
Assessing disability in morbidly obese individuals: the Italian Society of Obesity test for...
10
RESEARCH PAPER Assessing disability in morbidly obese individuals: the Italian Society of Obesity test for obesity-related disabilities LORENZO M. DONINI 1 , AMELIA BRUNANI 2 , ANNA SIRTORI 2 , CLAUDIA SAVINA 3 , SETTIMIO TEMPERA 1 , MASSIMO CUZZOLARO 1 , GIOVANNI SPERA 1 , VERONICA CIMOLIN 2,4 , HELMER PRECILIOS 2 , ALBERTO RAGGI 5 , PAOLO CAPODAGLIO 2 & THE SIO-ISDCA TASK FORCE* 1 Department of Medical Physiopathology (Food Science Section) –‘Sapienza’ University of Rome, Italy, 2 Rehabilitation Unit and Research Lab in Biomechanics and Rehabilitation, Istituto Auxologico Italiano IRCCS, Piancavallo, Verbania, Italy, 3 Villa delleQuerce Clinical Rehabilitation Institute – Nemi, RM – Italy, 4 Bioengnerring Department, Politecnico di Milano, Milano, Italy, and 5 Neurology, Public Health and Disability Unit, Neurological Institute C. Besta IRCCS Foundation, Milan, Italy Accepted March 2011 Abstract Purpose. To validate a new obesity-specific disability assessment test: the Obesity-related Disability test (Test SIO Disabilita ` Obesita ` Correlata, TSD-OC). Methods. Adult obese individuals were assessed with the TSD-OC, 36-Item Short-Form Health Survey (SF-36), 6-min walking test (6MWT) and grip strength. The TSD-OC is composed of 36 items divided into seven sections (pain, stiffness, activities of daily living and indoor mobility, housework, outdoor activities, occupational activities and social life). Statistical correlations between the TSD-OC, functional assessment (6MWT and grip strength) and quality of life parameters (SF-36) were analysed. Internal consistency was assessed with Cronbach’s a test. Test–retest reliability was evaluated in a subgroup of 30 individuals. A linking exercise between TSD-OC items and categories of the International Classification of Functioning, Disability and Health was performed. Results. Test–retest showed excellent stability (r ¼ 0.90) and excellent internal consistency was reported (Cronbach’s a 4 0.90). Significant low to moderate correlations between TSD-OC, SF-36 scores, 6MWT and grip strength were observed. A total of 26 ICF categories were linked, mostly related to the area of mobility. Conclusions. The TSD-OC is a reliable and valid instrument for measuring self-reported disability in obese subjects. It may represent an important tool for establishing rehabilitation needs in individuals with obesity-related disability, for planning appropriate rehabilitation programmes and for evaluating their effectiveness. Keywords: Obesity, assessment, TSD-OC Introduction Obesity is a clinical condition characterised by significant clinical implications, such as co-morbid- ities and somatic fragility, which seriously affect independence, psychological well being and overall quality of life (QoL) at all ages [1,2]. The 2000–2001 Health Survey for England [3] revealed that many of the encountered disabling conditions were signifi- cantly correlated with obesity. Conditions such as osteoarthritis, diabetes mellitus and chronic obstruc- tive pulmonary disease, which are often associated with obesity, were ranked among the 10 most burdensome diseases for high-income countries in the last update of WHO’s Global Burden of Disease study [4]. Obesity is in fact associated with an Correspondence: Veronica Cimolin, Department of Bioengineering, Politecnico di Milano, P.zza Leonardo Da Vinci 32, 20133, Milano, Italy. Tel: þ39 02 2399 3359. E-mail: [email protected] *SIO-SISDCA Task Force Collaborators are as follows: Maria RosaBollea, Emanuela Castellaneta, Roberto Dalle Grave, Ezio Di Flaviano, Maria Gabriella Gentile, FabrizioJacoangeli, Cecilia Invitti, Carla Lubrano, Fausto Manara, Barbara Mezzani, RobertoOstuzzi, GianluigiPanzolato, FabrizioPasanisi, Maria Letizia Petroni, Ferruccio Santini, Felice Strollo, Patrizia Todisco, and Mauro Zamboni. Disability and Rehabilitation, 2011; Early Online, 1–10 ISSN 0963-8288 print/ISSN 1464-5165 online ª 2011 Informa UK, Ltd. DOI: 10.3109/09638288.2011.575529 Disabil Rehabil Downloaded from informahealthcare.com by Dip di Bioingegneria - Bib on 05/04/11 For personal use only.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Assessing disability in morbidly obese individuals: the Italian Society of Obesity test for...

RESEARCH PAPER
Assessing disability in morbidly obese individuals: the Italian Society ofObesity test for obesity-related disabilities
LORENZO M. DONINI1, AMELIA BRUNANI2, ANNA SIRTORI2, CLAUDIA SAVINA3,
SETTIMIO TEMPERA1, MASSIMO CUZZOLARO1, GIOVANNI SPERA1,
VERONICA CIMOLIN2,4, HELMER PRECILIOS2, ALBERTO RAGGI5,
PAOLO CAPODAGLIO2 & THE SIO-ISDCA TASK FORCE*
1Department of Medical Physiopathology (Food Science Section) –‘Sapienza’ University of Rome, Italy, 2Rehabilitation Unit
and Research Lab in Biomechanics and Rehabilitation, Istituto Auxologico Italiano IRCCS, Piancavallo, Verbania, Italy,3Villa delleQuerce Clinical Rehabilitation Institute – Nemi, RM – Italy, 4Bioengnerring Department, Politecnico di Milano,
Milano, Italy, and 5Neurology, Public Health and Disability Unit, Neurological Institute C. Besta IRCCS Foundation,
Milan, Italy
Accepted March 2011
AbstractPurpose. To validate a new obesity-specific disability assessment test: the Obesity-related Disability test (Test SIO DisabilitaObesita Correlata, TSD-OC).Methods. Adult obese individuals were assessed with the TSD-OC, 36-Item Short-Form Health Survey (SF-36), 6-minwalking test (6MWT) and grip strength. The TSD-OC is composed of 36 items divided into seven sections (pain, stiffness,activities of daily living and indoor mobility, housework, outdoor activities, occupational activities and social life). Statisticalcorrelations between the TSD-OC, functional assessment (6MWT and grip strength) and quality of life parameters (SF-36)were analysed. Internal consistency was assessed with Cronbach’s a test. Test–retest reliability was evaluated in a subgroup of30 individuals. A linking exercise between TSD-OC items and categories of the International Classification of Functioning,Disability and Health was performed.Results. Test–retest showed excellent stability (r¼ 0.90) and excellent internal consistency was reported (Cronbach’sa4 0.90). Significant low to moderate correlations between TSD-OC, SF-36 scores, 6MWT and grip strength wereobserved. A total of 26 ICF categories were linked, mostly related to the area of mobility.Conclusions. The TSD-OC is a reliable and valid instrument for measuring self-reported disability in obese subjects. It mayrepresent an important tool for establishing rehabilitation needs in individuals with obesity-related disability, for planningappropriate rehabilitation programmes and for evaluating their effectiveness.
Keywords: Obesity, assessment, TSD-OC
Introduction
Obesity is a clinical condition characterised by
significant clinical implications, such as co-morbid-
ities and somatic fragility, which seriously affect
independence, psychological well being and overall
quality of life (QoL) at all ages [1,2]. The 2000–2001
Health Survey for England [3] revealed that many of
the encountered disabling conditions were signifi-
cantly correlated with obesity. Conditions such as
osteoarthritis, diabetes mellitus and chronic obstruc-
tive pulmonary disease, which are often associated
with obesity, were ranked among the 10 most
burdensome diseases for high-income countries in
the last update of WHO’s Global Burden of Disease
study [4]. Obesity is in fact associated with an
Correspondence: Veronica Cimolin, Department of Bioengineering, Politecnico di Milano, P.zza Leonardo Da Vinci 32, 20133, Milano, Italy.
Tel: þ39 02 2399 3359. E-mail: [email protected]
*SIO-SISDCA Task Force Collaborators are as follows: Maria RosaBollea, Emanuela Castellaneta, Roberto Dalle Grave, Ezio Di Flaviano, Maria Gabriella
Gentile, FabrizioJacoangeli, Cecilia Invitti, Carla Lubrano, Fausto Manara, Barbara Mezzani, RobertoOstuzzi, GianluigiPanzolato, FabrizioPasanisi, Maria
Letizia Petroni, Ferruccio Santini, Felice Strollo, Patrizia Todisco, and Mauro Zamboni.
Disability and Rehabilitation, 2011; Early Online, 1–10
ISSN 0963-8288 print/ISSN 1464-5165 online ª 2011 Informa UK, Ltd.
DOI: 10.3109/09638288.2011.575529
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dip
di B
ioin
gegn
eria
- B
ib o
n 05
/04/
11Fo
r pe
rson
al u
se o
nly.

increased risk of disability after the age of 50 years in
terms of limited mobility and activities of daily living
(ADL) and with a significantly lower number of
disability-free years (5.7 years for males and 5.02
years for females) [5]. As body mass index (BMI)
and age increase, these activities are bound to be
limited.
Disability associated with obesity may be predo-
minantly due to motor or cardiorespiratory compli-
cations, as well as a combination of the two
according to the coexistence of a range of related
conditions (i.e. osteoarthritis, cardiorespiratory dis-
orders, etc.). Some articles [6–10] reported difficul-
ties for obese subjects in ADL (i.e. personal hygiene
and dressing), indoor mobility, household chores
(i.e. rising from a couch, getting onto a high stool
and taking objects from a cupboard or picking them
up from the floor), outdoor activities (i.e. lifting and
carrying bags, walking4100 m and standing in a
queue) and occupational activities. As for the latter
point, obesity seems to be significantly related to sick
leave, reduction in productivity, the need to be
assigned to less demanding jobs and represents a
significant risk factor for work inability [11–14].
One of the major problems in the research area on
obesity-related disability is the lack of widely used
obesity-specific scales able to provide a thorough
understanding of the physical difficulties and limita-
tions in everyday life. Standardised functional
assessments are often non-specifically validated in
the obese population and are not designed to
measure clinical appropriateness, which heightens
the risk of underestimating the problems. Functional
status measures (i.e. the Barthel Index) assess only
physical disability as reflected by ADL or Instru-
mented ADL scales and thus fails to detect
functional status changes until disability is extreme
[15]. The association between the Functional In-
dependence Measure (FIM), the gold standard for
measuring outcomes in rehabilitation and BMI has
been recently investigated in unfit individuals with
medical complications who are undergoing intensive
rehabilitation: they showed higher gains in FIM
scores, mostly accounted for by the motor subscale,
as compared with normal weight patients [16].
Some evidence exists that obese individuals under-
going intensive rehabilitation do not have suboptimal
outcomes as compared with their leaner counterparts
[17]. Vincent and Vincent [18] showed that a high
BMI does not prevent FIM gains during inpatient
rehabilitation after total knee replacement. However,
these gains were achieved less efficiently and at a
higher cost than when BMI is normal. Two small
studies also reported no association between BMI
and FIM scores in post-acute stroke and joint
arthroplasty rehabilitation patients [19]. Since post-
acute rehabilitation individuals may encompass a
range of diagnoses, it is likely that the BMI-FIM
association may vary within subgroups. Those
studies investigate whether a high BMI might
actually impede the rehabilitation process after
surgery or stroke and the gains in physical function.
The FIM scale has never been used for the
assessment of obesity-related disability, which ap-
pears to be an entity backed by a consistent body of
recent literature, independent of recent acute events.
In 2002, the United States Task Force on Develop-
ing Obesity Outcomes and Learning Standards
(TOOLS) [20] recommended a summary of out-
come measures for the obese patient, which included
the use of the Medical Outcome Survey 36-Item
Short-Form Health Survey (SF-36) or its 12-items
version (SF-12) [21,22]. The use of such scales
allows researchers to compare the burden associated
with obesity against that associated with other
disorders. The SF-36 physical composite score
(PCS) also taps lower extremity functions likely to
be impaired by osteoarthritis and may be useful for
identifying obese individuals who would benefit from
a more intensive follow-up with disease-specific
scales. However, the SF-36 content is not restricted
to functional status, but includes a conflation of
symptom, function and health-perception scales or
items that, moreover, are not specific to the obese
individuals’ situation. Obesity-specific measures, on
the contrary, have the potential advantage of captur-
ing experiences frequently reported by obese indivi-
duals, which are not, in turn, assessed by generic
QoL or mood inventories measures, and tend to be
more sensitive to change [23].
The Impact of Weight on Quality of Life Ques-
tionnaire is a 74-item self-report obesity-specific
measure [24] that describes the effect of body weight
on functioning in areas such as health, social status,
work, mobility, self-esteem, sexual activities, ADL
and eating. Both the long and the reduced 31-item
versions of the questionnaire have shown good test–
retest reliability and internal consistency and re-
vealed significant improvements in all domains
following weight reduction [25]. Other obesity-
specific instruments suffer the disadvantage of being
used in limited settings and of lacking empirical
validation: the ORWELL97 suffers from limited and
unfocused content [26], and the Swedish Obese
Subjects Intervention Trial Battery is very psychoso-
cial oriented and lengthy [27]. The TOOLS Task
Force (2002) recommends the use of an existing
symptom-specific scale in addition to the more
general measure when the goal is to provide an in-
depth evaluation of one specific obesity-related
symptom.
In 2001, the WHO released the International
Classification of Functioning, Disability and Health
(ICF) as an international reference for understanding
2 L. M. Donini et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dip
di B
ioin
gegn
eria
- B
ib o
n 05
/04/
11Fo
r pe
rson
al u
se o
nly.

functioning and disability [28]. Disability in ICF is
understood as the relationships between impairments
at the level of the body, which determine limitations
and restrictions in undertaking activities and in
engaging in social situations and interaction with
environmental factors. Acting as facilitators, environ-
mental factors contribute to an increase in functional
level and a reduction in disability, if they are barriers
to the individual then they contribute to an increase in
disability. As a recent literature review has shown
[29], several experiences with the use of ICF in a
clinical context exist, and ICF-related tools like the
ICF-Core Set have been developed. The Compre-
hensive ICF-Core Set for obesity consists of 109
categories [30] mainly covering aspects related to
cardiovascular and metabolic functions (and their
related structures) as well as activities related to
mobility and self-care. The ICF is also useful as a
background to describe the content of existing
assessment tools, through standardised linking
rules [31].
Previous studies on obesity implications evidenced
different areas of impairments in body functions and
structures, as well as an increase in disability risk;
mobility limitations were reported in several studies
[9,23–27,32,33]. Daily activities appear to be re-
duced or limited as a direct expression of the
intrinsic health state, with a limited intervention of
external factors. Impairments in emotional func-
tions, even without a diagnosis of depression, are
reported together with impairments in body image as
well as in energy level. Such findings support known
evidence of the implications of emotional and
psychological factors in obese individuals’ eating
behaviours [34–37]. Disability in the area of inter-
personal interactions and social isolation, with
difficulties in creating and maintaining intimate
relationships, and in relating to strangers, are also
recognised features of obese individuals. Social
stigma and discrimination were frequently deemed
to underlie relational problems, jointly with personal
characteristics such as guilt and shame [34,35,38].
Multidimensional rehabilitation approaches have
been proposed to treat morbidly obese subjects [11].
Measuring disability with instruments reflecting the
full range of functional status appears therefore
crucial in order to initiate rehabilitation programmes
for obese subjects and to assess their effectiveness. In
2009, it was with this goal in mind that the Italian
Society of Obesity (SIO) developed a new scale for
assessing disability correlated to obesity in adult
populations, the short-form questionnaire the Obe-
sity-related Disability test (Test SIO Disabilita
Obesita Correlata, TSD.OC) [39]. This instrument
is intended to target the most important obesity-
specific functional status dimensions such as physi-
cal, emotional functioning and social functioning.
The aim of our study was to verify the extent to
which this new instrument is linked to the different
ICF components and to evaluate its validity and
reliability in a group of obese individuals.
Materials and methods
Subjects
A multi-centric study coordinated by the SIO and
involving 16 Italian hospitals (SIO-SISDCA Task
Force) was performed. Obese individuals under-
going multidisciplinary rehabilitation for obesity in
different settings (outpatient, day-hospital and in-
patient) were enrolled between January and June
2009. To be enrolled, individuals had to be aged over
20 years, have a BMI higher than 30 kg/m2 and be
able to walk a distance of at least 30 m indepen-
dently. Exclusion criteria were, to have undergone
orthopaedic surgery on the lower limbs and spine in
the 2 years prior to the start of the study, the presence
of neurological disturbances, the assumption of
pharmacological treatment for equilibrium and vestib-
ular disturbances, cardiological and respiratory dis-
turbances. The study protocol was approved by the
Ethical Committee of the Sapienza University of
Rome and all subjects gave written informed consent
prior to enrolment. A subsample of 30 randomly
selected individuals completed the TSD-OC a second
time 24 h after the first assessment.
Methods
The TSD-OC is composed of 36 items divided into
seven sections (pain: 5 items; stiffness: 2 items; ADL
and indoor mobility: 7 items; housework: 7 items;
outdoor activities: 5 items; occupational activities: 4
items and social life: 6 items), which reflect the
domains in which individuals experience the most
common problems. Individuals are requested to
provide a subjective assessment of their disability
for each item on a 0–10 visual analogue scale (VAS),
where 10 indicates the highest level of disability and
0 no difficulties in performing the task. In this
preliminary application, we decided to define arbi-
trary provisional ‘disability scores’ as the sum of each
item’s raw score divided by the maximum possible
score, expressed as a percentage according to the
following linear transformation: (raw score/max
score)6 100. For example, a raw score of 90, being
25% of the total possible score (which corresponds to
360), results in a final disability score of 25. In this
way, disability scores can be calculated for each
subsection, thus enabling a preliminary section-by-
section comparison.
The SIO test for obesity-related disabilities 3
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dip
di B
ioin
gegn
eria
- B
ib o
n 05
/04/
11Fo
r pe
rson
al u
se o
nly.
The SF-36 [40] is a multi-purpose general health
survey with 36 questions, generally used to evaluate
health-related quality of life (HRQoL). It is com-
posed of 36 items grouped into eight scales and of
two additional summary measures, the PCS and the
mental composite score (MCS). The scores of the
scales range between 0 and 100, with higher scores
reflecting greater HRQoL, while PCS and MCS are
norm-based scores with a mean of 50 and a standard
deviation of 10.
Objective measures of health status included
handgrip strength and walking speed. Grip strength
was measured by a handgrip (Jamar1 Hydraulic
Hand Dynamometer – 5030J1). The maximum
value (kg) out of three trials using the dominant
hand was recorded. Between two consecutive trials,
a 1-min recovery was provided. In the 6-min
walking test (6MWT) [41], subjects were in-
structed to walk as fast as they could along an
even, undisturbed 30 m hospital corridor marked
every 5 m with coloured tape on the floor. They
were allowed to stop or rest during the test if
necessary. The distance walked in 6 min was
computed. The subject’s pulse, respiratory rate,
blood pressure and perceived fatigue on Borg’s
scale were measured before the test, at 1, 3 and
5 min after the start and at test completion.
Statistics
For assessing retest reliability, Spearman’s rank
order correlation (rs) between the first and the
second administration of the TSD-OC in the
subsample was used. An rs of 0.80 was set as the
minimum level of acceptable stability [41]. Wilcox-
on’s signed-rank test was used to test the difference
between test and retest scores. Internal consistency
of the test was assessed using Cronbach’s a. The avalues of 0.6–0.7 indicate acceptable reliability,
while values higher than 0.8 indicate good reliability
[42]. To assess validity, Pearson’s correlation was
calculated between the TSD-OC score, SF-36
scores and objective physical assessments. Statistical
significance was set at P50.05. Data were analysed
using the SPSS for Windows 10.0 (SPSS Inc.,
1989–1999) statistical software package. SF-36,
6MWT and handgrip strength were also compared
against normative values [43–45], describing the
percentage of subjects who reported values lower
than normative ones.
Given the taxonomy of ICF and its coding rules,
‘rolling-up’ procedures have been applied to move
from detailed information to more generic, and
therefore to more wide open, second-level codes
(e.g. from d4200 to d420) that are more useful for
exploring the content of the questionnaire.
Results
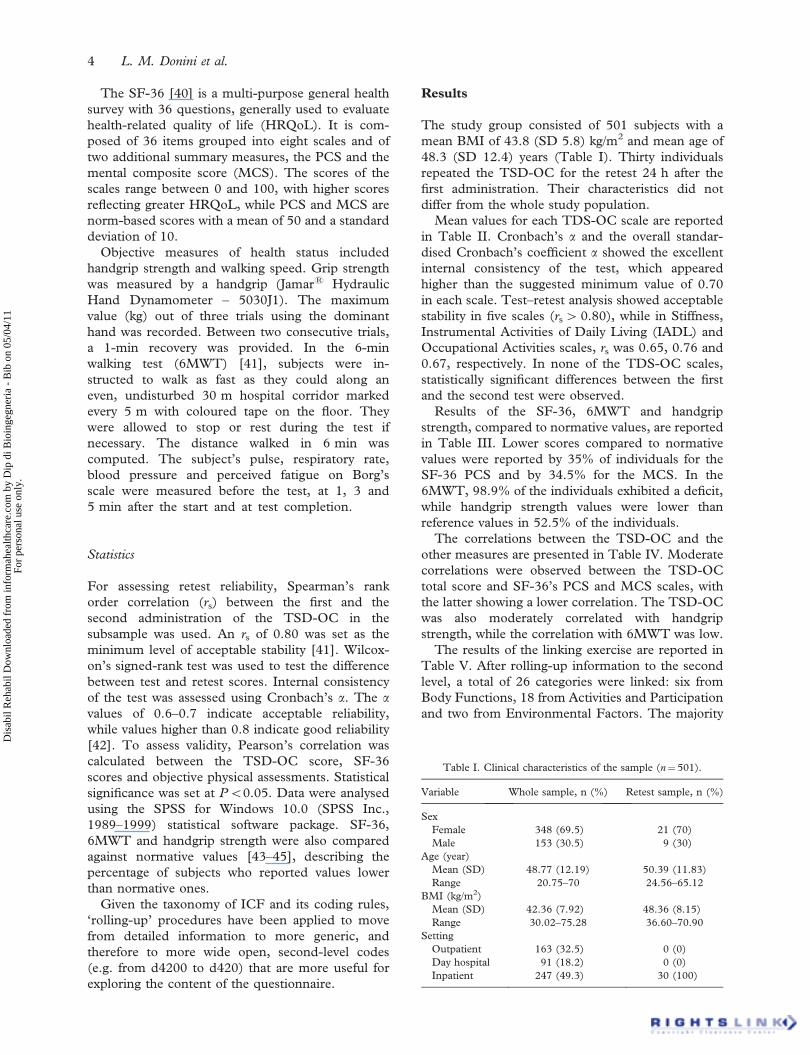
The study group consisted of 501 subjects with a
mean BMI of 43.8 (SD 5.8) kg/m2 and mean age of
48.3 (SD 12.4) years (Table I). Thirty individuals
repeated the TSD-OC for the retest 24 h after the
first administration. Their characteristics did not
differ from the whole study population.
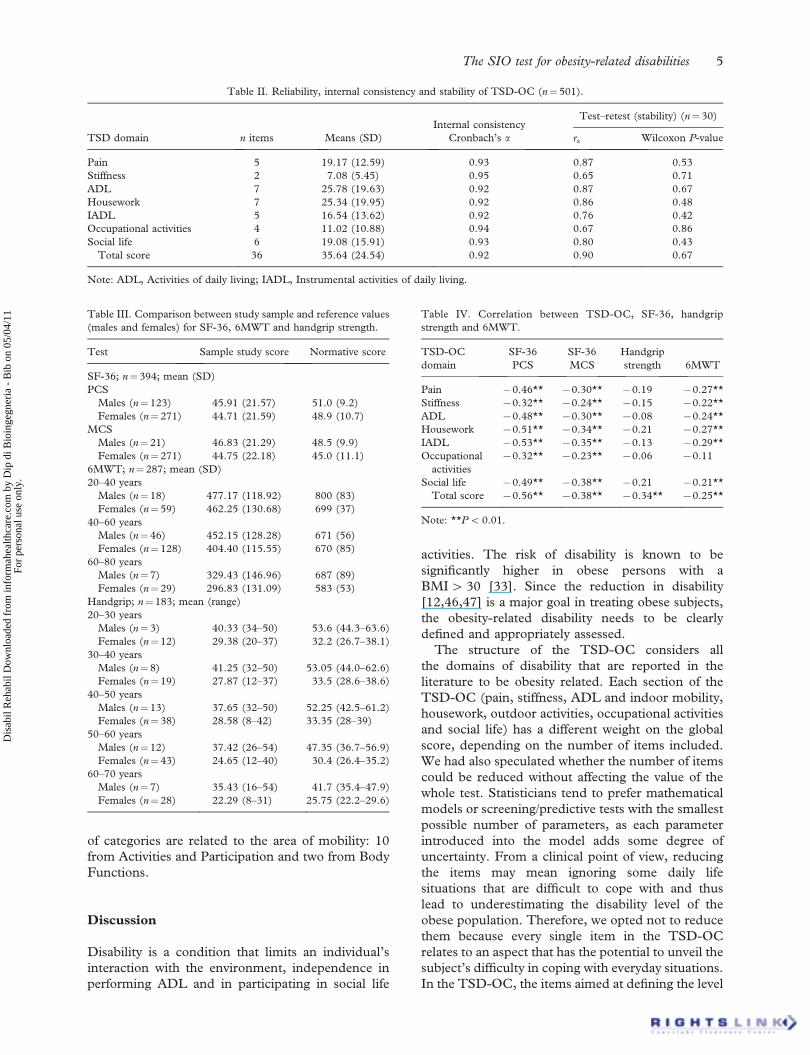
Mean values for each TDS-OC scale are reported
in Table II. Cronbach’s a and the overall standar-
dised Cronbach’s coefficient a showed the excellent
internal consistency of the test, which appeared
higher than the suggested minimum value of 0.70
in each scale. Test–retest analysis showed acceptable
stability in five scales (rs4 0.80), while in Stiffness,
Instrumental Activities of Daily Living (IADL) and
Occupational Activities scales, rs was 0.65, 0.76 and
0.67, respectively. In none of the TDS-OC scales,
statistically significant differences between the first
and the second test were observed.
Results of the SF-36, 6MWT and handgrip
strength, compared to normative values, are reported
in Table III. Lower scores compared to normative
values were reported by 35% of individuals for the
SF-36 PCS and by 34.5% for the MCS. In the
6MWT, 98.9% of the individuals exhibited a deficit,
while handgrip strength values were lower than
reference values in 52.5% of the individuals.
The correlations between the TSD-OC and the
other measures are presented in Table IV. Moderate
correlations were observed between the TSD-OC
total score and SF-36’s PCS and MCS scales, with
the latter showing a lower correlation. The TSD-OC
was also moderately correlated with handgrip
strength, while the correlation with 6MWT was low.
The results of the linking exercise are reported in
Table V. After rolling-up information to the second
level, a total of 26 categories were linked: six from
Body Functions, 18 from Activities and Participation
and two from Environmental Factors. The majority
Table I. Clinical characteristics of the sample (n¼ 501).
Variable Whole sample, n (%) Retest sample, n (%)
Sex
Female 348 (69.5) 21 (70)
Male 153 (30.5) 9 (30)
Age (year)
Mean (SD) 48.77 (12.19) 50.39 (11.83)
Range 20.75–70 24.56–65.12
BMI (kg/m2)
Mean (SD) 42.36 (7.92) 48.36 (8.15)
Range 30.02–75.28 36.60–70.90
Setting
Outpatient 163 (32.5) 0 (0)
Day hospital 91 (18.2) 0 (0)
Inpatient 247 (49.3) 30 (100)
4 L. M. Donini et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dip
di B
ioin
gegn
eria
- B
ib o
n 05
/04/
11Fo
r pe
rson
al u
se o
nly.
of categories are related to the area of mobility: 10
from Activities and Participation and two from Body
Functions.
Discussion
Disability is a condition that limits an individual’s
interaction with the environment, independence in
performing ADL and in participating in social life
activities. The risk of disability is known to be
significantly higher in obese persons with a
BMI4 30 [33]. Since the reduction in disability
[12,46,47] is a major goal in treating obese subjects,
the obesity-related disability needs to be clearly
defined and appropriately assessed.
The structure of the TSD-OC considers all
the domains of disability that are reported in the
literature to be obesity related. Each section of the
TSD-OC (pain, stiffness, ADL and indoor mobility,
housework, outdoor activities, occupational activities
and social life) has a different weight on the global
score, depending on the number of items included.
We had also speculated whether the number of items
could be reduced without affecting the value of the
whole test. Statisticians tend to prefer mathematical
models or screening/predictive tests with the smallest
possible number of parameters, as each parameter
introduced into the model adds some degree of
uncertainty. From a clinical point of view, reducing
the items may mean ignoring some daily life
situations that are difficult to cope with and thus
lead to underestimating the disability level of the
obese population. Therefore, we opted not to reduce
them because every single item in the TSD-OC
relates to an aspect that has the potential to unveil the
subject’s difficulty in coping with everyday situations.
In the TSD-OC, the items aimed at defining the level
Table II. Reliability, internal consistency and stability of TSD-OC (n¼501).
TSD domain n items Means (SD)
Internal consistency
Cronbach’s a
Test–retest (stability) (n¼ 30)
rs Wilcoxon P-value
Pain 5 19.17 (12.59) 0.93 0.87 0.53
Stiffness 2 7.08 (5.45) 0.95 0.65 0.71
ADL 7 25.78 (19.63) 0.92 0.87 0.67
Housework 7 25.34 (19.95) 0.92 0.86 0.48
IADL 5 16.54 (13.62) 0.92 0.76 0.42
Occupational activities 4 11.02 (10.88) 0.94 0.67 0.86
Social life 6 19.08 (15.91) 0.93 0.80 0.43
Total score 36 35.64 (24.54) 0.92 0.90 0.67
Note: ADL, Activities of daily living; IADL, Instrumental activities of daily living.
Table III. Comparison between study sample and reference values
(males and females) for SF-36, 6MWT and handgrip strength.
Test Sample study score Normative score
SF-36; n¼ 394; mean (SD)
PCS
Males (n¼123) 45.91 (21.57) 51.0 (9.2)
Females (n¼271) 44.71 (21.59) 48.9 (10.7)
MCS
Males (n¼21) 46.83 (21.29) 48.5 (9.9)
Females (n¼271) 44.75 (22.18) 45.0 (11.1)
6MWT; n¼287; mean (SD)
20–40 years
Males (n¼18) 477.17 (118.92) 800 (83)
Females (n¼59) 462.25 (130.68) 699 (37)
40–60 years
Males (n¼46) 452.15 (128.28) 671 (56)
Females (n¼128) 404.40 (115.55) 670 (85)
60–80 years
Males (n¼7) 329.43 (146.96) 687 (89)
Females (n¼29) 296.83 (131.09) 583 (53)
Handgrip; n¼ 183; mean (range)
20–30 years
Males (n¼3) 40.33 (34–50) 53.6 (44.3–63.6)
Females (n¼12) 29.38 (20–37) 32.2 (26.7–38.1)
30–40 years
Males (n¼8) 41.25 (32–50) 53.05 (44.0–62.6)
Females (n¼19) 27.87 (12–37) 33.5 (28.6–38.6)
40–50 years
Males (n¼13) 37.65 (32–50) 52.25 (42.5–61.2)
Females (n¼38) 28.58 (8–42) 33.35 (28–39)
50–60 years
Males (n¼12) 37.42 (26–54) 47.35 (36.7–56.9)
Females (n¼43) 24.65 (12–40) 30.4 (26.4–35.2)
60–70 years
Males (n¼7) 35.43 (16–54) 41.7 (35.4–47.9)
Females (n¼28) 22.29 (8–31) 25.75 (22.2–29.6)
Table IV. Correlation between TSD-OC, SF-36, handgrip
strength and 6MWT.
TSD-OC
domain
SF-36
PCS
SF-36
MCS
Handgrip
strength 6MWT
Pain 70.46** 70.30** 70.19 70.27**
Stiffness 70.32** 70.24** 70.15 70.22**
ADL 70.48** 70.30** 70.08 70.24**
Housework 70.51** 70.34** 70.21 70.27**
IADL 70.53** 70.35** 70.13 70.29**
Occupational
activities
70.32** 70.23** 70.06 70.11
Social life 70.49** 70.38** 70.21 70.21**
Total score 70.56** 70.38** 70.34** 70.25**
Note: **P5 0.01.
The SIO test for obesity-related disabilities 5
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dip
di B
ioin
gegn
eria
- B
ib o
n 05
/04/
11Fo
r pe
rson
al u
se o
nly.
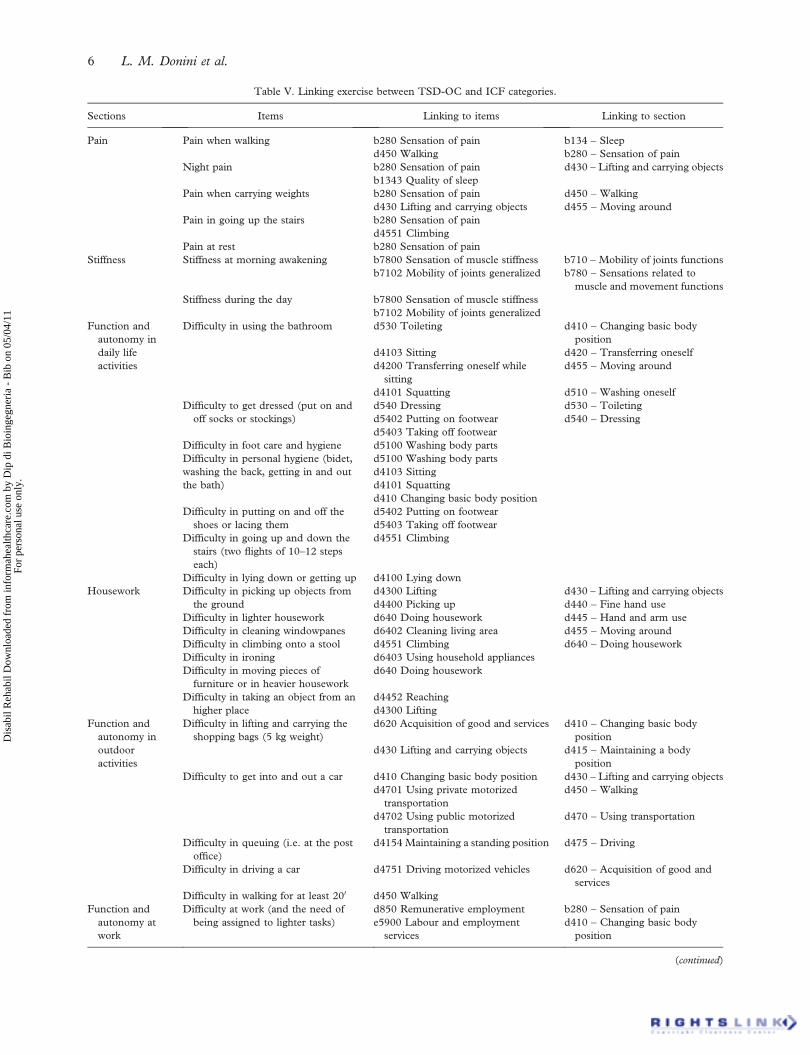
Table V. Linking exercise between TSD-OC and ICF categories.
Sections Items Linking to items Linking to section
Pain Pain when walking b280 Sensation of pain b134 – Sleep
d450 Walking b280 – Sensation of pain
Night pain b280 Sensation of pain d430 – Lifting and carrying objects
b1343 Quality of sleep
Pain when carrying weights b280 Sensation of pain d450 – Walking
d430 Lifting and carrying objects d455 – Moving around
Pain in going up the stairs b280 Sensation of pain
d4551 Climbing
Pain at rest b280 Sensation of pain
Stiffness Stiffness at morning awakening b7800 Sensation of muscle stiffness b710 – Mobility of joints functions
b7102 Mobility of joints generalized b780 – Sensations related to
muscle and movement functions
Stiffness during the day b7800 Sensation of muscle stiffness
b7102 Mobility of joints generalized
Function and
autonomy in
daily life
activities
Difficulty in using the bathroom d530 Toileting d410 – Changing basic body
position
d4103 Sitting d420 – Transferring oneself
d4200 Transferring oneself while
sitting
d455 – Moving around
d4101 Squatting d510 – Washing oneself
Difficulty to get dressed (put on and
off socks or stockings)
d540 Dressing d530 – Toileting
d5402 Putting on footwear d540 – Dressing
d5403 Taking off footwear
Difficulty in foot care and hygiene d5100 Washing body parts
Difficulty in personal hygiene (bidet,
washing the back, getting in and out
the bath)
d5100 Washing body parts
d4103 Sitting
d4101 Squatting
d410 Changing basic body position
Difficulty in putting on and off the
shoes or lacing them
d5402 Putting on footwear
d5403 Taking off footwear
Difficulty in going up and down the
stairs (two flights of 10–12 steps
each)
d4551 Climbing
Difficulty in lying down or getting up d4100 Lying down
Housework Difficulty in picking up objects from
the ground
d4300 Lifting d430 – Lifting and carrying objects
d4400 Picking up d440 – Fine hand use
Difficulty in lighter housework d640 Doing housework d445 – Hand and arm use
Difficulty in cleaning windowpanes d6402 Cleaning living area d455 – Moving around
Difficulty in climbing onto a stool d4551 Climbing d640 – Doing housework
Difficulty in ironing d6403 Using household appliances
Difficulty in moving pieces of
furniture or in heavier housework
d640 Doing housework
Difficulty in taking an object from an
higher place
d4452 Reaching
d4300 Lifting
Function and
autonomy in
outdoor
activities
Difficulty in lifting and carrying the
shopping bags (5 kg weight)
d620 Acquisition of good and services d410 – Changing basic body
position
d430 Lifting and carrying objects d415 – Maintaining a body
position
Difficulty to get into and out a car d410 Changing basic body position d430 – Lifting and carrying objects
d4701 Using private motorized
transportation
d450 – Walking
d4702 Using public motorized
transportation
d470 – Using transportation
Difficulty in queuing (i.e. at the post
office)
d4154 Maintaining a standing position d475 – Driving
Difficulty in driving a car d4751 Driving motorized vehicles d620 – Acquisition of good and
services
Difficulty in walking for at least 200 d450 Walking
Function and
autonomy at
work
Difficulty at work (and the need of
being assigned to lighter tasks)
d850 Remunerative employment b280 – Sensation of pain
e5900 Labour and employment
services
d410 – Changing basic body
position
(continued)
6 L. M. Donini et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dip
di B
ioin
gegn
eria
- B
ib o
n 05
/04/
11Fo
r pe
rson
al u
se o
nly.

of disability are based on VAS scores. The 10
(maximum level of disability) to 0 score (absence of
difficulty in performing a specific function) defines
the subjective/perceived level of disability. Future
studies should be aimed at defining the cut-off values
of the TSD-OC by comparing it with sensitive
performance tests in the obese population.
The validation of TSD-OC was performed against
the SF-36, which has several dimensions and,
although not obesity specific, has shown sensitivity
to the impact of weight loss on HRQoL in severely
obese persons [47]. Unsurprisingly, the TSD-OC
showed better correlations with the SF-36 items
related to physical than mental health component
and the mental health component. However, a
significant, although not so strong, correlation was
also found with the items describing the mental
health component. These data confirm that disability
in obesity is not only a physical issue, but one which
also brings about relevant psychological conse-
quences that also affect QoL.
The TSD-OC showed a significant correlation
also with the chosen functional parameters: grip
strength and distance walked in 6 min. The latter
test has been extensively used as an outcome
measure of the functional status and response to
treatment in individuals with cardiorespiratory dis-
orders as well as in the geriatric population and its
reproducibility in obese subjects has been recently
demonstrated [48].
The correlation between functional parameters
and the TSD-OC score, although statistically sig-
nificant, was not very strong. This may be due to the
fact that the TSD-OC and functional testing
measures two different aspects of disability: the
TSD-OC targets participation in the different
aspects of everyday life, while the latter measures
objective physical performance. The TSD-OC and
functional parameters therefore depict different but
complementary aspects of disability from a subjective
and an objective perspective, respectively, and
should both be used in a comprehensive assessment
of the disabling status of obesity. This also implies
that participation is not so strictly connected with
functional limitations: rather, it deals with the
engagement in social situations, which constitutes a
relevant problem for obese individuals. The relation-
ships found between disability profiles and HRQoL
are significant, but generally low or moderate,
meaning that QoL and disability reflect different
constructs, which therefore should not be considered
as transposable.
The linking exercise to ICF categories showed a
wide coverage in particular of activities related to
mobility and self-care, and of impairments of mental
functions. A few previous articles attempted to use or
Table V. (Continued).
Sections Items Linking to items Linking to section
Pain after a day of work b280 Sensation of pain d415 – Maintaining a body
position
Difficulty in maintaining a posture d415 Maintaining a body position d850 – Remunerative employment
d850 Remunerative employment e590 – Labour and employment
SSP
Need to be often absented from work e5901 Labour and employment
systems
d850 Remunerative employment
Function and
autonomy in the
social life
Necessity to avoid sofas, reclining
seats for fear of not getting up
d4103 Sitting b152 – Emotional functions
b152 Emotional functions b160 – Thought functions
Fear of falling and not being able to
get up
b152 Emotional functions d410 – Changing basic body
position
Feeling criticized for being obese b160 Thought functions d470 – Using transportation
Fear of having difficulty in going to the
cinema, to the theatre or in getting
on an airplane
b152 Emotional functions d750 – Informal social
relationships
d9202 Art and culture d920 – Recreation and leisure
d4702 Using public motorized
transportation
e115 – Products and technology
for personal use in daily living
Need to find armchairs to get up more
easily
e1150 General products and
technology for personal use in daily
living
d4103 Sitting
Difficulty in going round with ‘non-
obese’ friends or acquaintances
d7500 Informal relationship with
friends
d7502 Informal relationship with
acquaintances
Note: Linking to items was performed to the most specific category possible, linking to section was performed to second-level ICF
categories.
The SIO test for obesity-related disabilities 7
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dip
di B
ioin
gegn
eria
- B
ib o
n 05
/04/
11Fo
r pe
rson
al u
se o
nly.

implement the ICF in obesity rehabilitation pro-
grammes. A first experience mapped ICF categories
onto a full diagnostic and therapeutic protocol,
evidencing a total of 166 ICF cross-walked categories,
of which 106 mapped onto standardised assessment
tools [49]. An analysis of the prevalence of problems in
obese individuals showed that 43 ICF categories
reported relevant information (i.e. reported as a
problem) in at least 20% of subjects [50]. The
majority of these categories are covered by the TSD-
OC; however, some of them were not reported. In
particular, the TSD-OC covers information related to
two categories from Body Functions (b160 – Thought
Functions; b780 – Sensations related to muscle and
movement functions) and eight from Activities and
Participation (d420 – Transferring oneself, d440 –
Fine hand use, d445 – Hand and arm use, d470 –
Using transportation and d475 – Driving) that were
not reported in the ICF-based problems’ prevalence.
Finally, a third article [51] showed that impairments at
the level of the body are much more closely related to
limitations in performing activities than the effect of
environmental factors. All these studies support a
multidisciplinary approach to the evaluation of dis-
ability, which is a key element in the rehabilitation
programme, which however needs to rely upon valid
and solid assessment tools.
This study has some limitations. The first lies in
the cross-sectional design that does not allow us to
state that the TSD-OC is sensitive to change: future
studies should be planned to measure its reliability in
capturing differences in a pre- vs. post-rehabilitation
longitudinal design, at different time points. A
second limitation lies in the selection of our subjects
who were all individuals enrolled in specialty clinics
for obesity rehabilitation. However, age and BMI
range should reduce this limitation. For the linking
exercise, the instrument proposed appears in line
with the ICF bio-psychosocial model of disability.
However, only two environmental factors are con-
sidered while our previous results on the application
of such a methodology show that five categories were
more frequently rated as barriers and eight as
facilitators.
Conclusions
The results of the present study demonstrate the
validity of the TSD-OC as a tool able to measure the
aspects of disability described by obese subjects: in
particular, the TSD-OC proved to be significantly
correlated with functional and QoL parameters. Its
use within a multidisciplinary assessment should
be implemented by specific instruments able to
establish the role of environmental factors. This
new scale may represent an important instrument
for the description of obesity-related disability and
for planning and measuring the effectiveness of
rehabilitation programmes in obese subjects. Fu-
ture longitudinal studies should be planned to
assess its sensitivity to change at different time
points.
Acknowledgements
The authors are indebted to Prof GajVidmar for his
invaluable statistical assistance.
Declaration of interest: The authors report
no conflicts of interest. The authors alone are
responsible for the content and writing of the paper.
References
1. Kim JY, Oh DJ, Yoon TY, Choi JM, Choe BK. The impacts
of obesity on psychological well-being: a cross-sectional study
about depressive mood and quality of life. J Prev Med Publ
Health 2007;40:191–195.
2. Kostka T, Bogus K. Independent contribution of overweight/
obesity and physical inactivity to lower health-related quality
of life in community-dwelling older subjects. Z Gerontol
Geriatr 2007;40:43–51.
3. Lidstone JS, Ells LJ, Finn P, Whittaker VJ, Wilkinson JR,
Summerbell CD. Independent associations between weight
status and disability in adults: results from the health survey
for England. Publ Health 2006;120:412–417.
4. World Health Organization. The global burden of disease:
2004 update. Geneva: WHO; 2008.
5. Peeters A, Bonneux L, Nusselder WJ, De Laet C, Barendregt
JJ. Adult obesity and the burden of disability throughout life.
Obes Res 2004;12:1145–1151.
6. Menegoni F, Galli M, Tacchini E, Vismara L, Cavigioli M,
Capodaglio P. Gender-specific effect of obesity on balance.
Obesity (Silver Spring) 2009;17:1951–1956.
7. Xu X, Mirka GA, Hsiang SM. The effects of obesity on lifting
performance. Appl Ergon 2008;39:93–98.
8. Capodaglio P, Castelnuovo G, Brunani A, Vismara L, Villa
V, Capodaglio EM. Functional limitations and
occupational issues in obesity. Int J Occup Saf Ergon
2010;16:507–523.
9. Finkelstein EA, Chen H, Prabhu M, Trogdon JG, Corso PS.
The relationship between obesity and injuries among U.S.
adults. Am J Health Promot 2007;21:460–468.
10. Schmier JK, Jones ML, Halpern MT. Cost of obesity in the
workplace. Scand J Work Environ Health 2006;32:5–11.
11. Laskowski ER. Action on obesity and fitness: the physiatrist’s
role. PM R 2009;1:795–797.
12. Houston DK, Stevens J, Cai J. Abdominal fat distribution and
functional limitations and disability in a biracial cohort: the
Atherosclerosis Risk in Communities Study. Int J Obes
(Lond) 2005;29:1457–1463.
13. Ostbye T, Dement JM, Krause KM. Obesity and workers’
compensation: results from the Duke Health and
Safety Surveillance System. Arch Intern Med 2007;167:
766–773.
14. Karnehed N, Rasmussen F, Kark M. Obesity in young
adulthood and later disability pension: a population-based
8 L. M. Donini et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dip
di B
ioin
gegn
eria
- B
ib o
n 05
/04/
11Fo
r pe
rson
al u
se o
nly.

cohort study of 366,929 Swedish men. Scand J Public Health
2007;35:48–54.
15. Fortinksy RH, Granger CV, Seltzer GB. The use of functional
assessment in understanding home care needs. Med Care
1981;19:489–497.
16. Jain NB, Al-Adawi S, Dorvlo ASS, Burke DT. Association
between body mass index and functional independence
measure in patients with deconditioning. Am J Phys Med
Rehabil 2008;87:21–25.
17. Burke DT, Spinelli J, Al-Adawi S, Devora A, Hoaglin H, Jain
NB. Association between body mass index and gain in
functional independence measure for acute rehabilitation
patients. Arch Phys Med Rehabil 2007;86:5150.
18. Vincent HK, Vincent KR. Obesity and inpatient rehabilitation
outcomes following knee arthroplasty: a multicenter study.
Obesity 2008;16:130–136.
19. Vincent KR, Lee LW, Weng J, Alfano AP, Vincent HK. A
preliminary examination of the CMS eligibility criteria in
total-joint arthroplasty. Am J Phys Med Rehabil 2006;85:
872–881.
20. Ropka ME. Symptom status and functional status outcomes:
humanistic outcomes in obesity disease management. Obes
Res 2002;10(suppl 1):42S–49S.
21. Ware JE. SF-36 Health Survey update. Spine 2000;25:
3130–3139.
22. Ware JE, Kosinski M, Keller SD. A 12-item Short-Form
Health Survey: construction of scales and preliminary tests of
reliability and validity. Med Care 1996;34:220–233.
23. Kolotkin RL, Crosby RD, Kosloski KD, Williams GR.
Development of a brief measure to assess quality of life in
obesity. Obes Res 2001;9:102–111.
24. Kolotkin RL, Head S, Hamilton M, Tse CJ. Assessing the
impact of weight on quality of life. Obes Res 1995;3:49–56.
25. Kolotkin RL, Head S, Brookhart A. Construct validity of the
Impact of Weight on Quality of Life questionnaire. Obes Res
1997;5:434–441.
26. Mannucci E, Ricca V, Barciulli E, Di Bernardo M, Travaglini
R, Cabras PL, Rotella CM. Quality of life and overweight: the
obesity related well-being (Orwell 97) questionnaire. Addict
Behav 1999;24:345–357.
27. Sullivan M, Karlsson J, Sjostrom L, Backman L, Bengtsson C,
Bouchard C, Dahlgren S, Jonsson E, Larsson B, Lindstedt S.
Swedish obese subjects (SOS) – an intervention study of
obesity. Baseline evaluation of health and psychosocial
functioning in the first 1743 subjects examined. Int J Obes
Relat Metab Disord 1993;17:503–512.
28. World Health Organization. The International Classification
of Functioning, Disability and Health: ICF. Geneva: WHO;
2001.
29. Cerniauskaite M, Quintas R, Boldt C, Raggi A, Cieza A,
Bickenbach JE, Leonardi M. Systematic literature review on
ICF from 2001 to 2009: its use, implementation and
operationalisation. Disabil Rehabil 2011;33:281–309.
30. Stucki A, Daansen P, Fuessl M, Cieza A, Huber E, Atkinson
R, Kostanjsek N, Stucki G, Ruof J. ICF Core Set Obesity.
J Rehabil Med 2004;(suppl 44):107–113.
31. Cieza A, Geyh S, Chatterji S, Kstanjsek N, Ustun B, Stucki G.
ICF linking rules: an update based on lessons learned. J
Rehabil Med 2005;37:212–218.
32. Guyatt GH, Townsend M, Keller J, Singer J, Nogradi S.
Measuring functional status in chronic lung disease: conclu-
sions from a randomized control trial. Respir Med
1991;85(suppl B):17–21; discussion 33–37.
33. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J,
Stitt LW. Validation study of WOMAC: a health status
instrument for measuring clinically important patient
relevant outcomes to anti-rheumatic drug therapy in
patients with osteoarthritis of the hip or knee. J Rheumatol
1988;15:1833–1840.
34. Fairbank JC, Couper J, Davies JB, O’Brien JP. The Oswestry
low back pain disability questionnaire. Physiotherapy 1980;66:
271–273.
35. Schwartz AL. The Schwartz Cancer Fatigue scale: testing
reliability and validity. Oncol Nurs Forum 1998;25:711–
717.
36. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ.
The Pittsburgh Sleep Quality Index: a new instrument for
psychiatric practice and research. Psychiatry Res 1989;28:
193–213.
37. Beck AT, Steer RA, Garbin MG. Psychometric properties of
the beck depression inventory: twenty-five years of evaluation.
Clin Psychol Rev 1988;8:77–100.
38. Puhl RM, Heuer CA. The stigma of obesity: a review and
update. Obesity (Silver Spring) 2009;17:941–964.
39. Donini LM, Cuzzolaro M, Spera G, Badiali M, Basso N,
Bollea MR, Bosello O, Brunani A, Busetto L, Cairella G,
Cannella C, Capodaglio P, Carbonelli MG, Castellaneta E,
Castra R, Clini E, Contaldo F, Dalla Ragione L, Dalle
Grave R, D’Andrea F, Del Balzo V, De Cristofaro P, Di
Flaviano E, Fassino S, Ferro AM, Forestieri P, Franzoni E,
Gentile MG, Giustini A, Jacoangeli F, Lubrano C, Lucchin
L, Manara F, Marangi G, Marcelli M, Marchesini G, Marri
G, Marrocco W, Melchionda N, Mezzani B, Migliaccio P,
Muratori F, Nizzoli U, Ostuzzi R, Panzolato G, Pasanisi F,
Persichetti P, Petroni ML, Pontieri V, Prosperi E, Renna C,
Rovera G, Santini F, Saraceni V, Savina C, Scuderi N,
Silecchia G, Strollo F, Todisco P, Tubili C, Ugolini G,
Zamboni M. Documento di consensus. Obesita e disturbi
dell’alimentazione. Indicazioni per i diversi livelli di
trattamento. Eating Weight Disord 2010;15(suppl 1–2):1–
31.
40. Jenkinson C, Coulter A, Wright L. Short form 36 (SF36)
health survey questionnaire: normative data for adults of
working age. BMJ 1993;306:1437–1440.
41. ATS Committee on proficiency standards for clinical pul-
monary function laboratories. ATS statement: guidelines for
the six-minute walk test. Am J Respir Crit Care Med
2002;166:111–117.
42. Streiner DL, Norman GR, editors. Measurement Scales. A
practical guide to their development and use. 2nd ed. New
York: Oxford University Press; 1995.
43. Apolone G, Mosconi P, Quattrociocchi L, Gianicollo EAL,
Groth N, Ware JE jr, editors. Questionario sullo stato di salute
SF-12. Versione Italiana. Milano: Istituto di Ricerche Farm-
acologiche Mario Negri; 2005.
44. Gibbons WJ, Fruchter N, Sloan S, Levy RD. Reference
values for multiple repetitions 6-minute walk test in healthy
adults older than 20 years. J Cardiopulm Rehab 2001;21:
87–93.
45. Bohannon RW, Peolsson A, Massy-Westropp N, Desrosiers J,
Bear-Lehman J. Reference values for adult grip strength
measured with a Jamar dynamometer: a descriptive meta-
analysis. Physiotherapy 2006;92:11–15.
46. Houston DK, Stevens J, Cai J, Morey MC. Role of
weight history on functional limitations and disability in
late adulthood: the ARIC study. Obes Res 2005;13:1793–
1802.
47. Guallar-Castillon P, Sagardui-Villamor J, Banegas JR,
Graciani A, Fornes NS, LopezGarcıa E, Rodrıguez-Artalejo
F. Waist circumference as a predictor of disability
among older adults. Obesity (Silver Spring) 2007;15:233–
244.
48. Beriault K, Carpentier AC, Gagnon C, Menard J, Baillargeon
JP, Ardilouze JL, Langlois MF. Reproducibility of the
The SIO test for obesity-related disabilities 9
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dip
di B
ioin
gegn
eria
- B
ib o
n 05
/04/
11Fo
r pe
rson
al u
se o
nly.

6-minute walk test in obese adults. Int J Sports Med 2009;
30:725–727.
49. Brunani A, Liuzzi A, Sirtori A, Raggi A, Berselli ME, Villa V,
Ceriani F, Tacchini E, Vicari V, Parisio C, Vismara L, Zanini
A, Vinci C, Contini F, Braga E, Ricappi A, Camerlengo M,
Ristea M, Leonardi M. Mapping an obesity clinical evaluation
protocol to the International Classification of Functioning,
Disability and Health (ICF). Disabil Rehabil 2010;32:
417–423.
50. Raggi A, Sirtori A, Brunani A, Liuzzi A, Leonardi M.
Use of the ICF to describe functioning and disability in
obese patients. Disabil Rehabil 2009;31(suppl 1):S153–
S158.
51. Raggi A, Brunani A, Sirtori A, Liuzzi A, Berselli ME, Villa V,
Ceriani F, ICF-Obesity Group, Leonardi M. Obesity-related
disability: key factors identified by the International Classifi-
cation of Functioning, Disability and Health (ICF). Disabil
Rehabil 2010;32:2028–2034.
10 L. M. Donini et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Dip
di B
ioin
gegn
eria
- B
ib o
n 05
/04/
11Fo
r pe
rson
al u
se o
nly.




















