Symptom management and self-care for peripheral neuropathy in HIV/AIDS
11
Symptom management and self-care for peripheral neuropathy in HIV/AIDS P. K. NICHOLAS 1 , J. K. KEMPPAINEN 2 , G. E. CANAVAL 3 , I. B. CORLESS 1 , E. F. SEFCIK 4 , K. M. NOKES 5 , C. A. BAIN 6 , K. M. KIRKSEY 7 , L. SANZERO ELLER 8 , P. J. DOLE 9 , M. J. HAMILTON 4 , C. L. COLEMAN 10 , W. L. HOLZEMER 6 , N. R. REYNOLDS 11 , C. J. PORTILLO 6 , E. H. BUNCH 12 , D. J. WANTLAND 6 , J. VOSS 13 , R. PHILLIPS 5 , Y.-F. TSAI 14 , M. RIVERO MENDEZ 15 , T. G. LINDGREN 6 , S. M. DAVIS 16 , & D. M. GALLAGHER 17 1 Brigham and Women’s Hospital, MGH Institute of Health Professions, Boston, MA, USA, 2 University of North Carolina, Wilmington, NC, USA, 3 Universidad del Valle, Cali, Colombia, 4 Texas A & M University, Corpus Christi, TX, USA, 5 Hunter College, City University of New York, New York City, NY, USA, 6 University of California, San Francisco, San Francisco, CA, USA, 7 Ben Taub General Hospital, Houston, TX, USA, 8 Rutgers University, Newark, NJ, USA, 9 Greenwich House, New York City, NY, USA, 10 University of Pennsylvania, Philadelphia, PA, USA, 11 Ohio State University, Columbus, OH, USA, 12 University of Oslo, Oslo, Norway, 13 National Institutes of Health/National Institute of Neuromuscular Diseases Section, Bethesda, MD, USA, 14 Chang Gung University, Toa-Yuan, Taiwan, 15 University of Puerto Rico, San Juan, Puerto Rico, 16 Massachusetts General Hospital, Boston, MA, USA, and 17 New England AIDS Education and Training Center, Boston, MA, USA Abstract Peripheral neuropathy is the most common neurological complication in HIV and is often associated with antiretroviral therapy. As part of a larger study on self-care for symptoms in HIV disease, this study analyzed the prevalence and characteristics of peripheral neuropathy in HIV disease, sociodemographic and disease-related correlates and self-care strategies. A convenience sample of 1,217 respondents was recruited from data collection sites in several US cities, Puerto Rico, Colombia and Taiwan. Results of the study indicated that respondents with peripheral neuropathy (n /450) identified 20 self-care behaviors including complementary therapies, use of medications, exercise and rest and/or elevation of extremities. Ratings of frequency and effectiveness were also included. An activities checklist summarized into five categories of self-care behaviors including activities/thoughts, exercise, medications, complementary therapies and substance was used to determine self-care behaviors. Taking a hot bath was the most frequent strategy used by those with peripheral neuropathy (n /292) and received the highest overall rating of effectiveness of any self-management strategies included in this study at 8.1 (scale 1 10). Other self-care strategies to manage this symptom included: staying off the feet (n /258), rubbing the feet with cream (n /177), elevating the feet (n /236), walking (n /262), prescribed anti- epileptic agent (n /80), prescribed analgesics (n /84), over-the-counter medications (n /123), vitamin B (n /122), calcium supplements (n /72), magnesium (n /48), massage (n /156), acupuncture (n /43), reflexology (n /23) and meditation (n /80). Several behaviors that are often deemed unhealthy were included among the strategies reported to alleviate peripheral neuropathy including use of marijuana (n /67), cigarette smoking (n /139), drinking alcohol (n /81) and street drugs (n /30). Introduction Peripheral neuropathy is the most common neuro- logical complication in HIV disease (Dorsey & Morton, 2006; Ferrari et al., 2006). Involvement of the central or peripheral nervous system has been found in 30 63% of patients across the spectrum of HIV (Hall et al., 1991; Lichtenstein et al., 2005; Parry et al., 1997; Price, 1996; Schifitto et al., 2002, 2005; Swanson et al., 1998) and is often associated with antiretroviral therapy (Moore et al., 2000; Moyle & Sadler, 1998; Schifitto et al., 2002; Schooley, 1999; Simpson & Olney, 1992; Singer et al., 1993; Swanson et al., 1998). Few interna- tional studies exist that examine the global prevalence of neuropathy, however some studies (Nakagawa et al., 1997; Parry et al., 1997; Saarto & Wiffen, 2005) indicate that the pattern and Correspondence: Patrice K. Nicholas, DNSc., MPH., APRN., BC., MGH Institute of Health Professions, Graduate Program in Nursing, 36 1st Ave, Boston, MA 02129, USA. Tel: /1 (617) 726 1872. Fax: /1 (617) 724 6321. E-mail: [email protected] AIDS Care, February 2007; 19(2): 179 189 ISSN 0954-0121 print/ISSN 1360-0451 online # 2007 Taylor & Francis DOI: 10.1080/09540120600971083
Transcript of Symptom management and self-care for peripheral neuropathy in HIV/AIDS

Symptom management and self-care for peripheral neuropathyin HIV/AIDS
P. K. NICHOLAS1, J. K. KEMPPAINEN2, G. E. CANAVAL3, I. B. CORLESS1,
E. F. SEFCIK4, K. M. NOKES5, C. A. BAIN6, K. M. KIRKSEY7, L. SANZERO
ELLER8, P. J. DOLE9, M. J. HAMILTON4, C. L. COLEMAN10, W. L. HOLZEMER6,
N. R. REYNOLDS11, C. J. PORTILLO6, E. H. BUNCH12, D. J. WANTLAND6,
J. VOSS13, R. PHILLIPS5, Y.-F. TSAI14, M. RIVERO MENDEZ15, T. G. LINDGREN6,
S. M. DAVIS16, & D. M. GALLAGHER17
1Brigham and Women’s Hospital, MGH Institute of Health Professions, Boston, MA, USA, 2University of North Carolina,
Wilmington, NC, USA, 3Universidad del Valle, Cali, Colombia, 4Texas A & M University, Corpus Christi, TX, USA,5Hunter College, City University of New York, New York City, NY, USA, 6University of California, San Francisco, San
Francisco, CA, USA, 7Ben Taub General Hospital, Houston, TX, USA, 8Rutgers University, Newark, NJ, USA,9Greenwich House, New York City, NY, USA, 10University of Pennsylvania, Philadelphia, PA, USA, 11Ohio State
University, Columbus, OH, USA, 12University of Oslo, Oslo, Norway, 13National Institutes of Health/National Institute of
Neuromuscular Diseases Section, Bethesda, MD, USA, 14Chang Gung University, Toa-Yuan, Taiwan, 15University of Puerto
Rico, San Juan, Puerto Rico, 16Massachusetts General Hospital, Boston, MA, USA, and 17New England AIDS Education
and Training Center, Boston, MA, USA
AbstractPeripheral neuropathy is the most common neurological complication in HIV and is often associated with antiretroviraltherapy. As part of a larger study on self-care for symptoms in HIV disease, this study analyzed the prevalence andcharacteristics of peripheral neuropathy in HIV disease, sociodemographic and disease-related correlates and self-carestrategies. A convenience sample of 1,217 respondents was recruited from data collection sites in several US cities, PuertoRico, Colombia and Taiwan. Results of the study indicated that respondents with peripheral neuropathy (n�/450) identified20 self-care behaviors including complementary therapies, use of medications, exercise and rest and/or elevation ofextremities. Ratings of frequency and effectiveness were also included. An activities checklist summarized into fivecategories of self-care behaviors including activities/thoughts, exercise, medications, complementary therapies andsubstance was used to determine self-care behaviors. Taking a hot bath was the most frequent strategy used by thosewith peripheral neuropathy (n�/292) and received the highest overall rating of effectiveness of any self-managementstrategies included in this study at 8.1 (scale 1�10). Other self-care strategies to manage this symptom included: staying offthe feet (n�/258), rubbing the feet with cream (n�/177), elevating the feet (n�/236), walking (n�/262), prescribed anti-epileptic agent (n�/80), prescribed analgesics (n�/84), over-the-counter medications (n�/123), vitamin B (n�/122),calcium supplements (n�/72), magnesium (n�/48), massage (n�/156), acupuncture (n�/43), reflexology (n�/23) andmeditation (n�/80). Several behaviors that are often deemed unhealthy were included among the strategies reported toalleviate peripheral neuropathy including use of marijuana (n�/67), cigarette smoking (n�/139), drinking alcohol (n�/81)and street drugs (n�/30).
Introduction
Peripheral neuropathy is the most common neuro-
logical complication in HIV disease (Dorsey &
Morton, 2006; Ferrari et al., 2006). Involvement
of the central or peripheral nervous system has been
found in 30�63% of patients across the spectrum
of HIV (Hall et al., 1991; Lichtenstein et al., 2005;
Parry et al., 1997; Price, 1996; Schifitto et al., 2002,
2005; Swanson et al., 1998) and is often associated
with antiretroviral therapy (Moore et al., 2000;
Moyle & Sadler, 1998; Schifitto et al., 2002;
Schooley, 1999; Simpson & Olney, 1992; Singer
et al., 1993; Swanson et al., 1998). Few interna-
tional studies exist that examine the global
prevalence of neuropathy, however some studies
(Nakagawa et al., 1997; Parry et al., 1997; Saarto
& Wiffen, 2005) indicate that the pattern and
Correspondence: Patrice K. Nicholas, DNSc., MPH., APRN., BC., MGH Institute of Health Professions, Graduate Program in Nursing,
36 1st Ave, Boston, MA 02129, USA. Tel: �/1 (617) 726 1872. Fax: �/1 (617) 724 6321. E-mail: [email protected]
AIDS Care, February 2007; 19(2): 179�189
ISSN 0954-0121 print/ISSN 1360-0451 online # 2007 Taylor & Francis
DOI: 10.1080/09540120600971083

frequency of neuropathies are similar to those
reported from other continents. Research on neuro-
pathy in the pediatric population suggests that the
condition is under-recognized and under-reported
by clinicians (Floeter et al., 1997). In one study in
Brazil, peripheral neuropathy was found to occur
in one third of HIV-infected children but appeared
to have less severe features than the distal
sensory polyneuropathy described in adults (Araujo
et al., 2000).
Background
HIV-associated peripheral neuropathy is known to
exist in at least six patterns, with distal symmetrical
polyneuropathy (DSPN) as the most frequently
occurring type. Other patterns of peripheral
neuropathy include inflammatory demyelinating
polyneuropathy, progressive polyradiculopathy,
mononeuropathy multiplex, autonomic neuropathy
and diffuse infiltrative lymphocytosis syndrome
(Wulf et al., 2000). Lichtenstein et al. and the HIV
Outpatient Study Cohort (2005) found that of 2,515
patients in the sample, 329 (13.1%) received a
diagnosis of peripheral neuropathy.
Overview of DSPN
Distal symmetrical polyneuropathy is known to
occur mainly in patients with advanced immuno-
suppression and may also occur due to neurotoxicity
of antiretroviral therapy (Harrison & McArthur,
1995; Lichtenstein et al., 2005; Schifitto et al.,
2002, 2005; Swanson et al., 1998). Distal symme-
trical polyneuropathy can be a direct sequela of HIV
infection or a result of treatment with neurotoxic
drugs, particularly didanosine, dideoxycytidine,
stavudine, dapsone, metronidazole, isoniazid,
vincristine, pyridoxine and thalidomide (Verma
et al., 2004; Wulf et al., 2000). Recent literature
suggests that highly active antiretroviral therapy
(HAART) has changed the course of HIV-associated
DSPN (Schifitto et al., 2005) and that since
HAART was introduced, the incidence of peripheral
neuropathy has decreased (Lichtenstein et al.,
2004). In earlier studies, DSPN was found to occur
across the spectrum of HIV disease and its incidence
was increasing, most likely due to prolonged survival
rates, incidence of co-morbid conditions and the
development of HAART (Dal Pan & Mc Arthur,
1996; Senneff, 1999; Simpson & Olney, 1992;
Simpson & Tagliati, 1994; Simpson et al., 1994;
Swanson et al., 1998). In their review, Estanislao
et al. (2005) indicate that distal symmetric poly-
neuropathy is the most common form of peripheral
neuropathy in both HIV and hepatitis C mono-
infection (HCV); these authors suggest that further
study is needed to examine whether additive or
synergistic effects exist for those with co-infection
with HIV- and HCV-related neuropathy.
Role of antiretroviral medications in DSPN
Recent research indicates that HIV nucleoside
reverse transcriptase inhibitors (NRTIs) can cause
peripheral neuropathy that is a result of mitochon-
drial injury. Gerschenson and Brinkman (2004)
suggest that long-term exposure to antiretroviral
therapy and HIV exposure cause mitochondrial
toxicities, such as myopathies, neuropathy and other
complications. Futher, these authors suggest that
although mitochondrial pathogenesis has been pos-
tulated to be due exclusively to ‘NRTI-induced
inhibition DNA polymerase-gamma; it is now ap-
parent that the etiology is more complex involving
many effects and HIV per se’. Hulgan et al. (2005)
found that mitochondrial haplogroup T was more
frequent in subjects who developed peripheral neu-
ropathy. Among 137 white subjects randomized to
receive ddI plus d4T, 20.8% of those who developed
peripheral neuropathy belonged to mitochondrial
haplogroup T compared to 4.5% of control subjects;
independent predictors of peripheral neuropathy
were randomization to receive ddI plus d4T, older
age and mitochondrial haplogroup T (Hulgan et al.,
2005).
Clinical assessment of DSPN
Recently, clinical tools aimed at measuring HIV-
related neuropathy have been developed (Cherry et
al., 2005; Ellis et al., 2005; McArthur, 1998;
Venkataramana et al., 2005). The Brief Neuropathy
Screening Tool (BNST) was found to accurately
detect those HIV-infected individuals with the great-
est degree of neuropathy. The BNST is also viewed
as a valid neuropathy screening tool for use in HIV
infection and is simple enough to be applicable in
resource-limited settings (Cherry et al., 2005). Ellis
and associates (2005) found that the Brief Peripheral
Neuropathy Screen was a useful clinical tool for
measuring the neurological deficits related to neuro-
pathy. Venkataramana et al. (2005) found that a
subjective peripheral neuropathy screen was a reli-
able and valid tool for measurement of DSPN in
HIV disease.
Quality of life and symptom management of DSPN
Pandya et al. (2005) found that HIV-related neuro-
logical syndromes, including neuropathy, signifi-
cantly reduce quality of life. Griswold et al. (2005)
examined coping strategies of HIV patients with
peripheral neuropathy and found that these
180 P. K. Nicholas et al.

strategies may differ according to age, gender
and ethnic background in those living with HIV.
Griswold and associates (2005) found that catastro-
phizing as a negative coping strategy predicted
distress and interference with functioning in their
sample.
Symptom management research on HIV-related
neuropathy suggests that selecting appropriate phar-
macologic interventions is necessary (Verma et al.,
2004; 2005) and that self-management strategies are
important methods for managing neuropathy symp-
toms (Nicholas et al., 2002). Herbal medicines have
also been found to be widely used complementary
therapies in patients with HIV/AIDS and neuropathy
(Liu et al., 2005), although insufficient evidence
exists to support the use of herbal medicines in HIV/
AIDS patients. Finally, recent literature suggests that
substance use disorders are associated with higher
rates of DSPN (Berger et al., 1999; Morgello et al.,
2004) and that cannabis use is common in patients
with HIV disease (Woolridge et al., 2005). Thus, the
present study contributes to the limited body of
research available on the prevalence, characteristics
and self-care behaviors for DSPN.
Conceptual model
Theoretical framework. The theoretical perspective
guiding this analysis integrates the emotion regula-
tion principles identified by Leventhal’s common-
sense model perspective of health threat regulation
with those delineated in Scheier and Carver’s general
model of behavior self-regulation (Cameron, 2003).
Peripheral neuropathy is a common aspect of illness
in HIV disease, which can affect many aspects of
behavioral self-regulation or self-management across
the trajectory of illness. Although neuropathy is a
physiological phenomenon, it also represents
a perceptual process that may lead to the experience
of a health threat thus leading the individual
experiencing neuropathy to seek out behavioral
self-regulation through self-care.
Purpose of the study
As part of a larger study conducted by the UCSF
International HIV/AIDS Nursing Research Network
on self-care for symptoms in HIV disease, the
purpose of the present study was to analyze
the prevalence and characteristics of peripheral
neuropathy in HIV disease, the self-care strategies
and nature of the symptoms in this sample. A
descriptive quantitative design was employed for
the study. SPSS-PC version 11.0 was used to analyze
the descriptive data and categorize the symptom
management data. Quantitative methods were used
to analyze and summarize symptom management
data related to peripheral neuropathy.
Methods
Design and settings
This descriptive study used a cross-sectional design
to examine self-reported symptoms and self-care
behaviors in a sample of persons with HIV/AIDS.
Data were collected in 12 cities in eight states in the
US, Puerto Rico and three international sites.
The data collection sites were California (San
Francisco, Fresno), Massachusetts (Boston, Fall
River), New York (New York City), New Jersey
(Newark), North Carolina (Wilmington), Ohio
(Columbus), Texas (Corpus Christi, Harlingen,
Temple), Virginia (Richmond), Puerto Rico (San
Juan), Norway (Oslo), Taiwan (Taipei and Tao-
Yuan), and Colombia (Cali). The national and
international settings included community-based
organizations, university-based AIDS clinics, private
practices, public and for-profit hospitals, residential
and day care facilities and home care services.
Institutional Review Board approval was obtained
at each study site. Certificates of Confidentiality
were obtained when requested by institutional re-
view boards at specific sites.
Sample
The total sample included 1,217 HIV-infected men
and women from the US, the Commonwealth of
Puerto Rico, Taiwan, Norway and Colombia. Of the
larger sample of 1,217 participants, 450 individuals
reported experiencing peripheral neuropathy. Inclu-
sion criteria for the study were that participants had
to be (a) at least 18 years of age, (b) receiving AIDS-
related care at their respective facility, (c) able to
provide informed consent and (d) English, Spanish
or Chinese-speaking.
Instrumentation
The instruments used in the study included a
demographic survey, the Revised Sign and Symptom
Checklist for Persons with HIV Disease (SSC-
HIVrev) and the HIV/AIDS Targeted Quality of
Life (HAT-QOL) instrument. All instruments were
forward- and back-translated from the original
English-language instruments into Spanish and Chi-
nese versions and pilot tested.
Demographic survey. A survey booklet was used for
collecting information on personal and environmen-
tal characteristics including age, gender, years of
education, whether participants had adequate in-
come, whether they had children and other variables.
Peripheral neuropathy 181

In addition, data on biological/physiological factors,
such as whether participants had received an AIDS
diagnosis or had any comorbidities, were also col-
lected.
The revised sign and symptom checklist for persons with
HIV disease (SSC-HIVrev). The SCC-HIVrev
checklist is comprised of 64 items that capture the
frequency and severity of HIV signs and symptoms
that the participants were experiencing on a given
day. Items are rated on a 3-point Likert scale of
1�/mild, 2�/moderate or 3�/severe. Calculations
include the total number of symptoms (range�/0�64) and the mean severity of symptoms (range�/1�3). Reliability and validity of the instrument have
been previously reported for a US sample (Holzemer
et al., 2001). Likewise, a Chinese version of the
instrument has been tested with a Taiwanese sample
(Tsai et al., 2003). Slightly different Spanish ver-
sions of the SSC-HIVrev were used in Texas for a
predominately Mexican population, in San Juan for
a Puerto Rican population and in Cali for a
Colombian population. Researchers at each site
confirmed the content validity of the versions.
HIV/AIDS targets quality of life (HAT-QOL). The
HAT-QOL is a self-report scale that measures overall
functioning, life satisfaction, health worries, financial
worries and disclosure. The nine-dimensional scale
includes items that were initially tested in a sample of
201 HIV-seropositive persons. Only five of the nine
dimensions were used in this study: (a) overall
function, (b) financial worries, (c) health worries,
(d) disclosure worries and (e) life satisfaction. These
five dimensions exhibited favorable psychometric
properties including adequate internal consistency
and evidence of construct validity (Holmes & Shea,
1997; 1999). Evidence for the construct validity of
this instrument was provided by items that directly
reflected quality of life derived from reports by HIV-
positive persons. Items were rated on a 5-point scale
ranging from 1�/low to 5�/high. We computed
dimensional scores for the HAT-QOL scales by
summing all of the item responses in each dimen-
sion. Negatively worded items in the instrument
were reversed scored. Higher scores indicated more
favorable outcomes. The Cronbach’s alpha reliability
coefficient was above 0.80 for each scale, indicating
highly favorable internal consistency across items
(Nunnally & Bernstein, 1994).
Data analysis
Responses to the questionnaires were entered
into Statistical Package for the Social Sciences for
Windows Version software. Descriptive statistics (i.e.
means, standard deviations, frequencies and per-
cents) were used to examine demographic character-
istics of the sample, severity of illness, quality of life
and characteristics of peripheral neuropathy.
Results
Participants were recruited from data collection sites
in Boston, Massachusetts (n�/140; 11.5% of sam-
ple); San Francisco, California (n�/ 61; 5.0%);
Fresno, California (n�/ 80; 6.6%); Wilmington,
North Carolina (n�/ 34; 2.8%); Richmond, Virginia
(n�/ 90; 7.4%); Fall River, Massachusetts (n�/ 40;
3.3%); New York (two sites) (n�/ 84; 6.9% and n�/
43; 3.5%); Paterson, New Jersey (n�/ 92; 7.6%),
Corpus Christi, Texas (three sites) (n�/ 41; 3.4%,
n�/ 64; 5.3% and n�/ 50; 4.1%), Columbus, Ohio
(two sites) (n�/ 42; 3.5% and n�/ 15; 1.2%); Puerto
Rico (n�/ 44; 3.6%); Colombia (n�/102; 8.4%);
Taiwan (n�/ 118; 9.7%) and Norway (n�/ 77;
6.3%). In the broader study, a convenience sample
of 1,217 participants with HIV/AIDS was asked if
they experienced symptoms during the past week. If
yes, they were asked to check the activities on a 20-
item self-care activity checklist derived from previous
work. Survey questions were summarized into five
categories of self-care behaviors, including activities/
thoughts, exercise, medications, complementary
therapies and substance use. In addition to rating
self-care strategies, participants were also asked to
rate the frequency (daily, weekly, monthly) and
effectiveness of the self-care activity on a scale of
1�10 with 1�/very poor and 10�/excellent. In
addition to completing the self-care survey, partici-
pants were asked to rate the frequency, intensity and
impact of neuropathy symptoms on daily life on a
ten-point scale.
Neuropathy, the fourth most frequently identi-
fied symptom, was reported by 450 (36.9%)
participants. This subset of study participants in-
cluded 316 males (70.2%), 129 females (28.7%) and
three transgender (0.7%) with a mean age of 43.5
years (SD�/9.0). The ethnically diverse sample
included participants from Colombia (n�/ 27; 6.0%
of the total sample who reported neuropathy),
Norway (n�/ 38; 8.4% of total sample reporting
neuropathy), Puerto Rico (n�/14; 3.1% of total
sample reporting neuropathy), Taiwan (n�/ 44;
9.8% of total sample who reported neuropathy)
and the US (n�/ 327; 72.6% of total sample report-
ing neuropathy). Health status indicators included
an average of 11.1 years (SD�/5.8) since HIV-
positive diagnosis, with 41.6% of the sample who
reported neuropathy also self-reporting a diagnosis
of AIDS. Nearly eighty percent (77.9%) of those
with neuropathy were currently taking HIV medica-
tions, with the average length of time on HIV
medications reported as 8.9 years (SD�/4.7).
182 P. K. Nicholas et al.

Thirty-eight percent of the sample reported an
undetectable viral load. Sixty percent of the sample
had an education level of high school or less and
48% had at least one child living at home. The most
common co-existing medical or psychiatric disorders
reported were depression, hepatitis and hyperten-
sion. Over 14% (n�/ 64) indicated that they were
currently treated for depression. Nearly 71%
reported that they did not work for pay and only
19% reported having an adequate income. Twenty-
six percent of the sample reported a history of
injecting illicit drugs and the majority of the sample
indicated a history of substance use over the past six
months (see Table I).
For the total sample, neuropathy was experienced
a mean score of 4.9 days/week (SD 2.2). When
participants were also asked to rate the level of
impact of neuropathy on their lives on a scale of
1�10, they reported a mean score of 5.5 (SD�/3.3).
On the variable of ‘intensity’ related to neuropathy,
respondents reported a mean rating of 5.7 on a scale
of 1�10 (SD�/2.9) with 1�/very low and 10�/very
high. A self-rating of physical condition was
6.1 (SD�/2.3), psychological support was 6.3
(SD�/2.4) and the rating of social support at 6.8
(SD�/2.7) (each on scale of 1�10).
Across countries (US, Commonwealth of Puerto
Rico, Colombia, Norway, Taiwan), self-rating of
neuropathy varied significantly. Participants in
Norway had the highest reports of neuropathy
(50%), while those in the US reported similar rates
of neuropathy (36.2%) to those in Taiwan (37.3%).
For those in Colombia, 26.7% reported neuropathy
and participants from Puerto Rico reported the
lowest rate of neuropathy (10%). Thus self-report
of neuropathy differed significantly across countries
(p B/0.000) with 50% of respondents in Norway
indicating the presence of neuropathy and only 10%
in Puerto Rico reporting neuropathy. Participants in
Puerto Rico did, however, report significantly
increased rates of neuropathy intensity (7.1 for
Puerto Rico versus 6.5 for Colombia, 6.0 for US,
4.8 for Norway and 2.5 for Taiwan, p B/0.000) and
impact (7.3 for Puerto Rico versus 5.6 for Colombia,
5.9 for US, 4.3 for Norway and 2.7 for Taiwan,
p B/0.000) (see Table II).
Table III presents data on the frequency and
effectiveness of self-care strategies for the total
sample who reported neuropathy. The most com-
monly used strategies for managing neuropathy
included taking a hot bath (n�/260; 66%: 46.0%
daily, 7.3% monthly), walking (n�/ 234; 60.0%:
82.3%, daily, 9.2% monthly), staying off of feet
(n�/ 233; 59%: 78.9% daily, 78.9% monthly), eleva-
tion of feet (n�/ 214; 57%: 82.9%, daily, 15.1%
monthly) and rubbing the feet with cream (n�/ 159;
47%: 76.5% daily, 21.6% monthly).
Table I. Demographic data (n�/ 450).
Variable Range Mean SD Frequency
Age 21�84 years 43.58 years 9.0 439
CD4 Count (self report) 0�4800 397/mm3 364/mm3 315
Length of HIV (self report) 1�25 years 11.1 years 5.8 years 433
Length of AIDS diagnosis (self report) 2�23 years 8.9 years 4.7 years 187
Sex n (%)
Male 316 (70.2)
Female 129 (28.7)
Transgender 3 (0.70)
Ethnicity n (%)
African American/black 161 (35.8)
Caucasian 130 (28.9)
Hispanic/Latino 101 (22.4)
Asian/Pacific Islander 44 (9.8)
Native American Indian 6 (1.3)
Other 4 (0.9)
Risk Factors n (%)
Sex with man with HIV 279 (71.2)
Sharing needles 93 (26.1)
Sex with woman with HIV 89 (25.9)
Don’t know 58 (18.1)
Blood transfusion 21 (6.5)
Other 15 (4.7)
Income n (%)
Enough 81 (18.2)
Barely adequate 227 (51.1)
Current injection drug user 136 (30.6)
Peripheral neuropathy 183
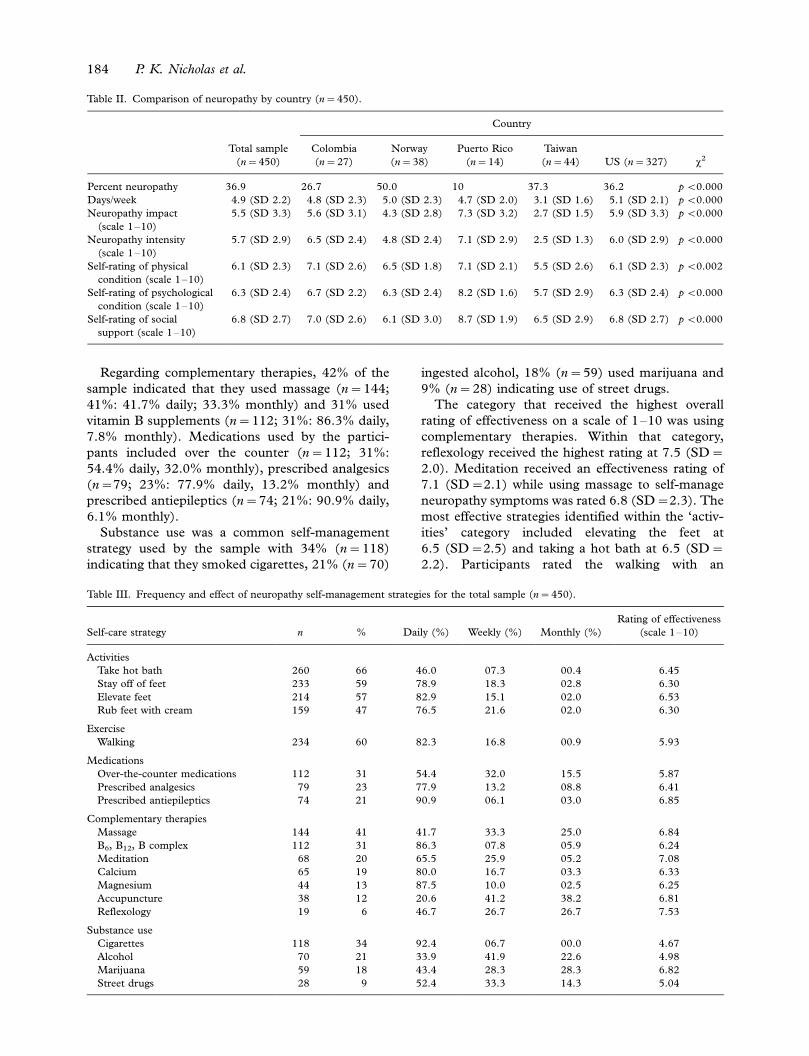
Regarding complementary therapies, 42% of the
sample indicated that they used massage (n�/ 144;
41%: 41.7% daily; 33.3% monthly) and 31% used
vitamin B supplements (n�/ 112; 31%: 86.3% daily,
7.8% monthly). Medications used by the partici-
pants included over the counter (n�/ 112; 31%:
54.4% daily, 32.0% monthly), prescribed analgesics
(n�/79; 23%: 77.9% daily, 13.2% monthly) and
prescribed antiepileptics (n�/ 74; 21%: 90.9% daily,
6.1% monthly).
Substance use was a common self-management
strategy used by the sample with 34% (n�/ 118)
indicating that they smoked cigarettes, 21% (n�/ 70)
ingested alcohol, 18% (n�/ 59) used marijuana and
9% (n�/ 28) indicating use of street drugs.
The category that received the highest overall
rating of effectiveness on a scale of 1�10 was using
complementary therapies. Within that category,
reflexology received the highest rating at 7.5 (SD�/
2.0). Meditation received an effectiveness rating of
7.1 (SD�/2.1) while using massage to self-manage
neuropathy symptoms was rated 6.8 (SD�/2.3). The
most effective strategies identified within the ‘activ-
ities’ category included elevating the feet at
6.5 (SD�/2.5) and taking a hot bath at 6.5 (SD�/
2.2). Participants rated the walking with an
Table II. Comparison of neuropathy by country (n�/ 450).
Country
Total sample
(n�/ 450)
Colombia
(n�/ 27)
Norway
(n�/ 38)
Puerto Rico
(n�/ 14)
Taiwan
(n�/ 44) US (n�/ 327) x2
Percent neuropathy 36.9 26.7 50.0 10 37.3 36.2 p B/0.000
Days/week 4.9 (SD 2.2) 4.8 (SD 2.3) 5.0 (SD 2.3) 4.7 (SD 2.0) 3.1 (SD 1.6) 5.1 (SD 2.1) p B/0.000
Neuropathy impact
(scale 1�10)
5.5 (SD 3.3) 5.6 (SD 3.1) 4.3 (SD 2.8) 7.3 (SD 3.2) 2.7 (SD 1.5) 5.9 (SD 3.3) p B/0.000
Neuropathy intensity
(scale 1�10)
5.7 (SD 2.9) 6.5 (SD 2.4) 4.8 (SD 2.4) 7.1 (SD 2.9) 2.5 (SD 1.3) 6.0 (SD 2.9) p B/0.000
Self-rating of physical
condition (scale 1�10)
6.1 (SD 2.3) 7.1 (SD 2.6) 6.5 (SD 1.8) 7.1 (SD 2.1) 5.5 (SD 2.6) 6.1 (SD 2.3) p B/0.002
Self-rating of psychological
condition (scale 1�10)
6.3 (SD 2.4) 6.7 (SD 2.2) 6.3 (SD 2.4) 8.2 (SD 1.6) 5.7 (SD 2.9) 6.3 (SD 2.4) p B/0.000
Self-rating of social
support (scale 1�10)
6.8 (SD 2.7) 7.0 (SD 2.6) 6.1 (SD 3.0) 8.7 (SD 1.9) 6.5 (SD 2.9) 6.8 (SD 2.7) p B/0.000
Table III. Frequency and effect of neuropathy self-management strategies for the total sample (n�/ 450).
Self-care strategy n % Daily (%) Weekly (%) Monthly (%)
Rating of effectiveness
(scale 1�10)
Activities
Take hot bath 260 66 46.0 07.3 00.4 6.45
Stay off of feet 233 59 78.9 18.3 02.8 6.30
Elevate feet 214 57 82.9 15.1 02.0 6.53
Rub feet with cream 159 47 76.5 21.6 02.0 6.30
Exercise
Walking 234 60 82.3 16.8 00.9 5.93
Medications
Over-the-counter medications 112 31 54.4 32.0 15.5 5.87
Prescribed analgesics 79 23 77.9 13.2 08.8 6.41
Prescribed antiepileptics 74 21 90.9 06.1 03.0 6.85
Complementary therapies
Massage 144 41 41.7 33.3 25.0 6.84
B6, B12, B complex 112 31 86.3 07.8 05.9 6.24
Meditation 68 20 65.5 25.9 05.2 7.08
Calcium 65 19 80.0 16.7 03.3 6.33
Magnesium 44 13 87.5 10.0 02.5 6.25
Accupuncture 38 12 20.6 41.2 38.2 6.81
Reflexology 19 6 46.7 26.7 26.7 7.53
Substance use
Cigarettes 118 34 92.4 06.7 00.0 4.67
Alcohol 70 21 33.9 41.9 22.6 4.98
Marijuana 59 18 43.4 28.3 28.3 6.82
Street drugs 28 9 52.4 33.3 14.3 5.04
184 P. K. Nicholas et al.
effectiveness rating of 5.93 (SD�/2.4) while using
prescribed antiepileptic medications to manage neu-
ropathy symptoms was rated at 6.85 (SD�/2.1).
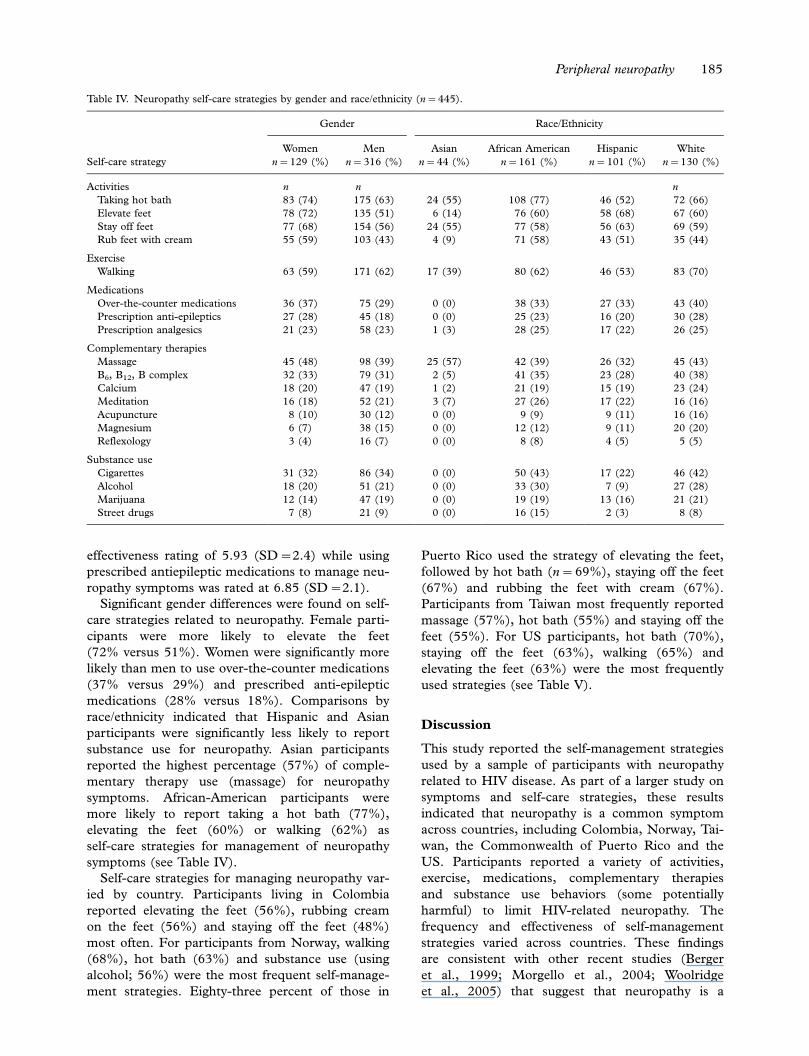
Significant gender differences were found on self-
care strategies related to neuropathy. Female parti-
cipants were more likely to elevate the feet
(72% versus 51%). Women were significantly more
likely than men to use over-the-counter medications
(37% versus 29%) and prescribed anti-epileptic
medications (28% versus 18%). Comparisons by
race/ethnicity indicated that Hispanic and Asian
participants were significantly less likely to report
substance use for neuropathy. Asian participants
reported the highest percentage (57%) of comple-
mentary therapy use (massage) for neuropathy
symptoms. African-American participants were
more likely to report taking a hot bath (77%),
elevating the feet (60%) or walking (62%) as
self-care strategies for management of neuropathy
symptoms (see Table IV).
Self-care strategies for managing neuropathy var-
ied by country. Participants living in Colombia
reported elevating the feet (56%), rubbing cream
on the feet (56%) and staying off the feet (48%)
most often. For participants from Norway, walking
(68%), hot bath (63%) and substance use (using
alcohol; 56%) were the most frequent self-manage-
ment strategies. Eighty-three percent of those in
Puerto Rico used the strategy of elevating the feet,
followed by hot bath (n�/ 69%), staying off the feet
(67%) and rubbing the feet with cream (67%).
Participants from Taiwan most frequently reported
massage (57%), hot bath (55%) and staying off the
feet (55%). For US participants, hot bath (70%),
staying off the feet (63%), walking (65%) and
elevating the feet (63%) were the most frequently
used strategies (see Table V).
Discussion
This study reported the self-management strategies
used by a sample of participants with neuropathy
related to HIV disease. As part of a larger study on
symptoms and self-care strategies, these results
indicated that neuropathy is a common symptom
across countries, including Colombia, Norway, Tai-
wan, the Commonwealth of Puerto Rico and the
US. Participants reported a variety of activities,
exercise, medications, complementary therapies
and substance use behaviors (some potentially
harmful) to limit HIV-related neuropathy. The
frequency and effectiveness of self-management
strategies varied across countries. These findings
are consistent with other recent studies (Berger
et al., 1999; Morgello et al., 2004; Woolridge
et al., 2005) that suggest that neuropathy is a
Table IV. Neuropathy self-care strategies by gender and race/ethnicity (n�/ 445).
Gender Race/Ethnicity
Self-care strategy
Women
n�/ 129 (%)
Men
n�/ 316 (%)
Asian
n�/ 44 (%)
African American
n�/ 161 (%)
Hispanic
n�/ 101 (%)
White
n�/ 130 (%)
Activities n n n
Taking hot bath 83 (74) 175 (63) 24 (55) 108 (77) 46 (52) 72 (66)
Elevate feet 78 (72) 135 (51) 6 (14) 76 (60) 58 (68) 67 (60)
Stay off feet 77 (68) 154 (56) 24 (55) 77 (58) 56 (63) 69 (59)
Rub feet with cream 55 (59) 103 (43) 4 (9) 71 (58) 43 (51) 35 (44)
Exercise
Walking 63 (59) 171 (62) 17 (39) 80 (62) 46 (53) 83 (70)
Medications
Over-the-counter medications 36 (37) 75 (29) 0 (0) 38 (33) 27 (33) 43 (40)
Prescription anti-epileptics 27 (28) 45 (18) 0 (0) 25 (23) 16 (20) 30 (28)
Prescription analgesics 21 (23) 58 (23) 1 (3) 28 (25) 17 (22) 26 (25)
Complementary therapies
Massage 45 (48) 98 (39) 25 (57) 42 (39) 26 (32) 45 (43)
B6, B12, B complex 32 (33) 79 (31) 2 (5) 41 (35) 23 (28) 40 (38)
Calcium 18 (20) 47 (19) 1 (2) 21 (19) 15 (19) 23 (24)
Meditation 16 (18) 52 (21) 3 (7) 27 (26) 17 (22) 16 (16)
Acupuncture 8 (10) 30 (12) 0 (0) 9 (9) 9 (11) 16 (16)
Magnesium 6 (7) 38 (15) 0 (0) 12 (12) 9 (11) 20 (20)
Reflexology 3 (4) 16 (7) 0 (0) 8 (8) 4 (5) 5 (5)
Substance use
Cigarettes 31 (32) 86 (34) 0 (0) 50 (43) 17 (22) 46 (42)
Alcohol 18 (20) 51 (21) 0 (0) 33 (30) 7 (9) 27 (28)
Marijuana 12 (14) 47 (19) 0 (0) 19 (19) 13 (16) 21 (21)
Street drugs 7 (8) 21 (9) 0 (0) 16 (15) 2 (3) 8 (8)
Peripheral neuropathy 185
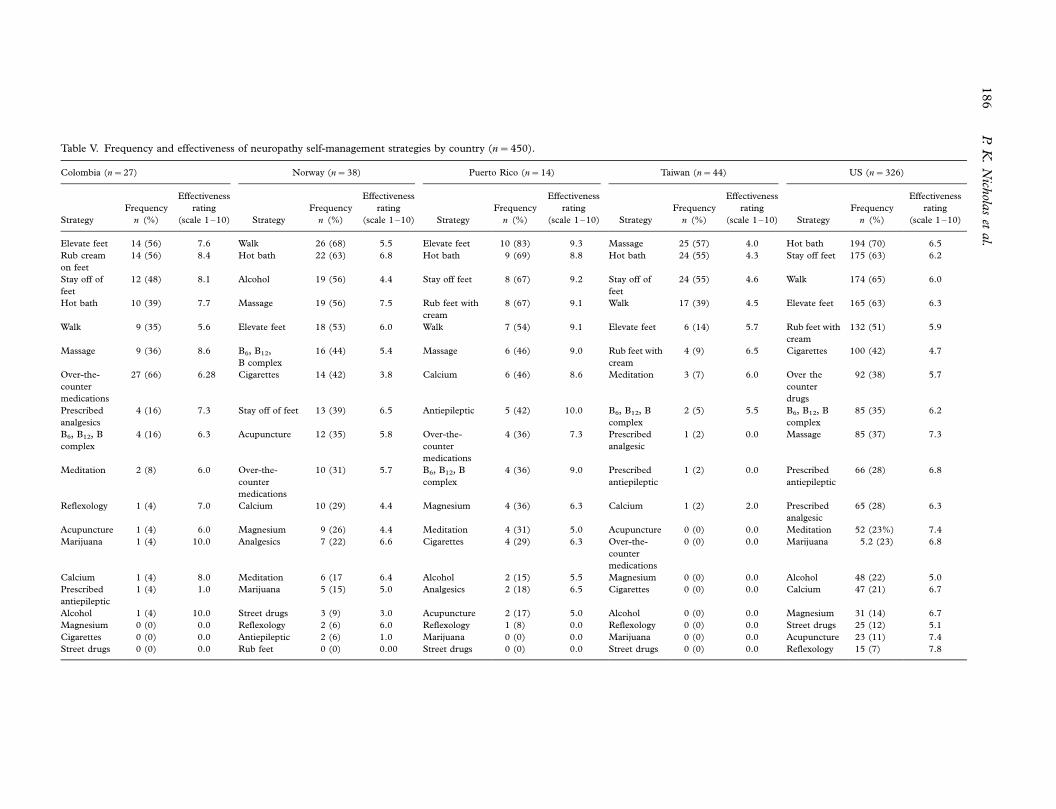
Table V. Frequency and effectiveness of neuropathy self-management strategies by country (n�/ 450).
Colombia (n�/ 27) Norway (n�/ 38) Puerto Rico (n�/ 14) Taiwan (n�/ 44) US (n�/ 326)
Strategy
Frequency
n (%)
Effectiveness
rating
(scale 1�10) Strategy
Frequency
n (%)
Effectiveness
rating
(scale 1�10) Strategy
Frequency
n (%)
Effectiveness
rating
(scale 1�10) Strategy
Frequency
n (%)
Effectiveness
rating
(scale 1�10) Strategy
Frequency
n (%)
Effectiveness
rating
(scale 1�10)
Elevate feet 14 (56) 7.6 Walk 26 (68) 5.5 Elevate feet 10 (83) 9.3 Massage 25 (57) 4.0 Hot bath 194 (70) 6.5
Rub cream
on feet
14 (56) 8.4 Hot bath 22 (63) 6.8 Hot bath 9 (69) 8.8 Hot bath 24 (55) 4.3 Stay off feet 175 (63) 6.2
Stay off of
feet
12 (48) 8.1 Alcohol 19 (56) 4.4 Stay off feet 8 (67) 9.2 Stay off of
feet
24 (55) 4.6 Walk 174 (65) 6.0
Hot bath 10 (39) 7.7 Massage 19 (56) 7.5 Rub feet with
cream
8 (67) 9.1 Walk 17 (39) 4.5 Elevate feet 165 (63) 6.3
Walk 9 (35) 5.6 Elevate feet 18 (53) 6.0 Walk 7 (54) 9.1 Elevate feet 6 (14) 5.7 Rub feet with
cream
132 (51) 5.9
Massage 9 (36) 8.6 B6, B12,
B complex
16 (44) 5.4 Massage 6 (46) 9.0 Rub feet with
cream
4 (9) 6.5 Cigarettes 100 (42) 4.7
Over-the-
counter
medications
27 (66) 6.28 Cigarettes 14 (42) 3.8 Calcium 6 (46) 8.6 Meditation 3 (7) 6.0 Over the
counter
drugs
92 (38) 5.7
Prescribed
analgesics
4 (16) 7.3 Stay off of feet 13 (39) 6.5 Antiepileptic 5 (42) 10.0 B6, B12, B
complex
2 (5) 5.5 B6, B12, B
complex
85 (35) 6.2
B6, B12, B
complex
4 (16) 6.3 Acupuncture 12 (35) 5.8 Over-the-
counter
medications
4 (36) 7.3 Prescribed
analgesic
1 (2) 0.0 Massage 85 (37) 7.3
Meditation 2 (8) 6.0 Over-the-
counter
medications
10 (31) 5.7 B6, B12, B
complex
4 (36) 9.0 Prescribed
antiepileptic
1 (2) 0.0 Prescribed
antiepileptic
66 (28) 6.8
Reflexology 1 (4) 7.0 Calcium 10 (29) 4.4 Magnesium 4 (36) 6.3 Calcium 1 (2) 2.0 Prescribed
analgesic
65 (28) 6.3
Acupuncture 1 (4) 6.0 Magnesium 9 (26) 4.4 Meditation 4 (31) 5.0 Acupuncture 0 (0) 0.0 Meditation 52 (23%) 7.4
Marijuana 1 (4) 10.0 Analgesics 7 (22) 6.6 Cigarettes 4 (29) 6.3 Over-the-
counter
medications
0 (0) 0.0 Marijuana 5.2 (23) 6.8
Calcium 1 (4) 8.0 Meditation 6 (17 6.4 Alcohol 2 (15) 5.5 Magnesium 0 (0) 0.0 Alcohol 48 (22) 5.0
Prescribed
antiepileptic
1 (4) 1.0 Marijuana 5 (15) 5.0 Analgesics 2 (18) 6.5 Cigarettes 0 (0) 0.0 Calcium 47 (21) 6.7
Alcohol 1 (4) 10.0 Street drugs 3 (9) 3.0 Acupuncture 2 (17) 5.0 Alcohol 0 (0) 0.0 Magnesium 31 (14) 6.7
Magnesium 0 (0) 0.0 Reflexology 2 (6) 6.0 Reflexology 1 (8) 0.0 Reflexology 0 (0) 0.0 Street drugs 25 (12) 5.1
Cigarettes 0 (0) 0.0 Antiepileptic 2 (6) 1.0 Marijuana 0 (0) 0.0 Marijuana 0 (0) 0.0 Acupuncture 23 (11) 7.4
Street drugs 0 (0) 0.0 Rub feet 0 (0) 0.00 Street drugs 0 (0) 0.0 Street drugs 0 (0) 0.0 Reflexology 15 (7) 7.8
186
P.K
.N
ichola
set
al.

common and complex symptom affecting those
living with HIV and that substance use is a common
self-care behavior.
Self-care strategies for neuropathy varied signifi-
cantly by country. The most frequently used self-
care measures reported by the participants from
Norway included walking, hot bath, alcohol use and
massage. Despite the potentially damaging effect of
alcohol related to neuropathy, many participants
indicated alcohol use as a self-care strategy. Alcohol
use is a potentially harmful self-care strategy for
neuropathy and may contribute to further
neuropathy for those with HIV disease. Additional
education about alcohol use for HIV-positive indivi-
duals may be needed in Norway and other countries.
The five most frequently used strategies in Taiwan
included massage, hot bath, staying off the feet,
walking and elevating the feet. Among the US
participants, the most frequently used self-care
strategies included hot bath, staying off the feet,
walking, elevating the feet and rubbing the feet with
cream. Over 40% (n�/ 100; 42%) of the US parti-
cipants also indicated that they smoked cigarettes to
self-manage neuropathy*another potentially harm-
ful self-care behavior. With the exception of partici-
pants from Taiwan, using over-the-counter
medications was a behavior used by participants in
several countries to manage neuropathy (Colombia,
66%; Norway, 31%; Puerto Rico, 36%; US, 38%).
In addition to receiving the highest frequency
rates, the neuropathy management strategy of taking
a hot bath received high ratings of effectiveness on a
scale of 1�10 for Colombia (rating of 7.7) and
Puerto Rico (rating of 8.8) but only moderate ratings
of effectiveness for participants from Norway (rating
of 6.8), the US (rating of 6.5) and Taiwan (rating
of 4.3).
A second self-care strategy, massage, also received
high frequency ratings across all countries (ranging
from 36% to 56% using this strategy) with high
ratings of effectiveness for participants in Norway
(7.5), US (7.3), Colombia (8.6) and Puerto Rico
(9.0) but low ratings of effectiveness in Taiwanese
participants (4.0). United States participants identi-
fied the unhealthy behavior of cigarette smoking
(n�/ 100; 42%) while Norwegian participants (n�/
19; 56%) identified alcohol use as a self-care
behavior for neuropathy. For Colombia or Puerto
Rico, unhealthy behaviors were not identified as
among the most frequent self-care behaviors in these
samples.
An examination of the data by gender and race/
ethnicity shows that women were more likely to
report activities (hot bath, elevating the feet, staying
off the feet, rubbing the feet with cream), massage
and use of some medications (over-the-counter and
prescription anti-epileptics) than men. African-
American respondents were more likely to use hot
bath as a self-care strategy for neuropathy than were
white, Asian or Hispanic participants.
Across all countries, medications were not identi-
fied as among the most frequently used strategies for
self-management of HIV. While 28% of the US
participants reported using prescribed medications
(analgesics and anti-epileptic medications), the med-
ication rate for participants in Taiwan was 2% for
both types of medications. For participants in Puerto
Rico, 42% identified prescribed antiepileptic medi-
cation usage, a higher percentage despite the small
sample size. In Colombia, 16% used prescribed
analgesics and in Norway, 6% identified prescribed
medications as a self-management strategy.
Studies suggest that appropriate pharmacologic
interventions should be based on efficacy, safety,
ease of administration and cost (Verma et al., 2005),
as well as accessibility to these pharmacologic agents
in the US and other countries. Saarto and Wiffen
(2005) in their systematic review found that tricyclic
antidepressants (TCAs) are an effective treatment
for neuropathic pain, while insufficient evidence
exists for the effectiveness of the newer selective
serotonin reuptake inhibitors (SSRIs). Paice and
associates (2000) found that capsaicin is ineffective
in relieving pain associated with HIV-related
neuropathy. In our study, few participants used
medications, thus additional patient assessment
and education are needed related to pharmacother-
apeutics and self-management in HIV disease.
Conclusion
Peripheral neuropathy is an important symptom in
HIV-infected individuals and requires assessment,
intervention and evaluation across the spectrum of
HIV disease. Neuropathy may also occur due to HIV
medications or disease progression and is often
associated with diminished quality of life. Healthcare
providers should assess for this common problem so
that appropriate interventions and follow-up can be
offered to patients. In addition, self-care behaviors
are frequently initiated by patients to manage
peripheral neuropathy, thus healthcare providers
should assess for these behaviors and help patients
to evaluate their effectiveness. The condition
is potentially debilitating and is often triggered
or aggravated by commonly used HIV therapies
(Hulgan et al., 2005; McArthur, 1998; Schifitto et
al., 2005; Swanson et al., 1998).
Future research should be conducted on new
therapies aimed at management of HIV-related
neuropathy including complementary therapies
(acupuncture and massage), medications including
pain medications and the TCAs that can minimize
neuropathic pain, vitamin therapies including B
Peripheral neuropathy 187

complex vitamins and magnesium and other self-
care strategies for peripheral neuropathy. However,
unhealthy behaviors that may exacerbate HIV-
related DSPN also require further investigation.
Woolridge et al. (2005) suggest that cannabis use
may be effective in limiting DSPN; other strategies
including medications require further study.
Additional research and clinical practice guide-
lines should address the need to develop and
promote effective self-care management of periph-
eral neuropathy. Further knowledge about the etiol-
ogy and management of peripheral neuropathy may
assist providers and patients to limit this common
HIV-related problem.
References
Araujo, A.P., Nascimento, O.J., & Garcia, O.S. (2000). Distal
sensory polyneuropathy in a cohort of HIV-infected children
over five years of age. Pediatrics , 106 , E35.
Berger, A.R., Schaumburg, H.H., Gourevitch, M.N., Freeman,
K., Herskovitz, S., & Arezzo, J.C. (1999). Prevalence of
peripheral neuropathy in injection drug users. Neuropathy,
53 , 592�597.
Cameron, L.D. (2003). Anxiety, cognition and responses to health
threats. In L. D. Cameron, & H. Leventhal (Eds.), The self-
regulation of health and illness behavior (pp. 157�183). New
York, NY: Routledge.
Cherry, C.L., Wesselingh, S.L., Lal, L., & McArthur, J.C. (2005).
Evaluation of a clinical screening tool for HIV-associated
sensory neuropathies. Neurology, 65 , 1778�1781.
Dal Pan, G.J., & McArthur, J.C. (1996). Neuroepidemiology of
HIV infection. Neurologic Clinics , 14 , 359�382.
Dorsey, S.G., & Morton, P.G. (2006). HIV peripheral neuro-
pathy: Pathophysiology and clinical implications. American
Association of Critical-Care Nurses Clinical Issues , 17 , 30�36.
Ellis, R.J., Evans, S.R., Clifford, D.B., Moo, L.R., McArthur,
J.C., Collier, A.C., et al. (2005). Clinical validation of the
NeuroScreen. Journal of Neurovirology, 11 , 503�511.
Estanislao, L.B., Morgello, S., & Simpson, D.M. (2005). Periph-
eral neuropathies associated with HIV and hepatitis C co-
infection: A review. AIDS , 19(Suppl.) , S135�S139.
Ferrari, S., Vento, S., Monaco, S., Cavallaro, T., Cainelli, F.,
Rizzuto, N., et al. (2006). Human immunodeficiency virus-
associated peripheral neuropathies. Mayo Clinic Proceedings , 81 ,
213�219.
Floeter, M.K., Civitello, L.A., Everett, C.R., Dambrosia, J., &
Luciano, C.A. (1997). Peripheral neuropathy in children with
HIV infection. Neurology, 49 , 207�212.
Gerschenson, M., & Brinkman, K. (2004). Mitochondrial dys-
function in AIDS and its treatment. Mitochondrion , 4 , 763�777.
Griswold, G.A., Evans, S., Spielman, L., & Fishman, B. (2005).
Coping strategies of HIV patients with peripheral neuropathy.
AIDS Care , 17 , 711�720.
Hall, C.D., Snyder, C.R., Messenheimer, J.A., Wilkins, J.W.,
Robertson, W.T., & Robertson, K.R. (1991). Peripheral
neuropathy in a cohort of human immunodeficiency virus-
infected patients: Incidence and relationship to nervous system
dysfunction. Archives of Neurology, 48 , 1273�1274.
Harrison, M.J.G., & McArthur, J.C. (1995). AIDS and neurology.
Edinburgh: Churchill Livingstone.
Holmes, W.C., & Shea, J.A. (1997). Performance of a new, HIV-
AIDS-targeted quality of life (HAT-QoL) instrument in
asymptomatic seropositive individuals. Quality of Life Research ,
6 , 561�571.
Holmes, W.C., & Shea, J.A. (1999). Two approaches to measuring
quality of life in the HIV/AIDS population: HAT-QoL and
MOS-HIV. Quality of Life Research , 8 , 515�527.
Holzemer, W.L., Hudson, A., Kirksey, K.M., Hamilton, M.J., &
Bakken, S. (2001). The revised Sign and Symptom Check-List
for HIV (SSC-HIVrev). Journal of the Association of Nurses in
AIDS Care , 12 , 60�70.
Hulgan, T., Haas, D.W., Haines, J.L., Ritchie, M.D., Robbins,
G.K., Shafer, R.W., et al. (2005). Mitochondrial haplogroups
and peripheral neuropathy during antiretroviral therapy: An
adult AIDS clinical trials group study. AIDS , 19 , 1341�1349.
Lichtenstein, K.A., Armon, C., Baron, A., Moorman, A.C.,
Wood, K.C., Holmberg, S. D., & The HIV Outpatient Study
Investigators (2005). Modification of the incidence of drug-
associated symmetrical peripheral neuropathy by host and
disease factors in the HIV outpatient study cohort. Clinical
Infectious Diseases , 40 , 148�157.
Liu, J.P., Manheimer, E., & Yang, M. (2005). Herbal medicines
for treating HIV infection and AIDS. Cochrane Database of
Systematic Reviews, Jul 20 (3), CD003937.
McArthur, J.H. (1998). The reliability and validity of the
subjective peripheral neuropathy screen. Journal of the Associa-
tion of Nurses in AIDS Care , 9 , 84�94.
Moore, R.D., Wong, W.M., Keruly, J.C., & McArthur, J.C.
(2000). Incidence of neuropathy in HIV-infected patients on
monotherapy versus those on combination therapy with dida-
nosine, stavudine and hydroxyurea. AIDS , 14 , 273�278.
Morgello, S., Estanislao, L., Simpson, D., Geraci, A., Dirocco, A.,
Gerits, P., et al., & Manhattan HIV Brain Bank (2004). HIV-
associated distal sensory polyneuropathy in the era of highly
active antiretroviral therapy: The Manhattan HIV Brain Bank.
Archives of Neurology, 61 , 546�551.
Moyle, G.J., & Sadler, M. (1998). Peripheral neuropathy with
nucleoside antiretroviral therapy: Risk factors, incidence and
management. Drug Safety, 19 , 481�494.
Nakagawa, M., Maruyama, Y., Sugita, H., & Osame, M. (1997).
Nationwide survey of neurologic manifestations of acquired
immunodeficiency syndrome in Japan. Internal Medicine , 36 ,
175�178.
Nicholas, P.K., Kemppainen, J., Holzemer, W.L., Nokes, K.M.,
Eller, L.S., Corless, I.B., et al. (2002). Self-care management
for peripheral neuropathy in HIV/AIDS. AIDS Care , 14 , 763�771.
Nunnally, J.C., & Bernstein, I.H. (1994). Psychometric theory.
New York, NY: McGraw-Hill.
Paice, J.A., Ferrans, C.E., Lashley, F.R., Shott, S., Vizgirda, V., &
Pitrak, D. (2000). Topical capsaicin in the management of HIV-
associated peripheral neuropathy. Journal of Pain and Symptom
Management , 19 , 45�52.
Pandya, R., Krentz, H.B., Gill, M.J., & Power, C. (2005). HIV-
related neurological syndromes reduce health-related quality of
life. Canadian Journal of Neurological Sciences , 32 , 201�204.
Parry, O., Mielke, J., Latif, A.S., Ray, S., Levy, L.F., & Siziya, S.
(1997). Peripheral neuropathy in individuals with HIV infec-
tion in Zimbabwe. Acta Neurologica Scandinavica , 96 , 218�222.
Price, R.W. (1996). Neurological complications of HIV infection.
Lancet , 348 , 445�452.
Saarto, T., & Wiffen, P.J. (2005). Antidepressants for neuropathic
pain. Cochrane Database of Systematic Review, July 20 (3),
CD005454.
Schifitto, G., McDermott, M.P., McArthur, J.C., Marder, K.,
Sacktor, N., Epstein, L., et al., & Dana Consortium on the
Therapy of HIV Dementia and Related Cognitive Disorders
(2002). Incidence of and risk factors for HIV-associated distal
sensory polyneuropathy. Neurology, 58 , 1764�1768.
188 P. K. Nicholas et al.

Schifitto, G., McDermott, M.P., McArthur, J.C., Marder, K.,
Sacktor, N., McClernon, D. R., et al., & The Nead Con-
sortium. (2005). Markers of immune activation and viral load
in HIV-associated sensory neuropathy. Neurology, 64 , 842�848.
Schooley, R.T. (1999). Longer-term immunologic effects and side
effects of successful antiretroviral therapy. Clinical Infectious
Diseases , 29 , 12�18.
Senneff, J.A. (1999). Numb toes and aching soles . San Antonio,
Texas: Medpress.
Simpson, D.M., & Olney, R.K. (1992). Peripheral neuropathies
associated with HIV infection. Neurologic Clinics , 10 , 685�711.
Simpson, D.M., & Tagliati, M. (1994). Neurologic manifestations
of HIV infection. Annals of Internal Medicine , 121 , 769�785.
Simpson, D.M., Tagliati, M., & Ramcharitar, S. (1994). Neuro-
logic complications of AIDS: New concepts and treatments.
Mount Sinai Journal of Medicine , 61 , 484�491.
Singer, E.J., Zorilla, C., Fahy-Chandon, B., Chi, S., Syndulko, K.,
& Rourtellotte, W.W. (1993). Painful symptoms reported by
ambulatory HIV-infected men in a longitudinal study. Pain , 54 ,
15�19.
Swanson, B., Zeller, J.M., & Paice, J.A. (1998). HIV-associated
distal symmetrical polyneuropathy: Clinical features and nur-
sing management. Journal of the Association of Nurses in AIDS
Care , 9 , 77�80.
Tsai, Y.F., Hsiung, P.C., & Holzemer, W.L. (2003). Validation of
a Chinese version of the Sign and Symptom Checklist for
persons with HIV disease. Journal of Pain and Symptom
Management , 25 , 363�368.
Venkataramana, A.B., Skolasky, R.L., Creighton, J.A., &
McArthur, J.C. (2005). Diagnostic utility of the subjective
peripheral neuropathy screen in HIV-infected persons with
peripheral sensory polyneuropathy. AIDS Reader , 15 , 341�344, 348�349 and 354.
Verma, S., Estanislao, L., Mintz, L., & Simpson, D. (2004).
Controlling neuropathic in HIV. Current HIV/AIDS Reports , 1 ,
136�141.
Verma, S., Estanislao, L., & Simpson, D. (2005). Controlling
neuropathic pain in HIV: Epidemiology, pathophysiology and
management. Central Nervous System drugs , 19 , 325�334.
Wulf, E.A., Wang, A.K., & Simpson, D.M. (2000). HIV-asso-
ciated peripheral neuropathy: Epidemiology, pathophysiology
and treatment. Drugs , 59 , 1251�1260 (abstract).
Woolridge, E., Barton, S., Samuel, J., Osorio, J., Dougherty, A., &
Holdcroft, A. (2005). Cannabis use in HIV for pain and other
medical symptoms. Journal of Pain and Symptom Management ,
29 , 358�367.
Peripheral neuropathy 189