
Noninvasive measurement of aortic aneurysm sac tension with vibrometry
Upload
independentCategory
view
0download
0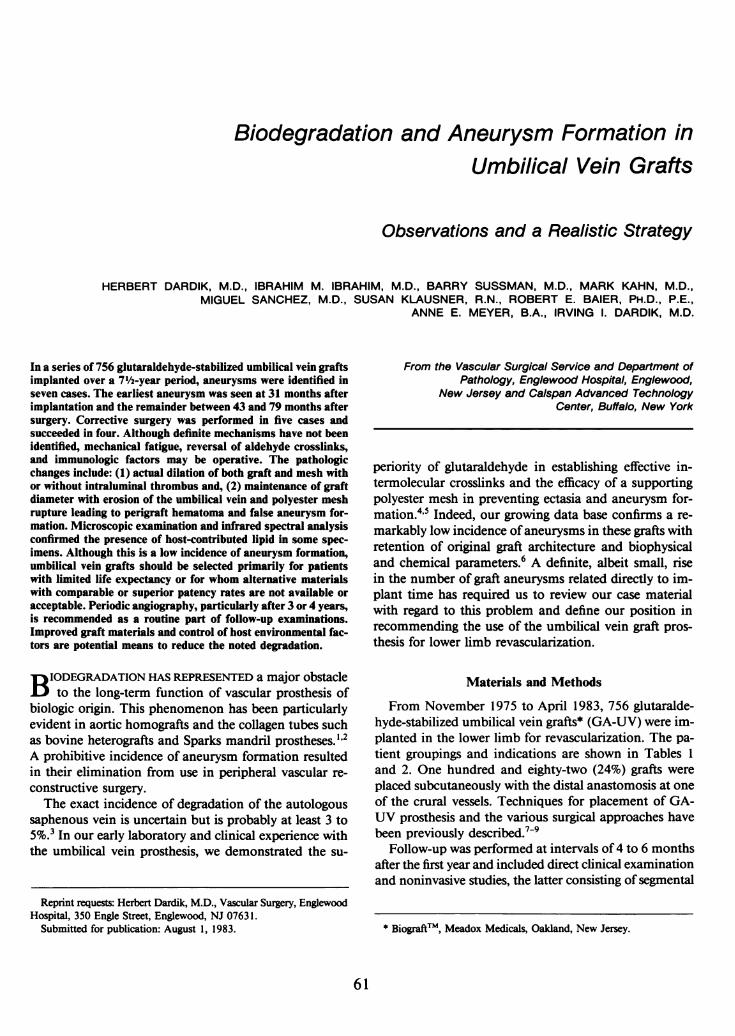
Biodegradation and Aneurysm Formation inUmbilical Vein Grafts
Observations and a Realistic Strategy
HERBERT DARDIK, M.D., IBRAHIM M. IBRAHIM, M.D., BARRY SUSSMAN, M.D., MARK KAHN, M.D.,MIGUEL SANCHEZ, M.D., SUSAN KLAUSNER, R.N., ROBERT E. BAIER, PH.D., P.E.,
ANNE E. MEYER, B.A., IRVING 1. DARDIK, M.D.
In a series of 756 glutaraldehyde-stabilized umbilical vein graftsimplanted over a 7½/2-year period, aneurysms were identified inseven cases. The earliest aneurysm was seen at 31 months afterimplantation and the remainder between 43 and 79 months aftersurgery. Corrective surgery was performed in five cases andsucceeded in four. Although definite mechanisms have not beenidentified, mechanical fatigue, reversal of aldehyde crosslinks,and immunologic factors may be operative. The pathologicchanges include: (1) actual dilation of both graft and mesh withor without intraluminal thrombus and, (2) maintenance of graftdiameter with erosion of the umbilical vein and polyester meshrupture leading to perigraft hematoma and false aneurysm for-mation. Microscopic examination and infrared spectral analysisconfirmed the presence of host-contributed lipid in some spec-imens. Although this is a low incidence of aneurysm formation,umbilical vein grafts should be selected primarily for patientswith limited life expectancy or for whom alternative materialswith comparable or superior patency rates are not available oracceptable. Periodic angiography, particularly after 3 or 4 years,is recommended as a routine part of follow-up examinations.Improved graft materials and control of host environmental fac-tors are potential means to reduce the noted degradation.
B IODEGRADATION HAS REPRESENTED a major obstacleto the long-term function of vascular prosthesis of
biologic origin. This phenomenon has been particularlyevident in aortic homografts and the collagen tubes suchas bovine heterografts and Sparks mandril prostheses." 2A prohibitive incidence of aneurysm formation resultedin their elimination from use in peripheral vascular re-constructive surgery.The exact incidence of degradation of the autologous
saphenous vein is uncertain but is probably at least 3 to5%.3 In our early laboratory and clinical experience withthe umbilical vein prosthesis, we demonstrated the su-
From the Vascular Surgical Service and Department ofPathology, Englewood Hospital, Englewood,
New Jersey and Calspan Advanced TechnologyCenter, Buffalo, New York
periority of glutaraldehyde in establishing effective in-termolecular crosslinks and the efficacy of a supportingpolyester mesh in preventing ectasia and aneurysm for-mation.4'5 Indeed, our growing data base confirms a re-markably low incidence ofaneurysms in these grafts withretention of original graft architecture and biophysicaland chemical parameters.6 A definite, albeit small, risein the number of graft aneurysms related directly to im-plant time has required us to review our case materialwith regard to this problem and define our position inrecommending the use of the umbilical vein graft pros-thesis for lower limb revascularization.
Materials and Methods
From November 1975 to April 1983, 756 glutaralde-hyde-stabilized umbilical vein grafts* (GA-UV) were im-planted in the lower limb for revascularization. The pa-tient groupings and indications are shown in Tables 1and 2. One hundred and eighty-two (24%) grafts wereplaced subcutaneously with the distal anastomosis at oneof the crural vessels. Techniques for placement of GA-UV prosthesis and the various surgical approaches havebeen previously described.7-9
Follow-up was performed at intervals of 4 to 6 monthsafter the first year and included direct clinical examinationand noninvasive studies, the latter consisting of segmental
* Biograft', Meadox Medicals, Oakland, New Jersey.
61
Reprint requests: Herbert Dardik, M.D., Vascular Surgery, EnglewoodHospital, 350 Engle Street, Englewood, NJ 07631.
Submitted for publication: August 1, 1983.

DARDIK AND OTHERS Ann. Surg. * January 1984
TABLE 1. Umbilical Vein Series
Clinical Data No. Age, Mean M: F Diabetes Prior Surgery
Popliteal AK 72 62 52: 20 34 (47%) 13 (18%)Popliteal BK 303 65 184: 119 158 (52%) 70 (23%)Post tibial 115 61 81: 34 49 (43%) 53 (46%)Ant tibial 60 64 39: 21 27 (45%) 38 (63%)Peroneal 101 69 70: 31 60 (59%) 33 (33%)Sequential 9 64 7: 2 3 (33%) 5 (56%)Trifurcation 30 67 23: 7 15 (50%) 8 (27%)AVF tibial 36 62 22: 14 13 (36%) 26 (72%)AVF peroneal 30 70 20: 10 13 (43%) 14 (47%)
Total 756 65 498: 258 372 (49%) 260 (34%)SubtotalsPOP 375 65 236: 139 192 (63%) 83 (22%)TIB 175 63 120: 55 76 (43%) 91 (52%)AVF 66 66 42: 24 26 (39%) 40 (60%)
limb pressures and pulse volume recordings. Subcuta-neous grafts were particularly easy to examine for thedevelopment of aneurysms. Postoperative arteriogramswere performed as indicated, such as for contralaterallimb ischemia. Because of patient reluctance, only a lim-ited number were obtained electively (Fig. 1). Recently,echography and digital subtraction arteriography havebeen performed selectively and may indeed represent ex-
cellent means for periodic review of graft morphology(Fig. 2).
Results
Seven aneurysms have been identified to date, the ear-
liest at 31 months after implantation with the remainderat 43 to 79 months (Table 3). Although these cases rep-resent a minute fraction of the entire series, this com-
plication looms increasingly larger as better risk patientssurvive for longer periods with functional grafts. Five ofthe aneurysms have been treated surgically by complete
TABLE 2. Umbilical Vein Series
Indications Limb Salvage Rest Pain Claudication Aneurysm
Popliteal AK 26 (36.1%) 39 (54.2%) 6 (8.3%) 1 (1.4%)Popliteal BK 114 (37.6%) 160 (52.8%) 12 (4.0%) 17 (5.6%)Post tibial 71 (61.7%) 38 (33.0%) 6 (5.2%) 0 (0.0%)Ant tibial 47 (78.3%) 11 (18.3%) 1 (1.7%) 1 (1.7%)Peroneal 99 (98.0%) 0 (0.0%) 0 (0.0%) 2 (2.0%)Sequential 5 (55.6%) 4 (44.4%) 0 (0.0%) 0 (0.0%)Trifurcation 14 (46.7%) 16 (53.3%) 0 (0.0%) 0 (0.0%)AVF tibial 36 (100.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%)AVF peroneal 30 (100.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%)
Totals 442 (58.5%) 268 (35.4%) 25 (3.3%) 21 (2.8%)
SubtotalsPOP 140 (37.3%) 199 (53.1%) 18 (4.8%) 18 (4.8%)TIB 118 (67.4%) 49 (28.0%) 7 (4.0%) 1 (0.6%)AVF 66 (100.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%)
resection and replacement with a new graft or by partialresection and interposition grafting. The former is our
procedure of choice in that degenerative changes, thoughnot apparent angiographically, may well be universal.Following complete replacement of a femoral poplitealgraft in case 1 15, distal closure of the crural circulationresulted in a below knee amputation despite continuedpatency of the new graft.
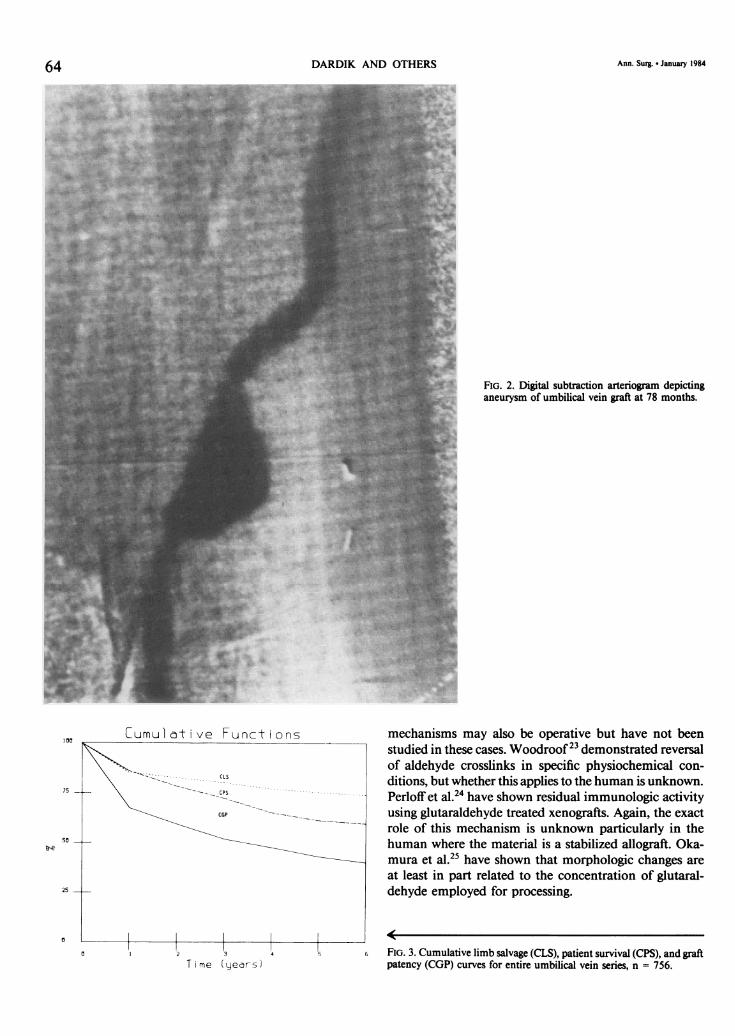
Cumulative graft patency, limb salvage, and patientsurvival rates for the entire series are depicted in figure3. This loss of graft patency, limb, and life are obviousfactors in decreasing the numbers of grafts available forin vivo morphologic study. Table 4 documents the numberof postoperative arteriograms in relation to the markeddecrease in grafts at risk from the beginning of the seriesthrough the subsequent years of follow-up. As more an-
giograms are performed remote from the operative date,it appears that the incidence of aneurysm formation in-creases in relationship to the number of grafts at risk.Two distinct morphologic types of aneurysms were
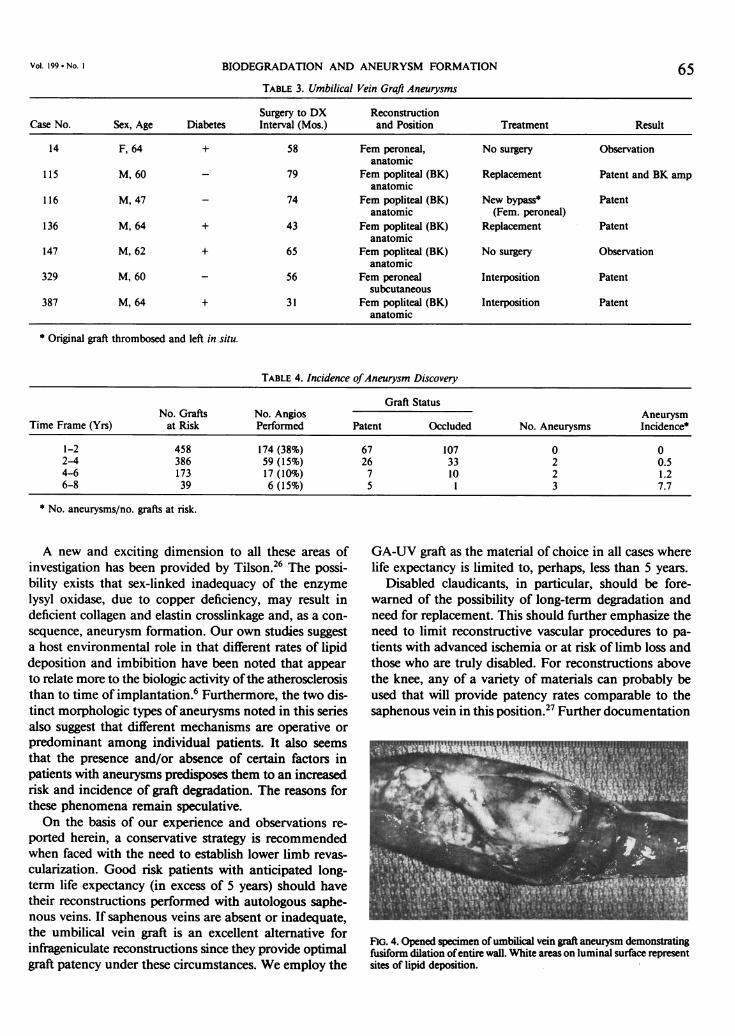
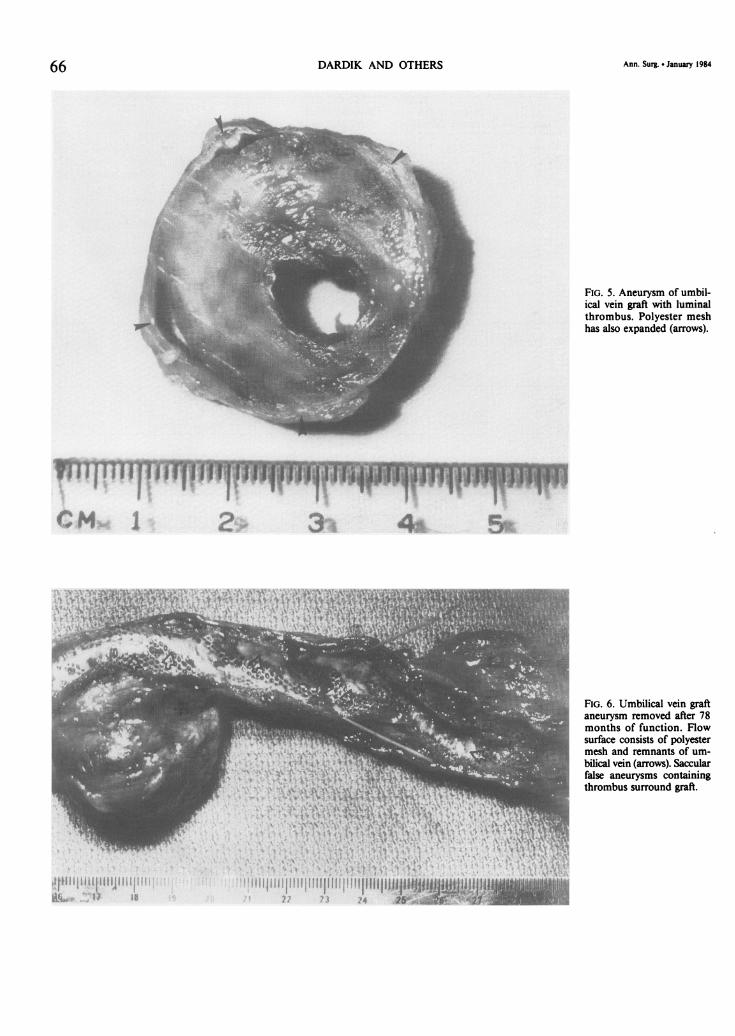
identified. The first consisted of actual dilation of thegraft and the polyester mesh (Fig. 4). Thrombus liningthe flow channel may be present (Fig. 5). The secondtype of aneurysm was caused by graft erosion withstretching and rupture of the polyester mesh resulting inmultiple false aneurysms about the graft (Fig. 6). Hostlipid uptake was increased in some grafts with aneurysmsas demonstrated by infrared spectral analysis (Fig. 7) andhistologically by lipid-laden macrophages (Fig. 8). How-ever, this was not a universal phenomenon in that min-imal lipid was identified in the 79-month specimen(Fig. 9).
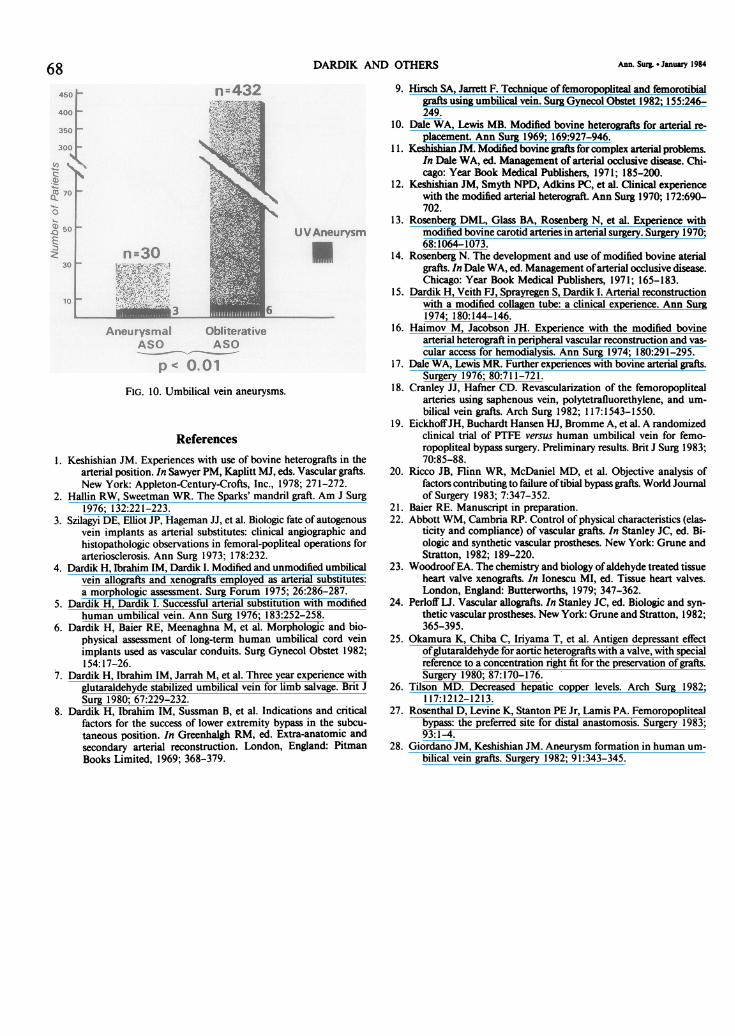
Another interesting observation was the relativelyhigher incidence of graft aneurysms in the patients in thisseries (Fig. 10) with aneurysmal disease (10.0%) as opposedto those with obliterative disease (1.4%).
62

BIODEGRADATION AND ANEURYSM FORMATION
Discussion
Initial enthusiasm for the dialdehyde tanned bovineheterograft'0-'4 was dampened by subsequent reportsdemonstrating a high incidence of early biodegradation,particularly aneurysms."5-7 Similar findings were soonnoted for the Sparks mandril prosthesis and led to thevirtual abandonment ofcollagen grafts for peripheral vas-cular reconstruction. Continued bias against all types ofbiologically derived grafts resulted in the large scale de-ployment of synthetic grafts, the most popular recentlybeing expanded PTFE. Published evidence suggests, how-ever, that a major disadvantage of these grafts is theirpoor long-term patency for distal reconstructions.18-20The application of glutaraldehyde as a crosslinking
agent marked a significant advance in the use of biologicstructures for human implantation. The porcine heartvalve and the human umbilical cord vein are the chiefexamples. Obviously, the hope that permanent tissue sta-bility and refractoriness to biodegradation could beachieved in all cases has not been realized. Nevertheless,the superiority ofthe GA-UV over the bovine heterograftand other collagen grafts is clear. Furthermore, the higherpatency rates achieved with GA-UV over PTFE in theinfrageniculate position still warrants its use for limb sal-vage in the absence of a suitable autologous vein, in thepatient with limited life expectancy, or where operativetime is critical. Improved technology and quality controlhave provided and will continue to provide better graftswith the hope that durability will increase.Management of these graft aneurysms has generally
been accomplished by resection and graft interpositionor replacement. Continued observation of the new im-plants will yield valuable information by noting stabilityor degradation in the same host environment. Two pa-tients have, to date, refused surgery. The natural historyof these aneurysms is unknown. One graft thrombosedduring the observation period and a new bypass was in-serted without removal of the original. Of the six patentgraft aneurysms, one was asymptomatic but easily pal-pable, another was in the subcutaneous position with thepatient aware of it, and the remaining four easily apparentto both patient and examiner. The incidence of aneu-rysmal degeneration in asymptomatic functioning graftsin the anatomic position without palpable enlargementis unknown but presumed to be low. Aneurysm formationis easily detectable in grafts placed subcutaneously. Todate, this has occurred only once.The mechanisms causing degradation and aneurysm
formation are uncertain. Physical forces causing fatigueof both the umbilical vein and the polyester mesh ob-viously play a role, but additional factors may also be
63
FIG. 1. Fifty-eight month postoperative arteriogram ofa femoral peronealbypass depicting aneurysmal biodegradation of umbilical vein graft.
operative. In vitro experimentation using pulsatile pumpssimulated to 1 l/2 years have so far failed to reproduce theclinical dilation of any of these grafts.2' Compliance andincreasing graft stiffness have been studied by Abbott andCambria,22 but the relationship of these factors to deg-radation and other morphologic changes needs clarifi-cation. Reversal of aldehyde links and immunologic
Vol. 199 * No. I
g:u..::
4. A.
1:
DARDIK AND OTHERS
Cumul ct ve Funct ons
Time (yeers)
FIG. 2. Digital subtraction arteriogram depictinganeurysm of umbilical vein graft at 78 months.
mechanisms may also be operative but have not beenstudied in these cases. Woodroof2' demonstrated reversalof aldehyde crosslinks in specific physiochemical con-ditions, but whether this applies to the human is unknown.Perloffet al.24 have shown residual immunologic activityusing glutaraldehyde treated xenografts. Again, the exactrole of this mechanism is unknown particularly in thehuman where the material is a stabilized allograft. Oka-mura et al.25 have shown that morphologic changes areat least in part related to the concentration of glutaral-dehyde employed for processing.
FIG. 3. Cumulative limb salvage (CLS), patient survival (CPS), and graftpatency (CGP) curves for entire umbilical vein series, n = 756.
64
,00
75 -
so -
25
Ann. Surg. * January 1984
BIODEGRADATION AND ANEURYSM FORMATION 65TABLE 3. Umbilical Vein Graft Aneurysms
Surgery to DX ReconstructionCase No. Sex, Age Diabetes Interval (Mos.) and Position Treatment Result
14 F, 64 + 58 Fem peroneal, No surgery Observationanatomic
115 M, 60 - 79 Fem popliteal (BK) Replacement Patent and BK ampanatomic
116 M, 47 - 74 Fem popliteal (BK) New bypass* Patentanatomic (Fem. peroneal)
136 M, 64 + 43 Fem popliteal (BK) Replacement Patentanatomic
147 M, 62 + 65 Fem popliteal (BK) No surgery Observationanatomic
329 M, 60 - 56 Fem peroneal Interposition Patentsubcutaneous
387 M, 64 + 31 Fem popliteal (BK) Interposition Patentanatomic
* Original graft thrombosed and left in situ.
TABLE 4. Incidence ofAneurysm Discovery
Graft StatusNo. Grafts No. Angios Aneurysm
Time Frame (Yrs) at Risk Performed Patent Occluded No. Aneurysms Incidence*
1-2 458 174 (38%) 67 107 0 02-4 386 59 (15%) 26 33 2 0.54-6 173 17 (10%) 7 10 2 1.26-8 39 6(15%) 5 1 3 7.7
* No. aneurysms/no. grafts at risk.
A new and exciting dimension to all these areas ofinvestigation has been provided by Tilson.6 The possi-bility exists that sex-linked inadequacy of the enzymelysyl oxidase, due to copper deficiency, may result indeficient collagen and elastin crosslinkage and, as a con-sequence, aneurysm formation. Our own studies suggesta host environmental role in that different rates of lipiddeposition and imbibition have been noted that appearto relate more to the biologic activity ofthe atherosclerosisthan to time of implantation.6 Furthermore, the two dis-tinct morphologic types of aneurysms noted in this seriesalso suggest that different mechanisms are operative orpredominant among individual patients. It also seemsthat the presence and/or absence of certain factors inpatients with aneurysms predisposes them to an increasedrisk and incidence of graft degradation. The reasons forthese phenomena remain speculative.On the basis of our experience and observations re-
ported herein, a conservative strategy is recommendedwhen faced with the need to establish lower limb revas-cularization. Good risk patients with anticipated long-term life expectancy (in excess of 5 years) should havetheir reconstructions performed with autologous saphe-nous veins. If saphenous veins are absent or inadequate,the umbilical vein graft is an excellent alternative forinfrageniculate reconstructions since they provide optimalgraft patency under these circumstances. We employ the
GA-UV graft as the material of choice in all cases wherelife expectancy is limited to, perhaps, less than 5 years.
Disabled claudicants, in particular, should be fore-warned of the possibility of long-term degradation andneed for replacement. This should further emphasize theneed to limit reconstructive vascular procedures to pa-tients with advanced ischemia or at risk of limb loss andthose who are truly disabled. For reconstructions abovethe knee, any of a variety of materials can probably beused that will provide patency rates comparable to thesaphenous vein in this position.27 Further documentation
FIG. 4. Opened specimen of umbilical vein graft aneurysm demonstratingfusiform dilation ofentire wall. White areas on luminal surface representsites of lipid deposition.
VOl. 199 . NO. I
DARDIK AND OTHERS Ann. Surg. * January 1984
FIG. 5. Aneurysm of umbil-ical vein graft with luminalthrombus. Polyester meshhas also expanded (arrows).
im 111T-i TrIT1IMM 1-4 b V
s' p j.{. ~' ~V > \ X r s
z i S\; t p*i
l I AAI,IpA I I 1JIIf d 4
II~ ~~~~~ ~ ~~~~~~~~~ ,/ -I 4 - __ ___ ;___
FIG. 6. Umbilical vein graftaneurysm removed after 78months of function. Flowsurface consists of polyestermesh and remnants of um-bilical vein (arrows). Saccularfalse aneurysms containingthrombus surround graft.
66
4
/ i .? i ?4 P.: -,.
I,j i i i I i i I I i i I i i I U I I i
iiA..., ii, I I i$

BIODEGRADATION AND ANEURYSM FORMATION
frequ
FIG. 7. Biograft explant-56 months. Infrared spectral analysis of anumbilical vein graft aneurysm removed after 56 months of function(case 329). Extensive lipid deposition is present.
of results will be required to establish the best alternativein this site.The development ofaneurysms in umbilical vein grafts
has been previously reported.628 The purpose of thismanuscript is to document the likelihood of increasedfrequency of this phenomenon as long-term function ismaintained in a particular host environment. Echography
FIG. 8. Photomicrograph oflipid laden macrophagesfound in graft removed at 56
months (case 329).
FIG. 9. Biograftexplant-79 months. Infiwed spectoam ofan umbilicalvein graft aneurysm removed after 79 months (case I 15) depicting virtualabsence of lipid. The significance of the presence or absence of lipiddeposition remains speculative.
and angiography should be considered in the follow-upexamination, perhaps as early as 3 years after surgery.Continued use of umbilical veins in peripheral vascularsurgery is appropriate in defined circumstances. Directionsfor future research include not only development of im-proved materials but of methods to control the host en-vironment.
Vol. 199 * No. I
micrometers (#m)67
DARDIK AND OTHERS Ann. Surg. * January 1984
40 nm432400
~70
, 50 UVAneurysm
3 nm30
Aneurysmal ObliterativASO ASO
p 0.01FIG. 10. Umbilical vein aneurysms.
References1. Keshishian JM. Experiences with use of bovine heterografts in the
arterial position. In Sawyer PM, Kaplitt MJ, eds. Vascular grafts.New York: Appleton-Century-Crofts, Inc., 1978; 271-272.
2. Hallin RW, Sweetman WR. The Sparks' mandril graft. Am J Surg1976; 132:221-223.
3. Szilagyi DE, Elliot JP, Hageman JJ, et al. Biologic fate of autogenousvein implants as arterial substitutes: clinical angiographic andhistopathologic observations in femoral-popliteal operations forarteriosclerosis. Ann Surg 1973; 178:232.
4. Dardik H, Ibrahim IM, Dardik I. Modified and unmodified umbilicalvein allografts and xenografts employed as arterial substitutes:a morphologic assessment. Surg Forum 1975; 26:286-287.
5. Dardik H, Dardik I. Successful arterial substitution with modifiedhuman umbilical vein. Ann Surg 1976; 183:252-258.
6. Dardik H, Baier RE, Meenaghna M, et al. Morphologic and bio-physical assessment of long-term human umbilical cord veinimplants used as vascular conduits. Surg Gynecol Obstet 1982;154:17-26.
7. Dardik H, Ibrahim IM, Jarrah M, et al. Three year experience withglutaraldehyde stabilized umbilical vein for limb salvage. Brit JSurg 1980; 67:229-232.
8. Dardik H, Ibrahim IM, Sussman B, et al. Indications and criticalfactors for the success of lower extremity bypass in the subcu-taneous position. In Greenhalgh RM, ed. Extra-anatomic andsecondary arterial reconstruction. London, England: PitmanBooks Limited, 1969; 368-379.
9. Hirsch SA, Jarrett F. Technique of femoropopliteal and femorotibialgrafts using umbilical vein. Surg Gynecol Obstet 1982; 155:246-249.
10. Dale WA, Lewis MB. Modified bovine heterografts for arterial re-placement. Ann Surg 1969; 169:927-946.
11. Kehishian JM. Modified bovine grafts for complex arterial problems.In Dale WA, ed. Management of arterial occlusive disease. Chi-cago: Year Book Medical Publishers, 1971; 185-200.
12. Keshishian JM, Smyth NPD, Adkins PC, et al. Clinical experiencewith the modified arterial heterograft. Ann Surg 1970; 172:690-702.
13. Rosenberg DML, Glass BA, Rosenberg N, et al. Experience withmodified bovine carotid arteries in arterial surgery. Surgery 1970;68:1064-1073.
14. Rosenberg N. The development and use of modified bovine aterialgrafts. In Dale WA, ed. Management ofarterial occlusive disease.Chicago: Year Book Medical Publishers, 1971; 165-183.
15. Dardik H, Veith FJ, Sprayregen S, Dardik I. Arterial reconstructionwith a modified collagen tube: a clinical experience. Ann Surg1974; 180:144-146.
16. Haimov M, Jacobson JH. Experience with the modified bovinearterial heterograft in peripheral vascular reconstruction and vas-cular access for hemodialysis. Ann Surg 1974; 180:291-295.
17. Dale WA, Lewis MR. Further experiences with bovine arterial grafts.Surgery 1976; 80:711-721.
18. Cranley JJ, Hafner CD. Revascularization of the femoropoplitealarteries using saphenous vein, polytetrafluorethylene, and um-bilical vein grafts. Arch Surg 1982; 117:1543-1550.
19. EickhoffJH, Buchardt Hansen HJ, Bromme A, et al. A randomizedclinical trial of PTFE versus human umbilical vein for femo-ropopliteal bypass surgery. Preliminary results. Brit J Surg 1983;70:85-88.
20. Ricco JB, Flinn WR, McDaniel MD, et al. Objective analysis offactors contributing to failure oftibial bypass grafts. World Journalof Surgery 1983; 7:347-352.
21. Baier RE. Manuscript in preparation.22. Abbott WM, Cambria RP. Control of physical characteristics (elas-
ticity and compliance) of vascular grafts. In Stanley JC, ed. Bi-ologic and synthetic vascular prostheses. New York: Grune andStratton, 1982; 189-220.
23. Woodroof EA. The chemistry and biology ofaldehyde treated tissueheart valve xenografts. In Ionescu MI, ed. Tissue heart valves.London, England: Butterworths, 1979; 347-362.
24. Perloff UJ. Vascular allografts. In Stanley JC, ed. Biologic and syn-thetic vascular prostheses. New York: Grune and Stratton, 1982;365-395.
25. Okamura K, Chiba C, Iriyama T, et al. Antigen depressant effectofglutaraldehyde for aortic heterografts with a valve, with specialreference to a concentration right fit for the preservation of grafts.Surgery 1980; 87:170-176.
26. Tilson MD. Decreased hepatic copper levels. Arch Surg 1982;117:1212-1213.
27. Rosenthal D, Levine K, Stanton PE Jr, Lamis PA. Femoropoplitealbypass: the preferred site for distal anastomosis. Surgery 1983;93:1-4.
28. Giordano JM, Keshishian JM. Aneurysm formation in human um-bilical vein grafts. Surgery 1982; 91:343-345.
Copyright © 2022 FDOKUMEN




















