40. Dialysis | Infection Prevention for Specialty Care Populations
Upload
independentCategory
view
1download
0
NEPHROLOGY - REVIEW
Arterial stiffness in dialysis patients: where are we now?
Mehmet Kanbay • Baris Afsar •
Paul Gusbeth-Tatomir • Adrian Covic
Received: 29 July 2009 / Accepted: 26 October 2009 / Published online: 19 November 2009
� Springer Science+Business Media, B.V. 2009
Abstract Patients with end-stage renal disease
treated by chronic dialysis have an impressive
mortality, which more than half of this mortality is
attributable to cardiovascular disease. Despite strat-
ification for sex, race, and the presence of diabetes,
cardiovascular disease mortality is 10–30 times
higher in dialysis patients compared to general
population. In dialysis patients, both atherosclerosis
(mainly affecting the intima of the arteries) and
arteriosclerosis (affecting predominantly the media
of large- and middle-sized arteries diffusely) are
highly prominent. Arteriosclerosis characterized by
reduced arterial compliance (i.e., reduced elasticity of
the arteries) is due to increased fibrosis, loss of elastic
fibers, and extensive vessel wall calcification. Arte-
riosclerosis is closely related to arterial stiffness. A
generally accepted mechanistic view is that an
increase in arterial stiffness causes a premature return
of reflected waves in late systole, increasing central
pulse pressure, thus systolic. An increased arterial
stiffness can increase the risk of stroke through
several mechanisms, including an increase in central
pulse pressure, influencing arterial remodeling both at
the site of the extracranial and intracranial arteries,
increasing carotid wall thickness, and the develop-
ment of stenosis and plaques, and the likelihood of
plaque rupture. Very importantly, it was also sug-
gested that arterial stiffness itself independently plays
a role in exacerbating chronic kidney disease pro-
gression. This review deals briefly with the definition
of arterial stiffness, methods of measuring arterial
stiffness and pathophysiology of arterial stiffness, and
factors related with arterial stiffness.
Keywords Arterial stiffness �Chronic kidney disease
Introduction
Patients with end-stage renal disease (ESRD) treated
by chronic dialysis have an impressive mortality, and
more than half of this mortality is attributable to
cardiovascular disease (CVD). Despite stratification
for sex, race, and the presence of diabetes, CVD
mortality is 10–30 times higher in dialysis patients
compared to general population [1]. Thus, it is
thought that apart from traditional risk factors/
uremia-related risk factors also play an important
role for the development of CVD. Emerging risk
factors include malnutrition, inflammation, oxidative
M. Kanbay (&) � B. Afsar
Department of Internal Medicine, Section of Nephrology,
Fatih University School of Medicine, Gokkusagi
Mahallesi 16. Cadde, No ? 16/21, Cevizlidere/Cankaya,
Ankara, Turkey
e-mail: [email protected]; [email protected]
P. Gusbeth-Tatomir � A. Covic
Department of Nephrology Clinic and Dialysis and
Transplantation Center, ‘‘C. I. PARHON’’ University
Hospital, Iasi, Romania
123
Int Urol Nephrol (2010) 42:741–752
DOI 10.1007/s11255-009-9675-1

stress, endothelial dysfunction, vascular calcification
(VC), and arterial stiffness. In dialysis patients, both
atherosclerosis (mainly affecting the intima of the
arteries) and arteriosclerosis (affecting predomi-
nantly the media of large- and middle-sized arteries
diffusely) are highly prominent. Arteriosclerosis
characterized by reduced arterial compliance (AC)
(i.e., reduced elasticity of the arteries) is due to
increased fibrosis, loss of elastic fibers, and extensive
vessel wall calcification [2]. Arteriosclerosis is
closely related to arterial stiffness. Increased stiffness
of large arteries has important clinical consequences:
raised systolic blood pressure (BP), increased pulse
pressure, left ventricular hypertrophy, and reduced
coronary perfusion [3]. A generally accepted mech-
anistic view is that an increase in arterial stiffness
causes a premature return of reflected waves in late
systole, increasing central pulse pressure, thus sys-
tolic BP. SBP increases the load on the left ventricle
(LV), increasing myocardial oxygen demand [4]. An
increased arterial stiffness can increase the risk of
stroke through several mechanisms, including an
increase in central pulse pressure (PP), influencing
arterial remodeling both at the site of the extracranial
and intracranial arteries, increasing carotid wall
thickness and the development of stenosis and
plaques [5, 6], and the likelihood of plaque rupture
[7]. Very importantly, it was also suggested that
arterial stiffness itself independently plays a role in
exacerbating chronic kidney disease progression [8].
Indeed, a large number of pathophysiological condi-
tions were associated with increased arterial stiffness.
For an extensive review, see Laurent et al. [4] .
This review deals briefly with the definition of
arterial stiffness, methods of measuring arterial
stiffness and pathophysiology of arterial stiffness,
and factors related with arterial stiffness.
Definition of arterial stiffness
Arteries are a unique system of distensible conduits
that contain the pulsatile output of the heart and
provide continuous flow to the tissues. During systole,
the transmitted flow of blood from the heart generates
a pressure wave that is propagated to all arteries of the
body. Pressure wave travels quickly at 5–15 m/s;
which is much faster than the speed of blood flow. On
arrival at branch points, pressure wave is reflected and
returned to the heart. The behavior of the pulse wave
is dependent on the ventricular contraction and the
compliance of the vascular system [9]. With the
influence of various factors such as age, high blood
pressure, and diabetes, the walls of large conduit
arteries undergo intense remodeling processes leading
to alteration in the viscoelastic properties. The result
is a diffuse process of arteriosclerosis, characterized
by stiffer arteries or, in other terms, reduced arterial
elasticity or compliance. Clinical consequences of
increased stiffness are higher SBP, lower diastolic BP,
and widened PP. All three changes are known as
major determinants for high CV morbidity and
mortality [3]. As arteries become stiffer, macroscopic
and microscopic changes are observed. Macroscopi-
cally, the arteries appear tortuous and dilated. Micro-
scopically, there is a loss of the orderly elastic
lamellae and disorganized thickening of the media
with glycosaminoglycan deposition, fibrosis, and
calcification. In the extreme, there is a medial necrosis
and aneurysm formation [9]. The causes and conse-
quences of arterial stiffness are shown in Fig. 1.
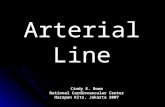
Methods to measure arterial stiffness
Ideally, such methods need to be safe, non-invasive,
quick, inexpensive, reliable, and reproducible; and
their results should correlate with the extent of
atherosclerotic disease and have high positive and
negative predictive values. The measurements should
integrate the deleterious effects of all genetic and
environmental cardiovascular (CV) risk factors in the
years of exposition [10]. Although several studies have
previously addressed the methodological issues con-
cerning the various indices of arterial stiffness cur-
rently available, and their clinical applications,
clinicians and researchers still report difficulties in
selecting the most appropriate methodology for their
specific use [4]. In clinical studies, several methods to
measure arterial stiffness have been investigated
including pulse wave velocity (PWV), systemic arte-
rial compliance (SAC), and augmentation index (AIx),
which are mostly used in clinical practice (Fig. 2).
A. Pulse wave velocity
Pulse wave velocity is defined as the speed of travel
of the pressure pulse along an arterial segment and
742 Int Urol Nephrol (2010) 42:741–752
123

can be obtained for any arterial segment accessible to
palpation. To measure PWV, continuous pulse wave
signals are recorded with pressure tonometers posi-
tioned over the arterial pulses [9]. Measurement of
PWV is generally accepted as the most simple, non-
invasive, robust, and reproducible method to deter-
mine arterial stiffness. Carotid-femoral PWV is a
direct measurement, and it corresponds to the widely
accepted propagative model of the arterial system [4].
The excellent reproducibility is demonstrated for
PWV, with intraobserver and interobserver variability
less than 5% [11]. Some limitations should be
underlined. The femoral pressure waveform may be
difficult to record accurately in patients with meta-
bolic syndrome, obesity, diabetes, and peripheral
artery disease. In the presence of aortic, iliac, or
proximal femoral stenosis, the pressure wave may be
attenuated and delayed. Abdominal obesity, particu-
larly in men, and large bust size in women can make
distance measurements inaccurate [12].
B. Augmentation index
The Augmentation index is derived from the arterial
pressure waveform and is a composite of the forward
pressure wave created by ventricular contraction and a
reflected wave. Waves are reflected from the periph-
ery, mainly at branch points. In elastic vessels, because
PWV is low, reflected wave tends to arrive back at the
aortic root during diastole. In the case of stiff arteries,
PWV rises, and the reflected wave arrives back at the
central arteries earlier, adding to the forward wave and
augmenting the systolic pressure. This phenomenon
can be quantitated through the AIx [4, 9].
Figure 2 demonstrates the schematic representa-
tion of AIx where the height of the late systolic peak
(P1) above the inflection (P2) defines the augmenta-
tion pressure, and the ratio of augmentation pressure
to PP defines the AIx (in percent), [6].
Measurement can be obtained directly from either
carotid artery or ascending aorta or using a transfer
Arteriosclerosis
Atherosclerosis
Systolic BP
Diastolic BP
Left ventricle hypertrophy Decompansated LVH
Ischemic heart disease
Peripheral artery disease
Decreased coronary reserveDecreased coronary perfusion
Cardiac failure
Volume overload
Cerebrovascular disease
Renal failure
Arteries becomes tortuous and dilated. Loss of elastic lamellae Disorganized thickening of the media Glycosaminoglycan deposition, Fibrosis Calcification
Medial necrosis and aneurysm formation
Widened PP
Reduced arterial elasticityor compliance
Death
Fig. 1 The causes and consequences of arterial stiffness
Int Urol Nephrol (2010) 42:741–752 743
123
function to derive aortic pressure waveforms from
recorded radial artery waveforms [13].
C. Arterial compliance
Arterial compliance is a measure of the elastic nature
of the arterial system, and it represents the relation-
ship between change in volume and change in
pressure during diastole. The AC requires measure-
ment of volumetric blood flow and associated driving
pressure to derive an estimated compliance over the
total systemic arterial tree. A hand-held Doppler flow
velocimeter placed on the suprasternal notch at the
base of the neck is used to estimate arterial blood
flow. Aortic driving pressure is estimated by appla-
nation tonometry of the right common carotid artery
using a non-invasive pressure transducer [9].
D. Arterial distensibility
Arterial distensibility (AD) is a quantitative evalua-
tion of arterial stiffness [14].
The distension of an artery refers to the change in
diameter during systole relative to diastole. Lower
distension suggests regional arterial stiffening. Ultra-
sound measurements of the distal common carotid
artery or aorta during the cardiac cycle can be used to
determine wall displacement and, thus, artery disten-
sion [9].
E. Ambulatory arterial stiffness index
It is the newly described method derived from
ambulatory blood pressure measurements [15].
Ambulatory arterial stiffness index (AASI) is a
Pressure tonometer
C=DxV
AC = Ad/R(Pes–Pd)
AIx = (DP/PP) X 100
PWV = D/Dt (m/s)
Fig. 2 Methods of measuring arterial stiffness
744 Int Urol Nephrol (2010) 42:741–752
123

method that aims to characterize the relationship of
systolic to diastolic BP during the day. By plotting
the individual values of systolic and diastolic BP
measurements obtained through 24-h non-invasive
ambulatory BP monitoring, the authors calculated the
regression slope of diastolic BP on systolic BP. The
slope was assumed as a global measure of AC, and its
reciprocal (1 minus the slope), named AASI, was
taken as a measure of arterial stiffness [16].
F. Arterial stiffness index
The Arterial stiffness index (ASI) is a quantitative
marker for arterial stiffness by measuring the volu-
metric changes of brachial artery in a computerized
oscillometry device [17]. ASI was proved to be
significantly correlated with aortic stiffness measured
by PWV and could serve as a reliable and convenient
method for arterial stiffness [18, 19]. However,
Kocak et al. [20] did not find a significant correlation
between FMD% and carotid-intima media thickness
in their peritoneal dialysis patient cohort. They
speculated that one possible explanation for their
results is that each method measures a different
aspect and stage of atherosclerosis.
G. X-ray vascular calcification score
Vascular calcifications were evaluated at baseline by
a single observer blind to clinical data, in plain X-ray
of pelvis and hands. Pelvis films were divided into
four sections by two imaginary lines: a horizontal line
over the upper limit of both femoral heads and a
median vertical line over the vertebral column [21].
The presence of VC in each section was rated as 1
and its absence as 0.
H. Cardiovascular magnetic resonance
This imaging modality also permits contemporaneous
visualization of large arteries and direct measurement
of aortic function, providing an integrated assessment
of both ventricular and vascular function in one
examination. Aortic distensibility (AD), the relative
change in aortic size throughout the cardiac cycle
relative to blood pressure, is readily assessed with
cardiovascular magnetic resonance [22].
Pathogenesis of arterial stiffness
The mechanisms for increased arterial stiffness in
renal patients are not entirely defined but may include
arterial calcification, chronic volume overload,
increased mechanical stress by hypertension, chronic
microinflammation, sympathetic overactivity, activa-
tion of the RAA axis, AGEs, lipid peroxidation, and
abnormalities of the nitric oxide system [23]. First of
all, it is important to note that even mild deterioration
in kidney function is a risk factor for the development
of arterial stiffness. Mourad et al. [24] investigated the
possibility that even mild deterioration in renal
function may cause increased arterial stiffness. In
1,290 subjects with normal BP or essential hyperten-
sion, they found that patients with the lowest tertile of
creatinine clearance (CrCl; but still normal serum
creatinine level) had a greater PWV, and this associ-
ation was independent of BP and other classic CV risk
factors. The negative association between PWV and
CrCl is stronger in subjects younger than 55 years.
Furthermore, a large longitudinal study of patients
with essential hypertension showed that the serum
creatinine level is a major determinant of accelerated
progression of aortic stiffness in treated patients with
hypertension [25]. CKD is a state characterized by
increased extracellular matrix collagen content and
proliferation of VSMCs in the setting of paracrine and
systemic activation of the RAA axis. Collagen and
elastin in the vessel wall of renal subjects are severely
altered by the increased generation of AGEs [26] and
augmented carbonyl stress [27]. Volume overload
(frequently encountered in ESRD subjects) also con-
tributes to the high PWV associated with stiffened
arteries [2]. However, volume reduction by hemodi-
alysis is not able to reverse/significantly decrease
arterial stiffness [28], although an increased extracel-
lular to intracellular fluid ratio is strongly associated
with arterial stiffness [29]. Further studies have to
determine if aggressive volume control in patients
with ESRD is able to reverse to certain extent arterial
stiffening. In patients with ESRD on chronic hemod-
ialysis, a strong relationship between stiffened arteries
and the microinflammatory state has been found [30].
In another study, Cheng et al. [31] demonstrated that
C-reactive protein is inversely correlated with PVW in
continuous ambulatory dialysis patients.
An inverse correlation between PWV and HDL
cholesterol levels has been reported [32]. Efficient
Int Urol Nephrol (2010) 42:741–752 745
123

removal of LDL cholesterol by lipid apheresis and
usage of vitamin E-coated hemodialysis membranes
improves arterial stiffness and reduces the serum
levels of several markers of inflammation [33].
Another important factor which is related with
increased in CKD is the presence of VC. VC results
from an imbalance between promoters and inhibitors
of mineralization, sharing similarities with the pro-
cess of skeletal mineralization. Different gene prod-
ucts seem to modulate the process of ectopic
calcification: matrix G1a protein, fetuin, osteopontin,
and the osteoprotegerin receptor activator of NF-KB
(RANK)–RANK ligand complex [34]. In particular,
serum fetuin, a potent in vitro inhibitor of calcifica-
tion, is strongly associated with valvular calcifica-
tions, but also with atherosclerosis, malnutrition, and
inflammation—a fatal triad in patients with ESRD
[35]. High levels of phosphate and/or calcium are
directly activating genes related to an osteoblastic
phenotype in the smooth muscle cells [36]. Hyper-
phosphatemia and increased calcium phosphate prod-
uct ([55 mg2/dl2) are important and clinically
evident contributors to VC in patients with ESRD
[37]. Low levels of inhibitors of calcification also
cause VSMC apoptosis; apoptotic cells and the
vesicles resulting from programmed cell death form
a nidus for the deposition of the calcium phosphate
salt (mainly hydroxyapatite). In the presence of a
medium with high level of calcium and phosphate (as
seen frequently in patients with ESRD ), exposed
VSMCs suffer rapid calcification [38]. According to
previous data, inflammation also contributes to the
calcification process [39]. Furthermore, pro-inflam-
matory cytokines have been shown to enhance in
vitro calcification of vascular cells [40], suggesting a
close relationship between inflammation and calcifi-
cation. There seems to be a direct link between
valvular calcification and inflammation in patients on
dialysis [41]. Arterial calcification is closely related
to arterial stiffness: more calcified arteries obviously
lose their elastic properties [42, 43]. Indeed, in
dialysis patients, studies persistently showed a
positive correlation between VC and arterial stiffness.
Guerin et al. [44] showed that the presence of VCs in
large arteries was associated with increased arterial
stiffness in dialysis patients. Furthermore, in pro-
spective studies, the same group showed that both
increased arterial stiffness and large-artery
calcifications were major predictors of general and
CV mortality in renal patients [45, 46]. Fang et al.
[47] found that elevated pulse pressure is associated
with an increased risk of all-cause and cardiovascular
death in patients on peritoneal dialysis. They con-
cluded that recognition of this characteristic as an
important predictor of mortality suggests that one
goal of antihypertensive therapy in patients with PD
should be to decrease elevated pulse pressure.
Moreover, Ogawa et al. [48] showed that arterioscle-
rosis assessed by stiffness parameter beta is associ-
ated with atherosclerotic changes of carotid arteries
and with the presence of silent cerebral infarction in
patients with HD . Haydar et al. [49] found that PWV
strongly correlates with total calcification scores
assessed by means of EBCT, even after correction
for age, dialysis therapy duration, prescribed dose of
calcium-containing phosphate binders, and microin-
flammatory status. Recently, in hemodialysis
patients, it was demonstrated that aortic stiffness
(assessed by PWV) was associated with bone activity.
London et al. [50] showed that patients with
adynamic bone disease were characterized by signif-
icantly higher aortic PWV. They also showed that in
patients with adynamic bone disease, significant
positive correlations between Ca dosage and aortic
calcification scores or aortic PWV were observed. In
their multivariate analysis, aortic PWV is indepen-
dently and positively associated with Ca dosage
(p \ 0.0001) and negatively with bone activity
(p = 0.03). They suggest that the positive associa-
tions between Ca load and PWV were stronger in
patients with adynamic bone disease (ABD), indicat-
ing that the presence of ABD conferred significantly
greater influence of Ca load on aortic calcifications
and stiffening. The presence of an active bone was
associated with lower aortic stiffness and better aortic
capacitive function.
Factors related with arterial stiffness
in end-stage renal disease
Apart from well-defined risk factors for the develop-
ment of arterial stiffness (e.g, hyperphosphatemia,
hyperparathyroidism, and hypercalcemia), other risk
factors also present that are thought to play a role for
the development of arterial stiffness.
746 Int Urol Nephrol (2010) 42:741–752
123

Malnutrition
Protein-energy malnutrition is a common problem in
patients with ESRD and is a powerful predictor of
morbidity and mortality [51]. Gu et al. [52] demon-
strated in 124 patients on peritoneal dialysis that
patients with malnutrition exhibited a significantly
higher PWV than those classified as well nourished by
subjective global assessment (p \ 0.05). They also
found that, in multivariate regression analysis, albu-
min, handgrip strength SGA, and bioelectrical imped-
ance analysis phase angle were each independently
associated with PWV after adjustment (p \ 0.0001).
Fetuin-A
This glycoprotein is a potent calcification inhibitor, and
absence of fetuin in fetuin-A knock-out mice results in
massive extra-osseous calcification [53]. Fetuin-A, a
negative acute-phase reactant, plays a pivotal role in the
inhibition of Cax P precipitation [54]. Moreover, low
fetuin-A levels were found to be related to increased
VCs in dialysis patients [55]. To determine whether
fetuin-A deficiency in dialysis patients is an indepen-
dent predictor for the development of vascular stiffness
as a consequence of VC in dialysis patients, Hermans
et al. [56] conducted a study in dialysis patients. They
could not identify fetuin-A as an independent predictor
of aortic stiffness as measured with PWV, and AI.
Sigrist et al. [57] also did not demonstrate any
relationship between fetuin-a and VC. However, we
believe that more studies are needed to determine the
relationship between fetuin-A and VC and its relation-
ship with arterial stiffness in dialysis patients.
Beta-blockers
Sigrist et al. [58] found that use of beta-blockers was
also associated with the progression of VC. Blockers
inhibit the beta adrenoreceptors in the heart and
peripheral vasculature and may promote VC through
modulating sympathetic activity and trophic effects
on peripheral vasculature. VC in patients with HD is
associated with reduced baroreflex sensitivity.
Asymmetric dimethylarginine
Wilkinson et al. [59] speculated that the endogenous
NO synthesis inhibitor asymmetric dimethylarginine
(ADMA) might participate in the pathogenesis of
arterial stiffness. Previous studies showed that he-
modialysis reduces ADMA levels and to improve
central pressure waveform [60, 61]. Recently, Soveri
et al. [62] examined the changes in ADMA levels and
central arterial pressure waveform during HD in 32
patients with HD. They found that HD reduced both
AIx (19%; p = 0.003) and ADMA levels (17%;
p \ 0.001). The magnitudes of changes in AIx and
ADMA during HD were correlated (r = 0.44;
p = 0.045). They suggest that the reduction in
ADMA level seen after HD is associated with
improvement in the central arterial pressure wave-
form, suggesting involvement of nitric oxide in the
regulation of arterial stiffness in patients with HD.
Homocysteine
The effect of homocysteine on arterial stiffness is
controversial. Plasma homocysteine levels were
independently correlated with arterial stiffness as
measured by lower limb PWV in patients with ESRD
[63]. Nevertheless, reducing plasma homocysteine
levels by folic acid did not change the carotid artery
stiffness in patients with ESRD [64]. Tsai et al. [65]
examined the independent association between
homocysteine and arterial stiffness in 109 hemodial-
ysis patients. Their multiple regression analyses
showed that plasma homocysteine had significant
associations with arterial stiffness index (ASI) and
with pulse pressure. They suggest that homocysteine
might cause increase arterial stiffness by enhancing
the growth of vascular smooth muscle cells, by
impairing cell growth and function of endothelium,
by inducing oxidative effect, and by reducing elastic
lamina tissue.
Bone mineral metabolism
Derangements in bone mineral metabolism are spec-
ulatively playing a role in the increased arterial
stiffness in hemodialysis patients. Indeed, some stud-
ies have demonstrated a correlation between PWV and
low bone mineral density [66, 67]. Toussaint et al. [68]
report cross-sectional data on 48 patients with CKD
(GFR 17–55 ml/min), assessing the associations
between VC, arterial stiffness, and bone mineral
density in chronic kidney disease. The authors did
not show any correlation between bone mineral
Int Urol Nephrol (2010) 42:741–752 747
123

density and PWV. As the evidence for associations
between arterial stiffness and bone mineral density
strengthens, focus must be shifted to understanding the
mechanism for these processes.
Hepatitis C
Adam et al. [69] conducted a study to analyze the
relationship between hepatitis c infection, arterial
stiffness, and insulin resistance in hemodialysis
patients. Thirty-seven HCV (?) and 30 HCV (-)
HD patients were enrolled. Arterial stiffness was
measured by ‘‘stiffness index b’’ and the elastic
modulus.’’ The authors found that insulin resistance
was associated with stiffness index b (r = ?0.547,
p = 0.001) and elastic modulus (r = ?0.532,
p = 0.001) only in HCV (?) patients. However, the
investigators did not find any difference between
seropositive and seronegative patients in terms of
‘‘stiffness index b’’ and ‘‘elastic modulus.’’ They
concluded that no direct effect of HCV infection on
arterial stiffness could be sustained.
Fibroblast growth factor-23
Fibroblast growth factor-23 (FGF23) is a secreted,
bone-derived factor that plays a fundamental role in
the regulation of phosphate and vitamin D metab-
olism [70]. FGF23 levels are elevated at later stages
of CKD as a response to persistent hyperphospha-
temia [71]. Circulating concentration of FGF-23
increases as renal function declines in patients with
chronic kidney disease, but does not change in
response to variation in phosphate intake in healthy
volunteers [72]. Gutierrez et al. [73] recently
demonstrated that FGF23 is independently associ-
ated with mortality in incident hemodialysis patients
although the mechanistic causes remain unknown.
Until recently, the association between FGF23 and
vascular function in ESRD patients was not known.
Mirza et al. [74] very recently demonstrated that
both in patients with and without renal failure
circulating FGF23 is independently associated with
increased arterial stiffness. Circulating fibroblast
growth factor-23 is associated with vascular dys-
function in the community. They suggest that further
research should be carried for determining the exact
role of fibroblast growth factor-23 for the develop-
ment of CVD.
Magnesium
Numerous studies now provide strong suggestive
evidence for a protective role of Mg in VC,
arrhythmias, and atherosclerosis in patients with
ESRD. These studies also suggest that serum Mg
concentrations in dialysis patients are independently
associated with PTH levels which is an independent
risk factor for VC. Previous studies allow us to
speculate on the possible salutary role of increasing
plasma levels of Mg to facilitate the healing of
vascular injuries, to prevent atherosclerosis, hyper-
tension, arrhythmia, and chronic myocardial ische-
mia. Magnesium-based compounds have an
additional further advantage of being very much
cheaper to use than some newer alternatives [75, 76].
Perspectives and conclusion
Raised blood pressure measured at the brachial site
is thought to be a major CV risk factor in the general
population. However, central BP (as opposed to
peripheral, brachial BP) is determined by several
factors other than those listed by classical textbooks
(i.e., cardiac output and peripheral vascular resis-
tance), such as the stiffness of conduit arteries and
the timing and magnitude of pressure wave reflec-
tions [3]. This nuance is crucial to any investigation
of BP therapy, as there is an intense discussion on
potential advantages of the BP-lowering therapy
beyond BP lowering. Recent publications have
suggested that central aortic pressures may be
independent predictors of CV outcomes. Recen-
tly,this has been confirmed first by a large prospec-
tive investigation – the CAFE study. The authors of
CAFE study showed that certain drugs (in this case,
the calcium channel blocker amlodipine ± perindop-
ril combination) are more favorable in reducing
central BP (i.e., arterial stiffness) than others (aten-
olol ± thiazide). They suggest that BP-lowering
drugs can have substantially different effects on
central aortic pressures and hemodynamics despite a
similar impact on brachial BP. Moreover, central
aortic pulse pressure may be a more important
determinant of clinical outcomes, and differences in
central aortic pressures may be a potential mecha-
nism to explain the different clinical outcomes. The
results of this study are groundbreaking, and as a
748 Int Urol Nephrol (2010) 42:741–752
123

result of the knowledge obtained from the CAFE
trial, clinicians should try to choose the antihyper-
tensive drug that achieves the best balance between
central and brachial BP in any particular patient.
Today, it was well demonstrated in several studies
that the independent predictive value of aortic
stiffness has been demonstrated after adjustment to
classical CV risk factors, including brachial pulse
pressure. This indicates that aortic stiffness has a
better predictive value than each of classical risk
factors. In addition, aortic stiffness retains its
predictive value for CVD events after adjustment
to the Framingham risk score, suggesting that aortic
stiffness has an added value to a combination of CV
risk factors. One reason may be that aortic stiffness
integrates the damage of CV risk factors on the
aortic wall over a long period of time, whereas BP,
glycemia, and lipids can fluctuate over time, and
their values, recorded at the time of risk assessment,
may not reflect the true values damaging the arterial
wall. Arterial stiffness attenuation may reflect the
true reduction of arterial wall damage, whereas BP,
glycemia, and lipids can be normalized in a few
weeks by using antihypertensive, antidiabetic, and
lipid-lowering drugs, leading to a strong reduction in
CV risk scores, but without yet any improvement of
atherosclerotic lesions and arterial stiffness, which
requires a long-lasting correction of biochemical
abnormalities. A temporal dissociation is thus
expected between the improvement of CV risk
factors and a still high arterial stiffness. A direct
answer to the issue of the predictive value of aortic
stiffness attenuation for the reduction of CV events
has not yet been afforded in the general population
widely [4]. Although there are indirect clues,
whether the reduction in central PP is associated
with a concomitant reduction in CV events, inde-
pendently of the normalization of classical CV risk
factors remains to be demonstrated. Thus, one major
goal of future clinical research will be to confirm
these data in large, well-designed trials. If the results
of these future trials do demonstrate a more favor-
able impact of some antihypertensives on central
blood pressure and on major CV end-points, it will
lead to a major shift in our understanding of BP, our
treatment of it, and also the way we measure blood
pressure. Arterial stiffness assessment (by applana-
tion tonometry or other methods) would become
mandatory in any clinical setting.
Thus, as mentioned earlier, there are many factors
that play a role for the development of arterial
stiffness. Some of them are unique to dialysis
patients, and some of them are also present in general
population. Our current knowledge does not enable
us to know exactly to what extend these factors play a
role for the development of arterial stiffness.
Although important research is going on, we still do
not know the answers to important questions. How do
these risk factors work, how they interact with each
other, at what stage can we stop the process? Finally,
which might be the protective factors related to
arterial stiffness prevention?
References
1. Foley RN, Parfrey PS, Sarnak MJ (1998) Clinical epide-
miology of cardiovascular disease in chronic renal disease.
Am J Kidney Dis 32:S112–S119
2. Gusbeth-Tatomir P, Covic A (2007) Causes and conse-
quences of increased arterial stiffness in chronic kidney
disease patients. Kidney Blood Press Res 30:97–107
3. Covic A, Gusbeth-Tatomir P, Goldsmith DJ (2005) Arte-
rial stiffness in renal patients: an update. Am J Kidney Dis
45:965–977
4. Laurent S et al (2006) Expert consensus document on
arterial stiffness: methodological issues and clinical
applications. Eur Heart J 27:2588–2605
5. Boutouyrie P, Bussy C, Hayoz D, Hengstler J, Dartois N,
Laloux B, Brunner H, Laurent S (2000) Local pulse pres-
sure and regression of arterial wall hypertrophy during
long term antihypertensive treatment. Circulation 101:
2601–2606
6. Zureik M, Ducimetiere P, Touboul PJ, Courbon D, Boni-
thon-Kopp C, Berr C, Magne C (2000) Common carotid
intima-media thickness predicts occurrence of carotid
atherosclerotic plaques longitudinal results from the ageing
vascular study (EVA) study. Arterioscler Thromb Vasc
Biol 20:1622–1629
7. Cheng GC, Loree HM, Kamm RD, Fishbein MC, Lee RT
(1993) Distribution of circumferential stress in ruptured
and stable atherosclerotic lesions: a structural analysis with
histopathological correlation. Circulation 87:1179–1187
8. Taal MW, Sigrist MK, Fakis A, Fluck RJ, McIntyre CW
(2007) Markers of arterial stiffness are risk factors for
progression to end-stage renal disease among patients with
chronic kidney disease stages 4 and 5. Nephron Clin Pract
107:c177–c181
9. Zoungas S, Asmar RP (2007) Arterial stiffness and
cardiovascular outcome. Clin Exp Pharmacol Physiol 34:
647–651
10. Celermajer DS (1998) Noninvasive detection of athero-
sclerosis. N Engl J Med 339:2014–2015
11. Asmar R, Benetos A, Topouchian J, Laurent P, Pannier B,
Brisac AM, Target R, Levy BI (1995) Assessment of
Int Urol Nephrol (2010) 42:741–752 749
123

arterial distensibility by automatic pulse wave velocity
measurement. Validation and clinical application studies.
Hypertension 26:485–490
12. Van Bortel LM, Duprez D, Starmans-Kool MJ, Safar ME,
Giannattasio C, Cockcroft J, Kaiser DR, Thuillez C (2002)
Applications of arterial stiffness, Task Force III: recom-
mendations for user procedures. Am J Hypertens 15:445–
452
13. McEniery CM, Yasmin HallIR, Qasem A, Wilkinson IB,
Cockcroft JR (2005) Normal vascular aging: differential
effects on wave reflection and aortic pulse wave velocity:
the Anglo-Cardiff Collaborative Trial (ACCT). J Am Coll
Cardiol 46:1753–1760
14. Nichols WW, O’Rourke MF (1998) Vascular impedance.
In: Nichols WW, O’Rourke MF (ed) McDonald’s blood
flow in arteries: theoretical, experimental and clinical
principles. 4th edn. London: Edward Arnold, pp 54–97,
243–283, 347–395
15. Ratto E, Leoncini G, Viazzi F, Vaccaro V, Falqui V, Pa-
rodi A, Conti N, Tomolillo C, Deferrari G, Pontremoli R
(2006) Ambulatory arterial stiffness index and renal
abnormalities in primary hypertension. J Hypertens 24:
2033–2038
16. Schillaci G, Parati G, Pirro M, Pucci G, Mannarino MR,
Sperandini L, Mannarino E (2007) Ambulatory arterial
stiffness ındex ıs not a specific marker of reduced arterial
compliance. Hypertension 49:986–991
17. Vogel RA, Benitez RM (2000) Noninvasive assessment of
cardiovascular risk: from Framingham to the future. Rev
Cardiovasc Med 1:34–42
18. Komai N, Ohishi M, Morishita R, Moriguchi A, Kaibe M,
Matsumoto K, Rakugi H, Higaki J, Ogihara T (2002)
Arterial stiffness index: a new evaluation for arterial
stiffness in elderly patients with essential hypertension.
Geriatric Geront Int 15:199–205
19. Hiramatsu K, Oiwa A, Shigematsu S et al (2004) A novel
arterial stiffness index (ASI) as a marker of arteriosclero-
sis. Am J Hypertens 17:131A
20. Kocak H, Gumuslu S, Sahin E, Ceken K, Ermis C, Gocmen
AY, Yakupoglu G, Ersoy FF, Suleymanlar G, Tuncer M
(2009) Relationship between carotid artery intima-media
thickness and brachial artery flow-mediated dilation in
peritoneal dialysis patients. Int Urol Nephrol 41(2):409–
416
21. Adragao T, Pires A, Birne R, Curto JD, Lucas C,
Goncalves M, Negrao AP (2009) A plain X-ray vascular
calcification score is associated with arterial stiffness and
mortality in dialysis patients. Nephrol Dial Transplant
24(3):997–1002
22. Mark PB, Doyle A, Blyth KG, Patel RK, Weir RA,
Steedman T, Foster JE, Dargie HJ, Jardine AG (2008)
Vascular function assessed with cardiovascular magnetic
resonance predicts survival in patients with advanced
chronic kidney disease. J Cardiovasc Magn Reson 10(1):39
23. London GM, Marchais SJ, Guerin AP, Metivier F (2002)
Impairment of arterial function in chronic renal disease:
prognostic impact and therapeutic approach. Nephrol Dial
Transplant 12:13–15
24. Mourad JJ, Pannier B, Blacher J et al (2001) Creatinine
clearance, pulse wave velocity, carotid compliance and
essential hypertension. Kidney Int 59:1834–1841
25. Benetos A, Adamopoulos C, Bureau JM et al (2002)
Determinants of accelerated progression of arterial stiff-
ness in normotensive subjects and in treated hypertensive
subjects over a 6-year period. Circulation 105:1202–1207
26. Makita Z, Bucala R, Rayfield EJ, Friedman EA, Kaufman
AM, Korbet SM, Barth RH, Winston JA, Fuh H, Manogue
KR et al (1994) Reactive glycosylation end-products in
diabetic uremia and treatment of renal failure. Lancet
343:1519–1522
27. Miyata T, de Strihou C, Kurokawa K, Baynes JW (1999)
Alterations in nonenzymatic biochemistry in uremia: origin
and significance of ‘carbonyl stress’ in long-term uremic
complications. Kidney Int 55:389–399
28. Tycho Vuurmans JL, Boer WH, Bos WJ, Blankestijn PJ,
Koomans HA (2002) Contribution of volume overload and
angiotensin II to the increase pulse wave velocity of he-
modialysis patients. J Am Soc Nephrol 13:177–183
29. Lin YP, Yu WC, Hsu TL, Ding PY, Yang WC, Chen CH
(2003) The extracellular fluid-to-intracellular fluid volume
ratio is associated with large-artery structure and function
in hemodialysis patients. Am J Kidney Dis 42:990–999
30. Kobayashi S, Okamoto K, Maesato K, Moriya H, Ohtake T
(2005) Important role of blood rheology in atherosclerosis
of patients with hemodialysis. Hemodial Int 9:268–274
31. Cheng LT, Tang LJ, Chen HM, Tang W, Wang T (2008)
Relationship between serum albumin and pulse wave
velocity in patients on continuous ambulatory peritoneal
dialysis. Vasc Health Risk Manag 4(4):871–876
32. London GM, Marchais SJ, Safar ME, Genest AF, Guerin
AP, Metivier F, Chedid K, London AM (1990) Aortic and
large artery compliance in end-stage renal failure. Kidney
Int 37:137–142
33. Nakamura T, Kawagoe Y, Matsuda T, Takahashi Y,
Sekizuka K, Ebihara I, Koide H (2003) Effects of LDL
apheresis and vitamin E-modified membrane on carotid
atherosclerosis in hemodialyzed patients with arterioscle-
rosis obliterans. Kidney Blood Press Res 26:185–191
34. Moe SM, Reslerova M, Ketteler M, O’Neill K, Duan D,
Koczman J, Westenfeld R, Jahnen-Dechent W, Chen NX
(2005) Role of calcification inhibitors in the pathogenesis
of vascular calcification in chronic kidney disease. Kidney
Int 67:2295–2304
35. Wang AY, Woo J, Lam CW, Wang M, Chan IH, Gao P,
Lui SF, Li PK, Sanderson JE (2005) Associations of serum
fetuin-A with malnutrition, inflammation, atherosclerosis
and valvular calcification syndrome and outcome in peri-
toneal dialysis patients. Nephrol DialTransplant 20:1676–
1685
36. Cozzolino M, Brancaccio D, Gallieni M, Slatopolsky E
(2005) Pathogenesis of vascular calcification in chronic
kidney disease. Kidney Int 68:429–436
37. Goldsmith DJ, Covic A, Sambrook PA, Ackrill P (1997)
Vascular calcification in long-term hemodialysis patients
in a single unit: a retrospective analysis. Nephron 77:37–43
38. Reynolds JL, Joannides AJ, Skepper JN, Mc-Nair R,
Schurgers LJ, Proudfoot D, Jahnen-Dechent W, Weissberg
PL, Shanahan CM (2004) Human vascular smooth muscle
cells undergo vesicle-mediated calcification in response to
changes in extracellular calcium and phosphate concen-
trations: a potential mechanism for accelerated vascular
calcification in ESRD. J Am Soc Nephrol 15:2857–2867
750 Int Urol Nephrol (2010) 42:741–752
123

39. Tintut Y, Patel J, Territo M, Saini T, Parhami F, Demer LL
(2002) Monocyte/macrophage regulation of vascular cal-
cification in vitro. Circulation 105:650–655
40. Tintut Y, Patel J, Parhami F, Demer LL (2000) Tumor
necrosis factor- alpha promotes in vitro calcification of
vascular cells via the cAMP pathway. Circulation 102:
2636–2642
41. Wang AY, Woo J, Wang M, Sea MM, Ip R, Li PK, Lui SF,
Sanderson JE (2001) Association of inflammation and
malnutrition with cardiac valve calcification in continuous
ambulatory peritoneal dialysis patients. J Am Soc Nephrol
12:1927–1936
42. Haydar AA, Hujairi NM, Covic AA, Pereira D, Rubens M,
Goldsmith DJ (2004) Coronary artery calcification is
related to coronary atherosclerosis in chronic renal disease
patients: a study comparing EBCT-generated coronary
artery calcium scores and coronary angiography. Nephrol
Dial Transplant 19:2307–2312
43. Kullo IJ, Bielak LF, Turner ST, Sheedy PF 2nd, Peyser PA
(2006) Aortic pulse wave velocity is associated with the
presence and quantity of coronary artery calcium. A
communitybased study. Hypertension 47:174–179
44. Guerin AP, London GM, Marchais SJ, Metivier F (2000)
Arterialstiffening and vascular calcifications in end-stage
renal disease. Nephrol Dial Transplant 15:1014–1021
45. London GM, Blacher J, Pannier B, Guerin AP, Marchais
SJ, Safar ME (2001) Impact of aortic stiffness attenuation
on survival of patients in endstage renal failure. Circulation
103:987–992
46. Blacher J, Guerin AP, Pannier B, Marchais SJ, London GM
(2001) Arterial calcifications, arterial stiffness, and car-
diovascular risk in end-stage renal disease. Hypertension
38:938–942
47. Fang W, Yang X, Bargman JM, Oreopoulos DG (2009)
Association between pulse pressure and mortality in
patients undergoing peritoneal dialysis. Perit Dial Int
29(2):163–170
48. Ogawa T, Shimada M, Ishida H, Matsuda N, Fujiu A,
Ando Y, Nitta K (2009) Relation of stiffness parameter
beta to carotid arteriosclerosis and silent cerebral infarction
in patients on chronic hemodialysis. Int Urol Nephrol
41(3):739–745
49. Haydar AA, Covic A, Colhoun H, Rubens M, Goldsmith
DJ (2004) Coronary artery calcification and aortic pulse
wave velocity in chronic kidney disease patients. Kidney
Int 65:1790–1794
50. London GM, Marchais SJ, Guerin AP, Boutouyrie P,
Metivier F, de Vernejoul MC (2008) Association of bone
activity, calcium load, aortic stiffness, and calcifications in
ESRD. J Am Soc Nephrol 19:1827–1835
51. Bossola M, Muscaritoli M, Tazza L, Giungi S, Tortorelli
A, Rossi Fanelli F, Luciani G (2005) Malnutrition in he-
modialysis patients: what therapy? Am J Kidney Dis
46:371–386
52. Gu Yue, Cheng Li-Tao, Chen Hui-Min, Sun Xiao-Yan,
Tang Li-Jun, Guo Li-Juan, Axelsson Jonas, Wang Tao
(2008) Strong association between nutritional markers and
arterial stiffness in continuous ambulatory peritoneal
dialysis patients. Blood Purif 26:340–346
53. Schafer C, Heiss A, Schwarz A et al (2003) The serum
protein alpha 2-Heremans-Schmid glycoprotein/fetuin-A is
a systemically acting inhibitor of ectopic calcification. J
Clin Invest 112:357–366
54. Jahnen-Dechent W, Schinke T, Trindl A, Muller-Esterl W,
Sablitzky F, Kaiser S, Blessing M (1997) Cloning and
targeted deletion of the mouse fetuin gene. J Biol Chem
272:31496–31503
55. Moe SM, Chen NX (2005) Inflammation and vascular
calcification. Blood Purif 23:64–71
56. Hermans MM, Brandenburg V, Ketteler M, Kooman JP,
van der Sande FM, Gladziwa U, Rensma PL, Bartelet K,
Konings CJ, Hoeks AP, Floege J, Leunissen KM (2006)
Study on the relationship of serum fetuin-A concentration
with aortic stiffness in patients on dialysis. Nephrol Dial
Transplant 21:1293–1299
57. Sigrist MhairiK, Taal MaartenW, Bungay Peter, Christo-
pher W (2007) McIntyre progressive vascular calcification
over 2 years ıs associated with arterial stiffening and
ıncreased mortality in patients with stages 4 and 5 chronic
kidney disease. Clin J Am Soc Nephrol 2:1241–1248
58. Chesterton LJ, Sigrist MK, Bennett T, Taal MW, McIntyre
CW (2005) Reduced baroreflex sensitivity is associated
with increased vascular calcification and arterial stiffness.
Nephrol Dial Transplant 20:1140–1147
59. Hermans MM, Vermeer C, Kooman JP, Brandenburg V,
Ketteler M, Gladziwa U, Rensma PL, Leunissen KM,
Schurgers LJ (2007) Undercarboxylated matrix GLA pro-
tein levels are decreased in dialysis patients and related to
parameters of calcium-phosphate metabolism and aortic
augmentation ındex. Blood Purif 25:395–401
60. Wilkinson IB, Franklin SS, Cockcroft JR (2004) Nitric
oxide and the regulation of large artery stiffness: from
physiology to pharmacology. Hypertension 44:112–116
61. Kielstein JT, Boger RH, Bode-Boger SM, Schaffer J,
Barbey M, Koch KM, Frolich JC (1999) Asymmetric
dimethylarginine plasma concentrations differ in patients
with endstage renal disease: Relationship to treatment
method and atherosclerotic disease. J Am Soc Nephrol
10:594–600
62. Mardare NG, Goldsmith DJ, Gusbeth-Tatomir P, Covic A
(2005) Intradialytic changes in reflective properties of the
arterial system during a single hemodialysis session. He-
modial Int 9:376–382
63. Wikstrom IngaSoveriLarsLindBjorn, Zilmer Mihkel, Zil-
mer Kersti, Fellstrom Bengt (2007) Improvement in central
arterial pressure waveform during hemodialysis ıs related
to a reduction in asymmetric dimethylarginine (ADMA)
levels. Nephron Clin Pract 106:c180–c186
64. Blacher J, Demuth K, Guerin AP, Safar ME, Moatti N,
London GM (1998) Influence of biochemical alterations on
arterial stiffness in patients with end-stage renal disease.
Arterioscler Thromb Vasc Biol 18:535–541
65. van Guldener C, Lambert J, ter Wee PM, Donker AJ,
Stehouwer CD (2000) Carotid artery stiffness in patients
with end-stage renal disease: no effect of long-term
homocysteine-lowering therapy. Clin Nephrol 53:33–41
66. Tsai JC, Kuo HT, Chiu YW, Hwang SJ, Chuang HY,
Chang JM, Chen HC, Lai YH (2005) Correlation of plasma
homocysteine level with arterial stiffness and pulse pres-
sure in hemodialysis patients. Atherosclerosis 182:121–127
67. London GM, Guerin AP, Verbeke FH, Pannier B, Bou-
touyrie P, Marchais SJ, Metivier F (2007) Mineral
Int Urol Nephrol (2010) 42:741–752 751
123

metabolism and arterial functions in end-stage renal dis-
ease: potential role of 25-hydroxyvitamin D deficiency. J
Am Soc Nephrol 18:369–373
68. Raggi P, Bellasi A, Ferramosca E, Block GA, Muntner P
(2007) Pulse wave velocity is inversely related to vertebral
bone density in hemodialysis patients. Hypertension
49:1278–1284
69. Toussaint ND, Lau KK, Strauss BJ, Polkinghorne KR, Kerr
PG (2008) Associations between vascular calcification,
arterial stiffness and bonemineral density in chronic kidney
disease. Nephrol Dial Transplant 23(2):586–593
70. Shimada T, Hasegawa H, Yamazaki Y, Muto T, Hino R,
Takeuchi Y, Fujita T, Nakahara K, Fukumoto S, Ya-
mashita T (2004) FGF-23 is a potent regulator of vitamin D
metabolism and phosphate homeostasis. J Bone Miner Res
19:429–435
71. Shimada T, Mizutani S, Muto T, Yoneya T, Hino R,
Takeda S, Takeuchi Y, Fujita T, Fukumoto S, Yamashita T
(2001) Cloning and characterization of FGF23 as a caus-
ative factor of tumor-induced osteomalacia. Proc Natl
Acad Sci USA 98:6500–6505
72. Larsson T, Nisbeth U, Ljunggren O, Juppner H, Jonsson
KB (2003) Circulating concentration of FGF-23 increases
as renal function declines in patients with chronic kidney
disease, but does not change in response to variation in
phosphate intake in healthy volunteers. Kidney Int 64(6):
2272–2279
73. Gutierrez OM, Mannstadt M, Isakova T, Rauh-Hain JA,
Tamez H, Shah A, Smith K, Lee H, Thadhani R, Juppner
H, Wolf M (2008) Fibroblast growth factor 23 and mor-
tality among patients undergoing hemodialysis. N Engl J
Med 359:584–592
74. Mirza MA, Larsson A, Lind L, Larsson TE (2009) Circu-
lating fibroblast growth factor-23 is associated with vas-
cular dysfunction in the community. Atherosclerosis 205:
385–390
75. Tzanakis IP, Oreopoulos DG (2009) Beneficial effects of
magnesium in chronic renal failure: a foe no longer. Int
Urol Nephrol 41(2):363–371
76. Turgut F, Kanbay M, Metin MR, Uz E, Akcay A, Covic A
(2008) Magnesium supplementation helps to improve
carotid intima media thickness in patients on hemodialysis.
Int Urol Nephrol 40(4):1075–1082
752 Int Urol Nephrol (2010) 42:741–752
123
Copyright © 2022 FDOKUMEN