A novel device for measuring arterial stiffness using finger-toe pulse wave velocity: Validation...
8
Please cite this article in press as: Alivon M, et al. A novel device for measuring arterial stiffness using finger-toe pulse wave velocity: Validation study of the pOpmètre ® . Arch Cardiovasc Dis (2015), http://dx.doi.org/10.1016/j.acvd.2014.12.003 ARTICLE IN PRESS +Model ACVD-793; No. of Pages 8 Archives of Cardiovascular Disease (2015) xxx, xxx—xxx Available online at ScienceDirect www.sciencedirect.com CLINICAL RESEARCH A novel device for measuring arterial stiffness using finger-toe pulse wave velocity: Validation study of the pOpmètre ® Un nouvel appareil de mesure de la rigidité artérielle utilisant la vitesse de l’onde de pouls doigt-orteil : étude de validation du pOpmètre ® Maureen Alivon a , Thao Vo-Duc Phuong a , Virginie Vignon a , Erwan Bozec b , Hakim Khettab a , Olivier Hanon c , Marie Briet a , Jean-Michel Halimi d , Magid Hallab e,∗ , Matthieu Plichart c , Kamel Mohammedi f , Michel Marre f , Pierre Boutouyrie a , Stéphane Laurent a a Inserm U970, HEGP, AP—HP, Université Paris-Descartes, Paris, France b CIC-Inserm, Hôpital Vandeouvre-lès-Nancy, Nancy, France c Hôpital Broca, AP—HP, Université Paris-Descartes, Paris, France d Nephrology Department, Franc ¸ois-Rabelais University, Tours, France e Gerontology Department, Nantes University, 1, place Alexis-Ricordeau, 44000 Nantes, France f Service d’Endocrinologie Diabétologie et Nutrition, Hôpital Bichat, AP—HP, Paris, France Received 22 June 2014; received in revised form 24 September 2014; accepted 5 December 2014 KEYWORDS Arterial stiffness; Pulse wave velocity; Finger-to-toe transit time Summary Background. — The finger-toe pathway could be a good alternative for assessing arterial stiffness conveniently. Aim. — To evaluate the accuracy of the pOpmètre ® — a new device that measures finger-toe pulse wave velocity (ft-PWV). Abbreviations: cf-PWV, Carotid-femoral pulse wave velocity; cf-TT, Carotid-to-femoral transit time; ft-TT, finger-to-toe transit time; ft-PWV, Finger-toe pulse wave velocity; ft-TT, Finger-to-toe transit time; PWV, Pulse wave velocity. ∗ Corresponding author. E-mail address: [email protected] (M. Hallab). http://dx.doi.org/10.1016/j.acvd.2014.12.003 1875-2136/© 2015 Elsevier Masson SAS. All rights reserved.
-
Upload
univ-paris5 -
Category
Documents
-
view
0 -
download
0
Transcript of A novel device for measuring arterial stiffness using finger-toe pulse wave velocity: Validation...

ARTICLE IN PRESS+ModelACVD-793; No. of Pages 8
Archives of Cardiovascular Disease (2015) xxx, xxx—xxx
Available online at
ScienceDirectwww.sciencedirect.com
CLINICAL RESEARCH
A novel device for measuring arterialstiffness using finger-toe pulse wavevelocity: Validation study of the pOpmètre®
Un nouvel appareil de mesure de la rigidité artérielle utilisant la vitesse del’onde de pouls doigt-orteil : étude de validation du pOpmètre®
Maureen Alivona, Thao Vo-Duc Phuonga,Virginie Vignona, Erwan Bozecb, Hakim Khettaba,Olivier Hanonc, Marie Brieta, Jean-Michel Halimid,Magid Hallabe,∗, Matthieu Plichartc,Kamel Mohammedi f, Michel Marref, PierreBoutouyriea, Stéphane Laurenta
a Inserm U970, HEGP, AP—HP, Université Paris-Descartes, Paris, Franceb CIC-Inserm, Hôpital Vandeouvre-lès-Nancy, Nancy, Francec Hôpital Broca, AP—HP, Université Paris-Descartes, Paris, Franced Nephrology Department, Francois-Rabelais University, Tours, Francee Gerontology Department, Nantes University, 1, place Alexis-Ricordeau, 44000 Nantes,Francef Service d’Endocrinologie Diabétologie et Nutrition, Hôpital Bichat, AP—HP, Paris, France
Received 22 June 2014; received in revised form 24 September 2014; accepted 5 December 2014
Please cite this article in press as: Alivon M, et al. A novel device for measuring arterial stiffness using finger-toe pulse wavevelocity: Validation study of the pOpmètre®. Arch Cardiovasc Dis (2015), http://dx.doi.org/10.1016/j.acvd.2014.12.003
KEYWORDSArterial stiffness;Pulse wave velocity;Finger-to-toe transittime
SummaryBackground. — The finger-toe pathway could be a good alternative for assessing arterial stiffnessconveniently.Aim. — To evaluate the accuracy of the pOpmètre® — a new device that measures finger-toepulse wave velocity (ft-PWV).
Abbreviations: cf-PWV, Carotid-femoral pulse wave velocity; cf-TT, Carotid-to-femoral transit time; ft-TT, finger-to-toe transit time;ft-PWV, Finger-toe pulse wave velocity; ft-TT, Finger-to-toe transit time; PWV, Pulse wave velocity.
∗ Corresponding author.E-mail address: [email protected] (M. Hallab).
http://dx.doi.org/10.1016/j.acvd.2014.12.0031875-2136/© 2015 Elsevier Masson SAS. All rights reserved.

ARTICLE IN PRESS+ModelACVD-793; No. of Pages 8
2 M. Alivon et al.
Methods. — The pOpmètre has two photodiode sensors, positioned on the finger and the toe.Pulse waves are recorded continuously for 20 seconds, and the difference in pulse wave transittime between toe and finger (ft-TT) is calculated. The travelled distance is estimated usingsubject height. Study 1 compared ft-PWV with carotid-femoral PWV (cf-PWV) obtained by thereference method (SphygmoCor®) in 86 subjects (mean age 53 ± 20 years), including 69 patientswith various pathologies and 17 healthy normotensives. Study 2 compared changes in ft-PWVand cf-PWV during a cold pressor test in 10 healthy subjects. Study 3 assessed repeatability in45 patients.Results. — ft-PWV correlated significantly with cf-PWV (R2 = 0.43; P < 0.0001). A better correla-tion was found in terms of transit time (R2 = 0.61; P < 0.0001). The discrepancy between transittimes was related to age. The cold pressor test induced parallel changes in cf-PWV and ft-PWV,with increased aortic stiffness that was reversible during recovery. Intra-session repeatabilitywas very good, with a coefficient of variation of 4.52%.Conclusion. — The pOpmètre® allows measurement of arterial stiffness in routine clinicalpractice. The greatest advantages of ft-PWV are simplicity, rapidity, feasibility, acceptabilityby patients and correct agreement with the reference technique. Further studies are neededto adjust for bias and to validate the pOpmètre in larger populations.© 2015 Elsevier Masson SAS. All rights reserved.
MOTS CLÉSLa rigidité artérielle ;Vitesse de l’onde depouls ;Temps de transitdoigt-orteil
RésuméContexte. — La voie doigt-orteil pourrait représenter une bonne alternative pour évaluer facile-ment la rigidité artérielle. Le but de cette étude était d’évaluer l’exactitude de pOpmètre(Axelife sas - France) un nouveau dispositif de mesure de la vitesse de l’onde de pouls doigt-orteil (ft-VOP).Méthodes. — pOpmètre® dispose de 2 capteurs photodiodes, placés sur le doigt et sur l’orteil.La différence (DOD) entre le pied de l’onde de l’orteil et celle du doigt est mesurée pendant20 s. La distance de parcours est estimée d’après la taille des patients. L’Étude 1 a comparé laft-VOP à la VOP carotidefémorale (cf-VOP) obtenu par la méthode de référence SphygmoCor®
dans 86 sujets (53 ± 20 ans), dont 69 patients atteints de diverses pathologies et 17 normotendussains. L’Étude 2 a comparé les changements de ft-VOP et cf-VOP lors d’un stress test à froiddans 10 sujets sains. L’Étude 3 a évalué la répétabilité chez 45 patients.Résultats. — ft-VOP était significativement corrélé avec cf-VOP (r2 = 0,43, p < 0,0001). Unemeilleure corrélation a été trouvée en termes de temps de transit (r2 = 0,61, p < 0,0001). Ladifférence entre les temps de transit a été liée à l’âge. Le stress test a induit des changementscomparables pour la cf-VOP et la ft-VOP: une augmentation de la rigidité aortique réversiblelors de la récupération. La répétabilité intra-session a été très bonne avec un coefficient devariation de 4,52 %.Conclusion. — pOpmètre® permet de mesurer la rigidité artérielle dans la pratique clinique. Lesplus grands avantages de ft-VOP sont la facilité, la rapidité, la faisabilité et l’acceptabilité parles patients, avec un agrément correct avec la technique de référence. D’autres études sontnécessaires pour tenir compte des biais afin de valider le pOpmètre dans des populations plusimportantes.© 2015 Elsevier Masson SAS. Tous droits réservés.
B
Aoot[(
siAf
ackground
ortic pulse wave velocity (PWV) is the ‘gold standard’f large artery stiffness. It is one of the best predictors
Please cite this article in press as: Alivon M, et al. A novel devicevelocity: Validation study of the pOpmètre®. Arch Cardiovasc D
f cardiovascular morbidity and mortality, independent ofraditional risk factors, in a large number of populations1—4]; this has been established with carotid-femoral PWVcf-PWV), a direct measurement of aortic stiffness [5,6].
fp(
Although cf-PWV is robust, reproducible and relativelyimple to use, it may be inconvenient for routine use in clin-cs because the measurement requires time and training.dditionally, access to the femoral artery might be difficultor cultural or clinical reasons. Other pathways have there-
for measuring arterial stiffness using finger-toe pulse waveis (2015), http://dx.doi.org/10.1016/j.acvd.2014.12.003
ore been investigated, such as brachial-ankle PWV, whichrovides interesting prognostic data [7,8]. The pOpmètre®
Axelife SAS, Saint Nicolas de Redon, France) is an original

IN+Model
gtMmpui
o
P
TatoottgimtimTmits
ctt
ctsc
S
DowU
iAtpTmf
mhd
ARTICLEACVD-793; No. of Pages 8
Finger-toe PWV to measure arterial stiffness
methodology, taking advantage of easy recording of thepulse wave at the finger and the toe using two photodiodessensors, and deriving finger-toe PWV (ft-PWV). This verysimple technique may be a good alternative for the mea-surement of arterial stiffness evaluation in outpatient andepidemiological settings. The pOpmètre has already beenstudied in the general population: ft-PWV correlates withageing [9] and is linked with carotid plaques in metabolicsyndrome [10]. However, ft-PWV has not yet been validatedagainst reference techniques. Moreover, the extent to whichft-PWV reflects central or peripheral arterial stiffness isunknown.
Accordingly, the aims of the present study were: to com-pare ft-PWV obtained with the pOpmètre with the goldstandard cf-PWV (Study 1); then to determine whether ft-PWV is altered similarly to cf-PWV during acute sympatheticstimulation (Study 2); and, finally, to study the repeatabilityof the pOpmètre PWV measurement (Study 3).
Methods
Study 1
A total of 86 subjects were included: 69 patients and 17healthy normotensives (42 men; mean age 53 ± 20 years;mean systolic blood pressure 130 ± 18 mmHg) from GeorgesPompidou European Hospital and Broca Hospital. Patientswere either well-controlled hypertensive patients (n = 49) orpatients with cognitive impairment (n = 20). In each subject,ft-PWV and cf-PWV were measured in a random order withthe pOpmètre and the SphygmoCor® (AtCor Medical, Sydney,Australia). Measurements were performed according to therecent expert consensus [6].
Additionally, carotid-radial PWV and femoral-post-tibialPWV were obtained in 30 subjects using the SphygmoCor.Blood pressure and heart rate were recorded by an auto-matic device (Colin BP-880; Colin Medical, TX, USA) every3 minutes to calculate the mean blood pressure value.
Study 2
The ‘cold pressor test’ was chosen as a sympathetic stim-ulation [11—13]; it was performed by immersing the righthand into an ice water container (4—5 ◦C) for 1 minute.Ten healthy subjects (4 men; mean age 30 ± 8.5 years;systolic blood pressure 118 ± 14.3 mmHg) were measured,and three sequences of measurements were performed: atbaseline (every minute during 4 minutes), during the test(at 0, 30 and 60 seconds) and during recovery (at 30, 60,90, 120 and 180 seconds). Blood pressures were recordedcontinuously with the oscillometric device during the test.We used the Complior® system (Alam Medical, Vincennes,France) for cf-PWV measurement, to obtain simultaneousmeasurement of cf-PWV and ft-PWV during these dynamicconditions.
Please cite this article in press as: Alivon M, et al. A novel devicevelocity: Validation study of the pOpmètre®. Arch Cardiovasc D
Study 3
The ft-PWV was measured in 45 patients in the nephrologyclinic of Tours Hospital; 38 patients with various patholo-
c
rt
PRESS3
ies and 7 healthy subjects were measured accordingo the guidelines [6] after 10 minutes of supine resting.easurements were done every 5 minutes. If the two firsteasures differed by more than 0.5 m/s, then a third waserformed and the median retained; the two closest meas-res were kept and the third discarded. All patients gavenformed consent.
The study designs were approved by the ethics committeef the Georges Pompidou European Hospital, Paris, France.
ulse wave velocity measurements
he pOpmètre was developed based on similar assumptionss those for brachial-ankle devices [14—16]. The pOpmètreakes advantage of two photodiode sensors, similar to pulseximeters [17] (see Fig. 1). The photodiodes are positionedn the finger and the toe, so that the pulpar arteries are inhe scope of the infrared ray. The pOpmètre measures theransit time between the foot of the pulse waves of the fin-er and the toe, approximating the aortic pulse transit timef the timings in the upper and lower limbs are similar; iteasures continuously for 20 seconds and simultaneously on
he same pulse wave. Two indices are computed: differencen pulse wave transit time between toe and finger (ft-TT; ins); and ft-PWV [in m/s; ft-PWV = k × subject’s height/ft-T], using a chart based on the height of 187 individualseasured in occupational medicine (personal data), where k
s dependent on height. The use of the height chart relates tohe fact that the aortic valves correspond to an anatomicaltable landmark [18].
For cf-PWV measurements, the SphygmoCor recordsarotid and femoral pulses successively and then, related tohe R wave of the electrocardiogram, calculates the transitime.
The Complior measures the arterial pulse wave at thearotid and femoral sites simultaneously. The travelled dis-ance is the direct distance between the carotid and femoralites of measurement multiplied by 0.8, according to theonsensus for the travelled distance measurement [6].
tatistical analysis
ata are expressed as means ± standard deviations. A valuef P < 0.05 was considered significant. The statistical analysisas performed using NCSS 2007 (NCSS LLC, Kaysville, UT,SA).
The correlation between measurement values wasnvestigated using Pearson regression coefficient. The Bland-ltman plot [19] was used to analyse the agreement betweenhe two methods. The relative differences between eachair of measurements were plotted against their mean.he discrepancy between two methods was studied usingultivariable correlation analyses between the relative dif-
erences and other variables.For Study 2, ft-PWV and cf-PWV were analysed by mixed
odels to demonstrate the evolution of blood pressure,eart rate and PWV in the same time frame. We alsoetermined the correlation between changes in ft-PWV and
for measuring arterial stiffness using finger-toe pulse waveis (2015), http://dx.doi.org/10.1016/j.acvd.2014.12.003
hanges in cf-PWV during the test and recovery period.In Study 3, we used the Bland-Altman method for graphic
epresentation, and we calculated the coefficient of varia-ion as the standard deviation divided by the mean.

ARTICLE IN PRESS+ModelACVD-793; No. of Pages 8
4 M. Alivon et al.
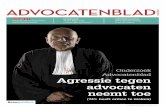
Figure 1. Pulse wave velocity (travelled distance/time of travel). A = k × height; B = k’ × height. The artery qualities in the upper andlower limb are similar (muscular arteries) and have quite similar transit times. The distance B—A is approximately equal to the aortic path.The transit time B—A = �t and reflects the aortic transit time; this measurement reflects the aortic pulse wave velocity. In the top leftc s.
R
S
TtFab
mdd
re
orner: infrared (IR) source and receptor around the pulp arteriole
esults
tudy 1
able 1 shows the descriptive variables for the main popula-ion of studies 1 and 2, and those of the study 3. As shown in
Please cite this article in press as: Alivon M, et al. A novel devicevelocity: Validation study of the pOpmètre®. Arch Cardiovasc D
ig. 2, ft-PWV correlated with cf-PWV (R2 = 0.43; P < 0.0001)nd the plot of the transit time of the two methods showed aetter correlation (R2 = 0.61; P < 0.0001). Table 2 shows the
aaC
Table 1 Descriptive variables for the main population of Stud
Variable Studies 1 and 2(n = 86; 42 men)
Age (years) 53.2 ± 20.0 [22.0—Height (cm) 167 ± 11 [147—19Weight (kg) 66 ± 16 [52—116BMI (kg/m2) 23.1 ± 5.1 [16.8—3SBP (mmHg) 130 ± 18 [98—192MBP (mmHg) 92 ± 13 [65—139DBP (mmHg) 72 ± 12 [52—113PP (mmHg) 67 ± 12 [45—121cf-PWV (m/s) 8.74 ± 2.15 [5.52—cf-TT (ms) 59 ± 14 [32—91]
ft-PWV (m/s) 8.52 ± 3.26 [3.58—ft-TT (ms) 76 ± 27 [23—150Normalized ft-PWV 8.77 ± 2.36 [4.48—
Data are mean ± standard deviation [range]. BMI: body mass index;
femoral transit time; DBP: diastolic blood pressure; ft-PWV: finger-toe
blood pressure; PP: pulse pressure; SBP: systolic blood pressure.
ean values and comparisons of the PWVs, transit times andistances measured by the two methods. Table 3 shows theetailed data for controls and patients.
In Fig. 3, the Bland-Altman plots show individualelative differences (i.e. [SphygmoCor—pOpmètre]/mean,xpressed as a percentage) observed between PWVs,
for measuring arterial stiffness using finger-toe pulse waveis (2015), http://dx.doi.org/10.1016/j.acvd.2014.12.003
nd transit time values obtained by the two methods,ccording to the mean level, calculated as (Sphygmo-or + pOpmètre)/2.
ies 1 and 2, and for the population of Study 3.
Study 3(n = 45; 28 men)
87.0] 49.7 ± 17.5 [19.1—78.9]8] 168 ± 8 [151—187]] 67 ± 12 [40—103]2.5] 23.5 ± 4.1 [17—34.4]] 137 ± 8 [96—174]] 109 ± 68 [43—100]] 79 ± 11 [51—98]] 58 ± 16 [26—98]16.24] —
—22.53] 11.25 ± 3.94 [5.03—28.20]] 66 ± 18 [16—127]14.79] —
cf-PWV: carotid-femoral pulse wave velocity; cf-TT: carotid-to-pulse wave velocity; ft-TT: finger-to-toe transit time; MBP: mean

Please cite this article in press as: Alivon M, et al. A novel device for measuring arterial stiffness using finger-toe pulse wavevelocity: Validation study of the pOpmètre®. Arch Cardiovasc Dis (2015), http://dx.doi.org/10.1016/j.acvd.2014.12.003
ARTICLE IN PRESS+ModelACVD-793; No. of Pages 8
Finger-toe PWV to measure arterial stiffness 5
0.0
4.0
8.0
12.0
16.0
20.0
24.0
0.0 4.0 8.0 12.0 16.0 20.0 24.0cf-PWV (m/s)
ft-P
WV
(m/s
)
0.0
40.0
80.0
120.0
160.0
0.0 40.0 80.0 120.0 160.0cf-TT (ms)
ft-TT
(ms)
Figure 2. Left chart: relationship between carotid-femoral pulse wave velocity (cf-PWV) (m/s) and finger-toe pulse wave velocity (ft-PWV) (m/s) (R2 = 0.43; ft-PWV = —0.16 + 0.79 × cf-PWV). Right chart: relationship between the difference in pulse wave transit time at toeand finger (ft-TT) (pOpmètre) and carotid-to-femoral transit time (cf-TT) (R2 = 0.61 finger-to-toe transit time [ft-TT] = —12 + 1.48 × cf-TT).
Table 2 Pulse wave velocities, transit times and differences between two methods.
Mean ± SD DifferenceSphygmoCor—pOpmètre
Percentagedifference (%)
R2 P
cf-PWV (m/s) 8.7 ± 2.2 0.22 ± 2.46 6.1 ± 24.5 0.43 < 0.0001ft-PWV (m/s) 8.5 ± 3.3cf-TT (ms) 59.4 ± 14.4 —17.5 ± 19.7 —20.3 ± 25.2 0.60 < 0.0001ft-TT (ms) 75.9 ± 27.6SphygmoCor distance (cm) 49.4 ± 5.4 —6.8 ± 4.9 —13.3 ± 10.1 0.21 < 0.0001pOpmètre distance (cm) 56.2 ± 3.6
cf-PWV: carotid- femoral pulse wave velocity; cf-TT: carotid-to-femoral transit time; ft-TT: finger-to-toe transit time; ft-PWV: finger-toepulse wave velocity; SD: standard deviation.
Table 3 Detailed descriptive values for the three populations.
Variable Healthy controls(n = 17; 29% women)
Patients with cognitive impairment(n = 20; 55% women)
Hypertensivepatients
Age (years) 28.6 ± 4.2 74.2 ± 13.1 53.2 ± 15.4Height (cm) 171 ± 12 161 ± 10 168 ± 10Weight (kg) 64 ± 15 67 ± 12 67 ± 17BMI (kg/m2) 21.5 ± 2.6 24.3 ± 6.9 23.2 ± 4.9SBP (mmHg) 115.8 ± 9.5 134.4 ± 17.6 132.4 ± 18.4MBP (mmHg) 81.1 ± 6.8 95.1 ± 10.5 93.9 ± 14.2DBP (mmHg) 64.1 ± 6.7 76.1 ± 9.0 73.1 ± 12.5HR (bpm) 66.2 ± 10.0 70.4 ± 14.7 65.9 ± 11.9cf-PWV (m/s) 6.73 ± 0.54 10.60 ± 2.35 8.68 ± 1.75cf-TT (ms) 73 ± 10 48 ± 11 60 ± 13ft-TT (ms) 102 ± 16 55 ± 24 75 ± 24ft-PWV (m/s) 7 5.76 ± 0.93 11.04 ± 3.54 8.46 ± 2.86cf-PWV—ft-PWV (m/s) 0.98 ± 1.01 —0.44 ± 3.00 0.23 ± 2.53Difference in TT (ms) —29.6 ± 14.7 —7.6 ± 6.8 —17.4 ± 20.3
Data are mean ± standard deviation [range]. BMI: body mass index; bpm: beats per minute; cf-PWV: carotid-femoral pulse wave velocity;cf-TT: carotid-to-femoral transit time; DBP: diastolic blood pressure; ft-PWV: finger- toe pulse wave velocity; ft-TT: finger-to-toe transittime; HR: heart rate; MBP: mean blood pressure; SBP: systolic blood pressure.

ARTICLE IN PRESS+ModelACVD-793; No. of Pages 8
6 M. Alivon et al.
Figure 3. Bland-Altman plot for the analysis of the difference between the two methods. Left chart: comparison of the pulse wavev rotid-femoral pulse wave velocity; Dtf: difference in pulse wave transitt standard deviation; TT-cf: carotid-to-femoral transit time.
bls(tav
S
TpeBec
S
Tvm2
Ftfi
Fi
elocities. Right chart: comparison of the transit times. cf-PWV: caime at toe and finger; ft-PWV: finger-toe pulse wave velocity; SD:
Additionally, the ft-TT correlated with the transit timeetween the femoral artery and the post-tibial artery (lowerimbs artery) (R2 = 0.16; P = 0.03), but not with the tran-it time between the carotid artery and the radial arteryupper limbs artery). The relative difference between theransit time obtained by the two methods correlated withge (R2 = 0.41; P = 0.0001) (Fig. 4), but not with other clinicalariables.
tudy 2
he cold pressor test led to significant increases in bloodressure and PWV followed by decreases during the recov-ry period. The changes in heart rate were not significant.oth cf-PWV and ft-PWV gave similar patterns (Fig. 5). How-ver, the correlation between the change in ft-PWV and thehange in cf-PWV was weak (R2 = 0.07; P = 0.02).
tudy 3
Please cite this article in press as: Alivon M, et al. A novel devicevelocity: Validation study of the pOpmètre®. Arch Cardiovasc D
he repeatability in the intra-session variability study wasery good: three measurements were made with the pOp-ètre in the same session, involving 38 patients (12 women,
6 men; mean age 53.8 ± 15 years) and seven controls (six
wfco
igure 5. Left chart: changes in pulse wave velocity (PWV) at baselinen systolic blood pressure (SBP) at B, CPT and R.
igure 4. Correlation between the relative difference in transitime and age. Dtf: difference in pulse wave transit time at toe andnger; TT-cf: carotid-to-femoral transit time.
for measuring arterial stiffness using finger-toe pulse waveis (2015), http://dx.doi.org/10.1016/j.acvd.2014.12.003
omen, one man; mean age 27 ± 10 years). In this group,t-PWV was 11.25 ± 3.94 m/s (range 5.03—28.2 m/s). Theoefficient of variation was 4.52%, with a mean differencef 0.02 ± 0.50 m/s.
(B), cold pressor test (CPT) and recovery (R). Right chart: changes

ARTICLE IN+ModelACVD-793; No. of Pages 8
Finger-toe PWV to measure arterial stiffness
0.0
3.0
6.0
9.0
12.0
15.0
18.0
0.0 3.0 6.0 9.0 12.0 15.0 18.0
Carotid to femoral PWV (m/s)
Nor
mal
ized
fing
er-to
e P
WV
(m/s
)
Figure 6. Correlation between normalized finger-toe pulse wavevelocity (ft-PWV) obtained with the pOpmètre and carotid-femoralPWV (cf-PWV) obtained with the SphygmoCor. Normalization wasdone on transit time by matching with the Z-score, and by using thedirect carotid-to-femoral distance. R2 = 0.54; coefficient of varia-
tdbceudtafiaPi
oirTuttd
vptcistcftDtuwa
vw
atrcbia
S
Tirrin depth, through precise modelling of the arterial tree, to
tion = 0.18; ft-PWV = 1.79 + 0.79 × cf-PWV.
Sensitivity analysis
Because we could see that the discrepancy between ft-PWVand cf-PWV was mainly caused by inadequacy of distanceestimation, we normalized ft-PWV by using the direct cf-distance measured for the SphygmoCor, and applied acorrection factor to the transit time, calculated by using theZ-score ([value—mean]/standard deviation). By doing this,the regression line of cf-PWV and ft-PWV came close to theidentity line, with no residual bias and mean difference = 0.The correlation coefficient R2 was equal to 0.54 (seeFig. 6).
No side effects were reported during the study, especiallywhile using the pOpmètre.
Discussion
In this present study, we were able to compare ft-PWVmeasured by the pOpmètre with cf-PWV measured byaccepted devices (SphygmoCor, Complior). We found thatthe agreement between the pOpmètre and the referencetechniques was good, especially when dealing with tran-sit time, whereas when transit times were translated intovelocities, the agreement decreased. Agreement for thetransit time with R2 in the range of 0.6 and coefficients ofvariation of 20%, in the presence of perfect distance mea-surements, would lead to the good category according tothe guidelines for validation of non-invasive haemodynamicmeasurement devices [20]. This bias could be corrected byadequate calibration as a function of age, but this new cali-
Please cite this article in press as: Alivon M, et al. A novel devicevelocity: Validation study of the pOpmètre®. Arch Cardiovasc D
bration would need further validation on a separate sample,ideally using magnetic resonance imaging, as this techniquecan truly measure distance [6,21]. This reflects that thetransit time from finger to toe is an acceptable proxy for
eTS
PRESS7
he carotid-to-femoral transit time (cf-TT), whereas theistance estimation initially proposed induces significantias. Distance measurement is problematic even for thearotid-to-femoral pathway [6,21,22]. Here, the distancestimation is complicated by the fact that it is impossible tose the anatomical landmarks of pulse measurements. Whenistance was estimated via the carotid-to-femoral direct dis-ance, obtained from the SphygmoCor measurement, afterdequate calibration of the distance measurement usingxed coefficients from Z-score analysis, the quality of thegreement of the transit time was translated into the ft-WV. This new estimation of distance needs to be validatedn a separate patient sample.
The fact that age is related to transit time bias (withverestimation of ft-TT at younger age compared with cf-TT)ndicates that ft-TT captures some additional informationelated to the ageing process, compared with cf-PWV.his feature has been noted previously by investigatorssing brachial-ankle PWV, which is often more sensitiveo metabolic risk factors than cf-PWV. Whether this par-icularity confers additional information or whether it isetrimental remains to be studied.
It was important to show that cf-PWV and ft-PWV couldary in the same direction during acute changes in bloodressure. We have shown that this is indeed the case,he two techniques providing similar patterns that followhanges in blood pressure. It must be noted that cf-PWVs more sensitive, and its differences versus baseline wereignificant at 0, 30 and 60 seconds during the cold pressorest, whereas ft-PWV was significant only at the end of theold exposure. This could be interpreted in two ways. Eithert-PWV is less robust than cf-PWV or it really is less sensi-ive to the time of measurement of blood pressure effect.espite this lesser reactivity to the pressor test, we shouldake into account that the pOpmètre is a really easy-to-se measurement device, totally investigator independent,hereas measurements with the Complior are demandingnd require two investigators.
The measurement repeatability with the pOpmètre wasery good, especially as repeatability was obtained over aide range of PWVs.
The fact that this measure is operator independentnd highly acceptable to patients helps to limit perturba-ions during the measurement session and facilitates goodepeatability. Further, the absence of manipulation of thearotid bifurcations makes involuntary activation of thearoreflex unlikely, and the absence of groin palpation lim-ts patient stress and subsequent variations in blood pressurend heart rate.
tudy limitations
his study has several limitations. The number of patientsncluded complied with the recommendations [20], but waselatively small (n = 86) and may have led to overoptimisticesults. The physical principles also need to be studied more
for measuring arterial stiffness using finger-toe pulse waveis (2015), http://dx.doi.org/10.1016/j.acvd.2014.12.003
xplain this level of agreement between ft-PWV and cf-PWV.he small number of subjects also limits interpretation oftudy 2.

IN+ModelA
8
C
IfTrmmmnstd
D
Ddt
R
[
[
[
[
[
[
[
[
[
[
[
[
ARTICLECVD-793; No. of Pages 8
onclusions
n conclusion, the results of this study indicate that thet-PWV is a promising means of assessing arterial stiffness.he greatest advantages of ft-PWV are probably simplicity,apidity, feasibility, patient acceptability and correct agree-ent with the reference technique. The good repeatabilityay lead to its use being considered in arterial stiffnessonitoring in long-term follow-up of patients. This tech-
ique is also affected by age-dependent bias in arterialtiffness assessment. Further studies are needed to adjusthe bias concerning peripheral stiffness and age, and to vali-ate the pOpmètre in a larger population.
isclosure of interest
r Magid Hallab is the owner of a patent. The other authorseclare that they have no conflicts of interest concerninghis article.
eferences
[1] Adji A, O’Rourke MF, Namasivayam M. Arterial stiffness, itsassessment, prognostic value, and implications for treatment.Am J Hypertens 2011;24:5—17.
[2] Boumaza S, Arribas SM, Osborne-Pellegrin M, et al. Fenes-trations of the carotid internal elastic lamina and structuraladaptation in stroke-prone spontaneously hypertensive rats.Hypertension 2001;37:1101—7.
[3] Laurent P, Albaladejo P, Blacher J, Rudnichi A, Smulyan H, SafarME. Heart rate and pulse pressure amplification in hypertensivesubjects. Am J Hypertens 2003;16:363—70.
[4] Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction ofcardiovascular events and all-cause mortality with arterialstiffness: a systematic review and meta-analysis. J Am CollCardiol 2010;55:1318—27.
[5] Laurent S, Cockcroft J, Van Bortel L, et al. Expert consen-sus document on arterial stiffness: methodological issues andclinical applications. Eur Heart J 2006;27:2588—605.
[6] Van Bortel LM, Laurent S, Boutouyrie P, et al. Expert consen-sus document on the measurement of aortic stiffness in dailypractice using carotid-femoral pulse wave velocity. J Hypertens2012;30:445—8.
Please cite this article in press as: Alivon M, et al. A novel devicevelocity: Validation study of the pOpmètre®. Arch Cardiovasc D
[7] Fowkes FG, Murray GD, Butcher I, et al. Ankle brachialindex combined with Framingham Risk Score to predict car-diovascular events and mortality: a meta-analysis. JAMA2008;300:197—208.
[
PRESSM. Alivon et al.
[8] Matsuoka O, Otsuka K, Murakami S, et al. Arterial stiffnessindependently predicts cardiovascular events in an elderlycommunity — Longitudinal Investigation for the Longevity andAging in Hokkaido County (LILAC) study. Biomed Pharmacother2005;59(Suppl 1):S40—4.
[9] Hallab M, Pichierri S, Boin JM, Tramblay M, Chevalet P, BerrutG. [A new index to evaluate arterial ageing independently ofarterial blood pressure: pOpscore((R))]. Ann Cardiol Angeiol(Paris) 2012;61:184—7.
10] Hallab M, Collette M, Terrier-Barbeau C, et al. [Regionaland peripheral arterial stiffness measured by pOpmetre(R) inpatients with Cvx risk factor, link with carotid plaques]. AnnCardiol Angeiol (Paris) 2013;62:189—92.
11] Bellinazzi VR, Sposito AC, Schreiber R, et al. Response to coldpressor test predicts long-term changes in pulse wave velocityin men. Am J Hypertens 2014;27:157—61.
12] Ben-Shlomo Y, Spears M, Boustred C, et al. Aortic pulse wavevelocity improves cardiovascular event prediction: an individ-ual participant meta-analysis of prospective observational datafrom 17,635 subjects. J Am Coll Cardiol 2014;63:636—46.
13] Stratton JR, Halter JB, Hallstrom AP, Caldwell JH, RitchieJL. Comparative plasma catecholamine and hemodynamicresponses to handgrip, cold pressor and supine bicycle exercisetesting in normal subjects. J Am Coll Cardiol 1983;2:93—104.
14] Kubo T, Miyata M, Minagoe S, Setoyama S, Maruyama I, Tei C. Asimple oscillometric technique for determining new indices ofarterial distensibility. Hypertens Res 2002;25:351—8.
15] Matsui Y, Eguchi K, Shibasaki S, et al. Impact of arterial stiffnessreduction on urinary albumin excretion during antihyperten-sive treatment: the Japan morning Surge-1 study. J Hypertens2010;28:1752—60.
16] Sugawara J, Hayashi K, Yokoi T, et al. Brachial-ankle pulse wavevelocity: an index of central arterial stiffness? J Hum Hypertens2005;19:401—6.
17] Allen J. Photoplethysmography and its application in clinicalphysiological measurement. Physiol Meas 2007;28:R1—39.
18] Hallab M, Chevalet P, Dahou A, Berrut G. Relationship betweenthe aortic valves and an anatomical landmark using chest CTscan. Artery Research 2012;6:55—7.
19] Bland JM, Altman DG. Statistical methods for assessing agree-ment between two methods of clinical measurement. Lancet1986;1:307—10.
20] Wilkinson IB, McEniery CM, Schillaci G, et al. ARTERY Societyguidelines for validation of non-invasive haemodynamic mea-surement devices: Part 1, arterial pulse wave velocity. ArteryResearch 2010;4:34—40.
21] Sugawara J, Hayashi K, Yokoi T, Tanaka H. Carotid-femoralpulse wave velocity: impact of different arterial path length
for measuring arterial stiffness using finger-toe pulse waveis (2015), http://dx.doi.org/10.1016/j.acvd.2014.12.003
measurements. Artery Res 2010;4:27—31.22] Vermeersch SJ, Rietzschel ER, De Buyzere ML, et al. Distance
measurements for the assessment of carotid to femoral pulsewave velocity. J Hypertens 2009;27:2377—85.