
Mapping Structural Brain Alterations in Obsessive-Compulsive Disorder

POMM
BoMqeRfppCpi
Kis
Og2(CfcRregsCwd2wit
vo1
F
DA
R
0d
renatal, Perinatal, and Postnatal Risk Factors inbsessive–Compulsive Disorder
arcos Salem Vasconcelos, Aline Santos Sampaio, Ana Gabriela Hounie, Fernando Akkerman,ariana Curi, Antonio Carlos Lopes, and Euripedes C. Miguel
ackground: The etiology of obsessive–compulsive disorder (OCD) remains unknown, although it is thought to involve an interactionf genetic and environmental factors. This study aimed to identify prenatal, perinatal, and postnatal risk factors in OCD.ethods: We compared retrospectively 68 OCD patients to 70 control subjects based on responses given on a standardized
uestionnaire. The questionnaire was designed to evaluate environmental factors, with a special focus on gestation, labor, birth, andarly infancy aspects.esults: The group of OCD patients had risk factors with greater frequency than the control group. Notable among the significant
indings (p � 0.001) were edema of the hands, feet, or face and excessive weight gain during gestation; hyperemesis gravidarum;rolonged labor; preterm birth; and jaundice. When socioeconomic class was used as a covariable in the logistic regression analysis,rolonged labor and edema during pregnancy remained statistically significant.onclusions: Some early risk factors may be associated with the expression of OCD later in life such as edema during pregnancy androlonged labor. If our findings are confirmed in future studies, greater attention should be given to such factors in predisposed
ndividuals, especially in prenatal care and delivery.ey Words: Compulsive behaviors, environmental factors, genet-cs, obsessive behaviors, obsessive– compulsive disorder (OCD), ob-tetric complications, perinatal complications
bsessive–compulsive disorder (OCD), once considereda rare disease is currently the fourth leading psychiatricdisorder, with a prevalence of approximately 3% in the
eneral population (Karno and Golding 1991; Torres and Lima005). Various authors have suggested that OCD is familialHanna et al 2005; Nestadt et al 2000; Pauls et al 1995; Rosario-ampos et al 2005), and twin studies support that the greater
requency within affected families is in part related to a geneticomponent (Carey and Gottesman 1981; Clifford et al 1984;asmussen and Tsuang 1986). Nevertheless, the variability in theesults obtained in these same studies implies the participation ofnvironmental factors. Some OCD subtypes may have greaterenetic loadings. Early-onset OCD appears to be a distinctubtype in which the genetic component is significant (Rosario-ampos et al 2005). Patients with early-onset OCD also presentith a higher frequency of Tourette syndrome (TS) and ticisorders (Rosario-Campos et al 2001, 2005; Hemmings et al004). Therefore, the genetic model of OCD that is currently mostidely accepted is designated mixed. In the mixed model, there
s an interaction between genes with major and minor effects andhe environment.
Perinatal risk factors for schizophrenia have been evaluated inarious studies. A recent meta-analysis revealed that three groupsf complications correlated significantly with schizophrenia:) prenatal (complications of pregnancy: bleeding, diabetes, Rh
rom the Department of Psychiatry (MSV, ASS, AGH, FA, ACL, ECM), Univer-sity of São Paulo Medical School, OCD Spectrum Disorders Program(PROTOC), and Mathematics and Statistics Institute (MC), University ofSão Paulo, São Paulo, Brazil.
rs. Vasconcelos and Sampaio contributed equally to the final manuscript.ddress reprint requests to Eurípedes C. Miguel, M.D., Ph.D., Department of
Psychiatry, University of São Paulo Medical School, Rua Dr. Ovídio Piresde Campos, 785, 4°.andar, s.03 – 05403-010, São Paulo – SP – Brazil;E-mail: [email protected].
eceived January 31, 2006; revised June 29, 2006; accepted July 6, 2006.
006-3223/07/$32.00oi:10.1016/j.biopsych.2006.07.014
incompatibility, preeclampsia, and prenatal infections); 2) peri-natal (complications of delivery: uterine atony, asphyxia, andemergency cesarean section); and 3) postnatal (abnormal fetalgrowth and development: low birth weight, congenital malfor-mations, and reduced head circumference; Cannon et al 2002). Inaddition, Gilmore et al (1998) concluded that mild ventriculo-megaly detected in the prenatal ultrasonography, as well asgreater age of the mother and lower gestational age, could berisk factors for schizophrenia.
Other studies have attempted to draw correlations betweenenvironmental factors and neuropsychiatric disorders. Glasson etal (2004) conducted such a study involving patients with autism.The authors found that the parents of autistic patients, comparedwith those of control subjects, were significantly older. Inaddition, patients with autism were more likely to be firstborn, tohave experienced fetal distress, to have been delivered by anelective or emergency cesarean section, and to have had a 1-minApgar score of � 6. In mothers of autistic patients, threatenedabortion, epidural caudal anesthesia, labor induction, and laborduration of less than 1 hour were all more frequent. Backer et al(2000) found that children with severe perinatal risks morefrequently suffered from deficits in visuomotor function, andpresented higher rates of somatic complaints, social withdrawal,and attention deficits. Children born between 32 and 35 weeks ofgestation more frequently experience problems at school, includ-ing those that fall within the spectrum of attention-deficit/hyperactivity disorder (Huddy et al 2001).
To date, there have been virtually no studies investigating theinfluence of environmental factors on the development of OCD.The only available data are those obtained from patients with TS,a neuropsychiatric disorder that, because of its similar pheno-typic characteristics and its greater frequency among OCDpatients and their relatives, has been considered to be etiologi-cally related to certain forms of OCD. For example, in a study ofsubjects with TS, Santangelo et al (1994) reported that laborcomplications (especially forceps) and maternal smoking, as wellas excessive consumption of caffeine or alcohol by the mother,were all correlated with the development of OCD. Kano et al(2001) found the frequency of TS and OCD to be lower in thefirst-degree relatives of TS probands whose mothers had expe-
rienced significant obstetric complications, such as forceps de-BIOL PSYCHIATRY 2007;61:301–307© 2007 Society of Biological Psychiatry

lpAmsO
tsmls
M
S
pSCC(Mpfcceiseep(a1t2apES
itv(a(t
swic
C
cPud1
302 BIOL PSYCHIATRY 2007;61:301–307 M.S. Vasconcelos et al
w
ivery, fetal distress, or premature birth, than in those of TSrobands whose mothers had experienced no such problems.lthough these findings did not hold up after correction forultiple testing they suggest that, in a subset of the probands
tudied, environmental factors were relevant in the expression ofCD.This study proposes to describe various environmental factors
hat might be correlated with OCD. On the basis of the suppo-ition that problems in the prenatal, perinatal, or postnatal perioday contribute to the expression of OCD over the course of a
ifetime (Santos 1999), such aspects were evaluated using atandardized questionnaire.
ethods and Materials
ubjectsThis was a retrospective study, involving analysis of data
reviously collected by the Obsessive–Compulsive Disorderpectrum Program (Projeto Transtornos do Espectro Obsessivo-ompulsivo [PROTOC]) at the Institute of Psychiatry of thelinical Hospital of the University of São Paulo Medical SchoolInstituto de Psiquiatria do Hospital das Clínicas da Faculdade deedicina da Universidade de São Paulo [FMUSP]). We includedatients diagnosed with OCD and referred to FMUSP or patientsrom private practices, excluding those who were unable toomplete the questionnaire for any reason. Written informedonsent was obtained in all cases. Of the 99 patient files, 31 werexcluded; 21 files were excluded because the questionnaire wasncomplete and the researchers were unable to contact theubject; 10 were excluded because the subjects lacked knowl-dge relating to gestational or perinatal history and the research-rs were unable to contact the mother or other reliable informedarty. Of the 68 OCD subjects included in the final sample, 4667.6%) had completed the questionnaire by proxy (the mother),nd 12 (17.6%) had completed it on their own. In the remaining0 cases (14.7%), it was unclear who had completed the ques-ionnaire. All these interviews were conducted between 1995 and003 in the course of other PROTOC research projects (Diniz etl 2004; Rosario-Campos et al 2001). These projects were ap-roved by institutional review boards (Ethics Committee forvaluation of Research Projects from Clinical Hospital, University ofão Paulo Medical School).
The control group comprised 70 gender- and age-matchedndividuals without OCD. Control group subjects were underreatment at the FMUSP Orthopedics Institute and were inter-iewed as part of a previous study conducted by our groupHounie at al 2004). Of the 70 control subjects, 41 (58.5%) weressisted by their mothers in completing the questionnaire and 2332.8%) required no assistance; it was not clear who completedhe questionnaire for the remaining 6 control subjects (8.5%).
Control subjects who had Yale–Brown Obsessive–Compul-ive Scale (Y-BOCS; Goodman et al 1989) scores higher that 7ere excluded to decrease the chance of including OCD subjects
n the control group, but none had a YBOCS score over 5. Fourontrol group subjects had a history of a tic disorder.
linical AssessmentAll patients were evaluated using research charts that in-
luded scales and questionnaires for psychiatric evaluation in theROTOC research setting. These charts were created through these of the Structured Clinical Interview for DSM-IV, Axis Iisorders—patient edition (SCID-I/P), version 2.0 (First et al
995) for adults. The Kiddie-Schizophrenia and Affective Disor-ww.sobp.org/journal
der Schedule (K-SADS; Orvaschel and Puig-Antich 1987) wasused for children between ages 5 and 15. These instruments weresupplemented with additional modules, designed by the PROTOCstaff, for the DSM-IV diagnosis of TS and tic disorders (Diniz et al2004; Hounie et al 2004; Rosario-Campos et al 2001). All ticdisorders or tics without other specifications according to theDSM-IV were included in the diagnosis of tic disorders. Thepresence and severity of obsessive–compulsive symptoms andtics were determined by using the checklists and rating scalesincorporated in the Y-BOCS and the Yale Global Tic SeverityScale (YGTSS; Leckman et al 1989), respectively.
To evaluate the obstetric, postnatal, and medical risk factorsof the subjects studied, the Medical and Risk Factor Question-naire (Rosario-Campos et al 2001), included in the chart, wasused. This questionnaire was created based on translations andadaptations of the Modified Schedule for Risk and ProtectiveFactors developed by the Yale Child Study Center of the YaleUniversity School of Medicine (Walkup and Leckman, personalcommunication). The newly created instrument (available uponrequest) evaluates a number of variables related to the prenatal,perinatal, and postnatal periods. In evaluating gestation, sometopics regarding the pre-pregnancy period are also addressed. Abrief description of this instrument is presented in Table 1.
The questionnaire was first completed by the patient or by aparent or relative of the patient, and its accuracy was thenchecked during the medical consultation, when any questions orambiguities were clarified. When the information was incom-plete or missing, a family member, preferably the mother, wascontacted by telephone.
Specific age at onset of obsessive–compulsive symptoms foreach subject were obtained from the patients or relatives when-ever possible. In this study, we defined age at onset as the age atwhich the patient, or a family member, remembered the obses-sive–compulsive symptoms beginning as described in our pre-vious studies (Rosario-Campos et al 2001). Briefly, we selectedthresholds of age 10 for the early-onset group and age 17 for thelate-onset group. These thresholds are consistent with the ageadvocated by Geller and colleagues (Geller et al 1998) to indicateprepubertal onset and are also in accordance with an OCDgenetic family study (Pauls et al 1995).
Demographic characteristics were obtained by direct inter-view. Subjects were classified as belonging to one of fivesocioeconomic classes (A, B, C, D, or E) based on a structuredinterview for Brazilian standards (Associação Brasileira de Anun-ciantes 1989). Marital status was defined as married, nevermarried, divorced, or widowed. Educational level was expressedas the number of years of schooling.
Statistical AnalysisStatistical analyses were performed using the SPSS program,
version 11. Categorical variables were described as relative andabsolute frequencies. Continuous variables were described asmeans and standard deviations if presenting normal distribution,or, if not, as medians and ranges.
In the univariate analysis, the demographic variables for theOCD and control groups were compared. Continuous demo-graphic variables were compared using the Student’s t test or theMann–Whitney U test, and categorical demographic variableswere compared using Pearson’s chi-square test or Fisher’s ExactTest. A multivariate analysis was also performed based on thelogistic regression model, using social class and schooling ascovariables in an attempt to identify which environmental factors
were, together with these covariables, more significantly corre-
lavstvm
R
D
rsnTmwOti
E
tmTT
a
T
Q
W
D
DDD
D
HW
WWW
D
DD
tive Fc
M.S. Vasconcelos et al BIOL PSYCHIATRY 2007;61:301–307 303
ated with OCD. The procedures previously described were alsodopted in the identification of factors correlating with thearious OCD subtypes. The associations between YBOCS totalcore and each qualitative variable were studied using Student’stest for OCD patients. The Normal distribution of the data waserified by Normal probability plots, Shapiro–Wilks, and Kol-ogorov–Smirnov tests.
esults
emographic DataWe found no significant differences between the two groups
egarding gender, age at the time of the interview, and maritaltatus; however, we did find such a difference regarding socioeco-omic class (p � .001) and level of education (p � .044; Table 2).his can be explained by the fact that OCD patients had, for theost part, been referred from private clinics and practices,hereas control group patients had been recruited from therthopedics Institute of the FMUSP, a public hospital, and
herefore the latter patients were more likely to have lowerncomes and less access to formal education.
nvironmental FactorsTable 3 shows the results of the comparisons made between
he OCD group and the control group in relation to the environ-ental factors that presented statistically significant differences.he studied variables found to be not significant are shown inable 4.
Prenatal Period. Among the environmental factors associ-
able 1. Summary of the Medical and Risk Factor Questionnaire
uestions
ere there any special circumstances/problems involved in getting or remmedication or special medical procedure necessary to initiate or continu
id any of the following specific problems occur in the child’s mother durinamount of weight gained in pounds); severe nausea/vomiting, severe anrubella diagnosis; vaginal bleeding; elevated blood pressure; protein in useizures; placenta separated from uterus too early (abruptio placenta); in
id you receive prenatal care?id your doctor prescribe any medication?id the doctor do any diagnostic tests (X-ray, ultrasound, other)? Specify tri
uring the pregnancy, did the child’s mother: a) drink more than three cupmore than 10 cigarettes in 24 hours? c) drink more than two drinks of alcother street drugs?
ow was the mother’s emotional state during pregnancy?here was the delivery?
hat was the child’s birth weight (grams)?as the delivery vaginal, vaginal with forceps, or by cesarian section?as there a) prolonged labor; b) unusual presentation (buttocks, face, footd) knotted cord?
id the doctor or nursing staff intervene in any way immediately after the bmedication, incubator, intensive care unit, surgery, blood transfusion, oth
evelopmental milestones: At what age did your child: a) sit? b) walk? c) beid you have any of these problems: seizures, convulsions; diabetes; head imeningitis; high blood pressure; migraine headaches; thyroid: overactiveautoimmune disorder; chicken pox; measles; mumps; polio; rubella; tonspneumonia; low blood pressure; strep infections; rheumatic fever; rheuminfection)?
This questionnaire is based on the Modified Schedule for Risk and Protecardiopulmonary resuscitation; Y/N/DK: yes/no/do not know.
ted to the period before conception, the most remarkable
difference was that related to maternal use of special medicationsor procedures to conceive, in the OCD group (p � .025). Theother factors indicated a trend to the level of significance.Mothers of individuals with OCD presented more difficulty inbecoming pregnant (p � .053) and a higher prevalence ofpreexisting medical problems (p � .051) than did those ofcontrol subjects (Table 3).
During the gestational period, mothers of individuals withOCD more frequently presented with excessive weight gain (p �.001); edema of the hands, feet, or face (p � .001); hyperemesisgravidarum (p � .001); and use of medication (p � .001).
Answers
pregnant with this child (infertility, need fornancy, preexisting medical problem, other)?
Y/NIf yes, explain
pregnancy? Excessive weight gain (totalelevated blood sugar; toxoplasmosis or
swelling of face, hands, or legs; convulsions/atible blood (Rh factor); other
(Y/N/DK)If yes, explain
Y/NY/N/DK
er, reason, and complications. Y/NSpecify
ffee/tea in 24 hours? b) on average smoken 24 hours? d) smoke marijuana? e) take
Y/N/DKSpecify
(Open answer)HospitalHome
nting first); c) cord around the baby’s neck; (Y/N)If Yes, please explain
birth (e.g., oxygen therapy, CPR, (Y/N/DK)Specify
toilet trained? e) talk? Agess with loss of consciousness; encephalitis;eractive, enlarged; heart disease; allergies;whooping cough; tremors; anemia; eczema;ever with chorea; skin disease; lung
(Y/N/DK)Specify
actors developed by Walkup and Leckman (personal communication). CPR:
Table 2. Demographic Data Comparing the Obsessive–CompulsiveDisorder Group to the Control Group
Variable OCD Control p
Number of Subjects: n (%) 68 (100) 70 (100) —Median age years (Range) 24.93 (11–44) 24.2 (11–43) .617Male: n (%) 47 (69.1) 45 (64.3) .547Median social classa B C �.001Marital status: n (%) 14 (21.2) married
51 (77.3) single1 (1.5) divorced2 (3) no data
25 (35.7) married43 (61.4) single
2 (2.9) divorced
.106
Mean level education(years of schooling) 13.25 11.67 .044
OCD, obsessive-compulsive disorder.aAs defined by the criteria used to classify socioeconomic status in the
questionnaire devised by the Associação Brasileira de Anunciantes (Brazilian
aininge pregg theemia;rine;comp
mest
s of coohol i
prese
aby’ser)?
comenjurie, und
illitis;atic f
Market Research Association).
www.sobp.org/journal
qcta(
nlOm.
L
sdSdistd[e1cTnsvE
TO
E
P
P
P
304 BIOL PSYCHIATRY 2007;61:301–307 M.S. Vasconcelos et al
w
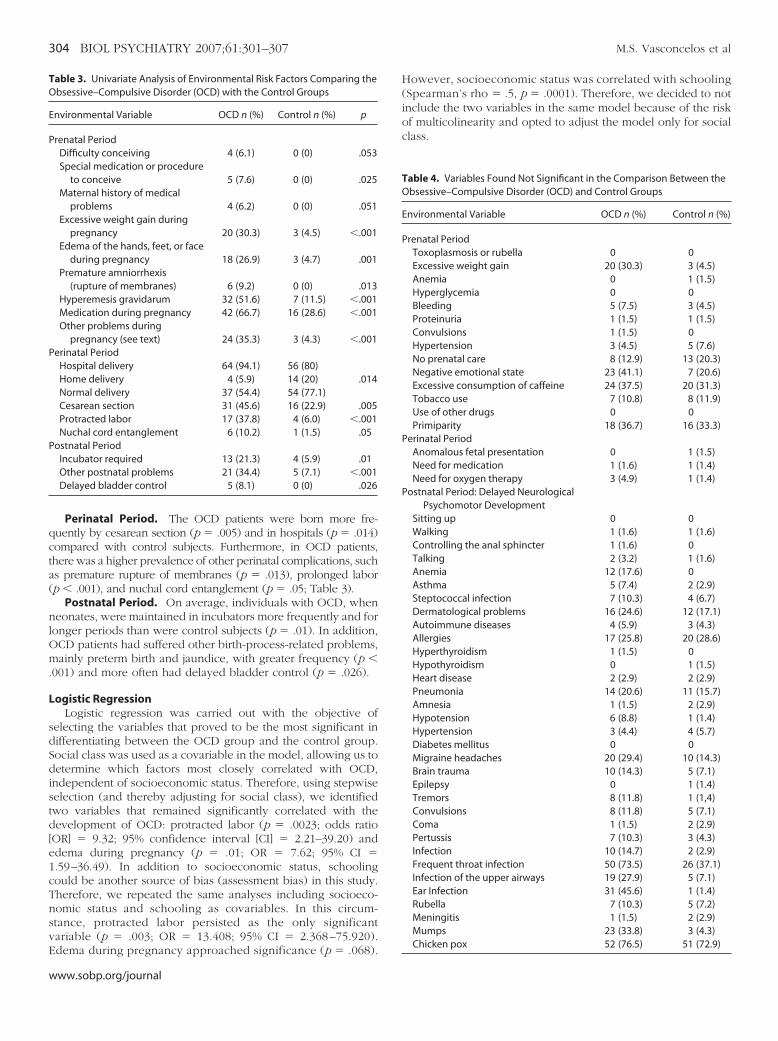
Perinatal Period. The OCD patients were born more fre-uently by cesarean section (p � .005) and in hospitals (p � .014)ompared with control subjects. Furthermore, in OCD patients,here was a higher prevalence of other perinatal complications, suchs premature rupture of membranes (p � .013), prolonged laborp � .001), and nuchal cord entanglement (p � .05; Table 3).
Postnatal Period. On average, individuals with OCD, wheneonates, were maintained in incubators more frequently and foronger periods than were control subjects (p � .01). In addition,CD patients had suffered other birth-process-related problems,ainly preterm birth and jaundice, with greater frequency (p �
001) and more often had delayed bladder control (p � .026).
ogistic RegressionLogistic regression was carried out with the objective of
electing the variables that proved to be the most significant inifferentiating between the OCD group and the control group.ocial class was used as a covariable in the model, allowing us toetermine which factors most closely correlated with OCD,ndependent of socioeconomic status. Therefore, using stepwiseelection (and thereby adjusting for social class), we identifiedwo variables that remained significantly correlated with theevelopment of OCD: protracted labor (p � .0023; odds ratioOR] � 9.32; 95% confidence interval [CI] � 2.21–39.20) anddema during pregnancy (p � .01; OR � 7.62; 95% CI �.59–36.49). In addition to socioeconomic status, schoolingould be another source of bias (assessment bias) in this study.herefore, we repeated the same analyses including socioeco-omic status and schooling as covariables. In this circum-tance, protracted labor persisted as the only significantariable (p � .003; OR � 13.408; 95% CI � 2.368–75.920).
able 3. Univariate Analysis of Environmental Risk Factors Comparing thebsessive–Compulsive Disorder (OCD) with the Control Groups
nvironmental Variable OCD n (%) Control n (%) p
renatal PeriodDifficulty conceiving 4 (6.1) 0 (0) .053Special medication or procedure
to conceive 5 (7.6) 0 (0) .025Maternal history of medical
problems 4 (6.2) 0 (0) .051Excessive weight gain during
pregnancy 20 (30.3) 3 (4.5) �.001Edema of the hands, feet, or face
during pregnancy 18 (26.9) 3 (4.7) .001Premature amniorrhexis
(rupture of membranes) 6 (9.2) 0 (0) .013Hyperemesis gravidarum 32 (51.6) 7 (11.5) �.001Medication during pregnancy 42 (66.7) 16 (28.6) �.001Other problems during
pregnancy (see text) 24 (35.3) 3 (4.3) �.001erinatal Period
Hospital delivery 64 (94.1) 56 (80)Home delivery 4 (5.9) 14 (20) .014Normal delivery 37 (54.4) 54 (77.1)Cesarean section 31 (45.6) 16 (22.9) .005Protracted labor 17 (37.8) 4 (6.0) �.001Nuchal cord entanglement 6 (10.2) 1 (1.5) .05
ostnatal PeriodIncubator required 13 (21.3) 4 (5.9) .01Other postnatal problems 21 (34.4) 5 (7.1) �.001Delayed bladder control 5 (8.1) 0 (0) .026
dema during pregnancy approached significance (p � .068).
ww.sobp.org/journal
However, socioeconomic status was correlated with schooling(Spearman’s rho � .5, p � .0001). Therefore, we decided to notinclude the two variables in the same model because of the riskof multicolinearity and opted to adjust the model only for socialclass.
Table 4. Variables Found Not Significant in the Comparison Between theObsessive–Compulsive Disorder (OCD) and Control Groups
Environmental Variable OCD n (%) Control n (%)
Prenatal PeriodToxoplasmosis or rubella 0 0Excessive weight gain 20 (30.3) 3 (4.5)Anemia 0 1 (1.5)Hyperglycemia 0 0Bleeding 5 (7.5) 3 (4.5)Proteinuria 1 (1.5) 1 (1.5)Convulsions 1 (1.5) 0Hypertension 3 (4.5) 5 (7.6)No prenatal care 8 (12.9) 13 (20.3)Negative emotional state 23 (41.1) 7 (20.6)Excessive consumption of caffeine 24 (37.5) 20 (31.3)Tobacco use 7 (10.8) 8 (11.9)Use of other drugs 0 0Primiparity 18 (36.7) 16 (33.3)
Perinatal PeriodAnomalous fetal presentation 0 1 (1.5)Need for medication 1 (1.6) 1 (1.4)Need for oxygen therapy 3 (4.9) 1 (1.4)
Postnatal Period: Delayed NeurologicalPsychomotor Development
Sitting up 0 0Walking 1 (1.6) 1 (1.6)Controlling the anal sphincter 1 (1.6) 0Talking 2 (3.2) 1 (1.6)Anemia 12 (17.6) 0Asthma 5 (7.4) 2 (2.9)Steptococcal infection 7 (10.3) 4 (6.7)Dermatological problems 16 (24.6) 12 (17.1)Autoimmune diseases 4 (5.9) 3 (4.3)Allergies 17 (25.8) 20 (28.6)Hyperthyroidism 1 (1.5) 0Hypothyroidism 0 1 (1.5)Heart disease 2 (2.9) 2 (2.9)Pneumonia 14 (20.6) 11 (15.7)Amnesia 1 (1.5) 2 (2.9)Hypotension 6 (8.8) 1 (1.4)Hypertension 3 (4.4) 4 (5.7)Diabetes mellitus 0 0Migraine headaches 20 (29.4) 10 (14.3)Brain trauma 10 (14.3) 5 (7.1)Epilepsy 0 1 (1.4)Tremors 8 (11.8) 1 (1,4)Convulsions 8 (11.8) 5 (7.1)Coma 1 (1.5) 2 (2.9)Pertussis 7 (10.3) 3 (4.3)Infection 10 (14.7) 2 (2.9)Frequent throat infection 50 (73.5) 26 (37.1)Infection of the upper airways 19 (27.9) 5 (7.1)Ear Infection 31 (45.6) 1 (1.4)Rubella 7 (10.3) 5 (7.2)Meningitis 1 (1.5) 2 (2.9)Mumps 23 (33.8) 3 (4.3)
Chicken pox 52 (76.5) 51 (72.9)
Ohp2ampaw(caf
D
pwrceSt
angcat2bcwhnpbhesen
shpca
Otactcporzn
M.S. Vasconcelos et al BIOL PSYCHIATRY 2007;61:301–307 305
Correlations Between Each of the Variables Studied and theCD Subtypes. Among the OCD patients, 29 (42.6%) had aistory of tics. In addition, 37 (54%) of the patients with OCD hadresented with early-onset OC symptoms (before age 10 years),5 (36.76%) were considered late-onset cases (OC symptomsppearing after age 17 years), and 2 (2.9%) provided no infor-ation regarding the age at onset of symptoms. Nineteenatients (50%) with early onset and no patient with late onsetlso had tic disorders. No statistically significant correlationsere found between the variables studied and the onset of OCD
early or late), with the presence of tics. There were no signifi-ant correlations with these early risk factors and the presence orbsence of familial history of tic disorders or OCD in theirst-degree relatives of the OCD subjects.
iscussion
This study describes a number of prenatal, perinatal, andostnatal variables associated with OCD, which, in interactionith other environmental or genetic factors, may play important
oles in the clinical expression of OCD. After controlling for possibleonfounding factors, protracted labor and edema during pregnancymerged as the most important risk factors associated with OCD.uch findings indicate that patients with OCD had more complica-ions during gestation and delivery than did control subjects.
A significant source of bias in this study is the fact that, onverage, the patients with OCD belonged to a higher socioeco-omic class than that of the control subjects. In addition, as aroup, the OCD patients had more schooling, which could raiseoncerns of assessment bias. As expected, socioeconomic statusnd schooling were correlated in this sample as they are reportedo be in the general population (Mengue et al 2004; Stein et al005). Therefore, some of the results obtained might reflect theseiases, rather than the presence or absence of OCD. Theseonfounders do not impede the evaluation of some findings forhich higher social status may have an attenuating effect,owever. For instance, because mothers with lower socioeco-omic status probably have more limited access to adequaterenatal and health care assistance (Coimbra et al 2003), it woulde expected that individuals from the control group would havead a higher number of problems during gestation, delivery, andarly infancy. This proposition is further evidenced by previoustudies associating premature rupture of membranes (Fergussont al 2002) and preterm birth (Lumley 1993) with low socioeco-omic status.
In contrast, we found that despite having access to a highertandard of health care, the mothers in the OCD group reportedaving more difficulty in becoming pregnant and a higherrevalence of preexisting medical problems and perinatal compli-ations, such as premature rupture of membranes, prolonged labornd nuchal cord entanglement, preterm birth, and jaundice.
Most likely reflecting the higher socioeconomic status in theCD group would be the results related to the location at which
he birth occurred (at home or in a hospital), the type of delivery,nd the use of medication. Despite the fact that the indicatingriteria for cesarean section are specific, the procedure is rou-inely performed in patients belonging to the upper sociallasses (A and B) in Brazil, even without a considered risk fromregnancy or delivery. In public hospitals, this procedure is alsoverrepresented because of economic factors (cesarian sectioneceives higher reimbursement from health maintenance organi-ations than natural delivery). In our finds, cesarian section was
ot associated with any previous medical problems or anyprocedure used to become pregnant, and the only risk duringpregnancy was the presence of vomiting and nausea (p � .056)and the use of medication (p � .004). Prenatal assistance wasassociated with socioeconomic status (p � .018) and with use ofmedication during pregnancy (p � .000). Likewise, the mothersof OCD patients had used more antiemetics and vitamins duringpregnancy, which might reflect greater access to health care (Men-gue et al 2004). The prenatal findings of excessive weight gain andhyperemesis gravidarum that were also higher in the OCD groupshould be investigated in future, better controlled studies.
As mentioned earlier, even after the logistic regression inwhich socioeconomic class was used as a covariable, protractedlabor and edema during pregnancy remained as risk factorssignificantly correlated with OCD.
Protracted delivery may be related to primiparity, dystocias,obstetric trauma, hypoxia, and fetal distress. This is consistentwith the findings of Santangelo et al (1994), who observed ahigher prevalence of OCD among individuals with TS who had agreater number of complications during delivery, especiallyamong those having undergone forceps deliveries. The use offorceps is typically indicated in dystocic deliveries, in whichthere is a clear need to reduce the duration of labor and fetaldistress. It is possible that the damage caused by hypoxia andfetal distress is more closely associated with increasing vulnera-bility to developing OCD than is the potential injury caused bythe use of forceps. The greater frequency of use of an incubatorand prematurity in the OCD group could also be correlated withthe greater number of neonatal problems.
Moreover, perinatal complications such as hypoxia are known toresult in smaller amygdala and hippocampus volumes (Murray etal 2004). Maternal stress, viral infections, and obstetric compli-cations, which trigger cytokine signaling, are hypothesized to beinvolved in schizophrenia and its related disorders. In an animalexperiment, infusing various cytokines in rat pups for 9 daysinduced behavioral abnormalities related to fear and anxietylevels, and sensorimotor gating emerged at different develop-mental stages depending on the cytokine species administered.Therefore, perinatal inflammatory events can induce future psy-chobehavioral and cognitive impairments with various latencies,although the pathologic mechanisms underlying these abnormal-ities remain to be determined (Tohmi et al 2004).
Edema during pregnancy is often a first sign of preeclampsia,especially when it affects face and hands and high bloodpressure is present. Furthermore, the diagnosis of preeclampsiais often difficult to be established in its mild forms. Preeclampsiaresults from poor placental perfusion, which releases a factor thatinjures the endothelium, causing activation of coagulation and anincreased sensitivity to pressors. It is usually associated withpremature labor, cesarian sections, and neonatal complications(Rey and Couturier 1994; Sibai et al 2005). Epidemiologic studiessuggest an immunological cause for preeclampsia (Lain andRoberts 2002). Because edema is also present in many normalpregnancies, it is not a reliable marker (Frishman et al 2005), andit is possible that mild forms of preeclampsia (or even hyperten-sion) and borderline prematurity might have been underdiag-nosed in our samples.
Another limitation of this study is its retrospective nature.Our findings are based on the recollections of the subjects andtheir parents regarding periods and events long past. There-fore, a certain degree of inaccuracy of the information exists.This may be offset, for the most part, by the fact that thisinformation was confirmed by the mother in more than half of
our subjects. We can assume that mothers of patients withwww.sobp.org/journal

moisdreirtaa
assshiatrfmtespcpdethesmffpbww
At0Ntn0Mt
A
B
B
306 BIOL PSYCHIATRY 2007;61:301–307 M.S. Vasconcelos et al
w
ental disorders tend to be more attentive to their ownbstetric histories and to the medical histories of their childrenn an attempt to find an explanation for the disorder. Previoustudies have suggested that there is a high degree of concor-ance between hospital records and the memories of mothersegarding prenatal, perinatal, and postnatal situations andvents (Buka et al 2004). The lack of correlation betweenndividual environmental factors and the early-onset or tic-elated OCD subtypes may also reflect the small sample size ofhe study. Also the high number of questions and variablesnalyzed, with multiple comparisons performed, could lead toType I error.In conclusion, even taking these potential limitations into
ccount, the examples provided by other mental disordersuch as schizophrenia lead us to believe that perinatal factorsuch as protracted labor and edema during pregnancy areignificant risk factors for the development of OCD. Because aistory of early environmental risk factors are associated withncreased risk for many psychiatric disorders (e.g., autism,norexia nervosa, schizophrenia, and affective disorders),hese data could have no specificity to suggest a causalelationship between prenatal, perinatal, and postnatal riskactors and OCD. Kano et al (2001) suggested that environ-ental factors such as severe perinatal problems could con-
ribute to the expression of phenocopies. Because this is anxploratory study and we have not performed genetic mea-ures in this study, we cannot conclude that edema duringregnancy or prolonged labor caused OCD in our sample. Thelinical expression of OCD induced by early risk factorsrobably depends on gene–environment interactions (Ver-oux 2004); however, the lack of correlation between thisarly risk factor and presence and absence of family history ofics or OCD in our study and the lower frequency of familyistory of OCD or tics in TS probands whose mothers hadxperienced obstetric complications in the (Kano et al 2001)tudy support the hypotheses that cases with early environ-ental risk factors may have less genetic loading. If our
indings are confirmed in future studies, there will be a needor greater investment in prophylactic measures during therenatal, perinatal, and postnatal periods for highly vulnera-le patients (such as those with a family history of OCD), asell as more careful follow-up for those whose conceptionas associated with these early risk factors.
This study was supported by grants from the Fundação demparo à Pesquisa do Estado de São Paulo (Foundation for
he Support of Research in the State of São Paulo) Grant Nos.3/04504 to MSV, Grant No. 99/08560-6 to ECM, and Granto. 98/15013-9 to AGH. Additional support was provided by
he Conselho Nacional de Desenvolvimento Científico e Tec-ológico (Grant Nos. 101408/2001-3 to Mr. MSV, 101579/3-9 to FA, and 521369/96-7 to ECM). The authors thank Dr.aria Conceição Rosário-Campos for her careful review of
his manuscript.
ssociação Brasileira de Anunciantes (1989): XXXI Estudos Marplan. SãoPaulo: Marplan Brasil Representações e Pesquisas.
acker A, Pauli-Pott U, Neuhauser G, Beckmann D (2000): Effects of signifi-cantly increased perinatal risks on developmental status in adolescence.Prax Kinderpsychol Kinderpsychiatr 49:385–398.
uka SL, Goldstein JM, Spartos E, Tsuang MT (2004): The retrospective mea-surement of prenatal and perinatal events: Accuracy of maternal recall.
Schizophr Res 71:417– 426.ww.sobp.org/journal
Cannon M, Jones PB, Murray RM (2002): Obstetric complication andschizophrenia: Historical and meta-analytical review. Am J Psychiatry159:1080 –1092.
Carey G, Gottesman LL (1981): Twin and family studies of anxiety, phobicand obsessive disorders. In: Klien DF, Rabkin J, editors. Anxiety: NewResearch and Changing Concepts. New York: Raven Press, 117–136.
Clifford CA, Murray RM, Fulker DW (1984): Genetic and environmental influ-ences in obsessional traits and symptoms. Psychol Med 14:791– 800.
Coimbra LC, Silva AAM, Mochel EG, Alves MTSSB, Ribeiro VS, Aragão VMF,et al (2003): Factors associated with inadequacy prenatal care utiliza-tion. Rev Saúde Publica 37: 456 – 462.
Diniz JB, Rosario-Campos MC, Shavitt RG, Curi M, Hounie AG, Brotto SA,Miguel EC (2004): Impact of age at onset and duration of illness on theexpression of comorbidities in obsessive– compulsive disorder. J ClinPsychiatry 65:22–27.
Ferguson SE, Smith GN, Salenieks ME, Windrim R, Walker MC (2002): Pretermpremature rupture of membranes. Nutritional and socioeconomic fac-tors. Obstet Gynecol 100:1250 –1256.
First MB, Spitzer RL, Gibbon M, Williams JBW (1995): Structured clinical inter-view for DSM-IV Axis I Disorders—patient edition (Version 2.0). New York:Biometric Research Department, New York State Psychiatric Institute.
Frishman WH, Schlocker SJ, Awad K, Tejani N (2005): Pathophysiology andmedical management of systemic hypertension in pregnancy. CardiolRev 3:274 –284.
Geller D, Biederman J, Jones J, Park K, Schwartz S, Shapiro S, Coffey B (1998):Is juvenile obsessive– compulsive disorder a developmental subtype ofthe disorder? A review of the pediatric literature. J Am Acad Child AdolescPsychiatry 37:420 – 427.
Gilmore JH, van Tol J, Kliewer MA, Silva SG, Cohen SB, Hertzberg BS, et al (1998):Mild ventriculomegaly detected in utero with ultrasound: clinical associa-tions and implications for schizophrenia. Schizophr Res 33:133–140.
Glasson EJ, Bower C, Petterson B, de Klerk N, Chaney G, Hallmayer JF (2004):Perinatal factors and the development of autism: A population study.Arch Gen Psychiatry 61:618 – 627.
Goodman WK, Price LH, Rasmussen AS, Mazure C, Fleischman RL, Hill CL, et al(1989): The Yale-Brown Obsessive–Compulsive Scale: I. Developmentuse and reliability. Arch Gen Psychiatry 26:1006 –1011.
Hanna GL, Himle JA, Curtis GC, Gillespie BW (2005): A family study of obses-sive– compulsive disorder with pediatric probands. Am J Med Genet BNeuropsychiatr Genet 134:13–19.
Hemmings SM, Kinnear CJ, Lochner C, Niehaus DJ, Knowles JA, Moolman-Smook JC, Corfield VA (2004): Early- versus late-onset obsessive– com-pulsive disorder: Investigating genetic and clinical correlates. PsychiatryRes 128:175–182.
Hounie AG, Pauls DL, do Rosario-Campos MC, Mercadante MT, Diniz JB, DeMathis MA, et al (2004): Obsessive– compulsive spectrum disorders inrheumatic fever with and without Sydenham’s chorea. J Clin Psychiatry65:994 –999.
Huddy CL, Johnson A, Hope PL (2001): Educational and behavioural prob-lems in babies of 32–35 weeks gestation. Arch Dis Child Fetal Neonatal Ed85:F23–28.
Kano Y, Ohta M, Nagai Y, Pauls D, Leckman J (2001): A family study ofTourette syndrome in Japan. Am J Med Genetics 105:414 – 421.
Karno M, Golding JM (1991): Obsessive– compulsive disorder. In: Robins LN,Regier DA, editors. Psychiatric Disorders in America. The EpidemiologicCatchment Area Study. New York: Free Press, 204 –219.
Lain KY, Roberts JM (2002). Contemporary concepts of the pathogenesisand management of preeclampsia. JAMA 287:3183–3186.
Leckman JF, Riddle MA, Hardin MT (1989): The Yale global tic severity scale:Initial testing of a clinician-rated scale of tic severity. J Am Acad ChildAdolesc Psychiatry 28:566 –573.
Lumley J (1993): The epidemiology of preterm birth. Baillieres Clin ObstetGynaecol. 7:477– 498.
Mengue SS, Schenkel EP, Schimidt MI, Duncan BB (2004): Factors related touse of medication during pregnancy in six Brazilian cities. Cad SaúdePública. 20:1602–1608.
Murray RM, Sham P, Van Os J, Zanelli J, Cannon M, McDonald C (2004): Adevelopmental model for similarities and dissimilarities between schizo-phrenia and bipolar disorder. Schizophr Res 71:405– 416.
Nestadt G, Samuels J, Riddle M, Bienvenu J, Liang KY, La Buda M, et al (2000)A family study of obsessive compulsive disorder. Arch Gen Psychiatry
57:358 –363.
O
P
R
R
R
R
S
M.S. Vasconcelos et al BIOL PSYCHIATRY 2007;61:301–307 307
rvaschel H, Puig-Antich J (1987): Schedule for affective disorder and schizo-phrenia for school-age children— epidemiologic (4th version). Ft. Lauder-dale, FL: Nova University, Center for Psychological Study.
auls DL, Alsobrook JP 2nd, Goodman W, Rasmussen S, Leckman JF(1995): A family study of obsessive– compulsive disorder. Am J Psychi-atry 152:76 – 84.
asmussen S, Tsuang MT (1986): Clinical characteristics and family history inDSM-III obsessive– compulsive disorder. Am J Psychiatry 143:317–322.
ey E, Couturier A (1994): The prognosis of pregnancy in women withchronic hypertension. Am J Obstet Gynecol 171:410 – 416.
osario-Campos MC, Leckman JF, Curi M, Quatrano S, Katsovitch L,Miguel EC, et al (2005): A family study of early-onset obsessive-compulsive disorder. Am J Med Genet B Neuropsychiatr Genet 5:92–97.
osario-Campos MC, Leckman JF, Mercadante MT, Shavitt RG, da Silva PradoH, et al (2001): Adults with early-onset obsessive– compulsive disorder.Am J Psychiatry 158:1899 –1903.
antangelo SL, Pauls DL, Goldstein JM, Faraone SV, Tsuang MT, Leckman JF(1994): Tourette’s syndrome: What are the influences of gender and
comorbid obsessive– compulsive disorder? J Am Acad Child AdolescPsychiatry 33:795– 804.
Santos AMN (1999): O Pediatra na Sala de Parto. Revista Diagnóstico andTratamento da Associação Paulista de Medicina 4:41– 48.
Sibai B, Dekker G, Kupferminc M (2005): Pre-eclampsia. Lancet 365:785–799.Stein AD, Behrman JR, DiGirolamo A, Grajeda R, Martorell R, Quisumbing A,
Ramakrishnan U (2005): Schooling, educational achievement, and cog-nitive functioning among young Guatemalan adults. Food Nutr Bul26(suppl 1):46 –54.
Tohmi M, Tsuda N, Watanabe Y, Kakita A, Nawa H (2004): Perinatal inflam-matory cytokine challenge results in distinct neurobehavioral alter-ations in rats: Implication in psychiatric disorders of developmental ori-gin. Neurosci Res 50:67–75.
Torres AR, Lima MC (2005): Epidemiology of obsessive-compulsive disorder.Rev Bras Psiquiatr 27:237–242.
Verdoux H (2004): Perinatal risk factors for schizophrenia: How specific are
they? Curr Psychiatry Rep 6:162–167.www.sobp.org/journal
Copyright © 2022 FDOKUMEN




















