Bone morphogenetic proteins in the non-healing of fractures ...
182
Clinical effectiveness and cost-effectiveness of bone morphogenetic proteins in the non-healing of fractures and spinal fusion: a systematic review KR Garrison, S Donell, J Ryder, I Shemilt, M Mugford, I Harvey and F Song Health Technology Assessment 2007; Vol. 11: No. 30 HTA Health Technology Assessment NHS R&D HTA Programme www.hta.ac.uk August 2007
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Bone morphogenetic proteins in the non-healing of fractures ...
Clinical effectiveness and cost-effectiveness of bone morphogenetic proteins in the non-healing of fractures and spinalfusion: a systematic review
KR Garrison, S Donell, J Ryder, I Shemilt, M Mugford, I Harvey and F Song
Health Technology Assessment 2007; Vol. 11: No. 30
HTAHealth Technology AssessmentNHS R&D HTA Programmewww.hta.ac.uk
The National Coordinating Centre for Health Technology Assessment,Mailpoint 728, Boldrewood,University of Southampton,Southampton, SO16 7PX, UK.Fax: +44 (0) 23 8059 5639 Email: [email protected]://www.hta.ac.uk ISSN 1366-5278
FeedbackThe HTA Programme and the authors would like to know
your views about this report.
The Correspondence Page on the HTA website(http://www.hta.ac.uk) is a convenient way to publish
your comments. If you prefer, you can send your comments to the address below, telling us whether you would like
us to transfer them to the website.
We look forward to hearing from you.
August 2007
Health Technology Assessm
ent 2007;Vol. 11: No. 30
Bone morphogenetic proteins in the non-healing of fractures and spinal fusion
Copyright notice
© Queen's Printer and Controller of HMSO 2007 HTA reports may be freely reproduced for the purposes of private research and study and may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising Violations should be reported to [email protected] Applications for commercial reproduction should be addressed to HMSO, The Copyright Unit, St Clements House, 2–16 Colegate, Norwich NR3 1BQ
How to obtain copies of this and other HTA Programme reports.An electronic version of this publication, in Adobe Acrobat format, is available for downloading free ofcharge for personal use from the HTA website (http://www.hta.ac.uk). A fully searchable CD-ROM isalso available (see below).
Printed copies of HTA monographs cost £20 each (post and packing free in the UK) to both public andprivate sector purchasers from our Despatch Agents.
Non-UK purchasers will have to pay a small fee for post and packing. For European countries the cost is£2 per monograph and for the rest of the world £3 per monograph.
You can order HTA monographs from our Despatch Agents:
– fax (with credit card or official purchase order) – post (with credit card or official purchase order or cheque)– phone during office hours (credit card only).
Additionally the HTA website allows you either to pay securely by credit card or to print out yourorder and then post or fax it.
Contact details are as follows:HTA Despatch Email: [email protected]/o Direct Mail Works Ltd Tel: 02392 492 0004 Oakwood Business Centre Fax: 02392 478 555Downley, HAVANT PO9 2NP, UK Fax from outside the UK: +44 2392 478 555
NHS libraries can subscribe free of charge. Public libraries can subscribe at a very reduced cost of £100 for each volume (normally comprising 30–40 titles). The commercial subscription rate is £300 per volume. Please see our website for details. Subscriptions can only be purchased for the current orforthcoming volume.
Payment methods
Paying by chequeIf you pay by cheque, the cheque must be in pounds sterling, made payable to Direct Mail Works Ltdand drawn on a bank with a UK address.
Paying by credit cardThe following cards are accepted by phone, fax, post or via the website ordering pages: Delta, Eurocard,Mastercard, Solo, Switch and Visa. We advise against sending credit card details in a plain email.
Paying by official purchase orderYou can post or fax these, but they must be from public bodies (i.e. NHS or universities) within the UK.We cannot at present accept purchase orders from commercial companies or from outside the UK.
How do I get a copy of HTA on CD?
Please use the form on the HTA website (www.hta.ac.uk/htacd.htm). Or contact Direct Mail Works (seecontact details above) by email, post, fax or phone. HTA on CD is currently free of charge worldwide.
The website also provides information about the HTA Programme and lists the membership of the variouscommittees.
HTA
Clinical effectiveness and cost-effectiveness of bonemorphogenetic proteins in the non-healing of fractures and spinalfusion: a systematic review
KR Garrison,1* S Donell,2 J Ryder,1 I Shemilt,1
M Mugford,1 I Harvey1 and F Song1,3
1 School of Medicine, Health Policy and Practice, University of East Anglia, Norwich, UK
2 Norwich and Norfolk University Hospital, Norwich, UK3 School of Allied Health Professions, University of East Anglia,
Norwich, UK
* Corresponding author
Declared competing interests of authors: S Donell has been involved in a trial of BMPfor Wyeth. Other than this, members of the review team have no economic relationshipwith sponsors.
Published August 2007
This report should be referenced as follows:
Garrison KR, Donell S, Ryder J, Shemilt I, Mugford M, Harvey I, et al. Clinical effectivenessand cost-effectiveness of bone morphogenetic proteins in the non-healing of fractures andspinal fusion: a systematic review. Health Technol Assess 2007;11(30).
Health Technology Assessment is indexed and abstracted in Index Medicus/MEDLINE,Excerpta Medica/EMBASE and Science Citation Index Expanded (SciSearch®) and Current Contents®/Clinical Medicine.

NIHR Health Technology Assessment Programme
The Health Technology Assessment (HTA) programme, now part of the National Institute for HealthResearch (NIHR), was set up in 1993. It produces high-quality research information on the costs,
effectiveness and broader impact of health technologies for those who use, manage and provide care inthe NHS. ‘Health technologies’ are broadly defined to include all interventions used to promote health,prevent and treat disease, and improve rehabilitation and long-term care, rather than settings of care.
The research findings from the HTA Programme directly influence decision-making bodies such as theNational Institute for Health and Clinical Excellence (NICE) and the National Screening Committee(NSC). HTA findings also help to improve the quality of clinical practice in the NHS indirectly in thatthey form a key component of the ‘National Knowledge Service’.
The HTA Programme is needs-led in that it fills gaps in the evidence needed by the NHS. There arethree routes to the start of projects.
First is the commissioned route. Suggestions for research are actively sought from people working in theNHS, the public and consumer groups and professional bodies such as royal colleges and NHS trusts.These suggestions are carefully prioritised by panels of independent experts (including NHS serviceusers). The HTA Programme then commissions the research by competitive tender.
Secondly, the HTA Programme provides grants for clinical trials for researchers who identify researchquestions. These are assessed for importance to patients and the NHS, and scientific rigour.
Thirdly, through its Technology Assessment Report (TAR) call-off contract, the HTA Programmecommissions bespoke reports, principally for NICE, but also for other policy-makers. TARs bring together evidence on the value of specific technologies.
Some HTA research projects, including TARs, may take only months, others need several years. They cancost from as little as £40,000 to over £1 million, and may involve synthesising existing evidence,undertaking a trial, or other research collecting new data to answer a research problem.
The final reports from HTA projects are peer-reviewed by a number of independent expert refereesbefore publication in the widely read monograph series Health Technology Assessment.
Criteria for inclusion in the HTA monograph seriesReports are published in the HTA monograph series if (1) they have resulted from work for the HTAProgramme, and (2) they are of a sufficiently high scientific quality as assessed by the referees and editors.
Reviews in Health Technology Assessment are termed ‘systematic’ when the account of the search,appraisal and synthesis methods (to minimise biases and random errors) would, in theory, permit thereplication of the review by others.
The research reported in this monograph was commissioned by the HTA Programme as project number04/34/02. The contractual start date was in November 2005. The draft report began editorial review inAugust 2006 and was accepted for publication in March 2007. As the funder, by devising a commissioningbrief, the HTA Programme specified the research question and study design. The authors have beenwholly responsible for all data collection, analysis and interpretation, and for writing up their work. TheHTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like tothank the referees for their constructive comments on the draft document. However, they do not acceptliability for damages or losses arising from material published in this report.
The views expressed in this publication are those of the authors and not necessarily those of the HTA Programme or the Department of Health.
Editor-in-Chief: Professor Tom WalleySeries Editors: Dr Aileen Clarke, Dr Peter Davidson, Dr Chris Hyde,
Dr John Powell, Dr Rob Riemsma and Dr Ken SteinProgramme Managers: Sarah Llewellyn Lloyd, Stephen Lemon, Stephanie Russell
and Pauline Swinburne
ISSN 1366-5278
© Queen’s Printer and Controller of HMSO 2007This monograph may be freely reproduced for the purposes of private research and study and may be included in professional journals providedthat suitable acknowledgement is made and the reproduction is not associated with any form of advertising.
Applications for commercial reproduction should be addressed to: NCCHTA, Mailpoint 728, Boldrewood, University of Southampton,Southampton SO16 7PX, UK.
Published by Gray Publishing, Tunbridge Wells, Kent, on behalf of NCCHTA.Printed on acid-free paper in the UK by St Edmundsbury Press Ltd, Bury St Edmunds, Suffolk. G

Objectives: To assess the clinical effectiveness andcost-effectiveness of bone morphogenetic protein(BMP) for the treatment of spinal fusions and thehealing of fractures compared with the currentstandards of care.Data sources: Electronic databases, related journalsand references from identified studies were searched in January 2006, with an updated search only forrandomised controlled trials (RCTs) in November 2006. Review methods: A systematic review of availabledata was conducted. The data from selected studieswere then analysed and graded according to quality andprocessed to give a value to the efficacy of BMP.Existing models were modified or updated to evaluatethe cost-effectiveness of BMP for open tibial fracturesand spinal fusion. Results: All selected trials were found to have severalmethodological weaknesses. Insufficient sample size inmost trials, meant that patient baseline comparabilitybetween trial arms was not achieved and the statisticalpower to detect a moderate effect was low. Data didindicate that BMP increased fracture union amongpatients with acute tibial fractures and found that high-dose BMP is more effective than a lower dose for opentibial fractures. The healing rate in the BMP group wasnot found to be statistically significantly different fromthat in the autogenous bone grafting group for patientswith tibial non-union fractures, but BMP reduced thenumber of secondary interventions in patients withacute tibial fractures compared with controls. Therewas very limited evidence that BMP in scaphoid non-union was safe and may help to accelerate non-unionhealing when used in conjunction with either autograftor allograft. There was evidence that BMP-2 is moreeffective than autogenous bone graft for radiographicfusion in patients with single-level degenerative disc
disease. No significant difference was found whenBMP-7 was compared with autograft for degenerativespondylolisthesis with spinal stenosis and spondylolysis.The use of BMP was associated with a reducedoperating time, improvement in clinical outcomes and ashorter hospital stay as compared with autograft. Theproportion of secondary interventions tended to belower in the BMP group than the control, but not ofstatistical significance. Trial data on time to return towork postoperatively were sometimes difficult tointerpret because of unclear or inappropriate dataanalysis methods. The incremental cost of BMP foropen tibial fractures was estimated to be about £3.5million per year in the UK. The estimated incrementalcost per quality-adjusted life-year (QALY) gained is£32,603. The probability that cost per QALY gained isless than £30,000 for open tibial fracture is 35.5%. Thecost-effectiveness ratio is sensitive to the price of BMPand the severity of open tibial fractures. The use ofrecombinant human bone morphogenetic protein forspinal fusion surgery may increase the cost to the UKNHS by about £1.3 million per year. The estimatedincremental cost per QALY gained was about£120,390. The probability that BMP is cost-effective(i.e. cost/QALY less than £30,000) was only 6.4%.From the societal perspective, the estimated total costof using BMP for spinal fusion is about £4.2 million peryear in the UK. Conclusions: Additional BMP treatment plusconventional intervention is more effective thanconventional intervention alone for union of acute open tibial fractures. The cost-effectiveness ofadditional BMP may be improved if the price of BMP is reduced or if BMP is mainly used in severecases. BMP may eliminate the need for autogenousbone grafting so that costs and complications related toharvesting autograft can be avoided. In non-unions,
Health Technology Assessment 2007; Vol. 11: No. 30
iii
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Abstract
Clinical effectiveness and cost-effectiveness of bonemorphogenetic proteins in the non-healing of fractures and spinal fusion: a systematic review
KR Garrison,1* S Donell,2 J Ryder,1 I Shemilt,1 M Mugford,1 I Harvey1 and F Song1,3
1 School of Medicine, Health Policy and Practice, University of East Anglia, Norwich, UK2 Norwich and Norfolk University Hospital, Norwich, UK3 School of Allied Health Professions, University of East Anglia, Norwich, UK* Corresponding author

there is no evidence that BMP is more or less effectivethan bone graft; however, it is currently used whenbone graft and other treatments have failed. The use ofBMP-2 in spinal fusion surgery seems to be moreeffective than autogenous bone graft in terms ofradiographic spinal fusion among patients with single-level degenerative disc disease. There is a lack ofevidence about the effectiveness of BMP for otherspinal disorders including spondylolisthesis and spinalstenosis. There was limited evidence showing that BMP
is associated with greater improvement in clinicaloutcomes. According to the results of economicevaluation, the use of BMP for spinal fusion is unlikely tobe cost-effective. The following areas would benefitfrom further research: clinical trials of BMP that includeformal economic evaluation, a multicentre RCT offracture non-union and of interbody and/orposterolateral spinal fusion, trials of non-tibial acute longbone fractures, and RCTs comparing BMP-2, BMP-7 andcontrols.
Abstract
iv
Health Technology Assessment 2007; Vol. 11: No. 30
v
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Contents
List of abbreviations .................................. vii
Executive summary .................................... ix
1 Background ................................................ 1Fractures ..................................................... 1Spinal fusion ............................................... 1Bone graft substitutes ................................. 2Bone morphogenetic protein ..................... 3Licensing .................................................... 4
2 Objectives and methods ............................ 5Review objectives ........................................ 5Methods ...................................................... 5
3 Results of effectiveness assessment: fracture healing .......................................... 9Number and characteristics of includedfracture healing RCTs ................................ 9Findings from RCTs on tibia fractures ....... 12Findings from RCT on scaphoid non-union ................................................... 21Summary of evidence on BMP for fractures ...................................................... 22
4 Results of effectiveness assessment: spinal fusion ................................................ 25Number and characteristics of included spinal fusion RCTs ..................................... 25Findings from RCTs on spinal fusions ....... 28Summary of evidence from randomised trials of BMP for spinal fusion ................... 43
5 Economic evaluation of BMP for tibial fracture and spinal fusion .......................... 45Review of published economic studies ....... 45Assessment of ABACUS models: economicevaluation of BMP for open tibial fractures 46Assessment of ABACUS model: economicevaluation of BMP for spinal fusion .......... 54Summary of economic evaluations ............ 60
6 Discussion and conclusions ........................ 63Methodological quality of included RCTs ........................................................... 63Effectiveness of BMP for tibial fractures .... 63Effectiveness of BMP for scaphoid non-union ................................................... 63Effectiveness of BMP for spinal fusion ...... 63Adverse effects and safety of BMP ............. 64
Different doses and types of BMPs ............ 64Cost-effectiveness ....................................... 65Conclusions ................................................ 65Recommendations for further research ...................................................... 65
Acknowledgements .................................... 67
References .................................................. 69
Appendix 1 Search strategies .................... 77
Appendix 2 Effectiveness data extraction forms .......................................................... 81
Appendix 3 Cost-effectiveness data extraction form ........................................... 85
Appendix 4 Checklist for quality assessment .................................................. 89
Appendix 5 List of excluded studies ......... 91
Appendix 6 RCT fracture study characteristics ............................................. 95
Appendix 7 RCT fracture quality assessment .................................................. 99
Appendix 8 RCT fracture adverse events .......................................................... 101
Appendix 9 Fracture case series and casereport findings ........................................... 103
Appendix 10 Fracture case series and casereport study characteristics ........................ 107
Appendix 11 Fracture case series and casereport interventions ................................... 111
Appendix 12 Fracture case series and casereport radiographic results ........................ 115
Appendix 13 Fracture case series and casereport clinical and other outcomes ............ 117
Appendix 14 Fracture case series and casereport secondary procedures and adverseevents .......................................................... 119

Appendix 15 RCT spine study characteristics ............................................. 121
Appendix 16 RCT spine quality assessment .................................................. 125
Appendix 17 RCT spine adverse events ... 129
Appendix 18 Spine fusion case series findings ....................................................... 131
Appendix 19 Spine case series characteristics ............................................. 135
Appendix 20 Spine case series interventions .............................................. 139
Appendix 21 Spine case series fusion results ......................................................... 143
Appendix 22 Spine case series study clinical and other outcomes ....................... 145
Appendix 23 Spine case series secondaryprocedures and adverse events .................. 147
Appendix 24 Patient statement ................. 149
Health Technology Assessment reportspublished to date ....................................... 151
Health Technology Assessment Programme ................................................ 165
Contents
vi
Health Technology Assessment 2007; Vol. 11: No. 30
vii
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
ACS absorbable collagen sponge
AICBG autogenous iliac crest bone graft
BCP biphasic calcium phosphate
BESTT BMP-2 Evaluation in Surgery forTibial Trauma
BMP bone morphogenetic protein
BSM bone substitute material
CEAC cost-effectiveness acceptability curve
CI confidence interval
CRD Centre for Reviews andDissemination
CRM compression-resistant matrix
CT computed tomography
DBM demineralised bone matrix
FDA Food and Drug Administration
HA–TCP hydroxyapatite and tricalciumphosphate
hBMP human bone morphogenetic protein
ICER incremental cost-effectiveness ratio
IM intramedullary
ITT intention-to-treat
NA not applicable
NNB natural non-organic bone
NR not reported
OP-1 osteogenic protein-1
OR odds ratio
OTF open tibial fracture
QALY quality-adjusted life-year
QoL quality of life
RCT randomised controlled trial
rhBMP recombinant human bonemorphogenetic protein
SC standard care
SF-36 Short Form with 36 Items
TGF transforming growth factor
TSRH Texas Scottish Rite Hospital
List of abbreviations
All abbreviations that have been used in this report are listed here unless the abbreviation is well known (e.g. NHS), or it has been used only once, or it is a non-standard abbreviation used only in figures/tables/appendices in which case the abbreviation is defined in the figure legend or at the end of the table.


ObjectivesThe objectives of this study were to assess theclinical effectiveness and cost-effectiveness of bone morphogenetic protein (BMP) for thetreatment of spinal fusions and the healing of fractures compared with the current standards of care.
MethodsElectronic literature databases, related journalsand references from identified studies weresearched for relevant studies in January 2006,then an updated search was performed only forrandomised controlled trials (RCTs) in November2006. The searches were not restricted bylanguage, publication status or date. Due to theanticipated paucity of relevant studies, all studiesthat reported on BMP for treatment of spinalfusion or fracture were included. However, in ouranalyses, we focused on evidence from RCTsbecause of the poor quality of data from identifiedcase series. All data were extracted by one reviewerand checked by another.
Models developed by ABACUS International weremodified or updated to evaluate the cost-effectiveness of BMP for open tibial fractures andspinal fusion.
ResultsQuantity and quality of included RCTsEight randomised trials of BMP for tibialfractures, one for scaphoid non-union and 12randomised trials of BMP for spinal fusion wereincluded. These trials had several methodologicalweaknesses, including unreported randomisationand allocation methods, incomparable baselinecharacteristics between the groups, failure toperform intention-to-treat analysis or to useindependent blinded assessors and failure toreport reasons for drop-outs. Some secondaryoutcomes were not measured and/or reported.Because of insufficient sample size in most trials,patient baseline comparability between trial armswas not achieved and the statistical power todetect a moderate effect was low.
Effectiveness of BMP for tibial fracturesAccording to the data from three trials (494patients in total), the use of BMP increasedfracture union among patients with acute tibialfractures [pooled odds ratio (OR) 1.65, 95%confidence interval (CI) 1.12 to 2.45]. This pooledanalysis was dominated by the data from a largetrial (n = 450). Data from the largest trial (n = 450) also indicated that high-dose BMP(1.5 mg/ml) is more effective than a lower dose(0.75 mg/ml) for open tibial fractures. Four smalltrials (245 patients in total) found that the healingrate in the BMP group was not statisticallysignificantly different from that in the autogenousbone grafting group for patients with tibial non-union fractures (pooled OR for union rate 0.82,95% CI 0.25 to 2.64). The use of BMP reduced thenumber of secondary interventions in patientswith acute tibial fractures compared with controls.
Effectiveness of BMP for scaphoid non-unionOnly one small RCT (n = 18) was identified. Verylimited evidence indicated that BMP in scaphoidnon-union was safe and may help to acceleratenon-union healing when used in conjunction witheither autograft or allograft.
Effectiveness of BMP for spinal fusionEvidence from seven trials (n = 631 in total)showed that BMP-2 is more effective thanautogenous bone graft for radiographic fusion inpatients with single-level degenerative disc disease(pooled OR 3.87, 95% CI 1.74 to 8.59). Two smalltrials (n = 56 in total) compared BMP-7 andautograft for degenerative spondylolisthesis withspinal stenosis and found no statisticallysignificant difference (pooled OR 0.87, 95% CI0.15 to 5.08). No statistically significant differencewas observed in one small trial (n = 20) thatcompared BMP-7 and autograft spondylolysis(pooled OR 0.38, 95% CI 0.05 to 2.77). The use ofBMP was associated with an average of 25-minutereduction (95% CI 11 to 37 minutes) in operatingtime and a shorter hospital stay (0.75 days, 95%CI 0.31 to 1.19 days) compared with autograft.BMP may be associated with improvement inclinical outcomes such as Oswestry Disability Indexscore, SF-36 score and back and leg pain. Theproportion of secondary interventions tended to
Health Technology Assessment 2007; Vol. 11: No. 30
ix
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Executive summary
be lower in the BMP group than that in thecontrol group, but the difference was notstatistically significant (pooled OR 0.62, 95% CI0.28 to 1.39). Data from trials on time to return towork postoperatively were sometimes difficult tointerpret because of unclear or inappropriatemethods used for data analysis and resultspresentation.
Cost-effectiveness assessmentsThe incremental cost of BMP for open tibialfractures is estimated to be about £3.5 million peryear in the UK. The estimated incremental costper quality-adjusted life-year (QALY) gained was£32,603, with a wide 95% CI from £14,085 to£61,257. The probability that cost per QALYgained is less than £30,000 for open tibial fracturewas 35.5%. The cost-effectiveness ratio is sensitiveto the price of BMP and the severity of open tibialfractures.
The use of rhBMP for spinal fusion surgery mayincrease the cost to the UK NHS by about £1.3 million per year. The estimated incrementalcost per QALY gained was about £120,390. Theprobability that BMP is cost-effective (i.e. that thecost/QALY is less than £30,000) was only 6.4%. Were-analysed data on time to return to work afterspinal surgery, and revealed that patients in theBMP group were not returning to work earlierthan those in the control group. From the societalperspective, the estimated total cost of using BMPfor spinal fusion is about £4.2 million per year inthe UK.
ConclusionsAdditional BMP treatment plus conventionalinterventions is more effective than the conventionalintervention alone for union of acute open tibial
fractures. The cost-effectiveness of additional BMPmay be improved if the price of BMP is reduced orBMP is mainly used in severe cases.
The use of BMP may eliminate the need forautogenous bone grafting so that costs andcomplications related to harvesting autograft canbe avoided. In non-unions, there is no evidencethat BMP is more or less effective than bone graft;however, it is currently used when bone graft andother treatments have failed.
The use of BMP-2 in spinal fusion surgery seemsmore effective than autogenous bone graft interms of radiographic spinal fusion amongpatients with single-level degenerative discdisease. There is a lack of evidence about theeffectiveness of BMP for other spinal disordersincluding spondylolisthesis and spinal stenosis.There was limited evidence showing that BMP is associated with greater improvement in clinical outcomes such as Oswestry DisabilityIndex score, SF-36 score and back and leg pain.According to the results of economic evaluation,the use of BMP for spinal fusion is unlikely to becost-effective.
Recommendations for furtherresearchThe following areas are recommended for furtherresearch:
● clinical trials of BMP that include formaleconomic evaluation
● a multicentre RCT covering fracture non-union ● a multicentre RCT covering interbody and/or
posterolateral spinal fusion ● RCTs covering non-tibial acute long bone
fractures ● RCTs comparing BMP-2, BMP-7 and controls.
x
Executive summary
FracturesA fracture is a broken bone. Most tibial fracturesheal within 20 weeks.1 The rate of fracture uniondepends on a number of factors, which include:
● violence of injury● presence of an open wound● number of fracture fragments● associated vascular injury● part of the tibia fractured● method of fracture treatment.2–4
A fracture that does not heal in the time expectedis considered a delayed union. The rate of delayedunions varies by fracture severity from 16–60% forless severe fractures (Gustilo–Anderson typesI–IIIA) to 43–100% for more severe fractures(Gustilo–Anderson types IIIB and IIIC).5–7 Afracture that demonstrates motion at the bonyends and is not completely healed within6 months is considered a non-union.8 Non-unionscan lead to significant pain, inhibition of functionand decreases in personal and professionalproductivity.9 The rate of non-unions has beenreported to range from 4 to 10%.1,10 The costs fortreating non-unions have been poorlyreported.11–14 Some factors that can contribute todelayed union or non-union are:
● severe comminution (broken into smallfragments)
● open fractures● association with tumour● infection● insufficient immobilisation● inadequate blood supply● poor nutrition● chronic disease.
A fracture is considered closed when the skin isnot breached. A fracture is open when the boneprotrudes through the skin or communicates witha wound and therefore has a significant risk ofinfection. It is estimated that there are 23 openfractures per 100,000 population, of which 54%involve either the phalangeal or tibial diaphysis.15
The severity of open fractures is graded using theGustilo–Anderson system. Grade I is a puncturewound and grade IIIC is a large, open, dirty
wound with an arterial injury. A higher grademeans a higher risk of amputation. In grade IIIBopen fractures there can be up to a 50% infectionrate.4 The severity of an open fracture isdetermined by:8
● energy level ● degree of contamination● degree of soft tissue injury● complexity of fracture pattern● vascular injury.
Spinal fusionSpinal fusion surgery is performed to stop motionat the painful vertebra segment,16 for a number ofconditions, including spinal stenosis,spondylolisthesis and degenerative lumbar discdisease.17–19 Between 10 and 40% of patients whoundergo spinal surgery fail to fuse.20,21
Spinal stenosis is caused by enlarged facet joints,which then place pressure on surrounding nervesand cause pain in the back, and sometimes thelegs. The usual treatment is modifying activities,such as using a stick or walker to walk and doinglow-impact exercise. Patients may also receiveepidural injections, of whom 50% will experiencetemporary relief. In certain patients, spinalsurgery is required to remove a portion of theenlarged facet joint to relieve pressure on thenerve in either an open decompression orlaminectomy.
Degenerative disc disease occurs when the outerring of the disc, the annulus fibrosus, becomesdamaged or worn. The contents of the disc maythen protrude and impinge on a spinal nerve root.This will cause pain in the lower back that radiatesto the hips and down the backs of the legs. Itusually occurs in healthy, active individualsbetween 30 and 50 years old. Diagnosis isconfirmed by magnetic resonance imaging scans.Cervical degenerative disc disease much lesscommonly causes symptoms than lumbardegenerative disc disease; however, the treatmentwhen symptomatic is much the same. The resultsof operations for cervical disc disease are lesssatisfactory than for lumbar disc disease.22
Health Technology Assessment 2007; Vol. 11: No. 30
1
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Chapter 1
Background

Spondylolysis is a discontinuity (defect) of the parsinterarticularis (a part of the bony arch that makesup the spinal canal). It may lead to instability ofthe spine with movement of one vertebra onanother. When symptomatic, it may result in pain,or (when severe) affect leg, bladder, bowel andsexual function. Spondylolisthesis is when onevertebra slips on another. Its causes are:
● dysplastic spondylolisthesis (includescongenital)
● degenerative spondylolisthesis (caused bydegenerative disc disease)
● traumatic spondylolisthesis (caused by fracture)● pathologic spondylolisthesis (caused by disease)● isthmic spondylolisthesis (includes lytic or stress
fracture, an elongated but intact pars or acutefracture of the pars).
The costs of back pain in the UK have beenreported to be a greater economic burden thanany other disease for which economic analysis hasbeen performed.23 Spinal fusion surgery is acontroversial procedure due to varying levels offusion success with surgery. Non-surgical treatmentis an alternative to surgery and the two have beencompared in randomised controlled clinical trials.One randomised controlled trial (RCT)24 found noclear evidence that surgery was more beneficialthan the use of multi-disciplinary rehabilitation.However, the authors reported that it was difficultto implement the multi-disciplinary rehabilitation,and that it is not usually available in the NHS.The advantages to rehabilitation are that it doesnot carry any risks or surgical costs. AnotherRCT25 found a significant improvement in painand disability in the surgery-treated groupcompared with those treated with physical therapy.Finally, Möller and Hedlund26 found that forpatients with isthmic spondylolisthesis treated witheither different surgical procedures or exerciseprogrammes, those who were treated with surgeryreported greater Oswestry score improvement atthe 2-year follow-up. From these studies, it isunclear whether non-surgical treatment iscomparable to surgical treatment, although theredoes seem to be greater improvement for thosepatients who received multi-disciplinaryrehabilitation over those who received onlyphysical therapy or exercise programmes.
Bone graft substitutesSpinal fusion (arthrodesis) is the most commonindication for bone graft. Currently, autogenousiliac crest bone graft (AICBG) is considered the
‘gold standard’ graft for bone induction. Becausethe bone is taken from the patient, it is bothhistocompatible and non-immunogenic.27 It hasthe three properties required for bone formation;osteogenicity, osteoconductivity andosteoinductivity. However, there are severaldisadvantages to using autogenous bone. Becausethe graft is taken from the patient, there is alimited amount. This usually becomes importantwhen they have had previous bone grafts and nolonger have an adequate volume of iliac crest boneto donate. They therefore require bone to beharvested from different sites or supplementedwith bone graft substitutes.28 Since harvestingbone creates a second surgical site, the use ofautogenous bone also increases operating timeand blood loss.27,29 Complications (morbidity) atthe donor site have been reported to be commonand enduring.30 The morbidity associated withAICBG includes patient donor site pain,dissatisfaction with donor site appearance andmany other complications, often classified as‘major’ and ‘minor’. The most common morbidityexperienced is donor site pain.30,31 The ratesreported of pain vary from one study to another.In a prospective study by Sasso and colleagues,99% of 202 patients had donor site pain at thetime of discharge from the hospital and some levelof donor site pain was reported in 31% of 140patients at 24 months after surgery.32 Goulet andcolleagues reported that 18.3% of 87 patients stillexperienced pain at the donor site at 24 monthsor more postoperatively.30 Using similar majorand minor complication definitions, aretrospective review by Arrington and colleagues27
and a prospective study by Banwart andcolleagues33 investigated the rate of complications.The studies classified a major complication asneeding lengthened hospitalisation orreoperation. Arrington and colleagues includedthe need for a major change in treatment whereasBanwart and colleagues included a problem thatcaused a significant disability. Minor complicationswere defined by both studies as those thatresponded to minor treatment. Banwart andcolleagues also described minor complications asthose that resolved without treatment or did notcause permanent disability. Based on thesedefinitions, 10% of 180 patients in the Banwartstudy and 5.8% of 414 patients in the Arringtonstudy experienced a major complication. Themajor complications included, but were notlimited to, donor defect hernias, vascular injuries,nerve injuries, deep infection haematoma, iliacwing fracture and chronic pain limiting activity.Some 39% of 180 patients in the Banwart studyand 10% of 414 patients in the Arrington study
Background
2

experienced a minor complication. Experiencedminor complications included, but were notlimited to, superficial infection, superficialseromas, minor haematomas, dysesthesia and scarunsightliness. The morbidities associated withAICBG and its limited supply have led to thedevelopment of bone graft substitutes.
Allograft bone (bone from another person), hasosteoconductive and weak osteoinductiveproperties. Its level of osteoinductivity depends onits preparation method. However, with allograftbone, there is an increased rate of infection,greater resorption rate, varying levels of immuneresponse and longer fusion times compared withautograft bone.
Demineralised bone matrix (DBM) is made fromallograft bone and is a composite of collagen, non-collagenous proteins and growth factors. Due to itsextensive processing, it is the least immunogenicof the types of allograft bone.34
Bone morphogenetic proteinBone morphogenetic proteins (BMPs) are part ofthe transforming growth factor beta (TGF-�)superfamily. The latter are proteins secreted bycells, which serve as signalling agents thatinfluence cell division, matrix synthesis and tissuedifferentiation. BMPs have an important role inbone and cartilage formation, fracture healing andrepair of other musculoskeletal tissues.
BMPs induce bone through two pathways. Theyrecruit mesenchymal cells from surroundingmuscle, bone marrow or blood vessels and eitherdifferentiate these cells into osteoblasts and makebone directly or via cartilage cells whichsubsequently change to bone cells. BMPs also helpin matrix production and vascularisation. In vivo,multiple BMPs are expressed during bonehealing.35 The combinatorial effects of BMP-2 andBMP-7 have been studied using gene therapy.36,37
Co-transfection with adenovirus vectors encodingBMP-2 and BMP-7 resulted in significantly greaterosteoblastic differentiation and spine fusion thanindividual gene transfection. Currently, singlerecombinant human bone morphogenetic proteins(rhBMPs) are used clinically in bone healing;however, the use of multiple BMPs with knownosteogenic activity may be more effective at lowerdoses.
There are two clinical BMPs available; BMP-7 [alsoknown as osteogenic protein-1 or (OP-1)],
supplied by Stryker UK Ltd, which uses a bovinecollagen carrier in granular form (Osigraft®), andBMP-2, supplied by Wyeth Research (UK) Ltd,which uses a collagen sponge carrier (InductOs™).These collagen carriers allow the slow release ofthe BMP over time. In simple terms, BMP-2 andBMP-7 are involved in the early stage of fracturerepair, but only BMP-2 acts throughout theprocess. With differentiation of bone cells, BMP-2is involved in the conversion of stem cells toosteoprogenitor cells and then throughout thedifferentiation process. BMP-7 is involved in thestages after the formation of osteoprogenitorcells.38
BMP has shown good results in preclinical non-human primate studies. In a study by Akamaruand colleagues,39 rhesus monkeys underwentbilateral posterolateral intertransverse processarthrodesis at L4–L5 and received either collagensponge 15:85 biphasic calcium phosphate (BCP)granules loaded with rhBMP-2, collagen spongeand allograft chips loaded with rhBMP-2 orAICBG. Both of the groups that received rhBMP-2achieved 100% fusion at 6 months whereas only33% of the control group were fused. Seehermanand colleagues40 found that a single percutaneousinjection of rhBMP-2 and �-bone substitutematerial (�-BSM) could accelerate fibularosteotomy healing by up to 40% in cynomolgusmonkeys. In another study by Seeherman andcolleagues,41 they also found that a percutaneousinjection of 0.5 ml of 1.5 mg/ml rhBMP-2 andcalcium phosphate matrix administered 1 weekpost-surgery accelerated osteotomy site healing by40–50% in cynomolgus monkeys.
BMP has also been evaluated for use in cranialdefects in non-human primates. Sheehan andcolleagues42 treated bilaterally created criticallysized calvarial defects and bilateral rectangularbone flaps with rhBMP-2 on a collagen sponge.Treatment with rhBMP-2 led to 71% closure ofdefects compared with 28% in the controlmonkeys. Five of the six bone flaps treated withrhBMP-2 had complete osteointegration whereasthe control experienced poor osteointegration ofbone flaps. Ferguson and colleagues43 found thatpartially purified bovine BMP led to a morecomplete regeneration of cranial trephine defectsthan the control bovine serum albumin in rhesusmonkeys.
Oral and maxillofacial studies have beenperformed in both primates and in humans.Blumenthal and colleagues44 evaluated the use ofrhBMP-2 with absorbable collagen sponge (ACS)
Health Technology Assessment 2007; Vol. 11: No. 30
3
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.

or �-BSM for the treatment of three-wall intrabonyperiodontal defects in the baboon. Compared withthe buffer control with both carriers, they foundthat rhBMP-2 significantly increased regeneration.Specifically, rhBMP-2/ACS led to significantlygreater new cementum formation. Chin andcolleagues45 used rhBMP-2 instead of autogenousbone to repair congenital facial clefts. Successfulosseous union was achieved in 98% of the cleftsites, and no systemic adverse events wereattributed to rhBMP-2.
LicensingIn the UK, Osigraft® (OP-1), produced by Stryker,is licensed for treatment of tibial non-unions of atleast 9 months’ duration, secondary to trauma, inskeletally mature patients in cases where previoustreatment with autograft has failed or the use of
autograft is infeasible. In the USA, OP-1 Putty™ isapproved by the Food and Drug Administration(FDA) for use in posterolateral spinal fusion inpatients who have had failed spinal fusions andare not able to provide their own bone for graftingdue to osteoporosis, diabetes or smoking.46
In the UK, InductOs™ (rhBMP-2), produced byWyeth, is licensed for the treatment of acute tibialfractures in adults, as an adjunct to the standard ofcare using open fracture reduction andintramedullary nail fixation. It is also licensed “forthe treatment of single level (L4–S1) anteriorlumbar spine fusions as a substitute for autogenousbone graft in adults with degenerative disc diseasewho have had at least six months of non-operativetreatment for this condition”.47 In the USA it isFDA approved with the name InFUSE™,Medtronic Sofamor Danek, for use in acute opentibial fractures with internal stabilisation.48
Background
4
Review objectivesThe objectives of this review were to assess theclinical effectiveness and cost-effectiveness of BMPfor the treatment of spinal fusions and non-healing fractures compared with the currentstandards of care. The outcomes of interestincluded healing rate, fusion rate, number ofsecondary interventions, adverse events, quality oflife and any other cost-effectiveness-relatedoutcomes.
MethodsThe search strategy was designed to look for any studies that are relevant to the effectivenessand cost-effectiveness of BMP in the treatment of either fractures or spinal fusion, includingclinical trials, literature reviews and economicevaluations.
The following electronic databases were initiallysearched from their default start dates to the end-point, January 2006: Cochrane Library (Central)from 1800, EMBASE (Ovid) from 1980,MEDLINE (Ovid) from 1966, Science CitationIndex from 1945, NeLH and the UK NationalResearch Register. Studies were limited to humans,with no language or date restrictions. Details ofsearches are given in Appendix 1.
The searches were not restricted by language,publication status or date.
A second search was then performed in MEDLINEand EMBASE, to determine the likelihood of BMPbeing referred to as TGF since it is part of theTGF family of proteins. EMBASE (Ovid) andMEDLINE (Ovid) were both searched from 1980to week 3 January 2006. Initially, in the BMP–TGFsearch, a similar number of papers were found asin the BMP search. Therefore, to assess morequickly whether there would be any relevantpapers, it was decided to reduce the number ofpapers by using the highly specific search strategyfor identifying RCTs.49 Thirty-one papers inMEDLINE and EMBASE were found using thisrefined search. The references were checked forrelevance. It was decided not to expand the search
or search the other databases when no relevantpapers were found.
A second search was then performed in November2006 for newly available RCTs in CochraneLibrary (Central) from 1800, Specialised Registerof the Cochrane Bone Joint and Muscle TraumaGroup, EMBASE (Ovid) from 1980, MEDLINE(Ovid) from 1966, Science Citation Index from1945, NeLH and the UK National ResearchRegister using a revised search strategy (seeAppendix 1).
Key journals were selected and handsearched from1995 to the most recently available at the time ofsearch. The following journals were handsearchedbased on them supplying the largest number ofrelevant papers identified from the search: ClinicalOrthopaedics and Related Research, January 1995 toFebruary 2006; European Spine Journal, February1995 to March 2006; Journal of Bone and JointSurgery – American, January 2000 to March 2006;Journal of Neurosurgery Spine, January 1999 toMarch 2006; and Spine, April 1995 to March 2006.
References extracted from the references in thepapers obtained were also handsearched for anypossibly relevant studies.
We also contacted relevant companies (Wyeth andStryker Biotech) and authors where appropriate toask for any missing or unpublished data (seeAcknowledgements).
Study inclusion and exclusionWe included any clinical trials and full or partialeconomic evaluation studies that assessed theeffectiveness and/or costs and/or cost-effectivenessof BMP for fracture and spinal fusion.
Stage 1Two reviewers independently assessed the papersfor inclusion or exclusion, using the title and,when available, the abstract.
Because it was expected that there would be alimited number of relevant studies and the BMPtreatment would vary considerably, includingfracture or fusion, degree of fracture or fusion,location, previous failed interventions, dosage,
Health Technology Assessment 2007; Vol. 11: No. 30
5
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Chapter 2
Objectives and methods
standard of care treatment method and BMPdelivery system, we included all varying BMPinterventions for treatment of fracture or fusion inhumans.
Stage 2Full copies of the studies identified in stage 1 wereobtained for assessment. Any studies that did notmeet the inclusion criteria were excluded at thisstage. The list of excluded papers is given inAppendix 5.
Data extraction strategyData from included studies were extracted by onereviewer and checked by another reviewer usingthe predesigned data extraction form. Multiplepublications of the same study were extracted asone study, and the sources noted. Theeffectiveness data extraction forms are shown inAppendix 2, the cost-effectiveness data extractionform in Appendix 3.
Clinical effectiveness reviewThe following data were extracted:
1. details of study population, including:(a) patient diagnoses(b) inclusion and exclusion criteria(c) surgical interventions(d) patient demographics
2. details of intervention, including:(a) type of BMP(b) dose(c) carrier
3. study design quality 4. details of follow-up lengths and patient
withdrawals5. details of outcomes measured, including:
(a) fusion rates(b) clinical scores(c) pain improvement(d) antibody response(e) adverse events(f) secondary procedures(g) return to work rate.
Cost-effectiveness reviewThe following data were extracted:1. details of study characteristics, including:
(a) type of study(b) dates data collected(c) setting
2. details on the source of effectiveness data,including:(a) where evidence is from(b) type of model used, if applicable(c) clinical evidence
3. details of economic analysis, including:(a) benefits measured and methods of
valuation(b) costs(c) statistical analysis(d) sensitivity analysis
4. details of results reported, including:(a) intervention and comparator costs(b) sensitive parameters.
Quality assessment strategyClinical effectivenessThe methodological quality of the selected studieswas assessed using the York Centre for Reviewsand Dissemination (CRD)50 criteria forexperimental and observational studies. Thecriteria were tested and the following quality issueswere considered to be important for RCTs:randomisation method, allocation concealment,blinding of outcome assessors, similar prognosticbaselines, clearly defined inclusion and exclusioncriteria, performance of intention-to-treat (ITT)analysis and the numbers lost to follow-up. For thenon-RCTs, the following quality criteria wereconsidered: explicit population definition, similarprognostic baselines, appropriate assessment ofoutcomes and number lost to follow-up. Qualityassessment criteria are given in Appendix 4.
Cost-effectivenessThe quality of published economics studies wasassessed using the Drummond checklist,51 whichincludes evaluation of study design, data collectionmethods, analysis and interpretation of results.Inclusion/exclusion of studies was based on theresearchers’ overall judgement of methodologicalquality, informed by the checklist.
Methods of analysis and synthesisDescriptive summaries of the included trials wereundertaken and relevant evidence was categorisedand summarised in tables. Summary tablesconstructed for trials included studycharacteristics, interventions, quality of studies,radiographic results, clinical results, adverseevents, antibody responses and secondaryinterventions. When possible, the ITT principleswere used to analyse the individual trial data.Where appropriate, results from individual studieswere quantitatively pooled by meta-analysis usingthe random effects model. Odds ratios (ORs) with95% confidence intervals (CIs) were used as theoutcome statistic for dichotomous data. Weightedmean differences with 95% CIs were used forcontinuous data. Heterogeneity across studies wastested. Publication bias was tested for using funnelplots. Where appropriate, sensitivity and/or
Objectives and methods
6

subgroup analyses were conducted. Results fromeconomic studies were also summarised and putinto tables where appropriate.
Quantity of available researchFigure 1 shows the process of identifying studies ineach stage of the search.
Number of included studiesSixty-eight publications reporting relevant trialswere identified, including eight abstracts, sevenabstracts from conference proceedings and 52published reports. Data from an unpublishedretrospective case series abstract on tibia fractureswere provided by Wyeth.52
Four publications reporting economic analyseswere identified, including one abstract and threepublished papers.53–55 Two of the published
papers53,54 reported the same study and weretreated as one. The remaining published paper55
and abstract56 did not have enough information tobe extracted, so the authors were contacted. Anabstract by McQueen and colleagues57 of arandomised clinical trial of radius malunions wasidentified. However, the results section containeda typo related to union success rates whichprevented data extraction; the authors werecontacted with no response. An abstract of anongoing study conducted at the Centre forMusculoskeletal Studies by Speck and Pike wasalso found; however, it is not included due to lackof data.
The studies were grouped according to study type(RCT or non-RCT), and within those groups bypopulation type (spinal fusion or fracture).Twenty-one reports of 13 RCTs evaluating the use
Health Technology Assessment 2007; Vol. 11: No. 30
7
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Papers identified by
RCT TGF–BMPsearch n = 31
Relevant included studies n = 0
Papers identified from
reference checking n = 3
Papers identified by electronic
search n = 2403
Duplicatesn = 717
Excluded non-relevant reports
n = 1576
Excluded literature reviews, non-
relevant studies and those without adequate data
n = 50
Unpublished study from
industry n = 1
Fracture9 RCTs from
14 reports18 non-RCTs
from 19 reports
Spine12 RCTs from
21 reports14 non-RCTs
from 16 reports1 economic
evaluation from 2 reports
Reports retrieved formore detailed
evaluation, includingliterature reviews
and abstractsn = 110
Included studiesn = 54 studies from
72 reports
FIGURE 1 Identification of relevant studies – flow chart

of BMP for spinal fusion were identified. Sixteenreports of 14 case series for use of BMP in spinalfusion were identified. Fourteen reports of nineRCTs evaluating the use of BMP for use infractures were identified. Nineteen reports of18 case series or case report studies for BMP usein fracture non-unions were identified.
Publication biasPublication bias was tested for using funnel plots(not shown). No significant asymmetry was found,
although there were only a small number ofstudies. The use of BMPs clinically is relativelyrecent. The risk of publication bias was unlikelydue to contact with manufacturers and theirknowledge of completed/ongoing trials. TheNational Research Register was also searched,which would contain any ongoing trials.
Objectives and methods
8
Number and characteristics ofincluded fracture healing RCTsNine RCTs are included, by Bilic and colleagues,58
Chen and colleagues,59 Cook,60 Friedlaender andcolleagues,9,10 Govender and colleagues,61 Jonesand colleagues28 and Maniscalco and colleagues.62
Abstracts of the study by McKee and colleagues63
and Perry and colleagues64 are included. Theincluded studies assessed BMP for use intreatment of fractures or non-unions.
Appendix 6 gives the table of generalcharacteristics of each fracture-healing RCTincluded in this review. All but one of the studiesincluded patients with either acute or non-uniontibial fractures. Due to the different characteristicsof the fractures, the studies were assessed based onfracture type.
Five of the studies were conducted in the USA,one in Italy, one in China and one in Croatia andone was a multi-centre trial in 11 countries(Australia, Belgium, Canada, UK, Finland, France,Germany, Israel, The Netherlands, Norway andSouth Africa). Five of the studies specified thattheir funding source was industry. One study59 wasgovernment sponsored and three studies58,62,64 didnot state their source of funding.
The Govender study61 had the most patients, witha total of 450 and the McKee study63 had thesecond highest number of patients (124).Friedlaender and colleagues9,10 reported data on122 patients with 124 non-unions. The numbers ofpatients in the remaining studies ranged from14 to 80.
One RCT58 assessed BMP in scaphoid non-unionsat the proximal pole and the surgical procedurewas not described.
The Chen,59 Cook,60 Perry64 and Friedlaender9,10
studies included patients with tibial non-unions. Afracture is generally considered a tibial non-unionafter a number of unsuccessful procedures, thusindicating a more difficult fracture to healsuccessfully. Although these are RCTs, patientsmay not be convincingly comparable between theBMP and the control groups in terms of certain
baseline prognostic factors. The Friedlaenderstudy9,10 reported a statistically significantdifference in the rate of atrophic non-unions atbaseline between the intervention and controlgroups, p = 0.048. Atrophic non-unions werefound in 26% of the BMP intervention group and15% of the control group. An atrophic non-unionhas an impaired blood supply and is thereforeeven more difficult to heal. Other reporteddifferences between the groups, although notstatistically significant, include a higher number ofpatients smoking tobacco in the interventiongroup (74%) compared with the control group(57%), p = 0.057. There were also more priorautografts in the intervention group (43%) thanthe control group (31%) (p = 0.177) and a highernumber of comminuted fractures in theintervention group (67%) than the control group(56%), p = 0.212. All of these populationcharacteristics could affect the healing ability ofthe non-union fractures and hence may affect thecomparability of the intervention group.
The remaining studies included patients withacute tibial fractures. The Govender study61
included patients with open fractures, of which themain component was diaphyseal. The McKeestudy63 included patients with open tibial shaftfractures which were suitable for intramedullarynailing procedure. The Jones study28 includedpatients with open or closed diaphyseal fracturesand the Maniscalco study62 patients with closedfractures.
The patients with non-unions were treated witheither intramedullary (IM) nails9,60,64 or thetreatment used was not reported.59 In theGovender study,61 IM nail fixation and routine softtissue management were used to treat the opentibial fractures (OTFs). The authors reported astatistically significant difference between thegroups of those treated with reamed andunreamed IM nails. Totals of 39 (27%) of thecontrol group, 48 (33%) of intervention group Aand 59 (41%) of intervention group B receivedreamed IM nails, p = 0.0371. Statically locking IMnailing was used in the McKee study.63 The Jonesstudy28 used staged reconstruction of the tibia asits surgical intervention for open or closed tibiafractures. Finally, monolateral external fixator
Health Technology Assessment 2007; Vol. 11: No. 30
9
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Chapter 3
Results of effectiveness assessment: fracture healing

treatment was performed for treatment of theclosed fractures in the Maniscalco study.62
Two studies28,61 reported the severity of the tibiafractures based on the Gustilo–Andersonclassification of open wounds. They included allgrades of fractures from I to IIIB. TheFriedlaender study9,10 reported different grades offractures ranging from III to IIIC, but did notspecify the grading system used. Finally, the tworemaining studies did not give details on theseverity of fractures included.
Where reported, the mean age of patients withtibia fractures ranged from 31 to 47 years. In theGovender study,61 there was a statisticallysignificant difference between the ages of theintervention groups and the control group, withmean ages in the control and 0.75 mg/ml(intervention A) groups of 37 years and a meanage in the 1.5 mg/ml (intervention B) group of33 years, p = 0.0384. The mean ages of patients inthe scaphoid non-union study58 ranged from 19 to23 years. Most of the studies reported outcomes atmultiple points of assessment. The follow-up timesranged from 6 to 24 months. Friedlaender andcolleagues9 specified a 24-month follow-up, butoutcomes were reported at the 9-month primaryfollow-up point, unless specified otherwise. TheManiscalco study62 did not clearly specify thefollow-up length but gave a mean length of follow-up.
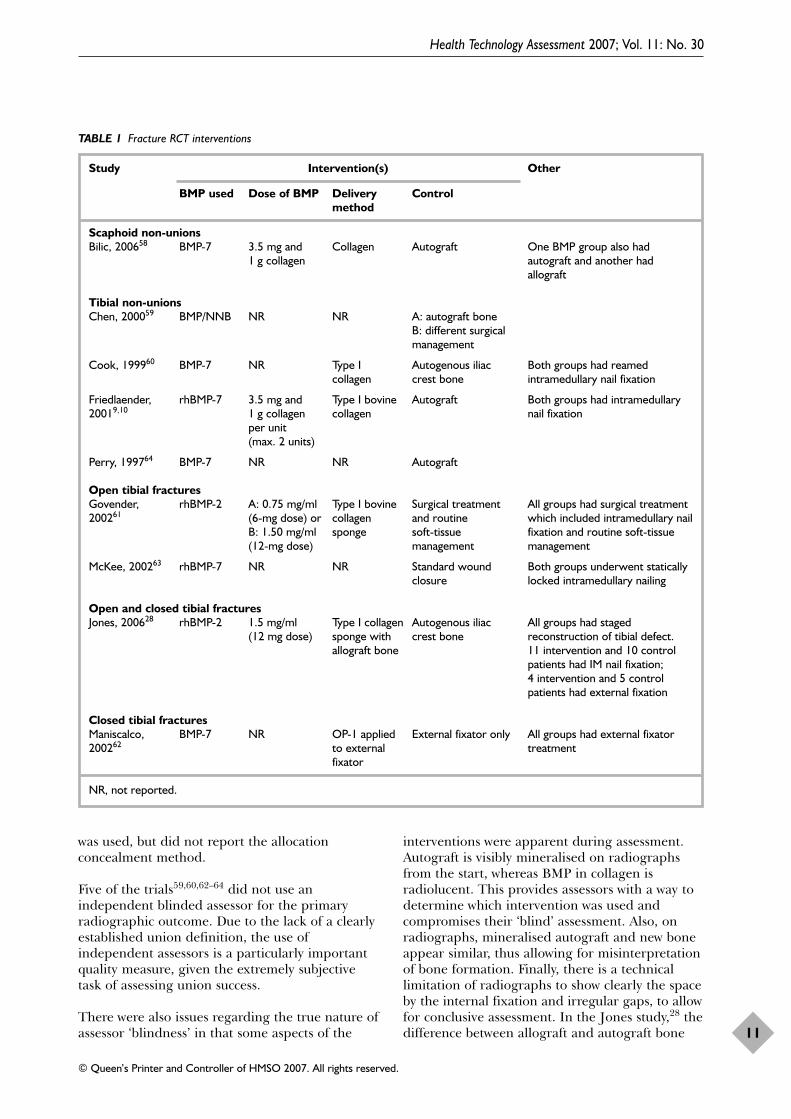
InterventionsTable 1 gives details on the interventionsinvestigated in the studies. Two studies28,61
investigated rhBMP-2 and six studies9,10,58,60,62–64
investigated BMP-7. One study59 used unspecifiedconcentrations of BMP and natural non-organicbone (NNB) in a complex.59 The concentrations ofrhBMP-2 used were 0.75 mg/ml61 and1.5 mg/ml.28,61 In the Govender study,61 therewere two intervention groups that received either a0.75 or 1.50 mg/ml concentration of BMP-2; 91%of patients in the 0.75 mg/ml group (interventionA) received the full dose of 6 g of rhBMP-2 and90% of intervention group B received the full1.50 mg/ml dose of 12 g of rhBMP-2. The patientswho did not receive the full dose did not because ofthe inability to close the wound because of the bulkof the BMP carrier. One fracture non-union study9
reported the concentration of BMP-7 used as 3.5mg per unit, with a maximum of two unitsimplanted (dependent on fracture size). Bilic andcolleagues58 reported that 3.5 mg of BMP-7 and 1 gof collagen were implanted in one group that alsoreceived autograft bone and another group that
received allograft bone. The remaining studies didnot report the dose of BMP-7 used.60,62–64 In theJones study,28 patients who received BMP-2 alsoreceived allograft bone. This is important becauseit is not possible to assign effectiveness to BMPalone compared with the control group.
Where reported, a collagen sponge was used todeliver the BMP-2 and collagen granules wereused to deliver the BMP-7. The control groups ofthe four studies9,10,28,60,64 that included patientswith non-unions received autograft bone inaddition to surgical treatment. One of thesestudies59 also had another control group thatreceived a different, unspecified, surgicaltreatment. Three studies61–63 that includedpatients with acute fractures used surgicaltreatment alone as the control intervention. In theremaining acute fracture study,28 the control grouppatients received AICBG. The scaphoid non-unioncontrol group received autograft bone only.
Quality assessment of studiesAppendix 7 summarises the quality of theincluded studies. Two of the studies arepreliminary reports60,62 and two63,64 are abstractsfrom conference presentations. The followingquality criteria were used to assess study designand methodology: randomisation method,allocation concealment, blinding of outcomeassessors, similar prognostic baselines, clearlydefined inclusion and exclusion criteria,performance of ITT analysis and the numbers andreasons of patients lost to follow-up reported.
The quality of the studies is variable, ranging fromlow to moderate, in that none of the studies meetall of the quality criteria. Based on the qualitycriteria, the studies in order of least to mostpossible bias is as follows: Govender andcolleagues;61 Bilic and colleagues,58 Jones andcolleagues,28 Friedlaender and colleagues9 andManiscalco and colleagues;62 Cook60 and Perryand colleagues;64 Chen and colleagues59 andMcKee and colleagues.63
In seven of the nine studies, the randomisationmethod was unclear in that they only used theterms ‘randomisation’ or ‘randomised’ and did notspecify the method used. For the same sevenstudies, the method of allocation concealment wasnot known. The remaining study, by Govenderand colleagues61 used a central, 24-hourautomated system, which was considered adequateand thus the allocation concealment was alsoconsidered adequate.65 Bilic and colleagues58
reported that computer-generated randomisation
Results of effectiveness assessment: fracture healing
10
was used, but did not report the allocationconcealment method.
Five of the trials59,60,62–64 did not use anindependent blinded assessor for the primaryradiographic outcome. Due to the lack of a clearlyestablished union definition, the use ofindependent assessors is a particularly importantquality measure, given the extremely subjectivetask of assessing union success.
There were also issues regarding the true nature ofassessor ‘blindness’ in that some aspects of the
interventions were apparent during assessment.Autograft is visibly mineralised on radiographsfrom the start, whereas BMP in collagen isradiolucent. This provides assessors with a way todetermine which intervention was used andcompromises their ‘blind’ assessment. Also, onradiographs, mineralised autograft and new boneappear similar, thus allowing for misinterpretationof bone formation. Finally, there is a technicallimitation of radiographs to show clearly the spaceby the internal fixation and irregular gaps, to allowfor conclusive assessment. In the Jones study,28 thedifference between allograft and autograft bone
Health Technology Assessment 2007; Vol. 11: No. 30
11
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 1 Fracture RCT interventions
Study Intervention(s) Other
BMP used Dose of BMP Delivery Controlmethod
Scaphoid non-unionsBilic, 200658 BMP-7 3.5 mg and Collagen Autograft One BMP group also had
1 g collagen autograft and another hadallograft
Tibial non-unionsChen, 200059 BMP/NNB NR NR A: autograft bone
B: different surgical management
Cook, 199960 BMP-7 NR Type I Autogenous iliac Both groups had reamed collagen crest bone intramedullary nail fixation
Friedlaender, rhBMP-7 3.5 mg and Type I bovine Autograft Both groups had intramedullary 20019,10 1 g collagen collagen nail fixation
per unit (max. 2 units)
Perry, 199764 BMP-7 NR NR Autograft
Open tibial fracturesGovender, rhBMP-2 A: 0.75 mg/ml Type I bovine Surgical treatment All groups had surgical treatment 200261 (6-mg dose) or collagen and routine which included intramedullary nail
B: 1.50 mg/ml sponge soft-tissue fixation and routine soft-tissue (12-mg dose) management management
McKee, 200263 rhBMP-7 NR NR Standard wound Both groups underwent statically closure locked intramedullary nailing
Open and closed tibial fracturesJones, 200628 rhBMP-2 1.5 mg/ml Type I collagen Autogenous iliac All groups had staged
(12 mg dose) sponge with crest bone reconstruction of tibial defect. allograft bone 11 intervention and 10 control
patients had IM nail fixation; 4 intervention and 5 controlpatients had external fixation
Closed tibial fracturesManiscalco, BMP-7 NR OP-1 applied External fixator only All groups had external fixator 200262 to external treatment
fixator
NR, not reported.

was apparent on the radiographs. Therefore, totest the ‘blindness’ of the blinded assessors, theradiographs were assessed in reverse chronologicalorder, and the point where the difference was nolonger apparent was identified. Six months wasdetermined as the point where ‘blindness’ wasconsistent and thus blinded assessors reviewed allof the images from 6 to 12 months.
Clinically, assessors use patient histories andclinical and radiographic outcomes to determinefracture healing.9 Therefore, relying on only oneaspect of clinical assessment may not provide anaccurate representation of clinical evaluation.Hence those studies28,61,62 that included clinicaloutcomes in their definition of successful healingmay provide a better representation of clinicalevaluations.
The Friedlaender study9 had a significantly highernumber of atrophic non-unions in the interventiongroup than control group, p = 0.048. Govenderand colleagues61 reported a statistically significantdifference in the ages between the interventiongroups and control group, where the mean age ofintervention group B was lower than those ofintervention group A and the control group,p = 0.0384. Three trials9,10,28,62 had a significantlyhigher number of males than females in theiroverall populations, but this was known to bebalanced between the intervention groups in allbut one of the studies.59 Three studies60,63,64 didnot report any population characteristics. Onestudy59 reported population characteristics, butdid not separate the characteristics between thetreatment groups. The inclusion and exclusioncriteria were clearly reported in four9,10,28,58,62 ofthe nine trials. The studies that did not adequatelyreport the inclusion and exclusion criteria gaveonly the patient diagnoses, and no furtherinformation.
Only two studies28,61 performed partial ITTanalyses in that the patients were assessed in thegroup to which they were randomised, but not allrandomised patients were included in the finalanalysis. Two studies did not mention patientdrop-outs.59,63 The drop-out rates in the Jonesstudy28 were 26.7% in the control group and13.3% in the BMP intervention group. TheGovender study61 reported an 8% drop-out rate inthe control group and 6 and 5.4% drop-outs inintervention groups A and B, respectively. Bilicand colleagues58 reported one patient drop-out inthe BMP–allograft group, but did not give areason. In the remaining studies, there were nopatient drop-outs.
Findings from RCTs on tibiafracturesRadiographic resultsTable 2 reports the union rates using ITT analysisof the studies and gives each study’s definition of asuccessful union.
The studies that reported a definition of successfulunion included the parameter of bridging boneseen on a certain number of radiographic views.Three of the studies28,61,62 also included clinicaloutcomes in their definition of successful union.Two studies59,64 did not report the definition ofunion used. The McKee study63 did not report theradiographic outcome or give a definition ofunion.
BMP for non-union tibial fractures:radiographic resultsChen and colleagues59 reported 100% union ratesin both the intervention group (n = 30) andautograft control group (n = 20). The secondcontrol group (n = 30) which received a different,unreported, surgical procedure had a 0% unionrate. The exact patient numbers are not reporteddue to the lack of information in the paperregarding drop-outs. Perry and colleagues64
reported a 95% union rate in the BMPintervention group and 81% in the control group.Two non-union studies9,10,60 reported higherunion rates in the control group. AlthoughFriedlaender and colleagues9 reported a follow-upof 24 months, they only reported radiographicunion rates at the 9-month follow-up point. It maybe that BMP is not as effective in severe cases ofnon-unions. Part of its action is to encourage ablood supply to form, which requires good localsoft tissue, especially muscle that may not bepresent in multiply-treated resistant non-unions.
The lengths of follow-up in these two studies9,10,60
were shorter than in the other non-union studies:9 months compared with 19 and 12 months. Thisshorter follow-up length could possibly have beentoo short, which therefore excluded some patientswho went on to heal within 12 months. Most ofthe acute fracture studies had a longer follow-uplength of 12 months. Data from the Jones study28
show that at the 8-month radiographic assessmentpoint the independent radiologist determined that60% (6/10) of control patients and 50% (6/12) ofintervention patients were healed. At the 12-month assessment, 67% (10/15) of controlpatients and 87% (13/15) of intervention patientswere considered healed. This example supportsthe view that a follow-up period of longer than
Results of effectiveness assessment: fracture healing
12
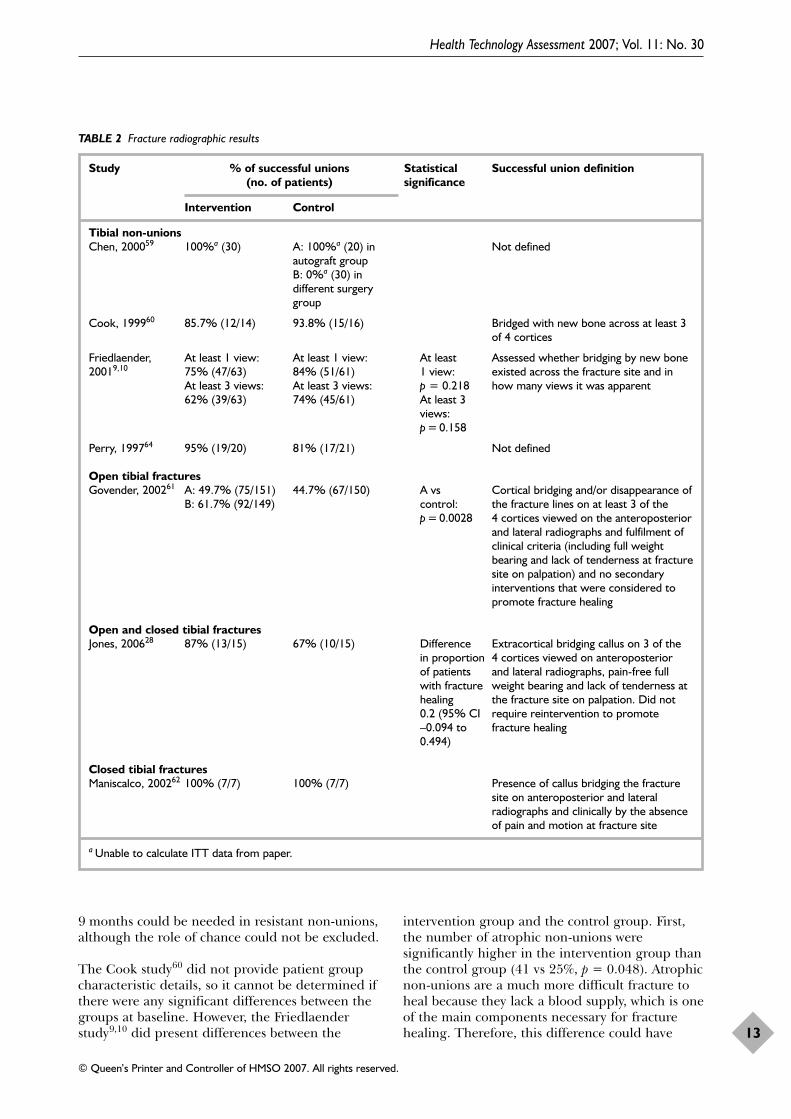
9 months could be needed in resistant non-unions,although the role of chance could not be excluded.
The Cook study60 did not provide patient groupcharacteristic details, so it cannot be determined ifthere were any significant differences between thegroups at baseline. However, the Friedlaenderstudy9,10 did present differences between the
intervention group and the control group. First,the number of atrophic non-unions weresignificantly higher in the intervention group thanthe control group (41 vs 25%, p = 0.048). Atrophicnon-unions are a much more difficult fracture toheal because they lack a blood supply, which is oneof the main components necessary for fracturehealing. Therefore, this difference could have
Health Technology Assessment 2007; Vol. 11: No. 30
13
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 2 Fracture radiographic results
Study % of successful unions Statistical Successful union definition(no. of patients) significance
Intervention Control
Tibial non-unionsChen, 200059 100%a (30) A: 100%a (20) in Not defined
autograft groupB: 0%a (30) in different surgery group
Cook, 199960 85.7% (12/14) 93.8% (15/16) Bridged with new bone across at least 3of 4 cortices
Friedlaender, At least 1 view: At least 1 view: At least Assessed whether bridging by new bone 20019,10 75% (47/63) 84% (51/61) 1 view: existed across the fracture site and in
At least 3 views: At least 3 views: p = 0.218 how many views it was apparent62% (39/63) 74% (45/61) At least 3
views: p = 0.158
Perry, 199764 95% (19/20) 81% (17/21) Not defined
Open tibial fracturesGovender, 200261 A: 49.7% (75/151) 44.7% (67/150) A vs Cortical bridging and/or disappearance of
B: 61.7% (92/149) control: the fracture lines on at least 3 of the p = 0.0028 4 cortices viewed on the anteroposterior
and lateral radiographs and fulfilment ofclinical criteria (including full weightbearing and lack of tenderness at fracturesite on palpation) and no secondaryinterventions that were considered topromote fracture healing
Open and closed tibial fracturesJones, 200628 87% (13/15) 67% (10/15) Difference Extracortical bridging callus on 3 of the
in proportion 4 cortices viewed on anteroposterior of patients and lateral radiographs, pain-free full with fracture weight bearing and lack of tenderness at healing the fracture site on palpation. Did not 0.2 (95% CI require reintervention to promote –0.094 to fracture healing0.494)
Closed tibial fracturesManiscalco, 200262 100% (7/7) 100% (7/7) Presence of callus bridging the fracture
site on anteroposterior and lateralradiographs and clinically by the absenceof pain and motion at fracture site
a Unable to calculate ITT data from paper.
affected the healing outcomes of the groups.Other differences to note, although not statisticallysignificant, were higher numbers of smokers(p = 0.057), prior autografts (p = 0.177),comminuted fractures (p = 0.212) and previousIM nail insertions (p = 0.280) in the interventiongroup compared with the control group. All ofthese characteristics increase the risk of resistantnon-union.
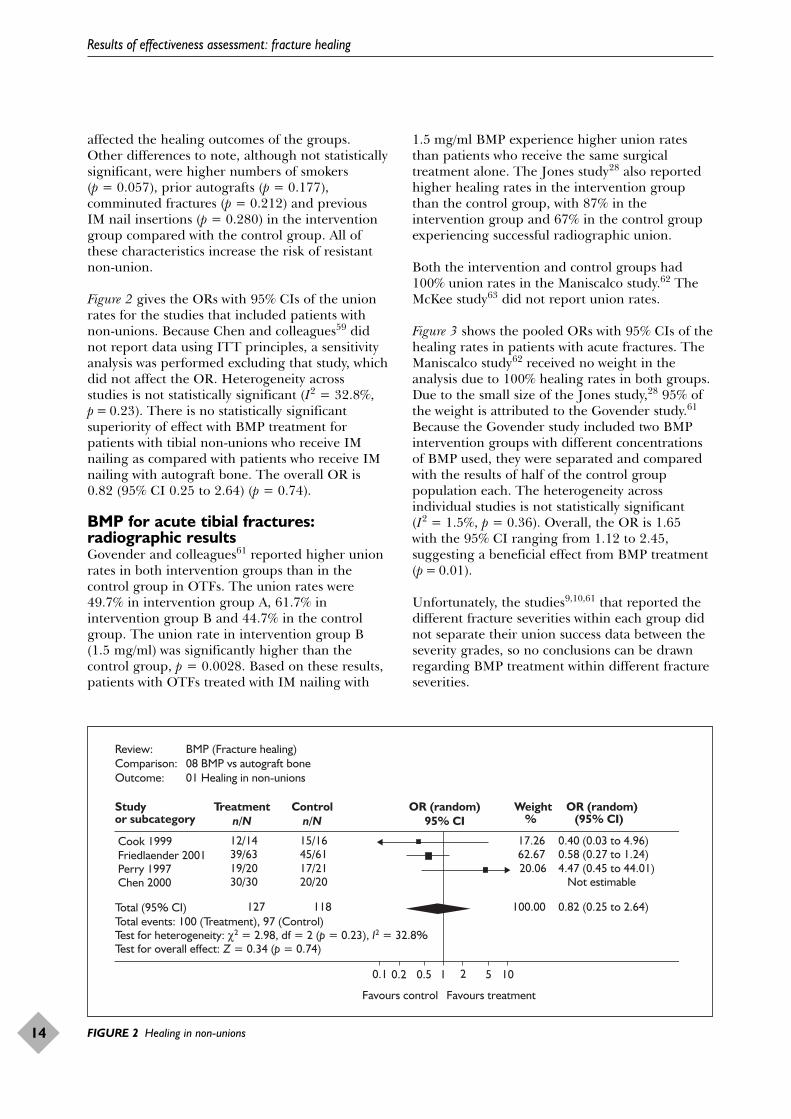
Figure 2 gives the ORs with 95% CIs of the unionrates for the studies that included patients withnon-unions. Because Chen and colleagues59 didnot report data using ITT principles, a sensitivityanalysis was performed excluding that study, whichdid not affect the OR. Heterogeneity acrossstudies is not statistically significant (I2 = 32.8%,p = 0.23). There is no statistically significantsuperiority of effect with BMP treatment forpatients with tibial non-unions who receive IMnailing as compared with patients who receive IMnailing with autograft bone. The overall OR is0.82 (95% CI 0.25 to 2.64) (p = 0.74).
BMP for acute tibial fractures:radiographic resultsGovender and colleagues61 reported higher unionrates in both intervention groups than in thecontrol group in OTFs. The union rates were49.7% in intervention group A, 61.7% inintervention group B and 44.7% in the controlgroup. The union rate in intervention group B(1.5 mg/ml) was significantly higher than thecontrol group, p = 0.0028. Based on these results,patients with OTFs treated with IM nailing with
1.5 mg/ml BMP experience higher union ratesthan patients who receive the same surgicaltreatment alone. The Jones study28 also reportedhigher healing rates in the intervention groupthan the control group, with 87% in theintervention group and 67% in the control groupexperiencing successful radiographic union.
Both the intervention and control groups had100% union rates in the Maniscalco study.62 TheMcKee study63 did not report union rates.
Figure 3 shows the pooled ORs with 95% CIs of thehealing rates in patients with acute fractures. TheManiscalco study62 received no weight in theanalysis due to 100% healing rates in both groups.Due to the small size of the Jones study,28 95% ofthe weight is attributed to the Govender study.61
Because the Govender study included two BMPintervention groups with different concentrationsof BMP used, they were separated and comparedwith the results of half of the control grouppopulation each. The heterogeneity acrossindividual studies is not statistically significant(I2 = 1.5%, p = 0.36). Overall, the OR is 1.65 with the 95% CI ranging from 1.12 to 2.45,suggesting a beneficial effect from BMP treatment(p = 0.01).
Unfortunately, the studies9,10,61 that reported thedifferent fracture severities within each group didnot separate their union success data between theseverity grades, so no conclusions can be drawnregarding BMP treatment within different fractureseverities.
Results of effectiveness assessment: fracture healing
14
Review: BMP (Fracture healing)Comparison: 08 BMP vs autograft boneOutcome: 01 Healing in non-unions
Study Treatmentn/N
Controln/N
OR (random)95% CI
Weight OR (random)or subcategory % (95% CI)
Cook 1999 12/14 15/16 17.26 0.40 (0.03 to 4.96) Friedlaender 2001 39/63 45/61 62.67 0.58 (0.27 to 1.24) Perry 1997 19/20 17/21 20.06 4.47 (0.45 to 44.01) Chen 2000 30/30 20/20 Not estimable
Total (95% CI) 127 118 100.00 0.82 (0.25 to 2.64)Total events: 100 (Treatment), 97 (Control)Test for heterogeneity: χ2 = 2.98, df = 2 (p = 0.23), I2 = 32.8%Test for overall effect: Z = 0.34 (p = 0.74)
0.1 0.2 0.5 1 2 5 10
Favours control Favours treatment
FIGURE 2 Healing in non-unions
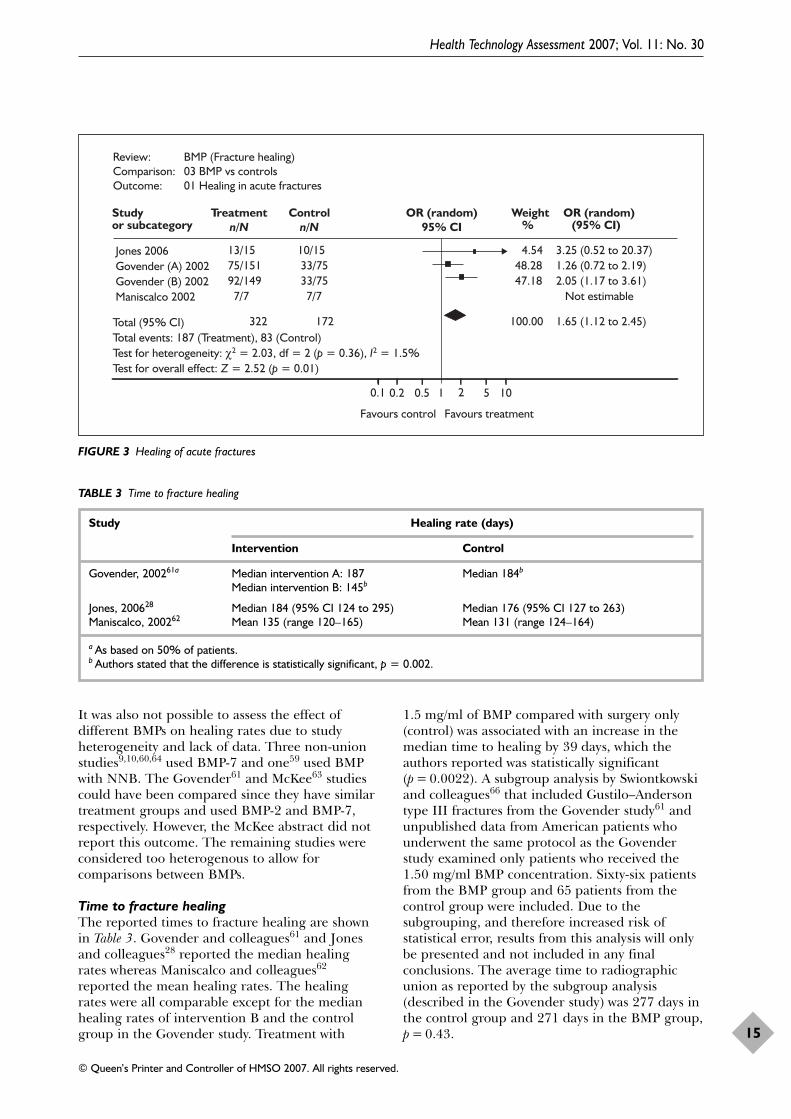
It was also not possible to assess the effect ofdifferent BMPs on healing rates due to studyheterogeneity and lack of data. Three non-unionstudies9,10,60,64 used BMP-7 and one59 used BMPwith NNB. The Govender61 and McKee63 studiescould have been compared since they have similartreatment groups and used BMP-2 and BMP-7,respectively. However, the McKee abstract did notreport this outcome. The remaining studies wereconsidered too heterogenous to allow forcomparisons between BMPs.
Time to fracture healingThe reported times to fracture healing are shownin Table 3. Govender and colleagues61 and Jonesand colleagues28 reported the median healingrates whereas Maniscalco and colleagues62
reported the mean healing rates. The healingrates were all comparable except for the medianhealing rates of intervention B and the controlgroup in the Govender study. Treatment with
1.5 mg/ml of BMP compared with surgery only(control) was associated with an increase in themedian time to healing by 39 days, which theauthors reported was statistically significant(p = 0.0022). A subgroup analysis by Swiontkowskiand colleagues66 that included Gustilo–Andersontype III fractures from the Govender study61 andunpublished data from American patients whounderwent the same protocol as the Govenderstudy examined only patients who received the1.50 mg/ml BMP concentration. Sixty-six patientsfrom the BMP group and 65 patients from thecontrol group were included. Due to thesubgrouping, and therefore increased risk ofstatistical error, results from this analysis will onlybe presented and not included in any finalconclusions. The average time to radiographicunion as reported by the subgroup analysis(described in the Govender study) was 277 days inthe control group and 271 days in the BMP group,p = 0.43.
Health Technology Assessment 2007; Vol. 11: No. 30
15
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Review: BMP (Fracture healing)Comparison: 03 BMP vs controlsOutcome: 01 Healing in acute fractures
Study Treatmentn/N
Controln/N
OR (random)95% CI
Weight OR (random)or subcategory % (95% CI)
0.1 0.2 0.5 1 2 5 10
Favours control Favours treatment
Jones 2006 13/15 10/15 4.54 3.25 (0.52 to 20.37) Govender (A) 2002 75/151 33/75 48.28 1.26 (0.72 to 2.19) Govender (B) 2002 92/149 33/75 47.18 2.05 (1.17 to 3.61) Maniscalco 2002 7/7 7/7 Not estimable
Total (95% CI) 322 172 100.00 1.65 (1.12 to 2.45)Total events: 187 (Treatment), 83 (Control)Test for heterogeneity: χ2 = 2.03, df = 2 (p = 0.36), I2 = 1.5%Test for overall effect: Z = 2.52 (p = 0.01)
FIGURE 3 Healing of acute fractures
TABLE 3 Time to fracture healing
Study Healing rate (days)
Intervention Control
Govender, 200261a Median intervention A: 187 Median 184b
Median intervention B: 145b
Jones, 200628 Median 184 (95% CI 124 to 295) Median 176 (95% CI 127 to 263)Maniscalco, 200262 Mean 135 (range 120–165) Mean 131 (range 124–164)
a As based on 50% of patients.b Authors stated that the difference is statistically significant, p = 0.002.
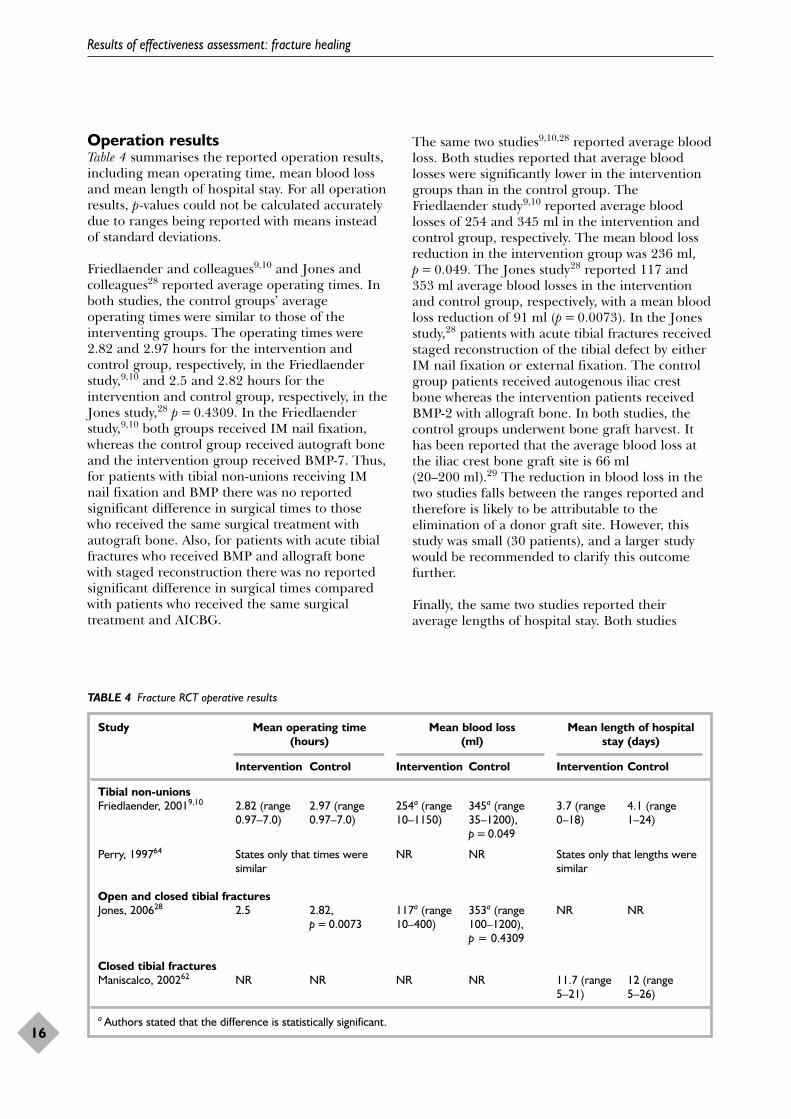
Operation resultsTable 4 summarises the reported operation results,including mean operating time, mean blood lossand mean length of hospital stay. For all operationresults, p-values could not be calculated accuratelydue to ranges being reported with means insteadof standard deviations.
Friedlaender and colleagues9,10 and Jones andcolleagues28 reported average operating times. Inboth studies, the control groups’ averageoperating times were similar to those of theinterventing groups. The operating times were2.82 and 2.97 hours for the intervention andcontrol group, respectively, in the Friedlaenderstudy,9,10 and 2.5 and 2.82 hours for theintervention and control group, respectively, in theJones study,28 p = 0.4309. In the Friedlaenderstudy,9,10 both groups received IM nail fixation,whereas the control group received autograft boneand the intervention group received BMP-7. Thus,for patients with tibial non-unions receiving IMnail fixation and BMP there was no reportedsignificant difference in surgical times to thosewho received the same surgical treatment withautograft bone. Also, for patients with acute tibialfractures who received BMP and allograft bonewith staged reconstruction there was no reportedsignificant difference in surgical times comparedwith patients who received the same surgicaltreatment and AICBG.
The same two studies9,10,28 reported average bloodloss. Both studies reported that average bloodlosses were significantly lower in the interventiongroups than in the control group. TheFriedlaender study9,10 reported average bloodlosses of 254 and 345 ml in the intervention andcontrol group, respectively. The mean blood lossreduction in the intervention group was 236 ml,p = 0.049. The Jones study28 reported 117 and353 ml average blood losses in the interventionand control group, respectively, with a mean bloodloss reduction of 91 ml (p = 0.0073). In the Jonesstudy,28 patients with acute tibial fractures receivedstaged reconstruction of the tibial defect by eitherIM nail fixation or external fixation. The controlgroup patients received autogenous iliac crestbone whereas the intervention patients receivedBMP-2 with allograft bone. In both studies, thecontrol groups underwent bone graft harvest. Ithas been reported that the average blood loss atthe iliac crest bone graft site is 66 ml(20–200 ml).29 The reduction in blood loss in thetwo studies falls between the ranges reported andtherefore is likely to be attributable to theelimination of a donor graft site. However, thisstudy was small (30 patients), and a larger studywould be recommended to clarify this outcomefurther.
Finally, the same two studies reported theiraverage lengths of hospital stay. Both studies
Results of effectiveness assessment: fracture healing
16
TABLE 4 Fracture RCT operative results
Study Mean operating time Mean blood loss Mean length of hospital (hours) (ml) stay (days)
Intervention Control Intervention Control Intervention Control
Tibial non-unionsFriedlaender, 20019,10 2.82 (range 2.97 (range 254a (range 345a (range 3.7 (range 4.1 (range
0.97–7.0) 0.97–7.0) 10–1150) 35–1200), 0–18) 1–24)p = 0.049
Perry, 199764 States only that times were NR NR States only that lengths were similar similar
Open and closed tibial fracturesJones, 200628 2.5 2.82, 117a (range 353a (range NR NR
p = 0.0073 10–400) 100–1200), p = 0.4309
Closed tibial fracturesManiscalco, 200262 NR NR NR NR 11.7 (range 12 (range
5–21) 5–26)
a Authors stated that the difference is statistically significant.

reported slightly longer lengths of stay for thecontrol groups compared with the interventiongroups, although the criteria for dischargingpatients was not described in either study. TheFriedlaender study9,10 reported an average hospitalstay of 3.7 days for the intervention group and4.1 days for the control group. The Jones study28
reported an average hospital stay length of 11.7days in the intervention group and 12 days in thecontrol group. There is not a significant differencebetween the reported lengths of hospital stay;therefore, based on reported data, treatment withBMP does not seem to affect this outcome for theincluded patients who received the specific surgicaltreatments as compared with their control groups.
For patients with tibial non-unions or acutefractures, there is no evidence to suggest adifference in surgical times or hospital stay lengthswith BMP treatment. However, there is astatistically significant reduction in blood losscompared with control autograft.
Other clinical outcomesTable 5 summarises the clinical outcomes mostfrequently reported, which were weight bearingand pain upon weight bearing.
Four studies9,10,60,62,63 reported results on weightbearing. Friedlaender and colleagues9,10 reportedsimilar percentages of patients’ weight bearing atthe final end-point (9 months) in the interventionand the control group. The method andparameters used to assess weight bearing were notdescribed. The McKee study63 reported 11% morepatients weight bearing in the intervention versusthe control group. However, it did not provide theactual number of patients weight bearing ornumber of drop-outs, so this result should betreated with caution. The Cook study60 onlyreported the total number of patients in the wholestudy weight bearing at the final end-point andthe Maniscalco study62 reported the averagenumber of days when each group was allowedpartial weight bearing. The Swiontkowskisubgroup analysis66 reported that the includedpatients’ time to full weight bearing was shorter inthe BMP group (95 ± 38 days) than the controlgroup (126 ± 61 days).
Due to the lack and variability of the data provided,it is not possible to determine whether treatmentwith BMP affects the patients’ ability to weightbear or the time at which they could weight bear.
Five studies9,10,60,61,63,64 reported on pain outcomes.The patients in the Friedlaender study9,10
reported mild pain at the surgical site in 89 and90% of the intervention and control groups,respectively, at the 9-month follow-up point. TheGovender study61 reported the number of patientswith overall body pain. The frequency of pain wassignificantly lower (67 and 68% in interventiongroups A and B, respectively) in both interventiongroups compared with the control group (79%),p = 0.0389. The statistical significance for theintervention B group compared to the controlgroup was p = 0.0343. The Govender studysuggests that there is an improvement in overallbody pain for patients with OTFs who receivesurgery with BMP as opposed to surgery alone.McKee and colleagues63 reported the proportionof patients without pain during activity; 24% fewerpatients in the BMP intervention groupexperienced pain with activity than in the controlgroup, p = 0.04. As with the weight bearingoutcome, this result should be treated with cautiondue to missing patient drop-out information.Cook60 reported the total number of patients withpain and their varying degrees of pain uponweight bearing regardless of their treatmentgroup. Owing to unstandardised methods ofcollecting data in some studies and lack of data inothers, it was not possible to conduct a meta-analysis to draw a better conclusion on the effectof BMP treatment on pain. Due to variablereporting in the non-union studies, it cannot bedetermined whether or not treatment with BMPaffects pain in patients with non-unions comparedwith treatment with autograft bone.
Three studies9,10,28,64 reported on donor site pain.Friedlaender and colleagues9,10 reported that allcontrol patients experienced pain at the donor siteand 80% of them reported that their pain wasmoderate or severe. At the 6-month follow-up,more than 20% still had mild or moderate pain atthe donor site, and at 12 months, 13% of patientsreported persistent pain. About 93% (14/15) of thecontrol group patients in the Jones study28
reported pain at the donor site, which rangedfrom 5 days to 4.5 months. At 12 months, onepatient reported residual tenderness at the graftsite. Perry and colleagues64 only reported that thecontrol patients experienced severe but temporarypain at the donor site. BMP has the advantage ofeliminating any donor site pain related toharvesting autograft bone.
The inconsistent reporting among the studiesraises concern about possible reporting bias. TheCook60 study reported the weight bearing andpain outcomes of the whole study population,regardless of treatment group.
Health Technology Assessment 2007; Vol. 11: No. 30
17
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
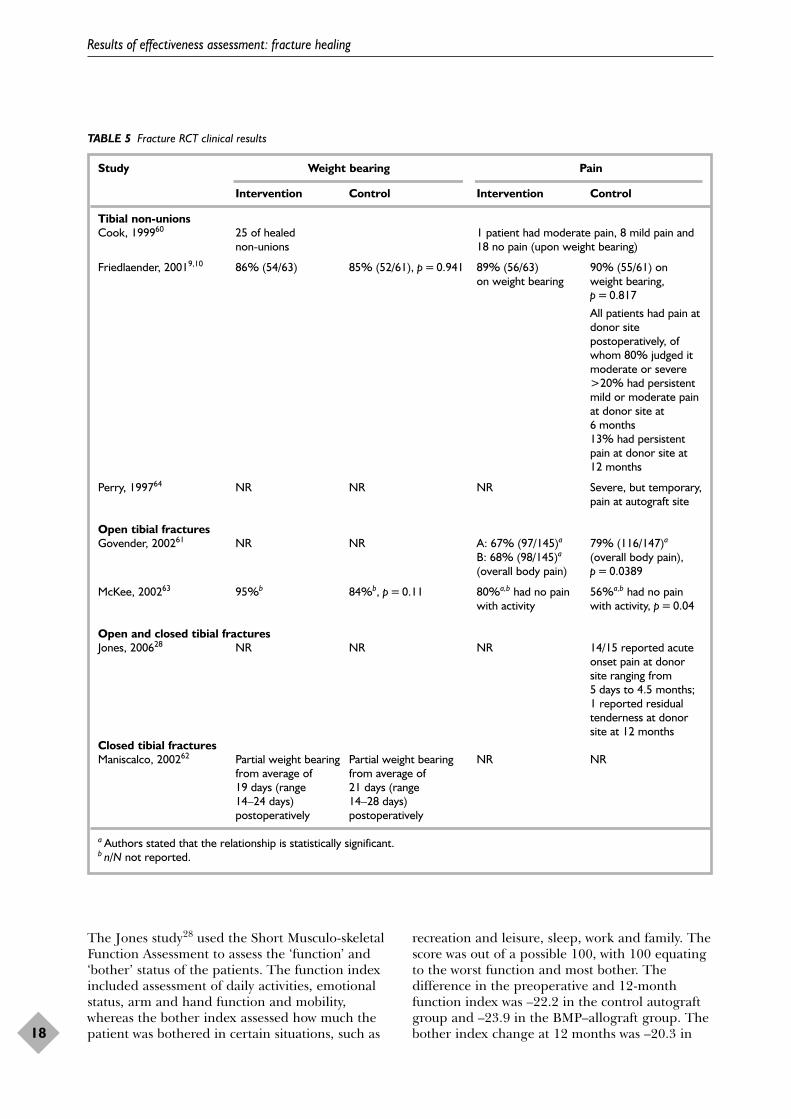
The Jones study28 used the Short Musculo-skeletalFunction Assessment to assess the ‘function’ and‘bother’ status of the patients. The function indexincluded assessment of daily activities, emotionalstatus, arm and hand function and mobility,whereas the bother index assessed how much thepatient was bothered in certain situations, such as
recreation and leisure, sleep, work and family. Thescore was out of a possible 100, with 100 equatingto the worst function and most bother. Thedifference in the preoperative and 12-monthfunction index was –22.2 in the control autograftgroup and –23.9 in the BMP–allograft group. Thebother index change at 12 months was –20.3 in
Results of effectiveness assessment: fracture healing
18
TABLE 5 Fracture RCT clinical results
Study Weight bearing Pain
Intervention Control Intervention Control
Tibial non-unionsCook, 199960 25 of healed 1 patient had moderate pain, 8 mild pain and
non-unions 18 no pain (upon weight bearing)
Friedlaender, 20019,10 86% (54/63) 85% (52/61), p = 0.941 89% (56/63) 90% (55/61) on on weight bearing weight bearing,
p = 0.817
All patients had pain atdonor sitepostoperatively, ofwhom 80% judged itmoderate or severe>20% had persistentmild or moderate painat donor site at6 months13% had persistentpain at donor site at12 months
Perry, 199764 NR NR NR Severe, but temporary,pain at autograft site
Open tibial fracturesGovender, 200261 NR NR A: 67% (97/145)a 79% (116/147)a
B: 68% (98/145)a (overall body pain), (overall body pain) p = 0.0389
McKee, 200263 95%b 84%b, p = 0.11 80%a,b had no pain 56%a,b had no pain with activity with activity, p = 0.04
Open and closed tibial fracturesJones, 200628 NR NR NR 14/15 reported acute
onset pain at donorsite ranging from5 days to 4.5 months;1 reported residualtenderness at donorsite at 12 months
Closed tibial fracturesManiscalco, 200262 Partial weight bearing Partial weight bearing NR NR
from average of from average of 19 days (range 21 days (range 14–24 days) 14–28 days) postoperatively postoperatively
a Authors stated that the relationship is statistically significant.b n/N not reported.
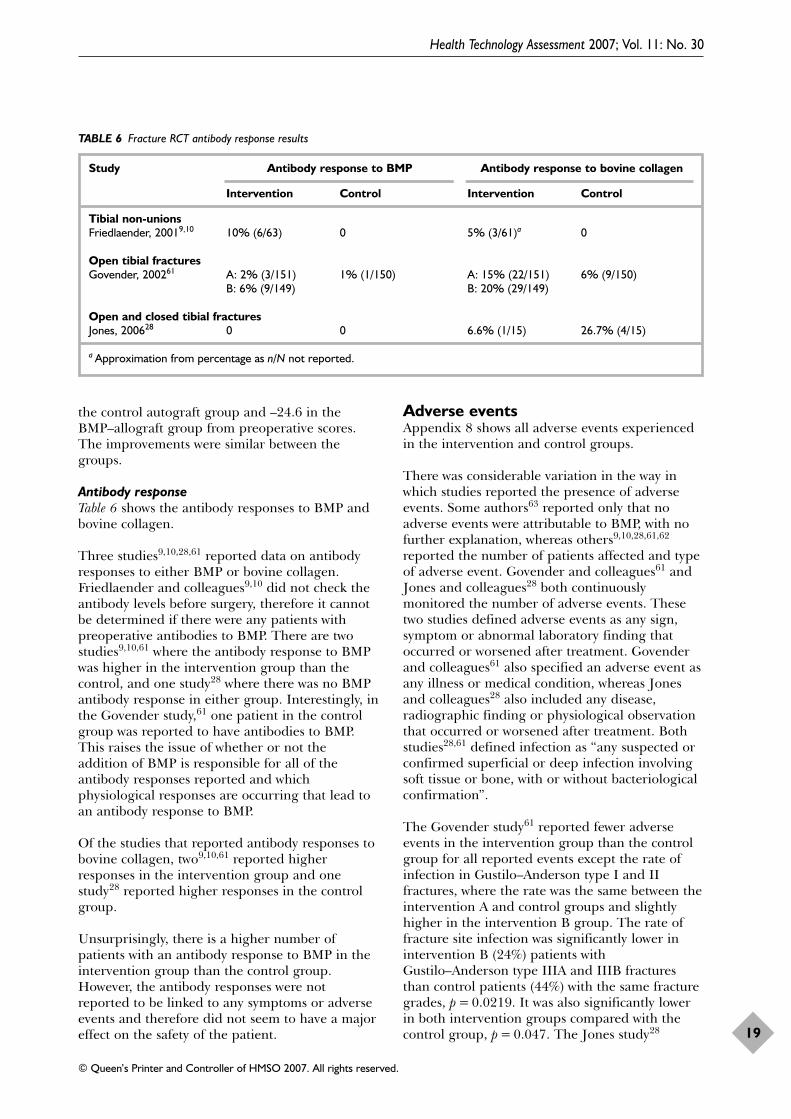
the control autograft group and –24.6 in theBMP–allograft group from preoperative scores.The improvements were similar between thegroups.
Antibody responseTable 6 shows the antibody responses to BMP andbovine collagen.
Three studies9,10,28,61 reported data on antibodyresponses to either BMP or bovine collagen.Friedlaender and colleagues9,10 did not check theantibody levels before surgery, therefore it cannotbe determined if there were any patients withpreoperative antibodies to BMP. There are twostudies9,10,61 where the antibody response to BMPwas higher in the intervention group than thecontrol, and one study28 where there was no BMPantibody response in either group. Interestingly, inthe Govender study,61 one patient in the controlgroup was reported to have antibodies to BMP.This raises the issue of whether or not theaddition of BMP is responsible for all of theantibody responses reported and whichphysiological responses are occurring that lead toan antibody response to BMP.
Of the studies that reported antibody responses tobovine collagen, two9,10,61 reported higherresponses in the intervention group and onestudy28 reported higher responses in the controlgroup.
Unsurprisingly, there is a higher number ofpatients with an antibody response to BMP in theintervention group than the control group.However, the antibody responses were notreported to be linked to any symptoms or adverseevents and therefore did not seem to have a majoreffect on the safety of the patient.
Adverse eventsAppendix 8 shows all adverse events experiencedin the intervention and control groups.
There was considerable variation in the way inwhich studies reported the presence of adverseevents. Some authors63 reported only that noadverse events were attributable to BMP, with nofurther explanation, whereas others9,10,28,61,62
reported the number of patients affected and typeof adverse event. Govender and colleagues61 andJones and colleagues28 both continuouslymonitored the number of adverse events. Thesetwo studies defined adverse events as any sign,symptom or abnormal laboratory finding thatoccurred or worsened after treatment. Govenderand colleagues61 also specified an adverse event asany illness or medical condition, whereas Jonesand colleagues28 also included any disease,radiographic finding or physiological observationthat occurred or worsened after treatment. Bothstudies28,61 defined infection as “any suspected orconfirmed superficial or deep infection involvingsoft tissue or bone, with or without bacteriologicalconfirmation”.
The Govender study61 reported fewer adverseevents in the intervention group than the controlgroup for all reported events except the rate ofinfection in Gustilo–Anderson type I and IIfractures, where the rate was the same between theintervention A and control groups and slightlyhigher in the intervention B group. The rate offracture site infection was significantly lower inintervention B (24%) patients withGustilo–Anderson type IIIA and IIIB fracturesthan control patients (44%) with the same fracturegrades, p = 0.0219. It was also significantly lowerin both intervention groups compared with thecontrol group, p = 0.047. The Jones study28
Health Technology Assessment 2007; Vol. 11: No. 30
19
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 6 Fracture RCT antibody response results
Study Antibody response to BMP Antibody response to bovine collagen
Intervention Control Intervention Control
Tibial non-unionsFriedlaender, 20019,10 10% (6/63) 0 5% (3/61)a 0
Open tibial fracturesGovender, 200261 A: 2% (3/151) 1% (1/150) A: 15% (22/151) 6% (9/150)
B: 6% (9/149) B: 20% (29/149)
Open and closed tibial fracturesJones, 200628 0 0 6.6% (1/15) 26.7% (4/15)
a Approximation from percentage as n/N not reported.

supported the results in the Govender study61 byalso reporting fewer adverse events. The groupshad similar adverse events in the Jones study,28
except for five patients who developed epidermalerythemas and one patient who had heterotopicbone formation in the BMP group and twopatients who had hardware failure in the controlgroup. The erythemas in BMP patients werereported to be mild or moderate and to haveresolved within 6–12 weeks postoperatively. Theheterotopic bone was described as an ‘anteriorbone spur’ and did not require removal. McKeeand colleagues63 did not report any specificsregarding adverse events but did say that anyadverse events were not related to BMP.Friedlaender and colleagues9,10 retrospectivelyclassified all adverse events as serious or non-serious according to the International Conferenceof Harmonization Guidelines.67 In both groups44% of patients had serious adverse events. Thestudy9,10 also reported a statistically significantdifference in the number of postoperativeosteomyelitis (bone infection) events, with 3%(n = 2) occurring in the BMP intervention groupand 21% (n = 13) in the control group, p = 0.002.The Maniscalco study62 reported that one patientin the BMP group had calcification of the tibio-fibular ligament and one control patient fell1 month after fixator removal and refractured thebone. The remaining studies reported moreadverse events in the intervention groups than thecontrol groups.
As previously reported, pain at the donor site wasa major issue for patients who underwent bonegrafting. Three patients in the control group ofthe Jones study28 also developed pustules ordrainage at the donor graft site, which lasted upto 2 weeks.
Overall, the evidence suggests that BMP reducesosteomyelitis in non-union fractures compared withautograft. It also reduces infections and pain inGustilo–Anderson type IIIA and IIIB openfractures compared with surgery alone. In studieswhere autograft bone was used as the control, BMPeliminated donor site pain and morbidity.Generally, the number and type of adverse eventsreported were similar between intervention groups,apart from one case of heterotopic bone formation,five cases of epidermal erythema and one case oftibio-fibular ligament calcification in BMP groups.
Secondary interventionsTable 7 gives the numbers and percentages ofpatients requiring secondary interventionsreported in the included RCTs of BMP for tibial
fractures. It also gives any details that wereprovided in the papers regarding the surgicalinterventions performed.
Four studies reported data on the number ofsecondary interventions in each group. In theJones study,28 the proportions of patients requiringsecondary interventions were similar between thegroups. In three studies,9,10,61,63 the proportion ofsecondary interventions was higher in the controlgroup than the intervention groups. Govender andcolleagues61 classified the secondary procedures asmost, less or non-invasive. The most invasiveprocedures included bone graft, exchange nailing,plate fixation, fibular osteotomy or bone transport;less invasive procedures included nail dynamisationor exchange from internal fixation to functionalbrace; and non-invasive procedures includedultrasound, electric stimulation or magnetic fieldstimulation. Fewer intervention patients requiredeither the most and less-invasive procedures thanthe control patients. There was a statisticallysignificant difference in the need for secondaryinterventions between the intervention groups66
(36 and 24% of BMP intervention groups A and B,respectively) and the control group (42%),p = 0.0326. There was also a statistically significantdifference between the number of ‘most invasive’procedures required between the groups,p = 0.0264. The Swiontkowski subgroup analysis66
reported significantly more control patients whoreceived invasive secondary procedures, with 28%(18/65) of the control group and 9% (6/66) of theBMP group, p = 0.0065. Similar statisticallysignificant findings were reported in the McKeestudy63 (p = 0.02). The Jones study28 reportedsimilar rates of secondary interventions in eachgroup; however, this study may lack power due tosmall sample sizes. From the above studies, there issome evidence that BMP treatment is associatedwith fewer secondary interventions compared withsurgery alone for patients with acute OTFs.
The Govender study61 also reported the proportionof secondary interventions based on woundseverity classification and smoking history. Therewere significantly fewer secondary interventions inpatients with both Gustilo–Anderson type IIIB andI, II and type IIIA fractures in intervention groupB compared with the control group, p < 0.01. Inpatients with a recent history of smoking, therewas a significantly lower rate of secondaryinterventions in intervention group B comparedwith the control group, p = 0.0138.
Among the patients with non-union fractures, theFriedlaender study9,10 reported a 2% difference in
Results of effectiveness assessment: fracture healing
20
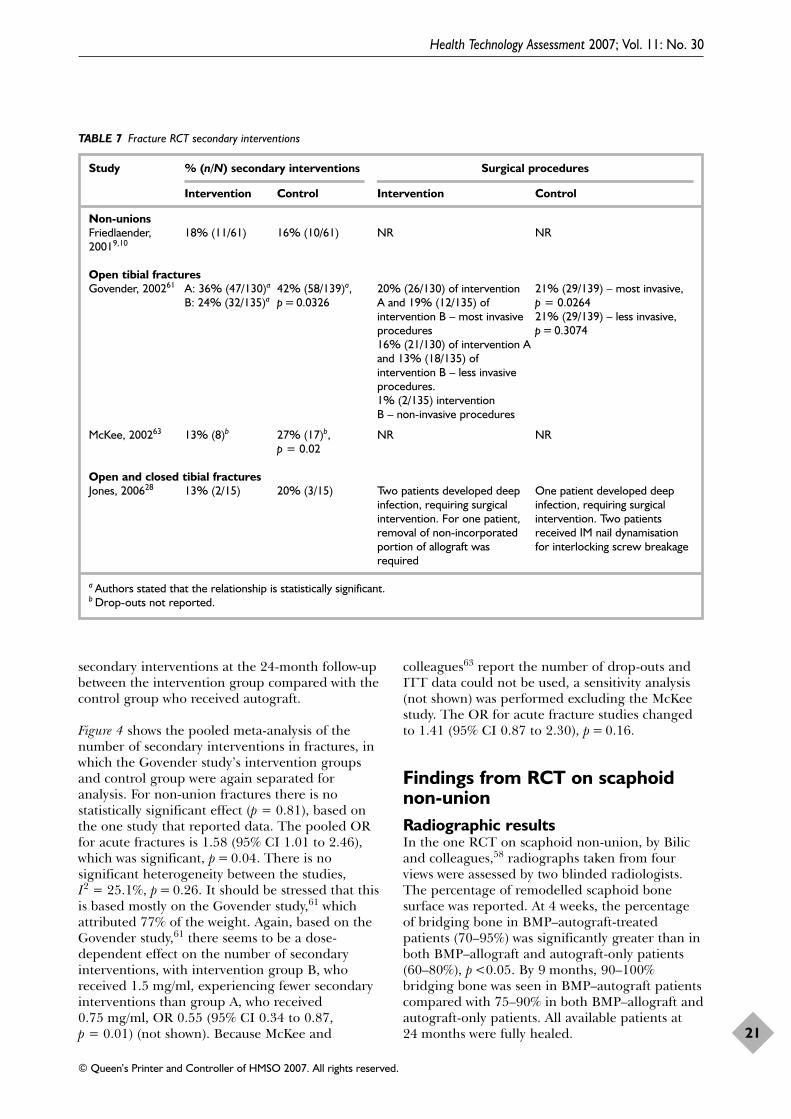
secondary interventions at the 24-month follow-upbetween the intervention group compared with thecontrol group who received autograft.
Figure 4 shows the pooled meta-analysis of thenumber of secondary interventions in fractures, inwhich the Govender study’s intervention groupsand control group were again separated foranalysis. For non-union fractures there is nostatistically significant effect (p = 0.81), based onthe one study that reported data. The pooled ORfor acute fractures is 1.58 (95% CI 1.01 to 2.46),which was significant, p = 0.04. There is nosignificant heterogeneity between the studies,I2 = 25.1%, p = 0.26. It should be stressed that thisis based mostly on the Govender study,61 whichattributed 77% of the weight. Again, based on theGovender study,61 there seems to be a dose-dependent effect on the number of secondaryinterventions, with intervention group B, whoreceived 1.5 mg/ml, experiencing fewer secondaryinterventions than group A, who received0.75 mg/ml, OR 0.55 (95% CI 0.34 to 0.87,p = 0.01) (not shown). Because McKee and
colleagues63 report the number of drop-outs andITT data could not be used, a sensitivity analysis(not shown) was performed excluding the McKeestudy. The OR for acute fracture studies changedto 1.41 (95% CI 0.87 to 2.30), p = 0.16.
Findings from RCT on scaphoidnon-unionRadiographic resultsIn the one RCT on scaphoid non-union, by Bilicand colleagues,58 radiographs taken from fourviews were assessed by two blinded radiologists.The percentage of remodelled scaphoid bonesurface was reported. At 4 weeks, the percentageof bridging bone in BMP–autograft-treatedpatients (70–95%) was significantly greater than inboth BMP–allograft and autograft-only patients(60–80%), p <0.05. By 9 months, 90–100%bridging bone was seen in BMP–autograft patientscompared with 75–90% in both BMP–allograft andautograft-only patients. All available patients at24 months were fully healed.
Health Technology Assessment 2007; Vol. 11: No. 30
21
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 7 Fracture RCT secondary interventions
Study % (n/N) secondary interventions Surgical procedures
Intervention Control Intervention Control
Non-unionsFriedlaender, 18% (11/61) 16% (10/61) NR NR20019,10
Open tibial fracturesGovender, 200261 A: 36% (47/130)a 42% (58/139)a, 20% (26/130) of intervention 21% (29/139) – most invasive,
B: 24% (32/135)a p = 0.0326 A and 19% (12/135) of p = 0.0264intervention B – most invasive 21% (29/139) – less invasive, procedures p = 0.307416% (21/130) of intervention Aand 13% (18/135) of intervention B – less invasive procedures. 1% (2/135) intervention B – non-invasive procedures
McKee, 200263 13% (8)b 27% (17)b, NR NRp = 0.02
Open and closed tibial fracturesJones, 200628 13% (2/15) 20% (3/15) Two patients developed deep One patient developed deep
infection, requiring surgical infection, requiring surgical intervention. For one patient, intervention. Two patients removal of non-incorporated received IM nail dynamisation portion of allograft was for interlocking screw breakagerequired
a Authors stated that the relationship is statistically significant.b Drop-outs not reported.
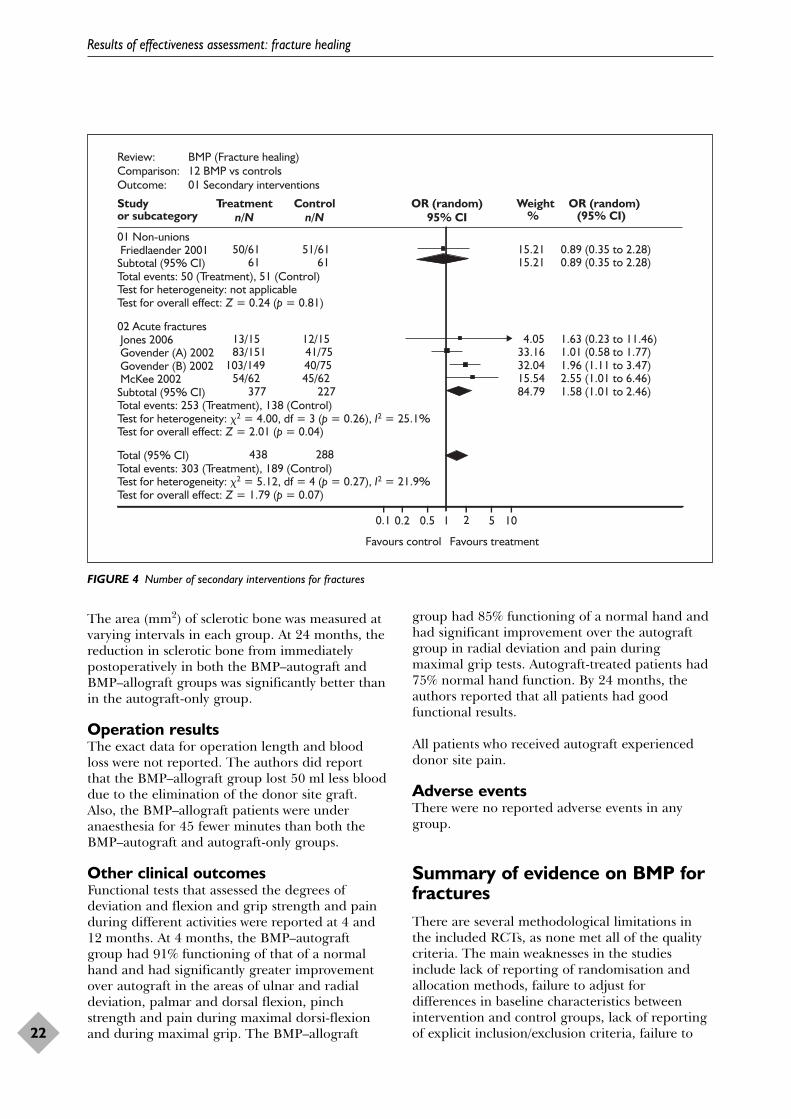
The area (mm2) of sclerotic bone was measured atvarying intervals in each group. At 24 months, thereduction in sclerotic bone from immediatelypostoperatively in both the BMP–autograft andBMP–allograft groups was significantly better thanin the autograft-only group.
Operation resultsThe exact data for operation length and bloodloss were not reported. The authors did reportthat the BMP–allograft group lost 50 ml less blooddue to the elimination of the donor site graft.Also, the BMP–allograft patients were underanaesthesia for 45 fewer minutes than both theBMP–autograft and autograft-only groups.
Other clinical outcomesFunctional tests that assessed the degrees ofdeviation and flexion and grip strength and painduring different activities were reported at 4 and12 months. At 4 months, the BMP–autograftgroup had 91% functioning of that of a normalhand and had significantly greater improvementover autograft in the areas of ulnar and radialdeviation, palmar and dorsal flexion, pinchstrength and pain during maximal dorsi-flexionand during maximal grip. The BMP–allograft
group had 85% functioning of a normal hand andhad significant improvement over the autograftgroup in radial deviation and pain duringmaximal grip tests. Autograft-treated patients had75% normal hand function. By 24 months, theauthors reported that all patients had goodfunctional results.
All patients who received autograft experienceddonor site pain.
Adverse eventsThere were no reported adverse events in anygroup.
Summary of evidence on BMP forfracturesThere are several methodological limitations inthe included RCTs, as none met all of the qualitycriteria. The main weaknesses in the studiesinclude lack of reporting of randomisation andallocation methods, failure to adjust fordifferences in baseline characteristics betweenintervention and control groups, lack of reportingof explicit inclusion/exclusion criteria, failure to
Results of effectiveness assessment: fracture healing
22
Review: BMP (Fracture healing)Comparison: 12 BMP vs controlsOutcome: 01 Secondary interventions
Study Treatmentn/N
Controln/N
OR (random)95% CI
Weight OR (random)or subcategory % (95% CI)
0.1 0.2 0.5 1 2 5 10
Favours control Favours treatment
01 Non-unions Friedlaender 2001 50/61 51/61 15.21 0.89 (0.35 to 2.28)Subtotal (95% CI) 61 61 15.21 0.89 (0.35 to 2.28)Total events: 50 (Treatment), 51 (Control)Test for heterogeneity: not applicableTest for overall effect: Z = 0.24 (p = 0.81)
02 Acute fractures Jones 2006 13/15 12/15 4.05 1.63 (0.23 to 11.46) Govender (A) 2002 83/151 41/75 33.16 1.01 (0.58 to 1.77) Govender (B) 2002 103/149 40/75 32.04 1.96 (1.11 to 3.47) McKee 2002 54/62 45/62 15.54 2.55 (1.01 to 6.46)Subtotal (95% CI) 377 227 84.79 1.58 (1.01 to 2.46)Total events: 253 (Treatment), 138 (Control)Test for heterogeneity: �2 = 4.00, df = 3 (p = 0.26), I2 = 25.1%Test for overall effect: Z = 2.01 (p = 0.04)
Total (95% CI) 438 288Total events: 303 (Treatment), 189 (Control)Test for heterogeneity: �2 = 5.12, df = 4 (p = 0.27), I2 = 21.9%Test for overall effect: Z = 1.79 (p = 0.07)
FIGURE 4 Number of secondary interventions for fractures
perform ITT analysis or to use independentblinded assessors and failure to report reasons fordrop-outs. Some outcomes were not measuredand/or reported in every included trial.
Tibial acute and non-union fracturesThere is no evidence that BMP treatment isassociated with shorter operating times or hospitalstays. There is evidence, however, that BMPintervention may be associated with a reduction inoperation blood loss, with reported meandecreases of 91 and 236 ml (p < 0.05). In patientswith non-unions, this may be attributable toelimination of blood loss from autograft removalfrom the donor site, which was conducted in thecontrol group.
According to evidence from three trials, BMPtreatment is associated with increasedradiographic healing amongst patients with acutetibial fractures (pooled OR 1.65, 95% CI 1.12 to2.45). This is based mainly on the data from onelarger study which carries 95% of the weight.
The available data from four clinical trials on non-union tibial fracture showed no statisticallysignificant difference between BMP and standardtreatment with autograft bone (pooled OR forradiographical union 0.82, 95% CI 0.25 to 2.64).
Furthermore, treatment with BMP eliminates theneed for bone grafting, where autograft bonewould normally be used, and thus eliminatesdonor site morbidities. The use of BMP reducesthe number of secondary interventions in patientswith acute tibial fractures compared with controls.
It was difficult to draw a conclusion on the impactof BMP treatment on weight bearing ability and/orpain as the data were scarce or collected in anunstandardised manner across the studies. Thereis some evidence that BMP treatment is associatedwith a lower number of adverse eventsexperienced in patients with non-unions and acutefractures in comparison with autograft and surgeryalone, respectively.
Appendix 24 reports a patient’s perspective on hisexperience and his suggestions regarding acutetibial fractures.
Scaphoid non-unionThere is little evidence on BMP in scaphoid non-union, although the evidence available suggeststhat BMP is safe and may help to accelerate non-union healing when used in conjunction witheither autograft or allograft. When used withallograft it eliminates the need for a donor site,thus preventing any associated morbidity.
Health Technology Assessment 2007; Vol. 11: No. 30
23
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.

Number and characteristics ofincluded spinal fusion RCTsTwelve RCTs are included, by Baskin andcolleagues,68 Boden and colleagues,69 Boden andcolleagues,70 Burkus and colleagues,71–73 Burkusand colleagues,74–76 Dimar and colleagues,77,78
Haid and colleagues,79 Johnsson and colleagues,80
Kanayama and colleagues81 and Vaccaro andcolleagues.82 Also included are abstracts by Assiriand colleagues83 and Shapiro and colleagues.84
The studies assess either BMP-2 or BMP-7 for usein spinal fusions. Appendix 15 reports the generalstudy characteristics of each included study.
Nine of the studies were conducted in the USA,one80 in Sweden and one83 in Canada.83 In onestudy,81 it was not clear where it was conducted,but the authors were from Japan and the USA.One study reported it was sponsored by NortonHealthcare78 and another stated that its fundingwas from a National Institutes of Health (NIH)award.81 Three studies74,83,84 did not state theirsources of funding and one study reported that itdid not receive any funds.77 The remaining studieswere sponsored by industry.
Seven studies included patients diagnosed withsingle-level degenerative disc disease. Four71–74,76,85
of these studies used anterior fusion andthree69,78,83 used posterolateral fusion. Anotherstudy80 included patients with L5 spondylolysis whowere treated with non-instrumented posterolaterallumbar fusion. Three studies81,82,84,86 includedpatients with spinal stenosis and degenerativespondylolisthesis who were treated withposterolateral fusion. Another study68 includedpatients with one- or two-level cervical disc diseasewho underwent anterior cervical discectomy. Theremaining study77 included patients with a varietyof diagnoses, with the majority includingdegenerative disc disease (n = 27) and grade Ispondylolisthesis (n = 27). Also included werepatients with herniation of nucleus pulposus (n = 6),instability (n = 13), spondylosis (n = 4) and stenosis(n = 21). All patients in this study were treated withposterolateral instrumented fusion.
The mean age of patients ranged from 40 to70 years. The length of follow-up for most trials
that included patients with disc disease was24 months. Although the Boden (2002) study69
specified a 24-month follow-up length, the meanfollow-up length was 17 months (range12–27 months). In the Kanayama study,81 themean follow-up lengths were 16 months for theBMP intervention group and 13 months for theautograft control group. The follow-up time was12 months in the study with spondylolysis patients.For patients with degenerative spondylolisthesiswith spinal stenosis, the follow-up time was12 months.
InterventionsTable 8 shows the interventions investigated in thestudies. Nine studies investigated BMP-2 andthree investigated BMP-7. Six studies68,71–74,76,79,85
used a BMP-2 concentration of 1.5 mg/ml. Wherereported, the doses used ranged from 8.4 to12 mg in the Burkus (2005) study,71–73 from 4.2 to8.4 mg in the Burkus (2002) study74,76 and from 4to 8 mg in the Haid (2004) study.79 Also used was2 mg/ml (dose of 20 mg each side of the spine) inthe Boden (2002)69 and Dimar Studies.77,78 TheShapiro study84 reported 4.2 mg/interspace used.The doses of BMP-7 used were 3.5 mg BMP-7/gcollagen vials on each side of the spine,81 3.5 mgper 3.5 ml80 and 3.5 mg per side of spine.82,86
Five BMP-2 studies68,71–74,76,79,85 used a collagensponge to deliver the BMP. The Shapiro study84
stated that it used BMP-2-soaked sponges, whichpresumably would have been made of collagen.One BMP-2 study used ceramic granules made ofhydroxyapatite and tricalcium phosphate(HA–TCP)69 and one used a compression resistantmatrix made of HA–TCP and collagensponges.77,78 HA–TCP, in the proportions of 15%hydroxyapatite and 85% tricalcium phosphate, hasbeen shown to enhance fusion in non-humanprimates.39 The ratio used in the Boden (2002)study69 was 60% hydroxyapatite and 40%tricalcium phosphate and was not specified in theDimar study.77,78 The carriers used in the BMP-7studies were a paste made of BMP-7, collagen andsaline,80 and a putty made of BMP-7, collagen andcarboxymethylcellulose.81,82,86 Eight studies usedAICBG as a control and the remaining twostudies81,84 used local autograft bone as thecontrol. The control group in the Kanayama
Health Technology Assessment 2007; Vol. 11: No. 30
25
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Chapter 4
Results of effectiveness assessment: spinal fusion

Results of effectiveness assessment: spinal fusion
26
TABLE 8 BMP interventions used in spine RCTs
Study BMP used Dose of BMP Delivery method Control Other
Assiri, 200483 rhBMP-2 NR NR Autogenous bone Both groups receivedTexas Scottish RiteHospital instrumentation
Baskin, 200368 rhBMP-2 1.5 mg/ml in Collagen sponge in Autograft bone Both groups received 3.2 ml water allograft in allograft ATLANTIS anterior then 0.4 ml cervical platesolution on collagen sponge
Boden, 200269 rhBMP-2 2 mg/ml (20 mg Ceramic granules AICBG with Texas Intervention groups per side of spine) distributed from a Scottish Rite received (A) Texas
glass syringe Hospital pedicle Scottish Rite Hospital screw pedicle screw instrumentation instrumentation or (B)
no instrumentation
Boden, 200085 rhBMP-2 1.5 mg/ml Collagen sponge in Autogenous iliac Both control and (2.6 ml used) fusion cage crest bone intervention groups had
tapered cylindricalthreaded fusion cages
Burkus, rhBMP-2 1.5 mg/ml Collagen sponge Autogenous iliac Both groups received a 200571–73 (dose range crest bone pair of threaded cortical
8.4–12 mg) allograft bone dowels
Burkus, rhBMP-2 1.5 mg/ml Collagen sponge Morcellised Both control and 200274–76 (dose range AICBG intervention groups
4.2–8.4 mg) received LT-CAGEs
Dimar, 200677 rhBMP-2 2 mg/ml Compression resistant Iliac crest graft (20 mg in each matrix consisting harvestlateral gutter) of HA–TCP with
collagen sponge
Haid, 200479,87 rhBMP-2 1.5 mg/ml Collagen sponges Morcellised Both control and (dose range AICBG intervention groups 4.0–8.0 mg) received stand-alone
cylindrical threadedtitanium fusion cages(INTER FIX cages)
Johnsson, 200280 BMP-7 3.5 mg (one BMP-7 paste made of Autograft iliac implant per side 3.5 mg BMP-7 with crest bone pasteof spine) 1 g of collagen and
2.5 ml saline
Kanayama, BMP-7 1 vial of 3.5 mg Collagen matrix Autograft bone Both control and 200681 BMP-7/g collagen and sodium with 5 g HA–TCP intervention groups
per side of spine carboxymethylcellulose granules per side received pedicle screw of spine instrumentation
Shapiro, 200584 rhBMP-2 4.2 mg/interspace Local bone wrapped in Local bone Both interventions rhBMP-2 sponges placed in interspace
between two wedges
Vaccaro, BMP-7 3.5 mg per side rhOP-1 with type I Iliac crest 200482,86,88 of spine collagen and 200 mg autograft
carboxymethylcellulose (OP-1 Putty)

study81 also received 5 g of HA–TCP on each sideof the spine. In the Burkus (2005)71–73 and Baskin68
studies, both groups received allograft bone.
Quality assessment of included RCTsAppendix 16 summarises the quality of theincluded studies. One of the studies was publishedin a preliminary report85 and two wereabstracts.83,84 We were unable to identify anyfurther publications from these trials.
The overall quality of the studies included in thisreview is substantially variable, ranging from lowto moderate. Based on the quality criteria, thestudies in order of least to most possible bias areas follows: Burkus and colleagues 200571–73 andBurkus and colleagues (2002);74–76 Boden andcolleagues (2000)85 and Vaccaro andcolleagues82,86,88 Boden and colleagues (2002)69
and Johnsson and colleagues (2002);80 Kanayamaand colleagues,81 Dimar and colleagues77 andBaskin and colleagues (2003);68 Haid andcolleagues;79,87 and finally Shapiro andcolleagues84 and Assiri and colleagues.83 It was notpossible to determine whether the quality criteriawere satisfied in the studies described in theabstracts83,84 due to the lack of information. TheBoden (2000)85 and Burkus (2005)71–73 studiesboth met all but one of the quality criteria.
In eight of the 12 studies, the randomisationmethod was unclear in that they only used theterms ‘randomisation’ or ‘randomised’, with nofurther explanation of the method used. In theother four studies, three different methods ofrandomisation were used and are consideredadequate and one method was found to beinadequate. The three methods of randomisationthat were considered adequate are the marginalbalancing method,85 sequentially numberedenvelopes71 and SAS PROC Plan.74 Assigning thepatients’ group at the time of surgery82 as arandomisation method was considered inadequate.In the Burkus (2005)71–73 and Burkus (2002)74–76
studies, the allocation concealments wereconsidered adequate based on their randomisationmethods as according to the guidelines in theCochrane Handbook for Systematic Reviews ofInterventions.65
One or more blinded independent assessors wereused to review radiographs in all but three trials.The Shapiro84 and Assiri83 studies did not reportthe assessment methods used and the Kanayamastudy81 did not report whether or not independentassessors were used. However, the actual ‘blinding’of assessors is questionable due to the ability of
assessors to visualise certain treatment elementson the radiographs and computed tomography(CT) scans. In the Boden (2002) study,69 thebiphasic calcium phosphate carrier andinstrumentation were visible on both radiographsand CT scans, thus allowing bias duringassessment.
The inclusion and exclusion criteria were clearlystated in six69,71–73,77,78,81,82,85,86 of the 10 trials.For the studies that did not explicitly report theinclusion and exclusion criteria, they onlyreported patient diagnoses and possibly broadinclusion criteria, but no exclusion criteria. TheShapiro84 and Assiri83 studies did not report anygroup characteristics.
There was a statistically significant differencebetween the BMP intervention group’s and controlgroup’s age in the Kanayama study,81 with a meanage of 70 ± 8.0 years in the BMP group and58.7 ± 9.0 years in the control group (p < 0.05). Inthe Boden (2002) study,69 two of the five patientsin the control group had diabetes whereas none inthe intervention group did. Diabetes leads to anincreased risk of infection and this may cause adecreased fusion rate. The infection rate was notreported; therefore, the effect of diabetes in thisstudy cannot be inferred.
Three studies79,83,84 reported no data on drop-outswhereas other studies reported comparable drop-outs. One exception is the Boden (2002) study,69
which reported an 18% drop-out rate in the BMP-only intervention group and 0% in both the BMPwith Texas Scottish Rite Hospital (TSRH) pediclescrew instrumentation and control groups. The18% drop-out rate was due to post-randomisationpatient exclusion when the investigatorsdiscovered that the exclusion criterion of greaterthan Grade 1 spondylolisthesis was met. One ofthe excluded patients had a solid bilateral fusionand the other developed a non-union. In thefusion analysis, these patients and their reportedfusion states were included in the assessment. Fourstudies69,74,76,81,82 reported the number andreasons patients were lost to follow-up. Twostudies68,71–73 gave the numbers lost to follow-up,but no reasons. Two studies80,85 did not lose anypatients to follow-up and three studies79,83,84,87 didnot report on whether any patients were lost tofollow-up. The Dimar study77 only reported thetotal number of patients initially randomised inthe whole study and the number of patientsavailable in each group at the final end-point.Therefore, the number of drop-outs and ITT datawere not calculable.
Health Technology Assessment 2007; Vol. 11: No. 30
27
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.

In summary, there were many methodologicalquality issues with the studies. Overall, the studiesfailed to meet many of the basic qualityexpectations of an RCT, such as describing therandomisation and allocation methods, analysingdata on an ITT basis, clearly defining inclusionand exclusion criteria and reporting reasons forany drop-outs.
Findings from RCTs on spinalfusionsFindings from RCTs for lumbar spinalfusionRadiographic resultsTable 9 shows the fusion rates of the spine studiesat their final end-points. It also gives thedefinition of successful fusion in each study. Dueto varying fusion rates and number of patientsavailable at each follow-up, the final radiographicassessments at the end-points of each study weredetermined to be the most reliable. Fusion ratesare shown based on an intention-to treat (numberslost considered failures) basis, when data werereported that allowed this.
Of the 11 studies, seven69,71–76,79,85,87 had a similardefinition of successful fusion. This definitionincludes; <5° angulation on flexion–extensionradiographs, �3 mm translation, radiolucent linescovering 50% or more of the implant andevidence of bridging trabecular bone. The Vaccarostudy82,86 had a minor difference in its definitionwhich included complete bridging bone and �2 mm translation. The Kanayama study81 alsoincluded <2 mm translation on radiographs andevidence of bridging bone on CT scan images.The Dimar study77 did not report a fusiondefinition, but instead classified fusion status witha grading system ranging from 1 (not fused) to 5(solid bilateral fusion). The authors did not reportthe exact scores of fusion at any end-pointsthroughout the study, but instead reported thenumber of patients with ‘solid fusions’ at the finalend-point. However, it was not specified whichgrades of fusion were considered solid fusions.Also included in two studies’ definition ofsuccessful fusion was the requirement that nosecondary surgeries were performed for eitherpersistent low back symptoms and clinicalsuspected non-unions74,76 or revision, removal orsupplemental fixations.71–73 It has been reportedthat a successful fusion does not always guaranteeimprovement in clinical outcomes.89–91 Therefore,it may not be appropriate to assess the success orfailure of fusion based on the fusion outcome
alone. The remaining study84 did not report itsdefinition of successful fusion.
Three small studies80–82,86 reported higher (butstatistically non-significant) fusion rates in thecontrol group versus the intervention group. Theremaining nine studies reported higher or equalfusion rates in the intervention versus controlgroup. Of these, two studies69,71 reportedstatistically significant differences between thefusion rates of intervention and control groups.Boden and colleagues69 reported that bothintervention groups had statistically significantlyhigher fusion rates than the control group withp = 0.018 and 0.028 for intervention groups A andB, respectively. Burkus and colleagues (2005)71–73
reported a significantly higher fusion rate in theintervention group compared with the controlgroup (p < 0.001).
Assessing the study characteristics andinterventions used there are a few differencesbetween the Johnsson study80 and the others.First, a BMP-7 paste made of BMP-7, collagen andsaline was used instead of the more commongranules. It could be that the paste is not a suitablecarrier and therefore BMP-7 was not as effective asit would have been with a different carrier. Also, theJohnsson study80 had the least specific definitionof fusion success, which leaves more room forinterpretation by the assessors, which could haveled to inconsistent assessment. The Vaccarostudy82,86 had the highest drop-out rate, with20.8% in the intervention group and 16.7% in thecontrol group. Since drop-outs were consideredfailures, this could have affected the results. In theKanayama study,81 one patient in the BMP groupdropped out and for this analysis was counted as afailure. Also, the authors reported that it wasdifficult to assess the status of new bone formationin the control group because the hydroxyapatiteparticles were slow to resorb. The investigatorssurgically explored the fusion area of those withsuccessful fusions when removing the screwinstrumentation and solid arthrodesis was foundin seven of nine control patients and four out ofseven intervention patients. New bone formationwas seen in six of seven of the interventionpatients. As with other studies, HA–TCP has beenshown to enhance fusion, and therefore ideallywould have been used in both treatment groups.In both treatment groups the authors suspectedbeneficial effects from HA–TCP, although thiscannot be supported by their findings.
Several papers69,71–74,76 have reported a tendencyfor fusion rates to decline over time. Possible
Results of effectiveness assessment: spinal fusion
28
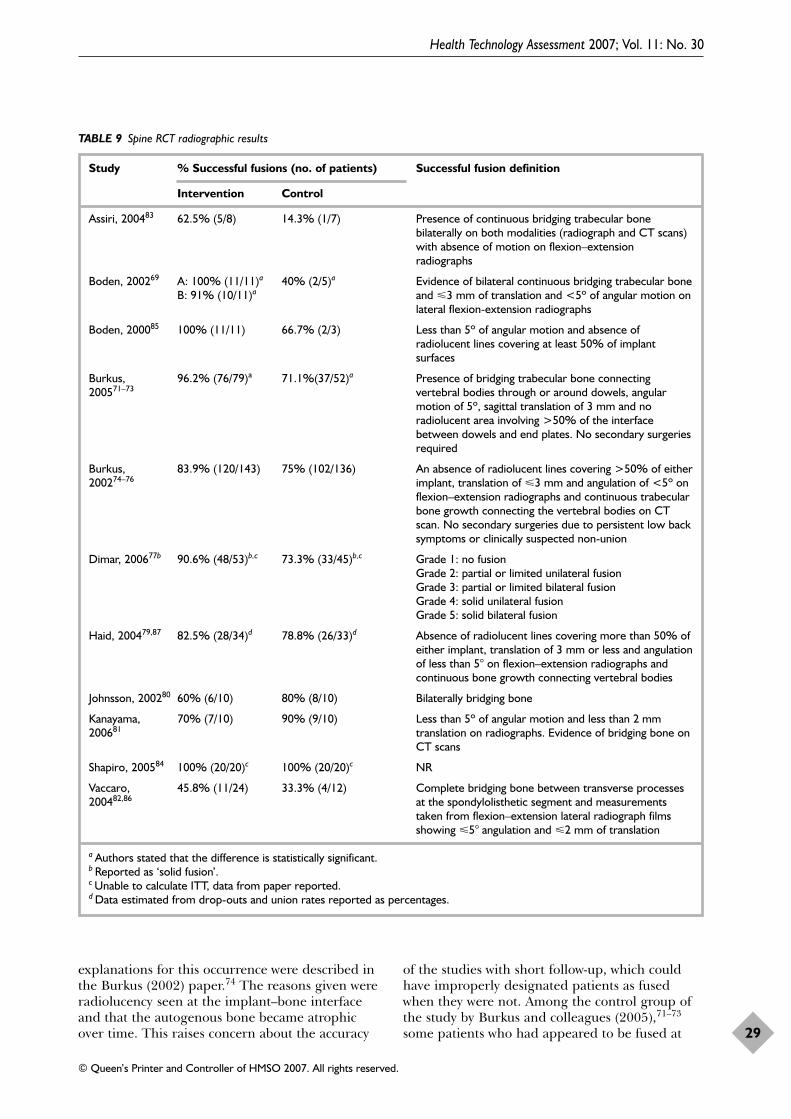
explanations for this occurrence were described inthe Burkus (2002) paper.74 The reasons given wereradiolucency seen at the implant–bone interfaceand that the autogenous bone became atrophicover time. This raises concern about the accuracy
of the studies with short follow-up, which couldhave improperly designated patients as fusedwhen they were not. Among the control group ofthe study by Burkus and colleagues (2005),71–73
some patients who had appeared to be fused at
Health Technology Assessment 2007; Vol. 11: No. 30
29
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 9 Spine RCT radiographic results
Study % Successful fusions (no. of patients) Successful fusion definition
Intervention Control
Assiri, 200483 62.5% (5/8) 14.3% (1/7) Presence of continuous bridging trabecular bonebilaterally on both modalities (radiograph and CT scans)with absence of motion on flexion–extensionradiographs
Boden, 200269 A: 100% (11/11)a 40% (2/5)a Evidence of bilateral continuous bridging trabecular bone B: 91% (10/11)a and �3 mm of translation and <5º of angular motion on
lateral flexion-extension radiographs
Boden, 200085 100% (11/11) 66.7% (2/3) Less than 5º of angular motion and absence ofradiolucent lines covering at least 50% of implantsurfaces
Burkus, 96.2% (76/79)a 71.1%(37/52)a Presence of bridging trabecular bone connecting 200571–73 vertebral bodies through or around dowels, angular
motion of 5º, sagittal translation of 3 mm and noradiolucent area involving >50% of the interfacebetween dowels and end plates. No secondary surgeriesrequired
Burkus, 83.9% (120/143) 75% (102/136) An absence of radiolucent lines covering >50% of either 200274–76 implant, translation of �3 mm and angulation of <5º on
flexion–extension radiographs and continuous trabecularbone growth connecting the vertebral bodies on CTscan. No secondary surgeries due to persistent low backsymptoms or clinically suspected non-union
Dimar, 200677b 90.6% (48/53)b,c 73.3% (33/45)b,c Grade 1: no fusionGrade 2: partial or limited unilateral fusionGrade 3: partial or limited bilateral fusionGrade 4: solid unilateral fusionGrade 5: solid bilateral fusion
Haid, 200479,87 82.5% (28/34)d 78.8% (26/33)d Absence of radiolucent lines covering more than 50% ofeither implant, translation of 3 mm or less and angulationof less than 5° on flexion–extension radiographs andcontinuous bone growth connecting vertebral bodies
Johnsson, 200280 60% (6/10) 80% (8/10) Bilaterally bridging bone
Kanayama, 70% (7/10) 90% (9/10) Less than 5º of angular motion and less than 2 mm 200681 translation on radiographs. Evidence of bridging bone on
CT scans
Shapiro, 200584 100% (20/20)c 100% (20/20)c NR
Vaccaro, 45.8% (11/24) 33.3% (4/12) Complete bridging bone between transverse processes 200482,86 at the spondylolisthetic segment and measurements
taken from flexion–extension lateral radiograph filmsshowing �5° angulation and �2 mm of translation
a Authors stated that the difference is statistically significant.b Reported as ‘solid fusion’.c Unable to calculate ITT, data from paper reported.d Data estimated from drop-outs and union rates reported as percentages.

the 12-month follow-up point were found not tobe fused at the 24-month follow-up. This was dueto previously unseen lucencies around theimplants that were thought to be obscured by thetightly packed autograft bone. The authorsreported that in the BMP group this was notobserved due to early integration of the allograftbone. Not all patients in the Boden (2002) study69
were followed up for 24 months, and hence thereis a chance of uncertainty regarding fusiondeterioration in patients who were not followed upfor the complete follow-up length.
In a report published by Glassman andcolleagues,78 the fusion results of 72 patients fromone centre of the multi-centre Dimar trial77 trialwere analysed based on the number of smokers.The numbers of smokers were comparablebetween the groups, with 22% in the BMPintervention group and 23% in the control group.At the 12-month final end-point, the mean fusiongrade in the control group was 3.25 for smokersand 3.93 for non-smokers. In the BMP group, themean fusion grades were 3.75 for smokers and4.86 for non-smokers. When both groups werecombined, smokers had a mean fusion grade of3.5 and non-smokers 4.42. Previous studies92 havefound evidence that smoking inhibits fusion andalthough not statistically significant, the data heresupport the prior findings.
Figure 5 shows data from individual trials andpooled estimates for fusion success outcome,according to subgroups of different patientdiagnoses. There is evidence for the effectivenessof BMP-2 with comparison with autograft bone forpatients with single-level degenerative discdisease. The pooled OR is 3.87 (95% CI 1.74 to8.59, p = 0.0009). However, there is also statisticallysignificant heterogeneity in this analysis(I2% = 53.8%, p = 0.04). This heterogeneity maynot be important, since the results of these trialswere consistently in favour of BMP-2. It is alsointeresting that the largest trial, (the Burkus(2002) study,69 showed the smallest treatmenteffect in Figure 5 (Egger’s test for funnel plot,p = 0.027; Begg’s test, p = 0.81). Some of theheterogeneity could be attributed to differentinterventions used. The Boden (2002)69 andDimar77 studies used HA–TCP granules indifferent proportions as bulking agents in the BMPgroup. HA–TCP has been shown to enhance fusionin non-human primates.39 Therefore, becauseHA–TCP was only used in the BMP group, thedifference in the fusion rates should be treatedwith caution. The Assiri study83 was excluded in asensitivity analysis (not shown) because the ITT
data were not reported and could not be calculated.The exclusion of this study made no difference tothe overall effect for single-level degenerative discdisease studies, so it was included.
Among patients with degenerativespondylolisthesis with spinal stenosis orspondylolysis, there is not enough evidence on theeffect of BMP-7 treatment compared withautograft bone in this analysis. The pooled OR is0.87 (95% CI 0.15 to 5.08, p = 0.88). Again, asensitivity analysis (not shown), excluding theShapiro study84 because it did not report ITTdata, did not affect the OR.
A sensitivity analysis (not shown) was conducted toinvestigate possible heterogeneity from combiningthe two BMP intervention groups in the Boden(2002) study.69 As mentioned above, theintervention group A and the control group bothreceived instrumentation whereas interventiongroup B did not. As a result, patients inintervention group B were excluded from thesensitivity analysis. This reduced the numbers inthe intervention group to 11/11. The conclusion onthe overall effect in single-level degenerative discdisease was the same when intervention group Bwas excluded, so all intervention patients areincluded. Overall, the analysis suggests that BMP-2is more effective than autograft for patients withsingle-level degenerative disc disease. However, forpatients with degenerative spondylolisthesis withspinal stenosis and spondylolysis treated with BMP-7, the data provide no statistically significant effect.
A sensitivity analysis was performed based onstudy quality (Figure 6). The analysis included fourstudies69,71–74,76,85 which met more than half of thequality criteria. The sensitivity analysis producedan OR of 6.55 (95% CI 1.48 to 29.06).
Anterior fusions are easier to defineradiographically because the fusion mass is visibleon the radiographs. Posterolateral fusions aremore difficult to define, and can be moreaccurately assessed using CT scans. All but two ofthe studies that used the posterolateral approachused CT scans to assess fusion. The Johnssonstudy80 used radiostereometric analysis to measurethe vertebral movement which was considered anadequate assessment method. The Vaccarostudy82,86 only used standard radiographs to assessthe fusion status, which may not have beenadequate to assess the fusion status clearly.
Figure 7 shows the analysis of spinal fusion successby the anterior approach. It is further
Results of effectiveness assessment: spinal fusion
30
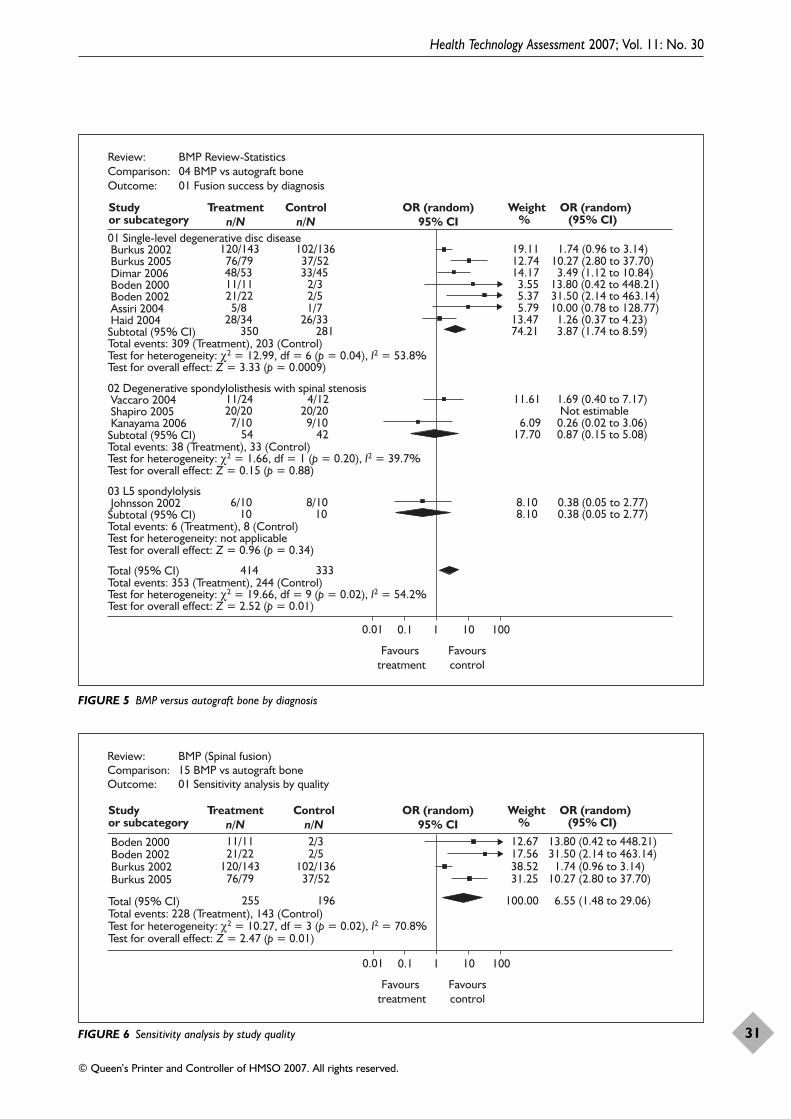
Health Technology Assessment 2007; Vol. 11: No. 30
31
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
01 Single-level degenerative disc disease Burkus 2002 120/143 102/136 19.11 1.74 (0.96 to 3.14) Burkus 2005 76/79 37/52 12.74 10.27 (2.80 to 37.70) Dimar 2006 48/53 33/45 14.17 3.49 (1.12 to 10.84) Boden 2000 11/11 2/3 3.55 13.80 (0.42 to 448.21) Boden 2002 21/22 2/5 5.37 31.50 (2.14 to 463.14) Assiri 2004 5/8 1/7 5.79 10.00 (0.78 to 128.77) Haid 2004 28/34 26/33 13.47 1.26 (0.37 to 4.23) Subtotal (95% CI) 350 281 74.21 3.87 (1.74 to 8.59)Total events: 309 (Treatment), 203 (Control)Test for heterogeneity: χ2 = 12.99, df = 6 (p = 0.04), I2 = 53.8%Test for overall effect: Z = 3.33 (p = 0.0009)
02 Degenerative spondylolisthesis with spinal stenosis Vaccaro 2004 11/24 4/12 11.61 1.69 (0.40 to 7.17) Shapiro 2005 20/20 20/20 Not estimable Kanayama 2006 7/10 9/10 6.09 0.26 (0.02 to 3.06) Subtotal (95% CI) 54 42 17.70 0.87 (0.15 to 5.08)Total events: 38 (Treatment), 33 (Control)Test for heterogeneity: χ2 = 1.66, df = 1 (p = 0.20), I2 = 39.7%Test for overall effect: Z = 0.15 (p = 0.88)
03 L5 spondylolysis Johnsson 2002 6/10 8/10 8.10 0.38 (0.05 to 2.77) Subtotal (95% CI) 10 10 8.10 0.38 (0.05 to 2.77)Total events: 6 (Treatment), 8 (Control)Test for heterogeneity: not applicableTest for overall effect: Z = 0.96 (p = 0.34)
Total (95% CI) 414 333Total events: 353 (Treatment), 244 (Control)Test for heterogeneity: χ2 = 19.66, df = 9 (p = 0.02), I2 = 54.2%Test for overall effect: Z = 2.52 (p = 0.01)
Review: BMP Review-StatisticsComparison: 04 BMP vs autograft boneOutcome: 01 Fusion success by diagnosis
Study Treatmentn/N
Controln/N
OR (random)95% CI
Weight OR (random)or subcategory % (95% CI)
0.01 0.1 1 10 100
Favourscontrol
Favours treatment
FIGURE 5 BMP versus autograft bone by diagnosis
Review: BMP (Spinal fusion)Comparison: 15 BMP vs autograft boneOutcome: 01 Sensitivity analysis by quality
Study Treatmentn/N
Controln/N
OR (random)95% CI
Weight OR (random)or subcategory % (95% CI)
0.01 0.1 1 10 100
Favourscontrol
Favours treatment
Boden 2000 11/11 2/3 12.67 13.80 (0.42 to 448.21) Boden 2002 21/22 2/5 17.56 31.50 (2.14 to 463.14) Burkus 2002 120/143 102/136 38.52 1.74 (0.96 to 3.14) Burkus 2005 76/79 37/52 31.25 10.27 (2.80 to 37.70)
Total (95% CI) 255 196 100.00 6.55 (1.48 to 29.06)Total events: 228 (Treatment), 143 (Control)Test for heterogeneity: χ2 = 10.27, df = 3 (p = 0.02), I2 = 70.8%Test for overall effect: Z = 2.47 (p = 0.01)
FIGURE 6 Sensitivity analysis by study quality
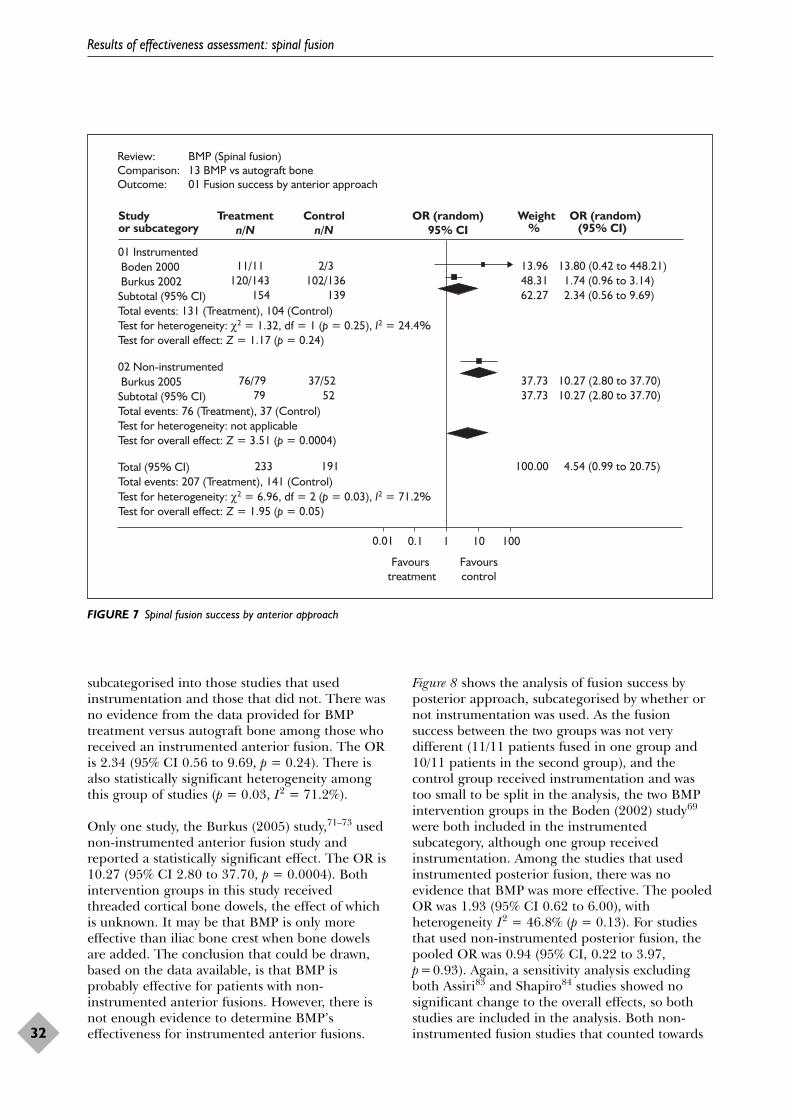
subcategorised into those studies that usedinstrumentation and those that did not. There wasno evidence from the data provided for BMPtreatment versus autograft bone among those whoreceived an instrumented anterior fusion. The ORis 2.34 (95% CI 0.56 to 9.69, p = 0.24). There isalso statistically significant heterogeneity amongthis group of studies (p = 0.03, I2 = 71.2%).
Only one study, the Burkus (2005) study,71–73 usednon-instrumented anterior fusion study andreported a statistically significant effect. The OR is10.27 (95% CI 2.80 to 37.70, p = 0.0004). Bothintervention groups in this study receivedthreaded cortical bone dowels, the effect of whichis unknown. It may be that BMP is only moreeffective than iliac bone crest when bone dowelsare added. The conclusion that could be drawn,based on the data available, is that BMP isprobably effective for patients with non-instrumented anterior fusions. However, there isnot enough evidence to determine BMP’seffectiveness for instrumented anterior fusions.
Figure 8 shows the analysis of fusion success byposterior approach, subcategorised by whether ornot instrumentation was used. As the fusionsuccess between the two groups was not verydifferent (11/11 patients fused in one group and10/11 patients in the second group), and thecontrol group received instrumentation and wastoo small to be split in the analysis, the two BMPintervention groups in the Boden (2002) study69
were both included in the instrumentedsubcategory, although one group receivedinstrumentation. Among the studies that usedinstrumented posterior fusion, there was noevidence that BMP was more effective. The pooledOR was 1.93 (95% CI 0.62 to 6.00), withheterogeneity I2 = 46.8% (p = 0.13). For studiesthat used non-instrumented posterior fusion, thepooled OR was 0.94 (95% CI, 0.22 to 3.97,p=0.93). Again, a sensitivity analysis excludingboth Assiri83 and Shapiro84 studies showed nosignificant change to the overall effects, so bothstudies are included in the analysis. Both non-instrumented fusion studies that counted towards
Results of effectiveness assessment: spinal fusion
32
Review: BMP (Spinal fusion)Comparison: 13 BMP vs autograft boneOutcome: 01 Fusion success by anterior approach
Study Treatmentn/N
Controln/N
OR (random)95% CI
Weight OR (random)or subcategory % (95% CI)
0.01 0.1 1 10 100
Favourscontrol
Favours treatment
01 Instrumented Boden 2000 11/11 2/3 13.96 13.80 (0.42 to 448.21) Burkus 2002 120/143 102/136 48.31 1.74 (0.96 to 3.14) Subtotal (95% CI) 154 139 62.27 2.34 (0.56 to 9.69)Total events: 131 (Treatment), 104 (Control)Test for heterogeneity: χ2 = 1.32, df = 1 (p = 0.25), I2 = 24.4%Test for overall effect: Z = 1.17 (p = 0.24)
02 Non-instrumented Burkus 2005 76/79 37/52 37.73 10.27 (2.80 to 37.70) Subtotal (95% CI) 79 52 37.73 10.27 (2.80 to 37.70)Total events: 76 (Treatment), 37 (Control)Test for heterogeneity: not applicableTest for overall effect: Z = 3.51 (p = 0.0004)
Total (95% CI) 233 191 100.00 4.54 (0.99 to 20.75)Total events: 207 (Treatment), 141 (Control)Test for heterogeneity: χ2 = 6.96, df = 2 (p = 0.03), I2 = 71.2%Test for overall effect: Z = 1.95 (p = 0.05)
FIGURE 7 Spinal fusion success by anterior approach

the odds ratio used BMP-7 in the dose of 3.5 mgper side of the spine. Where reported, theinstrumented fusion studies used BMP-2 in thedoses of 20 mg per side of spine and 4.2 mg perinterspace. The Kanayama study81 used BMP-7 ina dose of 3.5 mg per side of the spine also, andthe fusion rates were 20% lower in theintervention group versus the control group. Itcould be that a higher dose of BMP-7 is neededfor fusion or that BMP-7 is not as effective forspinal fusions. Based on the data presented, thereis no evidence of the effect of BMP for posteriorspinal fusion, instrumented or not.
It was not appropriate to analyse the studies basedon the BMP used (BMP-2 or BMP-7) due to highheterogeneity in the studies. All of the studies thatused BMP-2, except the Shapiro study,84 includedpatients with single-level degenerative discdisease. The Shapiro study84 included patientswith degenerative spondylolisthesis, similar to twostudies treated with BMP-7. However, in additionto BMP-2, intervention patients received local
bone with machined cortical wedges in theShapiro (2005) study.84 Patients who receivedBMP-7 were diagnosed with either degenerativespondylolisthesis or spondylolysis. Therefore, dueto the separation of diagnoses between BMPs, it isnot possible to compare effectiveness of BMP-2and BMP-7 for different diagnoses.
Operative resultsTable 10 summarises the reported operationresults, including mean operating time, meanblood loss and mean length of hospital stay.
Seven studies69,71,74,77,79,82,85 reported meanoperating times. In all but one intervention group[intervention A in the Boden (2002) study69] thereported mean operating time was equal to, orshorter than, the control group’s. Fourstudies69,71,77,85 reported statistically significantdifferent operating times, although the validity ofthe statistical tests is questionable. Due to differentsurgical procedures, there is a wide range of meanoperating times reported (1.4–3.7 hours).
Health Technology Assessment 2007; Vol. 11: No. 30
33
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
01 Instrumented Dimar 2006 48/53 33/45 25.28 3.49 (1.12 to 10.84) Assiri 2004 5/8 1/7 8.91 10.00 (0.78 to 128.77) Haid 2004 28/34 26/33 23.71 1.26 (0.37 to 4.23) Kanayama 2006 7/10 9/10 9.41 0.26 (0.02 to 3.06)Subtotal (95% CI) 105 95 67.30 1.93 (0.62 to 6.00)Total events: 88 (Treatment), 69 (Control)Test for heterogeneity: χ2 = 5.64, df = 3 (p = 0.13), I2 = 46.8%Test for overall effect: Z = 1.13 (p = 0.26)
02 Non-instrumented Johnsson 2002 6/10 8/10 12.95 0.38 (0.05 to 2.77) Vaccaro 2004 11/24 4/12 19.74 1.69 (0.40 to 7.17) Shapiro 2005 20/20 20/20 Not estimable Subtotal (95% CI) 54 42 32.70 0.94 (0.22 to 3.97)Total events: 37 (Treatment), 32 (Control)Test for heterogeneity: χ2 = 1.43, df = 1 (p = 0.23), I2 = 30.2%Test for overall effect: Z = 0.08 (p = 0.93)
Total (95% CI) 159 137 100.00 1.53 (0.65 to 3.58)Total events: 125 (Treatment), 101 (Control)Test for heterogeneity: χ2 = 8.05, df = 5 (p = 0.15), I2 = 37.9%Test for overall effect: Z = 0.98 (p = 0.33)
Review: BMP Review-StatisticsComparison: 05 BMP vs autograft boneOutcome: 01 Fusion success by posterior approach
Study Treatmentn/N
Controln/N
OR (random)95% CI
Weight %
OR (random)(95% CI)or subcategory
0.1 0.2 0.5 1 2 5 10
Favourscontrol
Favours treatment
FIGURE 8 Spinal fusion success by posterior approach
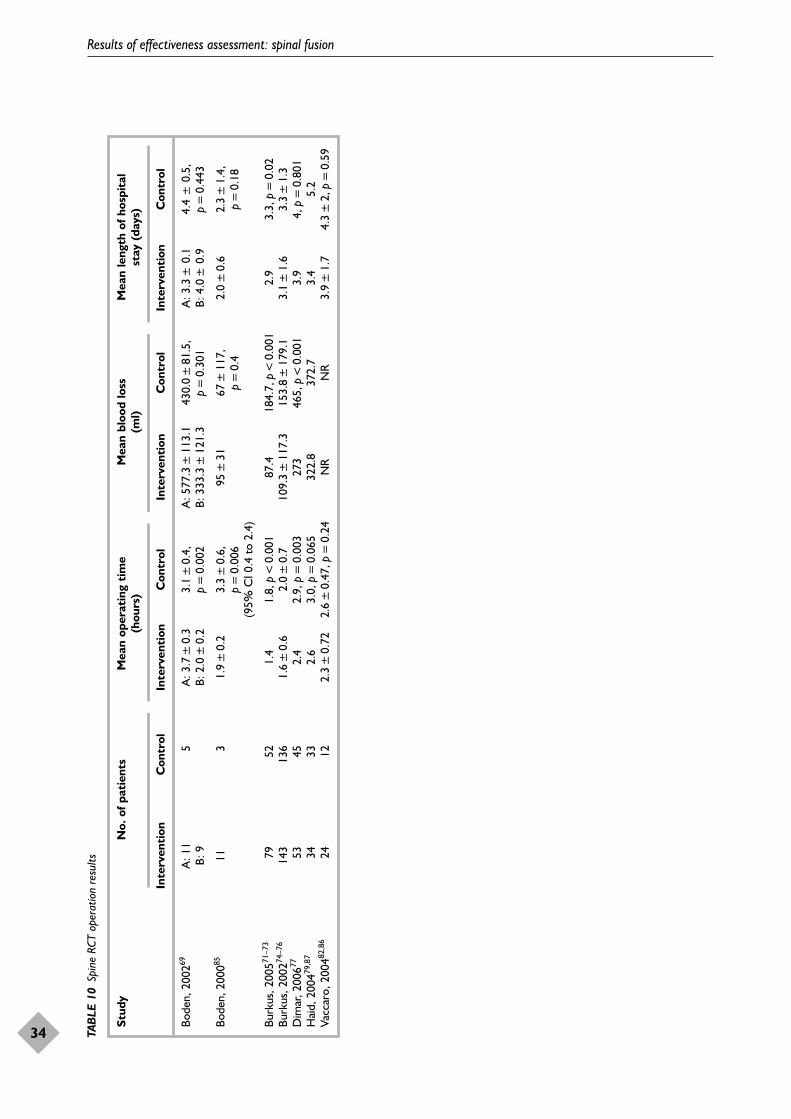
Results of effectiveness assessment: spinal fusion
34 TA
BLE
10
Spin
e RC
T op
erat
ion
resu
lts
Stud
yN
o. o
f pat
ient
sM
ean
oper
atin
g ti
me
Mea
n bl
ood
loss
M
ean
leng
th o
f hos
pita
l (h
ours
)(m
l)st
ay (
days
)
Inte
rven
tion
Con
trol
Inte
rven
tion
Con
trol
Inte
rven
tion
Con
trol
Inte
rven
tion
Con
trol
Bode
n, 2
00269
A: 1
15
A: 3
.7±
0.3
3.1
±0.
4,
A: 5
77.3
±11
3.1
430.
0±
81.5
, A
: 3.3
±0.
14.
4±
0.5,
B:
9B:
2.0
±0.
2p
=0.
002
B: 3
33.3
±12
1.3
p=
0.30
1B:
4.0
±0.
9p
=0.
443
Bode
n, 2
00085
113
1.9
±0.
23.
3±
0.6,
95
±31
67±
117,
2.
0±
0.6
2.3
±1.
4,
p=
0.00
6 p
=0.
4p
=0.
18(9
5% C
I 0.4
to
2.4)
Burk
us, 2
00571
–73
7952
1.4
1.8,
p<
0.00
187
.418
4.7,
p<
0.00
12.
93.
3, p
=0.
02Bu
rkus
, 200
274–7
614
313
61.
6±
0.6
2.0
±0.
710
9.3
±11
7.3
153.
8±
179.
13.
1±
1.6
3.3
±1.
3D
imar
, 200
67753
452.
42.
9, p
=0.
003
273
465,
p<
0.00
13.
94,
p=
0.80
1H
aid,
200
479,8
734
332.
63.
0, p
=0.
065
322.
837
2.7
3.4
5.2
Vacc
aro,
200
482,8
624
122.
3±
0.72
2.6
±0.
47, p
=0.
24N
RN
R3.
9±
1.7
4.3
±2,
p=
0.59
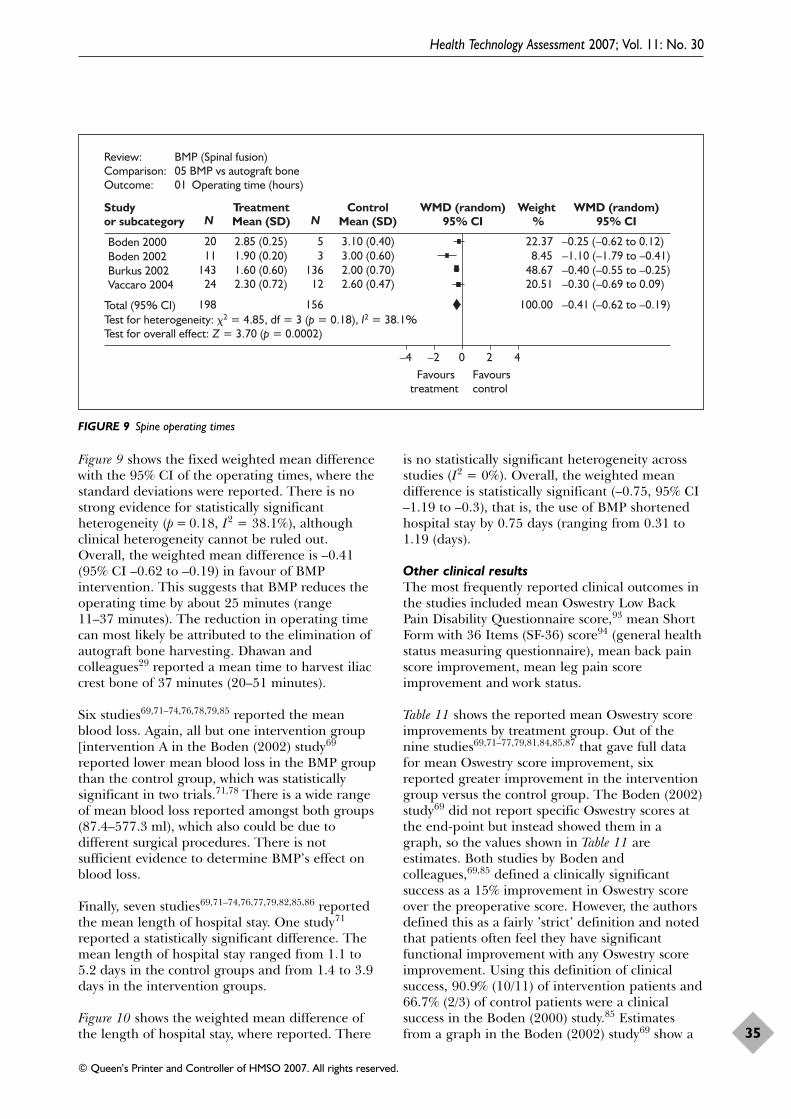
Figure 9 shows the fixed weighted mean differencewith the 95% CI of the operating times, where thestandard deviations were reported. There is nostrong evidence for statistically significantheterogeneity (p = 0.18, I2 = 38.1%), althoughclinical heterogeneity cannot be ruled out.Overall, the weighted mean difference is –0.41(95% CI –0.62 to –0.19) in favour of BMPintervention. This suggests that BMP reduces theoperating time by about 25 minutes (range11–37 minutes). The reduction in operating timecan most likely be attributed to the elimination ofautograft bone harvesting. Dhawan andcolleagues29 reported a mean time to harvest iliaccrest bone of 37 minutes (20–51 minutes).
Six studies69,71–74,76,78,79,85 reported the meanblood loss. Again, all but one intervention group[intervention A in the Boden (2002) study69
reported lower mean blood loss in the BMP groupthan the control group, which was statisticallysignificant in two trials.71,78 There is a wide rangeof mean blood loss reported amongst both groups(87.4–577.3 ml), which also could be due todifferent surgical procedures. There is notsufficient evidence to determine BMP’s effect onblood loss.
Finally, seven studies69,71–74,76,77,79,82,85,86 reportedthe mean length of hospital stay. One study71
reported a statistically significant difference. Themean length of hospital stay ranged from 1.1 to5.2 days in the control groups and from 1.4 to 3.9days in the intervention groups.
Figure 10 shows the weighted mean difference ofthe length of hospital stay, where reported. There
is no statistically significant heterogeneity acrossstudies (I2 = 0%). Overall, the weighted meandifference is statistically significant (–0.75, 95% CI–1.19 to –0.3), that is, the use of BMP shortenedhospital stay by 0.75 days (ranging from 0.31 to1.19 (days).
Other clinical resultsThe most frequently reported clinical outcomes inthe studies included mean Oswestry Low BackPain Disability Questionnaire score,93 mean ShortForm with 36 Items (SF-36) score94 (general healthstatus measuring questionnaire), mean back painscore improvement, mean leg pain scoreimprovement and work status.
Table 11 shows the reported mean Oswestry scoreimprovements by treatment group. Out of thenine studies69,71–77,79,81,84,85,87 that gave full datafor mean Oswestry score improvement, sixreported greater improvement in the interventiongroup versus the control group. The Boden (2002)study69 did not report specific Oswestry scores atthe end-point but instead showed them in agraph, so the values shown in Table 11 areestimates. Both studies by Boden andcolleagues,69,85 defined a clinically significantsuccess as a 15% improvement in Oswestry scoreover the preoperative score. However, the authorsdefined this as a fairly ’strict’ definition and notedthat patients often feel they have significantfunctional improvement with any Oswestry scoreimprovement. Using this definition of clinicalsuccess, 90.9% (10/11) of intervention patients and66.7% (2/3) of control patients were a clinicalsuccess in the Boden (2000) study.85 Estimatesfrom a graph in the Boden (2002) study69 show a
Health Technology Assessment 2007; Vol. 11: No. 30
35
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Review: BMP (Spinal fusion)Comparison: 05 BMP vs autograft boneOutcome: 01 Operating time (hours)
Studyor subcategory
TreatmentMean (SD)
ControlMean (SD)
WMD (random)95% CI
Weight %
WMD (random)95% CIN N
Boden 2000 20 2.85 (0.25) 5 3.10 (0.40) 22.37 –0.25 (–0.62 to 0.12) Boden 2002 11 1.90 (0.20) 3 3.00 (0.60) 8.45 –1.10 (–1.79 to –0.41)Burkus 2002 143 1.60 (0.60) 136 2.00 (0.70) 48.67 –0.40 (–0.55 to –0.25)Vaccaro 2004 24 2.30 (0.72) 12 2.60 (0.47) 20.51 –0.30 (–0.69 to 0.09)
Total (95% CI) 198 156 100.00 –0.41 (–0.62 to –0.19)Test for heterogeneity: �2 = 4.85, df = 3 (p = 0.18), I2 = 38.1%Test for overall effect: Z = 3.70 (p = 0.0002)
–4 –2 0 2 4 Favours
treatment Favourscontrol
FIGURE 9 Spine operating times
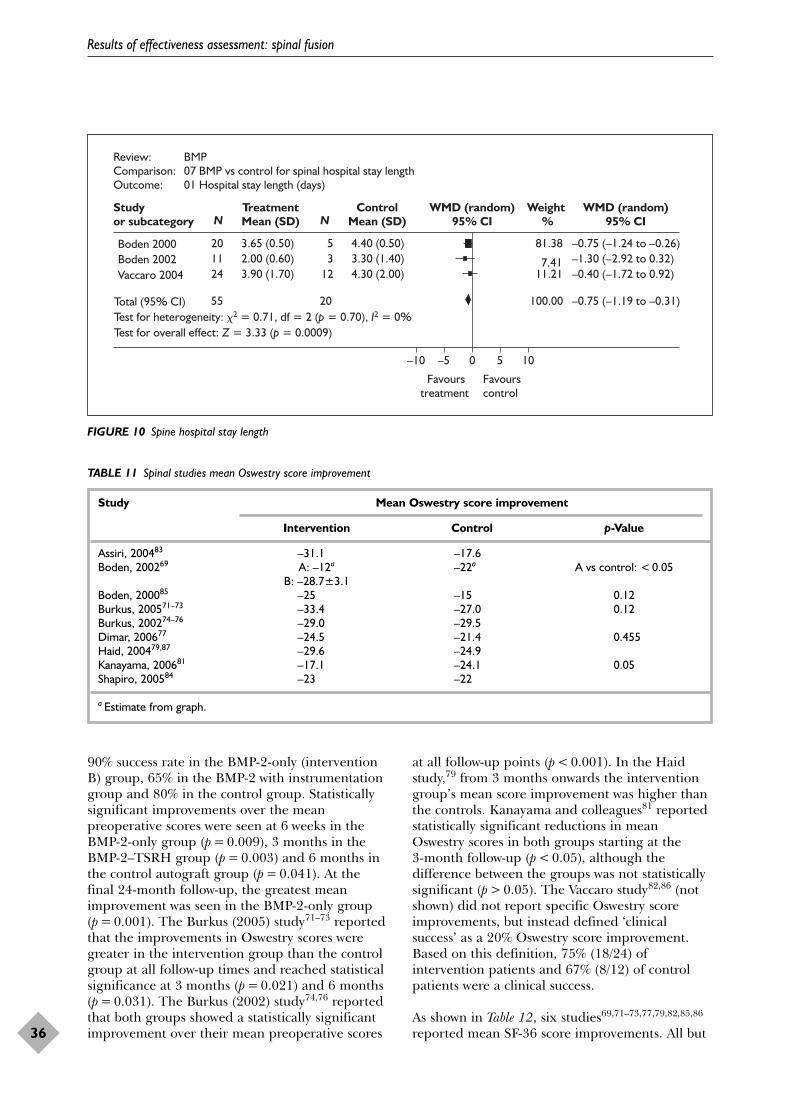
90% success rate in the BMP-2-only (interventionB) group, 65% in the BMP-2 with instrumentationgroup and 80% in the control group. Statisticallysignificant improvements over the meanpreoperative scores were seen at 6 weeks in theBMP-2-only group (p = 0.009), 3 months in theBMP-2–TSRH group (p = 0.003) and 6 months inthe control autograft group (p = 0.041). At thefinal 24-month follow-up, the greatest meanimprovement was seen in the BMP-2-only group(p = 0.001). The Burkus (2005) study71–73 reportedthat the improvements in Oswestry scores weregreater in the intervention group than the controlgroup at all follow-up times and reached statisticalsignificance at 3 months (p = 0.021) and 6 months(p = 0.031). The Burkus (2002) study74,76 reportedthat both groups showed a statistically significantimprovement over their mean preoperative scores
at all follow-up points (p < 0.001). In the Haidstudy,79 from 3 months onwards the interventiongroup’s mean score improvement was higher thanthe controls. Kanayama and colleagues81 reportedstatistically significant reductions in meanOswestry scores in both groups starting at the 3-month follow-up (p < 0.05), although thedifference between the groups was not statisticallysignificant (p > 0.05). The Vaccaro study82,86 (notshown) did not report specific Oswestry scoreimprovements, but instead defined ‘clinicalsuccess’ as a 20% Oswestry score improvement.Based on this definition, 75% (18/24) ofintervention patients and 67% (8/12) of controlpatients were a clinical success.
As shown in Table 12, six studies69,71–73,77,79,82,85,86
reported mean SF-36 score improvements. All but
Results of effectiveness assessment: spinal fusion
36
Review: BMP Comparison: 07 BMP vs control for spinal hospital stay lengthOutcome: 01 Hospital stay length (days)
Studyor subcategory
TreatmentMean (SD)
ControlMean (SD)
WMD (random)95% CI
Weight %
WMD (random)95% CIN N
Favourstreatment
Favourscontrol
Boden 2000 20 3.65 (0.50) 5 4.40 (0.50) 81.38 –0.75 (–1.24 to –0.26)Boden 2002 11 2.00 (0.60) 3 3.30 (1.40) 7.41 –1.30 (–2.92 to 0.32)Vaccaro 2004 24 3.90 (1.70) 12 4.30 (2.00) 11.21 –0.40 (–1.72 to 0.92)
Total (95% CI) 55 20 100.00 –0.75 (–1.19 to –0.31)Test for heterogeneity: �2 = 0.71, df = 2 (p = 0.70), I2 = 0%Test for overall effect: Z = 3.33 (p = 0.0009)
–10 –5 0 5 10
FIGURE 10 Spine hospital stay length
TABLE 11 Spinal studies mean Oswestry score improvement
Study Mean Oswestry score improvement
Intervention Control p-Value
Assiri, 200483 –31.1 –17.6Boden, 200269 A: –12a –22a A vs control: < 0.05
B: –28.7±3.1Boden, 200085 –25 –15 0.12Burkus, 200571–73 –33.4 –27.0 0.12Burkus, 200274–76 –29.0 –29.5Dimar, 200677 –24.5 –21.4 0.455Haid, 200479,87 –29.6 –24.9Kanayama, 200681 –17.1 –24.1 0.05Shapiro, 200584 –23 –22
a Estimate from graph.

two [intervention A group in the Boden (2002)study69 and physical component in the Dimarstudy77] studies showed higher mean scoreimprovement in the intervention versus controlgroups. Again, in the Boden (2002) study,69 thevalues were estimated from a graph. In the Boden(2002) study,69 statistically significantimprovements in the mean SF-36 physicalcomponent score over the preoperative valueswere seen at 3 months in intervention group B(p = 0.039) and 6 months in intervention group A(p = 0.033). At the last follow-up, the mean physicalscore for intervention group B was greater thanfor the control group (p = 0.07). In the same study,significant improvement in the bodily pain indexscore was seen at 6 weeks in intervention group B(p = 0.010), 3 months in intervention group B(p < 0.001) and 6 months in the control group(p = 0.034). However, this study is very small, withonly five patients in the control group and 11 ineach of the two intervention groups. In the Burkus(2005) study,71–73 mean score improvement for theintervention groups reached statistical significanceat 6 months (p = 0.001) and was significantlyhigher than the control group’s score (p = 0.017).The difference maintained significance at the final24-month follow-up, p = 0.015. The Boden (2000)study85 reported the mean improvements in alleight SF-36 categories; however, this study is alsovery small (14 patients). There is no significant
evidence to determine the effect of BMPtreatment compared with autograft bone.
Table 13 provides data reported on mean backpain score improvement. Out of the fivestudies69,71,74,77,79 that reported results for meanback pain, the score improvement was better inthe BMP intervention groups, except for anintervention group in the Boden (2002) study.69
All but one77 of the studies reported they used a20-point numerical rating scale to assess theintensity of the pain and either the type69 orduration71–74,76,79 of pain. Three of the studiesreported that the difference was statisticallysignificant.69,71,79 The Burkus (2005)71–73 andBurkus (2002)74,76 studies reported statisticallysignificant improvements in back pain scores inboth groups at all follow-up points. Theinterventions group’s mean score improvement inthe Burkus (2005) study71–73 was significantly betterthan that for the control group from the 3-monthfollow-up onwards (p < 0.05). Haid andcolleagues79,87 reported greater mean back painscores in the intervention group than the controlgroup at all follow-up points, with a significantdifference in the final follow-up mean scoreimprovement, p = 0.009. The available evidencepoints to a slightly greater improvement in backpain score in those treated with BMP comparedwith autograft.
Health Technology Assessment 2007; Vol. 11: No. 30
37
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 12 Spinal studies mean SF-36 score improvements
Study Mean SF-36 score improvement
Intervention Control p-Value
Boden, 200269 A: Physical = 6a Physical = 7a 0.049Bodily pain = 16a Bodily pain = 16a
B: Physical = 16a
Bodily pain = 37a
Boden, 200085 Physical = 37.7 Physical = 36.7Role–physical = 65.9 Role–physical = 41.7Pain index = 43.5 Pain index = 27General health perception = 5.7 General health perception = 8.3Vitality = 25 Vitality = 23.4Social function = 44.3 Social function = 37.5Role–emotional = 51.5 Role–emotional = 44.5Mental health = 15.6 Mental health = 13.3
Burkus, 200571–73 15.7 11.6 0.015
Dimar, 200677 Physical = 8.6 Physical = 10.7 0.378Bodily pain = 29.7 Bodily pain = 28.7 0.861
Haid, 200479,87 Physical = 14a Physical = 12a
Vaccaro, 200482,86 Physical = 15.3 Physical = 7.9Mental health = 9.6 Mental health = 6.8
a Estimate from graph.
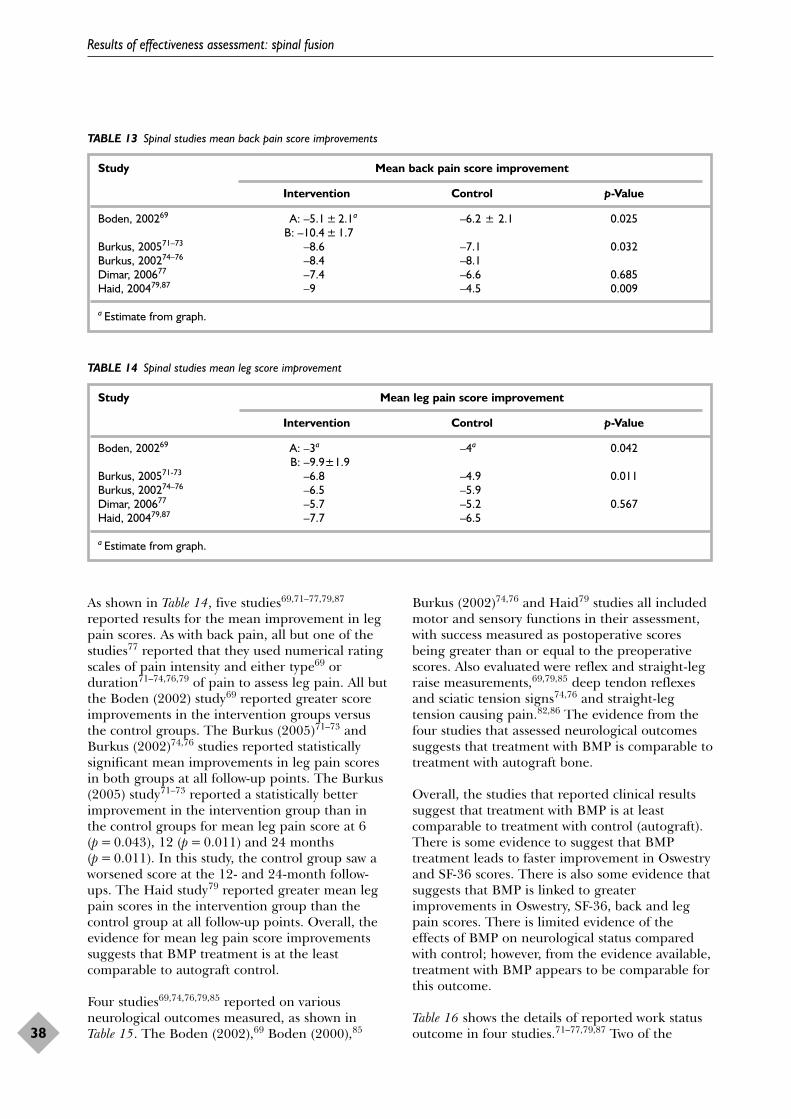
As shown in Table 14, five studies69,71–77,79,87
reported results for the mean improvement in legpain scores. As with back pain, all but one of thestudies77 reported that they used numerical ratingscales of pain intensity and either type69 orduration71–74,76,79 of pain to assess leg pain. All butthe Boden (2002) study69 reported greater scoreimprovements in the intervention groups versusthe control groups. The Burkus (2005)71–73 andBurkus (2002)74,76 studies reported statisticallysignificant mean improvements in leg pain scoresin both groups at all follow-up points. The Burkus(2005) study71–73 reported a statistically betterimprovement in the intervention group than inthe control groups for mean leg pain score at 6(p = 0.043), 12 (p = 0.011) and 24 months(p = 0.011). In this study, the control group saw aworsened score at the 12- and 24-month follow-ups. The Haid study79 reported greater mean legpain scores in the intervention group than thecontrol group at all follow-up points. Overall, theevidence for mean leg pain score improvementssuggests that BMP treatment is at the leastcomparable to autograft control.
Four studies69,74,76,79,85 reported on variousneurological outcomes measured, as shown inTable 15. The Boden (2002),69 Boden (2000),85
Burkus (2002)74,76 and Haid79 studies all includedmotor and sensory functions in their assessment,with success measured as postoperative scoresbeing greater than or equal to the preoperativescores. Also evaluated were reflex and straight-legraise measurements,69,79,85 deep tendon reflexesand sciatic tension signs74,76 and straight-legtension causing pain.82,86 The evidence from thefour studies that assessed neurological outcomessuggests that treatment with BMP is comparable totreatment with autograft bone.
Overall, the studies that reported clinical resultssuggest that treatment with BMP is at leastcomparable to treatment with control (autograft).There is some evidence to suggest that BMPtreatment leads to faster improvement in Oswestryand SF-36 scores. There is also some evidence thatsuggests that BMP is linked to greaterimprovements in Oswestry, SF-36, back and legpain scores. There is limited evidence of theeffects of BMP on neurological status comparedwith control; however, from the evidence available,treatment with BMP appears to be comparable forthis outcome.
Table 16 shows the details of reported work statusoutcome in four studies.71–77,79,87 Two of the
Results of effectiveness assessment: spinal fusion
38
TABLE 13 Spinal studies mean back pain score improvements
Study Mean back pain score improvement
Intervention Control p-Value
Boden, 200269 A: –5.1 ± 2.1a –6.2 ± 2.1 0.025B: –10.4 ± 1.7
Burkus, 200571–73 –8.6 –7.1 0.032Burkus, 200274–76 –8.4 –8.1Dimar, 200677 –7.4 –6.6 0.685Haid, 200479,87 –9 –4.5 0.009
a Estimate from graph.
TABLE 14 Spinal studies mean leg score improvement
Study Mean leg pain score improvement
Intervention Control p-Value
Boden, 200269 A: –3a –4a 0.042B: –9.9±1.9
Burkus, 200571-73 –6.8 –4.9 0.011Burkus, 200274–76 –6.5 –5.9Dimar, 200677 –5.7 –5.2 0.567Haid, 200479,87 –7.7 –6.5
a Estimate from graph.
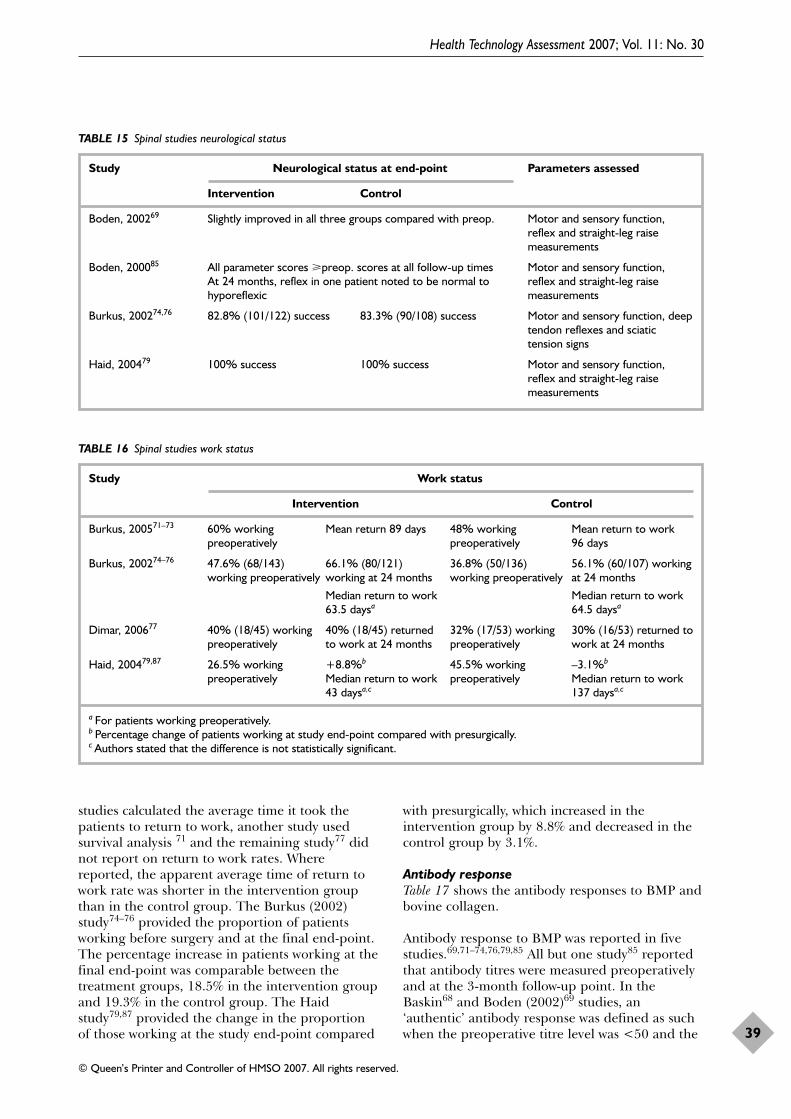
studies calculated the average time it took thepatients to return to work, another study usedsurvival analysis 71 and the remaining study77 didnot report on return to work rates. Wherereported, the apparent average time of return towork rate was shorter in the intervention groupthan in the control group. The Burkus (2002)study74–76 provided the proportion of patientsworking before surgery and at the final end-point.The percentage increase in patients working at thefinal end-point was comparable between thetreatment groups, 18.5% in the intervention groupand 19.3% in the control group. The Haidstudy79,87 provided the change in the proportionof those working at the study end-point compared
with presurgically, which increased in theintervention group by 8.8% and decreased in thecontrol group by 3.1%.
Antibody responseTable 17 shows the antibody responses to BMP andbovine collagen.
Antibody response to BMP was reported in fivestudies.69,71–74,76,79,85 All but one study85 reportedthat antibody titres were measured preoperativelyand at the 3-month follow-up point. In theBaskin68 and Boden (2002)69 studies, an‘authentic’ antibody response was defined as suchwhen the preoperative titre level was <50 and the
Health Technology Assessment 2007; Vol. 11: No. 30
39
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 15 Spinal studies neurological status
Study Neurological status at end-point Parameters assessed
Intervention Control
Boden, 200269 Slightly improved in all three groups compared with preop. Motor and sensory function,reflex and straight-leg raisemeasurements
Boden, 200085 All parameter scores �preop. scores at all follow-up times Motor and sensory function, At 24 months, reflex in one patient noted to be normal to reflex and straight-leg raise hyporeflexic measurements
Burkus, 200274,76 82.8% (101/122) success 83.3% (90/108) success Motor and sensory function, deeptendon reflexes and sciatictension signs
Haid, 200479 100% success 100% success Motor and sensory function,reflex and straight-leg raisemeasurements
TABLE 16 Spinal studies work status
Study Work status
Intervention Control
Burkus, 200571–73 60% working Mean return 89 days 48% working Mean return to work preoperatively preoperatively 96 days
Burkus, 200274–76 47.6% (68/143) 66.1% (80/121) 36.8% (50/136) 56.1% (60/107) working working preoperatively working at 24 months working preoperatively at 24 months
Median return to work Median return to work 63.5 daysa 64.5 daysa
Dimar, 200677 40% (18/45) working 40% (18/45) returned 32% (17/53) working 30% (16/53) returned to preoperatively to work at 24 months preoperatively work at 24 months
Haid, 200479,87 26.5% working +8.8%b 45.5% working –3.1%b
preoperatively Median return to work preoperatively Median return to work 43 daysa,c 137 daysa,c
a For patients working preoperatively.b Percentage change of patients working at study end-point compared with presurgically.c Authors stated that the difference is not statistically significant.
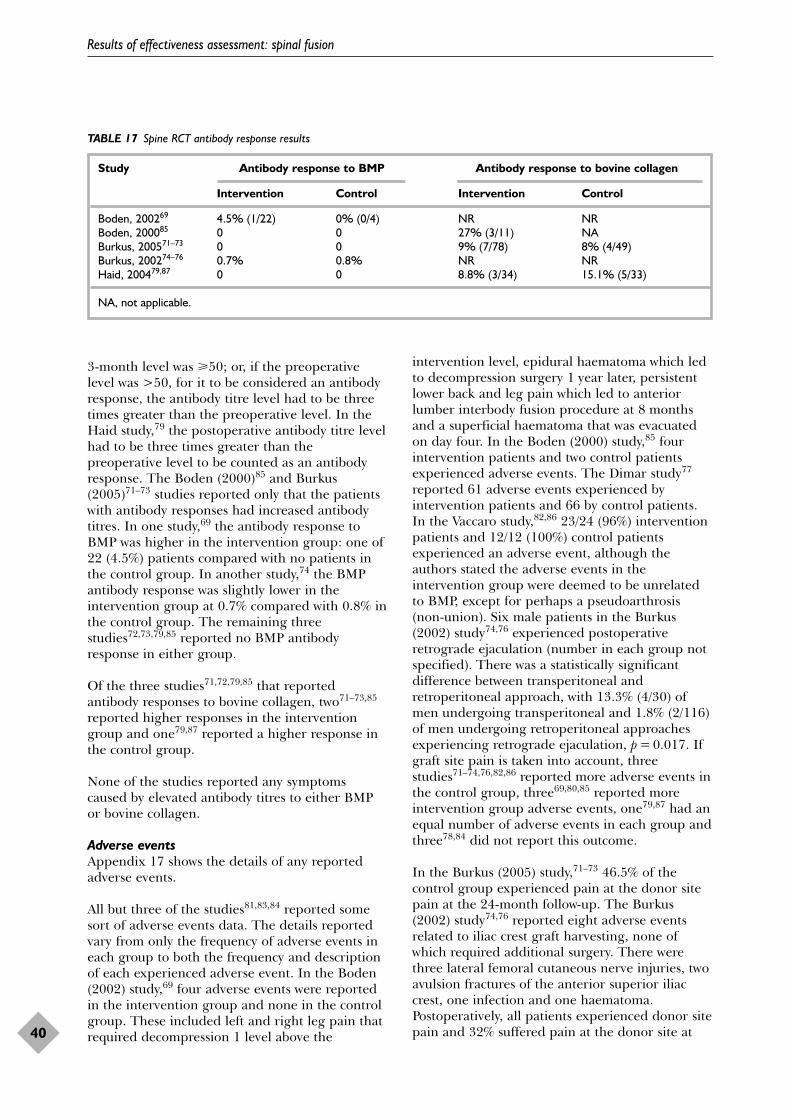
3-month level was �50; or, if the preoperativelevel was >50, for it to be considered an antibodyresponse, the antibody titre level had to be threetimes greater than the preoperative level. In theHaid study,79 the postoperative antibody titre levelhad to be three times greater than thepreoperative level to be counted as an antibodyresponse. The Boden (2000)85 and Burkus(2005)71–73 studies reported only that the patientswith antibody responses had increased antibodytitres. In one study,69 the antibody response toBMP was higher in the intervention group: one of22 (4.5%) patients compared with no patients inthe control group. In another study,74 the BMPantibody response was slightly lower in theintervention group at 0.7% compared with 0.8% inthe control group. The remaining threestudies72,73,79,85 reported no BMP antibodyresponse in either group.
Of the three studies71,72,79,85 that reportedantibody responses to bovine collagen, two71–73,85
reported higher responses in the interventiongroup and one79,87 reported a higher response inthe control group.
None of the studies reported any symptomscaused by elevated antibody titres to either BMPor bovine collagen.
Adverse eventsAppendix 17 shows the details of any reportedadverse events.
All but three of the studies81,83,84 reported somesort of adverse events data. The details reportedvary from only the frequency of adverse events ineach group to both the frequency and descriptionof each experienced adverse event. In the Boden(2002) study,69 four adverse events were reportedin the intervention group and none in the controlgroup. These included left and right leg pain thatrequired decompression 1 level above the
intervention level, epidural haematoma which ledto decompression surgery 1 year later, persistentlower back and leg pain which led to anteriorlumber interbody fusion procedure at 8 monthsand a superficial haematoma that was evacuatedon day four. In the Boden (2000) study,85 fourintervention patients and two control patientsexperienced adverse events. The Dimar study77
reported 61 adverse events experienced byintervention patients and 66 by control patients.In the Vaccaro study,82,86 23/24 (96%) interventionpatients and 12/12 (100%) control patientsexperienced an adverse event, although theauthors stated the adverse events in theintervention group were deemed to be unrelatedto BMP, except for perhaps a pseudoarthrosis(non-union). Six male patients in the Burkus(2002) study74,76 experienced postoperativeretrograde ejaculation (number in each group notspecified). There was a statistically significantdifference between transperitoneal andretroperitoneal approach, with 13.3% (4/30) ofmen undergoing transperitoneal and 1.8% (2/116)of men undergoing retroperitoneal approachesexperiencing retrograde ejaculation, p = 0.017. Ifgraft site pain is taken into account, threestudies71–74,76,82,86 reported more adverse events inthe control group, three69,80,85 reported moreintervention group adverse events, one79,87 had anequal number of adverse events in each group andthree78,84 did not report this outcome.
In the Burkus (2005) study,71–73 46.5% of thecontrol group experienced pain at the donor sitepain at the 24-month follow-up. The Burkus(2002) study74,76 reported eight adverse eventsrelated to iliac crest graft harvesting, none ofwhich required additional surgery. There werethree lateral femoral cutaneous nerve injuries, twoavulsion fractures of the anterior superior iliaccrest, one infection and one haematoma.Postoperatively, all patients experienced donor sitepain and 32% suffered pain at the donor site at
Results of effectiveness assessment: spinal fusion
40
TABLE 17 Spine RCT antibody response results
Study Antibody response to BMP Antibody response to bovine collagen
Intervention Control Intervention Control
Boden, 200269 4.5% (1/22) 0% (0/4) NR NRBoden, 200085 0 0 27% (3/11) NABurkus, 200571–73 0 0 9% (7/78) 8% (4/49)Burkus, 200274–76 0.7% 0.8% NR NRHaid, 200479,87 0 0 8.8% (3/34) 15.1% (5/33)
NA, not applicable.
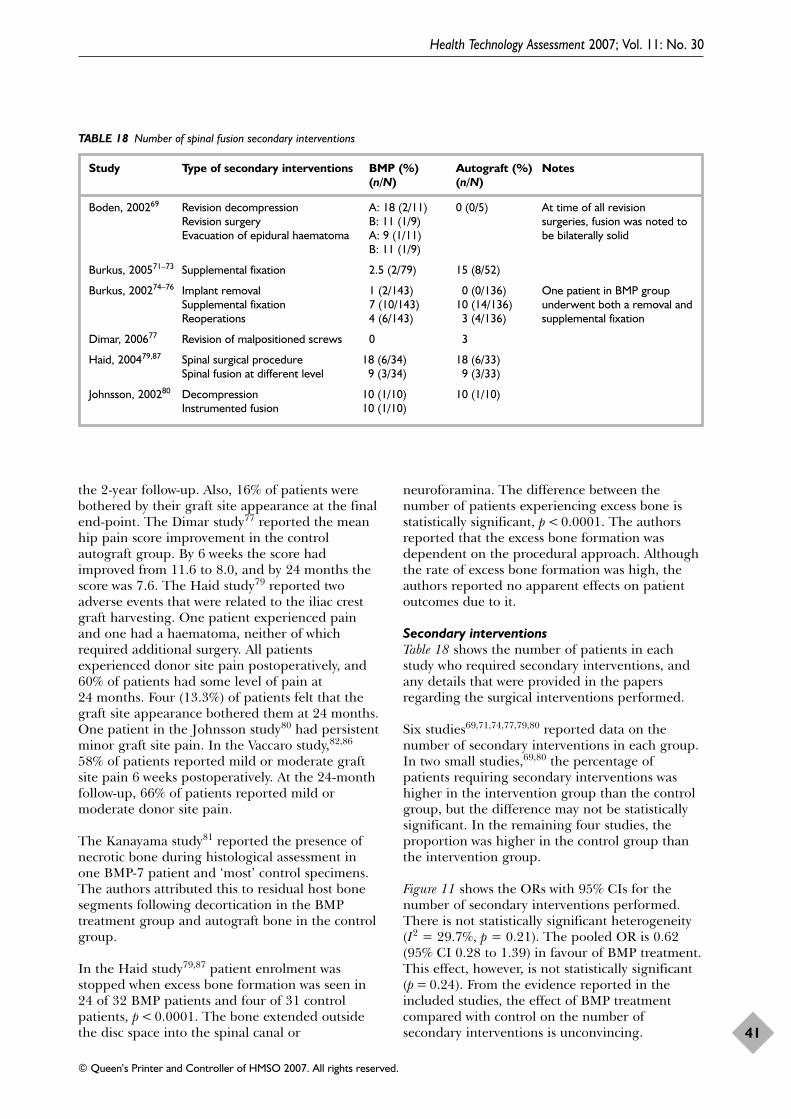
the 2-year follow-up. Also, 16% of patients werebothered by their graft site appearance at the finalend-point. The Dimar study77 reported the meanhip pain score improvement in the controlautograft group. By 6 weeks the score hadimproved from 11.6 to 8.0, and by 24 months thescore was 7.6. The Haid study79 reported twoadverse events that were related to the iliac crestgraft harvesting. One patient experienced painand one had a haematoma, neither of whichrequired additional surgery. All patientsexperienced donor site pain postoperatively, and60% of patients had some level of pain at24 months. Four (13.3%) of patients felt that thegraft site appearance bothered them at 24 months.One patient in the Johnsson study80 had persistentminor graft site pain. In the Vaccaro study,82,86
58% of patients reported mild or moderate graftsite pain 6 weeks postoperatively. At the 24-monthfollow-up, 66% of patients reported mild ormoderate donor site pain.
The Kanayama study81 reported the presence ofnecrotic bone during histological assessment inone BMP-7 patient and ‘most’ control specimens.The authors attributed this to residual host bonesegments following decortication in the BMPtreatment group and autograft bone in the controlgroup.
In the Haid study79,87 patient enrolment wasstopped when excess bone formation was seen in24 of 32 BMP patients and four of 31 controlpatients, p < 0.0001. The bone extended outsidethe disc space into the spinal canal or
neuroforamina. The difference between thenumber of patients experiencing excess bone isstatistically significant, p < 0.0001. The authorsreported that the excess bone formation wasdependent on the procedural approach. Althoughthe rate of excess bone formation was high, theauthors reported no apparent effects on patientoutcomes due to it.
Secondary interventionsTable 18 shows the number of patients in eachstudy who required secondary interventions, andany details that were provided in the papersregarding the surgical interventions performed.
Six studies69,71,74,77,79,80 reported data on thenumber of secondary interventions in each group.In two small studies,69,80 the percentage ofpatients requiring secondary interventions washigher in the intervention group than the controlgroup, but the difference may not be statisticallysignificant. In the remaining four studies, theproportion was higher in the control group thanthe intervention group.
Figure 11 shows the ORs with 95% CIs for thenumber of secondary interventions performed.There is not statistically significant heterogeneity(I2 = 29.7%, p = 0.21). The pooled OR is 0.62(95% CI 0.28 to 1.39) in favour of BMP treatment.This effect, however, is not statistically significant(p = 0.24). From the evidence reported in theincluded studies, the effect of BMP treatmentcompared with control on the number ofsecondary interventions is unconvincing.
Health Technology Assessment 2007; Vol. 11: No. 30
41
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 18 Number of spinal fusion secondary interventions
Study Type of secondary interventions BMP (%) Autograft (%) Notes(n/N) (n/N)
Boden, 200269 Revision decompression A: 18 (2/11) 0 (0/5) At time of all revision Revision surgery B: 11 (1/9) surgeries, fusion was noted to Evacuation of epidural haematoma A: 9 (1/11) be bilaterally solid
B: 11 (1/9)
Burkus, 200571–73 Supplemental fixation 2.5 (2/79) 15 (8/52)
Burkus, 200274–76 Implant removal 1 (2/143) 0 (0/136) One patient in BMP group Supplemental fixation 7 (10/143) 10 (14/136) underwent both a removal and Reoperations 4 (6/143) 3 (4/136) supplemental fixation
Dimar, 200677 Revision of malpositioned screws 0 3
Haid, 200479,87 Spinal surgical procedure 18 (6/34) 18 (6/33)Spinal fusion at different level 9 (3/34) 9 (3/33)
Johnsson, 200280 Decompression 10 (1/10) 10 (1/10)Instrumented fusion 10 (1/10)
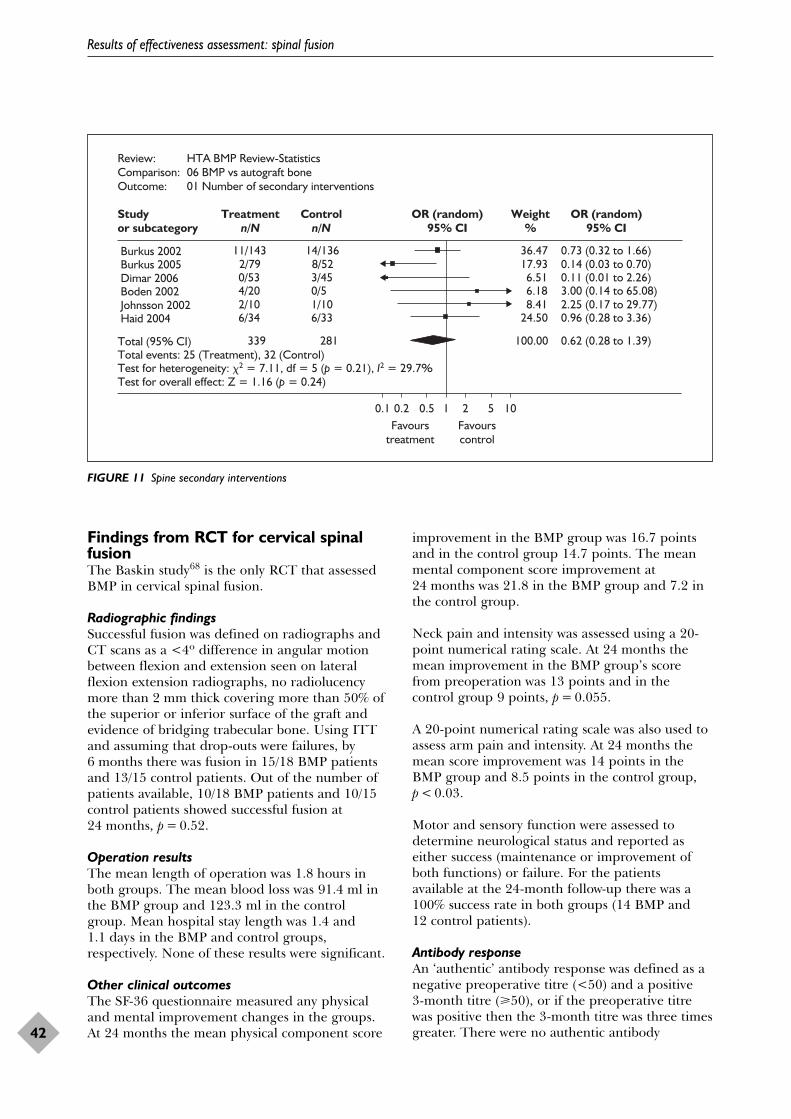
Findings from RCT for cervical spinalfusionThe Baskin study68 is the only RCT that assessedBMP in cervical spinal fusion.
Radiographic findingsSuccessful fusion was defined on radiographs andCT scans as a <4º difference in angular motionbetween flexion and extension seen on lateralflexion extension radiographs, no radiolucencymore than 2 mm thick covering more than 50% ofthe superior or inferior surface of the graft andevidence of bridging trabecular bone. Using ITTand assuming that drop-outs were failures, by6 months there was fusion in 15/18 BMP patientsand 13/15 control patients. Out of the number ofpatients available, 10/18 BMP patients and 10/15control patients showed successful fusion at24 months, p = 0.52.
Operation resultsThe mean length of operation was 1.8 hours inboth groups. The mean blood loss was 91.4 ml inthe BMP group and 123.3 ml in the controlgroup. Mean hospital stay length was 1.4 and1.1 days in the BMP and control groups,respectively. None of these results were significant.
Other clinical outcomesThe SF-36 questionnaire measured any physicaland mental improvement changes in the groups.At 24 months the mean physical component score
improvement in the BMP group was 16.7 pointsand in the control group 14.7 points. The meanmental component score improvement at24 months was 21.8 in the BMP group and 7.2 inthe control group.
Neck pain and intensity was assessed using a 20-point numerical rating scale. At 24 months themean improvement in the BMP group’s scorefrom preoperation was 13 points and in thecontrol group 9 points, p = 0.055.
A 20-point numerical rating scale was also used toassess arm pain and intensity. At 24 months themean score improvement was 14 points in theBMP group and 8.5 points in the control group,p < 0.03.
Motor and sensory function were assessed todetermine neurological status and reported aseither success (maintenance or improvement ofboth functions) or failure. For the patientsavailable at the 24-month follow-up there was a100% success rate in both groups (14 BMP and 12 control patients).
Antibody responseAn ‘authentic’ antibody response was defined as anegative preoperative titre (<50) and a positive 3-month titre (�50), or if the preoperative titrewas positive then the 3-month titre was three timesgreater. There were no authentic antibody
Results of effectiveness assessment: spinal fusion
42
Review: HTA BMP Review-StatisticsComparison: 06 BMP vs autograft boneOutcome: 01 Number of secondary interventions
Studyor subcategory
Treatmentn/N
Controln/N
OR (random)95% CI
Weight%
OR (random)95% CI
Burkus 2002 11/143 14/136 36.47 0.73 (0.32 to 1.66) Burkus 2005 2/79 8/52 17.93 0.14 (0.03 to 0.70) Dimar 2006 0/53 3/45 6.51 0.11 (0.01 to 2.26) Boden 2002 4/20 0/5 6.18 3.00 (0.14 to 65.08) Johnsson 2002 2/10 1/10 8.41 2.25 (0.17 to 29.77) Haid 2004 6/34 6/33 24.50 0.96 (0.28 to 3.36)
Total (95% CI) 339 281 100.00 0.62 (0.28 to 1.39)Total events: 25 (Treatment), 32 (Control)Test for heterogeneity: �2 = 7.11, df = 5 (p = 0.21), I2 = 29.7%Test for overall effect: Z = 1.16 (p = 0.24)
Favourstreatment
Favourscontrol
0.1 0.2 0.5 1 2 5 10
FIGURE 11 Spine secondary interventions

responses to BMP-2. One BMP and one controlpatient had responses to bovine type I collagen at3 months.
Adverse eventsPain at the donor site was measured usingnumerical rating scales. The control autograftgroup experienced significant graft site pain,p < 0.007, and were unhappy with the graft siteappearance. By 6 months, the groups werecomparable in terms of graft site pain andappearance. By 24 months an unreported numberof patients were still experiencing residual donorsite pain and rated the graft site appearance as‘fair’.
In two BMP group and one autograft controlgroup patients, bone formation anterior to thesegments adjacent to the treated level was visibleat the 12-month follow-up. The authors reportthat all three patients who experienced boneformation were treated by the same surgeon, andthe results may therefore be related to technique.Other possible explanations discussed wereacceleration of spondylitic bone growth inadjacent degenerated discs or blood at the surgical trauma site channelling BMP from thecarrier.
Secondary interventionsThere was one reported secondary intervention ina BMP-treated patient that was deemed unrelatedto the original procedure. A segment adjacent tothe original surgical site was operated on,requiring removal of the anterior cervical plate.
Summary of evidence fromrandomised trials of BMP forspinal fusionThe included RCTs have many methodologicalweaknesses as none met all of the quality criteria.The main methodological limitations of thestudies are lack of reporting of randomisation andallocation concealment methods, failure to analysedata using ITT analysis, unclear inclusion andexclusion criteria and failure to report reasons forpatient drop-outs. Some secondary outcomes werenot measured and/or reported in every trial.
Lumbar spinal fusionAccording to evidence from seven trials, the use ofBMP-2 increased radiographical fusion amongpatients with single-level degenerative disc disease(pooled OR: 3.87, 95% CI 1.59 to 9.46). Dataavailable from four trials of other spinal disorderswere insufficient to determine any difference ineffect between BMP and control treatments. Thepooled OR for patients with degenerativespondylolisthesis with spinal stenosis is 0.87 (95% CI 0.15 to 5.08) and for patients withspondylosis the OR is 0.38 (95%C CI 0.05 to 2.77).
The evidence suggests that BMP is associated witha 25-minute (range 11–37 minutes) reduction inoperating time compared with controls, which isprobably attributable to elimination of bone graftharvesting. BMP is also associated with a shorterhospital stay (pooled OR –0.75, 95% CI –0.31 to–1.19). There is no convincing evidence that theuse of BMP reduced blood loss.
Treatment with BMP eliminates donor sitemorbidities by replacing bone grafting. There wassome evidence to suggest that BMP is associatedwith greater improvement in clinical outcomessuch as Oswestry Disability Index score, SF-36score and back and leg pain. Available data on theimpact of BMP on the proportion of patients whoreturned to work was limited, unstandardised andsometime difficult to interpret. From the evidencereported in the studies, it was not possible todetermine convincingly the effect of BMP on the number of adverse events or secondaryinterventions. Further research and longer follow-up are required to evaluate the clinical importanceof excess bone formation seen in the Haid study.79
Cervical spinal fusionThere is little evidence for BMP in cervical spinalfusion. The evidence available indicates that BMPwith allograft is comparable to autograft withallograft for fusion rates, length of operation,blood loss, hospital stay length, SF-36 score andneurological improvement. However, there is someevidence to suggest that BMP may improve neckand arm pain scores over autograft control.Finally, the use of BMP with allograft eliminatesthe need for a donor site and thus consequentlyany donor site morbidity.
Health Technology Assessment 2007; Vol. 11: No. 30
43
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.

In this chapter, findings are presented from acritical review of published economic
evaluations on the use of BMP for fracture andspinal fusion. Two economic evaluation modelsprovided by ABACUS are then assessed andmodified.
Review of published economicstudiesThree published papers53–55 and one abstract56
were identified. However, one published shortstudy55 and the abstract56 did not provide enoughinformation for data extraction. The remainingtwo published papers reported the same set ofdata and were therefore treated as one study. Inthis review, we included only one study on theeconomic evaluation of BMP for spinal fusion,50,51
and we identified no published economicevaluations of BMP for fracture.
Data from the included study were extracted byone reviewer and checked by another. Theobjectives of the economic evaluation50,51 were(a) to compare the costs of stand-alone anteriorlumbar interbody fusion using either rhBMP-2 ona collagen sponge or autogenous iliac crest bonegraft in a tapered cylindrical cage or threadedcortical bone dowel and (b) to conduct a thresholdanalysis to estimate the cost (price) of BMP atwhich direct medical costs are entirely offset. Thepaper reported that it was conducted in a primarycare setting in the USA.
The study was judged to be of highmethodological quality based on assessment usingthe Drummond checklist.51 The only applicablechecklist items that were not met related to afailure to report whether discounting had beenundertaken, although this may be due to the shorttime horizon (2 years) considered by the model.All of the remaining quality criteria were eithermet or not applicable.
The study aimed to develop cost-offset models (i.e.a threshold analysis). Clinical outcomes considered
in the models were those relevant to medicalresource use, including fusion success rates, painand complications at the bone graft site. Datafrom two trials,75,95 along with peer-reviewedliterature and expert opinion, were used to createtwo different models comparing costs of BMP andcosts of AICBG. One model included hospitalcosts incurred during index hospitalisation onlyand the other additionally took into account directmedical costs 2 years after surgery.
Table 19 shows that a base price cost of BMP at$3380 was found to offset the index hospitalresources and 2-year resources (US$, 2001). Basedon effectiveness data extracted from the Burkus(2002) study,74–76 intervention with BMP over a 2-year period was found to cost $9 less thanAICBG intervention (US$, 2001).
Polly and colleagues54 included a sensitivityanalysis that was performed using data from the Burkus (2005) study.71–73,95 Costs wereinsensitive to changes in complication ratesassociated with bone harvesting, length of stay,autograft extender/harvester use, time horizon,autologous blood use and external electricalstimulation use. Table 20 shows results of thesensitivity analysis to changes in BMP price andfusion rate assumptions. The cost was found to besensitive to increases in the price of BMP anddecreases of fusion rates in the BMP patients.Based on the model presented in this study, costneutrality of BMP treatment compared withAICBG is reached at a BMP cost of $3389 (US$, 2001).
In summary, the economic evaluation by Polly andcolleagues54 suggests that the initial cost of usingBMP for spinal fusion is likely to be offset byavoiding autogenous bone graft and relatedcomplications and improved successful fusion.However, the models described in publishedpapers were not available electronically for us toassess detailed structures. The input estimateswere heavily based on expert opinion. In addition,the results of this US study may not begeneralisable to the UK setting.
Health Technology Assessment 2007; Vol. 11: No. 30
45
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Chapter 5
Economic evaluation of BMP for tibial fracture and spinal fusion
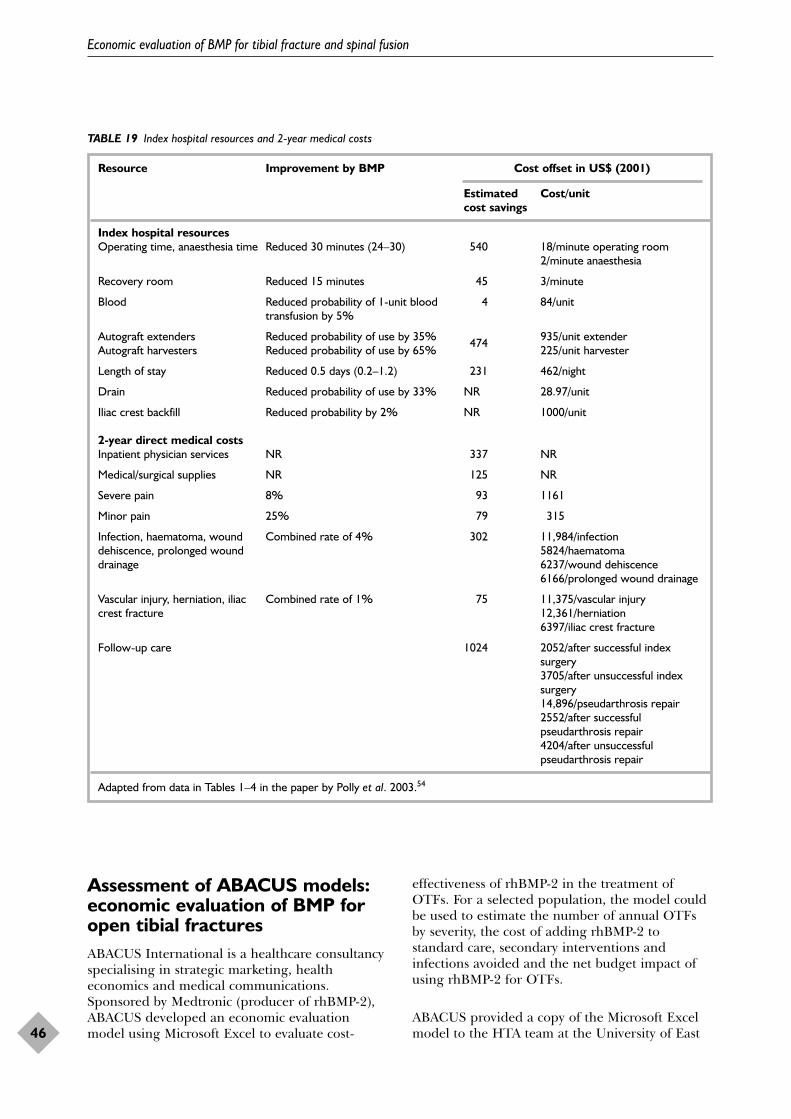
Assessment of ABACUS models:economic evaluation of BMP foropen tibial fractures ABACUS International is a healthcare consultancyspecialising in strategic marketing, healtheconomics and medical communications.Sponsored by Medtronic (producer of rhBMP-2),ABACUS developed an economic evaluationmodel using Microsoft Excel to evaluate cost-
effectiveness of rhBMP-2 in the treatment ofOTFs. For a selected population, the model couldbe used to estimate the number of annual OTFsby severity, the cost of adding rhBMP-2 tostandard care, secondary interventions andinfections avoided and the net budget impact ofusing rhBMP-2 for OTFs.
ABACUS provided a copy of the Microsoft Excelmodel to the HTA team at the University of East
Economic evaluation of BMP for tibial fracture and spinal fusion
46
TABLE 19 Index hospital resources and 2-year medical costs
Resource Improvement by BMP Cost offset in US$ (2001)
Estimated Cost/unitcost savings
Index hospital resourcesOperating time, anaesthesia time Reduced 30 minutes (24–30) 540 18/minute operating room
2/minute anaesthesia
Recovery room Reduced 15 minutes 45 3/minute
Blood Reduced probability of 1-unit blood 4 84/unittransfusion by 5%
Autograft extenders Reduced probability of use by 35% 474 935/unit extenderAutograft harvesters Reduced probability of use by 65% 225/unit harvester
Length of stay Reduced 0.5 days (0.2–1.2) 231 462/night
Drain Reduced probability of use by 33% NR 28.97/unit
Iliac crest backfill Reduced probability by 2% NR 1000/unit
2-year direct medical costsInpatient physician services NR 337 NR
Medical/surgical supplies NR 125 NR
Severe pain 8% 93 1161
Minor pain 25% 79 315
Infection, haematoma, wound Combined rate of 4% 302 11,984/infectiondehiscence, prolonged wound 5824/haematomadrainage 6237/wound dehiscence
6166/prolonged wound drainage
Vascular injury, herniation, iliac Combined rate of 1% 75 11,375/vascular injurycrest fracture 12,361/herniation
6397/iliac crest fracture
Follow-up care 1024 2052/after successful indexsurgery3705/after unsuccessful indexsurgery14,896/pseudarthrosis repair2552/after successfulpseudarthrosis repair4204/after unsuccessfulpseudarthrosis repair
Adapted from data in Tables 1–4 in the paper by Polly et al. 2003.54
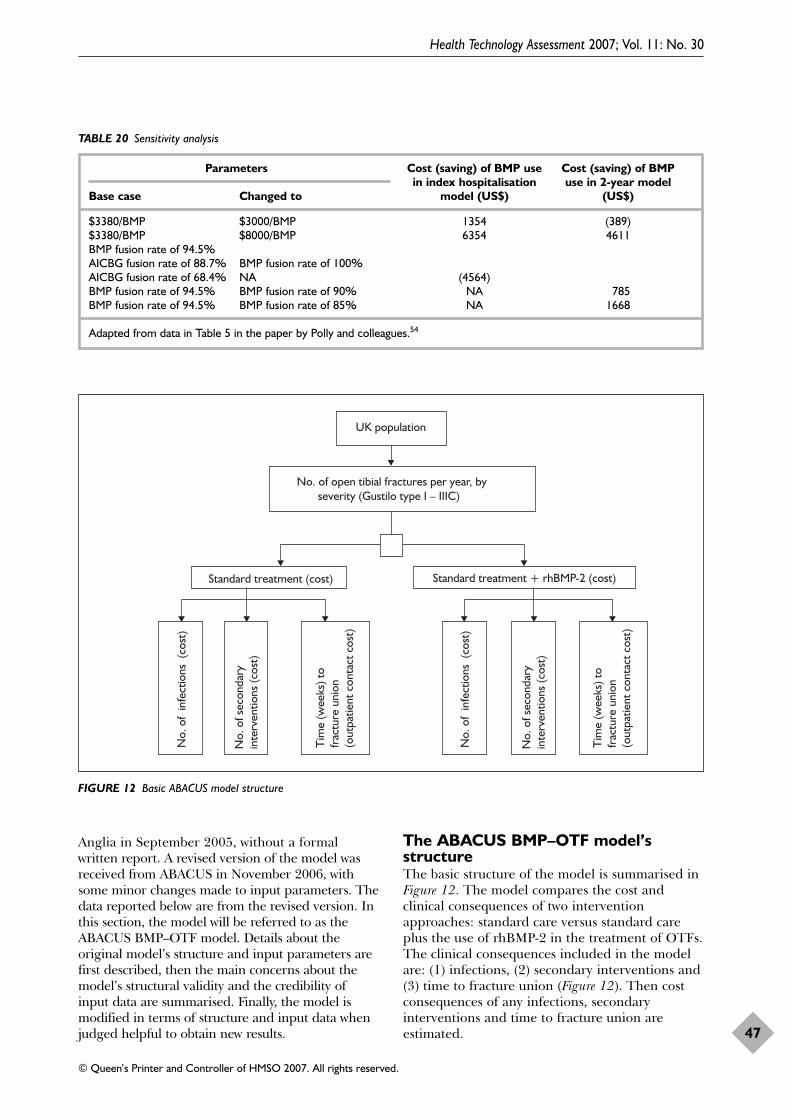
Anglia in September 2005, without a formalwritten report. A revised version of the model wasreceived from ABACUS in November 2006, withsome minor changes made to input parameters. Thedata reported below are from the revised version. Inthis section, the model will be referred to as theABACUS BMP–OTF model. Details about theoriginal model’s structure and input parameters arefirst described, then the main concerns about themodel’s structural validity and the credibility ofinput data are summarised. Finally, the model ismodified in terms of structure and input data whenjudged helpful to obtain new results.
The ABACUS BMP–OTF model’sstructureThe basic structure of the model is summarised inFigure 12. The model compares the cost andclinical consequences of two interventionapproaches: standard care versus standard careplus the use of rhBMP-2 in the treatment of OTFs.The clinical consequences included in the modelare: (1) infections, (2) secondary interventions and(3) time to fracture union (Figure 12). Then costconsequences of any infections, secondaryinterventions and time to fracture union areestimated.
Health Technology Assessment 2007; Vol. 11: No. 30
47
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 20 Sensitivity analysis
Parameters Cost (saving) of BMP use Cost (saving) of BMP in index hospitalisation use in 2-year model
Base case Changed to model (US$) (US$)
$3380/BMP $3000/BMP 1354 (389)$3380/BMP $8000/BMP 6354 4611BMP fusion rate of 94.5%AICBG fusion rate of 88.7% BMP fusion rate of 100%AICBG fusion rate of 68.4% NA (4564)BMP fusion rate of 94.5% BMP fusion rate of 90% NA 785BMP fusion rate of 94.5% BMP fusion rate of 85% NA 1668
Adapted from data in Table 5 in the paper by Polly and colleagues.54
UK population
No. of open tibial fractures per year, byseverity (Gustilo type I – IIIC)
Standard treatment (cost) Standard treatment + rhBMP-2 (cost)
No.
of
infe
ctio
ns (
cost
)
No.
of s
econ
dary
in
terv
entio
ns (c
ost)
Tim
e (w
eeks
) to
frac
ture
uni
on
(out
patie
nt c
onta
ct c
ost)
No.
of
infe
ctio
ns (
cost
)
No.
of s
econ
dary
in
terv
entio
ns (c
ost)
Tim
e (w
eeks
) to
frac
ture
uni
on
(out
patie
nt c
onta
ct c
ost)
FIGURE 12 Basic ABACUS model structure
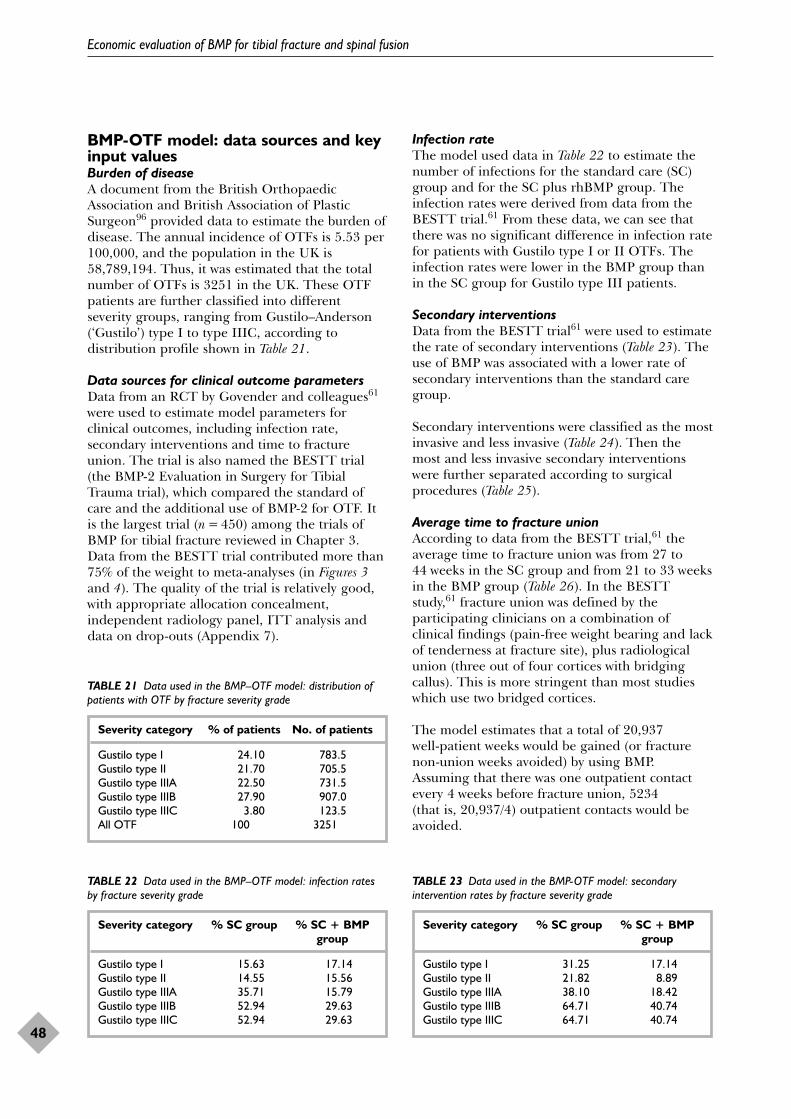
BMP-OTF model: data sources and keyinput valuesBurden of diseaseA document from the British OrthopaedicAssociation and British Association of PlasticSurgeon96 provided data to estimate the burden ofdisease. The annual incidence of OTFs is 5.53 per100,000, and the population in the UK is58,789,194. Thus, it was estimated that the totalnumber of OTFs is 3251 in the UK. These OTFpatients are further classified into differentseverity groups, ranging from Gustilo–Anderson(‘Gustilo’) type I to type IIIC, according todistribution profile shown in Table 21.
Data sources for clinical outcome parametersData from an RCT by Govender and colleagues61
were used to estimate model parameters forclinical outcomes, including infection rate,secondary interventions and time to fractureunion. The trial is also named the BESTT trial(the BMP-2 Evaluation in Surgery for TibialTrauma trial), which compared the standard ofcare and the additional use of BMP-2 for OTF. Itis the largest trial (n = 450) among the trials ofBMP for tibial fracture reviewed in Chapter 3.Data from the BESTT trial contributed more than75% of the weight to meta-analyses (in Figures 3and 4). The quality of the trial is relatively good,with appropriate allocation concealment,independent radiology panel, ITT analysis anddata on drop-outs (Appendix 7).
Infection rateThe model used data in Table 22 to estimate thenumber of infections for the standard care (SC)group and for the SC plus rhBMP group. Theinfection rates were derived from data from theBESTT trial.61 From these data, we can see thatthere was no significant difference in infection ratefor patients with Gustilo type I or II OTFs. Theinfection rates were lower in the BMP group thanin the SC group for Gustilo type III patients.
Secondary interventionsData from the BESTT trial61 were used to estimatethe rate of secondary interventions (Table 23). Theuse of BMP was associated with a lower rate ofsecondary interventions than the standard caregroup.
Secondary interventions were classified as the mostinvasive and less invasive (Table 24). Then themost and less invasive secondary interventionswere further separated according to surgicalprocedures (Table 25).
Average time to fracture unionAccording to data from the BESTT trial,61 theaverage time to fracture union was from 27 to44 weeks in the SC group and from 21 to 33 weeksin the BMP group (Table 26). In the BESTTstudy,61 fracture union was defined by theparticipating clinicians on a combination ofclinical findings (pain-free weight bearing and lackof tenderness at fracture site), plus radiologicalunion (three out of four cortices with bridgingcallus). This is more stringent than most studieswhich use two bridged cortices.
The model estimates that a total of 20,937 well-patient weeks would be gained (or fracturenon-union weeks avoided) by using BMP.Assuming that there was one outpatient contactevery 4 weeks before fracture union, 5234 (that is, 20,937/4) outpatient contacts would beavoided.
Economic evaluation of BMP for tibial fracture and spinal fusion
48
TABLE 21 Data used in the BMP–OTF model: distribution ofpatients with OTF by fracture severity grade
Severity category % of patients No. of patients
Gustilo type I 24.10 783.5Gustilo type II 21.70 705.5Gustilo type IIIA 22.50 731.5Gustilo type IIIB 27.90 907.0Gustilo type IIIC 3.80 123.5All OTF 100 3251
TABLE 22 Data used in the BMP–OTF model: infection ratesby fracture severity grade
Severity category % SC group % SC + BMP group
Gustilo type I 15.63 17.14Gustilo type II 14.55 15.56Gustilo type IIIA 35.71 15.79Gustilo type IIIB 52.94 29.63Gustilo type IIIC 52.94 29.63
TABLE 23 Data used in the BMP-OTF model: secondaryintervention rates by fracture severity grade
Severity category % SC group % SC + BMP group
Gustilo type I 31.25 17.14Gustilo type II 21.82 8.89Gustilo type IIIA 38.10 18.42Gustilo type IIIB 64.71 40.74Gustilo type IIIC 64.71 40.74
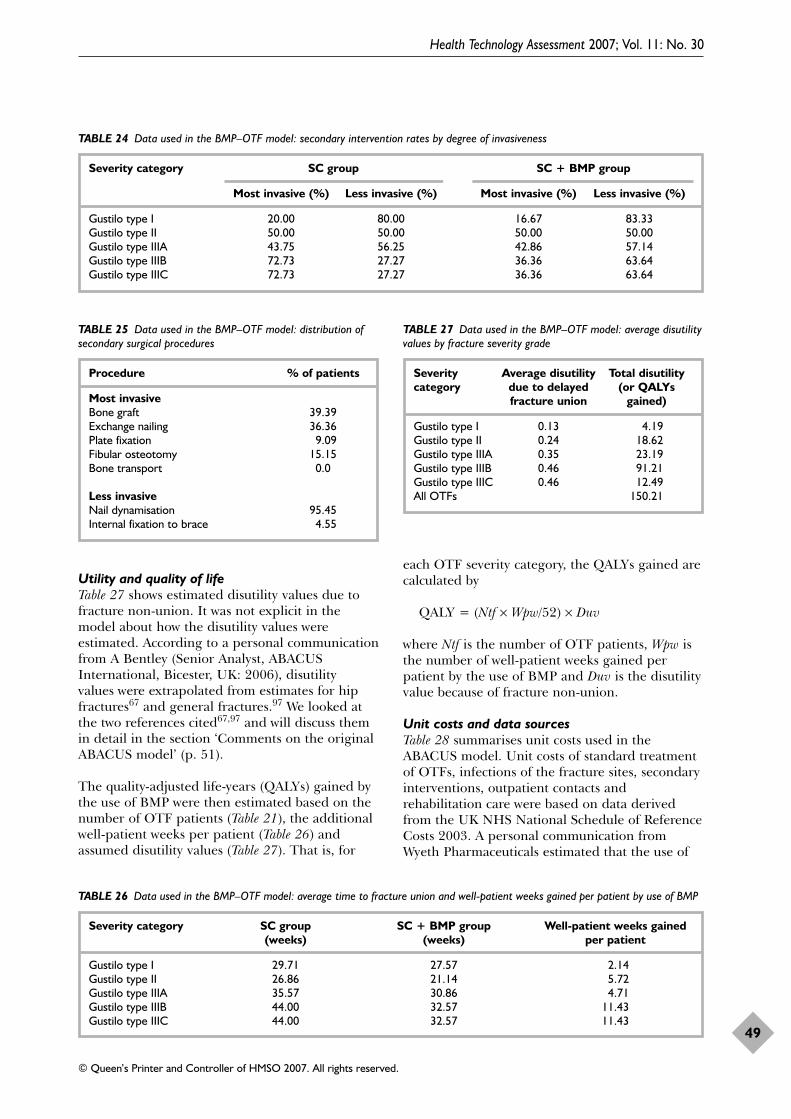
Utility and quality of lifeTable 27 shows estimated disutility values due tofracture non-union. It was not explicit in themodel about how the disutility values wereestimated. According to a personal communicationfrom A Bentley (Senior Analyst, ABACUSInternational, Bicester, UK: 2006), disutility values were extrapolated from estimates for hipfractures67 and general fractures.97 We looked atthe two references cited67,97 and will discuss themin detail in the section ‘Comments on the originalABACUS model’ (p. 51).
The quality-adjusted life-years (QALYs) gained bythe use of BMP were then estimated based on thenumber of OTF patients (Table 21), the additionalwell-patient weeks per patient (Table 26) andassumed disutility values (Table 27). That is, for
each OTF severity category, the QALYs gained arecalculated by
QALY = (Ntf × Wpw/52) × Duv
where Ntf is the number of OTF patients, Wpw isthe number of well-patient weeks gained perpatient by the use of BMP and Duv is the disutilityvalue because of fracture non-union.
Unit costs and data sourcesTable 28 summarises unit costs used in theABACUS model. Unit costs of standard treatmentof OTFs, infections of the fracture sites, secondaryinterventions, outpatient contacts andrehabilitation care were based on data derivedfrom the UK NHS National Schedule of ReferenceCosts 2003. A personal communication fromWyeth Pharmaceuticals estimated that the use of
Health Technology Assessment 2007; Vol. 11: No. 30
49
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 24 Data used in the BMP–OTF model: secondary intervention rates by degree of invasiveness
Severity category SC group SC + BMP group
Most invasive (%) Less invasive (%) Most invasive (%) Less invasive (%)
Gustilo type I 20.00 80.00 16.67 83.33Gustilo type II 50.00 50.00 50.00 50.00Gustilo type IIIA 43.75 56.25 42.86 57.14Gustilo type IIIB 72.73 27.27 36.36 63.64Gustilo type IIIC 72.73 27.27 36.36 63.64
TABLE 25 Data used in the BMP–OTF model: distribution ofsecondary surgical procedures
Procedure % of patients
Most invasiveBone graft 39.39Exchange nailing 36.36Plate fixation 9.09Fibular osteotomy 15.15Bone transport 0.0
Less invasiveNail dynamisation 95.45Internal fixation to brace 4.55
TABLE 27 Data used in the BMP–OTF model: average disutilityvalues by fracture severity grade
Severity Average disutility Total disutility category due to delayed (or QALYs
fracture union gained)
Gustilo type I 0.13 4.19Gustilo type II 0.24 18.62Gustilo type IIIA 0.35 23.19Gustilo type IIIB 0.46 91.21Gustilo type IIIC 0.46 12.49All OTFs 150.21
TABLE 26 Data used in the BMP–OTF model: average time to fracture union and well-patient weeks gained per patient by use of BMP
Severity category SC group SC + BMP group Well-patient weeks gained (weeks) (weeks) per patient
Gustilo type I 29.71 27.57 2.14Gustilo type II 26.86 21.14 5.72Gustilo type IIIA 35.57 30.86 4.71Gustilo type IIIB 44.00 32.57 11.43Gustilo type IIIC 44.00 32.57 11.43
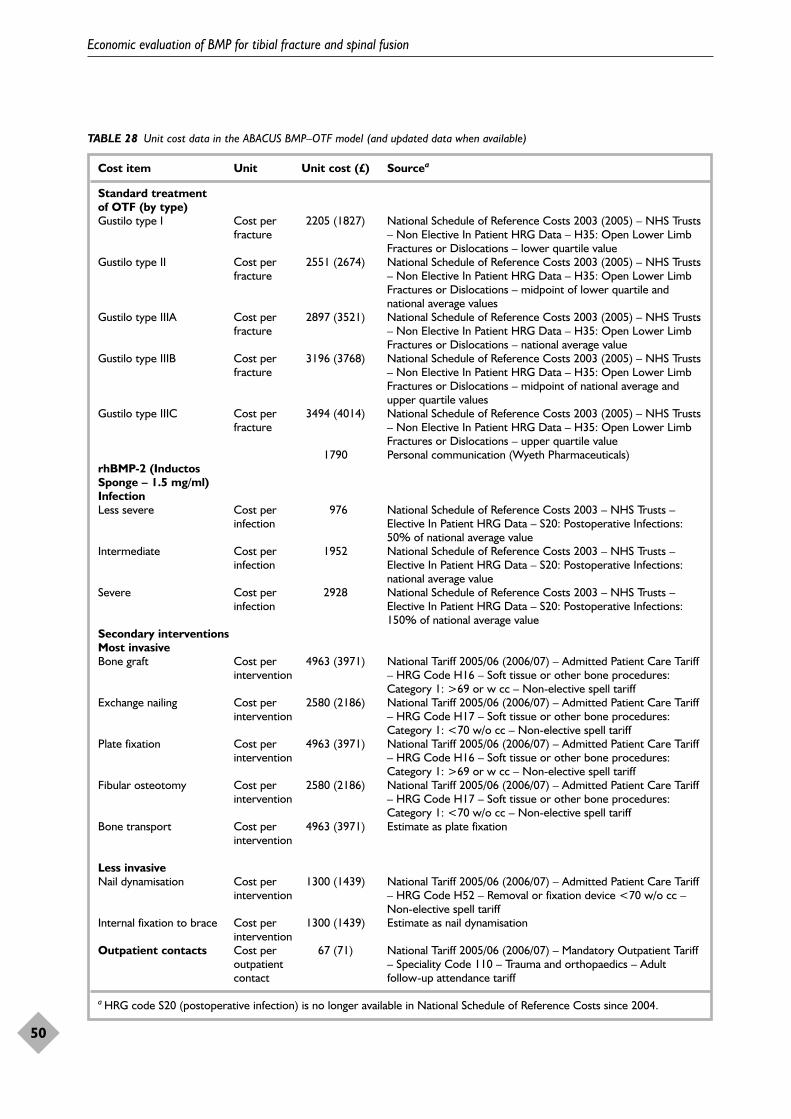
Economic evaluation of BMP for tibial fracture and spinal fusion
50
TABLE 28 Unit cost data in the ABACUS BMP–OTF model (and updated data when available)
Cost item Unit Unit cost (£) Sourcea
Standard treatment of OTF (by type)Gustilo type I Cost per 2205 (1827) National Schedule of Reference Costs 2003 (2005) – NHS Trusts
fracture – Non Elective In Patient HRG Data – H35: Open Lower LimbFractures or Dislocations – lower quartile value
Gustilo type II Cost per 2551 (2674) National Schedule of Reference Costs 2003 (2005) – NHS Trusts fracture – Non Elective In Patient HRG Data – H35: Open Lower Limb
Fractures or Dislocations – midpoint of lower quartile andnational average values
Gustilo type IIIA Cost per 2897 (3521) National Schedule of Reference Costs 2003 (2005) – NHS Trusts fracture – Non Elective In Patient HRG Data – H35: Open Lower Limb
Fractures or Dislocations – national average valueGustilo type IIIB Cost per 3196 (3768) National Schedule of Reference Costs 2003 (2005) – NHS Trusts
fracture – Non Elective In Patient HRG Data – H35: Open Lower LimbFractures or Dislocations – midpoint of national average andupper quartile values
Gustilo type IIIC Cost per 3494 (4014) National Schedule of Reference Costs 2003 (2005) – NHS Trusts fracture – Non Elective In Patient HRG Data – H35: Open Lower Limb
Fractures or Dislocations – upper quartile value1790 Personal communication (Wyeth Pharmaceuticals)
rhBMP-2 (Inductos Sponge – 1.5 mg/ml)InfectionLess severe Cost per 976 National Schedule of Reference Costs 2003 – NHS Trusts –
infection Elective In Patient HRG Data – S20: Postoperative Infections:50% of national average value
Intermediate Cost per 1952 National Schedule of Reference Costs 2003 – NHS Trusts – infection Elective In Patient HRG Data – S20: Postoperative Infections:
national average valueSevere Cost per 2928 National Schedule of Reference Costs 2003 – NHS Trusts –
infection Elective In Patient HRG Data – S20: Postoperative Infections:150% of national average value
Secondary interventionsMost invasiveBone graft Cost per 4963 (3971) National Tariff 2005/06 (2006/07) – Admitted Patient Care Tariff
intervention – HRG Code H16 – Soft tissue or other bone procedures:Category 1: >69 or w cc – Non-elective spell tariff
Exchange nailing Cost per 2580 (2186) National Tariff 2005/06 (2006/07) – Admitted Patient Care Tariff intervention – HRG Code H17 – Soft tissue or other bone procedures:
Category 1: <70 w/o cc – Non-elective spell tariffPlate fixation Cost per 4963 (3971) National Tariff 2005/06 (2006/07) – Admitted Patient Care Tariff
intervention – HRG Code H16 – Soft tissue or other bone procedures:Category 1: >69 or w cc – Non-elective spell tariff
Fibular osteotomy Cost per 2580 (2186) National Tariff 2005/06 (2006/07) – Admitted Patient Care Tariff intervention – HRG Code H17 – Soft tissue or other bone procedures:
Category 1: <70 w/o cc – Non-elective spell tariffBone transport Cost per 4963 (3971) Estimate as plate fixation
intervention
Less invasiveNail dynamisation Cost per 1300 (1439) National Tariff 2005/06 (2006/07) – Admitted Patient Care Tariff
intervention – HRG Code H52 – Removal or fixation device <70 w/o cc –Non-elective spell tariff
Internal fixation to brace Cost per 1300 (1439) Estimate as nail dynamisationintervention
Outpatient contacts Cost per 67 (71) National Tariff 2005/06 (2006/07) – Mandatory Outpatient Tariff outpatient – Speciality Code 110 – Trauma and orthopaedics – Adult contact follow-up attendance tariff
a HRG code S20 (postoperative infection) is no longer available in National Schedule of Reference Costs since 2004.

rhBMP-2 would cost £1790 per fracture additionalto the standard treatment.
Uncertainty and probabilistic simulationA range of values for important input parameterswere estimated for probabilistic simulations by theABACUS model. The model parameters that wererandomly investigated included severitydistribution of OTFs, infection rate, secondaryintervention rates/types, time to fracture union,disutility values and unit costs of interventions andclinical outcomes. In probabilistic simulations, therange (95% CIs) of input parameters could befrom 25% (or 50%) smaller and greater than thepoint estimates. Then input values were randomlysampled from a gamma or beta distribution toobtain random estimates for cost-effectivenessoutcomes. The random simulations were repeatedmany times to generate a large number of randomestimates, and the simulation results were used tocalculate average estimates and correspondingCIs. For estimating the incremental cost-effectiveness ratio (ICER), a cost-effectivenessacceptability curve (CEAC) can be created usingthe results of simulations.98
The BMP–OTF model’s original outputsThe main results of the original ABACUS modelare shown in Table 29. Based on input datadescribed above, the model estimated that therewere about 3251 OTFs in the UK each year. TheSC of these patients cost £8,976,951 and the SCplus rhBMP-2 cost £14,796,317. Hence the use ofrhBMP for the treatment of OTFs would cost theNHS an additional £5,819,366 each year.
However, the use of rhBMP-2 might prevent 367infections and 593 secondary interventions, whichwould result in saving of £497,906 and£1,911,972, respectively (Table 29). In addition,£350,692 could be saved by the use of BMPbecause reduced time to fracture union wouldavoid 5234 outpatient contacts. After taking awaysavings from the total costs, the use of rhBMP-2will cost the NHS £921 per OTF, or a total of£3,058,795 each year in the UK.
The original ABACUS model estimated that thecosts per QALYs gained by additional use of BMPfor OTFs is £20,364 (95% CI 11,683 to 31,321).
Comments on the original ABACUSmodelABACUS International sent a copy of the model,so the model can be considered as transparentgenerally in terms of its structure and inputparameters. The model was well developed andprogrammed; the ABACUS model was assessedand no programming and other errors werefound. The model’s structure seems reasonable,given the currently available research evidence.Clinical data for input parameters of the modelwas mainly from the BESTT trial61 and cost datafrom National Schedule of Reference costs (2003).Perhaps these are currently the best available datasources, although unit cost could be updated bydata from National Schedule of Reference costs2005.
The model could be used to conduct probabilisticsimulations. The range of input parameters wasarbitrarily decided to be 25% or 50% smaller orgreater than the point estimates of inputparameters. Therefore, it is unclear whetheruncertainty in estimates of input values had beenadequately accommodated in the analysis.
Possible duplicate counting of events and relatedcostsThe effects of the use of BMP were measured byits impact on infections of the fracture sites,secondary interventions and time to fractureunion, which reflect outcome measures used inclinical trials. However, the three outcomes maynot be completely independent. For example, apatient with infection may more likely requiresecondary interventions, and also with delayedfracture union. By personal communication (V Alt,Clinical Advisor, University Hospital Giessen-Marburg, Giessen, Germany: 2006), we receivedfurther data on secondary intervention andinfections for 44 patients in the BESTT trial. Ofthese patients, there were 18 who receivedsecondary interventions and 17 with infection
Health Technology Assessment 2007; Vol. 11: No. 30
51
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 29 Main results of the original BMP–OTF model
Point estimate (£) 95% CI (£) (based on 10,000 simulations)
Net cost impact in the UK 3,058,795 1,823,722 to 4,159,112Cost per OTF 941 561 to 1,279Incremental cost/QALY 20,364 11,683 to 31,321

events. Seven of the patients had both secondaryintervention and infection, although it is difficultto decide whether the two events were directlyassociated.
According to the Department of Health, England,the fundamental principle for costing in the NHSis that “reference costs should be produced usingfull absorption costing”.99 This means that eachreported unit cost will include the direct, indirectand overhead costs associated with providing thattreatment/care. Therefore, the cost ofpostoperative infection may already include thecost of corresponding secondary interventionsrequired due to infection. If so, savings related toinfections and secondary interventions may havebeen overestimated by duplicate counting.
Utility valuesDelayed union of an OTF will inevitably impact ona patient’s quality of life (QoL) (Appendix 24).There is a lack of objective data on patient utility.Utility values used in the ABACUS model wereextrapolated from estimates for older women withhip fractures67 and women with long-standingvertebral osteoporotic fractures.97 The two studieswere reviewed; more details and discussions areprovided below.
Salkeld and colleagues67 used the time trade-offtechnique to estimate the utility associated withhip fracture and fear of falling among olderwomen (aged �75 years). The baseline utilityvalue (EQ-50) was 0.77 for interviewed women.They found that a ‘bad’ hip fracture (which resultsin admission to a nursing home) was valued at0.05 and a ‘good’ hip fracture (maintainingindependent living in the community) 0.31. Thedis-utility value for a ‘good’ hip fracture could beestimated as 0.46 = 0.77 – 0.31, on which it seemsthat the disutility value used for Gustilo typeIIIB/C OTF non-union in the model was based.
Hall and colleagues97 measured QoL in womenwith long-standing vertebral osteoporotic fractureand age-matched normal women, using the SF-36.Then SF-36 scores were transformed to a utilityscore by the Fryback technique. It was found thatthe utility score was 0.64 for women with vertebralfracture and 0.72 for controls. The difference inthe utility scores between the two groups is 0.08(0.72–0.64). However, it is not clear how thisestimate has been used to estimate disutility valuesin the ABACUS model.
It is highly questionable whether the results fromSalkeld and colleagues’ study67 of hip fracture and
Hall and colleagues’ study97 of vertebralosteoporotic fracture are generalisable to patientswith OTF. We identified a further study ofeconomic evaluation of patients with closed tibialshaft fractures.100 Based on expert opinion, theutility value estimated was 0.9 for returning tonormal activities, 0.5 for non-union, 0.6 fordelayed union and 0.5 for experiencing apostoperative complication. This study estimatedthe utility value based on expert opinion, whichwas subjective and may not truly reflect patientopinion.
Fracture union in the BESTT trial was defined bya combination of pain-free weight bearing andlack of tenderness at fracture site plus radiologicalunion (three out of four cortices with bridgingcallus). Hence the QoL of patients may not bemuch different from normal many weeks beforethe defined fracture union. For example, a patientwith pain-free weight bearing and lack oftenderness at the fracture site did not meet thecriteria for fracture union if radiological union wasnot achieved. Therefore, the original ABACUSmodel may has overestimated the disutility valuesdue to delayed union.
Modified and updated ABACUS modelThe following changes were made in the modifiedABACUS model:
1. The population in the UK was 60,209,500 in2005.
2. Unit costs were updated by data from NationalSchedule of Reference Costs 2005/06 andNational Tariff 2006/07 when available.
3. Since the disutility values might be muchoverestimated in the original ABACUS modelbut there is no alternative objective data, wearbitrarily assumed the values to be 30%smaller.
4. To deal with possible multiple counting ofsavings, estimated costs of infections andoutpatient contacts were assumed to be 10%lower than those in the original model.
5. Considering great uncertainty, probabilisticsimulations were conducted by using a widerrange of input values: 50% greater or smallerthan the point estimates.
The results of the modified ABACUS model areshown in Table 30 and Figures 13 and 14.
The estimated direct cost of using rhBMP-2 is£5,959,958 each year in the UK. After consideringsavings from fewer clinical complications(infections and secondary interventions) and fewer
Economic evaluation of BMP for tibial fracture and spinal fusion
52
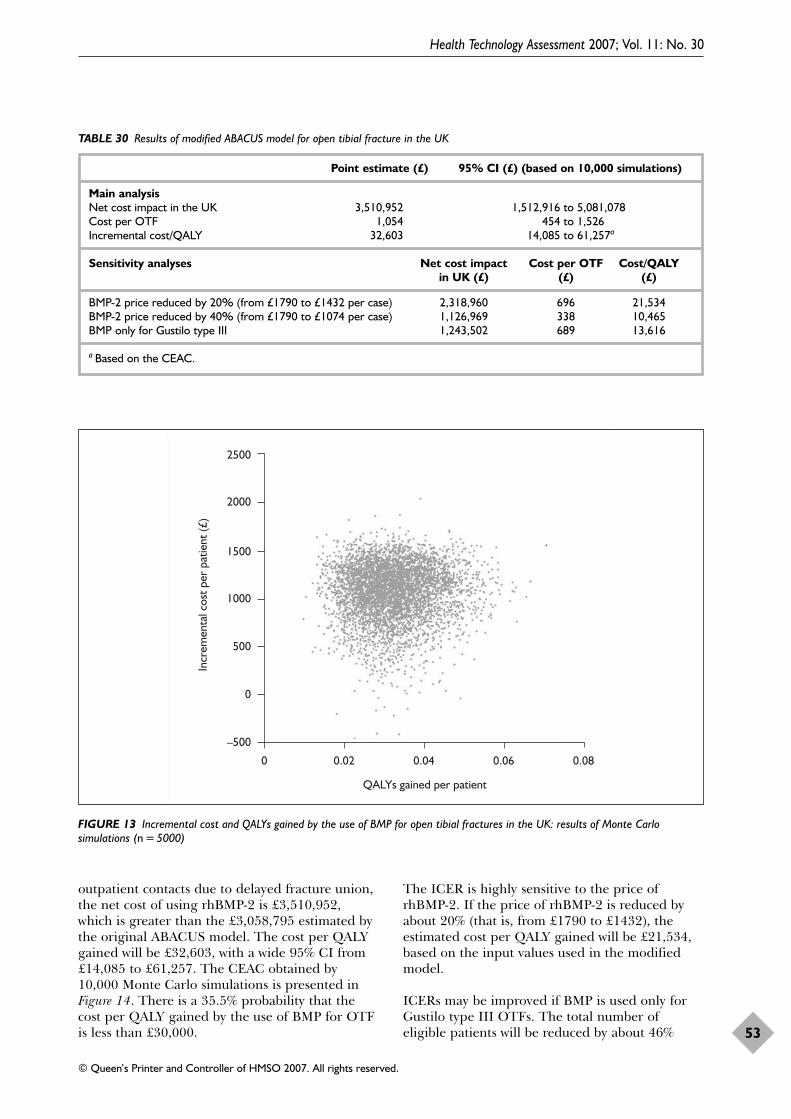
outpatient contacts due to delayed fracture union,the net cost of using rhBMP-2 is £3,510,952,which is greater than the £3,058,795 estimated bythe original ABACUS model. The cost per QALYgained will be £32,603, with a wide 95% CI from£14,085 to £61,257. The CEAC obtained by10,000 Monte Carlo simulations is presented inFigure 14. There is a 35.5% probability that thecost per QALY gained by the use of BMP for OTFis less than £30,000.
The ICER is highly sensitive to the price ofrhBMP-2. If the price of rhBMP-2 is reduced byabout 20% (that is, from £1790 to £1432), theestimated cost per QALY gained will be £21,534,based on the input values used in the modifiedmodel.
ICERs may be improved if BMP is used only forGustilo type III OTFs. The total number ofeligible patients will be reduced by about 46%
Health Technology Assessment 2007; Vol. 11: No. 30
53
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 30 Results of modified ABACUS model for open tibial fracture in the UK
Point estimate (£) 95% CI (£) (based on 10,000 simulations)
Main analysisNet cost impact in the UK 3,510,952 1,512,916 to 5,081,078Cost per OTF 1,054 454 to 1,526Incremental cost/QALY 32,603 14,085 to 61,257a
Sensitivity analyses Net cost impact Cost per OTF Cost/QALYin UK (£) (£) (£)
BMP-2 price reduced by 20% (from £1790 to £1432 per case) 2,318,960 696 21,534BMP-2 price reduced by 40% (from £1790 to £1074 per case) 1,126,969 338 10,465BMP only for Gustilo type III 1,243,502 689 13,616
a Based on the CEAC.
0 0.02 0.04 0.06 0.08
–500
0
500
1000
1500
2000
2500
QALYs gained per patient
Incr
emen
tal c
ost p
er p
atie
nt (£
)
FIGURE 13 Incremental cost and QALYs gained by the use of BMP for open tibial fractures in the UK: results of Monte Carlosimulations (n = 5000)
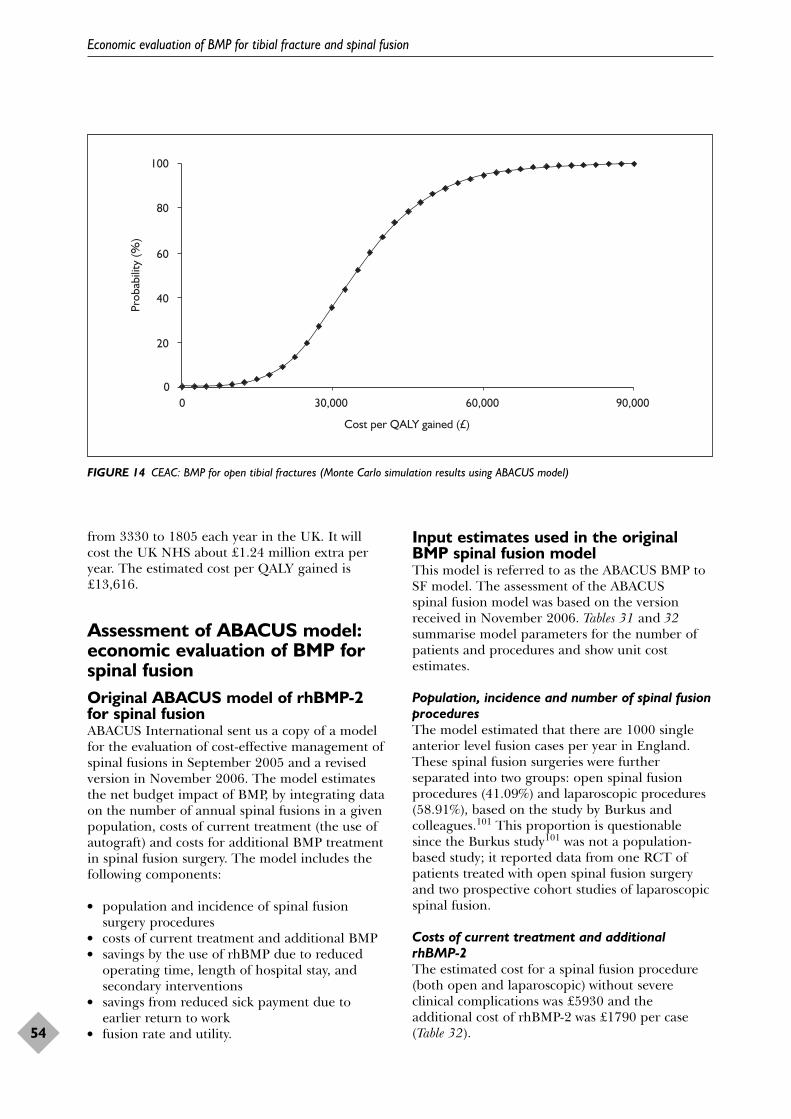
from 3330 to 1805 each year in the UK. It will cost the UK NHS about £1.24 million extra peryear. The estimated cost per QALY gained is£13,616.
Assessment of ABACUS model:economic evaluation of BMP forspinal fusionOriginal ABACUS model of rhBMP-2for spinal fusionABACUS International sent us a copy of a modelfor the evaluation of cost-effective management ofspinal fusions in September 2005 and a revisedversion in November 2006. The model estimatesthe net budget impact of BMP, by integrating dataon the number of annual spinal fusions in a givenpopulation, costs of current treatment (the use ofautograft) and costs for additional BMP treatmentin spinal fusion surgery. The model includes thefollowing components:
● population and incidence of spinal fusionsurgery procedures
● costs of current treatment and additional BMP● savings by the use of rhBMP due to reduced
operating time, length of hospital stay, andsecondary interventions
● savings from reduced sick payment due toearlier return to work
● fusion rate and utility.
Input estimates used in the originalBMP spinal fusion modelThis model is referred to as the ABACUS BMP toSF model. The assessment of the ABACUS spinal fusion model was based on the versionreceived in November 2006. Tables 31 and 32summarise model parameters for the number ofpatients and procedures and show unit costestimates.
Population, incidence and number of spinal fusionproceduresThe model estimated that there are 1000 singleanterior level fusion cases per year in England.These spinal fusion surgeries were furtherseparated into two groups: open spinal fusionprocedures (41.09%) and laparoscopic procedures(58.91%), based on the study by Burkus andcolleagues.101 This proportion is questionablesince the Burkus study101 was not a population-based study; it reported data from one RCT ofpatients treated with open spinal fusion surgeryand two prospective cohort studies of laparoscopicspinal fusion.
Costs of current treatment and additionalrhBMP-2The estimated cost for a spinal fusion procedure(both open and laparoscopic) without severeclinical complications was £5930 and theadditional cost of rhBMP-2 was £1790 per case(Table 32).
Economic evaluation of BMP for tibial fracture and spinal fusion
54
0 30,000 60,000 90,000
Cost per QALY gained (£)
0
20
40
60
80
100
Prob
abili
ty (%
)
FIGURE 14 CEAC: BMP for open tibial fractures (Monte Carlo simulation results using ABACUS model)
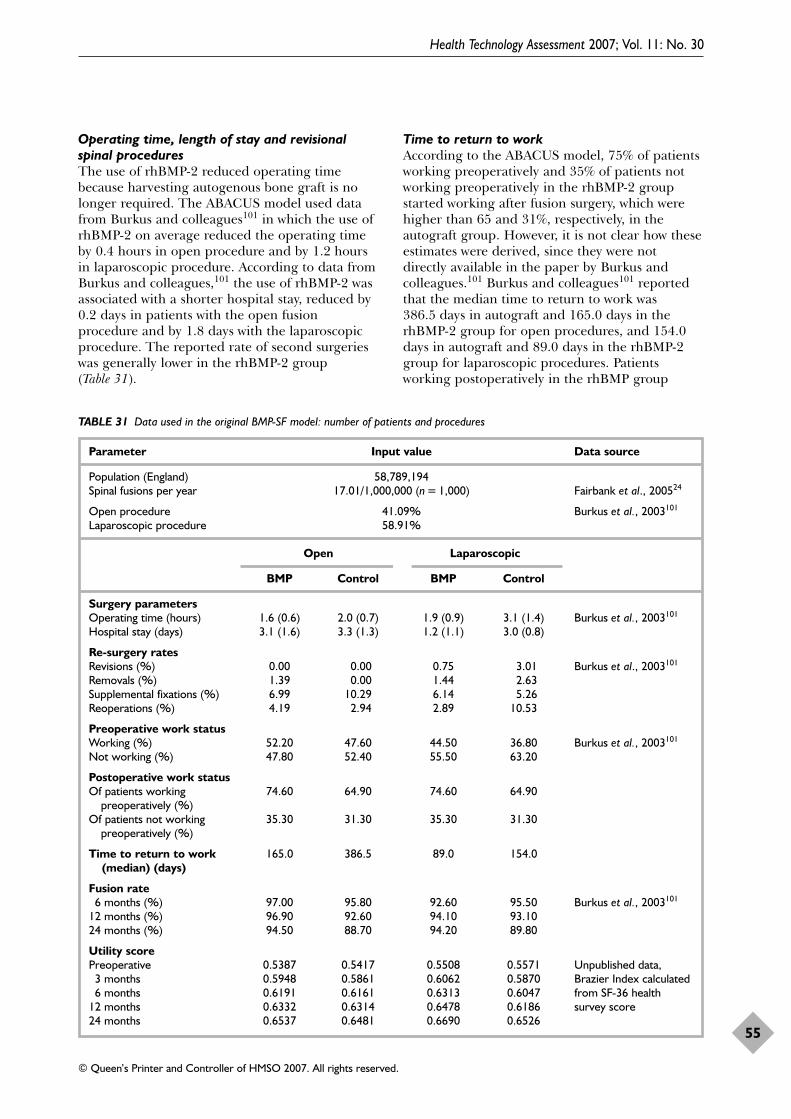
Operating time, length of stay and revisionalspinal proceduresThe use of rhBMP-2 reduced operating timebecause harvesting autogenous bone graft is nolonger required. The ABACUS model used datafrom Burkus and colleagues101 in which the use ofrhBMP-2 on average reduced the operating timeby 0.4 hours in open procedure and by 1.2 hoursin laparoscopic procedure. According to data fromBurkus and colleagues,101 the use of rhBMP-2 wasassociated with a shorter hospital stay, reduced by0.2 days in patients with the open fusionprocedure and by 1.8 days with the laparoscopicprocedure. The reported rate of second surgerieswas generally lower in the rhBMP-2 group(Table 31).
Time to return to workAccording to the ABACUS model, 75% of patientsworking preoperatively and 35% of patients notworking preoperatively in the rhBMP-2 groupstarted working after fusion surgery, which werehigher than 65 and 31%, respectively, in theautograft group. However, it is not clear how theseestimates were derived, since they were notdirectly available in the paper by Burkus andcolleagues.101 Burkus and colleagues101 reportedthat the median time to return to work was386.5 days in autograft and 165.0 days in therhBMP-2 group for open procedures, and 154.0days in autograft and 89.0 days in the rhBMP-2group for laparoscopic procedures. Patientsworking postoperatively in the rhBMP group
Health Technology Assessment 2007; Vol. 11: No. 30
55
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 31 Data used in the original BMP-SF model: number of patients and procedures
Parameter Input value Data source
Population (England) 58,789,194Spinal fusions per year 17.01/1,000,000 (n = 1,000) Fairbank et al., 200524
Open procedure 41.09% Burkus et al., 2003101
Laparoscopic procedure 58.91%
Open Laparoscopic
BMP Control BMP Control
Surgery parametersOperating time (hours) 1.6 (0.6) 2.0 (0.7) 1.9 (0.9) 3.1 (1.4) Burkus et al., 2003101
Hospital stay (days) 3.1 (1.6) 3.3 (1.3) 1.2 (1.1) 3.0 (0.8)
Re-surgery ratesRevisions (%) 0.00 0.00 0.75 3.01 Burkus et al., 2003101
Removals (%) 1.39 0.00 1.44 2.63Supplemental fixations (%) 6.99 10.29 6.14 5.26Reoperations (%) 4.19 2.94 2.89 10.53
Preoperative work statusWorking (%) 52.20 47.60 44.50 36.80 Burkus et al., 2003101
Not working (%) 47.80 52.40 55.50 63.20
Postoperative work statusOf patients working 74.60 64.90 74.60 64.90
preoperatively (%)Of patients not working 35.30 31.30 35.30 31.30
preoperatively (%)
Time to return to work 165.0 386.5 89.0 154.0(median) (days)
Fusion rate6 months (%) 97.00 95.80 92.60 95.50 Burkus et al., 2003101
12 months (%) 96.90 92.60 94.10 93.1024 months (%) 94.50 88.70 94.20 89.80
Utility scorePreoperative 0.5387 0.5417 0.5508 0.5571 Unpublished data,
3 months 0.5948 0.5861 0.6062 0.5870 Brazier Index calculated 6 months 0.6191 0.6161 0.6313 0.6047 from SF-36 health
12 months 0.6332 0.6314 0.6478 0.6186 survey score24 months 0.6537 0.6481 0.6690 0.6526
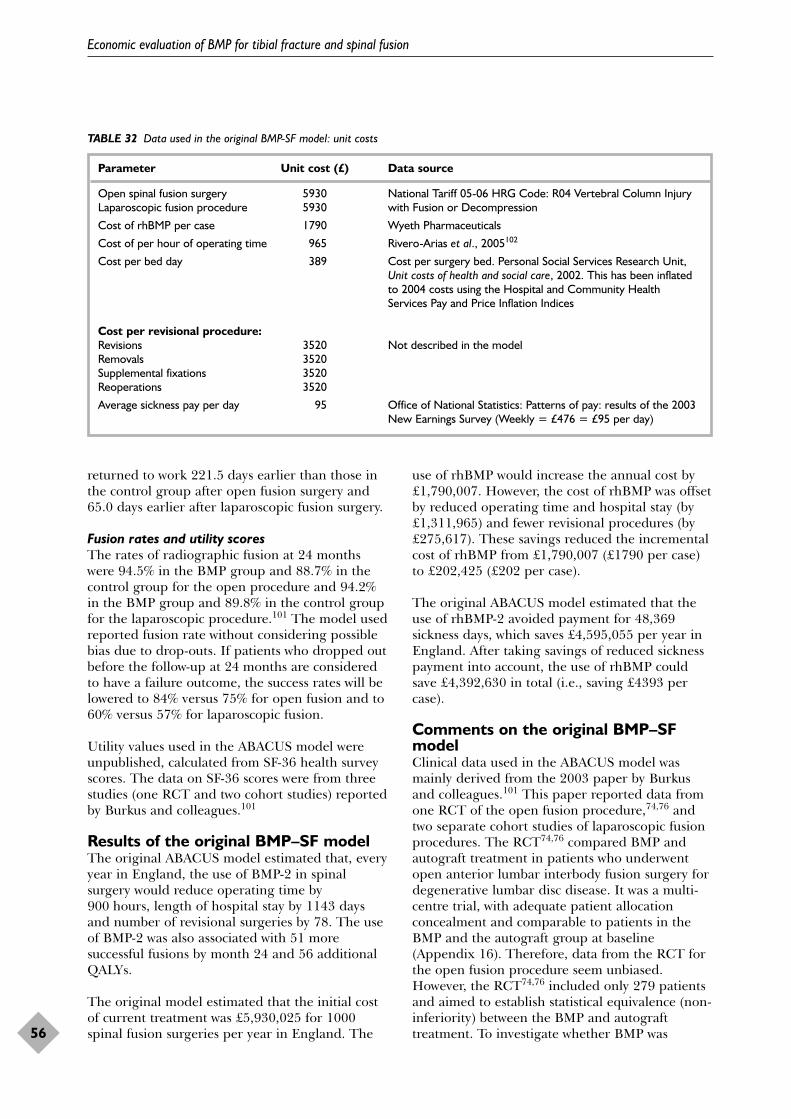
returned to work 221.5 days earlier than those inthe control group after open fusion surgery and65.0 days earlier after laparoscopic fusion surgery.
Fusion rates and utility scoresThe rates of radiographic fusion at 24 monthswere 94.5% in the BMP group and 88.7% in thecontrol group for the open procedure and 94.2%in the BMP group and 89.8% in the control groupfor the laparoscopic procedure.101 The model usedreported fusion rate without considering possiblebias due to drop-outs. If patients who dropped outbefore the follow-up at 24 months are consideredto have a failure outcome, the success rates will belowered to 84% versus 75% for open fusion and to60% versus 57% for laparoscopic fusion.
Utility values used in the ABACUS model wereunpublished, calculated from SF-36 health surveyscores. The data on SF-36 scores were from threestudies (one RCT and two cohort studies) reportedby Burkus and colleagues.101
Results of the original BMP–SF modelThe original ABACUS model estimated that, everyyear in England, the use of BMP-2 in spinalsurgery would reduce operating time by900 hours, length of hospital stay by 1143 daysand number of revisional surgeries by 78. The useof BMP-2 was also associated with 51 moresuccessful fusions by month 24 and 56 additionalQALYs.
The original model estimated that the initial costof current treatment was £5,930,025 for 1000spinal fusion surgeries per year in England. The
use of rhBMP would increase the annual cost by£1,790,007. However, the cost of rhBMP was offsetby reduced operating time and hospital stay (by£1,311,965) and fewer revisional procedures (by£275,617). These savings reduced the incrementalcost of rhBMP from £1,790,007 (£1790 per case)to £202,425 (£202 per case).
The original ABACUS model estimated that theuse of rhBMP-2 avoided payment for 48,369sickness days, which saves £4,595,055 per year inEngland. After taking savings of reduced sicknesspayment into account, the use of rhBMP couldsave £4,392,630 in total (i.e., saving £4393 percase).
Comments on the original BMP–SFmodelClinical data used in the ABACUS model wasmainly derived from the 2003 paper by Burkusand colleagues.101 This paper reported data fromone RCT of the open fusion procedure,74,76 andtwo separate cohort studies of laparoscopic fusionprocedures. The RCT74,76 compared BMP andautograft treatment in patients who underwentopen anterior lumbar interbody fusion surgery fordegenerative lumbar disc disease. It was a multi-centre trial, with adequate patient allocationconcealment and comparable to patients in theBMP and the autograft group at baseline(Appendix 16). Therefore, data from the RCT forthe open fusion procedure seem unbiased.However, the RCT74,76 included only 279 patientsand aimed to establish statistical equivalence (non-inferiority) between the BMP and autografttreatment. To investigate whether BMP was
Economic evaluation of BMP for tibial fracture and spinal fusion
56
TABLE 32 Data used in the original BMP-SF model: unit costs
Parameter Unit cost (£) Data source
Open spinal fusion surgery 5930 National Tariff 05-06 HRG Code: R04 Vertebral Column Injury Laparoscopic fusion procedure 5930 with Fusion or Decompression
Cost of rhBMP per case 1790 Wyeth Pharmaceuticals
Cost of per hour of operating time 965 Rivero-Arias et al., 2005102
Cost per bed day 389 Cost per surgery bed. Personal Social Services Research Unit,Unit costs of health and social care, 2002. This has been inflatedto 2004 costs using the Hospital and Community HealthServices Pay and Price Inflation Indices
Cost per revisional procedure:Revisions 3520 Not described in the modelRemovals 3520Supplemental fixations 3520Reoperations 3520
Average sickness pay per day 95 Office of National Statistics: Patterns of pay: results of the 2003New Earnings Survey (Weekly = £476 = £95 per day)
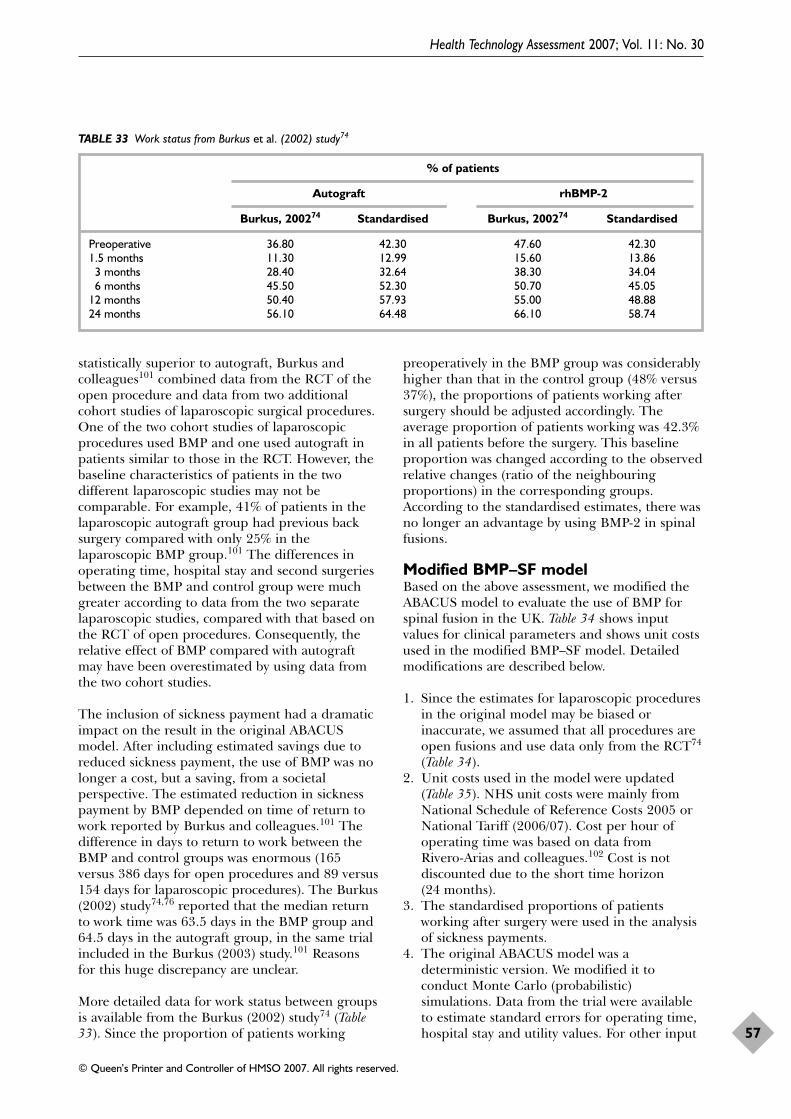
statistically superior to autograft, Burkus andcolleagues101 combined data from the RCT of theopen procedure and data from two additionalcohort studies of laparoscopic surgical procedures.One of the two cohort studies of laparoscopicprocedures used BMP and one used autograft inpatients similar to those in the RCT. However, thebaseline characteristics of patients in the twodifferent laparoscopic studies may not becomparable. For example, 41% of patients in thelaparoscopic autograft group had previous backsurgery compared with only 25% in thelaparoscopic BMP group.101 The differences inoperating time, hospital stay and second surgeriesbetween the BMP and control group were muchgreater according to data from the two separatelaparoscopic studies, compared with that based onthe RCT of open procedures. Consequently, therelative effect of BMP compared with autograftmay have been overestimated by using data fromthe two cohort studies.
The inclusion of sickness payment had a dramaticimpact on the result in the original ABACUSmodel. After including estimated savings due toreduced sickness payment, the use of BMP was nolonger a cost, but a saving, from a societalperspective. The estimated reduction in sicknesspayment by BMP depended on time of return towork reported by Burkus and colleagues.101 Thedifference in days to return to work between theBMP and control groups was enormous (165versus 386 days for open procedures and 89 versus154 days for laparoscopic procedures). The Burkus(2002) study74,76 reported that the median returnto work time was 63.5 days in the BMP group and64.5 days in the autograft group, in the same trialincluded in the Burkus (2003) study.101 Reasonsfor this huge discrepancy are unclear.
More detailed data for work status between groupsis available from the Burkus (2002) study74 (Table33). Since the proportion of patients working
preoperatively in the BMP group was considerablyhigher than that in the control group (48% versus37%), the proportions of patients working aftersurgery should be adjusted accordingly. Theaverage proportion of patients working was 42.3%in all patients before the surgery. This baselineproportion was changed according to the observedrelative changes (ratio of the neighbouringproportions) in the corresponding groups.According to the standardised estimates, there wasno longer an advantage by using BMP-2 in spinalfusions.
Modified BMP–SF modelBased on the above assessment, we modified theABACUS model to evaluate the use of BMP forspinal fusion in the UK. Table 34 shows inputvalues for clinical parameters and shows unit costsused in the modified BMP–SF model. Detailedmodifications are described below.
1. Since the estimates for laparoscopic proceduresin the original model may be biased orinaccurate, we assumed that all procedures areopen fusions and use data only from the RCT74
(Table 34). 2. Unit costs used in the model were updated
(Table 35). NHS unit costs were mainly fromNational Schedule of Reference Costs 2005 orNational Tariff (2006/07). Cost per hour ofoperating time was based on data from Rivero-Arias and colleagues.102 Cost is notdiscounted due to the short time horizon(24 months).
3. The standardised proportions of patientsworking after surgery were used in the analysisof sickness payments.
4. The original ABACUS model was adeterministic version. We modified it toconduct Monte Carlo (probabilistic)simulations. Data from the trial were availableto estimate standard errors for operating time,hospital stay and utility values. For other input
Health Technology Assessment 2007; Vol. 11: No. 30
57
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 33 Work status from Burkus et al. (2002) study74
% of patients
Autograft rhBMP-2
Burkus, 200274 Standardised Burkus, 200274 Standardised
Preoperative 36.80 42.30 47.60 42.301.5 months 11.30 12.99 15.60 13.86
3 months 28.40 32.64 38.30 34.046 months 45.50 52.30 50.70 45.05
12 months 50.40 57.93 55.00 48.8824 months 56.10 64.48 66.10 58.74
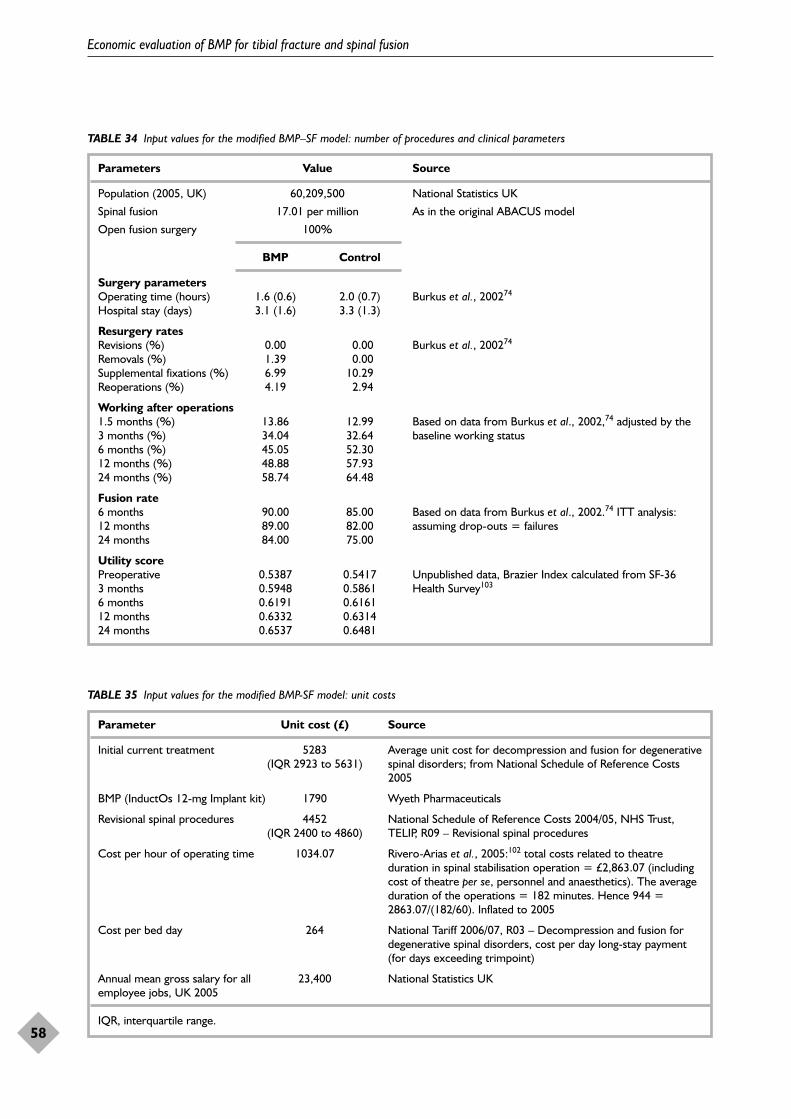
Economic evaluation of BMP for tibial fracture and spinal fusion
58
TABLE 34 Input values for the modified BMP–SF model: number of procedures and clinical parameters
Parameters Value Source
Population (2005, UK) 60,209,500 National Statistics UK
Spinal fusion 17.01 per million As in the original ABACUS model
Open fusion surgery 100%
BMP Control
Surgery parametersOperating time (hours) 1.6 (0.6) 2.0 (0.7) Burkus et al., 200274
Hospital stay (days) 3.1 (1.6) 3.3 (1.3)
Resurgery ratesRevisions (%) 0.00 0.00 Burkus et al., 200274
Removals (%) 1.39 0.00Supplemental fixations (%) 6.99 10.29Reoperations (%) 4.19 2.94
Working after operations1.5 months (%) 13.86 12.99 Based on data from Burkus et al., 2002,74 adjusted by the 3 months (%) 34.04 32.64 baseline working status6 months (%) 45.05 52.3012 months (%) 48.88 57.9324 months (%) 58.74 64.48
Fusion rate6 months 90.00 85.00 Based on data from Burkus et al., 2002.74 ITT analysis: 12 months 89.00 82.00 assuming drop-outs = failures24 months 84.00 75.00
Utility scorePreoperative 0.5387 0.5417 Unpublished data, Brazier Index calculated from SF-36 3 months 0.5948 0.5861 Health Survey103
6 months 0.6191 0.616112 months 0.6332 0.631424 months 0.6537 0.6481
TABLE 35 Input values for the modified BMP-SF model: unit costs
Parameter Unit cost (£) Source
Initial current treatment 5283 Average unit cost for decompression and fusion for degenerative (IQR 2923 to 5631) spinal disorders; from National Schedule of Reference Costs
2005
BMP (InductOs 12-mg Implant kit) 1790 Wyeth Pharmaceuticals
Revisional spinal procedures 4452 National Schedule of Reference Costs 2004/05, NHS Trust, (IQR 2400 to 4860) TELIP, R09 – Revisional spinal procedures
Cost per hour of operating time 1034.07 Rivero-Arias et al., 2005:102 total costs related to theatreduration in spinal stabilisation operation = £2,863.07 (includingcost of theatre per se, personnel and anaesthetics). The averageduration of the operations = 182 minutes. Hence 944 =2863.07/(182/60). Inflated to 2005
Cost per bed day 264 National Tariff 2006/07, R03 – Decompression and fusion fordegenerative spinal disorders, cost per day long-stay payment(for days exceeding trimpoint)
Annual mean gross salary for all 23,400 National Statistics UKemployee jobs, UK 2005
IQR, interquartile range.
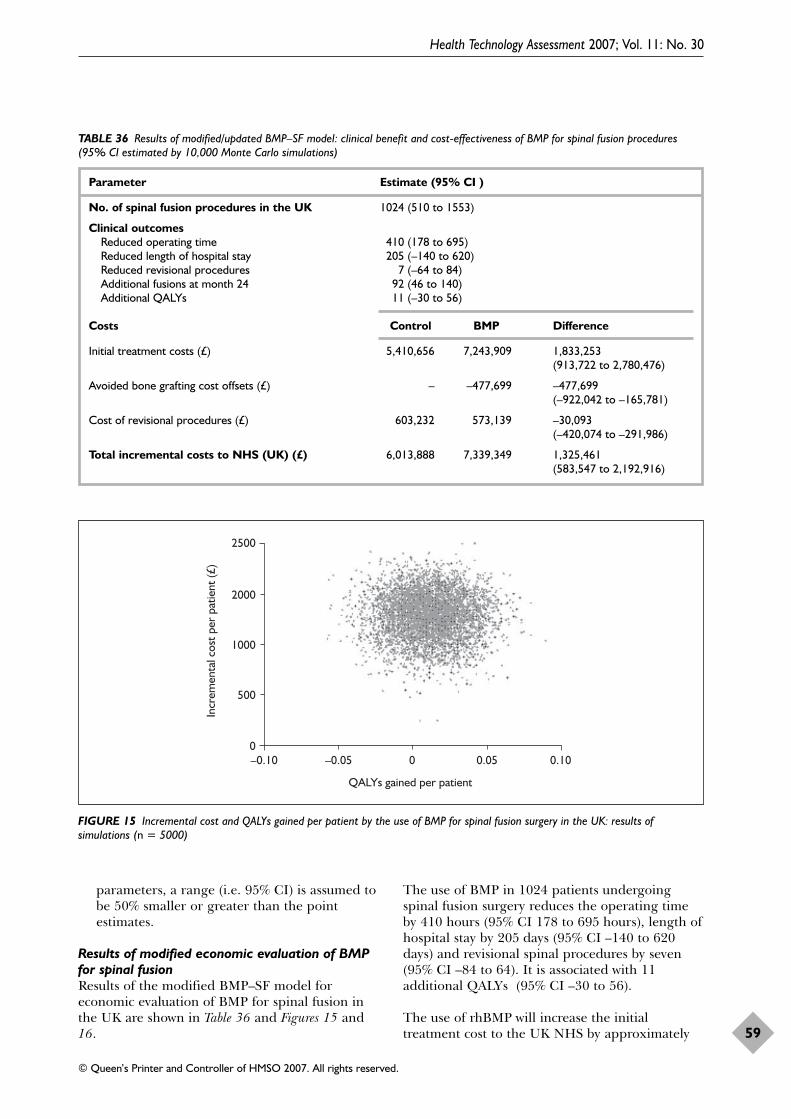
parameters, a range (i.e. 95% CI) is assumed tobe 50% smaller or greater than the pointestimates.
Results of modified economic evaluation of BMPfor spinal fusion Results of the modified BMP–SF model foreconomic evaluation of BMP for spinal fusion inthe UK are shown in Table 36 and Figures 15 and16.
The use of BMP in 1024 patients undergoingspinal fusion surgery reduces the operating timeby 410 hours (95% CI 178 to 695 hours), length ofhospital stay by 205 days (95% CI –140 to 620days) and revisional spinal procedures by seven(95% CI –84 to 64). It is associated with 11additional QALYs (95% CI –30 to 56).
The use of rhBMP will increase the initialtreatment cost to the UK NHS by approximately
Health Technology Assessment 2007; Vol. 11: No. 30
59
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 36 Results of modified/updated BMP–SF model: clinical benefit and cost-effectiveness of BMP for spinal fusion procedures(95% CI estimated by 10,000 Monte Carlo simulations)
Parameter Estimate (95% CI )
No. of spinal fusion procedures in the UK 1024 (510 to 1553)
Clinical outcomesReduced operating time 410 (178 to 695)Reduced length of hospital stay 205 (–140 to 620)Reduced revisional procedures 7 (–64 to 84)Additional fusions at month 24 92 (46 to 140)Additional QALYs 11 (–30 to 56)
Costs Control BMP Difference
Initial treatment costs (£) 5,410,656 7,243,909 1,833,253(913,722 to 2,780,476)
Avoided bone grafting cost offsets (£) – –477,699 –477,699 (–922,042 to –165,781)
Cost of revisional procedures (£) 603,232 573,139 –30,093 (–420,074 to –291,986)
Total incremental costs to NHS (UK) (£) 6,013,888 7,339,349 1,325,461(583,547 to 2,192,916)
2500
2000
1000
500
0–0.10 –0.05 0 0.05 0.10
QALYs gained per patient
Incr
emen
tal c
ost p
er p
atie
nt (£
)
FIGURE 15 Incremental cost and QALYs gained per patient by the use of BMP for spinal fusion surgery in the UK: results ofsimulations (n = 5000)
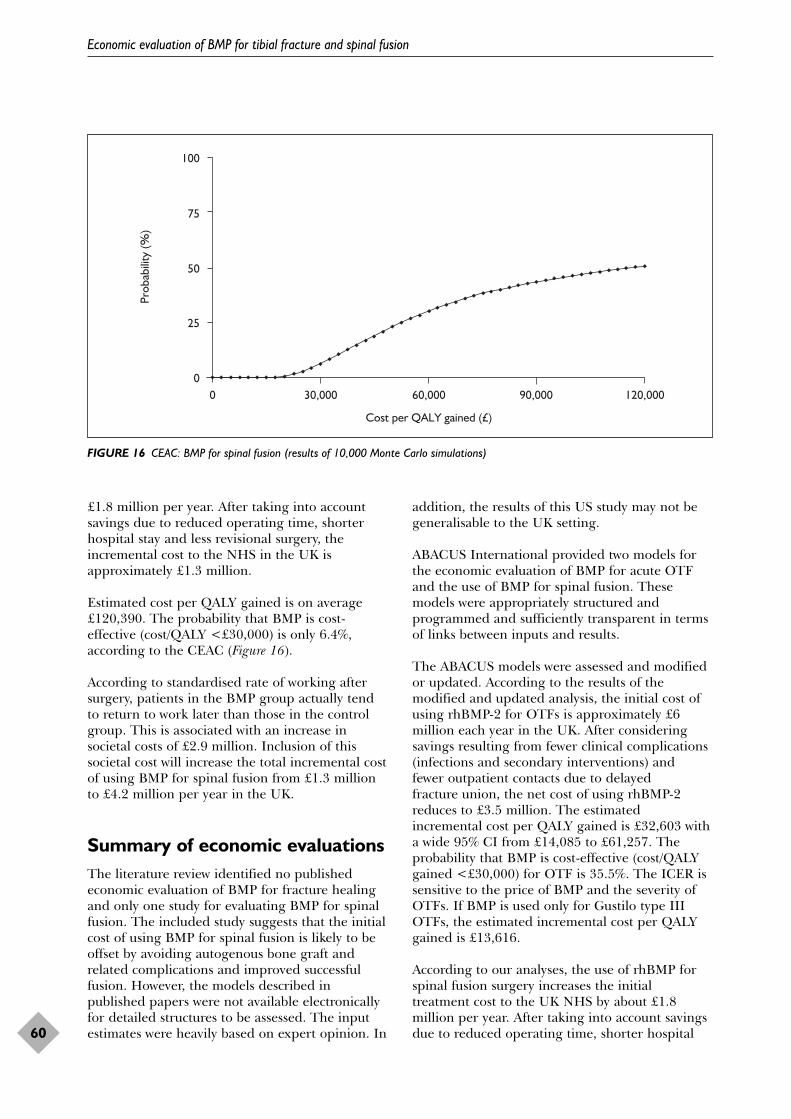
£1.8 million per year. After taking into accountsavings due to reduced operating time, shorterhospital stay and less revisional surgery, theincremental cost to the NHS in the UK isapproximately £1.3 million.
Estimated cost per QALY gained is on average£120,390. The probability that BMP is cost-effective (cost/QALY <£30,000) is only 6.4%,according to the CEAC (Figure 16).
According to standardised rate of working aftersurgery, patients in the BMP group actually tendto return to work later than those in the controlgroup. This is associated with an increase insocietal costs of £2.9 million. Inclusion of thissocietal cost will increase the total incremental costof using BMP for spinal fusion from £1.3 millionto £4.2 million per year in the UK.
Summary of economic evaluationsThe literature review identified no publishedeconomic evaluation of BMP for fracture healingand only one study for evaluating BMP for spinalfusion. The included study suggests that the initialcost of using BMP for spinal fusion is likely to beoffset by avoiding autogenous bone graft andrelated complications and improved successfulfusion. However, the models described inpublished papers were not available electronicallyfor detailed structures to be assessed. The inputestimates were heavily based on expert opinion. In
addition, the results of this US study may not begeneralisable to the UK setting.
ABACUS International provided two models forthe economic evaluation of BMP for acute OTFand the use of BMP for spinal fusion. Thesemodels were appropriately structured andprogrammed and sufficiently transparent in termsof links between inputs and results.
The ABACUS models were assessed and modifiedor updated. According to the results of themodified and updated analysis, the initial cost ofusing rhBMP-2 for OTFs is approximately £6million each year in the UK. After consideringsavings resulting from fewer clinical complications(infections and secondary interventions) and fewer outpatient contacts due to delayed fracture union, the net cost of using rhBMP-2reduces to £3.5 million. The estimatedincremental cost per QALY gained is £32,603 witha wide 95% CI from £14,085 to £61,257. Theprobability that BMP is cost-effective (cost/QALYgained <£30,000) for OTF is 35.5%. The ICER issensitive to the price of BMP and the severity ofOTFs. If BMP is used only for Gustilo type IIIOTFs, the estimated incremental cost per QALYgained is £13,616.
According to our analyses, the use of rhBMP forspinal fusion surgery increases the initialtreatment cost to the UK NHS by about £1.8million per year. After taking into account savingsdue to reduced operating time, shorter hospital
Economic evaluation of BMP for tibial fracture and spinal fusion
60
100
75
50
25
00 30,000 60,000 90,000 120,000
Cost per QALY gained (£)
Prob
abili
ty (%
)
FIGURE 16 CEAC: BMP for spinal fusion (results of 10,000 Monte Carlo simulations)

stay and less revisional surgery, the incrementalcost to the NHS in the UK is about £1.3 million.The estimated incremental cost per QALY gainedis on average £120,390. The probability that BMPis cost-effective (cost/QALY <£30,000) is only6.4%. In contrast to the original ABACUS model,patients in the BMP group actually tended to
return to work later than those in the controlgroup after standardisation by employment statusbefore spinal surgery. This is associated with anincreased societal cost of £2.9 million. From thesocietal perspective, the estimated totalincremental cost of using BMP for spinal fusion isabout £4.2 million per year in the UK.
Health Technology Assessment 2007; Vol. 11: No. 30
61
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.

The main purpose of this review was to evaluatethe effectiveness and cost-effectiveness of BMP
for the treatment of spinal fusions and fracturehealing. Although all types of studies were sought,only RCTs were used for analysis. This was becausecase series or case reports included heterogeneouspatient populations, had small sample sizes andwere generally of low quality. Also, some of thenon-RCTs included patients with serious co-morbidities and many received either autograftbone or other bone substitutes in addition to BMP.We decided not to include data from case series inthe analyses.
Methodological quality of includedRCTsWe identified eight RCTs of BMP for tibialfractures, one of scaphoid non-union and 12 ofBMP for spinal fusion. The included trials havesome methodological weaknesses, includingunreported randomisation and allocationmethods, incomparable baseline characteristicsbetween the groups, failure to perform ITTanalysis or to use independent blinded assessorsand failure to report reasons for drop-outs. Somesecondary outcomes were not measured and/or notreported. The sample size was small in most of theincluded trials, ranging from 14 to 450 in trials oftibial fracture and from 14 to 279 in trials ofspinal fusion. Because of insufficient sample size,patient baseline comparability between trial armsmay not be achieved and statistical power to detectmoderate effect and/or to establish equivalencebetween different interventions is low.
Effectiveness of BMP for tibialfracturesAmong the eight identified trials, the BMPintervention was evaluated in two trials for OTFs,one trial for closed tibial fracture, one trial forboth open and closed tibial fracture and four trialsfor tibial fracture non-union. Data from threetrials indicated that the use of BMP increasedfracture union among patients with acute tibialfractures (pooled OR 1.65, 95% CI 1.12 to 2.45).This pooled estimate is dominated by a large
multi-centre trial of acute OTF.61 Also in this largetrial, the high-dose BMP (1.5 mg/ml) showed ahigher union rate than the lower dose(0.75 mg/ml) (OR 1.64, 95% CI 1.03 to 2.59). Theproportion of secondary interventions in the BMPgroup is lower than that in the control group forpatients with acute tibial fractures (pooled OR0.53, 95% CI 0.37 to 0.78).
Evidence from four small trials providedinsufficient evidence to be certain whether BMPtreatment is more or less effective thanautogenous bone grafting for patients with tibialfracture non-union (pooled OR for union rate0.82, 95% CI 0.25 to 2.64). There are severalpossible explanations for this lack of effectivenessof BMP in fracture non-union. First, BMP may notbe more effective than autograft in atrophic non-union because of inadequate local blood supply.The trials included in the analysis were small (totalnumber of patients 30, 41 and 124), and patientsbetween trial arms may not be comparable. Therewere more atrophic non-unions at baseline in theBMP group than that in the control group in thelargest trial (n = 124). In addition, the length offollow-up (9 months) in some trials may not besufficiently long. However, the use of BMP avoidsthe need for autogenous bone grafting so thatcosts and complications related to harvestingautograft (e.g. pain, blood loss) can be prevented.
Effectiveness of BMP for scaphoidnon-unionOnly one small RCT (n = 18) was identified. Verylimited evidence indicated that BMP in scaphoidnon-union was safe and may help to acceleratenon-union healing when used in conjunction witheither autograft or allograft.
Effectiveness of BMP for spinalfusionThere are seven trials of BMP-2 in spinal fusionfor patients with symptomatic single-leveldegenerative disc disease, including four trials that used anterior fusion and three that usedposterolateral fusion. One trial80 of BMP-7
Health Technology Assessment 2007; Vol. 11: No. 30
63
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Chapter 6
Discussion and conclusions

included patients with L5 spondylolysis who weretreated with non-instrumented posterolaterallumbar fusion. Three trials81,82,84,86 of BMP-7included patients with spinal stenosis anddegenerative spondylolisthesis who were treatedwith posterolateral fusion. Evidence shows that theuse of BMP-2 is more effective than autogenousbone graft for radiographic fusion in patients withsingle-level degenerative disc disease (pooled OR3.87, 95% CI 1.74 to 8.59). The pooled OR forpatients with degenerative spondylolisthesis withspinal stenosis is 0.87 (95% CI 0.15 to 5.08) andfor patients with spondylolysis 0.38 (95% CI 0.05to 2.77).
BMP treatment replaces autogenous bone graftingand prevents donor site morbidities. The evidencesuggests that BMP is associated with a 25-minute(11–37 minutes) reduction in operating timecompared with controls, and a shorter hospitalstay (0.75 days, from 0.31 to 1.19 days). BMPtreatment may also be associated withimprovement in clinical outcomes such asOswestry Disability Index score, SF-36 score andback and leg pain. The proportion of secondaryinterventions tends to be lower in the BMP groupthan that in the control group, but the overalldifference is not statistically significant (pooledOR 0.62, 95% CI 0.28 to 1.39). Data from trials ontime to return to work after spinal fusion weresometimes difficult to interpret because of unclearor inappropriate methods used for data analysisand results presentation.
Several trials69,71–74,76 reported a tendency forfusion rates to decline over time. Possibleexplanations for this occurrence were described inthe Burkus (2002) study.74 The reasons given wereradiolucency seen at the implant–bone interfaceand that the autogenous bone became atrophicover time. In addition, patients who required asecondary operation for continuing low back paindespite evidence of radiographic fusion wereconsidered as a fusion failure. A secondaryoperation, not lack of new bone formation, wasreported as the reason for all fusion failures in theBMP group in the by Burkus (2002) trial.74
The effectiveness of BMP in spinal fusion alsodepends on the effectiveness of spinal fusionsurgery compared with other non-surgicalinterventions. A Cochrane systematic review104
concluded that there was only limited andheterogeneous evidence to support the use ofsurgery for degenerative lumbar spondylosis. Arecently published study in the UK found that “noclear evidence emerged that primary spinal fusion
surgery was any more beneficial than intensiverehabilitation” for patients with chronic low backpain, although 28% of patients initially allocatedto the rehabilitation group underwent spinalfusion surgery within 2 years.24 Therefore, futuretrials that compare BMP and autogenous bonegraft for spinal fusion should also include acontrol of intensive rehabilitation without surgery.
Adverse effects and safety of BMPMore patients in the BMP group developedantibody responses to BMP or bovine collagen.The clinical relevance of the antibody responses isnot clear. Carlisle and Fischgrund105 suggestedthat, because of these antibody responses, BMPshould not be used in pregnant women, andrepeat use of BMP should be avoided.
The largest trial of BMP for OTF61 provided nodata but mentioned that the use of BMP did notincrease soft-tissue calcification or heterotopicossification at remote sites. One case ofheterotopic bone formation was reported among15 BMP-treated patients with open or closed tibialfracture in the Jones trial.28 The patient had asolid tibiofibular synostosis, or joining of the tibiaand fibula bones. This event was a concern, butalso occurs in patients with severe fractures that donot receive BMP. In the Maniscalco trial,62
calcification of the tibio-fibular ligament wasobserved in one case among seven patients whoreceived BMP applied to external fixator forclosed tibial fracture. In a trial79,87 of BMP forspinal fusion, patient enrolment was stopped when excess bone formation was seen in 24 of 32 BMP patients and four of 31 control patients (p < 0.001), although the authorsreported no apparent effects on patient outcomes.Other trials of spinal fusion did not mentionexcess bone formation, and it is unclear whether excess bone formation was notinvestigated or not reported.
It is difficult to assess adverse effects and safety ofBMP for fracture and spinal fusion, partly becausedifferent trials often investigated and reporteddifferent adverse event outcomes.
Different doses and types of BMPsAccording to limited evidence, adequateconcentration is important for BMP to beeffective. The effect of different concentrations ofBMP for OTF was directly compared in one
Discussion and conclusions
64
study.61 It was found that high-dose BMP(1.5 mg/ml) is more effective than lower dose BMP(0.75 mg/ml) (OR 1.64, 95% CI 1.03 to 2.59).
Apart from one trial,59 which did not identifywhich BMP was used, two clinically available BMPproducts were used in the identified clinical trials:BMP-2 and BMP-7. They have not been directlycompared in randomised trials. For the treatmentof fractures, BMP-2 has been evaluated in twotrials (including one large trial with 450 patients,n = 480 total) and BMP-7 in six small trials(n = 351). For spinal fusion surgeries, BMP-2 wasevaluated in seven trials of 631 patients withsingle-level degenerative disc disease and one trialof 40 patients with degenerative spondylolisthesisand stenosis. BMP-7 was evaluated in two trials of56 patients with degenerative spondylolisthesiswith spinal stenosis and in one trial of 20 patientswith spondylolysis. Because great heterogeneity inpatients and surgical procedures, it is not possibleto make an indirect comparison of BMP-2 andBMP-7. Different doses/concentrations and typesof BMP should be compared in further RCTs.
Cost-effectiveness We assessed and modified two economic modelsdeveloped by ABACUS International to evaluatecost-effectiveness of BMP for OTF and spinalfusion.
The incremental cost of adopting the use of BMPin the treatment of OTFs is estimated to beapproximately £3.5 million per year from a UKNHS perspective. The estimated incremental costper QALY gained is £32,603 with a wide 95% CIfrom £14,085 to £61,257. The ICER is highlysensitive to the price of BMP and the severity ofOTFs. It should also be noted that utility valuesused in the model were extrapolated from studiesof general fractures (and elderly women for hipfractures). The estimate of health-related QoLused in the economic model may therefore beinaccurate. The effect of BMP on QoL needs to bedirectly evaluated with further research.
The use of rhBMP for spinal fusion surgery mayincrease the cost to the UK NHS by approximately£1.3 million per year. Estimated incremental costper QALY gained is about £120,390. We re-analysed data on time to return to work afterspinal surgery, and found that patients in the BMPgroup actually tended to return to work later thanthose in the control group. From a societalperspective, the estimated incremental total cost of
adopting use of BMP for spinal fusion isapproximately £4.2 million per year in the UK.
ConclusionsFor both fracture and spinal fusion indications, theuse of BMP may eliminate the need for autogenousbone grafting, so that costs and complicationsrelated to harvesting autograft can be avoided.
The main concerns about adverse effects and safetyof the use of BMP include antibody responses andsoft-tissue calcification or heterotopic ossification.No other serious adverse events or safety concernsabout the use of BMP have been consistentlyreported in the identified clinical trials, althoughwe may not be able to rule out rare but severeadverse events from using BMP.
BMP for tibial fractureAdditional BMP treatment plus conventionalinterventions is more effective than theconventional intervention alone for successful unionof acute OTFs. There is no evidence showing thatthe use of BMP is more or less effective thanconventional treatment for tibial fracture non-union or closed tibial fracture. The cost-effectiveness of additional BMP for open tibialfracture may be improved if the price of BMP isreduced or BMP is mainly used in severe cases.
BMP for spinal fusionThe use of BMP in spinal fusion surgery seemsmore effective than autogenous bone graft interms of radiographic spinal fusion amongpatients with single-level degenerative discdisease. There is a lack of evidence about theeffectiveness of BMP for other spinal disorders,including spondylolisthesis and spinal stenosis.There was limited evidence showing that BMP isassociated with greater improvement in clinicaloutcomes such as Oswestry Disability Index score,SF-36 score and back and leg pain. According tothe results of economic evaluation, the use of BMPfor spinal fusion is unlikely to be cost-effective.
Recommendations for furtherresearchThe following are our recommendations foradditional research:
● Clinical trials of BMP should include formaleconomic evaluation. More detailed data needto be collected on both costs (including relevant
Health Technology Assessment 2007; Vol. 11: No. 30
65
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
societal costs) and QoL (utilities) to inform sucheconomic evaluation.
● Multi-centre RCT of fracture non-union. Onlyone RCT of poor quality using BMP-7 has beenperformed. Since each study centre has smallrecruitment numbers, a non-inferiority design isneeded. Either BMP-2 or BMP-7 should bestudied, with autograft as control. Previousstudies have mixed BMP with other products. Itis recommended that BMP alone is testedagainst autograft, to demonstrate the true BMPeffect. It is also recommended that BMP istested in new non-union cases and not justwhere other therapies have failed. Ifequivalence can be shown between BMP andautograft, then donor site morbidity can beeliminated, decreasing pain and discomfort forpatients.
● Multi-centre RCT of interbody and/orposterolateral spinal fusion. Existing RCTsusing BMP-2 have methodological weaknesses.Further studies are recommended comparingBMP-2 against autograft. So far there have been
no RCTs using BMP-7. It is recommended thatthese should be undertaken. If equivalence canbe shown between BMP and autograft, thendonor site morbidity can be eliminated,decreasing pain and discomfort for patients.
● RCTs of non-tibial acute long bone fractures.One good-quality RCT has been performed ofBMP-2 in OTFs. Further similar studies onfractures at other sites are recommended. Weare aware that company-sponsored Phase 2 and3 studies of injectable BMP-2 are beingundertaken. The aim should be to demonstrateaccelerated fracture healing, reduction insecondary procedures and reduction inhealthcare and/or societal costs.
● RCTs comparing BMP-2/BMP-7/controls. Thereare no studies currently showing the relativeefficacy of BMP-2 versus BMP-7. Their differentmechanism of action may mean that they haveimportant clinical differences in differentcircumstances. Studies should be undertakencomparing these two products against controls.
Discussion and conclusions
66

We would like to thank all peer reviewers forcommenting on the manuscript, specifically
Abdullah Al-Taiar. Also, we thank Adam Frere-Smith for providing a patient’s perspective onacute tibia fractures. We also thank Wyeth forproviding a copy of an unpublished paper,ABACUS International for providing theeconomic models and Dr K Burkus for providingclarification of his included papers. Also, thanksare due to Rosie Filby, who providedadministrative support.
Contribution of authorsKimberly Garrison (Research Associate), Simon Donell (Consultant and Honorary Reader),Fujian Song (Reader in Research Synthesis),Miranda Mugford (Professor of Health Economics)and Ian Harvey (Professor of Epidemiology)developed and commented on the review protocol.Jon Ryder (Support Post in Information and
Quantitative Methods) and Kimberly Garrisondeveloped the search strategies and searchedelectronic databases. Kimberly Garrison and Fujian Song reviewed and assessed thestudies. Fujian Song, Ian Shemilt (ResearchCoordinator for Campbell and CochraneEconomics Methods Group) and MirandaMugford assessed and modified the ABACUSmodel. Simon Dorell, Miranda Mugford and Ian Harvey provided advice on the interpretationof evidence. Kimberly Garrison and Fujian Songprepared the report. All authors commented onthe draft manuscript.
Publication informationA protocol of Cochrane Systematic Review hasbeen accepted by Cochrane Collaboration, todevelop a Cochrane Systematic Review based onpart of the report (review of RCTs of the use ofBMP for tibial fracture).
Health Technology Assessment 2007; Vol. 11: No. 30
67
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Acknowledgements

1. Littenberg B, Weinstein LP, McCarren M. Closedfractures of the tibial shaft: a meta-analysis ofthree methods of treatment. J Bone Joint Surg Am1998;80:174–83.
2. Dervin GF. Skeletal fixation of grade IIIB tibialfractures: the potential of meta-analysis. ClinOrthop 1996;332:10–15.
3. Bhandari M, Adili A, Leone J, Lachowski RJ,Kwok DC. Early versus delayed operativemanagement of closed tibial fractures. Clin Orthop1999;368:230–9.
4. Bhandari M Guyatt GH, Swiontkowski MF,Schemitsch EH. Treatment of open fractures of theshaft of the tibia: a systematic overview and meta-analysis. J Bone Joint Surg Br 2001;83:62–8.
5. Sanders R, Jersinovich I, Anglen J, DiPasquale T,Herscovici D Jr. The treatment of open tibial shaftfractures using an interlocked intramedullary nailwithout reaming. J Orthop Trauma 1994;8:504–10.
6. Riemer BL, DiChristina DG, Cooper A, Savig S,Butterfield SL, Burke CJ III, et al. Nonreamednailing of tibial diaphyseal fractures in bluntpolytrauma patients. J Orthop Trauma 1995;9:66–75.
7. Caudle RJ, Stem PJ. Severe open fractures of thetibia. J Bone Joint Surg Am 1987;69:801–7.
8. Open fractures and trauma. http://www.limbcenter.com/disorders/indexasp. Accessed 20 March 2006.
9. Friedlaender G, Perry CR, Cole JD, Cook SD,Cierny G, Muschler GF, et al. Osteogenic protein-1(bone morphogenetic protein-7) in the treatmentof tibial nonunions. J Bone Joint Surg Am 2001;83Suppl 1: S151–8.
10. Friedlaender GE. Osteogenic protein-1 intreatment of tibial nonunions: current status. SurgTechnol Int 2004;13:249–52.
11. Heckman J D, Sarasohn-Kahn J. The economics oftreating tibia fractures: the cost of delayed unions.Bull Hosp Joint Dis 1997;56:63–72.
12. Downing ND, Griffin DR, Davis TRC. Acomparison of the relative costs of cast treatmentand intramedullary nailing for tibial diaphysealfractures in the UK. Injury 1997;28:373–5.
13. Beaver R, Brinker MR, Barrack RL. An analysis ofthe actual cost of tibial nonunions. J Louisiana StateMed Soc 1997;149:200–6.
14. Calvert N, Triffitt P, Johnstone S, et al. Internalfixation of fractures of the shaft of the tibia and ofthe distal radius in adults. Trent Institute for HealthServices Research Guidance Note for Purchasers1998;98(2).
15. Court-Brown CM, Cross AT, Hahn DM, Marsh DR,Willett K, Quaba AAWF, et al. The management ofopen tibial fractures. London: British OrthopaedicAssociation and British Association of PlasticSurgeons; 1997.
16. Modern lumbar spine fusion surgery. http://www.spine-health.com/topics/surg/mlsf/mlsf01.html. Accessed13 March 2006.
17. Katz JN, Lipson SJ, Lew R A, Grobler LJ,Weinstein JN, Brick GW, et al. Lumbarlaminectomy alone or with instrumented ornoninstrumented arthrodesis in degenerativelumbar spinal stenosis: patient selection, costs, andsurgical outcomes. Spine 1997;22:1123–31.
18. Niggemeyer O, Strauss JM, Schulitz KP.Comparison of surgical procedures fordegenerative lumbar spinal stenosis: a meta-analysis of the literature from 1975 to 1995. EurSpine J 1997;6:423–9.
19. Kuntz KM, Snider RK, Weinstein JN, Pope MH,Katz JN. Cost effectiveness of fusion with andwithout instrumentation for patients withdegenerative spondylolisthesis and spinal stenosis.Spine 2000;25:1132–9.
20. Boden SD. The ABCs of BMPs. Orthop Nurs2005;24(1):49–52.
21. Kirker-Head CA. Development and application ofbone morphogenetic proteins for the enhancementof bone healing. J Orthop Traumatol 2005;6:1–9.
22. Ullrich PF. Lumbar spinal fusion surgery.http://www.spine-health.com/topics/surg/overview/lumbar/lumb05.html. Accessed 15 May 2006.
23. Maniadakis N, Gray A. The economic burden ofback pain in the UK. Pain 2000;84:95–103.
24. Fairbank J, Frost H, Wilson-MacDonald J, Yu L,Barker K, Collins R. Randomised controlled trialto compare surgical stabilisation of the lumbarspine with an intensive rehabilitation programmefor patients with chronic low back pain: the MRCspine stabilisation trial. BMJ 2005;330:1233.
25. Fritzell P, Hagg O, Wessberg P, Nordwall A.Lumbar fusion versus nonsurgical treatment forchronic low back pain: a multicenter randomized
Health Technology Assessment 2007; Vol. 11: No. 30
69
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
References
controlled trial from the Swedish Lumbar SpineStudy Group. Spine 2006;31:245–9.
26. Möller H, Hedlund R. Surgery versus conservativetreatment in adult isthmic spondylolisthesis. Aprospective randomized study, Part 1. Spine2000;25:1171–5.
27. Arrington ED, Smith WJ, Chambers HG, BucknellAL, Davino NA. Complications of iliac crest bonegraft harvesting. Clin Orthop 1996;329:300–9.
28. Jones AL, Bucholz RW, Bosse MJ, Mirza SK, Lyon TR, Webb LX, et al. Recombinant humanBMP-2 and allograft compared with autogenousbone graft for reconstruction of diaphyseal tibialfractures with cortical defects. J Bone Joint Surg Am2006;88:1431–41.
29. Dhawan A, Kuklo TR, Bronfman E, Polly DW Jr.Analysis of iliac crest bone graft process measures.Scoliosis Research Society; 2002.
30. Goulet J, Senunas L, DeSilva G, Greenfield M.Autogenous iliac crest bone graft: complicationsand fuctional assessment. Clin Orthop 1997;339:76–81.
31. Robertson P, Wray A. Natural history of posterioriliac crest bone graft donation for spinal surgery.Spine 2001;26:1473–76.
32. Sasso RC, LeHuec JC, Shaffrey C. Iliac crest bonegraft donor site pain after anterior lumbarinterbody fusion – a prospective patientsatisfaction outcome assessment. J Spinal DisordTech 2005;18:S77–81.
33. Banwart J, Asher M, Hassanein R. Iliac crest bonegraft harvest donor site morbidity: a statisticalevaluation. Spine 1995;20:1055–60.
34. Vaccaro AR, Chiba K, Heller JG, Patel TC,Thalgott JS, Truumees E, et al. Bone graftingalternatives in spinal surgery. Spine J 2002;2:206–15.
35. Samartzis D, Khanna N, Shen FH, An HS. Updateon bone morphogenetic proteins and theirapplication in spine surgery. J Am Coll Surg 2005;200:236–48.
36. Zhu W, Rawlins B, Boachie-Adjei O, Myers ER,Arimizu J, Choi E, et al. Combined bonemorphogenetic protein-2 and -7 gene transferenhances osteoblastic differentiation and spinefusion in a rodent model. J Bone Miner Res2004;19:2021–32.
37. Zhao M, Zhao Z, Koh J, Jin T, Renny F.Combinatorial gene therapy for boneregeneration: cooperative interactions betweenadenovirus vectors expressing bonemorphogenetic proteins 2, 4, 7. J Cell Biochem2005;95:1–16.
38. Matthews SJ. Biological activity of bonemorphogenetic proteins (BMP’s). Injury 2005;36(Suppl 1):S34–7.
39. Akamaru T, Suh D, Boden SD, Kim HS,Minamide A, Louis-Ugbo J. Simple carrier matrixmodifications can enhance delivery ofrecombinant human bone morphogenetic protein-2 for posterolateral spine fusion. Spine 2003;28:429–34.
40. Seeherman HJ, Bouxsein M, Kim H, Li R, Li XJ,Aiolova M, et al. Recombinant human bonemorphogenetic protein-2 delivered in aninjectable calcium phosphate paste acceleratesosteotomy-site healing in a nonhuman primatemodel. J Bone Joint Surg Am 2004;86:1961–72.
41. Seeherman H, Li R, Bouxsein M, Kim H, Li XJ,Smith-Adaline EA, et al. rhBMP-2/calciumphosphate matrix accelerates osteotomy-sitehealing in a nonhuman primate model at multipletreatment times and concentrations. J Bone JointSurg Am 2006;88:144–60.
42. Sheehan JP, Sheehan JM, Seeherman H, Quigg M,Helm GA. The safety and utility of recombinanthuman bone morphogenetic protein-2 for cranialprocedures in a nonhuman primate model.J Neurosurg 2003;98 (1 Suppl):125–30.
43. Ferguson D, Davis WL, Urist MR, Hurt WC,Allen EP. Bovine bone morphogenetic protein(bBMP) fraction-induced repair of craniotomydefects in the rhesus monkey (Macaca speciosa). ClinOrthop 1987;219:251–8.
44. Blumenthal NM, Koh-Kunst G, Alves ME,Miranda D, Sorensen RG, Wozney JM, et al. Effectof surgical implantation of recombinant humanbone morphogenetic protein-2 in a bioabsorbablecollagen sponge or calcium phosphate puttycarrier in intrabony periodontal defects in thebaboon. J Periodontol 2002;73:1494–506.
45. Chin M, Ng T, Tom WK, Carstens M. Repair ofalveolar clefts with recombinant human bonemorphogenetic protein (rhBMP-2) in patients withclefts. J Craniofac Surg 2005;16:778–89.
46. New humanitarian device approval.http://www.fda.gov/cdrh/MDA/DOCS/h020008.html. Accessed 3 May 2006.
47. InductOsTM (rhBMP-2/ACS) receives additionalEuropean Commission marketing.http://www.prnewswire.co.uk/cgi/news/release?id=144283. Accessed 27 April 2006.
48. New device approval – infuse bone graft.http://www.fda.gov/cdrh/mda/docs/p000054.html.Accessed 3 May 2006.
49. Egger M, Smith GD, Altman DG. Systematic reviewsin health care: meta-analysis in context. London: BMJPublishing; 2001.
50. Khan K, ter Riet G, Glanville J, Sowden A,Kleijnen J. Undertaking systematic reviews of researchon effectiveness. York: York Publishing Services;2001.
References
70
51. Drummond M, Jefferson T. Guidelines for authorsand peer reviewers of economic submissions to theBMJ. BMJ 1996;313:275–83.
52. McKee MD, Schemitsch EH, Wild L, Waddell JP.The treatment of complex, recalcitrant long-bonenonunion with a human recombinant bonemorphogenetic protein: results of a prospectivepilot study. In Proceedings of Orthopedic TraumaAssociation 18th Annual Meeting. Toronto, Ontario:Orthopedic Trauma Association; 2002.
53. Ackerman SJ, Mafilios MS, Polly DW Jr. Economicevaluation of bone morphogenetic protein versusautogenous iliac crest bone graft in single-levelanterior lumbar fusion: an evidence-basedmodeling approach. Spine 2002;27(16 Suppl 1):S94–9.
54. Polly DW Jr, Ackerman SJ, Shaffrey CI, Ogilvie JW,Wang JC, Stralka SW, et al. A cost analysis of bonemorphogenetic protein versus autogenous iliaccrest bone graft in single-level anterior lumbarfusion. Orthopedics 2003;26:1027–37.
55. Jones AL. Recombinant human bone morphogenicprotein-2 in fracture care. J Orthop Trauma 2005;19:S23–5.
56. Meisel HJ. Cost variances in G-DRG groups. Theexample of rhBMP-2 in spine fusion surgery. ValueHealth 2004;7:712.
57. McQueen MM, Hajducka C, Court-Brown CM.A comparison of rhBMP-7 (ossigraft) andautogenous graft for treatment of metaphysealdefects after osteotomy of the distal radius. InProceedings of Orthopedic Trauma Association 19thAnnual Meeting. Salt Lake City; UT: OrthopedicTrauma Association; 2003.
58. Bilic R, Simic P, Jelic M, Stern-Padovan R, Dodig D, van Meerdervoort HP, et al. Osteogenicprotein-1 (BMP-7) accelerates healing of scaphoidnon-union with proximal pole sclerosis. Int Orthop2006;30:128–34.
59. Chen G, Yang JZ, Xu HM, Wang M. Theapplication of NNB/BMP complex in thetreatment of ununited-tibia fracture. Orthop J China2000;7:758–61.
60. Cook SD. Preclinical and clinical evaluation ofosteogenic protein-1 (BMP-7) in bony sites.Orthopedics 1999;22:669–71.
61. Govender S, Csimma C, Genant HK, Valentin-Opran A. Recombinant human bonemorphogenetic protein-2 for treatment of opentibial fractures – a prospective, controlled,randomized study of four hundred and fiftypatients. J Bone Joint Surg Am 2002;84:2123–34.
62. Maniscalco P, Gambera D, Bertone C, Rivera F,Crainz E, Urgelli S. Healing of fresh tibialfractures with OP-1. A preliminary report. ActaBiomed Ateneo Parmense 2002;73:27–33.
63. McKee MD, Schemitsch EH, Waddell JP,Kreder HJ, Stephen DJG, Leighton RK, et al. Theeffect of human recombinant bone morphogeneticprotein (rhBMP-7) on the healing of open tibialshaft fractures: results of a multi-center,prospective, randomized clinical trial. InProceedings of the Orthopedic Trauma Association 18thAnnual Meeting. Toronto, Ontario: OrthopedicTrauma Association; 2002.
64. Perry CR, Cole D, Perry M, Cierny G. Osteogenicprotein (OP-1) vs autograft in the management oftibial nonunions. In Proceedings of the OrthopedicTrauma Association 13th Annual Meeting. Louisville,KT: Orthopedic Trauma Association; 1997.
65. Higgins JPT, Green S, editors. Selection bias.Cochrane Handbook for Systematic Reviews ofInterventions 4.2.5 [updated May 2005]; Section6.3. The Cochrane Library, Issue 3, 2005.Chichester: J Wiley; 2005.
66. Swiontkowski MF, Hannu TA, Donell S,Esterhai JL, Goulet J, Jones A, et al. Recombinanthuman bone morphogenetic protein-2 in opentibial fractures: a subgroup analysis of datacombined from two prospective randomizedstudies. J Bone Joint Surg Am 2006;88:1258–65.
67. Salkeld G, Cameron I, Cumming R, Easter S,Seymour J, Kurrle SE, et al. Quality of life relatedto fear of falling and hip fracture in older women:a time trade off study. BMJ 2000;320:341–6.
68. Baskin DS, Ryan P, Sonntag V, Westmark R,Widmayer MA. A prospective, randomized,controlled cervical fusion study using recombinanthuman bone morphogenetic protein-2 with theCORNERSTONE-SR allograft ring and theATLANTIS anterior cervical plate. Spine2003;28:1219–25; discussion 25.
69. Boden SD, Kang J, Sandhu H, Heller JG. Use ofrecombinant human bone morphogenetic protein-2 to achieve posterolateral lumbar spine fusion inhumans: a prospective, randomized clinical pilottrial: 2002 Volvo Award in clinical studies. Spine2002;27:2662–73.
70. Boden SD, Martin GJ Jr, Morone MA, Ogbo JL,Moskovitz PA. Posterolateral lumbarintertransverse process spine arthrodesis withrecombinant human bone morphogenetic protein2/hydroxyapatite-tricalcium phosphate afterlaminectomy in the nonhuman primate. Spine1999;24:1179–85.
71. Burkus JK, Sandhu HS, Gornet MF, Longley MC.Use of rhBMP-2 in combination with structuralcortical allografts: clinical and radiographicoutcomes in anterior lumbar spinal surgery. J BoneJoint Surg Am 2005;87:1205–12.
72. Burkus JK, Transfeldt EE, Kitchel SH, Watkins RG,Balderston RA. Clinical and radiographicoutcomes of anterior lumbar interbody fusion
Health Technology Assessment 2007; Vol. 11: No. 30
71
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
using recombinant human bone morphogeneticprotein-2. Spine 2002;27:2396–408.
73. Burkus JK, Gornet M, Longley M. A largerandomized clinical evaluation of rhBMP-2 versusiliac crest bone graft combined with corticalallograft in lumbar spine fusion. Spine J 2004;4(5,Suppl 1):S35–6.
74. Burkus JK, Gornet MF, Dickman CA, Zdeblick TA.Anterior lumbar interbody fusion using rhBMP-2with tapered interbody cages. J Spinal Disord Tech2002;15:337–49.
75. Gornet MF BJ, Dickman CA, Zdeblick TA. rhBMP-2 with tapered cages: a prospective, randomizedlumbar fusion study. Presented at the NorthAmerican Society of Spine Surgeons Meeting, 30October–3 November 2001, Seattle, WA.
76. Burkus JK, Dorchak JD, Sanders DL.Radiographic assessment of interbody fusion usingrecombinant human bone morphogenetic proteintype 2. Spine 2003;15:372–7.
77. Dimar JR, Glassman SD, Burkus KJ, Carreon LY.Clinical outcomes and fusion success at 2 years ofsingle-level instrumented posterolateral fusionswith recombinant human bone morphogeneticprotein-2/compression resistant matrix versus iliaccrest bone graft. Spine 2006;31:2534–9.
78. Glassman SD, Dimar JR, Carreon LY,Campbell MJ, Puno RM, Johnson JR. Initialfusion rates with recombinant human bonemorphogenetic protein-2/compression resistantmatrix and a hydroxyapatite and tricalciumphosphate/collagen carrier in posterolateral spinalfusion. Spine 2005;30:1694–8.
79. Haid RW Jr, Branch CL Jr, Alexander JT, BurkusJK. Posterior lumbar interbody fusion usingrecombinant human bone morphogenetic proteintype 2 with cylindrical interbody cages. Spine J2004;4:527–38; discussion 38–9.
80. Johnsson R, Stromqvist B, Aspenberg P.Randomized radiostereometric study comparingosteogenic protein-1 (BMP-7) and autograft bonein human noninstrumented posterolateral lumbarfusion: 2002 Volvo Award in clinical studies. Spine2002;27:2654–61.
81. Kanayama M, Hashimoto T, Shigenobu K,Yamane S, Bauer T, Togawa D. A prospectiverandomized study of posterolateral lumbar fusionusing osteogenic protein-1 (OP-1) versus localautograft with ceramic bone substitute. Spine2006;31:1067–74.
82. Vaccaro AR, Patel T, Fischgrund J, Anderson DG,Truumees E, Herkowitz HN, et al. A pilot studyevaluating the safety and efficacy of OP-1 Putty(rhBMP-7) as a replacement for iliac crestautograft in posterolateral lumbar arthrodesis fordegenerative spondylolisthesis. Spine 2004;29:1885–92.
83. Assiri I, du Plessis S, Hurlbert J, Hu R, Salo P,Whittaker T. A prospective randomized clinicalstudy comparing instrumented lumbar fusion ratesor recombinant human bone morphogenicprotein-2 (rhBMP-2) with autogenous iliac crestbone graft in patients with symptomaticdegenerative disc disease. Calgary experience. CanJ Surg 2004;47 (Suppl):7–8.
84. Shapiro S, Rodgers RB, Sloan R, Altstadt T,Miller J. A randomized trial of instrumentedposterior lumbar interbody fusion using machinedcortical wedges/local bone with or without rhBMP2in the treatment of degenerative lumbarspondylolisthesis with stenosis. Neurosurgery2005;57:398.
85. Boden SD, Zdeblick TA, Sandhu HS, Heim SE.The use of rhBMP-2 in interbody fusion cages.Definitive evidence of osteoinduction in humans: apreliminary report. Spine 2000;25:376–81.
86. Vaccaro AR, Anderson DG, Patel T, Fischgrund J,Truumees E, Herkowitz HN, et al. Comparison ofOP-1 putty (rhBMP-7) to iliac crest autograft forposterolateral lumbar arthrodesis – a minimum 2-year follow-up pilot study. Spine2005;30:2709–16.
87. Alexander J, Branch, C Jr. Recombinant humanbone morphogenic protSD stem-2 in a posteriorlumbar interbody fusion construct: 2-year clinicaland radiologic outcomes. Spine J 2002;2 (5, Suppl1):48.
88. Coric D, Fischgrund JS, Patel T, Vaccaro AR,Eeric T, Herkowitz HN, et al. Two-year follow-upon patients in a pilot safety and efficacy study ofOP-1 (rhBMP-7) in posterolateral lumbar fusion asa replacement for iliac crest autograft. Neurosurgery2004;55:477.
89. Kuslich SD, Ulstrom CL, Griffith SL, Ahern JW,Dowdle JD. The Bagby and Kuslich method oflumbar interbody fusion. Spine 1998;23:1267–79.
90. Chow SP, Leong JC, Ma A, Yau AC. Anterior spinalfusion for deranged lumbar intervertebral disc.Spine 1980;5:452–8.
91. Blumenthal SL, Baker J, Dossett A, Selby DK. Therole of anterior lumbar fusion for internal discdisruption. Spine 1988;13:566–9.
92. Brown C, Orme T, Richardson H. The rate ofpseudarthrosis (surgical nonunion) in patients whoare smokers and patients who are nonsmokers: acomparison study. Spine 1986;9:942–3.
93. Fairbank JC, Couper J, Davies JB, O’Brien JP. TheOswestry low back pain disability questionnaire.Physiotherapy 1980;66:271–3.
94. Ware J, Sherbourne C. The MOS 36-item short-form health survey (SF-36): I. Conceptualframework and item selection. Med Care1992;30:473–83.
References
72
95. Burkus JK, Transfeldt EE, Kitchel SH, Watkins R,Balderston RA. rhBMP-2 and cortical dowels in thelumbar spine: long term outcomes. Presented at theNorth American Society of Spine Surgeons Meeting,30 October–3 November 2001, Seattle, WA.
96. BOA/BAPS Working Party. The Management of OpenTibial Fractures. Bexhill-on-Sea: BritishOrthopaedic Association; 1997.
97. Hall S, Criddle R, Comito T, Prince R. Acase–control study of quality of life and functionalimpairment in women with long-standingvertebral osteoporotic fracture. Osteoporos Int1999;9:508–15.
98. Briggs A, Gray A. Handling uncertainty whenperforming economic evaluation of healthcareinterventions. Health Technol Assess 1999;3(2).
99. Department of Health. NHS reference costs datacollection – instructions for NHS organisations abouthow to return all relevant cost data. London:Department of Health; 2006.
100. Sprague S, Bhandari M. An economic evaluationof early versus delayed operative treatment inpatients with closed tibial shaft fractures. ArchOrthop Trauma Surg 2002;122:315–23.
101. Burkus JK, Heim SE, Gornet MF, Zdeblick TA. IsINFUSE bone graft superior to autograft bone?An integrated analysis of clinical trials using theLT-CAGE lumbar tapered fusion device. J SpinalDisord Tech 2003;16:113–22.
102. Rivero-Arias O, Campbell H, Gray A, Fairbank J,Frost H, Wilson-MacDonald J. Surgicalstabilisation of the spine compared with aprogramme of intensive rehabilitation for themanagement of patients with chronic low backpain: cost utility analysis based on a randomisedcontrolled trial. BMJ 2005;330:1239.
103. Brazier J, Usherwood T, Harper R, Thomas K.Deriving a preference based single index from theUK SF-36 health survey. J Clin Epidemiol1998;51:1115–28.
104. Gibson J, Waddell G. Surgery for degenerativelumbar spondylolysis. Cochrane Database Syst Rev2005;4:CD001352.
105. Carlisle E, Fischgrund JS. Bone morphogeneticproteins for spinal fusion. Spine J 2005;5 (6Suppl):240S–9S.
106. Jones NF, Brown EE, Mostofi A, Vogelin E,Urist MR. Healing of a scaphoid nonunion usinghuman bone morphogenetic protein. J Hand Surg[Am] 2005;30:528–33.
107. Bai MH, Liu XY, Ge BF, Yallg C, Chen DA. Animplant of a composite of bovine bonemorphogenetic protein and plaster of Paris fortreatment of femoral shaft nonunions. Int Surg1996;81:390–2.
108. Benke G, Gorecki A. BMP-7 (OP-1) in humanorthopaedic surgery: Local and systemic effects ofapplication. Materialwiss Werkstofftech. 2004;35:980–2.
109. Bong MR, Capla EL, Egol KA, Sorkin AT,Distefano M, Buckle R, et al. Osteogenic protein-1(bone morphogenic protein-7) combined withvarious adjuncts in the treatment of humeraldiaphyseal nonunions. Bulletin Hosp Joint Dis2005;63:20–3.
110. Delloye C, Suratwala SJ, Cornu O, Lee FY.Treatment of allograft nonunions withrecombinant human bone morphogenetic proteins(rhBMP). Acta Orthop Belg 2004;70:591–7.
111. Dimitriou R, Dahabreh Z, Katsoulis E,Matthews SJ, Branfoot T, Giannoudis PV.Application of recombinant BMP-7 on persistentupper and lower limb non-unions. Injury 2005;36(Suppl. 4):S51–9.
112. Johnson EE, Urist MR. One-stage lengthening offemoral nonunion augmented with human bonemorphogenetic protein. Clin Orthop 1998;347:105–16.
113. Johnson EE, Urist MR. Human bonemorphogenetic protein allografting forreconstruction of femoral nonunion. Clin Orthop2000;371:61–74.
114. Johnson EE, Urist MR, Finerman GA. Bonemorphogenetic protein augmentation grafting ofresistant femoral nonunions. A preliminary report.Clin Orthop 1988;230:257–65.
115. Johnson EE, Urist MR, Finerman GA. Distalmetaphyseal tibial nonunion. Deformity and boneloss treated by open reduction, internal fixation,and human bone morphogenetic protein (hBMP).Clinical Orthop 1990;250:234–40.
116. Johnson EE, Urist MR. Distal metaphyseal tibialnonunions associated with significant bowingdeformity and cortical bone loss: treatment withhuman bone morphogenetic protein (h-BMP) andinternal fixation. Nippon Seikeigeka Gakkai Zasshi1989;63:613–20.
117. Johnson EE, Urist MR, Finerman GAM. Resistantnonunions and partial or complete segmentaldefects of long bones: treatment with implants of acomposite of human bone morphogenetic protein(BMP) and autolyzed, antigen-extracted,allogeneic (AAA) bone. Clinical Orthop1992;277:229–37.
118. Kujala S, Raatikainen T, Ryhanen J, Kaarela O,Jalovaara P. Composite implant of native bovinebone morphogenetic protein (BMP) and biocoralin the treatment of scaphoid nonunions – apreliminary study. Scand J Surg 2002;91:186–90.
Health Technology Assessment 2007; Vol. 11: No. 30
73
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.

119. Kujala S, Raatikainen T, Ryhänen J, Kaarela O,Jalovaara P. Composite implant of native bovinebone morphogenetic protein (BMP), collagencarrier and biocoral in the treatment of resistant ulnar nonunions: report of fivepreliminary cases. Arch Orthop Trauma Surg 2004;124:26–30.
120. Riedel GE, Valentin-Opran A. Clinical evaluationof rhBMP-2/ACS in orthopedic trauma: a progressreport. Orthopedics 1999;22:663–5.
121. Kuklo TR. Use of rhBMP-2 for open segmentaltibia fractures from Iraq. In Proceedings of theOrthopedic Trauma Association 21st Annual meeting.Ottowa, Ontario: Orthopedic Trauma Association;2005.
122. Schwartz ND, Hicks BM. Segmental bone defectstreated with recombinant human bone morphogeneticprotein-2. Chicago, IL: American Academy ofOrthopaedic Surgeons; 2006.
123. Johnson EE, Urist MR, Finerman GA. Repair ofsegmental defects of the tibia with cancellous bonegrafts augmented with human bonemorphogenetic protein. A preliminary report. ClinOrthop 1988;236:249–57.
124. Giannoudis PV, Tzioupis C. Clinical applicationsof BMP-7 – the UK perspective. Injury2005;36:47–50.
125. Kuklo TR, Rosner MK, Polly DW Jr. Computerizedtomography evaluation of a resorbable implantafter transforaminal lumbar interbody fusion.Neurosurgery 2004;16:E10.
126. Mankin HJ, Doppelt SH, Sullivan TR, TomfordWW. Osteoarticular and intercalary allografttransplantation in the management of malignanttumors of bone. Cancer 1982;50:613–30.
127. Boakye M, Mummaneni PV, Garrett M, Rodts G,Haid R. Anterior cervical discectomy and fusioninvolving a polyetheretherketone spacer and bonemorphogenetic protein. J Neurosurg Spine 2005;2:521–5.
128. Boden SD, Grob D, Damien C. Ne-Osteo bonegrowth factor for posterolateral lumbar spinefusion: results from a nonhuman primate studyand a prospective human clinical pilot study. Spine2004;29:504–14.
129. Govender PV, Rampersaud YR, Rickards L,Fehlings MG. Use of osteogenic protein-1 in spinalfusion: literature review and preliminary results ina prospective series of high-risk cases. NeurosurgFocus 2002;13:Article 4.
130. Jeppsson C, Saveland H, Rydholm U,Aspenberg P. OP-1 for cervical spine fusion:bridging bone in only 1 of 4 rheumatoid patientsbut prednisolone did not inhibit bone induction inrats. Acta Orthop Scand 1999;70:559–63.
131. Kleeman TJ, Ahn UM, Talbot-Kleeman A.Laparoscopic anterior lumbar interbody fusionwith rhBMP-2: a prospective study of clinical and radiographic outcomes. Spine 2001;26:2751–6.
132. Lanman TH, Hopkins TJ. Early findings in a pilotstudy of anterior cervical interbody fusion in whichrecombinant human bone morphogenetic protein-2 was used with poly(L-lactide-co-D,L-lactide)bioabsorbable implants. Neurosurgery 2004;16:E6.
133. Lanman TH, Hopkins TJ. Lumbar interbodyfusion after treatment with recombinant humanbone morphogenetic protein-2 added to poly(L-lactide-co-D,L-lactide) bioresorbableimplants. Neurosurgery 2004;16:E9.
134. Laursen M, Hoy K, Hansen ES, Gelineck J,Christensen FB, Bringer CE. Recombinant bonemorphogenetic protein-7 as an intracorporal bonegrowth stimulator in unstable thoracolumbar burstfractures in humans: preliminary results. Eur SpineJ 1999;8:485–90.
135. Luhmann SJ, Bridwell KH, Cheng I, Imamura T,Lenke LG, Schootman M. Use of bonemorphogenetic protein-2 for adult spinaldeformity. Spine 2005;30 (17 Suppl):S110–17.
136. Mummaneni PV, Pan J, Haid RW, Rodts GE.Contribution of recombinant human bonemorphogenetic protein-2 to the rapid creation ofinterbody fusion when used in transforaminallumbar interbody fusion: a preliminary report.Invited submission from the Joint Section Meetingon Disorders of the Spine and Peripheral Nerves, March 2004. J Neurosurg Spine 2004;1:19–23.
137. Vaccaro AR, Patel T, Fischgrund J, Anderson DG,Truumees E, Herkowitz H, et al. A 2-year follow-uppilot study evaluating the safety and efficacy of op-1 putty (rhbmp-7) as an adjunct to iliac crestautograft in posterolateral lumbar fusions. EurSpine J 2005;14:623–9.
138. Villavicencio AT, Burneikiene S, Nelson EL,Bulsara KR, Favors M, Thramann J. Safety oftransforaminal lumbar interbody fusion andintervertebral recombinant human bonemorphogenetic protein-2. J Neurosurg Spine2005;3:436–43.
139. Buttermann G. Prospective ACDF outcomes usingiliac crest autograft versus allograft with bonemorphogenetic protein. Seattle, WA: ScollosisResearch Society; 2002.
140. Mummaneni PV, Pan J, Rodts GE, Haid RW.Transforaminal lumbar interbody fusion: acomparison of Rh-BMP2 and iliac crest autograft –is Rh-BMP2 superior? Neurosurgery 2004;55:455–6.
References
74
141. Vaccaro AR, Patel T, Fischgrund J, Anderson DG,Truumees E, Herkowitz H, et al. A pilot safety andefficacy study of OP-1 putty (rhBMP-7) as anadjunct to iliac crest autograft in posterolaterallumbar fusions. Eur Spine J 2003;12:495–500.
142. Blount KJ, Krompinger WJ, Maljanian R,Browner BD. Moving toward a standard for spinalfusion outcomes assessment. J Spinal Disord Tech2002;15:16–23.
143. Eck KR, Lenke LG, Bridwell KH, Gilula LA,Lashgari CJ, Riew KD. Radiographic assessment ofanterior titanium mesh cages. J Spinal Disord Tech2000;13:501–9.
144. Lenke LG, Bridwell KH, Bullis D, Betz RR, BaldusC, Schoenecker PL. Results of in situ fusion foristhmic spondylolisthesis. J Spinal Disord Tech1992;5:433–42.
Health Technology Assessment 2007; Vol. 11: No. 30
75
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.

BMP for treatment of fractures orfusionMEDLINE (Ovid) 1966 to week 3January 2006 and EMBASE (Ovid) 1980to week 3 January 20061 bone morphogen$.ti,ab.2 osteogen$.ti,ab.3 osteoinduct$.ti,ab.4 protein$.ti,ab.5 factor$.ti,ab.6 polypeptide$.ti,ab.7 poly-peptide$.ti,ab.8 ((bone morphogen$ or osteogen$ or
osteoinduct$) adj (protein$ or factor$ orpolypeptide$ or poly-peptide$)).ti,ab.
9 (BMP or BMP2 or BMP-2 or BMP7 or BMP-7).ti,ab.
10 (rhBMP or rhBMP2 or rhBMP-2 or rhBMP7 orrhBMP-7).ti,ab.
11 (rh-BMP or rh-BMP2 or rh-BMP-2 or rh-BMP7or rh-BMP-7).ti,ab.
12 (rhop1 or rhop-1).ti,ab.13 (op1 or op-1).ti,ab.14 exp Bone Morphogenetic Proteins/15 fracture$.ti,ab.16 exp Fractures, Ununited/ or exp Skull
Fractures/ or exp Fractures, Malunited/ or expZygomatic Fractures/ or exp Orbital Fractures/or exp Fractures, Bone/ or exp SpinalFractures/ or exp Femoral Neck Fractures/ orexp Radius Fractures/ or exp FemoralFractures/ or exp Tibial Fractures/ or expMaxillary Fractures/ or exp Humeral Fractures/or exp Ulna Fractures/ or exp Fractures,Compression/ or exp Fractures, Cartilage/ orexp Fractures, Spontaneous/ or exp HipFractures/ or exp Shoulder Fractures/ or expJaw Fractures/ or exp Mandibular Fractures/ orexp Fractures, Open/ or exp Fractures, Closed/or exp Tooth Fractures/ or exp Rib Fractures/or exp Fractures, Stress/ or exp Fractures,Comminuted/
17 (nonunion or nonunion).ti,ab.18 (non-fusion or nonfusion).ti,ab.19 non-heal$.ti,ab.20 fusion.ti,ab.21 union.ti,ab.22 heal$.ti,ab.23 (allograft$ or autograft$).ti,ab.
24 spin$.ti,ab.25 tibial.ti,ab.26 or/8-1427 or/15-2528 26 and 2729 limit 28 to humans
Science Citation Index 1945 to week 2January 20061 TS=bone morphogen*2 TS=osteogen*3 TS=osteoinduct*4 TS=bmp or bmp2 or bmp-2 or bmp7 or bmp-
75 TS=rhbmp or rhbmp2 or rhbmp-2 or rhbmp7
or rhbmp-76 TS=rh-bmp or rh-bmp2 or rh-bmp-2 or rh-
bmp7 or rh-bmp-77 TS=rhop1 or rhop-18 TS=op1 or op-19 TS=fracture*10 TS=nonunion or nonunion11 TS=non-fusion or nonfusion12 TS=non-heal*13 TS=fusion14 TS=union15 TS=heal*16 TS=allograft or autograft17 TS=spin*18 TS=tibial19 #8 or #7 or #6 or #5 or #420 #18 or #17 or #16 or #15 or #14 or #13 or
#12 or #11 or #10 or #921 #20 and #19
NeLH on 19 January 2006Search terms: • Bmp• Op-1• Op1• Rhop-1• Rhop1• Rhbmp• Rhbmp2• Rhbmp-2• Rh-bmp• Rh-bmp-2• Rhop-1• Rhop1• Nonfusion
Health Technology Assessment 2007; Vol. 11: No. 30
77
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 1
Search strategies
• Non-fusion• Allograft*• Tibia• Bone morphogen*• Osteogen*• Bmp2• Bmp-2• Bmp7• Bmp-7• Rhbmp7• Rhbmp-7• Rh-bmp-7• Fracture*• Nonunion• Nonunion• Non-heal*• Fusion• Autograft*• Spin*
Cochrane Library Central 1800 to week 2 January 2006 (all in title andabstract)1 bone morphogen*2 osteogen*3 osteoinduct*4 protein*5 factor*6 polypeptide*7 poly-peptide*8 (bone morphogen* or osteogen* or
osteoinduct*) next (protein* or factor* orpolypeptide* or poly-peptide)
9 bmp or bmp2 or bmp-2 or bmp7 or bmp-710 rhbmp, rhbmp2, rhbmp-2, rhbmp7, rhbmp-711 rh-bmp, rh-bmp2, rh-bmp-2, rh-bmp7, rh-
bmp-712 rhop1 or rhop-113 op1 or op-114 MeSH descriptor Bone Morphogenetic
Proteins15 fracture*16 MeSH descriptor Fractures17 Non-union, nonunion18 non-fusion, nonfusion19 non-heal*20 fusion21 union22 heal*23 allograft* or autograft*24 spin*25 tibial26 #8 or #9 or #10 or #11 or #12 or #13 or
#1427 #15 or #16 or (#17 AND or#18) OR #19 or
#20 or #21 or #22 or #23 or #24 or #2528 #26 AND #27
BMP/TGF/RCT and clinical trialfilterMEDLINE (Ovid) 1980 to week 3January 2006 and EMBASE (Ovid) 1980to week 3 January 20061 bone morphogen$.ti,ab.2 osteogen$.ti,ab.3 osteoinduct$.ti,ab.4 protein$.ti,ab.5 factor$.ti,ab.6 polypeptide$.ti,ab.7 poly-peptide$.ti,ab.8 ((bone morphogen$ or osteogen$ or
osteoinduct$) adj (protein$ or factor$ orpolypeptide$ or poly-peptide$)).ti,ab.
9 (BMP or BMP2 or BMP-2 or BMP7 or BMP-7).ti,ab.
10 (rhBMP or rhBMP2 or rhBMP-2 or rhBMP7 orrhBMP-7).ti,ab.
11 (rh-BMP or rh-BMP2 or rh-BMP-2 or rh-BMP7or rh-BMP-7).ti,ab.
12 (rhop1 or rhop-1).ti,ab.13 (op1 or op-1).ti,ab.14 exp Bone Morphogenetic Proteins/15 fracture$.ti,ab.16 exp Fractures, Ununited/ or exp Skull
Fractures/ or exp Fractures, Malunited/ or expZygomatic Fractures/ or exp Orbital Fractures/or exp Fractures, Bone/ or exp SpinalFractures/ or exp Femoral Neck Fractures/ orexp Radius Fractures/ or exp FemoralFractures/ or exp Tibial Fractures/ or expMaxillary Fractures/ or exp Humeral Fractures/or exp Ulna Fractures/ or exp Fractures,Compression/ or exp Fractures, Cartilage/ orexp Fractures, Spontaneous/ or exp HipFractures/ or exp Shoulder Fractures/ or expJaw Fractures/ or exp Mandibular Fractures/ orexp Fractures, Open/ or exp Fractures, Closed/or exp Tooth Fractures/ or exp Rib Fractures/or exp Fractures, Stress/ or exp Fractures,Comminuted/
17 (nonunion or nonunion).ti,ab.18 (non-fusion or nonfusion).ti,ab.19 non-heal$.ti,ab.20 fusion.ti,ab.21 union.ti,ab.22 (heal or healed or heals or healing).ti,ab.23 (allograft$ or autograft$).ti,ab.24 (spine or spinal).ti,ab.25 tibial.ti,ab.26 or/8-1427 or/15-2528 26 and 2729 limit 28 to humans30 bone morphogen$.ti,ab.
Appendix 1
78
31 osteogen$.ti,ab.32 osteoinduct$.ti,ab.33 protein$.ti,ab.34 factor$.ti,ab.35 polypeptide$.ti,ab.36 poly-peptide$.ti,ab.37 ((bone morphogen$ or osteogen$ or
osteoinduct$) adj (protein$ or factor$ orpolypeptide$ or poly-peptide$)).ti,ab.
38 (BMP or BMP2 or BMP-2 or BMP7 or BMP-7).ti,ab.
39 (rhBMP or rhBMP2 or rhBMP-2 or rhBMP7 orrhBMP-7).ti,ab.
40 (rh-BMP or rh-BMP2 or rh-BMP-2 or rh-BMP7or rh-BMP-7).ti,ab.
41 (rhop1 or rhop-1).ti,ab.42 (op1 or op-1).ti,ab.43 (TGF or TGF-beta or transforming growth
factor beta or transforming growthfactor).ti,ab.
44 exp Bone Morphogenetic Proteins/45 fracture$.ti,ab.46 exp Fractures, Ununited/ or exp Skull
Fractures/ or exp Fractures, Malunited/ or expZygomatic Fractures/ or exp Orbital Fractures/or exp Fractures, Bone/ or exp SpinalFractures/ or exp Femoral Neck Fractures/ orexp Radius Fractures/ or exp FemoralFractures/ or exp Tibial Fractures/ or expMaxillary Fractures/ or exp Humeral Fractures/or exp Ulna Fractures/ or exp Fractures,Compression/ or exp Fractures, Cartilage/ orexp Fractures, Spontaneous/ or exp HipFractures/ or exp Shoulder Fractures/ or expJaw Fractures/ or exp Mandibular Fractures/ orexp Fractures, Open/ or exp Fractures, Closed/or exp Tooth Fractures/ or exp Rib Fractures/or exp Fractures, Stress/ or exp Fractures,Comminuted/
47 (nonunion or nonunion).ti,ab.48 (non-fusion or nonfusion).ti,ab.49 non-heal$.ti,ab.50 fusion.ti,ab.51 union.ti,ab.52 (heal or healed or heals or healing).ti,ab.53 (allograft$ or autograft$).ti,ab.54 (spine or spinal).ti,ab.55 tibial.ti,ab.56 or/37-4457 or/45-5558 56 and 5759 limit 58 to humans60 59 not 2961 randomized controlled trial.pt.62 controlled clinical trial.pt.63 exp Randomized Controlled Trials/64 exp Random Allocation/
65 exp Double-Blind Method/66 exp Single-Blind Method/67 or/61-6668 animal/ not human/“70 exp "Clinical Trial [Publicati”n Type]"/71 clinical-trial in PT.mp. [mp=title, original title,
abstract, name of substance word, subjectheading word]
72 (clin$ adj6 trial$).ti,ab.73 ((singl$ or doubl$ or trebl$ or tripl$) adj6
(blind$ or mask$)).mp. [mp=title, originaltitle, abstract, name of substance word, subjectheading word]
74 ((singl$ or doubl$ or trebl$ or tripl$) adj6(blind$ or mask$)).ti,ab.
75 exp Placebos/76 placebo$.ti,ab.77 random.ti,ab.78 exp Research Design/79 or/70-7880 animal/ not human/81 79 not (80 or 69)82 81 and 6083 Comparative Study/84 exp Evaluation Studies/85 exp Follow-Up Studies/86 exp Prospective Studies/87 (control$ or prospectiv$ or volunteer$).ti,ab.88 or/83-8789 animal/ not human/90 88 not (89 or 81 or 69)91 90 and 6092 from 91 keep 1-1093 from 82 keep 1-41
MEDLINE (Ovid) 1966 to week 2November 2006 and EMBASE (Ovid)1980 to week 2 November 20061 bone morphogen$.ti,ab.2 osteogen$.ti,ab.3 osteoinduct$.ti,ab.4 protein$.ti,ab.5 factor$.ti,ab.6 polypeptide$.ti,ab.7 poly-peptide$.ti,ab.8 ((bone morphogen$ or osteogen$ or
osteoinduct$) adj (protein$ or factor$ orpolypeptide$ or poly-peptide$)).ti,ab.
9 (BMP or BMP2 or BMP-2 or BMP7 or BMP-7).ti,ab.
10 (rhBMP or rhBMP2 or rhBMP-2 or rhBMP7 orrhBMP-7).ti,ab.
11 (rh-BMP or rh-BMP2 or rh-BMP-2 or rh-BMP7or rh-BMP-7).ti,ab.
12 (rhop1 or rhop-1).ti,ab.13 (op1 or op-1).ti,ab.14 exp Bone Morphogenetic Proteins/
Health Technology Assessment 2007; Vol. 11: No. 30
79
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
15 fracture$.ti,ab.16 exp Fractures, Ununited/ or exp Skull
Fractures/ or exp Fractures, Malunited/ or expZygomatic Fractures/ or exp Orbital Fractures/or exp Fractures, Bone/ or exp SpinalFractures/ or exp Femoral Neck Fractures/ orexp Radius Fractures/ or exp FemoralFractures/ or exp Tibial Fractures/ or expMaxillary Fractures/ or exp Humeral Fractures/or exp Ulna Fractures/ or exp Fractures,Compression/ or exp Fractures, Cartilage/ orexp Fractures, Spontaneous/ or exp HipFractures/ or exp Shoulder Fractures/ or expJaw Fractures/ or exp Mandibular Fractures/ orexp Fractures, Open/ or exp Fractures, Closed/or exp Tooth Fractures/ or exp Rib Fractures/or exp Fractures, Stress/ or exp Fractures,Comminuted/
17 (nonunion or non-union).ti,ab.18 (non-fusion or nonfusion).ti,ab.19 non-heal$.ti,ab.20 fusion.ti,ab.21 union.ti,ab.22 (heal or healed or heals or healing).ti,ab.23 (allograft$ or autograft$).ti,ab.24 spin$.ti,ab.25 tibial.ti,ab.26 or/8-1427 26 and (or/15-25)28 Randomized controlled trial.pt.
29 Controlled clinical trial.pt.30 exp Randomized Controlled Trials/31 exp Random Allocation/32 exp Double-Blind Method/33 exp Single-Blind Method/34 or/28-3335 animal/ not human/36 34 not 3537 exp “Clinical Trial [Publication Type]”/38 clinical-trial in PT.mp. 39 (clin$ adj6 trial$).ti,ab.40 ((singl$ or doubl$ or treb$ or trip$) adj6
(blind$ or mask$)).mp.41 exp Placebos/42 placebo$.ti,ab.43 random.ti,ab.44 exp Research Design/45 or/37-4446 animal/ not human/47 45 not (46 or 36)48 Comparative Study/49 exp Evaluation Studies/50 exp Follow-Up Studies/51 exp Prospective Studies/52 (control$ or prospectiv$ or volunteer$).ti,ab.53 or/ 48-5254 animal/ not human/55 53 not (54 or 47 or 32)56 27 and ((or/47,55) or 36)
Appendix 1
80

RCT data extraction formReviewer: __________________________________ Date: __________________________________
Author (year)
Title and source
Study objectives
Study characteristics
Country conducted
Patient diagnosis
Surgical interventions
Inclusion and exclusion criteria
Intervention A Intervention B Control
Interventions (mode of delivery, dose, duration, etc.)
No. of patients
Age
M/F
Weight
Length of follow-up
Principal outcome measure
Other outcome measures
Health Technology Assessment 2007; Vol. 11: No. 30
81
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 2
Effectiveness data extraction forms
Study design and quality (using the checklist Appendix 4)
1. Randomisation method
Allocation concealment?
2. Blinding
3. Baseline comparability
4. Inclusion/exclusion criteria explicit?
5. Intention-to-treat analysis?
6. Drop-outs
Patient withdrawals
Reasons
Total drop-outs: Intervention A Intervention B Control
Study results (including QoL and any adverse effects)
Outcome measures Intervention A Intervention B Control
Investigators’ conclusions
Reviewer’s comments and notes
Funding source
References checked
Appendix 2
82

Non-RCT data extraction form
Reviewer: __________________________________ Date: __________________________________
Author (year)
Title and source
Country conducted
Study type
Study objectives
Study characteristics
Patient diagnosis
Surgical intervention
BMP used Concentration Carrier
Inclusion/exclusion criteria
Follow-up length
Outcomes measured
Population characteristics
Number of patients
Age
M/F
Weigh
Quality assessment
Explicit population definition
Similar prognostic baseline
Appropriate assessment of outcomes
Study results
Outcome measures Outcome Statistical significance
Health Technology Assessment 2007; Vol. 11: No. 30
83
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Investigator’s conclusions
Reviewer’s comments and notes
Funding source
References checked
Appendix 2
84
Reviewer: __________________________________ Date: __________________________________
Author (year)
Title and source
Study objectives
Study characteristics
Economic study type(cost-effectiveness analysis; cost–utility analysis; cost–benefit analysis)
Setting:
Practice setting
Geographical location
Dates data collected:
Effectiveness analysis
Resources used
Prices used
Sources of effectiveness data
Evidence from (single study, expert opinion, peer reviewed literature)
Modelling used (if so, type)
Clinical evidence: Study 1 Study 2
Author
Title
Study design
Allocation method
Trial/study size
Follow-up duration
Loss to follow-up
Blinding methods (if any)
Health Technology Assessment 2007; Vol. 11: No. 30
85
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 3
Cost-effectiveness data extraction form
Primary outcomes
How primary outcomes were assessed
Trial summary
Confidence intervals
Clinical conclusions
Expert opinion:
Methods used to derive estimates of effectiveness
Estimates and assumptions made
Economic analysis
Health benefit measured
Basic method of valuation of intervention
When valued
Valuation tool used
Costs
Were resource quantities and costs reported separately?
Whose direct costs were analysed?
Source of direct cost data
Date which price data refer to
Estimation of prices from: (a guess, based on data, derived using modelling techniques)
Costs stated:
Discounting relevant?
Cost reported was (marginal, incremental or average)
Differential costing used
Appendix 3
86

Adjustments made to costs (i.e. new technology cost)
Costs adjusted for inflation (if so, method)
Statistical analysis
How resource use and/or costs were treated (i.e. point estimates or in a stochastic manner) give details
Descriptive statistics (if given, provide methodology)
Sensitivity analysis
Parameters (discount rate, estimates of effectiveness or cost data, etc.)
Areas of uncertainty investigated
Method used
Results
Estimated benefits Reported benefits p-Value and/or confidenceinterval
Duration of benefits
Side-effects considered in economic analysis
Total intervention cost and discount rate (in original currency)
Total comparator cost and discount rate (in original currency)
Statistical analysis results
Currency conversion
Incremental quantities/costs (discounted and not discounted)
Duration of intervention quantities/costs
Duration of comparator quantities/costs
How estimated benefits and costs were combined
Health Technology Assessment 2007; Vol. 11: No. 30
87
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.

Incremental analysis performed?
Summary findings
Any differences in cost-effectiveness of sub-populations?
Sensitive parameters
Authors’ comments on sensitive parameters and variation
Statistical testing results
Authors’ conclusions
Comments
Source of funding
Appendix 3
88
Quality assessment coding manualfor RCTs(yes, no, unknown/unclear, not applicable)
1. Was the randomisation method adequate?Yes: Random number tables
Computer and central officeCoded packagesSerially numbered sealed opaqueenvelopes
No: AlternationCase record numbers, birth dates, orsimilar approaches
Unknown/Unclear: only term ‘randomised’ or‘randomly allocated’
2. Were the outcome assessors blinded? Yes: There was a separate blinded panel of
assessors or independent assessorNo: No assessors were blindedUnknown/Unclear: No statements onprocedures and not deducible
3. Did patients have similar prognostic baselines?Yes: Groups are demonstrably comparableNo: Patient groups are not comparable
4. Were inclusion criteria explicitly stated?Yes: Clearly defined inclusion criteriaNo: Inclusion criteria not clearly defined,
unable to determine how sample wasmade up
Unknown/Unclear: Inadequately defined
5. Was an intention-to-treat analysis performed?Yes: Intention-to-treat analysis performed
according to ITT principleNo: No intention-to-treat analysis
performed
Unknown/Unclear: Intention-to-treat analysisnot performed to ITT principle
6. Loss to follow-upYes: Number of randomised stated. Numbers
lost stated (or calculable) from each groupwith reasons
Partial: Numbers stated, but no reasonsNo: Number randomised not stated or
specifiedUnknown: Not mentioned
Non-RCT quality assessment form(yes, no, unknown/unclear, not applicable)
1. Explicit group definition?Yes: There is a clear description of the group
characteristicsNo: The group is not clearly described
2. Similar prognostic baselines?Yes: Patients within group are comparableNo: Patients within group are not comparableUnknown/Unclear: Unsure whether patientgroup is comparable
3. Appropriate assessment of outcomes?Yes: Independent assessor(s) used to
determine outcomeNo: No independent assessor(s) usedUnknown/Unclear: No statements on outcomeassessment procedure or not deducible
4. Lost to follow-up?Yes: Number lost to follow-up and reasons
describedNo: Number lost to follow-up not givenPartial: Number stated but no reasons given
Health Technology Assessment 2007; Vol. 11: No. 30
89
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 4
Checklist for quality assessment

Appendix 4
90
Checklist for assessment of methodological quality in economic studies
Item Yes No Not Not clear appropriate
Study design1 The research question is stated2 The economic importance of the research question is stated3 The viewpoint(s) of the analysis are clearly stated and justified4 The rationale for choosing alternative programmes or interventions
compared is stated5 The alternatives being compared are clearly described6 The form of economic evaluation used is stated7 The choice of form of economic evaluation is justified in relation to the
questions addressed
Data collection8 The source(s) of effectiveness estimates used are stated9 Details of the design and results of effectiveness study are given
(if based on a single study)10 Details of the methods of synthesis or meta-analysis of estimates
are given (if based on a synthesis of a number of effectiveness studies)11 The primary outcome measure(s) for the economic evaluation are
clearly stated12 Methods to value benefits are stated13 Details of the subjects from whom valuations were obtained were given 14 Productivity changes (if included) are reported separately15 The relevance of productivity changes to the study question is discussed16 Quantities of resource use are reported separately from their unit costs17 Methods for the estimation of quantities and unit costs are described18 Currency and price data are recorded19 Details of currency of price adjustments for inflation or currency
conversion are given20 Details of any model used are given21 The choice of model used and the key parameters on which it is based
are justified.
Analysis and interpretation of results22 Time horizon of costs and benefits is stated23 The discount rate(s) is stated24 The choice of discount rate(s) is justified25 An explanation is given if costs and benefits are not discounted26 Details of statistical tests and confidence intervals are given for
stochastic data27 The approach to sensitivity analysis is given28 The choice of variables for sensitivity analysis is justified29 The ranges over which the variables are varied are justified30 Relevant alternatives are compared31 Incremental analysis is reported32 Major outcomes are presented in a disaggregated as well as
aggregated form33 The answer to the study question is given34 Conclusions follow from the data reported35 Conclusions are accompanied by the appropriate caveats
Source: Drummond MF, Jefferson TO. Guidelines for authors and peer reviewers of economic submissions to the BMJ. BMJ1996;313:275–83.
Health Technology Assessment 2007; Vol. 11: No. 30
91
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 5
List of excluded studies
Paper Reason for exclusion
Alden TD, Varady P, Kallmes DF, Jane JA Jr, Helm GA. Bone morphogenetic protein gene therapy. ReviewSpine 2002;27(16 Suppl 1):S87–93.
An HS, Phillips FM. Editorial. Are spine biologics the future in spinal surgery? Spine J Review2005;5(6 Suppl):207S–8S.
Anderson DG, Andersson GBJ, Boden SD, Damien C, Ebara S, Helm G, et al. ReviewSummary statement: clinical BMP programs. Spine 2002;27(16 Suppl.):S49.
Bailon-Plaza A, van der Meulen MC. A mathematical framework to study the effects of growth Mathematical modelfactor influences on fracture healing. J Theor Biol 2001;212:191–209
Baltzer AWA, Lieberman JR. Regional gene therapy to enhance bone repair. Gene Ther Review2004;11:344–50.
Becker W, Clokie C, Sennerby L, Urist MR, Becker BE. Histologic findings after implantation Diagnosis (extraction and evaluation of different grafting materials and titanium micro screws into extraction sockets: socket)case reports. J Periodontol 1998;69:414–21.
Overview of the biology of lumbar spine fusion and principles for selecting a bone graft Reviewsubstitute. Spine 2002;27(16 Suppl 1):S26–31.
Boden SD. The ABCs of BMPs. Orthop Nurs 2005;24:49–52; quiz 53-4. Review
Burkus JK, Schuler TC, Gornet MF, Zdeblick TA. Anterior lumbar interbody fusion for the Reviewmanagement of chronic lower back pain: current strategies and concepts. Orthop Clin North Am2004;35:25.
Carlisle E, Fischgrund JS. Bone morphogenetic proteins for spinal fusion. Spine J Review2005;5(6 Suppl):240S–9S.
Chin M, Ng T, Tom WK, Carstens M. Repair of alveolar clefts with recombinant human bone Diagnosis (alveolar morphogenetic protein (rhBMP-2) in patients with clefts. J Craniofac Surg 2005;16:778–89. clefts)
Cochran DL, Jones AA, Lilly LC, Fiorellini JP, Howell H. Evaluation of recombinant human bone Diagnosis (extraction morphogenetic protein-2 in oral applications including the use of endosseous implants: 3-year sites)results of a pilot study in humans. J Periodontol 2000;71:1241–57.
Csimma C, Swiontkowski MF. Large clinical trials in musculoskeletal trauma: are they possible? ReviewLessons learned from the international study of the use of rhBMP-2 in open tibial fractures. J Bone Joint Surg Am 2005;87:218–22.
De Biase P, Capanna R. Clinical applications of BMP. Injury 2005;36:43–6. Review
Derner R, Anderson AC. The bone morphogenic protein. Clin Podiatr Med Surg 2005;22:607–18. Review
Dickman CA. A prospective, randomized, controlled cervical fusion study using recombinant Point of viewhuman bone morphogenetic protein-2 with the CORNERSTONE-SR allograft ring and the ATLANTIS anterior cervical plate: point of view. Spine 2003;28:1225.
Einhorn TA. Clinical applications of recombinant human BMPs: early experience and future Reviewdevelopment. J Bone Joint Surg Am 2003;85 Suppl 3:82–8.
Geesink RGT, Hoefnagels NHM, Bulstra SK. Bone healing with OP-1 device in a human model. Unable to find in journal Bone 1999;24:423. (does not exist)
Geesink RG, Hoefnagels NH, Bulstra SK. Osteogenic activity of OP-1 bone morphogenetic Diagnosis (critically protein (BMP-7) in a human fibular defect. J Bone Joint Surg 1999;81:710–18. sized defect)
Giannoudis PV, Tzioupis C. Clinical applications of BMP-7 – the UK perspective. Retrospective analysis of Injury 2005;36:47–50. included studies
continued
Appendix 5
92
Paper Reason for exclusion
Granjeiro JM, Oliveira RC, Bustos-Valenzuela JC, Sogayar MC, Taga R. Bone morphogenetic Reviewproteins: From structure to clinical use. Braz J Med Biol Res 2005;38:1463–73.
Gupta MC, Maitra S. Bone grafts and bone morphogenetic proteins in spine fusion. ReviewCell Tissue Banking 2002;3:255–267.
Gupta MC, Khan SN. Application of bone morphogenetic proteins in spinal fusion. ReviewCytokine Growth Factor Rev 2005;16(3 Spec. Iss.):347–55.
Harwood PJ, Giannoudis PV. Application of bone morphogenetic proteins in orthopaedic practice: Reviewtheir efficacy and side effects. Expert Opin Drug Saf 2005;4:75–89.
Jones AL. Recombinant human bone morphogenic protein-2 in fracture care. J Orthop Trauma Inadequate data for 2005;19:S23–5. extraction (cost
analysis)
Khan SN, Lane JM. The use of recombinant human bone morphogenetic protein-2 (rhBMP-2) in Revieworthopaedic applications. Expert Opin Biol Ther 2004;4:741–8.
Kim DH, Jenis L, Berta SC, Vaccaro AR. Bone graft alternatives in spinal fusion surgery. ReviewCurr Opin Orthop 2003;14:127–37.
Kirker-Head CA. Development and application of bone morphogenetic proteins for the Reviewenhancement of bone healing. J Orthop Traumatol 2005;6:1–9.
Lieberman JR, Conduah A, Urist MR. Treatment of osteonecrosis of the femoral head with Diagnosis (hip core decompression and human bone morphogenetic protein. Clin Orthop Relat Res 2004:139–45. osteonecrosis)
Meisel HJ. Cost variances in G-DRG groups. The example of rhBMP-2 in spine fusion surgery. Inadequate data for Value Health 2004;7:712. extraction (abstract of
cost study)
McKay B, Sandhu HS. Use of recombinant human bone morphogenetic protein-2 in spinal Reviewfusion applications. Spine 2002;27(16 Suppl 1):S66–85.
McKee MD. Recombinant human bone morphogenic protein-7 – applications for clinical trauma. 2006 data requested J Orthop Trauma 2005;19:S26–8. from author
McQueen MM, Hajducka C, Court-Brown CM. A comparison of rhBMP-7 (ossigraft) and Unable to extract data autogenous graft for treatment of metaphyseal defects after osteotomy of the distal radius. (RCT)In: Orthopaedic Trauma Association; Salt Lake City, UT: 2003.
Mont MA, Ragland PS, Biggins B, Friedlaender G, Patel T, Cook S, et al. Use of bone Reviewmorphogenetic proteins for musculoskeletal applications. An overview. J Bone Joint Surg Am2004;86 Suppl 2:41–55.
Obert L, Deschaseaux F, Garbuio P. Critical analysis and efficacy of BMPs in long bones non-union. ReviewInjury 2005;36:38–42.
Poynton AR, Lane JM. Safety profile for the clinical use of bone morphogenetic proteins in the Reviewspine. Spine 2002;27(16 Suppl 1):S40–8.
Resnick DK, Choudhri TF, Dailey AT, Groff MW, Khoo L, Matz PG, et al. Guidelines for the Reviewperformance of fusion procedures for degenerative disease of the lumbar spine. Part 16: bone graft extenders and substitutes. J Neurosurg Spine 2005;2:733–6.
Samartzis D, Khanna N, Shen FH, An HS. Update on bone morphogenetic proteins and their Reviewapplication in spine surgery. J Am Coll Surg 2005;200:236–48.
Sandhu HS, Anderson DG, Andersson GBJ, Boden SD, Damien C, Ebara S, et al. Summary Commentstatement: Alternative delivery by gene therapy and cost justification of bone morphogenetic proteins for spine fusion. Spine 2002;27(16 Suppl):S86.
Sandhu H. Spinal fusion using bone morphogenetic proteins. Orthopedics 2004;27:717–18. Review
Sasso RC, LeHuec JC, Shaffrey C. Iliac crest bone graft donor site pain after anterior lumbar Contacted author about interbody fusion – a prospective patient satisfaction outcome assessment. J Spinal Disord Tech unreferenced studies2005;18:S77–81.
Seeherman H, Li R, Li XJ, Wozney J. Injectable rhBMP-2/CPM paste for closed fracture and Animal studyminimally invasive orthopaedic repairs. J Musculoskel Neuronal Interact 2003;3:317–19.
continued

Health Technology Assessment 2007; Vol. 11: No. 30
93
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Paper Reason for exclusion
Starr AJ. Recombinant human bone morphogenetic protein-2 for treatment of open tibial Commentfractures. J Bone Joint Surg Am 2003;85:2049; author replies, 2049–50.
Szpalski M, Gunzburg R. Recombinant human bone morphogenetic protein-2: a novel Reviewosteoinductive alternative to autogenous bone graft? Acta Orthop Belg 2005;71:133–48.
Termaat MF, Den Boer FC, Bakker FC, Patka P, Haarman HJTM. Bone morphogenetic proteins. ReviewDevelopment and clinical efficacy in the treatment of fractures and bone defects. J Bone Joint Surg Am 2005;87:1367–78.
Termaat MF, Den Boer FC, Barker FC, Patka P, Haarman H. Current concepts review bone Reviewmorphogenetic proteins development and clinical efficacy in the treatment of fractures and bone defects. J Bone Joint Surg Am 2005;87:1367–78.
Vaccaro AR, Chiba K, Heller JG, Patel TC, Thalgott JS, Truumees E, et al. Bone grafting Reviewalternatives in spinal surgery. Spine J 2002;2:206–15.
Valentin-Opran A, Wozney J, Csimma C, Lilly L, Riedel GE. Clinical evaluation of recombinant Reviewhuman bone morphogenetic protein-2. Clin Orthop Relat Res 2002:110–20.
Yin S. Use of OP-1 (BMP-7) in human tibial nonunions. Bone 1999;24:423. Not in journalreferenced

Health Technology Assessment 2007; Vol. 11: No. 30
95
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 6
RCT fracture study characteristics
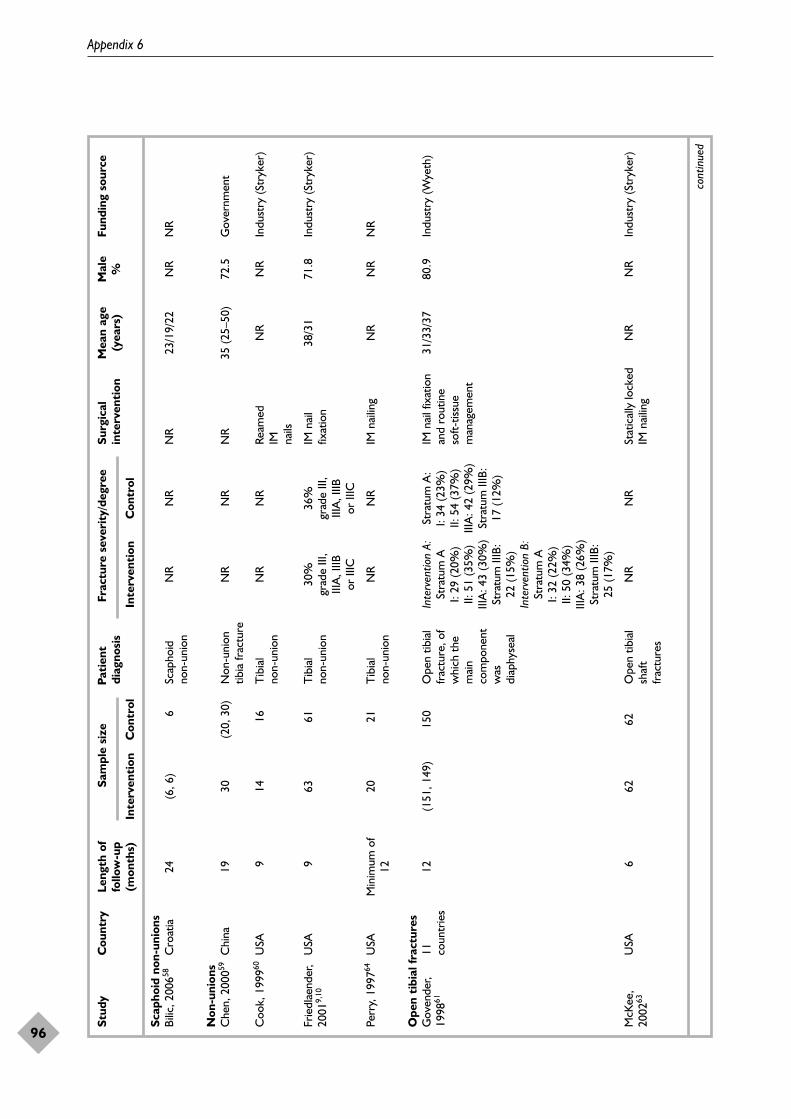
Appendix 6
96
Stud
yC
ount
ryLe
ngth
of
Sam
ple
size
Pati
ent
Frac
ture
sev
erit
y/de
gree
Surg
ical
M
ean
age
Mal
eFu
ndin
g so
urce
follo
w-u
pdi
agno
sis
inte
rven
tion
(yea
rs)
%(m
onth
s)In
terv
enti
onC
ontr
olIn
terv
enti
onC
ontr
ol
Scap
hoid
non
-uni
ons
Bilic
, 200
658C
roat
ia24
(6, 6
)6
Scap
hoid
N
RN
RN
R23
/19/
22N
RN
Rno
n-un
ion
Non
-uni
ons
Che
n, 2
00059
Chi
na19
30(2
0, 3
0)N
on-u
nion
NR
NR
NR
35 (2
5–50
)72
.5G
over
nmen
ttib
ia fr
actu
re
Coo
k, 1
99960
USA
914
16T
ibia
l N
RN
RRe
amed
N
RN
RIn
dust
ry (S
tryk
er)
non-
unio
nIM na
ils
Frie
dlae
nder
,U
SA9
6361
Tib
ial
30%
36
%
IM n
ail
38/3
171
.8In
dust
ry (S
tryk
er)
2001
9,10
non-
unio
ngr
ade
III,
grad
e III
, fix
atio
nIII
A, I
IIB
IIIA
, IIIB
or
IIIC
or II
IC
Perr
y, 1
99764
USA
Min
imum
of
2021
Tib
ial
NR
NR
IM n
ailin
gN
RN
RN
R12
non-
unio
n
Ope
n ti
bial
frac
ture
sG
oven
der,
11
12(1
51, 1
49)
150
Ope
n tib
ial
Inte
rven
tion
A:
Stra
tum
A:
IM n
ail f
ixat
ion
31/3
3/37
80.9
Indu
stry
(Wye
th)
1998
61co
untr
ies
frac
ture
, of
Stra
tum
AI:
34 (2
3%)
and
rout
ine
whi
ch t
he
I: 29
(20%
)II:
54
(37%
)so
ft-tis
sue
mai
n II:
51
(35%
)III
A: 4
2 (2
9%)
man
agem
ent
com
pone
nt
IIIA
: 43
(30%
)St
ratu
m II
IB:
was
St
ratu
m II
IB:
17 (1
2%)
diap
hyse
al22
(15%
)In
terv
entio
n B:
Stra
tum
AI:
32 (2
2%)
II: 5
0 (3
4%)
IIIA
: 38
(26%
)St
ratu
m II
IB:
25 (1
7%)
McK
ee,
USA
662
62O
pen
tibia
l N
RN
RSt
atic
ally
lock
ed
NR
NR
Indu
stry
(Str
yker
)20
0263
shaf
t IM
nai
ling
frac
ture
s
cont
inue
d
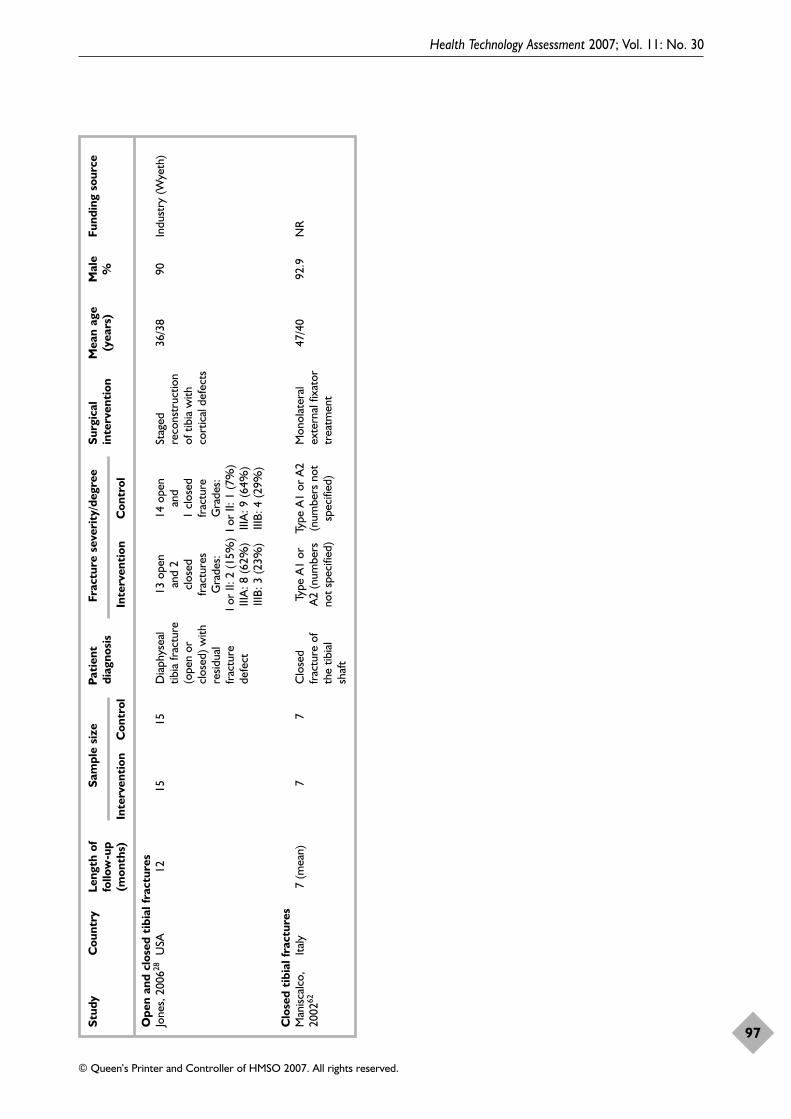
Health Technology Assessment 2007; Vol. 11: No. 30
97
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Stud
yC
ount
ryLe
ngth
of
Sam
ple
size
Pati
ent
Frac
ture
sev
erit
y/de
gree
Surg
ical
M
ean
age
Mal
eFu
ndin
g so
urce
follo
w-u
pdi
agno
sis
inte
rven
tion
(yea
rs)
%(m
onth
s)In
terv
enti
onC
ontr
olIn
terv
enti
onC
ontr
ol
Ope
n an
d cl
osed
tib
ial f
ract
ures
Jone
s, 2
00628
USA
1215
15D
iaph
ysea
l 13
ope
n 14
ope
n St
aged
36
/38
90In
dust
ry (W
yeth
)tib
ia fr
actu
re
and
2 an
d re
cons
truc
tion
(ope
n or
cl
osed
1 cl
osed
of
tib
ia w
ith
clos
ed) w
ith
frac
ture
sfr
actu
reco
rtic
al d
efec
tsre
sidua
l G
rade
s:G
rade
s:fr
actu
re
I or
II: 2
(15%
)I o
r II:
1 (7
%)
defe
ctIII
A: 8
(62%
)III
A: 9
(64%
)III
B: 3
(23%
)III
B: 4
(29%
)
Clo
sed
tibi
al fr
actu
res
Man
iscal
co,
Italy
7 (m
ean)
7 7
Clo
sed
Type
A1
or
Type
A1
or A
2M
onol
ater
al
47/4
092
.9N
R20
0262
frac
ture
of
A2
(num
bers
(n
umbe
rs n
ot
exte
rnal
fixa
tor
the
tibia
l no
t sp
ecifi
ed)
spec
ified
)tr
eatm
ent
shaf
t

Health Technology Assessment 2007; Vol. 11: No. 30
99
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 7
RCT fracture quality assessment
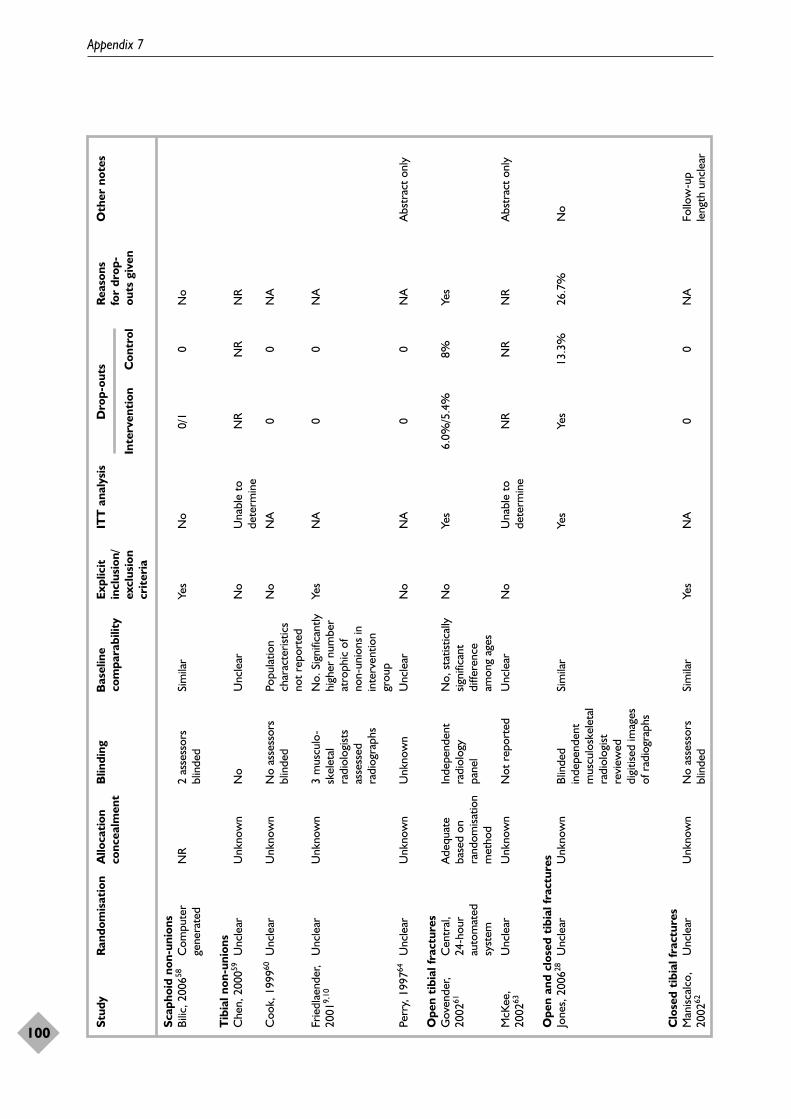
Appendix 7
100
Stud
yR
ando
mis
atio
nA
lloca
tion
B
lindi
ngB
asel
ine
Expl
icit
IT
T a
naly
sis
Dro
p-ou
tsR
easo
ns
Oth
er n
otes
conc
ealm
ent
com
para
bilit
yin
clus
ion/
for
drop
-ex
clus
ion
Inte
rven
tion
Con
trol
outs
giv
encr
iter
ia
Scap
hoid
non
-uni
ons
Bilic
, 200
658C
ompu
ter
NR
2 as
sess
ors
Sim
ilar
Yes
No
0/1
0N
oge
nera
ted
blin
ded
Tib
ial n
on-u
nion
sC
hen,
200
059U
ncle
arU
nkno
wn
No
Unc
lear
No
Una
ble
to
NR
NR
NR
dete
rmin
e
Coo
k, 1
99960
Unc
lear
Unk
now
nN
o as
sess
ors
Popu
latio
n N
oN
A0
0N
Abl
inde
dch
arac
teris
tics
not
repo
rted
Frie
dlae
nder
,U
ncle
arU
nkno
wn
3 m
uscu
lo-
No.
Sig
nific
antly
Ye
sN
A0
0N
A20
019,
10sk
elet
al
high
er n
umbe
r ra
diol
ogist
s at
roph
ic o
f as
sess
ed
non-
unio
ns in
ra
diog
raph
sin
terv
entio
n gr
oup
Perr
y, 1
99764
Unc
lear
Unk
now
nU
nkno
wn
Unc
lear
No
NA
00
NA
Abs
trac
t on
ly
Ope
n ti
bial
frac
ture
sG
oven
der,
Cen
tral
, A
dequ
ate
Inde
pend
ent
No,
sta
tistic
ally
N
oYe
s6.
0%/5
.4%
8%Ye
s20
0261
24-h
our
base
d on
ra
diol
ogy
signi
fican
t au
tom
ated
ra
ndom
isatio
n pa
nel
diffe
renc
e sy
stem
met
hod
amon
g ag
es
McK
ee,
Unc
lear
Unk
now
nN
ot r
epor
ted
Unc
lear
No
Una
ble
to
NR
NR
NR
Abs
trac
t on
ly20
0263
dete
rmin
e
Ope
n an
d cl
osed
tib
ial f
ract
ures
Jone
s, 2
00628
Unc
lear
Unk
now
nBl
inde
d Si
mila
rYe
sYe
s13
.3%
26.7
%N
oin
depe
nden
t m
uscu
losk
elet
al
radi
olog
ist
revi
ewed
di
gitis
ed im
ages
of
rad
iogr
aphs
Clo
sed
tibi
al fr
actu
res
Man
iscal
co,
Unc
lear
Unk
now
nN
o as
sess
ors
Sim
ilar
Yes
NA
00
NA
Follo
w-u
p 20
0262
blin
ded
leng
th u
ncle
ar
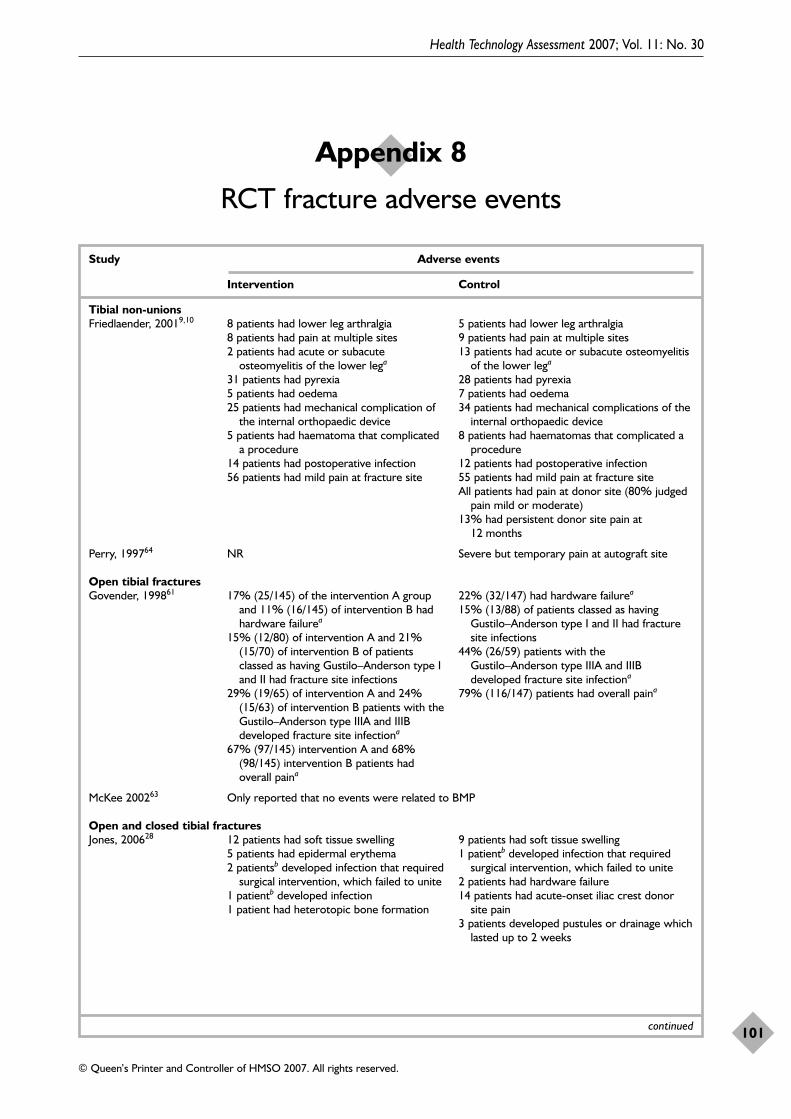
Health Technology Assessment 2007; Vol. 11: No. 30
101
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 8
RCT fracture adverse events
Study Adverse events
Intervention Control
Tibial non-unionsFriedlaender, 20019,10 8 patients had lower leg arthralgia 5 patients had lower leg arthralgia
8 patients had pain at multiple sites 9 patients had pain at multiple sites2 patients had acute or subacute 13 patients had acute or subacute osteomyelitis
osteomyelitis of the lower lega of the lower lega
31 patients had pyrexia 28 patients had pyrexia5 patients had oedema 7 patients had oedema25 patients had mechanical complication of 34 patients had mechanical complications of the
the internal orthopaedic device internal orthopaedic device5 patients had haematoma that complicated 8 patients had haematomas that complicated a
a procedure procedure14 patients had postoperative infection 12 patients had postoperative infection56 patients had mild pain at fracture site 55 patients had mild pain at fracture site
All patients had pain at donor site (80% judgedpain mild or moderate)
13% had persistent donor site pain at 12 months
Perry, 199764 NR Severe but temporary pain at autograft site
Open tibial fracturesGovender, 199861 17% (25/145) of the intervention A group 22% (32/147) had hardware failurea
and 11% (16/145) of intervention B had 15% (13/88) of patients classed as having hardware failurea Gustilo–Anderson type I and II had fracture
15% (12/80) of intervention A and 21% site infections(15/70) of intervention B of patients 44% (26/59) patients with the classed as having Gustilo–Anderson type I Gustilo–Anderson type IIIA and IIIB and II had fracture site infections developed fracture site infectiona
29% (19/65) of intervention A and 24% 79% (116/147) patients had overall paina
(15/63) of intervention B patients with the Gustilo–Anderson type IIIA and IIIB developed fracture site infectiona
67% (97/145) intervention A and 68% (98/145) intervention B patients had overall paina
McKee 200263 Only reported that no events were related to BMP
Open and closed tibial fracturesJones, 200628 12 patients had soft tissue swelling 9 patients had soft tissue swelling
5 patients had epidermal erythema 1 patientb developed infection that required 2 patientsb developed infection that required surgical intervention, which failed to unite
surgical intervention, which failed to unite 2 patients had hardware failure1 patientb developed infection 14 patients had acute-onset iliac crest donor 1 patient had heterotopic bone formation site pain
3 patients developed pustules or drainage which lasted up to 2 weeks
continued
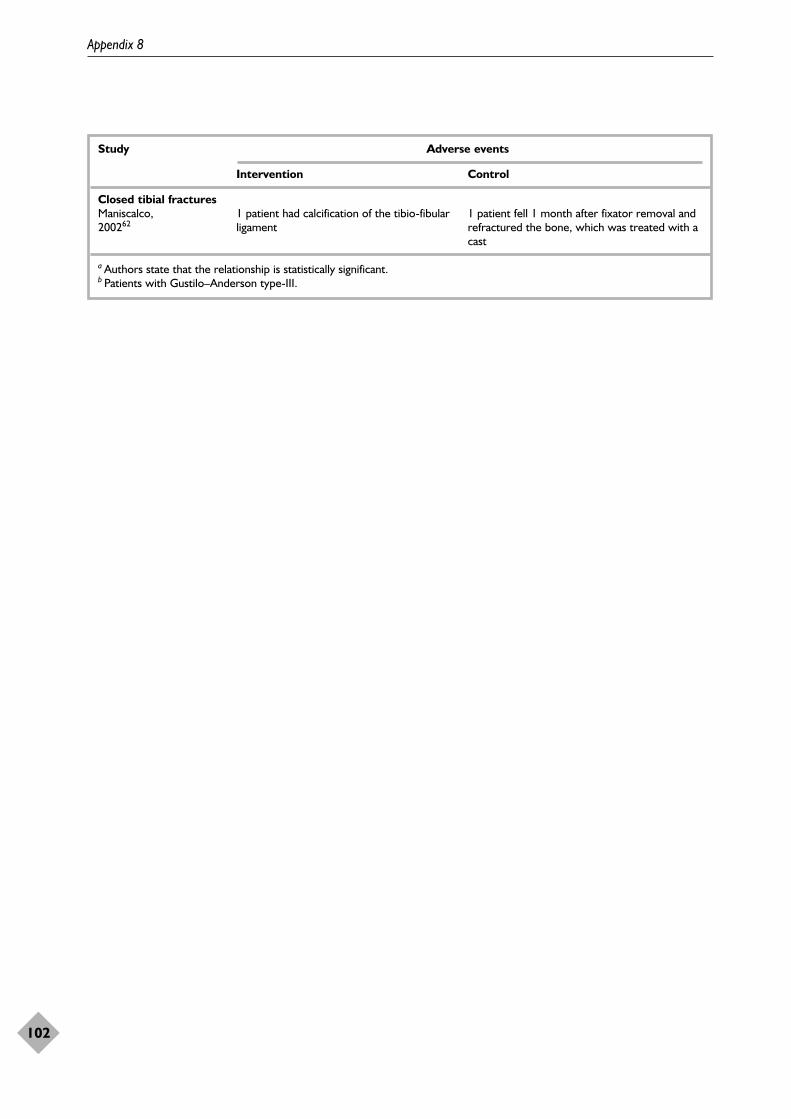
Appendix 8
102
Study Adverse events
Intervention Control
Closed tibial fracturesManiscalco, 1 patient had calcification of the tibio-fibular 1 patient fell 1 month after fixator removal and 200262 ligament refractured the bone, which was treated with a
cast
a Authors state that the relationship is statistically significant.b Patients with Gustilo–Anderson type-III.
Number and characteristics ofincluded studiesOne case report, by Jones and colleagues106 and14 case series, by Bai and colleagues,107 Benke andGorecki,108 Bong and colleagues,109 Delloye andcolleagues,110 Dimitriou and colleagues,111
Johnson and Urist (1998),112 Johnson and Urist(2000),113 Johnson and colleagues (1988),123
Johnson and colleagues (1988),114 Johnson andcolleagues (1990)115,116 Johnson and colleagues(1992),117 Kujala and colleagues (2002),118 Kujalaand colleagues (2004)119 Riedel and Valentin-Opran,120 were included. In addition threeabstracts from conference proceedings, by Kukloand colleagues,121 McKee and colleagues,52 andSchwartz and Hicks122 were also included.
Appendix 10 shows the main characteristics of theincluded studies. Thirteen of the studies wereconducted in the USA. The remaining studieswere conducted in England,111 Germany,108
Finland,118 China,107 and Belgium and theUSA.110 Of the studies that reported their fundingsource, three52,109,120 were sponsored by industryand two stated that they received no benefits fromany related commercial party.106,111 The remaining13 studies did not specify their funding source.
Four of the studies included patients with non-unions of the femur.112–114,122 The remainingstudies included non-unions of the tibia (n = 4),scaphoid (n = 2), humerus (n = 1), ulnar (n = 1) anda variety of different non-unions (n = 8). Eleven ofthe included studies performed some type ofinternal fixation. Another study121 performed bothexternal and internal fixation. Two studiesperformed one-stage lengthening112,113 and fivestudies did not clearly state their surgical methods.
The study sizes ranged from one patient to 653patients. The follow-up lengths ranged from3 months to six years and the mean ages rangedfrom 16 to 56.6 years.
QualityTable 37 shows the quality assessment of theincluded studies. Fifteen of the studies clearly
described their population. Nine of the studieshad similar patient populations. Only one studystated that an independent assessor was used foroutcome assessment. The Dimitriou study111 gavethe number and reasons for patients lost to follow-up. Two studies108,113 gave only the numbers ofpatients lost and two109,121 did not report onwhether any patients were lost to follow-up. Theremaining 11 studies did not lose any patients tofollow-up.
InterventionsAppendix 11 shows the interventions used in thenon-union studies.
Two studies108,109 used BMP-7 on collagengranules at a dose of 3.5 mg. The Dimitrioustudy111 also used BMP-7 at a dose of 3.5 mg butdid not report the carrier used. Two studies52,124
used rhBMP-7, but did not report the carrier ordose. Two studies110,120 used rhBMP-2 on acollagen sponge at doses ranging from 3.4 to12 mg. One study121 used rhBMP-2 but did notspecify the carrier or concentration used. Twostudies118,119 used bovine BMP on a collagensponge with doses ranging from 2 to 5 mg/cm3.Another study,107 used bovine BMP on a plaster ofParis carrier with a concentration range of50–200 mg. The remaining seven studies usedhuman BMP (hBMP), a BMP composite thoughtto contain mostly BMP-2 and BMP-7, at dosesbetween 50 and 100 mg, where reported. Thecarrier most used for hBMP was non-collagenousproteins (n = 5). Also used as a carrier wereallogenic, autolysed antigen-free cortical bone(n = 1) and gelatine capsules (n = 1). The casestudy, which used 50 mg of hBMP, also fixed thescaphoid with a K-wire and the patient wasimmobilised in a cast for 12 weeks.
In 12 of the studies, an additional bone graft orbone substitute was used in all or part of thepatient population. This included allograft bone,autograft bone or demineralised bone matrix(DBM). In the Delloye study,110 patients alsoreceived adjuvant chemotherapy and/or radiation.Two studies118,119 included biocoral frames in theirinterventions.
Health Technology Assessment 2007; Vol. 11: No. 30
103
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 9
Fracture case series and case report findings
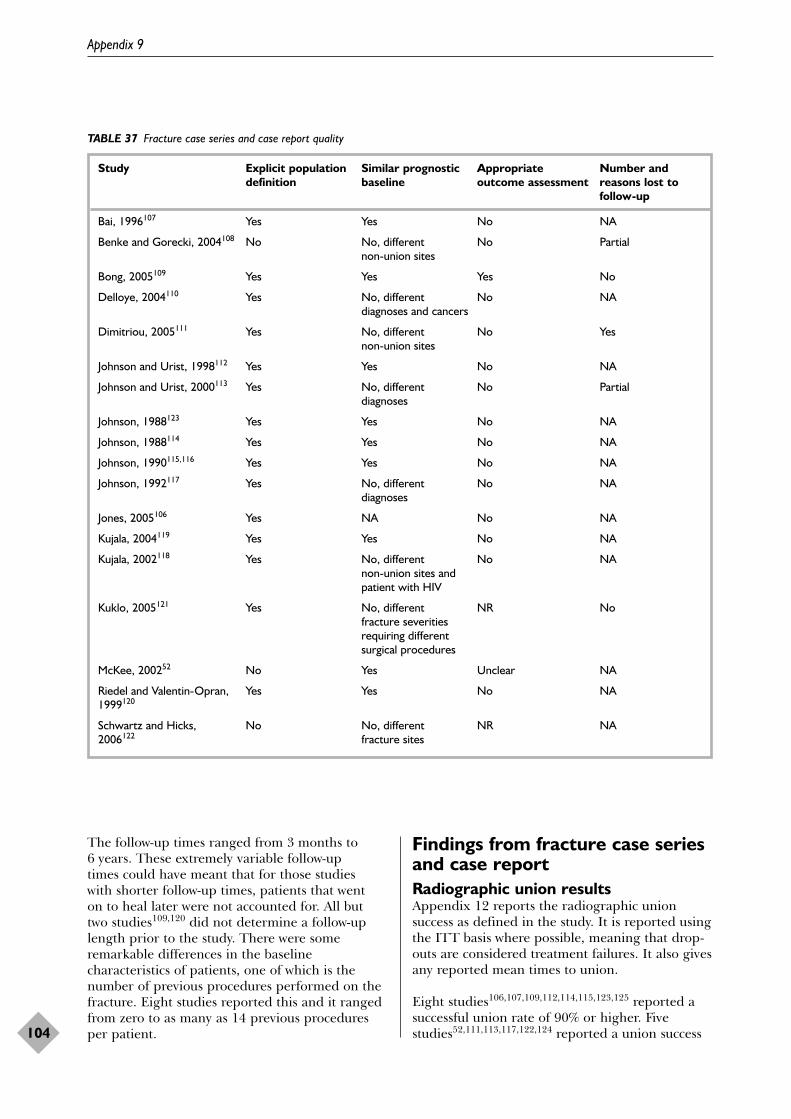
The follow-up times ranged from 3 months to6 years. These extremely variable follow-up times could have meant that for those studies with shorter follow-up times, patients that went on to heal later were not accounted for. All but two studies109,120 did not determine a follow-uplength prior to the study. There were someremarkable differences in the baselinecharacteristics of patients, one of which is thenumber of previous procedures performed on thefracture. Eight studies reported this and it rangedfrom zero to as many as 14 previous proceduresper patient.
Findings from fracture case seriesand case reportRadiographic union resultsAppendix 12 reports the radiographic unionsuccess as defined in the study. It is reported usingthe ITT basis where possible, meaning that drop-outs are considered treatment failures. It also givesany reported mean times to union.
Eight studies106,107,109,112,114,115,123,125 reported asuccessful union rate of 90% or higher. Fivestudies52,111,113,117,122,124 reported a union success
Appendix 9
104
TABLE 37 Fracture case series and case report quality
Study Explicit population Similar prognostic Appropriate Number and definition baseline outcome assessment reasons lost to
follow-up
Bai, 1996107 Yes Yes No NA
Benke and Gorecki, 2004108 No No, different No Partialnon-union sites
Bong, 2005109 Yes Yes Yes No
Delloye, 2004110 Yes No, different No NAdiagnoses and cancers
Dimitriou, 2005111 Yes No, different No Yesnon-union sites
Johnson and Urist, 1998112 Yes Yes No NA
Johnson and Urist, 2000113 Yes No, different No Partialdiagnoses
Johnson, 1988123 Yes Yes No NA
Johnson, 1988114 Yes Yes No NA
Johnson, 1990115,116 Yes Yes No NA
Johnson, 1992117 Yes No, different No NAdiagnoses
Jones, 2005106 Yes NA No NA
Kujala, 2004119 Yes Yes No NA
Kujala, 2002118 Yes No, different No NAnon-union sites and patient with HIV
Kuklo, 2005121 Yes No, different NR Nofracture severities requiring different surgical procedures
McKee, 200252 No Yes Unclear NA
Riedel and Valentin-Opran, Yes Yes No NA1999120
Schwartz and Hicks, No No, different NR NA2006122 fracture sites
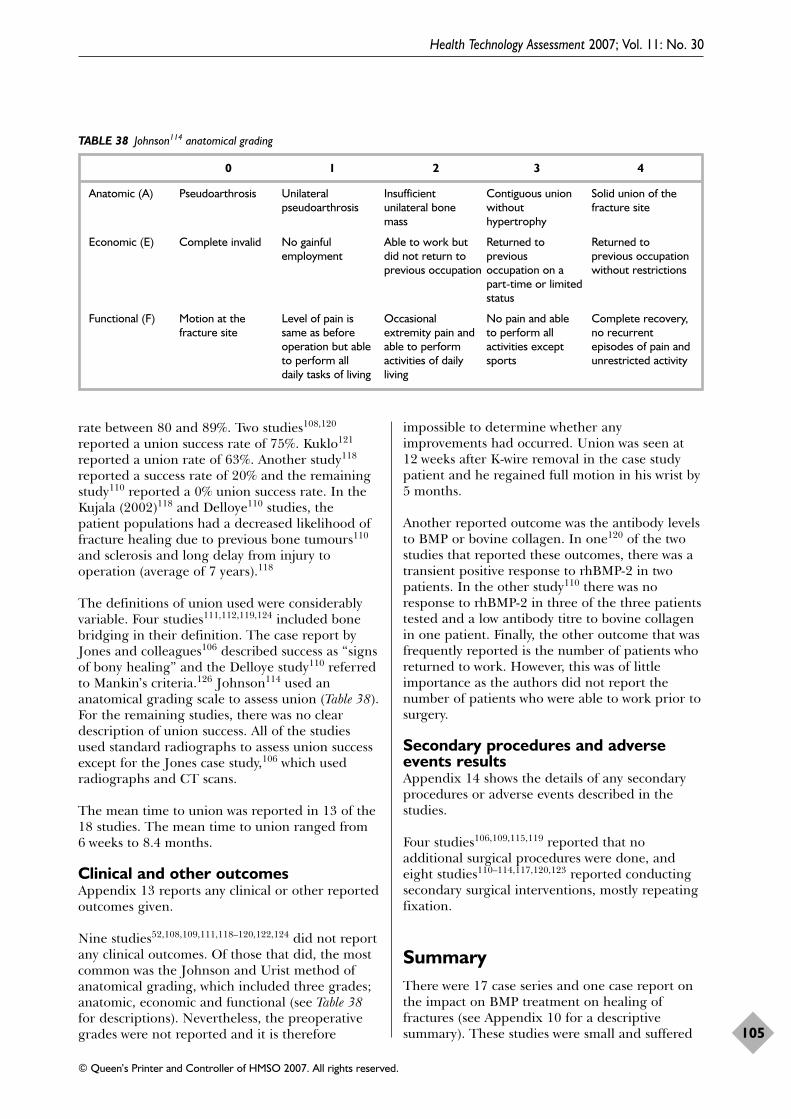
rate between 80 and 89%. Two studies108,120
reported a union success rate of 75%. Kuklo121
reported a union rate of 63%. Another study118
reported a success rate of 20% and the remainingstudy110 reported a 0% union success rate. In theKujala (2002)118 and Delloye110 studies, thepatient populations had a decreased likelihood offracture healing due to previous bone tumours110
and sclerosis and long delay from injury tooperation (average of 7 years).118
The definitions of union used were considerablyvariable. Four studies111,112,119,124 included bonebridging in their definition. The case report byJones and colleagues106 described success as “signsof bony healing” and the Delloye study110 referredto Mankin’s criteria.126 Johnson114 used ananatomical grading scale to assess union (Table 38).For the remaining studies, there was no cleardescription of union success. All of the studiesused standard radiographs to assess union successexcept for the Jones case study,106 which usedradiographs and CT scans.
The mean time to union was reported in 13 of the18 studies. The mean time to union ranged from6 weeks to 8.4 months.
Clinical and other outcomesAppendix 13 reports any clinical or other reportedoutcomes given.
Nine studies52,108,109,111,118–120,122,124 did not reportany clinical outcomes. Of those that did, the mostcommon was the Johnson and Urist method ofanatomical grading, which included three grades;anatomic, economic and functional (see Table 38for descriptions). Nevertheless, the preoperativegrades were not reported and it is therefore
impossible to determine whether anyimprovements had occurred. Union was seen at12 weeks after K-wire removal in the case studypatient and he regained full motion in his wrist by5 months.
Another reported outcome was the antibody levelsto BMP or bovine collagen. In one120 of the twostudies that reported these outcomes, there was atransient positive response to rhBMP-2 in twopatients. In the other study110 there was noresponse to rhBMP-2 in three of the three patientstested and a low antibody titre to bovine collagenin one patient. Finally, the other outcome that wasfrequently reported is the number of patients whoreturned to work. However, this was of littleimportance as the authors did not report thenumber of patients who were able to work prior tosurgery.
Secondary procedures and adverseevents resultsAppendix 14 shows the details of any secondaryprocedures or adverse events described in thestudies.
Four studies106,109,115,119 reported that noadditional surgical procedures were done, andeight studies110–114,117,120,123 reported conductingsecondary surgical interventions, mostly repeatingfixation.
SummaryThere were 17 case series and one case report onthe impact on BMP treatment on healing offractures (see Appendix 10 for a descriptivesummary). These studies were small and suffered
Health Technology Assessment 2007; Vol. 11: No. 30
105
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
TABLE 38 Johnson114 anatomical grading
0 1 2 3 4
Anatomic (A) Pseudoarthrosis Unilateral Insufficient Contiguous union Solid union of the pseudoarthrosis unilateral bone without fracture site
mass hypertrophy
Economic (E) Complete invalid No gainful Able to work but Returned to Returned to employment did not return to previous previous occupation
previous occupation occupation on a without restrictionspart-time or limited status
Functional (F) Motion at the Level of pain is Occasional No pain and able Complete recovery, fracture site same as before extremity pain and to perform all no recurrent
operation but able able to perform activities except episodes of pain and to perform all activities of daily sports unrestricted activitydaily tasks of living living

from several limitations in their designs. Ofparticular concern is the lack of a standarddefinition of the primary outcome andconsiderably different diagnoses. No concrete
evidence can be obtained from these studies onthe effectiveness of BMP treatment as manypatients had extreme co-morbidities, highlyvariable diagnoses and lack of a valid control.
Appendix 9
106

Health Technology Assessment 2007; Vol. 11: No. 30
107
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 10
Fracture case series and case report study characteristics
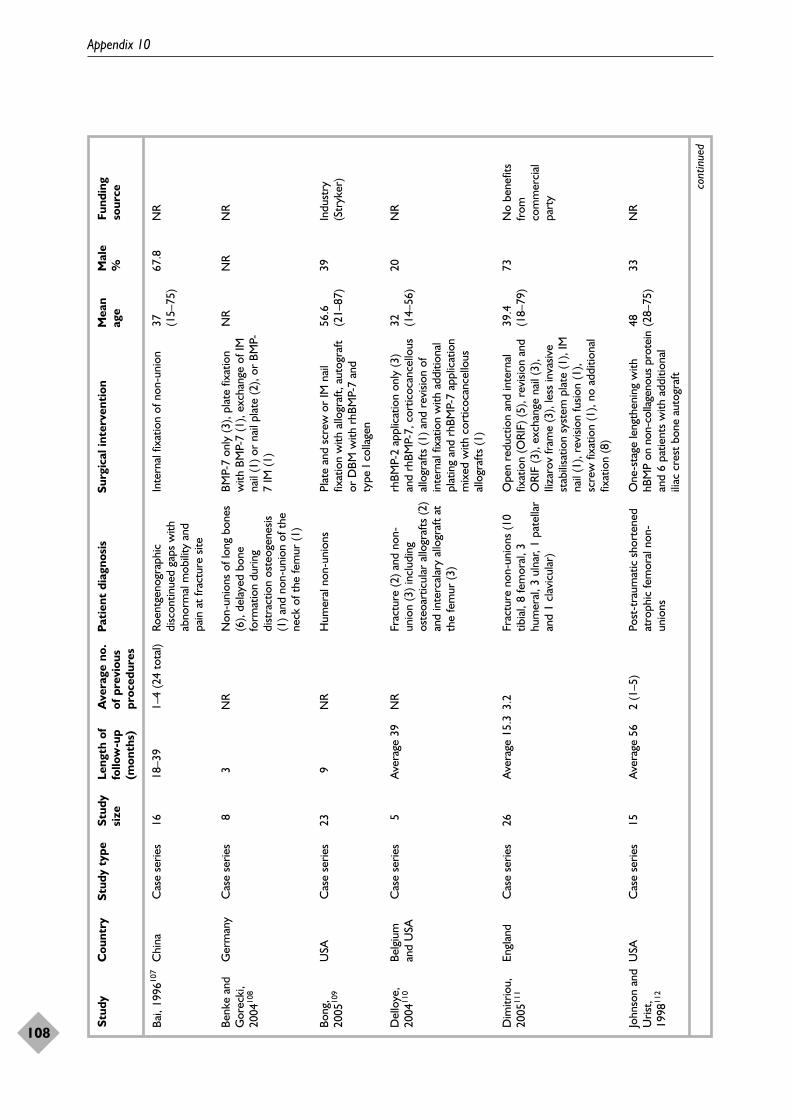
Appendix 10
108
Stud
yC
ount
rySt
udy
type
Stud
y Le
ngth
of
Ave
rage
no.
Pa
tien
t di
agno
sis
Surg
ical
inte
rven
tion
Mea
n M
ale
Fund
ing
size
follo
w-u
p of
pre
viou
s ag
e%
sour
ce(m
onth
s)pr
oced
ures
Bai,
1996
107
Chi
naC
ase
serie
s16
18–3
91–
4 (2
4 to
tal)
Roen
tgen
ogra
phic
disc
ontin
ued
gaps
with
abno
rmal
mob
ility
and
pain
at
frac
ture
site
Inte
rnal
fixa
tion
of n
on-u
nion
37 (15–
75)
67.8
NR
Benk
e an
dG
orec
ki,
2004
108
Ger
man
yC
ase
serie
s8
3N
RN
on-u
nion
s of
long
bon
es(6
), de
laye
d bo
nefo
rmat
ion
durin
gdi
stra
ctio
n os
teog
enes
is(1
) and
non
-uni
on o
f the
neck
of t
he fe
mur
(1)
BMP-
7 on
ly (3
), pl
ate
fixat
ion
with
BM
P-7
(1),
exch
ange
of I
Mna
il (1
) or
nail
plat
e (2
), or
BM
P-7
IM (1
)
NR
NR
NR
Bong
,20
0510
9U
SAC
ase
serie
s23
9N
RH
umer
al n
on-u
nion
sPl
ate
and
scre
w o
r IM
nai
lfix
atio
n w
ith a
llogr
aft,
auto
graf
tor
DBM
with
rhB
MP-
7 an
d ty
pe I
colla
gen
56.6
(21–
87)
39In
dust
ry(S
tryk
er)
Del
loye
,20
0411
0Be
lgiu
man
d U
SAC
ase
serie
s5
Ave
rage
39
NR
Frac
ture
(2) a
nd n
on-
unio
n (3
) inc
ludi
ngos
teoa
rtic
ular
allo
graf
ts (2
)an
d in
terc
alar
y al
logr
aft
atth
e fe
mur
(3)
rhBM
P-2
appl
icat
ion
only
(3)
and
rhBM
P-7,
cor
ticoc
ance
llous
allo
graf
ts (1
) and
rev
ision
of
inte
rnal
fixa
tion
with
add
ition
alpl
atin
g an
d rh
BMP-
7 ap
plic
atio
nm
ixed
with
cor
ticoc
ance
llous
allo
graf
ts (1
)
32 (14–
56)
20N
R
Dim
itrio
u,20
0511
1En
glan
dC
ase
serie
s26
Ave
rage
15.
33.
2Fr
actu
re n
on-u
nion
s (1
0tib
ial,
8 fe
mor
al, 3
hum
eral
, 3 u
lnar
, 1 p
atel
lar
and
1 cl
avic
ular
)
Ope
n re
duct
ion
and
inte
rnal
fixat
ion
(ORI
F) (5
), re
visio
n an
dO
RIF
(3),
exch
ange
nai
l (3)
,Ili
zaro
v fr
ame
(3),
less
inva
sive
stab
ilisa
tion
syst
em p
late
(1),
IMna
il (1
), re
visio
n fu
sion
(1),
scre
w fi
xatio
n (1
), no
add
ition
alfix
atio
n (8
)
39.4
(1
8–79
)73
No
bene
fits
from
com
mer
cial
part
y
John
son
and
Uris
t,19
9811
2
USA
Cas
e se
ries
15A
vera
ge 5
62
(1–5
)Po
st-t
raum
atic
sho
rten
edat
roph
ic fe
mor
al n
on-
unio
ns
One
-sta
ge le
ngth
enin
g w
ithhB
MP
on n
on-c
olla
geno
us p
rote
inan
d 6
patie
nts
with
add
ition
alili
ac c
rest
bon
e au
togr
aft
48 (28–
75)
33N
R
cont
inue
d
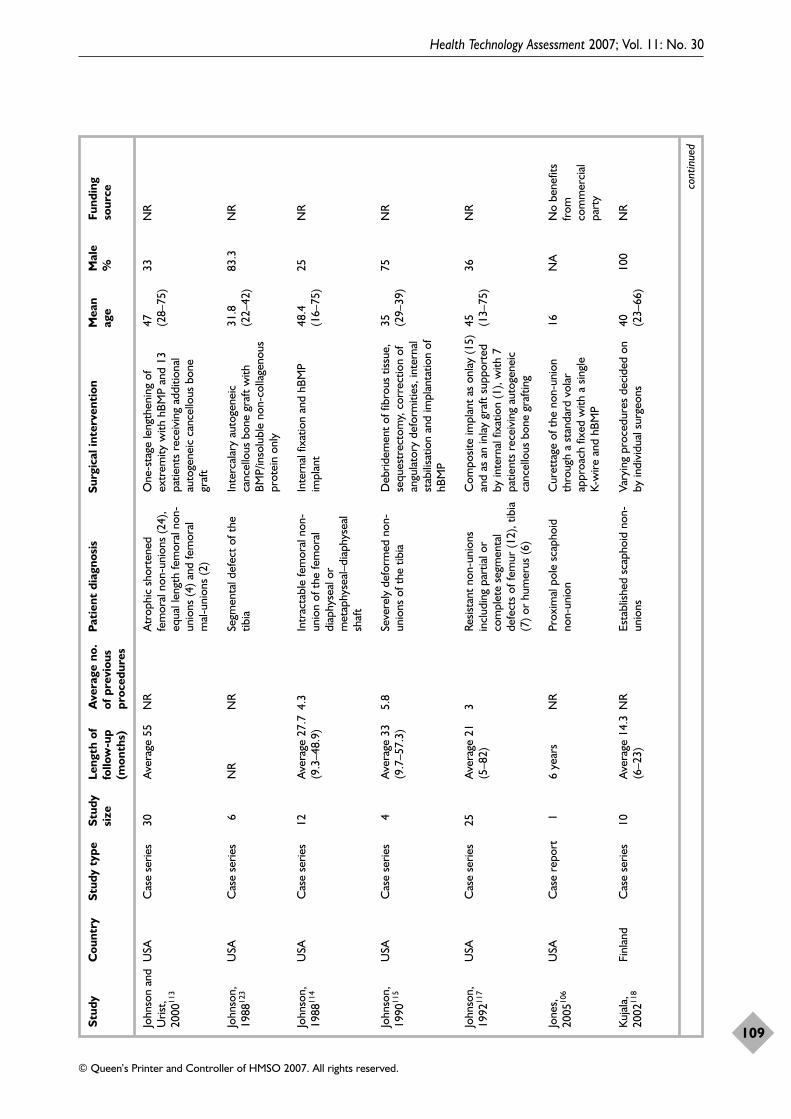
Health Technology Assessment 2007; Vol. 11: No. 30
109
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Stud
yC
ount
rySt
udy
type
Stud
y Le
ngth
of
Ave
rage
no.
Pa
tien
t di
agno
sis
Surg
ical
inte
rven
tion
Mea
n M
ale
Fund
ing
size
follo
w-u
p of
pre
viou
s ag
e%
sour
ce(m
onth
s)pr
oced
ures
John
son
and
Uris
t,20
0011
3
USA
Cas
e se
ries
30A
vera
ge 5
5N
RA
trop
hic
shor
tene
dfe
mor
al n
on-u
nion
s (2
4),
equa
l len
gth
fem
oral
non
-un
ions
(4) a
nd fe
mor
alm
al-u
nion
s (2
)
One
-sta
ge le
ngth
enin
g of
extr
emity
with
hBM
P an
d 13
patie
nts
rece
ivin
g ad
ditio
nal
auto
gene
ic c
ance
llous
bon
egr
aft
47 (28–
75)
33N
R
John
son,
1988
123
USA
Cas
e se
ries
6N
RN
RSe
gmen
tal d
efec
t of
the
tibia
Inte
rcal
ary
auto
gene
icca
ncel
lous
bon
e gr
aft
with
BMP/
inso
lubl
e no
n-co
llage
nous
prot
ein
only
31.8
(22–
42)
83.3
NR
John
son,
1988
114
USA
Cas
e se
ries
12A
vera
ge 2
7.7
(9.3
–48.
9)4.
3In
trac
tabl
e fe
mor
al n
on-
unio
n of
the
fem
oral
diap
hyse
al o
rm
etap
hyse
al–d
iaph
ysea
lsh
aft
Inte
rnal
fixa
tion
and
hBM
Pim
plan
t48
.4(1
6–75
)25
NR
John
son,
1990
115
USA
Cas
e se
ries
4A
vera
ge 3
3(9
.7–5
7.3)
5.8
Seve
rely
def
orm
ed n
on-
unio
ns o
f the
tib
iaD
ebrid
emen
t of
fibr
ous
tissu
e,se
ques
trec
tom
y, c
orre
ctio
n of
angu
lato
ry d
efor
miti
es, i
nter
nal
stab
ilisa
tion
and
impl
anta
tion
ofhB
MP
35
(29–
39)
75N
R
John
son,
1992
117
USA
Cas
e se
ries
25A
vera
ge 2
1(5
–82)
3Re
sista
nt n
on-u
nion
sin
clud
ing
part
ial o
rco
mpl
ete
segm
enta
lde
fect
s of
fem
ur (1
2), t
ibia
(7) o
r hu
mer
us (6
)
Com
posit
e im
plan
t as
onl
ay (1
5)an
d as
an
inla
y gr
aft
supp
orte
dby
inte
rnal
fixa
tion
(1),
with
7pa
tient
s re
ceiv
ing
auto
gene
icca
ncel
lous
bon
e gr
aftin
g
45 (13–
75)
36N
R
Jone
s,20
0510
6U
SAC
ase
repo
rt1
6 ye
ars
NR
Prox
imal
pol
e sc
apho
idno
n-un
ion
Cur
etta
ge o
f the
non
-uni
onth
roug
h a
stan
dard
vol
arap
proa
ch fi
xed
with
a s
ingl
e K-
wire
and
hBM
P
16N
AN
o be
nefit
sfr
omco
mm
erci
alpa
rty
Kuja
la,
2002
118
Finl
and
Cas
e se
ries
10A
vera
ge 1
4.3
(6–2
3)N
REs
tabl
ished
sca
phoi
d no
n-un
ions
Vary
ing
proc
edur
es d
ecid
ed o
nby
indi
vidu
al s
urge
ons
40 (23–
66)
100
NR
cont
inue
d
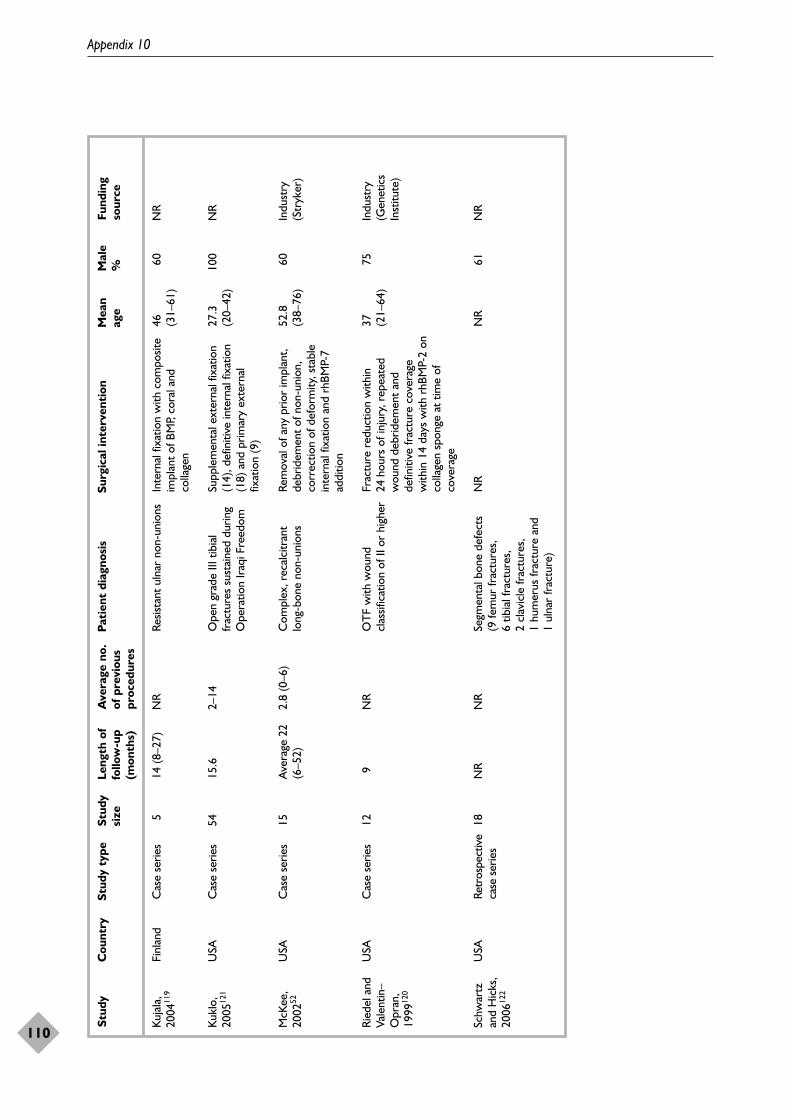
Appendix 10
110
Stud
yC
ount
rySt
udy
type
Stud
y Le
ngth
of
Ave
rage
no.
Pa
tien
t di
agno
sis
Surg
ical
inte
rven
tion
Mea
n M
ale
Fund
ing
size
follo
w-u
p of
pre
viou
s ag
e%
sour
ce(m
onth
s)pr
oced
ures
Kuja
la,
2004
119
Finl
and
Cas
e se
ries
514
(8–2
7)N
RRe
sista
nt u
lnar
non
-uni
ons
Inte
rnal
fixa
tion
with
com
posit
eim
plan
t of
BM
P, co
ral a
ndco
llage
n
46 (31–
61)
60N
R
Kukl
o,20
0512
1U
SAC
ase
serie
s54
15.6
2–14
Ope
n gr
ade
III t
ibia
lfr
actu
res
sust
aine
d du
ring
Ope
ratio
n Ir
aqi F
reed
om
Supp
lem
enta
l ext
erna
l fix
atio
n(1
4), d
efin
itive
inte
rnal
fixa
tion
(18)
and
prim
ary
exte
rnal
fixat
ion
(9)
27.3
(20–
42)
100
NR
McK
ee,
2002
52U
SAC
ase
serie
s15
Ave
rage
22
(6–5
2)2.
8 (0
–6)
Com
plex
, rec
alci
tran
tlo
ng-b
one
non-
unio
nsRe
mov
al o
f any
prio
r im
plan
t,de
brid
emen
t of
non
-uni
on,
corr
ectio
n of
def
orm
ity, s
tabl
ein
tern
al fi
xatio
n an
d rh
BMP-
7ad
ditio
n
52.8
(38–
76)
60In
dust
ry(S
tryk
er)
Ried
el a
ndVa
lent
in–
Opr
an,
1999
120
USA
Cas
e se
ries
129
NR
OT
F w
ith w
ound
clas
sific
atio
n of
II o
r hi
gher
Frac
ture
red
uctio
n w
ithin
24ho
urs
of in
jury
, rep
eate
dw
ound
deb
ridem
ent
and
defin
itive
frac
ture
cov
erag
ew
ithin
14
days
with
rhB
MP-
2 on
colla
gen
spon
ge a
t tim
e of
cove
rage
37 (21–
64)
75In
dust
ry(G
enet
ics
Inst
itute
)
Schw
artz
and
Hic
ks,
2006
122
USA
Retr
ospe
ctiv
eca
se s
erie
s18
NR
NR
Segm
enta
l bon
e de
fect
s (9
fem
ur fr
actu
res,
6
tibia
l fra
ctur
es,
2 cl
avic
le fr
actu
res,
1
hum
erus
frac
ture
and
1
ulna
r fr
actu
re)
NR
NR
61N
R

Health Technology Assessment 2007; Vol. 11: No. 30
111
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 11
Fracture case series and case report interventions

Appendix 11
112
Stud
yB
MP
use
dD
ose/
conc
entr
atio
nC
arri
erO
ther
How
use
d
cont
inue
d
Bai,
1996
107
bBM
P50
–200
mg
Plas
ter
of P
aris
6 ha
d ad
ditio
nal a
utog
enou
s bo
neC
ompo
site
appl
ied
dire
ctly
to
fill
inte
rfra
gmen
tary
def
ects
and
pac
k ar
ound
frac
ture
line
Benk
e an
dG
orec
ki 2
00410
8BM
P-7
3.5
mg
Col
lage
n sp
onge
NA
NR
Bong
, 200
5109
rhBM
P-7
3.5
mg
Col
lage
n gr
anul
esA
lso r
ecei
ved
allo
graf
t bo
ne, a
utog
raft
bone
or
DBM
NR
Del
loye
, 200
4110
rhBM
P-2
3.5–
12 m
gC
olla
gen
gran
ules
Four
pat
ient
s re
ceiv
ed a
djuv
ant
chem
othe
rapy
and
thre
e re
ceiv
ed r
adia
tion
ther
apy
Loca
l app
licat
ion
or im
plan
tatio
n
Dim
itrio
u, 2
00511
1rh
BMP-
73.
5 m
gN
R17
/25
patie
nts
rece
ived
BM
P an
d au
tolo
gous
bone
gra
ftN
R
John
son
and
Uris
t,19
9811
2hB
MP
(com
posit
eth
ough
t to
con
tain
mos
tly B
MP-
2 an
dBP
-7)
NR
NC
P6/
15 p
atie
nts
had
addi
tiona
l aut
ogen
eic
iliac
cre
stca
ncel
lous
bon
e gr
aft
Plac
ed a
long
med
ial s
ide
of in
terc
alar
yde
fect
John
son
and
Uris
t,20
0011
3hB
MP
100
mg
AA
A c
ortic
albo
ne13
/30
addi
tiona
l aut
ogen
eic
canc
ello
us b
one
graf
thB
MP/
AA
A im
plan
ts p
lace
d ac
ross
med
ial
inte
rcal
ary
fem
oral
sha
ft de
fect
John
son,
198
8123
hBM
P50
–100
mg
iNC
PA
ll pa
tient
s ha
d ili
ac c
rest
bon
e au
togr
aft
Plac
ed u
nder
neat
h th
e m
edia
l per
iost
eal
sleev
e of
the
def
ect
John
son,
198
8114
hBM
P50
–100
mg
iNC
P4/
12 p
atie
nts
rece
ived
aut
ogen
eic
canc
ello
usbo
ne a
utog
raft.
4 p
atie
nts
rece
ived
allo
gene
icbo
ne g
raft
Plac
ed a
s an
onl
ay a
cros
s th
e no
n-un
ion
gap
John
son,
199
0115
John
son,
199
2117
Jone
s, 2
00510
6
hBM
P
hBM
P
hBM
P
50–1
00 m
g
NR
50 m
g
NC
P
NC
P
Gel
atin
e ca
psul
e
1/4
patie
nts
had
cort
ical
allo
gene
ic b
one
All
had
AA
A b
one.
5/2
5 pa
tient
s re
ceiv
edA
ICBG
. 2/
25 p
atie
nts
had
ream
ings
from
the
can
al u
sed
as a
dditi
onal
gra
ft
K-w
ire t
o fix
Impl
ante
d ac
ross
frac
ture
site
Impl
ant
inco
rpor
ated
as
onla
y (1
5) a
ndin
lay
(10)
Impl
ante
d in
to s
caph
oid
non-
unio
n
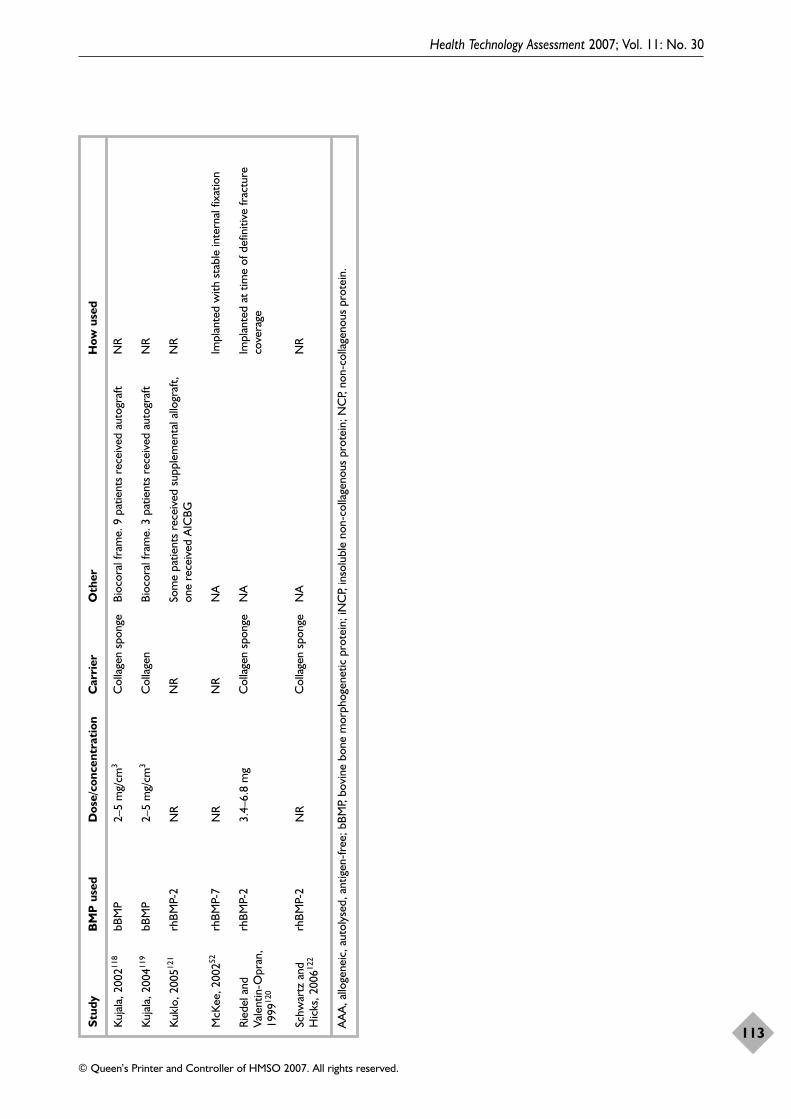
Health Technology Assessment 2007; Vol. 11: No. 30
113
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Stud
yB
MP
use
dD
ose/
conc
entr
atio
nC
arri
erO
ther
How
use
d
AA
A, a
lloge
neic
, aut
olys
ed, a
ntig
en-f
ree;
bBM
P, bo
vine
bon
e m
orph
ogen
etic
pro
tein
; iN
CP,
inso
lubl
e no
n-co
llage
nous
pro
tein
; NC
P, no
n-co
llage
nous
pro
tein
.
Kuja
la, 2
00211
8
Kuja
la, 2
00411
9
Kukl
o, 2
00512
1
McK
ee, 2
00252
Ried
el a
ndVa
lent
in-O
pran
,19
9912
0
Schw
artz
and
Hic
ks, 2
00612
2
bBM
P
bBM
P
rhBM
P-2
rhBM
P-7
rhBM
P-2
rhBM
P-2
2–5
mg/
cm3
2–5
mg/
cm3
NR
NR
3.4–
6.8
mg
NR
Col
lage
n sp
onge
Col
lage
n
NR
NR
Col
lage
n sp
onge
Col
lage
n sp
onge
Bioc
oral
fram
e. 9
pat
ient
s re
ceiv
ed a
utog
raft
Bioc
oral
fram
e. 3
pat
ient
s re
ceiv
ed a
utog
raft
Som
e pa
tient
s re
ceiv
ed s
uppl
emen
tal a
llogr
aft,
one
rece
ived
AIC
BG
NA
NA
NA
NR
NR
NR
Impl
ante
d w
ith s
tabl
e in
tern
al fi
xatio
n
Impl
ante
d at
tim
e of
def
initi
ve fr
actu
reco
vera
ge
NR

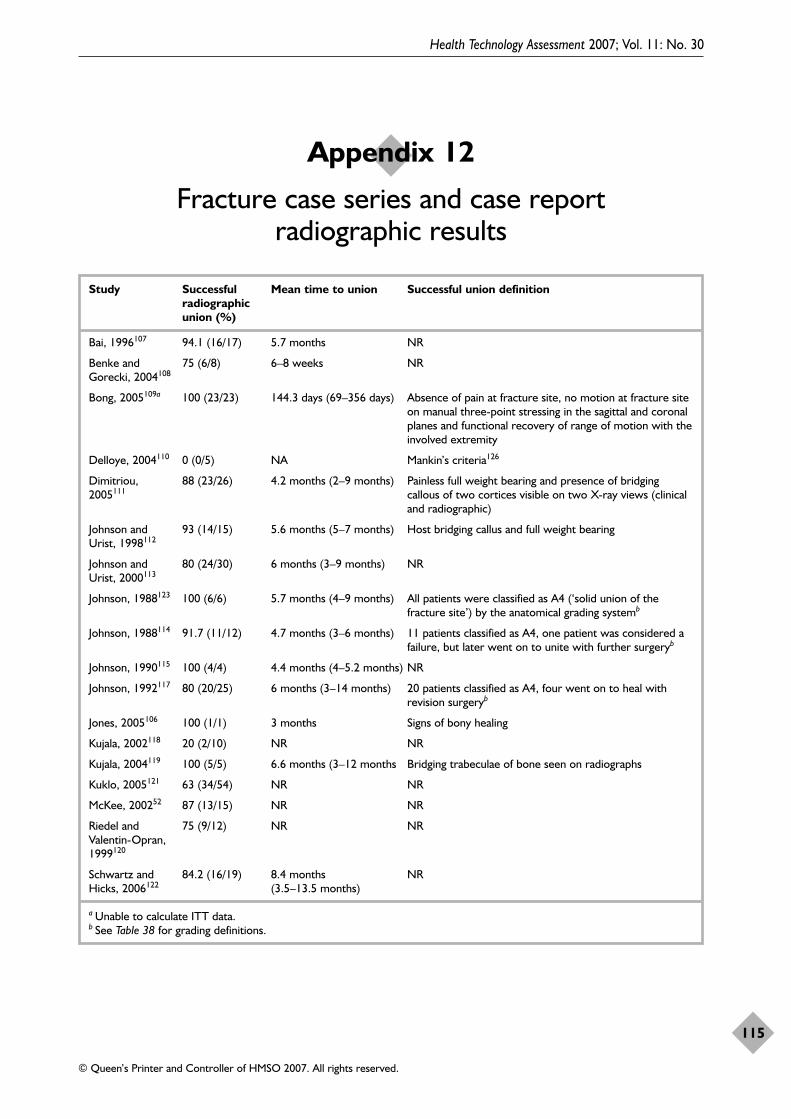
Health Technology Assessment 2007; Vol. 11: No. 30
115
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 12
Fracture case series and case report radiographic results
Study Successful Mean time to union Successful union definitionradiographic union (%)
Bai, 1996107 94.1 (16/17) 5.7 months NR
Benke and 75 (6/8) 6–8 weeks NRGorecki, 2004108
Bong, 2005109a 100 (23/23) 144.3 days (69–356 days) Absence of pain at fracture site, no motion at fracture siteon manual three-point stressing in the sagittal and coronalplanes and functional recovery of range of motion with theinvolved extremity
Delloye, 2004110 0 (0/5) NA Mankin’s criteria126
Dimitriou, 88 (23/26) 4.2 months (2–9 months) Painless full weight bearing and presence of bridging 2005111 callous of two cortices visible on two X-ray views (clinical
and radiographic)
Johnson and 93 (14/15) 5.6 months (5–7 months) Host bridging callus and full weight bearingUrist, 1998112
Johnson and 80 (24/30) 6 months (3–9 months) NRUrist, 2000113
Johnson, 1988123 100 (6/6) 5.7 months (4–9 months) All patients were classified as A4 (‘solid union of thefracture site’) by the anatomical grading systemb
Johnson, 1988114 91.7 (11/12) 4.7 months (3–6 months) 11 patients classified as A4, one patient was considered afailure, but later went on to unite with further surgeryb
Johnson, 1990115 100 (4/4) 4.4 months (4–5.2 months) NR
Johnson, 1992117 80 (20/25) 6 months (3–14 months) 20 patients classified as A4, four went on to heal withrevision surgeryb
Jones, 2005106 100 (1/1) 3 months Signs of bony healing
Kujala, 2002118 20 (2/10) NR NR
Kujala, 2004119 100 (5/5) 6.6 months (3–12 months Bridging trabeculae of bone seen on radiographs
Kuklo, 2005121 63 (34/54) NR NR
McKee, 200252 87 (13/15) NR NR
Riedel and 75 (9/12) NR NRValentin-Opran,1999120
Schwartz and 84.2 (16/19) 8.4 months NRHicks, 2006122 (3.5–13.5 months)
a Unable to calculate ITT data. b See Table 38 for grading definitions.

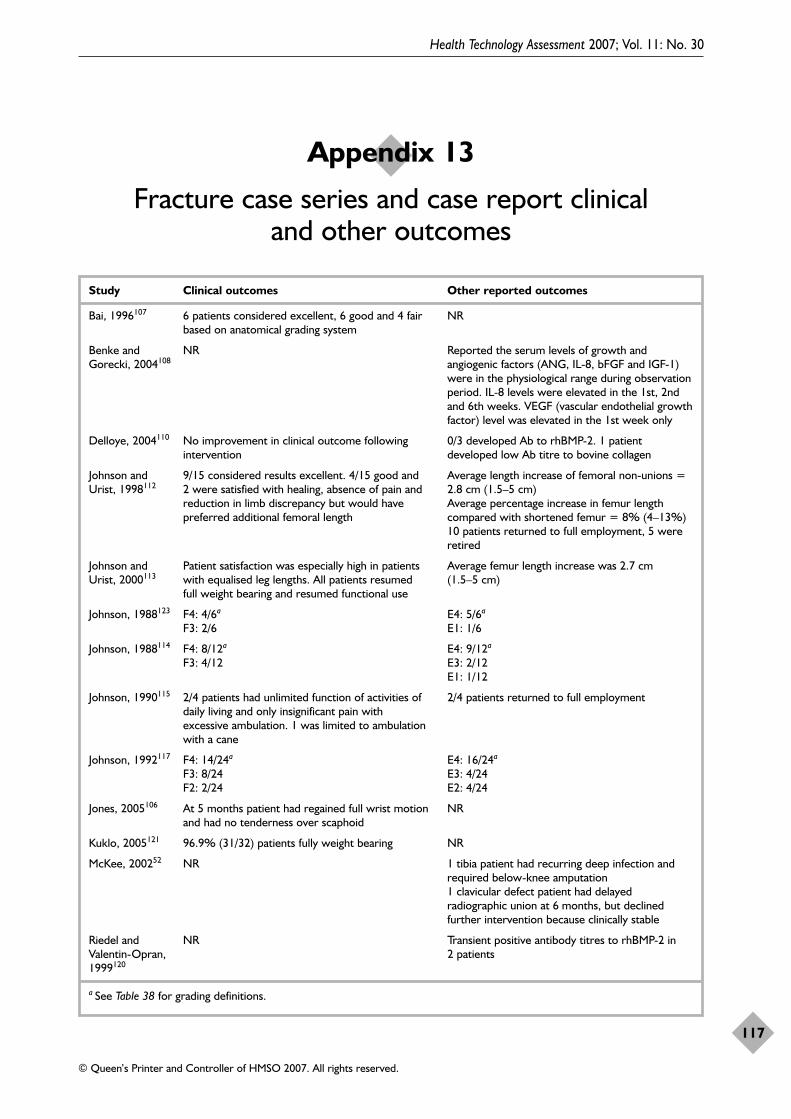
Health Technology Assessment 2007; Vol. 11: No. 30
117
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 13
Fracture case series and case report clinical and other outcomes
Study Clinical outcomes Other reported outcomes
Bai, 1996107 6 patients considered excellent, 6 good and 4 fair NRbased on anatomical grading system
Benke and NR Reported the serum levels of growth and Gorecki, 2004108 angiogenic factors (ANG, IL-8, bFGF and IGF-1)
were in the physiological range during observationperiod. IL-8 levels were elevated in the 1st, 2ndand 6th weeks. VEGF (vascular endothelial growthfactor) level was elevated in the 1st week only
Delloye, 2004110 No improvement in clinical outcome following 0/3 developed Ab to rhBMP-2. 1 patient intervention developed low Ab titre to bovine collagen
Johnson and 9/15 considered results excellent. 4/15 good and Average length increase of femoral non-unions = Urist, 1998112 2 were satisfied with healing, absence of pain and 2.8 cm (1.5–5 cm)
reduction in limb discrepancy but would have Average percentage increase in femur length preferred additional femoral length compared with shortened femur = 8% (4–13%)
10 patients returned to full employment, 5 wereretired
Johnson and Patient satisfaction was especially high in patients Average femur length increase was 2.7 cm Urist, 2000113 with equalised leg lengths. All patients resumed (1.5–5 cm)
full weight bearing and resumed functional use
Johnson, 1988123 F4: 4/6a E4: 5/6a
F3: 2/6 E1: 1/6
Johnson, 1988114 F4: 8/12a E4: 9/12a
F3: 4/12 E3: 2/12E1: 1/12
Johnson, 1990115 2/4 patients had unlimited function of activities of 2/4 patients returned to full employmentdaily living and only insignificant pain with excessive ambulation. 1 was limited to ambulation with a cane
Johnson, 1992117 F4: 14/24a E4: 16/24a
F3: 8/24 E3: 4/24F2: 2/24 E2: 4/24
Jones, 2005106 At 5 months patient had regained full wrist motion NRand had no tenderness over scaphoid
Kuklo, 2005121 96.9% (31/32) patients fully weight bearing NR
McKee, 200252 NR 1 tibia patient had recurring deep infection andrequired below-knee amputation1 clavicular defect patient had delayedradiographic union at 6 months, but declinedfurther intervention because clinically stable
Riedel and NR Transient positive antibody titres to rhBMP-2 in Valentin-Opran, 2 patients1999120
a See Table 38 for grading definitions.

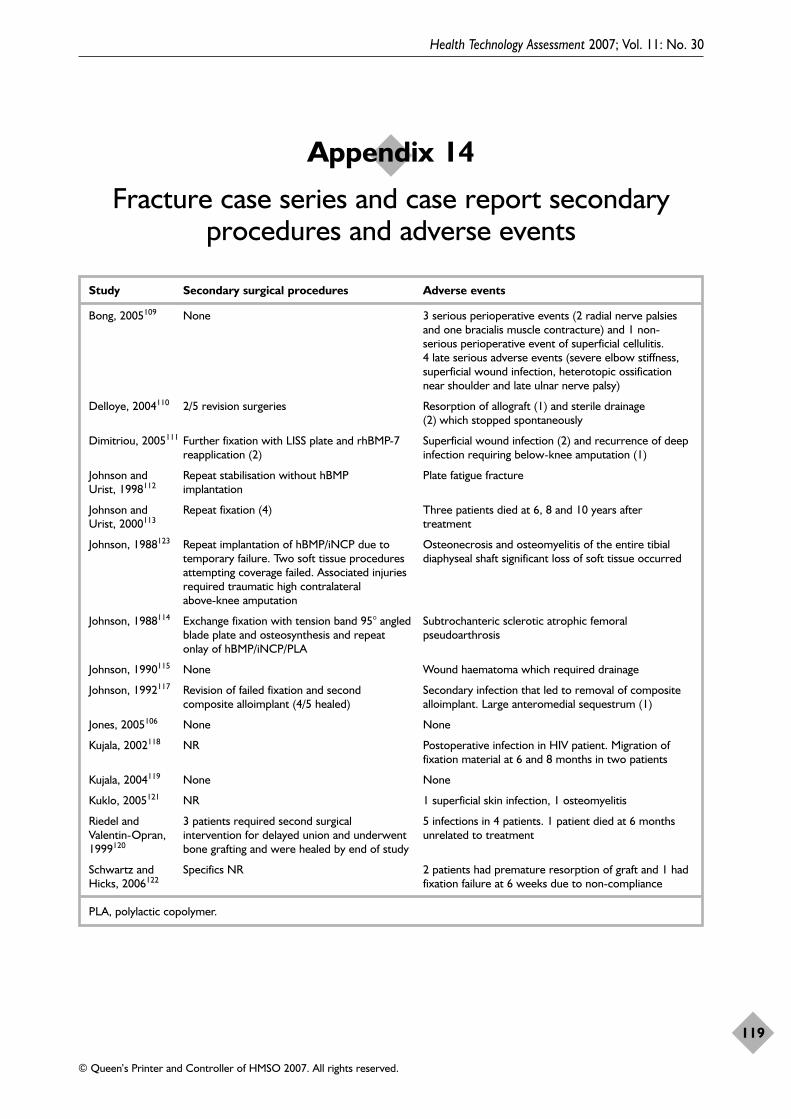
Health Technology Assessment 2007; Vol. 11: No. 30
119
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 14
Fracture case series and case report secondaryprocedures and adverse events
Study Secondary surgical procedures Adverse events
Bong, 2005109 None 3 serious perioperative events (2 radial nerve palsiesand one bracialis muscle contracture) and 1 non-serious perioperative event of superficial cellulitis. 4 late serious adverse events (severe elbow stiffness,superficial wound infection, heterotopic ossificationnear shoulder and late ulnar nerve palsy)
Delloye, 2004110 2/5 revision surgeries Resorption of allograft (1) and sterile drainage(2) which stopped spontaneously
Dimitriou, 2005111 Further fixation with LISS plate and rhBMP-7 Superficial wound infection (2) and recurrence of deep reapplication (2) infection requiring below-knee amputation (1)
Johnson and Repeat stabilisation without hBMP Plate fatigue fractureUrist, 1998112 implantation
Johnson and Repeat fixation (4) Three patients died at 6, 8 and 10 years after Urist, 2000113 treatment
Johnson, 1988123 Repeat implantation of hBMP/iNCP due to Osteonecrosis and osteomyelitis of the entire tibial temporary failure. Two soft tissue procedures diaphyseal shaft significant loss of soft tissue occurredattempting coverage failed. Associated injuries required traumatic high contralateral above-knee amputation
Johnson, 1988114 Exchange fixation with tension band 95° angled Subtrochanteric sclerotic atrophic femoral blade plate and osteosynthesis and repeat pseudoarthrosisonlay of hBMP/iNCP/PLA
Johnson, 1990115 None Wound haematoma which required drainage
Johnson, 1992117 Revision of failed fixation and second Secondary infection that led to removal of composite composite alloimplant (4/5 healed) alloimplant. Large anteromedial sequestrum (1)
Jones, 2005106 None None
Kujala, 2002118 NR Postoperative infection in HIV patient. Migration offixation material at 6 and 8 months in two patients
Kujala, 2004119 None None
Kuklo, 2005121 NR 1 superficial skin infection, 1 osteomyelitis
Riedel and 3 patients required second surgical 5 infections in 4 patients. 1 patient died at 6 months Valentin-Opran, intervention for delayed union and underwent unrelated to treatment1999120 bone grafting and were healed by end of study
Schwartz and Specifics NR 2 patients had premature resorption of graft and 1 had Hicks, 2006122 fixation failure at 6 weeks due to non-compliance
PLA, polylactic copolymer.


Health Technology Assessment 2007; Vol. 11: No. 30
121
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 15
RCT spine study characteristics
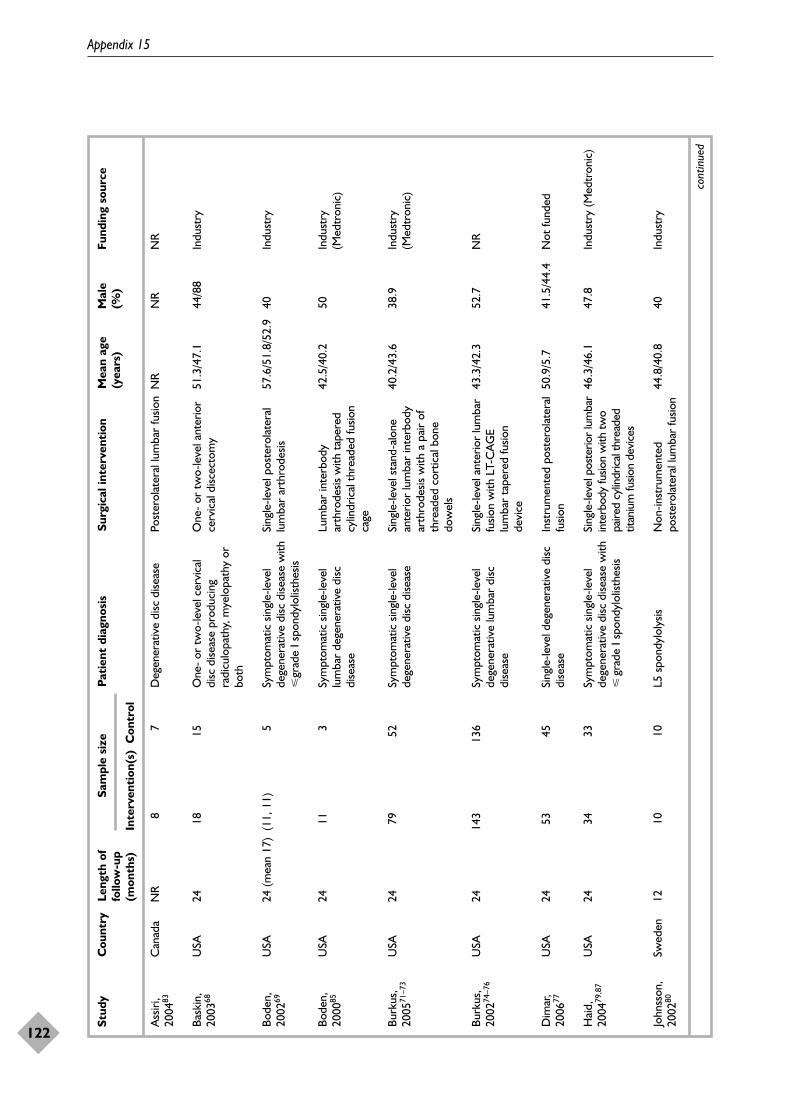
Appendix 15
122
Stud
yC
ount
ryLe
ngth
of
Sam
ple
size
Pati
ent
diag
nosi
sSu
rgic
al in
terv
enti
onM
ean
age
Mal
eFu
ndin
g so
urce
follo
w-u
p(y
ears
)(%
)(m
onth
s)In
terv
enti
on(s
)C
ontr
ol
cont
inue
d
Ass
iri,
2004
83
Bask
in,
2003
68
Bode
n,20
0269
Bode
n,20
0085
Burk
us,
2005
71–7
3
Burk
us,
2002
74–7
6
Dim
ar,
2006
77
Hai
d,20
0479
,87
John
sson
,20
0280
Can
ada
USA
USA
USA
USA
USA
USA
USA
Swed
en
NR
24 24 (m
ean
17)
24 24 24 24 24 12
8 18 (11,
11)
11 79 143 53 34 10
7 15 5 3 52 136 45 33 10
Deg
ener
ativ
e di
sc d
iseas
e
One
- or
tw
o-le
vel c
ervi
cal
disc
dise
ase
prod
ucin
gra
dicu
lopa
thy,
mye
lopa
thy
orbo
th
Sym
ptom
atic
sin
gle-
leve
lde
gene
rativ
e di
sc d
iseas
e w
ith�
grad
e I s
pond
ylol
isthe
sis
Sym
ptom
atic
sin
gle-
leve
llu
mba
r de
gene
rativ
e di
scdi
seas
e
Sym
ptom
atic
sin
gle-
leve
lde
gene
rativ
e di
sc d
iseas
e
Sym
ptom
atic
sin
gle-
leve
lde
gene
rativ
e lu
mba
r di
scdi
seas
e
Sing
le-le
vel d
egen
erat
ive
disc
dise
ase
Sym
ptom
atic
sin
gle-
leve
lde
gene
rativ
e di
sc d
iseas
e w
ith�
grad
e I s
pond
ylol
isthe
sis
L5 s
pond
ylol
ysis
Post
erol
ater
al lu
mba
r fu
sion
One
- or
tw
o-le
vel a
nter
ior
cerv
ical
disc
ecto
my
Sing
le-le
vel p
oste
rola
tera
llu
mba
r ar
thro
desis
Lum
bar
inte
rbod
yar
thro
desis
with
tap
ered
cylin
dric
al t
hrea
ded
fusio
nca
ge
Sing
le-le
vel s
tand
-alo
nean
terio
r lu
mba
r in
terb
ody
arth
rode
sis w
ith a
pai
r of
thre
aded
cor
tical
bon
edo
wel
s
Sing
le-le
vel a
nter
ior
lum
bar
fusio
n w
ith L
T-C
AG
Elu
mba
r ta
pere
d fu
sion
devi
ce
Inst
rum
ente
d po
ster
olat
eral
fusio
n
Sing
le-le
vel p
oste
rior
lum
bar
inte
rbod
y fu
sion
with
two
paire
d cy
lindr
ical
thre
aded
titan
ium
fusio
n de
vice
s
Non
-inst
rum
ente
dpo
ster
olat
eral
lum
bar
fusio
n
NR
51.3
/47.
1
57.6
/51.
8/52
.9
42.5
/40.
2
40.2
/43.
6
43.3
/42.
3
50.9
/5.7
46.3
/46.
1
44.8
/40.
8
NR
44/8
8
40 50 38.9
52.7
41.5
/44.
4
47.8
40
NR
Indu
stry
Indu
stry
Indu
stry
(Med
tron
ic)
Indu
stry
(Med
tron
ic)
NR
Not
fund
ed
Indu
stry
(Med
tron
ic)
Indu
stry
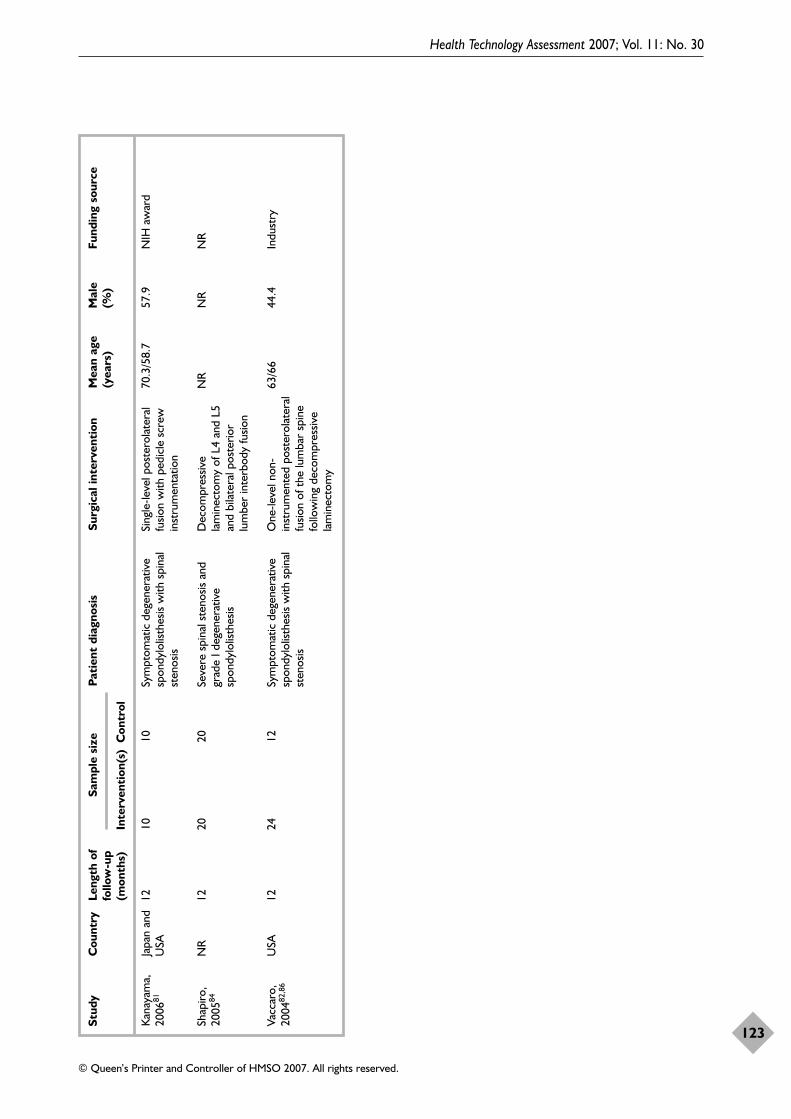
Health Technology Assessment 2007; Vol. 11: No. 30
123
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Stud
yC
ount
ryLe
ngth
of
Sam
ple
size
Pati
ent
diag
nosi
sSu
rgic
al in
terv
enti
onM
ean
age
Mal
eFu
ndin
g so
urce
follo
w-u
p(y
ears
)(%
)(m
onth
s)In
terv
enti
on(s
)C
ontr
ol
Kana
yam
a,20
0681
Shap
iro,
2005
84
Vacc
aro,
2004
82,8
6
Japa
n an
dU
SA
NR
USA
12
12 12
10 20 24
10 20 12
Sym
ptom
atic
deg
ener
ativ
esp
ondy
lolis
thes
is w
ith s
pina
lst
enos
is
Seve
re s
pina
l ste
nosis
and
grad
e I d
egen
erat
ive
spon
dylo
listh
esis
Sym
ptom
atic
deg
ener
ativ
esp
ondy
lolis
thes
is w
ith s
pina
lst
enos
is
Sing
le-le
vel p
oste
rola
tera
lfu
sion
with
ped
icle
scr
ewin
stru
men
tatio
n
Dec
ompr
essiv
ela
min
ecto
my
of L
4 an
d L5
and
bila
tera
l pos
terio
rlu
mbe
r in
terb
ody
fusio
n
One
-leve
l non
-in
stru
men
ted
post
erol
ater
alfu
sion
of t
he lu
mba
r sp
ine
follo
win
g de
com
pres
sive
lam
inec
tom
y
70.3
/58.
7
NR
63/6
6
57.9
NR
44.4
NIH
aw
ard
NR
Indu
stry

Health Technology Assessment 2007; Vol. 11: No. 30
125
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 16
RCT spine quality assessment

Appendix 16
126
Stud
yR
ando
mis
atio
nA
lloca
tion
B
lindi
ngB
asel
ine
com
para
bilit
yEx
plic
it
ITT
D
rop-
outs
(%
)co
ncea
lmen
tin
clus
ion/
anal
ysis
excl
usio
n cr
iter
iaIn
terv
enti
onC
ontr
olR
easo
ns g
iven
cont
inue
d
Ass
iri, 2
00483
Bask
in, 2
00368
Bode
n, 2
00269
Bode
n, 2
00085
Burk
us,
2005
71–7
3
Burk
us,
2002
74–7
6
Dim
ar, 2
00677
Unc
lear
Unc
lear
Unc
lear
Mar
gina
lba
lanc
ing
met
hod
Sequ
entia
llynu
mbe
red
enve
lope
s
SAS
PRO
C p
lan
stra
tifie
d by
inve
stig
ator
site
Unc
lear
Unk
now
n
Unk
now
n
Unk
now
n
Unk
now
n
Ade
quat
e(b
ased
on
rand
omisa
tion
met
hod)
Ade
quat
e(b
ased
on
rand
omisa
tion
met
hod)
Unk
now
n
Not
rep
orte
d
Two
inde
pend
ent
radi
olog
ists
revi
ewed
radi
ogra
phs
and
CT
scan
s
Two
inde
pend
ent
neur
orad
iolo
gist
sre
view
ed r
adio
grap
hsan
d C
T s
cans
Thr
ee r
adio
logi
sts
revi
ewed
rad
iogr
aphs
.T
hree
neu
rora
diol
ogist
san
d tw
o su
rgeo
nsre
view
ed C
T s
cans
Two
inde
pend
ent
radi
olog
ists
revi
ewed
radi
ogra
phs
and
CT
scan
s
Two
inde
pend
ent
radi
olog
ists
revi
ewed
radi
ogra
ph a
nd C
T
scan
s
One
rad
iolo
gist
and
tw
o or
thop
aedi
sts
revi
ewed
rad
iogr
aph
and
CT
sca
ns
Popu
latio
n ch
arac
teris
tics
not
repo
rted
Sim
ilar
Sim
ilar
exce
pt s
tatis
tical
lysig
nific
ant
diffe
renc
e in
diab
etes
rat
e (4
0% in
con
trol
grou
p, 0
% in
inte
rven
tion
grou
ps) a
nd e
duca
tion
>hi
ghsc
hool
(40%
in c
ontr
ol, 1
00%
in in
terv
entio
n A
and
87.
5% in
inte
rven
tion
B)
Sim
ilar
exce
pt fo
r st
atist
ical
lysig
nific
ant
diffe
renc
e in
mea
nw
eigh
t (2
11 lb
in c
ontr
olgr
oup
and
166
lb in
inte
rven
tion
grou
p)
Sim
ilar
Sim
ilar
Sim
ilar
No
No
Yes
Yes
Yes
No
Yes
No
No
No
No
No
No
No
NR
3 A: 0
B: 1
8
0 3.8
6.3
NR
NR
1 0 0 5.8
8.8
NR
NR
No
Yes
NA
No
Yes
NR
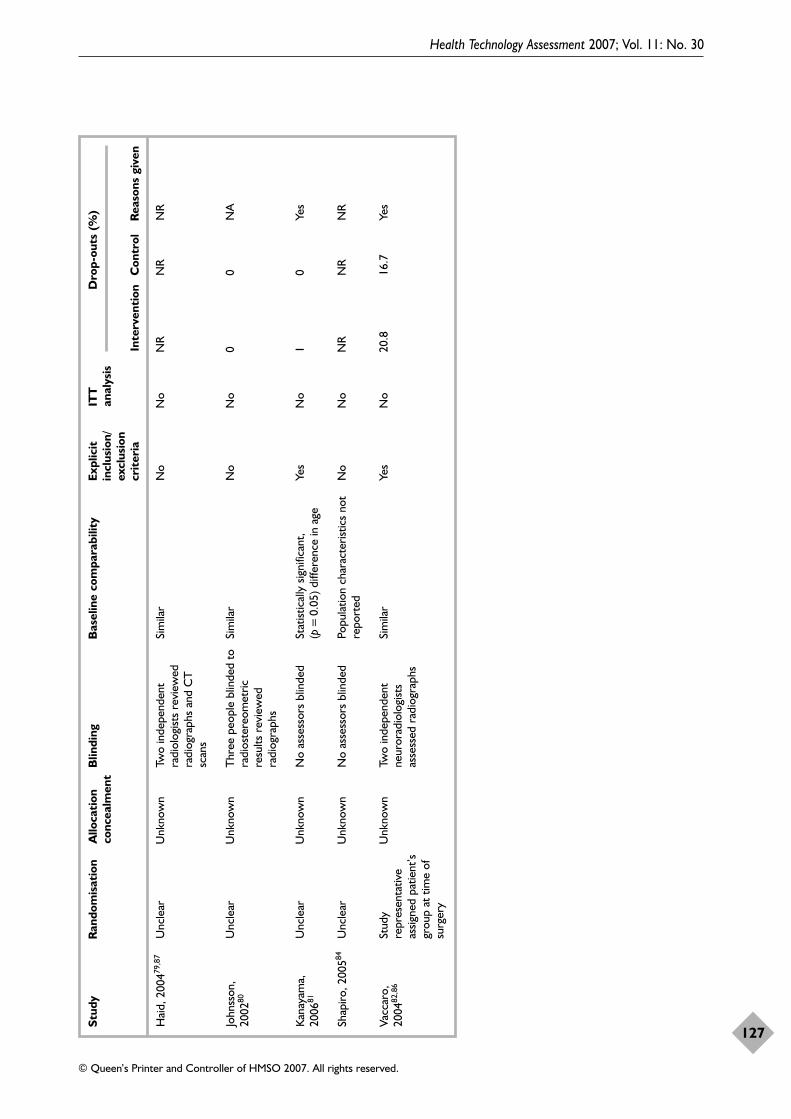
Health Technology Assessment 2007; Vol. 11: No. 30
127
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Stud
yR
ando
mis
atio
nA
lloca
tion
B
lindi
ngB
asel
ine
com
para
bilit
yEx
plic
it
ITT
D
rop-
outs
(%
)co
ncea
lmen
tin
clus
ion/
anal
ysis
excl
usio
n cr
iter
iaIn
terv
enti
onC
ontr
olR
easo
ns g
iven
Hai
d, 2
00479
,87
John
sson
,20
0280
Kana
yam
a,20
0681
Shap
iro, 2
00584
Vacc
aro,
2004
82,8
6
Unc
lear
Unc
lear
Unc
lear
Unc
lear
Stud
yre
pres
enta
tive
assig
ned
patie
nt’s
grou
p at
tim
e of
surg
ery
Unk
now
n
Unk
now
n
Unk
now
n
Unk
now
n
Unk
now
n
Two
inde
pend
ent
radi
olog
ists
revi
ewed
radi
ogra
phs
and
CT
scan
s
Thr
ee p
eopl
e bl
inde
d to
radi
oste
reom
etric
resu
lts r
evie
wed
radi
ogra
phs
No
asse
ssor
s bl
inde
d
No
asse
ssor
s bl
inde
d
Two
inde
pend
ent
neur
orad
iolo
gist
sas
sess
ed r
adio
grap
hs
Sim
ilar
Sim
ilar
Stat
istic
ally
sig
nific
ant,
(p=
0.05
) diff
eren
ce in
age
Popu
latio
n ch
arac
teris
tics
not
repo
rted
Sim
ilar
No
No
Yes
No
Yes
No
No
No
No
No
NR
0 1 NR
20.8
NR
0 0 NR
16.7
NR
NA
Yes
NR
Yes

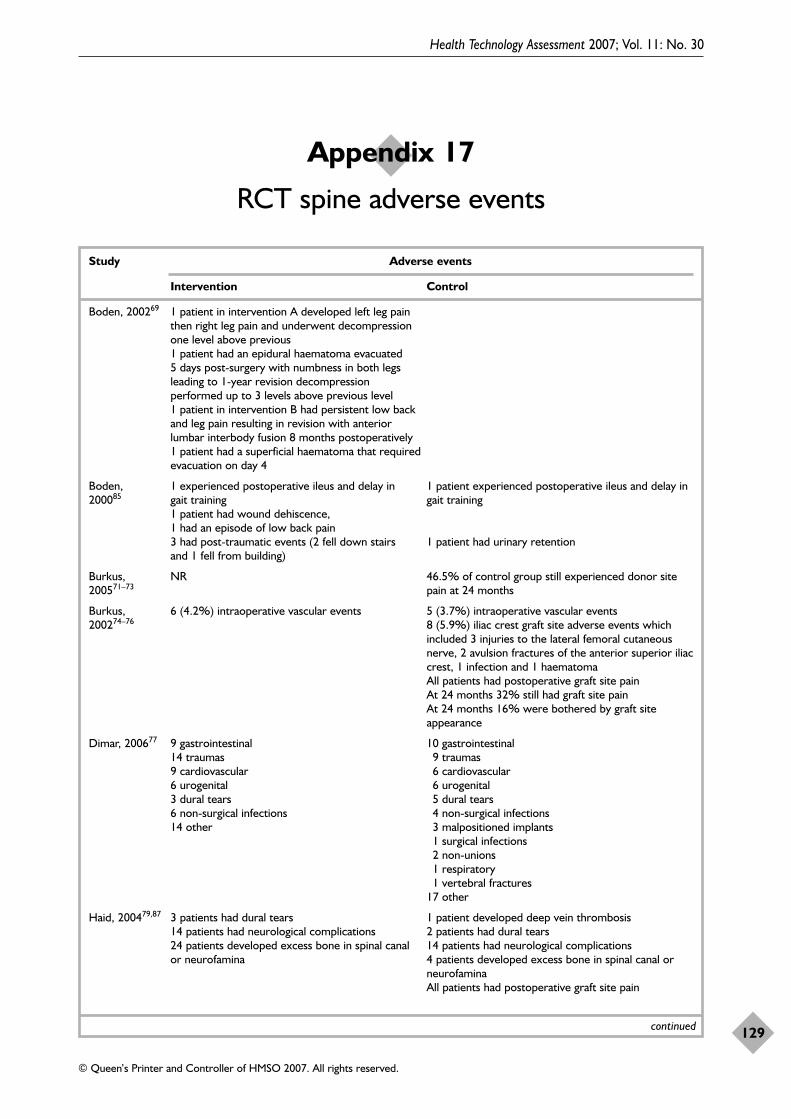
Health Technology Assessment 2007; Vol. 11: No. 30
129
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 17
RCT spine adverse events
Study Adverse events
Intervention Control
Boden, 200269 1 patient in intervention A developed left leg pain then right leg pain and underwent decompression one level above previous1 patient had an epidural haematoma evacuated 5 days post-surgery with numbness in both legs leading to 1-year revision decompression performed up to 3 levels above previous level1 patient in intervention B had persistent low back and leg pain resulting in revision with anterior lumbar interbody fusion 8 months postoperatively1 patient had a superficial haematoma that required evacuation on day 4
Boden, 1 experienced postoperative ileus and delay in 1 patient experienced postoperative ileus and delay in 200085 gait training gait training
1 patient had wound dehiscence, 1 had an episode of low back pain3 had post-traumatic events (2 fell down stairs 1 patient had urinary retentionand 1 fell from building)
Burkus, NR 46.5% of control group still experienced donor site 200571–73 pain at 24 months
Burkus, 6 (4.2%) intraoperative vascular events 5 (3.7%) intraoperative vascular events200274–76 8 (5.9%) iliac crest graft site adverse events which
included 3 injuries to the lateral femoral cutaneousnerve, 2 avulsion fractures of the anterior superior iliaccrest, 1 infection and 1 haematomaAll patients had postoperative graft site painAt 24 months 32% still had graft site painAt 24 months 16% were bothered by graft siteappearance
Dimar, 200677 9 gastrointestinal 10 gastrointestinal14 traumas 9 traumas9 cardiovascular 6 cardiovascular6 urogenital 6 urogenital3 dural tears 5 dural tears6 non-surgical infections 4 non-surgical infections14 other 3 malpositioned implants
1 surgical infections2 non-unions1 respiratory1 vertebral fractures
17 other
Haid, 200479,87 3 patients had dural tears 1 patient developed deep vein thrombosis14 patients had neurological complications 2 patients had dural tears24 patients developed excess bone in spinal canal 14 patients had neurological complicationsor neurofamina 4 patients developed excess bone in spinal canal or
neurofaminaAll patients had postoperative graft site pain
continued
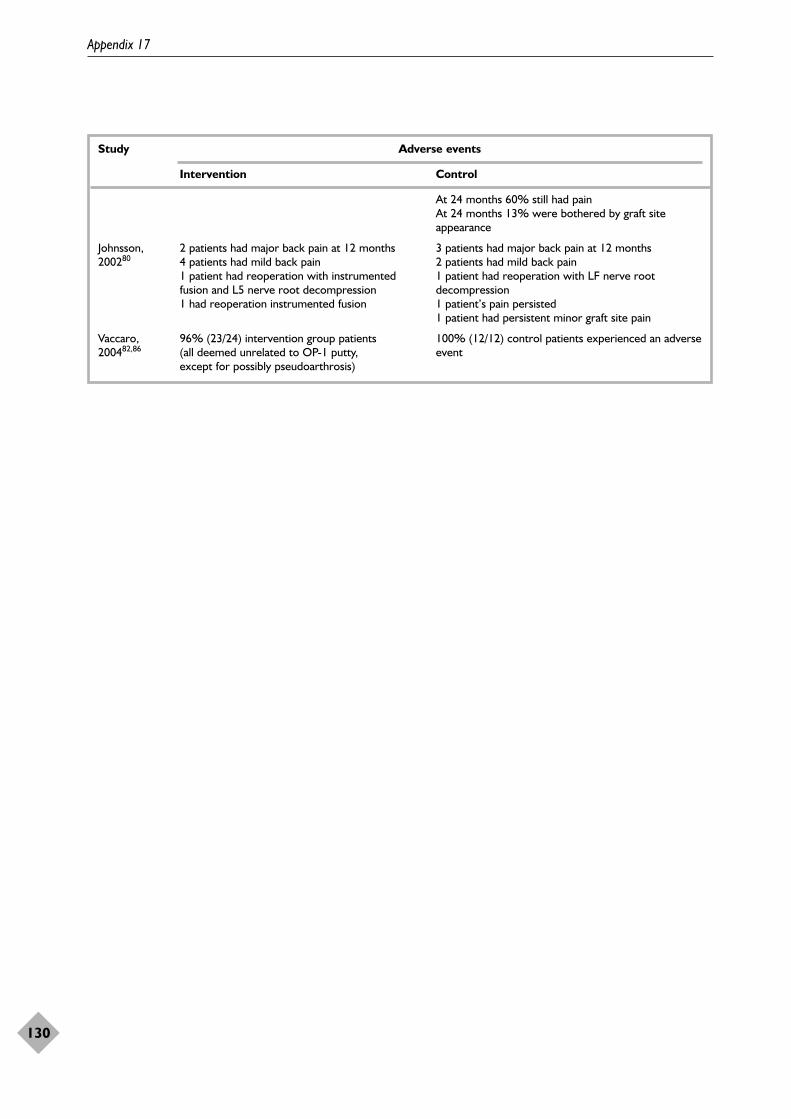
Appendix 17
130
Study Adverse events
Intervention Control
At 24 months 60% still had painAt 24 months 13% were bothered by graft siteappearance
Johnsson, 2 patients had major back pain at 12 months 3 patients had major back pain at 12 months200280 4 patients had mild back pain 2 patients had mild back pain
1 patient had reoperation with instrumented 1 patient had reoperation with LF nerve root fusion and L5 nerve root decompression decompression1 had reoperation instrumented fusion 1 patient’s pain persisted
1 patient had persistent minor graft site pain
Vaccaro, 96% (23/24) intervention group patients 100% (12/12) control patients experienced an adverse 200482,86 (all deemed unrelated to OP-1 putty, event
except for possibly pseudoarthrosis)

Spine case series studies: numberand characteristicsFourteen case series, by Boakye and colleagues,127
Boden and colleagues,128 Govender andcolleagues,129 Jeppsson and colleagues,130 Kleemanand colleagues,131 Kuklo and colleagues,125 Lanmanand Hopkins (2004),132 Lanman and Hopkins(2004),133 Laursen and colleagues,134 Luhmann andcolleagues,135 Mummaneni and colleagues,136
Vaccaro and colleagues137 and Villavicencio andcolleagues,138 and Buttermann139 (abstract only)were included.
General study characteristicsAppendix 19 shows the general studycharacteristics of each included spine case seriesstudy. Nine out of 14 studies were conducted inthe USA. The remaining studies were conductedin Switzerland,128 Sweden,130 Canada129 andDenmark.134 It was not clear where the conferenceabstract study139 was conducted. Two studies128,129
specified they were sponsored by industry andone130 by the Swedish Medical Research Counciland another135 stated that it received no funding.The remaining 10 studies did not report theirsource of funding.
The diagnoses included in the studies are highlyvariable between and within each study. Sixstudies125,131,132,136,138–140 included some type ofdisc disease in their patient population, andfour125,131,136,138,140 of those also included a levelof spondylolisthesis. The Buttermann abstract139
also included patients with herniated nucleuspulposus or stenosis. The Govender study129 usedthe following definition to describe their patientpopulation: “some form of spinal diseaserequiring spinal fusion with medical risk factorsknown to inhibit spinal fusion”. Of the remainingstudies, the diagnoses included radiculopathy,myeloradiculopathy or profound quadriparesis,127
lumbar spinal stenosis or spondylolisthesis,128
rheumatoid disease or psoriatic arthritis,130
discogenic pain, grade I spondylolisthesis or non-union from previous surgery132 and unstablethoracolumbar spine fractures.134 The Luhmannstudy135 did not specify patients’ diagnoses but
reported only that it included patients, requiringthe specific surgical procedures used.
The surgical interventions are also highly variablebetween and within the studies. Fourstudies125,133,136,138,140 used transforaminal lumbarinterbody fusion. The Lanman and Hopkins(2004)132 and Buttermann139 studies performedanterior cervical interbody fusion. The Kleemanstudy131 performed anterior lumbar interbodyfusion. Because of the variability in diagnoses inthe Govender study129 there were equally variablesurgical interventions performed. These includedlumbar decompression (1), lumbar decompression,posterior lumbar interbody fusion and pediclescrew fixation (1), craniocervical decompressionand fixation (1), suboccipital decompression,duraplasty and occipitocervical fusion (2), spinalcord untethering and lumbar pedicle screwfixation (1), atlantoaxial stabilisation (1), cervicallaminectomy and occipitocervical fusion (1) andlumbar pedicle subtraction osteotomy and pediclescrew fixation (1). The remaining studies useddiscectomy, anterior cervical discectomy andfusion at varying number of levels,127 one- or two-level spinal arthrodesis,128 atlanto-axial posteriorfusions,130 transpendicular BMP implantation,short segment instrumentation and posterolateralfusion,134 anterior, posterior or both fusions135 anddecompression following laminectomy andfacetectomy followed by intertransverse processfusions.137,141
The study sizes ranged from four to 74 patients.The follow-up lengths varied from 5 to 24 months.The mean ages ranged from 38 to 56.9 years.
QualityTable 39 summarises the quality of the includedstudies. Two are preliminary reports134,136,140 andone is an abstract from a conference.139
The quality of the studies is low. Six of thestudies125,128,131,134,135,137,141 meet at least three ofthe four quality criteria assessed.
Ten of the studies125,127,129,131,133–138,140,141 clearlydescribed their patient populations, whereas only
Health Technology Assessment 2007; Vol. 11: No. 30
131
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 18
Spine fusion case series findings
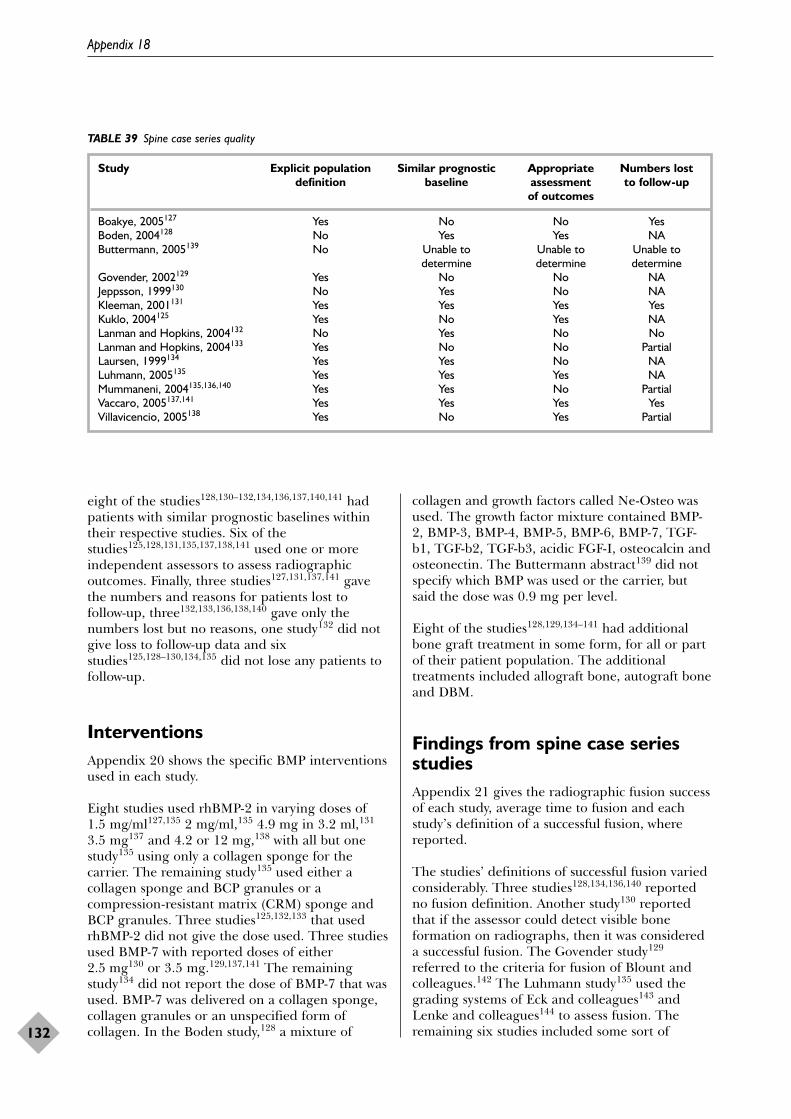
eight of the studies128,130–132,134,136,137,140,141 hadpatients with similar prognostic baselines withintheir respective studies. Six of thestudies125,128,131,135,137,138,141 used one or moreindependent assessors to assess radiographicoutcomes. Finally, three studies127,131,137,141 gavethe numbers and reasons for patients lost tofollow-up, three132,133,136,138,140 gave only thenumbers lost but no reasons, one study132 did notgive loss to follow-up data and sixstudies125,128–130,134,135 did not lose any patients tofollow-up.
InterventionsAppendix 20 shows the specific BMP interventionsused in each study.
Eight studies used rhBMP-2 in varying doses of1.5 mg/ml127,135 2 mg/ml,135 4.9 mg in 3.2 ml,131
3.5 mg137 and 4.2 or 12 mg,138 with all but onestudy135 using only a collagen sponge for thecarrier. The remaining study135 used either acollagen sponge and BCP granules or acompression-resistant matrix (CRM) sponge andBCP granules. Three studies125,132,133 that usedrhBMP-2 did not give the dose used. Three studiesused BMP-7 with reported doses of either2.5 mg130 or 3.5 mg.129,137,141 The remainingstudy134 did not report the dose of BMP-7 that wasused. BMP-7 was delivered on a collagen sponge,collagen granules or an unspecified form ofcollagen. In the Boden study,128 a mixture of
collagen and growth factors called Ne-Osteo wasused. The growth factor mixture contained BMP-2, BMP-3, BMP-4, BMP-5, BMP-6, BMP-7, TGF-b1, TGF-b2, TGF-b3, acidic FGF-I, osteocalcin andosteonectin. The Buttermann abstract139 did notspecify which BMP was used or the carrier, butsaid the dose was 0.9 mg per level.
Eight of the studies128,129,134–141 had additionalbone graft treatment in some form, for all or partof their patient population. The additionaltreatments included allograft bone, autograft boneand DBM.
Findings from spine case seriesstudiesAppendix 21 gives the radiographic fusion successof each study, average time to fusion and eachstudy’s definition of a successful fusion, wherereported.
The studies’ definitions of successful fusion variedconsiderably. Three studies128,134,136,140 reportedno fusion definition. Another study130 reportedthat if the assessor could detect visible boneformation on radiographs, then it was considereda successful fusion. The Govender study129
referred to the criteria for fusion of Blount andcolleagues.142 The Luhmann study135 used thegrading systems of Eck and colleagues143 andLenke and colleagues144 to assess fusion. Theremaining six studies included some sort of
Appendix 18
132
TABLE 39 Spine case series quality
Study Explicit population Similar prognostic Appropriate Numbers lost definition baseline assessment to follow-up
of outcomes
Boakye, 2005127 Yes No No YesBoden, 2004128 No Yes Yes NAButtermann, 2005139 No Unable to Unable to Unable to
determine determine determineGovender, 2002129 Yes No No NAJeppsson, 1999130 No Yes No NAKleeman, 2001131 Yes Yes Yes YesKuklo, 2004125 Yes No Yes NALanman and Hopkins, 2004132 No Yes No NoLanman and Hopkins, 2004133 Yes No No PartialLaursen, 1999134 Yes Yes No NALuhmann, 2005135 Yes Yes Yes NAMummaneni, 2004135,136,140 Yes Yes No PartialVaccaro, 2005137,141 Yes Yes Yes YesVillavicencio, 2005138 Yes No Yes Partial
bridging bone criteria in their definition, withvarying degrees of specificity for other criteria.The Buttermann abstract139 did not report that isassessed fusion status.
In seven of the studies,125,127,131–133,135,138 therewas a 90% or higher fusion rate. The Laursenstudy134 did not report fusion success rates and theBoden study128 gave no numerical data, butreported that the side of the spine the autograftwas used on showed better bone morphology,fusion quality and fusion success than the otherside. Three studies reported fusion rates of25%,130 42%137,141 and 44%.129 Of the studies thatreported lower fusion rates, two studies129,130
included populations with high-risk patients,including rheumatoid disease, psoriatic arthritis,those taking steroids and those with “medical riskfactors known to inhibit spinal fusion”. Fourstudies129,131,136,138,140 reported the mean times tofusion, which ranged from 3 to 6 months.
In a retrospective integrated analysis by Burkusand colleagues,101 the data from the Kleemanstudy131 along with unpublished data from othersites in the same study were compared with asimilar study using autograft bone. Both studiesincluded patients with single-level degenerativedisc disease and used an LT-CAGE inserted usinga laparoscopic approach. The inclusion andexclusion criteria were the same. The preoperativecharacteristics were similar except for thepreoperative working status, where 52% ofpatients who received InFUSE™ were workingpreoperatively, whereas only 45% of patients in theautograft study were working preoperatively.
The fusion rates in the InFUSE study were 94%(81/86) compared with 90% (150/167) in theautograft group at 24 months. Good fusion rateswere seen in both studies, although slightly higherin the study where patients received BMP.
Clinical and adverse events resultsAppendix 22 shows any clinical or other reportedoutcomes.
As reported in the Burkus integrated analysis,101
the mean operating time in the InFUSE study(1.9 ± 0.9 hours) was significantly lower than inthe autograft study (3.1 ± 1.4 hours). There wasalso less blood loss in the InFUSE study, with anaverage reduction of 146.1 ± 406.2 ml, comparedwith 213.6 ± 493 ml in the autograft study. Thehospital stay length was also lower in the InFUSE
study at 1.2 ± 1.1 days compared with 3.0 ± 3.8days in the autograft study.
In the Burkus analysis,101 the reportedimprovement in Oswestry score was greater in theInFUSE study than the autograft study, with amean reduction of 33.6 in the InFUSE study and23.9 in the autograft study. The SF-36 physicalcomponent score improvement was also greater inthe InFUSE study (+16.7) than the autograftstudy (+12.9). The SF-36 pain index was alsoimproved more in the InFUSE study (+41.3)compared with the autograft study (+32.7). Theclinical outcomes and the way in which they werereported were insufficient to come to anyconclusions regarding BMP’s effect on clinicaloutcomes. However, the trend in the clinicaloutcomes reported is an overall improvement infunction and pain, with the exception of the donorsites of iliac crest graft patients. In the twostudies136,137,140 that reported donor site pain,25–58% of patients reported pain at the lastfollow-up.
Appendix 23 shows the details of any secondarysurgical procedures and adverse events reported inthe studies.
Of the studies that reported data on the numberof secondary surgical procedures, threestudies125,132,137,141 reported one secondaryprocedure each, two131,138 reported two secondarysurgeries, one129 reported three second surgeriesand one128 reported four revision surgeries.
The Burkus analysis101 reported fewer secondaryinterventions in the InFUSE study, with 12secondary surgeries being performed in 134patients compared with the autograft study, where57 secondary surgeries were performed in 266patients. Also reported was the return to work ratein both studies. The InFUSE study reported amean return to work rate of 89 days whereas theautograft study reported a mean of 154 days,although it does not say from how many patientsthis was determined.
SummaryThere were 14 case series on the effect of BMPtreatment on spinal fusion (see Appendix 19 for adescriptive summary). These studies were small andhad many methodological weaknesses. No clearconclusions can be inferred from these studies asmany patients had extremely variable diagnosesand received differing surgical procedures.
Health Technology Assessment 2007; Vol. 11: No. 30
133
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.

Health Technology Assessment 2007; Vol. 11: No. 30
135
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 19
Spine case series characteristics
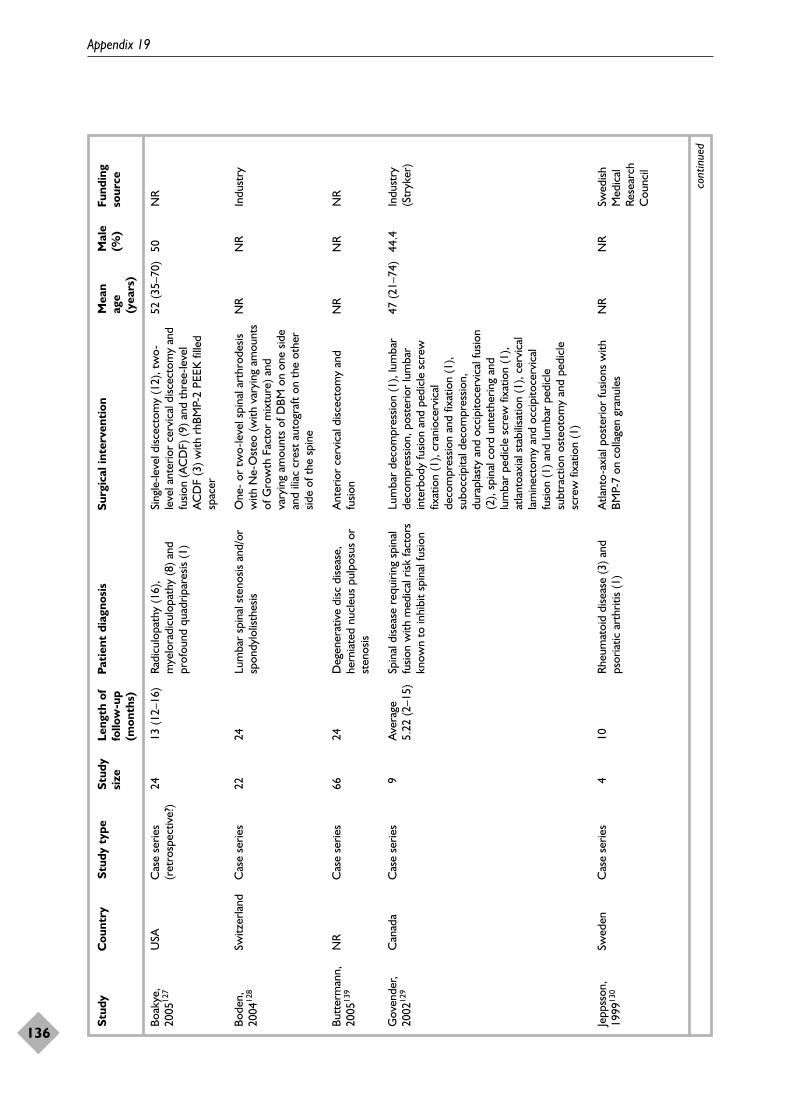
Appendix 19
136
Stud
yC
ount
rySt
udy
type
Stud
yLe
ngth
of
Pati
ent
diag
nosi
sSu
rgic
al in
terv
enti
onM
ean
Mal
e Fu
ndin
g si
zefo
llow
-up
age
(%)
sour
ce(m
onth
s)(y
ears
)
cont
inue
d
Boak
ye,
2005
127
Bode
n,20
0412
8
Butt
erm
ann,
2005
139
Gov
ende
r,20
0212
9
Jepp
sson
,19
9913
0
USA
Switz
erla
nd
NR
Can
ada
Swed
en
Cas
e se
ries
(ret
rosp
ectiv
e?)
Cas
e se
ries
Cas
e se
ries
Cas
e se
ries
Cas
e se
ries
24 22 66 9 4
13 (1
2–16
)
24 24 Ave
rage
5.22
(2–1
5)
10
Radi
culo
path
y (1
6),
mye
lora
dicu
lopa
thy
(8) a
ndpr
ofou
nd q
uadr
ipar
esis
(1)
Lum
bar
spin
al s
teno
sis a
nd/o
rsp
ondy
lolis
thes
is
Deg
ener
ativ
e di
sc d
iseas
e,he
rnia
ted
nucl
eus
pulp
osus
or
sten
osis
Spin
al d
iseas
e re
quiri
ng s
pina
lfu
sion
with
med
ical
risk
fact
ors
know
n to
inhi
bit
spin
al fu
sion
Rheu
mat
oid
dise
ase
(3) a
ndps
oria
tic a
rthr
itis
(1)
Sing
le-le
vel d
iscec
tom
y (1
2), t
wo-
leve
l ant
erio
r ce
rvic
al d
iscec
tom
y an
dfu
sion
(AC
DF)
(9) a
nd t
hree
-leve
lA
CD
F (3
) with
rhB
MP-
2 PE
EK fi
lled
spac
er
One
- or
tw
o-le
vel s
pina
l art
hrod
esis
with
Ne-
Ost
eo (w
ith v
aryi
ng a
mou
nts
of G
row
th F
acto
r m
ixtu
re) a
ndva
ryin
g am
ount
s of
DBM
on
one
side
and
iliac
cre
st a
utog
raft
on t
he o
ther
side
of t
he s
pine
Ant
erio
r ce
rvic
al d
iscec
tom
y an
dfu
sion
Lum
bar
deco
mpr
essio
n (1
), lu
mba
rde
com
pres
sion,
pos
terio
r lu
mba
rin
terb
ody
fusio
n an
d pe
dicl
e sc
rew
fixat
ion
(1),
cran
ioce
rvic
alde
com
pres
sion
and
fixat
ion
(1),
subo
ccip
ital d
ecom
pres
sion,
dura
plas
ty a
nd o
ccip
itoce
rvic
al fu
sion
(2),
spin
al c
ord
unte
ther
ing
and
lum
bar
pedi
cle
scre
w fi
xatio
n (1
),at
lant
oaxi
al s
tabi
lisat
ion
(1),
cerv
ical
lam
inec
tom
y an
d oc
cipi
toce
rvic
alfu
sion
(1) a
nd lu
mba
r pe
dicl
esu
btra
ctio
n os
teot
omy
and
pedi
cle
scre
w fi
xatio
n (1
)
Atla
nto-
axia
l pos
terio
r fu
sions
with
BMP-
7 on
col
lage
n gr
anul
es
52 (3
5–70
)
NR
NR
47 (2
1–74
)
NR
50 NR
NR
44.4
NR
NR
Indu
stry
NR
Indu
stry
(Str
yker
)
Swed
ishM
edic
alRe
sear
chC
ounc
il
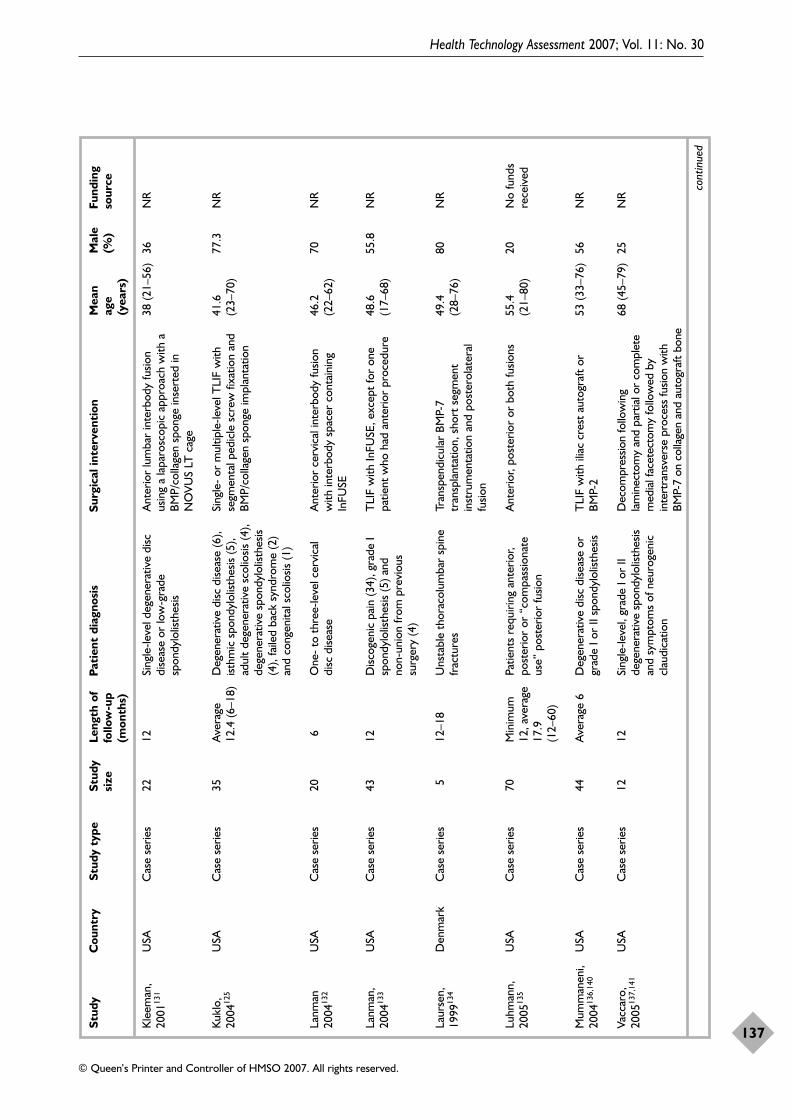
Health Technology Assessment 2007; Vol. 11: No. 30
137
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Stud
yC
ount
rySt
udy
type
Stud
yLe
ngth
of
Pati
ent
diag
nosi
sSu
rgic
al in
terv
enti
onM
ean
Mal
e Fu
ndin
g si
zefo
llow
-up
age
(%)
sour
ce(m
onth
s)(y
ears
)
cont
inue
d
Kle
eman
,20
0113
1
Kukl
o,20
0412
5
Lanm
an20
0413
2
Lanm
an,
2004
133
Laur
sen,
1999
134
Luhm
ann,
2005
135
Mum
man
eni,
2004
136,
140
Vacc
aro,
2005
137,
141
USA
USA
USA
USA
Den
mar
k
USA
USA
USA
Cas
e se
ries
Cas
e se
ries
Cas
e se
ries
Cas
e se
ries
Cas
e se
ries
Cas
e se
ries
Cas
e se
ries
Cas
e se
ries
22 35 20 43 5 70 44 12
12 Ave
rage
12.4
(6–1
8)
6 12 12–1
8
Min
imum
12, a
vera
ge17
.9(1
2–60
)
Ave
rage
6
12
Sing
le-le
vel d
egen
erat
ive
disc
dise
ase
or lo
w-g
rade
spon
dylo
listh
esis
Deg
ener
ativ
e di
sc d
iseas
e (6
),ist
hmic
spo
ndyl
olist
hesis
(5),
adul
t de
gene
rativ
e sc
olio
sis (4
),de
gene
rativ
e sp
ondy
lolis
thes
is(4
), fa
iled
back
syn
drom
e (2
)an
d co
ngen
ital s
colio
sis (1
)
One
- to
thr
ee-le
vel c
ervi
cal
disc
dise
ase
Disc
ogen
ic p
ain
(34)
, gra
de I
spon
dylo
listh
esis
(5) a
nd
non-
unio
n fr
om p
revi
ous
surg
ery
(4)
Uns
tabl
e th
orac
olum
bar
spin
efr
actu
res
Patie
nts
requ
iring
ant
erio
r,po
ster
ior
or “
com
pass
iona
teus
e” p
oste
rior
fusio
n
Deg
ener
ativ
e di
sc d
iseas
e or
grad
e I o
r II
spon
dylo
listh
esis
Sing
le-le
vel,
grad
e I o
r II
dege
nera
tive
spon
dylo
listh
esis
and
sym
ptom
s of
neu
roge
nic
clau
dica
tion
Ant
erio
r lu
mba
r in
terb
ody
fusio
nus
ing
a la
paro
scop
ic a
ppro
ach
with
aBM
P/co
llage
n sp
onge
inse
rted
inN
OVU
S LT
cag
e
Sing
le-
or m
ultip
le-le
vel T
LIF
with
segm
enta
l ped
icle
scr
ew fi
xatio
n an
dBM
P/co
llage
n sp
onge
impl
anta
tion
Ant
erio
r ce
rvic
al in
terb
ody
fusio
nw
ith in
terb
ody
spac
er c
onta
inin
gIn
FUSE
TLI
F w
ith In
FUSE
, exc
ept
for
one
patie
nt w
ho h
ad a
nter
ior
proc
edur
e
Tran
spen
dicu
lar
BMP-
7tr
ansp
lant
atio
n, s
hort
seg
men
tin
stru
men
tatio
n an
d po
ster
olat
eral
fusio
n
Ant
erio
r, po
ster
ior
or b
oth
fusio
ns
TLI
F w
ith il
iac
cres
t au
togr
aft
orBM
P-2
Dec
ompr
essio
n fo
llow
ing
lam
inec
tom
y an
d pa
rtia
l or
com
plet
em
edia
l fac
etec
tom
y fo
llow
ed b
yin
tert
rans
vers
e pr
oces
s fu
sion
with
BMP-
7 on
col
lage
n an
d au
togr
aft b
one
38 (2
1–56
)
41.6
(23–
70)
46.2
(22–
62)
48.6
(17–
68)
49.4
(28–
76)
55.4
(21–
80)
53 (3
3–76
)
68 (4
5–79
)
36 77.3
70 55.8
80 20 56 25
NR
NR
NR
NR
NR
No
fund
sre
ceiv
ed
NR
NR

Appendix 19
138
Stud
yC
ount
rySt
udy
type
Stud
yLe
ngth
of
Pati
ent
diag
nosi
sSu
rgic
al in
terv
enti
onM
ean
Mal
e Fu
ndin
g si
zefo
llow
-up
age
(%)
sour
ce(m
onth
s)(y
ears
)
TLI
F, tr
ansf
oram
inal
lum
bar
inte
rbod
y fu
sion.
Villa
vice
ncio
,20
0513
8U
SAC
ase
serie
s74
12D
egen
erat
ive
disc
dise
ase
TLI
F w
ith r
hBM
P-2
on c
olla
gen
with
auto
graf
t bo
ne a
nd o
ne o
r tw
ost
ruct
ural
bon
e al
logr
afts
56.9
(20–
82)
37.8
NR
Health Technology Assessment 2007; Vol. 11: No. 30
139
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 20
Spine case series interventions
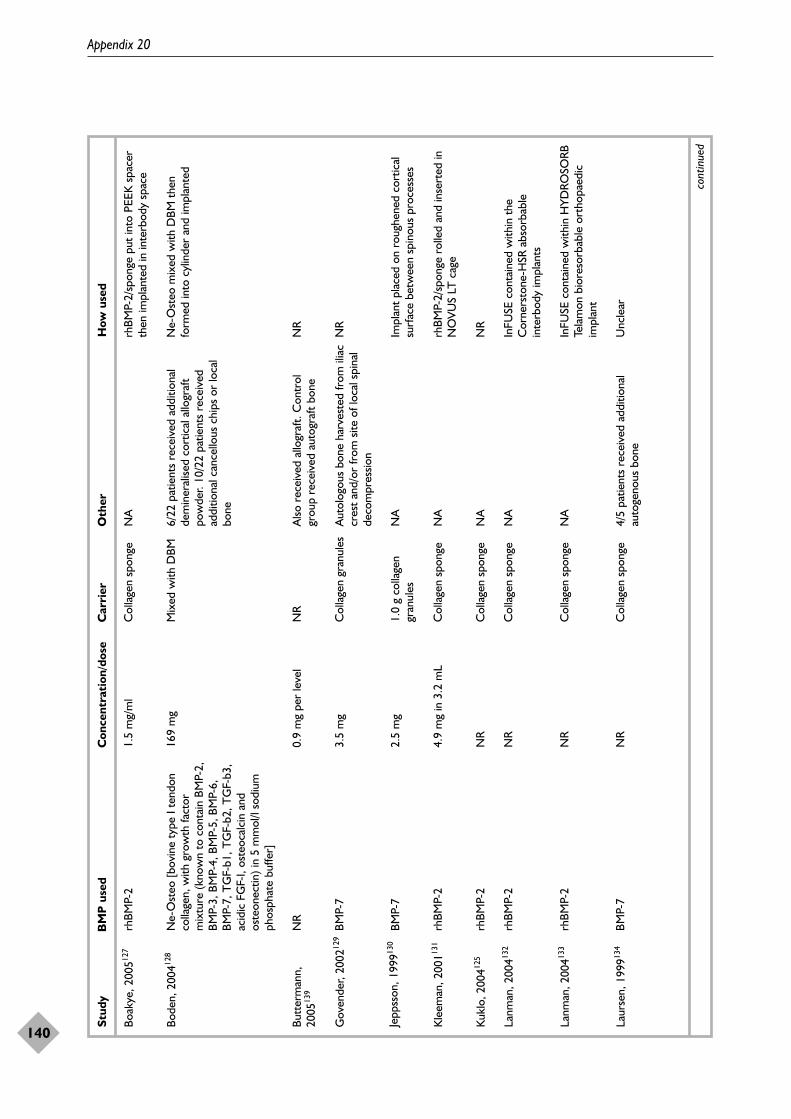
Appendix 20
140
Stud
yB
MP
use
dC
once
ntra
tion
/dos
eC
arri
erO
ther
How
use
d
cont
inue
d
Boak
ye, 2
00512
7rh
BMP-
21.
5 m
g/m
lC
olla
gen
spon
geN
Arh
BMP-
2/sp
onge
put
into
PEE
K s
pace
rth
en im
plan
ted
in in
terb
ody
spac
e
Bode
n, 2
00412
8N
e-O
steo
[bov
ine
type
I te
ndon
colla
gen,
with
gro
wth
fact
orm
ixtu
re (k
now
n to
con
tain
BM
P-2,
BMP-
3, B
MP-
4, B
MP-
5, B
MP-
6,BM
P-7,
TG
F-b1
, TG
F-b2
, TG
F-b3
,ac
idic
FG
F-I,
oste
ocal
cin
and
oste
onec
tin) i
n 5
mm
ol/l
sodi
umph
osph
ate
buffe
r]
169
mg
Mix
ed w
ith D
BM6/
22 p
atie
nts
rece
ived
add
ition
alde
min
eral
ised
cort
ical
allo
graf
tpo
wde
r. 10
/22
patie
nts
rece
ived
addi
tiona
l can
cello
us c
hips
or
loca
lbo
ne
Ne-
Ost
eo m
ixed
with
DBM
the
nfo
rmed
into
cyl
inde
r an
d im
plan
ted
Butt
erm
ann,
2005
139
NR
0.9
mg
per
leve
lN
RA
lso r
ecei
ved
allo
graf
t. C
ontr
olgr
oup
rece
ived
aut
ogra
ft bo
neN
R
Gov
ende
r, 20
0212
9BM
P-7
3.5
mg
Col
lage
n gr
anul
esA
utol
ogou
s bo
ne h
arve
sted
from
ilia
ccr
est
and/
or fr
om s
ite o
f loc
al s
pina
lde
com
pres
sion
NR
Jepp
sson
, 199
9130
BMP-
72.
5 m
g1.
0 g
colla
gen
gran
ules
NA
Impl
ant
plac
ed o
n ro
ughe
ned
cort
ical
surf
ace
betw
een
spin
ous
proc
esse
s
Kle
eman
, 200
1131
rhBM
P-2
4.9
mg
in 3
.2 m
LC
olla
gen
spon
geN
Arh
BMP-
2/sp
onge
rol
led
and
inse
rted
inN
OVU
S LT
cag
e
Kukl
o, 2
00412
5rh
BMP-
2N
RC
olla
gen
spon
geN
AN
R
Lanm
an, 2
00413
2rh
BMP-
2N
RC
olla
gen
spon
geN
AIn
FUSE
con
tain
ed w
ithin
the
Cor
ners
tone
-HSR
abs
orba
ble
inte
rbod
y im
plan
ts
Lanm
an, 2
00413
3rh
BMP-
2N
RC
olla
gen
spon
geN
AIn
FUSE
con
tain
ed w
ithin
HYD
ROSO
RBTe
lam
on b
iore
sorb
able
ort
hopa
edic
impl
ant
Laur
sen,
199
9134
BMP-
7N
RC
olla
gen
spon
ge4/
5 pa
tient
s re
ceiv
ed a
dditi
onal
auto
geno
us b
one
Unc
lear
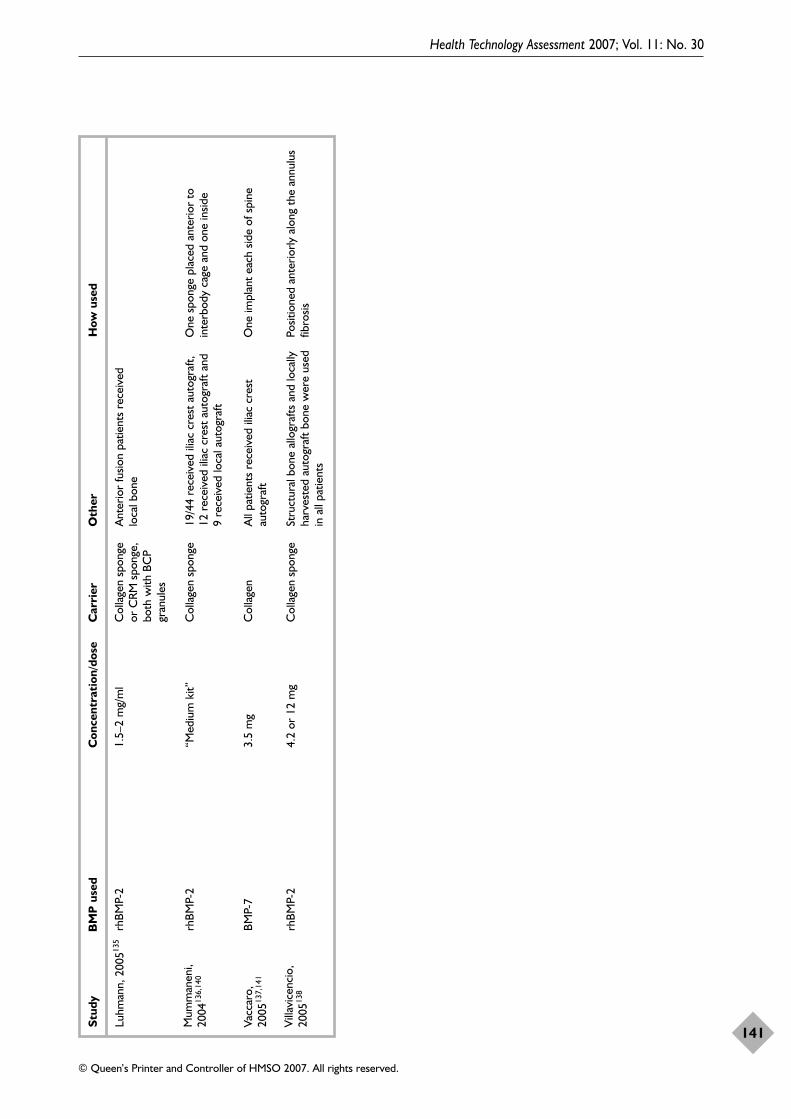
Health Technology Assessment 2007; Vol. 11: No. 30
141
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Stud
yB
MP
use
dC
once
ntra
tion
/dos
eC
arri
erO
ther
How
use
d
Luhm
ann,
200
5135
rhBM
P-2
1.5–
2 m
g/m
lC
olla
gen
spon
geor
CRM
spo
nge,
both
with
BC
Pgr
anul
es
Ant
erio
r fu
sion
patie
nts
rece
ived
loca
l bon
e
Mum
man
eni,
2004
136,
140
rhBM
P-2
“Med
ium
kit”
Col
lage
n sp
onge
19/4
4 re
ceiv
ed il
iac
cres
t au
togr
aft,
12 r
ecei
ved
iliac
cre
st a
utog
raft
and
9 re
ceiv
ed lo
cal a
utog
raft
One
spo
nge
plac
ed a
nter
ior
toin
terb
ody
cage
and
one
insid
e
Vacc
aro,
2005
137,
141
BMP-
73.
5 m
gC
olla
gen
All
patie
nts
rece
ived
ilia
c cr
est
auto
graf
tO
ne im
plan
t ea
ch s
ide
of s
pine
Villa
vice
ncio
,20
0513
8rh
BMP-
24.
2 or
12
mg
Col
lage
n sp
onge
Stru
ctur
al b
one
allo
graf
ts a
nd lo
cally
harv
este
d au
togr
aft
bone
wer
e us
edin
all
patie
nts
Posit
ione
d an
terio
rly a
long
the
ann
ulus
fibro
sis

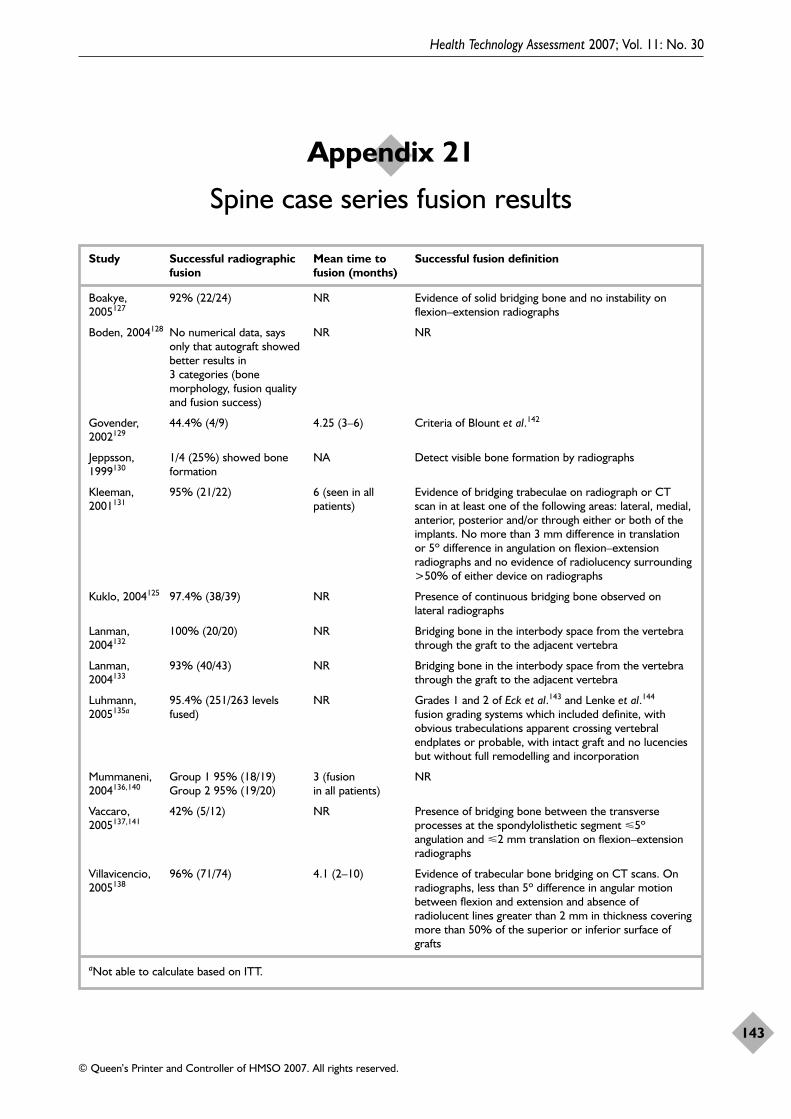
Health Technology Assessment 2007; Vol. 11: No. 30
143
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 21
Spine case series fusion results
Study Successful radiographic Mean time to Successful fusion definitionfusion fusion (months)
Boakye, 92% (22/24) NR Evidence of solid bridging bone and no instability on 2005127 flexion–extension radiographs
Boden, 2004128 No numerical data, says NR NRonly that autograft showed better results in 3 categories (bone morphology, fusion quality and fusion success)
Govender, 44.4% (4/9) 4.25 (3–6) Criteria of Blount et al.142
2002129
Jeppsson, 1/4 (25%) showed bone NA Detect visible bone formation by radiographs1999130 formation
Kleeman, 95% (21/22) 6 (seen in all Evidence of bridging trabeculae on radiograph or CT 2001131 patients) scan in at least one of the following areas: lateral, medial,
anterior, posterior and/or through either or both of theimplants. No more than 3 mm difference in translationor 5º difference in angulation on flexion–extensionradiographs and no evidence of radiolucency surrounding>50% of either device on radiographs
Kuklo, 2004125 97.4% (38/39) NR Presence of continuous bridging bone observed onlateral radiographs
Lanman, 100% (20/20) NR Bridging bone in the interbody space from the vertebra 2004132 through the graft to the adjacent vertebra
Lanman, 93% (40/43) NR Bridging bone in the interbody space from the vertebra 2004133 through the graft to the adjacent vertebra
Luhmann, 95.4% (251/263 levels NR Grades 1 and 2 of Eck et al.143 and Lenke et al.144
2005135a fused) fusion grading systems which included definite, withobvious trabeculations apparent crossing vertebralendplates or probable, with intact graft and no lucenciesbut without full remodelling and incorporation
Mummaneni, Group 1 95% (18/19) 3 (fusion NR2004136,140 Group 2 95% (19/20) in all patients)
Vaccaro, 42% (5/12) NR Presence of bridging bone between the transverse 2005137,141 processes at the spondylolisthetic segment �5º
angulation and �2 mm translation on flexion–extensionradiographs
Villavicencio, 96% (71/74) 4.1 (2–10) Evidence of trabecular bone bridging on CT scans. On 2005138 radiographs, less than 5º difference in angular motion
between flexion and extension and absence ofradiolucent lines greater than 2 mm in thickness coveringmore than 50% of the superior or inferior surface ofgrafts
aNot able to calculate based on ITT.

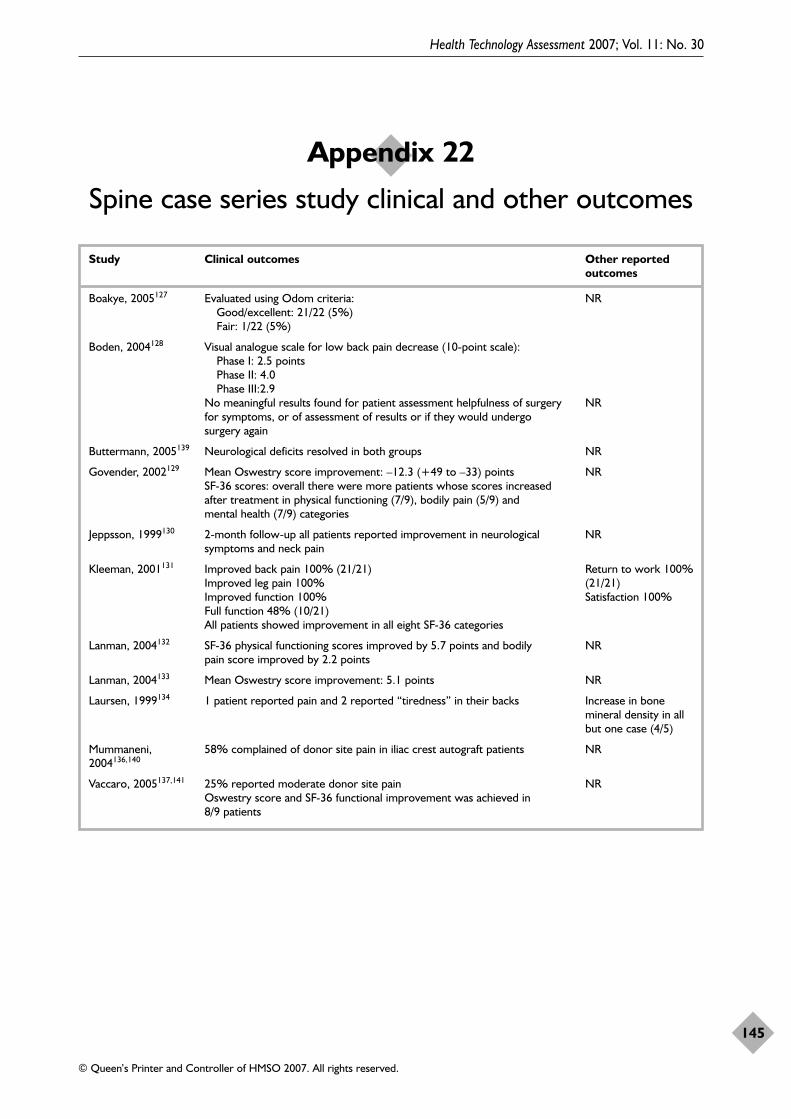
Health Technology Assessment 2007; Vol. 11: No. 30
145
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 22
Spine case series study clinical and other outcomes
Study Clinical outcomes Other reportedoutcomes
Boakye, 2005127 Evaluated using Odom criteria: NRGood/excellent: 21/22 (5%)Fair: 1/22 (5%)
Boden, 2004128 Visual analogue scale for low back pain decrease (10-point scale):Phase I: 2.5 points Phase II: 4.0Phase III:2.9
No meaningful results found for patient assessment helpfulness of surgery NRfor symptoms, or of assessment of results or if they would undergo surgery again
Buttermann, 2005139 Neurological deficits resolved in both groups NR
Govender, 2002129 Mean Oswestry score improvement: –12.3 (+49 to –33) points NRSF-36 scores: overall there were more patients whose scores increased after treatment in physical functioning (7/9), bodily pain (5/9) and mental health (7/9) categories
Jeppsson, 1999130 2-month follow-up all patients reported improvement in neurological NRsymptoms and neck pain
Kleeman, 2001131 Improved back pain 100% (21/21) Return to work 100% Improved leg pain 100% (21/21)Improved function 100% Satisfaction 100%Full function 48% (10/21)All patients showed improvement in all eight SF-36 categories
Lanman, 2004132 SF-36 physical functioning scores improved by 5.7 points and bodily NRpain score improved by 2.2 points
Lanman, 2004133 Mean Oswestry score improvement: 5.1 points NR
Laursen, 1999134 1 patient reported pain and 2 reported “tiredness” in their backs Increase in bonemineral density in allbut one case (4/5)
Mummaneni, 58% complained of donor site pain in iliac crest autograft patients NR2004136,140
Vaccaro, 2005137,141 25% reported moderate donor site pain NROswestry score and SF-36 functional improvement was achieved in 8/9 patients


Health Technology Assessment 2007; Vol. 11: No. 30
147
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 23
Spine case series secondary procedures and adverse events
Study Secondary surgical procedures Adverse events
Boakye, 2005127 NR 1 patient died 4 weeks postoperatively of medical complicationsincluding sepsis and respiratory distress. Transient dysphagia (2),CSF leakage with ossification of posterior longitudinal ligament(1), transient C-5 paresis (1) and transient vocal cord paresis (1).Clinically asymptomatic heterotopic bone formation (1)
Boden, 2004128 4/22 revision surgery Wound dehiscence, nerve root irritation, revision due toadjacent segment degeneration, pseudarthrosis caused by absentbone formation and dural tear (one each)
Buttermann, Control group had 1 pseudoarthrosis and 2 donor site 2005139 complications
Neck swelling was 4 times as likely in BMP group
Govender, Halo vest immobilisation for Cerebrospinal fluid leak and further spinal cord compression 2002129 3 months (1), further surgical leading to further deterioration
intervention not specified (1), insertion of temporary lumbar spinal drain (1)
Jeppsson, NR Impaired motion at neck (1), 8 mm redislocation in patient who 1999130 removed neck collar
Kleeman, Laparoscopic repair of two Bowel injury (1) and vascular injury (1) related to laparoscopic 2001131 adverse events technique
Kuklo, 2004125 Foraminal decompression to relieve 2 transient neurapraxia or mild motor weakness and persistent radiculopathy right-sided L-5 neurodynia. 1 intraoperative dural tear
Lanman, Second surgery for non-union Severe dysphagia2004132
Lanman, NR Dural tear on nerve root sleeve which led to numbness of right 2004133 leg which resolved in 3 weeks
Laursen, 1999134 NR Screw loosening. Resorption of whole anterior column atfracture level
Luhmann, NR 1 superficial wound dehiscence, 1 deep wound infection and 2005135 1 wound haematoma
Mummaneni, NR Pseudoarthrosis (1)2004136,140
Vaccaro, Revision instrumented surgical fusion Pseudoarthrosis (1)2005137,141
Villavicencio, Reoperation for screw position. 2005138 Removal of allograft at 15 months due
to migration into epidural space.Second surgery to extend fusion to an adjacent level (2 minimally invasive and 3 open)
CSF, cerebrospinal fluid.

The following is a statement by Adam Frere-Smith, consumer representative.
On the 9th of October, 2003, I had a sportingaccident that resulted in a double open compoundfracture to my left tibia and fibula. My fracture wastreated using intramedullary nail fixation. At thetime of the accident I was leading a very activelifestyle that revolved around surfing, mountainbiking, mountain boarding, fitness training andmartial arts, in which I was an assistant instructor.I was working as a hygiene technician and alsostudying at college. I had no car and travelled bybicycle and public transport.
After my release from hospital I spent 2 weeksconvalescing with family as I was living in a secondfloor flat; the first week I was confined to bed as Iwas still on pain management medication. I hadbeen issued with a pair of ‘walking sticks’, butfound these very difficult to use at first.
During the first couple of weeks back home manyfriends and family helped with transport andshopping, etc.; however, I was beginning to feelvery dependent and missed the social interactionof my hobbies. My income dropped to statutorysick pay, which hugely impacted my standard ofliving and quality of life.
During the study I had to attend regular checks at the orthopaedic clinic in the Norfolk andNorwich University Hospital (NNUH) where my progress was measured by X-ray. The two high points were when the clinician told me I had union of the fracture, although this had noaffect on my ability to walk, and when I was given the go-ahead to start load bearing on myleg.
As a patient, I think these two moments werepivotal to my perceived recovery rate. The first, because I was feeling so low at the time,missing work and activities, that it was a real boost to be told and to see on the X-ray, that mybone was getting ‘whole’ again; and the second,because learning to walk again felt like the endwas nearly in sight. It wasn’t though; it took many more weeks before I could walk without thesticks.
One aspect of my treatment that I think helpedwas the use of an internal fixation (intramedullarynail). It allowed me to wear my normal clothes, asopposed to patients who had casts or externalcages that are more obtrusive. Because of this, Ibelieve that I engaged in ‘normal’ lifestyle andsocial activities that helped my recovery, such asswimming, social outings and trips to thecountryside and beach, at a much earlier time,which I believe hastened my return to work andimproved my well-being.
After reading the draft report I was pleased to seethat it has highlighted some very encouragingpoints, from a patient’s point of view. Pain fromthe injured area over a prolonged period of timecan be very depressing and to have thiscompounded by additional pain from the donorsite when grafting is used would be doublydistressing and also increase the possibility ofinfections. If an alternative to grafting is available,and is shown to be just as effective, I believe itshould be used at every opportunity for thebenefit of the patient’s recovery, well-being andtheir quality of life.
It was very encouraging to read that BMP may beable to lower operation times, reduce blood loss,fracture and donor site pain, length of hospitalstay, reduce the risk of site infections and speedreturn to work and has no adverse affects onpatients. I feel these are all areas of distress for thepatient and their families and further investigationinto the use of BMP should be carried out ifprogress can be made to improve these outcomes,especially operation times, hospital stay andinfection risk, which are three major concerns topatients and their families.
As previously mentioned, the time of fractureunion and load bearing was to me, a major factorin my mental and physical recovery. To be able toaccelerate the time to union would be a verywelcome aspect. To be able to start to engage in‘normal’ activities again is very uplifting, to allparties involved, and no doubt speeds recoveryfurther.
Outpatient visits are another source of distress toboth patient and family, and as it will usually
Health Technology Assessment 2007; Vol. 11: No. 30
149
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Appendix 24
Patient statement

involve a third party for transportation reasons,incurs further economic hardship through thethird party’s loss of work that day and the patient’sfeelings of guilt and burden. The possibility of areduction in outpatient visits through acceleratedunion, reduction of the risk of infection and lowersecondary intervention rates are areas that I feelmost patients would like to see reduced.
I believe that research, which can help developgood or new practices and procedures, should be anecessity. From a patient’s point of view, if researchcan result in the improvement of front lineservices that will increase patient comfort andaccelerate healing then it should be carried out.Although I am not in the position to comment onthe economic findings of the report (how much istoo much to pay for a QALY and who is to decidethis figure), I believe the reasons for exploring thisarea of treatment are justified (societal costs andimproving patient recovery). Further research
would be a worthwhile investment especially if itwould clarify the discrepancies in the economicmodelling and bring greater uniformity whencomparing study results to identify good practice.
Although this study is looking at the economics ofBMP use, I feel strongly that the patient’s qualityof life is important in recovery and may alsoimpact on the economics of a treatment byfacilitating earlier return to work times.
Any treatments that can reduce areas such as pain,blood loss, treatment time, and the use of ‘visible’aids over similar treatments are important from apatient’s perspective, not only from the medicalpoint of view, but also in the way they can improvethe quality of the patient’s life. I believe thatresearch that includes investigation into quality oflife has the ability to highlight practices,procedures and treatments that may enhancemedical recovery due to their psychological affect.
Appendix 22
150
Health Technology Assessment 2007; Vol. 11: No. 30
151
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Volume 1, 1997
No. 1Home parenteral nutrition: a systematicreview.
By Richards DM, Deeks JJ, SheldonTA, Shaffer JL.
No. 2Diagnosis, management and screeningof early localised prostate cancer.
A review by Selley S, Donovan J,Faulkner A, Coast J, Gillatt D.
No. 3The diagnosis, management, treatmentand costs of prostate cancer in Englandand Wales.
A review by Chamberlain J, Melia J,Moss S, Brown J.
No. 4Screening for fragile X syndrome.
A review by Murray J, Cuckle H,Taylor G, Hewison J.
No. 5A review of near patient testing inprimary care.
By Hobbs FDR, Delaney BC,Fitzmaurice DA, Wilson S, Hyde CJ,Thorpe GH, et al.
No. 6Systematic review of outpatient servicesfor chronic pain control.
By McQuay HJ, Moore RA, EcclestonC, Morley S, de C Williams AC.
No. 7Neonatal screening for inborn errors ofmetabolism: cost, yield and outcome.
A review by Pollitt RJ, Green A,McCabe CJ, Booth A, Cooper NJ,Leonard JV, et al.
No. 8Preschool vision screening.
A review by Snowdon SK, Stewart-Brown SL.
No. 9Implications of socio-cultural contextsfor the ethics of clinical trials.
A review by Ashcroft RE, ChadwickDW, Clark SRL, Edwards RHT, Frith L,Hutton JL.
No. 10A critical review of the role of neonatalhearing screening in the detection ofcongenital hearing impairment.
By Davis A, Bamford J, Wilson I,Ramkalawan T, Forshaw M, Wright S.
No. 11Newborn screening for inborn errors ofmetabolism: a systematic review.
By Seymour CA, Thomason MJ,Chalmers RA, Addison GM, Bain MD,Cockburn F, et al.
No. 12Routine preoperative testing: a systematic review of the evidence.
By Munro J, Booth A, Nicholl J.
No. 13Systematic review of the effectiveness of laxatives in the elderly.
By Petticrew M, Watt I, Sheldon T.
No. 14When and how to assess fast-changingtechnologies: a comparative study ofmedical applications of four generictechnologies.
A review by Mowatt G, Bower DJ,Brebner JA, Cairns JA, Grant AM,McKee L.
Volume 2, 1998
No. 1Antenatal screening for Down’ssyndrome.
A review by Wald NJ, Kennard A,Hackshaw A, McGuire A.
No. 2Screening for ovarian cancer: a systematic review.
By Bell R, Petticrew M, Luengo S,Sheldon TA.
No. 3Consensus development methods, andtheir use in clinical guidelinedevelopment.
A review by Murphy MK, Black NA,Lamping DL, McKee CM, SandersonCFB, Askham J, et al.
No. 4A cost–utility analysis of interferon beta for multiple sclerosis.
By Parkin D, McNamee P, Jacoby A,Miller P, Thomas S, Bates D.
No. 5Effectiveness and efficiency of methodsof dialysis therapy for end-stage renaldisease: systematic reviews.
By MacLeod A, Grant A, Donaldson C, Khan I, Campbell M,Daly C, et al.
No. 6Effectiveness of hip prostheses inprimary total hip replacement: a criticalreview of evidence and an economicmodel.
By Faulkner A, Kennedy LG, Baxter K, Donovan J, Wilkinson M,Bevan G.
No. 7Antimicrobial prophylaxis in colorectalsurgery: a systematic review ofrandomised controlled trials.
By Song F, Glenny AM.
No. 8Bone marrow and peripheral bloodstem cell transplantation for malignancy.
A review by Johnson PWM, Simnett SJ,Sweetenham JW, Morgan GJ, Stewart LA.
No. 9Screening for speech and languagedelay: a systematic review of theliterature.
By Law J, Boyle J, Harris F, HarknessA, Nye C.
No. 10Resource allocation for chronic stableangina: a systematic review ofeffectiveness, costs and cost-effectiveness of alternativeinterventions.
By Sculpher MJ, Petticrew M, Kelland JL, Elliott RA, Holdright DR,Buxton MJ.
No. 11Detection, adherence and control ofhypertension for the prevention ofstroke: a systematic review.
By Ebrahim S.
No. 12Postoperative analgesia and vomiting,with special reference to day-casesurgery: a systematic review.
By McQuay HJ, Moore RA.
No. 13Choosing between randomised andnonrandomised studies: a systematicreview.
By Britton A, McKee M, Black N,McPherson K, Sanderson C, Bain C.
No. 14Evaluating patient-based outcomemeasures for use in clinical trials.
A review by Fitzpatrick R, Davey C,Buxton MJ, Jones DR.
Health Technology Assessment reports published to date
No. 15Ethical issues in the design and conductof randomised controlled trials.
A review by Edwards SJL, Lilford RJ,Braunholtz DA, Jackson JC, Hewison J,Thornton J.
No. 16Qualitative research methods in healthtechnology assessment: a review of theliterature.
By Murphy E, Dingwall R, GreatbatchD, Parker S, Watson P.
No. 17The costs and benefits of paramedicskills in pre-hospital trauma care.
By Nicholl J, Hughes S, Dixon S,Turner J, Yates D.
No. 18Systematic review of endoscopicultrasound in gastro-oesophagealcancer.
By Harris KM, Kelly S, Berry E,Hutton J, Roderick P, Cullingworth J, et al.
No. 19Systematic reviews of trials and otherstudies.
By Sutton AJ, Abrams KR, Jones DR,Sheldon TA, Song F.
No. 20Primary total hip replacement surgery: a systematic review of outcomes andmodelling of cost-effectivenessassociated with different prostheses.
A review by Fitzpatrick R, Shortall E,Sculpher M, Murray D, Morris R, LodgeM, et al.
Volume 3, 1999
No. 1Informed decision making: an annotatedbibliography and systematic review.
By Bekker H, Thornton JG, Airey CM, Connelly JB, Hewison J,Robinson MB, et al.
No. 2Handling uncertainty when performingeconomic evaluation of healthcareinterventions.
A review by Briggs AH, Gray AM.
No. 3The role of expectancies in the placeboeffect and their use in the delivery ofhealth care: a systematic review.
By Crow R, Gage H, Hampson S,Hart J, Kimber A, Thomas H.
No. 4A randomised controlled trial ofdifferent approaches to universalantenatal HIV testing: uptake andacceptability. Annex: Antenatal HIVtesting – assessment of a routinevoluntary approach.
By Simpson WM, Johnstone FD, BoydFM, Goldberg DJ, Hart GJ, GormleySM, et al.
No. 5Methods for evaluating area-wide andorganisation-based interventions inhealth and health care: a systematicreview.
By Ukoumunne OC, Gulliford MC,Chinn S, Sterne JAC, Burney PGJ.
No. 6Assessing the costs of healthcaretechnologies in clinical trials.
A review by Johnston K, Buxton MJ,Jones DR, Fitzpatrick R.
No. 7Cooperatives and their primary careemergency centres: organisation andimpact.
By Hallam L, Henthorne K.
No. 8Screening for cystic fibrosis.
A review by Murray J, Cuckle H,Taylor G, Littlewood J, Hewison J.
No. 9A review of the use of health statusmeasures in economic evaluation.
By Brazier J, Deverill M, Green C,Harper R, Booth A.
No. 10Methods for the analysis of quality-of-life and survival data in healthtechnology assessment.
A review by Billingham LJ, AbramsKR, Jones DR.
No. 11Antenatal and neonatalhaemoglobinopathy screening in theUK: review and economic analysis.
By Zeuner D, Ades AE, Karnon J,Brown J, Dezateux C, Anionwu EN.
No. 12Assessing the quality of reports ofrandomised trials: implications for theconduct of meta-analyses.
A review by Moher D, Cook DJ, JadadAR, Tugwell P, Moher M, Jones A, et al.
No. 13‘Early warning systems’ for identifyingnew healthcare technologies.
By Robert G, Stevens A, Gabbay J.
No. 14A systematic review of the role of humanpapillomavirus testing within a cervicalscreening programme.
By Cuzick J, Sasieni P, Davies P,Adams J, Normand C, Frater A, et al.
No. 15Near patient testing in diabetes clinics:appraising the costs and outcomes.
By Grieve R, Beech R, Vincent J,Mazurkiewicz J.
No. 16Positron emission tomography:establishing priorities for healthtechnology assessment.
A review by Robert G, Milne R.
No. 17 (Pt 1)The debridement of chronic wounds: a systematic review.
By Bradley M, Cullum N, Sheldon T.
No. 17 (Pt 2)Systematic reviews of wound caremanagement: (2) Dressings and topicalagents used in the healing of chronicwounds.
By Bradley M, Cullum N, Nelson EA,Petticrew M, Sheldon T, Torgerson D.
No. 18A systematic literature review of spiraland electron beam computedtomography: with particular reference toclinical applications in hepatic lesions,pulmonary embolus and coronary arterydisease.
By Berry E, Kelly S, Hutton J, Harris KM, Roderick P, Boyce JC, et al.
No. 19What role for statins? A review andeconomic model.
By Ebrahim S, Davey Smith G,McCabe C, Payne N, Pickin M, SheldonTA, et al.
No. 20Factors that limit the quality, numberand progress of randomised controlledtrials.
A review by Prescott RJ, Counsell CE,Gillespie WJ, Grant AM, Russell IT,Kiauka S, et al.
No. 21Antimicrobial prophylaxis in total hipreplacement: a systematic review.
By Glenny AM, Song F.
No. 22Health promoting schools and healthpromotion in schools: two systematicreviews.
By Lister-Sharp D, Chapman S,Stewart-Brown S, Sowden A.
No. 23Economic evaluation of a primary care-based education programme for patientswith osteoarthritis of the knee.
A review by Lord J, Victor C,Littlejohns P, Ross FM, Axford JS.
Volume 4, 2000
No. 1The estimation of marginal timepreference in a UK-wide sample(TEMPUS) project.
A review by Cairns JA, van der PolMM.
No. 2Geriatric rehabilitation followingfractures in older people: a systematicreview.
By Cameron I, Crotty M, Currie C,Finnegan T, Gillespie L, Gillespie W, et al.
Health Technology Assessment reports published to date
152

No. 3Screening for sickle cell disease andthalassaemia: a systematic review withsupplementary research.
By Davies SC, Cronin E, Gill M,Greengross P, Hickman M, Normand C.
No. 4Community provision of hearing aidsand related audiology services.
A review by Reeves DJ, Alborz A,Hickson FS, Bamford JM.
No. 5False-negative results in screeningprogrammes: systematic review ofimpact and implications.
By Petticrew MP, Sowden AJ, Lister-Sharp D, Wright K.
No. 6Costs and benefits of communitypostnatal support workers: arandomised controlled trial.
By Morrell CJ, Spiby H, Stewart P,Walters S, Morgan A.
No. 7Implantable contraceptives (subdermalimplants and hormonally impregnatedintrauterine systems) versus other formsof reversible contraceptives: twosystematic reviews to assess relativeeffectiveness, acceptability, tolerabilityand cost-effectiveness.
By French RS, Cowan FM, MansourDJA, Morris S, Procter T, Hughes D, et al.
No. 8An introduction to statistical methodsfor health technology assessment.
A review by White SJ, Ashby D, Brown PJ.
No. 9Disease-modifying drugs for multiplesclerosis: a rapid and systematic review.
By Clegg A, Bryant J, Milne R.
No. 10Publication and related biases.
A review by Song F, Eastwood AJ,Gilbody S, Duley L, Sutton AJ.
No. 11Cost and outcome implications of theorganisation of vascular services.
By Michaels J, Brazier J, PalfreymanS, Shackley P, Slack R.
No. 12Monitoring blood glucose control indiabetes mellitus: a systematic review.
By Coster S, Gulliford MC, Seed PT,Powrie JK, Swaminathan R.
No. 13The effectiveness of domiciliary healthvisiting: a systematic review ofinternational studies and a selective review of the Britishliterature.
By Elkan R, Kendrick D, Hewitt M,Robinson JJA, Tolley K, Blair M, et al.
No. 14The determinants of screening uptakeand interventions for increasing uptake:a systematic review.
By Jepson R, Clegg A, Forbes C,Lewis R, Sowden A, Kleijnen J.
No. 15The effectiveness and cost-effectivenessof prophylactic removal of wisdomteeth.
A rapid review by Song F, O’Meara S,Wilson P, Golder S, Kleijnen J.
No. 16Ultrasound screening in pregnancy: asystematic review of the clinicaleffectiveness, cost-effectiveness andwomen’s views.
By Bricker L, Garcia J, Henderson J,Mugford M, Neilson J, Roberts T, et al.
No. 17A rapid and systematic review of theeffectiveness and cost-effectiveness ofthe taxanes used in the treatment ofadvanced breast and ovarian cancer.
By Lister-Sharp D, McDonagh MS,Khan KS, Kleijnen J.
No. 18Liquid-based cytology in cervicalscreening: a rapid and systematic review.
By Payne N, Chilcott J, McGoogan E.
No. 19Randomised controlled trial of non-directive counselling,cognitive–behaviour therapy and usualgeneral practitioner care in themanagement of depression as well asmixed anxiety and depression inprimary care.
By King M, Sibbald B, Ward E, BowerP, Lloyd M, Gabbay M, et al.
No. 20Routine referral for radiography ofpatients presenting with low back pain:is patients’ outcome influenced by GPs’referral for plain radiography?
By Kerry S, Hilton S, Patel S, DundasD, Rink E, Lord J.
No. 21Systematic reviews of wound caremanagement: (3) antimicrobial agentsfor chronic wounds; (4) diabetic footulceration.
By O’Meara S, Cullum N, Majid M,Sheldon T.
No. 22Using routine data to complement andenhance the results of randomisedcontrolled trials.
By Lewsey JD, Leyland AH, Murray GD, Boddy FA.
No. 23Coronary artery stents in the treatmentof ischaemic heart disease: a rapid andsystematic review.
By Meads C, Cummins C, Jolly K,Stevens A, Burls A, Hyde C.
No. 24Outcome measures for adult criticalcare: a systematic review.
By Hayes JA, Black NA, Jenkinson C, Young JD, Rowan KM,Daly K, et al.
No. 25A systematic review to evaluate theeffectiveness of interventions to promote the initiation of breastfeeding.
By Fairbank L, O’Meara S, RenfrewMJ, Woolridge M, Sowden AJ, Lister-Sharp D.
No. 26Implantable cardioverter defibrillators:arrhythmias. A rapid and systematicreview.
By Parkes J, Bryant J, Milne R.
No. 27Treatments for fatigue in multiplesclerosis: a rapid and systematic review.
By Brañas P, Jordan R, Fry-Smith A,Burls A, Hyde C.
No. 28Early asthma prophylaxis, naturalhistory, skeletal development andeconomy (EASE): a pilot randomisedcontrolled trial.
By Baxter-Jones ADG, Helms PJ,Russell G, Grant A, Ross S, Cairns JA, et al.
No. 29Screening for hypercholesterolaemiaversus case finding for familialhypercholesterolaemia: a systematicreview and cost-effectiveness analysis.
By Marks D, Wonderling D,Thorogood M, Lambert H, HumphriesSE, Neil HAW.
No. 30A rapid and systematic review of theclinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIaantagonists in the medical managementof unstable angina.
By McDonagh MS, Bachmann LM,Golder S, Kleijnen J, ter Riet G.
No. 31A randomised controlled trial ofprehospital intravenous fluidreplacement therapy in serious trauma.
By Turner J, Nicholl J, Webber L,Cox H, Dixon S, Yates D.
No. 32Intrathecal pumps for giving opioids inchronic pain: a systematic review.
By Williams JE, Louw G, Towlerton G.
No. 33Combination therapy (interferon alfaand ribavirin) in the treatment ofchronic hepatitis C: a rapid andsystematic review.
By Shepherd J, Waugh N, Hewitson P.
Health Technology Assessment 2007; Vol. 11: No. 30
153
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
No. 34A systematic review of comparisons ofeffect sizes derived from randomisedand non-randomised studies.
By MacLehose RR, Reeves BC,Harvey IM, Sheldon TA, Russell IT,Black AMS.
No. 35Intravascular ultrasound-guidedinterventions in coronary artery disease:a systematic literature review, withdecision-analytic modelling, of outcomesand cost-effectiveness.
By Berry E, Kelly S, Hutton J,Lindsay HSJ, Blaxill JM, Evans JA, et al.
No. 36A randomised controlled trial toevaluate the effectiveness and cost-effectiveness of counselling patients withchronic depression.
By Simpson S, Corney R, Fitzgerald P,Beecham J.
No. 37Systematic review of treatments foratopic eczema.
By Hoare C, Li Wan Po A, Williams H.
No. 38Bayesian methods in health technologyassessment: a review.
By Spiegelhalter DJ, Myles JP, Jones DR, Abrams KR.
No. 39The management of dyspepsia: asystematic review.
By Delaney B, Moayyedi P, Deeks J,Innes M, Soo S, Barton P, et al.
No. 40A systematic review of treatments forsevere psoriasis.
By Griffiths CEM, Clark CM, ChalmersRJG, Li Wan Po A, Williams HC.
Volume 5, 2001
No. 1Clinical and cost-effectiveness ofdonepezil, rivastigmine andgalantamine for Alzheimer’s disease: arapid and systematic review.
By Clegg A, Bryant J, Nicholson T,McIntyre L, De Broe S, Gerard K, et al.
No. 2The clinical effectiveness and cost-effectiveness of riluzole for motorneurone disease: a rapid and systematicreview.
By Stewart A, Sandercock J, Bryan S,Hyde C, Barton PM, Fry-Smith A, et al.
No. 3Equity and the economic evaluation ofhealthcare.
By Sassi F, Archard L, Le Grand J.
No. 4Quality-of-life measures in chronicdiseases of childhood.
By Eiser C, Morse R.
No. 5Eliciting public preferences forhealthcare: a systematic review oftechniques.
By Ryan M, Scott DA, Reeves C, BateA, van Teijlingen ER, Russell EM, et al.
No. 6General health status measures forpeople with cognitive impairment:learning disability and acquired braininjury.
By Riemsma RP, Forbes CA, Glanville JM, Eastwood AJ, Kleijnen J.
No. 7An assessment of screening strategies forfragile X syndrome in the UK.
By Pembrey ME, Barnicoat AJ,Carmichael B, Bobrow M, Turner G.
No. 8Issues in methodological research:perspectives from researchers andcommissioners.
By Lilford RJ, Richardson A, StevensA, Fitzpatrick R, Edwards S, Rock F, et al.
No. 9Systematic reviews of wound caremanagement: (5) beds; (6) compression;(7) laser therapy, therapeuticultrasound, electrotherapy andelectromagnetic therapy.
By Cullum N, Nelson EA, FlemmingK, Sheldon T.
No. 10Effects of educational and psychosocialinterventions for adolescents withdiabetes mellitus: a systematic review.
By Hampson SE, Skinner TC, Hart J,Storey L, Gage H, Foxcroft D, et al.
No. 11Effectiveness of autologous chondrocytetransplantation for hyaline cartilagedefects in knees: a rapid and systematicreview.
By Jobanputra P, Parry D, Fry-SmithA, Burls A.
No. 12Statistical assessment of the learningcurves of health technologies.
By Ramsay CR, Grant AM, Wallace SA, Garthwaite PH, Monk AF,Russell IT.
No. 13The effectiveness and cost-effectivenessof temozolomide for the treatment ofrecurrent malignant glioma: a rapid andsystematic review.
By Dinnes J, Cave C, Huang S, Major K, Milne R.
No. 14A rapid and systematic review of theclinical effectiveness and cost-effectiveness of debriding agents intreating surgical wounds healing bysecondary intention.
By Lewis R, Whiting P, ter Riet G,O’Meara S, Glanville J.
No. 15Home treatment for mental healthproblems: a systematic review.
By Burns T, Knapp M, Catty J, Healey A, Henderson J, Watt H, et al.
No. 16How to develop cost-consciousguidelines.
By Eccles M, Mason J.
No. 17The role of specialist nurses in multiplesclerosis: a rapid and systematic review.
By De Broe S, Christopher F, Waugh N.
No. 18A rapid and systematic review of theclinical effectiveness and cost-effectiveness of orlistat in themanagement of obesity.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
No. 19The clinical effectiveness and cost-effectiveness of pioglitazone for type 2diabetes mellitus: a rapid and systematicreview.
By Chilcott J, Wight J, Lloyd JonesM, Tappenden P.
No. 20Extended scope of nursing practice: amulticentre randomised controlled trialof appropriately trained nurses andpreregistration house officers in pre-operative assessment in elective generalsurgery.
By Kinley H, Czoski-Murray C,George S, McCabe C, Primrose J, Reilly C, et al.
No. 21Systematic reviews of the effectiveness ofday care for people with severe mentaldisorders: (1) Acute day hospital versusadmission; (2) Vocational rehabilitation;(3) Day hospital versus outpatient care.
By Marshall M, Crowther R, Almaraz-Serrano A, Creed F, Sledge W, Kluiter H, et al.
No. 22The measurement and monitoring ofsurgical adverse events.
By Bruce J, Russell EM, Mollison J,Krukowski ZH.
No. 23Action research: a systematic review andguidance for assessment.
By Waterman H, Tillen D, Dickson R,de Koning K.
No. 24A rapid and systematic review of theclinical effectiveness and cost-effectiveness of gemcitabine for thetreatment of pancreatic cancer.
By Ward S, Morris E, Bansback N,Calvert N, Crellin A, Forman D, et al.
Health Technology Assessment reports published to date
154

No. 25A rapid and systematic review of theevidence for the clinical effectivenessand cost-effectiveness of irinotecan,oxaliplatin and raltitrexed for thetreatment of advanced colorectal cancer.
By Lloyd Jones M, Hummel S,Bansback N, Orr B, Seymour M.
No. 26Comparison of the effectiveness ofinhaler devices in asthma and chronicobstructive airways disease: a systematicreview of the literature.
By Brocklebank D, Ram F, Wright J,Barry P, Cates C, Davies L, et al.
No. 27The cost-effectiveness of magneticresonance imaging for investigation ofthe knee joint.
By Bryan S, Weatherburn G, BungayH, Hatrick C, Salas C, Parry D, et al.
No. 28A rapid and systematic review of theclinical effectiveness and cost-effectiveness of topotecan for ovariancancer.
By Forbes C, Shirran L, Bagnall A-M,Duffy S, ter Riet G.
No. 29Superseded by a report published in alater volume.
No. 30The role of radiography in primary carepatients with low back pain of at least 6weeks duration: a randomised(unblinded) controlled trial.
By Kendrick D, Fielding K, Bentley E,Miller P, Kerslake R, Pringle M.
No. 31Design and use of questionnaires: areview of best practice applicable tosurveys of health service staff andpatients.
By McColl E, Jacoby A, Thomas L,Soutter J, Bamford C, Steen N, et al.
No. 32A rapid and systematic review of theclinical effectiveness and cost-effectiveness of paclitaxel, docetaxel,gemcitabine and vinorelbine in non-small-cell lung cancer.
By Clegg A, Scott DA, Sidhu M,Hewitson P, Waugh N.
No. 33Subgroup analyses in randomisedcontrolled trials: quantifying the risks offalse-positives and false-negatives.
By Brookes ST, Whitley E, Peters TJ, Mulheran PA, Egger M,Davey Smith G.
No. 34Depot antipsychotic medication in thetreatment of patients with schizophrenia:(1) Meta-review; (2) Patient and nurseattitudes.
By David AS, Adams C.
No. 35A systematic review of controlled trialsof the effectiveness and cost-effectiveness of brief psychologicaltreatments for depression.
By Churchill R, Hunot V, Corney R,Knapp M, McGuire H, Tylee A, et al.
No. 36Cost analysis of child healthsurveillance.
By Sanderson D, Wright D, Acton C,Duree D.
Volume 6, 2002
No. 1A study of the methods used to selectreview criteria for clinical audit.
By Hearnshaw H, Harker R, CheaterF, Baker R, Grimshaw G.
No. 2Fludarabine as second-line therapy forB cell chronic lymphocytic leukaemia: a technology assessment.
By Hyde C, Wake B, Bryan S, BartonP, Fry-Smith A, Davenport C, et al.
No. 3Rituximab as third-line treatment forrefractory or recurrent Stage III or IVfollicular non-Hodgkin’s lymphoma: asystematic review and economicevaluation.
By Wake B, Hyde C, Bryan S, BartonP, Song F, Fry-Smith A, et al.
No. 4A systematic review of dischargearrangements for older people.
By Parker SG, Peet SM, McPherson A,Cannaby AM, Baker R, Wilson A, et al.
No. 5The clinical effectiveness and cost-effectiveness of inhaler devices used inthe routine management of chronicasthma in older children: a systematicreview and economic evaluation.
By Peters J, Stevenson M, Beverley C,Lim J, Smith S.
No. 6The clinical effectiveness and cost-effectiveness of sibutramine in themanagement of obesity: a technologyassessment.
By O’Meara S, Riemsma R, ShirranL, Mather L, ter Riet G.
No. 7The cost-effectiveness of magneticresonance angiography for carotidartery stenosis and peripheral vasculardisease: a systematic review.
By Berry E, Kelly S, Westwood ME,Davies LM, Gough MJ, Bamford JM,et al.
No. 8Promoting physical activity in SouthAsian Muslim women through ‘exerciseon prescription’.
By Carroll B, Ali N, Azam N.
No. 9Zanamivir for the treatment of influenzain adults: a systematic review andeconomic evaluation.
By Burls A, Clark W, Stewart T,Preston C, Bryan S, Jefferson T, et al.
No. 10A review of the natural history andepidemiology of multiple sclerosis:implications for resource allocation andhealth economic models.
By Richards RG, Sampson FC, Beard SM, Tappenden P.
No. 11Screening for gestational diabetes: asystematic review and economicevaluation.
By Scott DA, Loveman E, McIntyre L,Waugh N.
No. 12The clinical effectiveness and cost-effectiveness of surgery for people withmorbid obesity: a systematic review andeconomic evaluation.
By Clegg AJ, Colquitt J, Sidhu MK,Royle P, Loveman E, Walker A.
No. 13The clinical effectiveness of trastuzumabfor breast cancer: a systematic review.
By Lewis R, Bagnall A-M, Forbes C,Shirran E, Duffy S, Kleijnen J, et al.
No. 14The clinical effectiveness and cost-effectiveness of vinorelbine for breastcancer: a systematic review andeconomic evaluation.
By Lewis R, Bagnall A-M, King S,Woolacott N, Forbes C, Shirran L, et al.
No. 15A systematic review of the effectivenessand cost-effectiveness of metal-on-metalhip resurfacing arthroplasty fortreatment of hip disease.
By Vale L, Wyness L, McCormack K,McKenzie L, Brazzelli M, Stearns SC.
No. 16The clinical effectiveness and cost-effectiveness of bupropion and nicotinereplacement therapy for smokingcessation: a systematic review andeconomic evaluation.
By Woolacott NF, Jones L, Forbes CA,Mather LC, Sowden AJ, Song FJ, et al.
No. 17A systematic review of effectiveness andeconomic evaluation of new drugtreatments for juvenile idiopathicarthritis: etanercept.
By Cummins C, Connock M, Fry-Smith A, Burls A.
No. 18Clinical effectiveness and cost-effectiveness of growth hormone inchildren: a systematic review andeconomic evaluation.
By Bryant J, Cave C, Mihaylova B,Chase D, McIntyre L, Gerard K, et al.
Health Technology Assessment 2007; Vol. 11: No. 30
155
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
No. 19Clinical effectiveness and cost-effectiveness of growth hormone inadults in relation to impact on quality oflife: a systematic review and economicevaluation.
By Bryant J, Loveman E, Chase D,Mihaylova B, Cave C, Gerard K, et al.
No. 20Clinical medication review by apharmacist of patients on repeatprescriptions in general practice: arandomised controlled trial.
By Zermansky AG, Petty DR, RaynorDK, Lowe CJ, Freementle N, Vail A.
No. 21The effectiveness of infliximab andetanercept for the treatment ofrheumatoid arthritis: a systematic reviewand economic evaluation.
By Jobanputra P, Barton P, Bryan S,Burls A.
No. 22A systematic review and economicevaluation of computerised cognitivebehaviour therapy for depression andanxiety.
By Kaltenthaler E, Shackley P, StevensK, Beverley C, Parry G, Chilcott J.
No. 23A systematic review and economicevaluation of pegylated liposomaldoxorubicin hydrochloride for ovariancancer.
By Forbes C, Wilby J, Richardson G,Sculpher M, Mather L, Reimsma R.
No. 24A systematic review of the effectivenessof interventions based on a stages-of-change approach to promote individualbehaviour change.
By Riemsma RP, Pattenden J, Bridle C,Sowden AJ, Mather L, Watt IS, et al.
No. 25A systematic review update of theclinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIaantagonists.
By Robinson M, Ginnelly L, SculpherM, Jones L, Riemsma R, Palmer S, et al.
No. 26A systematic review of the effectiveness,cost-effectiveness and barriers toimplementation of thrombolytic andneuroprotective therapy for acuteischaemic stroke in the NHS.
By Sandercock P, Berge E, Dennis M,Forbes J, Hand P, Kwan J, et al.
No. 27A randomised controlled crossover trial of nurse practitioner versus doctor-led outpatient care in abronchiectasis clinic.
By Caine N, Sharples LD,Hollingworth W, French J, Keogan M,Exley A, et al.
No. 28Clinical effectiveness and cost –consequences of selective serotoninreuptake inhibitors in the treatment ofsex offenders.
By Adi Y, Ashcroft D, Browne K,Beech A, Fry-Smith A, Hyde C.
No. 29Treatment of established osteoporosis: a systematic review and cost–utilityanalysis.
By Kanis JA, Brazier JE, Stevenson M,Calvert NW, Lloyd Jones M.
No. 30Which anaesthetic agents are cost-effective in day surgery? Literaturereview, national survey of practice andrandomised controlled trial.
By Elliott RA Payne K, Moore JK,Davies LM, Harper NJN, St Leger AS,et al.
No. 31Screening for hepatitis C amonginjecting drug users and ingenitourinary medicine clinics:systematic reviews of effectiveness,modelling study and national survey ofcurrent practice.
By Stein K, Dalziel K, Walker A,McIntyre L, Jenkins B, Horne J, et al.
No. 32The measurement of satisfaction withhealthcare: implications for practicefrom a systematic review of theliterature.
By Crow R, Gage H, Hampson S,Hart J, Kimber A, Storey L, et al.
No. 33The effectiveness and cost-effectivenessof imatinib in chronic myeloidleukaemia: a systematic review.
By Garside R, Round A, Dalziel K,Stein K, Royle R.
No. 34A comparative study of hypertonicsaline, daily and alternate-day rhDNase in children with cystic fibrosis.
By Suri R, Wallis C, Bush A,Thompson S, Normand C, Flather M, et al.
No. 35A systematic review of the costs andeffectiveness of different models ofpaediatric home care.
By Parker G, Bhakta P, Lovett CA,Paisley S, Olsen R, Turner D, et al.
Volume 7, 2003
No. 1How important are comprehensiveliterature searches and the assessment oftrial quality in systematic reviews?Empirical study.
By Egger M, Jüni P, Bartlett C,Holenstein F, Sterne J.
No. 2Systematic review of the effectivenessand cost-effectiveness, and economicevaluation, of home versus hospital orsatellite unit haemodialysis for peoplewith end-stage renal failure.
By Mowatt G, Vale L, Perez J, WynessL, Fraser C, MacLeod A, et al.
No. 3Systematic review and economicevaluation of the effectiveness ofinfliximab for the treatment of Crohn’sdisease.
By Clark W, Raftery J, Barton P, Song F, Fry-Smith A, Burls A.
No. 4A review of the clinical effectiveness andcost-effectiveness of routine anti-Dprophylaxis for pregnant women whoare rhesus negative.
By Chilcott J, Lloyd Jones M, WightJ, Forman K, Wray J, Beverley C, et al.
No. 5Systematic review and evaluation of theuse of tumour markers in paediatriconcology: Ewing’s sarcoma andneuroblastoma.
By Riley RD, Burchill SA, Abrams KR,Heney D, Lambert PC, Jones DR, et al.
No. 6The cost-effectiveness of screening forHelicobacter pylori to reduce mortalityand morbidity from gastric cancer andpeptic ulcer disease: a discrete-eventsimulation model.
By Roderick P, Davies R, Raftery J,Crabbe D, Pearce R, Bhandari P, et al.
No. 7The clinical effectiveness and cost-effectiveness of routine dental checks: asystematic review and economicevaluation.
By Davenport C, Elley K, Salas C,Taylor-Weetman CL, Fry-Smith A, Bryan S, et al.
No. 8A multicentre randomised controlledtrial assessing the costs and benefits ofusing structured information andanalysis of women’s preferences in themanagement of menorrhagia.
By Kennedy ADM, Sculpher MJ,Coulter A, Dwyer N, Rees M, Horsley S, et al.
No. 9Clinical effectiveness and cost–utility ofphotodynamic therapy for wet age-relatedmacular degeneration: a systematic reviewand economic evaluation.
By Meads C, Salas C, Roberts T,Moore D, Fry-Smith A, Hyde C.
No. 10Evaluation of molecular tests forprenatal diagnosis of chromosomeabnormalities.
By Grimshaw GM, Szczepura A,Hultén M, MacDonald F, Nevin NC,Sutton F, et al.
Health Technology Assessment reports published to date
156
No. 11First and second trimester antenatalscreening for Down’s syndrome: theresults of the Serum, Urine andUltrasound Screening Study (SURUSS).
By Wald NJ, Rodeck C, Hackshaw AK, Walters J, Chitty L,Mackinson AM.
No. 12The effectiveness and cost-effectivenessof ultrasound locating devices forcentral venous access: a systematicreview and economic evaluation.
By Calvert N, Hind D, McWilliamsRG, Thomas SM, Beverley C, Davidson A.
No. 13A systematic review of atypicalantipsychotics in schizophrenia.
By Bagnall A-M, Jones L, Lewis R,Ginnelly L, Glanville J, Torgerson D, et al.
No. 14Prostate Testing for Cancer andTreatment (ProtecT) feasibility study.
By Donovan J, Hamdy F, Neal D,Peters T, Oliver S, Brindle L, et al.
No. 15Early thrombolysis for the treatment of acute myocardial infarction: asystematic review and economicevaluation.
By Boland A, Dundar Y, Bagust A,Haycox A, Hill R, Mujica Mota R,et al.
No. 16Screening for fragile X syndrome: a literature review and modelling.
By Song FJ, Barton P, Sleightholme V,Yao GL, Fry-Smith A.
No. 17Systematic review of endoscopic sinussurgery for nasal polyps.
By Dalziel K, Stein K, Round A,Garside R, Royle P.
No. 18Towards efficient guidelines: how tomonitor guideline use in primary care.
By Hutchinson A, McIntosh A, Cox S,Gilbert C.
No. 19Effectiveness and cost-effectiveness ofacute hospital-based spinal cord injuriesservices: systematic review.
By Bagnall A-M, Jones L, Richardson G, Duffy S, Riemsma R.
No. 20Prioritisation of health technologyassessment. The PATHS model:methods and case studies.
By Townsend J, Buxton M, Harper G.
No. 21Systematic review of the clinicaleffectiveness and cost-effectiveness of tension-free vaginal tape fortreatment of urinary stress incontinence.
By Cody J, Wyness L, Wallace S,Glazener C, Kilonzo M, Stearns S,et al.
No. 22The clinical and cost-effectiveness ofpatient education models for diabetes: a systematic review and economicevaluation.
By Loveman E, Cave C, Green C,Royle P, Dunn N, Waugh N.
No. 23The role of modelling in prioritisingand planning clinical trials.
By Chilcott J, Brennan A, Booth A,Karnon J, Tappenden P.
No. 24Cost–benefit evaluation of routineinfluenza immunisation in people 65–74years of age.
By Allsup S, Gosney M, Haycox A,Regan M.
No. 25The clinical and cost-effectiveness ofpulsatile machine perfusion versus coldstorage of kidneys for transplantationretrieved from heart-beating and non-heart-beating donors.
By Wight J, Chilcott J, Holmes M,Brewer N.
No. 26Can randomised trials rely on existingelectronic data? A feasibility study toexplore the value of routine data inhealth technology assessment.
By Williams JG, Cheung WY, Cohen DR, Hutchings HA, Longo MF, Russell IT.
No. 27Evaluating non-randomised interventionstudies.
By Deeks JJ, Dinnes J, D’Amico R,Sowden AJ, Sakarovitch C, Song F, et al.
No. 28A randomised controlled trial to assessthe impact of a package comprising apatient-orientated, evidence-based self-help guidebook and patient-centredconsultations on disease managementand satisfaction in inflammatory boweldisease.
By Kennedy A, Nelson E, Reeves D,Richardson G, Roberts C, Robinson A,et al.
No. 29The effectiveness of diagnostic tests forthe assessment of shoulder pain due tosoft tissue disorders: a systematic review.
By Dinnes J, Loveman E, McIntyre L,Waugh N.
No. 30The value of digital imaging in diabeticretinopathy.
By Sharp PF, Olson J, Strachan F,Hipwell J, Ludbrook A, O’Donnell M, et al.
No. 31Lowering blood pressure to preventmyocardial infarction and stroke: a new preventive strategy.
By Law M, Wald N, Morris J.
No. 32Clinical and cost-effectiveness ofcapecitabine and tegafur with uracil forthe treatment of metastatic colorectalcancer: systematic review and economicevaluation.
By Ward S, Kaltenthaler E, Cowan J,Brewer N.
No. 33Clinical and cost-effectiveness of new and emerging technologies for earlylocalised prostate cancer: a systematicreview.
By Hummel S, Paisley S, Morgan A,Currie E, Brewer N.
No. 34Literature searching for clinical andcost-effectiveness studies used in healthtechnology assessment reports carriedout for the National Institute forClinical Excellence appraisal system.
By Royle P, Waugh N.
No. 35Systematic review and economicdecision modelling for the preventionand treatment of influenza A and B.
By Turner D, Wailoo A, Nicholson K,Cooper N, Sutton A, Abrams K.
No. 36A randomised controlled trial toevaluate the clinical and cost-effectiveness of Hickman line insertions in adult cancer patients bynurses.
By Boland A, Haycox A, Bagust A,Fitzsimmons L.
No. 37Redesigning postnatal care: arandomised controlled trial of protocol-based midwifery-led carefocused on individual women’s physical and psychological health needs.
By MacArthur C, Winter HR, Bick DE, Lilford RJ, Lancashire RJ,Knowles H, et al.
No. 38Estimating implied rates of discount inhealthcare decision-making.
By West RR, McNabb R, Thompson AGH, Sheldon TA, Grimley Evans J.
Health Technology Assessment 2007; Vol. 11: No. 30
157
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.

No. 39Systematic review of isolation policies inthe hospital management of methicillin-resistant Staphylococcus aureus: a review ofthe literature with epidemiological andeconomic modelling.
By Cooper BS, Stone SP, Kibbler CC,Cookson BD, Roberts JA, Medley GF, et al.
No. 40Treatments for spasticity and pain inmultiple sclerosis: a systematic review.
By Beard S, Hunn A, Wight J.
No. 41The inclusion of reports of randomisedtrials published in languages other thanEnglish in systematic reviews.
By Moher D, Pham B, Lawson ML,Klassen TP.
No. 42The impact of screening on futurehealth-promoting behaviours and healthbeliefs: a systematic review.
By Bankhead CR, Brett J, Bukach C,Webster P, Stewart-Brown S, Munafo M,et al.
Volume 8, 2004
No. 1What is the best imaging strategy foracute stroke?
By Wardlaw JM, Keir SL, Seymour J,Lewis S, Sandercock PAG, Dennis MS, et al.
No. 2Systematic review and modelling of theinvestigation of acute and chronic chestpain presenting in primary care.
By Mant J, McManus RJ, Oakes RAL,Delaney BC, Barton PM, Deeks JJ, et al.
No. 3The effectiveness and cost-effectivenessof microwave and thermal balloonendometrial ablation for heavymenstrual bleeding: a systematic reviewand economic modelling.
By Garside R, Stein K, Wyatt K,Round A, Price A.
No. 4A systematic review of the role ofbisphosphonates in metastatic disease.
By Ross JR, Saunders Y, Edmonds PM,Patel S, Wonderling D, Normand C, et al.
No. 5Systematic review of the clinicaleffectiveness and cost-effectiveness ofcapecitabine (Xeloda®) for locallyadvanced and/or metastatic breast cancer.
By Jones L, Hawkins N, Westwood M,Wright K, Richardson G, Riemsma R.
No. 6Effectiveness and efficiency of guidelinedissemination and implementationstrategies.
By Grimshaw JM, Thomas RE,MacLennan G, Fraser C, Ramsay CR,Vale L, et al.
No. 7Clinical effectiveness and costs of theSugarbaker procedure for the treatmentof pseudomyxoma peritonei.
By Bryant J, Clegg AJ, Sidhu MK,Brodin H, Royle P, Davidson P.
No. 8Psychological treatment for insomnia inthe regulation of long-term hypnoticdrug use.
By Morgan K, Dixon S, Mathers N,Thompson J, Tomeny M.
No. 9Improving the evaluation of therapeuticinterventions in multiple sclerosis:development of a patient-based measureof outcome.
By Hobart JC, Riazi A, Lamping DL,Fitzpatrick R, Thompson AJ.
No. 10A systematic review and economicevaluation of magnetic resonancecholangiopancreatography comparedwith diagnostic endoscopic retrogradecholangiopancreatography.
By Kaltenthaler E, Bravo Vergel Y,Chilcott J, Thomas S, Blakeborough T,Walters SJ, et al.
No. 11The use of modelling to evaluate newdrugs for patients with a chroniccondition: the case of antibodies againsttumour necrosis factor in rheumatoidarthritis.
By Barton P, Jobanputra P, Wilson J,Bryan S, Burls A.
No. 12Clinical effectiveness and cost-effectiveness of neonatal screening forinborn errors of metabolism usingtandem mass spectrometry: a systematicreview.
By Pandor A, Eastham J, Beverley C,Chilcott J, Paisley S.
No. 13Clinical effectiveness and cost-effectiveness of pioglitazone androsiglitazone in the treatment of type 2 diabetes: a systematic review and economic evaluation.
By Czoski-Murray C, Warren E,Chilcott J, Beverley C, Psyllaki MA,Cowan J.
No. 14Routine examination of the newborn:the EMREN study. Evaluation of anextension of the midwife role including a randomised controlled trial of appropriately trained midwivesand paediatric senior house officers.
By Townsend J, Wolke D, Hayes J,Davé S, Rogers C, Bloomfield L, et al.
No. 15Involving consumers in research anddevelopment agenda setting for theNHS: developing an evidence-basedapproach.
By Oliver S, Clarke-Jones L, Rees R, Milne R, Buchanan P, Gabbay J, et al.
No. 16A multi-centre randomised controlledtrial of minimally invasive directcoronary bypass grafting versuspercutaneous transluminal coronaryangioplasty with stenting for proximalstenosis of the left anterior descendingcoronary artery.
By Reeves BC, Angelini GD, BryanAJ, Taylor FC, Cripps T, Spyt TJ, et al.
No. 17Does early magnetic resonance imaginginfluence management or improveoutcome in patients referred tosecondary care with low back pain? A pragmatic randomised controlledtrial.
By Gilbert FJ, Grant AM, GillanMGC, Vale L, Scott NW, Campbell MK,et al.
No. 18The clinical and cost-effectiveness ofanakinra for the treatment ofrheumatoid arthritis in adults: asystematic review and economic analysis.
By Clark W, Jobanputra P, Barton P,Burls A.
No. 19A rapid and systematic review andeconomic evaluation of the clinical andcost-effectiveness of newer drugs fortreatment of mania associated withbipolar affective disorder.
By Bridle C, Palmer S, Bagnall A-M,Darba J, Duffy S, Sculpher M, et al.
No. 20Liquid-based cytology in cervicalscreening: an updated rapid andsystematic review and economic analysis.
By Karnon J, Peters J, Platt J, Chilcott J, McGoogan E, Brewer N.
No. 21Systematic review of the long-termeffects and economic consequences oftreatments for obesity and implicationsfor health improvement.
By Avenell A, Broom J, Brown TJ,Poobalan A, Aucott L, Stearns SC, et al.
No. 22Autoantibody testing in children withnewly diagnosed type 1 diabetesmellitus.
By Dretzke J, Cummins C,Sandercock J, Fry-Smith A, Barrett T,Burls A.
Health Technology Assessment reports published to date
158
No. 23Clinical effectiveness and cost-effectiveness of prehospital intravenousfluids in trauma patients.
By Dretzke J, Sandercock J, Bayliss S,Burls A.
No. 24Newer hypnotic drugs for the short-term management of insomnia: asystematic review and economicevaluation.
By Dündar Y, Boland A, Strobl J,Dodd S, Haycox A, Bagust A, et al.
No. 25Development and validation of methodsfor assessing the quality of diagnosticaccuracy studies.
By Whiting P, Rutjes AWS, Dinnes J,Reitsma JB, Bossuyt PMM, Kleijnen J.
No. 26EVALUATE hysterectomy trial: amulticentre randomised trial comparingabdominal, vaginal and laparoscopicmethods of hysterectomy.
By Garry R, Fountain J, Brown J,Manca A, Mason S, Sculpher M, et al.
No. 27Methods for expected value ofinformation analysis in complex healtheconomic models: developments on thehealth economics of interferon-� andglatiramer acetate for multiple sclerosis.
By Tappenden P, Chilcott JB,Eggington S, Oakley J, McCabe C.
No. 28Effectiveness and cost-effectiveness ofimatinib for first-line treatment ofchronic myeloid leukaemia in chronicphase: a systematic review and economicanalysis.
By Dalziel K, Round A, Stein K,Garside R, Price A.
No. 29VenUS I: a randomised controlled trialof two types of bandage for treatingvenous leg ulcers.
By Iglesias C, Nelson EA, Cullum NA,Torgerson DJ on behalf of the VenUSTeam.
No. 30Systematic review of the effectivenessand cost-effectiveness, and economicevaluation, of myocardial perfusionscintigraphy for the diagnosis andmanagement of angina and myocardialinfarction.
By Mowatt G, Vale L, Brazzelli M,Hernandez R, Murray A, Scott N, et al.
No. 31A pilot study on the use of decisiontheory and value of information analysisas part of the NHS Health TechnologyAssessment programme.
By Claxton Kon K, Ginnelly L, SculpherM, Philips Z, Palmer S.
No. 32The Social Support and Family HealthStudy: a randomised controlled trial andeconomic evaluation of two alternativeforms of postnatal support for mothersliving in disadvantaged inner-city areas.
By Wiggins M, Oakley A, Roberts I,Turner H, Rajan L, Austerberry H, et al.
No. 33Psychosocial aspects of genetic screeningof pregnant women and newborns: a systematic review.
By Green JM, Hewison J, Bekker HL,Bryant, Cuckle HS.
No. 34Evaluation of abnormal uterinebleeding: comparison of threeoutpatient procedures within cohortsdefined by age and menopausal status.
By Critchley HOD, Warner P, Lee AJ, Brechin S, Guise J, Graham B.
No. 35Coronary artery stents: a rapid systematicreview and economic evaluation.
By Hill R, Bagust A, Bakhai A,Dickson R, Dündar Y, Haycox A, et al.
No. 36Review of guidelines for good practicein decision-analytic modelling in healthtechnology assessment.
By Philips Z, Ginnelly L, Sculpher M,Claxton K, Golder S, Riemsma R, et al.
No. 37Rituximab (MabThera®) for aggressivenon-Hodgkin’s lymphoma: systematicreview and economic evaluation.
By Knight C, Hind D, Brewer N,Abbott V.
No. 38Clinical effectiveness and cost-effectiveness of clopidogrel andmodified-release dipyridamole in thesecondary prevention of occlusivevascular events: a systematic review andeconomic evaluation.
By Jones L, Griffin S, Palmer S, MainC, Orton V, Sculpher M, et al.
No. 39Pegylated interferon �-2a and -2b incombination with ribavirin in thetreatment of chronic hepatitis C: asystematic review and economicevaluation.
By Shepherd J, Brodin H, Cave C,Waugh N, Price A, Gabbay J.
No. 40Clopidogrel used in combination withaspirin compared with aspirin alone inthe treatment of non-ST-segment-elevation acute coronary syndromes: asystematic review and economicevaluation.
By Main C, Palmer S, Griffin S, Jones L, Orton V, Sculpher M, et al.
No. 41Provision, uptake and cost of cardiacrehabilitation programmes: improvingservices to under-represented groups.
By Beswick AD, Rees K, Griebsch I,Taylor FC, Burke M, West RR, et al.
No. 42Involving South Asian patients inclinical trials.
By Hussain-Gambles M, Leese B,Atkin K, Brown J, Mason S, Tovey P.
No. 43Clinical and cost-effectiveness ofcontinuous subcutaneous insulininfusion for diabetes.
By Colquitt JL, Green C, Sidhu MK,Hartwell D, Waugh N.
No. 44Identification and assessment ofongoing trials in health technologyassessment reviews.
By Song FJ, Fry-Smith A, DavenportC, Bayliss S, Adi Y, Wilson JS, et al.
No. 45Systematic review and economicevaluation of a long-acting insulinanalogue, insulin glargine
By Warren E, Weatherley-Jones E,Chilcott J, Beverley C.
No. 46Supplementation of a home-basedexercise programme with a class-basedprogramme for people with osteoarthritisof the knees: a randomised controlledtrial and health economic analysis.
By McCarthy CJ, Mills PM, Pullen R, Richardson G, Hawkins N,Roberts CR, et al.
No. 47Clinical and cost-effectiveness of once-daily versus more frequent use of samepotency topical corticosteroids for atopiceczema: a systematic review andeconomic evaluation.
By Green C, Colquitt JL, Kirby J,Davidson P, Payne E.
No. 48Acupuncture of chronic headachedisorders in primary care: randomisedcontrolled trial and economic analysis.
By Vickers AJ, Rees RW, Zollman CE,McCarney R, Smith CM, Ellis N, et al.
No. 49Generalisability in economic evaluationstudies in healthcare: a review and casestudies.
By Sculpher MJ, Pang FS, Manca A,Drummond MF, Golder S, Urdahl H, et al.
No. 50Virtual outreach: a randomisedcontrolled trial and economic evaluationof joint teleconferenced medicalconsultations.
By Wallace P, Barber J, Clayton W,Currell R, Fleming K, Garner P, et al.
Health Technology Assessment 2007; Vol. 11: No. 30
159
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.

Volume 9, 2005
No. 1Randomised controlled multipletreatment comparison to provide a cost-effectiveness rationale for theselection of antimicrobial therapy inacne.
By Ozolins M, Eady EA, Avery A,Cunliffe WJ, O’Neill C, Simpson NB, et al.
No. 2Do the findings of case series studiesvary significantly according tomethodological characteristics?
By Dalziel K, Round A, Stein K,Garside R, Castelnuovo E, Payne L.
No. 3Improving the referral process forfamilial breast cancer geneticcounselling: findings of threerandomised controlled trials of twointerventions.
By Wilson BJ, Torrance N, Mollison J,Wordsworth S, Gray JR, Haites NE, et al.
No. 4Randomised evaluation of alternativeelectrosurgical modalities to treatbladder outflow obstruction in men withbenign prostatic hyperplasia.
By Fowler C, McAllister W, Plail R,Karim O, Yang Q.
No. 5A pragmatic randomised controlled trialof the cost-effectiveness of palliativetherapies for patients with inoperableoesophageal cancer.
By Shenfine J, McNamee P, Steen N,Bond J, Griffin SM.
No. 6Impact of computer-aided detectionprompts on the sensitivity and specificityof screening mammography.
By Taylor P, Champness J, Given-Wilson R, Johnston K, Potts H.
No. 7Issues in data monitoring and interimanalysis of trials.
By Grant AM, Altman DG, BabikerAB, Campbell MK, Clemens FJ,Darbyshire JH, et al.
No. 8Lay public’s understanding of equipoiseand randomisation in randomisedcontrolled trials.
By Robinson EJ, Kerr CEP, StevensAJ, Lilford RJ, Braunholtz DA, EdwardsSJ, et al.
No. 9Clinical and cost-effectiveness ofelectroconvulsive therapy for depressiveillness, schizophrenia, catatonia andmania: systematic reviews and economicmodelling studies.
By Greenhalgh J, Knight C, Hind D,Beverley C, Walters S.
No. 10Measurement of health-related qualityof life for people with dementia:development of a new instrument(DEMQOL) and an evaluation ofcurrent methodology.
By Smith SC, Lamping DL, Banerjee S, Harwood R, Foley B, Smith P, et al.
No. 11Clinical effectiveness and cost-effectiveness of drotrecogin alfa(activated) (Xigris®) for the treatment ofsevere sepsis in adults: a systematicreview and economic evaluation.
By Green C, Dinnes J, Takeda A,Shepherd J, Hartwell D, Cave C, et al.
No. 12A methodological review of howheterogeneity has been examined insystematic reviews of diagnostic testaccuracy.
By Dinnes J, Deeks J, Kirby J,Roderick P.
No. 13Cervical screening programmes: canautomation help? Evidence fromsystematic reviews, an economic analysisand a simulation modelling exerciseapplied to the UK.
By Willis BH, Barton P, Pearmain P,Bryan S, Hyde C.
No. 14Laparoscopic surgery for inguinalhernia repair: systematic review ofeffectiveness and economic evaluation.
By McCormack K, Wake B, Perez J,Fraser C, Cook J, McIntosh E, et al.
No. 15Clinical effectiveness, tolerability andcost-effectiveness of newer drugs forepilepsy in adults: a systematic reviewand economic evaluation.
By Wilby J, Kainth A, Hawkins N,Epstein D, McIntosh H, McDaid C, et al.
No. 16A randomised controlled trial tocompare the cost-effectiveness oftricyclic antidepressants, selectiveserotonin reuptake inhibitors andlofepramine.
By Peveler R, Kendrick T, Buxton M,Longworth L, Baldwin D, Moore M, et al.
No. 17Clinical effectiveness and cost-effectiveness of immediate angioplastyfor acute myocardial infarction:systematic review and economicevaluation.
By Hartwell D, Colquitt J, LovemanE, Clegg AJ, Brodin H, Waugh N, et al.
No. 18A randomised controlled comparison ofalternative strategies in stroke care.
By Kalra L, Evans A, Perez I, Knapp M, Swift C, Donaldson N.
No. 19The investigation and analysis of criticalincidents and adverse events inhealthcare.
By Woloshynowych M, Rogers S,Taylor-Adams S, Vincent C.
No. 20Potential use of routine databases inhealth technology assessment.
By Raftery J, Roderick P, Stevens A.
No. 21Clinical and cost-effectiveness of newerimmunosuppressive regimens in renaltransplantation: a systematic review andmodelling study.
By Woodroffe R, Yao GL, Meads C,Bayliss S, Ready A, Raftery J, et al.
No. 22A systematic review and economicevaluation of alendronate, etidronate,risedronate, raloxifene and teriparatidefor the prevention and treatment ofpostmenopausal osteoporosis.
By Stevenson M, Lloyd Jones M, De Nigris E, Brewer N, Davis S, Oakley J.
No. 23A systematic review to examine theimpact of psycho-educationalinterventions on health outcomes andcosts in adults and children with difficultasthma.
By Smith JR, Mugford M, Holland R,Candy B, Noble MJ, Harrison BDW, et al.
No. 24An evaluation of the costs, effectivenessand quality of renal replacementtherapy provision in renal satellite unitsin England and Wales.
By Roderick P, Nicholson T, ArmitageA, Mehta R, Mullee M, Gerard K, et al.
No. 25Imatinib for the treatment of patientswith unresectable and/or metastaticgastrointestinal stromal tumours:systematic review and economicevaluation.
By Wilson J, Connock M, Song F, YaoG, Fry-Smith A, Raftery J, et al.
No. 26Indirect comparisons of competinginterventions.
By Glenny AM, Altman DG, Song F,Sakarovitch C, Deeks JJ, D’Amico R, et al.
No. 27Cost-effectiveness of alternativestrategies for the initial medicalmanagement of non-ST elevation acutecoronary syndrome: systematic reviewand decision-analytical modelling.
By Robinson M, Palmer S, SculpherM, Philips Z, Ginnelly L, Bowens A, et al.
Health Technology Assessment reports published to date
160

No. 28Outcomes of electrically stimulatedgracilis neosphincter surgery.
By Tillin T, Chambers M, Feldman R.
No. 29The effectiveness and cost-effectivenessof pimecrolimus and tacrolimus foratopic eczema: a systematic review andeconomic evaluation.
By Garside R, Stein K, Castelnuovo E,Pitt M, Ashcroft D, Dimmock P, et al.
No. 30Systematic review on urine albumintesting for early detection of diabeticcomplications.
By Newman DJ, Mattock MB, DawnayABS, Kerry S, McGuire A, Yaqoob M, et al.
No. 31Randomised controlled trial of the cost-effectiveness of water-based therapy forlower limb osteoarthritis.
By Cochrane T, Davey RC, Matthes Edwards SM.
No. 32Longer term clinical and economicbenefits of offering acupuncture care topatients with chronic low back pain.
By Thomas KJ, MacPherson H,Ratcliffe J, Thorpe L, Brazier J,Campbell M, et al.
No. 33Cost-effectiveness and safety of epiduralsteroids in the management of sciatica.
By Price C, Arden N, Coglan L,Rogers P.
No. 34The British Rheumatoid Outcome StudyGroup (BROSG) randomised controlledtrial to compare the effectiveness andcost-effectiveness of aggressive versussymptomatic therapy in establishedrheumatoid arthritis.
By Symmons D, Tricker K, Roberts C,Davies L, Dawes P, Scott DL.
No. 35Conceptual framework and systematicreview of the effects of participants’ andprofessionals’ preferences in randomisedcontrolled trials.
By King M, Nazareth I, Lampe F,Bower P, Chandler M, Morou M, et al.
No. 36The clinical and cost-effectiveness ofimplantable cardioverter defibrillators: a systematic review.
By Bryant J, Brodin H, Loveman E,Payne E, Clegg A.
No. 37A trial of problem-solving by communitymental health nurses for anxiety,depression and life difficulties amonggeneral practice patients. The CPN-GPstudy.
By Kendrick T, Simons L, Mynors-Wallis L, Gray A, Lathlean J,Pickering R, et al.
No. 38The causes and effects of socio-demographic exclusions from clinicaltrials.
By Bartlett C, Doyal L, Ebrahim S,Davey P, Bachmann M, Egger M, et al.
No. 39Is hydrotherapy cost-effective? Arandomised controlled trial of combinedhydrotherapy programmes comparedwith physiotherapy land techniques inchildren with juvenile idiopathicarthritis.
By Epps H, Ginnelly L, Utley M,Southwood T, Gallivan S, Sculpher M, et al.
No. 40A randomised controlled trial and cost-effectiveness study of systematicscreening (targeted and total populationscreening) versus routine practice forthe detection of atrial fibrillation inpeople aged 65 and over. The SAFEstudy.
By Hobbs FDR, Fitzmaurice DA,Mant J, Murray E, Jowett S, Bryan S, et al.
No. 41Displaced intracapsular hip fractures in fit, older people: a randomisedcomparison of reduction and fixation,bipolar hemiarthroplasty and total hiparthroplasty.
By Keating JF, Grant A, Masson M,Scott NW, Forbes JF.
No. 42Long-term outcome of cognitivebehaviour therapy clinical trials incentral Scotland.
By Durham RC, Chambers JA, Power KG, Sharp DM, Macdonald RR,Major KA, et al.
No. 43The effectiveness and cost-effectivenessof dual-chamber pacemakers comparedwith single-chamber pacemakers forbradycardia due to atrioventricularblock or sick sinus syndrome: systematic review and economicevaluation.
By Castelnuovo E, Stein K, Pitt M,Garside R, Payne E.
No. 44Newborn screening for congenital heartdefects: a systematic review and cost-effectiveness analysis.
By Knowles R, Griebsch I, DezateuxC, Brown J, Bull C, Wren C.
No. 45The clinical and cost-effectiveness of leftventricular assist devices for end-stageheart failure: a systematic review andeconomic evaluation.
By Clegg AJ, Scott DA, Loveman E,Colquitt J, Hutchinson J, Royle P, et al.
No. 46The effectiveness of the HeidelbergRetina Tomograph and laser diagnosticglaucoma scanning system (GDx) indetecting and monitoring glaucoma.
By Kwartz AJ, Henson DB, Harper RA, Spencer AF, McLeod D.
No. 47Clinical and cost-effectiveness ofautologous chondrocyte implantationfor cartilage defects in knee joints:systematic review and economicevaluation.
By Clar C, Cummins E, McIntyre L,Thomas S, Lamb J, Bain L, et al.
No. 48Systematic review of effectiveness ofdifferent treatments for childhoodretinoblastoma.
By McDaid C, Hartley S, Bagnall A-M, Ritchie G, Light K,Riemsma R.
No. 49Towards evidence-based guidelines for the prevention of venousthromboembolism: systematic reviews of mechanical methods, oralanticoagulation, dextran and regionalanaesthesia as thromboprophylaxis.
By Roderick P, Ferris G, Wilson K,Halls H, Jackson D, Collins R,et al.
No. 50The effectiveness and cost-effectivenessof parent training/educationprogrammes for the treatment ofconduct disorder, including oppositionaldefiant disorder, in children.
By Dretzke J, Frew E, Davenport C,Barlow J, Stewart-Brown S, Sandercock J, et al.
Volume 10, 2006
No. 1The clinical and cost-effectiveness ofdonepezil, rivastigmine, galantamineand memantine for Alzheimer’s disease.
By Loveman E, Green C, Kirby J,Takeda A, Picot J, Payne E, et al.
No. 2FOOD: a multicentre randomised trialevaluating feeding policies in patientsadmitted to hospital with a recentstroke.
By Dennis M, Lewis S, Cranswick G,Forbes J.
No. 3The clinical effectiveness and cost-effectiveness of computed tomographyscreening for lung cancer: systematicreviews.
By Black C, Bagust A, Boland A,Walker S, McLeod C, De Verteuil R, et al.
Health Technology Assessment 2007; Vol. 11: No. 30
161
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
No. 4A systematic review of the effectivenessand cost-effectiveness of neuroimagingassessments used to visualise the seizure focus in people with refractoryepilepsy being considered for surgery.
By Whiting P, Gupta R, Burch J,Mujica Mota RE, Wright K, Marson A, et al.
No. 5Comparison of conference abstracts and presentations with full-text articles in the health technologyassessments of rapidly evolvingtechnologies.
By Dundar Y, Dodd S, Dickson R,Walley T, Haycox A, Williamson PR.
No. 6Systematic review and evaluation ofmethods of assessing urinaryincontinence.
By Martin JL, Williams KS, AbramsKR, Turner DA, Sutton AJ, Chapple C,et al.
No. 7The clinical effectiveness and cost-effectiveness of newer drugs for childrenwith epilepsy. A systematic review.
By Connock M, Frew E, Evans B-W, Bryan S, Cummins C, Fry-Smith A, et al.
No. 8Surveillance of Barrett’s oesophagus:exploring the uncertainty throughsystematic review, expert workshop andeconomic modelling.
By Garside R, Pitt M, Somerville M,Stein K, Price A, Gilbert N.
No. 9Topotecan, pegylated liposomaldoxorubicin hydrochloride andpaclitaxel for second-line or subsequenttreatment of advanced ovarian cancer: asystematic review and economicevaluation.
By Main C, Bojke L, Griffin S,Norman G, Barbieri M, Mather L, et al.
No. 10Evaluation of molecular techniques in prediction and diagnosis ofcytomegalovirus disease inimmunocompromised patients.
By Szczepura A, Westmoreland D,Vinogradova Y, Fox J, Clark M.
No. 11Screening for thrombophilia in high-risksituations: systematic review and cost-effectiveness analysis. The Thrombosis:Risk and Economic Assessment ofThrombophilia Screening (TREATS)study.
By Wu O, Robertson L, Twaddle S,Lowe GDO, Clark P, Greaves M, et al.
No. 12A series of systematic reviews to informa decision analysis for sampling andtreating infected diabetic foot ulcers.
By Nelson EA, O’Meara S, Craig D,Iglesias C, Golder S, Dalton J, et al.
No. 13Randomised clinical trial, observationalstudy and assessment of cost-effectiveness of the treatment of varicoseveins (REACTIV trial).
By Michaels JA, Campbell WB,Brazier JE, MacIntyre JB, PalfreymanSJ, Ratcliffe J, et al.
No. 14The cost-effectiveness of screening fororal cancer in primary care.
By Speight PM, Palmer S, Moles DR,Downer MC, Smith DH, Henriksson Met al.
No. 15Measurement of the clinical and cost-effectiveness of non-invasive diagnostictesting strategies for deep veinthrombosis.
By Goodacre S, Sampson F, StevensonM, Wailoo A, Sutton A, Thomas S, et al.
No. 16Systematic review of the effectivenessand cost-effectiveness of HealOzone®
for the treatment of occlusal pit/fissurecaries and root caries.
By Brazzelli M, McKenzie L, FieldingS, Fraser C, Clarkson J, Kilonzo M, et al.
No. 17Randomised controlled trials ofconventional antipsychotic versus newatypical drugs, and new atypical drugsversus clozapine, in people withschizophrenia responding poorly to, or intolerant of, current drugtreatment.
By Lewis SW, Davies L, Jones PB,Barnes TRE, Murray RM, Kerwin R, et al.
No. 18Diagnostic tests and algorithms used inthe investigation of haematuria:systematic reviews and economicevaluation.
By Rodgers M, Nixon J, Hempel S,Aho T, Kelly J, Neal D, et al.
No. 19Cognitive behavioural therapy inaddition to antispasmodic therapy forirritable bowel syndrome in primarycare: randomised controlled trial.
By Kennedy TM, Chalder T, McCrone P, Darnley S, Knapp M, Jones RH, et al.
No. 20A systematic review of the clinicaleffectiveness and cost-effectiveness ofenzyme replacement therapies forFabry’s disease andmucopolysaccharidosis type 1.
By Connock M, Juarez-Garcia A, FrewE, Mans A, Dretzke J, Fry-Smith A, et al.
No. 21Health benefits of antiviral therapy formild chronic hepatitis C: randomisedcontrolled trial and economicevaluation.
By Wright M, Grieve R, Roberts J,Main J, Thomas HC on behalf of theUK Mild Hepatitis C Trial Investigators.
No. 22Pressure relieving support surfaces: arandomised evaluation.
By Nixon J, Nelson EA, Cranny G,Iglesias CP, Hawkins K, Cullum NA, et al.
No. 23A systematic review and economicmodel of the effectiveness and cost-effectiveness of methylphenidate,dexamfetamine and atomoxetine for thetreatment of attention deficithyperactivity disorder in children andadolescents.
By King S, Griffin S, Hodges Z,Weatherly H, Asseburg C, Richardson G,et al.
No. 24The clinical effectiveness and cost-effectiveness of enzyme replacementtherapy for Gaucher’s disease: a systematic review.
By Connock M, Burls A, Frew E, Fry-Smith A, Juarez-Garcia A, McCabe C, et al.
No. 25Effectiveness and cost-effectiveness ofsalicylic acid and cryotherapy forcutaneous warts. An economic decisionmodel.
By Thomas KS, Keogh-Brown MR,Chalmers JR, Fordham RJ, Holland RC,Armstrong SJ, et al.
No. 26A systematic literature review of theeffectiveness of non-pharmacologicalinterventions to prevent wandering indementia and evaluation of the ethicalimplications and acceptability of theiruse.
By Robinson L, Hutchings D, CornerL, Beyer F, Dickinson H, Vanoli A, et al.
No. 27A review of the evidence on the effectsand costs of implantable cardioverterdefibrillator therapy in different patientgroups, and modelling of cost-effectiveness and cost–utility for thesegroups in a UK context.
By Buxton M, Caine N, Chase D,Connelly D, Grace A, Jackson C, et al.
Health Technology Assessment reports published to date
162
No. 28Adefovir dipivoxil and pegylatedinterferon alfa-2a for the treatment ofchronic hepatitis B: a systematic reviewand economic evaluation.
By Shepherd J, Jones J, Takeda A,Davidson P, Price A.
No. 29An evaluation of the clinical and cost-effectiveness of pulmonary arterycatheters in patient management inintensive care: a systematic review and arandomised controlled trial.
By Harvey S, Stevens K, Harrison D,Young D, Brampton W, McCabe C, et al.
No. 30Accurate, practical and cost-effectiveassessment of carotid stenosis in the UK.
By Wardlaw JM, Chappell FM,Stevenson M, De Nigris E, Thomas S,Gillard J, et al.
No. 31Etanercept and infliximab for thetreatment of psoriatic arthritis: a systematic review and economicevaluation.
By Woolacott N, Bravo Vergel Y,Hawkins N, Kainth A, Khadjesari Z,Misso K, et al.
No. 32The cost-effectiveness of testing forhepatitis C in former injecting drugusers.
By Castelnuovo E, Thompson-Coon J,Pitt M, Cramp M, Siebert U, Price A, et al.
No. 33Computerised cognitive behaviourtherapy for depression and anxietyupdate: a systematic review andeconomic evaluation.
By Kaltenthaler E, Brazier J, De Nigris E, Tumur I, Ferriter M,Beverley C, et al.
No. 34Cost-effectiveness of using prognosticinformation to select women with breast cancer for adjuvant systemic therapy.
By Williams C, Brunskill S, Altman D,Briggs A, Campbell H, Clarke M, et al.
No. 35Psychological therapies includingdialectical behaviour therapy forborderline personality disorder: a systematic review and preliminaryeconomic evaluation.
By Brazier J, Tumur I, Holmes M,Ferriter M, Parry G, Dent-Brown K, et al.
No. 36Clinical effectiveness and cost-effectiveness of tests for the diagnosisand investigation of urinary tractinfection in children: a systematic reviewand economic model.
By Whiting P, Westwood M, Bojke L,Palmer S, Richardson G, Cooper J, et al.
No. 37Cognitive behavioural therapy inchronic fatigue syndrome: a randomisedcontrolled trial of an outpatient groupprogramme.
By O’Dowd H, Gladwell P, Rogers CA,Hollinghurst S, Gregory A.
No. 38A comparison of the cost-effectiveness offive strategies for the prevention of non-steroidal anti-inflammatory drug-inducedgastrointestinal toxicity: a systematicreview with economic modelling.
By Brown TJ, Hooper L, Elliott RA,Payne K, Webb R, Roberts C, et al.
No. 39The effectiveness and cost-effectivenessof computed tomography screening forcoronary artery disease: systematicreview.
By Waugh N, Black C, Walker S,McIntyre L, Cummins E, Hillis G.
No. 40What are the clinical outcome and cost-effectiveness of endoscopy undertakenby nurses when compared with doctors?A Multi-Institution Nurse EndoscopyTrial (MINuET).
By Williams J, Russell I, Durai D,Cheung W-Y, Farrin A, Bloor K, et al.
No. 41The clinical and cost-effectiveness ofoxaliplatin and capecitabine for theadjuvant treatment of colon cancer:systematic review and economicevaluation.
By Pandor A, Eggington S, Paisley S,Tappenden P, Sutcliffe P.
No. 42A systematic review of the effectivenessof adalimumab, etanercept andinfliximab for the treatment ofrheumatoid arthritis in adults and aneconomic evaluation of their cost-effectiveness.
By Chen Y-F, Jobanputra P, Barton P,Jowett S, Bryan S, Clark W, et al.
No. 43Telemedicine in dermatology: a randomised controlled trial.
By Bowns IR, Collins K, Walters SJ,McDonagh AJG.
No. 44Cost-effectiveness of cell salvage andalternative methods of minimisingperioperative allogeneic bloodtransfusion: a systematic review andeconomic model.
By Davies L, Brown TJ, Haynes S,Payne K, Elliott RA, McCollum C.
No. 45Clinical effectiveness and cost-effectiveness of laparoscopic surgery forcolorectal cancer: systematic reviews andeconomic evaluation.
By Murray A, Lourenco T, de Verteuil R, Hernandez R, Fraser C,McKinley A, et al.
No. 46Etanercept and efalizumab for thetreatment of psoriasis: a systematicreview.
By Woolacott N, Hawkins N, Mason A, Kainth A, Khadjesari Z, Bravo Vergel Y, et al.
No. 47Systematic reviews of clinical decisiontools for acute abdominal pain.
By Liu JLY, Wyatt JC, Deeks JJ,Clamp S, Keen J, Verde P, et al.
No. 48Evaluation of the ventricular assistdevice programme in the UK.
By Sharples L, Buxton M, Caine N,Cafferty F, Demiris N, Dyer M, et al.
No. 49A systematic review and economicmodel of the clinical and cost-effectiveness of immunosuppressivetherapy for renal transplantation inchildren.
By Yao G, Albon E, Adi Y, Milford D,Bayliss S, Ready A, et al.
No. 50Amniocentesis results: investigation ofanxiety. The ARIA trial.
By Hewison J, Nixon J, Fountain J,Cocks K, Jones C, Mason G, et al.
Volume 11, 2007
No. 1Pemetrexed disodium for the treatmentof malignant pleural mesothelioma: a systematic review and economicevaluation.
By Dundar Y, Bagust A, Dickson R,Dodd S, Green J, Haycox A, et al.
No. 2A systematic review and economicmodel of the clinical effectiveness andcost-effectiveness of docetaxel incombination with prednisone orprednisolone for the treatment ofhormone-refractory metastatic prostatecancer.
By Collins R, Fenwick E, Trowman R,Perard R, Norman G, Light K, et al.
No. 3A systematic review of rapid diagnostictests for the detection of tuberculosisinfection.
By Dinnes J, Deeks J, Kunst H,Gibson A, Cummins E, Waugh N, et al.
No. 4The clinical effectiveness and cost-effectiveness of strontium ranelate forthe prevention of osteoporotic fragility fractures in postmenopausalwomen.
By Stevenson M, Davis S, Lloyd-Jones M, Beverley C.
Health Technology Assessment 2007; Vol. 11: No. 30
163
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.

No. 5A systematic review of quantitative andqualitative research on the role andeffectiveness of written informationavailable to patients about individualmedicines.
By Raynor DK, Blenkinsopp A,Knapp P, Grime J, Nicolson DJ, Pollock K, et al.
No. 6Oral naltrexone as a treatment forrelapse prevention in formerly opioid-dependent drug users: a systematicreview and economic evaluation.
By Adi Y, Juarez-Garcia A, Wang D,Jowett S, Frew E, Day E, et al.
No. 7Glucocorticoid-induced osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Stevenson M, McCloskey EV, Davis S, Lloyd-Jones M.
No. 8Epidemiological, social, diagnostic andeconomic evaluation of populationscreening for genital chlamydial infection.
By Low N, McCarthy A, Macleod J,Salisbury C, Campbell R, Roberts TE, et al.
No. 9Methadone and buprenorphine for themanagement of opioid dependence: a systematic review and economicevaluation.
By Connock M, Juarez-Garcia A,Jowett S, Frew E, Liu Z, Taylor RJ, et al.
No. 10Exercise Evaluation Randomised Trial(EXERT): a randomised trial comparingGP referral for leisure centre-basedexercise, community-based walking andadvice only.
By Isaacs AJ, Critchley JA, See Tai S, Buckingham K, Westley D,Harridge SDR, et al.
No. 11Interferon alfa (pegylated and non-pegylated) and ribavirin for thetreatment of mild chronic hepatitis C: a systematic review and economicevaluation.
By Shepherd J, Jones J, Hartwell D,Davidson P, Price A, Waugh N.
No. 12Systematic review and economicevaluation of bevacizumab andcetuximab for the treatment ofmetastatic colorectal cancer.
By Tappenden P, Jones R, Paisley S,Carroll C.
No. 13A systematic review and economicevaluation of epoetin alfa, epoetin betaand darbepoetin alfa in anaemiaassociated with cancer, especially thatattributable to cancer treatment.
By Wilson J, Yao GL, Raftery J,Bohlius J, Brunskill S, Sandercock J, et al.
No. 14A systematic review and economicevaluation of statins for the preventionof coronary events.
By Ward S, Lloyd Jones M, Pandor A,Holmes M, Ara R, Ryan A, et al.
No. 15A systematic review of the effectivenessand cost-effectiveness of differentmodels of community-based respite carefor frail older people and their carers.
By Mason A, Weatherly H, SpilsburyK, Arksey H, Golder S, Adamson J, et al.
No. 16Additional therapy for young childrenwith spastic cerebral palsy: a randomised controlled trial.
By Weindling AM, Cunningham CC,Glenn SM, Edwards RT, Reeves DJ.
No. 17Screening for type 2 diabetes: literaturereview and economic modelling.
By Waugh N, Scotland G, McNamee P, Gillett M, Brennan A,Goyder E, et al.
No. 18The effectiveness and cost-effectivenessof cinacalcet for secondaryhyperparathyroidism in end-stage renaldisease patients on dialysis: a systematicreview and economic evaluation.
By Garside R, Pitt M, Anderson R,Mealing S, Roome C, Snaith A, et al.
No. 19The clinical effectiveness and cost-effectiveness of gemcitabine formetastatic breast cancer: a systematicreview and economic evaluation.
By Takeda AL, Jones J, Loveman E,Tan SC, Clegg AJ.
No. 20A systematic review of duplexultrasound, magnetic resonanceangiography and computed tomographyangiography for the diagnosis and assessment of symptomatic, lowerlimb peripheral arterial disease.
By Collins R, Cranny G, Burch J,Aguiar-Ibáñez R, Craig D, Wright K, et al.
No. 21The clinical effectiveness and cost-effectiveness of treatments for childrenwith idiopathic steroid-resistantnephrotic syndrome: a systematic review.
By Colquitt JL, Kirby J, Green C,Cooper K, Trompeter RS.
No. 22A systematic review of the routinemonitoring of growth in children ofprimary school age to identify growth-related conditions.
By Fayter D, Nixon J, Hartley S,Rithalia A, Butler G, Rudolf M, et al.
No. 23Systematic review of the effectiveness ofpreventing and treating Staphylococcusaureus carriage in reducing peritonealcatheter-related infections.
By McCormack K, Rabindranath K,Kilonzo M, Vale L, Fraser C, McIntyre L,et al.
No. 24The clinical effectiveness and cost ofrepetitive transcranial magneticstimulation versus electroconvulsivetherapy in severe depression: a multicentre pragmatic randomisedcontrolled trial and economic analysis.
By McLoughlin DM, Mogg A, ErantiS, Pluck G, Purvis R, Edwards D, et al.
No. 25A randomised controlled trial andeconomic evaluation of direct versusindirect and individual versus groupmodes of speech and language therapyfor children with primary languageimpairment.
By Boyle J, McCartney E, Forbes J,O’Hare A.
No. 26Hormonal therapies for early breastcancer: systematic review and economicevaluation.
By Hind D, Ward S, De Nigris E,Simpson E, Carroll C, Wyld L.
No. 27Cardioprotection against the toxiceffects of anthracyclines given tochildren with cancer: a systematicreview.
By Bryant J, Picot J, Levitt G, Sullivan I, Baxter L, Clegg A.
No. 28Adalimumab, etanercept and infliximabfor the treatment of ankylosingspondylitis: a systematic review andeconomic evaluation.
By McLeod C, Bagust A, Boland A,Dagenais P, Dickson R, Dundar Y, et al.
No. 29Prenatal screening and treatmentstrategies to prevent group Bstreptococcal and other bacterialinfections in early infancy: cost-effectiveness and expected value ofinformation analyses.
By Colbourn T, Asseburg C, Bojke L,Philips Z, Claxton K, Ades AE,et al.
No. 30Clinical effectiveness and cost-effectiveness of bone morphogeneticproteins in the non-healing of fracturesand spinal fusion: a systematic review.
By Garrison KR, Donell S, Ryder J,Shemilt I, Mugford M, Harvey I, et al.
Health Technology Assessment reports published to date
164
Health Technology Assessment 2007; Vol. 11: No. 30
165
Health Technology AssessmentProgramme
Prioritisation Strategy GroupMembers
Chair,Professor Tom Walley, Director, NHS HTA Programme,Department of Pharmacology &Therapeutics,University of Liverpool
Professor Bruce Campbell,Consultant Vascular & GeneralSurgeon, Royal Devon & ExeterHospital
Professor Robin E Ferner,Consultant Physician andDirector, West Midlands Centrefor Adverse Drug Reactions,City Hospital NHS Trust,Birmingham
Dr Edmund Jessop, MedicalAdviser, National Specialist,Commissioning Advisory Group(NSCAG), Department ofHealth, London
Professor Jon Nicholl, Director,Medical Care Research Unit,University of Sheffield, School of Health and Related Research
Dr Ron Zimmern, Director,Public Health Genetics Unit,Strangeways ResearchLaboratories, Cambridge
Director, Professor Tom Walley, Director, NHS HTA Programme,Department of Pharmacology &Therapeutics,University of Liverpool
Deputy Director, Professor Jon Nicholl,Director, Medical Care ResearchUnit, University of Sheffield,School of Health and RelatedResearch
HTA Commissioning BoardMembers
Programme Director, Professor Tom Walley, Director, NHS HTA Programme,Department of Pharmacology &Therapeutics,University of Liverpool
Chair,Professor Jon Nicholl,Director, Medical Care ResearchUnit, University of Sheffield,School of Health and RelatedResearch
Deputy Chair, Dr Andrew Farmer, University Lecturer in GeneralPractice, Department of Primary Health Care, University of Oxford
Dr Jeffrey Aronson,Reader in ClinicalPharmacology, Department ofClinical Pharmacology,Radcliffe Infirmary, Oxford
Professor Deborah Ashby,Professor of Medical Statistics,Department of Environmentaland Preventative Medicine,Queen Mary University ofLondon
Professor Ann Bowling,Professor of Health ServicesResearch, Primary Care andPopulation Studies,University College London
Professor John Cairns, Professor of Health Economics,Public Health Policy, London School of Hygiene and Tropical Medicine, London
Professor Nicky Cullum,Director of Centre for EvidenceBased Nursing, Department ofHealth Sciences, University ofYork
Professor Jon Deeks, Professor of Health Statistics,University of Birmingham
Professor Jenny Donovan,Professor of Social Medicine,Department of Social Medicine,University of Bristol
Professor Freddie Hamdy,Professor of Urology, University of Sheffield
Professor Allan House, Professor of Liaison Psychiatry,University of Leeds
Professor Sallie Lamb, Director,Warwick Clinical Trials Unit,University of Warwick
Professor Stuart Logan,Director of Health & SocialCare Research, The PeninsulaMedical School, Universities ofExeter & Plymouth
Professor Miranda Mugford,Professor of Health Economics,University of East Anglia
Dr Linda Patterson, Consultant Physician,Department of Medicine,Burnley General Hospital
Professor Ian Roberts, Professor of Epidemiology &Public Health, InterventionResearch Unit, London Schoolof Hygiene and TropicalMedicine
Professor Mark Sculpher,Professor of Health Economics,Centre for Health Economics,Institute for Research in theSocial Services, University of York
Professor Kate Thomas,Professor of Complementaryand Alternative Medicine,University of Leeds
Professor David John Torgerson,Director of York Trial Unit,Department of Health Sciences,University of York
Professor Hywel Williams,Professor of Dermato-Epidemiology,University of Nottingham
Current and past membership details of all HTA ‘committees’ are available from the HTA website (www.hta.ac.uk)
© Queen’s Printer and Controller of HMSO 2007. All rights reserved.
Health Technology Assessment Programme
166
Diagnostic Technologies & Screening PanelMembers
Chair,Dr Ron Zimmern, Director ofthe Public Health Genetics Unit,Strangeways ResearchLaboratories, Cambridge
Ms Norma Armston,Freelance Consumer Advocate,Bolton
Professor Max Bachmann,Professor of Health CareInterfaces, Department ofHealth Policy and Practice,University of East Anglia
Professor Rudy BilousProfessor of Clinical Medicine &Consultant Physician,The Academic Centre,South Tees Hospitals NHS Trust
Ms Dea Birkett, Service UserRepresentative, London
Dr Paul Cockcroft, ConsultantMedical Microbiologist andClinical Director of Pathology,Department of ClinicalMicrobiology, St Mary'sHospital, Portsmouth
Professor Adrian K Dixon,Professor of Radiology,University Department ofRadiology, University ofCambridge Clinical School
Dr David Elliman, Consultant inCommunity Child Health,Islington PCT & Great OrmondStreet Hospital, London
Professor Glyn Elwyn, Research Chair, Centre forHealth Sciences Research,Cardiff University, Departmentof General Practice, Cardiff
Professor Paul Glasziou,Director, Centre for Evidence-Based Practice,University of Oxford
Dr Jennifer J Kurinczuk,Consultant ClinicalEpidemiologist, NationalPerinatal Epidemiology Unit,Oxford
Dr Susanne M Ludgate, Clinical Director, Medicines &Healthcare Products RegulatoryAgency, London
Mr Stephen Pilling, Director,Centre for Outcomes, Research & Effectiveness, Joint Director, NationalCollaborating Centre for MentalHealth, University CollegeLondon
Mrs Una Rennard, Service User Representative,Oxford
Dr Phil Shackley, SeniorLecturer in Health Economics,Academic Vascular Unit,University of Sheffield
Dr Margaret Somerville,Director of Public HealthLearning, Peninsula MedicalSchool, University of Plymouth
Dr Graham Taylor, ScientificDirector & Senior Lecturer,Regional DNA Laboratory, TheLeeds Teaching Hospitals
Professor Lindsay WilsonTurnbull, Scientific Director,Centre for MR Investigations &YCR Professor of Radiology,University of Hull
Professor Martin J Whittle,Clinical Co-director, NationalCo-ordinating Centre forWomen’s and Childhealth
Dr Dennis Wright, Consultant Biochemist &Clinical Director, The North West LondonHospitals NHS Trust, Middlesex
Pharmaceuticals PanelMembers
Chair,Professor Robin Ferner,Consultant Physician andDirector, West Midlands Centrefor Adverse Drug Reactions, City Hospital NHS Trust,Birmingham
Ms Anne Baileff, ConsultantNurse in First Contact Care,Southampton City Primary CareTrust, University ofSouthampton
Professor Imti Choonara,Professor in Child Health,Academic Division of ChildHealth, University ofNottingham
Professor John Geddes,Professor of EpidemiologicalPsychiatry, University of Oxford
Mrs Barbara Greggains, Non-Executive Director,Greggains Management Ltd
Dr Bill Gutteridge, MedicalAdviser, National SpecialistCommissioning Advisory Group(NSCAG), London
Mrs Sharon Hart, Consultant PharmaceuticalAdviser, Reading
Dr Jonathan Karnon, SeniorResearch Fellow, HealthEconomics and DecisionScience, University of Sheffield
Dr Yoon Loke, Senior Lecturerin Clinical Pharmacology,University of East Anglia
Ms Barbara Meredith,Lay Member, Epsom
Dr Andrew Prentice, SeniorLecturer and ConsultantObstetrician & Gynaecologist,Department of Obstetrics &Gynaecology, University ofCambridge
Dr Frances Rotblat, CPMPDelegate, Medicines &Healthcare Products RegulatoryAgency, London
Dr Martin Shelly, General Practitioner, Leeds
Mrs Katrina Simister, AssistantDirector New Medicines,National Prescribing Centre,Liverpool
Dr Richard Tiner, MedicalDirector, Medical Department,Association of the BritishPharmaceutical Industry,London
Current and past membership details of all HTA ‘committees’ are available from the HTA website (www.hta.ac.uk)
Therapeutic Procedures PanelMembers
Chair, Professor Bruce Campbell,Consultant Vascular andGeneral Surgeon, Departmentof Surgery, Royal Devon &Exeter Hospital
Dr Mahmood Adil, DeputyRegional Director of PublicHealth, Department of Health,Manchester
Dr Aileen Clarke,Consultant in Public Health,Public Health Resource Unit,Oxford
Professor Matthew Cooke,Professor of EmergencyMedicine, Warwick EmergencyCare and Rehabilitation,University of Warwick
Mr Mark Emberton, SeniorLecturer in OncologicalUrology, Institute of Urology,University College Hospital
Professor Paul Gregg,Professor of OrthopaedicSurgical Science, Department ofGeneral Practice and PrimaryCare, South Tees Hospital NHSTrust, Middlesbrough
Ms Maryann L Hardy, Lecturer, Division ofRadiography, University ofBradford
Dr Simon de Lusignan,Senior Lecturer, Primary CareInformatics, Department ofCommunity Health Sciences,St George’s Hospital MedicalSchool, London
Dr Peter Martin, ConsultantNeurologist, Addenbrooke’sHospital, Cambridge
Professor Neil McIntosh,Edward Clark Professor of ChildLife & Health, Department ofChild Life & Health, Universityof Edinburgh
Professor Jim Neilson,Professor of Obstetrics andGynaecology, Department ofObstetrics and Gynaecology,University of Liverpool
Dr John C Pounsford,Consultant Physician,Directorate of Medical Services,North Bristol NHS Trust
Dr Karen Roberts, NurseConsultant, Queen ElizabethHospital, Gateshead
Dr Vimal Sharma, ConsultantPsychiatrist/Hon. Senior Lecturer, Mental HealthResource Centre, Cheshire andWirral Partnership NHS Trust,Wallasey
Professor Scott Weich, Professor of Psychiatry, Division of Health in theCommunity, University ofWarwick
Disease Prevention PanelMembers
Chair, Dr Edmund Jessop, MedicalAdviser, National SpecialistCommissioning Advisory Group(NSCAG), London
Mrs Sheila Clark, ChiefExecutive, St James’s Hospital,Portsmouth
Mr Richard Copeland, Lead Pharmacist: ClinicalEconomy/Interface, Wansbeck General Hospital,Northumberland
Dr Elizabeth Fellow-Smith,Medical Director, West London Mental HealthTrust, Middlesex
Mr Ian Flack, Director PPIForum Support, Council ofEthnic Minority VoluntarySector Organisations, Stratford
Dr John Jackson, General Practitioner, Newcastle upon Tyne
Mrs Veronica James, ChiefOfficer, Horsham District AgeConcern, Horsham
Professor Mike Kelly, Director, Centre for PublicHealth Excellence, National Institute for Healthand Clinical Excellence, London
Professor Yi Mien Koh, Director of Public Health andMedical Director, London NHS (North West LondonStrategic Health Authority),London
Ms Jeanett Martin, Director of Clinical Leadership& Quality, Lewisham PCT,London
Dr Chris McCall, GeneralPractitioner, Dorset
Dr David Pencheon, Director,Eastern Region Public HealthObservatory, Cambridge
Dr Ken Stein, Senior ClinicalLecturer in Public Health,Director, Peninsula TechnologyAssessment Group, University of Exeter, Exeter
Dr Carol Tannahill, Director,Glasgow Centre for PopulationHealth, Glasgow
Professor Margaret Thorogood,Professor of Epidemiology,University of Warwick, Coventry
Dr Ewan Wilkinson, Consultant in Public Health,Royal Liverpool UniversityHospital, Liverpool
Health Technology Assessment 2007; Vol. 11: No. 30
167Current and past membership details of all HTA ‘committees’ are available from the HTA website (www.hta.ac.uk)

Health Technology Assessment Programme
168Current and past membership details of all HTA ‘committees’ are available from the HTA website (www.hta.ac.uk)
Expert Advisory NetworkMembers
Professor Douglas Altman,Professor of Statistics inMedicine, Centre for Statisticsin Medicine, University ofOxford
Professor John Bond,Director, Centre for HealthServices Research, University ofNewcastle upon Tyne, School ofPopulation & Health Sciences,Newcastle upon Tyne
Professor Andrew Bradbury,Professor of Vascular Surgery,Solihull Hospital, Birmingham
Mr Shaun Brogan, Chief Executive, RidgewayPrimary Care Group, Aylesbury
Mrs Stella Burnside OBE,Chief Executive, Regulation and ImprovementAuthority, Belfast
Ms Tracy Bury, Project Manager, WorldConfederation for PhysicalTherapy, London
Professor Iain T Cameron,Professor of Obstetrics andGynaecology and Head of theSchool of Medicine,University of Southampton
Dr Christine Clark,Medical Writer & ConsultantPharmacist, Rossendale
Professor Collette Clifford,Professor of Nursing & Head ofResearch, School of HealthSciences, University ofBirmingham, Edgbaston,Birmingham
Professor Barry Cookson,Director, Laboratory ofHealthcare Associated Infection,Health Protection Agency,London
Dr Carl Counsell, ClinicalSenior Lecturer in Neurology,Department of Medicine &Therapeutics, University ofAberdeen
Professor Howard Cuckle,Professor of ReproductiveEpidemiology, Department ofPaediatrics, Obstetrics &Gynaecology, University ofLeeds
Dr Katherine Darton, Information Unit, MIND – The Mental Health Charity,London
Professor Carol Dezateux, Professor of PaediatricEpidemiology, London
Dr Keith Dodd, ConsultantPaediatrician, Derby
Mr John Dunning,Consultant CardiothoracicSurgeon, CardiothoracicSurgical Unit, PapworthHospital NHS Trust, Cambridge
Mr Jonothan Earnshaw,Consultant Vascular Surgeon,Gloucestershire Royal Hospital,Gloucester
Professor Martin Eccles, Professor of ClinicalEffectiveness, Centre for HealthServices Research, University ofNewcastle upon Tyne
Professor Pam Enderby,Professor of CommunityRehabilitation, Institute ofGeneral Practice and PrimaryCare, University of Sheffield
Professor Gene Feder, Professorof Primary Care Research &Development, Centre for HealthSciences, Barts & The LondonQueen Mary’s School ofMedicine & Dentistry, London
Mr Leonard R Fenwick, Chief Executive, Newcastleupon Tyne Hospitals NHS Trust
Mrs Gillian Fletcher, Antenatal Teacher & Tutor andPresident, National ChildbirthTrust, Henfield
Professor Jayne Franklyn,Professor of Medicine,Department of Medicine,University of Birmingham,Queen Elizabeth Hospital,Edgbaston, Birmingham
Dr Neville Goodman, Consultant Anaesthetist,Southmead Hospital, Bristol
Professor Robert E Hawkins, CRC Professor and Director ofMedical Oncology, Christie CRCResearch Centre, ChristieHospital NHS Trust, Manchester
Professor Allen Hutchinson, Director of Public Health &Deputy Dean of ScHARR,Department of Public Health,University of Sheffield
Professor Peter Jones, Professorof Psychiatry, University ofCambridge, Cambridge
Professor Stan Kaye, CancerResearch UK Professor ofMedical Oncology, Section ofMedicine, Royal MarsdenHospital & Institute of CancerResearch, Surrey
Dr Duncan Keeley,General Practitioner (Dr Burch& Ptnrs), The Health Centre,Thame
Dr Donna Lamping,Research Degrees ProgrammeDirector & Reader in Psychology,Health Services Research Unit,London School of Hygiene andTropical Medicine, London
Mr George Levvy,Chief Executive, Motor Neurone Disease Association,Northampton
Professor James Lindesay,Professor of Psychiatry for theElderly, University of Leicester,Leicester General Hospital
Professor Julian Little,Professor of Human GenomeEpidemiology, Department ofEpidemiology & CommunityMedicine, University of Ottawa
Professor Rajan Madhok, Consultant in Public Health,South Manchester Primary Care Trust, Manchester
Professor Alexander Markham, Director, Molecular MedicineUnit, St James’s UniversityHospital, Leeds
Professor Alistaire McGuire,Professor of Health Economics,London School of Economics
Dr Peter Moore, Freelance Science Writer, Ashtead
Dr Andrew Mortimore, PublicHealth Director, SouthamptonCity Primary Care Trust,Southampton
Dr Sue Moss, Associate Director,Cancer Screening EvaluationUnit, Institute of CancerResearch, Sutton
Mrs Julietta Patnick, Director, NHS Cancer ScreeningProgrammes, Sheffield
Professor Robert Peveler,Professor of Liaison Psychiatry,Royal South Hants Hospital,Southampton
Professor Chris Price, Visiting Professor in ClinicalBiochemistry, University ofOxford
Professor William Rosenberg,Professor of Hepatology andConsultant Physician, Universityof Southampton, Southampton
Professor Peter Sandercock,Professor of Medical Neurology,Department of ClinicalNeurosciences, University ofEdinburgh
Dr Susan Schonfield, Consultantin Public Health, HillingdonPCT, Middlesex
Dr Eamonn Sheridan,Consultant in Clinical Genetics,Genetics Department,St James’s University Hospital,Leeds
Professor Sarah Stewart-Brown, Professor of Public Health,University of Warwick, Division of Health in theCommunity Warwick MedicalSchool, LWMS, Coventry
Professor Ala Szczepura, Professor of Health ServiceResearch, Centre for HealthServices Studies, University ofWarwick
Dr Ross Taylor, Senior Lecturer, Department ofGeneral Practice and PrimaryCare, University of Aberdeen
Mrs Joan Webster, Consumer member, HTA –Expert Advisory Network

How to obtain copies of this and other HTA Programme reports.An electronic version of this publication, in Adobe Acrobat format, is available for downloading free ofcharge for personal use from the HTA website (http://www.hta.ac.uk). A fully searchable CD-ROM isalso available (see below).
Printed copies of HTA monographs cost £20 each (post and packing free in the UK) to both public andprivate sector purchasers from our Despatch Agents.
Non-UK purchasers will have to pay a small fee for post and packing. For European countries the cost is£2 per monograph and for the rest of the world £3 per monograph.
You can order HTA monographs from our Despatch Agents:
– fax (with credit card or official purchase order) – post (with credit card or official purchase order or cheque)– phone during office hours (credit card only).
Additionally the HTA website allows you either to pay securely by credit card or to print out yourorder and then post or fax it.
Contact details are as follows:HTA Publications Email: [email protected] Box 642 Tel: 0870 1616662YORK YO31 7WX Fax: 0870 1616663UK
NHS libraries can subscribe free of charge. Public libraries can subscribe at a very reduced cost of £100 for each volume (normally comprising 30–40 titles). The commercial subscription rate is £300 per volume. Please see our website for details. Subscriptions can only be purchased for the current orforthcoming volume.
Payment methods
Paying by chequeIf you pay by cheque, the cheque must be in pounds sterling. Please see our website for details.
Paying by credit cardThe following cards are accepted by phone, fax, post or via the website ordering pages: Delta, Eurocard,Mastercard, Solo, Switch and Visa. We advise against sending credit card details in a plain email.
Paying by official purchase orderYou can post or fax these, but they must be from public bodies (i.e. NHS or universities) within the UK.We cannot at present accept purchase orders from commercial companies or from outside the UK.
How do I get a copy of HTA on CD?
Please use the form on the HTA website (www.hta.ac.uk/htacd.htm). Or contact our despatch agents(see contact details above) by email, post, fax or phone. HTA on CD is currently free of charge worldwide.
The website also provides information about the HTA Programme and lists the membership of the variouscommittees.
HTA

Clinical effectiveness and cost-effectiveness of bone morphogenetic proteins in the non-healing of fractures and spinalfusion: a systematic review
KR Garrison, S Donell, J Ryder, I Shemilt, M Mugford, I Harvey and F Song
Health Technology Assessment 2007; Vol. 11: No. 30
HTAHealth Technology AssessmentNHS R&D HTA Programmewww.hta.ac.uk
The National Coordinating Centre for Health Technology Assessment,Mailpoint 728, Boldrewood,University of Southampton,Southampton, SO16 7PX, UK.Fax: +44 (0) 23 8059 5639 Email: [email protected]://www.hta.ac.uk ISSN 1366-5278
FeedbackThe HTA Programme and the authors would like to know
your views about this report.
The Correspondence Page on the HTA website(http://www.hta.ac.uk) is a convenient way to publish
your comments. If you prefer, you can send your comments to the address below, telling us whether you would like
us to transfer them to the website.
We look forward to hearing from you.
August 2007
Health Technology Assessm
ent 2007;Vol. 11: No. 30
Bone morphogenetic proteins in the non-healing of fractures and spinal fusion