
7 Menstrual Dysfunction in Female Dialysis Patients
20
Therapeutic Apheresis and Dialysis 9(1):78–97, Blackwell Publishing, Inc. © 2005 International Society for Apheresis 78 Blackwell Science, LtdOxford, UKTAPTherapeutic Apheresis and Dialysis1744-99792005 International Society for ApheresisFebruary 2005 91 7897 Original Article AbstractsAbstracts Abstracts from the 3rd Slovenian Congress of Nephrology Dialysis and Apheresis Abstracts 1 Low Volume Exchange Protocol for Peritoneal Dialysis After Abdominal Surgery Z Plev nik, J Lavre, B Vujkovac and S Pe olar Department of Dialysis, General Hospital Slovenj Gradec, Slovenia Abdominal surgery is considered problematic if performed on dialysis patients who are on peritoneal dialysis. There is a common clinical practice to switch these patients to hemodialysis postoper- atively for a period of time. Our attempt was to keep these patients on peritoneal dialysis after abdominal surgery, using a modified protocol of low volume exchanges. During the last two years, three of our patients on peritoneal dialysis underwent abdominal sur- gery. In one patient, laparoscopic cholecystectomy was performed, and abdominal hernia repair was performed in the other two. The day after the operation, we started with low volume (500 mL) exchanges with solutions with 1.36% glucose. During the daytime we prescribed four exchanges, and during the nighttime we put patients on automatic peritoneal dialysis (APD), also with low volume exchanges. After 5 days, the volume of exchanges was gradually increased and after 3 weeks all three patients were on their standard preoperative dialysis regime. Periodically, we con- trolled the adequacy of dialysis with Kt/V, which was not changed during these procedures. There were no complications postopera- tively. We conclude that this modified protocol of peritoneal dial- ysis was useful and safe in all our patients and there was no need to switch patients to hemodialysis. Further clinical experience with a large number of patients might confirm the usefulness of low volume exchange protocol. 2 Renal Anemia Treatment In Peritoneal Dialysis Patients: A Multicenter Slovenian Study J Pajek 1 , K Grego 1 , A Gu ek 1 , S Bevc 2 , R Ekart 2 , B Vujkovac 3 , P Golob Kosmina 4 , A Kandus 1 and A F Bren 1 1 Department of Nephrology, University Medical Center, Ljubljana, Slovenia, 2 Department of Nephrology, University Hospital, Maribor, Slovenia, 3 Department of Nephrology, General Hospital, Slovenj Gradec, Slovenia, and 4 Department of Nephrology, General Hospital, Novo mesto, Slovenia Objectives The aim of our study was to: (i) assess the number of patients who need epoetin treatment and the adequacy of iron treatment, (ii) assess the influence of presence of diabetes mellitus, polycystic kidney disease and the influence of therapy with alumi- num phosphate binders and angiotensin system antagonists on the epoetin requirements, (iii) assess the role of other factors possibly influencing epoetin resistance – secondary hyperparathyroidism, inflammation, dialysis dose and residual renal function. s ˇ c ˇ c ˇ c ˇ Design and Methods Fifty-one stable peritoneal dialysis (PD) patients (mean age ± SD was 52 ± 13 years, 20 women) without recent bleeding, surgery, bone marrow disease, malignancy, or hypothyroidism were recruited in four Slovenian centers. The dose of epoetin was adjusted to maintain a target hemoglobin of above 110 g/L. At the time of inclusion (median 36 months of PD, range 3–124 months) the PET test results and relevant clinical and lab- oratory parameters were recorded. Index of epoetin resistance (IRE) was expressed as weekly epoetin dose/body weight/hemo- globin concentration. Results Twenty four percent of patients did not need epoetin treatment, the rest were treated with Epoetin-beta at a dose of 70 ± 56 U/kg/week s.c.; hemoglobin concentration was 124 ± 15 g/ L; 14% had hemoglobin below 110 g/L. Iron adequacy parameters (ferritin > 100 m g/L and TSAT > 20%) were fulfilled by 63% of patients, and their IRE was lower (0.43 ± 0.5 U/kg/week/g/L vs. 0.6 ± 0.72 U/kg/week/g/L), but not significantly ( P = 0.502). Patients with polycystic kidneys had lower IRE (0.13 ± 0.3 vs. 0.52 ± 0.55 U/kg/week/g/L, P = 0.011) and majority of them (71%) did not need epoetin treatment ( P = 0.006). No difference was found for diabetic patients. Treatment with angiotensin system antagonists, but not with aluminum phosphate binders, is associ- ated with increased IRE (0.56 ± 0.59 vs. 0.3 ± 0.4 U/kg/week/g/L, P = 0.038). A statistically significant correlation was found for IRE and CRP (r = 0.48, P = 0.001) and iPTH (r = 0.46, P = 0.001). No correlation between IRE and residual renal function was found (r = - 0.2, P = 0.173). Stepwise linear regression analysis for multi- ple variables (residual renal glomerular filtration rate, total weekly creatinine clearance, CRP, iPTH, iron adequacy, angiotensin sys- tem antagonist treatment, presence of polycystic kidneys) showed CRP and treatment with angiotensin system antagonists to be the most significant variables influencing IRE. Conclusion Our results show that systemic inflammation and angiotensin system antagonist treatment are the most important parameters affecting epoetin requirements in stable peritoneal dialysis patients. 3 Is Metabolism of Divalent Ions in Our Peritoneal Dialysis Population Optimal? M Benedik and A Gu ek Center for Dialysis, Department of Nephrology, University Medical Center, Ljubljana, Slovenia Introduction The problems of divalent ions, trace elements and bones are present in chronic dialysis patients despite optimal diet and therapy. Many patients have signs and symptoms of uremic osteopathy. Aim of the study To evaluate divalent ion metabolism and bone diseases in patients of our center for peritoneal dialysis. Methods In cross-section study, we studied 41 patients (14 women, 27 men, mean age 56.6 ± 14.2 years) who were at least for c ˇ
Transcript of 7 Menstrual Dysfunction in Female Dialysis Patients

Therapeutic Apheresis and Dialysis
9(1):78–97, Blackwell Publishing, Inc.© 2005 International Society for Apheresis
78
Blackwell Science, LtdOxford, UKTAPTherapeutic Apheresis and Dialysis1744-99792005 International Society for ApheresisFebruary 2005
91
7897
Original Article
AbstractsAbstracts
Abstracts from the 3rd Slovenian Congress of Nephrology
Dialysis and Apheresis Abstracts
1
Low Volume Exchange Protocol for Peritoneal Dialysis After Abdominal Surgery
Z Plev i nik, J Lavre, B Vujkovac and S Pe olar
Department of Dialysis, General Hospital Slovenj Gradec, Slovenia
Abdominal surgery is considered problematic if performed ondialysis patients who are on peritoneal dialysis. There is a commonclinical practice to switch these patients to hemodialysis postoper-atively for a period of time. Our attempt was to keep these patientson peritoneal dialysis after abdominal surgery, using a modifiedprotocol of low volume exchanges. During the last two years, threeof our patients on peritoneal dialysis underwent abdominal sur-gery. In one patient, laparoscopic cholecystectomy was performed,and abdominal hernia repair was performed in the other two. Theday after the operation, we started with low volume (500 mL)exchanges with solutions with 1.36% glucose. During the daytimewe prescribed four exchanges, and during the nighttime we putpatients on automatic peritoneal dialysis (APD), also with lowvolume exchanges. After 5 days, the volume of exchanges wasgradually increased and after 3 weeks all three patients were ontheir standard preoperative dialysis regime. Periodically, we con-trolled the adequacy of dialysis with Kt/V, which was not changedduring these procedures. There were no complications postopera-tively. We conclude that this modified protocol of peritoneal dial-ysis was useful and safe in all our patients and there was no needto switch patients to hemodialysis. Further clinical experience witha large number of patients might confirm the usefulness of lowvolume exchange protocol.
2
Renal Anemia Treatment In Peritoneal Dialysis Patients: A Multicenter Slovenian Study
J Pajek
1
, K Grego
1
, A Gu ek
1
, S Bevc
2
, R Ekart
2
, B Vujkovac
3
, P Golob Kosmina
4
, A Kandus
1
and A F Bren
1
1
Department of Nephrology, University Medical Center, Ljubljana, Slovenia,
2
Department of Nephrology, University Hospital, Maribor, Slovenia,
3
Department of Nephrology, General Hospital, Slovenj Gradec, Slovenia, and
4
Department of Nephrology, General Hospital, Novo mesto, Slovenia
Objectives
The aim of our study was to: (i) assess the numberof patients who need epoetin treatment and the adequacy of irontreatment, (ii) assess the influence of presence of diabetes mellitus,polycystic kidney disease and the influence of therapy with alumi-num phosphate binders and angiotensin system antagonists on theepoetin requirements, (iii) assess the role of other factors possiblyinfluencing epoetin resistance – secondary hyperparathyroidism,inflammation, dialysis dose and residual renal function.
s c c
c
Design and Methods
Fifty-one stable peritoneal dialysis (PD)patients (mean age
±
SD was 52
±
13 years, 20 women) withoutrecent bleeding, surgery, bone marrow disease, malignancy, orhypothyroidism were recruited in four Slovenian centers. The doseof epoetin was adjusted to maintain a target hemoglobin of above110 g/L. At the time of inclusion (median 36 months of PD, range3–124 months) the PET test results and relevant clinical and lab-oratory parameters were recorded. Index of epoetin resistance(IRE) was expressed as weekly epoetin dose/body weight/hemo-globin concentration.
Results
Twenty four percent of patients did not need epoetintreatment, the rest were treated with Epoetin-beta at a dose of70
±
56 U/kg/week s.c.; hemoglobin concentration was 124
±
15 g/L; 14% had hemoglobin below 110 g/L. Iron adequacy parameters(ferritin
>
100
m
g/L and TSAT
>
20%) were fulfilled by 63% ofpatients, and their IRE was lower (0.43
±
0.5 U/kg/week/g/L vs.0.6
±
0.72 U/kg/week/g/L), but not significantly (
P
=
0.502).Patients with polycystic kidneys had lower IRE (0.13
±
0.3 vs.0.52
±
0.55 U/kg/week/g/L,
P
=
0.011) and majority of them (71%)did not need epoetin treatment (
P
=
0.006). No difference wasfound for diabetic patients. Treatment with angiotensin systemantagonists, but not with aluminum phosphate binders, is associ-ated with increased IRE (0.56
±
0.59 vs. 0.3
±
0.4 U/kg/week/g/L,
P
=
0.038). A statistically significant correlation was found for IREand CRP (r
=
0.48,
P
=
0.001) and iPTH (r
=
0.46,
P
=
0.001). Nocorrelation between IRE and residual renal function was found(r
=
-
0.2,
P
=
0.173). Stepwise linear regression analysis for multi-ple variables (residual renal glomerular filtration rate, total weeklycreatinine clearance, CRP, iPTH, iron adequacy, angiotensin sys-tem antagonist treatment, presence of polycystic kidneys) showedCRP and treatment with angiotensin system antagonists to be themost significant variables influencing IRE.
Conclusion
Our results show that systemic inflammation andangiotensin system antagonist treatment are the most importantparameters affecting epoetin requirements in stable peritonealdialysis patients.
3
Is Metabolism of Divalent Ions in Our Peritoneal DialysisPopulation Optimal?
M Benedik and A Gu ek
Center for Dialysis, Department of Nephrology, University Medical Center, Ljubljana, Slovenia
Introduction
The problems of divalent ions, trace elements andbones are present in chronic dialysis patients despite optimal dietand therapy. Many patients have signs and symptoms of uremicosteopathy.
Aim of the study
To evaluate divalent ion metabolism and bonediseases in patients of our center for peritoneal dialysis.
Methods
In cross-section study, we studied 41 patients (14women, 27 men, mean age 56.6
±
14.2 years) who were at least for
c

Abstracts 79
Ther Apher Dial, Vol. 9, No. 1, 2005
6 months (mean 52.9
±
34.5 months) in our peritoneal dialysis(PD) program in the year 2003. Besides clinical, ultrasound, andX-ray data, we evaluated their laboratory data in the last 3 yearswhere available.
Results
Twenty-seven patients used CAPD, 14 CCPD methods,5/41 used PD
1
solution, 34/41 PD
4
and 2 both solutions. Thirty-fourpatients used CaCO
3
, 18 aluminum hydroxide, and 9 sevelamerhydrochloride as phosphate binder as monotherapy or in combi-nation. Sixteen patients used calcitriol and 9 sodium bicarbonate.Mean serum Ca in this population was 2.38
±
0.09 (range 2.16–2.56) mmol/L, mean serum PO
4
1.46
±
0.2 (range 1.13–2.23) mmol/L, mean serum alkaline phosphatase 1.44
±
0.74 (range 0.61–5.3)
m
kat/L, mean serum Al 21.7
±
12.1 (range 6.5–47.3)
m
g/L,mean i-PTH was 454.07
±
484 (range 1–1828) pg/mL and meanproduct of Ca and PO
4
was 3.48
±
0.53 mmol
2
/L
2
(range 2.52–4.84).We found positive correlation between alkaline phosphataseand i-PTH (
P
=
0.000153) and between i-PTH and serum Ca(
P
=
0.025291). 25/41 (61%) patients had maximum i-PTH higherthan 200 pg/mL, 13/41 (32%) patients had maximum i-PTH evenhigher than 600 pg/mL, 4 patients were waiting for parathyroidec-tomy, meanwhile 8/41 (19.5%) of patients had i-PTH
<
100 pg/mL,in 4 of them parathyroidectomy was done in the past.
Conclusions
Divalent metabolism is quite optimally achievedbut secondary hyperparathyroidism still prevails in our PDpatients. Management of divalent ions is very important beforethe beginning of peritoneal dialysis.
4
Endemic Nephropathy in Croatian Registry for Renal Replacement Therapy
S ala
Croatian Registry for Renal Replacement Therapy, “Sestre milosrdnice” Clinical Hospital, Zagreb, Croatia
In endemic regions along the River Sava, chronic progressivetubulointerstitial nephritis, driven by an unidentified environmen-tal factor, is the frequent cause of renal failure and need for renalreplacement therapy (RRT).The Croatian Registry for Renal Replacement Therapy (CRRRT)has collected individual patient data from the year 2000. Reportson 161 patients with endemic nephropathy (EN) are available for81 women and 80 men, 111 alive and 50 dead.The highest concentration of EN patients on dialysis is in Slavon-ski Brod (31%), Vinkovci (26%), and Sisak (13%). The overallfrequency of EN in Croatia is much lower. In the year 2002, ENwas the primary renal disease in 3.6% of 3100 patients on RRT,and in 3.1% patients starting dialysis. Prevalence was 25 cases permillion population (pmp) and incidence was 3.6 pmp.In EN patients starting RRT from 2000–2002, median age was64 years (62 years in all incident patients in 2002.). Endemic neph-ropathy patients live longer on RRT (median vintage 4.5 years,compared to 3.5 years for all patients on RRT). Favorable courseis evident in spite of older age and higher burden of neoplasms.Malignant disease is present in 7% of living patients, and in 20%of deceased patients.A trend of decline is indicated by a small but sustained decreasein the incidence and prevalence of EN patients on RRT. In theyears 2000, 2001, and 2002, the prevalence was 28 pmp, 27 pmp,and 25 pmp respectively. Incidence declined from 4.1 pmp to4.0 pmp, and to 3.6 pmp. Incident patients are getting older. Dur-ing the last 3 years, the youngest EN patient starting RRT was46 years old. The youngest patient in CRRRT was 33 years old atthe start of RRT in 1988.
C
Changes in life style may have lowered the exposure to the detri-mental environmental factor. Younger generations are spared, andin those entering RRT now, more time was needed to cumulate atoxic dose, producing progressive kidney sclerosis.
5
Ocular Changes in Hemodialysis Patients
D Pavlovi
1
, Z Vatavuk
2
, R Vrabec
2
, S ala
1
, A Sesar
2
, I Ratkovi -Gusi
1
and Z Mandi
2
1
Department of Nephrology and Dialysis,
2
Eye Clinic, University Hospital “Sestre milosrdnice” Zagreb, Croatia
Chronic renal failure is characterized by numerous disorders thatinvolve many organs. In dialysis patients, some disorders could bethe consequence of the dialysis treatment per se. The aim of ourstudy was to evaluate the ocular changes in hemodialysis patients.In 64 patients undergoing hemodialysis (30 female and 34 male),aged 24–83 years (mean 58 years) and on hemodialysis 1–213months (mean 47 months), complete ocular examination was per-formed: visual acuity (VA), intraocular pressure (IOP), biomicro-scopic examination, and fundoscopy. All patients were onhemodialysis 3 times a week, for 4 hours; bicarbonate dialysatewas used with 1.5 mmol/L Ca concentration. Most of the patientswere on calcitriol therapy and calcium carbonate were used asphosphate binders. Heparin was used during hemodialysis in allpatients in a dose up to 4000 i.u. Visual acuity was impaired in 84%of patients; mean IOP was 15 mmHg (right eye) and 14 mmHg(left eye) (normal vale 11–20 mmHg). Thirty-nine patients (60%)have cataracts, 6 of them were operated. Hypertensive vascularchanges were seen in 44 (68%) patients and in 6 patients agerelated macular degeneration was observed. Diabetic nonpro-lipherative or prolipherative changes were seen in 5 of 7 diabeticpatients. In 3 patients, argon laser coagulopathy was performed.Ocular calcifications were found in 14 patients. No correlation ofocular calcification and parathyroid hormone PTH level or cal-cium–phosphate product was observed.Patients with CRF or who are receiving dialysis represent a uniquegroup of patients. Pathologic changes could be found in manyorgans; therefore, we suggest more frequent complete ocularexamination in dialysis patients.
6
The Most Important Factor for Cardiovascular Morbidity in Hemodialysis Patients is Microinflammation
J Lavre
1
, B Vujkovac
1
and M abovi
2
1
Department of Nephrology and Dialysis, General Hospital Slovenj Gradec,
2
Department for Vascular Diseases, University Medical Center, Ljubljana, Slovenia
In hemodialysis (HD) patients, cardiovascular (CV) morbidity is10 to 20 times higher than in the general population. Dyslipidemia,malnutrition, and non-traditional CV risk factors are well-knownimportant determinants in the increased CV morbidity. We there-fore measured levels of serum high-sensitivity C-reactive protein(CRP), interleukin 6 (IL-6), tumor necrosis factor-
a
(TNF-
a
),albumin, ferritin, cholesterol (CHOL), triglyceride (TG), highdensity lipoprotein (HDL), low density lipoprotein (LDL), lipo-protein(a) (Lpa) and body mass index (BMI) in 22 HD patients(age 62.8
±
12.8) on maintenance HD for 65.16
±
33 months. Allpatients received standard dietary guidance with an average pro-tein intake of 1.2 g/kg/day, 35 kcal/kg, phosphate and potassium
c¢ Cc¢ c¢ c¢
S c¢

80 Abstracts
Ther Apher Dial, Vol. 9, No. 1, 2005
restriction. Twenty of 22 patients had well treated high bloodpressure. Two patients had non-insulin-dependent diabetes melli-tus treated only with diet. The patients were not treated with lipidlowering drugs, and only one patient was a smoker.The mean values of serum CHOL (4.31
±
0.88 mmol/L), TG(1.77
±
1.1 mmol/L), HDL (1.09
±
0.35 mmol/L) and LDL(2.43
±
0.53 mmol/L) were normal. The patients had elevated val-ues of serum CRP (10.63
±
12.56 mg/L), IL-6 (1.49
±
1.66 pg/mL),TNF-
a
(7.26
±
5.52 pg/mL) and Lpa (0.17
±
0.15
m
g/dL). The meanvalue of serum albumin (41.03
±
2.38 g/L) was also normal; themean value of BMI (26.32
±
4.34 kg/m
2
) was mildly elevated. Thepatients had elevated serum ferritin (518
±
342 mmol/L), butwithin the expected range. The mean value of Kt/V (1.86
±
0.23)was high normal.Our patients have elevated CRP, IL-6 and TNF-
a
. In contrast withother studies our patients had normal lipid status and also normalnutritional status. No significant relationships were found betweenCRP, IL-6, TNF-
a
, or ferritin and age, history of dialysis, albumin,and BMI. There was only a significant correlation between monthson dialysis and HDL (r
=
-
0.46,
P
=
0.048), but no significant cor-relation between months on dialysis and albumin, BMI, CHOL,TG, LDL, and Lp(a).We concluded that in our HD patients, the most important factorfor high CV morbidity was microinflammation. Dyslipidemia andmalnutrition are well controlled in optimally treated HD patientsand seems to be only a minor factor for CV morbidity.
7
Menstrual Dysfunction in Female Dialysis Patients
H Resi
1
, A Alajbegovi
3
, V Sahovi
1
, E Mesi
2
and E Sulji
3
1
Center for Hemodialysis, Clinical Center, University of Sarajevo,
2
Clinic for Nephrology, Dialysis and Kidney Transplantation, UCC, Tuzla, and
3
Neurology Clinics, Clinical Center, University of Sarajevo, Sarajevo, Bosnia and Herzegovina
Introduction
Uremia is associated with different endocrinologicabnormalities, which in some cases induce polyendocrinopathia.Female patients on dialysis are often subject to menstrual disor-ders that are variously manifested. The aim of our paper is toevaluate the etiology of menstrual dysfunctions in female dialysispatients.
Material and methods
Anamnesis, clinical and hormonal testswere performed on 25 female patients that were in chronic dialysisprograms 4 hours, 3 times per week. Oligomenorrhea is consid-ered as menstrual interval between 35 and 90 days and amenor-rhea as cease of menstruation in the last six months.
Results All patients had had normal menstrual cycles before thedialysis. Mean age of patients was 42.7 ± 9.96 years and meandialysis duration was 75.5 ± 62.41 months. Out of the 25 patients,10 developed amenorrhea when beginning dialysis and 5 of themregained regular menstrual cycle after one year. Seven patientshad oligomenorrhea and 8 patients had an early menopause. Pro-lactin concentration was significantly higher in the group whichdeveloped menopause (N = 8), cpr = 1222.3 ± 1013.4, amenorrhea(942.2 ± 1061.2), oligomenorrhea (860.4 ± 897.2), compared to thegroup with a regular menstruation cycle (444.8 ± 299.7). Theluteinizing hormone (LH) level in serum was increased in allgroups. FSH was insignificantly higher in groups with oligomenor-rhea and amenorrhea and amounted to 51.1 ± 69.9, while b-estradiol and progesterone were in normal ranges. Hemodialysisduration influenced the prolactin level and after one year of follow
c¢ c¢ c¢ c¢c¢
up prolactin level significantly decreased in the group with amen-orrhea that regained regular menstruation (cpr = 596.2 ± 297.2).Conclusion Different menstrual disorders are developed in dia-lyzed patients. Hyper prolactinemia was present in our dialysispopulation. Significant lowering of prolactin level in 20% ofpatients led to normalization of menstrual cycle.
8
Mixed Uremic Osteodystrophy – a Predominant Form of Renal Bone Disease in SloveniaM Legan1, M Benedik2, D Kova 2 and A Cör1
1Institute of Histology & Embryology, Medical Faculty University of Ljubljana, Slovenia 2Department of Nephrology, University Medical Center Ljubljana, Slovenia
Objectives To find out which form of renal osteodistrophy ispredominant in our population of patients with end-stage renalfailure. To elucidate the reasons of abnormal mineralization inmixed uremic osteodystrophy and low-turnover osteodystrophy.Design and methods Ninety-three consecutive patients (58males and 35 females, mean age 50.6 ± 12.2 years) with end-stagerenal failure underwent iliac bone biopsy (after double tetracy-cline labeling). Histomorphologic as well as histomorphometricanalyses were performed in bone tissue sections stained byGoldner, toluidin, Pearls’ blue, tiophlavin, Alumininon, andfluorescence.Results Thirty-eight (40.9%) of our patients had mixed renalbone disease, predominant hyperparathyroid bone disease wasfound in 31 (33.3%) patients, and low-turnover osteodystrophy in24 patients (25.8%). The deposits of aluminum on mineralizationfront were found in 10.8%, amyloid in 35.9%, and iron in 6.5%.The defective mineralization in patients with mixed and low-turnover forms of the disease was present in 22 patients due toamyloid, in 7 patients due to aluminum deposits, in 1 to irondeposits, whereas in 6 patients the reason was the combination of2 factors: amyloid and iron (3 patients), aluminum and iron (1patient), amyloid and aluminum (2 patients). In 26 patients, defec-tive mineralization was unknown (the bone sections were free ofaluminum, iron and amyloid).Conclusions In the Slovenian population of end-stage renal fail-ure patients, the predominant form of renal bone disease is mixedrenal osteodystrophy. The most important reason for defectivemineralization is amyloid deposits on the mineralization front.
9
The Effect of Handgrip Training and Intermittent Com-pression of Upper Arm Veins on Forearm Vessels in Patients With End-Stage Renal FailureR Rus1, R Ponikvar2, R B Kenda1 and J Buturovi -Ponikvar2
1Department of Pediatric Nephrology, 2Department of Nephrology, University Medical Center Ljubljana, Slovenia
Background It has already been shown that handgrip traininghas a beneficial effect on arteries and veins, and intermittent com-pression of upper arm veins alone improves the diameter of fore-arm veins. The purpose of our study was to investigate the additiveeffect of handgrip training and intermittent compression of upperarm veins on the forearm arteries and veins.Methods Eighteen chronic hemodialysis patients performeddaily handgrip training and intermittent compression of upper armby elastic band (Eschmarch) for 8 weeks. The activities were per-formed on the arm without vascular access. The forearm circum-
c
c¢

Abstracts 81
Ther Apher Dial, Vol. 9, No. 1, 2005
ference and maximal handgrip strength were measured beforeexercise, and after 4 and 8 weeks, together with arterial and veinparameters including endothelium-dependent and endothelium-independent vasodilatation obtained by ultrasonographymeasurements.Results The maximal handgrip strength and the forearm circum-ference increased significantly. The radial artery diameters weresignificantly higher after 8 weeks of training (1.89 mm ± 0.10 at thebeginning, 1.95 mm ± 0.10 after 8 weeks). Endothelium-depen-dent vasodilatation was also found to be markedly increased after4 and 8 weeks of training, but endothelium-independent vasodila-tation remained unchanged. The venous diameters before tourni-quet placement increased significantly after 8 weeks(2.40 mm ± 0.16 at the beginning, 2.62 mm ± 0.17 after 8 weeks).The venous diameters after tourniquet placement increased sig-nificantly after 4 and 8 weeks (3.36 mm ± 0.17 at the beginning,3.51 mm ± 0.18 after 4 weeks, 3.68 mm ± 0.18 after 8 weeks). Dis-tensibility of veins was preserved.Conclusion Our study suggests that both activities performeddaily, such as handgrip training and intermittent compression ofupper arm veins, increase the diameters of both arteries and veins.The endothelium-dependent vasodilatation was also improved.
10
Comparison of Four Prognostic Indexes in Severe Acute Renal FailureJ Guben ek, R Ponikvar and J Buturovi -PonikvarDialysis center, Department of Nephrology, University Medical Center, Ljubljana, Slovenia
Background Several prognostic indexes and models are in usefor acute renal failure (ARF) patients in intensive care units(ICU). Some were designed on general ICU populations (likeAPACHE II) and some were made specifically for ICU patientswith ARF.The purpose of our prospective clinical study was to compareAPACHE II and three ARF-specific prognostic indexes in theirability to discriminate survivors and non-survivors among criti-cally ill ARF patients requiring dialysis.Methods Forty-four critically ill patients with ARF requiringdialysis were included. Patients with chronic renal insufficiency(creatinine > 200 mmol/L), transplanted kidney or urinary tractobstruction were excluded. Four prognostic indexes were mea-sured at the time of first dialysis: APACHE II score (0–71), Cleve-land Clinic Foundation (CCF) score (0–20), predicted mortalityby Mehta and by Liano model. Primary end-points were ICUsurvival and recovery of renal function.Results Patients were 65 ± 5 years old, 75% were male, 50%recovered renal function (22/44). Mean APACHE II score was21.9 ± 6.5, CCF score was 9.2 ± 2.5, predicted mortality by Mehtamodel was 64 ± 5% and by Liano model 47 ± 20%. Patients thatrecovered renal function and those that died in ARF did not differsignificantly in any of the prognostic indexes measured. IntensiveCare Unit survival data was available for 32 patients, this groupwas not significantly different in prognostic indexes from thegroup for which ICU survival data was not available. IntensiveCare Unit mortality was 75% (24/32). There was significant differ-ence in APACHE II value in ICU survivors and non-survivors(16.6 ± 6.1 vs. 23.4 ± 6.5, P = 0.015), but no difference in the otherthree indexes.Conclusions Only the APACHE II values measured at first dial-ysis were significantly different between ICU survivors and non-survivors, whereas other three prognostic indexes were not.
s c¢
11
Thrombolysis of Permanent Hemodialysis CathetersV PremruCenter for hemodialysis, University Medical Center Ljubljana, Slovenia
Outline Occlusion of hemodialysis (HD) catheter and infectionare by far the most frequent reasons for removal of the catheter. Asan increasing number of patients depend on a catheter as a vascularaccess for an extended period, maintenance of HD catheter patencyis extremely important. One approach in case of catheter occlusionis thrombolysis. We describe our experience with HD catheterthrombolysis in rare patients with extreme access problems.Patients and methods In four patients (aged 77, 69, 64 and28 years, all female) hemodialyzed via permanent HD catheters,occlusion occurred and thrombolysis was attempted. Primarypatency periods were: 112 months for one surgically implantedsubclavian vein silastic catheter, 74 and 46 days for two percuta-neously inserted jugular vein catheters and 30 days for one surgi-cally implanted right intra-atrial catheter. Recombinant humantissue plasminogen activator (TPA) or urokinase was used 13times each as a thrombolytic agent in recommended doses forcatheter lysis. Heparin lock was also used three times.Results In the young patient with the intra-atrial catheter, r-TPAwas used 13 times with modest success even in the short-term:restoration of flow for average 11 (range, 1–23) days. Urokinasewas used 13 times in the other three patients: average secondarypatency time was 79 (3–109) days. Heparin was effective in restor-ing patency for 29 (22–34) days. No complications of thrombolytictherapy were noted.Discussion Thrombolysis of occluded HD catheter is sometimesthe only way to extend its functioning time. Especially in difficult-to-manage cases with exhausted vascular access sites, even forcatheter insertion, this might be of vital importance. In our expe-rience, in rare patients thrombolysis is needed frequently. It canbe repeated safely. Unfortunately, the effects of each treatmentseem to be only short-lived. Beside its allergogenic potential andlimited effectiveness, this therapy is also very expensive.
12
Genotype and Transmission of Hepatitis C Virus in Hemodialysis UnitsE Me i 1, N Tihi 1 and H Resi 2
1University Clinical Centre Tuzla, 2Clinical Centre of University Sarajevo, Sarajevo, Bosnia and Herzegovina
Objectives Hepatitis C virus (HCV) infection is spread world-wide with significant geographical differences in the prevalenceand genotypes. The aim of this study was to analyse HCV infectionin hemodialysis (HD) units in Bosnia and Herzegovina (BH),through genotypes and routes of transmission.Design and Methods We analysed data from Renal Registry ofBH for the years 2002 and 2003 in order to estimate prevalenceand incidence of anti-HCV positive patients in 23 HD units in BH(ELISA III). Then we tested 88 anti-HCV positive patients fromTuzla for HCV RNA using reverse transcription polymerase chainreaction (Amplicor Roche diagnostic commercial test) and geno-type with method of reverse hibridization of amplified samplematerial (Innolipa HCV II commercial test).Results In 2002 we registered a prevalence of 39.1 and an inci-dence of 3.1% of anti-HCV positive HD patients in 23 HD units,and in 2003 a prevalence of 29.3 and an incidence of 2.04% in 24HD units. Prevalence of anti-HCV positive patients was signifi-
s c¢ c¢ c¢

82 Abstracts
Ther Apher Dial, Vol. 9, No. 1, 2005
cantly different in HD units, from 14.3 to 69.1%. From 88 testedanti-HCV positive HD patients in Tuzla HD unit, we found 76HCV RNA positive patients (87.36%). The genotype of HCV wasanalysed in 59 of these patients and we found, unusual for Europe,genotype 4 in 37 (62.7%), genotype 1b in 17 (28.8%) and 1a infive patients (8.5%). A total of 61% of seroconversions happenedin 1999, 2000 and 2001. In 2001, we separated dialysis machinesfor anti-HCV positive and anti-HCV negative patients, and in2003 we had nine seroconversions (genotype 4 in five patients).These patients had no blood transfusions.Conclusions Prevalence and incidence of anti-HCV positivehemodialysis patients is still high in BH and origin of genotype 4HCV is not clear. Nosocomial spreading of HCV plays a signifi-cant and probably the most important role in transmission of HCVin HD units.
13
Survival of Hemodialysis Patients Older Than 65 years: Influence of Albumin, Hemoglobin, and Cholesterol ConcentrationL Orli , Mati Gla ar and B Sladoje MartinoviKlinika za internu medicinu, Odjel za dijalizu i nefrologiju, KBC Rijeka, Rijeka, Hrvatska
More and more patients over 65 years of age are starting dialysistreatment. It is understood that they are a special and more sen-sitive group, due to their age and correlated diseases. The aim of thiswork is to analyze the influence of albumin, hemoglobin, and cho-lesterol concentration at the beginning of treatment on survival ofpatients over 65 years. Between January 1, 1995 and December 31,1999, we followed 61 patients starting hemodialysis (31 male and 30female). All patients were over 65 years old. Their survival wasmonitored until June 30, 2002. They were divided into four groups,according to years of survival. In the first group were the patientswho died during the first year of treatment. The second group con-sisted of patients who died in the second year of treatment. In thethird group were patients still alive in the third year of treatmentand up to the fifth year. The fourth group consist of the patients whosurvived longer than five years. The average albumin values (g/L)for the first group at the beginning of dialysis were 31.9 ± 5.9; forthe second 35.3 ± 6.4; the third 38.1 ± 6.6 and the fourth 41.8 ± 6.7(P = 0.017). Initial hemoglobin (g/L) was, for the first group81.1 ± 14.3; the second group 85.7 ± 20.5; the third 86.4 ± 14.5 andthe fourth 97.2 ± 6.2 (P = 0.021). Cholesterol (mmol/L) in the firstgroup, when they started the treatment, was 4.7 ± 1.1, the second5.1 ± 1.8, the third 5.2 ± 1.5, and the fourth 5.1 ± 0.7 (P = 0.072).From these results it is obvious that shorter survival of olderpatients on hemodialysis is in correlation with lower albumin andhemoglobin values in the beginning of treatment. Also, patientswith shorter survival rates had lower cholesterol values, but hereare no statistically significant differences. It can be concluded thatthere is a better prognosis for patients starting dialysis when theyhave good albumin, hemoglobin and cholesterol values.
14
Tuberculosis Skin Test in Chronic Hemodialysis PatientsA Urban i , V Premru, B Knap, M Benedik, J Ponikvar-Buturovi , R Ponikvar and A F BrenDepartment of Nephrology, Dialysis Center, Clinical Center, Ljubljana, Slovenia
The incidence of tuberculosis (TB) is increasing worldwide due toincreasing number of immigrants during recent years. This
c¢ D- c¢ z c¢
c cc¢
increases the risk of TB in high risk groups of patients. Cellularimmunity has been demonstrated to be impaired in chronic hemo-dialysis (CHD) patients. Accordingly the incidence of TB indialysis patients was presumably higher than in the generalpopulation. In an attempt to detect patients at risk for TB amongCHD patients a crossover evaluation of tuberculosis skin test wasperformed in our dialysis center. Some preliminary results arepresented here. Among 203 tested CHD patients 139 (68.5%) didnot respond. In 64 (31.5%) patients, infiltrate was detected.The diameter of the infiltrate was 1 to <5 mm in 4/64 patients(6.25%); it was 5 to <10 mm in 18/64 pts (28.1%) and >10 mm in36/64 patients (56.3%). Mean age of tested patients on CHD formore than a year was similar in infiltrate positive subgroups ofpatients: 59.7, 58.7, and 55.9 years respectively. There are ques-tions whether younger CHD patients have a better preservedcellular immunity; whether markedly positive skin test reactionfor TB is connected with triggered cellular immune response toTB or is it a sign of subclinical TB disease. Chronic hemodialysispatients with highly positive skin TB test should be actively exam-ined for TB disease.
15
Circulating Levels of Interleukin-6 in Hemodialysis PatientsI Rus1, I Avber ek-Lu nik2
1Dialysis Center, 2Biochemical Laboratory, General Hospital Jesenice, Jesenice, Slovenia
Introduction Interleukin-6 (IL-6) has been described as bothpro–inflammatory and anti–inflammatory molecule, a hematopoi-etic factor, an inducer of plasma cell development and modulatorof bone resorption. Various studies reported that this cytokineinduces osteoclast–mediated bone resorption in vitro and in vivo.Few studies have been reported circulating IL-6 levels in hemodi-alysis (HD) patients so far. In the present study we measured IL-6 serum levels in a group of HD patients. We hypothesized directrelationship between parathyroid hormone (PTH) and IL-6 serumlevels.Methods Criteria for patient entry into the study were patientswith end stage renal failure without signs of inflammation(CRP < 5 mg/L). We enrolled 35 HD patients (mean age:60.2 years, HD duration: 6 to 384 months). Patients were dividedinto two subgroups with PTH below (N = 21) and above (N = 14)450 pg/mL. The mean value of two consecutive PTH measure-ments within 1 month was obtained for each patient. In all patientsIL-6 and intact PTH were measured by immunometric assays(Immulite, DPC, USA).Results We obtained higher serum IL-6 in HD patients(5.43 ± 3.52 pg/mL) than in healthy people (reference range: 2.0–3.3 pg/mL, presented by manufacturer). Pearson’s correlationbetween IL-6 and PTH was not significant (r = -0.039, P = 0.824).IL-6 levels differed significantly between low and high PTH sub-groups (5.28 ± 4.17 pg/mL vs 5.65 ± 2.35 pg/mL; P = 0.033). Thecorrelation between IL-6 and PTH was not significant in bothsubgroups.Conclusions Mean IL-6 serum levels were 1.6-fold higher in HDpatients than the upper level of reference range. They were alsosignificantly higher in HD patients with PTH above 450 pg/mL.The direct relationship between PTH and IL-6 was not confirmed.Our results provide only a brief insight into circulating levels ofIL-6 in uremic patients which might reflect resorptive phase ofbone remodeling process. This, however, has not yet been con-firmed.
s z

Abstracts 83
Ther Apher Dial, Vol. 9, No. 1, 2005
16
Treating of Nasal Carriers with Mupirocin and Prevention of Staphylococcus aureus Peritonitis and Esi/Ti in Peritoneal Dialysis PatientsA Gu ek, B Karas, J Pajek and M BenedikDepartment of Nephrology, University Medical Center, Ljubljana, Slovenia
Several studies found an increased risk of Staphylococcus aureus(SA) exit-site and/or tunnel infections (ESI/TI) or peritonitis (P)in SA nasal carriers. The aim of our study was to determine effi-cacy of local preventive therapy with mupirocin in nasal carriersof SA. In this prospective study, from January 1997 to December2003, 127 patients (pts) were included and observed for 4696 pt-months. The ones with one or more positive smears were treatedwith mupirocin for five consecutive days, twice daily, every month.In acute or chronic ESI/TI with SA, the mupirocin was appliedduring daily exit-site care. The pts with good or perfect exit-siteswere not treated. For statistic analysis, the proportion test andPearson¢s correlation test were used. Among our pts the numberof nasal carriers has decreased significantly (P < 0.05) from 1997(49.3%) to 2003 (18.0%). Simultaneously, the rates of SA perito-nitis dropped from 0.032 episode/pt year in 1997 to 0.022 in 2003(P = 0.25). Significantly less (P = 0.005) new SA ESI/TI were reg-istered, from 0.113 episode/pt-year in 1997 to 0.018 in 2001 and0.022 in 2003. Two cases of mupirocin-resistant SA were isolated,both in 2003, present in nasal as well as in ESI/TI swab. Diagnosisand treatment of SA nasal carriers among PD pts has proved tobe important. The decrease in incidence of new ESI/TI was statis-tically significant, while peritonitis rates decreased less signifi-cantly. Mupirocin-resistance in our study is low. When peritonealcatheter exit-site is good or perfect, treatment with mupirocin isnot necessary.
17
Osteoprotegerin and Bone Turnover Markers in Serum of Dialysis PatientsI Rus1, I Avber ek-Lu nik2 and J Marc3
1Nephrology Department, 2Laboratory Department, General Hospital Jesenice; 3Faculty of Pharmacy, University of Ljubljana, Slovenia
Introduction Recent studies have shown high circulating levelsof osteoprotegerin (OPG), one of the local regulators of boneremodelling in renal osteodystrophy. For non-invasive bone turn-over assessment several serum markers are used, therefore weinvestigated the relationship between OPG and some of estab-lished serum markers.Methods The 33 dialysis patients (age: 56.6 ± 12.2 years) and 20control individuals (age: 56.0 ± 20.6 years) were included in thisstudy. Dialysis patients were divided according PTH serum levels(below/above 300 pg/mL) into low (N = 23) and high (N = 10)PTH subgroups. Bone alkaline phosphatase (BALP), osteocalcin(OC), tartarate-resistant acid phosphatase 5b (TRAP 5b) andOPG were measured in all serum samples by specific immunoas-says, using commercially available reagent kits.Results Serum OPG levels in the whole group of dialysis patients(679.0 ± 213.0 pg/mL) were approximately two times higher thanin controls (337.1 ± 103.0 pg/mL). The difference in OPG levelsbetween low (708.8 ± 219.3 pg/mL) and high (613.3 ± 191.9 pg/mL) PTH subgroup was not significant (P = 0.223). In contrast,serum levels of OC and TRAP 5b differed significantly (P < 0.045)
c
s z
and BALP near the limit of significance (P = 0.065). We observednonsignificant correlation between OPG and measured bonemarkers in both PTH subgroups (r < 0.18). The relation betweenOPG and PTH was also inverse and nonsignificant (r < -0.365).Conclusions These results indicate that OPG alone does notmatch the requirements of a useful biochemical marker for differ-entiation between dialysis patients with low and high bone turn-over. However, established serum bone markers could serveclinicians in diagnosing specific types of renal osteodystrophy.
18
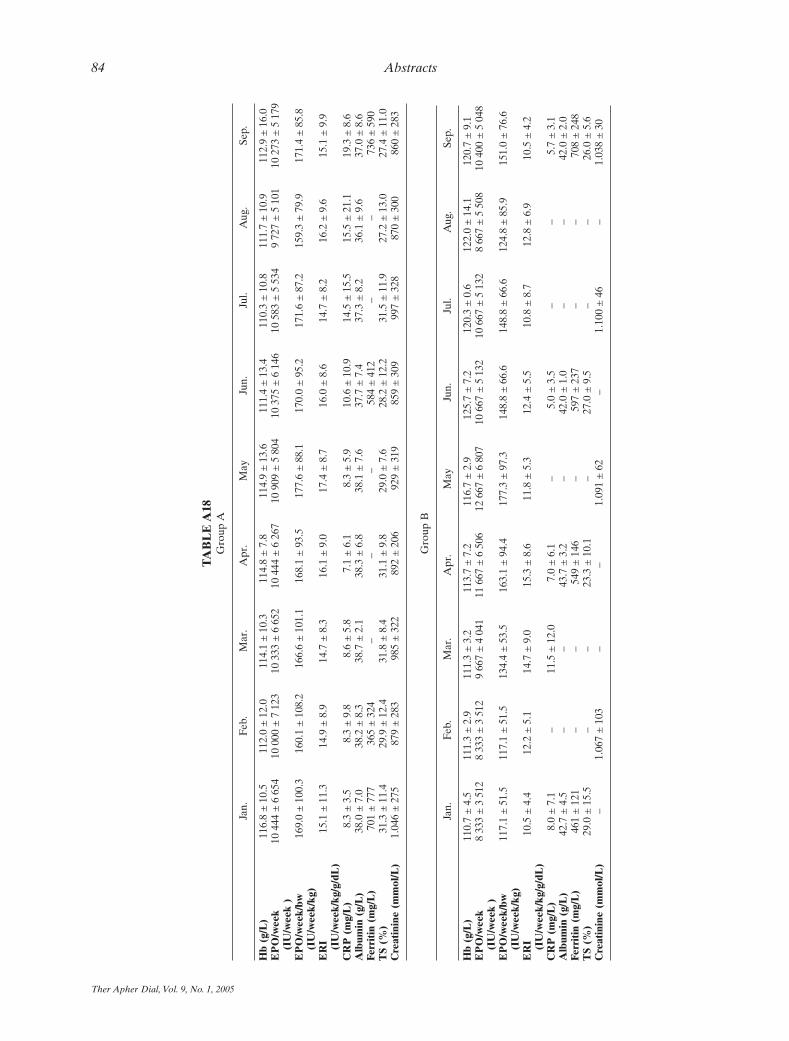
Erythropoietin Requirements in Chronic Hemodialysis Patients After Failure of Kidney TransplantN kofic, R Ponikvar, A F Bren, A Kandus, J Varl, M Malovrh and J Buturovi -PonikvarDialysis Center, Department of Nephrology, University Medical Center, Ljubljana, Slovenia
Introduction Studies have shown that presence of a failed kidneytransplant in patients returning to chronic hemodialysis followingfailure of their kidney transplant is associated with chronic inflam-matory state and erythropoietin resistance. The aim of our retro-spective clinical study was to analyze erythropoietin requirementsin chronic hemodialysis patients after failure of kidney transplant.Patients and methods Fifteen chronic hemodialysis patients afterfailure of kidney transplant, 11 males and 4 females, at the mean ageof 47.3 ± 13.3 years (range 21–65 years), were included in the study.Twelve patients had a failed kidney transplant still in place (groupA) and 3 patients were had had a failed transplant nephrectomy(group B). Hemoglobin level (Hb), erythropoietin dose per week(EPO/week), erythropoietin dose per week per dry body weight(EPO/week per bw), erythropoietin resistance index (ERI = EPO/week per bw per Hb), C-reactive protein (CRP), albumin level, fer-ritin level, transferrin saturation (TS) and creatinine level wereanalyzed monthly from January to September 2004.Results (see Table A18)Conclusion Our study showed that chronic hemodialysispatients with a failed kidney transplant still in place had increasederythropoietin requirements. They exhibited higher erythropoi-etin resistance with worse anemia and worse biochemical param-eters characteristic of chronic inflammatory state compared tochronic hemodialysis patients after a failed transplantnephrectomy.
19
Effect of Intermittent Compression of Upper Arm Veins on Forearm Vessels in Patients with End-Stage Renal DiseaseR R Rus, R Ponikvar2, R B Kenda1, A Urban i 2, J Buturovi -Ponikvar2
1Department of Pediatric Nephrology, 2Department of Nephrology, University Medical Center, Ljubljana, Slovenia
Background Native arteriovenous fistula is the best vascularaccess for chronic hemodialysis. Primary and long-term successdepends, in part, on the state of arteries and veins at the time ofthe operation. The aim of our study was to investigate the effectsof intermittent compression of upper arm veins on forearm vesselsin patients with terminal renal disease.Methods The study group comprised 16 chronic hemodialysispatients who performed daily intermittent compression of the
Sc¢
c cc¢
84 Abstracts
Ther Apher Dial, Vol. 9, No. 1, 2005
TAB
LE
A18
Gro
up A
Jan.
Feb.
Mar
.A
pr.
May
Jun.
Jul.
Aug
.Se
p.
Hb
(g/L
)11
6.8
± 1
0.5
112.
0 ±
12.
011
4.1
± 1
0.3
114.
8 ±
7.8
114.
9 ±
13.
611
1.4
± 1
3.4
110.
3 ±
10.
811
1.7
± 1
0.9
112.
9 ±
16.
0E
PO
/wee
k(I
U/w
eek
)10
444
± 6
654
10 0
00 ±
7 1
2310
333
± 6
652
10 4
44 ±
6 2
6710
909
± 5
804
10 3
75 ±
6 1
4610
583
± 5
534
9 72
7 ±
5 1
0110
273
± 5
179
EP
O/w
eek/
bw(I
U/w
eek/
kg)
169.
0 ±
100
.316
0.1
± 1
08.2
166.
6 ±
101
.116
8.1
± 9
3.5
177.
6 ±
88.
117
0.0
± 9
5.2
171.
6 ±
87.
215
9.3
± 7
9.9
171.
4 ±
85.
8
ER
I (IU
/wee
k/kg
/g/d
L)
15.1
± 1
1.3
14.9
± 8
.914
.7 ±
8.3
16.1
± 9
.017
.4 ±
8.7
16.0
± 8
.614
.7 ±
8.2
16.2
± 9
.615
.1 ±
9.9
CR
P (
mg/
L)
8.3
± 3
.58.
3 ±
9.8
8.6
± 5
.87.
1 ±
6.1
8.3
± 5
.910
.6 ±
10.
914
.5 ±
15.
515
.5 ±
21.
119
.3 ±
8.6
Alb
umin
(g/
L)
38.0
± 7
.038
.2 ±
8.3
38.7
± 2
.138
.3 ±
6.8
38.1
± 7
.637
.7 ±
7.4
37.3
± 8
.236
.1 ±
9.6
37.0
± 8
.6Fe
rrit
in (
mg/
L)
701
± 7
77 3
65 ±
324
––
– 5
84 ±
412
––
736
± 5
90T
S (%
)31
.3 ±
11.
429
.9 ±
12.
431
.8 ±
8.4
31.1
± 9
.829
.0 ±
7.6
28.2
± 1
2.2
31.5
± 1
1.9
27.2
± 1
3.0
27.4
± 1
1.0
Cre
atin
ine
(mm
ol/L
)1.
046
± 2
75 8
79 ±
283
985
± 3
22 8
92 ±
206
929
± 3
19 8
59 ±
309
997
± 3
28 8
70 ±
300
860
± 2
83
Gro
up B
Jan.
Feb.
Mar
.A
pr.
May
Jun.
Jul.
Aug
.Se
p.
Hb
(g/L
)11
0.7
± 4
.511
1.3
± 2
.911
1.3
± 3
.211
3.7
± 7
.211
6.7
± 2
.912
5.7
± 7
.212
0.3
± 0
.612
2.0
± 1
4.1
120.
7 ±
9.1
EP
O/w
eek
(IU
/wee
k )
8 33
3 ±
3 5
128
333
± 3
512
9 66
7 ±
4 0
4111
667
± 6
506
12 6
67 ±
6 8
0710
667
± 5
132
10 6
67 ±
5 1
328
667
± 5
508
10 4
00 ±
5 0
48
EP
O/w
eek/
bw(I
U/w
eek/
kg)
117.
1 ±
51.
511
7.1
± 5
1.5
134.
4 ±
53.
516
3.1
± 9
4.4
177.
3 ±
97.
314
8.8
± 6
6.6
148.
8 ±
66.
612
4.8
± 8
5.9
151.
0 ±
76.
6
ER
I (IU
/wee
k/kg
/g/d
L)
10.5
± 4
.412
.2 ±
5.1
14.7
± 9
.015
.3 ±
8.6
11.8
± 5
.312
.4 ±
5.5
10.8
± 8
.712
.8 ±
6.9
10.5
± 4
.2
CR
P (
mg/
L)
8.0
± 7
.1–
11.5
± 1
2.0
7.0
± 6
.1–
5.0
± 3
.5–
–5.
7 ±
3.1
Alb
umin
(g/
L)
42.7
± 4
.5–
–43
.7 ±
3.2
–42
.0 ±
1.0
––
42.0
± 2
.0Fe
rrit
in (
mg/
L)
461
± 1
21–
– 5
49 ±
146
– 5
97 ±
237
––
708
± 2
48T
S (%
)29
.0 ±
15.
5–
–23
.3 ±
10.
1–
27.0
± 9
.5–
–26
.0 ±
5.6
Cre
atin
ine
(mm
ol/L
)–
1.06
7 ±
103
––
1.09
1 ±
62
–1.
100
± 4
6–
1.03
8 ±
30

Abstracts 85
Ther Apher Dial, Vol. 9, No. 1, 2005
upper arm without vascular access by elastic band (Eschmarch).Ten chronic hemodialysis patients were included in the controlgroup which performed no specific activity.Forearm measurements were obtained at the beginning of thestudy and 4 and 8 weeks later during the course of intermittentcompression of the upper arm veins. The forearm circumferenceand maximal handgrip strength were measured. The arteryparameters, including endothelium-dependent vasodilatation andforearm vein parameters, were obtained by ultrasonographymeasurements.Results The forearm circumference, maximal handgrip strengthand artery parameters, including endothelium-dependent vasodi-latation, remained unchanged. The basal venous diameters(2.29 mm ± 0.19 at the beginning, 2.46 mm ± 0.19 after 4 weeksand 2.53 mm ± 0.18 after 8 weeks) were significantly increased inthe study group. The distensibility of veins was preserved in thestudy group. There were no significant changes in the controlgroup.Conclusions Our study demonstrated that daily intermittentcompression of the upper arm veins increases the forearm veindiameter and preserves the distensibility of veins in patients withend-stage renal failure.
20
Early Arteriovenous Fistula Construction–Late Beginning of Hemodialysis Treatment?M MalovrhDepartment of Nephrology, University Medical Center Ljubljana, Ljubljana, SloveniaIntroduction It was noticed that the decline of renal function wasslower in patients (pts) with end stage renal disease (ESRD) afterearly arteriovenous fistula (AVF) construction. The aim of thisprospective study was to find out the influence of AVF on theprogression of renal failure.Patients and methods Sixty ESRD pts with serum creatininelevel (SCL) between 400 and 500 mmol/L were included and ran-domized in two groups. One group of pts received AVF and theother did not. Serum creatinine level, creatinine clearance (CC),and mean arterial pressure (MAP) were followed every twomonths for one year. All pts were clinically evaluated for signs ofcardiac insufficiency. Hemodialysis (HD) was started when SCLwas 850 mmol/L or CC 10 mL/min or when signs of uremia werepresented.Results In Group A, 30 ESRD pts, 17 males and 13 females,age 61 ± 7.3 years, mean SCL 446.4 ± 30.5 mmol/L, mean CC29.3 ± 4.1 mL/min, native forearm AVFs were constructed. NoAVFs were constructed in Group B, 30 pts, 12 males and 18females, mean age 62.8 ± 8.2 years, mean SCL 447.6 ± 37.6 mmol/L,mean CC 29.1 ± 4.7 mL/min. Mean SCL during a 12 month periodin both groups is shown in Table A20.
After 12 months in Group A, 4/30 pts (13%) (1 after 6 months,2 after 8 months, 1 after 10 months) started hemodialysis (HD),26 pts had mean CC 23.1 ± 4.5 mL/min, MAP was 118 mmHg, nosign of cardiac insufficiency was found. In Group B, 11/30(37%)(P < 0.01) (1 after 4 months, 5 after 6 months, 4 after8 months, 1 after 10 months) started HD, central vein catheter wasused as a vascular access. In the remaining 19 pts mean CC15.6 ± 4.5 mL/min (P < 0.01), MAP was 123 mmHg (NS).Conclusions This prospective study confirmed our previousobservations of renal function after AVF construction. Besidesmatured AVF, the before-HD benefit of early AVF on progressionof renal insufficiency can be important. The reasons for this arenot well known. There are two possibilities: increased cardiac out-put and decreased resistance of intrarenal vessels. Measurementof renal perfusion and calculation of resistance index by duplexsonography is planned.
21
Review of Treatment with Vitamin D: Ten Month ObservationM Malovrh, V PremruDepartment of Nephrology, University Medical Center Ljubljana, Ljubljana, Slovenia
Introduction Hyperparathyroidism continues to be a majorproblem in patients with chronic kidney disease (CKD). Hypoc-alcemia and hyperphosphatemia are crucial for the developmentof secondary hyperparathyroidism (SHP). Preventing hyperphos-phatemia ameliorates the progression of SHP. Vitamin D analogs(Alpha D3) per oral after hemodialysis (HD) could be used in thetherapy of SHP. The purpose of this review in one dialysis centerwas to analyze the quality of such treatment.Patients and methods Patients (pts) on HD in one dialysis centerwere included in this analysis. Calcium (Ca) and phosphate (P)were followed during a 10 month period every 3 weeks and intactparathyroid hormone (iPTH) every three months. Vitamin D wasgiven after HD per oral under nurse control.Results Sixty-four pts, 34 female and 30 male, mean age59.9 ± 11.5 (range 32–82) years, HD treatment length mean8.8 ± 7.2 (range 0.7–30.7) years were observed. Mean Ca was2.46 ± 0.04 mmol/L, (range from 1.06 to 2.72), mean P1.52 ± 0.08 mmol/L (range from 0.62 to 3.53), mean iPTH211.9 ± 36.7 ng/L (range from 1 to 699). Mean calcium concentra-tion in dialysis fluid was 1.51 ± 0.02 mmol/L and mean dose ofvitamin D was 0.35 ± 0.11 mg.Mean values of parameters during the 10 months observation areshown in Table A21.
Conclusions Regular evaluation of Ca, P, iPTH and strict correc-tion of calcium concentration in dialysis fluid, per oral vitamin Dare very helpful in prevention of SHP. Critical elevation of iPTHwas in pts with low compliance in hypophosphatemic diet andtherapy. If concentration of phosphate is normal, elevated iPTHcould be diminished very effective by titration of vitamin D.
TABLE A20. Serum creatinine in a 12 month period (mmol/L)
Group A Group B
Start 446.4 ± 30 447.6 ± 372 months 451.9 ± 39 472.8 ± 39*4 months 466.4 ± 43 508.0 ± 60*6 months 482.8 ± 77 579.6 ± 123**8 months 493.1 ± 73 612.7 ± 127**10 months 494.3 ± 74 653.0 ± 141**12 months 509.2 ± 50 660.3 ± 123**
*P < 0.05, **P < 0.01.
TABLE A21
December2003
February2004
April2004
June 2004
Ca (mmol/L) 2.46 2.44 2.35 2.38P (mmol/L/ 1.52 1.56 1.71 1.53iPTH (ng/L) 204.8 173.1 272.3 196.5Ca in fluid (mmol/L) 1.52 1.53 1.49 1.49Dose of vitamin D (mg) 0.47 0.28 0.21 0.43

86 Abstracts
Ther Apher Dial, Vol. 9, No. 1, 2005
22
Subcutaneous Compared with Intravenous Epoetin in Patients Receiving Hemodialysis: One Center StudyM Malovrh and V PremruDepartment of Nephrology, University Medical Center Ljubljana, Ljubljana, SloveniaIntroduction There is strong evidence from randomized trialsthat subcutaneous (s.c.) epoetin is as effective as intravenous (i.v.)and may allow a lower dose to be used, thereby reducing costs.Dose requirements for s.c. are reported to be from 22–32% lowerthan those of i.v. epoetin. The purpose of these analyses was tofind out what was increasing the epotein dose after the beginningof i.v. administration.Patients and methods Patients (pts) on HD treated with epoetins.c. for 10 months (group A), and then with epoetin i.v. for10 months (group B) were included in this analysis. Hemoglobin(Hb), epoetin (alpha or beta) dose (EPO), and ferritin wereevaluated.Results 46 pts, 25 females and 21 males, mean age 58.2 ± 12.6(range 30–80) years, HD treatment mean 9.1 ± 7.7 (range 0.2–29.2) years were observed. In Group A, mean Hb was 123.8 g/L ± 2.4 (range 119–127), mean EPO 6914 ± 810 IE/week, ferritin603.5 ± 46.2 mg/L. In Group B mean Hb was 120.3 g/L ± 2.3 (range117–125) (P < 0.001), mean EPO 7433 ± 787 IE/week (NS),increasing for 7.5%, ferritin 534.2 ± 126.2 mg/L. Hemoglobin andEPO at different periods are shown in Table A22.
Conclusions We found minor difference between the doses ofs.c. and i.v. epoetin needed. There was no significant differencewhen mean value of whole group was compared, but in 50% thisdifference was statistically significant. Our results suggest that s.c.epoetin is more effective than i.v., but not in such huge amountsas some studies showed.
23
Review of Treatment with Epoetin: 10 Months ObservationM Malovrh, V PremruDepartment of Nephrology, University Medical Center Ljubljana, Ljubljana, Slovenia
Introduction Renal anemia is a major problem of patients withchronic kidney disease (CKD). Target hemoglobin concentration(Hb) in these patients should be >110 g/dL and hematocrit (Ht)
>0.33. Treatment of renal anemia with epoetin is a well estab-lished practice.The purpose of this review in one dialysis center was to analyzethe quality of such treatment and to find which parameters couldinfluence success of treatmentPatients and Methods Patients (pts) on HD were included in thisanalysis. The properties Hb, Ht, epoetin (alpha or beta intrave-nously) dose (EPO), ferritin, transferrin saturation (TSAT), hypo-chromic red cells (HYPO), CRP, albumin, parathyroid hormone(PTH) Kt/V were followed during 10 months period.Results 58 pts, 29 female and 29 male, mean age 60.5 ± 12.5(range 32–82) years, HD treatment mean 8.4 ± 7.8 (range 0.7–30.7) years were observed. Mean Hb was 119.9 g/L ± 2.1 (range79–142), mean Ht 0.36 ± 0.01, mean EPO 6970 ± 456.7 IE/week.EPO 110.3 ± 7.9 IE/kgBW/week, ferritin 603.5 ± 46.2 mg/L, TSAT25.8 ± 3.3%. HYPO 2.1 ± 0.1, CRP 7.4 ± 0.21, albumin41.9 ± 0.37 g/L, PTH 281.5 ± 47.9, Kt/V 1.68 ± 0.34. The female andmale groups were analyzed and compared (Table A23)
Conclusions Regular evaluation of crucial parameters for ane-mia correction and strict adaptation of EPO doses and iron ther-apy enable optimal maintenance of Hb and Ht, recommended byEuropean best practice guidelines. We found significant differencein EPO dose per week, but calculating to kg BW there was nosignificant difference between females and males.
24
Response on Epoetin Treatment is Poor in Hemodialysed Patients with Low Creatinine and Albumin ValuesB Knap1, M Lain ak2, J Varl1 and AF Bren1
1Department of Nephrology, Clinical Center Ljubljana, Ljubljana, Slovenia; 2Department of Internal Medicine, General Hospital Murska Sobota, Murska Sobota, Slovenia
Background Anemia frequently accompanies chronic renal fail-ure in patients treated with hemodialysis (HD). Despite treatmentwith erythropoetin up to 10% of patients still present with pro-nounced anemia. In the present study we wanted to identify sim-ple laboratory parameters or clinical characteristics, associated toanemia in patients treated with erythropoetin.Methods During May 2003 we screened all patients at our hemo-dialysis center for the presence of severe anemia (Hemoglobin(Hb) 100 or lower, Group 1) and compared them to the patientswithout anemia (Hb 120 or higher, Group 2). Patients with chronicbleeding or the ones receiving transfusion were excluded. Basicdemographic characteristics, blood pressure, and several biochem-ical markers were obtained for the enrolled patients. All data weretested for significance using Student’s t-test.
sc
TABLE A22
Group A Group B
Hb (g/L) EPO (IE/w) Hb (g/L) EPO (IE/w)
1 126.1 ± 10.9 8022 ± 5164 124.6 ± 11.1 5913 ± 3740*2 125.4 ± 9.5 7674 ± 5208 122.7 ± 11.1 6195 ± 38963 124.9 ± 9.9 7681 ± 5147 122.2 ± 12.8 7133 ± 49384 124.3 ± 11.3 7954 ± 4675 119.3 ± 13.3* 7282 ± 54395 124.0 ± 11.5 7340 ± 4435 118.2 ± 9.9* 7521 ± 46366 126.2 ± 11.6 7022 ± 44541 118.9 ± 10.7** 7804 ± 45587 127.3 ± 11.1 6022 ± 4427 120.2 ± 10.5 8043 ± 4584*8 125.3 ± 12.0 5777 ± 4567 121.2 ± 10.3 7913 ± 4554*9 121.2 ± 12.2 6222 ± 4851 118.3 ± 11.1* 8500 ± 4660*
10 119.0 ± 12.5 6232 ± 4374 117.3 ± 9.8 8239 ± 421211 120.5 ± 10.5 6200 ± 4634 119.2 ± 9.8 8431 ± 4189**12 118.9 ± 11.5 6466 ± 4148 121.0 ± 9.7 7717 ± 4166*
w, week; *P < 0.05 **P < 0.001.
TABLE A23
Female Male
Age 61.3 ± 14.6 59.7 ± 10.3HD 8.0 ± 7.9 8.7 ± 7.7Hb 119.8 ± 1.9 120.0 ± 1.8Ht 0.36 ± 0.01 0.36 ± 0.01EPO/w 6737 ± 336 7276 ± 404*EPO/kgBW/w 116.5 ± 3.9 111.7 ± 7.0Ferritin 589.0 ± 69.4 618.5 ± 36.5TSAT 27.5 ± 3.6 23.6 ± 3.1*CRP 7.4 ± 0.2 9.6 ± 0.1Kt/V 1.91 ± 0.31 1.47 ± 0.21**
w, week; *P < 0.05; **P < 0.001.

Abstracts 87
Ther Apher Dial, Vol. 9, No. 1, 2005
Results Out of 177 patients, 34 (Group 1) and 38 (Group 2) metthe inclusion criteria. There was no difference in age, gender, timeon HD and blood pressure (148 ± 22/81 ± 13 mm Hg vs. 151 ± 33/81 ± 15 mm Hg). Next to significant difference all hematologicalparameters (Hb 92 ± 8 vs. 127 ± 6; Ht 0.29 ± 0.03 vs. 0.40 ± 0.02;Ery 3.04 ± 0.32 vs. 4.17 ± 0.32; P < 0.001 for all) patients with ane-mia received a higher weekly dose of erythropoetin (12000 ± 5205IE vs. 7825 ± 4829 IE, P < 0.001), had lower albumin (35.6 ± 3.4 vs.38.1 ± 2.8, P < 0.001) and creatinine concentration (798 ± 218 vs.932 ± 266, P < 0.005). For other markers such as ferritin, iPTH,folic acid, and vitamin B12 we observed a trend to higher valuesin anemic patients.Conclusions Our data suggest that malnutrition and low musclemass are associated to poor response of treatment with erythro-poetin in patients with chronic renal failure treated with HD.Larger sample and prospective follow up could identify furthersimple markers of inadequate response to the treatment of anemia.
25
Frequent Low-Dose Iron Supplementation To Hemodialysis PatientsV Premru and M MalovrhCenter for hemodialysis Leoni e, University Medical Center Ljubljana, Slovenia
Outline Regular iron supplementation to most hemodialysis(HD) patients is necessary to ensure adequate response to epoetin(Epo). As enteral absorption of ferric compounds is insufficient inuremia, parenteral application is often needed. Usually, a dose ofelementary iron is injected intraveneously at the end of an HDsession once weekly to monthly according to the individualpatient’s needs. Doses range from usual 100 mg to several hundredmg. A surplus of iron immediately after application is transportedto physiologic stores but might also be deposited at other sites inthe body where it becomes inaccessible. In the long term, deposi-tion of iron might lead to hemosiderosis and organ malfunction.Increased oxidative stress and acute toxic effects might supervenealong with the increased susceptibility to infection, becoming fatal.Patients and methods In 59 patients on regular iron supplemen-tation, we examined the effects of frequent low-dose (25 mg) incomparison to usual regime of 100 mg post-dialysis i.v. iron on Hbconcentration and the required Epo dose to maintain the Hbtarget (120 g/L).Results (see Table A25)Conclusions Initial results suggest that stable Hb levels could bemaintained at the same Epo dosage with substantially lower doseof i.v. iron. Iron applied at the moment when the requirements arethe greatest (i.e., at the same time as Epo is being applied) couldenable higher iron bioavailability with less iron burden to body
sc
stores. This could possibly result in a better Epo response withavoidance of long-term iron sequestration and acute toxic effects.
26
Regional Citrate Anticoagulation During Hemodialysis: Our ExperiencesJ Buturovi -Ponikvar, S atak, M Benedik, J Varl, B Knap, A Marn Pernat, A Kandus, A Gu ek, V Premru, M Malovrh, J Guben ek, N kofic, L Gaber, A F Bren and R PonikvarDialysis Center, Department of Nephrology, University Medical Center Ljubljana, SloveniaBackground Regional citrate anticoagulation (RCA) duringhemodialysis is alternative to heparin in patients at high risk ofbleeding. It enables excellent antithrombotic effect in the circuit,but requires strict monitoring during the procedure. The aim ofour retrospective clinical study is to evaluate safety and efficacyof RCA performed according to our unit protocol.Methods Data from 40 protocols for RCA performed betweenApril and June 2004 were analyzed. Double-needle vascular accesswas obtained via either arteriovenous fistula or hemodialysis cath-eter. Hollow-fiber dialyzer Polyflux 14 S (Gambro, Lund, Sweden)was used in all dialysis sessions. Calcium-free dialysate was usedand set to: Na 137 mEq/L, bicarbonate 28 mEq/L, magnesium0.5 mEq/L, potassium 2.0 mEq/L, glucose 0 mEq/L. Potassiumand glucose were added into the dialysate or intravenously ifneeded, respectively. Blood flow rate was maintained between250–300 mL/min. 4% trisodium citrate was infused in the arterialline of the circuit, proximally from the arterial bubble trap, at theinitial rate 300 mL/hour and adjusted accordingly to the bloodflow rate and targeted clotting time (15–20 minutes in the circuit).One molar CaCl2 was infused in the venous line (distally from thevenous bubble trap) at the initial rate 13 mL/h and was adjustedto maintain ionized calcium concentration (iCa) within normalrange. Clotting time, iCa, Na, and bicarbonate were measuredduring hemodialysis. Clot formation in the dialyzer was estimatedby counting the number of clotted fibers and assessment of clotpresence in bubble traps.Results (see Table A26)
c¢ Cc
s S
TABLE A25
Fe++/month(mg)
Hb (g/L) Ht
Epo dose(I.U./week)
Period 1 267 119.4 0.361 6912Period 2 165 120.5 0.366 6895t-test (p) 0.002 0.278 0.905 0.609
TABLE A26
preHD At 60 min At 120 min At 180 min Post HD
Clotting time (min) – 11.0 ± 3.4 11.0 ± 3.3 11.2 ± 3.0 11.2 ± 2.7iCa (mmol/L) 1.15 ± 0.31 1.0 ± 0.12 1.03 ± 0.09 1.04 ± 0.10 1.07 ± 0.20Sodium (mmol/L) 137 ± 4 139 ± 3 139 ± 4 140 ± 3 140 ± 3Bicarbonate (mmol/L) 21.4 ± 3.0 – – – 25.02 ± 3.3pH 7.39 ± 0.04 – – – 7.45 ± 0.07
At 60 min At 120 min At 180 min At 240 min
Blood flow rate (mL/min) 268 ± 24 266 ± 25 267 ± 23 267 ± 23Citrate infusion rate (mL/h) 297 ± 11 298 ± 23 297 ± 22 300 ± 151M CaCl2 inf. rate (mL/h) 12.95 ± 0.45 13.12 ± 1.4 13.17 ± 1.55 13.35 ± 1.1

88 Abstracts
Ther Apher Dial, Vol. 9, No. 1, 2005
Assessment of clotting in the circuit 23/40 dialyzers (57.5%)were estimated as excellent (<10 clotted fibers), 14/40 (35%) asvery good (11–20 clotted fibers), 2/40 (5%) as good (21–50 clottedfibers) and one dialyzer (2.5%) was full of small thrombi (50–100clotted fibers capillaries). We noted significant clots in the venousbubble trap in two dialysis sessions. In addition, significant clotsin the arterial bubble trap was noted in two dialysis sessions. Nodialysis session was terminated prematurely because of technicalor clinical problems.Conclusion Regional citrate anticoagulation performed accord-ing to our protocol was safe and effective. Clotting time was lowerthan targeted, but excellent macroscopic antithrombotic activityin the circuit was achieved.
27
Citrate Anticoagulation for Single-Needle Hemodialysis: Safety and EfficacyJ Buturovi -Ponikvar, J Guben ek and R PonikvarDialysis Center, Department of Nephrology, University Medical Center, Ljubljana, Slovenia
Background Single-needle (SN) hemodialysis can be the onlyoption for selected patients with difficulties with vascular access.Full heparinization is required to avoid clotting in the circuit. Inpatients at risk of bleeding, citrate could be the alternative anti-coagulant. The aim of our retrospective clinical study was to eval-uate safety and efficacy of regional citrate anticoagulation (RCA)during SN hemodialysis.Patients and methods Regional citrate anticoagulation was per-formed using 4% trisodium citrate, 1M CaCl2 and dialysate with0 mmol/L Ca, 0.5 mmol/L Mg and 0 g/L glucose, Na was set at138 mmol/L and HCO3 at 28 mmol/L. Safety was assessed by per-cent of procedures that were terminated prematurely or changedto another modality due to RCA-related complications and byincidence of important hypocalcemia, defined as decrease of iCafrom start of dialysis >0.2 mmol/L or decrease >0.05 mmol/L to avalue of <0.8 mmol/L. Efficacy was evaluated by visual assessingof clot formation in arterial and venous bubble traps and dialyzer,after completing dialysis, by scoring: grade 5 (<10 fibers clotted)to 0 (>20% fibers clotted). It was considered insufficient if thegrade was £3 or a significant clot in bubble traps occurred.Results In retrospective analysis of 41 protocols, importanthypocalcemia was recorded in 34% of cases. 5% of procedureswere terminated prematurely. Median dialyzer grade was 5 (inter-quartile range 4–5, N = 36). Anticoagulation was insufficient in17% (6/36) of procedures, in these cases neither citrate infusionrate was lower nor coagulation time shorter. None of the systemsclotted. Thirty protocols were filled in completely; average param-eters are shown in the table below. In the first hour iCa decreasedin 67% of procedures for 0.08 ± 0.05 mmol/L, those procedureshad significantly lower starting calcium rate (6.4 ± 0.9 vs. 7.3 ± 1.1mmol/L, P = 0.02) and higher starting iCa (1.02 ± 0.13 vs.0.89 ± 0.14 mmol/L, P = 0.02). Over the entire procedure iCadecreased in 80% of cases for 0.17 ± 0.09 mmol/L, there was sig-nificant but small increase in Na (135 ± 4 vs. 137 ± 4 mmol/L,P £ 0.01) and no increase in HCO3 at the end of hemodialysis(Table A27).Conclusions Citrate anticoagulation during single-needle hemo-dialysis is a safe and effective procedure in the majority of patients.CaCl2 infusion rate should often be increased to correct hypocal-cemia. Close monitoring of iCa is mandatory. Increased startingdose of CaCl2 should be evaluated.
c¢ s
28
The Influence of Aerobic Training During Hemodialysis Procedure on Blood Pressure, Heart Rate and Aerobic Capacity of Chronic Hemodialysis PatientsS Fazli , R Ponikvar and J Buturovi -PonikvarDialysis Center, Department of Nephrology, University Medical Center, Ljubljana, Slovenia
Background Several studies have shown beneficial effect of aer-obic exercise performed during hemodialysis procedure. The aimof our prospective clinical study was to evaluate the effect of2 months aerobic exercise during hemodialysis procedure onblood pressure, heart rate and aerobic capacity of chronic hemo-dialysis patients.Methods Eleven adult chronic hemodialysis patients partici-pated the prospective clinical study. Nine of them completed a2 month aerobic exercise program. Exercise training was carriedout during hemodialysis procedure, three times a week, in lyingposition, on the “bed” cycle ergometer Thera-Joy (Medica, Ger-many). The exercise was prescribed based on aerobic capacity andBorg’s scale of subjective effort perceiving and corresponded tomoderate physical exercise (50–70% of the maximum target heartrate). Heart rate and blood pressure were monitored continuouslyduring the procedure. Aerobic capacity was tested before and afterthe 2 month exercise program.Results Mean values of systolic, diastolic blood pressure andheart rate before exercise were 146 ± 9 mmHg, 87 ± 5 mmHg, and77 ± 7 beats/min, respectively. After the exercise systolic and dias-tolic blood pressure were significantly lower and heart rate signif-icantly higher than before (142 ± 9 mmHg, 84 ± 6 mmHg, 82 ± 8,P < 0.05). If comparing systolic and diastolic blood pressure beforeand after the exercise in the first and eighth week of the exerciseprogram, no significant differences were found. However, heartrate was significantly lower before as well as after the exercise inthe eighth week compared to the first week of exercise. Mean VO2
increased from 29.2 ± 8.3 to 30.5 ± 9.3 mL/kg/min, mean doubleproduct increased from 29.7 ¥ 103 ± 6.4 to 32.0 ¥ 103 ± 6.2, bothdifferences not being statistically significant.Conclusion Controlled aerobic exercise during hemodialysisprocedure was safe and well tolerated. No significant difference inblood pressure, significantly lower heart rate and slight (althoughstatistically not significant) improvement in aerobic capacity wereobserved.
29
Temporary Hemodialysis Catheters as a Long Term Vascular Access in Chronic Hemodialysis PatientsR Ponikvar, C Likar, V Premru, M Benedik, J Varl, B Knap, A Urban i , A Marn- Pernat and J Buturovi - PonikvarDepartment of Nephrology, University Medical Center Ljubljana, Slovenia
Background In chronic hemodialysis patients with exhaustedarteries and veins in whom AV fistula or AV graft can not be
c¢ c¢
c cc¢
TABLE A27
Parameter Value
blood flow (mL/min) 244 ± 27starting rate of 4% Na citrate (mL/h) 191 ± 19citrate rate (percent of mean blood flow) 2.6% ± 0.4%starting rate of 1M CaCl2 (mL/h) 6.7 ± 1.1

Abstracts 89
Ther Apher Dial, Vol. 9, No. 1, 2005
performed any more, hemodialysis catheters become the lastresort, either tunneled, so called “permanent”, or non-tunneled,so called “temporary” catheters which can be usefully used for alonger period of time than a permanent vascular access.The aim of our clinical study was to asses temporary, precurved,jugular catheters as permanent vascular access in chronic hemo-dialysis patients.Methods Thirty chronic hemodialysis patients, 15 men, 16women, mean age 65.3 ± 13.5 years (range 30–90), with averagedialysis treatment time of 6.3 ± 8.1 years (range 1 month-30 years), have had single lumen, “temporary” precurved nontun-neled jugular catheters (Medcomp, USA) as permanent vascularaccess. Catheters were placed into right internal jugular vein, bySeldinger’s technique, in local anesthesia (2% lidocain), lockingsolution was 4% trisodium citrate. Catheters were placed by expe-rienced nephrologists, with ultrasound assistance, dressing wasperformed by dialysis nurses. Mupirocin was applied at the exitsite after each hemodialysis. In the case of malfunction, thrombo-sis or infection, the catheter was replaced with the new one, usinga guidewire. Prophylactic ceftazidime in a single dose was usedafter the catheter`s exchange. Unfractionated or fractionated hep-arin was anticoagulant.Results Hemodialysis catheters were used for vascular accesson average for 9.1 ± 6.5 months, range 1–22.7 months, total271.7 months or 8151 days. Average catheter running time was3.1 ± 1.9 months, range 0.5–10 months. Total number of sideeffects was 57, 7.0/1000 catheter days; 26 thrombosis, 3.2/ 1000catheter days; 9 ruptures of the catheter, 1.1/1000 catheter days;15 malfunction, 1.8/1000 catheter days; 2 exit site infections, 0.2/1000 catheter days; 2 bacteremias, 0.2/1000 catheter days; 1 avul-sion of the catheter, 0.1/1000 catheter days; and 2 catheters wereremoved because AV fistula was successfully used.In 21 patients single needle hemodialysis was performed, meanblood flow 251 ± 16 mL/minute, range 250–300, mean KT/V0.96 ± 0.16, range 0.72–1.27and in 9 patients double needle hemo-dialysis was performed (catheter and peripheral vein) with meanblood flow 252 ± 14 mL/minute, range 200–300, mean KT/V1.63 ± 0.25, range 1.21–1.96.Conclusions ‘Temporary’ jugular single lumen non-tunneledhemodialysis catheters provide good long term vascular accesswith acceptable functioning time and low infection rate. KT/V forsingle needle hemodialysis was rather low, however it significantlyimproved when double needle hemodialysis was performed. Themain reasons for catheter removal was thrombosis, malfunction,and mechanical damage of the catheter.
30
Increased Mercury Load in Protein A ImmunoadsorptionA Marn Pernat, M Horvat, M Logar and R PonikvarDepartment of Nephrology, University Clinical Center Ljubljana, Ljubljana, Slovenia
Background Immunoadsorption is an adsorption technique forextracorporeal removal of circulating autoantibodies in autoim-mune diseases such as myasthenia gravis and Guillain-Barré syn-drome. To prevent microbial growth during storage, the protein Acolumns are primed with thiomersal containing toxic ethylmercurywhich could be released during the immunoadsorption treatmentand potentially result in its accumulation and toxicity. To reducea thiomersal-related mercury release during immunoadsorptiontreatment we introduced a modified rinsing solution containing N-acetylcysteine which is an avid mercury scavenger.Methods Thirteen patients were treated by 17 protein A immu-noadsorption treatments and venous blood samples were collected
immediately before and after each session. Whole blood mercurylevels were measured by atomic absorption spectroscopy and eth-ylmercury levels by atomic fluorescent spectroscopy. According tothe manufacturer’s recommendations we used 600 mg of N-acetylcysteine to rinse the mercury from protein-loaded columnsbefore each immunoadsorption treatment.Results Following protein A immunoadsorption ethylmercurylevels increased from 0.148 ± 0.402 ng/g to 2.026 ± 1.944 ng/g(P < 0.001) and whole blood mercury increased from 2.447 ±3.065 ng/g to 20.437 ± 28.603 ng/g (P = 0.02). Post-treatment val-ues of whole blood mercury exceeded upper safety level of 5 ng/g in all 17 immunoadsorption treatments but no patient developedclinical signs of mercury toxicity.In one patient immunoadsorption treatment was repeated within7 days and the results of serial determinations of blood mercurylevels are shown in Table A30.
Conclusions The results of our study showed that whole bloodmercury and ethylmercury levels were increased during the immu-noadsorption treatments, suggesting mercury release from thi-omersal-primed columns even with addition of N-acetylcysteineto the rinsing solution. Mercury release was more pronounced atthe beginning of serial immunoadsorption treatments which indi-cates that mercury exposure might depend on the storage time ofprotein A columns containing thiomersal priming solution.
31
Plasma Exchange Therapy for Severe Hypertriglyceridemia with Acute PancreatitisR Ponikvar, A. Marn-Pernat, R. ugi , J Varl, M Benedik and J Buturovi -PonikvarDepartment of Nephrology, University Medical Center, Ljubljana, Slovenia
Background Serum triglyceride concentrations above 11 mmol/L can precipitate attacks of acute pancreatitis, although the patho-genesis of inflammation in this setting is unclear. In children withinherited disorders of lipoprotein metabolism that are associatedwith severe hypertriglyceridemia, attacks of acute pancreatitis canbe prevented by lowering their serum triglycerides to less than2.2 mmol/L. Some reports revealed favorable effects of membraneplasma exchange in severe hypertriglyceridemia and severe acutepancreatitis. The aim of our retrospective clinical study was toevaluate the efficacy of membrane plasma exchange (MPE) ther-apy in adult patients with severe hypertriglyceridemia and acutepancreatitis in terms of reduction of serum lipids, clinical improve-ment and reliability of the procedure itself.Methods 25 patients (pts; 24 men, 1 woman), aged 31–59 years(mean 44.6 ± 8.0) have been treated with MPE and LDL apheresis
Z c¢c¢
TABLE A30
Ethylmercury Whole blood mercury
(ng/g) (ng/g)
Before IA After IA Before IA After IA
Day 0 0.13 ± 0.03 1.35 ± 0.12 0.49 ± 0.06 76.8 ± 5.6Day 1 0.17 ± 0.00 0.10 ± 0.02 8.14 ± 1.24 19.4 ± 0.6Day 2 0.05 ± 0.00 0.09 ± 0.00 9.57 ± 0.80 11.8 ± 0.9Day 3 0.03 ± 0.00 0.08 ± 0.01 6.96 ± 0.09 8.52 ± 0.39Day 7 1.69 ± 0.00 4.23 ± 0.12 5.54 ± 0.32 9.04 ± 0.48
Data are presented as means ± standard deviation. IA,immunoadsorption.

90 Abstracts
Ther Apher Dial, Vol. 9, No. 1, 2005
(one procedure) for severe hypertriglyceridemia and acute pan-creatitis. Fresenius-Excorim PE monitor and PF 2000 plasmafilterwere used for MPE and Kaneka LDL monitor with dextran sul-phate columns for LDL apheresis. Vascular access was via femoralcatheter and peripheral vein in 16/25 pts (64%), 2 femoral cathe-ters in 8/25 pts (32%), and 2 peripheral veins in 1/25 pt (4%). Theanticoagulant used was heparin in 24/25 pts (96%) and citrate in1/25 (4%). The replacement solution was a mixture of humanalbumin and hemofiltration solution. One to two volumes ofplasma were exchanged per procedure.Results In total 42 procedures, 41 MPE and 1 LDL apheresiswere carried out, mean 1.68 ± 1.0 per patient, one procedure in 14/25 pts (56%), 2 procedures in 7/25 pts (28%), 3 procedures in 3/25 pts (12%) and 5 procedures in 1/25 pt (4%). One volume ofplasma was exchanged in 9/25 pts (36%), 1.5 volumes in 7/25 pts(28%) and 2 volumes in 9/25 pts (36%). From 3000–7200 mL ofplasma was exchanged per procedure, mean 4724 ± 1806 mL.Mean running time was 185 ± 64 min., range 95–440 min. Triglyc-eride concentration before and after MPE was 53 ± 29 mmol/L(range 15.3-109 mmol/L) and 12.9±10 mmol/L (range 1.5-33.1mmol/L), respectively. Total cholesterol before and after MPE was18.9±8.2 mmol/L (range 8-35) and 7.5 ± 5.4 mmol/L (range 0.6–22.6 mmol/L), respectively.Technical side effects were hemolysis in 1/42 MPE and pluggingof the plasma filter with lipids, with substantial drop of plasmafiltration rate in 3/42 MPEs. Hematoma after cannulation of theperipheral vein occurred in 2/42 MPE. Three patients had signs ofhypocalcemia and were given Ca gluconate or calcium chloride.Conclusions In 25 patients with severe hypertriglyceridemia andacute pancreatitis substantial reduction of triglyceride and choles-terol serum concentration was achieved during plasma exchangetherapy, along with clinical improvement of the patients.
32
Chronic LDL Apheresis in Children and Young AdultsR Ponikvar, R ugi , Fejzuli, H Dedi , L Gaber and J Buturovi -PonikvarDepartment of Nephrology, University Medical Center, Ljubljana, Slovenia
Background Familial homozygous hypercholesterolemia is aninherited disease which without therapy, leads to a lethal outcomebefore the age of 20 due to accelerated atherosclerosis. Therapy iseither “gene therapy”, liver transplantation, or chronic low densitylipoprotein (LDL) apheresis. The aim of the study is to asses theefficacy of LDL apheresis in two patients with familial homozy-gous hypercholesterolemia, who have been treated with chronicLDL apheresis in our Dialysis center for more than 10 years.Methods A girl, born in 1977 entered a chronic LDL apheresisprogram in 1990, aged 13 years. Apheresis sessions have beencarried out every two to three weeks. Vascular access was viacubital peripheral vein, and the anticoagulant used was heparin.LDL apheresis monitor was Kaneka, Japan, with dextran sulphatecolumn. Three volumes of plasma (each 8000 mL) were processedper session, which lasted for about 4 hours.A boy, born in 1988 entered an LDL apheresis programe in 1994,aged 6 years. Vascular access was at first via double lumen hemo-dialysis catheter, but at age 8, AV fistula was created because ofserious access problems. LDL apheresis was performed as mem-brane plasma exchange up to the age of 10. Since then a monitorKaneka with dextran sulphate column was used. LDL apheresiswas performed every 2 weeks, 3 volumes of plasma being pro-cessed, each 6000 mL.
Z c¢ C c¢c¢
Serum concentration of total cholesterol, LDL, high density lipo-protein (HDL), and triglycerides were monitored at the start andend of the LDL apheresis.Results The girl has been treated for 14 years. In total 302 LDLprocedures have been performed. In the year 2004 average con-centrations of total cholesterol at start (12.7 mmol/L) and at theend (2.1 mmol/L), as well as time average concentration (TAC;7.0 mmol/L) were stable and comparable with concentrations inthe past. The same was true for the average concentration of LDLcholesterol at the start (10.7 mmol/L), at the end (1.2 mmol/L),and for TAC (5.6 mmol/L).The boy has been treated for 10 years, a total of 135 LDL apher-esis procedures being carried out. Average concentration (at start,after LDL apheresis, and TAC) of total cholesterol and LDL cho-lesterol were 11.0 mmol/L, 2.3 mmol/L, 6.6 mmol/L and 9.4 mmol/L, 1.3 mmol/L, 5.1 mmol/L, respectively.Conclusion Chronic LDL apheresis performed every 2–3 weeksprovides stable metabolism of cholesterol and acceptable concen-tration of lipids. Up to now there has been no sign of acceleratedatherosclerosis in the patients.
33
Citrate Anticoagulation during Plasma Exchange in Patients with Thrombotic Thrombocytopenic Purpura – Short Heparin-Free Hemodialysis Helps to Remove Citrate LoadJ Buturovi -Ponikvar, Fejzuli and R PonikvarDepartment of Nephrology, University Medical Center Ljubljana, Slovenia
Background Treatment of thrombotic thrombocytopenic pur-pura (TTP) requires daily or even twice daily plasma exchanges(PE) with fresh frozen plasma as a replacement solution. If citrateanticoagulation is needed, citrate load (both from fresh frozenplasma and citrate as an anticoagulant) can be significant, causingsevere alkalosis. Citrate as a small molecule is easily dialyzable, soshort heparin-free hemodialyses performed periodically after orbetween PE procedures can help to remove citrate load. The aimof our report is to present our experience with citrate anticoagu-lation in patients with TTP treated with daily PEs.Methods Fifteen protocols of plasma exchange procedures per-formed in a 46-year-old female with TTP were analyzed. Bloodflow in all procedures was 100 mL/min, 4% trisodium citrate wasused as anticoagulant, infused into the arterial line at rate 130 mL/h. 1M CaCl2 was infused into the venous line in a dose adjusted tomaintain ionized calcium (iCa) within normal limits (mean doseof 11.5 ± 1.5 mL/h). Fresh frozen plasma was used as a replace-ment solution, 3258 ± 548 mL per procedure.Results Ionized calcium before PE ranged from 1.10–1.45 mmol/L (mean 1.27 ± 0.12). The initial iCa level gradually increased afterseveral procedures, as a consequence of citrate-calcium complexmetabolism between the procedures. Levels of iCa during PEwere: 1.15 ± 0.09 mmol/L after 1 hour, 1.18 ± 0.06 after 2 hours and1.16 ± 0.09 after 3 hours. Significant alkalosis occurred after sev-eral PEs with plasma pH 7.51 and bicarbonate 40.7 mmol/L. It wascorrected by a 2-hour heparin-free hemodialysis with dialysate: K4.0 mmol/L, calcium 1.5 mmol/L, sodium 140 mmol/L and bicar-bonate set to 24 mmol/L. After dialysis pH was 7.38 and bicarbon-ate 28.5 mmol/L. Such hemodialysis was repeated during PEtreatment.Conclusion Citrate anticoagulation can be safely performed inpatients treated with PE by daily plasma exchanges. Periodically
c¢ C

Abstracts 91
Ther Apher Dial, Vol. 9, No. 1, 2005
performed short heparin-free hemodialysis can remove excess cit-rate and help to correct and avoid severe metabolic alkalosis.
34
Chronic Immunoadsorption/Plasma Exchange in Patients With Recurrence of Focal Segmental Glomerular Sclerosis After Kidney TransplantationR Ponikvar, A Kandus, A Bren and J Buturovi -PonikvarDepartment of Nephrology, University Medical Center, Ljubljana, Slovenia
Background Recurrence of focal segmental glomerular sclerosis(FSGS) in a transplanted kidney can lead to graft failure. Mem-brane plasma exchange (PE) and immunoadsorption (IA) havebeen reported to be sometimes successful in preventing of FSGSrecurrence in transplanted kidneys. The aim of the study is toevaluate the effect of chronic PE/IA on graft function in twotransplanted patients with recurrence of FSGS in transplantedkidney.Methods A man, 45 years old, with biopsy proven FSGS innative kidneys was transplanted in January 2001. Soon after trans-plantation, recurrence of FSGS in transplanted kidney wasobserved and therefore several cycles of IA therapy were per-formed after transplantation. Since August 2001 he began chronicIA therapy every 3 weeks. Fresenius-Excorim membrane plasmaexchange monitor with PF 2000 plasmafilter, (Gambro), has beenused. One volume of plasma was exchanged per PE. Vascularaccess was by AV fistula.A woman, 42 years old, with biopsy proven FSGS in native kid-neys was transplanted in December 1998. Because of recurrenceof FSGS in transplanted kidney she began (after several cycles ofIA) with chronic IA in August 2001. Fresenius-Excorim immu-noadsorption monitor was used. One to 2 plasma volumes havebeen processed per session, and vascular access was by AV fistula.Results Daily proteinuria in the man decreased from 2.27 g in2001 to 1.13 g in 2004 (50.2% decrease) and serum creatinineincreased from 118 mmol/L to 130 mmol/L (9.2% increase).Daily proteinuria in the woman decreased from 3.89 g in 2001 to2.0 g in 2004 (48% decrease) and serum creatinine increased from96 mmol/L to 109 mmol/L (12% increase). PE/IA therapy was oth-erwise uneventful.Conclusions Chronic PE/IA therapy stabilized renal graft func-tion and substantially diminished daily proteinuria. The man livedwith kidney graft for more than 3.5 years and woman more than5.5 years after recurrence of FSGS occurred.
TRANSPLANTATION ABSTRACTS
35
The Survey of Kidney Transplantation in Slovenia: The First Four Years Since Joining The EurotransplantM Arnol, D Kova , A F Bren and A KandusDepartment of Nephrology, University Medical Center, Ljubljana, Slovenia
Objectives The aim of this retrospective study is a 4-year surveyof kidney transplantation since January 2000 when Sloveniabecame an active member of the Eurotransplant.Methods We reviewed all kidney transplants between January2000 and December 2003. All patients received equal immunosup-pression with basiliximab or daclizumab, cyclosporine, mycophe-nolate mofetil and steroids. Beside donor and recipient
c¢
c
demographic characteristics the incidence of delayed graft func-tion (DGF), acute rejection, and graft and patient survival wereanalyzed.Results During the observed period 189 patients (109 men, 80women), aged from 13 to 66 years (mean 46 ± 11 years) weretransplanted. Fifteen patients (7.9%) received second allograft.All kidney grafts came from cadaveric donors, aged from 6 to60 years (mean 37 ± 14 years). Eighty-seven grafts (46%) werefrom Slovenia. Mean HLA (A, B and DR) mismatches were2.7 ± 1.1 (range 0 to 5). Mean cold ischemia time was significantlylonger for grafts shipped from abroad compared with those pro-cured in Slovenia (25 ± 6.5 h vs. 18.5 ± 7.5 h, P < 0.01). The inci-dence of DGF was 31.2%. From January 2000 through May 2004(observation period 5 to 53 months) 9 recipients (4.7%) experi-enced acute rejection, successfully treated in 8 patients. Actuarialgraft survival at 1 and 3 years was 95.5%. Two patients (1.1%)died; both deaths were due to septic infection during the first6 months after transplantation.Conclusions In the last 4 years since joining the Eurotransplantuse of efficient and safe immunosuppression strategy resulted invery low incidence of acute rejection and high graft and patientsurvival rate. Slovenian membership in the Eurotransplant offersgood HLA matching and with this, probably long term benefit.Joining the Eurotransplant is also related to longer cold ischemiatime which can explain high incidence of DGF.
36
Prevention of Early Acute Rejection with Basiliximab and Triple Immunosuppression in Cadaveric Renal Allograft RecipientsA Kandus, K Grego, M Arnol, D Kova , J Kova , J Lindi , J Buturovi -Ponikvar, R Ponikvar and A F BrenDepartment of Nephrology, University Medical Center, Ljubljana, Slovenia
We assessed the efficacy and safety of basiliximab combined withtriple immunosuppression in adult recipients of at least 1 HLA-mismatched cadaveric renal allograft. All studied patients, trans-planted between October 1999 and December 2003, receivedequal immunosuppression: 20 mg infusion of basiliximab on day0 and on day 4, infusion of cyclosporine (CyA) (0.08 mg/kg/h)started at operation and continued by CyA-Neoral, 3 mg/kg b.i.d.on day 2, methylprednisolone, 0.4 mg/kg i.v. at operation, andmycophenolate mofetil started on day 1. CyA-Neoral dose wasadjusted to maintain blood trough levels of 150–250 ng/mL (FPIA,monoclonal). Oral methylprednisolone was tapered by 4 mg perweek to achieve a maintenance dose of 0.08 mg/kg/day. A total of153 patients, with mean age of 46 ± 11 years (SD; range 18–65 years), were studied. Thirteen of them received second renalallograft. The mean donor age was 37 ± 14 years (range 6–61 years). Mean cold ischemia time was 22.0 ± 8.0 h (range 7.0–41.0 h), mean value of HLA-antigen mismatches was 3.0 ± 0.9(range 1–5), mean latest PRA value was 8 ± 14% (range 0–85%).47 patients experienced delayed graft function. During a follow-up of 3 months no acute rejection episode occurred. Four renalallografts were removed, but not for rejection. One patient diedbecause of sepsis. In one patient life-threatening CMV disease wassuccessfully treated. One malignancy (skin basal cell carcinoma)was detected. Hypersensitivity reactions and cytokine-release syn-drome were not observed. After 3 months mean serum creatininewas 111 ± 36 mmol/L (range 53–238 mmol/L). Patient and graft sur-vival was 99.3% and 97.4%, respectively. We conclude that basil-iximab with this triple therapy is an efficient and safe
c cc c¢

92 Abstracts
Ther Apher Dial, Vol. 9, No. 1, 2005
immunosuppression strategy, demonstrated with absence of earlyacute rejection episodes, excellent allograft function, acceptableadverse event profile and high short-term survival rate.
37
Prevention of Early Acute Rejection with Daclizumab and Triple Immunosuppression in Cadaveric Renal Allograft RecipientsA Kandus, K Grego, M Arnol, D Kova , J Kova , J Lindi and A F BrenDepartment of Nephrology, University Medical center, Ljubljana, Slovenia
We assessed the safety and efficacy of daclizumab combined withtriple immunosuppression in adult recipients of at least 1 HLA-mismatched cadaveric renal allograft. All studied patientsreceived equal immunosuppression: daclizumab infusion of 1 mg/kg immediately before transplantation and at 2, 4, 6 and 8 weeksfollowing the transplantation, infusion of cyclosporine (CyA)(0.08 mg/kg/hr) started at operation and continued by CyA-Neoral, 3 mg/kg b.i.d. on day 2, methylprednisolone, 0.4 mg/kg i.v.at operation, and mycophenolate mofetil started on day 1. CyA-Neoral dose was adjusted to maintain blood trough levels of 100–170 ng/mL (FPIA, monoclonal). Oral methylprednisolone wastapered by 4 mg per week to achieve maintenance dose of 0.08 mg/kg/day. 39 patients, with mean age of 49 ± 10 years (SD; range 26–66 years), were studied. Three of them received a second renalallograft. The mean donor age was 38 ± 13 years (range 16–58 years). Mean cold ischemia time was 19.0 ± 6.5 h (range 9.5–39.5 h), mean value of HLA-antigen mismatches was 2.7 ± 1.0(range 1–5), mean latest PRA value was 3 ± 8% (range 0–47%).Ten patients experienced delayed graft function. During follow-upof 3 months one acute rejection episode was observed, vasculartype, treated with OKT3. One patient experienced a hypersensi-tivity reaction to daclizumab, which despite precautionary mea-sures required early interruption of the 5th infusion dose. In twopatients CMV disease, requiring hospitalisation, was successfullytreated. No malignancies were detected. After 3 months meanserum creatinine was 102.2 ± 24.0 mmol/L (range 63–152 mmol/L).2 renal allografts were removed, but not for rejection. Patient andgraft survival was 100% and 94.9%, respectively. We conclude thatdaclizumab with this triple therapy represents a safe and efficientimmunosuppression strategy, demonstrated with low incidence ofearly acute rejection episodes, excellent allograft function, accept-able adverse event profile and high short-term survival rate.
38
Long-term Follow-up of Renal Transplant Artery Stenosis: Case Controlled StudyA upunski, A Kandus, J Buturovi -PonikvarDepartment of Nephrology, University Medical Center, Ljubljana, Slovenia
Background Renal transplant artery stenosis is relatively fre-quent. It can cause hypertension, deterioration of renal functionor graft loss. It seems that it can be treated conservatively providedgraft perfusion is not jeopardized. The aim of our retrospectiveclinical study was to assess a long-term course of renal transplantartery stenosis by duplex-Doppler and its influence upon serumcreatinine, hemoglobin concentration, and hypertension, as well
c cc
Z c¢
as to investigate possible association between stenosis and thenumber of acute rejections.Methods Thirty-four renal transplant recipients, aged43 ± 13 years, with significant (>50%) renal transplant arterystenosis on Doppler were compared with 34 renal transplant recip-ients, in whom stenosis was excluded on Doppler; patients of bothgroups were matched by age, sex, time of transplantation, type ofrenal transplant and number of previous transplantations. We ana-lyzed peak systolic velocity in renal transplant artery, resistanceindex at the level of intrarenal arteries, serum creatinine, hemo-globin concentration, blood pressure, number of antihypertensivemedications, and number of acute rejections on a yearly basis.Results In the stenosis group, peak systolic velocity was2.1 ± 0.5 m/s at 1 year after transplantation (controls 1.1 ± 0.4 m/s), 1.9 ± 0.5 m/s at 2 years (0.9 ± 0.4 m/s), 1.9 ± 0.5 m/s at 3 years(0.9 ± 0.4 m/s); resistance index was 62 ± 10% at 1 year (controls68 ± 7%), 65 ± 9% at 2 years (67 ± 7%), 63 ± 9% at 3 years(67 ± 7); serum creatinine was 128 ± 58 mmol/L at 1 year (controls129 ± 43 mmol/L), 119 ± 47 mmol/L at 2 years (121 ± 33 mmol/L),125 ± 54 mmol/L at 3 years (127 ± 32).Conclusion Long-term course of renal transplant artery stenosis(>50%), treated medically or interventionally, seems to be stableand nonprogressive (during 3-year follow-up). Spontaneousregression of stenosis to nonsignificant level is possible. No signif-icant difference in graft function, blood pressure, or the numberof acute rejections was observed when comparing the stenotic andnonstenotic group.
39
De Novo Malignancies After Renal Transplantation – A Single Center ExperienceN Ivanovski1, Z Popov2, P Kolevski3, K akalaroski1, J Masin1 and K Zafirovska1
1Department of Nephrology, 2Department of Urology, 3Institute of Transfuziology, University Clinical Center, Skopje, Republic of Macedonia
Background The occurrence of malignancies after organ trans-plantation is a well known and very serious complication. Accord-ing to many authors, the overall prevalence of malignancies afterrenal transplantation is between 6 and 12%. Despite the fact thatmany factors could be involved, the etiopathogenesis is stillunclear. The aim of the authors is to present their own clinicalexperience in early diagnosis and treatment of de novo malignan-cies after renal transplantation.Patients and Methods Over a period of 12 years, 184 renal trans-plant (138 living related and 46 cadaveric) were performed andfollowed in our department on an outpatient basis. All patientswere treated by sequential quadruple immunosuppressive proto-col with mono (Il-2R antagonists) and polyclonal antibody (ATG)induction therapy and Cyclosporine A, Mycophenolate Mofetil or/and Azathioprine, and Prednisolone as maintenance therapy. Thestandard surgical and preservation procedure was performed inmost of the patients. The mean cold ischemia time in living renaltransplants was 3.6 h, while in cadaver was 25.6 h. About 20% ofthe patients developed acute rejection episodes, successfullytreated by steroid pulse therapy. According to the protocol in theDepartment the patients were regularly examined once-monthlyduring the whole period of follow up.Results Overall 18 malignancies (9.78%) in 14 patients (7.8%)were observed. All cases were clinically and histologically con-firmed. Of 14 transplant patients with malignancies, 4 were femaleand 10 male. The mean age of patients with cancer was 45 years
C

Abstracts 93
Ther Apher Dial, Vol. 9, No. 1, 2005
(range 21–53). Most of the malignancies were basal and/or squa-mous skin cancers (10 or 55%). Kaposi’s sarcomas were found in3 patients (16.6%, one visceral form). One breast cancer, oneseminoma, one cancer of the colon, one urogenital cancer infemale, one renal cell carcinoma and one plasmocytoma, weredetected to. Surprisingly no cases of post-transplant lymphopro-liferative disease (PTLD) were observed. All cancers were denovo malignancies presented in a mean time of 21 months (range2–52 months) after surgery. The overall mortality rate was 42.6%,most among the patients with solid organ cancers. Three graftswere lost because of reduction and cessation of immunosuppres-sion in patients with visceral form of Kaposi’s sarcoma, multipleskin cancers and plasmocytoma. We did not observe any correla-tion between the clinical occurrence of post-transplant malignan-cies and different HLA type, number of rejection episodes as wellas any specific bacterial, viral, or fungal infection.Conclusion The prevalence of post-transplant malignancies inour group of patients is similar to other authors. The predomi-nance of the skin cancers is understandable bearing in mind thesunny side of the country. Careful clinical examination and long-term screening protocols are needed for early detection and treat-ment of this mostly life threatening complication among the trans-plant population.
40
Does Mycophenolate Mofetil Increase the Incidence of Cytomegalovirus Disease Compared To Azathioprine After Cadaveric Kidney Transplantation?L Bubi -Filipi, N Ba i -Juki , Z Pureti , I Bari i , R malcelj, J Pasini and P KesDepartment of Dialysis, UHC Zagreb, Zagreb, Croatia
Although most published papers had not found an increase in theincidence of cytomegalovirus (CMV) disease with the use ofmycophenolate mophetil (MMF) in kidney transplant patients, wehad the feeling from our everyday practice that after its introduc-tion, the number of patients with the CMV disease increased. Inorder to test this hypothesis, we performed retrospective analysisof our database, comparing the incidence of CMV disease inpatients treated with azathioprine (AZA) and patients treatedwith MMF. Cytomegalovirus disease was defined as CMV antigen-emia (positive CMV pp65 determined by ELISA test) plus any offollowing: decreased leucocytes or thrombocytes, increased tran-saminases, or an increase in serum creatinine.The azathioprine treatred group (AZA group) included 280patients (132 female) treated for a total of 17,672 months withAZA + Cyclosporine A (CyA) + steroid, or AZA + steroid, whilethe MMF group included 219 patients (112 female) treated for atotal 5079 months with MMF + CyA + steroid, or MMF + steroid.There was no difference in acute rejection episodes between theAZA and the MMF groups. The AZA group had 51 CMV diseaseepisodes (1 episode per 346.5 treatment months), and the MMFgroup experienced 43 epizodes (1 per 118.1 months) (P < 0.01).Mean onset of the CMV disease was 32.65 ± 47.69 months (SD)after transplantation in the AZA group, and 3.72 ± 4.43 in theMMF group. There was no difference between two treatmentgroups regarding the donor–recipient CMV status mismatch.Despite having the increased incidence of CMV disease, the MMFgroup had less severe disease compared to the AZA group withdecrease in leucocyte count in 11.6% vs 15.7% of episodes,decrease in thrombocyte count in 20.9% vs 21.6%, elevation oftransaminases in 18.6% vs 29.4% respectively, and finally increasein serum creatinine greater than 20% in 51.2% in the MMF vs74.5% in the AZA group. Five patients from the AZA group
c¢ s c¢ c¢ c¢ s c¢S
experienced CMV pneumonitis with the mortality rate of 80%.Only one patient from the MMF group had CMV pneumonitis,and he survived.According to our results, patients treated with MMF have anincreased risk for development of the CMV disease. However, thedisease course is less severe, and less frequently accompanied withthe decrease in renal function in comparison to the AZA group.
41
Serum C-Reactive Protein in Kidney Transplant Patients – A Useful Marker of Immune ActivationL Bubi -Filipi, I Bari i , I Hr ak Pulji , N Ba i -Juki , Z Pureti and P KesDepartment of Dialysis, UHC Zagreb, Zagreb, Croatia
The clinical manifestations of different complications after kidneytransplantation are often vague and simple laboratory tests forearly diagnosis would be valuable. This study investigated whetherserial measurements of serum C-reactive protein could help dif-ferentiate episodes of transplant dysfunction due to rejection,infection, acute tubular necrosis, or cyclosporine A nephrotoxicityin renal allograft recipients. We retrospectively analyzed our dataon the daily measurements of serum C-reactive protein (sCRP) in117 renal allograft recipients (a total of 543 measurements wereperformed and 391 episodes of elevated sCRP were recorded) inthe diagnosis of acute rejections and other complications in theimmediate post-transplant period. Nineteen patients were treatedwith cyclosporine A, azathioprine, and prednisolone and 98patients with cyclosporine A, mycophenolate mophetil, and pred-nisolone. In patients with stable graft function the sCRP concen-trations were in the normal range.Serum C-reactive protein concentration was initially significantlyincreased in 23 episodes of rejection responsive to methylpred-nisolone (median of 54 mg/L) but fell very rapidly in response totreatment (median 15 mg/L). In episodes of rejection unrespon-sive to methylprednisolone, median initial sCRP levels were sig-nificantly higher, with a median of the 69 mg/L at the end of thetreatment. Twenty-nine patients with graft dysfunction caused byCsA nephrotoxicity showed no incraese in sCRP concentration. Asimilar pattern was seen in patients with acute tubular necrosis.Bacterial infections other than asymptomatic bacteriuria wereaccompained by the significant increase in sCRP (median of77 mg/L). The most significant elevations were associated withbacterial infections. Serum C-reactive protein seemed to be amore sensitive marker than fever or white blood cell count indiagnosis of all complications. Serial sCRP measurements provideeconomical and reproducible evidence of immune activation, helpdiscriminate renal dysfunction due to CsA nephrotoxicity or rejec-tion, and may be helpful in modification of immunosuppressivetherapy.
42
Follow-up of Kidney Graft Recipients with Cyclosporine Associated Hemolytic Uremic Syndrome and Thrombotic MicroangiopathyA Bren1, A Kandus1, J Buturovi -Ponikvar1, J Lindi 1, B Knap1, J Pajek1, K Grego1, A Vizjak2 and D Ferluga2
1Department of Nephrology, University Medical Center Ljubljana, 2Institute of Pathology, Faculty of Medicine, Ljubljana, Slovenia
The study was based on 462 patients who underwent kidney trans-plantation from 1986 through September 2003. Cyclosporine (Cs)
c¢ s c¢ s c¢ s c¢ c¢c¢
c¢ c

94 Abstracts
Ther Apher Dial, Vol. 9, No. 1, 2005
related thrombotic microangiopathy (TMA) was found in 15(3.3%) patients. Donors aged from 9 to 51 years. Cold ischemiatime ranged from 12 to 31 hours. Hemolytic uremic syndrome(HUS) developed in 2 weeks after transplantation in 14 patientsand in one later. Histopathologic examination demonstratedglomerular type of TMA in 3 patients, mixed type (glomerularand vascular) in 11 patients, and mesangial widening with nonspecific tubulo-interstitial lesions with progression to glomerulartype of TMA in repeated biopsy in one patient. Follow-up biop-sies revealed resolution of TMA in four patients and chronic vas-cular TMA in one patient. Six patients with mixed types of TMAneeded transient hemodialysis, nobody with glomerular typeneeded dialysis (P = 0.103) and 14/15 had good resolution of graftfunction after Cs dose reduction; only 1 graft with mixed typeTMA was lost due to irreversible HUS. Mean glomerular filtra-tion rate (GFR) as predicted by the Nankivell equation was76 ± 13 mL/min and 80 ± 27 mL/min 1 month after discharge forthe glomerular type of TMA and mixed type, respectively (NS).Glomerular filtration rates 1 year after HUS were 82 ± 12 and87 ± 21 mL/min (NS) for glomerular and mixed types, respec-tively. We concluded that mixed type of TMA was associated withmore severe early clinical course than glomerular type of TMA.Long-term prognosis seems good in majority of patients with nosignificant differences between the glomerular and mixed type ofTMA.
43
Conversion To Tacrolimus Due To Cyclosporine-Related Toxicity in Kidney Graft Recipients – Single Center StudyA F Bren, J Pajek and K Grego, A KandusDepartment of Nephrology, University Medical Center Ljubljana, Slovenia
Aim The aim of our study was to analyze cyclosporine (Cs)-related toxic effects that demanded conversion to tacrolimus (Tc),and the influence on blood pressure (BP), glucose control andgraft function.Methods From 1989 to 2003 10 patients (15 to 48 years), weretreated with Cs from 2 months to 11 years. The Cs dose wasadjusted to maintain the target blood trough levels of 100–170 mg/mL during first three post-transplant months and 70–100 mg/mLafterwards. Patients were switched to Tc due to following Cs-related toxic effects: gingival hypertrophy (8), hirsutism (1),hemolytic uremic syndrome (HUS) (3), and tremor (1). The Tcdose was adjusted to maintain a target whole blood trough levelof 10–20 ng/mL during the first 3 months after transplantation and5 to 15 ng/mL afterwards.Results After 3 to 46 months of follow-up Cs-related toxiceffects (gingival hypertrophy, hirsutism, HUS, tremor) signifi-cantly diminished, systolic and diastolic blood pressure weredecreased from 142 mmHg to 130 mmHg and from 87 mmHg to83 mmHg, respectively (P < 0.005 and P = 0.095, respectively),while no significant change was observed in plasma fasting glucoselevels. The calculated GFR (Nankivell formula) was 69 mL/min(range 91 to 44 mL/min) 3 to 6 months before conversion and67 mL/min (range 37 to 101 mL/min) 3 to 6 months after conver-sion (P = 0.279).Conclusion Our results show that kidney allograft function wasstable after conversion from Cs to Tc in the short-term period. Thebenefits of conversion from Cs to Tc included significant reductionin Cs-related toxic effects and also reduction of systolic bloodpressure.
44
Infection with Hepatitis B or Hepatitis C Viruses in Patients with Renal Transplants in SloveniaJ Kova , A Kandus, A F Bren and S Levi nikDepartment of Nephrology, University Medical Center, Ljubljana, Slovenia
In 214 patients (pts; 89 female and 125 male; mean age47.9 ± 10.6 years, 1SD) with functioning renal transplants andtransplanted between January 2000 and August 2004, results ofserologic markers of infection with hepatitis B virus (HBV) orhepatitis C virus (HCV) have been revised. Serologic markerswere checked routinely at transplantation and 3 and 12 monthsafter transplantation.Results (see Table A44)
c c
HBV infection One patient whose antigene-HBs were negativeat transplantation has been most probably infected via transfusionof packed red cells during the first year after transplantation. Bothantigene-HBs positive patients are now under supervision of aninfectologist and treated with lamivudine. In one of them viremiahas already ceased. In four of 13 patients with positive antibodiesagainst antigene-HBc it is not known, whether they had been incontact with HBV before transplantation or not. It is possible thatin one patient infection was transmitted from a donor who hadantibodies against antigene-HBc positive.Infection with HCV Five patients with positive antibodiesagainst-HCV had already been infected before transplantation.Two patients had been treated with interferon before transplanta-tion. They are both not viremic at present. In all five patients,chronic hepatitis was confirmed histopathologicaly before trans-plantation but liver biopsies have not been repeated later.In our group there are no patients infected with both viruses andno Delta antigene positive patients.Conclusionsa) Regular testing of serologic markers of viral hepatitis enablesearly recognition of infection with HBV or HCV in patients withrenal transplants.b) It is possible to transmit HBV infection with renal transplantsfrom donors positive for antibodies against antigene-HBc.c) In all patients with any positive result of serologic markers ofHBV or HCV infection (except antibodies against HBs antigene)viremia should be repeatedly excluded.d) Activity of viral hepatitis after renal transplantation should behistopathologicaly assessed in all HBV or HCV positive patients.
45
Renal Transplant Artery Stenosis: The Possible Association With Acute Rejection Episodes and Immunosuppressive TreatmentA upunski, A Kandus, AF Bren, J Buturovi -PonikvarZ c¢
TABLE A44. Patients with positive results of serologic markers of infection with HBV and HCV
Antigene-HBs Positive 2 (1)Antigene-HBs Negative
Antibodies against-HBc Positive 13 (9)Antibodies against-HBe Positive 1 (1)
Antibodies against HCV Positive 5 (5)
Number in brackets represents patients who were already pos-itive before transplantation (N = 214).

Abstracts 95
Ther Apher Dial, Vol. 9, No. 1, 2005
Department of Nephrology, University Medical Center, Ljubljana, Slovenia
Background Renal transplant artery stenosis is a relatively fre-quent complication after transplantation and is a potentially cor-rectable cause of hypertension and/or deterioration of renalfunction and graft loss. There were reports of the immunologicalmechanism playing a role in the pathogenesis of stenosis.Purpose The aim of our retrospective clinical study was to assessthe association of renal transplant artery stenosis with the acuterejection episodes and immunosuppressive treatment.Methods Thirty-four renal transplant recipients, 14 females and20 males, aged 42.7 ± 13 years, were found to have significant(>50%) stenosis. In the control group there were 34 patients with-out stenosis, matching the patients from stenosis group for age,sex, year of transplantation, type of graft and number of previousgrafts. Patients were followed for 3 years post-transplant. Acuterejection episodes were diagnosed histologically.Results In the stenosis group 8/34 (23%) patients had 10 acuterejection episodes compared to 5/34 (15%) patients having 6 epi-sodes in control group (P = 0.353). In stenosis group 20/34 (59%)patients have received double (cyclosporine A and methylpred-nisolone), and 14/34 (41%) patients triple immunosuppressivetreatment (cyclosporine A, methylprednisolone and azathioprineor mycophenolate mofetil), respectively. In the control group 28/34 (82%) patients have received double, and 6/34 (18%) patientstriple immunosuppressive treatment, respectively (P = 0.033).There were no significant differences in serum creatinine andblood pressure at 1, 2 and 3 years after transplantation betweenthe groups.Conclusions There was a tendency towards higher number ofacute rejection episodes in the stenosis group, however not statis-tically significant. Patients with stenosis have received more inten-sive immunosuppressive treatment.
NEPHROLOGY/ MISCELLANEOUS ABSTRACTS
46
Hypercalcemic Nephropathy and TNFa in Patients with Bronchial CarcinomaK akalaroski, S Crvenkova, N Ivanovski and D JovanovskiInstitute for Oncology and Radiotherapy; Department of Nephrology, Clinical Center, University “St Cyrill and Methodius”, Skopje, Republic of Macedonia
Background The phenomenon of “paraneocrinia” is very pro-nounced in patients (pts) with malignant tumors. Life-threateninghypercalcemia (H) is a very frequent condition in pts withplanocellular bronchial carcinoma (PBC), and many may berelated to “parahormonal” (PTH-RP), prostaglandins, TNFa, andOAF-activity.Aim of the Study The aim of the study is to demonstrate themechanisms of humoral hypercalcemia of malignancy (HHM)associated to PBC, their clinical presentation and our therapeuticpossibilities.Material and Methods In a 3 year period (1998–2001) wetreated 436 pts with primary lung carcinoma. Five pts (5/436;1.15%) suffering from PBC have developed bone metastases withclinically and laboratory evident HHM and hypercalcemic nephr-opathy (decreased PO4, metabolic alkalosis, hypochloremia,hypoalbuminemia, polyurodipsia, light reverse uremia, fatigue,
C
anorexia, nausea, itching, lethargy, and coma).The blood calciumconcentration and 24 h urinary Ca excretion were augmented(between 2.88 and 3.30 mmol/L for total calcemia and ll.80 to13.30 mmol/L for calciuria; diuresis, 2.9–4.6l /day) with character-istic electrocardiogram (ECG) signs (bradycardia, prolongedpulse rate and shortened ST-intervals) and moderately elevatedblood urea nitrogen (BUN; 10.11 ± 3.30 mmol/L), respectivelyserum creatinine (141.22 ± 38.73 mmol/L). The serum TNFawas significantly high in all hypercalcemic patients (N = 5)(105.40 ± 23.85 pg/L; RV = 10.80 ± 6.8 pg/L). The routinelyapplied nephrologic investigations (kidney ultrasonography, s.c.“kidney, ureter, bladder” X-ray radiography) were negative. Thetherapeutic measures consist in prohibition of oral Ca-intake,non-steroidal anti-inflammatory drugs (NAID), and H2-receptorantagonists. The volume expansion (300–500 mL/h saline, 0.9%),furosemide (20–80 mg/4–8 h), bisphosphonates (pamidronate,75 mg/i.v./every 4 weeks) and corticosteroids (1–2 mg/kg/bw/4–8 h) were introduced immediately when the diagnostic of HHMwas obvious. Two pts were complementarily treated with Salmoncalcitonin (5 IU/kg/bw).Results and Conclusion Laboratory improvement with completewithdrawal of clinical symptoms was noted in four pts. One patientdied because of irreversible coma. Humoral hypercalcemia ofmalignancy in PBC is a relatively rare condition and may bealmost certainly discovered and treated early if the serum TNFaconcentration is at least 10 times more in comparison with thereference values.
47
Glomerular Filtration Rate in Convalescents with Hemorrhagic Fever with Renal SyndromeD Tulumovi ,1 E Me i ,1 M Huki ,2 N ivkovi 3
1Clinic of Nephrology, Urology, Dialysis and Kidney Transplantation, University Clinical Center, Tuzla, 2Department of Microbiology, University Clinical Center, Sarajevo, and 3Department of Nuclear Medicine, University Clinical Center, Tuzla, Bosnia and Herzegovina
Objectives Bosnia and Herzegovina is a known endemic regionfor Hantavirus infection. In this region at least two different Han-taviruses, the Dobrava viruses (DOBV) and Puumala viruses(PUUV) have been found. The aim of the study was to determineglomerular filtration rate (GFR) in patients with a history of hem-orrhagic fever with renal syndrome (HFRS) 9 to 10 years after theacute phase of the disease.Design and Methods We prospectively reviewed clearance oftechnetium marked diethyl three amino pentacetic acid (Tc99mDTPA) in 42 male convalescents with serologically confirmedHFRS, 13 patients with PUUV infection and 29 patients withDOBV infection.Results The tubulosecretory phase of the GFR was prolonged insix patients (46%) with PUUV infection and 23 patients (79%)with DOBV infection (P < 0.05). Total and separate clearanceEDTA were significantly statistically lower (P < 0.001) in patientswith serologically confirmed DOBV infection. In patients withDOBV infection elimination of radio pharmac was prolonged.Conclusions Hemorrhagic fever with renal syndrome can causesustained renal damage that very rarely progresses into renal fail-ure. The tubulosecretory DTPA phase was prolonged in 46% ofexaminees with PUUV and in 79% of examinees with DOBVinfection. Elimination of radio pharmac from the kidney was pro-longed in both groups of patients. The DTPA clearance rate was
c¢ s c¢ c¢ Z c¢

96 Abstracts
Ther Apher Dial, Vol. 9, No. 1, 2005
lower in patients with serologically confirmed HFRS than in nor-mal populations, especially in patients with DOBV infection.
48
Polymorphisms In a-Adducin (G460w) and G-Protein b-3 Subunit (C825t) Genes In Essential HypertensionN Mar un Varda, B Zagradi nik, N Kokalj Voka and A GregoriDepartment of Paediatrics, Maribor Teaching Hospital, Maribor, Slovenia
Objectives Essential hypertension (EH) has a multifactorial ori-gin and is thought to arise from an interaction between suscepti-bility genes and environmental factors. A number of candidategenes have been proposed. In our study, the role of polymor-phisms in a-adducin (ADD1) and G-protein b-3 subunit (GNB3)genes in EH was investigated.Design and Methods Ninety-three children and young adults,aged from 4 to 27 years, with both parents, were included in ourstudy, giving 93 nuclear families. Two polymorphisms weredetected using the polymerase chain reaction technique (PCR).Investigating the C825T polymorphism of GNB3 the C allele wasidentified by the presence of 152 and 116 bp signals and the Tallele was present when a non-digested 268 bp long band wasdetected. The allele-specific polymerase chain reaction (PCR) wasused to study the G460W polymorphism of ADD1. For statisticalanalysis the transmission disequilibrium test (TDT) was used. Byusing non-transmitted alleles as the control population, problemsof population admixture and mismatched controls are avoided.Results The following genotype frequencies for G460W poly-morphism in ADD1gene were observed: 67 (72.0%) were GGhomozygotes, 23 (24.7%) were GW heterozygotes and 3 (3.3%)were WW homozygotes. Using the TDT test, 44 nuclear familieswere used. There were 63 transmitted G alleles, 25 transmitted Walleles, 60 non-transmitted G alleles and 28 non-transmitted Walleles. The observed difference was not statistically significant(c2 = 0.24, P = 0.62).The following genotype frequencies for theC825T polymorphism in GNB3 gene were found: 50 (53.8%) wereCC homozygotes, 35 (37.6%) were CT heterozygotes and 8 (8.6%)were TT homozygotes. 73 nuclear families were used. There were95 transmitted C alleles, 51 transmitted T alleles, 84 non-transmit-ted C alleles and 62 non-transmitted T alleles. The observed dif-ference again was not statistically significant (c2 = 1.75, P = 0.19).Conclusions Our study found no association of the polymor-phisms in ADD1 and GNB3 genes with EH, respectively. How-ever, our sample size was rather small. It seems very likely thatmany genes with small effects (such as the gene variants above)account for the heritability of EH.
49
Mutation Screening in Patients with Vesico-Ureteric RefluxB Zagradi nik,1 K Bra i ,2 N Mar un Varda,2 N Kokalj Voka 1 and A Gregori 2
1Laboratory of Medical Genetics, 2Department of Pediatrics, Teaching Hospital Maribor, Maribor, Slovenia
Objectives Primary vesico-ureteric reflux (VUR) is a very com-mon anomaly of urogenital tract which makes affected children
c s cc
s c c cc c
susceptible to repeated, severe urinary tract infections and possi-ble subsequent permanent damage to the kidney function. Thereflux is of genetic origin in most children but no candidate geneshave been identified as yet. Studies on knock-out mice with VURphenotype have put forward the uroplakin genes (UPK1a,UPK1b, UPK2 UPK3) and the AGTR2 (angiotensin II type 2receptor) gene as candidate genes for reflux in humans. Also, arecent genome wide linkage study detected several loci with sig-nificant LOD scores linked to VUR which included a locus for theuroplakin 1b gene. This study reports the results from screeningof the coding regions of genes AGTR2, UPK1b and UPK3 inpatients with primary vesico-ureteric reflux.Design and methods The sample of 85 patients diagnosed withVUR was included in the study. Sequence variation screening incoding regions of the UPK1B gene was performed with the het-eroduplex analysis followed by sequencing.Results No sequence variations were found in the coding exon3 of the gene AGTR2 and only polymorphisms were present inthe coding region of the gene UPK3. A sequence variation chang-ing asparagin to aspartatic acid at the codon 137 (N137D) in exon5 of the UPK1b gene was detected in 4.7% of patients with VURand in 0.83% of controls (OR = 5.87, 95% CI 1.54–22.33,P = 0.017).Conclusions These results suggest that in our sample of patientsthe AGTR2 gene is not involved in the pathogenesis of reflux, theyexclude the UPK3 gene as a candidate gene for VUR but they alsoassociate the UPK1b gene with primary vesico-ureteric reflux.
50
Twenty-four-hour Ambulatory Blood Pressure Monitoring in Healthy InfantsN Mar un Varda, A GregoriDepartment of Pediatrics, Maribor Teaching Hospital, Maribor, Slovenia
Objectives Ambulatory blood pressure monitoring (ABPM) hasbeen increasingly used in the assessment of elevated blood pres-sure (BP) in adults as well as in children. Normal ABPM referencevalues for school children have been published. However, there islittle reported experience with this method in children under theage of 6 years, especially in infants. The aim of our study was toinvestigate the feasibility of ABPM in healthy infants.Design and methods Ambulatory blood pressure monitoringrecordings were performed in 97 infants with no history of diseaseor drugs affecting BP. The medical history was taken and gender,age, height, and weight were recorded. A minimum of 22 hours ofrecording time and at least 40 recordings were required. An accu-rate oscillometric device (SpaceLabs 90207) was used in all infantswith an appropriate cuff, attached to the non-dominant arm. Mea-surements were performed every 20 minutes during the day andevery 30 minutes during the night.Results Ninety-seven infants, aged from 2 to 30 months (mean13 ± 3 months), were included. A satisfactory ABPM profile wasobtained in 84 (86.7%) infants. In five infants the number ofrecordings was <40, while in eight infants the recording time wastoo short. There were, on average, 54 (75.4%) satisfactory record-ings. The mean ± SD systolic and diastolic BP was 100 ± 6/63 ± 5 mmHg during the day-time and 96 ± 5/58 ± 4 mmHg atnight. The height of the infants ranged from 57 to 95 cm (mean75 ± 2 cm). The infants were divided into four groups according toheight. The mean systolic and diastolic values showed a slight, butsignificant increase with body height. The day to night decline of
c c

Abstracts 97
Ther Apher Dial, Vol. 9, No. 1, 2005
the mean systolic BP was 3.0 to 6.0% and the mean diastolic fallwas 3.4 to 10.6% in the different height groups.Conclusions Ambulatory blood pressure monitoring is a usefultool for the assessment of BP in very young children. The method
was well tolerated and the measurements were technically accept-able. We confirmed the increase in BP with body height and thenocturnal decrease in BP. To obtain normal data for ABPM forthis age group a much larger number of infants are needed.




















