
Obsessive compulsive font disorder': the challenge of supporting pupils writing with the computer
Upload
independentCategory
view
0download
0
Four-Factor Structure of Obsessive-CompulsiveDisorder Symptoms in Children, Adolescents,
and AdultsS. EVELYN STEWART, M.D., MARIA C. ROSARIO, M.D., PH.D., LEE BAER, PH.D.,
ALICE S. CARTER, PH.D., TIMOTHY A. BROWN, PSY.D., JEREMIAH M. SCHARF, M.D., PH.D.,CORNELIA ILLMANN, PH.D., JAMES F. LECKMAN, M.D., DENIS SUKHODOLSKY, PH.D.,
LILYA KATSOVICH, M.SC., STEVEN RASMUSSEN, M.D., WAYNE GOODMAN, M.D.,RICHARD DELORME, PH.D., MARION LEBOYER, M.D., NADIA CHABANE, M.D.,
MICHAEL A. JENIKE, M.D., DANIEL A. GELLER, M.B.B.S., AND DAVID L. PAULS, PH.D.
ABSTRACT
Objective: To determine whether the four-factor category-based obsessive-compulsive disorder (OCD) symptom
structure from a previous confirmatory factor analysis (CFA) may be appropriately used in child, adolescent, and adult
groups. Symptom dimensions are increasingly used as quantitative traits in genetic, neuroimaging, and treatment studies
of OCD across all ages. Identification of a category-based OCD symptom dimension structure that is validated for use
across child, adolescent, and adult age groups is necessary to guide ongoing translational research.Method: Four OCD
samples comprising 356 individuals were divided into child, adolescent, and adult groups. The fit of the only CFA-defined
four-factor model was compared across these independent age group samples. Multiple-group CFA using maximum
likelihood estimation assessed adequacy of fit comparing unconstrained and measurement weight-constrained models.
The fit of previous exploratory factor analysisYdefined three- and five-factor models on adults was also examined using
CFA.Results: A four-factor solution provided adequate but imperfect fit across age groups, with comparable indices to the
only previous OCD CFA: factor 1 (aggressive/sexual/religious/somatic/checking); factor 2 (symmetry/ordering/counting/
repeating); factor 3 (contamination/cleaning), and factor 4 (hoarding). Models in which factor loadings were constrained
and unconstrained across the three age groups yielded comparable model fit. Factors were highly correlated and were not
mutually exclusive. The four-factor solution provided an improved fit to both three- and five-factor solutions using CFA
across the three age groups. Conclusions: A four-factor, CFA-defined, category-based model of OCD symptom
dimensions is adequate for use in children, adolescents, and adult age groups. The factor structure of thismultiple age group
sample has limitations and is imperfect, but current findings support the comparability of the defined latent OCD dimensions
across age groups. Further work is needed to optimize a comprehensive symptom dimension model reflecting clinical
heterogeneity for use in emergent translational studies. J. Am. Acad. Child Adolesc. Psychiatry, 2008;47(7):763Y772.
Key Words: obsessive-compulsive disorder, age, factor analysis, symptom dimension, quantitative trait.
Accepted February 8, 2008.Reviewed and accepted by Deputy Editor John Walkup, M.D.Drs. Stewart, Baer, Scharf, Illmann, Geller, Jenike, and Pauls are with
Massachusetts General HospitalYHarvard Medical School; Dr. Rosario is with theFederal University of Sao Paulo; Dr. Carter is with the University ofMassachusetts; Dr. Brown is with Boston University; Drs. Leckman andSukhodolsky and Ms. Katsovitch are with Yale University; Dr. Rasmussen is withBrown University; Dr. Goodman is with the National Institutes of Health;Drs. Chabane and Delorme are with Robert Debre Hospital; and Dr. Leboyer iswith Mondor-Chenevier Hospital.
Grant support was provided by the Obsessive-Compulsive Foundation (S.E.S.,M.C.R., D.A.G.); McIngvale Foundation (S.E.S., D.L.P., D.A.G.); Harvard Scholar
in Medicine Award (S.E.S.); CIHR Postgraduate Fellowship (S.E.S.); University ofOttawa International Fellowship (S.E.S.); Tourette Syndrome Association (M.C.R.);NIMH-K08-MH01481 (D.A.G.); NINDS-R01-NS16648 (D.L.P.) andMH49351 (J.F.L.). The authors thank Erin Hendrickson and Casey Walsh for theirassistance with manuscript preparation and the reviewers for their valuable feedback.
This article is the subject of an editorial by Drs. Marc Riddle and MarcoGrados in this issue.
Correspondence to Dr. David Pauls, PNGU-Massachusetts General Hospital,185 Cambridge Street, Boston, MA 02114; e-mail: [email protected].
0890-8567/08/4707-0763�2008 by the American Academy of Child andAdolescent Psychiatry.
DOI: 10.1097/CHI.0b013e318172ef1e
WWW.JAACAP.COM 763J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:7, JULY 2008

Obsessive-compulsive disorder (OCD) is defined by thepresence of repetitive thoughts, images, impulses,behaviors, or mental acts that are performed to relieveanxiety or distress or are conducted according to certainrules. Obsessive-compulsive symptoms affect indivi-duals across the life span and typically start beforeadulthood. OCD has a distinctly heterogeneous clinicalexpression, not adequately captured by DSM-IV nosol-ogy, which may reflect a multitude of etiologic factors.Identification of more homogeneous OCD phenotypesis necessary for improved application of translationalresearch findings. One approach that is increasinglyused in the study of psychiatric disorders organizessymptoms into coexisting factors or dimensions withinindividuals. Yet it remains unclear whether the sameOCD dimensional structure found in adults is appro-priate for use in child and adolescent groups, nor is itclear whether the commonly used four-factor model ispreferable to three- and five-factor models whenexamining adult and nonadult age groups. Confirmingthe applicability of OCD symptom dimensions acrossage groups is necessary for future study of this frequentlylifelong disorder.Numerous strategies have been applied to reduce
OCD heterogeneity for use in clinical trials and ingenetic and neuroimaging studies. Tic-related and early-onset OCD subtypes1 have proved to be of heuristicvalue in subtyping OCD phenotypes. Dimensionalapproaches have also been successfully applied intranslational studies of other neuropsychiatric disorderssuch as depression and schizophrenia.2,3 In contrastwith categorical subtypes that fit individuals intoseparate, mutually exclusive groups, dimensions repre-sent coexisting symptom groupings within individuals.These symptom complexes may be used as quantitativetraits that may reflect distinct etiologic mechanisms andheritable components of the disorder. Clarification ofmore homogeneous OCD phenotypes based on thesedimensions may contribute to improved success infuture genetic studies,4,5 diagnostic nosology, andtreatments.6
Symptom dimensions of adult OCD have beenstudied almost exclusively via exploratory factor analysis(EFA).7Y13 Yet confirmatory factor analysis (CFA)is advantageous because it provides statistical good-ness-of-fit tests and allows comparison of competingmodels, in addition to cross-validating previouslyderived factor structures. Calculated fit indices evaluate
congruence between a theoretical model and the actualpatient data.14 One OCD CFA has been completed todate, and was conducted on an adult sample.7 The studyreported that the four-factor solution originallydescribed by Leckman et al.8 adequately convergedwith independently obtained data. This four-factorsolution was the only one providing an adequate fit fortheir adult sample, although one-, three-, and five-factormodels were also examined.Other adult studies using EFA have identified three-
and five-dimensional models characterizing OCDsamples, which explained between 42% and 66% ofsymptom variance.7Y13 Dimensions reported were notidentical but generally included a factor comprisingaggressive, sexual, somatic, and religious obsessions andchecking compulsions; a second factor comprisingsymmetry obsessions and ordering, counting, andrepeating compulsions; a third factor including con-tamination obsessions and cleaning compulsions; and afinal factor, including hoarding obsessions and compul-sions. In the first published OCD factor analysis study, athree-factor solution was reported in which hoardingsymptoms were included in the symmetry/ordering/counting/repeating factor.9 In studies reporting a five-factor solution, an additional emergent factor combinedeither repeating/counting10 or checking15 with aggres-sion13 or somatic obsession categories.11
The utility of OCD symptom dimensions in adultresearch has been validated by their use in treatmentstudies,13,16 functional neuroimaging,17Y19 genetic,10,20
and comorbidity studies.9,21,22 Specific symptomdimensions have also been associated with sex, age atonset, severity, and familiality of OCD in cross-sectionalstudies.11,21,23 However, there have been discrepanciesbetween results of adult OCD symptom dimensionstudies in the literature because not all of these studiesreported a four-factor model.10,11,13,15 This may beaccounted for in part by the fact that some factoranalyses have used current symptoms and others haveused lifetime symptoms to conduct analyses. Further-more, the four-factor category-based solution did notprovide a good fit when examined at the item level.7 Todate, no studies have used CFA to compare the five-factor model of Pinto et al.15 with the four-factor modelof Leckman et al.8 that was confirmed by Summerfeldtet al.7 in an independent sample.Although no current studies have conducted age
group comparisons of OCD symptom dimensions, a
STEWART ET AL.
764 WWW.JAACAP.COM J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:7, JULY 2008

few have examined the long-term stability of OCDsymptom dimensions among adults.24,25 In one study,the previously derived dimension structure13 wasrepeatedly applied to a sample over time. Most adultsdid not report changes across symptom dimensions,although specific symptoms within dimensions differedat follow-up.25 The second study examined phenotypicsubtype categories (autogenous, reactive, or mixed) in91 OCD patients over 3 years. They similarly reportedchanges of symptoms within subtypes but not acrosssubtypes.24 Finally, in the third study reassessing 48patients after 6 years, significant changes had occurredwithin symptom dimensions, but symptom shifts rarelyoccurred between dimensions.26
Although no child studies have examined OCDsymptom dimension stability, an early study reported apattern of symptom change over time that may mirroradult studies. Rettew et al.27 found that none of thechild patients maintained the same constellation ofOCD symptoms from presentation to follow-up.Because this study did not examine symptom dimen-sions, it is impossible to determine whether thesymptom instability was restricted to changes withindimensions (as reported for adults) or whether symptomchanges occurred between dimensions at these earlierdevelopmental levels.
More recently, two adequately powered EFA studieshave been reported for childhood OCD samples.28,29
One described a four-factor structure similar to thatin adult studies,29 whereas the other reported a sub-stantially different structure.28 Given that early- andlate-onset forms of OCD have distinct clinical character-istics, the associated symptom dimensions may hypothe-tically vary across age groups. Supporting this notion,clinical observation does suggest that frequencies ofspecific compulsions vary by age in both healthy30,31
and OCD-affected child populations.32 No attempt hasbeen made to replicate the Summerfeldt et al. CFA of afour-factor category-based model of adult OCD dimen-sions7 in a child or adolescent OCD sample.7
It is of considerable importance for future transla-tional genetic, neuroimaging, and treatment studies ofchildhood OCD to determine whether the frequentlyused symptom dimension structure derived for adults isappropriate for use across life span age groups. Thepresent study attempts to replicate findings from theonly OCD symptom CFA conducted to date, usingthree independent age group samples. It was hypothe-
sized that the four-factor categorically based solutionconfirmed by Summerfeldt et al.7 in an adult samplewould provide an adequate fit when applied toindependent child, adolescent, and adult samples.
METHOD
Participants
Participants were evaluated independently at one of the followingoutpatient clinics: the Harvard Pediatric OCD Clinic at McLeanHospital, Belmont, MA; the Service de psychopathologie de l`enfantet de l`adolescent (Child and Adolescent Psychopathology Clinic),Robert Debre Hospital, Paris; the TS/OCD clinic at the Yale ChildStudy Center, New Haven, CT; and the Adult OCD clinics at YaleUniversity and Brown University. All of the subjects had a definitivediagnosis of OCD according to DSM-IV or DSM-III-R criteria.Patients were excluded if they had ever received a diagnosis ofpervasive developmental disorder, schizophrenia, a major sensor-imotor handicap (e.g., deafness, blindness), or a major neurologicaldisorder other than tic disorder.The full sample was divided into the following age categories: the
child group (6Y12 years; n = 160), the adolescent group (13Y17years; n = 119), and the adult group (18+ years; n = 77). The childgroup was 49% (n = 79) male, the adolescent group was 54% (n =64) male, and the adult group was 58% (n = 45) male. The childgroup and a portion of the adolescent group were included in arecently published EFA.29 Of the present sample, 70 (from Yale andBrown) were previously included in an adult EFA12 and 286 (n = 90Harvard, n = 132 Yale, n = 64 Paris) were included in a child/adolescent EFA.There is no overlap between subjects included in the Summerfeldt
et al. CFA7 and those in the present study aiming to replicate theirfindings in different age groups, nor is there overlap with subjectsfrom Baer`s initial three-factor model9 or the more recent five-factormodel of Pinto et al.15 Each study was approved by the institutionalreview board of each study site. Parental consent and child assentwere obtained for each child and adolescent participant.
Symptom Evaluation and Diagnoses
Symptom severity ratings were derived from the Yale-BrownObsessive Compulsive Scale (Y-BOCS)33,34 and the Children`sYale-Brown Obsessive Compulsive Scale (CYBOCS).35 Subjects18 years of age and older were assessed with the Y-BOCS, and all ofthe others were assessed using the CYBOCS. Both instruments areclinician-rated, semistructured interviews used in rating the presenceand severity of obsessions and compulsions. They are divided intotwo major sections, including a symptom checklist and a symptomseverity scale. There is little difference between the adult and childseverity scales (both range from 0 to 40, with 16 indicating moderateseverity) other than the inclusion of child-friendly language in theCYBOCS symptom severity scale.Similar to the severity scales, the Y-BOCS symptom checklist and
the CYBOCS symptom checklist are similar and assess both presentand past symptoms. Both have more than 60 items, which areorganized into two miscellaneous categories and at least 13 othercategories according to their thematic content (including contam-ination, aggressive, sexual, hoarding, somatic, symmetry, andreligious obsessions and washing, checking, repeating, counting,ordering, and hoarding compulsions). The CYBOCS symptom
OCD FOUR-FACTOR STRUCTURE BY AGE GROUP
WWW.JAACAP.COM 765J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:7, JULY 2008
checklist also includes categories for magical thoughts, superstitions,and rituals involving others. Because this study aimed to compare anidentical factor model between age groups, categories and items thatwere not present in both adult (Y-BOCS symptom checklist) andchild (CYBOCS symptom checklist) OCD checklists were notconsidered in analyses. Thus, child magical thoughts/superstitionsand rituals with others were excluded. Following the approach takenby Summerfeldt et al., Baer, and others, miscellaneous categorieswere excluded because the study was designed and had sufficientpower to conduct categorical rather than item-level analyses.
Interviewers from the Yale, Harvard, and Brown sites held at leasta bachelor`s degree and went through a rigorous training program forthe conduct of structured interviews. Training included learningaboutDSM-IV diagnostic criteria, watching training tapes, observinginterviews performed by experienced raters, and rating severalsubjects under the direct supervision of an experienced rater.Interviewers from the Paris site were child and adolescentpsychiatrists with expertise in OCD. At all of the sites, interviewswere reviewed by two expert clinicians and a best estimate diagnosiswas assigned.
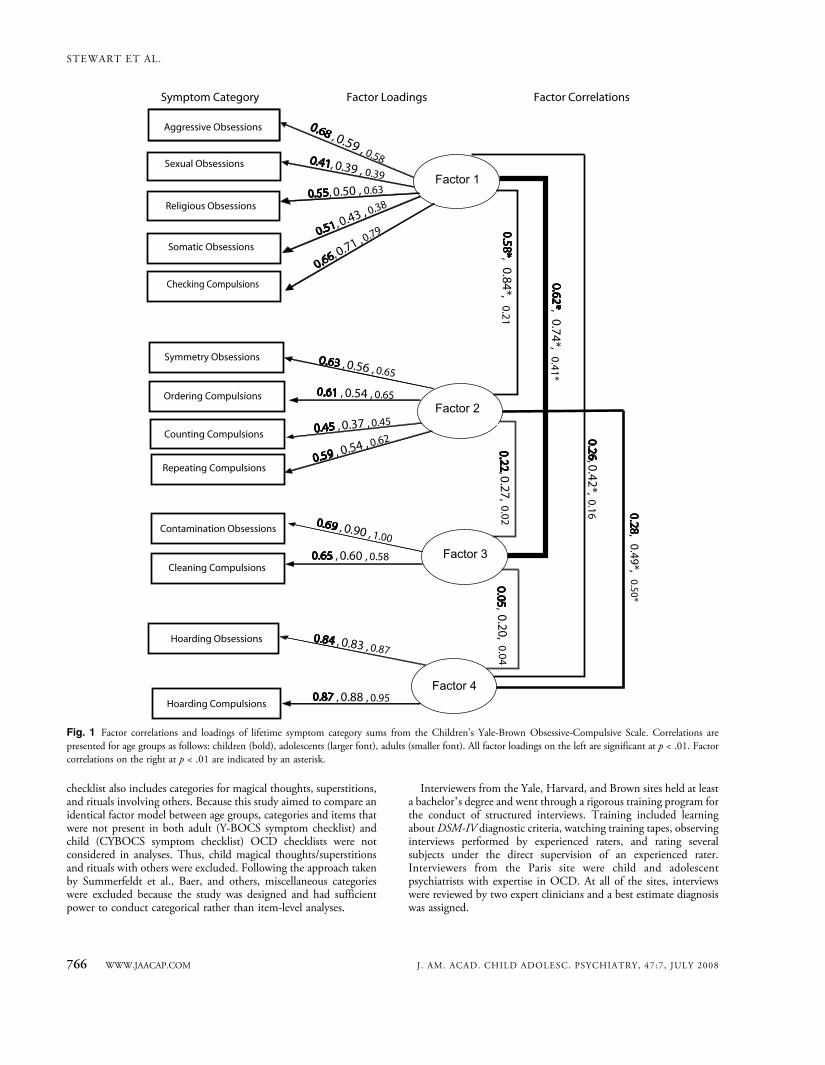
Fig. 1 Factor correlations and loadings of lifetime symptom category sums from the Children’s Yale-Brown Obsessive-Compulsive Scale. Correlations arepresented for age groups as follows: children (bold), adolescents (larger font), adults (smaller font). All factor loadings on the left are significant at p < .01. Factorcorrelations on the right at p < .01 are indicated by an asterisk.
STEWART ET AL.
766 WWW.JAACAP.COM J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:7, JULY 2008

Statistical Analysis
Confirmatory maximum likelihood-based factor analyses wereconducted using structural equation modeling via the AMOS 5program.36 Other statistical analyses were performed using SPSS.36
Items for the factors were chosen before model testing occurred, andchoices were guided by theoretical considerations as well as informedby previous studies.8,9 Similar to the approach of previous studies,miscellaneous categories were excluded, leaving 13 categories foranalyses. Lifetime symptom total and frequency for each Y-BOCS orCYBOCS symptom checklist category were determined for child,adolescent, and adult age groups. Age group comparisons wereconducted for mean symptom totals (using pairwise T tests) and forcategory symptom frequencies (using analysis of variance). Lifetimesymptoms rather than current symptoms were used in calculatingaggregate symptom category scores. These categories were treated assums of items within the categories rather than as dichotomousvariables. This method was guided by the hypothesis that theaccumulation of lifetime OCD symptoms forms a stable symptomdimension that may be subsequently used to identify underlyingconstructs and biological processes.The hypothesized four-factor structure tested in this study is
illustrated in Figure 1. Indices` cutoffs selected to indicate anadequate fit are identical to those from the previous OCD CFAstudy on adults.7 They are as follows: goodness-of-fit index (GFI)90.85, adjusted GFI (AGFI) 90.80, root mean square standardizedresidual (RMSSR) e0.10, and comparative fit index (CFI) 90.90.These criteria are more liberal than the ones suggested by Hu andBentler.37 Additional indices were also run including the Tucker
Lewis Index and the root mean square error of approximation. Whencompeting CFAs were not nested, the Akaike information criterion(AIC) was used to compare models, with the lower value preferred.38
Multiple-group CFAs were conducted first by assessing the overallfit of the unconstrained four-factor model across each of the three agegroups. Next, a model in which all of the factor loadings (i.e.,measurement weights) were constrained to be equal across the threeage groups was assessed, and the incremental W2 between thesenested models was then tested for significance. A statisticalcomparison of previously reported three-, four-, and five-factormodels was conducted using a CFA in this sample. To conduct aCFA on the five-factor model as described by Pinto et al.,15 theaggressive obsessions category was divided into fear of aggressiveimpulses and pathological doubt categories. Items used to form thepathological doubt categories for the adults were as follows: fear willbe responsible for something terrible and fear something terrible willhappen. For children and adolescents, items were as follows: fearsomething terrible will happen to others and fear of harm because ofbeing careless. The other item in the aggression category was notincluded in either subcategory because of its lack of specificity.
RESULTS
Descriptive Analyses
Lifetime mean symptom sums and lifetime frequen-cies of any symptom for each nonmiscellaneous Y-BOCS and CYBOCS checklist category for each age
TABLE 1Lifetime Mean Sums of Symptoms Endorsed and Lifetime Frequency of Any Symptom Endorsed Within Each Y-BOCS or CYBOCS Symptom
Checklist Category by Age Subgroup
Lifetime Mean Sum of Category Symptoms EndorsedLifetime Frequency of Any Category
Symptom Endorsed
Child(n = 160)Mean (SD)
Adolescent(n = 119),Mean (SD)
Adult(n = 77),Mean (SD)
F Statistic(Omnibus p,df = 2,353)
Child(n = 160)Mean (SD)
Adolescent(n = 119)Mean (SD)
Adult(n = 77),Mean (SD) Omnibus p
Obsession categoriesAggression 1.9 (1.9) 2.0 (2.1) 3.4 (2.4) 14.1 (<0.001a) 75% (120) 71% (84) 88% (68) .02a
Contamination 1.5 (1.6) 1.4 (1.6) 2.1 (2.0) 3.8 (0.02a) 62% (99) 58% (69) 66% (51) .51Sexual 0.4 (0.8) 0.3 (0.7) 0.6 (0.9) 2.8 (0.07) 19% (31) 16% (19) 30% (23) .06Hoarding 0.3 (0.5) 0.3 (0.5) 0.2 (0.4) 1.5 (0.23) 28% (45) 35% (41) 23% (18) .23Religious 0.5 (0.7) 0.4 (0.7) 0.3 (0.5) 1.2 (0.31) 38% (60) 32% (38) 31% (24) .51Symmetry 0.3 (0.5) 0.4 (0.5) 0.5 (0.5) 3.7 (0.03b) 33% (52) 39% (46) 51% (39) .03b
Somatic 0.6 (0.7) 0.6 (0.8) 0.5 (1.0) 0.9 (0.43) 50% (80) 41% (49) 38% (29) .14Compulsion categoriesOrdering 0.6 (0.5) 0.6 (0.5) 0.4 (0.5) 5.7 (0.004a) 57% (91) 59% (70) 36% (28) .004b
Counting 0.4 (0.5) 0.5 (0.5) 0.5 (0.5) 1.7 (0.18) 39% (63) 48% (57) 51% (39) .18Cleaning 0.8 (0.9) 1.0 (1.0) 1.8 (1.7) 19.5 (<0.001a) 54% (86) 61% (72) 68% (52) .12Hoarding 0.3 (0.5) 0.4 (0.5) 0.3 (0.4) 1.6 (0.20) 33% (52) 37% (44) 25% (19) .20Repeating 0.8 (0.8) 1.0 (0.8) 0.8 (0.7) 2.4 (0.09) 58% (92) 71% (84) 57% (44) .05Checking 1.6 (1.6) 1.6 (1.4) 2.6 (1.4) 13.0 (<0.001a) 67% (107) 77% (92) 94% (72) <.001b
Note: Y-BOCS = Yale-Brown Obsessive Compulsive Scale; CYBOCS = Children`s Yale-Brown Obsessive Compulsive Scale. Using post hocgroupwise comparisons: superscript a indicates that significant differences exist between adults and children and adults and adolescents (p < .05);superscript b indicates that significant differences exist only between adults and children (p < .05). All other comparisons were nonsignificant.
OCD FOUR-FACTOR STRUCTURE BY AGE GROUP
WWW.JAACAP.COM 767J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:7, JULY 2008

group, and related age group differences are listed inTable 1. Within all of the age groups, the presence ofany aggressive obsessions and any checking compulsionshad the highest lifetime frequencies compared withother symptom categories. Similarly, the presence of anysexual obsessions and any hoarding compulsions had thelowest lifetime frequencies compared with othersymptom categories within all of the age groups.There were significant age group differences betweenfrequencies of aggressive (p = .02), symmetry (p = .03),ordering (p = .004), and checking (p < .001) categorysymptoms. With respect to the mean number ofsymptoms endorsed per category, scores for aggressive,contamination, and symmetry obsessions and forordering, cleaning, and checking compulsions differedsignificantly across age groups (p < .05), with higherrates among adults for all of the categories exceptordering.
CFAs
Fit of the Unconstrained Four-Factor Model in theThree Age Groups. The hypothesized four-factorstructure tested in this study included the followingdimensionsVfactor 1: sexual/aggressive/religious/somatic/checking; factor 2: symmetry/ordering/repeating/counting;factor 3: contamination/cleaning; and factor 4: hoardingobsessions/compulsions.The initial step in the present multiple-group CFA
procedure (test of the unconstrained model) set out todetermine whether the hypothesis that the four-factorcategory-based model fit the data in each of the three agegroups could be rejected. This analysis yielded W2177 =299.1, p < 0.001. However, because the W2 value waslargely a reflection of the study sample size, othergoodness-of-fit measures were required to assess theadequacy of model fit (Table 2).38 Whereas the CFIvalue fell just below the cutoff criterion, the GFI, AGFI,and root mean square standardized residual values met
criteria indicating an adequately fitting model. Thus,based on the overall goodness-of-fit statistics, we couldnot reject the hypothesis that this model provided areasonable fit for the data in each age group. Thisunconstrained model was then used as the baselinemodel against which the next model was tested.Fit of the Four-Factor Model With Factor Loadings
Constrained to Be Equal Across the Three Age Groups.The next step in the multiple-group CFA (test ofmeasurement weight invariance) was to test a model inwhich each factor loading was constrained to be equalacross the three age groups. As shown in Table 2, theseadditional constraints resulted in a decreased W2 value(W218 difference = 22.1, p difference9 .23), with anonsignificant p value. This indicated that the observedsubject data were not significantly different from theexpected data based on the factor model; thus, theconstrained model was identified as more parsimonious.Like the unconstrained model, this model also yielded aCFI value just below the criterion but all GFI, AGFI,and RMSSR values met criteria, indicating an ade-quately fitting model. Factor loadings and interfactorcorrelations for each of the three age groups from thefour-factor model are presented in Figure 1. Significantcorrelations at p < .01 existed between factors 2 and 4(except in the child group) and between factor 1 andeach of the other factors (factor 3, factor 2 [except in theadult group], and factor 4 [in the adolescent group]).The model in which loadings were constrained fit thedata as well as the model in which loadings were free tovary across groups; we adopted the former as providingthe best fit because we also tested models with additionalconstraints on measurement intercepts, structuralcovariances, and measurement residuals, but found inall of the cases a highly significant increase in W2
(p < .001) and greatly reduced fit indices.Comparing the Four-Factor Model With a Three-Factor
Model. As in the present study, the three-factor model
TABLE 2Four-Factor Category-Based Obsessive-Compulsive Disorder Symptom Dimension Model Fit Summary
Model W2 df p GFI AGFI RMSSR CFI RMSEA TLI AIC
Initial (unconstrained) 4-factor model fit for 3 age groups 299.1 177 <.001 0.89 0.83 0.10 0.90 0.04 0.86 491.1Four-factor loadings constrained to be equal across 3 age groups 321.2 195 <.001 0.88 0.83 0.10 0.89 0.04 0.87 477.2Difference between fit of above models 22.1 18 .23 V V V V V V VSummerfeldt et al.7 4-factor model fit on an adults-only sample 153 59 <.001 0.90 0.84 0.08 0.86 V V V
Note: GFI = goodness-of-fit index; AGFI = adjusted goodness-of-fit index; RMSSR = root mean square standardized residual; CFI =comparative fit index; RMSEA = root mean square error of approximation; TLI = Tucker-Lewis index; AIC = Akaike information criterion.
STEWART ET AL.
768 WWW.JAACAP.COM J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:7, JULY 2008

proposed by Baer9 was developed from factor analysis ofthe same 13 � 13 correlation matrix based on the 13major symptom categories of the Y-BOCS symptomchecklist. It differed from the four-factor model in that itcontained no hoarding factor, but instead included thesymptom categories for hoarding obsessions and hoard-ing compulsions on the symmetry/ordering factor, andit included the somatic obsession symptom category onthe cleaning/contamination factor rather than theaggressive/sexual factor. When, as in this case, compet-ing CFAs are not nested, the AIC is used to compare themodels, with the lower value preferred.38 When weconducted the same CFA across the three age groups asdescribed in Table 2, the three-factor model withmeasurement weights constrained yielded AIC = 770.5,larger than the value of 477.2 observed for theunconstrained four-factor model; all of the othermajor fit indices also favored the four-factor modelversus the three-factor model.Comparing the Four-Factor Model With a Five-Factor
Model. Direct comparison of the model fits of our four-and the five-factor model proposed by Pinto et al.15 iscomplicated by the fact that the five-factor modeldivided the original aggressive obsessions symptomcategory in the Y-BOCS symptom checklist into twonew symptom categories (which they named Bfear ofaggressive impulses^ and Bpathological doubt^) yieldinga 14 � 14 correlation matrix of symptom categoriesrather than the 13 � 13 matrix used in the present andprevious factor analyses (e.g., Baer,9 Summerfeldtet al.7). The comparison began by modifying ourmultiage group data file to produce the same 14 � 14matrix as used by Pinto et al.15 to derive their five-factormodel.1 Then the same CFAs were conducted across thethree age groups as described in Table 2. The five-factormodel with measurement weights constrained yieldedan AIC of 652.8, larger than the value of 477.2 observedfor the four-factor model with measurement weightsconstrained, tested on a 13 � 13 correlation matrix;similarly, the constrained five-factor model yielded aCFI value of 0.86 compared to a CFI value of 0.89 forthe constrained four-factor model.
DISCUSSION
This study indicates that the four-factor category-based OCD symptom dimension structure defined inthe only previous symptom CFA provides an adequate
fit for the data in independent child, adolescent, andadult age groups (with equal factor loadings across agegroups). Fit indices across the three groups are similar tothose reported for the Summerfeldt et al.7 independentadult sample. As such, the first CFA study on adultOCD has now been replicated in an independentmultiple age group sample. Findings suggest that thisOCD dimensional structure can also be used in childrenand adolescents, emphasizing its heuristic value forfuture clinical, genetic, neuroimaging, and treatmentstudies. Furthermore, the fit of the four-factor modelinitially proposed by Leckman et al.8 was found toprovide a better fit than both the three-factor modelproposed by Baer9 and the five-factor model proposedby Pinto et al.15
This study is particularly relevant because symptomdimensions are increasingly used to define OCDphenotype, both clinically and in translational studies.Given the inherent heterogeneity in the presentation ofOCD, it is possible that significant research findingshave previously been diluted or lost without the use ofsuch a dimensional approach. Improved understandingof OCD symptom dimensions across age groups mayalso inform clinical treatment formulations. In fact, thepending DSM-V version will likely use dimensions inthe formal diagnosis and categorization of OCD.39,40
However, the few extant studies on children andadolescent factor analyses have not provided consistentresults. Given pending changes of OCD DSM criteria,the examination of symptom dimension validity acrossnonadult age groups has become a necessary objective toconfirm the appropriateness of its ongoing use in OCDresearch and clinical practice.The data presented here and elsewhere32 demonstrate
that categorically defined OCD symptom frequenciesdiffer between age groups. As reflected in Table 1,symptom frequencies for ordering, checking, symmetry,and aggression differed across age groups in this sample.However, factor loadings of individual symptomcategories were similar across age groups. These findingssupport the relevance of a four-factor category-baseddimensional model for use in nonadult and adult agegroups. This is also important in guiding future OCDresearch when symptom dimensions will likely bestudied to determine potential correlations with clinicalvariables such as treatment responsiveness16 andcomorbidity,21 with endophenotypes such as neuroima-ging findings,17,19 and with specific vulnerability genes.
OCD FOUR-FACTOR STRUCTURE BY AGE GROUP
WWW.JAACAP.COM 769J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:7, JULY 2008

Reflecting the findings of Summerfeldt et al.,7 someof the symptom dimensions in the studied four-factormodel were highly correlated (Fig. 1), reflecting thefrequent presentation of OCD with multiple rather thanisolated symptom types. Therefore, the statistical use ofvarimax rotation in numerous past OCD EFAs mayhave been inappropriate (if similar correlations werepresent) because this rotation type does not permitcovariance between factors. A preferable rotation for usein future OCD factor analyses is promax rotation, whichis not limited by this constraint.The modest GFIs in the present study and in the
Summerfeldt et al. CFA strongly suggest that despite itsusefulness, more work needs to be done to improve thedimensional model of OCD. To date, this structure hasbeen predominantly based on the general symptomcategories of the various Y-BOCS and CYBOCSsymptom checklists. These checklists are less preciseand more subjective than many personality measures,which have been the focus of many CFAs to date forother psychiatric illnesses.41 From modification indicesgenerated by our CFAs, checking, counting, andrepeating compulsions (all of which may be nonspecificresponses to various obsessions) appear to be reducingthe adequacy of fit of the four-factor model. Newermeasures such as the dimensional Y-BOCS may helpaddress this concern and also allow the measure ofdimension-specific severity, focusing on distress, fre-quency, and interference for each.42 We plan toinvestigate such modifications to improve our modelin future studies.Ideally, we would have conducted an item-level factor
analysis to clarify whether the Y-BOCS and CYBOCScategories were indeed homogeneous. There is anunderlying assumption among category-based factoranalyses to date that these are homogeneous. However,symptoms including checking, repeating, and countingmay be associated with diverse underlying thought andbehavioral content. Unfortunately, our sample did notprovide sufficient power to conduct item-level analyses.Although Pinto et al.15 noted that associated factors oftaboo thoughts and doubt/checking among adults aresupported by the item-level analyses of Summerfeldtet al.7 and Denys et al.,11 we found no evidence in oursample that their proposed five-factor model produced afit superior to that of the four-factor model that we tested.In this study, we sought to determine whether the
four-factor model described by the Summerfeldt et al. 7
CFA could be appropriately used in all age groups. In amanner similar to that of Summerfeldt et al.,7 ouranalyses did not include miscellaneous obsession andcompulsion categories. At the categorical level, mis-cellaneous obsessions and compulsions are heteroge-neous and are not built upon a theoretical construct.Moreover, subsequent work by Summerfeldt et al.43 andStorch et al.44 demonstrated high correlation of nearlyall miscellaneous symptoms with one or more factors inthe four-factor structure. Therefore, items from themiscellaneous categories do not necessarily represent anadditional overlooked symptom dimension, but thisremains to be tested empirically.Because the aim of this study was to compare a model
across age groups, categories and items that were notpresent in both adult (Y-BOCS) and child (CYBOCS)OCD checklists were excluded from analyses. Thus,child magical thoughts, superstitions, and rituals withothers were excluded. This is relevant because super-stitions and obsessions/checking and confessing formedindependent factors/clusters in a recent study of 213OCD-affected children.45 However, the goal of thestudy was to identify whether previously defined factorstructures are appropriate for future use across agegroups rather than to account for full similarity ordifferences between age groups. This study examinedthe appropriateness of a single set of OCD symptomdimensions for use across different age ranges. However,it did not address whether an OCD-affected individualwill have a stable symptom structure over time.Adequately powered longitudinal studies are necessaryto answer the more biologically relevant question ofwhether symptom stability occurs over the life span.Several limitations of this study must be acknowl-
edged. The fact that the adult group reported lowerlifetime rates of ordering suggests that retrospectivememory biases may have contributed error to themeasurement of some symptoms across the life span.Furthermore, this was not a longitudinal study ofcurrent symptoms, which would be necessary toultimately understand the progression or stability ofOCD dimensions from childhood through adulthood.However, this study did identify the utility of the four-factor structure across age groups by demonstratingcomparable model fit when holding factor loadingsconstant across age groups. Another major limitation isthe reliance on the symptom checklists of the Y-BOCSand CYBOCS and the categories that they use.
STEWART ET AL.
770 WWW.JAACAP.COM J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:7, JULY 2008

Although these scales are widely used, they containinherently ambiguous categories that fail to sort somefrequently encountered symptoms according to theirdimensional content. Another limitation was that thestudy sample was derived from different clinical sites andwould be best characterized as one of convenience,although this could arguably improve the general-izability of findings to a broader OCD population.Finally, despite their increasing popularity withinpsychiatry, the statistical approaches of CFA and EFAhave been criticized for several reasons. From atheoretical perspective, the utility of CFA has beencalled into question when the structure is not simple.46
These techniques are unable to provide definitive proofof factor structure, and all of the models are incorrect tosome degree.47 Acknowledging this, a goal of thisinvestigation was to determine whether a parsimoniousmodel that meaningfully explained the data forSummerfeldt et al.7 provided adequate fit for each ofthe three age groups. A second limitation of CFA is theabsence of a universally agreed-on measure of good fit.Different criteria have consequently been used acrossstudies to determine poor versus adequate versus goodfit. The criteria selected a priori for this study were moreliberal than those suggested by and Hu and Bentler.37
These criteria were intentionally selected to be identicalto those used by Summerfeldt et al.7 to determine themodel`s applicability in other age groups. Furthermore,our chosen indices were maximum likelihoodYbased fitindices, which outperform and are preferable to thoseobtained from generalized least squares or fromasymptotic distribution freeYbased indices, accordingto Hu and Bentler.37
In conclusion, this study has important clinical andresearch implications. It provides a determination of agegroup comparability of the four-factor category-basedOCD symptom dimension model as defined in theprevious CFA. This four-factor model of OCDsymptom dimensions provides an adequate but limitedquantitative representation of symptomatology in child,adolescent, and adult age groups. Moreover, the four-factor model originally described by Leckman et al.8
provided a better fit than the five-factor model recentlydescribed by Pinto et al.15 Thus, application of thissymptom dimension construct to subjects with OCDacross the life span is deemed appropriate, althoughimperfect. Furthermore, symptom factor loadings foreach dimension are not significantly different between
age groups, despite significant differences in rates ofsymptoms and correlations between factors across agegroups. This study may guide future OCD researchefforts to understand relationships between illnessphenotype, underlying etiology/genetics, and associatedclinical/treatment response factors. Although it may bepossible to identify separate etiologic factors for each ofthe dimensions, shared risk factors are also likely to bepresent. The identity of these factors requires elucidationbefore the pathophysiology of OCD is fully understood.Whether the model fit may be improved by item-basedrather than category-based OCD symptom dimensionsis a research question that remains to be answered.
Disclosure: Dr. Geller has received research support from, has been aspeaker for, or has served on the advisory boards of Shire, Eli Lilly, Pfizer,Bristol-Myers Squibb, Novartis, Forest Laboratories, and GlaxoSmithK-line. Dr. Carter receives royalties from Harcourt Assessment for theITSEA/BITSEA measures she codeveloped. The other authors report noconflicts of interest.
REFERENCES
1. do Rosario-Campos MC, Leckman JF, Curi M, et al. A family study ofearly-onset obsessive-compulsive disorder. Am J Med Genet B Neurop-sychiatr Genet. 2005;136:92Y97.
2. Korszun A, Moskvina V, Brewster S, et al. Familiality of symptomdimensions in depression. Arch Gen Psychiatry. 2004;61:468Y474.
3. Wickham H, Walsh C, Asherson P, et al. Familiality of symptomdimensions in schizophrenia. Schizophr Res. 2001;47:223Y232.
4. Miguel EC, Leckman JF, Rauch S, et al. Obsessive-compulsive disorderphenotypes: implications for genetic studies. Mol Psychiatry. 2005;10:258Y275.
5. Pato MT, Pato CN, Pauls DL. Recent findings in the genetics of OCD.J Clin Psychiatry. 2002;63(Suppl 6):30Y33.
6. Rosenberg DR, Hanna GL. Genetic and imaging strategies in obsessive-compulsive disorder: potential implications for treatment development.Biol Psychiatry. 2000;48:1210Y1222.
7. Summerfeldt LJ, Richter MA, Antony MM, Swinson RP. Symptomstructure in obsessive-compulsive disorder: a confirmatory factor-analyticstudy. Behav Res Ther. 1999;37:297Y311.
8. Leckman JF, Grice DE, Boardman J, et al. Symptoms of obsessive-compulsive disorder. Am J Psychiatry. 1997;154:911Y917.
9. Baer L. Factor analysis of symptom subtypes of obsessive compulsivedisorder and their relation to personality and tic disorders. J ClinPsychiatry. 1994(55 Suppl):18Y23.
10. Cavallini MC, DiBella D, Siliprandi F, Malchiodi F, Bellodi L.Exploratory factor analysis of obsessive-compulsive patients and associa-tion with 5-HTTLPR polymorphism. Am J Med Genet B NeuropsychiatrGenet. 2002;114:347Y353.
11. Denys D, de Geus F, van Megen HJ, Westenberg HG. Use of factoranalysis to detect potential phenotypes in obsessive-compulsive disorder.Psychiatry Res. 2004;128:273Y280.
12. Leckman JF, Zhang H, Alsobrook JP, Pauls DL. Symptom dimensions inobsessive-compulsive disorder: toward quantitative phenotypes. Am JMed Genet. 2001;105:28Y30.
13. Mataix-Cols D, Rauch SL, Manzo PA, Jenike MA, Baer L. Use of factor-analyzed symptom dimensions to predict outcome with serotonin
OCD FOUR-FACTOR STRUCTURE BY AGE GROUP
WWW.JAACAP.COM 771J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:7, JULY 2008

reuptake inhibitors and placebo in the treatment of obsessive-compulsivedisorder. Am J Psychiatry. 1999;156:1409Y1416.
14. Sanislow CA, Grilo CM,Morey LC, et al. Confirmatory factor analysis ofDSM-IV criteria for borderline personality disorder: findings from thecollaborative longitudinal personality disorders study. Am J Psychiatry.2002;159:284Y290.
15. Pinto A, Eisen JL, Mancebo MC, Greenberg BD, Stout RL, RasmussenSA. Taboo thoughts and doubt/checking: a refinement of the factorstructure for obsessive-compulsive disorder symptoms. Psychiatry Res.2007;151:255Y258.
16. Black DW, Monahan P, Gable J, Blum N, Clancy G, Baker P. Hoardingand treatment response in 38 nondepressed subjects with obsessive-compulsive disorder. J Clin Psychiatry. 1998;59:420Y425.
17. Mataix-Cols D, Wooderson S, Lawrence N, Brammer MJ, Speckens A,Phillips ML. Distinct neural correlates of washing, checking, andhoarding symptom dimensions in obsessive-compulsive disorder. ArchGen Psychiatry. 2004;61:564Y576.
18. Phillips ML, Marks IM, Senior C, et al. A differential neural response inobsessive-compulsive disorder patients with washing compared withchecking symptoms to disgust. Psychol Med. 2000;30:1037Y1050.
19. Rauch SL, Dougherty DD, Shin LM, et al. Neural correlates of factor-analyzed OCD symptom dimension: a PET study. CNS Spectr1998;3:37Y43.
20. Samuels J, Shugart YY, Grados MA, et al. Significant linkage tocompulsive hoarding on chromosome 14 in families with obsessive-compulsive disorder: results from the OCD Collaborative GeneticsStudy. Am J Psychiatry. 2007;64:493Y499.
21. Hasler G, LaSalle-Ricci VH, Ronquillo JG, et al. Obsessive-compulsivedisorder symptom dimensions show specific relationships to psychiatriccomorbidity. Psychiatry Res. 2005;135:121Y132.
22. Holtzer JC, Goodman WK, McDougle CJ, et al. Obsessive-compulsivedisorder with and without a chronic tic disorder. A comparison ofsymptoms in 70 patients. Br J Psychiatry. 1994;164:469Y473.
23. Hasler G, Pinto A, Greenberg BD, et al. Familiality of factor analysis-derived YBOCS dimensions in OCD-affected sibling pairs from theOCD Collaborative Genetics Study. Biol Psychiatry. 2007;61:617Y625.
24. Besiroglu L, Uguz F, Ozbebit O, et al. Longitudinal assessment ofsymptom and subtype categories in obsessive-compulsive disorder.Depress Anxiety. 2007;24:461Y466.
25. Mataix-Cols D, Rauch SL, Baer L, et al. Symptom stability in adultobsessive-compulsive disorder: data from a naturalistic two-year follow-up study. Am J Psychiatry. 2002;159:263Y268.
26. Rufer M, Grothusen A, Mass R, Peter H, Hand I. Temporal stability ofsymptom dimensions in adult patients with obsessive-compulsivedisorder. J Affect Disord. 2005;88:99Y102.
27. Rettew DC, Swedo SE, Leonard HL, Lenane MC, Rapoport JL.Obsessions and compulsions across time in 79 children and adolescentswith obsessive-compulsive disorder. J Am Acad Child Adolesc Psychiatry.1992;31:1050Y1056.
28. McKay D, Piacentini J, Greisberg S, Graae F, Jaffer M, Miller J. Thestructure of childhood obsessions and compulsions: dimensions in anoutpatient sample. Behav Res Ther. 2006;44:137Y146.
29. Stewart SE, Rosario MC, Brown TA, et al. Principal components analysis
of obsessive-compulsive disorder symptoms in children and adolescents.Biol Psychiatry. 2007;61:285Y291.
30. Evans DW, Leckman JF, Carter A, et al. Ritual, habit, and perfectionism:the prevalence and development of compulsive-like behavior in normalyoung children. Child Dev. 1997;68:58Y68.
31. Zohar AH, Felz L. Ritualistic behavior in young children. J Abnorm ChildPsychol. 2001;29:121Y128.
32. Geller DA, Biederman J, Faraone S, et al. Developmental aspects ofobsessive compulsive disorder: findings in children, adolescents, andadults. J Nerv Ment Dis. 2001;189:471Y477.
33. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-BrownObsessive Compulsive Scale. I. Development, use, and reliability. ArchGen Psychiatry. 1989;46:1006Y1011.
34. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-BrownObsessive Compulsive Scale. II. Validity. Arch Gen Psychiatry. 1989;46:1012Y1016.
35. Scahill L, Riddle MA, McSwiggin-Hardin M, et al. Children`s Yale-Brown Obsessive Compulsive Scale: reliability and validity. J Am AcadChild Adolesc Psychiatry. 1997;36:844Y852.
36. SPSS 12.0 for Windows; Chicago: SPSS Inc.; 2003.37. Hu L, Bentler P. Cutoff criteria for fit indices in covariance structure
analysis: Conventional criteria versus new alternatives. Struct EquationModel. 1999;6:1Y55.
38. Keith TZ. Multiple Regression and Beyond. Boston: Pearson Education;2006.
39. Leckman JF, Rauch SL, Mataix-Cols D. Symptom dimensions inobsessive-compulsive disorder: implications for the DSM-V. CNS Spectr.2007;12:376Y387, 400.
40. Mataix-Cols D, Pertusa A, Leckman JF. Issues for DSM-V: how shouldobsessive-compulsive and related disorders be classified? Am J Psychiatry.2007;164:1313Y1314.
41. Skodol AE, Oldham JM, Bender DS, et al. Dimensional representationsof DSM-IV personality disorders: relationships to functional impairment.Am J Psychiatry. 2005;162:1919Y1925.
42. Rosario-Campos MC, Miguel EC, Quatrano S, et al. The DimensionalYale-Brown Obsessive-Compulsive Scale (DY-BOCS): an instrument forassessing obsessive-compulsive symptom dimensions. Mol Psychiatry.2006;11:495Y504.
43. Summerfeldt LJ, Kloosterman PH, Antony MM, Richter MA, SwinsonRP. The relationship between miscellaneous symptoms and majorsymptom factors in obsessive-compulsive disorder. Behav Res Ther. 2004;42:1453Y1467.
44. Storch EA, Lack C, Merlo LJ, et al. Associations between miscellaneoussymptoms and symptom dimensions: an examination of pediatricobsessive-compulsive disorder. Behav Res Ther. 2007;45:2593Y2603.
45. Ivarsson T, Valderhaug R. Symptom patterns in children and adolescentswith obsessive-compulsive disorder (OCD). Behav Res Ther. 2006;44:1105Y1116.
46. McCrae R, Zonderman A, Costa P Jr. Evaluating replicability of factorsin the Revised NEO Personality Inventory: confirmatory factor analysisversus procrustes rotation. J Pers Soc Psychol. 2006;70:552Y566.
47. MacCallum RC, Austin JT. Applications of structural equation modelingin psychological research. Annu Rev Psychol. 2000;51:201Y226.
STEWART ET AL.
772 WWW.JAACAP.COM J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:7, JULY 2008
Copyright © 2022 FDOKUMEN




















