The Construction Bone's Sexual Identity throughout Her Life in ...

Infectious Diseases
� ���
� � �� ���� �� ���� ��
�
��� � � � � � � � � � � �
� �� �
�
�������������
���������������������������������������
16.14����
http://infection.thelancet.com
ReprintRationale for pertussis booster vaccination
throughout life in Europe
Fred Zepp, Ulrich Heininger, Jussi Mertsola, Ewa Bernatowska, Nicole
Guiso, John Roord, Alberto E Tozzi, Pierre Van Damme
Lancet Infect Dis 2011; 11: 557–70
Published Online May 19, 2011
DOI: DOI:10.1016/S1473-3099(11)70007-X
Previously published online
Copyright 2011 ELSEVIER LIMITED, 32 Jamestown Road, London, NW1 7BY UK.

Reprint Sales Representative
Greg Davies
T: +44 (0) 20 7424 4422
F: + 44 (0) 207424 4433
The Lancet Infectious Diseases is a
monthly subscription journal. For
further information on how to
subscribe please contact our
Subscription Department
T: +44 (0) 1865 843077
F: +44 (0) 1865 843970
(North America)
T: +1 (800) 462 6198
F: +1 (800) 327 9021
Printed in USA by Sheridan Reprints
LN1296
© 2011 Elsevier Ltd. All rights reserved. This journal and the individual contributions contained in it are protected under copyright by Elsevier Ltd, and the following terms and conditions apply to their use.
Publication information The Lancet Infectious Diseases (ISSN 1473-3099) is published monthly by Elsevier (The Boulevard, Langford Lane, Kidlington, Oxford, OX5 1GB, UK). Periodicals postage paid at Rahway, NJ, USA. POSTMASTER: send address corrections to The Lancet Infectious Diseases c/o Mercury International, 365 Blair Road, Avenel, NJ 07001, USA.
Photocopying Single photocopies of single articles may be made for
personal use as allowed by national copyright laws. Permission of the
Publisher and payment of a fee is required for all other photocopying,
including multiple or systematic copying, copying for advertising or
promotional purposes, resale, and all forms of document delivery.
Special rates are available for educational institutions that wish to
make photocopies for non-profit educational classroom use.Permissions may be sought directly from Elsevier Global Rights
Department, The Boulevard, Langford Lane, Kidlington, Oxford, OX5 1GB, UK, tel: +1 215 239 3804 or +44 (0)1865 843830, fax: +44 (0)1865 853333, email [email protected]
In the USA, users may clear permissions and make payments through the Copyright Clearance Center Inc, 222 Rosewood Drive, Danvers, MA 01923, USA; tel: +1 (978) 7508400, fax: +1 (978) 646-8600.
Other countries may have a local reprographic rights agency for payments.
Derivative works Subscribers may reproduce tables of contents or prepare lists of articles including abstracts for internal circulation within their institutions. Permission of the Publisher is required for resale or distribution outside the institution.
Permission of the Publisher is required for all other derivative works, including compilations and translations.
Electronic storage or usage Permission of the Publisher is required
to store or use electronically any material contained in this journal,
including any article or part of an article.
Except as outlined above, no part of this publication may be
reproduced, stored in a retrieval system, or transmitted in any form
or by any means, electronic, mechanical, photocopying, recording, or
otherwise, without prior written permission of the Publisher.
Address permissions requests to: Elsevier Health Sciences Rights
Department, at the mail, fax, and email addresses noted above.
No responsibility is assumed by Elsevier for any injury and/or dam-
age to persons or property as a matter of products liability, negligence
or otherwise, or from any use or operation of any methods, products,
instructions, or ideas contained in the material herein. Because of
rapid advances in the medical sciences, in particular, independent
verification of diagnoses and drug dosages should be made.

www.thelancet.com/infection Vol 11 July 2011 557
Review
Lancet Infect Dis 2011;
11: 557–70
Published Online
May 19, 2011
DOI:10.1016/S1473-
3099(11)70007-X
Department of Paediatrics and
Adolescent Medicine,
University Medical Centre,
Mainz, Germany
(Prof F Zepp MD); Division of
Paediatric Infectious Diseases
and Vaccines, University
Children’s Hospital, Basel,
Switzerland
(Prof U Heininger MD);
Department of Pediatrics,
University of Turku, Turku,
Finland (Prof J Mertsola MD);
Department of Immunology,
The Children’s Memorial Health
Institute, Warsaw, Poland
(Prof E Bernatowska MD);
Institut Pasteur, Molecular
Prevention and Therapy of
Infectious Diseases, Paris,
France (N Guiso PhD); Free
University Medical Centre,
Amsterdam, Netherlands
(Prof J Roord MD); Bambino
Gesù Hospital, Ospedale
Universitario Epidemiologia,
Rome, Italy (A E Tozzi MD); and
Vaccine and Infectious Disease
Institute, Centre for the
Evaluation of Vaccination,
University of Antwerp,
Belgium
(Prof P Van Damme MD)
Correspondence to:
Prof Fred Zepp, University
Medical Centre, Department of
Paediatrics, Johannes Gutenberg
University, Langenbeckstraße 1,
55131 Mainz, Germany
uni-mainz.de
Rationale for pertussis booster vaccination throughout life
in Europe
Fred Zepp, Ulrich Heininger, Jussi Mertsola, Ewa Bernatowska, Nicole Guiso, John Roord, Alberto E Tozzi, Pierre Van Damme
Although the introduction of universal pertussis immunisation in infants has greatly reduced the number of reported cases in infants and young children, disease incidence has been increasing in adolescents and adults in recent years. This changing epidemiological pattern is probably largely attributable to waning immunity after natural infection or vaccination. Furthermore, improved diagnostic testing, active surveillance, changes in disease susceptibility, vaccine characteristics, and increased awareness of the disease might also be contributing factors. Susceptibility to pertussis in adolescents and adults results not only in direct morbidity in these age groups, but also poses a transmission risk to susceptible non-immune infants who are often too young to be vaccinated. Because vaccination schedules vary across Europe, we review the pertussis situation in this region and propose considerations for use of pertussis booster vaccinations at diff erent ages to reduce individual morbidity and transmission from present rates and increase herd protection.
IntroductionDespite substantially improved disease prevention since the introduction of universal infant vaccination, pertussis (whooping cough) is one of the leading causes of vaccine-preventable deaths. Worldwide, an estimated 50 million cases of disease and 300 000 deaths occur every year.1 Although developed countries have generally achieved high rates of vaccination coverage in infants, the eff ect on circulating Bordetella pertussis has been limited, which is mainly attributable to waning immunity occurring 4–12 years after vaccination or 4–20 years after natural infection.2
The belief that pertussis is chiefl y a childhood disease is a common misconception. Whereas disease incidence in young children has been declining since the introduction of vaccination in paediatric age groups, the number of reported cases across all other age groups has increased in many European countries during the past decade. In particular, the incidence of pertussis in adolescents and adults has increased in Europe and the USA and these groups are now the main reservoir of infection (fi gure 1).3–14 This changing epidemiological pattern contributes to ongoing challenges for disease control. The apparent resurgence in pertussis might also be related to an increased awareness of the disease after the introduction of improved diagnostic tests and more active surveillance. Further more, changes in disease susceptibility and vaccine characteristics, shifting demographics, variations in vaccination coverage, and genetic variations of B pertussis could infl uence pertussis incidence. Untreated, pertussis is highly contagious during the fi rst few weeks of onset of disease symptoms, and one primary case can lead to 11–17 secondary cases in an immune-naive population.15,16 Because the clinical presentation of pertussis in adolescents and adults often goes unrecognised, the potential for disease transmission and risk of outbreaks in susceptible populations is high. In this Review, we assess the present pertussis situation with a specifi c focus on Europe and detail considerations for booster vaccinations in diff erent age groups.
The Consensus on Pertussis Booster Vaccination in Europe initiativeIn Europe, pertussis vaccination schedules vary between countries, and although many schedules routinely include booster vaccinations for preschool children, recom-mendations for adolescents and adults are less common and immunisation uptake is low in these groups (table 1). Recognising the need for pan-European guidance, a panel of European experts met in 2008 and 2009 to discuss and share evidence and expert opinions about clinical and biological diagnoses, epidemiology, and vaccination needs for pertussis across Europe. The meetings led to the development of a series of proposals about the use of pertussis booster vaccinations in diff erent age groups that are reported in this Review.
Burden of pertussisMorbidity and mortality associated with pertussis decreased substantially after the introduction of vaccination programmes;17,18 however, hospital admissions and fatalities are still evident, particularly in young infants. Pertussis-related case-fatality seems to be inversely associated with age, with most deaths occurring in unvaccinated or incompletely vaccinated infants who are younger than 12 months.19–21 In a retrospective analysis of 100 deaths attributable to community-acquired bacterial infection in children aged 10 days to 18 years in France, B pertussis caused 13% of all deaths, all of which occurred in children younger than 2 months.22
Reported complications of pertussis in adolescents and adults include sinusitis, otitis media, urinary incontinence, pneumonia, weight loss, rib fractures, encephalopathy, and fainting.23 Furthermore, underlying respiratory conditions might be worsened by pertussis. For example, investigators in one study24 reported that almost a third of adults (31%) with acute exacerbations of chronic bronchitis were also infected with B pertussis.
Pertussis also aff ects the patient’s family; for example, parents worry and lose sleep when caring for a child with the disease and might lose workdays or be less

558 www.thelancet.com/infection Vol 11 July 2011
Review
productive at work than normal.25 In addition to the burden placed on individuals and families, the broad socioeconomic burden of pertussis is notable.21,23,26,27 During an outbreak in France, more than half of 77 health-care workers with suspected infections missed 5 days of work and this lost productivity accounted for about 42% of total costs.27
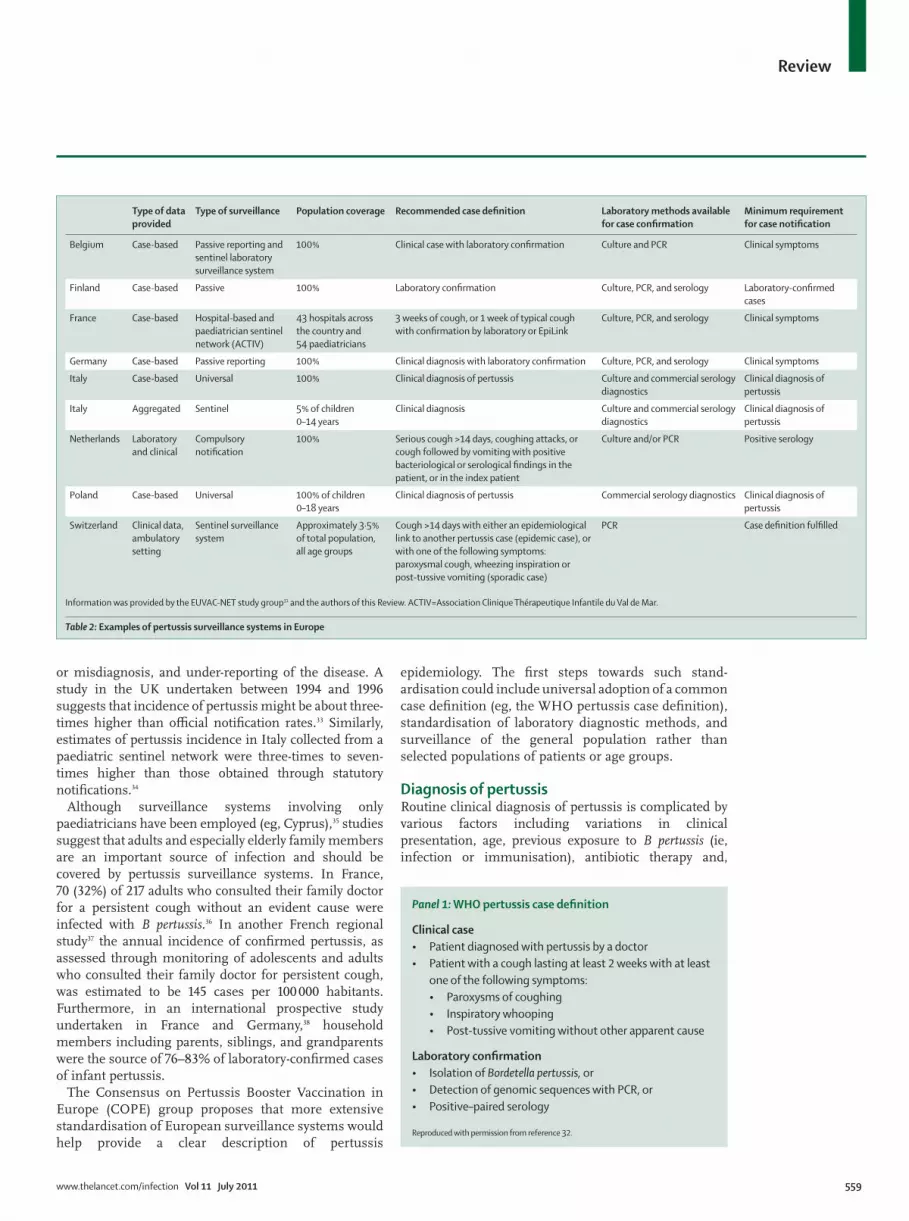
Epidemiology and surveillance across EuropeEpidemiological data collection varies between countries via surveillance of the general population, sentinel surveillance systems, voluntary notifi cations from health-care providers, and laboratory notifi cation. France employs a paediatric hospital-based surveillance system (Renacoq, established in 1996) for disease monitoring,28 with additional information provided by voluntary reporting from family doctors and mandatory nosocomial infection reports.29 Reporting of pertussis infection in Sweden has been obligatory since 1997 and clinically suspected or laboratory-confi rmed cases are reported to the Swedish Institute for Infectious Disease Control.30 Table 2 summarises characteristics of other European surveillance systems.
Diagnostic methods applied and case defi nitions for surveillance are also variable and include use of the WHO clinical case defi nition (panel 1), laboratory confi rmation or an epidemiological link to a confi rmed case, local case defi nitions, or doctors’ clinical diagnoses.
The European-wide programme, EUVAC-NET, was initiated in 1998 and funded by the European Community for the surveillance of vaccine-preventable diseases.3 During the 5 years between 1998 and 2002, 72 917 cases of pertussis were reported in 16 countries.31 The distribution of cases varied considerably between countries, with the highest number of cases reported by the Netherlands, Italy, Norway, Sweden, and Germany. This variation probably stems from diff erences in national surveillance systems, accessibility to sensitive diagnostic procedures, vaccination schedules, vaccines used, and vaccine coverage.
During the subsequent 5 years (2003–07), 43 482 cases of pertussis were reported in 20 European countries (table 3), equating to an incidence of about 4·1 per 100 000 people per year.4 Although various diff erent countries partici pated in this second phase of the EUVAC-NET project, a general trend towards a higher proportion of cases in older individuals has been reported over time (fi gure 1).
Disease incidence is probably higher than surveillance data suggest due to underconsulting, under-recognition
Figure 1: Age distribution of pertussis infection in Europe (A) and the USA (B), 1998–2007
Data from EUVAC-NET3,4 and the US Centers for Disease Control and Prevention.5–14
2003–07
2002
2001
2000
1999
1998
2007
2006
2005
2004
2003
2002
2001
2000
1999
1998
B
A
0% 20% 40% 60% 80% 100%
<1 year 1–4 years 5–14 years ≥15 years
<1 year 1–4 years 5–9 years 10–14 years ≥15 years
Age at primary series (months) Childhood and adolescent boosters Adult boosters
Austria 2, 4, and 6 12–24 months and 13–16 years Every 10 years
Belgium 2, 3, and 4 (same for
premature infants)
15 months, 5–7 years, and 14–16 years Cocoon, health-care workers, adults in contact with
young children, day-care personnel
Finland 3, 5, and 12 4 years and 14–15 years ··
France 2, 3, and 4 16–18 months and 11–13 years Adults (who did not receive any pertussis vaccination in
the past 10 years), all health-care workers, and cocoon
Germany 2, 3, and 4 11–14 months, 5–6 years, and 9–17 years Cocoon, all adults who received acellular pertussis
vaccine >10 years previously
Italy 3, 5, and 11 5–6 years and 11–15 years ··
Netherlands 2, 3, and 4 11 months and 4 years ··
Poland 2, 4, and 6 16–18 months and 6 years ··
Switzerland 2, 4, and 6 15–24 months and 4–7 years; (11–15 years catch-up) ··
Table 1: Examples of pertussis vaccination schedules in Europe
www.thelancet.com/infection Vol 11 July 2011 559
Review
or misdiagnosis, and under-reporting of the disease. A study in the UK undertaken between 1994 and 1996 suggests that incidence of pertussis might be about three-times higher than offi cial notifi cation rates.33 Similarly, estimates of pertussis incidence in Italy collected from a paediatric sentinel network were three-times to seven-times higher than those obtained through statutory notifi cations.34
Although surveillance systems involving only paediatricians have been employed (eg, Cyprus),35 studies suggest that adults and especially elderly family members are an important source of infection and should be covered by pertussis surveillance systems. In France, 70 (32%) of 217 adults who consulted their family doctor for a persistent cough without an evident cause were infected with B pertussis.36 In another French regional study37 the annual incidence of confi rmed pertussis, as assessed through monitoring of adolescents and adults who consulted their family doctor for persistent cough, was estimated to be 145 cases per 100 000 habitants. Furthermore, in an international prospective study undertaken in France and Germany,38 household members including parents, siblings, and grandparents were the source of 76–83% of laboratory-confi rmed cases of infant pertussis.
The Consensus on Pertussis Booster Vaccination in Europe (COPE) group proposes that more extensive standardisation of European surveillance systems would help provide a clear description of pertussis
epidemiology. The fi rst steps towards such stand-ardisation could include universal adoption of a common case defi nition (eg, the WHO pertussis case defi nition), standardisation of laboratory diagnostic methods, and surveillance of the general population rather than selected populations of patients or age groups.
Diagnosis of pertussisRoutine clinical diagnosis of pertussis is complicated by various factors including variations in clinical presentation, age, previous exposure to B pertussis (ie, infection or immunisation), antibiotic therapy and,
Type of data
provided
Type of surveillance Population coverage Recommended case defi nition Laboratory methods available
for case confi rmation
Minimum requirement
for case notifi cation
Belgium Case-based Passive reporting and
sentinel laboratory
surveillance system
100% Clinical case with laboratory confi rmation Culture and PCR Clinical symptoms
Finland Case-based Passive 100% Laboratory confi rmation Culture, PCR, and serology Laboratory-confi rmed
cases
France Case-based Hospital-based and
paediatrician sentinel
network (ACTIV)
43 hospitals across
the country and
54 paediatricians
3 weeks of cough, or 1 week of typical cough
with confi rmation by laboratory or EpiLink
Culture, PCR, and serology Clinical symptoms
Germany Case-based Passive reporting 100% Clinical diagnosis with laboratory confi rmation Culture, PCR, and serology Clinical symptoms
Italy Case-based Universal 100% Clinical diagnosis of pertussis Culture and commercial serology
diagnostics
Clinical diagnosis of
pertussis
Italy Aggregated Sentinel 5% of children
0–14 years
Clinical diagnosis Culture and commercial serology
diagnostics
Clinical diagnosis of
pertussis
Netherlands Laboratory
and clinical
Compulsory
notifi cation
100% Serious cough >14 days, coughing attacks, or
cough followed by vomiting with positive
bacteriological or serological fi ndings in the
patient, or in the index patient
Culture and/or PCR Positive serology
Poland Case-based Universal 100% of children
0–18 years
Clinical diagnosis of pertussis Commercial serology diagnostics Clinical diagnosis of
pertussis
Switzerland Clinical data,
ambulatory
setting
Sentinel surveillance
system
Approximately 3·5%
of total population,
all age groups
Cough >14 days with either an epidemiological
link to another pertussis case (epidemic case), or
with one of the following symptoms:
paroxysmal cough, wheezing inspiration or
post-tussive vomiting (sporadic case)
PCR Case defi nition fulfi lled
Information was provided by the EUVAC-NET study group31 and the authors of this Review. ACTIV=Association Clinique Thérapeutique Infantile du Val de Mar.
Table 2: Examples of pertussis surveillance systems in Europe
Panel 1: WHO pertussis case defi nition
Clinical case
• Patient diagnosed with pertussis by a doctor
• Patient with a cough lasting at least 2 weeks with at least
one of the following symptoms:
• Paroxysms of coughing
• Inspiratory whooping
• Post-tussive vomiting without other apparent cause
Laboratory confi rmation
• Isolation of Bordetella pertussis, or
• Detection of genomic sequences with PCR, or
• Positive–paired serology
Reproduced with permission from reference 32.

560 www.thelancet.com/infection Vol 11 July 2011
Review
possibly, concomitant infections. By contrast with the prevaccine era, atypical disease (often characterised by the absence of paroxysms and whoop) is noted more commonly today than are classic symptoms, especially in adolescents and adults.39 Data38,40 show that most pertussis infections in adults and adolescents are actually asymptomatic or oligo symptomatic, with the ratio of asymptomatic to symptomatic infections varying from 3·5 to 1·0 to 21·6 to 1·0.
Despite improvements in recent years, biological diagnosis of pertussis is challenging, with the requirement of specifi c sampling techniques and the limited availability of laboratory testing potentially contributing to under diagnosis or misdiagnosis. Two approaches are employed to detect bacteria in nasopharyngeal specimens: bacterial culture and PCR. Bacterial culture is highly specifi c and allows antibiotic susceptibility testing, but has low sensitivity (which declines with disease duration) and takes several days to complete. Real-time PCR is more rapid and signifi cantly more sensitive, although sensitivity also decreases with illness duration, and false-positive results might occur in the absence of stringent laboratory quality-control measurements.41–43 Training in appropriate sampling techniques is mandatory to avoid inadequate and incorrect specimen collection.
Serological diagnosis relies on determination of changes in the concentrations of B pertussis-specifi c antibodies in infected individuals. Although culture and PCR can be used early in the course of the disease, single-specimen serology is employed late in the course as serum antibodies do not usually peak until 3 weeks after the onset of cough.44 Although the kinetics of the immune response to pertussis infection vary between individuals, antibody titres (eg, pertussis toxin antibody) generally increase during the fi rst few weeks after onset of cough and then decline during the convalescent phase. Observation of this pattern supports consideration of decreased antibody con-centrations as part of the diagnostic process.45
Additionally, use of serology necessitates consideration of recent immunisation history, which might complicate assessment of the results. Indeed, more rapid increases and decreases of anti-pertussis toxin IgG antibody titres are noted in vaccinated groups than are in unvaccinated groups.45 This fi nding is likely to be of increasing importance if adolescent and adult booster vaccines become more widely used. In general, commercially available assays employ diff erent antigens and require diff erent interpretations; so far, none of the available assays has been validated.46 ELISA determination of serum antibody titres can be established with single-serum or paired-serum samples (ie, taken at diff erent
2003 2004 2005 2006 2007 Total
Cases Laboratory-
confi rmed
cases
Cases Laboratory-
confi rmed
cases
Cases Laboratory-
confi rmed
cases
Cases Laboratory-
confi rmed
cases
Cases Laboratory-
confi rmed
cases
Cases Laboratory-
confi rmed
cases
Austria* 170 170 (100%) 130 130 (100%) 135 135 (100%) 72 72 (100%) 133 133 (100%) 640 640 (100%)
Bulgaria* 180 0 222 0 313 313 (100%) 335 335 (100%) 269 238 (88%) 1319 886 (67%)
Cyprus 58 20 (34%) 15 12 (80%) 6 6 (100%) 8 3 (38%) 9 8 (89%) 96 49 (51%)
Czech Republic 342 340 (99%) 373 373 (100%) 412 412 (100%) 234 234 (100%) 186 144 (77%) 1547 1503 (97%)
Estonia† 623 489 (78%) 455 451 (99%) 63 62 (98%) 153 148 (97%) 409 399 (98%) 1703 1549 (91%)
Finland* 1264 1264 (100%) 1631 1631 (100%) 552 552 (100%) 536 536 (100%) 480 480 (100%) 4463 4463 (100%)
Hungary* 29 26 (90%) 31 30 (97%) 22 21 (95%) 17 17 (100%) 48 48 (100%) 147 142 (97%)
Iceland 4 3 (75%) 0 ·· 6 6 (100%) 6 3 (50%) 4 2 (50%) 20 14 (70%)
Ireland 40 NA 92 41 (45%) 83 33 (40%) 62 38 (61%) 78 47 (60%) 355 159 (45%)
Latvia† 99 55 (56%) 41 26 (63%) 25 15 (60%) 29 10 (34%) 27 15 (56%) 221 121 (55%)
Lithuania† 5 0 49 18 (37%) 64 41 (64%) 6 4 (67%) 17 14 (82%) 141 77 (55%)
Malta 7 2 (29%) 6 0 5 0 2 0 0 ·· 20 2 (10%)
Norway† 2768 2768 (100%) 1547 1542 (>99%) 4504 4492 (>99%) 6587 6585 (>99%) 5374 5367 (>99%) 20 780 20 754 (>99%)
Portugal 4 0 38 35 (92%) 78 73 (94%) 22 0 21 0 163 108 (66%)
Romania† 94 0 231 0 52 18 (35%) 37 4 (11%) 35 26 (74%) 449 48 (11%)
Slovakia* 47 47 (100%) 21 21 (100%) 17 17 (100%) 21 21 (100%) 21 21 (100%) 127 127 (100%)
Slovenia* 182 148 (81%) 113 94 (83%) 85 76 (89%) 551 446 (81%) 708 529 (75%) 1639 1293 (79%)
Spain 551 53 (10%) 530 102 (19%) 304 115 (38%) 383 101 (26%) 554 146 (26%) 2322 517 (22%)
Sweden* 664 574 (86%) 1567 1394 (89%) 1360 1072 (79%) 794 615 (77%) 690 554 (80%) 5075 4209 (83%)
UK 270 270 (100%) 370 312 (84%) 456 397 (87%) 476 476 (100%) 683 683 (100%) 2255 2138 (95%)
Total 7401 6229 (84%) 7462 6212 (83%) 8542 7856 (92%) 10331 9648 (93%) 9746 8854 (91%) 43 482 38 799 (89%)
Data are n or n (%). Data from reference 4. NA=not available. *Reported aggregated data for 2003–07. †Reported partly aggregated data for 2003–07.
Table 3: Number of reported cases of pertussis and laboratory-confi rmed cases, 2003–07

www.thelancet.com/infection Vol 11 July 2011 561
Review
times to assess the change in concentrations). Paired-sample serology is less practical for routine diagnosis and single-sample serology has therefore been the focus for a number of laboratories that assessed various cutoff levels.47 For example, a serum IgG titre of 100 U/mL or more against pertussis toxin has been regarded as indicative of recent or active pertussis infection in the Netherlands and the UK.48,49 This measure of seropositivity was employed as a comparator in a study in the UK, which investigated the potential of oral sampling as an alternative method to serum collection in young children. The investigators concluded that oral fl uid anti-pertussis toxin IgG titres of 70 arbitrary units or more provided a relatively high positive predictive value of 76·2–93·2% for pertussis in children with chronic coughs.49
There are several barriers to early diagnosis of pertussis. Symptoms of pertussis vary from mild respiratory symptoms to full-blown disease with characteristic paroxysmal coughing, inspiratory whooping, choking, and sometimes vomiting. Clinical symptoms that are predictive of pertussis include paroxysmal or severe prolonged cough, post-tussive vomiting, whoop, and obstructive apnoea, in addition to a long interval since the last pertussis vaccination.
The disease course can be infl uenced by various factors including immunisation history, age and sex of the patient. For example, women have been reported to present with more vomiting, whooping, and paroxysms than have men,50 whereas a study51 of children younger than 6 years of age reported the duration of spasmodic cough to be longer in girls than in boys. Such variation in presentation complicates or delays diagnosis, especially in adolescents and adults.
Atypical presentation of pertussis is increasingly common, with a persistent cough often the only sign to suggest the presence of the disease.52 However, coughing is a commonly encountered symptom in the general population and might be attributed to a number of underlying causes. Because vaccination programmes in infants and in early childhood are well established, pertussis is often thought to be low on the list of suspected infections and frequently goes unrecognised or misdiagnosed. Pertussis might be misidentifi ed as Mycoplasma pneumoniae, sinusitis, or upper respiratory tract infection.52 A study of schoolchildren aged 6–14 years with persistent cough in a region of Turkey, reported that 16·6% had serological evidence of a recent pertussis infection despite no cases having been diagnosed by a doctor.53 One epidemiological review40 suggested that rates of reported pertussis could be 40-fold to 160-fold lower than were actual disease rates. Furthermore, a study54 done in the Netherlands reported that pertussis infection rates, as noted by serological analysis were 685-times higher than were notifi ed infections (6·6% vs 0·01%, respectively) for people aged 3–79 years.
Presently, optimum rates of pertussis diagnosis are restricted by two key issues: fi rst, a mistaken and perhaps
widespread belief that this disease is controlled by contemporary vaccination programmes, and second, underestimation of clinical symptoms, especially in adults, by health-care providers. Raising of awareness among these providers and the general population to consider the possibility of pertussis for individuals with persistent cough is one of the steps to better recognition.
Early accurate diagnosis is important to control transmission of the disease and to enable prompt antibiotic treatment. Because atypical presentation is more common
Panel 2: Overview of considerations for diagnosis of pertussis
Clinical description
• Date of onset of symptoms
• Characteristics of the cough: duration, paroxysms, vomiting after cough, inspiratory
whoop, worse during the night
• Contact with a patient with pertussis with a compatible duration of incubation
(7–21 days)?
• Vaccine status: date of the preceding pertussis-containing vaccination
Biological confi rmation (for isolated cases or initial secondary cases in cluster or
outbreak situations)
Newborn babies and hospitalised infants
• Culture and real-time PCR on nasopharyngeal aspirates or pharyngeal swabs; culture
should continue to be done to analyse the evolution of the bacterial population
Children, adolescents, and adults
• Cough duration of 21 days or less:
• Real-time PCR and/or culture
• Cough duration more than 21 days:
• PCR and culture are no longer appropriate
• If secondary cases of disease are available in other patients after exposure to the
primary patient, PCR should be done for those secondary patients
• If there are no secondary patients, serological analysis should be undertaken for
anti-pertussis toxin antibodies if the patient has no history of pertussis vaccination
in the preceding 2 years
Culture
• Nasopharyngeal aspirate and immediate transportation to a laboratory
• Sensitivity is highest in early disease stages, severe disease, unvaccinated patients,
and infants
• Results of culture might be aff ected by antibiotics
PCR
• Likelihood of diagnosis improves when used in conjunction with culture
• PCR is most sensitive in early disease stages and in the paroxysmal stage
• Results are aff ected less by antibiotics than are results from culture
• Diagnostic accuracy might vary between laboratories
Serology
• Single-serum diagnosis might be useful for later stages of disease (3–4 weeks after
symptom onset); paired serology with the second specimen taken at later stage might
be useful for early specimens
• Antibodies (IgG and IgA) to pertussis toxin or fi lamentous haemagglutinin might be
reported in serum
• One result of a high titre of IgG against pertussis toxin (>100–125 U/mL on ELISA) is
highly sensitive and specifi c for diagnosis
• Interpretation of serology results might be diffi cult in recently immunised patients

562 www.thelancet.com/infection Vol 11 July 2011
Review
at present than it was in the prevaccination era, a shift away from pure reliance on clinical diagnosis and a move towards more regular laboratory testing is needed.55
The optimum diagnostic method according to age, immunisation, and duration of cough needs to be established. Accurate clinical and biological diagnoses of pertussis are challenging to make, and false-negative and false-positive results can occur. Panel 2 provides an overview of key considerations for diagnosis of pertussis. In terms of biological confi rmation, culture, PCR, and serology continue to have prominent places in the diagnostic process, but all have limitations, and their use is dependent on the age and history of the patient (panel 2). A standardisation of diagnostic methods is urgently needed throughout Europe.
Pertussis booster vaccinesPertussis vaccination schedules vary between countries; however, after primary vaccinations during infancy (usually three consecutive doses after the second month of life), a booster vaccination is usually given in the second year of life in addition to a preschool booster in many countries (table 1). Thereafter, only a few countries have introduced booster doses for adolescents (eg, Austria, Belgium, Finland, France, Germany, and Italy) and adults (eg, France and Germany).
Several vaccines are available for boosting immunity to pertussis. The immunogenicity of the combination tetanus–diphtheria acellular pertussis vaccine (DTPa) with or without inactivated poliovirus as a booster dose has been shown in studies of preschool children (aged 4–7 years) and young adolescents (aged 11–13 years) irrespective of vaccination history.56–58 Reactogenicity was considered acceptable (the most common adverse events being pain, redness, and swelling) and was lower than that associated with fourth or fi fth doses of combined tetanus–diphtheria whole-cell pertussis vaccine (DTPw).56 Duration of protection seems to be broadly the same between acellular and whole-cell pertussis vaccines (≥4 years postvaccination).2 In most industrialised countries, acellular vaccines have now replaced whole-cell vaccines.
Combined reduced antigen content tetanus–diphtheria and acellular pertussis vaccines (dTpa) were fi rst introduced for booster vaccination of adolescents and adults to help to reduce reactogenicity. Although these vaccines contain lower quantities of component antigens than do primary doses of pertussis vaccines, immunogenicity is unaff ected.59 Commercially available vaccines include Boostrix (a three-component vaccine produced by GlaxoSmithKline Biologicals, Rixensart, Belgium), Repevax (a fi ve-component vaccine produced by Sanofi Pasteur, Lyon, France), and Pediacel (a fi ve-component vaccine produced by Sanofi Pasteur).
Data from studies60–68 of several thousand adolescents and adults have shown the immunogenicity, safety, and acceptable reactogenicity of dTpa booster vaccination (with or without inactivated poliovirus). Many of these
studies also directly support the non-inferiority of the combined dTpa vaccine compared with reduced antigen content tetanus–diphtheria vaccine (dT) and acellular pertussis vaccines in terms of immunogenicity and adverse-event profi les in these age groups.63–66 A month after vaccination, high rates of seroprotection and seropositivity to all antigens (diphtheria and tetanus antigens ≥0·1 IU/mL and pertussis antigens ≥5 U/mL on ELISA) were reported with a seroprotection rate of more than 93% for diphtheria and tetanus and seropositivity of more than 98% for pertussis antigens in adults.66 Because there is no clear serological correlate of protection for pertussis antigens, immunogenicity is assessed by seropositivity and vaccine response (ie, seroconversion in previously sero negative individuals or a more than twofold increase in prevaccination titres in seropositive individuals).
Although the frequency of local injection-site reactions has been noted to increase in children receiving a fourth or fi fth dose of DTPa, a study investigating dTpa (simul-taneously with hepatitis A vaccine) as a sixth acellular pertussis-containing dose in adolescents showed that this outcome of increasing reactogenicity was reported for injection-site pain only.62 Reassuringly, a low prevelance (0·94%) of large injection-site swelling was seen in this study, which was consistent with the fi ndings of a large study of dTpa vaccination in adolescents in the USA.63
Long-term persistence (up to 5 years after combined dTpa) of seroprotection to diphtheria and tetanus has been shown in adolescents and adults, with much the same results as were noted in long-term follow-up after dT vaccination.69–71 Pertussis antibodies also remained detectable after 5 years of follow-up in most patients.69–71 Such study results support the replacement of dT with dTpa, because the combined booster vaccine has equivalent protection against diphtheria and tetanus with additional boosting of pertussis immunity.
Mathematical modelling of 5-year follow-up data from a dTpa trial in adolescents69 predicted that antibody decay would reach prevaccination rates between 9·5 and 15·0 years for the diff erent pertussis antibodies, a fi nding which supports proposals for decennial boosting to replace present dT schedules.72 Long-term vaccine trials are underway to further validate the fi ndings from these mathematical modelling studies.
Provision of a dTpa booster dose to adolescents who had previously not received a pertussis vaccination and had no history of pertussis led to an IgG immune response up to 49 days to pertussis toxoid in 88·6% of patients, to fi lamentous haemagglutinin in 91·9%, and to pertactin in 96·7%.73 These results suggest that one dTpa booster dose can be used in adolescent or adult populations with no history of pertussis disease or vaccinations.
In the following sections, we review the strategies available to countries wishing to improve their present pertussis immunisation programmes. Although these strategies could be implemented individually, they

www.thelancet.com/infection Vol 11 July 2011 563
Review
should be viewed as complementary and adoption of more than one approach to pertussis booster vaccination would make the most of opportunities to increase herd protection.
Cocooning immunisation strategyCocooning focuses on protecting newborn infants against pertussis by vaccination of family members and other adults in close contact with the infant. Studies report that family members (parents, grandparents, and siblings) can be the source of infection in newborn babies and young infants in a substantial proportion of cases (>33%) when an infection source could be identifi ed.38,74,75 Health-care workers can also be a source of infection when clusters of cases are reported in health-care settings.29 Molecular typing of B pertussis isolates recovered from Belgian children and their household members confi rmed that identical strains can cause full pertussal disease in children and asymptomatic infection in adults and adolescents.76
The COPE group therefore propose that adults (eg, parents, grandparents, child-care providers, and health-care providers) who have or who expect to have close contact with a non-immune or incompletely vaccinated infant who is younger than 12 months should receive a single dose of dTpa if they have not received dTpa within the previous 10 years. The updated WHO pertussis position paper77 also supports booster vaccination of health-care workers (especially those in maternity and paediatric units) in countries that have a high rate of nosocomial transmission.
A cost–eff ectiveness analysis78 undertaken in the Netherlands concluded that a cocooning immunisation strategy (for new parents) would be cost eff ective, and from a societal perspective, might even be cost-saving. The base-case analysis also suggested a reduction in the overall number of cases of pertussis in infants by 26%, although in this case infants would still be susceptible to transmission from other family members, such as the grandparents. In terms of immunisation of an elderly population,79 an Austrian study investigated the eff ect of a dTpa–inactivated poliovirus booster given to healthy adults (252 adults, median age 66 years). 5 weeks after vaccination, a humoral immune response was noted to the vaccine components. The magnitude of response, however, was infl uenced by prevaccination antibody titres, with patients who had lower prevaccination titres showing reduced responses. The study investigators note that routine booster programmes would be benefi cial to avoid loss of humoral protection.
Post-partum women are regarded as the most important group to immunise to protect newborn babies. In line with the US Centers for Disease Control and Prevention (CDC) recommendations, an initiative in the USA has been introduced to implement a standing protocol of dTpa immunisations to post-partum women before hospital discharge.80 Of the
targeted population, 72% received the booster dose, with various reasons given for those who were not immunised, such as those who had recently received a dTpa immunisation. Provision of appropriately tailored education to nurses, doctors, and patients was identifi ed as key to gaining support for the initiative, with nurses becoming powerful advocates for vaccination during the study.80 In the USA, the Advisory Committee on Immunization Procedures recommends that where possible women and their partners receive a dTpa booster before pregnancy as part of preconception planning.81 These recommendations also state that women of childbearing age should be a focal point for dTpa booster doses so that protection is provided in the event of unplanned pregnancy. Much the same recommendations have been made in Germany and France.82,83 The question of whether pertussis booster vaccination during pregnancy is viable or advisable is still under investigation. Although vaccination during pregnancy could potentially protect both mother and newborn baby, more data are needed for the extent of antibody transfer to the unborn child, the safety of such an approach, and whether there would be any implications for the infant’s subsequent primary immunisation schedule.
Whereas a cocoon strategy could have a small eff ect on the number of cases of adult pertussis, it can have a strong indirect eff ect on infants and young children if high rates of coverage can be achieved.28,84,85 Therefore, it is proposed that the cocoon strategy (ie, vaccination of close-contacts to newborns with dTpa) should continue and be further promoted until immunisation coverage in adults is suffi cient for herd protection.
Immunisation in preschool childrenProvision of booster vaccinations to preschool children would increase herd immunity and reduce rates of disease transmission to infants and neonates.86 Additionally, preschool booster vaccination might also reduce morbidity caused by pertussis in children up to the age of 8–12 years. Furthermore, if such preschool booster vaccination were linked to a school health system or other accessible public health system, coverage would be improved.
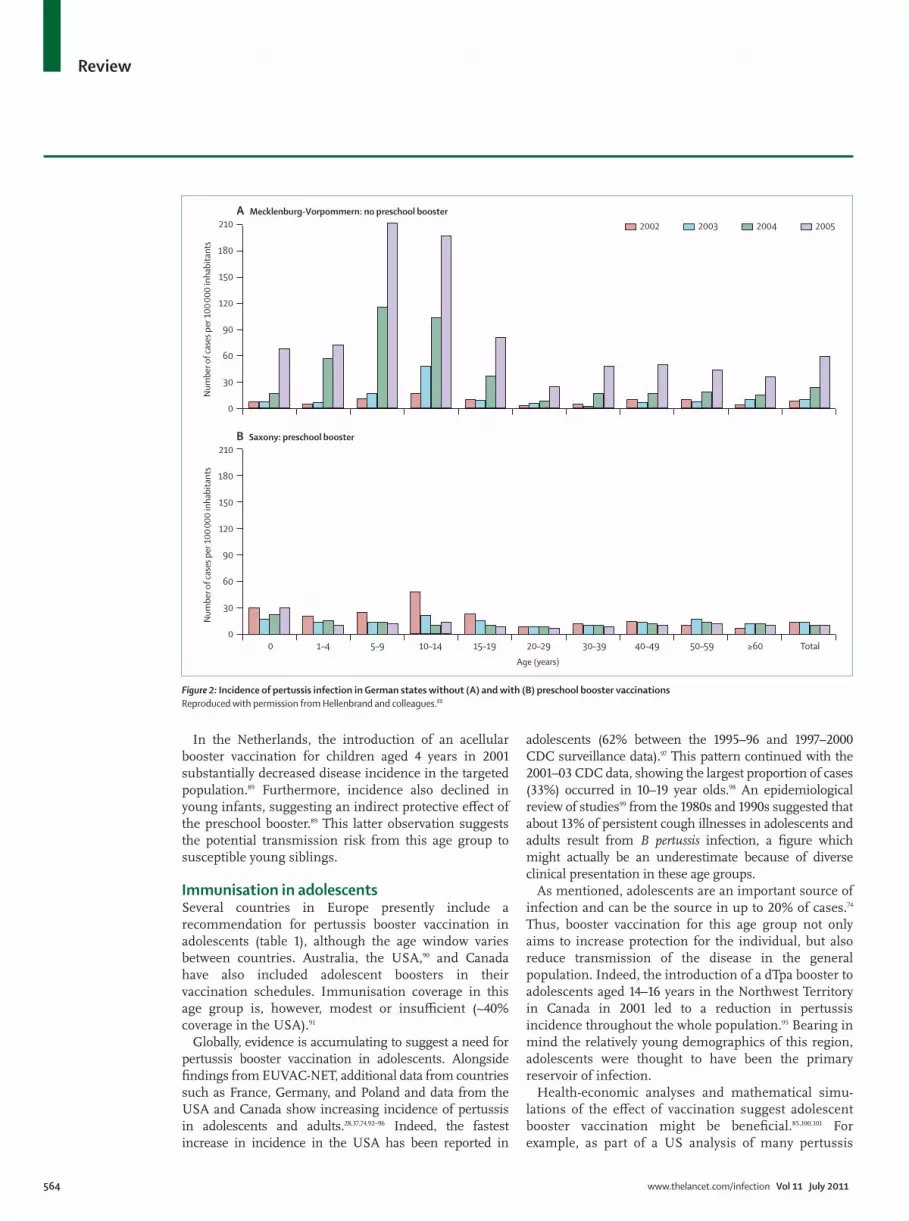
Use of a pertussis booster vaccination in preschool children may prevent more cases of pertussis than the primary immunisation schedule alone. Epidemiological data from various countries or regions suggest waning immunity of primary infant pertussis vaccinations and positive eff ects of preschool booster vaccinations.87–89 An epidemiological assessment of pertussis in diff erent regions of Germany reported a substantially increased incidence in children aged 5–14 years in a German state (Mecklenburg-Vorpommern) that did not advocate preschool boosters until 2006 compared with a state that did (Saxony; fi gure 2).88 Mecklenburg-Vorpommern introduced a preschool booster vaccination in 2005.
564 www.thelancet.com/infection Vol 11 July 2011
Review
In the Netherlands, the introduction of an acellular booster vaccination for children aged 4 years in 2001 substantially decreased disease incidence in the targeted population.89 Furthermore, incidence also declined in young infants, suggesting an indirect protective eff ect of the preschool booster.89 This latter observation suggests the potential transmission risk from this age group to susceptible young siblings.
Immunisation in adolescentsSeveral countries in Europe presently include a recommendation for pertussis booster vaccination in adolescents (table 1), although the age window varies between countries. Australia, the USA,90 and Canada have also included adolescent boosters in their vaccination schedules. Immunisation coverage in this age group is, however, modest or insuffi cient (~40% coverage in the USA).91
Globally, evidence is accumulating to suggest a need for pertussis booster vaccination in adolescents. Alongside fi ndings from EUVAC-NET, additional data from countries such as France, Germany, and Poland and data from the USA and Canada show increasing incidence of pertussis in adolescents and adults.28,37,74,92–96 Indeed, the fastest increase in incidence in the USA has been reported in
adolescents (62% between the 1995–96 and 1997–2000 CDC surveillance data).97 This pattern continued with the 2001–03 CDC data, showing the largest proportion of cases (33%) occurred in 10–19 year olds.98 An epidemiological review of studies99 from the 1980s and 1990s suggested that about 13% of persistent cough illnesses in adolescents and adults result from B pertussis infection, a fi gure which might actually be an underestimate because of diverse clinical presentation in these age groups.
As mentioned, adolescents are an important source of infection and can be the source in up to 20% of cases.74 Thus, booster vaccination for this age group not only aims to increase protection for the individual, but also reduce transmission of the disease in the general population. Indeed, the introduction of a dTpa booster to adolescents aged 14–16 years in the Northwest Territory in Canada in 2001 led to a reduction in pertussis incidence throughout the whole population.95 Bearing in mind the relatively young demographics of this region, adolescents were thought to have been the primary reservoir of infection.
Health-economic analyses and mathematical simu-lations of the eff ect of vaccination suggest adolescent booster vaccination might be benefi cial.85,100,101 For example, as part of a US analysis of many pertussis
Figure 2: Incidence of pertussis infection in German states without (A) and with (B) preschool booster vaccinations
Reproduced with permission from Hellenbrand and colleagues.88
0
30
60
90
120
150
A Mecklenburg-Vorpommern: no preschool booster
180
210
Nu
mb
er o
f ca
ses
per
10
0 0
00
inh
abit
ants
0
30
60
90
120
150
B Saxony: preschool booster
180
210
Nu
mb
er o
f ca
ses
per
10
0 0
00
inh
abit
ants
0 1–4 10–14 15–19 30–39 50–595–9 20–29 40–49 ≥60 Total
2002 2003 2004 2005
Age (years)

www.thelancet.com/infection Vol 11 July 2011 565
Review
vaccination strategies, immunisation of adolescents (aged 10–19 years) was projected to be the most cost-eff ective approach. The study investigators established that in 10 years, this strategy might prevent 0·4–1·8 million adolescent cases of pertussis in the USA and save US$0·3–1·6 billion (direct and indirect costs).100
Timing of booster vaccination in adolescents is important. On the basis of the aforementioned fi ndings, the COPE group propose that adolescents aged 10–17 years should receive a combined dTpa vaccine instead of dT, irrespective of complete primary vaccination schedule or type of previous pertussis booster vaccine. Adolescents aged 10–17 years who have a history of pertussis generally could receive a dTpa vaccine instead of dT, as such a history is an unreliable predictor of individual protection.
In the event of a pertussis outbreak, adolescents who received their previous pertussis immunisation more than 2 years earlier should receive dTpa.
Booster vaccination with dTpa has been well tolerated by adolescents who were immunised between 2 and 10 years after a previous diphtheria–tetanus-containing vaccine.102
Adolescents can be a hard-to-reach population and might have little perception of the outcomes of infectious disease and therefore a low interest in protection.103 Whenever feasible, integration of a dTpa vaccine strategy as part of the schooling system (ie, replacing the dT booster when appropriate) is likely to be one of the most promising methods of implementation. During an outbreak in a US high school, letters that were sent to parents emphasising the importance of vaccination for their children had a very small eff ect on the number of adolescents seeking vaccination from their doctor. A voluntary dTpa vaccination clinic was set up at the school, which resulted in an increase in coverage by about 31%.104
However, in locations where strong school health facilities are absent, other opportunities to provide vaccination should be considered, such as attendance at sports physicals or during health-care visits for other reasons.103 Implementation of dTpa boosters might be improved through coordination of the scheduling of vaccination to coincide with other immunisations, such as human papillomavirus vaccine.
Immunisation in adultsIn view of successful vaccination programmes for infants and children, pertussis incidence has been increasing in older age groups. Epidemiological data from Canada show a more than 20-fold increase in incidence in adults since 1990, which might be attributable in large part to use of an inadequate pertussis vaccine in the 1980s.96 From the US surveillance data (1997–2003), 20–23% of pertussis cases were reported in adults (≥20 years), a proportion that seems to be gradually increasing.19,98 Reports from Europe have also highlighted the growing burden of pertussis in adult populations.36,38,92
Pertussis is a frequent cause of longlasting cough in adults, with studies suggesting that the disease underlies 10–32% of persistent coughing in adults.36,99,105 The Adult Pertussis Trial (APERT, sponsored by the US National Institutes of Health) was initiated in 1997 to investigate several characteristics of the disease in patients aged 15–65 years and the eff ects of acellular pertussis vaccination. 2781 individuals were randomly allocated to two groups: a control group who received hepatitis A vaccine and an immunisation group who received an acellular pertussis vaccine. During follow-up, prolonged cough illness was commonly reported (63% of patients per year), with pertussis underlying between 0·7% and 5·7% of episodes in controls dependent on the duration of cough.106 Overall incidence for this age group was 370 cases per 100 000 people per year, suggesting a million pertussis cases every year in the USA in people older than 15 years if this rate were applied to the total population.106 The investigators also suggested that there are about fi ve patients who are asymptomatic or who have clinically insignifi cant infection for every classic case of clinical pertussis in adolescents and adults, a population which is a potential source of disease transmission.107 Vaccination reduced the risk for pertussis by 92%.106
From Markov modelling, a German study108 concluded that a dTpa vaccination programme for adults (aged 20–64 years) would be cost eff ective based on a disease incidence of 165 per 100 000 people per year and could even be cost-saving if the incidence were higher than 200 per 100 000 people per year. A US cost–benefi t analysis concluded that although more expensive than adolescent boosting, decennial adult (≥20 years old) booster vaccination could prevent 0·9–4·7 million adult cases of disease and save $1·3–6·4 billion in the USA every 10 years.100
Timing of booster vaccination in adults should be considered on the basis of previous vaccination history. In view of the restricted period of immunity conferred by natural infection or immunisation, and assuming that both preschool and adolescent boosters have been established, the COPE group proposes that adults aged 18 years or older could benefi t from a single dose of dTpa instead of dT for active booster vaccination, if they received their preceding dose of dT more than 10 years earlier irrespective of pertussis disease history. Although administration of a regular dTpa booster vaccine (eg, every 10 years) throughout adulthood could maintain pertussis immunity in this group, we recognise that a regular adult booster throughout life would pose a subtantial challenge for many countries at the moment.
Intervals of less than 10 years since the last dT vaccination may be used to protect against pertussis. However, further epidemiological studies are mandatory to defi ne the appropriate interval. In regions or situations where pertussis risk is increased, a single dose of dTpa at an interval of less than 10 years generally outweighs the risk for adverse reactions after

566 www.thelancet.com/infection Vol 11 July 2011
Review
vaccination. Studies have shown that intervals of 18 months in adolescents102 and as short as 4 weeks in adults109 since a previous dT-containing vaccine are well tolerated with no signifi cantly increased risk of adverse events.
In some European countries, booster vaccinations for health-care workers are recommended (table 1). Although vaccination of key health-care workers might be implemented as part of a cocooning strategy, more widespread targeting of health-care workers could be implemented in isolation or as a complementary strategy. The need for protection of health-care workers is supported by reports that outbreaks of pertussis in hospitals are common and these workers are usually the fi rst aff ected.29 Perhaps more importantly than the direct care of health-care workers, this group is often the source of infection for clusters of cases of disease occurring in patients in health-care settings.29
In addition to targeting of close family members of newborn babies as part of a cocooning strategy, opportun-ities to provide dTpa boosters with other vaccinations could be explored, such as individuals seeking travel vaccination or through occupational health visits, recipients of regular infl uenza immunisations, and in place of usual tetanus prophylaxis for wound management.110
Turning proposals into practiceFor the strategies discussed in this Review to be successfully implemented, national vaccination policy makers need to be convinced of the usefulness of present immunisation programmes and of the need to expand these programmes to improve control of pertussis. Education of the health-care community and increased public awareness of the existence and signifi cance of pertussis beyond childhood, the contagious nature of the disease, and the potential risks for individuals and their children will also be key. Although availability of disease information in health-care settings (eg, leafl ets and posters in doctors’ offi ces and hospitals) will be useful for people already within the health-care system, access to the media (newspapers, magazines, and internet advertising) will be needed to inform the outside community. Additionally, posters displayed in public
places, such as the workplace, could serve as useful reminders for the general public.
Computerised record reminders that automatically highlight when individuals are due or overdue for vaccination may be useful aids to doctors, particularly when linked to reminder and recall strategies (eg, postcards, emails, and SMS messages). Such reminders would likely have the greatest eff ect when combined with improved availability of vaccine services to prompt increased uptake. Increased availability might include reduction of the distance between vaccination clinics and target vaccinees, increased or more convenient hours during which vaccination services are provided, and setting up drop-in clinics or express-lane vaccination services. In some countries (eg, Germany), provision of vaccine passports or cards for individuals to keep a record of their own vaccination status also enables them to monitor their situations. The availability of vaccines that are free at the point of delivery will also improve vaccination uptake.
Some of the activities mentioned here were employed for 2·5 years in the Netherlands to try to improve rates of infl uenza immunisation.111 A coordinated collaborative nationwide programme of primary-care education and training, provision of patient information and reminder cards, employment of dedicated facilitators, and the introduction of supportive computer software served to signifi cantly increase infl uenza vaccine uptake from 9% to 16% (increase of 78%; p<0·001).111
Pertussis outbreaksManagement of pertussis outbreaks is labour and resource intensive and necessitates early diagnostic testing, aggressive antibiotic treatment and prophylaxis for high-risk contacts, accelerated infant vaccination, isolation of cases, and vaccination of potential contacts. As proposed in other sections of this Review, all potential contacts (eg, families or school and college students) in outbreak situations should be considered for booster vaccination. Intervals as short as 18 months in adolescents and even 1 month in adults since the last dT-containing vaccine can be considered in these patients to ensure protection for the individual and the community.
Primary objective Secondary objective
Universal adult Reduce morbidity in adults; develop herd immunity Reduce transmission to infants; reduce morbidity in children
Cocoon Reduce transmission to infants Reduce morbidity in adults
Health-care workers Reduce transmission to patients Reduce morbidity in health-care workers
Childcare workers Reduce transmission to infants Reduce morbidity in child-care workers
Universal adolescent Reduce morbidity in adolescents and adults; develop herd immunity Reduce transmission to infants
Preschool or school booster at 4–6 years of age Reduce morbidity in 4–6 year olds; develop herd immunity Reduce transmission to infants
Reinforce the present infant strategy Reduce morbidity in infants and toddlers; develop herd immunity Reduce spread in infants and children
Adapted with permission from Forsyth and colleagues.116 Although national vaccination policy makers can choose any one or more of the strategies listed, the Consensus on Pertussis Booster Vaccination in
Europe (COPE) group recommend that a step-by-step approach be taken. For example, fi rst preschool or school booster, then universal adolescent, cocoon, and fi nally universal adult strategies.
Table 4: Objectives of pertussis immunisation strategies

www.thelancet.com/infection Vol 11 July 2011 567
Review
ConclusionsNeither natural infection nor vaccination provides lifelong protection against pertussis, and, despite the existence of childhood immunisation programmes, B pertussis continues to circulate in all developed countries. Although B pertussis infection in adolescents and adults is prevalent, mild or atypical symptoms in these groups contribute to misdiagnosis and under-reporting. Pertussis should therefore be considered in the diff erential diagnosis of cough illnesses lasting more than 1–2 weeks.
As with the rest of the world, policy makers in European countries need to consider regular pertussis booster vaccination in preschool children, adolescents, and adults to protect individuals and interrupt transmission of infection, which will also protect susceptible infants who are incompletely vaccinated or unvaccinated. These considerations are in line with both the Advisory Committee on Immunization Procedures recom men da-tions for the USA and the recommendations from the Global Pertussis Initiative.112,113
Although recommendations are a fi rst step towards introduction of pertussis-booster vaccinations, in practice successful implementation in diff erent age groups is challenging. For example, an assessment of compliance with immunisation recommendations for adolescents in Erlangen, Germany reported that about 40% of the sample of students were not immunised against pertussis.114
To turn proposals into practice, the general public and health-care providers need to be trained or informed about pertussis. In Canada, for example, although adolescent pertussis booster vaccines are provided to students in school, continuation of medical education programmes for family doctors and paediatricians
ensured that doctors were well informed and supportive.115 Education of public health nurses and information provided to the general public in the lay press were also essential parts of the education programme.115 Reminder systems (by telephone, mail, or electronic media) and an increased number of opportunities for individuals to be immunised (eg, in schools, emergency departments, obstetrics and gynaecology departments, travel clinics, and occupational health services, or introduction of longer doctor’s offi ce hours) would also contribute to turn policy into practice.
Thus, the COPE group emphasises the need for pertussis booster vaccinations beyond childhood and, additionally, proposes implementation of a cocooning immunisation strategy to protect non-immune infants and replacement of dT boosters with dTpa for adolescents and adults in vaccination schedules across Europe. Table 4 provides a summary of objectives for immunisation strategies.116
Contributors
All authors discussed and agreed upon the concept and objectives of the
paper, contributed to the review and interpretation of the published work,
and reviewed and approved all versions of the report. All authors
contributed equally.
Confl icts of interest
EB has received honoraria and travel expenses from GlaxoSmithKline
(GSK) Biologicals for Consensus on Pertussis Booster Vaccination in
Europe (COPE) meetings and provided expert testimony for GSK
Biologicals. NG has received travel expenses and been paid for consultancy
for GSK Biologicals. UH been paid for consultancy and received honoraria
from GSK Biologicals and Sanofi Pasteur MSD. JM has been paid for
consultancy and received travel expenses from GSK Biologicals; JM’s
institution has received payment from GSK Biologicals for research into a
decennial administration of Boostrix vaccine in adults. JR has been paid
for consultancy and received honoraria and speakers’ bureau fees from
GSK Biologicals. AET has received travel expenses from Wyeth and GSK;
AET’s institution has received payment from Wyeth and GSK for trials on
conjugated pneumococcal polysaccharide and rotavirus vaccines. PVD is
the principal investigator for clinical trials done on behalf of the University
of Antwerp, for which the university obtains research grants from vaccine
manufacturers; PVD’s fees for presentations on vaccines are paid directly
to an educational fund held by the University of Antwerp. FZ received
travel expenses from GSK Biologicals, Novartis, and Sanofi Pasteur. The
University Medical Center Mainz received payments/honoraria from GSK
Biologicals, Novartis, and Sanofi Pasteur for lectures and expert
consultancy provided by FZ.
Acknowledgments
We thank the COPE group, including Kevin Connolly (Ireland),
Iris De Schutter (Belgium), Giovanni Gabutti (Italy), Roman Prymula
and Roman Chlibek (Czech Republic), Jacek Wysocki (Poland),
Anu Kantele (Finland), Amós García-Rojas and Lluis Salleras (Spain),
and Torbjörn Norén (Sweden) for their discussions and input into
these proposals. The COPE initiative has been supported by an
unrestricted educational grant from GlaxoSmithKline Biologicals.
Editorial and writing assistance for development of the manuscript was
provided by Jackie Bannister, Fishawack Communications (Abingdon,
Oxfordshire, UK).
References1 Vaccine Assessment and Monitoring team. WHO-recommended
standards for surveillance of selected vaccine-preventable diseases. Geneva, Switzerland: Department of Vaccines and Biologicals, World Health Organization, 2003.
2 Wendelboe AM, Van Rie A, Salmaso S, Englund JA. Duration of immunity against pertussis after natural infection or vaccination. Pediatr Infect Dis J 2005; 24: S58–61.
Search strategy and selection criteria
Data for this Review were identifi ed by searches of the
PubMed database and open-access websites of the
EUVAC-NET, World Health Organization, US Centers for
Disease Control and Prevention, and Robert Koch Institute.
We searched the PubMed database to identify articles
published in English between Jan 1, 2004, and July 30, 2009,
that reported on the following topics: burden of disease
(search terms “pertussis” AND “burden”, “economic burden”,
“hospitali*”, “impact”, “mortality”, OR “outbreak[s]”),
epidemiology and surveillance (“epidemiology” OR
“surveillance”), diagnosis (“diagnos*”), booster vaccines
(“booster” AND “adolescent[s]”, “adult[s]”, “preschool”, OR
“vaccin*”), resulting in about 850 results, which was reduced
to 274 after review of titles. After review of titles and
abstracts, the full text of every relevant article was reviewed.
Additional appropriate citations from these articles were also
retrieved. We searched open-access websites for relevant
content on July 30, 2009.

568 www.thelancet.com/infection Vol 11 July 2011
Review
3 EUVAC-NET pertussis surveillance fi nal report 1998–2002. 2003. http://www.euvac.net/graphics/euvac/pdf/pertussis1.pdf (accessed Feb 25, 2011).
4 EUVAC-NET. EUVAC-NET pertussis surveillance report 2003–2007. 2009. http://www.euvac.net/graphics/euvac/pdf/pertussis2.pdf (accessed Feb 25, 2011).
5 CDC. Summary of notifi able diseases—United States, 1998. MMWR Morb Mortal Wkly Rep 1999; 47: 1–92.
6 CDC. Summary of notifi able diseases—United States, 1999. MMWR Morb Mortal Wkly Rep 2001; 48: 1–101.
7 CDC. Summary of notifi able diseases—United States, 2000. MMWR Morb Mortal Wkly Rep 2002; 49: 1–100.
8 CDC. Summary of notifi able diseases—United States, 2001. MMWR Morb Mortal Wkly Rep 2003; 50: 1–108.
9 CDC. Summary of notifi able diseases—United States, 2002. MMWR Morb Mortal Wkly Rep 2004; 51: 1–84.
10 CDC. Summary of notifi able diseases—United States, 2003. MMWR Morb Mortal Wkly Rep 2005; 52: 1–85.
11 CDC. Summary of notifi able diseases—United States, 2004. MMWR Morb Mortal Wkly Rep 2006; 53: 1–79.
12 CDC. Summary of notifi able diseases—United States, 2005. MMWR Morb Mortal Wkly Rep 2007; 54: 1–92.
13 CDC. Summary of notifi able diseases—United States, 2006. MMWR Morb Mortal Wkly Rep 2008; 55: 1–94.
14 CDC. Summary of Notifi able Diseases—United States, 2007. MMWR Morb Mortal Wkly Rep 2009; 56: 1–94.
15 Anderson RM, May RM. Immunisation and herd immunity. Lancet 1990; 335: 641–45.
16 Wearing HJ, Rohani P. Estimating the duration of pertussis immunity using epidemiological signatures. PLoS Pathog 2009; 5: e1000647.
17 Tanaka M, Vitek CR, Pascual FB, Bisgard KM, Tate JE, Murphy TV. Trends in pertussis among infants in the United States, 1980–1999. JAMA 2003; 290: 2968–75.
18 Roush SW, Murphy TV. Historical comparisons of morbidity and mortality for vaccine-preventable diseases in the United States. JAMA 2007; 298: 2155–63.
19 Pertussis—United States, 1997–2000. MMWR Morb Mortal Wkly Rep 2002; 51: 73–76.
20 Celentano LP, Massari M, Paramatti D, Salmaso S, Tozzi AE. Resurgence of pertussis in Europe. Pediatr Infect Dis J 2005; 24: 761–65.
21 Cortese MM, Baughman AL, Zhang R, Srivastava PU, Wallace GS. Pertussis hospitalizations among infants in the United States, 1993 to 2004. Pediatrics 2008; 121: 484–92.
22 Floret D. Pediatric deaths due to community-acquired bacterial infection. Survey of French pediatric intensive care units. Arch Pediatr 2001; 8 (suppl 4): 705S–11S.
23 De Serres G, Shadmani R, Duval B, et al. Morbidity of pertussis in adolescents and adults. J Infect Dis 2000; 182: 174–79.
24 Bonhoeff er J, Bar G, Riff elmann M, Soler M, Heininger U. The role of Bordetella infections in patients with acute exacerbation of chronic bronchitis. Infection 2005; 33: 13–17.
25 Lee LH, Pichichero ME. Costs of illness due to Bordetella pertussis in families. Arch Fam Med 2000; 9: 989–96.
26 O’Brien JA, Caro JJ. Hospitalization for pertussis: profi les and case costs by age. BMC Infect Dis 2005; 5: 57.
27 Ward A, Caro J, Bassinet L, Housset B, O’Brien JA, Guiso N. Health and economic consequences of an outbreak of pertussis among healthcare workers in a hospital in France. Infect Control Hosp Epidemiol 2005; 26: 288–92.
28 Bonmarin I, Levy-Bruhl D, Baron N, Njamkepo E, Caro V. Pertussis surveillance in French hospitals: results from a 10 year period. Euro Surveill 2007; 12: 34–38.
29 Bonmarin I, Poujol I, Levy-Bruhl D. Nosocomial infections and community clusters of pertussis in France, 2000–2005. Euro Surveill 2007; 12: E11–12.
30 Carlsson RM, Trollfors B. Control of pertussis—lessons learnt from a 10-year surveillance programme in Sweden. Vaccine 2009; 27: 5709–18.
31 Tozzi AE, Pandolfi E, Celentano LP, Massari M, Salmaso S, Ciofi degli Atti ML. Comparison of pertussis surveillance systems in Europe. Vaccine 2007; 25: 291–97.
32 WHO-recommended surveillance standard of pertussis http://www.who.int/immunization_monitoring/diseases/pertussis_surveillance/en/index.html (accessed May 1, 2010).
33 Devine MJ, Bellis MA, Tocque K, Syed Q. Whooping cough surveillance in the north west of England. Commun Dis Public Health 1998; 1: 121–25.
34 Ciofi Degli Atti ML, Salmaso S, Bella A, et al. Pediatric sentinel surveillance of vaccine-preventable diseases in Italy. Pediatr Infect Dis J 2002; 21: 763–68.
35 Theodoridou M, Hadjipanagis A, Persianis N, Makri S, Hadjichristodoulou C. Pertussis outbreak detected by active surveillance in Cyprus in 2003. Euro Surveill 2007; 12: E11–12.
36 Gilberg S, Njamkepo E, Du Chatelet IP, et al. Evidence of Bordetella pertussis infection in adults presenting with persistent cough in a French area with very high whole-cell vaccine coverage. J Infect Dis 2002; 186: 415–18.
37 Lasserre A, Laurent E, Turbelin C, Hanslik T, Blanchon T, Guiso N. Pertussis among adolescents and adults followed in general practice in a regional French sample, in 2008. 28th Annual Meeting of the European Society for Paediatric Infectious Diseases (ESPID); Nice, France; May 4–8, 2010.
38 Wendelboe AM, Njamkepo E, Bourillon A, et al. Transmission of Bordetella pertussis to young infants. Pediatr Infect Dis J 2007; 26: 293–99.
39 Cherry JD, Grimprel E, Guiso N, Heininger U, Mertsola J. Defi ning pertussis epidemiology: clinical, microbiologic and serologic perspectives. Pediatr Infect Dis J 2005; 24: S25–34.
40 Cherry JD. Epidemiology of pertussis. Pediatr Infect Dis J 2006; 25: 361–62.
41 Qin X, Galanakis E, Martin ET, Englund JA. Multitarget PCR for diagnosis of pertussis and its clinical implications. J Clin Microbiol 2007; 45: 506–11.
42 Riff elmann M, Wirsing von Konig CH, Caro V, Guiso N. Nucleic acid amplifi cation tests for diagnosis of Bordetella infections. J Clin Microbiol 2005; 43: 4925–29.
43 Caro V, Guiso N, Alberti C, et al. Profi ciency program for real-time PCR diagnosis of Bordetella pertussis infections in French hospital laboratories and at the French National Reference Center for Whooping Cough and other Bordetelloses. J Clin Microbiol 2009; 47: 3197–203.
44 Heininger U, Cherry JD, Stehr K. Serologic response and antibody-titer decay in adults with pertussis. Clin Infect Dis 2004; 38: 591–94.
45 Simondon F, Iteman I, Preziosi MP, Yam A, Guiso N. Evaluation of an immunoglobulin G enzyme-linked immunosorbent assay for pertussis toxin and fi lamentous hemagglutinin in diagnosis of pertussis in Senegal. Clin Diagn Lab Immunol 1998; 5: 130–34.
46 Kosters K, Riff elmann M, Dohrn B, von Konig CH. Comparison of fi ve commercial enzyme-linked immunosorbent assays for detection of antibodies to Bordetella pertussis. Clin Diagn Lab Immunol 2000; 7: 422–26.
47 Mertens PL, Stals FS, Steyerberg EW, Richardus JH. Sensitivity and specifi city of single IgA and IgG antibody concentrations for early diagnosis of pertussis in adults: an evaluation for outbreak management in public health practice. BMC Infect Dis 2007; 7: 53.
48 de Melker HE, Versteegh FG, Conyn-Van Spaendonck MA, et al. Specifi city and sensitivity of high levels of immunoglobulin G antibodies against pertussis toxin in a single serum sample for diagnosis of infection with Bordetella pertussis. J Clin Microbiol 2000; 38: 800–06.
49 Litt DJ, Samuel D, Duncan J, Harnden A, George RC, Harrison TG. Detection of anti-pertussis toxin IgG in oral fl uids for use in diagnosis and surveillance of Bordetella pertussis infection in children and young adults. J Med Microbiol 2006; 55: 1223–28.
50 Jenkinson D. Natural course of 500 consecutive cases of whooping cough: a general practice population study. BMJ 1995; 310: 299–302.
51 Tozzi AE, Rava L, Ciofi degli Atti ML, Salmaso S. Clinical presentation of pertussis in unvaccinated and vaccinated children in the fi rst six years of life. Pediatrics 2003; 112: 1069–75.
52 Yaari E, Yafe-Zimerman Y, Schwartz SB, et al. Clinical manifestations of Bordetella pertussis infection in immunized children and young adults. Chest 1999; 115: 1254–58.

www.thelancet.com/infection Vol 11 July 2011 569
Review
53 Aksakal FN, Coplu N, Ceyhan MN, et al. High incidence of Pertussis among schoolchildren with prolonged cough in Turkey. Tohoku J Exp Med 2007; 211: 353–58.
54 de Melker HE, Versteegh FG, Schellekens JF, Teunis PF, Kretzschmar M. The incidence of Bordetella pertussis infections estimated in the population from a combination of serological surveys. J Infect 2006; 53: 106–13.
55 Bamberger E, Lahat N, Gershtein V, et al. Diagnosing pertussis: the role of polymerase chain reaction. Isr Med Assoc J 2005; 7: 351–54.
56 Jacquet JM, Begue P, Grimprel E, et al. Safety and immunogenicity of a combined DTPa-IPV vaccine administered as a booster from 4 years of age: a review. Vaccine 2006; 24: 2440–48.
57 Black S, Friedland LR, Ensor K, Weston WM, Howe B, Klein NP. Diphtheria-tetanus-acellular pertussis and inactivated poliovirus vaccines given separately or combined for booster dosing at 4–6 years of age. Pediatr Infect Dis J 2008; 27: 341–46.
58 Black S, Friedland LR, Schuind A, Howe B. Immunogenicity and safety of a combined DTaP-IPV vaccine compared with separate DTaP and IPV vaccines when administered as pre-school booster doses with a second dose of MMR vaccine to healthy children aged 4–6 years. Vaccine 2006; 24: 6163–71.
59 Jones T. Boostrix (GlaxoSmithKline). IDrugs 2005; 8: 656–61.
60 Grimprel E, von Sonnenburg F, Sanger R, Abitbol V, Wolter JM, Schuerman LM. Combined reduced-antigen-content diphtheria-tetanus-acellular pertussis and polio vaccine (dTpa-IPV) for booster vaccination of adults. Vaccine 2005; 23: 3657–67.
61 Blatter M, Friedland LR, Weston WM, Li P, Howe B. Immunogenicity and safety of a tetanus toxoid, reduced diphtheria toxoid and three-component acellular pertussis vaccine in adults 19–64 years of age. Vaccine 2009; 27: 765–72.
62 Zepp F, Knuf M, Habermehl P, Mannhardt-Laakmann W, Howe B, Friedland LR. Safety of reduced-antigen-content tetanus–diphtheria–acellular pertussis vaccine in adolescents as a sixth consecutive dose of acellular pertussis-containing vaccine. J Pediatr 2006; 149: 603–10.
63 Pichichero ME, Blatter MM, Kennedy WA, Hedrick J, Descamps D, Friedland LR. Acellular pertussis vaccine booster combined with diphtheria and tetanus toxoids for adolescents. Pediatrics 2006; 117: 1084–93.
64 Halperin SA, Smith B, Russell M, et al. An adult formulation of a fi ve-component acellular pertussis vaccine combined with diphtheria and tetanus toxoids is safe and immunogenic in adolescents and adults. Vaccine 2000; 18: 1312–19.
65 Van der Wielen M, Van Damme P, Joossens E, Francois G, Meurice F, Ramalho A. A randomised controlled trial with a diphtheria-tetanus-acellular pertussis (dTpa) vaccine in adults. Vaccine 2000; 18: 2075–82.
66 Van Damme P, Burgess M. Immunogenicity of a combined diphtheria-tetanus-acellular pertussis vaccine in adults. Vaccine 2004; 22: 305–08.
67 Mertsola J, Booy R, He Q, et al. The immunogenicity of repeated administration of reduced-antigen-content dTpa booster vaccine in adults. 6th World Congress of the World Society for Pediatric Infectious Diseases; Buenos Aires, Argentina; Nov 18–22, 2009 (poster 029).
68 Mertsola J, Booy R, Zepp F, et al. The safety of repeated administration of reduced-antigen-content dTpa boosters. 6th World Congress of the World Society for Pediatric Infectious Diseases; Buenos Aires, Argentina; Nov 18–22, 2009 (poster 045).
69 Barreto L, Guasparini R, Meekison W, Noya F, Young L, Mills E. Humoral immunity 5 years after booster immunization with an adolescent and adult formulation combined tetanus, diphtheria, and 5-component acellular pertussis vaccine. Vaccine 2007; 25: 8172–79.
70 McIntyre PB, Burgess MA, Egan A, Schuerman L, Hoet B. Booster vaccination of adults with reduced-antigen-content diphtheria, Tetanus and pertussis vaccine: immunogenicity 5 years post-vaccination. Vaccine 2009; 27: 1062–66.
71 McIntyre PB, Turnbull FM, Egan AM, Burgess MA, Wolter JM, Schuerman LM. High levels of antibody in adults three years after vaccination with a reduced antigen content diphtheria-tetanus-acellular pertussis vaccine. Vaccine 2004; 23: 380–85.
72 Bailleux F, Coudeville L, Kolenc-Saban A, Bevilacqua J, Barreto L, Andre P. Predicted long-term persistence of pertussis antibodies in adolescents after an adolescent and adult formulation combined tetanus, diphtheria, and 5-component acellular pertussis vaccine, based on mathematical modeling and 5-year observed data. Vaccine 2008; 26: 3903–08.
73 Knuf M, Zepp F, Meyer C, et al. Immunogenicity of a single dose of reduced-antigen acellular pertussis vaccine in a non-vaccinated adolescent population. Vaccine 2006; 24: 2043–48.
74 Bisgard KM, Pascual FB, Ehresmann KR, et al. Infant pertussis: who was the source? Pediatr Infect Dis J 2004; 23: 985–89.
75 Kowalzik F, Barbosa AP, Fernandes VR, et al. Prospective multinational study of pertussis infection in hospitalized infants and their household contacts. Pediatr Infect Dis J 2007; 26: 238–42.
76 De Schutter I, Malfroot A, Dab I, et al. Molecular typing of Bordetella pertussis isolates recovered from Belgian children and their household members. Clin Infect Dis 2003; 36: 1391–96.
77 WHO. Pertussis vaccines: WHO position paper. Wkly Epidemiol Rec 2010; 85: 385–400.
78 Westra TA, de Vries R, Tamminga JJ, Wilschut JC, Sauboin CJ, Postma MJ. Cost-eff ectiveness of a cocooning immunization strategy against pertussis for the Netherlands. International Society for Pharmacoeconomics and Outcomes Research 12th Annual Congress; Paris, France; Oct 24–27, 2009.
79 Kaml M, Weiskirchner I, Keller M, et al. Booster vaccination in the elderly: their success depends on the vaccine type applied earlier in life as well as on pre-vaccination antibody titers. Vaccine 2006; 24: 6808–11.
80 Healy CM, Rench MA, Castagnini LA, Baker CJ. Pertussis immunization in a high-risk postpartum population. Vaccine 2009; 27: 5599–602.
81 Kretsinger K, Broder KR, Cortese MM, et al. Preventing tetanus, diphtheria, and pertussis among adults: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine recommendations of the Advisory Committee on Immunization Practices (ACIP) and recommendation of ACIP, supported by the Healthcare Infection Control Practices Advisory Committee (HICPAC), for use of Tdap among health-care personnel. MMWR Recomm Rep 2006; 55: 1–37.
82 Impfempfehlungen der Ständigen Impfkommission am Robert Koch-Institut/Stand Juli 2009. Epidem Bull 2009; 30: 279–98.
83 Vaccination schedules and recommendations from the “Haut conseil de la santé publique” in France. Bulletin Épidémiologique Hebdomadaire 2009; 16–17: 146–76.
84 Coudeville L, van Rie A, Andre P. Adult pertussis vaccination strategies and their impact on pertussis in the United States: evaluation of routine and targeted (cocoon) strategies. Epidemiol Infect 2008; 136: 604–20.
85 Van Rie A, Hethcote HW. Adolescent and adult pertussis vaccination: computer simulations of fi ve new strategies. Vaccine 2004; 22: 3154–65.
86 Bamberger ES, Srugo I. What is new in pertussis? Eur J Pediatr 2008; 167: 133–39.
87 Andrews R, Herceg A, Roberts C. Pertussis notifi cations in Australia, 1991 to 1997. Commun Dis Intell 1997; 21: 145–48.
88 Hellenbrand W, Beier D, Jensen E, et al. The epidemiology of pertussis in Germany: past and present. BMC Infect Dis 2009; 9: 22.
89 de Greeff SC, Mooi FR, Schellekens JF, de Melker HE. Impact of acellular pertussis preschool booster vaccination on disease burden of pertussis in The Netherlands. Pediatr Infect Dis J 2008; 27: 218–23.
90 Broder KR, Cortese MM, Iskander JK, et al. Preventing tetanus, diphtheria, and pertussis among adolescents: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccines recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2006; 55: 1–34.
91 CDC. National, state, and local area vaccination coverage among adolescents aged 13–17 years—United States, 2008. MMWR Morb Mortal Wkly Rep 2009; 58: 997–1001.
92 Baron S, Njamkepo E, Grimprel E, et al. Epidemiology of pertussis in French hospitals in 1993 and 1994: thirty years after a routine use of vaccination. Pediatr Infect Dis J 1998; 17: 412–18.

570 www.thelancet.com/infection Vol 11 July 2011
Review
93 Guris D, Strebel PM, Bardenheier B, et al. Changing epidemiology of pertussis in the United States: increasing reported incidence among adolescents and adults, 1990–1996. Clin Infect Dis 1999; 28: 1230–37.
94 Gzyl A, Augustynowicz E, Rabczenko D, Gniadek G, Slusarczyk J. Pertussis in Poland. Int J Epidemiol 2004; 33: 358–65.
95 Kandola K, Lea A, White W, Santos M. A comparison of pertussis rates in the Northwest Territories: Pre- and postacellular pertussis vaccine introduction in children and adolescents. Can J Infect Dis Med Microbiol 2005; 16: 271–74.
96 Ntezayabo B, De Serres G, Duval B. Pertussis resurgence in Canada largely caused by a cohort eff ect. Pediatr Infect Dis J 2003; 22: 22–27.
97 Greenberg DP. Pertussis in adolescents: increasing incidence brings attention to the need for booster immunization of adolescents. Pediatr Infect Dis J 2005; 24: 721–28.
98 Pertussis—United States, 2001–2003. MMWR Morb Mortal Wkly Rep 2005; 54: 1283–86.
99 Cherry JD. The epidemiology of pertussis: a comparison of the epidemiology of the disease pertussis with the epidemiology of Bordetella pertussis infection. Pediatrics 2005; 115: 1422–27.
100 Purdy KW, Hay JW, Botteman MF, Ward JI. Evaluation of strategies for use of acellular pertussis vaccine in adolescents and adults: a cost-benefi t analysis. Clin Infect Dis 2004; 39: 20–28.
101 Caro JJ, Getsios D, El-Hadi W, Payne K, O’Brien JA. Pertussis immunization of adolescents in the United States: an economic evaluation. Pediatr Infect Dis J 2005; 24: S75–S82.
102 Halperin SA, Sweet L, Baxendale D, et al. How soon after a prior tetanus–diphtheria vaccination can one give adult formulation tetanus–diphtheria–acellular pertussis vaccine? Pediatr Infect Dis J 2006; 25: 195–200.
103 FitzSimons D, Vorsters A, Hoppenbrouwers K, Van Damme P. Prevention and control of viral hepatitis through adolescent health programmes in Europe. Vaccine 2007; 25: 8651–59.
104 CDC. Use of mass Tdap vaccination to control an outbreak of pertussis in a high school—Cook County, Illinois, September 2006–January 2007. MMWR Morb Mortal Wkly Rep 2008; 57: 796–99.
105 Riff elmann M, Littmann M, Hulsse C, O’Brien J, Wirsing von Konig CH. Pertussis: incidence, symptoms and costs. Dtsch Med Wochenschr 2006; 131: 2829–34.
106 Ward JI, Cherry JD, Chang SJ, et al. Effi cacy of an acellular pertussis vaccine among adolescents and adults. N Engl J Med 2005; 353: 1555–63.
107 Ward JI, Cherry JD, Chang SJ, et al. Bordetella pertussis infections in vaccinated and unvaccinated adolescents and adults, as assessed in a national prospective randomized Acellular Pertussis Vaccine Trial (APERT). Clin Infect Dis 2006; 43: 151–57.
108 Lee GM, Riff elmann M, Wirsing von Konig CH. Cost-eff ectiveness of adult pertussis vaccination in Germany. Vaccine 2008; 26: 3673–79.
109 Beytout J, Launay O, Guiso N, et al. Safety of Tdap-IPV given one month after Td-IPV booster in healthy young adults: a placebo-controlled trial. Hum Vaccin 2009; 5: 315–21.
110 Hoel T, Wolter JM, Schuerman LM. Combined diphtheria-tetanus-pertussis vaccine for tetanus-prone wound management in adults. Eur J Emerg Med 2006; 13: 67–71.
111 Hak E, Hermens RP, Hoes AW, Verheij TJ, Kuyvenhoven MM, van Essen GA. Eff ectiveness of a co-ordinated nation-wide programme to improve infl uenza immunisation rates in The Netherlands. Scand J Prim Health Care 2000; 18: 237–41.
112 Forsyth KD, Campins-Marti M, Caro J, et al. New pertussis vaccination strategies beyond infancy: recommendations by the global pertussis initiative. Clin Infect Dis 2004; 39: 1802–09.
113 Forsyth KD, Wirsing von Konig CH, Tan T, Caro J, Plotkin S. Prevention of pertussis: recommendations derived from the second Global Pertussis Initiative roundtable meeting. Vaccine 2007; 25: 2634–42.
114 Heininger U, Loos K, Lorenz I, Rascher W. Compliance with recommended immunizations in adolescents. Eur J Pediatr 2006; 165: 671–76.
115 Halperin SA. Canadian experience with implementation of an acellular pertussis vaccine booster-dose program in adolescents: implications for the United States. Pediatr Infect Dis J 2005; 24: S141–46.
116 Forsyth K, Tan T, von Konig CH, Caro JJ, Plotkin S. Potential strategies to reduce the burden of pertussis. Pediatr Infect Dis J 2005; 24: S69–74.

This article reprint is distributed with the support of GlaxoSmithKline Biologicals.
http://infection.thelancet.com
Copyright © 2022 FDOKUMEN