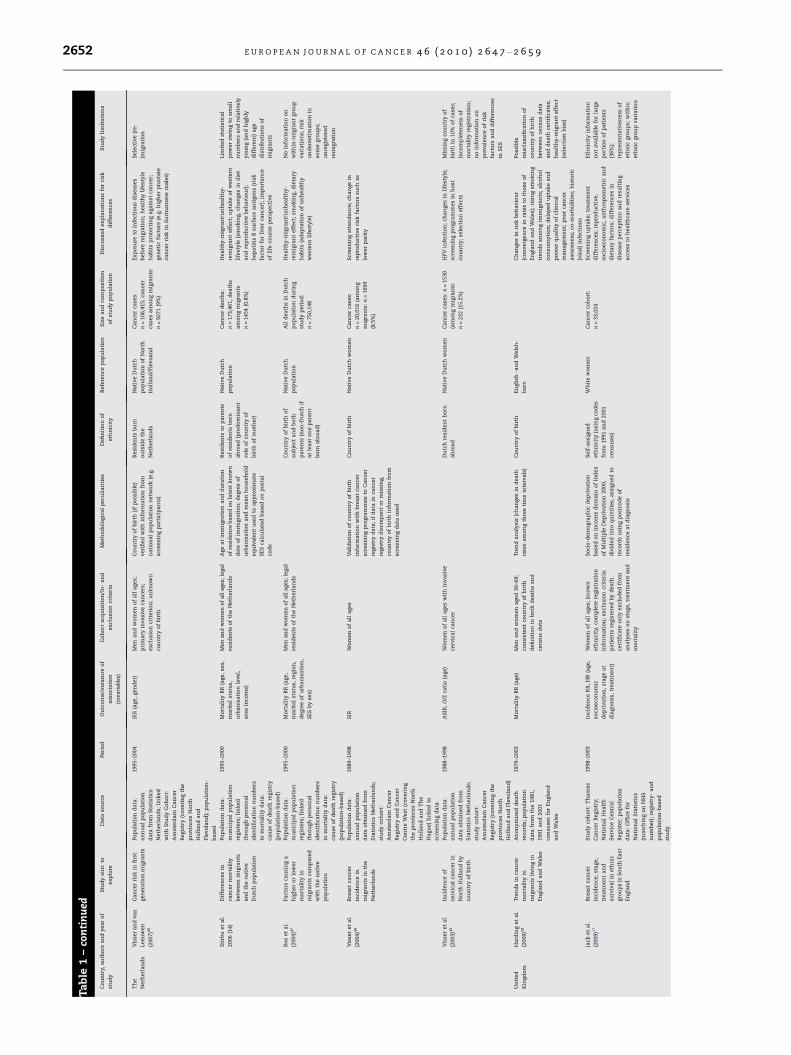
Table 1 – Methodological features of the studies included.
Country, authors and year
of study
Study aim: to explore Data source Period Outcome/measure of
association (covariables)
Cohort acquisition/In- and
exclusion criteria
Methodological peculiarities Definition of ethnicity Reference population Size and composition of
study population
Discussed explanations
for risk differences
Study limitations
Denmark Myrup et al.
(2008)13
The aetiology of
testicular cancer risk
Study population: civil
registration system linked
to Danish Cancer Registry
through unique personal
identification number
(population-based)
1968–2003 Incidence RR (Age,
calendar year, parental
birthplace, duration of stay,
age at immigration)
Males born between 1930 and
2003; residents of Denmark
between 2nd April 1968 and 31st
December 2003, born between 1st
January 1930 and 31st December
2003; known place of birth;
exclusion of individuals born in
Greenland
Adjustments for maternal and
paternal birthplace in different
strata; trend analyses for duration of
stay and age at immigration
(Parental) Country of birth
(collected by civil
registration system from
index cards in
municipality registration
offices)
Men born in Denmark of
parents born in
Denmark
Cohort: n = 2,109,459
Cancer cases in cohort:
n = 4216 (1st generation
migrants: n = 166 (3.9%),
2nd generation
migrants: n = 13 (0.3%)
Early environmental
exposures/period in uteri;
salmon bias
Small number of cases
in second-generation
immigrants
Norredam
et al. (2008)29
Differences in cancer
stage at diagnosis
between migrant
women and native
Danish women
Study population:
Statistical Department at
The Danish Immigration
Service; linkage of civil
registration numbers of
the study cohort with
Danish Cancer Registry
(population-/register-
based cohort)
1993–1999
(cohort)/2002
(cases)
Incidence OR (matching
procedure, age group,
cancer type at first
diagnosis)
Women aged 18+; migrants with
residence permit as refugees or
through family reunification in
Denmark between 1st January
1993 and 31st December 1999;
only first diagnosis cancers; only
cancer types allowing
categorisation of stage; exclusion
criteria: missing civil registration
number; duplicates; unclear or
missing data on nationality
1:6 matching on age and sex on
population level; 1:4 matching on an
individual level on age and sex
through a random sampling
procedure; comparison of local with
non-local stages of tumours;
migrant status as proxy for pre- and
post-migration circumstances
Nationality according to
WHO’s classification
system
Danish-born residents
with Danish-born
parents (identified
through Statistics DK)
Study cohort: Cases (1st
generation Migrants)
n = 62461; Controls
(Danish-born)
n = 249,839; Cancer
cohort: Cases n = 269;
Controls n = 1608
Differences in tumour
biology between migrants
and host populations;
barriers in access to
healthcare (language,
culture, health care
system); poor screening
uptake; salmon bias
Small number of cases;
high number of cases
with unknown stage;
nationality as poor bio-
socio-cultural proxy of
ethnicity; no SES
adjustments possible
Norredam
et al. (2007)30
Incidence of cancer
among 1st generation
migrants compared
with native Danes,
including time trends
Statistical Department at
The Danish Immigration
Service; linkage of civil
registration numbers of
the study cohort with
Danish Cancer Registry
(population-/register-
based cohort)
1993–2003 Incidence RR (age, region
of origin, migrant type,
duration of residence)
Men and women aged 30–80;
residence permit as refugees or
through family reunification in
Denmark between 1st January
1993 and 31st December 1999;
exclusion criteria: missing civil
registration number; duplicates;
unclear or missing data on
nationality; non-melanoma skin
cancers
1:6 matching on age and sex upon
arrival in Denmark and 1:4
matching on an individual level on
age and sex through a random
sampling procedure in the study
cohort; migrant status as proxy for
pre- and post-migration
circumstances
Nationality according to
WHO’s classification
system
Danish-born residents
with Danish-born
parents (identified
through Statistics DK)
Study cohort: cases (1st
generation migrants)
n = 62461; controls
(Danish-born)
n = 249,899; cancer cases
n = 3366 (16% migrants)
Lifestyle patterns (breast
and colorectal cancer),
smoking; decline in
incidence over time in
migrant women related to
increased cancer
diagnostic activities such
as screening and better
access to healthcare
services
Small number of cases;
no SES adjustments
possible; trend analysis
irrespective of duration
of stay which may dilute
effects
France Bouchardy
et al. (1996)31
Cancer mortality in
North African
migrants to France
Population data: ‘Institut
National de la Statistique
et des Etudes
Economiques’ (INSEE),
derived from the French
1982 census; mortality
data: ‘Institut National de
la sante et de la recherche
medicale’ (INSERM)
1979–1985 Mortality RR (age, gender,
social class, area of
residence)
Men and women of all ages;
records of deaths in resident
population of France from 1979 to
1985 (provided by INSERM)
Stratified analyses by
socioeconomic subgroup
Country of birth Individuals born in
metropolitan France
(native French)
Cancer deaths among
migrants: n = 27,352
(3.4% of all cancer
deaths)
Return of ill migrants to
country of origin prior to
death; healthy-migrant
effect; lower consumption
of alcohol and higher
tobacco intake; dietary
differences; reproductive
behaviour; cultural
factors related to Islam
Poor quality of French
mortality data; small
numbers of cancer
deaths among Egyptian
migrants; heterogeneity
within migrant groups
Bouchardy
et al. (1995)32
Cancer mortality in
sub-Saharan African
migrants to France
Population data: ‘Institut
National de la Statistique
et des Etudes
Economiques’ (INSEE),
derived from the French
1982 census; mortality
data: ‘Institut National de
la sante et de la recherche
medicale’ (INSERM)
1979–1985 Mortality RR (age group,
gender, social class, area
of residence)
Men and women of all ages;
records of deaths in resident
population of France from 1979 to
1985 (provided by INSERM)
Stratified analyses by
socioeconomic subgroup
Country of birth Individuals born in
metropolitan France
(native French)
Migrant study
population: n = 288,060;
Cancer deaths among
migrants: n = 1126 (0.1%)
Return of ill migrants to
country of origin; healthy
migrant effect; protective
lifestyle factors (tobacco,
alcohol consumption,
lower meat/fat intake,
high fibre diets); infection
with hepatitis B virus
during childhood/chronic
persistent hepatitis (liver
cancer); Schistosoma
haematobium infections
(bladder cancer); Burkitt’s
lymphoma (NHL)
Poor data quality;
heterogeneity within
migrant groups
Khlat
(1995)33
The cancer profile of
Maghrebian and Near
Eastern migrants
Two large migrant studies 1979–1991 Mortality RR (age, area of
residence, social class)
Men and women of all ages;
French mortality data
Review of studies Country of birth Native French
population
Cancer deaths among
Moroccan migrants:
n = 2062
Genetic factors, diet,
alcohol consumption,
childbearing patterns,
cultural factors, viral
causes
Bouchardy
et al. (1994)34
cancer patterns in
Chinese and South
East Asian migrants
to France
Population data: « Institut
National de la Statistique
et des Etudes
Economiques » (INSEE),
derived from the French
1982 census; mortality
data: « Institut National
de la sante et de la
recherche medicale »
(INSERM)
1979–1985 Mortality RR (age, social
class, area of residence)
Men and women of all ages;
records of deaths in resident
population of France from 1979–
1985 (provided by INSERM)
Computation of differences in risk
between migrants using a case-
control approach
Country of birth Metropolitan-born
population in France
Migrants in population
data: 3.2%; Cancer
deaths among migrants:
n = 8708
Consumption of salted
and preserved foods
(nasopharyngeal cancer);
genetic susceptibility;
high and early exposure
to infection with
hepatitis-B virus and
aflatoxin, chronic
infection with liver flukes
(liver cancer)
Poor quality of French
mortality data; Small
number of deaths in
Chinese-born migrants
continued on next page
EU
RO
PE
AN
JO
UR
NA
LO
FC
AN
CE
R4
6(2
01
0)
26
47
–2
65
92
64
9
Ta
ble
1–
con
tin
ued
Co
un
try,
au
tho
rsa
nd
yea
r
of
stu
dy
Stu
dy
aim
:to
ex
plo
re
Da
taso
urc
ePeri
od
Ou
tco
me/m
ea
sure
of
ass
oci
ati
on
(cov
ari
able
s)
Co
ho
rta
cqu
isit
ion
/In
-a
nd
ex
clu
sio
ncr
iteri
a
Meth
od
olo
gic
al
pecu
lia
riti
es
Defi
nit
ion
of
eth
nic
ity
Refe
ren
cep
op
ula
tio
nS
ize
an
dco
mp
osi
tio
n
of
stu
dy
po
pu
lati
on
Dis
cuss
ed
ex
pla
na
tio
ns
for
risk
dif
fere
nce
s
Stu
dy
lim
ita
tio
ns
Germ
an
yS
pa
llek
et
al.
(2009)1
6
Ca
nce
rin
cid
en
cein
Turk
ish
imm
igra
nts
inH
am
bu
rg
Stu
dy
coh
ort
:H
am
bu
rg
Ca
nce
rR
egis
try
;
Refe
ren
cep
op
ula
tio
n:
po
pu
lati
on
regis
try
1990–2
004
Inci
den
ceR
R(y
ea
ro
f
bir
th)
Men
an
dw
om
en
of
all
ages;
iden
tifi
cati
on
of
case
so
fTu
rkis
h
ori
gin
by
use
of
na
me-b
ase
d
alg
ori
thm
Str
ati
fica
tio
nb
yb
irth
coh
ort
sto
ad
just
for
age
an
dto
inve
stig
ate
the
life
cou
rse
pers
pect
ive
Na
me-b
ase
d
alg
ori
thm
Rep
rese
nta
tive
po
pu
lati
on
sam
ple
of
Ha
mb
urg
Ca
nce
rca
ses
in
Turk
ish
mig
ran
ts:
n=
1346
Dif
fere
nt
nu
trit
ion
al
pa
ttern
s
(ca
nce
ro
fd
igest
ive,
uri
na
rytr
act
an
dp
rost
ate
);ea
rly
life
ex
peri
en
ces
an
din
fect
ion
s(e
.g.
HP
Va
nd
EB
V);
hig
her
smo
kin
gp
rev
ale
nce
am
on
g
Turk
ish
ma
les;
dif
fere
nt
rep
rod
uct
ive
beh
av
iou
r
Mis
cla
ssifi
cati
on
an
d
inco
mp
lete
iden
tifi
cati
on
can
no
tb
e
rule
do
ut
du
eto
na
me-
ba
sed
ap
pro
ach
;sm
all
nu
mb
er
of
Turk
ish
case
s;p
oss
ible
un
dere
stim
ati
on
du
eto
rem
igra
tio
n
Win
kle
ret
al.
(2009)3
5
Ca
nce
rm
ort
ali
ty
an
din
cid
en
cein
FS
Um
igra
nts
in
Germ
an
y
Ca
nce
rm
ort
ali
ty:
sam
ple
of
mig
ran
t
coh
ort
inN
ort
hR
hin
e-
West
ph
ali
a;
can
cer
inci
den
ce:
sam
ple
of
mig
ran
tco
ho
rtin
Sa
arl
an
d;
Lin
ka
ge
wit
h
loca
lp
op
ula
tio
n
regis
trie
s,lo
cal
rece
pti
on
cen
tres,
Sa
arl
an
dC
an
cer
Regis
try,
NR
Wst
ati
stic
al
offi
cea
nd
loca
lh
ea
lth
offi
ces
1990–2
005
SM
R,
SIR
(age,ca
len
da
r
yea
r)
Ca
nce
rm
ort
ali
ty:
arr
iva
lin
Germ
an
yb
etw
een
1st
Jan
ua
ry
1990
an
d31st
Dece
mb
er
2001;
aged
15+
;ca
nce
rin
cid
en
ce:
arr
iva
lb
etw
een
1990
an
d2005;
ex
clu
sio
n:
mis
sin
gd
ata
,ca
nce
r
dia
gn
osi
sin
cou
ntr
yo
fo
rigin
Da
teo
fa
rriv
al
ap
pro
xim
ate
db
y
pa
ssp
ort
issu
ed
ate
;p
ers
on
-yea
r
est
ima
tio
nu
sin
gG
erm
an
mo
rta
lity
rate
s
Rese
ttle
rsfr
om
FS
U
of
Germ
an
eth
nic
ity
Th
een
tire
po
pu
lati
on
of
Germ
an
y
Mo
rta
lity
:S
tud
y
(mig
ran
t)co
ho
rt:
n=
34,3
93,
Dea
ths
in
coh
ort
:n
=2580,
Ca
nce
rd
ea
ths:
n=
708;
Inci
den
ce:
Stu
dy
(mig
ran
t)co
ho
rt:
n=
18,6
19,
Ca
nce
r
case
s:n
=586
Sim
ila
rS
IRa
nd
SM
Rp
att
ern
s
(pre
sum
ab
lyn
osu
rviv
al
dif
fere
nce
s);
big
imp
act
of
smo
kin
g
pre
va
len
ce(s
imil
ar
toco
un
try
of
ori
gin
);H
.pyl
ori
pre
va
len
ce
(sto
ma
chca
nce
r);
alc
oh
ol
con
sum
pti
on
an
dh
ep
ati
tis
infe
ctio
n
(liv
er
can
cer)
;h
igh
er
bir
thra
tes
(bre
ast
can
cer)
Sli
gh
tly
dif
fere
nt
po
pu
lati
on
su
sed
for
sta
nd
ard
isa
tio
n;
foll
ow
-
up
est
ima
tio
n
Ro
nell
en
fits
ch
et
al.
(2009)3
6
Sto
ma
chca
nce
r
mo
rta
lity
inFS
U
mig
ran
tsin
Germ
an
y
Stu
dy
po
pu
lati
on
:
sam
ple
of
mig
ran
tsfr
om
FS
Uto
Germ
an
fed
era
l
sta
teN
ort
hR
hin
e
West
ph
ali
a,
iden
tifi
ed
in
mu
nic
ipa
lp
op
ula
tio
n
regis
trie
s;li
nk
age
wit
h
mo
rta
lity
da
ta(c
au
seo
f
dea
thd
ata
ba
se)
thro
ugh
sex
,d
ate
so
fb
irth
an
d
dea
th,
last
resi
den
cea
s
iden
tifi
ers
(reg
istr
y-
ba
sed
)
1990–2
005
SM
R(a
ge,
cale
nd
ar
yea
r)
Arr
iva
lin
Germ
an
yb
etw
een
1st
Jan
ua
ry1990
an
d31st
Dece
mb
er
2001;
aged
15+
;su
ccess
full
y
iden
tifi
ed
inele
ctro
nic
mu
nic
ipa
l
po
pu
lati
on
regis
trie
s
Foll
ow
-up
ass
ura
nce
thro
ugh
ele
ctro
nic
reco
rdli
nk
age
wit
h
mu
nic
ipa
lp
op
ula
tio
nre
gis
trie
s
an
da
sta
teca
use
of
dea
th
da
tab
ase
;v
ita
lst
atu
s
asc
ert
ain
men
t;ca
use
of
dea
th
retr
ieva
l
Rese
ttle
rsfr
om
FS
U
of
Germ
an
eth
nic
ity
Th
een
tire
po
pu
lati
on
of
Germ
an
y
Stu
dy
(mig
ran
t)co
ho
rt:
n=
34,3
93,
dea
ths
in
coh
ort
:n
=2580;
sto
ma
chca
nce
r
dea
ths:
n=
68
Lo
ng
late
ncy
aft
er
ex
po
sure
tori
sk
fact
ors
inea
rly
life
(e.g
.HP
infe
ctio
n;
con
tin
ua
tio
no
fli
fest
yle
sa
nd
beh
av
iou
rs(e
.g.
die
tary
ha
bit
s);
cha
nge
inh
ygie
ne
con
dit
ion
s,
ea
rlie
rd
ete
ctio
n,
bett
er
trea
tmen
t
op
tio
ns,
imp
rov
ed
acc
ess
to
hea
lth
care
Rest
rict
ed
da
ta
av
ail
ab
ilit
y;
dif
fere
nce
s
inst
ud
yp
op
ula
tio
ns;
no
info
rma
tio
no
nex
act
tum
ou
rlo
cati
on
Ott
et
al.
(2008)3
7
Mo
rta
lity
of
can
cers
of
po
ssib
ly
infe
ctio
us
ori
gin
in
mig
ran
tsfr
om
FS
U
toG
erm
an
y
Stu
dy
po
pu
lati
on
:
sam
ple
of
mig
ran
tsfr
om
FS
Uto
Germ
an
fed
era
l
sta
teN
ort
hR
hin
e
West
ph
ali
a,
iden
tifi
ed
in
mu
nic
ipa
lp
op
ula
tio
n
regis
trie
s;li
nk
age
wit
h
mo
rta
lity
da
ta(c
au
seo
f
dea
thd
ata
ba
se)
thro
ugh
sex
,d
ate
so
fb
irth
an
d
dea
th,
last
resi
den
cea
s
iden
tifi
ers
(reg
istr
y-
ba
sed
)
1990–2
005
SM
R(s
ex
,5-y
ea
ra
ge
gro
up
,ca
len
da
ry
ea
r,
len
gth
of
stay,
imm
igra
tio
np
eri
od
),
mo
rta
lity
RR
Arr
iva
lin
Germ
an
yb
etw
een
1st
Jan
ua
ry1990
an
d31st
Dece
mb
er
2001;
aged
15+
;su
ccess
full
y
iden
tifi
ed
inele
ctro
nic
mu
nic
ipa
l
po
pu
lati
on
regis
trie
s
Age-,
sex
-,ca
use
-a
nd
cale
nd
ar
yea
rsp
eci
fic
mo
rta
lity
rate
so
fth
e
Germ
an
po
pu
lati
on
ob
tain
ed
usi
ng
WH
O’s
Mo
rta
lity
Da
tab
ase
;E
ffect
of
len
gth
of
resi
den
cea
na
lysi
s
Rese
ttle
rsfr
om
FS
U
of
Germ
an
eth
nic
ity
Th
een
tire
po
pu
lati
on
of
Germ
an
y
Stu
dy
coh
ort
:
n=
34,3
93,
dea
ths
in
coh
ort
:n
=2580
H.
pylo
ria
nd
hep
ati
tis
vir
us
infe
ctio
n,
nu
trit
ion
al
fact
ors
(lo
w
fru
it/v
egeta
ble
con
sum
pti
on
,h
igh
inta
ke
of
nit
rite
-co
nta
inin
gfo
od
s),
hig
ha
lco
ho
lco
nsu
mp
tio
n(g
ast
ric
an
dli
ver
can
cer)
;li
vin
gco
nd
itio
ns;
dif
fere
nce
sin
hea
lth
-seek
ing
beh
av
iou
r
Resu
lts
no
ta
dju
sted
for
pre
va
len
ceo
fri
sk
fact
ors
;o
nly
lim
ited
inte
rpre
tati
on
of
resu
lts
po
ssib
leo
win
gto
ab
sen
ceo
feth
nic
-
speci
fic
mo
rta
lity
da
tain
stu
die
su
sin
g
ad
min
istr
ati
ve
da
ta
Ky
ob
utu
ngi
et
al.
(2006)3
8
Dif
fere
nce
sin
can
cer
mo
rta
lity
betw
een
eth
nic
Germ
an
imm
igra
nts
an
dth
en
ati
ve
Germ
an
po
pu
lati
on
Stu
dy
po
pu
lati
on
:
sam
ple
of
mig
ran
tsfr
om
FS
Uto
Germ
an
fed
era
l
sta
teN
ort
hR
hin
e
West
ph
ali
a,
iden
tifi
ed
in
mu
nic
ipa
lp
op
ula
tio
n
regis
trie
s;li
nk
age
wit
h
mo
rta
lity
da
ta(c
au
seo
f
dea
thd
ata
ba
se)
thro
ugh
sex
,d
ate
so
fb
irth
an
d
dea
th,
last
resi
den
cea
s
iden
tifi
ers
(reg
istr
y
ba
sed
)
1990–2
001/2
002
SM
R(a
ge,
cale
nd
ar
yea
r,a
rriv
al
peri
od
),
Mo
rta
lity
RR
Arr
iva
lin
Germ
an
yb
etw
een
1st
Jan
ua
ry1990
an
d31st
Dece
mb
er
2001;
aged
15+
;su
ccess
full
y
iden
tifi
ed
inele
ctro
nic
mu
nic
ipa
l
po
pu
lati
on
regis
trie
s
Age-,
sex
-,ca
use
-a
nd
cale
nd
ar
yea
rsp
eci
fic
mo
rta
lity
rate
so
fth
e
Germ
an
po
pu
lati
on
ob
tain
ed
usi
ng
WH
O’s
Mo
rta
lity
Da
tab
ase
;
an
aly
sis
of
secu
lar
tren
ds
an
d
eff
ect
of
len
gth
of
resi
den
ce;
dir
ect
lyst
an
da
rdis
es
dea
thra
tes
calc
ula
ted
for
all
-ca
nce
rsa
nd
lun
g
can
cer
Rese
ttle
rsfr
om
FS
U
of
Germ
an
eth
nic
ity
Th
een
tire
po
pu
lati
on
of
Germ
an
y
Pers
on
-yea
rso
fFU
in
mig
ran
tst
ud
yco
ho
rt:
n=
247,1
43;
Ca
nce
r
dea
ths
inco
ho
rt:
n=
469
Dif
fere
nce
sin
risk
fact
or
dis
trib
uti
on
:sm
ok
ing,
alc
oh
ol
con
sum
pti
on
,d
iet,
ph
ysi
cal
act
ivit
y,
rep
rod
uct
ive
his
tory
,h
ea
lth
care
uti
lisa
tio
n,
gen
eti
cfa
cto
rs,
vir
al
infe
ctio
ns;
can
cer
mo
rta
lity
ma
inly
infl
uen
ced
by
pre
-mig
rati
on
risk
fact
ors
(co
un
try
of
ori
gin
eff
ect
)
Ass
ess
men
to
fcu
rren
t
or
pre
-mig
rati
on
ind
ivid
ua
lri
skp
rofi
les
of
mig
ran
tsim
po
ssib
le;
inco
mp
lete
FU
for
som
e
coh
ort
mem
bers
Zeeb
et
al.
(2002)2
1
Th
etr
an
siti
on
in
can
cer
mo
rta
lity
pa
ttern
sa
mo
ng
Turk
ish
mig
ran
ts
resi
din
gin
Germ
an
y
Mo
rta
lity
da
ta:
dea
th
regis
trati
on
reco
rds
(fo
rmer)
West
Germ
an
y;
inci
den
ced
ata
:S
aa
rla
nd
can
cer
regis
try
1970–1
998
(In
cid
en
ce)
an
d
1980–1
997
(Mo
rta
lity
)
AS
MR
,P
CIR
(age)
Men
an
dw
om
en
aged
0–6
4;
use
of
na
me-b
ase
da
pp
roa
ch(b
ase
d
on
Turk
ish
firs
ta
nd
surn
am
es)
as
pro
xy
for
eth
nic
ity
Tim
etr
en
ds
for
AS
MR
sa
na
lyse
din
thre
eeq
ua
lin
terv
als
;m
issi
ng
info
rma
tio
no
neth
nic
ity
in
inci
den
td
en
om
ina
tor
po
pu
lati
on
rem
ed
ied
by
calc
ula
tio
no
fP
CIR
s
(no
min
ato
ro
nly
),ex
pect
ed
pro
po
rtio
ns
ob
tain
ed
by
use
of
stra
tifi
ed
ran
do
msa
mp
leo
fth
e
en
tire
regis
try
Na
tio
na
lity
(mo
rta
lity
an
aly
sis)
;n
am
e-
ba
sed
alg
ori
thm
(in
cid
en
cea
na
lysi
s)
Na
tive
Germ
an
po
pu
lati
on
Ca
nce
rd
ea
ths
am
on
g
mig
ran
ts:
n=
6054;
inci
den
tca
nce
rca
ses
am
on
gm
igra
nts
:
n=
163
Po
ten
tia
lri
skfa
cto
rs:
un
fav
ou
rab
le
livin
gco
nd
itio
ns
inch
ild
ho
od
,h
igh
pre
va
len
ceo
fH
.py
lori
infe
ctio
ns
am
on
gTu
rks
(sto
ma
chca
nce
r);h
igh
die
tary
en
erg
yin
tak
e(b
rea
st
can
cer)
;sm
ok
ing
tren
ds;
hep
ati
tis
B
infe
ctio
n(l
iver
can
cer)
;h
ea
lth
y
mig
ran
teff
ect
;re
-mig
rati
on
of
ill
mig
ran
ts(s
alm
on
bia
s);
life
sty
le
cha
nges;
soci
o-c
ult
ura
lb
arr
iers
aff
ect
ing
up
tak
ea
nd
qu
ali
tyo
f
clin
ica
ltr
ea
tmen
t
Stu
dy
rest
rict
ed
to
pers
on
sb
elo
w65;
sma
ll
nu
mb
er
of
case
s
beca
use
of
yo
un
ga
ge
dis
trib
uti
on
of
Turk
ish
mig
ran
tsin
Germ
an
y;
no
gen
era
tio
n
ass
ign
men
tp
oss
ible
an
d
sub
ject
tob
ias
(e.g
.
inte
rcu
ltu
ral
ma
rria
ges)
2650 E U R O P E A N J O U R N A L O F C A N C E R 4 6 ( 2 0 1 0 ) 2 6 4 7 – 2 6 5 9
Sp
ain
Reg
ido
ret
al.
(2008)3
9
Wh
eth
er
mo
rta
lity
inim
mig
ran
tsin
the
regio
no
fM
ad
rid
dif
fers
fro
m
mo
rta
lity
inS
pa
nis
h
in-c
ou
ntr
ym
igra
nts
Mo
rta
lity
da
ta:
Mo
rta
lity
Reg
iste
r;p
op
ula
tio
n
da
ta:
Mu
nic
ipa
l
Po
pu
lati
on
Regis
ter,
cen
sus
da
ta(b
oth
sou
rces
pro
vid
ed
by
Ma
dri
dIn
stit
ute
of
Sta
tist
ics)
;u
nli
nk
ed
stu
dy
2000–2
004
Mo
rta
lity
RR
(age,
per
cap
ita
inco
me,
are
ao
f
resi
den
ce)
Men
aged
20–6
4Pe
rca
pit
ain
com
eest
ima
ted
ba
sed
on
inco
me
tax
retu
rns
for
the
yea
r
2000,
qu
art
iles
of
dis
trib
uti
on
ass
ign
ed
toea
chin
div
idu
al
ba
sed
on
cen
sus
tra
cto
fre
sid
en
ce
Co
un
try
of
bir
thS
pa
nis
hin
-co
un
try
mig
ran
ts;
po
pu
lati
on
bo
rnin
Ma
dri
d
Ca
nce
rd
ea
ths
am
on
g
mig
ran
ts:
n=
335
Hea
lth
y-m
igra
nt
eff
ect
;d
iffe
ren
ces
ind
em
ogra
ph
ics;
sta
ge
of
smo
kin
g
ep
idem
ic
Hete
rogen
eit
yw
ith
in
mig
ran
tgro
up
s;
info
rma
tio
no
n
po
pu
lati
on
an
dd
ea
ths
fro
md
iffe
ren
tso
urc
es
(nu
mera
tor/
den
om
ina
tor
info
rma
tio
nb
ias)
;n
o
info
rma
tio
no
nd
ura
tio
n
of
resi
den
ce
Sw
ed
en
Hem
min
ki
et
al.
(2010)4
0
Liv
er
an
d
ga
llb
lad
der
can
cer
inim
mig
ran
tsto
Sw
ed
en
Stu
dy
coh
ort
:S
wed
ish
Fam
ily
Ca
nce
rD
ata
ba
se;
lin
ka
ge
of
ad
min
istr
ati
ve
fam
ily
regis
ter
at
Sta
tist
ics
Sw
ed
en
toT
he
Sw
ed
ish
Ca
nce
rR
egis
try
1958–2
006
SIR
(5-y
ear
age
gro
up
,
sex
,p
eri
od
)
Fore
ign
-bo
rnm
en
an
dw
om
en
of
all
ages;
pri
ma
ryli
ver
can
cer
Co
un
try
of
bir
thN
ati
ve
Sw
ed
ish
po
pu
lati
on
Ca
nce
rca
ses
in
mig
ran
ts:
n=
1428
Ch
ron
icH
BV
infe
ctio
n,
oft
en
tra
nsm
itte
da
tb
irth
;li
ver
flu
ke
infe
ctio
ns;
po
or
liv
ing
con
dit
ion
s;
un
av
ail
ab
ilit
yo
fm
ed
ica
lca
re
Mo
usa
vi
et
al.
(2010)4
1
Ca
nce
rin
cid
en
cein
Ira
nia
nim
mig
ran
ts
toS
wed
en
Stu
dy
coh
ort
:S
wed
ish
Fam
ily
Ca
nce
rD
ata
ba
se
(cre
ate
db
yli
nk
age
of
ad
min
istr
ati
ve
fam
ily
regis
ter
at
Sta
tist
ics
Sw
ed
en
toT
he
Sw
ed
ish
Ca
nce
rR
egis
try
1958–2
006
SIR
(5-y
ear
age
gro
up
,
sex
,re
gio
n,
tim
e
peri
od
)
Men
an
dw
om
en
of
all
ages
Co
un
try
of
bir
thN
ati
ve
Sw
ed
ish
po
pu
lati
on
Ca
nce
rca
ses
in
mig
ran
ts:
n=
1293
En
vir
on
men
tal,
rep
rod
uct
ive
an
d
soci
oeco
no
mic
fact
ors
;H
ep
ati
tis
infe
ctio
nin
cou
ntr
yo
fo
rigin
;
smo
kin
g(b
lad
der
can
cer)
Mo
usa
vi
et
al.
(2010)4
2
Na
sop
ha
ryn
gea
l
an
d
hyp
op
ha
ryn
gea
l
can
cer
risk
in
imm
igra
nts
to
Sw
ed
en
Stu
dy
coh
ort
:S
wed
ish
Fam
ily
Ca
nce
rD
ata
ba
se
(cre
ate
db
yli
nk
age
of
ad
min
istr
ati
ve
fam
ily
regis
ter
at
Sta
tist
ics
Sw
ed
en
toT
he
Sw
ed
ish
Ca
nce
rR
egis
try
1958–2
006
SIR
(5-y
ear
age
gro
up
,
sex
,ti
me
peri
od
)
Men
an
dw
om
en
of
all
ages
Co
un
try
of
bir
thN
ati
ve
Sw
ed
ish
po
pu
lati
on
Ca
nce
rca
ses
in
mig
ran
ts:
n=
243
EB
Vin
fect
ion
inea
rly
life
;
dif
fere
nce
sin
smo
kin
ga
nd
die
tary
pa
ttern
s;ch
ewin
gto
ba
cco
Aze
rka
net
al.
(2008)4
3
Ris
ko
fin
va
siv
e
cerv
ica
lca
nce
r
am
on
gim
mig
ran
t
wo
men
Stu
dy
po
pu
lati
on
:
Sw
ed
ish
To
tal
Po
pu
lati
on
Regis
ter;
lin
ka
ge
wit
hS
wed
ish
Ca
nce
r,ca
use
of
dea
th
an
dm
igra
tio
nre
gis
ters
thro
ugh
na
tio
na
l
regis
tra
tio
nn
um
bers
1968–2
004
Inci
den
ceA
SR
,R
R(a
ge,
cale
nd
ar
peri
od
,S
ES
)
Wo
men
aged
13–7
9;
ex
clu
sio
n
crit
eri
a:
dea
th,
em
igra
tio
n,
his
tory
of
cerv
ica
lca
nce
rb
efo
re
en
try
into
coh
ort
;m
issi
ng
pla
ce
of
bir
tho
rm
igra
tio
nd
ate
;
wo
men
old
er
tha
n100
yea
rs
du
rin
gFU
Ca
tego
risa
tio
no
fm
igra
nt
ori
gin
s
into
low
-,m
ed
ium
-a
nd
hig
h-r
isk
are
as
for
cerv
ica
lca
nce
r,
acc
ou
nti
ng
for
inte
r-co
un
try
va
ria
tio
ns;
SE
So
bta
ined
fro
m1960,
1970,
1980
an
d1990
cen
suse
s,
cate
go
rise
din
tofi
ve
gro
up
s;eff
ect
of
du
rati
on
of
stay
(mo
reo
rle
ss
tha
n10
yea
rs);
stra
tifi
cati
on
by
age
at
imm
igra
tio
n
Bir
thre
gio
ns
Sw
ed
ish
-bo
rn
wo
men
Cerv
ica
lca
nce
rca
ses:
n=
19,5
42,
Ca
ses
am
on
gm
igra
nts
:
n=
1991
(10.2
%)
Ch
an
ges
inli
fest
yle
,se
xu
al
beh
av
iou
r;est
ab
lish
men
to
fce
rvic
al
can
cer
scre
en
ing
pro
gra
mm
es;
hea
lth
ym
igra
nt
eff
ect
;p
ers
iste
nt
HP
Vin
fect
ion
or
pre
can
cero
us
lesi
on
sb
efo
reim
mig
rati
on
Re-m
igra
tio
nw
ith
ou
t
reco
rdin
g,
lea
din
gto
un
dere
stim
ati
on
of
risk
s;y
ou
ng
mig
ran
t
po
pu
lati
on
s;h
igh
er
pro
po
rtio
no
f
un
cla
ssifi
ed
SE
Sa
mo
ng
imm
igra
nts
Mo
rad
iet
al.
(2008)4
4
Th
eo
ccu
rren
ceo
f
thyro
idca
nce
r
am
on
gS
wed
ish
resi
den
tsb
orn
in
Ira
nco
mp
are
dw
ith
tha
to
fS
wed
ish
-
bo
rnre
sid
en
ts
Stu
dy
coh
ort
:to
tal
Po
pu
lati
on
Regis
ter
held
by
Sta
tist
ics
Sw
ed
en
;
refe
ren
ceco
ho
rt:
Na
tio
na
lce
nsu
ses
1960–
1990,
lon
git
ud
ina
l
inte
gra
tio
nd
ata
ba
sefo
r
hea
lth
insu
ran
cea
nd
lab
ou
rm
ark
et
stu
die
s
1990–2
003;
lin
ka
ge
wit
h
Ca
nce
rR
egis
ter
thro
ugh
na
tio
na
lre
gis
trati
on
nu
mb
er
1969–2
004
Inci
den
ceR
R(a
ge,
cale
nd
ar
yea
r,
ed
uca
tio
n)
Men
an
dw
om
en
of
all
ages;
kn
ow
nd
ate
of
imm
igra
tio
n,
free
of
thy
roid
can
cer
at
sta
rto
fFU
Da
tao
np
are
nta
lp
lace
of
bir
th
thro
ugh
lin
ka
ge
wit
h
mu
ltig
en
era
tio
nre
gis
ter;
stra
tifi
cati
on
of
resu
lts
by
age
at
imm
igra
tio
n,
du
rati
on
of
stay
an
d
cale
nd
ar
yea
ro
fm
igra
tio
n(b
efo
re
or
aft
er
1990)
Co
un
try
of
bir
thN
ati
ve
Sw
ed
ish
po
pu
lati
on
Inci
den
tca
nce
rca
ses:
n=
9826;
am
on
g
mig
ran
ts:
n=
50
(0.5
%)
Ex
po
sure
toen
vir
on
men
tal
risk
fact
ors
du
rin
gea
rly
life
;io
din
e
defi
cien
cy;
hy
perp
last
icle
sio
ns
of
the
thy
roid
gla
nd
No
info
rma
tio
no
n
pre
va
len
ceo
fri
sk
fact
ors
;n
oin
form
ati
on
on
his
tolo
gic
al
cla
ssifi
cati
on
Hem
min
ki
et
al.
(2002)4
5
Ca
nce
rri
sks
in
ad
ult
imm
igra
nts
to
Sw
ed
en
Stu
dy
coh
ort
:S
wed
ish
Fam
ily
Ca
nce
rD
ata
ba
se
(cre
ate
db
yli
nk
age
of
ad
min
istr
ati
ve
fam
ily
regis
ter
at
Sta
tist
ics
Sw
ed
en
toT
he
Sw
ed
ish
Ca
nce
rR
egis
try
);
mo
rta
lity
da
ta:
dea
th
no
tifi
cati
on
da
ta;
ad
dit
ion
al
po
pu
lati
on
da
ta:
na
tio
na
lce
nsu
ses
of
1960,
1970,
1980
an
d
1990;
lin
ka
ge
thro
ugh
un
iqu
ete
chn
ica
l
iden
tifi
cati
on
nu
mb
er
1961–1
998
SIR
(5-y
ear
age
gro
up
,
sex
,re
gio
n,
peri
od
,
tum
ou
rty
pe)
Ad
ult
men
an
dw
om
en
;h
av
ing
chil
dre
nb
orn
inS
wed
en
(mem
ber
of
Fam
ily
Da
tab
ase
)
Co
un
try
of
bir
thS
wed
ish
na
tives
Ca
nce
rca
ses:
n=
673,4
24,
can
cer
case
sa
mo
ng
imm
igra
nts
:n
=32,7
22
(4.9
%)
Ma
rita
lst
atu
s;y
ou
ng
age
dis
trib
uti
on
of
imm
igra
nts
;to
ba
cco
con
sum
pti
on
(lu
ng,
uri
na
ry
bla
dd
er)
;p
igm
en
tati
on
,b
eh
av
iou
ral
dif
fere
nce
s(m
ela
no
ma
);
rep
rod
uct
ive
his
tori
es
(bre
ast
);
dia
gn
ost
ica
ctiv
ity
;m
ed
ica
lse
rvic
es
Mu
ltip
leco
mp
ari
son
pro
ble
m
Hem
min
ki
an
dLi
(2002)1
2
Ca
nce
rri
sks
in
Sw
ed
en
-bo
rn
desc
en
da
nts
of
imm
igra
nts
fro
m
Eu
rop
ea
na
nd
No
rth
Am
eri
can
cou
ntr
ies
Stu
dy
coh
ort
:S
wed
ish
Fam
ily
Ca
nce
rD
ata
ba
se
(cre
ate
db
yli
nk
age
of
ad
min
istr
ati
ve
fam
ily
regis
ter
at
Sta
tist
ics
Sw
ed
en
toT
he
Sw
ed
ish
Ca
nce
rR
egis
try
thro
ugh
un
iqu
ete
chn
ica
l
iden
tifi
cati
on
nu
mb
er)
1961–1
998
SIR
(5-y
ear
age
gro
up
,
sex
,re
gio
n,
peri
od
,
tum
ou
rty
pe)
Men
an
dw
om
en
aged
0–6
6S
epa
rate
an
aly
sis
by
fath
er’
sb
irth
cou
ntr
y,m
oth
er’
sb
irth
cou
ntr
y,fo
r
com
pa
trio
tp
are
nts
Pa
ren
tal
cou
ntr
yo
f
bir
th
Off
spri
ng
of
Sw
ed
ish
na
tiv
es
Ca
nce
rca
ses
by
fath
er’
sb
irth
cou
ntr
y:
n=
3460,
can
cer
case
s
by
mo
ther’
sb
irth
cou
ntr
y:
n=
4473
Lo
ng-l
ast
ing
en
vir
on
men
tal
an
d
heri
tab
leeff
ect
s(e
.g.
skin
pig
men
tati
on
);im
mu
ne
resp
on
se
Sm
all
nu
mb
er
of
case
s;
mu
ltip
leco
mp
ari
son
s
con
tin
ued
onn
ext
page
E U R O P E A N J O U R N A L O F C A N C E R 4 6 ( 2 0 1 0 ) 2 6 4 7 – 2 6 5 9 2651
Ta
ble
1–
con
tin
ued
Co
un
try,
au
tho
rsa
nd
yea
ro
f
stu
dy
Stu
dy
aim
:to
ex
plo
re
Da
taso
urc
ePeri
od
Ou
tco
me/m
ea
sure
of
ass
oci
ati
on
(cov
ari
able
s)
Co
ho
rta
cqu
isit
ion
/In
-a
nd
ex
clu
sio
ncr
iteri
a
Meth
od
olo
gic
al
pecu
lia
riti
es
Defi
nit
ion
of
eth
nic
ity
Refe
ren
cep
op
ula
tio
nS
ize
an
dco
mp
osi
tio
n
of
stu
dy
po
pu
lati
on
Dis
cuss
ed
ex
pla
na
tio
ns
for
risk
dif
fere
nce
s
Stu
dy
lim
ita
tio
ns
Th
e
Neth
erl
an
ds
Vis
ser
an
dva
n
Leeu
wen
(2007)4
6
Ca
nce
rri
skin
firs
t
gen
era
tio
nm
igra
nts
Po
pu
lati
on
da
ta:
an
nu
al
po
pu
lati
on
da
tafr
om
Sta
tist
ics
Neth
erl
an
ds;
lin
ked
wit
hS
tud
yC
oh
ort
:
Am
sterd
am
Ca
nce
r
Regis
try
(co
veri
ng
the
pro
vin
ces
No
rth
Ho
lla
nd
an
d
Fle
vo
lan
d);
po
pu
lati
on
-
ba
sed
1995–2
004
SIR
(age,
gen
der)
Men
an
dw
om
en
of
all
ages;
pri
ma
ryin
vasi
ve
can
cers
;
ex
clu
sio
ncr
iteri
on
:u
nk
no
wn
cou
ntr
yo
fb
irth
Co
un
try
of
bir
th(i
fp
oss
ible
)
ver
ified
wit
hin
form
ati
on
fro
m
na
tio
na
lp
op
ula
tio
nn
etw
ork
(e.g
.
scre
en
ing
pa
rtic
ipa
nts
)
Resi
den
tsb
orn
ou
tsid
eth
e
Neth
erl
an
ds
Na
tive
Du
tch
po
pu
lati
on
of
No
rth
Ho
lla
nd
/Fle
vo
an
d
Ca
nce
rca
ses:
n=
106,4
15;
can
cer
case
sa
mo
ng
mig
ran
ts:
n=
9271
(9%
)
Ex
po
sure
toin
fect
iou
sd
isea
ses
befo
rem
igra
tio
n;
hea
lth
yli
fest
yle
hab
its
pro
tect
ing
aga
inst
can
cer;
gen
eti
cfa
cto
rs(e
.g.
hig
her
pro
sta
te
can
cer
risk
inS
uri
na
mese
ma
les)
Sele
ctiv
e(r
e-
)mig
rati
on
Sti
rbu
et
al.
2006
(14)
Dif
fere
nce
sin
can
cer
mo
rta
lity
betw
een
mig
ran
ts
an
dth
en
ati
ve
Du
tch
po
pu
lati
on
Po
pu
lati
on
da
ta:
mu
nic
ipa
lp
op
ula
tio
n
regis
ters
;li
nk
ed
thro
ugh
pers
on
al
iden
tifi
cati
on
nu
mb
ers
tom
ort
ali
tyd
ata
:
cau
seo
fd
ea
thre
gis
try
(po
pu
lati
on
-ba
sed
)
1995–2
000
Mo
rta
lity
RR
(age,
sex
,
ma
rita
lst
atu
s,
urb
an
isa
tio
nle
vel,
are
ain
com
e)
Men
an
dw
om
en
of
all
ages;
lega
l
resi
den
tso
fth
eN
eth
erl
an
ds
Age
at
imm
igra
tio
na
nd
du
rati
on
of
resi
den
ceb
ase
do
nla
test
kn
ow
n
da
teo
fim
mig
rati
on
;d
egre
eo
f
urb
an
isa
tio
na
nd
mea
nh
ou
seh
old
eq
uiv
ale
nt
use
dto
ap
pro
xim
ate
SE
Sca
lcu
late
db
ase
do
np
ost
al
cod
e
Resi
den
tso
rp
are
nts
of
resi
den
tsb
orn
ab
roa
d(p
red
om
ina
nt
role
of
cou
ntr
yo
f
bir
tho
fm
oth
er)
Na
tive
Du
tch
po
pu
lati
on
Ca
nce
rd
ea
ths:
n=
173,4
61,
dea
ths
am
on
gm
igra
nts
n=
1454
(0.8
%)
Hea
lth
y-m
igra
nt/
un
hea
lth
y-
rem
igra
nt
eff
ect
;u
pta
ke
of
west
ern
life
sty
le(s
mo
kin
g,
cha
nges
ind
iet
an
dre
pro
du
ctiv
eb
eh
av
iou
r);
hep
ati
tis
Bsu
rfa
cea
nti
gen
s(r
isk
fact
or
for
liver
can
cer)
;im
po
rta
nce
of
life
-co
urs
ep
ers
pect
ive
Lim
ited
sta
tist
ica
l
po
wer
ow
ing
tosm
all
nu
mb
ers
an
dre
lati
vely
yo
un
g(a
nd
hig
hly
dif
fere
nt)
age
dis
trib
uti
on
so
f
mig
ran
ts
Bo
set
al.
(2004)4
7
Fact
ors
cau
sin
ga
hig
her
or
low
er
mo
rta
lity
in
mig
ran
tsco
mp
are
d
wit
hth
en
ati
ve
po
pu
lati
on
Po
pu
lati
on
da
ta:
mu
nic
ipa
lp
op
ula
tio
n
regis
ters
;li
nk
ed
thro
ugh
pers
on
al
iden
tifi
cati
on
nu
mb
ers
tom
ort
ali
tyd
ata
:
cau
seo
fd
ea
thre
gis
try
(po
pu
lati
on
-ba
sed
)
1995–2
000
Mo
rta
lity
RR
(age,
ma
rita
lst
atu
s,re
gio
n,
degre
eo
fu
rba
nis
ati
on
,
SE
Sb
yse
x)
Men
an
dw
om
en
of
all
ages;
lega
l
resi
den
tso
fth
eN
eth
erl
an
ds
Co
un
try
of
bir
tho
f
sub
ject
an
db
oth
pa
ren
ts(n
on
-Du
tch
if
at
lea
sto
ne
pa
ren
t
bo
rna
bro
ad
)
Na
tive
Du
tch
po
pu
lati
on
All
dea
ths
inD
utc
h
po
pu
lati
on
du
rin
g
stu
dy
peri
od
:
n=
750,1
48
Hea
lth
y-m
igra
nt/
un
hea
lth
y-
rem
igra
nt
eff
ect
;sm
ok
ing,
die
tary
hab
its
(ad
ap
tati
on
of
un
hea
lth
y
wes
tern
life
sty
le)
No
info
rma
tio
no
n
wit
hin
-mig
ran
tgro
up
va
ria
tio
ns;
risk
un
dere
stim
ati
on
in
som
egro
up
s;
un
regis
tere
d
rem
igra
tio
n
Vis
ser
et
al.
(2004)4
8
Bre
ast
can
cer
inci
den
cein
mig
ran
tsin
the
Neth
erl
an
ds
Po
pu
lati
on
da
ta:
an
nu
al
po
pu
lati
on
da
tao
bta
ined
fro
m
Sta
tist
ics
Neth
erl
an
ds;
stu
dy
coh
ort
:
Am
sterd
am
Ca
nce
r
Regis
try
an
dC
an
cer
Cen
tre
West
(co
veri
ng
the
pro
vin
ces
No
rth
Ho
lla
nd
an
dT
he
Ha
gu
e)
lin
ked
to
scre
en
ing
da
ta
1989–1
998
SIR
Wo
men
of
all
ages
Va
lid
ati
on
of
cou
ntr
yo
fb
irth
info
rma
tio
nw
ith
bre
ast
can
cer
scre
en
ing
pro
gra
mm
es
toC
an
cer
regis
try
da
ta;
ifd
ata
inca
nce
r
regis
try
dis
crep
an
to
rm
issi
ng,
cou
ntr
yo
fb
irth
info
rma
tio
nfr
om
scre
en
ing
da
tau
sed
Co
un
try
of
bir
thN
ati
ve
Du
tch
wo
men
Ca
nce
rca
ses:
n=
20,0
16
(am
on
g
mig
ran
ts:
n=
1699
(8.5
%)
Scr
een
ing
att
en
da
nce
;ch
an
ge
in
rep
rod
uct
ive
risk
fact
ors
such
as
low
er
pa
rity
Vis
ser
et
al.
(2003)4
9
Inci
den
ceo
f
cerv
ica
lca
nce
rin
No
rth
Ho
lla
nd
by
cou
ntr
yo
fb
irth
Po
pu
lati
on
da
ta:
an
nu
al
po
pu
lati
on
da
tao
bta
ined
fro
m
Sta
tist
ics
Neth
erl
an
ds;
stu
dy
coh
ort
:
Am
sterd
am
Ca
nce
r
Regis
try
(co
veri
ng
the
pro
vin
ces
No
rth
Ho
lla
nd
an
dFle
vo
lan
d)
1988–1
998
AS
IR,
O/E
rati
o(a
ge)
Wo
men
of
all
ages
wit
hin
va
sive
cerv
ica
lca
nce
r
Du
tch
resi
den
tb
orn
ab
roa
d
Na
tive
Du
tch
wo
men
Ca
nce
rca
ses:
n=
1530
(am
on
gm
igra
nts
:
n=
232
(15.2
%)
HP
Vin
fect
ion
;ch
an
ges
inli
fest
yle
;
scre
enin
gp
rogra
mm
es
inh
ost
cou
ntr
y;
sele
ctio
neff
ect
s
Mis
sin
gco
un
try
of
bir
thin
10%
of
case
s;
inco
mp
lete
ness
of
mo
rta
lity
regis
trati
on
;
no
info
rma
tio
no
n
pre
va
len
ceo
fri
sk
fact
ors
an
dd
iffe
ren
ces
inS
ES
Un
ited
Kin
gd
om
Ha
rdin
get
al.
(2009)2
8
Tre
nd
sin
can
cer
mo
rta
lity
in
mig
ran
tsli
vin
gin
En
gla
nd
an
dW
ale
s
An
on
ym
ised
dea
th
reco
rds;
po
pu
lati
on
da
tafr
om
the
1981,
1991
an
d2001
cen
suse
sfo
rE
ngla
nd
an
dW
ale
s
1979–2
003
Mo
rta
lity
RR
(age)
Men
an
dw
om
en
aged
30–6
9;
con
sist
en
tco
un
try
of
bir
th
defi
nit
ion
inb
oth
dea
ths
an
d
cen
sus
da
ta
Tre
nd
an
aly
sis
(ch
an
ges
ind
ea
th
rate
sa
mo
ng
thre
eti
me
inte
rva
ls)
Co
un
try
of
bir
thE
ngli
sh-a
nd
Wels
h-
bo
rn
Ch
an
ges
inri
skb
eh
av
iou
r
(co
nv
erg
en
cein
rate
sto
tho
seo
f
En
gla
nd
an
dW
ale
s);
risi
ng
smo
kin
g
tren
ds
am
on
gim
mig
ran
ts;
alc
oh
ol
con
sum
pti
on
;d
ela
yed
up
tak
ea
nd
po
ore
rq
ua
lity
of
clin
ica
l
ma
na
gem
en
t;p
oo
rca
nce
r
aw
are
ness
;co
-mo
rbid
itie
s;h
isto
ric
(vir
al)
infe
ctio
ns
Po
ssib
le
mis
cla
ssifi
cati
on
of
cou
ntr
yo
fb
irth
betw
een
cen
sus
da
ta
an
dd
ea
thce
rtifi
cate
s;
hea
lth
y-m
igra
nt
eff
ect
(sele
ctio
nb
ias)
Jack
et
al.
(2009)1
7
Bre
ast
can
cer
inci
den
ce,
sta
ge,
trea
tmen
ta
nd
surv
iva
lin
eth
nic
gro
up
sin
So
uth
Ea
st
En
gla
nd
Stu
dy
coh
ort
:T
ha
mes
Ca
nce
rR
egis
try
;
Na
tio
na
lH
ea
lth
Serv
ice
Cen
tra
l
Regis
ter;
po
pu
lati
on
da
ta:
Offi
cefo
r
Na
tio
na
lS
tati
stic
s
(ma
tch
ing
on
NH
S
nu
mb
er)
;re
gis
try
-a
nd
po
pu
lati
on
-ba
sed
stu
dy
1998–2
003
Inci
den
ceR
R,
HR
(age,
soci
oeco
no
mic
dep
riv
ati
on
,st
age
at
dia
gn
osi
s,tr
ea
tmen
t)
Wo
men
of
all
ages;
kn
ow
n
eth
nic
ity,
com
ple
tere
gis
trati
on
info
rma
tio
n;
ex
clu
sio
ncr
iteri
a:
pa
tien
tsre
gis
tere
db
yd
ea
th
cert
ifica
teo
nly
ex
clu
ded
fro
m
an
aly
ses
on
sta
ge,
trea
tmen
ta
nd
mo
rta
lity
So
cio
-dem
ogra
ph
icd
ep
riva
tio
n
ba
sed
on
inco
me
do
ma
ino
fIn
dex
of
Mu
ltip
leD
ep
riv
ati
on
2000,
div
ided
into
qu
inti
les,
ass
ign
ed
to
reco
rds
usi
ng
po
stco
de
of
resi
den
cea
td
iagn
osi
s
Self
-ass
ign
ed
eth
nic
ity
(usi
ng
cod
es
fro
m1991
an
d2001
cen
suse
s)
Wh
ite
wo
men
Ca
nce
rco
ho
rt:
n=
33,0
24
Scr
een
ing
up
tak
e;
trea
tmen
t
dif
fere
nce
s;re
pro
du
ctiv
e,
soci
oeco
no
mic
,a
nth
rop
om
etr
ica
nd
die
tary
fact
ors
;d
iffe
ren
ces
in
dis
ea
sep
erc
ep
tio
na
nd
resu
ltin
g
acc
ess
toh
ea
lth
care
serv
ices
Eth
nic
ity
info
rma
tio
n
no
tav
ail
ab
lefo
rla
rge
po
rtio
no
fp
ati
en
ts
(36%
);
rep
rese
nta
tiv
en
ess
of
eth
nic
gro
up
s;w
ith
in
eth
nic
gro
up
va
ria
tio
n
2652 E U R O P E A N J O U R N A L O F C A N C E R 4 6 ( 2 0 1 0 ) 2 6 4 7 – 2 6 5 9
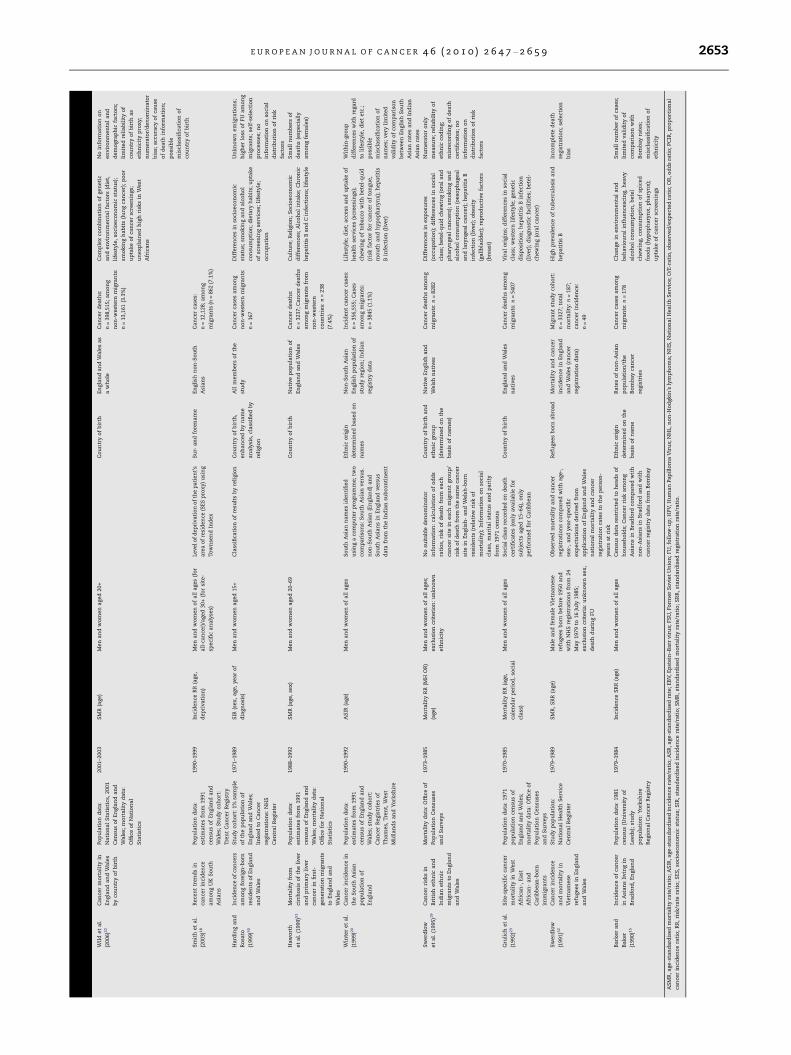
Wil
det
al.
(2006)2
2
Ca
nce
rm
ort
ali
tyin
En
gla
nd
an
dW
ale
s
by
cou
ntr
yo
fb
irth
Pop
ula
tio
nd
ata
:
Na
tio
na
lS
tati
stic
s,2001
Cen
sus
of
En
gla
nd
an
d
Wa
les;
mo
rta
lity
da
ta:
Offi
ceo
fN
ati
on
al
Sta
tist
ics
2001–2
003
SM
R(a
ge)
Men
an
dw
om
en
aged
20+
Co
un
try
of
bir
thE
ngla
nd
an
dW
ale
sa
s
aw
ho
le
Ca
nce
rd
ea
ths:
n=
398,5
15;
am
on
g
no
n-w
este
rnm
igra
nts
:
n=
13,1
61
(3.3
%)
Co
mp
lex
com
bin
ati
on
of
gen
eti
c
an
den
vir
on
men
tal
fact
ors
(die
t,
life
sty
le,
soci
oeco
no
mic
sta
tus)
;
smo
kin
gh
ab
its
(lu
ng
can
cer)
;p
oo
r
up
tak
eo
fca
nce
rsc
reen
ings;
un
ex
pla
ined
hig
hri
sks
inW
est
Afr
ica
ns
No
info
rma
tio
no
n
en
vir
on
men
tal
an
d
dem
ogra
ph
icfa
cto
rs;
lim
ited
reli
ab
ilit
yo
f
cou
ntr
yo
fb
irth
as
eth
nic
ity
pro
xy
;
nu
mera
tor/
den
om
ina
tor
bia
s;a
ccu
racy
of
cau
se
of
dea
thin
form
ati
on
;
po
ssib
le
mis
cla
ssifi
cati
on
of
cou
ntr
yo
fb
irth
Sm
ith
et
al.
(2003)1
8
Rece
nt
tren
ds
in
can
cer
inci
den
ce
am
on
gU
KS
ou
th
Asi
an
s
Pop
ula
tio
nd
ata
:
est
ima
tes
fro
m1991
cen
sus
of
En
gla
nd
an
d
Wa
les;
Stu
dy
coh
ort
:
Tre
nt
Ca
nce
rR
egis
try
1990–1
999
Inci
den
ceR
R(a
ge,
dep
riva
tio
n)
Men
an
dw
om
en
of
all
ages
(fo
r
all
-ca
nce
r)/a
ged
30+
(fo
rsi
te-
speci
fic
an
aly
ses)
Leve
lo
fd
ep
riv
ati
on
of
the
pa
tien
t’s
are
ao
fre
sid
en
ce(S
ES
pro
xy
)u
sin
g
To
wn
sen
dIn
dex
Su
r-a
nd
fore
na
me
En
gli
shn
on
-So
uth
Asi
an
s
Ca
nce
rca
ses:
n=
12,1
28;
am
on
g
mig
ran
ts(n
=862
(7.1
%)
Ha
rdin
ga
nd
Ro
sato
(1999)5
0
Inci
den
ceo
fca
nce
rs
am
on
gfo
reig
n-b
orn
resi
den
tso
fE
ngla
nd
an
dW
ale
s
Stu
dy
coh
ort
:1%
sam
ple
of
the
po
pu
lati
on
of
En
gla
nd
an
dW
ale
s;
lin
ked
toC
an
cer
regis
trati
on
s:N
HS
Cen
tra
lR
egis
ter
1971–1
989
SIR
(sex
,a
ge,
yea
ro
f
dia
gn
osi
s)
Men
an
dw
om
en
aged
15+
Cla
ssifi
cati
on
of
resu
lts
by
reli
gio
nC
ou
ntr
yo
fb
irth
,
en
ha
nce
db
yn
am
e
an
aly
sis,
cla
ssifi
ed
by
reli
gio
n
All
mem
bers
of
the
stu
dy
Ca
nce
rca
ses
am
on
g
no
n-w
este
rnm
igra
nts
:
n=
167
Dif
fere
nce
sin
soci
oeco
no
mic
sta
tus;
smo
kin
ga
nd
alc
oh
ol
con
sum
pti
on
;d
ieta
ryh
ab
its;
up
tak
e
of
scre
enin
gse
rvic
es;
life
sty
le;
occ
up
ati
on
Un
kn
ow
nem
igra
tio
ns;
hig
her
loss
of
FU
am
on
g
mig
ran
ts;
self
-sele
ctio
n
pro
cess
es;
no
info
rma
tio
no
nso
cia
l
dis
trib
uti
on
of
risk
fact
ors
Haw
ort
h
et
al.
(1999)5
1
Mo
rta
lity
fro
m
cirr
ho
sis
of
the
liver
an
dp
rim
ary
liver
can
cer
infi
rst-
gen
era
tio
nm
igra
nts
toE
ngla
nd
an
d
Wa
les
Pop
ula
tio
nd
ata
:
est
ima
tes
fro
m1991
cen
sus
of
En
gla
nd
an
d
Wa
les;
mo
rta
lity
da
ta:
Offi
cefo
rN
ati
on
al
Sta
tist
ics
1988–1
992
SM
R(a
ge,
sex
)M
en
an
dw
om
en
aged
20–6
9C
ou
ntr
yo
fb
irth
Na
tive
po
pu
lati
on
of
En
gla
nd
an
dW
ale
s
Ca
nce
rd
ea
ths:
n=
3237;C
an
cer
dea
ths
am
on
gm
igra
nts
fro
m
no
n-w
este
rn
cou
ntr
ies:
n=
238
(7.4
%)
Cu
ltu
re;
Reli
gio
n;
So
cio
eco
no
mic
dif
fere
nce
s;A
lco
ho
lin
tak
e;
Ch
ron
ic
hep
ati
tis
Ba
nd
Cin
fect
ion
s;li
fest
yle
Sm
all
nu
mb
ers
of
dea
ths
(esp
eci
all
y
am
on
gfe
ma
les)
Win
ter
et
al.
(1999)2
0
Ca
nce
rin
cid
en
cein
the
So
uth
Asi
an
po
pu
lati
on
of
En
gla
nd
Pop
ula
tio
nd
ata
:
est
ima
tes
fro
m1991
cen
sus
of
En
gla
nd
an
d
Wa
les;
stu
dy
coh
ort
:
Ca
nce
rR
egis
trie
so
f
Th
am
es,
Tre
nt,
West
Mid
lan
ds
an
dY
ork
shir
e
1990–1
992
AS
IR(a
ge)
Men
an
dw
om
en
of
all
ages
So
uth
Asi
an
na
mes
iden
tifi
ed
usi
ng
aco
mp
ute
rp
rogra
mm
e;
two
com
pa
riso
ns:
So
uth
Asi
an
vers
us.
no
n-S
ou
thA
sia
n(E
ngla
nd
)a
nd
So
uth
Asi
an
sin
En
gla
nd
vers
us
da
tafr
om
the
Ind
ian
sub
con
tin
en
t
Eth
nic
ori
gin
dete
rmin
ed
ba
sed
on
na
mes
No
n-S
ou
thA
sia
n
En
gli
shp
op
ula
tio
no
f
stu
dy
regio
n;
Ind
ian
regis
try
da
ta
Inci
den
tca
nce
rca
ses:
n=
356,5
55;
Ca
ses
am
on
gm
igra
nts
:
n=
3845
(1.1
%)
Lif
est
yle
;d
iet;
acc
ess
an
du
pta
ke
of
hea
lth
serv
ices
(scr
een
ings)
;
chew
ing
of
tob
acc
ow
ith
bete
l-q
uid
(ris
kfa
cto
rfo
rca
nce
ro
fto
ngu
e,
mo
uth
an
dh
yp
op
ha
ryn
x);
hep
ati
tis
Bin
fect
ion
(liv
er)
Wit
hin
-gro
up
dif
fere
nce
sw
ith
rega
rd
toli
fest
yle
,d
iet
etc
.;
po
ssib
le
mis
cla
ssifi
cati
on
of
na
mes;
very
lim
ited
va
lid
ity
of
com
pa
riso
n
betw
een
En
gli
shS
ou
th
Asi
an
rate
sa
nd
Ind
ian
Asi
an
rate
s
Sw
erd
low
et
al.
(1995)1
9
Ca
nce
rri
sks
in
Bri
tish
eth
nic
an
d
Ind
ian
eth
nic
mig
ran
tsto
En
gla
nd
an
dW
ale
s
Mo
rta
lity
da
ta:
Offi
ceo
f
Pop
ula
tio
nC
en
suse
s
an
dS
urv
eys
1973–1
985
Mo
rta
lity
RR
(MH
OR
)
(age)
Men
an
dw
om
en
of
all
ages;
ex
clu
sio
ncr
iteri
on
:u
nk
no
wn
eth
nic
ity
No
suit
ab
led
en
om
ina
tor
info
rma
tio
n:
calc
ula
tio
no
fo
dd
s
rati
os,
risk
of
dea
thfr
om
ea
ch
can
cer
site
inea
chm
igra
nt
gro
up
/
risk
of
dea
thfr
om
the
sam
eca
nce
r
site
inE
ngli
sh-
an
dW
els
h-b
orn
resi
den
ts(r
ela
tive
risk
of
mo
rta
lity
);In
form
ati
on
on
soci
al
cla
ss,
ma
rita
lst
atu
sa
nd
pa
rity
fro
m1971
cen
sus
Co
un
try
of
bir
tha
nd
eth
nic
gro
up
(dete
rmin
ed
on
the
ba
sis
of
na
mes)
Na
tive
En
gli
sha
nd
Wels
hn
ati
ves
Ca
nce
rd
ea
ths
am
on
g
mig
ran
ts:
n=
8282
Dif
fere
nce
sin
ex
po
sure
s
(occ
up
ati
on
);d
iffe
ren
ces
inso
cia
l
cla
ss;
bete
l-q
uid
chew
ing
(ora
la
nd
ph
ary
ngea
lca
nce
rs);
smo
kin
ga
nd
alc
oh
ol
con
sum
pti
on
(oeso
ph
agea
l
an
dla
ryn
gea
lca
nce
r);
hep
ati
tis
B
infe
ctio
n(l
iver)
;o
besi
ty
(ga
llb
lad
der)
;re
pro
du
ctiv
efa
cto
rs
(bre
ast
)
Nu
mera
tor
on
ly
mea
sure
;re
lia
bil
ity
of
eth
nic
cod
ing;
mis
reco
rdin
go
fd
ea
th
cert
ifica
tes;
no
info
rma
tio
no
n
dis
trib
uti
on
of
risk
fact
ors
Gru
lich
et
al.
(1992)2
3
Sit
e-s
peci
fic
can
cer
mo
rta
lity
inW
est
Afr
ica
n-,
Ea
st
Afr
ica
n-
an
d
Ca
rib
bea
n-b
orn
imm
igra
nts
Pop
ula
tio
nd
ata
:1971
po
pu
lati
on
cen
sus
of
En
gla
nd
an
dW
ale
s;
mo
rta
lity
da
ta:
Offi
ceo
f
Pop
ula
tio
nC
en
suse
s
an
dS
urv
eys
1970–1
985
Mo
rta
lity
RR
(age,
cale
nd
ar
peri
od
,so
cia
l
cla
ss)
Men
an
dw
om
en
of
all
ages
So
cia
lcl
ass
reco
rded
on
dea
th
cert
ifica
tes
(on
lyav
ail
ab
lefo
r
sub
ject
saged
15–6
4),
on
ly
perf
orm
ed
for
Ca
rib
bea
n
Co
un
try
of
bir
thE
ngla
nd
an
dW
ale
s
na
tives
Ca
nce
rd
ea
ths
am
on
g
mig
ran
ts:
n=
5407
Vir
al
ori
gin
s;d
iffe
ren
ces
inso
cia
l
cla
ss;
west
ern
life
sty
le;
gen
eti
c
dis
po
siti
on
;h
ep
ati
tis
Bin
fect
ion
(liv
er)
;d
iagn
ost
icfa
cili
ties;
bete
l-
chew
ing
(ora
lca
nce
r)
Sw
erd
low
(1991)5
2
Ca
nce
rin
cid
en
ce
an
dm
ort
ali
tyin
Vie
tna
mese
refu
gees
inE
ngla
nd
an
dW
ale
s
Stu
dy
po
pu
lati
on
:
Na
tio
na
lH
ea
lth
Serv
ice
Cen
tra
lR
egis
ter
1979–1
989
SM
R,
SR
R(a
ge)
Ma
lea
nd
fem
ale
Vie
tna
mese
refu
gees
bo
rnb
efo
re1950
an
d
wit
hN
HS
regis
trati
on
sfr
om
24
May
1979
to16
July
1985;
ex
clu
sio
ncr
iteri
a:
un
kn
ow
nse
x,
dea
thd
uri
ng
FU
Ob
serv
ed
mo
rta
lity
an
dca
nce
r
regis
trati
on
sco
mp
are
dw
ith
age-,
sex
-,a
nd
yea
r-sp
eci
fic
ex
pect
ati
on
sd
eri
ved
fro
m
ap
pli
cati
on
of
En
gla
nd
an
dW
ale
s
na
tio
na
lm
ort
ali
tya
nd
can
cer
regis
trati
on
rate
sto
the
pers
on
-
yea
rsa
tri
sk
Refu
gees
bo
rna
bro
ad
Mo
rta
lity
an
dca
nce
r
inci
den
cein
En
gla
nd
an
dW
ale
s(c
an
cer
regis
tra
tio
nd
ata
)
Mig
ran
tst
ud
yco
ho
rt:
n=
3327;
tota
l
mo
rta
lity
:n
=187;
can
cer
inci
den
ce:
n=
49
Hig
hp
reva
len
ceo
ftu
berc
ulo
sis
an
d
hep
ati
tis
B
Inco
mp
lete
dea
th
regis
trati
on
;se
lect
ion
bia
s
Ba
rker
an
d
Ba
ker
(1990)1
5
Inci
den
ceo
fca
nce
r
inA
sia
ns
liv
ing
in
Bra
dfo
rd,
En
gla
nd
Pop
ula
tio
nd
ata
:1981
cen
sus
(Un
ivers
ity
of
Leed
s);
stu
dy
po
pu
lati
on
:Y
ork
shir
e
Reg
ion
al
Ca
nce
rR
egis
try
1979–1
984
Inci
den
ceS
RR
(age)
Men
an
dw
om
en
of
all
ages
Cen
sus
da
tare
stri
cted
toh
ea
ds
of
ho
use
ho
lds;
Ca
nce
rri
ska
mo
ng
Asi
an
sin
Bra
dfo
rdco
mp
are
dw
ith
no
n-A
sia
ns
inB
rad
ford
an
dw
ith
can
cer
regis
try
da
tafr
om
Bo
mb
ay
Eth
nic
ori
gin
dete
rmin
ed
on
the
ba
sis
of
na
me
Ra
tes
of
no
n-A
sia
n
po
pu
lati
on
/th
e
Bo
mb
ay
can
cer
regis
trie
s
Ca
nce
rca
ses
am
on
g
mig
ran
ts:
n=
178
Ch
an
ge
inen
vir
on
men
tal
an
d
beh
av
iou
ral
infl
uen
cesc
ing,
hea
vy
alc
oh
ol
con
sum
pti
on
,b
ete
l
chew
ing,
con
sum
pti
on
of
spic
ed
foo
ds
(hy
po
ph
ary
nx
,p
ha
ryn
x);
up
tak
eo
fca
nce
rsc
reen
ings
Sm
all
nu
mb
er
of
case
s;
lim
ited
va
lid
ity
of
com
pa
riso
nw
ith
Bo
mb
ayra
tes;
mis
cla
ssifi
cati
on
of
eth
nic
ity
AS
MR
,age-s
tan
da
rdis
ed
mo
rta
lity
rate
/ra
tio
;AS
IR,a
ge-s
tan
da
rdis
ed
inci
den
cera
te/r
ati
o;A
SR
,age-s
tan
da
rdis
ed
rate
;E
BV
,Ep
stein
–Ba
rrv
iru
s;FS
U,F
orm
er
So
vie
tU
nio
n;F
U,f
oll
ow
-up
;HP
V,H
um
an
Pap
illo
ma
Vir
us;
NH
L,n
on
-Ho
dgk
in’s
lym
ph
om
a;N
HS
,Na
tio
na
lH
ea
lth
Serv
ice;O
/E-r
ati
o,o
bse
rved
/ex
pect
ed
rati
o;O
R,o
dd
sra
tio
;PC
IR,p
rop
ort
ion
al
can
cer
inci
den
cera
tio
;R
R,
risk
/ra
tera
tio
;S
ES
,so
cio
eco
no
mic
sta
tus;
SIR
,st
an
da
rdis
ed
inci
den
cera
te/r
ati
o;
SM
R,
sta
nd
ard
ised
mo
rta
lity
rate
/ra
tio
;S
RR
,st
an
da
rdis
ed
regis
tra
tio
nra
te/r
ati
o.
E U R O P E A N J O U R N A L O F C A N C E R 4 6 ( 2 0 1 0 ) 2 6 4 7 – 2 6 5 9 2653

2654 E U R O P E A N J O U R N A L O F C A N C E R 4 6 ( 2 0 1 0 ) 2 6 4 7 – 2 6 5 9
Only one study focused entirely on second-generation mi-
grants12 (based on the patient’s own and parental country of
birth) and two other studies included this group explicitly in
addition to first-generation migrants.13,14 Seven studies in-
cluded descendants indirectly, owing to the method used
for identifying migrants.15–21 For instance, the name-based
approach does not allow a distinction between generations,
which can only be estimated vaguely based on age. There
were 27 studies that were aimed at first-generation migrants
only.
For reasons of clarity, migrant origins have been pooled
into the following categories: Eastern Europe [Former Soviet
Union (FSU), Russia], Africa (North, West and East Africa), Mid-
dle East (most frequently referring to Iran, Iraq and adjacent
countries), Southern Europe/Turkey, Asia [divided into general
Asia (mostly China and Vietnam) and South Asia (including In-
dia, Bangladesh, Indonesia, Ceylon and Pakistan)] and South-
ern and Central America. Owing to inconsistent definitions
between the studies, some overlap cannot be excluded.
2.4. Applied methods
Studies investigating cancer incidence used mainly cancer
registry data (21/37). Studies assessing cancer mortality drew
mostly on vital statistics such as mortality or cause of death
registries and databases or surveys (17/37). Population data
were obtained from population registers/statistical bureaux
(17/37), census data (13/37) – which were primarily used in
studies from France and the United Kingdom (UK) – or a
population sample (7/37). Most studies were population-/
registry-based. In many studies linkage procedures had been
performed using a unique identifier such as the ‘Personal
Identity Number’ in Sweden and the ‘National Health Service
(NHS) number’ in the UK. Two studies used numerator-only
analyses.
Some studies adjusted for a socioeconomic proxy and also
took important covariables such as duration of stay, age at
immigration and calendar year into account.
Table 1 summarises the methodological features, explana-
tions and limitations of the studies included.
3. Findings
Table 2 provides an overview of all findings according to coun-
try of study, population of interest and cancer site, expressed
in tendencies.
The all-cancer comparison of most studies showed in par-
ticular on average a lower cancer risk for first-generation mi-
grants from non-western countries in terms of incidence and
mortality, although there were some studies that did not re-
veal significant differences, sometimes obviously due to small
study cohorts. However, male subjects originating from West
Africa exhibited significantly elevated cancer mortality in two
studies from the United Kingdom.22,23 Ambiguous results
were attained for migrants from Eastern Europe: Many stud-
ies revealed advantageous risks, although in several cases
they were not significant.
Since all-cancer morbidity reflects a summary of site-spe-
cific results, the aim is to point out cancers with significantly
elevated or lowered risks among migrants and to investigate
these results according to migrant origin.
3.1. Migrants from Southern Europe
In 35% of all studies (13/37) included from five different coun-
tries, migrants from Southern Europe, mostly Turkey, were
investigated. According to these studies, all malignant neo-
plasms together tended to occur significantly less often in
this group compared with the general population of the host
country.
Significantly elevated risks for this migrant group could be
observed for cancers of the stomach, liver, lung among males
and thyroid gland. In addition, increased risks were reported
for Hodgkin’s disease and lymphomas. In contrast, signifi-
cantly lower risks were found for cancers of the oesophagus,
colorectum, lung among females, skin, breast, prostate and
testis and bladder.
3.2. Migrants from Eastern Europe
In 32% of studies from five countries (12/37) migrants came
from the Eastern part of Europe, mostly parts of the former
Soviet Union. Lower all-cancer morbidity and mortality were
confirmed by the majority of these studies.
The site-specific results were ambiguous, but strongly con-
curred on the elevated risks for stomach and lung cancer in
males, whereas consistently decreased risks could be ob-
served for breast cancer in females and melanoma.
3.3. Migrants from Africa
Migrants originating from the African continent had to be cat-
egorised into ‘Africa’ (if no subgroups were available), ‘North
Africa’, ‘West Africa’ and ‘East Africa’.
In 16% of studies from four countries (6/37) migrants from
Africa without further regional classifications were investi-
gated. However, only three studies covered all-cancer morbid-
ity which resulted in advantageous risks for migrants. The
most striking similarities in the study results could be ob-
served for liver cancer due to strongly elevated risks and colo-
rectal cancer as well as cancer of male and female genital
organs due to decreased risks.
North African migrants were studied in 12 studies (32%)
from five countries (Denmark, France, Sweden, Netherlands
and the UK). All-cancer morbidity was lower or not significant
in all studies. Elevated risks were observed for cancers of the
nasopharynx, liver, gallbladder and cervix uteri. Significantly
decreased risks were found for almost all other cancer sites,
especially for colorectal, lung and breast cancer as well as
melanoma.
Migrants from the western part of Africa represent an
exceptional group among migrants from non-industrialised
countries. Only 4 out of 37 studies (11%) from France and the
UK looked at this group but all of them presented quite detailed
results that allowed us to look at many possible parallels. All-
cancer mortality was significantly elevated among males
residing in the United Kingdom, but the opposite was the case
for males living in France. The studies coincide in increased
risks for cancers of the liver, pancreas and prostate as well as
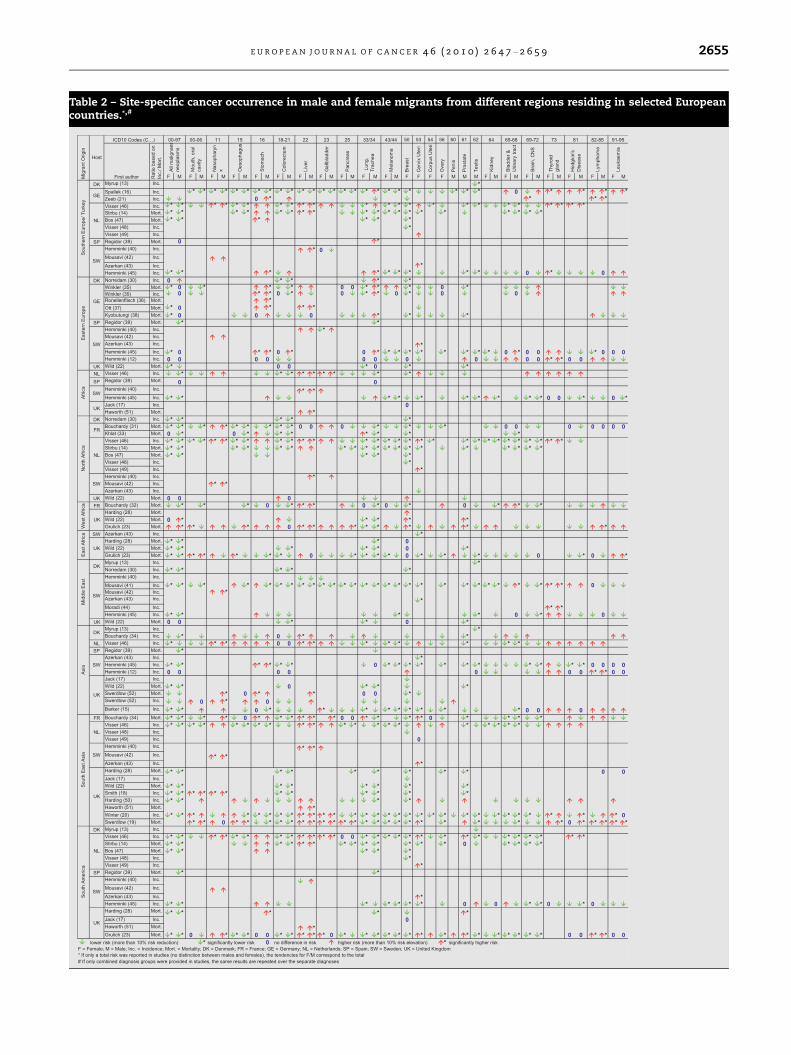
Table 2 – Site-specific cancer occurrence in male and female migrants from different regions residing in selected Europeancountries.*,#
E U R O P E A N J O U R N A L O F C A N C E R 4 6 ( 2 0 1 0 ) 2 6 4 7 – 2 6 5 9 2655
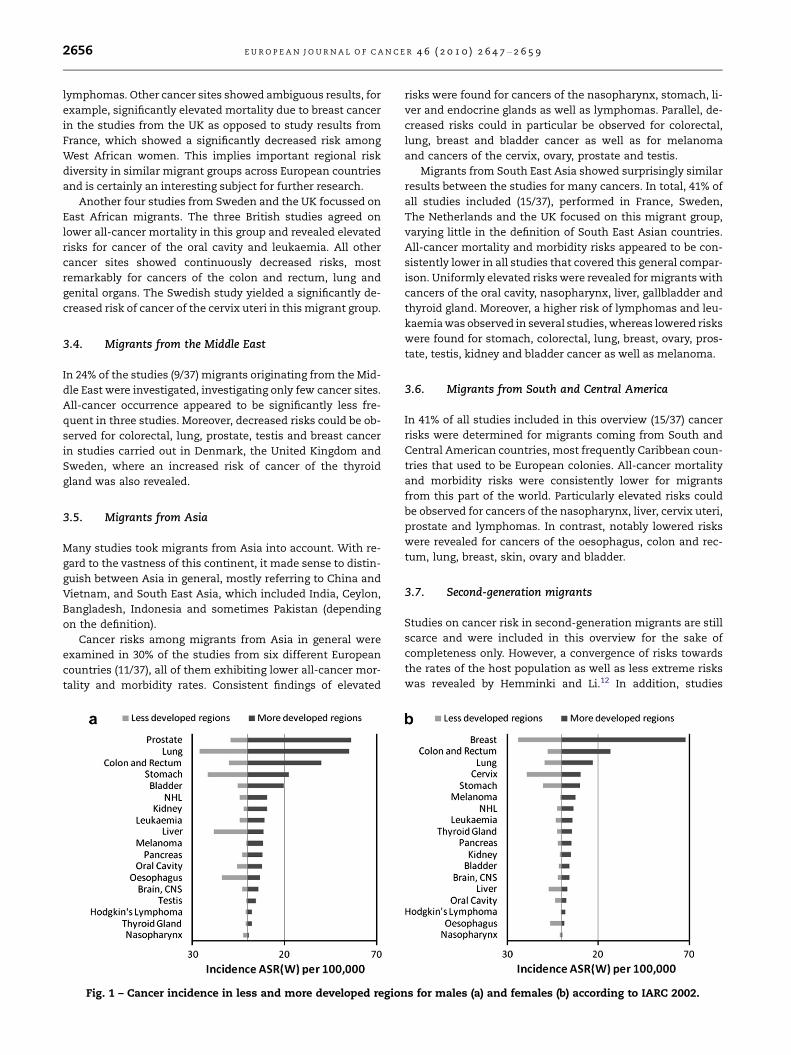
2656 E U R O P E A N J O U R N A L O F C A N C E R 4 6 ( 2 0 1 0 ) 2 6 4 7 – 2 6 5 9
lymphomas. Other cancer sites showed ambiguous results, for
example, significantly elevated mortality due to breast cancer
in the studies from the UK as opposed to study results from
France, which showed a significantly decreased risk among
West African women. This implies important regional risk
diversity in similar migrant groups across European countries
and is certainly an interesting subject for further research.
Another four studies from Sweden and the UK focussed on
East African migrants. The three British studies agreed on
lower all-cancer mortality in this group and revealed elevated
risks for cancer of the oral cavity and leukaemia. All other
cancer sites showed continuously decreased risks, most
remarkably for cancers of the colon and rectum, lung and
genital organs. The Swedish study yielded a significantly de-
creased risk of cancer of the cervix uteri in this migrant group.
3.4. Migrants from the Middle East
In 24% of the studies (9/37) migrants originating from the Mid-
dle East were investigated, investigating only few cancer sites.
All-cancer occurrence appeared to be significantly less fre-
quent in three studies. Moreover, decreased risks could be ob-
served for colorectal, lung, prostate, testis and breast cancer
in studies carried out in Denmark, the United Kingdom and
Sweden, where an increased risk of cancer of the thyroid
gland was also revealed.
3.5. Migrants from Asia
Many studies took migrants from Asia into account. With re-
gard to the vastness of this continent, it made sense to distin-
guish between Asia in general, mostly referring to China and
Vietnam, and South East Asia, which included India, Ceylon,
Bangladesh, Indonesia and sometimes Pakistan (depending
on the definition).
Cancer risks among migrants from Asia in general were
examined in 30% of the studies from six different European
countries (11/37), all of them exhibiting lower all-cancer mor-
tality and morbidity rates. Consistent findings of elevated
Fig. 1 – Cancer incidence in less and more developed regio
risks were found for cancers of the nasopharynx, stomach, li-
ver and endocrine glands as well as lymphomas. Parallel, de-
creased risks could in particular be observed for colorectal,
lung, breast and bladder cancer as well as for melanoma
and cancers of the cervix, ovary, prostate and testis.
Migrants from South East Asia showed surprisingly similar
results between the studies for many cancers. In total, 41% of
all studies included (15/37), performed in France, Sweden,
The Netherlands and the UK focused on this migrant group,
varying little in the definition of South East Asian countries.
All-cancer mortality and morbidity risks appeared to be con-
sistently lower in all studies that covered this general compar-
ison. Uniformly elevated risks were revealed for migrants with
cancers of the oral cavity, nasopharynx, liver, gallbladder and
thyroid gland. Moreover, a higher risk of lymphomas and leu-
kaemia was observed in several studies, whereas lowered risks
were found for stomach, colorectal, lung, breast, ovary, pros-
tate, testis, kidney and bladder cancer as well as melanoma.
3.6. Migrants from South and Central America
In 41% of all studies included in this overview (15/37) cancer
risks were determined for migrants coming from South and
Central American countries, most frequently Caribbean coun-
tries that used to be European colonies. All-cancer mortality
and morbidity risks were consistently lower for migrants
from this part of the world. Particularly elevated risks could
be observed for cancers of the nasopharynx, liver, cervix uteri,
prostate and lymphomas. In contrast, notably lowered risks
were revealed for cancers of the oesophagus, colon and rec-
tum, lung, breast, skin, ovary and bladder.
3.7. Second-generation migrants
Studies on cancer risk in second-generation migrants are still
scarce and were included in this overview for the sake of
completeness only. However, a convergence of risks towards
the rates of the host population as well as less extreme risks
was revealed by Hemminki and Li.12 In addition, studies
ns for males (a) and females (b) according to IARC 2002.

E U R O P E A N J O U R N A L O F C A N C E R 4 6 ( 2 0 1 0 ) 2 6 4 7 – 2 6 5 9 2657
assessing the effects of duration of residence or age at migra-
tion indicate an adaptation of rates, which also indicates a
change of risk over time, i.e. after migration. Investigating
cancer occurrence in second-generation migrants will be-
come more relevant in future, due to the increasing age and
size of this population group.
4. Discussion
Our findings suggest that migrants from non-western coun-
tries were more likely to develop cancers that are related to
infectious diseases, compared with the general population
of their industrialised host country. This is especially true
for cancers of the oral cavity, nasopharynx, stomach, liver,
gallbladder, cervix uteri, prostate and lymphomas. In con-
trast, almost all studies found lower risks for cancers that
are strongly related to a ‘western’ lifestyle (poor diet, physical
inactivity, reproductive factors, etc.), irrespective of the mi-
grant origin. This is in particular the case for colorectal cancer
and cancers of the pancreas, lung, breast, ovary, kidney and
bladder. Some elevated risks could also be explained partly
by important covariables such as socioeconomic status, espe-
cially for migrants originating from West Africa.
We also found that in most studies, migrants show cancer
risks that are in between the corresponding risk of the native
populations in their home and their host country. The major-
ity of the findings tend to be in accordance with the rates, vis-
ualised in Fig. 1.
Whereas all-cancer incidence in the more developed coun-
tries amounts to 314 [age-standardised rate (ASR(W)) per
100,000] among males and 228 among females, less well-
developed countries show an average of 159 for males and
129 for females.24
It can be observed that cancer sites with a comparatively
high incidence in less well-developed regions also exhibit a
high incidence for migrant populations from non-western
countries residing in industrialised countries. This applies
particularly for cancers of the liver, oesophagus, stomach
and nasopharynx among males and cervix, stomach, liver,
oesophagus and nasopharynx among females. In the same
manner, low incidences in less well-developed regions are re-
flected by low incidences among migrant groups originating
from these countries. This pattern could be confirmed in a re-
cent study by Zanetti and colleagues,25 who analysed cancer
incidence in North Africa.
Mortality data show a similar picture, although the differ-
ences are less clear, which is mainly attributable to disparities
in access to care and suboptimal communication on the
dilemmas of treatment.
Our findings also concur with those of others from non-
European countries and continents that host non-western
migrants. McCredie and colleagues26 for instance observed
lower cancer incidences for migrants from various non-wes-
tern origins in Australia and McDonald and Neily27 could con-
firm similar results for migrant women in the United States.
A close relationship with individual exposure experienced
during a life span could be confirmed for migrants of various
origins. In addition to individual factors and health behav-
iour, the causal roles of exposure in the home country, i.e. be-
fore migration, during migration itself and in the host
country, as well as the influence of social factors, certainly
represent key factors in carcinogenesis.
Exposure to risk factors and adaptation to changing envi-
ronments evolve over time and therefore cancer risk diversi-
fies with the duration of residence, new exposures and new
generations. Prospectively, a convergence of cancer risk (a
simultaneous decrease in cancers with high incidence in mi-
grants and an increase in those with a currently low inci-
dence) towards the level of the rates in the native
population of the host country can be expected over time
and across migrant generations.6,14,16,28
Of course there are limitations to the comparisons con-
ducted in this overview. Firstly, the definitions of the migrant
groups and the study populations varied among studies and
countries. Ethnicity proxies, such as ‘self-assigned ethnicity’
and name-based approaches, are in particular prone to mis-
classification bias, since a distinction between generations
or for example intercultural marriages is not possible. Sec-
ond, the comparability of studies is also limited with regard
to the size, composition and time window of the study popu-
lations. It is also important to note that in some studies pop-
ulation data from censuses or surveys were used (instead of
population-based registers), which is always a biased under-
estimate of the population at risk because as a rule only the
head of the household is considered.
Third, migrant origins may sometimes have been collected
in an inconsistent way, which was unavoidable in some cases
(e.g. the allocation of Pakistan or Turkey).
Fourth, studies investigating both mortality and morbidity
have been included, given the assumption of parallel effects,
although mortality is mainly driven by (access to) treatment
and the varying fatality rates of different cancers. Consequently,
different measures of association have been pooled and
compared on the basis of tendencies. The comparisons
therefore lack a magnitude and only provide a rough estimation
of risk disparities. Meta-analysis was not the aim of this
overview.
The healthy migrant effect could partly explain the advan-
tageous risks of migrants, but since effects seem to persist, its
influence is probably marginal. Several studies also discussed
the possible effects of the so-called salmon-bias, which
assumes that migrants tend to return to their roots when they
become ill. This is in most instances unlikely due to the fact
that health services and treatment are often better in the host
country and many migrants have already been joined by and
settled with their families.
This is to our knowledge the first direct comparison of
studies on cancer occurrence in migrant populations in
Europe. Despite the limitations mentioned above, broad
comparisons are feasible and will gain importance in the
future. Prospectively, a transnational study of cancer occur-
rence in migrant populations could surmount many of these
difficulties. This primarily concerns the definition of migrant
groups requiring close networking between countries. In
doing so, the results would be more reliable and the magni-
tude of the risk diversity could be studied in more detail. In
order to appreciate the change in risk after migration, a
comparison with data from the country of birth would be
ideal.
2658 E U R O P E A N J O U R N A L O F C A N C E R 4 6 ( 2 0 1 0 ) 2 6 4 7 – 2 6 5 9
Conflict of interest statement
None declared.
Acknowledgement
Melina Arnold’s work has partly been funded by EU SANCO
(MEHO project: Migrant and Ethnic Minorities Health Obser-
vatory; Contract number: 2005122).
R E F E R E N C E S
1. World Migration 2008: managing labour mobility in theevolving global economy; 2009.
2. Bhopal RS. Ethnicity, race, and health in multicultural societies:foundations for better epidemiology, public health, and healthcare. Oxford University Press; 2007.
3. Spallek J, Razum O. Health of migrants: deficiencies in thefield of prevention. Med Klin (Munich) 2007;102(6):451–6.
4. Omran AR. The epidemiologic transition. A theory of theepidemiology of population change. Milbank Mem Fund Q1971;49(4):509–38.
5. Marmot M. Changing places changing risks: the study ofmigrants. Public Health Rev 1993;21(3–4):185–95.
6. Razum O, Twardella D. Time travel with Oliver Twist – towardsan explanation for a paradoxically low mortality amongrecent immigrants. Trop Med Int Health 2002;7(1):4–10.
7. Razum O, Rohrmann S. The healthy migrant effect: role ofselection and late entry bias. Gesundheitswesen2002;64(2):82–8.
8. Parkin DM, Khlat M. Studies of cancer in migrants: rationaleand methodology. Eur J Cancer 1996;32A(5):761–71.
9. Zeeb H, Spallek J, Razum O. Epidemiological perspectives ofmigration research: the example of cancer. PsychotherPsychosom Med Psychol 2008;58(3–4):130–5.
10. Spallek J, Razum O. Erklarungsmodelle fur diegesundheitliche Situation von Migrantinnen und Migranten.In: Bauer U, Bittlingmayer UH, Richter M, editors. Healthinequalities: Determinanten und Mechanismen gesundheitlicherUngleichheit. Wiesbaden: Vs Verlag; 2008. p. 271–88.
11. Stronks K, Kulu-Glasgow I, Agyemang C. The utility of‘country of birth’ for the classification of ethnic groups inhealth research: the Dutch experience. Ethn Health2009;14(3):1–14.
12. Hemminki K, Li X. Cancer risks in second-generationimmigrants to Sweden. Int J Cancer 2002;99(2):229–37.
13. Myrup C, Westergaard T, Schnack T, et al. Testicular cancerrisk in first- and second-generation immigrants to Denmark. JNatl Cancer Inst 2008;100(1):41–7.
14. Stirbu I, Kunst AE, Vlems FA, et al. Cancer mortality ratesamong first and second generation migrants in theNetherlands: convergence toward the rates of the nativeDutch population. Int J Cancer 2006;119(11):2665–72.
15. Barker RM, Baker MR. Incidence of cancer in Bradford Asians.J Epidemiol Community Health 1990;44(2):125–9.
16. Spallek J, Arnold M, Hentschel S, Razum O. Cancerincidence rate ratios of Turkish immigrants in Hamburg,Germany: a registry based study. Cancer Epidemiol2009;33(6):413–8.
17. Jack RH, Davies EA, Moller H. Breast cancer incidence, stage,treatment and survival in ethnic groups in South EastEngland. Br J Cancer 2009;100(3):545–50.
18. Smith LK, Botha JL, Benghiat A, Steward WP. Latest trends incancer incidence among UK South Asians in Leicester. Br JCancer 2003;89(1):70–3.
19. Swerdlow AJ, Marmot MG, Grulich AE, Head J. Cancermortality in Indian and British ethnic immigrants from theIndian subcontinent to England and Wales. Br J Cancer1995;72(5):1312–9.
20. Winter H, Cheng KK, Cummins C, et al. Cancer incidence inthe south Asian population of England (1990–92). Br J Cancer1999;79(3–4):645–54.
21. Zeeb H, Razum O, Blettner M, Stegmaier C. Transition incancer patterns among Turks residing in Germany. Eur JCancer 2002;38(5):705–11.
22. Wild SH, Fischbacher CM, Brock A, Griffiths C, Bhopal R.Mortality from all cancers and lung, colorectal, breast andprostate cancer by country of birth in England and Wales,2001–2003. Br J Cancer 2006;94(7):1079–85.
23. Grulich AE, Swerdlow AJ, Head J, Marmot MG. Cancermortality in African and Caribbean migrants to England andWales. Br J Cancer 1992;66(5):905–11.
24. GLOBOCAN database database on the Internet. IARC; 2002.25. Zanetti R, Tazi MA, Rosso S. New data tells us more about
cancer incidence in North Africa. Eur J Cancer 2010;46(3):462–6.26. McCredie M, Coates MS, Ford JM. Cancer incidence in
migrants to New South Wales. Int J Cancer 1990;46(2):228–32.27. McDonald JT, Neily J. Race, immigrant status, and cancer
among women in the United States. J Immigr Minor Health2009. doi:10.1007/s10903-009-9268-1.
28. Harding S, Rosato M, Teyhan A. Trends in cancer mortalityamong migrants in England and Wales, 1979–2003. Eur JCancer 2009;45(12):2168–79.
29. Norredam M, Krasnik A, Pipper C, Keiding N. Differences instage of disease between migrant women and native Danishwomen diagnosed with cancer: results from a population-based cohort study. Eur J Cancer Prev 2008;17(3):185–90.
30. Norredam M, Krasnik A, Pipper C, Keiding N. Cancerincidence among 1st generation migrants compared to nativeDanes – a retrospective cohort study. Eur J Cancer2007;43(18):2717–21.
31. Bouchardy C, Parkin DM, Wanner P, Khlat M. Cancer mortalityamong north African migrants in France. Int J Epidemiol1996;25(1):5–13.
32. Bouchardy C, Wanner P, Parkin DM. Cancer mortality amongsub-Saharan African migrants in France. Cancer Causes Control1995;6(6):539–44.
33. Khlat M. Cancer in Mediterranean migrants-based on studiesin France and Australia. Cancer Causes Control1995;6(6):525–31.
34. Bouchardy C, Parkin DM, Khlat M. Cancer mortality amongChinese and South-East Asian migrants in France. Int J Cancer1994;58(5):638–43.
35. Winkler V, Ott JJ, Holleczek B, Stegmaier C, Becher H. Cancerprofile of migrants from the Former Soviet Union in Germany:incidence and mortality. Cancer Causes Control 2009.doi:10.1007/s10552-009-9381-4.
36. Ronellenfitsch U, Kyobutungi C, Ott JJ, et al. Stomachcancer mortality in two large cohorts of migrants from theFormer Soviet Union to Israel and Germany: are thereimplications for prevention? Eur J Gastroenterol Hepatol2009;21(4):409–16.
37. Ott JJ, Paltiel AM, Winkler V, Becher H. Chronic diseasemortality associated with infectious agents: a comparativecohort study of migrants from the Former Soviet Union inIsrael and Germany. BMC Public Health 2008;8:110.
38. Kyobutungi C, Ronellenfitsch U, Razum O, Becher H. Mortalityfrom cancer among ethnic German immigrants from theFormer Soviet Union, in Germany. Eur J Cancer2006;42(15):2577–84.
E U R O P E A N J O U R N A L O F C A N C E R 4 6 ( 2 0 1 0 ) 2 6 4 7 – 2 6 5 9 2659
39. Regidor E, de La Fuente L, Martinez D, Calle ME, Dominguez V.Heterogeneity in cause-specific mortality according tobirthplace in immigrant men residing in Madrid, Spain. AnnEpidemiol 2008;18(8):605–13.
40. Hemminki K, Mousavi SM, Brandt A, Ji J, Sundquist J. Liver andgallbladder cancer in immigrants to Sweden. Eur J Cancer2010;46(5):926–31.
41. Mousavi SM, Brandt A, Weires M, et al. Cancer incidenceamong Iranian immigrants in Sweden and Iranian residentscompared to the native Swedish population. Eur J Cancer2010;46(3):599–605.
42. Mousavi SM, Sundquist J, Hemminki K. Nasopharyngeal andhypopharyngeal carcinoma risk among immigrants inSweden. Int J Cancer 2010. doi:10.1002/ijc.25287.
43. Azerkan F, Zendehdel K, Tillgren P, Faxelid E, Sparen P. Risk ofcervical cancer among immigrants by age at immigration andfollow-up time in Sweden, from 1968 to 2004. Int J Cancer2008;123(11):2664–70.
44. Moradi T, Nordqvist T, Allebeck P, Galanti MR. Risk of thyroidcancer among Iranian immigrants in Sweden. Cancer CausesControl 2008;19(3):221–6.
45. Hemminki K, Li X, Czene K. Cancer risks in first-generationimmigrants to Sweden. Int J Cancer 2002;99(2):218–28.
46. Visser O, van Leeuwen FE. Cancer risk in first generationmigrants in North-Holland/Flevoland, The Netherlands, 1995–2004. Eur J Cancer 2007;43(5):901–8.
47. Bos V, Kunst AE, Keij-Deerenberg IM, Garssen J, MackenbachJP. Ethnic inequalities in age- and cause-specific mortality inThe Netherlands. Int J Epidemiol 2004;33(5):1112–9.
48. Visser O, van der Kooy K, van Peppen AM, Ory FG, vanLeeuwen FE. Breast cancer risk among first-generationmigrants in the Netherlands. Br J Cancer 2004;90(11):2135–7.
49. Visser O, Busquet EH, van Leeuwen FE, Aaronson NK, Ory FG.Incidence of cervical cancer in women in North-Holland bycountry of birth from 1988–1998. Ned Tijdschr Geneeskd2003;147(2):70–4.
50. Harding S, Rosato M. Cancer incidence among first generationScottish, Irish, West Indian and South Asian migrants livingin England and Wales. Ethn Health 1999;4(1–2):83–92.
51. Haworth EA, Soni Raleigh V, Balarajan R. Cirrhosis andprimary liver cancer amongst first generation migrants inEngland and Wales. Ethn Health 1999;4(1–2):93–9.
52. Swerdlow A. Mortality and cancer incidence in Vietnameserefugees in England and Wales: a follow-up study. Int JEpidemiol 1991;20(1):13–9.