
Prevalence of infection with hantavirus in rodent populations of central Argentina

ORIGINAL PAPER
Human papillomavirus (HPV) 16 and the prognosis of headand neck cancer in a geographical region with a low prevalenceof HPV infection
Rossana Veronica Mendoza Lopez • Jose Eduardo Levi • Jose Eluf-Neto •
Rosalina Jorge Koifman • Sergio Koifman • Maria Paula Curado •
Pedro Michaluart-Junior • David Livingstone Alves Figueiredo • Fabiano Pinto Saggioro •
Marcos Brasilino de Carvalho • Luiz Paulo Kowalski • Marcio Abrahao •
Francisco de Gois-Filho • Eloiza Helena Tajara • Tim Waterboer •
Paolo Boffetta • Paul Brennan • Victor Wunsch-Filho
Received: 27 June 2013 / Accepted: 15 January 2014 / Published online: 29 January 2014
� Springer International Publishing Switzerland 2014
Abstract
Background The role of human papillomavirus (HPV) on
head and neck squamous cell carcinoma (HNSCC) survival
in regions with low HPV prevalence is not yet clear. We
evaluated the HPV16 infection on survival of HNSCC
Brazilian patient series.
Methods This cohort comprised 1,093 HNSCC cases
recruited from 1998 to 2008 in four Brazilian cities and
followed up until June 2009. HPV16 antibodies were
analyzed by multiplex Luminex assay. In a subset of 398
fresh frozen or paraffin blocks of HNSCC specimens, we
analyzed for HPV16 DNA by L1 generic primer poly-
merase chain reaction. HNSCC survival according to
HPV16 antibodies was evaluated through Kaplan–Meier
method and Cox regression.
Results Prevalence of HPV16 E6 and E6/E7 antibodies
was higher in oropharyngeal cancer than in other head and
neck tumor sites. HPV16 DNA positive in tumor tissue was
also higher in the oropharynx. Seropositivity for HPV16 E6
antibodies was correlated with improved HNSCC survival
and oropharyngeal cancer. The presence of HPV16 E6/E7
R. V. M. Lopez (&) � V. Wunsch-Filho
Faculdade de Saude Publica, Universidade de Sao Paulo,
Av. Dr. Arnaldo, 715, Sao Paulo CEP 01246-904, Brazil
e-mail: [email protected]
R. V. M. Lopez
Instituto de Ensino e Pesquisa, Hospital de Cancer de Barretos,
Barretos, Brazil
J. E. Levi
Instituto de Medicina Tropical, Universidade de Sao Paulo,
Sao Paulo, Brazil
J. Eluf-Neto
Faculdade de Medicina, Universidade de Sao Paulo, Sao Paulo,
Brazil
R. J. Koifman � S. Koifman
Escola Nacional de Saude Publica, Fundacao Oswaldo Cruz,
Rio de Janeiro, Brazil
M. P. Curado
Hospital Araujo Jorge, Goiania, Brazil
M. P. Curado � P. Boffetta
International Prevention Research Institute, Lyon, France
P. Michaluart-Junior
Hospital das Clınicas, Faculdade de Medicina, Universidade de
Sao Paulo, Sao Paulo, Brazil
D. L. A. Figueiredo � F. P. Saggioro
Hospital das Clınicas, Faculdade de Medicina de Ribeirao Preto,
Universidade de Sao Paulo, Ribeirao Preto, Brazil
M. B. de Carvalho
Hospital Heliopolis, Sao Paulo, Brazil
L. P. Kowalski
Hospital do Cancer A.C. Camargo, Sao Paulo, Brazil
M. Abrahao
Hospital Sao Paulo, Universidade Federal de Sao Paulo,
Sao Paulo, Brazil
F. de Gois-Filho
Instituto do Cancer Arnaldo Viera de Carvalho, Sao Paulo,
Brazil
E. H. Tajara
Faculdade de Medicina de Sao Jose do Rio Preto, Sao Paulo,
Brazil
123
Cancer Causes Control (2014) 25:461–471
DOI 10.1007/s10552-014-0348-8

antibodies was correlated with improved HNSCC survival
and oropharyngeal cancer survival. The death risk of oro-
pharyngeal squamous cell carcinoma patients HPV16 E6/
E7 antibodies positive was 78 % lower than to those who
test negative.
Conclusion Oropharyngeal squamous cell carcinoma is
less aggressive in the HPV16 E6/E7 positive serology
patients. HPV16 E6/E7 antibody is a clinically sensible
surrogate prognostic marker of oropharyngeal squamous
cell carcinoma.
Keywords Human papillomavirus � Serology �Prognosis � Head and neck cancer � Prevalence
Introduction
Head and neck squamous cell carcinomas (HNSCC)
include tumors of the oral cavity, oropharynx, and larynx,
which vary with respect to their etiology and prognosis.
Worldwide, these tumors account for 650,000 new cases
and 350,000 deaths every year [1]. Latin America, partic-
ularly Brazil, has a relatively high incidence of HNSCC.
Among both sexes, the rates of oral cavity and larynx
cancer were 2.8 and 2.2/100,000, respectively, in 2008 [2].
The relative survival rate for HNSCC is approximately
50–70 %, including all sites, clinical stages, and forms of
treatment. In Brazil, the 5-year survival rate for oral and
oropharyngeal cancer is \50 % [3].
Tobacco smoking and alcohol consumption are the most
important risk factors for HNSCC [4]. The International
Agency for Research on Cancer recognizes human papil-
lomavirus (HPV) type 16 as the only type of HPV that is
carcinogenic to organs other than the cervix uteri, includ-
ing the anus, penis, vagina, vulva, oral cavity, oropharynx,
and tonsils [5]. HPV16 has been associated with increased
risk of head and neck cancer, particularly oropharynx and
tonsil tumors in high as well as low HPV prevalence
regions [6–10]. In regions with high HPV prevalence,
studies have shown that HPV16-positive patients have a
better HNSCC prognosis than those who are HPV16-neg-
ative [11–14]. However, the impact of HPV16 on HNSCC
survival in regions with low HPV prevalence is not known.
We analyzed the relationship between HPV16 infection
and the overall survival of patients with HNSCC and
cancer in specific sites (oral cavity, oropharynx, hypo-
pharynx, and larynx) in Brazil, a country with a low
prevalence of HPV infection.
Materials and methods
Study subjects
This study includes incident HNSCC cases confirmed by
histology and diagnosed between 1998 and 2008. The cases
originated from two multicentre studies in Brazil. The
Latin American study was conducted from 1998 to 2002 in
seven cities; for the present study, we only included cases
from the cities of Goiania, Rio de Janeiro, and Sao Paulo.
The Gencapo study was conducted from 2003 to 2008 in
the cities of Ribeirao Preto and Sao Paulo. Both studies
were approved by the clinical centres’ ethics committees
and by the National Commission on Ethics in Research.
Written consent was given by each patient participating in
the studies.
HNSCC was classified into one of four categories
according to anatomical subsites, each of which has a
distinct prognosis: oral cavity, oropharynx, hypopharynx,
and larynx. The International Classification of Diseases,
version 10 [15], was used to classify the tumor subsite
according to the method used by Hashibe and colleagues
[16]: oral cavity (C00.3–C00.9, C02.0–C02.3, C02.8,
C02.9, C03.0, C03.1, C03.9, C04.0, C04.1, C04.8, C04.9,
C05.0, C05.8, C05.9, C06.0–C06.2, C06.8, C06.9, C14.0,
C14.2, and C14.8), oropharynx (C01.9, C02.4, C05.1,
C05.2, C09.0, C09.1, C09.8, C09.9, C10.0–C10.4, C10.8,
and C10.9), hypopharynx (C12.9, C13.0–C13.2, C13.8, and
C13.9), and larynx (C32.0–C32.3, C32.8, and C32.9).
All patients underwent face-to-face interviews immedi-
ately after diagnosis with trained interviewers who used a
structured questionnaire to obtain information about vari-
ables that could affect HNSCC survival, including tobacco
smoking, alcohol consumption, and education. Patient
hospital records were reviewed to obtain additional infor-
mation on tumor clinical stage, treatment, and time since
diagnosis until dead or last information. The tumor’s
clinical stage was classified as CS I–IV according to the
TNM classification system, 6th edition [17]. Additional
information on cause of death was validated through death
certificates obtained from the Sao Paulo State Death Reg-
istry (for patients from Ribeirao Preto and Sao Paulo) and
from the Goiania Population Cancer Registry (for patients
from Goiania). In Rio de Janeiro, death certificates were
included in the hospital medical records.
T. Waterboer
German Cancer Research Center (DKFZ), Heidelberg, Germany
P. Boffetta
The Tisch Cancer Institute, Mount Sinai School of Medicine,
New York, NY, USA
P. Brennan
International Agency for Research on Cancer, Lyon, France
462 Cancer Causes Control (2014) 25:461–471
123
Patients were recruited into the study from November
1998 to December 2008, and they were followed until 30
June 2009. Of the 1,275 eligible cases at the start of the
study, 182 were excluded because no information was
available on tobacco smoking, alcohol consumption, edu-
cation, tumor clinical stage, or treatment. Ultimately, 1,093
cases with complete follow-up records were included in the
analysis.
Biological samples
In both studies, blood was obtained from each patient at the
time of the interview. Tumor tissue samples from biopsies
or surgical procedures were obtained for a subset of 398
cases (36 %), including 198 fresh-frozen samples and 200
paraffin-embedded samples.
DNA extraction and detection of HPV DNA
For patient samples from the Gencapo study, DNA was
extracted from paraffin slices using the Nucleon HT kit
(GE Life Sciences, Sao Paulo, Brazil) and examined using
the Inno-LiPA HPV Genotyping kit (Innogenetics, Gent,
Belgium) [18]. For patient samples from the Latin Amer-
ican study, DNA was extracted from fresh tumor tissue
using the QIAamp DNA Mini kit (Qiagen, Valencia, CA,
Table 1 Baseline characteristics of HNSCC study patients, Brazil, 1998–2008
All patients Oral cavity Oropharynx Hypopharynx Larynx
n = 1,093 n = 321 n = 252 n = 115 n = 405
n (%) n (%) n (%) n (%) n (%)
Study
Latin America 727 (66.5) 181 (56.4) 200 (79.4) 84 (73.0) 262 (64.7)
GENCAPO 366 (33.5) 140 (43.6) 52 (20.6) 31 (27.0) 143 (35.3)
Sex
Female 148 (13.5) 56 (17.4) 39 (15.5) 7 (6.1) 46 (11.4)
Male 945 (86.5) 265 (82.6) 213 (84.5) 108 (93.9) 359 (88.6)
Age (years)
\55 435 (39.8) 145 (45.2) 115 (45.6) 43 (37.4) 132 (32.6)
55–64 373 (34.1) 101 (31.5) 91 (36.1) 39 (33.9) 142 (35.1)
65–75 225 (20.6) 55 (17.1) 37 (14.7) 24 (20.9) 109 (26.9)
C75 60 (5.5) 20 (6.2) 9 (3.6) 9 (7.8) 22 (5.4)
Education (years)
0 160 (14.6) 41 (12.8) 37 (14.7) 18 (15.7) 64 (15.8)
1–7 589 (53.9) 163 (50.8) 144 (57.1) 63 (54.8) 219 (54.1)
8–10 226 (20.7) 73 (22.7) 39 (15.5) 25 (21.7) 89 (22.0)
C11 118 (10.8) 44 (13.7) 32 (12.7) 9 (7.8) 33 (8.1)
Tobacco smoking
Nonsmoker 53 (4.8) 21 (6.5) 15 (6.0) 3 (2.6) 14 (3.5)
Former smoker 273 (25.0) 61 (19.0) 50 (19.8) 30 (26.1) 132 (32.6)
Current smoker 767 (70.2) 239 (74.5) 187 (74.2) 82 (71.3) 259 (64.0)
Alcohol consumption
Nondrinker 97 (8.9) 35 (10.9) 13 (5.2) 5 (4.3) 44 (10.9)
Former drinker 390 (35.7) 82 (25.5) 101 (40.1) 50 (43.5) 157 (38.8)
Current drinker 606 (55.4) 204 (63.6) 138 (54.8) 60 (52.2) 204 (50.4)
Tumor stage
T1/T2 366 (33.5) 133 (41.4) 83 (32.9) 24 (20.9) 126 (31.1)
T3 325 (29.7) 60 (18.7) 84 (33.3) 44 (38.3) 137 (33.8)
T4 402 (36.8) 128 (39.9) 85 (33.7) 47 (40.9) 142 (35.1)
Treatment
Surgery 347 (31.7) 129 (40.2) 39 (15.5) 20 (17.4) 159 (39.3)
Radiotherapy 214 (19.6) 36 (11.2) 73 (29.0) 35 (30.4) 70 (17.3)
Surgery ? radiotherapy 335 (30.6) 114 (35.5) 66 (26.2) 31 (27.0) 124 (30.6)
Other 197 (18.0) 42 (13.1) 74 (29.4) 29 (25.2) 52 (12.8)
Cancer Causes Control (2014) 25:461–471 463
123

USA). HPV DNA detection was performed by polymerase
chain reaction (PCR) with the generic primers PGMY09/
11, which amplify a fragment spanning *450 bp of the L1
region of most mucosal HPV types [19], in the presence of
human b-globin primers, which amplify a fragment of
268 bp as a positive control. The reaction conditions were
as follows: 200 lM dNTPs, 4 mM magnesium chloride,
80 nM PGMY09/11, and 20 nM PCO4/GH20 (b-globin)
oligonucleotides, 250 ng of template DNA, and 1 U of Taq
polymerase (Invitrogen, Sao Paulo, Brazil). The thermo-
cycling profile consisted of an initial incubation of 5 min at
94 �C, followed by 40 cycles of 94 �C (1 min), 55 �C
(1 min), and 72 �C (1 min) and a final elongation step of
5 min at 72 �C in a PE 2400 (Applied Biosystems, Foster
City, CA, USA) or a MasterCycler gradient thermal cycler
(Eppendorf AG, Hamburg, Germany). The PCR products
were analyzed by electrophoresis on a 2 % agarose gel
stained with ethidium bromide and observed under
ultraviolet light. Further genotyping of PGMY09/11-posi-
tive samples was conducted by restriction fragment length
polymorphism using the enzymes and patterns described by
Bernard et al. [20]. These procedures and analyses were
conducted at the Institute of Tropical Medicine at the
University of Sao Paulo in Brazil.
Detection of HPV antibodies
Antibodies against HPV were analyzed by multiplex
Luminex serology assay. This antibody detection method is
based on a glutathione S-transferase capture ELISA [21] in
combination with fluorescent bead technology [22]. To
determine a positive serological response, mean fluores-
cence intensity values were dichotomised as antibody
positive or negative for the serological response to onco-
proteins E1, E2, E4, E6, E7, and L1 of HPV16; oncopro-
teins E6, E7, and L1 of HPV 18, 31, 33, and 35;
Table 2 Characteristics of HNSCC patients by HVP DNA and HPV16 DNA status, Brazil, 1998–2008
Total n = 398 HPV DNA p HPV16 DNA p
Negative Positive Negative Positive
n = 363 n = 35 n = 384 n = 14
n (%) n (%) n (%) n (%)
Sex 0.0631 0.0851
Female 50 42 (84.0) 8 (16.0) 46 (92.0) 4 (8.0)
Male 348 321 (92.2) 27 (7.8) 338 (97.1) 10 (2.9)
Age (years) 0.0782 0.9411
\55 162 141 (87.0) 21 (13.0) 155 (95.7) 7 (4.3)
55–64 141 132 (93.6) 9 (6.4) 136 (96.5) 5 (3.5)
65–75 76 71 (93.4) 5 (6.6) 74 (97.4) 2 (2.6)
C75 19 19 (100.0) 0 19 (100.0) 0
Tobacco smoking 0.4382 0.1061
Nonsmoker 15 13 (86.7) 2 (13.3) 13 (86.7) 2 (13.3)
Former smoker 107 95 (88.8) 12 (11.2) 103 (96.3) 4 (3.7)
Current smoker 276 255 (92.4) 21 (7.6) 268 (97.1) 8 (2.9)
Alcohol consumption 0.0102 0.0751
Nondrinker 38 32 (84.2) 6 (15.8) 34 (89.5) 4 (10.5)
Former drinker 140 122 (87.1) 18 (12.9) 136 (97.1) 4 (2.9)
Drinker 220 209 (95.0) 11 (5.0) 214 (97.3) 6 (2.7)
Tumor Site 0.2462 0.9591
Oral cavity 121 113 (93.4) 8 (6.6) 117 (96.7) 4 (3.3)
Oropharynx 91 85 (93.4) 6 (6.6) 87 (95.6) 4 (4.4)
Hypopharynx 44 41 (93.2) 3 (6.8) 43 (97.7) 1 (2.3)
Larynx 142 124 (87.3) 18 (12.7) 137 (96.5) 5 (3.5)
Treatment 0.0262 0.1861
Surgery 143 128 (89.5) 15 (10.5) 136 (95.1) 7 (4.9)
Radiotherapy 76 76 (100) 0 76 (100) 0
Surgery ? radiotherapy 122 109 (89.3) 13 (10.7) 118 (96.7) 4 (3.3)
Other 57 50 (87.7) 7 (12.3) 54 (94.7) 3 (5.3)
1 Fisher’s exact test. 2 chi-square test
464 Cancer Causes Control (2014) 25:461–471
123

oncoproteins E6 and L1 of 45, 52, and 58; and oncoprotein
L1 of HPV 6, 11, and 77. Means plus three standard
deviations were calculated to define cutoffs, excluding
outliers [23]. These procedures and analyses were con-
ducted at the German Cancer Research Center in Heidel-
berg, Germany.
Statistical analysis
Frequencies and percentages were calculated for categori-
cal variables, and the associations between variables were
tested using Fisher’s exact test or chi-square tests. The
concordance between HPV DNA and serological response
was calculated using the Kappa statistic. Cox model
regression was performed to calculate the hazard ratios
(HR) and 95 % confidence intervals (95 % CI) for the
association of HPV on HNSCC overall survival, adjusting
for gender, age (years\55, 55–64, 65–74, and C75), study
group (Latin America or Gencapo), education (years of
schooling: 0, 1–7, 8–10, and C11), tobacco smoking
(nonsmoker, former smoker, current smoker), alcohol
consumption (nondrinker, former drinker, current drinker),
Table 3 Characteristics of HNSCC patients by HPV16 E6, E7, L1, E6/E7 serology antibodies, Brazil, 1998–2008
Total HPV16 E6 HPV16 E7 HPV16 L1 HPV16 E6/E7
Negative Positive Negative Positive Negative Positive Negative Positive
n = 1,013 n = 80 n = 833 n = 260 n = 1,018 n = 75 n = 1,066 n = 27
n (%) n (%) n (%) n (%) n (%) n (%) n (%) n (%)
Sex
Female 148 136 (91.9) 12 (8.1) 116 (78.4) 32 (21.6) 132 (89.2) 16 (10.8) 141 (95.3) 7 (4.7)
Male 945 877 (92.8) 68 (7.2) 717 (75.9) 228 (24.1) 886 (93.8) 59 (6.2) 925 (97.9) 20 (2.1)
p1 0.692 0.506 0.041 0.080
Age (years)
\55 435 395 (90.8) 40 (9.2) 337 (77.5) 98 (22.5) 403 (92.6) 32 (7.4) 420 (96.6) 15 (3.4)
55–64 373 345 (92.5) 28 (7.5) 285 (76.4) 88 (23.6) 349 (93.6) 24 (6.4) 365 (97.9) 8 (2.1)
65–75 225 216 (96.0) 9 (4.0) 164 (72.9) 61 (27.1) 208 (92.4) 17 (7.6) 221 (98.2) 4 (1.8)
C75 60 57 (95.0) 3 (5.0) 47 (78.3) 13 (21.7) 58 (96.7) 2 (3.3) 60 (100.0) 0
p1 0.093 0.592 0.657 0.277
Tobacco smoking
Nonsmoker 53 43 (81.1) 10 (18.9) 36 (67.9) 17 (32.1) 47 (88.7) 6 (11.3) 47 (88.7) 6 (11.3)
Former smoker 273 253 (92.7) 20 (7.3) 208 (76.2) 65 (23.8) 255 (93.4) 18 (6.6) 265 (97.1) 8 (2.9)
Current smoker 767 717 (93.5) 50 (6.5) 589 (76.8) 178 (23.2) 716 (93.4) 51 (6.6) 754 (98.3) 13 (1.7)
p1 0.004 0.341 0.420 \0.001
Alcohol
Nondrinker 97 90 (92.8) 7 (7.2) 77 (79.4) 20 (20.6) 88 (90.7) 9 (9.3) 95 (97.9) 2 (2.1)
Former drinker 390 370 (94.9) 20 (5.1) 302 (77.4) 88 (22.6) 365 (93.6) 25(6.4) 384 (98.5) 6 (1.5)
Drinker 606 553 (91.3) 53 (8.7) 454 (74.9) 152 (25.1) 565 (93.2) 41 (6.8) 587 (96.9) 19 (3.1)
p1 0.101 0.492 0.601 0.275
Tumor Site
Oral cavity 321 301 (93.8) 20 (6.2) 246 (76.6) 75 (23.4) 302 (94.1) 19 (5.9) 316 (98.4) 5 (1.6)
Oropharynx 252 225 (89.3) 27 (10.7) 191 (75.8) 61 (24.2) 237 (94.0) 15 (6.0) 238 (94.4) 14 (5.6)
Hypopharynx 115 113 (98.3) 2 (1.7) 86 (74.8) 29 (25.2) 105 (91.3) 10 (8.7) 115 (100.0) 0
Larynx 405 374 (92.3) 31 (7.7) 310 (76.5) 95 (23.5.) 374 (92.3) 31 (7.7) 397 (98.0) 8 (2.0)
p1 0.017 0.976 0.620 0.002
Treatment
Surgery 347 319 (91.9) 28 (8.1) 254 (73.2) 93 (26.8) 319 (91.9) 28 (8.1) 339 (97.7) 8 (2.3)
Radiotherapy 214 200 (93.5) 14 (6.5) 166 (77.6) 48 (22.4) 199 (93.0) 15 (7.0) 210 (98.1) 4 (1.9)
Surgery ? radiotherapy 335 310 (92.5) 25 (7.5) 259 (77.3) 76 (22.7) 313 (93.4) 22 (6.6) 324 (96.7) 11 (3.3)
Other 197 184 (93.4) 13 (6.6) 154 (78.2) 43 (21.8) 187 (94.9) 10 (5.1) 193 (98.0) 4 (2.0)
p1 0.887 0.458 0.609 0.697
1 chi-square test or Fisher’s exact test
Cancer Causes Control (2014) 25:461–471 465
123

tumor clinical stage (T1/T2, T3, and T4), and treatment
(surgery, radiotherapy, surgery plus radiotherapy, another
treatment). The dependence between oral cavity, hypo-
pharynx, and larynx cancer (combined) survival and oro-
pharynx cancer (separately) survival on the presence of
HPV16 antibodies was evaluated using the Kaplan–Meier
method, and the differences between the curves were
assessed using log-rank tests. For the descriptive analysis
and multiple survival analyses, we used IBM� SPSS�
Statistics version 18 (IBM Corp, Somers, NY, USA) and
Stata/SE 11.0 for Windows (StataCorp LP, College Station,
TX, USA). All reported p values are two-sided with a
significance level of 0.05.
Results
At the end of the follow-up period, 356 of the study
patients were alive, 626 had died, and 111 were lost to
follow-up. The median survival of the cohort members was
32 months (95 % CI 27–37 months). HNSCC 5-year
overall survival after diagnosis was 38 %, and disease-
specific survival was 43 %.
The description of study group, demographic charac-
teristics, tobacco and alcohol consumption, clinical stage
and treatment for all patients with serological response to
HPV is presented in Table 1 and corresponding to all
patients with serological samples. Of the HNSCC cases,
321 (29.4 %) affected the oral cavity, 252 (23.1 %)
affected the oropharynx, 115 (10.5 %) affected the
hypopharynx, and 405 (37.1 %) affected the larynx. The
majority of the patients were male, and 37 % were between
51 and 60 years old. The education level was low; 68.5 %
had \8 years of schooling. Only 4.8 % of the HNSCC
patients reported that they did not smoke, and 8.9 % did
not report alcohol consumption at the time of the interview.
An advanced clinical tumor stage (T3 or T4) at diagnosis
was observed in many of the HNSCC cases, and the most
common treatment approach was surgery or a combination
of surgery plus radiotherapy.
The overall prevalence of HPV DNA was 8.8 % and for
HPV16 DNA was 3.5 % in tumor tissue. Table 2 shows the
prevalence of HPV DNA and HPV16 DNA according to
gender, age, tobacco smoking, alcohol consumption, ana-
tomical site, and treatment. Association statistically sig-
nificant was observed in alcohol consumption and
treatment with HPV DNA status. The HPV16 DNA prev-
alence in tumor tissue was higher in women, patients
50 years old or younger, nonsmokers, and nondrinkers. In
addition, the prevalence of HPV16 DNA was higher in
patients with oropharyngeal cancer than in patients with
cancers of other head and neck sites. No association was
observed between treatment and HPV16 DNA status;
however, we observed that all patients who received
radiotherapy were negative to HPV16 DNA. A total of
8.8 % of HNSCC patients tested positive for HPV DNA in
tumor tissue (35/398), of which 40 % had HPV16 (14/35).
Table 3 displays the prevalence of HPV16 antibodies
by gender, age, tobacco smoking, alcohol consumption,
anatomical site, and treatment. The overall prevalence of
Table 4 Concordance between HPV16 DNA and HPV16 serological antibodies by HNSCC subsite, Brazil, 1998–2008
Oral cavity Kappap1
Oropharynx Kappap1
Hypopharynx Kappap1
Larynx Kappap1
HPV16 DNA HPV16 DNA HPV16 DNA HPV16 DNA
Negative Positive Negative Positive Negative Positive Negative Positiven = 117 n = 4 n = 87 n = 4 n = 43 n = 1 n = 137 n = 5n (%) n (%) n (%) n (%) n (%) n (%) n (%) n (%)
HPV16 E6 -0.044 0.578 NA 0.145
Negative 110 (94.0) 4 (100.0) 0.614 84 (96.6) 1 (25.0) \0.001 43(100.0)
1 (100.0) 123 (89.8) 3 (60.0) 0.039
Positive 7 (6.0) 0 3 (3.4) 3 (75.0) 0 0 14 (10.2) 2 (40.0)
HPV16 E7 0.040 0.062 -0.044 0.033
Negative 82 (70.1) 2 (50.0) 0.391 63 (72.4) 2 (50.0) 0.332 30 (69.8) 1 (100.0) 0.512 101 (73.7) 3 (60.0) 0.496
Positive 35 (29.9) 2 (50.0) 24 (27.6) 2 (50.0) 13 (30.2) 0 36 (26.3) 2 (40.0)
HPV16 L1 -0.048 0.416 -0.039 0.063
Negative 108 (92.3) 4 (100.0) 0.564 84 (96.6) 2 (50.0) \0.001 38 (88.4) 1 (100.0) 0.717 125 (91.2) 4 (80.0) 0.392
Positive 9 (7.7) 0 3 (3.4) 2 (50.0) 5 (11.6) 0 12 (8.8) 1 (20.0)
HPV16E6/E7
-0.029 0.477 NA 0.171
Negative 114 (97.4) 4 (100.0) 0.746 85 (97.7) 2 (50.0) \0.001 43(100.0)
1 (100.0) 133 (97.1) 4 (80.0) 0.042
Positive 3 (2.6) 0 2 (2.3) 2 (50.0) 0 0 4 (2.9) 1 (20.0)
1 p for Kappa statistic
NA not available
466 Cancer Causes Control (2014) 25:461–471
123
HPV16 antibodies among HNSCC patients was as fol-
lows: E6 (7.3 %), E7 (23.8 %), L1 (6.9 %), and E6/E7
(2.5 %). HPV16 E6 and E6/E7 antibodies had the lowest
prevalence overall among the HNSCC patients, but the
prevalence of these antibodies was higher among younger
patients, nonsmokers, and those with oropharyngeal can-
cer. According to treatment, the data showed no associ-
ation with serological response to HPV. Relative
frequencies were distributed similarly in each treatment
and antibodies.
In general, the concordance of HPV16 DNA and HPV16
serological antibodies was low. However, in cases of oro-
pharyngeal cancer, the concordance between HPV16 DNA
and HPV16 E6, L1, and E6/E7 was moderate (0.578, 0.416,
and 0.477, respectively) (Table 4).
Seropositivity for antibodies against HPV16 E6 and E6/
E7 was significantly associated with a better HNSCC
prognosis. Oropharyngeal cancer patients with HPV16 E6/
E7 seropositivity had a 78 % lower risk of death compared
with those with negative serology (HR = 0.22; 95 % CI
0.06–0.76). No association between HPV16 DNA in tumor
tissue and HNSCC survival was observed (HR = 0.74;
95 % CI 0.27–2.07). Greater survival rates were observed
among patients with oropharyngeal tumors who were
HPV16 DNA-positive, but this result was not precise
(HR = 0.04; 95 % CI 0.001–1.75) (Table 5). We observed
a poorer prognosis among men, among patients with
advanced clinical tumor stage (T3 and T4), and among
those treated with surgery and radiotherapy. Considering
only oropharyngeal cancer, older patients and smokers
(former and current) had lower overall survival (data no
showed).
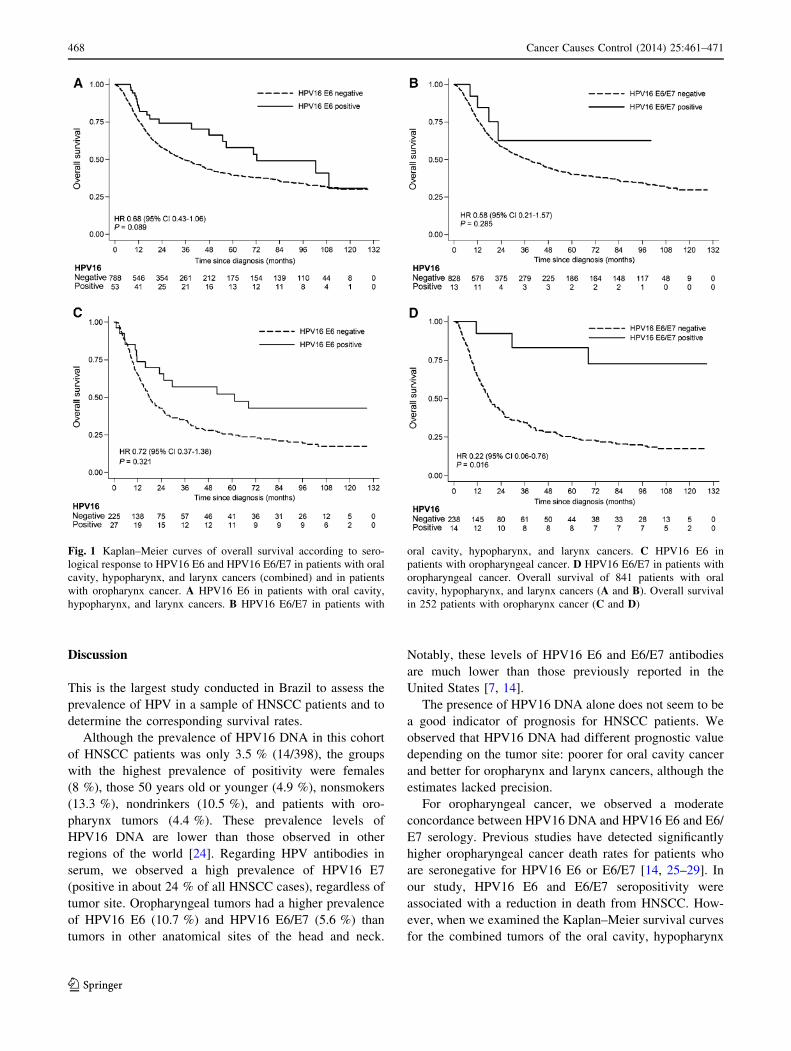
Based on the results in Table 5, Kaplan–Meier survival
curves were calculated for oral cavity, hypopharyngeal,
and laryngeal cancers combined (Fig. 1a, b) and for oro-
pharyngeal cancer cases separately (Fig. 1c, d), consider-
ing seropositivity for HPV16 E6 (Fig. 1a, c) and E6/E7
(Fig. 1b, d), respectively. The prognosis was clearly better
for oropharyngeal cancer patients with a positive serolog-
ical response to HPV16 E6/E7 (Log-rank test; p = 0.016)
(Fig. 1d).
Seropositivity for antibodies against HPV16 E6 and E6/
E7 was significantly associated with a better HNSCC
prognosis. Oropharyngeal cancer patients with HPV16 E6/
E7 seropositivity had a 78 % lower risk of death compared
with those with negative serology.
Table 6 shows the characteristics of HNSCC patients by
availability of biological samples for HPV DNA status. No
differences were observed in patients according to gender,
age, tobacco and alcohol consumption, anatomical site, and
tumor stage. Tumor tissue samples were only available for
surgery cases and association was observed for HPV16
DNA (p = 0.041).Ta
ble
5O
ver
all
surv
ival
of
HN
SC
Cp
atie
nts
by
HP
V1
6se
rolo
gic
alan
tib
od
ies
and
HP
V1
6D
NA
,B
razi
l,1
99
8–
20
08
nH
NS
CC
pn
Ora
lca
vit
yp
nO
rop
har
yn
xp
nH
yp
op
har
yn
xp
nL
ary
nx
pH
R1
(95
%C
I)H
R1
(95
%C
I)H
R1
(95
%C
I)H
R1
(95
%C
I)H
R1
(95
%C
I)
HP
V1
6E
6
Neg
ativ
e1
,01
31
30
11
22
51
11
31
37
41
Po
siti
ve
80
0.6
3(0
.44
–0
.89
)0
.01
02
00
.98
(0.5
1–
1.8
9)
0.9
47
27
0.7
0(0
.37
–1
.32
)0
.26
82
0.7
7(0
.08
–7
.96
)0
.82
93
10
.58
(0.3
0–
1.1
5)
0.1
19
HP
V1
6E
7
Neg
ativ
e8
33
12
46
11
91
18
61
31
01
Po
siti
ve
26
01
.00
(0.8
3–
1.2
2)
0.9
75
75
1.0
7(0
.74
–1
.56
)0
.71
56
10
.73
(0.5
0–
1.0
9)
0.1
21
29
1.2
3(0
.73
–2
.08
)0
.43
19
51
.02
(0.7
1–
1.4
7)
0.9
24
HP
V1
6L
1
Neg
ativ
e1
,01
81
30
21
23
71
10
51
37
41
Po
siti
ve
75
0.9
3(0
.67
–1
.30
)0
.66
81
90
.98
(0.5
1–
1.8
9)
0.9
62
15
0.7
5(0
.34
–1
.65
)0
.47
61
00
.91
(0.4
1–
2.0
3)
0.8
10
31
1.0
3(0
.57
–1
.85
)0
.92
6
HP
V1
6E
6/E
7
Neg
ativ
e1
,06
61
31
61
23
81
11
5N
A3
97
1
Po
siti
ve
27
0.3
4(0
.16
–0
.73
)0
.00
65
1.8
5(0
.56
–6
.13
)0
.31
41
40
.22
(0.0
6–
0.7
5)
0.0
16
0N
A8
0.2
2(0
.03
–1
.58
)0
.13
2
HP
V1
6D
NA
Neg
ativ
e3
84
11
17
18
71
43
NA
13
71
Po
siti
ve
14
0.7
4(0
.27
–2
.07
)0
.56
64
2.0
2(0
.39
–1
0.5
7)
0.4
07
40
.05
(0.0
01
–1
.77
)0
.09
81
NA
50
.76
(0.0
9–
6.2
3)
0.7
96
1H
azar
dra
tio
adju
sted
for
stu
dy
,g
end
er,
age,
edu
cati
on
,to
bac
cosm
ok
ing
,al
coh
ol
con
sum
pti
on
,cl
inic
altu
mo
rst
age,
and
trea
tmen
t.N
A:
no
tav
aila
ble
Cancer Causes Control (2014) 25:461–471 467
123
Discussion
This is the largest study conducted in Brazil to assess the
prevalence of HPV in a sample of HNSCC patients and to
determine the corresponding survival rates.
Although the prevalence of HPV16 DNA in this cohort
of HNSCC patients was only 3.5 % (14/398), the groups
with the highest prevalence of positivity were females
(8 %), those 50 years old or younger (4.9 %), nonsmokers
(13.3 %), nondrinkers (10.5 %), and patients with oro-
pharynx tumors (4.4 %). These prevalence levels of
HPV16 DNA are lower than those observed in other
regions of the world [24]. Regarding HPV antibodies in
serum, we observed a high prevalence of HPV16 E7
(positive in about 24 % of all HNSCC cases), regardless of
tumor site. Oropharyngeal tumors had a higher prevalence
of HPV16 E6 (10.7 %) and HPV16 E6/E7 (5.6 %) than
tumors in other anatomical sites of the head and neck.
Notably, these levels of HPV16 E6 and E6/E7 antibodies
are much lower than those previously reported in the
United States [7, 14].
The presence of HPV16 DNA alone does not seem to be
a good indicator of prognosis for HNSCC patients. We
observed that HPV16 DNA had different prognostic value
depending on the tumor site: poorer for oral cavity cancer
and better for oropharynx and larynx cancers, although the
estimates lacked precision.
For oropharyngeal cancer, we observed a moderate
concordance between HPV16 DNA and HPV16 E6 and E6/
E7 serology. Previous studies have detected significantly
higher oropharyngeal cancer death rates for patients who
are seronegative for HPV16 E6 or E6/E7 [14, 25–29]. In
our study, HPV16 E6 and E6/E7 seropositivity were
associated with a reduction in death from HNSCC. How-
ever, when we examined the Kaplan–Meier survival curves
for the combined tumors of the oral cavity, hypopharynx
Fig. 1 Kaplan–Meier curves of overall survival according to sero-
logical response to HPV16 E6 and HPV16 E6/E7 in patients with oral
cavity, hypopharynx, and larynx cancers (combined) and in patients
with oropharynx cancer. A HPV16 E6 in patients with oral cavity,
hypopharynx, and larynx cancers. B HPV16 E6/E7 in patients with
oral cavity, hypopharynx, and larynx cancers. C HPV16 E6 in
patients with oropharyngeal cancer. D HPV16 E6/E7 in patients with
oropharyngeal cancer. Overall survival of 841 patients with oral
cavity, hypopharynx, and larynx cancers (A and B). Overall survival
in 252 patients with oropharynx cancer (C and D)
468 Cancer Causes Control (2014) 25:461–471
123

and larynx and, separately, oropharynx tumors, the strong
association of HPV16 E6/E7 with oropharyngeal cancer
prognosis became clear.
There are some limitations to our study. We were not
able to obtain information on crucial covariates for 14.3 %
(182/1,275) of the initial cases, and we were also unable to
follow up with 10.2 % (111/1,093) of the patients included
in the study. The patients who were lost might have
affected the study’s precision. Another limitation is that
tissue samples, from which HPV16 DNA was extracted,
were only available for a portion of the cases (36.4 %),
which could compromise the evaluation of the association
of HPV16 DNA and HNSCC survival. Tumor tissue
availability depends of the tumor size and also if the patient
was submitted to surgery or not. However, the subset for
which no tissue samples were available was comparable to
the entire sample with respect to demographics, lifestyle,
and clinical characteristics (Table 6).
We observed that patients who are positive for HPV16
E6/E7 antibodies represent a group with a higher percent-
age of oropharyngeal cancer, females and nonsmokers.
This profile explains the better prognosis of this group.
However, the survival advantage associated with HPV16
infection in patients with oropharyngeal squamous cell
Table 6 Characteristics of HNSCC patients by availability of HPV16 DNA, Brazil, 1998–2008
Total
n = 1,093
n (%)
No samples
n = 695
n (%)
Samples available n = 398 p1
HPV16 DNA
Negative Positive
n = 384 n = 14
n (%) n (%)
Sex 0.475
Female 148 (13.5) 98 (14.1) 46 (12.0) 4 (28.6)
Male 945 (86.5) 597 (85.9) 338 (88.0) 10 (71.4)
Age (years) 0.637
\55 435 (39.8) 273 (39.3) 155(40.4) 7 (50.0)
55–64 373 (34.1) 232 (33.4) 136 (35.4) 5 (35.7)
65–75 225 (20.6) 149 (21.4) 74 (19.3) 2 (14.3)
C75 60 (5.5) 41 (5.9) 19 (4.9) 0
Tobacco smoking 0.290
Nonsmoker 53 (4.8) 38 (5.5) 13 (3.4) 2 (14.3)
Former smoker 273 (25.0) 166 (23.9) 103 (26.8) 4 (28.6)
Current smoker 767 (70.2) 491 (70.6) 268 (69.8) 8 (57.1)
Alcohol consumption 0.832
Nondrinker 97 (8.9) 59 (8.5) 34 (8.9) 4 (28.6)
Former drinker 390 (35.7) 250 (36.0) 136 (35.4) 4 (28.6)
Drinker 606 (55.4) 386 (55.5) 214 (55.7) 6 (42.9)
Site 0.867
Oral cavity 321 (29.4) 200 (28.8) 117 (30.5) 4 (28.6)
Oropharynx 252 (23.1) 161 (23.2) 87 (22.7) 4 (28.6)
Hypopharynx 115 (10.5) 71 (10.2) 43 (11.2) 1 (7.1)
Larynx 405 (37.1) 263 (37.8) 137 (35.7) 5 (35.7)
Tumor stage 0.233
T1/T2 366 (33.5) 228 (32.8) 133 (34.6) 5 (35.7)
T3 325 (29.7) 219 (31.5) 102 (26.6) 4 (28.6)
T4 402 (36.8) 248 (35.7) 149 (38.8) 5 (35.7)
Treatment 0.041
Surgery 347 (31.7) 204 (29.4) 136 (35.4) 7 (50.0)
Radiotherapy 214 (19.6) 138 (19.9) 76 (19.8) 0
Surgery ? radiotherapy 335 (30.7) 213 (30.6) 118 (30.7) 4 (28.6)
Other 197 (18.0) 140 (20.1) 54 (14.1) 3 (21.4)
1 chi-square test for association between availability of tumor tissues (with samples or not) and characteristic
Cancer Causes Control (2014) 25:461–471 469
123

carcinoma likely reflects the interplay between the virus
and lymphoid tissue, accounting for the differences in the
biology of the disease and the treatment response [30].
In conclusion, patients with oropharyngeal cancer who
test positive for HPV16 E6/E7 antibodies survived longer
than those who test negative, then HPV16 E6/E7 antibodies
are a clinically relevant indicator of prognosis for oro-
pharyngeal squamous cell carcinoma. This result, which
was obtained in a geographical region with a low preva-
lence of HPV infection, is similar to results reported in
regions with a high prevalence of HPV infection. Test for
HPV 16 E6/E7 antibodies may highlight to clinicians those
patients who could be treated for a shorter duration and
lowering the risk of unnecessary toxic effects.
Acknowledgments This work was supported by Fundacao de
Amparo a Pesquisa do Estado de Sao Paulo (FAPESP) [10/50733-6;
09/52031-1 and 04/12054-9] and by the European Commission
[IC18-CT97-0222].
Conflict of interest None declared.
References
1. Argiris A, Karamouzis MV, Raben D, Ferris RL (2008) Head and
neck cancer. Lancet 371:1695–1709
2. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM
(2010) GLOBOCAN 2008 v2.0, Cancer Incidence and Mortality
Worldwide: IARC CancerBase No 10 [Internet]. Lyon, France:
International Agency for Research on Cancer; [cited 2012 Aug
30]. http://globocan.iarc.fr
3. Carvalho AL, Ikeda MK, Magrin J, Kowalski LP (2004) Trends
of oral and oropharyngeal cancer survival over five decades in
3267 patients treated in a single institution. Oral Oncol 40:71–76
4. Szymanska K, Hung RJ, Wunsch Filho V, Eluf Neto J, Curado
MP, Koifman S et al (2011) Alcohol and tobacco, and the risk of
cancers of the upper aerodigestive tract in Latin America: a case–
control study. Cancer Causes Control 22:1037–1046
5. Human papillomaviruses (2007) Lyon, France: International
Agency for Research on Cancer- IARC Monograph on the
Evaluation of Carcinogenic Risks to Humans
6. Herrero R, Castellsague X, Pawlita M, Lissowska J, Kee F,
Balaram P et al (2003) Human papillomavirus and oral cancer:
The International Agency for Research on Cancer Multicenter
Study. J Natl Cancer Inst 95:1772–1783
7. Smith EM, Ritchie JM, Pawlita M, Rubenstein LM, Haugen TH,
Turek LP et al (2006) Human papillomavirus seropositivity and
risks of head and neck cancer. Int J Cancer 120:825–832
8. D’Souza G, Kreimer AR, Viscidi R, Pawlita M, Fakhry C, Koch
WM et al (2007) Case-control study of human papillomavirus and
oropharyngeal cancer. N Engl J Med 356:1944–1956
9. Nasman A, Attner P, Hammarstedt L, Du J, Eriksson M, Giraud
G et al (2009) Incidence of human papillomavirus (HPV) positive
tonsillar carcinoma in Stockholm, Sweden: an epidemic of viral-
induced carcinoma? Int J Cancer 125:362–366
10. Ribeiro KB, Levi JE, Pawlita M, Koifman S, Matos E, Eluf-Neto
J et al (2011) Low human papillomavirus prevalence in head and
neck cancer: results from two large case–control studies in high-
incidence regions. Int J Epidemiol 40:489–502
11. Fakhry C, Westra WH, Li S, Cmelak A, Ridge JA, Pinto H et al
(2008) Improved survival of patients with human papillomavi-
rus–positive head and neck squamous cell carcinoma in a pro-
spective clinical trial. J Natl Cancer Inst 100:261–269
12. Smith EM, Rubenstein LM, Ritchie JM, Lee JH, Haugen TH,
Hamsikova E et al (2008) Does treatment seropositivity to human
papillomavirus have prognostic significance for head and neck
cancers? Cancer Epidemiol Biomarkers Prev 17:2087–2096
13. Ang KK, Harris J, Wheeler R, Weber R, Rosenthal DI, Nguyen-
Tan PF et al (2010) Human papillomavirus and survival of
patients with oropharyngeal cancer. N Engl J Med 363:24–35
14. Liang C, Marsit CJ, McClean MD, Nelson HH, Christensen BC,
Haddad RI et al (2012) Biomarkers of HPV in head and neck
squamous cell carcinoma. Cancer Res 72:5004–5013
15. World Health Organization (1992) International statistical clas-
sification of diseases and related health problems. 10th rev. World
Health Organization, Washington, DC
16. Hashibe M, Brennan P, Benhamou S, Castellsague X, Chen C,
Curado MP et al (2007) Alcohol drinking in never users of
tobacco, cigarette smoking in never drinkers, and the risk of head
and neck cancer: pooled analysis in the International Head and
Neck Cancer Epidemiology Consortium. J Natl Cancer Inst
99:777–789
17. Sobin LH, Wittekind C (2002) TNM classification of malignant
tumours. International Union Against Cancer, 6th edn. Wiley-
Liss, New York
18. Kleter B, Van Doorn LJ, Schrauwen L, Molijn A, Sastrowijoto S,
Ter Schegget J et al (1999) Development and clinical evaluation
of a highly sensitive PCR-reverse hybridization line probe assay
for detection and identification of anogenital human papilloma-
virus. J Clin Microbiol 37:2508–2517
19. Coutlee F, Gravitt P, Kornegay J, Hankins C, Richardson H,
Lapointe N et al (2002) Use of PGMY primers in L1 consensus
PCR improves detection of human papillomavirus DNA in gen-
ital samples. J Clin Microbiol 40:902–907
20. Bernard HU, Chan SY, Manos MM, Ong CK, Villa LL, Delius H
et al (1994) Identification and assessment of known and novel
human papillomaviruses by polymerase chain reaction amplifica-
tion, restriction fragment length polymorphisms, nucleotide
sequence, and phylogenetic algorithms. J Infec Dis 170:1077–1085
21. Sehr P, Zumbach K, Pawlita M (2001) A generic capture ELISA
for recombinant proteins fused to glutathione-S-transferase: val-
idation for HPV serology. J Immunol Methods 253:153–162
22. Waterboer T, Sehr P, Michael KM, Franceschi S, Nieland JD,
Joos TO et al (2005) Multiplex human papillomavirus serology
based on in situ-purified glutathione s-transferase fusion proteins.
Clin Chem 51:1845–1853
23. Clifford GM, Shin HR, Oh JK, Waterboer T, Ju YH, Vaccarella S
et al (2007) Serologic response to oncogenic human papilloma-
virus types in male and female university students in Busan,
South Korea. Cancer Epidemiol Biomarkers Prev 16:1874–1879
24. Kreimer AR, Clifford GM, Boyle P, Franceschi S (2005) Human
papillomavirus types in head and neck squamous cell carcinomas
worldwide: a systematic review. Cancer Epidemiol Biomarkers
Prev 14:467–475
25. Dayyani F, Etzel CJ, Liu M, Ho CH, Lippman SM, Tsao AS
(2010) Meta-analysis of the impact of human papillomavirus
(HPV) on risk and overall survival in head and neck squamous
cell carcinomas (HNSCC). Head Neck Oncol 2:15. doi:10.1186/
1758-3284-2-15
26. Smith EM, Pawlita M, Rubenstein LM, Haugen TH, Hamsikova
E, Turek LP (2010) Risk factors and survival by HPV-16 E6 and
E7 antibody status in human papillomavirus positive head and
neck cancer. Int J Cancer 127:111–117
27. Rotnaglova E, Tachezy R, Salakova M, Prochazka B, Kosl’abova
E, Vesela E et al (2011) HPV involvement in tonsillar cancer:
470 Cancer Causes Control (2014) 25:461–471
123

prognostic significance and clinically relevant markers. Int J
Cancer 129:101–110
28. Rubenstein LM, Smith EM, Pawlita M, Haugen TH, Hamsikova
E, Turek LP (2011) Human papilomavırus serologic follow-up
response and relationship to survival in head and neck cancer: a
case-comparison study. Infec Agent Cancer 6:9. doi:10.1186/
1750-9378-6-9
29. Smith EM, Rubenstein LM, Haugen TH, Pawlita M, Turek LP
(2012) Complex etiology underlies risk and survival in head and
neck cancer human papillomavirus, tobacco, and alcohol: a case
for multifactor disease. J Oncol. doi:10.1155./2012/571862
30. Mendez E (2012) Biomarkers of HPV infection in oropharyngeal
carcinomas: can we find simplicity in the puzzle of complexity?
Cancer Res 72:4896–4898
Cancer Causes Control (2014) 25:461–471 471
123
Copyright © 2022 FDOKUMEN




















