Budd-Chiari syndrome: illustrated review of current management
12
REVIEW ARTICLE Budd^Chiari syndrome: illustrated review of current management John D. Horton 1 , Francisco L. San Miguel 1 and Jorge A. Ortiz 2 1 William Beaumont Army Medical Center, Department of Surgery, El Paso, TX, USA 2 Texas Transplant Institute, Methodist Specialty and Transplant Hospital, San Antonio, TX, USA Keywords Budd–Chiari – hepatic vein thrombosis – liver transplantation – portasystemic shunt, surgical – portasystemic shunt, transjugular intrahepatic – review Correspondence John D. Horton, MD, William Beaumont Army Medical Center, Department of Surgery, 5005 North Piedras St., El Paso, TX 79920-5001, USA Tel: 1210 286 9292 Fax: 1915 569 2602 e-mail: [email protected] Received 26 September 2007 Accepted 6 December 2007 DOI:10.1111/j.1478-3231.2008.01684.x Abstract Budd–Chiari syndrome (BCS) is characterized by hepatic venous outflow obstruc- tion at any level from the small hepatic veins to the atriocaval junction. BCS is a complex disease with a wide spectrum of aetiologies and presentations. This article reviews the current literature with respect to presentation, management and prognosis of the disease. Medical, interventional and surgical management of BCS is discussed. Particular attention is paid to interventional and surgical aspects of management. The review is augmented by images, which provide a clinical corollary to the text. In 1845, an internist named George Budd described the classic triad of abdominal pain, hepatomegaly and ascites. In 1899, pathologist Hans Chiari documented the histopathological features of what is now known as the Budd–Chiari syndrome (BCS) (1, 2). BCS is characterized by hepatic venous outflow obstruction at any level from the small hepatic veins to the atriocaval junction, regardless of the cause of obstruc- tion (3, 4). The natural history of BCS is poorly understood (5). Described treatment modalities for BCS include antic- oagulation and treatment of underlying disease, per- cutaneous interventional techniques, transjugular intrahepatic portosystemic shunt (TIPS), surgical shunts and liver transplantation. Because of the rarity of BCS, there have been no randomized prospective trials comparing medical with surgical treatment of this disease (3). Currently, clinical judgment and local expertise play a large role in the management of BCS. This review article discusses the presentation, manage- ment and prognosis of BCS with particular attention focused on the interventional and surgical aspects of treatment. Pathophysiology Obstruction is usually caused by a thrombus, but may result from extrinsic compression (tumour, abscess, cysts), membranous webs within the inferior vena cava (IVC) (3), or postoperative complications following liver transplantation (6–8). Membranous web occlu- sion of the IVC is much more common in the Asian population than in Western countries (1, 9). Membra- nous web occlusion was once thought to be a con- genital lesion, but more recent evidence suggests that membranous webs are the sequelae of thrombus for- mation (10–12). Additionally, membranous webs have been associated with hepatocellular carcinoma (11). Posthepatic obstruction leads to increased sinusoidal pressure, sinusoidal congestion, hepatomegaly, hepatic pain, portal hypertension and ascites. Without venous outflow, the elevated sinusoidal pressure leads to perisinusoidal necrosis of hepatocytes in Rappaport zone 3 and eventually to liver failure (3). Ischaemic injury is compounded by oxidative injury caused by the release of free radicals from sinusoidal cells (13). BCS results from the occlusion of three hepatic veins in about 2/3 of the cases, isolated occlusion of the IVC The views expressed in this document are those of the author(s) and do not reflect the official policy of William Beaumont Army Medical Center, the Department of the Army, the Department of Defense, or the United States Government. Liver International (2008) c 2008 The Authors. Journal compilation c 2008 Blackwell Munksgaard 455 Liver International ISSN 1478-3223
-
Upload
universidaddelavida -
Category
Documents
-
view
0 -
download
0
Transcript of Budd-Chiari syndrome: illustrated review of current management

REVIEW ARTICLE
Budd^Chiari syndrome: illustrated reviewof currentmanagementJohn D. Horton1, Francisco L. San Miguel1 and Jorge A. Ortiz2
1 William Beaumont Army Medical Center, Department of Surgery, El Paso, TX, USA
2 Texas Transplant Institute, Methodist Specialty and Transplant Hospital, San Antonio, TX, USA
Keywords
Budd–Chiari – hepatic vein thrombosis – liver
transplantation – portasystemic shunt,
surgical – portasystemic shunt, transjugular
intrahepatic – review
Correspondence
John D. Horton, MD, William Beaumont Army
Medical Center, Department of Surgery, 5005
North Piedras St., El Paso, TX 79920-5001, USA
Tel: 1210 286 9292
Fax: 1915 569 2602
e-mail: [email protected]
Received 26 September 2007
Accepted 6 December 2007
DOI:10.1111/j.1478-3231.2008.01684.x
AbstractBudd–Chiari syndrome (BCS) is characterized by hepatic venous outflow obstruc-
tion at any level from the small hepatic veins to the atriocaval junction. BCS is a
complex disease with a wide spectrum of aetiologies and presentations. This article
reviews the current literature with respect to presentation, management and
prognosis of the disease. Medical, interventional and surgical management of
BCS is discussed. Particular attention is paid to interventional and surgical aspects
of management. The review is augmented by images, which provide a clinical
corollary to the text.
In 1845, an internist named George Budd describedthe classic triad of abdominal pain, hepatomegaly andascites. In 1899, pathologist Hans Chiari documentedthe histopathological features of what is now knownas the Budd–Chiari syndrome (BCS) (1, 2). BCS ischaracterized by hepatic venous outflow obstructionat any level from the small hepatic veins to theatriocaval junction, regardless of the cause of obstruc-tion (3, 4).
The natural history of BCS is poorly understood (5).Described treatment modalities for BCS include antic-oagulation and treatment of underlying disease, per-cutaneous interventional techniques, transjugularintrahepatic portosystemic shunt (TIPS), surgicalshunts and liver transplantation. Because of the rarityof BCS, there have been no randomized prospectivetrials comparing medical with surgical treatment ofthis disease (3). Currently, clinical judgment and localexpertise play a large role in the management of BCS.This review article discusses the presentation, manage-ment and prognosis of BCS with particular attention
focused on the interventional and surgical aspects oftreatment.
Pathophysiology
Obstruction is usually caused by a thrombus, but mayresult from extrinsic compression (tumour, abscess,cysts), membranous webs within the inferior vena cava(IVC) (3), or postoperative complications followingliver transplantation (6–8). Membranous web occlu-sion of the IVC is much more common in the Asianpopulation than in Western countries (1, 9). Membra-nous web occlusion was once thought to be a con-genital lesion, but more recent evidence suggests thatmembranous webs are the sequelae of thrombus for-mation (10–12). Additionally, membranous webs havebeen associated with hepatocellular carcinoma (11).Posthepatic obstruction leads to increased sinusoidalpressure, sinusoidal congestion, hepatomegaly, hepaticpain, portal hypertension and ascites. Without venousoutflow, the elevated sinusoidal pressure leads toperisinusoidal necrosis of hepatocytes in Rappaportzone 3 and eventually to liver failure (3). Ischaemicinjury is compounded by oxidative injury caused bythe release of free radicals from sinusoidal cells (13).BCS results from the occlusion of three hepatic veinsin about 2/3 of the cases, isolated occlusion of the IVC
The views expressed in this document are those of the author(s) and do
not reflect the official policy of William Beaumont Army Medical Center,
the Department of the Army, the Department of Defense, or the United
States Government.
Liver International (2008)c� 2008 The Authors. Journal compilation c� 2008 Blackwell Munksgaard 455
Liver International ISSN 1478-3223

in 10% of cases and combined occlusion in almost 1/3of the cases (1). Caudate lobe hypertophy (Fig. 1),which may further compress the IVC, can occur in upto 50% of chronic presentations (1).
Presentation
The majority of patients with BCS present withhepatomegaly, right upper quadrant pain and abdom-inal ascites (5, 14). Lower extremity oedema is anothercommon finding on physical exam. Some patients mayfeature signs of portal hypertension such as varicealbleeding and refractory ascites without a significantimpact on liver function. A high serum–ascites gradi-ent (Z1.1 g/dl) is usually found (1).
Young children (o 10 years of age) account for1–7% of all cases of BCS. This group often presentslate in the course of disease, by which time irreversiblepathology may be present (15).
The most common underlying disorders in patientswith BCS are myeloproliferative disorders such aspolycythaemia vera and essential thrombocytosis (1).The prevalence of myeloproliferative disorders in thispopulation can be as high as 53%. In Western nations,factor V Leiden (25%) and factor II gene mutation(5%) are other common aetiologies. Some patients mayhave a combination of thrombophilias (5). Othercommon associations include oral contraceptive use,protein C and S deficiencies, antiphospholipid syn-drome, antithrombin III deficiency, paroxysmal noc-
turnal haemoglobinuria, cancer, Bechet’s syndrome andtrauma (16). BCS after pregnancy has been describedand is associated with a particularly poor prognosis(17). Twenty per cent of cases of BCS are idiopathic (1).
The Budd–Chiari syndrome is termed primary orsecondary based on the aetiology and site of venousoutflow obstruction. Primary BCS originates fromwithin the lumen of the veins or venules and resultsfrom thrombus, webs or endophlebitis. SecondaryBCS results from an extra-luminal lesion such astumour, abscess or cyst, which can invade the lumenor cause extrinsic compression of the hepatic venousoutflow tract (4).
Patients with BCS present with varying degrees ofsymptomatology and acuity. The clinical presentationof patients with BCS is governed by the extent andswiftness of hepatic outflow obstruction juxtaposed tothe body’s ability to decompress the liver via develop-ment of collateral blood flow. Based on this pathophy-siology, patients can be divided into the followingcategories: fulminant, acute, subacute or chronic (13).The subacute form is the most common presentationand is characterized by slow accumulation of ascites.Hepatocellular damage is minimal due to the develop-ment of hepatic and portal venous collaterals. Thefulminant form is rare and is defined as the develop-ment of hepatic encephalopathy within 8 weeks of theonset of jaundice. Acute BCS has a rapid onset,intractable ascites and a short duration of symptoms.Collateral venous channels do not develop in the acuteform of BCS. Chronic BCS usually occurs in thebackground of cirrhosis. A report by Dilawari included177 patients with BCS and used a variation of theabove classification scheme. This patient populationpresented with the following distribution: 7% acutefulminant, 28% acute and 65% chronic (18).
Presentation of BCS has been classified using a varietyof schemes. Langlet’s recent clinicopathological classifi-cation demonstrated prognostic value. This schemedivides patients into the following types: type I (acuteinjury only, corresponding to onset of hepatic outflowobstruction), type II (chronic lesions only, correspond-ing to the sequelae of remote hepatic outflow obstruc-tion) and type III (acute injury superimposed onchronic lesions). This patient population had the follow-ing distribution: 7% type I, 45% type II and 48% typeIII. Patients with type I BCS had the best prognosiswhereas those with type III had the worst (19).
Diagnostic evaluation
Work-up of suspected BCS begins with imagingmodalities such as Doppler ultrasound, computed
Fig. 1. Coronal computed tomography (CT) showing caudatelobe hypertrophy (white arrow) and inferior vena cava (IVC)compression (black arrow).
Liver International (2008)456 c� 2008 The Authors. Journal compilation c� 2008 Blackwell Munksgaard
Budd–Chiari review Horton et al.
tomography (CT) scan and magnetic resonance ima-ging (MRI). Radiographic analysis should attempt todetermine the patency of the hepatic veins, IVC andportal vein because this information will determinetherapeutic options. Other radiographic findings seenin BCS include inhomogeneous parenchymal en-hancement, presence of intrahepatic collaterals, hyper-vascular nodules and caudate lobe hypertrophy (Fig.1) (20). Doppler ultrasound, often the first studyobtained, has a sensitivity and specificity as high as85% (21). CT scans allow for the evaluation of ascites,hepatic vein patency, vena cava patency and caudatelobe hypertrophy. MRI may differentiate chronic fromacute disease and provide further delineation of vas-cular anatomy. On MRI, patients with chronic BCSdemonstrate heterogeneous signal intensity through-out the liver, while those with acute BCS showdivergent signal intensities and decreased contrastenhancement in the periphery relative to the centralregion of the liver (22). Other investigations that mayaid in management include infra- and suprahepaticcaval pressures (Fig. 2), hepatic venography and liverbiopsy (16). Imaging studies also play an important
role in postoperative evaluation and surveillance ofsurgical shunts (Fig. 3).
Underlying hypercoagulable states should be inves-tigated in all patients (16). Patients found to havemembranous obstruction should also undergo hyper-coagulable work-up, as recent evidence suggests thatthrombosis may be the inciting event for membranousweb formation (10–12). Of note, low levels of antith-rombin III, protein C and protein S may be seen inpatients with any disease resulting in hepatocellulardysfunction. Bone marrow biopsy should be consid-ered to identify occult myeloproliferative diseases (23).Some authors recommend testing for JAK2 mutationsin all patients with BCS in order to uncover a possiblelatent myeloproliferative disorder (1).
Liver biopsy may reveal a wide range of histologicalfindings from sinusoidal congestion and inflammationto cirrhosis and parenchymal necrosis. Extravasation
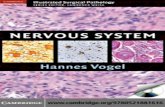
Fig. 2. Pressure gradient of 9 mm Hg measured across aninferior vena cava (IVC) stenosis (large arrow).
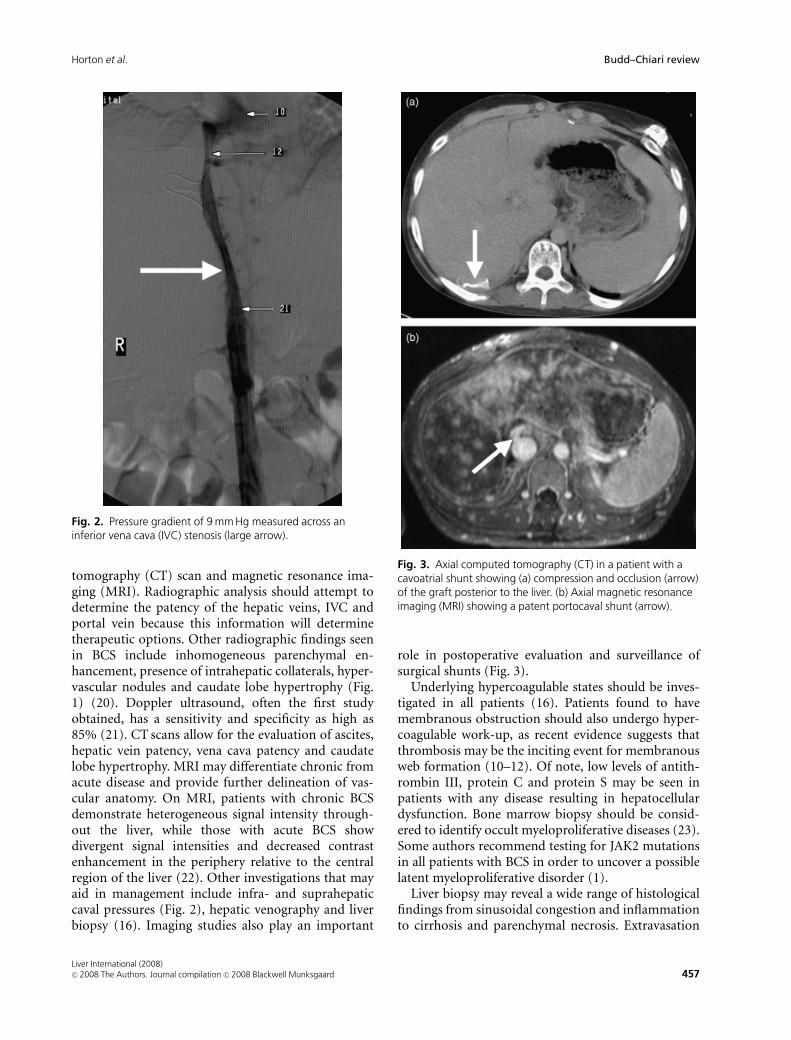
Fig. 3. Axial computed tomography (CT) in a patient with acavoatrial shunt showing (a) compression and occlusion (arrow)of the graft posterior to the liver. (b) Axial magnetic resonanceimaging (MRI) showing a patent portocaval shunt (arrow).
Liver International (2008)c� 2008 The Authors. Journal compilation c� 2008 Blackwell Munksgaard 457
Horton et al. Budd–Chiari review

of red cells into the liver-cell plate and space of Disseis a characteristic feature of BCS. Sample error duringbiopsy may occur as parenchymal changes may beheterogeneous. No correlation has been observedbetween histological findings and patient outcomes(16, 19, 24). Moreover, some authors argue that biopsyresults should not play a dominant role in decisionmaking because patients with fibrosis at initial pre-sentation may do well with procedures other thantransplantation (25).
Management strategies
Treatment of BCS generally follows a least invasive tomost invasive strategy. However, this paradigm is notabsolute and circumstances may dictate immediatesurgery or even transplantation depending on thepresentation. Algorithms for management of BCS havebeen reported (26, 27).
Plessier’s algorithm, which was applied to 51patients over a 7-year period, resulted in overall 1-,3- and 5-year survival rates of 96%, 89% and 89%respectively (27). This algorithm included medicalmanagement, recanalization, TIPS and liver trans-plant. Surgical shunts were not part of the algorithm.
Medical management
Medical management consists of anticoagulation, so-dium restriction, diuretic therapy and paracentesis.Anticoagulation can be achieved with heparin in theacute setting and with warfarin for long-term treat-ment. Sodium should be restricted to approximately60–90 mEq/day (1500–2000 mg of salt). Moderateascites can be treated with oral diuretics such asfurosemide (20–40 mg/day) and spironolactone(50–200 mg/day). Patients with symptomatic large-volume ascites can undergo periodic abdominal para-centesis (16). Some clinicians recommend medicaltherapy alone for patients with few symptoms, rela-tively normal liver-function tests and easily controlledascites (13).
A report by McCarthy in 1985 showed that medicalmanagement alone resulted in death within 6 monthsin 12 of 14 patients (28). However, Khuroo reportedmore promising results from a case series where 8 of 20patients treated with medical therapy alone had sig-nificant clinical and biochemical improvement with53% of all medically treated patients alive after 24months (29). Both these studies were retrospectivecase series from a single institution.
Plessier reported their experience with 51 cases ofBCS and found that nine of their patients weresuccessfully treated with medical therapy alone. Inter-
estingly, this study found a 15% rate of heparin-induced thrombocytopaenia, which is 10-fold higherthan the rates from large clinical trials (27).
For patients who present with BCS several monthsafter liver transplantation, medical management maybe a viable option. Parrilla’s series reported that onlythree out of 1112 transplants suffered delayed hepaticoutflow obstruction, and all three patients were suc-cessfully managed with diuretics for control of theirascites (7).
Interventional techniques and transjugularintrahepatic portosystemic shunt
In recent years, percutaneous interventions haveplayed an increasing role in the management ofpatients with BCS. Indeed, most institutions are morelikely to possess the capability to perform TIPS thanto employ a surgeon with the expertise to perform amesenteric-systemic shunt (9). Consequently, TIPShas become the first option when a shunting proce-dure is indicated (30). Catheter-directed thrombolytictherapy, angioplasty and stent placement can be effec-tive in the acute setting (16), while TIPS may beemployed in the acute or chronic setting.
A recent 10 patient case series and literature reviewby Sharma concluded that systemic thrombolytictherapy is of little value and that catheter-directedthrombolysis is more efficacious for acute thrombusthat is not completely occlusive. The authors also feltthat tissue plasminogen activator is the preferred agentand that it should be delivered just proximal to orwithin the thrombus (31).
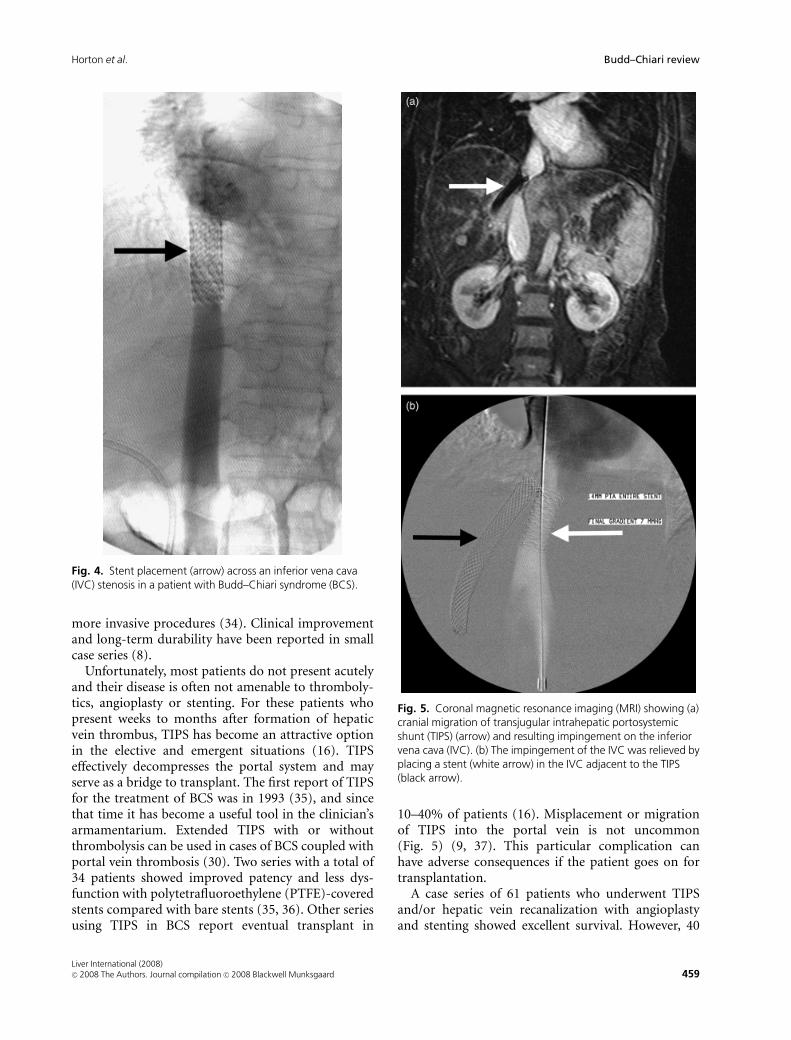
Angioplasty and stenting are additional adjunctsthat may be used. Angioplasty often suffers from highreocclusion rates. Thus, placement of stents in the IVCor hepatic veins has been recommended (Fig. 4) (31).A study out of China recently reported a case series of115 in which stents were placed in the IVC and hepaticveins with success rates of 94% and 87% respectively.Patency reached 90% after a mean follow-up of morethan 45 months (32). The proportion of patients withmembranous occlusion, which may be more amenableto angioplasty and stenting, was much more prevalentin this population (57%) than would be expected inmost Western institutions.
Angioplasty and stenting may offer certain advan-tages to patients who suffer from BCS after livertransplantation. The aetiology in this subset of pa-tients is usually secondary to technical problems (33).Assuming hepatic function has not been lost, correc-tion of the technical issue may be accomplished bypercutaneous means and may obviate the need for
Liver International (2008)458 c� 2008 The Authors. Journal compilation c� 2008 Blackwell Munksgaard
Budd–Chiari review Horton et al.
more invasive procedures (34). Clinical improvementand long-term durability have been reported in smallcase series (8).
Unfortunately, most patients do not present acutelyand their disease is often not amenable to thromboly-tics, angioplasty or stenting. For these patients whopresent weeks to months after formation of hepaticvein thrombus, TIPS has become an attractive optionin the elective and emergent situations (16). TIPSeffectively decompresses the portal system and mayserve as a bridge to transplant. The first report of TIPSfor the treatment of BCS was in 1993 (35), and sincethat time it has become a useful tool in the clinician’sarmamentarium. Extended TIPS with or withoutthrombolysis can be used in cases of BCS coupled withportal vein thrombosis (30). Two series with a total of34 patients showed improved patency and less dys-function with polytetrafluoroethylene (PTFE)-coveredstents compared with bare stents (35, 36). Other seriesusing TIPS in BCS report eventual transplant in
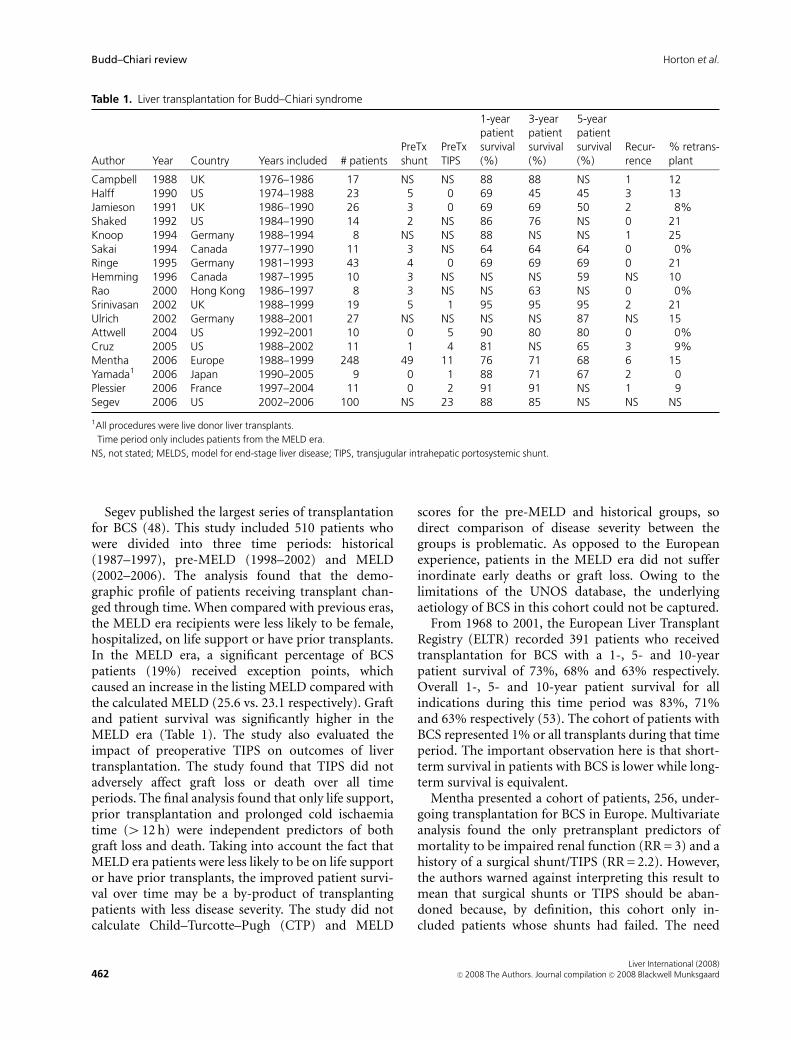
10–40% of patients (16). Misplacement or migrationof TIPS into the portal vein is not uncommon(Fig. 5) (9, 37). This particular complication canhave adverse consequences if the patient goes on fortransplantation.
A case series of 61 patients who underwent TIPSand/or hepatic vein recanalization with angioplastyand stenting showed excellent survival. However, 40
Fig. 4. Stent placement (arrow) across an inferior vena cava(IVC) stenosis in a patient with Budd–Chiari syndrome (BCS).
Fig. 5. Coronal magnetic resonance imaging (MRI) showing (a)cranial migration of transjugular intrahepatic portosystemicshunt (TIPS) (arrow) and resulting impingement on the inferiorvena cava (IVC). (b) The impingement of the IVC was relieved byplacing a stent (white arrow) in the IVC adjacent to the TIPS(black arrow).
Liver International (2008)c� 2008 The Authors. Journal compilation c� 2008 Blackwell Munksgaard 459
Horton et al. Budd–Chiari review

patients required repeated radiological interventions.An important conclusion from this study was thatshort-length stenosis of hepatic veins is under-recog-nized and percutaneous recanalization is under-uti-lized in the management of patients with BCS. Thisstudy suggested that when stratified by disease severity,interventional radiology techniques may have themost impact on the sickest patients (compared withsurvival in patients treated with surgical shunts).Forty-four patients treated initially with surgicalshunts, transplantation or medical therapy alone werenot included for analysis in this study (26).
Interpretation of the literature in this area can bedifficult. Results from a case series in Asia may notapply to the patient population in Western countriesbecause the incidence of membranous obstruction ismuch higher in the Asian series. Also, technologyevolves quickly and today’s stents used for TIPS andother percutaneous interventions may have very dif-ferent properties than those from only a few years ago.As stated before, no prospective trials in patients withBCS exist and conclusions from any published reportshould be viewed with caution.
Surgical shunts
The role of surgical shunts in the treatment of BCS isa controversial topic. A wide range of perioperativemortality has been reported (0–50%) (3). However,long-term survival rates (5–14 years) after variousshunting procedures have been reported to be as highas 90% (16). There are multiple factors that make itdifficult to interpret the literature on this subject.Studies that compare surgical shunts to medical orminimally invasive techniques are often difficult tointerpret because they are usually retrospective, mayhave significant time bias and, maybe most impor-tantly, the sickest patients are usually managed non-operatively (38). Also, in recent years, experience withthese procedures has begun to dwindle. For example,chief residents at a large academic centre such as JohnsHopkins only performed four portosystemic decom-pression surgeries between 1995 and 1999 (9).
Shunting procedures are indicated in patientswith reversible liver injury. However, identifyingthis population of patients is not straightforward(39). Anatomic considerations such as extensiveIVC thrombus may make TIPS difficult and favourplacement of a surgical shunt. While several cases ofBCS with portal vein and/or mesenteric vein throm-bosis have been successfully managed with TIPS andthrombolysis (30), open surgical intervention maybe required.
Selection of which surgical shunt to perform re-quires consideration of several factors. For patientswithout IVC obstruction, the portocaval or mesocavalshunts are reasonable options. Previous portocavalshunts can make the hilar dissection during transplan-tation particularly challenging. In patients with cau-date lobe hypertrophy (Fig. 1), portocaval shunts maybe difficult and even require caudate lobe resectionbefore construction (9). Orloff et al. (40) reportedgreat success with portocaval shunts with 31 of 32patients alive at 3.5–27 years after surgery. Unfor-tunately, their success has not been replicated byothers (9).
For patients with IVC obstruction and/or an infra-hepatic to right atrium pressure gradient of4 20 mm Hg, mesocaval and portocaval shunts maynot effectively decompress the liver. Some authorsreport improved long-term outcomes with a pressuregradient of greater than 10 mm Hg between the portalvein and IVC (40). The most important pressuregradient is not between the infra and suprahepaticvena cava, but between the two vascular structures thatare to be connected (3). Consequently, many authorsconsider mesoatrial or cavoatrial shunts in these cases(Fig. 6) (9). While the primary patency rate ofmesoatrial shunts is relatively low, 5-year survival hasbeen acceptable (9, 41).
Wang (2) reported good 1-, 3- and 5-year patencyrates for mesoatrial (90.7%, 77.1%, 61.1%) andcavoatrial (97.2%, 86.0%, 79.8%) shunts. Orloffreported 18 cases of BCS with IVC and hepatic veinocclusion. In their early experience, eight of thesepatients were treated with mesoatrial shunts. Five ofthese patients died after the graft thrombosed. The
Fig. 6. Intraoperative photo taken during a cavoatrial shuntprocedure showing the anastomosis of the graft to theinfrahepatic vena cava (arrow). The liver is retracted mediallyand the graft is then brought posteriorly through the diaphragmand into the right hemithorax.
Liver International (2008)460 c� 2008 The Authors. Journal compilation c� 2008 Blackwell Munksgaard
Budd–Chiari review Horton et al.

authors then began to use a combined side–to-sideportocaval shunt and cavoatrial shunt in these pa-tients. Results were much better with all 10 patientssurviving to their last follow-up (mean follow-up 9years) (40).
The literature is unclear with regard to which shuntshould be used in any particular situation. No pro-spective studies exist. Retrospective studies are hetero-geneous and often include data from three or moretypes of surgical shunts. Many comparative studieshave either no control group or a small control group(3). Clinical judgment and technical expertise oftendominate the decision-making process.
Portocaval shunts require disconnection duringliver transplantation. This can result in increasedoperative time and blood loss. Alternatively, mesocavalshunts are not part of the operative field duringtransplantation, can be divided easily and may simplifythe procedure by providing portal and systemic de-compression during intraoperative venovenousbypass through a single femoral vein cannula (9).
Two case series with a total of 73 patients underwentsurgical shunting procedures before transplantation.Both of these studies showed worse outcomes in thepatients who had a portocaval shunt. Additionally, thelarger of the two studies showed a 5-year survivaladvantage of mesocaval shunts compared withpatients without previous shunt procedures (95% vs.65%) (42, 43).
In Langlet’s extensive review of the literature onsurgical shunting, only two studies assessed survivalafter correcting for prognostic factors. Neither of thesestudies could demonstrate any favourable effects ofsurgical shunts on survival. Thus, the review arguesthat the late beneficial effects of relieving hepaticcongestion may be balanced by the high early mortal-ity of the procedure (3). Murad’s multivariate analysisstratified 205 patients with BCS treated by a variety ofmodalities into three classes and found that surgicalshunting and TIPS was associated with increasedmortality as the interval between diagnosis andshunting lengthened. The study also showed a trendtoward improved survival in class II patients (RR, 0.63;P = 0.29) (44).
Another surgical option is radical resection withanatomic reconstruction (45). This approach may bemore applicable in Asian countries, where the aetiol-ogy is often IVC or hepatic vein membranes.
Liver transplantation
The first successful liver transplant for a patientwith BCS was performed in 1974 (46). Since that
time, several series and registry analyses of livertransplantation for BCS have been reported (Table 1).Recently, two large series have been published docu-menting the European and U.S. experience (47, 48).For patients with BCS and acute fulminant liver failureor cirrhosis and decompensated disease with poorsynthetic function, liver transplantation is the treat-ment of choice (9). Evidence of poor hepatocytesynthetic function includes albumin o3 g/dl, pro-thrombin time 3 s greater than control, and conju-gated bilirubin 43 mg/dl (23). When compared withpatients who receive shunting procedures, trans-planted patients maintain higher serum albumin levelsand improved synthetic function (25). In patients withcertain synthetic deficiencies such as antithrombin IIIor protein C, liver transplantation offers the additionaladvantage of curing these genetic defects (9, 49, 50).While liver transplantation has emerged as a safetherapeutic option for patients with BCS, its applica-tion should not be used liberally. Patients withBCS have multiple therapeutic options that maynot be available to many patients on the transplantwaiting list.
Calculating model for end-stage liver disease(MELD) scores in patients with chronic BCS may beproblematic because many of these patients are onwarfarin or some other form of anticoagulation. Inthis patient population, international normalized ratio(INR) is not an accurate indicator of hepatic syntheticfunction. It has recently been suggested that the INRbe capped at 2.5 for patients on warfarin. Additionally,it has been proposed that patients with fulminanthepatic failure resulting from BCS should be listedas United Network for Organ Sharing (UNOS) status1A (51).
Several technical considerations make the trans-plantation procedure itself especially challenging inpatients with BCS. Haemostasis can be particularlychallenging, and above average blood loss is oftenreported (39). Some centres employ venovenous by-pass during all transplants in patients who havesignificant portal hypertension and prior shunt sur-gery. Caudate lobe enlargement (Fig. 1) may presentproblems during transplantation by making mobiliza-tion of the liver difficult and increasing the difficultyof the piggyback technique (9). BCS may cause adiffuse fibrotic reaction in the retroperitoneum, whichmay increase the complexity of steps requiringcontrol of the IVC (9, 38). Additionally, dense adhe-sions between the liver and diaphragm surroundingthe suprahepatic IVC have been described (38, 52).The portal vein may be thickened, narrowed and eventhrombosed (39).
Liver International (2008)c� 2008 The Authors. Journal compilation c� 2008 Blackwell Munksgaard 461
Horton et al. Budd–Chiari review
Segev published the largest series of transplantationfor BCS (48). This study included 510 patients whowere divided into three time periods: historical(1987–1997), pre-MELD (1998–2002) and MELD(2002–2006). The analysis found that the demo-graphic profile of patients receiving transplant chan-ged through time. When compared with previous eras,the MELD era recipients were less likely to be female,hospitalized, on life support or have prior transplants.In the MELD era, a significant percentage of BCSpatients (19%) received exception points, whichcaused an increase in the listing MELD compared withthe calculated MELD (25.6 vs. 23.1 respectively). Graftand patient survival was significantly higher in theMELD era (Table 1). The study also evaluated theimpact of preoperative TIPS on outcomes of livertransplantation. The study found that TIPS did notadversely affect graft loss or death over all timeperiods. The final analysis found that only life support,prior transplantation and prolonged cold ischaemiatime (412 h) were independent predictors of bothgraft loss and death. Taking into account the fact thatMELD era patients were less likely to be on life supportor have prior transplants, the improved patient survi-val over time may be a by-product of transplantingpatients with less disease severity. The study did notcalculate Child–Turcotte–Pugh (CTP) and MELD
scores for the pre-MELD and historical groups, sodirect comparison of disease severity between thegroups is problematic. As opposed to the Europeanexperience, patients in the MELD era did not sufferinordinate early deaths or graft loss. Owing to thelimitations of the UNOS database, the underlyingaetiology of BCS in this cohort could not be captured.
From 1968 to 2001, the European Liver TransplantRegistry (ELTR) recorded 391 patients who receivedtransplantation for BCS with a 1-, 5- and 10-yearpatient survival of 73%, 68% and 63% respectively.Overall 1-, 5- and 10-year patient survival for allindications during this time period was 83%, 71%and 63% respectively (53). The cohort of patients withBCS represented 1% or all transplants during that timeperiod. The important observation here is that short-term survival in patients with BCS is lower while long-term survival is equivalent.
Mentha presented a cohort of patients, 256, under-going transplantation for BCS in Europe. Multivariateanalysis found the only pretransplant predictors ofmortality to be impaired renal function (RR = 3) and ahistory of a surgical shunt/TIPS (RR = 2.2). However,the authors warned against interpreting this result tomean that surgical shunts or TIPS should be aban-doned because, by definition, this cohort only in-cluded patients whose shunts had failed. The need
Table 1. Liver transplantation for Budd–Chiari syndrome
Author Year Country Years included # patientsPreTxshunt
PreTxTIPS
1-yearpatientsurvival(%)
3-yearpatientsurvival(%)
5-yearpatientsurvival(%)
Recur-rence
% retrans-plant
Campbell 1988 UK 1976–1986 17 NS NS 88 88 NS 1 12Halff 1990 US 1974–1988 23 5 0 69 45 45 3 13Jamieson 1991 UK 1986–1990 26 3 0 69 69 50 2 8%Shaked 1992 US 1984–1990 14 2 NS 86 76 NS 0 21Knoop 1994 Germany 1988–1994 8 NS NS 88 NS NS 1 25Sakai 1994 Canada 1977–1990 11 3 NS 64 64 64 0 0%Ringe 1995 Germany 1981–1993 43 4 0 69 69 69 0 21Hemming 1996 Canada 1987–1995 10 3 NS NS NS 59 NS 10Rao 2000 Hong Kong 1986–1997 8 3 NS NS 63 NS 0 0%Srinivasan 2002 UK 1988–1999 19 5 1 95 95 95 2 21Ulrich 2002 Germany 1988–2001 27 NS NS NS NS 87 NS 15Attwell 2004 US 1992–2001 10 0 5 90 80 80 0 0%Cruz 2005 US 1988–2002 11 1 4 81 NS 65 3 9%Mentha 2006 Europe 1988–1999 248 49 11 76 71 68 6 15Yamada1 2006 Japan 1990–2005 9 0 1 88 71 67 2 0Plessier 2006 France 1997–2004 11 0 2 91 91 NS 1 9Segev 2006 US 2002–2006� 100 NS 23 88 85 NS NS NS
1All procedures were live donor liver transplants.�Time period only includes patients from the MELD era.
NS, not stated; MELDS, model for end-stage liver disease; TIPS, transjugular intrahepatic portosystemic shunt.
Liver International (2008)462 c� 2008 The Authors. Journal compilation c� 2008 Blackwell Munksgaard
Budd–Chiari review Horton et al.

for emergency transplant was not associated withincreased mortality. Eighty-seven per cent of deathsoccurred during the first year and the authors con-cluded that the slow course of myeloproliferativedisorders was not significantly affected by transplanta-tion (47). However, two other series report cases ofpolycythaemia vera transforming into acute leukaemiaseveral years after transplant (49, 54). The life expec-tancy for patients with polycythaemia who have devel-oped myelofibrosis is approximately 3 years. Thus,transplantation does not offer a survival advantage inpatients with myelofibrosis (54). Based on Murad’sclassification system of patients with BCS, patients inclass III from Mentha’s cohort had improved survivalwith transplantation compared with Murad’s cohorttreated without transplant (5-year survival 71% vs.42%) (44, 47).
Yamada presented nine patients with BCS treatedwith living donor liver transplantation. This seriesreported an 88% 1-year and 71% 3-year survival, withtwo patients suffering recurrence of BCS (55).
Liver transplants complicated by postoperative BCSmay not always be amenable to minimally invasiveinterventions (34). In a review of 1112 patients whounderwent liver transplantation with the piggybacktechnique, nine patients suffered from early post-operative BCS. Retransplantation was performed inseven of these patients, and four of the nine diedwithin 2 months of their operation (7). Other largeseries have reported a 24% mortality rate for thiscomplication (6). Other than retransplantation andpercutaneous interventions, alternate managementstrategies include surgical shunts (56), simple rotationof the graft, caval thrombectomy, anastomosis recon-struction or diaphragmatic placement of the graft (6).
Budd–Chiari syndrome following liver transplanta-tion with the piggyback technique is a well-describedcomplication with a reported incidence of 1–7% (8).Venous outflow obstruction is often considered morecommon after the piggyback technique (33). However,two recent retrospective studies were unable to detect adifference in the rate of BCS between the piggybacktechnique and the standard technique (57, 58).Furthermore, there is little difference in postoperativeBCS when comparing large case series utilizing eitherthe standard or piggyback technique, 1.7% vs.1.1–1.5% respectively (6, 7, 59). This complicationusually presents in the early postoperative period.However, approximately 25% of cases may presentafter the first postoperative week (7). Technical factorsthat have been associated with this complication areinadequate graft size and use of two hepatic veins forthe venous anastomosis (6, 7). The rate of BCS after
construction of the venous anastomosis with two veinsis 2.3% while the use of three veins decreases the rateto 0.7% (7). Compared with the conventional piggy-back technique, the side-to-side variation of the piggy-back technique has been associated with a decreasedincidence of BCS, 2.4% vs. 0.7% respectively(P = 0.014) (6).
As recurrent BCS after transplantation has beenreported, lifelong anticoagulation is recommended(4). Recurrence of BCS after transplantation has beenreported to be as high as 27% and may requireretransplantation (49). Patients are often startedon heparin postoperatively (total daily dose7500–30 000 U intravenously) and converted to cou-madin a week later (23, 54, 60). In patients withmyeloproliferative disorders, coumadin does not ad-dress their underlying pathophysiology. In these pa-tients, administration of hydroxyurea and aspirin canbe given instead of traditional anticoagulation to treatthe aetiology of BCS. The newer drug, anagrelide, hasreplaced hydroxyurea in some centres (23). Post-transplant anticoagulation may not be necessary inpatients who possessed synthetic defects such as pro-tein C deficiency corrected by transplantation (23, 50).While life-long anticoagulation after transplantationis routine for most patients, it does come with a price.Campbell (47) and Mentha (52) reported clinicallysignificant haemorrhage in many patients, 44% and11% respectively.
Prognosis
Outcomes in patients with BCS have improved since1985 (19). Approximately 25% of patients remainasymptomatic after treatment, and spontaneous reso-lution has been reported (16). Several authors haveinvestigated prognostic indicators in patients withBCS.
Khuroo (29) analysed 47 consecutive patients withBCS and found the following factors to adversely affectsurvival: florid clinical presentation, male sex, no TIPSperformed and CTP score.
Langlet updated previous work on their prognosticindex (PI) and found that ascites score, Pugh score,age, creatinine and type III presentation (acute injurysuperimposed on chronic lesions) were all indepen-dent predictors of survival. After including 123patients who underwent surgical shunts, this analysiswas unable to show a survival benefit to surgicalshunts whether performed early (within 2 monthsafter diagnosis) or not. Short-term and long-termsurvival was good regardless of treatment modality inpatients with PIo 5.1. However, the authors caution
Liver International (2008)c� 2008 The Authors. Journal compilation c� 2008 Blackwell Munksgaard 463
Horton et al. Budd–Chiari review

that this study was underpowered to detect a possiblebenefit to surgical shunts in patients who present withtype I BCS (acute injury only, corresponding to theonset of hepatic outflow obstruction) (19). A weaknessof the PI is that only two of its variables incorporateobjective data.
Murad reported the results of an internationalmulti-institutional study, which included 237 patients(205 included in multivariate analysis) treated with avariety of modalities. This cohort achieved transplant-free survival rates of 82%, 69% and 62% at 1, 5 and10 years respectively. The following factors were foundby multivariate analysis to be independent predictorsof 5-year transplant-free survival: presence of ascites,presence of encephalopathy, INR and bilirubin. Basedon these variables, the authors constructed an equa-tion that assigned patients into one of three classes(Table 2). The 5-year transplant-free survival was 89%,74% and 42% for class I, class II and class IIIrespectively (44). The strengths of this analysis werethat it included more patients than the Langlet study,and its variables were either objective or binary. Thedegree of ascites and encephalopathy were not vari-ables. Only the presence or absence of ascites andencephalopathy was considered in the multivariateanalysis. A possible weakness of this study is that itexcluded patients who underwent transplant.
Conclusion
Budd–Chiari syndrome is a complex disease with awide spectrum of aetiologies and presentations. Amultidisciplinary approach to diagnosis and treatmentis advantageous in patients with BCS. Medical therapyconsists of treatment of underlying disease, anticoagu-lation and symptom control. Emerging technologieshave offered new minimally invasive treatment mod-alities such as percutaneous catheter-directed throm-bolysis, angioplasty, stenting and TIPS. While surgical
shunting continues to play a role in the treatment ofpatients with BCS, its place in treatment strategies isunclear. Surgical shunting is best reserved to thoseinstitutions with significant operative experience, TIPScapability and a liver transplant programme. Livertransplantation is the treatment of choice for patientswith fulminant hepatic failure or those with chroniccirrhosis and poor synthetic function. As technologycontinues to progress, new diagnostic and therapeuticoptions will likely enhance the clinician’s ability to carefor patients with this challenging disease.
References
1. Chung RT, Iafrate AJ, Amrein PC, Sahani DV, Misdraji J.
Case records of the Massachusetts general hospital. Case 15-
2006. A 46-year-old woman with sudden onset of abdominal
distention. N Engl J Med 2006; 354: 2166–75.
2. Wang ZG, Zhang FJ, Yi MQ, Qiang LX. Evolution of
management for Budd-Chiari syndrome: a team’s view from
2564 patients. ANZ J Surg 2005; 75: 55–63.
3. Langlet P, Valla D. Is surgical portosystemic shunt the
treatment of choice in Budd-Chiari syndrome? Acta Gastro-
enterol Belg 2002; 65: 155–60.
4. Janssen HL, Garcia-Pagan JC, Elias E, Mentha G, Hadengue
A, Valla DC. Budd-Chiari syndrome: a review by an expert
panel. J Hepatol 2003; 38: 364–71.
5. Valla DC. The diagnosis and management of the Budd–
Chiari syndrome: consensus and controversies. Hepatology
2003; 38: 793–803.
6. Navarro F, Le Moine MC, Fabre JM, et al. Specific vascular
complications of orthotopic liver transplantation with pre-
servation of the retrohepatic vena cava: review of 1361 cases.
Transplantation 1999; 68: 646–50.
7. Parrilla P, Sanchez-Bueno F, Figueras J, et al. Analysis of the
complications of the piggy-back technique in 1,112 liver
transplants. Transplantation 1999; 67: 1214–7.
8. Wang SL, Sze DY, Busque S, et al. Treatment of hepatic
venous outflow obstruction after piggyback liver transplanta-
tion. Radiology 2005; 236: 352–9.
9. Klein AS. Management of Budd–Chiari syndrome. Liver
Transpl 2006; 12(Suppl 2): S23–8.
10. Kage M, Arakawa M, Kojiro M, Okuda K. Histopathology
of membranous obstruction of the inferior vena cava
in the Budd–Chiari syndrome. Gastroenterology 1992; 102:
2081–90.
11. Kew MC, Hodkinson HJ. Membranous obstruction of the
inferior vena cava and its causal relation to hepatocellular
carcinoma. Liver Int 2006; 26: 1–7.
12. Terabayashi H, Okuda K, Nomura F, Ohnishi K, Wong P.
Transformation of inferior vena caval thrombosis to mem-
branous obstruction in a patient with the lupus anticoagu-
lant. Gastroenterology 1986; 91: 219–24.
13. Menon KV, Shah V, Kamath PS. The Budd–Chiari syndrome.
N Engl J Med 2004; 350: 578–85.
Table 2. Murad’s Budd–Chiari syndrome prognostic classification
Score�% ofcohort (%)
5-yearsurvival (%)
% withsurgicalshunt
Class I 0–1.1 27 89 29Class II 1.1–1.5 46 74 55Class III 4 1.5 27 42 60
�Equation:1.27� encephalopathy11.04� ascites10.72�prothrombin
time10.004�bilirubin.
Ascites and hepatic encephalopathy were scored as present (1) or absent
(0) and prothrombin time as higher (1) or lower (0) than 2.3 INR. Bilirubin
was included as a continuous variable.
INR, international normalized ratio.
Liver International (2008)464 c� 2008 The Authors. Journal compilation c� 2008 Blackwell Munksgaard
Budd–Chiari review Horton et al.
14. Senzolo M, Cholongitas EC, Patch D, Burroughs AK. Update
on the classification, assessment of prognosis and therapy of
Budd–Chiari syndrome. Nat Clin Pract Gastroenterol Hepatol
2005; 2: 182–90.
15. Cauchi JA, Oliff S, Baumann U, et al. The Budd–Chiari
syndrome in children: the spectrum of management. J
Pediatr Surg 2006; 41: 1919–23.
16. Zimmerman MA, Cameron AM, Ghobrial RM. Budd–Chiari
syndrome. Clin Liver Dis 2006; 10: 259–73, viii.
17. Khuroo MS, Datta DV. Budd–Chiari syndrome following
pregnancy. Report of 16 cases, with roentgenologic, hemo-
dynamic and histologic studies of the hepatic outflow tract.
Am J Med 1980; 68: 113–21.
18. Dilawari JB, Bambery P, Chawla Y, et al. Hepatic outflow
obstruction (Budd–Chiari syndrome). Experience with 177
patients and a review of the literature. Medicine 1994; 73:
21–36.
19. Langlet P, Escolano S, Valla D, et al. Clinicopathological
forms and prognostic index in Budd–Chiari syndrome. J
Hepatol 2003; 39: 496–501.
20. Brancatelli G, Vilgrain V, Federle MP, et al. Budd–Chiari
syndrome: spectrum of imaging findings. Am J Roentgenol
2007; 188: W168–76.
21. Bolondi L, Gaiani S, Li Bassi S, et al. Diagnosis of
Budd–Chiari syndrome by pulsed Doppler ultrasound.
Gastroenterology 1991; 100(Pt 1): 1324–31.
22. Noone TC, Semelka RC, Siegelman ES, et al. Budd–Chiari
syndrome: spectrum of appearances of acute, subacute, and
chronic disease with magnetic resonance imaging. J Magn
Reson Imaging 2000; 11: 44–50.
23. Melear JM, Goldstein RM, Levy MF, et al. Hematologic
aspects of liver transplantation for Budd–Chiari syndrome
with special reference to myeloproliferative disorders. Trans-
plantation 2002; 74: 1090–5.
24. Valla D, Benhamou JP. Obstruction of the hepatic
veins or suprahepatic inferior vena cava. Dig Dis 1996; 14:
99–118.
25. Shaked A, Goldstein RM, Klintmalm GB, Drazan K, Husberg
B, Busuttil RW. Portosystemic shunt versus orthotopic liver
transplantation for the Budd–Chiari syndrome. Surg Gynecol
Obstet 1992; 174: 453–9.
26. Eapen CE, Velissaris D, Heydtmann M, Gunson B, Olliff S,
Elias E. Favourable medium term outcome following hepatic
vein recanalisation and/or transjugular intrahepatic porto-
systemic shunt for Budd Chiari syndrome. Gut 2006; 55:
878–84.
27. Plessier A, Sibert A, Consigny Y, et al. Aiming at minimal
invasiveness as a therapeutic strategy for Budd–Chiari syn-
drome. Hepatology 2006; 44: 1308–16.
28. McCarthy PM, van Heerden JA, Adson MA, Schafer LW,
Wiesner RH. The Budd–Chiari syndrome. Medical and
surgical management of 30 patients. Arch Surg 1985; 120:
657–62.
29. Khuroo MS, Al-Suhabani H, Al-Sebayel M, et al. Budd–-
Chiari syndrome: long-term effect on outcome with transju-
gular intrahepatic portosystemic shunt. J Gastroenterol
Hepatol 2005; 20: 1494–502.
30. Olliff SP. Transjugular intrahepatic portosystemic shunt in
the management of Budd Chiari syndrome. Eur J Gastro-
enterol Hepatol 2006; 18: 1151–4.
31. Sharma S, Texeira A, Texeira P, Elias E, Wilde J, Olliff SP.
Pharmacological thrombolysis in Budd Chiari syndrome: a
single centre experience and review of the literature. J Hepatol
2004; 40: 172–80.
32. Zhang CQ, Fu LN, Xu L, et al. Long-term effect of stent
placement in 115 patients with Budd–Chiari syndrome.
World J Gastroenterol 2003; 9: 2587–91.
33. Aucejo F, Winans C, Henderson JM, et al. Isolated right
hepatic vein obstruction after piggyback liver transplanta-
tion. Liver Transpl 2006; 12: 808–12.
34. Settmacher U, Nussler NC, Glanemann M, et al. Venous
complications after orthotopic liver transplantation. Clin
Transplant 2000; 14: 235–41.
35. Hernandez-Guerra M, Turnes J, Rubinstein P, et al. PTFE-
covered stents improve TIPS patency in Budd–Chiari syn-
drome. Hepatology 2004; 40: 1197–202.
36. Gandini R, Konda D, Simonetti G. Transjugular intrahepatic
portosystemic shunt patency and clinical outcome in patients
with Budd–Chiari syndrome: covered versus uncovered
stents. Radiology 2006; 241: 298–305.
37. Clavien PA, Selzner M, Tuttle-Newhall JE, Harland RC,
Suhocki P. Liver transplantation complicated by misplaced
TIPS in the portal vein. Ann Surg 1998; 227: 440–5.
38. Halff G, Todo S, Tzakis AG, Gordon RD, Starzl TE. Liver
transplantation for the Budd–Chiari syndrome. Ann Surg
1990; 211: 43–9.
39. Jamieson NV, Williams R, Calne RY. Liver transplantation
for Budd–Chiari syndrome, 1976–1990. Ann Chir 1991; 45:
362–5.
40. Orloff MJ, Daily PO, Orloff SL, Girard B, Orloff MS. A 27-
year experience with surgical treatment of Budd–Chiari
syndrome. Ann Surg 2000; 232: 340–52.
41. Slakey DP, Klein AS, Venbrux AC, Cameron JL. Budd–Chiari
syndrome: current management options. Ann Surg 2001; 233:
522–7.
42. Brems JJ, Hiatt JR, Klein AS, et al. Effect of a prior
portasystemic shunt on subsequent liver transplantation.
Ann Surg 1989; 209: 51–6.
43. Mazzaferro V, Todo S, Tzakis AG, Stieber AC, Makowka L,
Starzl TE. Liver transplantation in patients with previous
portasystemic shunt. Am J Surg 1990; 160: 111–6.
44. Murad SD, Valla DC, de Groen PC, et al. Determinants of
survival and the effect of portosystemic shunting in patients
with Budd—Chiari syndrome. Hepatology 2004; 39: 500–8.
45. Zhang XM, Li QL. Radical surgery under genuine direct
vision for the treatment of Budd–Chiari syndrome. Hepato-
biliary Pancreat Dis Int 2006; 5: 65–9.
46. Putnam CW, Porter KA, Weil R III, Reid HA, Starzl TE. Liver
transplantation of Budd–Chiari syndrome. JAMA 1976; 236:
1142–3.
Liver International (2008)c� 2008 The Authors. Journal compilation c� 2008 Blackwell Munksgaard 465
Horton et al. Budd–Chiari review
47. Mentha G, Giostra E, Majno PE, et al. Liver transplantation
for Budd–Chiari syndrome: a European study on 248
patients from 51 centres. J Hepatol 2006; 44: 520–8.
48. Segev DL, Nguyen GC, Locke JE, et al. Twenty years of liver
transplantation for Budd–Chiari syndrome: a national reg-
istry analysis. Liver Transpl 2007; 13: 1285–94.
49. Cruz E, Ascher NL, Roberts JP, Bass NM, Yao FY. High
incidence of recurrence and hematologic events following
liver transplantation for Budd–Chiari syndrome. Clin Trans-
plant 2005; 19: 501–6.
50. Tan HP, Markowitz JS, Maley WR, Merritt WT, Klein AS.
Successful liver transplantation in a patient with Budd–
Chiari syndrome caused by homozygous factor V Leiden.
Liver Transpl 2000; 6: 654–6.
51. Washburn WK, Gish RG, Kamath PS. Model for end-stage
liver disease (MELD) exception for Budd–Chiari syndrome.
Liver Transpl 2006; 12(Suppl 3): S93–4.
52. Campbell DA Jr., Rolles K, Jamieson N, et al. Hepatic
transplantation with perioperative and long term anticoagu-
lation as treatment for Budd–Chiari syndrome. Surg Gynecol
Obstet 1988; 166: 511–8.
53. Adam R, McMaster P, O’Grady JG, et al. Evolution of liver
transplantation in Europe: report of the European liver
transplant registry. Liver Transpl 2003; 9: 1231–43.
54. Srinivasan P, Rela M, Prachalias A, et al. Liver transplanta-
tion for Budd–Chiari syndrome. Transplantation 2002; 73:
973–7.
55. Yamada T, Tanaka K, Ogura Y, et al. Surgical techniques
and long-term outcomes of living donor liver transplanta-
tion for Budd–Chiari syndrome. Am J Transplant 2006; 6:
2463–9.
56. Molmenti EP, Grover DS, Thuluvath PJ, et al. Cavoa-
trial shunt in the treatment of suprahepatic vena cava
stricture after liver transplantation. Liver Transpl 2004; 10:
1216–7.
57. Barshes NR, Lee T, Kilic M, Goss JA. Reconstruction of the
hepatic venous outflow in piggyback liver transplantation.
Exp Clin Transplant 2004; 2: 189–95.
58. Miyamoto S, Polak WG, Geuken E, et al. Liver transplanta-
tion with preservation of the inferior vena cava. A compar-
ison of conventional and piggyback techniques in adults. Clin
Transplant 2004; 18: 686–93.
59. Glanemann M, Settmacher U, Langrehr JM, et al. Results of
end-to-end cavocavostomy during adult liver transplanta-
tion. World J Surg 2002; 26: 342–7.
60. Knoop M, Lemmens HP, Langrehr JM, et al. Liver transplan-
tation for Budd–Chiari syndrome. Transplant Proc 1994; 26:
3577–8.
Liver International (2008)466 c� 2008 The Authors. Journal compilation c� 2008 Blackwell Munksgaard
Budd–Chiari review Horton et al.