
ARTICLE IN PRESS G Model
13
UNCORRECTED PROOF Please cite this article in press as: Beeson P, et al. Hallux rigidus: A cross-sectional study to evaluate clinical parameters. Foot (2009), doi:10.1016/j.foot.2008.12.001 ARTICLE IN PRESS G Model YFOOT 1064 1–13 The Foot xxx (2009) xxx–xxx 1 Contents lists available at ScienceDirect The Foot journal homepage: www.elsevier.com/locate/foot Hallux rigidus: A cross-sectional study to evaluate clinical parameters 1 P. Beeson ∗ , C. Phillips, S. Corr, W.J. Ribbans 2 Division of Podiatry, School of Health, The University of Northampton, United Kingdom 3 4 a rticle info 5 6 Article history: 7 Received 18 September 2008 8 Received in revised form 2 December 2008 9 Accepted 4 December 2008 10 11 Keywords: 12 Hallux rigidus 13 Clinical 14 Parameters 15 History 16 Physical examination 17 abstract Background: Hallux rigidus (HR) is a common condition with history and physical examination used to help evaluate pathology, grade clinical changes and to inform treatment. Method: A cross-sectional study was undertaken to evaluate the demographics of and clinical parameters encountered in HR. In 110 subjects (180 feet) aged 18–70 years (mean 52 years) a standardized history and physical examination was undertaken. Clinical parameters associated with HR were evaluated. The Foot Health Status Questionnaire (FHSQ) was used to measure health-related quality-of-life dimensions. Results: Seventy (64%) subjects had bilateral HR and 73 (66%) were female. Mean HR onset was 44 (14–68 years) years and median HR duration 6 years (1–33 years). A history of 1st MTPJ trauma presented in 22% of subjects; 74% of whom had unilateral HR. Eighty-four (47%) feet had pes planus based on a positive Foot Posture Index. A correlation between pes planus and 1st MTPJ pain was found (r = 0.84, p = 0.05). In 74% of feet, hallux abductus interphalangeus angle (HAI ◦ ) was greater than normal (≤10 ◦ ). A correlation between HAI and reduced 1st MTPJ ROM was found (r = 0.92, p = 0.05). Second toe length was the same as the hallux in 111 feet (62%). A correlation between valgus hallucal rotation and 1st MTP joint pain in HR was found (r = .78, p =.05). A positive relationship was found between 2nd toe length and 1st MTPJ pain (p = 0.001 < 0.05). A correlation between hallucal interphalangeal joint (IPJ) hyperextension and 1st MTPJ pain was found (r = 0.78, p =0.01). A positive relationship was found between lesser MTPJ pain and supination at propulsion (p <0.001). There was no evidence of Achilles tendon contracture. The FHSQ results concur with clinical findings. Conclusions: HR was associated with female gender, bilateral involvement, older age groups, increased HAI ◦ , 2nd toe length similar to hallux, hallucal IPJ hyperextension, lesser MTP joint pain, flat foot and certain gait alterations. HR was not associated with Achilles tendon tightness or footwear. The content validity of clinical parameters of HR needs to be established by formal research prior to their inclusion in a classification of HR. © 2009 Published by Elsevier Ltd. 1. Introduction 18 Hallux rigidus is a term used to describe symptoms commonly Q1 19 associated with degenerative arthritis of the 1st metatarsopha- 20 langeal (MTP) joint. HR is associated with painful, progressive loss of 21 dorsiflexion, and proliferative bone response, leading to increased 22 bulk of the joint. 23 The minimum physiological dorsiflexion of the 1st MTP joint 24 that is necessary for normal gait is unknown however, the val- 25 ues reported in the literature range from 15 ◦ to 90 ◦ [1]. There is 26 no known study which validates a clinical or diagnostic threshold 27 separating the terms hallux limitus and hallux rigidus. In patients 28 with less advanced joint disease hallux limitus may more accurately 29 ∗ Corresponding author at: School of Health, The University of Northampton, Park Campus, Boughton Green Road, Northampton NN2 7AL, United Kingdom. Tel.: +44 1604 735500. E-mail address: [email protected] (P. Beeson). describe the condition. These arbitrary divisions are most likely to 30 be part of a continuum. Contemporary definitions utilize hallux lim- 31 itus and hallux rigidus interchangeably. For ease of discussion the 32 later definition was chosen for this study. 33 HR is a common 1st MTP joint problem, second only in incidence 34 to hallux valgus [2]. Symptoms associated with HR were initially 35 reported by Davies-Colley [3], although Cotterill [4] is credited with 36 proposing the term hallux rigidus. The pathological changes of the 37 1st MTP joint and metatarso-sesamoid compartment in HR differs 38 from hallux valgus [5] due to its different biomechanical proper- 39 ties [6]. Since Davies-Colley’s description in 1887 numerous authors 40 have reported on the clinical parameters of HR [7–16]. Symptoms 41 and objective information from history and physical examination 42 of HR are well documented (Table 1). There is, however, con- 43 flicting information on demographics and clinical evaluation, as 44 well as widespread disagreement on certain clinical parameters 45 (Table 2). 46 The mean age of onset of HR is variable between studies. Early 47 studies indicate a lower mean age of HR (Table 3) while more recent 48 0958-2592/$ – see front matter © 2009 Published by Elsevier Ltd. doi:10.1016/j.foot.2008.12.001
-
Upload
northampton -
Category
Documents
-
view
0 -
download
0
Transcript of ARTICLE IN PRESS G Model
Y
1
H1
P2
D3
4
a5
6
A7
R8
R9
A10
11
K12
H13
C14
P15
H16
P17
118
Q119
a20
l21
d22
b23
24
t25
u26
n27
s28
w29
CT
0d
D P
RO
OF
ARTICLE IN PRESSG ModelFOOT 1064 1–13
The Foot xxx (2009) xxx–xxx
Contents lists available at ScienceDirect
The Foot
journa l homepage: www.e lsev ier .com/ locate / foot
allux rigidus: A cross-sectional study to evaluate clinical parameters
. Beeson ∗, C. Phillips, S. Corr, W.J. Ribbansivision of Podiatry, School of Health, The University of Northampton, United Kingdom
r t i c l e i n f o
rticle history:eceived 18 September 2008eceived in revised form 2 December 2008ccepted 4 December 2008
eywords:allux rigiduslinicalarametersistoryhysical examination
a b s t r a c t
Background: Hallux rigidus (HR) is a common condition with history and physical examination used tohelp evaluate pathology, grade clinical changes and to inform treatment.Method: A cross-sectional study was undertaken to evaluate the demographics of and clinical parametersencountered in HR. In 110 subjects (180 feet) aged 18–70 years (mean 52 years) a standardized historyand physical examination was undertaken. Clinical parameters associated with HR were evaluated. TheFoot Health Status Questionnaire (FHSQ) was used to measure health-related quality-of-life dimensions.Results: Seventy (64%) subjects had bilateral HR and 73 (66%) were female. Mean HR onset was 44 (14–68years) years and median HR duration 6 years (1–33 years). A history of 1st MTPJ trauma presented in 22%of subjects; 74% of whom had unilateral HR. Eighty-four (47%) feet had pes planus based on a positiveFoot Posture Index. A correlation between pes planus and 1st MTPJ pain was found (r = 0.84, p = 0.05). In74% of feet, hallux abductus interphalangeus angle (HAI◦) was greater than normal (≤10◦). A correlationbetween HAI and reduced 1st MTPJ ROM was found (r = 0.92, p = 0.05). Second toe length was the sameas the hallux in 111 feet (62%). A correlation between valgus hallucal rotation and 1st MTP joint pain inHR was found (r = .78, p = .05). A positive relationship was found between 2nd toe length and 1st MTPJpain (p = 0.001 < 0.05). A correlation between hallucal interphalangeal joint (IPJ) hyperextension and 1stMTPJ pain was found (r = 0.78, p = 0.01). A positive relationship was found between lesser MTPJ pain and
TE
supination at propulsion (p < 0.001). There was no evidence of Achilles tendon contracture. The FHSQresults concur with clinical findings.Conclusions: HR was associated with female gender, bilateral involvement, older age groups, increasedHAI◦, 2nd toe length similar to hallux, hallucal IPJ hyperextension, lesser MTP joint pain, flat foot andcertain gait alterations. HR was not associated with Achilles tendon tightness or footwear. The contentvalidity of clinical parameters of HR needs to be established by formal research prior to their inclusion in
30
31
32
33
34
35
36
37
38
ORRE
Ca classification of HR.
. Introduction
Hallux rigidus is a term used to describe symptoms commonlyssociated with degenerative arthritis of the 1st metatarsopha-angeal (MTP) joint. HR is associated with painful, progressive loss oforsiflexion, and proliferative bone response, leading to increasedulk of the joint.
The minimum physiological dorsiflexion of the 1st MTP jointhat is necessary for normal gait is unknown however, the val-
UN
C
Please cite this article in press as: Beeson P, et al. Hallux rigidus: Adoi:10.1016/j.foot.2008.12.001
es reported in the literature range from 15◦ to 90◦ [1]. There iso known study which validates a clinical or diagnostic thresholdeparating the terms hallux limitus and hallux rigidus. In patientsith less advanced joint disease hallux limitus may more accurately
∗ Corresponding author at: School of Health, The University of Northampton, Parkampus, Boughton Green Road, Northampton NN2 7AL, United Kingdom.el.: +44 1604 735500.
E-mail address: [email protected] (P. Beeson).
39
40
41
42
43
958-2592/$ – see front matter © 2009 Published by Elsevier Ltd.oi:10.1016/j.foot.2008.12.001
© 2009 Published by Elsevier Ltd.
describe the condition. These arbitrary divisions are most likely tobe part of a continuum. Contemporary definitions utilize hallux lim-itus and hallux rigidus interchangeably. For ease of discussion thelater definition was chosen for this study.
HR is a common 1st MTP joint problem, second only in incidenceto hallux valgus [2]. Symptoms associated with HR were initiallyreported by Davies-Colley [3], although Cotterill [4] is credited withproposing the term hallux rigidus. The pathological changes of the1st MTP joint and metatarso-sesamoid compartment in HR differsfrom hallux valgus [5] due to its different biomechanical proper-ties [6]. Since Davies-Colley’s description in 1887 numerous authorshave reported on the clinical parameters of HR [7–16]. Symptomsand objective information from history and physical examinationof HR are well documented (Table 1). There is, however, con-
cross-sectional study to evaluate clinical parameters. Foot (2009),
flicting information on demographics and clinical evaluation, as 44
well as widespread disagreement on certain clinical parameters 45
(Table 2). 46
The mean age of onset of HR is variable between studies. Early 47
studies indicate a lower mean age of HR (Table 3) while more recent 48
Original text:
Inserted Text
England⁎
Original text:
Inserted Text
18-70 yrs (mean 52 yrs)
Original text:
Inserted Text
(14-68 yrs)
Original text:
Inserted Text
(1-33 yrs).
Original text:
Inserted Text
IPJ hyperextension and 1st
Original text:
Inserted Text
MTP
Original text:
Inserted Text
fifteen to ninety degrees
Original text:
Inserted Text
author. Senior Lecturer,
Original text:
Inserted Text
England. Tel.: +1604

E
ARTICLE IN PRESSG ModelYFOOT 1064 1–13
2 P. Beeson et al. / The Foot xxx (2009) xxx–xxx
Table 1Documented findings.
History Examination
Pain with joint motion [1,14,16,18] Restricted joint motion [7,14,23–25]Intolerance of footwear [14,21,22] Increased joint size [14,20,26]; soft tissue
swelling [19,20]Everted or supinated gait [1,18,20,27–30]
Table 2Disputed findings of HR.
Demographic data Clinical data
Family history Functional hallux limitusEarly onset of disease [10] Supports concept [28,42–44]Great toe problems [14] Questions concept [14,45]
Age of onset ArchAdult [14,19,20,31–34] Pes planus [4,7,23,40,46–50]Adolescent [7,23,27,35,36] Normal [51]
Presentation Achilles tendonUnilteral [10,20,37]; bilateral [1,14,38] Contracture [23,52]
Normal [14]
Gender predilectionMale [38,39]; female [14,20,30–33,36,40,41]
Table 3Age range of HR in earlier studies (1940–1978).
Author No. of cases Age range (years) Mean age (years)
Jack [51] 15 11–44 18.7Bingold and Collins
(1952) [23] Q633 18 cases <25 years No mean
15 cases >25 yearsKGM
s49
w50
51
o52
h53
p54
[55
[56
57
i58
j59
s60
V61
d62
i63
a64
TA
S
MDFHTEC
GKM
Table 5Exclusion criteria.
Hallux valgus-rigidus (intermetatarsal angle ≥12◦)Severe multiple forefoot deformitiesSignificant trauma sustained to foot/leg in previous 12 monthsNeuropathy1st ray/forefoot surgery (including digital/excluding soft tissue)Morton’s neuroma affecting any inter-metatarsal spaceSeptic arthritis of 1st MTP jointInflammatory arthritidesNeuromuscular disordersInsulin dependent Diabetes MellitusHypermobility syndromes
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
EC
T
essel and Bonney [27] 9 9–18 12.4oodfellow [35] 3 13–18 15cMaster [36] 7 12–33 21
tudies consistently present higher proportions of older patientsith HR (Table 4).
It is clear that there are conflicting notions about the aetiologyf HR [2–4,7–11,13–24,26–40,43–51]. The traumatic origin of HRas been proposed by several authors [20,38,37] while Jack (1940)roposed a spontaneous onset. Poor footwear [3,23], ankle equinus23], pes planus [4,7,23,26,40,46–51] and functional hallux limitus28–45] has also been cited.
A number of complaints can be associated with HR. Thesenclude generalized foot pain, 1st MTP joint or metatarsosesamoidoint pain, 1st MTP joint stiffness, locking and spasm/cramp. Inome cases, significant synovitis may accompany these complaints.
UN
CO
RR
Please cite this article in press as: Beeson P, et al. Hallux rigidus: Adoi:10.1016/j.foot.2008.12.001
ariability of the severity and location of 1st MTP joint pain may beependent upon a number of factors including lifestyle and activ-
ty levels. In the early stages, discomfort predominates at the dorsalspect of the joint and becomes more diffuse with the progression
able 4ge range of HR in later studies (1979–2003).
tudy No. of cases Age range(years)
Mean age(years)
ann et al. [20] 20 35–77 56.8rago et al. [40] 42 17–80 45eltham et al. [34] 67 23–80 None givenamilton et al. [41] 34 None given 56.2homas and Smith [31] 17 20–69 47asley et al. [18] 57 36–70 51oughlin and Shurnas [14] 114 (5.3%)
<20 years13–70 43
eldwert et al. [32] 47 26–69 52urtz et al. [33] 33 35–75 50.6ackay et al. [19] 39 18–79 56
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
D P
RO
OF
Long-term steroid useHistory of severe peripheral vascular diseaseMetabolic bone disease
of the disease. Other complaints including metatarsalgia (due toa compensatory increase in weight bearing to unload the 1st rayduring gait), inability to rise up on toes and altered gait have beendocumented [2,14,15,20,21].
This study aims to identify the demographics and key clini-cal parameters associated with a group of subjects with HR. Themethodological process used and its impact on the accuracy ofseverity and grading of HR will be discussed.
2. Methodology
An observational, cross-sectional study was undertaken. Thisinvolved a quantification of specific variables applied to a sample ofsubjects with varying severity. It was undertaken to evaluate clini-cal parameters in 110 HR subjects (180 feet) aged 18–70 years withvarying degrees of restricted 1st MTP joint dorsiflexion <65◦ (mea-sured with a standard full-circle plastic goniometer, calibrated to 1◦
increments) with either pain, deformity or both. Ethical approval(Leicestershire, Northants, Rutland) was obtained, subjects gaveinformed consent and a pilot study was undertaken.
Careful preliminary examination of subjects’ clinical noteswas undertaken to remove those possessing criteria of exclusion(Table 5). An invitation letter and study information sheet was sentto suitable subjects giving them time for consideration prior toinclusion in the study.
Detailed exclusion criteria were reviewed at the time of datacollection.
A standardized questionnaire and examination were used. Sub-jects were questioned about their history including the following:family history of great toe problems, age of onset (denoted by1st MTP joint deformity or restriction/pain), duration of pain orsymptoms (including stiffness, locking, spasm/cramp), variabilityof pain, factors aggravating symptoms, factors providing relief ofsymptoms, affect on activity levels and types of activities restricted,contribution of occupation to HR and footwear restrictions. Thebody mass index (BMI) for each subject was documented to deter-mine its effect on the clinical parameters. Repetitive 1st MTP jointtrauma can result in joint damage precipitating HR. The subject’stype and frequency of sporting activities was documented. Theassociation of 1st MTP joint OA (HR) and OA at other sites wasdocumented.
A standardized questionnaire (FHSQ) [59,60] was also com-pleted by each subject and used to measure health-relatedquality-of-life dimensions: foot pain, physical function, appearance,footwear and general perceptions of foot health.
cross-sectional study to evaluate clinical parameters. Foot (2009),
The physical examination included inspection of the foot non- 108
weight bearing and weight-bearing. Both feet were examined 109
(exclusion criteria permitting). The following clinical data was 110
obtained: Rearfoot position in stance was evaluated using the Foot 111
Posture Index (FPI) [53]. The FPI was used to quantify the degree 112
Original text:
Inserted Text
Demographic
Original text:
Inserted Text
.Normal [51].Presentation
Original text:
Inserted Text
Bilateral
Original text:
Inserted Text
.Gender predilectionNormal
Original text:
Inserted Text
(1940 – 1978).
Original text:
Inserted Text
(yrs)Mean age (yrs)Jack (1940)
Original text:
Inserted Text
25yrsno
Original text:
Inserted Text
25yrsKessel & Bonney (1958)
Original text:
Inserted Text
(1979 – 2003).
Original text:
Inserted Text
(yrs)Mean age(yrs)Mann et al
Original text:
Inserted Text
al (1997)
Original text:
Inserted Text
& Smith (1999) [31]1720-69
Original text:
Inserted Text
20yrs13-70
Original text:
Inserted Text
al (1992) [32]4726-6952Kurtz
Original text:
Inserted Text
al (1997) [19]3918-79
Original text:
Inserted Text
months.Neuropathy.1st
Original text:
Inserted Text
18-70

DO
OF
ARTICLE IN PRESSG ModelYFOOT 1064 1–13
P. Beeson et al. / The Foot xxx (2009) xxx–xxx 3
t113
[114
e115
b116
e117
118
a119
u120
H121
u122
v123
s124
t125
M126
s127
128
a129
p130
p131
b132
p133
d134
m135
i136
w137
p138
s139
140
2141
u142
p143
t144
fl145
r146
T147
m148
A149
1150
3151
152
f153
W154
(155
l156
D157
≤
Table 6Observed gait parameters.
PropulsionMid-tarsal joint pronationSupinationDelayed heel liftVertical toe-offAb/Adductory twist at toe-offKnee flexionInability to push through ground at toe-off
Table 7Sample characteristics. Q7
Subjects (feet) 110 (180)
GenderFemale 73 (66%)Male 37 (34%)
Age (years)Mean (range) 52 (23–70)Median 55
Age of onset, mean (range) 44 (14–68)
Duration of symptoms years (range) 6 (1–33)
Table 8Age groups.
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
The mean age of HR onset in the bilateral group was 50 years and 181
unilateral group 53 years. Bilateral foot involvement was similar 182
between genders (62% females, 68% males). 183
Table 9Foot involvement.
NC
OR
RE
CTE
Fig. 1. Measurement of ankle joint dorsiflexion.
o which the foot was pronated, supinated or in a neutral position53]. Six foot parameters (three rearfoot and three forefoot) werevaluated for each subject. Each parameter was graded as describedy Redmond et al. [53]. Final aggregate scores were applied to cat-gorize type of foot posture.
Location, magnitude and timing of 1st MTP joint pain weressessed. Passive 1st MTP joint range of motion ROM was measuredsing the method described by Ronconi et al. [54] and Greene andeckman [55]. The total ROM (dorsiflexion and plantarflexion) wassed to calculate reduction in motion and compared with normalalues [55]. Active 1st MTP joint dorsiflexion was measured in atatic weight bearing position. Subjects were asked to push up ontohe ball of the foot (avoiding supinating) to obtain maximum 1st
TP joint dorsiflexion. Subjects’ ability to rise up on toes withoutupinating was also evaluated.
Hallucal IPJ pain (using system described by Coughlin [22]) wasssessed. Frontal plane hallucal position was determined by com-aring the angle of the hallucal nail plate with the ground. Sagittallane position (hallucal IPJ hyperextension) was measured weightearing with a goniometer using the medial mid-axial line of theroximal and distal phalanges as reference points. Transverse planeeformity of the hallucal IPJ (hallux abductus interphalangeus) waseasured with a goniometer using the dorsal mid-axial line of prox-
mal and distal phalanges as reference points. Hallucal flexor poweras measured by assessing the ability of the hallux to prevent aiece of paper from being pulled away from under it during statictance.
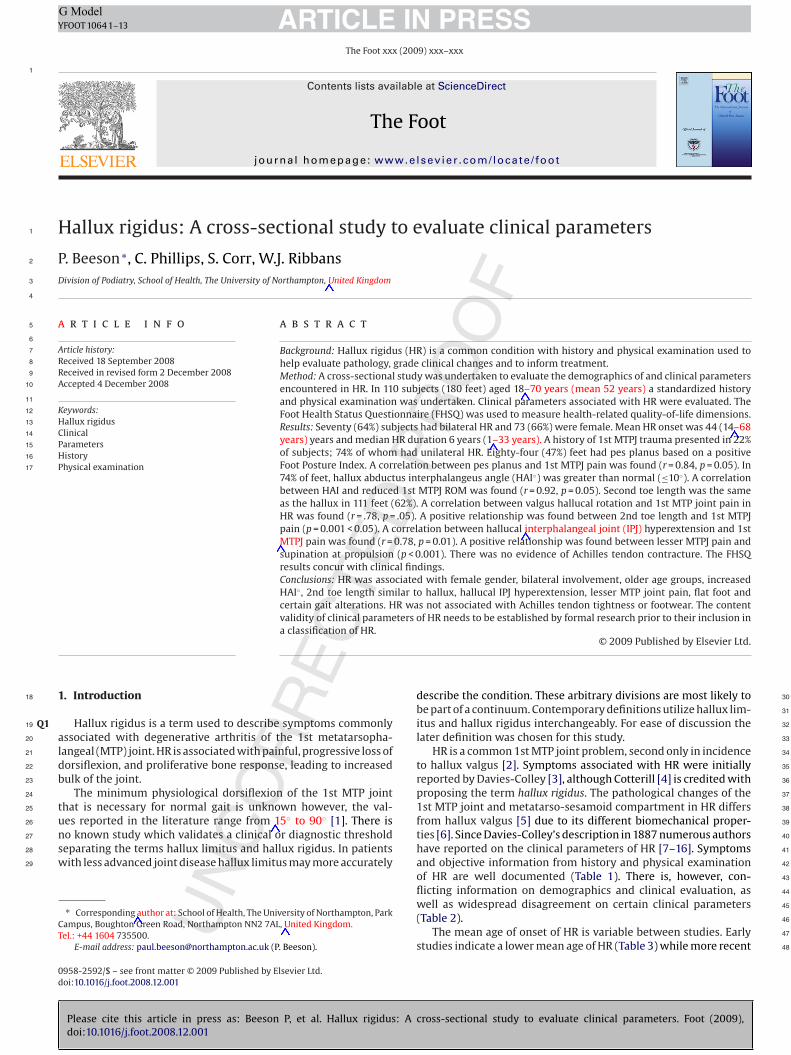
The location of callosities, lesser toe deformities, comparison ofnd toe length with hallux and lesser MTP joint pain were doc-mented. Ankle joint dorsiflexion was measured with a standardlastic full-circle goniometer (calibrated to 1◦ increments) usinghe technique described by Silfverskiold [56] (knee extended andexed position). The foot was held with the talonavicular jointeduced to eliminate transverse tarsal or subtalar motion [57,58].he fibula and plantar-lateral border of the foot were used as land-arks (Fig. 1). A right angle was considered to be neutral position.brief subjective assessment of the subjects’ gait at propulsion (by
st author) was undertaken (Table 6).
. Results
Descriptive and comparative statistical analyses were per-ormed using SPSS for Windows version 15.0) (SPSS Inc., 233 S.
UPlease cite this article in press as: Beeson P, et al. Hallux rigidus: Adoi:10.1016/j.foot.2008.12.001
acker Drive, Chicago, IL 60606, USA). Standard chi-square analysis�2) was performed on categorical data. Pearson and binary corre-ation coefficients were used to evaluate the non-continuous data.ifferences were considered to be significant when the p-value was0.05.
PRYears 18–30 31–40 41–50 51–60 61–70
% 5.7 10.7 18.6 37.1 27.9F:M ratio 7:1 7:1 1:1 2:1 3:1
3.1. Demographic data
The findings of the current study demonstrate that HR was asso-ciated with increased female prevalence, bilateral involvement, andolder age of subjects at onset (Tables 7–9). These findings concurwith those of previous research [14]. Few subjects in the currentstudy had adolescent onset. It is recognised that this may be influ-enced by the minimum age of subjects (18 years) used and the factthat subjects were only taken from an adult orthopaedic clinic.
The mean age of onset of symptoms (1st MTP joint deformity orrestriction/pain) was 44 years. This is 11 years prior to the medianage of presentation at a foot and ankle clinic (55 years) and supportsthe concept that this condition may be one of insidious develop-ment. Foot biomechanics, footwear type and activity levels mayhave some bearing on the development of symptoms and sub-sequent progression of disease. Overall subjects were marginallyoverweight (>25 kg/m2 = overweight), indicated by a mean BMI of25.93 kg/m2 (19.53–37.26) but with no gender difference for thisvariable (male: 26.48, female: 25.70).
In the current study there was a pronounced difference betweengender; more females presented with HR (Table 7), the mean age ofHR onset was less in females (43 years) than males (51 years) andthe ratio of females to males was greater in the younger age groups(Table 8).
cross-sectional study to evaluate clinical parameters. Foot (2009),
Bilateral (subjects) % Unilateral (subjects) % Trauma history (feet) %
(70) 64% (40) 36% (39) 22%L (18) 45% Unilateral 74%R (22) 55% Bilateral 26%
Original text:
Inserted Text
(3 rearfoot and 3
Original text:
Inserted Text
&
Original text:
Inserted Text
&
Original text:
Inserted Text
1 degree
Original text:
Inserted Text
x2
Original text:
Inserted Text
P value
Original text:
Inserted Text
GenderAge (yrs)Age of onset
Original text:
Inserted Text
yrs (range)FemaleMaleMean (rang)
Original text:
Inserted Text
18-3031-4041-5051-6061-70
Original text:
Inserted Text
eleven
Original text:
Inserted Text
yrs)
Original text:
Inserted Text
25 Kg/m
Original text:
Inserted Text
25.93 Kg/m2 (19.53-37.26)
Original text:
Inserted Text
R (22) 55%Unilateral 74%
E P
RO
OF
ARTICLE IN PRESSG ModelYFOOT 1064 1–13
4 P. Beeson et al. / The Foot xxx (2009) xxx–xxx
Table 10ACategorical history findings (based on 110 subjects or 180 feet).
Parameters Count (%)
Never Rarely Some days Most days Everyday
Activity levels restricted by HR 8 (7) 16 (14.5) 17 (15.5) 35 (31.8) 33 (30)Footwear contributing to 1st MTPJ pain 4 (3.6) 20 (18.1) 25 (22.7) 40 (36.3) 21 (19.3)Variability of 1st MTPJ pain 6 (5.4) 8 (7.2) 37 (33.6) 42 (38.3) 17 (15.4)1st MTPJ pain on movement 9 (8.1) 2 (1.8) 24 (21.8) 35 (31.8) 40 (36.3)1st MTPJ pain at rest 42 (38.1) 14 (12.7) 32 (29) 16 (14.5) 6 (5.4)Presence of 1st MTPJ stiffness 15 (13.6) 10 (9) 26 (23.6) 36 (32.7) 23 (20.9)Morning 1st MTPJ stiffness only 38 (34.5) 7 (6.3) 15 (13.7) 29 (26.4) 21 (19.1)Evening 1st MTPJ stiffness only 31 (28.1) 14 (12.2) 24 (21.8) 28 (25.4) 13 (11.8)1st MTPJ stiffness all day 39 (35.4) 11 (10) 23 (20.9) 21 (19) 16 (14.5)1st MTPJ spasm/cramp 50 (45.4) 18 (16.3) 32 (29) 9 (8.3) 1 (0.9)Locking of 1st MTPJ 70 (63.6) 13 (11.8) 23 (20.9) 3 (2.7) 1 (0.9)Ability to rise up on toes 23 (20.9) 24 (21.8) 20 (18.1) 21 (19) 22 (20)Lesser MTPJ pain 111 (61.6) 16 (8.8) 33 (18.3) 12 (6.6) 8 (4.4)Change in walking pattern 11 (10) 13 (11.8) 29 (26.1) 21 (19) 36 (32.7)A (20) 50 (27.7) 22 (12.2) 51 (28.3)R (13.3) 38 (21.1) 31 (17.2) 42 (23.3)
3184
185
a186
a187
u188
189
j190
t191
j192
2193
i194
t195
1196
d197
a198
p199
f200
n201
o202
3203
204
(205
206
f207
c208
f209
p210
s211
h212
o213
(214
i215
216
j217
Table 11Mean clinical findings (based on 180 feet).
Parameters (counts*) Mean ±S.D. 95% CI Range
Lower Upper
Passive 1st MTPJ ROMDorsiflexion 41◦ 19◦ 37 43 0–82◦
Plantar flexion 15◦ 5◦ 11 17 0–25◦
Active 1st MTPJ ROMDorsiflexion 58◦ 19◦ 53 60 0–90◦
Ankle joint equines
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
TC
P
D
C
RR
EC
Tbility to push off through ground 21 (11.6) 36oll out during propulsion 45 (25) 24
.2. History data
No statistically significant association was found between HRnd a history of trauma (p = 0.1). Trauma history was only found insmall proportion of subjects and was more common in those withnilateral HR (Table 9).
Onset of HR was reported to be insidious in 86 (78%) of sub-ects and acute in 24 (22%) subjects. 1st MTP joint pain (withinhe last 6 months) was reported to be severe in 26 (23.6%) sub-ects, moderate in 42 (38.2%), mild in 22 (20%) and not present in0 (18.2%) of subjects. Historical categorical findings are presented
n Tables 10A and 10B. Subjects stated that footwear contributedo the development of HR in 23% of cases, however, pain in thest MTP joint was found to be associated with footwear on mostays in 40 patients (36%). Short, tight, loose fitting, high-heelednd new footwear was found to aggravate symptoms of HR. Occu-ation contributed to HR in 29% of subjects and other factorsound to aggravate HR are outlined in the discussion. There waso statistically significant correlation between HR and footwear orccupation (p > 0.1).
.3. Clinical data
Table 11 shows mean clinical findings. The confidence intervalCI) illustrates the range of measures drawn from the study sample.
The hallucal position (frontal plane) was rectus in 91 (50.5%)eet, valgus in 75 (41.6%) feet and varus in 13 (7.2%) feet. Hallu-al flexor power was weak in 10 (5.5%) feet, medium in 20 (11.1%)eet and strong in 150 (83.3%) feet. The length of the 2nd toe com-ared with the hallux was found to be longer in 54 (30%) feet, theame length as the hallux in 111 (61.6%) feet and shorter than theallux in 15 (8.3%). During passive 1st MTP joint dorsiflexion pain
UN
CO
Please cite this article in press as: Beeson P, et al. Hallux rigidus: Adoi:10.1016/j.foot.2008.12.001
ccurred at the end-of-range in 29 (26.3%) subjects, mid-range in 4137.2%) subjects, beginning in 35 (31.8%) subjects and all-of-rangen 5 (4.5%) subjects.
Osteoarthritis was present in joints other than the 1st MTPoint in 32 (29.1%) subjects; hips were affected in 14 (12.7%) sub-
able 10Bategorical history findings (based on 110 subjects).
arameter Count (%)
None CLO GS GS + C G
rugs used for 1st MTPJ pain 51 (46) 7 (6) 13 (12) 12 (11) 1
LO, Cod liver oil; GS, glucosamine sulphate; C, chondroitin; Gels, topical non-steroidals; P,
DKnee extended 10◦ 2◦ 8◦ 10◦ 5–17◦
Knee flexed 13◦ 3◦ 12◦ 15◦ 8–25◦
*, Nominal data; S.D., standard deviation; ROM, range of motion.
jects, knees in 40 (36.3%) subjects and finger joints in 56 (50.9%)subjects.
Tables 12A and 12B show categorical clinical findings.
3.4. Foot Health Status Questionnaire
Questions relating to foot pain and physical function wereassessed during the last week whereas perceptions of foot healthwere assessed during the last month (Table 13). General health wasrated as very good by 90 (88%) subjects, fair by 18 (16%) subjectsand poor by 2 (2%) subjects. Severe foot pain was experienced by41 (37%) subjects, moderate pain by 22 (20%), mild pain by 20 (18%),very mild by 9 (10%) and 17 (15%) experienced no pain. Condition offeet was rated as excellent by 4 (4%) subjects, very good by 18 (16%)subjects, good by 58 (53%) subjects, fair by 20 (18%) subjects andpoor by 10 (9%) subjects. Overall foot health was rated as excellentby 5 (5%) subjects, very good by 17 (15%) subjects, good by 58 (53%)
cross-sectional study to evaluate clinical parameters. Foot (2009),
subjects, fair by 20 (18%) subjects and poor by 10 (9%) subjects. The 233
amount of time that foot pain affected subjects emotionally was 234
rated as no time at all by 10 (9%) subjects, a small amount of time 235
25 (23%) subjects, moderate amount of time 53 (48%) subjects, quite 236
a bit of time 17 (15%) subjects and all of the time 5 (5%) subjects. 237
els P B V A CD CC
(1) 4 (3.5) 11 (10) 5 (4.5) 2 (1.8) 2 (1.8) 2 (1.8)
paracetamol; B, brufen; V, volterol; A, arthrotec; CD, Co-dydramol; CC, Co-codamol.
Original text:
Inserted Text
(Based
Original text:
Inserted Text
(7)
Original text:
Inserted Text
SD95%
Original text:
Inserted Text
0-82°- Plantar
Original text:
Inserted Text
0-25
Original text:
Inserted Text
0-90
Original text:
Inserted Text
equinus- Knee
Original text:
Inserted Text
°-17°- Knee
Original text:
Inserted Text
°-25°Table
Original text:
Inserted Text
(Based
Original text:
Inserted Text
Table 11Mean Clinical findings

DR
OO
F
ARTICLE IN PRESSG ModelYFOOT 1064 1–13
P. Beeson et al. / The Foot xxx (2009) xxx–xxx 5
Table 12ACategorical clinical findings (based on 110 subjects or 180 feet*).
Parameter Count (%)
Normal Delayed heel lift Supination Vertical toe-off Abductory twist Knee flexion
Gait at propulsion 37 (20.5) 50 (27.7) 68 (37.7) 11 (6.1) 12 (6.6) 2 (1.1)
Parameter Count (%)
None Hallux IPJ 2nd MTPJ 3rd MTPJ 5th MTPJ 1st MH
Location of callosities* 58 (32.2) 67 (37.2) 18 (10) 10 (5.5) 18 (10) 9 (5)
Parameter Count (%)
Severely supinated Supinated Neutral Pronated Severely pronated
Foot Posture Index* 6 (3.3) 12 (6.6) 78 (43.3) 64 (35.5) 20 (11.1)
Parameter Count (%)
None Hammer Claw Mallet AV
Lesser toe deformities* 9 (5) 13 (7.2) 77 (42.7) 18 (10) 63 (35)
Parameter Count (%)
≤20◦ DF ≤15◦ DF ≤10◦ DF ≤5◦ DF ≤0◦ DF
Ankle joint (AJ) equines* 5 (2.7) 58 (32.2) 107 (59.4) 10 (5.5) 0 (0)
Parameter Count (%)
Absent Mild, >5◦ Moderate, >10◦ Severe, >15◦
Hallucal IPJ hyperextension* 60 (33.3) 66 (36.6) 46 (25.5) 8 (4.4)H ◦ 50 (H 18 (
H xion;
4238
239
w240
l241
[242
[243
t244
w245
o246
4247
4248
249
f250
TC
P
L
E
251
252
253
254
255
256
257
258
259
260
261
CTE
AI * 51 (28.3)allucal IPJ pain* 144 (80)
AI◦ , Hallux abductus interphalangeus angle; IPJ, interphalangeal joint; DF, dorsifle
. Discussion
A number of findings are commonly reported in patientsith HR, these include pain on 1st MTP joint motion (particu-
arly dorsiflexion) [1,14,16–18], restriction of 1st MTP joint motion7,14,23–25], joint enlargement with dorsal bony proliferation14,20,26], intolerance of constricting footwear [14,21,22], inabilityo raise up on toes and a modified gait [14,17,18,20,27–30,61]. Theseere verified in the current study and will be discussed alongside
ther demographic, history and clinical factors.
.1. Demographics and history findings
UN
CO
RR
E
Please cite this article in press as: Beeson P, et al. Hallux rigidus: Adoi:10.1016/j.foot.2008.12.001
.1.1. Family historyBonney and MacNab [10] reported that patients with a positive
amily history (FH) of great toe arthritis had an earlier onset of dis-
able 12Bategorical clinical findings (based on 180 feet*).
arameters Count Percentage
ocation of HR pain*Dorsal bump (DB) 75 41.61st MTP joint 21 11.6Sesamoids 10 5.5Proximal phalanx (PP) 4 2.2PP + DC/EHL 3 1.6DB + 1st MTP joint 12 6.6DB + PP 9 5DB + DC/EHL 2 1.1DB + sesamoids 13 7.2DB + joint + sesamoids 7 3.8DB + DC/EHL + sesamoids 11 6.1Joint + DC/EHL 11 6.1Joint + PP 2 1.1
HL, extensor hallucis longus; DC, dorsal capsule; ROM, range of motion.
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
P27.7) 57 (31.6) 22 (12.2)10) 16 (8.8) 2 (1.2)
MT, metatarsal head; AV, adducto-varus.
ease and Coughlin and Shurnas [14] found an association betweenHR and a positive FH of great toe problems in almost two-thirds ofpatients. What is not clear is how many of these were in fact halluxvalgus (HV). In the current study 24% reported a positive FH, butthey could not differentiate between HR and HV. Future HR studiesmay need to consider a properly controlled family study before apositive FH is concluded.
4.1.2. Age of onsetMuch has been written about the age of HR onset but not all
authors are in agreement (Table 2). Some early studies (Table 3)state that HR starts spontaneously in childhood or adolescence[35,51] while others suggest it is categorized as either primary(adolescent) or secondary (adult) [7]. Few studies have reported onadolescent patients with HR [6,23,27,35,36]. In reviewing studiesthat report on age [14,18–20,31–34,40,41,62] the mean age at onsetwas 51 years. The mean age at onset in the current study was 44(14–68) years; only 3 subjects developed symptoms at an age of lessthan 18 years. Given the small number of adolescent subjects withHR reported by our study and others [14,18–20,31–34,40,41,62]and the fact that pathological specimens from both adults andadolescent patients with HR were found to be consistent withdegenerative arthritis [14,23] it is concluded that artificially divid-ing patients into primary and secondary categories is unnecessary.
4.1.3. Gender predilectionGould [38] and Hattrup and Johnson [39] both found a male
predilection to HR. Gould [38] reported that 64% of HR patientswere males and that gender predilection depended upon age. Their
cross-sectional study to evaluate clinical parameters. Foot (2009),
results were only based on 15,000 out of 45,000 returned ques- 278
tionnaires sent to shoe shops, where briefed shoe fitters, asked and 279
marked the questions. No clinical examination was undertaken. The 280
findings were then projected into the total United States population 281
(186 million at the time). 282
Original text:
Inserted Text
(Based
Original text:
Inserted Text
None
Original text:
Inserted Text
Severely
Original text:
Inserted Text
None
Original text:
Inserted Text
≤20
Original text:
Inserted Text
equinus*
Original text:
Inserted Text
AbsentMild > 5°Moderate >10
Original text:
Inserted Text
Legend: HAI̊:
Original text:
Inserted Text
angle, IPJ: interphalangeal joint,
Original text:
Inserted Text
joint
Original text:
Inserted Text
&
Original text:
Inserted Text
History
Original text:
Inserted Text
(Based on 180 feet)Parameters
Original text:
Inserted Text
- Sesamoids105.5- Proximal
Original text:
Inserted Text
- PP+DC/EHL31.6- DB
Original text:
Inserted Text
- DB+PP95- DB+DC/EHL21.1-
Original text:
Inserted Text
- Joint+DC/EHL116.1- Joint
Original text:
Inserted Text
longus, DC: Dorsal capsule, ROM:
Original text:
Inserted Text
&
Original text:
Inserted Text
(14-68)
Original text:
Inserted Text
Normal [14].Male [38,39];
Original text:
Inserted Text
&

EO
OF
ARTICLE IN PRESSG ModelYFOOT 1064 1–13
6 P. Beeson et al. / The Foot xxx (2009) xxx–xxx
Table 13Foot Health Status Questionnaire (110 questionnaires).
Foot pain Count (%)
Never Occasionally Often Very often Always
Frequency of foot pain 6 (5) 9 (10) 30 (27) 57 (52) 7 (6)Frequency of aching feet 6 (5) 18 (16) 25 (23) 51 (46) 10 (9)Frequency of sharp pains 25 (23) 53 (48) 22 (20) 6 (5) 4 (4)
Physical function Count (%)
Not at all Slightly Moderately Quite a bit Extremely
Feet limit work activity 15 (14) 22 (20) 33 (30) 25 (22) 15 (14)Feet limit type of work 65 (59) 25 (23) 6 (5) 2 (2) 2 (2)Foot health limits walking 13 (12) 22 (20) 35 (32) 25 (22) 15 (14)Feet limit climbing stairs 9 (10) 22 (20) 37 (34) 21 (19) 19 (17)
Footwear Count (%)
Strongly agree Agree (A) Neither A or D Disagree (D) Strongly disagree
Hard to find comfy shoes 9 (8) 11 (10) 27 (25) 50 (45) 13 (12)Hard to find shoes to fit 11 (10) 9 (8) 27 (25) 50 (45) 13 (12)Limited in shoes worn 13 (12 50 (45) 27 (25) 9 (8) 11 (10)
Perceptions foot health Count (%)
All the time Most of the time Some of the time Little of the time None of the time
DDDD
283
d284
a285
c286
287
f288
w289
a290
S291
f292
t293
b294
w295
r296
o297
m298
p299
g300
f301
y302
4303
304
t305
t306
c307
n308
c309
4310
311
D312
f313
c314
(315
O316
t317
318
319
320
321
322
323
324
325
326
327
328
329
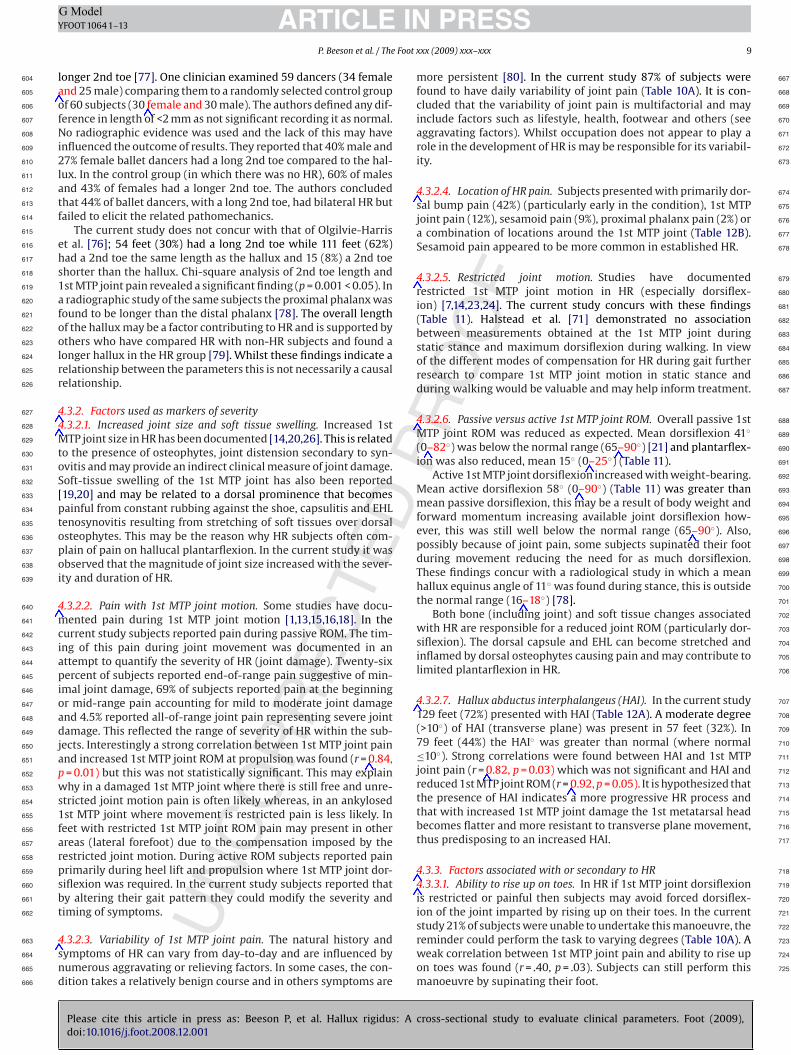
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
NC
OR
RE
CT
id foot problems tire 10 (9) 25 (23)id you have lots of energy 5 (5) 18 (16)id you feel worn out 9 (8) 25 (23)id you feel full of life 5 (5) 18 (16)
In complete contrast, virtually all recent HR studies (pre-ominantly surgical intervention) [14,20,30,31,33,36,40,41] showhigher female predilection (62%), a percentage comparable to theurrent study (66%).
This female predilection to HR may not be due to biological dif-erences but to social and cultural factors that result in womenearing footwear that aggravate a predisposition to develop HR or
ggravate pain in deformities of similar magnitude. Coughlin andhurnas [14], in a self-selected review of 18 post-surgery HR studies,ound that 62% of females were affected by HR, a finding similar toheir own results (63%) and concluded that there was an associationetween HR and female gender. In addition they found that femalesere more commonly affected in all age groups, a finding compa-
able with the current study (Table 8). However, this finding maynly reflect the higher number of females receiving surgical treat-ent for HR, but not the true male/female incidence in the general
opulation, who have the condition but have not as yet, had sur-ical intervention. The current study shows a much higher ratio ofemales in the younger age groups (Table 8): Is this because 18–40ear-old females are more likely to wear inappropriate footwear?
.1.4. Body mass indexIt was considered that an increased BMI may predispose subjects
owards HR and contribute towards levels of pain experienced. Inhe current study subjects were only marginally overweight, indi-ated by a mean BMI of 25.93 kg/m2 (19.53–37.26) and there waso gender difference (male: 26.48, female: 25.70). BMI was notonsidered to be a predisposing factor for HR.
.1.5. Bilateral involvementUnilateral HR has been reported by some authors [10,20,37].
rago et al. [40] reported increased unilateral involvement in
UPlease cite this article in press as: Beeson P, et al. Hallux rigidus: Adoi:10.1016/j.foot.2008.12.001
emales, but presented no demographic data to support this. In theurrent study unilateral involvement presented in 40 (36%) subjectsequal numbers of left or right feet); 38% were female (Table 9).ther studies report bilateral HR [1,14,38] or bilateral presenta-
ion with unilateral symptoms. In this study bilateral involvement
D P
R53 (48) 17 (15) 5 (5)52 (47) 26 (24) 9 (8)51 (46) 17 (16) 8 (7)52 (47) 26 (24) 9 (8)
presented in 70 (64%) subjects (Table 9), which may reflect thepredominance of older subjects (Table 7) rather than the true inci-dence as, with the passage of time, a higher percentage of patientsare likely to exhibit bilateral disease. It may also reflect the typeof clinic (surgical) from which subjects were taken. In the currentstudy analysis was undertaken at the point of referral. Coughlin andShurnas [14] found bilateral HR at final follow-up (79%) comparedto 19% at initial examination.
In the current study a history of trauma was common in subjectswho developed unilateral HR (positive trauma history in 22% studysample; 74% of whom had unilateral involvement) (Table 9). Noassociation between HR as a whole and a history of trauma (p = 0.1)was found. These findings concur with that of other researchers[14]. A statistically significant association between unilateral HRand trauma (p < 0.05) was found.
A small proportion of unilateral HR subjects had the asymp-tomatic foot examined. In these cases it was apparent thatdifferences between the feet existed and that they may result in dif-ferent biomechanical function of the 1st MTP joint. Although thesefindings suggest a trend the numbers of subjects where such a com-parison was possible was too small to enable definitive conclusionsto be drawn. Further research in this area is warranted.
4.1.6. FootwearPoor footwear has been implicated in the development of HR for
many decades. Davis-Colley [3] first proposed a link in 1887. Bingoldand Collins [23] and DuVries [63] cited footwear that is too short,Lorimer et al. [64] footwear that is too loosely fitting and Cracchi-olo [65] footwear that causes hyperextension of the great toe asa cause of HR. Some authors reported that patients with HR wereintolerant to footwear [14,21,22]. Unfortunately, the vast majorityof ‘evidence’ over the years has been anecdotal. The few studies that
cross-sectional study to evaluate clinical parameters. Foot (2009),
addressed the issue, found that the association between footwear 349
and HR was not statistically significant [14,66]. Sim-Fook and Hodg- 350
son [66] examined 118 shod and 107 unshod Chinese subjects. Only 351
17% of those wearing footwear and 10.3% not wearing footwear were 352
affected by HR. There was a marked gender bias in that 84% of the 353
Original text:
Inserted Text
FOOT PAIN Count
Original text:
Inserted Text
PHYSICAL FUNCTIONNot
Original text:
Inserted Text
FOOTWEARStrongly
Original text:
Inserted Text
PERCEPTIONS FOOT HEALTHAll
Original text:
Inserted Text
&
Original text:
Inserted Text
18-40
Original text:
Inserted Text
25.93 Kg/m2 (19.53-37.26)
Original text:
Inserted Text
&
Original text:
Inserted Text
&
Original text:
Inserted Text
&

D
INY
Foot x
u354
S355
t356
s357
(358
359
a360
j361
o362
f363
(364
p365
(366
s367
p368
s369
s370
e371
d372
n373
n374
r375
w376
4377
378
r379
(380
f381
u382
i383
t384
f385
b386
t387
o388
v389
i390
4391
392
H393
o394
m395
p396
r397
b398
l399
i400
w401
i402
j403
g404
o405
406
t407
t408
m409
4410
411
s412
m413
i414
h415
s416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
NC
OR
RE
CTE
ARTICLEG ModelFOOT 1064 1–13
P. Beeson et al. / The
nshod were female and 67% of the shod were male. Coughlin andhurnas [14] found that 16% of patients considered their footwearo be a contributory cause of their HR. They found no statisticallyignificant correlation between footwear and HR to confirm thisr = 0.08, p > 0.1) [14].
In the current study only 23% subjects considered their footwearcontributory cause of their HR. However, the frequency of 1st MTP
oint pain in HR associated with footwear was found to affect 36%f subjects on most days (Table 10A). The most common types ofootwear restrictions reported by females were high-heeled shoes31%) probably because the 1st MTP joint is held in an extendedosition during gait. Slip-on shoes (16%) and Wellington boots3%) may cause FHB overuse to maintain stability and subsequentesamoid pain. In 14% of subjects dress shoes were found to com-ress the forefoot, this may alter 1st MTP joint biomechanics. Flathoes (5%) may increase the requirement for dorsiflexion at propul-ion. Shoes with a seam over 1st MTP joint (3%) rub the jointspecially if dorsal osteophytes are present and can compress theorsomedial cutaneous nerve resulting in dysesthesia or numb-ess along the medial border of the hallux. Walking boots (2%) andew shoes (1%) only contributed to HR in a few cases. No footwearestrictions were reported in a quarter of subjects, most of whichere males.
.1.7. Factors aggravating HRIn the current study subjects reported a number of factors
esponsible for aggravating the symptoms of HR. Whilst footwear23%) was the most common (in 67% women and 33% of men) otheractors were also reported: cold/damp weather (11%), walking onneven terrain (10%) or for long distances (9.5%), normal walk-
ng (8.2%), running (6.4%), descending stairs (6.4%), stubbing HRoe joint (4.6%), not wearing insoles (4.6%), kneeling (4.5%), drivingor long periods (3.6%), standing for long periods (2.8%), weight ofed covers (2.7%), increased body weight (0.9%). Subjects reportedhat prolonged activity while barefoot or in soft-soled shoes wasften difficult. Only 1.8% of subjects reported that no factors aggra-ated their HR. Factors aggravating HR are likely to be idiosyncratic,nfluenced by lifestyle and general health.
.1.8. Relief of HR symptomsSubjects reported strategies responsible for immediate relief of
R symptoms. Sitting (23.6%), removal of footwear (23%), wearingf insoles with trainers (9%) and use of painkillers (5.7%) were theost common. It is interesting that so few subjects opted to use
ainkillers although this is reflected in the small number of subjectseporting severe 1st MTP joint pain (23.6%). A strong correlationetween the use of painkillers and symptoms in these particu-
ar subjects was found (r = 0.82, p = 0.05). Other strategies reportedncluded: 1st MTP joint distraction (5%), immersing joint in warmater (4.3%), use of flat stiff soled shoes (3.5%), modified gait (walk-
ng on outer border of foot) (3.4%), foot exercises (3%), massagingoint (2.9%), walking on flat surfaces (2.6%) and use of non-steroidalel (1%). In subjects with well-advanced disease no measure wouldbtain immediate pain relief (13%).
Subjects presented with a wide range of HR pathology and symp-oms but the majority took either no pain medication (46%) or overhe counter drugs (44%) whilst a few (11%) took prescription only
edicines (Table 10B).
.1.9. Restriction of activity levels1st MTP joint pain in HR was found to restrict activity levels in
UPlease cite this article in press as: Beeson P, et al. Hallux rigidus: Adoi:10.1016/j.foot.2008.12.001
ubjects on most days (31.8%) (Table 10A) and 30% of subjects wereoderately affected in their activities (Table 13). The types of activ-
ties restricted by HR included: running, long walks (particularlyill walking), walking on uneven surfaces, dancing, multidirectionalports and aerobic exercise. Predominantly activities requiring a
PR
OO
F
PRESSxx (2009) xxx–xxx 7
forced excursion of the 1st MTP joint in the sagittal and/or frontalplane may precipitate pain. Transverse plane movement however,is resisted because of increased transverse plane stability promotedby bony changes in HR.
4.1.10. OccupationIn the current study 42% of subjects lead an active occupation
but only 29% considered that their occupation contributed to HR.This concurs with the FHSQ data (30% of subjects reported beingaffected at work by their HR) and that of other studies who foundno statistically significant correlation between HR and occupation(r = 0.08, p > 0.1) [14].
In the current study, just over one-quarter (27%) of subjects wereretired, which may influence their activity levels and subsequent HRpain. In retirement some subjects may be more active while othersmay be less active because of ill health. This factor has not beenconsidered in other studies.
4.1.11. 1st MTP joint symptomsIn the current study subjects reported moderate (38.2%) and
severe (23.6%) 1st MTP joint pain within the last 6 months and only18% of subjects reported no pain (Table 10A). A painful 1st MTP jointwas reported for 67% of waking hours on movement and variableon most days for 38% of subjects (Table 10A). Some subjects (29%)presented with pain at rest (Table 10A).
Subjects were asked to grade their 1st MTP joint stiffness andindicate the period during the day when they experienced jointstiffness. This was graded on a continuum between 0 and 10 (0 = nostiffness, 10 = unable to move). In the current study 86% of sub-jects reported 1st MTP joint stiffness (Table 10A) and if variable,at its worst, 45% were graded as 5 out of 10. Only 20% of subjectsreported no 1st MTP joint stiffness. There was a strong correlationbetween 1st MTP joint pain and stiffness (r = 0.79, p = 0.01) but thiswas not statistically significant. Morning stiffness was reported in66% of subjects; evening stiffness in 71% and 64% had 1st MTP jointstiffness throughout the day (Table 10A).
Locking of the 1st MTP joint was reported in 36% subjects butwas variable and short lasting in nature. More commonly 55% ofsubjects experienced cramp/spasm of the 1st MTP joint and hallux(Table 10A) a consequence of capsulitis and FHL/FHB tenosynovitis.Subjects reported 1st MTP joint symptoms to be worse during theheel-rise and propulsion phases of gait.
4.1.12. Subject’s perception of their gaitIn the current study 90% of subjects considered that their walk-
ing pattern had changed during the development of their HR, ofwhich 33% considered that this change affected them everyday(Table 10A). Only 51 (28%) of feet were able to push through theground at propulsion everyday, the remainder were affected tovarying degrees of severity (Table 10A) and 135 feet (75%) rolledoutwards during propulsion. The differences in frequency for eachof the above variables of gait are outlined in Table 12A.
4.1.13. Presence of OA in other jointsAn association between radiological foot OA and radiological
OA at other sites has been reported [67]. In the current clinicalstudy 29% of subjects (mainly females) with HR (1st MTP joint OA)reported OA in other joints. This was found to be most commonin finger joints (51%). Whilst these findings indicate a relationshipbetween the parameters this is not necessarily a causal relation-
cross-sectional study to evaluate clinical parameters. Foot (2009),
ship. Future epidemiological studies would be useful to determine 473
whether a systemic aetiology is involved in the development of HR 474
and provide an enhanced ability to describe the respective influ- 475
ences of mechanical and systemic factors in the development of 476
this condition. 477
Original text:
Inserted Text
&
Original text:
Inserted Text
high heeled
Original text:
Inserted Text
&
Original text:
Inserted Text
.82,
Original text:
Inserted Text
well advanced
Original text:
Inserted Text
.08, p>.1)
Original text:
Inserted Text
zero and ten
Original text:
Inserted Text
.79, p=.01)

E
INY
8 Foot
4478
479
a480
t481
o482
t483
i484
p485
4486
487
f488
c489
c490
(491
v492
r493
t494
(495
t496
t497
j498
w499
a500
501
w502
p503
a504
d505
i506
h507
M508
l509
r510
w511
t512
(513
p514
a515
t516
4517
4518
4519
c520
u521
p522
1523
s524
t525
526
a527
J528
w529
p530
r531
o532
o533
r534
a535
S536
c537
538
l539
540
541
542
543
544
545
546
547
548
549
550
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
575
576
577
578
579
580
581
582
583
584
585
586
587
588
589
590
591
592
593
594
595
596
597
598
NCOR
RE
CT
ARTICLEG ModelFOOT 1064 1–13
P. Beeson et al. / The
.1.14. SportIt is recognized that certain sports impart 1st MTP joint trauma
nd may be responsible for precipitating HR development whilstheir frequency may exacerbate symptoms. In the current study 69%f subjects reported undertaking a range of sports (football, rugby,ennis, golf, badminton, rock climbing, running, walking, horse rid-ng, yoga, aerobics and swimming) of variable frequency (1–5 timeser week) prior to HR onset.
.2. Foot Health Status Questionnaire (FHSQ)
The FHSQ evaluated health related quality-of-life dimensions ofoot pain, physical function/appearance, footwear and general per-eptions of foot health. Findings from the FHSQ (Table 13) broadlyoncur with the history and physical results of the current studyTables 10–12). The severity (37% – severe) and frequency (42% –ery often) of foot pain documented was greater than that verballyeported (clinical study). This may be because the FHSQ data relatedo foot pain within the previous week rather than the last 6 monthsclinical study). Interestingly the frequency of foot pain was foundo vary (52% – very often) more often in the short term (1 week)han over a longer period of 6 months (38% most days). Some sub-ects reported that their 1st MTP joint pain made them feel tired andorn out and that their pain appeared to affect them both physically
nd emotionally (Table 13).The restrictions of physical function documented by subjects
ere related to similar activities as those found in the clinical com-onent of the study (aggravating factors). Subjects reported thatlthough it was possible to find footwear to fit their feet and whichoes not hurt their feet the number and type of footwear was lim-
ted (Table 13). A number of subjects (particularly females) were notappy with the appearance of their feet because of the enlarged 1stTP joint/s and considered that this factor as well as joint pain
imited them in their choice of footwear. The majority of subjectseported their general health as good except for two subjects whoere restricted by heart disease (angina). It was interesting to note
hat the subject’s perception of their general foot health was goodapart from 1st MTP joint) but many felt that their 1st MTP joint/sathology limited them in vigorous physical and social activitiesnd were concerned about the impact this may have on their long-erm general health.
.3. Clinical findings
.3.1. Factors thought to contribute to development of HR
.3.1.1. Pes planus. Pes planus as a cause of HR has been impli-ated by a number of authors [4,7,23,26,40,46–51,61] with thenderstanding that excessive foot pronation results in increasedlantar fascia tension and increased dorsiflexion force under thest metatarsal head, and thus a reduced ability of the hallux to dor-iflex. No demographic data were reported in any of these studieso substantiate the notion that pes planus is a cause of HR.
Jack [51] assessed foot posture by observing the weight-bearingrch of the foot but no criteria were documented to quantify this.ack [51] considered an association between pes planus and HR butas unclear which comes first or whether the two develop pari
assu. Coughlin and Shurnas [14] assessed foot posture using a Har-is Beath mat to measure arch height or excess heel valgus. Only 11%f their patients had pes planus. Their results were similar to thosef Harris and Beath [57] (15%) who examined 3619 normal militaryecruits. The Harris and Beath mat has not been tested for reliability
UPlease cite this article in press as: Beeson P, et al. Hallux rigidus: Adoi:10.1016/j.foot.2008.12.001
nd validity and it was considered that the results of Coughlin andhurnas which were based on previous studies were not reliable oronclusive.
Scherer [68] suggested that calcaneal eversion can theoreticallyimit 1st MTP joint motion. Harradine and Bevan [69] appeared to
D P
RO
OF
PRESSxxx (2009) xxx–xxx
validate this conjecture by examining the effect of static rearfooteversion (using 3◦, 5◦ and 8◦ valgus wedges in a standard shoe) on1st MTP joint ROM. A reduced joint ROM with increasing calcanealeversion was found. This artificially replicated three magnitudes ofpronation; therefore, the findings may not be representative of thefull continuum of foot pronation seen in the general population.Mahiquez et al. [70] examined the relationship between rearfootvalgus and 1st MTP joint OA and found 23% of subjects more likelyto develop 1st MTP joint OA with hindfoot valgus. Halstead et al. [71]found patients with 1st MTP joint OA demonstrated higher medialforefoot pressures and more pronated foot postures. Grady et al.[72] retrospectively analysed 772 HR patients and found 5.5% hadaetiologies of both trauma and excessive pronation while 21.7% hadexcess pronation only. The measurement criteria included excesspronation at mid-stance/toe-off and Kite’s angle >45◦.
Payne and Dananberg [29] contend that blockade of 1st MTPjoint sagittal plane motion (sagittal plane facilitation theory) pro-duces compensation within other planes. Compensatory subtalarand mid-tarsal joint pronation (frontal plane) with forefoot abduc-tion (transverse plane) can ensue, producing flatfoot in some HRpatients. Whilst the above studies provide interesting theories link-ing pes planus with HR none use a validated tool to quantify footposture.
In the current study the Foot Posture Index (FPI) [53] was used toquantify the degree of pronation or supination. This is a valid, reli-able and objective measure of foot function [53]. The FPI quantifiesfoot posture in a relaxed stance position, requiring no manipulationof the foot, marking of lines or measurement with instrumentation.Thus the controversial issues relating to goniometer assessmentand validity of neutral subtalar joint positioning are avoided [73,74].In the current study 84 (47%) feet had pes planus (11% of whichwere severely pronated). The remaining 78 (43%) feet had a nor-mal foot posture and 20 (10%) feet had a high arched supinated foot(Table 12A). A strong correlation between a pronated (pes planus)foot and 1st MTP joint pain was found (r = 0.84, p = 0.05). It is theo-rized that in a pes planus foot forefoot hypermobility at propulsionmay promote 1st MTP joint instability, increasing ROM and pain.A correlation between increased 1st MTP joint ROM and pronatedfeet (r = 0.72, p = 0.1) support this concept although this was not sta-tistically significant. Whilst these findings indicate a relationshipbetween the parameters this is not necessarily causal.
4.3.1.2. Functional hallux limitus. Functional hallux limitus (FHLim)is defined as reduced 1st MTP joint dorsiflexion on foot loadingcompared with passive non-weight-bearing and has been proposedas a cause of HR [28,42–45]. None of these authors mention anklejoint position when assessing for FHLim. If the ankle is plantarflexedwhen passive 1st MTP joint dorsiflexion is tested then hallux dor-siflexion is likely to increase as the flexor hallucis longus (FHL) istaken off stretch [16]. Coughlin and Shurnas [75] also question theconcept of FHLim as reported in the literature, which remains the-oretical conjecture and a subjective diagnosis [45], conceived toexplain abnormalities seen on in-shoe pressure readings and visualgait assessments [68]. Coughlin and Shurnas [14] hypothesized thatFHLim may represent the residual elevatus occasionally noted ondorsiflexion stress X-rays of patients with severe HR. In early stageHR FHLim may be a consequence of tenosynovitis of the FHL tendonwhich limits its excursion and subsequently that of 1st MTP jointdorsiflexion on foot loading [16]. The findings of the current studyconcur with those of other authors [14,16].
cross-sectional study to evaluate clinical parameters. Foot (2009),
4.3.1.3. 2nd toe length. Three foot types are seen in the general pop- 599
ulation. Square foot (hallux and 2nd toe equal length), Morton’s or 600
Greek foot (hallux shorter than 2nd toe) and Egyptian foot (hal- 601
lux longer than 2nd toe). Ogilvie-Harris et al. [76] assessed 2nd toe 602
length in ballet dancers and found a correlation between HR and a 603
Original text:
Inserted Text
(1-5
Original text:
Inserted Text
-
Original text:
Inserted Text
-
Original text:
Inserted Text
six
Original text:
Inserted Text
-very
Original text:
Inserted Text
(one
Original text:
Inserted Text
six
Original text:
Inserted Text
long term
Original text:
Inserted Text
Planus
Original text:
Inserted Text
&
Original text:
Inserted Text
&
Original text:
Inserted Text
&
Original text:
Inserted Text
&
Original text:
Inserted Text
&
Original text:
Inserted Text
therefore the
Original text:
Inserted Text
[70
Original text:
Inserted Text
&
Original text:
Inserted Text
.84, p=.05).
Original text:
Inserted Text
.72,
Original text:
Inserted Text
&
Original text:
Inserted Text
&
Original text:
Inserted Text
x-rays
D
INY
Foot x
l604
a605
o606
f607
N608
i609
2610
l611
a612
t613
f614
615
e616
h617
s618
1619
a620
f621
o622
o623
l624
r625
r626
4627
4628
M629
t630
o631
S632
[633
p634
t635
o636
p637
o638
i639
4640
m641
c642
i643
a644
p645
i646
o647
a648
d649
j650
a651
p652
w653
s654
1655
f656
a657
r658
p659
s660
b661
t662
4663
s664
n665
d666
667
668
669
670
671
672
673
674
675
676
677
678
679
680
681
682
683
684
685
686
687
688
689
690
691
692
693
694
695
696
697
698
699
700
701
702
703
704
705
706
707
708
709
710
711
712
713
714
715
716
717
718
719
720
ion of the joint imparted by rising up on their toes. In the current 721
NC
OR
RE
CTE
ARTICLEG ModelFOOT 1064 1–13
P. Beeson et al. / The
onger 2nd toe [77]. One clinician examined 59 dancers (34 femalend 25 male) comparing them to a randomly selected control groupf 60 subjects (30 female and 30 male). The authors defined any dif-erence in length of <2 mm as not significant recording it as normal.o radiographic evidence was used and the lack of this may have
nfluenced the outcome of results. They reported that 40% male and7% female ballet dancers had a long 2nd toe compared to the hal-ux. In the control group (in which there was no HR), 60% of malesnd 43% of females had a longer 2nd toe. The authors concludedhat 44% of ballet dancers, with a long 2nd toe, had bilateral HR butailed to elicit the related pathomechanics.
The current study does not concur with that of Olgilvie-Harrist al. [76]; 54 feet (30%) had a long 2nd toe while 111 feet (62%)ad a 2nd toe the same length as the hallux and 15 (8%) a 2nd toehorter than the hallux. Chi-square analysis of 2nd toe length andst MTP joint pain revealed a significant finding (p = 0.001 < 0.05). Inradiographic study of the same subjects the proximal phalanx was
ound to be longer than the distal phalanx [78]. The overall lengthf the hallux may be a factor contributing to HR and is supported bythers who have compared HR with non-HR subjects and found aonger hallux in the HR group [79]. Whilst these findings indicate aelationship between the parameters this is not necessarily a causalelationship.
.3.2. Factors used as markers of severity
.3.2.1. Increased joint size and soft tissue swelling. Increased 1stTP joint size in HR has been documented [14,20,26]. This is related
o the presence of osteophytes, joint distension secondary to syn-vitis and may provide an indirect clinical measure of joint damage.oft-tissue swelling of the 1st MTP joint has also been reported19,20] and may be related to a dorsal prominence that becomesainful from constant rubbing against the shoe, capsulitis and EHLenosynovitis resulting from stretching of soft tissues over dorsalsteophytes. This may be the reason why HR subjects often com-lain of pain on hallucal plantarflexion. In the current study it wasbserved that the magnitude of joint size increased with the sever-ty and duration of HR.
.3.2.2. Pain with 1st MTP joint motion. Some studies have docu-ented pain during 1st MTP joint motion [1,13,15,16,18]. In the
urrent study subjects reported pain during passive ROM. The tim-ng of this pain during joint movement was documented in anttempt to quantify the severity of HR (joint damage). Twenty-sixercent of subjects reported end-of-range pain suggestive of min-
mal joint damage, 69% of subjects reported pain at the beginningr mid-range pain accounting for mild to moderate joint damagend 4.5% reported all-of-range joint pain representing severe jointamage. This reflected the range of severity of HR within the sub-
ects. Interestingly a strong correlation between 1st MTP joint painnd increased 1st MTP joint ROM at propulsion was found (r = 0.84,= 0.01) but this was not statistically significant. This may explainhy in a damaged 1st MTP joint where there is still free and unre-
tricted joint motion pain is often likely whereas, in an ankylosedst MTP joint where movement is restricted pain is less likely. Ineet with restricted 1st MTP joint ROM pain may present in otherreas (lateral forefoot) due to the compensation imposed by theestricted joint motion. During active ROM subjects reported painrimarily during heel lift and propulsion where 1st MTP joint dor-iflexion was required. In the current study subjects reported thaty altering their gait pattern they could modify the severity andiming of symptoms.
UPlease cite this article in press as: Beeson P, et al. Hallux rigidus: Adoi:10.1016/j.foot.2008.12.001
.3.2.3. Variability of 1st MTP joint pain. The natural history andymptoms of HR can vary from day-to-day and are influenced byumerous aggravating or relieving factors. In some cases, the con-ition takes a relatively benign course and in others symptoms are
PR
OO
F
PRESSxx (2009) xxx–xxx 9
more persistent [80]. In the current study 87% of subjects werefound to have daily variability of joint pain (Table 10A). It is con-cluded that the variability of joint pain is multifactorial and mayinclude factors such as lifestyle, health, footwear and others (seeaggravating factors). Whilst occupation does not appear to play arole in the development of HR is may be responsible for its variabil-ity.
4.3.2.4. Location of HR pain. Subjects presented with primarily dor-sal bump pain (42%) (particularly early in the condition), 1st MTPjoint pain (12%), sesamoid pain (9%), proximal phalanx pain (2%) ora combination of locations around the 1st MTP joint (Table 12B).Sesamoid pain appeared to be more common in established HR.
4.3.2.5. Restricted joint motion. Studies have documentedrestricted 1st MTP joint motion in HR (especially dorsiflex-ion) [7,14,23,24]. The current study concurs with these findings(Table 11). Halstead et al. [71] demonstrated no associationbetween measurements obtained at the 1st MTP joint duringstatic stance and maximum dorsiflexion during walking. In viewof the different modes of compensation for HR during gait furtherresearch to compare 1st MTP joint motion in static stance andduring walking would be valuable and may help inform treatment.
4.3.2.6. Passive versus active 1st MTP joint ROM. Overall passive 1stMTP joint ROM was reduced as expected. Mean dorsiflexion 41◦
(0–82◦) was below the normal range (65–90◦) [21] and plantarflex-ion was also reduced, mean 15◦ (0–25◦) (Table 11).
Active 1st MTP joint dorsiflexion increased with weight-bearing.Mean active dorsiflexion 58◦ (0–90◦) (Table 11) was greater thanmean passive dorsiflexion, this may be a result of body weight andforward momentum increasing available joint dorsiflexion how-ever, this was still well below the normal range (65–90◦). Also,possibly because of joint pain, some subjects supinated their footduring movement reducing the need for as much dorsiflexion.These findings concur with a radiological study in which a meanhallux equinus angle of 11◦ was found during stance, this is outsidethe normal range (16–18◦) [78].
Both bone (including joint) and soft tissue changes associatedwith HR are responsible for a reduced joint ROM (particularly dor-siflexion). The dorsal capsule and EHL can become stretched andinflamed by dorsal osteophytes causing pain and may contribute tolimited plantarflexion in HR.
4.3.2.7. Hallux abductus interphalangeus (HAI). In the current study129 feet (72%) presented with HAI (Table 12A). A moderate degree(>10◦) of HAI (transverse plane) was present in 57 feet (32%). In79 feet (44%) the HAI◦ was greater than normal (where normal≤10◦). Strong correlations were found between HAI and 1st MTPjoint pain (r = 0.82, p = 0.03) which was not significant and HAI andreduced 1st MTP joint ROM (r = 0.92, p = 0.05). It is hypothesized thatthe presence of HAI indicates a more progressive HR process andthat with increased 1st MTP joint damage the 1st metatarsal headbecomes flatter and more resistant to transverse plane movement,thus predisposing to an increased HAI.
4.3.3. Factors associated with or secondary to HR4.3.3.1. Ability to rise up on toes. In HR if 1st MTP joint dorsiflexionis restricted or painful then subjects may avoid forced dorsiflex-
cross-sectional study to evaluate clinical parameters. Foot (2009),
study 21% of subjects were unable to undertake this manoeuvre, the 722
reminder could perform the task to varying degrees (Table 10A). A 723
weak correlation between 1st MTP joint pain and ability to rise up 724
on toes was found (r = .40, p = .03). Subjects can still perform this 725
manoeuvre by supinating their foot.
Original text:
Inserted Text
&
Original text:
Inserted Text
female,
Original text:
Inserted Text
4.4Factors
Original text:
Inserted Text
4.4.1
Original text:
Inserted Text
4.4.2
Original text:
Inserted Text
.84, p=.01)
Original text:
Inserted Text
4.4.3
Original text:
Inserted Text
4.4.4
Original text:
Inserted Text
4.4.5
Original text:
Inserted Text
4.4.6
Original text:
Inserted Text
(0-82
Original text:
Inserted Text
°-90
Original text:
Inserted Text
(0-25
Original text:
Inserted Text
(0-90
Original text:
Inserted Text
°-90
Original text:
Inserted Text
°-18
Original text:
Inserted Text
4.4.7
Original text:
Inserted Text
.82, p=.03)
Original text:
Inserted Text
.92, p=.05).
Original text:
Inserted Text
4.5Factors
Original text:
Inserted Text
4.5.1

E
ARTICLE ING ModelYFOOT 1064 1–13
10 P. Beeson et al. / The Foot
4726
i727
l728
h729
i730
(731
j732
733
(734
h735
a736
w737
l738
w739
a740
t741
v742
l743
4744
I745
i746
[747
w748
t749
h750
3751
f752
(753
t754
h755
i756
4757
t758
759
760
761
762
763
764
765
766
767
768
769
770
771
772
773
774
775
776
777
778
779
780
781
782
783
784
785
786
787
788
789
790
791
792
793
794
795
796
797
798
799
800
801
802
803
804
805
806
807
808
809
810
811
812
813
814
NC
OR
RE
CT
Fig. 2. Valgus hallucal rotation in HR.
.3.3.2. Hallucal position (frontal plane). Medial 1st ray deviation,ncreased 1/2 intermetatarsal angle and lateral deviation of the hal-ux may alter the pull of abductor hallucis causing it to rotate theallux and medial sesamoid into valgus. Valgus hallucal rotation
s normally associated with hallux valgus but may present in HRFig. 2) where it may influence sagittal plane motion at the 1st MTPoint and sesamoid tracking.
In the current study valgus hallucal rotation presented in 75 feet42%), hallux varus in 13 feet (7%) and 91 feet (51%) had a rectusallux. A moderate correlation between valgus hallucal rotationnd limited 1st MTP joint ROM (r = 0.59, p = 0.01) was found butas not statistically significant. A correlation between valgus hal-
ucal rotation and 1st MTP joint pain was found (r = .78, p = .05). Itas concluded that hallucal valgus rotation may biomechanically
lter 1st MTP joint function in HR. It is unclear whether this fea-ure progresses with time, however, in the small number of halluxalgus-rigidus subjects excluded from this study a more severe andate stage HR was seen.
.3.3.3. Hallucal interphalangeal joint (IPJ) hyperextension. HallucalPJ hyperextension (dorsal sagittal plane deviation) can be seen dur-ng early stages of HR when MTP joint motion is still good. Lynn81] considered that IPJ hyperextension is another causal factorhich increases susceptibility to HR rather than being secondary
o reduced MTP joint motion. In the current study 120 feet (62%)ad a hyperextended hallucal IPJ of varying degrees of severity and0% of these were greater than 10◦ (Table 12A). A correlation wasound between hallucal IPJ hyperextension and 1st MTP joint painr = 0.78, p = 0.01) but this was not statistically significant. This rela-ionship is not necessarily causal. In the current study the degree of
UPlease cite this article in press as: Beeson P, et al. Hallux rigidus: Adoi:10.1016/j.foot.2008.12.001
allucal IPJ hyperextension did not appear to increase with increas-ng severity of HR.
.3.3.4. Hallucal interphalangeal joint pain. As sagittal plane restric-ion of the 1st MTP joint can result in compensatory transverse
D P
RO
OF
PRESSxxx (2009) xxx–xxx
and/or sagittal plane deformity of the hallucal IPJ it was assumedthat hallucal IPJ pain may develop. In the current study a painful IPJwas reported in 36 subjects (20%) and only 18 (10%) of these hadmoderate to severe pain (Table 12A). Chi-square analysis of hallu-cal IPJ pain and 1st MTP joint pain revealed no significant finding(0.24 > p > 0.05). In this group of subject’s hallucal IPJ pain was notconsidered to be a feature associated with HR.
4.3.3.5. Hallucal flexor function. Tenosynovitis of the hallucal flexortendons in HR may influence hallucal purchase power. The abilityof the hallux to prevent a piece of paper from being pulled awayfrom under it during static stance was not found to be impaired inHR where 150 (83%) feet had a strong (not moveable) response.
4.3.3.6. Location of plantar callosities. These were related to abnor-malities of gait (pronation and inverted step). Increasing severityof 1st MTP joint pain results in more supinatory compensation andsubsequently more laterally placed callosities. In 67 (37%) feet calluspresented over the plantar medial hallucal IPJ. This may be relatedto 47% of subjects who presented with a pronated gait in whichthere is likely to be increased hallucal IPJ propulsion. Of the remain-ing 46 (26%) feet callus was located under the lateral metatarsalheads (2nd–5th), 9 (5%) feet under the 1st metatarsal head and 58(32%) feet presented with no callosities (Table 12A). The severity ofcallosities may be influenced by lifestyle and activity levels.
4.3.3.7. Lesser toe position. Coughlin [82] and Roukis et al. [2] notedthat the medial angulation of the 2nd toe can result from compen-sation during gait. In an attempt to provide medial column stabilitythe flexor digitorum longus (FDL) muscle contracts. A “windswept”appearance to the entire forefoot, rather than just the 2nd toe mayresult. In the current study lesser toe clawing in 77 (43%) feet, medi-alisation (adduct-varus) of 3rd–5th toes in 63 (35%) feet, and othertoe deformities presented (Table 12A).
4.3.3.8. Ankle equinus. A recent study concludes that gastrocne-mius contracture plays a vital biomechanical role in chronic footproblems [58]. Bingold and Collins [23] suggested an associationbetween Achilles tendon contracture and HR. Isolated gastrocne-mius tightness has been reported in up to 24% of “normal” patientswhen defined as less than 5◦ dorsiflexion with the knee fullyextended and the condition was implicated in the pathogenesisof midfoot, hind foot, and forefoot pathology [52] although it wasunclear how many patients had HR. Coughlin and Shurnas [14]found no association between Achilles tendon tightness and HR.They defined gastrocnemius contracture as <0◦ dorsiflexion whenthe knee was fully extended with the foot in neutral. Only 3.5% oftheir subjects had 5◦ or less of dorsiflexion although the study hadno control group with which to correlate the results. In the currentstudy 10 (5.5%) feet had 5◦ or less dorsiflexion with the knee fullyextended and foot held in neutral (to eliminate subtalar and mid-tarsal joint involvement) (Table 12A). No subject had an Achillestendon contracture <0◦. The mean ankle dorsiflexion with the kneeextended was 9◦ (5–17◦) this increased to 13◦ (8–25◦) with the kneeflexed (Table 11). It is concluded that ankle equinus secondary toAchilles tendon tightness is not associated with HR.
4.3.3.9. Lesser metatarsal overload. Supinated gait in response torestricted 1st MTP joint motion can cause overload and pain in theregion of the lesser metatarsal heads [45]. In the current study lesserMTP joint pain (transfer metatarsalgia) was in reported in 69 (38%)
cross-sectional study to evaluate clinical parameters. Foot (2009),
feet with varying degrees of frequency (Table 10A). A strong cor- 815
relation between lesser MTP joint pain and a change in walking 816
pattern (r = 0.80, p = 0.05) was found. Chi-square analysis of lesser 817
MTP joint pain and supination at propulsion revealed a statistically 818
significant finding (p < 0.001). It is hypothesized that 1st MTP joint 819
Original text:
Inserted Text
4.5.2
Original text:
Inserted Text
.59, p=.01)
Original text:
Inserted Text
4.5.3
Original text:
Inserted Text
MTPJ pain was found (r=0.78,
Original text:
Inserted Text
4.5.4
Original text:
Inserted Text
4.5.5
Original text:
Inserted Text
4.5.6
Original text:
Inserted Text
(2nd- 5th),
Original text:
Inserted Text
4.5.7
Original text:
Inserted Text
3rd-5th
Original text:
Inserted Text
4.5.8
Original text:
Inserted Text
&
Original text:
Inserted Text
&
Original text:
Inserted Text
<0
Original text:
Inserted Text
& midtarsal
Original text:
Inserted Text
°-17
Original text:
Inserted Text
°-25
Original text:
Inserted Text
4.5.9
Original text:
Inserted Text
.80, p=.05)
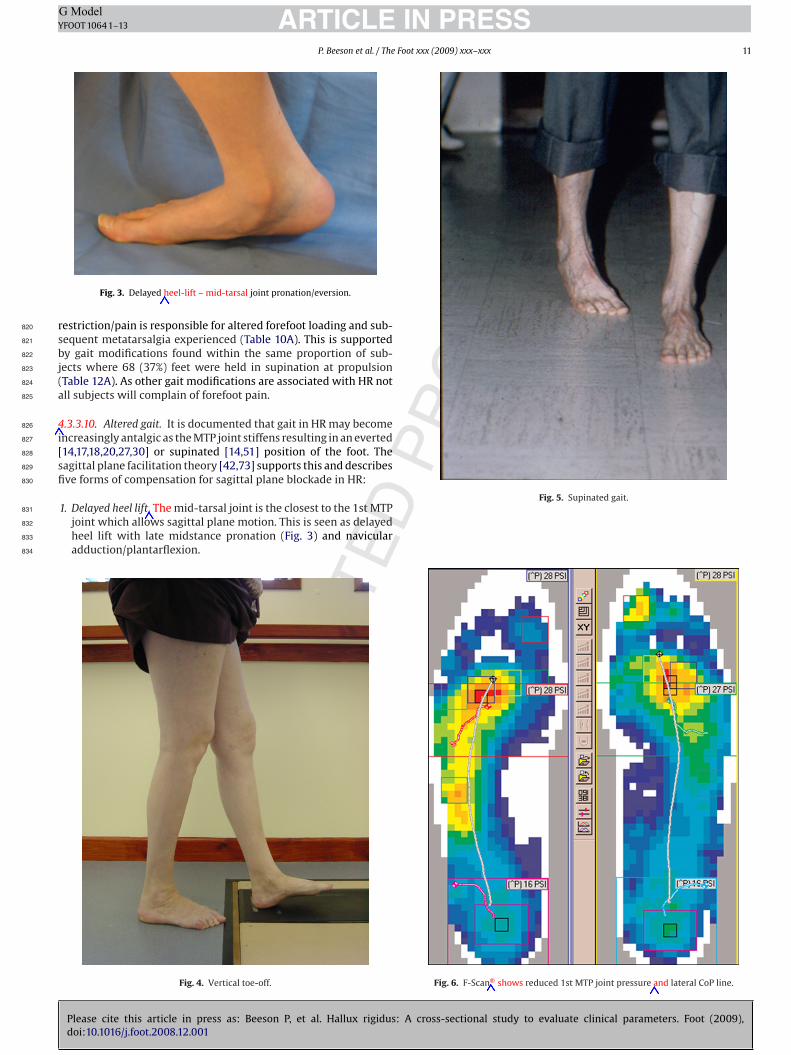
PR
OO
F
ARTICLE IN PRESSG ModelYFOOT 1064 1–13
P. Beeson et al. / The Foot xxx (2009) xxx–xxx 11
r820
s821
b822
j823
(824
a825
4826
i827
[828
s829
fi830
831
832
833
834
Fig. 3. Delayed heel-lift – mid-tarsal joint pronation/eversion.
estriction/pain is responsible for altered forefoot loading and sub-equent metatarsalgia experienced (Table 10A). This is supportedy gait modifications found within the same proportion of sub-ects where 68 (37%) feet were held in supination at propulsionTable 12A). As other gait modifications are associated with HR notll subjects will complain of forefoot pain.
.3.3.10. Altered gait. It is documented that gait in HR may becomencreasingly antalgic as the MTP joint stiffens resulting in an everted14,17,18,20,27,30] or supinated [14,51] position of the foot. Theagittal plane facilitation theory [42,73] supports this and describesve forms of compensation for sagittal plane blockade in HR:
UN
CO
RR
EC
TED
Please cite this article in press as: Beeson P, et al. Hallux rigidus: A cross-sectional study to evaluate clinical parameters. Foot (2009),doi:10.1016/j.foot.2008.12.001
1. Delayed heel lift. The mid-tarsal joint is the closest to the 1st MTPjoint which allows sagittal plane motion. This is seen as delayedheel lift with late midstance pronation (Fig. 3) and navicularadduction/plantarflexion.
Fig. 4. Vertical toe-off.
Fig. 5. Supinated gait.
Fig. 6. F-Scan® shows reduced 1st MTP joint pressure and lateral CoP line.
Original text:
Inserted Text
–mid-tarsal
Original text:
Inserted Text
4.5.10
Original text:
Inserted Text
The
Original text:
Inserted Text
F-Scan shows
Original text:
Inserted Text
&

E
ARTICLE ING ModelYFOOT 1064 1–13
12 P. Beeson et al. / The Foot
835
836
837
838
839
840
841
842
843
844
845
846
847
848
849
850
851
852
853
5854
855
856
857
858
5859
860
k861
a862
m863
864
S865
m
866
867
868
869
870
871
872
873
874
875
876
877
878
879
880
881
882
883
884
885
886
887
888
889
890
891
892
893
894
895
896
897
898
899
900
901
902
903
904
905
906
Q2 907
908
909
910
911
912
913
914
915
916
917
[ 918
919
920
921
922
923
924
925
926
927
928
929
930
931
NC
OR
RE
CT
Fig. 7. Failure of knee to fully extend.
2. Vertical toe-off. Denotes continuation of delayed heel-lift wherefoot is lifted vertically off the ground. An apropulsive, laborious,slow gait can present where there is a lack of heel-off by the timeof the contra-lateral heel contact (Fig. 4).
3. Inverted step. Patients with increasingly severe HR supinatetheir foot during gait [14] to avoid extending the 1st MTP jointand propulse from the lateral four toes (Fig. 5). Weight-flow isdirected to the lateral column and fails to shift medially to thefirst web space prior to heel lift. Lateral shoe wear results despiteexcessive foot pronation. This explains the paradox of a flexi-ble pronated foot with lateral forefoot shoe wear and bulging.Dynamic in-shoe pressure measurement systems such as the F-Scan® show reduced pressure under the 1st MTP joint and lateraldeviation of centre of pressure (CoP) line (Fig. 6).
4. Abductory (external) or adductory (internal) hip rotation twist attoe-off. Seen during mid-stance/propulsion producing ‘medialroll-off’ following path of least resistance. This form of compen-sation is associated with FHLim as advocated by Dananberg [28];it is responsible for medial hallucal IPJ pinch callus.
. Flexion compensation of the body (seen during single limb supportFig. 7). In the current study all five forms of HR gait compensationwere observed. At propulsion 68 (38%) feet were supinated, 50(28%) delayed heel lift (mid-tarsal joint pronation) and 37 (20.5%)had a normal gait (Table 12A).
. Conclusion
The purpose of this cross-sectional study was to document theey clinical parameters associated with HR. A number of difficulties
UPlease cite this article in press as: Beeson P, et al. Hallux rigidus: Adoi:10.1016/j.foot.2008.12.001
nd limiting factors associated with clinical evaluation and assess-ent of the foot were highlighted.Only certain clinical parameters were useful to evaluate HR.
ome features were either too time-consuming (plantar pressureeasurement), too difficult to measure, or the reliability of their
932
D P
RO
OF
PRESSxxx (2009) xxx–xxx
measurement [83,84] (particularly angular measurements) was indoubt.
The findings of this research are based on the defined studypopulation. HR was associated with female gender, bilateralinvolvement, older age groups (a condition which develops overtime), increased HAI angle, FHL tenosynovitis, a 2nd toe of simi-lar length to the hallux and restricted and/or painful 1st MTP jointdorsiflexion. HR was also associated with pain located over thedorsal bump (particularly in the early stages), hallucal IPJ hyper-extension, lesser MTP joint pain (when supinating at propulsion),medial angulation of the 2nd toe, flat foot and various specific gaitalterations. Unilateral involvement was less common, and mostlyassociated with trauma. In bilateral cases, a positive family his-tory could not be concluded, however a properly constructed familystudy may prove such an association. An association between HR(1st MTP joint OA) and OA at other sites (finger joints) particularlyin women was found but not tested statistically. Future epidemi-ological studies would be useful to determine whether a systemicaetiology is involved in HR development and clarify the respec-tive influences of mechanical and systemic factors in the conditionsdevelopment.
HR was not associated with Achilles tendon tightness. Footwearwas not found to be a contributory cause, however, it was reportedto be an aggravating factor (particularly in women). There were fewsubjects with adolescent onset HR.
For clinical parameters of the foot to be considered valid forinclusion in a classification of HR their content validity needs tobe firstly established by formal research [84]. The purpose of thisresearch study was to establish such validity.
References
[1] Shereff M, Baumhauer J. Hallux rigidus and osteoarthritis of the first metatar-sophalangeal joint: instructional course lecture. Current concepts review. J BoneJoint Surg 1988;80-A:898–909.
[2] Roukis TS, Jacobs PM, Dawson DM, Erdmann BB, Ringstrom JB. A prospectivecomparison of clinical, radiographic, intraoperative features of hallux rigidus. JFoot Ankle Surg 2002;41:76–95.
[3] Davies-Colley M. Contraction of the metatarsophalangeal joint of the great toe.Br Med J 1887;1:728.
[4] Cotterill J. Stiffness of the great toe in adolescents. Br Med J 1887;1:1158.[5] Bock P, Kristen K-H, Kroner A, Engel A. Hallux valgus and cartilage degeneration
in the first metatarsophalangeal joint. J Bone Joint Surg 2004;86B:669–73.[6] Beeson P, Phillips C, Corr S, Ribbans WJ. Radiological evaluation of hallux
rigidus: problems and pitfalls. Podiatry; submitted for publication.[7] Nilsonne H. Hallux rigidus and its treatment. Acta Orthop Scand
1930;1:295–303.[8] Lambrinudi P. metatarsus primus elevatus. Proc R Soc Med 1938;31:1273.[9] Lapidus P. Dorsal bunion: its mechanics and operative correction. J Bone Joint
Surg 1940;22-B:627–37.[10] Bonney G, MacNab I. Hallux valgus and hallux rigidus. A critical survey of oper-
ative results. J Bone Joint Surg 1952;34:366–85.[11] Rzonca E, Levitz S, Luc B. Hallux equines. The stages of hallux limitus and hallux
rigidus. JAPMA 1984;74:390–3.12] Regnauld B. Disorders of the great toe. In: Elson R, editor. The foot: pathol-
ogy, aetiology, seminology, clinical investigation and treatment. New York:Springer-Verlag; 1986. p. 269–281, 344–349.
[13] Durrant MN, Siepert KK. Role of soft tissue structures as an etiology of halluxlimitus. JAPMA 1993;83:173–80.
[14] Coughlin MJ, Shurnas PS. Hallux rigidus: dermographics, etiology and radio-graphic assessment. Foot Ankle Int 2003;24:731–43.
[15] Vanore JV, Christensen JC, Kravitz SR, Schuberth JM, Thomas JL, Weil LS, etal. Clinical practice guideline first metatarsophalangeal joint disorders Panelof the American College of Foot & Ankle Surgeons. Diagnosis and treatment offirst metatarsophalangeal joint disorders. Section 2: Hallux rigidus. J Foot AnkleSurg 2003;42:124–36.
[16] Michelson J, Dunn L. Tenosynovitis of the flexor hallucis longus: a clini-cal study of the spectrum of presentation and treatment. Foot Ankle Int2005;26:291–303.
cross-sectional study to evaluate clinical parameters. Foot (2009),
[17] Mann R, Clanton T. Hallux rigidus: treatment by cheilectomy. J Bone Joint Surg 933
1988;70-A:400–6. 934
[18] Easley M, Davis W, Anderson R. Intermediate to long-term follow-up of medial- 935
approach dorsal cheilectomy for hallux rigidus. Foot Ankle Int 1999;20:147–52. 936
[19] Mackay D, Blyth M, Rymaszewaski L. The role of cheilectomy in the treatment 937
of hallux rigidus. J Foot Ankle Surg 1997;36:337–40. 938
Original text:
Inserted Text
Denotes
Original text:
Inserted Text
Patients
Original text:
Inserted Text
Seen
Original text:
Inserted Text
In
Original text:
Inserted Text
–A
Original text:
Inserted Text
Problems
Original text:
Inserted Text
Submitted
Original text:
Inserted Text
Its
Original text:
Inserted Text
–B
Original text:
Inserted Text
equines,
Original text:
Inserted Text
Foot:
Original text:
Inserted Text
344349
Original text:
Inserted Text
Dermographics,
Original text:
Inserted Text
A
Original text:
Inserted Text
Treatment
Original text:
Inserted Text
–A

D
INY
Foot x
[939
940
[941
942
[943
944
[945
[946
947
[948
949
950
[951
952
[953
954
[955
956
[Q3957
958
[Q4959
960
[961
962
[963
964
[965
966
[967
968
[969
[970
971
[972
973
[974
[975
976
[977
978
[979
980
[981
982
[983
984
985
[986
987
[988
989
[990
991
[992
993
[994
995
[996
997
[998
999
[1000
[1001
1002
[1003
1004
1005
[1006
1007
[ 1008
1009
[ 1010
1011
[ 1012
1013
[ 1014
1015
[ 1016
1017
1018
[ 1019
1020
1021
[ 1022
1023
[ 1024
1025
1026
[ 1027
1028
[ 1029
1030
[ 1031
1032
1033
[ 1034
1035
1036
[ 1037
1038
1039
[ 1040
1041
[ 1042
1043
[ 1044
1045
1046
[ 1047
1048
1049
[ 1050
1051
[ 1052
1053
[ 1054
1055
1056
[ 1057
1058
[ 1059
1060
[ 1061
1062
[ Q5 1063
1064
[ 1065
1066
1067
[ 1068
[ 1069
[82] Coughlin MJ. Second metatarsophalangeal joint instability in the athlete. Foot 1070
Ankle Int 1993;14:309–19. 1071
RE
CTE
ARTICLEG ModelFOOT 1064 1–13
P. Beeson et al. / The
20] Mann RA, Coughlin MJ, DuVries HL. Hallux rigidus: a review of the literatureand a method of treatment. Clin Orthop 1979;142:57–63.
21] Camasta CA. Hallux limitus and hallux rigidus. Clin Podiat Med Surg1996;13:431–7.
22] Coughlin M. Arthritides. In: Coughlin MJ, Mann RA, editors. Surgery of the footand ankle. 7th ed. St. Louis: Mosby; 1999. p. 605–50.
23] Bingold A, Collins D. Hallux rigidus. J Bone Joint Surg 1950;32-B:214–22.24] Smith R, Katchis S, Ayson L. Outcomes in hallux rigidus treated non-operatively:
a long-term follow-up study. Foot Ankle Int 2000;21:906–13.25] Kilmartin TE. Metatarsal osteotomy for hallux rigidus. An outcome study of
three different osteotomy techniques compared with Keller’s excisional arthro-plasty. Br J Pod 2000;3:95–101.
26] Giannestras N. Hallux rigidus. In: Giannestras N, editor. Foot disorders: medicaland surgical management. Philadelphia: Lea & Febiger; 1973. p. 400–2.
27] Kessell L, Bonney G. Hallux rigidus in the adolescent. J Bone Joint Surg 1958;40-B:668–73.
28] Dananberg HJ. Gait style as an etiology to chronic postural pain. Part I: functionalhallux limitus. JAPMA 1993;83:433–41.
29] Payne CB, Dananberg HJ. Sagittal plane facilitation of the foot. AJPM1997;31:7–11.
30] Mulier T, Steenwerckx A, Thienpont E, et al. Results after cheilectomy in athleteswith hallux rigidus. Foot Ankle Int 1999;20:232–7.
31] Thomas P, Smith R. Proximal phalanx osteotomy for the surgical treatment ofhallux rigidus. Foot Ankle Int 1999;20:3–12.
32] Geldwert J, Rocj G, McGrath M, Mancuso J. Cheilectomy: still a useful techniquefor grade I and grade II hallux limitus/rigidus. J Foot Surg 1992;31:154–9.
33] Kurtz D, Harrill J, Kaczander B, Solomon M. The Valenti procedure for halluxlimitus: a long-term follow-up and analysis. J Foot Ankle Surg 1999;38:123–30.
34] Feltham G, Hanks S, Marcus R. Age-based outcomes of cheilectomy for thetreatment of hallux rigidus. Foot Ankle Int 2001;22:192–7.
35] Goodfellow J. Etiology of hallux rigidus. Proc R Soc Med 1966;59:821–4.36] McMaster MJ. The pathogenesis of hallux rigidus. J Bone Joint Surg
1978;60B:82–7.37] Bryant A, Tinley P, Singer K. A comparison of radiographic measurements in
normal, hallux valgus and hallux limitus feet. J Foot Ankle Surg 2000;39:39–43.38] Gould N. Hallux rigidus: cheilectomy or implant? Foot Ankle Int 1981;1:315–20.39] Hattrup S, Johnson K. Subjective results of hallux rigidus following treatment
with cheilectomy. Clin Orthop 1988;226:182–91.40] Drago JJ, Oloff L, Jacobs AM. A comprehensive review of hallux limitus. J Foot
Ankle Surg 1984;23:213–20.41] Hamilton W, O’Malley M, Thompson F, Kovatis P. Capsular interposition arthro-
plasty for severe hallux rigidus. Foot Ankle Int 1997;18:68–70.42] Dananberg HJ. Gait style as an etiology to chronic postural pain. Part II: proximal
compensatory process. JAPMA 1993;83:615–24.43] Di Napoli D. Gait analysis based on first MTPJ function: the functional hallux
limitus concept. In: Tucker GA, editor. Reconstructive surgery of the foot andleg update 93. The Podiatry Institute; 1993. p. 27–32.
44] Payne C, Chuter V, Miller K. Sensitivity and specificity of the functional halluxlimitus test to predict foot function. JAPMA 2002;92:269–71.
45] Clough JG. Functional hallux limitus and lesser metatarsal overload. JAPMA2005;95:593–601.
46] Cavolo D, Cavallaro D, Arrington L. The Watermann osteotomy for hallux limitus.Clin Podiatr Med Surg 1979;69:52–7.
47] Cohen I, Kanat I. Functional limitation of motion at the first metatarsopha-langeal joint. J Foot Surg 1984;23:477–84.
48] Meyer J, Nishon L, Weiss L, Docks G. Metatarsus primus elevatus and the etiologyof hallux rigidus. J Foot Surg 1987;26:237–41.
49] Saxena A. The Valenti procedure for hallux limitus/rigidus. J Foot Ankle Surg1995;34:485–8.
50] Viegas G. Reconstruction of hallux limitus deformity using a 1st metatarsalsagittal-Z osteotomy. J Foot Ankle Surg 1998;37:204–11.
51] Jack EA. The aetiology of hallux rigidus. Br J Surg 1940;27:492–7.52] DiGiovanni C, Kuo R, Tejwani N, Price R, Hansen S, Criernecki J, et al. Isolated
gastrocnemius tightness. J Bone Joint Surg 2002;84–A:962–70.
UN
CO
R
Please cite this article in press as: Beeson P, et al. Hallux rigidus: Adoi:10.1016/j.foot.2008.12.001
53] Redmond A, Crosbie J, Ouvrier RA. Development and validation of a novel ratingsystem for scoring standing foot posture: the Foot Posture Index. Clin Biomech2005;21:89–98.
54] Ronconi P, Monachino P, Baleanu P, Favilli G. Distal oblique osteotomy of thefirst metatarsal for the correction of hallux limitus and rigidus deformity. J FootAnkle Surg 2000;39:154–60.
[
[
PR
OO
F
PRESSxx (2009) xxx–xxx 13
55] Greene WB, Hecknam JD. The clinical measurement of joint motion. AmericanAcademy of Orthopedic Surgeons; 1994. p. 29–31.
56] Silfverskiold N. Reduction of the two-joints muscles of the leg in one jointmuscles in spastic conditions. Acta Chir Scand 1924;56:315–30.
57] Harris R, Beath T. Hypermobile flatfoot with short tendo-achilles. J Bone JointSurg 1948;30-A:116–38.
58] Grebing BR, Coughlin MJ. Evaluation of Morton’s theory of 2nd metatarsalhypertrophy. J Bone Joint Surg 2004;86A:1376–85.
59] Bennett PJ, Patterson C, Wearing S, Baglioni T. Development and validationof a questionnaire designed to measure foot health status. JAPMA 1998;88:419–28.
60] Bennett PJ, Patterson C. The Foot Health Status questionnaire (FHSQ): anew instrument for measuring outcomes of footcare. Aust J Podiatr Med1998;32:87–92.
61] Feldman R, Hutter J, Lapow L, Pour B. Cheilectomy and hallux rigidus. J FootSurg 1983;22:170–4.
62] Pontell D, Gudas C. Retrospective analysis of surgical treatment of hallux lim-itus/rigidus: clinical and radiographic follow-up of hinged, silastic implantarthroplasty and cheilectomy. J Foot Surg 1988;27:503–10.
63] DuVries H. Static deformities. In: DuVries H, editor. Surgery of the foot. St Louis:Mosby; 1959. p. 392–8.
64] Lorimer D, French G, O’Donnell M, Burrow G. Neale’s disorders of the foot.Edinburgh: Churchill Livingstone; 2002. p. 193.
65] Cracchiolo A, Weltmer JB, Lian G, et al. Arthroplasty of the first metatar-sophalangeal joint with double-stem silicone implant. J Bone Joint Surg1992;74A:552–63.
66] Sim-Fook L, Hodgson AR. A comparison of foot forms among the non-shoe and shoe wearing Chinese population. J Bone Joint Surg 1958;40-A:1058–62.
67] Wilder FV, Barrett JP, Farina EJ. The association of radiographic foot osteoarthri-tis and radiographic osteoarthritis at other sites. Osteoarthritis Cartilage2005;13:211–5.
68] Scherer PR. Heel spur syndrome: pathomechanics and nonsurgical treatment.JAPMA 1991;81:68–72.
69] Harradine PD, Bevan LS. The effect on rearfoot eversion on maximal halluxdorsiflexion: a preliminary study. JAPMA 2000;90:390–3.
70] Mahiquez MY, Wilder FV, Stephens HM. Positive hindfoot valgus andosteoarthritis of the first metatarsophalangeal joint. Foot Ankle Int2006;27:1055–9.
71] Halstead J, Turner DE, Redmond AC. The relationship between hallux dorsiflex-ion and ankle joint complex frontal plane kinematics: a preliminary study. ClinBiomech 2005;20:526–31.
72] Grady JF, Axe TM, Zager EJ, et al. A retrospective analysis of 772 patients withhallux limitus. JAPMA 2002;92:102–8.
73] Menz HB. Clinical hindfoot measurement: a critical review of the literature. TheFoot 1995;5:57–64.
74] McPoil TG, Cornwall MW. The relationship between subtalar joint neu-tral position and rearfoot motion during walking. Foot Ankle Int 1994;15:141–5.
75] Coughlin MJ, Shurnas PS. Hallux rigidus: grading and long-term results of oper-ative treatment. J Bone Joint Surg 2003;85A:2072–88.
76] Ogilvie-Harris DJ, Carr MM, Fleming PJ. The foot in ballet dancers: the impor-tance of 2nd toe length. Foot Ankle Int 1995;16:144–7.
77] Magee DJ. Orthopedic physical assessment. St. Louis: Saunders Elsevier; 2006.p. 73.
78] Beeson P, Phillips C, Corr S, Ribbans WJ. Cross-sectional study to evaluate theradiological parameters in hallux rigidus. The Foot; in press.
79] Munuera PV, Dominguez G, Castillo JM. Radiographic study of the size of thefirst metatarso-digital segment in feet with incipient hallux limitus. JAPMA2007;97:460–8.
80] Yee G, Lau J. Current concepts: hallux rigidus. Foot Ankle Int 2008;29:637–46.81] Lynn MD. Letter to editor. Foot Ankle Int 2004;25:605.
cross-sectional study to evaluate clinical parameters. Foot (2009),
83] Coughlin MJ, Freund E. The reliability of angular measurements in hallux valgus 1072
deformities. Foot Ankle Int 2001;22:369–79. 1073
84] Beeson P, Phillips C, Corr S, Ribbans WJ. Classification systems for hallux rigidus: 1074
a review of the literature. Foot Ankle Int 2008;29:407–14. 1075
Original text:
Inserted Text
Clinics Podiatric Medicine & Surgery
Original text:
Inserted Text
Foot and Ankle7th Ed.1999Mosby
Original text:
Inserted Text
–B
Original text:
Inserted Text
Disorders: Medical and Surgical
Original text:
Inserted Text
Functional
Original text:
Inserted Text
& Ankle Int.20
Original text:
Inserted Text
–term
Original text:
Inserted Text
Proximal
Original text:
Inserted Text
The
Original text:
Inserted Text
Clinical Biomechanics21
Original text:
Inserted Text
Clinical Measurement of Joint
Original text:
Inserted Text
19942931
Original text:
Inserted Text
–A
Original text:
Inserted Text
A
Original text:
Inserted Text
Foot
Original text:
Inserted Text
Disorders of the Foot
Original text:
Inserted Text
193
Original text:
Inserted Text
waering
Original text:
Inserted Text
Pathomechanics
Original text:
Inserted Text
A
Original text:
Inserted Text
Clinical Biomechanics20
Original text:
Inserted Text
Grading
Original text:
Inserted Text
The
Original text:
Inserted Text
Physical Assessment
Original text:
Inserted Text
St Louis73
Original text:
Inserted Text
Phillips,
Original text:
Inserted Text
Foot. In Press 2008.
Original text:
Inserted Text
Concepts: Hallux RigidusFoot
Original text:
Inserted Text
Ed*itorFoot &

















![[SPECIAL ARTICLE] Modernities Through Art and Design: Printing Press as a Source of Examining Penang’s Modernity](https://static.fdokumen.com/doc/165x107/6326f4c5cf3e39ceab049c48/special-article-modernities-through-art-and-design-printing-press-as-a-source.jpg)

