
Maternal Immunity Provides Protection against Pertussis in Newborn Piglets

Bordetella pertussis
http://www.hhmi.princeton.edu/sw/2002/psidelsk/Microlinks.htm
Dr. M. Noofeli

Outline
Bordetella Pertussis microbiology
Whooping Cough/Pertussis
Vaccine
Current problems with B. pertussis
2

Bordetella pertussis Basics
Aerobic, Gram negative coccobacillus
Alcaligenaceae Family
Specific to Humans
Colonizes the respiratory tract
Whooping Cough (Pertussis)
3 http://microvet.arizona.edu/Courses/MIC420/lecture_notes/bordetella_pertussis/
gram_pertussis.html

What is Pertussis?
Whooping cough, “The Cough of 100 Days”
4

Transmission
Very Contagious
Transmission occurs via respiratory droplets
5 http://www.ratbags.com/rsoles/history/2000/12december.htm http://www.universityscience.ie/imgs/scientists/whoopingcough.gif

Spread of Pertussis: Then vs. Now
6

7
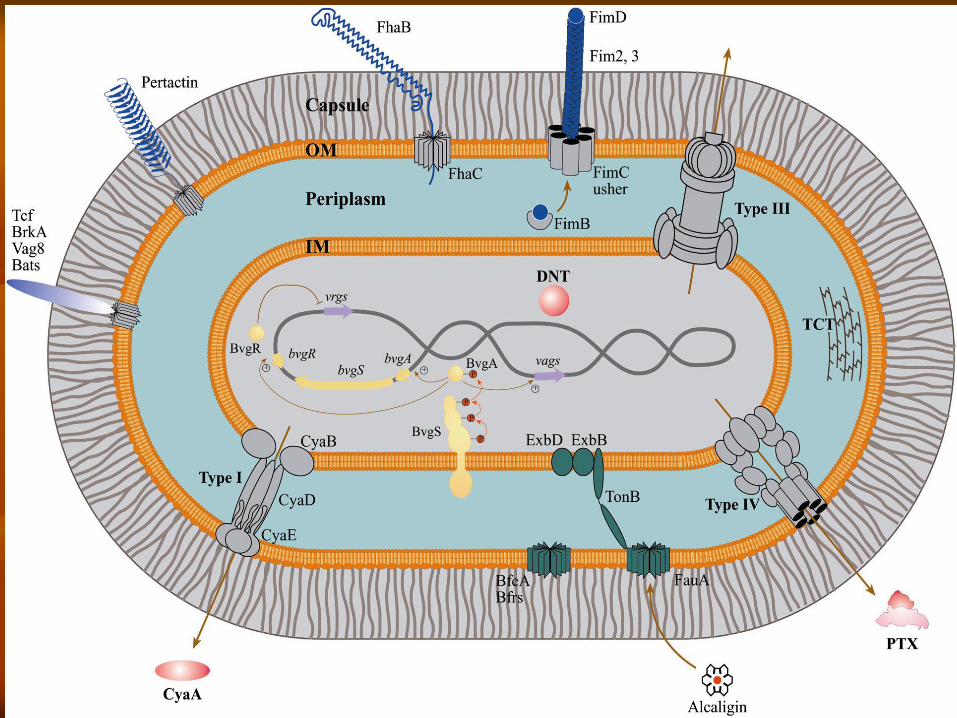
Virulence Factors
Adhesions
Filamentous hemagglutinin (FHA)
Pertactin
Fimbriae
Colonization of tracheal epithelial cells
by Bordetella pertussis
*Filamentous hemagglutinin is an adhesin that allows the bacterium
to adhere to galactose residues of the glycolipids on the membrane
of ciliated epithelial cells of the respiratory tract.
*Pertussis toxin also functions as an adhesin. One subunit of the
pertussis toxin remains bound to the bacterial cell wall while another
subunit binds to the glycolipids on the membrane of ciliated epithelial
cells of the respiratory tract.
*B. Pertussis also produces an adhesin called pertactin that further
enables the bacterium to adhere to cells.

8
Virulence Factors Cont..
Toxins
Pertussis Toxin (PTX)
Colonizing factor
Cell Bound
Extracellular
Adenylate Cyclase Toxin (CYA)
Invasive toxin
Activated by host cell calmodulin
Tracheal Cytotoxin (TCT)
Disaccharide tetrapeptide

Adhesions
Filamentous hemagglutinin
Pertactin
Fimbriae
9 http://www.rivm.nl/infectieziektenbulletin/bul1306/kinkhoest.jpg
http://www.my-pharm.ac.jp/~yishibas/research/Pertussis1.jpg

Toxins
Pertussis Toxin
Adenylate Cyclase Toxin
Tracheal cytotoxin
Dermonecrotic toxin
Heat-labile toxin
10 www.ibl.fr/u447/u447.htm

Pertussis Toxin
Colonizing factor and endotoxin
Cell bound and extracellular
11
gsbs.utmb.edu/ microbook/ch031.htm www.med.sc.edu:85/ ghaffar/pertussis.jpg

Adenylate Cyclase Toxin
Invasive toxin
Activated by host cell calmodulin
Impairment of immune effector cells
12
Babu et al., 2001
13
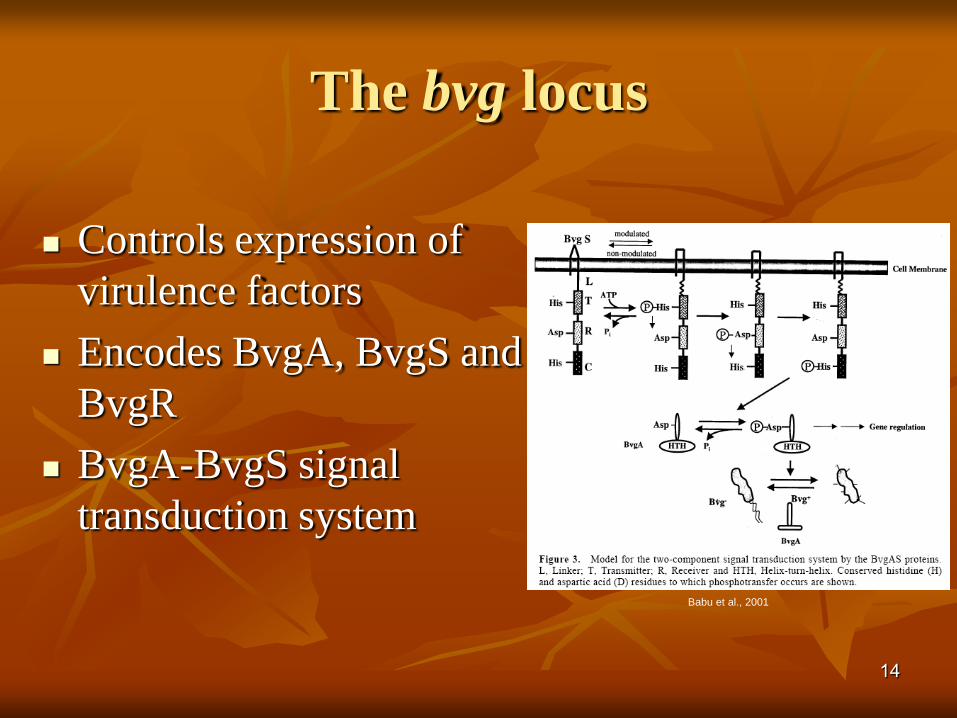
The bvg locus
Controls expression of
virulence factors
Encodes BvgA, BvgS and
BvgR
BvgA-BvgS signal
transduction system
14
Babu et al., 2001

Whooping Cough
Also known as Pertussis
Outbreaks first described in the 16th Century
Major cause of childhood fatality prior to
vaccination
15 paaap.org/immunize/ course/slide27.html

16
Pertussis Among Adolescents and
Adults Disease often milder than in infants and children
Infection may be asymptomatic, or may present as classic pertussis
Persons with mild disease may transmit the infection
Older persons often source of infection for children
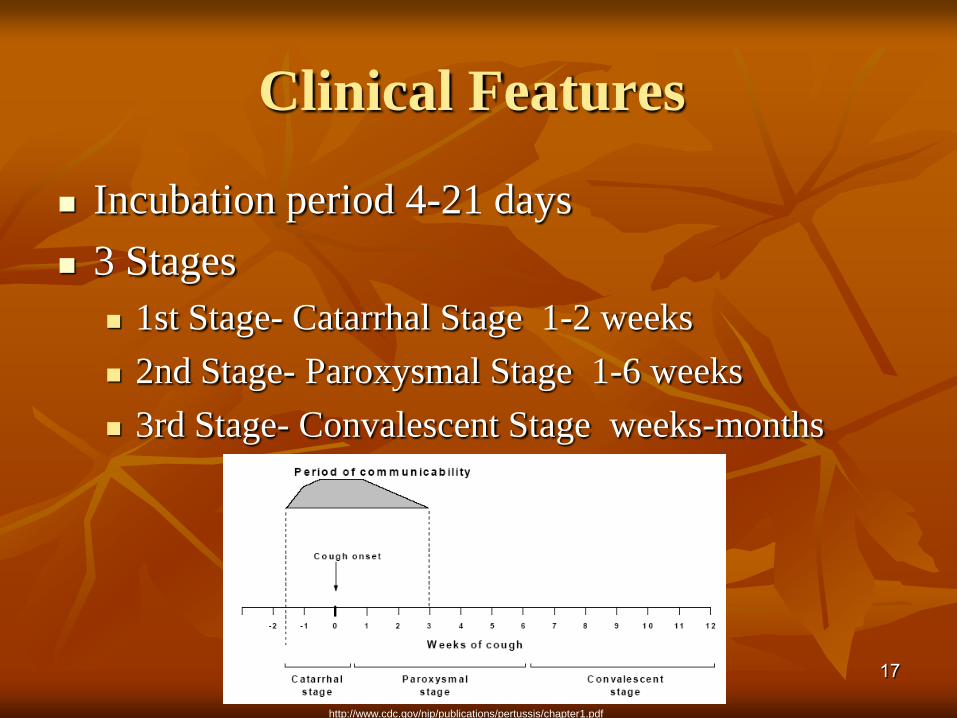
Clinical Features
Incubation period 4-21 days
3 Stages
1st Stage- Catarrhal Stage 1-2 weeks
2nd Stage- Paroxysmal Stage 1-6 weeks
3rd Stage- Convalescent Stage weeks-months
17
http://www.cdc.gov/nip/publications/pertussis/chapter1.pdf
18
Incubation period 4-21 days
3 Stages
1st Stage- Catarrhal Stage 1-2 weeks
runny nose, sneezing, low fever, and a mild cough (common mistaken for cold)
2nd Stage- Paroxysmal Stage 1-6 weeks
whooping cough, which consists of bursts or paroxysms of numerous, rapid coughs,
severity of the infection is at its greatest
3rd Stage- Covalescent Stage weeks-months
gradual recovery starts

19
Pertussis Complications*
Condition
Pneumonia
Seizures
Encephalopathy
Hospitalization
Death
Percent reported
4.9
0.7
0.1
16
0.2
*Cases reported to CDC 2001-2003 (N=28,998)

Diagnosis
Isolation by culture
PCR
Direct fluorescent antibody
Serological testing
20 http://medinfo.ufl.edu/year2/mmid/bms5300/images/d7053.jpg
21
Test only patients with signs and symptoms of pertussis
Within 3 weeks of cough onset
Nasopharyngeal swab or aspirate
Prepare and administer vaccines in areas separate from pertussis specimen collection
Wear gloves immediately before and during specimen collection or vaccine preparation and administration with immediate disposal of gloves after the procedure, and
Clean surfaces using a 10% bleach solution to reduce the amount of nucleic acids in the clinic environment.
Treatment
Antibiotic therapy
Erythromycin
Azithromycin and clarithromycin
22
http://www.aboutthatbug.com/AboutThatBug/files/CCLIBRARYFILES/
FILENAME/0000000032/033_lg.jpg http://www.vet.purdue.edu/bms/courses/lcme510/chmrx/macrohd.htm

Pertussis Vaccine
1st Pertussis vaccine- whole cell
Acellular vaccine now used
Combination vaccines
23 http://www.nfid.org/publications/clinicalupdates/pediatric/pertussis.html
http://www.tdh.state.tx.us/immunize/providers.htm

24
Pertussis-containing Vaccines
DTaP (pediatric)
approved for children 6 weeks through 6 years (to
age 7 years)
Tdap (adolescent and adult)
approved for persons 10 through 64 years
(Boostrix) and 11 through 64 years (Adacel)

Vaccine Schedule:
Expanded to Adults!
DTaP
2, 4, 6 months
15-18 months
4-6 years
Tdap
11-12 years
One dose between 19-
64 (instead of Td)
Any adult in contact
with infant <1 y.o.
25
26
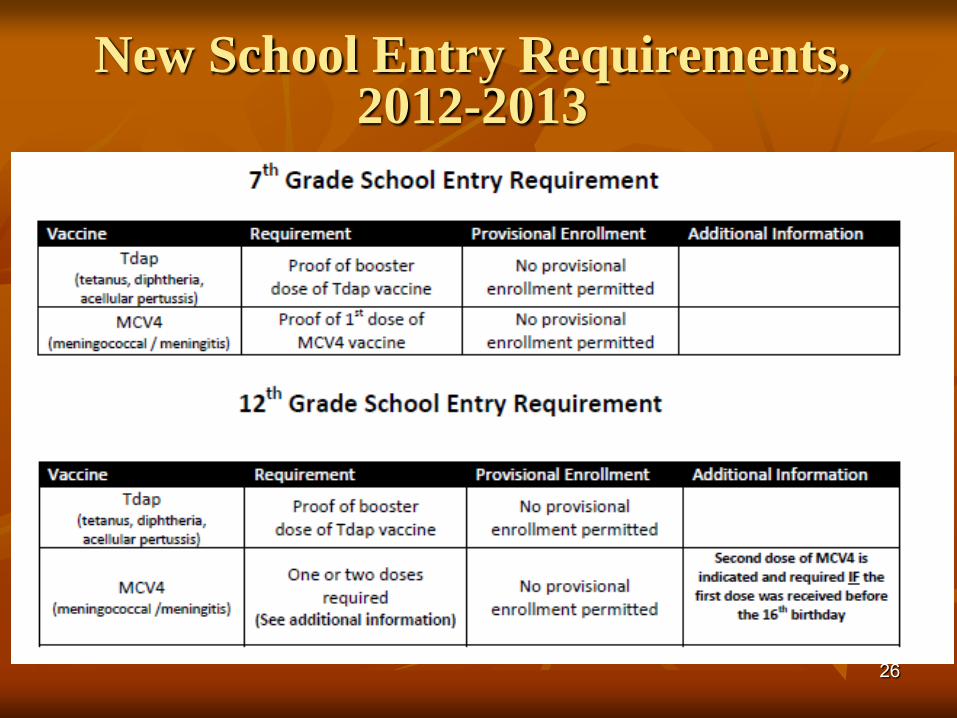
New School Entry Requirements, 2012-2013
27

28
Pertussis Vaccination of (Teens and) Adults
Who What
Pregnant or post-
partum women not
previously
vaccinated with
Tdap
• one dose of Tdap during the third trimester or late second
trimester*
• One dose of Tdap in the immediate postpartum period before
discharge from hospital or birthing center if not previously
vaccinated with Tdap or status unknown*
Healthcare personnel
who have not
previously received
Tdap as an adult
• A single dose of Tdap is recommended for health care
personnel and who have direct patient contact*
• Prioritize those who have direct contact with infants
28
*can be administered regardless of interval since the previous Td dose. Shorter
intervals may be appropriate if your patient is at high risk for contracting pertussis,
or has close contact with infants.
29
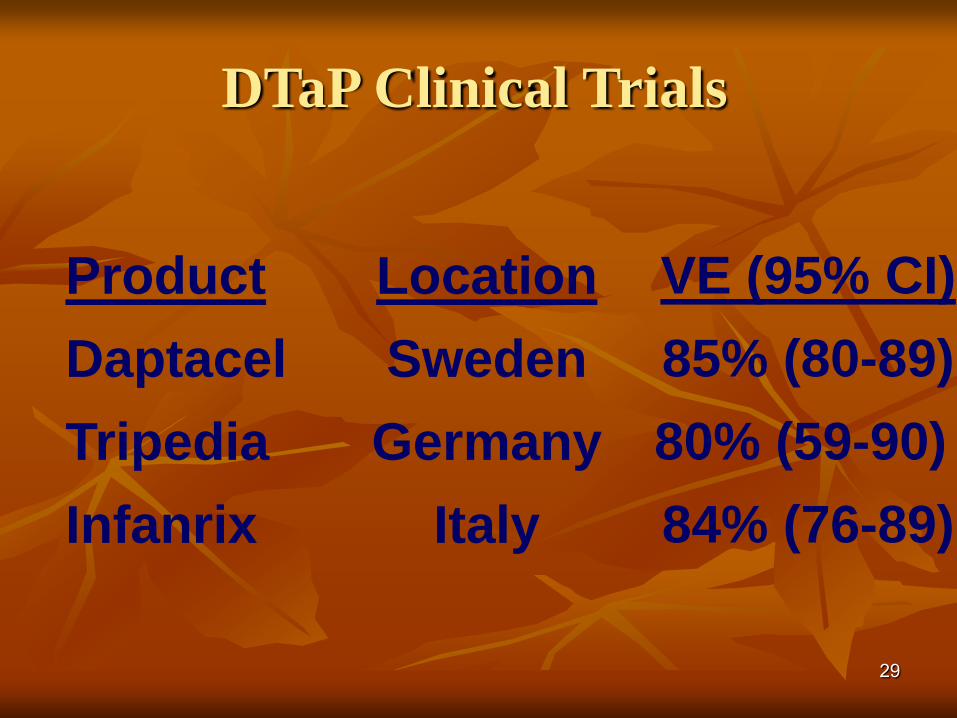
DTaP Clinical Trials
Product
Daptacel
Tripedia
Infanrix
Location
Sweden
Germany
Italy
VE (95% CI)
85% (80-89)
80% (59-90)
84% (76-89)
30
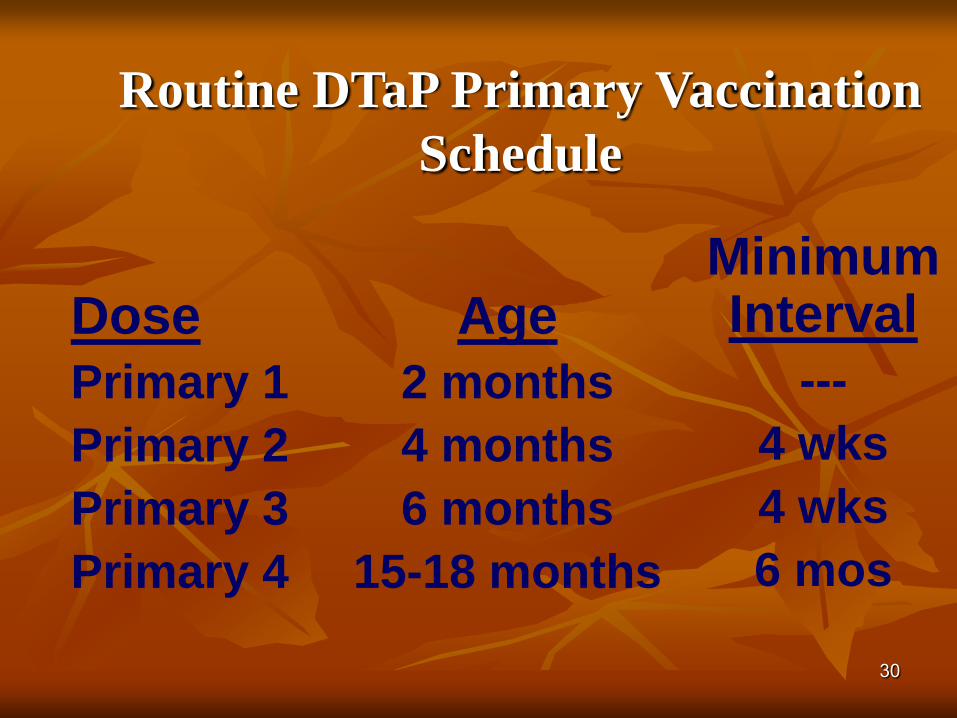
Routine DTaP Primary Vaccination
Schedule
Dose
Primary 1
Primary 2
Primary 3
Primary 4
Age
2 months
4 months
6 months
15-18 months
Minimum Interval
---
4 wks
4 wks
6 mos
31
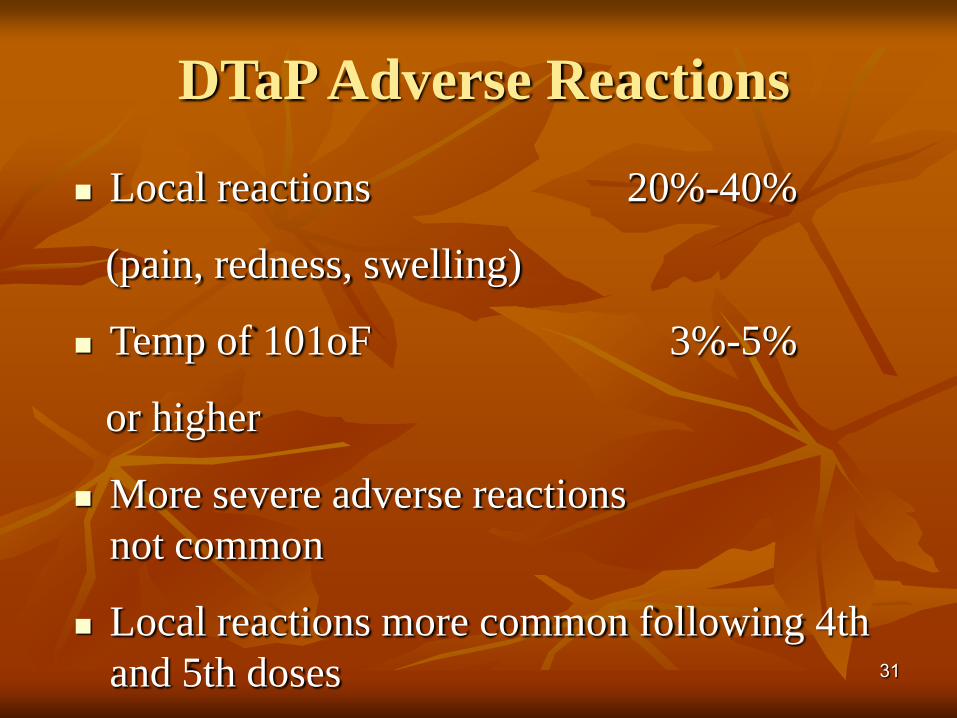
DTaP Adverse Reactions
Local reactions 20%-40%
(pain, redness, swelling)
Temp of 101oF 3%-5%
or higher
More severe adverse reactions
not common
Local reactions more common following 4th
and 5th doses

32
Adverse Reactions Following the 4th
and 5th DTaP Dose
Local adverse reactions and fever increased with
4th and 5th doses
of DTaP
Reports of swelling of entire limb
Extensive swelling after 4th dose NOT a
contraindication to 5th dose

33
DTaP Contraindications
Severe allergic reaction to vaccine
component or following a prior dose
Encephalopathy not due to another
identifiable cause occurring within 7 days
after vaccination
34
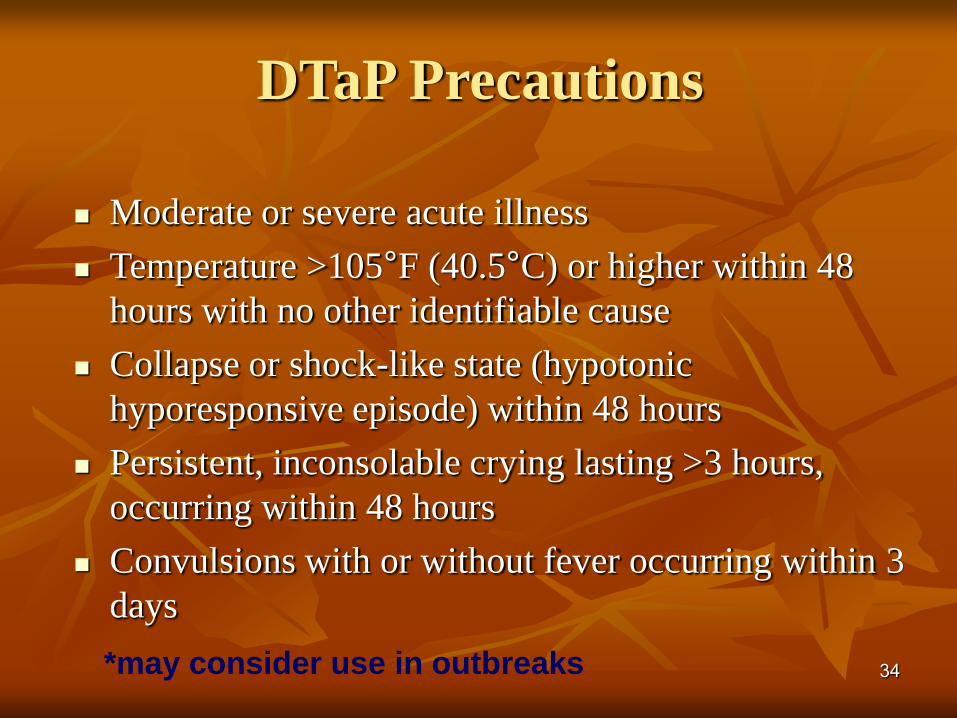
DTaP Precautions
Moderate or severe acute illness
Temperature >105°F (40.5°C) or higher within 48
hours with no other identifiable cause
Collapse or shock-like state (hypotonic
hyporesponsive episode) within 48 hours
Persistent, inconsolable crying lasting >3 hours,
occurring within 48 hours
Convulsions with or without fever occurring within 3
days
*may consider use in outbreaks

35
Pertussis Among Adolescents
and Adults
Prolonged cough (3 months or longer)
Post-tussive vomiting
Multiple medical visits and extensive medical evaluations
Complications
Hospitalization
Medical costs
Missed school and work
Impact on public health system

36
Recommendations for Tdap
Vaccination of Adolescents
Adolescents 11 or 12 years of age should receive a
single dose of Tdap instead of Td*
Adolescents 13 through 18 years who have not
received Tdap should receive a single dose of Tdap
as their catch-up booster instead of Td*
*if the person has completed the recommended childhood
DTaP/DTP vaccination series, and has not yet received a
Td booster
MMWR 2006;55(RR-3):1-43.

37
Tdap Vaccination of Adults
19 Through 64 Years of Age
Single dose of Tdap to replace a single dose of Td
May be given at an interval less than 10 years
since receipt of last tetanus toxoid-containing
vaccine
Special emphasis on adults with close contact with
infants (e.g., childcare and healthcare personnel,
and parents)
MMWR 2006;55(RR-17):1-37.

Increase in Pertussis cases
Incidence of disease increasing in countries
with high vaccination levels
US- Massachusetts
Netherlands
France
Finland
38
http://www.cdc.gov/nip/publications/pertussis/chapter1.pdf

Increased awareness and reporting
Better tests
Waning immunity in adults
39
Why is the Incidence of Pertussis
Increasing?

Cases in 2003
40 http://www.pertussis.com/digest/index.html

41
0
5000
10000
15000
20000
25000
30000
1980 1985 1990 1995 2000 2005
Ca
se
sPertussis—United States, 1980-2007
Year
42
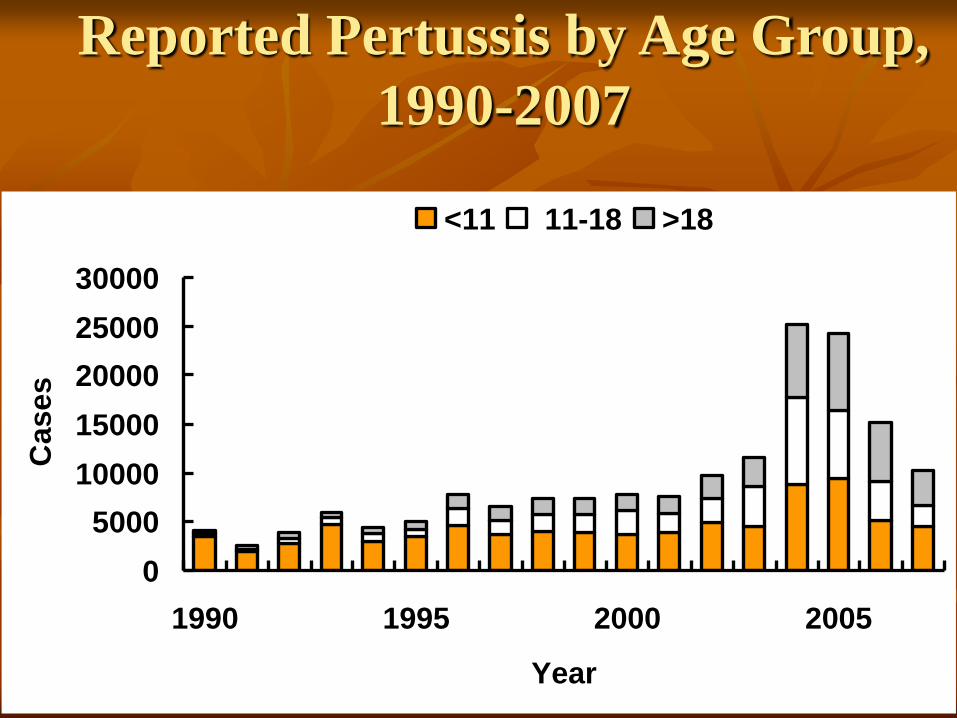
Reported Pertussis by Age Group,
1990-2007
0
5000
10000
15000
20000
25000
30000
1990 1995 2000 2005
Year
Cas
es
<11 11-18 >18

Netherlands
Mismatch between
vaccine strains and
circulating strains
played role in
reemergence
43
Mooi et al., 2001

Strain Variation
B. pertussis population has changed
significantly since vaccine introduction
Adaptation to vaccine
Antigenic divergence
44 Mooi et al., 2001

Vaccine problems
Complications/Safety
Multiple administration
Waning adolescent and adult immunity
Strain Variability
45
http://www.healthcareforhoosiers.com/Member/vaccineschedule.html

46
Live attenuated pertussis vaccines
Are they the future of
pertussis control ?

47
Live attenuated B. pertussis for intranasal
administration
Mucosal administration Induction of systemic and mucosal immune responses
Ease of administration
Persistence of the bacteria in the host
Long-lived immune responses
Reduced number of administrations to induce
protection
Potential as a multivalent vaccine

Conclusions
Reemerging in adult and adolescent
populations as worldwide vaccination rates
increase
High vaccination rates not enough
Better vaccine development needed
48
References
Ahuja, N., Kumar, P., Bhatnagar, R. The Adenylate Cyclase Toxins. Critical Reviews in Microbiology.
2004; 30(3): 187-196.
Babu, MM., Bhargavi, J., Singh Saund, R., Singh, S.K. Virulence Factors in Bordetella pertussis. Current
Science. June 2001; 80(12): 1512-1522.
Coote, JG. Environmental Sensing Mechanisms in Bordetella. Advances in Microbial Physiology. 2001;
44: 141-181.
Dalet, K., Weber, C., Guillemot, L., Njamkepo, E., Guiso, N. Characterization of Adenylate Cyclase-
Hemolysin Gene Duplication in a Bordetella pertussis isolate. Infection and Immunity. Aug 2004; 72(8):
4874-4877.
Forsyth, K.D., Campins-Marti, M., Caro, J., Cherry, J.D., Greenberg, D., Guiso, N., Heininger, U.,
Schellenkens, J., Tan, T., von Konig, C., Plotkin, S. New Pertussis Vaccination Strategies beyond Infancy:
Recommendations by the Global Pertussis Initiative. Clinical Infectious Diseases. Dec 2004: 39: 1802-
1809.
Hardwick, T.H., Cassiday, P., Weyant, R.S., Bisgard, K.M., Sanden, G.N. Changes in the Predominance
and Diversity of Genomic Subtypes of Bordetella pertussis Isolated in the United States, 1935-1999.
Emerging Infectious Diseases. Jan 2002; 8(1): 44-49.
Mattoo, S., Foreman-Wykert, A., Cotter, P., Miller, J. Mechanisms of Bordetella Pathogenesis. Frontiers
in Bioscience. Nov 2001; 6: E168-186
Merkel, T.J., Stibitz, S., Keith, J.M., Leef, M., Shahin, R. Contribution of Regulation by the bvg Locus to
Respiratory Infection of Mice by Bordetella pertussis. Infection and Immunity. Sept 1998; 66(9): 4367-
4373.
49
Reference cont.
Mooi, F.R., van Loo, I.H.M., King, A.J. Adaptation of Bordetella pertussis to Vaccination: A Cause for Its
Reemergence? Emerging Infectious Disease. June 2001; 7(No. 3 Supplement): 526-528.
Pishko, E.J., Betting, D.J., Hutter, C.S., Harvill, E.T. Bordetella pertussis Aquires Resistance to
Complement Mediated Killing In Vivo. Infection and Immunity. Sept 2003; 71(9): 4936-4942.
Robbins, J.B., Schneerson, R., Trollfors, B., Sato, H., Sato, Y., Rappuoli, R., Keith., J.M. The Diphtheria
and Pertussis Components of the Diphtheria-Tetanus Toxoids-Pertussis Vaccine Should Be Genetically
Inactivated Mutant Toxins. The Journal of Infectious Diseases. 2005;191: 81-88.
Schouls, L.M., van der Heide, H.G.J., Vauterin, L., Vaurerin, P., Mooi, F.R. Multiple-Locus Variable-
Number Tandem Repeat Analysis of Dutch Bordetella pertussis Strains Reveals Rapid Genetic Changes
with Clonal Expansion during the Late 1990s. Journal of Bacteriology. Aug 2004; 186(16): 5496-5505.
Shumilla, J.A., Lacaille, V., Hornell, M.C., Haung, J., Narasimhan, S., Relman, D.A., Mellins, E.D.
Bordetella Pertussis Infection of Primary Human Monocytes Alters HLA-DR Expression. Infection and
Immunity. Mar 2004; 72(3): 1450-1462.
Steele, RW. Pertussis: Is Eradication Achievable? Pediatric Annals. Aug 2004; 33(8): 525-534.
Veal-Carr, W., Stibitz, S. Demonstration of differential virulence gene promoter activation in vivo in
Bordetella pertussis using RIVET. Molecular Microbiology. 2005; 55(3): 788-798.
Yih, W.K., Lett, S.M., des Vignes, F.N., Garrison, K.M., Sipe, P.L., Marchant, C.D. The Increasing
Incidence of Pertussis in Massachusetts Adolescents and Adults, 1989-1998. The Journal of Infectious
Diseases. 2000; 182: 1409-1416.
50
Copyright © 2022 FDOKUMEN




















