
HIF-1 Stabilization in Flagellin-Stimulated Human Bronchial ...
Upload
univ-lille2Category
view
0download
0
Bronchial obstructive phenotypes in the firstyear of life among Paris birth cohort infants
In developed countries, both the incidence andprevalence of asthma during childhood haveincreased dramatically in the last few decades(1). According to the International Study onAllergies and Asthma in Childhood (ISAAC),asthma was experienced in France by 6.7–9.3% of6–7-yr-old children and by 10.5–15.1% of 13–14-yr-old adolescents in 1997, while prevalence ofallergic rhinitis and atopic eczema symptomsvaried from 12% to 25% and 9% to 13%respectively (2). Although the prevalence of pae-diatric asthma and allergy seems to have steadiedover the last 10 yr (3), asthma remains the mostcommon infantile chronic illness. As most cases
develop asthma during childhood (4), many birthcohort studies have been implemented worldwideto try to explain the reasons for this epidemic.However, data on incidence and prevalence ofrespiratory/allergic disorders among pre-schoolchildren are heterogeneous, making it difficult tocompare wheezing and allergic phenotypes at thisage. The natural history of respiratory symptomsremains unclear but associations between earlychildhood respiratory symptoms (as soon asinfancy) and the subsequent risk of asthma haveyet to be established (5).A growing interest in birth cohort studies has
recently been shown when assessing the aetiology
Clarisse B, Demattei C, Nikasinovic L, Just J, Daures J-P, Momas I.Bronchial obstructive phenotypes in the first year of life among Parisbirth cohort infants.Pediatr Allergy Immunol 2008.� 2008 The AuthorsJournal compilation � 2008 Blackwell Munksgaard
As the natural history of respiratory and allergic manifestations is un-clear, our ongoing Paris birth cohort study prospectively assesses theonset of these symptoms in early childhood. Data were collected by fivequestionnaires sent at regular intervals during the first year of life.Partitioning around medoids (PAM) was used to classify infantsaccording to their bronchial obstructive symptoms. A polytomous lo-gistic regression was performed to assess the eventual predictable powerof various respiratory events and perinatal factors. Results are given for2698 infants. Atopic dermatitis occurred in 17.9% of infants. The mainrespiratory symptoms in infancy were wheeze in the chest (22%),dyspnoea responsible for sleep disturbance (23.7%), nocturnal drycough (14.5%) and shortness of breath (4.2%). The PAM methodidentified three groups of infants. Apart from the G0 group of infantsmostly asymptomatic, two distinct clinical phenotypes (G1 and G2:8.7% and 23.5% of total infants respectively) emerged. G2 was definedby severe bronchial obstructive disorders as all cases of dyspnoea withsleep disturbance were included in this group, while all infants assignedin G1 suffered from nocturnal dry cough. G2 group infants had sig-nificantly higher rates of respiratory events while a parental history ofasthma, symptoms suggestive of rhino-conjunctivitis and birth seasonclearly differentiated the G1 group. Finally, G1 and G2 group infantsshould be closely followed up as they are expected to develop allergicand asthmatic phenotypes, possibly in relation to environmental andbehavioural risk factors.
B�n�dicte Clarisse1,2, ChristopheDemattei3, Lydia Nikasinovic1,Jocelyne Just1,4, Jean-Pierre Daures5
and Isabelle Momas1,2
1Laboratoire Sant� Publique et Environnement,
Facult� des Sciences Pharmaceutiques et
Biologiques, Universit� Paris Descartes, Paris, France,2Cellule « Epid�miologie », Direction de l�Action
Sociale, de l�Enfance et de la Sant� de la Mairie de
Paris, Paris, France, 3D�partement de l�Information
M�dicale, Centre Hospitalier Universitaire de N�mes,
N�mes, France, 4Centre de l�Asthme et des Allergies,
Groupe Hospitalier Trousseau-La Roche Guyon,
Assistance Publique - H�pitaux de Paris, Universit�
Pierre et Marie Curie-Paris6, Paris, France, 5Institut
Universitaire de Recherche Clinique, Universit�
Montpellier I, Montpellier, France
Key words: wheeze; phenotype; eczema; infant;
occurrence; prospective birth cohort
Prof. Isabelle Momas, Laboratoire Sant� Publique et
Environnement, EA 4064 – Facult� des Sciences
Pharmaceutiques et Biologiques – 4 avenue de
l�Observatoire 75270 Paris Cedex 06 – France
Tel.: 33 1-53-73-97-26
Fax: 33 1-43-25-38-76
E-mail: [email protected]
Accepted XX Xxxxxxx1 Xxxxxxxx
P A I 7 4 3 B Dispatch: 26.2.08 Journal: PAI CE: Bharathy
Journal Name Manuscript No. Author Received: No. of pages: 8 PE: PUSHPA
Pediatr Allergy Immunol 2008
DOI: 10.1111/j.1399-3038.2008.00743.x
� 2008 The AuthorsJournal compilation � 2008 Blackwell Munksgaard
PEDIATRIC ALLERGY AND
IMMUNOLOGY
1
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657
of various wheezing and atopic phenotypes.These studies have been conducted worldwide,and while half of them have been carried out inEuropean countries, none as far as we are awarehave taken place in France. Our team hastherefore implemented the Paris prospective birthcohort study (6) that plans to follow-up enrolledchildren until their sixth birthday. Health datacollection is based upon short time interval self-administered questionnaires in order to describeas exactly as possible all respiratory and allergicsymptoms, their chronology and chronicity.The purpose of this study was to analyse, in
the Paris birth cohort, the incidence of wheezeand respiratory symptoms during the first12 months of life and to try to identify bronchialobstructive phenotypes in infancy.
Methods
Population
This study deals with the first 2698 infantsenrolled in the Paris birth cohort, who wererecruited in five maternity hospitals in the Parisarea from 2003 to 2006 (6). Eligible children aresingleton full-term newborns with a birth weightover 2500 g, who had no complications duringbirth or the neonatal period. The parents of thesechildren have to reside in the Paris area, and themothers must be able to speak French. Partici-pating infants represent 63% of the eligiblenewborns. The study was approved by thenational ethics committee and parents gave theirwritten informed consent.
Data collection
At birth, history of allergic conditions [asthma,atopic dermatitis (AD), allergic rhinitis] in bothparents was recorded by a structured interviewwith the mother. Gender, anthropometric mea-sures and parity were also registered.During the first year of follow up, parents were
sent a questionnaire when their child was 1, 3, 6,9 and 12 months old. When data were incom-plete, the missing information was elicited bytelephone. Non-responders were sent question-naires twice.Most questions were abstracted from previ-
ously validated questionnaires, such as the2AMICS (7) and the French version of the ISAACquestionnaires. Parents were regularly ques-tioned on the occurrence of infectious diseases,episodes of �wheezing and whistling in the chest�and symptoms indicating AD. At 1 yr of age,questions concerned asthma-like symptoms,
especially shortness of breath, �dyspnoea respon-sible for sleep disturbance�, �dry cough at nightapart from a cough associated with a cold orchest infection� as well as symptoms suggestingrhino-conjunctivitis such as �problems withsneezing, or a runny or blocked nose apart froma cold or the flu� associated with �itchy-wateryeyes� whether coupled with allergen exposure ornot. Parents were also asked details aboutsymptom frequencies, associated disorders, gen-erated disturbances (impact on sleep and inter-ference with daily activities), and physiciandiagnoses of allergic diseases.
Definition of health outcomes
Each kind of respiratory infection was consid-ered as recurrent when the child experienced atleast three infections before 1 yr of age. Wheezerswere defined as children with at least one attackof wheezing in their first 12 months of life.According to the frequency of wheezing attacks,children with three or more episodes of wheezingwere categorized as recurrent wheezers, whilethose who experienced less than three attacks ofwheezing were regarded as infrequent wheezers.AD was defined by reported doctor-diagnosedeczema or by a parental report of both an �itchyrash intermittently coming and going� andeczema.
Statistical analysis
Statistical analyses were performed using STA-TA� and R 2.4.1 (R Foundation for StatisticalComputing, 2006, http://www.R-project.org)software. Type I error rate was 0.05 for allanalysis.First, incidence rates of respiratory tract
infections, wheeze and AD were estimated.Incidence rates of respiratory infections, bron-chial obstructive symptoms, nasal manifestationsand AD were calculated. Contingency tableanalyses and chi-squared tests were performedto investigate associations between health out-come occurrence and gender or frequency ofwheeze attacks.The classification of bronchial obstructive
symptoms (binary or ordinal data) was achievedby the partitioning around medoids (PAM)method (8). The data were partitioned into threegroups (G0, G1, G2) from four symptom vari-ables: (i) wheeze (no, infrequent, recurrent); (ii)an ordinal symptom; (iii) shortness of breath,dyspnoea responsible for sleep disturbance anddry cough at night; (iv) three binary symptoms(no, yes). The groups were built around the
Clarisse et al.
2
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657
medoids (or centrotypes) specified as follows: (i)an observation without any symptom for G0; (ii)an infrequent wheezer with no other associatedbronchial obstructive symptom for G1; (iii) arecurrent wheezer with at most one associatedbronchial obstructive symptom for G2. ThePAM algorithm was based on the search forthese three representative medoids among theobservations of the data set. These observationsshould represent the structure of the data. Afterfinding a set of three medoids, three clusters wereconstructed by assigning each observation to thenearest medoid. The goal was to find threerepresentative objects which minimize the sumof the dissimilarities of the observations to theirclosest representative object. The handling ofordinal and binary data was achieved by usingthe Gower�s general dissimilarity coefficient (9).Each variable was first standardized by dividingeach entry by the range of the correspondingvariable.Differences between groups with regard to
gender, parity, anthropometric measures, paren-tal history of allergy, and infectious and allergicevents were assessed using a univariate polytom-ous logistic regression model comparing the twomutually exclusive groups (G1, G2), with G0group as the unique comparison group. Multi-variate modelling was achieved using a polytom-ous logistic regression containing all variableswith a p-value lower than 20% in univariateanalysis. The associations were expressed asadjusted odds ratios (ORa) with 95% confidenceintervals (95% CIs).
Results
Results are given for 2698 children over 1 yr ofage, who all had questionnaires at 1, 3, 6, 9and 12 months of age filled out and for 2632infants with regard to wheeze frequency be-cause of incomplete data for 66 infants. Thetotal sample comprised 1400 (51.9%) boys and1298 (48.1%) girls. The participant was the firstborn in 57.0% of cases and had at least twosiblings in 9.3% of cases. The mothers of theinfants studied were of high socioeconomicstatus and of intermediate3 white-collar statusfor 46% and 37% respectively. At inclusion,63.1% of families lived in central Paris, the restresiding in the Parisian suburbs. A parentalhistory of allergy (asthma, AD, allergic rhinitis)was noted for 51.8% of newborns, 18% ofthem having both parents allergic. As forasthma predisposition, 18.2% and 1.1% ofinfants were born to one and both asthmaticparents respectively.
First incidence rates of respiratory and allergic disorders by
period of follow up
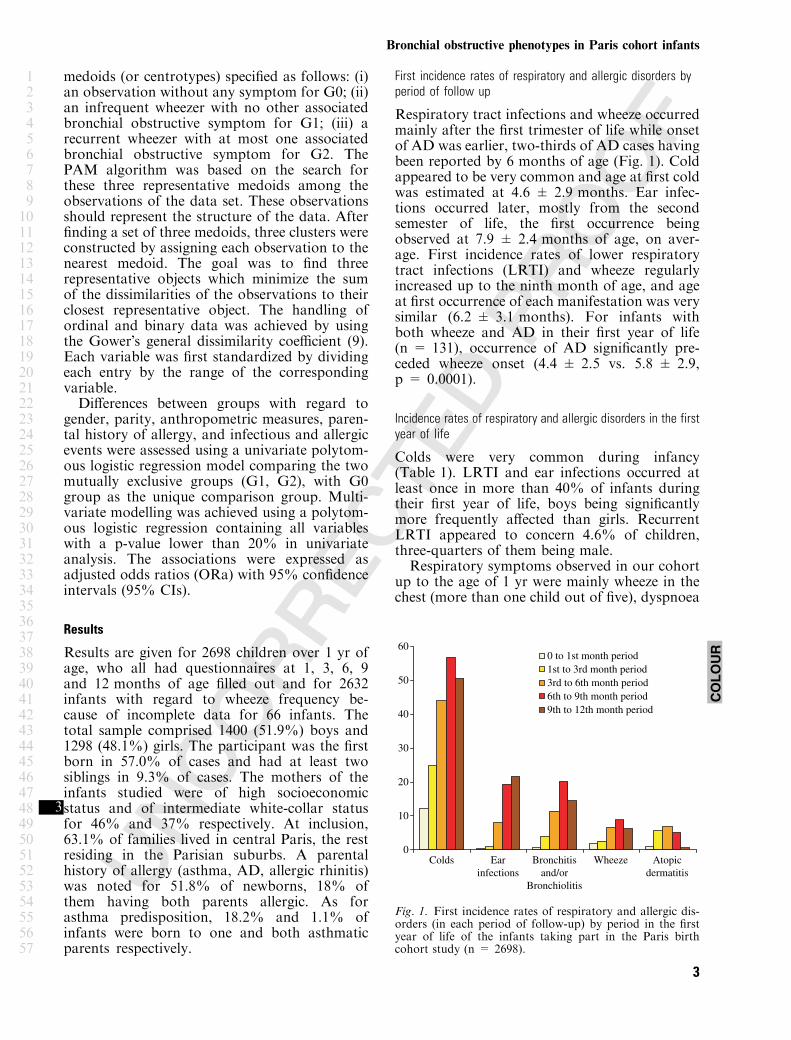
Respiratory tract infections and wheeze occurredmainly after the first trimester of life while onsetof AD was earlier, two-thirds of AD cases havingbeen reported by 6 months of age (Fig. 1). Coldappeared to be very common and age at first coldwas estimated at 4.6 ± 2.9 months. Ear infec-tions occurred later, mostly from the secondsemester of life, the first occurrence beingobserved at 7.9 ± 2.4 months of age, on aver-age. First incidence rates of lower respiratorytract infections (LRTI) and wheeze regularlyincreased up to the ninth month of age, and ageat first occurrence of each manifestation was verysimilar (6.2 ± 3.1 months). For infants withboth wheeze and AD in their first year of life(n = 131), occurrence of AD significantly pre-ceded wheeze onset (4.4 ± 2.5 vs. 5.8 ± 2.9,p = 0.0001).
Incidence rates of respiratory and allergic disorders in the first
year of life
Colds were very common during infancy(Table 1). LRTI and ear infections occurred atleast once in more than 40% of infants duringtheir first year of life, boys being significantlymore frequently affected than girls. RecurrentLRTI appeared to concern 4.6% of children,three-quarters of them being male.Respiratory symptoms observed in our cohort
up to the age of 1 yr were mainly wheeze in thechest (more than one child out of five), dyspnoea
0
10
20
30
40
50
60
Colds Ear
infections
Bronchitis
and/or
Bronchiolitis
Wheeze Atopic
dermatitis
0 to 1st month period
1st to 3rd month period
3rd to 6th month period
6th to 9th month period
9th to 12th month period
Fig. 1. First incidence rates of respiratory and allergic dis-orders (in each period of follow-up) by period in the firstyear of life of the infants taking part in the Paris birthcohort study (n = 2698).
COLOUR
Bronchial obstructive phenotypes in Paris cohort infants
3
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657

responsible for sleep disturbance (one quarter ofchildren), dry cough at night apart from a cold ora chest infection (14.5%) and shortness of breath(around 4%). Except for nocturnal dry coughand dyspnoea, boys had significantly higherincidence rates of these respiratory symptomswhen compared with girls.Parents estimated that wheeze onset was
mainly associated with a cold, chest infection orbronchiolitis (87.7%). Change in weather wasalso frequently assumed responsible for wheezing(27.2%). Wheeze was sometimes reported asresulting from exposure to pollens, dust and petallergens (5.9%).
Impact of wheezing on quality of life and wheeze-associated
bronchial obstructive symptoms in the first year of life
According to the frequency of wheezing attacks,33% of children with wheeze were classified asrecurrent wheezers, while 67% of them wereinfrequent wheezers (Table 2). Increased fre-quency of wheezing had an impact on sleepdisturbance (almost half of recurrent wheezershad sleep disturbed by wheezing, when comparedwith 37.3% in case of infrequent wheeze). Sim-ilarly, wheezing interfered with daily activities for47.9% of recurrent wheezers and only 34.7% ofinfrequent wheezers.Focusing on other bronchial obstructive symp-
toms, shortness of breath, dyspnoea with sleepdisturbance and nocturnal dry cough apart froma cold or a chest infection were all more commonamong recurrent wheezers than among infre-quent wheezers. Furthermore, recurrent wheezerswere significantly at higher risk (25.8% vs.11.1%, p < 0.0001) of suffering from at leasttwo of these wheeze-associated symptomswhen compared with their pairs4 with infrequentwheezing.
Classification of bronchial obstructive symptoms in the first
year of life using the PAM method
The PAM method partitioned our population(n = 2632) in three groups according to wheezeand other bronchial obstructive symptomsreported in the first year of life (Fig. 2). Themost numerous group (G0) was composed of1786 infants, most of them (83.7%) with nobronchial obstructive symptoms up to the age of1 yr. However, more than 15% of these G0group infants had wheeze, most of the timeinfrequent and without any other obstructivesymptom (Fig. 2). Another group (G2) including
Table 1. Incidence rates (%) of respiratory and allergic disorders in the first
year of life of infants taking part in the Paris birth cohort study (n = 2698)
Total
(n = 2698)
Boys
(n = 1400)
Girls
(n = 1298) p-value*
Colds 92.1 91.6 92.6 0.29
Recurrent� colds 38.6 37.1 40.2 0.10
Ear infections 42.6 45.1 39.9 0.006
Recurrent� ear infections 6.2 6.7 5.6 0.24
Bronchitis and/or
bronchiolitis
42.2 45.5 38.7 <0.0001
Recurrent� bronchitis
and/or bronchiolitis
4.6 5.6 3.4 0.005
Wheeze� 21.6 24.6 18.5 <0.0001
Number of wheeze attacks�
Infrequent wheezers 14.4 15.7 13.0 0.09
Recurrent� wheezers 7.2 8.9 5.4
Dyspnoea with sleep having
been disturbed
23.7 24.1 23.3 0.59
Dry cough at night apart from
a cold or a chest infection
14.5 13.8 15.3 0.28
Shortness of breath 4.2 5.1 3.2 0.01
Symptoms indicating allergic
rhino-conjunctivitis
8.2 8.3 8.2 0.91
Atopic dermatitis 17.9 20.0 15.7 0.004
*p for gender comparison; �recurrent: ‡3 episodes; �data available for
n = 2632.
Table 2. Impact of wheeze on quality of life and wheeze-associated bronchial obstructive symptoms in the first year of life of infants taking part in the Paris birth
cohort study (n = 2632), n (%)
Total wheezers,
n = 569 (21.6)
Infrequent wheezers,
n = 379 (14.4)
Recurrent wheezers,
n = 190 (7.2) p-value*
Impact of wheeze on quality of life�
Sleep having been disturbed due to wheeze
<1 night per week 110 (24.7) 69 (24.5) 41 (25.0) <10)4
‡1 night per week 74 (16.6) 36 (12.8) 38 (23.2)
Daily activities interfered by wheeze
A little 126 (28.3) 81 (28.7) 45 (27.6) <10)4
A moderate amount/a lot 50 (11.2) 17 (6.0) 33 (20.3)
Wheeze-associated symptoms
Shortness of breath 43 (9.6) 14 (5.0) 29 (17.5) <10)4
Dyspnoea with sleep having been disturbed 214 (37.6) 129 (34.0) 85 (44.7) 0.01
Dry cough at night apart from a cold or a chest infection 135 (23.7) 71 (18.7) 64 (33.7) <10)4
*p for infrequent/recurrent wheezers comparison.
�Data available for n = 446.
Clarisse et al.
4
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657
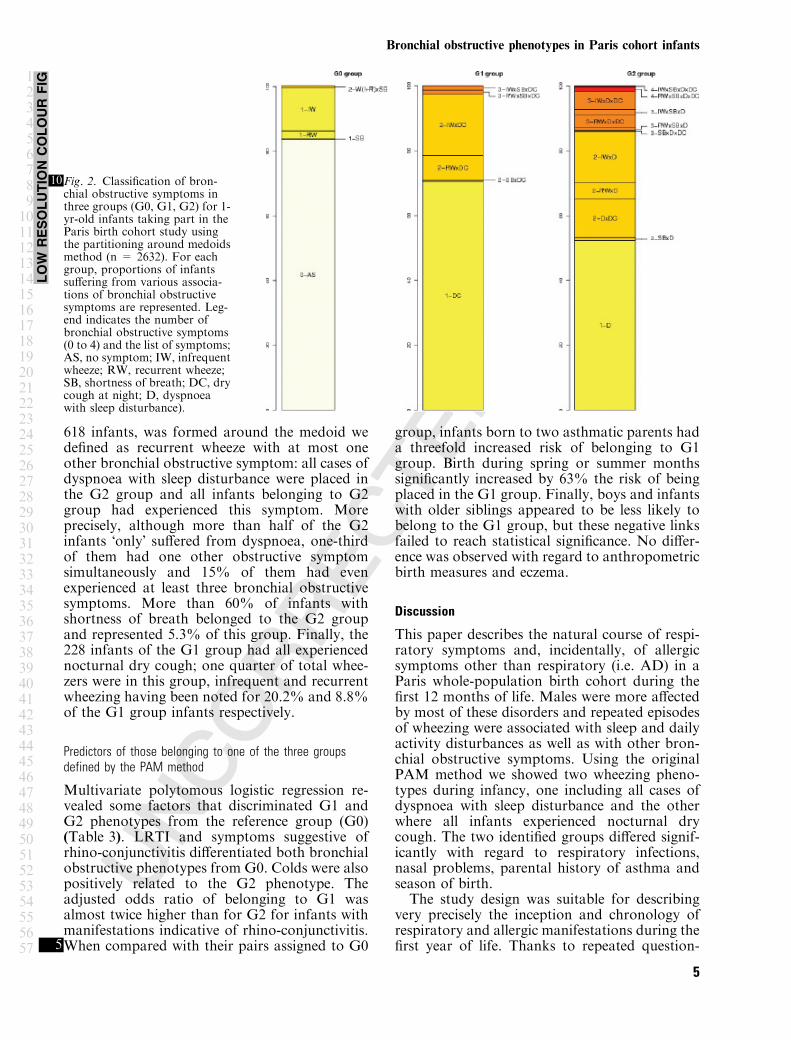
618 infants, was formed around the medoid wedefined as recurrent wheeze with at most oneother bronchial obstructive symptom: all cases ofdyspnoea with sleep disturbance were placed inthe G2 group and all infants belonging to G2group had experienced this symptom. Moreprecisely, although more than half of the G2infants �only� suffered from dyspnoea, one-thirdof them had one other obstructive symptomsimultaneously and 15% of them had evenexperienced at least three bronchial obstructivesymptoms. More than 60% of infants withshortness of breath belonged to the G2 groupand represented 5.3% of this group. Finally, the228 infants of the G1 group had all experiencednocturnal dry cough; one quarter of total whee-zers were in this group, infrequent and recurrentwheezing having been noted for 20.2% and 8.8%of the G1 group infants respectively.
Predictors of those belonging to one of the three groups
defined by the PAM method
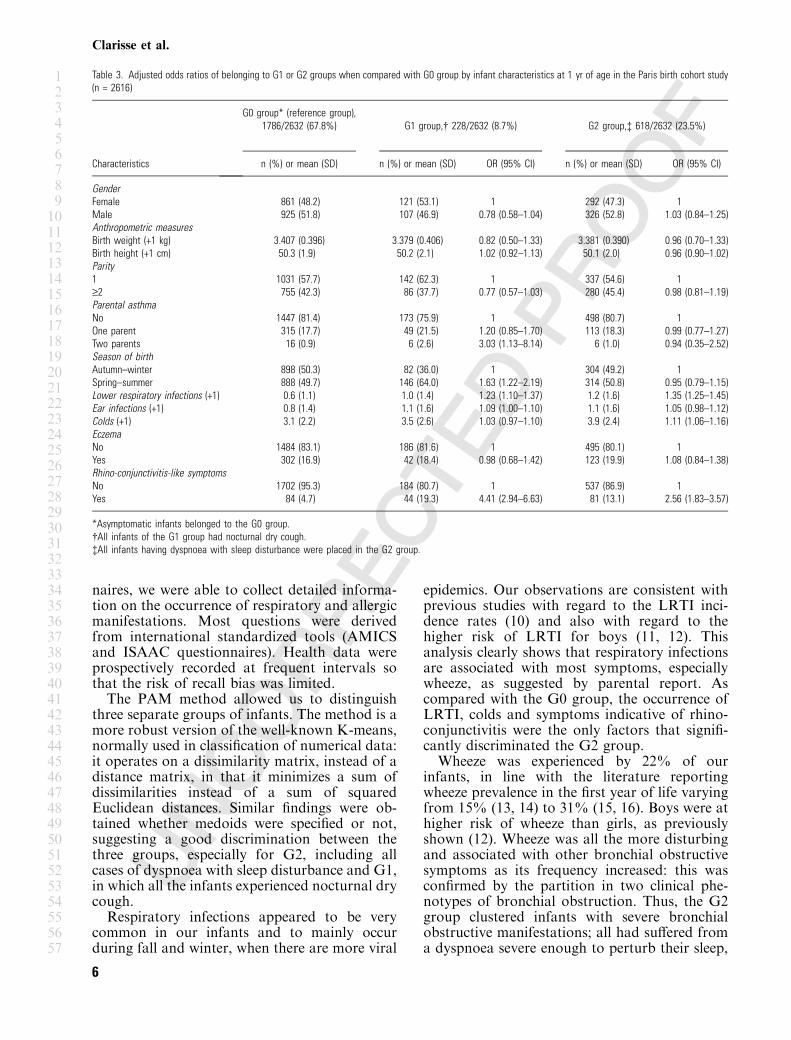
Multivariate polytomous logistic regression re-vealed some factors that discriminated G1 andG2 phenotypes from the reference group (G0)(Table 3). LRTI and symptoms suggestive ofrhino-conjunctivitis differentiated both bronchialobstructive phenotypes from G0. Colds were alsopositively related to the G2 phenotype. Theadjusted odds ratio of belonging to G1 wasalmost twice higher than for G2 for infants withmanifestations indicative of rhino-conjunctivitis.When compared with their pairs5 assigned to G0
group, infants born to two asthmatic parents hada threefold increased risk of belonging to G1group. Birth during spring or summer monthssignificantly increased by 63% the risk of beingplaced in the G1 group. Finally, boys and infantswith older siblings appeared to be less likely tobelong to the G1 group, but these negative linksfailed to reach statistical significance. No differ-ence was observed with regard to anthropometricbirth measures and eczema.
Discussion
This paper describes the natural course of respi-ratory symptoms and, incidentally, of allergicsymptoms other than respiratory (i.e. AD) in aParis whole-population birth cohort during thefirst 12 months of life. Males were more affectedby most of these disorders and repeated episodesof wheezing were associated with sleep and dailyactivity disturbances as well as with other bron-chial obstructive symptoms. Using the originalPAM method we showed two wheezing pheno-types during infancy, one including all cases ofdyspnoea with sleep disturbance and the otherwhere all infants experienced nocturnal drycough. The two identified groups differed signif-icantly with regard to respiratory infections,nasal problems, parental history of asthma andseason of birth.The study design was suitable for describing
very precisely the inception and chronology ofrespiratory and allergic manifestations during thefirst year of life. Thanks to repeated question-
10Fig. 2. Classification of bron-chial obstructive symptoms inthree groups (G0, G1, G2) for 1-yr-old infants taking part in theParis birth cohort study usingthe partitioning around medoidsmethod (n = 2632). For eachgroup, proportions of infantssuffering from various associa-tions of bronchial obstructivesymptoms are represented. Leg-end indicates the number ofbronchial obstructive symptoms(0 to 4) and the list of symptoms;AS, no symptom; IW, infrequentwheeze; RW, recurrent wheeze;SB, shortness of breath; DC, drycough at night; D, dyspnoeawith sleep disturbance).
LOW
RESOLUTIO
NCOLOUR
FIG
Bronchial obstructive phenotypes in Paris cohort infants
5
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657
naires, we were able to collect detailed informa-tion on the occurrence of respiratory and allergicmanifestations. Most questions were derivedfrom international standardized tools (AMICSand ISAAC questionnaires). Health data wereprospectively recorded at frequent intervals sothat the risk of recall bias was limited.The PAM method allowed us to distinguish
three separate groups of infants. The method is amore robust version of the well-known K-means,normally used in classification of numerical data:it operates on a dissimilarity matrix, instead of adistance matrix, in that it minimizes a sum ofdissimilarities instead of a sum of squaredEuclidean distances. Similar findings were ob-tained whether medoids were specified or not,suggesting a good discrimination between thethree groups, especially for G2, including allcases of dyspnoea with sleep disturbance and G1,in which all the infants experienced nocturnal drycough.Respiratory infections appeared to be very
common in our infants and to mainly occurduring fall and winter, when there are more viral
epidemics. Our observations are consistent withprevious studies with regard to the LRTI inci-dence rates (10) and also with regard to thehigher risk of LRTI for boys (11, 12). Thisanalysis clearly shows that respiratory infectionsare associated with most symptoms, especiallywheeze, as suggested by parental report. Ascompared with the G0 group, the occurrence ofLRTI, colds and symptoms indicative of rhino-conjunctivitis were the only factors that signifi-cantly discriminated the G2 group.Wheeze was experienced by 22% of our
infants, in line with the literature reportingwheeze prevalence in the first year of life varyingfrom 15% (13, 14) to 31% (15, 16). Boys were athigher risk of wheeze than girls, as previouslyshown (12). Wheeze was all the more disturbingand associated with other bronchial obstructivesymptoms as its frequency increased: this wasconfirmed by the partition in two clinical phe-notypes of bronchial obstruction. Thus, the G2group clustered infants with severe bronchialobstructive manifestations; all had suffered froma dyspnoea severe enough to perturb their sleep,
Table 3. Adjusted odds ratios of belonging to G1 or G2 groups when compared with G0 group by infant characteristics at 1 yr of age in the Paris birth cohort study
(n = 2616)
Characteristics
G0 group* (reference group),
1786/2632 (67.8%) G1 group,� 228/2632 (8.7%) G2 group,� 618/2632 (23.5%)
n (%) or mean (SD) n (%) or mean (SD) OR (95% CI) n (%) or mean (SD) OR (95% CI)
Gender
Female 861 (48.2) 121 (53.1) 1 292 (47.3) 1
Male 925 (51.8) 107 (46.9) 0.78 (0.58–1.04) 326 (52.8) 1.03 (0.84–1.25)
Anthropometric measures
Birth weight (+1 kg) 3.407 (0.396) 3.379 (0.406) 0.82 (0.50–1.33) 3.381 (0.390) 0.96 (0.70–1.33)
Birth height (+1 cm) 50.3 (1.9) 50.2 (2.1) 1.02 (0.92–1.13) 50.1 (2.0) 0.96 (0.90–1.02)
Parity
1 1031 (57.7) 142 (62.3) 1 337 (54.6) 1
‡2 755 (42.3) 86 (37.7) 0.77 (0.57–1.03) 280 (45.4) 0.98 (0.81–1.19)
Parental asthma
No 1447 (81.4) 173 (75.9) 1 498 (80.7) 1
One parent 315 (17.7) 49 (21.5) 1.20 (0.85–1.70) 113 (18.3) 0.99 (0.77–1.27)
Two parents 16 (0.9) 6 (2.6) 3.03 (1.13–8.14) 6 (1.0) 0.94 (0.35–2.52)
Season of birth
Autumn–winter 898 (50.3) 82 (36.0) 1 304 (49.2) 1
Spring–summer 888 (49.7) 146 (64.0) 1.63 (1.22–2.19) 314 (50.8) 0.95 (0.79–1.15)
Lower respiratory infections (+1) 0.6 (1.1) 1.0 (1.4) 1.23 (1.10–1.37) 1.2 (1.6) 1.35 (1.25–1.45)
Ear infections (+1) 0.8 (1.4) 1.1 (1.6) 1.09 (1.00–1.10) 1.1 (1.6) 1.05 (0.98–1.12)
Colds (+1) 3.1 (2.2) 3.5 (2.6) 1.03 (0.97–1.10) 3.9 (2.4) 1.11 (1.06–1.16)
Eczema
No 1484 (83.1) 186 (81.6) 1 495 (80.1) 1
Yes 302 (16.9) 42 (18.4) 0.98 (0.68–1.42) 123 (19.9) 1.08 (0.84–1.38)
Rhino-conjunctivitis-like symptoms
No 1702 (95.3) 184 (80.7) 1 537 (86.9) 1
Yes 84 (4.7) 44 (19.3) 4.41 (2.94–6.63) 81 (13.1) 2.56 (1.83–3.57)
*Asymptomatic infants belonged to the G0 group.
�All infants of the G1 group had nocturnal dry cough.
�All infants having dyspnoea with sleep disturbance were placed in the G2 group.
Clarisse et al.
6
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657
and half of them had experienced wheeze, noc-turnal dry cough and/or shortness of breath inaddition. Consequently, infants placed in the G2group would be at higher risk of asthma later inlife.The second clinical phenotype is characterized
by a nocturnal dry cough reported for all theinfants of the G1 group, one-third of themhaving experienced wheeze in addition. A par-ticular profile of these children was revealed bymultivariate analysis. First, the G1 group waspartitioned on parental history of asthma.Parental inheritance was previously demon-strated among older children. In the Danishbirth cohort (17), parental asthma thusincreased the incidence of wheeze before18 months of age. Although we could not showsuch an association, the Avon longitudinalstudy (ALSPAC) team (18) noted a 1.6increased risk of wheeze before 3.5 yr of agefor children born to asthmatic mothers. Simi-larly, in the Oslo birth cohort, bronchialobstruction at age 2 yr and asthma at age 4 yrwere strongly linked to maternal asthma (19).As for the association with symptoms evocativeof rhino-conjunctivitis, it was much strongerthan the one observed for the G2 group.Moreover, as colds discriminated the G2 groupbut not the G1 group, symptoms suggestive ofrhino-conjunctivitis could clearly represent aspecific phenotype, possibly allergic. These find-ings therefore argue for taking into accountthese nasal problems, distinct from colds, assoon as from infancy (20). Our follow up showsthat symptoms indicative of rhino-conjunctivitisexist in almost 8% of infants as early as in thefirst year of life. In the literature, prevalence ofrhino-conjunctivitis in infancy varied from29.1% (4) to 0% (21). The discrepanciesbetween the figures resulted from heterogeneousdefinitions, sometimes very strict – includingrepeated episodes of rhinitis or conjunctivitisafter exposure to a particular allergen andunrelated to infection (21) or even associatedwith a positive skin prick test (22) – andsometimes, conversely,6 very large (4, 14). Ourdefinition was intermediate, as it accounted forconjunctive symptoms whether associated withallergen exposure or not. Finally, the discrimi-native power of symptoms suggestive of rhino-conjunctivitis for both the G1 and G2 groupscould illustrate the bronchial and nasal epithe-lial hyper-reactivity speculated in the hypothesisof united airway diseases (23). G1 infants weremore likely to be born during spring andsummer, when there is more exposure to pollen.The role of birth season is poorly documented
and was mainly tested on wheeze and asthma,leading to controversial results. In the UK, noimpact of birth season on asthma before age1 yr was observed in the Isle of Wight study(24), whereas the ALSPAC infants bornbetween April and December were at higherrisk of early wheezing as compared with theirpairs7 born during January to March period (18).Finally, a parental history of asthma, symptomsindicative of rhino-conjunctivitis and birth dur-ing spring or summer were obviously morefrequent in the G1 group, which should be morelikely to develop allergy.Atopic dermatitis was the main reported
allergic manifestation during infancy, beingexperienced by 17.9% of our infants as previ-ously observed (13, 21, 25–28), most of thembeing males (27, 29, 30). AD occurred very earlyin life (17, 26), and is often considered as theinitial clinical manifestation of an atopic consti-tution while the presence of wheezing is usually amarker for bronchial hyper-reactivity (26). Weobserved that AD preceded wheeze as soon as inthe first year of life, which could be consistentwith the allergic march8 described among childrenfollowed up for a longer period (31). Althoughwe noted a positive association between AD andwheeze (p = 0.06) as reported elsewhere (17, 29),
9AD could not discriminate our groups. But whiletesting if wheezing and AD represent differentphenotypes, Linneberg et al. (17) noted somedifferential effects of risk factors on each symp-tom, emphasizing that these phenotypes have adifferent aetiology.Finally, the robust PAM method enabled us to
partition our population into three groupsaccording to the occurrence of bronchial obstruc-tive symptoms. Apart from asymptomaticinfants, we identified two different clinical phe-notypes: the G2 group included all infantssuffering from dyspnoea with sleep disturbance,and the G1 group included all infants who hadnocturnal dry cough. Infants of the G2 grouphad significantly higher rates of respiratoryevents and could represent future asthmaticchildren. As a parental history of asthma, symp-toms suggestive of rhino-conjunctivitis, and birthduring spring and summer clearly differentiatedthe G1 group, it is possible that these childrencould have an allergic profile later in life. As aconsequence, these two specific groups of infantsdeserve to be followed up very carefully, as theyare expected to develop asthmatic or allergicphenotypes, and will probably be more suscep-tible to environmental and behavioural riskfactors. Further analysis of our birth cohort willaim to test these hypotheses.
Bronchial obstructive phenotypes in Paris cohort infants
7
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657
AcknowledgmentsThis study was supported by a grant from the FrenchHealth Ministry within the context of the PRIMEQUALresearch project, carried out by the French Ministry incharge of the Environment. This survey is supported by theParis council, within its Social, Childhood and HealthDirection (DASES). We express gratitude to the Parismaternity hospitals, especially Tenon, Rothschild, Necker,Pitie-Salpetriere and the Institut Mutualiste Montsourishospital for their welcome during newborn enrolment.We are grateful to the administrative staff, Chrystele
Grouas, Dominique Viguier, Isabelle Folmer, and LeilaBlusseau for their involvement in the Paris cohort study, aswell as to Nancy Keufer and Catherine Fillol for theenrolment of infants. We would like to thank all parents andchildren who participated in the Paris study.
References
1. Kuehni CE, Davis A, Brooke AM, Silverman M. Areall wheezing disorders in very young (preschool) chil-dren increasing in prevalence? Lancet 2001: 357: 1821–5.
2. Asher M. Worldwide variations in the prevalence ofasthma symptoms: the International Study of Asthmaand Allergies in Childhood (ISAAC). Eur Respir J 1998:12: 315–35.
3. Asher MI, Montefort S, Bjorksten B, et al. World-wide time trends in the prevalence of symptoms ofasthma, allergic rhinoconjunctivitis, and eczema inchildhood: ISAAC Phases One and Three repeat mul-ticountry cross-sectional surveys. Lancet 2006: 368:733–43.
4. Martinez FD,Wright AL, Taussig LM,Holberg CJ,HalonenM,MorganWJ. Asthma and wheezing in thefirst six years of life. The Group Health Medical Asso-ciates. N Engl J Med 1995: 332: 133–8.
5. Dodge R, Martinez FD, Cline MG, Lebowitz MD,Burrows B. Early childhood respiratory symptoms andthe subsequent diagnosis of asthma. J Allergy ClinImmunol 1996: 98: 48–54.
6. Clarisse B, Nikasinovic L, Poinsard R, Just J,Momas I. The Paris prospective birth cohort study:Which design and who participates? Eur J Epidemiol2007: ???: ???.
7. Sunyer J, Puig C, Torrent M, et al. Nitrogen dioxideis not associated with respiratory infection during thefirst year of life. Int J Epidemiol 2004: 33: 116–20.
8. Kaufman L, Rousseeuw PJ. Finding Groups in Data:An Introduction to Cluster Analysis – Wiley Series inProbability and Mathematical Statistics – AppliedProbability and Statistics. New York: Wiley, 1990.
9. Gower JC. A general coefficient of similarity and someof its properties. Biometrics 1971: 27: 857–72.
10. Park JH, Gold DR, Spiegelman DL, Burge HA,Milton DK. House dust endotoxin and wheeze in thefirst year of life. Am J Respir Crit Care Med 2001: 163:322–8.
11. Koopman LP, Smit HA, Heijnen ML, et al. Respira-tory infections in infants: interaction of parental allergy,child care, and siblings – The PIAMA study. Pediatrics2001: 108: 943–8.
12. Marbury MC, Maldonado G, Waller L. The indoorair and children�s health study: methods and incidencerates. Epidemiology 1996: 7: 166–74.
13. Gehring U, Bolte G, Borte M, et al. Exposureto endotoxin decreases the risk of atopic eczema in
infancy: a cohort study. J Allergy Clin Immunol 2001:108: 847–54.
14. Gehring U, Cyrys J, Sedlmeir G, et al. Traffic-relatedair pollution and respiratory health during the first 2 yrsof life. Eur Respir J 2002: 19: 690–8.
15. Linehan MF, Hazell ML, Frank TL, Frank PI.Prevalence of respiratory symptoms in under 5s: 1993 to2001. Arch Dis Child 2005: 90: 516–9.
16. Lopez N, de Barros-Mazon S, Vilela MM, CondinoNeto A, Ribeiro JD. Are immunoglobulin E levelsassociated with early wheezing? A prospective study inBrazilian infants. Eur Respir J 2002: 20: 640–5.
17. Linneberg A, Simonsen JB, Petersen J, StensballeLG, Benn CS. Differential effects of risk factors oninfant wheeze and atopic dermatitis emphasize a differ-ent etiology. J Allergy Clin Immunol 2006: 117: 184–9.
18. Sherriff A, Peters TJ, Henderson J, Strachan D.Risk factor associations with wheezing patterns inchildren followed longitudinally from birth to 3(1/2)years. Int J Epidemiol 2001: 30: 1473–84.
19. Jaakkola JJ, Nafstad P, Magnus P. Environmentaltobacco smoke, parental atopy, and childhood asthma.Environ Health Perspect 2001: 109: 579–82.
20. Sole D, Camelo-Nunes IC, Wandalsen GF, Melo
KC, Naspitz CK. Is rhinitis alone or associated withatopic eczema a risk factor for severe asthma in chil-dren? Pediatr Allergy Immunol 2005: 16: 121–5.
21. Vasar M, Julge K, Bjoksto B. Development of atopicsensitization and allergic diseases in early childhood.Acta Paediatr 2000: 89: 523–7.
22. Biagini JM, LeMasters GK, Ryan PH, et al. Envi-ronmental risk factors of rhinitis in early infancy.Pediatr Allergy Immunol 2006: 17: 278–84.
23. Grossman J. One airway, one disease. Chest 1997: 111:11S–6S.
24. Arshad SH, Hide DW. Effect of environmental factorson the development of allergic disorders in infancy.J Allergy Clin Immunol 1992: 90: 235–41.
25. Dunlop AL, Reichrtova E, Palcovicova L, et al.Environmental and dietary risk factors for infantileatopic eczema among a Slovak birth cohort. PediatrAllergy Immunol 2006: 17: 103–11.
26. Illi S, von Mutius E, Lau S, et al. The natural courseof atopic dermatitis from birth to age 7 years and theassociation with asthma. J Allergy Clin Immunol 2004:113: 925–31.
27. Moore MM, Rifas-Shiman SL, Rich-Edwards JW,et al. Perinatal predictors of atopic dermatitis occurringin the first six months of life. Pediatrics 2004: 113: 468–74.
28. Rothenbacher D, Weyermann M, Beermann C,Brenner H. Breastfeeding, soluble CD14 concentrationin breast milk and risk of atopic dermatitis and asthmain early childhood: birth cohort study. Clin Exp Allergy2005: 35: 1014–21.
29. Bohme M, Lannero E, Wickman M, Nordvall SL,Wahlgren CF. Atopic dermatitis and concomitantdisease patterns in children up to two years of age. ActaDerm Venereol 2002: 82: 98–103.
30. Hagendorens MM, Bridts CH, Lauwers K, et al.Perinatal risk factors for sensitization, atopic dermatitisand wheezing during the first year of life (PIPO study).Clin Exp Allergy 2005: 35: 733–40.
31. Spergel JM, Paller AS. Atopic dermatitis and theatopic march. J Allergy Clin Immunol 2003: 112: S118–27.
Clarisse et al.
8
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657
Author Query Form
Journal: PAI
Article: 743
Dear Author,During the copy-editing of your paper, the following queries arose. Please respond to these by markingup your proofs with the necessary changes/additions. Please write your answers on the query sheet ifthere is insufficient space on the page proofs. Please write clearly and follow the conventions shown onthe attached corrections sheet. If returning the proof by fax do not write too close to the paper’s edge.Please remember that illegible mark-ups may delay publication.
Many thanks for your assistance.
Queryreference
Query Remarks
1 Production Editor: Please supply accepted date.
2 Au: Please define: ‘AMICS�
3 Au: Please check: ‘intermediate� or ‘middle class�
4 Au: Please check: ‘their pairs�
5 Au: Please be clear: ‘with their pairs�
6 Au: Please check and use the correct term: ‘very large�
7 Au: Please be clear: ‘with their pairs�
8 Au: Please check: ‘allergic march�
9 Au: Please check: ‘AD could not discriminate our groups� or ‘the groupscould not be discriminated on the basis of AD�
10 Au: Figure 2 has supplied as Low Resolution images. Please supply highresolution images. For guidelines on electronic graphics, please see http://www.blackwellpublishing.com/bauthors/illustratio ns.asp
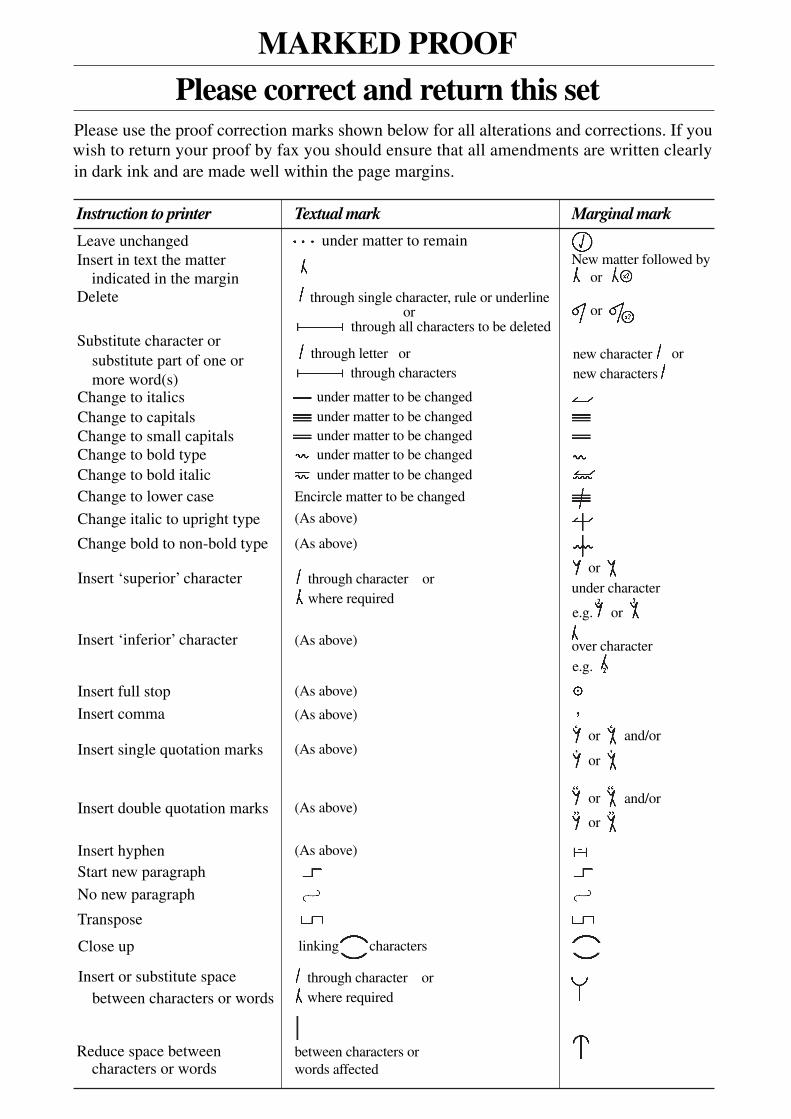
MARKED PROOF
Please correct and return this set
Instruction to printer
Leave unchanged under matter to remain
through single character, rule or underline
New matter followed by
or
or
or
or
or
or
or
or
or
and/or
and/or
e.g.
e.g.
under character
over character
new character
new characters
through all characters to be deleted
through letter or
through characters
under matter to be changed
under matter to be changed
under matter to be changed
under matter to be changed
under matter to be changed
Encircle matter to be changed
(As above)
(As above)
(As above)
(As above)
(As above)
(As above)
(As above)
(As above)
linking characters
through character or
where required
between characters or
words affected
through character or
where required
or
indicated in the margin
Delete
Substitute character or
substitute part of one or
more word(s)Change to italics
Change to capitals
Change to small capitals
Change to bold type
Change to bold italic
Change to lower case
Change italic to upright type
Change bold to non-bold type
Insert ‘superior’ character
Insert ‘inferior’ character
Insert full stop
Insert comma
Insert single quotation marks
Insert double quotation marks
Insert hyphen
Start new paragraph
No new paragraph
Transpose
Close up
Insert or substitute space
between characters or words
Reduce space betweencharacters or words
Insert in text the matter
Textual mark Marginal mark
Please use the proof correction marks shown below for all alterations and corrections. If you
in dark ink and are made well within the page margins.
wish to return your proof by fax you should ensure that all amendments are written clearly
Copyright © 2022 FDOKUMEN




















