
The characteristics of unacceptable/taboo thoughts in obsessive–compulsive disorder
Upload
independentCategory
view
0download
0
FEATURE REVIEW
Obsessive-compulsive disorder phenotypes: implicationsfor genetic studiesEC Miguel1, JF Leckman2, S Rauch3, MC do Rosario-Campos1, AG Hounie1, MT Mercadante1,4,5,
P Chacon1 and DL Pauls3,4
1Department of Psychiatry, University of Sao Paulo Medical School, Sao Paulo, SP, Brazil; 2Child Study Center, Yale UniversitySchool of Medicine, New Haven, CT, USA; 3Psychiatric Unit, Massachusetts General Hospital, Harvard Medical School, USA;4Neurodevelopmental Genetics Unit, Massachusetts General Hospital, Harvard Medical School, Charlestown, MA, USA;5Pervasive Development Disorder Program, Mackenzie Presbyterian University, Sao Paulo, SP, Brazil
Obsessive-compulsive disorder (OCD) clinical presentation is remarkably diverse, and canvary both within and across patients over time. This variability in the phenotypic expressionhas led to the hypothesis that OCD is a heterogeneous disorder and that this heterogeneityobscures the findings of clinical, natural history and treatment response studies andcomplicates the search for vulnerability genes. A complete understanding of what comprisesOCD and the underlying etiological mechanisms will require a dramatic change in how thedisorder is conceptualized. In this review, several different approaches that may represent thefirst steps in this reconceptualization are discussed. These approaches include (1) narrowingthe phenotype to identify categorically defined more homogeneous and mutually exclusivesubtypes of OCD, (2) considering OC symptom dimensions as quantitative components of themore complex OCD phenotype and (3) broadening the phenotype to include other etiologicallyrelated conditions. A combined dimensional approach within distinctive subgroups isproposed as probably the most effective in helping to identify the heritable components ofOCD. By identifying heritable components of OCD, it should be possible to find genes for theseseparate components. The review continues with the illustration of the possible role of someepigenetic risk and protective factors in the OCD presentation and the relevance of examiningassociated traits and/or endophenotypes to enhance our ability to understand the geneticbasis of OCD. To conclude, we discuss the variability in treatment outcome and thesignificance of the development of specific pharmacological and/or behavioral basedtherapies tailored to each of these phenotypes.Molecular Psychiatry (2005) 10, 258–275. doi:10.1038/sj.mp.4001617Published online 21 December 2004
Keywords: obsessive-compulsive disorder; obsessive behaviors; compulsive behaviors;genetics; molecular genetics
Obsessive-compulsive disorder (OCD) is a chronic,neuropsychiatric disorder that affects approximately2% of the world population and significantly inter-feres with social, family and work functioning.1
OCD is characterized by intrusive unwantedthoughts, fears or images (obsessions) and/or ritualizedbehaviors or mental acts (compulsions), generallyperformed to relieve the anxiety and/or distress causedby the obsessions.2 The DSM IV2 criteria for OCD havebeen shown to be reliable and well replicated amongdifferent cultures. However, the current concept,adopted by DSM-IV2 and ICD-10,3 of defining OCD asa unitary nosological entity may be misleading. In fact,obsessive-compulsive (OC) symptoms are remarkably
diverse, and the clinical presentation can vary bothwithin and across patients over time.4
This variability in the phenotypic expression hasled to the hypothesis that OCD is a heterogeneousdisorder and that this heterogeneity obscures thefindings of clinical, natural history and treatmentresponse studies and complicates the search forvulnerability genes.
Success in refining the measurement of OC pheno-types is likely to lead to greater clarity concerningcourse, treatment strategies and outcome. Likewise, abetter description of clinical phenotypes shouldfacilitate genetic, neurobiological, environmentaland treatment response studies. In fact, dissectingthe phenotype into less complex components may bean important tool for the identification of suscept-ibility genes for OCD.
The main objective of this paper is to summarizethe available data describing the clinical heterogene-ity of OCD and review the studies that suggest that
Received 01 September 2004; revised 27 September 2004;accepted 29 September 2004
Correspondence: Prefessor EC Miguel, MD, PhD, Department ofPsychiatry, University of Sao Paulo Medical School, Rua Dr.Ovıdio Pires de Campos, s/n, 05403-010, Sao Paulo, SP, Brazil.E-mail: [email protected]
Molecular Psychiatry (2005) 10, 258–275& 2005 Nature Publishing Group All rights reserved 1359-4184/05 $30.00
www.nature.com/mp

this clinical heterogeneity may be due to an under-lying genetic heterogeneity. Furthermore, differentstrategies (including both categorical and dimen-sional approaches) of phenotype description will bediscussed. The review continues with the illustrationof the possible role of some epigenetic risk andprotective factors in the OCD presentation. Specifi-cally, data regarding streptococcal infection andrheumatic fever (RF) (given recent findings suggestingtheir association with OCD) will be summarized. Wehypothesize that these and other as yet unidentifiedepigenetic factors are likely to be etiologicallyimportant and that the illnesses currently identifiedas OCD are most likely the result of complexinteractions between genes and environment overthe course of brain development.
The paper proceeds with a discussion of therelevance of examining associated traits and/or en-dophenotypes for linkage and association studies andof the likelihood that they will enhance our ability tounderstand the genetic basis of OCD. The rationale forthe use of endophenotypes, which are traits associatedwith specific conditions but not including any aspectof the clinical manifestation of the syndrome understudy, is based on the assumption that the number ofgenes required to produce variations in OCD traits maybe fewer than those involved in producing the OCDdiagnosis.5 In addition, these intermediate phenotypescould be less influenced by environmental factors andbe a better way to define affected and nonaffectedindividuals in a given family.
To conclude, we discuss the variability in treatmentoutcome as additional evidence of OCD heterogeneityand propose a combined dimensional conceptualiza-tion within distinct subgroups as probably the mosteffective means of identifying the heritable compo-nents of OCD as well as new treatment strategies.
Brief overview of genetic studies of OCDThe results from twin and family studies suggest thattransmission and expression of OCD and lesserphenotypes are genetically mediated.6–8 Furthermore,there may be an ‘OCD spectrum’ of related disordersthat share some of the same vulnerability genes.While the extent of this spectrum remains unknown,there are some compelling data supporting the geneticassociation between OCD and disorders such as Gillesde la Tourette syndrome (TS), body dysmorphicdisorder (BDD) and grooming behaviors.6,9,10 Addi-tional studies also suggest (see below) that obsessive-compulsive personality disorder (OCPD), currentlyconceived as a personality disorder, is also potentiallya condition within the OCD spectrum.11
Patterns of transmission within families are con-sistent with genetic transmission, although segrega-tion analyses of OCD family data7,12–14 have yieldeddivergent results. Some studies are consistent with asimple Mendelian mode of transmission, while otherssuggest a more complex pattern of transmission that
may be due to multifactorial components that arelikely present in the expression of OCD.7
Molecular genetic research in OCD has been largelylimited to candidate gene studies.15 The majority ofstudies conducted to date have focused on genesimportant in the serotonin and dopaminergic neuro-transmitter systems due to the efficacy of serotoninreuptake inhibitors (SRIs) and dopamine antagonistsin the treatment of OCD patients.16–18
In summary, even though the genetic transmissionof OCD is indisputable, the mode of transmission andthe genes involved are still unknown. A majordifficulty in genetic studies of complex disorderssuch as OCD has been sample heterogeneity. There-fore, it is believed that the identification of subgroupsthat are genetically valid is extremely important forOCD research.
Strategies for identifying valid OCD phenotypes
Several strategies have been employed in the searchfor more homogeneous phenotypes, and some of thesestudies will be presented below.
The categorical approach: the identification ofhomogeneous and mutually exclusive subgroupsThe categorical approach describes specific clinicaland phenomenological characteristics of OCD inorder to identify those that may be associated withan independent pattern of inheritance. The rationalefor this approach is that elucidation of specifichomogeneous subgroups might lead to the identifica-tion of a subtype of OCD that is distinctivelytransmitted within families and might be due tounique genetic factors that could be more easilyidentified with genetic linkage studies.
Some clinical and phenomenological characteris-tics have been shown to be related to familial risk andthus could represent different OCD subtypes. Amongthese are age at onset of OC symptoms, comorbiditywith tic disorders and higher frequencies of sensoryphenomena associated with compulsions.
Early-onset OCD phenotypeAlthough DSM-IV and ICD-10 use the same diagnosticcriteria for children and adults, recent studies havesuggested that age at onset of OC symptoms is animportant factor in subtyping OCD, and that childrenwith OCD as well as adults with an early onset of theirsymptoms may represent a more etiologically homo-geneous subset of patients.19–22
This hypothesis was emphasized in clinical studiesreporting that OCD age of onset is bimodal. Beforepuberty, there is a peak among male patients.19,20,23
During adolescence, there is an increase in thenumber of girls diagnosed with OCD, reaching a 1 : 1sex ratio in adulthood.24
As in adult patients,22,25 high rates of comorbidityare seen in children and adolescents with OCD, andsome studies report that 90% of patients in their OCDsamples had at least one other neuropsychiatric
Obsessive-compulsive disorder phenotypesEC Miguel et al
259
Molecular Psychiatry

diagnosis.26 Even though other disorders, such asdepression, simple phobias, separation anxiety anddisruptive behavior disorders, are also very fre-quent,27 the association with tics is the most striking.In studies of children with OCD, it has been reportedthat 20–59% have tics.28 Similarly, 48% of early-onsetOCD patients presented tics or TS, compared to 10%of OCD subjects with a later onset.21
Some of the most frequent findings described inearly-onset patients (both children and adults) arepresented in Table 1.
In a recent study, Diniz et al22 examined therelationship between comorbidity patterns and ageat onset, as well as illness duration, in adult OCDpatients. These investigators found that an earlier ageat onset of OC symptoms was associated with ticdisorders, whereas longer illness duration was asso-ciated with depressive disorder and social phobia.22
There have been few studies incorporating age atonset into neurobiological investigations of OCD.Busatto et al,34 using regional cerebral blood flow(rCBF) SPECT, found that early-onset patients showeddecreased rCBF in the right thalamus, left anteriorcingulate cortex and bilateral inferior prefrontal cortex,as well as increased rCBF in the right cerebellum.Moreover, OC symptom severity was positively corre-lated with left orbitofrontal rCBF in early-onset patients.
Studies with adult patients have suggested that anearly age of onset may be a predictor of poorresponse to treatment with clomipramine or other
SRIs,21,35,36 although other studies found no suchrelationship.37,38
Age at onset also appears to be related to differ-ential familial recurrence risk of OCD.6,7,9 In a recentstudy of 106 families of children and adolescentswith OCD, Rosario-Campos et al32 studied 325 first-degree family members of childhood and adolescentOCD probands and 140 first-degree relatives of controlchildren and adolescents. The results from this studywere consistent with earlier reports from families ofadult OCD probands with early onset. The rates of OCDobserved among first-degree relatives were significantlyhigher than those seen in family studies of adult OCDprobands (see Table 2). The rate of OCD among caserelatives was 25.2 times higher than the rate amongcontrol relatives. Other interesting findings were asignificant positive correlation between the ages at onsetof OCD in case probands and their affected relatives anda significantly higher rate of TS and tics among caserelatives, when compared to control relatives (OR¼ 7.8).Interestingly, although the recurrence risks among caserelatives were high, only 57% of the probands had apositive family history of OCD or tics, reinforcing thehypothesis that OCD is in fact a genetically hetero-geneous condition. Some cases are familial (associatedor not to tics), and others have no family history.
To date, there have been no segregation analysescompleted on data from early-onset OCD families.Similarly, there is a paucity of molecular studiesperformed with samples composed of individualswith early-onset OCD (see Table 5). One associationstudy39 found significant differences between OCDsubjects and controls in genotype and allele frequen-cies of the A allele of the 5-HT2A receptor gene. Agenome-wide linkage analysis40 suggested evidencefor linkage on chromosome 9p. The same groupsequenced the LOD score peak region identified inthis genome scan and found no evidence for afunctional mutation in the SLC1A1 gene.41
In sum, the early-onset phenotype is characterizedby a male preponderance24,42, a higher frequency ofcompulsions not preceded by obsessions,19,21 highercomorbidity with tics and TS20,28 and worse responseto monotherapy treatment with clomipramine orSRI.21,35 Furthermore, the early-onset phenotype hasbeen associated with increased familial loading forOCD.6,7,30,32 Taken together, these data suggest that the
Table 1 Phenotypic features frequently described in early-onset OCD patients
Phenotypic features Study
Higher familial risk 28–33Fears of contamination, of harming oneselfor others, sexual obsessions, washing orcleaning, checking, repetition, symmetryobsessions and order/arranging rituals
33
Higher frequency of tic -like compulsions 21, 31Higher frequency of compulsions notpreceded by obsessions but sensoryphenomena; worse treatment response
21
Higher number of comorbidities 26Higher comorbidity with tic disorders 21–23, 26
Table 2 Comparison of prevalence rates of OCD and tic disorders (TSþ chronic motor and vocal tics) in family studies
Study Age of probands Morbid risk in relativesof late OCD probands
(age at onset 418)
Morbid risk in relatives ofearly-onset OCD (probands
with age at onset o18)
Morbid risk for ticdisorders in relatives of
OCD probands
6 Adults 8.772.9 10.771.6 4.671.07, 9 Adults 0.0* 13.8* 4.95**32 Children and
adolescents— 22.772.6 11.7
*Study 7.**Study 9.
Obsessive-compulsive disorder phenotypesEC Miguel et al
260
Molecular Psychiatry
early-onset OCD phenotype might represent a moregenetically homogeneous subgroup.
Tic-related OCD phenotypeClinical and epidemiological studies have shown thatapproximately 30% of OCD patients also have a ticdisorder (usually chronic tics or TS).43,44 Familystudies have shown not only higher rates of OCsymptoms and OCD in relatives of TS patients,45–51
but also higher rates of tics or TS in first-degreerelatives of OCD patients6,9,28,32 when compared tocontrols. These results suggest that at least someforms of OCD are etiologically related to TS and mighttherefore be variant expressions of the same genesthat are important for the expression of tics.
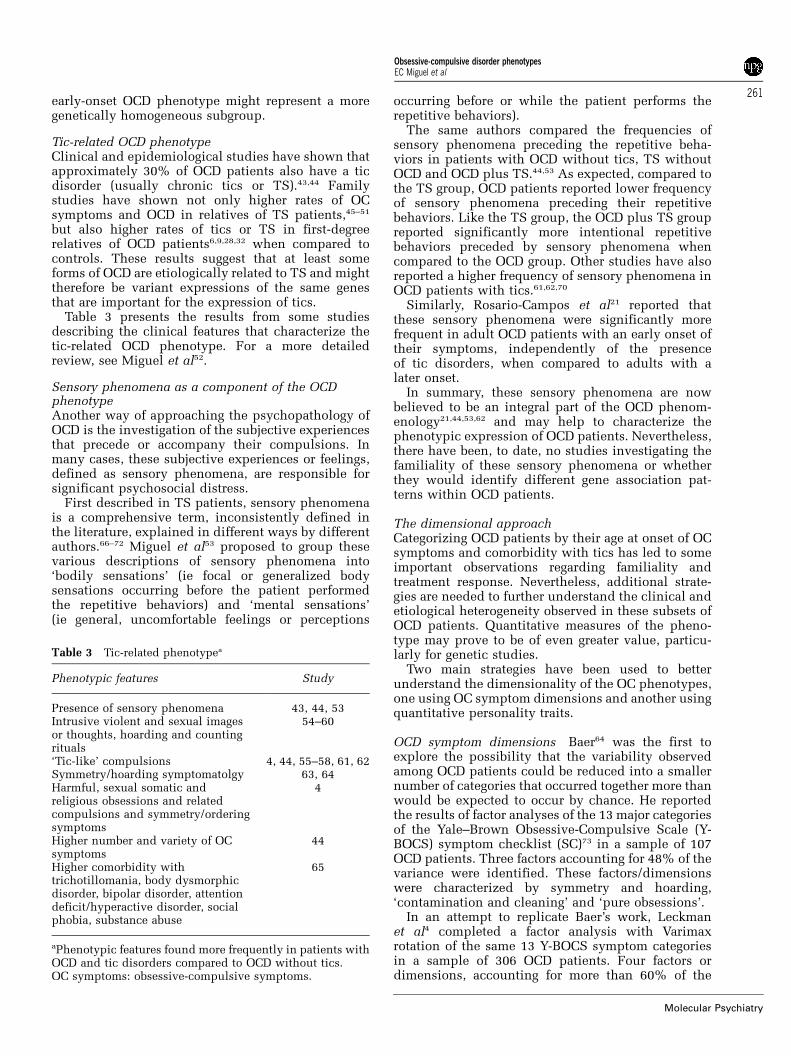
Table 3 presents the results from some studiesdescribing the clinical features that characterize thetic-related OCD phenotype. For a more detailedreview, see Miguel et al52.
Sensory phenomena as a component of the OCDphenotypeAnother way of approaching the psychopathology ofOCD is the investigation of the subjective experiencesthat precede or accompany their compulsions. Inmany cases, these subjective experiences or feelings,defined as sensory phenomena, are responsible forsignificant psychosocial distress.
First described in TS patients, sensory phenomenais a comprehensive term, inconsistently defined inthe literature, explained in different ways by differentauthors.66–72 Miguel et al53 proposed to group thesevarious descriptions of sensory phenomena into‘bodily sensations’ (ie focal or generalized bodysensations occurring before the patient performedthe repetitive behaviors) and ‘mental sensations’(ie general, uncomfortable feelings or perceptions
occurring before or while the patient performs therepetitive behaviors).
The same authors compared the frequencies ofsensory phenomena preceding the repetitive beha-viors in patients with OCD without tics, TS withoutOCD and OCD plus TS.44,53 As expected, compared tothe TS group, OCD patients reported lower frequencyof sensory phenomena preceding their repetitivebehaviors. Like the TS group, the OCD plus TS groupreported significantly more intentional repetitivebehaviors preceded by sensory phenomena whencompared to the OCD group. Other studies have alsoreported a higher frequency of sensory phenomena inOCD patients with tics.61,62,70
Similarly, Rosario-Campos et al21 reported thatthese sensory phenomena were significantly morefrequent in adult OCD patients with an early onset oftheir symptoms, independently of the presenceof tic disorders, when compared to adults with alater onset.
In summary, these sensory phenomena are nowbelieved to be an integral part of the OCD phenom-enology21,44,53,62 and may help to characterize thephenotypic expression of OCD patients. Nevertheless,there have been, to date, no studies investigating thefamiliality of these sensory phenomena or whetherthey would identify different gene association pat-terns within OCD patients.
The dimensional approachCategorizing OCD patients by their age at onset of OCsymptoms and comorbidity with tics has led to someimportant observations regarding familiality andtreatment response. Nevertheless, additional strate-gies are needed to further understand the clinical andetiological heterogeneity observed in these subsets ofOCD patients. Quantitative measures of the pheno-type may prove to be of even greater value, particu-larly for genetic studies.
Two main strategies have been used to betterunderstand the dimensionality of the OC phenotypes,one using OC symptom dimensions and another usingquantitative personality traits.
OCD symptom dimensions Baer64 was the first toexplore the possibility that the variability observedamong OCD patients could be reduced into a smallernumber of categories that occurred together more thanwould be expected to occur by chance. He reportedthe results of factor analyses of the 13 major categoriesof the Yale–Brown Obsessive-Compulsive Scale (Y-BOCS) symptom checklist (SC)73 in a sample of 107OCD patients. Three factors accounting for 48% of thevariance were identified. These factors/dimensionswere characterized by symmetry and hoarding,‘contamination and cleaning’ and ‘pure obsessions’.
In an attempt to replicate Baer’s work, Leckmanet al4 completed a factor analysis with Varimaxrotation of the same 13 Y-BOCS symptom categoriesin a sample of 306 OCD patients. Four factors ordimensions, accounting for more than 60% of the
Table 3 Tic-related phenotypea
Phenotypic features Study
Presence of sensory phenomena 43, 44, 53Intrusive violent and sexual imagesor thoughts, hoarding and countingrituals
54–60
‘Tic-like’ compulsions 4, 44, 55–58, 61, 62Symmetry/hoarding symptomatolgy 63, 64Harmful, sexual somatic andreligious obsessions and relatedcompulsions and symmetry/orderingsymptoms
4
Higher number and variety of OCsymptoms
44
Higher comorbidity withtrichotillomania, body dysmorphicdisorder, bipolar disorder, attentiondeficit/hyperactive disorder, socialphobia, substance abuse
65
aPhenotypic features found more frequently in patients withOCD and tic disorders compared to OCD without tics.OC symptoms: obsessive-compulsive symptoms.
Obsessive-compulsive disorder phenotypesEC Miguel et al
261
Molecular Psychiatry
variance, were identified. Factor I is characterized byaggressive, sexual, somatic and religious obsessions,as well as related compulsions. Factor II includessymmetry, ordering and counting, as well as arrangingobsessions and compulsions. Factor III involvescontamination obsessions and cleaning compulsions.Factor IV is characterized by hoarding obsessions andcompulsions. Of interest is the fact that high scores onfactors I and II were associated with a personal orfamily history of tics in these OCD patients.
To date, there have been 11 factor analysis studiespublished, assessing more than 2000 patients.4,63,64,74–82
In all of these studies, 3–5 OC factors or dimensionshave been identified, accounting for almost 70% ofthe variance.83
Additionally, there is a growing body of evidencefrom various fields suggesting that these OCD symp-tom dimensions are valid and reliable constructs.As noted above, the factors identified in all studiesare fairly consistent4,63,76 and temporally stable.77
In addition, these factors have been shown to becorrelated with a number of biometric vari-ables14,79,82,84–86 as well as with treatment re-sponse.63,77,85,87,89 Furthermore, recent neuroimagingstudies have provided additional support for thevalidity of these factors; different patterns of activa-tion have been observed for different OC symptomdimensions.90 In contrast, initial volumetric MRIstudies show only modest differences across symp-tom dimensions.
Alsobrook et al14 were the first to use OC symptomdimensions in a family/genetic study. They reportedthat the relatives of OCD probands who had highscores on either the factor characterized by aggres-sive/sexual/religious obsessions and related compul-sions or factors characterized by symmetry/ordering(factors I and II as described by Leckman et al4) weretwice as likely to have first-degree family memberswith OCD compared to individuals with low scoreson these factors.14
In a more recent study,82 the familiality of OCDsymptom dimensions was examined in a sample ofTS affected sibpairs from the Tourette SyndromeAssociation International Consortium for Genetics(TSAICG).91 Significant correlations were observedbetween sibpairs as well as mother–child pairs for theaggressive, sexual and religious obsessions andchecking compulsions factor, and for the symmetryand ordering obsessions and compulsions factor.Furthermore, the results from segregation analysesin this sample were consistent with dominant majorgene effects for the aggressive, sexual and religiousobsessions and checking compulsions factor, and forthe symmetry and ordering obsessions and compul-sions factor, and recessive major gene effects for thecontamination/cleaning factor and the hoarding ob-sessions and compulsions factor. It is not clearwhether these results will generalize to individualswith OCD who do not have TS, but the inclusion ofTS sibpairs is of heuristic value because the OCsymptoms observed in these families generally have
an early onset, and therefore are more likely to beetiologically homogeneous.
Using the same TSAICG data set, Zhang et al86
analyzed genotypic data from a genome scan usingthe hoarding factor as a quantitative phenotype.Significant allele sharing was observed for markersat 4q34–35, 5q35.2–35.3 and 17q25. The 4q site is inproximity to D4S1625, the marker that was identifiedby TSAICG as being in a genomic region withsuggestive linkage to the TS phenotype. The 17q sitehas also been implicated in some TS families. Thus,the 4p and 17q results could simply be coming fromlinkage to the TS phenotype and not represent aseparate locus for hoarding; however, the chromo-some 5 site has not been implicated in any other studyof TS and might suggest a separate locus for hoarding.
A recent case–control study in patients with ticsfound a significant association between the long/longhaplotype polymorphism of the promoter region ofthe serotonin transporter gene (5-HTTLPR) and highscores on the ‘repeating/counting’ factor, located onchromosome 17q11.1–12.79
In conclusion, the complex clinical presentation ofOCD can be summarized using a few consistent andtemporally stable symptom dimensions. These can beunderstood as a spectrum of potentially overlappingvulnerabilities that do not establish an absolute,qualitative break between ‘normal’ and ‘abnormal’,cutting across diagnostic boundaries. This character-istic of the dimensional approach is particularlyimportant for genetic studies, in which familymembers presenting with OC symptoms below thethreshold for a DSM-IV diagnosis should also beassessed and included in research studies.6,82
A dimensional approach is also not mutuallyexclusive of other methods, and may indeed encom-pass previous attempts of subdividing patients ac-cording to age at onset or comorbidity with tics.Indeed, the combined use of categorical and dimen-sional approaches is likely to offer the greatestpromise. In fact, the use of quantitative traits mayprovide a powerful approach to detect the geneticsusceptibility loci that contribute to OCD presenta-tions. Thus far, this approach has provided especiallypromising leads with regard to the hoarding OCphenotype. Although the dimensional structure ofOC symptoms is still imperfect, this quantitativeapproach to phenotypic traits has the potential toadvance our understanding of OCD and may aid inthe identification of more robust endophenotypes.
Quantitative personality traits related to OCD It hasbeen suggested that some patients may be vulnerableto OCD because of their affective disposition (egtemperament), which could ultimately contribute tothe expression of the condition. These individuals are‘abnormal’ only in degree, not in kind.92 For instance,a person who diverges to an extreme along theneuroticism dimension (which identifies thoseindividuals who tend to have intense emotions)would be expected to respond with a dysphoric
Obsessive-compulsive disorder phenotypesEC Miguel et al
262
Molecular Psychiatry

emotion such as anxiety or OC symptoms when facinga challenge that would not trouble a less affectivelyvulnerable individual.92
Recent family data suggest that there may be somerelationship between these personality dimensionsand OCD. Samuels et al11 reported that high neuroti-cism (measured by The Revised NEO PersonalityInventory developed by Costa and McCrae93), andOCPD were more frequent in relatives of OCD casescompared with relatives of controls.
Thus, these personality characteristics may share acommon familial etiology with OCD. It is possiblethat neuroticism, OCPD and OCD are alternativeexpressions of the same underlying vulnerability.Each of these phenotypes may represent a differentlevel of severity along a continuum, or additionalfactors may be necessary for differentiation into thespecific clinical phenomena. Alternatively, thesethree phenotypes could represent distinct geneticentities, one being a direct expression of the geneticvulnerability and the other emerging secondarily.11
It is important to note that the results frommolecular genetic studies suggest that there may besome genes that are associated with some of thesequantitative traits. The low-activity allele of thepromoter region of the serotonin transporter gene (5-HTTLPR) has been reported to be associated withneuroticism and harm avoidance in normal volun-teers.94,95 In another study, carriers of the same alleleexhibited higher scores for neuroticism and harmavoidance than noncarriers, although only within asubgroup of patients with avoidant, dependent andOCPD diagnosis and not among those with otherDSM-IV personality disorders.96
Broadening the OCD phenotype
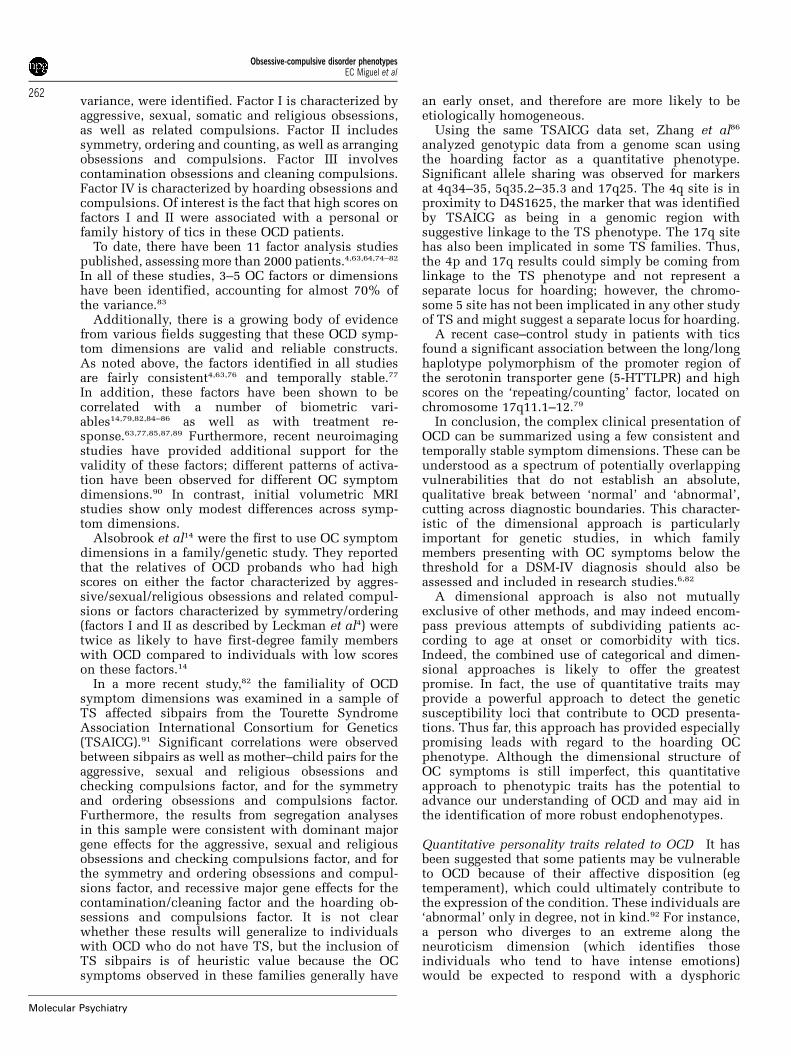
OCD and OCD spectrum disorders In contrast todisaggregating OCD into smaller quantitativecomponents, another strategy that could enhancethe probability of finding susceptibility genes forOCD would be the identification of other conditionsthat were etiologically related and due to the sameunderlying mechanisms. Thus, broadening thediagnostic boundaries could enhance the chance ofdetecting genes related to OCD. Several disordershave been proposed as part of an OCD spectrum ofdisorders because they have been observed morefrequently among relatives of OCD probands whencompared to controls (see Table 4).
Nestadt et al,101 using the latent class analysis anddata from previous studies of The Johns Hopkins OCDFamily Study Group, identified two subgroups: onecharacterized by panic disorder/agoraphobia (PD/AG)and tic disorders (TD) and another characterized bygeneralized anxiety disorder (GAD), recurrent majordepressive disorder (RMDD) and OCD spectrumdisorders (eg body dysmorphic disorder, eating dis-orders and grooming behaviors). Relatives of pro-bands in the second group were at greater risk forOCD and OCD-related comorbid diagnoses. Further-
more, age of onset was progressively lower for thosesubjects with more OCD-related comorbidity. Thegroup with PD/AG and TD presented a later age ofonset of OCD and tended to have lower familialloading.
Recently, Chacon et al102 elaborated on some ofthese conclusions and suggested that TD should alsobe included in the OCD spectrum disorders group.The rationale for this was based on data from previousclinical studies22,65 indicating an association betweenTD and other OCD spectrum disorders such as bodydysmorphic disorder and trichotillomania. Further-more, there are consistent findings suggesting anassociation between TD and early OCD age of onset inthe proband21 and higher familial risk for OCD in theirrelatives.6,32 In addition, these authors speculated thatone possible explanation for this divergence could bethe fact that the presence of TS was an exclusionarycriterion in the John Hopkins OCD Family Study.7
The different phenotypes expressed in this sub-group could reflect the interaction of the same geneticvulnerability factors modified by life events orenvironmental factors, consistent with the conceptof clinical heterogeneity.103 The second subgroupwould be characterized by the presence of separationanxiety and PD/AG and a lower genetic risk and laterage of onset.
Additional data suggest that hypochondria,104 at-tention-deficit/hyperactivity disorder65 and eatingdisorders105 should also be considered as part of theOCD spectrum disorders constellation. The proposedmodel is graphically represented in Figure 1.
OCD and other syndromes
As discussed above, phenomenological, clinical andfamily/genetic studies have yielded data suggestingthat a spectrum of behaviors is related to OCD andthat there may be common etiological factors im-portant for the expression of some components ofthese behaviors. To date, there have been fewmolecular genetic findings identifying specific sus-ceptibility genes for these phenotypes (see Table 5).However, recent studies showing that OC symptomsmay be associated with other syndromes couldprovide clues for the location of some susceptibilitygenes for OCD. For instance, some interesting find-ings have come from studies of idiopathic focaldystonia (IFD) and Prader–Willi syndrome (PWS).
Table 4 Neuropsychiatric disorders found more frequentlyin relatives of OCD probands
Disorders Studies
Tic disorders 6, 9, 32Depressive and anxiety disorders 97Trichotillomania, skin picking, onicophagia(grooming behaviors)
98
Body dysmorphic disorder 98, 99Idiopathic focal dystonia 100
Obsessive-compulsive disorder phenotypesEC Miguel et al
263
Molecular Psychiatry
Cavallaro et al100 reported the results of a familystudy with 76 IFD patients and 129 controls. Thepresence of OCD was higher in the patients with IFDcompared to controls (20 vs 0.77%). Nearly all IFDpatients with OCD showed poor insight and reducedegodystonia regarding OCD symptoms, which werelong standing. These investigators also found a highermorbid risk for OCD but only among family membersof probands of IFD plus OCD when compared tofamily members of probands of IFD without OCD andto controls. Since IFD is rare, the high frequency ofOCD in IFD reported suggests that a subgroup of IFD(IFD/OCD subgroup) has a higher probability ofsharing biological mechanisms for both IFD andOCD. A few different hereditary backgrounds havebeen suggested for several types of dystonia (muta-tions at DYT1, DYT6, DYT7 and DYT13—some of thegenes involved in dystonia). Candidate genes fordystonia could be tested in OCD patients.
PWS is a genetic disorder caused by an abnormalityin chromosome 15. Approximately 70% of casesresult from a paternally derived deletion at 15(q11–q13), whereas a maternal disomy is found in 30% ofcases. Interestingly, the disorder is manifested whenthe father is the parent transmitting the anomalousgene.106 Some OC symptoms, as well as OCD, havebeen described in PWS populations.106–108 Wigren andHansen108 reported that the compulsions found inPWS were more often related to insistence onsameness, external routines and repetition rituals.They also reported high comorbidity with trichotillo-mania and skin picking. A study by Dykens et al109
found almost the same pattern of OC symptoms, usingthe Y-BOCS symptoms: hoarding, ordering andarranging, just right compulsions, concern withsymmetry and exactness, and redoing things. Clarkeet al107 also found insistence on routines, hoardingand ordering objects and repetitive actions and
speech, pointing to the lack of more typical OCsymptoms such as cleaning, checking and countingrituals. Altogether, these data suggest that the me-chanisms underlying compulsions in PWS may besomewhat different from typical OCD. State et al110
compared subjects with PWS to subjects with PWS-like features but who lacked the PWS genotype (ie aphenocopy) and confirmed that OC symptoms weremore frequent in the former group, suggesting that OCsymptoms may be part of the phenotype related todeletions in chromosome 15.
Chromosome 15 has also been implicated inautism,111 a disorder in which compulsive featureshave also been described. The most common chro-mosomal abnormality reported to be associated withautism is a duplication of the 15q11–13 regions,although deletions have also been described. Thus,chromosome 15 could be a target of investigation inthe search for candidate regions of OCD genes.Hollander et al112 investigated relatives of 176 autisticprobands of 57 multiplex families and found thatprobands with high rates of repetitive behaviors weremore likely to have one or both parents with OCsymptoms or OCD than probands with low rates ofrepetitive behaviors.
In conclusion, broadening the diagnostic bound-aries of OCD represents another heuristic approach toenhance the chance of detecting genes related to OCD.Several psychiatric disorders were proposed as part ofan OCD spectrum of disorders because they have beenobserved more frequently among relatives of OCDprobands than among controls (Table 4). In familymembers of probands with some neurologic disorderssuch as IFD, OCD has also been reported. Thesefindings suggest that OCD may be better conceptua-lized from a genetic standpoint as a quantitative trait,whereby the same genes may predispose to a varietyof phenotypes. In addition, genes found relevant to
Figure 1 OCD and related disorders.
Obsessive-compulsive disorder phenotypesEC Miguel et al
264
Molecular Psychiatry
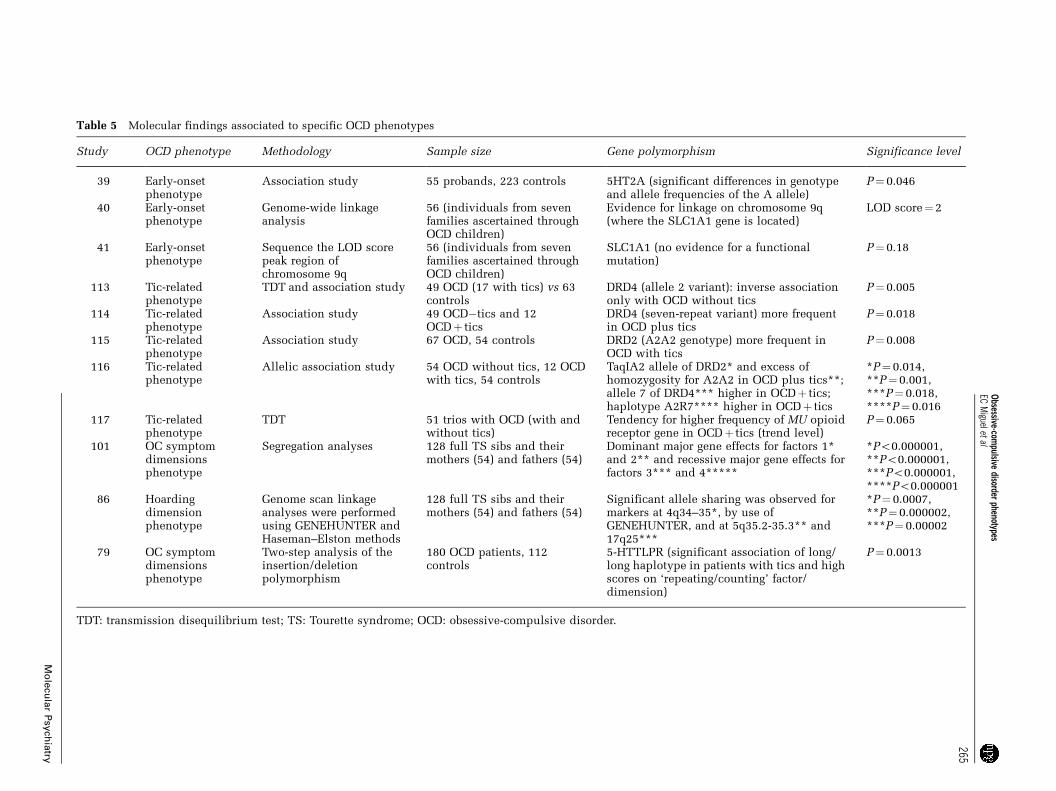
Table 5 Molecular findings associated to specific OCD phenotypes
Study OCD phenotype Methodology Sample size Gene polymorphism Significance level
39 Early-onsetphenotype
Association study 55 probands, 223 controls 5HT2A (significant differences in genotypeand allele frequencies of the A allele)
P¼ 0.046
40 Early-onsetphenotype
Genome-wide linkageanalysis
56 (individuals from sevenfamilies ascertained throughOCD children)
Evidence for linkage on chromosome 9q(where the SLC1A1 gene is located)
LOD score¼ 2
41 Early-onsetphenotype
Sequence the LOD scorepeak region ofchromosome 9q
56 (individuals from sevenfamilies ascertained throughOCD children)
SLC1A1 (no evidence for a functionalmutation)
P¼ 0.18
113 Tic-relatedphenotype
TDT and association study 49 OCD (17 with tics) vs 63controls
DRD4 (allele 2 variant): inverse associationonly with OCD without tics
P¼ 0.005
114 Tic-relatedphenotype
Association study 49 OCD�tics and 12OCDþ tics
DRD4 (seven-repeat variant) more frequentin OCD plus tics
P¼ 0.018
115 Tic-relatedphenotype
Association study 67 OCD, 54 controls DRD2 (A2A2 genotype) more frequent inOCD with tics
P¼ 0.008
116 Tic-relatedphenotype
Allelic association study 54 OCD without tics, 12 OCDwith tics, 54 controls
TaqIA2 allele of DRD2* and excess ofhomozygosity for A2A2 in OCD plus tics**;allele 7 of DRD4*** higher in OCDþ tics;haplotype A2R7**** higher in OCDþ tics
*P¼ 0.014,**P¼ 0.001,***P¼ 0.018,****P¼ 0.016
117 Tic-relatedphenotype
TDT 51 trios with OCD (with andwithout tics)
Tendency for higher frequency of MU opioidreceptor gene in OCDþ tics (trend level)
P¼ 0.065
101 OC symptomdimensionsphenotype
Segregation analyses 128 full TS sibs and theirmothers (54) and fathers (54)
Dominant major gene effects for factors 1*and 2** and recessive major gene effects forfactors 3*** and 4*****
*Po0.000001,**Po0.000001,***Po0.000001,****Po0.000001
86 Hoardingdimensionphenotype
Genome scan linkageanalyses were performedusing GENEHUNTER andHaseman–Elston methods
128 full TS sibs and theirmothers (54) and fathers (54)
Significant allele sharing was observed formarkers at 4q34–35*, by use ofGENEHUNTER, and at 5q35.2-35.3** and17q25***
*P¼ 0.0007,**P¼ 0.000002,***P¼ 0.00002
79 OC symptomdimensionsphenotype
Two-step analysis of theinsertion/deletionpolymorphism
180 OCD patients, 112controls
5-HTTLPR (significant association of long/long haplotype in patients with tics and highscores on ‘repeating/counting’ factor/dimension)
P¼ 0.0013
TDT: transmission disequilibrium test; TS: Tourette syndrome; OCD: obsessive-compulsive disorder.
Obsessive-com
pulsivedisorder
phenotypesEC
Miguelet
al
265
Mo
lecu
lar
Psy
chia
try

other neuropsychiatric disorders, such as thosedescribed above, could be targeted in future OCDmolecular studies.
Molecular findings associated with specific OCDphenotypesAs reported earlier, molecular studies in OCD havefocused mostly on candidate genes from the serotoninand dopaminergic system. Table 5 describes severalstudies showing molecular findings associated withsome of the subgroups presented above. Usually,initial results are received with great enthusiasm.However, most have not been successfully corrobo-rated via replication.
Environmental factors
Complex traits are most likely to be generated bycomplex interactions of environmental and experien-tial factors with a number of genes and their products.Even pivotal regulatory proteins of cellular path-ways and neurocircuits are most likely to have only avery modest impact, while noise from nongeneticmechanisms obstructs identification of relevantgene variants. Finally, epigenetic phenomena mightalso substantially contribute to the molecular biologyof behavior.118,119
Epigenetic risk and protective factorsTwin studies of OCD have consistently indicated thepresence of unique environmental factors associatedwith the expression of the syndrome.120,121 Limiteddata have been presented on a variety of risk factorsincluding pre- and perinatal adverse events, sex-specific hormonal factors, pregnancy and birth,psychosocial stressors and postinfectious immune-based factors. Additional longitudinal twin andsingleton studies are needed to explore developmen-tal trajectories within distinct subgroups of patientsand to determine whether significant new genetic andenvironmental effects and interactions emerge duringthe course of adolescence and adulthood.
For more than a quarter of a century, it has beenbelieved that perinatal factors play a role in OCD.122
There is some indication that perinatal difficultiesmight predispose to earlier onset of OCD in males123
and be associated with chronic tic disorders.124 Forexample, in one study of individuals with TS,delivery complications, especially forceps deliveries,were associated with OCD.124 Similarly, fetal expo-sure to relatively high levels of caffeine, nicotine oralcohol also predicted OCD in these same TSprobands.124
As mentioned above, males are more frequentlyaffected with early-onset OCD than are females. Whilethis could be due to genetic mechanisms, frequentmale-to-male transmission within families appears torule out the presence of an X-linked vulnerabilitygene. This observation has led to the hypothesis thatandrogenic steroids during critical periods in fetaldevelopment may play a role in the later development
of tic-related OCD.125 It has also led investigators totest the efficacy of antiandrogenic agents in treatingOCD. It is of interest that the selective androgenantagonist flutamide had a positive effect in oneOCDþTS patient.125 This finding, however, was notreplicated in a larger open study.126
Another interesting observation is that the rates ofOCD among new mothers is substantially higher thanrates among the population and vary from 11 to47%.127–131 Most of these cases begin during latepregnancy or a few days to 2 weeks after delivery andinvolve intrusive worries of the mother doing harm tothe newborn. Indeed, there are even anecdotal reportsthat new fathers may also be at increased risk.132 Theneurobiological basis for this phenomenon remains indoubt. One tenable hypothesis is that these changesinvolve possible alterations in the central oxytocinand serotonergic pathways.133,134 Others have specu-lated that the postpartum period may be a normalperiod of heightened sensitivity to threat that, evenamong normal parents, has features of OCD.135
The role of recent life events in influencing theonset and course of psychiatric disorders has beenwidely examined, and OCD has long been identifiedas a ‘stress-sensitive’ condition. However, only a fewstudies have investigated the occurrence of stressfulor potentially triggering events in the history ofindividuals with OCD.127–129,131,136,137 Frequentlyreported precipitants include a recent move, sexualor marital problems and the illness or death of a nearrelative.127–129 However, these studies have methodo-logical weaknesses such as assessment of eventoccurrence without reliable and valid schedules,investigation of ill-defined premorbid study periodsand absence of comparison groups. Neverthe-less, most controlled studies have shown similareffects.136,137 Preliminary work also suggests a rele-vant relationship between the expression of symp-toms of OCD and post-traumatic stress disorder(PTSD). For instance, Gershuny et al,138 in a caseseries, reported that symptoms of OCD and PTSDwere connected such that decreases in OCD-specificsymptoms related to increases in PTSD-specificsymptoms, and increases in OCD-specific symptomsrelated to decreases in PTSD-specific symptoms withimportant clinical implications.138,139
Streptococcal infection, RF and the impact onfuture studies
Based on reports of a higher prevalence of OCD inpatients with Sydenham’s chorea (SC, the neurologi-cal manifestation of RF), a number of studies wereundertaken and the results suggest a possible relation-ship between streptococcus infection and OCD.140
Additional studies reported a higher prevalence ofOCD and TS in RF, even without SC, both inactive141,142 and nonactive143 phases. Furthermore,familial aggregation of OCD/TS has been describedin relatives of RF cases (Hounie et al, personalcommunication).
Obsessive-compulsive disorder phenotypesEC Miguel et al
266
Molecular Psychiatry

Given these findings, Swedo140 proposed that thereis a subgroup of prepubertal children, who, afterexposure to streptococcal infection, did not developRF but instead had an abrupt onset of OCD and TSsymptoms. Swedo140 referred to this group of childrenas Pediatric Autoimmune Neuropsychiatric DisordersAssociated with Streptococcal infections (PANDAS).The hypothesized mechanism underlying the rela-tionship between streptococcal infection, RF and theOCD spectrum manifestations is the molecular mimi-cry between bacteria and host. This assumption hasbeen widely supported by several studies showinghigher levels of autoantibodies in OCD patients.144
However, the sole presence of autoantibodies is notsufficient to explain the hypothetic symptom induc-tion. Indeed, there are several unanswered questionsabout the connection between infection and neurop-sychiatric symptoms. In rheumatic heart disease,crossreactive antibodies binding to streptococcal Mproteins and to myosin have been identified. Thesame has not been demonstrated in SC or PANDASpatients. In addition, the presence of T cells at the siteof damaged cardiac valves may explain the immunemechanism in rheumatic carditis,145 although nothingsimilar has been demonstrated in SC. Crossreactivityhas been found between N-acetyl-glucosamine (astreptococcal antigen) and lysoganglioside (a trans-membrane molecule highly enriched in the CNS)using SC monoclonal antibodies.146 However, it is stillunclear how antibodies could cross the blood–brainbarrier. The selective permeability of the blood–brainbarrier presumably protects the brain from immuno-logical insult. However, it has been demonstrated thatantibody access into the brain can occur whenimmune-regulatory substances, such as cytokines oractivated B or T cells, disrupt the barrier.
To further explore the genetics of this possibleassociation between the immune system response andOCD/TS, studies focusing on the human leucocyteantigen (HLA) alleles, which are related to autoim-mune susceptibility, have been conducted. Diffe-rent populations have exhibited associations betweenRF and different HLA genotypes, such as HLA-DR6,DR7 and DQB1.147,148 There are several other asso-ciations, and data suggest that these might be relatedto clinical manifestations of RF.149 To date, very fewstudies examining the relation between HLA andOCD have been published and the results have beeninconclusive. In early studies, the presence of theD8/17 B cell marker, claimed as a non-HLA RFmarker, was reported to be increased in OCD/TS andPANDAS patients.140 However, these early findingshave not been consistently replicated, and there isnow considerable controversy regarding this rela-tionship.150,151
Finally, one recent study152 found an associationbetween a variant in the myelin oligodendrocyteglycoprotein (MOG) gene, a component of the myelinsheath, and OCD. The authors suggested that thepotentially autoimmune demyelinating role of thismolecule, as a target autoantigen, could hypotheti-
cally be as an inductor of OCD, via demyelination inthe frontal lobe or in other neuroanatomical re-gions.152 The complexity of this model, in which atrue autoimmune mechanism would be causing OCD,as well as the lack of evidence supporting it, arguesfor further studies.
It was initially proposed that exposure to strepto-coccus represented an ‘environmental cause’ of OCDand related disorders.140 However, this does notappear to be the case, given that familial aggregationfor OCD/TS has been described in relatives ofPANDAS probands.153 The rate of OCD found inrelatives of OCD triggered by streptococcal infectioncases (PANDAS/OCD) was the same as that found forOCD in relatives of children with OCD. It has beenproposed that early-onset OCD shares underlyingmechanisms with OCD triggered by streptococcalinfections. On the other hand, it is also possible that,given the high frequency of exposure to streptococcusof prepubertal children, the reported associationbetween OCD and exposure to streptococcus couldbe spurious. The same may be true for TS.
In summary, it has been demonstrated that there isan association between OCD/TS and streptococcalinfections with and without RF (Table 6). However, itis not currently known if PANDAS, OCD, TS, RF andSC result from common susceptibility genes and, ifso, what the common pathophysiological mechan-isms might be. More work is needed and futureresearch should focus on the role of functionalcytokine polymorphisms and autoimmune mechan-isms in the manifestation of OCD and relateddisorders in RF and PANDAS patients. If some ofthese polymorphisms are related to the manifestationof OCD, it would allow future studies to examine theimpact of specific environmental factors involved inthese disorders. Furthermore, establishing the role ofstreptococcal infections, if any, in the genesis of someneuropsychiatric disorders should allow clinicians to
Table 6 Phenotypic features of OCD related to streptococcalinfection
OCD related tostreptococcal Infection
Phenotypic features
RF-related phenotype Early-onsetAssociation with ticsAssociations with other OCDspectrum disorders
PANDAS-relatedphenotype
Early onsetPresence of OCD and/or TSAbrupt symptom onsetPresence of streptococcalinfectionChoreiform movements
RF: rheumatic fever; PANDAS: Pediatric AutoimmuneNeuropsychiatric Disorders Association with Streptococcalinfections.
Obsessive-compulsive disorder phenotypesEC Miguel et al
267
Molecular Psychiatry

develop adequate treatments and preventive strate-gies for this subgroup of patients.
Endophenotypes
Another approach to enhance the discriminativecapacity of linkage and association studies for under-standing the genetic basis of OCD would be to identifyendophenotypes associated with OCD. Endopheno-types can include neurophysiological, biochemical,endocrinological, neuropsychological, cognitive andneuroimaging (neuroanatomical) phenotypes.5 Verylittle work has been carried out to identify endophe-notypes for OCD, with the possible exception ofstructural and functional neuroimaging studies.
Neuroimaging as a useful tool for identifying OCDendophenotypesThis section extends previous writings on this topicby Rauch and co-workers.154,155 To date, neuroimagingresearch has been highly influential in advancingneurobiological models of OCD (see Saxena andRauch156). Looking forward, however, there is as yetuntapped potential for utilizing these methods tofacilitate advances in genetic research. As illustratedin the earlier sections of this review, phenotypiccharacterization is an absolutely critical element ofgenetic studies. Perhaps, particularly in the area ofpsychiatric genetics, there has been increasing inter-est in the possibility of establishing endophenotypes(sometimes called extended phenotypes) that couldserve as objectively derived, quantitative phenotypicparameters for use in genetic studies.
‘Endophenotypes’ are also defined as ‘measurablecomponents unseen by the unaided eye along thepathway between disease and distal genotype’.5 Brainimaging measures have attributes that are well suitedto this enterprise, enabling both objective andquantitative characterization of study participants.Perhaps more importantly, structural, functional andneurochemical brain measures promise to provideinformation that is truly mediating and intermediatebetween genes and corresponding clinical pheno-types. Explicitly, the premise is that a given gene orgenetic profile will more directly correspond to aparticular neural profile, which then in turn willmore directly correspond to a clinical/behavioralphenotype (see Kosslyn and Plomin157 and Gottesmanand Gould).5 That is, whereas there exist a range ofdivergent and convergent correspondences betweengenes and behavior, identifying the mediating neuralprofile will help to clarify these correspondences.
To elaborate, the challenge of delineating thegenetics of OCD would be greatly simplified if therewere a direct correspondence between a single geneand the categorical designation of meeting clinicaldiagnostic criteria for the disorder. However, as notedabove, the case for OCD (and most other psychiatricdisorders) is certainly not so simple. Consequently, ithas been appealing to attempt to disaggregate the OCDphenotype into dimensions that might have a more
direct correspondence to various genes. One way bywhich neuroimaging can assist in this process is tovalidate the supposition that a given phenotypicdimension or attribute directly corresponds to aspecific neural profile, or in some cases to highlightwhere convergences or divergences from neuralprofile to clinical phenotype exist. In fact, if it canbe shown via neuroimaging that a dimensionalscheme for characterizing clinical OCD phenotypesmaps well on to discrete, specific, correspondingneural profiles, then this would lend credence tousing such a dimensional scheme for characterizingphenotypic variance within an OCD sample, andpotentially mitigate the need to actually acquire brainimaging information as part of future genetic studies.
Here it is noteworthy that several imaging studieshave been performed to test hypotheses regardingdifferences in brain function between categoricallydefined subsets of OCD subjects, including studies ofpatients with/without comorbid major depression,158
early/later onset of OCD,159 or pure presentations ofwashing vs checking160 or hoarding.161
Few studies to date, however, have sought toestablish neural profiles that quantitatively covarywith the prominence/severity of factor analyticallyderived symptom dimensions in OCD.90 Thisapproach has been recently employed in a recentstudy. Mataix-cols et al162 used a symptom provocationparadigm with functional magnetic resonance imagingto investigate the neural correlates of washing, check-ing and hoarding symptom dimensions in OCD, andfound a distinct pattern of activation associated witheach symptom dimension. Patients demonstratedsignificantly greater activation than controls in bilat-eral ventromedial prefrontal regions and right caudatenucleus (washing); putamen/globus pallidus, thalamusand dorsal cortical areas (checking); left precentralgyrus and right orbitofrontal cortex (hoarding). Basedon these findings, the authors propose that OCD couldbe better understood as a spectrum of multiplepotentially overlapping syndromes that are likely tobe continuous with ‘normal’ worries and extendbeyond the traditional nosologic boundaries of OCD.However, in a separate volumetric study from Barce-lona, few if any differences were observed.163
Such preliminary data foreshadow the type ofneuroimaging studies that need to be performed inorder to validate current dimensional approaches aspowerful surrogate indices of neural profiles, orconversely to confirm these brain imaging measuresas robust biomarkers of the dimensional phenotypes.In this regard, it is important to emphasize thatneuroimaging research could help to refine how theclinical phenotypes are characterized, so as tooptimize concordance between clinical phenotypicdesignations and mediating neural profiles.
Nonetheless, it may turn out that sufficient un-explained variance exists between clinical subpheno-types and neural profiles that it would be mostpowerful to rely directly on neuroimaging measuresas endophenotypes for genetic studies of OCD. Major
Obsessive-compulsive disorder phenotypesEC Miguel et al
268
Molecular Psychiatry

drawbacks of such an approach include high cost(B$500–5000 per subject for various imaging mea-sures) as well as increased subject burden (eg time,discomfort, and in some cases radiation exposure).Alternative indices of brain function (eg neuro-psychological tests, evoked potentials, endocrinemeasures) might also be considered for use asendophenotypes in genetic studies. However, ingeneral, these are cruder, less direct measures ofbrain function than can be provided by contemporaryimaging methods.
Whereas brain imaging measures have been referredto generically up to this point, there are profoundissues to consider regarding which measures mightactually be of use in genetic studies. As genotypesper se are lasting, relatively static, parameters, theideal endophenotypes should likewise be temporallystable as trait markers. This is no small challenge,as essentially all measures of brain structure, functionand chemistry are dynamic over the human lifetime.In particular, measures of regional brain activity arerelatively state dependent.
Therefore, in order to develop brain imagingmeasures as useful phenotypes for genetic research,it would be important to demonstrate test/retestreliability, to standardize state variables duringacquisition and to consider characterizing indivi-duals against a normative trajectory to control forage/stage of development and sex, as well as possiblysalient environmental factors (eg years of education).
A vast range of different brain imaging measuresremains feasible as candidates for characterizing OCDphenotypes. These include (1) structural indices suchas regional volumes, (2) functional indices such asregional metabolism at rest or regional brain activa-tion during standardized behavioral tasks, (3) regionalconcentrations of neurochemical or metabolic pro-ducts, such as n-acetyl aspartate, choline or glutamateand (4) regional indices of receptor binding poten-tials. It is a daunting task to explore this parameterspace by brute force alone. The most rational startingpoint is to consider those measures and those brainelements for which between-group differences (OCDvs normal control subjects) have already been reliablyfound. This approach directs us to a circuit comprisedof the orbitofrontal cortex, anterior cingulate cortex,striatum and thalamus. However, findings of structur-al abnormalities within these regions have beeninconsistent, and functional abnormalities withinthis circuitry have largely been shown to resolve withsuccessful treatment. Therefore, much work remainsto be carried out if we are to identify brain imagingindices that can be readily leveraged as endopheno-types for the genetic study of OCD.
Finally, brain imaging can also be used to investi-gate the neural correlates of functional geneticpolymorphisms.164 That is, once candidate geneshave been identified for OCD vulnerability, brainimaging studies can be used to delineate the struc-tural, functional and neurochemical consequences ofsuch genotypes. Hariri et al165 have provided a
pioneering example of such an approach, by illustrat-ing differential brain activation profiles in subjectswith one vs two copies of the short allele of theserotonin transporter (5-HTT) promoter polymorph-ism, which has been associated with reduced 5-HTTexpression and function. This is a particularlygermane example, given the central role of serotoninin the pharmacological treatment of OCD, andprevailing questions about the role of this transmittersystem in OCD pathophysiology.
Treatment implications
Variability in treatment outcome of OCD consists ofadditional evidence supporting the notion that OCDis heterogeneous. Although the underlying causativeprocess may not be addressed by pharmacotherapy, itmight be useful to examine whether specific OCDphenotypes respond differently to drug treatmentsand whether polymorphisms associated with themechanism of action of specific drugs may be in factvulnerability genes related to the disorder. Given thepossible multifactorial pathogenesis of OCD, thesepolymorphic genes could influence at least a smallpart of the phenotypic variance. Finally, genesassociated with susceptibility to OCD might representpossible targets for future drug development.
Several studies have searched for phenotypicfeatures that could predict treatment response inOCD. Table 7 describes some phenotypic featuresthat were reported as predictive of worse treatmentresponse in OCD. Most of these variables were notreplicated in subsequent studies. One of the mostcited papers in this area,166 however, provided
Table 7 Phenotypic features described as predictors ofworse treatment response (pharmacological and cognitive-behavioral) in OCD
Phenotypic Features Study
Presence of tics 166, 167Early onset of OC symptoms 21, 36, 168Absence of sensory phenomena 37Predominance of compulsions withoutobsessions
169
Presence of hoarding 63, 87, 89, 132Presence or high score on sexual/religious obsession dimension
63, 88
Somatic obsessions 168, 170Poor insight of OC symptoms 168, 170Higher severity of OC symptoms 169Schizotypal, borderline and paranoidpersonality disorders
171–174
Being single 37Lack of family history of OCD 168Family history of tic disorder 37, 175Overvalued ideation 170, 176Post-traumatic stress disorder 138
OC symptoms: obsessive-compulsive symptoms.
Obsessive-compulsive disorder phenotypesEC Miguel et al
269
Molecular Psychiatry

some evidence of a tic-related OCD phenotypebased on treatment response. McDougle et al166 foundthat OCD patients with tics benefited from theaugmentation with typical antipsychotics to SRIs,whereas OCD patients without tics did not. As shownin Table 2, some molecular studies support theinvolvement of the dopaminergic system in thisOCD subtype.113,114
In addition, based on the efficacy of SRIs in OCD,polymorphisms in the promoter region of the seroto-nin transporter have been studied in OCD pedi-grees.18,177,178 However, no differences in SRIresponses were found among the different genotypesstudied.178 In sum, the data on phenotypic featuresand knowledge of candidate genes that could predicttreatment response in OCD are still very preliminaryand represent additional evidence that a betterdefinition of the OCD phenotype is needed. Futurestudies attempting to identify the pharmacogenetictargets that mediate antiobsessive effects on keyneuronal functions may provide a theoretical founda-tion for important changes in the antiobsessiveparadigm (today modeled based on specific actionsof antidepressants).179
Conclusions and future studies
Many studies have provided strong evidence thatOCD is clinically heterogeneous and that this clinicalheterogeneity is likely due to etiologic heterogeneity.Gaining a complete understanding of what comprisesOCD and the underlying etiological mechanisms willrequire a dramatic change in how the disorder isconceptualized. This is also probably true for allpsychiatric disorders. In this review, several differentapproaches that may represent the first steps inthis reconceptualization were discussed. Theseapproaches include (1) narrowing the phenotype toidentify categorically defined more homogeneous andmutually exclusive subtypes of OCD, (2) consideringOC symptom dimensions as quantitative componentsof the more complex OCD phenotype and (3) broad-ening the phenotype to include other etiologicallyrelated conditions.
A combined dimensional approach within distinc-tive subgroups may be the most effective in helpingidentify the heritable components of OCD. In contrastto the categorical approach, factors or dimensions arenot mutually exclusive. Therefore, each patient canexhibit one or more symptom dimensions at any giventime.4,85 These symptom dimensions may cut acrosstraditional diagnostic boundaries and thus couldprovide a more powerful approach for the detectionof genetic susceptibility loci that contribute to OCDbehaviors. However, to appreciate fully these quanti-tative dimensions, it is important that future studiesexamine the relationship between these dimensionsand the clinical and phenomenological variables,such as tic-related vs non-tic-related OCD and earlyvs late-onset OCD, that suggest the existence ofdifferent subtypes of OCD.
If these dimensional quantitative phenotypes are tobe used in subsequent molecular genetic studies, it isalso imperative to determine which ones are heritableand transmitted within families. Once heritablecomponents are identified, they could prove to beextremely beneficial in genetic linkage studies andother molecular genetic research.
New instruments capable of documenting this OCDdimensionality as well as specific aspects of theclinical presentation need to be developed. Progresshas been made with respect to the assessment of OCsymptom dimensions. A new instrument that incor-porates Y-BOCS and adds additional items to betterdefine these dimensions has been developed. TheDimensional Yale–Brown Obsessive-CompulsiveScale (DY-BOCS) has been piloted and the results ofinitial psychometric analyses are promising.180
Furthermore, another instrument has been developedfor the assessment of sensory phenomena: theUniversity of Sao Paulo Sensory Phenomena Scale(USP-SPS); a validation study is currently underway.
The ultimate goal is to delineate heritable OCDphenotypes that will facilitate the identification ofsusceptibility loci important for the manifestation ofthese behaviors. Recent genetic studies have beenunsuccessful in identifying the susceptibility genesfor OCD or the most likely mode of transmission ofthe disorder. This is probably because OCD is anetiologically heterogeneous disorder. By identifyingheritable components of OCD, it should be possibleto find genes for these separate components. It isexpected that different susceptibility genes wouldpredispose to the different components of behavior.
In addition to the efforts of identifying the genesinvolved in the etiology and expression of OCD,future studies are also needed to provide moreefficient tools for the investigation of the environ-mental and cultural factors involved in the expressionof these different phenotypes. Likewise, new brain-based markers, including brain imaging profiles, areexpected to provide endophenotypes for candidategene studies, which may also be helpful in clarifyingthe genetic heterogeneity of OCD.
Finally, it is also hoped that the identification ofmore homogeneous OCD phenotypes will facilitatethe development of new treatment strategies. Thecharacterization of the pathophysiological mechan-isms of OCD components could contribute to thedevelopment of specific pharmacological and beha-vioral therapies tailored to each of these phenotypes.A cure might one day be defined as specific treatmentor prevention of an identifiable combination ofgenetic variation and environmental events179 thatare responsible for each OCD phenotype.
Acknowledgements
This work was supported by grants from Fundacao deAmparo a Pesquisa do Estado de Sao Paulo (FAPESP):#99/08560-6 to Dr Miguel, #99/08560-6 to Dr Merca-dante, #98/15013-9 to Dr Hounie, #03/07451-6 to
Obsessive-compulsive disorder phenotypesEC Miguel et al
270
Molecular Psychiatry
Dr Rosario-Campos and #06697-6 to Dr Chacon. Thiswork was supported by Conselho Nacional deDesenvolvimento Cientıfico e Tecnologico (CNPQ),Brazil (grant #521369/96-7) to Dr Miguel and Mack-Pesquisa to Dr Mercadante.
References
1 Karno M, Golding JM, Sorenson SB, Burnam MA. The epidemiol-ogy of obsessive-compulsive disorder in five US communities.Arch Gen Psychiatry 1988; 45: 1094–1099.
2 American Psychiatric Association. Diagnostic and StatisticalManual of Mental Disorders, 4th edn. American PsychiatricAssociation: Washington, DC, 1994, p 886.
3 World Health Organization. The ICD-10 Classification of Mentaland Behavioural Disorders: Clinical Descriptions and DiagnosticGuidelines. World Health Organization: Geneva, 1992.
4 Leckman JF, Grice DE, Boardman J, Zhang H, Vitale A, Bondi Cet al. Symptoms of obsessive-compulsive disorder. Am JPsychiatry 1997; 154: 911–917.
5 Gottesman II, Gould TD. The endophenotype concept inpsychiatry: etymology and strategic intentions. Am J Psychiatry2003; 160: 636–645.
6 Pauls DL, Alsobrook JP, Goodman W, Rassmussen S, Leckman JF.A family study of obsessive-compulsive disorder. Am J Psychiatry1995; 152: 76–84.
7 Nestadt G, Samuels J, Riddle M, Bienvenu JO, Liang KY, LaBudaM et al. A family study of obsessive-compulsive disorder. ArchGen Psychiatry 2000; 57: 358–363.
8 Rasmussen SA, Tsuang MT. The epidemiology of obsessivecompulsive disorder. Clin Psychiatry 1984; 45: 450–457, (review).
9 Grados M, Riddle MA, Samuels JF, Liang KY, Hoehn-Saric R,Bienvenu OJ et al. The familial phenotype of obsessive-compulsive disorder in relation to tic disorders. Biol Psychiatry2001; 50: 559–565.
10 Bienvenu OJ, Samuels J, Riddle MA, Hoehn-Saric R, Liang KY,Cullen BAM et al. The relationship of obsessive-compulsivedisorder to possible spectrum disorders: results from a familystudy. Biol Psychiatry 2000; 48: 287–293.
11 Samuels J, Nestadt G, Bienvenu OJ, Costa Jr PT, Riddle MA, LiangKY et al. Personality disorders and normal personality dimen-sions in obsessive-compulsive disorder. Br J Psychiatry 2000;177: 457–462.
12 Nicolini H, Hanna G, Baxter L, Schwartz J, Weissbacker K,Spence MA. Segregation analysis of obsessive-compulsive andassociated disorders. Preliminary results. Ursus Medicus 1991; 1:25–28.
13 Cavallini MC, Perna G, Caldirola D, Bellodi L. A segregationstudy of panic disorder in families of panic patients responsive tothe 35% CO2 challenge. Biol Psychiatry 1999; 46: 815–820.
14 Alsobrook JP, Leckman JF, Goodman WK, Rasmussen SA, PaulsDL. Segregation analysis of obsessive-compulsive disorderusing symptom-based factor scores. Am J Med Genet 1999; 88:669–675.
15 Pato MT, Pato CN, Pauls DL. Recent findings in the genetics ofOCD. J Clin Psychiatry 2002; 63(Suppl 6): 30–33.
16 McDougle CJ, Goodman WK, Leckman JF, Lee NC, Heninger GR,Price LH. Haloperidol addition in fluvoxamine-refractory ob-sessive-compulsive disorder. A double-blind, placebo-controlledstudy in patients with and without tics. Arch Gen Psychiatry1994; 51: 302–308.
17 Nordstron EJ, Burton FH. A transgenic model of comorbidTourette’s syndrome and obsessive-compulsive disorder circui-try. Mol Psychiatry 2002; 7: 617–625, 524.
18 Rosenberg D, Hanna G. Genetic and imaging strategies inobsessive-compulsive disorder: potential implications for treat-ment development. Biol Psychiatry 2000; 48: 1210–1222.
19 Geller D, Biederman J, Jones J, Park K, Schwartz S, Shapiro Set al. Is juvenile obsessive-compulsive disorder a developmentalsubtype of the disorder? A review of the pediatric literature. J AmAcad Child Adolesc Psychiatry 1998; 37: 420–427.
20 Eichstedt JA, Arnold SL. Childhood-onset obsessive-compulsivedisorder: a tic-related subtype of OCD? Clin Psychol Rev 2001; 21:137–158.
21 Rosario-Campos MC, Leckman F, Mercadante MT, Shavitt G,Prado HS, Sada P et al. Adults with early-onset obsessive-compulsive disorder. Am J Psychiatry 2001; 158: 1899–1903.
22 Diniz J, Rosario-Campos MC, Shavitt RG, Curi M, Hounie AG,Brotto SA et al. Impact of age of onset and duration of illnessin the expression of comorbidities in obsessive-compulsivedisorder. J Clin Psychiatry 2004; 65: 22–27.
23 Swedo SE, Rapoport JL. Phenomenology and differential diag-nosis of obsessive-compulsive disorder in children and ado-lescents. In: Rapoport JL (ed) Obsessive-compulsive Disorderin Children and Adolescents. American Psychiatric Press:Washington, DC, 1989, pp 13–32.
24 Zohar AH, Pauls DL, Ratzone G, Apter A, Dycian A, Binder Met al. Obsessive-compulsive disorder with and without tics in anepidemiological sample of adolescents. Am J Psychiatry 1997;154: 274–276.
25 Geller DA, Biederman J, Faraone SV, Cradock K, Hagermoser L,Zaman N et al. Attention-deficit/hyperactivity disorder inchildren and adolescents with obsessive-compulsive disorder:fact or artifact? J Am Acad Child Adolesc Psychiatry 2002; 41:52–58.
26 Geller DA, Biederman J, Griffin S, Jones J, Lefkowitz TR.Comorbidity of juvenile obsessive-compulsive disorder withdisruptive behavior disorders. J Am Acad Child AdolescPsychiatry 1996; 35: 1637–1646.
27 Piacentini J. Cognitive behavioral therapy of childhood OCD.Child Adolesc Psychiatric Clin N Am 1999; 8: 599–616.
28 Leonard HL, Lenane MC, Swedo SE, Rettew DC, Gershon ES,Rapopport JL. Tics and Tourette’s disorder: a 2- to 7- year follow-up of 54 obsessive-compulsive children. Am J Psychiatry 1992;149: 1244–1251.
29 Reddy PS, Reddy YC, Srinath S, Khanna S, Sheshadri SP,Girimaji SR. A family study of juvenile obsessive-compulsivedisorder. Can J Psychiatry 2001; 46: 346–351.
30 Lenane MC, Swedo SE, Leonard H, Pauls DL, Sceery W, RapoportJ. Psychiatric disorders in first degree relatives of children andadolescents with obsessive-compulsive disorder. J Am AcadChild Adolesc Psychiatry 1990; 29: 407–412.
31 Riddle MA, Scahill L, King R, Hardin MT, Towbin KE, Ort SIet al. Obsessive-compulsive disorder in children and adoles-cents: phenomenology and family history. J Am Acad ChildAdolesc Psychiatry 1990; 29: 766–772.
32 Rosario-Campos MC, Leckman JF, Curi M, Quatrano S, KatsovitchL, Miguel EC et al. A family study of early-onset obsessive-compulsive disorder. Am J Med Genet, in press.
33 March JS, Leonard HL. Obsessive-compulsive disorder inchildren and adolescents: a review of the past 10 years. J AmAcad Child Adolesc Psychiatry 1996; 35: 1265–1273.
34 Busatto GF, Zamignani DR, Buchpiguel CA, Garrido GEJ, GlabusMF, Rocha ET et al. A voxel based investigation of regionalcerebral blood flow abnormalities in obsessive-compulsive dis-order using single photon emission computed tomography(SPECT). Psychiatry Res 2000; 99: 15–27.
35 Ackerman DL, Greenland S, Bystritsky A, Morgenstern H,Katz RJ. Predictors of treatment response in obsessive-compulsive disorder: multivariate analyses from a multi-center trial of clomipramine. J Clin Psychopharmacol 1994; 14:247–254.
36 Ravizza L, Barzega G, Bellino S, Bogetto F, Maina G. Predictors ofdrug treatment response in obsessive-compulsive disorder. J ClinPsychiatry 1995; 56: 368–373.
37 Shavitt RG, Belotto C, Curi M, Hounie AG, Rosario-Campos MC,Diniz JB et al. Sensory phenomena and treatment response inobsessive-compulsive disorder, submitted.
38 Miguel EC, Shavitt RG, Ferrao YA, Brotto SA, Diniz JB. How totreat OCD in patients with Tourette’s syndrome. J Psychosom Res2003; 55: 49–57.
39 Walitza S, Wewetzer C, Warnke A, Gerlach M, Geller F, Gerber Get al. 5-HT2A promoter polymorphism �1438G/A in childrenand adolescents with obsessive-compulsive disorders. MolPsychiatry 2002; 7: 1054–1057.
Obsessive-compulsive disorder phenotypesEC Miguel et al
271
Molecular Psychiatry
40 Hanna GL, Piacentini J, Cantwell DP, Fischer DJ, Himle JA, VanEtten M. Obsessive-compulsive disorder with and without tics ina clinical sample of children and adolescents. Depress Anxiety2002; 16: 59–63.
41 Veenstra-VanderWeele J, Kim SJ, Gonen D, Hanna GL, LeventhalBL, Cook EH. Genomic organization of the SLC1A1/EAAC1 geneand mutation screening in early-onset obsessive-compulsivedisorder. Mol Psychiatry 2001; 6: 160–167.
42 Fontanelle L, Marques C, Versiani M. The effect of gender onthe clinical features and therapeutic response in obsessive-compulsive disorder. Rev Bras Psiquiatria 2002; 24: 7–11.
43 Miguel EC, Coffey BJ, Baer L, Savage CR, Rauch SL, Jenike MA.Phenomenology of intentional repetitive behaviors in obsessive-compulsive disorder and Tourette’s syndrome. J Clin Psychiatry1995; 56: 246–255.
44 Miguel EC, Rauch SL, Jenike MA. Obsessive-compulsivedisorder. Psychiatric Clin N Am 1997; 20: 863–883.
45 Pauls DL, Towbin KE, Leckman JF, Zahner GE, Cohen DJ. Gillesde la Tourette’s syndrome and obsessive-compulsive disorder:evidence supporting a genetic relationship. Arch Gen Psychiatry1986; 43: 1180–1182.
46 Pauls DL, Raymond CL, Stevenson JM, Leckman JF. A familystudy of Gilles de la Tourette syndrome. Am J Hum Genet 1991;48: 154–163.
47 Comings DE, Comings BG. A controlled study of Tourettesyndrome. IV. Obsessions, compulsions, and schizoid behaviors.Am J Hum Genet 1987; 41: 782–803.
48 Robertson MM, Trimble MR, Lees AJ. The psychopathology ofthe Gilles de la Tourette syndrome. A phenomenological analysis.Br J Psychiatry 1988; 152: 383–390.
49 Pauls DL, Leckman JF. The inheritance of Gilles de laTourette’s syndrome and associated behaviors: evidence forautosomal dominant transmission. N Engl J Med 1986; 315:993–997.
50 Eapen V, Pauls DL, Robertson MM. Evidence for autosomaldominant transmission in Tourette’s syndrome—United King-dom Cohort Study. Br J Psychiatry 1993; 162: 593–596.
51 Van de Wetering BJM. The Gilles de la Tourette syndrome. Apsychiatric–genetic study. PhD theses, Erasmus University,Rotterdam.
52 Miguel EC, do Rosario-Campos MC, Shavitt RG, Hounie AG,Mercadante MT. The tic-related obsessive-compulsive disorderphenotype and treatment implications. Adv Neurol 2001; 85:43–55, (review).
53 Miguel EC, Rosario-Campos MC, Shavitt RG, Hounie AG,Mercadante MT. The tic-related obsessive-compulsive disorderphenotype. Adv Neurol 2000; 85: 43–55.
54 Swerdlow NR, Zinner S, Farber RH, Seacrist C, Hartston H.Symptoms in obsessive-compulsive disorder and Tourette syn-drome: a spectrum? CNS Spectrums 1999; 4: 21–33.
55 Petter T, Richter MA, Sandor P. Clinical features distinguishingpatients with Tourette’s syndrome and obsessive-compulsivedisorder from patients with obsessive-compulsive disorder with-out tics. J Clin Psychiatry 1998; 59: 456–459.
56 Eapen V, Robertson MM, Alsobrook II JP, Pauls DL. Obsessive-compulsive symptoms in Gilles de la Tourette’s syndrome andobsessive-compulsive disorder: differences by diagnosis andfamily history. Am J Med Genet 1997; 74: 432–438.
57 Holzer JC, Goodman WK, McDougle CJ, Baer L, Boyarsky BK,Leckman JF et al. Obsessive-compulsive disorder with andwithout a chronic tic disorder: a comparison of symptoms in 70patients. Br J Psychiatry 1994; 164: 469–473.
58 George MS, Trimble MR, Ring HA, Sallee FR, RobertsonMM. Obsessions in obsessive-compulsive disorder with andwithout Gilles de la Tourette’s syndrome. Am J Psychiatry 1993;105: 93–97.
59 Pitman RK. Pierre Janet on obsessive-compulsive disorder (1903).Arch Gen Psychiatry 1987; 44: 226–232.
60 Rasmussen AS, Tsuang MT. Clinical characteristics and familyhistory in DSM-III obsessive compulsive disorder. Am J Psychia-try 1986; 143: 317–322.
61 Leckman JF, Walker DE, Goodman WK, Pauls DL, Cohen DJ. ‘Just-right’ perceptions associated with compulsive behavior inTourette’s syndrome. Am J Psychiatry 1994; 151: 675–680.
62 Leckman JF, Goodman WK, Anderson GM, Riddle MA,Chappell PB, McSwiggan-Hardin Mt et al. Cerebrospinal fluidbiogenic amines in obsessive compulsive disorder, Tourette’ssyndrome, and healthy controls. Neuropsychopharmacology1995; 12: 73–86.
63 Mataix-Cols D, Rauch SL, Manzo PA, Jenike MA, Baer L. Use offactor-analyzed symptom dimensions to predict outcome withserotonin reuptake inhibitors and placebo in the treatment ofobsessive-compulsive disorder. Am J Psychiatry 1999; 156:1409–1416.
64 Baer L. Factor analysis of symptom subtypes of obsessivecompulsive disorder and their relation to personality and ticdisorders. J Clin Psychiatry 1994; 55: 18–23.
65 Coffey BJ, Miguel EC, Biederman J, Baer L, Rauch SL, O’SullivanRL et al. Tourette’s disorder with and without obsessive-compulsive disorder in adults: are they different? J Nerv MentDis 1998; 186: 201–206.
66 Bliss J. Sensory experiences of Gilles de la Tourette syndrome.Arch Gen Psychiatry 1980; 37: 1343–1347.
67 Shapiro AK, Shapiro ES, Young JG, Feinberg TE. Gilles de laTourette Syndrome. Raven Press: New York, 1988.
68 Kurlan R, Lichter D, Hewitt D. Sensory tics in Tourette’ssyndrome. Neurology 1989; 39: 731–734.
69 Cohen AJ, Leckman JF. Sensory phenomena associated withGilles de la Tourette’s syndrome. J Clin Psychiatry 1992; 53:319–323.
70 Leckman JF, Walker DE, Cohen DJ. Premonitory urges inTourette’s syndrome. Am J Psychiatry 1993; 150: 98–102.
71 Chee KY, Sachdev P. A controlled study of sensory tics in Gillesde la Tourette syndrome and obsessive-compulsive disorderusing a structured interview. J Neurol Neurosurg Psychiatry1997; 62: 188–192.
72 Rosario-Campos MC. Transtorno obsessivo-compulsivo de inıcioprecoce e de inıcio tardio: caracterısticas clınicas, psicopatolo-gicas e de comorbidade. Dissertacao de mestrado, Faculdade deMedicina da Universidade de Sao Paulo, Sao Paulo, 1998, p 99.
73 Goodman WK, Price LH, Rasmussen SA, Mazure C, FleischmanRL, Hill CL et al. The Yale–Brown obsessive-compulsive scale: I.development use and reliability. Arch Gen Psychiatry 1989; 46:1006–1011.
74 Hantouche EG, Lancrenon S. Modern typology of symptoms andobsessive-compulsive syndromes: results of a large French studyof 615 patients. Encephale 1996; 22: 9–21.
75 Summerfeldt LJ, Richter MA, Anthony MM, Huta VM, SwinsonRP. Symptom structure in obsessive-compulsive disorder: factoranalytic evidence for subgroups. Poster presented at the 150thAnnual Meeting of the American Psychiatric Association, SanDiego, CA, May 1997.
76 Summerfeldt LJ, Richter MA, Antony MM, Swinson RP. Symp-tom structure in obsessive-compulsive disorder: a confirmatoryfactor-analytic study. Behav Res Ther 1999; 37: 297–311.
77 Mataix-Cols D, Rauch SL, Baer L, Eisen JL, Shera DM, GoodmanWK et al. Symptom stability in adult obsessive compulsivedisorder: data from a naturalistic two-year follow-up study. Am JPsychiatry 2002; 159: 263–268.
78 Tek C, Ulug B. Religiosity and religious obsessions in obsessive-compulsive disorder. Psychiatry Res 2001; 104: 99–108.
79 Cavallini MC, Di Bella D, Siliprandi F, Malchiodi F, Bellodi L.Exploratory factor analysis of obsessive-compulsive patients andassociation with 5-HTTLPR polymorphism. Am J Med Genet2002; 114: 347–353.
80 Foa EB, Huppert JD, Leiberg S, Langner R, Kichic R, Hajcak Get al. The obsessive-compulsive inventory: development andvalidation of a short version. Psychol Assess 2002; 14: 485–496.
81 Feinstein SB, Fallon BA, Petkova E, Liebowitz MR. Item-by-itemfactor analysis of the Yale–Brown Obsessive Compulsive ScaleSymptom Checklist. J Neuropsychiatry Clin Neurosci 2003; 15:187–193.
82 Leckman JF, Pauls DL, Zhang H, Rosario-Campos MC,Katsovich L, Kidd KK et al. Tourette Syndrome AssociationInternational Consortium for Genetics. Obsessive-compulsivesymptom dimensions in affected sibling pairs diagnosedwith Gilles de la Tourette syndrome. Am J Med Genet 2003;116B: 60–68.
Obsessive-compulsive disorder phenotypesEC Miguel et al
272
Molecular Psychiatry
83 Mataix-Cols D, Rosario-Campos MC, Leckman JF. A multidimen-sional model of obsessive-compulsive disorder. Am J Psychiatry,in press.
84 Mataix-Cols D, Cullen S, Lange K, Zelaya F, Andrew C, Amaro Eet al. Neural correlates of anxiety associated with obsessive-compulsive symptom dimensions in normal volunteers. BiolPsychiatry 2003; 53: 482–493.
85 Mataix-Cols D, Fullana MA, Alonso P, Menchon JM, VallejoJ. Convergent and discriminate validity of the Yale–BrownObsessive-Compulsive Scale Symptom Checklist. PsychotherPsychosom, in press.
86 Zhang H, Leckman JF, Tsai C-P, Kidd KK, Rosario Campos MC.The Tourette Syndrome Association International Consortium forGenetics: genome wide scan of hoarding in sibling pairs bothdiagnosed with Gilles de la Tourette syndrome. Am J Hum Genet2002; 70: 896–904.
87 Black DW, Monahan P, Gable J, Blum N, Clancy G, Baker P.Hoarding and treatment response in 38 nondepressed subjectswith obsessive-compulsive disorder. J Clin Psychiatry 1998; 59:420–425.
88 Alonso P, Menchon JM, Pifarre J, Mataix-Cols D, Torres L, SalgadoP et al. Long-term follow-up and predictors of clinical outcome inobsessive-compulsive patients treated with serotonin reuptakeinhibitors and behavioral therapy. J Clin Psychiatry 2001; 62:535–540.
89 Saxena S, Maidment KM, Vapnik T, Golden G, Rishwain T, RosenRM et al. Obsessive-compulsive hoarding: symptom severityand response to multimodal treatment. J Clin Psychiatry 2002; 63:21–27.
90 Rauch SL, Dougherty DD, Shin LM, Alpert NM, Manzo P, Leahy Let al. Neural correlates of factor-analyzed OCD symptom dimen-sions: a PET study. CNS Spectrums 1998; 3: 37–43.
91 The Tourette Syndrome International Consortium for Genetics.A complete genome screen in sib pairs affected by Gilles de laTourette syndrome. Am J Hum Genet 1999; 65: 1428–1436.
92 McHugh PR, Slavney PR (eds). The Perspectives of Psychiatry.Johns Hopkins: Baltimore, 1988.
93 Costa Jr PT, McCrae RR. Revised NEO Personality Inventory (NEOPI-R) Professional Manual. Psychological Assessment Resources:Odessa, FL, 1992.
94 Lesch K-P, Bengel D, Heils A, Sabol SZ, Greenberg BD, Petri Set al. Association of anxiety-related traits with a polymorphismin the serotonin transporter gene regulatory region. Science 1996;274: 1527–1531.
95 Greenberg BD, Li Q, Lucas FR, Hu S, Sirota LA, Benjamin J et al.Association between the serotonin transporter promoter poly-morphism and personality traits in a primarily female populationsample. Am J Med Genet 2000; 96: 202–216.
96 Jacob CP, Strobel A, Hohenberger K, Ringel T, Gutknecht L, Reif Aet al. Association between allelic variation of serotonin transpor-ter function and neuroticism in anxious cluster C personalitydisorders. Am J Psychiatry 2004; 161: 569–572.
97 Nestadt G, Samuels J, Riddle MA, Liang K-Y, Bienvenu OJ,Hoehn-Saric R et al. The relationship between obsessive-compulsive disorder and anxiety and affective disorders: resultsfrom the Johns Hopkins OCD family study. Psychol Med 2001; 31:481–487.
98 Bienvenu OJ, Samuels JF, Riddle MA, Hoehn-Saric R, Liang KY,Cullen BAM et al. The relationship of obsessive-compulsivedisorder to possible spectrum disorders: results from a familystudy. Biol Psychiatry 2000; 48: 287–293.
99 Gonzales CH. Estudo de famılias no transtorno obse-ssivo-compulsivo. Tese de doutorado—Escola Paulista deMedicina, Universidade Federal de Sao Paulo, Sao Paulo, 2003,p 227.
100 Cavallaro R, Galardi G, Cavallini MC, Henin M, Amodio S,Bellodi L et al. Obsessive compulsive disorder among idiopathicfocal dystonia patients: an epidemiological and family study. BiolPsychiatry 2002; 52: 356–361.
101 Nestadt G, Addington A, Samuels J, Liang K, Bienvenu OJ, RiddleM et al. The identification of OCD-related subgroups based oncomorbidity. Biol Psychiatry 2003; 53: 914–920.
102 Chacon P, Rosario-Campos MC, Hounie AG, Lopes AC, Curi M,Miguel EC. Comment on ‘the identification of OCD-related
subgroups based on comorbidity’. Biol Psychiatry 2004; 55:960–961.
103 Faraone SV, Tsuang MT, Tsuang DW (eds). Genetics of MentalDisorders: A Guide for Students, Clinicians, and Researchers.The Guilford Press: New York, 1999, p 272.
104 Torres AR, Dedomenico AM, Crepaldi AL, Miguel EC. Obsessive-compulsive symptoms in patients with panic disorder. ComprPsychiatry 2004; 45: 219–224.
105 Bellodi L, Cavallini MC, Bertelli S, Chiapparino D, Riboldi C,Smeraldi E. Morbidity risk for obsessive-compulsive spectrumdisorders in first-degree relatives of patients with eatingdisorders. Am J Psychiatry 2001; 158: 563–569.
106 Dykens E, Shah B. Psychiatric disorders in Prader–Willisyndrome: epidemiology and management. CNS Drugs 2003;17: 167–178.
107 Clarke DJ, Boer H, Whittington A, Holland JB. Prader–Willisyndrome, compulsive and ritualistic behaviors: the first popula-tion-based survey. Br J Psychiatry 2002; 180: 358–362.
108 Wigren M, Hansen S. Rituals and compulsivity in Prader–Willisyndrome: profile and stability. J Intellect Disabil Res 2003; 47:428–438.
109 Dykens EM, Leckman JF, Cassidy SB. Obsessions and compul-sions in Prader–Willi syndrome. J Child Psychol Psychiatry 1996;37: 995–1002.
110 State MW, Dykens EM, Rosner B, Martin A, King BH. Obsessive-compulsive symptoms in Prader–Willi and ‘Prader–Willi-like’patients. J Am Acad Child Adolesc Psychiatry 1999; 38: 329–334.
111 Wassink TH, Piven J, Patil SR. Chromosomal abnormalities in aclinic sample of individuals with autistic disorder. PsychiatrGenet 2001; 11: 57–63.
112 Hollander E, King A, Delaney K, Smith CJ, Silverman JM.Obessive-compulsive behaviors in parents of multiplex autismfamilies. Psychiatry Res 2003; 117: 11–16.
113 Millet B, Chabane N, Delorme R, Leboyer M, Leroy S, Poirier MFet al. Association between the dopamine receptor D4 (DRD4)gene and obsessive-compulsive disorder. Am J Med Genet 2003;116B: 55–59.
114 Cruz C, Camarena B, King N, Paez F, Sidenberg D, Fuente JR et al.Increased prevalence of the seven- variant of the dopamine D4receptor gene in patients with obsessive-compulsive disorderswith tics. Neurosci Lett 1997; 231: 1–4.
115 Nicolini H, Cruz C, Camarena B, Orozco B, Kennedy JL, King Net al. DRD2, DRD3, and 5HTDA receptor genes polymorphismsin obsessive-compulsive disorder. Mol Psychiatry 1996; 1:461–465.
116 Nicolini H, Cruz C, Paez F, Camarena B. Los genes de losreceptores a dopamina D2 y D4 distinguen la presencia clınica detics en el trastorno obsesivo-compulsivo. Gac Med Mex 1998; 8:163–169.
117 Urraca N, Camarena B, Gomez-Caudillo L, Esmer MC, Nicolini H.Micro opioid receptor gene as a candidate for the study ofobsessive compulsive disorder with and without tics. Am J MedGenet 2004; 127B: 94–96.
118 Kelsoe JR. Arguments for the genetic basis of the bipolarspectrum. J Affect Disord 2003; 73: 183–197.
119 Reif A, Lesch KP. Toward a molecular architecture of personality.Behav Brain Res 2003; 139: 1–20.
120 Jonnal AH, Gardner CO, Prescott CA, Kendler KS. Obsessive andcompulsive symptoms in a general population sample of femaletwins. Am J Med Genet 2000; 96: 791–796.
121 Eley TC, Bolton D, O’Connor TG, Perrin S, Smith P, Plomin R.A twin study of anxiety-related behaviours in pre-schoolchildren. J Child Psychol Psychiatry 2003; 44: 945–960.
122 Capstick N, Seldrup J. Obsessional states. A study in therelationship between abnormalities occurring at the time of birthand the subsequent development of obsessional symptoms. ActaPsychiatr Scand 1977; 56: 427–431.
123 Lensi P, Cassano GB, Correddu G, Ravagli S, Kunovac JL, AkiskalHS. Obsessive-compulsive disorder—familial–developmentalhistory, symptomatology, comorbidity and course with specialreference to gender-related differences. Br J Psychiat 1996; 169:101–107.
124 Santangelo SL, Pauls DL, Goldstein J, Faraone SV, Tsuang MT,Leckman JF. Tourette’s syndrome: what are the influences of
Obsessive-compulsive disorder phenotypesEC Miguel et al
273
Molecular Psychiatry

gender and comorbid obsessive-compulsive disorder? J Am AcadChild Adolesc Psychiatry 1994; 33: 795–804.
125 Peterson BS, Leckman JF, Scahill L, Naftolin F, Keefe D, CharestNJ et al. Hypothesis: steroid hormones and sexual dimorphismsmodulate symptom expression in Tourette’s syndrome. Psycho-neuroendocrinology 1992; 17: 553–563.
126 Altemus M, Greenberg BD, Keuler D, Jacobson KR, Murphy DL.Open trial of flutamide for treatment of obsessive-compulsivedisorder. J Clin Psychiatry 1999; 60: 442–445.
127 Pollitt J. Natural history of obsessional states. BMJ 1957; 9:133–140.
128 Ingram IM. Obsessional illness in mental hospital patients.J Mental Sci 1961; 107: 382–402.
129 Lo WH. A follow-up study of obsessional neurotics in Hong KongChinese. Br J Psychiatry 1967; 113: 823–832.
130 Neziroglu F, Anemone R, Yaryura-Tobias J. Onset of obsessive-compulsive disorder in pregnancy. Am J Psychiatry 1992; 149:947–950.
131 Maina G, Albert U, Bogetto F, Vaschetto P, Ravizza L. Recent lifeevents and obsessive-compulsive disorder (OCD): the role ofpregnancy/delivery. Psychiatry Res 1999; 89: 49–58.
132 Abramowitz JS, Schwartz SA, Moore KM, Luenzmann KR.Obsessive-compulsive symptoms in pregnancy and the puer-perium: a review of the literature. J Anxiety Disord 2003; 17:461–478.
133 Abramowitz J, Moore K, Carmin C, Wiegartz PS, Purdon C. Acuteonset of obsessive-compulsive disorder in males followingchildbirth. Psychossomatics 2001; 42: 429–431.
134 Leckman JF, Goodman WK, North WG, Chappell PB, Price LH,Pauls DL et al. Elevated levels of CSF oxytocin in obsessivecompulsive disorder: comparison with Tourette’s syndrome andhealthy controls. Arch Gen Psychiatry 1994; 51: 782–792.
135 Leckman JF, Mayes LC, Feldman R, Evans D, King RA, Cohen DJ.Early parental preoccupations and behaviors and their possiblerelationship to the symptoms of obsessive-compulsive disorder.Acta Psychiat Scand 1999; 100(Suppl 396): 1–26.
136 McKeon J, Roa B, Mann A. Life events and personality traitsin obsessive-compulsive neurosis. Br J Psychiatry 1984; 144:185–189.
137 Khanna S, Rajendra PN, Channabasavanna SM. Live events andonset of obsessive-compulsive disorder. Int J Soc Psychiatry1988; 34: 305–309.
138 Gershuny BS, Baer L, Radomsky AS, Wilson KA, Jenike MA.Connections among symptoms of obsessive-compulsive disorderand posttraumatic stress disorder: a case series. Behav Res Ther2003; 41: 1029–1041.
139 Gershuny BS, Baer L, Radomsky AS, Wilson KA, Jenike MA.Comorbid posttraumatic stress disorder: impact on treatmentoutcome for obsessive-compulsive disorder. Am J Psychiatry2002; 159: 852–854.
140 Swedo SE. Pediatric autoimmune neuropsychiatric disordersassociated with streptococcal infections (PANDAS). Mol Psy-chiatry 2002; 7(Suppl 2): S24–S25.
141 Asbahr FR, Negrao AB, Gentil V, Zanetta DM, da Paz JA,Marques-Dias MJ et al. Obsessive-compulsive and relatedsymptoms in children and adolescents with rheumatic feverwith and without chorea: a prospective 6-month study. Am JPsychiatry 1998; 155: 1122–1124.
142 Mercadante MT, Busatto GF, Lombroso PJ, Prado L, Rosario-Campos MC, do Valle R et al. The psychiatric symptoms ofrheumatic fever. Am J Psychiatry 2000; 157: 2036–2038.
143 Hounie AG, Pauls DL, Mercadante MT, Rosario-Campos MC,Shavitt RG, De Mathis MA et al. Obsessive-compulsive spectrumdisorders in rheumatic fever with and without Sydenham’schorea. J Clin Psychiatry 2004; 65: 994–999.
144 Mercadante MT, Hounie AG, Muniz JB, Miguel EC, Lombroso PJ.The basal ganglia and immune-based neuropsychiatric disorders.Psychiatric Annals 2001; 31: 534–540.
145 Guilherme L, Kalil J. Rheumatic fever: the T cell response leadingto autoimmune aggression in the heart. Autoimmun Rev 2002; 1:261–266.
146 Kirvan CA, Swedo SE, Heuser JS, Cunningham MW. Mimicry andautoantibody-mediated neuronal cell signaling in Sydenhamchorea. Nat Med 2003; 9: 914–920.
147 Donadi EA, Smith AG, Louzada-Junior P, Voltarelli JC, NepomGT. HLA class I and class II profiles of patients presenting withSydenham’s chorea. J Neurol 2000; 247: 122–128.
148 Stanevicha V, Eglite J, Sochnevs A, Gardovska D, Zavadska D,Shantere R. HLA class II associations with rheumatic heartdisease among clinically homogeneous patients in children inLatvia. Arthritis Res Ther 2003; 5: R340–R346.
149 Cunningham MW. Pathogenesis of groups A streptococcalinfections. Microbiol Rev 2000; 13: 470–511.
150 Murphy T, Goodman W. Genetics of childhood disorders: XXXIV.Autoimmune disorders, part 7: D8/17 reactivity as an immuno-logical marker of susceptibility to neuropsychiatric disorders.J Am Acad Child Adolesc Psychiatry 2002; 41: 98–100.
151 Inoff-Germain G, Rodriguez RS, Torres-Alcantara S, Diaz-JimenezMJ, Swedo SE, Rapoport JL. An immunological marker (D8/17)associated with rheumatic fever as a predictor of childhoodpsychiatric disorders in a community sample. J Child PsycholPsychiatry 2003; 44: 782–790.
152 Zai G, Bezchlibnyk YB, Richter MA, Arnold P, Burroughs E,Barr CL et al. Myelin oligodendrocyte glycoprotein (MOG) gene isassociated with obsessive-compulsive disorder. Am J Med Genet2004; 129: 64–68.
153 Lougee L, Perlmutter SJ, Nicolson R, Garvey MA, Swedo SE.Psychiatric disorders in first-degree relatives of children withpediatric autoimmune neuropsychiatric disorders associatedwith streptococcal infections (PANDAS). J Am Acad ChildAdolesc Psychiatry 2000; 39: 1120–1126.
154 Rauch SL. Preparing for psychiatry in the 21st century. In: SternTA, Herman JB (eds) Psychiatry Update and Board Preparation.McGraw-Hill: New York, 2000, pp 579–583.
155 Rauch SL, Shin LM, Dougherty DD, Alpert NM, Fischman AJ,Jenike MA. Predictors of fluvoxamine response in contamination-related obsessive-compulsive disorder: a PET symptom provoca-tion study. Neuropsychopharmacology 2002; 27: 782–791.
156 Saxena S, Rauch SL. Functional neuroimaging and the neuro-anatomy of obsessive-compulsive disorder. Psychiatr Clin N Am2000; 23: 563–586.
157 Kosslyn SM, Plomin R. Toward a neurocognitive genetics: goalsand issues. In: Dougherty DD, Rauch SL (eds) PsychiatricNeuroimagaign Research: Contemporary Strategies. AmericanPsychiatric Publishing Inc.: Washington, DC, 2001, pp 383–402.
158 Saxena S, Brody AL, Ho ML, Alborzian S, Ho MK, Maidment KMet al. Cerebral metabolism in major depression and obsessive-compulsive disorder occurring separately and concurrently. BiolPsychiatry 2001; 50: 159–170.
159 Busatto GF, Buchpiguel CA, Zamignani DR, Garrido GEJ, GlabusMF, Rosario-Campos MC et al. Regional cerebral blood flowdifferences in obsessive-compulsive disorder subtyped accordingto the age of illness onset. J Am Acad Child Adolesc Psychiatry2001; 40: 347–354.
160 Phillips ML, Marks IM, Senior C, Lythgoe D, O’Dwyer A-M,Meehan O et al. A differential neural response in obse-ssive-compulsive disorder patients with washing comparedwith checking symptoms to disgust. Psychol Med 2000; 30:1037–1050.
161 Saxena S, Brody AL, Maidment KM, Smith EC, Zohrabi N, Katz Eet al. Cerebral glucose metabolism in obsessive-compulsivehoarding. Am J Psychiatry 2004; 161: 1038–1048.
162 Mataix-Cols D, Woonderson S, Lawrence N, Brammer MJ,Speckens A, Phillips ML. Distinct neural correlates of washing,checking, and hoarding symptom dimensions in obsessive-compulsive disorder. Arch Gen Psychiatry 2004; 61: 564–576.
163 Pujol J, Soriano-Mas C, Alonso P, Cardoner N, MenchonJM, Deus J et al. Mapping structural brain alterations inobsessive-compulsive disorder. Arch Gen Psychiatry 2004; 61:720–730.
164 Hariri AR, Weinberger DR. Imaging genomics. Br Med Bull 2003;65: 259–270.
165 Hariri AR, Mattay VS, Tessitore A, Kolachana B, Fera F, GoldmanD et al. Serotonin transporter genetic variation and the responseof the human amygdala. Science 2002; 297: 400–403.
166 McDougle CJ, Goodman WK, Leckman JF, Lee NC, Heninger GR,Price LH. Haloperidol addition in fluvoxamine-refractoryobsessive-compulsive disorder: a double-blind placebo-controlled
Obsessive-compulsive disorder phenotypesEC Miguel et al
274
Molecular Psychiatry

study in patients with and without tics. Arch Gen Psychiatry1994; 51: 302–308.
167 McDougle CJ, Goodman WK, Leckman JF, Barr LC, Heninger GR,Price LH. The efficacy of fluvoxamine in obsessive-compulsivedisorder: effects of comorbid chronic tic disorder. J ClinPsychopharmacol 1993; 13: 354–358.
168 Erzegovesi S, Cavallini MC, Cavedini P, Diaferia G, Locatelli M,Bellodi L. Clinical predictors of drug response in obsessive-compulsive disorder. J Clin Psychopharmacol 2001; 21: 488–492.
169 Alarcon LD, Llibb JW, Spitler D. A predictive study of obsessive-compulsive disorder response to clomipramine. J Clin Psycho-pharmacol 1993; 13: 210–213.
170 Neziroglu FA, Stevens PK, Yaryura-Tobias JA. Overvalued ideasand their impact on treatment outcome. Rev Bras Psiquiatr 1999;21: 209–216.
171 Mundo E, Erzegovesi S, Bellodi L. Follow-up of obsessive-compulsive patients treated with proserotonergi agents. J ClinPsychopharmacol 1995; 15: 288–289.
172 Baer L, Jenike MA, Black DW, Treece C, Rosenfeld R, Greist J.Effects of Axis II diagnoses on treatment outcome withclomipramine in 55 patients with obsessive-compulsive disorder.Arch Gen Psychiatry 1992; 49: 862–866.
173 McDougle CJ, Goodman WK, Price LH, Delgado PL, Krystal JH,Charney DS et al. Neuroleptic addition in fluvoxamine-refractoryobsessive-compulsive disorder. Am J Psychiatry 1990; 147:652–654.
174 Minichiello WE, Baer L, Jenike MA. Schizotypal personalitydisorder: a poor prognostic indicator for behavior therapy in thetreatment of obsessive-compulsive disorder. J Anxiety Disord1987; 1: 273–276.
175 Hollander E, Bienstock CA, Koran LM, Pallanti S, Marazziti D,Rasmussen SA et al. Refractory obsessive-compulsive disorderstate-of-art treatment. J Clin Psychiatry 2002; 63(Suppl 6): 20–29,(review).
176 Neziroglu F, Pinto A, Yaryura-Tobias JA, McKay D. Overvaluedideation as a predictor of fluvoxamine response in patientswith obsessive-compulsive disorder. Psychiatry Res 2004; 125:53–60.
177 McDougle CJ, Epperson CN, Price LH, Gelernter J. Evidence forlinkage disequilibrium between serotonin transporter proteingene (SLC6A4) and obsessive-compulsive disorder. Mol Psychia-try 1998; 3: 270–273.
178 Di Bella D, Erzegovesi S, Cavallini MC, Bellodi L. Obsessive-compulsive disorder, 5-HTTLPR polymorphism and treatmentresponse. Pharmacogenomics J 2002; 2: 176–181.
179 Wong ML, Licinio J. From monoamines to genomic targets: aparadigm shift for drug discovery in depression. Nat Rev DrugDiscov 2004; 3: 136–151.
180 Rosario-Campos MC, Miguel EC, Quatrano S, Chacon P, Ferrao Y,Findley D et al. The Dimensional Yale–Brown ObsessiveCompulsive Scales (DY-BOCS): a new instrument for assessingobsessive-compulsive symptom dimensions, submitted.
Obsessive-compulsive disorder phenotypesEC Miguel et al
275
Molecular Psychiatry
Copyright © 2022 FDOKUMEN




















