
Exercise self-efficacy intervention in overweight and obese
12
http://hpq.sagepub.com/ Journal of Health Psychology http://hpq.sagepub.com/content/early/2014/08/20/1359105314545096 The online version of this article can be found at: DOI: 10.1177/1359105314545096 published online 21 August 2014 J Health Psychol Jude Buckley Exercise self-efficacy intervention in overweight and obese women Published by: http://www.sagepublications.com can be found at: Journal of Health Psychology Additional services and information for http://hpq.sagepub.com/cgi/alerts Email Alerts: http://hpq.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - Aug 21, 2014 OnlineFirst Version of Record >> at The University of Auckland Library on October 1, 2014 hpq.sagepub.com Downloaded from at The University of Auckland Library on October 1, 2014 hpq.sagepub.com Downloaded from
Transcript of Exercise self-efficacy intervention in overweight and obese

http://hpq.sagepub.com/Journal of Health Psychology
http://hpq.sagepub.com/content/early/2014/08/20/1359105314545096The online version of this article can be found at:
DOI: 10.1177/1359105314545096
published online 21 August 2014J Health PsycholJude Buckley
Exercise self-efficacy intervention in overweight and obese women
Published by:
http://www.sagepublications.com
can be found at:Journal of Health PsychologyAdditional services and information for
http://hpq.sagepub.com/cgi/alertsEmail Alerts:
http://hpq.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Aug 21, 2014OnlineFirst Version of Record >>
at The University of Auckland Library on October 1, 2014hpq.sagepub.comDownloaded from at The University of Auckland Library on October 1, 2014hpq.sagepub.comDownloaded from

Journal of Health Psychology 1 –11© The Author(s) 2014Reprints and permissions: sagepub.co.uk/journalsPermissions.navDOI: 10.1177/1359105314545096hpq.sagepub.com
Introduction
Obesity levels are rapidly increasing throughout the world (International Obesity Task Force Data on Levels of Overweight and Obesity, 2005) and are concomitant with increased automation of daily life activities and more passive leisure pur-suits (World Health Organization (WHO), 2003). These changes have led to diminished activity-related energy expenditure (EE) (Sallis and Owen, 1999). The average reduction in EE over the past few decades is estimated at 800 kcal/day (James, 1995). The rate of increase in obesity appears to be greater for women (Annesi and Whitaker, 2010). Obesity is a well-established risk factor for major chronic illnesses such as cardiovascular diseases, type 2 diabetes, and cancer (Arkin et al., 2008).
Exercise plays a prominent role in promot-ing optimal health (Erlichman et al., 2002;
Jerome and McAuley, 2012). The positive effects of increased EE from exercise on health outcomes are independent of weight loss (Blair et al., 1993; Gaesser et al., 2011; Hu et al., 2004). Weight-loss independent benefits of exercise for overweight and obese women include reduced blood lipids and improved insulin sensitivity (Gaesser et al., 2011), increased body satisfaction, and positive mood (Annesi, 2010). Yet, a majority of overweight women do not meet the recommended levels of
Exercise self-efficacy intervention in overweight and obese women
Jude Buckley
AbstractThis study investigated the effects of a brief tailored intervention on self-efficacy beliefs and exercise energy expenditure in active and inactive overweight and obese women. Participants were randomly assigned to either control (N = 50) or intervention (N = 47) conditions, and their exercise self-efficacy was assessed three times over a 12-week period. Results showed that the intervention increased schedule, physical, exercise-worries efficacy, and energy expenditure in the previously inactive group. The results suggest that self-efficacy interventions are effective at increasing exercise energy expenditure in inactive overweight and obese women.
Keywordsenergy expenditure, exercise, obesity, self-efficacy, women
The University of Auckland, New Zealand
Corresponding author:Jude Buckley, School of Psychology, The University of Auckland, Private Bag 92019, Auckland, New Zealand. Email: [email protected]
545096 HPQ0010.1177/1359105314545096Journal of Health PsychologyBuckleyresearch-article2014
Article
at The University of Auckland Library on October 1, 2014hpq.sagepub.comDownloaded from

2 Journal of Health Psychology
physical activity for health (Pelis and Lucas, 2009). Reasons underlying suboptimal exercise levels include that initiating and adhering to regular exercise pose a daunting challenge for overweight and obese individuals and are often experienced negatively (Ekkekakis et al., 2010). Nonetheless, overweight and obese women are a high priority for interventions that increase exercise EE, as an active way of life may have important health benefits even for those who remain overweight.
Health benefits of exercise are accrued through varying quantities of activity ranging from 150 to 400 kcal/day (American College of Sports Medicine (ACSM), 2000). While many different intervention approaches to promoting exercise lead to acceptable increases in exercise behavior (Heath et al., 2012), responses to increasing EE in overweight and obese individ-uals have been poor (Mann et al., 2007). Research supports Social Cognitive Theory’s (SCT; Bandura, 1986, 1997) proposal that self-management interventions are effective at pro-moting health behavior change (reviewed in Bandura, 2004). Given increased time pressure and information overload demands of daily life, intervention efforts may need to be simplified if they are to provide greater flexibility for indi-viduals to increase their exercise EE. Recent work in the nutrition literature demonstrates that health advice that does not rely on health professional support or computer literacy is effective at promoting health behaviors (Lally et al., 2008).
Interventions derived from SCT that enhance self-efficacy beliefs have proved effective at increasing initiation and adherence to exercise in a variety of populations (Napolitano et al., 2008). Building on SCT, exercise self-efficacy beliefs are construed as beliefs in one’s abilities to carry out the steps involved in exercise, such as scheduling regular exercise sessions, com-pleting physical activities, and overcoming worries about exercise. Self-efficacy beliefs are dynamic (Bandura, 1997), and evidence sug-gests that the relationship between self-efficacy and physical activity behavior is reciprocally determined (McAuley et al., 2011). Moreover,
self-efficacy beliefs determine the degree of effort individuals expend when engaging in activities (Bandura, 1997). Thus, SCT provides a promising framework for interventions aimed at increasing exercise self-efficacy and exercise EE in overweight and obese women.
Although increases in self-efficacy have been associated with greater physical activity in healthy weight individuals (Williams and French, 2011), the effectiveness of self-efficacy interventions at increasing physical activity behaviors in overweight and obese individuals appears equivocal. Some research shows that self-efficacy-based interventions are associated with improvements in physical activity perfor-mance in overweight and obese adults (e.g. Dallow and Anderson, 2003; Schlenk et al., 2011). In contrast, a recent systematic review and meta-analysis (Olander et al., 2013) reported that changes in self-efficacy were not significantly associated with changes in physi-cal activity. The researchers concluded that tar-geting self-efficacy in interventions may not be important for physical activity change in obese populations. According to SCT, however, self-efficacy is a focal determinant of health behav-ior change because it is the common pathway through which self-regulatory efforts influence health functioning (Bandura, 1997, 2004). Enactive mastery experiences at executing self-regulation plans are the most dependable way to cultivate a resilient sense of self-efficacy (Bandura, 1997; Scholz et al., 2007). Thus, investigating whether intervention-induced increases in self-efficacy are associated with greater exercise EE in overweight and obese populations is a research priority.
The primary aim of this study was to investi-gate the effects of a 12-week self-efficacy inter-vention to increase exercise EE by boosting scheduling, physical, and exercise-worries self-efficacy in overweight and obese women. A prospective, randomized control design was used to examine the effects of the intervention over a 12-week period. It was expected that increases in self-efficacy would lead to an increase in exercise EE. The intervention required participants to formulate action plans
at The University of Auckland Library on October 1, 2014hpq.sagepub.comDownloaded from

Buckley 3
for exercise outcome expectancies, goal setting, relapse management, and exercise self-incentives. It was predicted that the intervention would lead to greater increases from baseline to 12 weeks in scheduling, physical, and exercise-worries self-efficacy relative to the control con-dition for previously inactive women. It was also predicted that previously inactive women in the intervention group would have greater net exercise EE per exercise session compared with inactive participants in the control group. Recent research on exercise self-efficacy sug-gests that intervention-induced changes in exer-cise self-efficacy may be different for specific subgroups of a population (McAuley et al., 2011). In this study, the extent to which the intervention influenced self-efficacy and exer-cise EE in active women was also explored as little is known about the association between self-efficacy and exercise EE in active over-weight and obese women.
Methods
Participants
Active and inactive overweight and obese women (age M = 37 years, standard deviation (SD) = 9) attending a commercial weight loss program (Weight Watchers (WW)) volunteered to be part of this research by responding face to face to the investigator. Inclusion criteria are as follows: (1) aged between 18 and 56 years, (2) body mass index (BMI) of greater than 25 kg/m2, and (3) able to be physically active. Those who were excluded included women (1) who had BMI values less than 25 kg/m2 and (2) who were unable to be physically active. Written informed consent was obtained from all partici-pants, and appropriate Human Participants Ethics Committee approval was received. Women agreed to complete study-related self-report measures of scheduling, physical, and exercise-worries self-efficacy at baseline, week 6 and week 12. After withdrawals prior to the start of the investigation due in the main to either change of circumstances (n = 11) or stressful and disruptive family circumstances
(n = 18), 97 women (77%) fulfilling inclusion requirements were randomly assigned to either intervention conditions (N = 50) or control con-ditions (N = 47). Overall, the BMI range was 25.6–51.50 kg/m2, and the majority of partici-pants were of European ethnicity (93%) and were in full- or part-time employment (91%). There were no significant group differences on any of these participant characteristics.
Intervention and control protocols
Participants in the intervention groups received an intervention derived from SCT (Bandura, 1986, 1997) that comprised six components. Participants were required to make action plans for exercise around the following six compo-nents: (1) in the outcome expectancy task, par-ticipants identified five reasons why exercise was important to them and three types of exer-cise that they enjoyed doing; (2) in the goal set-ting task, participants set both realistic and ideal exercise goals for the 12-week study period; (3) in the self-regulation task, participants identi-fied two to three main physical and scheduling difficulties and worries they had with regard to regular exercise and identified two to three pos-itive things to say or do to overcome those dif-ficulties; (4) in the relapse management task, participants reviewed strategies they could used to reinstate regular exercise; (5) in the exercise achievements task, participants reflected on their exercise achievements and identified rewards for achieving their goals. Participants also completed a cognitive restructuring task that required them to say stop in a commanding manner, either out loud or to themselves when-ever they had a negative thought about exercise and to replace that thought with a positive exer-cise thought; and (6) participants were phoned by the investigator in the seventh week to review the intervention components and address any issues that may have arisen. Participants were instructed to set aside 30 minutes on the day that they received their intervention to read the intervention materials and complete the actions plans. Participants were also instructed to put their actions plans in a prominent place
at The University of Auckland Library on October 1, 2014hpq.sagepub.comDownloaded from

4 Journal of Health Psychology
and review them regularly. The intervention groups also received the standard WW exercise booklet. Participants in the control condition received the standard WW information about exercise only. The booklet described how to exercise safely and how to choose activities to suit whether participants preferred to exercise indoors or outdoors, alone or in a group. The booklet also informed participants who exercise burns kilocalories and elevates mood.
Procedure
The investigator met with participants in the intervention and control groups separately, either individually or in pairs, to administer the baseline questionnaire and either the interven-tion or control materials. Participants in both groups returned the baseline questionnaire at the end of the WW meeting. To ensure equivalence of the two groups, the investigator interacted with the control group for the same length of time as the intervention group. In place of the intervention procedure, the investigator reviewed each of the points in the WW booklet on exercise. For all participants, the investigator explained how to fill out a daily exercise log.
Measures
Assessments were conducted at baseline, 6 and 12 weeks post intervention via question-naires that were mailed to participants at 6 and 12 weeks.
Exercise status. Exercise status was assessed with two items each with a yes or no rating scale. Participants were asked to indicate (1) whether they were currently exercising and, if yes, (2) the number of times they had exercised in the past 2 weeks. Participants were classified as inactive if they responded no or active if they responded yes.
Exercise self-efficacy. Three measures of exercise self-efficacy were employed. A measure of schedule efficacy (11 items; α = .93 − .54) was adapted from DuCharme and Brawley (1995) to
assess beliefs in one’s abilities to organize and schedule regular exercise. An 8-item measure (α = .94 − .66) was developed to assess exercise-related worries self-efficacy. Participants rated their confidence to overcome worries about exercise pertinent to overweight individuals. Items for the scale were generated using factors identified as relevant to overweight and obese populations (Grilo, 1995; Grilo et al., 1993). Example items are “exercise when I’ve had pre-vious negative exercise experiences,” “when I feel embarrassed in exercise clothes,” and “when I feel shame of being seen exercising.”
An 18-item (α = .92 − .68) measure was developed according to Bandura’s (2006) guidelines for constructing self-efficacy scales to assess confidence in physical ability for exer-cise. Items for the scale were generated in line with evidence that weight-related impediments to physical activity are commonly reported by overweight and obese women (Ball et al., 2000). To overcome potential impediments to exercise, the scale assessed physical activity of increasing difficulty, using both weight bearing and non-weight bearing physical activities items. Participants rated their confidence they could complete physical activities. Example items are “walk briskly on the flat for 30 min,” “walk briskly on a hilly route for 30 min,” “ped-dle fast on a stationary cycle for 20 min without stopping,” “walk up 3 flights of 15 stairs with-out stopping,” and “complete 10 sit-ups without stopping.” For each of the exercise self-efficacy scales, ratings ranged from 1 (I cannot do it at all) to 7 (certain I can do it), and they were aver-aged to generate scores. Higher scores reflected greater exercise self-efficacy.
Daily exercise log
The daily exercise log required participants to record the type, duration, and rate of perceived exertion (intensity) for all exercise they under-took during the 12-week study. The self-report of exercise was used to calculate net exercise EE. Evidence suggests that EE can be meas-ured with reasonable reliability from self-report of exercise (Kriska and Caspersen, 1997;
at The University of Auckland Library on October 1, 2014hpq.sagepub.comDownloaded from

Buckley 5
Montoye et al., 1996). Completed exercise was assigned an intensity unit based on the rate of EE and expressed as rate of physical activity to resting metabolic rate (MET) (Kotz and Levine, 2005; McArdle et al., 1996). Exercise under-taken by participants was classified as multi-ples of one MET. For example, exercise performed at three METs required three times the resting EE. MET values were assigned to physical activity, using the Compendium of Energy Costs of Physical Activity compiled by Ainsworth et al. (1993).
Calculation net exercise energy expenditure
Net exercise EE (Net exercise EE (kcal/min)) was calculated in kilocalories per minute, per exercise session using the calculation protocols detailed by McArdle et al. (1996). Net exercise EE (kcal/min) was computed by subtracting mean resting metabolic rate (RMR) from gross mean exercise EE. Mean resting metabolic rate was computed using the following equation: surface area (m2) × basal metabolic rate (BMR) (kcal/m2/h). Mean gross exercise EE for the control and intervention groups was calculated from physical activity log records. The gross mean exercise EE was 10.01 for the control group and 13.17 for interventions group. The equations for mean resting metabolic rate for the control and interventions groups were com-puted as follows
ControlgroupRMR m= ×=1 94 36
69 84
2.
.
kcal/m /h
kcal/h
2
which equated to 1.16 kcal/min
Intervention groupRMR m=
×=
1 92
36
69 12
2.
.
kcal/m /h
kcal/h
2
which equated to 1.16 kcal/min.The equations for mean Net exercise EE
(kcal/min) were computed as follows
Controlgroup mean Net exercise EE
(kcal / min) = 10.01-1.16 = 8.85
Inttervention group Net exercise EE
(kcal / min) = 13.17 -1.16 = 12.01
Data analyses
Data were analyzed using the Statistical Packages for Social Sciences (SPSS, version 7.5). Preliminary analyses revealed that all exercise self-efficacy measures met assump-tions of repeated measures analysis of variance (ANOVA) and factorial ANOVA.
Exercise self-efficacy
A series of repeated measures ANOVAs were used to assess the main and interactive effects of Exercise status (inactive, active), Condition (intervention, control), and Time (baseline, 6, 12 weeks) on scheduling, physical, and exer-cise-worries self-efficacy. Significant Exercise status × Condition × Time interactions were fol-lowed up with simple effects analyses assessing differences among intervention effects within each of the exercise status groups.
Exercise energy expenditure
A series of factorial ANOVAs were used to assess the main and interactive effects of Exercise status, Condition, and Time on net EE over the 12-week study period. Significant Exercise status × Condition × Time interactions were followed up with simple effects analyses assessing differences among intervention effects within each of the exercise status groups.
Results
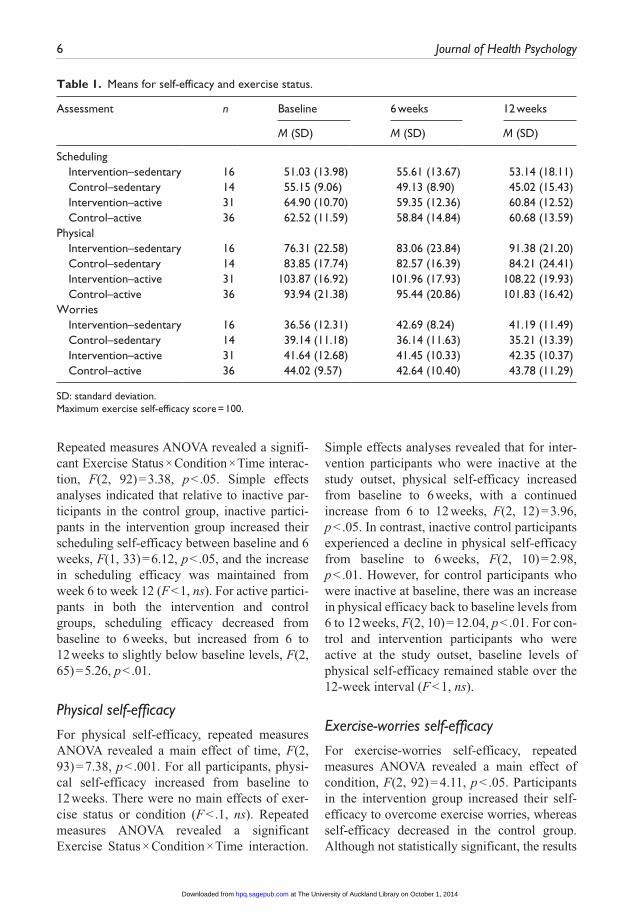
Table 1 presents the means and SDs of self- efficacy and exercise status.
Schedule self-efficacy
For schedule efficacy, there were no main effects of exercise status, condition, or time (F < .1, ns).
at The University of Auckland Library on October 1, 2014hpq.sagepub.comDownloaded from
6 Journal of Health Psychology
Repeated measures ANOVA revealed a signifi-cant Exercise Status × Condition × Time interac-tion, F(2, 92) = 3.38, p < .05. Simple effects analyses indicated that relative to inactive par-ticipants in the control group, inactive partici-pants in the intervention group increased their scheduling self-efficacy between baseline and 6 weeks, F(1, 33) = 6.12, p < .05, and the increase in scheduling efficacy was maintained from week 6 to week 12 (F < 1, ns). For active partici-pants in both the intervention and control groups, scheduling efficacy decreased from baseline to 6 weeks, but increased from 6 to 12 weeks to slightly below baseline levels, F(2, 65) = 5.26, p < .01.
Physical self-efficacy
For physical self-efficacy, repeated measures ANOVA revealed a main effect of time, F(2, 93) = 7.38, p < .001. For all participants, physi-cal self-efficacy increased from baseline to 12 weeks. There were no main effects of exer-cise status or condition (F < .1, ns). Repeated measures ANOVA revealed a significant Exercise Status × Condition × Time interaction.
Simple effects analyses revealed that for inter-vention participants who were inactive at the study outset, physical self-efficacy increased from baseline to 6 weeks, with a continued increase from 6 to 12 weeks, F(2, 12) = 3.96, p < .05. In contrast, inactive control participants experienced a decline in physical self-efficacy from baseline to 6 weeks, F(2, 10) = 2.98, p < .01. However, for control participants who were inactive at baseline, there was an increase in physical efficacy back to baseline levels from 6 to 12 weeks, F(2, 10) = 12.04, p < .01. For con-trol and intervention participants who were active at the study outset, baseline levels of physical self-efficacy remained stable over the 12-week interval (F < 1, ns).
Exercise-worries self-efficacy
For exercise-worries self-efficacy, repeated measures ANOVA revealed a main effect of condition, F(2, 92) = 4.11, p < .05. Participants in the intervention group increased their self-efficacy to overcome exercise worries, whereas self-efficacy decreased in the control group. Although not statistically significant, the results
Table 1. Means for self-efficacy and exercise status.
Assessment n Baseline 6 weeks 12 weeks
M (SD) M (SD) M (SD)
Scheduling Intervention–sedentary 16 51.03 (13.98) 55.61 (13.67) 53.14 (18.11) Control–sedentary 14 55.15 (9.06) 49.13 (8.90) 45.02 (15.43) Intervention–active 31 64.90 (10.70) 59.35 (12.36) 60.84 (12.52) Control–active 36 62.52 (11.59) 58.84 (14.84) 60.68 (13.59)Physical Intervention–sedentary 16 76.31 (22.58) 83.06 (23.84) 91.38 (21.20) Control–sedentary 14 83.85 (17.74) 82.57 (16.39) 84.21 (24.41) Intervention–active 31 103.87 (16.92) 101.96 (17.93) 108.22 (19.93) Control–active 36 93.94 (21.38) 95.44 (20.86) 101.83 (16.42)Worries Intervention–sedentary 16 36.56 (12.31) 42.69 (8.24) 41.19 (11.49) Control–sedentary 14 39.14 (11.18) 36.14 (11.63) 35.21 (13.39) Intervention–active 31 41.64 (12.68) 41.45 (10.33) 42.35 (10.37) Control–active 36 44.02 (9.57) 42.64 (10.40) 43.78 (11.29)
SD: standard deviation.Maximum exercise self-efficacy score = 100.
at The University of Auckland Library on October 1, 2014hpq.sagepub.comDownloaded from

Buckley 7
revealed a trend toward an Exercise Status × Condition × Time interaction, F2, 91) = 2.54, p < .08 in the predicted direction. The pattern of effects from simple effects analyses revealed that relative to inactive control partici-pants, there was a trend for inactive intervention participants to increase their self-efficacy to overcome exercise worries from baseline to 6 weeks, F(1, 19) = 6.72, p < .05, and maintain this increase from 6 to 12 weeks (F < 1, ns). In contrast, inactive control participants tended to decrease their self-efficacy, F(1, 14) = 6.94, p < .05, over the first 6 weeks, and this decrease remained from 6 to 12 weeks (F < 1, ns).
Energy expenditure
Table 2 presents the means and SDs for net EE. A factorial ANOVA of the differences in net EE per exercise session revealed a Time × Condition × Exercise Status interaction, F(1, 73) = 6.48 p < .05. Simple effects analysis revealed that relative to inactive participants in the control group, inactive participants in the intervention group expended significantly more kilocalories per exercise session over the 12-week period, F(1, 19) = 6.89, p < .05.
Discussion
This research investigated the effects of an exercise self-efficacy intervention in inactive and active overweight and obese women. Taken
together, the results support the predictions that the intervention would lead to greater changes in exercise self-efficacy and higher net EE in inactive intervention participants compared with those in the control condition. Consistent with findings that improving self-regulation skills influences self-efficacy (Annesi, 2010) and exercise (Carels et al., 2011), the results showed that self-generated plans for exercise are effective at providing enactive mastery self-efficacy experiences. For previously inactive participants, the intervention significantly increased self-efficacy for scheduling exercise and completing physical activities, and there was a trend toward significance for overcoming worries about exercise. Regardless of exercise status, the intervention (vs control condition) enhanced participants’ confidence to overcome worries about exercise that are pertinent to overweight and obese individuals.
Exercise status significantly moderated the effects of the intervention. The intervention increased exercise self-efficacy in previously inactive intervention participants relative to inactive participants in the control condition but had little impact on the self-efficacy beliefs of women who were active at the study outset. For previously inactive intervention participants, the intervention had the greatest impact on self-efficacy in the first 6 weeks. From week 6 to 12, increased levels of scheduling and exercise-worries efficacy remained stable whereas phys-ical self-efficacy increased. In contrast, levels of exercise self-efficacy decreased for inactive control participants over the first 6 weeks of the study. For these participants, decreases in scheduling and exercise-worries self-efficacy were maintained from 6 to 12 weeks, but physi-cal efficacy increased back to baseline.
The fact that the intervention was most influ-ential on schedule, physical, and worries effi-cacy in previously inactive women during the first 6 weeks of the study is consistent with evi-dence that the influence of self-efficacy on exercise behavior is strongest during the early stages of an exercise program (DuCharme and Brawley, 1995; McAuley, 1992; McAuley et al., 2011). The findings accord with SCT’s
Table 2. Means for net exercise energy expenditure per exercise session and exercise status over 12 weeks.
Condition n Net exercise energy expenditure (kcal/min)
M SD
Intervention–sedentary
10 950.4 705.7
Control–sedentary 11 321.7 350.6Intervention–active 27 659.0 460.2Control–active 29 633.8 397.4
SD: standard deviation.
at The University of Auckland Library on October 1, 2014hpq.sagepub.comDownloaded from

8 Journal of Health Psychology
premise that cognitive guidance systems are especially influential in the early stages of behavior change, and as long as individuals continue to believe in their abilities to perform an activity, they act habitually on that belief without having to reappraise their efficacy for every performance. This contention is sup-ported by recent evidence that suggests apprais-als of exercise self-efficacy can become automatic (Buckley and Cameron, 2010, 2011). It is suggested, therefore, that given the stability of scheduling and exercise-worries efficacy from 6 to 12 weeks, previously inactive inter-vention participants may have been habitually acting on enhanced beliefs about these exercise abilities.
The finding that physical self-efficacy con-tinued to increase over the study duration sug-gests that previously inactive intervention participants reappraised their self-efficacy beliefs to increase their confidence in their physical abilities. In contrast, there were no sig-nificant changes in physical efficacy over the 12 weeks for intervention and control partici-pants who were active at baseline.
Evidence that exercise self-efficacy decreased for inactive control participants is suggestive that overweight and obese women may overestimate their exercise self-regulation abilities perhaps due to exaggerated self-efficacy judgments and inadequate knowledge of the self-regulatory demands of exercise (Bandura, 1997; DuCharme and Brawley, 1995). This finding is consistent with recent evidence that previously inactive older adults overestimate their exercise capabilities prior to initiating an exercise program (McAuley et al., 2011). It appears, therefore, that without appropriate exercise experience to inform self-efficacy expectations, previously inactive people tend to overestimate their exercise capabilities.
There were no significant changes in physi-cal efficacy over the 12 weeks for intervention and control participants who were active at baseline. However, for active participants, scheduling efficacy decreased during the first 6 weeks of the study, but increased over the final 6 weeks, although it remained below
baseline. The increase in scheduling efficacy over the final 6 weeks is suggestive that enac-tive experiences at scheduling exercise into their daily routine prompted these participants to reappraise their scheduling efficacy more favorably.
Consistent with SCT that self-efficacy influ-ences the degree of effort individuals expend in an endeavor, the finding that net EE was signifi-cantly higher for previously inactive interven-tion participants compared with those in the control group is suggestive that self-management experiences prompted these women to increase the amount of energy they expended while exercising. Although women who were active at the study outset had higher exercise self-effi-cacy, their EE remained below that of previ-ously inactive women throughout the 12 weeks. In previously active participants, the lower EE per exercise session may be due to these par-ticipants exercising at lower intensities or for less duration than those who were inactive at baseline. Future research could profitably investigate the interrelationships between self-efficacy, self-regulation, and EE to determine whether once active, overweight and obese women use compensatory mechanisms to main-tain exercise.
Taken together, the findings are suggestive that overweight and obese women are not a homogeneous group. Consequently, exercise interventions for overweight and obese women may be more effective at increasing health-related EE if they consider initial exercise sta-tus. Moreover, the findings add to evidence that interventions that consider action planning and self-efficacy (e.g. Luszczynska and Tryburcy, 2008; Wilson et al., 2012) are effectual at elicit-ing change in physical activity.
The study findings should be considered within the context of the methodological con-straints. First, the study relied on self-report measures of exercise, and evidence suggests that over-reporting of physical activity occurs in overweight and obese populations (Dishman, 1994; Rzewnicki et al., 2003). Future research could include objective measures of exercise and EE to establish concurrent validity of
at The University of Auckland Library on October 1, 2014hpq.sagepub.comDownloaded from

Buckley 9
self-report of exercise. The study was conducted with women attending a commercial WW pro-gram; the results may not generalize to commu-nity dwelling overweight and obese women who are not motivated to attend WW sessions. Another limitation is that previously inactive women may have perceived themselves to be exercising at greater intensity than those who were active at the study outset. A further con-straint of the study is the small sample size of the inactive intervention and control groups rel-ative to participants who were active at the study outset. Considering exercise status proved to be an important moderator of intervention effects on self-efficacy, a replication study with a larger sample of inactive women is warranted to con-firm the findings of this investigation. The results of this study provide implications for interventions and future research. They empha-size the utility of self-generated plans to foster mastery self-efficacy experiences. Interventions could be broadened to include plans to assure mastery of emotional self-efficacy as over-weight and obese individuals often experience exercise negatively. Furthermore, overweight and obese individuals could be encouraged to increase exercise effort to accrue health bene-fits. This research suggests that self-directed mastery experiences are essential components of interventions aimed at increasing exercise self-efficacy and EE in overweight and obese women.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Ainsworth BE, Haskell WL, Leon AS, et al. (1993) Compendium of physical activities: Classification of energy costs of human physi-cal activities. Medicine and Science in Sports and Exercise 25(1): 71–80.
American College of Sports Medicine (ACSM) (2000) ACSM’s Guidelines for Exercise Testing and Prescription (6th edn). Philadelphia, PA: Lippincott Williams & Wilkins.
Annesi JJ (2010) Relations of changes in self-reg-ulatory efficacy and physical self-concept with improvements in body satisfaction in obese women initiating exercise with cognitive-behavioral support. Body Image 7: 356–359.
Annesi JJ and Whitaker AC (2010) Psychological factors associated with weight loss in obese and severely obese women in a behavioral physi-cal activity intervention. Health Education & Behavior 37(4): 593–606.
Arkin JM, Alsdorf R, Sherman B, et al. (2008) Relations of cumulative weight burden to vascu-lar endothelial dysfunction in obesity. American Journal of Cardiology 10: 98–101.
Ball K, Crawford D and Owen N (2000) Obesity as a barrier to physical activity. Australian and New Zealand Journal of Public Health 24(3): 331–333.
Bandura A (1986) Social Foundations of Thought and Action. Upper Saddle River, NJ: Prentice Hall, Inc.
Bandura A (1997) Self-Efficacy: The Exercise of Control. New York: W.H. Freeman and Company.
Bandura A (2004) Health promotion by social cog-nitive means. Health Education & Behavior 31(2): 143–164.
Bandura A (2006) Guide to the construction of self-effi-cacy scales. In: Pajares F and Urdan T (eds) Self-Efficacy Beliefs of Adolescents, vol. 5. Greenwich, CT: Information Age Publishing, pp. 307–337.
Blair SN, Powell KE, Bazzarre TL, et al. (1993) Physical inactivity workshop. Circulation 88(3): 1402–1405.
Buckley J and Cameron LD (2010) Automatic judgements of exercise self-efficacy and exer-cise disengagement in adults with high and low exercise self-regulation experience. Psychology of Sport and Exercise 12(3): 324–332.
Buckley J and Cameron LD (2011) Automaticity of exercise self-efficacy beliefs in adults with high and low exercise self-regulation experience. Journal of Sport & Exercise Psychology 33(3): 325–348.
Carels RA, Young KM, Koball A, et al. (2011) Transforming your life: An environmental modification approach to weight loss. Journal of Health Psychology 16: 430–438.
Dallow CB and Anderson J (2003) Using self-effi-cacy and a transtheoretical model to develop a physical activity intervention for obese women. American Journal of Health Promotion 17(6): 373–381.
at The University of Auckland Library on October 1, 2014hpq.sagepub.comDownloaded from
10 Journal of Health Psychology
Dishman RK (1994) Prescribing exercise intensity for healthy adults using perceived exertion. Medicine and Science in Sports and Exercise 26: 1087–1094.
DuCharme K and Brawley L (1995) Predicting the intentions and behavior of exercise initiates using two forms of self-efficacy. Journal of Behavioral Medicine 18(5): 479–497.
Ekkekakis P, Lind E and Vazou S (2010) Affective responses to increasing levels of exercise intensity in normal-weight, overweight and obese middle-aged women. Obesity 18(1): 79–85.
Erlichman J, Kerbey AL and James WPT (2002) Physical activity and its impact on health outcomes: Paper 2: Prevention of unhealthy weight gain and obesity by physical activity: An analysis of the evidence. Obesity Review 3: 273–287.
Gaesser GA, Angadi SS and Sawyer BJ (2011) Exercise and diet, independent of weight loss, improve cardiometabolic risk profile in over-weight and obese individuals. The Physician and Sportsmedicine 39(2): 87–97.
Grilo CM (1995) The role of physical activity in weight loss and weight loss management. Medicine, Exercise, Nutrition and Health 4: 60–76.
Grilo CM, Brownell KD and Stunkard AJ (1993) The metabolic and psychological importance of exercise in weight control. In: Stunkard AJ and Wadden T (eds) Obesity: Theory and Therapy. New York: Raven Press, pp. 253–273.
Heath GW, Parra DC, Sarmiento OL, et al. (2012) Evidence-based intervention in physical activ-ity: Lessons from around the world. Lancet 380: 272–281.
Hu FB, Willett CW, Li T, et al. (2004) Adiposity as compared with physical activity in predicting mortality among women. New England Journal of Medicine 351: 2694–2703.
International Obesity Task Force Data on Levels of Overweight and Obesity (2005) http://www.iotf.org/database/GlobalAdults (accessed 18 July 2007).
James WPT (1995) A public health approach to the problem of obesity. International Journal of Obesity 19(Suppl. 3): S37–S45.
Jerome GJ and McAuley E (2012) Enrollment and participation in a pilot walking programme: The role of self-efficacy. Journal of Health Psychology 18(2): 236–244.
Kotz CM and Levine JA (2005) Role of non-exer-cise activity thermogenesis (NEAT) in obesity. Minnesota Medicine 88: 54–57.
Kriska AM and Caspersen CJ (1997) Introduction to a collection of physical activity questionnaires. Medicine and Science in Sports and Exercise 25(1): S5–S9.
Lally P, Chipperfield A and Wardle J (2008) Healthy habits: Efficacy of simple advice on weight control based on a habit-formation model. International Journal of Obesity 32: 700–707.
Luszczynska A and Tryburcy M (2008) Effects of a self-efficacy intervention on exercise: The moderating role of diabetes and cardiovascular diseases. Applied Psychology: An International Review 57(4): 644–659.
McArdle WD, Katch FI and Katch VL (1996) Exercise Physiology Energy, Nutrition and Human Performance (4th edn). Baltimore, MD: Williams & Wilkins.
McAuley E (1992) The role of efficacy cognitions in the prediction of exercise behavior in middle-aged adults. Journal of Behavioral Medicine 15(1): 65–88.
McAuley E, Mailey EL, Mullen SP, et al. (2011) Growth trajectories of exercise self-efficacy in older adults: Influence of measures and initial status. Health Psychology 30(1): 75.
Mann T, Tomiyama J, Westling E, et al. (2007) Medicare’s search for effective obesity treat-ments: Diets are not the answer. American Psychologist 62: 220–233.
Montoye HJ, Kemper HCG, Saris W, et al. (1996) Measuring Physical Activity and Energy Expenditure. Champaign, IL: Human Kinetics.
Napolitano MA, Papandonatos GD, Lewis BA, et al. (2008) Mediators of physical activity behav-ior change: A multivariate approach. Health Psychology 27(4): 409.
Olander EK, Fletcher H, Williams S, et al. (2013) What are the most effective techniques in changing obese individuals’ physical activ-ity self-efficacy and behaviour: A system-atic review and meta-analysis. International Journal of Behavioral Nutrition and Physical Activity 10: 29.
Pelis JR and Lucas JW (2009) Summary health sta-tistics for U.S adults: National health interview survey. 2007 National Center for Health Statistics. Vital Health Stat 10(240).
Rzewnicki R, Vanden AY and De Bourdeaudhuij I (2003) Addressing overreporting on the
at The University of Auckland Library on October 1, 2014hpq.sagepub.comDownloaded from

Buckley 11
International Physical Activity Questionnaire (IPAQ) telephone survey with a population sample. Public Health Nutrition 6(3): 299–305.
Sallis JF and Owen N (1999) Physical Activity and Behavioral Medicine. Thousand Oaks, CA: SAGE.
Schlenk EA, Lias JL, Sereika SM, et al. (2011) Improving physical activity and function in overweight and obese older adults with osteoarthritis of the knee: A feasibility study. Rehabilitation Nursing 36(1): 32–42.
Scholz U, Sniehotta F, Schüz B, et al. (2007) Dynamics in self-regulation: Plan execu-tion self-efficacy and mastery of action plans. Journal of Applied Social Psychology 37(11): 2706–2725.
Williams SL and French DP (2011) What are the most effective intervention techniques for chang-ing physical activity self-efficacy and physical activity behavior and are they the same? Health Education Research 26: 308–322.
Wilson AJ, Jung ME, Cramp A, et al. (2012) Effects of a group-based exercise and self-regulatory intervention on obese adolescents’ physical activity, social cognitions, body composition and strength: A randomized feasibility study. Journal of Health Psychology 17(8): 1223–1237.
World Health Organization (WHO) (2003) Global Strategy on Diet, Physical Activity, and Health: Fact Sheet: Obesity and Overweight. Geneva: World Health Organization.
at The University of Auckland Library on October 1, 2014hpq.sagepub.comDownloaded from


















![[Hepatic steatosis, visceral fat and metabolic alterations in apparently healthy overweight/obese individuals]](https://static.fdokumen.com/doc/165x107/6324f8237fd2bfd0cb03375f/hepatic-steatosis-visceral-fat-and-metabolic-alterations-in-apparently-healthy.jpg)

