
Asthma symptom re-emergence after omalizumab withdrawal correlates well with increasing IgE and...
10
Original article Asthma symptom re-emergence after omalizumab withdrawal correlates well with increasing IgE and decreasing pharmacokinetic concentrations Raymond G. Slavin, MD, a Caterina Ferioli, BSc, b Stacey J. Tannenbaum, PhD, c Carmen Martin, PhD, d Martin Blogg, BSc, d and Philip J. Lowe, PhD b St Louis, Mo, Basel, Switzerland, East Hanover, NJ, and Horsham, United Kingdom Background: Physicians have questioned whether omalizumab can be discontinued or the dose reduced after clinical improvement is seen in patients with severe asthma. Objectives: To examine the relationships among omalizumab, free IgE, and clinical outcomes in a randomized, placebo- controlled trial in patients with severe persistent allergic asthma following a posology based on pretreatment total IgE and body weight. Methods: A pharmacokinetic-pharmacodynamic binding model was used to calculate free IgE, omalizumab, and total IgE concentrations during the 28-week treatment and 16-week follow-up of the INvestigation of Omalizumab in seVere Asthma TrEatment (INNOVATE) study. These were plotted against the mean changes in the total asthma symptom score, morning peak expiratory flow, and rescue medication use for physician-defined treatment responders and nonresponders. Results: The model accurately fitted omalizumab and free and total IgE, allowing reconstruction of the entire time course for each patient. Free IgE was rapidly suppressed below the 50 ng/ mL (20.8 IU/mL) target, although there was a notable period before clinical measures stabilized. After treatment cessation, free IgE and omalizumab returned toward baseline and, after a delay, asthma symptoms re-emerged. Model-derived omalizumab and free IgE concentrations correlated well with changes in clinical outcomes, particularly in omalizumab- treated responders. Asthma symptoms exhibited different correlations during response onset compared with response offset (hysteresis), indicative of physiological time delays between changes in IgE levels and pulmonary function. Conclusion: Omalizumab and free IgE correlated well with clinical symptoms. Reducing omalizumab doses below those in the dosing table cannot be recommended; the resulting increase in free IgE would cause a deterioration in asthma control. (J Allergy Clin Immunol 2009;123:107-13.) Key words: Asthma, omalizumab, pharmacokinetics, pharmacody- namics, IgE Allergic (IgE-mediated) asthma is characterized by the pres- ence of IgE antibodies against common allergens. 1-3 When aller- gen cross-links specific IgE bound to high-affinity IgE (FceRI) receptors on the surface of basophils and mast cells, proinflamma- tory mediators are released that trigger and perpetuate airway symptomatology. 4,5 Omalizumab, an anti-IgE mAb, binds to the Fc region of all forms of circulating IgE, regardless of IgE speci- ficity, preventing IgE-mediated responses, 6,7 and downregulating FceRI expression on mast cells and basophils. 8 The efficacy and tolerability of omalizumab have been demonstrated in patients with moderate-to-severe and severe persistent allergic (IgE-medi- ated) asthma. 9-11 Clinical benefit with omalizumab is observed when serum free IgE levels are reduced to 50 ng/mL or less. 12,13 Omalizumab dosing is based on pretreatment total serum IgE level and body weight, and calculated using a dosing table. Omalizumab binds to IgE to reversibly form IgG-IgE complexes (omalizumab 1 IgE % IgG-IgE). In binding, omalizumab pushes the reaction toward the IgG-IgE complex, which is incapable of binding to IgE receptors, thereby suppressing free IgE and reducing the clinical symptoms of allergic asthma. Pharmacoki- netic-pharmacodynamic (PK-PD) models based on this binding reaction have been published. 14,15 However, although the causal role of IgE in allergic disease is well established, the relationship between free IgE and clinical symptoms of asthma has not been ac- curately quantified. We reconstructed for each patient the full time courses of omalizumab, free IgE, and total IgE from collected sam- ples including, importantly, the posttreatment follow-up period by using a PK-PD binding model of the same form as previously pub- lished. 15 From these time courses, model-derived omalizumab and free IgE levels could be determined for time points when no di- rectly sampled data were available, from the initial state, through IgE suppression, to the return to baseline at the end of the fol- low-up period when symptoms were returning. We then examined the relationship between the model-derived omalizumab and free IgE concentrations with changes in clinical outcomes in patients with severe persistent allergic asthma. METHODS A robust PK-PD model 15 was used to calculate serum concentrations of free IgE, omalizumab, and total IgE at any point during treatment with From a the St Louis University School of Medicine; b Modeling and Simulation, Novartis Pharma AG, Basel; c Novartis Pharmaceuticals Corp, East Hanover; and d Novartis Horsham Research Center. Supported by Novartis Pharma AG. Disclosure of potential conflict of interest: R. G. Slavin receives grant support from Schering-Plough and Accentia and is on the speakers’ bureau for Genentech-Novartis. C. Ferioli is employed by Novartis Pharma AG. S. J. Tannenbaum owns stock in Novartis and is employed by Novartis Pharmaceuticals. C. Martin owns stock in Novartis and is employed by Novartis Horsham Research Center. M. Blogg owns stock in Novartis and is employed by Novartis. P. J. Lowe owns stock in Novartis and is employed by Novartis Pharmaceuticals. Received for publication November 8, 2007; revised September 3, 2008; accepted for publication September 4, 2008. Reprint requests: Philip J. Lowe, PhD, Modeling and Simulation, Novartis Pharma AG, Lichtstrasse 35, CH-4056 Basel, Switzerland. E-mail: [email protected]. 0091-6749/$36.00 Ó 2009 American Academy of Allergy, Asthma & Immunology doi:10.1016/j.jaci.2008.09.050 107
Transcript of Asthma symptom re-emergence after omalizumab withdrawal correlates well with increasing IgE and...

Original article
Asthma symptom re-emergence after omalizumabwithdrawal correlates well with increasing IgE anddecreasing pharmacokinetic concentrations
Raymond G. Slavin, MD,a Caterina Ferioli, BSc,b Stacey J. Tannenbaum, PhD,c Carmen Martin, PhD,d Martin Blogg, BSc,d
and Philip J. Lowe, PhDb St Louis, Mo, Basel, Switzerland, East Hanover, NJ, and Horsham, United Kingdom
Background: Physicians have questioned whether omalizumabcan be discontinued or the dose reduced after clinicalimprovement is seen in patients with severe asthma.Objectives: To examine the relationships among omalizumab,free IgE, and clinical outcomes in a randomized, placebo-controlled trial in patients with severe persistent allergic asthmafollowing a posology based on pretreatment total IgE and bodyweight.Methods: A pharmacokinetic-pharmacodynamic binding modelwas used to calculate free IgE, omalizumab, and total IgEconcentrations during the 28-week treatment and 16-weekfollow-up of the INvestigation of Omalizumab in seVere AsthmaTrEatment (INNOVATE) study. These were plotted against themean changes in the total asthma symptom score, morning peakexpiratory flow, and rescue medication use for physician-definedtreatment responders and nonresponders.Results: The model accurately fitted omalizumab and free andtotal IgE, allowing reconstruction of the entire time course foreach patient. Free IgE was rapidly suppressed below the 50 ng/mL (20.8 IU/mL) target, although there was a notable periodbefore clinical measures stabilized. After treatment cessation,free IgE and omalizumab returned toward baseline and, after adelay, asthma symptoms re-emerged. Model-derivedomalizumab and free IgE concentrations correlated well withchanges in clinical outcomes, particularly in omalizumab-treated responders. Asthma symptoms exhibited differentcorrelations during response onset compared with responseoffset (hysteresis), indicative of physiological time delaysbetween changes in IgE levels and pulmonary function.Conclusion: Omalizumab and free IgE correlated well withclinical symptoms. Reducing omalizumab doses below those in
From athe St Louis University School of Medicine; bModeling and Simulation, Novartis
Pharma AG, Basel; cNovartis Pharmaceuticals Corp, East Hanover; and dNovartis
Horsham Research Center.
Supported by Novartis Pharma AG.
Disclosure of potential conflict of interest: R. G. Slavin receives grant support from
Schering-Plough and Accentia and is on the speakers’ bureau for Genentech-Novartis.
C. Ferioli is employed by Novartis Pharma AG. S. J. Tannenbaum owns stock in
Novartis and is employed by Novartis Pharmaceuticals. C. Martin owns stock in
Novartis and is employed by Novartis Horsham Research Center. M. Blogg owns stock
in Novartis and is employed by Novartis. P. J. Lowe owns stock in Novartis and is
employed by Novartis Pharmaceuticals.
Received for publication November 8, 2007; revised September 3, 2008; accepted for
publication September 4, 2008.
Reprint requests: Philip J. Lowe, PhD, Modeling and Simulation, Novartis Pharma AG,
Lichtstrasse 35, CH-4056 Basel, Switzerland. E-mail: [email protected].
0091-6749/$36.00
� 2009 American Academy of Allergy, Asthma & Immunology
doi:10.1016/j.jaci.2008.09.050
the dosing table cannot be recommended; the resulting increasein free IgE would cause a deterioration in asthma control.(J Allergy Clin Immunol 2009;123:107-13.)
Key words: Asthma, omalizumab, pharmacokinetics, pharmacody-namics, IgE
Allergic (IgE-mediated) asthma is characterized by the pres-ence of IgE antibodies against common allergens.1-3 When aller-gen cross-links specific IgE bound to high-affinity IgE (FceRI)receptors on the surface of basophils and mast cells, proinflamma-tory mediators are released that trigger and perpetuate airwaysymptomatology.4,5 Omalizumab, an anti-IgE mAb, binds to theFc region of all forms of circulating IgE, regardless of IgE speci-ficity, preventing IgE-mediated responses,6,7 and downregulatingFceRI expression on mast cells and basophils.8 The efficacy andtolerability of omalizumab have been demonstrated in patientswith moderate-to-severe and severe persistent allergic (IgE-medi-ated) asthma.9-11 Clinical benefit with omalizumab is observedwhen serum free IgE levels are reduced to 50 ng/mL or less.12,13
Omalizumab dosing is based on pretreatment total serum IgE leveland body weight, and calculated using a dosing table.
Omalizumab binds to IgE to reversibly form IgG-IgE complexes(omalizumab 1 IgE % IgG-IgE). In binding, omalizumab pushesthe reaction toward the IgG-IgE complex, which is incapable ofbinding to IgE receptors, thereby suppressing free IgE andreducing the clinical symptoms of allergic asthma. Pharmacoki-netic-pharmacodynamic (PK-PD) models based on this bindingreaction have been published.14,15 However, although the causalrole of IgE in allergic disease is well established, the relationshipbetween free IgE and clinical symptoms of asthma has not been ac-curately quantified. We reconstructed for each patient the full timecourses of omalizumab, free IgE, and total IgE from collected sam-ples including, importantly, the posttreatment follow-up period byusing a PK-PD binding model of the same form as previously pub-lished.15 From these time courses, model-derived omalizumab andfree IgE levels could be determined for time points when no di-rectly sampled data were available, from the initial state, throughIgE suppression, to the return to baseline at the end of the fol-low-up period when symptoms were returning. We then examinedthe relationship between the model-derived omalizumab and freeIgE concentrations with changes in clinical outcomes in patientswith severe persistent allergic asthma.
METHODSA robust PK-PD model15 was used to calculate serum concentrations of
free IgE, omalizumab, and total IgE at any point during treatment with
107

J ALLERGY CLIN IMMUNOL
JANUARY 2009
108 SLAVIN ET AL
Abbreviations used
PEF: Peak expiratory flow
PK-PD: Pharmacokinetic-pharmacodynamic
omalizumab, from information on the patient’s body weight, baseline (total)
IgE concentration, dosing history, and concentrations of omalizumab, free
IgE, and total IgE during treatment. Model-derived omalizumab and free IgE
concentrations were then correlated with mean changes in clinical measures
(total asthma symptom score, morning peak expiratory flow [PEF], and rescue
medication use) from a clinical trial in patients with severe persistent allergic
asthma. The correlation between omalizumab and free IgE with clinical
measures was further examined according to whether the patient responded to
omalizumab.
Clinical dataThe analysis included data from 2 clinical studies: a randomized, double-
blind, placebo-controlled study in patients with inadequately controlled severe
persistent allergic (IgE-mediated) asthma (INNOVATE study),10 and a single-
dose bioequivalence study.16 Both studies were approved by Institutional Re-
view Boards, and all patients gave informed written consent. The studies were
conducted in accordance with the declaration of Helsinki and Good Clinical
Practice guidelines.
The INNOVATE study was composed of a 28-week treatment period and a
16-week follow-up after cessation of treatment. Omalizumab was adminis-
tered by subcutaneous injection according to a dosing table.17 Further details
of the INNOVATE study have been published previously.10
The bioequivalence study was a single-dose, parallel-group study of
omalizumab (150 mg and 300 mg subcutaneously) in healthy but atopic
volunteers with IgE above normal levels at baseline, in the range 30 to 300 IU/
mL at the screening visit.
Measurement of omalizumab and total IgE and free
IgE concentrationsSamples were obtained from 476 patients in the INNOVATE study and
analyzed for total omalizumab, free IgE, and total IgE at weeks 1, 2, 12, 28, 32,
and 44 and applied to the PK-PD model. Given that there were only limited
concentration data available from the INNOVATE study, data from 152
subjects in the richly sampled bioequivalence study were also included.
Samples were collected just before dosing, then at 6 and 12 hours postdose,
then on days 2, 3, 4, 6, 8, 11, 15, 22, 29, 42, 57, 71, and 85.
Details of techniques for measuring omalizumab and free and total IgE
have been reported previously.12,15
Omalizumab-IgE modelThe nonlinear mixed-effect model of omalizumab-IgE turnover and
binding, including validation through posterior predictive checking, has
been published previously.15 The same model was used in this analysis to es-
timate omalizumab and free IgE concentrations at time points when clinical
measures were assessed. The model was fitted simultaneously to the data
from both studies, producing individually fitted curves for each patient by us-
ing a post hoc Bayesian procedure conditioned on each patient’s data. Differ-
ences between this study model and the model previously published15 were the
following: (1) an interpatient variance was introduced in the omalizumab-IgE
dissociation constant, Kd, before examination of the clinical outcome, to ac-
count for the possibility that varying expression levels of competing factors
(eg, unquantifiable FceRI and II expressed in the body) may exist for omali-
zumab binding with IgE; and (2) given the larger population available for pa-
rameter estimation, body weight covariates were introduced on the IgE
production and clearance parameters in addition to the covariates previously
described.15
Correlation between omalizumab/free IgE
concentration and clinical measuresMean changes from baseline (in the INNOVATE study) were determined
for total asthma symptom score (sum of the daytime [range, 0–4], nighttime
[0–4] and morning [0–1] scores), mean morning PEF, and rescue mediation
use (mean number of daily puffs). For each patient, the changes from baseline
in clinical measures were summarized into 28-day arithmetic means. The
midpoint of each of the averaged periods—that is, day 14, 42, 70, 98, and so
forth—was then used to plot clinical measures against model-derived
omalizumab and free IgE concentrations at those time points. To account
for patients receiving differing doses (as a function of body weight and
baseline IgE according to the dosing table), omalizumab concentrations were
expressed as a percentage of the steady-state average concentration for each
patient, then summarized to arithmetic means. The steady-state average
concentration was calculated from the model estimates of each patient’s
parameters.
Responders to omalizumab treatmentMean changes from baseline in clinical measures were also determined for
patients who responded to omalizumab after 28 weeks of therapy, according to
a validated assessment,18 and correlated with model-derived omalizumab and
free IgE concentrations. In this study, 62% of the omalizumab-treated patients
and 43% of the placebo-treated patients were defined as responders. Further
information on the assessment of response is provided in this article’s Online
Repository at www.jacionline.org.
RESULTSThere were a total of 10,872 observations (3221 omalizumab,
4450 total IgE, and 3201 free IgE) from 152 volunteers in thesingle-dose bioequivalence study and 476 patients in the multiple-dose INNOVATE study. Baseline demographic data are summa-rized in Table I.
Omalizumab and free IgE concentrationsThe model fit both single-dose data from healthy atopic
volunteers and longer-term multiple-dose data from patientswith severe persistent allergic asthma well. Example fits of themodel to data from 2 individual patients are shown in Fig 1, Aand B. After a single omalizumab dose, omalizumab concentra-tions rose above 10,000 ng/mL, whereas free IgE was sup-pressed to approximately 10 ng/mL. Free IgE was further
TABLE I. Patient numbers and baseline demographic data for
studies contributing to the population pharmacokinetic analysis
INNOVATE study
Parameter
Bioequivalence
study
Omalizumab
group
Placebo
group
No. of patients included
in the analyses
152 245 231
Age (y)
Mean (SD) 35 (12) 42 (14) 43 (14)
Range 18-64 12-79 14-74
Body weight (kg)
Mean (SD) 71 (12) 79 (20) 78 (18)
Range 48-91 45-148 39-146
Baseline total serum
IgE (ng.mL-1)
Mean (SD) 186 (124) 488 (371) 463 (381)
Range 47-620 51-1692 53-2173

J ALLERGY CLIN IMMUNOL
VOLUME 123, NUMBER 1
SLAVIN ET AL 109
FIG 1. Example fits of the model for a single 300-mg dose (A) and multiple 4-weekly 150-mg doses (B) to
samples collected from 2 individual patients showing model fits for each patient’s plasma omalizumab,
total IgE, and free IgE. Individual patient predictions for free IgE in all omalizumab-treated patients from
the INNOVATE study (C).
suppressed with multiple dosing as the drug accumulated. At thesame time, total IgE increased, because of the formation of oma-lizumab-IgE complexes, which have a longer half-life than freeIgE.14,15 Sampled free IgE from the INNOVATE study popula-tion produced a narrow range of concentrations (5-50 ng/mL;Fig 1, C). Using the model to reconstruct each patient’s individ-ual curve gave a broader range of IgE concentrations with whichto correlate clinical measures (Fig 1, C). All 3 markers were ac-curately described by the model, and each contributed informa-tion to the others through the molecular binding equation, soeven when data were not available for free IgE when it wentabove the 150 ng/mL upper limit of quantitation during the fol-low-up period, it was estimable from the total IgE and omalizu-mab measurements. Interestingly, omalizumab only justachieves steady-state by the end of the 28-week treatment period(Fig 1, B), indicating that there may be slow kinetic componentsin the omalizumab-IgE system beyond that of the conventionallyreported 26-day terminal half-life of the total antibody (free drugplus drug-IgE complex).17
Because the model fitted the observed data well, the entire timecourse of omalizumab, free IgE, and total IgE could bereconstructed for patients in the INNOVATE study, even thoughsamples were collected on only 6 visits. From Fig 1, C, it can beseen that the omalizumab dosing table successfully maintains freeIgE below 50 ng/mL for the majority of the patients with severeasthma over the 28-week treatment period with omalizumab.The omalizumab dosing table successfully maintained measuredtrough free IgE below 50 ng/mL (20.8 IU/mL) over the 28 weeksin 95% (198/209) of omalizumab-treated patients compared with6% (12/200) placebo-treated patients. From the model fittedcurves, which eliminated the residual (mostly assay-related) er-ror, 99% of omalizumab-treated responders and 98% of nonre-sponders achieved free IgE <50 ng/mL.
Data for those patients who discontinued omalizumab duringthe treatment period were retained, because they continued toprovide information on the relationship between free IgE andclinical outcomes. In these patients, omalizumab concentrations
decreased and, at the same time, free IgE increased towardbaseline levels (Fig 1, C).
After treatment cessation, free IgE returns toward baselinearound 18 to 20 weeks after the last dose in the majority ofpatients. Unfortunately, for a conventional analysis based ondirect sampling and assay, free IgE rises above the 150 ng/mLupper limit of quantitation in the majority of patients. Thislimitation can be overcome, because omalizumab and free IgEconcentrations can be calculated for individual patients at anytime point in the study by using the individually fitted curves,supported with information from the other measurements acrosstime, across the 3 markers, and across patients.
Correlation of omalizumab and free IgE
concentrations with clinical measuresAlthough free IgE is extensively and very rapidly suppressed
after commencing omalizumab (Fig 1, A-C), there was a notableperiod before total symptom score (Figs 2, A and 3, A), PEF (Figs2, B and 3, B), and rescue medication use (Figs 2, C and 3, C)achieved their new equilibrium values in the overall omalizu-mab-treated patients and omalizumab-treated responder popula-tions at around 12 to 16 weeks. The omalizumab concentrationspredicted by the model are shown in Figs 2, D and 3, D and 2,E and 3, E, which also show the corresponding predictions forfree serum IgE. It can be seen from Fig 3, E, that IgE levels inboth responders and nonresponders are equally suppressed. Aftercessation of treatment, omalizumab concentrations fall back tobaseline (Figs 2, D and 3, D), free IgE returns to baseline (Figs2, E and 3, E) and, after a slight delay, the clinical symptoms ofasthma re-emerge (Figs 2, A-C and 3, A-C). The extent of the oma-lizumab-induced treatment effect was notably greater than that ofthe placebo, although neither had returned completely to baselineby the final measurement time in the study. Whether this repre-sents a persistent effect remains to be established.
Once the time courses of the clinical responses were estab-lished, model-derived concentrations of omalizumab and free IgE

J ALLERGY CLIN IMMUNOL
JANUARY 2009
110 SLAVIN ET AL
could be plotted against the clinical measurements. The correla-tions of omalizumab and free IgE with changes from baseline inclinical measures are shown in Fig 4. At the start of the study, freeIgE is at baseline and omalizumab at 0% of the steady-state level.With treatment, omalizumab concentrations increase and free IgEconcentrations fall, with the first point plotted at 14 days the mid-point of the first 28-day data collection period. Omalizumab andfree IgE concentrations then equilibrate as the patients approachsteady-state, and the changes in symptom score, PEF, and rescuemedication use follow. When omalizumab is discontinued, oma-lizumab decreases, free IgE increases, and the 3 symptommeasures return toward their pretreatment values. That the trajec-tory of the return curve is not the same as that of the on-treatmentcurve—forming a hysteresis loop—is indicative of a delay in thebiological system whereby pulmonary function takes some timeto respond to changes in free IgE levels. The gap between theon-treatment and off-treatment curves will be related to the lengthof time it takes for the signal from IgE to be translated into a mea-surable clinical response; with a shorter translation time, the on-curves and off-curves will be closer together.
The correlation is even more pronounced in responders toomalizumab (Fig 5). Unlike responders, nonresponders present a
FIG 2. Symptom scores (A), PEF (B), and rescue medication use (C) in the
overall omalizumab-treated population compared with placebo. The black
bar above each plot designates the treatment duration. Model-predicted
omalizumab concentrations (D) and free IgE concentrations (E) are also
shown.
random path centered on no change in the 3 variables (Figs 3 and5). It was interesting to note that the omalizumab concentrationsreached higher absolute values in the responder group (Fig 3, D).However, on closer examination, it was apparent that the meanbaseline IgE levels were significantly lower for the nonresponder(least-squares mean, 299 ng/mL) than the responder group (least-squares mean, 379 ng/mL; P < .01). Although both respondersand nonresponders reached close to 100% of their steady-state av-erage concentrations (Fig 5), nonresponders received lower abso-lute doses, because the dosing table adjusts dose by milligram perkilogram per unit of baseline IgE. Free IgE and omalizumablevels did not correlate with the 3 symptom measures in the pla-cebo group; a version of Fig 5 that includes placebo-treated pa-tients is available as Fig E1 in the Online Repository atwww.jacionline.org.
DISCUSSIONA previous mechanism-based population PK-PD model of the
binding of an anti-IgE mAb15 has been used to calculate individualpatient concentrations of drug and free IgE throughout and aftertreatment with omalizumab in a phase III clinical study,10 even
FIG 3. Symptom scores (A), PEF (B), rescue medication use (C), model-pre-
dicted omalizumab concentrations (D), and model-predicted free IgE con-
centrations (E) in response to omalizumab in physician-evaluated
responders and nonresponders.

J ALLERGY CLIN IMMUNOL
VOLUME 123, NUMBER 1
SLAVIN ET AL 111
FIG 4. The change from the baseline (time zero) value of the total symptom score, morning PEF (L/min), and
rescue medication use (puffs) correlate with free IgE (A) and omalizumab (B) concentrations in the overall
omalizumab-treated population. To allow comparison across many different dosing levels, omalizumab is
expressed as a percentage of each individual patient’s steady-state average concentration.
FIG 5. Correlation between levels of free IgE (A) and omalizumab (B) and clinical outcomes in responders
(circles) and nonresponders (crosses) while on treatment and after cessation of omalizumab therapy. To
allow comparison across many different dosing levels, omalizumab is expressed as a percentage of each
individual patient’s steady-state average concentration.
though actual sampling was limited. To achieve this with good es-timates of drug absorption parameters and to demonstrate that themodel accurately describes the return of free IgE to baseline, datafrom a richly sampled bioequivalence study were merged with thephase III study dataset. The model was fitted simultaneously to theomalizumab, total IgE, and free IgE; because both the increase intotal IgE and the suppression of free IgE are responsive to
omalizumab, the use of the model allows a more precise estimateof each patient’s free IgE than would be possible with a single freeIgE assay. As previously demonstrated,15 such models enable therange of free IgE suppression to be calculated for any combinationof dose, regimen, and the major covariates, body weight and base-line IgE. Administration of the appropriate dose of omalizumabdetermined by using the dosing table appears to suppress free

J ALLERGY CLIN IMMUNOL
JANUARY 2009
112 SLAVIN ET AL
IgE adequately below the target 50 ng/mL, as previously demon-strated.15 When examining our model-predicted relationship, it isnoteworthy that as free IgE is suppressed even further (toward 10ng/mL), clinical measures appear to continue to improve.
The suppression of IgE appears to precede the clinical effectsof omalizumab on clinical measures. This is analogous to thedelay seen between the psoriasis activity and severity indexresponse to the rapid suppression of free CD11a induced withefalizumab.19 As free IgE returns to baseline, clinical symptomsof asthma re-emerge. The delays in both onset of clinical responseand the resumption of symptoms after withdrawal of omalizumabare most likely a result of the time taken for the physiologic sys-tem to readjust to the changed steady-state levels of IgE—in ef-fect, healing once IgE is lowered to normal levels, and reinjuryafter treatment cessation. These physiologic responses includethe known desensitization of effector cells with omalizumab,where reduced free serum IgE causes a slow downregulation ofthe FceRI receptor; thus, at least 12 weeks’ omalizumab treatmentis needed before evaluation of clinical benefit.8,18,20,21 Indeed,data from the INNOVATE study presented here show a plateauin the improvements in asthma symptoms and lung function ataround 12 to 16 weeks.
When omalizumab and free IgE concentrations were correlatedwith clinical outcomes, the classical curvilinear or logarithmicsigmoidal S-shaped relationship typical of ligand-receptor bind-ing and pharmacologic responses was apparent. The smooth na-ture of these clinical pharmacodynamic responses for all 3clinical measures in omalizumab-treated responders clearly indi-cates the presence of a real phenomenon. This is similar to thephysiological responses noted by other authors examining there-expression of FceRI on basophils after reduction or discontin-uation of omalizumab.8,22 Measurement of FceRIa expression onbasophils in subjects who received omalizumab for 52 weeksshowed that 8 weeks after omalizumab discontinuation, freeIgE levels rose (but did not reach baseline), paralleled by a risein basophil FceRIa expression to 80% of baseline, and histaminerelease responses, which returned to baseline.22 Therefore, ifdoses of omalizumab were to be reduced, free IgE would no lon-ger be adequately suppressed, and clinical symptoms might in-crease. Examination of Fig 5 also suggests that if patients whocould potentially respond to omalizumab are underdosed accord-ing to body weight and/or baseline total IgE, free IgE levels willbe partially suppressed, and a corresponding partial improvementin clinical outcomes may be seen, although not to the threshold atwhich they would be defined as responders. The probability of im-provement in symptoms decreases as the degree of underdosingincreases. Because the clinical symptoms of nonrespondersshow random fluctuations around baseline without any tendencytoward improvement despite adequate suppression of free IgE(Fig 5), further IgE suppression is unlikely to achieve a clinicalbenefit. IgE may not be the driving factor behind asthma in thesepatients. Although beyond the scope of this study, it could behypothesized that patients’ ratio of specific IgE to total IgE orinterpatient variability in the expression of FceRI on effectorcells, with subsequent reduction in the patient’s sensitivity tofree IgE reduction with omalizumab, may have some influenceon response or lack thereof.
The results presented here represent an average response acrossmany patients. It must be remembered that within any 1 cell of theomalizumab dosing table, there will exist a range of doses whenexpressed as milligram per kilogram body weight per IU/mL IgE.
This will generate a range of effective doses, especially in someregions of the table, such as 30 to 100 IU/mL and 30 to 60 kg,where there is a 7-fold range in mg/kg/IgE (IU/mL). The omali-zumab-IgE model automatically takes this into account when es-timating individual free IgE levels; higher mg/kg/IgE (IU/mL),caused by lower body weight and/or baseline IgE, will translateinto greater suppression of free IgE beyond the target level andtherefore, given the correlation between free IgE and symptoms,a greater chance of clinical benefit.
In summary, we used a robust PK-PD model that allowed thecalculation of free IgE, omalizumab, and total IgE concentrationsat any point in time during omalizumab therapy—revealing freeIgE concentrations at a series of time points, away from theplanned investigator visits, to match diary-derived asthma symp-tom data. In patients treated with omalizumab and dosed inaccordance with the dosing table, model-derived omalizumab andfree IgE concentrations correlated well with changes in clinicalmeasures of asthma, particularly in responders, revealing for thefirst time both the time-dependent and concentration-dependentrelationship between free IgE and clinical outcomes. This rela-tionship exhibited classic pharmacologic hysteresis loops indic-ative of delays between IgE and downstream physiological eventsthat are manifest as clinical symptoms of asthma. In conclusion,this model-based analysis demonstrates that reducing omalizu-mab concentrations below those achieved with the dosing tablewould not suppress free IgE effectively, and would likely result inthe re-emergence of symptoms. Although it remains to bedetermined whether prolonged use of omalizumab has anydisease-modifying properties, on the basis of this evidence, adose reduction after 6 months of treatment cannot be recom-mended in patients judged to have responded to omalizumab.
We thank professional medical writers Dr Dominic Hague (contracted
writer) and Thomas McMurray (ACUMED) for editorial assistance with the
manuscript, and Dr Frank Albers for his critical review and helpful comments
on the manuscript.
Key messages
d Free IgE is correlated with symptoms of asthma, albeit ina time-dependent manner.
d Reduction in omalizumab buffering allows free IgE to in-crease and therefore increases asthma symptoms.
REFERENCES
1. Burrows B, Martinez FD, Halonen M, Barbee RA, Cline MG. Association of
asthma with serum IgE levels and skin-test reactivity to allergens. N Engl J Med
1989;320:271-7.
2. Holgate S, Casale T, Wenzel S, Bousquet J, Deniz Y, Reisner C. The anti-inflam-
matory effects of omalizumab confirm the central role of IgE in allergic inflamma-
tion. J Allergy Clin Immunol 2005;115:459-65.
3. Global Initiative for Asthma (GINA). Global strategy for asthma management and
prevention. Issued 1995 (NIH pub no. 02–3659); updated 2002–2007. Available at:
http://www.ginasthma.org. Accessed July 23, 2008.
4. Prussin C, Metcalfe DD. IgE, mast cells, basophils, and eosinophils. J Allergy Clin
Immunol 2003;111:S486-94.
5. Novak N, Bieber T. Allergic and nonallergic forms of atopic diseases. J Allergy
Clin Immunol 2003;112:252-62.
6. Presta LG, Lahr SJ, Shields RL, Porter JP, Gorman CM, Fendly BM, et al. Human-
ization of an antibody directed against IgE. J Immunol 1993;151:2623-32.
7. Presta L, Shields R, O’Connell L, Lahr S, Porter J, Gorman C, et al. The binding site on
human immunoglobulin E for its high-affinity receptor. J Biol Chem 1994;269:26368-73.

J ALLERGY CLIN IMMUNOL
VOLUME 123, NUMBER 1
SLAVIN ET AL 113
8. MacGlashan DW Jr, Bochner BS, Adelman DC, Jardieu PM, Togias A, McKenzie-
White J, et al. Down-regulation of FceRI expression on human basophils during in
vivo treatment of atopic patients with anti-IgE antibody. J Immunol 1997;158:1438-45.
9. Bousquet J, Cabrera P, Berkman N, Buhl R, Holgate S, Wenzel S, et al. The effect
of treatment with omalizumab, an anti-IgE antibody, on asthma exacerbations and
emergency medical visits in patients with severe persistent asthma. Allergy 2005;
60:302-8.
10. Humbert M, Beasley R, Ayres J, Slavin R, Hebert J, Bousquet J, et al. Benefits of
omalizumab as add-on therapy in patients with severe persistent asthma who are
inadequately controlled despite best available therapy (GINA 2002 step 4 treat-
ment): INNOVATE. Allergy 2005;60:309-16.
11. Corren J, Casale T, Lanier BQ, Blogg M, Reisner C, Gupta N. Omalizumab is well
tolerated in adolescent/adult patients (�12 years) with moderate-to-severe persis-
tent asthma [abstract]. J Allergy Clin Immunol 2005;115:S75.
12. Adelroth E, Rak S, Haahtela T, Aasand G, Rosenhall L. Recombinant humanized
mAb-E25, an anti-IgE mAb, in birch pollen-induced seasonal allergic rhinitis. J Al-
lergy Clin Immunol 2000;106:253-9.
13. Hochhaus G, Brookman L, Fox H, Johnson C, Matthews J, Ren S, et al. Pharma-
codynamics of omalizumab: implications for optimised dosing strategies and clin-
ical efficacy in the treatment of allergic asthma. Curr Med Res Opin 2003;19:
491-8.
14. Meno-Tetang GML, Lowe PJ. On the prediction of the human response: a recycled
mechanistic PK/PD approach. Basic Clin Pharmacol Tox 2005;96:182-92.
15. Hayashi N, Tsukamoto Y, Sallas WM, Lowe PJ. A mechanism-based binding
model for the population pharmacokinetics and pharmacodynamics of omalizu-
mab. Br J Clin Pharmacol 2006;63:548-61.
16. Data on file. Novartis Pharma AG, Basel, Switzerland.
17. Omalizumab (Xolair) summary of product characteristics. 2007. Available at:
http://www.fda.gov/cder/foi/label/2007/103976s5102lbl.pdf. Accessed March 18,
2008.
18. Bousquet J, Rabe K, Humbert M, Chung KF, Berger W, Fox H, et al. Predicting and
evaluating response to omalizumab in patients with severe persistent allergic
asthma. Respir Med 2007;101:1483-92.
19. Ng C, Joshi A, Dedrick RL, Garovoy MR, Bauer RJ. Pharmacokinetic-pharmaco-
dynamic-efficacy analysis of efalizumab in patients with moderate to severe psori-
asis. Pharm Res 2005;22:1088-100.
20. Lin H, Boesel KM, Griffith DT, Prussin C, Foster B, Romero FA, et al. Omalizu-
mab rapidly decreases nasal allergic response and FceRI on basophils. J Allergy
Clin Immunol 2004;113:297-302.
21. Beck LA, Marcotte GV, MacGlashan D, Togias A, Saini S. Omalizumab-induced
reductions in mast cell FceRI expression and function. J Allergy Clin Immunol
2004;114:527-30.
22. Saini SS, MacGlashan DW Jr, Sterbinsky SA, Togias A, Adelman DC, Lichtenstein
LM, et al. Down-regulation of human basophil IgE and FC epsilon RI alpha surface
densities and mediator release by anti-IgE-infusions is reversible in vitro and in
vivo. J Immunol 1999;162:5624-30.

J ALLERGY CLIN IMMUNOL
JANUARY 2009
113.e1 SLAVIN ET AL
METHODS
Response assessmentAnalyses of data from the omalizumab clinical trials program have shown
that there is no reliable baseline characteristic predictive of a therapeutic
response to omalizumab. The physician’s overall assessment was the most
meaningful measure of response to omalizumab therapy because it identified
61% of omalizumab-treated patients as responders, whereas other single and
composite measures only identified up to 50% of true responders.E1 This com-
posite measure encompasses multiple aspects of response; it is based on clin-
ical assessments including patient interviews, review of medical notes,
spirometry and diaries of symptoms, rescue medication use, and PEF. The
physician’s overall assessment was graded in a 5-level evaluation of asthma
control: complete control, marked improvement in control, discernable but
limited control, no appreciable change, and worsening in control. Responders
were defined as those with marked improvement or complete control.
In this study, 62% of the evaluable omalizumab-treated patients in the
modeling dataset and 43% of placebo-treated patients were defined as re-
sponders. The number of omalizumab-treated and placebo-treated patients in
each response level is shown in Table E1. Responders are not uniformly distrib-
uted across the groups; as expected, omalizumab appears to shift a larger number
of patients toward the complete control and marked improvement in control
levels. Response to therapy in the placebo group in this analysis was also noted
and may be attributable to the well documented placebo effect observed in
asthma studies caused by increased physician contact compliance with concom-
itant medications.E2
Exploratory analysis: Association between baseline
total IgE and response to omalizumabDuring development of the model, exploratory analysis of the association
between baseline total IgE and response to omalizumab was carried out by
subgrouping patients by baseline IgE. The proportions of responders and non-
responders in each group were similar (results not shown). Response to oma-
lizumab therefore appears to be independent of baseline total IgE.
Correlation between free IgE level and omalizumab
concentrations and asthma symptoms in the
placebo groupThere was no correlation between mean free IgE levels or mean
omalizumab concentrations and asthma symptoms in the placebo group. In
Fig E1, mean free IgE can be seen to hover around baseline, and omalizumab
concentrations remain at 0. Changes in total symptom score, rescue medica-
tion use, and PEF are seen to hover close to baseline in those placebo-treated
patients defined as nonresponders, whereas more pronounced changes can be
observed in those placebo-treated patients who were defined as responders.
REFERENCES
E1. Bousquet J, Rabe K, Humbert M, Chung KF, Berger W, Fox H, et al. Predicting
and evaluating response to omalizumab in patients with severe persistent allergic
asthma. Respir Med 2007;101:1483-92.
E2. Joyce DP, Jackevicius C, Chapman KR, McIvor RA, Kesten S. The placebo effect
in asthma drug therapy trials: a meta-analysis. J Asthma 2000;37:303-18.

J ALLERGY CLIN IMMUNOL
VOLUME 123, NUMBER 1
SLAVIN ET AL 113.e2
FIG E1. Correlation between levels of free IgE and omalizumab and clinical outcomes in responders (circles)
and nonresponders (crosses) while on treatment and after cessation of omalizumab therapy, including data
from placebo-treated patients. To allow comparison across many different dosing levels, omalizumab is
expressed as a percentage of each individual patient’s steady-state average concentration.
J ALLERGY CLIN IMMUNOL
JANUARY 2009
113.e3 SLAVIN ET AL
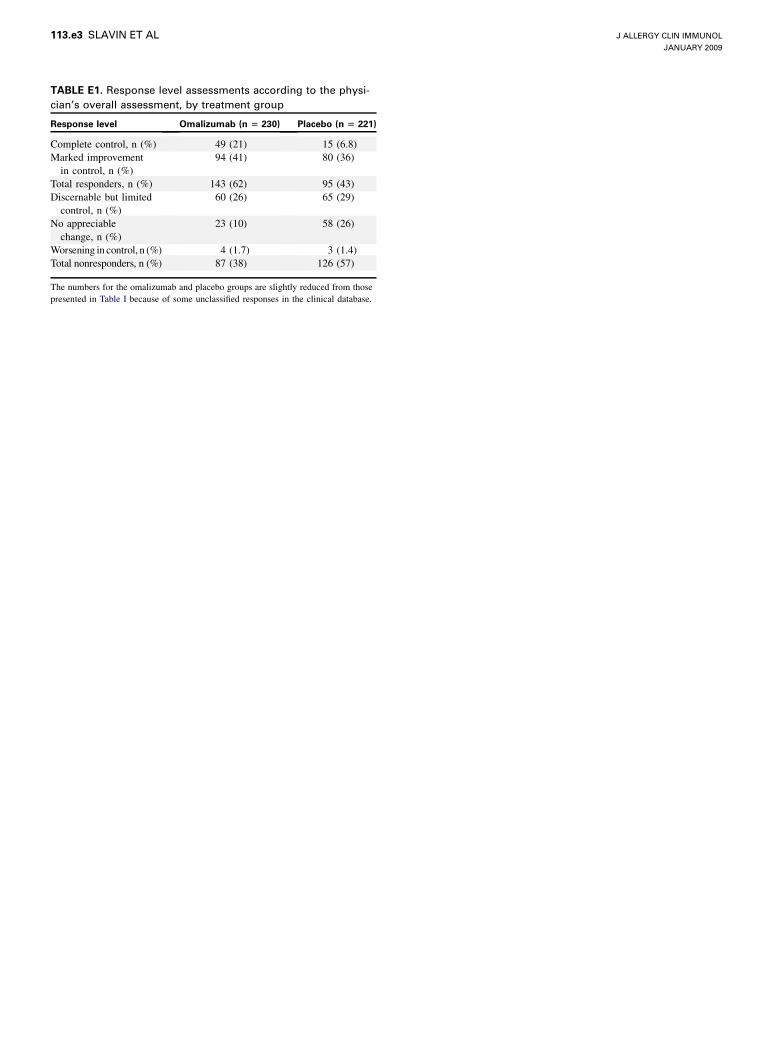
TABLE E1. Response level assessments according to the physi-
cian’s overall assessment, by treatment group
Response level Omalizumab (n 5 230) Placebo (n 5 221)
Complete control, n (%) 49 (21) 15 (6.8)
Marked improvement
in control, n (%)
94 (41) 80 (36)
Total responders, n (%) 143 (62) 95 (43)
Discernable but limited
control, n (%)
60 (26) 65 (29)
No appreciable
change, n (%)
23 (10) 58 (26)
Worsening in control, n (%) 4 (1.7) 3 (1.4)
Total nonresponders, n (%) 87 (38) 126 (57)
The numbers for the omalizumab and placebo groups are slightly reduced from those
presented in Table I because of some unclassified responses in the clinical database.




















