
Mapping Structural Brain Alterations in Obsessive-Compulsive Disorder

227
Progress in Neurotherapeutics and Neuropsychopharmacology, 3:1, 227–240 © 2008 Cambridge University PressDOI: 10.1017/S1748232107000146 Printed in the United Kingdom
Serotonin Related Genes AffectAntidepressant Treatment inObsessive–Compulsive Disorder
F. Van NieuwerburghLaboratory of Pharmaceutical Biotechnology, Ghent University, Ghent, Belgium;Email:[email protected]
D. DeforceLaboratory of Pharmaceutical Biotechnology, Ghent University, Ghent, Belgium;Email:[email protected]
D.A.J.P. DenysAMC, University of Amsterdam, Amsterdam, The Netherlands;Email:[email protected]
A B S T RAC T
Up to 60% of OCD patients do not respond to a regular serotonin reuptakeinhibitor (SRI) treatment. The purpose of the present study was to determinewhether polymorphisms of the serotonin transporter (5-HTT), 5-HT1D�, and5-HT2A receptor genes affect the efficacy of SRI treatment in OCD. Ninety-one outpatients with primary OCD according to DSM-IV criteria consentedto the study were randomly assigned a 12-week, double-blind trial to receivedosages titrated upward to 300 mg/day of venlafaxine, or 60 mg/day of paroxe-tine. Primary efficacy was assessed by the change from baseline on the Yale-Brown obsessive–compulsive scale (Y-BOCS), and response was defined as a �25% reduction on the Y-BOCS. All of the paroxetine treated patients,with the G/G genotype of the 5-HT2A polymorphism were responders (�2 � 8.66, df � 2, p � 0.013). In the venlafaxine treated patients, the majorityof responders carried the S/L genotype of the 5-HTTLPR polymorphism (�2 � 9.71, df � 2, p � 0.008). The small group of patients who both carriedthe S/L genotype of the 5-HTTLPR polymorphism and the G/G genotype ofthe 5-HT2A polymorphism responded all to treatment.
The results of this study suggest that the response in paroxetine and in venlafaxine treated OCD patients is associated with the G/G genotype of the
Correspondence should be addressed to: Damiaan Denys, AMC, University of Amsterdam, PA.2-179, PO Box 75867, 1070AW Amsterdam, The Netherlands; Email: [email protected]

5-HT2A polymorphism and with the S/L genotype of the 5-HTTLPR poly-morphism, respectively.
Key words: 5-HT1D�, 5-HT2A , 5-HTT, 5-HTTLPR, association study, obsessive–compulsive disorder,pharmacogenetics, serotonin, serotonin reuptake inhibitor, SSRI.
Introduction and Overview
Although serotonin reuptake inhibitors (SRIs) are the mainstay of treatment forOCD, up to 40–60% of OCD patients do not respond to an initial medicationtrial (Hollander et al., 2002; Goodman et al., 1998). Moreover, patients who failto respond to a treatment with a SRI have 25% less chance to achieve responsewith another SRI compared to a patient who previously responded to a SRI(Denys et al., 2003a). It is often necessary to switch between different selectiveSRIs (SSRIs) to find a more suitable alternative. This trial and error approach,where patients often do not display a full therapeutic response until several weeksafter initiation, is unfavorable. This makes SSRI treatment of OCD a classicexample where pharmacogenetics could bring a solution.
Reviews by Veenstra-VanderWeele et al. (2000) and Mancama & Kerwin (2003)give an overview of the role of pharmacogenetics in individualizing treatment withSSRIs and possible genetic influences on therapeutic response to drugs affecting theserotonin system. In OCD, three studies have investigated the role of the 5-HTTLPRand treatment response. McDougle et al. (1998) found an association of the L-allele with poorer response to SRIs, whereas Billett et al. (1997) and Di Bella et al.(2000) failed to find a relation between response and 5-HTT genotypes. Otherreceptors that might be involved in the therapeutic efficacy of SRIs are the terminal5-HT1D� auto-receptor and the postsynaptic 5-HT2A receptor. Except for Tot et al.who failed to find an association between the -1438G/A and T102C polymorphismof the 5-HT2A receptor in 52 OCD patients following a 12-week trial with fluvox-amine, fluoxetine, or sertraline, no further study has investigated the 5-HT2A or5-HT1D� receptor genes with regard to treatment response of SRIs in OCD.
Purpose of the Trial
In this study we tested the hypothesis that polymorphisms of the 5-HTT (L-alleleof the 5-HTTLPR), 5-HT1D�, and 5-HT2A gene are associated with treatmentresponse with SRIs in OCD. We report the results of 91 patients who participatedin 12-week, double-blind trial with paroxetine and venlafaxine and were assessedfor the 44 bp insertion/deletion 5-HTTLPR, the 5-HT1D� G861C, and the 5-HT2A 1438G/A polymorphism.
228 F. Van Nieuwerburgh et al.

Agents
The usefulness of the tricyclic antidepressant (TCA) clomipramine and SSRIs inOCD has been well established. Like the other SSRIs, paroxetine is better toler-ated than the TCAs, causing few anticholinergic adverse effects.Like clomipramine,venlafaxine, and its active metabolite O-desmethyl venlafaxine, are potentinhibitors of the neuronal uptake of both serotonin and norepinephrine, and weakinhibitors of the reuptake of dopamine. Contrary to clomipramine, venlafaxinelacks the anticholinergic, antihistaminergic, and alpha-adrenergic blockingeffects. Therefore, venlafaxine is less likely to produce adverse side effects relatedto these pharmacological properties (Denys et al., 2003b).
A randomized double-blind comparison study of paroxetine and venlafaxinein patients with obsessive–compulsive disorder showed no significant differencesbetween venlafaxine and paroxetine with regard to response or responder rates.The incidence of adverse events for venlafaxine and paroxetine was comparable(Denys et al., 2003b).
Clinical Trial
Subjects
Ninety-one outpatients gave written informed consent to participate in this studywhich had been approved by the University of Utrecht Medical Ethical Reviewcommittee (Utrecht, The Netherlands). All patients were diagnosed with OCDaccording to DSM-IV criteria and the M.I.N.I., a clinical and structured interview,was used to confirm the diagnosis (Sheehan et al., 1998) Severity of obsessive–compulsive symptoms was rated with the Y-BOCS, depressive symptoms withthe HAM-D, and anxiety with the HAM-A (Goodman et al., 1989; Hamilton,1959; 1960). Only patients with a score of at least 18 on the Y-BOCS, or at least12, if only obsessions or only compulsions were present, were included. Patientswith a major depressive disorder or patients with a total score of 15 or more on the 17-item Hamilton depression rating scale (HAM-D) on admission wereexcluded. Information on family history of OCD and other psychiatric disorderswas obtained by direct interviews with the patients and the presence of vocaland/or motor tics was assessed during the clinical interview.
Trial Methods
Patients were randomly assigned to receive either paroxetine or venlafaxine XRfor 12 weeks in a single-center, double-blind controlled, and parallel-group studydesign. Paroxetine treatment was initiated at a dose of 15 mg/day, and graduallyincreased to 60 mg/day using a fixed dosing schedule. Venlafaxine treatment
Serotonin Related Genes Affect Antidepressant Treatment 229

was initiated at a dose of 75 mg/day and gradually increased to 300 mg/day.Psychotropic drugs or psychotherapy were not allowed. Obsessive–compulsivesymptoms were measured with the Y-BOCS, and response to treatment wasprospectively defined as a �25% decrease in Y-BOCS score. Three out of 91patients dropped out during the study because of lack of motivation or sideeffects. A detailed description of the study has been published earlier (Denys et al.,2003b; Sheehan et al., 1998; Goodman et al., 1989; Hamilton, 1959; 1960).
Genotyping
Blood samples were collected from each subject and frozen at �80°C. DNA wasextracted from 10 � l of peripheral blood according to standard procedures. Thetotal number of subjects genotyped for the genes in this study was 88. In sevencases, the genotyping of the 5-HT1D� polymorphism failed, and in one case thegenotyping of the 5-HTT polymorphism. All subjects were genotyped at theUniversity of Ghent (Belgium) based on a coded identification number. The 5-HTT, 5-HT1D�, and 5-HT2A genotyping was performed following a standard-ized protocol.
5-HTT
For the detection of the 44 bp insertion/deletion 5-HTTLPR polymorphism, theoligonucleotide primers were 5�-6FAM-GGCGTTGCCGCTCTGAATGC-3�
and 5�-AGGGACTGAGCTGGACAAC.CAC-3� were used to amplify a 484/528 bp fragment comprising the 5-HTT-
linked polymorphic region. The PCR reaction was performed according to fol-lowing conditions: 94°C for 1 min, 60°C for 1 min, 72°C for 1 min 40 s per cycle,for a total of 35 cycles. The PCR products were analyzed by capillary electro-phoresis on an Applied Biosystems 3100 Genetic Analyzer.
5-HT1D�
For detection of the 5-HT1D� G861C polymorphism, the oligonucleotideprimers 5�-GAAACAGACGCCCAACAGGAC-3� and 5�-CCAGAAACCGC-GAAAGAAGAT-3� were used to amplify a 548 bp region comprising the G861Cpolymorphism site. The PCR reaction was performed under the following condi-tions: 90°C for 1 min, 55°C for 2 min, 72°C for 3 min per cycle, for a total of 32cycles. Digestion of 10 � l of PCR product was accomplished by incubation for4 h with 10 units of Hinc II restriction enzyme at 37°C. Digestion with Hinc IIyields either two fragments (452 bp and 96 bp) for the G-allele or three fragments(310 bp, 142 bp and 96 bp) for the C-allele. The fragments resulting from thedigestion were resolved on a 1.5% agarose gel and visualized by ethidium bro-mide staining.
230 F. Van Nieuwerburgh et al.

5-HT2A
For the detection of the 5-HT2A 1438G/A polymorphism within the promoterregion of the 5-HT2A receptor gene, the oligonucleotide primers 5�-6FAM-AAGCTGCAAGGTAGCAACAGC-3� and 5�-NED-AACCAACTTATTTC-CTACCAC-3� were used to amplify a 468 bp region comprising the 5-HT2A
1438G/A polymorphism site. The PCR reaction was performed under the fol-lowing conditions: 95°C for 1 min, 47°C for 1 min, 72°C for 1 min 20 s per cycle,for a total of 40 cycles. Digestion of 10 � l of PCR product was accomplished by overnight incubation with 10 units of Msp I restriction enzyme at 37°C. Afterincubation with Msp I, the 1438A allele remains intact while the 1438G allele iscut into a 223 bp piece (6FAM-labelled) and a 243 bp piece (NED-labelled). Thefragments resulting from the digestion were analyzed by capillary electrophoresison an Applied Biosystems 3100 Genetic Analyzer.
Analysis
The following statistical procedure was pursued. Firstly, the genotypic pattern ofdistribution and the allele frequencies of the 5-HTT, 5-HT1D�, and 5-HT2A poly-morphisms were analyzed in the whole sample (n � 88). Secondly, an analogousanalysis was performed in the paroxetine treated patients (n � 40), and in the ven-lafaxine treated patients (n � 44) separately. Medication use and dose was uncer-tain in four patients and they were excluded from the treatment groups. Theassociation between the distribution of the genotypes and allele frequencies withthe responders and non-responders were assessed by cross-tabulation and �2
analyses. One way ANOVAs were calculated to determine whether significant dif-ferences were present between genotypes in mean decrease of Y-BOCS scores.Considering a partial Bonferroni’s correction, the p-value for statistical signifi-cance would be 0.020 with an alpha of 0.05, 6 tests, 2 degrees of freedom, and acorrelation correction factor of 0.5. The data are presented as mean � SD, andperformed at 5% level of significance. All statistical analyses were conducted withthe SPSS statistical package version 11.5.
Results
Demographic variables and outcome measures are presented in Table 1. Thepatient sample was slightly skewed towards the female population (63%). Fifty-six out of 88 patients (63%) were rated as responders, 31 out of 40 patients in the paroxetine group, and 24 out of 44 patients in the venlafaxine group. Fourpatients were not assigned to a particular treatment group (see Methods section).There were no statistically significant differences between responders and non-responders as regards gender, age, age of onset, family history, and baseline Y-BOCS, HAM-A, or HAM-D measures.
Serotonin Related Genes Affect Antidepressant Treatment 231

In the whole sample (Table 2), a difference in genotype distribution of the 5-HTTLPR polymorphism was found between responders and non-responders.Sixty-four percent of the responders carried the S/L genotype of the 5-HTTLPRpolymorphism compared to 18% carrying the S/S genotype and 18% carrying the L/L genotype. The difference just failed to be statistically significant afterBonferroni’s correction (�2 � 7.17, df � 2, p � 0.028). When the mean Y-BOCSdecrease was stratified by 5-HTTLPR genotype, a superior response was observedin the S/L genotype (37% decrease) versus the S/S genotype (28%) and the L/Lgenotype (29%), but the ANOVA failed to reach statistical significance (F2,84 � 1.2,p � 0.30). Allele frequencies of the 5-HTTLPR polymorphism between respondersand non-responders were not statistically significant different (�2 � 0.05, df � 1,p � 0.71), and there were no significant differences between responders and non-responders in allele or genotype frequencies for the 5-HT1D� and 5-HT2A poly-morphisms in the whole sample.
In the paroxetine treated patients (Table 3 and Figure 1), the majority of respon-ders carried the G/G genotype of the 5-HT2A polymorphism (�2 � 8.66, df � 2,p � 0.013). The association of a superior response with the G/G genotype wasconfirmed in the ANOVA when the mean Y-BOCS decrease was broken downaccording to the genotypes. Patients carrying the G/G genotype of the 5-HT2A
polymorphism had a mean decrease of 51% on the Y-BOCS compared to 34%with the A/A genotype and 29% with the A/G genotype (F2,39 � 4.95, p � 0.012).In general, responders carried predominantly the G-allele compared to non-responders (�2 � 8.43, df � 1, p � 0.004) (OR 4.89 95% CI 1.59–15.02).
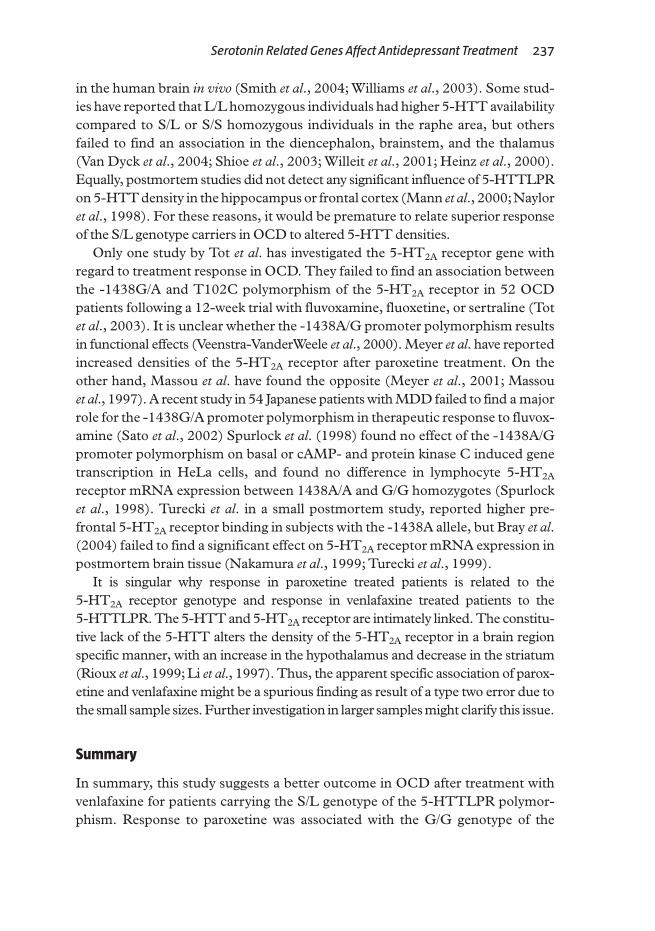
In the venlafaxine treated patients (Table 4 and Figure 2), the majority ofresponders carried the S/L genotype of the 5-HTTTLPR polymorphism (�2 �
9.72, df � 2, p � 0.008). The ANOVA showed a difference in favor of the S/Lgenotype with a mean Y-BOCS decrease of 38% compared to 24% in patients
232 F. Van Nieuwerburgh et al.
Table 1. Demographic and Clinical Characteristics of the Patients Sample
NON-RESPONDERS (n � 32) RESPONDERS (n � 56)
Gender (male/female) 14/18 20/36Age on admission 31.7 � 12.0 34.1 � 11.3Positive family history 11 19Mean age of onset 14.7 � 9.3 17.2 � 7.4
15 years age of onset 12 3320 years age of onset 20 23
Y-BOCS baseline 26.8 � 5.8 25.2 � 5.2Y-BOCS endpoint 24.8 � 5.7 13.2 � 5.4Y-BOCS mean % decrease 6.8 � 11.0 48.6 � 18.0HAM-D 5.6 � 10.7 7.8 � 10.8HAM-A 7.4 � 6.7 9.8 � 7.5Paroxetine (n � 40) 9 31Venlafaxine (n � 44) 20 24

Serotonin Related Genes Affect Antidepressant Treatment 233
Tabl
e 2.
Alle
le F
req
uen
cies
an
d G
eno
typ
e D
istr
ibu
tio
n o
f th
e 5
-HT 1
D�-,
5-H
T 2A
Rec
epto
r, a
nd
5-H
TT P
oly
mo
rph
ism
s in
the
Wh
ole
Sam
ple
(n
��8
8)
nA
LL
EL
Ep-
VA
LU
EG
EN
OT
YP
ES
p-V
AL
UE
FR
EQ
UE
NC
ES
5-H
T1D
�C
GC
CC
GG
GN
on-r
espo
nder
s 30
0.23
0.74
0.27
31
(3.3
%)
12 (
40.0
%)
17 (
56.7
%)
0.51
0R
espo
nder
s51
0.31
0.69
4 (7
.8%
)24
(47
.1%
)23
(45
.1%
)5-
HT
2AA
GA
AA
GG
GN
on-r
espo
nder
s 32
0.48
0.52
0.41
85
(15.
6%)
21 (
65.6
%)
6 (1
8.8%
)0.
144
Res
pond
ers
560.
420.
5811
(19
.6%
)25
(44
.6%
)20
(35
.7%
)5-
HT
TL
SL
LL
/SS
SN
on-r
espo
nder
s32
0.55
0.45
0.55
112
(37
.5%
)11
(34
.4%
)9
(28.
1%)
0.02
8R
espo
nder
s55
0.50
0.50
10 (
18.2
%)
35 (
63.6
%)
10 (
18.2
%)
Tabl
e 3.
Alle
le F
req
uen
cies
an
d G
eno
typ
e D
istr
ibu
tio
n o
f th
e 5
-HT 1
D�-,
5-H
T 2A
Rec
epto
r, a
nd
5-H
TT P
oly
mo
rph
ism
s in
the
Par
oxe
tin
e Tr
eate
d G
rou
p (
n ��
40
)
nA
LL
EL
Ep-
VA
LU
EG
EN
OT
YP
ES
p-V
AL
UE
FR
EQ
UE
NC
IES
5-H
T1D
�C
GC
CC
GG
GN
on-r
espo
nder
s8
0.19
0.81
0.51
30
(0.0
%)
3 (3
7.5%
)5
(62.
50%
)0.
625
Res
pond
ers
280.
270.
733
(10.
7%)
9 (3
2.1%
)16
(57
.1%
)5-
HT
2AA
GA
AA
GG
GN
on-r
espo
nder
s9
0.67
0.33
0.00
43
(33.
3%)
5 (6
6.7%
)0
(0.0
%)
0.01
3R
espo
nder
s31
0.29
0.71
4 (1
2.9%
)10
(32
.3%
)17
(54
.8%
)5-
HT
TL
SL
LL
/SS
SN
on-r
espo
nder
s9
0.56
0.44
0.77
23
(33.
3%)
4 (4
4.4%
)2
(22.
2%)
0.78
7R
espo
nder
s30
0.52
0.48
7 (2
3.3%
)17
(56
.7%
)6
(20.
0%)

with the S/S genotype and 15% in patients with the LL genotype, who had the worst outcome, but failed to be statistically significant after correction (F2,43 � 3.27, p � 0.04).
Since the number of responders appeared to be correlated to the G/G genotypeof the 5-HT2A polymorphism in the paroxetine treated patients, and to the S/Lgenotype of the 5-HTTLPR polymorphism in the venlafaxine treated patients, weanalyzed thereupon responder rates in patients who had either one of the geno-types in the full sample. More than 81% of the responders (45 out of 55) carriedeither the G/G genotype of the 5-HT2A polymorphism or the S/L genotype of the5-HTTLPR polymorphism (�2 � 8.1, df � 1, p � 0.004). All of patients (n � 9)who carried both the G/G genotype of the 5-HT2A polymorphism and to the S/L genotype of the 5-HTTLPR polymorphism were responders. There was astatistically significant difference between the mean Y-BOCS decrease of 49% inthese patients compared to the remainder of patients (�2 � 16.0, df � 8, p � 0.01).
Conclusion and Translation to Clinical Practice
The main finding of this study is that in paroxetine treated OCD patients, themajority of responders carried the G/G genotype of the 5-HT2A polymorphism,whereas in the venlafaxine treated patients, the majority of responders carried theS/L genotype of the 5-HTTLPR polymorphism. The small group of patients (n � 9) who both carried the S/L genotype of the 5-HTTLPR polymorphism andthe G/G genotype of the 5-HT2A polymorphism responded all to treatment.
234 F. Van Nieuwerburgh et al.
0
10
20
30
40
50
60
70
AA AG GG
Responders Non-responders
Genotypes
Par
oxet
ine
trea
ted
patie
nts
(%)
Fig. 1.
In the paroxetine treated patients (n � 37), the majority of responders (green) carried the GG
genotype of the 5-HT2A polymorphism (�2 � 8.66, df � 2, p � 0.013).

Serotonin Related Genes Affect Antidepressant Treatment 235
Tabl
e 4.
Alle
le F
req
uen
cies
an
d G
eno
typ
e D
istr
ibu
tio
n o
f th
e 5
-HT 1
D��-,
5-H
T 2A
Rec
epto
r, a
nd
5-H
TT P
oly
mo
rph
ism
s in
the
Ven
lafa
xin
e Tr
eate
d G
rou
p (
n ��
44
)
nA
LL
EL
Ep-
VA
LU
EG
EN
OT
YP
ES
p-V
AL
UE
FR
EQ
UE
NC
IES
5-H
T1D
�C
GC
CC
GG
GN
on-r
espo
nder
s 19
0.24
0.76
0.21
41
(5.3
%)
7 (3
6.8%
)11
(57
.9%
)0.
221
Res
pond
ers
220.
360.
641
(4.5
%)
14 (
63.6
%)
7 (3
1.8%
)5-
HT
2AA
GA
AA
GG
GN
on-r
espo
nder
s20
0.40
0.60
0.08
72
(10.
0%)
12 (
60.0
%)
6 (3
0.0%
)0.
165
Res
pond
ers
240.
580.
427
(29.
2%)
14 (
58.3
%)
3 (1
2.5%
)5-
HT
TL
SL
LL
/SS
SN
on-r
espo
nder
s21
0.55
0.45
0.39
38
(40.
0%)
6 (3
0.0%
)6
(30.
0%)
0.00
8R
espo
nder
s 23
0.46
0.54
2 (8
.3%
)18
(75
.0%
)4
(16.
7%)

Three previous studies have investigated the role of the 5-HTTLPR and treat-ment response in OCD. Our results are in line with the findings of McDougle et al. who found a trend for an association of the L-allele with poorer response to SRIs (clomipramine, fluvoxamine, fluoxetine, sertraline, and paroxetine) in asample of 33 patients (McDougle et al., 1998). Billett et al. (1997) and Di Bella et al. (2000) failed to find an association between SRI response and 5-HTTLPRgenotypes (Di Bella et al., 2000; Billett et al., 1997).
Our results are in contradiction with the majority of reports in mood disordersin which the presence of the L variant of the 5-HTTLPR has been associated witha more favorable and faster response to SRIs (Smits et al., 2004). It is possible thatthis discrepancy is due to pathophysiologic and neurobiological dissimilaritiesbetween OCD and mood disorders. It has been suggested that SRIs exert theirbeneficial effects with their typical delay of 6–8 weeks in OCD by down regulating5-HT1D� receptors in the orbito-frontal whereas in MDD, a faster response isobserved probably due 5-HT auto-receptor desensitization in other brain areassuch as the hippocampus and hypothalamus (Elmansari et al., 1995). This sup-position is appealing, but still needs to be confirmed.
It is unclear exactly why the S/L genotype of the 5-HTTLPR could cause a better response with SRIs in OCD. The L/L genotype has been related to higher 5-HTT densities and hence an increased efficacy of SRIs. However, it still needsto be clarified whether or not the 5-HTTLPR determines the number of 5-HTT
236 F. Van Nieuwerburgh et al.
0
10
20
30
40
50
60
70
80
LL LS SS
Responders Non-responders
Genotypes
Ven
lafa
xine
trea
ted
patie
nts
(%)
Fig. 2.
In the venlafaxine treated patients (n � 44), the majority of responders (green) carried the S/L
genotype of the 5-HTTLPR polymorphism (�2 � 9.71, df � 2, p � 0.008).
in the human brain in vivo (Smith et al., 2004; Williams et al., 2003). Some stud-ies have reported that L/L homozygous individuals had higher 5-HTT availabilitycompared to S/L or S/S homozygous individuals in the raphe area, but othersfailed to find an association in the diencephalon, brainstem, and the thalamus(Van Dyck et al., 2004; Shioe et al., 2003; Willeit et al., 2001; Heinz et al., 2000).Equally, postmortem studies did not detect any significant influence of 5-HTTLPRon 5-HTT density in the hippocampus or frontal cortex (Mann et al., 2000;Nayloret al., 1998). For these reasons, it would be premature to relate superior responseof the S/L genotype carriers in OCD to altered 5-HTT densities.
Only one study by Tot et al. has investigated the 5-HT2A receptor gene withregard to treatment response in OCD. They failed to find an association betweenthe -1438G/A and T102C polymorphism of the 5-HT2A receptor in 52 OCDpatients following a 12-week trial with fluvoxamine, fluoxetine, or sertraline (Totet al., 2003). It is unclear whether the -1438A/G promoter polymorphism resultsin functional effects (Veenstra-VanderWeele et al., 2000). Meyer et al. have reportedincreased densities of the 5-HT2A receptor after paroxetine treatment. On theother hand, Massou et al. have found the opposite (Meyer et al., 2001; Massou et al., 1997). A recent study in 54 Japanese patients with MDD failed to find a majorrole for the -1438G/A promoter polymorphism in therapeutic response to fluvox-amine (Sato et al., 2002) Spurlock et al. (1998) found no effect of the -1438A/Gpromoter polymorphism on basal or cAMP- and protein kinase C induced genetranscription in HeLa cells, and found no difference in lymphocyte 5-HT2A
receptor mRNA expression between 1438A/A and G/G homozygotes (Spurlocket al., 1998). Turecki et al. in a small postmortem study, reported higher pre-frontal 5-HT2A receptor binding in subjects with the -1438A allele, but Bray et al.(2004) failed to find a significant effect on 5-HT2A receptor mRNA expression inpostmortem brain tissue (Nakamura et al., 1999; Turecki et al., 1999).
It is singular why response in paroxetine treated patients is related to the 5-HT2A receptor genotype and response in venlafaxine treated patients to the 5-HTTLPR. The 5-HTT and 5-HT2A receptor are intimately linked. The constitu-tive lack of the 5-HTT alters the density of the 5-HT2A receptor in a brain region specific manner, with an increase in the hypothalamus and decrease in the striatum(Rioux et al., 1999; Li et al., 1997). Thus, the apparent specific association of parox-etine and venlafaxine might be a spurious finding as result of a type two error due tothe small sample sizes. Further investigation in larger samples might clarify this issue.
Summary
In summary, this study suggests a better outcome in OCD after treatment withvenlafaxine for patients carrying the S/L genotype of the 5-HTTLPR polymor-phism. Response to paroxetine was associated with the G/G genotype of the
Serotonin Related Genes Affect Antidepressant Treatment 237

5-HT2A polymorphism. The small group of patients who both carried the S/Lgenotype of the 5-HTTLPR polymorphism and the G/G genotype of the 5-HT2A
polymorphism responded all to treatment. Our results indicate that 5-HT2A and5-HTTLPR polymorphisms may be markers for treatment outcome in OCD.
References
Billett, E.A., Richter, M.A., King, N., Heils, A., Lesch, K.P., & Kennedy, J.L. (1997).Obsessive compulsive disorder, response to serotonin reuptake inhibitors and the serotonintransporter gene. Molecular Psychiatry, 2(Suppl. 5), 403–406.
Bray, N.J., Buckland, P.R., Hall, H., Owen, M.J., & O’Donovan, M.C. (2004). Theserotonin-2A receptor gene locus does not contain common polymorphism affecting mRNAlevels in adult brain. Molecular Psychiatry, 9, 109–114.
Denys, D., Burger, H., van Megen, H., de Geus, F., & Westenberg, H. (2003a). A score forpredicting response to pharmacotherapy in obsessive–compulsive disorder. International ClinicalPsychopharmacology, 18(Suppl. 6), 315–322.
Denys, D., van der Wee, N., van Megen, H.J.G.M., & Westenberg, H.G.M. (2003b).A double blind comparison of venlafaxine and paroxetine in obsessive–compulsive disorder.Journal of Clinical Psychopharmacology, 23(Suppl. 6), 568–575.
Denys, D., van Megen, H.J.G.M., van der Wee, N., & Westenberg, H.G.M. (2004).A double-blind switch study of paroxetine and venlafaxine in obsessive–compulsive disorder.Journal of Clinical Psychiatry, 65(Suppl. 1), 37–43.
Di Bella, D., Erzegovesi, S., Cavallini, M.C., d’Annucci, A., & Bellodi, L. (2000).Obsessive–compulsive disorder, treatment response and the 5htt gene. American Journal ofMedical Genetics, 96(Suppl. 4), 536–536.
Elmansari, M., Bouchard, C., & Blier, P. (1995). Alteration of serotonin release in the guinea-pig orbitofrontal cortex by selective serotonin reuptake inhibitors – relevance totreatment of obsessive–compulsive disorder. Neuropsychopharmacology, 13(Suppl. 2),117–127.
Goodman, W.K., Price, L.H., Rasmussen, S.A., Mazure, C., Fleischmann, R.L., Hill, C.L.,Heninger, G.R., & Charney, D.S. (1989). The yale-brown obsessive compulsive scale. 1.Development, use, and reliability. Archives of General Psychiatry, 46(Suppl. 11), 1006–1011.
Goodman, W.K., Ward, H.E., & Murphy, T.K. (1998). Biologic approaches to treatment-refractory obsessive–compulsive disorder. Psychiatric Annals, 28(Suppl. 11), 641–649.
Hamilton, M. (1959). The assessment of anxiety states by rating. British Journal of MedicalPsychology, 32, 50–55.
Hamilton, M. (1960). A rating scale for depression. Journal of Neurology, Neurosurgery andPsychiatry, 23, 56–62.
Heinz, A., Jones, D.W., Mazzanti, C., Goldman, D., Ragan, P., Hommer, D.,Linnoila, M., & Weinberger, D.R. (2000). A relationship between serotonin transportergenotype and in vivo protein expression and alcohol neurotoxicity. Biological Psychiatry,47(Suppl. 7), 643–649.
Hollander, E., Bienstock, C.A., Koran, L.M., Pallanti, S., Marazziti, D.,Rasmussen, S.A., Ravizza, L., Benkelfat, C., Saxena, S., Greenberg, B.D.,Sasson, Y., & Zohar, J. (2002). Refractory obsessive–compulsive disorder: state-of-the-arttreatment. Journal of Clinical Psychiatry, 63, 20–29.
Li, Q., Muma, N.A., Battaglia, G., & Van der Kar, L.D. (1997). Fluoxetine graduallyincreases [i-125]doi-labelled 5-ht2a/2c receptors in the hypothalamus without changing thelevels of g(q)- and g(11)-proteins. Brain Research, 775(Suppl. 1–2), 225–228.
238 F. Van Nieuwerburgh et al.

Mancama, D., & Kerwin, R.W. (2003). Role of pharmacogenomics in individualising treatmentwith ssris. CNS Drugs, 17(Suppl. 3), 143–151.
Mann, J.J., Huang, J.Y., Underwood, M.D., Kassir, S.A., Oppenheim, S., Kelly, T.M.,Dwork, A.J., & Arango, V. (2000). A serotonin transporter gene promoter polymorphism (5-httlpr) and prefrontal cortical finding in major depression and suicide. Archives of GeneralPsychiatry, 57(Suppl. 8), 729–738.
Massou, J.M., Trichard, C., AttarLevy, D., Feline, A., Corruble, E., Beaufils, B., &Martinot, J.L. (1997). Frontal 5-ht2a receptors studied in depressive patients during chronictreatment by selective serotonin reuptake inhibitors. Psychopharmacology, 133(Suppl. 1), 99–101.
McDougle, C.J., Epperson, C.N., Price, L.H., & Gelernter, J. (1998). Evidence for linkagedisequilibrium between serotonin transporter protein gene (slc6a4) and obsessive compulsivedisorder. Molecular Psychiatry, 3(Suppl. 3), 270–273.
Meyer, J.H., Kapur, S., Eisfeld, B., Brown, G.M., Houle, S., DaSilva, J., Wilson, A.A.,Rafi-Tari, S., Mayberg, H.S., & Kennedy, S.H. (2001). The effect of paroxetine on 5-ht2areceptors in depression: an [f-18]setoperone pet imaging study. American Journal of Psychiatry,158(Suppl. 1), 78–85.
Nakamura, T., Matsushita, S., Nishiguchi, N., Kimura, M., Yoshino, A., & Higuchi, S.(1999). Association of a polymorphism of the 5ht2a receptor gene promoter region with alcoholdependence. Molecular Psychiatry, 4(Suppl. 1), 85–88.
Naylor, L., Dean, B., Pereira, A., Mackinnon, A., Kouzmenko, A., & Copolov, D. (1998).No association between the serotonin transporter-linked promoter region polymorphism andeither schizophrenia or density of the serotonin transporter in human hippocampus.Molecular Medicine, 4(Suppl. 10), 671–674.
Rioux, A., Fabre, V., Lesch, K.P., Moessner, R., Murphy, D.L., Lanfumey, L.,Hamon, M., & Martres, M.P. (1999). Adaptive changes of serotonin 5-ht2a receptors inmice lacking the serotonin transporter. Neuroscience Letters, 262(Suppl. 2), 113–116.
Sato, K., Yoshida, K., Takahashi, H., Ito, K., Kamata, M., Higuchi, H., Shimizu, T.,Itoh, K., Inoue, K., Tezuka, T., Suzuki, T., Ohkubo, T., Sugawara, K., & Otani, K.(2002). Association between-1438g/a promoter polymorphism in the 5-ht2a receptor gene andfluvoxamine response in Japanese patients with major depressive disorder. Neuropsychobiology,46(Suppl. 3), 136–140.
Sheehan, D.V., Lecrubier, Y., Sheehan, K.H., Amorim, P., Janavs, J., Weiller, E.,Hergueta, T., Baker, R., & Dunbar, G.C. (1998). The mini-international neuropsychiatricinterview (mini): The development and validation of a structured diagnostic psychiatricinterview for dsm-iv and icd-10. Journal of Clinical Psychiatry, 59, 22–33.
Shioe, K., Ichimya, T., Suhara, T., Takano, A., Sudo, Y., Yasuno, F., Hirano, M.,Shinohara, M., Kagami, A., Okubo, Y., Nankai, M., & Kanba, S. (2003). No associationbetween genotype of the promoter region of serotonin transporter gene and serotonintransporter binding in human brain measured by pet. Synapse, 48(Suppl. 4), 184–188.
Spurlock, G., Heils, A., Holmans, P., Williams, J., D’Souza, U.M., Cardno, A.,Murphy, K.C., Jones, L., Buckland, P.R., McGuffin, P., Lesch, K.P., & Owen, M.J.(1998). A family based association study of t102c polymorphism in 5ht2a and schizophrenia plusidentification of new polymorphisms in the promoter. Molecular Psychiatry, 3(Suppl. 1), 42–49.
Smith, G.S., Lotrich, F.E., Malhotra, A.K., Lee, A.T., Ma, Y.L., Kramer, E.,Gregersen, P.K., Eidelberg, D., & Pollock, B.G. (2004). Effects of serotonin transporter promoter polymorphisms on serotonin function. Neuropsychopharmacology,29(Suppl. 12), 2226–2234.
Smits, K.M., Smits, L.J.M., Schouten, J.S.A.G., Stelma, F.F., Nelemans, P., & Prins, M.H.(2004). Influence of sertpr and stin2 in the serotonin transporter gene on the effect of selectiveserotonin reuptake inhibitors in depression: a systematic review. Molecular Psychiatry,9(Suppl. 5), 433–441.
Serotonin Related Genes Affect Antidepressant Treatment 239

240 F. Van Nieuwerburgh et al.
Tot, S., Erdal, M.E., Yazici, K., Yazici, A.E., & Metin, O. (2003). T102c and -1438 g/apolymorphisms of the 5-ht2a receptor gene in turkish patients with obsessive–compulsivedisorder. European Psychiatry, 18(Suppl. 5), 249–254.
Turecki, G., Briere, R., Dewar, K., Antonetti, T., Lesage, A.D., Seguin, M., Chawky, N.,Vanier, C., Alda, M., Joober, R., Benkelfat, C., & Rouleau, G.A. (1999). Prediction oflevel of serotonin 2a receptor binding by serotonin receptor 2a genetic variation in postmortembrain samples from subjects who did or did not commit suicide. American Journal of Psychiatry,156(Suppl. 9), 1456–1458.
Van Dyck, C.H., Malison, R.T., Staley, J.K., Jacobsen, L.K., Seibyl, J.P., Laruelle, M.,Baldwin, R.M., Innis, R.B., & Gelernter, J. (2004). Central serotonin transporteravailability measured with [i-123]beta-cit spect in relation to serotonin transporter genotype.American Journal of Psychiatry, 161(Suppl. 3), 525–531.
Veenstra-VanderWeele, J., Anderson, G.M., & Cook, E.H. (2000). Pharmacogenetics andthe serotonin system: initial studies and future directions. European Journal of Pharmacology,410(Suppl. 2–3), 165–181.
Willeit, M., Stastny, J., Pirker, W., Praschak-Rieder, N., Neumeister, A., Asenbaum, S.,Tauscher, J., Fuchs, K., Sieghart, W., Hornik, K., Aschauer, H.N., Brucke, T., &Kasper, S. (2001). No evidence for in vivo regulation of midbrain serotonin transporteravailability by serotonin transporter promoter gene polymorphism. Biological Psychiatry,50(Suppl. 1), 8–12.
Williams, R.B., Marchuk, D.A., Gadde, K.M., Barefoot, J.C., Grichnik, K., Helms, M.J.,Kuhn, C.M., Lewis, J.G., Schanberg, S.M., Stafford-Smith, M., Suarez, E.C.,Clary, G.L., Svenson, I.K., & Siegler, I.C. (2003). Serotonin-related gene polymorphismsand central nervous system serotonin function. Neuropsychopharmacology, 28(Suppl. 3), 533–541.
Copyright © 2022 FDOKUMEN




















