
Comorbidity in obsessive–compulsive disorder (OCD): A report from the International College of...
21
Comorbidity in Obsessive-Compulsive Disorder (OCD): A Report from the International College of Obsessive-Compulsive Spectrum Disorders (ICOCS) Christine Lochner, Naomi A. Fineberg, Joseph Zohar, Michael van Amerin- gen, Alzbeta Juven-Wetzler, Alfredo Carlo Altamura, Natalie L. Cuzen, Eric Hollander, Damiaan Denys, Humberto Nicolini, Bernardo Dell‘Osso, Stefano Pallanti, Dan J. Stein, Jose Menchon Magrina, Lucheza Hranov, Oguz Karamustafalioglu, Donatella Marazziti PII: S0010-440X(14)00145-X DOI: doi: 10.1016/j.comppsych.2014.05.020 Reference: YCOMP 51325 To appear in: Comprehensive Psychiatry Received date: 27 May 2013 Revised date: 8 May 2014 Accepted date: 28 May 2014 Please cite this article as: Lochner Christine, Fineberg Naomi A., Zohar Joseph, van Ameringen Michael, Juven-Wetzler Alzbeta, Altamura Alfredo Carlo, Cuzen Natalie L., Hollander Eric, Denys Damiaan, Nicolini Humberto, Dell‘Osso Bernardo, Pallanti Ste- fano, Stein Dan J., Magrina Jose Menchon, Hranov Lucheza, Karamustafalioglu Oguz, Marazziti Donatella, Comorbidity in Obsessive-Compulsive Disorder (OCD): A Report from the International College of Obsessive-Compulsive Spectrum Disorders (ICOCS), Comprehensive Psychiatry (2014), doi: 10.1016/j.comppsych.2014.05.020 This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Transcript of Comorbidity in obsessive–compulsive disorder (OCD): A report from the International College of...

�������� ����� ��
Comorbidity in Obsessive-Compulsive Disorder (OCD): A Report from theInternational College of Obsessive-Compulsive Spectrum Disorders (ICOCS)
Christine Lochner, Naomi A. Fineberg, Joseph Zohar, Michael van Amerin-gen, Alzbeta Juven-Wetzler, Alfredo Carlo Altamura, Natalie L. Cuzen,Eric Hollander, Damiaan Denys, Humberto Nicolini, Bernardo Dell‘Osso,Stefano Pallanti, Dan J. Stein, Jose Menchon Magrina, Lucheza Hranov, OguzKaramustafalioglu, Donatella Marazziti
PII: S0010-440X(14)00145-XDOI: doi: 10.1016/j.comppsych.2014.05.020Reference: YCOMP 51325
To appear in: Comprehensive Psychiatry
Received date: 27 May 2013Revised date: 8 May 2014Accepted date: 28 May 2014
Please cite this article as: Lochner Christine, Fineberg Naomi A., Zohar Joseph, vanAmeringen Michael, Juven-Wetzler Alzbeta, Altamura Alfredo Carlo, Cuzen Natalie L.,Hollander Eric, Denys Damiaan, Nicolini Humberto, Dell‘Osso Bernardo, Pallanti Ste-fano, Stein Dan J., Magrina Jose Menchon, Hranov Lucheza, Karamustafalioglu Oguz,Marazziti Donatella, Comorbidity in Obsessive-Compulsive Disorder (OCD): A Reportfrom the International College of Obsessive-Compulsive Spectrum Disorders (ICOCS),Comprehensive Psychiatry (2014), doi: 10.1016/j.comppsych.2014.05.020
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
1 | P a g e
Comorbidity in Obsessive-Compulsive Disorder (OCD):
A Report from the International College of Obsessive-Compulsive Spectrum Disorders (ICOCS)
Christine Lochner1*
; Naomi A. Fineberg2,3,4
; Joseph Zohar5; Michael van Ameringen
6; Alzbeta Juven-
Wetzler5; Alfredo Carlo Altamura
7; Natalie L. Cuzen
8, Eric Hollander
9; Damiaan Denys
10,11; Humberto
Nicolini12
; Bernardo Dell‘Osso7; Stefano Pallanti
13; Dan J. Stein
1,8
1. MRC Unit on Anxiety and Stress Disorders, Department of Psychiatry, University of
Stellenbosch, South Africa
2. Behavioural and Clinical Neuroscience Institute, University of Cambridge, Cambridge
3. Department of Psychiatry (NAF), Queen Elizabeth II Hospital, Welwyn Garden City,
Hertfordshire
4. Postgraduate Medical School (NAF), University of Hertfordshire, Hatfield, United Kingdom
5. Chaim Sheba Medical Center, Department of Psychiatry, Israel
6. Department of Psychiatry and Behavioural Neurosciences, McMaster University, Ontario, Canada
7. Department of Psychiatry, University of Milan, Fondazione IRCCS Policlinico, Milano
8. Department of Psychiatry and Mental Health, University of Cape Town, South Africa
9. Department of Psychiatry, Montefiore Medical Center University Hospital, Albert Einstein College of
Medicine, New York, New York
10. Department of Psychiatry, Academic Medical Center, University of Amsterdam, the Netherlands
11. The Netherlands Institute for Neuroscience, an Institute of the Royal Netherlands Academy of Arts
and Sciences, Amsterdam, the Netherlands
12. Carracci Medical Centre, Mexico City, Mexico
13. Department of Psychiatry, University of Florence, Florence, Italy
ICOCS Project Group:
Jose Menchon Magrina1, Lucheza Hranov
2, Oguz Karamustafalioglu
3, Donatella Marazziti
4
1. Neuroscience Group-Institut d'Investigació Biomèdica de Bellvitge, Psychiatry Department, Bellvitge
University Hospital-Catalan Health Institute, University of Barcelona, Centro de Investigación Biomédica
en Red de Salud Mental
2. Department of Psychiatry, University Hospital of Neurology and Psychiatry, St. Naum, Sofia, Bulgaria

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
2 | P a g e
3. Sisli Etfal Research and Teaching Hospital, Department of Psychiatry, Istanbul, Turkey.
4. Dipartimento d Medicina Clinica e Sperimentale, University of Pisa, Pisa, Italy
* To whom correspondence should be addressed:
PO Box 19063, Tygerberg, 7505
South Africa
Email: [email protected]

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
3 | P a g e
ABSTRACT
Background: Obsessive-compulsive disorder (OCD) is often associated with significant psychiatric
comorbidity. Comorbid disorders include mood and anxiety disorders as well as obsessive-
compulsive spectrum disorders (OCSDs). This paper aims to investigate comorbidity of DSM Axis I-
disorders, including OCSDs, in patients with OCD from 10 centers affiliated with the International
College of Obsessive-Compulsive Spectrum Disorders (ICOCS).
Methods: This is a cross-sectional study of comorbidity of Axis I disorders including OCSDs in 457
outpatients with primary OCD (37% male; 63% female), with ages ranging from 12 to 88 years (mean:
39.8 ± 13). Treating clinicians assessed Axis I disorders using the Mini International Neuropsychiatric
Interview and assessed OCSDs using the Structured Clinical Interview for OCD related/spectrum
disorders (SCID-OCSD).
Results: In terms of the OCSDs, highest comorbidity rates were found for tic disorder (12.5%), BDD
(8.71%) and self-injurious behaviour (7.43%). In terms of the other Axis I-disorders, major depressive
disorder (MDD; 15%), social anxiety disorder (SAD; 14%), generalized anxiety disorder (GAD; 13%)
and dysthymic disorder (13%) were most prevalent.
Discussion: High comorbidity of some OCSDs in OCD supports the formal recognition of these
conditions in a separate chapter of the nosology. Rates of other Axis I disorders are high in both the
general population and in OCSDs, indicating that these may often also need to be the focus of
intervention in OCD.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
4 | P a g e
BACKGROUND
Obsessive-compulsive disorder (OCD) is often associated with significant psychiatric comorbidity, in
both epidemiological [[1,2]] and clinical studies [[3]]. DSM-IV Axis I comorbidity in OCD consists not
only of anxiety and mood disorders but also of obsessive-compulsive spectrum (including impulse-
control), substance use and psychotic disorders. In the National Comorbidity Survey Replication
(NCS-R), a nationally representative survey of U.S. adults [[2]], the most common comorbid conditions
in OCD were anxiety disorders (75.8%), followed by mood disorders (63.3%), impulse-control
disorders (55.9%), and substance use disorders (38.6%). Clinical samples (e.g. [[4-7]]) have
demonstrated similar patterns.
The relationship between OCD and the putative OCD spectrum disorders (OCSDs) has been the
focus of considerable discussion. The OCSDs are thought to be related to OCD insofar as they have
similar phenomenological and psychobiological features, are assessed and evaluated in analogous
ways, and may respond to a somewhat similar set of interventions. In DSM-5, several of the putative
OCD spectrum disorders were included in the new chapter of obsessive-compulsive and related
disorders [[8]], reflecting the literature on the diagnostic validity and clinical utility of this construct.
While many studies have discussed the relationship between OCD and specific OCD spectrum
disorders, surprisingly few studies have systematically investigated the comorbidity of OCDSDs in
OCD patients. An early study by Du Toit and colleagues [[4]] showed that 57.6% of their sample
currently met criteria for at least one putative OCSD, and that 67.1% had a lifetime history of at least
one comorbid OCSD. In that study, the OCSDs with the highest prevalence were compulsive self-
injury (22.4%), compulsive buying (10.6%), and intermittent explosive disorder (10.6%). More
recently, a cluster analysis of OCSDs in a sample of 210 OCD patients identified 3 separate clusters
that were named: i.) “Reward deficiency” (including hair-pulling disorder [trichotillomania, or HPD],
pathological gambling, hypersexual disorder and Tourette’s disorder [TD]), ii.) “Impulsivity” (including
compulsive shopping, kleptomania, eating disorders, self-injury and intermittent explosive disorder,
and iii.) “Somatic” (including body dysmorphic disorder [BDD] and hypochondriasis) [[9]]. However,
there is a need to assess whether such comorbidity findings also hold in different contexts. There is
also a need to determine the relationship between such comorbidity and OCD severity.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
5 | P a g e
Further investigation of comorbidity in OCD is important for a number of reasons. First, comorbidity
may influence treatment decisions (e.g. [[10]]); for example, patients with severe depression require
robust antidepressant treatment [[11]], or modified psychotherapy since they may find exposure and
response prevention (ERP) - a specialized form of cognitive behavioral therapy (CBT) – difficult [[10]],
Also, patients with comorbid tic disorders may require pharmacotherapy augmentation with a D2
antagonist (e.g. [[12]]). Second, comorbidity patterns may shed light on the pathogenesis of OCD and
OCSDs; for example, findings that TD is common in OCD patients and family members while OCD is
common in TD patients and family members have led to strong interest in genetic overlap between the
conditions [[13,14]] . Third, comorbidity patterns may impact on discussions about the nosology of
OCD and OCSDs; high comorbidity of a particular putative OCSD in OCD may suggest a more
specific relationship between such a condition and OCD (e.g. [[9,15,16]]).
The International College of Obsessive-Compulsive Spectrum Disorders (ICOCS) includes clinical
research sites from across the globe - i.e. North America (Canada, the United States and Mexico),
Africa (South Africa), Europe (Spain, Italy, Turkey, Bulgaria), and the Middle East (Israel) – providing a
unique database of 504 OCD patients with demographic, diagnostic, treatment and symptom severity
data. This cross-sectional study of OCD aimed at obtaining a “snap shot” view of the rates of
comorbidity of DSM Axis I-disorders, including the OCSDs.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
6 | P a g e
METHODS
Consecutive patients at different stages of treatment were recruited at nine of the ICOCS sites. Out of
the total of 504, there were some comorbidity data for 462 consecutive outpatients with a primary
diagnosis OCD. Data from patients with a current diagnosis of schizophrenia or other psychotic
disorders were excluded from the analyses (N=5).
Written informed consent was obtained from all patients. The Institutional Review Boards of the
participating sites approved the relevant protocol and consent procedures at each site. Socio-
demographic and clinical data were collected after the project was approved by the IRB’s of the
respective sites and the data were subsequently included in a common web-database.
Measures:
OCD participants were interviewed by clinical psychologists, psychiatrists or other mental health
professionals with expertise in the field (but including trainees who work under the supervision of
experienced clinicians). A basic demographics questionnaire to assess age, gender, nationality,
educational status, current professional status and level of income was included. The Mini-
International Neuropsychiatric Interview (MINI) [[17,18]], a short structured diagnostic interview. was
administered to diagnose OCD and any current psychiatric (non-OCSD) comorbidity (DSM-IV criteria
[[19,20]]). This instrument is used widely in psychiatric settings and has been shown to have sound
psychometric properties [[18,21,22]]. If a comorbid disorder was present, OCD had to be the primary
diagnosis, i.e. causing the most impairment and distress. The SCID-OCSD [[4]] was used (at some
sites) to assess for the presence of comorbid OCSDs. This instrument follows the structure of the
established SCID-I/P [23]), but the psychometric properties of this scale have not been evaluated yet.
The Yale-Brown Obsessive Compulsive Scale (YBOCS) [[24]] is a rater-administered 10-item scale
that was included as the OCD severity measure. It focuses on 5 domains for obsessions and
compulsions, including time, distress, interference, resistance, and control. The YBOCS has
established reliability and validity, is widely accepted as the major outcome measure for OCD [[24]].
The different sites used either validated assessment scales, or the English versions of scales.
Data analysis:
For the present investigation, comorbidity of mood, anxiety, and substance use disorders as well as a

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
7 | P a g e
broad range of selected putative OCSDs (anorexia nervosa, bulimia nervosa, binge-eating disorder,
BDD, compulsive shopping, kleptomania, pathological gambling, intermittent explosive disorder,
hypersexual disorder, tic disorder, TD, and HPD) (using DSM-IV criteria [[19,20]]) were assessed. In
addition, patients at the participating sites were compared in terms of available demographic and
clinical variables (i.e. age, gender, educational level, income, professional status and
pharmacotherapy type) which may affect comorbidity,
Data analysis was performed using Statistica software (Statsoft 12, version 2, 2013). Chi-square
analyses and analysis of variance (ANOVA) were used to examine the associations between
variables. Bootstrap analysis were used where the assumption of normal data distribution could not
be made.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
8 | P a g e
RESULTS
Demographics:
The sample included 457 consecutive outpatients consisting of 171 males (37%) and 286 females
(63%), with ages ranging from 12 to 88 years (mean: 39.8 ± 13 years). The mean number of years in
education for the whole sample was 13.16 (SD: 3.66). Participants from the different sites differed
significantly in terms of age, gender and level of education (all p<0.001).
In terms of their professional status (with options: working / unemployed / student / retired),
approximately 70% of the sample reported that they were currently employed (54%) or were studying
(16.6%). Twenty two percent were unemployed and 7.3 % reported retirement. Income varied widely
in the sample, with 53.5% reporting above average, 19.4% average, and 26.8% below average
income. Study sites differed significantly on both these variables (both p<0.001).
Comorbidity findings:
The numbers of patients for whom comorbidity data were available varied from disorder to disorder
(the exact numbers of patients for whom data were available are included in the tables).
Comorbidity: Axis I-disorders (non-OCSDs)
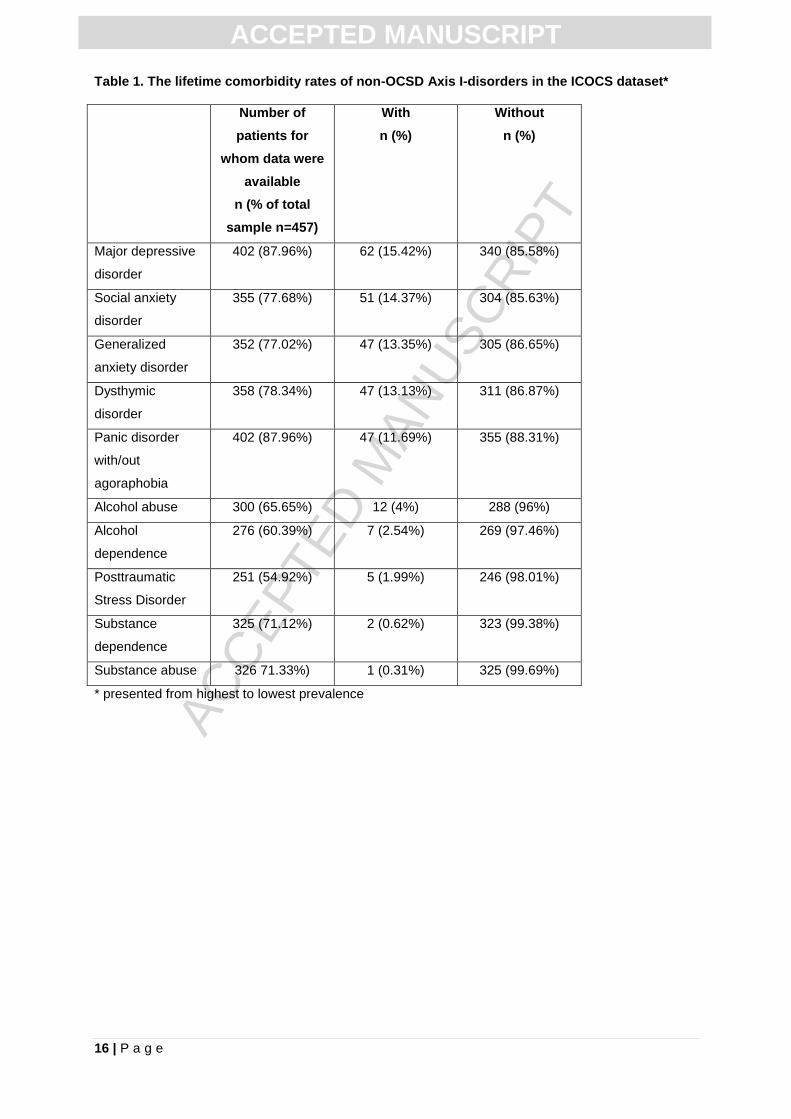
Table 1 depicts the mean current comorbidity rates of Axis I-disorders (i.e., non-OCSDs) in the ICOCS
dataset. Highest comorbidity rates were noted for major depressive disorder (MDD; 15.42%), social
anxiety disorder (SAD; 14.37%), generalized anxiety disorder (GAD; 13.35%) and dysthymic disorder
(13.13%).
[Insert Table 1 here]
Data for all of the above non-OCSD Axis-I disorders were available for 149 individuals. The total
number of these comorbid conditions per patient ranged between 0 and 6. There were 63 (42.3% of
the total) patients with 1 or more of these comorbid conditions. The correlation between the number of
comorbid non-OCSD Axis I-disorders per patient and age was not significant. There was a significant
positive correlation between the number of comorbid non-OCSD Axis I-disorders and OCD severity
(r=0.26; p<0.01).

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
9 | P a g e
Comorbidity: OCSDs
Lifetime comorbidity rates of OCSDs in the ICOCS dataset are depicted in Table 2. Highest
comorbidity rates were found for tic disorder (12.5%), BDD (8.71%) and self-injurious behaviours
(7.43%). Five percent (5.3%) had intermittent explosive disorder and HPD, respectively.
[Insert Table 2 here]
Data for all the comorbid conditions (i.e. OCSD and non-OCSD) were available for 118 individuals.
The total number of comorbid conditions per patient ranged between 0 and 7, with 64 (54.2%) having
one or more. The number of comorbid OCSDs per patient, and age and OCD severity, respectively,
were not significantly correlated.
Cross-national comorbidity rates:
Comorbidity rates of some Axis I-disorders differed significantly across sites (Table 3). These were
MDD (p=0<001), dysthymic disorder (p<0.001), SAD (p<0.001), GAD (p=0.02) and panic disorder
(p=0.006). The number of Axis I disorders also differed significantly across sites (p=0.03); post hoc
analyses indicated that the South African sample had significantly larger number of comorbid Axis I
compared to Spain (p=0.007).
Comorbidity rates of OCSDs also differed significantly across sites (Table 3), for tic disorder
(p<0.001), BDD (p<0.001), self-injurious behaviours (p<0.001), anorexia nervosa (p=0.002), bulimia
nervosa (p<0.001), binge-eating disorder (p=0.003), HPD (p<0.001) and compulsive shopping
(p=0.001). However, the different sites did not differ significantly in terms of the total number of
comorbid OCSDs.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
10 | P a g e
DISCUSSION
This study provides rates of comorbidity of DSM Axis I-disorders, including the OCSDs, in a large
sample of OCD patients from 9 ICOCS centers from around the globe. The highest comorbidity rates
of anxiety and mood disorders were for MDD, SAD, GAD and dysthymic disorder. The highest
comorbidity rates of OCSDs were for tic disorder, BDD and self-injurious behaviours. The number of
comorbid disorders correlated positively with OCD severity.
There is much evidence to suggest high prevalence of anxiety and mood disorders in OCD. Previous
clinical studies reports high rates of lifetime comorbidity between OCD and other anxiety disorders;
ranging from 18% for SAD and 12% for panic disorder (e.g. [25,26]), and 20% and higher for GAD
(e.g. [[25,27]]). Similarly, many clinical OCD studies have found high rates of current depression (e.g.
between 13-73% of children with OCD have comorbid depression [[28,29]] and approximately 50-80%
of adults with OCD have comorbid depression [[30]]). In our study, rates of anxiety and mood
disorders were generally slightly lower (e.g. 14.37% with SAD, 11.69% with panic disorder, 13.35%
with GAD and 15.42% with depression) than in a number of these previous publications, perhaps
reflecting that many of the patients included in our study were already on effective treatment. Notably,
of the 361 participants with available data on psychopharmacotherapy, 317 (87.81%) were on
psychotropic medication at the time of the assessments [[31]], and clinical improvement rates for the
SSRIs indeed indicated relatively good treatment response. Alternatively, however, we may have
missed some of the lifetime diagnoses owing to the ‘snapshot’ single interview method, which is
subject to recall bias. Prospective longitudinal studies, such as the Brown Longitudinal Obsessive-
Compulsive study [[6]] and the Zurich cohort study [[1]] that found rates of depression around 67% and
60%, respectively, may be less subject to such bias.
Rates of comorbid substance use disorders (SUDs) in our sample were less than 1%. This finding
also stands in contrast to earlier clinical studies that found much higher rates (e.g. 27% of 323 OCD
patients in another study [[32]]). However, our results are consistent with those of Denys et al [[33]]
and a prospective longitudinal cohort study of OCD [[1]], in which the rate of either alcohol or drug
abuse disorder was not elevated. In addition, a recent large-scale case-control family-based study
was unable to show a direct association between OCD and substance abuse [[34]]. Indeed, it has

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
11 | P a g e
been suggested that while there is a high rate of SUDs in community studies of OCD, in patients with
more severe illness, seen in specialized clinics, there is less such comorbidity [[35]].
Rates of comorbid OCSDs were also high, particularly given the relatively low base rate of many such
disorders in the general population. This is consistent with earlier work [[4]], which has emphasized
the high prevalence of tic disorders as well as OCDS in OCD. However, comorbidity in the current
sample was lower than in some previous work [[36,37]]. Indeed, there were differences in comorbidity
rates across sites in our sample, consistent with different thresholding of the clinical significance
criteria or other methodological differences across sites.
Nevertheless, the relative high comorbidity of some of the OCSDs in OCD found here arguably
supports the formal recognition of some of these conditions in a separate chapter of the nosology; i.e.
that on obsessive-compulsive and related disorders. Our data on the high rates of tics in OCD, for
example, support the DSM-5 proposal to have a subtype of tic-related OCD; individuals with OCD and
tics often have earlier onset of OCD, are more likely to be male, and may be less likely to respond to
standard first line treatments [[38]].
It is notable that the severity of OCD symptoms correlated strongly with the number of comorbid
anxiety and mood disorders. Comorbid anxiety and affective disorders have previously been
associated with increased OCD severity and duration of illness, respectively [[1]]. However there are
surprisingly few randomized controlled trials on the treatment of OCD with comorbid anxiety and mood
disorders. For example, it is important to know, say, whether OCD with comorbid anxiety is
associated with a greater response to adjunctive antipsychotic agents, or whether comorbid substance
abuse is associated with a greater response to adjunctive treatment with mood-stabilizing agents.
Our findings are tempered by a few limitations, including the relatively small sample size and the
relative paucity of data on comorbid Axis I-disorders (non-OCSDs) on the ICOCS database. Thus
there is insufficient statistical power to make strong claims about differences in comorbidity across
site, and there is a need for additional work on the relationship between OCD and a range of other
conditions such as bipolar disorder [[39]]. In addition, information on the specific stages of medication
treatment (i.e. whether patients were at the beginning of, or at the end of a course of
pharmacotherapy) which may have influenced comorbidity rates, was not available for analysis.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
12 | P a g e
Information on response to CBT or whether the CBT trials were optimal (e.g. adequate number of
sessions, with expert clinicians etc.) was also not available. Nevertheless, the pharmacotherapy
response data that were available generally suggested good treatment response in the majority of the
sample, perhaps explaining the lower rates of comorbidity found here compared to previous literature.
The lack of validated translations of assessment scales in some countries is another important study
limitation. Nevertheless, the fact that this was an international sample is one of the strengths of the
project and the findings here are consistent with those which have emerged from prior single site
studies. Moreover, the international nature of our sample puts us in a position to address the question
whether comorbidity in OCD differs across regions. However, as noted above, such differences may
reflect differences in varous factors across sites, including differences in terms of socio-demographic
variables, which cannot be fully investigated here. For example, the very high prevalence rates of
mood disorders (MDD and dysthymia) and some of the anxiety disorders (GAD and PD) at the Turkish
site, and the very high prevalence of BDD in participants from Canada, deserves further consideration.
In conclusion, high comorbidity of (some) OCSDs in OCD arguably supports the formal recognition of
these conditions in a separate chapter of the nosology and pathogenesis. On the other hand, rates of
other non-OCSD (Axis I-) disorders are also high, indicating that these may often also need to be the
focus of intervention in OCD. Future longitudinal studies should examine risk factors for comorbidity in
OCD, as well as its impact on treatment outcomes.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
13 | P a g e
Reference List
[1] N. A. Fineberg, M. P. Hengartner, C. Bergbaum, T. Gale, W. Rossler, and J. Angst, Lifetime comorbidity of obsessive-compulsive disorder and sub-threshold obsessive-compulsive symptomatology in the community: impact, prevalence, socio-demographic and clinical characteristics, Int J Psychiatry Clin Pract., 17 (2013), pp. 188-196.
[2] A. M. Ruscio, D. J. Stein, W. T. Chiu, and R. C. Kessler, The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication, Mol. Psychiatry, 15 (2010), pp. 53-63.
[3] G. Nestadt, C. Z. Di, M. A. Riddle, M. A. Grados, B. D. Greenberg, A. J. Fyer, J. T. McCracken, S. L. Rauch, D. L. Murphy, S. A. Rasmussen, B. Cullen, A. Pinto, J. A. Knowles, J. Piacentini, D. L. Pauls, O. J. Bienvenu, Y. Wang, K. Y. Liang, J. F. Samuels, and K. B. Roche, Obsessive-compulsive disorder: subclassification based on co-morbidity, Psychol. Med., 39 (2009), pp. 1491-1501.
[4] P. L. du Toit, J. van Kradenburg, D. Niehaus, and D. J. Stein, Comparison of obsessive-compulsive disorder patients with and without comorbid putative obsessive-compulsive spectrum disorders using a structured clinical interview, Compr Psychiatry, 42 (2001), pp. 291-300.
[5] V. H. LaSalle, K. R. Cromer, K. N. Nelson, D. Kazuba, L. Justement, and D. L. Murphy, Diagnostic interview assessed neuropsychiatric disorder comorbidity in 334 individuals with obsessive-compulsive disorder, Depress. Anxiety., 19 (2004), pp. 163-173.
[6] A. Pinto, M. C. Mancebo, J. L. Eisen, M. E. Pagano, and S. A. Rasmussen, The Brown Longitudinal Obsessive Compulsive Study: clinical features and symptoms of the sample at intake, J Clin Psychiatry, 67 (2006), pp. 703-711.
[7] C. S. Rubenstein, T. A. Pigott, F. L'Heureux, J. L. Hill, and D. L. Murphy, A preliminary investigation of the lifetime prevalence of anorexia and bulimia nervosa in patients with obsessive compulsive disorder, J Clin Psychiatry, 53 (1992), pp. 309-314.
[8] American Psychiatric Association, DSM-5: Diagnostic and Statistical Manual of Mental Disorders, American Psychiatric Publishing, Washington DC 2013.
[9] C. Lochner, S. M. Hemmings, C. J. Kinnear, D. J. Niehaus, D. G. Nel, V. A. Corfield, J. C. Moolman-Smook, S. Seedat, and D. J. Stein, Cluster analysis of obsessive-compulsive spectrum disorders in patients with obsessive-compulsive disorder: clinical and genetic correlates, Compr. Psychiatry, 46 (2005), pp. 14-19.
[10] K. H. Walsh and C. J. McDougle, Psychotherapy and medication management strategies for obsessive-compulsive disorder, Neuropsychiatr. Dis. Treat., 7 (2011), pp. 485-494.
[11] G. E. Anholt, I. M. Aderka, A. J. van Balkom, J. H. Smit, H. Hermesh, H. E. de, and O. P. van, The impact of depression on the treatment of obsessive-compulsive disorder: results from a 5-year follow-up, J Affect Disord, 135 (2011), pp. 201-207.
[12] T. K. Murphy, P. J. Mutch, J. M. Reid, P. J. Edge, E. A. Storch, M. Bengtson, and M. Yang, Open label aripiprazole in the treatment of youth with tic disorders, J Child Adolesc. Psychopharmacol, 19 (2009), pp. 441-447.
[13] J. C. Holzer, W. K. Goodman, C. J. McDougle, L. Baer, B. K. Boyarsky, J. F. Leckman, and L. H. Price, Obsessive-compulsive disorder with and without a chronic tic disorder. A comparison of symptoms in 70 patients, Br J Psychiatry, 164 (1994), pp. 469-473.
[14] D. L. Pauls, J. P. Alsobrook, W. Goodman, S. Rasmussen, and J. F. Leckman, A family study of obsessive-compulsive disorder, Am J Psychiatry, 152 (1995), pp. 76-84.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
14 | P a g e
[15] C. Lochner and D. J. Stein, Does work on obsessive-compulsive spectrum disorders contribute to understanding the heterogeneity of obsessive-compulsive disorder?, Prog Neuropsychopharmacol Biol Psychiatry, 30 (2006), pp. 353-361.
[16] C. Lochner and D. J. Stein, Obsessive-compulsive spectrum disorders in obsessive-compulsive disorder and other anxiety disorders, Psychopathology, 43 (2010), pp. 389-396.
[17] D. V. Sheehan, Y. Lecrubier, J. Janavs, and et al, Mini-international neuropsychiatric interview (MINI)., University of South Florida Institute for Research in Psychiatry and INSERM-Hopital de la Salpetriere, Paris, Tampa, Florida, USA, and Paris, Florence 1994.
[18] D. V. Sheehan, Y. Lecrubier, K. H. Sheehan, P. Amorim, J. Janavs, E. Weiller, T. Hergueta, R. Baker, and G. C. Dunbar, The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10, J Clin Psychiatry, 59 Suppl 20 (1998), pp. 22-33.
[19] American Psychiatric Association, Diagnostic and statistical manual of mental disorders IV, 1994.
[20] American Psychiatric Association, American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders 4th edition - Text revision (DSM-IV-TR), American Psychiatric Association, Washington, DC 2000.
[21] Y. Lecrubier, D. Sheehan, E. Weiller, and et al, The Mini International Neuropsychiatric Interview (M.I.N.I.): a short diagnostic structured interview: reliability and validity according to the CIDI., European Psychiatry, 12 (1997), pp. 224-231.
[22] D. V. Sheehan, Y. Lecrubier, K. H. Sheehan, and et al, The validity of the Mini International Neuropsychiatric Interview (M.I.N.I.) according to the SCID-P and its reliability. European Psychiatry, 12 (1997), pp. 232-241.
[23] M. B. First, R. L. Spitzer, M. Gobbon, and J. B. W. Williams, Structured clinical interview for DSM-IV Axis I disorders - Patient edition (SCID-I/P, Version 2.0, 8/98 revision), New York State Psychiatric Institute, Biometrics Research Department, New York 1998.
[24] W. K. Goodman, L. Price, Rasmussen SA, C. Mazure, R. Fleischmann, C. Hill, and et al, The Yale-Brown Obsessive Compulsive Scale. I. Development, use, and reliability., Arch Gen Psychiatry, 46 (1989), pp. 1006-1011.
[25] V. Brakoulias, V. Starcevic, P. Sammut, D. Berle, D. Milicevic, K. Moses, and A. Hannan, Obsessive-compulsive spectrum disorders: a comorbidity and family history perspective, Australas. Psychiatry, 19 (2011), pp. 151-155.
[26] T. A. Pigott, F. L'Heureux, B. Dubbert, S. Bernstein, and D. L. Murphy, Obsessive compulsive disorder: comorbid conditions, J Clin Psychiatry, 55 Suppl (1994), pp. 15-27.
[27] J. L. Eisen, W. K. Goodman, M. B. Keller, M. G. Warshaw, L. M. DeMarco, D. D. Luce, and S. A. Rasmussen, Patterns of remission and relapse in obsessive-compulsive disorder: a 2-year prospective study, J Clin Psychiatry, 60 (1999), pp. 346-351.
[28] D. A. Geller, J. Biederman, S. Griffin, J. Jones, and T. R. Lefkowitz, Comorbidity of juvenile obsessive-compulsive disorder with disruptive behavior disorders, J Am Acad. Child Adolesc. Psychiatry, 35 (1996), pp. 1637-1646.
[29] D. A. Geller, B. Coffey, S. Faraone, L. Hagermoser, N. K. Zaman, C. L. Farrell, B. Mullin, and J. Biederman, Does comorbid attention-deficit/hyperactivity disorder impact the clinical expression of pediatric obsessive-compulsive disorder?, CNS. Spectr., 8 (2003), pp. 259-264.
[30] L. Besiroglu, F. Uguz, M. Saglam, M. Y. Agargun, and A. S. Cilli, Factors associated with major depressive disorder occurring after the onset of obsessive-compulsive disorder, J Affect. Disord., 102 (2007), pp. 73-79.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
15 | P a g e
[31] Van Ameringen M., W. Simpson, B. Patterson, B. Dell'Osso, N. Fineberg, E. Hollander, L. Hranov, G. Hranov, C. Lochner, O. Karamustafalioglu, D. Marazziti, J. M. Menchon, H. Nicolini, S. Pallanti, D. J. Stein, and J. Zohar, Pharmacological treatment strategies in obsessive compulsive disorder: A cross-sectional view in nine international OCD centers, J Psychopharmacol, (2014).
[32] M. C. Mancebo, J. E. Grant, A. Pinto, J. L. Eisen, and S. A. Rasmussen, Substance use disorders in an obsessive compulsive disorder clinical sample, J Anxiety. Disord., 23 (2009), pp. 429-435.
[33] D. Denys, N. Tenney, H. J. van Megen, G. F. de, and H. G. Westenberg, Axis I and II comorbidity in a large sample of patients with obsessive-compulsive disorder, J Affect. Disord., 80 (2004), pp. 155-162.
[34] R. MacDonald, R. M. Crum, C. L. Storr, A. Schuster, and O. J. Bienvenu, Sub-clinical anxiety and the onset of alcohol use disorders: longitudinal associations from the Baltimore ECA follow-up, 1981-2004, J Addict. Dis., 30 (2011), pp. 45-53.
[35] N. L. Cuzen, D. J. Stein, C. Lochner, and N. A. Fineberg, Comorbidity of obsessive-compulsive disorder and substance use disorder: a new heuristic, Hum. Psychopharmacol, 29 (2014), pp. 89-93.
[36] H. L. Leonard, M. C. Lenane, S. E. Swedo, D. C. Rettew, E. S. Gershon, and J. L. Rapoport, Tics and Tourette's disorder: a 2- to 7-year follow-up of 54 obsessive-compulsive children, Am J Psychiatry, 149 (1992), pp. 1244-1251.
[37] R. K. Pitman, R. C. Green, M. A. Jenike, and M. M. Mesulam, Clinical comparison of Tourette's disorder and obsessive-compulsive disorder, Am J Psychiatry, 144 (1987), pp. 1166-1171.
[38] C. Lochner and D. J. Stein, Heterogeneity of obsessive-compulsive disorder: a literature review, Harv. Rev. Psychiatry, 11 (2003), pp. 113-132.
[39] N. A. Fineberg, D. S. Baldwin, J. M. Menchon, D. Denys, E. Grunblatt, S. Pallanti, D. J. Stein, and J. Zohar, Manifesto for a European research network into obsessive-compulsive and related disorders, Eur Neuropsychopharmacol, 23 (2013), pp. 561-568.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
16 | P a g e
Table 1. The lifetime comorbidity rates of non-OCSD Axis I-disorders in the ICOCS dataset*
Number of
patients for
whom data were
available
n (% of total
sample n=457)
With
n (%)
Without
n (%)
Major depressive
disorder
402 (87.96%) 62 (15.42%) 340 (85.58%)
Social anxiety
disorder
355 (77.68%) 51 (14.37%) 304 (85.63%)
Generalized
anxiety disorder
352 (77.02%) 47 (13.35%) 305 (86.65%)
Dysthymic
disorder
358 (78.34%) 47 (13.13%) 311 (86.87%)
Panic disorder
with/out
agoraphobia
402 (87.96%) 47 (11.69%) 355 (88.31%)
Alcohol abuse 300 (65.65%) 12 (4%) 288 (96%)
Alcohol
dependence
276 (60.39%) 7 (2.54%) 269 (97.46%)
Posttraumatic
Stress Disorder
251 (54.92%) 5 (1.99%) 246 (98.01%)
Substance
dependence
325 (71.12%) 2 (0.62%) 323 (99.38%)
Substance abuse 326 71.33%) 1 (0.31%) 325 (99.69%)
* presented from highest to lowest prevalence

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
17 | P a g e
Table 2. Lifetime comorbidity rates of OCSDs in the ICOCS dataset*
Number of
patients for
whom data were
available
n (% of total
sample n=457)
With
n (%)
Without
N (%)
Tic disorder 376 (82.28%) 47 (12.5%) 329 (87.5%)
Body dysmorphic
disorder
241 (52.73%) 21 (8.71%) 220 (91.29%)
Self-injurious
behaviours
269 (80.74%) 20 (7.43%) 249 (92.57%)
Compulsive
shopping
244 (53.39%) 17 (6.97%) 227 (93.03%)
Intermittent
explosive disorder
244 (53.39%) 13 (5.33%) 231 (94.67%)
Hair-pulling
disorder
(trichotillomania)
245 (53.61%) 13 (5.31%) 232 (94.69%)
Tourette’s
disorder
261 (57.11%) 11 (4.21%) 250 (95.79%)
Binge-eating
disorder
387 (84.68%) 14 (3.62%) 373 (96.38%)
Anorexia Nervosa 249 (54.49%) 8 (3.21%) 241 (96.79%)
Kleptomania 247 (54.05%) 5 (2.02%) 242 (97.98%)
Bulimia Nervosa 243 (53.17%) 4 (1.64%) 239 (98.35%)
Pathological
gambling
242 (52.95%) 3 (1.24%) 239 (98.76%)
Hypersexual
disorder
241 (52.74%) 1 (0.4%) 240 (99.59%)
* presented from highest to lowest prevalence

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
18 | P a g e
Table 3. Lifetime comorbidity rates of non-OCSD Axis I-disorders and OCSDs across sites
Comorbi
d
conditio
ns
ICOCS sites (N (%)) Chi
-
squ
are
d
f
p
Mexi
co
Ne
w
Yo
rk*
Can
ada
Isra
el
Italy
(Mila
n)
Italy
(Flor
ence)
Bulg
aria
Spai
n
Turk
ey
Sout
h
Afric
a
Major
depressi
ve
disorder
2/13
(15.3
8%)
0/0 8/67
(11.9
4%)
5/55
(9.09
%)
1/51
(1.96
%)
9/46
(19.5
7%)
0/11 3/39
(7.69
%)
11/2
0
(55
%)
23/1
00
(23
%)
40.
16
9 <0.
001
Dysthymi
c
disorder
0/6 0/0 2/58
(3.45
%)
9/49
(18.3
7%)
0/47 6/41
(14.6
3%)
1/8
(12.5
%)
2/38
(5.26
%)
4/11
(36.3
6%)
23/1
00
(23
%)
36.
15
9 <0.
001
Social
anxiety
disorder
1/6
(16.6
7%)
0/0 21/6
2
(33.8
7%)
7/46
(15.2
2%)
2/44
(4.55
%)
0/45 1/8
(12.5
%)
3/37
(8.11
%)
1/7
(14.2
9%)
15/1
00
(15
%)
34.
77
9 <0.
001
Generali
zed
anxiety
disorder
1/8
(12.5
%)
0/0 4/59
(6.78
%)
5/41
(12.2
%)
9/50
(18
%)
5/39
(12.8
2%)
2/10
(20
%)
2/37
(5.41
%)
6/9
(66.6
7%)
13/9
9
(13.1
3%)
19.
97
9 0.0
2
Panic
disorder
with/out
agoraph
obia
2/13
(15.3
8%)
0/0 13/6
7
(19.4
%)
1/55
(1.82
%)
6/52
(11.5
4%)
9/52
(17.3
1%)
1/11
(9.09
%)
1/38
(2.63
%)
5/14
(35.7
1%)
9/10
0
(9%)
23.
12
9 0.0
06
Posttrau
matic
Stress
Disorder
0/5 0/0 0/4 3/46
(6.52
%)
0/6 0/35 0/9 0/36 0/10 2/10
0
(2%)
7.2
7
9 0.6
1
Alcohol
abuse
2/9
(22.2
0/0 2/23
(8.7
2/45
(4.44
4/44
(9.09
0/28 0/8 0/35 0 2/98
(2.04
14.
94
9 0.0
9

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
19 | P a g e
%) %) %) %) %)
Alcohol
depende
nce
1/5
(20
%)
0/0 1/19
(5.26
%)
2/39
(5.13
%)
0/46 0/22 0/2 0/37 1/7
(14.2
9%)
2/99
(2.02
%)
11.
34
9 0.2
5
Substanc
e abuse
0/12 0/0 0/27 0/43 1/43
(2.33
%)
0/33 0/9 0/38 0/23 0/98 4.0
7
9 0.9
1
Substanc
e
depende
nce
0/12 0/0 0/32 0/36 0/50 1/39
(2.56
%)
0/6 1/38
(2.63
%)
0/13 0/99 5.8 9 0.7
6
Tic
disorder
8/13
(61.5
4%)
0/0 5/62
(8.06
%)
13/2
7
(48.1
5%)
0/49 5/54
(9.26
%)
1/9
(11.1
1%)
4/36
(11.1
1%)
4/26
(15.3
8%)
7/10
0
(7%)
56.
09
9 <0.
001
Tourette’
s
disorder
1/10
(10
%)
0/0 1/5
(20
%)
5/54
(9.26
%)
0/5 1/37
(2.7%
)
0/4 1/39
(2.56
%)
1/8
(12.5
%)
1/99
(1.01
%)
10.
67
9 0.3
Hair-
pulling
disorder
(trichotill
omania)
4/4
(75
%)
0/0 2/3
(66.6
7%)
3/53
(5.66
%)
1/1
(100
%)
0/38 0/2 0/39 0/6 4/99
(4.04
%)
36.
76
9 <0.
001
Body
dysmorp
hic
disorder
1/3
(33.3
3%)
0/0 7/9
(77.7
8%)
1/55
(1.82
%)
0/0 0/30 0/2 3/39
(7.69
%)
0/7 9/96
(9.38
%)
38.
37
9 <0.
001
Binge-
eating
disorder
1/13
(7.69
%)
0/0 9/65
(13.8
5%)
2/55
(3.64
%)
1/50
(2%)
0/36 0/6 1/38
(2.63
%)
0/26 0/98 24.
86
9 0.0
03
Anorexia
Nervosa
0/1 0/0 4/11
(36.3
6%)
0/56 0/2 1/32
(3.13
%)
0/3 3/39
(7.69
%)
0/6 0/97 26.
28
9 0.0
02
Bulimia
Nervosa
0/1 0/0 3/10 0/53 1/1 0/31 0/3 0/38 0/9 0/97 28. 9 <0.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
20 | P a g e
(30
%)
57 001
Self-
injurious
behaviou
rs
1/2
(50
%)
0/0 14/2
7
(51.8
5%)
1/55
(1.82
%)
1/1
(100
%)
0/38 0/3 1/39
(2.56
%)
0/6 2/98
(2.04
%)
63.
44
9 <0.
001
Compulsi
ve
shopping
1/2
(50
%)
0/0 5/7
(71.4
3%)
1/53
(1.89
%)
0/1 1/34
(2.94
%)
0/3 2/37
(5.41
%)
0/7 7/10
0
(7%)
26.
98
9 0.0
01
Kleptom
ania
0/2 0/0 2/4
(50
%)
0/54 0/1 0/38 0/2 2/39
(5.13
%)
0/8 1/99
(1.01
%)
16.
4
9 0.0
6
Pathologi
cal
gambling
0/1 0/0 0/2 0/53 0/0 2/39
(5.13
%)
0/3 1/39
(2.56
%)
0/6 0/99 7.2
3
9 0.6
1
Intermitte
nt
explosive
disorder
0/3 0/0 3/9
(33.3
3%)
1/52
(1.92
%)
0/1 1/33
(3.03
%)
0/1 2/39
(5.13
%)
2/7
(28.5
7%)
4/99
(4.04
%)
13.
57
9 0.1
4
Hyperse
xual
disorder
0/0 0/0 1/4
(25
%)
0/53 0/1 0/36 0/3 0/39 0/6 0/99 8.4
7
9 0.4
9
* The New York site contributed 1 case with a primary diagnosis of OCD, of whom comorbidity data
were not available.




















