1997 peritoneal dialysis–core indicators study: Dialysis adequacy and nutritional indicators...
12
SPECIAL REPORT 1997 Peritoneal Dialysis–Core Indicators Study: Dialysis Adequacy and Nutritional Indicators Report Michael J. Flanigan, MD, Michael V. Rocco, MD, Diane Frankenfield, DrPH, George Bailie, PhD, Pamela Frederick, MSB, Barbara Prowant, MSN, and Lisa Taylor, RN ● The 1997 Peritoneal Dialysis–Core Indicators Study: Dialysis Adequacy and Nutritional Indicators Report documents the current status of peritoneal dialysis within the United States. A national random sample of adult peritoneal dialysis (PD) patients participating in the United States End Stage Renal Disease (ESRD) program was surveyed. PD subjects were large, with a mean body weight of 76 18.9 kg (mean 1 SD) and a body mass index (BMI) of 27 6.4. The dialysis prescriptions documented achieved a mean weekly Kt/V urea (wKt/V) and weekly creatinine clearance (wCrCl) of 2.45 2.29 and 65.5 35.2 L/wk/1.73m 2 , respectively. The serum albumin of these patients was 3.5 0.48 g/dL, their normalized protein equivalent of nitrogen appearance (nPNA) 1.0 0.63 g/kg/d, and their normalized creatinine appearance rate (nCAR) 14 6.0 mg/kg/d. Serum albumin correlated meagerly but in a positive fashion with BMI, nPNA, and nCAR, and negatively with wCrCl. Among adult US PD patients, serum albumin values appear to correlate poorly with alternative measures of nutritional status and are inversely related to the intensity of renal replacement therapy. The presumptive dietary protein intake (nPNA) and creatinine appear- ance rate (nCAR) derived for PD patients do correlate in a positive fashion with dialysis delivery, at least up to a wCrCl of 60 to 80 L/wk/1.73 m 2 and wKt/V 2.1, but their values suggest that 30% to 50% of PD patients have marginal nutritional status. 1999 by the National Kidney Foundation, Inc. INDEX WORDS: CAPD; CCPD; peritoneal dialysis; 1997 PD-CIS; clearances, adequacy. M ALNUTRITION is reportedly common among dialysis patients, 1-4 and both mal- nutrition and hypoalbuminemia, a presumed sur- rogate for poor nutrition, are powerful predictors of increased morbidity and mortality in the dialy- sis population. 5-8 Observational reports have long noted that uremia results in reduced food con- sumption and protein-calorie malnutrition. 9-13 The National Cooperative Dialysis Study established that ‘‘inadequate dialysis’’is also associated with reduced dietary protein intake and increased pa- tient morbidity. 14,15 Subsequent reports have pro- posed that ‘‘inadequate dialysis,’’ ‘‘malnutri- tion,’’ and anemia are the major modifiable risk factors influencing the morbidity and mortality risks of dialysis patients. 16-18 Peritoneal dialysis (PD) patients are also be- lieved to have a high incidence of malnutrition, 4,5 which may contribute to excessive ‘‘technique failure,’’ 19 morbidity, and mortality. 20-23 Similar to the hemodialysis experience, it has been pos- sible to correlate ‘‘malnutrition’’ indices with both reduced dialysis clearance and a heightened risk of morbidity and mortality. 5-8 Defining a numerical equivalent of ‘‘inadequate dialysis’’ has been more difficult. There are reports, some center specific, correlating poor patient outcome with limited urea and creatinine removal, 2,23-25 and there are even proposed minimal desired values for combined dialysis and renal fractional urea removal (wKt/V) and creatinine clearance (wCrCl), 26 but the proposition that greater ‘‘dialy- sis adequacy’’ improves ‘‘nutritional indices’’ remains controversial. 27-29 The number of US residents using PD contin- ues to increase, and in 1997 the Health Care From the University of Iowa College of Medicine, Iowa City, IA; Wake Forest University School of Medicine, Wake Forest University, Winston-Salem, NC; Quality Measure- ment and Health Assessment Group, Offıce of Clinical Standards & Quality, Health Care Financing Administra- tion, Baltimore, MD; the Department of Pharmacy Practice, State University of New York at Albany, Albany, NY; Univer- sity of Missouri-Columbia School of Medicine, Dialysis Clinics, Columbia, MO; and ESRD Network 12, Kansas City, MO. Received December 4, 1998; accepted in revised form February 16, 1999. The data described in this report are supplied by the Health Care Financing Administration (HCFA) ESRD Core Indicators Study and the United States Renal Data System. Interpretation and reporting of this data is the responsibility of the authors and not an offıcial policy or interpretation of the US Government. Address reprint requests to Michael J. Flanigan, MD, Department of Medicine, T-305-GH, University of Iowa Hospitals and Clinics, 200 Hawkins Dr, Iowa City, IA 52242-4060. E-mail: [email protected] 1999 by the National Kidney Foundation, Inc. 1523-6838/99/3306-0035$3.00/0 American Journal of Kidney Diseases, Vol 33, No 6 (June), 1999: E3 1
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of 1997 peritoneal dialysis–core indicators study: Dialysis adequacy and nutritional indicators...

SPECIAL REPORT
1997 Peritoneal Dialysis–Core Indicators Study: Dialysis Adequacyand Nutritional Indicators Report
Michael J. Flanigan, MD, Michael V. Rocco, MD, Diane Frankenfield, DrPH, George Bailie, PhD,Pamela Frederick, MSB, Barbara Prowant, MSN, and Lisa Taylor, RN
● The 1997 Peritoneal Dialysis–Core Indicators Study: Dialysis Adequacy and Nutritional Indicators Reportdocuments the current status of peritoneal dialysis within the United States. A national random sample of adultperitoneal dialysis (PD) patients participating in the United States End Stage Renal Disease (ESRD) program wassurveyed. PD subjects were large, with a mean body weight of 76 � 18.9 kg (mean � 1 SD) and a body mass index(BMI) of 27 � 6.4. The dialysis prescriptions documented achieved a mean weekly Kt/V urea (wKt/V) and weeklycreatinine clearance (wCrCl) of 2.45 � 2.29 and 65.5 � 35.2 L/wk/1.73m 2, respectively. The serum albumin of thesepatients was 3.5 � 0.48 g/dL, their normalized protein equivalent of nitrogen appearance (nPNA) 1.0 � 0.63 g/kg/d,and their normalized creatinine appearance rate (nCAR) 14 � 6.0 mg/kg/d. Serum albumin correlated meagerly butin a positive fashion with BMI, nPNA, and nCAR, and negatively with wCrCl. Among adult US PD patients, serumalbumin values appear to correlate poorly with alternative measures of nutritional status and are inversely related tothe intensity of renal replacement therapy. The presumptive dietary protein intake (nPNA) and creatinine appear-ance rate (nCAR) derived for PD patients do correlate in a positive fashion with dialysis delivery, at least up to awCrCl of 60 to 80 L/wk/1.73 m 2 and wKt/V � 2.1, but their values suggest that 30% to 50% of PD patients havemarginal nutritional status.
� 1999 by the National Kidney Foundation, Inc.
INDEX WORDS: CAPD; CCPD; peritoneal dialysis; 1997 PD-CIS; clearances, adequacy.
MALNUTRITION is reportedly commonamong dialysis patients,1-4 and both mal-
nutrition and hypoalbuminemia, a presumed sur-rogate for poor nutrition, are powerful predictorsof increased morbidity and mortality in the dialy-sis population.5-8 Observational reports have longnoted that uremia results in reduced food con-sumption and protein-calorie malnutrition.9-13TheNational Cooperative Dialysis Study establishedthat ‘‘inadequate dialysis’’ is also associated withreduced dietary protein intake and increased pa-tient morbidity.14,15Subsequent reports have pro-posed that ‘‘inadequate dialysis,’’ ‘‘malnutri-tion,’’ and anemia are the major modifiable riskfactors influencing the morbidity and mortalityrisks of dialysis patients.16-18
Peritoneal dialysis (PD) patients are also be-lieved to have a high incidence of malnutrition,4,5
which may contribute to excessive ‘‘techniquefailure,’’19 morbidity, and mortality.20-23 Similarto the hemodialysis experience, it has been pos-sible to correlate ‘‘malnutrition’’ indices withboth reduced dialysis clearance and a heightenedrisk of morbidity and mortality.5-8 Defining anumerical equivalent of ‘‘inadequate dialysis’’has been more difficult. There are reports, somecenter specific, correlating poor patient outcomewith limited urea and creatinine removal,2,23-25
and there are even proposed minimal desired
values for combined dialysis and renal fractionalurea removal (wKt/V) and creatinine clearance(wCrCl),26but the proposition that greater ‘‘dialy-sis adequacy’’ improves ‘‘nutritional indices’’remains controversial.27-29
The number of US residents using PD contin-ues to increase, and in 1997 the Health Care
From the University of Iowa College of Medicine, IowaCity, IA; Wake Forest University School of Medicine, WakeForest University, Winston-Salem, NC; Quality Measure-ment and Health Assessment Group, Offıce of ClinicalStandards & Quality, Health Care Financing Administra-tion, Baltimore, MD; the Department of Pharmacy Practice,State University of New York at Albany, Albany, NY; Univer-sity of Missouri-Columbia School of Medicine, DialysisClinics, Columbia, MO; and ESRD Network 12, KansasCity, MO.
Received December 4, 1998; accepted in revised formFebruary 16, 1999.
The data described in this report are supplied by theHealth Care Financing Administration (HCFA) ESRD CoreIndicators Study and the United States Renal Data System.Interpretation and reporting of this data is the responsibilityof the authors and not an offıcial policy or interpretation ofthe US Government.
Address reprint requests to Michael J. Flanigan, MD,Department of Medicine, T-305-GH, University of IowaHospitals and Clinics, 200 Hawkins Dr, Iowa City, IA52242-4060. E-mail: [email protected]
� 1999 by the National Kidney Foundation, Inc.1523-6838/99/3306-0035$3.00/0
American Journal of Kidney Diseases, Vol 33, No 6 (June), 1999: E3 1

Financing Administration (HCFA) Facility Sur-vey indicated that 30,673 Medicare recipients(16% of the US dialysis population) used PD tomanage their end-stage renal disease.30 The 1997Peritoneal Dialysis–Core Indicators Study (1997PD-CIS) is a cross-sectional prevalence surveydepicting the status of PD within the UnitedStates. The current analysis is undertaken tobetter define the status of these patients relativeto their ‘‘dialysis adequacy’’ and ‘‘nutritionalstatus.’’
METHODS
The data contained in this report are available from theQuality Measurement and Health Assessment Group, Officeof Clinical Standards and Quality, Health Care FinancingAdministration (HCFA), US Department of Health and Hu-man Services, 7500 Security Blvd, Baltimore, MD, and areidentified as the 1997 Peritoneal Dialysis–Core IndicatorsStudy (1997 PD-CIS). In February 1997, HCFA’s RenalBeneficiary Utilization System identified a national randomsample of 1,375 adult PD patients (�5% of the adult USperitoneal dialysis population) age 18 years or older onSeptember 30, 1996, and alive on December 31, 1996. InJuly 1997, a two-page questionnaire was distributed to thedialysis facilities providing care to these subjects. Facilitystaff abstracted clinical information from the patient’s medi-cal record for each subject receiving peritoneal dialysisduring the months of November through December 1996,January through February 1997, and March through April1997. Completed questionnaires were forwarded to regionalESRD Network Offices for data verification and electronicsubmission to the Office of Clinical Standards and Quality.
The data collected included information about patientdemographics, dialysis prescription, dialysis dose, residualrenal function, anemia management, albumin, and bloodpressure control. The data were imported into a spreadsheetprogram. Body mass index (BMI) in kg/m2, total renal anddialysis weekly fractional urea clearance (wKt/V), totalweekly renal glomerular filtration rate, dialysate creatinineclearance (wCrCl) in L/wk/1.73m2, protein equivalent ofnitrogen appearance (nPNA) in mg/kg/d, creatinine appear-ance rate (nCAR) in mg/kg/d, and percent lean body mass(LBM) as a percent of actual body weight were calculated instandard fashion31,32and normalized to standard body weightand surface area, using the Watson total body water andGehan body surface area calculations.33 Statistical analyses,including descriptive statistics, two-tailedt-tests, linear re-gression and correlation, and chi-square analysis, were con-ducted using the computer software package Microsoft Ex-cel v 5.1 (Microsoft Corp, Redmond, WA) for the Macintosh(Apple Computer, Cupertino, CA), and multivariant compari-sons used the SPSS software package Sigma Stat v 1.0(SPSS Inc, Chicago, IL). Comparative results were consid-ered significant if theP value (Bonferroni’s correction usedfor multiple t-test comparisons) was below 0.05.
RESULTS
Completed forms were received for 1,219 sub-jects (89% of the sample), 57% of whom used
continuous ambulatory peritoneal dialysis(CAPD) and 39% automated peritoneal dialysis(APD) in the forms of chronic cycling peritonealdialysis (CCPD) and PD-Plus therapy. The re-maining 4% of patients used intermittent perito-neal dialysis, tidal peritoneal dialysis, or otherhybrid dialysis formulae, and these patients arenot included in subsequent analyses. There werefew differences between the patients performingCAPD and those using APD. Table 1 displayssome of the demographic and dialysis character-istics of these groups and contrasts them with acontemporary group of adult hemodialysis pa-tients, the 1997 Hemodialysis–Core IndicatorsStudy cohort. The APD and CAPD groups differin the number of dialysis exchanges per day, thequantity of dialysis fluid used daily, and thelikelihood of having African American ethnicity,but not in residual renal function or total deliv-ered dialysis dose. In comparison with hemodi-alysis (HD) patients; PD patients are younger,heavier, more likely to be white and to have aprimary diagnosis of glomerulonephritis, and lesslikely to have a primary diagnosis of hyperten-sive renal failure. HD patients have more dialysisexperience than PD patients, are more likely tomeet the National Kidney Foundation–DialysisOutcomes Quality Initiative (DOQI) ClinicalPractice Guidelines for Dialysis Adequacy, andare more likely to have a serum albumin exceed-ing 3.5 g/dL by bromcresol green than are PDpatients.34,35
APD and CAPD subjects vary primarily indialysis prescription and not in delivered dialysisefficiency or demographics; thus, this analysispresents the dialysis outcomes for the combinedgroup of all CAPD and APD peritoneal dialysis(PD) patients (Fig 1). The mean patient age is54.5� 14.8 years, with a range of 18 to 90 years.The mean weight of PD patients is 76.1� 18.9kg, and men are heavier than women (81.2 kgv70.6 kg, respectively). If a BMI greater than 28 isused to define obesity, then 36% of PD patientsare obese, and the likelihood of a BMI greaterthan 28 is higher among female PD subjects(Fig 2).
The serum albumin of PD patients is lowerthan that of their hemodialysis counterparts, and,as noted in Fig 3, more than 50% of PD patientshave an average serum albumin below 3.5 g/dLby bromcresol purple or 3.2 g/dL by bromcresol
2 FLANIGAN ET AL

green. Table 2 notes that the mean 6-monthserum albumin levels of PD patients correlatepositively with the nPNA, the nCAR, and energyintake represented as the BMI, but inversely withthe results of the 4-hour peritoneal equilibrationtest for creatinine and dialysis intensity, ex-pressed as either the total wCrCl or the dialysis-only component of weekly creatinine clearance(wdCrCl). Although these associations are statis-tically significant, their correlation coefficientsare low enough (r � 0.2) to suggest that they arelargely devoid of clinical consequence. Whenmultivariant analyses relate patient age, durationof dialysis experience, BMI, nPNA, nCAR, PET
test, wKt/V, and wdCrCl to serum albumin, onlywdCrCl and nCAR are important predictors ofthe serum albumin value (P � 0.0001).
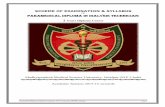
Independent calculation of wKt/V and wCrClwas possible for 867 (72%) and 844 (70%) ofreporting subjects, respectively. Figure 1 showsthat the amount of dialysis delivered to PDsubjects, or dialysis adequacy, varies substan-tially. Although the mean delivered wKt/V was2.54, the median value is only 2.11, and 41% ofPD patients have a wKt/V below 2.0. In theabsence of residual kidney function, only 35% ofPD patients would achieve a wKt/V of 2.0 orgreater using their current prescriptions. Simi-
Table 1. Results of 1997 Core Indicators Surveys
CAPD APD All PD HD-CIS
Number 695 476 1,219 6,858Male/Female 342/353 257/219 626/593 3,591/3,266
(%M) (49) (54) (51) (52)Age (y)* 54.5 � 14.5 54.5 � 15.5 54.5 � 14.8 59.9 � 15.3
18-44 (%) 27 28 27 1845-64 (%) 47 42 45 3765� (%) 26 30 28 45
Primary diagnosis*Diabetes (%) 35 34 34 38Hypertension (%) 22 22 22 27Glomerulonephritis (%) 19 16 18 14Other/unknown (%) 24 27 26 21
Ethnicity*†Black (%) 27 21 25 37Caucasian (%) 63 69 66 51Other (%) 10 10 9 12
ESRD experience (y) 2.8 � 3.5 2.6 � 3.2 2.7 � 3.4 3.5 � 3.8Weight (kg)* 76.4 � 18.7 75.5 � 19.1 76.1 � 18.9 71.6 � 18.8PET—4 h (D/P creatinine) 0.69 � 0.31 0.67 � 0.14 0.68 � 0.26Exchanges/d† 4.2 � 0.5 5.6 � 1.6 4.6 � 1.6Dialysate volume (L/d)† 10.5 � 2.6 13.3 � 3.1 11.6 � 3.1wCrCl 65 � 33.7 67 � 37.4 66 � 35.2wKt/V 2.4 � 1.9 2.5 � 2.8 2.5 � 2.3
wCrCl � DOQI‡ (%) 47 46 47wKt/V � DOQI‡ (%) 55 57 56 74
nPNA 1.0 � 0.62 1.0 � 0.64 1.0 � 0.63nCAR 14.2 � 5.80 14.7 � 6.26 14.4 � 5.99Albumin (BCG) G/dL* 3.5 � 0.5 3.6 � 0.5 3.5 � 0.48 3.8 � 0.41Exchange vol �2 L (%) 38 42�4 Exchanges/d CAPD (%) or 23�1 AM Exchange/d APD (%) 37
NOTE. APD and CAPD patients are similar in patient characteristics and dialysis results. Relatively fewer blacks use APDthan CAPD, and still fewer use peritoneal dialysis than hemodialysis. Hemodialysis patients weight less, are older, are morelikely to have a diagnosis of hypertensive nephrosclerosis, and are more likely to achieve DOQI adequacy goals than are PDpatients. APD patients use more dialysis fluid than CAPD patients, but similar proportions of APD and CAPD patients achieveDOQI-recommended wKt/V and wCrCl indices.
*P � .05 PD v HD.†P � .05 APD v CAPD.‡Percentage of reporting subjects.
1997 PD-CIS 3
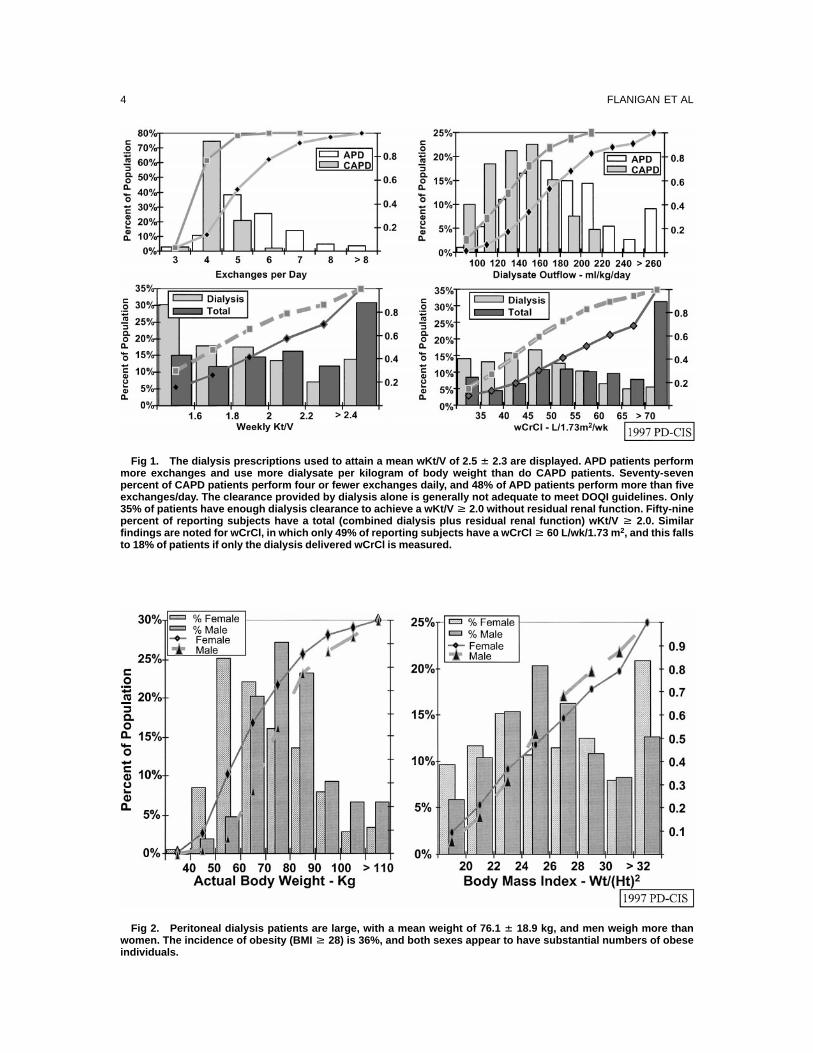
Fig 1. The dialysis prescriptions used to attain a mean wKt/V of 2.5 � 2.3 are displayed. APD patients performmore exchanges and use more dialysate per kilogram of body weight than do CAPD patients. Seventy-sevenpercent of CAPD patients perform four or fewer exchanges daily, and 48% of APD patients perform more than fiveexchanges/day. The clearance provided by dialysis alone is generally not adequate to meet DOQI guidelines. Only35% of patients have enough dialysis clearance to achieve a wKt/V H 2.0 without residual renal function. Fifty-ninepercent of reporting subjects have a total (combined dialysis plus residual renal function) wKt/V H 2.0. Similarfindings are noted for wCrCl, in which only 49% of reporting subjects have a wCrCl H 60 L/wk/1.73 m 2, and this fallsto 18% of patients if only the dialysis delivered wCrCl is measured.
Fig 2. Peritoneal dialysis patients are large, with a mean weight of 76.1 � 18.9 kg, and men weigh more thanwomen. The incidence of obesity (BMI H 28) is 36%, and both sexes appear to have substantial numbers of obeseindividuals.
4 FLANIGAN ET AL

larly, the mean delivered wCrCl is 65.5 L/wk/1.73 m2, but when the dialysis exclusive contribu-tion is measured, the mean wdCrCl falls to 49.3L/wk/1.73 m2. The median values for total anddialysis-only wCrCl are 59.0 and 46.9 L/wk/1.73m2, respectively.
Twenty-four–hour dialysis and urine collec-tions were used to determine daily creatinine andprotein equivalent nitrogen appearance. The mean
nPNA or protein catabolic rate was 1.0� 0.63g/kg/d, and the mean nCAR� 14 � 6.0 mg/kg/d. When the protein equivalent of nitrogenappearance is indexed to the patient’s actualbody weight (PNA-N), estimated dietary proteinintake drops to 0.87� 0.54 g/kg/d, and fewerthan 10% of patients have a PNA-N exceeding1.2 g/kg/d (solid bars in Fig 4). Figures 4 and 5illustrate that the distribution of nPNA differsfrom the more normal distribution of nCAR.Although the mean and median values for nPNAdiffer at 1.0 and 0.9 g/kg/d, respectively, themean and median values for nCAR are equal toone another.
Creatinine appearance can be used to deter-mine a ‘‘lean body mass index’’ or LBM as apercentage of body weight. This value is math-ematically linked to nCAR (nCAR in mg/kg/d � 30.69� LBM; r2 � 0.86). Whereas nPNAand serum albumin vary between male and fe-male patients, nCAR is not significantly differentbetween men and women. Serum albumin, nCAR,and lean body mass as a percent of body weight(LBM) all decline with age (Table 3). Figure 6presents the distribution of LBM for the 844patients evaluated, and Fig 7 shows the relation-ship between LBM and nPNA:
LBM � 20 � ln (nPNA) � 49; r2 � 0.18
The relationship is not linear over the rangeevaluated, and the slope of regression in thelower range (LBM� 0.15� 0.37[nPNA],r2 � 0.18 for nPNA 0.2 to 0.8 mg/kg/d) is 5times greater than when nPNA exceeds 1.0 mg/kg/d (LBM � 0.46� 0.07[nPNA], r2 � 0.01).nCAR is mathematically linked to wCrCl, and
Fig 3. The mean serum al-bumin values measured bybromcresol green (BCG) andbromcresol purple (BCP)assay are depicted. Thesevalues represent the meanserum albumin for each pa-tient over the 6-month studyperiod. The mean serum al-bumin values of 3.5 g/dL and3.2 g/dL for the BCG and BCPmethodologies, respectively,are below those of hemodi-alysis patients.
Table 2. The Relationship of Serum Albumin toDialysis Adequacy and Protein Metabolism Indices
LinearRegression
Results Significance Correlation
Alb � 3.40 �
0.121 � nPNA P � 0.032 r2 � 0.0043Alb � 3.37 �
0.010 � nCAR P � 0.001 r2 � 0.0159Alb � 3.23 �
0.010 � (BMI) P � 0.001 r2 � 0.0149Alb � 3.78
0.416 � PET P � 0.014 r2 � 0.008Alb � 3.70
0.002 � wCrCl P � 0.050 r2 � 0.005Alb � 3.86
0.006 � wdCrCl P � 0.001 r2 � 0.03
NOTE. The mean serum albumin of each patient wascorrelated with that person’s nutritional and dialysis indi-ces. The large number of patients examined permits theserelationships to reach statistical significance; however, thecorrelation coefficients are low. This suggests that effortsdirected at changing the dialysis indices, nPNA, energyintake, and nCAR are unlikely to have a major influence onthe population serum albumin over the range of valuesinvestigated (albumin, 2.0 to 4.5 g/dL). The parametermost closely associated with serum albumin is wdCrCl, ameasure combining membrane permeability with theamount of dialysate used.
1997 PD-CIS 5

thus nCAR and wCrCl will correlate with oneanother. The same would be true for LBM andwCrCl. There is, however, no direct mathemati-cal coupling between wKt/V and nCAR or LBM.Evaluation of the LBM–dialysis dose associa-tion, represented as wKt/V, also appears to benonlinear:
LBM � 13.1� ln (wKt/V) � 36.6; r2 � 0.065
and increases in wKt/V are associated with mean-ingful increases in LBM up to a wKt/V range
of 2.0 to 2.1 (LBM� 0.21� 0.14[wKt/V],r2 � 0.20 for wKt/V � 2.0). Further increases inwKt/V are associated with minimal LBM in-creases (LBM� 0.32� 0.06[wKt/V], r2 � 0.04for wKt/V � 2.1).
In a similar fashion, higher dialysis doses,represented by wCrCl, are associated with in-creases in nPNA (Fig 8), and again the relation-ship is best modeled by nonlinear regressionover the range evaluated. The influence of wCrClseems to be greatest when the delivered dialysis
Fig 4. The protein equiva-lent of nitrogen appearanceapproximates dietary proteinintake under steady-state con-ditions. This value can be nor-malized to actual body weight(PNA-N) or to a standard bodyweight based on the Watsonlean body mass (nPNA).Based on this sample of 855patients, 50% of PD subjectshave a daily protein intake(nPNA) at or below 0.9 g/kg/d.If this is expressed as di-etary protein intake per kilo-gram of actual body weight(PNA-N), then fewer than 50%of PD patients have a PNA-Ngreater than 0.8 g/kg/d.These values are signifi-cantly less than the 1.1 g/kg/drecommended for protein ho-meostasis. 43
Fig 5. Creatinine, the end metabolite of muscle creatine metabolism, generally appears in the urine of healthyyoung adults in a range of 15 to 20 mg/kg/d in women and 20 to 25 mg/kg/d in men. These generation rates arepresumably related to the lean body mass and diet of an individual. Among peritoneal dialysis patients, 30% of 845reporting individuals have a normalized creatinine appearance rate (nCAR) below 12 mg/kg/d, a value associatedwith malnutrition and increased risk of hospitalization, whereas only 20% have an nCAR exceeding 17.5 mg/kg/d, avalue associated with normal nutritional status.
6 FLANIGAN ET AL

dose is below a transition zone of 60 to 80L/wk/1.73 m2:
nPNA � 0.266� ln (wCrCl) 0.168;
· r2 � 0.129
DISCUSSION
General clinical observations substantiate thepremise that peritoneal dialysis alters the uremiccondition. Acutely uremic individuals becomemore alert and vital and show improved appetiteand weight gain after initiation of PD. The quan-tity of renal replacement therapy necessary toachieve and maintain this outcome remains in-completely defined, and estimates of a minimaldesired renal replacement dose vary. The Na-tional Kidney Foundation’s DOQI guidelines26
suggest that PD should provide urea removalequal that attained by an endogenous creatinineclearance of 10 to 15 mL/min. During CAPD,these recommended minimal values are awKt/V � 2.0 and a wCrCl� 60 L/wk/1.73 m2.36
These recommendations increase to a wKt/V�2.1 and wCrCl� 63 L/wk/1.73 m2 when patientsuse continuous APD.37
In 1997, 76% of sampled PD patients had atleast one dialysis adequacy test performed dur-ing the 6-month survey period. This represents asignificant increase from the 48% reporting inci-dence of 1995.38 Among reporting subjects, only47% achieve the DOQI recommended wCrCl of60 L/wk/1.73 m2 or greater. PD patients tend tobe heavier than hemodialysis patients and oftendepend upon residual renal function to achieve
Table 3. Age-Related Changes in Nutritional Indices
Age(y)
nPNA(mg/kg/d)*
nCAR(mg/kg/d)† LBM (%Wt)†
Albumin(g/dL)†
Female Male Female Male Female Male Female Male
20-40 1.17 0.89 16.5 15.8 52 56 3.50 3.6640-60 1.08 0.92 15.1 15.0 47 50 3.46 3.56�60 1.06 0.92 11.8 13.6 39 46 3.29 3.43
NOTE. Serum albumin and nCAR or percent lean body mass (LBM) decrease with age. Additionally, serum albumin,nPNA, and LBM are different between men and women. These differences mimic the directional changes noted innondialysis subjects. Despite relatively normal protein intakes, peritoneal dialysis patients have depressed serum albuminvalues, LBM, and nCAR values. These alterations are not uniform in all age ranges, and are most striking for patients aged 20to 40 years in whom the nCAR and LBM are 20% to 30% below those expected for nondialysis, healthy subjects. The 40- to60-years-old group has mean nCAR and LBM results 10% to 15% below expectations, whereas patients older than age 60years have LBM, and nCAR values equal those of an age-matched nonuremic population.
*P � 0.05 differs with gender.†P � 0.05 differs with age.
Fig 6. The creatinine ap-pearance rates of 844 PD pa-tients are used to derive alean body mass estimate(percentage of actual bodyweight) as per Keshaviah etal.3 Fewer than half of pa-tients have a LBM exceeding50% of body weight.
1997 PD-CIS 7

dialysis efficiency equal to that of hemodialysis.In this series, 30% to 50% of the patients meet-ing DOQI guidelines for wKt/V and wCrCl,respectively, do so only with the assistance ofresidual renal function. Despite substantial num-bers of large patients, fewer than 50% of CAPDpatients deviate from a standard prescription offour 2-L exchanges per day, and only 55% achievea wKt/V exceeding the DOQI expectations. Stillfewer (47%) meet the DOQI wCrCl goal. Previ-ous analyses have suggested that limitations onperitoneal membrane efficiency might make it
difficult to attain a wCrCl of 60 L/wk/1.73 m2 orgreater as endogenous kidney function de-clines.39,40 In this situation, DOQI guidelinessuggest that priority be given to attaining thegoal wKt/V of 2.0 or greater.
Serum albumin is a powerful statistical indica-tor of morbidity and mortality risk in the dialysispopulation.5-8 This association is even more ro-bust when trends are analyzed.41 It has beenpopular to refer to serum albumin as a ‘‘nutri-tional indicator,’’ inferring that the excess morbid-ity and mortality associated with a low serum
Fig 7. Creatinine appearance derived from the wCrCl measurement can be used to determine both nCAR andLBM. Both measures can be used to approximate body composition and the static protein nutritional state of apopulation. LBM appears to increase in proportion to estimated dietary protein intake (nPNA), and this associationis best modeled by a nonlinear relationship. This association would predict that an nPNA below 0.8 g/kg/d will leadto a LBM below 45%, a level previously associated with excess morbidity and evidences of malnutrition bysubjective global assessment. Similarly, LBM falls to less desirable levels as the delivered ‘‘dialysis dose’’ isreduced. The slope of these correlations is 3.5- to 5-fold higher below the transition levels of wKt/V � 2.0 to 2.2 andnPNA � 1.0 to 1.2 g/kg/d than at higher values of nPNA and wKt/V.
Fig 8. The estimated di-etary protein intake (nPNA)falls to less desirable levelsas the delivered ‘‘dialysisdose’’ is reduced (nPNA �0.27*ln(wCrCl) � 0.17; r �0.36) below a wCrCl of 60 to80 L/wk/1.73 m 2. The regres-sion analysis, which mini-mizes systematic error, isnonlinear, suggesting athreshold phenomena, butthe correlation coefficient isnot as high as would be ex-pected if dialysis dose werethe overwhelming determi-nant of protein appetite.
8 FLANIGAN ET AL

albumin are manifestations of malnutrition. Re-cent reports2,28,42 question the validity of thisinterpretation, and this analysis provides furtherimpetus for skepticism. In this report, meanserum albumin values increase only marginallyas BMI, nPNA, nCAR, and LBM increase. Thesecorrelations are so fragile that it seems unlikelythat serum albumin can be used as a clinicalpredictor of nutritional status.
Additionally, serum albumin levels are in-versely correlated with wdCrCl, a composite mea-sure of peritoneal membrane permeability (4-hour creatinine peritoneal equilibration testresults) and dialysate use. The overall situationmimics previous findings amongst HD1 and PDpatients,2,5 and it appears that in cross-sectionalsurveys unmeasured parameters are more influen-tial in determining serum albumin than are di-etary protein intake, body composition, or dialy-sis dose.
Thus, although serum albumin levels are influ-enced by dietary protein intake, they offer neithersensitivity nor specificity as a measure of nutri-tional status in PD patients. Alternatively, nonal-bumin nutritional surrogates do improve withincreasing dialysis delivery. Both nPNAand LBMdecrease as the dialysis dose falls, and this isparticularly notable when the wKt/V is below 2.0or the wCrCl is below 60 L/wk/1.73 m2. Reviewof residual plots suggests that these correlationsare nonlinear and that above a wCrCl of 60 to 80L/wk/1.73 m2 or a wKt/V of 2.1, increasing‘‘dialysis intensity’’ is no longer predictably asso-ciated with major increases in nPNA, nCAR, orLBM.
Urea appearance in dialysate and urine can beused to derive the nPNA, which under steady-state conditions approximates a patient’s dietaryprotein intake. Among chronic renal failure pa-tients not on dialysis, nPNA falls spontaneouslywith advancing renal impairment9,12 and is oftenless than 0.7 g/kg/d. At this level of proteinintake, others have shown that patients developevidences of malnutrition, including reducedLBM, weight loss, low serum transferrin, andlow cholesterol levels.9,10,12Among PD patients,the mean nPNA is 1.0 g/kg/d, but, as Fig 5shows, nPNA is not normally distributed, andonly 25% of PD patients have an nPNA exceed-ing 1.0 g/kg/d. Blumenkrantz et al43 once re-ported that PD patients uniformly attained posi-
tive nitrogen balance when their daily dietscontained more than 1.1 g protein per kilogrambody weight, and Flanigan et al44 have shownthat nitrogen use changes when PD patients havean nPNA below 0.8 to 1.0 g/kg/d.43,44 Usingthese criteria, few PD patients have a dailyprotein intake high enough to assure a positivenitrogen balance, and 34% of PD patients have aprotein intake below the stress range of 0.8 to 1.0g/kg/d. Other surveys have reported positivecorrelations between nPNA, serum albumin, leanbody mass, and dialysis efficiency and haverelated patient health to nPNA and LBM, as wellas albumin and dialysis adequacy.4,22-25,28In thesereports, patients with an nPNA less than 0.9g/kg/d show increased morbidity. Based on thisassessment, 50% of the patients herein reportedare at risk for excessive hospitalization.
Creatinine appearance has been used to deter-mine body composition and the completeness of24-hour urine and dialysate collections.3,45-47Re-cently, the biological variability of creatinineappearance has been assessed in PD populations,and nCAR has been found to be insensitive tosubtle, patient-specific changes in body composi-tion and dialysis performance.48,49Creatinine ap-pearance does, however, correlate with othermeasures of body composition and in epidemio-logic studies of PD patients the nCAR-estimatedLBM compares favorably with body composi-tion estimates by anthropometric measurement,near-infrared analysis, bioimpedence, underwa-ter weighing, dual-energy x-ray absorptiometry(DEXA), and total body potassium.3,4,29,49,50
The 1997 PD-CIS patient cohort is among thelargest reported in the literature, and with a meanbody weight of 76.1� 18.9 kg and BMI of27.1� 6.4 kg/m2, this group exceeds the weightsreported by Canada-United States (CANUSA) orJones et al by 15% to 20%.5,24,29 This patientgroup also has a creatinine appearance rate be-low that reported by the CANUSA group,5 Kesha-viah et al,3 and Jones et al29 but similar to thatnoted by Johansson et al.49 This occurs becausewe have chosen to ignore the ‘‘metabolic degra-dation’’ hypothesis, which adds complexity butlittle else to LBM predictions.49 If this derivationdifference is rectified, the daily creatinine genera-tion or nCAR for the 1997 PD-CIS cohort is14.4 � 5.99 mg/kg/d and is not different fromthose of CANUSA, 15.5 mg/kg/d5; Keshaviah et
1997 PD-CIS 9

al,314.4 mg/kg/d; Jones et al,29 14.8 mg/kg/d;Nolph et al,2 14.5 mg/kg/d; Johansson et al,49
16.3 mg/kg/d; Lo et al,50 14.2 mg/kg/d; andBhatla et al,51 15.2 mg/kg/d.
Normal subjects have creatinine appearancerates exceeding those of uremic individuals.44,48,51
The roles of diet, enteric creatinine degradation,variable muscle metabolism, and day-to-day al-terations in renal function have been postulatedto account for these differences but do not ex-plain why the discrepancy is most prominent inyoung men and women. Among 20- to 40-year-olds, the anticipated nCAR is 20% to 30% abovethat recorded for PD-CIS participants, whereasin 40- to 60-year-olds this discrepancy is reducedto 10% to 15%, and when patients exceed 60years of age, the recorded nCAR equals thatexpected in normals.45 In a comparison of leanbody mass measurement techniques, Johanssonet al49 report that 48 PD patients had an LBMequal to 93% of predicted when LBM was mea-sured by total body potassium counting. In thatreport, creatinine kinetics consistently underesti-mated the LBM determined by potassium count-ing and the mean creatinine-estimated LBM was53% � 11% of total body weight.49 In similarfashion, Churchill and the CANUSAstudy group5
report that the mean LBM of 650 CAPD patientscorresponds to an nCAR of 15.5 mg/kg/d with25th and 75th percentiles of 12.6 mg/kg/d and18.0 mg/kg/d, respectively. McCusker et al24
further analyzed these data and noted that annCAR less than 15.5 mg/kg/d when startingdialysis is associated with excess mortality risk.In total, 20% of the 1997 PD-CIS cohort have annCAR exceeding 17.5 mg/kg/d, a value associ-ated with the reduced morbidity and normalnutritional status by subjective global assess-ment (SGA), and 30% of the 1997 PD-CIScohort have an nCAR below 12.5 mg/kg/d, arange associated with malnutrition by SGA, anda creatinine-derived LBM below 41% of bodyweight, a level associated with an excess risk ofmorbidity and mortality.3,5,29,49
Creatinine appearance has previously beencorrelated in a positive and significant fashionwith increases in nPNA, wKt/V, wCrCl, serumalbumin, and nutritional status by SGA scor-ing.2,3,5,24,29This report confirms the associationsof nCAR with nPNA, wKt/V, and serum albuminand confirms a decrease in nCAR with age.
Gender differences in creatinine appearance areacknowledged, but normalization to a Watsonstandard body size dissipates this distinction.The nCAR of young adult PD patients is farbelow that anticipated, and significant numbersof patients probably have an LBM more than15% below desired levels, but the general depres-sion of nCAR among dialysis patients must beviewed in accord with a mean patient age of 55years. Subjects in this age range have a reducednCAR and LBM because of aging processes, andthe differences between expected and observedindices of body composition are less impressive.
The association between LBM and nPNA ap-pears compelling but may, in part, representgreater creatinine generation as a result of agreater dietary creatine content among ‘‘meateaters’’ or individuals with a high dietary proteinintake and not a true relationship between leanmuscle mass and estimated dietary protein in-take.49 In general, a direct relationship betweendietary creatine content and creatinine genera-tion would be expected to yield a linear relation-ship and not the nonlinear, ‘‘threshold,’’ or ‘‘first-order’’ kinetics shown in Fig 7. The associationsbetween nPNA and LBM and dialysis deliveryare, however, less compelling, and although wehave avoided regressions of nPNA on wKt/V andLBM on wCrCl to avoid direct mathematicalcoupling, it is possible that the relationshipsdetermined represent an indirect coupling be-cause of the ‘‘fixed’’ ratio of peritoneal urea tocreatinine diffusion determined by innate perito-neal membrane characteristics.39 In this case, thenonlinear clearance to mass removal relationshipmight well yield a nonlinear relationship, account-ing for the correlation coefficients ofr � 0.4 andr � 0.3 for nPNA wCrCl and LBM wKt/V,respectively.
CONCLUSION
The data reported here represent a prevalencereport and cannot be used to determine causality.Longitudinal follow-up would be necessary toassociate patient outcome with the variables mea-sured in this report. Similarly, assessing the ef-fects of any intervention that changes one of thereported variables on patient welfare is not pos-sible with this data set. The information reportedhere does, however, describe the status of USperitoneal dialysis patients in 1997. These pa-
10 FLANIGAN ET AL

tients exhibit a mixed picture of nutritional indi-cator variables. They are obese but have a dietaryprotein intake or nPNA that appears marginal.The nPNA generally improves as wCrCl in-creases up to 60 to 80 L/wk/1.73 m2, but fewerthan 50% of patients have dialysis adequacymeasures in this range, and the median nPNA isonly 0.9 g/kg/d. This value falls to 0.8 g/kg/d ifPNA is indexed to actual body weight (PNA-N).Serum albumin values are depressed and below3.5 g/dL in 50% of PD subjects. IncreasingnPNA values are only feebly correlated withhigher serum albumin values, and serum albu-min is inversely related to dialysis delivery. Thisis presumably because increases in wCrCl resultin greater dialysate protein losses. Increases innPNA are correlated with a higher daily creati-nine appearance rate (nCAR) and LBM, butthese values remain below those expected innormals. This suggests that lean body mass isindeed depressed, particularly among young adultPD patients. These reductions may be the resultof depressed dietary protein intake, and nCARappears to approach normal values only whenthe nPNA is 1.0 g/kg/d or greater and the wKt/Vis at least 2.0. Fewer than 45% of PD patientshave a wKt/V high enough to support the desireddietary protein intake goal of 1.0 g/kg/d andmaintain a serum blood urea nitrogen below 60mg/dL. In general, there is opportunity to im-prove dialysis delivery and some aspects of pro-tein nutrition for this patient population, al-though serum albumin may not changeappreciably even with attention to dietary treat-ment and dialysis adequacy.
REFERENCES
1. Qureshi RA, Alvestrand A, Danielsson A, Divino-Filho JC, Gutierrez A, Lindholm B, Bergstrom J: Factorspredicting malnutrition in hemodialysis patients: A crosssectional study. Kidney Int 53:773-782, 1998
2. Nolph KD, Moore HL, Prowant B, Meyer M, Tward-owski ZJ, Khanna R, Ponferrada L, Keshaviah P: Crosssectional assessment of weekly urea and creatinine clear-ances and indices of nutrition in continuous ambulatoryperitoneal dialysis patients. Perit Dial Int 13:178-183, 1993
3. Keshaviah PR, Nolph KD, Moore HL, Prowant B,Emerson PF, Meyer M, Twardowski ZJ, Khanna R, Ponfer-rada L, Collins A: Lean body mass estimation by creatininekinetics. J Am Soc Nephrol 4:1475-1485, 1994
4. Young GA, Kopple JD, Lindholm B, Vonesh EF, DeVecchi A, Scalamogna A, Castelnova C, Oreopoulos DG,Anderson GH, Bergstrom J, DiChiro J, Gentile D, NissensonA, Sakhrani L, Brownjohn AM, Nolph KD, Prowant BF,
Algrim CE, Martis L, Serkes KD: Nutritional assessment ofcontinuous ambulatory peritoneal dialysis patients: An inter-national study. Am J Kidney Dis 17:462-471, 1991
5. Churchill DN, Taylor DW, Keshaviah PR: Adequacyof dialysis and nutrition in continuous peritoneal dialysis:Association with clinical outcomes. J Am Soc Nephrol7:198-207, 1996
6. Blake PG, Flowerdew G, Blake RM, Oreopoulos DG:Serum albumin in patients on continuous ambulatory perito-neal dialysis: Predictors and correlations with outcomes. JAm Soc Nephrol 3:1501-1507, 1993
7. Spiegel DM, Breyer JA: Serum albumin: A predictorof long-term outcome in peritoneal dialysis patients. Am JKidney Dis 23:283-285, 1994
8. Struijk DG, Krediet RT, Koomen GCM, BoeschotenEW, Arisz L: The effect of serum albumin at the start ofcontinuous ambulatory peritoneal dialysis treatment on pa-tient survival. Perit Dial Int 14:121-126, 1994
9. Pollock CA: Protein intake. J Am Soc Nephrol 8:777-783, 1997
10. Kopple JD, Levey AS, Greene T, Chumlea WC,Gassman JJ, Hollinger DL, Maroni BJ, Merrill D, ScherchLK, Schulman G, Wang SR, Zimmer GS: Effect of dietaryprotein restriction on nutritional status in the Modification ofDiet in Renal Disease Study. Kidney Int 52:778-791, 1997
11. Lusvarghi E, Fantuzzi AL, Medici G, Barbi L,D’Amelio A: Natural history of nutrition in chronic renalfailure. Nephrol Dial Transplant 11:75S-84S, 1996 (suppl 9)
12. Ikizler TA, Greene JH, Wingard RL, Parker RA,Hakim RM: Spontaneous dietary protein intake during pro-gression of chronic renal failure. J Am Soc Nephrol 6:1386-1391, 1995
13. Rigalleau V, Combe C, Blanchetier V, Aubertin J,Aparicio M, Gin H: Low protein diet in uremia: Effects onglucose metabolism and energy production rate. Kidney Int51:1222-1227, 1997
14. Parker TF, Laird NM, Lowrie EG: Comparison of thestudy groups in the National Cooperative Dialysis Study anda description of morbidity, mortality, and patient with-drawal. Kidney Int 23:S42-S49, 1983 (suppl 13)
15. Lowrie EG, Laird NM, Parker TF, Sargent JA: Effectof the hemodialysis prescription on patient morbidity: Re-port from the National Cooperative Dialysis Study. N Engl JMed 305:1176-1181, 1981
16. Lowrie EG, Lew NL: Death risk in hemodialysispatients: The predictive value of commonly measured vari-ables and an evaluation of death rate differences betweenfacilities. Am J Kidney Dis 15:458-482, 1990
17. Foley RN, Parfrey PS, Harnett JD, Kent GM, MurrayDC, Barre PE: The impact of anemia on cardiomyopathy,morbidity, and mortality in end-stage renal disease. Am JKidney Dis 28:53-61, 1996
18. Auer J, Simon G, Stevens J, Griffiths P, Howarth D,Anastassiades E, Gokal R, Oliver D: Quality of life improve-ments in CAPD patients treated with subcutaneously admin-istered erythropoietin for anemia. Perit Dial Int 12:40-42,1992
19. Woodrow G, Turney JH, Brownjohn AM: Techniquefailure in peritoneal dialysis and its impact on patient sur-vival. Perit Dial Int 17:360-364, 1997
20. Maiorca R, Cancarini GC, Brunori G, Zubani R,
1997 PD-CIS 11

Camerini C, Manili L, Movilli E: Comparison of long-termsurvival between hemodialysis and peritoneal dialysis. AdvPerit Dial 12:79-88, 1996
21. Fenton SS, Schaubel DE, Desmeules M, MorrisonHI, Mao Y, Copleston P, Jeffery JR, Kjellstrand CM: Hemo-dialysis versus peritoneal dialysis: A comparison of adjustedmortality rates. Am J Kidney Dis 30:334-342, 1997
22. Port FK: Morbidity and mortality in dialysis patients.Kidney Int 46:1728-1737, 1994
23. Selgas R, Bajo MA, Fernandez-Reyes MJ, Bosque E,Lopez-Revuelta K, Jimenez C, Borrego JF, de Alvaro F: Ananalysis of adequacy of dialysis in a selected population onCAPD for over 3 years: The influence of urea and creatininekinetics. Nephrol Dial Transplant 8:1244-1253, 1993
24. McCusker FM, Teehan BP, Thorpe K, Keshaviah P,Churchill D: How much peritoneal dialysis is required forthe maintenance of a good nutritional state? Kidney Int50:S56-S61, 1996 (suppl 56)
25. Teehan BP, Schleifer CR, Brown JM, Sigler MH,Raimondo J: Urea kinetic analysis and clinical outcome onCAPD: A five year longitudinal study. Adv Perit Dial 6:181-185, 1990
26. NKF-DOQI Clinical Practice Guidelines for Perito-neal Dialysis Adequacy. Am J Kidney Dis 30:S74-S85, 1997(suppl 2)
27. Davies SJ, Russell L, Bryan J, Phillips L, Russell GI:Comorbidity, urea kinetics, and appetite in continuous ambu-latory peritoneal dialysis patients: Their interrelationshipand prediction of survival. Am J Kidney Dis 26:353-361,1995
28. Maiorca R, Brunori G, Zubani R, Cancarini GC,Manili L, Camerini C, Movilli E, Pola A, d’Avolio G, GelattiU: Predictive value of dialysis adequacy and nutritionalindices for mortality and morbidity in CAPD and HDpatients: A longitudinal study. Nephrol Dial Transplant 10:2295-2305, 1995
29. Jones CH, Newstead CG, Will EJ, Smye SW, Davi-son AM: Assessment of nutritional status in CAPD patients:Serum albumin is not a useful measure. Nephrol Dial Trans-plant 12:1406-1413, 1997
30. 1996 Facility Survey File. Available at http://www.hcfa.gov/stats/pufiles.htm. Accessed February 4, 1998
31. DOQI Clinical Practice Guidelines for PeritonealDialysis Adequacy. Available at http://www.kidney.org/doqi/doqi/pdg6.htlm. Accessed February 5, 1998
32. DOQI Clinical Practice Guidelines for PeritonealDialysis Adequacy. Available at http://www.kidney.org/doqi/doqi/pdg12.html. Accessed February 5, 1998
33. DOQI Clinical Practice Guidelines for PeritonealDialysis Adequacy. Available at http://www.kidney.org/doqi/doqi/pdg9.html. Accessed February 5, 1998
34. Health Care Financing Administration: 1997 AnnualReport, End Stage Renal Disease Core Indicators Project.Available at http://www.hcfa.gov/medicare/hsqb/hsqb3c.htm.Accessed March 15, 1998
35. The USRDS Dialysis Morbidity and Mortality Study(Wave 2). Available at http://monroe.mcit.med.umich.edu/usrds/chapters97/ch04.html. Accessed April 22, 1998
36. Clinical Practice Guidelines for Peritoneal DialysisAdequacy. Guideline 15—Weekly Dose of CAPD (Evi-dence). Available at http://www.kidney.org/doqi/doqi/pdg15.html. Accessed June 4, 1998
37. Clinical Practice Guidelines for Peritoneal DialysisAdequacy. Guideline 16—Weekly Dose of NIPD and CCPD(Opinion). Available at http://www.kidney.org/doqi/doqi/pdg16.html. Accessed June 4, 1998
38. Rocco MV, Flanigan MJ, Beaver S, Frederick P,Gentile DE, McClellan WM, Polder J, Prowant BF, TaylorL, Helgerson SD: Report from the 1995 Core Indicators forPeritoneal Dialysis Study Group. Am J Kidney Dis 30:165-173, 1997
39. Flanigan MJ: Peritoneal dialysis indices: Weekly CrCland weekly Kt/V are linked. Am J Kidney Dis 31:495-501,1998
40. Tzamaloukas AH, Murata GH, Piraino B, Rao P,Bernardini J, Malhotra D, Oreopoulos DG: Peritoneal ureaand creatinine clearances in continuous ambulatory perito-neal dialysis patients with different types of peritoneal solutetransport. Kidney Int 53:1405-1411, 1998
41. Culp K, Flanigan M, Lowrie EG, Lew N, Zimmer-man B: Modeling mortality risk in hemodialysis patientsusing laboratory values as time-dependent covariates. Am JKidney Dis 28:741-746, 1996
42. Cueto-Manzano AM, Espinosa A, Hernandez A, Cor-rea-Rotter R: Peritoneal transport kinetics correlate withserum albumin but not the overall nutritional status in CAPDpatients. Am J Kidney Dis 30:229-236, 1997
43. Blumenkrantz MJ, Kopple JD, Moran JK, CoburnJW: Metabolic balance studies and dietary protein require-ments in patients undergoing continuous ambulatory perito-neal dialysis. Kidney Int 21:849-861, 1982
44. Flanigan MJ, Lim VS, Pflederer TA: Tidal peritonealdialysis: Kinetics and protein balance. Am J Kidney Dis22:700-707, 1993
45. Schuster VL, Seldon DW: Renal clearance, in SeldonDW, Giebisch G (eds): The Kidney: Physiology and Patho-physiology. New York, NY, Raven Press, 1985, pp 369-373
46. Forbes GB, Bruning GJ: Urinary creatinine excretionand lean body mass. Am J Clin Nutr 29:1359-1366, 1976
47. Keen M, Lipps B, Gotch F: The measured creatininegeneration rate in CAPD suggests only 78% of prescribeddialysis is delivered. Adv Perit Dial 9:73-75, 1993
48. Goel S, Nolph KD, Moore HL, Prowant BF, KhannaR, Twardowski ZJ: A prospective study of the effects ofnoncompliance on small solute removal in continuous ambu-latory peritoneal dialysis. Trans ASAIO 41:M452-456, 1995
49. Johansson AC, Attman PO, Haraldsson B: Creatininegeneration rate and lean body mass: A critical analysis inperitoneal dialysis patients. Kidney Int 51:855-859, 1997
50. Lo Wk, Prowant BF, Moore HL, Gamboa SB, NolphKD, Flynn MA, Londeree BL, Keshaviah PK, Emerson PE:Comparison of different measurements of lean body mass innormal individuals and in chronic peritoneal dialysis pa-tients. Am J Kidney Dis 23:74-85, 1994
51. Bhatla B, Moore H, Emerson P, Keshaviah P, Prow-ant B, Nolph KD, Singh A: Lean body mass estimation bycreatinine kinetics, bioimpedance, and dual energy x-rayabsorptiometry in patients on continuous ambulatory perito-neal dialysis. Trans ASAIO 41:M442-M446, 1995
52. Mitch WE, Walser M: A proposed mechanism forreduced creatinine excretion in severe chronic renal failure.Nephron 21:248-254, 1978
12 FLANIGAN ET AL