Annual Report October 1, 2018 to September 30, 2019
351
Copyright 2019. EngenderHealth/Fistula Care Plus. All rights reserved. Fistula Care Plus (FC+) c/o EngenderHealth 505 9th Street NW, Suite 601 Washington, DC 20004 Telephone: (202) 902 2000 Fax: (202) 783 0281 E-mail:[email protected] www.fistulacare.org This publication is made possible by the generous support of the American people through the Office of Maternal and Child Health, U.S. Agency for International Development (USAID), under the terms of cooperative agreement AID-OAA-A14-00013. The contents are the responsibility of the Fistula Care Plus project and do not necessarily reflect the views of USAID or the United States Government. Fistula Care Plus Associate Cooperative Agreement AID-OAA-A14-00013 Annual Report October 1, 2018 to September 30, 2019 Managing Partner: EngenderHealth; Associate Partners: The Population Council, Dimagi, Direct Relief, Fistula Foundation, Maternal Health Task Force, TERREWODE Submitted to United States Agency for International Development Washington, D.C. November 30, 2019 EngenderHealth U.S. / Washington, D.C. Office 505 9th Street NW, Suite 601 Washington, DC 20004 Telephone: (202) 902 2000 Fax: (202) 783 0281 E-mail: [email protected]
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Annual Report October 1, 2018 to September 30, 2019

Copyright 2019. EngenderHealth/Fistula Care Plus. All rights reserved. Fistula Care Plus (FC+) c/o EngenderHealth 505 9th Street NW, Suite 601 Washington, DC 20004 Telephone: (202) 902 2000 Fax: (202) 783 0281 E-mail:[email protected] www.fistulacare.org This publication is made possible by the generous support of the American people through the Office of Maternal and Child Health, U.S. Agency for International Development (USAID), under the terms of cooperative agreement AID-OAA-A14-00013. The contents are the responsibility of the Fistula Care Plus project and do not necessarily reflect the views of USAID or the United States Government.
Fistula Care Plus Associate Cooperative Agreement AID-OAA-A14-00013
Annual Report October 1, 2018 to September 30, 2019
Managing Partner: EngenderHealth; Associate Partners: The Population Council, Dimagi, Direct Relief, Fistula Foundation, Maternal Health Task Force, TERREWODE Submitted to United States Agency for International Development Washington, D.C. November 30, 2019
EngenderHealth U.S. / Washington, D.C. Office 505 9th Street NW, Suite 601 Washington, DC 20004 Telephone: (202) 902 2000 Fax: (202) 783 0281 E-mail: [email protected]
Annual Report • October 2018 – September 2019 Fistula Care Plus 2
TABLE OF CONTENTS
TABLE OF CONTENTS ........................................................................................................................... 2
ACRONYMS AND ABBREVIATIONS ................................................................................................... 5
TABLES ....................................................................................................................................................... 7
FIGURES ..................................................................................................................................................... 8
EXECUTIVE SUMMARY ........................................................................................................................ 9
INTRODUCTION ..................................................................................................................................... 11
SECTION I: MANAGEMENT ACTIVITIES ....................................................................................... 12 OVERVIEW............................................................................................................................................... 12 STAFFING AND RECRUITMENT ................................................................................................................ 12 PROJECT MANAGEMENT ......................................................................................................................... 12 PARTNERSHIP: GLOBAL AND COUNTRY-LEVEL ..................................................................................... 13 LEVERAGING FC+ FOR ADDITIONAL FISTULA PROGRAMMING .............................................................. 15 INTERNATIONAL CLINICAL SUPPORT AND TECHNICAL ASSISTANCE (TA) TRAVEL .............................. 15 MEETINGS ............................................................................................................................................... 16 FUNDING ................................................................................................................................................. 19
SECTION II: GLOBAL ACCOMPLISHMENTS ................................................................................ 20 FISTULA CARE PLUS ACHIEVEMENTS ..................................................................................................... 20 OBJECTIVE 1: STRENGTHENED ENABLING ENVIRONMENT TO INSTITUTIONALIZE FISTULA PREVENTION, TREATMENT, AND REINTEGRATION IN THE PUBLIC AND PRIVATE SECTORS ........................................... 21 OBJECTIVE 2: ENHANCED COMMUNITY UNDERSTANDING AND PRACTICES TO PREVENT FISTULA, IMPROVE ACCESS TO FISTULA TREATMENT, REDUCE STIGMA, AND SUPPORT REINTEGRATION OF WOMEN
AND GIRLS WITH FISTULA ........................................................................................................................ 28 OBJECTIVE 3: REDUCED TRANSPORTATION, COMMUNICATIONS, AND FINANCIAL BARRIERS TO
ACCESSING PREVENTIVE CARE, DETECTION, TREATMENT, AND REINTEGRATION SUPPORT ................... 29 OBJECTIVE 4: STRENGTHENED PROVIDER AND HEALTH FACILITY CAPACITY TO PROVIDE AND SUSTAIN
QUALITY SERVICES FOR FISTULA PREVENTION, DETECTION, AND TREATMENT...................................... 33 OBJECTIVE 5: STRENGTHENED EVIDENCE BASE FOR APPROACHES TO IMPROVE FISTULA CARE AND
SCALED UP APPLICATION OF STANDARD MONITORING AND EVALUATION (M&E) INDICATORS FOR
PREVENTION AND TREATMENT................................................................................................................ 42
SECTION III: COUNTRY REPORTS ................................................................................................... 49 BANGLADESH .......................................................................................................................................... 49 DEMOCRATIC REPUBLIC OF CONGO ....................................................................................................... 58 MOZAMBIQUE ......................................................................................................................................... 64 UGANDA .................................................................................................................................................. 71 WEST AFRICA/NIGER (WAN) ................................................................................................................. 84
APPENDIX A: FC+ PLANNED AND ACTUAL SUPPORTED SITES, FY18/19............................. 89
APPENDIX B: FC+ PARTNERSHIPS, BY COUNTRY ...................................................................... 91
APPENDIX C: FC+ PARTNERSHIPS WITH FAITH-BASED ORGANIZATIONS (FBOS) ....... 93
APPENDIX D: NUMBER OF USAID-SUPPORTED FISTULA REPAIR SURGERIES BY COUNTRY, SITE AND YEAR ............................................................................................................... 96
Annual Report • October 2018 – September 2019 Fistula Care Plus 3
APPENDIX E: FC/ FC+ PEER REVIEWED PUBLICATIONS ....................................................... 103
APPENDIX F: FC/FC+ PUBLICATION READERSHIP METRICS* ............................................ 118
APPENDIX G: FIGO SUMMARY TRIP REPORT ........................................................................... 120
APPENDIX H: FC+ PARTICIPATION AT ISOFS AND IOFWG ................................................... 126
APPENDIX I: SCIENTIFIC PROGRAM OF THE 7TH INTERNATIONAL ISOFS CONFERENCE....................................................................................................................................... 130
APPENDIX J: TANZANIA CESAREAN SECTION POLICY BRIEF ............................................ 137
APPENDIX K: IOFWG ROAD MAP .................................................................................................. 139
APPENDIX L: ISOFS PLENARY PRESENTATION ........................................................................ 150
APPENDIX M: USAID RESEARCH BRIEFING............................................................................... 155
APPENDIX N: UGANDA BARRIERS INTERVENTION RESEARCH BRIEF ............................ 165
APPENDIX O: KATSINA BARRIERS INTERVENTION RESEARCH BRIEF ........................... 172
APPENDIX P: EBONYI BARRIERS INTERVENTION RESEARCH BRIEF .............................. 177
APPENDIX Q: FC+ TRIBUTE TO DR. DENIS MUKWEGE .......................................................... 182
APPENDIX R: FC+ URODAK 2019 PRESENTATION .................................................................... 183
APPENDIX S: INTERNATIONAL CONSULTATION ON THE REGIONAL STRATEGY FOR THE ELIMINATION OF OBSTETRIC FISTULA – MEETING REPORT ................................... 188
APPENDIX T: ECSACOG PANEL PRESENTATION: BOATIN ................................................... 195
APPENDIX U: ECSACOG PRESENTATION: MASWIME ............................................................ 200
APPENDIX V: ECSACOG PRESENTATION: ROA ........................................................................ 202
APPENDIX W: ECSACOG PRESENTATION: SHIVERA .............................................................. 206
APPENDIX X: ECSACOG PRESENTATION: LUGAZIA ............................................................... 208
APPENDIX Y: FC+ ANNUAL PARTOGRAPH MONITORING: FY 14/15................................... 212
APPENDIX Z: FC+ ANNUAL PARTOGRAPH MONITORING: FY 15/16 ................................... 215
APPENDIX AA: FC+ ANNUAL PARTOGRAPH MONITORING: FY 16/17 ................................ 218
APPENDIX BB: FC+ ANNUAL PARTOGRAPH MONITORING: FY 17/18 ................................ 221
APPENDIX CC: FC+ ANNUAL PARTOGRAPH MONITORING: FY 18/19 ................................ 223
APPENDIX DD: AFLATEEN TECHNICAL BRIEF ......................................................................... 224
APPENDIX EE: HEALTH WORKERS TECHNICAL BRIEF ........................................................ 232
APPENDIX FF: RELIGIOUS LEADERS TECHNICAL BRIEF ..................................................... 238
APPENDIX GG: SUCCESS STORIES TECHNICAL BRIEF .......................................................... 246
APPENDIX HH: TERREWODE RESEARCH TECHNICAL BRIEF............................................. 254
APPENDIX II: 4Q CHECKLIST TECHNICAL BRIEF ................................................................... 262

Annual Report • October 2018 – September 2019 Fistula Care Plus 4
APPENDIX JJ: USG BRIEF ON RECOGNIZING U.S. ACHIEVEMENTS IN GLOBAL FISTULA CARE ..................................................................................................................................... 268
APPENDIX KK: IDEOF FIVE YEARS OF FC+ BRIEF .................................................................. 270
APPENDIX LL: LANCET COMMENTARY ..................................................................................... 278
APPENDIX MM: REMOVING BARRIERS JOURNAL ARTICLE ............................................... 280
APPENDIX NN: UN REPORT ON FISTULA .................................................................................... 294
APPENDIX OO: RCOG PRESENTATION ........................................................................................ 312
APPENDIX PP: FC+ URODAK PRESENTATION ........................................................................... 317
APPENDIX QQ: FC+ PRESENTATION AT INTERNATIONAL CONSULTATION ON THE REGIONAL STRATEGY FOR OBSTETRIC FISTULA ELIMINATION IN WEST AND CENTRAL AFRICA .............................................................................................................................. 323
APPENDIX RR: FC+ SUPPORTED TREATMENT SITES MEETING TO DISCUSS DATA ... 329
APPENDIX SS: FC+ CORE INDICATORS: ANNUAL ACHIEVEMENTS .................................. 330
Annual Report • October 2018 – September 2019 Fistula Care Plus 5
ACRONYMS AND ABBREVIATIONS
ACOG ........................................ American College of Obstetricians and Gynecologists AGOTA ..................................... Tanzanian Association of Gynaecologists and Obstetricians ANC ........................................... Antenatal Care BMGF ........................................ Bill and Melinda Gates Foundation BSMMU ..................................... Bangabandhu Sheikh Mujib Medical University C-Section ................................... Cesarean Section CBO ........................................... Community Based Organization CDDM ....................................... Clinical data for decision-making COSECSA ................................. College of Surgeons of East, Central and Southern Africa CPR ............................................ Country program review CSME ......................................... Maternal and Child Health Center (Centre de Santé Mère / Enfant) CNRFO ...................................... Centre National de Référence pour la Fistules Obstétricales CYP ............................................ Couple-Years of Protection DDM .......................................... Data for Decision Making DGHS ......................................... Directorate General of Health Services DHIS .......................................... District Health Information System DHS ........................................... Demographic and Health Survey DRC ........................................... Democratic Republic of the Congo ECOWAS ................................... Economic Community of West African States ECSA ...................................... East, Central, and Southern Africa ECSACOGS ............................... East, Central, and Southern Association College of Obstetricians and
Gynecologists EmOC ........................................ Emergency Obstetric Care EmONC ..................................... Emergency Obstetric and Neonatal Care ETOO ......................................... Essential Training in Operative Obstetrics FBO ............................................ Faith Based Organization FC ............................................... Fistula Care FC+ ............................................ Fistula Care Plus FF ............................................... Fistula Foundation FFM ........................................... Focus Fistula Mozambique FIGO .......................................... International Federation of Gynecology and Obstetrics FP ............................................... Family planning FY .............................................. Fiscal year GIEESC ..................................... Global Initiative for Emergency and Essential Surgical Care GOB ........................................... Government of Bangladesh HC .............................................. Health Center HGR ........................................... General Reference Hospital HMIS ......................................... Health Management Information System HSD ........................................... Health Services Delivery IDEOF ........................................ International Day to End Obstetric Fistula IGL ............................................. Imagerie des Grand Lacs IHI .............................................. Institute for Healthcare Improvement IOFWG ...................................... International Obstetric Fistula Working Group ISOFS ......................................... International Society of Obstetric Fistula Surgeons IUCD .......................................... Intrauterine contraceptive device IVR ............................................. Interactive voice response MCH .......................................... Maternal and Child Health MCSP ......................................... Maternal and Child Survival Program ME&R ........................................ Monitoring, evaluation and research
Annual Report • October 2018 – September 2019 Fistula Care Plus 6
M&E .......................................... Monitoring and evaluation MHTF ........................................ Maternal Health Task Force MNCH ....................................... Maternal, Newborn and Child Health MOH .......................................... Ministry of Health MSRK ........................................ Maternité Sans Risque de Kindu NCE ........................................... No cost extension NFTWG ..................................... National Fistula Technical Working Group NOFIC ....................................... National Obstetric Fistula Center NSOAP ...................................... National Surgical, Obstetric, and Anesthesia Plans OBGYN ..................................... Obstetricians and gynecologists OF .............................................. Obstetric fistula OGSB ......................................... Obstetrical and Gynaecological Society of Bangladesh PGSSC ....................................... Harvard Program on Global Surgery and Social Change PHC ............................................ Primary Health Center PMP ........................................... Performance Management Plan POP ............................................ Pelvic organ prolapse PPP ............................................. Public Private Partnership PRH ............................................ Population and reproductive health PROSANI .................................. Le Projet de Santé Intégré RCOG ........................................ Royal College of Obstetricians and Gynecologists REF ............................................ Réseau pour l’Eradication des Fistules (Niger) SBCC ......................................... Social and behavior change communication SDI ............................................. Service delivery improvement SJH ............................................. St. Joseph Hospital (DRC) SMNE ........................................ Santé de la mère, du nouveau né et de l‘enfant SOO ........................................... Structured Operative Obstetrics SST ............................................. Surgical safety toolkit SWT ........................................... Site Walk-Through TA .............................................. Technical Assistance TOT ............................................ Training of trainers TF ............................................... Traumatic fistula TSHIP ........................................ Targeted States High Impact Project (Nigeria) UFC…………. .......................... University Fistula Center UNFPA ...................................... United Nations Population Fund UROMAP .................................. Urology Maputo Conference USAID ....................................... United States Agency for International Development USAID/W .................................. USAID/Washington VHT ........................................... Village health team volunteer VVF ........................................... Vesico Vaginal Fistula WA ............................................. West Africa WACS ........................................ West and Central Africa College of Surgeons WAHO ....................................... West African Health Organization WCAGEOF ................................ West and Central African Group to End Obstetric Fistula WDI ........................................... Women Deemed Incurable
Annual Report • October 2018 – September 2019 Fistula Care Plus 7
TABLES
Title Page Table 1: Active Subawards as of September 30, 2019 14 Table 2: International Technical Assistance Travel, FY 18/19 15 Table 3: Meetings and Presentations, FY 18/19 16 Table 4: Select Fistula Care Plus Achievements and Benchmarks, as of September 30, 2019 20 Table 5: Total Number of Clinical Training Participants, by Country, by Topic, FY 18/19 21 Table 6: FC+ Twitter Account Metrics, FY 18/19 27 Table 7: Community Outreach/Education Events, by Country, FY 18/19 28 Table 8: Community Volunteer/Educator Training, Participants by Country, FY 18/19 Table 9: Number of USAID-Supported Surgical Fistula Repairs, by Country, FY 18/19
29 37
Table 10: Training in Surgical Fistula Repair, Participants by Quarter, FY 18/19 39 Table 11: Training for Health System Personnel (excluding fistula/POP surgery), Participants by Quarter, FY 18/19
40
Table 12: Number Seeking, Requiring, and Receiving POP Treatment, by Country, FY 18/19 41 Table 13: Peer-Reviewed Articles Published, FY 18/19 43 Table BGD1: Community Outreach/Education/Advocacy Events, FY 18/19 53 Table BGD2: Community Volunteer/Educator Training, Participants, By Quarter, FY 18/19 53 Table BGD3: USAID-Supported Surgical Fistula Repairs, by Site, FY 18/19 54 Table BGD4: Surgical Fistula Repair Training, Participants by Trainee Institution, FY 18/19 55 Table BGD5: Non-Surgical Health System Personnel Training, Participants by Topic, FY 18/19 56 Table BGD6: Family Planning Counseling Sessions and CYP, by Site, FY 18/19 56 Table DRC1: Community Outreach/Education/Advocacy Events, FY 18/19 59 Table DRC2: USAID-Supported Surgical Fistula Repairs, by Site, FY 18/19 61 Table DRC3: Non-Surgical Health System Personnel Training, Participants by Topic, FY 18/19 62 Table DRC4: Family Planning Counseling Sessions and CYP, by Site, FY 18/19 62 Table MOZ1: Community Outreach/Education/Advocacy Events, FY 18/19 67 Table MOZ2:Community Volunteer/Educator Training, FY 18/19 67 Table MOZ3: USAID-Supported Surgical Fistula Repairs, by Site, By Quarter, FY 18/19 68 Table MOZ4: Non-Surgical Health System Personnel Training, Participants by Topic, By Quarter, FY 18/19
69
Table MOZ5: Surgical Fistula Repair Training, Participants by Trainee Institution, FY 18/19 70 Table UGA1: Community Outreach/Education/Advocacy Events, FY 18/19 75 Table UGA2: USAID-Supported Surgical Fistula Repairs, by Site, FY 18/19 79 Table UGA3: Family Planning Counseling Sessions and CYP, FY 18/19 80 Table WAN1: USAID-Supported Surgical Fistula Repairs, by Site, FY 18/19 87
Annual Report • October 2018 – September 2019 Fistula Care Plus 8
FIGURES
Title Page Figure 1: Fistula Care Plus Project Framework 11 Figure 2: Fistula Care Plus Website Views, by Month 28 Figure 3: Cesarean Section Rates, by Country, FY 18/19 35 Figure 4: Number of Women Seeking and Requiring Fistula Treatment, and Number of Surgical Repairs, By Country, FY 18/19
37
Figure 5: USAID-Supported Surgical Fistula Repairs, by Quarter, FY 18/19 37 Figure 6: Outcome Rates for Fistula Surgical Repairs, by Country, FY 18/19 39 Figure 7: Family Planning Counseling Sessions, by Country, FY 18/19 40 Figure 8: Family Planning CYP, Short-Term vs. Long-Term/Permanent Methods, by Country, FY 18/19
41
Figure BGD1: Number of Women Seeking and Requiring Fistula Treatment, and Number of Surgical Repairs, by Site, FY 18/19
54
Figure BGD2: Outcome Rates for Surgical Repairs, by Site, FY 18/19 55 Figure BGD3: Number of Obstetric Deliveries, by Site, FY 18/19 57 Figure BGD4: Cesarean Section Rates, by Site, FY 18/19 57 Figure DRC1: Number of Women Seeking and Requiring Fistula Treatment, and Number of Surgical Repairs, by Site, FY 18/19
61
Figure DRC2: Outcome Rates for Surgical Repairs, by Site, FY 18/19 62 Figure DRC3: Number of Obstetric Deliveries, by Site, FY 18/19 63 Figure DRC4: Cesarean Section Rates, by Site, FY 18/19 63 Figure MOZ1: Number of Women Seeking and Requiring Fistula Treatment, and Number of Surgical Repairs, by Site, FY 18/19
68
Figure MOZ2: Outcome Rates for Surgical Repairs, by Site, FY 18/19 69 Figure UGA1: Number of Women Seeking and Requiring Fistula Treatment, and Number of Surgical Repairs, by Site, FY 18/19
79
Figure UGA2: Outcome Rates for Surgical Repairs, by Site, FY 18/19 80 Figure UGA3: Number of Obstetric Deliveries, by Site, FY 18/19 81 Figure UGA4: Cesarean Section Rates, by Site, October 2018 – March 2019 82 Figure WAN1: Number of Women Seeking and Requiring Fistula Treatment, and Number of Surgical Repairs, by Site, FY 18/19
86
Figure WAN2: Outcome Rates for Surgical Repairs, by Site, FY 18/19 87
Annual Report • October 2018 – September 2019 Fistula Care Plus 9
EXECUTIVE SUMMARY
The annual report presents key accomplishments and activities for the sixth fiscal year (October 1, 2018 to September 30, 2019) of Fistula Care Plus (FC+). EngenderHealth manages the project in collaboration with international and national partners. During FY 18/19, USAID supported fistula treatment and prevention services through the FC+ project in five countries—Bangladesh, the Democratic Republic of the Congo (DRC), Mozambique, Niger, and Uganda. USAID also supported fistula activities in Ethiopia, Guinea, Mali, and Pakistan through bilateral funding. EngenderHealth implements fistula prevention and care activities in Guinea with funds from other sources, including the Jhpiego-implemented, USAID-funded Health Services Delivery (HSD) project (activity ended September 30, 2019).
Key accomplishments during the October 1, 2018 to September 30, 2019 period included:
Objective 1: Strengthened enabling environment FC+ participation in the National Surgical, Obstetric, and Anesthesia Planning (NSOAP) Conference
for High-Level Global, Regional, and Country Authorities and Funders and the Utstein Meeting on Indicators and Reporting Criteria for Surgery, Obstetrics and Anaesthesia Patient Safety
Delivery of Fistula Repair Modules containing disposable supplies by project partner Direct Relief International – as of September 30, 2019 kits have been delivered to a total of 11 FC+ supported sites in DRC, Mozambique, Niger, and Uganda
Three plenary oral presentations, 21 oral presentations, and 14 posters at the meetings of the International Society of Obstetric Fistula Surgeons (ISOFS) and the International Obstetric Fistula Working Group (IOFWG)
15 oral presentations and convening of the panel “Cesarean section safety in low-resource settings: Ensuring quality in a context of rapidly increasing volume” at the International Federation of Gynecology and Obstetrics (FIGO) World Congress
Production of two briefs for International Day to End Obstetric Fistula (IDEOF) on U.S. investments in fistula care and FC+ achievements for the first five years of implementation
Collaboration with Harvard Program in Global Surgery and Social Change (PGSSC) to expand documentation and measurement of sequelae of prolonged/obstructed labor
Co-sponsored International Consultation on the Regional Strategy for Obstetric Fistula Elimination in West and Central Africa
Five presentations and inauguration of the Isaac Achwal Research Award at the joint Association of Gynaecologists and Obstetricians of Tanzania (AGOTA) and East, Central, Southern Africa (ECSA) College of Obstetrics and Gynecology (ECSACOG) Conference
Objective 2: Enhanced community understanding and practices 1,246 in-person community awareness-raising activities/events conducted by program partners,
reaching 149,585 participants; two mass media events reaching over 600,000 people Objective 3: Reduced transportation, communications, and financial barriers Completion of endline data collection of the Barriers Intervention Study in Katsina State, Nigeria Dissemination events held in Katsina and Ebonyi, Nigeria in December 2018; and in Uganda in
March 2019 through the National Fistula Technical Working Group Global dissemination of findings and lessons learned through presentations at ISOFS and Africa
region conferences, technical briefs, and peer-reviewed journal publications Objective 4: Strengthened provider and health facility capacity 24 sites supported by FC+ for fistula treatment and prevention activities; 9 sites supported through
other USAID bilateral support 605 surgical fistula repairs and 6 non-surgical repairs supported through FC+; 597 surgical repairs
supported by other bilateral USAID programs; this has brought the total USAID-supported surgical

Annual Report • October 2018 – September 2019 Fistula Care Plus 10
fistula repairs since 2005 to 54,697 and the total EngenderHealth-supported surgical fistula repairs to 43,085
19 sites supported by FC+ for prevention-only activities, 44 sites supported through other USAID bilateral support
46,373 family planning (FP) counseling sessions provided at supported sites, with FP services resulting in 33,469 Couple Years of Protection (CYP)
29 clinicians trained in fistula surgical repair; 12 clinicians trained in pelvic organ prolapse (POP) repair
938 health system personnel trained in non-surgical fistula repair and prevention topics Objective 5: Strengthened evidence base Publication of “Caesarean section provision and readiness in Tanzania: analysis of cross-sectional
surveys of women and health facilities over time” in BMJ as well as a policy brief summarizing key findings from analysis of Tanzanian DHS and SPA data, commissioned by FC+ and executed by the London School for Hygiene and Tropical Medicine
Publication of “Removing barriers to fistula care: Applying appreciative inquiry to improve access to screening and treatment in Nigeria and Uganda” on the research-to-action partnership to address fistula treatment barriers in Health Care for Women International
Publication of a commentary in Lancet Global Health entitled “Meeting the SDG challenge to end fistula and preventable childbirth-related morbidity and mortality” which emphasizes the critical role of universal access to skilled care at birth
Publication of six technical briefs: five summarizing project activities in Uganda including the Site Walk Through approach, research with Ugandan organization TERREWODE, partnering with local religious leaders, and piloting of work with adolescents using the Aflateen curriculum; and one brief on the 4Q checklist for fistula screening in Bangladesh

Annual Report • October 2018 – September 2019 Fistula Care Plus 11
INTRODUCTION
This annual report provides a summary of accomplishments for the sixth fiscal year (October 1, 2018 – September 30, 2019) of Fistula Care Plus (FC+), a five-year Associate Cooperative Agreement (No. AID-OAA-A14-00013) supported by USAID that has been extended through two no-cost extensions (NCEs) until March 31, 2021. In this report, we present data on quantitative project indicators as well as narrative updates organized into: Section I: Management Activities, Section II: Global Accomplishments, and Section III: Country Accomplishments. Global and country accomplishments are reported against the objectives of the FC+ Project Framework (see Figure 1 and Appendix SS) and in alignment with the USAID-approved Project Monitoring Plan (PMP). Section II is further organized by sub-objective.
Figure 1: Fistula Care Plus Project Framework
GOAL: To strengthen health system capacity for fistula prevention, detection, treatment, and reintegration in priority countries in sub-Saharan Africa and South Asia Obj. 1: Strengthened enabling environment to institutionalize fistula prevention, treatment, and reintegration in the public and private sectors
Obj. 2: Enhanced community understanding and practices to prevent fistula, improve access to fistula treatment, reduce stigma, and support reintegration of women and girls with fistula
Obj. 3: Reduced transportation, communications, and financial barriers to accessing preventive care, detection, treatment, and reintegration support
Obj. 4: Strengthened provider and health facility capacity to provide and sustain quality services for fistula prevention, detection, and treatment
Obj. 5: Strengthened evidence base for approaches to improve fistula care and scaled up application of standard monitoring and evaluation (M&E) indicators for prevention and treatment
USAID support to EngenderHealth for fistula services began in FY 04/05 under the Access, Quality, and Use in Reproductive Health (ACQUIRE) and Action for West Africa Region (AWARE) Projects and continued through the Fistula Care (FC) project, which ended on December 31, 2013.
USAID/Washington (USAID/W) awarded the FC+ project to EngenderHealth, in partnership with the Population Council, Dimagi, Direct Relief International, Fistula Foundation, Maternal Health Task Force, and TERREWODE, on December 12, 2013. FC+ seeks to strengthen health system capacity for fistula prevention, detection, treatment, and reintegration in priority countries in Sub-Saharan Africa and South Asia.
During FY 18/19, FC+ supported fistula prevention and treatment activities with USAID funding at a total of 43 sites in Bangladesh, the Democratic Republic of the Congo (DRC), Mozambique, Niger, and Uganda: 24 treatment and prevention sites and 19 prevention-only sites. The number of supported sites varied over the course of FY 18/19, due to close-out of activity in Uganda. See Appendix A for a full list of FC+ planned and actual supported sites for the fiscal year.
In addition to the support provided via FC+, USAID provided bilateral support to fistula work carried out at 53 sites (nine treatment, 44 prevention-only) in four countries: Ethiopia (through Pathfinder); Guinea (through Jhpiego); Mali (through IntraHealth); and Pakistan (through the Jinnah Post Graduate Medical Center). Support for fistula work in Mali ended in February 2019, and in Guinea in September 2019. An integrated health project is beginning implementation in DRC but not yet carrying out fistula activity.
During FY 18/19, EngenderHealth continued fistula activities in Guinea through the Jhpiego-led Health Services Delivery (HSD) project, as well as support from the Alcoa Foundation. Recently awarded funding from Fistula Foundation complements HSD activities in Guinea for training providers, prevention activities, and care of women with fistula in Guinea. HSD fistula activities have concluded as of September 30, 2019.

Annual Report • October 2018 – September 2019 Fistula Care Plus 12
SECTION I: MANAGEMENT ACTIVITIES
Overview During FY 18/19, the global FC+ team’s management activities focused on revision and implementation of project subawards, workplan and budget development, application and implementation of a project No-Cost Extension (NCE), and preparation of a competed subaward in Niger. Management activities provided the oversight and operational framework that enabled the achievements described in Sections II and III.
Staffing and Recruitment During FY 18/19, the FC+/Global team was comprised of the following staff: Lauri Romanzi: Project Director Vandana Tripathi: Deputy Director Jarryd Botha: Financial Management and Administrative Specialist Nazmul Huda: Global Activities Manager Isaac Achwal: Senior Clinical Advisor and Regional Strategy Specialist Altiné Diop: Program Associate Karen Levin: Senior Program Associate, Monitoring and Evaluation (50% LOE) In February 2019, Dr. Isaac Achwal, FC+ Senior Clinical Advisor and Regional Strategy Specialist, passed away. His contributions to the project, and to global health broadly, were great and he is deeply missed.
Project Management FC+ leadership oversaw project management through participation in meetings with USAID/W; finalization of FY 18/19 workplans and budgets; preparation and submission of FY 19/20 workplans and budgets; execution of an NCE application to USAID; securing USAID Mission concurrence and USAID/W approvals for subawards and country level programming; and working with partners and country-level staff to facilitate FC+ finance and M&E systems, and staffing and program support. USAID/W granted approval of an 18-month NCE in March 2019, extending the project through March 31, 2021.
At the request of USAID/Washington, FC+ has continued to work with several projects supporting fistula work through USAID-supported bilateral funding in order to coordinate reporting of fistula data to USAID. During FY 18/19, FC+ was able to gather data from three bilateral projects: Pathfinder in Ethiopia, Jhpiego in Guinea, and IntraHealth in Mali. As of the end of FY 18/19, the USAID-funded MCSP project in Rwanda, IntraHealth’s work in Mali, and the fistula work under the JHPIEGO project in Guinea have all concluded. USAID’s new Integrated Health Project in DRC has not yet begun fistula activity.
Throughout FY 18/19, FC+ continued to hold coordinated country program reviews (CPR) involving monthly teleconferences between Clinical, Program Management, M&E, and Finance staff from global and country offices to streamline and harmonize staff and programmatic functions in relation to objectives, indicators, and program innovations.
The FC+ Global Activities Manager worked with the FP compliance point persons in each office to ensure FP compliance plans and status are up to date. They are stored centrally on EngenderHealth’s intranet. All staff and partners completed the online training courses for Protecting Life in Global Health Assistance (PLGHA) and US Abortion and Family Planning Requirements. These certificates are also stored on the project intranet.
Annual Report • October 2018 – September 2019 Fistula Care Plus 13
FC+, at the request of the USAID Mission in Maputo, Mozambique, has partnered with Maputo-based NGO Focus Fistula, to build the NGO’s administrative capacity, support fistula repair, and reinforce clinical capacity at partner facilities through the leadership of Dr. Igor Vaz. The first subaward with Focus Fistula was awarded on February 1, 2018, covering activity through November 2018. A second subaward governs activity from April 1, 2019 onward. The goal of this partnership is to strengthen the clinical capacity of selected ministry and private facilities and staff to provide accessible, quality obstetric, iatrogenic and traumatic fistula surgical and non-surgical treatment services in Mozambique. Through the subaward, Focus Fistula works with the Ministry of Health, UNFPA Mozambique, and USAID/Mozambique mission staff to support fistula service provision that is focused on complex caseload while also supervising surgical treatment for simple fistula cases. This is achieved through a concentrated repair model that concurrently supports capacity building for routine fistula services.
Partnership: Global and Country-Level In the sixth project year of FC+, engagement with collaborative partners to build the project’s sustainability and legacy platform has been a key priority, as has documentation of project achievements and challenges.
FC+ conversations with project partner Fistula Foundation have not yet engaged the Foundation’s commitments to sustain fistula service delivery at selected treatment sites at the end of the FC+ project. This is partly due to the extension of the FC+ project through two NCEs, and because the Foundation’s priorities shift from year to year. Once FC+ is closer to the end of project, the Foundation is ready to consider this sustainability engagement. However, in FY 19/20, FC+ will focus advocacy for Foundation engagement on fistula treatment sites in Nigeria and Uganda, where project support has already ended.
FC+ continues to contribute to the global safe surgery community of practice through technical consultation activities and collaboration with the WHO Global Initiative for Essential and Emergency Surgical Care (GIEESC). FC+ has participated in and provided technical support to organizations and institutions involved in regional surgical safety efforts, particularly the College of Surgeons of East, Southern and Central Africa (COSECSA); the East, Central, Southern Africa (ECSA) College of Obstetrics and Gynecology; and the West African College of Surgeons (WACS); see Section II, Objective 1 for details. FC+ also continues to collaborate with the Harvard Program in Global Surgery and Social Change (PGSSC).
FC+ has also continued partnership with the American College of Obstetricians and Gynecologists (ACOG), to provide technical assistance for monitoring and evaluation of a program to strengthen surgical obstetrics in Uganda (see Section II, Objective 1 as well as Section III: Uganda).
During FY 18/19, FC+ worked with global partners to strengthen and disseminate the evidence base for improved fistula care. FC+ has continued collaboration with the Population Council to implement and evaluate interventions in response to the completed research study that identified barriers faced by women seeking fistula repair services in Nigeria and Uganda. This work is described in detail in Section II, Objectives 3 and 5 as well as in Section III: and Uganda.
FC+ continues to monitor the activity of the nascent East, Central, Southern Africa (ECSA) College of Obstetrics and Gynecology (ECSACOG), supporting and participating in the June 2019 joint Tanzanian Association of Gynaecologists and Obstetricians (AGOTA) and ECSACOG Conference in Dar es Salaam.
The West and Central African Group to End Obstetric Fistula (WCAGEOF) advocacy coalition meeting, to have been held, with FC+ support, concurrent with the annual 2019 January general meeting and
Annual Report • October 2018 – September 2019 Fistula Care Plus 14
scientific conference of the West African College of Surgeons (WACS) in Dakar, Senegal was canceled due to the USG government shutdown. Instead, FC+ supported and participated in the West Africa Regional Fistula Strategy meeting held in June 2019 in Senegal, see Section II, Objective 1 for details.
FC+ continues to collaborate with global maternal health stakeholders, including the M&E Technical Working Group of the WHO Quality, Equity, and Dignity Network and the WHO Think Tank on Maternal and Newborn Health Effective Coverage Measures. See Section II, Objective 1 for details.
FC+ also works with a variety of faith-based organizations (FBOs) in several countries, to advance objectives across the project results framework. These FBO partnerships are summarized in Appendix C.
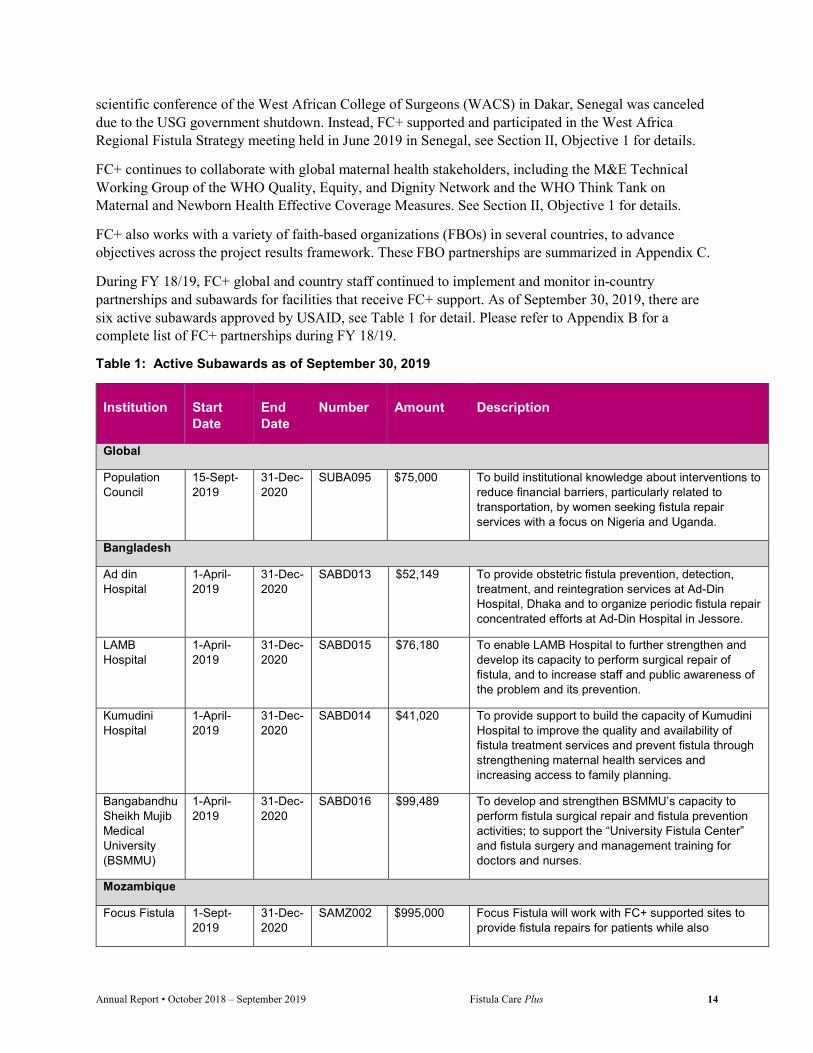
During FY 18/19, FC+ global and country staff continued to implement and monitor in-country partnerships and subawards for facilities that receive FC+ support. As of September 30, 2019, there are six active subawards approved by USAID, see Table 1 for detail. Please refer to Appendix B for a complete list of FC+ partnerships during FY 18/19.
Table 1: Active Subawards as of September 30, 2019
Institution Start Date
End Date
Number Amount Description
Global
Population Council
15-Sept-2019
31-Dec-2020
SUBA095 $75,000 To build institutional knowledge about interventions to reduce financial barriers, particularly related to transportation, by women seeking fistula repair services with a focus on Nigeria and Uganda.
Bangladesh
Ad din Hospital
1-April-2019
31-Dec-2020
SABD013 $52,149 To provide obstetric fistula prevention, detection, treatment, and reintegration services at Ad-Din Hospital, Dhaka and to organize periodic fistula repair concentrated efforts at Ad-Din Hospital in Jessore.
LAMB Hospital
1-April-2019
31-Dec-2020
SABD015 $76,180 To enable LAMB Hospital to further strengthen and develop its capacity to perform surgical repair of fistula, and to increase staff and public awareness of the problem and its prevention.
Kumudini Hospital
1-April-2019
31-Dec-2020
SABD014 $41,020 To provide support to build the capacity of Kumudini Hospital to improve the quality and availability of fistula treatment services and prevent fistula through strengthening maternal health services and increasing access to family planning.
Bangabandhu Sheikh Mujib Medical University (BSMMU)
1-April-2019
31-Dec-2020
SABD016 $99,489 To develop and strengthen BSMMU’s capacity to perform fistula surgical repair and fistula prevention activities; to support the “University Fistula Center” and fistula surgery and management training for doctors and nurses.
Mozambique
Focus Fistula 1-Sept-2019
31-Dec-2020
SAMZ002 $995,000 Focus Fistula will work with FC+ supported sites to provide fistula repairs for patients while also

Annual Report • October 2018 – September 2019 Fistula Care Plus 15
Institution Start Date
End Date
Number Amount Description
coordinating prevention activities to reduce the number of fistula cases in Mozambique
In addition to work with project partners, FC+ staff participated in several meetings and coordination processes led by USAID and its flagship projects. These include meetings of the USAID PRH Service Delivery Improvement (SDI) CAs, the USAID/JHUCCP Service Delivery Communication Community of Practice, the USAID Research and Policy Division and the USAID PRH Gender CAs. FC+ sought opportunities to support USAID-led and global initiatives addressing maternal health, see Table 3 for details of meetings in which FC+ participated during the fiscal year.
Leveraging FC+ for Additional Fistula Programming EngenderHealth continues to support fistula services in Guinea. EngenderHealth successfully raised funds from the Alcoa Foundation, which has significant mining interests in Guinea, as well as the Islamic Development Bank/Islamic Solidarity Fund for Development and the Fistula Foundation. In January 2016, the USAID Guinea RFA-OAA-15-000024 Guinea Health Service Delivery (HSD) project for FP and MNCH was awarded to the Jhpiego-led consortium. EngenderHealth and Save the Children are partners on the five-year project and EngenderHealth led fistula prevention and repair activities for a “fistula free generation” in Guinea. HSD support for fistula activity concluded at the end of this fiscal year.
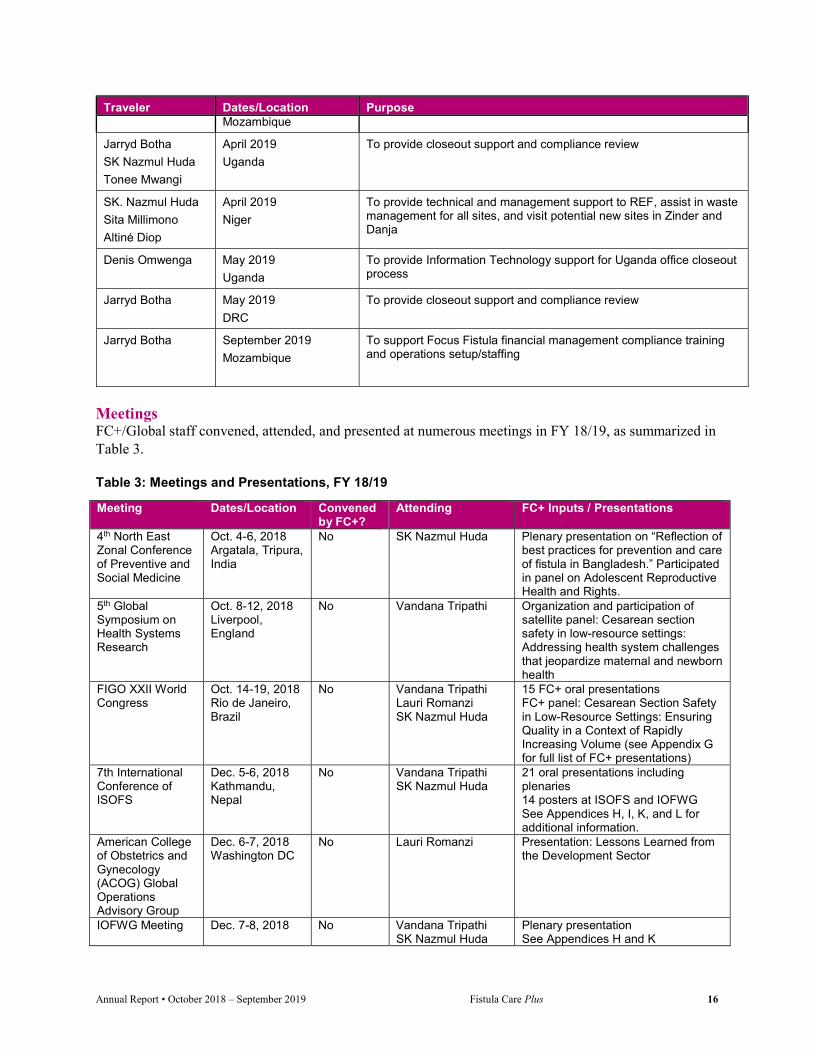
International Clinical Support and Technical Assistance (TA) Travel FC+ global staff and consultants have carried out international clinical support and TA visits to seven countries during FY 18/19 (see Table 2). This travel included management visits to Bangladesh, DRC, Niger, Nigeria, Mozambique, and Uganda and technical assistance for the planning of the 7th ISOFS Conference in Nepal.
Table 2: International Technical Assistance Travel, FY 18/19
Traveler Dates/Location Purpose
Jarryd Botha
Lauri Romanzi
October 2018
Nigeria
FC+ office closeout support
Isaac Achwal October 2018
DRC
Workplan implementation and clinical monitoring visit
SK Nazmul Huda November 2018
Nepal
Technical assistance to the local organizing committee of the 7th ISOFS Conference
Jarryd Botha November 2018
Bangladesh
FC+ field office support
Isaac Achwal November 2018
DRC
Workplan implementation and clinical monitoring follow up visit
SK Nazmul Huda February 2019
Mozambique
Support to subaward partner Focus Fistula financial and programmatic systems.
Jarryd Botha March 2019 Support to subaward partner Focus Fistula financial and programmatic systems
Annual Report • October 2018 – September 2019 Fistula Care Plus 16
Traveler Dates/Location Purpose Mozambique
Jarryd Botha
SK Nazmul Huda
Tonee Mwangi
April 2019
Uganda
To provide closeout support and compliance review
SK. Nazmul Huda
Sita Millimono
Altiné Diop
April 2019
Niger
To provide technical and management support to REF, assist in waste management for all sites, and visit potential new sites in Zinder and Danja
Denis Omwenga May 2019
Uganda
To provide Information Technology support for Uganda office closeout process
Jarryd Botha May 2019
DRC
To provide closeout support and compliance review
Jarryd Botha September 2019
Mozambique
To support Focus Fistula financial management compliance training and operations setup/staffing
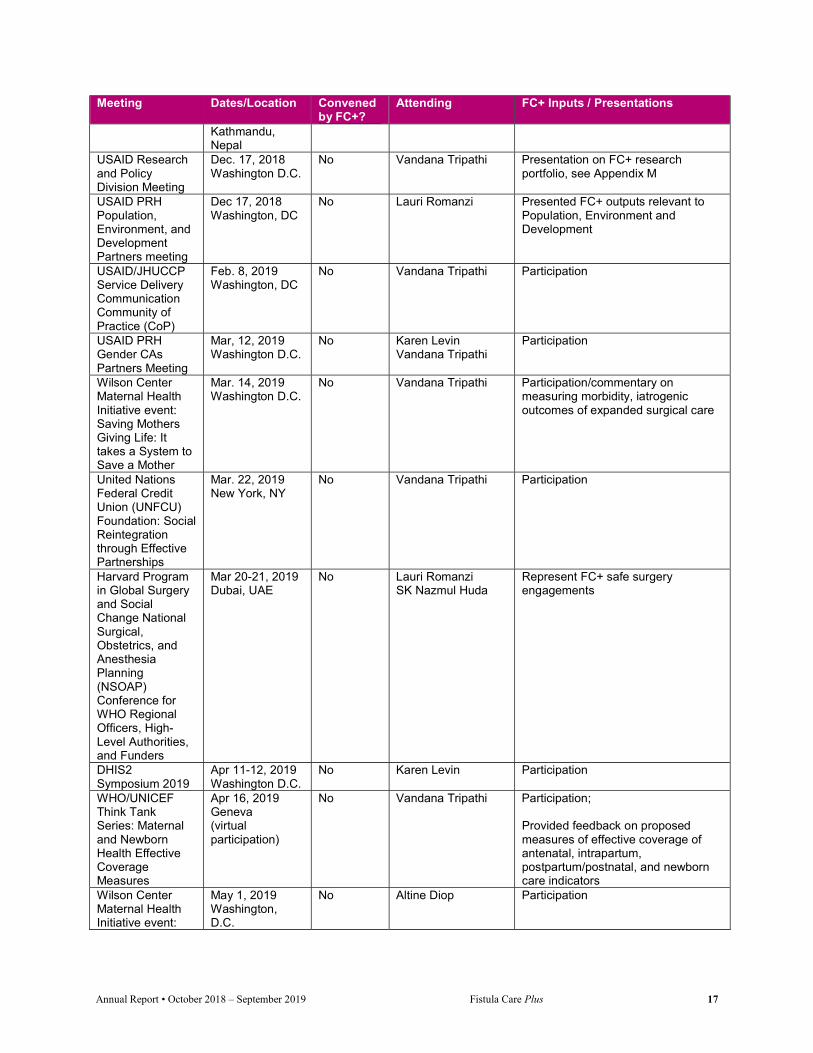
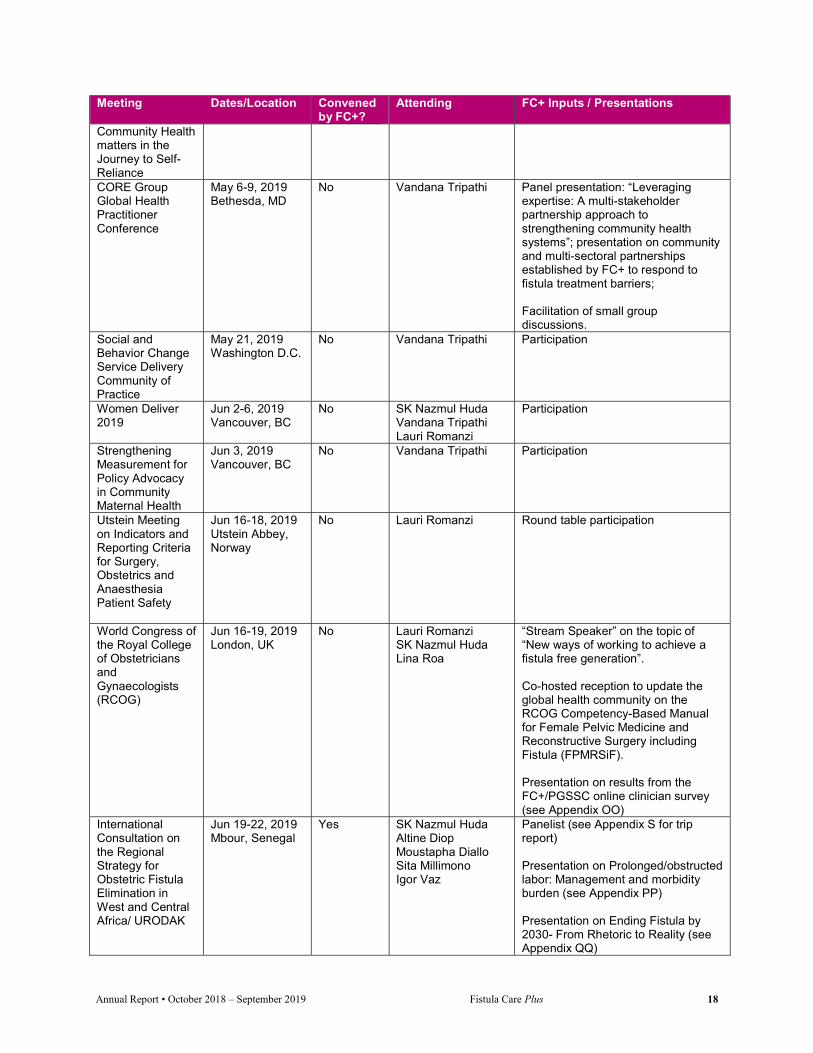
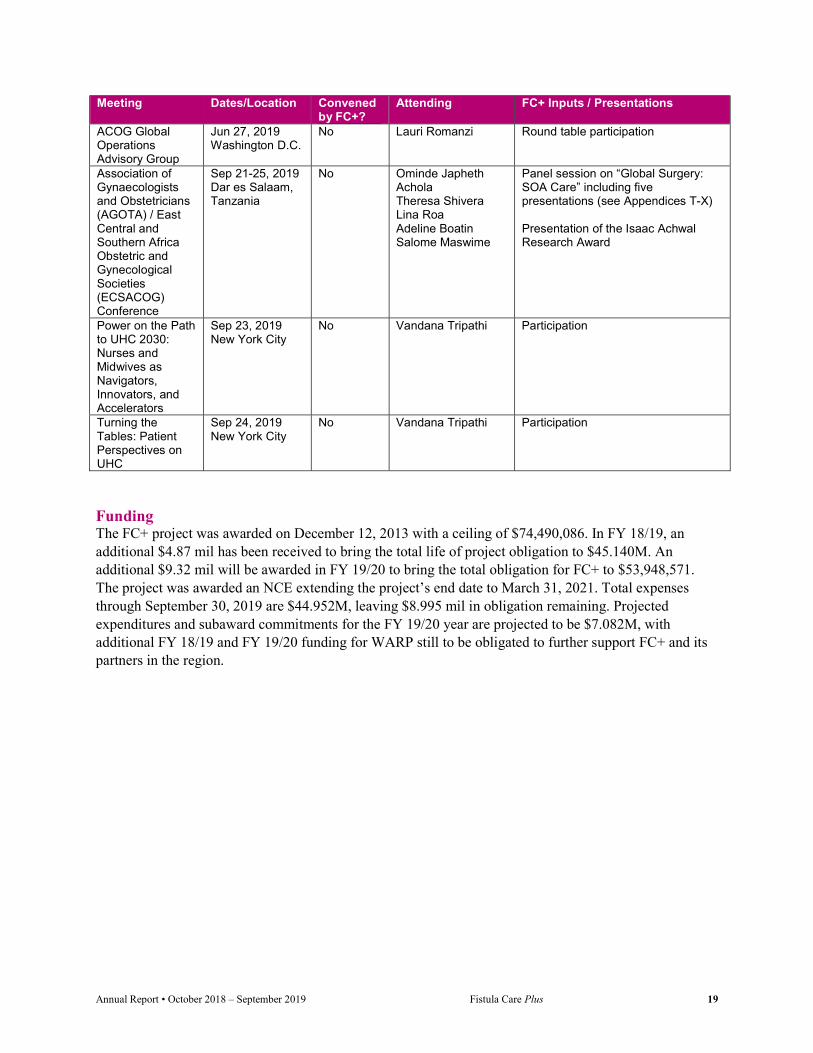
Meetings FC+/Global staff convened, attended, and presented at numerous meetings in FY 18/19, as summarized in Table 3.
Table 3: Meetings and Presentations, FY 18/19
Meeting Dates/Location Convened by FC+?
Attending FC+ Inputs / Presentations
4th North East Zonal Conference of Preventive and Social Medicine
Oct. 4-6, 2018 Argatala, Tripura, India
No SK Nazmul Huda Plenary presentation on “Reflection of best practices for prevention and care of fistula in Bangladesh.” Participated in panel on Adolescent Reproductive Health and Rights.
5th Global Symposium on Health Systems Research
Oct. 8-12, 2018 Liverpool, England
No Vandana Tripathi Organization and participation of satellite panel: Cesarean section safety in low-resource settings: Addressing health system challenges that jeopardize maternal and newborn health
FIGO XXII World Congress
Oct. 14-19, 2018 Rio de Janeiro, Brazil
No Vandana Tripathi Lauri Romanzi SK Nazmul Huda
15 FC+ oral presentations FC+ panel: Cesarean Section Safety in Low-Resource Settings: Ensuring Quality in a Context of Rapidly Increasing Volume (see Appendix G for full list of FC+ presentations)
7th International Conference of ISOFS
Dec. 5-6, 2018 Kathmandu, Nepal
No Vandana Tripathi SK Nazmul Huda
21 oral presentations including plenaries 14 posters at ISOFS and IOFWG See Appendices H, I, K, and L for additional information.
American College of Obstetrics and Gynecology (ACOG) Global Operations Advisory Group
Dec. 6-7, 2018 Washington DC
No Lauri Romanzi Presentation: Lessons Learned from the Development Sector
IOFWG Meeting Dec. 7-8, 2018 No Vandana Tripathi SK Nazmul Huda
Plenary presentation See Appendices H and K
Annual Report • October 2018 – September 2019 Fistula Care Plus 17
Meeting Dates/Location Convened by FC+?
Attending FC+ Inputs / Presentations
Kathmandu, Nepal
USAID Research and Policy Division Meeting
Dec. 17, 2018 Washington D.C.
No Vandana Tripathi Presentation on FC+ research portfolio, see Appendix M
USAID PRH Population, Environment, and Development Partners meeting
Dec 17, 2018 Washington, DC
No Lauri Romanzi Presented FC+ outputs relevant to Population, Environment and Development
USAID/JHUCCP Service Delivery Communication Community of Practice (CoP)
Feb. 8, 2019 Washington, DC
No Vandana Tripathi Participation
USAID PRH Gender CAs Partners Meeting
Mar, 12, 2019 Washington D.C.
No Karen Levin Vandana Tripathi
Participation
Wilson Center Maternal Health Initiative event: Saving Mothers Giving Life: It takes a System to Save a Mother
Mar. 14, 2019 Washington D.C.
No Vandana Tripathi Participation/commentary on measuring morbidity, iatrogenic outcomes of expanded surgical care
United Nations Federal Credit Union (UNFCU) Foundation: Social Reintegration through Effective Partnerships
Mar. 22, 2019 New York, NY
No Vandana Tripathi Participation
Harvard Program in Global Surgery and Social Change National Surgical, Obstetrics, and Anesthesia Planning (NSOAP) Conference for WHO Regional Officers, High-Level Authorities, and Funders
Mar 20-21, 2019 Dubai, UAE
No Lauri Romanzi SK Nazmul Huda
Represent FC+ safe surgery engagements
DHIS2 Symposium 2019
Apr 11-12, 2019 Washington D.C.
No Karen Levin Participation
WHO/UNICEF Think Tank Series: Maternal and Newborn Health Effective Coverage Measures
Apr 16, 2019 Geneva (virtual participation)
No Vandana Tripathi Participation; Provided feedback on proposed measures of effective coverage of antenatal, intrapartum, postpartum/postnatal, and newborn care indicators
Wilson Center Maternal Health Initiative event:
May 1, 2019 Washington, D.C.
No Altine Diop Participation
Annual Report • October 2018 – September 2019 Fistula Care Plus 18
Meeting Dates/Location Convened by FC+?
Attending FC+ Inputs / Presentations
Community Health matters in the Journey to Self-Reliance CORE Group Global Health Practitioner Conference
May 6-9, 2019 Bethesda, MD
No Vandana Tripathi Panel presentation: “Leveraging expertise: A multi-stakeholder partnership approach to strengthening community health systems”; presentation on community and multi-sectoral partnerships established by FC+ to respond to fistula treatment barriers; Facilitation of small group discussions.
Social and Behavior Change Service Delivery Community of Practice
May 21, 2019 Washington D.C.
No Vandana Tripathi Participation
Women Deliver 2019
Jun 2-6, 2019 Vancouver, BC
No SK Nazmul Huda Vandana Tripathi Lauri Romanzi
Participation
Strengthening Measurement for Policy Advocacy in Community Maternal Health
Jun 3, 2019 Vancouver, BC
No Vandana Tripathi Participation
Utstein Meeting on Indicators and Reporting Criteria for Surgery, Obstetrics and Anaesthesia Patient Safety
Jun 16-18, 2019 Utstein Abbey, Norway
No Lauri Romanzi Round table participation
World Congress of the Royal College of Obstetricians and Gynaecologists (RCOG)
Jun 16-19, 2019 London, UK
No Lauri Romanzi SK Nazmul Huda Lina Roa
“Stream Speaker” on the topic of “New ways of working to achieve a fistula free generation”. Co-hosted reception to update the global health community on the RCOG Competency-Based Manual for Female Pelvic Medicine and Reconstructive Surgery including Fistula (FPMRSiF). Presentation on results from the FC+/PGSSC online clinician survey (see Appendix OO)
International Consultation on the Regional Strategy for Obstetric Fistula Elimination in West and Central Africa/ URODAK
Jun 19-22, 2019 Mbour, Senegal
Yes SK Nazmul Huda Altine Diop Moustapha Diallo Sita Millimono Igor Vaz
Panelist (see Appendix S for trip report) Presentation on Prolonged/obstructed labor: Management and morbidity burden (see Appendix PP) Presentation on Ending Fistula by 2030- From Rhetoric to Reality (see Appendix QQ)
Annual Report • October 2018 – September 2019 Fistula Care Plus 19
Meeting Dates/Location Convened by FC+?
Attending FC+ Inputs / Presentations
ACOG Global Operations Advisory Group
Jun 27, 2019 Washington D.C.
No Lauri Romanzi Round table participation
Association of Gynaecologists and Obstetricians (AGOTA) / East Central and Southern Africa Obstetric and Gynecological Societies (ECSACOG) Conference
Sep 21-25, 2019 Dar es Salaam, Tanzania
No Ominde Japheth Achola Theresa Shivera Lina Roa Adeline Boatin Salome Maswime
Panel session on “Global Surgery: SOA Care” including five presentations (see Appendices T-X) Presentation of the Isaac Achwal Research Award
Power on the Path to UHC 2030: Nurses and Midwives as Navigators, Innovators, and Accelerators
Sep 23, 2019 New York City
No Vandana Tripathi Participation
Turning the Tables: Patient Perspectives on UHC
Sep 24, 2019 New York City
No Vandana Tripathi Participation
Funding The FC+ project was awarded on December 12, 2013 with a ceiling of $74,490,086. In FY 18/19, an additional $4.87 mil has been received to bring the total life of project obligation to $45.140M. An additional $9.32 mil will be awarded in FY 19/20 to bring the total obligation for FC+ to $53,948,571. The project was awarded an NCE extending the project’s end date to March 31, 2021. Total expenses through September 30, 2019 are $44.952M, leaving $8.995 mil in obligation remaining. Projected expenditures and subaward commitments for the FY 19/20 year are projected to be $7.082M, with additional FY 18/19 and FY 19/20 funding for WARP still to be obligated to further support FC+ and its partners in the region.

Annual Report • October 2018 – September 2019 Fistula Care Plus 20
SECTION II: GLOBAL ACCOMPLISHMENTS
Fistula Care Plus Achievements During its sixth fiscal year, FC+ made progress in line with the aims and targets of its global workplan. Table 4 provides a snapshot of FC+ achievements in FY 18/19. Full reporting on FC+ benchmarks for core indicators can be found in Appendix SS. Appendix D provides information on all USAID-supported fistula repair surgeries from 2005-present.
Suspension of activity for a large proportion of the fiscal year in DRC and Niger, as well as the financial non-participation of the Uganda Mission in the NCE, had a significant impact on the project’s ability to achieve planned benchmarks, as illustrated in Table 4. These challenges are described in Section III and the FC+ management team is addressing them so that the seventh fiscal year is not similarly affected.
Table 4: Select Fistula Care Plus Achievements and Benchmarks as of September 30, 2019
Clinical training outputs are summarized in Table 5. Training accomplishments are described in greater detail in Objective 4, and in Section III, by country.
1 Does not include training of surgeons to provide fistula repair.
FY13/14 Actual
FY14/15 Actual
FY15/16 Actual
FY16/17 Actual
FY17/18 Actual
FY18/19 Benchmark
FY18/19 Actual
Number of countries supported by FC+ 5 6 6 5 6 5 5
Number of sites supported by FC+ for fistula repair and prevention
25 31 37 33 37 23 24
Number of prevention-only sites supported by FC+
16 249 500 former TSHIP
289 500 former TSHIP
252 500 former TSHIP
210 500 former TSHIP
13 19
Number of participants in community volunteer/educator training in tools and approaches to raise awareness regarding fistula prevention and repair
114 776 679 850 749 1,074 71
Number of community awareness-raising activities/events conducted by program partners
12 1,990 10,352 (in person) 41 (mass media)
33,425 (in person) 659 (mass media)
17,678 (in person) 53 (mass media)
6,064 1,246 (in person) 2 (mass media)
Number of participants reached through community awareness-raising events/activities conducted by program partners
10,745 414,067 2,862,124 (in person) 3,676,406 (mass media)
557,186 (in person) 15,289,736 (mass media)
681,597 (in person) 20,919,065 (mass media)
203,000 (in person) 600,000 (mass media)
149,585 (in person) 600,000 (mass media)
Number of surgical fistula repairs 873 2,876 3,514 3,250 3,104 1,224 605
Number of participants in health systems personnel training, by topic, for fistula and/or POP prevention and treatment (disaggregated by training topic, sex and cadre of provider)1
161 1,065 1,414 1,391 1,289 439 938
Number of FP counseling sessions provided
38,373 149,610 167,424 (FC+) 198,614 (Former TSHIP)
205,048 (FC+) 218,688 (Former TSHIP)
233,840 (FC+) 223,090 (Former TSHIP)
31,010 46,373
Number of CYP provided 40,039 107,986 106,645 (FC+) 89,341 (Former TSHIP)
170,019 (FC+) 93,187 (Former TSHIP)
197,273 (FC+) 117,956 (Former TSHIP)
36,500 33,469

Annual Report • October 2018 – September 2019 Fistula Care Plus 21
Table 5: Total Number of Clinical Training Participants, by Country, by Topic, FY 18/19
Bangladesh DRC Mozambique WA/
Niger Uganda Total
First Training in Surgical Fistula Repair
0 0 0 0 0 0
Continuing Training in Surgical Fistula Repair
0 0 0 0 0 0
Surgical Fistula TOT 0 0 0 0 0 0 First Training in Surgical POP Repair 0 0 0 0 0 0 Continuing Training in Surgical POP Repair
0 0 0 0 0 0
ANC 0 0 0 0 0 0 Catheterization for fistula prevention 0 0 0 0 0 0 Community, outreach and advocacy 0 0 0 0 0 0 Data management 0 0 0 0 0 0 EmONC 0 0 0 0 0 0 EmONC and labor monitoring 0 16 0 0 0 16 FP counseling 0 0 0 0 0 0 FP methods 0 0 0 0 0 0 FP and fistula counseling 0 0 0 0 0 0 Fistula counseling 0 0 0 0 0 0 Gender 0 0 0 0 0 0 Infection Prevention 0 0 0 0 0 0 Non-surgical POP treatment 0 0 0 0 0 0 Pre- and Post-Operative Care2 637 0 285 0 0 922 Quality Assurance 0 0 0 0 0 0 Other 0 0 0 0 0 0 TOTAL 637 16 285 0 0 938
Objective 1: Strengthened enabling environment to institutionalize fistula prevention, treatment, and reintegration in the public and private sectors FC+ strengthens the enabling environment to institutionalize fistula prevention, treatment, and reintegration in the public and private sectors by improving country and facility policies, guidelines, and resources allocated to fistula prevention and treatment, including addressing the needs of particularly vulnerable women (e.g., women deemed incurable (WDI) and those with traumatic fistula (TF)).
Sub-Objective 1.1: Establish sustainability plans: from policy to implementation During FY 18/19, FC+ continued to develop Public Private Partnerships (PPPs) with a focus on ensuring the sustainability of these efforts beyond the project.
FC+’s collaboration with Laborie led to the procurement and delivery of a urodynamics unit and disposable supplies at St. Joseph Hospital in Kinshasa, supported and coordinated by the USAID Mission. A multidisciplinary training for clinicians from supported sites in DRC is planned for FY 19/20.
FC+ continued conversations with Bard Medical towards supporting implementation of non-surgical, catheter-based fistula treatment to support the project’s translation and distribution of the Nigeria FMOH catheter protocol. Bard Medical was originally engaged through referral from USAID’s Susan Rae Ross. At the time, the project was scheduled to end in September 2019, and Bard was unable to accommodate engagements at the 2019 meeting of the West African College of Surgeons nor any other appropriate
2 Trainings are reported under the category that best describes their overall content. The trainings reported here covered myriad other topics, including family planning, catheterization, EmONC, etc. but are reported only under their “primary” category.
Annual Report • October 2018 – September 2019 Fistula Care Plus 22
stakeholder meeting. In May 2019, FC+ provided an updated PPP concept to Becton-Dickinson, which has acquired Bard Medical and is also supporting clinical research on the Odon device. FC+ is now working with Bard Medical to provide sponsorship to the 2020 West African College of Surgeons (WACS) meeting, where Bard and FC+ can jointly host a session and workshop on the catheter protocol and procurement procedures.
FC+ engagement of pessary supply chain in DRC with Bioteque, a medical device distributor, has stalled due to lack of uptake by patients who have difficulty with post-pessary fitting follow up. FC+ will seek opportunities to reinforce training and advocacy related to pessary in future visits from project-supported experts, such as physical therapy trainers.
FC+ activities to support collaborations between Wake Forest University and University of Kinshasa for low-cost, non-cellular regenerative medicine therapies to improve fistula treatment outcomes have post-engagement activity, not supported by the project, in the form of ongoing communications between the two academic departments.
FC+ participated in the National Surgical, Obstetric, and Anesthesia Planning (NSOAP) Conference for High-level Global, Regional and Country Authorities and Funders, held in March 2019 in Dubai, United Arab Emirates. The conference attendees included a multi-disciplinary group of international stakeholders representing nine ministries of health, the World Health Organization, the World Bank Group, bilateral and multilateral development agencies, philanthropic organizations, professional societies, non-governmental institutions, and academia. The conference covered global and regional collaboration for NSOAP development, financing, and implementation in Asian, African, and Western Pacific nations.
During FY 18/19, FC+ continued advocacy and participation in the development of a costed fistula strategy in Uganda and the National Fistula Strategy in Bangladesh, dissemination of a national strategic plan for fistula in DRC, and advocacy with the Ministry of Health in Mozambique for a national fistula strategy.
FC+ is working with project partner Direct Relief International to streamline enrollment, MOUs, and materials receipt so that all eligible FC+ supported sites may benefit from sustainable Direct Relief International donation of disposable supplies in Fistula Repair Modules to facilitate best-quality fistula services worldwide. A Fistula Repair Module is a standardized pack of high-quality medicines and disposable surgical and anesthesia supplies necessary for fistula repair surgery. These modules are available to qualified health facilities providing fistula care services at no cost. This donation process requires FC+ supported sites to first register with Direct Relief International via an online application prior to receiving the modules. As of the end of FY 18/19, 11 supported sites have received fistula modules from Direct Relief International: five in DRC, three in Uganda, one in Mozambique, and two in Niger. One additional site in Niger has an application currently pending. After experiencing supply delays, Direct Relief International is finishing the procurement of additional equipment for DRC. Direct Relief has also provided dignity kits for distribution to fistula clients in Mozambique; see Section III: Mozambique for details.
FC+ has supported Direct Relief’s efforts, in collaboration with Fistula Foundation and UNFPA, to develop a Global Fistula Map (http://globalfistulamap.org/). The utility of the map is to provide information on the geographical landscape and surgical capacity of the known global fistula repair network. FC+ has reached out to project partners and country contacts to help bolster Direct Relief’s efforts to ensure that the map has the most complete and up to date information about facilities providing fistula repair.

Annual Report • October 2018 – September 2019 Fistula Care Plus 23
As part of global advocacy efforts to encourage international support for fistula prevention and treatment, FC+ worked with USAID/W to prepare materials and handle logistics for a Hill Briefing planned for May 2019. While this briefing was not ultimately convened, the project produced a brief on U.S. government investments and a brief on FC+ project achievements in fistula care (see Appendices JJ and KK). FC+ country and global teams continue to maintain and expand partnerships with private entities, such as media outlets, for cost share and other support to FC+ activities. See Section III, by country, and project efforts building sustainability described in Objectives 1 and 4.
In September 2019, FC+ participated in a series of meetings convened by Harvard’s PGSSC. One of the meetings, scheduled with Monique Wubbenhorst, Deputy Assistant Administrator BGH, USAID, had to be postponed until later in the year. Discussions were held with ACOG’s Office of Global Women’s Health, focusing on PGSSC-ACOG collaborations for quality of surgical care, as well as discussions the World Bank Group regarding potential collaboration. FC+ joined ACOG representatives to attend a Water, Sanitation, and Hygiene (WASH) event on Capitol Hill that promoted current work on water production and stewardship. No further project-specific engagement has emerged with these groups, apart from the ongoing M&ER partnerships with ACOG and PGSSC.
Sub-Objective 1.2: Improve data available on OF to facilitate planning FC+ has carried out several activities during FY 18/19 to promote improved availability of fistula data for program implementation and improvement.
The FC+ Director and Deputy Director continued to provide technical assistance to the FC+/Harvard PGSSC collaboration to expand the documentation and measurement of sequelae of prolonged/obstructed labor (P/OL). With the Harvard team, the Director and Deputy Director reviewed the results of a survey of FC+ supported sites and other clinicians to understand the prevalence and estimated severity of clinical and psychosocial sequelae. Preliminary findings were presented at the RCOG annual meeting in London in June 2019 (see Table 3). The team will use these results to generate a new model of years lost to disability (YLD) from prolonged/obstructed labor.
At the International Society of Obstetric Fistula Surgeons (ISOFS) and the International Obstetric Fistula Working Group (IOFWG) meetings in Kathmandu, Nepal, in December 2018, the FC+ Deputy Director shared the results of FC+ supported efforts to document fistula and POP prevalence in Bangladesh using the 4Q checklist. Noting the similarity of results from these efforts to those documented through much more resource-intensive national surveys, it was proposed that others working to document the fistula burden and improve data for programming consider such tools. The FC+ Project Director participated in the Utstein Meeting on: Indicators and Reporting Criteria for Surgery, Obstetrics and Anaesthesia Patient Safety, held June 16-19, 2019 in Norway. In 2015, the Lancet Commission on Global Surgery (LCoGS) published six indicators as a model for monitoring and evaluation platforms related to unmet surgical burden of disease in low and middle income countries. The Laerdel Foundation supported this meeting for review of LCoGS indicators, resulting in the upcoming publication of an Utstein consensus paper on metrics and reporting criteria for surgery, obstetrics, and anaesthesia patient safety. This will both reinforce and clarify the global indicator set, as well as define next steps for dissemination and data collection. An eventual output of this process could be directly actionable for the United Nations Statistical Commission, with broad and long-term international impact.
The FC+ Deputy Director participated in the WHO/UNICEF Think Tank Series on Maternal and Newborn Health Effective Coverage Measures in April 2019. The Deputy Director provided feedback on proposed measures of effective coverage of antenatal, intrapartum, postpartum/postnatal, and newborn
Annual Report • October 2018 – September 2019 Fistula Care Plus 24
care indicators. The Deputy Director subsequently provided review to a Joint Statement on Effective Coverage and co-authorship to a manuscript by the Think Tank group. The manuscript has been submitted to Lancet Global Health and the Statement is expected to be circulated by the end of the year.
The United Nations released a report on obstetric fistula in September 2018, outlining efforts made by the international community at the global, regional and national levels to end obstetric fistula, and offers recommendations to intensify those efforts with a human rights-based approach. The report, which includes work supported by FC+, is presented in Appendix NN and can also be accessed at: http://www.endfistula.org/publications/un-report-obstetric-fistula-2018.
Sub-Objective 1.3: Advocate for a fistula-free generation Activities to strengthen the enabling environment for fistula services and advocate for prevention and treatment needed to achieve a fistula-free generation have been taking place nationally and regionally throughout the first half of the fiscal year. National and regional working groups have met with FC+ support and participation during FY 18/19 in Bangladesh, Mozambique, and Uganda to strengthen communication and collaboration between partners working towards the elimination of fistula and to strengthen national strategies.
The FC+ Deputy Director and FC+/Uganda worked with the USAID/W Communications team to support production of a USAID Stories video about a fistula patient who received services supported by FC+. FC+ has worked to identify appropriate clients for the video, address USAID questions about logistics, and plan the filming trip. The resulting video was released on the International Day to End Obstetric Fistula (IDEOF) through USAID’s Stories website (https://stories.usaid.gov/justines-fresh-start/) as well as websites and social media of FC+ and our partners (e.g., Fistula Foundation).
Regional and International Advocacy
Globally, FC+ has continued advocacy efforts within the global safe surgery community to capitalize on potential within this community to accelerate the achievement of the United Nations Secretary General’s 2016 call to action to “end fistula within a generation” through surgical systems strengthening within the maternal health community. FC+ is working to strengthen regional institutions through support for working groups and colleges of surgeons, promoting a sustainable legacy for safe surgery and fistula elimination efforts.
FC+ continues to support the Economic Community of West African States (ECOWAS) Assembly of Health Ministers’ (AMS) September 2018 ECOWAS Member States Resolution on the Elimination of Fistula from the ECOWAS Region (https://wcaro.unfpa.org/en/publications/ecowas-member-states-resolution-fistula-elimination). This Resolution was derived from the FC+ facilitated Banjul Call to Action meeting, first proposed by the West African Health Organization (WAHO) and its Banjul Call to Action partners during the project-supported launch of the March 2018 High Level Meeting of the West and Central African Group to End Obstetric Fistula (WCAGEOF) held in Banjul, Republic of The Gambia. The Resolution sets goals for the elimination of obstetric fistula in ECOWAS member countries by 2030. FC+ has been supporting WAHO and its Banjul Call to Action partners for the implementation of the Resolution, and had planned to convene a follow-on meeting of the West African Group to End Obstetric Fistula. However, due to the United States Government shutdown, the meeting originally planned for January 2019 during the WACS conference was postponed until June 2019.
The International Consultation on the Regional Strategy for Obstetric Fistula Elimination in West and Central Africa was held in Senegal in June 2019, see Appendix S. The Consultation was sponsored by

Annual Report • October 2018 – September 2019 Fistula Care Plus 25
regional partners including Fistula Care Plus/EngenderHealth, the West African Health Organization (WAHO), UNFPA, and URODAK. The overall objective of the consultation was to share the approved Banjul Call to Action resolution, signed and adopted by the health ministers of 15 members of the ECOWAS region, with all stakeholders and operationalize the resolution with action plans focusing on pillars such as capacity building of health providers, monitoring, evaluation, and resource mobilization. The operationalization of the resolution will be done in partnership with academic institutions, professional associations and NGOs for identification and referral of cases, surgical and non-surgical treatment, reintegration and rehabilitation of women with fistula in the region. This strategy must be underpinned by quality assurance and an evidence-based, flexible framework that includes data for decision-making.
The three-day meeting took place June 19-21, 2019 in Saly Portugal, Senegal. Opening ceremonies were led by Professor Serigne Magueye Gueye, Professor at Cheikh Anta Diop University and Grand Yoff General Hospital, Vice President of WACS; Dr. Sosthene Dougrou, UNFPA Representative; Dr. Aissa Bouwawe, WAHO; and Dr. Moustapha Diallo representing FC+/EngenderHealth. Presentations during the first day of the meeting covered topics including the history of global resolutions related to fistula and the “Banjul Call to Action 2018”, the roles of ECOWAS and UNFPA in obstetric fistula elimination in the region, capacity building efforts for midwives and nurses, and specific strategic approaches to speed up obstetric fistula elimination including costing data and country-level situation analyses.
The second day of the meeting focused on academic institutional roles in obstetric fistula efforts, including presentations from the West African College of Surgeons (WACS), the West African Postgraduate College of Pharmacists (WAPCP), and the West African College of Nursing (WACN). The third and final day of the meeting included a presentation by the FC+ Global Activities Manager summarizing FC+ project strategies and achievements (see Appendix QQ), followed by development of countries’ road maps and preparation of the Saly resolution for fistula elimination.
This regional meeting was immediately followed by URODAK, an annual meeting of urologists in the region. The FC+ Global Activities Manager made a presentation on behalf of the FC+ Deputy Director at the URODAK meeting that addressed the management and morbidity burden of prolonged and obstructed labor (see Appendix PP).
As part of regional advocacy, FC+ participated in the Fourth North East Zonal Conference of the Indian Association on Preventive and Social Medicine (NEZCON) in October 2018, held in Agartala, India. The conference focuses on common reproductive health challenges in South East Asia; the FC+ Global Activities Manager presented on “The Fistula Program Experience in Bangladesh” as well as taking part in a panel on “Adolescent Health and Pregnancy.” The FC+/Bangladesh team jointly presented a plenary on “Reflections of Best Practices for Prevention and Care of Fistula in Bangladesh.”
Globally, FC+ had a robust presence at the International Federation of Gynecology and Obstetrics (FIGO) World Congress in October 2018 in Rio de Janeiro, Brazil. FC+ moderated and presented at the panel: Cesarean section safety in low-resource settings: Ensuring quality in a context of rapidly increasing volume. Panel participants included the FC+ Director and Deputy Director, Dr. Francesca Cavallaro of the London School of Hygiene and Tropical Medicine Health, and Dr. John Varallo of Jhpiego. System challenges contribute to poor quality, inequitably distributed surgical obstetric care in low-resource settings. Increasing iatrogenic fistula from unsafe cesarean sections demonstrates the impact of these gaps. Panelists presented evidence regarding the systems contexts and pressures affecting cesarean care and the recommendations of a global consultation to examine these challenges. The full report of this consultation and a study commissioned by FC+ from the London School of Hygiene and Tropical

Annual Report • October 2018 – September 2019 Fistula Care Plus 26
Medicine (LSHTM) are available at: https://fistulacare.org/resources/program-reports/cesarean-section-technical-consultation/. Approximately 70 FIGO delegates attended the session which was filmed for circulation through the FC+ and EngenderHealth websites. In addition to this panel, FC+ staff made 15 oral presentations during the FIGO Free Communication Sessions (see Objective 5 and Appendix G).
FC+ also contributed significant logistical and financial support for the planning and execution of the 7th Biennial Conference of the International Society of Obstetric Fistula Surgeons (ISOFS), held in Kathmandu, Nepal in December 2018 (see Appendices H, I, and L). Over 500 attendees took part in the conference, jointly hosted by ISOFS, the Nepal Society of Obstetrics and Gynaecologists (NESOG), FC+/EngenderHealth, UNFPA, Fistula Foundation, Direct Relief International, Operation Fistula, and the Islamic Development Bank. Pre- and post-conference workshops were held, and UNFPA hosted a meeting of the International Obstetric Fistula Working Group immediately following the conference (see Appendices H and K). FC+ supported attendance of 26 participants at the conference and gave three plenary oral presentations, 21 oral presentations, and 14 posters at ISOFS and IOFWG.
FC+ sponsored three preconference and conference workshops that included a live fistula surgery workshop, a scientific writing workshop, and a urodynamics workshop. FC+ also supported a side event, hosted by the South Asian Group on Fistula and Other Related Disorders (SAGFORD) and ISOFS, entitled “An Evening on the Kathmandu and Banjul Calls to Action.” Professor Sayeba Akhter, the ISOFS Asian Representative and Chair of SAGFORD, chaired the event, which included the participation of EngenderHealth President Traci Baird, and Professor Oladosu Ojengbeded and Dr. Shershah Syed, President and President-Elect of ISOFS. Past ISOFS Presidents Dr. Kees Waldjik and Dr. Tom Rassen also were in attendance. At ISOFS, the FC+ Deputy Director made remarks at the plenary honoring 2018 Nobel Peace Prize recipient and FC+ partner, Dr. Denis Mukwege in absentia (see Appendix Q).
The FC+ Project Director and Global Activities Manager attended the World Congress of the Royal College of Obstetricians and Gynaecologists (RCOG) meeting held Jun 16-19, 2019 in London. The Project Director was a “Stream Speaker” at the conference on the topic of “New ways of working to achieve a fistula free generation.” The Project Director also co-hosted, with Maisha Syed of the RCOG Global Health team, a reception to update the global health community on the RCOG Competency-Based Manual for Female Pelvic Medicine and Reconstructive Surgery including Fistula (FPMRSiF). Lina Roa, an ObGyn and Harvard PGSSC fellow, presented on results from the FC+/PGSSC online clinician survey on the full spectrum of preventable maternal/newborn prolonged and obstructed labor morbidities/mortality, see Appendix OO.
FC+ country and global staff supported events commemorating the International Day to End Obstetric Fistula (IDEOF) throughout the world on May 23, 2019. Country-specific events are described in Section III of this report. At the global level, FC+ worked with USAID/Washington to prepare a two-page brief on “United States Achievements in Global Fistula Care,” see Appendix JJ. FC+ also prepared a technical brief “Five Years of Fistula Care Plus: Looking Back at Key Achievements and the Way Forward to End Fistula,” see Appendix KK.
Together with UNFPA, the FC+ Project Director co-authored a commentary in the Lancet Global Health entitled “Meeting the SDG challenge to end fistula and preventable childbirth-related morbidity and mortality” which emphasizes the critical role of universal access to skilled care at birth (see Appendix XX or accessible at https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(19)30198-6/fulltext). Drawing upon recommendations from the Lancet Commission on High Quality Health Systems in the SDG Era and the Lancet Commission on Global Surgery, it puts forward that ensuring all women and girls in need receive timely, high quality, life-saving obstetric surgery (whether cesarean section or fistula

Annual Report • October 2018 – September 2019 Fistula Care Plus 27
repair) is a fundamental human rights issue and a key strategy for achieving the Sustainable Development Goals.
FC+ continues to monitor the activity of the nascent East, Central, Southern Africa (ECSA) College of Obstetrics and Gynecology (ECSACOG). FC+ supported attendance of an EngenderHealth Senior Clinical Associate as well as four key regional ECSA Ob/Gyn leaders and one fellow from Harvard’s PGSSC to represent the project’s interests at the joint Association of Gynaecologists and Obstetricians of Tanzania (AGOTA) and ECSACOG Conference held September 22-24, 2019 in Dar es Salaam, Tanzania. FC+ supported attendees made five presentations (see Appendices T–X) as part of an organized panel session on “Global Surgery: SOA Care”. Presentations from the panelists covered findings from a study conducted in Africa that highlighted the leading causes of mortality in Africa and challenges in perioperative care including lack of access and poor quality of care. The panel also provided information about the National Surgery, Obstetrics, and Anesthesia Planning (NSOAP) initiative, which promotes collaboration of the different disciplines to ensure safe surgery and the commitment of the Southern African Development Community (SADC) countries to develop NSOAPs that will then be integrated into national health sector strategic plans. The session provided the opportunity for ECSACOG members in countries not currently engaged in NSOAP to hear about the process, understand the motivations for engaging in this process, and learn from other countries already engaged in this process.
EngenderHealth has worked with ECSACOG to establish the Isaac Achwal Research Award, in honor of the late Dr. Isaac Michel Owino Achwal who was the Senior Clinical Advisor at FC+/EngenderHealth. Prior to his death, Dr. Achwal provided significant support to the newly established ECSACOG within the ECSA Health Community Secretariat. In addition to his support for this college, Dr. Achwal was a family planning and reproductive health champion who was instrumental in building the capacity of and mentoring in-country staff and assisting them in establishing national FP/RH services and, where applicable, also introducing new approaches. The award has been established for a period of five years, with EngenderHealth helping to provide support for the first three years. The award includes a small monetary prize as well as a certificate from the College and is intended for new and emerging voices within ECSA-region obstetrics and gynecology interns and residents to best celebrate Dr. Achwal as a champion of training, capacity building, and bringing new voices into the fold.
FC+ External Relations
As part of a coordinated external relations strategy, the FC+ blog and Twitter account have been updated throughout the fiscal year. In FY 18/19, the blog featured two postings highlighting current issues in maternal health and FC+ activities (see Objective 5). Website viewing data for this fiscal year could not be obtained, due to technical difficulties, but will be accessible starting in the beginning of FY 19/20. Past views are presented in Figure 2, by month. The FC+ Twitter account metrics are presented in Table 6.
Table 6. FC+ Twitter Account Metrics, FY 18/19 Metric FY 18/19 Total since April 2015 Twitter Followers 818 818 Impressions (number of times tweets appear on feeds) 1.7 million 2.8 million Link clicks 36 555 Retweets 52 1,357 Favorites/Likes 161 1,440 Mentions 109 1,081 Total Engagements (number of times someone interacts with a tweet)
453 5,264

Annual Report • October 2018 – September 2019 Fistula Care Plus 28
Figure 2. Fistula Care Plus Website Views by Month
Objective 2: Enhanced community understanding and practices to prevent fistula, improve access to fistula treatment, reduce stigma, and support reintegration of women and girls with fistula FC+ enhances community understanding and practices to prevent fistula, improve access to fistula treatment, reduce stigma, and support reintegration of women and girls with fistula by building community awareness, skills, and mobilization regarding the behaviors and services that can prevent fistula, as well as those that enable treatment.
The FC+ project aims to address gender inequalities as a root cause of fistula, for instance through barriers to prevention and care, and maximize overall impact. The FC+ Gender Focal Point worked with the EngenderHealth Gender team to develop a Gender Action Plan to address the training, capacity, and programmatic needs of the project and ensure gender mainstreaming. The action plan was based on input from country programs, documented best practices, USAID guidance and gender priorities, and recommendations from the EngenderHealth Gender team. During FY 18/19, countries continued to implement their components of the action plan.
Sub-Objective 2.1 Create awareness and reduce stigma about OF Country-level activities to increase community understanding and practices related to preventing fistula and the availability of fistula repair services were undertaken in Bangladesh, DRC, Mozambique, and Uganda in FY 18/19. A total of 1,248 community outreach/education/advocacy events were carried out, reaching 749,585 people. Two of these were mass media events reaching over 600,000 people. Additional detail by country can be found in Table 7, as well as in Section III.
Table 7: Community Outreach/ Education Events, by Country, FY 18/19
Country Oct-Dec 2018 Jan-Mar 2019 Apr–Jun 2019 Jul-Sep 2019 FY 18/19 #
Events # Reached
# Events
# Reached
# Events
# Reached
# Events
# Reached
# Events
# Reached
Bangladesh -in person -mass media
2 1
117 N/A
8 0
628 0
1 1
108 600,000
13 0
561 0
24 2
1,414 600,000
DRC -in person
3
110
0
0
0
0
0
0
3
110
WA/Niger -in person
0
0
0
0
0
0
0
0
0
0
Mozambique -in person
1
283
1
311
1
77
1
266
4
937
Uganda -in person
349
23,494
866
123,630
NS
NS
NS
NS
1,215
147,124
Total 355 24,004 875 124,569 3 600,185 14 827 1,248 749,585 -in person -mass media
355 1
24,004 N/A
875 0
124,569 0
2 1
185 600,000
14 0
827 0
1,246 2
149,585 600,000
9831
8439
10632
49216026 6145 6675
5437 5562 6111 6470 6764
Oct-Dec15
Jan-Mar16
Apr-Jun16
Jul- Sep16
Oct-Dec16
Jan-Mar17
Apr-Jun17
Jul- Sep17
Oct-Dec17
Jan-Mar18
Apr-Jun18
Jul-Sep18
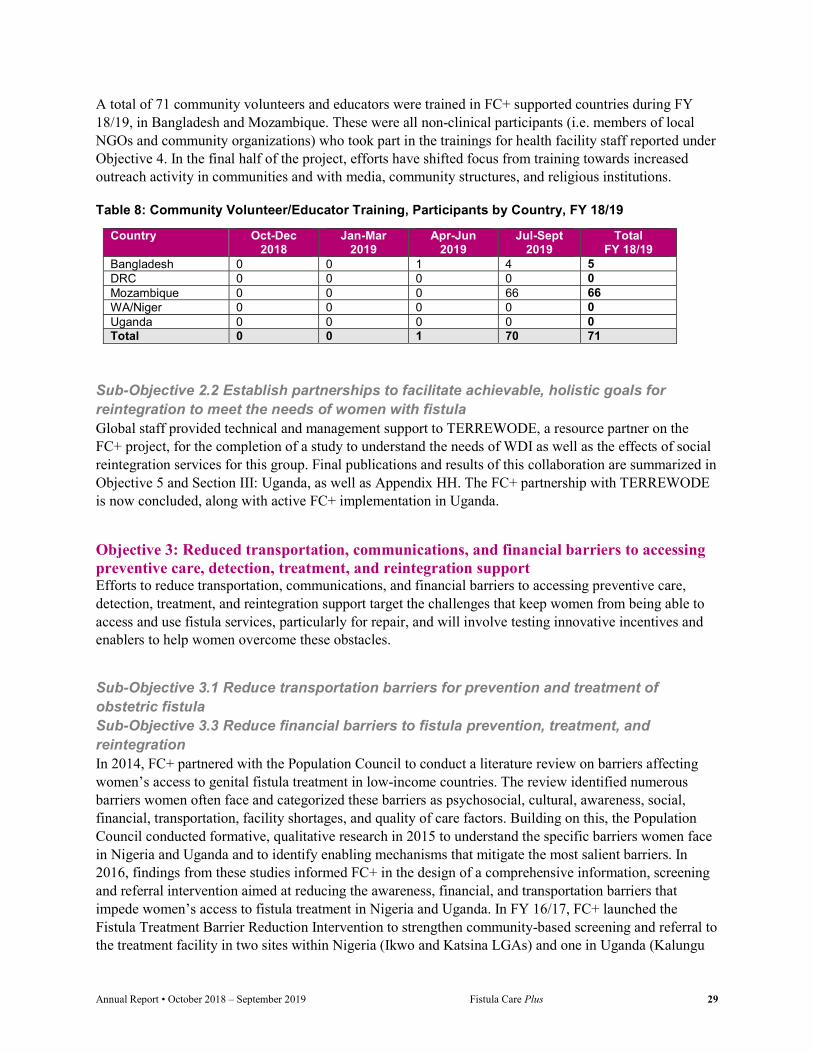
Annual Report • October 2018 – September 2019 Fistula Care Plus 29
A total of 71 community volunteers and educators were trained in FC+ supported countries during FY 18/19, in Bangladesh and Mozambique. These were all non-clinical participants (i.e. members of local NGOs and community organizations) who took part in the trainings for health facility staff reported under Objective 4. In the final half of the project, efforts have shifted focus from training towards increased outreach activity in communities and with media, community structures, and religious institutions.
Table 8: Community Volunteer/Educator Training, Participants by Country, FY 18/19
Country Oct-Dec 2018
Jan-Mar 2019
Apr-Jun 2019
Jul-Sept 2019
Total FY 18/19
Bangladesh 0 0 1 4 5 DRC 0 0 0 0 0 Mozambique 0 0 0 66 66 WA/Niger 0 0 0 0 0 Uganda 0 0 0 0 0 Total 0 0 1 70 71
Sub-Objective 2.2 Establish partnerships to facilitate achievable, holistic goals for reintegration to meet the needs of women with fistula Global staff provided technical and management support to TERREWODE, a resource partner on the FC+ project, for the completion of a study to understand the needs of WDI as well as the effects of social reintegration services for this group. Final publications and results of this collaboration are summarized in Objective 5 and Section III: Uganda, as well as Appendix HH. The FC+ partnership with TERREWODE is now concluded, along with active FC+ implementation in Uganda.
Objective 3: Reduced transportation, communications, and financial barriers to accessing preventive care, detection, treatment, and reintegration support Efforts to reduce transportation, communications, and financial barriers to accessing preventive care, detection, treatment, and reintegration support target the challenges that keep women from being able to access and use fistula services, particularly for repair, and will involve testing innovative incentives and enablers to help women overcome these obstacles.
Sub-Objective 3.1 Reduce transportation barriers for prevention and treatment of obstetric fistula Sub-Objective 3.3 Reduce financial barriers to fistula prevention, treatment, and reintegration In 2014, FC+ partnered with the Population Council to conduct a literature review on barriers affecting women’s access to genital fistula treatment in low-income countries. The review identified numerous barriers women often face and categorized these barriers as psychosocial, cultural, awareness, social, financial, transportation, facility shortages, and quality of care factors. Building on this, the Population Council conducted formative, qualitative research in 2015 to understand the specific barriers women face in Nigeria and Uganda and to identify enabling mechanisms that mitigate the most salient barriers. In 2016, findings from these studies informed FC+ in the design of a comprehensive information, screening and referral intervention aimed at reducing the awareness, financial, and transportation barriers that impede women’s access to fistula treatment in Nigeria and Uganda. In FY 16/17, FC+ launched the Fistula Treatment Barrier Reduction Intervention to strengthen community-based screening and referral to the treatment facility in two sites within Nigeria (Ikwo and Katsina LGAs) and one in Uganda (Kalungu

Annual Report • October 2018 – September 2019 Fistula Care Plus 30
District). The Population Council conducted implementation research to evaluate the effects of this Intervention.
The Intervention utilized a consistent fistula screening algorithm across multiple communication and referral channels, including community agents, primary health facilities, and mass media; and a transportation voucher to enable positively screened women to travel for free to and from an accredited fistula treatment facility. In each of the three sites, FC+ supported activities that sought to strengthen community-based screening and referral to the treatment facility. In FY 16/17, FC+ trained community agents (CBO volunteers in Nigeria and VHTs in Uganda) and health workers (doctors, midwives, nurses, and community health care workers) at primary health facilities to identify potential fistula clients and refer these women for treatment. A total of 94 PHC workers from 41 facilities were trained across Ikwo and Katsina LGAs in Nigeria and 42 PHC workers were trained from 21 facilities across Kalungu District in Uganda. Community volunteers participated in two-day trainings on identifying fistula patients, promoting healthy pregnancies, and community engagement activities; and a total of 82 volunteers were trained across Ikwo and Katsina LGAs in Nigeria and 275 volunteers were trained across Kalungu District in Uganda. By July 2017, the barrier intervention was fully launched in all three intervention sites (Ebonyi and Katsina States in Nigeria and Kalungu District in Uganda).
FC+ also collaborated with Viamo (formerly VOTO Mobile) to design a free interactive voice response (IVR) fistula screening hotline that collected data on positively screened callers. The fistula hotline was widely advertised through graphic flyers disseminated by the community agents and PHC workers at community venues. Community agents followed-up with women who called into the hotline and facilitated their free transport to the fistula treatment facility using a transportation voucher designed for the intervention. Community agents also used the fistula hotline to screen women using their own phones during their community mobilization activities (home visits, community forums, etc.); while primary health facility workers used a paper-based job aid to screen patients at primary health facilities. Community agents and primary health workers followed up with positively screened women and facilitated their free transport to the fistula treatment facility using the transportation voucher. All three screening channels – community agents, health workers, and the hotline - collected the same data, and used the same fistula symptom-screening question.
At the intervention’s midline, the Population Council and FC+/Global M&E/R staff conducted a mid-course visit to disseminate to local and national stakeholders findings from the intervention’s baseline data and conduct qualitative data collection with the aim of identifying challenges experienced by the intervention’s facilitators and recommending mid-course corrections to improve the intervention’s effectiveness. The visit to Nigeria occurred in the fourth quarter of FY 16/17 and to Uganda in the first quarter of FY 17/18. Based on analysis of the data collected, the Population Council and FC+ teams jointly developed recommendations for mid-course changes based on these findings. The key recommendation developed was to reinforce facilitator’s roles and responsibilities within these newly established screening and referral mechanisms and to strengthen linkages between the community agents and PHC providers working within the same catchment area. Activities to implement recommendations identified from the midline findings were conducted through the third quarter of FY17/18.
FC+ concluded the implementation of the Intervention in both Nigeria and Uganda in FY17/18. Population Council completed endline data collection in Uganda and Ebonyi State in Nigeria in the fourth quarter of FY 17/18. In FY 18/19, Population completed endline data collection in Katsina State in Nigeria. Research briefs summarizing the intervention process and outputs were published and shared at dissemination meetings in Uganda and Nigeria (see Appendices N-P).

Annual Report • October 2018 – September 2019 Fistula Care Plus 31
In Nigeria, primary healthcare (PHC) center provider surveys at endline demonstrated variable improvements in provider knowledge of fistula causes, symptoms, and referrals. Analysis of the fistula center register data, alongside FC+ program monitoring data, show increases in admissions and surgeries, which may be in part attributed to the levels of referrals from one or more FC+ intervention components in Ebonyi, and at least to some extent in Katsina. The proportion change/variability explained may be less in Katsina given the already high volume of patients present at the fistula center (Babbar Ruga). Moreover, program monitoring data and qualitative interviews suggests that the interventions may have had influences beyond the intervention local government areas (LGAs). Endline client surveys also show reductions in some barriers at the community level, notably in stigma, lack of social support, and finance and transportation in accessing care. Qualitative data on the intervention process and experience further reveal successes including the helpful nature of numerous intervention components: trainings that informed and linked PHC providers and community volunteers with the fistula center, job aid utility in PHC centers, the confidentiality of community screening through the mobile hotline, the transportation voucher (in areas where it was used), and other free transportation options. Challenges related to the hotline’s sustainability, transportation, and integrating intervention components within the larger health system, without proper funding, were identified in qualitative interviews.
In the first quarter of FY 18/19, Population Council led two dissemination events in Katsina and Ebonyi, on December 11 and 14, 2018, with 22 and 23 stakeholders, respectively. In both states, stakeholders included the Commissioners of Health, Executive Secretaries of the State PHC Development Agency, RH focal persons, Directors of Public Health, Directors of Medical Services, Local Government Primary Health Coordinators, National Obstetric Fistula Centers (NOFICs) representatives, the Secretary of the Nigerian Red Cross (in Katsina), community-based organizations (FOMWAN in Katsina and DOVENET in Ebonyi), community agents, PHC facility staff, and direct beneficiaries of the barrier reduction interventions. The disseminations were well received, garnered ample discussion, and elicited varying degrees of commitment from stakeholders to sustain aspects of and learnings from the barrier reduction intervention, particularly in the context of both states adopting the PHC Under One Roof (PHCUOR) Policy, an output of Nigeria’s National Health Act 2014, aimed at restructuring and strengthening PHC. The State PHC Development Agency (SPHCDA), tasked with ensuring supplies and human resource capacity, agreed to use FC+ training materials—including job aids for screening—in orientations to the restructured PHCs and training of health workers at secondary facilities, and in Katsina, in training LGA health educators who give health talks during routine antenatal care (ANC).
Sustaining fistula awareness building campaigns was highly prioritized in Katsina; media houses vested in corporate social responsibility affirmed their interest in speaking on television and radio about fistula to raise awareness of care options. In Ebonyi, the SPHCDA advocated for the placement of a desk officer at the LGA level to connect clients to facilities, the state ministry expressed plans to leverage UNFPA funds for safe-motherhood and the Saving One Million Lives Initiative, and the NOFIC is seeking collaboration with the state to continue outreach campaigns. The hotline—although unsustainable without national support—spurred interest in the need to widely educate communities about fistula to shift norms and empower women to seek care.
Though the transport voucher was deemed unsustainable, stakeholders understood and were motivated to address the financial and geographic access barriers to fistula repair. Katsina’s recent establishment of a social insurance scheme includes transportation to secondary facilities and repair sites; the state procured and deployed tricycles and motorcycles to health facilities that can be utilized to transport women with fistula. Additionally, the National Union for Road Transport Workers remains committed to transporting women with fistula, in collaboration with PHC departments, in select LGAs. In Ebonyi, the state

Annual Report • October 2018 – September 2019 Fistula Care Plus 32
government procured ambulances as a part of the PHCUOR implementation and will consider fistula an emergency condition eligible for free transportation to a secondary facility or fistula center. Challenges persist for how to engage community agents more effectively, given their positive contributions to the intervention.
The Uganda dissemination meeting was held through the National Fistula Technical Working Group, which convened its meeting in late March 2019. Final reports on Uganda dissemination were published in April and May 2019 and are available at https://fistulacare.org/resources/publications/technical-briefs/ as well as in Appendices DD-HH. FC+ Uganda and Population Council staff jointly presented the study findings at the working group meeting where the National Fistula Strategy revision was a topic of discussion. Their discussions with critical stakeholders focused on the findings in the research brief. The FTWG and MoH, in particular, were enthusiastic about the findings and incorporated the research brief as part of Uganda’s National Fistula Strategy.
Preliminary analyses in Uganda (in the research brief) complement findings from Nigeria, with fistula surgeries appearing to generally increase over the intervention period, and number of hotline calls and positive screenings throughout the intervention following a similar pattern of high to low to moderate use. Clients referred through the intervention were in discrete time periods, given the pooled/camp-based model, compared to Nigeria, where routine services exist. Although there was some improvement in PHC provider knowledge and practices of screening and referral for fistula, the intervention implementation’s success came from VHT engagement with the hotline to directly link communities to the Kitovu Mission Hospital. Moreover, the timeliness of these findings can directly contribute to the National Fistula Strategy and Community Health Strategy discourse; the latter of which has vacillated with respect to roles of VHTs and other community health worker cadres in the country.
In addition to country-specific research briefs presented at the dissemination meetings described above, completed dissemination products from FY 18/19 include:
A presentation at the first Social Behavioral Change (SBC) Africa Conference in Nairobi, Kenya (February 2019): “Integrating an Innovative Mobile Hotline to Improve Awareness of and Access to Fistula Repair” by Pooja Sripad, Caroline Johnson, Charity Ndwiga, Emmanuel Nwala, and Elly Arnoff (Appendix D).
A chapter accepted for the forthcoming book, Obstetric Fistula: A Preventable Tragedy entitled “Comparing Three Models of Fistula Care Among Five Facilities in Nigeria and Uganda” by Pooja Sripad, Caroline Johnson, Vandana Tripathi, and Charlotte Warren.
A manuscript describing the process of developing the Intervention published in HealthCare for Women International in July 2019, entitled “Removing barriers to fistula care: Applying appreciative inquiry to improve access to screening and treatment in Nigeria and Uganda” by Vandana Tripathi, Elly Arnoff, and Pooja Sripad (see Appendix MM and accessible online at: https://www.tandfonline.com/doi/full/10.1080/07399332.2019.1638924).
A manuscript describing the processes and outputs of the IVR hotline, entitled “Use of interactive voice response technology to address barriers to fistula care in Nigeria and Uganda” by Vandana Tripathi, Elly Arnoff, Ben Bellows, and Pooja Sripad, accepted for a special issue of mHealth focusing on digital health interventions to promote reproductive health. This is expected to be published in the first quarter of FY 19/20.
A presentation about the Intervention entitled “Leveraging Expertise: A Multi-Stakeholder Partnership Approach to Strengthening Community Health Systems” by Vandana Tripathi, as part of a USAID/Population Council/Aga Khan Foundation panel on stakeholder partnerships for the CORE Group Conference and meeting held in Bethesda, Maryland in May 2019.

Annual Report • October 2018 – September 2019 Fistula Care Plus 33
A full day analysis and manuscript workshop was held at Population Council’s New York office in March 2019. Several additional manuscripts, as well as the full final research report, are at various stages of analysis, writing, and internal review. All completed technical briefs and reports developed to date through this partnership are available at: https://www.popcouncil.org/research/fistula-care-plus, also see Appendices N, O, and P. Objective 4: Strengthened provider and health facility capacity to provide and sustain quality services for fistula prevention, detection, and treatment FC+ strengthens clinician and health facility capacity to provide and sustain quality services for fistula prevention, detection, and treatment, supporting health facilities and their staff to deliver effective clinical care and monitoring of topics ranging from FP counseling to fistula repair outcomes.
Sub-Objective 4.1 Strengthen facility-level capacity to prevent fistula Good quality obstetric care, including timely recognition and management of prolonged/obstructed labor, is the cornerstone of fistula prevention. FC+ efforts to strengthen fistula prevention at the facility level primarily relate to increasing capacity for FP, labor monitoring, and EmONC. Training efforts and provision of FP counseling and services are described below.
To assess the quality of labor monitoring and management of prolonged/obstructed labor, FC+ conducts partograph reviews annually at facilities that receive FC+ support for labor and delivery care. When possible, reviews are also conducted at facilities where FC+ plans to provide such support during the life of the project, even if the support is not currently being provided. Such support may include training, supervision or other inputs related to EmONC, BEmONC, partograph/labor monitoring, and cesarean section. Support may also include provision of supplies, equipment and/or expendables, through a formal agreement, for labor and delivery services as well as improving infrastructure and/or systems (i.e. data capture, supervision, monitoring). As noted in Section 3: Uganda, FC+/Uganda carried out a documentation of its efforts to scale up partograph usage for labor monitoring at 12 HC IIIs and two district hospitals (Kagando and Bwera) that receive referrals from lower level facilities in Bukonzo East and West health sub districts. Findings are highlighted in the FC+ technical brief “Fistula Care Plus in Uganda: Success Stories” accessible here: https://fistulacare.org/wp-fcp/wp-content/uploads/2019/05/FCPlus-Success-Stories_v3.pdf and in Appendix GG.
A record review tool was developed by FC+ M&E and clinical staff, during FY 14/15, to be completed as either a stand-alone data collection activity or in conjunction with clinical visits/medical monitoring visits at facilities supported for L&D services and treatment. The review focuses on the partograph as a labor monitoring tool, for the purpose of identification of and timely response to obstructed labor specifically. The review looks at a sampling of patient files to determine whether essential elements of the partograph form have been completed correctly and utilized in decision making for the patient. The tool also includes questions related to facility and workforce labor and delivery capacity.
Records review summaries from FY 14/15 through FY 18/19 can be found in Appendices Y through CC. A total of 200 records from FY 18/19 were reviewed at a total of eight facilities in two countries (Bangladesh and DRC), see Appendix CC for detailed scores by site. Reviews were not carried out in Niger or Mozambique where partograph support has not been implemented, or in Uganda where the project closed-out activities during this fiscal year.
Record review indicated wide variety in rates and quality of partograph completion between sites, and between countries. DRC completion rates were overall consistent with the findings in the previous year,

Annual Report • October 2018 – September 2019 Fistula Care Plus 34
with 83% of files containing a partograph compared to 81% in FY 17/18, 73% in FY 16/17 and 74% in FY 15/16. In Bangladesh, rates of completion have remained steady at 54%, the same as in FY 17/18, and similar to earlier rates of 57% in FY 16/17 and 59% in FY 15/16. In Bangladesh, when partographs were not present in a patient file, relevant data was still recorded in the file, but not using the partograph form. The vast majority of records reviewed were not referral cases, or not clearly identified as referral cases, which made it difficult to measure the number of records that included a partograph from the referring facility.
The review tool examined four specific parts of the partograph for completion: Contractions monitored half-hourly; fetal heart rate monitored half-hourly; and maternal blood pressure and pulse monitored either at admission or throughout labor. In Bangladesh, contractions and fetal heart rate were monitored in 54% of records, with the other components recorded in 90-100% of records, which reflects an increase from the previous year. In DRC, contractions and fetal heart rate monitoring were found in 80 and 76% of records, respectively, an increase over the previous year’s 55-56%. Maternal blood pressure and pulse were recorded at a slight decrease from the previous year (77 and 79%, compared to 84% for both in FY 17/18).
Records were also assessed to determine whether the partograph included a crossed action line, and if so, whether action was taken to address the prolonged or obstructed labor. Very few records included partographs with crossed action lines, but in all but two of those cases, action was taken.
Overall, the record review for FY 18/19 covered a smaller number of sites compared with previous years, and indicated that partograph implementation at supported sites continues to vary in terms of completeness and correctness, as it has in previous years. There has been steady improvement over the years in the indicators for supported sites in DRC, attributable to on-going efforts to strengthen partograph use through trainings. FC+ will continue to utilize these findings in programmatic activities for FY 18/19.
During FY 18/19, FC+ supported sites reported a total of 55,798 deliveries in three program countries (Bangladesh, DRC, and Uganda). Data was not available from Mozambique or Niger, where the project is not working directly to support obstetric services.
FC+ supported sites tend to be higher-level facilities that are more likely to receive referrals and complications; this contributes to a high proportion of cesarean section deliveries relative to the national average cesarean section rates in these countries. The total cesarean section rate across all FC+ supported sites reporting data was 51.4% (Figure 3). Cesarean section rates at supported sites vary widely at the country level (from 29% in Uganda to 69% in Bangladesh) and at the facility level, due to the varied patient profiles and clinical mandates of different facilities.
Across supported sites, 1.2% of all deliveries were reported as prolonged/obstructed labors, with 7.1% of those prolonged/obstructed labors receiving catheterization for fistula prevention. The reported numbers range by country and by site, with a high of 3% of labors reported as prolonged/obstructed in Uganda and less than <1% reported in Bangladesh. Site-level data can be found in Section III, by country.

Annual Report • October 2018 – September 2019 Fistula Care Plus 35
Figure 3: Cesarean Section Rates, by Country, FY 18/19 (n=55,798 deliveries)
Sub-Objective 4.2 Increase capacity for treatment FC+ continues its leadership role in the IUGA-ICS Joint Report on the Terminology for Female Pelvic Floor Fistulae, currently in its 12th round of review. FC+ has inserted the fistula COP’s working definitions of fistula etiologies for congenital and acquired fistula (obstetric, iatrogenic, mixed obstetric/iatrogenic, traumatic, cancer, infection and inflammatory disease) into the drafts of the IUGA-ICS Joint Report. The Joint Report will also include sections on definitions of women deemed incurable and women with persistent incontinence, while also introducing definitions for women with residual incontinence, chronic fistula definitions for WDI, persistent fistula, and residual fistula. It is anticipated that a working draft will be circulated to an invited group of external reviewers chosen from the ISOFS academic senior fistula surgeon community in February 2020.
Royal College of Obstetricians and Gynecologists (RCOG) Global Health Division
Since FY 16/17, FC+ and RCOG Global Health have been collaborating to create a competency-based educational manual, anchored in RCOG teaching product protocols, to support accredited multi-disciplinary sub-specialty fellowship programs for urogynaecology/female pelvic medicine emerging under the leadership of senior academic fistula surgeons in Africa and South Asia. FC+ continues to hold an MOU with RCOG and a draft is expected in early 2020.
Surgical Safety Toolkit
In response to gaps in clinical records, challenges understanding M&E data trends, and in response to specific clinical staff requests at supported facilities, FC+ introduced the Surgical Safety Toolkit (SST) in FY 16/17. The SST includes a set of clinical trackers and quality assurance checklists. The SST is designed to support the provision of surgical care at a minimum acceptable standard, as outlined by global actors such as the World Health Organization and the Lancet Commission on Global Surgery. The SST contributes to a platform for ongoing quality assurance in fistula services past the duration of the project. The SST is a novel, integrated package that includes a client tracker of clinical outcomes for surgical and non-surgical care for fistula, pelvic organ prolapse (POP), and incontinence; a surgical skills tracker designed to document return on investment of funded clinician training, for fistula, prolapse, and incontinence; a sentinel event tracker designed to identify time trends of near-miss morbidity events that will augment the existing system of mortality review and help target quality improvement support to
30.7
63.4
71.1
48.6
69.3
36.6
28.9
51.4
Bangladesh
DRC
Uganda
FC+ Total
Vaginal delivery
C-Section
Annual Report • October 2018 – September 2019 Fistula Care Plus 36
facilities. The SST also guides and supports staff teamwork behaviors with seven surgical safety checklists covering topics ranging from candidacy for surgery to daily post-operative care and discharge follow-up planning. The checklists are integrated into the client tracker and were designed to meet specific requests from supported sites that shared internally identified gaps within facility care systems.
FC+ activities to monitor, analyze and learn from the SST data continue to evolve. Previously supported by an external consultant now unavailable to the project, SST data review will be revitalized commensurate with staffing and country project closeouts.
Preliminary learning from SST implementation indicates three categories of facilities revealed by SST checklist gap analysis: 1) strong clinical data systems and strong staff engagement; 2) weak clinical data systems and strong staff engagement; and 3) weak clinical data systems and weak staff engagement. This grouping has guided FC+ support efforts including systems analysis and coaching of facility staff by FC+ clinical officers. The anesthesia portion of the intra-op checklist and the post-op daily rounds checklist have both emerged as particularly important in sentinel event analysis and associated systems strengthening. An in-depth analysis of SST data is planned for FY 19/20.
Clinical services at supported treatment and prevention sites
During FY 18/19, a total of 988 women with severe incontinence symptoms sought fistula care services at FC+ supported sites. Of these women, 721 were diagnosed with fistula (73% of those seeking, compared with 66% in FY 17/18). Of those diagnosed, 675 were medically eligible for surgical repair (94%). FC+ supported the provision of 605 surgical fistula repairs in FY 18/19 (90% of those eligible, compared with 89% in FY 17/18). The number of surgical repairs supported during FY 18/19 represents a significant decrease from the number supported in FY 17/18 (605 repairs compared with 3,089 repairs). This decrease is due to the end of program activity in Nigeria, which was the project’s largest country in terms of number of repairs; the months-long suspension of activity in DRC due to the de-scoping associated with Trafficking Victims Protection Act provisions; and suspension of activities in Niger due to financial and administrative review of our subaward partner and the need to focus on medical waste management at supported sites; and the end of clinical support activity in Uganda early in FY 18/19. See Figure 4 for data on women seeking and requiring fistula treatment and the number of surgical repairs supported, by country. Site level information is presented in Section III, by country.
Some women may be diagnosed with fistula in one quarter, and repaired in the next. Because FC+ does not track individual women through established monitoring and evaluation data collection, we are unable to present a definitive percentage of women requiring repair who receive it. We are also unable to report the number of women repaired because women may have multiple repairs over the life of project, or repairs at multiple sites. However, within a given quarter, the number of repairs generally reflects the number of women.
Including projects receiving bilateral funding, a total of 1,202 surgical repairs were supported by USAID in ten countries (Bangladesh, DRC, Ethiopia, Guinea, Mali, Mozambique, Niger, and Uganda) during FY 18/19, of which 605 (50%) were supported through FC+ (see Figure 5 and Table 9 for detail). The remaining 597 surgical repairs were supported by USAID bilateral projects. Site level repair data is presented in Section III, by country.
In addition to these surgical repairs, FC+ supported non-surgical treatment of fistula using catheterization for a total of six women during FY 18/19, in Bangladesh, DRC, and Niger. It is important to note that much prevention and early treatment of fistula using catheterization is likely to occur outside of fistula treatment centers in maternity service sites.

Annual Report • October 2018 – September 2019 Fistula Care Plus 37
Figure 4: Number of Women Seeking and Requiring Fistula Treatment, and Number of Surgical Repairs, By Country, FY 18/193
Figure 5: USAID-Supported Surgical Fistula Repairs, by Quarter, FY 18/19 (n=1,202)
Table 9: Number of USAID-Supported Surgical Fistula Repairs, by Country, FY 18/19
Site Oct-Dec 2018
Jan-Mar 2019
Apr–Jun 2019
Jul-Sept 2019
Total FY 18/19
Bangladesh 63 89 88 36 276 DRC 107 51 0 0 158 Mozambique 38 21 0 53 112 WA/Niger 45 0 0 0 45 Uganda 6 8 0 0 14 Total FC+ 259 169 88 89 605 Mali: IntraHealth (bilateral) 78 0 0 0 78 Ethiopia: Pathfinder (bilateral) 103 129 71 56 359 Guinea: Jhpiego HSD project 78 25 20 37 160 Total USAID bilateral 259 154 91 93 597 Total All USAID-supported 518 323 179 182 1,202
In FY 18/19, FC+ was able to collect etiology data for 99% (n=714) of all diagnosed cases. Data reported during this period indicate that for diagnosed cases, the etiology of the fistula was: obstructed/prolonged
3 For this reporting period, in Niger, the total number of surgeries is greater than the number of women eligible, due to women receiving surgery during the period who had been diagnosed and deemed eligible in previous quarters.
259
169
88 89
259
15491 93
518
323
179 182
0
100
200
300
400
500
Q1 Q2 Q3 Q4
FC+
Bilateral
Total USAIDsupported
0
100
200
300
400
500
Bangladesh DRC Mozambique Niger Uganda
Seeking
Eligible
Repairs

Annual Report • October 2018 – September 2019 Fistula Care Plus 38
labor 69% (n=495); iatrogenic 27% (n=195); traumatic 1% (n=7); and other causes (primarily cancer or congenital) 2% (n=17).
Clinician error during medical procedures has emerged as an important contributor to the fistula burden (iatrogenic fistula), causing a higher proportion of cases than traumatic fistula in most settings. FC+ collected data from supported sites on the number of cases deemed by the operating surgeon to be iatrogenic fistula. During this reporting period, 20 supported sites reported this data; as noted above, reporting that 27% of all diagnosed fistula cases were identified as iatrogenic in nature. The percent of cases identified as iatrogenic varied widely between countries: highest in Bangladesh (40%) and DRC (29%), and lower in Mozambique (7%), Niger (2%), and Uganda (0%) (see Section III, by country). Bangladesh and DRC have consistently reported the highest iatrogenic rates throughout the life of the project. Bangladesh consistently reports significantly higher rates of cesarean section births at supported facilities. However, case reviews in Bangladesh suggest that most iatrogenic fistula is linked to hysterectomy, in contrast to most sub-Saharan African countries, where it is linked to cesarean section.
FC+ emphasizes the importance of routine, high quality service provision and encourages and supports efforts in each facility towards the optimal model of routine repairs year round for cases that are well within the surgeon skill set and facility spectrum of care, combined with concentrated repair efforts for cases that require master surgeon consultants and/or require transfer to higher level facility for anticipated complex peri-operative care beyond the scope of the home facility. Concentrated repair efforts are also utilized as a strategic approach to address the overwhelming backlog of clients. During FY 18/19, provision of repairs at supported sites was predominantly carried out through routine services (66%) with a smaller proportion occurring through concentrated repair efforts (34%).
During FY 18/19, 94.9% of all discharged FC+ repair cases were closed at the time of discharge (compared with 88.4% in FY 17/18). 92% of all cases were closed and continent (i.e., dry in the case of fistula resulting in leakage of urine) at discharge, 2.9% were closed with remaining incontinence, and 5.1% were not closed, see Figure 6 for outcome rates by country.
Closed and continent rates are a potentially non-informative indicator for quality of care, in that a patient can have suboptimal outcome even when the quality of fistula care meets or exceeds an acceptable standard. This is exacerbated by variations in case mix, i.e., if some facilities are caring for many more patients with complex fistulas and complicating incontinence co-morbidities. However, in tandem with other clinical indicators (e.g., complications), this indicator may be useful in identifying settings where audit and analysis of the case mix, skills and materials that underpin evaluation and management of post-fistula incontinence, overall quality of care, and other issues may be warranted. Historically, the project has set a benchmark of 75% for the proportion of discharged cases deemed closed and continent. When rates fall below benchmarks, FC+ investigates the causes to determine whether follow-up action is necessary.
Of the 551 discharged cases during the fiscal year, data on level of fistula complexity were available for 97% of cases. 30.7% were classified as simple fistula and 65.9% were not simple. During the fiscal year, simple fistula made up 21% of reported cases in Mozambique, 19% in Bangladesh, approximately half of reported cases in DRC and Niger, and 100% of those reported in Uganda, proportions that have remained relatively consistent throughout the project, with the exception of Bangladesh where the percentage of simple cases has previously been higher than that reported during this period.
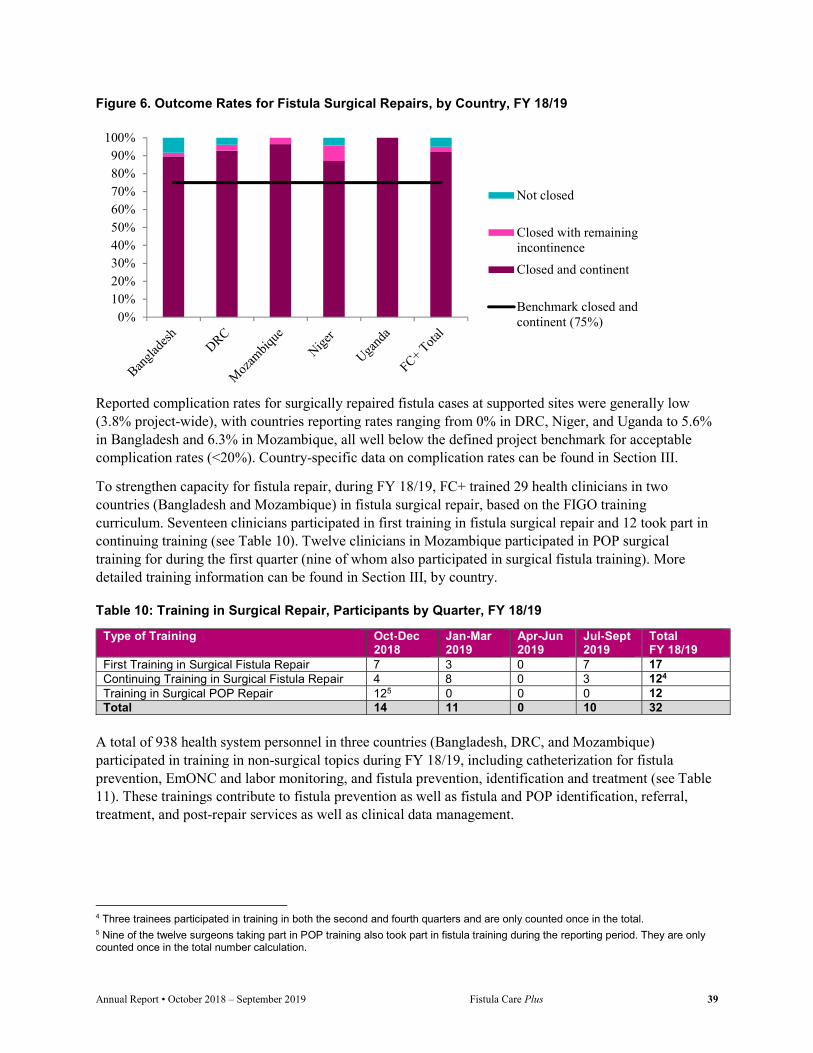
Annual Report • October 2018 – September 2019 Fistula Care Plus 39
Figure 6. Outcome Rates for Fistula Surgical Repairs, by Country, FY 18/19
Reported complication rates for surgically repaired fistula cases at supported sites were generally low (3.8% project-wide), with countries reporting rates ranging from 0% in DRC, Niger, and Uganda to 5.6% in Bangladesh and 6.3% in Mozambique, all well below the defined project benchmark for acceptable complication rates (<20%). Country-specific data on complication rates can be found in Section III.
To strengthen capacity for fistula repair, during FY 18/19, FC+ trained 29 health clinicians in two countries (Bangladesh and Mozambique) in fistula surgical repair, based on the FIGO training curriculum. Seventeen clinicians participated in first training in fistula surgical repair and 12 took part in continuing training (see Table 10). Twelve clinicians in Mozambique participated in POP surgical training for during the first quarter (nine of whom also participated in surgical fistula training). More detailed training information can be found in Section III, by country.
Table 10: Training in Surgical Repair, Participants by Quarter, FY 18/19
Type of Training Oct-Dec 2018
Jan-Mar 2019
Apr-Jun 2019
Jul-Sept 2019
Total FY 18/19
First Training in Surgical Fistula Repair 7 3 0 7 17 Continuing Training in Surgical Fistula Repair 4 8 0 3 124 Training in Surgical POP Repair 125 0 0 0 12 Total 14 11 0 10 32
A total of 938 health system personnel in three countries (Bangladesh, DRC, and Mozambique) participated in training in non-surgical topics during FY 18/19, including catheterization for fistula prevention, EmONC and labor monitoring, and fistula prevention, identification and treatment (see Table 11). These trainings contribute to fistula prevention as well as fistula and POP identification, referral, treatment, and post-repair services as well as clinical data management.
4 Three trainees participated in training in both the second and fourth quarters and are only counted once in the total. 5 Nine of the twelve surgeons taking part in POP training also took part in fistula training during the reporting period. They are only counted once in the total number calculation.
0%10%20%30%40%50%60%70%80%90%
100%
Not closed
Closed with remainingincontinence
Closed and continent
Benchmark closed andcontinent (75%)

Annual Report • October 2018 – September 2019 Fistula Care Plus 40
Table 11: Training for Health System Personnel (excluding fistula/POP surgery), Participants by Quarter, FY 18/19
Type of Training Oct-Dec 2018
Jan-Mar 2019
Apr-Jun 2019
Jul-Sept 2019
Total FY 18/19
ANC 0 0 0 0 0 Catheterization for fistula prevention 0 0 0 0 0 Community, outreach and advocacy 0 0 0 0 0 Data management 0 0 0 0 0 EmONC 0 0 0 0 0 EmONC and labor monitoring 16 0 0 0 16 FP counseling 0 0 0 0 0 FP methods 0 0 0 0 0 FP and fistula counseling 0 0 0 0 0 Fistula counseling 0 0 0 0 0 Gender 0 0 0 0 0 Infection Prevention 0 0 0 0 0 Labor monitoring 0 0 0 0 0 Non-surgical POP treatment 0 0 0 0 0 Pre- and Post-Operative Care 112 214 28 568 9226 Quality Assurance 0 0 0 0 0 Other 0 0 0 0 0 Total 128 214 28 568 938
Sub-Objective 4.3 Integrate family planning (FP) services to respond to client needs FC+ supports efforts to strengthen integration of FP in fistula treatment services and broader maternal health care at supported sites. During FY 18/19, a total of 46,373 counseling sessions were provided at supported sites, and FP services resulted in a total of 33,469 Couple Years of Protection (CYP). The method mix contributing to this total CYP includes tubal ligation (41%), implants (31%), injectables (9%), IUCD (8%), and oral pills (5%). Country specific counseling information is provided in Figure 7 and CYP information in Figure 8, with additional country- and site-specific information provided in Section III.
Figure 7. Family Planning Counseling Sessions, by Country, FY 18/19 (n=46,373)
6 Trainings are reported under the category that best describes their overall content. The trainings reported here covered myriad other topics, including family planning, catheterization, EmONC, etc. but are reported only under their “primary” category.
33,363
1,213
11,797
46,373
Bangladesh
DRC
Uganda
FC+ Total

Annual Report • October 2018 – September 2019 Fistula Care Plus 41
Figure 8. Family Planning CYP, Short-Term vs. Long-Term/Permanent Methods, by Country, FY 18/19 (n=33,469)
Sub-Objective 4.4 Support and establish treatment/care programs for WDI and POP During FY 18/19, FC+ has continued the establishment and support of treatment for WDI and women suffering from POP. FC+ has been working to establish functioning supply chains for pessaries in supported countries. A pessary supply chain was established with Bioteque, a FC+ PPP partner, in DRC and Uganda after competitive bidding among suppliers meeting standards for quality and vetting for donor procurement compliance. Panzi and St. Joseph Hospital have received pessaries, however uptake has been very limited. Pessary uptake failure in DRC is directly related to geopolitical instability and transport costs that create barriers to returning for follow-up care which is mandatory to pessary treatment and long-term management. The utility of pessaries in outreach facilities for women with POP who are awaiting surgery is under investigation. However, in facilities in North and South Kivu, and in Kinshasa, return for follow-up emerged as the main barrier to success. FC+ will continue to incorporate opportunities for training and advocacy regarding pessary use in future visits from project-supported experts.
During FY18/19, four FC+ supported sites (three in DRC and one in Uganda) provided routine data on non-surgical and surgical POP treatment. During the reporting period, these sites reported that 316 women sought treatment for possible POP symptoms with 238 women diagnosed with and eligible for treatment for POP (75% of those seeking). A total of 238 women received POP treatment during this period (100% of those eligible). Supported sites reported providing 442 non-surgical POP treatments and 238 surgical POP treatments (some women may receive both non-surgical and surgical treatment). Non-surgical POP treatments at reporting sites presently overwhelmingly consist of counseling and physical therapy with no pessaries reported. POP treatment data is presented by country in Table 12.
Table 12. Number Seeking, Requiring, and Receiving POP Treatment, by Country, FY 18/19
Country #Seeking #Eligible % of Seeking #Receiving % of Eligible DRC 315 237 75% 237 100% Uganda 1 1 100% 1 100% Total 316 238 75% 238 100%
Supported facilities reported no complications for women receiving surgical POP treatment. Given the nature of surgical POP repair, it is to be expected that all treated women would be considered “cured” at
3,171
210
3,139
13,481
2,068
11,399
Bangladesh
DRC
Uganda
STM LTM+PM
Annual Report • October 2018 – September 2019 Fistula Care Plus 42
the time of discharge. The project is not currently able to gather longer term follow up data to monitor repair breakdown after discharge.
Objective 5: Strengthened evidence base for approaches to improve fistula care and scaled up application of standard monitoring and evaluation (M&E) indicators for prevention and treatment FC+ strengthens the evidence base for approaches to improve fistula care and promotes M&E scale-up by ensuring that FC+ activities are appropriately documented and disseminated and by learning from and contributing to the knowledge of the fistula community as well as the broader maternal health sector.
Throughout the fiscal year, FC+ ensures compliance with USAID and EngenderHealth policies and procedures for research and evaluation dissemination by including all studies and reports on the relevant internal and external databases. Sub-Objective 5.1 Increase standardization in terminology, classification, and indicators FC+ conducted a documentation of the process by which standard indicators for fistula treatment, developed and promoted under the previous FC project, were integrated and adopted in the Health Management Information Systems (HMIS) of select FC+ countries (Bangladesh, Niger, Nigeria, and Uganda) and in Guinea, where EngenderHealth implements fistula programming as a sub-awardee. The process documentation sought to understand the degree to which recently selected fistula indicators have been adopted and/or operationalized by national HMIS as well as the use of HMIS fistula data by health workers/managers at facility, regional and national levels. Key professional respondents for this process documentation included national, regional, and sub-regional health office staff involved in reviewing, synthesizing, and acting on data on HMIS fistula indicators, and health facility staff involved in monitoring, collecting, and reporting data on these indicators. In FY 17/18, FC+ completed data collection in Bangladesh, Nigeria, Uganda, and Guinea, with a total of 35 professional respondent interviews. Analysis of these data could not be completed as anticipated due to the departure of the FC+ Program Associate – Research & Evaluation. FC+ will complete this analysis in FY 19/20 through a practicum partnership with research graduate students at the Columbia University Mailman School of Public Health.
Sub-Objective 5.2 Strengthen monitoring and evaluation/research (ME&R) systems and use of data To operationalize the FC+ PMP, a key activity through the life of the project has been developing and updating FC+ M&E and data management and review systems. FC+ has built a DHIS2 platform to function as the global M&E database for the current project. The FC+ Senior M&E Associate has continued to be active in the global DHIS2 community during FY 18/19, sharing FC+/EngenderHealth’s experience and learning about the latest developments in the field. This included participation in a BAO Systems-led training on the functionality of DHIS2’s tracker program in January 2019 and participation in the annual DHIS2 Global Symposium held in April 2019 in Washington D.C.
FC+ conducts internal DDM exercises after the close of each quarter to discuss program data and identify issues in need of follow-up. FC+ has continuously updated the indicators and visualizations reviewed during global DDMs to reflect emerging project priorities (e.g., fistula etiology trends) or learning from other projects and partners (e.g., approaches recommended at the Institute for Healthcare Improvement First Africa Forum on Quality and Safety). This practice has been carried out in Bangladesh, DRC, Niger, Nigeria, and Uganda as well, both within the FC+ country office and with partner sites through annual
Annual Report • October 2018 – September 2019 Fistula Care Plus 43
clinician and partner network meetings, generally convened by FC+ and the MOH, which provide opportunity to reflect on both national and site level data trends.
FC+ works with supported treatment sites to encourage ongoing review of site-specific data to identify and act upon areas of clinical and programmatic concern and opportunities to improve fistula services. While it is ideal for sites to review data on a monthly or quarterly basis, depending on service volume, experience from the original FC project indicates that this is very difficult for sites to achieve, given shortages in human and other resources. In FY 18/19, 63% of FC+ supported treatment sites met at least once during the fiscal year to review their data, a decline when compared to FY 17/18 (94%); 33% (compared to 56% in FY 17/18) met at least twice (see Appendix RR for country and site details). This decline is attributed to close out in Uganda and activity suspensions in DRC and Niger that curtailed activities.
Sub-Objective 5.3 Use research findings to improve practice Conference presentations and publications continue to foster evidence-based change in research and FC+ program practices. Throughout the fiscal year, FC+ convened and presented at multiple meetings and conferences to disseminate findings from research and program evaluations; see Table 3 for details.
The FC+ Deputy Director organized and participated in a satellite panel at the 5th Global Symposium on Health Systems Research in October 2018, in Liverpool, England. The panel, “Cesarean section safety in low-resource settings: Addressing health system challenges that jeopardize maternal and newborn health”, was well attended, with numerous participants from Bangladesh and Uganda in particular expressing great interest in the cesarean section safety/quality action agenda and FC+’s support to the ACOG ETOO pilot.
FC+ presented 15 oral presentations and one panel, “Cesarean Section Safety in Low-Resource Settings: Ensuring Quality in a Context of Rapidly Increasing Volume” at the FIGO XXII World Congress held in October 2018 in Rio de Janeiro, Brazil (see Appendix G).
Two staff members from FC+/Uganda attended the fifth International Conference on Family Planning (ICFP) in Kigali, Rwanda in November 2018. The FC+ Uganda team made four poster presentations covering their work with religious leaders, strengthening data for decision making, improving contraceptive method mix through a rights-based approach, and family planning integration at a hospital pediatric unit. They also presented one oral presentation on family planning service integration at fistula prevention and treatment sites.
FC+’s program experiences and research were prominently represented at the 7th International Conference of ISOFS and the IOFWG meeting in December 2018 in Kathmandu, Nepal. A total of 21 oral presentations and 14 posters were presented on FC+ supported work (see Appendices H, I, K, and L).
As described in Objective 4, FC+ presented at the World Congress of the Royal College of Obstetricians and Gynaecologists (RCOG) meeting held Jun 16-19, 2019 in London on the topics of “New ways of working to achieve a fistula free generation” and on progress to date from collaboration with the Harvard PGSSC to document and measure the sequelae of prolonged/obstructed labor (see Appendix OO). FC+ made a presentation on FC+ global achievements at the International Consultation on the Regional Strategy for Obstetric Fistula Elimination in West and Central Africa which was held in Senegal in June 2019, and on the management and morbidity burden of prolonged/obstructed labor at the subsequent URODAK meeting (see Appendices PP and QQ).
Annual Report • October 2018 – September 2019 Fistula Care Plus 44
FC+ participated in several USAID-organized briefings and working groups in order to disseminate findings and share updates on activities with USAID/Washington staff including the USAID SDI CAs meeting and the USAID/JHUCCP Service Communication Community of Practice meetings in September 2018, and the USAID Research and Policy Division meeting in December 2018 (see Table 3 for details).
FC+ has also contributed to the evidence informing fistula and related programs through the continued publication of reports, briefs, and journal articles. During FY 18/19, four articles related to FC+ support activity were accepted or published in peer-reviewed journals (see Table 13). FC+ ensures that all articles supported with project resources and included in approved workplans are published open-access, in line with USAID policy on research.
The FC+ Deputy Director has continued to work with the Population Council on analysis of the fistula treatment barriers intervention endline data collection. FY 18/19 knowledge products resulting from this collaboration have been detailed in Section II Objective 3. Peer-reviewed journal articles are included in Appendix E and research briefs and reports are available on the FC+ and Population Council websites (https://www.popcouncil.org/research/fistula-care-plus). See Objective 3 for additional updates on this study as well as Appendices N, O, and P.
As part of the July 2017 technical consultation on cesarean section in low-resource settings, convened by FC+ and Maternal Health Task Force, FC+ commissioned an analysis of DHS and SPA data from the London School for Hygiene and Tropical Medicine to synthesize as much information as possible about the current profile of cesarean section services. This report, The Landscape of Cesarean Section in Sub-Saharan Africa and South and Southeast Asia (https://fistulacare.org/wp-fcp/wp-content/uploads/2015/10/LSHTM-report_Nov-8_final_for-web.pdf) was published in November 2017, and assesses the landscape of cesarean sections in low and middle income countries using recent, comparable, nationally representative DHS survey data from 44 countries. This collaboration also resulted in the October 2018 publication of a paper, “Caesarean section provision and readiness in Tanzania: analysis of cross-sectional surveys of women and health facilities over time”, in BMJ Open, as well as publication in December 2018 of a policy brief (https://fistulacare.org/wp-fcp/wp-content/uploads/2018/12/Tanzania_CSPolicyBrief_2018-3.pdf) summarizing key findings from analysis of Tanzanian DHS/SPA, see Appendix J.
As described in Objective 1, the FC+ Project Director co-authored a commentary in Lancet Global Health entitled “Meeting the SDG challenge to end fistula and preventable childbirth-related morbidity and mortality” which emphasizes the critical role of universal access to skilled care at birth (see Appendix LL and here: https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(19)30198-6/fulltext).
Table 13: Peer-Reviewed Articles Published, FY 18/19
Authors Title Journal El Ayadi, A.; Barageine, J.;, Korn, A.; Kakaire, O.; Turan, J.; Obore, S.; Byamugisha, J.; Lester, F.; Nalubwama, H.; Mwanje, H.; Tripathi, V.; and Miller, S.
Trajectories of women's physical and psychosocial health following obstetric fistula repair in Uganda: A longitudinal study.
Tropical Medicine & International Health. October 2018 24(Suppl 1) DOI: 10.1111/tmi.13178 https://www.researchgate.net/publication/328585886_Trajectories_of_Women's_Physical_and_Psychosocial_Health_Following_Obstetric_Fistula_Repair_in_Uganda_A_Longitudinal_Study

Annual Report • October 2018 – September 2019 Fistula Care Plus 45
Authors Title Journal Cavallaro F.; Pembe, A.; Campbell O.; et al.
Caesarean section provision and readiness in Tanzania: analysis of cross-sectional surveys of women and health facilities over time
BMJ Open. 2018;8(9):e024216. Published 2018 Oct 4. doi:10.1136/bmjopen-2018-024216 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6173245/
Romanzi L.; Meara J.; Anastasi E.; Knutsson A.
Meeting the SDG challenge to end fistula and preventable childbirth-related morbidity and mortality.
Lancet Glob Health. 2019; 7: e835–36 https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(19)30198-6/fulltext
Tripathi V.; Arnoff E.; Sripad P. Removing barriers to fistula care: Applying appreciative inquiry to improve access to screening and treatment in Nigeria and Uganda.
Health Care Women Int. 2019 Jul 23:1-16. doi: 10.1080/07399332.2019.1638924. (Epub ahead of print) https://www.ncbi.nlm.nih.gov/pubmed/31335303
As detailed in Section 3: Uganda, FC+ has published multiple technical briefs capturing various project activities in Uganda, as part of the project’s close out there (see Appendices DD-HH and https://fistulacare.org/resources/publications/technical-briefs/). These include:
“Fistula Care Plus in Uganda: Success Stories”: a compilation of success stories from clients, clinicians, and others involved with FC+ Uganda;
“Improving Quality of Life for Women with Incurable Fistula: A Fistula Care Plus and TERREWODE Research Partnership in Uganda” describing FC+’s partnering with a Ugandan organization, the Association for the Rehabilitation and Re-orientation of Women for Development (TERREWODE), to conduct research on the social reintegration needs of these women and evaluate the effects of interventions responding to these needs;
“Communities and Health Workers Improving Maternal Health Together in Jinja District” describing the experiencing of implementing the site walk-through (SWT) model in Jinja, Uganda;
“Engaging Religious Leaders in Support of Maternal Health in Uganda” documenting the FC+ Uganda program experience and key lessons learned leveraging existing communication strengths by engaging religious leaders and fostering their support for maternal health and family planning services to raise awareness;
“Empowering Youth through Social and Financial Life Skills and Healthy Behaviors: Lessons from a Ugandan Pilot” describing FC+’s Aflateen PLUS youth engagement strategy paired an integrated curriculum with dual strategies for in- and out-of school youth. This approach could be replicated in Uganda and other low-resource settings to support youth in developing life skills and planning a healthy future.
In August 2019, FC+ published a technical brief describing its 4Q Checklist for fistula screening and referral, and noting the utility of this approach for improving information at the local level about fistula burden, essential for targeting of outreach and planning of services, see Appendix II.
Also in August 2019, FC+ developed two technical briefs for International Day to End Obstetric Fistula. A two-page summary of USG investments in fistula care, produced together with USAID/W (see Appendix JJ) and a brief summarizing achievements from the first five years of FC+ (see Appendix KK).

Annual Report • October 2018 – September 2019 Fistula Care Plus 46
The FC+ Deputy Director and FC+/DRC finalized a manuscript from the study of non-obstetric fistula. This study documented that 19% of fistulas treated across several FC+ supported sites in DRC were non-obstetric in origin. These cases were primary iatrogenic fistulas, most related to cesarean section. The manuscript was reviewed and approved by USAID/W, and submitted to the International Journal of Gynecology and Obstetrics (IJGO) in the third quarter of this fiscal year. The manuscript was not accepted, and will be submitted to an alternative publication in the first quarter of FY 19/20.
The FC+ Deputy Director authored two abstracts accepted for the ICM 2020 World Congress of Midwives: a poster presenting the results of the global midwives survey of practices related to bladder care and management of prolonged/obstructed labor; and an oral presentation on the cesarean section/ iatrogenic fistula consultation and action agenda.
The Deputy Director also reviewed and provided feedback on the WHO/UNICEF Joint Statement on Measuring Effective Coverage in Maternal, Newborn, Child, and Adolescent Health. This statement, and the accompanying manuscript submitted to Lancet Global Health, follows a series of discussions about effective coverage as well as reviews of indicators for effective coverage. The statement and manuscript are expected to be published in the first quarter of FY 19/20.
Appendix E provides a list of FC/FC+ peer-reviewed journal publications and Appendix F provides metrics for readership of articles published by FC/FC+. While metrics are only available for some FC/FC+ articles, these have been viewed more than 54,000 times.
The project’s online presence has helped foster relationships with peer organizations, including resource partners such as MHTF. FC+ is increasingly engaged by partner organizations to participate in Twitter chats and other forms of online discourse focused on maternal health and morbidity. During FY 18/19, the project shared two posts on the FC+ blog (https://fistulacare.org/blog).
Sub-Objective 5.4 Contribute to the evidence for improved programming and care As described under Objective 2, FC+ and TERREWODE applied validated quality of life (QoL) assessment tools and develop indicators and data collection tools for a joint study on the psychosocial reintegration of women deemed incurable (WDI). Data analysis was completed in the fourth quarter of FY 17/18, documenting substantial improvements in QoL among WDI. These findings have been summarized in a preliminary report in the first quarter of FY 18/19, and were presented at the ISOFS biennial conference in Kathmandu in December 2018. The findings were documented in a technical brief published in May 2019. Study findings, including recommendations regarding optimal tools for QoL assessment and for fistula services supporting WDI were shared with partners in Uganda during FC+ closeout and dissemination meetings. The technical brief on this partnership can be found in Appendix HH and here: https://fistulacare.org/resources/publications/technical-briefs.
In FY 17/18, the FC+ core team supported the Uganda team to complete a process documentation of a youth engagement strategy centered on the Aflateen PLUS curriculum, developed by EngenderHealth in collaboration with Private Development Education Network (PEDN). This initiative aimed to empower in and out of school youth to engage in behaviors that increase their ability to make responsible financial, social, and reproductive health decisions, including messages on voluntary FP and where to access services. Trained facilitators collaborated with health workers to conduct youth outreach events using sports, edutainment and drama, incorporating services such as HIV/AIDS testing, and provision of condoms and other FP methods. Details of Aflateen PLUS outputs in FY 18/19 are provided in Section III: Uganda.
Annual Report • October 2018 – September 2019 Fistula Care Plus 47
During the process documentation, teachers reported highly valuing the financial education component (e.g. savings tools, planning and budgeting, financial enterprises) of the curriculum; peer educators appreciated the increase in their capacity to make health referrals, and health workers reported increased skills in communicating with and serving adolescents and youth. All cadres of facilitators appreciated the learner-centered/empowerment training approach, which was novel relative to other, more didactic training approaches they had been exposed to. In considering tangible changes in health knowledge and behaviors, respondents noted a decline in pregnancy-related school drop-outs, increased confidence among youth to seek out information on FP and to request condoms, and an increased ‘savings’ culture and use of savings to address financial challenges such as transportation costs and school fees. Respondents also described supply-side barriers that made it challenging for youth and community members to follow up on referrals (e.g., inadequate supplies at health facilities). Outputs of and lessons learned from Aflateen PLUS implementation were shared through presentations at the ISOFS biennial conference in Kathmandu in December 2018, and in a technical brief published in March 2019 (see Appendix DD and https://fistulacare.org/resources/publications/technical-briefs).
FC+ has provided technical review and commentary to clinical research initiatives implemented by partners, which advance project evidence interests. During FY 18/19, these included a survey led by Harvard’s PGSSC to estimate burden of disease associated with prolonged/obstructed labor. FC+ is providing technical support to these research activities, which are led by other institutions. These are not FC+ research activities, should this level of engagement change, FC+ will submit concept and protocol materials to AORs for review/approval in accordance with PMP and USAID policy. The Harvard survey was launched in September 2018, and circulated to fistula surgeons and clinicians attending P/OL cases around the world, including at FC+ supported sites. FC+ staff have reviewed the survey results and provided the Harvard team with guidance on how to use the findings to develop a new model estimating Years Lost to Disability (YLD) as a result of prolonged/obstructed labor. The survey results were presented at the RCOG World Congress held in June 2019 (see Appendix OO).
During FY 18/19, FC+ and ACOG continued collaboration on ACOG Global Program’s cesarean section/EmONC training in Uganda, Essential Training in Operative Obstetrics (ETOO), formerly known as the Structured Operative Obstetrics (SOO) pilot. This ACOG Global Programs (http://www.acog.org/About-ACOG/ACOG-Departments/Global-Womens-Health) initiative builds on the Canadian Network for International Surgeons (www.CNIS.ca) cesarean skills program in Uganda and is geared toward assuring minimum acceptable levels of cesarean delivery skills among clinical trainees. In the first quarter, the FC+ Deputy Director presented a review of ETOO program M&E data at FIGO 2018. FC+/Uganda participated in an ETOO meeting in Kampala, along with government partners. Further details of collaboration on the ground are provided in Section III: Uganda. While FC+ has closed out in Uganda, the Deputy Director has continued to provide technical assistance for analysis of continued rounds of training through ETOO in FY 18/19, to ensure a sustained project legacy for fistula prevention in Uganda.
FC+ provided technical review and commentary on the physiotherapy (PT) section adapted by Laura Keyser for the WHO/UNFPA fistula booklet revision (the Orange Manual). This text was adapted from an integrated physiotherapy manual developed by Mama LLC, designed to educate and train available health care workers and provide standardized general and specific PT treatment to women with fistula. The integrated physiotherapy manual “Implementing Physical Rehabilitation Services into Comprehensive Fistula and Maternity Care: A Training Guide for Health Care Workers” was finalized in August 2019 and can be accessed at: https://drive.google.com/file/d/1pscwUQkNLx1WWjzRaw8s60HUVGht5gWx/view. In FY 19/20, FC+
Annual Report • October 2018 – September 2019 Fistula Care Plus 48
plans to support the publication of this manual as a physical resource and disseminate it through a Fistula Community of Practice (FCoP) webinar.

Annual Report • October 2018 – September 2019 Fistula Care Plus 49
SECTION III: COUNTRY REPORTS
Please note: reports are provided only for objectives that were actively addressed in FY 18/19. All sub-objectives are consolidated for reporting.
Bangladesh USAID-supported fistula repair services in Bangladesh began in July 2005 through the previous FC project and continue through FC+, with seven hospitals providing fistula treatment and five prevention-only sites during FY 18/19. In Bangladesh, FC+ works with private hospitals and public sector institutions, including Medical College Hospitals and District Hospitals. The FC+ project is working in partnership with the Bangabandhu Sheikh Mujib Medical University (BSMMU) to set up a Fistula Prevention, Treatment, and Training Center on-site. All currently supported fistula treatment sites in Bangladesh provide referrals to fistula clients for social and medical services and five sites provide reintegration services.
In FY 17/18, the Bangladesh Country Project Manager (CPM) took on additional duties within the project, and is now also serving as the FC+ Global Activities Manager (GAM). Objective 1: Strengthened enabling environment to institutionalize fistula prevention, treatment, and reintegration in the public and private sectors In January and February 2019, the USAID/Bangladesh Mission undertook an assessment of USAID-funded fistula prevention, treatment, repair, and rehabilitation activities in Bangladesh over the last 13 years to identify and prioritize the most relevant interventions to be implemented under its portfolio going forward. Strengths and challenges of the current project are being identified as well as opportunities for fistula programming beyond the life of the current project. The assessment team used a variety of data collection methods, including key informant and group interviews, focus groups, and a survey. Several visits to FC+ supported fistula care facilities took place throughout the country as well as visits to UNFPA Bangladesh, Save the Children, and the Directorate Generals of Health Services and of Family Planning.
In May 2019, the Directorate General of Health Services (DGHS) organized a launch workshop for the National Strategy for Obstetric Fistula (2017-2022), with support from USAID and UNFPA. The strategy provides guidelines for different levels of fistula care provided through various tiers of the health system. The strategy specifically supports the role of community clinics for prevention, care, referral, and rehabilitation of fistula clients. During the workshop, the Honorable State Minister for Health, Dr. Murad Hasan, reiterated the government’s commitment to end obstetric fistula by 2030.
As part of efforts to celebrate the International Day to End Obstetric Fistula (IDEOF), the University Fistula Center at BSMMU, in collaboration with FC+, organized a radio talk show on maternal health promotion and fistula prevention in May 2019. An estimated 600,000 people were reached through the community radio program (see Table BGD1).
Launch workshop for the National Strategy for Obstetric Fistula (2017-2022). Credit: N. Biswas.

Annual Report • October 2018 – September 2019 Fistula Care Plus 50
During FY 18/19, FC+/Bangladesh continued efforts to bring together the multiple actors providing fistula-related services in Bangladesh to share experiences, discuss challenges, and identify priorities for the future. During the second quarter, FC+/Bangladesh organized the second three-day National Annual Partners’ Forum with a theme of “Supporting Each Other for Enhancing Sustainability.” Participants included professional organizations, the Ministry of Health and Family Welfare, academic institutions, United Nations organizations, USAID/Bangladesh, fistula surgeons, gynecologists, obstetricians, public health experts, nurses, midwives, print and electronic media, and civil society representatives.
Topics covered included iatrogenic fistula and the rising numbers of cesarean sections, the role of international development agencies in setting up UFCs within Bangladesh, rehabilitation and reintegration efforts, South-South cooperation and opportunities to share experiences and successful strategies.
As part of the Partners’ Forum, the FC+/Bangladesh CPM/GAM moderated a workshop on the Robson classification system for cesarean section, with the goal of discussing its implementation in Bangladesh as well as its challenges. Dr. Beatrice Ambauen-Berger of LAMB Hospital presented on the question, “Is Caesarean Section Safer” and focused on global and national cesarean section rates and explanations for the particularly high rates in Bangladesh. She discussed complications of normal vaginal delivery and of cesarean sections and emphasized the need to follow proper indication for cesarean sections to reduce maternal and child mortality and morbidity. Ms. Stacy Saha of LAMB Hospital discussed the Robson classification in detail and how the implementation of this system in Bangladesh can play a significant role in reduction unnecessary cesarean section rates.
In March 2019, FC+ organized several meetings at Ad-Din Jashore to discuss the rehabilitation and reintegration of fistula clients in the Southwestern districts of Bangladesh. Representatives of the Ad-Din Foundation and BSMMU joined FC+ for this meeting and decided the following:
Community-based registry data will be cleaned and edited. Paramedics will provide additional information regarding the number of villages and population
covered by each union’s services. Fistula orientation program for paramedics rescheduled for end of March 2019. International Fistula Day will be celebrated on May 18, 2019 due to Ramadan, at BSMMU with
participation from FC+, Ad-Din Foundation and BSMMU.
As part of efforts to continue advocacy and policy discussion on services for women whose fistula are deemed incurable, FC+/Bangladesh supported a workshop hosted by SAGFORD and Mamm’s Institute of Fistula and Women’s Health on the topic, “Revisiting the Global Concept of Persistent Fistula Related Disorders in the Context of Bangladesh” in November 2018. The workshop covered a range of issues related to women whose fistula are deemed incurable and a panel discussion addressed the specific roles of different actors including anesthesiologists, obstetricians and gynecologists, urologists, pediatric surgeons and general surgeons. Workshop participants included the President and members of the Obstetrical and Gynecological Society of Bangladesh (OGSB), the Chief of the University Fistula Center (UFC) of Bangabandhu Sheikh Mujib Medical University (BSMMU), the President of the Urological Association of Bangladesh, the Director of Primary Health Care in the Directorate General of Health Services (DGHS), and the Asian representative to ISOFS. The purposes of the workshop were to consider the spectrum of care needed by women with persistent fistula related disorder in Bangladesh and to develop recommendations that professional associations, ministries of health, and other key institutions could use as a foundation for professional guidelines, standards, and protocols.

Annual Report • October 2018 – September 2019 Fistula Care Plus 51
The Workshop Consensus, entitled “Jashore Recommendations for Persistent Fistula Related Disorders” calls for the recognition that women with persistent fistula related disorder are individuals with the agency and ability to make informed decisions about their care. The goal of the recommendations was to ensure the best possible quality of life for women with persistent fistula-related disorders in the Bangladeshi context.
FC+ Bangladesh participated in a regionally-focused conference in October 2018: the 4th North East Frontier Zonal Conference on Preventive and Social Medicine in Agartala, India. The FC+/Bangladesh team presented on Fistula Programming Experience in Bangladesh, as well as partaking in a panel on Reflections of Best Practices for Prevention and Care of Fistula in Bangladesh. The FC+/Bangladesh CPM/GAM also took part in a panel on Adolescent Health and Pregnancy.
Globally, the FC+/Bangladesh CPM/GAM was the primary support to and liaison between the International Society of Obstetric Fistula Surgeons (ISOFS) and FC+. In November, he participated in an ISOFS coordination meeting to provide technical assistance to the local organizing committee’s efforts in their planning for the upcoming ISOFS Conference.
The 7th International ISOFS Conference was held in Kathmandu, Nepal on December 5-6, 2018 (see Section II, Objective 5 and Appendices H, I, and L). On December 4th, FC+/Bangladesh supported a side event, hosted by the South Asian Group on Fistula and Other Related Disorders (SAGFORD) and ISOFS, titled “An Evening on Kathmandu and Banjul Calls to Action.” This event was chaired by Professor Sayeba Akhter, the Asian Representative of ISOFS and Chair of the SAGFORD with participation from EngenderHealth and FC+ leadership. The event included 53 participants from different countries including past and present ISOFS leadership and prominent fistula surgeons. The FC+/Bangladesh CPM/GAM co-hosted the closing plenary presentation with current ISOFS President Professor Oladosu Ojengbede and incoming ISOFS President Dr. Shershah Syed, entitled “From Kathmandu, the way Forward: Ending Fistula on a Changing Path and Merging Boundaries.”
In collaboration with BSMMU, as part of ongoing efforts to engage and motivate journalists to cover the topic of fistula, FC+/Bangladesh organized orientations on the topic of female genital fistula prevention and treatment with several different groups. In October 2018, orientations were held in Khulna for rural journalists and female leaders. The 81 participants included lo cal journalists and members of the Health Reporters Forum, as well as local health officials. In April 2019, a workshop was held in Dhaka for 108 representatives from electronic and print media outlets. The workshop was co-hosted by both BSMMU and the Female Journalists Association.
In July 2019, FC+, BSMMU, and the Press Institute of Bangladesh co-organized an experience-sharing workshop around the theme of “Ending fistula in Bangladesh” for 60 electronic and print media journalists, as well as development partners. Speakers included Mr. Zafar Wazed, Director General of the Press Institute of Bangladesh; Joseph Monehin, Deputy Director, Health, Population and Education, USAID; Mr. Kazi Mohiul Hoque, Directorate General of Family Planning; Prof. Dr. Tripti Rani Das,
April 2019 press orientation on the prevention and treatment of female genital fistula. Credit: M. Rahman.
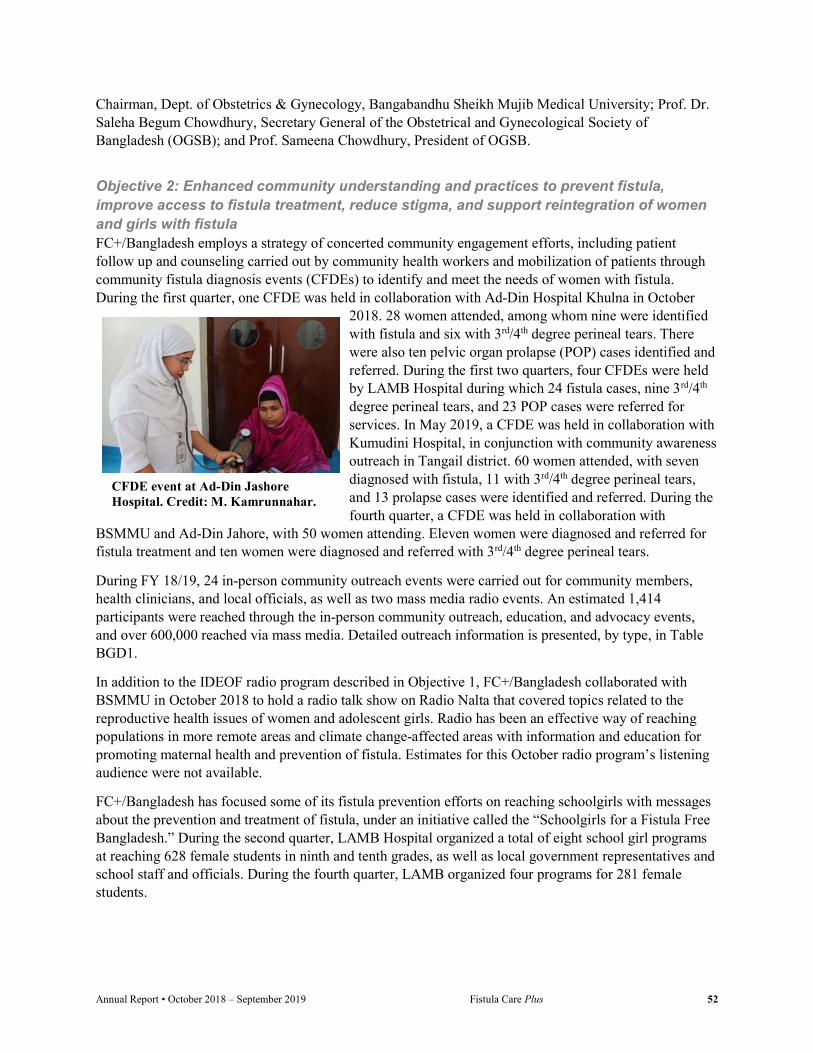
Annual Report • October 2018 – September 2019 Fistula Care Plus 52
Chairman, Dept. of Obstetrics & Gynecology, Bangabandhu Sheikh Mujib Medical University; Prof. Dr. Saleha Begum Chowdhury, Secretary General of the Obstetrical and Gynecological Society of Bangladesh (OGSB); and Prof. Sameena Chowdhury, President of OGSB.
Objective 2: Enhanced community understanding and practices to prevent fistula, improve access to fistula treatment, reduce stigma, and support reintegration of women and girls with fistula FC+/Bangladesh employs a strategy of concerted community engagement efforts, including patient follow up and counseling carried out by community health workers and mobilization of patients through community fistula diagnosis events (CFDEs) to identify and meet the needs of women with fistula. During the first quarter, one CFDE was held in collaboration with Ad-Din Hospital Khulna in October
2018. 28 women attended, among whom nine were identified with fistula and six with 3rd/4th degree perineal tears. There were also ten pelvic organ prolapse (POP) cases identified and referred. During the first two quarters, four CFDEs were held by LAMB Hospital during which 24 fistula cases, nine 3rd/4th degree perineal tears, and 23 POP cases were referred for services. In May 2019, a CFDE was held in collaboration with Kumudini Hospital, in conjunction with community awareness outreach in Tangail district. 60 women attended, with seven diagnosed with fistula, 11 with 3rd/4th degree perineal tears, and 13 prolapse cases were identified and referred. During the fourth quarter, a CFDE was held in collaboration with
BSMMU and Ad-Din Jahore, with 50 women attending. Eleven women were diagnosed and referred for fistula treatment and ten women were diagnosed and referred with 3rd/4th degree perineal tears.
During FY 18/19, 24 in-person community outreach events were carried out for community members, health clinicians, and local officials, as well as two mass media radio events. An estimated 1,414 participants were reached through the in-person community outreach, education, and advocacy events, and over 600,000 reached via mass media. Detailed outreach information is presented, by type, in Table BGD1.
In addition to the IDEOF radio program described in Objective 1, FC+/Bangladesh collaborated with BSMMU in October 2018 to hold a radio talk show on Radio Nalta that covered topics related to the reproductive health issues of women and adolescent girls. Radio has been an effective way of reaching populations in more remote areas and climate change-affected areas with information and education for promoting maternal health and prevention of fistula. Estimates for this October radio program’s listening audience were not available.
FC+/Bangladesh has focused some of its fistula prevention efforts on reaching schoolgirls with messages about the prevention and treatment of fistula, under an initiative called the “Schoolgirls for a Fistula Free Bangladesh.” During the second quarter, LAMB Hospital organized a total of eight school girl programs at reaching 628 female students in ninth and tenth grades, as well as local government representatives and school staff and officials. During the fourth quarter, LAMB organized four programs for 281 female students.
CFDE event at Ad-Din Jashore Hospital. Credit: M. Kamrunnahar.
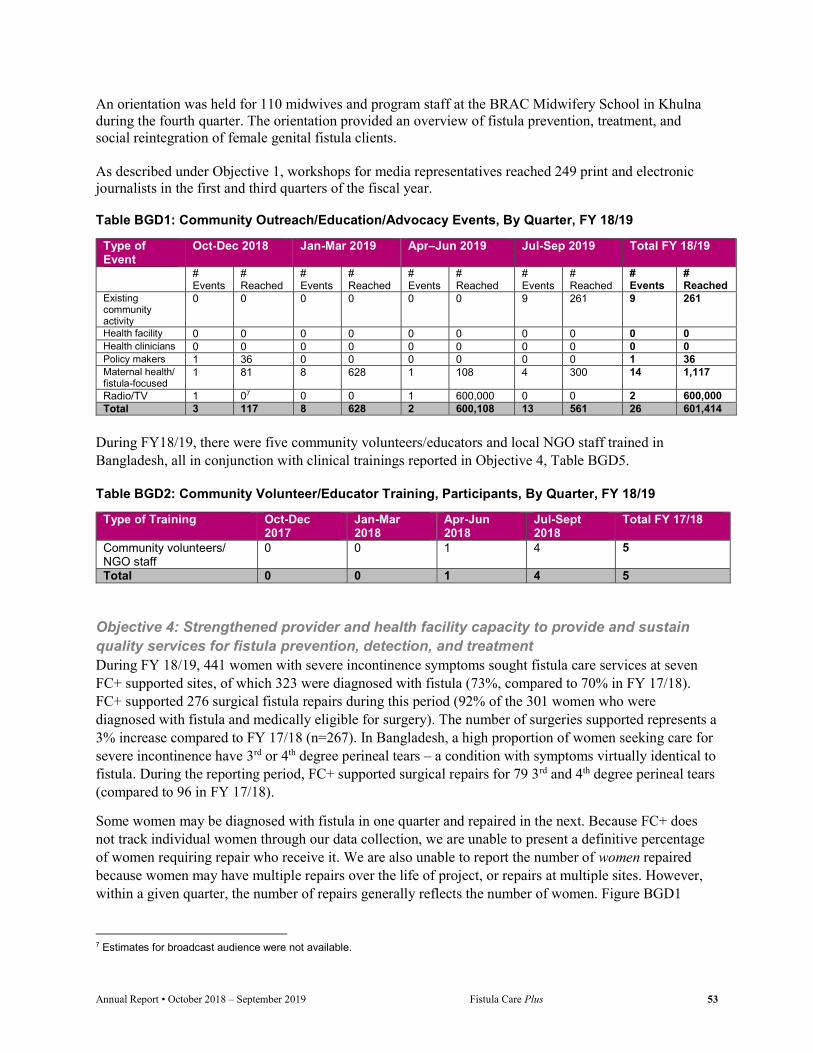
Annual Report • October 2018 – September 2019 Fistula Care Plus 53
An orientation was held for 110 midwives and program staff at the BRAC Midwifery School in Khulna during the fourth quarter. The orientation provided an overview of fistula prevention, treatment, and social reintegration of female genital fistula clients. As described under Objective 1, workshops for media representatives reached 249 print and electronic journalists in the first and third quarters of the fiscal year.
Table BGD1: Community Outreach/Education/Advocacy Events, By Quarter, FY 18/19
Type of Event
Oct-Dec 2018 Jan-Mar 2019 Apr–Jun 2019 Jul-Sep 2019 Total FY 18/19
# Events
# Reached
# Events
# Reached
# Events
# Reached
# Events
# Reached
# Events
# Reached
Existing community activity
0 0 0 0 0 0 9 261 9 261
Health facility 0 0 0 0 0 0 0 0 0 0 Health clinicians 0 0 0 0 0 0 0 0 0 0 Policy makers 1 36 0 0 0 0 0 0 1 36 Maternal health/ fistula-focused
1 81 8 628 1 108 4 300 14 1,117
Radio/TV 1 07 0 0 1 600,000 0 0 2 600,000 Total 3 117 8 628 2 600,108 13 561 26 601,414
During FY18/19, there were five community volunteers/educators and local NGO staff trained in Bangladesh, all in conjunction with clinical trainings reported in Objective 4, Table BGD5.
Table BGD2: Community Volunteer/Educator Training, Participants, By Quarter, FY 18/19
Type of Training Oct-Dec 2017
Jan-Mar 2018
Apr-Jun 2018
Jul-Sept 2018
Total FY 17/18
Community volunteers/ NGO staff
0 0 1 4 5
Total 0 0 1 4 5
Objective 4: Strengthened provider and health facility capacity to provide and sustain quality services for fistula prevention, detection, and treatment During FY 18/19, 441 women with severe incontinence symptoms sought fistula care services at seven FC+ supported sites, of which 323 were diagnosed with fistula (73%, compared to 70% in FY 17/18). FC+ supported 276 surgical fistula repairs during this period (92% of the 301 women who were diagnosed with fistula and medically eligible for surgery). The number of surgeries supported represents a 3% increase compared to FY 17/18 (n=267). In Bangladesh, a high proportion of women seeking care for severe incontinence have 3rd or 4th degree perineal tears – a condition with symptoms virtually identical to fistula. During the reporting period, FC+ supported surgical repairs for 79 3rd and 4th degree perineal tears (compared to 96 in FY 17/18).
Some women may be diagnosed with fistula in one quarter and repaired in the next. Because FC+ does not track individual women through our data collection, we are unable to present a definitive percentage of women requiring repair who receive it. We are also unable to report the number of women repaired because women may have multiple repairs over the life of project, or repairs at multiple sites. However, within a given quarter, the number of repairs generally reflects the number of women. Figure BGD1
7 Estimates for broadcast audience were not available.

Annual Report • October 2018 – September 2019 Fistula Care Plus 54
presents data on women seeking and eligible for fistula treatment, and the number of fistula surgeries supported, by site.
Figure BGD1: Number of Women Seeking and Requiring Fistula Treatment, and Number of Surgical Repairs, by Site, FY 18/19
These 276 fistula repair surgeries were conducted at six FC+ supported hospitals: Ad-Din Dhaka, BSMMU, Dr. Muttalib Community Hospital, Kumudini, LAMB, and Mamm’s Institute of Fistula and Women’s Health (see Table BGD3 for detail by quarter). LAMB Hospital conducted concentrated repair efforts in during all four quarters of the fiscal year, during which 48 fistula cases and 16 3rd/4th degree perineal tear cases were repaired. Repairs performed at the concentrated effort carried out in the fourth quarter were not directly supported by FC+ and are not counted in the quarterly totals reported for LAMB. FC+ supported only the travel expenses for the surgeons due to limited funds.
Table BGD3: USAID-Supported Surgical Fistula Repairs, by Site, FY 18/19
Site Oct-Dec 2018
Jan-Mar 2019
Apr–Jun 2019
Jul-Sep 2019
Total FY 18/19
Ad-Din Dhaka 3 8 6 2 19 BSMMU 11 7 6 4 28 Dr. Muttalib 3 2 6 2 13 Kumudini 5 8 4 4 21 LAMB 20 43 43 0 106 Mamm’s Institute 21 21 23 24 89 Total 63 89 88 36 276
Etiology data was available for 99% of the 323 diagnosed fistula cases. Just over half of fistulas diagnosed were the result of prolonged/obstructed labor (54%), followed by iatrogenic causes (40%). 2% of diagnosed fistula were the result of trauma and the remaining “other” etiology (4%) was primarily congenital and cancer. The proportion of fistula deemed iatrogenic continues to be very high in Bangladesh, consistently higher than other countries where FC+ supports fistula repair. The proportion was high at all supported sites, with variation: from a low of 12.5% at Kumudini to highs of 62% at Dr. Muttalib, 54% at BSMMU, and 47% at Ad-Din Dhaka.
Discharged fistula repairs in FY 18/19 were more often classified as not simple cases (74%), with only 19% classified as simple (7% of cases did not have this data reported). 91.6% of all fistula surgery cases discharged in this time period were closed at discharge (compared with 89% in FY 17/18); with 89.6%
0
20
40
60
80
100
120
140
Ad-DinDhaka
Ad-DinKhulna
BSMMU Dr. Muttalib Kumudini LAMB Mamm'sInstitute
Seeking
Eligible
Repairs
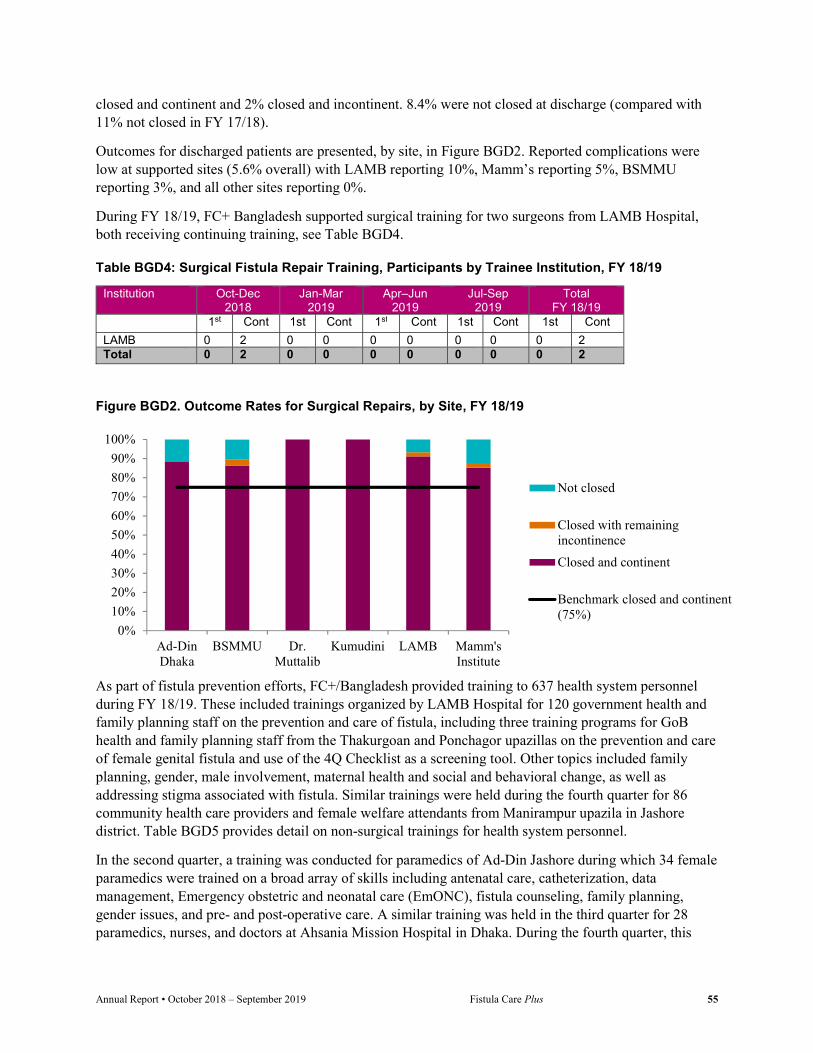
Annual Report • October 2018 – September 2019 Fistula Care Plus 55
closed and continent and 2% closed and incontinent. 8.4% were not closed at discharge (compared with 11% not closed in FY 17/18).
Outcomes for discharged patients are presented, by site, in Figure BGD2. Reported complications were low at supported sites (5.6% overall) with LAMB reporting 10%, Mamm’s reporting 5%, BSMMU reporting 3%, and all other sites reporting 0%.
During FY 18/19, FC+ Bangladesh supported surgical training for two surgeons from LAMB Hospital, both receiving continuing training, see Table BGD4.
Table BGD4: Surgical Fistula Repair Training, Participants by Trainee Institution, FY 18/19
Institution Oct-Dec 2018
Jan-Mar 2019
Apr–Jun 2019
Jul-Sep 2019
Total FY 18/19
1st Cont 1st Cont 1st Cont 1st Cont 1st Cont
LAMB 0 2 0 0 0 0 0 0 0 2 Total 0 2 0 0 0 0 0 0 0 2
Figure BGD2. Outcome Rates for Surgical Repairs, by Site, FY 18/19
As part of fistula prevention efforts, FC+/Bangladesh provided training to 637 health system personnel during FY 18/19. These included trainings organized by LAMB Hospital for 120 government health and family planning staff on the prevention and care of fistula, including three training programs for GoB health and family planning staff from the Thakurgoan and Ponchagor upazillas on the prevention and care of female genital fistula and use of the 4Q Checklist as a screening tool. Other topics included family planning, gender, male involvement, maternal health and social and behavioral change, as well as addressing stigma associated with fistula. Similar trainings were held during the fourth quarter for 86 community health care providers and female welfare attendants from Manirampur upazila in Jashore district. Table BGD5 provides detail on non-surgical trainings for health system personnel.
In the second quarter, a training was conducted for paramedics of Ad-Din Jashore during which 34 female paramedics were trained on a broad array of skills including antenatal care, catheterization, data management, Emergency obstetric and neonatal care (EmONC), fistula counseling, family planning, gender issues, and pre- and post-operative care. A similar training was held in the third quarter for 28 paramedics, nurses, and doctors at Ahsania Mission Hospital in Dhaka. During the fourth quarter, this
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Ad-DinDhaka
BSMMU Dr.Muttalib
Kumudini LAMB Mamm'sInstitute
Not closed
Closed with remainingincontinence
Closed and continent
Benchmark closed and continent(75%)

Annual Report • October 2018 – September 2019 Fistula Care Plus 56
training was held for 47 paramedics at Ad-Din Jashore and 82 paramedics, doctors, and program staff from Gono Shastho Kendro in Cox’s Bazaar and Charfashion in Bhola..
During the fourth quarter, LAMB and Kumudini Hospitals organized two training programs on the prevention and care of female genital fistula for 87 government health and family planning staff from community clinics and the upazila health complexes of Parbatipur and Mirzapur districts. Also in the fourth quarter, four trainings for doctors, nurses, and community health care providers were held in Gono Sasthya Kendra; Mirzapur, Tangail; and Ad-din Jashore, during which 153 clinicians were trained on topics including antenatal care, catheterization, EmONC, family planning, and fistula pre- and post-operative care. Table BGD5: Non-Surgical Health System Personnel Training, Participants by Topic, FY 18/19
Topic Oct-Dec 2018
Jan-Mar 2019
Apr–Jun 2019
Jul-Sep 2019
Total FY 18/19
Fistula orientation, Pre- and post-operative care 0 154 28 455 637 Total 0 154 28 455 642
FC+ supports FP counseling and service provision at most supported sites in Bangladesh. During FY 18/19, 33,363 counseling sessions took place at supported sites and 16,653 CYP were provided; see Table BGD6 for detail, by site. Method mix in Bangladesh during this fiscal year was primarily comprised of tubal ligation (71% of CYP), oral contraceptives (10%), Implanon (7%), and Depo (6%).
Table BGD6: Family Planning Counseling Sessions and CYP, by Site, By Quarter, FY 18/19
Site Oct-Dec 2018 Jan-Mar 2019 Apr–Jun 2019 Jul-Sep 2019 Total FY 18/19 #sessions CYP #sessions CYP #sessions CYP #sessions CYP #sessions CYP8 Ad-Din Dhaka
3,585 2,376 4,400 2,322 4,300 2,026 5,000 2,836 17,285 9,560
Ad-Din Khulna
1,047 510 723 429 1,157 535 1,265 591 4,192 2,065
Kumudini 1,435 868 2,408 856 1,150 708 2,300 673 7,293 3,106 LAMB 1,134 588 2,100 764 1,359 572 NA9 NA 4,593 1,923 Total 7,201 4,314 9,631 4,371 7,966 3,841 8,565 4,100 33,363 16,653
FC+ supported sites reported 30,385 total obstetric deliveries with an overall cesarean section rate of 69.3% during the fiscal year. Information on number of deliveries, by site, is represented in Figure BGD3 and cesarean section rates, by site, are presented in Figure BGD4.
Six FC+ supported facilities report current use of catheterization as a prevention intervention following prolonged/obstructed labor. Due to record keeping at the facilities, it is difficult to collect accurate data on the number of prolonged and obstructed labors.
8 Due to rounding, totals may differ slightly from the sum of individual quarters. 9 Due to funding issues, support to LAMB in the fourth quarter was discontinued as the project approaches close out in Bangladesh.
Fistula orientation training at Ahsania Mission Hospital. Credit: I. Jahan.

Annual Report • October 2018 – September 2019 Fistula Care Plus 57
Obj. 5: Strengthened evidence base for approaches to improve fistula care and scaled up application of standard monitoring and evaluation (M&E) indicators for prevention and treatment Each quarter, the FC+/Bangladesh team conducts data quality assurance visits to supported facilities, as well as prepares internal data-for-decision making summaries that are shared and discussed with each supported facility.
In August 2019, FC+ published a technical brief describing its 4Q Checklist for fistula screening and referral, and noting the utility of this approach for improving information at the local level about fistula burden, essential for targeting of outreach and planning of services (https://fistulacare.org/wp-fcp/wp-content/uploads/2019/11/FCPlus_4Q-checklist_v3.pdf).
Figure BGD3. Number of Obstetric Deliveries, by Site, FY 18/19 (n=30,385)
Figure BGD4. Cesarean Section Rates, by Site, FY 18/19
72.3
74.3
83
83.1
61.8
21.1
0% 100%
Ad-din Dhaka
Ad-Din Khulna
BSSMU
Dr. Muttalib
Kumudini
LAMB
Vaginal delivery C-Section
15,461
6,431
2,085
249
4,549
1,610
Ad-din Dhaka
Ad-Din Khulna
BSMMU
Dr. Muttalib
Kumudini
LAMB
Annual Report • October 2018 – September 2019 Fistula Care Plus 58
Democratic Republic of Congo USAID-supported fistula services in DRC began in 2008 through the previous FC project and continued through FC+ in FY 18/19 in four hospitals: HEAL Africa, Panzi Hospital, Saint Joseph Hospital (SJH) and Beniker Hospital.
Support to Beniker was suspended following concerns about the site’s capacity to maintain adequate clinical quality and ensure appropriate financial oversight. The site will be assessed again in FY 19/20 and support will only be renewed if the site’s capacity is deemed appropriate. Support has ended to two previously supported sites, MSRK and IGL. USAID has also provided bilateral support to the Project de Santé Integré (ProSani) for fistula repair at Kaziba General Reference Hospital in DRC. ProSani ended in the previous fiscal year and has been followed by a comprehensive integrated health project that has not yet begun to provide fistula services.
In DRC, FC+ has partnered with health centers and hospitals to support fistula repairs, train doctors and nurses in fistula-related skills and topics, improve EmONC, and conduct outreach to rural clinics to ensure that women in need of medical attention are referred to the hospitals for repair.
Throughout the life of the project, the city of Beni and its surroundings have remained subject to insecurity due to violence in the area. This permanent instability and insecurity causes frequent displacements of the population. Elections at the end of the previous fiscal year accentuated tensions and the Ebola epidemic in the province of North Kivu and the Ecuador region has constrained travel and government resources.
Programmatic activities in the first two quarters of FY18/19 were significantly impacted by severely delayed obligations and a required ‘pause’ in activity in January and part of February 2019 due to USG deliberations regarding DRC status. A de-scoping process related to the provisions of the Trafficking Victims Protection Act took place beginning in January 2019, through the leadership of USAID/Washington. Support is no longer provided to DRC government entities or activities. Program activities were suspended during the de-scoping period (the second, third, and fourth quarters of FY 18/19), with activities resuming at the very end of the fiscal year. Activities reported below involving direct support to government entities are only from the period before this pause and de-scoping process began. Objective 1: Strengthened enabling environment to institutionalize fistula prevention, treatment, and reintegration in the public and private sectors During the first quarter of FY 18/19, FC+/DRC participated in the Santé de la Mère, du Nouveau né et de L‘Enfant – Maternal, Newborn and Infant Health Task Force (SMNE Task Force) along with experts from the MOH and professionals working in the field of maternal, neonatal, and child health (MNCH) and fistula. The Task Force has provided a platform for reflection, designing standards and guidelines, and monitoring activities and progress. FC+/DRC has previously worked with UNFPA to spearhead efforts to create a National Multidisciplinary Working Group for the Elimination of Obstetric Fistula within the Task Force.
The National Strategy for the Elimination of Obstetric Fistula has been published and printed. However, its official presentation and distribution is still pending because of health emergencies in the eastern region of the country.
During the first quarter, FC+/DRC supported the Ministry of Health in training on the norms and guidelines of Maternal, Newborn, Child and Adolescent Health (SRMNEA) in Lubumbashi at Beniker Hospital. This followed trainings that occurred in the previous fiscal year for supported sites in the eastern

Annual Report • October 2018 – September 2019 Fistula Care Plus 59
part of the country (HEAL Africa, HGR Panzi and clinicians from surrounding structures) and for SJH and six other faith-based and public sector facilities. At the conclusion of the briefing, 100 kits of the SRMNEA standards and guidelines were distributed to the facilities and the Provincial Divisions of Health.
FC+/DRC supported facilities have leveraged support from several other sources for fistula-related activities. Panzi continues its partnership with the radio station SVEN to support awareness raising in the community and during certain outreach. SJH, in partnership with the Ministry of Gender, Family and Children organized a National Campaign for the repair of obstetric fistula with funding from the Vodacom/DRC Foundation and UNFPA. This campaign, held during the first quarter of the fiscal year, operated on 65 clients suffering from fistula. The Christoffel Blind Mission (CBM) DRC, a German organization, provided funding for community outreach activities, including community meetings and television spots, as well as the payment of fees for special imaging and laboratory examinations.
Objective 2: Enhanced community understanding and practices to prevent fistula, improve access to fistula treatment, reduce stigma, and support reintegration of women and girls with fistula During the first quarter of FY 18/19, two supported fistula treatment sites conducted awareness raising campaigns in their communities to improve knowledge about fistula, access to treatment, male involvement, FP, and the fight against stigma (HEAL Africa and SJH). FC+ supported sites in DRC carried out three in-person community outreach efforts reaching 110 people, see Table DRC1.
FC+ DRC partners HEAL Africa and Hospital St. Joseph conducted community mobilization activities in Goma and nearby territories as well as Kinshasa, convening structured dialogues among community members, religious leaders, and students. These events brought together 110 people from NGOs, local governance, churches, schools, and community volunteers. These community dialogues included extensive participatory discussion of how men contribute to the health risks faced by women and how male involvement can ameliorate these risks. Facilitators discussed male decision making in women’s health care seeking and access, lack of communication between partners, and male opposition to partners’ FP use. Community members described obstacles to male involvement including traditional values that discourage men engaging in maternal health issues, men’s lack of knowledge of maternal health and women’s non-communication about their health problems, male discomfort in settings seen as “women’s environments,” male fear of side effects related to modern contraceptive methods, and health service settings that discourage men’s presence.
After a discussion of these issues, community members identified the consequences of male non-involvement in maternal health, including fistula, prolapse, unwanted pregnancy, abortion, and maternal and newborn death. The dialogues generated ideas about behavior change among both men and women that could improve maternal health and prevent these adverse outcomes.
There were no community volunteer/educator trainings in DRC during FY 18/19.
Table DRC1: Community Outreach/Education/Advocacy Events, By Quarter, FY 181/19
Type of Event Oct-Dec 2018 Jan-Mar 2019 Apr–Jun 2019 Jul-Sep 2019 Total FY 18/19 #
Events # Reached
# Events
# Reached
# Events
# Reached
# Events
# Reached
# Events
# Reached
Existing community activity
0 0 0 0 0 0 0 0 0 0

Annual Report • October 2018 – September 2019 Fistula Care Plus 60
Type of Event Oct-Dec 2018 Jan-Mar 2019 Apr–Jun 2019 Jul-Sep 2019 Total FY 18/19 Health facility 0 0 0 0 0 0 0 0 0 0 Health clinicians
0 0 0 0 0 0 0 0 0 0
Policy makers 0 0 0 0 0 0 0 0 0 0 Maternal health/ fistula-focused
3 110 0 0 0 0 0 0 3 110
Radio/TV 0 0 0 0 0 0 0 0 0 0 Total -in person -mass media
3 0
110 0
0 0
0 0
0 0
0 0
0 0
0 0
3 0
110 0
Objective 4: Strengthened provider and health facility capacity to provide and sustain quality services for fistula prevention, detection, and treatment
FC+/DRC carried out clinical monitoring visits at all four supported facilities in the first quarter, in addition to financial administration follow-up visits and capacity building efforts. The clinical monitoring visit to Beniker Polyclinic in Lubumbashi was followed by dissemination of the SMNEA guidelines by the MOH and a briefing on their use. During the fourth quarter, clinical monitoring was repeated during which medical waste management and partograph monitoring was carried out at supported sites.
As noted, programmatic activity during the reporting period was significantly reduced due to financial and political challenges, as well as the de-scoping process associated with Trafficking Victims Protection Act provisions. During the first two quarters of FY 18/19, 214 women with severe incontinence symptoms arrived seeking fistula care at FC+ supported sites, of which 189 were diagnosed with fistula (88%). Of these diagnosed cases, 182 were medically eligible for surgical repair (96%). FC+ supported 158 fistula repair surgeries during this period (87% of those eligible). During the third and fourth quarters, supported sites continued to provide fistula repairs with support from the Fistula Foundation and UNFPA.
Some women may be diagnosed with fistula in one quarter, and repaired in the next. Because FC+ does not track individual women through our data collection, we are unable to present a definitive percentage of women requiring repair who receive it. We are also unable to report the number of women repaired because women may have multiple repairs over the life of project, or repairs at multiple sites. However, within a given quarter, the number of repairs generally reflects the number of women. Figure DRC1 presents data on women seeking and requiring fistula treatment, and the number of fistula surgeries supported, by site.
Construction of a new cured brick incinerator at HEAL Africa. Credit: M. Mpunga.

Annual Report • October 2018 – September 2019 Fistula Care Plus 61
Figure DRC1: Number of Women Seeking and Eligible for Fistula Treatment, and Number of Surgical Repairs, by Site, FY 18/19
These 158 fistula repair surgeries were conducted at four FC+ supported hospitals: Beniker, HEAL Africa, Panzi, and SJH, see Table DRC2 for detail by quarter. 131 of these repairs (83%) were provided via routine service provision, with 27 repairs (17%) carried out via outreach efforts. During this period, SJH performed repairs via both routine services and outreach efforts, Beniker and HEAL provided only routine repairs and Panzi provided only outreach repairs. In addition to the surgical repairs reported here, two women received non-surgical catheter treatment for fistula at HEAL Africa and were not closed at discharge.
Information on the etiology of diagnosed fistula was available for all diagnosed cases (189, 100%). Of those cases, 69% were identified as being caused by obstructed or prolonged labor; 29% identified as iatrogenic in nature; and 2% due to cervical cancer.
Table DRC2: USAID-Supported Surgical Fistula Repairs, by Site, By Quarter, FY 18/19
Site Oct-Dec 2018
Jan-Mar 2019
Apr–Jun 2019
Jul-Sep 2019
Total FY 18/19
Beniker 9 64 0 0 73 HEAL Africa 15 19 0 0 34 Panzi 0 18 0 0 18 SJH 27 6 0 0 33 FC+ Total 51 107 0 0 158
A total of 152 fistula cases were discharged during the first two quarters of FY 18/19. 49% (n=74) were classified as simple fistula and 51% (n=78) as not simple. 96.1% of all discharged fistula surgery cases were closed at time of discharge: 92.8% were closed and continent and 3.3% were closed and incontinent. Outcomes for discharged patients are presented, by site, in Figure DRC2.
There were no reported complications at supported sites during the reporting period.
0
10
20
30
40
50
60
70
80
90
100
Beniker HEAL Africa Panzi SJH
Seeking
Eligible
Repairs

Annual Report • October 2018 – September 2019 Fistula Care Plus 62
Figure DRC2. Outcome Rates for Surgical Repairs, by Site, October 2018 – March 2019
During the first two quarters of FY 18/19, three supported sites (HEAL, Panzi, and SJH) reported providing POP treatment to 237 women. The sites reported 237 surgical POP treatments and 442 non-surgical treatments. SJH has developed a client card and a protocol for surgical practice for the care of women with POP.
There were no surgical repair trainings carried out in DRC during FY 18/19.
As part of fistula prevention and treatment efforts, FC+/DRC provided training to 16 health care clinicians and facility staff at Beniker on the new SMNEA guidelines, described under Objective 1, during the first quarter of FY 18/19; see Table DRC3.
Table DRC3: Non-Surgical Health System Personnel Training, Participants by Topic, By Quarter, FY 18/19
Topic Oct-Dec 2018
Jan-Mar 2019
Apr–Jun 2019
Jul-Sep 2019
Total FY 18/19
EmONC and labor monitoring 16 0 0 0 16 Total 16 0 0 0 16
In the first two quarters of FY 18/19, FC+/DRC continued support to ensure that FP services are provided and integrated with fistula service provision at supported sites. FP activities have been integrated into all supported sites, including SJH which is a Catholic facility. During the first half of FY 18/19, over 1,200 counseling sessions took place at these supported sites and 2,058 CYP were provided (see Table DRC4 for detail, by site). Family planning data was not collected from supported sites during the period of activity suspension in the third and fourth quarters.
Table DRC4: Family Planning Counseling Sessions and CYP, by Site, By Quarter, FY 18/19
Site Oct-Dec 2018 Jan-Mar 2019 Apr–Jun 2019 Jul-Sep 2019 Total FY 18/19 #sessions CYP #sessions CYP #sessions CYP #sessions CYP #sessions CYP10 Beniker 0 0 45 41 - - - - 45 41 HEAL Africa
39 384 26 311 - - - - 65 696
Panzi 318 432 331 639 - - - - 649 1,070 SJH 247 106 207 145 - - - - 454 251 Total 604 922 609 1,136 - - - - 1,213 2,058
FC+/DRC supported sites reported an overall cesarean section rate of 37% in the first two quarters of FY 18/19, with a total of 3,414 deliveries. Information on number of deliveries, by site, is presented in Figure
10 Due to rounding, totals may differ slightly from the sum of individual quarters.
0%
20%
40%
60%
80%
100%Not closed
Closed with remainingincontinenceClosed and continent

Annual Report • October 2018 – September 2019 Fistula Care Plus 63
DRC3 and cesarean section rates, by site, are presented in Figure DRC4. Just over 1% of reported deliveries were prolonged/obstructed labor and of those, 13% received catheterization for fistula prevention. Obstetric data was not collected from supported sites during the period of activity suspension in the third and fourth quarters.
Figure DRC3. Number of Obstetric Deliveries, by Site, FY 18/19 (n=3,414)
Figure DRC4. Cesarean Section Rates, by Site, FY 18/19
Obj. 5: Strengthened evidence base for approaches to improve fistula care and scaled up application of standard monitoring and evaluation (M&E) indicators for prevention and treatment FC+/DRC participated in the FIGO World Congress held in Rio De Janeiro, Brazil in October 2018, contributing three presentations to the conference (see Appendix G). FC+/DRC also made four presentations and presented two posters at the ISOFS Conference in Kathmandu, Nepal in December 2018 (see Appendix H). The project sponsored attendance of six people from FC+/DRC and supported facilities at the two conferences: three to FIGO and three to ISOFS.
57
68.5
60.6
43
31.5
39.4
0% 100%
HEAL Africa
Panzi
SJH
Vaginal delivery C-Section
894
1,614
906
HEAL Africa
Panzi
SJH

Annual Report • October 2018 – September 2019 Fistula Care Plus 64
Mozambique FC+ activity in Mozambique began in December 2017 and is supported through a subaward with the Mozambique-based organization Focus Fistula. The goal of this sub-award is to strengthen the clinical capacity of selected ministry and private health facilities and staff to provide accessible, quality obstetric, iatrogenic, and traumatic fistula surgical and non-surgical treatment services in Mozambique. Due to a delay in initial funding of the newly established sub-award in April 2019, Focus Fistula was not able to complete any surgical campaigns during the third quarter of FY 18/19. The new sub agreement was fully executed by both parties on April 24 and the funds made available on May 9, 2019.
During FY18/19, FC+ and Focus Fistula continued efforts to establish effective communication, financial reporting, and routine monitoring and evaluation systems. Concentrated repair efforts took place at Hospital Central Maputo and Nampula Central Hospital during the first quarter, Inhambane District Hospital during the second quarter, and Lichinga Provincial Hospital during the fourth quarter.
On March 18, 2019, Focus Fistula Mozambique (FFM) received a visit from the local USAID Mozambique Mission including USAID Program Management Specialists Ms. Denise Calado and Raquel Zaqueu and Agreement Officer Mr. Robin Mardeusz. The entire FFM staff was present, as well as a founding member of FFM, Mrs. Marylene Spezzati, and the FC+ Global Activities Manager. The meeting was an opportunity to share information on FFM’s activity thus far and establish linkages with the mission. Discussions also covered future expectations regarding USAID’s implementation of obstetric fistula activities in Mozambique and FFM’s plans to develop internal organizational capacity.
Objective 1: Strengthened enabling environment to institutionalize fistula prevention, treatment, and reintegration in the public and private sectors Focus Fistula is in discussions with the Mozambique Ministério da Saúde (MISAU – Ministry of Health) and UNFPA to develop a national strategy for the prevention, treatment, and reintegration of women with fistula. Through negotiations, MISAU has agreed that Focus Fistula will be able to work with public health units, provincial health directorates, and medical and paramedical staff, as well as have access to housing, infection prevention and waste management resources. MISAU and Focus Fistula will also work together on the transport of patients to and from treatment facilities. UNFPA will provide disposable supplies to concentrated fistula repair efforts and seek out consultation from Focus Fistula on the national fistula program.
A Memorandum of Understanding was drafted between MISAU and Focus Fistula to lay out terms of collaboration including agreements regarding use of public hospitals and cost shares on activities. The ministry has expressed an interest that Focus Fistula focus on repair of complex cases, while surgical technicians repair simple cases under Dr. Vaz’s supervision. This may impact the number of cases that are repaired by Focus Fistula, as complex cases require more time and will be fewer in number. The MOU continues to be under review with the ministry.
Focus Fistula Mozambique is currently creating a position for a focal point and coordinator of operated patients in coordination with UNFPA and MISAU in order to record the new cases operated and the postoperative follow-up needs.
Representative from the Ministry of Health addressing participants at International Day to End Obstetric Fistula event on May 23, 2019. Credit: Anicha.

Annual Report • October 2018 – September 2019 Fistula Care Plus 65
On November 12-13, 2018, Focus Fistula participated in the National Obstetric Fistula Workshop held in Maputo. The workshop looked back at achievement to date and forward towards the future of obstetric fistula efforts in Mozambique. There were 79 participants with attendees from throughout Mozambique’s district and provincial levels. Representatives of various Mozambique governmental ministries participated in the workshop including the Minister of Health as well as representatives of the Ministries of Gender, Children, Social Action and Justice, and Religious Affairs. The United Nations and various non-governmental organizations (NGOs) were also represented, as well as skilled fistula surgeons and professors from the region. Participants also included obstetricians/gynecologists, urologists, general surgeons, and obstetric nurses.
Topics covered during the workshop included: use of the partograph for fistula prevention; use of catheterization during labor; review of abdominal and pelvic anatomy in term women; regular prenatal checkup for risk evaluation and reduction with maternal child health department; family planning provision and logistics; overview of the current fistula landscape in Mozambique; development of a National Obstetric Fistula Implementation Strategy; obstetric fistula advocacy; social reintegration of obstetric fistula patients; organization of obstetric fistula treatment campaigns; FIGO conference recommendations; and best practices for fistula care.
Following this workshop, the Urology Maputo Congress (UROMAP) was held on November 15-16, 2018 in Maputo. The Congress brought together physicians from Portuguese-speaking (Lusophone) countries including Mozambique, Portugal, Angola, Guinea Bissau, and Nigeria. This year’s theme was “Improving Women’s Health” and topics covered included urology challenges in member states, the relationship between urology and gynecology, and common challenges experienced in both urology and gynecology.
Focus Fistula’s Dr. Igor Vaz and UNFPA’s Mozambique representative Andrea Wojnar opened the Congress. They shared information on the national deficit of medical specialists in Mozambique where there are less than 50 countrywide and only six urological specialists, two of whom graduated in November 2018. The urology department at Maputo Central Hospital alone registers more than two thousand cases seeking specialized attention annually, with increasing demand in the country.
On the second day of the Congress, participants had the opportunity to take part in a live session at the Central Hospital of Maputo on surgical approaches to complex obstetric fistula. Surgery was performed by Prof. Dr. Igor Vaz, assisted by Dr. Diamantino Perreira, a gynecologist from Angola, and Dr. Malamu Sasali, a general surgeon from Guinea Bissau. Dr. Vaz also provided instruction on how to physically classify fistulas and how to surgically approach them based on their complexities. Next years’ UroMAP Congress is planned for June 2019 in Maputo.
As part of international celebrations to commemorate the International Day to End Obstetric Fistula (IDEOF) on May 23, 2019, Focus Fistula partnered with a local bank in Maputo to hold an event for the general community, civil society organizations, governmental institutions, and local businessmen. The 77 participants included the National Director of Medical Assistance, on behalf of the Health Minister, who spoke about the importance of clinical training for fistula prevention. Focus Fistula’s Dr. Igor Vaz also spoke at the event, addressing topics including the prevention and treatment of obstetric fistula, the

Annual Report • October 2018 – September 2019 Fistula Care Plus 66
importance of prenatal consultations and family planning, the factors of early marriage, poverty and education in fistula, weaknesses of the national health system and difficulties operationalizing surgical missions due to high cost, especially for complex fistula cases and women who have fistula deemed
incurable. Two women who had received fistula surgeries told their stories and provided encouragement for those attending to get involved in support for fistula treatment and prevention.
Focus Fistula’s Dr. Igor Vaz attended the International Consultation on the Regional Strategy for Obstetric Fistula Elimination in West and Central Africa held June 19-21, 2019 in Saly Portugal, Senegal. The Consultation was sponsored by regional partners including Fistula Care
Plus/EngenderHealth, the West African Health Organization (WAHO), UNFPA, and URODAK. The overall objective of the consultation was to share the approved Banjul Call to Action resolution, signed and adopted by the health ministers of 15 members of the ECOWAS region. The operationalization of the resolution will be done in partnership with academic institutions, professional associations and NGOs for identification and referral of cases, surgical and non-surgical treatment, reintegration and rehabilitation of women with fistula in the region.
Dr. Vaz also participated in the Indonesia Genitourinary Reconstructive Society (InaGURS) meeting held in Bali, Indonesia in September 2019, in conjunction with 12th Malang Continuing Urology Education.
MISAU, in coordination with Dr. Vaz, Prof. Serigne Gueye, and UNFPA, participated in an evaluation mission to Mocuba, Zambezia Province in July 2019 to assess the feasibility of implementing a fistula surgical training program for health technicians. Training courses are under development and are expected to be implemented in the first quarter of FY 19/20. This activity is not funded by FC+.
Focus Fistula is working with Direct Relief International to facilitate deliveries of materials and medicines. Focus Fistula and Direct Relief International assisted with Cyclone Idai relief efforts at the end of March 2019 by redirecting their donation of 150 dignity kits from their original shipment to facilities in Beira treating those affected by the cyclone. The dignity kits provide materials for patient hygiene and health and food supplies. Direct Relief International subsequently shipped additional dignity kits to Focus Fistula who was able to deliver the kits to patients during the concentrated repair efforts in Lichinga during the fourth quarter.
Attendees viewing exhibition of fistula patients’ success stories during IDEOF event. Credit: Anicha.
Dr. Nelson Tchamo of Lichinga Provincial Hospital delivers a dignity kit to a post-operative client. Credit: I. Vaz.
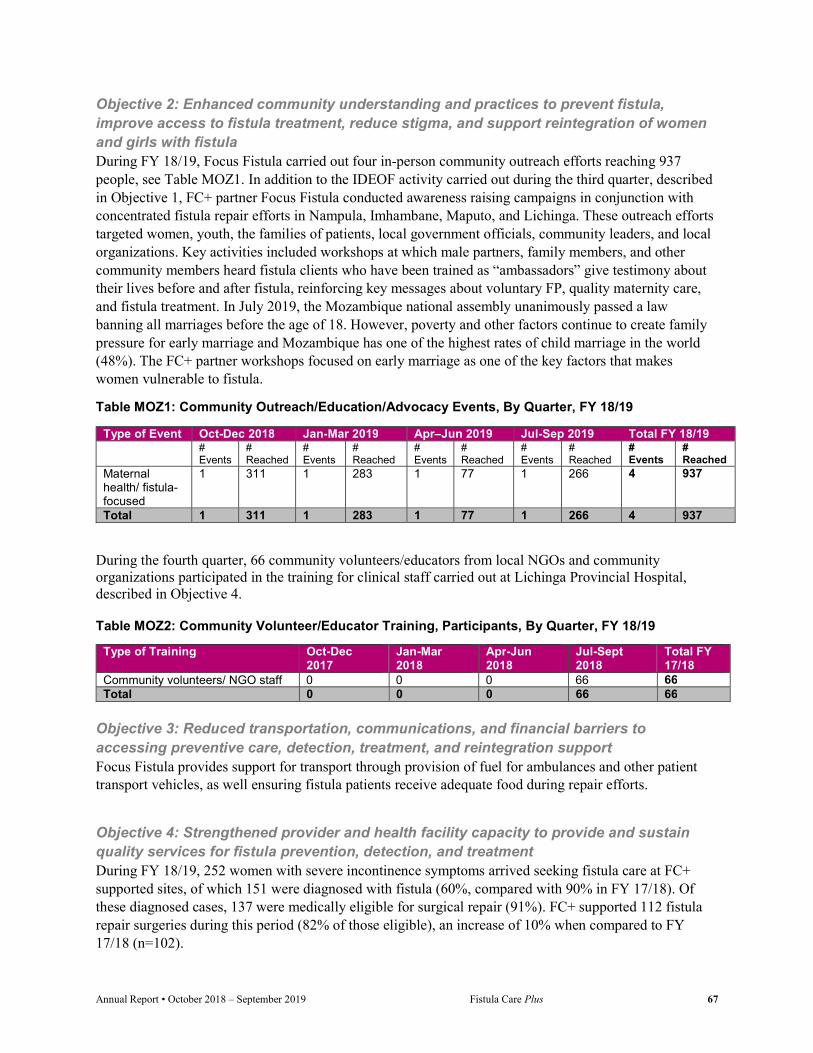
Annual Report • October 2018 – September 2019 Fistula Care Plus 67
Objective 2: Enhanced community understanding and practices to prevent fistula, improve access to fistula treatment, reduce stigma, and support reintegration of women and girls with fistula During FY 18/19, Focus Fistula carried out four in-person community outreach efforts reaching 937 people, see Table MOZ1. In addition to the IDEOF activity carried out during the third quarter, described in Objective 1, FC+ partner Focus Fistula conducted awareness raising campaigns in conjunction with concentrated fistula repair efforts in Nampula, Imhambane, Maputo, and Lichinga. These outreach efforts targeted women, youth, the families of patients, local government officials, community leaders, and local organizations. Key activities included workshops at which male partners, family members, and other community members heard fistula clients who have been trained as “ambassadors” give testimony about their lives before and after fistula, reinforcing key messages about voluntary FP, quality maternity care, and fistula treatment. In July 2019, the Mozambique national assembly unanimously passed a law banning all marriages before the age of 18. However, poverty and other factors continue to create family pressure for early marriage and Mozambique has one of the highest rates of child marriage in the world (48%). The FC+ partner workshops focused on early marriage as one of the key factors that makes women vulnerable to fistula.
Table MOZ1: Community Outreach/Education/Advocacy Events, By Quarter, FY 18/19
Type of Event Oct-Dec 2018 Jan-Mar 2019 Apr–Jun 2019 Jul-Sep 2019 Total FY 18/19 #
Events # Reached
# Events
# Reached
# Events
# Reached
# Events
# Reached
# Events
# Reached
Maternal health/ fistula-focused
1 311 1 283 1 77 1 266 4 937
Total 1 311 1 283 1 77 1 266 4 937
During the fourth quarter, 66 community volunteers/educators from local NGOs and community organizations participated in the training for clinical staff carried out at Lichinga Provincial Hospital, described in Objective 4.
Table MOZ2: Community Volunteer/Educator Training, Participants, By Quarter, FY 18/19
Type of Training Oct-Dec 2017
Jan-Mar 2018
Apr-Jun 2018
Jul-Sept 2018
Total FY 17/18
Community volunteers/ NGO staff 0 0 0 66 66 Total 0 0 0 66 66
Objective 3: Reduced transportation, communications, and financial barriers to accessing preventive care, detection, treatment, and reintegration support Focus Fistula provides support for transport through provision of fuel for ambulances and other patient transport vehicles, as well ensuring fistula patients receive adequate food during repair efforts.
Objective 4: Strengthened provider and health facility capacity to provide and sustain quality services for fistula prevention, detection, and treatment During FY 18/19, 252 women with severe incontinence symptoms arrived seeking fistula care at FC+ supported sites, of which 151 were diagnosed with fistula (60%, compared with 90% in FY 17/18). Of these diagnosed cases, 137 were medically eligible for surgical repair (91%). FC+ supported 112 fistula repair surgeries during this period (82% of those eligible), an increase of 10% when compared to FY 17/18 (n=102).
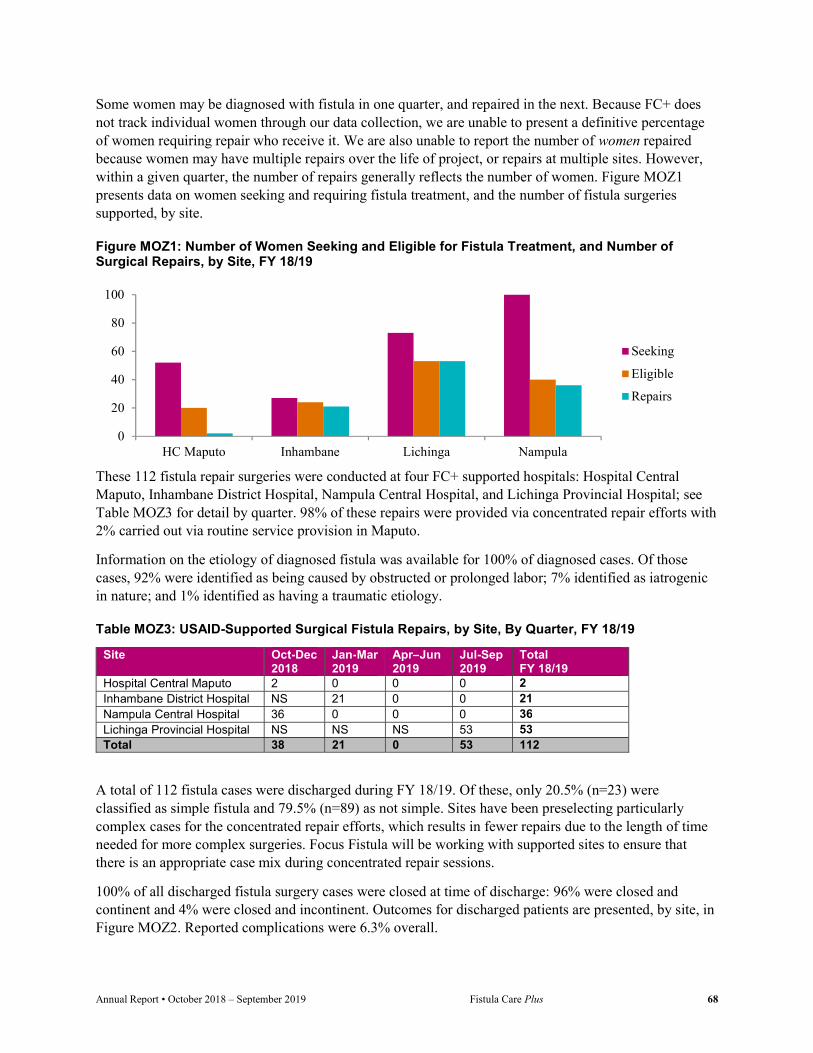
Annual Report • October 2018 – September 2019 Fistula Care Plus 68
Some women may be diagnosed with fistula in one quarter, and repaired in the next. Because FC+ does not track individual women through our data collection, we are unable to present a definitive percentage of women requiring repair who receive it. We are also unable to report the number of women repaired because women may have multiple repairs over the life of project, or repairs at multiple sites. However, within a given quarter, the number of repairs generally reflects the number of women. Figure MOZ1 presents data on women seeking and requiring fistula treatment, and the number of fistula surgeries supported, by site.
Figure MOZ1: Number of Women Seeking and Eligible for Fistula Treatment, and Number of Surgical Repairs, by Site, FY 18/19
These 112 fistula repair surgeries were conducted at four FC+ supported hospitals: Hospital Central Maputo, Inhambane District Hospital, Nampula Central Hospital, and Lichinga Provincial Hospital; see Table MOZ3 for detail by quarter. 98% of these repairs were provided via concentrated repair efforts with 2% carried out via routine service provision in Maputo.
Information on the etiology of diagnosed fistula was available for 100% of diagnosed cases. Of those cases, 92% were identified as being caused by obstructed or prolonged labor; 7% identified as iatrogenic in nature; and 1% identified as having a traumatic etiology.
Table MOZ3: USAID-Supported Surgical Fistula Repairs, by Site, By Quarter, FY 18/19
Site Oct-Dec 2018
Jan-Mar 2019
Apr–Jun 2019
Jul-Sep 2019
Total FY 18/19
Hospital Central Maputo 2 0 0 0 2 Inhambane District Hospital NS 21 0 0 21 Nampula Central Hospital 36 0 0 0 36 Lichinga Provincial Hospital NS NS NS 53 53 Total 38 21 0 53 112
A total of 112 fistula cases were discharged during FY 18/19. Of these, only 20.5% (n=23) were classified as simple fistula and 79.5% (n=89) as not simple. Sites have been preselecting particularly complex cases for the concentrated repair efforts, which results in fewer repairs due to the length of time needed for more complex surgeries. Focus Fistula will be working with supported sites to ensure that there is an appropriate case mix during concentrated repair sessions.
100% of all discharged fistula surgery cases were closed at time of discharge: 96% were closed and continent and 4% were closed and incontinent. Outcomes for discharged patients are presented, by site, in Figure MOZ2. Reported complications were 6.3% overall.
0
20
40
60
80
100
HC Maputo Inhambane Lichinga Nampula
Seeking
Eligible
Repairs

Annual Report • October 2018 – September 2019 Fistula Care Plus 69
Figure MOZ2. Outcome Rates for Surgical Repairs, by Site, FY 18/19
Focus Fistula Mozambique carries out weekly phone calls to physicians involved in the campaigns and serving as FFM focal points and coordinators at the provincial levels. These interactions also involve the surgical technicians of the districts' health centers from which the patients come. These surgical technicians are responsible for preparing patients for upcoming repair efforts and following them post-operatively.
The Focus Fistula monitoring and evaluation assistant makes calls on a weekly or bi-monthly basis to each of the surgical technicians and also calls twice a month to each of the repaired patients. All patients are informed of dates of upcoming campaigns, and given advice as needed regarding complications or the need to return to a fistula surgeon at the provincial level.
During each concentrated repair effort, Focus Fistula provides orientations and basic training to local clinicians that covers information on fistula physiopathology, treatment, prevention and pre- and post-operative care. This training also focuses on use of catheterization during labor as a simple technique to help prevent fistula as well as the importance of appropriate fistula classification in identifying which cases need to be reserved for surgery by an advanced fistula surgeon. As part of fistula prevention and treatment efforts, FC+ supported hands on training as well as decentralized training of 285 health care clinicians and facility staff in Mozambique during FY 18/19; see Table MOZ4.
Table MOZ4: Non-Surgical Health System Personnel Training, Participants by Topic, By Quarter, FY 18/19
Topic Oct-Dec 2018
Jan-Mar 2019
Apr–Jun 2019
Jul-Sep 2019
Total FY 18/19
Pre- and Post-Operative Care 112 60 0 113 285 Total 112 60 0 113 285
0%
20%
40%
60%
80%
100%
Maputo Inhambane Lichinga Nampula
Not closed
Closed with remainingincontinenceClosed and continent
Task Shifting for Surgical Fistula Repair
Focus Fistula’s training approach utilizes a task shifting model that is innovative in the fistula care community. While senior surgeons perform the most complex and labor-intensive surgical cases, concurrent fistula surgeries on-site are task-shifted to nurses, midwives, and other non-surgeon clinicians, commensurate with their individual skill levels. FC+ will document the process and outcomes of this task shifting in FY 19/20.

Annual Report • October 2018 – September 2019 Fistula Care Plus 70
A total of 27 clinicians were trained in fistula surgical repair during FY18/19; see Table MOZ5. During the first quarter, nine clinicians participated in surgical repair training for fistula, and an additional three Obstetrician/ Gynecologists were invited to join the training for several prolapse cases that presented during the concentrated repair effort at Nampula Central Hospital. During the second quarter, 11 surgeons and surgeon technicians participated in surgical repair training for fistula during the concentrated repair effort at Inhambane District Hospital. During both
training sessions, the caseload of patients was predominantly complicated repairs which was not ideal for training purposes. Continued training is recommended for all participants, with access to a greater number of simple fistula repairs. During the fourth quarter, 10 clinicians were trained in conjunction with the concentrated repair effort at Lichinga Provincial Hosptial. Three of the trainees had also participated in training during the second quarter.
Table MOZ5: Surgical Fistula Repair Training, Participants by Trainee Institution, FY 18/19
Institution Oct-Dec 2018
Jan-Mar 2019
Apr–Jun 2019
Jul-Sep 2019
Total FY 18/19
Total # surgeons trained
1st Cont 1st Cont 1st Cont 1st Cont 1st Cont Total
Nampula Central Hospital
2 3 0 0 0 0 0 0 2 3 5
Namapa 1 0 0 0 0 0 0 0 1 0 1 Monapo 1 0 0 0 0 0 0 0 1 0 1 Nacala 1 0 0 0 0 0 0 0 1 0 1 Marere 0 1 0 0 0 0 0 0 0 1 1 Inhambane 0 0 3 3 0 0 0 0 3 3 6 Vilankulos 0 0 0 3 0 0 0 3 0 311 3 Zavala 0 0 0 1 0 0 0 0 0 1 1 Massinga 0 0 0 1 0 0 0 0 0 1 1 Lichinga 0 0 0 0 0 0 7 0 7 0 7 Total 5 4 3 8 0 0 7 3 15 12 27
Obj. 5: Strengthened evidence base for approaches to improve fistula care and scaled up application of standard monitoring and evaluation (M&E) indicators for prevention and treatment FC+ continues to work with Focus Fistula to ensure that M&E systems are adequate and functional for project reporting and for tracking patients and providing quality services. The Focus Fistula team also carries out daily meetings during concentrated repair efforts where each day’s data is reviewed and discussed.
11 The same three clinicians participated in training in the second and fourth quarters.
Surgeon training at Inhambane District Hospital. Credit: S. Lenny.

Annual Report • October 2018 – September 2019 Fistula Care Plus 71
Uganda USAID-supported fistula services in Uganda began in 2004 through the previous FC project and continued through FC+ in six treatment and prevention sites and 14 prevention-only sites. FC+ activities in Uganda ended in May 2019.
In Uganda, FC+ supported fistula repair services, POP treatment services, clinical training, efforts to improve the quality of obstetric care and FP services, and building community awareness. The project increased emphasis on the integration of FP services with fistula and maternal health care and piloting efforts to meet the reintegration needs of women who have undergone fistula repair. FC+ Uganda’s efforts during FY 18/19 focused on winding down activities and documenting best practices for the project’s work in Uganda.
Objective 1: Strengthened enabling environment to institutionalize fistula prevention, treatment, and reintegration in the public and private sectors FC+/Uganda worked to strengthen the enabling environment for fistula services through cultivation of partnerships with governmental and non-governmental agencies, participation in technical working groups and professional meetings and conferences, and by convening relevant stakeholders in Uganda through partner meetings and updates.
During FY18/19, FC+/Uganda supported multiple efforts spearheaded by the Ugandan Ministry of Health. FC+/Uganda provided support to the National Ugandan Fistula Technical Working Group (FTWG) over the life of the project. The FTWG is comprised of select fistula surgeons, officials from the Ministry of Health, and representatives from implementing partners supporting fistula work in the country. The FTWG met in December 2018 during which the group received an update on the progress of the National Fistula Strategy. The consultant carrying out the work reported that the strategy document was progressing but that costing had to be carried out by an economist, which was not included in the original budget for the assignment. Funding needs to come from other resources for the costing exercise. FC+/Uganda advocated for the inclusion of data on iatrogenic fistula prevalence in the data collected by the MOH. The group chairperson agreed and tasked FC+ to design a reporting format to be approved for use at hospitals and aggregated by the Fistula Secretariat.
The FTWG met again in March 2019, during which FC+/Uganda and the Population Council presented findings from the research study carried out on barriers to fistula care. The FC+/Uganda Senior Clinical Associate made a presentation on a fistula partners mapping exercise that had been requested by USAID/Uganda in order to get a broader understanding of the current fistula services coverage and support in the country. The exercise included a list of all facilities reporting fistula surgery in DHIS2, a list of fistula surgeons and organizations supporting the facilities and their performance over the last three years. This exercise revealed gaps in the quality of information in the national DHIS2 and also engendered questions about the fistula secretariat’s oversite role on fistula activities in the country. A number of hospitals have been registering fistula repair in the national DHIS2 but not reporting to the fistula secretariat, and a number of Health Center (HC) IIs and IIIs had registered repairs, which contravenes the National Policy Guidelines and Service Standards for Reproductive Health Services which limits their functions to history-taking, examination, IEC/counseling, investigation, prevention, and referral. There were marked data quality issues in the DHIS2, while the currently cited fistula prevalence of 1% is based on that HMIS data. Based on these findings, the following recommendations were made:
The fistula secretariat should follow up facilities that are operating “under the radar” for Quality Assurance (QA) /Quality Improvement (QI) purposes as mandated by the National Fistula Strategy.

Annual Report • October 2018 – September 2019 Fistula Care Plus 72
The secretariat should investigate HC IIs and HC IIIs that register fistula repair to determine who is actually attempting repair.
The MOH’s division of Health Information needs to address obstetric fistula data quality issues. The FTWG should compile, and keep updated, a list of districts served through outreach screening
and/or treatment. FC+/Uganda was requested to design a simplified fistula reporting form, which fistula treatment sites
will use to send quarterly reports to the secretariat.
The MOH, with support from WHO, developed a Sexual and Reproductive Health/Family Planning (RH/FP) Monitoring and Evaluation framework in 2015 to guide programs implementation. Given new developments in the sector since that time, it was necessary to review and update the framework to incorporate new updates and align it to new program indicators that have been included in the recently revised Health Management Information System (HMIS) system. Stakeholders from different program areas were invited to present updates and proposed revisions to be considered for incorporation into the framework. FC+ program presented updates on program activity and indicators proposed for inclusion following the FTWG’s approved recommendations. The indicators are under consideration and a team from the MOH and WHO are working on finalizing and sharing the revised SRH/RP M&E Framework.
FC+/Uganda participated in the development of national adolescent health service standards, through a meeting in Mukono, Uganda in December 2018. The Reproductive Health Division spearheaded the development of guidelines and service standards to ensure provision of youth friendly services and to standardize services. The standards were adopted from the WHO framework for the accelerated action for the health of adolescents (AA-AH!) to improve access to health care services by young people in alignment with the country’s health sector development plan 2020. Following the exercise, a roadmap to improve programming was developed and endorsed by the Minister of Health.
FC+/Uganda participated in meetings during the first quarter organized by the Ugandan Bureau of Statistics, with support from the MOH and UNFPA, as part of government efforts to calculate current expenditures on family planning and what resources are needed to meet Family Planning 2020 partnership goals. A survey designed to capture current resource flow was disseminated and data collection carried out for FY16/17 and FY17/18. Results will be shared when the survey is concluded and ready for dissemination. FC+/Uganda also participated in monthly MCH Technical Working Group meetings and the Reproductive Health partners’ coordination meetings, convened by the MOH.
The Ugandan MOH has embarked on a campaign to raise public awareness about cancer, install new radiotherapy machines, and increase support to the Expanded Program for Immunization (UNEPI) as part of efforts to stem the growth of cancer deaths in the country. These efforts have thus far had limited success in increasing Human Papilloma Virus (HPV) immunization coverage. Some of the challenges sighted for the low coverage include significant knowledge gaps in the training of health care workers, conducting immunization as a special activity rather than as a routine service,
Officials examining HPV vaccination cards printed with the support of FC+/EH/MSD. Credit: G. Kiwanjago.
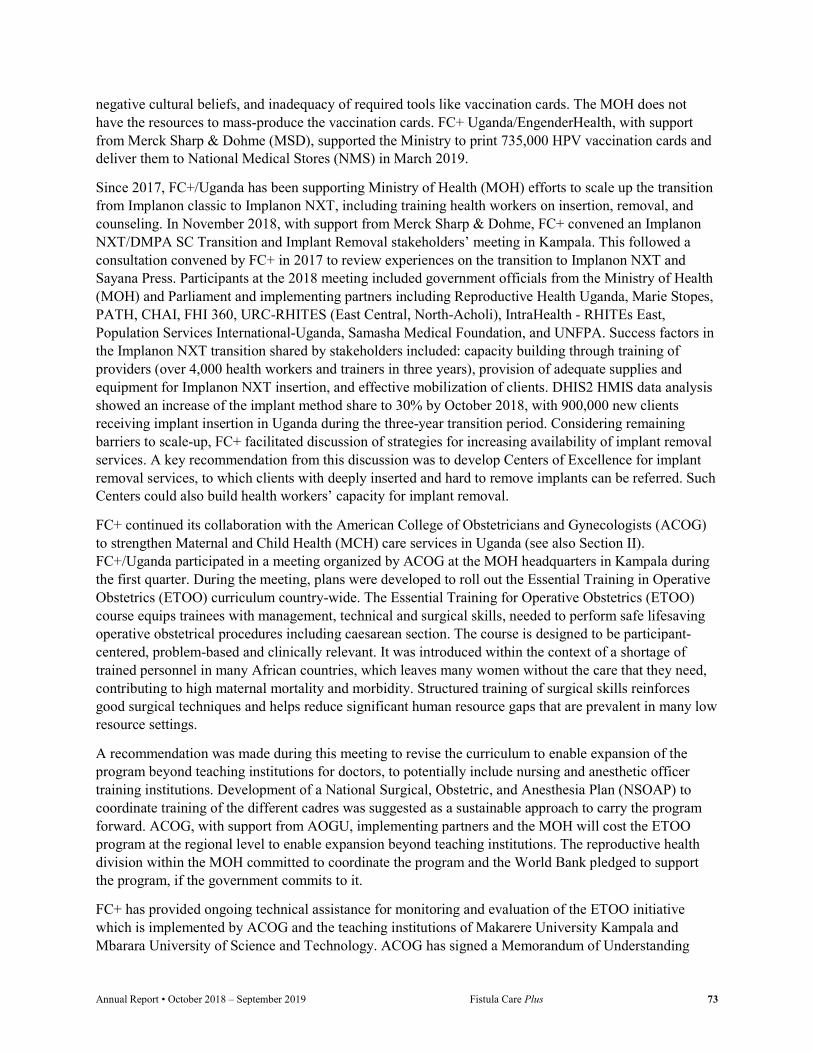
Annual Report • October 2018 – September 2019 Fistula Care Plus 73
negative cultural beliefs, and inadequacy of required tools like vaccination cards. The MOH does not have the resources to mass-produce the vaccination cards. FC+ Uganda/EngenderHealth, with support from Merck Sharp & Dohme (MSD), supported the Ministry to print 735,000 HPV vaccination cards and deliver them to National Medical Stores (NMS) in March 2019.
Since 2017, FC+/Uganda has been supporting Ministry of Health (MOH) efforts to scale up the transition from Implanon classic to Implanon NXT, including training health workers on insertion, removal, and counseling. In November 2018, with support from Merck Sharp & Dohme, FC+ convened an Implanon NXT/DMPA SC Transition and Implant Removal stakeholders’ meeting in Kampala. This followed a consultation convened by FC+ in 2017 to review experiences on the transition to Implanon NXT and Sayana Press. Participants at the 2018 meeting included government officials from the Ministry of Health (MOH) and Parliament and implementing partners including Reproductive Health Uganda, Marie Stopes, PATH, CHAI, FHI 360, URC-RHITES (East Central, North-Acholi), IntraHealth - RHITEs East, Population Services International-Uganda, Samasha Medical Foundation, and UNFPA. Success factors in the Implanon NXT transition shared by stakeholders included: capacity building through training of providers (over 4,000 health workers and trainers in three years), provision of adequate supplies and equipment for Implanon NXT insertion, and effective mobilization of clients. DHIS2 HMIS data analysis showed an increase of the implant method share to 30% by October 2018, with 900,000 new clients receiving implant insertion in Uganda during the three-year transition period. Considering remaining barriers to scale-up, FC+ facilitated discussion of strategies for increasing availability of implant removal services. A key recommendation from this discussion was to develop Centers of Excellence for implant removal services, to which clients with deeply inserted and hard to remove implants can be referred. Such Centers could also build health workers’ capacity for implant removal.
FC+ continued its collaboration with the American College of Obstetricians and Gynecologists (ACOG) to strengthen Maternal and Child Health (MCH) care services in Uganda (see also Section II). FC+/Uganda participated in a meeting organized by ACOG at the MOH headquarters in Kampala during the first quarter. During the meeting, plans were developed to roll out the Essential Training in Operative Obstetrics (ETOO) curriculum country-wide. The Essential Training for Operative Obstetrics (ETOO) course equips trainees with management, technical and surgical skills, needed to perform safe lifesaving operative obstetrical procedures including caesarean section. The course is designed to be participant-centered, problem-based and clinically relevant. It was introduced within the context of a shortage of trained personnel in many African countries, which leaves many women without the care that they need, contributing to high maternal mortality and morbidity. Structured training of surgical skills reinforces good surgical techniques and helps reduce significant human resource gaps that are prevalent in many low resource settings.
A recommendation was made during this meeting to revise the curriculum to enable expansion of the program beyond teaching institutions for doctors, to potentially include nursing and anesthetic officer training institutions. Development of a National Surgical, Obstetric, and Anesthesia Plan (NSOAP) to coordinate training of the different cadres was suggested as a sustainable approach to carry the program forward. ACOG, with support from AOGU, implementing partners and the MOH will cost the ETOO program at the regional level to enable expansion beyond teaching institutions. The reproductive health division within the MOH committed to coordinate the program and the World Bank pledged to support the program, if the government commits to it.
FC+ has provided ongoing technical assistance for monitoring and evaluation of the ETOO initiative which is implemented by ACOG and the teaching institutions of Makarere University Kampala and Mbarara University of Science and Technology. ACOG has signed a Memorandum of Understanding

Annual Report • October 2018 – September 2019 Fistula Care Plus 74
with the Association of Obstetricians and Gynaecologists of Uganda (AOGU) whereby AOGU will follow up with residents at teaching hospitals to ensure they fulfill all course requirements and will possibly track the number of women that require repeat surgery due to complications following surgery conducted by trainees.
During the remainder of the fiscal year, ACOG organized surgical skills training at Mbarara and Busitema Universities. FC+ has continued to analyze the knowledge and competence outputs resulting from these trainings for dissemination to stakeholders at periodic stakeholder meetings; a summary of these results will be shared in the next semi-annual report, following a stakeholder meeting in the first quarter of FY 19/20.
ACOG has met with the Minister of Education through introduction from the AOGU. They discussed the importance of surgical skills training and received commitment from the Minister to support the program.
FC+ Uganda participated in IDEOF activities held in conjunction with a concentrated repair effort at Kisiizi Hospital supported by UNFPA and other partners including TERREWODE and Medical Teams International. On May 28, 2019 the Government of Uganda represented by the MoH hosted the FC+ Technical Close-Out event at its headquarters. The objective of the event was to disseminate knowledge products and best practices developed over the life of the project. Key activities included remarks from representatives of the MoH, USAID, and EngenderHealth; an FC+ project presentation; a plenary discussion; and a knowledge management gallery walk. The meeting was attended by 49 participants, including representatives from the MoH and Ministry of Education and Sports, USAID, local government representatives, religious leaders, clinical staff, and FC+ Uganda project staff.
Along with an opportunity for government stakeholders to discuss adoption of project strategies, the meeting served as an opportunity to consider how successful approaches can be transferred to the USAID RHITES projects in the future. The USAID/Uganda Family Health Team Leader highlighted the institutionalization of routine fistula care at supported sites as a key achievement of the project. Routine fistula care provision is a model that enables health systems to locally plan and deliver fistula treatment, rather than relying on sporadic visits from external clinicians. The USAID Family Health Team Leader also noted that the USAID RHITES projects will be tasked with planning for fistula treatment and reporting on fistula indicators going forward. The Director of Curative Services at the MOH noted that the National Fistula Technical Working Group will be a nationally owned platform for building on and locally sustaining FC+ achievements
FC+ Uganda shared findings from the project’s work including topics such as iatrogenic fistula, urinary catheterization, use of the partograph, and efforts to improve fistula data quality. In addition, the project’s work with youth and religious leaders, and research on reducing barriers to accessing fistula repair were highlighted. The following technical briefs were shared (see Appendices DD, EE, FF and HH and here: https://fistulacare.org/resources/publications/technical-briefs/).
Father Raphael Kahwa explains how religious leaders advanced maternal health messaging through FC+ Uganda’s work. Credit: FC+ Uganda.
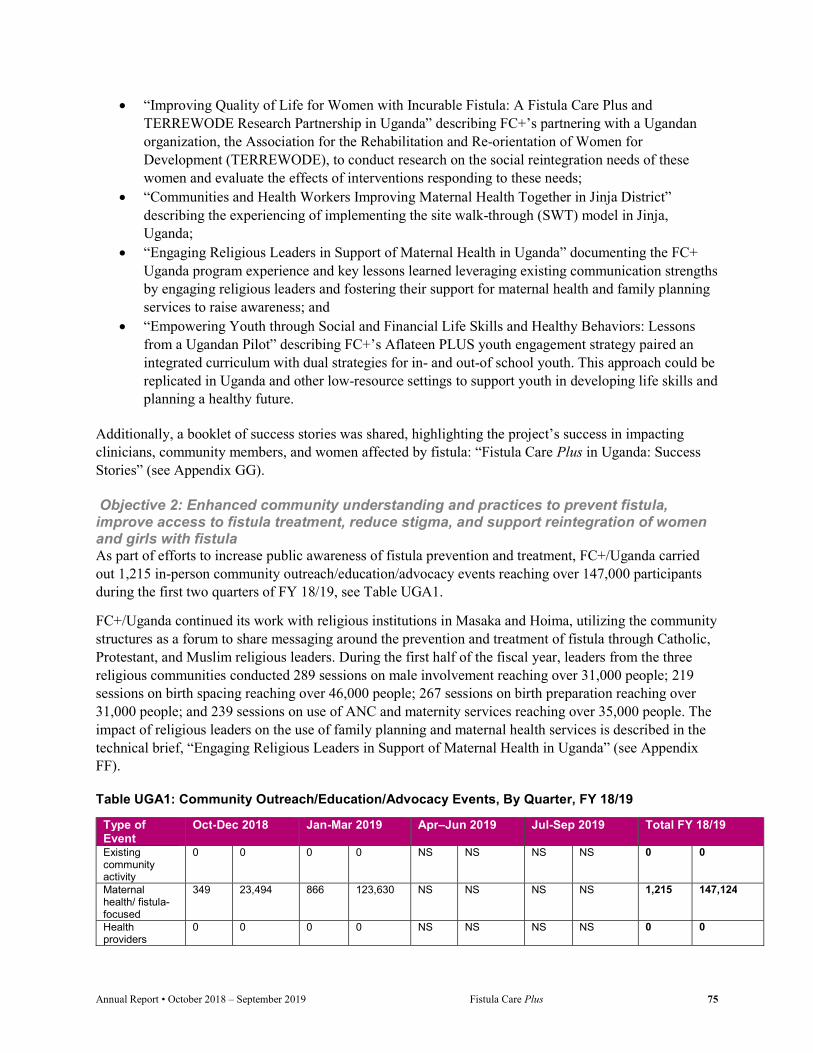
Annual Report • October 2018 – September 2019 Fistula Care Plus 75
“Improving Quality of Life for Women with Incurable Fistula: A Fistula Care Plus and TERREWODE Research Partnership in Uganda” describing FC+’s partnering with a Ugandan organization, the Association for the Rehabilitation and Re-orientation of Women for Development (TERREWODE), to conduct research on the social reintegration needs of these women and evaluate the effects of interventions responding to these needs;
“Communities and Health Workers Improving Maternal Health Together in Jinja District” describing the experiencing of implementing the site walk-through (SWT) model in Jinja, Uganda;
“Engaging Religious Leaders in Support of Maternal Health in Uganda” documenting the FC+ Uganda program experience and key lessons learned leveraging existing communication strengths by engaging religious leaders and fostering their support for maternal health and family planning services to raise awareness; and
“Empowering Youth through Social and Financial Life Skills and Healthy Behaviors: Lessons from a Ugandan Pilot” describing FC+’s Aflateen PLUS youth engagement strategy paired an integrated curriculum with dual strategies for in- and out-of school youth. This approach could be replicated in Uganda and other low-resource settings to support youth in developing life skills and planning a healthy future.
Additionally, a booklet of success stories was shared, highlighting the project’s success in impacting clinicians, community members, and women affected by fistula: “Fistula Care Plus in Uganda: Success Stories” (see Appendix GG). Objective 2: Enhanced community understanding and practices to prevent fistula, improve access to fistula treatment, reduce stigma, and support reintegration of women and girls with fistula As part of efforts to increase public awareness of fistula prevention and treatment, FC+/Uganda carried out 1,215 in-person community outreach/education/advocacy events reaching over 147,000 participants during the first two quarters of FY 18/19, see Table UGA1.
FC+/Uganda continued its work with religious institutions in Masaka and Hoima, utilizing the community structures as a forum to share messaging around the prevention and treatment of fistula through Catholic, Protestant, and Muslim religious leaders. During the first half of the fiscal year, leaders from the three religious communities conducted 289 sessions on male involvement reaching over 31,000 people; 219 sessions on birth spacing reaching over 46,000 people; 267 sessions on birth preparation reaching over 31,000 people; and 239 sessions on use of ANC and maternity services reaching over 35,000 people. The impact of religious leaders on the use of family planning and maternal health services is described in the technical brief, “Engaging Religious Leaders in Support of Maternal Health in Uganda” (see Appendix FF).
Table UGA1: Community Outreach/Education/Advocacy Events, By Quarter, FY 18/19
Type of Event
Oct-Dec 2018 Jan-Mar 2019 Apr–Jun 2019 Jul-Sep 2019 Total FY 18/19
Existing community activity
0 0 0 0 NS NS NS NS 0 0
Maternal health/ fistula-focused
349 23,494 866 123,630 NS NS NS NS 1,215 147,124
Health providers
0 0 0 0 NS NS NS NS 0 0

Annual Report • October 2018 – September 2019 Fistula Care Plus 76
Type of Event
Oct-Dec 2018 Jan-Mar 2019 Apr–Jun 2019 Jul-Sep 2019 Total FY 18/19
Health facility 0 0 0 0 NS NS NS NS 0 0 Radio/TV 0 0 0 0 NS NS NS NS 0 0 Total 349 23,494 866 123,630 NS NS NS NS 1,215 147,124
Recognizing that lifelong habits are often formed during early years of a person’s life, FC+/Uganda prioritized adolescents and youth in its community engagement efforts. Reaching young people with reproductive health and FP information in a manner that is relevant to their needs and empowers young people with knowledge and skills to make responsible choices is one way in which FC+/Uganda addresses fistula prevention. In partnership with the Private Education Development Network (PEDN) and Aflatoun International, EngenderHealth adapted the evidence-based Aflateen curriculum, integrating sexual health, FP, and fistula prevention content with the existing social and financial education modules. By connecting the Aflateen learner-centered, social and financial approach with EngenderHealth’s gender-transformative interventions, the enhanced Aflateen PLUS curriculum seeks to enhance the capacity of young people to empower themselves to make positive decisions about their education, health, social, and financial well-being. The curriculum was rolled out to ten in-school and ten out-of-school youth groups distributed equally across the Districts of Jinja and Kamuli and this dual in- and out-of-school strategy aims to offer-friendly environments, where young people have genuine opportunities to engage in dialogue and personal exploration in order to foster sense of efficacy.
In the two previous fiscal years, FC+ conducted a needs assessment and mapping of schools and out-of-school youth groups in Kamuli and Jinja districts; supported training of teachers and peer-educators to roll out the Aflateen PLUS curriculum with youth groups and of school nurses and community health workers to provide adolescent/youth friendly SRH services; provided continuous supportive supervision to teachers, peer-educators, nurses, and community health workers; and supported additional community mobilization activities implemented by trained peer-educators. Throughout, FC+/Uganda has monitored the activity, including participation of youth in the clubs, whether they pass on information to their communities, and youth receiving health services.
During FY 18/19, 359 Aflateen PLUS club members participated in club meetings; 1,154 individuals were reached during club outreaches; 356 club members were sensitized about reproductive health; 523 individuals were referred to health facilities for services; 315 club members participated in community activities; and club members implemented 223 financial enterprises. In December 2018, the FC+ core team supported FC+/Uganda to report on the preliminary findings of a process documentation of the pilot phase of the Aflateen PLUS implementation (July 2017-July 2018) at the seventh biennial conference of the International Society of Obstetric Fistula Surgeons, held in Kathmandu. In May 2019, the FC+ core team supported FC+ Uganda in developing and publishing a technical brief detailing the more extensive qualitative and quantitative findings of the pilot documentation: Empowering Youth through Social and Financial Life Skills and Healthy Behaviors: Lessons from a Ugandan Pilot” (see Appendix DD and https://fistulacare.org/wp-fcp/wp-content/uploads/2019/05/FC_Plus_TechBrief-UgandanPilot-4.pdf).
Along with describing the Aflateen PLUS strategy and processes, the brief summarizes service outputs from the pilot period and the perspectives of program implementers and users. Particularly notable were the results achieved by peer educators in education, empowering, and mobilizing out-of-school youth. Describing the outcomes of her work with out-of-school youth, a peer educator noted:
“They are discussing about STIs and counseling their peers to open up in case they have any disease. Sometimes the [health facility] in-charge calls me to let me know how one of my group

Annual Report • October 2018 – September 2019 Fistula Care Plus 77
members managed to take a colleague to access treatment from the health center, so I see that as tremendous change among the youth.”
Another peer educator described the changes effected through the financial education and savings components of the Aflateen PLUS strategy:
“We have come up with a saving club within our group, whereby we started with only 20,000 shillings. Today we have raised 350,000 shillings…We are just looking for how to multiply that money…we have also been successful with the knowledge we have from Aflateen as far as financial enterprise strategy is concerned, and we have come up with a financial enterprise of tents and chairs. And, indeed it’s working for the community, and it’s working for us, because it’s bringing money to the group.”
The brief also includes recommendations for improvement as the Aflateen PLUS strategy is scaled up and replicated elsewhere.
There were no community volunteer/educator trainings supported in Uganda during FY18/19.
Obj. 3: Reduced transportation, communications, and financial barriers to accessing preventive care, detection, treatment, and reintegration support As described in Section II, Objectives 3 and 5, FC+/Uganda continued working with the Population Council during FY 18/19 to evaluate an intervention package designed using the results of the formative research on barriers to fistula treatment conducted during FY 15/16. The Fistula Treatment Barriers Reduction Intervention sought to address the barriers identified through formative research, specifically low awareness, high stigma, high cost of accessing services, and clinician “gate-keeping” at lower levels of the health system. After two years of implementation, the Population Council conducted an end-line evaluation to assess intervention outcomes.
The intervention was carried out in Kalungu District and offered treatment services to women at Kitovu Mission Hospital in the neighboring Masaka District. The intervention utilized multiple communication channels for fistula messaging, screening, and referral, a consistent screening algorithm for fistula screening, and a transportation voucher to enable positively screened women to travel for free to and from Kitovu Mission Hospital. FC+ and Viamo (formerly VOTO Mobile) partnered to develop a free fistula screening hotline, whereby village health team (VHT) volunteers and women from the community call to find out about fistula – its causes, prevention, and services available. At the community level, VHTs circulated targeted messages about fistula symptoms and available treatment services; and the IVR hotline, widely advertised by VHTs, radio messages, and flyers, screened women for fistula using mobile devices. At primary health care facilities, health workers identified potential fistula clients for referral and facilitated free transportation to appropriate treatment facilities. Positively screened women identified through primary health care workers, VHTs, and the hotline all received a voucher for free transportation to and from the fistula treatment facility as well as case-management support from either the VHT or primary health care worker.
Endline data collection of the study was completed and a dissemination event was conducted through the National Fistula Working Group meeting in Uganda in late March, 2019. See Section II, Objective III for details. Preliminary analysis of intervention processes and outputs demonstrates increases in health system capacity to provide fistula treatment, robust use of the transportation voucher, and increased demand for fistula care. These findings are provided in Appendix N. Technical briefs and reports developed to date through this partnership are available at: https://www.popcouncil.org/research/fistula-
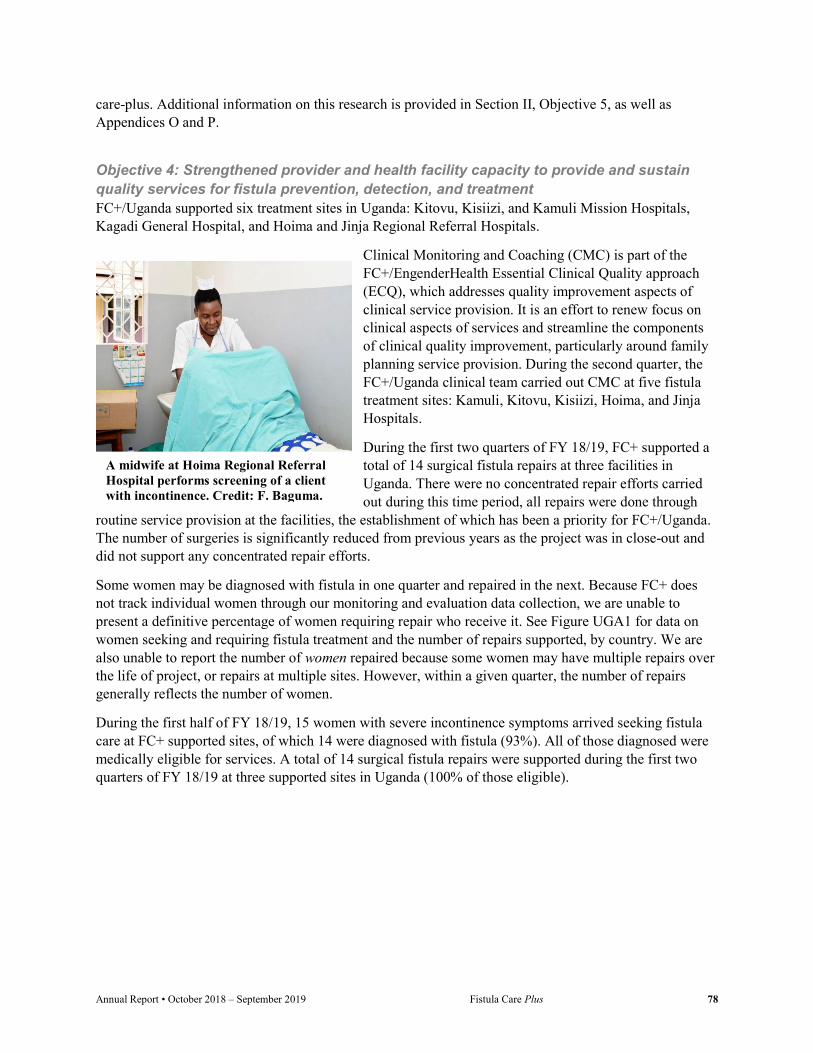
Annual Report • October 2018 – September 2019 Fistula Care Plus 78
care-plus. Additional information on this research is provided in Section II, Objective 5, as well as Appendices O and P.
Objective 4: Strengthened provider and health facility capacity to provide and sustain quality services for fistula prevention, detection, and treatment FC+/Uganda supported six treatment sites in Uganda: Kitovu, Kisiizi, and Kamuli Mission Hospitals, Kagadi General Hospital, and Hoima and Jinja Regional Referral Hospitals.
Clinical Monitoring and Coaching (CMC) is part of the FC+/EngenderHealth Essential Clinical Quality approach (ECQ), which addresses quality improvement aspects of clinical service provision. It is an effort to renew focus on clinical aspects of services and streamline the components of clinical quality improvement, particularly around family planning service provision. During the second quarter, the FC+/Uganda clinical team carried out CMC at five fistula treatment sites: Kamuli, Kitovu, Kisiizi, Hoima, and Jinja Hospitals.
During the first two quarters of FY 18/19, FC+ supported a total of 14 surgical fistula repairs at three facilities in Uganda. There were no concentrated repair efforts carried out during this time period, all repairs were done through
routine service provision at the facilities, the establishment of which has been a priority for FC+/Uganda. The number of surgeries is significantly reduced from previous years as the project was in close-out and did not support any concentrated repair efforts.
Some women may be diagnosed with fistula in one quarter and repaired in the next. Because FC+ does not track individual women through our monitoring and evaluation data collection, we are unable to present a definitive percentage of women requiring repair who receive it. See Figure UGA1 for data on women seeking and requiring fistula treatment and the number of repairs supported, by country. We are also unable to report the number of women repaired because some women may have multiple repairs over the life of project, or repairs at multiple sites. However, within a given quarter, the number of repairs generally reflects the number of women.
During the first half of FY 18/19, 15 women with severe incontinence symptoms arrived seeking fistula care at FC+ supported sites, of which 14 were diagnosed with fistula (93%). All of those diagnosed were medically eligible for services. A total of 14 surgical fistula repairs were supported during the first two quarters of FY 18/19 at three supported sites in Uganda (100% of those eligible).
A midwife at Hoima Regional Referral Hospital performs screening of a client with incontinence. Credit: F. Baguma.
Annual Report • October 2018 – September 2019 Fistula Care Plus 79
Figure UGA1: Number of Women Seeking and Eligible for Fistula Treatment, and Number of Surgical Repairs, by Site, FY 18/19
FC+/Uganda made a concerted effort with supported sites to institute and support routine repair services; these efforts have borne fruit with a growing number of repairs being conducted through routine service provision (see Table UGA2 for detail by quarter). All FC+ supported repairs during this reporting period were carried out through routine service provision. The Fistula Foundation supported a concentrated repair effort at Kitovu during the first quarter through which 43 patients received surgery, and during the second quarter whereby 32 patients received surgery. Child Injury Birth supported a concentrated effort in the second quarter at Kitovu during which 63 surgical repairs were conducted. Kamuli Mission Hospital organized its own concentrated repair effort during the second quarter whereby 26 patients received surgery.
Table UGA2: USAID-Supported Surgical Fistula Repairs, by Site, By Quarter, FY 18/19
During FY 18/19, 100% of all fistula repair surgeries supported by FC+ were reported as closed and continent at time of discharge. This very high rate of optimal outcome (closed and continent) has remained consistent over the course of the project and may reflect excellent surgical skills and/or patient selection practices, and is also subject to on-going audit. Outcomes for discharged patients are presented in Figure UGA2. There were no reported complications at supported sites during the reporting period.
Etiology data was available for 100% of the 14 diagnosed fistula cases. All diagnosed fistula cases were reported to have resulted from obstructed or prolonged labor.
FC+/Uganda provided support to Jinja, Kamuli, and Kitovu for the provision of routine pelvic organ prolapse (POP) services. In the first two quarters of FY 18/19, one surgical POP treatment procedure was reported from Jinja Regional Referral Hospital.
There were no trainings in surgical fistula repair supported during the reporting period. FC+/Uganda did not carry out and trainings for health care clinicians during FY 18/19.
0
2
4
6
8
10
Hoima RRH Jinja RRH Kisiizi
Seeking
Eligible
Repairs
Site Oct-Dec 2018
Jan-Mar 2019
Apr–Jun 2019
Jul-Sep 2019
Total FY 18/19
Hoima Regional Referral Hospital 2 1 NS NS 3 Jinja Regional Referral Hospital 2 5 NS NS 7 Kisiizi Mission Hospital 2 2 NS NS 4 Total 6 8 NS NS 14

Annual Report • October 2018 – September 2019 Fistula Care Plus 80
Figure UGA2. Outcome Rates for Surgical Repairs, by Site, FY 18/19
FC+/Uganda carried out in-depth FP compliance visits at selected facilities in Masaka and Kalungu districts during the first two quarters of FY18/19. The visits included discussion related to contraceptive choices, review of existing clients’ records for documentation of key counselling components, and review of existing data in files and registers to ascertain client choice, method adoption and continuity. Following review, the team discussed the implications of gaps identified on client choice, method adoption and continuity as well as how to routinely use the facility data to identify “red flags” in FP service provision.
The clinical team conducted on-site orientation meetings and discussed compliance issues related to contraceptive choice at Kalungu HC III, Kiyumba HC IV, Kyanamukaka HC IV, Kitovu Hospital and Masaka Regional Referral Hospital. Areas of concern included poor method mix due to frequent stock outs of contraceptives (particularly oral contraceptives); low utilization of all methods at all facilities due to missed opportunities to mobilize clients; and unavailability of permanent method services at hospitals and HC IVs. Based on the findings the team recommended continuous follow up and supportive supervision to encourage integration of FP services, strengthening alternative distribution channels for contraceptives, and on site mentoring and coaching among staff, particularly on record keeping and monitoring their own facility data.
During the third quarter, FC+ Uganda held a dissemination meeting in Kasese district to share key findings from project efforts to scale up partograph use in lower health centers in the Bukonzo East and West health sub-districts. Participants from the implementing facilities were invited to share their experiences, including partograph champions and in-charges at the sites. Participants reported an improvement in both partograph use and maternal health outcomes in Bukonzo East and West and well as improved midwife attitudes towards partograph use.
FC+/Uganda supported FP counseling and service provision at 17 sites in Uganda during the first two quarters of FY 18/19. 11,797 counseling sessions took place at supported sites and 14,539 CYP were provided, see Table UGA3 for detail, by site. Method mix contributing to this CYP in Uganda was primarily implants (57%), IUD (14%), Depo Provera (13%), and tubal ligation (7%).
Table UGA3: Family Planning Counseling Sessions and CYP, by Site, By Quarter, FY 18/19
Site Oct-Dec 2018 Jan-Mar 2019 Apr–Jun 2019 Jul-Sep 2019 Total FY 18/19 #sessions CYP #sessions CYP #sessions CYP #sessions CYP #sessions CYP12 Azur HCIV 85 257 224 434 NS NS NS NS 309 691 Buraru HCIII 549 230 516 275 NS NS NS NS 1,065 505
12 Due to rounding, totals may differ slightly from the sum of individual quarters.
0%
100%
Hoima Jinja Kisiizi
Not closed
Closed with remainingincontinenceClosed and continent
Benchmark closed andcontinent (75%)

Annual Report • October 2018 – September 2019 Fistula Care Plus 81
Site Oct-Dec 2018 Jan-Mar 2019 Apr–Jun 2019 Jul-Sep 2019 Total FY 18/19 #sessions CYP #sessions CYP #sessions CYP #sessions CYP #sessions CYP12
Buseruka HCIII
149 178 314 146 NS NS NS NS 463 324
Bwera GH 569 821 608 557 NS NS NS NS 1,177 1,378 Hoima RH 796 422 927 556 NS NS NS NS 1,723 978 Jinja RRH 878 1,473 835 629 NS NS NS NS 1,713 2,103 Kagando 647 1,327 133 774 NS NS NS NS 780 2,100 Kalungu HCIII 127 183 143 254 NS NS NS NS 270 438 Kamuli 0 0 172 258 NS NS NS NS 172 258 Karambi HCIII NA 100 45 11 NS NS NS NS 45 112 Kigorobya HCIV
476 459 315 377 NS NS NS NS 791 836
Kikuube HCIV 569 222 201 472 NS NS NS NS 770 694 Kitovu 38 50 50 75 NS NS NS NS 88 125 Kiyumba HCIV
79 103 112 164 NS NS NS NS 191 266
Kyanamukaka HCIV
122 221 200 116 NS NS NS NS 322 337
Masaka RRH 635 1,062 737 1,435 NS NS NS NS 1,372 2,497 Rwesande HCIV
376 649 170 251 NS NS NS NS 546 899
Total 6,095 7,756 5,702 6,783 NS NS NS NS 11,797 14,539
Supported sites reported an overall cesarean section rate of 28.9% during the first two quarters of FY 18/19, based on 21,999 reported deliveries. Information on number of deliveries, by site, is represented in Figure UGA3 and cesarean section rates, by site, are presented in Figure UGA4. Sites reported that 2.9% of all labors were prolonged/obstructed, 12% of which received catheterization for fistula prevention.
Figure UGA3. Number of Obstetric Deliveries, by Site, FY 18/19 (n=21,999)
96377
2222008
39593263
1521187
982326
594418
996850
196158137
4975167
Azur HCIVBuraru HCIII
Buseruka HCIIIBwera GHHoima RH
JinjaKagando
Kalungu HCIIIKamuli
Karambi HCIIIKigorobya HCIV
Kikuube HCIVKisiiziKitovu
Kiyumba HCIVKyanamukaka HCIV
LukoloMasaka RRH
Rwesande HCIV
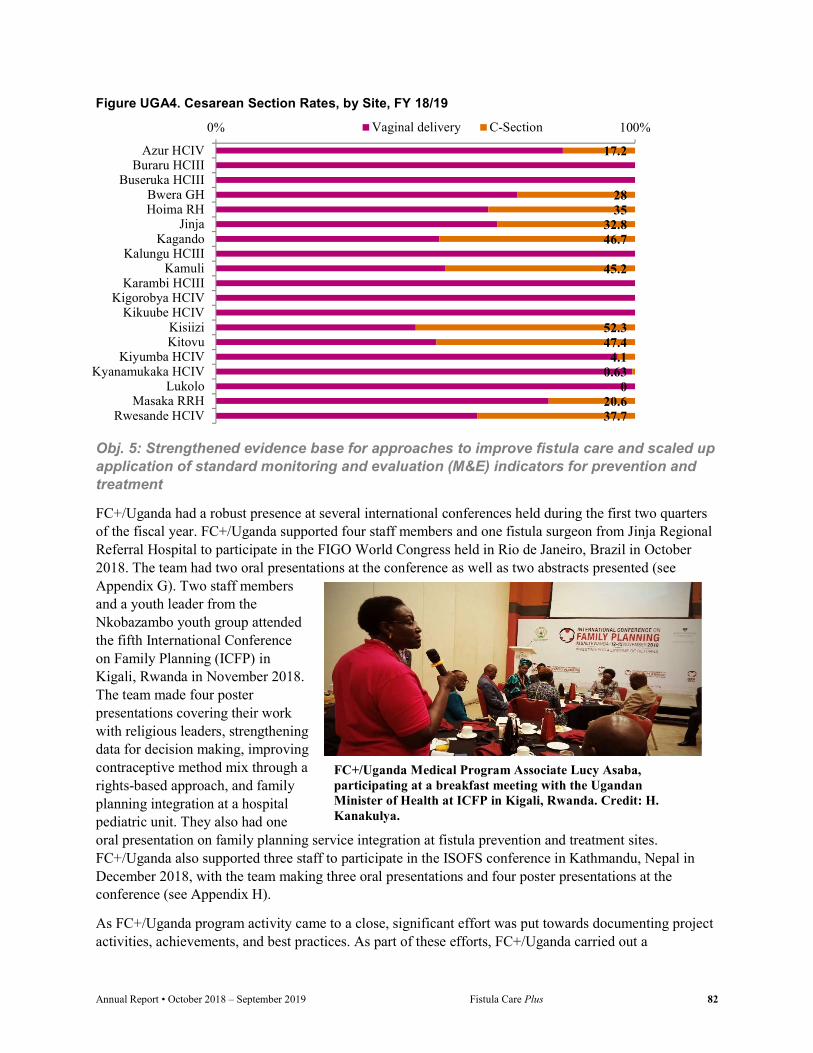
Annual Report • October 2018 – September 2019 Fistula Care Plus 82
Figure UGA4. Cesarean Section Rates, by Site, FY 18/19
Obj. 5: Strengthened evidence base for approaches to improve fistula care and scaled up application of standard monitoring and evaluation (M&E) indicators for prevention and treatment
FC+/Uganda had a robust presence at several international conferences held during the first two quarters of the fiscal year. FC+/Uganda supported four staff members and one fistula surgeon from Jinja Regional Referral Hospital to participate in the FIGO World Congress held in Rio de Janeiro, Brazil in October 2018. The team had two oral presentations at the conference as well as two abstracts presented (see Appendix G). Two staff members and a youth leader from the Nkobazambo youth group attended the fifth International Conference on Family Planning (ICFP) in Kigali, Rwanda in November 2018. The team made four poster presentations covering their work with religious leaders, strengthening data for decision making, improving contraceptive method mix through a rights-based approach, and family planning integration at a hospital pediatric unit. They also had one oral presentation on family planning service integration at fistula prevention and treatment sites. FC+/Uganda also supported three staff to participate in the ISOFS conference in Kathmandu, Nepal in December 2018, with the team making three oral presentations and four poster presentations at the conference (see Appendix H).
As FC+/Uganda program activity came to a close, significant effort was put towards documenting project activities, achievements, and best practices. As part of these efforts, FC+/Uganda carried out a
17.2
2835
32.846.7
45.2
52.347.4
4.10.63
020.637.7
0% 100%
Azur HCIVBuraru HCIII
Buseruka HCIIIBwera GHHoima RH
JinjaKagando
Kalungu HCIIIKamuli
Karambi HCIIIKigorobya HCIV
Kikuube HCIVKisiiziKitovu
Kiyumba HCIVKyanamukaka HCIV
LukoloMasaka RRH
Rwesande HCIV
Vaginal delivery C-Section
FC+/Uganda Medical Program Associate Lucy Asaba, participating at a breakfast meeting with the Ugandan Minister of Health at ICFP in Kigali, Rwanda. Credit: H. Kanakulya.
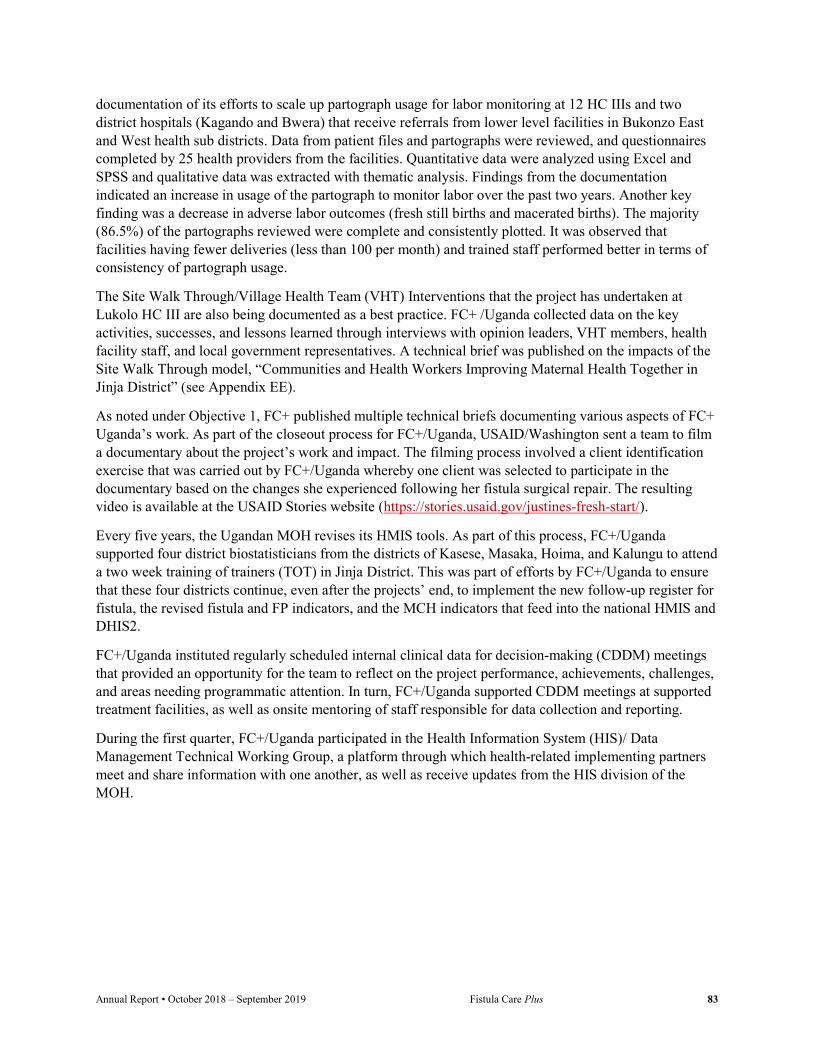
Annual Report • October 2018 – September 2019 Fistula Care Plus 83
documentation of its efforts to scale up partograph usage for labor monitoring at 12 HC IIIs and two district hospitals (Kagando and Bwera) that receive referrals from lower level facilities in Bukonzo East and West health sub districts. Data from patient files and partographs were reviewed, and questionnaires completed by 25 health providers from the facilities. Quantitative data were analyzed using Excel and SPSS and qualitative data was extracted with thematic analysis. Findings from the documentation indicated an increase in usage of the partograph to monitor labor over the past two years. Another key finding was a decrease in adverse labor outcomes (fresh still births and macerated births). The majority (86.5%) of the partographs reviewed were complete and consistently plotted. It was observed that facilities having fewer deliveries (less than 100 per month) and trained staff performed better in terms of consistency of partograph usage.
The Site Walk Through/Village Health Team (VHT) Interventions that the project has undertaken at Lukolo HC III are also being documented as a best practice. FC+ /Uganda collected data on the key activities, successes, and lessons learned through interviews with opinion leaders, VHT members, health facility staff, and local government representatives. A technical brief was published on the impacts of the Site Walk Through model, “Communities and Health Workers Improving Maternal Health Together in Jinja District” (see Appendix EE).
As noted under Objective 1, FC+ published multiple technical briefs documenting various aspects of FC+ Uganda’s work. As part of the closeout process for FC+/Uganda, USAID/Washington sent a team to film a documentary about the project’s work and impact. The filming process involved a client identification exercise that was carried out by FC+/Uganda whereby one client was selected to participate in the documentary based on the changes she experienced following her fistula surgical repair. The resulting video is available at the USAID Stories website (https://stories.usaid.gov/justines-fresh-start/).
Every five years, the Ugandan MOH revises its HMIS tools. As part of this process, FC+/Uganda supported four district biostatisticians from the districts of Kasese, Masaka, Hoima, and Kalungu to attend a two week training of trainers (TOT) in Jinja District. This was part of efforts by FC+/Uganda to ensure that these four districts continue, even after the projects’ end, to implement the new follow-up register for fistula, the revised fistula and FP indicators, and the MCH indicators that feed into the national HMIS and DHIS2.
FC+/Uganda instituted regularly scheduled internal clinical data for decision-making (CDDM) meetings that provided an opportunity for the team to reflect on the project performance, achievements, challenges, and areas needing programmatic attention. In turn, FC+/Uganda supported CDDM meetings at supported treatment facilities, as well as onsite mentoring of staff responsible for data collection and reporting.
During the first quarter, FC+/Uganda participated in the Health Information System (HIS)/ Data Management Technical Working Group, a platform through which health-related implementing partners meet and share information with one another, as well as receive updates from the HIS division of the MOH.

Annual Report • October 2018 – September 2019 Fistula Care Plus 84
West Africa/Niger (WAN) EngenderHealth began support for fistula services in the West Africa Region with implementation of a BMGF grant in Niger in 2005. USAID-supported fistula services in the region began in 2007 through the AWARE and FC projects and continues through FC+ in Niger in three treatment sites. As of September 30, 2019, FC+ provides support to three treatment and prevention sites in Niger: CSME Maradi, CSME Tahoua, and Centre National de Référence pour la Fistule Obstétricale (CNRFO).
FC+ closed its office in Niger on June 30, 2018. FC+ supported fistula work in Niger and the West Africa Region during the first quarter of FY 18/19 through a subaward to the Réseau pour l’Eradication des Fistule (REF). Activity through REF has been suspended as FC+ completes a financial and administrative review and addresses significant waste management challenges identified at supported sites. FC+ will compete a new subaward in the first quarter of FY 19/20 to select the best local partner for future activities. Delays and challenges reconciling the financial reports for subawardee REF and the subsequent decision to compete a new subaward led to a significant slowdown in program implementation during FY 18/19.
FC+’s work in Niger is part of a larger West Africa regional focus with the goal of continuing to support Niger as a regional hub for fistula treatment and prevention. Emphasis is on collaboration with regional partners such as WACS, ISOFS, and UNFPA, to strengthen fistula prevention, treatment, and reintegration efforts throughout West Africa.
Objective 1: Strengthened enabling environment to institutionalize fistula prevention, treatment, and reintegration in the public and private sectors FC+ continues to support the Economic Community of West African States (ECOWAS) Assembly of Health Ministers’ (AMS) September 2018 ECOWAS Member States Resolution on the Elimination of Fistula from the ECOWAS Region (https://wcaro.unfpa.org/en/publications/ecowas-member-states-resolution-fistula-elimination). This Resolution was derived from the FC+ facilitated Banjul Resolution, first proposed by the West African Health Organization (WAHO) during the project-supported launch of the March 2018 High Level Meeting of the West and Central African Group to End Obstetric Fistula (WCAGEOF) held in Banjul, Republic of The Gambia. The Resolution sets goals for the elimination of obstetric fistula in ECOWAS member countries by 2030. FC+ has been supporting WAHO and its Banjul Call to Action partners for the implementation of the Resolution, and had planned to convene a follow-on meeting of the West African Group to End Obstetric Fistula. However, due to the United States Government shutdown, the meeting originally planned for January 2019 during the WACS conference was postponed until June 2019.
The International Consultation on the Regional Strategy for Obstetric Fistula Elimination in West and Central Africa was held in Senegal in June 2019, see Appendix S. The Consultation was sponsored by regional partners including Fistula Care Plus/EngenderHealth, the West African Health Organization (WAHO), UNFPA, and URODAK. The overall objective of the consultation was to share the Banjul Call to Action resolution from the 2018 Banjul ECOWAS conference on obstetric fistula elimination with all stakeholders and operationalize the resolution with action plans focusing on pillars such as capacity building of health providers, monitoring, evaluation and resource mobilization. The operationalization of the resolution will be done in partnership with academic institutions, professional associations and NGOs for identification and referral of cases, surgical and non-surgical treatment, reintegration and rehabilitation of women with fistula in the region. This strategy must be underpinned by quality assurance and an evidence-based, flexible framework that includes data for decision-making.

Annual Report • October 2018 – September 2019 Fistula Care Plus 85
The three-day meeting took place June 19-21, 2019 in Saly Portugal, Senegal. Opening ceremonies were led by Professor Serigne Magueye Gueye, Professor at Cheikh Anta Diop University and Grand Yoff General Hospital, President of WACS; Dr. Sosthene Dougrou, UNFPA Representative; Dr. Aissa Bouwawe, WAHO; and Mr. Moustapha Diallo representing FC+/EngenderHealth. Presentations during the first day of the meeting covered topics including the history of global resolutions related to fistula and the “Banjul Call to Action 2018”, the roles of ECOWAS and UNFPA in obstetric fistula elimination in the region, capacity building efforts for midwives and nurses, and specific strategic approaches to speed up obstetric fistula elimination including costing data and country-level situation analyses.
The second day of the meeting focused on academic institutional roles in obstetric fistula efforts, including presentations from the West African College of Surgeons (WACS), the West African Postgraduate College of Pharmacists (WAPCP), and the West African College of Nursing (WACN). The third and final day of the meeting included a presentation by the FC+ Global Activities Manager summarizing FC+ project strategies and achievements (see Appendix QQ), followed by development of countries’ road maps and preparation of the Saly resolution for fistula elimination.
This regional meeting was immediately followed by URODAK, an annual meeting of urologists in the region. The FC+ Global Activities Manager made a presentation on behalf of the FC+ Deputy Director at the URODAK meeting that addressed the management and morbidity burden of prolonged and obstructed labor (see Appendix PP).
During the first quarter, FC+ received confirmation from Direct Relief International that donated fistula modules were shipped to Maradi and the facility confirmed receipt in the second quarter. Tahoua received their modules in the third quarter. During the third quarter, CNRFO began submission of their application for Direct Relief fistula modules and the request is currently being processed.
Objective 2: Enhanced community understanding and practices to prevent fistula, improve access to fistula treatment, reduce stigma, and support reintegration of women and girls with fistula After the closure of the FC+/WA office in Niger, REF managed community activities through their subaward. Due to the current activity suspension, no community outreach activities were implemented during FY 18/19.
As described further in Objective 5, FC+ has finalized and shared with USAID/WA a program learning report on the implementation of Site Walk Throughs (SWTs) to strengthen community-facility linkages in Niger. Findings will be applied to programmatic decisions regarding refresher trainings for the community volunteers, to identify additional support needs related to implementation of the action plans, and to inform future FC+ implementation of the SWT approach.
Obj. 3: Reduced transportation, communications, and financial barriers to accessing preventive care, detection, treatment, and reintegration support Under the REF subaward, FC+/WAN reimbursed the roundtrip transportation costs and client repair fees for all clients in need referred to CNRFO, CSME Tahoua, and CSME Maradi for fistula repair. Delays in finalizing financial reports and implementing a new subaward resulted in challenges for timely fund transfers. As noted above, activity through REF has been suspended as FC+ completes a financial and administrative review. FC+ will compete a new subaward in the first quarter of FY 19/20 to select the best local partner for future activities.

Annual Report • October 2018 – September 2019 Fistula Care Plus 86
Objective 4: Strengthened provider and health facility capacity to provide and sustain quality services for fistula prevention, detection, and treatment In April 2019, an FC+ Senior Clinical Advisor, the FC+ Global Activities Manager and an FC+ Program Associate took part in a caravan group of several donors, including USAID/WA, making site visits to assess the current environment for fistula prevention and treatment at supported facilities. The FC+ team visited CNRFO; Provincial Mother and Child Hospitals at Maradi, Tahoua, and Zinder; and the Danja Fistula Center at Maradi. Severe gaps in medical waste management and infection prevention practice were observed at supported sites. Following consultation with governmental authorities and USAID colleagues, FC+ committed to installing a pit hole system for medical waste management at CNRFO, Maradi and Tahoua. Following a local bidding process, vendors have been identified to manage these installations, which will be completed by December 2019. During the fourth quarter of FY 18/19, the FC+ Global team has also worked through a local consultant to ensure drainage and evacuate spoiled water at CNRFO.
In addition to these waste management and infection prevention issues and recommendations, the FC+ team recommended a financial audit of the CNRFO health facility and the potential of supporting Danja, a private health facility, in the future. Due to the aforementioned subaward challenges, surgical repairs were only supported during the first quarter of the fistula year. In the first quarter of FY 18/19, 66 women with severe incontinence symptoms sought fistula care services at FC+ supported sites, of which 44 were diagnosed with fistula (67%) and 41 of those women were medically eligible for surgery. FC+ supported 45 surgical fistula repairs during this period. The number of repairs exceeds the number of women diagnosed during the period because several women had received diagnoses in previous quarters when there was no surgeon available at CNRFO for repairs.
Some women may be diagnosed with fistula in one quarter and repaired in the next. Because FC+ does not track individual women through our data collection, we are unable to present a definitive percentage of women requiring repair who receive it. We are also unable to report the number of women repaired because women may have multiple repairs over the life of project, or repairs at multiple sites. However, within a given quarter, the number of repairs generally reflects the number of women. Figure WAN1 presents data on women seeking and eligible for fistula treatment, and the number of fistula surgeries supported, by site.
Figure WAN1: Number of Women Seeking and Requiring Fistula Treatment, and Number of Surgical Repairs, by Site, FY 18/19
0
20
40
CSME Tahoua CSME Maradi CNRFO
Seeking
Eligible
Repairs

Annual Report • October 2018 – September 2019 Fistula Care Plus 87
These 45 fistula repair surgeries were conducted at three FC+ supported hospitals: CSME Maradi, CSME Tahoua,and Centre National de Référence de la Fistule Obstétricale (CNRFO), see Table WAN1 for detail by quarter. All surgeries performed occurred during routine service provision.
In addition to the surgical repairs supported, three women received non-surgical catheter treatment (catheterization) for fistula during the fiscal year at CSME Tahoua, all of whom were closed and continent at discharge.
Table WAN1: USAID-Supported Surgical Fistula Repairs, by Site, By Quarter, FY 18/19
Site Oct-Dec 2018
Jan-Mar 2019
Apr–Jun 2019
Jul-Sep 2019
Total FY 18/19
CSME Tahoua 7 0 0 0 7 CSME Maradi 4 0 0 0 4 CNRFO 34 0 0 0 34 Total 45 0 0 0 45
Etiology data was available for 39 diagnosed fistula cases (89% of those diagnosed). The vast majority of fistulas diagnosed were the result of prolonged/obstructed labor (86.4%), followed by iatrogenic causes (2.3%).
Discharged fistula repairs during the first quarter of FY 18/19 were nearly evenly split between simple and not simple cases (48% and 52% respectively). 96% of all fistula surgery cases discharged in this time period were closed at discharge; with 87% closed and continent and 9% closed and incontinent. 4% were not closed at discharge. Outcomes for discharged patients are presented, by site, in Figure WAN2. No complications were reported.
No surgeons or other health facility personnel were trained during FY 18/19.
Figure WAN2. Outcome Rates for Surgical Repairs, by Site, FY 18/19
With the closure of the FC+ office in Niger in FY 17/18, FC+ support for family planning counseling and service provision and obstetric services at supported sites was suspended.
0%
20%
40%
60%
80%
100%
CSME Tahoua CSME Maradi CNRFO
Not closed
Closed with remainingincontinence
Closed and continent
Benchmark closed andcontinent (75%)

Annual Report • October 2018 – September 2019 Fistula Care Plus 88
Obj. 5: Strengthened evidence base for approaches to improve fistula care and scaled up application of standard monitoring and evaluation (M&E) indicators for prevention and treatment In 2014, with support from EngenderHealth technical advisors, the Tahoua and Maradi Districts in Niger were selected as pilot sites for community engagement activities, focusing on the training of community volunteers to promote utilization of preventive and maternal health services and family planning, and the implementation of Site Walk-Throughs/Visites Guidees (SWT) to strengthen community-facility linkages. SWTs were implemented in August 2016 in four locations within the Integrated Health Centers in Gradoume Tajae, Chadakori and Dan Issa. The SWT participants (community leaders, community volunteers, and facility staff) jointly analyzed problems and proposed locally relevant solutions to improve uptake of maternal, preventive and family planning services.
FC+ has finalized and shared with USAID/WA the program learning report on the SWTs in Niger. Findings will be applied to programmatic decisions regarding refresher trainings for the community volunteers, to identify additional support needs related to implementation of the action plans, and to inform future FC+ implementation of the SWT approach.
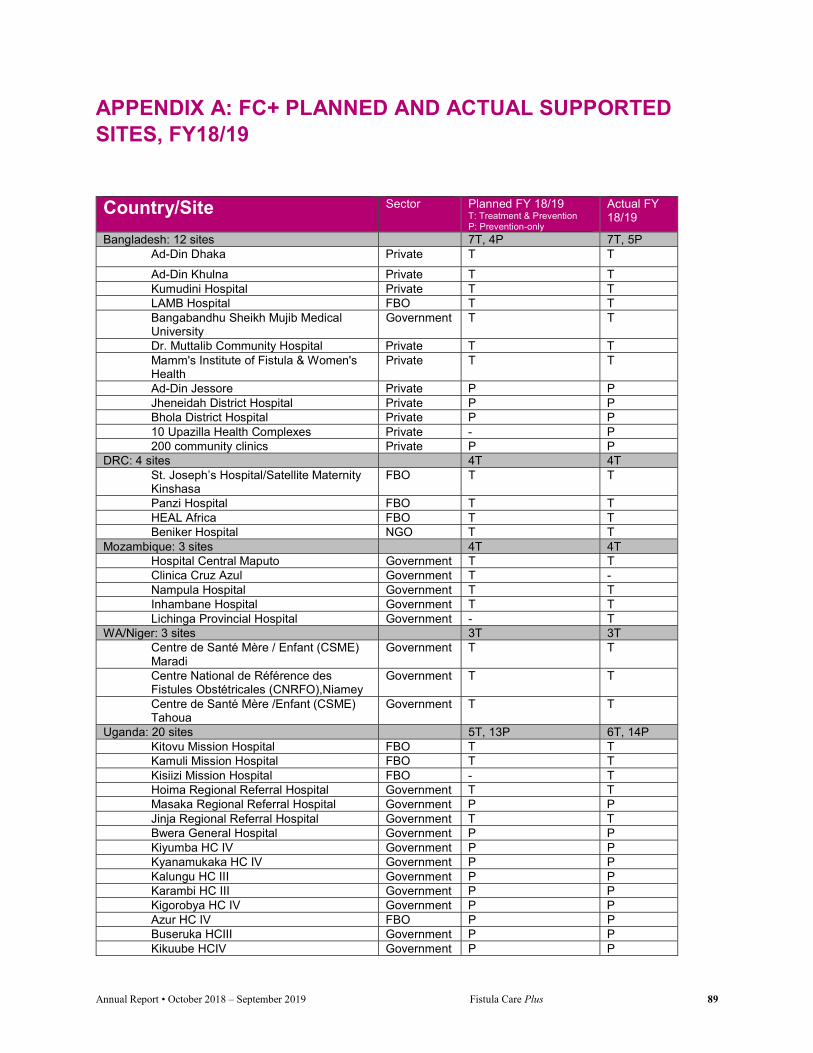
Annual Report • October 2018 – September 2019 Fistula Care Plus 89
APPENDIX A: FC+ PLANNED AND ACTUAL SUPPORTED SITES, FY18/19
Country/Site Sector Planned FY 18/19 T: Treatment & Prevention P: Prevention-only
Actual FY 18/19
Bangladesh: 12 sites 7T, 4P 7T, 5P Ad-Din Dhaka Private T T
Ad-Din Khulna Private T T Kumudini Hospital Private T T LAMB Hospital FBO T T Bangabandhu Sheikh Mujib Medical University
Government T T
Dr. Muttalib Community Hospital Private T T Mamm's Institute of Fistula & Women's Health
Private T T
Ad-Din Jessore Private P P Jheneidah District Hospital Private P P Bhola District Hospital Private P P 10 Upazilla Health Complexes Private - P 200 community clinics Private P P
DRC: 4 sites 4T 4T St. Joseph’s Hospital/Satellite Maternity Kinshasa
FBO T T
Panzi Hospital FBO T T HEAL Africa FBO T T Beniker Hospital NGO T T
Mozambique: 3 sites 4T 4T Hospital Central Maputo Government T T Clinica Cruz Azul Government T - Nampula Hospital Government T T Inhambane Hospital Government T T Lichinga Provincial Hospital Government - T
WA/Niger: 3 sites 3T 3T Centre de Santé Mère / Enfant (CSME) Maradi
Government T T
Centre National de Référence des Fistules Obstétricales (CNRFO),Niamey
Government T T
Centre de Santé Mère /Enfant (CSME) Tahoua
Government T T
Uganda: 20 sites 5T, 13P 6T, 14P Kitovu Mission Hospital FBO T T Kamuli Mission Hospital FBO T T Kisiizi Mission Hospital FBO - T Hoima Regional Referral Hospital Government T T Masaka Regional Referral Hospital Government P P Jinja Regional Referral Hospital Government T T Bwera General Hospital Government P P Kiyumba HC IV Government P P Kyanamukaka HC IV Government P P Kalungu HC III Government P P Karambi HC III Government P P Kigorobya HC IV Government P P Azur HC IV FBO P P Buseruka HCIII Government P P Kikuube HCIV Government P P

Annual Report • October 2018 – September 2019 Fistula Care Plus 90
Country/Site Sector Planned FY 18/19 T: Treatment & Prevention P: Prevention-only
Actual FY 18/19
Buraru HCIII Government P P Rwesande HCIV FBO P P Kagando Hospital FBO T P Lukolo HCIII Government P P Kagadi General Hospital Government - T
USAID Supported, Non Fistula Care Plus IntraHealth (Mali) JHPIEGO (Guinea) Jinnah Post Graduate Medical Center (Pakistan) Pathfinder (Ethiopia)
9T, 44P 4T, 44P 4T 1T NA
TOTAL USAID supported FC+ = 5 Countries
23T, 17P = 40 sites 24T, 19P= 43 sites
TOTAL USAID supported, bilateral (non FC+) = 4 Countries
9T, 44P= 53 sites
TOTAL USAID supported, All Projects = 9 countries
33T, 63P= 96 sites
T: Treatment and Prevention, P: Prevention-only

Annual Report • October 2018 – September 2019 Fistula Care Plus 91
APPENDIX B: FC+ PARTNERSHIPS, BY COUNTRY13 Country Partners Nature of Partnership Bangladesh Government of Bangladesh
Ministry of Health and Family Welfare (MOHFW)
Endorsement and dissemination of National Fistula Strategy and National Action Plan, participation in National Task Force on Obstetric Fistula, Vouchers
Directorate General of Health Services (DGHS)
National Task Force and Action Plan development, Government Medical College and District Hospitals, partograph use, C-Section, strengthening HMIS, surgical training
Directorate General of Family Planning (DGFP)
FP integration, community outreach
Ministry of Social Welfare (MOSW) and Ministry of Women and Children’s Affairs (MCWC) Quality Improvement Secretariat (QIS), Health Economics Unit, Ministry of Health
Reintegration, WDI Establishment of Technical Committee on Fistula
Obstetrical and Gynecological Society of Bangladesh (OGSB)
Partograph use, C-Section
UNFPA National Task Force, strengthening HMIS, policy, Increase treatment capacity, Surgical training
Direct Relief International Drugs and disposable surgical supplies Hope Foundation Hospital Strengthening HMIS and FP services
DRC Ministry of Health Fistula prevention and treatment Coordination SMNEA (Health of the Mother, Newborn, Child and Adolescent) Task Force Dissemination of SMNEA standards and guidelines
Access to Primary Health Care Project (ASSP) (DFID)
Fistula prevention and treatment, Community outreach
PROSANI Plus (Projet de Santé Intégré), Integrated Health Project (IHP), USAID
Fistula prevention and treatment
UNFPA Fistula prevention and treatment Direct Relief International Drugs and disposable surgical supplies
WA/Niger Ministry of Health Coordination, strategy Centre National de Référence des Fistules Obstétricales (CRNFO)
Training, treatment and research
UNFPA Fistula prevention and treatment REF Fistula treatment, community outreach
Mozambique Focus Fistula Fistula prevention and treatment Ministry of Health Fistula prevention and treatment
Uganda Ministry of Health(MoH) including all FC+ supported public facilities
Fistula prevention and treatment, National technical working groups PPFP integration into National Program Review of National RH Policy guidelines
District Health Offices (Masaka, Kasese, Kalungu, Hoima, Jinja, Kamuli)
Fistula prevention and treatment interventions; Quality improvement in facilities
TERREWODE Social reintegration, particularly with WDI/Persistent fistula-related disorder
AMREF Resource mobilization Population Council Barriers to treatment study
13 This list reflects partnerships in FY 18/19. This list does not include supported sites or other fistula projects supported by USAID bilateral funds.

Annual Report • October 2018 – September 2019 Fistula Care Plus 92
Country Partners Nature of Partnership Direct Relief International Drugs and medical supplies UNFPA Fistula prevention and treatment, FTWG UHMG FP Commodities Village Health Teams, Religious groups, Women’s groups
Community outreach and sensitizations
JPHIEGO Postpartum FP programming including capacity building of health workers,
Ministry of Gender, Labour and Social Development
Integrating gender into advocacy for obstetric prevention
PNFP Hospitals health facilities Fistula prevention and treatment Radio stations Public-private partnerships; Promoting fistula
awareness Private Education Development Network (PEDN)
Implementation of youth-focused interventions
Uganda Village project Fistula prevention and treatment FHI 360 Communications initiative USAID RHITES South West Fistula treatment, follow-up/reintegration USAID RHITES East Central Fistula treatment, follow-up/reintegration JSI Resource mobilization Merck, Sharp, and Dohme Implanon NXT/ DMPA transition and implant
removal stakeholders’ meeting
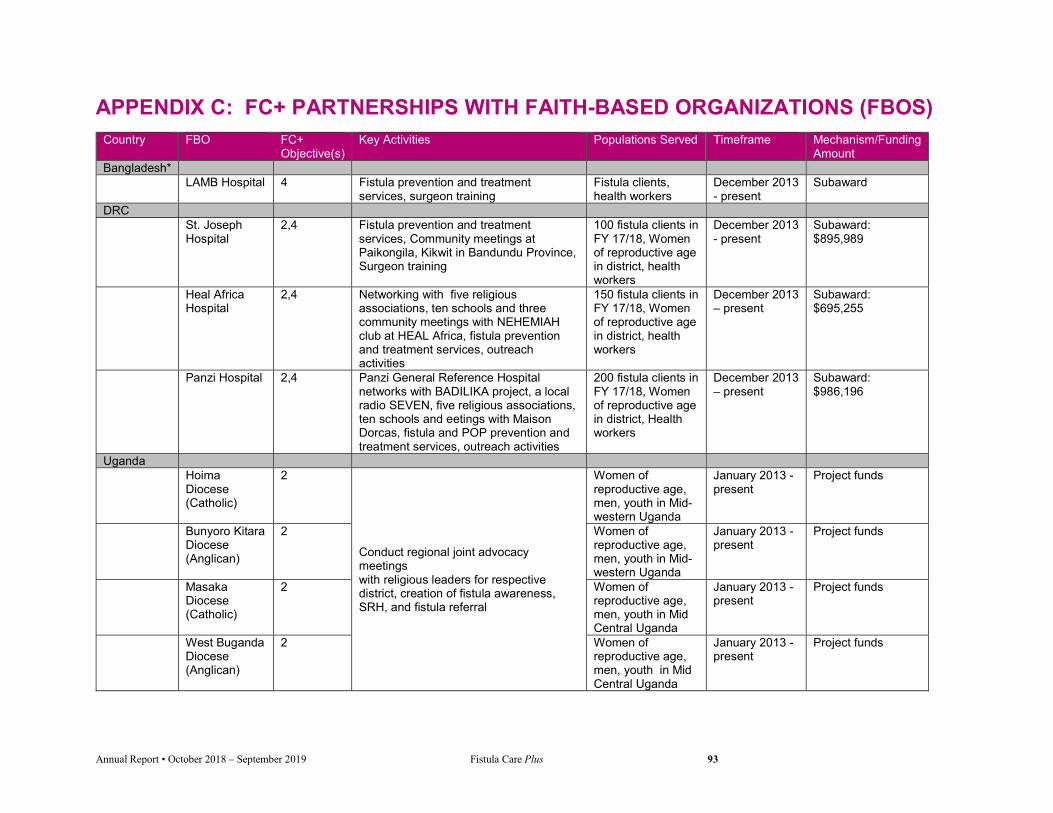
Annual Report • October 2018 – September 2019 Fistula Care Plus 93
APPENDIX C: FC+ PARTNERSHIPS WITH FAITH-BASED ORGANIZATIONS (FBOS) Country FBO FC+
Objective(s) Key Activities Populations Served Timeframe Mechanism/Funding
Amount Bangladesh* LAMB Hospital 4 Fistula prevention and treatment
services, surgeon training Fistula clients, health workers
December 2013 - present
Subaward
DRC St. Joseph
Hospital 2,4 Fistula prevention and treatment
services, Community meetings at Paikongila, Kikwit in Bandundu Province, Surgeon training
100 fistula clients in FY 17/18, Women of reproductive age in district, health workers
December 2013 - present
Subaward: $895,989
Heal Africa Hospital
2,4 Networking with five religious associations, ten schools and three community meetings with NEHEMIAH club at HEAL Africa, fistula prevention and treatment services, outreach activities
150 fistula clients in FY 17/18, Women of reproductive age in district, health workers
December 2013 – present
Subaward: $695,255
Panzi Hospital 2,4 Panzi General Reference Hospital networks with BADILIKA project, a local radio SEVEN, five religious associations, ten schools and eetings with Maison Dorcas, fistula and POP prevention and treatment services, outreach activities
200 fistula clients in FY 17/18, Women of reproductive age in district, Health workers
December 2013 – present
Subaward: $986,196
Uganda Hoima
Diocese (Catholic)
2
Conduct regional joint advocacy meetings with religious leaders for respective district, creation of fistula awareness, SRH, and fistula referral
Women of reproductive age, men, youth in Mid-western Uganda
January 2013 - present
Project funds
Bunyoro Kitara Diocese (Anglican)
2 Women of reproductive age, men, youth in Mid-western Uganda
January 2013 - present
Project funds
Masaka Diocese (Catholic)
2 Women of reproductive age, men, youth in Mid Central Uganda
January 2013 - present
Project funds
West Buganda Diocese (Anglican)
2 Women of reproductive age, men, youth in Mid Central Uganda
January 2013 - present
Project funds

Annual Report • October 2018 – September 2019 Fistula Care Plus 94
Country FBO FC+ Objective(s)
Key Activities Populations Served Timeframe Mechanism/Funding Amount
Masaka District Muslim Council
2 Women of reproductive age, men, youth in Mid Central Uganda
January 2013 - present
Project funds
Kamuli Mission Hospital
2,4,5 Fistula treatment, prevention and surgeon training; Capacity building on institutionalization of the partograph/ EMNOC; Integration of FP information, counselling and referral in MCH and fistula treatment; Support for IPC; Data for decision making, data quality assessment
Women of reproductive age in East Central Uganda, fistula clients, men; Health workers; Fistula clients; Patients and clients attending MCH services
January 2016 - present
Sub award Project funds
Kitovu Mission Hospital
2,4,5 Fistula treatment, prevention and surgeon training; Capacity building on institutionalization of the partograph/ EMNOC; Integration of FP information, counselling and referral in MCH and fistula treatment; Support for IPC; Data for decision making, data quality assessment
Women of reproductive age in East Central Uganda, fistula clients, men; Health workers; Fistula clients; Patients and clients attending MCH services
January 2016 - present
Sub award Project funds
Kagando Mission Hospital
4 Capacity building on institutionalization of the partograph /EMNOC; Integration of FP information, counselling and referral in MCH and fistula treatment; Support for IPC Building capacity of seven lower level health facilities (HSD) for scaling up institutionalization of the partograph /EMNOC
Health workers; Women on maternity wards for delivery and immediate postpartum care; Patients and clients attending MCH/FP services
December 2013 - present
Project funds
Kisiizi Mission Hospital
4 Fistula treatment, prevention and surgeon training
Women of reproductive age in South Western
January 2018 - present
Sub award Project funds

Annual Report • October 2018 – September 2019 Fistula Care Plus 95
Country FBO FC+ Objective(s)
Key Activities Populations Served Timeframe Mechanism/Funding Amount
Uganda, fistula clients
Azur Christian HC IV
4 Capacity building on institutionalization of the partograph/ EMNOC; Integration of FP information, counselling and referral in MCH and fistula treatment; Support for IPC
Health workers; Women on maternity wards for delivery and immediate postpartum care; Patients and clients attending MCH/FP services
December 2013 - present
Project funds
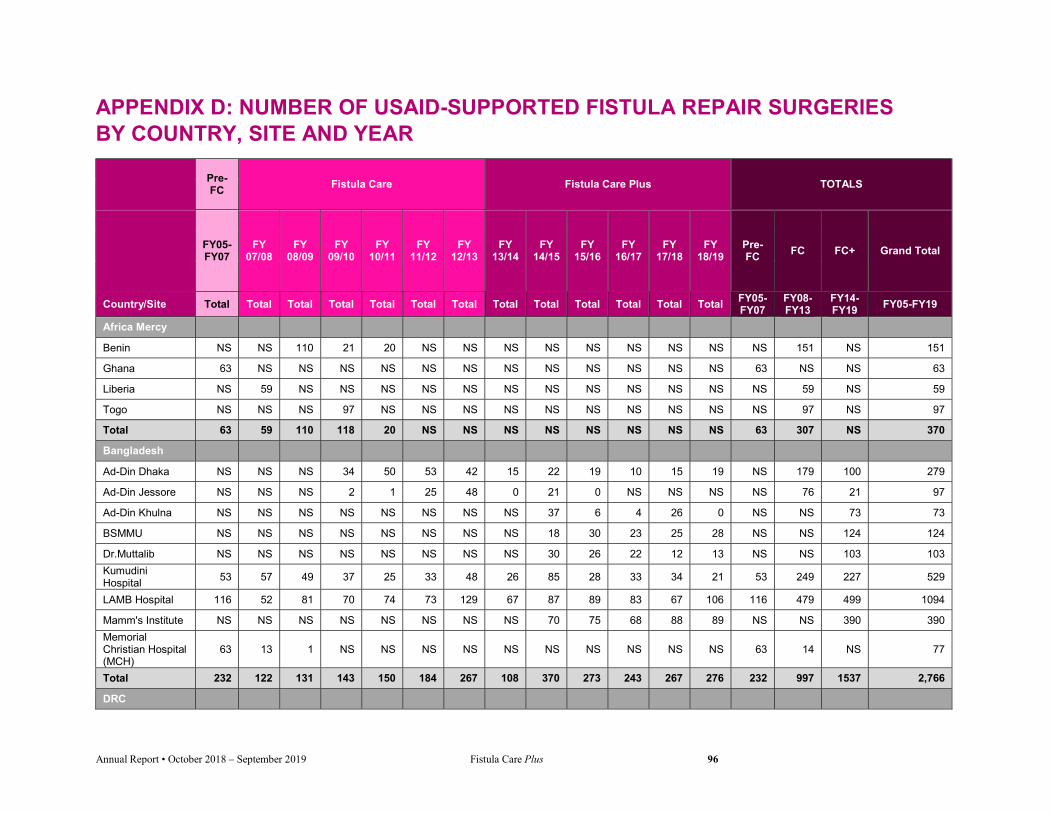
Annual Report • October 2018 – September 2019 Fistula Care Plus 96
APPENDIX D: NUMBER OF USAID-SUPPORTED FISTULA REPAIR SURGERIES BY COUNTRY, SITE AND YEAR
Pre-FC
Fistula Care Fistula Care Plus TOTALS
FY05-FY07
FY 07/08
FY 08/09
FY 09/10
FY 10/11
FY 11/12
FY 12/13
FY 13/14
FY 14/15
FY 15/16
FY 16/17
FY 17/18
FY 18/19
Pre-FC
FC FC+ Grand Total
Country/Site Total Total Total Total Total Total Total Total Total Total Total Total Total FY05-FY07
FY08-FY13
FY14-FY19
FY05-FY19
Africa Mercy
Benin NS NS 110 21 20 NS NS NS NS NS NS NS NS NS 151 NS 151
Ghana 63 NS NS NS NS NS NS NS NS NS NS NS NS 63 NS NS 63
Liberia NS 59 NS NS NS NS NS NS NS NS NS NS NS NS 59 NS 59
Togo NS NS NS 97 NS NS NS NS NS NS NS NS NS NS 97 NS 97
Total 63 59 110 118 20 NS NS NS NS NS NS NS NS 63 307 NS 370
Bangladesh
Ad-Din Dhaka NS NS NS 34 50 53 42 15 22 19 10 15 19 NS 179 100 279
Ad-Din Jessore NS NS NS 2 1 25 48 0 21 0 NS NS NS NS 76 21 97
Ad-Din Khulna NS NS NS NS NS NS NS NS 37 6 4 26 0 NS NS 73 73
BSMMU NS NS NS NS NS NS NS NS 18 30 23 25 28 NS NS 124 124
Dr.Muttalib NS NS NS NS NS NS NS NS 30 26 22 12 13 NS NS 103 103
Kumudini Hospital
53 57 49 37 25 33 48 26 85 28 33 34 21 53 249 227 529
LAMB Hospital 116 52 81 70 74 73 129 67 87 89 83 67 106 116 479 499 1094
Mamm's Institute NS NS NS NS NS NS NS NS 70 75 68 88 89 NS NS 390 390
Memorial Christian Hospital (MCH)
63 13 1 NS NS NS NS NS NS NS NS NS NS 63 14 NS 77
Total 232 122 131 143 150 184 267 108 370 273 243 267 276 232 997 1537 2,766
DRC

Annual Report • October 2018 – September 2019 Fistula Care Plus 97
Pre-FC
Fistula Care Fistula Care Plus TOTALS
FY05-FY07
FY 07/08
FY 08/09
FY 09/10
FY 10/11
FY 11/12
FY 12/13
FY 13/14
FY 14/15
FY 15/16
FY 16/17
FY 17/18
FY 18/19
Pre-FC
FC FC+ Grand Total
Country/Site Total Total Total Total Total Total Total Total Total Total Total Total Total FY05-FY07
FY08-FY13
FY14-FY19
FY05-FY19
HEAL Africa Hospital
268 200 214 210 163 288 264 NS 44 183 128 147 34 268 1339 536 2,143
Imagerie Des Grands-Lacs
NS NS NS NS 38 78 89 NS 40 127 75 NS NS NS 205 242 447
Maternité Esengo de Kisenso
NS NS NS NS NS NS 27 NS NS NS NS NS NS NS 27 NS 27
Maternite Sans Risque Kindu
NS NS NS NS 35 151 82 NS 68 226 46 NS NS NS 268 340 608
Mutombo NS NS NS NS 104 80 119 NS NS NS NS NS NS NS 303 NS 303
Beniker NS NS NS NS NS NS NS NS NS NS NS 80 73 NS NS 73 73
Panzi Hospital 371 134 268 262 180 500 567 NS 105 223 157 200 18 371 1911 703 2,985
St. Joseph NS NS NS NS 45 124 208 NS 128 241 141 133 33 NS 377 676 1,053
DRC Bilaterals
Project AXxes NS 361 442 514 NS NS NS NS NS NS NS NS NS NS 1317 NS 1,317
PS Kabongo NS NS NS NS NS 50 NS NS NS NS NS NS NS NS 50 NS 50
PS Katako Kombe
NS NS NS NS NS 87 NS NS NS NS NS NS NS NS 87 NS 87
PS HGR Katana NS NS NS NS NS NS 50 NS NS NS NS NS NS NS 50 NS 50
PS Kaziba NS NS NS NS NS 152 135 60 158 240 207 44 0 NS 287 709 996
PS Lodja NS NS NS NS NS 82 NS NS NS NS NS NS NS NS 82 NS 82
PS Luiza NS NS NS NS NS 28 NS NS NS NS NS NS NS NS 28 NS 28
PS Malemba Kulu NS NS NS NS NS 60 NS NS NS NS NS NS NS NS 60 NS 60
PS Tshikaji NS NS NS NS NS 49 NS NS NS NS NS NS NS NS 49 NS 49
PS Uvira NS NS NS NS NS 13 37 NS NS NS NS NS NS NS 50 NS 50
Total 639 695 924 986 565 1742 1,578 60 543 1240 754 604 158 639 6490 3279 10,408
Ethiopia

Annual Report • October 2018 – September 2019 Fistula Care Plus 98
Pre-FC
Fistula Care Fistula Care Plus TOTALS
FY05-FY07
FY 07/08
FY 08/09
FY 09/10
FY 10/11
FY 11/12
FY 12/13
FY 13/14
FY 14/15
FY 15/16
FY 16/17
FY 17/18
FY 18/19
Pre-FC
FC FC+ Grand Total
Country/Site Total Total Total Total Total Total Total Total Total Total Total Total Total FY05-FY07
FY08-FY13
FY14-FY19
FY05-FY19
Arba Minch Hospital
NS NS NS 27 NS NS NS NS NS NS NS NS NS NS 27 NA 27
Bahir Dar Fistula Center
564 596 297 383 307 392 NS NS NS NS NS NS NS 564 1975 NA 2,539
Mekelle Center NS NA 166 177 195 198 NS NS NS NS NS NS NS NS 736 NA 736
Ethiopia Bilateral
Pathfinder Project NS NS NS NS NS NS NS NS NS NS NS 366 359 NS NS 359 359
Total 564 596 463 587 502 590 NS NS NS NS NS 366 359 564 2,738 359 3,661
Guinea
Ignace Deen 193 63 49 20 NS NS 0 NS NS NS NS NS NS 193 132 NS 325
Jean Paul II NS 36 88 126 144 185 90 NS NS NS NS 11 0 NS 669 NS 669
Kissidougou 298 130 148 132 193 189 173 NS 15 49 122 111 78 298 965 375 1638
Labe NS NS 31 114 122 123 132 NS 5 37 69 43 34 NS 522 188 710
Boke NS NS NS NS NS NS NS NS NS 6 24 19 8 NS NS 57 57
Faranah NS NS NS NS NS NS NS NS NS NS NS 10 7 NS NS NS 7
Kindia NS NS NS NS NS NS NS NS NS NS 27 28 33 NS NS 88 88
Mercy Ships training repairs
NS NS NS NS NS NS 25 NS NS NS NS NS NS NS 25 NS 25
Total 491 229 316 392 459 497 420 NS 20 92 242 222 160 491 2,313 708 3519
Mali
Gao Regional Hospital
NS NS 46 40 91 53 NS NS NS NS NS NS NS NS 230 NA 230
Kayes Hospital NS NS NS NS NS NS 70 NS NS NS NS NS NS NS 70 NA 70
Mopti NS NS NS NS NS NS 20 NS NS NS NS NS NS NS 20 NA 20
Sikasso NS NS NS NS NS NS 140 NS NS NS NS NS NS NS 140 NA 140
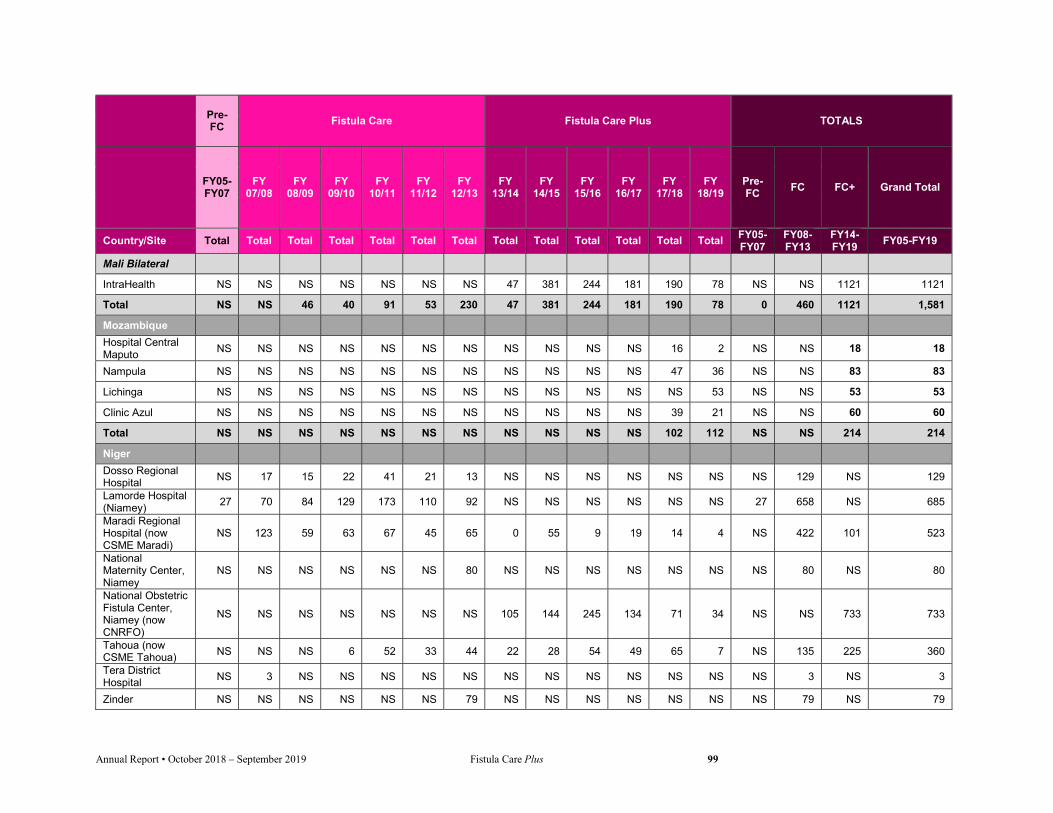
Annual Report • October 2018 – September 2019 Fistula Care Plus 99
Pre-FC
Fistula Care Fistula Care Plus TOTALS
FY05-FY07
FY 07/08
FY 08/09
FY 09/10
FY 10/11
FY 11/12
FY 12/13
FY 13/14
FY 14/15
FY 15/16
FY 16/17
FY 17/18
FY 18/19
Pre-FC
FC FC+ Grand Total
Country/Site Total Total Total Total Total Total Total Total Total Total Total Total Total FY05-FY07
FY08-FY13
FY14-FY19
FY05-FY19
Mali Bilateral
IntraHealth NS NS NS NS NS NS NS 47 381 244 181 190 78 NS NS 1121 1121
Total NS NS 46 40 91 53 230 47 381 244 181 190 78 0 460 1121 1,581
Mozambique
Hospital Central Maputo
NS NS NS NS NS NS NS NS NS NS NS 16 2 NS NS 18 18
Nampula NS NS NS NS NS NS NS NS NS NS NS 47 36 NS NS 83 83
Lichinga NS NS NS NS NS NS NS NS NS NS NS NS 53 NS NS 53 53
Clinic Azul NS NS NS NS NS NS NS NS NS NS NS 39 21 NS NS 60 60
Total NS NS NS NS NS NS NS NS NS NS NS 102 112 NS NS 214 214
Niger
Dosso Regional Hospital
NS 17 15 22 41 21 13 NS NS NS NS NS NS NS 129 NS 129
Lamorde Hospital (Niamey)
27 70 84 129 173 110 92 NS NS NS NS NS NS 27 658 NS 685
Maradi Regional Hospital (now CSME Maradi)
NS 123 59 63 67 45 65 0 55 9 19 14 4 NS 422 101 523
National Maternity Center, Niamey
NS NS NS NS NS NS 80 NS NS NS NS NS NS NS 80 NS 80
National Obstetric Fistula Center, Niamey (now CNRFO)
NS NS NS NS NS NS NS 105 144 245 134 71 34 NS NS 733 733
Tahoua (now CSME Tahoua)
NS NS NS 6 52 33 44 22 28 54 49 65 7 NS 135 225 360
Tera District Hospital
NS 3 NS NS NS NS NS NS NS NS NS NS NS NS 3 NS 3
Zinder NS NS NS NS NS NS 79 NS NS NS NS NS NS NS 79 NS 79

Annual Report • October 2018 – September 2019 Fistula Care Plus 100
Pre-FC
Fistula Care Fistula Care Plus TOTALS
FY05-FY07
FY 07/08
FY 08/09
FY 09/10
FY 10/11
FY 11/12
FY 12/13
FY 13/14
FY 14/15
FY 15/16
FY 16/17
FY 17/18
FY 18/19
Pre-FC
FC FC+ Grand Total
Country/Site Total Total Total Total Total Total Total Total Total Total Total Total Total FY05-FY07
FY08-FY13
FY14-FY19
FY05-FY19
Total 27 213 158 220 333 209 373 127 227 308 202 150 45 27 1,506 1059 2,592
Nigeria
National Obstetric Fistula Centre Abakaliki
NS NS 189 330 268 277 316 71 283 134 197 188 NS NS 1,380 873 2253
Babbar Ruga Hospital (Katsina)
356 536 331 359 330 416 359 160 309 244 357 279 NS 356 2,331 1349 4036
Faridat Yakubu General Hospital (Zamfara)
180 150 187 115 114 116 126 21 49 95 77 100 NS 180 808 342 1330
General Hospital Ogoja (Cross River State)
NS NS NS NS NS 114 50 14 17 17 63 33 NS NS 164 144 308
UTH Ibadan NS NS NS NS NS NS 37 18 6 6 20 0 NS NS 37 50 87
Gesse VVF Center (Kebbi)
102 122 151 207 216 215 152 55 140 171 153 114 NS 102 1,063 633 1798
Laure Fistula Center at Murtala Mohammed Specialist Hospital (Kano)
339 473 337 265 379 288 313 122 386 270 293 251 NS 339 2,055 1322 3716
Maryam Abacha Women’s and Children’s Hospital (Sokoto)
104 156 152 200 137 138 132 93 183 103 186 197 NS 104 915 762 1781
Ningi General Hospital (Bauchi)
NS NS NS NS 63 78 74 NS 131 164 186 156 NS NS 215 637 852
Other NS NS NS 136 NS 43 NS NS NS 20 23 0 NS NS 179 43 222
Maryam Abacha (Yobe)
NS NS NS NS NS NS NS NS NS NS NS 40 NS NS NS 40 40
Adeoyo GH NS NS NS NS NS NS NS NS 18 18 56 100 NS NS NS 192 192
Jahun VVF Center
NS NS NS NS NS NS NS NS 79 204 179 NS NS NS NS 462 462

Annual Report • October 2018 – September 2019 Fistula Care Plus 101
Pre-FC
Fistula Care Fistula Care Plus TOTALS
FY05-FY07
FY 07/08
FY 08/09
FY 09/10
FY 10/11
FY 11/12
FY 12/13
FY 13/14
FY 14/15
FY 15/16
FY 16/17
FY 17/18
FY 18/19
Pre-FC
FC FC+ Grand Total
Country/Site Total Total Total Total Total Total Total Total Total Total Total Total Total FY05-FY07
FY08-FY13
FY14-FY19
FY05-FY19
Sobi General Hospital (Kwara State)
NS NS NS NS NS 35 21 NS 44 13 50 22 NS NS 56 129 185
Family Life VVF Center
NS NS NS NS NS NS NS NS NS 52 NS NS NS NS NS 52 52
Hajiya Gambo Sawaba VVF Center
NS NS NS NS NS NS NS NS NS 72 113 58 NS NS NS 243 243
Wesley Guilds NS NS NS NS NS NS NS NS NS NS NS 22 NS NS NS NS 0
Total 1,081 1,437 1,347 1,612 1,507 1,720 1,580 554 1645 1583 1953 1560 0 1,081 9,203 7,295 17,579
Rwanda
CHUK 100 36 51 126 109 4 9 NS NS NS NS NS NS 100 335 NS 435
Kanombe Hospital
NS NS 14 48 38 55 35 NS NS NS NS NS NS NS 190 NS 190
Kibogora NS NS NS NS NS 21 0 NS NS NS NS NS NS NS 21 NS 21
Ruhengeri 192 47 102 85 131 34 4 NS NS NS NS NS NS 192 403 NS 595
Rwanda Bilateral
MCSP Project NS NS NS NS NS NS NS NS NS NS NS 249 0 NS NS 0 0
Total 292 83 167 259 278 114 48 NS NS NS NS 249 0 292 949 0 1,241
Sierra Leone
Aberdeen 272 363 253 166 211 244 115 NS NS NS NS NS NS 272 1,352 NS 1,624
Total 272 363 253 166 211 244 115 NS NS NS NS NS 0 272 1,352 NS 1,624
Tanzania
Vodafone/CCBRT NS NS NS NS NS NS NS 705 828 1048 885 NS NS NS NS 3466 3,466
Total NS NS NS NS NS NS NS 705 828 1048 885 NS 0 NS NS 3,466 3,466
Uganda
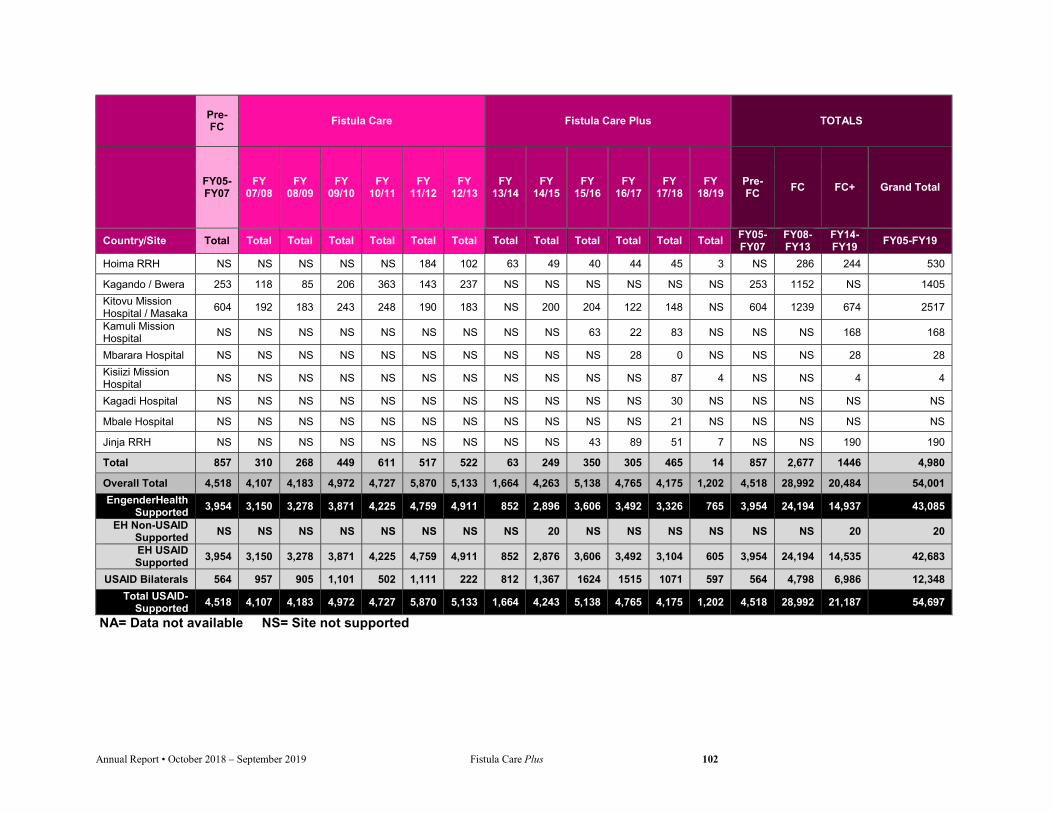
Annual Report • October 2018 – September 2019 Fistula Care Plus 102
Pre-FC
Fistula Care Fistula Care Plus TOTALS
FY05-FY07
FY 07/08
FY 08/09
FY 09/10
FY 10/11
FY 11/12
FY 12/13
FY 13/14
FY 14/15
FY 15/16
FY 16/17
FY 17/18
FY 18/19
Pre-FC
FC FC+ Grand Total
Country/Site Total Total Total Total Total Total Total Total Total Total Total Total Total FY05-FY07
FY08-FY13
FY14-FY19
FY05-FY19
Hoima RRH NS NS NS NS NS 184 102 63 49 40 44 45 3 NS 286 244 530
Kagando / Bwera 253 118 85 206 363 143 237 NS NS NS NS NS NS 253 1152 NS 1405
Kitovu Mission Hospital / Masaka
604 192 183 243 248 190 183 NS 200 204 122 148 NS 604 1239 674 2517
Kamuli Mission Hospital
NS NS NS NS NS NS NS NS NS 63 22 83 NS NS NS 168 168
Mbarara Hospital NS NS NS NS NS NS NS NS NS NS 28 0 NS NS NS 28 28
Kisiizi Mission Hospital
NS NS NS NS NS NS NS NS NS NS NS 87 4 NS NS 4 4
Kagadi Hospital NS NS NS NS NS NS NS NS NS NS NS 30 NS NS NS NS NS
Mbale Hospital NS NS NS NS NS NS NS NS NS NS NS 21 NS NS NS NS NS
Jinja RRH NS NS NS NS NS NS NS NS NS 43 89 51 7 NS NS 190 190
Total 857 310 268 449 611 517 522 63 249 350 305 465 14 857 2,677 1446 4,980
Overall Total 4,518 4,107 4,183 4,972 4,727 5,870 5,133 1,664 4,263 5,138 4,765 4,175 1,202 4,518 28,992 20,484 54,001
EngenderHealth Supported
3,954 3,150 3,278 3,871 4,225 4,759 4,911 852 2,896 3,606 3,492 3,326 765 3,954 24,194 14,937 43,085
EH Non-USAID Supported
NS NS NS NS NS NS NS NS 20 NS NS NS NS NS NS 20 20
EH USAID Supported
3,954 3,150 3,278 3,871 4,225 4,759 4,911 852 2,876 3,606 3,492 3,104 605 3,954 24,194 14,535 42,683
USAID Bilaterals 564 957 905 1,101 502 1,111 222 812 1,367 1624 1515 1071 597 564 4,798 6,986 12,348
Total USAID-Supported
4,518 4,107 4,183 4,972 4,727 5,870 5,133 1,664 4,243 5,138 4,765 4,175 1,202 4,518 28,992 21,187 54,697
NA= Data not available NS= Site not supported

Annual Report • October 2018 – September 2019 Fistula Care Plus 103
APPENDIX E: FC/ FC+ PEER REVIEWED PUBLICATIONS14
I. Published Anastasi E, Romanzi L, Ahmed S, Knuttson AT, Ojengbede O, Grant K; Campaign to End Fistula. Ending fistula
within a generation: making the dream a reality. Lancet Glob Health. 2017 Aug;5(8):e747-e748. [COMMENTARY – NO ABSTRACT]
Arrowsmith SD, Ruminjo J, Landry EG. Current practices in treatment of female genital fistula: a cross sectional study. BMC Pregnancy and Childbirth. 2010 Nov 10;10:73.
BACKGROUND: Background: Maternal outcomes in most countries of the developed world are good. However, in many developing/resource-poor countries, maternal outcomes are bleaker: Every year, more than 500,000 women die in childbirth, mostly in resource-poor countries. Those who survive often suffer from severe and long-term morbidities. One of the most devastating injuries is obstetric fistula, occurring most often in south Asia and sub-Saharan Africa. Fistula treatment and care are available in many countries across Africa and Asia, but there is a lack of reliable data around clinical factors associated with the success of fistula repair surgery. Most published research has been retrospective. While these studies have provided useful information about the care and treatment of fistula, they are limited by the design. This study was designed to identify practices in care that could lead to the design of prospective and randomized controlled trials. METHODS: Self-administered questionnaires were completed by 40 surgeons known to provide fistula treatment services in Africa and Asia at private and government hospitals. The questionnaire was divided into three parts to address the following issues: prophylactic use of antibiotics before, during, and after fistula surgery; urethral catheter management; and management practices for patients with urinary incontinence following fistula repair. RESULTS: The results provide a glimpse into current practices in fistula treatment and care across a wide swath of geographic, economic, and organizational considerations. There is consensus in treatment in some areas (routine use of prophylactic antibiotics, limited bed rest until the catheter is removed, nonsurgical treatment for postsurgical incontinence), while there are wide variations in practice in other areas (duration of catheter use, surgical treatments for postsurgical incontinence). These findings are based on a small sample and do not allow for recommending changes in clinical care, but they point to issues for possible clinical trial research that would contribute to more efficient and effective fistula care. CONCLUSIONS: The findings from the survey allowed us to consider clinical practices most influential in the cost, efficacy, and safety of fistula treatment. These considerations led us to formulate recommendations for eight randomized controlled trials on the following subjects: 1) Efficacy/safety of short-term catheterization; 2) efficacy of surgical and nonsurgical therapies for urinary incontinence; 3) technical measures during fistula repair to reduce the incidence of post-surgery incontinence; 4) identification of predictive factors for "incurable fistula"; 5) usefulness of urodynamic studies in the management of urinary incontinence; 6) incidence and significance of multi-drug resistant bacteria in the fistula population; 7) primary management of small, new fistulas by catheter drainage; and 8) antibiotic prophylaxis in fistula repair. Arrowsmith SD, Barone MA, Ruminjo J. Outcomes in obstetric fistula care: a literature review. Current Opinion
in Obstetrics and Gynecology. 2013 Oct;25(5):399-403.
PURPOSE OF REVIEW: To highlight the lack of consistency in the terminology and indicators related to obstetric fistula care and to put forward a call for consensus. RECENT FINDINGS: Recent studies show at least some degree of statistical correlation between outcome and the following clinical factors: degree of scarring/fibrosis, fistula location, fistula size, damage to the urethra, presence of circumferential fistula, bladder capacity, and prior attempt at fistula repair. SUMMARY: Consensus about basic definitions of clinical success does not yet exist. Opinions vary widely about the prognostic parameters for success or failure. Commonly agreed upon definitions and outcome measures will help ensure that site reviews are accurate and conducted fairly. To properly compare technical innovations with existing methods, agreement must be reached on definitions of success. Standardized
14 This summarizes all peer-reviewed publications throughout the life of both the FC and FC+ projects, as of September 2019.

Annual Report • October 2018 – September 2019 Fistula Care Plus 104
indicators for mortality and morbidity associated with fistula repair will improve the evidence base and contribute to quality of care. Barone M, Widmer M, Arrowsmith S, Ruminjo J, Seuc A, Landry E, Hamidou Barry T, Danladi D, Djangnikpo L,
Gbawuru-Mansaray T, Harou I, Lewis A, Muleta M, Nembunzu D, Olupot R, Sunday-Adeoye I, Wakasiaka WK, Landoulsi S, Delamou A, Were L, Frajzyngier V, Beattie K, A Gülmezoglu AM. 7 day bladder catheterization is not inferior to 14 day catheterization following repair of female genital fistula: a randomized controlled, non-inferiority trial. Lancet. 2015 Jul 4;386(9988):56-62.
BACKGROUND: Duration of bladder catheterization after female genital fistula repair varies widely. We aimed to establish whether 7 day bladder catheterization was not inferior to 14 days in terms of incidence of fistula repair breakdown among women with simple fistula. METHODS: We conducted a non-inferiority randomized controlled trial at eight hospitals in eight African countries. Women with a simple fistula that was closed after surgery and that remained closed until postoperative day 7 were eligible. Participants were randomized in a 1:1 ratio to 7 or 14-day bladder catheterization. The primary outcome was fistula repair breakdown, based on dye test results, any time after day 7 after catheter removal up to 3 months post-surgery. Secondary outcomes included: repair breakdowns at 7 days after catheter removal or thereafter, urinary retention on day 1, 3 and/or 7 after catheter removal; infections and febrile episodes potentially related to the treatment; catheter blockage; prolonged hospitalization; and residual incontinence at 3 months. The trial is registered with ClinicalTrials.gov, Identifier NCT01428830. FINDINGS: 524 participants were randomized and followed up between January 2012 and August 2013; 261 in the 7-day group and 263 in the 14-day group. The analysis population included 250 participants in the 7-day group and 251 in the 14-day group. There was no significant difference in the rate of fistula repair breakdown between the groups (risk difference 0.8%; 95% CI -2.8-4.5). There were no significant differences in the secondary outcomes between the groups. INTERPRETATION: 7 day bladder catheterization after repair of simple fistula was non-inferior to 14 day catheterization. It is safe and effective for managing women following repair of simple fistula without a significant increased risk of repair breakdown, urinary retention or residual incontinence through 3 months after surgery. Barone MA, Frajzyngier V, Arrowsmith S, Ruminjo J, Seuc A, Landry E, Beattie K, Barry TH, Lewis A, Muleta M,
Nembunzu D, Olupot R, Sunday-Adeoye I, Wakasiaka WK, Widmer M, Gülmezoglu AM. Non-inferiority of short-term urethral catheterization following fistula repair surgery: study protocol for a randomized controlled trial. BMC Womens Health. 2012 Mar 20;12:5.
BACKGROUND: A vaginal fistula is a devastating condition, affecting an estimated 2 million girls and women across Africa and Asia. There are numerous challenges associated with providing fistula repair services in developing countries, including limited availability of operating rooms, equipment, surgeons with specialized skills, and funding from local or international donors to support surgeries and subsequent post-operative care. Finding ways of providing services in a more efficient and cost-effective manner, without compromising surgical outcomes and the overall health of the patient, is paramount. Shortening the duration of urethral catheterization following fistula repair surgery would increase treatment capacity, lower costs of services, and potentially lower risk of healthcare-associated infections among fistula patients. There is a lack of empirical evidence supporting any particular length of time for urethral catheterization following fistula repair surgery. This study will examine whether short-term (7 day) urethral catheterization is not worse by more than a minimal relevant difference to longer-term (14 day) urethral catheterization in terms of incidence of fistula repair breakdown among women with simple fistula presenting at study sites for fistula repair service. METHODS/DESIGN: This study is a facility-based, multicenter, non-inferiority randomized controlled trial (RCT) comparing the new proposed short-term (7 day) urethral catheterization to longer-term (14 day) urethral catheterization in terms of predicting fistula repair breakdown. The primary outcome is fistula repair breakdown up to three months following fistula repair surgery as assessed by a urinary dye test. Secondary outcomes will include repair breakdown one week following catheter removal, intermittent catheterization due to urinary retention and the occurrence of septic or febrile episodes, prolonged hospitalization for medical reasons, catheter blockage, and self-reported residual incontinence. This trial will be conducted among 512 women with simple fistula presenting at 8 study sites for fistula repair surgery over the

Annual Report • October 2018 – September 2019 Fistula Care Plus 105
course of 24 months at each site. DISCUSSION: If no major safety issues are identified, the data from this trial may facilitate adoption of short-term urethral catheterization following repair of simple fistula in sub-Saharan Africa and Asia. TRIAL REGISTRATION: ClinicalTrials.gov Identifier NCT01428830. Barone MA, Frajzyngier V, Ruminjo J, Asiimwe F, Barry TH, Bello A, Danladi D, Ganda SO, Idris S, Inoussa M,
Lynch M, Mussell F, Podder DC. Determinants of postoperative outcomes of female genital fistula repair surgery. Obstetrics and Gynecology. 2012 Sep;120(3):524-31.
OBJECTIVE: To determine predictors of fistula repair outcomes 3 months postsurgery. METHODS: We conducted a multicountry prospective cohort study between 2007 and 2010. Outcomes, measured 3 months postsurgery, included fistula closure and residual incontinence in women with a closed fistula. Potential predictors included patient and fistula characteristics and context of repair. Multivariable generalized estimating equation models were used to generate adjusted risk ratios (RRs) and 95% confidence intervals (CIs). RESULTS: Women who returned for follow-up 3-month postsurgery were included in predictors of closure analyses (n=1,274). Small bladder size (adjusted RR 1.57, 95% CI 1.39-1.79), prior repair (adjusted RR 1.40, 95% CI 1.11-1.76), severe vaginal scarring (adjusted RR 1.56, 95% CI 1.20-2.04), partial urethral involvement (adjusted RR 1.36, 95% CI 1.11-1.66), and complete urethral destruction or circumferential defect (adjusted RR 1.72, 95% CI 1.33-2.23) predicted failed fistula closure. Women with a closed fistula at 3-month follow-up were included in predictors of residual incontinence analyses (n=1,041). Prior repair (adjusted RR 1.37, 95% CI 1.13-1.65), severe vaginal scarring (adjusted RR 1.35, 95% CI 1.10-1.67), partial urethral involvement (adjusted RR 1.78, 95% CI 1.27-2.48), and complete urethral destruction or circumferential defect (adjusted RR 2.06, 95% CI 1.51-2.81) were significantly associated with residual incontinence. CONCLUSION: The prognosis for genital fistula closure is related to preoperative bladder size, previous repair, vaginal scarring, and urethral involvement. Bedwell C, Levin K, Pett C, Lavender DT. A realist review of the partograph: when and how does it work for
labour monitoring? BMC Pregnancy and Childbirth. 2017 Jan 13;17(1):31.
BACKGROUND: The partograph (or partogram) is recommended by the World Health Organisation (WHO), for monitoring labour wellbeing and progress. Concerns about limitations in the way the partograph is used in the clinical context and the potential impact on its effectiveness have led to this realist systematic review of partograph use. METHODS: This review aimed to answer two key questions, 1) What is it about the partograph that works (or does not work); for whom does it work; and in what circumstances? 2) What are the essential inputs required for the partograph to work? A comprehensive search strategy encompassed key databases; including papers of varying methodologies. Papers were selected for inclusion if the focus of the paper was the partograph and related to context, mechanism or outcome. Ninety five papers were included for data synthesis. Two authors completed data extraction and synthesis. RESULTS: The evidence synthesis relates the evidence to identified theories of health worker acceptability, health system support, effective referral systems, human resources and health worker competence, highlighting barriers and facilitators. CONCLUSIONS: This first comprehensive realist synthesis of the partograph, provides the international community of maternity clinicians with a picture of potential issues and solutions related to successful labour recording and management, which is also translatable to other monitoring approaches.
Brazier E, Fiorentino R, Barry MS, Diallo M. The value of building health promotion capacities within communities: Evidence from a maternal health intervention in Guinea. Health Policy and Planning. 2015 Sep;30(7):885-94.
BACKGROUND: This paper presents results from a community-level intervention that promoted use of maternal health services as a means of preventing obstetric fistula. Implemented in the Republic of Guinea, the intervention aimed to build the capacity of community-level committees to heighten awareness about maternal health risks and to promote use of professional maternal health services. METHODS: Data were collected through a population-based survey. A total of 2,335 women of reproductive age were interviewed, including 878 with a live birth or stillbirth since the launch of the intervention. An index of community capacity was created to explore the
Annual Report • October 2018 – September 2019 Fistula Care Plus 106
effect of living in a community with strong community-level resources and support for maternal health. Other composite variables were created to measure the content of women’s antenatal counseling and their individual exposure to maternal health promotion activities at the community level. Multivariate logistic regression was used to explore the effect of community capacity and individual exposure variables on women’s use of antenatal care (> 4 visits), institutional delivery, and care for complications. RESULTS: Women living in communities with a high score on the community capacity index were more than twice as likely as women in communities with low score to attend at least four ANC visits, to deliver in a health facility, and to seek care for perceived complications. CONCLUSIONS: Building the capacity of community-level cadres to promote maternity care-seeking by women in their villages is an important complement to facility-level interventions to increase the availability, quality, and utilization of essential health services.
Brazier E, Fiorentino R, Barry S, Kasse Y, Millimono S. Rethinking how to promote maternity care-seeking: factors associated with institutional delivery in Guinea. Health Care for Women International. 2014 Sep;35(7-9):878-95.
This paper presents findings from a study on women’s delivery care-seeking in two regions of Guinea. We explored exposure to interventions promoting birth preparedness and complication readiness among women with recent live births and stillbirths. Using multivariate regression models, we identified factors associated with women’s knowledge and practices related to birth preparedness, as well as their use of health facilities during childbirth. We found that women’s knowledge about preparations for any birth (normal or complicated) was positively associated with increased preparation for birth, which itself was associated with institutional delivery. Knowledge about obstetric risks and danger signs, was not associated with birth preparation or with institutional delivery. The study findings highlight the importance of focusing on preparation for all births—and not simply obstetric emergencies—in interventions aimed at increasing women’s use of skilled maternity care.
Cavallaro FL, Pembe AB, Campbell O, Hanson C, Tripathi V, Wong KL, Radovich E, Benova L. Caesarean section provision and readiness in Tanzania: analysis of cross-sectional surveys of women and health facilities over time. BMJ Open. 2018 Oct 4;8(9):e024216.
OBJECTIVES: To describe trends in caesarean sections and facilities performing caesareans over time in Tanzania and examine the readiness of such facilities in terms of infrastructure, equipment and staffing. DESIGN: Nationally representative, repeated cross-sectional surveys of women and health facilities. SETTING: Tanzania. PARTICIPANTS: Women of reproductive age and health facility staff. MAIN OUTCOME MEASURES: Population-based caesarean rate, absolute annual number of caesareans, percentage of facilities reporting to perform caesareans and three readiness indicators for safe caesarean care: availability of consistent electricity, 24 hour schedule for caesarean and anaesthesia providers, and availability of all general anaesthesia equipment. RESULTS: The caesarean rate in Tanzania increased threefold from 2% in 1996 to 6% in 2015-16, while the total number of births increased by 60%. As a result, the absolute number of caesareans increased almost fivefold to 120 000 caesareans per year. The main mechanism sustaining the increase in caesareans was the doubling of median caesarean volume among public hospitals, from 17 caesareans per month in 2006 to 35 in 2014-15. The number of facilities performing caesareans increased only modestly over the same period. Less than half (43%) of caesareans in Tanzania in 2014-15 were performed in facilities meeting the three readiness indicators. Consistent electricity was widely available, and 24 hour schedules for caesarean and (less systematically) anaesthesia providers were observed in most facilities; however, the availability of all general anaesthesia equipment was the least commonly reported indicator, present in only 44% of all facilities (34% of public hospitals). CONCLUSIONS: Given the rising trend in numbers of caesareans, urgent improvements in the availability of general anaesthesia equipment and trained anaesthesia staff should be made to ensure the safety of caesareans. Initial efforts should focus on improving anaesthesia provision in public and faith-based organization hospitals, which together perform more than 90% of all caesareans in Tanzania. Delamou A, Delvaux T, El Ayadi AM, Tripathi V, Camara BS, Beavogui AH, Romanzi L, Cole B, Bouedouno P,
Diallo M, Barry TH, Camara M, Diallo K, Leveque A, Zhang WH, De Brouwere V. Fistula recurrence, pregnancy,

Annual Report • October 2018 – September 2019 Fistula Care Plus 107
and childbirth following successful closure of female genital fistula in Guinea: a longitudinal study. Lancet Glob Health. 2017 Nov;5(11):e1152-e1160.
Background: Female genital fistula is a devastating maternal complication of delivery in developing countries. We sought to analyse the incidence and proportion of fistula recurrence, residual urinary incontinence, and pregnancy after successful fistula closure in Guinea, and describe the delivery-associated maternal and child health outcomes. Methods: We did a longitudinal study in women discharged with a closed fistula from three repair hospitals supported by EngenderHealth in Guinea. We recruited women retrospectively (via medical record review) and prospectively at hospital discharge. We used Kaplan-Meier methods to analyse the cumulative incidence, incidence proportion, and incidence ratio of fistula recurrence, associated outcomes, and pregnancy after successful fistula closure. The primary outcome was recurrence of fistula following discharge from repair hospital in all eligible women who consented to inclusion and could provide follow-up data. Findings: 481 women eligible for analysis were identified retrospectively (from Jan 1, 2012, to Dec 31, 2014; 348 women) or prospectively (Jan 1 to June 20, 2015; 133 women), and followed up until June 30, 2016. Median follow-up was 28·0 months (IQR 14·6–36·6). 73 recurrent fistulas occurred, corresponding to a cumulative incidence of 71 per 1000 person-years (95% CI 56·5–89·3) and an incidence proportion of 18·4% (14·8–22·8). In 447 women who were continent at hospital discharge, we recorded 24 cases of post-repair residual urinary incontinence, equivalent to a cumulative incidence of 23·1 per 1000 person-years (14·0–36·2), and corresponding to 10·3% (5·2–19·6). In 305 women at risk of pregnancy, the cumulative incidence of pregnancy was 106·0 per 1000 person-years, corresponding to 28·4% (22·8–35·0) of these women. Of 50 women who had delivered by the time of follow-up, only nine delivered by elective caesarean section. There were 12 stillbirths, seven delivery-related fistula recurrences, and one maternal death. Interpretation: Recurrence of female genital fistula and adverse pregnancy-related maternal and child health outcomes were frequent in women after fistula repair in Guinea. Interventions are needed to safeguard the health of women after fistula repair. Delamou A, Utz B, Delvaux T, Beavogui AH, Shahabuddin A, Koivogui A, Levêque A, Zhang WH, De Brouwere V.
Pregnancy and childbirth after repair of obstetric fistula in sub-Saharan Africa: Scoping Review. Tropical Medicine & International Health. 2016 Nov;21(11):1348-1365.
OBJECTIVE: To synthesise the evidence on pregnancy and childbirth after repair of obstetric fistula in sub-Saharan Africa and to identify the existing knowledge gaps. METHODS: A scoping review of studies reporting on pregnancy and childbirth in women who underwent repair for obstetric fistula in sub-Saharan Africa was conducted. We searched relevant articles published between 1 January 1970 and 31 March 2016, without methodological or language restrictions, in electronic databases, general Internet sources and grey literature. RESULTS: A total of 16 studies were included in the narrative synthesis. The findings indicate that many women in sub-Saharan Africa still desire to become pregnant after the repair of their obstetric fistula. The overall proportion of pregnancies after repair estimated in 11 studies was 17.4% (ranging from 2.5% to 40%). Among the 459 deliveries for which the mode of delivery was reported, 208 women (45.3%) delivered by elective caesarean section (CS), 176 women (38.4%) by emergency CS and 75 women (16.3%) by vaginal delivery. Recurrence of fistula was a common maternal complication in included studies while abortions/miscarriage, stillbirths and neonatal deaths were frequent foetal consequences. Vaginal delivery and emergency cesarean section were associated with increased risk of stillbirth, recurrence of the fistula or even maternal death. CONCLUSION: Women who get pregnant after repair of obstetric fistula carry a high risk for pregnancy complications. However, the current evidence does not provide precise estimates of the incidence of pregnancy and pregnancy outcomes post-repair. Therefore, studies clearly assessing these outcomes with the appropriate study designs are needed.
Delamou, A., Delvaux, T., Utz, B., Camara, B. S., Beavogui, A. H., Cole, B., Levin, K., Diallo, M., Millimono, S.,
Barry, T. H., El Ayadi, A. M., Zhang, W.-H. and De Brouwere, V. Factors associated with loss to follow-up in women undergoing repair for obstetric fistula in Guinea. Tropical Medicine & International Health. 2015 Nov;20(11):1454-1461.
Annual Report • October 2018 – September 2019 Fistula Care Plus 108
Objectives: To analyse the trend of loss to follow-up over time and identify factors associated with women being lost to follow-up after discharge in three fistula repair hospitals in Guinea. Methods: This retrospective cohort study used data extracted from medical records of fistula repairs conducted from 1 January 2007 to 30 September 2013. A woman was considered lost to follow-up if she did not return within 4 months post-discharge. Factors associated with loss to follow-up were identified using a subsample of the data covering the period 2010–2013. Results: Over the study period, the proportion of loss to follow-up was 21.5% (448/2080) and varied across repair hospitals and over time with an increase from 2% in 2009 to 52% in 2013. After adjusting for other variables in a multivariate logistic regression model, women who underwent surgery at Labe hospital and at Kissidougou hospital were more likely to be lost to follow-up than women operated at Jean Paul II hospital (OR: 50.6; 95% CI: 24.9–102.8) and (OR: 11.5; 95% CI: 6.1–22.0), respectively. Women with their fistula closed at hospital discharge (OR: 3.2; 95% CI: 2.1–4.8) and women admitted for repair in years 2011–2013 showed higher loss to follow-up as compared to 2010. Finally, loss to follow-up increased by 2‰ for each additional kilometre of distance a client lived from the repair hospital (OR: 1.002; 95% CI: 1.001–1.003). Conclusion: Reimbursement of transport was the likely reason for change over time of LTFU. Reducing geographical barriers to care for women with fistula could sustain fistula care positive outcomes.
Delamou, A., Diallo, M., Beavogui, A. H., Delvaux, T., Millimono, S., Kourouma, M., Beattie, K., Barone, M.,
Barry, T. H., Khogali, M., Edginton, M., Hinderaker, S. G., Ruminjo, J., Zhang, W.-H. and De Brouwere, V. Good clinical outcomes from a 7-year holistic programme of fistula repair in Guinea. Tropical Medicine & International Health. 2015 20: 813–819.
OBJECTIVES: Female genital fistula remains a public health concern in developing countries. From January 2007 to September 2013, the Fistula Care project, managed by EngenderHealth in partnership with the Ministry of Health and supported by USAID, integrated fistula repair services in the maternity wards of general hospitals in Guinea. The objective of this article was to present and discuss the clinical outcomes of 7 years of work involving 2116 women repaired in three hospitals across the country. METHODS: This was a retrospective cohort study using data abstracted from medical records for fistula repairs conducted from 2007 to 2013. The study data were reviewed during the period April to August 2014. RESULTS: The majority of the 2116 women who underwent surgical repair had vesicovaginal fistula (n = 2045, 97%) and 3% had rectovaginal fistula or a combination of both. Overall 1748 (83%) had a closed fistula and were continent of urine immediately after surgery. At discharge, 1795 women (85%) had a closed fistula and 1680 (79%) were dry, meaning they no longer leaked urine and/or faeces. One hundred and fifteen (5%) remained with residual incontinence despite fistula closure. Follow-up at 3 months was completed by 1663 (79%) women of whom 1405 (84.5%) had their fistula closed and 80% were continent. Twenty-one per cent were lost to follow-up. CONCLUSION: Routine programmatic repair for obstetric fistula in low resources settings can yield good outcomes. However, more efforts are needed to address loss to follow-up, sustain the results and prevent the occurrence and/or recurrence of fistula.
Delamou, A, Samadari, G, Camara BS, Traore P, Diallo F, Millimono S, Wane D, Toliver M, Laffe K, Verani F.
Prevalence and correlates of intimate partner violence among family planning clients in Conakry, Guinea. BMC Research Notes. 2015 8:814
Intimate partner violence (IPV) is a global public health problem that affects women’s physical, mental, sexual and reproductive health. Very little data on IPV experience and FP use is available in resource-poor settings, such as in West Africa. The aim of this study was to describe the prevalence, patterns and correlates of IPV among clients of an adult Family Planning clinic in Conakry, Guinea. The study data was collected for four months (March to June 2014) from women’s family planning charts and from an IPV screening form at the Adult Family Planning and Reproductive Health Clinic of “Association Guinéenne pour le Bien-Etre Familial”, a non-profit organization in Conakry, Guinea. 232 women out of 245 women who attended the clinic for services during the study period were screened for IPV and were included in this study. Of the 232 women screened, 213 (92 %) experienced IPV in one form or another at some point in their lifetime. 169 women reported psychological violence (79.3 %), 145 reported sexual violence (68.1 %) and 103 reported physical violence (48.4 %). Nearly a quarter of women reported joint

Annual Report • October 2018 – September 2019 Fistula Care Plus 109
occurrence of the three forms of violence (24 %).Half of the IPV positive women were current users of family planning (51.2 %) and of these, 77.9 % preferred injectable contraceptives. The odds of experiencing IPV was higher in women with secondary or vocational level of education than those with higher level of education (AOR: 8.4; 95 % CI 1.2–58.5). Women residing in other communes of Conakry (AOR: 5.6; 95 % CI 1.4–22.9) and those preferring injectable FP methods (AOR: 4.5; 95 % CI 1.2–16.8) were more likely to experience lifetime IPV. IPV is prevalent among family planning clients in Conakry, Guinea where nine out of ten women screened in the AGBEF adult clinic reported having experienced one or another type of IPV. A holistic approach that includes promotion of women’s rights and gender equality, existence of laws and policies is needed to prevent and respond to IPV, effective implementation of policies and laws, and access to quality IPV services in Guinea and countries with higher rates of IPV.
El Ayadi AM, Barageine J, Korn A, Kakaire O, Turan J, Obore S, Byamugisha J, Lester F, Nalubwama H, Mwanje H, Tripathi V, Miller S. Trajectories of Women's Physical and Psychosocial Health Following Obstetric Fistula Repair in Uganda: A Longitudinal Study. Trop Med Int Health. 2018 Oct 29.
OBJECTIVES: To explore trajectories of physical and psychosocial health, and their interrelationship, among women completing fistula repair in Uganda for one-year post-surgery. METHODS: We recruited a 60-woman longitudinal cohort at surgical hospitalization from Mulago Hospital in Kampala Uganda (Dec 2014-June 2015) and followed them for one year. We collected survey data on physical and psychosocial health at surgery and at 3, 6, 9, and 12 months via mobile phone. Fistula characteristics were abstracted from medical records. All participants provided written informed consent. We present univariate analysis and linear regression results. RESULTS: Across post-surgical follow-up, most women reported improvements in physical and psychosocial health, largely within the first six months. By 12 months, urinary incontinence had declined from 98% to 33%, and general weakness from 33% to 17%, while excellent to good general health rose from 0% to 60%. Reintegration, self-esteem, and quality of life all increased through six months and remained stable thereafter. Reported stigma reduced, yet some negative self-perception remained at twelve months (mean 17.8). Psychosocial health was significantly impacted by report of physical symptoms; at 12 months, physical symptoms were associated with a 21.9 lower mean reintegration score (95% CI -30.1, -12.4) CONCLUSIONS: Our longitudinal cohort experienced dramatic improvements in physical and psychosocial health after surgery. Continuing fistula-related symptoms and the substantial differences in psychosocial health by physical symptoms supports additional intervention to support women's recovery or more targeted psychosocial support and reintegration services to ensure that those coping with physical or psychosocial challenges are appropriately supported. El Ayadi A, Nalubwama H, Barageine J, Neilands TB, Obore S, Byamugisha J, Kakaire O, Mwanje H, Korn A,
Lester F, Miller S. Development and preliminary validation of a post-fistula repair reintegration instrument among Ugandan women. Reproductive Health. 2017 Sep 2;14(1):109.
BACKGROUND: Obstetric fistula is a debilitating and traumatic birth injury affecting 2-3 million women globally, mostly in sub-Saharan Africa and Asia. Affected women suffer physically, psychologically and socioeconomically. International efforts have increased access to surgical treatment, yet attention to a holistic outcome of post-surgical rehabilitation is nascent. We sought to develop and pilot test a measurement instrument to assess post-surgical family and community reintegration. METHODS: We conducted an exploratory sequential mixed-methods study, beginning with 16 in-depth interviews and four focus group discussions with 17 women who underwent fistula surgery within two previous years to inform measure development. The draft instrument was validated in a longitudinal cohort of 60 women recovering from fistula surgery. Qualitative data were analyzed through thematic analysis. Socio-demographic characteristics were described using one-way frequency tables. We used exploratory factor analysis to determine the latent structure of the scale, then tested the fit of a single higher-order latent factor. We evaluated internal consistency and temporal stability reliability through Raykov's ρ and Pearson's correlation coefficient, respectively. We estimated a series of linear regression models to explore associations between the standardized reintegration measure and validated scales representing theoretically related constructs. RESULTS: Themes central to women's experiences following surgery included resuming mobility, increasing social interaction, improved self-esteem, reduction of internalized stigma, resuming work, meeting their own needs and the needs of dependents, meeting other expected and desired roles, and negotiating larger life

Annual Report • October 2018 – September 2019 Fistula Care Plus 110
issues. We expanded the Return to Normal Living Index to reflect these themes. Exploratory factor analysis suggested a four-factor structure, titled 'Mobility and social engagement', 'Meeting family needs', 'Comfort with relationships', and 'General life satisfaction', and goodness of fit statistics supported a higher-order latent variable of 'Reintegration.' Reintegration score correlated significantly with quality of life, depression, self-esteem, stigma, and social support in theoretically expected directions. CONCLUSION: As more women undergo surgical treatment for obstetric fistula, attention to the post-repair period is imperative. This preliminary validation of a reintegration instrument represents a first step toward improving measurement of post-surgical reintegration and has important implications for the evidence base of post-surgical reintegration epidemiology and the development and evaluation of fistula programming.
Frajzyngier V, Ruminjo J, Asiimwe F, Barry TH, Bello A, Danladi D, Ganda SO, Idris S, Inoussa M, Lynch M,
Mussell F, Podder DC, Barone MA. Factors influencing choice of surgical route of repair of genitourinary fistula, and the influence of route of repair on surgical outcomes: findings from a prospective cohort study. BJOG. 2012 Oct;119(11):1344-53.
OBJECTIVE: The abdominal route of genitourinary fistula repair may be associated with longer-term hospitalisation, hospital-associated infection and increased resource requirements. We examined: (1) the factors influencing the route of repair; (2) the influence of the route of repair on fistula closure 3 months following surgery; and (3) whether the influence of the route of repair on repair outcome varied by whether or not women met the published indications for abdominal repair. DESIGN: Prospective cohort study. SETTING: Eleven health facilities in sub-Saharan Africa and Asia. POPULATION: The 1274 women with genitourinary fistula presenting for surgical repair services. METHODS: Risk ratios (RRs) and 95% confidence intervals (95% CIs) were generated using log-binomial and Poisson (log-link) regression. Multivariable regression and propensity score matching were employed to adjust for confounding. MAIN OUTCOME MEASURES: Abdominal route of repair and fistula closure at 3 months following fistula repair surgery. RESULTS: Published indications for abdominal route of repair (extensive scarring or tissue loss, genital infibulation, ureteric involvement, trigonal, supratrigonal, vesico-uterine or intracervical location or other abdominal pathology) predicted the abdominal route [adjusted risk ratio (ARR), 15.56; 95% CI, 2.12-114.00]. A vaginal route of repair was associated with increased risk of failed closure (ARR, 1.41; 95% CI, 1.05-1.88); stratified analyses suggested elevated risk among women meeting indications for the abdominal route. CONCLUSIONS: Additional studies powered to test effect modification hypotheses are warranted to confirm whether the abdominal route of repair is beneficial for certain women. Frajzyngier V, Ruminjo J, Barone MA. Factors influencing urinary fistula repair outcomes in developing
countries: a systematic review. American Journal of Obstetrics & Gynecology. 2012 Oct;207(4):248-58. We reviewed literature examining predictors of urinary fistula repair outcomes in developing country settings, including fistula and patient characteristics, and perioperative factors. We searched Medline for articles published between January 1970 and December 2010, excluding articles that were (1) case reports, cases series or contained 20 or fewer subjects; (2) focused on fistula in developed countries; and (3) did not include a statistical analysis of the association between facility or individual-level factors and surgical outcomes. Twenty articles were included; 17 were observational studies. Surgical outcomes included fistula closure, residual incontinence after closure, and any incontinence (dry vs wet). Scarring and urethral involvement were associated with poor prognosis across all outcomes. Results from randomized controlled trials examining prophylactic antibiotic use and repair outcomes were inconclusive. Few observational studies examining perioperative interventions accounted for confounding by fistula severity. We conclude that a unified, standardized evidence-base for informing clinical practice is lacking. Frajzyngier V, Li G, Larson E, Ruminjo J, Barone MA. Development and comparison of prognostic scoring
systems for surgical closure of genitourinary fistula. American Journal of Obstetrics & Gynecology. 2013 Feb;208(2):112.e1-11.
OBJECTIVE: The purpose of this study was to test the diagnostic performance of 5 existing classification systems (developed by Lawson, Tafesse, Goh, Waaldijk, and the World Health Organization) and a prognostic scoring

Annual Report • October 2018 – September 2019 Fistula Care Plus 111
system that was derived empirically from our data to predict fistula closure 3 months after surgery. STUDY DESIGN: Women with genitourinary fistula (n = 1274) who received surgical repair services at 11 health facilities in sub-Saharan Africa and Asia were enrolled in a prospective cohort study. Using one-half of the sample, we created multivariate generalized estimating equation models to obtain weighted prognostic scores for components of each existing classification system and the empirically derived scoring system. With the second one-half, we developed receiver operating characteristic curves using the prognostic scores and calculated areas under the curves (AUCs) and 95% confidence intervals (CIs) for each system. RESULTS: Among existing systems, the scoring systems that represented the World Health Organization, Goh, and Tafesse classifications had the highest predictive accuracy: AUC, 0.63 (95% CI, 0.57-0.68); AUC, 0.62 (95% CI, 0.57-0.68), and AUC, 0.60 (95% CI, 0.55-0.65), respectively. The empirically derived prognostic score achieved similar predictive accuracy (AUC, 0.62; 95% CI, 0.56-0.67); it included significant predictors of closure that are found in the other classification systems, but contained fewer, nonoverlapping components. The differences in AUCs were not statistically significant. CONCLUSION: The prognostic values of existing urinary fistula classification systems and the empirically derived score were poor to fair. Further evaluation of the validity and reliability of existing classification systems to predict fistula closure is warranted; consideration should be given to a prognostic score that is evidence-based, simple, and easy to use. Keya KT, Sripad P, Nwala E, Warren CE. "Poverty is the big thing": exploring financial, transportation, and
opportunity costs associated with fistula management and repair in Nigeria and Uganda. Int J Equity Health. 2018 Jun 1;17(1):70.
Background: Women living with obstetric fistula often live in poverty and in remote areas far from hospitals that offer surgical repair. These women and their families incur a range of costs, some of which include: management of their condition, lost productivity and time, and transport to facilities – all of which prevent them from accessing fistula repair. This study explores, through women, community, and provider lenses, the financial, transport, and opportunity cost barriers and enablers to seeking repair services. Methods: A qualitative approach was applied in Kano and Ebonyi, Nigeria and Hoima and Masaka, Uganda. The study team conducted in-depth interviews (IDIs) with women affected by fistula (n=52) – including those awaiting repair, living with fistula and post-repair, their spouses and other family members (n=17), and health service providers involved in fistula repair and counseling (n=38). Focus group discussions (FGDs) with male and female community stakeholders (n=8) and post-repair clients (n=6) were also conducted. Results: Women’s experiences indicate that costs associated with the obstetric fistula condition reflect a combined set of costs associated with delivery, repair, transport, forgone income, and companion expenses that altogether is often catastrophic. Medical and non-medical ancillary costs such as food, medications, and water are not borne evenly across fistula care centers or camps due to funding shortages. In Uganda, most women spent Ugandan Shilling 10,000 to 90,000 (US$3.00-US$25.00) for a single trip to the camp for two people, while Nigerian women (Kano) spent Naira 250 to 2000 (US$0.80-US$6.41) for transportation. Factors influencing the cost of fistula care access include education and vocational skills of women and their family, community-based savings mechanisms, available resources in repair centers, client counselling, and subsidized care and transport. Conclusions: The concentration of women in poverty and the catastrophic costs associated with fistula repair speak to an inability to prioritize accessing fistula treatment over household expenditures. Findings recommend innovative approaches to financial assistance, transport, information of the available repair centers, rehabilitation, and reintegration in overcoming cost barriers.
Landry E, Pett C, Forentino R, Ruminjo J, Mattison C. Assessing the quality of record keeping for cesarean deliveries: results from a multicenter retrospective record review in five low-income countries. BMC Pregnancy and Childbirth. 2014 Apr 12;14:139.
BACKGROUND: Reliable, timely information is the foundation of decision making for functioning health systems; the quality of decision making rests on quality data. Routine monitoring, reporting, and review of cesarean section (CS) indications, decision-to-delivery intervals, and partograph use are important elements of quality improvement for maternity services. METHODS: In 2009 and 2010, a sample of CS delivery records from calendar year 2008 was

Annual Report • October 2018 – September 2019 Fistula Care Plus 112
reviewed at nine facilities in Bangladesh, Guinea, Mali, Niger, and Uganda. Data from patient records and hospital registers were collected on key aspects of care (e.g., timing of key events, indications, partograph use, maternal and fetal outcomes). Qualitative interviews were conducted with key informants at all study sites. RESULTS: A total of 2,941 records were reviewed. Fifty-seven key informant interviews were conducted to learn about record-keeping practices. Patient record-keeping systems were of varying quality across study sites: at five sites, more than 20% of records could not be located. Across all sites, patient files were missing key aspects of CS delivery care: timing of key events (e.g., examination, decision to perform CS), administration of prophylactic antibiotics, maternal complications, and maternal and fetal outcomes. Rates of partograph use were disappointingly low at six sites: 0 to 23.9% of patient files at these sites had a completed partograph on file, and among those found, 2.1% to 65.1% were completed correctly. Information on fetal outcomes was missing in up to 40% of patient files. CONCLUSIONS: Deficits in CS patient record data quality across a broad range of health facilities in low-resource settings in four sub-Saharan Africa countries and Bangladesh indicate an urgent need to improve record keeping.
Landry E, Frajzyngier V, Ruminjo J, Asiimwe F, Barry TH, Bello A, Danladi D, Ganda SO, Idris S, Inoussa M, Kanoma B, Lynch M, Mussell F, Podder DC, Wali A, Mielke E, Barone MA. Profiles and experiences of women undergoing genital fistula repair: findings from five countries. Global Public Health. 2013;8(8):926-42.
This article presents data from 1354 women from five countries who participated in a prospective cohort study conducted between 2007 and 2010. Women undergoing surgery for fistula repair were interviewed at the time of admission, discharge, and at a 3-month follow-up visit. While women's experiences differed across countries, a similar picture emerges across countries: women married young, most were married at the time of admission, had little education, and for many, the fistula occurred after the first pregnancy. Median age at the time of fistula occurrence was 20.0 years (interquartile range 17.3-26.8). Half of the women attended some antenatal care (ANC); among those who attended ANC, less than 50% recalled being told about signs of pregnancy complications. At follow-up, most women (even those who were not dry) reported improvements in many aspects of social life, however, reported improvements varied by repair outcome. Prevention and treatment programmes need to recognise the supportive role that husbands, partners, and families play as women prepare for safe delivery. Effective treatment and support programmes are needed for women who remain incontinent after surgery.
Longombe AO, Claude KM, Ruminjo J. Fistula and traumatic genital injury from sexual violence in a conflict
setting in Eastern Congo: case studies. Reproductive Health Matters. 2008 May;16(31):132-41. The Eastern region of the Democratic Republic of Congo (DRC) is currently undergoing a brutal war. Armed groups from the DRC and neighbouring countries are committing atrocities and systematically using sexual violence as a weapon of war to humiliate, intimidate and dominate women, girls, their men and communities. Armed combatants take advantage with impunity, knowing they will not be held to account or pursued by police or judicial authorities. A particularly inhumane public health problem has emerged: traumatic gynaecological fistula and genital injury from brutal sexual violence and gang-rape, along with enormous psychosocial and emotional burdens. Many of the women who survive find themselves pregnant or infected with STIs/HIV with no access to treatment. This report was compiled at the Doctors on Call for Service/Heal Africa Hospital in Goma, Eastern Congo, from the cases of 4,715 women and girls who suffered sexual violence between April 2003 and June 2006, of whom 702 had genital fistula. It presents the personal experiences of seven survivors whose injuries were severe and long-term, with life-changing effects. The paper recommends a coordinated effort amongst key stakeholders to secure peace and stability, an increase in humanitarian assistance and the rebuilding of the infrastructure, human and physical resources, and medical, educational and judicial systems. Mallick L, Tripathi V. The association between female genital fistula symptoms and gender-based violence: A
multicountry secondary analysis of household survey data. Trop Med Int Health. 2018 Jan;23(1):106-119.

Annual Report • October 2018 – September 2019 Fistula Care Plus 113
OBJECTIVE: The Demographic and Health Surveys (DHS), which include standardised questions on female genital fistula symptoms, provide a unique opportunity to evaluate the epidemiology of fistula. This study sought to examine associations between self-reported fistula symptoms and experience of gender-based violence (GBV) among women interviewed in DHS surveys. METHODS: This study used data from thirteen DHS surveys with standardised fistula and domestic violence modules. Data from the most recent survey in each country were pooled, weighting each survey equally. Multivariable logistic regressions controlled for maternal and demographic factors. RESULTS: Prevalence of fistula symptoms in this sample of 95 625 women ranges from 0.3% to 1.8% by country. The majority of women reporting fistula symptoms (56%) have ever experienced physical violence, and more than one-quarter have ever experienced sexual violence (27%), compared with 38% and 13% among women with no symptoms, respectively. Similarly, 16% of women with fistula symptoms report recently experiencing sexual violence-twice the percentage among women not reporting symptoms (8%). Women whose first experience of sexual violence was from a non-partner have almost four times the odds of reporting fistula symptoms compared with women who never experienced sexual violence. These associations indicate a need to investigate temporal and causal relationships between violence and fistula. CONCLUSIONS: The increased risk of physical and sexual violence among women with fistula symptoms suggests that fistula programmes should incorporate GBV into provider training and services.
Ngongo C, Levin K, Landry E, Sutton I, Ndizeye S. What to measure and why? Experience developing and using novel monitoring indicators in maternal health: the case of obstetric fistula. Journal of Health Informatics in Developing Countries. 2015 9(1): 14-22.
The field of obstetric fistula has historically lacked common definitions for measuring outcomes. This paper recounts the process of developing, refining, and using standardized monitoring indicators and approaches as part of a fistula prevention and repair project working in fourteen countries. The process included the development and refinement of clinical indicators, the introduction of standardizing data collection and reporting at partner health facilities, building capacity to use data for decision making locally, nationally, and within the project, institutionalizing data review meetings and partner health facilities, and supporting the introduction of fistula treatment indicators into national Health Management Information Systems to enable continued measurement and support for fistula treatment services. As monitoring in the field of obstetric fistula continues to become more standardized and routine, the multi-country scope of the project enabled a wide-ranging effort through which indicators for a “new” maternal health content area were developed and applied. This experience provides lessons for other initiatives seeking to strengthen monitoring and reporting related to novel or emerging topics in maternal health services. Ngongo C, Christie K, Holden J, Ford C, Pett C. Striving for excellence: nurturing midwives' skills in Freetown,
Sierra Leone. Midwifery. 2013 Oct;29(10):1230-4. Midwives provide critical, life-saving care to women and babies. Effective midwives must be clinically competent, with the required knowledge, skills, and attitudes to provide quality care. Their success depends on an environment of supportive supervision, continuing education, enabling policies, and access to equipment and referral facilities. In Freetown, Sierra Leone, the Aberdeen Women's Centre launched a maternity unit with an emphasis on striving for excellence and providing ongoing professional development to its staff midwives. Its success was built upon fostering a sense of responsibility and teamwork, providing necessary resources, conforming to evidence-based standards, and building partnerships. An explicit philosophy of care was crucial for guiding clinical decision making. In its first two years of operation, the Aberdeen Women's Centre assisted 2076 births with two maternal deaths and 92 perinatal deaths. In-service education and supportive supervision facilitated the midwives' professional growth, leading to capable future leaders who are providing exemplary care to delivering mothers and their newborns in Freetown.
Annual Report • October 2018 – September 2019 Fistula Care Plus 114
Raassen TJ, Ngongo CJ, Mahendeka MM. Iatrogenic genitourinary fistula: an 18-year retrospective review of 805 injuries. International Urogynecology Journal. 2014 Dec;25(12):1699-706.
INTRODUCTION: Genitourinary fistula poses a public health challenge in areas where women have inadequate access to quality emergency obstetric care. Fistulas typically develop during prolonged, obstructed labor, but clinicians can also inadvertently cause a fistula when performing obstetric or gynecological surgery. METHODS: This retrospective study analyzes 805 iatrogenic fistulas from a series of 5,959 women undergoing genitourinary fistula repair in 11 countries between 1994 and 2012. Injuries fall into three categories: ureteric, vault, and vesico-[utero]/-cervico-vaginal. This analysis considers the frequency and characteristics of each type of fistula and the risk factors associated with iatrogenic fistula development. RESULTS: In this large series, 13.2% of genitourinary fistula repairs were for injuries caused by clinician error. A range of cadres conducted procedures resulting in iatrogenic fistula. Four out of five iatrogenic fistulas developed following surgery for obstetric complications: cesarean section, ruptured uterus repair, or hysterectomy for ruptured uterus. Others developed during gynecological procedures, most commonly hysterectomy. Vesico-[utero]/-cervico-vaginal fistulas were the most common (43.6%), followed by ureteric injuries (33.9%) and vault fistulas (22.5%). One quarter of women with iatrogenic fistulas had previously undergone a laparotomy, nearly always a cesarean section. Among these women, one quarter had undergone more than one previous cesarean section. CONCLUSIONS: Women with previous cesarean sections are at increased risk for iatrogenic injury. Work environments must be adequate to reduce surgical error. Training must emphasize the importance of optimal surgical techniques, obstetric decision-making, and alternative ways to deliver dead babies. Iatrogenic fistulas should be recognized as a distinct genitourinary fistula category.
Romanzi L, Meara JG, Anastasi E, Knutsson AT. Meeting the SDG challenge to end fistula and preventable childbirth-related morbidity and mortality. Lancet Global Health. 2019 Jul;7(7):e835-e836. [COMMENTARY – NO ABSTRACT]
Ruminjo JK, Frajzyngier V, Bashir Abdullahi M, Asiimwe F, Hamidou Barry T, Bello A, Danladi D, Oumarou Ganda S, Idris S, Inoussa M, Lynch M, Mussell F, Chandra Podder D, Wali A, Barone MA. Clinical procedures and practices used in the perioperative treatment of female genital fistula during a prospective cohort study. BMC Pregnancy Childbirth. 2014 Jul 5;14:220.
BACKGROUND: Treatment and care for female genital fistula have become increasingly available over the last decade in countries across Africa and South Asia. Before the International Federation of Gynaecology and Obstetrics (FIGO) and partners published a global fistula training manual in 2011 there was no internationally recognized, standardized training curriculum, including perioperative care. The community of fistula care practitioners and advocates lacks data about the prevalence of various perioperative clinical procedures and practices and their potential programmatic implications are lacking. METHODS: Data presented here are from a prospective cohort study conducted between September 2007 and September 2010 at 11 fistula repair facilities supported by Fistula Care in five countries. Clinical procedures and practices used in the routine perioperative management of over 1300 women are described. RESULTS: More than two dozen clinical procedures and practices were tabulated. Some of them were commonly used at all sites (e.g., vaginal route of repair, 95.3% of cases); others were rare (e.g., flaps/grafts, 3.4%) or varied widely depending on site (e.g. for women with urinary fistula, the inter-quartile range for median duration of post-repair bladder catheterization was 14 to 29 days). CONCLUSIONS: These findings show a wide range of clinical procedures and practices with different program implications for safety, efficacy, and cost-effectiveness. The variability indicates the need for further research so as to strengthen the evidence base for fistula treatment in developing countries.
Ruminjo R, Landry E, Beattie K, Isah A, Faisel AJ, Millimono S. Mortality risk associated with surgical treatment of female genital fistula. International Journal of Gynecology and Obstetrics. 2014 Apr 18. pii: S0020-7292(14)00194-5.
OBJECTIVE: Most surgeries proceed without incident, but all major surgeries have inherent risks for adverse events, including death. Some deaths are attributable to the condition requiring surgery, concurrent morbidity, or

Annual Report • October 2018 – September 2019 Fistula Care Plus 115
the surgery itself. For fistula treatment, published literature on mortality risk is extremely limited. This article describes the mortality risk associated with surgical treatment of female genital fistula and the contributory and contextual factors. METHODS: Confidential inquiries and clinical audits were conducted at 14 fistula repair sites in seven resource-poor countries. Data collection included interviews with key personnel involved in the clinical management of the deceased and a review of hospital records and client files following an audit protocol. RESULTS: Thirty deaths occurred from 26,060 fistula repair surgeries from 2005 to 2013, 21 attributable to surgery; the case fatality was 0.08 per 100 procedures. The causes of death for nearly half of the cases were various manifestations of sepsis and inflammation. CONCLUSIONS: This case fatality rate for fistula repair surgery is in the same range as comparable gynecologic operations in high-resource settings. Clinical and systemic issues should be addressed to minimize chances of recurrence, improve perioperative care and follow-up, assure prudent referral or deferral of difficult cases, and maintain better records.
Ruminjo J. 2007. Obstetric fistula and the challenge to maternal health care systems. IPPF Medical Bulletin 41(4):3-4. [COMMENTARY – NO ABSTRACT]
Tripathi V, Arnoff E, Sripad P. Removing barriers to fistula care: Applying appreciative inquiry to improve access to screening and treatment in Nigeria and Uganda. Healthcare for Women International. 2019 Jul 23:1-16.
A research-to-action collaboration sought to understand and respond to barriers to female genital fistula treatment in Nigeria and Uganda. This was guided by appreciative inquiry, a participatory approach for transformative programming with four phases: 1) inquire, 2) imagine, 3) innovate, and 4) implement. Through this process, partners designed and refined a treatment barrier reduction intervention using multiple communication channels to disseminate a consistent fistula screening algorithm and provide transportation vouchers to those screening positive. Partnership between an implementation organization, a research institution, and local community partners enabled data-driven design and patient-centered implementation to address specific barriers experienced by women. Tripathi V, Stanton C, Strobino D, Bartlett L. Measuring the quality of maternal and care processes at the time
of delivery in sub-Saharan Africa: development and validation of a short index. BMC Pregnancy Childbirth. 2019 Apr 16;19(1):133.
BACKGROUND: There is a growing recognition that quality of care must improve in facility-based deliveries to achieve further global reductions in maternal and newborn mortality and morbidity. Better measurement of care quality is needed, but the unpredictable length of labor and delivery hinders the feasibility of observation, the gold standard in quality assessment. This study evaluated whether a measure restricted to actions at or immediately following delivery could provide a valid assessment of the quality of the process of intrapartum and immediate postpartum care (QoPIIPC), including essential newborn care. METHODS: The study used a comprehensive QoPIIPC index developed through a modified Delphi process and validated by delivery observation data as a starting point. A subset of items from this index assessed at or immediately following delivery was identified to create a "delivery-only" index. This delivery-only index was evaluated across content and criterion validation domains using delivery observation data from Kenya, Madagascar, and Tanzania, including Zanzibar. RESULTS: The delivery-only index included 13 items and performed well on most validation criteria, including correct classification of poorly and well-performed deliveries. Relative to the comprehensive QoPIIPC index, the delivery-only index had reduced content validity, representing fewer dimensions of QoPIIPC. The delivery-only index was also less strongly associated with overall quality performance in observed deliveries than the comprehensive QoPIIPC index. CONCLUSIONS: Where supervision resources are limited, a measure of the quality of labor and delivery care targeting the time of delivery may mitigate challenges in observation-based assessment. The delivery-only index may enable increased use of observation-based quality assessment within maternal and newborn care programs in low-resource settings.

Annual Report • October 2018 – September 2019 Fistula Care Plus 116
Tripathi V, Elneil S, Romanzi L. Demand and capacity to integrate pelvic organ prolapse and genital fistula services in low-resource settings. Int Urogynecol J. 2018 Feb 6. [Epub ahead of print]
INTRODUCTION AND HYPOTHESIS: There is a need for expanded access to safe surgical care in low- and middle-income countries (LMICs) as illustrated by the report of the 2015 Lancet Commission on Global Surgery. Packages of closely-related surgical procedures may create platforms of capacity that maximize impact in LMIC. Pelvic organ prolapse (POP) and genital fistula care provide an example. Although POP affects many more women in LMICs than fistula, donor support for fistula treatment in LMICs has been underway for decades, whereas treatment for POP is usually limited to hysterectomy-based surgical treatment, occurring with little to no donor support. This capacity-building discrepancy has resulted in POP care that is often non-adherent to international standards and in non-integration of POP and fistula services, despite clear areas of similarity and overlap. The objective of this study was to assess the feasibility and potential value of integrating POP services at fistula centers. METHODS: Fistula repair sites supported by the Fistula Care Plus project were surveyed on current demand for and capacity to provide POP, in addition to perceptions about integrating POP and fistula repair services. RESULTS: Respondents from 26 hospitals in sub-Saharan Africa and South Asia completed the survey. Most fistula centers (92%) reported demand for POP services, but many cannot meet this demand. Responses indicated a wide variation in assessment and grading practices for POP; approaches to lower urinary tract symptom evaluation; and surgical skills with regard to compartment-based POP, and urinary and rectal incontinence. Fistula surgeons identified integration synergies but also potential conflicts. CONCLUSIONS: Integration of genital fistula and POP services may enhance the quality of POP care while increasing the sustainability of fistula care. Tripathi V. A literature review of quantitative indicators to measure the quality of labor and delivery care.
International Journal of Gynecology and Obstetrics. 2016 Feb:132(2): 139-45. BACKGROUND: Strengthening measurement of the quality of labor and delivery (L&D) care in low-resource countries requires an understanding of existing approaches. OBJECTIVES: To identify quantitative indicators of L&D care quality and assess gaps in indicators. SEARCH STRATEGY: PubMed, CINAHL Plus, and Embase databases were searched for research published in English between January 1, 1990, and October 31, 2013, using structured terms. SELECTION CRITERIA: Studies describing indicators for L&D care quality assessment were included. Those whose abstracts contained inclusion criteria underwent full-text review. DATA COLLECTION AND ANALYSIS: Study characteristics, including indicator selection and data sources, were extracted via a standard spreadsheet. MAIN RESULTS: The structured search identified 1224 studies. After abstract and full-text review, 477 were included in the analysis. Most studies selected indicators by using literature review, clinical guidelines, or expert panels. Few indicators were empirically validated; most studies relied on medical record review to measure indicators. CONCLUSIONS: Many quantitative indicators have been used to measure L&D care quality, but few have been validated beyond expert opinion. There has been limited use of clinical observation in quality assessment of care processes. The findings suggest the need for validated, efficient consensus indicators of the quality of L&D care processes, particularly in low-resource countries.
Tripathi V, Stanton C, Strobino D, Bartlett L. Development and Validation of an Index to Measure the Quality of
Facility-Based Labor and Delivery Care Processes in Sub-Saharan Africa. PLoS ONE. 2015. 10(6): e0129491.
BACKGROUND: High quality care is crucial in ensuring that women and newborns receive interventions that may prevent and treat birth-related complications. As facility deliveries increase in developing countries, there are concerns about service quality. Observation is the gold standard for clinical quality assessment, but existing observation-based measures of obstetric quality of care are lengthy and difficult to administer. There is a lack of consensus on quality indicators for routine intrapartum and immediate postpartum care, including essential newborn care. This study identified key dimensions of the quality of the process of intrapartum and immediate postpartum care (QoPIIPC) in facility deliveries and developed a quality assessment measure representing these dimensions. METHODS & FINDINGS: Global maternal and neonatal care experts identified key dimensions of

Annual Report • October 2018 – September 2019 Fistula Care Plus 117
QoPIIPC through a modified Delphi process. Experts also rated indicators of these dimensions from a comprehensive delivery observation checklist used in quality surveys in sub-Saharan African countries. Potential QoPIIPC indices were developed from combinations of highly-rated indicators. Face, content, and criterion validation of these indices was conducted using data from observations of 1,145 deliveries in Kenya, Madagascar, and Tanzania (including Zanzibar). A best-performing index was selected, composed of 20 indicators of intrapartum/immediate postpartum care, including essential newborn care. This index represented most dimensions of QoPIIPC and effectively discriminated between poorly and well-performed deliveries. CONCLUSIONS: As facility deliveries increase and the global community pays greater attention to the role of care quality in achieving further maternal and newborn mortality reduction, the QoPIIPC index may be a valuable measure. This index complements and addresses gaps in currently used quality assessment tools. Further evaluation of index usability and reliability is needed. The availability of a streamlined, comprehensive, and validated index may enable ongoing and efficient observation-based assessment of care quality during labor and delivery in sub-Saharan Africa, facilitating targeted quality improvement.
Tunçalp O, Tripathi V, Landry E, Stanton CK, Ahmed S. Measuring the incidence and prevalence of obstetric
fistula: approaches, needs, and recommendations. Bulletin of the World Health Organization. 2015 Jan; 93(1):60-62. [COMMENTARY - NO ABSTRACT]
Tunçalp Ö, Isah A, Landry E, Stanton CK. Community-based screening for obstetric fistula in Nigeria: a novel approach. BMC Pregnancy Childbirth. 2014 Jan 24;14:44.
BACKGROUND: Obstetric fistula continues to have devastating effects on the physical, social, and economic lives of thousands of women in many low-resource settings. Governments require credible estimates of the backlog of existing cases requiring care to effectively plan for the treatment of fistula cases. Our study aims to quantify the backlog of obstetric fistula cases within two states via community-based screenings and to assess the questions in the Demographic Health Survey (DHS) fistula module. METHODS: The screening sites, all lower level health facilities, were selected based on their geographic coverage, prior relationships with the communities and availability of fistula surgery facilities in the state. This cross-sectional study included women who presented for fistula screenings at study facilities based on their perceived fistula-like symptoms. Research assistants administered the pre-screening questionnaire. Nurse-midwives then conducted a medical exam. Univariate and bivariate analyses are presented. RESULTS: A total of 268 women attended the screenings. Based on the pre-screening interview, the backlog of fistula cases reported was 75 (28% of women screened). The backlog identified after the medical exam was 26 fistula cases (29.5% of women screened) in Kebbi State sites and 12 cases in Cross River State sites (6.7%). Verification assessment showed that the DHS questionnaire had 92% sensitivity, 83% specificity with 47% positive predictive value and 98% negative predictive value for identifying women afflicted by fistula among women who came for the screenings. CONCLUSIONS: This methodology, involving effective, locally appropriate messaging and community outreach followed up with medical examination by nurse-midwives at lower level facilities, is challenging, but represents a promising approach to identify the backlog of women needing surgery and to link them with surgical facilities.

Annual Report • October 2018 – September 2019 Fistula Care Plus 118
APPENDIX F: FC/FC+ PUBLICATION READERSHIP METRICS*
TITLE VIEWS JOURNAL PUB YEAR
Obstetric fistula and the challenge to maternal health care systems n/a* IPPF Medical Bulletin 2007 Fistula and traumatic genital injury from sexual violence in a conflict setting in Eastern Congo: case studies n/a Reproductive Health Matters 2008 Current practices in treatment of female genital fistula: a cross sectional study 8,995
BMC Pregnancy and Childbirth 2010
Determinants of postoperative outcomes of female genital fistula repair surgery. n/a Obstetrics and Gynecology 2012 Factors influencing choice of surgical route of repair of genitourinary fistula, and the influence of route of repair on surgical outcomes: findings from a prospective cohort study n/a BJOG 2012 Factors influencing urinary fistula repair outcomes in developing countries: a systematic review n/a
American Journal of Obstetrics and Gynecology 2012
Non-inferiority of short-term urethral catheterization following fistula repair surgery: study protocol for a randomized controlled trial 5,260 BMC Women's Health 2012 Development and comparison of prognostic scoring systems for surgical closure of genitourinary fistula. n/a
American Journal of Obstetrics and Gynecology 2013
Outcomes in obstetric fistula care: a literature review n/a Current Opinion in Obstetrics and Gynecology 2013
Profiles and experiences of women undergoing genital fistula repair: findings from five countries 1,457 Global Public Health 2013 Striving for excellence: nurturing midwives' skills in Freetown, Sierra Leone. n/a Midwifery 2013 Assessing the quality of record keeping for cesarean deliveries: results from a multicenter retrospective record review in five low-income countries. 2,393
BMC Pregnancy and Childbirth 2014
Clinical Procedures and Practices Used in the Perioperative Treatment of Female Genital Fistula during a Prospective Cohort Study. 2,654
BMC Pregnancy and Childbirth 2014
Community-based screening for obstetric fistula in Nigeria: a novel approach 3,825
BMC Pregnancy and Childbirth 2014
Iatrogenic genitourinary fistulas: An 18-year retrospective review of 801 iatrogenic injuries n/a
International Journal of Urogynecology 2014
Rethinking how to promote careseeking: Factors associated with institutional delivery in Guinea 1,459
Health Care for Women International 2014
Measuring the incidence and prevalence of obstetric fistula: approaches, needs, and recommendations n/a
Bulletin of the World Health Organization 2014
Mortality risk associated with surgical treatment of female genital fistula. 228***
International Journal of Gynecology and Obstetrics 2014
The value of building health promotion capacities within communities: Evidence from a maternal health intervention in Guinea. n/a Health Policy and Planning 2014 A literature review of quantitative indicators to measure the quality of labor and delivery care** n/a
International Journal of Gynecology and Obstetrics 2015
Breakdown of simple female genital fistula repair after 7 day versus 14 day postoperative bladder catheterisation: a randomised, controlled, open-label, non-inferiority trial n/a The Lancet 2015 Development and validation of an index to measure facility-based labor and delivery care processes in sub-Saharan Africa** 10,673 PLOS ONE 2015 Prevalence and correlates of intimate partner violence among family planning clients in Conakry, Guinea. 696 BMC Research Notes 2015
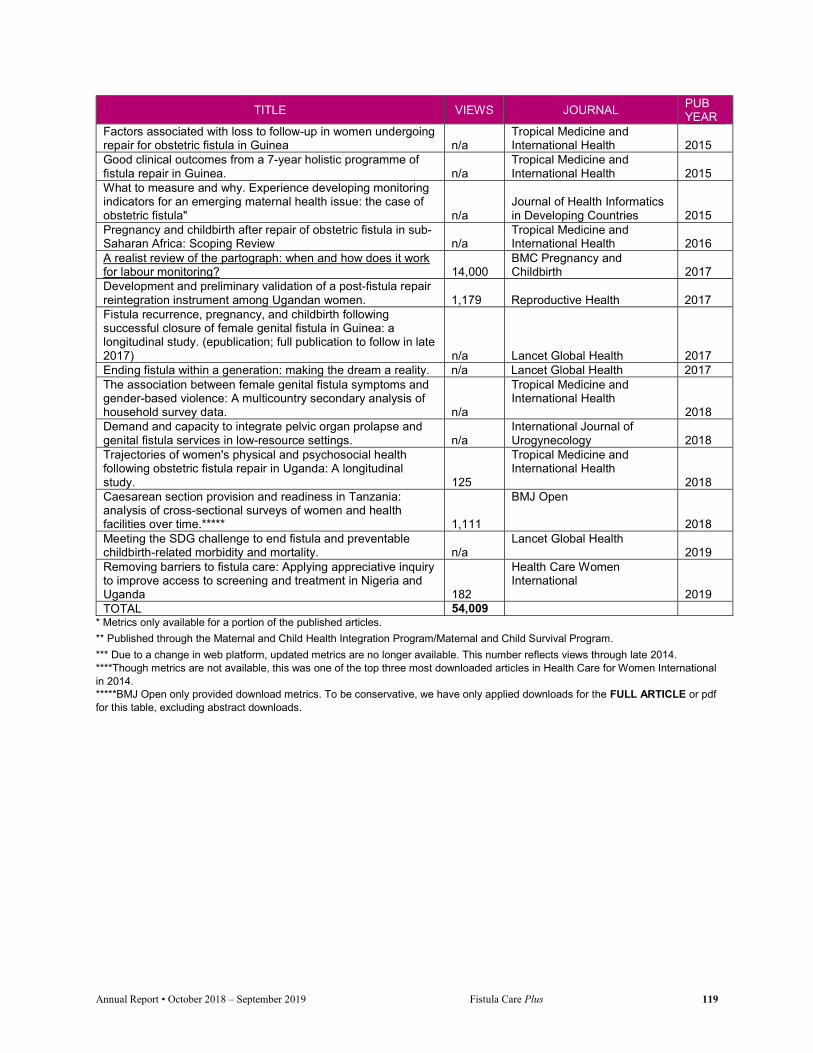
Annual Report • October 2018 – September 2019 Fistula Care Plus 119
TITLE VIEWS JOURNAL PUB YEAR
Factors associated with loss to follow-up in women undergoing repair for obstetric fistula in Guinea n/a
Tropical Medicine and International Health 2015
Good clinical outcomes from a 7-year holistic programme of fistula repair in Guinea. n/a
Tropical Medicine and International Health 2015
What to measure and why. Experience developing monitoring indicators for an emerging maternal health issue: the case of obstetric fistula" n/a
Journal of Health Informatics in Developing Countries 2015
Pregnancy and childbirth after repair of obstetric fistula in sub-Saharan Africa: Scoping Review n/a
Tropical Medicine and International Health 2016
A realist review of the partograph: when and how does it work for labour monitoring? 14,000
BMC Pregnancy and Childbirth 2017
Development and preliminary validation of a post-fistula repair reintegration instrument among Ugandan women. 1,179 Reproductive Health 2017 Fistula recurrence, pregnancy, and childbirth following successful closure of female genital fistula in Guinea: a longitudinal study. (epublication; full publication to follow in late 2017) n/a Lancet Global Health 2017 Ending fistula within a generation: making the dream a reality. n/a Lancet Global Health 2017 The association between female genital fistula symptoms and gender-based violence: A multicountry secondary analysis of household survey data. n/a
Tropical Medicine and International Health
2018 Demand and capacity to integrate pelvic organ prolapse and genital fistula services in low-resource settings. n/a
International Journal of Urogynecology 2018
Trajectories of women's physical and psychosocial health following obstetric fistula repair in Uganda: A longitudinal study. 125
Tropical Medicine and International Health
2018 Caesarean section provision and readiness in Tanzania: analysis of cross-sectional surveys of women and health facilities over time.***** 1,111
BMJ Open
2018 Meeting the SDG challenge to end fistula and preventable childbirth-related morbidity and mortality. n/a
Lancet Global Health 2019
Removing barriers to fistula care: Applying appreciative inquiry to improve access to screening and treatment in Nigeria and Uganda 182
Health Care Women International
2019 TOTAL 54,009
* Metrics only available for a portion of the published articles.
** Published through the Maternal and Child Health Integration Program/Maternal and Child Survival Program.
*** Due to a change in web platform, updated metrics are no longer available. This number reflects views through late 2014. ****Though metrics are not available, this was one of the top three most downloaded articles in Health Care for Women International in 2014. *****BMJ Open only provided download metrics. To be conservative, we have only applied downloads for the FULL ARTICLE or pdf for this table, excluding abstract downloads.

Annual Report • October 2018 – September 2019 Fistula Care Plus 120
APPENDIX G: FIGO SUMMARY TRIP REPORT

Annual Report • October 2018 – September 2019 Fistula Care Plus 121

Annual Report • October 2018 – September 2019 Fistula Care Plus 122
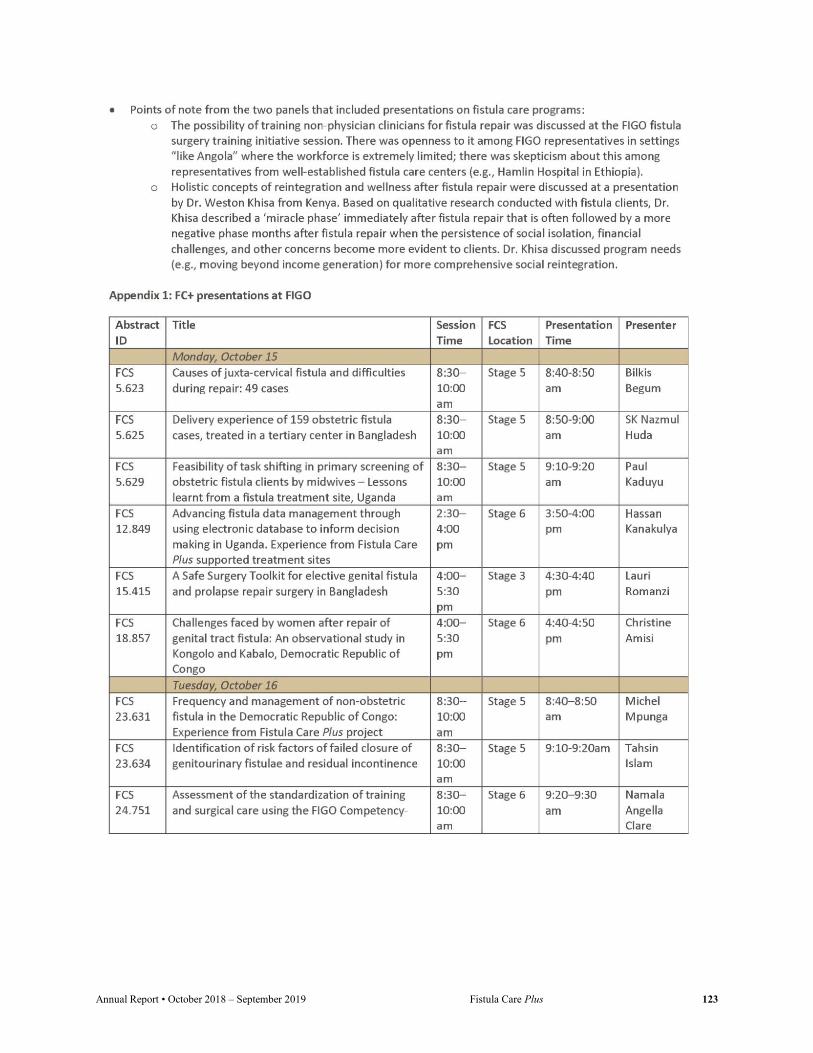
Annual Report • October 2018 – September 2019 Fistula Care Plus 123

Annual Report • October 2018 – September 2019 Fistula Care Plus 124

Annual Report • October 2018 – September 2019 Fistula Care Plus 125

Annual Report • October 2018 – September 2019 Fistula Care Plus 126
APPENDIX H: FC+ PARTICIPATION AT ISOFS AND IOFWG
FC+ presentations and posters at the 2018 International Society of Obstetric Fistula Surgeons
(ISOFS) and International Obstetric Fistula Working Group (IOFWG) Meetings
Summary: FC+ staff and supported partners gave 3 plenary oral presentations, 21 oral presentations, and 14 posters at ISOFS and IOFWG
Submitting country
Title Lead Author
Other Authors Format
Bangladesh Private initiative to treat fistula Sayeba Akhter
Plenary oral
Bangladesh Experience of using Community Radio for Fistula Communication in Bangladesh
Nitta Biswas
SK Nazmul Huda Poster
Bangladesh Report of a Prevalence survey on Female Genital Fistula in a large district in Bangladesh
Lucky Ghose
SK Nazmul Huda, Vandana Tripathi
Oral
Bangladesh Surgical Safety Toolkit based Quality Monitoring of Fistula Surgery in Bangladesh
Israt Jahan SK Nazmul Huda Lauri Romanzi
Oral
Bangladesh Media Leaders Workshop on Fistula Communication: An Innovation for capacity building of Bangladesh Press
Ashifur Rahman
Nazmul Huda, Nitta Biswas
Oral
Bangladesh Why has the Caesarean Rate Increased Dramatically in Bangladesh?
Nazmul Huda
John Richards, Labin Rahman
Oral
Bangladesh Rehabilitation and reintegration of Fistula Clients through Micro credit linked services
Sheikh Mohiuddin
Fazlul Haque, SK Nazmul Huda
Oral
Bangladesh Contribution of Ad-din Micro-credit program in Fistula case identification, referral and community based rehabilitation
Fazlul Haque
Sheikh Mohiuddin, SK Nazmul Huda
Poster
Bangladesh Role of a community clinic to prevent fistula
Anirudha Karmakar
SK Nazmul Huda Poster
Bangladesh Female Genital Fistula Repair Performance of Ad-din Hospitals 2013-2018
Nahid Yesmin
Farzana Yesmin,
Sheela Podder, Lucky Ghose
Poster (Accepted as oral, but poster prepared)

Annual Report • October 2018 – September 2019 Fistula Care Plus 127
Submitting country
Title Lead Author
Other Authors Format
Bangladesh Doctors beyond the wall of the hospital: Reflections of Community Based Actions of University Fistula Center, BSMMU
Begum Nasrin
Saleha Begum Chowdhury, Farhana Alam
Oral
Bangladesh Experience of Partnership with Fistula Program in Bangladesh: University Fistula Center, BSMMU
Farhana Alam
Saleha Begum Chowdhury, Sharmeen Mahmud
Oral
Bangladesh Fistula Champions leading local actions for Ending Fistula in Bangladesh
Ashorjo Karmaker
Shampad Karmaker, SK Nazmul Huda
Poster
Bangladesh Fistula Communication by Print and Electronic Media in Bangladesh as facilitated by Bangladesh Health Reporters Forum
Sebika Debnath
Nitta Biswas, SK Nazmul Huda
Poster
Bangladesh Community Radio Supporting Maternal and Child Health and Preventing obstetric Fistula in an area impacted by climate change
Selim Shahriar
Abdullah al Mahmood, Nitta Biswas, SK Nazmul Huda
Poster
Bangladesh Iatrogenic Fistula: Types, Causes and Post-repair outcome – 70 Cases
Bilkis Begum Chowdhury
Oral
Bangladesh Baseline knowledge of female genital fistula symptoms, causes and treatment among a rural population in Northern Bangladesh
Stacy Saha
Bea Ambauen-Berger, Shirajum Munira
Poster
Bangladesh Preliminary analysis of quality of life (QOL) before and after surgery for female genital fistula. A prospective cohort study
Stacy Saha
Bea Ambauen-Berger, Shirajum Munira
Oral
Bangladesh Incidence and characteristics of surgical fistula patients at LAMB hospital from 2011 to 2017
Bea Ambauen-Berger
Stacy Saha, Alison Seadon
Oral
DRC Facteurs de risques et prise en charge de la fistule obstétricale compliquée de calcul vésical à l’hôpital Saint Joseph de Kinshasa RD Congo
Dolores Nembunzu
Michel Mpunga, Felicien Banze, B. Tena Tena, Vandana Tripathi
Oral
DRC Childbirth injuries encountered on outreach in remote RDCongo
Justin Paluku Lussy
Esther KAHAMBU KITAMBALA, Eugénie KAMABU MUKEKULU
Oral
DRC The Mobile Surgical Outreach Model for
Kenny Raha AMISI NOTIA1, L. KEYSER3, J. MCKINNEY 3, M.
Oral

Annual Report • October 2018 – September 2019 Fistula Care Plus 128
Submitting country
Title Lead Author
Other Authors Format
women with genital fistula in the Democratic Republic of Congo
BERG4, D. MUKWEGE1,2
DRC Frequency and management of non-obstetric fistula in the Democratic Republic of Congo: experience from Fistula Care Plus project
Alexandre Delamou
Michel Mpunga2, Félicien Banze2, Dolores Nembunzu3, Kenny Raha4, Justin Paluku5, Rachel Kinja4, Esther Kitambala5, Brian Tena-Tena Aussak3, Ruth Bulu Bobina5, Notia A4, Mukuliboy Anne3, Altine Diop6, Vandana Tripathi6, Lauri Romanzi6
Oral
DRC IMPLEMENTING PHYSIOTHERAPY SERVICES INTO FISTULA CARE AT PANZI HOSPITAL, BUKAVU, DRC
Laura Keyser
Mc Kinney J., Amisi Ch., Mukwege D., Kinja Rachel
Poster
Niger
Fistula Prevention Awareness Activities of Community Volunteers in Niger
Ibrahim Souley
Diop Ndeye Altine2,
Mounkaila, Habsatou Traore3, Tripathi Vandana
Oral
Uganda Improving fistula data reporting through collaboration, learning and adaptation of fistula tools and indicators in Uganda
Hassan Kanakulya
Paul Kaduyu, Elly Arnoff, Rose Mukisa, Vandana Tripathi
Poster
Uganda Assessment of health worker knowledge in fistula management in Uganda
Hassan Kanakulya
C. Ndwiga, P. Sripad, E. Arnoff, R. Mukisa, S. Warren, J. Barageine
Poster
Uganda Facilitating Data for Decision Making to improve Health Management Information Systems reporting at four supported sites in Uganda
Hassan Kanakulya
Carol Kyozira, Paul Kaduyu, Rose Mukisa
Oral
Uganda Building the capacity of teachers to facilitate sexual reproductive information increases their confidence levels – the case of in school Aflateen plus Clubs, Uganda.
Molly Tumusiime
Dr. Paul Kaduyu, Hassan Kanakulya, Dr. Rose Mukisa,
Poster
Uganda Establishing Depression Levels among Women Seeking Pelvic
Paul Kaduyu
Rose Mukisa, Veronica Ibanda
Oral

Annual Report • October 2018 – September 2019 Fistula Care Plus 129
Submitting country
Title Lead Author
Other Authors Format
Floor Disorder Treatment at Fistula Care Plus Supported Sites in Uganda.
Uganda Increasing opportunities for obstetric fistula case detection and treatment by using multifactorial approaches – the case of Kalungu district –Uganda.
Molly Tumusiime
Paul Kaduyu Hassan Kanakulya Rose Mukisa
Oral
Uganda Using a communication strategy to empower youths make responsible social, economic, and sexual and reproductive health decision.
Molly Tumusiime
Paul Kaduyu Hassan Kanakulya Rose Mukisa
Poster
Uganda (Pop Council)
Enhancing primary health care providers’ capacity in screening and referral of women with fistula.
Charity Ndwiga
Pooja Sripad, George Odwe and Charlotte Warren
Oral
Global Improving quality of life for women with incurable fistula in Uganda
Vandana Tripathi
Uganda & TERREWODE teams
Oral
Global The association between female genital fistula symptoms and gender-based violence
Vandana Tripathi
Lindsay Mallick Oral
Global Bladder care and management of prolonged/obstructed labor for obstetric fistula: A global survey of intrapartum and postpartum clinical practices
Vandana Tripathi
Elly Arnoff Poster
Global Emerging global evidence about fistula – what do we know and how can fistula programs respond?
Vandana Tripathi
Plenary oral
Global Key learnings and highlights from the Fistula Care Plus project to inform a global road map**
Vandana Tripathi
IOFWG Plenary oral
**Presented at IOFWG meeting following ISOFS

Annual Report • October 2018 – September 2019 Fistula Care Plus 130
APPENDIX I: SCIENTIFIC PROGRAM OF THE 7TH INTERNATIONAL ISOFS CONFERENCE
December 5-6, 2018. Kathmandu, Nepal Day 1: 5thDec 2018, Wednesday Hall A 7:00-9:00 : Registration 9:00-9:15 : Scientific Opening 9:15-10:15am: Free Paper on surgical management of OF Chairpersons: Kees Waaldijk/ Steven Arrowsmith
S Time Topic Presenter 1. 9:15-9:25 Dr. Why I am still not dry? (urodynamic changes
after successful VVF repair) Aziz Adbullah
2. 9:25- 9:35 Doctor! Will I be dry? Factors determining recurrence after vesicovaginal fistula repair
Sajjad Ahmed Siddique
3. 9:35-9:45 Randomized Control Trial: Prophylactic autologous Fascia Sling for women at risk of urethral incontinence
Rachel J Pope
4. 9:45- 9:55 Genitourinary Fistula, A series of 1704 cases Haq Nawaz 5. 9:55-10:05 An experience of Abdominal repair of high
genitourinary fistula Tanveer Shafqat
6. 10:05-10:15 Assessment of etiology and outcome of fistula cases (VVF RVF) operated at Shaikh Zaid Women Hospital
Rafia Baloch
10:15- 11:15 Training and Capacity Building Chairpersons: Shershah Syed/Gillian Slinger/ Kiran Bajracharya
S No Time Topic Presenter 1. 10:15-10:25 Enhancing primary health care providers’ capacity
in screening and referral of women with fistula. Charity Ndwiga
2. 10:25-10:35 Stones before touching the Sharpen Knives Bello OO 3. 10:35-10:45 A Health Systems Strengthening Approach to
Female Genital Fistula in Kenya Elizabeth Amakove Wala
4. 10:45-10:55 Obstetric Fistula Orientation Program in Nepal Tara M Shakya 5. 10:55-11:05 Profile of obstetric and Iatrogenic Fistula Surgeries
at Kathmandu Model Hospital Ranjana Shrestha
6. 11:05-11:15 Discussion 11:15-11:30 TEA TIME
11:30-12:30 Public Health Session Chairperson: Serigne M Gueye/ Kate Grant/ Bhola Rijal
S No Time Topic Presenter 1. 11:30-11:40 Reason for delay in seeking medical care among
women with obstetric anal sphincter injuries Francis Ogwang Banya
2. 11:40-11:50 Fistula prevention in Niger: A way to improve access to information and care
Altine Diop
3. 11:50-12:00 Abandonment and isolation of Fistula Clients by spouses/partner and society
Jacob Malungo
4. 12:00-12:10 Use of Bladder diary as diagnostic and therapeutic tool for Overactive bladder
Raheela Mohsin/ Novera Chughtai
5. 10:10-12:20 Vesico-vaginal Fistula a leading cause of Traumatic Stress in sufferers
Sadaf Ahmed
6. 12:20-12:30 Fistula as a Public Health Challenge in Pakistan Shamoon Noushad 12:30-13:00 Medical Informatics Chairpersons: Erin Mielke/ Seth Cochran/Sajjad Ahmed
Annual Report • October 2018 – September 2019 Fistula Care Plus 131
S No Time Topic Presenter 1. 12:30-12:40 Fistula care in the digital era: A discussion
on digitization of fistula care in five UNFPA countries
Bryony Michaelson
2. 12:40-14:50 How operation fistula uses data visualization to help women with operative fistula
Naledi Hollbruegge
3. 14:50-13:00 How the use of business intelligence tools in the fistula sector can improve surgical performance
Seth Cochran
13:00-14:00 LUNCH BREAK/ Poster Presentation 14:00-15:05 Key Note Speakers (Plenary) Chairpersons: Oladosu Ojengbede/ Sayeba Akhter/ Shershah Syed
S No Time Topic Presenter 1. 14:00-14:25
(25min) Obstetric trauma surgery art and science: The corpus interpelvinum with endopelvic diaphragm with regards to prolapse and (in)continence in reconstructive pelvis surgery
Kees Waaldijk
2. 14:25-14:50 (25 min)
Global Fistula Map Update: Direct Relief International Fistula Module Program Update: A New Telemedicine Initiative for Fistula Care : from Direct Relief International- the primary sponsor of ISOFS 2018
Jessica White Steven Arrowsmith Rachel Pope
3. 14:50-15:05 (15 min)
Fistula in 2018: Moving Forward in a Season of Change
Steven Arrowsmith
15:05-16:00 ISOFS Session- Meet the Leaders (Panel Discussion) Moderator: Nazmul Huda Participants:
1. President ISOFS- Dr Oladosu Ojengbede 2. President Elect. ISOFS- Dr Shershah Syed 3. CEO, Fistula Foundation- Ms. Kate Grant 4. Dr Steven Arrowsmith( Direct Relief International, FF, ISOFS) 5. Ms. Erin Anastasia,UNFPA 6. Ms. Erin Mielke, USAID 7. President Engender Health-_Ms Traci Baird 8. CEO- Operation Fistula-Mr Seth Cochran
16:00-17:30 Plenary Session (GUEST SPEAKERS) Chairperson: Sunday Langman/ Heera Tuladhar
S No Time Topic Presenter 1. 16:00-16:15 Genital Tract Fistula: Changing Trends in
presentation and outcome Oladosu Ojengbede
2. 16:15-16:30 Private initiative in addressing fistula problem in Bangladesh
Sayeba Akhter
3. 16:30-16:45 Midwifery Tutors Training Programme Shershah Syed 4. 16:45-17:00 How the use of business intelligence tools in
the fistula sector can improve surgical performance
Seth Cochran
5. 17:00-17:15 Addressing the shortage of fistula surgeons: Update from FIGO training initiative
Gillian Slinger
6. 17:15-17:30 Emerging evidence about the global fistula burden what do we know and how can fistula programs respond?
Vandana Tripathi

Annual Report • October 2018 – September 2019 Fistula Care Plus 132
18:00-19:30 INAGURATION followed by Dinner at Radisson Hotel Hall B 7:00-9:00 am: Registration 9:00-9:15 am: Scientific Opening 9:15-10:15am: Free Paper on surgical management Chairperson: Erin Anastasi/ Sherley Haywood/ Paban Sharma
S No
Time Topic Presenter
1. 9:15-9:25 Social integration and rehabilitation of obstetric fistula patients before and after repair in sub-saharan Africa: A systematic review
Shallon Atuhaire/ Oladosu Ojengbede
2. 9:25-9:35 Management of Obstetric Fistula: Experience of the Schiphra Hospital
D Ouedraogo
3. 9:35-9:45 Surgical proficiency grading and outcome of fistula repair; does it really matter?
Tolulope Babawarun/ Blawal OO
4. 9:45-9:55 Outcome and predictors of surgical repair of obstetric vasicovaginal fistula in a Teaching Hospital in Ethiopia: Retrospective cohort study
Demisew Amenu
5. 9:55-10:05 Success of Local Fistula Mentorship: Review of Route in Repairs At Referral Hospital in Uganda
Angella Clare Namala
6. 10:05-10:15 Fistula Presentation Awareness Sajjad Ahmed Siddiqui
10:15-11:15 Training and Capacity Building Chairperson: Lindsay Pollaczek/ Rashna Chinoy/ Swaraj Rajbhandari
S No Time Topic Presenter 1. 10:15-10:25 Fistula Programme Management using
DHIS2: Experience of Fistula Care Plus Project in Bangladesh
Masum Salah Uddin
2. 10:25-10:35 It takes a village: The Vital role of community oraganizations in enhancing fistula patient identification, referral and reintegration in Kenya
Lindsay P/Habiba C. Mohamed
3. 10:35-10:45 Enhancing Holistic Care of patients with Obstetric Fistula and other childbirth injuries- TERREWODE’s Experience of developing a dedicated fistula Hospital in Uganda
Alice Emasu
4. 10:45-10:55 The Mobile Surgical Outreach Model for women with genital fistula in DR Congo
Kenny Raha
5. 10:55-11:00 Discussion 11:00-11:30 TEA TIME 11:30-12:30 Public Health Session Chairperson: Kusum Thapa/ Nazmul Huda
S No Time Topic Presenter 1. 11:30-11:40 Evidence based classification/staging system
for Obstetric Fistula: Planning and preliminary intervention in Nigeria
Oladosu Ojengbede
2. 11:40-11:50 Prevalence findings from a community-based female genital fistula screening programme in Bangladesh
Licky Ghosh
3. 11:50-12:00 Situation of obstetric fistula in a marginalized teagarden community in Bangladesh: A Qualitative Study
Abu Sayeed Md. Abdullah

Annual Report • October 2018 – September 2019 Fistula Care Plus 133
4. 12:00-12:10 Profile of Obstetric Fistula Clients: Is the trend changing?
Moharson Bello IO
5. 12:10-12:20 Assessment of the impact of non-state actors in the support of obstetric fistula care: Matters arising
Abdus-Salam RA
6. 12:20-12:30 Experience of using Community Radio for Fistula Communication in Bangladesh
Nitta Biswas
12:30-13:00 Medical Informatics Chairperson: Bryony Michaelson / Gehanath Baral
S No Time Topic Presenter 1. 12:30-12:40 Using GOFER to digitize patient records in
Kathmandu Model Hospital Hema K Pradhan
2. 12:40-12:50 Facilitating data for decision making to improve health management information systems reporting four supported sites in Uganda
Hassan Kanakulya
3. 12:50-13:00 Eradication of neglected surgical diseases in Kenya: A study Protocol
Henry Jaymie
13:00-14:00 LUNCH BREAK / Poster Presentation Followed by Plenary Sessions Day 2: 6thDec 2018, Thursday Hall A 8:00-9:00 Free Paper Session Chairperson: Sanu M Dali/ Naresh P KC/Sheela Verma
S No Time Topic Presenter 1. 8:00-8:10 Improving quality of life for women with
incurable fistula in Uganda Vandana Tripathi
2. 8:10-8:20 Persistent Depression after Obstetric Fistula Repair
Mary Juanita Stokes
3. 8:20-8:30 Reasons for delay in decision making and reaching health facility among obstetric fistula and pelvic organ prolapse patients in Gondar University Hospital, Northwest Ethiopia
Mulat Adefris
4. 8:30-8:40 Factors associated with obstetric fistula repair failure among women admitted at Gynocare Women’s and fistula Hospital in Kenya 2012-2016: case control
Antholy Wanjala Nakhisa/Henry RM
5. 8:40-8:50 Making the dream a reality: how are we going to end fistula within a generation?
Erin Anastasi
6. 8:50-9:00 The association between female genital fistula symptoms and gender based violence
Vandana Tripathi
9:00-10:00 Free Papers on surgical management Chairperson: Ashudeep Sharma/ Michael Breen/ Geeta Gurung
S No Time Topic Presenter 1. 9:00-9:10 Fistula prevention Awareness Activities of
Community Volunteerism in Niger: A way to improve access to information and care
Altine Diop
2. 9:10-9:20 Risk factors and management of obstetric fistula association with bladder calculus Saint Joseph Hospital, Kinshasa- RD Congo
Dolores M. Nembunzu
3. 9:20-9:30 Iatrogenic fistula in Luapula province, Inadequate distribution of good surgical skills
Kenipher Mijere (Aubrey Shanzi)
4. 9:30-9:40 Experience of managing Ureterovaginal Fistulas following Obstetrical and gynecological surgeries
Amit Mani Upadhyay
Annual Report • October 2018 – September 2019 Fistula Care Plus 134
5. 9:40-9:50 Management of the Obstetric Fistula in Burundi: The experience from a multidisciplinary approach over 5 years
Gaetan Mareschal
6. 9:50-10:00 Iatrogenic Genitourinary Fistula: Changing Trends
Tarun Pradhan
10:00-11:00 Mix Bag Session Chairperson: Sunday-Adeoye/ Jayant Sharma/ Madhu Tumbhahangphe
S No Time Topic Presenter 1. 10:00-10:10 Frequency and management of non-obstetric
fistula in the Democratic Republic of Congo: experience from Fistula Care Plus Project
Alexandre Delamou
2. 10:10-10:20 Characteristics of obstetric fistula women repaired at Kissi Gynocare Fistula Center
John Omboga
3. 10:20-10:30 Prevalence, aetiology and management of ureteric injuries in Mulago National Referral hospital, Kampala, Uganda
Susan Obore Abiar
4. 10:30-10:40 Incidence and characteristics of surgical fistula patients at LAMB Hospital from 2011 to 2017
Beatrice Ambauen-B
5. 10:40-10:50 Doctors beyond wall of hospital: Reflections of community based actions of University Fistula Center BSSMU
Shuily Chowdhury
6. 10:50-11:00 Plastic Surgery Techniques for the Improvement of Outcomes of Complex Obstetric Fistula Repairs
Rachel J Pope
11:00-11:15 TEA TIME 11:15-12:15 Clinical Plus Chairperson: Kundu Yangzom/ Barageine Justus
S No Time Topic Presenter 1. 11:15-11:25 The medical and psychological morbidity of
patients with urogenital fistulae Pushpa Srichand
2. 11:25-11:35 Establishing Depression Levels among women seeking Obstetric Fistula Treatment at Fistula Care Plus Supported sites in Uganda
Paul Kaduyu
3. 11:35-11:45 Childbirth injuries encountered on outreach in remote RD Congo
Justin Paluku L
4. 11:45-11:55 Rectovaginal fistula due to missing Intra Uterine Contraceptive device
Alexander Bambala Kawimbe
5. 11:55-12:05 Management of complex fistula Pushpa Srichand 6. 12:05-12:15 Discussion
12:15-13:15 Public Health Session Chairperson: Dibya S Malla/Aziz Abdulla/Punya Poudel
S No Time Topic Presenter 1. 12:15-12:25 Rehabilitation and reintegration of Fistula
Clients through Micro Credit linked services Sheikh Mohiuddin
2. 12:25-12:35 Role of a community clinic for prevention of Female Genital Fistula
Anirudha Karmakar
3. 12:35-12:45 Fistula Champions leading local action for ending fistula in Bangladesh
Aysarjo Karmakar
4. 12:45-12:55 Human resource development for prevention and care of fistula: Experience of University fistula Center BSSMU
Saleha Begum Chowdhary
5. 12:55-13:05 Building a Countrywide Treatment Network: Lessons from Kenya and Zambia
Lindsey Pollaczek
6. 13:05-13:15 Discussion 13:15-14:00 LUNCH BREAK/ Poster Presentation

Annual Report • October 2018 – September 2019 Fistula Care Plus 135
14:00-15:00 Clinical Plus Chairpersons: Anjana Karki/ Joseph Monehin/ Andrew Browning
S No Time Topic Presenter 1. 14:00-14:10 What is happening with Obstetric fistula in
the Western Nepal? Shirley Heywood
2. 14:10-14:20 Burden of obstetric Fistula on Rohingya refugees in Cox's Bazar, Bangladesh- A call for action
Iftikher Mahmood
3. 14:20-14:30 A retrospective survey of the duration of leakage and patient perceived bottlenecks to seeking fistula treatment in Uganda
Asiimwe Ian Shane
4. 14:30-14:40 Women’s experience of fistula-related stigma in Uganda: Application of a conceptual framework to inform stigma-reduction intervention
Alison M EiAyede
5. 14:40-14:50 Causes and prevention of Iatrogenic fistula during Gynaecologic Surgery
Ashudeep Sharma
6. 14:50-15:00 Management of Genital Fistula in Women with Meyer-Rokitansky-Kuster-Hauser Syndrome
Sunday Jenner Lengmang
15:00-16:00 Business Meeting of ISOFS 16:00-16:45: CLOSING CEREMONY- MC: Dr Astha Shrestha/ Dr Monica Gurung FOLLOWED BY DINNER and Cultural Program AT HOTEL MANASLU (INFRONT OF RADISSON GATE) Day 2: 6thDec 2018, Thursday Hall B 9:00-10:00 Free Papers Chairperson: Lata Bajracharya/ Traci L Baird
S No Time Topic Presenter 1. 9:00-9:10 Self Audit as part time Fistula Surgeon Aziz Addullah 2. 9:10-9:20 Iatrogenic Fistula: Types, Causes and Post-repair
outcome – 70 cases Bilkis Begum Chaudhary
3. 9:20-9:30 Increasing Frequency of iatrogenic fistula a new challenge
Nasira Tasnim
4. 9:30-9:40 Genital Fistula: Successes, challenges and way forward in a facility specialization in fistula management in Bangladesh
Nrinmoy Biswas
5. 9:40-9:50 Preliminary analysis of Quality of Life (QOL) before and after surgery for female genital fistula: A Prospective cohort study
Stacy Lea Saha
6. 9:50-10:00 Translation of Data in action: Exploring Data Documentation process and further Scope for Improvement in Bangladesh
Animesh Biswas
10:00-11:00 Free Paper Session Chairperson: Bimala Malla/ Andrew Browning/Rachana Shah
S No Time Topic Presenter 1. 10:00-10:10 Post-repair residual incontinence: Assessing
the severity and impact on quality of life for Ugandan women
Bonnie J Ruder
2. 10:10-10:20 Surgical Safety Toolkit based Quality Monitoring of Fistula Surgery in Bangladesh
Israt Jahan
3. 10:20-10:30 Surgical success of patients presenting for repair of VVF- Data from fistula repair center, Ayub Teaching Hospital, Abottabad, Pakistan
Azizun Nisa Abbasi
4. 10:30-10:40 Prevention of Iatrogenic Fistula Suman Sharma 5. 10:40-10:50 Experience of partnership with Fistula
Program in Bangladesh: University Fistula Frahan Alam

Annual Report • October 2018 – September 2019 Fistula Care Plus 136
Center, Bangabandhu Sheikh Mujib Medical University
6. 10:50-11:00 Increasing opportunities for obstetric fistula case detection and treatment by using a multifaceted approach – the case of Kalungu district –Uganda
Tumusiime Molly/ Paul Kaduyu
11:00-11:15 TEA TIME 11:15-11:45 Free Paper Session Chairperson: Bilkis Begum Chaudhury/Vandana Tripathi
S No Time Topic Presenter 1. 11:15-11:25 Epidemiological profile of obstetric fistula women
at the National Obstetric Fistula Reference Center in Niamey; from January 2016 to 31 December 2017
Abdoulaye Idrissa
2. 11:25-11:35 Why has the Caesarean Rate Increased Dramatically in Bangladesh?
John Richards
3. 11:35-11:45 Female Genital Fistula Repair Performance of Ad-din Hospitals 2013-2018
Nahid Yesmin/ Farzana Yesmin
4. 11:45-11:55 Prevalence findings from a community-based female genital fistula screening program in Bangladesh
Lucky Ghose, SkNazmul Huda, Vandana Tripathi
11:55-13:00 IsDB Session Chairperson: Shershah Syed/ Kristonia Lockhart Implementation Workshop on the Islamic Development Bank/Islamic Solidarity Fund for Development Coalition to Stop Obstetric Fistula Program ( For a smaller session for participants from Afghanistan, Pakistan, Somalia, The Gambia and Sierra Leone)
1. 11:55-12:00 Introduction by IsDB Kristonia Lockhart 2. 12:00-12:15 Brief Introduction by country teams-
- Pakistan, Somalia, The Gambia Country Team
3. 12:55-12:30 Presentation by International Fistula Alliance (IFA) on Introduction of IFA, proposed methodology, proposed schedule
Martin Andrews / Bonnie Ruder
4. 12:30-13:00 Questions and Answers session Facilitated by Martin Andrews
13:00-14:00 LUNCH BREAK/ Poster Presentation
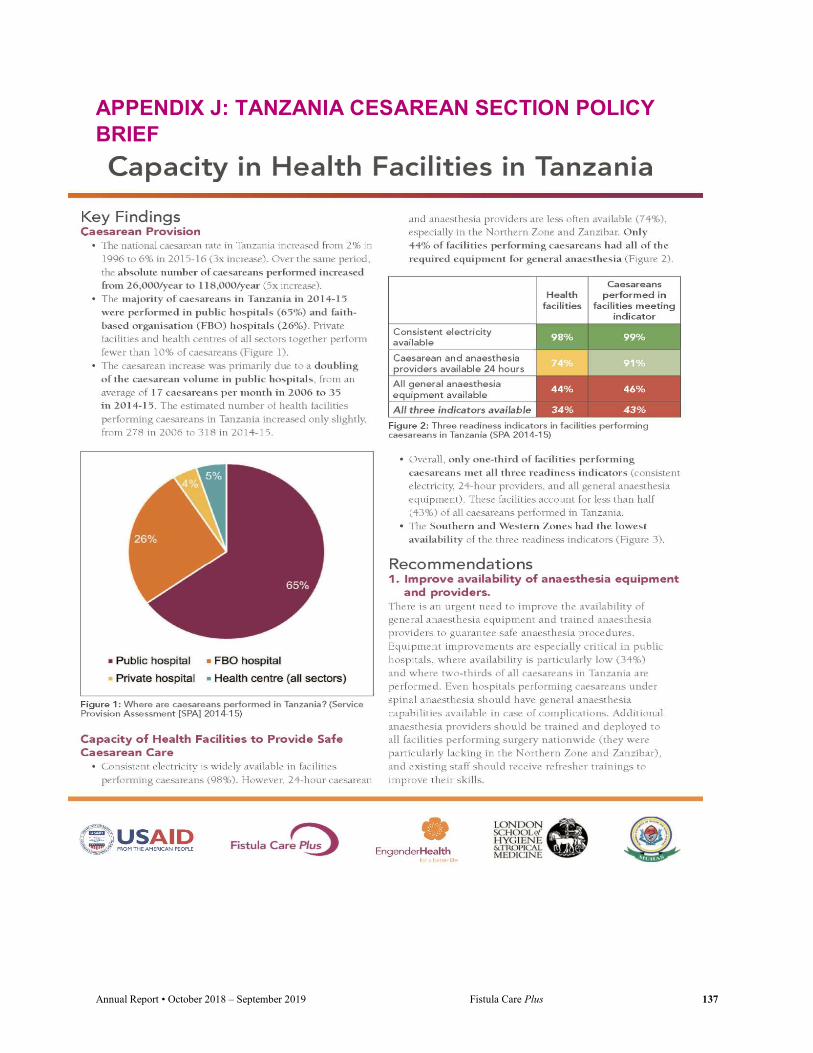
Annual Report • October 2018 – September 2019 Fistula Care Plus 137
APPENDIX J: TANZANIA CESAREAN SECTION POLICY BRIEF

Annual Report • October 2018 – September 2019 Fistula Care Plus 138

Annual Report • October 2018 – September 2019 Fistula Care Plus 139
APPENDIX K: IOFWG ROAD MAP

Annual Report • October 2018 – September 2019 Fistula Care Plus 140

Annual Report • October 2018 – September 2019 Fistula Care Plus 141

Annual Report • October 2018 – September 2019 Fistula Care Plus 142

Annual Report • October 2018 – September 2019 Fistula Care Plus 143

Annual Report • October 2018 – September 2019 Fistula Care Plus 144

Annual Report • October 2018 – September 2019 Fistula Care Plus 145

Annual Report • October 2018 – September 2019 Fistula Care Plus 146

Annual Report • October 2018 – September 2019 Fistula Care Plus 147

Annual Report • October 2018 – September 2019 Fistula Care Plus 148

Annual Report • October 2018 – September 2019 Fistula Care Plus 149

Annual Report • October 2018 – September 2019 Fistula Care Plus 150
APPENDIX L: ISOFS PLENARY PRESENTATION
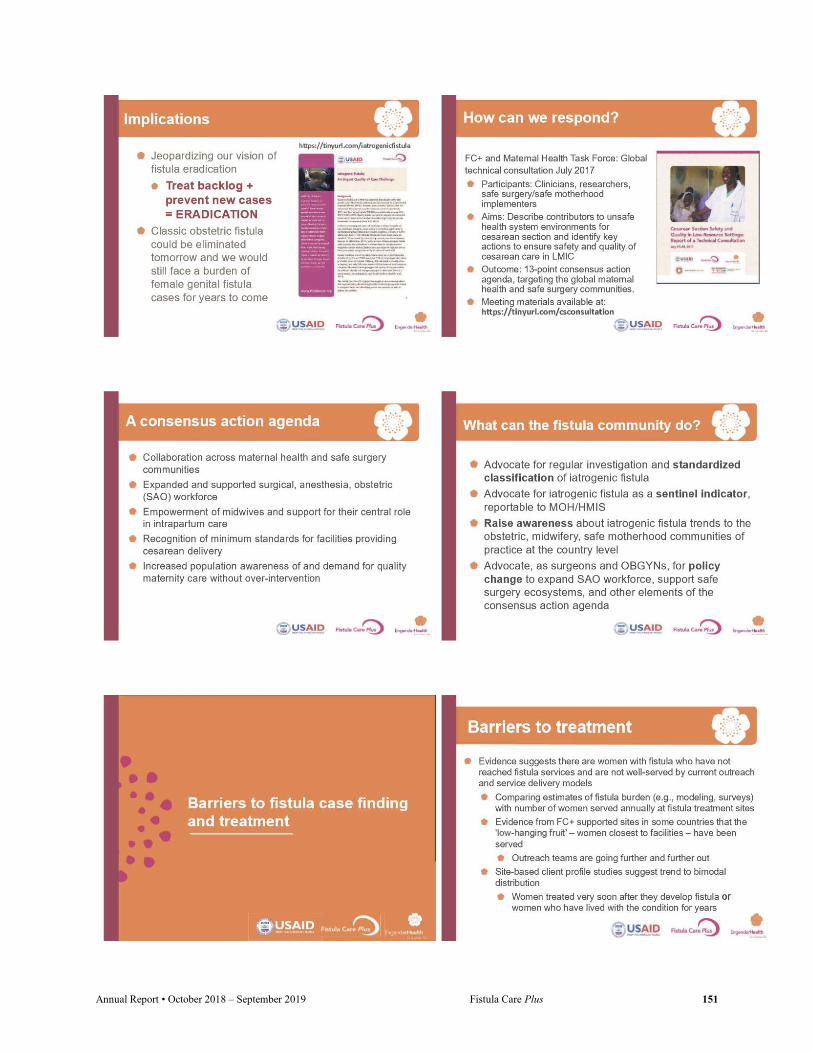
Annual Report • October 2018 – September 2019 Fistula Care Plus 151

Annual Report • October 2018 – September 2019 Fistula Care Plus 152

Annual Report • October 2018 – September 2019 Fistula Care Plus 153
Annual Report • October 2018 – September 2019 Fistula Care Plus 154
Annual Report • October 2018 – September 2019 Fistula Care Plus 155
APPENDIX M: USAID RESEARCH BRIEFING

Annual Report • October 2018 – September 2019 Fistula Care Plus 156

Annual Report • October 2018 – September 2019 Fistula Care Plus 157

Annual Report • October 2018 – September 2019 Fistula Care Plus 158

Annual Report • October 2018 – September 2019 Fistula Care Plus 159

Annual Report • October 2018 – September 2019 Fistula Care Plus 160

Annual Report • October 2018 – September 2019 Fistula Care Plus 161

Annual Report • October 2018 – September 2019 Fistula Care Plus 162

Annual Report • October 2018 – September 2019 Fistula Care Plus 163
Annual Report • October 2018 – September 2019 Fistula Care Plus 164

Annual Report • October 2018 – September 2019 Fistula Care Plus 165
APPENDIX N: UGANDA BARRIERS INTERVENTION RESEARCH BRIEF

Annual Report • October 2018 – September 2019 Fistula Care Plus 166

Annual Report • October 2018 – September 2019 Fistula Care Plus 167

Annual Report • October 2018 – September 2019 Fistula Care Plus 168

Annual Report • October 2018 – September 2019 Fistula Care Plus 169

Annual Report • October 2018 – September 2019 Fistula Care Plus 170
Annual Report • October 2018 – September 2019 Fistula Care Plus 171

Annual Report • October 2018 – September 2019 Fistula Care Plus 172
APPENDIX O: KATSINA BARRIERS INTERVENTION RESEARCH BRIEF

Annual Report • October 2018 – September 2019 Fistula Care Plus 173

Annual Report • October 2018 – September 2019 Fistula Care Plus 174

Annual Report • October 2018 – September 2019 Fistula Care Plus 175

Annual Report • October 2018 – September 2019 Fistula Care Plus 176
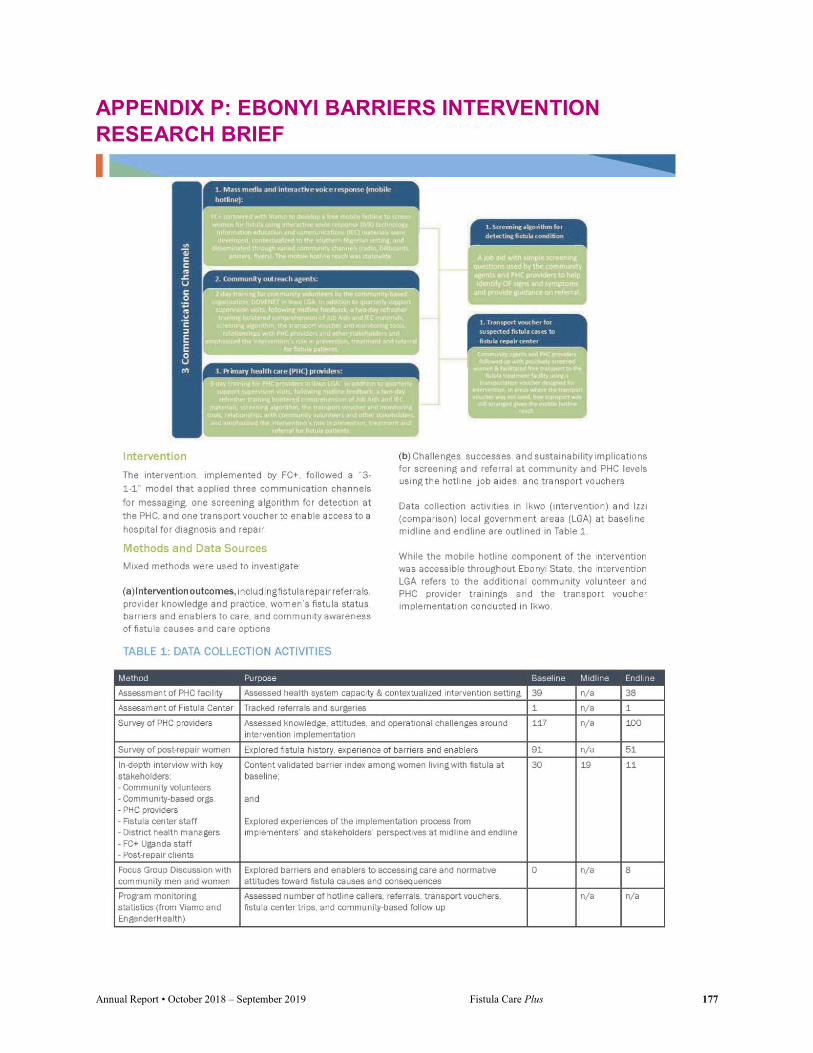
Annual Report • October 2018 – September 2019 Fistula Care Plus 177
APPENDIX P: EBONYI BARRIERS INTERVENTION RESEARCH BRIEF

Annual Report • October 2018 – September 2019 Fistula Care Plus 178
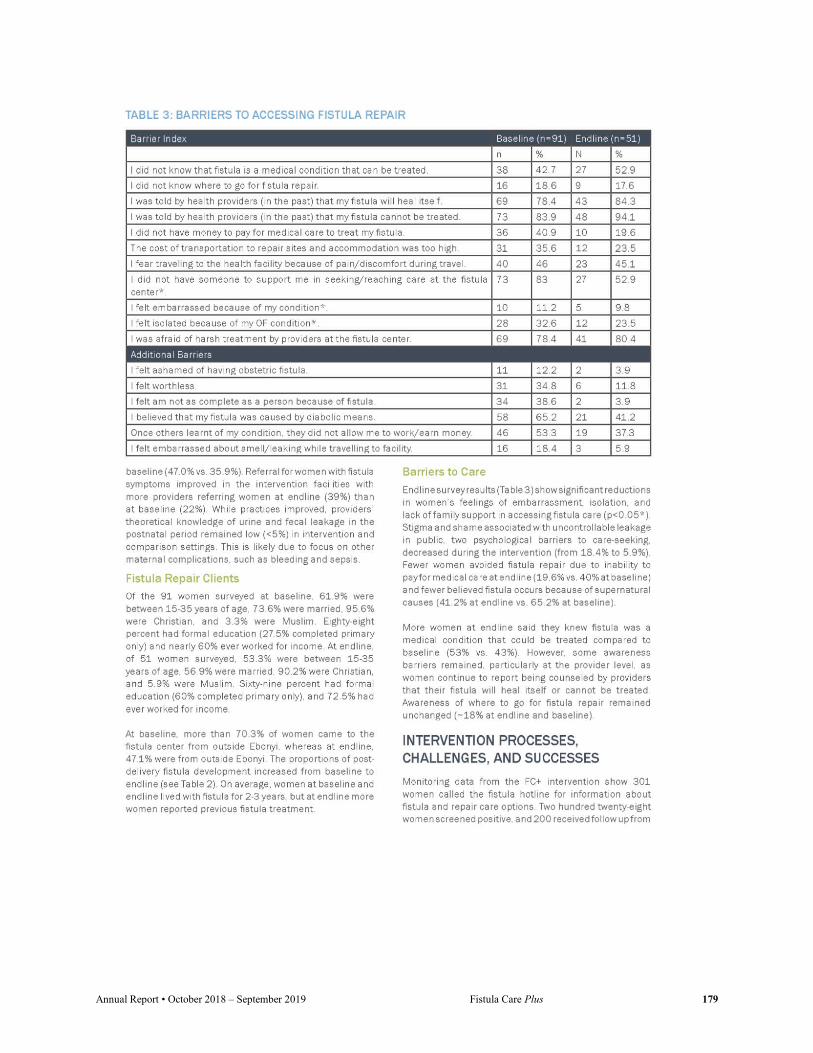
Annual Report • October 2018 – September 2019 Fistula Care Plus 179

Annual Report • October 2018 – September 2019 Fistula Care Plus 180

Annual Report • October 2018 – September 2019 Fistula Care Plus 181
Annual Report • October 2018 – September 2019 Fistula Care Plus 182
APPENDIX Q: FC+ TRIBUTE TO DR. DENIS MUKWEGE
Introductory remarks honoring Denis Mukwege at the 7th ISOFS Conference in Kathmandu, Nepal, December 2018 – Vandana Tripathi, Deputy Director, Fistula Care Plus Project
Prof Dr. Denis Mukwege is a world-renowned gynecological surgeon and the founder and director of Panzi Hospital in Bukavu, Democratic Republic of the Congo. Dr. Mukwege was awarded the 2018 Nobel Peace Prize alongside Nadia Murad for his advocacy against rape as a weapon of war and his services to survivors of sexual violence.
Dr. Mukewege founded Panzi Hospital in Bukavu in 1999. Initially envisioned as a center for OBGYN care, the epidemic of sexual and gender based violence in DRC brought women with many other urgent needs to the Panzi doorstep. Since its doors opened, Dr. Mukwege and his staff have helped to care for more than 50,000 survivors of sexual violence. No matter where the women are from, their social standing, or their ability to pay, they come to Panzi knowing that they will find a safe place to heal.
At the risk of his own safety, Dr. Mukwege has consistently urged the international community to become more involved in the fight to end sexual and gender based violence. He is on the advisory committee for the International Campaign to Stop Rape and Gender Violence in Conflict. He has been the recipient of numerous awards before the Nobel Peace Prize, including the United Nations Human Rights Prize in 2008 and the European Parliament’s Sakharov Prize for Freedom of Thought in 2014. He was named one of Time Magazine's Most Influential People in the World in 2016, as well as one of Fortune Magazine's 50 of the World's Greatest Leaders.
Dr. Mukwege has described himself as a “true son of the soil” to Fistula Care Plus staff. And it is certain that no one is more proud than the women of eastern Congo that Dr. Mukwege and Panzi Hospital serve. EngenderHealth staff recount walking alongside Dr. Mukwege in Bukavu and seeing person after person cheer, stopping to greet him with a touch of the hand and a heartfelt thanks.
EngenderHealth is deeply proud to partner with Panzi Hospital through the Fistula Care Plus project. We join all of you in honoring this great leader of the global fistula community.
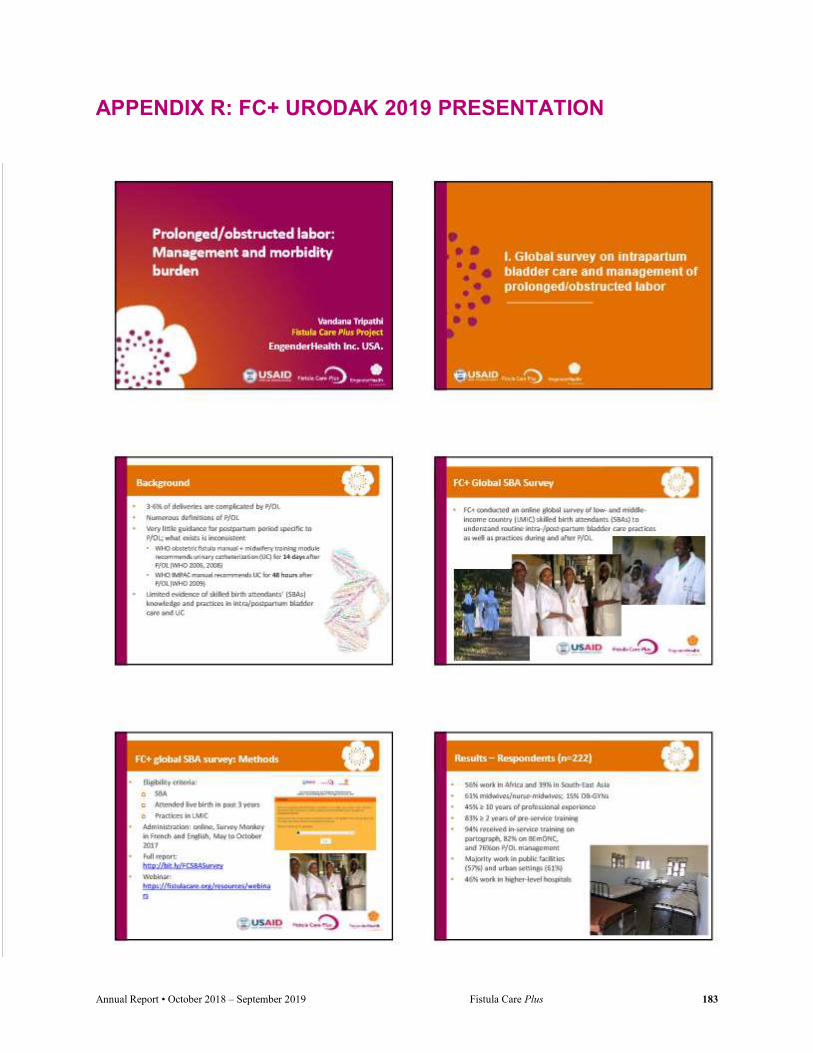
Annual Report • October 2018 – September 2019 Fistula Care Plus 183
APPENDIX R: FC+ URODAK 2019 PRESENTATION

Annual Report • October 2018 – September 2019 Fistula Care Plus 184

Annual Report • October 2018 – September 2019 Fistula Care Plus 185

Annual Report • October 2018 – September 2019 Fistula Care Plus 186

Annual Report • October 2018 – September 2019 Fistula Care Plus 187
Annual Report • October 2018 – September 2019 Fistula Care Plus 188
APPENDIX S: INTERNATIONAL CONSULTATION ON THE REGIONAL STRATEGY FOR THE ELIMINATION OF OBSTETRIC FISTULA – MEETING REPORT
International Consultation on the Regional Strategy for the Elimination of Obstetric Fistula June 19-21, 2019 | Dakar, Senegal
Travelers:
Dr. Sk. Nazmul Huda, Global Manager, FC+ Project, EngenderHealth Inc. (June 20-22) Ms. Altiné Diop, Program Associate El Hadj Moustapha Diallo, Guinea program Manager (June 18-22) Dr. Sita Millimono, Senior Clinical Advisor (June 18-22)
Date: June 19-21, 2019 Country: Senegal Distribution: FC+ Core and Mustafa Kudrati Objectives The overall objective is to share the resolution from the 2018 Banjul ECOWAS conference on obstetric fistula elimination with all stakeholders and operationalize the resolution with action plans focusing on pillars such as capacity building of health providers, monitoring, evaluation and resource mobilization. The resolution is known as “Banjul Call to Action” which was subsequently signed and adopted by the Health Ministers of ECOWAS region. The operationalization of the resolution will be done in partnership with academic institutions, professional associations and NGOs for identification and referral of cases, surgical and non-surgical treatment, reintegration and rehabilitation of women with fistula in the region. This strategy must be underpinned by quality assurance and evidence-based, flexible framework that includes data for decision-making.
Specific objectives: • Disseminate the "Banjul Call to Actions 2018" of the ECOWAS Assembly of Ministers of Health; • Advocate for the political and financial commitment of States, technical and financial partners and
the private sector for the elimination of fistula in West Africa. • Develop action plans to operationalize the resolution for fistula elimination by group of countries in
the sub region. o Plan of action to prevent obstetric fistula o Plan of action to build the capacity of fistula surgeons to prevent cases of iatrogenic fistulas
and thus take care of pending cases in the region o Action plan to mobilize resources for the sustainability of prevention and treatment
activities o Develop a mechanism for monitoring and evaluation of tools including key indicators for
monitoring progress at regional and country level to contribute to the elimination Establish a coordination system of action plans for concrete results

Annual Report • October 2018 – September 2019 Fistula Care Plus 189
Develop a strategy plan for the next resource mobilization meeting to be held in the same year; Develop a budget to establish cost discrepancies associated with the implementation of fistula
action plans in the region. Present business case and return data on investment in fistula care in West Africa.
Wednesday June 19, 2019: First Day
Opening ceremony: The opening ceremony took place in the morning (9:00-9:30) with the presence of Pr. Serigne Magueye Gueye, Professor at Cheikh Anta Diop University and Grand Yoff General Hospital, Vice President of WACS, Dr. Sosthene Dougrou, the UNFPA Representative, Dr. Aissa Bouwawe, OOAS, and El Hadj Moustapha Diallo, on behalf of Dr. Sk. Nazmul Huda, Global Manager, Fistula Care Plus Project, EngenderHealth Inc. The Consultant delineated the meeting objectives and then 45 mn were allocated to the presentation of participants, their experience and current role regarding obstetric fistula.
Prof. Serigne Magueye Gueye highlighted the expected results of the conference:
Conditions for OF treatment and prevention are created; Regional and national partnership reinforced; Constraints and challenges for implementation identified; Coordination mechanism elaborated; Monitoring and evaluation mechanism developed; Country wise costed action plan established.
Session 1:
Presentation of resolutions on obstetric fistula (Resolution of the UN Secretary General): Dr. Sosthene Dodourou the UNFPA Representative provided detailed information on the report which highlighted the major global initiatives about OF since 1994 (with the adoption of the Program of Action of the ICPD Conference on Population and Development in Cairo); the report also detailed several ECOWAS initiatives. Dr. Sosthene pointed-out that 15 years after the declaration to end fistula, the situation has not been changed significantly; therefore more than ever, there is an urgent need to accelerate the efforts and

Annual Report • October 2018 – September 2019 Fistula Care Plus 190
develop an international road map to be presented in July 2019 to the Niamey summit of ECOWAS presidents.
Presentation of “Banjul call to Actions 2018” of the ECOWAS Ministries of Health: Dr. Aissa Bouwawe from WAHO presented the resolution, which recognizes that the ECOWAS region has over 80% of fistula burden; this therefore requires a clear roadmap by 2030, a strong engagement of States and the Technical and Financial Partners for resource mobilization and for addressing the root causes of OF.
Session 2: Regional Strategies for the elimination of obstetric fistula Role of the ECOWAS Center for Gender Development in the OF elimination in the ECOWAS
region ECOWAS implements an ambitious program to eliminate obstetric fistula in West Africa. Specific Objectives include: (1) Provide treatment and care to OF victims; (2) assist victims to return to normal productive and reproductive lives through Income Generation Activities {3) conduct outreach and advocacy activities for mechanisms, legislation, and policies for OF elimination.
Annual budget ranges from 50,000 to 60,000 USD granted each year to each Member State; between 40 to 50 women are supported annually in each Member State. ECOWAS plans to capitalize on the roadmaps already developed by countries to accelerate the reduction of maternal, neonatal and child mortality supported by UNFPA. ECOWAS will improve Reference Centers, to enable women to seek treatment in their countries, to have a family environment conducive to healing and to reduce the costs of medical evacuation to foreign countries.
The UNFPA regional strategy for OF elimination Dr. Sosthene Dodourou presented the strategy which recognizes that the Persistence of Obstetric Fistula is undermining regional efforts to Harnessing the demographic dividend and Women Empowerment in West and Central Africa.
Regional context: Exact number of women living with OF still unknown. Prevalence: 600K- 1000K; Incidence:30,000 new cases per year. Top 10 countries are: Nigeria, Niger, Ghana, Cameroon, Mali, Burkina Faso, Cote D’Ivoire, Chad, Senegal, Guinea.
IF NOTHING IS DONE it will take 300 years to end Obstetric Fistula! Need to change our approach. The New Paradigm is : ELIMINATION. Prevention of New Cases. Treatment of current cases UNFPA objectives and strategies in Annex 1.
The program of capacity building for midwives and nurses
Dr. Badara N’Diaye Regional Manager from Amref Health Africa conducted a well-received PPT presentation on the E-learning solution in the training of health workers:

Annual Report • October 2018 – September 2019 Fistula Care Plus 191
o Develop and sustain human resources for health in order to catalyze the achievement of universal health coverage in West Africa
o Develop and provide sustainable health services and solutions to improve access to and use of quality preventive, curative and promotional health services in West Africa
o Contribute to increased investments in health to achieve universal coverage in 2030 Amref Approach
o Help countries increase the number of midwives and nurses trained; o Work in partnership with Professional Associations o Rely on innovative approaches; Scale up successful innovations.
o Midwifes involved in E-learning: Cohorts from 150 to 500, Success rate: 80%, Diploma: License (Bs), Integration of audio/video solutions, Mobile app, Offline version
Role of civil society in the OF elimination in Africa (Example of Benin) Prof. René Xavier PERRIN presented the Foundation Claude Talion interventions in Benin.
Actions of the Foundation include: Prevention, Sensitization, Active identification of women with obstetric fistula, Social mobilization, resource mobilization, Socio-economic reintegration.
The prevention focusses on improving access to quality prenatal care, fight against female genital mutilation and boosting girls’ education.
Achievements include: Distribution of "dignity kits"; Media campaigns: radio spots, Creation of a telephone line: toll free number; Training of 500 community relays (Klouékanmin, Toviklin, Lalo, Ouinhi, Zagnanado, Pobè, Kétou, Adjaouèrè); identification of 5 NGOs working for OF.
Opening of a Reception Center with a capacity of 40 people in the locality of Biakou in Tanguiéta for healed women; Opening of a Training Center in weaving, sewing, beading, knitting and soap making. Financial support for income-generating activities (100,000 FCFA); Accompaniment of healed women for their empowerment and their acceptance by society (awareness). Session 3: Adequate strategic approaches for speeding up the OF elimination
Economic Cost of Obstetric Fistula Dr. Sosthene Dodourou, from UNFPA, conducted this presentation. o Average age of onset of fistula = 22 years o Initiation of the treatment = 8 years later (Mutela in 2009): That is to say at 30 years; o Life expectancy of women in Ethiopia = 59 years. Each surgery allow 29 DALY gain. o The average cost of repair in Ethiopia is $ 1,163 o $ 1,163 / 29 = $ 40 for avoiding one DALY.Surgery is cost effective.
Coalition to stop Obstetric Fistula: Islamic Development Bank (IDB)
Situational Analysis of Obstetric Fistula in the countries The rest of the day was entirely dedicated to the presentations of different fistula elimination strategies of 18countries of the region. Most countries have similar components including prevention, treatment and reintegration; however strategies differed from one country to another. THURSDAY, JUNE 20, 2019: Second Day

Annual Report • October 2018 – September 2019 Fistula Care Plus 192
Session 1: Role of academic institutions in the speeding up of the elimination of Obstetric Fistula. West African College of Surgeons (WACS) Prof. Philip Mishelbwala, the Secretary of WACS conducted the presentation on behalf of Prof. Serigne Magueye Gueye, Président, WACS and Prof. Joseph Ikechebelu – Chairman, Obs/Gyn, WACS
WACS was established in 1960 and has 18 member countries, 7 Faculties and has over 6,000 fellows; domain of interventions include: Anesthesia, Dental Surgery, Ob&Gyn, Ophthalmology, ORL, Radiology & Surgery. WACS role in OF elimination focusses on treatment, Database & Research, Capacity building, and advocacy. (Presentation in Annex III). West African Postgraduate College of Pharmacists (WAPCP): Dr Markieu Kaira Janneh, President
Role of pharmacists in the prevention/elimination of OF: o Participation in the treatment process, before and after the surgery. o Provide support in Procurement and Supply Chain Management o Implement a pooled procurement system of countries within the Region o Adapt/ selection of appropriate kits and supplies for the management of OF in the Region o Opportunity to create a Regional warehouse; o Identification & Referral Services o Promoting access to family planning commodities and use of emergency contraceptive pills.
West African College of Nursing (WACN): Prof. Fatoumate Daffeh, president, made the presentation. Action Plan includes:
o Include prevention of Obstetric Fistula (OF) in training Curricula o Develop specific training programs in the prevention of OF o Include Emergency OC in training programs for Nurses o Conduct in-service / continuing education programs on OF; o Conduct committee sensitization programs in the eradication of OF o Build capacity of healthcare workers in the provision of proper antenatal care o Work with Government/ Ministries of Health for distribution of trained workforce. o Promote institutional deliveries and proper use of partographs o Proper management of women in the first and second stages of labor o Participate in rehabilitation of patients with OF o Provide psychological support to women with OF o Promote use of family planning services o Create awareness in the risk of early marriage o Facilitate the elimination of FGM in committee programs o Increase public awareness on preventive measures
Works by thematic groups Participants were divided into 3 thematic groups: Prevention (MoH representatives), Treatment and Training (Surgeons and academic institutions), Social reintegration (Minister of Gender representatives). At the end of the day, the thematic groups presented their respective reports.
FRIDAY, JUNE 21, 2019: Third Day
Annual Report • October 2018 – September 2019 Fistula Care Plus 193
Dr. Sk. Nazmul Huda, Global Manager, FC+ project presented the Fistula Care + project strategies and achievements. The rest of the 3rd and last day of the conference was devoted to the development of countries’ road map and to the preparation of the Saly resolution for fistula eradication. The regional meeting was followed by URODAK- a annual event of the urologists of the region. Dr. Nazmul on behalf of Dr. Vandana Tripathi made a presentation in a session of URODAK on June 22nd. ANNEXES: 1. UNFPA regional strategy to end OF; PPT presentation
2. Annex II: IDB PPT Presentation 3. Annex III: West African College of Surgeons (WACS) PPT presentation
Dr. Nazmul Huda had two important side meetings in Dakar. Following is a note for record of the meetings: Meeting with Dr Mbayi Kangudie (Dr. Didier), MD, MPH; Senior Health Advisor; USAID West Africa about Niger program:
1. I reflected on my recent visit to Niger. Discussed thoroughly about the situation in Zinder, Maradi, Danja, Tahoua and CNRFO. He endorsed my observations on Niger situation.
2. He advised to engage consultant/s ASAP for facilitating clinical waste management at CNRFO (Pit hole method) and do an audit of resource management. He is NOT in favor of taking any risk of finance management in different level (Ministry and facility level).
3. Dr. Didier strongly recommended to enhance fistula repair performance in Niger. He expected at least 20-30 repairs reported from Niger in July-October period. Following options were discussed:
a. He was keen in a per case partial repair cost support (USD 200) system in at least one suitable facility. Danja was thought to be the most potential site. He asked to immediately go for an understanding with Danja in this regard.
b. I discussed the possible challenges for repair cost reimbursement to Danja. Following options he agreed to explore:
i. To use existing REF pipeline if possible. ii. To explore any option to directly pay to Danja.
iii. To explore channeling repair cost to Danja through their key donor of Danja. Meaning give this amount to Danja’s source organization in USA.
iv. To explore channeling the repair cost to Danja through one of FC+ existing partner.
v. He advised to go for an understanding with Danja ASAP, they start repair performance for USAID and then in the next three workout/complete payment options.
Annual Report • October 2018 – September 2019 Fistula Care Plus 194
4. Dr. Didier advised West African Countries as one unit in the rest of the project period. In a separate meeting with Prof. Serigne, he (Dr. Didier) advised Prof. to submit a note for capacity building inputs for the region as a whole. Prof. Serigne promised to submit the note ASAP.
5. Dr. Didier advised Dr. Nazmul to visit Niger soon to follow up Danja engagement. Key points:
Consultant ASAP– for audit and pit holes at CNRFO; Enhance repair performance immediately in Q4,
Per case payment (USD 200) agreement with Danja effective ASAP, work out reimbursement options. In future address West African Countries as one unit.

Annual Report • October 2018 – September 2019 Fistula Care Plus 195
APPENDIX T: ECSACOG PANEL PRESENTATION: BOATIN

Annual Report • October 2018 – September 2019 Fistula Care Plus 196

Annual Report • October 2018 – September 2019 Fistula Care Plus 197

Annual Report • October 2018 – September 2019 Fistula Care Plus 198
Annual Report • October 2018 – September 2019 Fistula Care Plus 199

Annual Report • October 2018 – September 2019 Fistula Care Plus 200
APPENDIX U: ECSACOG PRESENTATION: MASWIME
Annual Report • October 2018 – September 2019 Fistula Care Plus 201

Annual Report • October 2018 – September 2019 Fistula Care Plus 202
APPENDIX V: ECSACOG PRESENTATION: ROA

Annual Report • October 2018 – September 2019 Fistula Care Plus 203

Annual Report • October 2018 – September 2019 Fistula Care Plus 204
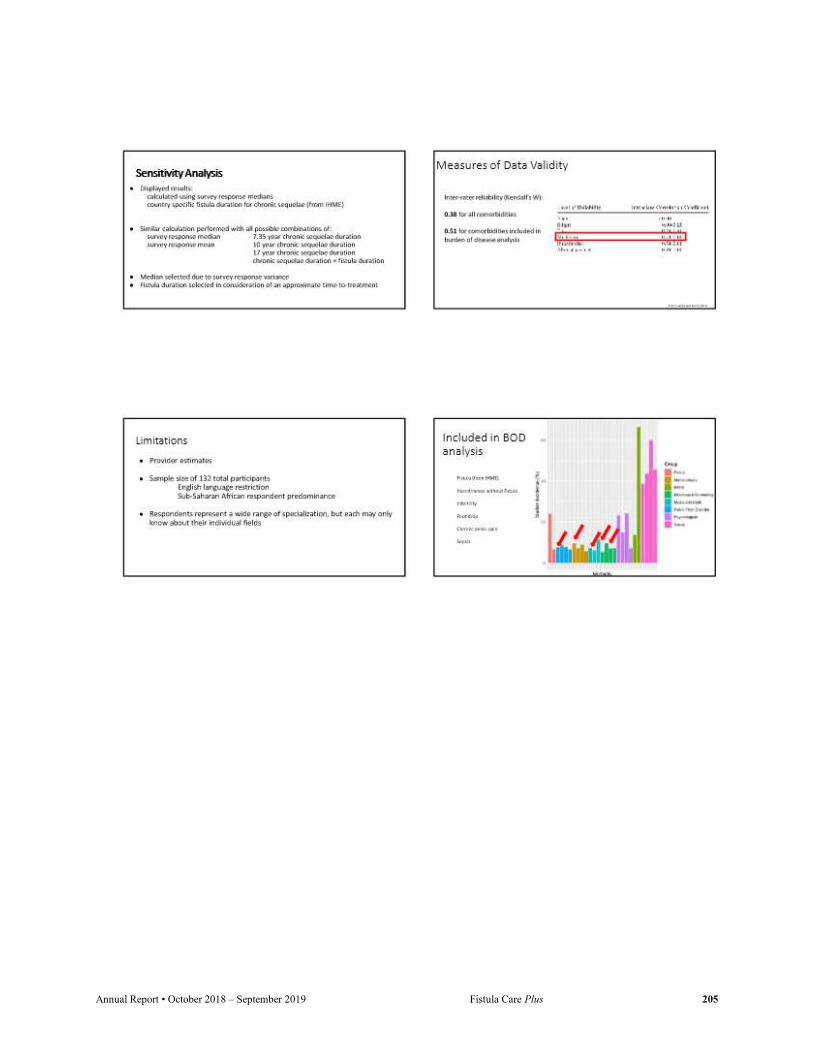
Annual Report • October 2018 – September 2019 Fistula Care Plus 205

Annual Report • October 2018 – September 2019 Fistula Care Plus 206
APPENDIX W: ECSACOG PRESENTATION: SHIVERA

Annual Report • October 2018 – September 2019 Fistula Care Plus 207

Annual Report • October 2018 – September 2019 Fistula Care Plus 208
APPENDIX X: ECSACOG PRESENTATION: LUGAZIA
Annual Report • October 2018 – September 2019 Fistula Care Plus 209
Annual Report • October 2018 – September 2019 Fistula Care Plus 210

Annual Report • October 2018 – September 2019 Fistula Care Plus 211

Annual Report • October 2018 – September 2019 Fistula Care Plus 212
APPENDIX Y: FC+ ANNUAL PARTOGRAPH MONITORING: FY 14/15 Fa
cilit
y na
me
Num
ber r
ecor
ds re
view
ed
5. P
arto
grap
h in
pat
ient
file
?
6. P
arto
grap
h fr
om a
re
ferr
ing
faci
lity
in p
atie
nt
file?
7. C
ontr
actio
ns (1
/2hr
ly
thro
ugho
ut la
bor)
8. F
etal
Hea
rt R
ate
(1/2
hrly
th
roug
hout
labo
r)
9. M
ater
nal B
lood
Pre
ssur
e (E
ITH
ER A
. - a
t adm
issi
on o
r B.
- th
roug
hout
labo
r)
10. M
ater
nal P
ulse
(EIT
HER
A
. - a
t adm
issi
on o
r B. -
th
roug
hout
labo
r)
11. C
ross
Act
ion
line?
12. A
ctio
ns T
aken
? (Q
uant
itativ
e)
Indicator A (Mean Score)
Indicator B (% Correct Action)
0: No, not in file 1: Yes, in file
0: No, not in file; 1: Yes, in file; N/A: not referred; DK: source cannot be determined
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not crossed; 1: crossed
0: No, appropriate actions not taken; 1:Yes, appropriate actions taken
Maximum = 5
Maximum = 100%
Bangladesh 175 0.45 n/a 0.41 0.41 0.41 0.38 0.10 0.10 2.05 100.00%
LAMB 25 1.00 n/a 0.88 0.88 0.88 0.88 0.04 0.04 4.52 100.00% Ad-din Dhaka 25 1.00 n/a 0.84 0.84 0.84 0.84 0.00 0.00 4.36 n/a
Ad-din Jessore 25 0.32 n/a 0.32 0.32 0.32 0.28 0.32 0.32 1.56 100.00% Ad-din Khulna 25 0.32 n/a 0.32 0.32 0.32 0.24 0.32 0.32 1.52 100.00%
BSMMU 25 0.00 n/a 0.00 0.00 0.00 0.00 0.00 0.00 0.00 n/a Kumudini 25 0.48 n/a 0.48 0.48 0.48 0.44 0.04 0.04 2.36 100.00% Muttalib 25 0.00 n/a 0.00 0.00 0.00 0.00 0.00 0.00 0.00 n/a
Niger 50 1.00 0.70 0.88 1.00 1.00 1.00 0.00 0.00 4.88 n/a CSME Maradi 25 1.00 0.92 0.76 1.00 1.00 1.00 0.00 0.00 4.76 n/a CSME Tahoua 25 1.00 0.48 1.00 1.00 1.00 1.00 0.00 0.00 5.00 n/a
Nigeria 276 0.17 0.00 0.00 0.01 0.00 0.00 0.00 0.00 0.18 0.00%
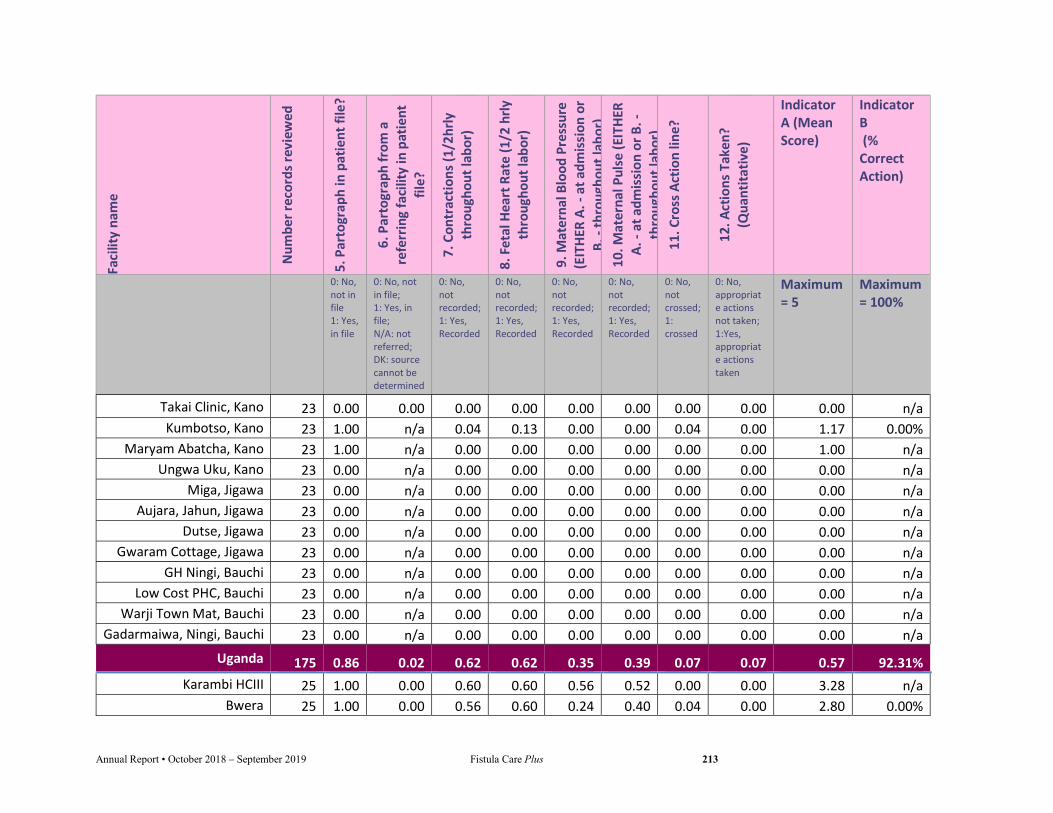
Annual Report • October 2018 – September 2019 Fistula Care Plus 213
Faci
lity
nam
e
Num
ber r
ecor
ds re
view
ed
5. P
arto
grap
h in
pat
ient
file
?
6. P
arto
grap
h fr
om a
re
ferr
ing
faci
lity
in p
atie
nt
file?
7. C
ontr
actio
ns (1
/2hr
ly
thro
ugho
ut la
bor)
8. F
etal
Hea
rt R
ate
(1/2
hrly
th
roug
hout
labo
r)
9. M
ater
nal B
lood
Pre
ssur
e (E
ITH
ER A
. - a
t adm
issi
on o
r B.
- th
roug
hout
labo
r)
10. M
ater
nal P
ulse
(EIT
HER
A
. - a
t adm
issi
on o
r B. -
th
roug
hout
labo
r)
11. C
ross
Act
ion
line?
12. A
ctio
ns T
aken
? (Q
uant
itativ
e)
Indicator A (Mean Score)
Indicator B (% Correct Action)
0: No, not in file 1: Yes, in file
0: No, not in file; 1: Yes, in file; N/A: not referred; DK: source cannot be determined
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not crossed; 1: crossed
0: No, appropriate actions not taken; 1:Yes, appropriate actions taken
Maximum = 5
Maximum = 100%
Takai Clinic, Kano 23 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 n/a Kumbotso, Kano 23 1.00 n/a 0.04 0.13 0.00 0.00 0.04 0.00 1.17 0.00%
Maryam Abatcha, Kano 23 1.00 n/a 0.00 0.00 0.00 0.00 0.00 0.00 1.00 n/a Ungwa Uku, Kano 23 0.00 n/a 0.00 0.00 0.00 0.00 0.00 0.00 0.00 n/a
Miga, Jigawa 23 0.00 n/a 0.00 0.00 0.00 0.00 0.00 0.00 0.00 n/a Aujara, Jahun, Jigawa 23 0.00 n/a 0.00 0.00 0.00 0.00 0.00 0.00 0.00 n/a
Dutse, Jigawa 23 0.00 n/a 0.00 0.00 0.00 0.00 0.00 0.00 0.00 n/a Gwaram Cottage, Jigawa 23 0.00 n/a 0.00 0.00 0.00 0.00 0.00 0.00 0.00 n/a
GH Ningi, Bauchi 23 0.00 n/a 0.00 0.00 0.00 0.00 0.00 0.00 0.00 n/a Low Cost PHC, Bauchi 23 0.00 n/a 0.00 0.00 0.00 0.00 0.00 0.00 0.00 n/a
Warji Town Mat, Bauchi 23 0.00 n/a 0.00 0.00 0.00 0.00 0.00 0.00 0.00 n/a Gadarmaiwa, Ningi, Bauchi 23 0.00 n/a 0.00 0.00 0.00 0.00 0.00 0.00 0.00 n/a
Uganda 175 0.86 0.02 0.62 0.62 0.35 0.39 0.07 0.07 0.57 92.31% Karambi HCIII 25 1.00 0.00 0.60 0.60 0.56 0.52 0.00 0.00 3.28 n/a
Bwera 25 1.00 0.00 0.56 0.60 0.24 0.40 0.04 0.00 2.80 0.00%

Annual Report • October 2018 – September 2019 Fistula Care Plus 214
Faci
lity
nam
e
Num
ber r
ecor
ds re
view
ed
5. P
arto
grap
h in
pat
ient
file
?
6. P
arto
grap
h fr
om a
re
ferr
ing
faci
lity
in p
atie
nt
file?
7. C
ontr
actio
ns (1
/2hr
ly
thro
ugho
ut la
bor)
8. F
etal
Hea
rt R
ate
(1/2
hrly
th
roug
hout
labo
r)
9. M
ater
nal B
lood
Pre
ssur
e (E
ITH
ER A
. - a
t adm
issi
on o
r B.
- th
roug
hout
labo
r)
10. M
ater
nal P
ulse
(EIT
HER
A
. - a
t adm
issi
on o
r B. -
th
roug
hout
labo
r)
11. C
ross
Act
ion
line?
12. A
ctio
ns T
aken
? (Q
uant
itativ
e)
Indicator A (Mean Score)
Indicator B (% Correct Action)
0: No, not in file 1: Yes, in file
0: No, not in file; 1: Yes, in file; N/A: not referred; DK: source cannot be determined
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not crossed; 1: crossed
0: No, appropriate actions not taken; 1:Yes, appropriate actions taken
Maximum = 5
Maximum = 100%
Hoima 25 1.00 0.12 0.96 0.96 0.24 0.12 0.08 0.08 3.28 100.00% Kitovu 25 1.00 0.00 0.68 0.68 0.28 0.24 0.12 0.12 2.88 100.00%
Masaka RRH 25 1.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 1.00 n/a Kalungu HCIII 25 0.00 0.00 0.72 0.72 0.44 0.72 0.00 0.00 2.60 n/a
Kagando 25 1.00 0.00 0.84 0.76 0.68 0.72 0.28 0.28 4.00 100.00%
FC+ TOTAL 676 0.62 0.24 0.48 0.51 0.44 0.44 0.05 0.04 1.92 0.95

Annual Report • October 2018 – September 2019 Fistula Care Plus 215
APPENDIX Z: FC+ ANNUAL PARTOGRAPH MONITORING: FY 15/16
Faci
lity
nam
e
Num
ber r
ecor
ds re
view
ed
5. P
arto
grap
h in
pat
ient
fil
e?
6. P
arto
grap
h fr
om a
re
ferr
ing
faci
lity
in p
atie
nt
file?
7. C
ontr
actio
ns (
1/2h
rly
thro
ugho
ut la
bor)
8. F
etal
Hea
rt R
ate
(1/2
hrly
th
roug
hout
labo
r)
9. M
ater
nal B
lood
Pre
ssur
e (E
ITH
ER A
. - a
t adm
issi
on o
r B.
- th
roug
hout
labo
r)
10. M
ater
nal P
ulse
(EIT
HER
A.
- at
adm
issi
on o
r B. -
th
roug
hout
labo
r)
11. C
ross
Act
ion
line?
12. A
ctio
ns T
aken
? (Q
uant
itativ
e)
Indicator A (Mean Score)
Indicator B (% Correct Action)
0: No, not in file 1: Yes, in file
0: No, not in file; 1: Yes, in file; N/A: not referred; DK: source cannot be determined
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not crossed; 1: crossed
0: No, appropriate actions not taken; 1:Yes, appropriate actions taken
Maximum = 5
Maximum = 100%
Bangladesh 136 0.59 n/a 0.56 0.81 0.98 0.98 0.34 0.34 3.92 100.00%
LAMB 25 1.00 0.92 1.00 1.00 1.00 1.00 1.00 4.92 100.00% Ad-din Dhaka 25 0.92 0.88 0.92 0.88 0.88 0.00 0.00 4.48 n/a
Ad-din Khulna 11 1.00 1.00 1.00 1.00 1.00 1.00 1.00 5.00 100.00% BSMMU 25 0.00 0.00 1.00 1.00 1.00 0.00 0.00 3.00 n/a
Kumudini 25 0.60 0.56 0.96 1.00 1.00 0.04 0.04 4.12 100.00% Muttalib 25 0.00 0.00 0.00 1.00 1.00 0.00 0.00 2.00 n/a
Niger 50 1.00 0.00 0.50 0.50 1.00 1.00 0.00 0.00 4.00 n/a
CSME Maradi 25 1.00 0.40 0.40 1.00 1.00 0.00 0.00 3.80 n/a CSME Tahoua 25 1.00 0.60 0.60 1.00 1.00 0.00 0.00 4.20 n/a
Uganda 397 0.51 0.00 0.71 0.68 0.39 0.35 0.12 0.09 2.59 78.43%
Karambi HCIII 25 0.00 0.80 0.80 0.28 0.28 0.00 0.00 1.36 n/a Bwera 25 0.88 0.48 0.44 0.20 0.20 0.16 0.16 2.20 100.00%

Annual Report • October 2018 – September 2019 Fistula Care Plus 216
Faci
lity
nam
e
Num
ber r
ecor
ds re
view
ed
5. P
arto
grap
h in
pat
ient
fil
e?
6. P
arto
grap
h fr
om a
re
ferr
ing
faci
lity
in p
atie
nt
file?
7. C
ontr
actio
ns (
1/2h
rly
thro
ugho
ut la
bor)
8. F
etal
Hea
rt R
ate
(1/2
hrly
th
roug
hout
labo
r)
9. M
ater
nal B
lood
Pre
ssur
e (E
ITH
ER A
. - a
t adm
issi
on o
r B.
- th
roug
hout
labo
r)
10. M
ater
nal P
ulse
(EIT
HER
A.
- at
adm
issi
on o
r B. -
th
roug
hout
labo
r)
11. C
ross
Act
ion
line?
12. A
ctio
ns T
aken
? (Q
uant
itativ
e)
Indicator A (Mean Score)
Indicator B (% Correct Action)
0: No, not in file 1: Yes, in file
0: No, not in file; 1: Yes, in file; N/A: not referred; DK: source cannot be determined
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not crossed; 1: crossed
0: No, appropriate actions not taken; 1:Yes, appropriate actions taken
Maximum = 5
Maximum = 100%
Hoima 25 0.64 0.56 0.56 0.08 0.08 0.04 0.04 1.92 100.00% Kiyumba HCIV 25 0.00 0.92 0.96 0.68 0.64 0.32 0.32 3.20 100.00%
Jinja 25 0.96 0.28 0.24 0.12 0.12 0.08 0.08 1.72 100.00% Kamuli 25 1.00 0.76 0.60 0.52 0.44 0.08 0.00 3.32 0.00%
Kigorobya HCIV 25 0.00 0.96 0.92 0.68 0.64 0.28 0.24 3.20 85.71% Kyanamukaaka
HCIV 25 0.00 1.00 1.00 0.52 0.56 0.08 0.08 3.08 100.00%
Buraru HCIII 22 0.00 0.88 0.88 0.72 0.16 0.28 0.28 2.64 100.00% Azur HCIV 25 1.00 0.68 0.72 0.04 0.00 0.24 0.12 2.44 50.00%
Buseruka HCIII 25 0.00 0.96 0.84 0.56 0.52 0.28 0.20 2.88 71.43% Kikuube HCIV 25 0.48 0.92 0.88 0.64 0.68 0.00 0.00 3.60 n/a
Kitovu 25 1.00 0.68 0.68 0.32 0.48 0.00 0.00 3.16 n/a Masaka RRH 25 1.00 0.92 0.88 0.44 0.24 0.04 0.04 3.48 n/a
Kalungu HCIII 0 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 n/a Rwesande HCIV 25 0.72 0.56 0.52 0.36 0.36 0.04 0.00 2.52 0.00%
Kagando 25 1.00 0.68 0.68 0.44 0.48 0.12 0.04 3.28 33.33%

Annual Report • October 2018 – September 2019 Fistula Care Plus 217
Faci
lity
nam
e
Num
ber r
ecor
ds re
view
ed
5. P
arto
grap
h in
pat
ient
fil
e?
6. P
arto
grap
h fr
om a
re
ferr
ing
faci
lity
in p
atie
nt
file?
7. C
ontr
actio
ns (
1/2h
rly
thro
ugho
ut la
bor)
8. F
etal
Hea
rt R
ate
(1/2
hrly
th
roug
hout
labo
r)
9. M
ater
nal B
lood
Pre
ssur
e (E
ITH
ER A
. - a
t adm
issi
on o
r B.
- th
roug
hout
labo
r)
10. M
ater
nal P
ulse
(EIT
HER
A.
- at
adm
issi
on o
r B. -
th
roug
hout
labo
r)
11. C
ross
Act
ion
line?
12. A
ctio
ns T
aken
? (Q
uant
itativ
e)
Indicator A (Mean Score)
Indicator B (% Correct Action)
0: No, not in file 1: Yes, in file
0: No, not in file; 1: Yes, in file; N/A: not referred; DK: source cannot be determined
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not recorded; 1: Yes, Recorded
0: No, not crossed; 1: crossed
0: No, appropriate actions not taken; 1:Yes, appropriate actions taken
Maximum = 5
Maximum = 100%
DRC 75 0.74 0.00 0.48 0.35 0.72 0.72 0.01 0.01 3.01 100.00%
Heal Africa 25 1 0.44 0.24 0.92 0.92 0.00 0.00 3.52 n/a St. Joseph 25 0.96 0.72 0.72 1.00 1.00 0.04 0.04 4.40 100%
Esengo 25 1 0.76 0.44 0.96 0.96 0.00 0.00 4.12 n/a MSRK 0 0 0.00 0.00 0.00 0.00 0.00 0.00 0.00 n/a
FC+ TOTAL 658 0.71 0.56 0.59 0.77 0.76 0.12 0.11 3.38 0.94

Annual Report • October 2018 – September 2019 Fistula Care Plus 218
APPENDIX AA: FC+ ANNUAL PARTOGRAPH MONITORING: FY 16/17 Fa
cilit
y na
me
Num
ber r
ecor
ds re
view
ed
5. P
arto
grap
h in
pat
ient
fil
e?
6. P
arto
grap
h fr
om a
re
ferr
ing
faci
lity
in p
atie
nt
file?
7. C
ontr
actio
ns (
1/2h
rly
thro
ugho
ut la
bor)
8. F
etal
Hea
rt R
ate
(1/2
hrly
th
roug
hout
labo
r)
9. M
ater
nal B
lood
Pre
ssur
e (E
ITH
ER A
. - a
t adm
issi
on o
r B.
- th
roug
hout
labo
r)
10. M
ater
nal P
ulse
(EIT
HER
A
. - a
t adm
issi
on o
r B. -
th
roug
hout
labo
r)
11. C
ross
Act
ion
line?
12. A
ctio
ns T
aken
? (Q
uant
itativ
e)
Indicator A (Mean Score)
Indicator B (% Correct Action)
0: No, not in file
1: Yes, in file
0: No, not in file; 1: Yes, in file;
N/A: not referred;
DK: source cannot be
determined
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not crossed; 1:
crossed
0: No, appropriate actions not
taken; 1:Yes,
appropriate actions
taken
Maximum = 5 Maximum = 100%
Bangladesh 150 0.57 n/a 0.55 0.82 0.99 0.93 0.03 0.03 3.86 100.00% LAMB 25 1.00 n/a 0.96 0.96 1.00 1.00 0.16 0.16 4.92 100.00% Ad-din Dhaka 25 1.00 n/a 1.00 1.00 1.00 1.00 0.00 0.00 5.00 n/a Ad-din Khulna 25 0.64 n/a 0.64 0.92 0.92 0.60 0.00 0.00 3.72 n/a BSMMU 25 0.00 n/a 0.00 1.00 1.00 1.00 0.00 0.00 3.00 n/a Kumudini 25 0.76 n/a 0.72 1.00 1.00 1.00 0.00 0.00 4.48 n/a Muttalib 25 0.00 n/a 0.00 0.04 1.00 1.00 0.00 0.00 2.04 n/a
Niger 25 0.84 0.00 0.32 0.72 0.80 0.80 0.00 0.00 3.48 n/a CSME Maradi NA NA NA NA NA NA NA NA NA NA NA CSME Tahoua 25 0.84 0.00 0.32 0.72 0.80 0.80 0.00 0.00 3.48 n/a
Uganda 409 0.94 0.01 0.83 0.80 0.55 0.52 0.05 0.02 3.60 45.45% Karambi HCIII 25 1.00 0 0.72 0.68 0.32 0.48 0.00 0.00 2.48 n/a Bwera 25 1.00 n/a 0.76 0.76 0.40 0.32 0.12 0.04 3.24 33.33%

Annual Report • October 2018 – September 2019 Fistula Care Plus 219
Faci
lity
nam
e
Num
ber r
ecor
ds re
view
ed
5. P
arto
grap
h in
pat
ient
fil
e?
6. P
arto
grap
h fr
om a
re
ferr
ing
faci
lity
in p
atie
nt
file?
7. C
ontr
actio
ns (
1/2h
rly
thro
ugho
ut la
bor)
8. F
etal
Hea
rt R
ate
(1/2
hrly
th
roug
hout
labo
r)
9. M
ater
nal B
lood
Pre
ssur
e (E
ITH
ER A
. - a
t adm
issi
on o
r B.
- th
roug
hout
labo
r)
10. M
ater
nal P
ulse
(EIT
HER
A
. - a
t adm
issi
on o
r B. -
th
roug
hout
labo
r)
11. C
ross
Act
ion
line?
12. A
ctio
ns T
aken
? (Q
uant
itativ
e)
Indicator A (Mean Score)
Indicator B (% Correct Action)
0: No, not in file
1: Yes, in file
0: No, not in file; 1: Yes, in file;
N/A: not referred;
DK: source cannot be
determined
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not crossed; 1:
crossed
0: No, appropriate actions not
taken; 1:Yes,
appropriate actions
taken
Maximum = 5 Maximum = 100%
Hoima 25 0.96 0.08 0.72 0.76 0.32 0.20 0.12 0.04 2.96 33.33% Kiyumba HCIV 25 1.00 0.00 1.00 0.96 0.48 0.60 0.24 0.12 4.04 50.00% Jinja 25 0.96 0.05 0.68 0.64 0.40 0.36 0.04 0.04 3.04 100.00% Kamuli 25 1.00 0.00 0.96 0.96 0.72 0.76 0.08 0.04 4.40 50.00% Kigorobya HCIV 25 1.00 n/a 0.92 0.64 0.68 0.72 0.00 0.00 3.96 n/a Kyanamukaaka HCIV 25 1.00 0.00 0.96 0.96 0.88 0.84 0.04 0.00 4.64 0.00% Buraru HCIII 20 1.00 n/a 1.00 1.00 0.85 0.80 0.00 0.00 4.65 n/a Azur HCIV 25 0.96 n/a 0.76 0.68 0.08 0.04 0.00 0.00 2.52 n/a Buseruka HCIII 16 1 n/a 0.94 0.94 0.88 0.81 0.00 0.00 4.57 n/a Kikuube HCIV 23 1.00 n/a 0.96 0.96 0.61 0.52 0.00 0.00 4.05 n/a Kitovu 25 0.96 0.04 0.72 0.68 0.36 0.28 0.04 0.00 3.00 0.00% Masaka RRH 25 0.64 0.00 0.60 0.60 0.16 0.04 0.00 0.00 2.04 n/a Rwesande HCIV 25 1.00 n/a 0.76 0.72 0.72 0.56 0.00 0.00 3.76 n/a Lukolo HCIII 25 0.52 n/a 1.00 1.00 0.96 0.92 0.08 0.04 4.40 n/a Kagando 25 1.00 0.00 0.72 0.72 0.52 0.52 0.12 0.08 3.48 66.67%
DRC 124 0.73 0.00 0.46 0.44 0.72 0.66 0.07 0.05 2.85 69.44%
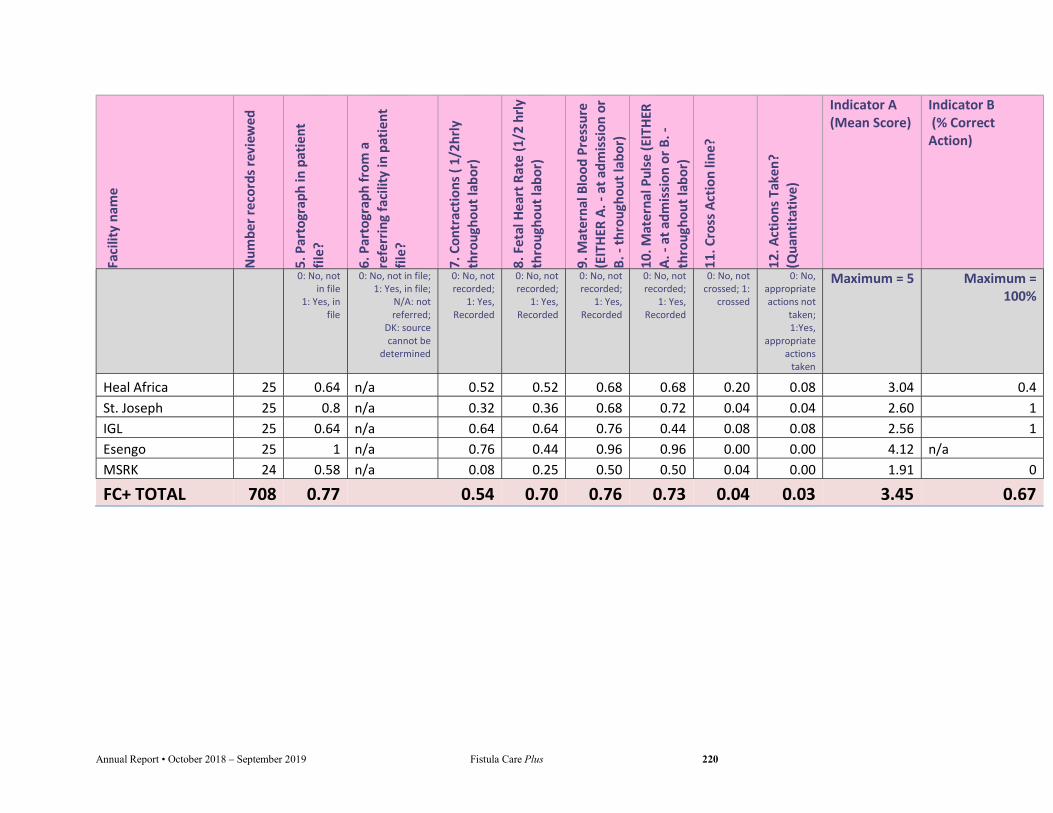
Annual Report • October 2018 – September 2019 Fistula Care Plus 220
Faci
lity
nam
e
Num
ber r
ecor
ds re
view
ed
5. P
arto
grap
h in
pat
ient
fil
e?
6. P
arto
grap
h fr
om a
re
ferr
ing
faci
lity
in p
atie
nt
file?
7. C
ontr
actio
ns (
1/2h
rly
thro
ugho
ut la
bor)
8. F
etal
Hea
rt R
ate
(1/2
hrly
th
roug
hout
labo
r)
9. M
ater
nal B
lood
Pre
ssur
e (E
ITH
ER A
. - a
t adm
issi
on o
r B.
- th
roug
hout
labo
r)
10. M
ater
nal P
ulse
(EIT
HER
A
. - a
t adm
issi
on o
r B. -
th
roug
hout
labo
r)
11. C
ross
Act
ion
line?
12. A
ctio
ns T
aken
? (Q
uant
itativ
e)
Indicator A (Mean Score)
Indicator B (% Correct Action)
0: No, not in file
1: Yes, in file
0: No, not in file; 1: Yes, in file;
N/A: not referred;
DK: source cannot be
determined
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not crossed; 1:
crossed
0: No, appropriate actions not
taken; 1:Yes,
appropriate actions
taken
Maximum = 5 Maximum = 100%
Heal Africa 25 0.64 n/a 0.52 0.52 0.68 0.68 0.20 0.08 3.04 0.4 St. Joseph 25 0.8 n/a 0.32 0.36 0.68 0.72 0.04 0.04 2.60 1 IGL 25 0.64 n/a 0.64 0.64 0.76 0.44 0.08 0.08 2.56 1 Esengo 25 1 n/a 0.76 0.44 0.96 0.96 0.00 0.00 4.12 n/a MSRK 24 0.58 n/a 0.08 0.25 0.50 0.50 0.04 0.00 1.91 0
FC+ TOTAL 708 0.77 0.54 0.70 0.76 0.73 0.04 0.03 3.45 0.67

Annual Report • October 2018 – September 2019 Fistula Care Plus 221
APPENDIX BB: FC+ ANNUAL PARTOGRAPH MONITORING: FY 17/18 Fa
cilit
y na
me
Num
ber r
ecor
ds
revi
ewed
5. P
arto
grap
h in
pa
tient
file
?
6. P
arto
grap
h fr
om a
re
ferr
ing
faci
lity
in
patie
nt fi
le?
7. C
ontr
actio
ns (
1/2h
rly th
roug
hout
la
bor)
8. F
etal
Hea
rt R
ate
(1/2
hrly
thro
ugho
ut
labo
r)
9. M
ater
nal B
lood
Pr
essu
re (E
ITH
ER A
. -
at a
dmis
sion
or B
. -
thro
ugho
ut la
bor)
10
. Mat
erna
l Pul
se
(EIT
HER
A. -
at
adm
issi
on o
r B. -
th
roug
hout
labo
r)
11. C
ross
Act
ion
line?
12. A
ctio
ns T
aken
? (Q
uant
itativ
e)
Indicator A (Mean Score)
Indicator B (% Correct Action)
0: No, not in file
1: Yes, in file
0: No, not in file; 1: Yes, in file;
N/A: not referred;
DK: source cannot be
determined
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not crossed; 1:
crossed
0: No, appropriate actions not
taken; 1:Yes,
appropriate actions
taken
Maximum = 5 Maximum = 100%
Bangladesh 149 0.54 n/a 0.56 0.56 0.81 0.78 0.09 0.83 3.25 n/a LAMB 25 1.00 n/a 0.92 1.00 1.00 1.00 0.00 1.00 4.92 n/a Ad-din Dhaka 24 0.96 n/a 0.96 0.96 0.96 0.96 0.00 1.00 4.80 n/a Ad-din Khulna 25 0.76 n/a 0.52 0.44 0.52 0.28 0.56 0.00 2.52 0.00% BSMMU 25 0.00 n/a 0.08 0.40 0.40 0.44 0.00 1.00 1.32 n/a Kumudini 25 0.52 n/a 0.88 0.52 1.00 1.00 0.00 1.00 3.92 n/a Muttalib 25 0.00 n/a 0.00 0.04 1.00 1.00 0.00 1.00 2.04 n/a
Uganda 450 0.99 0.01 0.80 0.79 0.66 0.60 0.07 0.05 3.79 69.84% Karambi HCIII 25 1.00 0 0.96 0.88 0.92 0.92 0.00 0.00 3.72 n/a Bwera 25 1.00 n/a 0.88 0.88 0.88 0.88 0.12 0.12 4.52 100.00% Hoima 25 0.96 0.08 0.68 0.68 0.52 0.52 0.24 0.20 3.36 83.33% Kiyumba HCIV 25 1.00 n/a 0.96 0.92 0.88 0.76 0.16 0.16 4.52 100.00% Jinja 25 1.00 n/a 0.56 0.52 0.20 0.16 0.04 0.00 2.44 0.00% Kamuli 25 1.00 n/a 0.80 0.80 0.88 0.84 0.10 0.08 4.32 80.00% Kalungu 25 1.00 n/a 0.96 0.88 0.80 0.80 0.00 0.00 4.44 n/a

Annual Report • October 2018 – September 2019 Fistula Care Plus 222
Faci
lity
nam
e
Num
ber r
ecor
ds
revi
ewed
5. P
arto
grap
h in
pa
tient
file
?
6. P
arto
grap
h fr
om a
re
ferr
ing
faci
lity
in
patie
nt fi
le?
7. C
ontr
actio
ns (
1/2h
rly th
roug
hout
la
bor)
8. F
etal
Hea
rt R
ate
(1/2
hrly
thro
ugho
ut
labo
r)
9. M
ater
nal B
lood
Pr
essu
re (E
ITH
ER A
. -
at a
dmis
sion
or B
. -
thro
ugho
ut la
bor)
10
. Mat
erna
l Pul
se
(EIT
HER
A. -
at
adm
issi
on o
r B. -
th
roug
hout
labo
r)
11. C
ross
Act
ion
line?
12. A
ctio
ns T
aken
? (Q
uant
itativ
e)
Indicator A (Mean Score)
Indicator B (% Correct Action)
0: No, not in file
1: Yes, in file
0: No, not in file; 1: Yes, in file;
N/A: not referred;
DK: source cannot be
determined
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not crossed; 1:
crossed
0: No, appropriate actions not
taken; 1:Yes,
appropriate actions
taken
Maximum = 5 Maximum = 100%
Kigorobya HCIV 25 1.00 n/a 0.72 0.68 0.64 0.36 0.04 0.04 3.40 n/a Kyanamukaaka HCIV 25 1.00 n/a 1.00 1.00 0.76 0.88 0.04 0.04 4.64 100.00% Buraru HCIII 25 1.00 n/a 1.00 1.00 1.00 0.76 0.08 0.00 4.76 0.00% Azur HCIV 25 1.00 n/a 0.76 0.76 0.32 0.08 0.08 0.04 2.92 50.00% Buseruka HCIII 25 1 n/a 0.92 0.92 0.80 0.80 0.00 0.00 4.44 n/a Kikuube HCIV 25 0.92 n/a 0.84 0.84 0.32 0.16 0.04 0.04 3.08 100.00% Kitovu 25 0.96 0.04 0.68 0.68 0.48 0.28 0.00 0.00 3.08 n/a Masaka RRH 25 1.00 0.00 0.28 0.32 0.16 0.20 0.08 0.00 1.96 0.00% Rwesande HCIV 25 1.00 n/a 0.84 0.84 0.84 0.84 0.16 0.12 4.36 75.00% Lukolo HCIII 25 1.00 n/a 0.96 1.00 0.92 0.96 0.00 0.00 4.84 n/a Kagando 25 1.00 0.00 0.64 0.68 0.60 0.56 0.08 0.04 3.48 50.00%
DRC 75 0.81 0.00 0.55 0.56 0.84 0.84 0.01 0.47 3.40 100.00% Heal Africa 25 1 n/a 0.40 0.44 0.88 0.88 0.00 0.32 3.60 n/a St. Joseph 25 0.72 n/a 0.64 0.64 0.64 0.64 0.04 0.08 2.68 100% Panzi 25 0.72 n/a 0.60 0.60 1.00 1.00 0.00 1.00 3.92 n/a
FC+ TOTAL 674 0.78 0.64 0.64 0.77 0.74 0.06 0.45 3.48 n/a
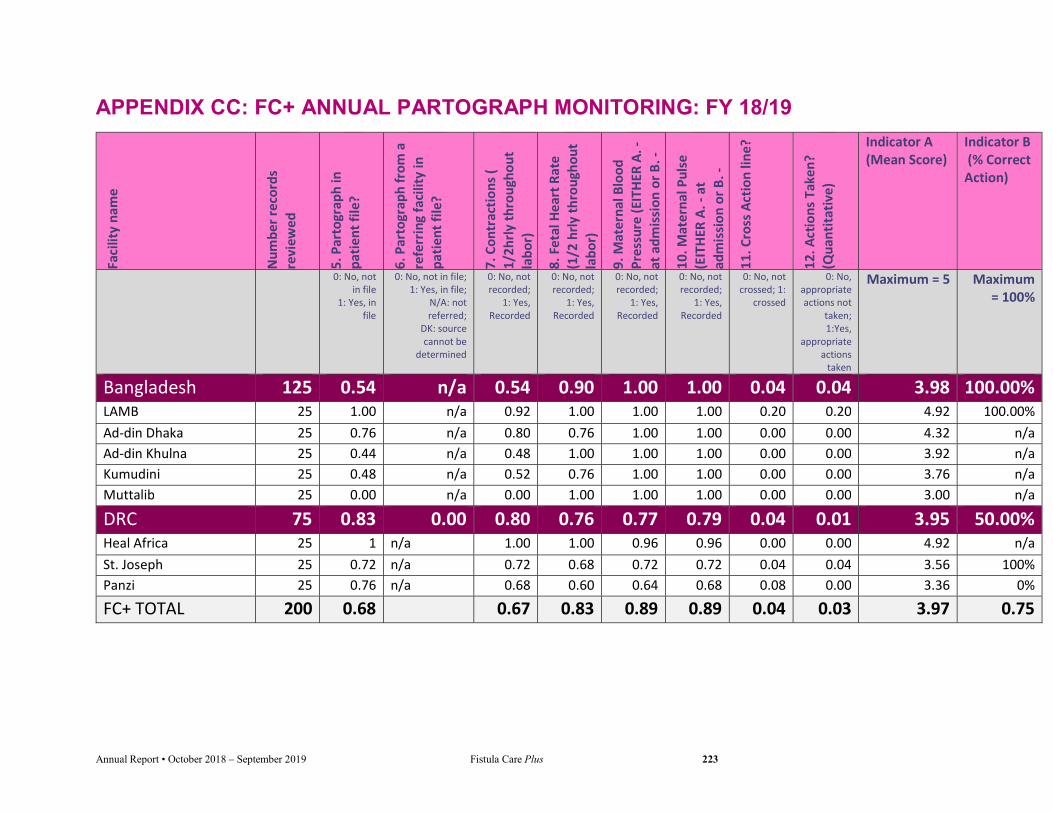
Annual Report • October 2018 – September 2019 Fistula Care Plus 223
APPENDIX CC: FC+ ANNUAL PARTOGRAPH MONITORING: FY 18/19 Fa
cilit
y na
me
Num
ber r
ecor
ds
revi
ewed
5. P
arto
grap
h in
pa
tient
file
?
6. P
arto
grap
h fr
om a
re
ferr
ing
faci
lity
in
patie
nt fi
le?
7. C
ontr
actio
ns (
1/2h
rly th
roug
hout
la
bor)
8. F
etal
Hea
rt R
ate
(1/2
hrly
thro
ugho
ut
labo
r)
9. M
ater
nal B
lood
Pr
essu
re (E
ITH
ER A
. -
at a
dmis
sion
or B
. -
thro
ugho
ut la
bor)
10
. Mat
erna
l Pul
se
(EIT
HER
A. -
at
adm
issi
on o
r B. -
th
roug
hout
labo
r)
11. C
ross
Act
ion
line?
12. A
ctio
ns T
aken
? (Q
uant
itativ
e)
Indicator A (Mean Score)
Indicator B (% Correct Action)
0: No, not in file
1: Yes, in file
0: No, not in file; 1: Yes, in file;
N/A: not referred;
DK: source cannot be
determined
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not recorded;
1: Yes, Recorded
0: No, not crossed; 1:
crossed
0: No, appropriate actions not
taken; 1:Yes,
appropriate actions
taken
Maximum = 5 Maximum = 100%
Bangladesh 125 0.54 n/a 0.54 0.90 1.00 1.00 0.04 0.04 3.98 100.00% LAMB 25 1.00 n/a 0.92 1.00 1.00 1.00 0.20 0.20 4.92 100.00% Ad-din Dhaka 25 0.76 n/a 0.80 0.76 1.00 1.00 0.00 0.00 4.32 n/a Ad-din Khulna 25 0.44 n/a 0.48 1.00 1.00 1.00 0.00 0.00 3.92 n/a Kumudini 25 0.48 n/a 0.52 0.76 1.00 1.00 0.00 0.00 3.76 n/a Muttalib 25 0.00 n/a 0.00 1.00 1.00 1.00 0.00 0.00 3.00 n/a
DRC 75 0.83 0.00 0.80 0.76 0.77 0.79 0.04 0.01 3.95 50.00% Heal Africa 25 1 n/a 1.00 1.00 0.96 0.96 0.00 0.00 4.92 n/a St. Joseph 25 0.72 n/a 0.72 0.68 0.72 0.72 0.04 0.04 3.56 100% Panzi 25 0.76 n/a 0.68 0.60 0.64 0.68 0.08 0.00 3.36 0%
FC+ TOTAL 200 0.68 0.67 0.83 0.89 0.89 0.04 0.03 3.97 0.75

Annual Report • October 2018 – September 2019 Fistula Care Plus 224
APPENDIX DD: AFLATEEN TECHNICAL BRIEF

Annual Report • October 2018 – September 2019 Fistula Care Plus 225

Annual Report • October 2018 – September 2019 Fistula Care Plus 226
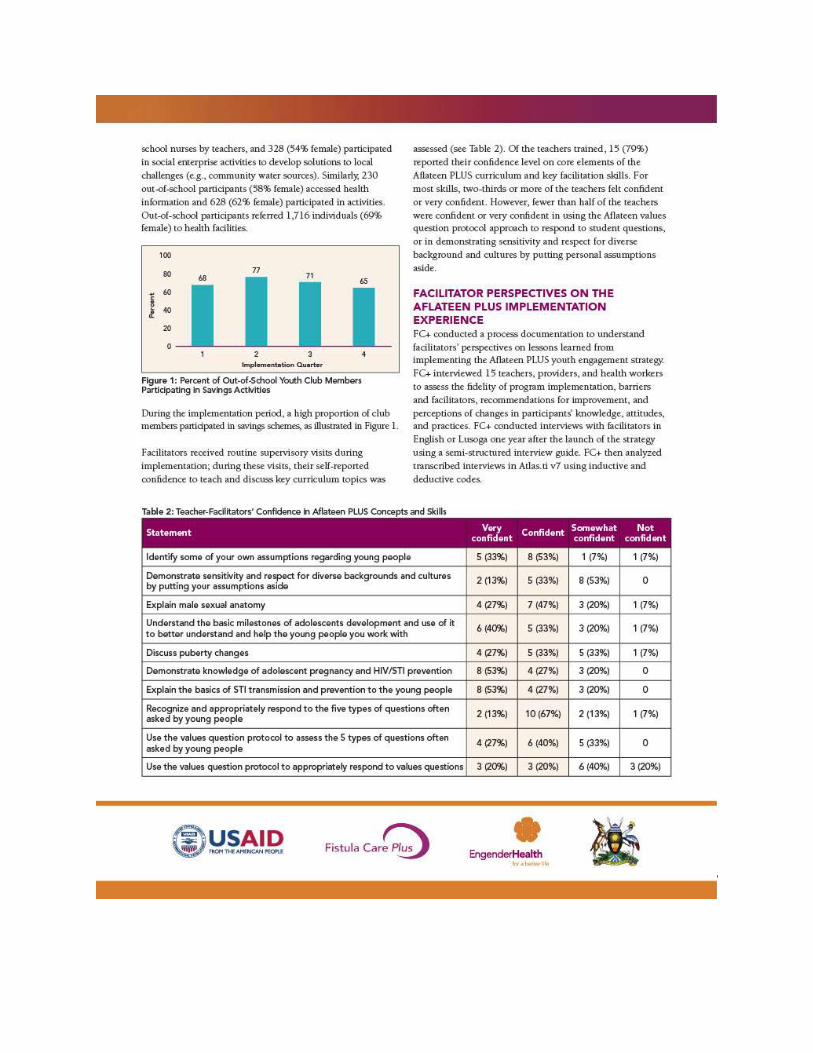
Annual Report • October 2018 – September 2019 Fistula Care Plus 227
Annual Report • October 2018 – September 2019 Fistula Care Plus 228

Annual Report • October 2018 – September 2019 Fistula Care Plus 229

Annual Report • October 2018 – September 2019 Fistula Care Plus 230

Annual Report • October 2018 – September 2019 Fistula Care Plus 231
Annual Report • October 2018 – September 2019 Fistula Care Plus 232
APPENDIX EE: HEALTH WORKERS TECHNICAL BRIEF
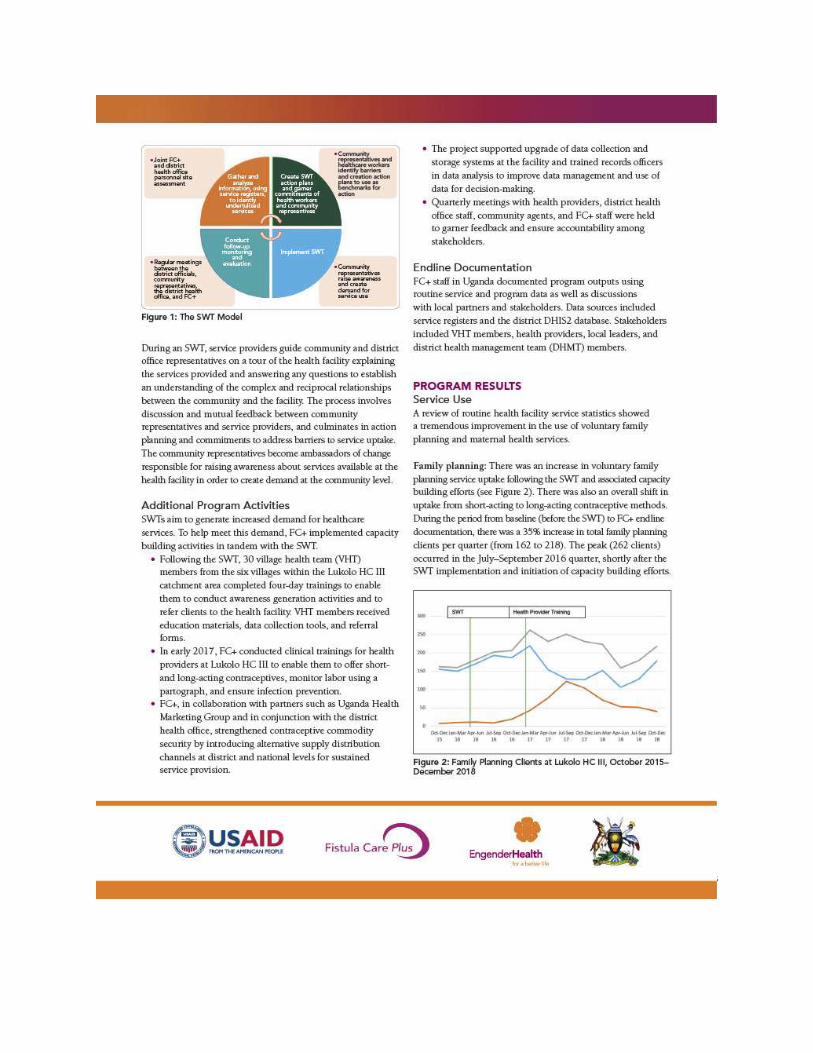
Annual Report • October 2018 – September 2019 Fistula Care Plus 233

Annual Report • October 2018 – September 2019 Fistula Care Plus 234
Annual Report • October 2018 – September 2019 Fistula Care Plus 235

Annual Report • October 2018 – September 2019 Fistula Care Plus 236

Annual Report • October 2018 – September 2019 Fistula Care Plus 237
Annual Report • October 2018 – September 2019 Fistula Care Plus 238
APPENDIX FF: RELIGIOUS LEADERS TECHNICAL BRIEF
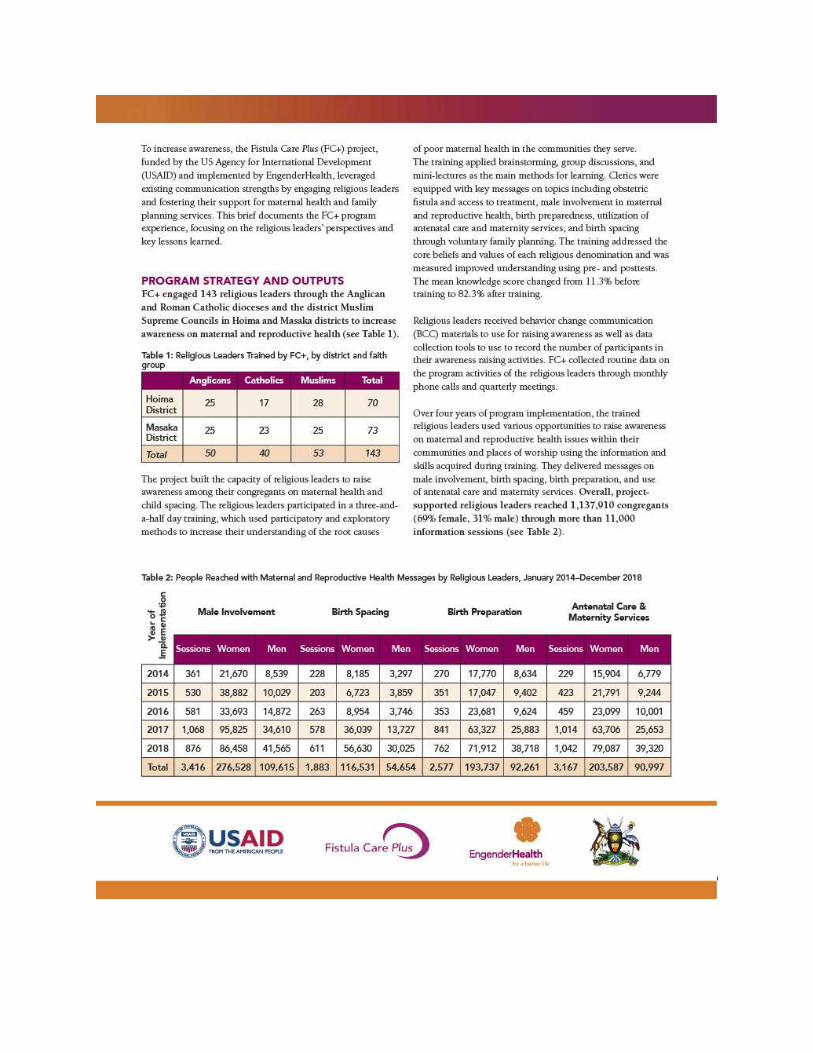
Annual Report • October 2018 – September 2019 Fistula Care Plus 239

Annual Report • October 2018 – September 2019 Fistula Care Plus 240
Annual Report • October 2018 – September 2019 Fistula Care Plus 241

Annual Report • October 2018 – September 2019 Fistula Care Plus 242

Annual Report • October 2018 – September 2019 Fistula Care Plus 243

Annual Report • October 2018 – September 2019 Fistula Care Plus 244

Annual Report • October 2018 – September 2019 Fistula Care Plus 245

Annual Report • October 2018 – September 2019 Fistula Care Plus 246
APPENDIX GG: SUCCESS STORIES TECHNICAL BRIEF

Annual Report • October 2018 – September 2019 Fistula Care Plus 247
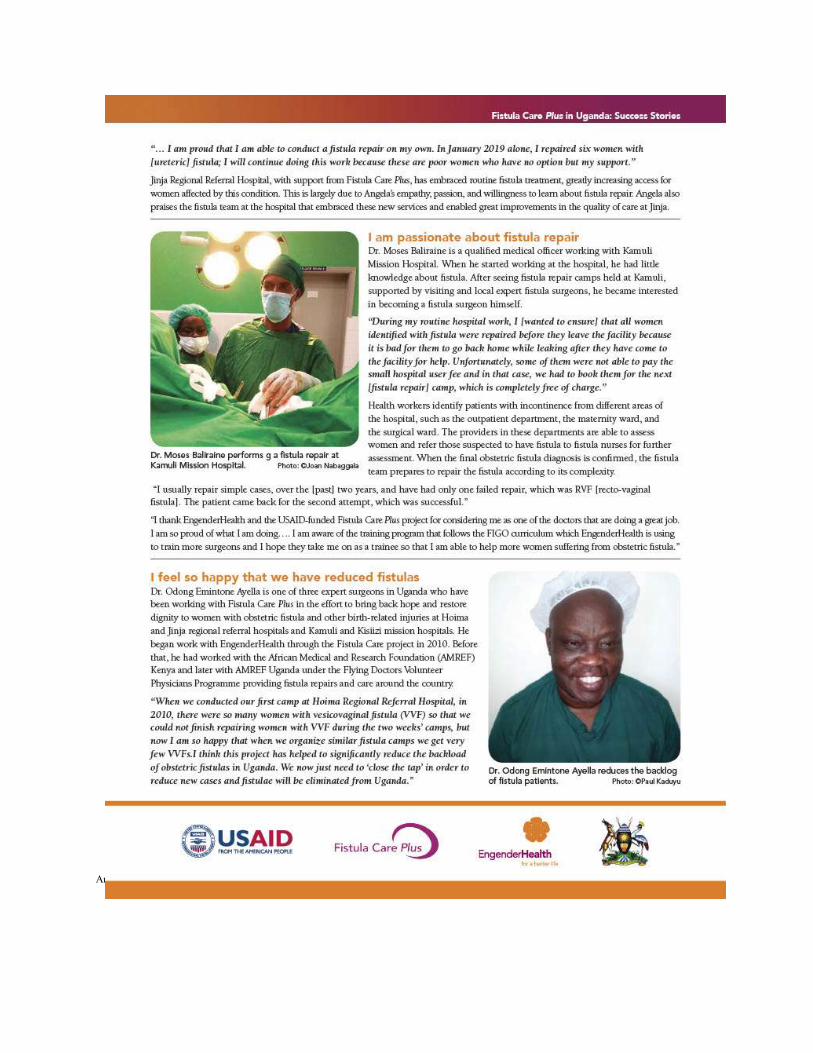
Annual Report • October 2018 – September 2019 Fistula Care Plus 248

Annual Report • October 2018 – September 2019 Fistula Care Plus 249

Annual Report • October 2018 – September 2019 Fistula Care Plus 250
Annual Report • October 2018 – September 2019 Fistula Care Plus 251

Annual Report • October 2018 – September 2019 Fistula Care Plus 252

Annual Report • October 2018 – September 2019 Fistula Care Plus 253

Annual Report • October 2018 – September 2019 Fistula Care Plus 254
APPENDIX HH: TERREWODE RESEARCH TECHNICAL BRIEF
Annual Report • October 2018 – September 2019 Fistula Care Plus 255

Annual Report • October 2018 – September 2019 Fistula Care Plus 256

Annual Report • October 2018 – September 2019 Fistula Care Plus 257

Annual Report • October 2018 – September 2019 Fistula Care Plus 258
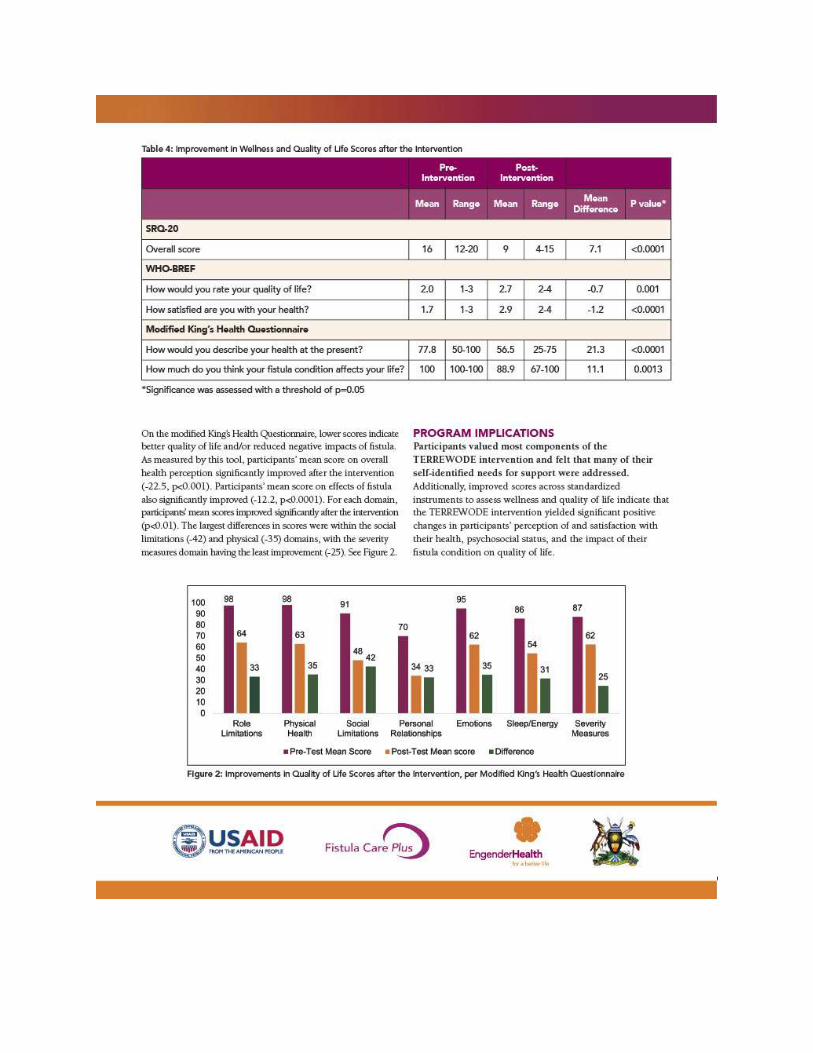
Annual Report • October 2018 – September 2019 Fistula Care Plus 259

Annual Report • October 2018 – September 2019 Fistula Care Plus 260

Annual Report • October 2018 – September 2019 Fistula Care Plus 261

Annual Report • October 2018 – September 2019 Fistula Care Plus 262
APPENDIX II: 4Q CHECKLIST TECHNICAL BRIEF

Annual Report • October 2018 – September 2019 Fistula Care Plus 263
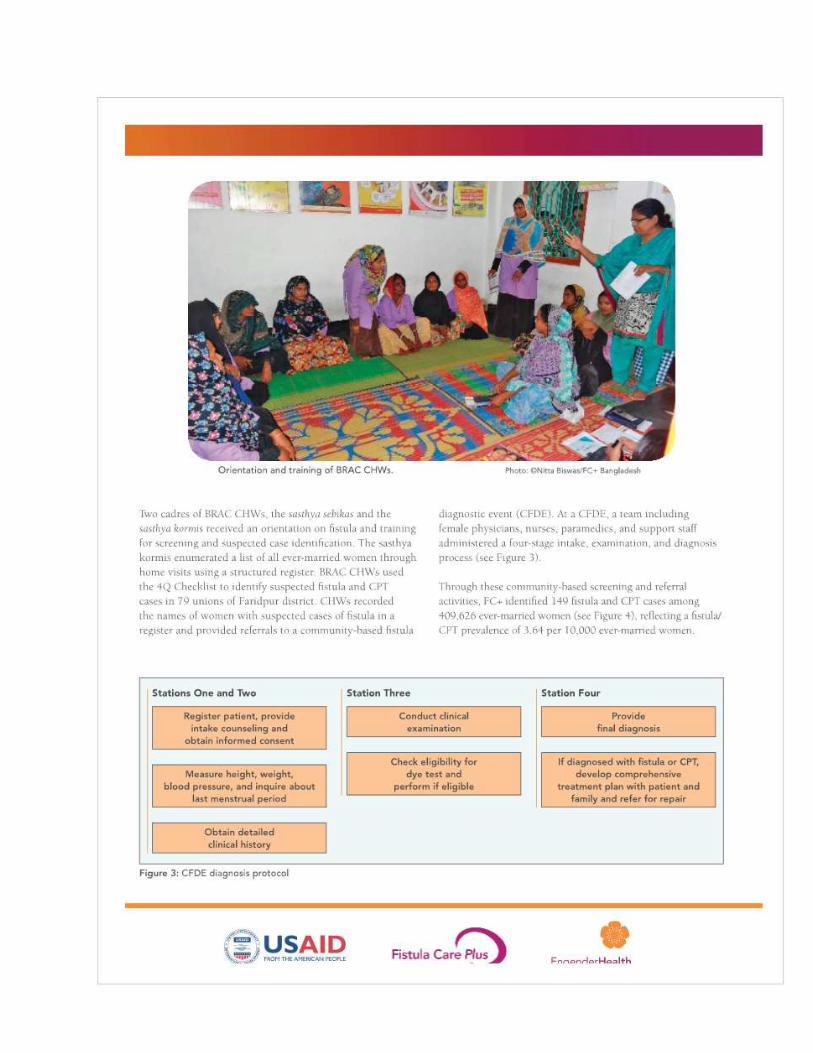
Annual Report • October 2018 – September 2019 Fistula Care Plus 264

Annual Report • October 2018 – September 2019 Fistula Care Plus 265

Annual Report • October 2018 – September 2019 Fistula Care Plus 266

Annual Report • October 2018 – September 2019 Fistula Care Plus 267

Annual Report • October 2018 – September 2019 Fistula Care Plus 268
APPENDIX JJ: USG BRIEF ON RECOGNIZING U.S. ACHIEVEMENTS IN GLOBAL FISTULA CARE

Annual Report • October 2018 – September 2019 Fistula Care Plus 269

Annual Report • October 2018 – September 2019 Fistula Care Plus 270
APPENDIX KK: IDEOF FIVE YEARS OF FC+ BRIEF

Annual Report • October 2018 – September 2019 Fistula Care Plus 271

Annual Report • October 2018 – September 2019 Fistula Care Plus 272

Annual Report • October 2018 – September 2019 Fistula Care Plus 273

Annual Report • October 2018 – September 2019 Fistula Care Plus 274

Annual Report • October 2018 – September 2019 Fistula Care Plus 275

Annual Report • October 2018 – September 2019 Fistula Care Plus 276

Annual Report • October 2018 – September 2019 Fistula Care Plus 277

Annual Report • October 2018 – September 2019 Fistula Care Plus 278
APPENDIX LL: LANCET COMMENTARY

Annual Report • October 2018 – September 2019 Fistula Care Plus 279

Annual Report • October 2018 – September 2019 Fistula Care Plus 280
APPENDIX MM: REMOVING BARRIERS JOURNAL ARTICLE

Annual Report • October 2018 – September 2019 Fistula Care Plus 281

Annual Report • October 2018 – September 2019 Fistula Care Plus 282

Annual Report • October 2018 – September 2019 Fistula Care Plus 283

Annual Report • October 2018 – September 2019 Fistula Care Plus 284

Annual Report • October 2018 – September 2019 Fistula Care Plus 285

Annual Report • October 2018 – September 2019 Fistula Care Plus 286

Annual Report • October 2018 – September 2019 Fistula Care Plus 287
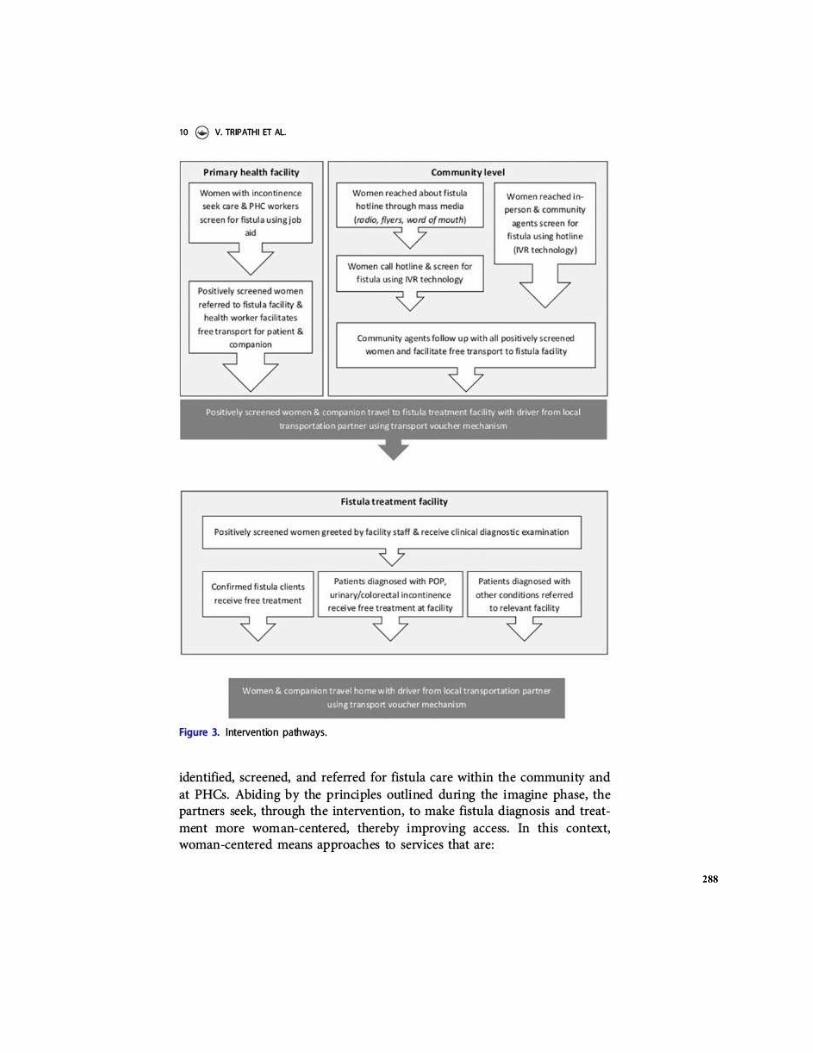
Annual Report • October 2018 – September 2019 Fistula Care Plus 288

Annual Report • October 2018 – September 2019 Fistula Care Plus 289

Annual Report • October 2018 – September 2019 Fistula Care Plus 290

Annual Report • October 2018 – September 2019 Fistula Care Plus 291

Annual Report • October 2018 – September 2019 Fistula Care Plus 292

Annual Report • October 2018 – September 2019 Fistula Care Plus 293

Annual Report • October 2018 – September 2019 Fistula Care Plus 294
APPENDIX NN: UN REPORT ON FISTULA

Annual Report • October 2018 – September 2019 Fistula Care Plus 295

Annual Report • October 2018 – September 2019 Fistula Care Plus 296

Annual Report • October 2018 – September 2019 Fistula Care Plus 297

Annual Report • October 2018 – September 2019 Fistula Care Plus 298
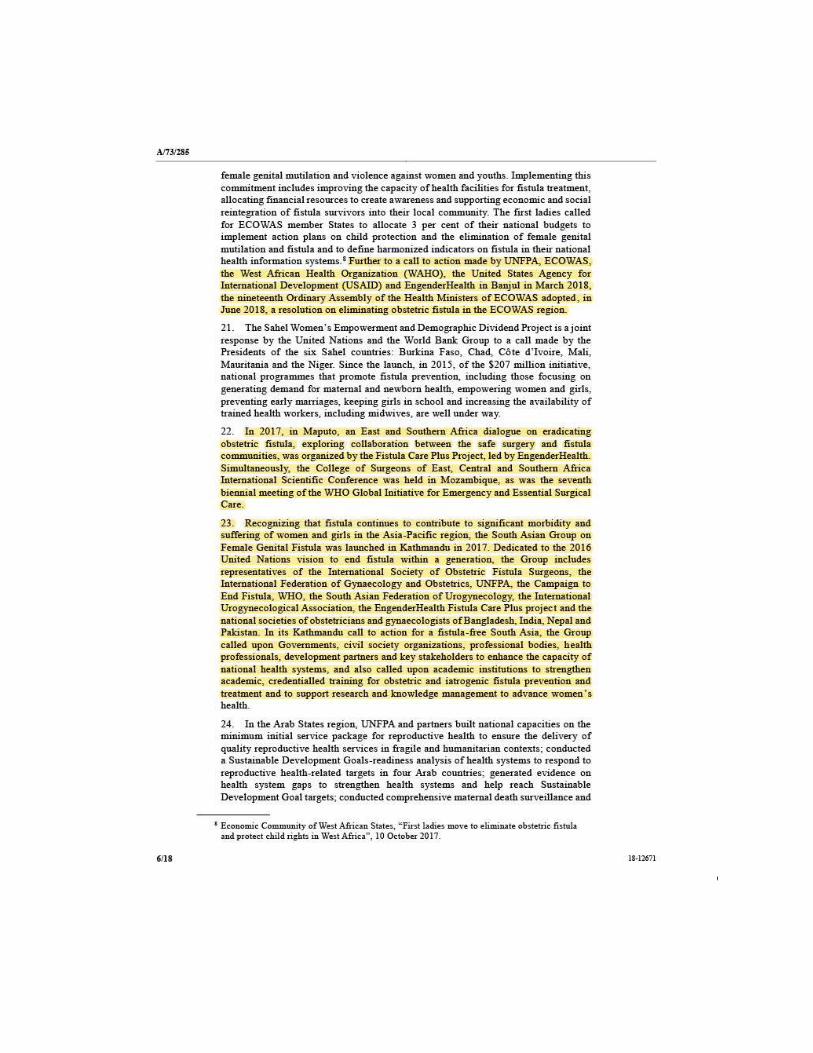
Annual Report • October 2018 – September 2019 Fistula Care Plus 299

Annual Report • October 2018 – September 2019 Fistula Care Plus 300

Annual Report • October 2018 – September 2019 Fistula Care Plus 301

Annual Report • October 2018 – September 2019 Fistula Care Plus 302

Annual Report • October 2018 – September 2019 Fistula Care Plus 303

Annual Report • October 2018 – September 2019 Fistula Care Plus 304

Annual Report • October 2018 – September 2019 Fistula Care Plus 305

Annual Report • October 2018 – September 2019 Fistula Care Plus 306

Annual Report • October 2018 – September 2019 Fistula Care Plus 307

Annual Report • October 2018 – September 2019 Fistula Care Plus 308

Annual Report • October 2018 – September 2019 Fistula Care Plus 309

Annual Report • October 2018 – September 2019 Fistula Care Plus 310

Annual Report • October 2018 – September 2019 Fistula Care Plus 311

Annual Report • October 2018 – September 2019 Fistula Care Plus 312
APPENDIX OO: RCOG PRESENTATION
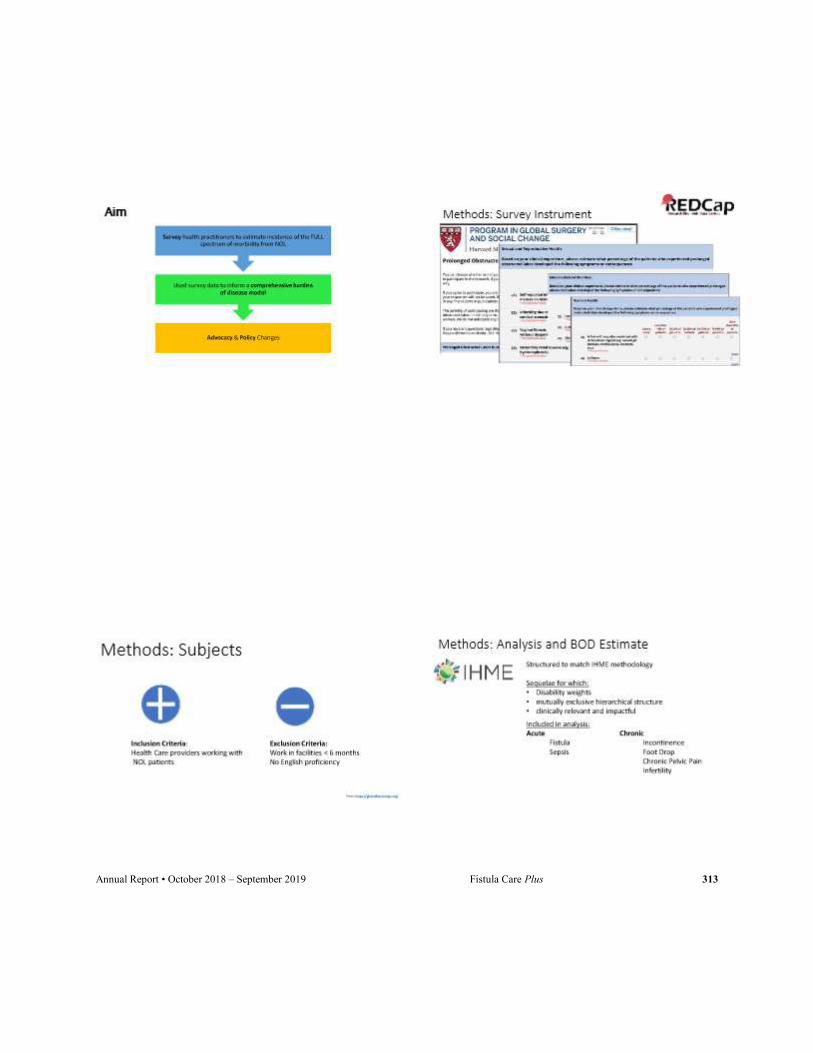
Annual Report • October 2018 – September 2019 Fistula Care Plus 313

Annual Report • October 2018 – September 2019 Fistula Care Plus 314

Annual Report • October 2018 – September 2019 Fistula Care Plus 315

Annual Report • October 2018 – September 2019 Fistula Care Plus 316
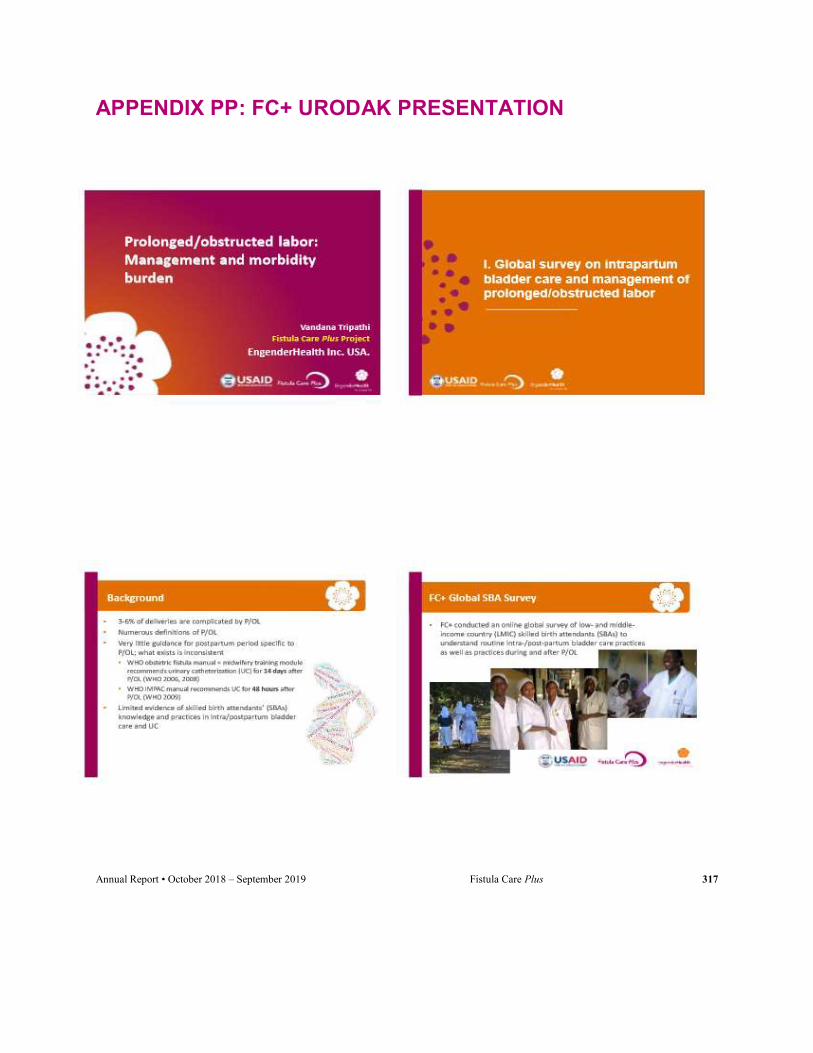
Annual Report • October 2018 – September 2019 Fistula Care Plus 317
APPENDIX PP: FC+ URODAK PRESENTATION

Annual Report • October 2018 – September 2019 Fistula Care Plus 318

Annual Report • October 2018 – September 2019 Fistula Care Plus 319
Annual Report • October 2018 – September 2019 Fistula Care Plus 320

Annual Report • October 2018 – September 2019 Fistula Care Plus 321

Annual Report • October 2018 – September 2019 Fistula Care Plus 322
Annual Report • October 2018 – September 2019 Fistula Care Plus 323
APPENDIX QQ: FC+ PRESENTATION AT INTERNATIONAL CONSULTATION ON THE REGIONAL STRATEGY FOR OBSTETRIC FISTULA ELIMINATION IN WEST AND CENTRAL AFRICA
Annual Report • October 2018 – September 2019 Fistula Care Plus 324

Annual Report • October 2018 – September 2019 Fistula Care Plus 325

Annual Report • October 2018 – September 2019 Fistula Care Plus 326

Annual Report • October 2018 – September 2019 Fistula Care Plus 327

Annual Report • October 2018 – September 2019 Fistula Care Plus 328
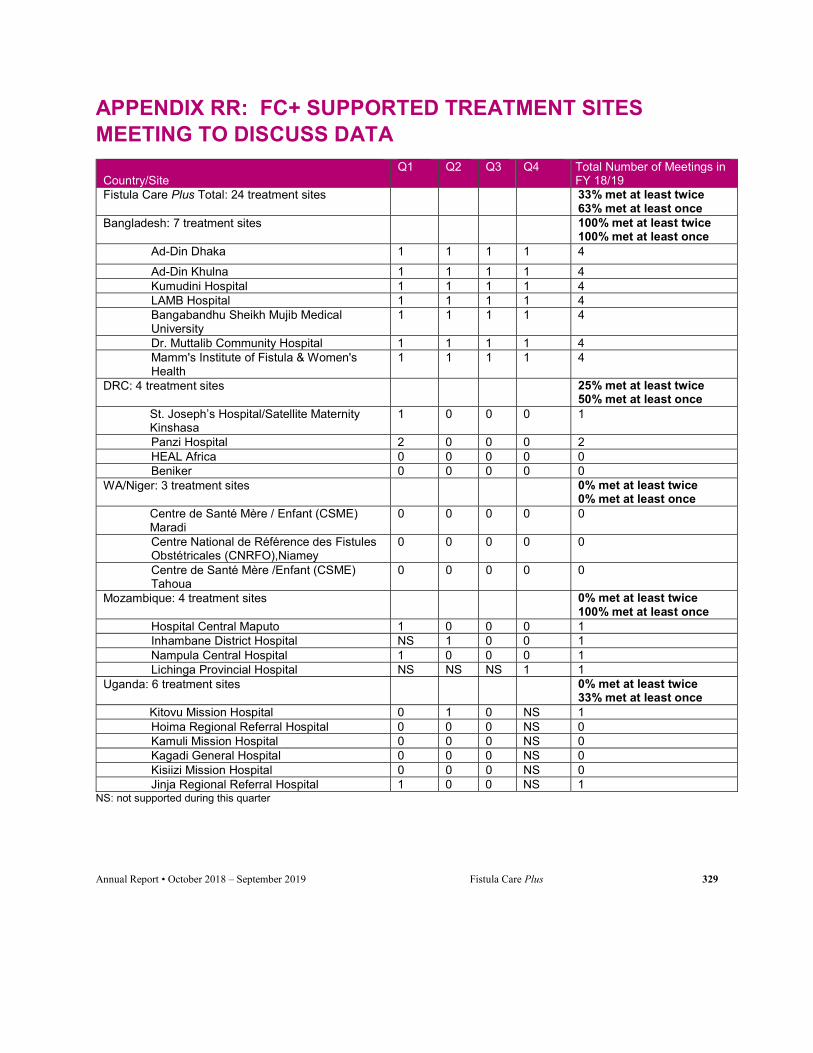
Annual Report • October 2018 – September 2019 Fistula Care Plus 329
APPENDIX RR: FC+ SUPPORTED TREATMENT SITES MEETING TO DISCUSS DATA
Country/Site
Q1 Q2 Q3 Q4 Total Number of Meetings in FY 18/19
Fistula Care Plus Total: 24 treatment sites 33% met at least twice 63% met at least once
Bangladesh: 7 treatment sites 100% met at least twice 100% met at least once
Ad-Din Dhaka 1 1 1 1 4
Ad-Din Khulna 1 1 1 1 4 Kumudini Hospital 1 1 1 1 4 LAMB Hospital 1 1 1 1 4 Bangabandhu Sheikh Mujib Medical University
1 1 1 1 4
Dr. Muttalib Community Hospital 1 1 1 1 4 Mamm's Institute of Fistula & Women's Health
1 1 1 1 4
DRC: 4 treatment sites 25% met at least twice 50% met at least once
St. Joseph’s Hospital/Satellite Maternity Kinshasa
1 0 0 0 1
Panzi Hospital 2 0 0 0 2 HEAL Africa 0 0 0 0 0 Beniker 0 0 0 0 0
WA/Niger: 3 treatment sites 0% met at least twice 0% met at least once
Centre de Santé Mère / Enfant (CSME) Maradi
0 0 0 0 0
Centre National de Référence des Fistules Obstétricales (CNRFO),Niamey
0 0 0 0 0
Centre de Santé Mère /Enfant (CSME) Tahoua
0 0 0 0 0
Mozambique: 4 treatment sites 0% met at least twice 100% met at least once
Hospital Central Maputo 1 0 0 0 1 Inhambane District Hospital NS 1 0 0 1 Nampula Central Hospital 1 0 0 0 1 Lichinga Provincial Hospital NS NS NS 1 1
Uganda: 6 treatment sites 0% met at least twice 33% met at least once
Kitovu Mission Hospital 0 1 0 NS 1 Hoima Regional Referral Hospital 0 0 0 NS 0 Kamuli Mission Hospital 0 0 0 NS 0 Kagadi General Hospital 0 0 0 NS 0 Kisiizi Mission Hospital 0 0 0 NS 0 Jinja Regional Referral Hospital 1 0 0 NS 1
NS: not supported during this quarter

Annual Report • October 2018 – September 2019 Fistula Care Plus 330
APPENDIX SS: FC+ CORE INDICATORS: ANNUAL ACHIEVEMENTS Note: Benchmarks for FY 15/16 are the approved benchmarks based on approved country workplans. Benchmarks for FY 17/18 are drawn from the original project approved FC+ PMP. Blanks indicate indicators/years for which benchmarks have not been finalized.
Goal: To strengthen health system capacity for fistula prevention, detection, treatment, and reintegration in priority countries in Sub-Saharan Africa and South Asia.
Indicator 1: Number of countries supported by Fistula Care Plus (FC+)
Definition: # of countries in which FC+ is supporting fistula repair sites and other activities to strengthen fistula-related policy, community capacity, and services
Additional description/context: FC+ will support countries to strengthen capacity for obstetric fistula prevention, detection, repair, and reintegration of affected women.
Data source and collection: Collected quarterly from project reports by FC+ staff
Benchmark Values15
Year Target Actual Notes
FY2013/14 5 5
FY2014/15 5 6 FC+ supported activities in Togo through the USAID/WARP mission
FY2015/16 6 6 FC+ supported activities in Togo through the USAID/WARP mission
FY2016/17 6 5 FC+ supported activities in Togo ended in FY 15/16.
FY2017/18 6 6 FC+ support to Mozambique initiated in FY17/18.
FY2018/19 5 5 Support to Nigeria ended in FY17/18. Support to Uganda ended in May 2019.
Indicator 2: Number of sites supported by FC+ for fistula repair and prevention
Definition: # of facilities to which FC+ is providing support for fistula repair services.
Additional description/context: FC+ will support facilities to provide fistula repair services. The majority of these sites will also provide some level of prevention care. Support can include: provider
15 Benchmarks are aggregated for all indicators unless otherwise stated.

Annual Report • October 2018 – September 2019 Fistula Care Plus 331
Indicator 2: Number of sites supported by FC+ for fistula repair and prevention
training and clinical mentoring, equipment, and/or other site strengthening activities such as quality improvement (QI) and management capacity building. Support to clients at these sites can include: transport costs to hospitals for surgery, temporary shelter, costs for repair, post-operative hospitalization costs, pre and post operative counseling. and client rehabilitation services during post-operative recovery. Supported sites will provide data to FC+ on clinical indicators including numbers of clients seeking and requiring fistula repair services, the number of repairs performed, and the outcomes for those clients. Supported sites may also be engaged in fistula prevention activities, as defined in indicator 3. However, in reporting, sites will be disaggregated into prevention-only sites and repair/prevention sites. Sites that provide both are reported via indicator 2.
Data source and collection: Collected quarterly from project reports by FC+ project staff and in-country partners
Benchmark Values
Year Target Actual Notes
FY2013/14 26 25
FY2014/15 32 31
FY2015/16 34 37
FY2016/17 36 33
FY2017/18 36 37
FY2018/19 23 24
Indicator 3: Number of prevention-only sites supported by FC+
Definition: # of facilities to which FC+ is providing support only for fistula prevention services.
Additional description: FC+ will support facility sites to provide services that prevent fistula. Support can include: include provider training and clinical mentoring, equipment, minor renovation or rehabilitation of facilities, other site strengthening activities such as quality improvement (QI) and management capacity building; and/or community outreach for awareness, screening, detection, and referral activities. FC+ will focus prevention interventions in three areas: a. Emergency obstetric services (EmOC) with immediate interventions to help prevent fistula. We will track three key immediate term interventions which will be a focus of strengthening at selected sites:
Correct use of the partograph to manage labors Availability of C-section services Routine use of catheterization for women who had prolonged/obstructed labor. b. Family Planning (FP) services as a medium term fistula prevention intervention
c. Screening, detection, and referral of women needing fistula treatment to repair sites.

Annual Report • October 2018 – September 2019 Fistula Care Plus 332
Indicator 3: Number of prevention-only sites supported by FC+
As noted above, facilities will be classified as either prevention-only or repair/prevention sites. Repair sites may also be engaged in any or all of the prevention activities outlined here.
Data source and collection: Collected quarterly from project reports by FC+ staff and in-country partners
Benchmark Values
Year Target Actual Notes
FY2013/14 43 16 Delays in funds release and subaward agreements negatively affected prevention-only site support
FY2014/15 39 749 FC+ has temporarily taken on support of a large number of prevention-only sites in Nigeria following the close of the TSHIP project.
FY2015/16 790 789
FY2016/17 791 752 Support to sites in Jigawa State in Nigeria was discontinued during the FY.
FY2017/18 787 710 Expected increases in Nigeria prevention only sites did not occur during the FY.
FY2018/19 17 19 Support to sites in Nigeria ended in FY17/18. Support to sites in Uganda ended in FY 18/19.
Objective 1: Strengthened enabling environment to institutionalize fistula prevention, treatment and reintegration in the public and private sectors
Indicator 4: Number of countries receiving support from FC+ where governments or supported facilities have revised/adopted/ initiated/implemented policies or guidelines for fistula prevention or treatment
Definition: # of supported countries or facilities (some private sites may develop their own policies/guidelines) that have revised/adopted, initiated, or are continuing to implement policies in support of fistula prevention and treatment services.
Additional description/context: The FC+ Annual Report will include the name of policy/guideline, location, and status (e.g., under development or review, approved, implemented). Fistula-specific polices or guidelines can be part of broader reproductive and/or maternal health documents. For the purposes

Annual Report • October 2018 – September 2019 Fistula Care Plus 333
Indicator 4: Number of countries receiving support from FC+ where governments or supported facilities have revised/adopted/ initiated/implemented policies or guidelines for fistula prevention or treatment
of FC+, a policy16 is an official statement by a government or health authority that provides an overall direction for a health issue by defining a vision, values, principles, and objectives, and establishing a broad model of action to achieve that vision. Policies may address financing, coordination among agencies and programs, necessary legislation, organization of services, procurement of material resources, required human resources, quality standards, and/or information systems. A guideline is a statement that provides a framework or course of action through which to implement policy objectives, including recommendations and best practices that ensure quality within services to be provided. This indicator includes countries that have fistula policies/guidelines in place at the start of the project.
Data source and collection: Collected annually from project reports and policy/guideline documents by FC+ staff and in-country partners
Benchmark Values
Year Target Actual Notes
FY2013/14 5 5
FY2014/15 5 5
FY2015/16 6 5
FY2016/17 6 5
FY2017/18 5 5
FY2018/19 4 4
Indicator 5: Number of countries receiving support from FC+ where governments or supported facilities have addressed WDI, women with TF and/or POP in their fistula and/or broader reproductive/maternal health policies or guidelines
Definition: # of supported countries or facilities (some private sites may develop their own policies/guidelines) that have addressed the needs of WDI, women with TF, and/or women with POP in their relevant policies/guidelines.
Additional description/context: This incorporation can be within fistula-specific documents or broader policies/guidelines on reproductive and/or maternal health services.
Annual report will include the name of policy/guideline, location, and status (e.g., under development or review, approved, implemented). The definitions of policies and guidelines described under indicator 5 will be applied here.
16 Adapted from World Health Organization definitions. Available at: http://www.who.int/mental_health/policy/services/1_MHPolicyPlan_Infosheet.pdf. Accessed January 22, 2014.

Annual Report • October 2018 – September 2019 Fistula Care Plus 334
Indicator 5: Number of countries receiving support from FC+ where governments or supported facilities have addressed WDI, women with TF and/or POP in their fistula and/or broader reproductive/maternal health policies or guidelines
Data source and collection: Collected annually from project reports and policy/guideline documents by FC+ staff and in-country partners
Benchmark Values
Year Target Actual Notes
FY2013/14 0 0 Policy efforts related to WDI/TF/POP to begin in FY14/15
FY2014/15 1 2 Nigeria and Uganda have both held national level meetings drafting policy related to treatment and reintegration of WDI
FY2015/16 2 2 Bangladesh and Niger
FY2016/17 2 4 Bangladesh, Niger, Nigeria, and Uganda
FY2017/18 5 5 Bangladesh, DRC, Niger, Nigeria and Uganda
FY2018/19 4 4 Bangladesh, DRC, Niger, and Uganda
Indicator 6: Number of countries receiving support from FC+ in which governments have budget line item for fistula care
Definition: # of supported countries with a specific annual budget allocation to fund fistula prevention, detection, repair, and/or reintegration services.
Additional description/context: This is an annual, rather than aggregated, indicator.
Data source and collection: Collected annually from project reports and key informant interviews by FC+ staff and in-country partners
Benchmark Values
Year Target Actual Notes
FY2013/14 2 2 Budget allocations made in Nigeria and Uganda
FY2014/15 2 2 Budget allocations made in Nigeria and Uganda
FY2015/16 3 2 Bangladesh and Nigeria
FY2016/17 3 3 Bangladesh, Niger, Nigeria
FY2017/18 3 3 Bangladesh, Niger, Nigeria
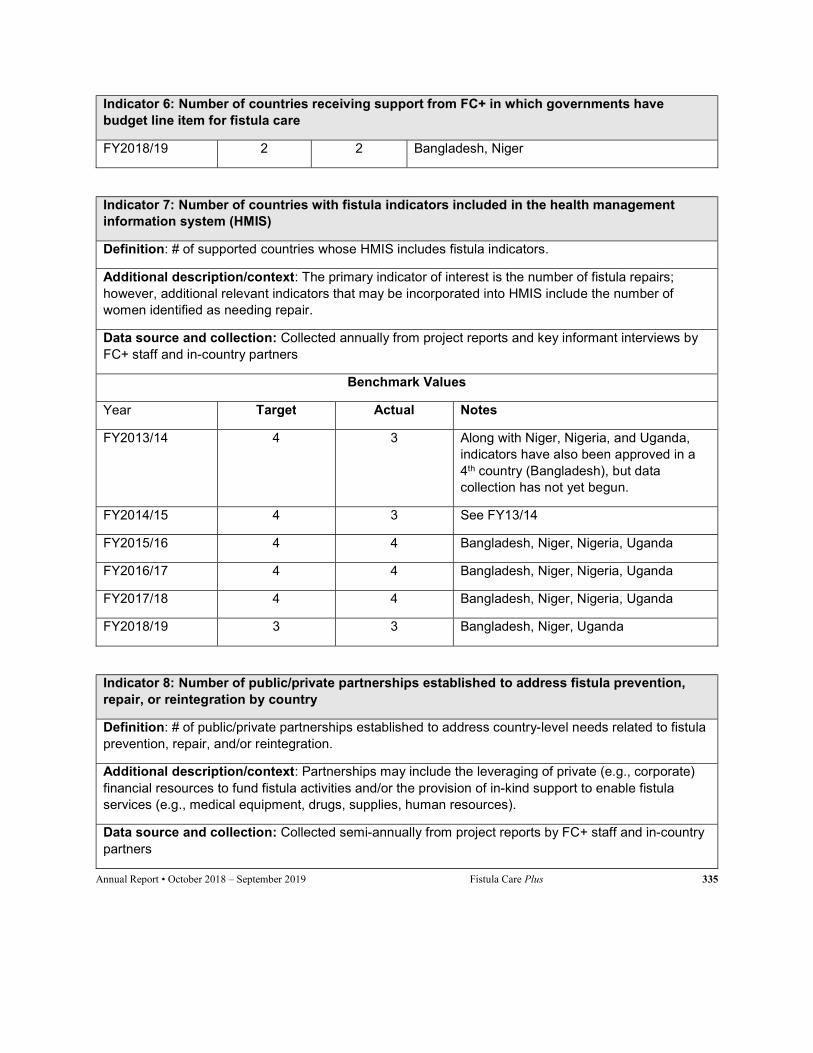
Annual Report • October 2018 – September 2019 Fistula Care Plus 335
Indicator 6: Number of countries receiving support from FC+ in which governments have budget line item for fistula care
FY2018/19 2 2 Bangladesh, Niger
Indicator 7: Number of countries with fistula indicators included in the health management information system (HMIS)
Definition: # of supported countries whose HMIS includes fistula indicators.
Additional description/context: The primary indicator of interest is the number of fistula repairs; however, additional relevant indicators that may be incorporated into HMIS include the number of women identified as needing repair.
Data source and collection: Collected annually from project reports and key informant interviews by FC+ staff and in-country partners
Benchmark Values
Year Target Actual Notes
FY2013/14 4 3 Along with Niger, Nigeria, and Uganda, indicators have also been approved in a 4th country (Bangladesh), but data collection has not yet begun.
FY2014/15 4 3 See FY13/14
FY2015/16 4 4 Bangladesh, Niger, Nigeria, Uganda
FY2016/17 4 4 Bangladesh, Niger, Nigeria, Uganda
FY2017/18 4 4 Bangladesh, Niger, Nigeria, Uganda
FY2018/19 3 3 Bangladesh, Niger, Uganda
Indicator 8: Number of public/private partnerships established to address fistula prevention, repair, or reintegration by country
Definition: # of public/private partnerships established to address country-level needs related to fistula prevention, repair, and/or reintegration.
Additional description/context: Partnerships may include the leveraging of private (e.g., corporate) financial resources to fund fistula activities and/or the provision of in-kind support to enable fistula services (e.g., medical equipment, drugs, supplies, human resources).
Data source and collection: Collected semi-annually from project reports by FC+ staff and in-country partners

Annual Report • October 2018 – September 2019 Fistula Care Plus 336
Indicator 8: Number of public/private partnerships established to address fistula prevention, repair, or reintegration by country
Benchmark Values
Year Target Actual Notes
FY2013/14 117 3 In addition to the 3 PPPs (Bangladesh, Nigeria, and Uganda), an individual has also donated commodities in Uganda
FY2014/15 2 3 Partnerships for private contribution to fistula activities are active in DRC, Nigeria, and Uganda. Proposals for such partnership are pending in Bangladesh and Niger.
FY2015/16 3 4 Bangladesh, DRC, Nigeria, Uganda
FY2016/17 4 4 Bangladesh, DRC, Nigeria, Uganda
FY2017/18 5 3 DRC, Nigeria, Uganda (with global partners Laborie Inc., Gradian Health Systems, and Bioteque)
FY2018/19 3 1 DRC (Laborie Inc)
Objective 2: Enhanced community understanding and practices to prevent fistula, improve access to fistula treatment, reduce stigma, and support reintegration of women and girls with fistula
Indicator 9: Number of community volunteers/educators trained in tools and approaches to raise awareness regarding fistulae prevention and repair
Definition: # of community volunteers/educators trained in topics and approaches and approaches, such as social and behavior change communication (SBCC), stigma, gender-based barriers, and male involvement to mobilize communities for fistula prevention, the use of safe motherhood services including family planning and EmOC, and fistula screening/detection/referral for repair.
Additional description/context: Community volunteers/educators are individuals affiliated with or employed by community-based organizations, non-governmental organizations, and/or faith-based organizations. In some countries, they are affiliated with government agencies (e.g., Ethiopia’s Health Development Army); however, while these individuals may liaise with health facilities and providers, their role is restricted to health promotion and they are not formally attached to specific health facilities. These are considered to be distinct from the community health workers discussed in Indicator 18 below.
17 This will be achieved in Y2 due to the shortened Y1.

Annual Report • October 2018 – September 2019 Fistula Care Plus 337
Indicator 9: Number of community volunteers/educators trained in tools and approaches to raise awareness regarding fistulae prevention and repair
Data source and collection: Collected quarterly from training reports by FC+ staff and in-country partners
Benchmark Values
Year Target Actual Notes
FY2013/14 227 0 Delays in funds release and subaward approvals negatively affected ability to implement community volunteer/educator trainings in FY13/14
FY2014/15 494 77
FY2015/16 607 679
FY2016/17 725 850
FY2017/18 1,423 749 Expected refresher trainings in Niger did not take place due to office closure.
FY2018/19 1,074 71 Planned refresher trainings in Niger did not take place due to suspended activity in DRC and Niger.
Indicator 10: Number of community awareness-raising activities/events conducted by program partners
Definition: # events carried out by program partners to provide information about EmOC availability, fistula prevention, screening and detection, repair, and other safe motherhood issues.
Additional description/context: Events may include community gatherings and broadcast messages.
Data source and collection: Collected quarterly from program monitoring reports by FC+ staff and in-country partners.
Benchmark Values
Year Target Actual Notes
FY2013/14 570 12 Delays in funds release and subaward approvals negatively affected ability to implement community outreach and education in FY13/14.
FY2014/15 586 1,990
FY2015/16 1,695 10,393

Annual Report • October 2018 – September 2019 Fistula Care Plus 338
Indicator 10: Number of community awareness-raising activities/events conducted by program partners
FY2016/17 6,130 In person:33,425
Mass media: 659
Home visits in Niger and Aflateen activities in Uganda resulted in achievements far above benchmarks.
FY2017/18 10,666 In person: 17,678
Mass media: 53
FY2018/19 6,064 In person:
Mass media:
1,246
2
Indicator 11: Number of participants reached through community awareness-raising events/activities conducted by program partners
Definition: # of participants reached through community awareness raising events/activities conducted by program partners.
Additional description/context: Participants may include attendees at events in the community, as well as those listening to/watching broadcast messages. Numbers of persons reached will be estimates for some activities; e.g., radio partners will provide estimates of the listenership for broadcast events.18
Data source and collection: Collected quarterly from program monitoring reports by FC+ staff and in-country partners.
Benchmark Values
Year Target Actual Notes
FY2013/14 155,150 10,745 Delays in funds release and subaward approvals negatively affected ability to implement community outreach and education in FY13/14
FY2014/15 232,100 414,067
FY2015/16 In person: 306,750
Mass media: 1,550,000
In person: 2,862,124
Mass media: 3,676,406
FY2016/17 In person: 327,000
In person: 557,186
Mass media reach numbers were not available in all countries.
18 FC+ has expanded its definition of the reach of community activities to include the audience for radio broadcasts; not all countries have been able to establish baseline estimates of these audiences yet; these benchmarks may thus be revised based on Y1 experience.

Annual Report • October 2018 – September 2019 Fistula Care Plus 339
Indicator 11: Number of participants reached through community awareness-raising events/activities conducted by program partners
Mass media: 102,150,000
Mass media: 15,289,736
FY2017/18 In person: 676,000
Mass media: 27,339,750
In person: 681,597
Mass media: 20,919,065
FY2018/19 In person: 203,000
Mass media: 600,000
In person: 149,585
Mass media: 600,000
Objective 3: Reduced transportation, communication, and financial barriers to accessing preventive care, detection, treatment, and reintegration support
Indicator 12: Number and type of transportation initiatives introduced, enhanced, and/or tested
Definition: # of initiatives introduced enhanced, and/or tested to reduce barriers faced by women in traveling to fistula services, particularly repair, in the catchment areas of FC+ sites.
Additional description/context: Initiatives may include vouchers, support from local transportation networks, and other strategies to enable transportation to fistula services.
Data source and collection: Collected semi-annually from program monitoring and evaluation reports by FC+ staff and in-country partners
Benchmark Values
Year Target Actual Notes
FY2013/14 0 0
FY2014/15 2 0 Delays in approvals/conduct of Pop Council study have negatively impacted ability to move forward with designing and piloting initiatives
FY2015/16 2 0 Initiatives planned but not yet implemented, will take place in FY 16/17
FY2016/17 2 2 Nigeria and Uganda
FY2017/18 2 2 Nigeria and Uganda

Annual Report • October 2018 – September 2019 Fistula Care Plus 340
Indicator 12: Number and type of transportation initiatives introduced, enhanced, and/or tested
FY2018/19 0 0 Documentation of results of initiatives, active implementation ended in FY 17/18
Indicator 13: Number and type of communication technologies introduced, enhanced, and/or tested for improving communication with patients and/or providers
Definition: # of initiatives introduced enhanced, and/or tested to improve communication with providers and/or patients engaged through FC+ sites.
Additional description/context: Initiatives may target health behavior and service utilization messages for women, follow-up support and mentoring for trained providers, and/or monitoring of service provision/uptake by patients and providers.
Data source and collection: Collected semi-annually from program monitoring and evaluation reports by FC+ staff and in-country partners
Benchmark Values
Year Target Actual Notes
FY2013/14 0 0
FY2014/15 1 0 Delays in approval and conduct of Pop Council study have negatively impacted ability to design/test new technologies
FY2015/16 2 0 Initiatives developed but will be implemented in FY 16/17
FY2016/17 2 2 Nigeria and Uganda
FY2017/18 2 2 Nigeria and Uganda
FY2018/19 0 0
Objective 4: Strengthened provider and health facility capacity to provide and sustain quality services for fistula prevention, detection, and treatment
Indicator 14: Number of women requiring fistula repairs
Definition: # of women diagnosed with obstetric fistula at supported repair sites

Annual Report • October 2018 – September 2019 Fistula Care Plus 341
Indicator 14: Number of women requiring fistula repairs
Additional description/context: This will be a subset of women seeking treatment at repair sites; women will be screened to determine whether their incontinence is due to obstetric fistula. This indicator encompasses all types of fistula, including urinary and RVF together, and RVF alone.19
Data source and collection: Collected quarterly from hospital registers/ client records/program reports by FC+ staff and partner staff
Benchmark Values
Year Target Actual Notes
FY2013/14 2,131 912
FY2014/15 4,000 3,790
FY2015/16 18,000 4,798
FY2016/17 N/A 4,031
FY2017/18 N/A 3,847
FY2018/19 N/A 721
Indicator 15a: Number of surgical fistula repairs
Definition: # of fistula repair surgeries performed at supported sites.
Additional description/context: This includes all types of fistula repairs, including urinary alone, urinary and RVF together, and RVF alone. Each time a woman has surgery it will be counted; however, it is unlikely that any woman would get more than one repair surgery per quarter. Therefore the quarterly figure for the number of surgeries should therefore equal the number of women getting fistula repair.
Data source and collection: Collected quarterly from hospital registers/ client records/program reports by FC+ staff and partner staff
Benchmark Values
Year Target Actual Notes
19 We have included this indicator in our approved PMP instead of number of women seeking fistula repairs. We know from experience that many women seeking care are often not diagnosed with fistula, but rather have some other condition that results in some incontinence. FC+ will collect information on the number of women seeking care for urinary incontinence as part of our routine clinical monitoring as was done under Fistula Care. If the difference between the number seeking and the number requiring is large then we will know that work needs to be done to improve messages about fistula treatment. We believe for USAID reporting to Congress, the number requiring is more powerful. We are using the term urinary fistula instead of VVF since it more accurately describes the range of typical fistula cases seen at sites. Urinary type fistula includes: vesicovaginal, urethro-vaginal, uretero-vaginal, vesico-uterine.

Annual Report • October 2018 – September 2019 Fistula Care Plus 342
Indicator 15a: Number of surgical fistula repairs
FY2013/14 1,30020 852 Delays in funds release and subaward approvals negatively affected ability to support fistula repairs during FY13/14.
FY2014/15 3.830 2,876 Repairs benchmark increased due to requests from Bangladesh and Nigeria missions
FY2015/16 4,121 3,514
FY2016/17 3,780 3,250
FY2017/18 2,950 3,104
FY2018/19 1,224 605
Indicator 15b: Number of conservative fistula treatments (catheterization)
Definition: # of conservative fistula treatments (catheterization) performed at supported sites.
Note: There is no annual benchmark assigned to this indicator.
Additional description/context: This includes the number of catheterizations performed on an existing fistula, as a conservative approach to fistula repair, provided by supported sites.
Data source and collection: Collected quarterly from hospital registers/ client records/program reports by FC+ staff and partner staff.
Benchmark Values
Year Target Actual Notes
FY2013/14 N/A 4
FY2014/15 N/A 304
FY2015/16 N/A 323
FY2016/17 N/A 294
FY2017/18 N/A 162
FY2018/19 N/A 6
20 Release of MCH funds were delayed in Nigeria and Uganda; these two countries account for a large proportion (73%) of the estimated repairs. This benchmark was calculated based on the provision of repairs for two quarters. However, repairs in Uganda were only carried out in the final quarter of the FY.

Annual Report • October 2018 – September 2019 Fistula Care Plus 343
Indicator 16: Outcomes of fistula repair (percentage closed and dry)
Definition: Numerator: # of women who received any type of fistula repair surgery (urinary alone, urinary and RVF together, and RVF alone) who when discharged, had a closed fistula and were dry at time of discharge / Denominator: # women who had any type of fistula repair surgery and were discharged X 100
Additional description/context: N/A
Data source and collection: Collected quarterly from hospital registers/ client records/program reports by FC+ staff and partner staff
Benchmark Values
Year Target Actual Notes
FY2013/14 75% 76% Closed and continent data is incomplete for FY13/14 due to new data collection tools. Data presented is what is available for this time period.
FY2014/15 75% 67% 79% of fistulas successfully closed (67% closed and continent, 12% closed and incontinent)
21% not closed
FY2015/16 75% 77% 88% of fistulas successfully closed (77% closed and continent; 11% closed and incontinent)
12% not closed
FY2016/17 75% 78% 89% of fistulas successfully closed (78% closed and continent; 11% closed and incontinent)
11% not closed
FY2017/18 75% 80% 89% of fistulas successfully closed (80% closed and continent; 9% closed and incontinent)
11% not closed
FY2018/19 75% 92% 95% of fistulas successfully closed (92% closed and continent; 2.9% closed and incontinent)
5% not closed
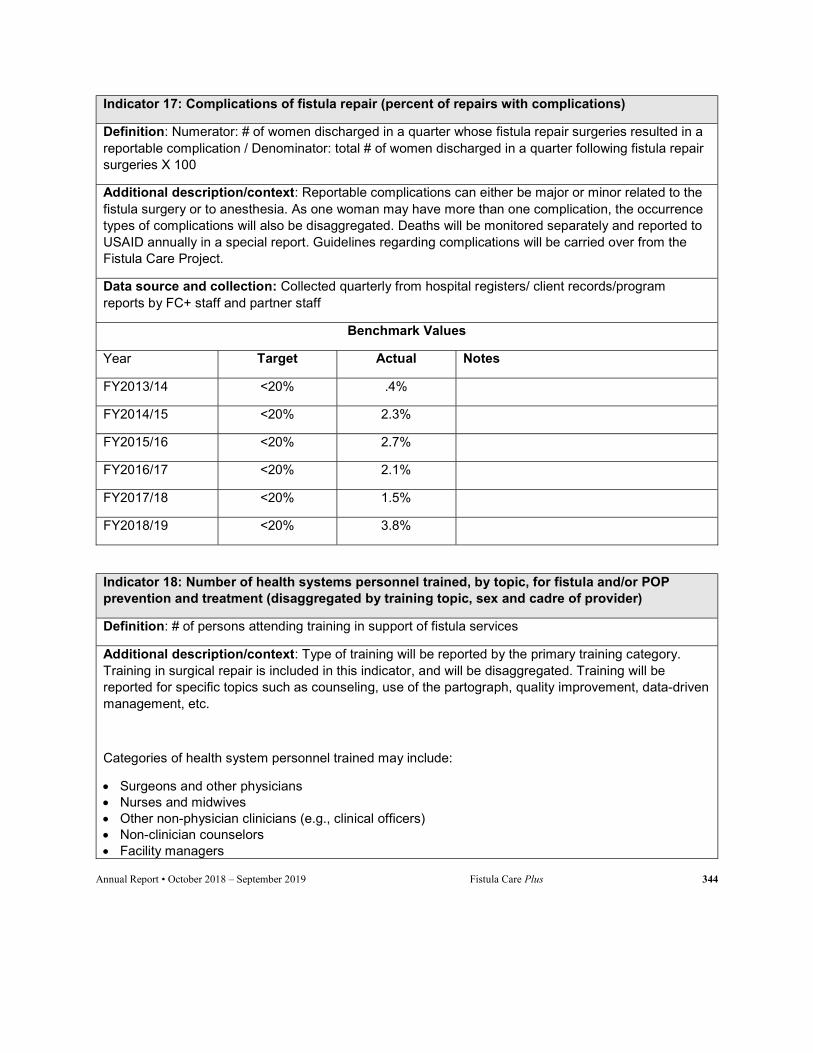
Annual Report • October 2018 – September 2019 Fistula Care Plus 344
Indicator 17: Complications of fistula repair (percent of repairs with complications)
Definition: Numerator: # of women discharged in a quarter whose fistula repair surgeries resulted in a reportable complication / Denominator: total # of women discharged in a quarter following fistula repair surgeries X 100
Additional description/context: Reportable complications can either be major or minor related to the fistula surgery or to anesthesia. As one woman may have more than one complication, the occurrence types of complications will also be disaggregated. Deaths will be monitored separately and reported to USAID annually in a special report. Guidelines regarding complications will be carried over from the Fistula Care Project.
Data source and collection: Collected quarterly from hospital registers/ client records/program reports by FC+ staff and partner staff
Benchmark Values
Year Target Actual Notes
FY2013/14 <20% .4%
FY2014/15 <20% 2.3%
FY2015/16 <20% 2.7%
FY2016/17 <20% 2.1%
FY2017/18 <20% 1.5%
FY2018/19 <20% 3.8%
Indicator 18: Number of health systems personnel trained, by topic, for fistula and/or POP prevention and treatment (disaggregated by training topic, sex and cadre of provider)
Definition: # of persons attending training in support of fistula services
Additional description/context: Type of training will be reported by the primary training category. Training in surgical repair is included in this indicator, and will be disaggregated. Training will be reported for specific topics such as counseling, use of the partograph, quality improvement, data-driven management, etc.
Categories of health system personnel trained may include:
Surgeons and other physicians Nurses and midwives Other non-physician clinicians (e.g., clinical officers) Non-clinician counselors Facility managers
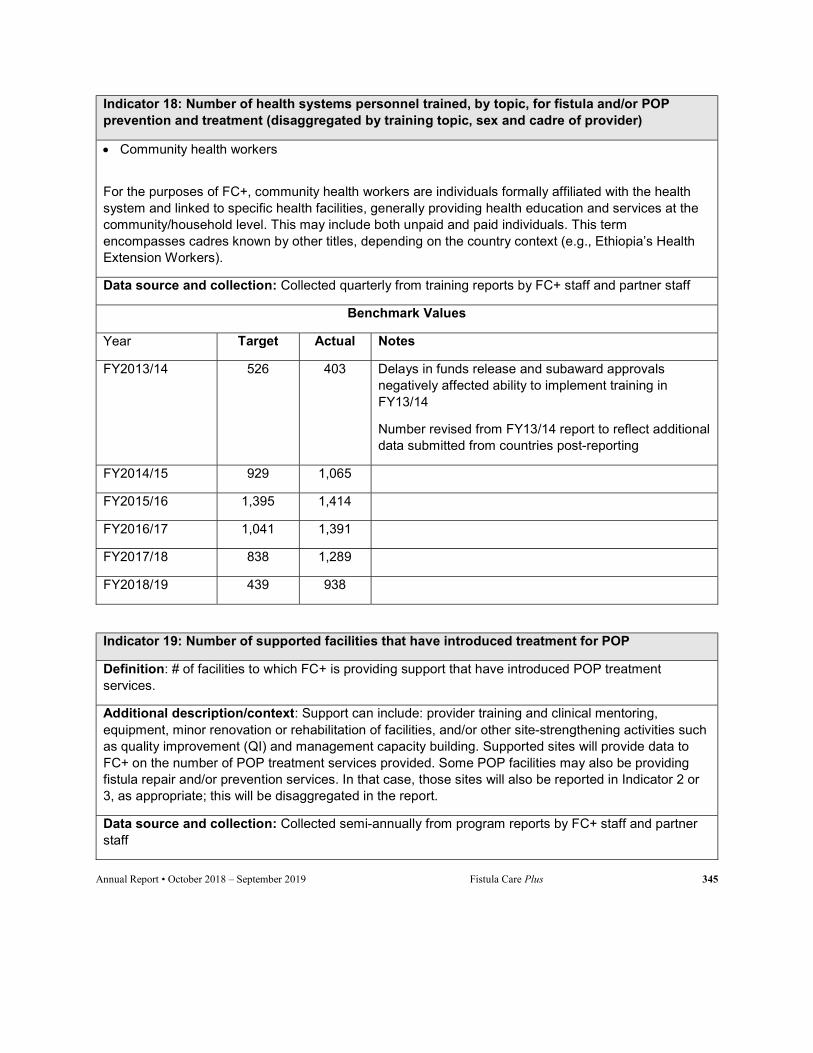
Annual Report • October 2018 – September 2019 Fistula Care Plus 345
Indicator 18: Number of health systems personnel trained, by topic, for fistula and/or POP prevention and treatment (disaggregated by training topic, sex and cadre of provider)
Community health workers
For the purposes of FC+, community health workers are individuals formally affiliated with the health system and linked to specific health facilities, generally providing health education and services at the community/household level. This may include both unpaid and paid individuals. This term encompasses cadres known by other titles, depending on the country context (e.g., Ethiopia’s Health Extension Workers).
Data source and collection: Collected quarterly from training reports by FC+ staff and partner staff
Benchmark Values
Year Target Actual Notes
FY2013/14 526 403 Delays in funds release and subaward approvals negatively affected ability to implement training in FY13/14
Number revised from FY13/14 report to reflect additional data submitted from countries post-reporting
FY2014/15 929 1,065
FY2015/16 1,395 1,414
FY2016/17 1,041 1,391
FY2017/18 838 1,289
FY2018/19 439 938
Indicator 19: Number of supported facilities that have introduced treatment for POP
Definition: # of facilities to which FC+ is providing support that have introduced POP treatment services.
Additional description/context: Support can include: provider training and clinical mentoring, equipment, minor renovation or rehabilitation of facilities, and/or other site-strengthening activities such as quality improvement (QI) and management capacity building. Supported sites will provide data to FC+ on the number of POP treatment services provided. Some POP facilities may also be providing fistula repair and/or prevention services. In that case, those sites will also be reported in Indicator 2 or 3, as appropriate; this will be disaggregated in the report.
Data source and collection: Collected semi-annually from program reports by FC+ staff and partner staff

Annual Report • October 2018 – September 2019 Fistula Care Plus 346
Indicator 19: Number of supported facilities that have introduced treatment for POP
Benchmark Values
Year Target Actual Notes
FY2013/14 0 0 0
FY2014/15 1 0 9 supported sites providing ongoing POP treatment21
FY2015/16 6 4 10 supported sites providing ongoing POP treatment
FY2016/17 N/A 2 15 supported sites providing ongoing POP treatment
FY2017/18 4 N/A 11 supported sites providing ongoing POP treatment
FY2018/19 N/A N/A 4 supported sites providing ongoing POP treatment
Indicator 20: Number of POP treatment services provided
Definition: # of POP treatment services performed at supported sites.
Additional description/context: This includes both conservative treatment (e.g., treatment with a pessary) and all types of surgical treatment (e.g., hysterectomy with pelvic support repair, mesh, etc.). Reports will disaggregate by type of treatment.
Data source and collection: Collected quarterly from hospital registers/ client records/program reports by FC+ staff and partner staff
Benchmark Values
Year Target Actual Notes
FY2013/14 0 NA
FY2014/15 30 1,334
FY2015/16 505 2,681
FY2016/17 N/A 2,884
FY2017/18 400 2,886
FY2018/19 N/A 680
21 Reported through FC+ routine M&E; not necessarily introduced or strengthened through FC+ supported fistula/POP integration activities. See indicator 20 for clinical outputs at these sites.

Annual Report • October 2018 – September 2019 Fistula Care Plus 347
Indicator 21: Couple-years of protection in sites supported by FC+
Definition: The estimated protection provided by family planning services, based upon the volume of all contraceptives distributed to clients during the reporting period
Additional description/context: USAID-endorsed conversion factors for each family planning method will be used to calculate CYP.22 All CYP will be credited to the year in which the method was distributed, rather than annualizing CYP.
Data source and collection: Collected semi-annually from facility FP registers by FC+ staff and in-country partners
Benchmark Values
Year Target Actual Notes
FY2013/14 28,430 40,039
FY2014/15 90,500 107,985
FY2015/16 153,261 195,986
FY2016/17 145,496 263,206
FY2017/18 184,755 315,229
FY2018/19 36,500 33,469 Support to Nigeria sites ended in FY 17/18
Indicator 22: Number of FP counseling sessions provided to clients
Definition: # of counseling sessions provided to clients at FC+ sites regarding FP methods.
Additional description/context: As a woman may receive more than one FP counseling session in a given quarter, this indicator represents number of service encounters, rather than numbers of individual clients.
Data source and collection: Collected semi-annually from facility FP registers by FC+ staff and in-country partners
Benchmark Values
Year Target Actual Notes
FY2013/14 53,698 38,373
FY2014/15 117,800 149,610
FY2015/16 204,532 366,038
22 Office of Sustainable Development, Bureau for Africa, USAID. Health and Family Planning Indicators: A Tool for Results Frameworks Volume I. Accessed: January 20, 2014.
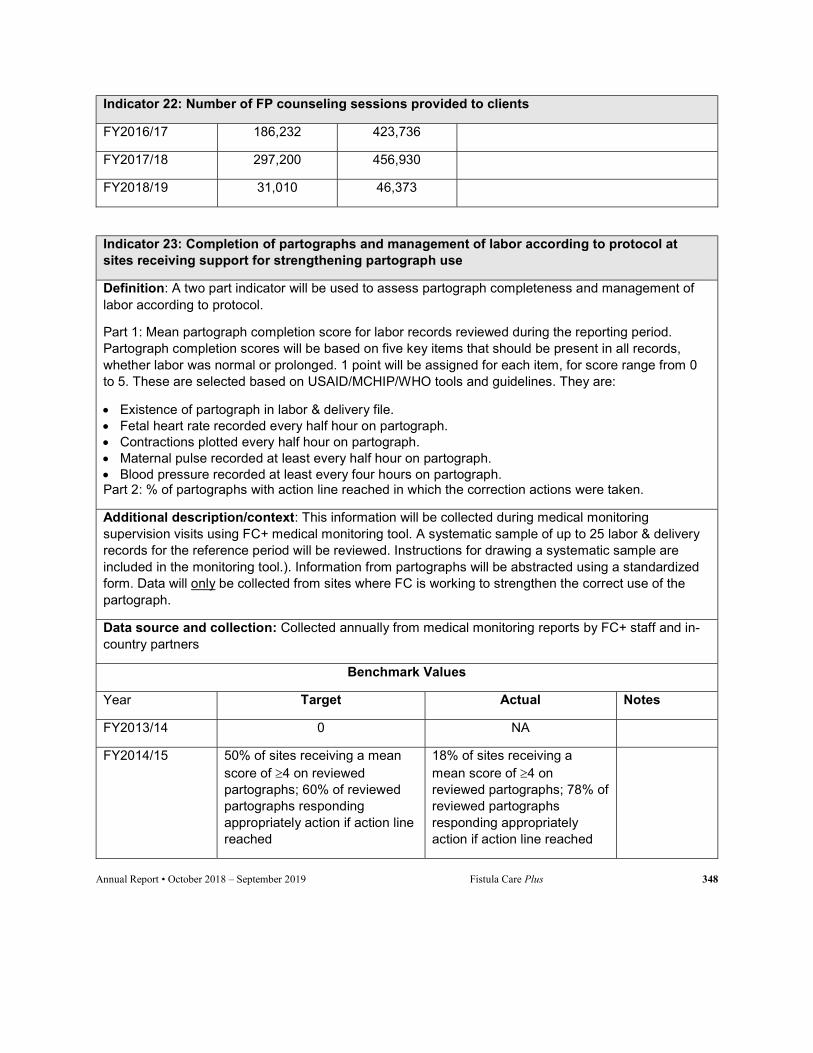
Annual Report • October 2018 – September 2019 Fistula Care Plus 348
Indicator 22: Number of FP counseling sessions provided to clients
FY2016/17 186,232 423,736
FY2017/18 297,200 456,930
FY2018/19 31,010 46,373
Indicator 23: Completion of partographs and management of labor according to protocol at sites receiving support for strengthening partograph use
Definition: A two part indicator will be used to assess partograph completeness and management of labor according to protocol.
Part 1: Mean partograph completion score for labor records reviewed during the reporting period. Partograph completion scores will be based on five key items that should be present in all records, whether labor was normal or prolonged. 1 point will be assigned for each item, for score range from 0 to 5. These are selected based on USAID/MCHIP/WHO tools and guidelines. They are:
Existence of partograph in labor & delivery file. Fetal heart rate recorded every half hour on partograph. Contractions plotted every half hour on partograph. Maternal pulse recorded at least every half hour on partograph. Blood pressure recorded at least every four hours on partograph. Part 2: % of partographs with action line reached in which the correction actions were taken.
Additional description/context: This information will be collected during medical monitoring supervision visits using FC+ medical monitoring tool. A systematic sample of up to 25 labor & delivery records for the reference period will be reviewed. Instructions for drawing a systematic sample are included in the monitoring tool.). Information from partographs will be abstracted using a standardized form. Data will only be collected from sites where FC is working to strengthen the correct use of the partograph.
Data source and collection: Collected annually from medical monitoring reports by FC+ staff and in-country partners
Benchmark Values
Year Target Actual Notes
FY2013/14 0 NA
FY2014/15 50% of sites receiving a mean score of 4 on reviewed partographs; 60% of reviewed partographs responding appropriately action if action line reached
18% of sites receiving a mean score of 4 on reviewed partographs; 78% of reviewed partographs responding appropriately action if action line reached
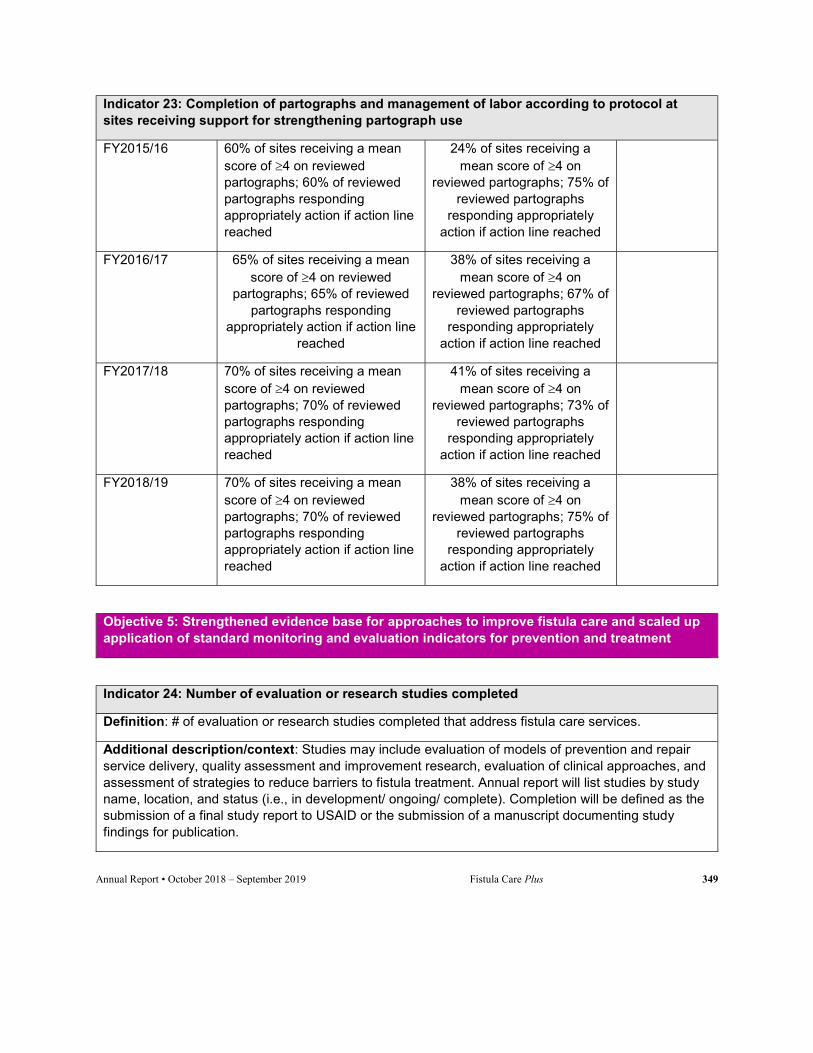
Annual Report • October 2018 – September 2019 Fistula Care Plus 349
Indicator 23: Completion of partographs and management of labor according to protocol at sites receiving support for strengthening partograph use
FY2015/16 60% of sites receiving a mean score of 4 on reviewed partographs; 60% of reviewed partographs responding appropriately action if action line reached
24% of sites receiving a mean score of 4 on
reviewed partographs; 75% of reviewed partographs
responding appropriately action if action line reached
FY2016/17 65% of sites receiving a mean score of 4 on reviewed
partographs; 65% of reviewed partographs responding
appropriately action if action line reached
38% of sites receiving a mean score of 4 on
reviewed partographs; 67% of reviewed partographs
responding appropriately action if action line reached
FY2017/18 70% of sites receiving a mean score of 4 on reviewed partographs; 70% of reviewed partographs responding appropriately action if action line reached
41% of sites receiving a mean score of 4 on
reviewed partographs; 73% of reviewed partographs
responding appropriately action if action line reached
FY2018/19 70% of sites receiving a mean score of 4 on reviewed partographs; 70% of reviewed partographs responding appropriately action if action line reached
38% of sites receiving a mean score of 4 on
reviewed partographs; 75% of reviewed partographs
responding appropriately action if action line reached
Objective 5: Strengthened evidence base for approaches to improve fistula care and scaled up application of standard monitoring and evaluation indicators for prevention and treatment
Indicator 24: Number of evaluation or research studies completed
Definition: # of evaluation or research studies completed that address fistula care services.
Additional description/context: Studies may include evaluation of models of prevention and repair service delivery, quality assessment and improvement research, evaluation of clinical approaches, and assessment of strategies to reduce barriers to fistula treatment. Annual report will list studies by study name, location, and status (i.e., in development/ ongoing/ complete). Completion will be defined as the submission of a final study report to USAID or the submission of a manuscript documenting study findings for publication.
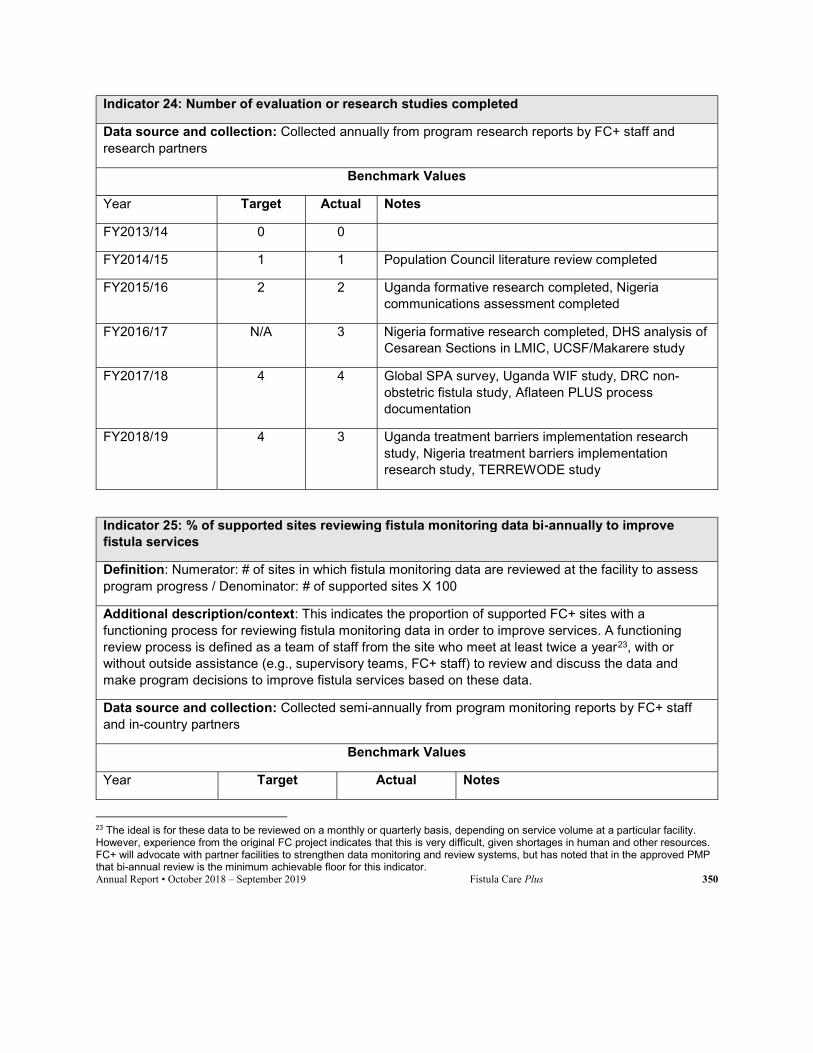
Annual Report • October 2018 – September 2019 Fistula Care Plus 350
Indicator 24: Number of evaluation or research studies completed
Data source and collection: Collected annually from program research reports by FC+ staff and research partners
Benchmark Values
Year Target Actual Notes
FY2013/14 0 0
FY2014/15 1 1 Population Council literature review completed
FY2015/16 2 2 Uganda formative research completed, Nigeria communications assessment completed
FY2016/17 N/A 3 Nigeria formative research completed, DHS analysis of Cesarean Sections in LMIC, UCSF/Makarere study
FY2017/18 4 4 Global SPA survey, Uganda WIF study, DRC non-obstetric fistula study, Aflateen PLUS process documentation
FY2018/19 4 3 Uganda treatment barriers implementation research study, Nigeria treatment barriers implementation research study, TERREWODE study
Indicator 25: % of supported sites reviewing fistula monitoring data bi-annually to improve fistula services
Definition: Numerator: # of sites in which fistula monitoring data are reviewed at the facility to assess program progress / Denominator: # of supported sites X 100
Additional description/context: This indicates the proportion of supported FC+ sites with a functioning process for reviewing fistula monitoring data in order to improve services. A functioning review process is defined as a team of staff from the site who meet at least twice a year23, with or without outside assistance (e.g., supervisory teams, FC+ staff) to review and discuss the data and make program decisions to improve fistula services based on these data.
Data source and collection: Collected semi-annually from program monitoring reports by FC+ staff and in-country partners
Benchmark Values
Year Target Actual Notes
23 The ideal is for these data to be reviewed on a monthly or quarterly basis, depending on service volume at a particular facility. However, experience from the original FC project indicates that this is very difficult, given shortages in human and other resources. FC+ will advocate with partner facilities to strengthen data monitoring and review systems, but has noted that in the approved PMP that bi-annual review is the minimum achievable floor for this indicator.
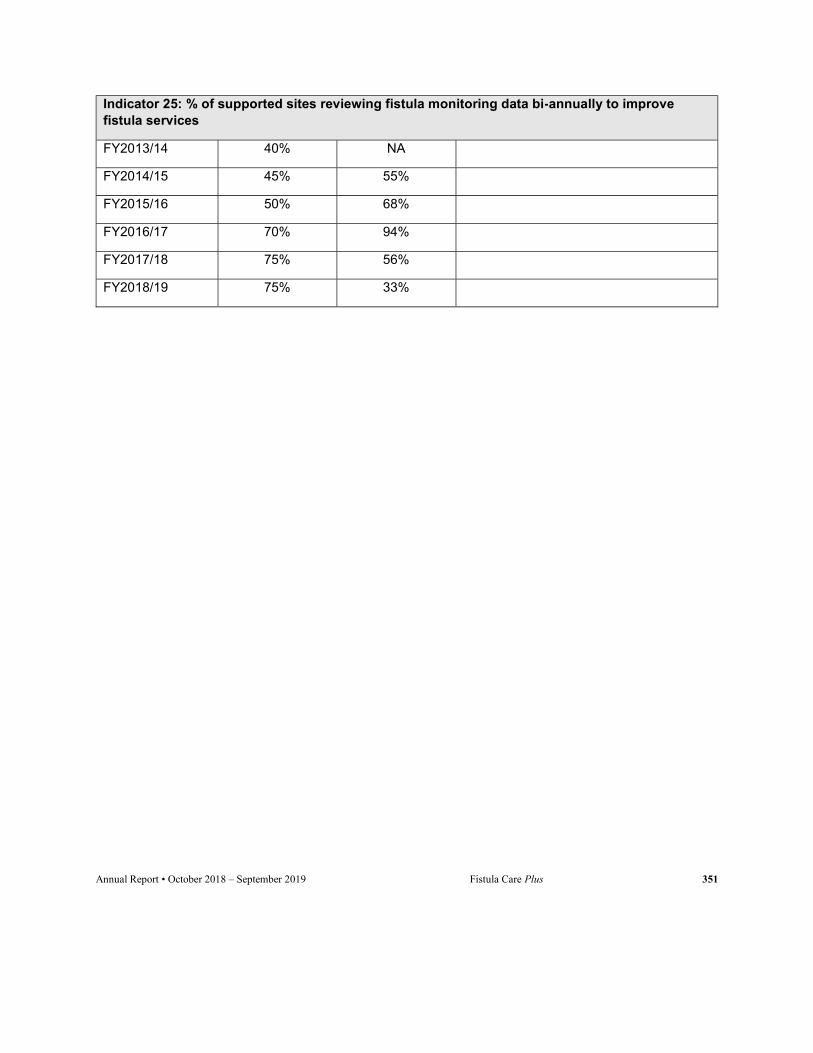
Annual Report • October 2018 – September 2019 Fistula Care Plus 351
Indicator 25: % of supported sites reviewing fistula monitoring data bi-annually to improve fistula services
FY2013/14 40% NA
FY2014/15 45% 55%
FY2015/16 50% 68%
FY2016/17 70% 94%
FY2017/18 75% 56%
FY2018/19 75% 33%