Angiotensin-(1-7) modulates angiotensin II-induced vasoconstriction in human mammary artery
Upload
independentCategory
view
0download
0
Kidney International, Vol. 56 (1999), pp. 1442–1454
Angiotensin-converting enzyme in non-neoplastic kidney diseases
ROMAN METZGER, RAINER M. BOHLE, KATHARINA PAULS, GERRIT EICHNER,FRANCOIS ALHENC-GELAS, SERGEI M. DANILOV, and FOLKER E. FRANKE
Department of Pediatric Surgery, Ludwig-Maximilians-University of Munich, Munich, and Department of Pathology,Mathematical Institute, Justus-Liebig-University of Giessen, Giessen, Germany; INSERM U 367, Paris, France; andDepartment of Anesthesiology, University of Illinois at Chicago, Chicago, Illinois, USA
Angiotensin-converting enzyme in non-neoplastic kidney diseases. as a dipeptidylpeptidase and has a broad specificity capa-Background. The angiotensin I-converting enzyme (ACE, ble of hydrolyzing a wide range of peptide substrates in
CD143, kininase II) plays a critical role in controlling the level vitro. ACE plays an important role in the regulation ofof vasoactive peptides such as angiotensins and kinins in theblood pressure and the control of regional blood flowlocal circulations and tissue interstitium. Because recent workthrough the generation of angiotensin II (Ang II) fromhas documented a vessel-, organ-, and species-specific pattern
of endothelial ACE expression in the vascular system, we have angiotensin I and the degradation of bradykinin. Twoanalyzed whether or not changes of this pattern occur in vessels, isoforms of the molecule are known: a somatic and atubules, and interstitium of the human kidney that is affected testicular form. In contrast to testicular ACE, exclusivelyby different non-neoplastic diseases.
expressed by germinal cells, the somatic isoform of ACEMethods. Using a set of well-characterized monoclonal anti-is found in different cell types as a transmembrane ecto-bodies (mAbs), ACE was assessed on renal tissue of 135 pa-
tients by immunohistochemistry, including an additional analy- enzyme [1, 2]. Besides its vascular localization on thesis at the ultrastructural level. A semiquantitative evaluation luminal surface of endothelial cells [3, 4], somatic ACEallowed the estimation and comparison of ACE content in is present in other cell types such as neuroneal cells,different renal compartments. These data were compared with
absorptive epithelial cells, and mononuclear cells of theseveral clinical findings, diagnosis, therapeutic modalities, andimmune system [1, 2, 5, 6, 9] [abstracts: Chumachenkohistological features.
Results. In contrast to the normal human kidney, where et al, Arteriosclerosis 115(Suppl):S63, 1995; Metzger etACE is abundant in the brush border of the proximal tubule al, Pathol Res Pract 192:364, 1996]. Especially the kidneybut is usually absent in endothelial cells of any vessel type, an
is well known to contain high amounts of ACE. Formerendothelial neoexpression of ACE was observed in differentstudies localized the enzyme mainly to the brush borderdiseases. In general, this neoexpression was associated with
histological sites of interstitial fibrosis and showed some selec- of the proximal tubular segment in humans and othertivity for glomerular endothelial cells in diabetes mellitus and species [10–14].chronic arterial hypertension. There was also a loss of epithelial By newly introduced monoclonal antibodies (mAbs),ACE in the proximal tubule in certain pathological conditions,
the detection of immunoreactive ACE has become reli-for example, in chronic fibroplastic processes, acute pyelone-able [5, 14], and consequently, the antigen was assignedphritis, and different stages of acute renal failure.
Conclusions. Neoexpression of ACE by renal endothelial to CD143 [15, 16]. Some of these mAbs are also suitablecells, as well as changes of the tubular ACE content, is a for formalin-fixed, paraffin-embedded tissue specimens,common finding in diseased human kidneys. As associated with
allowing studies on human tissue archives of certain or-certain tissue sites, clinical and/or morphological features, thesegan systems or a multitude of diseases (abstract; Metzgerchanges may be involved in parenchymal remodeling and renal
pathophysiology. et al, Pathol Res Pract 192:364, 1996). Thus, we haverecently shown that the expression of ACE within thehuman vascular system is heterogeneous, largely depend-
Angiotensin-converting enzyme (ACE, kininase II, ing on the localization of the endothelial cell and theE.C.3.4.15.1) is a zinc metallopeptidase that mainly acts vessel type. Only endothelial cells of small muscular ar-
teries and arterioles show a strong anti-ACE immunore-activity in the systemic circulation combined with anKey words: kidney, endothelium, ACE, CD143, vascular system, inter-
stitium, interstitial fibrosis. organ as well as species dependent pattern (Franke etal, manuscript submitted for publication).Received for publication July 16, 1998
One of the most remarkable exceptions that has beenand in revised form March 31, 1999Accepted for publication May 19, 1999 documented during these studies concerns the kidney.
In contrast to the overall systemic circulation and animal 1999 by the International Society of Nephrology
1442
Metzger et al: ACE in non-neoplastic kidney diseases 1443
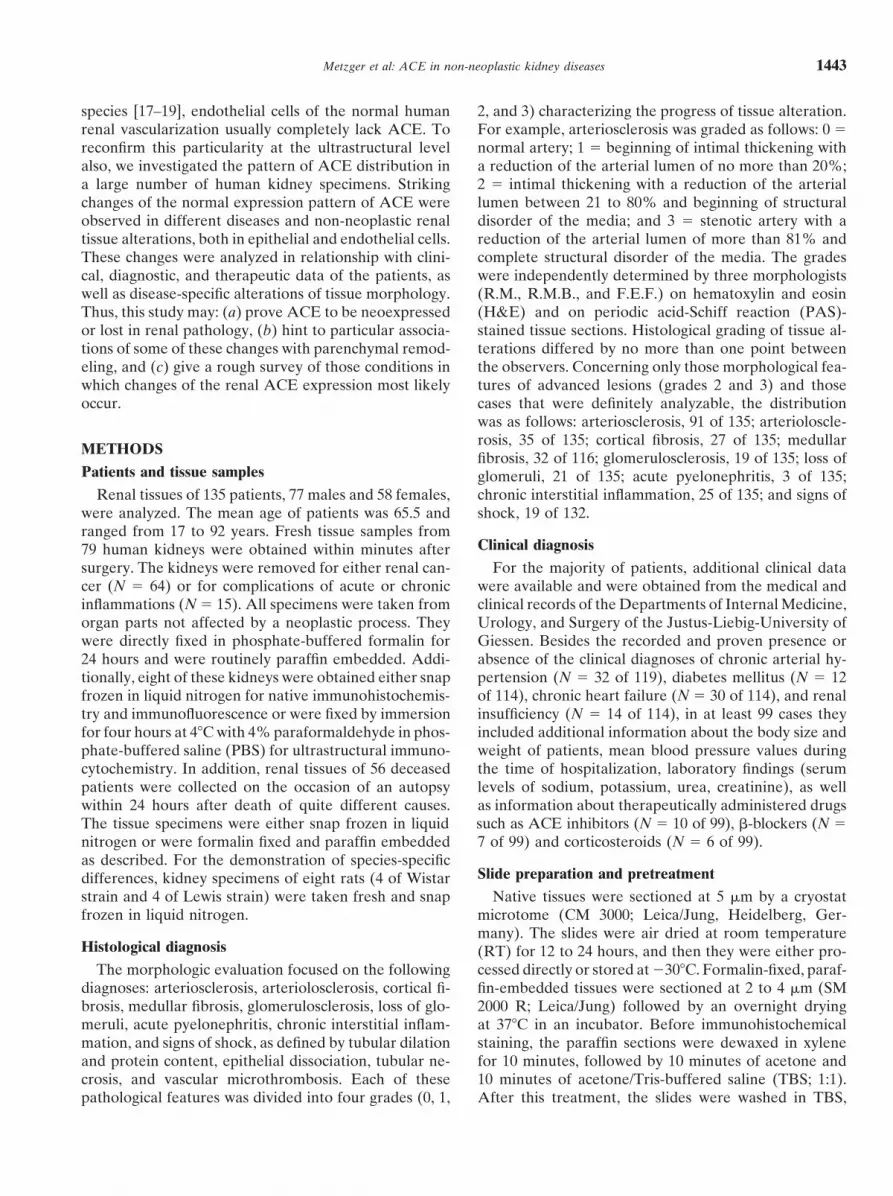
species [17–19], endothelial cells of the normal human 2, and 3) characterizing the progress of tissue alteration.For example, arteriosclerosis was graded as follows: 0 5renal vascularization usually completely lack ACE. To
reconfirm this particularity at the ultrastructural level normal artery; 1 5 beginning of intimal thickening witha reduction of the arterial lumen of no more than 20%;also, we investigated the pattern of ACE distribution in
a large number of human kidney specimens. Striking 2 5 intimal thickening with a reduction of the arteriallumen between 21 to 80% and beginning of structuralchanges of the normal expression pattern of ACE were
observed in different diseases and non-neoplastic renal disorder of the media; and 3 5 stenotic artery with areduction of the arterial lumen of more than 81% andtissue alterations, both in epithelial and endothelial cells.
These changes were analyzed in relationship with clini- complete structural disorder of the media. The gradeswere independently determined by three morphologistscal, diagnostic, and therapeutic data of the patients, as
well as disease-specific alterations of tissue morphology. (R.M., R.M.B., and F.E.F.) on hematoxylin and eosin(H&E) and on periodic acid-Schiff reaction (PAS)-Thus, this study may: (a) prove ACE to be neoexpressed
or lost in renal pathology, (b) hint to particular associa- stained tissue sections. Histological grading of tissue al-terations differed by no more than one point betweentions of some of these changes with parenchymal remod-
eling, and (c) give a rough survey of those conditions in the observers. Concerning only those morphological fea-tures of advanced lesions (grades 2 and 3) and thosewhich changes of the renal ACE expression most likely
occur. cases that were definitely analyzable, the distributionwas as follows: arteriosclerosis, 91 of 135; arterioloscle-rosis, 35 of 135; cortical fibrosis, 27 of 135; medullar
METHODSfibrosis, 32 of 116; glomerulosclerosis, 19 of 135; loss of
Patients and tissue samples glomeruli, 21 of 135; acute pyelonephritis, 3 of 135;chronic interstitial inflammation, 25 of 135; and signs ofRenal tissues of 135 patients, 77 males and 58 females,
were analyzed. The mean age of patients was 65.5 and shock, 19 of 132.ranged from 17 to 92 years. Fresh tissue samples from
Clinical diagnosis79 human kidneys were obtained within minutes aftersurgery. The kidneys were removed for either renal can- For the majority of patients, additional clinical data
were available and were obtained from the medical andcer (N 5 64) or for complications of acute or chronicinflammations (N 5 15). All specimens were taken from clinical records of the Departments of Internal Medicine,
Urology, and Surgery of the Justus-Liebig-University oforgan parts not affected by a neoplastic process. Theywere directly fixed in phosphate-buffered formalin for Giessen. Besides the recorded and proven presence or
absence of the clinical diagnoses of chronic arterial hy-24 hours and were routinely paraffin embedded. Addi-tionally, eight of these kidneys were obtained either snap pertension (N 5 32 of 119), diabetes mellitus (N 5 12
of 114), chronic heart failure (N 5 30 of 114), and renalfrozen in liquid nitrogen for native immunohistochemis-try and immunofluorescence or were fixed by immersion insufficiency (N 5 14 of 114), in at least 99 cases they
included additional information about the body size andfor four hours at 48C with 4% paraformaldehyde in phos-phate-buffered saline (PBS) for ultrastructural immuno- weight of patients, mean blood pressure values during
the time of hospitalization, laboratory findings (serumcytochemistry. In addition, renal tissues of 56 deceasedpatients were collected on the occasion of an autopsy levels of sodium, potassium, urea, creatinine), as well
as information about therapeutically administered drugswithin 24 hours after death of quite different causes.The tissue specimens were either snap frozen in liquid such as ACE inhibitors (N 5 10 of 99), b-blockers (N 5
7 of 99) and corticosteroids (N 5 6 of 99).nitrogen or were formalin fixed and paraffin embeddedas described. For the demonstration of species-specific
Slide preparation and pretreatmentdifferences, kidney specimens of eight rats (4 of Wistarstrain and 4 of Lewis strain) were taken fresh and snap Native tissues were sectioned at 5 mm by a cryostat
microtome (CM 3000; Leica/Jung, Heidelberg, Ger-frozen in liquid nitrogen.many). The slides were air dried at room temperature
Histological diagnosis (RT) for 12 to 24 hours, and then they were either pro-cessed directly or stored at 2308C. Formalin-fixed, paraf-The morphologic evaluation focused on the following
diagnoses: arteriosclerosis, arteriolosclerosis, cortical fi- fin-embedded tissues were sectioned at 2 to 4 mm (SM2000 R; Leica/Jung) followed by an overnight dryingbrosis, medullar fibrosis, glomerulosclerosis, loss of glo-
meruli, acute pyelonephritis, chronic interstitial inflam- at 378C in an incubator. Before immunohistochemicalstaining, the paraffin sections were dewaxed in xylenemation, and signs of shock, as defined by tubular dilation
and protein content, epithelial dissociation, tubular ne- for 10 minutes, followed by 10 minutes of acetone and10 minutes of acetone/Tris-buffered saline (TBS; 1:1).crosis, and vascular microthrombosis. Each of these
pathological features was divided into four grades (0, 1, After this treatment, the slides were washed in TBS,

Metzger et al: ACE in non-neoplastic kidney diseases1444
Table 1. Antibodies to human angiotensin-converting enzyme (ACE; CD143) and endothelial cells
ConcentrationClone/serum Immunogen lg /ml Source/references
9B9 Human lung ACE (CD143) 0.4 Chemicon, CA [20]3G8 Human lung ACE (CD143) 5.0 Chemicon, CA [20]i1A8 Human lung ACE (CD143) 33.0 Chemicon, CA [20]i2H5 Human lung ACE (CD143) 1.0 Chemicon, CA [20]3A5 Human lung ACE (CD143) 6.7 Chemicon, CA [20]5F1 Human lung ACE (CD143) 10.0 Chemicon, CA [20]
CG1a Human kidney ACE (CD143) 10.0 [20]CG2a Human kidney ACE (CD143) 5.0 BMA, Augst [20]CG4a Human kidney ACE (CD143) 10.0 [20]
Y4b Human kidney ACE (CD143) 2.0 [13]
JC/70A CD31 (PECAM-I) 2.3 DAKO, Glostrup10F3 CD54 (ICAM-I) 1.0 GLT Biotrack, NYQBEND/10 CD34 2.0 Dianova, HamburgF8/86 vWF 11.6 DAKO, GlostrupBMA 120 Endothelium 10.0 Behring, MarburgBNH 9 BUR cell line Pre-diluted Dianova, HamburgMRC OX-43 Rat endothelium 1:50,000 Serotec, Wiesbaden
MR12/53c Rabbit Ig 1.0 DAKO, Glostrupa Reactive on microwave pretreated formalin fixed tissue sectionsb Purified immunoglobulin fraction from rabbit antiserumc Used as negative control in APAAP technique
placed in microwave-proofed tubes (Sigma, Deisenho- (Franke et al, manuscript submitted for publication). Thefinal concentrations used are given in Table 1.fen, Germany) containing 0.01 mol citrate buffer solution
(pH 7.0) and were boiled for five minutes at 600 W inImmunohistochemistrythe microwave (SS 566H; Bosch, Munich, Germany).
The alkaline-phosphatase-antialkaline-phosphatase (AP-The evaporated volume was replaced with distilled wa-AAP) technique was applied according to the methodter, and the procedure was repeated four times. Afterof Cordell et al [22]. On native and formalin-fixed tissuemicrowave treatment, the slides were left to cool downsections, the technique was applied with the followingand were washed in TBS. Frozen sections were fixed inmodifications: To prevent nonspecific reactivity [23], theacetone for 10 minutes at RT and were air dried.polyclonal rabbit antimouse Ig (“link”-antibody; Dako,Glostrup, Denmark) was used at a dilution of 1:40. WhenAntibodiesstaining native tissues of rat, the polyclonal rabbit anti-Nine well-characterized mouse mAbs to the somaticmouse Ig was preabsorbed by an admixture of purifiedisoform of human ACE (CD143) were used [20]. Onerat serum. Here, a 1:750 dilution of redistilled lyophilizedset of these mAb (9B9, i2H5, 5F1, 3G8, 1A8, and 3A5)rat serum (Dianova, Heidelberg, Germany) was foundhas been generated to the native, conformational intactto be optimal to abolish any background. The APAAP
ACE molecule of the lung. The other set (CG1, CG2,complex (Dako) was used at a dilution of 1:50. The
and CG4) generated to human kidney ACE recognizes alkaline phosphatase substrate reaction with new fuchsinthe slightly denatured molecule. In addition, one highly (100 mg/ml) and levamisole (400 mg/ml) was performedpurified polyclonal antibody (pAb) to human kidney for 20 minutes at RT. Additionally, other immunohisto-ACE made in rabbit, Y4, was used [13]. To ensure endo- chemical methods such as the silver-amplified immuno-thelial cell integrity, mAbs known as endothelial cell- gold technique [24] and conventional immunofluorescencespecific markers were applied: CD31, CD34, CD54, fac- were performed to confirm the results of immunostainingtor 8, BMA 120, and BNH 9. A mouse antirabbit-Ig allowing double-labeling experiments.mAb (MR 12/53) was used as negative control (Table
Ultrastructural immunocytochemistry1). For the detection of ACE in the kidney of rat, mAb9B9, cross reacting with ACE of rat on native tissues To analyze ACE in renal tissues at the subcellular[5], was used. Here, the reactivity was compared with level, the pre-embedding method combined with the per-an endothelial cell marker of rat (mAb MRC OX-43) oxidase-antiperoxidase (PAP) staining method was ap-[21]. The proper concentration of each mAb was thor- plied [25]. Fixed human kidneys, cryoprotected in 2.3oughly tested for the optimal staining signal on native molar sucrose in PBS, were snap frozen in liquid nitrogen
and sectioned into 25 to 30 mm thick slices by a cryostatand formalin-fixed tissues as recently described in detail

Fig. 1. Angiotensin-converting enzyme (ACE; CD143) in the normal kidney of humans (A–D) and of rat (E and F). (A) The typical apical cellulardistribution of ACE is shown on epithelial cells of the proximal tubule, whereas those of the distal tubule are negative. Also not labeled for ACEare all endothelial cells, as shown by an interlobular artery (A), a vas afferens (arrow), a glomerulus, and a vein (V). Compare with the serialsection and endothelial marker CD31 at the right side (anti-ACE mAb CG1, APAAP, paraffin-section 340). (B) A serial section of the sametopography is showing all endothelial cells homogeneously stained by CD31. Compare with ACE expression sites on the left by the help of thesame indicated morphological structures (anti-CD31 mAb JC/70A, APAAP, paraffin-section 340). (C) Double labeling to ACE (CG2, black) andto CD31 (JC/70A, red) at the border of the renal cortex and the medullary ray. Endothelial ACE immunoreactivity is not detectable (anti-ACEmAb CG2 and anti-CD31 mAb JC/70A, silver-amplified immunogold and APAAP, paraffin-section 340). (D) Ultrastructural detection of ACEis limited exclusively to the apical brush borders of the proximal tubular epithelial cells (E). No protein precursors in cytoplasmic vesicles and noACE on basolateral cell membranes are visible. Insert 1 shows a magnification of the upper part of a single epithelial cell with the heavily markedbrush-border. Insert 2 shows a magnification of the surface of a capillary endothelial cell (arrow) lacking ACE, as well as a plasma cell in thelumen of the capillary (anti-ACE mAb CG2, pre-embedding method with PAP, X 600/insert 1 and 2 3 1200). (E) The epithelial ACE distributionin the kidney of rat shows a moderate expression only at the distal part of the proximal tubule. Also, endothelial ACE is clearly present in aninterlobular artery (A) and a vas afferens (arrow), whereas endothelial cells of the glomerule, the capillary network, and a vein (V) are not labeled.Compare with serial section and endothelial marker MRC OX-43 on the right hand and with the different expression pattern of humans above(anti-ACE mAb 9B9, APAAP, cryostat-section, 340). (F) Serial section of the same topography is showing all endothelial cells stained by MRCOX-43. Note that this mAb also cross-reacts with stromal cells and blood ingredients. Compare with ACE expression sites on the left by the helpof the same indicated morphological structures (mAb MRC OX-43, APAAP, cryostat-section, 340).

Metzger et al: ACE in non-neoplastic kidney diseases1446
microtome. After descending and ascending alcohol with Fisher’s exact test. This procedure was used to gainhints of possible relationships of the analyzed variables.steps in PBS, the slices were incubated for one hour at
RT with a blocking solution of 10% normal goat serum/ Furthermore, the same method was used to inform ofpossible dependencies on other variables by cross-corre-PBS (Sigma, St. Louis, MO, USA). The slices were then
incubated with the primary mAb CG2 at a dilution of lation, splitting of the test collective according to thefactors of interest, or by the exclusion of special cases,20 mg/ml in PBS for one hour. This was followed by
incubation with the polyclonal rabbit antimouse Ig, used for example, patients suffering from sepsis prior to death.at a dilution of 1:20 in PBS and finally by incubation
Effect of postmortem autolysis on renal angiotensin-with mouse PAP (Dako) used at a dilution of 1:80 inconverting enzyme immunoreactivityPBS. Each incubation step was done for one hour at RT
and was followed by washing three times for 10 minutes. To determine the influence of autolysis on the renalmorphology as well as on the immunoreactivity of anti-The sections were then rinsed for 20 minutes in 0.05 m
Tris-HCl buffer, pH 7.6, and the peroxidase activity was ACE mAbs, freshly obtained renal tissue specimens offive individuals were placed in a refrigerator at 48C in arevealed by incubation with 10 mg diaminobenzidine
(DAB; Sigma) in 10 ml 0.05 m Tris-HCl buffer, pH 7.6, humid atmosphere (the storing temperature of deceasedpatients) or in an incubator at 378C. At certain time inter-containing 5 ml of H2O2 (30%). After fixation and DAB
amplification in 1.25% osmium tetroxide [26], the slices vals, parts of the specimens were taken and were immedi-ately prepared for immunohistochemical analysis.were dehydrated and flat embedded in standard Spurr.
Contrasted thin sections were examined in a Zeiss EM9 S-2 electron microscope at 60 kV.
RESULTS
Angiotensin-converting enzyme and the effect ofSemiquantitative evaluation and statisticspostmortem alterationsThe renal expression of ACE was evaluated regarding
different anatomic structures as mentioned earlier in this At saturating concentrations, all anti-ACE mAbsshowed an identical pattern of staining in the differentarticle. The tubular compartment was analyzed in 135
cases by immunohistochemistry; the complete renal vas- human organs tested, including kidney. No differenceswere found between antibodies predominantly reactingcularization, including all parenchymal vessel types, was
assessed in 106 of these cases. The levels of immunoreac- on native tissues (mAb 9B9, i2H5, 5F1, 3G8, 1A8, 3A5,pAb Y4) and those predominantly reacting on formalin-tivity in different renal cells and compartments were
scored as previously described [27, 28] by three morphol- fixed tissues (CG1, CG2, and CG4) [16]. ACE in thehuman kidney was found to be very stable with all mAbsogists (discussed earlier in this article) into four sub-
groups as follows: 0 5 no expression detectable; 1 5 tested (mAb 9B9, i2H5, 3G8, CG1, CG2, and CG4).Even after four days of observation, the tissues storedslight expression; 2 5 moderate expression; and 3 5
strong expression. For example, the score value of 3 was at 48C showed no alterations of the intensity of immuno-staining or in the pattern of distribution. Progressiveequivalent to the immunostaining of proximal tubule
epithelial cells by mAb CG1 (Fig. 1A) or immunostain- autolysis occurred in renal tissues stored at 378C. Here,even if disintegration of the renal morphology occurred,ing of endothelial cells by the mAb to CD31 (PECAM-I;
Fig. 1B). Again, the scoring differed not essentially be- immunoreactivity was not diminished during the first12 hours (not shown). The decrease in the intensity oftween the three observers. The statistical evaluations
were performed using a computer program [SPSSe for immunostaining with anti-ACE mAbs occurred in a pro-portional manner, both for cells expressing high levelsWindows 95e (release 8)]. Clinical and morphological
diagnoses as well as patients data were correlated with of ACE (for example, proximal tubular epithelial cells)and cells expressing low or intermediate levels (for exam-the level of ACE (score values) in anatomic structures
using the Spearman rank correlation method, which is ple, endothelial cells in perirenal tissue; data not shown).We and other authors have recently described the strongappropriate for ordered categorical data. The Spearman
rank correlation coefficient [r(s), possible values from 21 molecular resistance of ACE to autolysis in human tis-sues [16, 29]. These data show that immunohistochemicalto 1] measures the degree of monotone associations be-
tween two variables: A large positive value of r(s) indi- analysis of ACE is possible on routine autopsy specimensand not only on specimens obtained from rapid autopsycates that large (small) values of one of the ordinal vari-
ables tends to be associated with large (small) values of or surgery.the other. A large negative value of r(s) indicates just the
Angiotensin-converting enzyme in normalopposite scenario. This method gave information abouthuman kidneythe strength and direction of associations between the
variables. It was combined with Pearson’s chi-square test In all analyzed cases with a normal appearance of therenal parenchyma, a dense immunostaining with all anti-for independence and, in the case of small subgroups,

Metzger et al: ACE in non-neoplastic kidney diseases 1447
ACE mAbs lined the luminal surface of the proximal Changes of tubular angiotensin-converting enzyme(CD143). A gross reduction of detectable tubular ACEtubule. Some epithelial cells of the parietal layer of the
Bowman’s capsule at the urinary pole were accessory was caused by any loss of intact renal proximal tubulesand ACE-bearing epithelial cells. This was especiallylabeled. Other segments and structures of the nephron
were found to be negative (Fig. 1 A–D). No endothelial true for advanced lesions of parenchymal remodeling,and, combined with the loss of glomerules, cortical and/ACE was detectable in the vasculature of the human
kidney. ACE was not detectable in medium- or small- or medullar fibrosis (Fig. 2 A, B), raised laboratory val-ues of retention as well as renal insufficiency (data notsized arteries, in arterioles, in the glomerular tuft, or on
the venous side of the renal parenchymal vasculature shown). Advanced lesions of parenchymal remodeling,including most cases of chronic pyelonephritis, also more(Fig. 1 A–D). This lack of ACE was still evident when
mAb concentrations were disproportionately increased, often showed a reduced expression of ACE at the brushborder sites of remaining epithelial cells (Fig. 2D andcausing a strong “background” reactivity (data not
shown). These findings in the renal vasculature contrast Table 2). A strictly different pattern was found in threecases of acute pyelonephritis (Fig. 2E). Unrelated toto those made in other peripheral circulations where
endothelial cells were predominantly labeled by anti- other analyzed variables, a significant loss of ACE at theepithelial brush border site and even a relative dimin-ACE mAbs in small arteries and arterioles and some
capillaries (Franke et al, manuscript submitted for publi- ished detection of released tubular ACE were recorded(Table 2). This tubular reduction of detectable ACE incation). The typical expression pattern of the peripheral
microcirculation occurred immediately outside the pa- acute inflammation histologically coincided with the lo-cal presence of neutrophilic granulocytes, and a residualrenchymal vasculature in the loose connective tissues
surrounding the calyces and the capsule (data not expression of ACE was sometimes only observed in addi-tionally invaded macrophages (Fig. 2F).shown). The electronmicroscopical analysis confirmed
the microscopical findings. Ultrastructurally, the labeling Moreover, by analyzing different stages of renal shock,we found an increasing content of released and non–cell-was confined to the cell membrane of the brush border
in the epithelial cells of proximal tubule. Structures bound ACE in the lumen of renal tubules (Fig. 3). Theimmunoreactivity of all anti-ACE mAbs was not dimin-within the cytoplasm and the basolateral wall of the
epithelial cells as well as the endothelial cells of the ished and was found in the form of intratubular precipi-tates and on the surface of cytoplasmatic blebs releasedvasculature were not labeled (Fig. 1D).by the apical membranes of the epithelial cells even in
Angiotensin-converting enzyme in normal rat kidney early proximal tubular injury (Fig. 3 A–D). In advancedstages of tubular damage and necrosis with loss of cellu-In comparison and in contrast to the human in which
intense labeling was observed all along the proximal lar polarity, integrity of tight junctions and cytoskeletalnetworks in proximal tubular cells, ACE appeared ontubule, epithelial ACE in the rat was restricted to the
straight portion of the proximal tubule located at the the whole cellular surface (Fig. 3 E, F). This contrastedsharply with the polarized apical immunostaining in nor-outer zone of the medulla (Fig. 1E). By opposition to
the endothelial cells of the human renal vasculature, rat mal tubules (Fig. 1 A, C). The immunohistological find-ing of a probably intact molecule within the tubular lu-kidney vessels showed a strong ACE immunoreactivity
in endothelial cells of renal arteries and preglomerular men correlated well with the histological signs of renalshock (Table 2). In only cases of chronic arterial hyper-arterial vessels, including the vas afferens (Fig. 1 E, F).
Endothelial cells of the glomerular tuft, the capillary tension and administered corticosteroids [r(S) 5 0.239,P 5 0.017, N 5 99] was a relative increase of tubularnetwork, and the veins were mostly negative (Fig. 1 E, F).released ACE also recorded. Interestingly, both were
Angiotensin-converting enzyme in human found to be not influenced by other variables, includingkidney diseases the morphological signs of shock (in applying cross-cor-
relation and/or exclusion of cases from analysis, for ex-In contrast to the normal human kidney, the patternof ACE distribution in different renal disorders was al- ample, with signs of shock). Further clinical and thera-
peutical data were not associated with significant changestered. In general, a neoexpression of endothelial ACEwithin the vascular tree of kidney (Fig. 2 A–C) and a of tubular ACE.
Changes of endothelial angiotensin-converting enzymereduction or rearrangement of epithelial ACE in theproximal tubule were observed (Fig. 2 D–F and Fig. 3 (CD143). In different diseases, an unexpected and often
only scattered and inhomogeneous neoexpression ofA–F). These changes of ACE expression were scored inup to 135 adult kidneys at defined tissue sites and were ACE by endothelial cells was observed in almost all
parts of the renal vascularization. Sometimes apparentcorrelated with each of several clinical findings, diagno-sis, and histological tissue alterations. The most impor- even in medium- and small-sized parenchymal arteries
(Fig. 2A), this neoexpression was found to more oftentant results are summarized in Tables 2 and 3.

Metzger et al: ACE in non-neoplastic kidney diseases1448
Fig. 2. Human kidney diseases with neoexpression of endothelial angiotensin-converting enzyme (ACE; CD143; A–C) and reduction or loss ofepithelial ACE (D–F). (A) Cortical fibrosis in a case of a chronic interstitial nephritis is going along with a remarkable neoexpression of ACE inendothelial cells of a parenchymal artery (A). Endothelial cells of some glomeruli also show scattered ACE (anti-ACE mAb CG1, APAAP,paraffin-section, 340). (B) Medullar fibrosis in another case of chronic interstitial nephritis shows endothelial neoexpression of ACE in vasa recta(anti-ACE mAb CG2, APAAP, paraffin-section, 340). (C) Diabetic glomerulosclerosis shows neoexpression of endothelial ACE especially withinthe glomerular tuft. Note the diffuse enlargement of the capillary loops and the beginning of nodular capillary obliteration (anti-ACE mAb CG2,APAAP, paraffin-section, 3160). (D) Loss and reduction of epithelial ACE (arrow) is shown in a zone of atrophic tubules in a case of advancedarteriosclerosis. Note the intimal thickening of the parenchymal artery in the center (anti-ACE mAb CG4, APAAP, paraffin-section, 340). (E)Almost complete loss and down regulation of tubular ACE in a case of acute pyelonephritis. In the acute phase of inflammation, no endothelialneoexpression is observed (arrow). Compare with the intense tubular ACE expression of normal cortical tissue (Fig 1A; anti-ACE mAb CG2,APAAP, paraffin-section, 325). (F) Despite the massive loss of tubular ACE in acute pyelonephritis, invading activated macrophages may show anexpression. Note that the tubular loss of ACE coincides with the presence of granulocytes (anti-ACE mAb CG2, APAAP, paraffin-section, 340).

Metzger et al: ACE in non-neoplastic kidney diseases 1449
Fig. 3. Epithelial angiotensin-converting enzyme (ACE; CD143) in early (A–D) and advanced (E and F) stages of renal shock in humans. (A) Onsetof tubular insufficiency with tubular enlargement. ACE-immunoreactive luminal precipitates and immunoreactive cytoplasmatic blebs released by theepithelial cells of proximal tubules are found (arrows; anti-ACE mAb CG2, APAAP, paraffin-section, 3160). (B) Free ACE-positive cytoplasmaticblebs and fragments are more prominent in this case of early shock stage. Note that the general tissue morphology is intact and compare withnormal appearance (Fig. 1A; anti-ACE mAb CG2, APAAP, paraffin-section, 3160). (C) More intense ACE-containing precipitates and swollenblebs are shown in this early stage of shock kidney. The cellular integrity of proximal tubular epithelium is still preserved. Note the strict ACE-negative epithelium of the distal tubule (anti-ACE mAb CG2, APAAP, paraffin-section, 3160). (D) In this stage of early kidney shock, the spaceof Bowman’s capsule is filled with ACE-reactive cellular detritus (arrows), presumably caused by flow black (anti-ACE mAb CG2, APAAP,paraffin-section, 340). (E) The cellular ACE expression site changes with the onset of cellular dissociation in this more advanced stage of renalshock [now see the pericellular and cytoplasmatic distribution of immunoreactivity (arrow) in contrast to the normal apical expression site; Fig.1A and discussed earlier in this article; anti-ACE mAb CG2, APAAP, paraffin-section, 3160]. (F) The cellular detachment from basal membranes,the complete loss of polarity, and the beginning of necrosis are conjoined with a circular cellular distribution of ACE (arrows). Note that even inthis advanced stage of shock, the immunoreactivity to ACE obviously is not diminished (anti-ACE mAb CG2, APAAP, paraffin-section, 340).

Metzger et al: ACE in non-neoplastic kidney diseases1450
Table 2. Changes of tubular angiotensin-converting enzyme (ACE; the presented correlations were not found to neutralizeCD143) in correlation to clinical diagnosis and renal morphology
one another or were found to be influenced by advancedLocalization of morphological alterations of the glomerule (in applying
anti-ACE immunoreactivity cross-correlation and/or exclusion of cases from analy-Brush borders Lumen sis). However, of those clinical and therapeutical data(apical pole of of tubules
that were additionally compared, only the administrationepithelium) (released ACE)of ACE inhibitors in the course of the clinical presenta-
Clinical diagnosistion of the affected hypertonic patients was found sig-Arterial hypertension NS r(s) 5 0.187be
Diabetes mellitus NS NS nificantly associated with the detection of endothelialCardiac insufficiency NS NS ACE and, here, only at the site of glomerules [r(s) 5Chronic renal insufficiency NS NS
0.314, P 5 0.008, N 5 71].Vascular alterationsArteriosclerosis NS NSArteriolosclerosis NS NSGlomerular sclerosis NS NS DISCUSSION
Parenchymal remodelingThe abundant expression of ACE in the human kidneyLoss of glomerules r(s) 5 20.214b NS
Cortical fibrosis r(s) 5 20.177b NS tubule observed in this study is essentially in agreementMedullar fibrosis r(s) 5 20.205b NS with previous studies [10–14]. ACE, as proven by ultra-
Inflammatory changesstructural analysis, was found to be strictly confined toAcute pyelonephritis r(s) 5 20.337de r(s) 5 20.211be
Chronic pyelonephritis r(s) 5 20.260c NS the epithelial brush borders of the proximal tubule. WeSigns of shocka NS r(s) 5 0.453de
could not confirm an additional expression on the baso-The analysis of those variables presented in rows and columns was performed lateral cell membrane, the endoplasmatic reticulum, or
according to Spearman’s rank correlation test. r(s) 5 Spearman’s rank correlationthe nuclear envelope, as reported by other authors [10,coefficient (possible values from 21 to 1). Abbreviation NS is no significant
correlation. 12, 13, 30]. This may be due to the use of mAb anda As defined by tubular dilation, tubular protein, epithelial dissociation, necro-
different tissue-fixation procedures. Despite the abun-sis, and microthrombosisb P , 0.05, c P , 0.01, d P , 0.001, depending on the availability of data sets dance of the enzyme on tubular brush borders, its local
of each individual case, all correlations are based on the minimum of N 5 114and systemic function is not clearly understood. ACE,and the maximum of N 5 135
e Correlations that were found not essentially affected by other variables (see as a peptidase with a broad substrate specificity, is abletext)
to hydrolyze a wide range of peptide substrates in vitro,liberating different dipeptides or tripeptides [2]. Ang IIis most likely one of the products of tubular ACE. Foundin high local concentrations [31], Ang II was shown toaffect smaller vessels such as arterioles, vasa afferentiabe formed in the proximal tubular lumen [32] and wasand efferentia, glomerular capillaries, vasa recta, andshown to stimulate the sodium and bicarbonate transportalso the endothelial cells of veins (Fig. 2B). The endothe-[33, 34]. Ang II receptors also have been identified inlial neoexpression of ACE was not specific for certainthe renal brush border and basolateral cell membranestissue sites in most cases, but was observed in vessels[35, 36]. Recently, concerning possible resorptive func-next to fibrotic remodeling of kidney parenchyma andtions of ACE in addition, two high-affinity oligopeptideoccurred, for example, more frequently in endothelialtransporters were identified in the brush borders of intes-cells of vasa recta in the case of medullary fibrosis (Table 3).tine and proximal tubules of kidney: PepT1 and PepT2,Although found to be not specific for a certain typerespectively [37–41]. Because of similar cellular and sub-of disease, the glomerular neoexpression of ACE corre-cellular localization, ACE and other peptidases mightlated with the incidence of diabetes mellitus (Fig. 2Calso participate in the terminal digestion and reabsorp-and Table 3). In a total of 86 patients analyzable fortion of proteins and peptides in the tubule lumen, to-both features, for dichotomized data this means thatgether with the dipeptide and tripeptide transporterACE expression was immunohistochemically detected
in glomeruli of 6 out of 11 kidneys of diabetic patients PepT2.In different diseases associated with an acute damagebut only in those of 4 out of 75 kidneys of nondiabetic
patients. Interestingly, moreover, a slight glomerular to the proximal tubular epithelium, we found a luminalrelease of ACE. Especially in advanced stages of renalneoexpression of ACE was also found to be associated
more frequently with patients having the recorded diag- shock, this non–cell-bound immunoreactivity was foundto diffuse to proximal and distal segments of the nephronnosis of chronic arterial hypertension (Table 3). For 91
analyzable patients again this means that glomerular (Fig. 3 A–D). It has been proposed that urinary ACEand ACE activity may be a marker of proximal tubuleACE was present in 7 out of 27 hypertonic patients
versus only 3 out of 64 nonhypertonic patients. Despite a damage [42, 43]. Our data are in agreement with theseclinical and experimental findings and confirm that thepartial coincidence of both diseases in patients suffering
from diabetes mellitus and chronic arterial hypertension, urinary enzyme is released from the proximal tubular

Metzger et al: ACE in non-neoplastic kidney diseases 1451
Table 3. Changes of endothelial angiotensin-converting enzyme (ACE; CD143) in correlation to clinical diagnosis and renal morphology
Localization of anti-ACE immunoreactivity
Arteriolesa Glomerules Vasa recta
Clinical diagnosisArterial hypertension NS r(s) 5 0.310df NSDiabetes mellitus NS r(s) 5 0.513ef r(s) 5 0.241c
Cardiac insufficiency NS NS NSChronic renal insufficiency NS r(s) 5 0.252c NS
Vascular alterationsArteriosclerosis NS NS NSArteriolosclerosis NS r(s) 5 0.217c NSGlomerular sclerosis r(s) 5 0.272d r(s) 5 0.248c r(s) 5 0.317d
Parenchymal remodelingLoss of glomerules r(s) 5 0.270d NS r(s) 5 0.304d
Cortical fibrosis r(s) 5 0.271d NS r(s) 5 0.316d
Medullar fibrosis r(s) 5 0.258c r(s) 5 0.285d r(s) 5 0.485ef
Inflammatory changesAcute pyelonephritis NS NS NSChronic pyelonephritis r(s) 5 0.274d NS r(s) 5 0.230c
Signs of shockb NS NS NS
The analysis of those variables presented in rows and columns was performed according to Spearman’s rank correlation test; r(s) 5 Spearman’s rank correlationcoefficient (possible values from 21 to 1); abbreviation NS is no significant correlation.
a Vasa afferentia and efferentiab As defined by tubular dilation, tubular protein, epithelial dissociation, necrosis, and microthrombosisc P , 0.05; d P , 0.01; e P , 0.001; depending on the availability of data sets of each individual case, all correlations are based on the minimum of N 5 86 and
the maximum of N 5 106.f Correlations that were found not essentially affected by other variables (see text)
epithelium [44]. The loss of all brush border enzymes Thus, the remarkable absence of ACE in vessels of thenormal human kidney in contrast to other circulationsduring ischemia occurs in general. In this respect, how-
ever, the strong molecular resistance of ACE even in supports the concept of the heterogeneity of endothelialcell populations with tissue- and organ-specific functionsadvanced cellular damage and necrosis is remarkable
(Fig. 3F). Only in cases of chronic arterial hypertension [46–48]. This organ-specific lack of endothelial ACE maycontribute to a relatively lower vascular resistance ofor therapy with corticosteroids was a tendency to a slight
increase of luminal ACE also recorded. Sharply con- human kidney and the high renal blood flow. Further-more, the absence of endothelial ACE may protect thetrasting with this cellular detachment of still conserved
ACE, a marked reduction or even complete loss of any renal circulation against excess Ang II formation andkinin inactivation. In this respect, however, species-spe-detectable ACE in renal tubules occurred in acute pyelo-
nephritis (Fig. 2 E, F). This loss of immunoreactivity in cific differences have to be considered, as illustrated bythe different localization of renal ACE in humans andthe absence of cellular necrosis may be best explained
by a drastic conformational change or even molecular in rats (discussed in scheme of Fig. 4).Interestingly, we found a neoexpression of ACE ondestruction of ACE in the close neighborhood of acti-
vated neutrophilic granulocytes. Liberated peroxides in endothelial cells in different diseases of the human kid-ney affecting certain parts of the renal vascular system,the granulocytic burst reaction have clearly been shown
to decrease ACE activity of endothelial cells in animal for example, arteries, capillaries of the glomerular tuft,or vasa recta. Inconstantly and independent from themodels [45]. Interestingly, this granulocytic burst and
peroxide-induced decrease of ACE activity may indeed nature of the underlying diseases, these changes werealways seen beside local fibrotic remodeling of the af-be paralleled by the loss of immunohistochemically de-
tectable ACE in a cell culture model, and the reduction fected tissue compartments. In general, a neoexpressionof ACE occurs also in other cell types and diseases,or loss of detectable endothelial ACE was found also in
acute inflammations of other organ systems (Franke, for example, in sarcoidosis, atherosclerosis, myocardialinfarction, and renal cell carcinoma and indicates a po-unpublished data).
The complete lack of endothelial ACE in the normal tential function of ACE in the angiogenesis and fibroticparenchymal remodeling [5, 9, 16, 49, 50] [abstracts: Chu-human kidney was already mentioned in some former
studies using polyclonal antibodies [10, 11]. However, in machenko et al, Arteriosclerosis 115(Suppl):S63, 1995;Metzger et al, Pathol Res Pract 192:364, 1996]. Besidessome studies, the enzyme was detected in the interstitial
capillaries of the vasa recta [12–14]. We have found ACE vasoconstrictory effects, Ang II has potent fibrogenic andmitogenic effects [51–53], and it has been shown that thein these particular endothelial cells in only certain patho-
logical conditions such as medullar or cortical fibrosis. inhibition of ACE may prevent these effects in athero-

Metzger et al: ACE in non-neoplastic kidney diseases1452
Fig. 4. Schematic diagram of the normal renal angiotensin-converting enzyme (ACE; CD143) distribution in humans and rat regarding the specialendothelial as well as epithelial expression sites. Note that exceptions to this rule, caused by pathological alterations, unknown individual factors,or in rat, by strain differences, might occur.
sclerosis and vascular restenosis [54–56]. In animal stud- tion of ACE, which is abnormally expressed by endothe-ies, it has been suggested that Ang II is involved in lial cells of the renal vasculature.nephrogenesis and renal vascular development [57–59]. Up- and down-regulation or loss of ACE was observedAngiotensins are also probably responsible for the devel- in different non-neoplastic kidney diseases, as well as inopment of glomerular sclerosis, interstitial sclerosis, and different renal tissue compartments. Even in the com-proteinuria in some diseases [58, 60, 61]. plexity of an altered renal morphology, renal function,
In this study, diabetes mellitus, for example, was sig- clinical presentation of patients, as well as therapeuticalnificantly associated with a neoexpression of ACE in the intervention, some of these changes of ACE expressionglomerular tuft (Fig. 2C). This was confirmed in animal were found clearly associated with certain pathologicalmodels [62] and was recently corroborated by others conditions: (a) fibrotic remodeling of renal tissues, (b)[63]. The onset and progression of diabetic nephropathy
chronic arterial hypertension, (c) diabetes mellitus, (d)was found to be associated with the genetic polymor-
ischemic renal shock, and (e) acute pyelonephritis. Semi-phism of ACE and elevated plasma levels of the enzymequantitative immunohistochemistry and the employed[64, 65]. On the other hand, several studies in humansstatistical method may both tend to incorrectly estimateand animals indicate that ACE inhibitors have beneficialthe exact changes of functionally effective ACE mole-effects on diabetic nephropathy, and it has been pro-cules. However, as changes and interesting associationsposed that these protective effects are independent ofwere detectable even using these relatively rough meth-the reduction of blood pressure [66, 67]. ACE inhibitorsods, we would like to point out that ACE is an importantreduce the progression of albuminuria and the degrada-molecule in the pathophysiology of diseases affecting thetion of renal function in type I diabetes and in incipienthuman kidney. In the future, new technical approachesrenal failure of several origins [62, 68–72]. The beneficial
effects of ACE inhibition may be mediated by the inhibi- will help to study molecular changes more exactly even

Metzger et al: ACE in non-neoplastic kidney diseases 1453
M, Moretta L, Okumura K, Shaw S, Springer TA, Sugamuraon the level of single cells in normal as well as diseasedK, Zola H, New York and London, Garland Publishing, 1997, pp
tissues [73]. 749–75117. Hall ER, Kato J, Erdos EG, Robinson CJ, Oshima G: Angioten-
sin I-converting enzyme in the nephron. Life Sci 18:1299–1303,ACKNOWLEDGMENTS1976
This work was supported in part by a Bristol Myers Squibb Insti- 18. Taugner R, Ganten D: The localization of converting enzyme intute—INSERM grant, and by DAKO A/S. We thank Mr. Luke Kerk- kidney vessels of the rat. Histochemistry 75:191–201, 1982man, M.D., for his excellent technical support, Mrs. Monika Nickolaus 19. Ikemoto F, Song GB, Tominaga M, Kanayama Y, Yamamoto K:for helpful discussions, and Mrs. Irene Ruocco for her admirable pa- Angiotensin-converting enzyme in the rat kidney: Activity, distri-tience and skill in reading and correcting the manuscript. Furthermore, bution, and response to angiotensin-converting enzyme inhibitors.we thank Dr. Harry Towbin, Novartis, Switzerland, for his help in Nephron 55(Suppl 1):S3–S9, 1990providing antibodies used in this study. 20. Danilov S, Jaspard E, Churakova T, Towbin H, Savoie F, Wei
L, Alhenc-Gelas F: Structure-function analysis of angiotensinReprint requests to Folker E. Franke, M.D., Department of Pathol- I-converting enzyme using monoclonal antibodies: Selective inhibi-
ogy, Justus-Liebig University of Giessen, Langhansstrasse 10, D-35392 tion of the amino-terminal active site. J Biol Chem 269:26806–Giessen, Germany. 26814, 1994E-mail: [email protected] 21. Robinson A, White T, Mason D: MRC OX-43: A monoclonal
antibody which reacts with all vascular endothelium in the ratexcept that of brain capillaries. Immunology 57:231–237, 1985REFERENCES
22. Cordell JL, Falini B, Erber WN, Ghosh AK, Abdulaziz Z,MacDonald S, Pulford KA, Stein H, Mason DY: Immunoenzy-1. Soffer RL: Angiotensin-converting enzyme and the regulation ofmatic labeling of monoclonal antibodies using immune complexesvasoactive peptides. Annu Rev Biochem 45:73–94, 1976of alkaline phosphatase and monoclonal anti-alkaline phosphatase2. Skidgel RA, Erdos EG: Biochemistry of angiotensin-I converting(APAAP complexes). J Histochem Cytochem 32:219–229, 1984enzyme, in Renin Angiotensin System, edited by Robertson JIS,
23. Franke FE, Schachenmayr W, Osborn M, Altmannsberger M:Nichols MG, London, Gower Medical Publishers, 1993, pp 10.1–10.10 Unexpected immunoreactivities of intermediate filament antibod-
3. Ryan US, Ryan JW, Whitaker C, Chiu A: Localization of angio- ies in human brain and brain tumors. Am J Pathol 139:67–79, 1991tensin converting enzyme (kininase II). II. Immunocytochemistry 24. Roth J, Saremaslani P, Warhol MJ, Heitz PU: Improved accu-and immunofluorescence. Tissue Cell 8:125–145, 1976 racy in diagnostic immunohistochemistry, lectin histochemistry and
4. Caldwell PR, Seegal BC, Hsu KC, Das M, Soffer RL: Angioten- in situ hybridization using a gold-labeled horseradish peroxidasesin-converting enzyme: Vascular endothelial localization. Science antibody and silver intensification. Lab Invest 67:263–269, 1992191:1050–1051, 1976 25. Wendelschafer-Crabb G, Erlandsen SL, Walker DH: Ultra-
5. Falkenhahn M, Franke F, Bohle RM, Zhu YC, Stauss HM, structural localization of viral antigens using the unlabeled anti-Bachmann S, Danilov S, Unger T: Cellular distribution of angio- body-enzyme method. J Histochem Cytochem 24:517–526, 1976tensin-converting enzyme after myocardial infarction. Hyperten- 26. Lascano EF, Berria MI: PAP labeling enhancement by osmiumsion 25:219–226, 1995 tetroxide-potassium ferrocyanide treatment. J Histochem Cyto-
6. Sun Y, Weber KT: Angiotensin-converting enzyme and wound chem 36:697–699, 1988healing in diverse tissues of the rat. J Lab Clin Med 127:94–101, 27. Zeiher AM, Goebel H, Schachinger V, Ihling C: Tissue1996 endothelin-1 immunoreactivity in the active coronary atheroscle-
7. Deleted in proof rotic plaque: A clue to the mechanism of increased vasoreactivity8. Deleted in proof of the culprit lesion in unstable angina. Circulation 91:941–947,9. Diet F, Pratt RE, Berry GJ, Momose N, Gibbons GH, Dzau VJ: 1995
Increased accumulation of tissue ACE in human atherosclerotic 28. Haberbosch W, Bohle RM, Franke FE, Danilov S, Alhenc-coronary artery disease. Circulation 94:2756–2767, 1996 Gelas F, Braun-Dullaeus R, Holschermann H, Waas W, Till-
10. Takada Y, Hiwada K, Unno M, Kokubu T: Immunological local- manns H, Gardemann A: The expression of angiotensin-I con-ization of angiotensin converting enzyme at ultrastructural level verting enzyme in human atherosclerotic plaques is not related toin the human lung and kidney. Biomed Res 3:169–174, 1982 the deletion/insertion polymorphism but to the risk of restenosis
11. Defendini R, Zimmerman EA, Weare JA, Alhenc-Gelas F, after coronary interventions. Atherosclerosis 130:203–213, 1997Erdos EG: Angiotensin-converting enzyme in epithelial and neu- 29. MacGregor DP, Murone C, Mendelsohn FA: The stability ofroepithelial cells. Neuroendocrinology 37:32–40, 1983angiotensin receptors and angiotensin converting enzyme in post12. Alhenc-Gelas F, Baussant T, Hubert C, Soubrier F, Corvolmortem brain. Neurochem Int 25:413–417, 1994P: The angiotensin converting enzyme in the kidney. J Hypertens
30. Marchetti J, Roseau S, Alhenc-Gelas F: Angiotensin I con-7(Suppl):S9–S13, 1989verting enzyme and kinin-hydrolyzing enzymes along the rabbit13. Bruneval P, Hinglais N, Alhenc-Gelas F, Tricottet V, Corvolnephron. Kidney Int 31:744–751, 1987P, Menard J, Camilleri JP, Bariety J: Angiotensin I converting
31. Seikaly MG, Arant BS Jr, Seney FD Jr: Endogenous angiotensinenzyme in human intestine and kidney: Ultrastructural immunohis-concentrations in specific intrarenal fluid compartments of the rat.tochemical localization. Histochemistry 85:73–80, 1986J Clin Invest 86:1352–1357, 199014. Danilov SM, Faerman AI, Printseva OY, Martynov AV, Sak-
32. Braam B, Mitchell KD, Fox J, Navar LG: Proximal tubularharov IY, Trakht IN: Immunohistochemical study of angiotensin-secretion of angiotensin II in rats. Am J Physiol 264:F891–F898,converting enzyme in human tissues using monoclonal antibodies.1993Histochemistry 87:487–490, 1987
33. Schuster VL, Kokko JP, Jacobson HR: Angiotensin II directly15. Danilov SM, Franke FE, Erdos EG: CD143 (angiotensin-con-stimulates sodium transport in rabbit proximal convoluted tubules.verting enzyme) workshop panel report, in Leucocyte Typing VI,J Clin Invest 73:507–515, 1984edited by Kishimoto T, Kikutani H, von dem Borne AEG, Goyert
34. Liu FY, Cogan MG: Angiotensin II stimulates early proximalSM, Mason DY, Miyasaka M, Moretta L, Okumura K, Shaw S,bicarbonate absorption in the rat by decreasing cyclic adenosineSpringer TA, Sugamura K, Zola H, New York and London,monophosphate. J Clin Invest 84:83–91, 1989Garland Publishing, 1997, pp 746–749
35. Brown GP, Douglas JG: Angiotensin II-binding sites in rat and16. Franke FE, Metzger R, Bohle RM, Kerkman L, Alhenc-Gelasprimate isolated renal tubular basolateral membranes. Endocrinol-F, Danilov SM: CD143 workshop: Angiotensin-I-converting en-ogy 112:2007–2014, 1983zyme (CD143) on endothelial cells in normal and in pathological
36. Clauser E, Curnow KM, Davies E, Conchon S, Teutsch B,conditions, in Leucocyte Typing VI, edited by Kishimoto T, Kiku-tani H, von dem Borne AEG, Goyert SM, Mason DY, Miyasaka Vianello B, Monnot C, Corvol P: Angiotensin II receptors: Pro-

Metzger et al: ACE in non-neoplastic kidney diseases1454
tein and gene structures, expression and potential pathological 56. Wolf G: Angiotensin as a renal growth promoting factor. AdvExp Med Biol 377:225–236, 1995involvements. Eur J Endocrinol 134:403–411, 1996
57. Tufro-McReddie A, Romano LM, Harris JM, Ferder L, Gomez37. Fei YJ, Kanai Y, Nussberger S, Ganapathy V, Leibach FH,RA: Angiotensin II regulates nephrogenesis and renal vascularRomero MF, Singh SK, Boron WF, Hediger MA: Expressiondevelopment. Am J Physiol 269:F110–F115, 1995cloning of a mammalian proton-coupled oligopeptide transporter.
58. Hilgers KF, Reddi V, Krege JH, Smithies O, Gomez A: AberrantNature 368:563–566, 1994renal vascular morphology and renin expression in mutant mice38. Liu W, Liang R, Ramamoorthy S, Fei YJ, Ganapathy ME, Hed-lacking angiotensin-converting enzyme. Hypertension 29:216–221,iger MA, Ganapathy V, Leibach FH: Molecular cloning of PEPT19972, a new member of the H1/peptide cotransporter family, from
59. Esther CR Jr, Howard TE, Marino EM, Goddard JM, Capecchihuman kidney. Biochim Biophys Acta 1235:461–466, 1995MR, Bernstein KE: Mice lacking angiotensin-converting enzyme39. Boll M, Herget M, Wagener M, Weber WM, Markovich D,have low blood pressure, renal pathology, and reduced male fertil-Biber J, Clauss W, Murer H, Daniel H: Expression cloning ity. Lab Invest 74:953–965, 1996
and functional characterization of the kidney cortex high-affinity 60. Okada H, Suzuki H, Kanno Y, Ikenaga H, Saruta T: Renalproton-coupled peptide transporter. Proc Natl Acad Sci USA responses to angiotensin receptor antagonist and angiotensin-con-93:284–289, 1996 verting enzyme inhibitor in partially nephrectomized spontane-
40. Nussberger S, Hediger MA: How peptides cross biological mem- ously hypertensive rats. J Cardiovasc Pharmacol 26:564–569, 1995branes. (editorial) Exp Nephrol 3:211–218, 1995 61. Rosenberg ME, Smith LJ, Correa-Rotter R, Hostetter TH: The
41. Leibach FH, Ganapathy V: Peptide transporters in the intestine paradox of the renin-angiotensin system in chronic renal disease.and the kidney. Annu Rev Nutr 16:99–119, 1996 Kidney Int 45:403–410, 1994
42. Kato I, Takada Y, Nishimura K, Hiwada K, Kokubu T: Increased 62. Anderson S, Jung FF, Ingelfinger JR: Renal renin-angiotensinurinary excretion of angiotensin converting enzyme in patients system in diabetes: Functional, immunohistochemical, and molecu-with renal diseases. J Clin Chem Clin Biochem 20:473–476, 1982 lar biological correlations. Am J Physiol 265:F477–F486, 1993
63. Mizuiri S, Yoshikawa H, Tanegashima M, Miyagi M, Kobayashi43. Hosojima H, Miyauchi E, Morimoto S: Urinary excretion of angio-M, Sakai K, Hayashi I, Aikawa A, Ohara T, Hasegawa A: Renaltensin-converting enzyme in NIDDM patients with nephropathy.ACE immunohistochemical localization in NIDDM patients withDiabetes Care 12:580–582, 1989nephropathy. Am J Kidney Dis 31:301–307, 199844. Pedraza-Chaverri J, Cruz C, del Socorro-Blancas M, Hernan-
64. Marre M, Bernadet P, Gallois Y, Savagner F, Guyene TT,dez-Pando R, Ibarra-Rubio ME, Larriva-Sahd J, Tapia E: An-Hallab M, Cambien F, Passa P, Alhenc Gelas F: Relationshipsgiotensin I converting enzyme activity in uranyl nitrate inducedbetween angiotensin I converting enzyme gene polymorphism,acute renal failure in rats. Renal Fail 17:377–388, 1995plasma levels, and diabetic retinal and renal complications. Diabe-45. Chen X, Catravas JD: Neutrophil-mediated endothelial angioten-tes 43:384–388, 1994sin-converting enzyme dysfunction: Role of oxygen-derived free
65. Jardine AG, Padmanabhan N, Connell JM: Angiotensin con-radicals. Am J Physiol 265:L243–L249, 1993verting enzyme gene polymorphisms and renal disease. Curr Opin46. Kumar S, West DC, Ager A: Heterogeneity in endothelial cellsNephrol Hypertens 7:259–264, 1998from large vessels and microvessels. Differentiation 36:57–70, 1987 66. Erley CM, Harrer U, Kramer BK, Risler T: Renal hemodynam-
47. Kuzu I, Bicknell R, Fletcher CD, Gatter KC: Expression of ics and reduction of proteinuria by a vasodilating beta blockeradhesion molecules on the endothelium of normal tissue vessels versus an ACE inhibitor. Kidney Int 41:1297–1303, 1992and vascular tumors. Lab Invest 69:322–328, 1993 67. Remuzzi A, Imberti O, Puntorieri S, Malanchini B, Macconi
48. Risau W: Differentiation of endothelium. FASEB J 9:926–933, D, Magrini L, Bertani T, Remuzzi G: Dissociation between anti-1995 proteinuric and antihypertensive effect of angiotensin converting
49. Silverstein E, Pertschuk LP, Friedland J: Immunofluorescent enzyme inhibitors in rats. Am J Physiol 267:F1034–F1044, 1994localization of angiotensin converting enzyme in epithelioid and 68. Praga M, Hernandez E, Montoyo C, Andres A, Ruilope LM,giant cells of sarcoidosis granulomas. Proc Natl Acad Sci USA Rodicio JL: Long-term beneficial effects of angiotensin-converting76:6646–6648, 1979 enzyme inhibition in patients with nephrotic proteinuria. Am J
50. Takada Y, Hiwada K, Yokoyama M, Ochi K, Takeuchi M, Ko- Kidney Dis 20:240–248, 199269. Lewis EJ, Hunsicker LG, Bain RP, Rohde RD: The effect ofkubu T: Angiotensin converting enzyme: A possible histologic
angiotensin-converting-enzyme inhibition on diabetic nephropa-indicator for human renal cell carcinoma. Cancer 56:130–133, 1985thy: The Collaborative Study Group. N Engl J Med 329:1456–1462,51. Campbell-Boswell M, Robertson AL Jr: Effects of angiotensin1993II and vasopressin on human smooth muscle cells in vitro. Exp
70. Ruilope LM: Effects of angiotensin converting enzyme inhibitorsMol Pathol 35:265–276, 1981on the progression of diabetic nephropathy. J Hypertens 1352. Naftilan AJ: The role of angiotensin II in vascular smooth muscle(Suppl):S91–S93, 1995cell growth. J Cardiovasc Pharmacol 20(Suppl 1):S37–S40, 1992
71. Maschio G, Alberti D, Janin G, Locatelli F, Mann JF, Mo-53. Weber H, Webb ML, Serafino R, Taylor DS, Moreland S, Nor-tolese M, Ponticelli C, Ritz E, Zucchelli P: Effect of the angio-man J, Molloy CJ: Endothelin-1 and angiotensin-II stimulate de-tensin-converting-enzyme inhibitor benazepril on the progressionlayed mitogenesis in cultured rat aortic smooth muscle cells: Evi-of chronic renal insufficiency: The Angiotensin-Converting-dence for common signaling mechanisms. Mol Endocrinol 8:148– Enzyme Inhibition in Progressive Renal Insufficiency Study Group.
158, 1994 N Engl J Med 334:939–945, 199654. Powell JS, Clozel JP, Muller RK, Kuhn H, Hefti F, Hosang M, 72. The GISEN Group: Randomised placebo-controlled trial of effect
Baumgartner HR: Inhibitors of angiotensin-converting enzyme of ramipril on decline in glomerular filtration rate and risk ofprevent myointimal proliferation after vascular injury. Science terminal renal failure in proteinuric, non-diabetic nephropathy.245:186–188, 1989 Lancet 349:1857–1863, 1997
55. Rakugi H, Wang DS, Dzau VJ, Pratt RE: Potential importance 73. Fink L, Seeger W, Ermert L, Hanze J, Stahl U, Grimminger F,of tissue angiotensin-converting enzyme inhibition in preventing Kummer W, Bohle RM: Real-time quantitative RT-PCR after
laser-assisted cell picking. Nature Med 4:1329–1333, 1998neointima formation. Circulation 90:449–455, 1994
Copyright © 2022 FDOKUMEN