Bivalirudin in patients undergoing primary angioplasty for acute myocardial infarction...
11
Articles www.thelancet.com Vol 374 October 3, 2009 1149 Bivalirudin in patients undergoing primary angioplasty for acute myocardial infarction (HORIZONS-AMI): 1-year results of a randomised controlled trial Roxana Mehran, Alexandra J Lansky, Bernhard Witzenbichler, Giulio Guagliumi, Jan Z Peruga, Bruce R Brodie, Dariusz Dudek, Ran Kornowski, Franz Hartmann, Bernard J Gersh, Stuart J Pocock, S Chiu Wong, Eugenia Nikolsky, Louise Gambone, Lynn Vandertie, Helen Parise, George D Dangas, Gregg W Stone, for the HORIZONS-AMI Trial Investigators* Summary Background In the HORIZONS-AMI trial, patients with acute ST-segment elevation myocardial infarction (STEMI) undergoing percutaneous coronary intervention (PCI) who were treated with the thrombin inhibitor bivalirudin had substantially lower 30-day rates of major haemorrhagic complications and net adverse clinical events than did patients assigned to heparin plus a glycoprotein IIb/IIIa inhibitor (GPI). Here, we assess whether these initial benefits were maintained at 1 year of follow-up. Methods Patients aged 18 years or older were eligible for enrolment in this multicentre, open-label, randomised controlled trial if they had STEMI, presented within 12 h after the onset of symptoms, and were undergoing primary PCI. 3602 eligible patients were randomly assigned by interactive voice response system in a 1:1 ratio to receive bivalirudin (0·75 mg/kg intravenous bolus followed by 1·75 mg/kg per h infusion; n=1800) or heparin plus a GPI (control; 60 IU/kg intravenous bolus followed by boluses with target activated clotting time 200–250 s; n=1802). The two primary trial endpoints were major bleeding and net adverse clinical events (NACE; consisting of major bleeding or composite major adverse cardiovascular events [MACE; death, reinfarction, target vessel revascularisation for ischaemia, or stroke]). This prespecified analysis reports data for the 1-year follow-up. Analysis was by intention to treat. Patients with missing data were censored at the time of withdrawal from the study or at last follow-up. This trial is registered with ClinicalTrials.gov, number NCT00433966. Findings 1-year data were available for 1696 patients in the bivalirudin group and 1702 patients in the control group. Reasons for participant dropout were loss to follow-up and withdrawal of consent. The rate of NACE was lower in the bivalirudin group than in the control group (15·6% vs 18·3%, hazard ratio [HR] 0·83, 95% CI 0·71–0·97, p=0·022), as a result of a lower rate of major bleeding in the bivalirudin group (5·8% vs 9·2%, HR 0·61, 0·48–0·78, p<0·0001). The rate of MACE was similar between groups (11·9% vs 11·9%, HR 1·00, 0·82–1·21, p=0·98). The 1-year rates of cardiac mortality (2·1% vs 3·8%, HR 0·57, 0·38–0·84, p=0·005) and all-cause mortality (3·5% vs 4·8%, HR 0·71, 0·51–0·98, p=0·037) were lower in the bivalirudin group than in the control group. Interpretation In patients with STEMI undergoing primary PCI, anticoagulation with bivalirudin reduced the rates of net adverse clinical events and major bleeding at 1 year compared with treatment with heparin plus a GPI. This finding has important clinical implications for the selection of optimum treatment strategies for patients with STEMI. Funding Cardiovascular Research Foundation, with unrestricted grant support from Boston Scientific Corporation and The Medicines Company. Introduction Glycoprotein IIb/IIIa inhibitors (GPIs) are frequently used in the USA and Europe in patients with ST- segment elevation myocardial infarction (STEMI) who are undergoing primary percutaneous coronary intervention (PCI) to reduce ischaemic complications. 1–3 These agents, however, increase the rates of haemorrhagic events and of thrombocytopenia, 4–7 both of which have been strongly associated with early and late mortality. 8–12 The direct thrombin inhibitor bivalirudin, when used instead of heparin plus a GPI during PCI, reduces the rates of major and minor bleeding and thrombocytopenia across a broad range of patients with coronary artery disease. 13–17 In the large- scale prospective HORIZONS-AMI (Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction) trial, patients with high-risk STEMI undergoing primary PCI were randomly assigned to receive bivalirudin alone or heparin plus a GPI. Patients in the bivalirudin group had lower 30-day rates of major bleeding and thrombocytopenia, similar rates of composite ischaemic events, and improved survival compared with those in the heparin plus GPI group. 17 Whether the beneficial effects of bivalirudin seen at 30 days are preserved, increased, or diminished at 1 year is not known. We report the prespecified analysis of 1-year outcomes from the HORIZONS-AMI trial. Lancet 2009; 374: 1149–59 Published Online August 30, 2009 DOI:10.1016/S0140- 6736(09)61484-7 See Comment page 1125 *Members listed at end of paper Columbia University Medical Center/New York-Presbyterian Hospital and the Cardiovascular Research Foundation, New York, NY, USA (R Mehran MD, A J Lansky MD, E Nikolsky MD, L Gambone, L Vandertie, H Parise ScD, G D Dangas MD, Prof G W Stone MD); Charité Campus Benjamin Franklin, Berlin, Germany (B Witzenbichler MD); Ospedali Riuniti di Bergamo, Bergamo, Italy (G Guagliumi MD); Silesian Center for Heart Disease, Lodz, Poland (J Z Peruga MD); LeBauer Cardiovascular Research Foundation and Moses Cone Hospital, Greensboro, NC, USA (B R Brodie MD); Jagiellonian University, Krakow, Poland (D Dudek MD); Rabin Medical Center, Petach Tikva, Israel (R Kornowski MD); Universitätsklinikum Schleswig-Holstein, Lübeck, Germany (F Hartmann MD); Mayo Clinic, Rochester, MN, USA (Prof B J Gersh MB); London School of Hygiene and Tropical Medicine, London, UK (Prof S J Pocock PhD); and New York-Presbyterian Hospital/ Weill Cornell Medical Center, New York, NY, USA (S C Wong MD) Correspondence to: Dr Roxana Mehran, Columbia University Medical Center, 161 Fort Washington Avenue (5th Floor), New York, NY 10032, USA [email protected]
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Bivalirudin in patients undergoing primary angioplasty for acute myocardial infarction...

Articles
www.thelancet.com Vol 374 October 3, 2009 1149
Bivalirudin in patients undergoing primary angioplasty for acute myocardial infarction (HORIZONS-AMI): 1-year results of a randomised controlled trialRoxana Mehran, Alexandra J Lansky, Bernhard Witzenbichler, Giulio Guagliumi, Jan Z Peruga, Bruce R Brodie, Dariusz Dudek, Ran Kornowski, Franz Hartmann, Bernard J Gersh, Stuart J Pocock, S Chiu Wong, Eugenia Nikolsky, Louise Gambone, Lynn Vandertie, Helen Parise, George D Dangas, Gregg W Stone, for the HORIZONS-AMI Trial Investigators*
SummaryBackground In the HORIZONS-AMI trial, patients with acute ST-segment elevation myocardial infarction (STEMI) undergoing percutaneous coronary intervention (PCI) who were treated with the thrombin inhibitor bivalirudin had substantially lower 30-day rates of major haemorrhagic complications and net adverse clinical events than did patients assigned to heparin plus a glycoprotein IIb/IIIa inhibitor (GPI). Here, we assess whether these initial benefi ts were maintained at 1 year of follow-up.
Methods Patients aged 18 years or older were eligible for enrolment in this multicentre, open-label, randomised controlled trial if they had STEMI, presented within 12 h after the onset of symptoms, and were undergoing primary PCI. 3602 eligible patients were randomly assigned by interactive voice response system in a 1:1 ratio to receive bivalirudin (0·75 mg/kg intravenous bolus followed by 1·75 mg/kg per h infusion; n=1800) or heparin plus a GPI (control; 60 IU/kg intravenous bolus followed by boluses with target activated clotting time 200–250 s; n=1802). The two primary trial endpoints were major bleeding and net adverse clinical events (NACE; consisting of major bleeding or composite major adverse cardiovascular events [MACE; death, reinfarction, target vessel revascularisation for ischaemia, or stroke]). This prespecifi ed analysis reports data for the 1-year follow-up. Analysis was by intention to treat. Patients with missing data were censored at the time of withdrawal from the study or at last follow-up. This trial is registered with ClinicalTrials.gov, number NCT00433966.
Findings 1-year data were available for 1696 patients in the bivalirudin group and 1702 patients in the control group. Reasons for participant dropout were loss to follow-up and withdrawal of consent. The rate of NACE was lower in the bivalirudin group than in the control group (15·6% vs 18·3%, hazard ratio [HR] 0·83, 95% CI 0·71–0·97, p=0·022), as a result of a lower rate of major bleeding in the bivalirudin group (5·8% vs 9·2%, HR 0·61, 0·48–0·78, p<0·0001). The rate of MACE was similar between groups (11·9% vs 11·9%, HR 1·00, 0·82–1·21, p=0·98). The 1-year rates of cardiac mortality (2·1% vs 3·8%, HR 0·57, 0·38–0·84, p=0·005) and all-cause mortality (3·5% vs 4·8%, HR 0·71, 0·51–0·98, p=0·037) were lower in the bivalirudin group than in the control group.
Interpretation In patients with STEMI undergoing primary PCI, anticoagulation with bivalirudin reduced the rates of net adverse clinical events and major bleeding at 1 year compared with treatment with heparin plus a GPI. This fi nding has important clinical implications for the selection of optimum treatment strategies for patients with STEMI.
Funding Cardiovascular Research Foundation, with unrestricted grant support from Boston Scientifi c Corporation and The Medicines Company.
IntroductionGlycoprotein IIb/IIIa inhibitors (GPIs) are frequently used in the USA and Europe in patients with ST-segment elevation myocardial infarction (STEMI) who are undergoing primary percutaneous coronary intervention (PCI) to reduce ischaemic complications.1–3 These agents, however, increase the rates of haemorrhagic events and of thrombocytopenia,4–7 both of which have been strongly associated with early and late mortality.8–12 The direct thrombin inhibitor bivalirudin, when used instead of heparin plus a GPI during PCI, reduces the rates of major and minor bleeding and thrombocytopenia across a broad range of patients with coronary artery disease.13–17 In the large-
scale prospective HORIZONS-AMI (Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction) trial, patients with high-risk STEMI undergoing primary PCI were randomly assigned to receive bivalirudin alone or heparin plus a GPI. Patients in the bivalirudin group had lower 30-day rates of major bleeding and thrombocytopenia, similar rates of composite ischaemic events, and improved survival compared with those in the heparin plus GPI group.17 Whether the benefi cial eff ects of bivalirudin seen at 30 days are preserved, increased, or diminished at 1 year is not known. We report the prespecifi ed analysis of 1-year outcomes from the HORIZONS-AMI trial.
Lancet 2009; 374: 1149–59
Published OnlineAugust 30, 2009DOI:10.1016/S0140-6736(09)61484-7
See Comment page 1125
*Members listed at end of paper
Columbia University Medical Center/New York-Presbyterian Hospital and the Cardiovascular Research Foundation, New York, NY, USA (R Mehran MD, A J Lansky MD, E Nikolsky MD, L Gambone, L Vandertie, H Parise ScD, G D Dangas MD, Prof G W Stone MD); Charité Campus Benjamin Franklin, Berlin, Germany (B Witzenbichler MD); Ospedali Riuniti di Bergamo, Bergamo, Italy (G Guagliumi MD); Silesian Center for Heart Disease, Lodz, Poland (J Z Peruga MD); LeBauer Cardiovascular Research Foundation and Moses Cone Hospital, Greensboro, NC, USA (B R Brodie MD); Jagiellonian University, Krakow, Poland (D Dudek MD); Rabin Medical Center, Petach Tikva, Israel (R Kornowski MD); Universitätsklinikum Schleswig-Holstein, Lübeck, Germany (F Hartmann MD); Mayo Clinic, Rochester, MN, USA (Prof B J Gersh MB); London School of Hygiene and Tropical Medicine, London, UK (Prof S J Pocock PhD); and New York-Presbyterian Hospital/Weill Cornell Medical Center, New York, NY, USA (S C Wong MD)
Correspondence to: Dr Roxana Mehran, Columbia University Medical Center, 161 Fort Washington Avenue (5th Floor), New York, NY 10032, [email protected]
Articles
1150 www.thelancet.com Vol 374 October 3, 2009
MethodsParticipantsThe study design of the HORIZONS-AMI trial has been reported elsewhere.17,18 Briefl y, consecutive patients aged 18 years or older were eligible for enrolment if they presented within 12 h after the onset of symptoms with STEMI of 1 mm or more in two or more contiguous leads, new left bundle branch block, or true posterior myocardial infarction. Exclusion criteria included contraindications to any of the study drugs; previous administration of fi brinolytic therapy, bivalirudin, GPI, low-molecular-weight heparin, or fondaparinux for the present admission (previous unfractionated heparin was allowed); current use of coumadin; history of bleeding diathesis, conditions predisposing to haemorrhagic risk or refusal to receive blood transfusions; stroke or transient ischaemic attack within 6 months or any permanent neurological defi cit; recent or known platelet count less than 100 000 cells per μL or haemoglobin concentration less than 100 g/L; planned elective surgical procedure that would necessitate thienopyridine interruption within 6 months of enrolment; coronary stent implantation within 30 days; and non-cardiac
comorbid conditions with life expectancy less than 1 year or that might result in protocol non-compliance. The study was approved by the institutional review board or ethics committee at each participating centre, and all patients provided written informed consent.
Randomisation and maskingPatients were randomly assigned in the emergency department, in an open-label manner, to receive bivalirudin (Angiomax, The Medicines Company, Parsippany, NJ, USA) alone (intervention) or un-fractionated heparin plus a GPI (control) in a 1:1 ratio. The randomisation codes were generated by use of a dynamic randomisation algorithm implemented by a computerised interactive voice response system (E-trials, Morrisville, NC, USA). The trial was single blinded for the pharmacology and stent arms. The following groups were masked to antithrombotic treatment and stent assignments: programmers, data analysis staff , statisticians, all core laboratories (angiographic, intra-vascular ultrasound, and electrocardiographic), and an independent clinical events committee.
ProceduresIn patients assigned to intervention, bivalirudin was given as an intravenous bolus of 0·75 mg/kg followed by an infusion of 1·75 mg/kg per h. In controls, heparin was given as an intravenous bolus of 60 IU/kg, with subsequent boluses titrated by nomogram to a target activated clotting time of 200–250 s. Both bivalirudin and heparin were discontinued, as specifi ed by the protocol, at the completion of angiography or PCI but could be continued at low doses if required at the discretion of the operator. A GPI was given before PCI to all patients in the control group, but was to be given only to those patients in the bivalirudin group who had refractory no refl ow or giant thrombus after PCI. Abciximab (0·25 mg/kg bolus plus 0·125 μg/kg per min infusion, maximum 10 μg/min) or double bolus eptifi batide (180 μg/kg bolus plus 2·0 μg/kg per min infusion, with a second bolus given in 10 min) were allowed as the GPI at the discretion of the investigator, adjusted for renal impairment as appropriate according to the US Food and Drug Administration label, and continued for 12 h (abciximab) or 12–18 h (eptifi batide).
Aspirin (324 mg chewed or 500 mg intravenous) was given in the emergency room, after which 300–325 mg was given orally every day during the hospital stay, and 75–81 mg every day thereafter indefi nitely. A loading dose of clopidogrel (either 300 mg or 600 mg at the discretion of the investigator) was given before insertion of the catheter, followed by 75 mg orally every day for at least 6 months; dual antiplatelet therapy was recommended for 1 year or longer. A dynamic (minimisation) allocation scheme was used to balance randomisation for administration of prerandomisation heparin, administration of clopidogrel 300 mg or
First randomisation (1:1)1800 assigned to bivalirudin
Second randomisation (3:1)1146 assigned to paclitaxel-eluting stent
381 assigned to bare-metal stent273 no second randomisation
3602 enrolled and randomised
29 not true myocardial infarction*
75 dropped out22 withdrew53 lost to follow-up
72 dropped out26 withdrew46 lost to follow-up
28 not true myocardial infarction*
13 dropped out 7 withdrew 6 lost to follow-up
11 dropped out 4 withdrew 7 lost to follow-up
1787 (99·3%) followed-up at day 30
1771 eligible for follow-up at 1 year
1696 (95·8%) followed-up at 1 year
1800 included in ITT analysis
1774 eligible for follow-up at 1 year
1702 (95·9%) followed-up at 1 year
1802 included in ITT analysis
1791 (99·4%) followed-up at day 30
First randomisation (1:1)1802 assigned to control
Second randomisation (3:1)1111 assigned to paclitaxel-eluting stent368 assigned to bare-metal stent323 no second randomisation
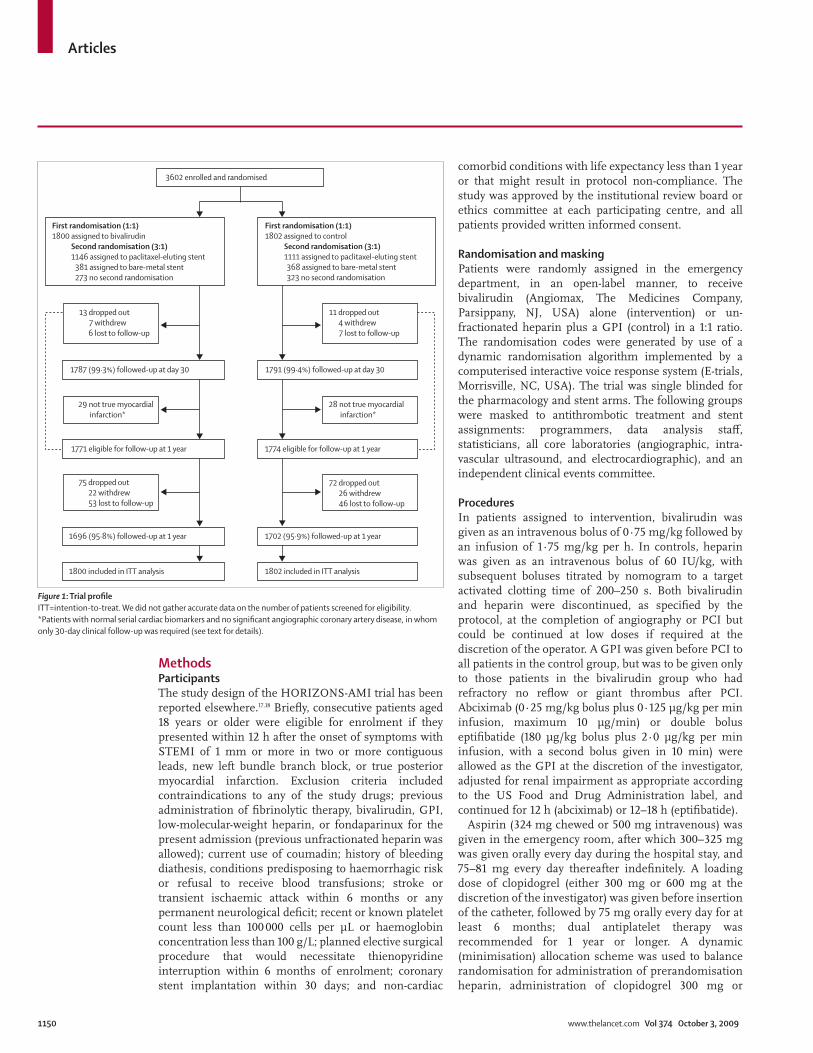
Figure 1: Trial profi leITT=intention-to-treat. We did not gather accurate data on the number of patients screened for eligibility. *Patients with normal serial cardiac biomarkers and no signifi cant angiographic coronary artery disease, in whom only 30-day clinical follow-up was required (see text for details).

Articles
www.thelancet.com Vol 374 October 3, 2009 1151
600 mg or ticlopidine 500 mg before insertion of the catheter, planned administration of abciximab versus eptifi batide if randomised to control, and US or non-US study site.
Emergency coronary angiography with left ventriculography was done after randomisation, followed by triage, at the discretion of the physician, to PCI, coronary artery bypass graft surgery (CABG), or medical management, as previously described.18 After angiography, patients undergoing PCI were randomly assigned again, in 3:1 ratio, to either paclitaxel-eluting stents (TAXUS Express, Boston Scientifi c, Natick, MA, USA) or otherwise identical uncoated bare-metal stents (Express, Boston
Scientifi c). However, in patients who had all measured cardiac biomarkers within normal limits and no coronary artery lesions with a diameter stenosis of more than 50% (by core laboratory determination), only 30-day follow-up was required.
Two primary endpoints were prespecifi ed: major bleeding (not related to coronary artery bypass graft surgery), and net adverse clinical events (NACE; major bleeding or composite major adverse cardiovascular events [MACE; consisting of death, reinfarction, target vessel revascularisation for ischaemia, or stroke]). This prespecifi ed analysis reports these endpoint measures and their components at 1 year of follow-up. Major bleeding was defi ned as intracranial or intraocular haemorrhage, bleeding at the access site with a haematoma that was 5 cm or larger in diameter or that required intervention, a decrease in haemoglobin concentration of 40 g/L or more without an overt source of bleeding or 30 g/L or more with an overt source of bleeding, reoperation for bleeding, or blood product transfusion.
Control group (n=1802)
Bivalirudin group (n=1800)
Age (years, median [range]) 60·7 (21·6–91·6) 59·8 (26·0–92·3)
Male 1372/1802 (76%) 1388/1800 (77%)
Diabetes 312/1800 (17%) 281/1799 (16%)
Insulin dependent 87/1800 (5%) 72/1799 (4%)
Hypertension 993/1800 (55%) 931/1799 (52%)
Hyperlipidaemia 769/1800 (43%) 781/1799 (43%)
Current smoker 807/1792 (45%) 845/1789 (47%)
Previous myocardial infarction
205/1800 (11%) 187/1799 (10%)
Previous PCI 198/1800 (11%) 188/1798 (10%)
Previous CABG 46/1800 (3%) 59/1799 (3%)
Creatinine clearance <60 mL/min
292/1676 (17%) 262/1661 (16%)
Baseline anaemia* 182/1693 (11%) 177/1696 (10%)
Time from symptom onset to hospital arrival, (h, median [IQR])
2·1 (1·3–3·9) 2·2 (1·3–4·0)
Time from symptom onset to fi rst balloon infl ation (h, median [IQR])
3·7 (2·7–5·6) 3·7 (2·7–5·6)
Killip class II–IV 152/1797 (8%) 153/1795 (8%)
Index procedure
PCI 1666/1802 (93%) 1679/1800 (93%)
Stent implanted 1591/1802 (88%) 1611/1800 (90%)
Stent implanted (in patients undergoing PCI)
1591/1666 (95%) 1611/1679 (96%)
Aspirin use
At discharge 1697/1748 (97%) 1729/1762(98%)
At 30 days† 1634/1690 (97%) 1648/1694 (97%)
At 6 months† 1570/1631 (96%) 1592/1642 (97%)
At 1 year† 1537/1606 (96%) 1562/1625 (96%)
Thienopyridine use
At discharge 1621/1748 (93%) 1652/1764 (94%)
At 30 days† 1573/1695 (93%) 1585/1698 (93%)
At 6 months† 1425/1634 (87%) 1443/1644 (88%)
At 1 year† 1059/1609 (66%) 1105/1626 (68%)
Data are n/N (%), unless otherwise indicated. PCI=percutaneous coronary intervention. CABG=cornonary artery bypass graft surgery. *Haematocrit value at initial presentation less than 39% for men and less than 36% for women. †Taken on more than 50% of days since the last visit.
Table 1: Baseline characteristics of study participants
Control group (n=1802)
Bivalirudin group (n=1800)
p value (log-rank)
NACE 325 (18·3%) 275 (15·6%) 0·022
MACE 210 (11·9%) 209 (11·9%) 0·98
Mortality, all-cause 86 (4·8%) 61 (3·5%) 0·037
Cardiac 67 (3·8%) 38 (2·1%) 0·005
Non-cardiac 19 (1·1%) 23 (1·3%) 0·56
Reinfarction 76 (4·4%) 62 (3·6%) 0·22
Q wave 36 (2·1%) 38 (2·2%) 0·81
Non-Q wave 45 (2·7%) 24 (1·4%) 0·009
Death or reinfarction 151 (8·5%) 118 (6·7%) 0·041
Ischaemic TVR 100 (5·9%) 123 (7·2%) 0·12
Ischaemic TLR 77 (4·5%) 103 (6·0%) 0·051
Ischaemic remote TVR 34 (2·0%) 39 (2·3%) 0·60
Stroke 20 (1·2%) 20 (1·1%) 0·99
Stent thrombosis (defi nite or probable) 50 (3·2%) 57 (3·6%) 0·53
Defi nite 37 (2·4%) 52 (3·3%) 0·12
Probable 13 (0·8%) 5 (0·3%) 0·055
Bleeding endpoints
Protocol major, non-CABG 165 (9·2%) 103 (5·8%) <0·0001
Protocol major, all 210 (11·8%) 137 (7·7%) <0·0001
Blood transfusion 71 (4·0%) 47 (2·7%) 0·024
TIMI (major or minor) 182 (10·2%) 115 (6·5%) <0·0001
TIMI major 98 (5·5%) 63 (3·6%) 0·005
TIMI minor 85 (4·8%) 54 (3·0%) 0·008
GUSTO (life-threatening, severe, or moderate) 107 (6·0%) 77 (4·4%) 0·023
GUSTO life-threatening or severe 12 (0·7%) 14 (0·8%) 0·70
GUSTO moderate 96 (5·4 %) 65 (3·7%) 0·013
Data are number of events (rate [%], expressed as Kaplan-Meier estimate). No adjustment for alpha has been done. NACE=net adverse clinical events. MACE=major adverse cardiovascular events. TVR=target vessel revascularisation. TLR=target lesion revascularisation. CABG=coronary artery bypass graft surgery. TIMI=thrombolysis in myocardial infarction. GUSTO=Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries. Stent thrombosis was defi ned according to the Academic Research Consortium classifi cation,19 and determined only in patients in whom stents were implanted (1591 patients assigned to control and 1611 patients assigned to bivalirudin).
Table 2: Adverse events at 1 year

Articles
1152 www.thelancet.com Vol 374 October 3, 2009
Bleeding was also assessed and adjudicated by the thrombolysis in myocardial infarction (TIMI) and Global Utilization of Streptokinase and Tissue Plasminogen
Activator for Occluded Coronary Arteries (GUSTO) scales. The component defi nitions of MACE have been defi ned previously.17,18 Cardiac mortality was defi ned as death from myocardial infarction, cardiac perforation or pericardial tamponade, arrhythmia or conduction abnormality, stroke, procedural complications, or any death in which a cardiac cause could not be excluded. Non-cardiac death was defi ned as a death not caused by cardiac causes, including bleeding-related death. Stent thrombosis was defi ned as the defi nite or probable occurrence of a stent-related thrombotic event according to the Academic Research Consortium classifi cation.19 An independent clinical events committee, which was masked to treatment assignment, adjudicated all primary endpoint and stent thrombosis events using original source documents throughout the 1-year follow-up period.
Statistical analysisThe study was powered for two independent randomisations. For the fi rst (pharmacology) random-isation described in this report, the primary NACE endpoint and the primary safety endpoint of major bleeding (not related to CABG) were evaluated with sequential non-inferiority followed by superiority tests. We initially calculated that randomisation of 3332 patients in a 1:1 ratio aff orded 80% power to show non-inferiority for death, reinfarction, ischaemic target vessel revascularisation, stroke, or major bleeding at 30 days, assuming rates of 12% in both groups and delta 3·2%, using a one-sided binomial test of proportions, α=0·025. Additionally, randomisation of 3332 patients aff orded 99% power to show non-inferiority for major bleeding at 30 days, assuming rates of 6% in the bivalirudin group and 9% in the unfractionated heparin plus GPI group, delta 1%, using a one-sided binomial test of proportions, α=0·025. This number was increased to 3400 patients to account for a 2% anticipated loss to follow-up at 30 days. During the course of the trial, it was necessary to increase the overall number of randomised patients to 3600 to enrol at least 3000 patients into the stent group of the study (power and endpoints described elsewhere).17
Analysis was by intention to treat (all patients were analysed according to treatment assignment, irrespective of treatment received). Secondary analyses included patients who were randomised again to paclitaxel-eluting stent or bare-metal stent. Categorical outcomes were compared by χ² or Fisher’s exact test. Continuous variables were compared by the Wilcoxon rank sum test. The primary event analyses were done with time-to-event data (for which patients were censored at the time of withdrawal from the study or at last follow-up), determined with Kaplan-Meier methods, and compared by use of the log-rank test. 1-year event rates are expressed
A
C
B
18·3%
15·6%
9·2%
5·8%
11·9%11·9%
HR 0·83 (95% CI 0·71–0·97)p=0·022
HR 0·61 (95% CI 0·48–0·78)p<0·0001
HR 1·00 (95% CI 0·82–1·21)p=0·98
Number at riskBivalirudin
Control18001802
22
20
18
16
14
NAC
E (%
)
12
10
8
6
4
2
0
12
11
10
9
8
7
Maj
or b
leed
ing
even
ts (%
)
6
5
4
3
2
1
0
12131415
1110
987
MAC
E (%
)
6543210
15591498
15141458
14831426
13431281
Number at riskBivalirudin
Control18001802
16201543
16011531
15861514
14481368
Number at riskBivalirudin
Control18001802
16271619
15791573
15441540
13941380
0 1 2 3 4 5 6Time (months)
7 8 9 10 11 12
Bivalirudin (n=1800)Control (n=1802)
Figure 2: Time-to-event curves (primary and major secondary endpoints) for patients in bivalirudin and control groups up to 1 year(A) Net adverse clinical events (NACE; major bleeding or composite major adverse cardiovascular events [MACE]). (B) Major bleeding (not related to coronary artery bypass surgery). (C) MACE (death, reinfarction, target vessel revascularisation for ischaemia, or stroke). HR=hazard ratio.

Articles
www.thelancet.com Vol 374 October 3, 2009 1153
as Kaplan-Meier estimates. For the patients randomly assigned to paclitaxel-eluting stent or bare-metal stent, formal interaction testing was done to establish whether any interactions were present between stent type and assigned drug on the two primary endpoints and the major secondary endpoint at 1 year. Cox proportional hazards regression was done to adjust for baseline diff erences between the groups. An interaction with time was included in the model to assess proportionality. Also, interactions were examined for the primary and major secondary endpoints for the two groups of the factorial design. Statistical analysis was done with SAS version 9.1. This trial is registered with ClinicalTrials.gov, number NCT00433966.
Role of the funding sourceThe sponsors of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had fi nal responsibility for the decision to submit for publication.
ResultsBetween March 25, 2005, and May 7, 2007, 3602 eligible patients at 123 centres in 11 countries were randomly assigned to receive bivalirudin (n=1800) or control (n=1802). Figure 1 shows the trial profi le. Following emergency angiography, the primary management strategy was primary PCI in 92·9% of patients (bivalirudin, n=1679; control, n=1666), deferred PCI in 0·1% (bivalirudin, n=2; control, n=0), CABG in 1·7% (bivalirudin, n=24; control, n=38), and medical management in 5·4% (bivalirudin, n=95; control, n=98).
Table 1 shows the baseline characteristics of the study participants. The proportion of patients with hypertension was higher in the control group than in the bivalirudin group. Compliance with protocol-specifi ed study drugs was high in both groups (reported elsewhere17), as was antithrombotic drug use. 126 (7·5%) of 1675 patients in the bivalirudin group undergoing primary PCI received a GPI during the procedure for ischaemic or thrombotic complications. 1625 (97·7%) of 1664 patients in the control group undergoing primary PCI received a GPI, including abciximab (864 [52·0%]), eptifi batide (758 [45·6%]), and tirofi ban (three [0·2%]; data were missing for four patients in the bivalirudin group and two in the control group).
Compared with patients with 1-year follow-up (n=3398), patients without 1-year follow-up (n=204) were younger (median 60·2 years [range 21·6–91·6] vs 59·0 years [28·8–92·3], p=0·015), less frequently had hyperlipid ae-mia (44% vs 33%, p=0·003), and less frequently had Killip class II or more on admission (9% vs 4%, p=0·019). Additionally, patients without 1-year follow-up received a clopidogrel loading dose of 300 mg less frequently (35% vs 28%, p=0·038) and a loading dose of 600 mg more frequently (65% vs 72%, p=0·050).
At 1 year, patients assigned to bivalirudin had a lower rate of NACE than did controls (15·6% vs 18·3%, HR 0·83, 95% CI 0·71–0·97, p=0·022), as a result of a lower rate of major bleeding in the bivalirudin group (5·8% vs 9·2%, HR 0·61, 0·48–0·78, p<0·0001), with a similar rate of MACE between groups (11·9% vs 11·9%, HR 1·00, 0·82–1·21, p=0·98; table 2 and fi gure 2). The lower rate of protocol-defi ned major bleeding in the bivalirudin group than in controls was caused by fewer patients with haematomas 5 cm or larger (1·2% vs control 2·6%, p=0·003) or a decrease in haemoglobin concentration of 40 g/L or more without an overt source of bleeding (2·8% vs 4·7%, p=0·002), and fewer patients who had blood transfusions (2·7% vs 4·0%, p=0·02). Additionally, the rate of a decrease in haemoglobin 30 g/L or more with an overt source of bleeding was lower in the bivalirudin group than in the control group, although the diff erence was not signifi cant (1·7% vs 2·5%, p=0·08). Rates of major and minor bleeding were also lower in patients assigned to bivalirudin than in controls according to TIMI and GUSTO criteria (table 2).
3006 patients were randomly assigned to paclitaxel-eluting stents or bare-metal stents (fi gure 1). Logistic regression showed no signifi cant interactions between assigned pharmacological intervention and assigned stent type on the relative rates of major bleeding, MACE, and NACE (table 3). There was also no interaction between stent type, assigned pharmacological intervention, and the occurrence of target lesion revascularisation for ischaemia at 1 year, as previously reported.20
At 1 year, the rate of cardiac mortality was lower in patients assigned to bivalirudin than in controls (2·1% vs 3·8%, HR 0·57, 0·38–0·84, p=0·005). All-cause mortality was also lower in the bivalirudin group than in the control group (3·5% vs 4·8%, HR 0·71, 0·51–0·98, p=0·037; table 2 and fi gure 3). The reduction in mortality at 1 year in the bivalirudin group was independent of stent type (p value for interaction 0·64; fi gure 3). Assignment to bivalirudin rather than to control remained an
Control group Bivalirudin group Hazard ratio (95% CI) pint
NACE (1 year)
Bare-metal stent 62/368 (16·8%) 57/381 (15·0%) 0·89 (0·64–1·24) 0·96
Paclitaxel-eluting stent 183/1111 (16·5%) 169/1146 (14·7%) 0·90 (0·74–1·08) ··
MACE (1 year)
Bare-metal stent 42/368 (11·4%) 49/381 (12·9%) 1·13 (0·77–1·66) 0·77
Paclitaxel-eluting stent 113/1111 (10·2%) 123/1146 (10·7%) 1·06 (0·83–1·34) ··
Major bleeding (1 year)
Bare-metal stent 28/368 (7·6%) 18/381 (4·7%) 0·66 (0·49–0·88) 0·88
Paclitaxel-eluting stent 102/1111 (9·2%) 69/1146 (6·0%) 0·62 (0·35–1·10) ··
Data are n/N (%). Major bleeding: not related to coronary artery bypass grafting. pint=p value for interaction. NACE=net adverse clinical events. MACE=major adverse cardiovascular events.
Table 3: Occurrence of the primary and major secondary endpoint events at 1 year by assigned pharmacological and stent groups

Articles
1154 www.thelancet.com Vol 374 October 3, 2009
independent predictor of survival in a prespecifi ed multivariable analysis that accounted for diff erences in baseline covariates (adjusted HR 0·68, 0·47–0·98, p=0·04). At 1 year, patients assigned to bivalirudin also had fewer events of non-Q-wave myocardial infarction, and had a lower rate of composite death or reinfarction than did controls (table 2). The rate of stent thrombosis was similar between study groups at 1 year (fi gure 3). The rate of target lesion revascularisation for ischaemia was higher in the bivalirudin group than in the control group, although the diff erence did not reach signifi cance (p=0·051). Rates of target vessel revascularisation, non-cardiac mortality, Q-wave myocardial infarction, and stroke did not diff er between the study groups (table 2).
Table 4 shows the adverse events between 30 days and 1 year. Cardiac death, reinfarction, and composite death or reinfarction occurred less frequently between 30 days and 1 year in patients assigned to bivalirudin than in patients assigned to control. Patients who had major bleeding had substantially higher 1-year rates of mortality (both cardiac and non-cardiac), reinfarction (both Q wave and non-Q wave), and stroke than did patients without major bleeding (table 5).
DiscussionIn this large-scale, prospective, randomised controlled trial of patients with STEMI undergoing primary PCI, procedural anticoagulation with the direct thrombin
Figure 3: Time-to-event curves (mortality and stent thrombosis outcomes) for patients in bivalirudin and control groups up to 1 year(A) All-cause mortality. (B) Cardiac and non-cardiac mortality. (C) All-cause mortality according to stent randomisation. (D) Defi nite or probable stent thrombosis. HR=hazard ratio. PES=paclitaxel-eluting stent. BMS=bare-metal stent.
Number at riskBivalirudin
Control
BivalirudinControl
6
4·8%
3·5%
5
All-c
ause
mor
talit
y (%
)
4
3
2
1
0
6
5
4·4%4·0%
3·6%
Bivalirudin (n=1611)Control (n=1591)
Bivalirudin (n=1800)Control (n=1802)
Bivalirudin (n=1800)Control (n=1802)
3·2%
HR 1·13 (95% CI 0·77–1·65) p=0·53
3·0%2·6%
All-c
ause
mor
talit
y (%
)
4
3
2
1
0
0 1 2 3 4 5 6Time (months)
7 8 9 10 11 12 0 1 2 3 4 5 6Time (months)
7 8 9 10 11 12
6
5
Mor
talit
y (%
) 4
3
3·8%
CardiacHR 0·57 (95% CI 0·38–0·84) p=0·005
Non-cardiacp=0·56
2·1%
1·3%1·1%
2
1
0
5
Sten
t thr
ombo
sis (%
)
4
3
2
1
0
HR 0·71 (95% CI 0·51–0·98)p=0·037
18001802
17041678
16841663
16691646
15201486
Number at risk Number at riskControl/PES
Control/BMSBivalirudin/PES
Bivalirudin/BMS
Control/PES (n=1111)Control/BMS (n=368)Bivalirudin/BMS (n=1146)Bivalirudin/PES (n=381)
1111368
1146381
1064349
1116367
1058348
1103364
1049343
1098359
948313
1001335
16111591
15251495
15031475
14851457
13551315
18001802
17041678
16841663
16691646
15201486
A
C
B
D

Articles
www.thelancet.com Vol 374 October 3, 2009 1155
inhibitor bivalirudin reduced the rates of net adverse clinical events and major bleeding at 1 year compared with treatment with heparin plus routine use of a GPI. All-cause mortality and cardiac mortality at 1 year were also substantially reduced in patients assigned to bivalirudin compared with those assigned to heparin plus a GPI. Although the benefi ts of bivalirudin treatment were present at 30 days (including improved survival),
cardiac death, reinfarction, and composite death or reinfarction also occurred less frequently in the bivalirudin group than in the control group between 30 days and 1 year, contributing to the improved outcomes at 1 year. The diff erence in survival between study groups widened between 30 days and 1 year, with approximately 17 cardiac deaths and 13 all-cause deaths prevented per 1000 patients treated at 1 year (number needed to treat to prevent one cardiac death and one all-cause death approximately 59 and 77 patients, respectively). The benefi cial eff ects of bivalirudin were independent of stent type (paclitaxel-eluting stent or bare-metal stent).
The reduction in mortality in the bivalirudin group compared with the control group might be attributable to the prevention of iatrogenic haemorrhagic complications. The rates of all-cause mortality, cardiac mortality, and stroke were all fi ve times higher in patients who had major bleeding than in those who did not. Additionally, the rate of reinfarction in patients who had major bleeding was twice the rate in those without major bleeding. Previous trials have reported an independent association between major bleeding (with or without blood transfusions) and subsequent mortality in patients with acute coronary syndrome and in those undergoing PCI.8–12 Major bleeding was a more powerful predictor of mortality than periprocedural myocardial infarction after PCI in the double-blind, randomised REPLACE-2 trial.21 The reduction in bleeding with bivalirudin compared with heparin plus a GPI resulted in reduced mortality at 1 year after PCI in the fairly low-risk patients in that study; however, diff erences in mortality between groups did not reach signifi cance.14 Additionally, treatment with bivalirudin reduces the occurrence of severe thrombo cytopenia,13,17,22 the develop-ment of which has also been associated with mortality in patients with STEMI and after PCI.4–7 Moreover, reinfarction is one of the most common causes of death after primary PCI,23,24 and the reduction in non-Q-wave myocardial infarction with bivalirudin might have contributed to the survival advantage at 1 year in patients treated with this agent. Patients without STEMI who were assigned to treatment with fondaparinux had a lower rate of major bleeding at 9 days and improved 6-month survival compared with patients assigned to enoxaparin.25
The REPLACE-2,21 ACUITY,16 and HORIZONS-AMI17 trials assessed the use of bivalirudin compared with heparin plus a GPI in patients with stable and unstable ischaemic syndromes, unstable angina and non-STEMI, and STEMI, respectively. In a large meta-analysis (N=18 819) of these three randomised trials, mortality at
Control group (n=1802)
Bivalirudin group (n=1800)
p value
NACE 131 (7·8%) 123 (7·3%) 0·52
MACE 123 (7·3%) 115 (6·8%) 0·52
Mortality, all-cause 30 (1·8%) 24 (1·4%) 0·38
Cardiac 15 (0·9%) 6 (0·4%) 0·046
Non cardiac 15 (0·9%) 18 (1·1%) 0·63
Reinfarction 46 (2·8%) 29 (1·7%) 0·041
Q wave 14 (0·8%) 13 (0·8%) 0·82
Non-Q wave 34 (2·1%) 16 (1·0%) 0·009
Death or reinfarction 74 (4·4%) 51 (3·0%) 0·031
Ischaemic TVR 71 (4·3%) 79 (4·7%) 0·57
Ischaemic TLR 48 (2·9%) 61 (3·6%) 0·24
Ischaemic remote TVR 28 (1·7%) 33 (2·0%) 0·56
Stroke 8 (0·5%) 7 (0·4%) 0·77
Stent thrombosis (defi nite or probable) 17 (1·1%) 15 (1·0%) 0·66
Defi nite 15 (1·0%) 14 (0·9%) 0·79
Probable 2 (0·1%) 1 (0·1%) 0·55
Bleeding endpoints
Protocol major, non-CABG 10 (0·6%) 13 (0·8%) 0·55
Protocol major, all 14 (0·8%) 17 (1·0%) 0·62
Blood transfusion 7 (0·4%) 10 (0·6%) 0·49
TIMI major or minor 9 (0·5%) 12 (0·7%) 0·53
TIMI major 5 (0·3%) 7 (0·4%) 0·58
TIMI minor 4 (0·2%) 5 (0·3%) 0·75
GUSTO (life-threatening, severe, or moderate) 7 (0·4%) 14 (0·8%) 0·13
GUSTO life-threatening or severe 1 (0·1%) 5 (0·3%) 0·11
GUSTO moderate 6 (0·4%) 11 (0·7%) 0·24
Data are number of events (rate [%], expressed as Kaplan-Meier estimate). No adjustment for alpha has been done. NACE=net adverse clinical events. MACE=major adverse cardiovascular events. TVR=target vessel revascularisation. TLR=target lesion revascularisation. CABG=coronary artery bypass graft surgery. TIMI=thrombolysis in myocardial infarction. GUSTO=Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries. Stent thrombosis was defi ned according to the Academic Research Consortium classifi cation,19 and determined only in patients in whom stents were implanted (1591 patients assigned to control and 1611 patients assigned to bivalirudin).
Table 4: Adverse events between 30 days and 1 year
Patients with major bleeding (n=268)
Patients without major bleeding (n=3334)
p value
Mortality, all-cause 44 (16·6%) 103 (3·1%) <0·0001
Cardiac 29 (11·0%) 76 (2·3%) <0·0001
Non-cardiac 15 (6·3%) 27 (0·9%) <0·0001
Reinfarction 20 (8·0%) 118 (3·7%) 0·0003
Q wave 12 (4·7%) 62 (1·9%) 0·002
Non-Q wave 9 (3·7%) 60 (1·9%) 0·036
Stroke 11 (4·5%) 29 (0·9%) <0·0001
Ischaemic TVR 32 (13·1%) 191 (6·0%) <0·0001
MACE 87 (32·8%) 332 (10·2%) <0·0001
Data are number of events (rate [%], expressed as Kaplan-Meier estimate). TVR=target vessel revascularisation. MACE=major adverse cardiovascular events.
Table 5: Major adverse cardiovascular events within 1 year according to the occurrence of major bleeding not related to coronary artery bypass graft surgery

Articles
1156 www.thelancet.com Vol 374 October 3, 2009
30 days and at 1 year was examined by use of a fi xed eff ects Mantel-Haenszel model. Bivalirudin was associated with a non-signifi cant 9% reduction in 30-day mortality and a signifi cant 15% reduction in 1-year mortality in invasively managed patients across a wide cross-section of clinical acuity.26
We have previously reported that stent thrombosis within the fi rst 24 h occurred more frequently in patients assigned to bivalirudin than in those assigned to heparin plus a GPI.17 However, between 24 h and 1 year, stent thrombosis was more frequent in the heparin plus GPI group than in the bivalirudin group (46 vs 36 stent thrombosis events, respectively). As a result, at the end of the 1-year follow-up, the rate of stent thrombosis was similar in the two groups (3·1% vs 3·5%, respectively, p=0·53). Moreover, the hazard ratio for death within the fi rst month was greater after major bleeding than after reinfarction or stent thrombosis,17 emphasising the importance of selecting an anticoagulation regimen that will reduce the rate of haemorrhagic complications to a minimum (most of which are iatrogenic, occurring as a result of intense anticoagulation after femoral artery access) as well as reducing the rate of recurrent ischaemia.
Although the mechanisms through which bleeding complications either cause or are associated with mortality are unknown, they are likely to be multifactorial. Mechanisms might include the following: the rare occurrence of truly life-threatening or fatal bleeding, such as intracranial haemorrhage; hypotension, ischaemia, or arrhythmias as a result of volume depletion and decreased oxygen delivery (which might be especially relevant in vulnerable STEMI patients); procedures needed to treat major haemorrhage, which could themselves be complicated; systemic infl ammation, vasoconstriction, and apoptosis from red blood cell transfusions;27–31 discontinuation of medications such as antiplatelet agents, β blockers, and angiotensin-converting enzyme inhibitors to treat bleeding and hypotension;32–35 and the presence of other unmeasured confounders associated with bleeding (although the concordant reduction in both bleeding and mortality with bivalirudin, without any other obvious mechanism to explain this eff ect, suggests that the relation is at least in part causal).
Fewer patients in the bivalirudin group died between 30 days and 1 year of follow-up than did patients in the control group. Although this fi nding might be a result of chance, a similar observation was reported in the REPLACE-2 and ACUITY trials.13,14,16 Moreover, in the ACUITY trial,36 the occurrence of bleeding within 30 days was found to be an independent determinate of subsequent mortality occurring between 30 days and 1 year. These results, now replicated in three consecutive prospective trials in more than 23 000 patients, suggest that the prevention of early bleeding complications reduces the occurrence of both late and early mortality. Early bleeding might lead to late mortality through a
variety of mechanisms, including longlasting adverse eff ects from transfusions and the discontinuation of antiplatelet agents, β blockers, and angiotensin-converting enzyme inhibitors, which might not be restarted.37 Moreover, the fi nding of fewer episodes of late reinfarction in patients in the bivalirudin group than in controls has not previously been described, and requires confi rmation and further investigation into the possible mechanisms of this eff ect.
Although HORIZONS-AMI is one of the largest completed prospective, randomised trials in patients with STEMI undergoing primary PCI, this study has several limitations. The logistic complexities of the trial necessitated an open-label design. Potential bias was mitigated by masking laboratory technicians and clinical event adjudication committees to treatment assignment. Moreover, bias introduced by the open-label study design would be expected to diminish over time. In this regard, the early and even greater late reduction in mortality caused by bivalirudin—an endpoint less subject to ascertainment bias than other MACE components—provides reassurance that the results are reliable. Additionally, the mechanistic underpinnings for the observed reduction in mortality in the bivalirudin group (reduced bleeding, transfusions, and thrombocytopenia), together with the consistency of this fi nding in previous trials, further substantiate the validity of our results. Although the incremental reduction in rates of death and reinfarction between 30 days and 1 year in patients assigned to bivalirudin is encouraging, longer-term follow-up is needed to establish the robustness of this fi nding.
Thus, this 1-year analysis of the HORIZONS-AMI trial shows that in high-risk patients with STEMI undergoing primary PCI, procedural anticoagulation with bivalirudin alone seemed to reduce haemorrhagic complications, late reinfarction, and early and late cardiac and all-cause mortality compared with unfractionated heparin plus the routine use of a GPI.
ContributorsRM, GWS, and EN formed the core writing team for the report. GWS,
RM, BJG, and SJP contributed to study conception and design. GWS,
RM, BCJ, SJP, SCW, JZP, GG, BW, AJL, BRB, DD, EN, RK, FH, LG, LV,
HP, and GDD participated in acquisition of data, statistical analyses, or
interpretation of data. All authors reviewed and commented on a draft
of the report and gave fi nal approval to submit for publication.
The HORIZONS-AMI Trial InvestigatorsThe following investigators and institutions participated in the
HORIZONS-AMI trial:
Executive Committee: USA G W Stone (principal investigator and chair;
Columbia University Medical Center and the Cardiovascular Research
Foundation, New York, NY); B R Brodie (LeBauer Cardiovascular
Research Foundation and Moses Cone Hospital, Greensboro, NC);
D A Cox (Mid Carolina Cardiology, Charlotte, NC); C L Grines (William
Beaumont Hospital, Royal Oak, MI); B D Rutherford (St Luke’s Hospital,
Kansas City, MO).
Pharmacology Committee: USA D Bhatt (Cleveland Clinic Foundation,
Cleveland, OH); G Dangas (Columbia University Medical Center and
the Cardiovascular Research Foundation, New York, NY); F Feit
(New York University, New York, NY); M Ohman (Duke University
Medical Center, Durham, NC).

Articles
www.thelancet.com Vol 374 October 3, 2009 1157
European Steering Committee: Italy A Colombo (Colombus Hospital,
Milan); G Guagliumi (Ospedali Riuniti di Bergamo, Bergamo); E Garcia
(Hospital Universitario Gregorio Maranon, Madrid). Germany E Grube
(Heart Center Siegburg, Siegburg); A Kastrati (Deutsches Herzzentrum,
Technische Universität, Munich). Netherlands H Bonnier (Catharina
Hospital, Eindhoven); P Serruys (Thoraxcenter, Rotterdam);
H Suryapranata (Hospital De Weezenlanden, Zwolle).
Country Leaders: Argentina J Belardi, L Grinfeld. Austria K Huber.
Denmark L Rasmussen. Germany E Grube, A Kastrati. Israel Y Almagor.
Italy A Colombo, G Guagliumi. Netherlands H Bonnier, H Suryapranata.
Norway D Nilsen. Poland D Dudek. Spain E Garcia. Sweden
G Olivecrona. UK A Banning.
Clinical Endpoints Committee: Cardiovascular Research Foundation Data
Center, New York, NY, USA (S C Wong; chair).
Field Offi cers: M Farkouh (chair), M Attubato, G Dangas, F Feit,
R Mehran.
Site Management and Data Monitoring Europe: D-Target. South America
Tango. USA J Tyson and Associates.
Data Management: E-trials, Morrisville, NC, USA, D Winsted (manager).
Data Coordination and Analysis: Cardiovascular Research Foundation
Data Center, New York, NY, USA, R Mehran (director), I Bihl
(operations), H Parise (statistics).
Data Safety and Monitoring Board: UK S J Pocock (London School of
Hygiene and Tropical Medicine, London). USA B J Gersh (chair; Mayo
Clinic, Rochester, MN); D Faxon (Brigham and Women’s Hospital,
Boston, MA); S King (Fuqua Heart Center, Atlanta, GA); D O Williams
(Rhode Island Hospital, Providence, RI).
Qualitative and Quantitative Coronary Angiographic Core Laboratory Analysis: Cardiovascular Research Foundation, New York, NY, USA,
A J Lansky (director), E Cristea (operations).
Qualitative and Quantitative Electrocardiographic Core Laboratory Analysis: Cardiovascular Research Foundation, New York, NY, USA, J Reiff el
(director).
Intravascular Ultrasound Core Laboratory Analysis: Cardiovascular
Research Foundation, New York, NY, USA, G Mintz (director).
Biomarker Substudy Core Laboratory: BioSite, San Diego, CA, USA.
Participating countries (total enrolment) and hospitals (principal investigator): Argentina (207) Fundación Favaloro, Capital Federal, Buenos
Aires (Oscar A Mendiz); Hospital Alemán, Buenos Aires (Jose Amadeo
Alvarez); Hospital Britanico, Buenos Aires (Jose Alvarez); Hospital
Espanol de La Plata, La Plata, Buenos Aires (Diego David Grinfeld);
Hospital Gral de Agudos (Cosme Argerich); Capital Federal, Buenos
Aires (Miguel Angel Riccitelli); Hospital Italiano de Buenos Aires,
Capital Federal, Buenos Aries (Daniel Berrocal); Instituto Cardiovascular
de Buenos Aires, Capital Federal, Buenos Aires (Jorge Belardi); Instituto
Cardiovascular de Rosario, Rosario, Santa Fe (Anibal Agustin Damonte);
Sanatorio Argentino de la Plata, La Plata, Buenos Aires (Guillermo
Cugat); Sanatorio Otamendi, Buenos Aires (A Rodriguez); Sanatorio
Modelo Quilmes, Quilmes, Buenos Aires (Ernesto M Torresani);
Sanatorio Allende, Cordoba (Hugo F Londero). Austria (143) AKH Wien,
Vienna (Dietmar Glogar); Wilhelminen Hospital, Vienna (Kurt Huber);
Hanusch-Krankenhaus, Vienna (George Gaul); St Johanns-Spital,
Landesklinik fur Innere Medizin II und Kardiologie, Salzburg (Johann
Altenberger); Universitätsklinik für Innere Medizin II, Innsbruk
(Othmar Pachinger). Germany (791): Asklepios Klinik Langer, Langen
(Hans-Georg Olbrich); Charité Campus Benjamin Franklin, Berlin
(Bernhard Witzenbichler); Charité/CVK, Berlin (Martin Moeckel);
Charité Universitätsmedizin Campus Mitte, Berlin (Wolfgang Rutsch);
Heart Center Siegburg, Siegburg (Eberhard Grube); Herzzentrum
Segeberger Kliniken GmbH, Bad Segeberg (Gert Richardt); Klinik
Innere Medizin I Friedrich-Schiller-University Jena, Jena (Klaus Pethig);
Klinikum Dachau d Amperkliniken AG Kardiologie, Dachau
(Martin Desaga); Klinikum Darmstadt Medizinisch Klinik I, Darmstadt
(Gerald Werner); Klinikum Coburg, Coburg (Johannes Brachmann);
Universitätsklinikum Heidelberg/Kardiologie, Heidelberg
(Helmut Kuecherer); University Hospital Aachen, Aachen
(Rainer Hoff mann); Universitätsklinikum Schleswig-Holstein, Lübeck
(Franz Hartmann); University Hospital Eppendorf Department of
Cardiology, Hamburg (Stefan Willems); University of Ulm Head
Interventional Cardiology Leiter Forschungsgruppe Interventionelle,
Ulm (Jochen Wöhrle); Silesian Medical Academy, Munich
(Adnan Kastrati). Israel (526) Assaf Harofe Medical Center
Catheterization Laboratory, Cardiology Department, Zrifi n
(Ricardo Krakover); Bnei Zion Medical Center, Haifa (Uri Rosenschein);
Carmel Medical Center, Haifa (Basil S Lewis); Hadassah Hebrew
University Medical Center-Jerusalem, Jerusalem (Morris Mosseri);
Rabin Medical Center-Belinson Campus (Ran Petach-Tikva Kornowski);
Rambam Medical Center-Department of Radiology, Haifa
(Luis Gruberg); Shaare Zedek Medical Center-Jerusalem, Jerusalem
(Yaron Almagor); Sheba Medical Center-Tel-Hashomer Heart Institute,
Ramat-Gan (Victor Guetta); Sourasky Medical Center-Tel Aviv Head Dept
of Cardiology, Tel Aviv (Ariel Finkelstein); Wolfson Holon, Holon
(Yoseph Rozenman). Italy (219) Ospedali Riuniti di Bergamo,
Bergamo (Giulio Guagliumi); Ospedale San Raff aele Milano U O di
Emodinamica e di Cardiologia Interventistic, Milan (Antonio Colombo).
Netherlands (133) Catharina Hospital Dept R&D, Eindhoven
(Hans Bonnier); Hospital De Weezenlanden, Zwolle
(Harry Suryapranata) Medisch Centrum Rijnmond-Zuid, Rotterdam
(Peter Smits). Norway (79) Haukeland University Hospital, Department
of Heart Disease, Bergen (Jan Erik Nordrehaug); Stavanger University
Hospital, Rogaland (Dennis Nilsen). Poland (582) Institute of Cardiology-
Haemodynamics Dept, Warsawa, Witold Ruzyllo (Adam Witkowski);
Jagiellonian University, Krakow (Dariusz Dudek); Medical University of
Gdask, Gdask (Andrzej Rynkiewicz); Silesian Center for Heart Disease,
Lodz (Jan Z Peruga); Silesian Medical Academy, Katowice
(Andrzej Ochala); Szpital Jana PawlaII-Dept of Hemo and Angio,
Krakow (Krzysztof Zmudka); Klinika Kardiologii Inwazyjnej CSK
MSWiA, Warsaw (Robert Gil). Spain (6) Hospital General Universitario
de Alicante, Alicante (Pascual Bordes). UK (102) John Radcliff e Hospital,
Oxford (Adrian Banning); Leeds Teaching Hospital NHS Trust, Leeds
(Daniel Blackman); Manchester Heart Centre, Manchester
(Magdi El-Omar); Royal Sussex County Hospital, Brighton, East Sussex
(Adam De Belder); Northern General Hospital, Sheffi eld (Ever Grech);
Wythenshawe Hospital, Manchester (Bernard Prendergast). USA (814)
Alexian Brothers Medical Center, Elk Grove Village, IL (Sarah Johnson);
Anderson Area Medical Center, Anderson, SC (Brent McLaurin);
Bakersfi eld Memorial Hospital, Bakersfi eld, CA (Tommy Lee);
Beth Israel Deaconess Medical, Cardiovascular Division, Boston, MA
(Duane S Pinto); Bethesda North Hospital, Montgomery, OH (Joe Choo);
Brotman Medical Center, Culver City, CA (Ronald Karlsberg); Cannon
Cardiac & Vascular Research Ctr of Northern Michigan, Petoskey, MI
(Louis A Cannon); Cardiovascular Medicine Associates, Middleburg
Heights, OH (Trilok Sharma); Christiana Care Health Services, Newark,
DE (James Ritter); Columbia University, New York, NY (Leroy Rabbani);
Deaconess Medical Center, Spokane, WA (Pierre P Leimgruber); Doctors
Hospital at Renaissance, Edinburg, TX (Ofsman Quintana); Doylestown
Hospital, Doylestown, PA (Joseph McGarvey Jr); El Paso Heart Clinic,
El Paso, TX (Oscar Aguilar); Emory University School of Medicine
Emory Crawford, Atlanta, GA (Henry Liberman); Geisinger Medical
Center, Danville, PA (Jim Blankenship); Good Samaritan Hospital,
Cincinnati, OH (Ali Razavi); Harrisburg Hospital/Pinnacle Health,
Harrisburg, PA (Rajesh Dave); Heart Care Midwest/St Francis Medical
Center, Peoria, IL (John Rashid); Heart Care Research Foundation,
Merrionette Park, IL (Joseph F Stella); Innovis Health, South Fargo, ND
(Edmund Finkinski); Jersey Shore University Medical Center, Neptune,
NJ (Matthew Bach); LeBauer CV Research Foundation/Moses Cone
Hospital, Greensboro, NC (Bruce Brodie); Maine Medical Center,
Portland, ME (Mirle A Kellett Jr); McAllen Heart Hospital, McAllen, TX
(Ofsman Quintana); MedStar Research Institute, Cardiovascular
Research, Washington, DC (Ron Waksman); Mid Carolina Cardiology/
Presbyterian Hospital, Charlotte, NC (Robert Iwaoka); Mid Ohio Heart
Clinic Inc, Mansfi eld, OH (Gregory M Eaton); Northwest Indiana
Cardiovascular Physicians, Valparaiso, IN (Keith Atassi); NYU Medical
Center, New York, NY (Michael Attubato); Oklahoma Heart Institute,
Tulsa, OK (Raj Chandwaney); Providence Heart and Vascular Institute,
Portland, OR (Bradley Evans); Providence Memorial Hospital, El Paso,
TX (Oscar Aguilar); Research Associates of Jackson, Jackson, TN
(Henry Lui); Scottdale Healthcare-Osborn, Scottsdale, AZ, (David Rizik);
Scottsdale Healthcare-Shea, Scottsdale, AZ (David Rizik); Sentara
Virginia Beach General Hospital, Virginia Beach, VA (John Griffi n);
Somerset Medical Center, Bridgewater, NJ (Jason O Hall); South
Carolina Heart Center, Columbia, SC (Michael C Foster); Sparks

Articles
1158 www.thelancet.com Vol 374 October 3, 2009
Regional Medical Center, Fort Smith, AR (Jorge A Hernandez);
St James Hospital & Health Centers Chicago Heights, Chicago Heights,
IL (Noel Camba); St John Hospital, Detroit, MI (Thomas LaLonde);
St Josephs Regional Medical Center, Paterson, NJ (Mahesh Bikkina);
St Luke’s Hospital MAHI, Kansas City, MO (Barry Rutherford); Suncoast
Cardiovascular Research, Saint Petersburg, FL (Vibhuti Singh);
Tennessee Cardiovascular Research Institute, Nashville, TN
(John McPherson); Cardiovascular Specialists/Cape Cod Hospital,
Hyannis, MA (Richard B Zelman); Care Group Hospital: Heart Center of
Indiana Clinical Laboratory/St Vincent’s Hospital, Indianapolis, Indiana
(James B Hermiller); Charlton Memorial Hospital, Fall River, MA
(Kenneth S Korr); Heart Center/Cardiovascular Associates, PC,
Kingsport, TN (Christopher Metzger); Miriam Hospital, Providence, RI
(Paul Gordon); Valley Hospital, Ridgewood, NJ (Cary Hirsch); Western
Pennsylvania Hospital, Pittsburgh, PA (Venkatraman Srinivasan); Valley
Baptist Medical Center, Brownsville, TX (Kalim Habet); Washington
Adventist Hospital, Takoma Park, MD (Mark A Turco); Watson Clinic
Center for Research Inc, Lakeland, FL (Douglas Ebersole); William
Beaumont Hospital, Royal Oak, MI (Cindy L Grines).
Confl icts of interestRM has received lecture fees from Boston Scientifi c and The Medicines
Company. AJL has received grant support from The Medicines Company
and Boston Scientifi c. GG has received consulting fees from or has
served on advisory boards for Abbott Vascular and Boston Scientifi c and
has received grant support from Medtronic and Boston Scientifi c.
DD has received lecture fees from Nycomed. BJG has received
consulting fees from or has served on advisory boards for AstraZeneca,
Bristol-Myers Squibb, Abbott Laboratories, and Boston Scientifi c, and
has equity interest in CV Therapeutics. SJP has received consulting fees
from and has served on an advisory board for The Medicines Company.
EN, LG, LV, and HP are employed by the Cardiovascular Research
Foundation. GWS has received grant support from Boston Scientifi c,
The Medicines Company, and Abbott Vascular. The other authors declare
that they have no confl icts of interest.
AcknowledgmentsThe trial was sponsored by the Cardiovascular Research Foundation,
with unrestricted grant support from Boston Scientifi c Corporation and
The Medicines Company.
References1 Stone GW, Grines CL, Cox DA, et al. Comparison of angioplasty
with stenting, with or without abciximab, in acute myocardial infarction. N Engl J Med 2002; 346: 957–66.
2 Kandzari DE, Hasselblad V, Tcheng JE, et al. Improved clinical outcomes with abciximab therapy in acute myocardial infarction: a systematic overview of randomized clinical trials. Am Heart J 2004; 147: 457–62.
3 Montalescot G, Barragan P, Wittenberg O, et al. Platelet glycoprotein IIb/IIIa inhibition with coronary stenting for acute myocardial infarction. N Engl J Med 2001; 344: 1895–903.
4 Kereiakes DJ, Berkowitz SD, Lincoff AM, et al. Clinical correlates and course of thrombocytopenia during percutaneous coronary intervention in the era of abciximab platelet glycoprotein IIb/IIIa blockade. Am Heart J 2000; 140: 74–80.
5 Merlini PA, Rossi M, Menozzi A, et al. Thrombocytopenia caused by abciximab or tirofi ban and its association with clinical outcome in patients undergoing coronary stenting. Circulation 2004; 109: 2203–06.
6 Nikolsky E, Sadeghi HM, Eff ron MB, et al. Impact of in-hospital acquired thrombocytopenia in patients undergoing primary angioplasty for acute myocardial infarction. Am J Cardiol 2005; 96: 474–81.
7 Tamhane UU, Gurm HS. The chimeric monoclonal antibody abciximab: a systematic review of its safety in contemporary practice. Expert Opin Drug Saf 2008; 7: 809–19.
8 Eikelboom JW, Mehta SR, Anand SS, Xie C, Fox KA, Yusuf S. Adverse impact of bleeding on prognosis in patients with acute coronary syndromes. Circulation 2006; 114: 774–82.
9 Kinnaird TD, Stabile E, Mintz GS, et al. Incidence, predictors, and prognostic implications of bleeding and blood transfusion following percutaneous coronary interventions. Am J Cardiol 2003; 92: 930–35.
10 Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA 2004; 292: 1555–62.
11 Kirtane AJ, Piazza G, Murphy SA, et al. Correlates of bleeding events among moderate- to high-risk patients undergoing percutaneous coronary intervention and treated with eptifi batide: observations from the PROTECT-TIMI-30 trial. J Am Coll Cardiol 2006; 47: 2374–79.
12 Manoukian SV, Feit F, Mehran R, et al. Impact of major bleeding on 30-day mortality and clinical outcomes in patients with acute coronary syndromes: an analysis from the ACUITY Trial. J Am Coll Cardiol 2007; 49: 1362–68.
13 Lincoff AM, Bittl JA, Harrington RA, et al. Bivalirudin and provisional glycoprotein IIb/IIIa blockade compared with heparin and planned glycoprotein IIb/IIIa blockade during percutaneous coronary intervention: REPLACE-2 randomized trial. JAMA 2003; 289: 853–63.
14 Lincoff AM, Kleiman NS, Kereiakes DJ, et al. Long-term effi cacy of bivalirudin and provisional glycoprotein IIb/IIIa blockade vs heparin and planned glycoprotein IIb/IIIa blockade during percutaneous coronary revascularization: REPLACE-2 randomized trial. JAMA 2004; 292: 696–703.
15 Stone GW, McLaurin BT, Cox DA, et al. Bivalirudin for patients with acute coronary syndromes. N Engl J Med 2006; 355: 2203–16.
16 Stone GW, Ware JH, Bertrand ME, et al. Antithrombotic strategies in patients with acute coronary syndromes undergoing early invasive management: one-year results from the ACUITY trial. JAMA 2007; 298: 2497–506.
17 Stone GW, Witzenbichler B, Guagliumi G, et al. Bivalirudin during primary PCI in acute myocardial infarction. N Engl J Med 2008; 358: 2218–30.
18 Mehran R, Brodie B, Cox DA, et al. The Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction (HORIZONS-AMI) Trial: study design and rationale. Am Heart J 2008; 156: 44–56.
19 Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized defi nitions. Circulation 2007; 115: 2344–51.
20 Stone GW, Lansky AJ, Pocock SJ, et al. Paclitaxel-eluting stents versus bare-metal stents in acute myocardial infarction. N Engl J Med 2009; 360: 1946–59.
21 Feit F, Voeltz MD, Attubato MJ, et al. Predictors and impact of major hemorrhage on mortality following percutaneous coronary intervention from the REPLACE-2 Trial. Am J Cardiol 2007; 100: 1364–69.
22 Stone GW, Bertrand ME, Moses JW, et al. Routine upstream initiation vs deferred selective use of glycoprotein IIb/IIIa inhibitors in acute coronary syndromes: the ACUITY Timing trial. JAMA 2007; 297: 591–602.
23 Ohman EM, Califf RM, Topol EJ, et al. Consequences of reocclusion after successful reperfusion therapy in acute myocardial infarction. TAMI Study Group. Circulation 1990; 82: 781–91.
24 Orn S, Cleland JG, Romo M, Kjekshus J, Dickstein K. Recurrent infarction causes the most deaths following myocardial infarction with left ventricular dysfunction. Am J Med 2005; 118: 752–58.
25 Fifth Organization to Assess Strategies in Acute Ischemic Syndromes Investigators, Yusuf S, Mehta SR, Chrolavicius S, et al. Comparison of fondaparinux and enoxaparin in acute coronary syndromes. N Engl J Med 2006; 354: 1464–76.
26 Stone GW, Pocock SJ, Moses JW, et al. Mortality of patients treated with bivalirudin compared to heparin plus glycoprotein IIb/IIIa inhibitors after clopidogrel pre-treatment: A meta-analysis from randomized trials. Eur Heart J (in press).
27 Zallen G, Moore EE, Ciesla DJ, Brown M, Biffl WL, Silliman CC. Stored red blood cells selectively activate human neutrophils to release IL-8 and secretory PLA2. Shock 2000; 13: 29–33.
28 Fransen E, Maessen J, Dentener M, Senden N, Buurman W. Impact of blood transfusions on infl ammatory mediator release in patients undergoing cardiac surgery. Chest 1999; 116: 1233–39.
29 Biedler AE, Schneider SO, Seyfert U, et al. Impact of alloantigens and storage-associated factors on stimulated cytokine response in an in vitro model of blood transfusion. Anesthesiology 2002; 97: 1102–09.

Articles
www.thelancet.com Vol 374 October 3, 2009 1159
30 Twomley KM, Rao SV, Becker RC. Proinfl ammatory, immunomodulating, and prothrombotic properties of anemia and red blood cell transfusions. J Thromb Thrombolysis 2006; 21: 167–74.
31 Kahn RC, Zaroulis C, Goetz W, Howland WS. Hemodynamic oxygen transport and 2,3-diphosphoglycerate changes after transfusion of patients in acute respiratory failure. Intensive Care Med 1986; 12: 22–25.
32 Nikolsky E, Mehran R, Aymong ED, et al. Impact of anemia on outcomes of patients undergoing percutaneous coronary interventions. Am J Cardiol 2004; 94: 1023–27.
33 Ferrari E, Benhamou M, Cerboni P, Marcel B. Coronary syndromes following aspirin withdrawal: a special risk for late stent thrombosis. J Am Coll Cardiol 2005; 45: 456–59.
34 Biondi-Zoccai GG, Lotrionte M, Agostoni P, et al. A systematic review and meta-analysis on the hazards of discontinuing or not adhering to aspirin among 50 279 patients at risk for coronary artery disease. Eur Heart J 2006; 27: 2667–74.
35 Grines CL, Bonow RO, Casey DE, et al. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. Circulation 2007; 115: 813–18.
36 Mehran R, Pocock SJ, Stone GW, et al. Associations of major bleeding and myocardial infarction with the incidence and timing of mortality in patients presenting with non-ST-elevation acute coronary syndromes: a risk model from the ACUITY Trial. Eur Heart J 2009; 30: 1457–66.
37 Wang TY, Xiao L, Alexander KP, et al. Antiplatelet therapy use after discharge among acute myocardial infarction patients with
in-hospital bleeding. Circulation 2008; 118: 2139–45.