Loss of FHIT Function in Lung Cancer and Preinvasive Bronchial Lesions1
7
ICANCER RESEARCH 58. 50.12-5037. November 15. 1998] Advances in Brief Loss of FHIT Function in Lung Cancer and Preinvasi ve Bronchial Lesions1 Gabriella Sozzi, Ugo Pastorino, Luisa Moiraghi, Elda Tagliabue, Francesco Pezzella, Cristina Ghirelli, Silvana Tornielli, Laura Sard, Kay Huebner, Marco A. Pierotti, Carlo M. Croce,2 and Silvana Pilotti Division of Experimental Oncology A. E und Anatomical Pathology, istituto Nazionale Tumori. 20133 Milan. Italy ¡G.S.. L. M.. E. T.. C. G.. S. T.. L S.. M. A. P.. S. P.l; Division oj Thoracic Surgery. Jaropean Inclinile of 'Oncology. 20141 Milan. Italy ¡U.P.I; Department of Pathology. University College of London, Ltmdon. United Kingdom ¡F.P.¡;and the Kimmel Cancer Center. Jefferson Medical College. Philadelphia. Pennsylvania IVI07 ¡K.H.. C. M. C.¡ Abstract We previously cloned and characterized the tumor suppressor gene /•'////' (fragile histidine triad) at chromosome 3pl4.2 and found that this gene is altered In deletions in human tumors, including lung cancer. To assess the frequency and specificity of inactivation and its relevance in a clinical setting, we have produced antibodies against the Fhit protein and studied its expression in a series of non-small cell lung cancers and normal hronchial mucosa and a spectrum of preinvasive lesions by immunohis- tochemislry. The data indicate that the loss of Phil protein is the most frequent alteration in non-small cell lung cancer (73%} and precancerous lesions (93% ), is significantly higher in the tumors of smokers (75% ) than in those of nonsmokers (39%; /' < (1.001)51, and is an independent and more frequent event than p53 overexpression in tumors and precancerous lesions (73 versus 46%). The percentage of cases lacking Fhit expression was higher in the squamous type compared to adenocarcinoma (87 versus 57%; P < (1.0(1(1011. whereas other histotypes (large cell, mucoepidermal) showed an intermediate value (69%). Loss of Fhil expression in a very high percentage of primary lung carcinomas and precancerous lesions supports the notion that FHIT alterations play an important role in the growth control of bronchial cells. FHIT inactivation is particularly important in squamous cell carcinomas that are often associated with precursor dysplastic lesions. The overall high frequency and precocity of Fhit loss in lung carcinogenesis and the development of the presently described immunohistochemical approach suggest a potential use of this gene in the early detection of lung cancer and in chemopreventive studies as an intermediate biomarker. Introduction Deletions of the short arm of chromosome 3 are considered critical events in the pathogenesis of lung cancer (1-3). The observation of 3p alterations in preinvasive lesions of the bronchus suggests that one or more tumor suppressor gene(s) may act as gatekeepers for lung carcinogenesis (4-8). FHIT, the tumor suppressor gene at 3pl4.2 (9), encompasses the FRA3B fragile site and is a common target of deletions in primary human cancers of epithelial origin, including those of the lung, head and neck, stomach, cervix, breast, and kidney (9-12). The analysis of FHIT RNA expression has shown FHIT alterations in these tumor types to be correlated with deletions within the FHIT gene (9. 13-17). Structural changes and abnormal mRNA expression have been reponed in cell lines and primary tumors of Received 9/9/98; accepted 10/1/98. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1Supported in part by the Associa/ione and Federazione Italiana per la Ricerca sul Cancro (AIRC/FIRC) and the Special Project of the Consiglio Nazionale delle Ricerche Applica/ioni Cllniche della Ricerca Oncologica. C. M. C. and K. H. were supported by NIH Grants CA56336. CA21124. and CA39860. ' To whom requests for reprints should be addressed, at Kimmel Cancer Center. Jefferson Medical College. Thomas Jefferson University. 233 South 10th Street. Phila delphia, PA 19107. Phone: (215) 503-4645; Fax: (215) 923-3528; E-mail: C_Croce@ lac.jci.tju.edu. SCLC1 and NSCLC (18-20). In addition, Fhit protein expression was markedly reduced or absent in the great majority of primary SCLCs and in tumor-derived cell lines showing FHIT gene abnormalities (21). The transfection of a FHIT transgene into lung, renal, and gastric cancer cell lines lacking endogenous FHIT because of homozygous deletions resulted in a very low yield of Fhit-cxpressing clones (22). Moreover, the ability of wild-type Fhit transfectants to form tumors in nude mice was suppressed (22), supporting a role for FHIT us a tumor suppressor gene. The crystallographic structure of Fhit, a diadenosine 5'.5'"-P'.Pn- polyphosphate hydrolase (23), suggests that in its active form, FHIT is bound to its preferred substrate, Ap3A, in a dimeric state (24). This binding seems to be critical for tumorigenicity because the hydrolase "dead" Fhit mutant protein still suppresses tumorigenicity, suggesting that hydrolase activity is not required for tumor suppression (22). Although the biological function of the Fhit protein is still unknown, it is conceivable that FHIT plays a role in cell proliferation and/or apoptotic pathways. NSCLC represents a major cause of mortality worldwide; it ac counts for 75-80% of all lung tumors and includes three main histological subtypes: (a) adenocarcinoma; (b) squamous cell carci noma; and (c) large cell carcinoma (25). The progression from normal epithelium to invasive neoplasia develops through the occurrence of morphological lesions of various grades, which are considered risk factors for tumor development. The detection of molecular changes in these samples would thus provide useful markers for early diagnosis of lung cancer and for the assessment of individuals at higher risk for this type of tumor. Inactivation of the suppressor gene p53 and overexpression of EGFR as well as more generali/.ed allelic losses (LOH) at several chomosomal regions on the short arm of chromo some 3 (3p) have been reported in preinvasive lesions (4, 5, 7, 8, 26. 27). However, in spite of the high frequency of LOH on 3p in precancerous lesions (7. 8). the involvement of specific tumor sup pressor gene(s) in any 3p region has not been demonstrated. This would be extremely important to increase the sensitivity of the mo lecular assays of preinvasive lesions in routine clinicopathological diagnosis as well as to better clarify the pathogenesis of lung tumors. Materials and Methods Study Patients. From January 1974 to December 1990. 608 consecutive patients at the Division of Thoracic Surgery of the Istituto Na/ionale Tumori (Milan. Italy) underwent surgical resection for pathological stage I (pT,_2NOMORO) NSCLC (28, 29). After pathological review, 474 cases were considered adequate for the present analysis, and new sections were obtained from paraffin blocks. The remaining cases were excluded due to the inade quacy of paraffin blocks or a diagnosis other than NSCLC (carcinoid, SCLC). The main clinical features of these patients are listed in Table 1. The periop erative mortality rate was 3.9%. The vast majority of the patients were treated 1 The abbreviations used are: SCLC, small cell lung carcinoma; NSCLC. non-SCLC: EGFR, epidermal growth factor receptor: LOH, loss of helerozygosity: GST. glulathione S-transferase; RT. room temperature; CIS. carcinoma in situ. 5032 on May 20, 2015. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Loss of FHIT Function in Lung Cancer and Preinvasive Bronchial Lesions1

ICANCER RESEARCH 58. 50.12-5037. November 15. 1998]
Advances in Brief
Loss of FHIT Function in Lung Cancer and Preinvasi ve Bronchial Lesions1
Gabriella Sozzi, Ugo Pastorino, Luisa Moiraghi, Elda Tagliabue, Francesco Pezzella, Cristina Ghirelli,Silvana Tornielli, Laura Sard, Kay Huebner, Marco A. Pierotti, Carlo M. Croce,2 and Silvana Pilotti
Division of Experimental Oncology A. E und Anatomical Pathology, istituto Nazionale Tumori. 20133 Milan. Italy ¡G.S.. L. M.. E. T.. C. G.. S. T.. L S.. M. A. P.. S. P.l; Divisionoj Thoracic Surgery. Jaropean Inclinile of 'Oncology. 20141 Milan. Italy ¡U.P.I; Department of Pathology. University College of London, Ltmdon. United Kingdom ¡F.P.¡;and
the Kimmel Cancer Center. Jefferson Medical College. Philadelphia. Pennsylvania IVI07 ¡K.H.. C. M. C.¡
Abstract
We previously cloned and characterized the tumor suppressor gene/•'////'(fragile histidine triad) at chromosome 3pl4.2 and found that this
gene is altered In deletions in human tumors, including lung cancer. To
assess the frequency and specificity of inactivation and its relevance in aclinical setting, we have produced antibodies against the Fhit protein andstudied its expression in a series of non-small cell lung cancers and normalhronchial mucosa and a spectrum of preinvasive lesions by immunohis-
tochemislry.The data indicate that the loss of Phil protein is the most frequent
alteration in non-small cell lung cancer (73%} and precancerous lesions
(93% ), is significantly higher in the tumors of smokers (75% ) than in thoseof nonsmokers (39%; /' < (1.001)51, and is an independent and more
frequent event than p53 overexpression in tumors and precancerouslesions (73 versus 46%). The percentage of cases lacking Fhit expressionwas higher in the squamous type compared to adenocarcinoma (87 versus57%; P < (1.0(1(1011.whereas other histotypes (large cell, mucoepidermal)
showed an intermediate value (69%).Loss of Fhil expression in a very high percentage of primary lung
carcinomas and precancerous lesions supports the notion that FHITalterations play an important role in the growth control of bronchial cells.FHIT inactivation is particularly important in squamous cell carcinomasthat are often associated with precursor dysplastic lesions. The overallhigh frequency and precocity of Fhit loss in lung carcinogenesis and thedevelopment of the presently described immunohistochemical approachsuggest a potential use of this gene in the early detection of lung cancerand in chemopreventive studies as an intermediate biomarker.
Introduction
Deletions of the short arm of chromosome 3 are considered criticalevents in the pathogenesis of lung cancer (1-3). The observation of 3p
alterations in preinvasive lesions of the bronchus suggests that one ormore tumor suppressor gene(s) may act as gatekeepers for lungcarcinogenesis (4-8). FHIT, the tumor suppressor gene at 3pl4.2 (9),
encompasses the FRA3B fragile site and is a common target ofdeletions in primary human cancers of epithelial origin, includingthose of the lung, head and neck, stomach, cervix, breast, and kidney(9-12). The analysis of FHIT RNA expression has shown FHIT
alterations in these tumor types to be correlated with deletions withinthe FHIT gene (9. 13-17). Structural changes and abnormal mRNA
expression have been reponed in cell lines and primary tumors of
Received 9/9/98; accepted 10/1/98.The costs of publication of this article were defrayed in part by the payment of page
charges. This article must therefore be hereby marked advertisement in accordance with18 U.S.C. Section 1734 solely to indicate this fact.
1Supported in part by the Associa/ione and Federazione Italiana per la Ricerca sul
Cancro (AIRC/FIRC) and the Special Project of the Consiglio Nazionale delle RicercheApplica/ioni Cllniche della Ricerca Oncologica. C. M. C. and K. H. were supported byNIH Grants CA56336. CA21124. and CA39860.
' To whom requests for reprints should be addressed, at Kimmel Cancer Center.
Jefferson Medical College. Thomas Jefferson University. 233 South 10th Street. Philadelphia, PA 19107. Phone: (215) 503-4645; Fax: (215) 923-3528; E-mail: C_Croce@
lac.jci.tju.edu.
SCLC1 and NSCLC (18-20). In addition, Fhit protein expression was
markedly reduced or absent in the great majority of primary SCLCsand in tumor-derived cell lines showing FHIT gene abnormalities
(21). The transfection of a FHIT transgene into lung, renal, and gastriccancer cell lines lacking endogenous FHIT because of homozygousdeletions resulted in a very low yield of Fhit-cxpressing clones (22).Moreover, the ability of wild-type Fhit transfectants to form tumors in
nude mice was suppressed (22), supporting a role for FHIT us a tumorsuppressor gene.
The crystallographic structure of Fhit, a diadenosine 5'.5'"-P'.Pn-
polyphosphate hydrolase (23), suggests that in its active form, FHITis bound to its preferred substrate, Ap3A, in a dimeric state (24). Thisbinding seems to be critical for tumorigenicity because the hydrolase"dead" Fhit mutant protein still suppresses tumorigenicity, suggesting
that hydrolase activity is not required for tumor suppression (22).Although the biological function of the Fhit protein is still unknown,it is conceivable that FHIT plays a role in cell proliferation and/orapoptotic pathways.
NSCLC represents a major cause of mortality worldwide; it accounts for 75-80% of all lung tumors and includes three main
histological subtypes: (a) adenocarcinoma; (b) squamous cell carcinoma; and (c) large cell carcinoma (25). The progression from normalepithelium to invasive neoplasia develops through the occurrence ofmorphological lesions of various grades, which are considered riskfactors for tumor development. The detection of molecular changes inthese samples would thus provide useful markers for early diagnosisof lung cancer and for the assessment of individuals at higher risk forthis type of tumor. Inactivation of the suppressor gene p53 andoverexpression of EGFR as well as more generali/.ed allelic losses(LOH) at several chomosomal regions on the short arm of chromosome 3 (3p) have been reported in preinvasive lesions (4, 5, 7, 8, 26.27). However, in spite of the high frequency of LOH on 3p inprecancerous lesions (7. 8). the involvement of specific tumor suppressor gene(s) in any 3p region has not been demonstrated. Thiswould be extremely important to increase the sensitivity of the molecular assays of preinvasive lesions in routine clinicopathologicaldiagnosis as well as to better clarify the pathogenesis of lung tumors.
Materials and Methods
Study Patients. From January 1974 to December 1990. 608 consecutivepatients at the Division of Thoracic Surgery of the Istituto Na/ionale Tumori(Milan. Italy) underwent surgical resection for pathological stage I(pT,_2NOMORO) NSCLC (28, 29). After pathological review, 474 cases wereconsidered adequate for the present analysis, and new sections were obtainedfrom paraffin blocks. The remaining cases were excluded due to the inadequacy of paraffin blocks or a diagnosis other than NSCLC (carcinoid, SCLC).The main clinical features of these patients are listed in Table 1. The perioperative mortality rate was 3.9%. The vast majority of the patients were treated
1 The abbreviations used are: SCLC, small cell lung carcinoma; NSCLC. non-SCLC:
EGFR, epidermal growth factor receptor: LOH, loss of helerozygosity: GST. glulathioneS-transferase; RT. room temperature; CIS. carcinoma in situ.
5032
on May 20, 2015. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

LOSS OF Fhit IN LUNG CANCER
Table 1 Frequenc\ of Fhit reactivity in ¡hetumor according to the main clinicalfeatures
Fhit reactivity
Age<6060SexMaleFemaleSize<2
cm2cmPT12Typesee"AdenocarcinomaGrade12-3TotalPositive6564115144089488131845922129Negative159186324211162297826720211213287345Total224250430351563181263482331961911094747t
Fhitnegative71747460747262778757698073P0.460.110.580.00130.000010.06
" SCC. squamous cell carcinoma.
with surgery alone. For the present analysis, the follow-up period was updated
to August 1997. with a median observation time of 64 months overall and 102months tor surviving patients. The diagnosis of NSCLC was made by histo-
logical examination according to the WHO (30) and to the Armed Forces
Institute of Pathology (31).Immunohistochemistry. Staining was performed on paraffin sections with
the use of a rabbit polyclonal anti-GST-Fhit antiserum (15. 22. 23). The specificityof this antiserum was previously demonstrated by immunoblot and by the immu-
nocytochemical detection of exogenous Fhit protein in transfected Cos and humantumor cell lines (15. 22). Additionally, absorption of the antiserum with purifiedGST did not reduce the detection of endogenous and exogenous Fhit (21). Todetermine the relationship and the temporal sequence of Fhit and p53 alterations,consecutive sections from tumor and bronchial mucosa specimens that wereshown to contain precancerous lesions of various grades by morphological examination were serially cut and stained with anti-Fhit serum. anti-p53. and Mibl
antibody directed against a nuclear proliferation antigen to help complement theassessment of the grading of the preinvasive lesions.
Briefly, formalin- or Bouin-fixed paraffin-embedded tumor and bronchial mucosa sections were serially cut and mounted in poly-L-lysine (Sigma. St. Louis.MO) -coated slides, deparaffined in xylene. and rehydrated in graded alcohols.Endogenous peroxidase activity was blocked by treatment for 30 min with 0.3%-
hydrogen peroxide in methanol. Antigen enhancement was performed by steamingthe sections at 100°Cin 5 mmol/liter sodium citrate buffer in distilled water (pH
6.0) for 2 min. The slides were cooled under tap water and washed three times in0.05 M PBS-0.1% Triton and then incubated with blocking serum (normal goat ata 1:50 dilution in PBS-1 % BSA-0.1 % sodium azide) for 30 min at RT. The slideswere incubated overnight with primary rabbit polyclonal anti-GST-Fhit serum at a1:4000 dilution in PBS. D07 monoclonal antibody (at a 1:400 dilution in PBS-19Õ-
BSA-0.1% sodium a/.ide: Ylem-Novocastra. Newcastle upon Tyne. United Kingdom) and Mibl (diluted 1:100 in PBS-1% BSA-0.\% sodium a/ide; Immunotech.Marseille. France). The slides were washed again three times in PBS-0. IVr Tritonand then incubated with secondary antibody (biotinylated goat antirabbit or anti-mouse IgG diluted at 1:200 and 1:100. respectively, in PBS-1% BSA-0.1%sodium azide; DAKO) for 30 min at RT. After washings in PBS-0.1% Triton, afinal incubation with streptavidin-conjugated horseradish peroxidase (DAKO) at a
dilution of 1:300 in PBS for 30 min at RT was performed, and after subsequentPBS washings, peroxidase activity was detected by aminoethyl carbazole for 10min in the dark. The slides were counterstained with Cara/zi hematoxylin. Staining without the antibody was routinely performed as a negative control procedure.
Bronchial and tumor sections were routinely stained with nonimmune rabbitserum ( 1:4000 dilution) to control for nonspecific antibody binding. Slides didnot show immunoreactivity in any of these immunohistochemical stainingcontrol assays.
Immunostaining was classified in the following three groups according toboth intensity and extent: («)negative, no staining was present, or positive
staining was detected in <IO% of the cells; (b) weak, staining was moderatein all of the cells (i.e., less intense than that in the internal control), or a rangeof 10-30% of the cells stained positive; and (c) strong, immunostaining was asstrong as that of the internal control and was present in >309{- of the cells. Two
independent readers, a pathologist (S. P.) and a scientist (G. S.). were involvedin the assessment of expression.
Statistical Analysis. To examine the association of the various categoricalvariables, we used the \2 test with a two-sided Fisher's exact test for the
comparison of small groups. P < 0.05 was considered to be statisticallysignificant. Statistical analysis was performed using EPI Info Version 5.
Survival curves were calculated by Kaplan-Meier estimate, using log-rank
testing for the assessment of statistical significance.
Results
Loss of Fhit Expression in NSCLC. Table 1 lists the frequency ofFhit reactivity (strong and weak expression were combined as positive) inthe tumor samples. Of the 474 tumors analyzed. 345 (73%) were completely negative for Fhit protein expression (Fig. 1). The percentage ofnegative cases was higher in the squamous-type carcinoma compared
with adenocarcinoma (87 versus 57%: P < 0.00001 ), whereas the otherhistotypes (large cell carcinoma, mucoepidermoid carcinoma) showed anintermediate value (69%). In the adenocarcinoma specimens with positive Fhit immunostaining, the pattern of protein expression was clearlyassociated with the more differentiated cells, whereas less differentiatedareas within the same tumor showed weaker Fhit protein expression (Fig.2, B and C). Fhit immunostaining in squamous tumors also showedpositive reactivity restricted to the more differentiated, keratinized, andsometimes apoptotic cells, whereas the basal hyperproliferative tumorcells showed prevalent negative staining (Fig. 1, C and D). These findingsdemonstrate that the loss of Fhit protein expression is a very frequentchange in lung tumors, particularly in the squamous type of lung carcinoma. No association was found between Fhit-negative immunostaining
and the size of the tumor, whereas an association with pT, or pT2pathological stage (62 versus 77%; P = 0.0013) and tumor grading [49(grade 1) versus 74% (grades 2 and 3); P = 0.009] among the patients as
a whole and in the group with adenocarcinoma, respectively, was observed.
Loss of Fhit Expression and Smoking Habits. When Fhit expression was compared with smoking habits (cigarette/year andcigarette number/day), the frequency of Fhit-negative tumors in
smokers was significantly higher than it was in tumors fromnonsmokers (75 versus 39%: P < 0.0005; Table 2). Of note,tumors from patients who smoked for less then 20 years showed anintermediate rate of Fhit-negative immunostaining (50%). The
correlation between lack of Fhit expression and smoking was alsoobserved in the subset of adenocarcinoma patients (Table 2). Theseresults indicate that FHIT alterations preferentially occur in thetumors of heavy smokers.
There was no difference in overall survival between the patientswith Fhit-negative tumors and those with Fhit-positive tumors(P = 0.5; Fig. 3A). When the patients with adenocarcinoma were
studied separately, a slight difference in survival was observed in thepatients with Fhit-negative tumors [40 versus 53% at 5 years(P = 0.05) and 33 versus 42% at 10 years (P = 0.1): Fig. 3ß].Noassociation with overall survival was found in early-stage disease
(pT,) or with time to recurrence in the whole group.Comparison of the Frequency of Fhit Loss and of Other Alter
ations Observed in Lung Cancer. Absence of the Fhit protein intumor samples (73%) was a more frequent alteration then p53 (46%),EGFR (50%), and Bcl2 (19%) overexpression (Table 3). Fhit and p53alterations were found to be independent events, because the frequency of Fhit-negative cases in the groups of p53-positive and-negative tumors, respectively, was very similar (Table 3). The fact
5033
on May 20, 2015. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

LOSS OF Fhil IN LUNG CANCER
Fig. I. Phil-negative immunoslaining in squamous cell carcinomas. A. squamous cellimmunoreactivity in normal bronchial mucosa. B. Fhil-negalive immunostaining in a squamous cen carcinoma containing rnC and D. squamous cell carcinomas showing Fhil immunoreactivity restricted to the more difterenlialed. keraliniml cells
... _^ carcinoma showing Phil-negative immunostaining in tumor cells and Fhit-posiliveimmunostaining in a squamous cell carcinoma containing Phil-positive immunoslaining in trapped bronchialb.ed alveoli.
that the FHIT und TP53 genes are both mutated in a large number ofthe same tumors suggests that the two proteins do not participate inthe same biochemical pathway. p53 analysis by immunohistochemis-
try can underestimate the frequency of p53 alterations due to the
occurrence of deletion or stop codon mutations in the p53 generesulting in negative immunostaining; however, missense mutations(especially G to T trans versions) accompanied by stabilization of thep53 protein represent the most frequent change in lung tumors (32).
Fig. 2. Fhil immunostaining modulation in adeno-
carcinoma. A, hronchoalveolar carcinoma showingareas with strong and weak immunoreaclivity. Noiethe increasing cytological grading from K lo C, i.e.,the larger nuclear si/c and increased chromasia aswell as milotic rale in ('. which parallels the decreased
immunoreactivily of Fhit staining.
; -v^
£
I
I
5034
on May 20, 2015. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

LOSS OF Fhit IN LUNG CANCER
Table 2 Smoking habits and Fhit reactivity
Fhit reactivity
AllcasesNonsmokersSmokersAdenocarcinoma
onlyNonsmokersSmokersPositive141151074Negative93364108Total2345114182%
Fhitnegative39752959P0.00050.049
metaplasia lesions either within the tumor or at the resection marginof the surgical specimens (Fig. 4, A and B); however, in several casesof incomplete metaplasia, Fhit immunostaining was weaker than thatin the normal bronchus (Fig. 4C). The modulation of Fhit expressionin the bronchial lesions of increasing grade, occurring in 34 patients,is reported in Table 4. A progressive loss of Fhit protein expressionoccurred in 3 of 5 cases of moderate dysplasia lesions and in 14 of 14severe dysplasia lesions, whereas the single case of mild dysplasiaanalyzed showed positive immunoreactivity. (Figs. 5 and 6). Negative
100-|
80-
60-
40-
20-
100-
80-
60-
40-
20-
Fhit-, Fhit +
T
60 120months
180
B
FhitFhit
p = 0.1
60 120months
180
Fig. 3. Survival curves of the series. Overall survival according to Fhit expression inthe whole series (A) and in the subset of adenocarcinoma (ß).Curves were calculated byKaplan-Meier estimate, using log-rank testing for the assessment of statistical signifi
cance.
The overall frequency of the tumors showing either Fhit-negativeimmunostaining or p53-positive immunoreactivity was 83%; thus, the
use of these two markers could be a remarkably sensitive tool for lungcancer screening. An even higher sensitivity, i.e., 91%, could beachieved by adding EGFR immunostaining of the tumor samples.
Loss of Fhit Expression in Precancerous Lesions. The Fhit protein was clearly detectable by immunohistochemistry in the normalbronchial mucosa at the resection margin of the 309 patients analyzed.Fhit immunoreactivity was homogeneously observed in the cytoplasmof basal cells as well as in the differentiated columnar cells. The highlevel of Fhit expression in the normal bronchus suggests a possiblerole in the control of cell proliferation of bronchial cells that isdisrupted during tumorigenesis. Positive Fhit immunostaining wasobserved in 326 hyperplastic bronchial mucosa and in 78 squamous
Table 3 Correlation between Fhit anil other markers in the tumor
Fhit reactivity
p53PositiveNegativeEgFRPositiveNegativeBcI2PositiveNegativePositive4681537415110Negative16617717716362270Total21225823023777380%
Fhitnegative786977698171P0.0180.0470.67
¿
Fig. 4. Fhit immunoreactivity in bronchial mucosa. Strong Fhit immunostaining isshown in (A) early subcolumnar hyperplasia and (B) micropapillary hyperplasia. C,incomplete squamous metaplasia displaying a weaker Fhit immunoreactivity.
5035
on May 20, 2015. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

LOSS OF Fhic IN LUNG CANCER
Table 4 Ciirrelalitm henrren f-'hil ami p5i in preinvasine bronchial lesions
Fhit reactivity Fhit negative
CISDysplasiaAny
lesionTotalp_53PositiveNegativeNot
évaluablePositiveNegativePositiveNegativePositive000!2123Negative1573710221742Total1573812231945%
Overall %P"1001001008883%899310083
1.093
0.58
"Two-sided Fisher's exaet test.
immunostaining was observed in all 25 (100%) CIS lesions occurringcither adjacent to the tumor or at the resection margin of the surgicalsamples. Overall. 17 of 20 (85%) dysplastic lesions and 42 of 45(93%) precancerous lesions showed negative Fhit immunostaining.
A high (81%) concordance was observed between the results ofFhit immunostaining in the high-grade precancerous lesions and the
invasive tumor occurring in the same patient.When the same serially cut sections containing the preinvasive
lesions were immunostuined for p53. an inverse correlation betweenFhit and p53 immunostaining was observed in dysplastic and CISlesions (Table 4; Fig. 6). In fact, p53 overexpression and loss of Fhitprotein expression were concordant in these lesions. However, thefrequency of Fhit-negative high-grade preinvasive lesions (dysplasia
and CIS) was significantly higher than that of p53 overexpression (93versus 55%: P = 0.00013) and reflected that observed in tumors of the
squamous type. Thus, the level of sensitivity of Fhit immunostainingis higher than that achieved by p53 immunoreactivity in precancerouslesions. These findings reinforce the hypothesis that FHIT may act asa gatekeeper in the lung carcinogenetic process, and the similartemporal sequence of Fhit and p53 alterations in lung carcinogenesispoints to a role for both pathways in lung carcinogenesis.
Discussion
In the present study, we analy/.ed the largest series of lung tumors andbronchial mucosa samples reported thus far for the expression of a novel
tumor suppressor gene. FHIT, and its correlation with three other well-
established molecular markers of lung cancer: (a) p53; (h) EGFR; and (c)BCL2. The series was homogeneous by stage and treatment and wasenriched by prolonged and intensive clinical follow-up. With the number
of patients available, the power of the statistical test should have detectedany correlation of major significance. The results show that altered Fhitexpression is the most frequent genetic change in lung tumors and is anindependent biological marker. We did not observe a major impact ofFhit expression on prognosis, a finding similar to that reported for p53abnormal expression in the same series (28). This is not surprising,because the inactivation of both genes is involved in the early phases oflung carcinogenesis and hence is more likely related to the initiation ofthe neoplastic process rather than to the progression to invasive tumor anddistant metastasis.
Our observations of the loss of Fhit protein expression in a substantialpercentage of primary NSCLCs and in precancerous lesions that wereeither adjacent or distant from the tumor suggest that FHIT alterationsplay an important role in the growth control of bronchial cells. This isparticularly true for squamous cell carcinoma, which is often associatedwith precursor dysplastic lesions of various types, where the progressiveloss of Fhit protein was demonstrated to be an early event, likely leadingto altered control of cell growth and/or apoptosis. The assessment of themechanisms of Fhit action will permit the elucidation of specific pathways by which Fhit affects the tumorigenic process.
Loss of Fhit expression was significantly associated with tumorsoccurring in heavy smokers, a finding consistent with our previousobservation of a higher rate of LOH at the FHIT locus in the lung tumorsof smokers versus those of nonsmokers (33). This suggests that FHITplays a specific role as a sensor of smoke-related carcinogenic damage
leading to the loss of FHIT function. One has to take into account thedifferent prevalence of female lung cancer in the United States andNorthern Europe; nonetheless, the excess of male lung cancers is associated with smoking. In our data, the loss of Fhit expression amongsmoking females was very similar to that observed in males (65 versus75%).
In conclusion, this study demonstrates in a large series of stage INSCLCs. precancerous lesions, and bronchial tissues that loss of the
Fig. 5. Fhit and Mihl immunoreactivity in bronchial lesions occurring at the bronchial resectionmargin of a lung cancer patient. A. a progressivedecrease in Fhit immunoreactivity starting fromhasal cell hvperplasia to moderate/severe dysplasiaand questionable early invasive squamous carcinoma (leßin riffln). H. a progressive increase inMihl-positive nuclei in the same lesions.
5036
on May 20, 2015. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
LOSS OF Fhil IN LUNG CANCER
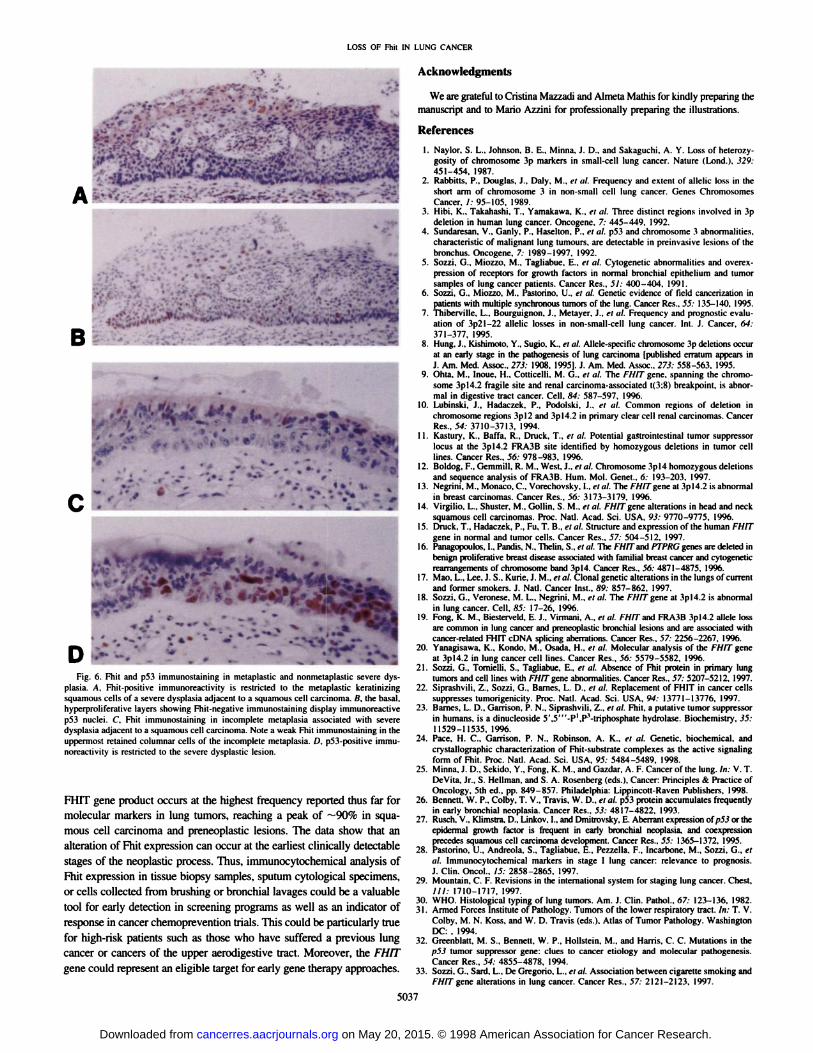
Fig. 6. Fhit and p53 immunostaining in metaplaslic and nonniclaplastic severe dys-plasia. A. Fhit-positivc immunoreaclivily is restricted lo the melaplastic keratinizingsquamous cells of a severe dysplasia adjacent to a squamous cell carcinoma, fl. the hasal.hyperproliferative layers showing Fhit-negative inimunosiaining display immunoreactive
p53 nuclei. C. Fhil immunostammg in incomplete metaplasia associated with severedysplasia adjacent to a squamous cell carcinoma. Note a weak Fhit immunostaining in theuppermosl retained columnar cells of the incomplete metaplasia. /). p53-positive immu-
noreactivity is restricted to the severe dysplastic lesion.
FHIT gene product occurs at the highest frequency reported thus far formolecular markers in lung tumors, reaching a peak of —¿�90%in squa
mous cell carcinoma and preneoplastic lesions. The data show that analteration of Fhit expression can occur at the earliest clinically detectablestages of the neoplastic process. Thus, immunocytochemical analysis ofFhit expression in tissue biopsy samples, sputum cytological specimens.or cells collected from brushing or bronchial lavages could be a valuabletool for early detection in screening programs as well as an indicator ofresponse in cancer chemoprevention trials. This could be particularly truefor high-risk patients such as those who have suffered a previous lung
cancer or cancers of the upper aerodigestive tract. Moreover, the FHITgene could represent an eligible target for early gene therapy approaches.
Acknowledgments
We are grateful to Cristina Ma/zadi and Almeta Mathis tor kindly preparing themanuscript and to Mario A//.ini for professionally preparing the illustrations.
References
1. Naylor. S. L.. Johnson. B. E.. Minna, ¡.D.. and Sakaguchi. A. Y. Loss of heieiw.y-gosity of chromosome 3p markers in small-cell lung cancer. Nature (Lond.), 329:451-454. 1987.
2. Rabbins. P.. Douglas. !.. Daly. M., et al. Frequency and extent of allelic loss in theshort arm of chromosome 3 in non-small cell lung cancer. Genes ChromosomesCancer. I: 95-105. 1989.
3. Hihi. K.. Takahashi. T.. Yamakawa. K.. el ill. Three distinct regions involved in 3pdeletion in human lung cancer. Oncogene. 7: 445-449. 1992.
4. Sundaresan. V., Ganly. P.. Haselton. P.. el ill. p53 and chromosome 3 abnormalities,characteristic of malignant lung tumours, are detectable in preinvasive lesions of thebronchus. Oncogene. 7: 1989-1997. 1992.
5. Sozzi. G.. Miozzo. M.. Tagliabue. E., el al. Cytogenelic abnormalities and overex-
pression of receptors for growth factors in normal bronchial epithelium and tumorsamples of lung cancer patients. Cancer Res., 51: 4(X)-4()4. 1991.
6. So//.¡.G.. Mioz/o, M.. Pastorino. U., el al. Genetic evidence of field canceri/ation inpatients with multiple synchronous tumors of the lung. Cancer Res.. 55: 135-140. 1995.
7. Thiberville. L.. Bourguignon. !.. Metayer. J.. ft til. Frequency and prognostic evaluation of 3p21-22 allelic losses in non-small-cell lung cancer. Int. J. Cancer. 64:371-377. 1995.
8. Hung. J.. Kishimoto. Y.. Sugio. K.. et al. Allelc-spccific chromosome 3p deletions txxurat an early stage in the pathogenesis of lung carcinoma [published erratum appears inJ. Am. Med. Assoc.. 271: 1908. 1995]. J. Am. Med. Assoc.. 273: 558-563. 1995.
9. Ohta. M.. Inoue. H.. Cottieelli. M. G.. et al. The /-V//7"gene, spanning the chromo
some 3pl4.2 fragile site and renal carcinoma-associated 1(3:8) breakpoint, is abnormal in digestive tract cancer. Cell. 84: 587-597. 1996.
10. Lubinski. J.. Hadaczck. P.. Podolski. J.. i-t til. Common regions of deletion in
chromosome regions 3pl2 and 3pl4.2 in primary clear cell renal carcinomas. CancerRes.. 54: 3710-3713. 1994.
11. Kastury. K.. Batta. R.. Druck, T., et al. Potential gastrointestinal tumor suppressorlocus at the 3pl4.2 FRA3B site identified by homo/ygous deletions in tumor celllines. Cancer Res.. 56: 978-983, 1996.
12. Boldog. F.. Gemmili. R. M.. West. J.. et al. Chromosome 3pl4 homozygous deletionsand sequence analysis of FRA3B. Hum. Mol. Genet., fi: 193-203. 1997.
13. Negrini. M.. Monaco. C.. Vorechovsky. I., el ni. The /-'/y/7gene at 3pl4.2 is abnormal
in breast carcinomas. Cancer Res.. 56: 3173-3179. 1996.14. Virgilio. L.. Shuster. M.. Gollin. S. M., et al. FHIT gene alterations in head and neck
squamous cell carcinomas. Proc. Nati. Acad. Sci. USA. 93: 9770-9775. 1996.15. Druck. T.. Hadac/ek. P., Fu, T. B., et ni. Structure and expression of the human FHIT
gene in normal and tumor cells. Cancer Res., 57: 504-512. 1997.16. Panagopoulos. I.. Pandis. N.. Thelin. S.. el al. The I-HIT and PTPRC genes are deleted in
benign proliferarne breast disease associated with familial breast cancer and cylogeneticrearrangements of chromosome band 3pl4. Cancer Res.. 56: 4871—1875,1996.
17. Mao. L.. Lee. J. S.. Kurie. J. M..elal. Clonal genetic alterations in the lungs of currentand former smokers. J. Nail. Cancer Inst.. Ä9:857-862. 1997.
18. So//.i. G.. Veronese. M. L., Negrini, M.. el al. The /-Y//rgene at 3pl4.2 is abnormalin lung cancer. Cell. 85: 17-26. 1996.
19. Fong. K. M.. Biestcrveld. E. J.. Virmani, A., el al. FHIT and FRA3B 3pl4.2 alÃelelossare common in lung cancer and preneoplastic bronchial lesions and are associated withcancer-related FHIT cDNA splicing aberrations. Cancer Res.. 57: 2256-2267, 19%.
20. Yanagisawa. K.. Kondo. M.. Osada. H., el al. Molecular analysis of the FHIT geneat 3pl4.2 in lung cancer cell lines. Cancer Res.. 56: 5579-5582. 1996.
21. Soz/.i. G.. Tornielli, S.. Tagliabue. E., et al. Absence of Fhit protein in primary lungtumors and cell lines with FHIT gene abnormalities. Cancer Res.. 57: 5207-5212. 1997.
22. Siprashvili. Z.. Sozzi. G.. Barnes. L. D.. el al. Replacement of FHIT in cancer cellssuppresses tumorigenicity. Proc. Nati. Acad. Sci. USA. 94: 13771-13776. 1997.
23. Bames. L. D.. Garrison, P. N.. Siprashvili. Z.. et al. Fhit. a putative tumor suppressorin humans, is a dinucleoside 5'.5"'-P',P'-triphosphate hydrolase. Biochemistry. 35:
11529-11535. 1996.24. Pace. H. C., Garrison. P. N., Robinson, A. K., et al. Genetic, biochemical, and
crystallographic characterization of Fhit-substrate complexes as the active signalingform of Fhit. Proc. Nati. Acad. Sci. USA, M: 5484-5489. 1998.
25. Minna. J. D., Sckido, Y.. Hong. K. M.. and Cia/dar. A. F. Cancer of the lung. In: V. T.DeVtta. Jr., S. Hellman. and S. A. Rosenberg (eds.). Cancer: Principles & Practice ofOncology. 5th éd..pp. 849-857. Philadelphia: Lippincolt-Raven Publishers. 1998.
26. Bennett. W. P.. Colby. T. V.. Travis. W. D., el al. p53 protein accumulates frequentlyin early bronchial neoplasia. Cancer Res.. 53: 4817-4822. 1993.
27. Rusch. V., Klimstra. D.. Linkov. I., and Dmitrovsky, E. Aberrant expression of ;>5.for theepidermal growth factor is frequent in early bronchial neoplasia, and coexpressionprecedes squamous cell carcinoma development. Cancer Res.. 55: 1365-1372. 1995.
28. Pastorino. U.. Andreola. S.. Tagliabue. E.. Pezzetta. F.. Incarbone. M.. Sozzi. G., elal. Immunocylocheniical markers in stage I lung cancer: relevance to prognosis.J. Clin. Oncol.. /5: 2858-2865. 1997.
29. Mountain. C. F. Revisions in the international system for staging lung cancer. Chest.///: 1710-1717. 1997.
30. WHO. Histológica! typing of lung tumors. Am. J. Clin. Pathol.. 67: 123-136. 1982.31. Armed Forces Institute of Pathology. Tumors of the lower respiratory tract. In: T. V.
Colby, M. N. Koss. and W. D. Travis (eds.). Atlas of Tumor Pathology. WashingtonDC: . 1994.
32. Greenblatt. M. S.. Bennett. W. P., Hollstein. M., and Harris. C. C. Mutations in thep53 tumor suppressor gene: clues to cancer etiology and molecular pathogenesis.Cancer Res.. 54: 4855-4878. 1994.
33. Sozzi. G., Sard. L.. De Gregorio, L., el al. Association between cigarette smoking andgene alterations in lung cancer. Cancer Res.. 57: 2121-2123. 1997.
5037
on May 20, 2015. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
1998;58:5032-5037. Cancer Res Gabriella Sozzi, Ugo Pastorino, Luisa Moiraghi, et al. Bronchial Lesions
Function in Lung Cancer and PreinvasiveFHITLoss of
Updated version
http://cancerres.aacrjournals.org/content/58/22/5032
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
To request permission to re-use all or part of this article, contact the AACR Publications
on May 20, 2015. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from