
Decrease of Prefrontal Metabolism After Subthalamic Stimulation in Obsessive-Compulsive Disorder: A...
7
Decrease of Prefrontal Metabolism After Subthalamic Stimulation in Obsessive-Compulsive Disorder: A Positron Emission Tomography Study Florence Le Jeune, Marc Vérin, Karim N’Diaye, Dominique Drapier, Emmanuelle Leray, Sophie Tezenas Du Montcel, Nicolas Baup, Antoine Pelissolo, Mircea Polosan, Luc Mallet, Jérome Yelnik, Bertrand Devaux, Denys Fontaine, Isabelle Chereau, Aurélie Bourguignon, Julie Peron, Paul Sauleau, Sylvie Raoul, Etienne Garin, Marie-Odile Krebs, Nematollah Jaafari, and Bruno Millet, for the French Stimulation dans le trouble obsessionnel compulsif (STOC) study group Background: High-frequency bilateral subthalamic nucleus (STN) deep brain stimulation (DBS) is a promising treatment in refractory obsessive-compulsive disorder (OCD). Method: Using the crossover, randomized, and double-blind procedure adopted by the STOC study, 10 patients treated with high- frequency bilateral STN DBS underwent am 18-fluorodeoxyglucose positron emission tomography (PET) investigation to highlight the neural substratum of this therapeutic approach. Results: The median Yale–Brown Obsessive Compulsive Scale (Y-BOCS) scores for all 10 patients were 31 (minimum 18, maximum 36) with “Off-Stimulation” status and 19 (minimum 0, maximum 30) with “On-Stimulation” status (p .05). The OCD patients in Off-Stimulation status showed a hypermetabolism in the right frontal middle and superior gyri, right parietal lobe, postcentral gyrus, and bilateral putamen compared with healthy control subjects. A significant decrease in cerebral metabolism was observed in the left cingulate gyrus and the left frontal medial gyrus in On-Stimulation conditions compared with Off-Stimulation conditions. In addition, the improvement assessed by Y-BOCS scores during the On-Stimulation conditions was positively correlated with PET signal changes at the boundary of the orbitofrontal cortex and the medial prefrontal cortex, between PET signal changes and the Y-BOCS scores modifications in On-Stimulation status. Conclusion: This study suggests that the therapeutic effect of STN DBS is related to a decrease in prefrontal cortex metabolism. Key Words: Cingulate gyrus, deep brain stimulation, 18 FDG-PET, obsessive compulsive disorder, orbitofrontal cortex, subthalamic nucleus S evere obsessive-compulsive disorder (OCD) remains a chronic and disabling condition, despite the use of classic treatments associating serotonin reuptake inhibitors with be- havioral and cognitive therapy (BCT) (1). This disorder rarely disap- pears, and alternatives to the classic treatments are needed (2). Deep brain stimulation (DBS) has been used for resistant patients, experimenting with various targets according to the rationale de- veloped by each team. The published results of ongoing trials of DBS in OCD concerning the ventral portion of the anterior limb of the internal capsule have suggested that stimulation may be effec- tive (1,3–7). The French Research Consortium (Stimulation dans le Trouble Obsessionnel Compulsif [STOC] study group) recently de- cided to target the subthalamic nucleus (STN), with successful re- sults. This technique was assessed using a crossover, randomized, and double-blind procedure, with each patient undergoing with a 3-month “Off-Stimulation” period and a 3-month “On-Stimulation” period. Results suggested that high-frequency STN stimulation im- proves obsessive-compulsive severity and overall function in se- vere OCD patients (8). Apart from gauging the effectiveness of this novel treatment, it is also crucial to improve our understanding of the physiopathologic mechanism involved in OCD and the way in which therapeutic tools act. Positron emission tomography (PET) studies of OCD patients have been performed to this end, with most results indicating increased activity of the prefrontal cortex, especially the orbitofrontal cortex (OFC), in OCD patients, compared with healthy subjects (9 –13). Regarding the action of DBS, previous studies using the ventral striatum target in severe OCD patients have reported hy- pometabolism of the anterior cingulate gyrus (14,15), all the while failing to distinguish the effects of DBS on brain structures from those related to the therapeutic effect. From the Department of Nuclear Medicine (FLJ, EG), Centre Eugène Marquis, the “Behavior and Basal Ganglia” University Research Department (FLJ, MV, DD, EL, AB, JP, PS, BM), Université Rennes 1, and the Department of Neurology (MV, JP), University Hospital, Rennes; Pierre et Marie Curie—Paris 06 University (KND, LM, JY), Centre de Recherche de l’Institut du Cerveau et de la Moëlle épinière, Unité mixte de recherche-S975, and Institut national de la Santé et de la Recherche Médicale (INSERM) (KND, LM, JY), U975, Centre national de la Recherche Scientifique (CNRS) (KND, LM, JY), UMR 7225, Paris; University Department of Adult Psychiatry (DD, AB, BM), Guillaume Régnier Hospital, and Department of Epidemiology and Public Health (EL), University Hospital, Rennes; Biostatistics and Medical Informatics Unit and Clinical Research Unit (STDM), Pitié-Salpétrière University Hospital, INSERM (NB, BD, MO-K), University of Paris Descartes, Department of Psychiatry, Sainte Anne Hospital, and Clinical Investigation Centre (AP, LM, JY), Pitié-Salpêtrière University Hospital, Assistance Publique-Hôpitaux de Paris, Paris; Department of Psychiatry (MP), University Hospital, Grenoble; Department of Neurosurgery (DF), University Hospital, Nice; Department of Psychiatry (IC, PS), University Hospital, Clermont-Ferrand; Department of Physiology (SR), University Hospital, Rennes; Department of Neurosurgery (NJ), University Hospital, Nantes; and Department of Psychiatry, Centre hospitalier Henri Laborit, Center Investiga- tion Clinique-Psychiatry INSERM U 802, University Hospital, 86000 Poitiers, France. Address correspondence to Florence Le Jeune, M.D., Ph.D., Department of Nuclear Medicine—Centre Eugène Marquis, Bd Flandres, Dunkerque, 35062 Rennes, Cedex, France; E-mail: [email protected]. Received Nov 13, 2009; revised May 4, 2010; accepted Jun 8, 2010. BIOL PSYCHIATRY 2010;68:1016 –1022 0006-3223/$36.00 doi:10.1016/j.biopsych.2010.06.033 © 2010 Society of Biological Psychiatry
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Decrease of Prefrontal Metabolism After Subthalamic Stimulation in Obsessive-Compulsive Disorder: A...

DSAFSBSS
Bo
Mfn
R“swgOc
C
Kon
ShpDevDttTc
F
A
R
0d
ecrease of Prefrontal Metabolism After Subthalamictimulation in Obsessive-Compulsive Disorder:Positron Emission Tomography Study
lorence Le Jeune, Marc Vérin, Karim N’Diaye, Dominique Drapier, Emmanuelle Leray,ophie Tezenas Du Montcel, Nicolas Baup, Antoine Pelissolo, Mircea Polosan, Luc Mallet, Jérome Yelnik,ertrand Devaux, Denys Fontaine, Isabelle Chereau, Aurélie Bourguignon, Julie Peron, Paul Sauleau,ylvie Raoul, Etienne Garin, Marie-Odile Krebs, Nematollah Jaafari, and Bruno Millet, for the Frenchtimulation dans le trouble obsessionnel compulsif (STOC) study group
ackground: High-frequency bilateral subthalamic nucleus (STN) deep brain stimulation (DBS) is a promising treatment in refractorybsessive-compulsive disorder (OCD).
ethod: Using the crossover, randomized, and double-blind procedure adopted by the STOC study, 10 patients treated with high-requency bilateral STN DBS underwent am 18-fluorodeoxyglucose positron emission tomography (PET) investigation to highlight theeural substratum of this therapeutic approach.
esults: The median Yale–Brown Obsessive Compulsive Scale (Y-BOCS) scores for all 10 patients were 31 (minimum � 18, maximum � 36) withOff-Stimulation” status and 19 (minimum � 0, maximum � 30) with “On-Stimulation” status (p � .05). The OCD patients in Off-Stimulation statushowed a hypermetabolism in the right frontal middle and superior gyri, right parietal lobe, postcentral gyrus, and bilateral putamen comparedith healthy control subjects. A significant decrease in cerebral metabolism was observed in the left cingulate gyrus and the left frontal medialyrus in On-Stimulation conditions compared with Off-Stimulation conditions. In addition, the improvement assessed by Y-BOCS scores during then-Stimulation conditions was positively correlated with PET signal changes at the boundary of the orbitofrontal cortex and the medial prefrontal
ortex, between PET signal changes and the Y-BOCS scores modifications in On-Stimulation status.
onclusion: This study suggests that the therapeutic effect of STN DBS is related to a decrease in prefrontal cortex metabolism.
, they (MV
le épide laal, an
rch Uspita
sychiHospind Drs, Frf Nu
ey Words: Cingulate gyrus, deep brain stimulation, 18FDG-PET,bsessive compulsive disorder, orbitofrontal cortex, subthalamicucleus
evere obsessive-compulsive disorder (OCD) remains achronic and disabling condition, despite the use of classictreatments associating serotonin reuptake inhibitors with be-
avioral and cognitive therapy (BCT) (1). This disorder rarely disap-ears, and alternatives to the classic treatments are needed (2).eep brain stimulation (DBS) has been used for resistant patients,xperimenting with various targets according to the rationale de-eloped by each team. The published results of ongoing trials ofBS in OCD concerning the ventral portion of the anterior limb of
he internal capsule have suggested that stimulation may be effec-ive (1,3–7). The French Research Consortium (Stimulation dans lerouble Obsessionnel Compulsif [STOC] study group) recently de-ided to target the subthalamic nucleus (STN), with successful re-
rom the Department of Nuclear Medicine (FLJ, EG), Centre Eugène MarquisEL, AB, JP, PS, BM), Université Rennes 1, and the Department of Neurolog(KND, LM, JY), Centre de Recherche de l’Institut du Cerveau et de la Moëlla Recherche Médicale (INSERM) (KND, LM, JY), U975, Centre nationalDepartment of Adult Psychiatry (DD, AB, BM), Guillaume Régnier HospitRennes; Biostatistics and Medical Informatics Unit and Clinical ReseaUniversity of Paris Descartes, Department of Psychiatry, Sainte Anne HoHospital, Assistance Publique-Hôpitaux de Paris, Paris; Department of PUniversity Hospital, Nice; Department of Psychiatry (IC, PS), UniversityRennes; Department of Neurosurgery (NJ), University Hospital, Nantes; ation Clinique-Psychiatry INSERM U 802, University Hospital, 86000 Poitie
ddress correspondence to Florence Le Jeune, M.D., Ph.D., Department oRennes, Cedex, France; E-mail: [email protected].
eceived Nov 13, 2009; revised May 4, 2010; accepted Jun 8, 2010.
006-3223/$36.00oi:10.1016/j.biopsych.2010.06.033
sults. This technique was assessed using a crossover, randomized,and double-blind procedure, with each patient undergoing with a3-month “Off-Stimulation” period and a 3-month “On-Stimulation”period. Results suggested that high-frequency STN stimulation im-proves obsessive-compulsive severity and overall function in se-vere OCD patients (8). Apart from gauging the effectiveness of thisnovel treatment, it is also crucial to improve our understanding of thephysiopathologic mechanism involved in OCD and the way in whichtherapeutic tools act. Positron emission tomography (PET) studies ofOCD patients have been performed to this end, with most resultsindicating increased activity of the prefrontal cortex, especially theorbitofrontal cortex (OFC), in OCD patients, compared with healthysubjects (9–13). Regarding the action of DBS, previous studies usingthe ventral striatum target in severe OCD patients have reported hy-pometabolism of the anterior cingulate gyrus (14,15), all the whilefailing to distinguish the effects of DBS on brain structures from thoserelated to the therapeutic effect.
“Behavior and Basal Ganglia” University Research Department (FLJ, MV, DD,, JP), University Hospital, Rennes; Pierre et Marie Curie—Paris 06 University
nière, Unité mixte de recherche-S975, and Institut national de la Santé et deRecherche Scientifique (CNRS) (KND, LM, JY), UMR 7225, Paris; Universityd Department of Epidemiology and Public Health (EL), University Hospital,nit (STDM), Pitié-Salpétrière University Hospital, INSERM (NB, BD, MO-K),l, and Clinical Investigation Centre (AP, LM, JY), Pitié-Salpêtrière Universityatry (MP), University Hospital, Grenoble; Department of Neurosurgery (DF),tal, Clermont-Ferrand; Department of Physiology (SR), University Hospital,epartment of Psychiatry, Centre hospitalier Henri Laborit, Center Investiga-ance.clear Medicine—Centre Eugène Marquis, Bd Flandres, Dunkerque, 35062
BIOL PSYCHIATRY 2010;68:1016–1022© 2010 Society of Biological Psychiatry
tbl
M
P
cpumStTwwBmA(MtM(
T
PN
swsr
F. Le Jeune et al. BIOL PSYCHIATRY 2010;68:1016–1022 1017
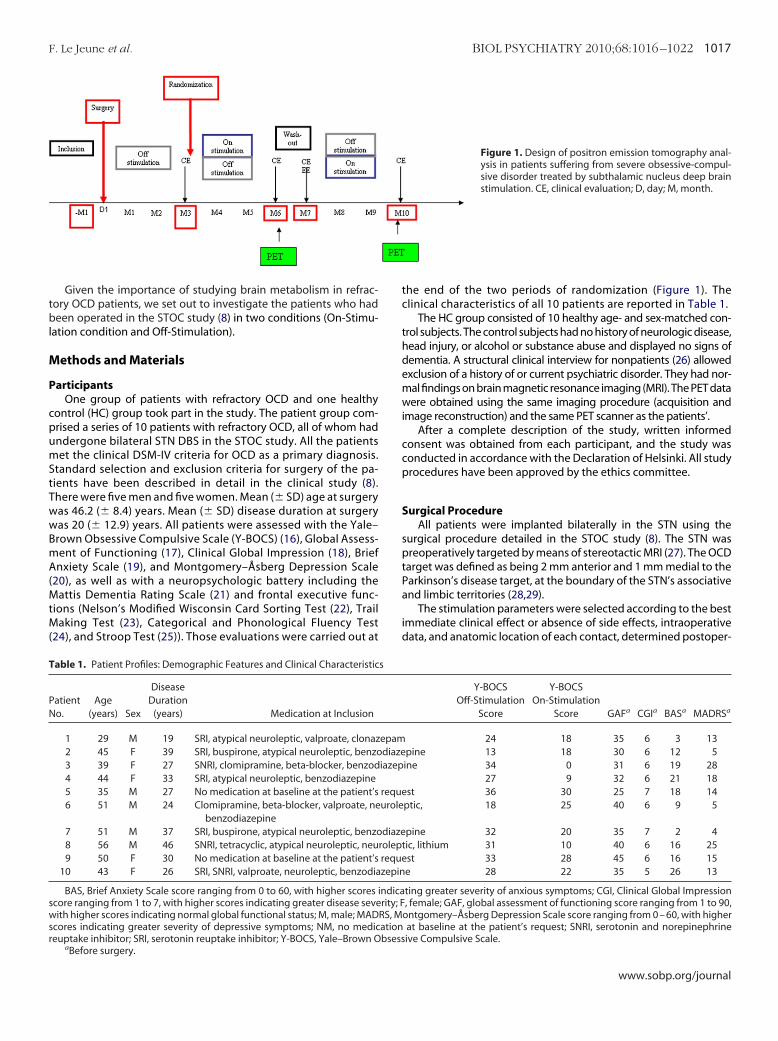
Given the importance of studying brain metabolism in refrac-ory OCD patients, we set out to investigate the patients who hadeen operated in the STOC study (8) in two conditions (On-Stimu-
ation condition and Off-Stimulation).
ethods and Materials
articipantsOne group of patients with refractory OCD and one healthy
ontrol (HC) group took part in the study. The patient group com-rised a series of 10 patients with refractory OCD, all of whom hadndergone bilateral STN DBS in the STOC study. All the patientset the clinical DSM-IV criteria for OCD as a primary diagnosis.
tandard selection and exclusion criteria for surgery of the pa-ients have been described in detail in the clinical study (8).here were five men and five women. Mean (� SD) age at surgeryas 46.2 (� 8.4) years. Mean (� SD) disease duration at surgeryas 20 (� 12.9) years. All patients were assessed with the Yale–rown Obsessive Compulsive Scale (Y-BOCS) (16), Global Assess-ent of Functioning (17), Clinical Global Impression (18), Brief
nxiety Scale (19), and Montgomery–Åsberg Depression Scale20), as well as with a neuropsychologic battery including the
attis Dementia Rating Scale (21) and frontal executive func-ions (Nelson’s Modified Wisconsin Card Sorting Test (22), Trail
aking Test (23), Categorical and Phonological Fluency Test24), and Stroop Test (25)). Those evaluations were carried out at
able 1. Patient Profiles: Demographic Features and Clinical Characteristic
atiento.
Age(years) Sex
DiseaseDuration
(years) Medication at Inclusion
1 29 M 19 SRI, atypical neuroleptic, valproate, clonaz2 45 F 39 SRI, buspirone, atypical neuroleptic, benzo3 39 F 27 SNRI, clomipramine, beta-blocker, benzod4 44 F 33 SRI, atypical neuroleptic, benzodiazepine5 35 M 27 No medication at baseline at the patient’s6 51 M 24 Clomipramine, beta-blocker, valproate, ne
benzodiazepine7 51 M 37 SRI, buspirone, atypical neuroleptic, benzo8 56 M 46 SNRI, tetracyclic, atypical neuroleptic, neu9 50 F 30 No medication at baseline at the patient’s
10 43 F 26 SRI, SNRI, valproate, neuroleptic, benzodia
BAS, Brief Anxiety Scale score ranging from 0 to 60, with higher scorescore ranging from 1 to 7, with higher scores indicating greater disease seveith higher scores indicating normal global functional status; M, male; MAD
cores indicating greater severity of depressive symptoms; NM, no mediceuptake inhibitor; SRI, serotonin reuptake inhibitor; Y-BOCS, Yale–Brown O
aBefore surgery.
the end of the two periods of randomization (Figure 1). Theclinical characteristics of all 10 patients are reported in Table 1.
The HC group consisted of 10 healthy age- and sex-matched con-trol subjects. The control subjects had no history of neurologic disease,head injury, or alcohol or substance abuse and displayed no signs ofdementia. A structural clinical interview for nonpatients (26) allowedexclusion of a history of or current psychiatric disorder. They had nor-mal findings on brain magnetic resonance imaging (MRI). The PET datawere obtained using the same imaging procedure (acquisition andimage reconstruction) and the same PET scanner as the patients’.
After a complete description of the study, written informedconsent was obtained from each participant, and the study wasconducted in accordance with the Declaration of Helsinki. All studyprocedures have been approved by the ethics committee.
Surgical ProcedureAll patients were implanted bilaterally in the STN using the
surgical procedure detailed in the STOC study (8). The STN waspreoperatively targeted by means of stereotactic MRI (27). The OCDtarget was defined as being 2 mm anterior and 1 mm medial to theParkinson’s disease target, at the boundary of the STN’s associativeand limbic territories (28,29).
The stimulation parameters were selected according to the bestimmediate clinical effect or absence of side effects, intraoperativedata, and anatomic location of each contact, determined postoper-
Figure 1. Design of positron emission tomography anal-ysis in patients suffering from severe obsessive-compul-sive disorder treated by subthalamic nucleus deep brainstimulation. CE, clinical evaluation; D, day; M, month.
Y-BOCSOff-Stimulation
Score
Y-BOCSOn-Stimulation
Score GAFa CGIa BASa MADRSa
24 18 35 6 3 13pine 13 18 30 6 12 5ine 34 0 31 6 19 28
27 9 32 6 21 18st 36 30 25 7 18 14
ptic, 18 25 40 6 9 5
pine 32 20 35 7 2 4tic, lithium 31 10 40 6 16 25
st 33 28 45 6 16 15e 28 22 35 5 26 13
ting greater severity of anxious symptoms; CGI, Clinical Global Impression, female; GAF, global assessment of functioning score ranging from 1 to 90,
ontgomery–Åsberg Depression Scale score ranging from 0 – 60, with higherat baseline at the patient’s request; SNRI, serotonin and norepinephrineive Compulsive Scale.
s
epamdiazeiazep
requeurole
diazeroleprequezepin
indicarity; F
RS, Mationbsess
www.sobp.org/journal

a(
P
sctswtottopkpee“et
ea
nwts3xaotpid
Fmdni
1018 BIOL PSYCHIATRY 2010;68:1016–1022 F. Le Jeune et al.
w
tively with a digital three-dimensional (3D) deformable atlas29,30) (see Figure 2 in Mallet et al.) (8).
ET Data AcquisitionAll OCD patients and healthy control subjects underwent PET
cans at the same center in Rennes (Department of Nuclear Medi-ine, Eugène Marquis Center). The neuroradiologist was blind tohe stimulation conditions of each patient. All OCD patients weretudied using 18fluorodeoxyglucose (18FDG)-PET in a resting stateith eyes open, having fasted for at least 6 hours. They underwent
wo scans at the end of each phase of randomization (M6 and M10f the protocol). Thus, for each patient, one scan was performed in
he Off-Stimulation condition and one in the On-Stimulation condi-ion, and the order of the PET examination was the same as therder of the surgery procedure determined by the randomizedrocedure used in the STOC study (Figure 1). All the patients wereept on their usual medication for the total duration of study; twoatients underwent only minor changes: in one patient, benzodiaz-pine dosage was slightly augmented (from 50 to 60 mg of cloraz-pate) from the middle of the “On” period until the middle of theOff” period, and in another patient had benzodiazepine (bromaz-pam 15 mg) and olanzapine (10 mg) introduced in the middle ofhe “Off” period at M8.
PET measurements were performed using a dedicated Discov-ry ST PET scanner (GEMS, Milwaukee, Wisconsin) in 3D mode, withn axial field of view of 15.2 cm.
A 144 to 160 MBq injection of 18FDG was administered intrave-ously under standardized conditions (in a quiet, dimly lit roomith the patient’s eyes and ears open). During acquisition, the pa-
ient’s head was immobilized using a head-holder. A cross-laserystem was used to achieve stable and reproducible positioning. AD emission scan was performed 30 min postinjection and after-ray-based attenuation correction. Following scatter, dead time,nd random corrections, PET images were reconstructed by 3Drdered subset expectation maximization providing 47 contiguous
ransaxial 3.75-mm-thick slices. Because the PET images of the OCDatients were acquired more than 3 months after the electrode
mplantation, we were able to exclude the microlesional effects
igure 2. Significant increase in glucose metabolism in the right frontaliddle gyrus (Brodmann’s area 10) in Off-Stimulation obsessive-compulsive
isorder patients compared with healthy control subjects (p � .005). Coro-al views projected onto brain slices of a standard magnetic resonance
maging (x,y,z Talairach coordinates).
escribed by Hilker (31).
ww.sobp.org/journal
PET Data AnalysisThe data were analyzed in unblinded conditions and were di-
vided into two groups, On-Stimulation and Off-Stimulation, usingSMP2 software (Wellcome Department of Cognitive Neurology,London, United Kingdom) implemented in MATLAB, version 7(MathWorks, Sherborn, Massachusetts). Statistical parametric mapswere spatially extended statistical processes used to characterizespecific regional effects in imaging data. They combine the generallinear model (to create the statistical map) with Gaussian field the-ory to draw statistical inferences about regional effects (32).
All subject data were standardized on the Montreal NeurologicalInstitute (MNI) atlas using 12-parameter affine transformation, fol-lowed by nonlinear transformations and a trilinear interpolation.Dimensions of the resulting voxels were 2 � 2 � 2 mm. Standard-ized data were then smoothed by a 12-mm full width at half maxi-mum isotropic Gaussian filter. The general linear model analysiswas applied on globally normalized data using standard propor-tional scaling. Reported effects are given in the Talairach and Tour-noux referential (33) computed from the MNI coordinates usingMatthew Brett’s script (http://www.mrc-cbu.cam.ac.uk/Imaging).
Three contrasts were analyzed:
1. We compared the data of the Off-Stimulation OCD patientswith those of HCs to determine the modifications in glucosemetabolism in refractory OCD, using the “compare-popula-tions one scan/subject” routine, which performed a fixed-effects simple t test for each voxel. Clusters of a minimum of 50contiguous voxels, with a threshold of p � .005 were consid-ered significantly different.
2. To determine direct STN DBS effects, we compared the data ofthe Off-Stimulation OCD patients with the data of the On-Stimulation patients and used the “population main effect, 2cond’s, 1scan/cond (paired t test)” SPM routine. Clusters of aminimum of 50 contiguous voxels, with a threshold of two-tailed p � .005, were considered significantly different.
3. To investigate the neural correlates of the clinical improve-ment in patients, we correlated the change in the Y-BOCSscore between the “On” and the “Off” state and the differentialcontrast between the PET images acquired in each condition.Whole-brain correlations were considered significant at thep � .005 threshold (uncorrected) and for clusters with a mini-mum size of 50 voxels.
Statistical Analysis of Clinical DataBecause of the small number of subjects, nonparametric analy-
ses were carried out. The primary outcome was the clinical benefitaccording to the Y-BOCS score, comparing the On-Stimulation andOff-Stimulation conditions. As for the analysis of the whole STOCstudy on 16 patients, analysis was performed by testing three ef-fects: carryover (some effects of the first treatment were still presentwhen the patient entered the second treatment period), period (theeffect of stimulation was different in the On–Off group than in theOff–On group), and treatment effects (34). For all comparisons,p values � .05 were considered significant (except for the carryovereffect, which was .10). Statistical analysis was performed with SPSS15.0 for Windows.
Results
Clinical and Neuropsychological Effect of STN StimulationNo significant differences were found between the On-Stimula-
tion and Off-Stimulation conditions for the neuropsychologic back-ground tests and the Montgomery–Åsberg Depression Scale score
ranging from 0 to 60.
3aTt
ido
C
c
pw(4
soer(
MO
iT
c
sessiv
F. Le Jeune et al. BIOL PSYCHIATRY 2010;68:1016–1022 1019
The median YBOCS scores for all 10 patients taken together were1 (minimum � 18, maximum � 36) with Off-Stimulation statusnd 19 (minimum � 0, maximum � 30) with On-Stimulation status.he difference was statistically significant (p � .05). We found nei-her a carryover effect (p � .16) nor a period effect (p � .23).
Because clinical scores of the two patients, with minor changesn treatment, did not depart from the rest of the group (within threeeciles around the median), we can safely ascribe the effects webserved at the group level to the STN stimulation.
omparison of Glucose Metabolism Between Patients and HCAreas of significant difference in glucose metabolism found by
omparing the OCD patients and the HC are shown in Table 2.When we studied the increases in the metabolism in the OCD
atients, six clusters were significant at p � .005. Hypermetabolismas observed in the right frontal lobe, middle and superior gyri
Brodmann’s areas [BA] 10 and 47; Figure 2), postcentral gyrus (BA3), and bilateral putamen.
Regarding the decreases in metabolism in OCD patients,even clusters were significant at p � .005. Hypometabolism wasbserved in the right limbic lobe (cingulate gyrus, BA 31), bilat-ral frontal lobe (medial gyrus, BA 6) and superior gyrus, BA 8),ight temporal lobe (right insula, BA 13), and right parietal lobeBA 7).
etabolic Effects of STN DBS: On-Stimulation Versusff-Stimulation Conditions
Areas of significant difference found by comparing the patientsn the On-Stimulation and Off-Stimulation conditions are shown inable 3.
In the On-Stimulation condition, there was a significant de-rease in cerebral metabolism (p � .005) in the left limbic lobe
Table 2. Comparison of Regional Glucose Metabolic Ra
Region
Decrease in Glucose Metabolism in OCD Off vs. HCsRight limbic lobe, cingulate gyrus, BA 31Left frontal lobe, medial gyrus, BA 6 �Left frontal lobe, superior gyrus, BA 8 �Right frontal lobe, medial gyrus, BA 6Right frontal lobe, superior gyrus, BA 8Right temporal lobe, insula, BA 13Right parietal lobe, BA 7
Increase in Glucose Metabolism in OCD Off vs. HCsRight frontal lobe, superior gyrus, BA 47Right frontal lobe, middle gyrus, BA 10Right putamenLeft putamen �Right parietal lobe, postcentral gyrus, BA 43
BA, Brodmann’s area; HCs, healthy controls; OCD, ob
Table 3. Regions with Decreased Glucose Metabolismp � .005, multiple-comparison corrected)
Regions BA
Left Limbic Lobe, Cingulate Gyrus 32 �Left Limbic Lobe, Cingulate Gyrus 24 �Left Frontal Lobe, Medial Gyrus 6 �
BA, Brodmann’s area.
(cingulate gyrus, BA 24 and 32) and left frontal lobe (medial gyrus,BA 6; Figure 3).
No increase was found in cerebral metabolism in the On-Stimu-lation condition (no cluster significant at p � .005).
Finally, we investigated the neural correlates of the clinical im-provement by correlating the decrease in Y-BOCS score and thechanges in PET signal between the two sessions (On vs. Off). Thisanalysis revealed that the decrease in Y-BOCS score was correlatedwith a decrease of metabolic activity in the orbitofrontal cortex–ventral medial prefrontal region (�10, �38, �10 Talairach coordi-nates, BA 10 –11) (Figure 4).
Discussion
To our knowledge, this study is the first to describe the meta-bolic effects of STN DBS in refractory OCD patients. It is also the firstto have used a double-blind randomized PET investigation to assesspatients suffering from refractory OCD conducted within the frame-work of the STOC study. This study allowed us to investigate refrac-tory OCD patients using functional neuroimaging. Whereas othertechniques, such as functional MRI, require specific conditions foracquisitions in stimulated patients, these patients can be assessedby means of metabolic imaging techniques, such as 18FDG-PET,without any modifications of their stimulation parameters.
We began by studying modifications in severe OCD patients inthe Off-Stimulation condition compared with HCs. The PET scansacquired in the Off-Stimulation state were performed 3 monthsafter surgery so that we could exclude the possibility that the met-abolic changes were due to the microlesional effects of STN implan-tation (31). We confirmed the increase in glucose metabolism in theright frontal middle and superior gyri (BA 10 and BA 47) of patientswith severe and refractory OCD. Those areas have been described
tween OCD and HCs (p � .051, corrected)
airach Coordinates
Z Value Voxel No.y z
–36 30 4.14 3832 54 4.32 786
18 40 3.83 78612 48 4.14 41124 46 3.67 411
0 2 4.29 536�44 38 5.32 383
38 �6 4.00 11058 �10 3.68 103
�8 �4 3.86 198�10 �4 3.45 80�6 18 3.65 127
e-compulsive disorder; Off, Off-Stimulation.
-Stimulation Compared with Off-Stimulation (k � 50,
rach Coordinates
t Value Cluster Sizey z
15 38 3.45 2850 39 3.10 285
14 45 3.70 285
tes Be
Tal
x
16141818144226
5226322864
in On
Talai
x
226
www.sobp.org/journal

apeT1
ani
pttofrgid(acS
ccdlfctcmnOagtcti
1020 BIOL PSYCHIATRY 2010;68:1016–1022 F. Le Jeune et al.
w
s a part of orbitofrontal cortex (35). In this sense, we replicatedrevious findings showing increased functional activity in this area,ither bilaterally (10) or restricted to the left (9,13) or right (12) side.hese seemingly discrepant results of previous studies using8FDG-PET in the resting state could be due to both demographicnd clinical differences between the sample groups (11,36). Theseeuroimaging data have influenced current models of pathophys-
ology in OCD (1,37).We then determined the metabolic effects of STN DBS by com-
aring patients in the On-Stimulation and Off-Stimulation condi-ions. A significant decrease in glucose metabolism was observed inhe anterior cingulate gyrus (BA 24 and 32) following STN DBS. Inther disorders, such as Parkinson’s disease, STN DBS has also been
ound to modify the glucose metabolism of this area (38). Theseesults suggest a strong link between the STN and the cingulateyrus, with a metabolic modification directly related to STN DBS,
ndependently of the disorder. Such a link has already beenemonstrated in monkeys, in which areas equivalent to BA 24
rostral cingulate motor area, which controls higher cognitivespects of movement) and to BA 23 (caudal cingulate area, whichontrols movement execution) both send projections into theTN (39).
Finally, we observed a positive correlation between the de-rease of 18FDG metabolism at the boundary of the orbitofrontalortex and the medial prefrontal cortex (BA 10 and 11) and theecrease of Y-BOCS scores secondary to the stimulation. This corre-
ation strongly suggests that the benefit therapeutic effect of high-requency STN stimulation is related to the decrease of prefrontalortex activity, especially in orbitofrontal cortex. Previous func-ional neuroimaging studies using 18FDG-PET have highlightedhanges in glucose metabolism when patients respond to treat-ent, be it selective serotonin reuptake inhibitors (SSRIs), BCT, or
eurosurgery. Most of these studies have revealed a decrease inFC and/or caudate nuclei in responders to treatment (3,40 – 43),lthough a few have found a decrease in the anterior cingulateyrus (44) or thalamus (45). With regard to the clinical efficacy of this
reatment, STN DBS acts similarly to the other treatments, and thelinical improvement was associated to a decrease of glucose me-abolism in OFC. It should be mentioned that the patients includedn this study belong to a specific subgroup of refractory OCD pa-
ww.sobp.org/journal
tients: they respond to STN DBS but are resistant to SSRIs, BCT, andother therapies, as required by the definition of treatment resis-tance. This suggests that although the mechanism underneaththe clinical benefit is similar to other therapies, STN-DBS mayalso act through other mechanisms. The results of our studysuggest that STN DBS may act directly on the OFC through thehyperdirect circuit described in animal studies (rat) (46,47). Theauthors of these studies suggest that “via the reciprocal connec-tions between the STN and the cerebral cortex, STN DBS mightmodulate rather directly the excitability of prefrontal corticalareas and in that way contribute to the effects of stimulation.”Our metabolic results obtained in OCD refractory patients couldprovide an argument on the functionality of this hyperdirectpathway in humans. An additional argument for this hypothesisis that no glucose metabolism changes were highlighted in basalganglia as had been described with BCT or SSRIs. To achieve thesame beneficial effect on clinical signs, STN DBS would act ondifferent circuits compared with other drugs.
STN DBS would therefore appear to have a beneficial impact viacircuits connecting the STN and OFC in severe refractory patientsfor whom other common treatments have failed.
This study has potential limitations. By using the standardanatomic template from the SPM toolbox, we did not take intoaccount possible structural abnormalities in OCD patients. Arecent meta-analysis has indeed shown consistent volumechanges in anterior cingulate cortex, OFC, and thalamus in thesepatients (48). Although this might represent an additionalsource of variance in the comparison of patient data with that ofhealthy control subjects (contrast 1), the within-patient analysis(comparing On- and Off-Stimulation states) is immune to thisproblem. In all cases, the possibility of anatomic alterations inOCD calls for caution in interpreting the anatomic localization ofthe activation patterns resulting from SPM analysis resting ontemplate-based normalization.
In conclusion, our results objectively demonstrate that high-frequency STN DBS induced a decrease of anterior cingulate gyrusmetabolism in refractory OCD patients and that the therapeuticeffects is correlated to a decrease in orbitofrontal cortex metabo-lism.
Figure 3. Significant decrease in glucose metabolism inOn-Stimulation compared with Off-Stimulation in the cin-gulate gyrus (Brodmann’s area 24 and 32) and left frontallobe (medial gyrus Brodmann’s area 6) (p � .005). Trans-versal, sagittal, and coronal views projected onto brainslices of a standard magnetic resonance imaging (x,y,zTalairach coordinates).
Figure 4. Correlation between metabolic change in-duced by stimulation and concomitant clinical improve-ment. Whole-brain analysis shows a significant cluster ofcorrelation in the ventromedial prefrontal cortex with thedecrease in the Yale–Brown Obsessive Compulsive Scalescore.

WOJtDc
bp(fi
C
CSbLHPtbDDWMgoPA(GWdCDC(AR(PMCMMTMNc
gt
F. Le Jeune et al. BIOL PSYCHIATRY 2010;68:1016–1022 1021
This study was supported by a grant from Medtronic to Dr. Millet.e thank Elizabeth Portier for English editing and proofreading anddile Audrain for bibliography management. We thank S. Brousse and
. Soulabaille, clinical research nurses, for their help in referring pa-ients to us and accompanying them during the study. We also thankr. Pierre Payoux (CHU Purpan, Toulouse, France) for his thoughtful
omments on the SPM methodology.Bruno Millet received the grant from Medtronic to explore deep
rain stimulation in resistant and chronic depressive patients. He alsoarticipated on boards for Medtronic and pharmaceutical companies
Bristol-Myers-Squibb, Janssen). All other authors report no biomedicalnancial interests or potential conflicts of interest.
ClinicalTrials.gov: Subthalamic Nucleus Stimulation in Severe Obsessiveompulsive Disorder; http://www.clinicaltrials.gov; NCT00169377.
Members of the French STOC Study Group are as follows: Trialoordination: L. Mallet (Center d’investigation Clinique, CHU Pitié-alpêtrière, Paris). Steering Committee: Y. Agid, B. Aouizerate, C. Ar-us, T. Bougerol, P. Damier, D. Fontaine, J.L. Houeto, M.O. Krebs, J.J.emaire, L. Mallet, B. Millet, P. Pollak. Logistics and Monitoring: D.ourton, S. Aprelon, C. Jourdain (Assistance Publique-Hôpitaux dearis, Direction de la Recherche Clinique, Paris). Coordinatingeams—Anatomy: E. Bardinet, J. Yelnik; Electrophysiology: P. Bur-aud, M.L. Welter, A.H. Clair; Neuropsychology: V. Czernecki, M. Vérin.ata Management and Statistical Analysis: S. Tézenas du Montcel,. Madar (Unité de Recherche Clinique, CHU Pitié-Salpêtrière, Paris).riting Committee: L. Mallet, A. Pelissolo, S. Tezenas du Montcel,.L. Welter, J. Yelnik. Centers (Principal Investigator, PI; Coinvesti-
ators: psychiatrist, P; neurosurgeon, N; neurologist, Nl; electrophysi-logist, E; radiologist, R; neuropsychologist, Np): Coordinating Center,aris; Pitié-Salpêtrière Hospital: L. Mallet (PI, P), A. Pelissolo (PI, P), Y.gid (Nl), P. Cornu (N), S. Navarro (N), M.L. Welter (E, Nl), A. Hartmann
Nl), B. Pidoux (E), D. Grabli (Nl), V. Czernecki (Np), D. Dormont (R), D.alanaud (R), J. Yelnik, E. Bardinet (neuroanatomists), C. Béhar (Np), Y.orbe (Nl), A.H. Clair (Np), B. Moutaud, CIC staff and nurses; Bor-
eaux: B. Aouizerate (PI, P), P. Burbaud (E), E. Cuny (N), D. Guehl (Nl);lermont-Ferrand: P.M. Llorca (PI, P), I Chéreau (P), J.J. Lemaire (N), F.urif (Nl), P. Derost (Nl), J. Coste (E); J. Gabrillargues, M. Barget, I. dehazeron; Grenoble: T. Bougerol (PI, P), M. Polosan (P), A.L. Benabid
N), S. Chabardès (N), E. Seigneuret (N), P. Krack (Nl), P. Pollak (Nl), C.rdouin (Np), J.F. Le Bas (R); Nantes: P. Damier (PI, Nl), Y. Lajat (N), S.aoul (N); Nice: V. Mattei (PI, P), D. Fontaine (N), M. Borg (Nl), P. Paquis
Nl), E. Michel (Np), P. Robert (P); Marie-Noelle Magnié-Mauro, (E), F.apetti (P); Paris Sainte-Anne Hospital: N. Baup (PI, P), B. Devaux (N),.O. Krebs (P), C. Oppenheimer (R); JP. Olié (P), D. Ranoux (Nl), M.
hayet (Np); Poitiers: J.L. Houeto (PI, Nl), N. Jaafari (P), B. Bataille (N), V.esnage (Nl); R. Gil (Nl), V. Audouin (Np), J.L. Senon (P); Rennes: B.illet (PI, P), M. Vérin (Nl), D. Drapier (P), P. Sauleau (E); S. Drapier (Nl);
oulouse: C. Arbus (PI, P), Y. Lazorthe (N), P. Chaynes (N), N. Fabre (Nl),. Simonetta (E), L. Schmitt (P), J.A. Lotterie (R), C. Camassel. Sponsor:. Best (Assistance Publique-Hôpitaux de Paris, Direction de la Recher-
he Clinique, Paris).Independent Safety Committee: J.C. Aussilloux, S. Blond, J. Fein-
old, D. Sicard. Independent Selection Committee: J. Adès, J. Cot-raux, M. Goudemand.
1. Aouizerate B, Guehl D, Cuny E, Rougier A, Bioulac B, Tignol J, Burbaud P(2004): Pathophysiology of obsessive-compulsive disorder: A necessarylink between phenomenology, neuropsychology, imagery and physiol-ogy. Prog Neurobiol 72:195–221.
2. Pallanti S, Quercioli L (2006): Treatment-refractory obsessive-compul-sive disorder: Methodological issues, operational definitions and thera-
peutic lines. Prog Neuropsychopharmacol Biol Psychiatry 30:400 – 412.3. Abelson JL, Curtis GC, Sagher O, Albucher RC, Harrigan M, Taylor SF, et al.(2005): Deep brain stimulation for refractory obsessive-compulsive dis-order. Biol Psychiatry 57:510 –516.
4. Greenberg BD, Malone DA, Friehs GM, Rezai AR, Kubu CS, Malloy PF, et al.(2006): Three-year outcomes in deep brain stimulation for highly resis-tant obsessive-compulsive disorder. Neuropsychopharmacology 31:2384–2393.
5. Nuttin B, Cosyns P, Demeulemeester H, Gybels J, Meyerson B (1999):Electrical stimulation in anterior limbs of internal capsules in patientswith obsessive-compulsive disorder. Lancet 354:1526.
6. Nuttin B, Gybels J, Cosyns P, Gabriels L, Meyerson B, Andreewitch Set al.(]?�2003): Deep brain stimulation for psychiatric disorders. NeurosurgClin N Am 14:xv–xvi.
7. Sturm V, Lenartz D, Koulousakis A, Treuer H, Herholz K, Klein JC,Klosterkötter J (2003): The nucleus accumbens: A target for deep brainstimulation in obsessive-compulsive- and anxiety-disorders. J ChemNeuroanat 26:293–299.
8. Mallet L, Polosan M, Jaafari N, Baup N, Welter ML, Fontaine D, et al.(2008): Subthalamic nucleus stimulation in severe obsessive-compul-sive disorder. N Engl J Med 359:2121–2134.
9. Baxter LR Jr, Phelps ME, Mazziotta JC, Guze BH, Schwartz JM, Selin CE(1987): Local cerebral glucose metabolic rates in obsessive-compulsivedisorder. A comparison with rates in unipolar depression and in normalcontrols. Arch Gen Psychiatry 44:211–218.
10. Baxter LR Jr, Schwartz JM, Mazziotta JC, Phelps ME, Pahl JJ, Guze BH,Fairbanks L (1988): Cerebral glucose metabolic rates in nondepressedpatients with obsessive-compulsive disorder. Am J Psychiatry 145:1560 –1563.
11. Menzies L, Chamberlain SR, Laird AR, Thelen SM, Sahakian BJ, Bullmore ET(2008): Integrating evidence from neuroimaging and neuropsychologicalstudies of obsessive-compulsive disorder: The orbitofronto-striatal modelrevisited. Neurosci Biobehav Rev 32:525–549.
12. Nordahl TE, Benkelfat C, Semple WE, Gross M, King AC, Cohen RM (1989):Cerebral glucose metabolic rates in obsessive compulsive disorder.Neuropsychopharmacology 2:23–28.
13. Swedo SE, Schapiro MB, Grady CL, Cheslow DL, Leonard HL, Kumar A, etal. (1989): Cerebral glucose metabolism in childhood-onset obsessive-compulsive disorder. Arch Gen Psychiatry 46:518 –523.
14. Rauch SL, Dougherty DD, Malone D, Rezai A, Friehs G, Fischman AJ, et al.(2006): A functional neuroimaging investigation of deep brain stimula-tion in patients with obsessive-compulsive disorder. J Neurosurg 104:558 –565.
15. Van Laere K, Nuttin B, Gabriels L, Dupont P, Rasmussen S, Greenberg BD,Cosyns P (2006): Metabolic imaging of anterior capsular stimulation inrefractory obsessive-compulsive disorder: A key role for the subgenualanterior cingulate and ventral striatum. J Nucl Med 47:740 –747.
16. Goodman WK, Price LH, Rasmussen SA, Mazure C, Delgado P, HeningerGR, Charney DS (1989): The Yale–Brown Obsessive Compulsive Scale. II.Validity. Arch Gen Psychiatry 46:1012–1016.
17. APA (2000): DSM-IV-TR: Diagnostic and Statistical Manual of Mental Dis-orders, 4th ed. Washington, DC: American Psychiatric Association.
18. Guy W (1976): Clinical global impression. In: ECDEU Assessment Manualfor Psychopharmacology. Rockville, MD: US Department of Health Edu-cation and Welfare Publishing Group.
19. Tyrer P, Owen RT, Cicchetti DV (1984): The brief scale for anxiety: Asubdivision of the comprehensive psychopathological rating scale.J Neurol Neurosurg Psychiatry 47:970 –975.
20. Montgomery SA, Asberg M (1979): A new depression scale designed tobe sensitive to change. Br J Psychiatry 134:382–389.
21. Mattis S (1988): Dementia Rating Scale Professional Manual. Odessa, FL:Psychological Assessment Resources.
22. Nelson HE (1976): A modified card sorting test sensitive to frontal lobedefects. Cortex 12:313–324.
23. Reitan RM (1958): Validity of the Trail Making Test as an indicator oforganic brain damage. Percept Mot Skills 8:271–276.
24. Cardebat D, Doyon B, Puel M, Goulet P, Joanette Y (1990): Evocationlexicale formelle et sémantique chez des sujets normaux. Performanceset dynamiques de production en fonction du sexe, de l’age et du niveaud’étude. Acta Neurol Belg 90:207–217.
25. Stroop J (1935): Studies of interference on serial verbal reaction. J Exp
Psychol 18:643– 662.www.sobp.org/journal

2
2
2
2
3
3
3
3
3
3
3
1022 BIOL PSYCHIATRY 2010;68:1016–1022 F. Le Jeune et al.
w
6. First M, Spitzer RL, Gibbon M, Williams JB (1996): Structured clinicalinterview for the DSM-IV Axis I disorders—Patient edition, version 2.0.New York: New York State Psychiatric Institute.
7. Bejjani BP, Dormont D, Pidoux B, Yelnik J, Damier P, Arnulf I, et al. (2000):Bilateral subthalamic stimulation for Parkinson’s disease by using three-dimensional stereotactic magnetic resonance imaging and electro-physiological guidance. J Neurosurg 92:615– 625.
8. Karachi C, Francois C, Parain K, Bardinet E, Tande D, Hirsch E, Yelnik J(2002): Three-dimensional cartography of functional territories in thehuman striatopallidal complex by using calbindin immunoreactivity.J Comp Neurol 450:122–134.
9. Yelnik J, Bardinet E, Dormont D, Malandain G, Ourselin S, Tande D, et al.(2007): A three-dimensional, histological and deformable atlas of thehuman basal ganglia. I. Atlas construction based on immunohistochem-ical and MRI data. Neuroimage 34:618 – 638.
0. Bardinet E, Bhattacharjee M, Dormont D, Pidoux B, Malandain G, Schup-bach M, et al. (2009): A three-dimensional histological atlas of the hu-man basal ganglia. II. Atlas deformation strategy and evaluation in deepbrain stimulation for Parkinson disease. J Neurosurg 110:208 –219.
1. Hilker R, Voges J, Weisenbach S, Kalbe E, Burghaus L, Ghaemi M, et al.(2004): Subthalamic nucleus stimulation restores glucose metabolismin associative and limbic cortices and in cerebellum: Evidence from aFDG-PET study in advanced Parkinson’s disease. J Cereb Blood FlowMetab 24:7–16.
2. Friston KJ, Holmes AP, Worsly KJ, Poline JP, Frith CD, Frackowiak RS(1995): Statistical parametric maps in functional imaging: A generallinear approach. Hum Brain Mapp 2:189 –210.
3. Talairach J, Tournoux P (1988): Co-Planar Stereotaxic Atlas of the HumanBrain: 3-Dimensional Proportional System: An Approach to Cerebral Imag-ing. New York: Thieme Medical Publishers.
4. Jones B, Kenward M (2003): The 2 � 2 cross-over trial with continuousdata. In: Design and Analysis of Cross-Over Trials, 2nd ed. New York: Chap-man & Hall.
5. Kringelbach ML, Rolls ET (2004): The functional neuroanatomy of thehuman orbitofrontal cortex: Evidence from neuroimaging and neuro-psychology. Prog Neurobiol 72:341–372.
6. Mataix-Cols D, Wooderson S, Lawrence N, Brammer MJ, Speckens A,Phillips ML (2004): Distinct neural correlates of washing, checking, andhoarding symptom dimensions in obsessive-compulsive disorder. Arch
Gen Psychiatry 61:564 –576.ww.sobp.org/journal
37. Saxena S, Brody AL, Schwartz JM, Baxter LR (1998): Neuroimaging andfrontal-subcortical circuitry in obsessive-compulsive disorder. Br J Psy-chiatry Suppl:26 –37.
38. Le Jeune F, Peron J, Biseul I, Fournier S, Sauleau P, Drapier S, et al. (2008):Subthalamic nucleus stimulation affects orbitofrontal cortex in facialemotion recognition: A PET study. Brain 131:1599 –1608.
39. Takada M, Tokuno H, Hamada I, Inase M, Ito Y, Imanishi M, et al. (2001):Organization of inputs from cingulate motor areas to basal ganglia inmacaque monkey. Eur J Neurosci 14:1633–1650.
40. Baxter LR Jr, Schwartz JM, Bergman KS, Szuba MP, Guze BH, MazziottaJC, et al. (1992): Caudate glucose metabolic rate changes with both drugand behavior therapy for obsessive-compulsive disorder. Arch Gen Psy-chiatry 49:681– 689.
41. Saxena S, Brody AL, Maidment KM, Dunkin JJ, Colgan M, Alborzian S, etal. (1999): Localized orbitofrontal and subcortical metabolic changesand predictors of response to paroxetine treatment in obsessive-com-pulsive disorder. Neuropsychopharmacology 21:683– 693.
42. Saxena S, Brody AL, Ho ML, Alborzian S, Maidment KM, Zohrabi N, et al.(2002): Differential cerebral metabolic changes with paroxetine treat-ment of obsessive-compulsive disorder vs major depression. Arch GenPsychiatry 59:250 –261.
43. Schwartz JM, Stoessel PW, Baxter LR Jr, Martin KM, Phelps ME (1996):Systematic changes in cerebral glucose metabolic rate after successfulbehavior modification treatment of obsessive-compulsive disorder.Arch Gen Psychiatry 53:109 –113.
44. Perani D, Colombo C, Bressi S, Bonfanti A, Grassi F, Scarone S, et al. (1995)[18F]FDG PET study in obsessive-compulsive disorder. A clinical/meta-bolic correlation study after treatment. Br J Psychiatry 166:244 –250.
45. Saxena S (2003): Neuroimaging and the pathophysiology of obsessivecompulsive disorder (OCD). In: Fu C, Senior C, Russel T, Weinberger D,Murray R, editors. Neuroimaging in psychiatry. London and New York:Martin Dunitz, 191–224.
46. Degos B, Deniau JM, Le Cam J, Mailly P, Maurice N (2008): Evidence for adirect subthalamo-cortical loop circuit in the rat. Eur J Neuosci 27:2599–2610.
47. Maurice N, Deniau JM, Glowinski J, Thierry AM (1999): Relationshipbetween the prefrontal cortex and the basal ganglia in the rat: Physiol-ogy of the cortico-nigral circuits. J Neurosci 19:4674 – 4681.
48. Rotge JY, Dilharreguy B, Aouizerate B, Martin-Guehl C, Guehl D, Jaafari N, etal. (2009): Inverse relationship between thalamic and orbitofrontal volumes
in obsessive-compulsive disorder. Prog Neuropsychopharmacol Biol Psychi-atry 15:682–687.



















