
Assessment of clinical outcomes in breast cancer patients treated with taxanes: multi-analytical...
7
Assessment of clinical outcomes in breast cancer patients treated with taxanes: multi-analytical approach Sonam Tulsyan a , Pankaj Chaturvedi a , Abhishek Kumar Singh a , Gaurav Agarwal b , Punita Lal c , Sushma Agrawal c , Rama Devi Mittal d , Balraj Mittal a, ⁎ a Department of Genetics, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow 226014, India b Department of Endocrine & Breast Surgery, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow 226014, India c Department of Radiotherapy, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow 226014, India d Department of Urology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow 226014, India abstract article info Article history: Received 9 November 2013 Received in revised form 30 January 2014 Accepted 1 April 2014 Available online 2 April 2014 Keywords: ABCB1 Cytochrome P450 Polymorphisms Clinical response Myelosuppression Polymorphisms in genes encoding CYPs (Phase I) and ABCB1 (Phase III) enzymes may attribute to variability of efficacy of taxanes. The present study aims to find the influence of CYP and ABCB1 gene polymorphisms on taxanes based clinical outcomes. 132 breast cancer patients treated with taxanes based chemotherapy were ge- notyped for CYP3A4*1B, CYP3A5*3, CYP1B1*3, CYP2C8*3, ABCB1 1236CNT, 2677GNT/A and 3435CNT polymor- phisms using PCR-RFLP. Associations of genetic variants with clinical outcomes in terms of response in 58 patients receiving neo-adjuvant chemotherapy (NACT), and chemo-toxicity in 132 patients were studied. Multi- factor dimensionality reduction (MDR) analysis was performed to evaluate higher order gene–gene interactions with clinical outcomes. Pathological response to taxane based NACT was associated with GA genotype as well as A allele of CYP3A5*3 polymorphism (P corr = 0.0465, P corr = 0.0465). Similarly, association was found in domi- nant model of CYP3A5*3 polymorphism with responders (P corr = 0.0465). Haplotype analysis further revealed A CYP3A4 –A CYP3A5 haplotype to be significantly associated with responders (P corr = 0.048). In assessing toxicity, sig- nificant association of variant (TT) genotype and T allele of ABCB1 2677GNT/A polymorphism, was found with ‘grade 1 or no leucopenia’ (P corr = 0.0465, P corr = 0.048). On evaluating higher order gene–gene interaction models by MDR analysis, CYP3A5*3; ABCB11236CNT and ABCB1 2677GNT/A; ABCB1 3435CNT and CYP1B1*3 showed significant association with treatment response, grade 2–4 anemia and dose delay/reduction due to neutropenia (P = 0.024, P = 0.004, P = 0.026), respectively. Multi-analytical approaches may provide a better assessment of pharmacogenetic based treatment outcomes in breast cancer patients treated with taxanes. © 2014 Elsevier B.V. All rights reserved. 1. Introduction Taxanes are commonly used cyto-toxic drugs in breast cancer treat- ment. Paclitaxel and docetaxel — the two common taxanes interfere with the microtubules at the mitotic spindle, resulting in cell cycle arrest during mitosis and finally cell death (Abal et al., 2003). Taxanes are part of the adjuvant treatment of breast cancer, as well as neo-adjuvant che- motherapy (NACT) for locally advanced breast cancers (LABC). Howev- er, there is a considerable inter-individual variation in the response to taxanes based chemotherapy, and many breast cancer patients have taxanes resistant tumors (Gehrmann et al., 2008). The severity of drug toxicity and adverse events, mostly in the form of myelosuppression also varies considerably. Pharmacogenetic studies can help identify in- dividuals predisposed to a high risk of toxicity and resistance to taxanes containing chemotherapeutic regimen. Polymorphisms in genes encoding taxane metabolizing enzymes and transporters can affect drug treatment outcomes. Both paclitaxel and docetaxel are metabolized by CYP3A4, CYP3A5 and CYP2C8 to inactive hydroxylated metabolites in the liver (Marsh, 2006). Taxanes are sub- strates for CYP1B1 enzymes (Bournique and Lemarie, 2002) and are re- sponsible for their catalytic activity (Hanna et al., 2000; Li et al., 2000; Shimada et al., 1999). The drug metabolites are substrates for ABCB1 transporters or P-glycoprotein which are located at the biliary canalicular membrane, enabling taxanes elimination from hepatocytes (Sparreboom et al., 1997). Polymorphisms in CYPs and ABCB1 genes have been studied in context with taxanes dependent toxicities (Dong et al., 2012; Rizzo et al., 2010; Tsai et al., 2009). As noted for anthracyclines, some studies have found ABCB1 genotypes and haplotypes to correlate with taxanes Gene 543 (2014) 69–75 Abbreviations: NACT, neo-adjuvant chemotherapy; ACT, adjuvant chemotherapy; NCI, National Cancer Institute; CTCAE, Common Toxicity Criteria for Adverse Events; PCR, poly- merase chain reaction; RFLP, restriction fragment length polymorphism; OR, odds ratios; CI, confidence intervals; FDR, False Discovery Rate Test; MDR, multifactor dimensionality reduction; CVC, cross-validation consistency; LABC, locally advanced breast cancer. ⁎ Corresponding author at: Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raebareli Road, Lucknow 226014, India. E-mail address: [email protected] (B. Mittal). http://dx.doi.org/10.1016/j.gene.2014.04.004 0378-1119/© 2014 Elsevier B.V. All rights reserved. Contents lists available at ScienceDirect Gene journal homepage: www.elsevier.com/locate/gene
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Assessment of clinical outcomes in breast cancer patients treated with taxanes: multi-analytical...

Gene 543 (2014) 69–75
Contents lists available at ScienceDirect
Gene
j ourna l homepage: www.e lsev ie r .com/ locate /gene
Assessment of clinical outcomes in breast cancer patients treated withtaxanes: multi-analytical approach
Sonam Tulsyan a, Pankaj Chaturvedi a, Abhishek Kumar Singh a, Gaurav Agarwal b, Punita Lal c,Sushma Agrawal c, Rama Devi Mittal d, Balraj Mittal a,⁎a Department of Genetics, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow 226014, Indiab Department of Endocrine & Breast Surgery, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow 226014, Indiac Department of Radiotherapy, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow 226014, Indiad Department of Urology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow 226014, India
Abbreviations:NACT, neo-adjuvant chemotherapy; ACNational Cancer Institute; CTCAE, Common Toxicity Criterimerase chain reaction; RFLP, restriction fragment length pCI, confidence intervals; FDR, False Discovery Rate Test; Mreduction; CVC, cross-validation consistency; LABC, locally⁎ Corresponding author at: Sanjay Gandhi Post Gradua
Raebareli Road, Lucknow 226014, India.E-mail address: [email protected] (B. Mittal).
http://dx.doi.org/10.1016/j.gene.2014.04.0040378-1119/© 2014 Elsevier B.V. All rights reserved.
a b s t r a c t
a r t i c l e i n f oArticle history:Received 9 November 2013Received in revised form 30 January 2014Accepted 1 April 2014Available online 2 April 2014
Keywords:ABCB1Cytochrome P450PolymorphismsClinical responseMyelosuppression
Polymorphisms in genes encoding CYPs (Phase I) and ABCB1 (Phase III) enzymes may attribute to variability ofefficacy of taxanes. The present study aims to find the influence of CYP and ABCB1 gene polymorphisms ontaxanes based clinical outcomes. 132 breast cancer patients treated with taxanes based chemotherapy were ge-notyped for CYP3A4*1B, CYP3A5*3, CYP1B1*3, CYP2C8*3, ABCB1 1236CNT, 2677GNT/A and 3435CNT polymor-phisms using PCR-RFLP. Associations of genetic variants with clinical outcomes in terms of response in 58patients receiving neo-adjuvant chemotherapy (NACT), and chemo-toxicity in 132 patients were studied. Multi-factor dimensionality reduction (MDR) analysis was performed to evaluate higher order gene–gene interactionswith clinical outcomes. Pathological response to taxane based NACT was associated with GA genotype as well asA allele of CYP3A5*3 polymorphism (Pcorr = 0.0465, Pcorr = 0.0465). Similarly, association was found in domi-nant model of CYP3A5*3 polymorphism with responders (Pcorr = 0.0465). Haplotype analysis further revealedACYP3A4–ACYP3A5haplotype to be significantly associatedwith responders (Pcorr= 0.048). In assessing toxicity, sig-nificant association of variant (TT) genotype and T allele of ABCB1 2677GNT/A polymorphism, was found with‘grade 1 or no leucopenia’ (Pcorr = 0.0465, Pcorr = 0.048). On evaluating higher order gene–gene interactionmodels by MDR analysis, CYP3A5*3; ABCB11236CNT and ABCB1 2677GNT/A; ABCB1 3435CNT and CYP1B1*3showed significant association with treatment response, grade 2–4 anemia and dose delay/reduction due toneutropenia (P = 0.024, P = 0.004, P = 0.026), respectively. Multi-analytical approaches may provide a betterassessment of pharmacogenetic based treatment outcomes in breast cancer patients treated with taxanes.
© 2014 Elsevier B.V. All rights reserved.
1. Introduction
Taxanes are commonly used cyto-toxic drugs in breast cancer treat-ment. Paclitaxel and docetaxel — the two common taxanes interferewith themicrotubules at themitotic spindle, resulting in cell cycle arrestduringmitosis and finally cell death (Abal et al., 2003). Taxanes are partof the adjuvant treatment of breast cancer, as well as neo-adjuvant che-motherapy (NACT) for locally advanced breast cancers (LABC). Howev-er, there is a considerable inter-individual variation in the response totaxanes based chemotherapy, and many breast cancer patients have
T, adjuvant chemotherapy; NCI,a for Adverse Events; PCR, poly-olymorphism; OR, odds ratios;DR, multifactor dimensionalityadvanced breast cancer.
te Institute of Medical Sciences,
taxanes resistant tumors (Gehrmann et al., 2008). The severity of drugtoxicity and adverse events, mostly in the form of myelosuppressionalso varies considerably. Pharmacogenetic studies can help identify in-dividuals predisposed to a high risk of toxicity and resistance to taxanescontaining chemotherapeutic regimen.
Polymorphisms in genes encoding taxane metabolizing enzymes andtransporters can affect drug treatment outcomes. Both paclitaxel anddocetaxel are metabolized by CYP3A4, CYP3A5 and CYP2C8 to inactivehydroxylated metabolites in the liver (Marsh, 2006). Taxanes are sub-strates for CYP1B1 enzymes (Bournique and Lemarie, 2002) and are re-sponsible for their catalytic activity (Hanna et al., 2000; Li et al., 2000;Shimada et al., 1999). The drug metabolites are substrates for ABCB1transporters or P-glycoprotein which are located at the biliary canalicularmembrane, enabling taxanes elimination from hepatocytes (Sparreboomet al., 1997). Polymorphisms in CYPs and ABCB1 genes have been studiedin context with taxanes dependent toxicities (Dong et al., 2012; Rizzoet al., 2010; Tsai et al., 2009). As noted for anthracyclines, some studieshave found ABCB1 genotypes and haplotypes to correlate with taxanes

70 S. Tulsyan et al. / Gene 543 (2014) 69–75
dependent toxicities (Bosch et al., 2006; Sissung et al., 2006; Yamaguchiet al., 2006), while other studies have not shown any correlation (Gohet al., 2002;Kimet al., 2012;Marsh andMcLeod, 2007;Marsh et al., 2007).
Considering that these candidate genes have a role in taxane activa-tion, metabolism and transportation, we aimed to find out the influenceof 7 SNPs (CYP3A4*1B, CYP3A5*3, CYP1B1*3, CYP2C8*3, ABCB11236CNT, ABCB1 2677GNT/A and ABCB1 3435CNT) with taxanes basedbreast cancer treatment outcomes in terms of response to NACT andchemo-toxicity using multi-analytical approaches.
2. Methodology
2.1. Patient selection
This prospective studywas approved by the research ethics commit-tee of SGPGIMS, Lucknow, India. A total of 132 histologically confirmedbreast cancer patients treated with taxanes based chemotherapy in theDepartments of Endocrine & Breast Surgery and Radiotherapy, SanjayGandhi Post Graduate Institute of Medical Sciences (SGPGIMS), Luck-now, were recruited in the study after taking their informed consent.Patients were staged according to AJCC-TNM classification system(Edge and Compton, 2010). Patients who did not complete their treat-ment as planned, or those for whom complete clinical, pathologic, oper-ative or outcome data were unavailable were excluded.
2.2. Drug administration
Study patients either received Docetaxel or Paclitaxel as adjuvantor NACT in sequential manner after four cycles of combination chemo-therapy consisting of anthracyclines (doxorubicin or epirubicin), 5-fluorouracil and cyclophosphamide. Patients treated with concomitantanthracyclines and taxanes were excluded. Paclitaxel was administeredat the standard dose of 80 mg/m2 infused i.v. over 1 h q 1 weekly for12 cycles, and docetaxel was administered at the dose of 100mg/m2 in-fused i.v. over 2 h q 3 weekly for four cycles.
2.3. Evaluation of treatment outcomes
According to the Response Evaluation Criteria in Solid Tumors(RECIST criteria) (Therasse et al., 2000), response was assessed in 58breast cancer patients treated with taxanes based NACT at the end oftaxanes therapy. The patientswith complete and partial pathological re-sponse were considered as responders while patients with static andprogressive disease were considered as non-responders. Chemo-toxicity in 132 patients receiving taxanes based adjuvant or NACT wasgraded according to the National Cancer Institute (NCI) CommonToxicity Criteria for Adverse Events (CTCAE), version 3.0 (http://ctep.cancer.gov). According to the NCI-CTCAE, grade 2–4 toxicitywas recorded in terms of grade 2–4 anemia (hemoglobin b 10 g/dl),leucopenia (TLC b 3000/mcL) and thrombocytopenia (platelets countb 75,000/mcL). Patients who suffered fromno or grade 1 toxicity are in-cluded in “No grade 2–4 toxicity”. Chemo-toxicity in the form of dosedelay or reduction due to febrile neutropenia was also recorded.
2.4. Genotyping
Venous blood (5 ml) was collected from each patient and the geno-mic DNAwas extracted fromperipheral blood using the standard saltingout method (Miller et al., 1988). The quality and quantity of DNA werechecked by using Nanodrop spectrophotometer (Thermo Fisher Scien-tific/Nanodrop Products, Wilmington, Delaware, USA).
Polymorphisms in CYP3A4, CYP3A5, CYP1B1, CYP2C8 and ABCB1were determined by Polymerase chain reaction (PCR)-Restriction frag-ment length polymorphism (RFLP) (Supplementary Table S1). Ten per-cent of the samples from patients including samples of each genotype
were re-genotyped by other laboratory personnel. No discrepancy wasfound after sequencing randomly selected 5% samples.
2.5. Statistical evaluation
Descriptive statistics of patients was presented as mean and stan-dard deviations for continuous measures and frequencies and percent-ages for categorical measures. Correlation between various genotypesand treatment outcomeswas examined using binary logistic regression.Association was expressed as odds ratios (OR) or risk estimates with95% confidence intervals (CI). Statistical analysis was done using SPSSstatistical analysis software, version 17.0 (SPSS Inc., Chicago, IL, USA).Statistical analysis of the haplotype estimation and linkage disequilibri-um was conducted using the SNPstat Software (Sole et al., 2006).Benjamini–Hochberg FalseDiscovery Rate Test (FDR) is used inmultiplehypothesis testing to correct for multiple comparisons. In a list ofrejected hypotheses, FDR controls the expected proportion of incorrect-ly rejected null hypothesis (type I errors). Multifactor dimensionalityreduction (MDR) analysis was done for the detection and characteriza-tion of gene–gene interactions (Hahn et al., 2003). The best gene–geneinteraction model was selected across all multi-locus models on thebasis of maximum testing accuracy (rounded up to 2 decimal places),cross-validation consistency (CVC) and permutation results were con-sidered to be statistically significant at the 0.05 level (rounded up to 3decimal places).
3. Results
3.1. Patient characteristics
The mean age of breast cancer patients was 48.06 ± 10.97 years.Detailed characteristics of patients including assessment of hormone re-ceptors (estrogen and progesterone) and HER 2-neu status; lymphnodes involved, metastasis, menopausal status and histology are sum-marized in Table 1. Out of 132 patients recruited in the study, paclitaxelwas administered to 68 (51.51%) patients while docetaxel was given to64 (48.48%). 58 patients in all received NACT.
3.2. Association of genetic variants with treatment response
Of the 58 locally advanced breast cancer (LABC) patients treatedwith taxanes based NACT, 22 (37.9%) were non-responders whereas36 (62.1%) patients were responders (Table 2). For CYP3A5*3 poly-morphism, border-line association of AG genotype was observed withresponders (Pcorr = 0.0465, OR = 0.29). Similarly, significant associa-tion of variant allele A (Pcorr = 0.0465, OR = 0.31) and in dominantmodel (Pcorr = 0.0465, OR= 0.26) was seen with responders. Howev-er, no association was found with other genetic variants of CYP andABCB with response (Table 2).
3.3. Association of genetic variants with chemo-toxicity
Out of 132 patients treated with taxanes based adjuvant or NACT,overall grade 2–4 chemo-toxicity was observed in 78 (59.1%) patients.No association of CYP or ABCB1 polymorphismswas observedwith che-motherapy induced grade 2–4 toxicity (Table 3).
Grade 2–4 anemia was noticed in 72 (54.5%) patients. For geneticvariants in either CYP or ABCB1, no association was observed withgrade 2–4 anemia at the genotypic level or at the allelic level (Sup-plementary Table S2). Furthermore, grade 2–4 leucopenia and thrombo-cytopenia were recorded in 32 (24.2%) and 7 (5.3%) patients,respectively. For ABCB1 2677GNT/A, significant association of GT geno-type was observed with patients having grade 1 or no leucopenia(Pcorr = 0.0465, OR = 0.15). Similarly, a marginal association of Tallele was seen (Pcorr = 0.0465, OR = 0.54) with grade 1 or no leu-copenia (Supplementary Table S3). However, due to less patient

Table 1Base-line characteristics of breast cancer patients.
Characteristics Number of patientsN = 132
Percentage(%)
Age in years (mean ± SD) 48.06 ± 10.97
GenderFemale 130 98.5Male 2 1.5
Menstrual statusPre-menopause 58 43.9Post-menopause 72 54.5Not applicable 2 1.5
HistotypeDuctal 126 95.5Lobular 2 1.5Mixed 4 3.0
Pathological lymph node statusN0 40 30.3N1 46 34.8N2 36 27.3N3 10 7.6
MetastasisM0 118 89.4M1 13 9.8Unknown 1 0.8
Hormone receptor statusPositive 72 54.5Negative 59 44.7Unknown 1 0.8
Her 2 neu statusPositive 57 43.2Negative 71 53.8Unknown 4 3.0
Taxanes based chemotherapyPaclitaxel (68)Adjuvant 50 (73.5)Neo-adjuvant 18 (26.5)
Docetaxel (64)Adjuvant 24 (37.5)Neo-adjuvant 40 (62.5)
71S. Tulsyan et al. / Gene 543 (2014) 69–75
number in thrombocytopenia we could not perform statistical analysis.Dose delay or reduction due to febrile neutropenia was also noticed in20 (15.2%) patients. Similarly, we were unable to find any association ofthe genetic variants of the genes studiedwith dose delay/reduction (Sup-plementary Table S4).
3.4. Association of haplotypes with treatment response and chemo-toxicity
Haplotype analysis was done in three ways — polymorphismsin same gene as that of ABCB1 1236CNT–2677GNT/A–3435CNT (D′ =0.620) (data not shown); polymorphisms present in the same CYPgroup of genes as that of CYP3A4*1B–CYP3A5*3 and polymorphismspresent on the same chromosome (chromosome 7) in the order ofCYP3A4*1B–CYP3A5*3–ABCB1 1236CNT–2677GNT/A–3435CNT(D′ =0.778) (data not shown).
CYP3A4*1B and CYP3A5*3 polymorphisms are in strong linkagedisequilibriumwith a D′= 0.779. The analysis revealed that the haplo-type ACYP3A4–ACYP3A5 was significantly associated with responders intreatment response (Pcorr = 0.048, OR = 0.16). Global haplotypeanalysis indicated significant difference between non-responders andresponders based on the distribution pattern of the 4 haplotypes (P =0.0035) (Table 4). Additionally, no significant association of the haplo-types with grade 2–4 toxicity was found (Supplementary Table S5).
3.5. Higher order gene–gene interaction by MDR analysis
MDR analysis was performed for the characterization of gene–geneinteractions with clinical outcomes. Simply, it was used to predict thebest gene–gene interaction model. The best prediction model for eachclinical outcome is illustrated in Table 5. The best interaction modelfor predicting treatment response was CYP3A5*3 (testing accuracy =0.55, CVC = 7/10, permutation p = 0.024). Further applying the MDRanalysis on grade 2–4 toxicity and anemia, wewere unable tofind a sta-tistically significant interaction model. For predicting grade 2–4 leuco-penia, ABCB1 1236CNT, ABCB1 2677GNT/A was considered as the bestinteraction model (testing accuracy = 0.50, CVC = 6/10, permutationp = 0.004). Similarly for dose delay/reduction, ABCB1 3435CNT,CYP1B1*3was considered as the best interactionmodel (testing accura-cy = 0.54, CVC = 8/10, permutation p = 0.026).
4. Discussion
Taxanes are effective anti-cancer drugs believed to prolong survivalin breast cancer patients (Crown, 2001; Esposito et al., 1999; Salminenet al., 1999). These are associated with risk of myelo-toxic side effectsin form of anemia, leucopenia, thrombocytopenia and febrile neutrope-nia. Further, the treatment response in breast cancer, as can be assessedin LABC patients treatedwithNACT varies from patient to patient. PhaseI (CYPs) and Phase III (ABCB1) drug metabolizing enzymes play an im-portant role in the metabolism of paclitaxel and docetaxel, and mayhave role in ascertaining the extent of disease response and toxicity oftaxanes (Fromm, 2002; Marsh, 2006; Tran et al., 2006). This study wasconducted with the aim to determine the role of genetic variants ofthese enzymes in taxanes based treatment outcomes.
We evaluated the association of drug transporters (ABCB1) and drugmetabolizing enzyme (CYPs) polymorphisms with treatment outcomesin 58 breast cancer patients treated with taxanes based NACT. We ob-served that GA genotype as well as A allele of CYP3A5*3 were signifi-cantly associated with responders in treatment response group alongwith the haplotype combination ACYP3A4–ACYP3A5. Our results were con-sistent on applying MDR analysis as well. The A to G nucleotide changecauses an alternative splice site in the pre-mRNA. This leads to the pro-duction of aberrant mRNA due to a premature stop codon, resulting inthe absence of functional CYP3A5 from liver tissue. GG homozygotesof CYP3A5*3 lack CYP3A5 enzyme expression, while the presence of atleast one A allele is involved in the expression of CYP3A5 enzyme.Many studies have explored the role of GG genotype of CYP3A5*3 andfound to be associated with decreased clearance of its substrates in dif-ferent ethnicity (Hustert et al., 2001; Kuehl et al., 2001). Our results canbe explained by the fact that the presence of A allele of CYP3A5*3 poly-morphism is responsible for the normal expression of the enzyme, thusmetabolizing taxanes with pathological response. However, A allele istheminor allele in Asian population (http://hapmap.org). Somuch can-not be said about the role of this polymorphism in the chemotherapeu-tic drug clinical outcomes, individually in the North Indian ethnicity.Recently, a study on 69 metastatic breast cancer patients who weretreatedwith docetaxel plus capecitabine, foundno significant associationof 79 SNPs in CYP450 with both response and progression free survival(PFS) (Dong et al., 2012). Among the enzymes involved in taxanemetab-olism, ATP-binding cassette transporters, are the most studied. Kafkaet al. (2003) reported significant correlation between the 3435T variantand better clinical response to anthracyclines with or without taxanes inLABC patients (n = 68) (Kafka et al., 2003). Further, association of theABCB1 gene polymorphisms 2677GNT/A and 3435CNT with treatmentresponse of paclitaxel monotherapy in metastatic breast cancer patientswas also reported (Chang et al., 2009). However, we could not find anyassociation of ABCB1 polymorphisms with treatment response.
We also studied the association of CYPs and ABCB1 genetic variantswith chemo-toxicity in terms of anemia, leucopenia and dose delay/reduction due to febrile neutropenia following taxane administration.

Table 2Frequency distribution of CYPs and ABCB1 polymorphisms between responders and non-responders.
Genotype/allele Non-respondersN = 22 (37.9%)
RespondersN = 36 (62.1%)
ORa (95% CIb) P value Pcorr
CYP3A4*1B polymorphismAA 20(90.9) 35(97.2) 1(Reference) – –
AG 2(9.1) 1(2.8) 3.50(0.29–41.07) 0.319 –
A 42(95.5) 71(98.6) 1(Reference) – –
G 2(4.5) 1(1.4) 3.38(0.29–38.42) 0.326 –
AG + GG 2(9.1) 1(2.8) 3.50(0.29–41.07) 0.319 –
CYP3A5*3 polymorphismGG 17(77.3) 17(47.2) 1(Reference) – –
GA 5(22.7) 17(47.2) 0.29 (0.08–0.97) 0.046 0.0465AA 0(0) 2(5.6) 0.00 0.999 –
G 39(88.6) 51(70.8) 1(Reference) – –
A 5(11.4) 21(29.2) 0.31(0.10–0.89) 0.031 0.0465GA + AA 5(22.7) 19(52.8) 0.26(0.08–0.86) 0.028 0.0465
CYP1B1*3 polymorphismCC 7(31.8) 15(41.7) 1(Reference) – –
CG 15(68.2) 19(52.8) 1.69(0.55–5.20) 0.359 –
GG 0(0) 2(5.6) 0.00 0.999 –
C 29(65.1) 49(68.1) 1(Reference) – –
G 15(34.1) 23(31.9) 1.10(0.49–2.44) 0.811 –
CG + GG 15(68.2) 21(58.3) 1.53(0.50–4.66) 0.454 –
CYP2C8*3 polymorphismGG 18(81.8) 30(83.3) 1(Reference) – –
GA 4(18.2) 6(16.7) 1.11(0.27–4.47) 0.882 –
G 40(90.9) 66(91.7) 1(Reference) – –
A 4(9.1) 6(8.3) 1.10(0.29–4.13) 0.888 –
GA + AA 4(18.2) 6(16.7) 1.11(0.27–4.47) 0.882 –
ABCB1 1236CNT polymorphismCC 2(9.1) 9(25.0) 1(Reference) – –
CT 10(45.5) 15(41.7) 3.00(0.53–16.89) 0.213 –
TT 10(45.5) 12(33.3) 3.75(0.65–21.51) 0.138 –
C 14(31.8) 33(45.8) 1(Reference) – –
T 30(68.2) 39(54.2) 1.81(0.82–3.97) 0.138 –
CT + TT 20(90.9) 27(75.0) 3.33(0.64–17.14) 0.150 –
ABCB1 2677GNT/A polymorphismGG 0(0) 2(5.6) 1(Reference) – –
GT 9(40.9) 18(50.0) 0.00 0.999 –
TT 12(54.5) 12(33.3) 0.00 0.999 –
AT 1(4.5) 4(11.1) 0.00 0.999 –
G 9(20.5) 22(30.6) 1(Reference) – –
T 34(77.3) 46(63.9) 1.80(0.74–4.41) 0.194 –
A 1(2.3) 4(5.6) 0.61(0.06–6.24) 0.678 –
GT + TT + AT + GA + AA 22(100) 34(94.4) 0.00 0.999 –
ABCB1 3435CNT polymorphismCC 1(4.5) 4(11.1) 1(Reference) – –
CT 8(36.4) 20(55.6) 1.60(0.15–16.60) 0.694 –
TT 13(59.1) 12(33.3) 4.33(0.42–44.42) 0.217 –
C 10(22.7) 28(38.9) 1(Reference) – –
T 34(77.3) 44(61.1) 2.16(0.92–5.06) 0.075 –
CT + TT 21(95.5) 32(88.9) 2.62(0.27–25.14) 0.402 –
Significant P values are given in bold.a OR—odds ratio.b CI—confidence interval; Benjamini Hochberg FDR test—Pcorr.
72 S. Tulsyan et al. / Gene 543 (2014) 69–75
For ABCB1 2677GNT/A, significant association was seen for GT genotypeand T allele with grade 1 or no leucopenia (Pcorr = 0.0465; Pcorr =0.048). On applying MDR analysis, we found ABCB11236CNT, ABCB12677GNT/A as the best interaction model for grade 2–4 leucopeniaand ABCB1 3435CNT, CYP1B1*3 for dose delay/reduction due to febrileneutropenia. ABCB1 2677GNT/A is a non-synonymous polymorphism,producing Ala893Thr and Ala893Ser, respectively (Tanabe et al.,2001). Individualswith homozygous 2677A/T genotype had significant-ly decreased intestinal P-gp expression and increased drug serum levelsafter chemotherapy. A number of studies have stated the role of ABCB1polymorphisms with breast cancer dependent toxicity. But, our resultsare not in agreement with some of the reported literature. In a studyfor CYP3A5*3 polymorphismon breast cancer patientswith TEC chemo-therapy, the patients carrying the GA genotype had more side effects of
fever, pleural effusion, and febrile neutropenia than those with the GGgenotype (Tsai et al., 2009). The authors further correlated the ABCB1genotypes with toxicity and found GG genotype of ABCB1 2677GNT/Ato be significantly associated with febrile neutropenia (Tsai et al.,2009). However, Chang et al. (2009) reported that none of the ABCB1genotypes were correlated with toxicity (Chang et al., 2009). Most ofthe studies published so far have considered only neutropenia as amea-sure of myelo-toxicity. Rizzo et al. (2010) reported that CYP2C8*3,CYP1B1*3 and ABCB1 (1236 CNT; 2677GNT/A; 3435 CNT) polymor-phisms in taxane metabolism pathway are not associated with neutro-penia (Rizzo et al., 2010). Another study reported CYP3A5 *1/*3 andABCB1 2677 G/G genotype to be significantly associated with febrileneutropenia in docetaxel treated breast cancer patients (Tsai et al.,2009). In a study on Korean patients, it was found that ABCB1 3435 T/T
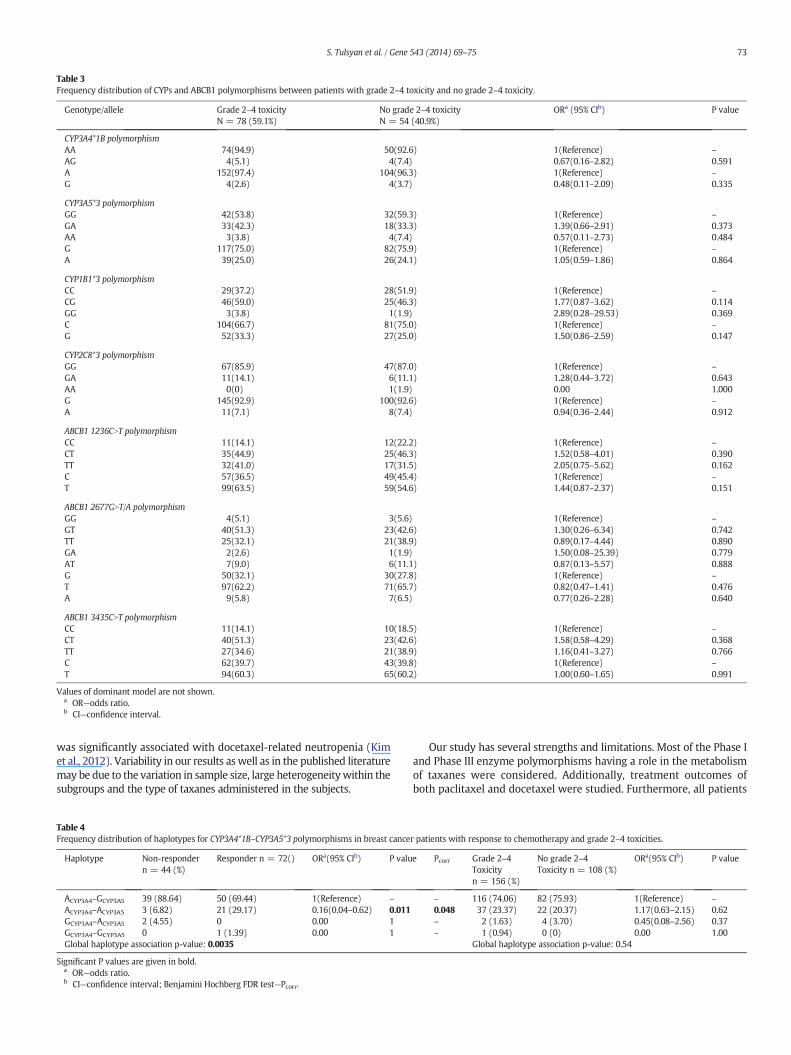
Table 3Frequency distribution of CYPs and ABCB1 polymorphisms between patients with grade 2–4 toxicity and no grade 2–4 toxicity.
Genotype/allele Grade 2–4 toxicityN = 78 (59.1%)
No grade 2–4 toxicityN = 54 (40.9%)
ORa (95% CIb) P value
CYP3A4*1B polymorphismAA 74(94.9) 50(92.6) 1(Reference) –
AG 4(5.1) 4(7.4) 0.67(0.16–2.82) 0.591A 152(97.4) 104(96.3) 1(Reference) –
G 4(2.6) 4(3.7) 0.48(0.11–2.09) 0.335
CYP3A5*3 polymorphismGG 42(53.8) 32(59.3) 1(Reference) –
GA 33(42.3) 18(33.3) 1.39(0.66–2.91) 0.373AA 3(3.8) 4(7.4) 0.57(0.11–2.73) 0.484G 117(75.0) 82(75.9) 1(Reference) –
A 39(25.0) 26(24.1) 1.05(0.59–1.86) 0.864
CYP1B1*3 polymorphismCC 29(37.2) 28(51.9) 1(Reference) –
CG 46(59.0) 25(46.3) 1.77(0.87–3.62) 0.114GG 3(3.8) 1(1.9) 2.89(0.28–29.53) 0.369C 104(66.7) 81(75.0) 1(Reference) –
G 52(33.3) 27(25.0) 1.50(0.86–2.59) 0.147
CYP2C8*3 polymorphismGG 67(85.9) 47(87.0) 1(Reference) –
GA 11(14.1) 6(11.1) 1.28(0.44–3.72) 0.643AA 0(0) 1(1.9) 0.00 1.000G 145(92.9) 100(92.6) 1(Reference) –
A 11(7.1) 8(7.4) 0.94(0.36–2.44) 0.912
ABCB1 1236CNT polymorphismCC 11(14.1) 12(22.2) 1(Reference) –
CT 35(44.9) 25(46.3) 1.52(0.58–4.01) 0.390TT 32(41.0) 17(31.5) 2.05(0.75–5.62) 0.162C 57(36.5) 49(45.4) 1(Reference) –
T 99(63.5) 59(54.6) 1.44(0.87–2.37) 0.151
ABCB1 2677GNT/A polymorphismGG 4(5.1) 3(5.6) 1(Reference) –
GT 40(51.3) 23(42.6) 1.30(0.26–6.34) 0.742TT 25(32.1) 21(38.9) 0.89(0.17–4.44) 0.890GA 2(2.6) 1(1.9) 1.50(0.08–25.39) 0.779AT 7(9.0) 6(11.1) 0.87(0.13–5.57) 0.888G 50(32.1) 30(27.8) 1(Reference) –
T 97(62.2) 71(65.7) 0.82(0.47–1.41) 0.476A 9(5.8) 7(6.5) 0.77(0.26–2.28) 0.640
ABCB1 3435CNT polymorphismCC 11(14.1) 10(18.5) 1(Reference) –
CT 40(51.3) 23(42.6) 1.58(0.58–4.29) 0.368TT 27(34.6) 21(38.9) 1.16(0.41–3.27) 0.766C 62(39.7) 43(39.8) 1(Reference) –
T 94(60.3) 65(60.2) 1.00(0.60–1.65) 0.991
Values of dominant model are not shown.a OR—odds ratio.b CI—confidence interval.
73S. Tulsyan et al. / Gene 543 (2014) 69–75
was significantly associated with docetaxel-related neutropenia (Kimet al., 2012). Variability in our results as well as in the published literaturemay be due to the variation in sample size, large heterogeneitywithin thesubgroups and the type of taxanes administered in the subjects.
Table 4Frequency distribution of haplotypes for CYP3A4*1B–CYP3A5*3 polymorphisms in breast cance
Haplotype Non-respondern = 44 (%)
Responder n = 72() ORa(95% CIb) P valu
ACYP3A4–GCYP3A5 39 (88.64) 50 (69.44) 1(Reference) –
ACYP3A4–ACYP3A5 3 (6.82) 21 (29.17) 0.16(0.04–0.62) 0.011GCYP3A4–ACYP3A5 2 (4.55) 0 0.00 1GCYP3A4–GCYP3A5 0 1 (1.39) 0.00 1Global haplotype association p-value: 0.0035
Significant P values are given in bold.a OR—odds ratio.b CI—confidence interval; Benjamini Hochberg FDR test—Pcorr.
Our study has several strengths and limitations. Most of the Phase Iand Phase III enzyme polymorphisms having a role in the metabolismof taxanes were considered. Additionally, treatment outcomes ofboth paclitaxel and docetaxel were studied. Furthermore, all patients
r patients with response to chemotherapy and grade 2–4 toxicities.
e Pcorr Grade 2–4Toxicityn = 156 (%)
No grade 2–4Toxicity n = 108 (%)
ORa(95% CIb) P value
– 116 (74.06) 82 (75.93) 1(Reference) –
0.048 37 (23.37) 22 (20.37) 1.17(0.63–2.15) 0.62– 2 (1.63) 4 (3.70) 0.45(0.08–2.56) 0.37– 1 (0.94) 0 (0) 0.00 1.00
Global haplotype association p-value: 0.54

Table 5Higher order gene–gene interaction by MDR analysis.
Clinical outcomes Best interaction model CV testing accuracya,b CV consistencya P for permutation testingc OR(CI)b
Treatment response CYP3A5*3 0.55 7/10 0.024 2.29 (1.01–5.21)Grade 2–4 toxicity CYP1B1*3 0.53 9/10 0.094 1.43 (0.82–2.48)Grade 2–4 anemia CYP1B1*3 0.57 10/10 0.072 2.81 (1.10–7.22)Grade 2–4 leucopenia ABCB11236CNT, ABCB1 2677GNT/A 0.50 6/10 0.004 2.45 (0.93–6.50)Dose delay/reduction ABCB1 3435CNT, CYP1B1*3 0.54 8/10 0.026 2.53 (1.10–5.82)
Model with maximum CV testing accuracy and consistency was considered as the best interaction model.Significant P values are in bold.
a CV—cross validation.b Values rounded up to 2 decimal places.c Values rounded up to 3 decimal places.
74 S. Tulsyan et al. / Gene 543 (2014) 69–75
recruited in the study were histopathologically confirmed matchedsubjects. Study endpoint considered in case of responderswas objectivepathological response rather than more subjective clinical response,as has been used in most previous studies. Correlation of response totaxanes is compounded by the fact that all patients had previouslyreceived anthracyclines based combination chemotherapy. However,as taxane monotherapy is not an accepted treatment regime, studyingcorrelations of the taxane based metabolizing and transporter genepolymorphisms with response to taxanes alone is not possible. Further-more, in the patients evaluated by us, the groups of patients with andwithout genetic variant had all other things equal, and were found tobe having significant difference in treatment outcomes, when correlat-ed with the polymorphisms.
The sample size is one of themajor limitations of this study, particu-larly in the case of response to chemotherapy. However, this limitationhad been overcome by applying Benjamini–Hochberg FDR test for mul-tiple comparisons andMDRanalysiswhich cross validates the results 10times and reduces the chances of false positive association in small sam-ple sized study. Our study needs further validation to ascertain the roleof drug metabolizing and transporter enzyme polymorphisms in breastcancer treatment outcomes, which can potentially raise the possibilityof individualized treatment by identification of the patients with possi-bility of poor response to chemotherapy and an increased risk of chemo-toxicity.
Conflict of interest
All authors have no conflicts of interest.
Acknowledgments
We are thankful to the Indian Council of Medical Research (ICMR-BMS/NTF/1/2010-2-11) and Department of Science and Technology(DST-SSD/SS/005/2009) for providing financial support to carry outthis study.
Appendix A. Supplementary data
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.gene.2014.04.004.
References
Abal, M., Andreu, J.M., Barasoain, I., 2003. Taxanes: microtubule and centrosome targets,and cell cycle dependent mechanisms of action. Current Cancer Drug Targets 3,193–203.
Bosch, T.M., Huitema, A.D., Doodeman, V.D., Jansen, R., Witteveen, E., Smit, W.M., Jansen,R.L., van Herpen, C.M., Soesan, M., Beijnen, J.H., Schellens, J.H., 2006. Pharmacogeneticscreening of CYP3A and ABCB1 in relation to population pharmacokinetics of doce-taxel. Clinical Cancer Research 12, 5786–5793.
Bournique, B., Lemarie, A., 2002. Docetaxel (Taxotere) is not metabolized by recombinanthuman CYP1B1 in vitro, but acts as an effector of this isozyme. Drug Metabolism andDisposition 30, 1149–1152.
Chang, H., Rha, S.Y., Jeung, H.C., Im, C.K., Ahn, J.B., Kwon,W.S., Yoo, N.C., Roh, J.K., Chung, H.C., 2009. Association of the ABCB1 gene polymorphisms 2677GNT/A and 3435CNTwith clinical outcomes of paclitaxel monotherapy in metastatic breast cancer pa-tients. Annals of Oncology 20, 272–277.
Crown, J., 2001. Docetaxel: overview of an active drug for breast cancer. The Oncologist 6(Suppl. 3), 1–4.
Dong, N., Yu, J., Wang, C., Zheng, X., Wang, Z., Di, L., Song, G., Zhu, B., Che, L., Jia, J., Jiang, H.,Zhou, X., Wang, X., Ren, J., 2012. Pharmacogenetic assessment of clinical outcome inpatients with metastatic breast cancer treated with docetaxel plus capecitabine. Jour-nal of Cancer Research and Clinical Oncology 138, 1197–1203.
Edge, S.B., Compton, C.C., 2010. The American Joint Committee on Cancer: the 7th editionof the AJCC cancer stagingmanual and the future of TNM. Annals of Surgical Oncology17, 1471–1474.
Esposito, M., Venturini, M., Vannozzi, M.O., Tolino, G., Lunardi, G., Garrone, O., Angiolini, C.,Viale, M., Bergaglio, M., Del Mastro, L., Rosso, R., 1999. Comparative effects of paclitax-el and docetaxel on the metabolism and pharmacokinetics of epirubicin in breastcancer patients. Journal of Clinical Oncology 17, 1132.
Fromm, M.F., 2002. The influence of MDR1 polymorphisms on P-glycoprotein expressionand function in humans. Advanced Drug Delivery Reviews 54, 1295–1310.
Gehrmann, M., Schmidt, M., Brase, J.C., Roos, P., Hengstler, J.G., 2008. Prediction of pacli-taxel resistance in breast cancer: is CYP1B1*3 a new factor of influence?Pharmacogenomics 9, 969–974.
Goh, B.C., Lee, S.C., Wang, L.Z., Fan, L., Guo, J.Y., Lamba, J., Schuetz, E., Lim, R., Lim, H.L., Ong,A.B., Lee, H.S., 2002. Explaining interindividual variability of docetaxel pharmacoki-netics and pharmacodynamics in Asians through phenotyping and genotyping strat-egies. Journal of Clinical Oncology 20, 3683–3690.
Hahn, L.W., Ritchie, M.D., Moore, J.H., 2003. Multifactor dimensionality reduction softwarefor detecting gene–gene and gene–environment interactions. Bioinformatics 19,376–382.
Hanna, I.H., Dawling, S., Roodi, N., Guengerich, F.P., Parl, F.F., 2000. Cytochrome P450 1B1(CYP1B1) pharmacogenetics: association of polymorphisms with functional differ-ences in estrogen hydroxylation activity. Cancer Research 60, 3440–3444.
Hustert, E., Haberl, M., Burk, O., Wolbold, R., He, Y.Q., Klein, K., Nuessler, A.C., Neuhaus, P.,Klattig, J., Eiselt, R., Koch, I., Zibat, A., Brockmoller, J., Halpert, J.R., Zanger, U.M.,Wojnowski, L., 2001. The genetic determinants of the CYP3A5 polymorphism. Phar-macogenetics 11, 773–779.
Kafka, A., Sauer, G., Jaeger, C., Grundmann, R., Kreienberg, R., Zeillinger, R., Deissler,H., 2003. Polymorphism C3435T of the MDR-1 gene predicts response topreoperative chemotherapy in locally advanced breast cancer. Int J Oncol 22,1117–1121.
Kim, K.P., Ahn, J.H., Kim, S.B., Jung, K.H., Yoon, D.H., Lee, J.S., Ahn, S.H., 2012. Prospectiveevaluation of the drug-metabolizing enzyme polymorphisms and toxicity profile ofdocetaxel in Korean patients with operable lymph node-positive breast cancerreceiving adjuvant chemotherapy. Cancer Chemotherapy and Pharmacology 69,1221–1227.
Kuehl, P., Zhang, J., Lin, Y., Lamba, J., Assem, M., Schuetz, J., Watkins, P.B., Daly, A.,Wrighton, S.A., Hall, S.D., Maurel, P., Relling, M., Brimer, C., Yasuda, K.,Venkataramanan, R., Strom, S., Thummel, K., Boguski, M.S., Schuetz, E., 2001.Sequence diversity in CYP3A promoters and characterization of the genetic basis ofpolymorphic CYP3A5 expression. Nature Genetics 27, 383–391.
Marsh, S., 2006. Taxane pharmacogenetics. Personalized Medicine 3, 33–43.Marsh, S., McLeod, H.L., 2007. Pharmacogenetics and oncology treatment for breast
cancer. Expert Opinion on Pharmacotherapy 8, 119–127.Marsh, S., Somlo, G., Li, X., Frankel, P., King, C.R., Shannon,W.D., McLeod, H.L., Synold, T.W.
, 2007. Pharmacogenetic analysis of paclitaxel transport and metabolism genes inbreast cancer. Pharmacogenomics Journal 7, 362–365.
Miller, S.A., Dykes, D.D., Polesky, H.F., 1988. A simple salting out procedure for extractingDNA from human nucleated cells. Nucleic Acids Research 16, 1215.
Rizzo, R., Spaggiari, F., Indelli, M., Lelli, G., Baricordi, O.R., Rimessi, P., Ferlini, A., 2010. As-sociation of CYP1B1 with hypersensitivity induced by taxane therapy in breast cancerpatients. Breast Cancer Research and Treatment 124, 593–598.
Salminen, E., Bergman,M., Huhtala, S., Ekholm, E., 1999. Docetaxel: standard recommend-ed dose of 100 mg/m(2) is effective but not feasible for some metastatic breast can-cer patients heavily pretreated with chemotherapy-A phase II single-center study.Journal of Clinical Oncology 17, 1127.
Shimada, T., Watanabe, J., Kawajiri, K., Sutter, T.R., Guengerich, F.P., Gillam, E.M., Inoue, K.,1999. Catalytic properties of polymorphic human cytochrome P450 1B1 variants. Car-cinogenesis 20, 1607–1613.

75S. Tulsyan et al. / Gene 543 (2014) 69–75
Sissung, T.M., Mross, K., Steinberg, S.M., Behringer, D., Figg, W.D., Sparreboom, A., Mielke,S., 2006. Association of ABCB1 genotypes with paclitaxel-mediated peripheral neu-ropathy and neutropenia. European Journal of Cancer 42, 2893–2896.
Sole, X., Guino, E., Valls, J., Iniesta, R., Moreno, V., 2006. SNPStats: a web tool for the anal-ysis of association studies. Bioinformatics 22, 1928–1929.
Sparreboom, A., van Asperen, J., Mayer, U., Schinkel, A.H., Smit, J.W., Meijer, D.K., Borst, P.,Nooijen, W.J., Beijnen, J.H., van Tellingen, O., 1997. Limited oral bioavailability and ac-tive epithelial excretion of paclitaxel (Taxol) caused by P-glycoprotein in the intes-tine. Proceedings of the National Academy of Sciences of the United States ofAmerica 94, 2031–2035.
Tanabe,M., Ieiri, I., Nagata, N., Inoue, K., Ito, S., Kanamori, Y., Takahashi, M., Kurata, Y., Kigawa,J., Higuchi, S., Terakawa, N., Otsubo, K., 2001. Expression of P-glycoprotein in humanplacenta: relation to genetic polymorphism of the multidrug resistance (MDR)-1gene. Journal of Pharmacology and Experimental Therapeutics 297, 1137–1143.
Therasse, P., Arbuck, S.G., Eisenhauer, E.A., Wanders, J., Kaplan, R.S., Rubinstein, L., Verweij,J., Van Glabbeke, M., van Oosterom, A.T., Christian, M.C., Gwyther, S.G., 2000. New
guidelines to evaluate the response to treatment in solid tumors. European Organiza-tion for Research and Treatment of Cancer, National Cancer Institute of the UnitedStates, National Cancer Institute of Canada. Journal of the National Cancer Institute92, 205–216.
Tran, A., Jullien, V., Alexandre, J., Rey, E., Rabillon, F., Girre, V., Dieras, V., Pons, G.,Goldwasser, F., Treluyer, J.M., 2006. Pharmacokinetics and toxicity of docetaxel: roleof CYP3A, MDR1, and GST polymorphisms. Clinical Pharmacology and Therapeutics79, 570–580.
Tsai, S.M., Lin, C.Y., Wu, S.H., Hou, L.A., Ma, H., Tsai, L.Y., Hou, M.F., 2009. Side effects afterdocetaxel treatment in Taiwanese breast cancer patients with CYP3A4, CYP3A5, andABCB1 gene polymorphisms. Clinica Chimica Acta 404, 160–165.
Yamaguchi, H., Hishinuma, T., Endo, N., Tsukamoto, H., Kishikawa, Y., Sato, M., Murai, Y.,Hiratsuka, M., Ito, K., Okamura, C., Yaegashi, N., Suzuki, N., Tomioka, Y., Goto, J.,2006. Genetic variation in ABCB1 influences paclitaxel pharmacokinetics inJapanese patients with ovarian cancer. International Journal of Gynecological Cancer16, 979–985.




















