
The Relationship between IL-10 Levels and Cardiovascular Events in Patients with CKD
Upload
independentCategory
view
1download
0
Article
Association of IL-6 and a Functional Polymorphismin the IL-6 Gene with Cardiovascular Events inPatients with CKD
Belinda Spoto,* Francesco Mattace-Raso,† Eric Sijbrands,† Daniela Leonardis,* Alessandra Testa,* Anna Pisano,*Patrizia Pizzini,* Sebastiano Cutrupi,* Rosa M. Parlongo,* Graziella D’Arrigo,* Giovanni Tripepi,*Francesca Mallamaci,* and Carmine Zoccali*
AbstractBackground and objectivesHigh serum IL-6 is a major risk factor for cardiovascular disease (CVD) in the generalpopulation. This cytokine is substantially increased in patients with CKD, but it is still unknownwhether the linkbetween IL-6 and CVD in CKD is causal in nature.
Design, setting, participants, & measurements In a cohort of 755 patients with stages 2–5 CKD, consecutivelyrecruited from 22 nephrology units in southern Italy, this study assessed the relationship of serum IL-6 withhistory of CVD, as well as with incident cardiovascular (CV) events (mean follow up6SD, 31610 months) andused the functional polymorphism (2174 G/C) in the promoter of the IL-6 gene to investigate whether the linkbetween IL-6 and CV events is causal.
Results In adjusted analyses, serum IL-6 above the median value was associated with history of CVD (P,0.001)and predicted the incidence rate of CV events (hazard ratio, 1.66; 95% confidence interval [95% CI], 1.11 to 2.49;P=0.01). Patients homozygous for the risk allele (C) of the2174G/Cpolymorphismhad higher levels of IL-6 thandid those with other genotypes (P=0.04). Homozygous CC patients more frequently had a history of CVD (oddsratio, 2.15; 95% CI, 1.15 to 4.00; P=0.02) as well as a 87% higher rate of incident CV events (hazard ratio, 1.87; 95%CI, 1.02 to 3.44; P=0.04) compared with other genotypes.
Conclusions In patients with stages 2–5 CKD, high serum IL-6 is associated with history of CVD and predictsincident CV events. The parallel relationship with history of CVD and incident CV events of the 2174 G/Cpolymorphism in the IL-6 gene suggests that IL-6may be causally involved in the high CV risk in this population.
Clin J Am Soc Nephrol 10: ccc–ccc, 2014. doi: 10.2215/CJN.07000714
IntroductionClassic experimental studies by Russel Ross et al. inthe 1990s solidly established inflammation as a criticalcomponent of the atherosclerosis process (1). Duringthe last two decades, large cohort studies in the gen-eral population have shown strong links between bio-markers of inflammation and cardiovascular (CV)outcomes in the general population (2–5) and in patientswith CV disease (CVD) (6,7). Observational studies aremethodologically vulnerable for testing causality be-cause these studies are open to various sources ofbias and confounding. Mendelian randomization—i.e.,the random assortment of alleles at conception—offersan intriguing opportunity to limit problems inherent toobservational studies because categorization of patientsaccording to pertinent alleles is a sort of genetic ran-domization. Genetic variants may thus be used as indi-cators of environmental exposures in the observationalcontext (8). Large-scale Mendelian randomization stud-ies applying genetic polymorphisms of inflammatorycytokines (9) strongly support the hypothesis that, as
seen in experimental animals (10,11), the link betweeninflammation and atherosclerosis complication iscausal in nature.CV risk is a multifactorial problem in patients with
CKD (12). Systemic inflammation is common in thesepatients, particularly those with stage 5 CKD under-going dialysis (13,14). In line with studies in the gen-eral population (5,15), IL-6, a major proinflammatorycytokine, is an established strong predictor of adverseclinical outcomes in patients with stage 5D CKD (16–20).However, the relationship between IL-6 and CVD atearlier CKD stages was investigated in just one rela-tively small study by Barreto et al. (21), which was basedon a limited number of CV events (just 22 events). Inaddition, to date we lack specific proof that this relation-ship in the CKD population is causal.Circulating levels of IL-6 are genetically regulated.
Because transmission of genes is a random phenom-enon, gene polymorphisms modulating IL-6 synthesismay represent an unbiased means for testing whetherthe link between IL-6 and CV outcomes in patients
*National ResearchCouncil of Italy-Institute of ClinicalPhysiology & Instituteof Biomedicineand MolecularImmunology &Nephrology, Dialysisand TransplantationUnit of Reggio,Calabria, Italy; and†Department ofInternal Medicine,Erasmus UniversityMedical Center,Rotterdam, TheNetherlands.
Correspondence:Professor CarmineZoccali, CNR-IFC andNephrology, Dialysisand TransplantationUnit, Ospedali Riuniti,89124 ReggioCalabria, Italy, c/oEUROLINE, ViaVallone Petrara 55-57,89100 ReggioCalabria, Italy. [email protected]
www.cjasn.org Vol 10 February, 2014 Copyright © 2014 by the American Society of Nephrology 1
. Published on December 9, 2014 as doi: 10.2215/CJN.07000714CJASN ePress

with CKD is causal (Mendelian randomization). The 2174G/C single-nucleotide polymorphism is a functional vari-ant located in the promoter region of the IL-6 gene thatregulates the rate of IL-6 gene transcription (22–28) andtherefore represents a reliable research tool for testingthe nature (causal versus noncausal) of the link betweenIL-6 and CV outcomes in CKD. With this background inmind, we set out to confirm findings by Barreto et al. (21)in a large observational study with a carefully character-ized cohort of 755 patients with stages 2–5 CKD and to testwhether this relationship may underlie a causal link byapplying the Mendelian randomization approach (i.e., bystratifying the study population according to the func-tional 2174 G/C polymorphism in the IL-6 gene).
Materials and MethodsStudy ProtocolThe study protocol conformedwith the ethical guidelines
of our institution and was approved by ethical committeesof all participating units. Each participant provided writteninformed consent.
Patients with CKDOur study population included a genetically homogenous
series of 755 white patients from the same geographic area(southern Italy) (29), consecutively recruited from 22 ne-phrology units between October 2005 and September 2008.Eligible patients were age 18–75 years and in stable clinicalcondition. Exclusion criteria included acute or rapidly evolv-ing renal disease, kidney transplant, acute intercurrent infec-tions or acute inflammatory processes, pregnancy, cancer, ordiseases in the terminal phase. This cohort was described indetail elsewhere (30).
Control PopulationTo compare the allelic frequencies of the 2174 G/C
polymorphism observed in patients with CKD, westudied a sample of 463 consecutive blood donors of thegeneral population from the same geographical area ofpatients with CKD.
Follow-up and Study OutcomeAfter the initial assessment, patients were monitored for
a mean6SD of 31610 months (range, 0.3–48 months). Thestudy endpoint was fatal and nonfatal CV events as de-scribed elsewhere (30). These events included myocardialinfarction, documented by electrocardiography and bio-markers of myocardial injury; heart failure, defined asdyspnea in addition to two of the following conditions:raised jugular pressure, bi-basilar crackles, pulmonaryvenous hypertension, or interstitial edema on chest radi-ography requiring hospitalization; electrocardiography-documented arrhythmia; stroke; peripheral vascular disease;and major arterial or venous thrombotic episodes. Theseevents were accurately recorded during the follow-up period.The history of CVD was defined as the presence of at least
one of the following comorbidities at enrollment: myocar-dial infarction, heart failure, peripheral vascular disease,stroke, transient ischemic attack, or coronary surgery/angioplasty.
Laboratory MeasurementsIn the whole study population, blood sampling was
performed in the early morning after an overnight fast andplasma was stored at 280°C until analysis. Serum glucose,lipids, hemoglobin, albumin, creatinine, and C-reactiveprotein (CRP) were measured by standard methods in theroutine clinical laboratory. Serum IL-6 was measured byELISA (R&D Systems, Inc., Minneapolis, MN). The eGFRwas calculated by using the four-variables Modification ofDiet in Renal Disease study equation (31) and not by theCKD-Epidemiology Collaboration formula because the cre-atinine data were not traceable by isotope dilution massspectrophotometry during the study period. All patientswith CKD underwent a 24-hour urinary collection for themeasurement of proteinuria.
Genotyping of 2174G/C PolymorphismAllelic discrimination of 2174 G/C polymorphism was
performed using a custom TaqMan SNP Genotyping As-say provided by Applied Biosystems (Foster City, CA). Inthis assay, primers were designed to amplify a region thatincluded the mutation site specifically recognized by a fewprobes able to discriminate wild-type and mutated alleles.The sequences of primers and probes were: 59-CGACC-TAAGCTGCACTTTTCC-39 (forward primer) and 59-GGGCTGATTGGAAACCTTATTAAGATTG-39 (reverseprimer); 59-CCTTTAGCAT[G]GCAAGAC-39 (C allele-specificprobe) and 59- CCTTTAGCAT[C]GCAAGAC-39 (G allele-specific probe). Allelic discrimination was performed on a7900HT Fast Real-Time PCR platform and its accompany-ing Sequence Detection System software, version 2.4 (Ap-plied Biosystems). Briefly, genomic DNA was extractedfrom peripheral blood mononuclear cells using standardsalting out procedure (32). The reaction system contained20 ng of genomic DNA, 12.5 ml of 2X TaqMan UniversalPCR Master Mix No AmpErase UNG, 1,25 ml of 40X AssayMix (including unlabeled PCR primers, FAM and VIC dye-labeled TaqMan MGB probes), and H2O for a total volumeof 25 ml. A random 10% of samples were independentlyrepeated to confirm genotyping results. The genotype re-sults for these samples were completely consistent. Allanalyses were done blinded to clinical information.
Statistical AnalysesData were expressed as mean6SD, median and interquar-
tile range, or percentage frequency. Comparisons betweentwo groups were made by t-test, Mann–Whitney test, orchi-square test, as appropriate. The comparison amongmore than two groups was performed by ANOVA forlog-transformed variables, when appropriate. The devia-tion from Hardy–Weinberg equilibrium was assessed bythe chi-square test comparing observed and expected geno-type frequencies. The 95% confidence interval (95% CI) ofthe risk allele frequency was calculated as suggested by thestandard method (33).The functional form of serum IL-6 (as continuous, binary,
quartile, or quintile data) was formally investigated by theanalysis of Martingale residuals, and the binary form(below/above the median) provided the best data fitting.The relationships between serum levels of IL-6 and CVD
was evaluated by two approaches. First, we analyzed thebaseline association between serum IL-6 and history of
2 Clinical Journal of the American Society of Nephrology

CVD. Second, we investigated the predictive power ofserum IL-6 in the prospective cohort study. In both logisticand survival analyses, we considered variables that metcriteria to be confounders (i.e., variables related [P#0.10] toboth the exposure under investigation [serum IL-6 levelsbelow/above the median value] and history of CVD orincident fatal and nonfatal CV events, which are not aneffect of the exposure and are not in the causal pathwaybetween the exposure and outcome) (34). Tested covariatesincluded traditional risk factors (age, sex, smoking, dia-betes and glucose, cholesterol, and BP), factors specific toCKD (hemoglobin, albumin, eGFR, and urinary protein),antihypertensive treatment, body mass index, and CRP. Inboth logistic and Cox regression models, eGFR was alwaysforced because of the strong and significant correlationbetween eGFR and serum IL-6 (Table 1). To further inves-tigate the causal role of IL-6 in the pathway leading to CVevents in patients with CKD, we applied a Mendelian ran-domization approach (i.e., we stratified the study popu-lation according to the 2174 G/C polymorphism). Theseanalyses were appropriately adjusted for variables thatdiffered between CC and GC or GG patients and that ap-peared to be potential confounders (i.e., age, sex, choles-terol) for the interpretation of the link between the riskgenotype (CC) and the study outcomes.In the prospective cohort study, the potential distortion
on the study results due to the competing risks of deathwas assessed by comparing the incidence rate of death inexposed patients (high IL-6 levels or CC risk genotype) andunexposed patients (low IL-6 levels or GC/GG genotype).If a difference was found, the competing risk of death wasaccounted for by carrying out a survival analysis consid-ering a combined outcome: death/CV events (35). Datawere expressed as odds ratios (ORs; logistic regressionanalysis), hazard ratios (HRs; Cox regression model), 95%CIs, and P values. To internally validate the independentrelationships of serum IL-6 and 2174 G/C polymorphismswith history of CVD and incident CV events, a bootstrapresampling technique of 1000 samples (randomly extractedfrom the original sample) was performed (36). All potentialeffect modifications exerted by covariates on the relation-ship between the key exposures (serum IL-6 and2174 G/Cpolymorphism) and study outcomes were formally testedby introducing a multiplicative term into the models; nosignificant interaction was found.All calculations were made by using a standard statis-
tical package (IBM SPSS Statistics for Windows, version21.0. 0.1, IBM, Armonk, NY).
ResultsWe studied 755 patients with stages 2–5 CKD (stage 2,
3%; stage 3a, 22%; stage 3b, 38%; stage 4, 34%; stage 5, 3%).Four hundred fifty-three patients were male (60%), 263had type 2 diabetes (35%), and 98 were current smokers(13%). Two-hundred twenty-one patients (29%) had a his-tory of CVD (Table 1). One hundred nine patients had onlyone previous CV event, and 112 of them had two or moreprevious CV events. The first CV event in this populationwas myocardial infarction in 19 patients, heart failure in 26patients, peripheral vascular disease in 29 patients, strokein 12 patients, transient ischemic attack in 12 patients, and
coronary surgery/angioplasty in 11 patients. Six hundredninety-one patients (92%) were receiving antihypertensivetreatment: one medication in 19%, two medications in 29%,three medications in 28%, and four or more medications in16%. The mean eGFR was 36613 ml/min per 1.73 m2, andthe median 24-hour urinary protein excretion was 0.6 mg/24hours (interquartile range, 0.2–1.5 mg/24 hours). The medianIL-6 level was 2.5 pg/ml (interquartile range, 1.6–4.0 pg/ml).
Analyses Based on Serum IL-6 LevelsPatients with IL-6 above the median value were signif-
icantly older, more frequently had diabetes, and had higherserum glucose and 24-hour urinary protein values thanthose with IL-6 below this threshold (Table 1). Values foreGFR, hemoglobin, and albumin were lower in patientswith higher IL-6 than in those with IL-6 below the medianvalue. Systolic BP was higher and diastolic BP was lowerin patients with IL-6 levels above the median (Table 1). Asexpected, serum CRP levels were directly associated withIL-6 levels (r=0.57; P,0.001). On bivariate, multivariate,and bootstrapping validation analyses, patients with anIL-6 level above the median were more likely to havehad a history of CVD (P#0.01) than those with an IL-6level below the median (Table 2).During the follow-up, 42 patients died. The incidence
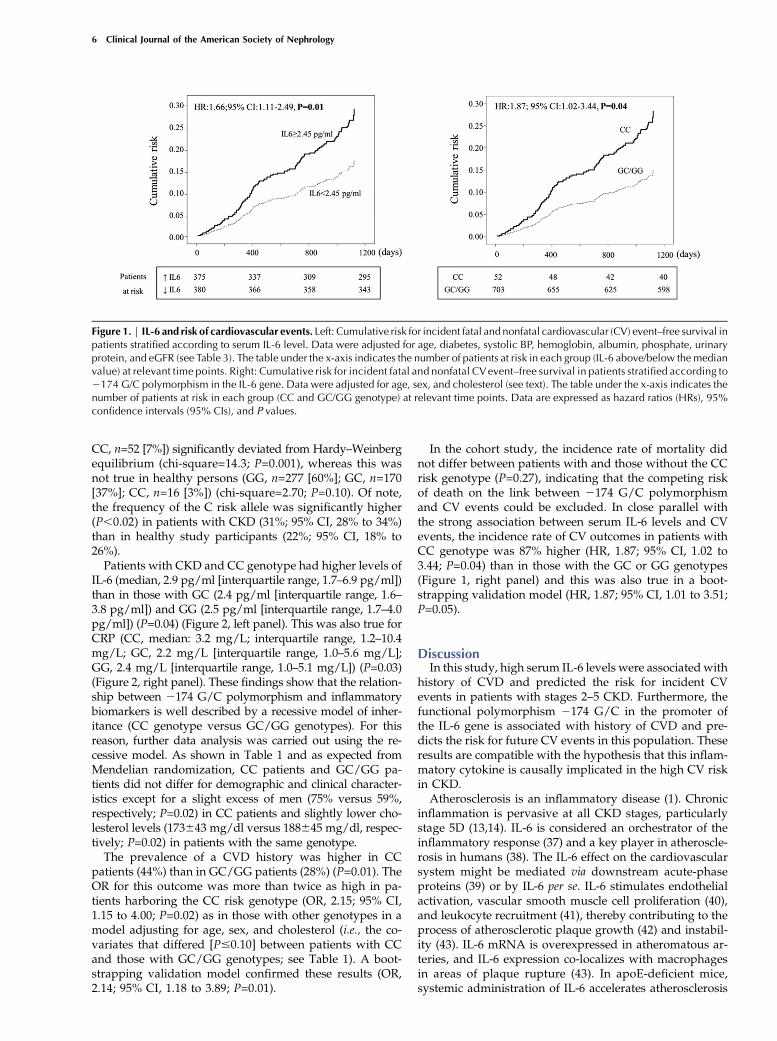
rate of mortality was three times higher (P=0.01) in patientswith IL-6 above the median (3 deaths per 100 person-years; 95% CI, 2.0 to 4.1 deaths per 100 patient-years)than in those with IL-6 below this threshold (1 death per100 person-years; 95% CI, 0.6 to 2.1 deaths per 100 patient-years). Overall, 117 patients had fatal and nonfatal CVevents. As shown in Table 3, on bivariate, multivariate,and bootstrapping validation analyses, the incidence rateof fatal and nonfatal CV outcomes was significantly higher(P#0.02) in patients with IL-6 levels above the median (8.6CV events per 100 person-years; 95% CI, 2.5 to 5.0 CVevents per 100 patient-years) than in those with IL-6 levelsbelow this threshold (3.6 CV events per 100 person-years;95% CI, 6.9 to 10.8 CV events per 100 patient-years) (Fig-ure 1, left panel). CKD stages did not modify the relation-ship between IL-6 and CV risk (P for interaction=0.33).Further analyses investigating IL-6 as a continuous vari-able confirmed this biomarker as a strong and indepen-dent risk factor for study outcomes (history of CVD:bivariate analysis OR (1 pg/ml), 1.16 [95% CI, 1.10 to 1.26],P,0.001, and multivariate analysis OR, 1.10 [95% CI, 1.02 to1.20], P=0.02; incident CV events, bivariate analysis HR(1 pg/ml), 1.14 [95% CI, 1.07 to 1.22], P,0.001, and multi-variate analysis HR, 1.12 [95% CI, 1.03 to 1.22], P,0.001).To account for the potential effect of competing risks due
to death on the relationship between IL-6 and CV out-comes, an additional adjusted analysis that considered acombined endpoint of death/CV events was performed.This multivariate analysis showed that the HR of thecombined endpoint was about 1.5 times higher (HR, 1.54;95% CI, 1.05 to 2.26; P=0.03) in patients with IL-6 levelsabove the median as compared with the remaining ones.
Analyses Based on the 2174 G/C PolymorphismIn patients with CKD, the genotype distribution of 2174
G/C polymorphism (GG, n=333 [44%]; GC, n=370 [49%];
Clin J Am Soc Nephrol 10: ccc–ccc, February, 2014 IL-6 and CV Risk in CKD, Spoto et al. 3

Tab
le1.
Maindem
ograp
hic
andclinical
charac
teristicsofthestudypopulationac
cordingto
serum
IL-6
leve
lsan
d2174G/C
polymorphism
Cha
racteristic
Who
leGroup
(n=75
5)Se
rum
IL-6
Lev
elGen
otyp
e
,2.5pg
/ml(n=
380)
$2.5pg
/ml(n=
375)
PValue
CC(n=52
)GC/GG
(n=70
3)PValue
Age
(yr)
62611
59612
6469
,0.00
159
613
62610
0.09
Men
(%)
453(60)
224(59)
229(61)
0.55
39(75)
414(59)
0.02
Diabe
tes(%
)26
3(35)
105(28)
158(42)
,0.00
121
(40)
242(34)
0.38
Current
smok
ers(%
)98
(13)
55(14)
43(11)
0.22
9(17)
89(13)
0.34
CVcomorbidities(%
)22
1(29)
82(22)
139(37)
,0.00
123
(44)
198(28)
0.01
Bod
ymassindex
(kg/
m2 )
28.264.7
27.364.3
29.064.8
,0.00
127
.963.8
28.264.7
0.54
SystolicBP(m
mHg)
1346
1813
2617
1356
190.03
1326
1613
4618
0.41
DiastolicBP(m
mHg)
78611
79610
77611
0.01
76610
78610
0.15
Antihyp
ertens
ivetreatm
ent(%)
691(92)
341(90)
350(93)
0.89
44(85)
647(92)
0.69
Glucose
(mg/
dl)
1166
4910
9641
1226
56,0.00
198
(87–
127)
99(88–
120)
0.65
Total
cholesterol(mg/
dl)
1876
4518
9643
1846
460.12
1736
4318
8645
0.02
Hem
oglobin(g/dl)
12.861.8
13.161.8
12.661.8
,0.00
112
62.0
1361.8
0.29
Album
in(g/dl)
4.26
0.5
4.26
0.5
4.16
0.5
0.01
4.16
0.4
4.26
0.5
0.53
CRP(m
g/L)
2.4(1.0–5.5)
1.4(0.7–2.8)
4.3(1.9–9.0)
,0.00
13.2(1.2–10
)2.3(1.0–5.4)
0.06
Phosph
ate(m
g/dl)
3.76
0.8
3.66
0.7
3.8 6
0.8
0.02
3.71
60.68
3.72
60.78
0.92
eGFR
(ml/min
per1.73
m2 )
36613
38613
34613
,0.00
134
612
36613
0.32
Urina
ryprotein(m
g/24
hr)
0.6(0.2–1.5)
0.5(0.2–10.2)
0.6(0.2–1.7)
0.01
0.7(0.2–1.6)
0.6(0.2–1.5)
0.53
Dataareexpressedas
mean6
SD,m
edianan
dinterqua
rtile
rang
e,or
percen
tage
freq
uen
cy,a
sap
prop
riate.CV,cardiova
scular;C
RP,C
-reactiveprotein.
4 Clinical Journal of the American Society of Nephrology

Tab
le2.
Logistic
regressionmodelsofhistory
ofca
rdiova
sculardisea
se
Variable
Bivariate
Multiva
riate
Boo
tstrap
ping
Validation
OR(95%
CI)
PValue
OR(95%
CI)
PValue
OR(95%
CI)
PValue
Serum
IL-6
value(0
[,2.5pg
/ml];1
[$2.5pg
/ml])a
2.14
(1.55to
2.95
),0.00
11.58
(1.11to
2.24
)0.01
1.58
(1.12to
2.24
)0.01
Age
(inyr)
1.05
(1.03to
1.07
),0.00
11.05
(1.03to
1.07
),0.00
1Diabe
tes(0=no
;1=ye
s)2.83
(1.99to
4.03
),0.00
12.83
(1.97to
4.08
),0.00
1Sy
stolicBP(inmmHg)
1.00
(0.99to
1.01
)0.93
1.00
(0.99to
1.01
)0.94
Hem
oglobin(ing/
dl)
1.04
(0.94to
1.16
)0.47
1.04
(0.93to
1.16
)0.49
Album
in(ing/
dl)
0.74
(0.50to
1.11
)0.15
0.74
(0.50to
1.11
)0.14
Phosph
ate(inmg/
dl)
1.02
(0.80to
1.30
)0.86
1.02
(0.78to
1.34
)0.87
Urina
ryprotein(inmg/
24hr)
1.01
(0.89to
1.13
)0.93
1.01
(0.88to
1.14
)0.93
eGFR
(ml/min
per1.73
m2 )
1.00
(0.98to
1.01
)0.57
1.00
(0.98to
1.01
)0.57
OR,o
ddsratio;
95%
CI,95
%confi
den
ceinterval.
a Below
/ab
ovethemed
ianva
lue(inpa
renthe
ses).T
hedescription
ofthemod
elbu
ildingstrategy
isrepo
rted
intheMaterialsan
dMetho
dssection.
Tab
le3.
Coxregressionmodelsofinciden
tca
rdiova
scularev
ents
Variable
Bivariate
Multiva
riate
Boo
tstrap
pingValidation
HR(95%
CI)
PValue
HR(95%
CI)
PValue
HR(95%
CI)
PValue
Serum
IL-6
value(0
[,2.5pg
/ml];1
[$2.5pg
/ml])a
2.37
(1.61to
3.51
),0.00
11.66
(1.11to
2.49
)0.01
1.66
(1.10to
2.52
)0.02
Age
(inyr)
1.07
(1.04to
1.10
),0.00
11.07
(1.03to
1.10
),0.00
1Diabe
tes(0=no
;1=ye
s)1.59
(1.09to
2.32
)0.02
1.59
(1.06to
2.37
)0.02
SystolicBP(inmmHg)
1.00
(1.00to
1.02
)0.31
1.00
(1.00to
1.02
)0.31
Hem
oglobin(ing/
dl)
0.91
(0.80to
1.02
)0.10
0.91
(0.81to
1.02
)0.09
Album
in(ing/
dl)
0.82
(0.53to
1.27
)0.38
0.82
(0.52to
1.29
)0.39
Phosph
ate(inmg/
dl)
1.13
(0.88to
1.44
)0.34
1.13
(0.88to
1.45
)0.35
Urina
ryprotein(inmg/
24hr)
1.05
(0.94to
1.17
)0.38
1.05
(0.93to
1.18
)0.44
eGFR
(ml/min
per1.73
m2 )
1.01
(0.99to
1.02
)0.44
1.01
(0.99to
1.02
)0.49
HR,h
azardratio.
a Below
/ab
ovethemed
ianva
lue(inpa
renthe
ses).T
hedescription
ofthemod
elbu
ildingstrategy
isrepo
rted
intheMaterialsan
dMetho
dssection.
Clin J Am Soc Nephrol 10: ccc–ccc, February, 2014 IL-6 and CV Risk in CKD, Spoto et al. 5
CC, n=52 [7%]) significantly deviated from Hardy–Weinbergequilibrium (chi-square=14.3; P=0.001), whereas this wasnot true in healthy persons (GG, n=277 [60%]; GC, n=170[37%]; CC, n=16 [3%]) (chi-square=2.70; P=0.10). Of note,the frequency of the C risk allele was significantly higher(P,0.02) in patients with CKD (31%; 95% CI, 28% to 34%)than in healthy study participants (22%; 95% CI, 18% to26%).Patients with CKD and CC genotype had higher levels of
IL-6 (median, 2.9 pg/ml [interquartile range, 1.7–6.9 pg/ml])than in those with GC (2.4 pg/ml [interquartile range, 1.6–3.8 pg/ml]) and GG (2.5 pg/ml [interquartile range, 1.7–4.0pg/ml]) (P=0.04) (Figure 2, left panel). This was also true forCRP (CC, median: 3.2 mg/L; interquartile range, 1.2–10.4mg/L; GC, 2.2 mg/L [interquartile range, 1.0–5.6 mg/L];GG, 2.4 mg/L [interquartile range, 1.0–5.1 mg/L]) (P=0.03)(Figure 2, right panel). These findings show that the relation-ship between 2174 G/C polymorphism and inflammatorybiomarkers is well described by a recessive model of inher-itance (CC genotype versus GC/GG genotypes). For thisreason, further data analysis was carried out using the re-cessive model. As shown in Table 1 and as expected fromMendelian randomization, CC patients and GC/GG pa-tients did not differ for demographic and clinical character-istics except for a slight excess of men (75% versus 59%,respectively; P=0.02) in CC patients and slightly lower cho-lesterol levels (173643 mg/dl versus 188645 mg/dl, respec-tively; P=0.02) in patients with the same genotype.The prevalence of a CVD history was higher in CC
patients (44%) than in GC/GG patients (28%) (P=0.01). TheOR for this outcome was more than twice as high in pa-tients harboring the CC risk genotype (OR, 2.15; 95% CI,1.15 to 4.00; P=0.02) as in those with other genotypes in amodel adjusting for age, sex, and cholesterol (i.e., the co-variates that differed [P#0.10] between patients with CCand those with GC/GG genotypes; see Table 1). A boot-strapping validation model confirmed these results (OR,2.14; 95% CI, 1.18 to 3.89; P=0.01).
In the cohort study, the incidence rate of mortality didnot differ between patients with and those without the CCrisk genotype (P=0.27), indicating that the competing riskof death on the link between 2174 G/C polymorphismand CV events could be excluded. In close parallel withthe strong association between serum IL-6 levels and CVevents, the incidence rate of CV outcomes in patients withCC genotype was 87% higher (HR, 1.87; 95% CI, 1.02 to3.44; P=0.04) than in those with the GC or GG genotypes(Figure 1, right panel) and this was also true in a boot-strapping validation model (HR, 1.87; 95% CI, 1.01 to 3.51;P=0.05).
DiscussionIn this study, high serum IL-6 levels were associated with
history of CVD and predicted the risk for incident CVevents in patients with stages 2–5 CKD. Furthermore, thefunctional polymorphism 2174 G/C in the promoter ofthe IL-6 gene is associated with history of CVD and pre-dicts the risk for future CV events in this population. Theseresults are compatible with the hypothesis that this inflam-matory cytokine is causally implicated in the high CV riskin CKD.Atherosclerosis is an inflammatory disease (1). Chronic
inflammation is pervasive at all CKD stages, particularlystage 5D (13,14). IL-6 is considered an orchestrator of theinflammatory response (37) and a key player in atheroscle-rosis in humans (38). The IL-6 effect on the cardiovascularsystem might be mediated via downstream acute-phaseproteins (39) or by IL-6 per se. IL-6 stimulates endothelialactivation, vascular smooth muscle cell proliferation (40),and leukocyte recruitment (41), thereby contributing to theprocess of atherosclerotic plaque growth (42) and instabil-ity (43). IL-6 mRNA is overexpressed in atheromatous ar-teries, and IL-6 expression co-localizes with macrophagesin areas of plaque rupture (43). In apoE-deficient mice,systemic administration of IL-6 accelerates atherosclerosis
Figure 1. | IL-6 and risk of cardiovascular events. Left: Cumulative risk for incident fatal and nonfatal cardiovascular (CV) event–free survival inpatients stratified according to serum IL-6 level. Data were adjusted for age, diabetes, systolic BP, hemoglobin, albumin, phosphate, urinaryprotein, and eGFR (see Table 3). The table under the x-axis indicates the number of patients at risk in each group (IL-6 above/below the medianvalue) at relevant time points. Right: Cumulative risk for incident fatal and nonfatal CVevent–free survival in patients stratified according to2174 G/C polymorphism in the IL-6 gene. Data were adjusted for age, sex, and cholesterol (see text). The table under the x-axis indicates thenumber of patients at risk in each group (CC and GC/GG genotype) at relevant time points. Data are expressed as hazard ratios (HRs), 95%confidence intervals (95% CIs), and P values.
6 Clinical Journal of the American Society of Nephrology

(10). Elevated levels of IL-6 are predictive of future CVevents in healthy men (15) and women (44) and are mark-ers of poor prognosis in patients with chronic angina (45)and acute coronary syndrome (46). IL-6 levels are mark-edly elevated in CKD, a phenomenon only in part ex-plained by reduced renal clearance of this cytokine.Furthermore, the observation of a parallel increase in IL-6and CRP in our study is in keeping with the notion that IL-6drives the synthesis of CRP. High IL-6 has been solidly as-sociated with mortality in patients with stage 5 CKD whoare being maintained on long-term dialysis (16–20).To the best of our knowledge, only one study has tested
the relationship between IL-6 and CV mortality in CKD(21). This seminal study was carried out in a small cohortof 125 patients, was based on a limited number of CVevents (n=22), and also included dialysis patients (34% ofthe whole cohort) (21). Our study, based on a large CKDcohort composed exclusively of predialysis patients andincluding a large number of CV events, confirmed pilotdata by Barreto et al. (21) and showed that high IL-6 iscoherently associated both with history of CVD as wellas with incident CV events.Being observational in nature, findings in studies discussed
above, including our analysis based on circulating IL-6,remain hypothesis-generating and as such leave unresolvedthe critical question of whether this cytokine is causally im-plicated in CV complications in patients with predialysis CKD.This question can be resolved only by a full-fledged clinical trial.The Mendelian randomization approach is useful step in
the pathway to discovery in clinical research. Since geneticpolymorphisms are distributed randomly at gamete for-mation and since genotypes precede phenotypes and donot change over time, comparing individuals harboring agiven risk allele for the expression of a corresponding riskfactor with those without the risk allele in question mayallow unbiased assessment of the link between the attendantrisk factor and relevant clinical outcomes. In this perspective,we used the functional polymorphism2174 G/C in the pro-moter of the IL-6 gene as a marker to further investigate thelink between IL-6 and CV events in patients with CKD. The
2174 G/C polymorphism is a common variant that regu-lates the serum concentration of IL-6 (22–28). In keepingwith previous studies in patients with CVD (28), coronaryartery bypass grafting surgery (23,25), carotid atherosclero-sis (24), abdominal aortic aneurysm (22), and dialysis (26),we found that patients with CKD and CC genotype hadhigher circulating levels of IL-6 and CRP than those harbor-ing GC or GG genotypes, specifically legitimating the use ofthis genetic marker as an unbiased means for assessing thecausal nature of the link between the gene product (IL-6) ofthis polymorphism and CV complications in CKD. Interest-ingly, this analysis showed that this polymorphism is inde-pendently associated both with the history of CVD as wellas with incident CV events. Such associations, which wentalong with the previously described relationships of serumIL-6 with the same outcomes, further strengthen the hypoth-esis that IL-6 is a direct player in atherosclerotic complicationsin CKD. Moreover, the observation that the distribution ofgenotypes frequency of the 2174 G/C polymorphism in pa-tients with CKD was not in Hardy–Weinberg equilibriumand that the frequency of the C allele was significantly higherin patients CKD compared with general population of thesame geographic area, offers additional circumstantial evi-dence that IL-6 is a causal risk factor for CV events in thispopulation (47).Mendelian randomization studies support causal inter-
pretations but do not constitute definitive proof for cau-sality, which demands specific experimental evidence (i.e.,a formal randomized clinical trial). In this respect, meta-analytic data from two genetic consortia exploring the ef-fect of a polymorphism in the IL-6 receptor on the risk ofcoronary artery disease showed the allele that attenuatedIL-6 signaling was significantly associated with reducedrisk of coronary heart disease (48). Notably, the relevanceof this genetic association for the control of inflammation isshown by a meta-analysis of clinical trials testing a mono-clonal antibody against the IL-6 receptor (tocilizumab) inrheumatoid arthritis and documenting that lowering serumlevels of IL-6 is an effective strategy to induce the remissionof this chronic inflammatory disease (49).
Figure 2. | Inflammatory biomarkers and 2 174 G/C polymorphism. Serum levels of IL-6 (left panel) and C-reactive protein (right panel)according to2174 G/C polymorphism in IL-6 gene. Data are expressed as medians. The interquartile ranges are indicated in parentheses. Thecomparison among groups was made by ANOVA.
Clin J Am Soc Nephrol 10: ccc–ccc, February, 2014 IL-6 and CV Risk in CKD, Spoto et al. 7

Some limitations should be acknowledged. First, eventhough our cohort study registered a sizable number ofcardiovascular events, the number of deaths (n=42) waslimited, preventing adequately adjusted analyses focusingon this major outcome. However, the analysis of the pri-mary outcome in this study, incident CV events, whichwas robustly based on 117 events, showed parallel linksbetween serum IL-6 and the genetic marker of this cyto-kine with the same events.Second, although Mendelian randomization is a powerful
approach for inferring causality in observational studies, itsapplication has potential limitations. Genetic variants can beindicators of environmental exposures on condition thatthere is no genetic admixture, pleiotropy or linkage disequi-librium. However, it is reasonable to believe that in our studyall these assumptions are fulfilled. Our population is genet-ically homogeneous (29) and the 2174G/C polymorphismis a functional variant directly responsible for serum levelsof IL-6 (22–28). Furthermore, pleiotropy seems highly un-likely because of the location of 2174 G/C polymorphismin the promoter region of the gene.Third, although we demonstrated that our findings had
high internal validity by bootstrap modeling, replication ofthe results in a second cohort is a required proof for theexternal generalizability of findings in observational studies.In this respect, our observational study in a large southernEuropean cohort confirms findings in a small central Europeancohort (21). Furthermore, our study is the first applying agenetic marker of IL-6 to express the nature (causal versusnot causal) of the link between IL-6 and CV events in pa-tients with CKD.In conclusion, high serum IL-6 is associated with both a
history of CVD and future CV events in patients with CKD,and these associations are fully confirmed by the applica-tion of a functional polymorphism in the IL-6 gene. Overall,this study is compatible with the hypothesis that the IL-6plays a causal role in the high CV risk of patients with CKD.
AcknowledgmentsWe thank Cristina Politi andMaria Cristina Sanguedolce for their
technical collaboration in genetic study.This study is part of the Syskid project, which is supported through
European Union’s FP7, grant agreement number HEALTH-F2-2009-241544.
Contributors: members of the Southern Italy CKD CohortWorking Group (in alphabetical order): Audino A, Bruzzese V,Caglioti A, Campo S, Caridi G, Catalano F, Chiarella S, Cicchetti T,D’Anello E, Enia G, Fabiano F, Fatuzzo P, Ferini S, Garozzo M,Grandinetti F, GulloM,MafricaA,Maimone I,Mancuso F,ManninoM,Marino F, Natale G, Palma L, Papalia T, ParlongoG, Pinciaroli A,PinnaM, Plutino D, PostorinoM, Pugliese A, Rapisarda F, SantoroO,Tramontana D.
DisclosuresNone.
References1. Ross R: Atherosclerosis—an inflammatory disease. N Engl J Med
340: 115–126, 19992. Ridker PM, Cushman M, Stampfer MJ, Tracy RP, Hennekens CH:
Inflammation, aspirin, and the risk of cardiovascular disease inapparently healthy men. N Engl J Med 336: 973–979, 1997
3. Ridker PM, Hennekens CH, Buring JE, Rifai N: C-reactiveprotein and other markers of inflammation in the prediction ofcardiovascular disease in women. N Engl J Med 342: 836–843,2000
4. Pai JK, Pischon T, Ma J, Manson JE, Hankinson SE, Joshipura K,Curhan GC, Rifai N, Cannuscio CC, Stampfer MJ, Rimm EB: In-flammatorymarkers and the risk of coronary heart disease inmenand women. N Engl J Med 351: 2599–2610, 2004
5. Danesh J, Kaptoge S, Mann AG, Sarwar N, Wood A, AnglemanSB, Wensley F, Higgins JP, Lennon L, Eiriksdottir G, Rumley A,Whincup PH, Lowe GD, Gudnason V: Long-term interleukin-6levels and subsequent risk of coronary heart disease: two newprospective studies and a systematic review. PLoS Med 5: e78,2008
6. Ridker PM, Rifai N, Pfeffer MA, Sacks FM, Moye LA, Goldman S,Flaker GC, Braunwald E; Cholesterol and Recurrent Events(CARE) Investigators: Inflammation, pravastatin, and the risk ofcoronary events after myocardial infarction in patients with av-erage cholesterol levels. Circulation 98: 839–844, 1998
7. Libby P, Ridker PM, Maseri A: Inflammation and atherosclerosis.Circulation 105: 1135–1143, 2002
8. Davey Smith G, Hemani G: Mendelian randomization: geneticanchors for causal inference in epidemiological studies. HumMol Genet 23[R1]: R89–R98, 2014
9. Hingorani AD, Casas JP; Interleukin-6 Receptor MendelianRandomisation Analysis (IL6R MR) Consortium: The interleukin-6 receptor as a target for prevention of coronary heart disease:a mendelian randomisation analysis. Lancet 379: 1214–1224,2012
10. Huber SA, Sakkinen P, Conze D, HardinN, Tracy R: Interleukin-6exacerbates early atherosclerosis in mice. Arterioscler ThrombVasc Biol 19: 2364–2367, 1999
11. Schuett H, Oestreich R, Waetzig GH, AnnemaW, Luchtefeld M,Hillmer A, Bavendiek U, von Felden J, Divchev D, Kempf T,Wollert KC, Seegert D, Rose-John S, Tietge UJ, Schieffer B, GroteK: Transsignaling of interleukin-6 crucially contributes to ath-erosclerosis inmice.Arterioscler ThrombVasc Biol 32: 281–290,2012
12. Zoccali C: Traditional and emerging cardiovascular and renalrisk factors: An epidemiologic perspective.Kidney Int 70: 26–33,2006
13. Stenvinkel P, KettelerM, Johnson RJ, LindholmB, Pecoits-Filho R,RiellaM,HeimburgerO, Cederholm T,GirndtM: IL-10, IL-6, andTNF-alpha: Central factors in the altered cytokine network ofuremia—the good, the bad, and the ugly. Kidney Int 67: 1216–1233, 2005
14. Zoccali C, Mallamaci F, Tripepi G: Inflammatory proteins aspredictors of cardiovascular disease in patients with end-stagerenal disease. Nephrol Dial Transplant 19[Suppl 5]: V67–V72,2004
15. Ridker PM, Rifai N, Stampfer MJ, Hennekens CH: Plasma con-centration of interleukin-6 and the risk of future myocardial in-farction among apparently healthy men. Circulation 101: 1767–1772, 2000
16. Pecoits-Filho R, Barany P, LindholmB,HeimburgerO, StenvinkelP: Interleukin-6 is an independent predictor of mortality in pa-tients starting dialysis treatment. Nephrol Dial Transplant 17:1684–1688, 2002
17. Zoccali C, Tripepi G, Mallamaci F: Dissecting inflammation inESRD: Do cytokines and C-reactive protein have a complemen-tary prognostic value for mortality in dialysis patients? J Am SocNephrol 17[Suppl 3]: S169–S173, 2006
18. Honda H, Qureshi AR, Heimburger O, Barany P, Wang K,Pecoits-Filho R, Stenvinkel P, Lindholm B: Serum albumin, C-reactive protein, interleukin 6, and fetuin a as predictors ofmalnutrition, cardiovascular disease, and mortality in patientswith ESRD. Am J Kidney Dis 47: 139–148, 2006
19. Meuwese CL, Snaedal S, Halbesma N, Stenvinkel P, Dekker FW,Qureshi AR, Barany P, Heimburger O, Lindholm B, Krediet RT,Boeschoten EW, Carrero JJ: Trimestral variations of C-reactiveprotein, interleukin-6 and tumour necrosis factor-a are similarlyassociated with survival in haemodialysis patients.Nephrol DialTransplant 26: 1313–1318, 2011
20. Rao M, Guo D, Perianayagam MC, Tighiouart H, Jaber BL,Pereira BJ, Balakrishnan VS: Plasma interleukin-6 predicts
8 Clinical Journal of the American Society of Nephrology

cardiovascular mortality in hemodialysis patients. Am J KidneyDis 45: 324–333, 2005
21. Barreto DV, Barreto FC, Liabeuf S, Temmar M, Lemke HD,Tribouilloy C, Choukroun G, Vanholder R, Massy ZA; EuropeanUremic Toxin Work Group (EUTox): Plasma interleukin-6 is in-dependently associated with mortality in both hemodialysis andpre-dialysis patients with chronic kidney disease. Kidney Int 77:550–556, 2010
22. Jones KG, Brull DJ, Brown LC, Sian M, Greenhalgh RM,Humphries SE, Powell JT: Interleukin-6 (IL-6) and the prognosis ofabdominal aortic aneurysms. Circulation 103: 2260–2265, 2001
23. Brull DJ, Montgomery HE, Sanders J, Dhamrait S, Luong L,Rumley A, LoweGD,Humphries SE: Interleukin-6 gene -174g.cand -572g.c promoter polymorphisms are strong predictors ofplasma interleukin-6 levels after coronary artery bypass surgery.Arterioscler Thromb Vasc Biol 21: 1458–1463, 2001
24. Jerrard-Dunne P, Sitzer M, Risley P, Steckel DA, Buehler A, vonKegler S, Markus HS; Carotid Atherosclerosis Progression Study:Interleukin-6 promoter polymorphism modulates the effects ofheavy alcohol consumption on early carotid artery atheroscle-rosis: the Carotid Atherosclerosis Progression Study (CAPS).Stroke 34: 402–407, 2003
25. Wypasek E, Undas A, Sniezek-Maciejewska M, Kapelak B,PlicnerD, Stepien E, Sadowski J: The increased plasmaC-reactiveprotein and interleukin-6 levels in patients undergoingcoronary artery bypass grafting surgery are associated withthe interleukin-6-174G . C gene polymorphism. Ann ClinBiochem 47: 343–349, 2010
26. Liu Y, Berthier-Schaad Y, Fallin MD, Fink NE, Tracy RP, Klag MJ,Smith MW, Coresh J: IL-6 haplotypes, inflammation, and riskfor cardiovascular disease in a multiethnic dialysis cohort. J AmSoc Nephrol 17: 863–870, 2006
27. Gillerot G, Goffin E, Michel C, Evenepoel P, BiesenWV, TintillierM, Stenvinkel P, Heimburger O, Lindholm B, Nordfors L,Robert A, Devuyst O: Genetic and clinical factors influence thebaseline permeability of the peritonealmembrane.Kidney Int 67:2477–2487, 2005
28. Jenny NS, Tracy RP, Ogg MS, Luong A, Kuller LH, Arnold AM,Sharrett AR, Humphries SE: In the elderly, interleukin-6 plasmalevels and the -174G.C polymorphism are associated with thedevelopment of cardiovascular disease. Arterioscler ThrombVasc Biol 22: 2066–2071, 2002
29. Di Gaetano C, Voglino F, Guarrera S, Fiorito G, Rosa F, Di BlasioAM, Manzini P, Dianzani I, Betti M, Cusi D, Frau F, Barlassina C,Mirabelli D, Magnani C, Glorioso N, Bonassi S, Piazza A,Matullo G: An overview of the genetic structure within the Italianpopulation from genome-wide data. PLoS ONE 7: e43759, 2012
30. Zoccali C, Leonardis D, Enia G, Postorino M, Mallamaci F;MAURO study working group: The MAURO study: Multiple in-tervention and audit in renal diseases to optimize care. J Nephrol21: 20–22, 2008
31. Levey AS, Coresh J, Greene T, Stevens LA, Zhang YL, HendriksenS, Kusek JW, Van Lente F; Chronic Kidney Disease EpidemiologyCollaboration: Using standardized serum creatinine values inthe modification of diet in renal disease study equation for esti-mating glomerular filtration rate. Ann Intern Med 145: 247–254,2006
32. Miller SA, Dykes DD, PoleskyHF: A simple salting out procedurefor extracting DNA from human nucleated cells. Nucleic AcidsRes 16: 1215, 1988
33. Newcombe RG: Confidence Intervals for Proportion and RelatedMeasures of Effect Size. Boca Raton, FL: CRC Press, 2013, pp181–182
34. Jager KJ, Zoccali C, Macleod A, Dekker FW: Confounding: Whatit is and how to deal with it. Kidney Int 73: 256–260, 2008
35. Varadhan R,Weiss CO, Segal JB,Wu AW, Scharfstein D, Boyd C:Evaluating health outcomes in the presence of competing risks: Areview of statistical methods and clinical applications.Med Care48[Suppl]: S96–S105, 2010
36. Steverberg EW:Clinical PredictionModels. A Practical Approachto Development,Validation, and Updating, New York, Springer,2009. pp. 93–98 and 303–304
37. Naka T,NishimotoN, Kishimoto T: The paradigmof IL-6: Frombasicscience to medicine. Arthritis Res 4[Suppl 3]: S233–S242, 2002
38. Hartman J, Frishman WH: Inflammation and atherosclerosis: Areview of the role of interleukin-6 in the development of ath-erosclerosis and the potential for targeted drug therapy. CardiolRev 22: 147–151, 2014
39. Baumann H, Gauldie J: Regulation of hepatic acute phaseplasma protein genes by hepatocyte stimulating factors andother mediators of inflammation. Mol Biol Med 7: 147–159,1990
40. Morimoto S, Nabata T, Koh E, Shiraishi T, Fukuo K, Imanaka S,Kitano S, Miyashita Y, Ogihara T: Interleukin-6 stimulatesproliferation of cultured vascular smooth muscle cells in-dependently of interleukin-1 beta. J Cardiovasc Pharmacol 17[Suppl 2]: S117–S118, 1991
41. Romano M, Sironi M, Toniatti C, Polentarutti N, Fruscella P,Ghezzi P, Faggioni R, Luini W, van Hinsbergh V, Sozzani S,Bussolino F, Poli V, Ciliberto G, Mantovani A: Role of IL-6 and itssoluble receptor in induction of chemokines and leukocyte re-cruitment. Immunity 6: 315–325, 1997
42. Schieffer B, Selle T, Hilfiker A, Hilfiker-Kleiner D, Grote K, TietgeUJ, Trautwein C, Luchtefeld M, Schmittkamp C, Heeneman S,Daemen MJ, Drexler H: Impact of interleukin-6 on plaque de-velopment and morphology in experimental atherosclerosis.Circulation 110: 3493–3500, 2004
43. Schieffer B, Schieffer E, Hilfiker-Kleiner D, Hilfiker A, KovanenPT, Kaartinen M, Nussberger J, Harringer W, Drexler H:Expression of angiotensin II and interleukin 6 in humancoronary atherosclerotic plaques: Potential implications for in-flammation and plaque instability. Circulation 101: 1372–1378,2000
44. Volpato S, Guralnik JM, Ferrucci L, Balfour J, Chaves P, Fried LP,Harris TB: Cardiovascular disease, interleukin-6, and risk ofmortality in older women: TheWomen’sHealth andAging Study.Circulation 103: 947–953, 2001
45. Ikonomidis I, Andreotti F, Economou E, Stefanadis C, ToutouzasP, Nihoyannopoulos P: Increased proinflammatory cytokinesin patients with chronic stable angina and their reduction byaspirin. Circulation 100: 793–798, 1999
46. Ikeda U, Ito T, Shimada K: Interleukin-6 and acute coronarysyndrome. Clin Cardiol 24: 701–704, 2001
47. Wang J, Shete S: A test for genetic association that incorporatesinformation about deviation from Hardy-Weinberg proportionsin cases. Am J Hum Genet 83: 53–63, 2008
48. Sarwar N, Butterworth AS, Freitag DF, Gregson J, Willeit P,Gorman DN, Gao P, Saleheen D, Rendon A, Nelson CP, BraundPS, Hall AS, Chasman DI, Tybjærg-Hansen A, Chambers JC,Benjamin EJ, Franks PW, Clarke R, Wilde AA, Trip MD, Steri M,Witteman JC, Qi L, van der Schoot CE, de Faire U, Erdmann J,Stringham HM, Koenig W, Rader DJ, Melzer D, Reich D, PsatyBM, Kleber ME, Panagiotakos DB, Willeit J, Wennberg P,Woodward M, Adamovic S, Rimm EB, Meade TW, Gillum RF,Shaffer JA, Hofman A, Onat A, Sundstrom J, Wassertheil-SmollerS, Mellstrom D, Gallacher J, Cushman M, Tracy RP, Kauhanen J,KarlssonM, Salonen JT,Wilhelmsen L, Amouyel P, Cantin B, BestLG, Ben-Shlomo Y, Manson JE, Davey-Smith G, de Bakker PI,O’Donnell CJ, Wilson JF, Wilson AG, Assimes TL, Jansson JO,Ohlsson C, Tivesten A, Ljunggren O, Reilly MP, Hamsten A,Ingelsson E, Cambien F, Hung J, Thomas GN, Boehnke M,Schunkert H, Asselbergs FW, Kastelein JJ, Gudnason V, SalomaaV, Harris TB, Kooner JS, Allin KH, Nordestgaard BG, HopewellJC, Goodall AH, Ridker PM, Holm H, Watkins H, OuwehandWH, SamaniNJ, Kaptoge S,Di Angelantonio E,HarariO,DaneshJ; IL6R Genetics Consortium Emerging Risk Factors Collabora-tion: Interleukin-6 receptor pathways in coronary heart disease:A collaborative meta-analysis of 82 studies. Lancet 379: 1205–1213, 2012
49. Navarro G, Taroumian S, Barroso N, Duan L, Furst D: Tocilizu-mab in rheumatoid arthritis: A meta-analysis of efficacy and se-lected clinical conundrums. Semin Arthritis Rheum 43: 458–469, 2014
Received: July 14, 2014 Accepted: October 24, 2014
Published online ahead of print. Publication date available at www.cjasn.org.
Clin J Am Soc Nephrol 10: ccc–ccc, February, 2014 IL-6 and CV Risk in CKD, Spoto et al. 9
Copyright © 2022 FDOKUMEN




















