
Monitoring cerebral oxygenation during balloon occlusion with multichannel NIRS
Upload
independentCategory
view
1download
0
Accepted Manuscript
Balloon Mitral Valvuloplasty in United States: A 13 year perspective
Apurva O. Badheka , M.D Neeraj Shah , M.D Abhijit Ghatak , M.D Nileshkumar J.Patel , M.D Ankit Chothani , M.D Kathan Mehta , M.D Vikas Singh , M.D Nilay Patel ,M.D Peeyush Grover , M.D Abhishek Deshmukh , M.D Sidakpal S. Panaich , M.DGhanshyambhai T. Savani , M.D Vipulkumar Bhalara , M.D Shilpkumar Arora , M.DAnkit Rathod , M.D Harit Desai , M.D Saibal Kar , M.D Carlos Alfonso , M.D Igor F.Palacios , M.D Cindy Grines , M.D Theodore Schreiber , M.D Charanjit S. Rihal ,M.D Raj Makkar , M.D Mauricio G. Cohen , M.D William O'Neill , M.D Eduardo deMarchena , M.D
PII: S0002-9343(14)00401-X
DOI: 10.1016/j.amjmed.2014.05.015
Reference: AJM 12531
To appear in: The American Journal of Medicine
Received Date: 24 March 2014
Revised Date: 13 May 2014
Accepted Date: 13 May 2014
Please cite this article as: Badheka AO, Shah N, Ghatak A, Patel NJ, Chothani A, Mehta K, Singh V,Patel N, Grover P, Deshmukh A, Panaich SS, Savani GT, Bhalara V, Arora S, Rathod A, Desai H,Kar S, Alfonso C, Palacios IF, Grines C, Schreiber T, Rihal CS, Makkar R, Cohen MG, O'Neill W, deMarchena E, Balloon Mitral Valvuloplasty in United States: A 13 year perspective, The American Journalof Medicine (2014), doi: 10.1016/j.amjmed.2014.05.015.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Balloon Mitral Valvuloplasty in United States: A 13 year perspective
Authors: Apurva O. Badheka M.Da*, Neeraj Shah M.Db*, Abhijit Ghatak M.Dc*, Nileshkumar J Patel
M.Db*, Ankit Chothani M.Dd*, Kathan Mehta M.De*, Nilay Patel M.Da, Vikas Singh M.Dc, Peeyush
Grover M.Dc, Abhishek Deshmukh M.Df, Sidakpal S. Panaich M.Da , Ghanshyambhai T. Savani M.Dc,
Vipulkumar Bhalara M.Da, Shilpkumar Arora M.Da, Ankit Rathod M.Dg, Harit Desai M.Dc, Saibal Kar
M.Dg, Carlos Alfonso M.Dc, Igor F. Palacios M.Dh, Cindy Grines M.Da, Theodore Schreiber, M.Da,
Charanjit S. Rihal M.Di, Raj Makkar M.Dg, Mauricio G. Cohen M.Dc, William O'Neill M.Dj, Eduardo de
Marchena M.Dc.
a: Detroit Medical Center, Detroit, MI; b: Staten Island University Hospital, Staten Island, NY;
c:University of Miami Miller School of Medicine, Miami, FL; d: MedStar Washington Hospital Center,
Washington, DC; e: UPMC Shadyside Hospital, Pittsburgh, PA; f: University of Arkansas for Medical
Sciences, Little Rock, AR; g: Cedars-Sinai Medical Centre, LA, CA; h: Massachusetts General hospital,
Boston, MA; i: Mayo Clinic, Rochester, MN; j: Henry Ford Hospital, Detroit, MI.
* Authors share equal contribution to this manuscript.
Acknowledgment: None declared.
Disclosures: None of the authors have any disclosures relevant to the content of the manuscript.
Funding sources: No study specific funding was used to support this work. The authors are solely
responsible for the study design, conduct and analyses, drafting and editing of the manuscript and its final
contents. No statement should be construed as an official position of the AHRQ or the US Department of
Health and Human Services. All authors had access to the data and a role in writing the manuscript.
Running title: Balloon Mitral Valvuloplasty.
Key Words: Balloon, mitral valve, valvuloplasty, cost, hospital stay, mortality, complications.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2
Word Count: 3244
Corresponding Author:
Eduardo De Marchena, MD, F.A.C.C., F.A.C.P
Associate Dean for International Medicine,
University of Miami Miller School of Medicine.
Dominion Towers, 1400 NW 10th Ave, Suite 206A
Miami, Fl33136
Phone: (305) 243 5535
Email: [email protected]
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
3
ABSTRACT
Background: Incidence and prevalence of mitral stenosis is declining in USA. We performed this study
to determine recent trends in utilization, complications, mortality, length of stay and cost associated with
balloon mitral valvuloplasty(BMV).
Methods: Utilizing the nationwide inpatient sample (NIS) database from 1998 to 2010 we identified
patients using the international classification of diseases, 9th Revision, clinical modification (ICD 9-CM)
procedure code for “percutaneous valvuloplasty". Patients≥18 years of age with mitral stenosis were
included. Patients with concomitant aortic, tricuspid or pulmonic stenosis were excluded. Primary
outcome included death and procedural complications.
Results: A total of 1308 balloon mitral valvuloplasty (weighted n= 6540) were analyzed. There was a
7.5% decline in utilization of the procedure from 24.6 procedures/10 million population in 1998-01 to
22.7 procedures/10 million population in 2008-10, (p for trend=0.098).We observed a 15.9% overall
procedural complication rate and 1.7% mortality rate. The procedural complication rates have increased
in recent years (p= 0.001) corresponding to increasing age and burden of comorbidities in patients. The
mean cost per admission for BMV has gone up significantly over the 10 years from $11668 ± 1046 in
2001 to $ 23651 ± 301 in 2010 (p<0.001).
Conclusions: In a large cross sectional study of balloon mitral valvuloplasty in USA, we have reported
trends of decreasing overall utilization and increasing procedural complication rates and cost over a
period of 13 years.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
4
INTRODUCTION
Since its introduction in 1984,1 Balloon Mitral Valvuloplasty has established itself as the
procedure of choice for patients with severe symptomatic rheumatic mitral stenosis with excellent
immediate, intermediate and long term results.2-9 Although there has been a steady decline in the
incidence of rheumatic heart disease in industrialized nations, rheumatic mitral stenosis still causes
significant mortality and morbidity worldwide. This is especially true in nations with significant numbers
of immigrants from regions with endemic rheumatic heart disease.10
We conducted this study with the aim of examining the trends of over the last decade and study
the effect of hospital and operator procedure volume on outcomes, using the USA’s largest all payer
insurance inpatient database.
METHODS
Data Source:
We analyzed 13 year data (from 1998-2010) of the nationwide inpatient sample (NIS), a subset of
the Healthcare Cost and Utilization Project sponsored by the Agency for Healthcare Research and
Quality (AHRQ). This is the largest publicly available all-payer inpatient care database in the United
States, including 7 to 8 million discharges/year, and is a 20% stratified sample of US community
(nonfederal, short-term, general, and specialty) hospitals. Each individual hospitalization is de-identified
and maintained in the database as a unique entry with 1 primary discharge diagnosis and <14 secondary
diagnosis. Each entry has information on demographic details, insurance status, comorbidities,
procedures, hospitalization outcome, and length of stay with safeguards to protect the privacy of
individual patients, physicians, and hospitals. These data undergo annual quality assessments.
Furthermore, comparisons against the following data sources strengthen the external validity of the
Nationwide Inpatient Sample: the American Hospital Association Annual Survey Database, the National
Hospital Discharge Survey from the National Center for Health Statistics, and the MedPAR inpatient data
from the Centers for Medicare and Medicaid Services.11,12
Study population and design:

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
5
We queried this database from 1998 to 2010 using the International Classification of Diseases, 9th
Revision, Clinical Modification (ICD-9-CM) procedure code designating “Percutaneous Balloon
Valvuloplasty" (ICD-9: 35.96). We included patient ≥18 years of age with mitral stenosis (ICD-9:394.0,
394.2, 396.1, 746.5, 424.0). Patients with concomitant aortic, tricuspid or pulmonic stenosis were
excluded (ICD-9: 395.0, 395.2, 396.0, 396.2, 396.8, 397.0, 397.1, 746.0, 746.1, 746.3, 424.2, 424.3).
Census data was used to determine population estimates of adults ≥18 years of age in order to calculate
the national utilization rates. Since nationwide inpatient sample represents a 20% stratified random
sample of US hospitals17, the population at risk forming the denominator is 20% of the US census
population of adults ≥18 years age for any given year.13 Therefore, utilization rates were calculated by
dividing the number of procedures performed in a given year divided by 20% of the US census
population ≥18 years of age for that year.
We defined severity of comorbid conditions using Deyo modification of Charlson Comorbidity
Index (CCI)15 which contains 17 comorbid conditions with differential weights.(Supplementary table 1)
Preventable procedural complications were identified by Patient Safety Indicators (PSIs) which
have been established by the AHRQ to monitor preventable hospital adverse events. These indicators are
based on ICD-9-CM codes and Medicare severity Diagnosis-Related Groups and each PSI has specific
inclusion and exclusion criteria.14,15 PSI individual technical specifications, were used to identify post-
procedure respiratory failure, post-procedure physiologic and metabolic derangement with acute renal
failure requiring dialysis studied separately, post-procedure pulmonary embolism or deep vein
thrombosis, procedural infectious complications which included post-procedure sepsis and central venous
catheter related bloodstream infection, iatrogenic pneumothorax, complications of anesthesia, pressure
ulcers, and accidental puncture or laceration.16
Other procedure related complications which included hemorrhage requiring blood transfusion,
iatrogenic cardiac complications, implantation of permanent pacemaker implying complete heart block,
pericardial complications, conversion to open heart surgery, other iatrogenic respiratory complications
(which included ventilator associated pneumonia, post-procedure aspiration pneumonia and other
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
6
respiratory complications not elsewhere classified), procedural stroke or transient ischemic attack (TIA)
and vascular complications were identified using ICD-9-CM codes in any secondary diagnosis field
(Supplementary table2). Vascular complications were defined as PSI code for accidental puncture or
ICD-9-CM codes for injury to blood vessels, creation of arteriovenous fistula, injury to
theretroperitoneum, vascular complications requiring surgery and other vascular complications not
elsewhere classified. “Any complications” was defined as occurrence of one or more procedural
complications listed in Table 2.
Hospital and operator procedure volume:
Annual hospital volume was determined using the unique hospital identification number to
calculate the total number of procedures performed by a particular institution in a given year. Hospital
volume and operator volume was incorporated as a continuous variables in the multivariate model in 5
and 3 units per year increments respectively. Two multivariate models were created, one with hospital
volume alone and another incorporating both hospital and operator volume with a term to adjust for
interaction effect between hospital and operator volume. Hospital ID was incorporated as a random effect
in the model to account for the effect of hospital clustering. Of note, operator volume data was available
for only 727 (55.6%) subjects.
Length of stay, Disposition & cost of hospitalization:
The total duration of hospital stay in days was estimated, after excluding in the hospital deaths,
using the length of stay information in the dataset. Disposition was classified into 3 categories: patients
discharged home or with home care services, those discharged to short or long term nursing home or
transferred to another facility and those who died in-hospital.
The Healthcare Cost and Utilization Project (HCUP) contains data on total charges billed by each
hospital. In order to enable users to see how hospital charges translate into actual costs, the HCUP cost-
to-charge ratio files were created. In order to calculate estimated cost of hospitalizations the nationwide
inpatient sample data were merged with cost-to-charge ratios available from HCUP.24 Cost of each
inpatient stay was estimated by multiplying hospital charge with cost-to-charge ratios. Adjusted cost for
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
7
each year was calculated in terms of the 2010 cost, after adjusting for inflation according to the latest
consumer price index (CPI) data. Of note, cost data were available only from 2001 to 2010.
Statistical analysis:
Stata IC 11.0 (Stata-Corp, College Station, TX) and SAS 9.3 (SAS Institute Inc, Cary, North
Carolina) were utilized for analyses. We accounted for complex survey design and clustering in the
analyses using the weights provided for each discharge record in the dataset. Weighted values of patient
level observations were generated to produce a nationally representative estimate of the entire US
population of hospitalized patients. Differences between categorical variables were tested using the chi-
square test and differences between continuous variables were tested using student’s t test. P-value of <
0.05 was considered significant.
Tests for year wise trend:
For categorical variables like utilization rates, procedural complication rates and in-hospital
mortality rates, we used the chi-square test of trend for proportions or Cochrane Armitage test using
‘ptrend’ command in STATA.17,18 For continuous variables like cost and length of stay, we used the non-
parametric test for trend by Cuzick (which is similar to Wilcoxon rank sum test) using the ‘nptrend’
command in STATA.19
Hierarchical modeling:
Hierarchical mixed effects models were generated in order to identify independent multivariate
predictors of in-hospital mortality, procedural complications, length of stay and cost of hospitalization.
Two level hierarchical models (with patient level factors nested within hospital level factors) were
created with the unique hospital identification number incorporated as random effects within the model.
Hierarchical mixed effects logistic regression models were used for categorical dependent variables like
in-hospital mortality and procedural complications and hierarchical mixed effects linear regression
models were used for continuous dependent variables like cost of hospitalization and length of stay.
Variables with >10% missing data were not included in the multivariate models e.g. we excluded race
(27.8% missing data) and admission type (14.8% missing data). In all models, we included hospital level
variables like hospital region (Northeast, South, Midwest with West as referent), teaching vs. non-

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
8
teaching hospital and patient level variables like age, sex, Deyo modification of CCI, use of intra-cardiac
echocardiography (ICE), occurrence of procedural complications, admission over the weekend and
primary payer (with Medicare/Medicaid considered as referent) in addition to hospital/operator procedure
volume. All interactions were thoroughly tested. We assessed multicollinearity using variance inflation
factor (VIF), with VIF greater than 20 suggestive of multicollinearity, and found that none of the
variables were collinear.
RESULTS
Utilization rates:
There were 1308 BMV procedures available for analysis (1998-2010) in patients ≥ 18years,
representing an estimated 6542 procedures in United States over 13 years. The mean age of the patients
was 58.1 ± 15.9 years with majority females (77%). The mean age rose from 58.4 + 16.7 years in 1998 to
62.9 + 17.0 years in 2010 (p for trend<0.001). Although data on race was missing on 27.8% of cases,
among the rest whites constituted the majority (45.5%) (Table1). The mean Charlson (CCI) score for the
cohort was calculated as 0.8 ± 1.1 (0.6+ 1.2 in 1998 to 1.5+ 1.5 in 2010 p for trend<0.001). Most of the
admissions for the procedure (95.8%) were over the weekdays with majority been done electively
(53.4%) with majority in urban teaching hospitals (>90%). There was a 7.5% decline in utilization of the
procedure from 24.60 procedures/10 million population in 1998-01 to 22.76 procedures/10 million
population in 2008-10 (p trend =0.09)(Figure 1).
Mortality:
Among 1308 procedures, we reported 23 (crude mortality rate-1.7%) deaths. Increasing age
(OR1.71 for every 10 year increase in age, 95% CI 1.08-2.72, p=0.022) and occurrence of any procedural
complication (OR 22.19, 95% CI 6.06-81.16, p<0.001) were independent predictors of mortality. The
overall crude mortality rate was consistent across 1998 to 2007 (average mortality rate from 1998-2007
was 1.36%); however there was a significant increase in the mortality rate from 2008-2010 (mortality rate
from 2008-10 was 2.61%), p=0.001. This is in conjunction with the increase in the mean age and means
CCI score (Figure 2).
Complications:
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
9
The incidence of procedural complication rate was 15.9% (Table 2). Vascular adverse events
accounted for 2.7% of these procedural complications. (Table 2 and Supplementary table 2). Cardiac
complications occurred in 4.5% of these cases with majority been coded as iatrogenic cardiac
complications (2.7%). Complete heart block requiring permanent pacing (<0.5%) and pericardial
tamponade (0.6%) accounted for rest. The ICD-9 codes for the individual categories are reported in
Supplementary table 2. During admission, 5.8% patients required open heart surgery. Respiratory
complications included pneumothorax (<0.5%), post-operative respiratory failure (1.9%) and other
iatrogenic respiratory complications (<0.5%). Post-procedure neurological events (stroke or TIA)
accounted for 2.8% of complications. Remaining procedural complications were coded as renal and
metabolic complications (<0.5%), post-procedure deep vein thrombosis or pulmonary embolism (0.8%),
post-op infectious complications (0.8%), and pressure ulcers (0.7%).
As illustrated in Table 3, increasing CCI was an independent predictor of the combined endpoint
of procedural complications and death. Increase in operator volume was an independent predictor of
decreased risk of death and procedural complications (HR 0.39 for every 3 unit increase in the operator
volume, p=0.001) or complications (HR 0.42 for every 3 units increase in the operator volume, p=0.002).
Increasing hospital volume showed statistically non-significant trends towards decreased combined end
points. (Supplementary table 3).
Overall, there was annual 0.4% (p=0.001) increase in the procedural complication rate from 1998 to 2010
correlating with simultaneous rise in age and mean CCI score over the study period (Figure 2).
Length of stay, disposition and cost:
The mean length of stay (±SE) for patients discharged alive was 3.9 ± 0.2 days. Any
complication during the procedure (+6.87 days, 95% CI 5.41-8.33 days, p<0.001), weekend admissions
(+4.86 days, 95% CI 2.59-7.12 days, p=0.001) were strongly predictive of extended length of stay (Table
3). On the contrary, increase in operator volume was associated with reduced length of stay. Similar to
the combined model, in the hospital volume only model, increase in hospital volume although showed a
non-significant trend towards decreasing length of stay (Supplementary table 3).
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
10
The mean length of stay in 1998 was significantly higher as compared to 2010 (5.30± 0.70 days
vs. 3.92 ± 0.45 days, p=0.001) (Figure3). As shown in Table 1, most of the patients (86.8%) were
discharged with only 5.8% requiring disposition to assisted facilities.
As illustrated in Table 1, medicare and medicaid were the primary payers for the procedure
(46.9%). The cost data were available for only 423 procedures (which corresponds to 2115 weighted
procedures), from 2001-2010. The mean cost per admission for the procedure has gone up significantly
(Figure 4) {2001: $11,668 ± 1046 vs. 2010: $23,651 ±308, p<0.001}.The only independent predictor of
increased cost of hospitalization (in the model with both operator and hospital volume) was occurrence of
any procedural complications (Table3). In the hospital volume model, weekend admissions were also
predictive of increased cost of hospitalization (Supplementary table3).
DISCUSSION
Our study represents one of the largest studies to summarize the overall trends of balloon mitral
valvuloplasty over a 13 year period from 1998-2010. We observed a slow and steady decline in the
utilization of procedure representing the overall gradual decline in mitral stenosis in USA and a shift in
the paradigm of utilization towards patients with increasing age and comorbidities. The demographics of
the patients included in our study are markedly different as compared to those from developing
nations.20,21 In addition to a higher percentage of females in our study, the mean age and the underlying
comorbidities of patients undergoing BMV were higher and comparable to previous studies.3,22,23 This
data is in conjunction with the NHLBI24 registry where mortality rate was highest among patients above
70 years of age which usually implies unfavorable valve anatomy and increase in the comorbidities.
Complications:
In prior studies10,23-26 mortality rates of 0-3% have been reported and are usually related to
vascular complications, hemopericardium and shock. We report an in-patient mortality rate of 1.7%
significantly associated with occurrence of any procedural complications, and increasing age.
The overall procedural complication rate was 15.9% of patients admitted for the procedure. The
overall procedural complication rates are slightly higher than those reported in the NHLBI24 registry
(12%) which had a similar heterogeneous patient distribution. This difference in the complication rate is
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
11
related to reporting of an comparatively more exhaustive list of complications, as identified by PSI and
ICD-9 CM codes in patients with advanced age and significant comorbidities. The percentage of patients
with post-op hemorrhage requiring transfusion in our series was similar to those reported by Nobuyoshi
et al (2%)26 in their series of 106 patients. Similar rates (1%) of vascular complications have been
reported in the in the NHLBI registry albeit with a much higher rate of transfusion requirement (8.5%).
Cardiac complications: The incidence of cardiac tamponade/requirement for urgent
pericardiocentesis has been reported in up to 4-7% of the procedures in prior studies.24,25 In our study
pericardial complications occurred only in 0.6% of the cases which could partly be attributed to a certain
proportion of patients with cardiac tamponade being coded under either “iatrogenic cardiac
complications” or “requiring open heart surgery”. Episodes of complete heart block as reported in our
study are uncommon during the procedure and are usually related to trauma incurred by the conduction
system either during the trans-septal puncture or balloon dilatation. We report a 5.8% rate of cardiac
surgery during the admission which are comparable to prior study (4-6.7%)24,25 and likely related to peri-
procedural complications.
Left atrial (LA) or left atrial appendage (LAA) thrombus formation is not uncommon in patients
with mitral stenosis despite warfarin therapy27 and intra-procedural strokes are usually secondary to
embolization from the catheters, wires, and dislodgement of a intracardic thrombus stroke rates of up to
2%24 has been reported in the past and are usually higher in elderly patients with calcified valves and
increased comorbidities.28 The rates of neurological complications in our study (2.8%) are in keeping
with those reported in the literature.24,28 Utilization of imaging especially TEE or ICE prior to the
procedure to document absence of intracardiac thrombus is mandatory per the ACC/AHA guidelines29.
We observed the use of ICE in only 4% of the cases. Use of the same ICD-9 codes identifying
transthoracic and TEE precluded any comment on use of TEE. Post procedural respiratory complications
are usually secondary to worsening mitral regurgitation leading to pulmonary edema. Our rates of post-
operative respiratory failure of 2% are slightly lower than previously reported peri-procedural intubation
rates of up to 3.8% by the NHLBI registry.24

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
12
The overall increase in the complication rate as observed from 1998 to 2010 may be explained by
the simultaneously increasing trend in age and comorbidity burden. In addition, the overall decline in
rheumatic heart disease and utilization of the procedure over the years, may lead to decreased annual
operator volume possibly accounting for the increased trend in complications. We observed that the
average annual operator volume declined from (mean + SE) 2.8 + 0.4 in 1998 to 1.6+0.1 in 2009
(p=0.003).
We have demonstrated increasing operator volume to be independently predictive of favorable
outcomes. Similar association of reduced complications, increased technical success and improved
outcome with increasing operator volume has been reported in the literature.30-32 Although increased
hospital procedural volume did not reach statistical significance in our report, it showed a favorable trend
towards reducing complication rates, supporting the conclusions from the NHLBI registry.24
In keeping with these trends our data supports recently updated guidelines29 on valvular heart
disease strongly recommend that mitral valvuloplasty should be performed in higher volume centers with
skilled and experienced operators. As the utilization rate of BMV is gradually decreasing over years,
these centers would not only play a pivotal role in reducing the complication rates, but would also be
indispensable towards providing and maintaining adequate volume required for training physicians.
Length of stay, disposition and cost:
Length of stay reported in our cohort was comparable to that reported in the NHLBI data
(3.6±6.8 days). Patients admitted over the weekend and those experiencing any procedural complications
had extended stay. Increasing operator volume translated into reduced length of stay. Post procedure most
of these patients were discharged home with only a very small proportion of patients going to another
facility. We observed a significant rise in the cost for in-hospital care for patients over study period
without any significant change in the mean stay. This could largely be secondary to advanced age along
with an increase in the burden of comorbidities and the associated cost of management of chronic illness
in patients.
Limitations:

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
13
Our study has several important limitations, which are inherent to administrative databases. It is
possible that procedure volume was misrepresented by the sample. Similarly, we identified complications
using the standardized ICD-9 and PSI codes which may not cover all procedural complications. Although
principal diagnosis is accurately coded in administrative data, secondary or comorbid diagnoses are often
under-reported. The operator volume data could be misrepresented as operators could be performing the
procedure in hospitals, which were not part of the database. We observed a decreasing trend of missing
secondary diagnoses from 1998 to 2010 (9.7% vs. 1.1%, p<0.001). More complete data entry with
increased reporting of the comorbid conditions over the years may be the sole reason for the observed
trend of increase in the Charlson comorbidity index over the years, which is a possible limitation of our
study.
In conclusion, there has been a very steady, albeit statistically non-significant, trend of decline in
utilization of balloon mitral valvuloplasty in US in concordance with the downward trend in incidence of
mitral stenosis. The procedure is increasingly being performed on patients with higher comorbidities and
increasing age. Operator experience significantly reduces the risk of death and procedural complications
and plays a pivotal role in reducing the overall length of stay and indirectly influences the cost
effectiveness of the procedure.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
14
REFERENCES
1. Inoue K, Owaki T, Nakamura T, Kitamura F, Miyamoto N. Clinical application of transvenous mitral
commissurotomy by a new balloon catheter. The Journal of thoracic and cardiovascular surgery
1984;87:394-402.
2. Abascal VM, Wilkins GT, O'Shea JP, Choong CY, Palacios IF, Thomas JD, Rosas E, Newell JB,
Block PC, Weyman AE. Prediction of successful outcome in 130 patients undergoing percutaneous
balloon mitral valvotomy. Circulation 1990;82:448-456.
3. Multicenter experience with balloon mitral commissurotomy. NHLBI Balloon Valvuloplasty Registry
Report on immediate and 30-day follow-up results. The National Heart, Lung, and Blood Institute
Balloon Valvuloplasty Registry Participants. Circulation 1992;85:448-461.
4. Iung B, Nicoud-Houel A, Fondard O, Hafid A, Haghighat T, Brochet E, Garbarz E, Cormier B, Baron
G, Luxereau P, Vahanian A. Temporal trends in percutaneous mitral commissurotomy over a 15-year
period. European heart journal 2004;25:701-707.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
15
5. Palacios IF, Block PC, Wilkins GT, Weyman AE. Follow-up of patients undergoing percutaneous
mitral balloon valvotomy. Analysis of factors determining restenosis. Circulation 1989;79:573-579.
6. Dean LS, Mickel M, Bonan R, Holmes DR, Jr., O'Neill WW, Palacios IF, Rahimtoola S, Slater JN,
Davis K, Kennedy JW. Four-year follow-up of patients undergoing percutaneous balloon mitral
commissurotomy. A report from the National Heart, Lung, and Blood Institute Balloon Valvuloplasty
Registry. Journal of the American College of Cardiology 1996;28:1452-1457.
7. Trevino AJ, Ibarra M, Garcia A, Uribe A, de la Fuente F, Bonfil MA, Feldman T. Immediate and long-
term results of balloon mitral commissurotomy for rheumatic mitral stenosis: comparison between Inoue
and double-balloon techniques. American heart journal 1996;131:530-536.
8. Pavlides GS, Nahhas GT, London J, Gangadharan C, Troszak E, Barth-Jones D, Puchrowicz-Ochocki
S, O'Neill WW. Predictors of long-term event-free survival after percutaneous balloon mitral
valvuloplasty. The American journal of cardiology 1997;79:1370-1374.
9. Fawzy ME, Fadel B, Al-Sergani H, Al Amri M, Hassan W, Abdulbaki K, Shoukri M, Canver C. Long-
term results (up to 16.5 years) of mitral balloon valvuloplasty in a series of 518 patients and predictors of
long-term outcome. Journal of interventional cardiology 2007;20:66-72.
10. Nobuyoshi M, Arita T, Shirai S, Hamasaki N, Yokoi H, Iwabuchi M, Yasumoto H, Nosaka H.
Percutaneous balloon mitral valvuloplasty: a review. Circulation 2009;119:e211-219.
11. http://www.hcup-us.ahrq.gov/db/nation/nis/nisrelatedreports.jsp.
12. Epstein AJ, Polsky D, Yang F, Yang L, Groeneveld PW. Coronary revascularization trends in the
United States, 2001-2008. JAMA : the journal of the American Medical Association 2011;305:1769-1776.
13. U.S. Census Bureau - Population Division. Annual estimates of the resident population by sex and
selected age groups for the United States: April 1, 2000 to July 1, 2009 (NC-EST2009-02) [Accessed
March 2, 2011]; .
14. McDonald KM, Romano PS, Geppert J, Davies SM, Duncan BW, Shojania KG, Hansen A. Measures
of Patient Safety Based on Hospital Administrative Data - The Patient Safety Indicators. Rockville (MD),
2002.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
16
15. Romano PS, Geppert JJ, Davies S, Miller MR, Elixhauser A, McDonald KM. A national profile of
patient safety in U.S. hospitals. Health Aff (Millwood) 2003;22:154-166.
16. http://www.qualityindicators.ahrq.gov/modules/PSI_TechSpec.aspx.Accessed March 2, 2011.
17. Murphy MM, Ng SC, Simons JP, Csikesz NG, Shah SA, Tseng JF. Predictors of major complications
after laparoscopic cholecystectomy: surgeon, hospital, or patient? Journal of the American College of
Surgeons 2010;211:73-80.
18. Armitage P. Tests for Linear Trends in Proportions and Frequencies.
19. Cuzick J. A Wilcoxon-type test for trend. Statistics in medicine 1985;4:87-90.
20. Carroll JD, Feldman T. Percutaneous mitral balloon valvotomy and the new demographics of mitral
stenosis. JAMA : the journal of the American Medical Association 1993;270:1731-1736.
21. Joswig BC, Glover MU, Handler JB, Warren SE, Vieweg WV. Contrasting progression of mitral
stenosis in Malayans versus American-born Caucasians. American heart journal 1982;104:1400-1403.
22. Herrmann HC, Wilkins GT, Abascal VM, Weyman AE, Block PC, Palacios IF. Percutaneous balloon
mitral valvotomy for patients with mitral stenosis. Analysis of factors influencing early results. The
Journal of thoracic and cardiovascular surgery 1988;96:33-38.
23. Palacios I, Block PC, Brandi S, Blanco P, Casal H, Pulido JI, Munoz S, D'Empaire G, Ortega MA,
Jacobs M, et al. Percutaneous balloon valvotomy for patients with severe mitral stenosis. Circulation
1987;75:778-784.
24. Complications and mortality of percutaneous balloon mitral commissurotomy. A report from the
National Heart, Lung, and Blood Institute Balloon Valvuloplasty Registry. Circulation 1992;85:2014-
2024.
25. Herrmann HC, Kleaveland JP, Hill JA, Cowley MJ, Margolis JR, Nocero MA, Zalewski A, Pepine
CJ. The M-Heart percutaneous balloon mitral Valvuloplasty Registry: initial results and early follow-up.
The M-Heart Group. Journal of the American College of Cardiology 1990;15:1221-1226.
26. Nobuyoshi M, Hamasaki N, Kimura T, Nosaka H, Yokoi H, Yasumoto H, Horiuchi H, Nakashima H,
Shindo T, Mori T, et al. Indications, complications, and short-term clinical outcome of percutaneous
transvenous mitral commissurotomy. Circulation 1989;80:782-792.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
17
27. Shaw TR, Northridge DB, Sutaria N. Mitral balloon valvotomy and left atrial thrombus. Heart
2005;91:1088-1089.
28. Shaw TR, Sutaria N, Prendergast B. Clinical and haemodynamic profiles of young, middle aged, and
elderly patients with mitral stenosis undergoing mitral balloon valvotomy. Heart 2003;89:1430-1436.
29. Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Jr., Faxon DP, Freed MD, Gaasch WH, Lytle
BW, Nishimura RA, O'Gara PT, O'Rourke RA, Otto CM, Shah PM, Shanewise JS. 2008 Focused update
incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart
disease: a report of the American College of Cardiology/American Heart Association Task Force on
Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients
With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for
Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation
2008;118:e523-661.
30. Iung B, Cormier B, Ducimetiere P, Porte JM, Nallet O, Michel PL, Acar J, Vahanian A. Immediate
results of percutaneous mitral commissurotomy. A predictive model on a series of 1514 patients.
Circulation 1996;94:2124-2130.
31. Hung JS, Lau KW, Lo PH, Chern MS, Wu JJ. Complications of Inoue balloon mitral
commissurotomy: impact of operator experience and evolving technique. American heart journal
1999;138:114-121.
32. Rihal CS, Nishimura RA, Holmes DR, Jr. Percutaneous balloon mitral valvuloplasty: the learning
curve. American heart journal 1991;122:1750-1756.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
18
FIGURE TITLES AND LEGENDS
Figure 1: Utilization trends for Balloon Mitral Valvuloplasty per 10 million populations from 1998
2010.
Figure 2: Trends in procedural complication and mean Charlson/Deyo score for BMV 1998-2010.
CCI: Charlson comorbidity index
Figure 3: Length of stay & Cost trends for BMV admission from 2001-2010.
Figure 4: Utilization cost (in dollars) & complications trends adjusted for 2010 for BMV from
2001-2010.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
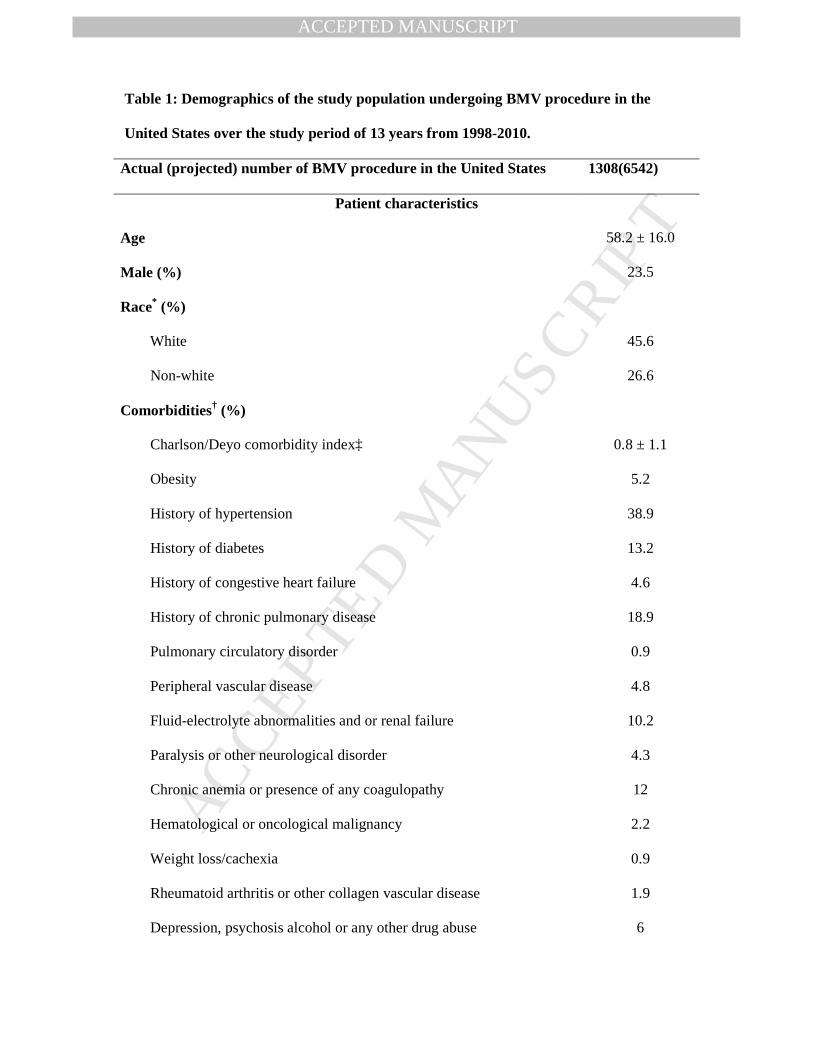
Table 1: Demographics of the study population undergoing BMV procedure in the
United States over the study period of 13 years from 1998-2010.
Actual (projected) number of BMV procedure in the United States 1308(6542)
Patient characteristics
Age 58.2 ± 16.0
Male (%) 23.5
Race* (%)
White 45.6
Non-white 26.6
Comorbidities† (%)
Charlson/Deyo comorbidity index‡ 0.8 ± 1.1
Obesity 5.2
History of hypertension 38.9
History of diabetes 13.2
History of congestive heart failure 4.6
History of chronic pulmonary disease 18.9
Pulmonary circulatory disorder 0.9
Peripheral vascular disease 4.8
Fluid-electrolyte abnormalities and or renal failure 10.2
Paralysis or other neurological disorder 4.3
Chronic anemia or presence of any coagulopathy 12
Hematological or oncological malignancy 2.2
Weight loss/cachexia 0.9
Rheumatoid arthritis or other collagen vascular disease 1.9
Depression, psychosis alcohol or any other drug abuse 6

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Median household income
category for patient's zip code§
1. 0-25th percentile 16.5
2. 26-50th percentile 25.4
3. 51-75th percentile 25.3
4. 76-100th percentile 32.8
Primary Payer (%)
Medicare / Medicaid 47.2
Private including HMO 43.2
Self pay/no charge/other 9.6
Hospital characteristics
Hospital bed size (%)
Small 5.5
Medium 10.5
Large 84.0
Urban hospitals (%) 99.1
Hospital region (%)
Northeast 29.7
Midwest or North Central 21.4
South 22.9
West 26.0
Teaching hospitals (%) 90.6
Emergent/ urgent admission (%) 31.8
Weekend admission (%) 4.2

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Other major cardiac procedures performed
during hospitalization (ICD 9 procedure code) (%)
Coronary angiography (88.55, 88.56) 42.6
Percutaneous coronary intervention (36.06, 36.07) 1.7
Intraaortic balloon pump (37.68,37.62) 1.5
Left ventricular assist device (37.68,37.62) <0.5%
Morbidity, mortality, cost and outcome
Length of stay(Means ± SE) 3.92 ± 0.2
Total charges# ($)(Means ± SE) 20,499 ± 886
Disposition
Home 92.5
Facility 5.8
Death 1.7
* Race was missing in 27.8% of the patient population.
† Variables are AHRQ comorbidity measures, which were available for year 2002 -2010 (n =
900).
‡ Charlson/Deyo comorbidity index was calculated as per Deyo classification.
§ This represents a quartile classification of the estimated median household income of
residents in the patient's ZIP Code. These values are derived from ZIP Code-demographic
data obtained from Claritas. The quartiles are identified by values of 1 to 4, indicating the
poorest to wealthiest populations. Because these estimates are updated annually, the value
ranges vary by year. http://www.hcupus.ahrq.gov/db/vars/zipinc_qrtl/nisnote.jsp
|| Admission type was missing in 14.8% of the population.
# For each year, cost was adjusted for inflation according to reference 2010 cost. Cost was
missing in 27.2% cases.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
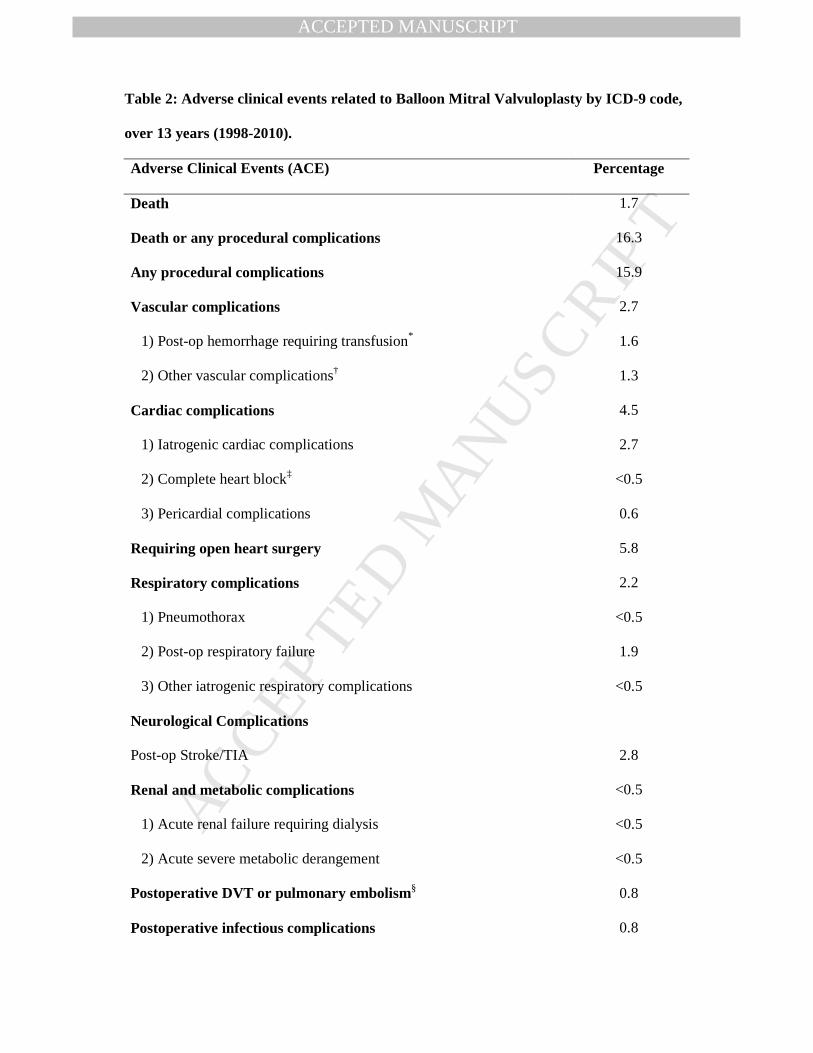
Table 2: Adverse clinical events related to Balloon Mitral Valvuloplasty by ICD-9 code,
over 13 years (1998-2010).
Adverse Clinical Events (ACE) Percentage
Death 1.7
Death or any procedural complications 16.3
Any procedural complications 15.9
Vascular complications 2.7
1) Post-op hemorrhage requiring transfusion* 1.6
2) Other vascular complications† 1.3
Cardiac complications 4.5
1) Iatrogenic cardiac complications 2.7
2) Complete heart block‡ <0.5
3) Pericardial complications 0.6
Requiring open heart surgery 5.8
Respiratory complications 2.2
1) Pneumothorax <0.5
2) Post-op respiratory failure 1.9
3) Other iatrogenic respiratory complications <0.5
Neurological Complications
Post-op Stroke/TIA 2.8
Renal and metabolic complications <0.5
1) Acute renal failure requiring dialysis <0.5
2) Acute severe metabolic derangement <0.5
Postoperative DVT or pulmonary embolism§ 0.8
Postoperative infectious complications 0.8

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Pressure ulcer rate 0.7
Anesthetic complications 0.0
* Hemorrhage requiring transfusion was identified as having any patient having post-
operative hemorrhage and also got transfusion.
† Details in supplementary Table 2.
‡ ICD-9 codes for permanent pacemaker were used to identify post procedure patients with
complete heart block.
§ Infectious complications were identified as composite of post-operative sepsis, septic shock
or catheter related infection.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
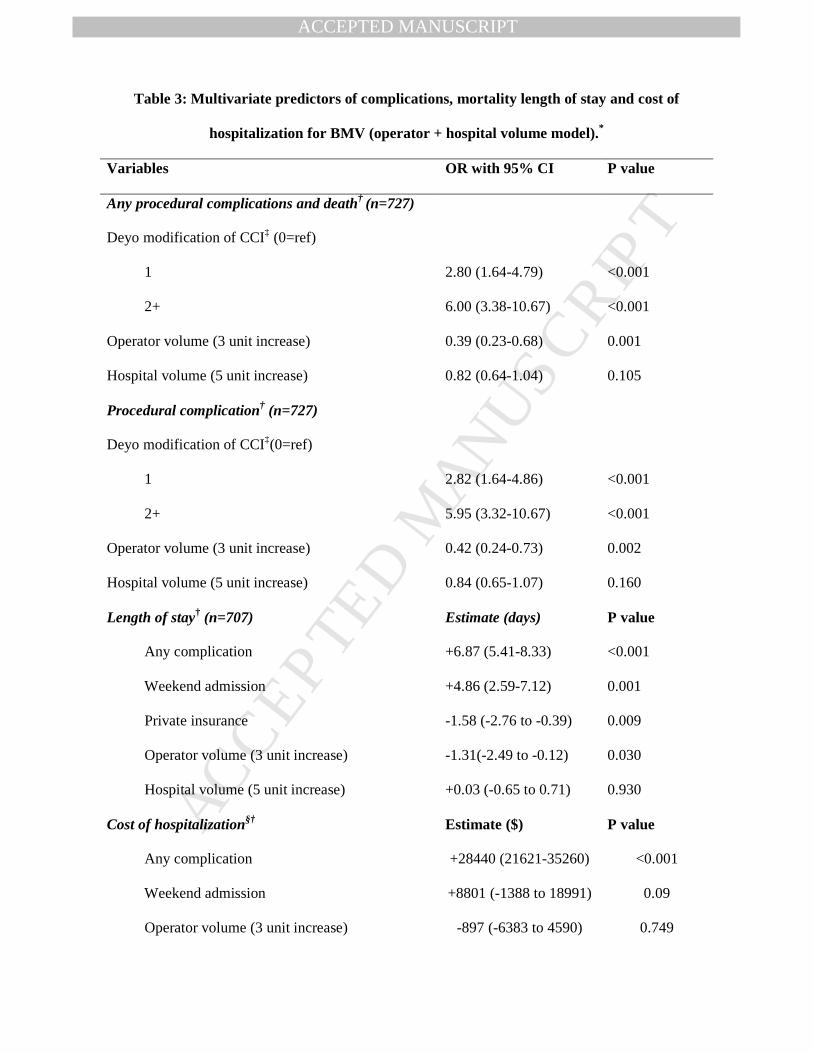
Table 3: Multivariate predictors of complications, mortality length of stay and cost of
hospitalization for BMV (operator + hospital volume model).*
Variables OR with 95% CI P value
Any procedural complications and death† (n=727)
Deyo modification of CCI‡ (0=ref)
1 2.80 (1.64-4.79) <0.001
2+ 6.00 (3.38-10.67) <0.001
Operator volume (3 unit increase) 0.39 (0.23-0.68) 0.001
Hospital volume (5 unit increase) 0.82 (0.64-1.04) 0.105
Procedural complication† (n=727)
Deyo modification of CCI‡(0=ref)
1 2.82 (1.64-4.86) <0.001
2+ 5.95 (3.32-10.67) <0.001
Operator volume (3 unit increase) 0.42 (0.24-0.73) 0.002
Hospital volume (5 unit increase) 0.84 (0.65-1.07) 0.160
Length of stay† (n=707) Estimate (days) P value
Any complication +6.87 (5.41-8.33) <0.001
Weekend admission +4.86 (2.59-7.12) 0.001
Private insurance -1.58 (-2.76 to -0.39) 0.009
Operator volume (3 unit increase) -1.31(-2.49 to -0.12) 0.030
Hospital volume (5 unit increase) +0.03 (-0.65 to 0.71) 0.930
Cost of hospitalization§† Estimate ($) P value
Any complication +28440 (21621-35260) <0.001
Weekend admission +8801 (-1388 to 18991) 0.09
Operator volume (3 unit increase) -897 (-6383 to 4590) 0.749

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Hospital volume (5 unit increase) +1149 (-2142 to4440) 0.494
We could not analyze the entire study population due to limited availability of operator ID for
all hospitals in HCUS NIS dataset.
* Apart from cost of hospitalization data rest of the data is from 1998-2010.
† Variables included for the multivariable analysis included age (in 10 years increment),
gender, any procedural complications, use of intra-cardiac echocardiography (ICE), Deyo
modification of CCI, Operator volume (3 unit increase), Weekend admission, primary payer,
teaching hospital, hospital regions (South, North-East, Mid-West, West), and Hospital
volume in 5 unit increments.
‡ CCI denotes Charlson comorbidity index
§ Cost data were recorded beginning 2001 and hence we have information on hospitalization
cost from 2001 to 2010 only. For each year, cost was adjusted for inflation according to the
2010 value. (http://www.usinflationcalculator.com).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 1: Utilization trends for Balloon Mitral Valvuloplasty per 10 million population
from 1998 2010.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 2: Trends in procedural complication and mean Chalson Deyo score for BMV 1998-
2010.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 3: Length of stay & cost trends for BMV admission from 2001-2010.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 4: Utilization cost (in dollars) & complications trends adjusted for 2010 for BMV
from 2001-2010.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Clinical Significance:
• Utilization of balloon mitral valvuloplasty (BMV) declined by 7.5% in the last decade (p for
trend=0.098).
• The procedural complication rates have increased in recent years (p= 0.001) corresponding to
increasing age and burden of comorbidities in patients undergoing this procedure.
• The mean cost per admission for BMV has significantly increased from $11,668 ± 1,046 in 2001
to $ 2,3651 ± 301 in 2010 (p<0.001).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Supplementary table 1: Deyo modification of Charlson comorbidity index (CCI).
Reported ICD-9 CM Codes Condition Charlson Score
410 – 410.9 Myocardial infarction 1
428 – 428.9 Congestive heart failure 1
433.9, 441 – 441.9, 785.4, V43.4 Peripheral vascular disease 1
430 – 438 Cerebrovascular disease 1
290 – 290.9 Dementia 1
490 – 496, 500 – 505, 506.4 Chronic pulmonary disease 1
710.0, 710.1, 710.4, 714.0 – 714.2,
714.81, 725
Rheumatologic disease 1
531 – 534.9 Peptic ulcer disease 1
571.2, 571.5, 571.6, 571.4 – 571.49 Mild liver disease 1
250 – 250.3, 250.7 Diabetes 1
250.4 – 250.6 Diabetes with chronic
complications
2
344.1, 342 – 342.9 Hemiplegia or paraplegia 2
582 – 582.9, 583 – 583.7, 585, 586, 588 –
588.9
Renal disease 2
140-172.9, 174-195.8, 200-208.9 Any malignancy including
leukemia and lymphoma
2
572.2 – 572.8 Moderate or severe liver disease 3
196-199.1 Metastatic solid tumor 6
042 – 044.9 AIDS 6

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
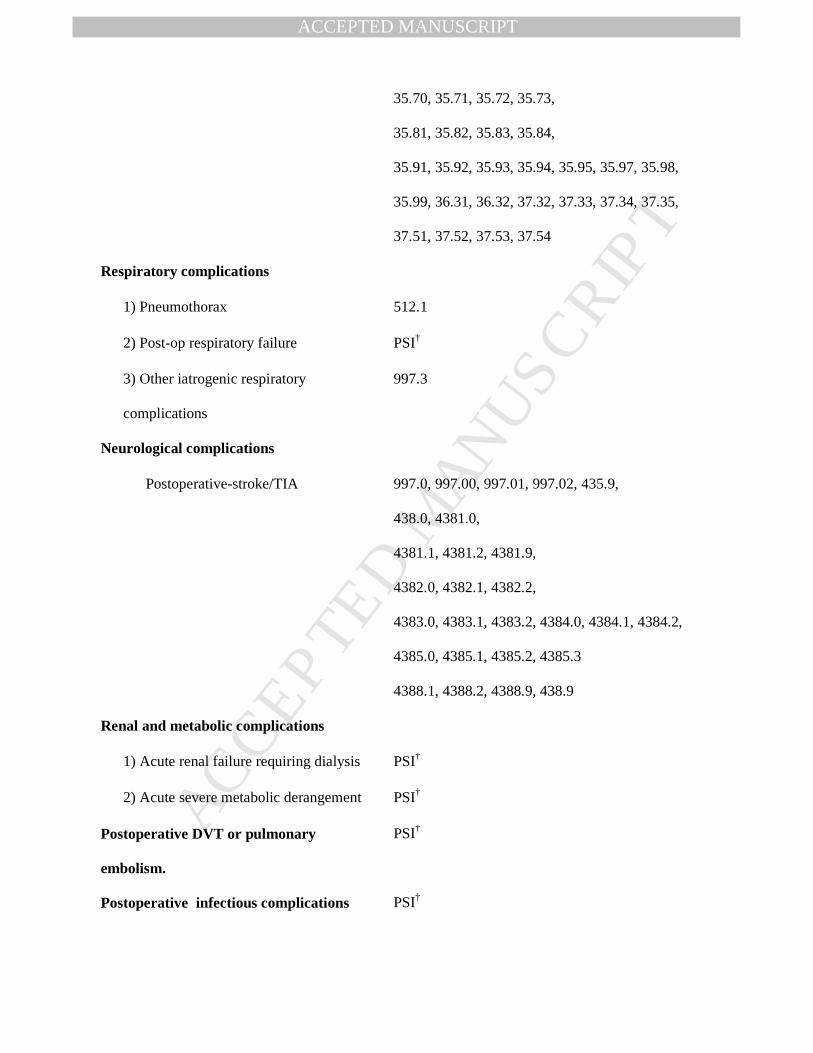
Supplementary table 2: Procedural complications of BMV by ICD 9 code.
Any procedural complications ICD CODE
Vascular complications
1) Post-op hemorrhage requiring
transfusion
99.0
2) Vascular complications including -Injury to blood vessels-900-904
-Accidental puncture-998.2, e8700-8709 (PSI)
-AV fistula-447
-Injury to retro-peritoneum 8680.4
-Vascular complications requiring surgery-39.31,
39.41, 39.49, 39.52, 39.53, 39.56, 39.57, 39.58,
39.59, 39.79
-Other vascular complications-999.2, 997.7
Cardiac complications
1) Iatrogenic cardiac complications 997.1*
2) Complete heart block 37.71, 37.73, 37.81, 37.82, 37.83, 0051,v450.1
3) Pericardial complications 423.0-Hemopericardium
423.3-Cardiac tamponade
37.0-Pericardiocentesis
37.12-Pericardiotomy or pericardial window
Requiring open heart surgery 35.10, 35.11, 35.12, 35.13, 35.14,
35.20, 35.21, 35.22, 35.23, 35.24, 35.25, 35.26,
35.27, 35.28, 35.32, 35.33,35.34, 35.35,35.42,
35.50, 35.51, 35.52, 35.53, 35.54,
35.60, 35.61, 35.62, 35.63,
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
35.70, 35.71, 35.72, 35.73,
35.81, 35.82, 35.83, 35.84,
35.91, 35.92, 35.93, 35.94, 35.95, 35.97, 35.98,
35.99, 36.31, 36.32, 37.32, 37.33, 37.34, 37.35,
37.51, 37.52, 37.53, 37.54
Respiratory complications
1) Pneumothorax 512.1
2) Post-op respiratory failure PSI†
3) Other iatrogenic respiratory
complications
997.3
Neurological complications
Postoperative-stroke/TIA 997.0, 997.00, 997.01, 997.02, 435.9,
438.0, 4381.0,
4381.1, 4381.2, 4381.9,
4382.0, 4382.1, 4382.2,
4383.0, 4383.1, 4383.2, 4384.0, 4384.1, 4384.2,
4385.0, 4385.1, 4385.2, 4385.3
4388.1, 4388.2, 4388.9, 438.9
Renal and metabolic complications
1) Acute renal failure requiring dialysis PSI†
2) Acute severe metabolic derangement PSI†
Postoperative DVT or pulmonary
embolism.
PSI†
Postoperative infectious complications PSI†
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
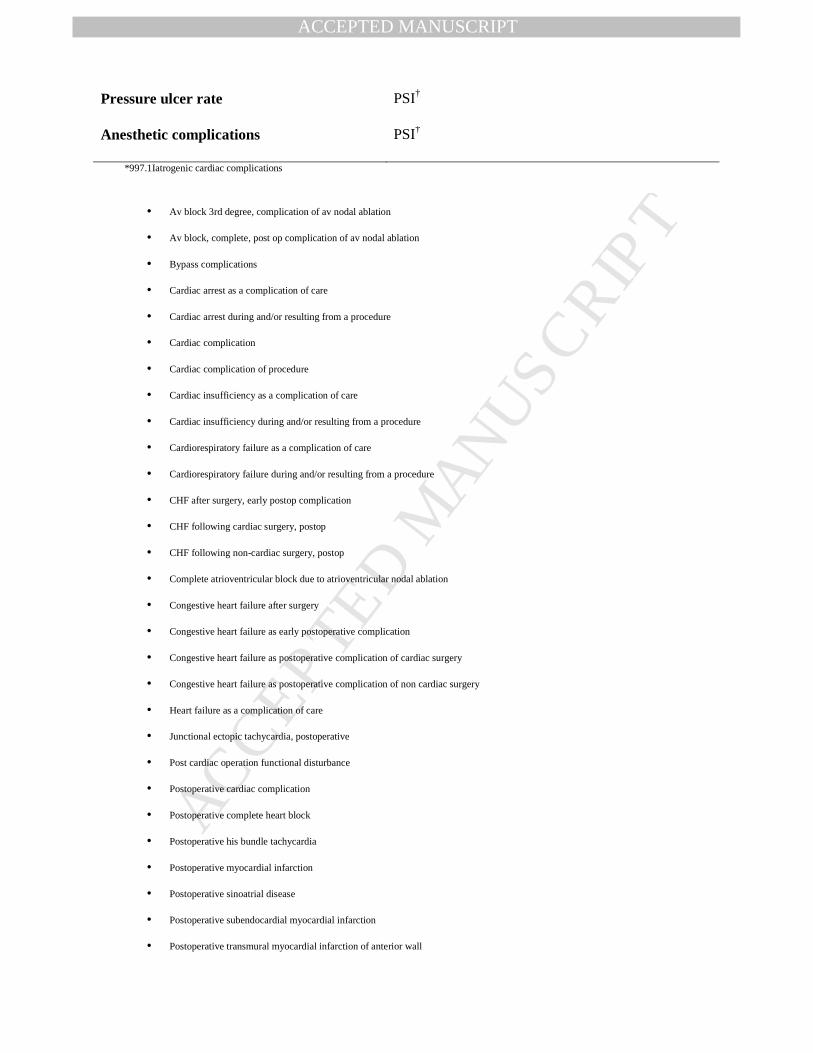
*997.1Iatrogenic cardiac complications
• Av block 3rd degree, complication of av nodal ablation
• Av block, complete, post op complication of av nodal ablation
• Bypass complications
• Cardiac arrest as a complication of care
• Cardiac arrest during and/or resulting from a procedure
• Cardiac complication
• Cardiac complication of procedure
• Cardiac insufficiency as a complication of care
• Cardiac insufficiency during and/or resulting from a procedure
• Cardiorespiratory failure as a complication of care
• Cardiorespiratory failure during and/or resulting from a procedure
• CHF after surgery, early postop complication
• CHF following cardiac surgery, postop
• CHF following non-cardiac surgery, postop
• Complete atrioventricular block due to atrioventricular nodal ablation
• Congestive heart failure after surgery
• Congestive heart failure as early postoperative complication
• Congestive heart failure as postoperative complication of cardiac surgery
• Congestive heart failure as postoperative complication of non cardiac surgery
• Heart failure as a complication of care
• Junctional ectopic tachycardia, postoperative
• Post cardiac operation functional disturbance
• Postoperative cardiac complication
• Postoperative complete heart block
• Postoperative his bundle tachycardia
• Postoperative myocardial infarction
• Postoperative sinoatrial disease
• Postoperative subendocardial myocardial infarction
• Postoperative transmural myocardial infarction of anterior wall
Pressure ulcer rate PSI†
Anesthetic complications PSI†

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
• Postoperative transmural myocardial infarction of inferior wall
• Recurrent coronary arteriosclerosis after percutaneous transluminal coronary angioplasty
997.1 Excludes
• the listed conditions as long-term effects of cardiac surgery or due to the presence of cardiac prosthetic device ( 429.4)
Applies To
• Cardiac:
o arrest during or resulting from a procedure
o insufficiency during or resulting from a procedure
• Cardiorespiratory failure during or resulting from a procedure
Heart failure during or resulting from a procedure
†Post-procedural complications were identified by Patient Safety Indicators (PSIs) which have been established by the Agency for
Healthcare Research and Quality to monitor preventable adverse events during hospitalization. These indicators are based on ICD-9-CM
codes and Medicare severity Diagnosis-Related Groups and each PSI has specific inclusion and exclusion criteria PSI individual measure
technical specifications, Version 4.4, March 2012 was used to identify and define preventable complications.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Supplementary table 3: Multivariate predictors of complications, mortality length of
stay and cost of hospitalization for BMV (hospital volume model).*
Variables OR with 95% CI P value
Any procedural complications and
death†(n=1303)
Deyo modification of CCI‡ (0=ref)
1 2.76 (1.87-4.09) <0.001
2+ 5.62 (3.67-8.60) <0.001
Female gender 0.66 (0.46-0.94) 0.021
Hospital volume (5 unit increase) 0.93 (0.78-1.09) 0.37
Procedural complications†:(n=1303)
Deyo modification of CCI‡(0=ref)
1 2.80 (1.88-4.15) <0.001
2+ 5.50 (3.59-8.45) <0.001
Female gender 0.70(0.50-1.02) 0.062
Hospital volume (5 unit increase) 0.94 (0.80-1.11) 0.478
Length of stay†: (n=1270) Estimate (days) P value
Any complication +6.38 (5.40-7.37) <0.001
Deyo modification of CCI‡ (0=ref)
1 +0.96 (0.14-1.78) 0.022
2+ +1.98 (0.99-2.98) <0.001
Weekend admission +4.83 (3.12-6.54) <0.001

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Private insurance -1.52 (-2.34 to -0.7) <0.001
Hospital volume (5 unit increase) -0.31 (-0.66 to 0.05) 0.09
Cost of hospitalization§†:(n=779) Estimate ($) P value
Any complication +27265 (22953-31576) <0.001
Weekend admission +11940 (4459-19421) 0.002
Hospital volume (5 unit increase) -1243 (-2921 to 435) 0.146
* Apart from cost of hospitalization data rest of the data is from 1998-2010.
† Variables included for the multivariable analysis included age (in 10 year increments),
gender, any procedural complications, use of intra-cardiac echocardiography (ICE), Deyo
modification of CCI, Weekend admission, primary payer, teaching hospital, hospital regions
(South, North-East, Mid-West, West), and Hospital volume in 5 unit increments.
‡ CCI denotes Charlson comorbidity index
§ Cost data were recorded beginning 2001 and hence we have information on hospitalization
cost from 2001 to 2010 only. For each year, cost was adjusted for inflation according to the
2010 value. (http://www.usinflationcalculator.com).
Copyright © 2022 FDOKUMEN




















