Anesthesia: Essays and Researches - JournalOnWeb
126
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 i EDITORIAL BOARD Editor-in-Chief Mohamad Said Maani Takrouri Riyadh, KSA [email protected] Arab National Editors Yehia H. Khater Egypt [email protected] Bashir A. Atiyat Amman, Jordan [email protected] Izdiad Badran Amman, Jordan i[email protected] Jamal Sharif Alshanableh Amman, Jordan [email protected] Maroun Ghabach Beirut, Lebanon [email protected] Marie-Claire Antakly Beirut Lebanon [email protected] Mohamed A. Seraj Riyadh, KSA Dhafer Alkhudairi Riyadh, KSA Bassam Al-Barzangi UAE Email. [email protected] Members Mohammed Saleh Ben Ammar Tunisia Bourhan Al Abed Syria Mohamad Taha Al Jasir Syria Hussein Abukhudeir Jordan Abdelmajid Daoud Tunisia Ahmad Sibti Morocco Dina Baroudi Syria, USA, KSA Anesthesia: Essays and Researches Official Publication of Pan Arab Federation of Societies of Anesthologists July - December 2011, Vol. 5, Issue 2 ISSN: 0259-1162, E-ISSN: 2229-7685 The journal Anesthesia: Essays and Researches (ISSN: Print-0259-1162; Online 2229-7685) is peer-reviewed journal published on behalf of Pan Arab Federation of Societies of Anesthesiologists. The journal publishes articles on the subject of Anesthesia, pharmacology, physiology. pain management and intensive care. The Journal is published semiannually (in the third week of June and December). Abstracting and indexing information The journal is indexed with Caspur, EBSCO Publishing’s Electronic Databases, Expanded Academic ASAP, Genamics JournalSeek, Google Scholar, Health & Wellness Research Center, Health Reference Center Academic, Hinari, Index Copernicus, OpenJGate, PrimoCentral, ProQuest, SCOLOAR, SIIC databases, Summon by Serial Solutions and Ulrich’s International Periodical Directory. Information for authors There are no page charges for submissions to the journals. Please check http://www.aeronline.org for details. All manuscripts must be submitted online at www. journalonweb.com/aer Subscription information Copies of the journal provided free of cost to the members of Pan Arab Federation of Societies of Anesthesiologists. A subscription to Anesthesia: Essays and Researches comprises 2 issues. Prices include postage. Annual Subscription Rate for non-members- • Institutional: INR 2000.00 for India USD 160.00 for outside India • Personal: INR 1000.00 for India USD 100.00 for outside India For mode of payment and other details, please visit www. medknow.com/subscribe.asp. Claims for missing issues will be serviced at no charge if received within 60 days of the cover date for domestic subscribers, and 3 months for subscribers outside India. Duplicate copies cannot be sent to replace issues not delivered because of failure to notify publisher of change of address. The journal is published and distributed by Medknow Publications and Media Pvt. Ltd. Copies are sent to subscribers directly from the publisher’s address. It is illegal to acquire copies from any other source. If a copy is received for personal use as a member of the association/society, one cannot resale or give-away the copy for commercial or library use. The copies of the journal to the members of the association are sent by ordinary post. The editorial board, association or publisher will not be responsible for non receipt of copies. If any member/subscriber wishes to receive the copies by registered post or courier, kindly contact the publisher’s office. If a copy returns due to incomplete, incorrect or changed address of a member/subscriber on two consecutive occasions, the names of such members will be deleted from the mailing list of the journal. Providing complete, correct and up-to-date address is the responsibility of the member/subscriber. Advertising policies The journal accepts display and classified advertising. Frequency discounts and special positions are available. Inquiries about advertising should be sent to Medknow Publications, [email protected]. The journal reserves the right to reject any advertisement considered unsuitable according to the set policies of the journal. GENERAL INFORMATION The appearance of advertising or product information in the various sections in the journal does not constitute an endorsement or approval by the journal and/or its publisher of the quality or value of the said product or of claims made for it by its manufacturer. Copyright The entire contents of the Anesthesia: Essays and Researches are protected under Indian and international copyrights. The Journal, however, grants to all users a free, irrevocable, worldwide, perpetual right of access to, and a license to copy, use, distribute, perform and display the work publicly and to make and distribute derivative works in any digital medium for any reasonable non-commercial purpose, subject to proper attribution of authorship and ownership of the rights. The journal also grants the right to make small numbers of printed copies for their personal non-commercial use. Permissions For information on how to request permissions to reproduce articles/information from this journal, please visit http://www. aeronline.org Disclaimer The information and opinions presented in the Journal reflect the views of the authors and not of the Journal or its Editorial Board or the Publisher. Publication does not constitute endorsement by the journal. Neither the Anesthesia: Essays and Researches nor its publishers nor anyone else involved in creating, producing or delivering the Anesthesia: Essays and Researches or the materials contained therein, assumes any liability or responsibility for the accuracy, completeness, or usefulness of any information provided in the Anesthesia: Essays and Researches, nor shall they be liable for any direct, indirect, incidental, special, consequential or punitive damages arising out of the use of the Anesthesia: Essays and Researches. The Anesthesia: Essays and Researches, nor its publishers, nor any other party involved in the preparation of material contained in the Anesthesia: Essays and Researches represents or warrants that the information contained herein is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from the use of such material. Readers are encouraged to confirm the information contained herein with other sources. Addresses Editorial office Mohamad Said Maani Takrouri, Department of Anesthesia, King Fahad Medical City, P.O. Box 59046, Riyadh 11525, Kingdom Saudi Arabia. Phone: +96612889999 Fax: +96612889999 E-mail: [email protected] Website: www.aeronline.org Published by Medknow Publications and Media Pvt. Ltd. B5-12, Kanara Business Centre, Off Link Road, Ghatkopar (East), Mumbai – 400075, India. Phone: 91-22-66491818 Website: www.medknow.com Printed at ???
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Anesthesia: Essays and Researches - JournalOnWeb

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
ii
EDITORIAL BOARDEditor-in-ChiefMohamad Said Maani TakrouriRiyadh, [email protected]
Arab National EditorsYehia H. [email protected]
Bashir A. AtiyatAmman, [email protected]
Izdiad BadranAmman, [email protected]
Jamal Sharif AlshanablehAmman, [email protected]
Maroun GhabachBeirut, [email protected]
Marie-Claire Antakly Beirut [email protected]
Mohamed A. SerajRiyadh, KSA
Dhafer AlkhudairiRiyadh, KSA
Bassam Al-BarzangiUAEEmail. [email protected]
MembersMohammed Saleh Ben Ammar Tunisia
Bourhan Al AbedSyria
Mohamad Taha Al Jasir Syria
Hussein Abukhudeir Jordan
Abdelmajid Daoud Tunisia
Ahmad Sibti Morocco
Dina BaroudiSyria, USA, KSA
Anesthesia: Essays and ResearchesOfficial Publication of Pan Arab Federation of Societies of Anesthologists
July - December 2011, Vol. 5, Issue 2 ISSN: 0259-1162, E-ISSN: 2229-7685
The journalAnesthesia: Essays and Researches (ISSN: Print-0259-1162; Online 2229-7685) is peer-reviewed journal published on behalf of Pan Arab Federation of Societies of Anesthesiologists. The journal publishes articles on the subject of Anesthesia, pharmacology, physiology. pain management and intensive care. The Journal is published semiannually (in the third week of June and December).
Abstracting and indexing informationThe journal is indexed with Caspur, EBSCO Publishing’s Electronic Databases, Expanded Academic ASAP, Genamics JournalSeek, Google Scholar, Health & Wellness Research Center, Health Reference Center Academic, Hinari, Index Copernicus, OpenJGate, PrimoCentral, ProQuest, SCOLOAR, SIIC databases, Summon by Serial Solutions and Ulrich’s International Periodical Directory.
Information for authorsThere are no page charges for submissions to the journals. Please check http://www.aeronline.org for details.All manuscripts must be submitted online at www.journalonweb.com/aer
Subscription informationCopies of the journal provided free of cost to the members of Pan Arab Federation of Societies of Anesthesiologists. A subscription to Anesthesia: Essays and Researches comprises 2 issues. Prices include postage. Annual Subscription Rate for non-members-
• Institutional: INR2000.00forIndia USD 160.00 for outside India• Personal: INR1000.00forIndia USD 100.00 for outside India
For mode of payment and other details, please visit www.medknow.com/subscribe.asp.
Claims for missing issues will be serviced at no charge if received within 60 days of the cover date for domestic subscribers, and 3 months for subscribers outside India. Duplicate copies cannot be sent to replace issues not delivered because of failure to notify publisher of change of address.
The journal is published and distributed by Medknow Publications and Media Pvt. Ltd. Copies are sent to subscribers directly from the publisher’s address. It is illegal to acquire copies from any other source. If a copy is received for personal use as a member of the association/society, one cannot resale or give-away the copy for commercial or library use.
The copies of the journal to the members of the association are sent by ordinary post. The editorial board, association or publisher will not be responsible for non receipt of copies. If any member/subscriber wishes to receive the copies by registered post or courier, kindly contact the publisher’s office. If a copy returns due to incomplete, incorrect or changed address of a member/subscriber on two consecutive occasions, the names of such members will be deleted from the mailing list of the journal. Providing complete, correct and up-to-date address is the responsibility of the member/subscriber.
Advertising policiesThe journal accepts display and classified advertising. Frequency discounts and special positions are available. Inquiries about advertising should be sent to Medknow Publications, [email protected].
The journal reserves the right to reject any advertisement considered unsuitable according to the set policies of the journal.
G E N E R A L I N F O R M A T I O NThe appearance of advertising or product information in the various sections in the journal does not constitute an endorsement or approval by the journal and/or its publisher of the quality or value of the said product or of claims made for it by its manufacturer.
Copyright
The entire contents of the Anesthesia: Essays and Researches are protected under Indian and international copyrights. The Journal, however, grants to all users a free, irrevocable, worldwide, perpetual right of access to, and a license to copy, use, distribute, perform and display the work publicly and to make and distribute derivative works in any digital medium for any reasonable non-commercial purpose, subject to proper attribution of authorship and ownership of the rights. The journal also grants the right to make small numbers of printed copies for their personal non-commercial use.
Permissions
For information on how to request permissions to reproduce articles/information from this journal, please visit http://www.aeronline.org
Disclaimer
The information and opinions presented in the Journal reflect the views of the authors and not of the Journal or its Editorial Board or the Publisher. Publication does not constitute endorsement by the journal. Neither the Anesthesia: Essays and Researches nor its publishers nor anyone else involved in creating, producing or delivering the Anesthesia: Essays and Researches or the materials contained therein, assumes any liability or responsibility for the accuracy, completeness, or usefulness of any information provided in the Anesthesia: Essays and Researches, nor shall they be liable for any direct, indirect, incidental, special, consequential or punitive damages arising out of the use of the Anesthesia: Essays and Researches. The Anesthesia: Essays and Researches, nor its publishers, nor any other party involved in the preparation of material contained in the Anesthesia: Essays and Researches represents or warrants that the information contained herein is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from the use of such material. Readers are encouraged to confirm the information contained herein with other sources.
Addresses
Editorial officeMohamad Said Maani Takrouri, Department of Anesthesia, King Fahad Medical City, P.O. Box 59046, Riyadh 11525, Kingdom Saudi Arabia. Phone: +96612889999 Fax: +96612889999 E-mail: [email protected] Website: www.aeronline.org
Published by Medknow Publications and Media Pvt. Ltd. B5-12, Kanara Business Centre, Off Link Road, Ghatkopar (East), Mumbai – 400075, India. Phone: 91-22-66491818 Website: www.medknow.com
Printed at
???

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
ii
C O N T E N T S
EditorialPediatric Neurosurgery, special attention is required!Raed A. Alsatli ....................................................................................................................... 127
Review ArticleCurrent role of dexmedetomidine in clinical anesthesia and intensive careManpreet Kaur, P. M. Singh ........................................................................................................ 128
Original ArticlesPalonosetron and palonosetron plus dexamethasone to prevent postoperative nausea and vomiting in patients undergoing laparoscopic cholecystectomy: A prospective, randomized, double-blind comparative studySoumyendu Ghosh, Anirban Pal, Amita Acharya, Chaitali Biswas, Tirtha Ratan Ghosh, Subhabrata Ghosh ........... 134
Efficacy of thoracic epidural anesthesia for laparoscopic cholecystectomyAmit Gupta, Kumkum Gupta, Prashant K. Gupta, Nivesh Agarwal, Bhawna Rastogi ...................................... 138
Wound infiltration with plain bupivacaine as compared with bupivacaine fentanyl mixture for postoperative pain relief after abdominal surgeryReetika Chander, Dootika Liddle, Baljinder Kaur, Mary Varghese ............................................................ 142
A double-blind study on analgesic effects of fentanyl combined with bupivacaine for extradural labor analgesiaGaurav S. Tomar, Rajan B. Godwin, Neeraj Gaur, Ashish Sethi, Neeraj Narang, Veena Kachhwaha, T. C. Kriplani, Akhilesh Tiwari .................................................................................................... 147
Coma in the elderly: Etiological factors, management, and prognosis in the department of anesthesia and intensive careD. Diango, M. Moghomaye, Y. Maiga, S. A. Beye, A. S. Dembele, Y. Coulibaly, A. Diallo ................................. 153
A comparative study of efficacy of oral nonsteroidal antiinflammatory agents and locally injectable steroid for the treatment of plantar fasciitisChaitali Biswas, Anirban Pal, Amita Acharya .................................................................................... 158
Do pencil-point spinal needles decrease the incidence of postdural puncture headache in reality? A comparative study between pencil-point 25G Whitacre and cutting-beveled 25G Quincke spinal needles in 320 obstetric patientsAnirban Pal, Amita Acharya, Nidhi Dawar Pal, Satrajit Dawn Jhuma Biswas ............................................... 162
Comparison between preemptive gabapentin and paracetamol for pain control after adenotonsillectomy in childrenSabry M. Amin, Yasser M. Amr ..................................................................................................... 167
Intrathecal nalbuphine as an adjuvant to subarachnoid block: What is the most effective dose?Arghya Mukherjee, Anirban Pal, Jitendra Agrawal, Amrita Mehrotra, Nidhi Dawar ....................................... 171
Comparison of sodium diclofenac, ketamine and propofol with fentanyl and midazolam in balanced anaesthesiaMozaffar Rabiee, Ebrahim Alijanpour, Ali Jabbari, Farzan Khirkhah, Yousof Mortazavi, Ali Bijani ..................... 176
Ondansetron, ramosetron, or palonosetron: Which is a better choice of antiemetic to prevent postoperative nausea and vomiting in patients undergoing laparoscopic cholecystectomy?Sarbari Swaika, Anirban Pal, Surojit Chatterjee, Debashish Saha, Nidhi Dawar ........................................... 182
Continuous spinal anesthesia with epidural catheters: An experience in the peripheryS. Parthasarathy, M. Ravishankar ................................................................................................. 187
July-December2011 Volume5 Issue2
Anesthesia: Essays and ResearchesOfficial Publication of Pan Arab Federation of Societies of Anesthologists

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
iiiiii
Comparison of intrathecal bupivacaine-fentanyl and bupivacaine-butorphanol mixtures for lower limb orthopedic proceduresBinay Kumar, Aparna Williams, Dootika Liddle, Mary Verghese .............................................................. 190
A comparison between intravenous paracetamol plus fentanyl and intravenous fentanyl alone for postoperative analgesia during laparoscopic cholecystectomyAnirban Hom Choudhuri, Rajeev Uppal .......................................................................................... 196
Case ReportsHeimlich’s maneuver-assisted bronchoscopic removal of airway foreign bodySohan Lal Solanki, Shivendu Bansal, Arvind Khare, Amit Jain ................................................................ 201
Giant cervical lipoma excision under cervical epidural anesthesia: A viable alternative to general anesthesiaRam Pal Singh, Aparna Shukla, Satyajeet Verma ............................................................................... 204
A very common case become rare: Anesthetic considerations of lepromatous leprosySandeep Sahu, Vipin Goyal, Sanjay Dhiraaj, Kamal Kishore, P. K. Singh ................................................... 207
Bronchospasm following supraclavicular brachial plexus blockRohini V. Bhat Pai, Harihar V. Hegde, M. C. B. Santosh, S. Roopa ........................................................... 211
Postoperative tension pneumocephalus following cerebral aneurysm surgery in supine position without prior lumbar drainageChaitali Biswas, Saswata Bharati, Anirban Pal .................................................................................. 214
Adrenal incidentaloma: Anesthetic management, the challenge and the outcomeReema M. Al-Hadhrami, Nehal Gahndour, Sherine Qudeera, Maher Moazin, Razan Nafakh ............................. 217
Dexmedetomidine and fentanyl combination for procedural sedation in a case of Duchenne muscular dystrophyAshish Kulshrestha, Sukhminder Jit Singh Bajwa, Amarjit Singh, Vinod Kapoor ........................................... 224
Amniotic fluid embolism: A diagnostic dilemmaAshish Kulshrestha, Megha Mathur ............................................................................................... 227
Commentary Amniotic fluid embolism: A catastrophic problem in need of a prepared team with a plan Karen Nelson DO, Michael S. Firstenberg ................................................................................ 230
Hemoglobin drop after anesthesia in craniosynstosis – Dilemma of operate or not to operateNihal El-Ghandour, Salah Kassem, Abdelrahman J. Al Sabbagh, Ayman Al-Banyan, Firas A. Shubbak, Ahmad Hassib, Hazem Zaki ....................................................................................................... 233
Historical ReportHistorical report account on the development of anesthesiology and medical services in Kingdom Saudi Arabia 1956–1987: M. I. Al-Khawashki’s letter dated April 25th 1997Mohamad Said Maani Takrouri, Farah Maani Takrouri .......................................................................... 236
Letters to EditorBone cement implantation syndrome: A rare catastropheNikhil Mudgalkar, K. V. Ramesh ................................................................................................... 240
Central venous catheter placement: An alternative of Certodyn® (Universal Adapter)Manish Jain, Bhavana Rastogi, V. P. Singh, Kumkum Gupta ................................................................... 242
Rare artifacts mimicking sinus tachycardia in a case of vaginal hysterectomy with situs inversus totalisSukhminder Jit Singh Bajwa, Sukhwinder Kaur Bajwa, Jasbir Kaur, Amarjit Singh ....................................... 244
An unusual foreign body in breathing circuit detected by capnographyShivendu Bansal, Sohan Lal Solanki, Rupesh Yadav ............................................................................ 245
Anesthesia view of hematuria associated with cell saver use during scoliosis surgeryManal Bakhsh, Muaz Al Ghadir, Razan Naffakh, Nahid El-Bakri .............................................................. 247
Author Index, 2011 .............................................................................................................. 249
Title Index, 2011 .................................................................................................................. 250

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
iv
Anesthesia: Essays and Researches on Web
http://www.journalonweb.com/aer
Anesthesia: Essays and Researches now accepts articles electronically. It is easy, convenient and fast. Check following steps:
Advantages
•Any-time, any-where access•Faster review•Cost saving on postage•No need for hard-copy submission (except
on acceptance images should be sent)•Ability to track the progress•Ease of contacting the journal
•Submission of new articles with images•Submission of revised articles•Checking of proofs•Track the progress of article in review
process
Facilities
Help
•Check Frequently Asked Questions (FAQs) on the site
•In case of any difficulty contact the editor
Online submission checklist
•First Page File (text/rtf/doc/pdf file) with title page, covering letter, acknowledge-ment, etc.
•Article File (text/rtf/doc/pdf file) - text of the article, beginning from Title, Abstract till References (including tables). File size limit 1 MB. Do not include images in this file.
•Images (jpeg): Submit good quality colour images. Each image should be less than 4096 kb (4 MB) in size.
Requirements for usage
•Computer and internet connection•Web-browser (preferably newer versions -
IE 5.0 or NS 4.7 and above)•Cookies and javascript to be enabled in
web-browser
1 Registration•Register from http://www.journalonweb.com/aer as a new
author (Signup as author)•Two-step self-explanatory process
2 New article submission
•Prepare your files (Article file, First page file and Images, if any)
•Login into your area•Click on ‘Submit a new article’ under ‘New Article’•Follow the steps (three steps for article without images and five
for with images)•On successful submission you will receive an acknowledgement
quoting the manuscript numbers
3 Tracking the progress•Click on ‘In Review Article’ under ‘Submitted Articles’•The table gives status of the article and its due date to move to
next phase•More details can be obtained by clicking on the ManuscriptID•Comments sent by the editor and referee will be available from
these pages
4 Submitting a revised article
•Click on ‘Article for Revision’ under ‘Submitted Articles’•Click on ‘Revise’•From the first window, you can modify Article Title, Article Type•First Page file and Images could be modified from second and
third window, respectively•The fourth step is uploading the revised article file.•Include the referees’ comments along with the point to point
clarifications at the beginning of the revised article file. •Do not include authors’ name in the article file. •Upload the revised article file against New Article File - Browse,
choose your file and then click Upload OR Click Finish•On completion of revision process you will be able to check the
latest file uploaded from Article Cycle (In Review Articles-> Click on manuscript id -> Latest file will have a number with ‘R’)

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
127
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
lung atelectases and ventilatory difficulties, respiratory acidosis, and sepsis.
Bonhomme et al., reported a hematocrit threshold of 21%, below which transfusion is indicated, but the above-mentioned blood salvage techniques should be appropriately implemented, to avoid or reduce homologous blood transfusion.[3]
It is very important to build up an anesthesia management plan before surgery; this plan has to consider the perioperative risk factors related to the operation in this specific child, evaluation of the preoperative condition, airway assessment, and invasive management techniques, such as, arterial line and central venous catheter. Important information can be obtained from the surgeon about the surgical plan, which may affect the anesthetic plan. Finally, the parents of the child have to be informed about the possible intra- and postoperative anesthesia risks.
Good preoperative assessment, correct intraoperative and ICU management plan, and teamwork with the surgeon and intensivist are the key issues to achieve a successful end result.
Raed A. AlsatliDepartment of Cardiac Science,
King Saud University, College of Medicine, Riyadh, Kingdom of Saudi Arabia
E-mail: [email protected]
REFERENCES
1. Velardi F, Di Chirico A, Di Rocco C. Blood salvage in craniosynostosis surgery. Child Nerv Syst 1999;15:695-710.
2. El-Ghandour N, Kassem S, Al Sabbagh AJ, Al-Banyan A, Shubbak FA, Hassib A, et al. Hemoglobin drop after anesthesia in craniosynstosis: Dilemma of operate or not to operate. Anesth Essays Res 2011;5:233-5.
3. Bonhomme V, Damas F, Born JD, Hans P. Perioperative management of blood loss during surgical treatment for craniosynostosis. Ann Fr Anesth Reanim 2002;21:119-25.
Pediatric neurosurgical operations carry a considerable risk of bleeding in the perioperative period. This risk is related to several factors, such as, the nature of surgery, preoperative hemoglobin level, and body weight of the patient.
Bleeding is a major risk intra- and postoperatively, affecting the hemodynamic stability, oxygen carrying capacity, and consequently morbidity and mortality.
The anesthetist has to have a clear plan regarding the perioperative management of blood loss, including preoperative autologous blood donation, erythropoietin administration, and normovolemic hemodilution. Intraoperative management during surgery should include precise evaluation of blood losses, hematocrit measurements at regular intervals, autologous blood transfusion and homologous blood transfusion, which has to extend into the postoperative phase.[1]
In this issue, a case report of craniosynostosis undergoing a corrective surgery has been reported.[2] Difficult intubation due to high larynx was encountered. The surgery was quite complicated: Pansynostosis orbital bar advancement, frontal expansion, and right optic canal deroofing. The operation lasted for 10 hours with blood loss of about 90% of the patient’s estimated red cell mass.
Apart from postoperative blood loss in the Intensive Care Unit, the postoperative course was complicated with sever
Editorial
Pediatric Neurosurgery, special attention is required!
AER_73_11
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AP Done 27th Jan

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
128
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Review Article
Current role of dexmedetomidine in clinical anesthesia and intensive careManpreet Kaur, P. M. Singh1
Department of Anaesthesia and Critical Care, All India Institute of Medical Sciences, J.P.N.A Trauma Centre, 1Department of Anaesthesia and Critical Care, All India Institute of Medical Sciences, New Delhi, India
Corresponding author: Dr. Manpreet Kaur, Department of Anaesthesia, All India Institute of Medical Sciences, J.P.N.A Trauma Centre, New Delhi - 110 029, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_30_11R16
AbstractDexmedetomidine is a new generation highly selective α2-adrenergic receptor (α2-AR) agonist that is associated with sedative and analgesic sparing effects, reduced delirium and agitation, perioperative sympatholysis, cardiovascular stabilizing effects, and preservation of respiratory function. The aim of this review is to present the most recent topics regarding the advantages in using dexmedetomidine in clinical anesthesia and intensive care, while discussing the controversial issues of its harmful effects.
Key words: Dexmedetomidine, intensive care unit sedation, α2-adrenergic receptor agonist
INTRODUCTION
α2-adrenergic receptor (α2-AR) agonists have been successfully used in several clinical settings in view of diverse actions which include sedation, analgesia, anxiolysis, perioperative sympatholysis, cardiovascular stabilizing effects, reduced anesthetic requirements, and preservation of respiratory function.[1] Dexmedetomidine is a relatively new drug approved at the end of 1999 by the Food and Drug Administration (FDA) for humans use for short-term sedation and analgesia (<24 hours) in the intensive care unit (ICU). Dexmedetomidine is a useful sedative agent with analgesic properties, hemodynamic stability and ability to recover respiratory function in mechanically ventilated patients facilitating early weaning.[2] Besides being a new modality of sedation and analgesia in
ICU patient management,[3] it has been studied in several other perioperative settings, which will be discussed.
CHEMICAL STRUCTURE
Dexmedetomidine is the dextrorotatory S-enantiomer of medetomidine, an agent used in veterinary medicine. [4] It is chemically (S)-4-[1-(2,3-dimethylphenyl) ethyl]-3H-imidazole [Figure 1].
Figure 1: Chemical structure of dexmedetomidine

129
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Kaur and Singh: Current role of dexmedetomidine in clinical anesthesia and intensive care
MECHANISM OF ACTION
α2-AR agonists produce clinical effects after binding to G-Protein-coupled α2-AR, of which there are three subtypes (α2A, α2B, and α2C) with each having different physiological functions and pharmacological activities. These receptor subtypes are found ubiquitously in the central, peripheral, and autonomic nervous systems, as well as in vital organs and blood vessels. [5] Dexmedetomidine is 8 to 10 times more selective towards α2-AR than clonidine.[6] Neither clonidine nor dexmedetomidine is totally selective for any one of the α2-AR subtypes, but dexmedetomidine seems to have higher α2A-AR and α2C-AR affinity than clonidine.[7] Major differences in the pharmacology of clonidine and dexmedetomidine have been described in [Table 1].
Locus ceruleus of the brain stem is the principal site for the sedative action and spinal cord is the principal site for the analgesic action, both acting through α2A-AR. In the heart, the dominant action of α2-AR agonists is a decrease in tachycardia (through blocking cardioaccelerator nerve) and bradycardia via α2A-AR (through a vagomimetic action). In the peripheral vasculature, there is sympatholysis-mediated vasodilatation and smooth muscle cells receptor-mediated vasoconstriction.[8] The mechanism for the antishivering and diuretic actions has yet to be established firmly[9] [Figure 2].
The responses to activation of the receptors in other areas include decreased salivation, decreased secretion, and decreased bowel motility in the gastrointestinal
tract; contraction of vascular and other smooth muscle; inhibition of renin release, increased glomerular filtration, and increased secretion of sodium and water in the kidney; decreased intraocular pressure; and decreased insulin release from the pancreas.[10] Combining all these effects, dexmedetomidine avoids some of the side effects of multiagent therapies.
PHARMACOKINETICS
Absorption and distributionDexmedetomidine exhibits linear pharmacokinetics in the recommended dose range of 0.2 to 0.7 μg/ kg/ hr administered as intravenous infusion up to 24 hours. The distribution phase is rapid, with a half-life of distribution of approximately 6 minutes and elimination half life of 2 hours. The steady-state volume of distribution is 118 L. The average protein binding is 94% and is constant across the different plasma concentrations and also similar in males and females. It has negligible protein binding displacement by drugs commonly used during anesthesia and in the ICU like fentanyl, ketorolac, theophylline, digoxin, and lidocaine. [10] Context-sensitive half life ranges from 4 minutes after a 10-minute infusion to 250 minutes after an 8-hour infusion. Oral bioavailability is poor because of extensive first-pass metabolism. However, bioavailability of sublingually administered dexmedetomidine is high (84%), offering a potential role in pediatric sedation and premedication.[11]
Metabolism and excretionDexmedetomidine undergoes almost complete biotransformation through direct N-glucuronidation and cytochrome P-450 (CYP 2A6)-mediated aliphatic hydroxylation to inactive metabolites. Metabolites are excreted in the urine (about 95%) and in the feces (4%). [10] Dose adjustments are required in patients with hepatic failure because of lower rate of metabolism.
Table 1: Comparison of clonidine with dexmedetomidineClonidine DexmedetomidineDeveloped in the 1960s Developed in the 1980s
Clinically used first as antihypertensive in 1966
Clinically approved as sedative and analgesic used in ICU in 1999
Ratio α 2:α 1 receptor binding is 220:1
Dexmedetomidine is 7-8 times more specific for a2.Ratio α 2:α 1 receptor binding is 1620:1
Clonidine is a partial agonist at the α 2 adrenergic receptor
Dexmedetomidine is a full agonist at the α 2 adrenergic receptor
Octanol/buffer partition coefficient: 0.8
Octanol/buffer partition coefficient: 2.8 more lipophilic (3.5-fold) than clonidine
The maximum reduction in inhalational anesthetic requirement to maintain 1 MAC provided by clonidine is 50%
Dexmedetomidine has been shown to result in approximately a 90% reduction in inhalational anesthetic requirement to maintain 1 MAC
Plasma half-life is T½: 9-12 hours Plasma half-life T½: 2-2.5 hours
Protein binding: 50% Protein binding: 94%
Elimination half life is 8 hrs Elimination half life is 2 hrs
Distribution half life is >10 min Distribution half life is 5 min Figure 2: Physiology of various α2-adrenergic receptors

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
130
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Kaur and Singh: Current role of dexmedetomidine in clinical anesthesia and intensive care
CLINICAL PHARMACOLOGY
Cardiovascular systemDexmedetomidine evokes a biphasic blood pressure response: A short hypertensive phase and subsequent hypotension. The two phases are considered to be mediated by two different α2-AR subtypes: the α-2B AR is responsible for the initial hypertensive phase, whereas hypotension is mediated by the α2A-AR.[12] In younger patients with high levels of vagal tone, bradycardia and sinus arrest have been described which were effectively treated with anticholinergic agents (atropine, glycopyrrolate).
Central nervous systemDexmedetomidine reduces cerebral blood flow and cerebral metabolic requirement of oxygen but its effect on intracranial pressure (ICP) is not yet clear. Dexmedetomidine modulates spatial working memory, enhancing cognitive performance besides having sedative, analgesic, and anxiolytic action through the α2-AR.[13] Studies suggest the likelihood of its neuroprotective action by reducing the levels of circulating and brain catecholamines and thus balancing the ratio between cerebral oxygen supplies, reducing excitotoxicity, and improving the perfusion in the ischemic penumbra. It reduces the levels of the glutamate responsible for cellular brain injury, especially in subarachnoid hemorrhage.[14] It has been shown to limit the morphologic and functional effects after ischemic (focal and global) and traumatic injury to the nervous system.
Respiratory effectsDexmedetomidine affect on respiration appears to be similar in order of magnitude to those seen in the heavy sleep state. [15] Dexmedetomidine does not suppress respiratory function, even at high doses.[16] It has no adverse effects on respiratory rate and gas exchange when used in spontaneously breathing ICU patients after surgery.[15] It helps in maintaining sedation without cardiovascular instability or respiratory drive depression and hence may facilitate weaning and extubation in trauma/surgical ICU patients who have failed previous attempts at weaning because of agitation and hyperdynamic cardiopulmonary response.[2,17]
Endocrine and renal effectsDexmedetomidine activates peripheral presynaptic α2- AR which reduces the release of catecholamines, and hence reduces sympathetic response to surgery.[18] Animal studies have demonstrated the occurrence of natriuresis and diuresis. Dexmedetomidine is an imidazole agent but unlike etomidate, it does not appear to inhibit steroidogenesis when used as an infusion for short-term sedation.[19]
ADVERSE EFFECTS
The various reported side effects are hypotension, hypertension, nausea, vomiting, dry mouth, bradycardia,
atrial fibrillation, pyrexia, chills, pleural effusion, atelectasis, pulmonary edema, hyperglycemia, hypocalcaemia, acidosis, etc. Rapid administration of dexmedetomidine infusion (Loading dose of 1 μ/ kg/ hr if given in less than 10 minutes) may cause transient hypertension mediated by peripheral α2B- AR vasoconstriction.[5] But hypotension and bradycardia may occur with ongoing therapy mediated by central
α2A-AR, causing decreased release of noradrenaline from the sympathetic nervous system. Long-term use of dexmedetomidine leads to super sensitization and upregulation of receptors; so, with abrupt discontinuation, a withdrawal syndrome of nervousness, agitation, headaches, and hypertensive crisis can occur.[20] Dexmedetomidine is not recommended in patients with advanced heart block and ventricular dysfunction.[5] FDA has classified it as a category C pregnancy risk, so the drug should be used with extreme caution in women who are pregnant.
CLINICAL APPLICATIONS OF DEXMEDETOMIDINE
PremedicationDexmedetomidine is used as an adjuvant for premedication, especially in patients susceptible to preoperative and perioperative stress because of its sedative, anxiolytic, analgesic, sympatholytic, and stable hemodynamic profile. Dexmedetomidine decreases oxygen consumption in intraoperative period (up to 8%) and in postoperative period (up to 17%).[21] Premedication dose is 0.33 to 0.67 mg/kg IV given 15 minutes before surgery (this dose minimizes side effects of hypotension and bradycardia).
Intraoperative useDexmedetomidine attenuates hemodynamic stress response to intubation and extubation by sympatholysis. [15,22-24] In view of absent respiratory depression, it can be continued at extubation period unlike other drugs. Dexmedetomidine potentiates anesthetic effect of all the anesthetic agents irrespective of the mode of administration (intravenous, inhalation, regional block). Intraoperative administration of dexmedetomidine in lower concentrations has reduced the requirement of other anesthetic agents; fewer interventions to treat tachycardia; and a reduction in the incidence of myocardial ischemia.[23] However, side effects like bradycardia and hypotension are limitations to its use necessitating need for pharmacological rescue therapy. These effects may be attributed to the combined properties of volatile anesthetics such as vasodilatation and myocardial depression. Dexmedetomidine administered in high concentrations may cause systemic and pulmonary hypertension because of direct peripheral vascular effects or may compromise myocardial function and blood pressure.

131
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Kaur and Singh: Current role of dexmedetomidine in clinical anesthesia and intensive care
Locoregional analgesiaHighly lipophilic nature of dexmedetomidine allows rapid absorption into the cerebrospinal fluid and binding to α2-AR of spinal cord for its analgesic action. It prolongs the duration of both sensory and motor blockade induced by local anesthetics irrespective of the route of administration (e.g., epidural,[25] caudal,[26] or spinal[27]). Dexmedetomidine though enhances both central and peripheral neural blockade by local anesthetics;[27] however, the peripheral neural blockade is due to its binding to α2A-AR.[28] Dexmedetomidine has been successfully used in intravenous regional anesthesia (IVRA),[29] brachial plexus block,[30] and intraarticularly. [31,32] Addition of 0.5 μg/kg dexmedetomidine to lidocaine for IVRA improves quality of anesthesia and improves intraoperative-postoperative analgesia without causing side effects.[29] Dexmedetomidine added to levobupivacaine for axillary brachial plexus block shortens the onset time and prolongs the duration of the block and postoperative analgesia.[30] Intraarticular dexmedetomidine in patients undergoing arthroscopic knee surgery improves the quality and duration of postoperative analgesia.[31,32]
Sedation in intensive care unitDexmedetomidine has become popular sedative agent in ICU because of its ability to produce cooperative sedation, i.e., patients remain awake, calm, and are able to communicate their needs. It does not interfere with the respiratory drive or produce any agitation, hence facilitating early weaning from ventilator, thereby reducing overall ICU stay costs.[33] The maintenance of natural sleep during sedation might speed recovery time in the ICU. Dexmedetomidine currently is approved by FDA for use in ICU for not more than 24 hours; though many studies have reported its safe use for longer duration.[34] Dexmedetomidine, when compared with conventional sedatives and opiates [Table 2], has been demonstrated to be associated with both sedative and analgesic sparing effects, reduced delirium and agitation, minimal respiratory depression, and desirable cardiovascular effects.[2,35,36]
Procedural sedationDexmedetomidine is an attractive agent for short-term procedural sedation and has been safely used in transesophageal echocardiography,[37] colonoscopy,[38] awake carotid endarterectomy,[39] shockwave lithotripsy,[34] vitreoretinal surgery,[40] elective awake fiberoptic intubation,[41] pediatric patients undergoing tonsillectomy,[42] and pediatric MRI.[43] The usual dose of dexmedetomidine for procedural sedation is 1 μg/ kg, followed by an infusion of 0.2 μg/kg/h. Its onset of action is less than 5 minutes and the peak effect occur within 15 minutes. As the pharmacologic effects of dexmedetomidine can be reversed by the α2-AR antagonist atipamezole,[44] dexmedetomidine provides a titratable form of hypnotic sedation that can be readily reversed.
Controlled hypotensionDexmedetomidine is an effective and safe agent for controlled hypotension mediated by its central and peripheral sympatholytic action. Its easy administration, predictability with anesthetic agents, and lack of toxic side effect while maintaining adequate perfusion of the vital organs makes it a near-ideal hypotensive agent. Spinal fusion surgery for idiopathic scoliosis,[45] septoplasty and tympanoplasty operations,[46] and maxillofacial surgery[47] have been safely done with dexmedetomidine-controlled hypotension.
AnalgesiaDexmedetomidine activates α2-AR in the spinal cord reducing transmission of nociceptive signals like substance P. It has significant opioid sparing effect and is useful in intractable neuropathic pain.[14]
Cardiac surgeryDexmedetomidine in addition to blunting the hemodynamic response to endotracheal intubation also reduces the extent of myocardial ischemia during cardiac surgery.[48] Dexmedetomidine has been successfully used to manage patients with pulmonary hypertension undergoing mitral valve replacement, with reduction in pulmonary vascular resistance, pulmonary artery pressure, and pulmonary capillary wedge pressures.[5]
Table 2: Comparison of dexmedetomidine with other ICU sedativesEffects Dexmedetomidine Benzodiazepines Propofol Opioids HaloperidolSedation √ √ √ √ √
Analgesia √ √
Alleviation of anxiety √ √
Cooperative sedation √
Facilitation of ventilation during weaning
√
No respiratory depression √ √
Control of delirium √ √
Organ protection √ √
Control of stress response √
Antishivering agent √
Mimicking of natural sleep √ Based on data from Pandharipande et al.[36]

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
132
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Kaur and Singh: Current role of dexmedetomidine in clinical anesthesia and intensive care
NeurosurgeryDexmedetomidine provides stable cerebral hemodynamics without sudden increase in ICP during intubation, extubation, and head pin insertion. It attenuates neurocognitive impairment (delirium and agitation) allowing immediate postoperative neurological evaluation. It exerts its neuroprotective effects through several mechanisms which make the usage of this drug a promising tool during cerebral ischemia.[14] It does not interfere with neurological monitors[5] and has an upcoming role in “functional” neurosurgery. This includes awake craniotomy for the resection of tumors or epileptic foci in eloquent areas, and the implantation of deep brain stimulators for Parkinson’s disease.[5]
ObesityDexmedetomidine does not cause respiratory depression and has been infused at a dose of 0.7 μg/kg intraoperatively to avoid respiratory depression due to narcotic usage in a morbidly obese patient.[49]
ObstetricsDexmedetomidine has been successfully used as an adjunct to unsatisfactory analgesia by systemic opioids in laboring parturients who could not benefit from epidural analgesia.[50] It provides maternal hemodynamic stability, anxiolysis, and stimulation of uterine contractions. It is retained in placental tissue and passes less readily into the fetal circulation than clonidine because of high lipophilicity and thereby has less susceptibility to cause fetal bradycardia.
PediatricsIt is currently being used off-label as an adjunctive agent in pediatric patients for sedation and analgesia in the critical care unit and for sedation during noninvasive procedures in radiology like computed tomography and magnetic resonance imaging.[43]
Other usesThe literature suggests other potential uses for dexmedetomidine, for example• Dexmedetomidine has been used successfully in
the treatment of withdrawal from benzodiazepines, opioids, alcohol, and recreational drugs.
• As an adjunct in otorhinolaryngology anesthesia formiddle ear surgery and rhinoplasty.
• Asanadjunctintherepairofaorticaneurysms.• ManagementoftetanusinICU.• Asanantishiveringagent.• Dexmedetomidine is effective in preventing ethanol-
induced neurodegeneration.
CONCLUSION
Dexmedetomidine because of its unique properties offers its promising use in wide spectrum of clinical settings and
ICUs. It is a part of fast-tracking anesthesia regimens and offers anesthetic sparing and hemodynamic stabilizing effects. As pharmacological effects of dexmedetomidine can be reversed by α2-AR antagonist atipamezole, combination of dexmedetomidine and atipamezole can provide titratable form of sedation in the future.
REFERENCES
1. Kemp KM, Henderlight L, Neville M. Precedex: Is it the future of cooperative sedation? Nursing 2008;38 Suppl Critical:7-8.
2. Takrouri MS, Seraj MA, Channa AB, el-Dawlatly AA, Thallage A, Riad W, et al. Dexmedetomidine in intensive care unit: A study of hemodynamic changes. Middle East J Anesthesiol 2002;16:587-95.
3. Takrouri MS. New concepts in intensive care: Dexmedetomidine and immunonutrition. Middle East J Anesthesiol 2002;16:567-72.
4. Dexmedetomidine. Available from: http://en.wikipedia.org/wiki/Dexmedetomidine [Last accessed on 2011 March 18].
5. Afsani N. Clinical application of dexmedetomidine. S Afr J Anaesthesiol Analg 2010;16:50-6.
6. Wagner DS, Brummett CM. Dexmedetomidine: As safe as safe can be. Semin Anesth Perioper Med Pain 2006;25:77-83.
7. Fairbanks CA, Stone LS, Wilcox GL. Pharmacological profiles of alpha 2 adrenergic receptor agonists identified using genetically altered mice and isobolographic analysis. Pharmacol Ther 2009;123:224-38.
8. Macdonald E, Koblka BK, Scheinin M. Gene targeting–homing in on alpha 2-adrenoceptor-subtype function. Trends Pharmacol Sci 1997;18:211-9.
9. Kamibayashi T, Maze M. Clinical Uses of a2-Adrenergic Agonists. Anesthesiology 2000;93:1345-9.
10. Gertler R, Brown HC, Mitchell DH, Silvius EN. Dexmedetomidine: A novel sedative-analgesic agent. Proc (Bayl Univ Med Cent) 2001;14:13-21.
11. Anttila M, Penttilä J, Helminen A, Vuorilehto L, Scheinin H. Bioavailability of dexmedetomidine after extravascular doses in healthy subjects. Br J Clin Pharmacol 2003;56:691-3.
12. Philipp M, Brede M, Hein L. Physiological significance of alpha(2)-adrenergic receptor subtype diversity: One receptor is not enough. Am J Physiol Regul Integr Comp Physiol 2002;283: R287-95.
13. Franowicz JS, Arnsten AF. The alpha-2a noradrenergic agonist, guanfacine, improves delayed response performance in young adult rhesus monkeys. Psychopharmacology (Berl) 1998;136:8-14.
14. Bekker A, Sturaitis MK. Dexmedetomidine for neurological surgery. Neurosurgery 2005;57:1-10.
15. Venn RM, Hell J, Grounds RM. Respiratory effects of dexmedetomidine in the surgical patient requiring intensive care. Crit Care 2000;4:302-8.
16. Hsu YW, Cortinez LI, Robertson KM, Keifer JC, Sum-Ping ST, Moretti EW, et al. Dexmedetomidine pharmacodynamics: Part I: Cross-over comparison of the respiratory effects of dexmedetomidine and remifentanil in healthy volunteers. Anesthesiology 2004;101:1066-76.
17. Siobal MS, Kallet RH, Kivett VA, Tang JF. Use of dexmedetomidine to facilitate extubation in surgical intensive-care-unit patients who failed previous weaning attempts following prolonged mechanical ventilation: A pilot study. Respir Care 2006;51:492-6.
18. Ebert TJ, Hall JE, Barney JA, Uhrich TD, Colinco MD. The effects of increasing plasma concentrations of dexmedetomidine in humans. Anesthesiology 2000;93:382-94.
19. Venn R, Bryant A, Hall GM, Grounds RM. Effects of dexmedetomidine on adrenocortical function and the cardiovascular, endocrine and inflammatory responses in post-operative patients needing sedation in the intensive care unit. Br J Anaesth 2001;86:650-6.
20. Morgan GE, Mikhail MS, Murray MJ. Preoperative Medication in Clinical Anaethesia. In: Morgan GE, Mikhail MS, Murray MJ, Editors. 4th ed. New York: Mc graw Hill; 2006. p. 248.
21. Taittonen MT, Kirvela OA, Aantaa R, Kanto JH. Effect of clonidine and dexmedetomidine premedication on perioperative oxygen consumption and haemodynamic state. Br J Anaesth 1997;78:400-6.
22. Scheinin B, Lindgren L, Randell T, Scheinin H, Scheinin M. Dexmedetomidine attenuates sympathoadrenal responses to tracheal intubation and reduces the need for thiopentone and peroperative fentanyl. Br J Anaesth 1992;68:126-31.
23. Aho M, Lehtinen AM, Erkola O, Kallio A, Korttila K. The effect of intravenously administered dexmedetomidine on perioperative hemodynamics and

133
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Kaur and Singh: Current role of dexmedetomidine in clinical anesthesia and intensive care
isoflurane requirements in patients undergoing abdominal hysterectomy. Anesthesiology 1991;74:997-1002.
24. Guler G, Akin A, Tosun E, Eskitafloglu E, Mizrak A, Boyaci A. Single-dose dexmedetomidine attenuates airway and circulatory reflexes during extubation. Acta Anaesthesiol Scand 2005;49:1088-91.
25. Schnaider TB, Vieira AM, Brandao AC, Lobo MV. Intraoperative analgesic effect of epidural ketamine, clonidine or dexmedetomidine for upper abdominal surgery. Rev Bras Anestesiol 2005;55:525-31.
26. El-Hennawy AM, Abd-Elwahab AM, Abd-Elmaksoud AM, El-Ozairy HS, Boulis SR. Addition of clonidine or dexmedetomidine to bupivacaine prolongs caudal analgesia in children. Br J Anaesth 2009;103:268-74.
27. Kanazi GE, Aouad MT, Jabbour-Khoury SI, Al Jazzar MD, Alameddine MM, Al-Yaman R, et al. Effect of low-dose dexmedetomidine or clonidine on the characteristics of bupivacaine spinal block. Acta Anaesthesiol Scand 2006;50:222-7.
28. Yoshitomi T, Kohjitani A, Maeda S, Higuchi H, Shimada M, Miyawaki T. Dexmedetomidine enhances the local anesthetic action of lidocaine via an alpha-2A adrenoceptor. Anesth Analg 2008;107:96-101.
29. Memiş D, Turan A, Karamanlıoglu B, Pamukçu Z, Kurt I. Adding Dexmedetomidine to Lidocaine for Intravenous Regional Anesthesia. Anesth Analg 2004;98:835-40.
30. Esmaoglu A, Yegenoglu F, Akin A, Turk CY. Dexmedetomidine added to levobupivacaine prolongs axillary brachial plexus block. Anesth Analg 2010;111:1548-51.
31. Al-Metwalli RR, Mowafi HA, Ismail SA, Siddiqui AK, Al-Ghamdi AM, Shafi MA, et al. Effect of intra-articular dexmedetomidine on postoperative analgesia after arthroscopic knee surgery. Br J Anaesth 2008;101:395-9.
32. Paul S, Bhattacharjee DP, Ghosh S, Dawn S, Chatterjee N. Efficacy of intra-articular dexmedetomidine for postoperative analgesia in arthroscopic knee surgery. Ceylon Med J 2010;55:111-5.
33. Short J. Use of Dexmedetomidine for Primary Sedation in a General Intensive Care Unit. Crit Care Nurse 2010;30:29-38.
34. Kaygusuz K, Gokce G, Gursoy S, Ayan S, Mimaroglu C, Gultekin Y. A comparison of sedation with dexmedetomidine or propofol during shockwave lithotripsy: A randomized controlled trial. Anesth Analg 2008;106:114-9.
35. Shehabi Y, Botha JA, Ernest D, Freebairn RC, Reade M, Roberts BL, et al. Clinical application, the use of dexmedetomidine in intensive care sedation. Crit Care Shock 2010;13:40-50.
36. Pandharipande PP, Pun BT, Herr DL, Maze M, Girard TD, Miller RR, et al. Effect of sedation with dexmedetomidine vs lorazepam on acute brain dysfunction in mechanically ventilated patients: The MENDS randomized controlled trial. JAMA 2007;298:2644-53.
37. Cooper L, Candiotti K, Gallagher C, Grenier E, Arheart KL, Barron ME. A Randomized, Controlled Trial on Dexmedetomidine for Providing Adequate Sedation and Hemodynamic Control for Awake, Diagnostic Transesophageal
Echocardiography. J Cardiothorac Vasc Anesth 2011;25:233-7.38. Jalowiecki P, Rudner R, Gonciarz M, Kawecki P, Petelenz M, Dziurdzik P. Sole
use of dexmedetomidine has limited utility for conscious sedation during outpatient colonoscopy. Anesthesiology 2005;103:269-73.
39. Bekker AY, Basile J, Gold M, Riles T, Adelman M, Cuff G, et al. Dexmedetomidine for awake carotid endarterectomy: Efficacy, hemodynamic profile, and side effects. J Neurosurg Anesthesiol 2004;16:126-35.
40. Ghali A, Mahfouz AK, Ihanamäki T, El Btarny AM. Dexmedetomidine versus propofol for sedation in patients undergoing vitreoretinal surgery under sub-Tenon’s anesthesia. Saudi J Anaesth 2011;5:36-41.
41. Bergese SD, Khabiri B, Roberts WD, Howie MB, McSweeney TD, Gerhardt MA, et al. Dexmedetomidine for conscious sedation in difficult awake fiberoptic intubation cases. J Clin Anesth 2007;19:141-4.
42. Olutoye OA, Glover CD, Diefenderfer JW, McGilberry M, Wyatt MM, Larrier DR, et al. The effect of intraoperative dexmedetomidine on postoperative analgesia and sedation in pediatric patients undergoing tonsillectomy and adenoidectomy. Anesth Analg 2010;111:490-5.
43. Phan H, Nahata MC. Clinical uses of dexmedetomidine in pediatric patients. Paediatr Drugs 2008;10:49-69.
44. Aho M, Erkola O, Kallio A, Scheinin H, Korttila K. Comparison of dexmedetomidine and midazolam sedation and antagonism of dexmedetomidine with atipamezole. J Clin Anesth 1993;5:194-203.
45. El-Gohary MM, Arafa AS. Dexmedetomidine as a hypotensive agent: Efficacy and hemodynamic response during spinal surgery for idiopathic scoliosis in adolescents. Egyp J Anaesth 2010;26:305-11.
46. Ayoglu H, Yapakci O, Ugur MB, Uzun L, Altunkaya H, Ozer Y, et al. Effectiveness of dexmedetomidine in reducing bleeding during septoplasty and tympanoplasty operations. J Clin Anesth 2008;20:437-41.
47. Richa F, Yazigi A, El Hage C, Jebara S, Hokayem N, Antakly MC. Dexmedetomidine: An agent for controlled hypotension in maxilla-facial surgery. Eur J Anaesthesiol 2004;21:902-6.
48. Wijeysundera DN, Naik JS, Beattie WS. Alpha-2 adrenergic agonists to prevent perioperative cardiovascular complications: A meta analysis. Am J Med 2003;114:742-52.
49. Hofer RE, Sprung J, Sarr MG, Wedel DJ. Anesthesia for a patient with morbid obesity using dexmedetomidine without narcotics. Can J Anesth 2005;52:176-80.
50. Abu-Halaweh SA, Al Oweidi AK, Abu-Malooh H, Zabalawi M, Alkazaleh F, Abu-Ali H, et al. Intravenous dexmedetomidine infusion for labour analgesia in patient with preeclampsia. Eur J Anaesthesiol 2009;26:86-7.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.
134
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Original Article
Palonosetron and palonosetron plus dexamethasone to prevent postoperative nausea and vomiting in patients undergoing laparoscopic cholecystectomy: A prospective, randomized, double-blind comparative studySoumyendu Ghosh, Anirban Pal, Amita Acharya1, Chaitali Biswas, Tirtha Ratan Ghosh, Subhabrata Ghosh
Department of Anesthesiology, Calcutta National Medical College (CNMC), Kolkata, 1Department of Anesthesiology, Bangur Institute of Neurology (BIN), Kolkata, India
Corresponding author: Dr. Anirban Pal, 43/6/5 Jheel Road, Kolkata - 700 031, West Bengal, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_68_11R5 AP Done 27th Jan
AbstractBackground: Laparoscopic cholecystectomy (LC) is associated with a high risk of postoperative nausea and vomiting (PONV). Palonosetron is a newer 5HT3 receptor antagonist, which is routinely used in our institution to prevent PONV in patients scheduled for LC, under general anesthesia (GA). We formulated this study to find out whether the palonosetron and dexamethasone combination will be a better choice than palonosetron alone in the prevention of PONV.Materials and Methods: Sixty American Society of Anesthesiologists (ASA) physical status I and II patients, scheduled for LC under GA, were randomized to receive either palonosetron or a combination of palonosetron and dexamethasone. The number of complete responders (no emesis, no requirement of rescue anti-emetic medication) and the four-point nausea score was recorded at 2, 6, 24, 48 h postoperatively and the data was analyzed statistically.Results: The number of complete responders, as well as the nausea score, did not vary significantly (P=0.718) between the two groups over the 48-h postoperative period.Conclusions: The palonosetron and dexamethasone combination was not more effective than palonosetron alone in the prevention of PONV, in patients undergoing LC under GA.
Key words: Complete responders, four-point nausea score, 5HT3 receptor antagonist
INTRODUCTION
Laparoscopic cholecystectomy (LC) is one of the most
approved. please proceed with publication
commonly performed procedures in general surgery. It is the most preferred procedure for symptomatic cholelithiasis, because of less morbidity and mortality associated with it. The advantages of LC may be counteracted by a high incidence of distressing side-effects like postoperative nausea and vomiting (PONV). PONV is more undesirable than pain[1] and can lead to delay in recovery, wound dehiscence and prolonged hospitalization.[2] Creation of pneumo-peritoneum is an essential part of laparoscopy, leading to stretching of mechano receptors, increased serotonin (5HT) synthesis and PONV.

135
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Ghosh, et al.: Palonosetron and dexamethasone versus palonosetron in PONV
5HT3 receptor antagonists (5HT3RA) have a definite role in the prevention of PONV. 5HT3 receptors are found in the gut and in areas of the central nervous system (CNS), being abundant in the chemoreceptor trigger zone (CTZ) of the area postrema,[3] which has projections to the vomiting center located in the lateral reticular formation of the medulla oblongata. Peripheral 5HT3 receptors are located in vagal nerve terminals, which are linked to the vomiting center via the nucleus tractus solitarius. [4] Competitive antagonism with 5HT3RA at these sites, and probably others, can block initiation of the vomiting reflex, caused by emetogenic stimuli.
Palonosetron is a newer 5HT3RA, recently introduced in clinical usage, with reduced need for repeat dosage. Palonosetron is a single stereoisomer isoquinoline based on a fused tricyclic ring system attached to a quinuclidine moiety. A single dose is widely distributed in the tissues (mean ± SD volume of distribution 8.3 ± 2.4 L/kg), moderately bound to plasma proteins (62%) and has a long terminal half-life of approximately 40 h.[5]
Dexamethasone causes better control of late PONV probably by inhibiting prostaglandin synthesis, decreasing 5HT levels in the nervous system, and anti-inflammatory action at the operative site.[6] Moreover, a single dose of dexamethasone is not associated with any significant side-effects.[7]
A meta-analysis concluded that the best prophylaxis of PONV is by combining dexamethasone with a selective 5HT3RA.[8] Previous studies have shown that dexamethasone when added to 5HT3 antagonist ondansetron, increases its efficacy.[9] In this research work, we wanted to study whether a combination of palonosetron and dexamethasone would be more effective than palonosetron alone in the prevention of PONV, in patients undergoing LC under general anesthesia (GA).
MATERIALS AND METHODS
After obtaining institutional approval and informed consent from participating patients, we studied 60 American Society of Anesthesiologists (ASA) physical Status I and II patients, aged 18 to 60 years, weighing 40-70 kg, scheduled for elective laparoscopic surgery under GA. The study was a prospective, randomized, double-blind one.
Patients who were pregnant or menstruating, with gastrointestinal or renal disease, who received cancer chemotherapy within past four weeks, emetogenic radiotherapy within past eight weeks, who had experienced nausea, vomiting or taken anti-emetic medication within 24 h before surgery, were excluded from the study.
The patients were randomly (computer-generated numbers inserted into opaque envelope) allocated to two groups P and PD. Group P patients received 0.075 mg palonosetron and Group PD received a combination of 0.075 mg palonosetron with 8 mg dexamethasone. One
of the authors, who took no further part in the study, prepared the study drugs in identical syringes, containing either 0.075 mg palonosetron or 0.075 mg palonosetron and 8 mg dexamethasone (total volume of 5 ml made with normal saline). The study drugs were known to be compatible when mixed and administered just before induction of anesthesia.
A consultant anesthesiologist who performed general anesthesia and used the study drug, was unaware of the type of study drug used and did not participate in the study. A standard institutional protocol for general anesthesia was followed in all the patients. All patients were advised overnight fasting and were premedicated with tablet midazolam 7.5 mg, 2 h before surgery, injection (Inj) ranitidine 50 mg and glycopyrolate 0.2 mg, and fentanyl 2 mcg/kg given by intravenous (IV) route, before start of the anesthetic procedure. Monitoring of pulse, non-invasive blood pressure, electrocardiography ECG, oxygen saturation, and end-tidal carbon dioxide (ET CO2) was done. The study drugs were administered slow IV, just before induction of anesthesia. The patients were pre-oxygenated with oxygen for 3 min, induction done with IV thiopentone 5 mg/kg, followed by IV rocuronium 0.6 mg/kg and direct laryngoscopy with intubation by endo-tracheal tube of appropriate size. Oro-gastric tube was introduced after endo-tracheal intubation and suction through tube was done. Maintenance of anesthesia was done with 33% oxygen with nitrous oxide with 0.5-1.5% isoflurane and 8 liters of total gas flow. Inj rocuronium was repeated at 25% of the initial dose and Inj fentanyl 1 mcg/kg at 30-min interval. Ventilation was done to maintain ET CO2 at 30-35 mm Hg. Intra-abdominal pressure was maintained below 15 mm Hg. Inj tramadol 100 mg IV and diclofenac 75 mg intramuscular (IM) was given to all patients, 30 min before the end of surgery and diclofenac repeated eight-hourly. At end of the operation, residual neuromuscular blockade was antagonized with Inj neostigmine 0.05 mg/kg with glycopyrolate (0.2 mg for each 1 mg of neostigmine). Extubation was done after suction of the oropharynx and adequate recovery from GA, judged on a clinical basis. Patient was sent to post anaesthesia care unit (PACU) and oxygen administered at 3 l/min. There was provision of rescue analgesic in the form of IV paracetamol 1 g (100 ml).
Patients were asked about nausea, vomiting, retching and any side-effects, at 2, 6, 24, 48 h by an investigator. The investigator and the patients were blinded to the study drug used. The severity of PONV was measured on a four-point (0-3) scoring system. PONV score 0 = no nausea and no retching; 1 = complaining of sickness and retching; 2 = vomiting one or two time in 30 min; 3 = vomiting more than two times in 30 min.[10] Nausea was defined as the subjectively unpleasant sensation associated with awareness of the urge to vomit, retching was defined as the labored, spastic, rhythmic contraction

136
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Ghosh, et al.: Palonosetron and dexamethasone versus palonosetron in PONV
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
of the respiratory muscles without the expulsion of the gastric contents, and vomiting was defined as the forceful expulsion of gastric contents from the mouth. The number of complete responders was recorded. Complete response is defined as no nausea, vomiting or retching and no need of rescue anti-emetic medicines within postoperative 48 h. If vomiting occurred or PONV score was 2 or more, IV ondansetron 4 mg was given as rescue anti-emetic. Any need for rescue drug and side-effects like headache, dizziness and drowsiness were noted. Data was analyzed using graph-pad software using Chi square test and t test where appropriate. Results were expressed in mean±SD. A P value<0.05 was considered as statistically significant.
RESULTS
The groups P and PD were comparable in respect of age, sex, weight, ASA physical status and duration of surgery [Table 1].
The number of complete responders (no vomiting, no rescue anti-emetics) was 25/30 (83.33%) in Group P and 24/30 (86.66%) in Group PD over the time period of 48 h and the difference was not statistically significant (P=0.718) [Table 2].
The four-point nausea score (0-3) recorded over the time period 0-2, 2-6, 6-24, 24-48 h did not differ significantly (P=0.718) between the two groups. Only five patients (16.66%) in Group P and four patients (13.33%) in Group PD experienced nausea and retching (Score 1). None of the patients had any vomiting episodes [Table 2]. There was provision of rescue anti-emetic but none of the patients required it.
The hemodynamic parameters, oxygen saturation, ECG changes were recorded intra-operatively and no significant difference between the groups was recorded. No incidence of hypotension was noted in any of patients in the postoperative 48-h period.
The patients were observed for side-effects during the 48-h postoperative period. None of the patients had any clinically serious side-effects; one patient in Group PD reported slight dizziness, which was insignificant and not of much clinical concern.
DISCUSSION
Laparoscopic cholecystectomy is associated with a high incidence of PONV ranging from 53-72%.[11] PONV is an unpleasant sensation which is associated with poor patient satisfaction.[12] PONV is multi-factorial, the important factors being patient age, sex, smoking habits, duration and type of surgery, pain, opioid requirements, inhalation agents used, use of nitrous oxide, and inadequate intravenous fluid therapy.[13,14]
Anesthetic agents initiate the vomiting reflex by stimulating the central 5HT3 receptors on the
chemoreceptor trigger zone (CTZ). The relation between pneumoperitoneum and PONV is not exactly known. The abdominal insufflation during LC increases the abdominal pressure with subsequent dilatation of intestinal loops which could influence the secretion of 5HT.[15] The mucosal enterochromaffin cells of the intestinal tract contain approximately 90% of 5HT present in the body.[16]
Palonosetron is a “second-generation” 5HT3RA, reported to be superior to the “first-generation” 5HT3RAs, because it binds at the allosteric site of 5HT3 receptor and this binding may prevent attachment of 5HT at the orthosteric site of the receptor, explaining its long-lasting effects. [17] Palonosetron is not simply a competitive antagonist at the 5HT3 receptor. Its high affinity is accompanied by high selectivity for 5HT3 receptors. The metabolism of palonosetron is primarily in the liver, by the Cytochrome P450 enzyme system, with CYP2D6 being the predominant isoenzyme. Following initial rapid distribution, IV palonosetron undergoes a slow elimination phase, primarily handled by the kidney.[18]
Dexamethasone, a long-acting glucocorticoid with some mineralocorticoid effects, has been reported as an effective anti-emetic in cancer chemotherapy patients[19] and has been found to have a prophylactic effect on
Table 1: Demographic profile, duration of surgery and ASA physical status
Gr P (n=30) Gr PD (n=30) P valueAge (years) 36.33 ± 10 35.03 ± 10.15 0.627
Sex (M:F) 3:27 5:25 0.448
Body weight (kg) 57.47 ± 8.25 56.67 ± 9.81 0.7239
Duration of surgery (min) 59 ± 13.35 61.33 ± 15.42 0.5340
ASA physical status (I:II) 25:5 25:5 1
Table 2: Complete responders and nausea score over the time periods
Group P (n=30)
Group PD (n=30)
P value
Complete responders (number of patients)
25 (83.33%) 26 (86.66%) 0.718
Nausea
0-2 h 0 score = 301 score = 02 score = 03 score = 0
0 score = 301 score = 02 score = 03 score = 0
2-6 h 0 score = 301 score = 02 score = 03 score = 0
0 score = 301 score = 02 score = 03 score = 0
6-24 h 0 score = 301 score = 02 score = 03 score = 0
0 score = 301 score = 02 score = 03 score = 0
24-48 h 0 score = 251 score = 52 score = 03 score = 0
0 score = 261 score = 42 score = 03 score = 0
0.718

137
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Ghosh, et al.: Palonosetron and dexamethasone versus palonosetron in PONV
PONV in adults undergoing laparoscopic surgery.[20] It has a low cost and a prolonged biological half-life of 36 to 48 h. Dexamethasone appears to have an excellent side-effect profile after a single dose, although its effects on immune function, and the potential for adverse outcomes such as wound infection, have not been studied.
A study by Song et al., demonstrated that combined dexamethasone and ondansetron is more effective in reducing severe nausea and vomiting than ondansetron alone in patients receiving fentanyl-based intravenous patient-controlled analgesia.[21] Rusch et al., found that addition of dexamethasone to different anti-emetics significantly decreases the incidence of PONV.[22] Bisgaard et al., observed that preoperative dexamethasone compared to placebo, reduces the incidence of PONV in patients undergoing LC and recommended its routine use in LC.[23] Maemondo et al., in their study of the combination of palonosetron and dexamethasone to prevent chemotherapy-induced nausea and vomiting found this combination to be very effective.[24] We therefore formulated our study to find out whether the combination of palonosetron and dexamethasone is more beneficial than palonosetron to prevent PONV. As PONV is a common occurrence after LC under GA, we believed it would be unethical to include a placebo group. Our selections of drug dosages are based on previous research works that demonstrated that these doses are effective. Our study results show that the number of complete responders and the nausea score in the periods 2, 6, 24 and 48 h postoperative, in the two groups P and PD, did not differ significantly (P=0.718). Blitz et al., in their study of 118 patients undergoing laparoscopic surgery, randomized to receive a combination of 8 mg dexamethasone plus 0.075 mg palonosetron, and 0.075 mg palonosetron alone found no significant difference in the incidence of PONV between the groups.[25] Our study results are in accordance with their study.
CONCLUSION
A combination of palonosetron and dexamethasone does not decrease the incidence of PONV compared to palonosetron alone. We recommend not to add dexamethasone to palonosetron as it will further increase the cost, expose the patient to the risk of added side-effects, without any extra benefit, in patients undergoing LC under GA.
REFERENCES
1. Macario A, Weinger M, Carney S, Kim A. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesth Analg 1999;89:652-8.
2. Kenny GN. Risk factors for postoperative nausea and vomiting. Anaesthesia 1994;49:6-10.
3. Bunce KT, Tyers MB. The role of 5 HT in postoperative nausea and vomiting. Br J Anesth 1992;69(suppl. 1):S60-2.
4. Watcha MF, White PF. Postoperative nausea and vomiting. Its etiology, treatment, and prevention. Anesthesiology1992;77:162-84.
5. Stoltz R, Cyong JC, Shah A, Parisi S. Pharmacokinetic and safety evaluation of palonosetron, a 5-hydroxytryptamine-3 receptor antagonist, in US and Japanese healthy subjects. J Clin Pharmacol 2004;44:520-31.
6. McKenzie R, Tantisira B, Karambelkar DJ, Riley TJ, Abdelhady H. Comparison of ondansetron with ondansetron plus dexamethasone in prevention of postoperative nausea vomiting. Anesth Analg 1994;79:961-4.
7. Madan R, Bhatia A, Chakithandy S, Subramaniam R, Rammohan G, Desphande S, et al. Prophylactic dexamethasone for postoperative nausea and vomiting in pediatric strabismus surgery: A Dose ranging and safety evaluation study. Anesth Analg 2005;100:1622-6.
8. Henzi I, Walder B, Tramer MR. Dexamethasone for prevention of postoperative nausea and vomiting: A quantitative systemic review. Anesth Analg 2000;90:186-94.
9. D’souza N, Swami M, Bhagwat S. Comparative study of dexamethasone and ondansetron for prophylaxis of postoperative nausea and vomiting in laparoscopic gynecologic surgery. Int J Gynaecol Obstet 2011;113:124-7.
10. Ummenhofer W, Frei FJ, Urwyler A, Kern C, Drewe J. Effects of ondansetron on prevention of postoperative nausea and vomiting in children. Anesthesiology 1994;81:804-10.
11. Fuji Y, Saitoh Y, Tanaka H. Ramosetron versus granisetron for prevention of post operative nausea and vomiting after laparoscopic cholecystectomy. Can J Anaesth 1999;46:991-3.
12. Klockgesthes-Radke A, Piorek V, Crozier TC, Kettler D. Nausea and vomiting after laparoscopic surgery: A comparison of propofol and thiopentone/halothane anaesthesia. Eur J anaesthesthiol 1996;13:3-9.
13. Sinclair DR, Chung F, Mezei G. Can postoperative nausea and vomiting be predicted? Anesthesiology 1999;91:109-18.
14. Maharaj CH, Kallam SR, Malik A, Hassett P, Grady D, Laffey JG. Preoperative intravenous fluid therapy decreases postoperative nausea and pain in high risk patients. Anesth Analg 2005;100:675-82.
15. Cunningham AJ, McCoy D. Anesthetic implications of laparoscopic surgery. Adv Anesth 1994;11:137-72.
16. Hindle AT. Recent developments in the physiology and pharmacology of 5hydroxytryptamine. Br J Anesth 1994;73:395-407.
17. Rojas C, Stathis M, Thomas A, Massuda E, Alt J, Zhang J, et al. Palonosetron exhibits unique molecular interactions with the 5-HT3 receptor. Anesth Analg 2008;107:469-78.
18. Wallenborn J, Kranke P. Palonosetron hydrochloride in the prevention and treatment of postoperative nausea and vomiting. Clinical Medicine Insights. Therapeutics 2010;2:387-99.
19. Aapro MS, Alberts DS. Dexamethasone as an antiemetic in patients treated with cisplatine. N Engl J Med 1981;30:520.
20. Wang JJ, Ho ST, Liu YH, Lee SC, Liu YC, Liao YC, et al. Dexamethasone reduces nausea and vomiting after laparoscopic cholecystectomy. Br J Anaesth 1999;83:772-5.
21. Song JW, Park EY, Lee JG, Park YS, Kang BC, Shim YH. The effect of combining dexamethasone with ondansetron for nausea and vomiting associated with fentanyl-based intravenous patient-controlled analgesia. Anaesthesia 2011;66:263-7.
22. Rüsch D, Arndt C, Martin H, Kranke P. The addition of dexamethasone to dolasetron or haloperidol for treatment of established postoperative nausea and vomiting. Anaesthesia 2007;62:810-7.
23. Bisgaard T, Klarskov B, Kehlet H, Rosenberg J. Preoperative dexamethasone improves surgical outcome after laparoscopic cholecystectomy-a randomized double blind placebo controlled trial. Ann Surg 2003;238:651-60.
24. Maemondo M, Masuda N, Sekine I, Kubota K, Segawa Y, Shibuya M, et al. A phase II study of palonosetron combined with dexamethasone to prevent nausea and vomiting induced by highly emetic chemotherapy. Ann Oncol 2009;20:1860-6.
25. Blitz JD, Haile M, Kline R, Franco L, Didehvar S, Pachter HL, et al. Arandomized double blind study to evaluate efficacy of palonosetron with dexamethasone versus palonosetron alone for prevention of postoperative and postdischarge nausea and vomiting in subjects undergoing laparoscopic surgeries with high emetogenic risk. Am J Ther 2011 [In Press].
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.

138
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Original Article
Efficacy of thoracic epidural anesthesia for laparoscopic cholecystectomy Amit Gupta, Kumkum Gupta, Prashant K. Gupta1, Nivesh Agarwal2, Bhawna Rastogi
Departments of Anaesthesiology and Critical Care, 1Radio-diagnosis, Imaging and Interventional Radiology, 2Surgery, N. S. C. B. Subharti Medical College, Subhartipuram, NH-58, Meerut, Uttar Pradesh, India
Corresponding author: Prof. Kumkum Gupta, 108, Chanakyapuri, Shastri Nagar, Meerut - 250 004, Uttar Pradesh, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_63_11R6
AbstractBackground: Laparoscopic cholecystectomy is performed to minimize the postoperative morbidity and early return to work. This study was planned to evaluate the efficacy and feasibility of thoracic epidural anesthesia for laparoscopic cholecystectomy, so that it can be later used as anesthetic technique in patients when general anesthesia is not feasible.Materials and Methods: Forty-eight adult consented patients of ASA grade I and II of either sex scheduled for elective laparoscopic cholecystectomy were enrolled for thoracic epidural anesthesia with 15 ml of 0.75% ropivacaine and 50 µg fentanyl. Intraoperative hemodynamic parameters and respiratory efficiency were recorded. Intra-operatively patient anxiety, pain, vomiting, hypotension or any other adverse event was managed with appropriate drug regime. Postoperative pain management with epidural analgesia, and bowel recovery were also recorded.Results: The thoracic epidural anesthesia was effective for laparoscopic cholecystectomy in all except in two patients where conversion to general anesthesia was required. The hemodynamic parameters and respiratory efficiency were maintained within physiological limits. Only 4 patients required treatment for hypotension with vasopressor and 15 patients experienced shoulder pain, which was effectively managed with small doses of ketamine. The midazolam was required only in 11 patients for anxiety. The mean surgical time was 56.8 ± 51.6 min. The 24-hour postoperative epidural infusion for analgesia was effective with limited effects on bowel and bladder function. Postoperatively only 3 patients had an episode of vomiting. There was good surgeon and patient’s satisfaction.Conclusions: The thoracic epidural anesthesia with 0.75% ropivacaine and fentanyl for elective laparoscopic cholecystectomy is efficacious and has preserved ventilation and hemodynamic changes within physiological limits during pneumoperitoneum with minimal treatable side effects.
Key words: Epidural anesthesia, fentanyl, laparoscopic cholecystectomy, pneumoperitoneum, ropivacaine
INTRODUCTION
Laparoscopic cholecystectomy is advantageous due to reduction of postoperative pain, better cosmetic results with quicker return to normal activities. It is usually performed under general anesthesia with controlled ventilation due to pathophysiological changes of carbon dioxide pneumoperitoneum and extreme of patient

139
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Gupta, et al.: Epidural anesthesia for laproscopic cholecystectomy
positioning. In recent years, advanced laparoscopic surgery has targeted older and high risk sick patients for general anesthesia. In these patients, regional anesthesia offers several advantages with improved patient satisfaction.[1-4] However, this anesthetic approach requires a relaxed and cooperative patient, low intra-abdominal pressure (IAP) to reduce shoulder pain and ventilator disturbances, reduced table tilt with a precise and gentle surgical technique.[5]
Ropivacaine, a long acting local anesthetic, is a better alternative to bupivacaine due to its lower toxicity and greatest margin of safety of all long acting local anesthetics at present.[6,7] After epidural injection, it shows biphasic absorption with an initial rapid phase half -life of 4.2 ± 0.9 minutes. The total plasma concentration increases during continuous epidural infusion of ropivacaine because of an increase in the degree of protein binding and subsequent decrease in clearance of ropivacaine.[8] Epidural administration of the ropivacaine with fentanyl has been shown to accelerate the onset of sensory and motor blocks without significant fentanyl-related side effects.[9]
Encouraged by these facts, this study was aimed to assess the efficacy of thoracic epidural anesthesia with 0.75% ropivacaine and 50 µg fentanyl for elective laparoscopic cholecystectomy, so later it can be used as anesthetic technique in patients who are at risk for general anesthesia.
MATERIALS AND METHODS
After approval from the Ethical Committee of the Institution and informed consent for the procedure, 48 adult patients aged between 22 and 56 years of either sex with ASA physical status I and II, scheduled for elective laparoscopic cholecystectomy under thoracic epidural anesthesia from January 2010 to March 2011 were enrolled for this prospective study. Patients who were unable to co-operate, had a body mass index >32 kg m2, acute cholecystitis, suspected common bile duct stones, history of cardiac, pulmonary or renal disease, history of drug or alcohol abuse, chronic pain or daily intake of analgesics, and allergy to amide local anesthetic were not included. Patients who preferred general anesthesia and in patients where surgeon suspect technical difficulty or patients had contraindications to perform epidural block were also excluded from the study. Patients were explained during the preoperative assessment about the procedure technique and were assured that any pain, anxiety or discomfort, during surgery would we treated effectively. The surgeons were free to request for general anesthesia if they felt technical difficulty for the surgery.
Anesthesia and surgical techniqueIn the operating room, an intravenous infusion of 500 mL of Ringer lactate was commenced and base
line values of heart rate, mean arterial blood pressure, electrocardiography, respiratory rate and pulse oximetry reading were recorded. All patients were premedicated with midazolam 1 mg, ondansetron 4 mg and metoclopramide 10 mg intravenously.
Thoracic epidural anesthesia was performed in left lateral decubitus position. Under all aseptic precautions, 2 ml of 2% lignocaine with epinephrine was infiltrated at the T10-T11 inter-spinous space and an 18-gauge Touhy needle was introduced in midline to identify the epidural space using ‘loss of resistance’ to air method. The epidural catheter was then threaded and taped in place, leaving 4 cm in epidural space. A test dose of 3 ml of 2% lignocaine with epinephrine 5 µg/ml was injected through the epidural catheter. If no intrathecal or intravascular injection was evident up to 5 min, a bolus dose of 15 ml 0.75% ropivacaine with 50 µg fentanyl was given slowly over 5 min. The level of sensory block, assessed with pin-prick stimulus, covering the area of the proposed incision (T4-5) was confirmed before surgery. If needed, the incremental dose of 2 ml of 0.75% ropivacaine was given. The patients were breathing spontaneously with oxygen supplementation at the rate of 5 L/minutes. The nasogastric tube was inserted to decompress the stomach on surgeon demand. Pneumoperitoneum was established with low pressure carbon dioxide of 10 mm Hg at a flow rate of 1 L/min. After the creation of pneumoperitoneum but prior to gall bladder dissection, 12 ml of 0.25% Bupivacaine was instilled into the right sub-diaphragmatic space and over the gall bladder.[10] Head up and left lateral tilt of the operating table was employed as minimal as possible in order to minimize diaphragmatic irritation. Intra-operatively, the patients were monitored for heart rate, blood pressure, respiratory rate, arterial oxygen saturation (SpO2) and end tidal carbon dioxide (EtCO2). The parameters were recorded at 5 min intervals. Hypotension, defined as a fall in blood pressure by more than 20% of pre-anesthetic value, was managed by rapid crystalloid infusion and/or intravenous bolus of 6 mg mephentermine. Bradycardia (<50 beats/min) was treated with IV 0.6 mg atropine. Respiratory insufficiency was defined as a respiratory rate at or below 8 breaths/min, pulse oximetry value of less than 94% at any given time and/ or subjective breathing difficulty not relieved by reassurance. Duration of pneumoperitoneum as well as surgery was kept minimal. Anxiety was treated with midazolam 2 mg. The ketamine 0.25 mg/kg was given intravenously for shoulder pain. Any conversion of anesthetic or surgical technique was noted with reasons to do so.
Postoperative analgesia was provided as a continuous epidural infusion of 0.2% ropivacaine with fentanyl 2 µg/ ml, at a rate of 10 ml/hour and removed after 24 hours. Pain was assessed using visual analogue score (VAS) of 0 (no pain) -100 mm (worst pain imaginable). The other

140
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Gupta, et al.: Epidural anesthesia for laproscopic cholecystectomy
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
parameters included pulse rate, arterial blood pressure, headache, nausea, vomiting, pruritis, and retention of urine with bowel recovery. Patients were asked to rank their satisfaction with regards to the anesthetic procedure on a score scale ranging from 0 to 10.[11]
RESULTS
The present study enrolled 48 adult consented patients of either sex (male-12 and female-36) with ASA Grade I and II scheduled for elective laparoscopic surgery under thoracic epidural anesthesia with 0.75% ropivacaine and 50 µg fentanyl. Their average age was 41.8 years. An effective sensory block was developed with average of 15 (12-21) minutes. The median highest level of sensory blockade achieved was at T4-T5, and lower level was L1-L3. The dermatome level of analgesia achieved was satisfactory in all patients [Table 1].
Transient hypotension was recorded in 8 patients who were treated effectively with one dose of 6 mg IV mephentermine. None of them required continuous pharmacological support. There was no observed change in the respiratory rate. The end tidal carbon dioxide increased over the first 10 minutes from 30.65 ± 4.12 to 35.47 ± 5.3 mm Hg (P<0.002) and declined after deflation. All other observed changes were within physiological limits. The 11 anxious patients needed IV midazolam supplementation and 15 patients complained of shoulder pain which was effectively treated with small doses of IV ketamine while all others were comfortable throughout the laparoscopic cholecystectomy. Only 2 patients required conversion to general anesthesia due to technical difficulty [Table 2].
Postoperative analgesia was well maintained and intravenous opioid analgesic was not required. Only 1 patient had postoperative hypotension and 3 patients have experienced one or more vomiting episodes. No patient has complained of headache, pruritis and retention of urine. The bowel recovery was not altered [Table 3].
All patients gave an overall satisfaction score 8 or above and all resumed normal activities within few days. Only in 2 patients, the surgeon found technical difficulty for laparoscopic surgery hence conversion to general anaesthesia was done. Average time to discharge was 1.8 days.
DISCUSSION
Epidural anesthesia was considered safe for laparoscopic cholecystectomy without associated respiratory depression as the respiratory control mechanism remains intact to allow the patients to adjust their minute ventilation. Moreover, the respiratory changes are less evident in awaken patients under regional anesthesia and patients maintain an unchanged end tidal carbon dioxide.[12] The central neuraxial anesthesia has been found beneficial
Table 1: Patients demographic data and surgical out comeParameters Number of patients/
incidenceSex (male:female) (n) 12/36
Age (years) 41.8 (22-56)
BMI (kg m–2) 30.2 (27-32)
ASA I:II (n) 33:15
Time for induction (min) 15 (12-21)
Operative time (min) 56.8 ± 51.6
End tidal carbon dioxide (mm Hg) 30.65 ± 4.12 to 35.47 ± 5.3
Pneumoperitoneum time (min) 42.73 (38-54)
Conversion to general anaesthesia (n) 2
Patient satisfaction score at discharge (10:9:8)
(n) 22:18:8
Table 2: Intraoperative eventsParameters Number of patients (%)Shoulder pain 15 (31.25)
Hypotension 08 (16.67)
Bradycardia None
Anxiety 11 (20.28)
Conversion to GA 02 (4.16)
Table 3: Postoperative eventsParameters Number of patientsNausea/vomiting 03
Postoperative hypotension 01
Respiratory depression None
VAS score in first 24 hrs 2 (0-3)
usually in patients with significant medical diseases when low intra-abdominal pressure and less degree of patient tilt during surgical procedure is used.[5] The shoulder pain, secondary to diaphragmatic irritation from carbon dioxide pneumoperitoneum, is incompletely alleviated using epidural anesthesia alone and extensive sensory block from T4 to L5 is needed for the laparoscopic procedure.
This present prospective study was aimed to evaluate the efficacy of epidural anesthesia with 0.75% ropivacaine with fentanyl for laparoscopic cholecystectomy. Lack of complications and morbidity encourage us to share our preliminary experience of thoracic epidural anaesthesia for laparoscopic cholecystectomy.
Many researchers have observed that laparoscopic cholecystectomy performed under regional analgesia is advantageous due to reduction of surgical stress response. Avoidance of airway instrumentation and lower incidence of deep vein thrombosis are other few advantages.[1] The low intra-abdominal pressure with low insufflation flow rate contributes only few hemodynamic changes. Critchley et al. reported 29% increase in mean arterial blood pressure after gas insufflation under general anesthesia.[13]

141
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Gupta, et al.: Epidural anesthesia for laproscopic cholecystectomy
In the present study, the low incidence of right shoulder pain was observed which could be attributed to low intra-abdominal pressure of 10 mm Hg combined with minimal table tilt and the instillation of 0.25% bupivacaine into right sub-diaphragmatic space and over the gall bladder. Van Zundert et al.[14] also noted shoulder and neck pain in 2 of their 6 patients operated under epidural anesthesia. Minai et al. attributed the high incidence of shoulder pain to the physical and chemical stimulation of the diaphragm by pneumoperitoneum.[15] No patient experienced breathing difficulty during abdominal insufflation, perhaps due to low gas pressure flow rate.
During the present study, the hemodynamic changes were also minimal due to preloading with 15 ml/kg of ringer lactate over 20 minutes, low intra-abdominal pressure, minimal table tilt and absence of any cardiovascular disease. The study also did not show any notable events apart from hypotension which was easily treated by vasopressor drugs. The regional sympathetic block have compensated for the increased sympathetic tone resulting from pneumoperitoneum in a head-up tilt position.[16] Although regional anesthesia facilitates the unopposed vagal reflex, but none of our patients suffered bradycardia.
Postoperative nausea and vomiting was reported in 3 patients who were treated with intravenous ondansetron. [17] Low incidence in the present study could be attributed to antiemetic prophylaxis with metoclopramide and ondansetron, avoidance of hypotension, adequate pain control and avoidance of postoperative parenteral opioids medication. At the time of discharge, all patients reported being satisfied with the anesthetic technique, good postoperative pain control and minimal nausea and vomiting.
Bejarano et al. used spinal anesthesia with midazolam sedation for laparoscopic ventral hernia repair and concluded that spinal anesthesia is feasible and well tolerated.[18]
Van Zundert et al. stated that segmental spinal anesthesia can be used safely for patients with impaired organ function. [14] Lau et al. also quoted that laparoscopic hernia can be performed successfully under spinal anesthesia.[19]
However, there are several disadvantages of the regional technique due to sympathetic denervation of high regional block which may lead to bradycardia, hypotension and decreased cardiac output. The vigilant monitoring is essential for prevention and treatment. Continuous infusion of low dose epidural analgesia with 0.2% ropivacaine and 2 µg/ml fentanyl provided good postoperative analgesia and no patient demanded for parenteral opioids.[20,21]
CONCLUSION
The thoracic epidural anesthesia for elective laparoscopic cholecystectomy is efficacious. The continuous infusion of 0.2% ropivacaine, with fentanyl 2 µg/ml has provided
effective postoperative analgesia. Success of the technique necessitates relaxed and co-operative patient and gentle surgical procedure with low intra-abdominal pressure technique.
REFERENCES
1. Tzovaras G, Fafoulakis F, Pratsas K, Georgopoulou S, Stamatiou G, Hatzitheofilou C. Laparoscopic cholecystectomy under spinal anesthesia: A pilot study. Surg Endosc 2006;20:580-2.
2. Gramatica L Jr, Brasesco OE, Luna AM, Martinessi V, Panebianco G, Labaque F, et al. Laparoscopic cholecystectomy performed under regional anesthesia in patients with chronic obstructive pulmonary disease. Surg Endosc 2002;16:472-5.
3. Kim YI, Lee JS, Jin HC, Chae WS, Kim SH. Thoracic epidural anesthesia for laparoscopic cholecystectomy in an elderly patient with severely impaired pulmonary function tests. Acta Anaesthesiol Scand 2007;51:1394-6.
4. Savas JF, Litwack R, Davis K, Miller TA. Regional anesthesia as an alternative to general anesthesia for abdominal surgery in patients with severe pulmonary impairment. Am J Surg 2004;188:603-5.
5. Sarli L, Costi R, Sansebastiano G, Trivelli M, Roncoroni L. Prospective randomized trial of low-pressure pneumoperitoneum for reduction of shoulder tip pain following laparoscopy. Br J Surg 2000;87:1161-5.
6. Agarwal A, Verma RK, Srivastava S. Ropivacaine – the latest local anesthetic in the Indian market. JOACP 2010;26:223-8.
7. Akerman B, Hellberg B, Trossvik C. Primary evaluation of the local anaesthetic properties of the amino amide agent ropivacaine (LEA 103). Acta Anaesthesiol Scand 1988;32:571-8.
8. McClellan KJ, Faulds D. Ropivacaine-an update of its use in regional anesthesia. Drugs 2000;60:1065-93.
9. Scott DA, Blake D, Buckland M, Etches R, Halliwell R, Marsland C, et al. A comparison of epidural ropivacaine infusion alone and in combination with 1,2, and 4 g/ml Fentanyl for seventy two hour of postoperative analgesia after major abdominal surgery. Anaesth Analg 1999;88:857-64.
10. Boddy AP, Mehta S, Rhodes M. The effect of intra-peritoneal local anesthesia in laparoscopic cholecystectomy: A systemic review and meta-analysis. Anesth Analg 2006;103:682-8.
11. Grass JA. The role of epidural anesthesia and analgesia in postoperative outcome. Anesthesiol Clin North America 2000;18:407-28.
12. Raju NP, Sivasashanmugam T, Ravishankar M. Respiratory changes during spinal anesthesia for gynacological laparoscopic surgery. J Anaesth Clin Pharmacol 2010;26:475-9.
13. Critchley LA, Critchley JA, Gin T. Haemodynamic changes in patients undergoing laparoscopic cholecystectomy: Measurement by transthoracic bioimpedance. Br J Ansesth 1993;70:681-3.
14. Van Zundert AA, Stultiens G, Jakimowicz JJ, Peek D, van der Ham WG, Korsten HH, et al. Laparoscopic cholecystectomy under segmental thoracic spinal anaesthesia: A feasibility study. Br J Anaesth 2007;98:682-6.
15. Minai H, Yamada K, Tashiro K, Yamamoto K. Anesthetic management for awake laparoscopic surgery for ectopic pregnancy in a patient with heterotopic pregnancy. Masui 2005;54:1313-4.
16. Wheatly RG, Schug SA, Waston D. Safety and efficacy of postoperative epidural analgesia. Br J Anesth 2001;87:47-61.
17. Malins AF, Field JM, Nesting PM, Cooper GM. Nausea and vomiting oral ondansetron metoclopraide and placebo. Br J Anaesth 1994;72:231-3.
18. Bejarano Gonzalez- Serna D, Utera A, Gallego JI, Rodiguez R, De La Portilla F, Espinosa JE, et al. Laparoscopic treatment of ventral hernia under spinal anesthesia. Cir Esp 2006;80:168-70.
19. Lau H, Wong C, Chu K, Patil NG. Endoscopic totally extraperitoneal inguinal hernioplasty under spinal anesthesia. J Laparoendosc Adv Tech 2005;15:121-4.
20. McLeod Ga, Dell K, Smith C, Wildsmith JA. Measuring the quality of continuous epidural block for abdominal surgery. Br J Anaesth 2006;96:521-3.
21. Bisgaard T. Analgesic treatment after laparoscopic cholecystectomy: A critical assessment of the evidence. Anesthesiology 2006;104:835-46.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
142
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Original Article
Wound infiltration with plain bupivacaine as compared with bupivacaine fentanyl mixture for postoperative pain relief after abdominal surgeryReetika Chander, Dootika Liddle, Baljinder Kaur, Mary Varghese
Department of Anaesthesia, CMC & Hospital, Ludhiana, India
Corresponding author: Dr. Dootika Liddle, Associate Professor, Department of Anaesthesia, Christian Medical College, Ludhiana, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_18_11R5
AbstractAim: To compare the efficacy of wound infiltration with Bupivacaine or Bupivacaine with fentanyl for post operative analgesia.Background: The role of Bupivacaine and fentanyl mixture as wound infiltration for post operative analgesia is less explored in human subjects.Material and methods: This prospective, randomized included 60 ASA grade I, II, and III patients in the age group of 20-75 years of age. The patients were randomized into two groups of 30 patients each: Group A received wound infiltration with a solution containing 0.5% bupivacaine (2 mg/kg), while, group B received infiltration with a solution containing fentanyl 25 μg added to 0.5% bupivacaine (2 mg/kg).Results: None of the patients in both groups had unbearable incisional pain but addition of fentanyl to 0.5% bupivacaine reduced analgesic consumption in the postoperative period. (P<0.05)Conclusion: Addition of opioids to local anesthetics results in better postoperative analgesia and reduced opioid requirement post operatively.
Key words: Bupivacaine, fentanyl, wound infiltration
INTRODUCTION
Postoperative pain remains prevalent and is the greatest concern for a patient. Effective paid relief is not only human but also has a positive impact on recovery as postoperative pain is associated with increased morbidity and mortality.
Pain after abdominal surgeries leads to restricted breathing effort and inability to adequately cough out secretion[1] which leads to a decrease in functional residual capacity, early airway closure, segmental or lobar collapse, retention of secretions leading to bronchopneumonia.[2]
Wound infiltration provides good postoperative analgesia, facilitating a rapid and smooth recovery. Local anesthetics are potent long lasting and act through several mechanisms including inhibition of the effects of prostaglandins, inhibition of the migration of leucocytes, and reduction of vascular permeability. It has proven effective in various surgical procedures especially in herniorrhaphies,[3] gynecological surgeries,[4] thoracotomies, etc.
It was found that combination of local anesthetic with

143
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Chander, et al.: Wound inflitration analgesia
opioid for wound infiltration in a patient undergoing cholecystectomy was associated with better postoperative analgesia, reduced analgesic consumption, and better lung function.[5]
MaTeRIals aND MeThODs
After obtaining approval from the institutional ethical committee and informed written consent from the patients, 60 patients, aged 20-75 years ASA I-III undergoing abdominal surgical procedures, were randomly allocated into two equal groups.
Patient with severe cardiovascular or liver disease, those who received opioids as premedication, and those with known allergic response to local anesthetics were excluded from the study.
The study was conducted as a randomized double-blind study using two solutions:a. Solution containing 0.5% bupivacaine (2 mg/kg).b. Solution containing added fentanyl 25 mg to 0.5%
bupivacaine (2 mg/kg).
Coding of the solutions was done by a senior anesthetist and the person administering the drug was unaware of its constituents.
All patients received Tab Diazepam 10 mg 1h prior to induction as preanesthetic medication. After precurarization with 1 mg of vecuronium to prevent fasciculations, the patients were induced with thiopentone (4 mg/kg) and tracheal intubation was done with succinyl choline (1-2 mg/kg). Anesthesia was maintained using O2, N2O, and halothane (0.5%) or isoflurane (1-2%). Intermittent vecuronuim (0.1 mg/kg) was given when required. No opiods were used during the surgery. Prior to skin suturing wound was infiltrated using one of the solutions. At the end of the surgery muscle relaxation was reversed using neostigmine (0.05 mg/kg) and glycopyrrolate (0.01 mg/kg).
The assessment of pain was done in each patient at 0, 1, 2, 4, 6, 8, 12, and 24 h after surgery and three types of pain were analyzed:a. Constant incisional pain.b. Movement-associated pain.c. Pain upon pressure on the surgical wound.
Rescue analgesiaThe patient was given Inj. Tramadol 50 mg iv on complaint of pain. The time of first request of analgesia was recorded. The total narcotic requirement in mg in the first 24 h was calculated and used for statistical purpose.
ResUlTs
We compared the analgesic effects of Bupivacaine and Bupivacaine Fentanyl admixture when used for wound infiltration in post operative patients. The patients in
Figure 1: Comparison of heart rate in patients of both groups
Figure 2: Comparison of respiratory rate in patients of both groups
Figure 3: Comparison of systolic blood pressure in patients of both groups
Table I: Patient characteristicsGroup A Group B
n=30 n=30Age (in years) 44.87 ± 12.2 43.70 ± 14.1
Sex (M/F) 9/21 7/23
Weight (kg) 61.23 ± 8.173 58.57 ± 8.43
Duration of surgery (hours) 1.917 ± 0.54 2.26 ± 1.30

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
144
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Chander, et al.: Wound inflitration analgesia
Figure 4: Comparison of diastolic blood pressure in patients of both groups
Figure 5: Comparison of constant incision pain post op in patients of both groups
Figure 6: Comparison of movement associated pain post-op in patients of both groups
both groups were comparable in terms of age, sex, weight and duration of surgery [Table 1]. The hemodynamic parameters i.e. heart rate, systolic and diastolic blood pressure and respiratory rate were compared in patients of both groups at regular intervals [Figures 1, 2, 3, 4]. Group B was found to have significant tachycardia,higher systolic and diastolic blood pressure compared to patients in group A. There was no stastical difference in both groups in terms of respiratory rates [Fgure 2]. Our study had statistically significant difference in terms of constant incisional pain when comparing both groups with more patients in group A complaining of moderate pain [Figure 5].
While comparing pain upon movement we found statistically significant difference from 1 hour post-op to 6 hours post-op with patients in Group A having more pain compared to Group B [Figure 6]. The difference between both groups in terms of pain upon pressure on the wound was statistically significant with patients in the plain bupivacaine group having more pain compared to the buivacaine fentanyl group at all times except at 24h [Figure 7]. There was also a difference in the number of patients in both groups who required analgesia as early
as 2h postoperatively. The difference was marked as 40% in group A compared to 3% in group B [Figure 8]. At 24h the opioid requirement (number of dose) was found to be less in group B (mean 105 ± 24.03) compared to group A (mean 218 ± 62.26) [Figure 9].
DIsCUssION
Several studies have been done for finding efficacious drugs to combat pain. Narcotics have been the main stay of postoperative pain management and morphine as the standard drug despite its various side effects. NSAIDS are also associated with gastric ulceration and bleeding complications and a concern in renal dysfunction. TENS, ALENS, conventional acupuncture[6] relaxation technique, and cryoanalgesics have also shown inconsistent results. [7] However, there has been renewed interest in local anesthetic wound instillation for postoperative pain control. Eriksson studied the in vivo effects of lidocaine on leucocyte function in the surgical wound. He found significantly lower leucocyte counts in the wounds treated with lidocaine.[8]
Figure 7: Comparison of pain upon pressure post-op in patients of both groups

145
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Chander, et al.: Wound inflitration analgesia
Figure 8: Comparison of time for first request for analgesia in patients of both groups
Figure 9: Comparison of total no of doses of rescue analgesia in initial 24 hours post operatively in patients of both groups
Various studies have been done to assess the pain and comparing effect of plain anesthetic as compared to anesthetic opioid mixture for wound infiltration. [9] By using plain lignocaine and lignocaine fentanyl mixture in wound infiltration, three types of pain were assessed spontaneous pain, movement-associated pain, and pain upon pressure—and they found that they were significantly higher in the plain lignocaine group compared to the lignocaine fentanyl at all times of observation. We did a similar study; our patients in both groups were comparable in terms of age, sex, weight, and duration of surgery. Our study had comparable results as we also had a statistically significant difference in terms of constant incisional pain when comparing both groups. Also pain upon movement was statistically significant at 4 h in the bupivacaine fentanyl group. The difference between both groups in terms of pain upon pressure on the wound was statistically significant with patients in the plain bupivacaine group having more pain compared to the buivacaine fentanyl group at all times except at 24 h.
There was also a difference in the number of patients in both groups who required analgesia as early as 2 h postoperatively. The difference was marked as 40% in group A compared to 3% in group B and this correlated well with the studies done before by Likar et al.[10] and Tverosky et al.[11] who also showed a better analgesic effect with added opioids to local analgesics.
At 24 h the opioid requirement (number of dose) was found to be less in group B (mean 105 ± 24.03) compared to group A (mean 218 ± 62.26) which was similar to studies done by Kumar et al. and Tverosky et al.
Opioid over the years were thought to have a central action only but recent researches have shown that opioid agonists have peripheral action as well.[12,13] The peripheral opiate antinociception is mediated through l as well as k receptors located on primary afferent veins.[14]
Fentanyl with its less histamine releasing property may be a better drug than morphine or meperidine for peripheral analgesia. Being an opioid of the phenol peperidine group
it could have a local anesthetic effect on the nerves. But the dose required for this effect would be much larger and a dose of 25 mg used by us cannot account for this effect. The primary clinical effect of fentanyl may be related to the central opiate receptors and thus can occur at a very small dose.
The mean duration of analgesia was higher in the fentanyl bupivacaine group compared to the bupivacaine group. Further the mean rescue analgesic doses were significantly less in group B as compared to group A. This supports the peripheral analgesic effect of opioids. The presence of inflammation has been found to enhance the efficacy of peripherally applied opioids.[15] This is because inflammation disrupts the perineuriun as well as increases the number of peripheral sensory nerve terminals. The favorable results in our study may be because of infiltration being performed after completion of surgery when inflammatory response may have begun. The negative results by some authors may be related to the infiltration of opioid prior to surgery when inflammation has not yet started.
In conclusion, combination of bupivacaine and fentanyl for wound infiltration in abdominal surgeries was associated with better postoperative analgesia and reduced analgesic consumption.
ReFeReNCes
1. Patel JM, Lanzalene RJ, William JS, Mullen BV, Hinshaw JR. The effect of incisional infiltration of bupivacaine hydrochloride upon pulmonary function, atelectaisis and narcotic need following elective cholecystectomy. Surg Gynacol Obst 1983;15:338-40.
2. Egan TM, Harman SJ, Doucette EJ, Normand SL, McLeod RS. A randomized controlled trial to determine effectiveness of fascial infiltration of Bupivacaine in preventing respiratory complication after elective abdominal surgery. Surgery 1988;104:734-40.
3. Tverosky M, Carlos Cozcor, Mikhal Ayaiche. Postoperative pain relief after inguinal herniorraphies different types of Anaesthesia. Anesthesia Analgesia (American journal) 1990;70:29-35.
4. Goldstien A, Grimant P, Henifuer A, Keller M, Fortin A, Darai E. Preventing postoperative pain by LA instillation after laparoscopic gynaecology surgery. A placebo controlled comparison of bupivacaine and ropivacaine. Anesth Analg 2001;91:403-7.
5. Karman L, Singh JR, Jindal SK. Postoperative pulmonary function in

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
146
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Chander, et al.: Wound inflitration analgesia
laproscopic versus open cholecystectomy: A preoperative, comparative study. Indian J Gastroenterol 2005;24:608.
6. Ekbolm A, Hanson P, Thomsson M, Thomas M. Increase postoperative pain and consumption of analgesic following acupuncture. Pain 1991;44:241-7.
7. Khiroya RC. Davenport HT, Jones JG. Cryoanalgesia for pain after herniorraphy. Anaesthesia 1986;41:73-6.
8. Eriksson AS, Sinclair R, Cassuto J, Thomson P. Influence of lidocaine on leukocyte function in the surgical wound. Anaesthesiology 1992;77:74-8. 9. Kumar PT, Bhardwaj N, Sharma K, Bhatia YK. Peripheral analgesic effect of wound infiltration with lignocaine, fentanyl and combination of lignocaine-fentanyl on postoperative pain. J Anaesth Clin Pharmacol 2006;22:161-7.
10. Likar R, Stitl R, Gragger K, Pipam W, Blatnig H, Breschan C, et al. Peripheral morphine analgesia in dental surgery. Pain 1998;76:145-50.
11. Tverosky RS, Lebovits A, Williams C, Sexton TR. Ketorole verus fentanyl for postoperative pain management in out patient. Clin J Pain 1995;11:127-33.
12. Tverosky M, Braslavsky A, Mazor A, Ferman R, Kissin l. The peripheral effect of fentanyl on postoperative pain. Anesth Analg 1998;87:1121-4.
13. Stein C. Periheral mechanisms of opioid analgesia. Anesth Analg 1993;76:182-91.14. Stein C, Millan MJ, Shippenberg TS, Peter K, Herz A. Peripheral opioid receptors
mediating antinociception in inflammation. Evidence for involvement of mu delta and kappa receptors. J Pharmacol Exp Ther 1989;248:1269-75.
15. Hahnenkamp K, Theilmeier G, Van Aken HK, Hoenemann CW. The effect of local anaesthesia on perioperative coagulation, inflammation and microcirculation. Anesth Analg 2002;94:1441-7.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.

147
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Original Article
A double-blind study on analgesic effects of fentanyl combined with bupivacaine for extradural labor analgesiaGaurav S. Tomar, Rajan B. Godwin1, Neeraj Gaur3, Ashish Sethi1, Neeraj Narang1, Veena Kachhwaha1, T. C. Kriplani1, Akhilesh Tiwari2
Department of Anesthesia and Critical Care, St. Stephen’s Hospital, 2Sushruta Trauma Centre, New Delhi, 1NSCB Medical College, Jabalpur, 3Department of Community Medicine, GRMC Medical College, Gwalior, Madhya Pradesh, India
Corresponding author: Dr. Gaurav S. Tomar, Department of Anesthesia and Critical Care, St. Stephen’s Hospital, New Delhi, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_37_11R4 AP Done 28th Jan
AbstractBackground: The intermittent technique of labor extradural analgesia has been showing promising results over other techniques. This study was done to assess and compare the efficacy of two different doses of fentanyl mixed with low doses of bupivacaine in intermittent labor extradural analgesia.Materials and Methods: 90 ASA grade I-II parturients in active labor with a cervical dilatation of 3–5 cm were randomly allocated to three different groups:• Group A: 10 ml bupivacaine 0.125% + fentanyl 10 µg (1 µg/ml).• Group B: 10 ml bupivacaine 0.125% + fentanyl 20 µg (2 µg/ml).• Group C: 10 ml bupivacaine 0.125% (the control group).All patients were preloaded with 10-15 ml/kg Lactated Ringer’s solution. Labor analgesia was maintained by intermittent boluses of the drug combination.Results: The mean time of the onset of analgesia was significantly lower (P<0.05) and the duration of analgesia was significantly higher (P<0.01) in Group B when compared with Groups A and C (P<0.001). Patient satisfaction was considerably better in Group B (P<0.01). However, in both groups, the progression of labor was found to be slightly more prolonged than Group C. The level of the sensory and motor block was comparable in both the groups and was at the T8–T10 level; it was comparable and the level of motor blockade (Bromage score = 0, 1) in each group was also not significant (P>0.05).Conclusion: The addition of fentanyl (2 µg/ml) to bupivacaine 0.125% decreases the time of the onset of analgesia and increases the duration of analgesia and level of maternal satisfaction during labor as compared to fentanyl (1 µg/ml).
Key words: Fentanyl, intermittent extradural technique, labor analgesia
INTRODUCTION
The joy of child birth is always accompanied with a fear of pain. A negative birth experience is associated with subsequent infertility, and women’s experiences should therefore be considered seriously in the provision of maternity care.[1] The concept of a walking epidural during labor is worthwhile as confining a parturient

148
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Tomar, et al.: Fentanyl with bupivacaine in labor epidural analgesia
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
to bed may lead to painful and prolonged labor with higher incidences of abnormal presentations and fetal distress.[1,2] Nowadays, it’s considered to be the gold standard for labor pains. Epidural analgesia has been used extensively in developed countries and now getting popular in developing countries like India, etc., with some modification in the traditional epidural technique.
Over the past 10 years, there have been remarkable changes in the field of obstetric anesthesia. Anesthesiologists have improved upon their techniques to alleviate pain during labor while at the same time increasing the safety for both mother and the baby. Newer techniques such as combined spinal-epidural anesthesia, continuous epidural infusions, walking epidurals, and patient-controlled epidural analgesia (PCEA) are now available.
In contrast, continuous infusion extradural analgesia (CIEA) has been associated with significant motor blockade.[3] However, newer modalities, such as CSE and PCEA, are more expensive, technically more difficult, and associated with an increased incidence of side effects such as nausea, vomiting, and pruritus along with the use of opioids.[4] Although rarely meningitis has also been reported.[5]
The greatest advantage of implementing intermittent lumbar extradural for labor analgesia is the lack of need of a volume elastomeric extradural infusion pump, making its role worthwhile in conducting deliveries in emergency settings, and primary, secondary, and tertiary health centers of developing countries (India, etc.) where these facilities are not easily available but do have the human resources to provide the intermittent top-ups.
Our study was designed to evolve an appropriate dose combination of bupivacaine and fentanyl in extradural labor analgesia using an intermittent bolus technique and to evaluate the maternal and neonatal outcomes with its effect on the progress of labor.
MaTeRIals aND MeTHODs
After obtaining approval from the institutional ethics committee, the present study was conducted after taking informed written consent from all the parturients.
A total of 90 patients were randomly assigned to one of the two intervention groups A and B, and control group C:• Group A (n=30): 10 ml of 0.125% bupivacaine and
1 µg/ ml fentanyl as a first bolus followed by intermittent top-ups of 0.0625% bupivacaine 10 ml + fentanyl 1 µg/mlatvisualanalogscore(VAS)≥3.
• GroupB(n=30): 10 ml of 0.125% bupivacaine and 2 µg/ ml fentanyl as a first bolus followed by intermittent top-ups of 0.0625% bupivacaine 10 ml + fentanyl 2 µg/ ml at VAS≥3.
• GroupC(n=30): 10 ml of 0.125% bupivacaine as a first bolus followed by intermittent top-ups of 0.0625% bupivacaine10mlatVAS≥3.
Patients were explained regarding the possible risks and complications. Women were placed in a left lateral position when the cervix was 3–5 cm dilated and with strict aseptic precautions; the mid-lumbar extradural space L3–L4/L4–L5 was identified by using a loss of resistancetechniquewitha16–18GTuohyneedleandanepiduralcatheter (Perifix16Gor18Gcatheter;B.Braun,Melsungen,Germany)was sited4–5cm in the space.Theepidural test dose was avoided in the study.
This was a prospective, double-blind, hospital-based study done from -August 10, 2009, December 10, 2009. A total of 90 patients admitted in the obstetric labor room were selected for the study of 200 cases. A time-based simple random sampling technique was used. Subjects and other study personnel were blinded as per group assignment.
Inclusion criteria were full-term (37–42 weeks) parturients of ASA class I and II having fixed cephalic presentation and cervical dilatation of 3–5 cm in spontaneous labor.
Exclusion criteria- were parturients with PIH, preterm labor, breech presentation, history of previous cesarean delivery, bad obstetric history, bleeding dyscrasia, and spinal deformities, patients on anticoagulants, hypotensive patients, morbid obese and elderly patients >35 years of age and patients having cervical dilatation >5 cm before epidural catheter insertion, patients having allergy to local anesthetics and opioids, and patients who refused on consent agreement were excluded from this study.
Data collectionFor the collection of samples, all the variables were assessed and a pretested semistructured Performa was used containing information regarding sociodemographic details of patient variables.• Preoperative data collection: A complete preanesthetic
evaluation was carried out, and maternal baseline pulse rate, blood pressure, respiratory rate, and SpO2 and fetal heart rate were recorded.
• Drug preparation and top-up administration: The drug solution containing the analgesic was prepared by an OT assistant or a junior resident. The top-up administration on the request of analgesia by the parturient by recording VAS was given by the resident (junior/senior) on duty. These were completely blinded from the study.
After collection, data were put in an Excel sheet and analyzed with the intention to treat using SPSS, 17th version.
Statistical analysis usedThe statistical significance for categorical variables was determined by Chi-square analysis. Fisher’s exact t-test was used in case one or more expected cell count was less than 5. For continuous variables, a two-sample

149
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Tomar, et al.: Fentanyl with bupivacaine in labor epidural analgesia
t-test was applied. Differences among the group means were compared using analysis of variance. Results were expressed as mean ± SD (standard deviation). A P value <0.05 was considered statistically significant.
Taking a sample size of 30 in each group with a = 0.05, the power of the study is approximately 80%.
In Group A (n=30), the first dose of 10 ml containing 0.125% bupivacaine mixed with 1 µg/ml fentanyl (0.0001%) was administered via the catheter into the epidural space. In Group B (n=30), the first dose containing a similar concentration of bupivacaine along with 2 µg/ml fentanyl (0.0002%) was given. Top-up doses (10 ml containing 0.0625% bupivacaine with a similar concentration of fentanyl respective to each group) were given when patient’s VAS ≥3. After each drug administration,patient vitals (pulse, BP, RR, SPO2), maximum sensory/motor blockade level achieved, and fetal heart rate were monitored at 5, 10, 15, 30, 45, 60, 90, 120, 150, 180 min intervals or till delivery. Following every top-up dose, patients were monitored carefully for 10 min to detect any weakness or inadequacy of analgesia.
Motor blockade was assessed by the modified Bromage score[6] (0 = no impairment; 1 = unable to raise extended leg but able to move knees and foot; 2 = unable to raise extended leg as well as flex knees, but able to move foot; 3 = not able to flex ankle, feet, or knees) which was determined every 60 min during the first stage of labor. Maximum levels of sensory blockade achieved were assessed by the pinprick method and ice cube method.
Observed parameters were onset of analgesia, duration of analgesia, and time to the first top-up requirement assessed by VAS and verbal pain score (VPS) for pain at every 10 min, numbers of top-ups required, duration of the first and second stage of labor, mode of delivery, and APGARscoreat1and5min.
On the day after delivery, maternal satisfaction level assessed by parturient acceptance regarding the quality of analgesia throughout labor was assessed by the following scoring system: 0, failure; 1, incomplete; 2, good; 3, excellent; and not possible to evaluate (NPE) due to delivery by cesarean section.[6,7] All the obstetricians, attending the parturient were asked regarding the maintenance of maternal expulsive power during the second stage of labor.
ResUlTs
The onset and duration of analgesia when compared to the intervention groups A and B was found to be statistically significant (P<0.0001). Twenty parturients in Group B had profound analgesia within 10min; inGroup A, it took around 15–20min to achievemaximum
analgesiawhile inGroupC,maximumanalgesiawasseenafter 20–30 min [Table 1]. VAS and VPS showed a faster onset of complete analgesia in Group B. The duration ofanalgesia of the first bolus dose (time interval between the bolus dose and the first maternal analgesia request) washigherinGroupB(i.e.,120±20.26minascomparedto 100 ± 10.04min of Group A and 75 ± 12.24min ofGroupC).
The duration and progression of labor (first and second stage) from the insertion of the epidural (i.e., study time) was found to be slightly prolonged by approximately less than 15min in Group B as compared to Groups A and Cthat was statistically nonsignificant (P>0.05). There was no difference in the degree of sensory blockade as assessed by the pinprick method or ice cube method, maximum at the T8 level in around 60% parturients, and motor blockade assessed by the modified Bromage score (score = 0) in among 93.34% parturients inGroupA and 90% parturientsof Group C which means that they were able to walk upto a certain distance and were able to void by themselves. Only two parturients in Group A and three parturients inGroup B had a score = 1 as compared to eight (26.67%)parturients of the control group that was statistically significant (P=0.024;Table1).APGARscoresat1and5minwere found to be comparable and statistically nonsignificant in both intervention groups (P=0.99; Table 1). Top-up requirements because of shorter duration of action was quite higher in control group C than intervention groups A and B in the order of C>A>B (P=0.001; Table 2).
The total dose of bupivacaine and fentanyl used in our study was 67.42 ± 20.25 mg bupivacaine and 74.34 ± 30.34 µgfentanyl inGroupA,53.20±18.15mgbupivacaine and 65.12+25.65 µg fentanyl in Group B,and 76.24 ± 12.34 mg bupivacaine in the control group C which was statistically significant (P<0.05; Table 2).
Therewas one accidental dural puncture inGroup B andthe patient was excluded from the study.
The mode of delivery was spontaneous, i.e., normal vaginal delivery (NVD) in both the intervention groups; only one patient in Group A (3.33%), two in GroupB (6.66%), and four parturients in Group C (13.34%)were converted to cesarean section because of the prolongation of the labor (statistically nonsignificant P value, 0.337).
Maternal nausea and vomiting were reported in two cases (6.66%) in Group B and in one parturient (3.33%)in Group A as compared to nil among control group C[Table 1]. The incidence of urinary retention (13.34%) and hypotension (6.66%) was quite higher in the control group than any intervention group. Fetal distress was reported inonefetus inGroupsAandC(3.33%),andtwoinGroupB(6.66%).

150
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Tomar, et al.: Fentanyl with bupivacaine in labor epidural analgesia
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
The maternal satisfaction level was significantly higher (90%) in Group B; 20 parturients reported excellentanalgesia, while 7 explained a good score when compared toa60%satisfaction level inGroupAand just40% in thecontrol group (P<0.0001; Table 1).
DIsCUssION
In this prospective, randomized, double-blind study between two different doses of fentanyl for labor analgesia; doses chosen were based on a pilot study
Table 1: Comparison of various studied parameters among three groupsParameters studied Control group
Group C (%)Intervention groups Test applied (Chi-square analysis)
Group A (B+F10) (%)
Group B (B+F20) (%)
c2 value P value
Onset of action0-10 min10-15 min15-30 min
1 (3.33)4 (13.34)26 (86.67)
2 (6.66)9 (30)
19 (63.33)
18 (60)11 (36.66)01 (3.33)
51.01 <0.0001
Highest sensory blockade T6T8T10
2 (6.66)18 (60)
10 (33.33)
3 (10)16 (53.34)11 (36.66)
4 (13.33)16 (53.34)10 (33.33)
0.89 0.925
Max. motor blockadeMod. bromage score 0Mod. bromage score 1
22 (73.33)08 (26.66)
29 (96.66)01 (3.33)
27 (90)03 (10)
7.5 0.024 (between C and A/B)
Mode of delivery NVDLSCS
26 (86.67)04 (13.34)
29 (96.66)01 (3.33)
28 (93.33)02 (6.66)
2.17 0.337
APGAR scoreAt 1 min = +5At 5 min = +7
27 (90)28 (93.33)
28 (93.33)29 (96.66)
28 (93.33)28 (93.33)
0.00 0.99
Side effects (maternal)Nausea/vomitingHypotensionUrinary retention
000204
1 (3.33)00
2 (6.66)00
5.19 0.07
Side effects (Fetal)Distress/bradycardia 00 1 (3.33) 2 (6.66) 2.07 0.355
Mater. satisfaction levelOverall NPE FailureIncompleteGoodExcellent
12 (40)03 (10)
03 (9.99)12 (40)10 (30)
02 (6.66)
18 (60)01 (3.33)02 (6.6)09 (30)12 (40)06 (20)
27 (90)02 (6.66)00 (00)
01 (3.33)07 (23.33)20 (66.66)
33.07 0.00006
Table 2: Comparison of duration of labor and amount of drugs used among three groupsParameters studied Control group Intervention groups Test applied
Group C (mean ± SD)
Group A (mean ± SD)
Group B (mean ± SD)
ANOVA
Study duration of labor (h)
1st stage 2.76 ± 0.34 2.80 ± 0.35 2.87 ± 0.36 F value = 0.759P value = 0.471
2nd stage 1.26 ± 0.26 1.24 ± 0.24 1.32 ± 0.32 F value = 0.685P value = 0.507
Total dose, bupivacaine (mg) 76.24 ± 12.34 67.42 ± 20.25 53.20 ± 18.15 F value = 13.639P value<0.0001
Total dose, fentanyl (mcg) NA 74.34 ± 30.34 65.12 ± 25.65 T value = 2.59P value = 0.03
No. of top-ups 3.12 ± 1.23 2.48 ± 1.29 1.82 ± 1.35 F value = 7.606P value = 0.001
Duration of action (1st top-up requirement; min)
75 ± 12.24 100 ± 10.04 120 ± 20.26 F value = 69.20P value<0.0001

151
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Tomar, et al.: Fentanyl with bupivacaine in labor epidural analgesia
assessing clinical impression of efficacy, motor blockade, and duration of action. We decreased the volume and concentration of the drug injected extradurally, keeping in view the difference in demographic data (age, height) in the Indian population as compared to the western parturients [Table 3].[7-9] Our aim was to minimize the concentration of the local anesthetic along with an appropriate dose of the opioid, so as to provide maximal labor analgesia along with active maternal participation during labor without affecting fetal well-being.
The test dose was avoided in this study because in a laboring patient, maternal heart rate variability from the pain of uterine contractions may confuse the interpretation of the heart rate response, and intravenous epinephrine may have deleterious effects on the uterine blood flow.[10,11]
The time interval from the initial bolus dose to the maternal analgesia request in our study was significantly increased in Group B. The longer latency to demand foranalgesia in parturients of Group B could be attributedto a comparatively higher concentration of the opioid (fentanyl) used with the diluted low concentration of the local anesthetic (bupivacaine) since an increase in doses of the opioid and local anesthetic is directly proportional to the quality and duration of satisfactory analgesia and anesthesia but inversely to the time of the onset of block. [7]
The VAS and VPS at 10min were lower in Group Bindicating an early onset of analgesia. There was no difference in the degree of motor blockade in both intervention groups.
In our study, 93.33% parturients in Group A and 90% inGroup B were mobile during 25–50% of the study time.Ambulation was achieved in 70% of the fentanyl epidural group and 68% in the bupivacaine, epinephrine, and fentanyl (BEF) group by Breen et al.[8] The incidence of sparing of motor blockade in both intervention groups in the present study is likely explained by the use of a lower concentration bupivacaine solution. Because motor blockade is considered undesirable during labor analgesia, the potential local anesthetic (bupivacaine) sparing effect of an intermittent bolus technique may be more clinically relevant than other continuous extradural techniques such as CIEA, PCEA, and CSEA.[3]
Several mechanisms have been proposed to explain the advantages of bolus compared with the continuous infusion of extradural solutions. When injected as a bolus through a multiorifice epidural catheter, the solution exits the distal end of the epidural catheter through all the orifices.[12] In contrast, when a continuous infusion of the same volume is injected through the catheter, it primarily exits through the proximal orifice. Another possible explanation of reduced bupivacaine consumption with the bolus technique may be the distribution of solutions in extradural space which is nonuniform but which spreads uniformly when delivered in large volumes with high injectable pressure.[13]
Our most significant findings were the reduction in the number of boluses and the overall reduction in the local anesthetic use in Group B (2 µg/ml fentanyl).[14-16] Local anesthetic sparing by a magnitude of 15–20% is also characteristic of PCEA[17] whereby patients self-administer the local anesthetic according to their level of pain. However, a potential criticism of the PCEA system is that patients will only demand a bolus when developing pain as the sensory block regresses. This is compounded by the lag time between the administration and action of epidural drugs. In contrast, regular intermittent bolus administration endeavors to prevent pain by injecting the local anesthetic at time intervals chosen so that the majority of patients remain pain free.[17-19]
In addition to bupivacaine, we found a dose sparing effect of fentanyl.[3,14,15,20,21] The systemic absorption of extradural fentanyl may result in fetal depression.[22,23] In Group B,there were two reported cases of fetal bradycardia seen as compared to group A in which only one case was seen. Incidence maternal side effects like urinary retention and hypotension were quite higher in the control group than any intervention group that possibly justified with the higher consumption of the local anesthetic (bupivacaine). Maternal analgesia satisfaction was higher (90% reported good/excellent) in Group B (with 2µg/ml fentanyl group) thaninGroupA(1µg/ml fentanyl) showing a 60% satisfied level which was merely 40% in Group C. This differencewas found to be clinically significant when measured by a 100-mm VAS and VPS.[24,25]
There are few limitations in our study. By study design, subjects randomized to each group were nulliparae
Table 3: Comparison of anthropometric variables and age of parturients between three groupsVariables Intervention groups Control group Test
applied ANOVA
Group A (B+F10) Group B (B+F20) Group CNo. Mean SD Mean SD Mean SD
Age (years) 30 22.4 1.86 23 2.24 22 1.80 F value = 1.94 P value = 0.149
Height (cm) 30 154.64 3.24 156.28 4.22 155.20 3.84 F value = 1.45 P value = 0.24
Weight (kg) 30 54.42 5.20 56.80 6.40 55.88 5.90 F value = 1.261 P value = 0.289
152
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Tomar, et al.: Fentanyl with bupivacaine in labor epidural analgesia
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
and multiparae; in multiparae there was lesser drug requirement because of shorter duration of labor as compared to nulliparae. In the current study, the salutary effect of the intermittent bolus technique was higher in women with longer duration of labors and in nulliparae. So, its use was found to be of greater significance in primigravida or nulliparous women.[16] Another limitation is a small sample size.
In summary, we found that 2 µg/ml extradural fentanyl is better than 1 µg/ml when combined with bupivacaine in the intermittent bolus technique, as it leads to faster onset, longer duration of analgesia, higher maternal satisfaction, and lesser drug requirement of the local anesthetic with a comparable side effect profile.
aCKNOWleDGMeNT
The authors are thankful to Dr. (Prof.) Rekha Mahendra, MD; Dr. Shankar Agrawal, MD, Department of Anesthesiology and Critical Care, NSCB Medical College, Jabalpur, Madhya Pradesh, India.
ReFeReNCes
1. Mendez-Bauer C, Arroyo J, Garcia Ramos C, Menendez A, Lavilla M, Izquierdo F, et al. Effects of standing position on spontaneous uterine contractility and other aspects of labor. J Perinat Med 1975;3:89-100.
2. Flynn AM, Kelly J, Hollins G, Lynch PF. Ambulation in labor. Br Med J 1978;2:591-3.
3. Wong CA, Ratliff JT, Sullivan JT, Scavone BM, Toledo P, McCarthy RJ. A randomized comparison of programmed intermittent epidural bolus with continuous epidural infusion for labor analgesia. Anesth Analg 2006;102:904-9.
4. Norris MC, Grieco WM, Borkowski M, Leighton BL, Arkoosh VA, Huffnagle HJ, et al. Complications of labor analgesia: Epidural versus combined spinal epidural analgesia techniques. Anesth Analg 1994;79:529-37.
5. Harding SA, Collis RE, Morgan BM. Meningitis after combined spinal-extradural anaesthesia in obstetrics. Br J Anaesth 1994;73:545-7.
6. Bromage PR. A comparison of the hydrochloride and carbon dioxide salt of lidocaine and prilocaine in epidural analgesia. Acta Anaesthesiol Scand Suppl 1965;16:55-69.
7. Gupta S, Raiger LK, Raman V. Ambulatory labor Analgesia - Comparison of two regional techniques. Indian J Anaesth 2002;46:44-8.
8. Breen TW, Shapiro T, Glass B, Payne DF, Oriol NE. Epidural anaesthesia for labor in an ambulatory patient. Anesth Analg 1993;77:919-24.
9. Cohen SE, Yeh JY, Riley ET, Vogel TM. Walking with labor epidural analgesia: The impact of bupivacaine concentration and a lidocaine-epinephrine test dose. Anesthesiology 2000;92:387-92.
10. Norris MC, Ferrenbach D, Dalman H, Fogel ST, Borrenpohl S, Hoppe W, et al. Does epinephrine improve the diagnostic accuracy of aspiration during labor epidural analgesia?. Anesth Analg 1999;88:1073-6.
11. Hood DD, Dewan DM, James FM 3rd. Maternal and fetal effect of epinephrine in gravid ewes. Anesthesiology 1986;64:610-3.
12. Kayner AM, Shankar KB. Epidural infusion: continuous or bolus? Anesth Analg 1999;89:534.
13. Hogan Q. Distribution of solution in the epidural space: Examination by cryomicrotome section. Reg Anesth Pain Med 2002;27:150-6.
14. Murphy JD, Henderson K, Bowden MI, Lewis M, Cooper GM. Bupivacaine versus bupivacaine plus fentanyl for epidural analgesia: Effect on maternal satisfaction. BMJ 1991;302:564-7.
15. Lyons G, Columb M, Hawthorne L, Dresner M. Extradural pain relief in labor: Bupivacaine sparing by extradural fentanyl is dose dependent. Br J Anaesth 1997;78:493-7.
16. Chua SM, Sia AT. Automated intermittent epidural boluses improve analgesia induced by intrathecal fentanyl during labor. Can J Anaesth 2004;51:581-5.
17. Boutros A, Blary S, Bronchard R, Bonnet F. Comparison of intermittent epidural bolus, continuous epidural infusion and patient controlled-epidural analgesia during labor. Int J Obstet Anesth 1999;8:236-41.
18. Bogod DG, Rosen M, Rees GA. Extradural infusion of 0.125% bupivacaine at 10 ml h-1 to women during labor. Br J Anaesth 1987;59:325-30.
19. Smedstad KG, Morison DH. A comparative study of continuous and intermittent epidural analgesia for labor and delivery. Can J Anaesth 1988;35:234-41.
20. James KS, McGrady E, Quasim I, Patrick A. Comparison of epidural bolus administration of 0.25% bupivacaine and 0.1% bupivacaine with 0.0002% fentanyl for analgesia during labor. Br J Anaesth 1998;81:507-10.
21. Celleno D, Capogna G. Epidural fentanyl plus bupivacaine 0.0125% for labor: Analgesic effects. Can J Anaesth 1988;35:375-8.
22. Loftus JR, Hill H, Cohen SE. Placental transfer and neonatal effects of epidural sufentanil and fentanyl administered with bupivacaine during labor. Anesthesiology 1995;83:300-8.
23. Kumar M, Paes B. Epidural opioid analgesia and neonatal respiratory depression. J Perinatol 2003;23:425-7.
24. Singer AJ, Thode HC Jr. Determination of the minimal clinically significant difference on a patient visual analog satisfaction scale. Acad Emerg Med 1988;5:1007-11.
25. Nikkola E, Läärä A, Hinkka S, Ekblad U, Kero P, Salonen M. Patient-controlled epidural analgesia in labor does not always improve maternal satisfaction. Acta Obstet Gynecol Scand 2006;85:188-94.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.
153
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Original Article
Coma in the elderly: Etiological factors, management, and prognosis in the department of anesthesia and intensive careD. Diango, M. Moghomaye, Y. Maiga1, S. A. Beye2, A. S. Dembele3, Y. Coulibaly4, A. Diallo4
Department of Anesthesia and Intensive Care of Gabriel, 1Department of Neurology of Gabriel, TOURE Teaching Hospital, Bamako,2Department of Anesthesia and Resuscitation in Hospital of Segou, 3Department of Anesthesia in Ophthalmological Tropical African Institute Teaching Hospital, Bamako, 4Department of Anesthesia Resuscitation Emergency of Point G Teaching Hospital, Bamako, Mali
Corresponding author: Dr. Diango Djibo, Anaesthesiologist, Senior Lecturer, Department of Anesthesia and Intensive Care of Gabriel, TOURE Teaching Hospital, Bamako, Mali. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_22_11R8
AbstractObjective: To study the etiologies, therapeutic and prognosis factors of coma in the elderly in the Department of Anesthesia and Intensive Care of Gabriel TOURE Teaching Hospital, Mali.Materials and Methods: This was a prospective descriptive study of all cases of coma in the elderly, registered from February 1, 2008 to January 31, 2009 at the Department of Anesthesiology CHU Gabriel Touré, Bamako.Results: During the study period, 564 patients were admitted to the intensive care unit (ICU) in which 174 (30.85%) were older people. We collected 100 subjects with impaired consciousness, the object of our study, which represented 17.73% of all admissions in the Department of Anesthesiology during the study period and 57.47% of all admissions of older people; 66% of our subjects were male. Hypertensive patients accounted for 60% of cases. In 46% of cases, it was a coma from cardiovascular causes and in 28% of cases; it was a coma of metabolic origin. The diagnoses made in the wake of the care of the elderly in ICU were predominantly stroke (46%) and electrolyte disturbances (13%). The coma was sudden onset in 58% of cases, including 28 cases of stroke whether 48.27%. The prognosis was marked by a fatality with 51% of deaths in our sample.Conclusion: The prognosis improvement of the elderly in coma through to the introduction of proxy measures.
Key words: Comatose, elderly, management, prognosis
the elderly and increases the consumption level of care. Due to this fact, the increase in life expectancy of the population accounts from more frequent care of the elderly intensive care units (ICUs),[1] the capital of the old age, according to WHO is generally set at 60 years. In a recent study in North America, including 10 900 patients, approximately 50% were aged over 60 years. [2] In 1996 in the Ivory Coast compiled 300 cases of impaired consciousness on 6875 admissions[3] whether 5.06%. In Department of Anaesthesia and Intensive Care of Gabriel TOURE Teaching Hospital in Mali a similar study to the
INTRODUCTION
The physiological changes induced by age tend to weaken

154
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Diango, et al.: Coma in the elderly
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
above[4] found 53.4% of cases of impaired consciousness with 25.38% of coma in particular. Different disorders of consciousness are generally understood as deficits or the mechanical effects of exogenous.[5] These disorders of consciousness create an emergency that must be overcome immediately. However, in our context, the lack of technical equipment makes it difficult and mostly hypothetical etiologic diagnosis.
Even if the definition of elderly is more physiological than chronological, support the elderly poses several problems:• In terms of frequency, improvedmedical and surgical
techniques and increased life expectancy are increasing the admission of elderly patients in ICU.
• Intermsofethics,thediscussionabouttheprobabilityof survival of the “patient” limits “aggressive therapy.”
• In economic terms, the cost of intensive care is veryhigh.
In view of this difficulty that hinders etiologic consistently support our comatose patients, our attention will focus on providing a better knowledge on the etiology and treatment of cases of coma observed in the SAR of Gabriel TOURE Teaching Hospital. This prospective study aims to investigate the etiologies, management, and prognostic factors of coma in the elderly.
MATERIALS AND METHODS
Study framework and operationThe ICU (SAR) adult versatile of Gabriel TOURE Teaching Hospital is a 9-bed unit, which receives on average 420 patients per year. The effective medical management of patients is provided daily by three anesthesiologists, 2 internal and students making function internally. At the paramedical per 12 h, groups of nurses and caregivers to help provide care to patients.
MethodologyThis was a prospective descriptive study of a 12-month period from February 2008 to January 2009.
Inclusion criteriaAll patients aged ≥60 years, irrespective of gender, inwhom the impairment of consciousness was clinically GlasgowComaScale(GCS)≤8confirmedwerechosen.
Non-inclusion criteria• Patientsagedbelow60years• PatientswithaGCS>8• Patientswhoseadmissionhasbeenmadeoutsideour
study period.
Data reviewedAge, gender, the source, medical history, the mode of onset of coma, the GCS at admission, etiology of coma, the main diagnosis, additional tests carried, established
treatment, the duration of the stay, severity scores calculated within the first 24 h, T-RTS, IGSA, Trauma Index-output mode.
Capture and analysisEntry and data analysis, statistical tests were performed using SPSS 16.0. The results were presented in theform of tables and graphs using Microsoft software and Microsoft Excel and Word 2007.
RESULTS
Male sex was predominant in 66% of cases with a sex ratio of 1.94; extreme ages being of 60 and 90 years. Subjects in the age group of 60–65 years were most represented amounting to 35% of the cases, out of which 18 were sent by the SAU (home emergency service) and 10 were from other hospital services of Gabriel TOURE Teaching Hospital, respectively, 51.42% and 28.57% [Table 1].
The diagnosis made in the wake of the care of elderly patients in the ICU was predominantly stroke (46%). Stroke was more common in men than in women, respectively, 67.39% and 32.60% [Table 2].
The hypertensive patients accounted for 60% of the subjects; 63.33% were male. Patients with a historyof diabetes and/or hypertension accounted for 67% of subjects in the sample. The subjects of the age group of 60–65 years were most affected by the cardiovascular and metabolic diseases associated or not, including hypertension, diabetes, and hypertension and stroke, respectively, 25.71%, 11.42%, and 14.28% [Table 3].
Support the SAR was made between 12 and 24 h after the onset of impaired consciousness in 42% of subjects [Table 4].
The antipyretic and analgesic were administered, respectively, in 79% and 69% of cases [Table 5].
According to the T-RTS score, the majority of subjects in our sample had a probability of death or above 50% with a T-RTS score between 9 and 11. We identified 51% of deaths in our study, which may be superimposed on the T-RTS score predictor. IGSA score showed 39% of subjects in our sample with a probability of death equal to 70% [Table 6].
Patients admitted with a GCS scale between 3 and 5 diedwithin 12% of cases and 23.53% of all subjects died [Table 7].
DISCUSSION
Constraints of the studyAll the difficulties we have encountered throughout our study may be attributed to a lack of documented scientific data on the elderly and a lack of comparative data, because there are no studies prospectively evaluating the benefit of resuscitation for these patients.[6]

155
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Diango, et al.: Coma in the elderly
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Table 2: Leading diagnoses of patients who diedDiagnosis Outcome from
comaTotal (n)
Died (n) %Stroke 23 50 46
Hypovolemic shock 3 43 7
Acidocetosic coma 1 25 4
Hyperosmolar coma 0 0 3
Severe acute malaria 5 62 8
ICEP 5 83 6
Polytrauma 4 66 6
Sepsis 1 50 2
Head injury 1 20 5
Electrolytic disorders 10 77 13
ICEP: Intracranial expansive process
Table 1: Characteristics of patients hospitalizedMen/women (n) 66/34
Average age (years)Extreme age (years)
75 ± 1560–90
OriginEmergency Service (%)Gabriel TOURE Teaching Hospital (%)Private Medical Center (%)Other health facilities (CHC, HCRef) (%)
5328118
Average stay 1-5 days (%) 56
Mortality (%) 51CHC: Community Health Center; HCRef: Health Center for Reference
Table 3: Clinical featuresMedical history
Cardiovascular (hypertension, stroke)Metabolic (diabetes)None
601531
Admission glasgow coma scale
3–56–8
2179
Complementary tests
BiologyComputed tomography
9861
Etiologies of coma
CardiovascularMetabolicTraumaticInfectious
4628179
Values are given in percentage
Table 6: Mortality and severity indicatorSeverity indicator Died PercentageT-RTS
6–89–11
1340
6550
IGSA≤8>8
2033
3384
Champion3–910–14
449
10051
Table 7: Evolution of patients according to initial glasgow coma scaleAdmission glasgow coma scale
Outcome of coma TotalDied Not dead
Between 3 and 5 12 9 21
Between 6 and 8 39 40 79
Total 51 49 100 Chi-square of Pearson = 1.993; ddl = 1; P=0.158
Table 4: Distribution of patients according to the time between the onset of impaired consciousness and admissionDelay between the onset of impaired consciousness and admission
Frequency of admission
[1 H and 6 H] 12
[6 H and 12 H] 17
[12 H and 24 H] 42
[24 H and 48 H] 29
Total 100
Table 5: Distribution of patients according to established treatmentTreatment instituted FrequencyCrystalloids 100
Antipyretic 79
Analgesic 69
Antibiotic 59
Antihypertensive 37
Antimalarials 23
Colloids 20
Anticoagulants 19
Tonic cardiac sympathomimetic 17
Insulin 16
Liquefying bronchial 15
Antiplatelet aggregation 13
Anticerebral edema 9
Antiparasitic 8
Anticonvulsing 7
Corticoids 6
Epidemiological dataDuring the study period which lasted 12 months, 564 patients were admitted to the ICU of whom 174 (30.85%) were older people. In this sample of 174 elderly, we collected 100 subjects with impaired consciousness, the object of our study, who represented 17.73% of all admissions in the Department of Anaesthesiology during the study period and 57.47% of all admissions of older people.
The frequency of coma in ICUs varies in the literature and is related to admission, transfer of patients, and

156
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Diango, et al.: Coma in the elderly
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
management of available resources and financing of care. This effect could possibly increase in the next few years if nothing is done, given the delay in the management of many diseases that can cause impaired consciousness.
Male sex was predominant in 66% of the cases with a sex ratio of 1.94; extreme ages being 60 and 90 years. Subjects in the age group of 60-65 years were most represented 35% of the cases, of which 18 were sent by the SAU (home emergency service) and 10 were from other hospital services of Gabriel TOURE Teaching Hospital, accounting for 51.42% and 28.57%, respectively.
Clinical and management dataMedical historyThe hypertensive patients accounted for 60% of the subjects of whom 63.33% were male. Patients with ahistory of diabetes and/or hypertension accounted for 67% of the subjects in the sample. The subjects of the age group of 60–65 years were most affected by the cardiovascular and metabolic diseases associated or not, including hypertension, diabetes, and hypertension and stroke, respectively, 25.71%, 11.42%, and 14.28%.
Our results differ from those of[3] who found that 44% of patients had a history of diabetes and/or hypertension. The frequency of cardiovascular and metabolic diseases alone or in combination could be related to the age of our comatose patients (60–90 years).
Onset of altered consciousness and admissionThe management was made between 1 and 24 h in 71% of cases. The evacuation could be done within 24 h for patients from private institutions and other health facilities if there was an early warning system (telephone, radio, and others) and rapid transit.
Glasgow coma scalePatients admitted in emergency with a GCS between 6and 8 represented 79%. Our results are similar to those [4] who found in his study, 80.8% of patients with a GCS between 6 and 8.
Additional testsIn our study, laboratory tests and CT (computed tomography) were the main complementary tests performed in 98% and 61% of cases, respectively. In 8% of cases the cause of coma was not confirmed because of the lack of paraclinical facility, which was in part due to the economic condition of the families. This could also explain the fact that in our study, treatment was instituted in 82% of the cases.
Our results are similar to those[7] who found that the coma was confirmed by additional tests in 85.2% of cases.
Treatment institutedThe treatment was instituted in 82% of cases. This was mainly antipyretic and analgesic in 79% and 69% of cases,
respectively. It was mainly symptomatic and nonspecific, especially as the additional tests for a large majority were not made for lack of financial means and third-party payment. The appropriate management of elderly patients in the ICU depends on both adequate financial means available to the patient’s family and the resources available to the SAR (equipment, drugs).
Etiological dataCause of comaIn our series, three groups of causes dominated our study: coma from cardiovascular origin (46%), metabolic (28%), and coma caused by trauma (17%). Cases of cardiovascular disease could be explained by the frequency of certain risk factors in the Malian population, such as hypertension and diabetes. In Mali, hypertension is the most common diseases in adults and its prevalence reaches 10% of the population.[8] Regarding diabetes, 1.4% of the population is diabetic, 8.4% of patients have postprandial blood glucose limit to suspect diabetes,[9] diabetes being a precursor to infection. There is therefore an emergence of these risk factors in Mali.
DiagnosisThe diagnoses made in the wake of the care of the elderly in the ICU were predominantly stroke (46%) and these were more common in men than in women, respectively, 67.39% and 32.60%. The coma was sudden onset in 58% of cases, including 28 cases (48.27%) of stroke. In 42% of the cases, it was gradual onset in 18 stroke cases and 6 cases of metabolic disorders, respectively, 42.85% and 14.28%, of all the progressive onset of coma. Cases of cardiovascular disease could be explained by the emergence of risk factors, such as hypertension and diabetes in Mali.[8,10]
Support medicThe treatment instituted was made in full in 18% of the cases and mostly in comas of metabolic origin, that is, 50% and was done partly in 82% of cases, mostly in comas of cardiovascular origin, 48.78%. This difference could be explained by the heaviness of the investigations, sometimes very expensive in a neurologic coma, which is not the case in the coma of metabolic origin.
Facts about the evolution of comaWe identified 51% of deaths in the SAR and 49% of patients were transferred to other inpatient services UHC or allowed to return home at the request of the family. The percentage of deaths (51%) is explained by the predominance of elderly patients with a precarious financial situation and the difficulty of care due to lack of appropriate service level for effective resuscitation in the intensive care setting.
T-RTS scoreAccording to the T-RTS score, the majority of subjects in our sample had a probability of death or above 50% whether a T-RTS score between 9 and 11. We identified

157
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Diango, et al.: Coma in the elderly
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
51% of deaths in our study, which may be superimposed on the T-RTS score predictor. Our results differ from those [11] found that 55.8% of patients with T-RTS score between 9 and 11.
Score IGSAIGSA score showed 39% of subjects in our sample with a probability of death equal to 70%. Our results corroborate a study made by[12] showing that total mortality increased with the value of the IGS, whatever the type of patient. This mortality is higher for medical patients.
Score championBy score of champion, 96% of subjects in our sample had a mixed prognosis with a score between 10 and 14. Our results are similar to those[11] in which 78.9% of patients had a score of champion severe or critical.
Length of stayThe length of stay was an average of 1–5 days and involving 58% of subjects. We identified 51 deaths among the elderly of which 34 died within 5 days after admission to the SAR. The mortality rate is significantly higher here, in the case of a coma from cardiovascular causes (46%), which is the leading cause of death in our etiology.
This could be due to late detection and correction of poor risk factors, such as hypertension and diabetes.
Outcome of comaIn our series, 51% of patients had died. The majority of patients in whom treatment was done in part had died—88.68% of all deceased patients.
This result could be explained by the fact that in most cases, treatment was not necessarily set the specific treatment needed. Initially, it was recognized symptomatic rotated to the clinical signs and circumstances of occurrence; the second time, this treatment was often based on the level of patient’s life. For a GCS between 6 and 8, the death rate was 73.59%.
According to a study conducted,[13] mortality in the elderly in the ICU is higher than that of younger patients (mortality with patients 20-29 years is half of the mortality ofpatientswhoseage>60years).
CONCLUSION
Coma in the elderly, as defined, is a medical emergency and treatment. The cost-benefit ratio is unfavorable for
the elderly because its more productive life expectancy is shorter and rehabilitation to longer life. In order to improve the prognosis of coma significantly in the elderly, a better understanding of the etiology and a review is necessary complementary precise, fast, and focused.
Maybe we should set up centers to take better care of elderly patients.
REFERENCES
1. Spoljar P. Les troubles de l’éveil de coma:Déficit ou défense [en ligne].Déc 2002. Consultable à l’Avalable from: http://www.cairn.info/load_pdf.php?ID_ARTICLE = CPSY_034_0093 [Last accessed on 2008 June 20].
2. Muller L, Lefrant J Y, Gache A, DE LA Coussaye J E. Critères d’admission du sujet âgé en réanimation. Médecine d’urgence Elsevier[en ligne], Paris 2003, p. 29-37. Consultable à l’ Available from: http://www.sfmu.org/documents/consensus/cc_avc.pdf [Last accessed on 2008 Dec 28].
3. Gbobia RE. Etude de 300 cas de coma admis aux urgences médicales du Chu de Treichville. Université de cote d’ivoire, Faculté de médecine. Th d med, Abidjan; 1996. Nº1648.
4. Imboua Edget A. J. Aspects épidémiologiques et étiologiques des comas au service de réanimation de l’hôpital Gabriel Touré. Th d med, Bamako; N°64 Consultable à l’ Available from: http://www.keneya.net/fmpos/theses.pdf [Last accessed on 2005].
5. Lehot J-J, Bonhomme F. Urgence- Réanimation Anesthésie- Douleur. Editions PRADEL, Paris 2003, p. 1-187.
6. Soury-lavergne Aude, Guidet B. L’admission des patients âgés en réanimation médicale. 37ème Congrès de la Société de Réanimation de Langue Française[en ligne], Paris Janvier 2009. Consultable à l’ Available from: http://www.blogexpert.info/doc/srlfdp.pdf [Last accessed on 2009 Jan 24].
7. Dembele Sidibe M. Aspects épidémiologiques et cliniques des comas dans le SAR du CHU GT. Th d Med, Bamako; N°477 Consultable à l’ Available from: http://www.keneya.net/fmpos/theses.pdf [Last accessed on 2008].
8. Guindo Y D. Prise en charge des AVC en unité de soins intensifs de l’HNPG. Th d Med, Bamako; N°78. Consultable à l’ Available from: http://www.keneya.net/fmpos/theses.pdf [Last accessed on 2001].
9. Toure F. Complications dégénératives du diabète au Mali. Th d Med, Bamako; N°63. Consultable à l’ Available from: http://www.keneya.net/fmpos/theses.pdf [Last accessed on 1989].
10. Boire M. Motifs de consultation dans le service de cardiologie de l’HGT à propos de 500 cas. Th d med, Bamako; N° 18. Consultable à l’ Available from: http://www.keneya.net/fmpos/theses.pdf [Last accessed on 1998].
11. Diango D, Wega Kwekam N, Diallo A, Diallo G, Diallo A. Polytraumatisme au service des urgences chirurgicales de l’hôpital gabriel touré Mali Medical 2002 T XVII N° 3and4.
12. Tchoua R, Vemba A, Taty koumba C, Ngaka nsafu D. Gravite des malades de réanimation à la fondation jeanne EBORI de Libreville. Med Af Noire[en ligne], 1999, Vol. 5, p. 497. Consultable à l’ Available from: http://www.santetropicale.com/resume/114602.pdf [Last accessed on 2008 Dec 28].
13. Tagan D. La réanimation de la personne âgée[en ligne]. Janvier 2003. Consultable à l’Available from: http://www.hopital-riviera.ch/soins-intensifs/AA%20Dias%20Poweroint/Rea_age.ppt [Last accessed on 2008 Dec 18].
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
158
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Original Article
A comparative study of efficacy of oral nonsteroidal antiinflammatory agents and locally injectable steroid for the treatment of plantar fasciitisChaitali Biswas, Anirban Pal, Amita Acharya1
Department of Anaesthesiology, Calcutta National Medical College, 1Department of Anaesthesiology, Bangur Institute of Neurosciences, Kolkata, India
Corresponding author: Dr. Chaitali Biswas, 135, P K Guha Lane, Jora-Pukur, Dum Dum Cantt, Kolkata - 700 028, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_49_11R8 AP Done 27th Jan
AbstractObjectives: To compare the effectiveness of oral nonsteroidal antiinflammatory drugs (NSAIDs) and locally injectable steroid (methylprednisolone) in the treatment of plantar fasciitis.Materials and Methods: One hundred and twenty subjects with unilateral plantar fasciitis were recruited and randomly allocated to two study groups. Group I (NSAIDs group) (n=60) received oral tablet diclofenac (50 mg) and paracetamol (500 mg) twice a day (BD) along with tab. ranitidine 150 mg BD. Group II (injectable steroid group) (n=60) received injection of 1 ml of methylprednisolone (Depomedrol) (40 mg) and 2 ml of 0.5% bupivacaine into the inflammed plantar fascia. Pain intensity was measured using 10 cm visual analog scale (VAS). Subjects were evaluated clinically before, and 1 week, 2 weeks, 4 weeks, and 8 weeks (2 months) after the initiation of treatment in both the groups. The outcome was assessed in terms of VAS score and recurrence of the heel pain.Statistical Analysis Used: “Z” test and Chi-square test were used wherever applicable.Results: Pain relief was significant after steroid injection (P<0.001) and the improvement was sustained. The recurrence of heel pain was significantly higher in the oral NSAIDS group (P<0.001).Conclusion: Local injection of steroid is more effective in the treatment of plantar fasciitis than oral NSAIDs.
Key words: Nonsteroidal antiinflammatory drugs, plantar fasciitis, steroid injection, visual analog scale
INTRODUCTION
Plantar fasciitis is the one of the most common causes of painful heel in adults. It is assumed to be
caused by inflammation and is typically precipitated by biomechanical stress. It is very difficult to treat this condition as the causation is not exactly diagnosed.
Plantar fascia is a broad band of fibrous tissue which originates from the anteromedial plantar aspect of the calcaneal tuberosity and inserts through several slips into the plantar aspects of the metatarsophalangeal joints, the flexor tendon sheaths, and the bases of the proximal phalanges of the digits. Athletic population has a high frequency of plantar fasciitis[1] and in the non-athletic population it is most frequently seen in weight bearing occupations.

159
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Biswas, et al.: NSAIDS and local steroid injection for plantar fasciitis
Excessive pulling and stretching of plantar fascia either from excessive exercise or overuse, repeated trauma, aging, obesity, poor fitting shoe gear or poor foot alignment while running or prolong standing, produce microscopic tear of collagen or cystic degeneration in the origin of plantar fascia causing pain and inflammation.
The classic presentation of plantar fasciitis is pain on the sole of foot at the inferior region of the heel which is particularly worse with the first step taken on rising in the morning.
Numerous treatment measures have been used for plantar fasciitis, but there is no definitive treatment. Non surgical techniques include orthoses, stretching, splinting, taping, topical medications with or without iontophoresis, oral nonsteroidal antiinflammatory medications (NSAIDs), extra corporeal shock wave therapy, laser, percutaneous injections with steroid, botulinum toxin type A, autologous blood or platelet rich plasma.[2] Surgical option includes plantar fascia release, ultrasound guided needle fasciotomy, coablation surgery (topaz procedure).
The present study was undertaken with the intention to compare the effectiveness of NSAIDs and injectable steroid in conjunction with conventional supportive measures in the treatment of plantar fasciitis.
MATERIALS AND METHODS
This randomized, prospective, comparative study was conducted at the pain clinic of a tertiary level health care center over a period of nine months. After obtaining institutional ethical committee clearance and patients’ written informed consent, 120 adult patients, aged between 25-60 years, without any significant systemic disorder (The American Society of Anesthesiologists (ASA) grade I and II), of both sexes, with unilateral plantar fasciitis of less than three months duration, without any prior proper treatment, with moderate to severe intensity of pain (visual analog scale (VAS) score 5–9 in 10 cm scale) and willing to be in follow-up regularly for two months, were enrolled for the study.
Subjects selected for the study were randomly allocated into two groups - group I (NSAIDs group) who were prescribed oral tablet diclofenae (50 mg) and paracetamol (500 mg) - one tab. twice a day along with tab. ranitidine (150 mg) - one tab. twice a day for 4 weeks and group II (injectable steroid group) in whom a single injection of 40 mg (1 ml) of methylprednisolone (Depomedrol) and 2 ml of 0.5% bupivacaine was injected into the tender most point of inflammed plantar fascia. For this purpose, randomization was done by allocating subjects with odd number to group I and even number to group II.
The group II patients were placed in the lateral recumbent position with the affected side down. The medial aspect of the foot was identified and soft tissue just distal to the calcaneous was palpated to locate the point of maximal
tenderness or swelling where a 25-gauge, 1.5 inch needle was inserted perpendicular to the skin. The needle was directed down past the midline of the width of the foot. Methylprednisolone (Depomedrol) was injected slowly and evenly through the middle one third of the width of the foot while the needle was being withdrawn. Injection through the base of the foot into the fat pad was avoided. These patients were advised to apply ice locally and avoid strenuous activity involving the injected region for at least 48 hours and to start stretching exercises after 1 week of local steroid injection.
All the subjects in both the groups were advised to use soft heel foot wear, not to stand for long time, and not to walk bare foot.
All patients were familiarized with 0-10 cm visual analogue scale (VAS) for pain; 0 equal to “no pain” and 10 equal to “worst possible pain”. In both groups, pain intensity was measured before treatment, and 1 week, 2 weeks, 4 weeks, and 8 weeks (2 months) after the initiation of the treatment. The recurrence or increase in severity of heel pain was also assessed after 2 months of initiation of treatment. Complications, if any, occurred in any of the groups were also noted.
Statistical analysisStatistical analysis was done by the graph pad prism software 4 version and also manually which was done to cross check the outcomes. Sample size was decided on consultation with the statistician: Fifty was the smallest number in each group, where any results could be statistically significant (with power of 80%). Hence sample size of 60 (sixty) was selected for both the groups. Statistical measures such as “Z” test and Chi-square test were used to analyze the data. Results were reported as mean ± standard deviation (SD). The results were considered to be statistically significant at the 5% critical level (P<0.05).
RESULTS
All the patient parameters and the results from the two groups (group I and group II) were entered in the pre-designed study pro forma sheet.
There was no significant difference in demographic profile for both the groups [Table 1].
Statistically significant reduction in heel pain was seen in group II patients, as average VAS score improved from 7.05 ± 1.02 at the initiation of treatment to 2.01 ± 1.12 at 1 weekand 1.12 ± 1.32 at 2 weeks. The improvement was sustained throughout the study; at 2 months, the average VAS score was 1.92 ± 1.22 [Table 2].
In group I patients, after initial improvement in average VAS score (at 1-week outcome measure 5.14 ± 1.86 from basal VAS score of 7.15 ± 1.08), no statistically

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
160
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Biswas, et al.: NSAIDS and local steroid injection for plantar fasciitis
significant reduction in VAS score was seen throughout the study. Infact, VAS score increased after discontinuation of oral NSAIDs as 2 month outcome measure showed average VAS score of 5.76 ± 1.62 [Table 2].
The P value for VAS scores before the initiation of treatment for both groups was >0.1 and at 1 week was <0.001, at 2 week (<0.001), at 4 weeks (<0.001), and at 2 months was (<0.001), which showed a highly significant statistical difference in VAS scores throughout the study period between the two study groups [Table 2].
The recurrence of heel pain was significantly higher in group I (33/60 i.e. 55%) than that of group II (6/60 i.e. 10%) (P<0.001) [Table 3].
Occurrence of complications was more in group I patients (58/60 i.e. 96.66%) as compared to group II patients (10/60 i.e. 16.66%; only 2 patients presented with plantar fascia rupture) [Table 4].
DISCUSSION
Plantar fasciitis is an inflammatory condition and the use of NSAIDs and local steroid injection are both logical and effective modalities for symptom relief. In our study, we intended to investigate that which would be a better treatment option for plantar fasciitis among these two.
In this study, it was found that a single local injection of steroid with local anesthetic caused statistically significant relief in heel pain and improvement in VAS score throughout the study period as compared to oral NSAIDs therapy (P<0.001). A double-blind randomized controlled trial by Crawford et al.,[3] in 106 patients with heel pain at a rheumatology clinic concluded that a statistically significant reduction in pain was detected at 1 month (P=0.02) in favor of steroid injection. As
evidenced by Gudeman et al.,[4] in a study on 40 patients, iontophoresis of dexamethasone for plantar fasciitis should be considered when more immediate results are needed. Other studies showed that when more conservative management was unsuccessful, steroid injection was a preferred option.[5-7] Studies[6] have found steroid treatments to have a success rate of 70% or more.
The recurrence of heel pain was found to be significantly low in the injectable steroid group than that of oral NSAIDs group (P<0.001).
NSAIDs mainly act by inhibition of prostaglandin synthesis, but they do not suppress the production of other inflammatory mediators like leukotrienes, cytokines, platelet activating factor etc. Steroids interfere at several steps in the inflammatory response, but the most important overall mechanism appears to be limitation of recruitment of inflammatory cells at the local site. So their actions are both direct and local.
Long-term use of oral NSAIDs can cause serious systemic side effects like gastritis, peptic ulcer, esophagitis, gastrointestinal (GI) bleeding, interstitial nephritis, Na+ and water retention, thrombocytopenia, bleeding, pruritus, central nervous system, and hepatic complications.[8] As steroid is injected locally in the treatment of plantar fasciitis, chances of systemic side effects are very rare. But the potential risks for local steroid injection for plantar fasciitis include local site erythema, plantar fascia rupture, and fat pad atrophy. [9,10] In our study, the overall incidence of adverse side effects were more frequent with oral NSAIDs than local injection of steroid, but two patients presented with plantar fascia rupture later and were treated accordingly. These complications are uncommon and preventable and rupture may occur without steroid injections.[10]
CONCLUSION
On the basis of this study, it can be concluded that in comparison to oral NSAIDs, local steroid injection is a better treatment modality as it causes early, rapid and sustained relief of pain and inflammation in plantar fasciitis and is associated with lower recurrence of heel pain and lesser complications.
Table 1: Demographic profile of groups (mean ± SD)
Group I Group IINo. of patient 60 60
ASA grade (I/II) 32/28 29/31
Age (years) 38.40 ± 11.6321 41.70 ± 8.8680
Weight (kg) 59.60 ± 8.7684 55.40 ± 5.6233
Male/female 34/26 38/22P value >0.05 (not significant); ASA: American Society of Anesthesiologists
Table 2: Pain intensity (mean change in VAS score)Groups VAS score (mean ± standard deviation)
Before initiation of treatment
At 1 week At 2 weeks At 4 weeks At 8 weeks
Group I (NSAIDs) n=60 7.15 ± 1.08 5.14 ± 1.86 4.78 ± 1.74 4.15 ± 1.18 5.76 ± 1.62
Group II (steroid inj.) n=60 7.05 ± 1.02 2.01 ± 1.12 1.12 ± 1.32 1.09 ± 1.16 1.92 ± 1.22
P value (‘Z’ test) 0.29 <0.001 <0.001 <0.001 <0.001VAS: Visual analog scale

161
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Biswas, et al.: NSAIDS and local steroid injection for plantar fasciitis
REFERENCES
1. Simon J. Bartold. The plantar fascia as a source of pain-biomechanics, presentation and treatment. J Body Work Mov Thera 2004;8:214-26.
2. Gill LH. Plantar fasciitis: Diagnosis and conservative management. J Am Acad Orthop Surg 2004;350:2159-66.
3. Crawford F, Atkins D, Young P, Edwards J. Steroid injection for heel pain: Evidence of short-term effectiveness. A randomized controlled trial. Rheumatology (Oxford) 1999;38:974-7.
4. Gudeman SD, Eisele SA, Heidt RS Jr, Colosimo AJ, Stroupe AL. Treatment of plantar fasciitis by iontophoresis of 0.4% dexamethasone. A randomized, double-blind, placebo-controlled study. Am J Sports Med 1997;25:312-6.
5. Cardone DA, Tallia AF. Joint and Soft tissue injection. Am Fam Physician 2002;66:283-8.
6. Kane D, Greaney T, Bresnihan B, Gibney R, FitzGerald O. Ultrasound guided injection of recalcitrant plantar fasciitis. Ann Rheum Dis 1998;57:383-4.
7. Tsai WC, Wang CL, Tang FT, Hsu TC, Hsu KH, Wong MK. Treatment of proximal plantar fasciitis with ultrasound-guided steroid injection. Arch Phys Med Rehabil 2000;81:1416-21.
8. Donley BG, Moore T, Sferra J, Gozdanovic J, Smith R. The efficacy of oral non-steroidal anti-inflammatory medication in the treatment of plantar fasciitis. A randomized, prespective, placebo-controlled study. Foot Ankle Int 2007;28:20-3.
9. Tatli YZ, Kapasi S. The real risks of steroid injection for plantar fasciitis, with a review of conservative therapies. Curr Rev Musculoskelet Med 2009;2:3-9.
10. Acevedo JI, Beskin JL. Complications of plantar fascia rupture associated with corticosteroid injection. Foot Ankle Int 1998;19:91-7.
Table 3: Recurrence (or increase in severity) of heel pain after 2 monthsGroups Recurrence No recurrence
No. Percentage No. PercentageGroup I (NSAIDs) n=60 33 55 27 45
Group II (inj. steroid) n=60 6 10 54 90
Chi-square value (χ2) = 27.69 (P <0.001)
Table 4: Occurrence of complicationsComplications Group I (n=60) Group II (n=60)Gastritis 40 0
Esophagitis 5 0
Pruritus 8 0
Feeling of bloating 5 0
Injection site erythema 0 6
Injection site infection 0 2
Plantar fascia rupture 0 2
Total no. of complications 58 (96.66%) 10 (16.66%)
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.
Author Help: Online submission of the manuscripts
Articles can be submitted online from http://www.journalonweb.com. For online submission, the articles should be prepared in two files (first page file and article file). Images should be submitted separately.1) First Page File: Prepare the title page, covering letter, acknowledgement etc. using a word processor program. All information related to your identity
should be included here. Use text/rtf/doc/pdf files. Do not zip the files.2) Article File: The main text of the article, beginning with the Abstract to References (including tables) should be in this file. Do not include any information
(such as acknowledgement, your names in page headers etc.) in this file. Use text/rtf/doc/pdf files. Do not zip the files. Limit the file size to 1 MB. Do not incorporate images in the file. If file size is large, graphs can be submitted separately as images, without their being incorporated in the article file. This will reduce the size of the file.
3) Images: Submit good quality color images. Each image should be less than 4 MB in size. The size of the image can be reduced by decreasing the
actual height and width of the images (keep up to about 6 inches and up to about 1800 x 1200 pixels). JPEG is the most suitable file format. The image quality should be good enough to judge the scientific value of the image. For the purpose of printing, always retain a good quality, high resolution image. This high resolution image should be sent to the editorial office at the time of sending a revised article.
4) Legends: Legends for the figures/images should be included at the end of the article file.

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
162
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Original Article
Do pencil-point spinal needles decrease the incidence of postdural puncture headache in reality? A comparative study between pencil-point 25G Whitacre and cutting-beveled 25G Quincke spinal needles in 320 obstetric patientsAnirban Pal, Amita Acharya1, Nidhi Dawar Pal2, Satrajit Dawn Jhuma Biswas3
Department of Anesthesiology, Calcutta National Medical College (CNMC), Kolkata, 1Department of Anesthesiology, Bangur Institute of Neurology(BIN), Kolkata, 2Specialist Medical officer (Anesthesiology), West Bengal Health Service, West Bengal, 3Department of Gynaecology and Obstetrics, Institute of Post-Graduation Medical Education and Research (IPGME and R), Kolkata, India
Corresponding author: Dr. Anirban Pal, 43/6/5 Jheel Road, Kolkata - 700 031, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_56_11R5 AP Done 27th Jan
AbstractBackground: Postdural puncture headache (PDPH) is a distressing complication of the subarachnoid block. The previous studies conducted, including the recent ones, do not conclusively prove that pencil-point spinal needles decrease the incidence of PDPH. In this study, we have tried to find out whether a pencil-point Whitacre needle is a better alternative than the classic cutting beveled, commonly used, Quincke spinal needle, in patients at risk of PDPH.Materials and Methods: Three hundred and twenty obstetric patients, 20–36 years of age, ASA I and II, posted for Cesarean section under subarachnoid block, were randomly assigned into two groups W and Q, where 25G Whitacre and 25G Quincke spinal needles were used, respectively. The primary objective of the study was to find out the difference in incidence of PDPH, if any, between the two groups, by using the t test and Chi square test.Results: The incidence of PDPH was 5% in group W and 28.12% in group Q, and the difference in incidence was statistically significant (P<0.001).Conclusion: The pencil-point 25G Whitacre spinal needle causes less incidence of PDPH compared to the classic 25G Quincke needle, and is recommended for use in patients at risk of PDPH.
Key words: Cesarean section, postdural puncture headache, Quincke spinal needle, subarachnoid block, Whitacre spinal needle
INTRODUCTION
Cesarean section (CS) under subarachnoid block (SAB) is practiced worldwide, due to several advantages over epidural or general anesthesia. The greatest drawback of SAB is the postdural puncture headache (PDPH). In an obstetric anesthesiology closed claim study, published in the American Society of Anesthesiology newsletter, 1999,

163
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Pal, et al.: Quincke versus Whitacre spinal needles in postdural puncture headache
PDPH was the third most common claim, accounting for 15% of the obstetric claims.[1]
A postdural puncture headache is caused by leakage of the cerebrospinal fluid (CSF) through the dural hole formed by the spinal needle. Therefore, decreasing the size of the hole may be a logical solution to decreasing the incidence of PDPH, as suggested by different studies.[2-4] Cruickshank and colleagues have demonstrated that there is little or no dural leak with a 29G spinal needle.[5] However, all the authors have reported both practical and manufacturing difficulties as loss of feel, danger of bending or damage even when using an introducer, and CSF is very slow to appear at the needle hub, unless aspirated.[2-5] The 25G Quincke needle, with a medium cutting bevel, is still the most popular and in widespread use, due to the ease of handling. However the incidence of PDPH is 25% with the 25G Quincke needle.[6,7]
In the 1950s, Hart and Whitacre[8] suggested the use of pencil-point spinal needles, without a cutting edge, to reduce trauma to the dural fibers. Clinical[9] and laboratory studies[5] have indicated that pencil-point needles may produce fewer PDPH symptoms, but none of the recent studies clearly state that Whitacre pencil-point spinal needles are better than Quincke needles, in respect to PDPH.[10,11] We decided to compare the incidence of PDPH and find out the difference, if any, in 320 obstetric patients undergoing CS under SAB using 25G Whitacre spinal needle and an equivalent size Quincke needle.
MATERIALS AND METHODS
Three hundred and twenty ASA I and II parturients, aged 20–36 years, weighing 58–87 kilograms, with a of height 123–174 cm, undergoing CS under SAB were recruited for this randomized double blind study, which was approved by the institutional ethical committee. A patient information sheet was given to patients attending the antenatal clinic at 36 weeks gestation. At the pre-anesthetic visit, the patients were counseled about SAB and PDPH, and written informed consent was obtained.
Exclusion criteria of the patients included contraindication to neuraxial anesthesia, history of recurrent headache, occipital neuralgia or migraine. In addition patients requiring more than three attempts of lumbar puncture were excluded from the study. Subjects were randomly (computer generated numbers inserted into opaque envelope) and evenly allocated to one of the two groups to receive SAB, either with 25G Whitacre spinal needle (group W, n=120) or 25G Quincke spinal needle (group Q, n=120). The patients were unaware of the type of spinal needle used to perform the SAB.
The patients fasted from midnight, for at least eight hours, and received oral ranitidine 150 mg the night
before and on the morning of the surgery. In addition they also received 30 ml of non-particulate antacid 30 minutes prior to surgery. The patients were transported to the operation theater (OT) in the left lateral position. Before starting the anesthetic procedure monitors of pulse-oximetry (SpO2), echocardiogram (ECG), and non-invasive blood pressure (NIBP) were attached and monitored throughout the intraoperative period. An intravenous access was established with an 18G i.v. cannula in the dorsum of the left hand and preloading with Ringer’s lactate solution 20 ml/kg was done in all the patients.
The patients were placed in flexed sitting position, a midline skin wheal was raised with 2 ml 2% lignocaine and SAB was performed in the L2-3 or L3-4 interspace. The bevel of the Quincke needle was inserted parallel to the longitudinal axis of the spinal cord and after penetration of the dura, the needle was rotated to make the opening in the cephalad direction. After obtaining free flow of CSF, the patients received 0.5% hyperbaric bupivacaine 10 mg and fentanyl 25 mcg intrathecally. The patients were then turned supine with a wedge under right hip. Anesthesia was considered adequate for surgery when there was loss of cold sensation at the T4 level, tested with ethyl chloride. In case of failure of the dural puncture or inadequate SAB, the patients were administered general anesthesia. Oxygen was administered via the Hudson mask at 4 l/minute throughout the procedure and 10 units of oxytocin given i.v. after delivery of the fetus. Mean arterial blood pressure was monitored at regular five-minute intervals. If the systolic blood pressure decreased by more than 20% from the baseline, then 300–500 ml of colloids and incremental bolus of 5 mg intravenous ephedrine were used.
Postoperatively, all the patients were questioned for five consecutive days about the onset, characteristics, duration, and associated symptoms of any headache. The replies to the questionnaires were assessed by one of the authors who was blinded to the type of needle used. PDPH is characterized by, (1) postural, aggravated by sitting or standing, relieved by lying supine (2) frontal or occipital (3) may be accompanied by nausea, vomiting, neck stiffness, diplopia, tinnitus. If the patient’s headache did not satisfy the criteria for PDPH, we excluded other serious intracranial causes of headache. PDPH was treated initially with bed rest, hydration, and paracetamol 15 mg per kg orally, four times daily. If PDPH persisted longer than 24 hours with the same severity, the decision to perform an epidural blood patch was taken by a consultant anesthesiologist. The primary objective of the study was to find out any difference in the incidence of PDPH between the two groups. The secondary objective was to find out the incidence of failure of lumbar puncture and the number of attempts required to achieve lumbar puncture.

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
164
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Pal, et al.: Quincke versus Whitacre spinal needles in postdural puncture headache
Power analysis based on a similar previous study[12]
revealed that a sample size of 160 patients per group was sufficient to achieve a power of 80% and an alpha error of 0.05 to detect a 20% reduction in incidence of PDPH (software version 2.1; 30 February, 2003). Results were expressed as a mean (SD), the number of patients or percentage of patients. Unpaired student’s two-tailed was used to compare the demographic data between the two groups. The Chi square test and t test were used to find out any difference in the incidence of PDPH between the two groups. A P-value of less than 0.05 was considered statistically significant.
RESULTS
Three hundred and twenty consecutive patients posted for Cesarean section who fulfilled the inclusion criteria were included in the study. All patients allocated were able to complete the study.
There were no differences in patient characteristics between the groups [Table 1].
The heart rate, mean blood pressure, and oxygen saturation did not differ between the groups, at all the measured time intervals.
In both the groups, the dural puncture was performed successfully in less than three attempts. The number of attempts was comparable in both groups, as seen by the t test [Table 2]. Out of 160 patients in each group, the dura could be punctured in the first attempt in 143 patients in group Q (89.37%) and 146 patients in group W (91.25%).
Three patients in group Q and one patient of group W required general anesthesia, due to inadequate SAB. Failure of SAB was similar in both groups (t test used, P value = 0.3135) [Table 2].
Forty-five out of 160 patients in group Q (28.12%) developed PDPH, whereas, only eight out of 160 patients in group W (5%) developed PDPH (t test and Chi square test applied, P value < 0.001) [Table 2]. Non-specific headaches, not fulfilling the criteria of PDPH were comparable in both groups (P value = 0.1284) [Table 2].
Incidence of side effects like nausea and vomiting were similar in both groups (t test applied, P value = 0.7716). No patient in any of the groups reported visual or auditory symptoms [Table 3].
DISCUSSION
In 1898, Karl August Bier, a German surgeon and his assistants were the first to report the symptoms associated with PDPH. Bier presumed that the headache was due to loss of CSF.[13] Later the presence of a CSF leak
had been confirmed with radionuclide cisternography,[14]
radionuclide myelography, manometric studies, epiduroscopy, and direct visualization at laminectomy.[15]
The present trend of the anesthetic technique in CS worldwide is SAB, because it is safe to the mother and newborn, easier to perform, and has a high degree of success rate. However, among the side effects of SAB, PDPH is the most distressing one and results in increased morbidity, prolonged hospital stay, increased cost, and patient dissatisfaction. Therefore, PDPH remains a ‘big problem’ for the anesthesiologist.
Obstetric patients are at high risk of PDPH because of their sex and young age.[7] After delivery of the fetus, the reduced epidural pressure increases the rate of CSF leakage through the dural opening leading to loss of buoyant support of the brain, thereby causing traction on the meninges, a pain-sensitive structure. In addition as a consequence of the decreased CSF volume, there is compensatory vasodilatation and increased intracranial blood volume, according to Monro Kellie hypothesis, leading to a headache.[16]
Obstetric patients with a past history of PDPH[17] or migraine, or requiring more than three attempts to
Table 1: Patient characteristics; values are mean (range or SD)Variables Group Q (n=160) Group W (n=160)Age (years) 27.95 (20-36) 28.18 (22-34)
Weight (kilograms) 71.18 (4.82) 70.99 (4.68)
Height (cm) 154.2 (8.7) 152.4 (8.7)
Gestation (weeks) 38.5 (0.9) 38.6 (1)
Table 2: Attempts of dural puncture, failure of SAB, incidence of PDPH, and other headaches; values are given as number of patients (%)Variables Group Q (n=160) Group W (n=160)Attempts of dural puncture
1 143 (89.375) 146 (91.25)
2 13 (8.125) 12 (7.5)
3 4 (2.5) 2 (1.25)
Failure of SAB 3 (1.87) 1 (1.62)
PDPH 45 (28.12) 8 (5)
Other headaches 15 (9.3) 8 (5)
Table 3: Accompanying symptoms; values are given as number of patients (%)Variables Group Q (n=160) Group W (n=160)Nausea 4 (8.8) 1 (12.5)
Vomiting 4 (8.8) 1 (12.5)
Blurred vision 0 (0) 0 (0)
Tinnitus 0 (0) 0 (0)
165
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Pal, et al.: Quincke versus Whitacre spinal needles in postdural puncture headache
achieve lumbar puncture were excluded from the study as they were at an increased risk of headache in the postoperative period. Therefore, the observed differences in the incidence of PDPH between the groups could be solely attributed to the type of spinal needle used.
Incidence and severity of PDPH is proportional to the rate of CSF leakage through the dural hole made by the spinal needle, so in high-risk obstetric patients, the use of finer gauge needles is justified. Even as the incidence of PDPH is 0–2% with a 29G Quincke needle, failure of SAB is common due to technical difficulties with finer gauge needles.[2,4,18] Therefore, 25G, 26G, and 27G Quincke needles are in widespread use. The incidence of PDPH is 3–25%,[18] 0.3–20%,[2] and 1.5–5.6%[19] with 25G, 26G, and 27G needles, respectively. We chose the 25G spinal needle because of the technical ease of insertion over the finer spinal needles.
Kang S B and his colleagues noted that some PDPH were severe enough to require an epidural blood patch.[20] The therapy of epidural blood patch is invasive, cumbersome, and hazardous. Thus, there is no doubt, that prevention is a better option than definitive therapy, in case of PDPH. None of our patients in either group required an epidural blood patch.
A few authors suggested that Quincke needles, if introduced with the bevel parallel to the longitudinal axis of the dural fibers, as standard technique, could reduce the incidence of PDPH.[2,19] However, Cruickshank and colleagues could not demonstrate any significant difference in CSF leakage by aligning the bevel of the needle either parallel or across the dural fibers, in vitro, and their observation was that the CSF leakage rate was related to the needle size.[5] However, we chose to insert the Quincke needle with the bevel parallel to the longitudinal axis of the spinal cord, as per the classical teaching.
Several studies were carried out worldwide with different types of needle tip designs, to find out any difference in incidence of PDPH. Hart and Whitacre, in the 1950s, designed the first pencil-point needle and claimed a decrease in incidence of PDPH from 5 to 2%, using 20 gauge needles.[8] Vallejo et al., in their study of one thousand and two obstetric patients, undergoing elective Cesarean delivery, studied the difference in incidence of PDPH, using five different types of spinal needles, and found that the 25G Quincke needle had a higher frequency of PDPH compared to the pencil-point needles (which included 25G Whitacre). Nevertheless, they concluded that in addition to PDPH, cost consideration, ease of insertion, rate of CSF flow, and the ease with which the needle bends or breaks when excessive forward force is applied, be taken into consideration when choosing the spinal needle.[12] Hwang et al., in their study with 93 Cesarean section patients, using 25G Whitacre and 25G and 26G
Quincke needles, found that 25G Whitacre caused a lower incidence of PDPH, but their results were not statistically significant. [10] Shaikh et al., in their study of 480 post Cesarean section patients, used 25G and 27G Quincke needles and 27G Whitacre spinal needles and found that 27G Whitacre spinal needles had better outcomes.[11] These above-mentioned studies do not clearly state that pencil-point 25G Whitacre was a better option than the 25G Quincke spinal needle in respect to PDPH. We observed a statistically significant reduction in the incidence of PDPH by using the 25G Whitacre spinal needle compared to the 25G Quincke needle (5% versus 28.12%, P value < 0.001). However, there was no difference in the two groups with respect to the number of attempts of lumbar puncture, failure of SAB, and the accompanying symptoms.
CONCLUSION
The 25G Whitacre spinal needle is recommended for SAB in the CS of obstetric patients at high risk of PDPH, to reduce the incidence of PDPH. However, the cost of the Whitacre spinal needle has to be balanced against the risk of PDPH, the associated cost of a longer hospital stay, and the hazardous therapy of an epidural blood patch.
REFERENCES
1. Chadwick HS. Obstetric anesthesia closed claim update II. — ASA Newsletter 1999;63:6.
2. Flaatten H, Rodt SA, Vamnes J, Rosland J, Wisborg T, Koller ME. Postdural puncture headache. A comparison between 26 and 29 gauge needles in young patients. Anesthesia 1989;44:147-9.
3. Dahl JB, Schultz E, Anker-Moller E, Christensen EF, Staunstrup HG, Carlsson P. Spinal anesthesia in young patients using 29 gauge needles: Technical considerations and an evaluation of post operative complaints compared with general anesthesia. Br J Anesth 1990;64:178-82.
4. Lesser P, Bembridge M, Lyons G, MacDonald R. An evaluation of 30 gauge needle for spinal anesthesia for Cesarean section. Anesthesia 1990;45:767-8.
5. Cruickshank RH, Hopkinson JM. Fluid flow through dural puncture sites: An in vitro comparison of needle point types. Anesthesia 1989;44:415-8.
6. Barker P. Headache after dural puncture. Anesthesia 1989;44:696-7.7. Flaatten H, Rodt SA, Rosland J, Vamnes J. Postoperative headache in young
patients after spinal anesthesia. Anesthesia 1987;42:202-5.8. Hart JR, Whitacre RJ. Pencil-point needle in prevention of postspinal
headache. J Am Med Assoc 1951;147:657-8.9. Halpern S, Preston R. Postdural puncture headache and spinal needle design:
Meta-analyses. Anesthesiology 1994;81:1376-83.10. Hwang JJ, Ho ST, Wang JJ, Liu HS. Post dural puncture headache in cesarean
section: Comparison of 25-gauge Whitacre with 25- and 26-gauge Quincke needles. Acta Anesthesiol Sin 1997;35:33-7.
11. Shaikh JM, Memon A, Memon MA, Khan M. Post dural puncture headache after spinal anesthesia for Cesarean section: A comparison of 25 g Quincke, 27 g Quincke and 27 g Whitacre spinal needles. J Ayub Med Coll Abbottabad 2008;20:10-3.
12. Vallejo MC, Mandell GL, Sabo DP, Ramanathan S. Post-dural puncture headache: A randomized comparison of five spinal needles in obstetric patients. Anesth Analg 2000;91:916-20.
13. Wulf HF. The centennial of spinal anesthesia. Anesthesiology 1998;89:500-6.
14. Rando TA, Fishman RA. Spontaneous intracranial hypotension report of two cases and review of literature. Neurology 1992;42:481-7.
15. Turnbull DK, Shepherd DB. Postdural puncture headache: Pathogenesis, prevention and treatment. Br J Anesth 2003;91:718-29.
16. Grant R, Condon B, Hart I, Teasdale GM. Changes in intracranial CSF

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
166
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Pal, et al.: Quincke versus Whitacre spinal needles in postdural puncture headache
volume after lumbar puncture and their relationship to post L P headache. J Neurol Neurosurg Psychiatry 1991;54:440-2.
17. Lybecker H, Moller JT, May O, Nielsen HK. Incidence and prediction of postdural puncture headache: A prospective study of 1021 spinal anesthesias. Anesth Analg 1990;70:389-94.
18. Geurts JW, Haanschoten MC, Van Wijk RM, Kraak H, Besse TC. Postdural puncture headache in young patients. A comparative study between the use of 0.52 mm (25 gauge) and 0.33 mm (29 gauge) spinal needles. Acta Anesthesiol Scand 1990;34:350-3.
19. Corbey MP, Bach AB, Lech K, Frorup AM. Grading of severity of postdural
puncture headache after 27 gauge Quincke and Whitacre needles. Acta Anesthesiol Scand 1997;41:779-84.
20. Kang SB, Goodenough DE, Lee YK, Olson RA. Comparison of 26 and 27G needles for spinal anesthesia for ambulatory surgery patients. Anesthesiology 1992;76:734-8.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.
Author Help: Reference checking facility
The manuscript system (www.journalonweb.com) allows the authors to check and verify the accuracy and style of references. The tool checks the references with PubMed as per a predefined style. Authors are encouraged to use this facility, before submitting articles to the journal.
• The style as well as bibliographic elements should be 100% accurate, to help get the references verified from the system. Even a single spelling error or addition of issue number/month of publication will lead to an error when verifying the reference.
• Example of a correct style Sheahan P, O’leary G, Lee G, Fitzgibbon J. Cystic cervical metastases: Incidence and diagnosis using fine needle aspiration biopsy.
Otolaryngol Head Neck Surg 2002;127:294-8. • Only the references from journals indexed in PubMed will be checked. • Enter each reference in new line, without a serial number.• Add up to a maximum of 15 references at a time.• If the reference is correct for its bibliographic elements and punctuations, it will be shown as CORRECT and a link to the correct
article in PubMed will be given.• If any of the bibliographic elements are missing, incorrect or extra (such as issue number), it will be shown as INCORRECT and link to
possible articles in PubMed will be given.

167
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Original Article
Comparison between preemptive gabapentin and paracetamol for pain control after adenotonsillectomy in childrenSabry M. Amin, Yasser M. Amr
Department of Anesthesia, Tanta University Hospital, Tanta University, Tanta, Egypt
Corresponding author: Dr. Sabry M. Amin, Department of Anesthesia, Tanta University Hospital, Tanta University, Tanta - 31527, Egypt. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_44_11R9
AbstractBackground: Tonsillectomy is the most commonly performed surgical procedure in ENT practice. Postoperative pain remains the major problem following tonsillectomy, if not treated. Different methods and many drugs have been used to control the postoperative pain. In this study, we evaluate the role of gabapentin premedication vs paracetamol in management of postoperative pain following adenotonsillectomy in children.Materials and Methods: In a double blind randomized study, 70 children were subjected for adenotonsillectomy classified into two equal groups. Group I: Gabapentin 10 mg/kg was given orally 2 hours before induction of anesthesia (Gabapentin syrup 250 mg/5 ml); Group II: Oral paracetamol 20 mg/kg was given orally 2 hours before induction of anesthesia. All children underwent general anesthesia. Pain score was assisted postoperatively 2 hours, 4 hours, 6 hours, 8 hours, 12 hours, and 18 hours after recovery using visual analogue scale (VAS).Result: Pain score in gabapentin group was significantly less in 2 hours, 4 hours, 6 hours, and 8 hours postoperatively than in paracetamol group (P=0.0003, <0.0001, 0.0004, <0.0001, respectively). The time to first analgesia was longer in the gabapentin group than paracetamol group (7.95 ± 2.06 hours vs 5.85 ± 1.87 hours; P<0.0001) and the total amount of pethedine was less in gabapentin group than in paracetamol group (8 ± 10.05 mg vs 16.25 ± 11.57 mg; P=0.002).Conclusion: Gabapentin premedication improves postoperative analgesia following adenotonsillectomy in children and reduce analgesic requirements in comparison with paracetamol premedication, with no reported side effects.
Key words: Adenotonsillectomy, gabapentin, paracetamol, postoperative pain
INTRODUCTION
Tonsillectomy is one of the most commonly performed children’s surgeries and produces a considerable degree of pain postoperatively.[1] These characters make this surgery ideal for the investigation of pain-relieving medications.[2]
Opiates, which provide the most effective pain relief, are associated with a high incidence of nausea and

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
168
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Amin and Amr: Gabapentin, paracetamol for pain control after adenotonsillectomy in children
vomiting, respiratory depression, and sedation.[3] These side effects are hazardous in children; thus, alternatives to opiates have been sought for postoperative analgesia in tonsillectomy. Gabapentin was introduced in 1993 and had been used in the treatment of children’s seizures and chronic pain syndromes.[4]
Gabapentin has been used in management of acute conditions in the perioperative period. Gabapentin has role in postoperative analgesia, preoperative anxiolysis, prevention of chronic postoperative neuropathic pain, attenuation of hemodynamic changes during intubation, and prevention of postoperative nausea, vomiting, and delirium.[5] This clinical study compares effect of gabapentin premedication with paracetamol premedication on postoperative pain following adenotonsillectomy in children.
MATERIALS AND METHODS
This study was carried out on 70 children ASA I and II who underwent adenotonsillectomy after obtaining approval from the hospital ethics committee and written informed consent from the parents of each child.
Age group was between 4 and 6 years. Exclusion criteria included diabetes, liver and/or kidney disease, hypersensitivity to drugs used, peritonsillar abscess, swallowing disorder, epilepsy or previous treatment with gabapentin or opioids analgesia. Tonsillectomy dissection was done using the bipolar diathermy and was performed in all patients by the four surgeons with the same experience and qualifications. Patients were randomly allocated equally (35 patients) in each group as follows:• GroupI:Gabapentin10mg/kgwasgivenorally2hours
before induction of anesthesia (Gabapentin syrup 250 mg/5 ml).[6]
• GroupII:Oralparacetamol20mg/kgwasgivenorally2 hours before induction of anesthesia.[7]
The randomization was performed using sealed numbered envelopes indicating the group of each patient. A blind nurse who did not participate in patients’ follow up read the number and made group assignments.
A blinded chief nurse who did not participate in data collection confirmed that each patient ingested the medications as was scheduled. The process of inclusion in the study went on until the required number of patients was reached.
Anesthesia technique General anesthesia was induced by sevoflurane (7 vol.%,). After the patients’ loss of consciousness, intravenous line was inserted. Central orotracheal intubation was performed with 1 µg/kg fentanyl and rocronium 0.6 mg/Kg. Anesthesia was maintained with sevoflurane 2 to 3 vol.% in N2O/O2 (70:30 vol.%) and ventilation was controlled to maintain normocapnia. Standard patient monitoring (electrocardiogram, non-invasive arterial pressure, heart
rate, pulse oximetry, and end-tidal CO2) were used during anesthesia.
After the surgeon had completed the operation, residual neuromuscular blockade was antagonized with atropine 0.01 mg/kg and neostigmine 0.05 mg/kg. Oropharyngeal suction was done under direct vision, all patients were extubated in tonsillectomy position with or without nasopharyngeal or oropharyngeal airway in place to prevent airway obstruction, and were transported to the post-anesthesia recovery room.
Metoclopramide 0.15 mg/kg was administered for treatment of postoperative nausea and vomiting (PONV). If PONV still persisted, ondansetron 0.1 mg/kg was administered.
Measurements The pain intensity was assisted by a person who was blind to study by using visual analogue scale graded from 0 to 10 (0 = no pain, 10 = the worst possible pain) in the following time in the post-anesthesia recovery room 2 hours, 4 hours, 6 hours, 8 hours, 12 hours, and 18 hours after recovery.
During the preoperative visit, all children were shown the visual analogue toy containing different animal figures increasing in size from bird (0, bottom = no pain) to elephant (10, top = worst pain), in ten steps.
Postoperative analgesia was given in all patients depending on VAS score.
If the VAS value was less than 5 rectal, paracetamol 20 mg/kg was given; if VAS value was more than 5, pethedine 0.5 mg/kg was given intra-muscular and recorded. The time to first dose of analgesia and total amount of pethedine used was recorded in all patients.
Patients will be discharged postoperative when they had no or mild pain (VAS around 3), were able to tolerate clear fluids and soft food, and had no bleeding or nausea and vomiting.
Primary outcome measure of this study was the total postoperative pethedine consumption (from the time of extubation). Secondary outcome measures were pain scores, presence of nausea/vomiting, and sedation.
Sample size was chosen based on the previous study in our institute, which had determined that 35 patients in each group were enough for detection of significant changes in analgesic requirements.[8]
Statistical analysis All data are expressed as mean ± SD. To study the pattern of changes in individual variables in each group during various phase of study, an analysis of variance for repeated measure was performed. P value <0.05 was regarded as statistically significant. Unpaired t-test was used to compare between both groups and Mann-Whitney U test was used for pain scores.

169
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Amin and Amr: Gabapentin, paracetamol for pain control after adenotonsillectomy in children
RESULTS
This study was carried out on 70 patients divided into two groups, 35 in each group. The groups were comparable with regards to demographic data including age, gender, weight, and duration of anesthesia [Table 1].
Time to first request for analgesia was significantly longer in group I than group II (7.95 ± 2.06 hours vs 5.85 ± 1.87 hours; P<0.0001) [Table 1].
The amount of pethedine was less in group I than group II (8 ± 10.05 mg vs 16.25 ± 11.57 mg; P = 0.002) [Table 1].
Pain score in gabapentin group was significantly less in 2 hours, 4 hours, 6 hours, and 8 hours postoperatively than in paracetamol group (P = 0.0003, <0.0001, 0.0004, <0.0001, respectively). At 12 hours, VAS score was comparable between groups and patients received analgesia (pethedine in dose 0.5 mg/kg). Also, at 18 hours, the VAS was comparable between groups [Table 2].
Incidence of nausea, vomiting, and sedation was comparable in both groups. Six patients in group I received metoclopramide for controlling vomiting vs four patients in group II.
DISCUSSION
Tonsillectomy is one of the most common operation performed in children; it is associated with significant postoperative pain which if not treated well can cause significant risk including increasing heart rate, blood pressure, respiratory rate, difficulty swallowing, increased risk of postoperative bleeding, and prolong hospital stay.
In our study, we use either gabapentin 10 mg/kg 2 hours before anesthesia or oral paracetamol 20 mg/kg for controlling the postoperative pain following adenotonsillectomy in children and revealed that gabapentin premedication reduced VAS, prolonged the time for first analgesic requirement, and decreased its requirements.
The mechanism of gabapentin on pain is thought to involve voltage-gated N-type calcium ion channels. It is thought to bind to the alpha 2_ delta subunit of the voltage-dependent calcium channel in the central nervous system. This reduces calcium influx into the nerve terminals and decreases the release of neurotransmitters such as glutamate.[9,10]
These findings are consistent with that of Jeon et al. who concluded that premedication with gabapentin decreased post-tonsillectomy pain during swallowing in adult patients.[11]
A number of reports from many groups have revealed that preemptive gabapentin may play a considerable role in controlling postoperative pain. However, many of these
studies used it preoperatively and postoperatively.[12-14]
The present study showed that the total pethedine requirements were less in gabapentin group. This is concordant with the findings of other studies. [12,14] Mikkelsen et al.[15] reported that gabapentin reduced opioid consumption in the first 24 hours after tonsillectomy. However, the benefits of reduced opioid intake were overwhelmed by side effects of large doses of gabapentin used. They were unable to demonstrate any reduction in postoperative pain scores and postulated the lack of effect of gabapentin in post-tonsillectomy pain.
On the other hand, gabapentin is expensive and may increase the incidence of postoperative dizziness which may limit its use in day case surgery. However, incidence of nausea, vomiting, and sedation was comparable in both groups.
CONCLUSION
Gabapentin 10 mg/kg administrated orally 2 hours before adenotonsillectomy in children significantly decreased postoperative pain score and pethedine requirements vs paracetamol premedication, with no reported side effects.
REFERENCES
1. Page GG. The immune-supressive effects of pain. Adv Exp Med Biol 2003;521:117-25.
2. Joshi GP, Ogunnaike BO. Consequences of inadequate postoperative pain relief and chronic persistent pain. Anesthesiol Clin North America 2005;23:21-36.
3. Michaloliakou C, Chung F, Sharma S. Preoperative multimodal analgesia facilitates recovery after laparoscopic choecystectomy. Anesth Analg 1996;82:44-51.
4. Fullerton CA, Busch AB, Frank RG. The rise and fall of gabapentin for bipolar disorder: A case study on off-label pharmaceutical diffusion. Med Care 2010;48:372-9.
Table 2: Visual analogue scaleTime (h) Group (I) Group (II) P value2 0.98 ± 0.73 1.7 ± 0.86 0.0003
4 1.55 ± 1.19 3.55 ± 0.95 <0.0001
6 4.050 ± 1.61 5.20 + 0.89 0.0004
8 4.30 ± 0.27 5.90 ± 0.79 <0.0001
12 5.3 ± 0.83 5.65 ± 1.08 0.29
18 4.45 ± 0.9 4.30 ± 0.65 0.43
Table 1: Demographic data; pethedine consumption; time of first analgesic requirement; and duration of anesthesia
Group (I) Group (II) P valueAge (yr) 5.3 ± 1.08 4.8 ± 1.24 0.15
Weight (kg) 16.4 ± 1.93 16.10 ± 1.71 0.68
Sex (M/F) 19/16 20/15
Duration of anesthesia (min) 32 ± 6.16 32.75 ± 6.58 0.71
Pethedine consumption (mg) 8 ± 10.05 16.25 ± 11.57 <0.0001
Time to first analgesic request (h) 7.95 ± 2.06 5.85 ± 1.87 0.002

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
170
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Amin and Amr: Gabapentin, paracetamol for pain control after adenotonsillectomy in children
5. Kong VK, Irwin MG. Gabapentin: A multimodal perioperative drug? Br J Anesth 2007;99:775-86.
6. Haig GM, Bockbrader HN, Wesche DL, Boellner SW, Ouellet D, Brown RR, et al. Single-dose gabapentin pharmacokinetics and safety in healthy infants and children. J Clin Pharmacol 2001;41:507-14.
7. Lönnqvist PA, Morton NS. Postoperative analgesia in infants and children. Br J Anaesth 2005:95;59-68.
8. Amr YM, Yousef AA. Evaluation of efficacy of the perioperative administration of Venlafaxine or gabapentin on acute and chronic postmastectomy pain. Clin J Pain 2010;26:381-5.
9. Davies A, Hendrich J, Van Minh AT, Wratten J, Douglas L, Dolphin AC. Functional biology of the alpha (2) delta subunits of voltage-gated calcium channels. Trends Pharmacol Sci 2007;28:220-8.
10. Loo ZD, Calcutt NA, Higuera ES, Valder CR, Song YH, Svensson CI, et al. Injury type-specific calcium channel alpha2delta-1 subunit up-regulation in rat neuropathic pain models correlates with antiallodynic effects of gabapentin. J Pharmcol Exp Ther 2002;303:1199-205.
11. Jeon EJ, Park YS, Park SS, Lee SK, Kim DH. The effectiveness of gabapentin on post-tonsillectomy pain control. Eur Arch Otorhinolaryngol 2009;266:1605-9.
12. Dirks J, Fredensborg BB, Christensen D, Fomsgaard JS, Flyger H, Dahl JB. A randomized study of the effects of single-dose gabapentin versus placebo on postoperative pain and morphine consumption after mastectomy. Anesthesiology 2002;97:560-4.
13. Fassoulaki A, Patris K, Sarantopoulos C, Hogan Q. The analgesic effect of gabapentin and mexiletine after breast surgery for cancer. Anesth Analg 2002;95:985-91.
14. Turan A, Memiş D, Karamanlioglu B, Yagiz R, Pamukçu Z, Yavuz E. The analgesic effects of gabapentin in monitored anesthesia care for ear-nose-throat surgery. Anesth Analg 2004;99:375-8.
15. Mikkelsen S, Hilsted KL, Andersen PJ, Hjortso NC, Enggard TP, Jorgensen DG, et al. The effect of gabapentin on postoperative pain following tonsillectomy in adults. Acta Anaesthesiol Scand 2006;50:809-15.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.
Staying in touch with the journal
1) Table of Contents (TOC) email alert Receive an email alert containing the TOC when a new complete issue of the journal is made available online. To register for TOC alerts go
towww.aeronline.org/signup.asp.
2) RSS feeds Really Simple Syndication (RSS) helps you to get alerts on new publication right on your desktop without going to the journal’s website.
You need a software (e.g. RSSReader, Feed Demon, FeedReader, My Yahoo!, NewsGator and NewzCrawler) to get advantage of this tool. RSS feeds can also be read through FireFox or Microsoft Outlook 2007. Once any of these small (and mostly free) software is installed, add www.aeronline.org/rssfeed.asp as one of the feeds.

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
171
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Original Article
Intrathecal nalbuphine as an adjuvant to subarachnoid block: What is the most effective dose?Arghya Mukherjee, Anirban Pal1, Jitendra Agrawal, Amrita Mehrotra, Nidhi Dawar2
Department of Anesthesiology, GR Medical College, Gwalior, Madhya Pradesh, 1Department of Anesthesiology, Calcutta National Medical College (CNMC), Kolkata, West Bengal, 2Specialist Medical Officer (Anaesthesiology), West Bengal Health Service, West Bengal, India
Corresponding author: Dr. Anirban Pal, 43/6/5 Jheel Road, Kolkata - 700 031, West Bengal, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_59_11R5 AP Done 27th Jan
AbstractBackground: Nalbuphine has been used intrathecally as an adjuvant in previous studies, but none clearly state the most effective dose of nalbuphine. The purpose of our study was to establish the effectiveness of intrathecal nalbuphine as an adjuvant, compare three different doses and determine the optimum dose with prolonged analgesic effect and minimal side-effects.Materials and Methods: In this prospective, randomized, double-blinded, controlled study, 100 ASA I and II patients undergoing lower limb orthopedic surgery under subarachnoid block (SAB), were randomly allocated to four groups: A, B, C and D, to receive 0.5 ml normal saline (NS) or 0.2, 0.4 and 0.8 mg nalbuphine made up to 0.5 ml with NS added to 0.5% hyperbaric bupivacaine 12.5 mg (total volume 3 ml), respectively. The onset of sensory and motor blockade, two-segment regression time of sensory blockade, duration of motor blockade and analgesia, visual analogue scale (VAS) pain score and side-effects were compared between the groups.Results: Two-segment regression time of sensory blockade and duration of effective analgesia was prolonged in groups C (0.4 mg nalbuphine) and D (0.8 mg nalbuphine) (P<0.05), and the incidence of side-effects was significantly higher in group D (P<0.05) compared with the other groups.Conclusion: Nalbuphine used intrathecally is a useful adjuvant in SAB and, in a dose of 0.4 mg, prolongs postoperative analgesia without increased side-effects.
Key words: Hyperbaric bupivacaine, nalbuphine, subarachnoid block
INTRODUCTION
The first report on the use of intrathecal opioids (ITO) for acute pain treatment was in 1979 by Wang and colleagues.[1] Use of ITO as adjuncts has a definite place
in the present regional anesthesia practice. Various opioids have been used along with bupivacaine to prolong its effect, to improve the quality of analgesia and minimize the requirement of postoperative analgesics. [2,3] Nalbuphine is a semisynthetic opioid with mixed mu antagonist and k agonist properties.[4] Previous studies have shown that epidural or intrathecal administration of nalbuphine produces a significant analgesia accompanied by minimal pruritus and respiratory depression.[5,6] Culebras et al. in 2002 used intrathecal nalbuphine in doses 0.2, 0.8 and 1.6 mg with 10 mg of 0.5% hyperbaric bupivacaine in patients undergoing caesarean section under subarachnoid block (SAB) and found 0.8 mg of nalbuphine as an effective dose.[7] But, they have not used

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
172
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Mukherjee, et al.: Optimal dose of intrathecal nalbuphine
0.4 mg nalbuphine. Lin et al. found that the addition of intrathecal nalbuphine 0.4 mg to hyperbaric tetracaine, compared with intrathecal morphine 0.4 mg for SAB, improved the quality of intraoperative and postoperative analgesia, with fewer side-effects.[5] In this prospective, double-blind, randomized, controlled study, we tried to establish the effectiveness of intrathecal nalbuphine as an additive by comparing with the control and determining the optimal dose of intrathecal nalbuphine using 0.2, 0.4 and 0.8 mg added to 12.5 mg hyperbaric bupivacaine 0.5% (total volume 3 ml) to have prolonged pain relief with minimal side-effects in patients undergoing lower limb orthopedic surgical procedures under SAB.
MATERIALS AND METHODS
The study was approved by the local institutional ethics committee and written informed consent was obtained from all patients before participation. One hundred patients, ASA physical status I and II, aged 20–60 years, scheduled for elective lower limb orthopedic surgeries, of duration less than 3 h, under SAB, were included in the study. Patients were randomly allocated to one of four groups (n=25). They received either normal saline (NS) 0.5 ml (group A), nalbuphine 0.2 mg (group B), nalbuphine 0.4 mg (group C) or nalbuphine 0.8 mg (group D), made up to 0.5 ml volume with NS, mixed with 12.5 mg of hyperbaric bupivacaine 0.5% (total volume 3 ml). The baricity of the study drugs was comparable. The drugs were prepared by one of the authors who did not take further part in the study. An experienced anesthesiologist who did not participate in the study performed the SAB and was blinded to the study drug used. Both patients and observers, who recorded and analyzed the data, were blinded to the study drug received.
Patients with a history of adverse response to bupivacaine or nalbuphine, pregnant patients, patients receiving phenothiazine, other tranquilizers, hypnotics or other central nervous system depressants (including alcohol) or suffering from peripheral or central neurological, cardiac, respiratory, hepatic, renal disease or with body weight more than 100 kg or less than 40 kg and height less than 145 cm or more than 160 cm and patients having contraindication to SAB were excluded from study.
All the patients fasted for at least 6 h before the procedure. After securing intravenous (18G) access in dorsum of the left hand and attaching routine monitors, preloading with Ringer’s lactate solution 15 ml/kg over 10 min was done. SAB was performed with 3 ml of the study drug injected in L3/4 or L4/5 intervertebral space, using a 25 gauge Quincke spinal needle, in the sitting position, maintaining aseptic precautions, according to the standard institutional protocol. Thereafter, patients were placed in the supine or lateral position for surgery. Intraoperative fluid replacements were given as necessary depending on the blood loss and
hemodynamic parameters. Intraoperative hypotension and bradycardia was managed with colloids and atropine 0.6 mg, respectively. In case of any respiratory depression, oxygen through facemask at 6 l was administered. Advanced equipments and drugs for resuscitation, airway management and ventilation were kept ready.
The onset of sensory blockade (time taken from the end of injection to loss of pin prick sensation at T10 dermatome) and complete motor blockade (time taken from the end of injection to development of grade IV motor block, modified Bromage’s criteria[8]), highest level of sensory blockade, duration of sensory blockade (two-segment regression time from highest level of sensory blockade), duration of motor blockade (time required for motor blockade return to Bromage’s grade I from the time of onset of motor blockade) and duration of effective analgesia (time from the intrathecal injection to the first analgesic requirement, visual analogue scale [VAS] score 3.5 or more) were recorded.
The changes in pulse rate, systolic and diastolic blood pressure, oxygen saturation (SpO2) and respiratory rate were recorded at 0, 2, 5,10 and 15 min and then at 15-min intervals up to 300 min after SAB, or up to the end point of study. Any side-effects in the form of post-operative hypotension, bradycardia, respiratory depression (judged by respiratory rate less than 10 or SpO2 <90%) nausea and vomiting (in presence of stable hemodynamic parameters) and pruritus were recorded. Those patients who did not develop sensory block up to T10 and Grade IV motor block were excluded from the study.
Intensity of pain was assessed by VAS[9] at 0, 10, 15, 30 and 60 min and then at 30-min intervals till 300 min after injection or until the patient received a rescue analgesic. Patients reporting a VAS score 3.5 or more received rescue analgesics in the form of injection (Inj) Diclofenac 75 mg IM. Incidence of nausea, vomiting and pruritus was noted. Nausea and vomiting was treated with Inj Ondansetron 4 mg i.v. and pruritus with anti-histaminics. Data were analyzed using Student’s t-test (paired and unpaired), one-way ANOVA and Fisher’s test with the help of Epical C2000 software. A P value less than 0.05 was considered statistically significant.
RESULTS
All the demographic variables like age, weight, height, sex ratio and duration of surgery were comparable in all the four groups; P>0.05 [Table 1].
The onset time of sensory and motor blockade were found to be statistically insignificant (P>0.05) among all the four groups [Table 2]. There was no case of failure or inadequate blockade after SAB. Maximum sensory level achieved by all groups was T6, and a T10 level was achieved by all patients. Two-segment regression time of sensory

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
173
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Mukherjee, et al.: Optimal dose of intrathecal nalbuphine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
blockade was prolonged progressively in groups A, B, C and D [Table 2]. The duration of analgesia was progressively prolonged in groups B, C and D as compared with group A; P<0.05 [Table 2]. Group D recorded the longest duration of analgesia with a mean of 278.5 min compared with 237.3 min in group C [Table 2]. Duration of motor blockade was comparable in all the four groups; P=0.592 [Table 2].
The patients recorded a mean VAS score of 3.475 at 270 min (group D), 3.477 at 240 min (group C), 3.26 at 210 min (group B) and 3.14 at 150 min after starting of anesthesia and were given rescue analgesics when VAS was 3.5 or more [Table 3].
On intragroup comparison after SAB, there was no statistically significant difference in the intraoperative mean pulse rate, systolic blood pressure and diastolic blood pressure, respiratory rate and SpO2 between the groups (Table not provided).
The side-effects, postoperative hypotension (P=0.010), bradycardia (P=0.004), nausea and vomiting with stable hemodynamic parameters (P=0.023) and pruritus (P=0.004), were significantly higher in group D. We did not come across any case of respiratory depression in any of the groups [Table 4].
DISCUSSION
ITO used as adjuncts are capable of producing analgesia of prolonged duration but allow early ambulation of patients because of their sympathetic and motor nerve-sparing activities.[10,11] The popularity of ITO was undermined by reports of side-effects, such as respiratory depression,
pruritus and postoperative nausea and vomiting.[12]
Nalbuphine is an opioid (393Da) structurally related to oxy-morphone. It is a highly lipid-soluble opioid with an agonist action at the k opioid receptor and an antagonist activity at the mu opioid receptor.[13,14] Nalbuphine and other k agonists had provided reasonably potent analgesia in certain models of visceral nociception. [4] They have a short duration of action, consistent with their lipid solubility and rapid clearance compared with other opioids like morphine. Recent reports suggest that the safety of ITO are more assured than previously published studies.[15] Nalbuphine given systemically has a reduced incidence of respiratory depression and has been used to antagonize the side-effects of spinal opiates. [16- 18] There are a few studies of neuraxial administration of nalbuphine that have shown to produce a significant analgesia accompanied by minimal pruritus and respiratory depression.[6]
Yoon et al. studied 60 obstetric patients scheduled for caesarean section under SAB to receive morphine 0.1 mg or nalbuphine 1 mg or morphine 0.1 mg with nalbuphine 1 mg in addition to 0.5% bupivacaine 10 mg and concluded that effective analgesia was prolonged in the morphine group and morphine with nalbuphine group, but the incidence of pruritus was significantly lower in the nalbuphine group, while the incidence of nausea and vomiting did not differ in the different groups.[19]
Fournier et al. studied the analgesic effects of intrathecal morphine 160 mcg and nalbuphine 400 mcg in geriatric patients scheduled for elective total hip replacement under continuous spinal anesthesia, given in the postoperative period, in the recovery room, and
Table 1: Demographic data and duration of surgery in groups A, B, C and D (mean ± SD)Variable Group A (n=25) Group B (n=25) Group C (n=25) Group D (n=25) F test P valueAge (years) 40.9 ± 11.14 39.3 ± 10.67 41.0 ± 11.16 43.2 ± 11.34 0.525 0.666
Weight (kg) 64.9 ± 5.21 66.0 ± 10.38 63.7 ± 11.26 65.0 ± 10.06 0.244 0.865
Height (cm) 164.3 ± 5.72 166.0 ± 3.08 165.0 ± 6.50 164.8 ± 6.64 0.396 0.756
Sex (M: F) 14:11 15:10 15:10 13:12 0.929
Duration of surgery (min)
119.1 ± 17.10 120.9 ± 26.46 121.4 ± 25.47 121.7 ± 25.16 0.060 0.981
Table 2: Sensory block, motor block and analgesia in groups A, B, C and D (mean ± SD)Parameters Group A (n=25) Group B (n=25) Group C (n=25) Group D (n=25) F test P valueOnset time of sensory blockade (min)
1.75 ± 0.27 1.69 ± 0.20 1.63 ± 0.24 1.59 ± 0.18 2.415 0.071
Two-segment regression time of sensory blockade (min)
118.2 ± 6.80 134.4 ± 6.95 141.5 ± 5.83 153.3 ± 6.05 130.4 0.000
Onset time of complete motor blockade (min)
5.9 ± 0.57 5.8 ± 0.76 5.7 ± 0.62 5.6 ± 0.53 1.063 0.369
Duration of motor blockade (min)
138.8 ± 5.84 139.4 ± 7.75 140.6 ± 6.02 141.0 ± 5.83 0.639 0.592
Duration of effective analgesia (min)
170.0 ± 5.85 213.8 ± 6.70 237.3 ± 5.64 278.5 ± 6.04 1393.891 0.000
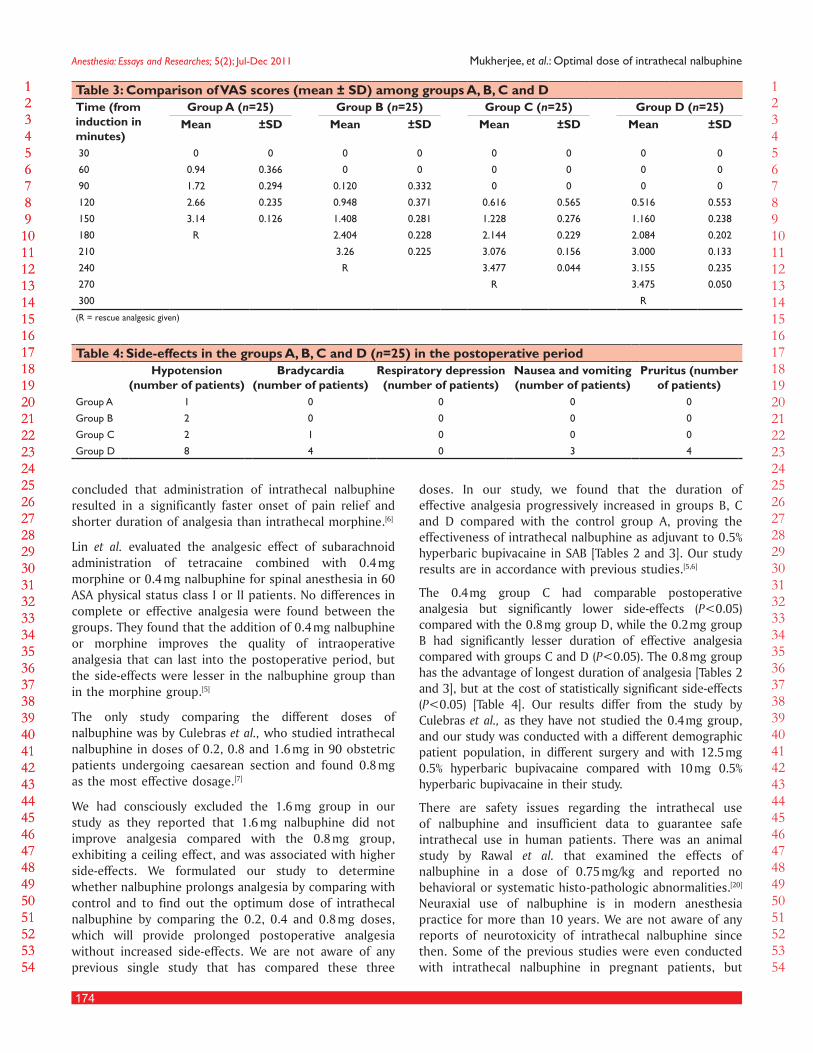
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
174
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Mukherjee, et al.: Optimal dose of intrathecal nalbuphine
concluded that administration of intrathecal nalbuphine resulted in a significantly faster onset of pain relief and shorter duration of analgesia than intrathecal morphine.[6]
Lin et al. evaluated the analgesic effect of subarachnoid administration of tetracaine combined with 0.4 mg morphine or 0.4 mg nalbuphine for spinal anesthesia in 60 ASA physical status class I or II patients. No differences in complete or effective analgesia were found between the groups. They found that the addition of 0.4 mg nalbuphine or morphine improves the quality of intraoperative analgesia that can last into the postoperative period, but the side-effects were lesser in the nalbuphine group than in the morphine group.[5]
The only study comparing the different doses of nalbuphine was by Culebras et al., who studied intrathecal nalbuphine in doses of 0.2, 0.8 and 1.6 mg in 90 obstetric patients undergoing caesarean section and found 0.8 mg as the most effective dosage.[7]
We had consciously excluded the 1.6 mg group in our study as they reported that 1.6 mg nalbuphine did not improve analgesia compared with the 0.8 mg group, exhibiting a ceiling effect, and was associated with higher side-effects. We formulated our study to determine whether nalbuphine prolongs analgesia by comparing with control and to find out the optimum dose of intrathecal nalbuphine by comparing the 0.2, 0.4 and 0.8 mg doses, which will provide prolonged postoperative analgesia without increased side-effects. We are not aware of any previous single study that has compared these three
doses. In our study, we found that the duration of effective analgesia progressively increased in groups B, C and D compared with the control group A, proving the effectiveness of intrathecal nalbuphine as adjuvant to 0.5% hyperbaric bupivacaine in SAB [Tables 2 and 3]. Our study results are in accordance with previous studies.[5,6]
The 0.4 mg group C had comparable postoperative analgesia but significantly lower side-effects (P<0.05) compared with the 0.8 mg group D, while the 0.2 mg group B had significantly lesser duration of effective analgesia compared with groups C and D (P<0.05). The 0.8 mg group has the advantage of longest duration of analgesia [Tables 2 and 3], but at the cost of statistically significant side-effects (P<0.05) [Table 4]. Our results differ from the study by Culebras et al., as they have not studied the 0.4 mg group, and our study was conducted with a different demographic patient population, in different surgery and with 12.5 mg 0.5% hyperbaric bupivacaine compared with 10 mg 0.5% hyperbaric bupivacaine in their study.
There are safety issues regarding the intrathecal use of nalbuphine and insufficient data to guarantee safe intrathecal use in human patients. There was an animal study by Rawal et al. that examined the effects of nalbuphine in a dose of 0.75 mg/kg and reported no behavioral or systematic histo-pathologic abnormalities. [20] Neuraxial use of nalbuphine is in modern anesthesia practice for more than 10 years. We are not aware of any reports of neurotoxicity of intrathecal nalbuphine since then. Some of the previous studies were even conducted with intrathecal nalbuphine in pregnant patients, but
Table 3: Comparison of VAS scores (mean ± SD) among groups A, B, C and DTime (from induction in minutes)
Group A (n=25) Group B (n=25) Group C (n=25) Group D (n=25)Mean ±SD Mean ±SD Mean ±SD Mean ±SD
30 0 0 0 0 0 0 0 0
60 0.94 0.366 0 0 0 0 0 0
90 1.72 0.294 0.120 0.332 0 0 0 0
120 2.66 0.235 0.948 0.371 0.616 0.565 0.516 0.553
150 3.14 0.126 1.408 0.281 1.228 0.276 1.160 0.238
180 R 2.404 0.228 2.144 0.229 2.084 0.202
210 3.26 0.225 3.076 0.156 3.000 0.133
240 R 3.477 0.044 3.155 0.235
270 R 3.475 0.050
300 R
(R = rescue analgesic given)
Table 4: Side-effects in the groups A, B, C and D (n=25) in the postoperative periodHypotension
(number of patients)Bradycardia
(number of patients)Respiratory depression (number of patients)
Nausea and vomiting (number of patients)
Pruritus (number of patients)
Group A 1 0 0 0 0
Group B 2 0 0 0 0
Group C 2 1 0 0 0
Group D 8 4 0 3 4

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
175
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Mukherjee, et al.: Optimal dose of intrathecal nalbuphine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
no neurotoxicity was reported in them.[7,18] The FDA in 2005 advised that nalbuphine may be used during labor and delivery only if clearly indicated and if the potential benefit outweighs the risk. We are unaware of any definite caution in the use of nalbuphine by any statutory authority in nonpregnant patients and in subjects more than 18 years old. We have excluded pregnant patients from our study and obtained clearance from the local institutional ethical committee.
CONCLUSION
Intrathecal nalbuphine prolongs the duration of postoperative analgesia when used as an adjunct, and 0.4 mg is the most effective dose that prolongs early postoperative analgesia without increasing the risk of side-effects. We recommend 0.4 mg as the optimal dose of nalbuphine if used intrathecally along with 12.5 mg 0.5% hyperbaric bupivacaine for SAB in patients undergoing lower limb orthopedic surgeries.
REFERENCES
1. Wang JK, Nauss LA, Thomas JE. Pain relief by Intrathecally applied morphine in man. Anesthesiology 1979;50:149-51.
2. Veering B. Focus on Adjuvants in regional Anesthesia. Euro Anesthesia 2005;28-31:217-21.
3. Morgan M. The rational use of intrathecal and extradural opioids. Br J Anaesth 1989;63:165-88.
4. Schmauss C, Doherty C, Yaksh TL. The analgesic effects of an intrathecally administered partial opiate agonist, nalbuphine hydrochloride. Eur J Pharmacol 1982;86:1-7.
5. Lin ML. The analgesic effect of subarachnoid administration of tetracaine combined with low dose of morphine or nalbuphine for spinal anaesthesia. Ma Zui Xue Za Zhi 1992;30:101-5.
6. Fournier R, Gamulin Z, Macksay M, Van Gessel E. Intrathecal morphine versus nalbuphine for post operative pain relief after total hip replacement. Anesthesiology 1998;89:867.
7. Culebras X, Gaggero G, Zatloukal J, Kern C, Marti RA. Advantages of Intrathecal nalbuphine, compared with intrathecal morphine, after Cesarean delivery: An evaluation of postoperative analgesia and adverse effects. Anesth Analg 2000;91:601-5.
8. Bromage PR. Epidural analgesia. Philadelphia: WB Saunders; 1978.9. Crichton N. Information point: Visual analogue scale (VAS). J Clin Nursing
2001;10:697-706.10. Tawfik MO. Mode of action of intraspinal opioids. Pain Rev 1994;1:275-94.11. Terajima K, Onodera H, Kobayashi M, Yamanaka H, Ohno T, Konuma S,
et al. Efficacy of intrathecal morphine for analgesia following elective cesarean section: Comparison with previous delivery. J Nippon Med Sch 2003;70:327-33.
12. Chaney MA. Side effects of intrathecal and epidural opioids. Can J Anesth 1995;42:891-903.
13. Zarr GD, Werling LL, Brown SR, Cox BM. Opioid ligand binding sites in the spinal cord of the guinea-pig. Neuropharmacology 1986;25:47-80.
14. De Souza EB, Schmidt WK, Kuhar MJ. Nalbuphine: An autoradiographic opioid receptor binding profile in the central nervous system of an agonist/antagonist analgesic. J Pharmacol Exp Ther 1988;244:391-402.
15. Ready LB, Loper KA, Nessly M, Wild L. Postoperative epidural morphine is safe on surgical wards. Anesthesiology 1991;75:452-6.
16. Henderson SK, Cohen H. Nalbuphine augmentation of analgesia and reversal of side effects following epidural hydromorphone. Anesthesiology 1986;65:216-8.
17. Penning JP, Samson B, Baxter AD. Reversal of epidural morphine-induced respiratory depression and pruritus with nalbuphine. Can J Anaesth 1988;35:599-604.
18. Yang T, Breen TW, Archer D, Fick G. Comparison of 0.25 mg and 0.1 mg intrathecal morphine for analgesia after cesarean section. Can J Anaesth 1999;46:856-60.
19. Yoon JY, Jee YS, Hong JY. A Comparison of Analgesic Effects and side effects of intrathecal morphine, nalbuphine and morphine-nalbuphine mixture for pain relief during a caesarean section. Korean J Anaesthesiol 2002;42:627-33.
20. Rawal N, Nuutinen L, Raj PP, Lovering SL, Gobuty AH, Hargardine J, et al. Behavioral and histopathologic effects following intrathecal administration of butorphanol, sufentanil, and nalbuphine in sheep. Anesthesiology 1991;75:1025-34.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
176
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Original Article
Comparison of sodium diclofenac, ketamine and propofol with fentanyl and midazolam in balanced anaesthesiaMozaffar Rabiee, Ebrahim Alijanpour, Ali Jabbari1, Farzan Khirkhah2, Yousof Mortazavi, Ali Bijani3
Department of Anaesthesiology and Intensive Care, Babol University of Medical Sciences, 1Researcher of Deputy of Treatment, Golestan University of Medical Sciences, Golestan, Babol University of Medical Sciences, 2Department of Psychiatry, 3Non Communicable Paediatric Research Center, Babol University of Medical Sciences, Babol, Iran
Corresponding author: Dr. Ebrahim Alijanpour, Department of Anaesthesiology and Intensive Care, Flat 2, Rohani Hospital, Ganj, AfrozBlv, DaneshgahSq, Babol City, Mazandaran Province, Iran. E-mail:[email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_32_11R16
AbstractContext: Analgesia is based on balanced anaesthesia, which is usually maintained by administration of narcotic agents. In some patients, it is not possible to use narcotics. We compared hemodynamic changes, anaesthesia depth, emetic sequelae and post-operative pain between sodium Diclofenac, Ketamine-Propofol (DKP) and Fentanyl-Midazolam (FM).Aims: The effectiveness of an anaesthetic technique employing sodium was compared against in patients undergoing elective surgery.Settings and Design: In a clinical trial study, 82 patients who attended for an elective surgery were randomly divided into two groups.Materials and Methods: In DKP group pre-medication included Sodium Diclofenac 1 mg/kg and Midazolam 0.02 mg/kg, whereas, in FM group they were Fentanyl 2 µg/kg and Midazolam 0.02 mg/ kg. Anaesthesia induction in both groups was the same. Anaesthesia was conserved in DKP group by using Propofol plus Ketamine infusion plus N2O 50% and in FM group with Fentanyl plus Midazolam plus N2o 50%. Hemodynamic changes, depth of anaesthesia, nausea and vomiting, post operative analgesic effects were recorded.Results: Hemodynamic changes and depth of anaesthesia were similar throughout the maintenance phase in two groups. In FM group, significant increase in heart rate was recorded in recovery room. Pain score according to visual analogue scale (VAS) and need for analgesics, was significantly more in FM group compared to DKP group (P = 0.000). No patient suffered from nausea, vomiting or hallucinations.Conclusions: This study revealed that intravenous administration of Sodium Diclofenac along with Ketamine and Propofolplus N2O 50% for general anaesthesia provides a balanced anaesthesia as

177
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Rabiee, et al.: Diclofenac, ketamine and propofol versus fentanyl and midazolam
well as hemodynamic stability, and adequate depth of anaesthesia. It also reduces the postoperative pain and need for narcotics. We recommended DKP plus N2O 50% method for patients prohibited from opioid administration. It will be an acceptable method in sensitive patients.
Key words: Balanced anaesthesia, ketamine, propofol, sodium diclofenac
a premedication for balanced anaesthesia; however, there is often a disparity in the level of sedation compared with the presence of amnesia.[14]
The study was designed to test the hypothesis that administration of sodium diclofenac and ketamine accompanied with propofol instead of fentanyl in balanced anaesthesia may adversely affect the quality of anaesthesia and postoperative outcome in patients receiving the total intra venous anaesthesia (TIVA) method plus N2O 50%, in patients prohibited from opioid administration. To attempt this, hemodynamic changes, anaesthesia depth, emetic sequelae and post-operative pain were studied in usual methods for opioid administration (fentanyl and midazolam - FM group) and the other group without administration of opioids by sodium diclofenac, ketamine and propofol (DKP). We substituted fentanyl by sodium diclofenac and ketamine in patients undergoing surgery who received TIVA in balanced anaesthesia.
MATERIALS AND METHODS
This experimental study was conducted on a single surgical population of patients undergoing elective inguinal hernioraphy with duration of surgery under 1 hour. The study was approved by our institutional review board, and the written informed consent was obtained from all of the participants. Some of our exclusion criteria were a history of current NSAIDs use, analgesic or psychotropic drug therapy, alcohol or substance abuse, NSAID allergy, bronchial asthma, peptic ulcer disease, renal disease, or bleeding disorders, end stage disease and confounding underlying diseases. Patients who had the above mentioned criteria were excluded from the study, and 82 patientsof American Society of Anesthesiologists (ASA) Class I, between 15 and 55 years of age old were included.
The patients were divided into two groups randomized. In DKP group, premedication included sodium diclofenac 1 mg/kg and midazolam 0.02 mg/kg, whereas in FM group fentanyl 2 µg/kg and midazolam 0.02 mg/kg were administered. Hemodynamic factors like systolic and diastolic Blood Pressure (BP), Heart Rate (HR) and Bispectrial index monitoring (with Danmeter CSM 06 Denmark instrument), emetic sequelae were evaluated and recorded before, during and after the surgery up to discharge time from post anaesthetic care unit (PACU).
INTRODUCTION
The term balanced anaesthesia was introduced by Lundy in 1926 which consists of amnesia, analgesia, muscle relaxation and autonomic reflexes suppression as well as hemodynamic stability. The use of opioids in general anaesthesia is a key component in the current notion of “balanced anaesthesia”. Opioid administration in balanced anaesthesia reduces anxiety and pain before the operation, decreases somatic and autonomic responses of airway stimulations, corrects hemodynamic stability and lowers the need for vaporizing anaesthetic drugs as well as a post-operation analgesia.[1] Fentanyl is one of the most common parenteral opioid analgesics administered in balanced anaesthesia because it allows smooth emergence from anaesthesia without coughing and bucking, and provides residual postoperative analgesia.[2,3]
In some conditions like surgical squint correction, the anaesthesiologist prefers to avoid opioid analgesic agents to reduce the post-operation nausea and vomiting (PONV);[4,5] Also, concern over opioid side effects can cause practitioners to hesitate to use opioids. In patients undergoing ultra rapid opiate detoxification who are applied with naltrexone, there are some limitations for opioids, but not for other analgesic such as Ketamine and Non steroidalanti inflammatory drugs (NSAIDs);[6,7] thus, opioids cannot be used always, and therefore, the need for anaesthetic technique with no opioid side effects emerges.[5]
Propofol is the most frequently used intravenous (IV) anaesthetic today. It is suitable for the induction and maintenance of anaesthesia. Compared with volatile anaesthetics, the use of propofol for general anaesthesia has been purported to reduce postoperative emesis and requirements for antiemetic[8,9] Sodium diclofenac is one of the common NSAIDs with anti inflammatory, analgesic and anti pyretic effects, which can be used to reduce pain.[10] Ketamine is a non barbiturate anaesthetic drug with analgesic effects, which is fast-acting and used for premedication, sedation, induction or maintenance of anaesthesia and postoperative analgesia.[11] There has been increased interest in the routine use of ketamine in small doses for preventive analgesia and for the treatment or prevention of opiate tolerance and hyperalgesia. [12- 14] Benzodiazepines are among the most frequently prescribed drugs. Midazolam is often used for sedation as
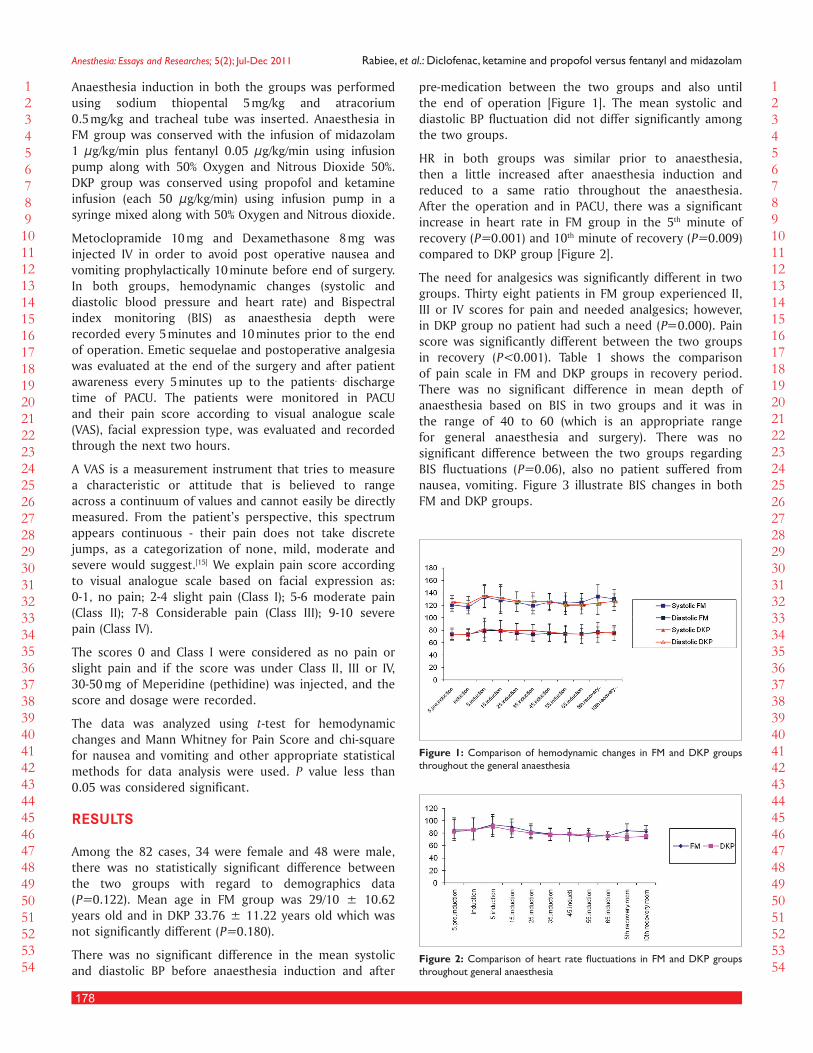
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
178
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Rabiee, et al.: Diclofenac, ketamine and propofol versus fentanyl and midazolam
Anaesthesia induction in both the groups was performed using sodium thiopental 5 mg/kg and atracorium 0.5 mg/ kg and tracheal tube was inserted. Anaesthesia in FM group was conserved with the infusion of midazolam 1 µg/kg/min plus fentanyl 0.05 µg/kg/min using infusion pump along with 50% Oxygen and Nitrous Dioxide 50%. DKP group was conserved using propofol and ketamine infusion (each 50 µg/kg/min) using infusion pump in a syringe mixed along with 50% Oxygen and Nitrous dioxide.
Metoclopramide 10 mg and Dexamethasone 8 mg was injected IV in order to avoid post operative nausea and vomiting prophylactically 10 minute before end of surgery. In both groups, hemodynamic changes (systolic and diastolic blood pressure and heart rate) and Bispectral index monitoring (BIS) as anaesthesia depth were recorded every 5 minutes and 10 minutes prior to the end of operation. Emetic sequelae and postoperative analgesia was evaluated at the end of the surgery and after patient awareness every 5 minutes up to the patients, discharge time of PACU. The patients were monitored in PACU and their pain score according to visual analogue scale (VAS), facial expression type, was evaluated and recorded through the next two hours.
A VAS is a measurement instrument that tries to measure a characteristic or attitude that is believed to range across a continuum of values and cannot easily be directly measured. From the patient’s perspective, this spectrum appears continuous - their pain does not take discrete jumps, as a categorization of none, mild, moderate and severe would suggest.[15] We explain pain score according to visual analogue scale based on facial expression as: 0-1, no pain; 2-4 slight pain (Class I); 5-6 moderate pain (Class II); 7-8 Considerable pain (Class III); 9-10 severe pain (Class IV).
The scores 0 and Class I were considered as no pain or slight pain and if the score was under Class II, III or IV, 30-50 mg of Meperidine (pethidine) was injected, and the score and dosage were recorded.
The data was analyzed using t-test for hemodynamic changes and Mann Whitney for Pain Score and chi-square for nausea and vomiting and other appropriate statistical methods for data analysis were used. P value less than 0.05 was considered significant.
RESULTS
Among the 82 cases, 34 were female and 48 were male, there was no statistically significant difference between the two groups with regard to demographics data (P=0.122). Mean age in FM group was 29/10 ± 10.62 years old and in DKP 33.76 ± 11.22 years old which was not significantly different (P=0.180).
There was no significant difference in the mean systolic and diastolic BP before anaesthesia induction and after
pre-medication between the two groups and also until the end of operation [Figure 1]. The mean systolic and diastolic BP fluctuation did not differ significantly among the two groups.
HR in both groups was similar prior to anaesthesia, then a little increased after anaesthesia induction and reduced to a same ratio throughout the anaesthesia. After the operation and in PACU, there was a significant increase in heart rate in FM group in the 5th minute of recovery (P=0.001) and 10th minute of recovery (P=0.009) compared to DKP group [Figure 2].
The need for analgesics was significantly different in two groups. Thirty eight patients in FM group experienced II, III or IV scores for pain and needed analgesics; however, in DKP group no patient had such a need (P=0.000). Pain score was significantly different between the two groups in recovery (P<0.001). Table 1 shows the comparison of pain scale in FM and DKP groups in recovery period. There was no significant difference in mean depth of anaesthesia based on BIS in two groups and it was in the range of 40 to 60 (which is an appropriate range for general anaesthesia and surgery). There was no significant difference between the two groups regarding BIS fluctuations (P=0.06), also no patient suffered from nausea, vomiting. Figure 3 illustrate BIS changes in both FM and DKP groups.
Figure 1: Comparison of hemodynamic changes in FM and DKP groups throughout the general anaesthesia
Figure 2: Comparison of heart rate fluctuations in FM and DKP groups throughout general anaesthesia

179
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Rabiee, et al.: Diclofenac, ketamine and propofol versus fentanyl and midazolam
DISCUSSION
This research was aimed to evaluate the effects of sodium diclofenac, ketamine and propofol versus fentanyl and midazolam in balance analgesia during and after operation based on usual and standard monitoring to evaluate efficacy of two methods. There was no significant difference in hemodynamic fluctuations and depth of anaesthesia (as seen by the BIS values) throughout maintenance of general anaesthesia between the two groups. There was merely a heart rate increase in recovery period of FM group which can be justified with the post operation pain. A similar result was found in a study conducted by Oztekin, et al. in 2002.[6] IV prescription of NSAIDs as a sole analgesic failed to control postoperative pain following major surgery,[16] but we could get a good response in combination of NSAID and ketamine in our study. Postoperative nausea and vomiting continue to be problematic areas in anaesthesia.[17] Regarding clinical signs and symptoms (nausea, vomiting), there was no significant difference between FM and DKP groups; perhaps due to prophylactic drug administration of midazolame in pre-medication and metoclopramide plus dexamethasone 10 minutes prior to the end of the operation.
Fuji study on preventing postoperative nausea and vomiting after middle ear surgery in adult patients showed that none of the available antiemetic is entirely effective, perhaps because most of them act through the blockage on one type of receptor.[18] Maybe combined antiemetic with different sites of activity would be more effective.[19] Riad, et al. demonstrated that the prophylactic administration of combination of midazolam and dexamethasione was superior to each drug alone in reduction of nausea and vomiting.[20] Multi disciplinary approach is advisable for prevention and therapy of PONV nowadays;[21,22] and it is similar to our results.
Anaesthetic techniques have a major role in post operative nausea and vomiting (PONV), and without prescription of antiemetic drugs for prophylaxis of PONV, the incidence of the latter is highest in balanced anaesthesia, followed by inhalational based anaesthesia and least for total intra venous anaesthesia (TIVA) based on propofol.[23,24] In our study, we used TIVA technique plus N2O 50%, based on fentanyl, midazolam (FM) and sodium diclofenace, ketamine andpropofol (DKP), with a premedication
induction policy and anti emetic drugs for prophylaxis during the anaesthesia period, because of which we could achieve an overall low incidence of PONV.
In the group receiving sodium diclofenac and ketamine, there was no need for pethidine post-operatively due to significantly low pain score. A similar finding was reported by a study conducted by Oztekin, et al. which showed that patients, who received 1 mg/kg sodium diclofenac intravenously, had a lesser pain and the need for morphine was also redcued.[6] Dhawan et al. conducted a study which showed the effect of rectal sodium diclofenac in reducing post-operative pain after cardiac surgery.[25]
Achariyapota, et al. and their collaborated study showed similar results about efficacy of rectal suppositories of sodium diclofenac in perinea pain after perinearhaphy. [26] In contrast, Canbay, et al. have reported that there was no significant difference in post-operative pain and necessary dosage of analgesics when sodium diclofenac 1 mg/kg intramuscular (IM) were added to ketamine and remifentanyl.[27]
In an investigation, 0.5 mg/kg ketamine was prescribed prior to incision in major abdominal surgeries and ketamine was repeated at a dose of 0.2 mg/kg after 20 minutes of operation. Good responses were obtained in comparison with placebo in their investigation.[28]
It has been reported that ketamine reduces postoperative pain and morphine consumption in post- thoracotomy. [12,13,29]
A comparison between propofol-ketamine versus protocol-fentanyl combinations for deep sedation and analgesia in pediatric patient in 2008 showed superiority of propofol-ketamine combination over propofol-fentanyl combination, because of more restlessness in patients given propofol-fentanyl. A clinical investigation in 2008 showed that sub dissociative-dose ketamine is safer than fentanyl for analgesia during propofol procedural sedation.[30,31] A study showed that use of NSAIDS instead of opioid or reduction of opioid dose could be reducing the complication of opioids without qualification impairment. In addition they discoveredthat intravenous NSAIDs and fentanyl could produce a greater decrease in the propofol sedation requirement during anaesthesia, and the use of NSAID in combination with propofol for anaesthesia was associated
Figure 3: BIS changes in both FM and DKP groups
Table 1: Comparison of pain scale in FM and DKP groups in recoveryGroup VAS P value
0 I II III IVFM 2 0 9 25 4 0.000
DKP 11 31 0 0 0DKP: Diclofenac, Ketamine-Propofol; FM: Fentanyl-Midazolam; VAS: Visual analogue scale

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
180
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Rabiee, et al.: Diclofenac, ketamine and propofol versus fentanyl and midazolam
with an improved recovery profile.[32] These results are further emphasized in our study as well. Two different groups of clinical investigators evaluated the efficacy of total intravenous anaesthesia with propofol, pentazocine and ketamine in mastectomy. They reported that patients had hemodynamic stability, rapid recovery and effective postoperative pain relief. [33,34]
Several studies have been shown that midazolam and ketamine seem to be acceptable drugs for use during assisted reproduction[35,36] and recent data also suggests that propofol may be a safe alternative for use during assisted reproduction.[37-39] Felfering et al. reported that no unpleasant emergence phenomenon could be observed in patients who received total intravenous anaesthesia with ketamine and propofol;[40] and in our study, no patient suffered from hallucination in the recovery room or other side effects of ketamine which are especially related to the psychological aspects, maybe due to benzodiazepine administration.
In the present study, we compared the clinical efficacy and safety of two different kind of balanced anaesthesia; anaesthesia by fentanyl and midazolam (FM) administration and a kind of TIVA anaesthesia by helping intravenous sodium diclofenac along with ketamine and propofol (DKP) without opioids. There were no noticeable effects on the depth of anaesthesia and hemodynamic stability during TIVA method plus N2O 50% accompanied with DKP, and balanced anaesthesia was also achieved. The incidence of PONV with respect to our policy was also low, so our method can be regarded as acceptable in susceptible patients.DKP significantly leads to a reduced post operative pain and need for opioid prescription. We recommended TIVA method plus N2O 50% accompany with DKP for patients with prohibited opioid administration.
REFERENCES
1. Bovill JG, Sebel PS, Stanley TH. Opiod Analgesics in anaesthesia: With special reference to their use in cardiovascular anaesthesia. Anesthesiology 1984;61:731-55.
2. Kido K, Aoi A, Konno T, Yasuda M, Sato M, Shimoda H, et al. Balance Anaesthesia Using Sevoflurane and Fentanyl Based on Site Concentration Model Compared to Sevoflurane/N2O Anaesthesia for Oral Surgery. Anesth Prog 2008;36:162-6.
3. Iwakiri H, Nagata O, Matsukawa T, Ozaki M, Sessler DI. Effective concentration of propofol for recovery of consciousness is virtually independent of fentanyl Effectiveconcentration. Anesth Analg 2003;96:1651-5.
4. Aftab S, Khan AB, Raza G. Assessment of risk factors for postoperative nausea and vomiting. J Coll Physicians Surg Pak 2008;18:137-41.
5. Vanderburg AA, Lambourne A, Yazjin S, Laghari NA. Vomiting after ophthalmic surgery: Effects of intra-operative anti-emetics and postoperative fluid restriction. Anaesthesia 1987;42:270-6.
6. Oztekin S, Hepaguslar H, Karr AA, Ozzeybek D, Artikaslan O, Elar Z. Preemptivediclofenac reduces morphine use afterremifentanilbased anaesthesia for tonsillectomy. Pediatr Anesth 2002;12:694-9.
7. Kaye AD, Gevirtz C, Bosscher HA, Duke JB, Frost EA, Richards TA, et al. Ultrarapid opiate detoxification: A review. Can J Anesth 2003;50:663-71.
8. Watcha MF, Simeon RM, White PF, Stevens JL. Effect of propofol on the incidence of postoperative vomiting after strabismus surgery in pediatric outpatients. Anesthesiology 1991;75:204-9.
9. Weir PM, Munro HM, Reynolds PI, Lewis IH, Wilton NC. Propofol infusion
and the incidence of emesis in pediatric outpatient strabismus surgery. Anesth Analg 1993;76:760-4.
10. Legeby M, Sandelin K, Wickman M, Olofsson C. Analgesic efficacy of diclofenac in combination with morphine and paracetamol after mastectomy and immediate breast reconstruction. Acta Anaesthesiol Scand 2005;49:1360-6.
11. Vallejo MC, Romeo RC, Davis DJ, Ramanathan S. Propofol-Ketamine versus propofol-fentanyl for outpatient laparoscopy: Comparison of postoperative nausea, emesis, analgesia, and recovery. J Clin Anesth 2002;14:426-31.
12. Nesher N, Serovian I, Marouani N, Chazan S, Weinbroum AA. Ketamine spares morphine consumption after transthoracic lung and heart surgery without adverse hemodynamic effects. Pharmacol Res 2008;58:38-44.
13. Kollender Y, Bickels J, Stocki D, Maruoani N, Chazan S, Nirkin A, et al. Subanesthetic Ketamine spares postoperative morphine and controls pain better than standard morphine does alone in orthopaedic-oncological patients. Eur J Cancer 2008;44:954-62.
14. Greves J, Glass PS, David A, Lubars KY, Matthew D, McEvoy, et al. Intravenous Anesthetic. In: Miller RD, editors. Anaesthesia 7th ed. Philadelphia: Churchill Livingstone; 2010. p. 746-7.
15. Wewers ME, Lowe NK. A critical review of visual analogue scales in the measurement of clinical phenomena. Res Nurs Health 1990;13:227-36.
16. Parke TJ, Millett S, Old S, Goodwin AP, Rice AS. Ketorolac for early postoperative analgesia. J Clin Anaesth 1995;7:465-9.
17. White PF. practical issues in outpatient anaesthesia: Management of post operative pain and emesis. Can J Anesth 1995;42:1053-8.
18. Fujii Y. Current management of vomiting after tonsillectomy in children. Curr Drug Saf 2009;4:62-73.
19. Splinter WM. Prevention of vomiting after strabismus surgery in children: Dexamethasone alone versus dexamethasone plus low-dose ondansetron. Pediatr Anaesth 2001;11:591-5.
20. Riad W, Altaf R, Abdulla A, Oudan H. Effect of Midazolam, dexamethasone and their combination on the prevention of nausea and vomiting following strabismus repair in children. Eur J Anaesthesiol 2007;24:697-701.
21. Elhakim M, Ali N, Rashed I, Riad M, Refat M. Dexamethasone reduces postoperative vomiting and pain after pediatric tonsillectomy. Can J Anesth 2003;50:392-7.
22. Unlugenc H, Guler T, Gunes Y, Isik G. Comparative study of the antiemetic efficacy of ondansetron,propofol and midazolam in the early postoperative period. Eur J Anesthesiol 2004;21:60-5.
23. Lim BL, Low TC. Total intravenous versus inhalational anaesthesia for dental day surgery. Anesth Intensive Care 1992;20:475-9.
24. Jellish SW, Leonetti JP, Murdoch JR, Fowles S. propofol-based anaesthesia as compared with standard anesthetic techniques for middle ear surgery. J Clin Anesth 1995;7:292-6.
25. Dhawan N, Das S, Kiran U, Chauhan S, Bisoi AK, Makhija N. Effect of rectal diclofenac in reducing postoperative pain and rescue analgesia requirement after cardiac surgery. Pain Pract 2009;9:385-93.
26. Achariyapota V, Titapant V. Relieving perineal pain after perineorrhaphy by diclofenacrctalsuppositories: Arandomized double-blinded placebo controlled trial. J Med Assoc Thai 2008;91:799-804.
27. Canbay O, Karakas O, Celebi N, Peker L, Coskun F, Aypar U. The preemptiveuse of diclofenac sodium in combination with ketamine and remifentanildose not enhance postoperative analgesia after laparoscopic gynecological procedures. Saudi Med J 2006;27:642-5.
28. Argiriadou H, Himmelseher S, Papagiannopoulou P, Georgiou M, Kanakoudis F, Giala M, et al. Improvement of pain treatment after major abdominal surgery by intravenous S+ ketamine. Anesth Analg 2004;98:1413-8.
29. Nesher N, Ekstein MP, Paz Y, Marouani N, Chazan S, Weinbroum AA. Morphine with adjuvant ketamine vs higher dose of morphine alone for immediate post thoracotomy analgesia. Chest 2009;136:245-52.
30. Tosun Z, Yeesmaoglu A, Coruh A. Propofol-ketamine vspropofol-fentanyl combinations for deep sedation and analgesia in pediatric patients undergoing burn dressing changes. PediatrAnaesth 2008;18:43-7.
31. Messenger DW, Murray HE, Dungey PE, van Vlymen J, Sivilotti ML. Sub dissociativedose ketamine versus fentanyl for analgesia during propofol procedural sedation: A randomized clinical trial. Acad Emerg Med 2008;15:877-86.
32. Ramirez-Ruiz M, Smith I, White PF. Use of analgesics during propofol sedation: A comparison of ketorolac, dezocine and fentanyl. J Clin Anesth 1995;7:481-5.
33. Nonaka A, Suzuki S, Masamune T, Imamura M, Abe F. Anesthetic management by total intravenous anaesthesia with propofol, pentazocine and ketamine. Masui 2005;54:133-7.
34. Badrinath S, Avramov MN, Shadrick M, Witt TR, Ivankovich AD. The use of propofolcombination during monitored anaesthesia care. Anaesth Analg 2000;90:858-62.

181
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Rabiee, et al.: Diclofenac, ketamine and propofol versus fentanyl and midazolam
35. Ben-Shlomo I, Moskovich R, Katz Y, Shalev E. Midazolam/ketamine sedative combination compared with fentanyl/propofol/isoflurane anaesthesia for oocyte retrieval. Hum Reprod 1999;14:1757-9.
36. B-Shlomo I, Moskovich R, Golan J, Eyali V, Tabak A, Shalev E. The effect of propofol anaesthesia on oocyte fertilization and early embryo quality. Hum Reprod 2000;15:2197-9.
37. Christiaens F, Janssenswillen C, Van Steirteghem AC, Devroey P, Verborgh C, Camu F. Comparison of assisted reproductive technology performance after oocyte retrieval under general anaesthesia (propofol) versus paracervical local anaesthetic block: A case-controlled study. Hum Reprod 1998;13:2456-60.
38. Tomioka S, Nakajo N. No genotoxic effect of propofol in Chinese hamster ovary cells: Analysis by sister chromatid exchanges. Acta Anaesthesiol Scand 2000;44:2161-5.
39. Hammadeh ME, Wilhelm W, Huppert A, Rosenbaum P, Schmidt W. Effects of general anaesthesia vs. sedation on fertilization cleavage and pregnancy rates in an IVF program. Arch Gynecol Obstet 1999;263:56-9.
40. Felfernig M, Andel D, Weintraud M, Connor D, Andel H, Blaicher AM. Postoperative vigilance in patients with total intravenous anaesthesia with ketamine/propofol. J R Nav Med Serv 2006;92:64-8.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.
“Quick Response code” link foR full text aRticles
The journal issue has a unique new feature for reaching to the journal’s website without typing a single letter. Each article on its first page has a “Quick Response Code”. Using any mobile or other hand-held device with camera and GPRS/other internet source, one can reach to the full text of that particular article on the journal’s website. Start a QR-code reading software (see list of free applications from http://tinyurl.com/yzlh2tc) and point the camera to the QR-code printed in the journal. It will automatically take you to the HTML full text of that article. One can also use a desktop or laptop with web camera for similar functionality. See http://tinyurl.com/2bw7fn3 or http://tinyurl.com/3ysr3me for the free applications.
Announcement
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
182
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Original Article
Ondansetron, ramosetron, or palonosetron: Which is a better choice of antiemetic to prevent postoperative nausea and vomiting in patients undergoing laparoscopic cholecystectomy?Sarbari Swaika, Anirban Pal1, Surojit Chatterjee, Debashish Saha2, Nidhi Dawar3
Department of Anesthesiology, Bankura Sammilani Medical College (BSMC), Bankura, West Bengal, 1Department of Anesthesiology, Calcutta National Medical College (CNMC), Kolkata, West Bengal, 2Burdwan Medical College (BMC), Burdwan, West Bengal, 3Specialist Medical Officer (Anesthesiology) West Bengal Health Service, West Bengal, India
Corresponding author: Dr. Anirban Pal, 43/6/5 Jheel Road, Kolkata - 700 031, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_53_11R10 AP Done 27th Jan
AbstractBackground: Postoperative nausea and vomiting (PONV) is a serious concern in patients undergoing laparoscopic cholecystectomy (LC), with an incidence of 46 to 72%. The purpose of this study was to compare the antiemetic efficacy of intravenous (iv) ondansetron 8 mg, ramosetron 0.3 mg, and palonosetron 0.075 mg for prophylaxis of PONV in high-risk patients undergoing LC.Materials and Methods: In this prospective, randomized, double-blinded study, 87 female patients, 18 to 70 years of age (ASA I and II) and undergoing elective LC under general anesthesia were randomly allocated into three equal groups, the ondansetron group (8 mg iv; n=29), the ramosetron group (0.3 mg iv; n=29), and the palonosetron group (0.075 mg iv; n=29), and the treatments were given just after completion of surgery before extubation. The incidence of complete response (patients who had no PONV and needed no other rescue antiemetic medication), nausea, vomiting, retching, and need for rescue antiemetics over 24 hours after surgery were evaluated.Results: The number of complete responders were 19 (65.5%) for ramosetron, 11 (37.9%) for palonosetron, and 10 (34.5%) for ondansetron, representing a significant difference overall (P=0.034) as well as between ramosetron and ondansetron (P=0.035). Comparison between ramosetron and palonosetron also showed a clear trend favoring the former (P=0.065).Conclusion: Ramosetron 0.3 mg iv was more effective than palonosetron 0.075 mg and ondansetron 8 mg in the early postoperative period, but there was no significant difference in the overall incidence of nausea suffered.
Key words: Laparoscopic cholecystectomy, ondansetron, palonosetron, postoperative nausea and vomiting, ramosetron
INTRODUCTION
Laparoscopic cholecystectomy (LC) has rapidly emerged as an alternative to open cholecystectomy and is a routinely performed procedure for symptomatic cholelithiasis.[1] But, postoperative nausea and vomiting (PONV) is a distressing and frequent adverse events of anesthesia and surgery, and the incidence following LC is as high as 46 to 72%.[2,3]

183
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Swaika, et al.: Ondansetron, ramosetron or palonosetron?
5-HT3 receptor antagonists (5HT3RA) belong to the Cys-loop superfamily of ligand-gated ion channels and are first-line therapies in the prevention of PONV.[4,5] 5HT3RA have an enviable safety profile, with minor side-effects and rare cardiac conduction abnormalities. Ondansetron was the first 5HT3RA with a relatively short half-life of 3 to 5 hours and may be given several times a day depending on the severity of the symptoms. Ramosetron is a recently developed 5HT3RA that exhibits significantly greater binding affinity for 5-HT3 receptors and a slower dissociation rate from receptor binding, resulting in more potent and longer receptor antagonizing, which may last up to 48 hours.[6] Palonosetron is the first of “second-generation” 5HT3RA and is superior to the “first generation” 5HT3RAs in respect of high receptor-binding affinity and it may also bind to the receptor at an allosteric site. It has a prolonged mean elimination half-life of about 40 hours.[7] 5HT3RA undergo Phase I metabolism in the liver by the cytochrome P450 enzyme system; ondansetron, ramosetron, and palonosetron are primarily metabolized by CYP3A4, CYP1A2, and CYP2D6, respectively.[8]
This study was conducted to determine the efficacy of three 5HT3RA—ondansetron, ramosetron, and palonosetron—in the prevention of PONV for patients undergoing LC.
MATERIALS AND METHODS
For this study, 87 female patients scheduled to undergo LC were randomized in a double-blind manner to receive ondansetron 8 mg (group O, n=29), ramosetron 0.3 mg (group R, n=29), and palonosetron 0.075 mg (group P, n=29) intravenously just after completion of surgery before extubation. The study was commenced after obtaining approval from the institutional ethical committee and written informed consent from patients. Our patients were American Society of Anaesthesiologists (ASA) I and II. We have deliberately excluded ASA III and IV patients as uremic patients, patients with cardiovascular disease with hypotension, neurological disease, advanced liver disease and gastro-intestinal disease have a definite association with nausea and vomiting irrespective of surgical and anesthetic technique. Patients who have received antiemetic drug within the preceding 24 hours, those with a history of alcohol or drug abuse within last 3 months, those who were allergic to any of the study medications, and those with a body weight more than 30% of the ideal body weight were also excluded as these may either alter or hamper our study results.
A standardized anesthesia regimen was followed. All patients received midazolam 1 mg intravenous (iv), glycopyrrolate 0.2 mg iv, and butorphanol 1 mg iv for premedication 10 minutes before surgery. Butorphanol’s onset of analgesia is within a few minutes for iv administration, with peak analgesic activity occurring within 30 to 60 minutes, and
the duration of analgesia is generally 3 to 4 hours. In our institution, the duration of LC was approximately 1 hour and so no other opioids were required intraoperatively.
General anesthesia was induced with thiopentone sodium 3 to 5 mg/kg and tracheal intubation was facilitated with suxamethonium 1.5 mg/kg. Propofol itself has an antiemetic property, and we consciously avoided its use in this study. Thiopentone also gives better hemodynamic stability than propofol, and is helpful regarding hypotensive PONV. Anesthesia was maintained with sevoflurane (0.5–1%), nitrous oxide (60%), and atracurium (0.5 mg/kg). We are using the closed system to deliver anesthetic gases and are using nitrous as the carrier gas. 1 MAC is necessary for maintenance of anesthesia, and 1 MAC of sevoflurane is between 1.71 and 2.05%, which is reduced to 0.66% by the addition of 60% nitrous oxide.[9] At the end of surgery, residual neuromuscular block was reversed with neostigmine (0.05 mg/kg) and glycopyrrolate (0.005 mg/kg) in all patients. The study medication (ondansetron, ramosetron, or palonosetron) was administered intravenously just at the end of surgery before extubation. For postoperative pain control, diclofenac 75 mg im was administered 30 minutes before the end of surgery and repeated 8-hourly for postoperative analgesia.[10] We had provision of postoperative rescue analgesic in the form of repeat dose of injection butorphanol 2 mg im, but none of our patients required it. Patients were observed in the postanesthesia care unit before being transferred to the ward.
The incidence of complete response, vomiting, and intensity of nausea using a 100-mm visual analogue scale (0, none; 100, maximum), retching, and need for rescue antiemetics was evaluated for 24 hours, divided into three intervals: 0–2 hours, 2–6 hours, and 6–24 hours.
Complete response was defined as no PONV and no need for another rescue antiemetic medication.
Vomiting was defined as the forceful expulsion of gastric contents from the mouth.
Nausea was defined as the subjectively unpleasant sensation associated with awareness of the urge to vomit.
Retching was defined as the labored, spastic, rhythmic contraction of the respiratory muscles without the expulsion of gastric contents.
Patients were asked to communicate their degree of nausea during the interval of assessment. Rescue antiemetics, injection ondansetron 4 mg iv, were provided on ranging of nausea intensity from moderate to severe (VAS score >50), patients request, and on vomiting. The hemodynamic data were noted both during the intraoperative and postoperative periods at regular intervals. Adverse events were evaluated and recorded by the investigator during the

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
184
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Swaika, et al.: Ondansetron, ramosetron or palonosetron?
24-hour observation period. In our institution, the surgeons did not usually ask for intraoperative nasogastric tube insertion. Only two of the 87 patients studied required nasogastric tube insertion. But, routine use of nasogastric tube does not affect the incidence of PONV.[11]
For the purpose of sample size calculation, the number of complete responders was taken as the primary outcome measure. It was estimated that 24 subjects would be required per group in order to detect 40% improvement in complete responder rate for the better-performing drug, assuming that a minimum of one-third of the subjects would be complete responders, whatever the drug. We therefore set our recruitment target at 30 subjects per group to account for a possible 20% dropout rate.
Numerical data have been summarized by mean and standard deviation. Median and interquartile values have also been presented for nausea visual analogue score (VAS) scores as this variable was nonparametric. Numerical variables have been compared between groups by one-way analysis of variance when normally distributed and by the Kruskal-Wallis test if otherwise. Categorical variables have been summarized as percentages and compared between groups by the Chi-square test or Fisher’s exact test, as appropriate. All analyses have been two-tailed and P<0.05 has been considered statistically significant. Analysis was performed by Statistica version 6 (StatSoft Inc., 2001; Tulsa, OK USA) software.
RESULTS
We recruited 29 subjects per group, and all of them completed the scheduled evaluation.
The groups were comparable with respect to age, weight, and duration of surgery, but the data showed no statistical significance, as shown in Table 1.
The hemodynamic data were noted both during the intraoperative and postoperative periods at regular intervals. There was no statistically significant difference in the measurements of vitals of the three groups.
The number of complete responders was 19 (65.5%) for ramosetron, 11 (37.9%) for palonosetron, and 10 (34.48%) for ondansetron, representing a significant difference overall (P=0.034) as well as between ramosetron and ondansetron (P=0.035). Comparison between ramosetron and palonosetron also showed a trend favoring the former (P=0.065). Palonosetron and ondansetron were comparable [Table 2].
The evolution of nausea intensity, as rated by VAS scoring, has been depicted in Table 3.
There was no significant difference in nausea between groups in any of the three time intervals.
The number of subjects in each of the three study groups
experiencing at least one vomiting episode within the relevant time intervals is summarized in Table 4. This Table shows that a significantly greater number of subjects suffered vomiting in the early (0–2 hours) postoperative period if they were in the palonosetron or ondansetron groups compared with the ramosetron group, which actually had no vomiting during this period. However, this difference between groups were no longer found in the later periods, when small and comparable numbers in all three groups experienced vomiting. So far, as retching was concerned, small and comparable numbers experienced such episodes in the different postoperative periods, which are shown in Table 5. Table 6 depicts the requirement of rescue antiemetic medication for subjects experiencing more than trivial nausea-vomiting. These numbers were also comparable between the ramosetron, palonosetron, and ondansetron groups.
Summary for retching episodes is presented in Table 5.
DISCUSSION
PONV remains a significant problem in modern anesthetic practice, and has adverse consequences such as delayed
Table 1: Patient’s characteristics and duration of surgery
Ramosetron (n=29)
Palonosetron (n=29)
Ondansetron (n=29)
Age (years)Weight (kg)
41.5 (14.52)51.93 (7.31)
38.9 (13.09)52.8 (6.92)
45.9 (16.07)53.45 (9.18)
Duration of surgery (min)
56.04 (10.24) 56.08 (8.02) 57.08 (8.38)
Table 3: Change in nausea score over time in the three study groups
Ramosetron (n=29)
Palonosetron (n=29)
Ondansetron (n=29)
Nausea score(0–2 h)
Mean (SD)Median (IQR)
0.14 (0.351)0.0 (0.0-0.0)
0.17 (0.468)0.0 (0.0-0.0)
0.07 (0.258)0.0 (0.0-0.0)
Nausea score (2–6 h)
Mean (SD)Median (IQR)
0.41 (0.946)0.0 (0.0-0.0)
0.59 (0.983)0.0 (0.0-1.0)
0.55 (0.827)0.0 (0.0-1.0)
Nausea score (6–24 h)
Mean (SD)Median (IQR)
0.14 (0.441)0.0 (0.0-0.0)
0.07 (0.258)0.0 (0.0-0.0)
0.41 (0.824)0.0 (0.0-0.0)
SD: Standard deviation; IQR: Interquartile range
Table 2: Number of complete respondersRamosetron
(n=29)Palonosetron
(n=29)Ondansetron
(n=29)No. of complete responders
19 (65.5%) 11 (37.9%) 10 (34.48%)

185
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Swaika, et al.: Ondansetron, ramosetron or palonosetron?
recovery, unexpected hospital admission, delayed return to work of ambulatory patients, pulmonary aspiration, wound dehiscence, and dehydration.[12] Therefore, prevention of PONV in surgical patients gets similar priority to that of alleviating postoperative pain.[13]
The vomiting center is an indiscrete area located in the lateral reticular formation of the medulla, which is responsible for controlling and coordinating nausea and vomiting. The center receives a wide range of afferent inputs from receptors in the gastrointestinal tract, peripheral pain receptors, the nucleus solitarius, vestibular system, the cerebral cortex, and the chemoreceptor trigger zone (CTZ). The exact mechanism of PONV caused by pneumoperitoneum is not known. Pneumoperitoneum probably stimulates the mechanoreceptors in the gut, and this increases the risk of PONV. Pneumoperitoneum-induced intestinal ischemia may release serotonin and other neurotransmitters, which could lead to PONV. But Kim et al. found that lowering the pneumoperitoneum pressure to 8 mmHg does not reduce the incidence of PONV.[14]
Acetylcholine and histamine are two important neurotransmitters of the vomiting center and dopamine and 5-hydroxytryptamine are two important neurotransmitters located in the CTZ. The 5HT3RA act on
the 5-HT3 receptor, a subtype of serotonin receptor found in terminals of the vagus nerve and in certain areas of the brain.
Although ondansetron 4 or 8 mg has been recommended for preventing PONV, the meta-analysis by Tramer et al. suggested that an 8 mg dose of ondansetron was optimal for the prevention of PONV.[15] A study by Ryu et al. also suggests that ondansetron 8 mg is more effective than 4 mg.[16] Therefore, we selected ondansetron 8 mg for this study.
According to Fujii et al., ramosetron is effective in preventing PONV after gynecological surgery, and ramosetron 0.3 mg is an effective dose for preventing PONV. In addition, the manufacturer’s recommended dose is 0.3 mg iv once a day.[17,18] Therefore, ramosetron at the 0.3 mg dose was chosen for our study.
Based on the studies of Candiotti et al., the minimum effective dose of palonosetron in the prophylaxis of PONV is 0.075 mg, and this has been approved by the food drug agency (FDA). They used palonosetron 0.025 mg, 0.05 mg, and 0.075 mg groups, and the incidence of early emesis was lower in the palonosetron 0.075 mg group compared with placebo. [5] In our study, we have decided to use palonosetron 0.075 mg.
We are unaware of any study where ondansetron, ramosetron, and palonosetron have been compared together for their respective efficacy.
Previous studies conducted using ramosetron had favorable outcomes. Feng et al. reported that ramosetron was more effective than granisetron in preventing emesis, nausea, and anorexia in the time period of 18 to 24 hours after chemotherapy.[19] Takenaka et al. concluded that ramosetron had been the most effective in comparison with granisetron and ondansetron in reducing chemotherapy-induced nausea and vomiting.[20] Fuji et al. showed that the complete response during the first 24 hours after anesthesia was 85% with granisetron and 93% with ramosetron.[21] Kim et al. showed that ramosetron 0.3 mg was as effective as ondansetron 8 mg in decreasing the incidence of PONV in female patients during the first 24 hours after gynecological surgery. [22]
In another study, Ryu et al. reported that ramosetron 0.3 mg and ondansetron 8 mg are more effective than ondansetron 4 mg for the prevention of PONV after LC.[16]
Studies conducted with palonosetron are mainly placebo based. According to Candiotti et al., patients with Apfel score >2, undergoing day-case laparoscopy, received prophylaxis against PONV with palonosetron 0.025 mg, 0.05 mg, 0.075 mg, or placebo. Nitrous oxide was used but no other prophylactic antiemetics were administered. A dose-dependent increase in complete response was observed, with rates in the 0- to 24-hour period for the placebo, palonosetron 0.025 mg, 0.05 mg, and 0.075 mg
Table 4: Frequency of vomiting in the study groupsPostoperative time period (h)
Ramosetron (n=29) (%)
Palonosetron (n=29) (%)
Ondansetron (n=29) (%)
0–2 0 6 (20.7) 3 (10.3)
2–6 7 (24.1) 6 (20.7) 6 (20.7)
6–24 1 (3.5) 3 (10.3) 5 (17.2)
Values denote count (%). The difference between groups was statistically significant for the 0–2 hours postoperative period (P=0.037), but not during the later periods
Table 5: Frequency of retching in the study groupsPostoperative time period (h)
Ramosetron (n=29) (%)
Palonosetron (n=29) (%)
Ondansetron (n=29) (%)
0–2 2 (6.9) 6 (20.7) 2 (6.9)
2–6 4 (13.8) 3 (10.3) 3 (10.3)
6–24 0 0 3 (10.3)
Values denote count (%). The difference between groups was not statistically significant in any of the postoperative periods
Table 6: Number of subjects requiring rescue antiemetics in the study groupsPostoperative time period (h)
Ramosetron (n=29) (%)
Palonosetron (n=29) (%)
Ondansetron (n=29) (%)
0–2 1 (3.5) 5 (17.2) 1 (3.5)
2–6 5 (17.2) 8 (27.6) 6 (20.7)
6–24 1 (3.5) 3 (10.3) 6 (20.7)
Values denote count (%). The difference between groups was not statistically significant in any of the postoperative periods

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
186
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Swaika, et al.: Ondansetron, ramosetron or palonosetron?
groups of 26%, 33%, 39%, and 43%, respectively. The incidence of early emesis was lower in the palonosetron 0.075 mg group compared with placebo (33% vs 44%), as was the severity of nausea.[5] In a study by Saito et al., 1143 cancer patients who were receiving highly emetogenic chemotherapy were randomly assigned to either single-dose palonosetron (0.75 mg) or granisetron (40 mg/kg) 30 minutes before chemotherapy, both in conjunction with dexamethasone. According to this study, the efficacy of palonosetron in preventing chemotherapy-induced vomiting is not inferior to that of granisetron in the acute phase (75.3% vs 73.3%), and is better than that of granisetron in the delayed phase (56.8% vs 44.5%; P<0.001) when administered in combination with dexamethasone.[23]
Aspinall and Goodman suggested that if active drugs are available, placebo-controlled trials are unethical because PONV are very much distressing after laparoscopic surgery.[24] In our study, three prominent 5-HT3RAs, namely ramosetron, palonosetron, and ondansetron, were used as antiemetics for the prophylaxis of PONV during the first 24 hours in patients undergoing LC. The number of complete responders was higher in the ramosetron group (P=0.034), while that in the ondansetron and palonosetron groups was comparable [Table 2]. In the early postoperative period (0–2 hours), the ramosetron group showed very less or almost no vomiting as compared with the ondansetron and palonosetron groups (P=0.037) [Table 4]. Therefore, ramosetron was a better antiemetic in this period. But, in the time periods 2–6 hours and 6–24 hours, there was no statistically significant difference between the vomiting episodes of the three groups. Parameters like intensity of nausea, retching, and requirements of rescue antiemetics were comparable in all groups, with no significant difference over the three time periods [Tables 3, 5 and 6].
CONCLUSION
Ramosetron 0.3 mg is a better choice as an antiemetic in the prophylaxis of PONV compared with ondansetron 8 mg and palonosetron 0.075 mg in the early postoperative period (0–2 hours) after LC.
REFERENCES
1. NIH Consensus conference. Gallstones and laparoscopic cholecystctomy. JAMA 1993;269:1018-24.
2. Fuji Y. The utility of Antiemetics and Treatment of postoperative nausea and vomiting in patients scheduled for laparoscopic cholecystectomy. Curr Pharm Des 2005;11:3173-83.
3. Wang JJ, Ho ST, Liu YH, Lee SC, Liu YC, Liao YC, et al. Dexamethasone reduces nausea and vomiting after laparoscopic cholecystectomy. Br J Anaesth 1999;83:772-5.
4. Habib AS, Gan TJ. Evidence-based management of postoperative nausea and
vomiting: A review. Can J Anaesth 2004;51:326-41.5. Candiotti KA, Kovac AL, Melson TI, Clerici G, Joo Gan T. A randomized,
double-blind study to evaluate the efficacy and safety of three different doses of palonosetron versus placebo for preventing postoperative nausea and vomiting. Anesth Analg 2008;107:445-51.
6. Rabasseda X. Ramosetron, a 5-HT3 receptor antagonist for the control of nausea and vomiting. Drugs Today (Barc) 2002;38:75-89.
7. Wallenborn J, Kranke P. Palonosetron hydrochloride in the prevention and treatment of postoperative nausea and vomiting. Clinical medicine insights. Therapeutics 2010;2:387-99.
8. Muchatuta NA, Michael JP. Management of post-operative nausea and vomiting: Focus on palonosetron. Ther Clin Risk Manag 2009;5:21-34.
9. Smith I, Nathanson M, White PF. Sevoflurane - a long-awaited volatile anaesthetic. Br J Anaesth 1996;76:435-45.
10. Wilson YG, Rhodes M, Ahmed R, Daugherty M, Cawthorn SJ, Armstrong CP. Intramuscular diclofenac sodium for postoperative analgesia after laparoscopic cholecystectomy: A randomised, controlled trial. Surg Laparosc Endosc 1994;4:340-4.
11. Kerger KH, Mascha E, Steinbrecher B, Frietsch T, Radke OC, Stoecklein K, et al. Routine use of nasogastric tubes does not reduce postoperative nausea and vomiting. Anesth Analg 2009;109:768-73.
12. Gan TJ. Risk factors for postoperative nausea and vomiting. Anesth Analg 2006;102:1884-98.
13. Macario A, Weinger M, Carney S, Kim A. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesth Analg 1999;89:652-8.
14. Kim DK, Cheong IY, Lee GY, Cho JH. Low Pressure (8 mmHg) Pneumoperitoneum does not Reduce the Incidence and Severity of Postoperative Nausea and Vomiting (PONV) following Gynecologic Laparoscopy. Korean J Anesthesiol 2006;50:36-7.
15. Tramer MR, Reynolds DJ, Moore RA, McQuay HJ. Efficacy, dose-response, and safety of ondansetron in prevention of postoperative nausea and vomiting: A quantitative systematic review of randomized placebo-controlled trials. Anesthesiology 1997;87:1277-89.
16. Ryu J, So YM, Hwang J, Do SH. Ramosetron vs ondansetron for the prevention of post-operative nausea and vomiting after laparoscopic cholecystectomy. Surg Endosc 2010;24:812-7.
17. Fujii Y, Saitoh Y, Tanaka H, Toyooka H. Ramosetron for preventing postoperative nausea and vomiting in women undergoing gynecological surgery. Anesth Analg 2000;90:472-5.
18. Fujii Y, Tanaka H. Double-blind, placebo-controlled, dose-ranging study of ramosetron for the prevention of nausea and vomiting after thyroidectomy. Clin Ther 2002;24:1148-53.
19. Feng FY, Zhang P, He YJ, Li YH, Zhou MZ, Cheng G, et al. Comparison of the selective serotonin3 antagonists ramosetron and granisetron in treating acute chemotherapy induced emesis, nausea, and anorexia: A single blind, randomized, crossover study. Curr Ther Res 2000;61:901-9.
20. Takenaka M, Okamoto Y, Ikeda K, Hashimoto R, Ueda T, Kurokawa N, et al. Comparison of anti-emetic efficacy of 5-HT3RA in orthopedics cancer patients receiving high dose chemotherapy. Gan To Kagaku Ryoho 2007;34:403-7.
21. Fuji Y, Saitoh Y, Tanaka H, Toyooka H. Ramosetron vs granisetron for the prevention of postoperative nausea and vomiting after laparoscopic cholecystectomy. Can J Anesth 1999:46:991-3.
22. Kim SI, Kim SC, Baek YH, Ok SY, Kim SH. Comparison of ramosetron with ondansetron for prevention of postoperative nausea and vomiting in patients undergoing gynaecological surgery. Br J Anaesth 2009;103:549-53.
23. Saito M, Aogi K, Sekine I, Yoshizawa H, Yanagita Y, Sakai H, et al. Palonosetron plus dexamethasone versus granisetron plus dexamethsone for prevention of nausea and vomiting during chemotherapy: A double-blind, double-dummy, randomized, comparative phase III trial. Lancet Oncol 2009;10:115-24.
24. Aspinall RL, Goodman NW. Denial of effective treatment and poor quality of clinical information in placebo control trials of ondansetron for postoperative nausea and vomiting: A review of published trials. BMJ 1995;311:844-6.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.

187
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Original Article
Continuous spinal anesthesia with epidural catheters: An experience in the peripheryS. Parthasarathy, M. Ravishankar
Department of Anesthesiology, Mahatma Gandhi Medical College and Research Institute, Puducherry, India
Corresponding author: Dr. S. Parthasarathy, Department of Anesthesiology, Mahatma Gandhi Medical College and Research Institute, Puducherry, India E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_67_11R2
Abstract Background and Aim: Continuous spinal anesthesia (CSA) offers considerable advantages over “singleshot” spinal or epidural anesthesia since it allows administration of well-controlled anesthesia using small doses of local anesthetics and a definite end point with less failure rate. There are described technical difficulties with introduction of spinal micro catheters and hence this study was undertaken by using epidural catheters.Materials and Methods: Sixty patients of ASA grade II to III were selected and they were administered continuous spinal anesthesia with Portex 18-G epidural catheters.Results: The introduction was done in first attempt and was easy in all cases. The intraoperative period was uneventful in all cases. Early postoperative analgesia was achieved in all cases. Only two patients (3%) had postdural puncture headache controlled with simple analgesics. In a 3 month postoperative followup, the incidence of neurological complication is nil.Conclusion: We conclude CSA with epidural catheters is a simple and safe alternative for prolonged procedures with negligible failure rate especially in high-risk patients and in patients with possible difficulties in administration of general anesthesia.
Key words: Continuous spinal anesthesia, epidural catheters, high risk patients
INTRODUCTION
Continuous spinal anesthesia is the technique of initiating and maintaining spinal anesthesia with small doses of local anesthetic injected intermittently into the subsubarachnoid space.[1] Its use has been reported for various procedures such as Cesarean section, orthopaedic,
trauma or peripheral vascular procedures in the lower limb, urological, gynecological, rectal and perineal surgeries. It has been used in old and high-risk patients. [2- 5] However, CSA has not gained wide popularity because of the fear of postanaesthetic cauda equina syndrome, and the difficulty in placing microcatheters into the subarachnoid space. As there are technical difficulties in introduction of spinal catheters and inaccessibility to such catheters in peripheral South India we resorted to this study of introduction of epidural catheters into the subarachnoid space. We selected high-risk patients with possible prolonged duration of surgery to perform the study.
MATERIALS AND METHODS
Sixty patients of ASA II and III were selected for the

188
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Parthasarathy and Ravishankar: Continuous spinal with epidural catheters
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
study. All patients were informed about the study and approval from the institutional ethics committee was obtained. All patients had a few systemic diseases and the projected time of surgery was more than 2 hours. Out of the 60 patients, 12 had anticipated dificult airway. They were premedicated with Inj. Pentazoine 30 mg and promethazine 12.5 mg IM 30 minutes before anesthesia. They were positioned in the right lateral position and after a local anaesthetic injection in L3-L4 interspace in midline, insertion of 16-G epidural needle was done to get a free flow of CSF. 2.5-3 ml of Bupivacaine heavy (Anawin – Neon labs) with 1 mg of preservative free midazolam was injected into the subarachanoid space and the 18-G epidural catheter was introduced in all cases in the first attempt. The anaesthetic protocol were otherwise similar to a spinal anesthetic. Inj. Bupivacaine heavy was administered again when there was a recession in level or if there is patient discomfort. In all the patients the catheters were removed at the end of surgery. Routine monitoring included pulse oximetry, ECG and noninvasive blood pressure measurement (NIBP). For all patients, the following variables were recorded: age, weight, ASA physical status, duration of procedure, anesthetic drugs and doses, the most cephalad sensory level to pinprick, the use of additional systemic sedatives and analgesics, baseline and changes in BP and heart rate (HR), the use of sympathomimetic drugs, volume of IV fluid, and perianesthetic complications. The last included technical failure to thread the catheter, evidence of inadequate anesthesia (either insufficient sensory level or quality of the block), “high” spinal anesthesia, hypotension, bradycardia, postdural puncture headache (PDPH) and adverse neurological sequelae including persistent pain, motor or sensory deficits, haematoma or infection.They were followed up for a three month period for any adverse neurological sequalae.
RESULTS
Out of the 60 patients, 41 were male (68.3%). All the 60 patients had different combinations of systemic illness [Table 1]. The types of surgery is detailed in Table 2. The mean age of the patients was 54.2 ± 12.4 years (SD) and weight was 76.2 ± 17.8 kg (SD). All the patients were pre planned to administer continuous spinal anesthesia with epidural catheters. Hyperbaric bupivacaine with preservative-free midazolam was given to all patients and the dose of local anesthetic adjusted to achieve the desired level. The level was between T4 and T6 in all the cases. Forty patients required second dose of local anesthetic because of complaints and they received 1.5 ml of hyperbaric 0.5% bupivacaine through the catheter with an air flush to empty the drug within the catheter tubing. The anesthetic management was according to practice protocols followed. Anesthetic duration, fluid administration, the use of sympathomimetic drugs, the
appearance of PDPH and other side effects if significant were noted. The hemodynamic changes were within acceptable limits. They are tabled below [Tables 3 and 4]. During the first dose of spinal anesthetic, sympathomimetics were necessary in 46 patients and ephedrine was used in all. One patient received 6 mg, 10 patients needed 12 mg, 10 needed 18 mg, 11 patients needed 24 mg, 11 needed 30 mg and the rest three needed 36 mg of ephedrine. All the patients (TURP with hernioplasy) who were positioned in lithotomy did not need sympathomimetics. None of the 60 patients needed additional systemic analgesics or sedatives. In all the 40 patients who required second anesthetic dose, the level was adequate and below T4. Thirty out the 40 needed one or two shots of 6 mg Inj. Ephedrine for hypotension. As most of the patients were catheterized, the problem of voiding did not arise in our study. PDPH was observed only in two patients which resolved in 2 days with oral analgesics. No postanesthetic neurological deficit was detected in any of our cases.
DISCUSSION
This study describes the use of continuous spinal
Table 1: Various systemic illnessesSystemic illness No. of patientsDiabetes mellitus and bronchial asthma 20
Diabetes mellitus and hypertension 21
Diabetes mellitus and IHD 12
Anemia with COPD 02
Parkinsonism with COPD 5IHD: Ishemic heart disease; COPD: Chronic obstructive pulmonary disease
Table 2: Types of surgeryType of surgery No. of patients Incisional hernia repair 11
Hysterectomy with incisional hernia repair 14
TURP with inguinal hernia (bilateral) 14
Orthopedic hip surgeries 16
Vascular surgery (lower limb) 05TURP: Transurethral resection of prostate
Table 3: Hemodynamic variablesBaseline systolic BP (mmHg) 137.8 ± 22.9
Maximal systolic BP decrease 35.1 ± 9.8
Baseline diastolic BP (mmHg) 84.5 ± 12.4
Maximal diastolic BP decrease 13.4 ± 10.3
Baseline HR (beats per minute) 85.3 ± 13.2
Maximal HR decrease 9.2 ± 8.4
Table 4: Clinical detailDuration (min)* 125.6 ± 34.5
Fluids (ml)* 1830 ± 578
Sympathomimetics (n) 46 (77%)
PDPH (n) 2 (3%)*Mean ± SD; PDPH: Postdural puncture headache

189
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Parthasarathy and Ravishankar: Continuous spinal with epidural catheters
anesthesia with a standard 18-G epidural catheter as an effective and safe anesthetic approach especially in high-risk patients.Continuous spinal anesthesia combines the advantages of both epidural and spinal anesthesia. The failure rate is very low as placement of the Tuohy needle in the subarachnoid space is easily ascertained by the escape of CSF. We did not encounter any failure and the catheter was inserted in the first attempt in all cases (100%). Rabonowitz reported 85% success in placing the catheter in the first attempt. In all his cases, he succesfully used 20-G epidural catheter,[6] but we used an 18-G catheter and this difference of 15% may be due to a bigger sized catheter. Onset of anesthesia is easy to control and can be either gradual, or rapid, depending on the sequence of injection of the local anesthetic (LA). The administered dose of LA is small reducing the possibility of systemic toxicity if the catheter is accidentally inserted intravascularly. We did not titrate to use LA in the fear of failure of insertion of the catheter later and the consequences. We gave the required anesthetic dose for the particular surgery in the first attempt to get the level and all our cases reported significant but acceptable haemodynamic disturbances. In forty of our patients, the duration of surgery went beyond the acceptable time limit of the first dose and hence we administered the second dose of the local anaesthetic. In all the cases, the second dose worked well to prove the catheter was in situ.The administration of the second dose effected an early postoperative analgesia as the surgery was completed in another half hour in many cases. This is an incidental observation and we cant comment that it instituted postoperative analgesia as the effect is an obvious result. Our study is deficient in that it neither had controls with single shot spinal anesthesia nor continuous epidural anesthesia to comment either on postoperative pain or hemodynamic disturbances. We removed the catheter in all the cases at the end of surgery for the fear of position and intrathecal infection especially in peripheral set ups like us. There is a general fear of PDPH with the use of epidural catheters in intrathecal space but we encountered this complication only in two cases. This clearly demonstrates that PDPH is less common when we insert catheter into the spinal compartment. Ng A reported the insertion of epidural catheter for prophylaxis for PDPH in accidental dural puncture during epidural attempts.[7] The insertion of epidural catheter was regarded as a treatment to prevent PDPH in accidental dural punctures during attempted epidural anesthesia.[8] This fact of incidence of PDPH goes along with our
findings. There was another fear that the presence of a “big” catheter may initiate neurological sequalae like cauda equina syndrome. It is to be highlighted at this juncture that we used only hyperbaric bupivacaine as repeated doses of lignocaine[9] has established neurotoxicity in such instances. Shenkman et al.[10] reported succesful use of epidural catheters in subarachnoid space in patients for ESWL and they did not have any neurological side effects. We did not encounter any adverse neurological complaints in any of our 60 cases.
CONCLUSIONS
Continuous spinal anesthesia with standard epidural catheters is feasible and successful. The technique can be used in patients with extended duration of surgery where administration of general anesthesia is associated with risks. The hemodynamic effects are acceptable. The incidence of PDPH is negligble. There are no adverse neurological outcomes. There is an effective early postoperative analgesia.
REFERENCES
1. Hurley RJ. Continuous spinal anesthesia. Int Anesthesiol Clin 1989;27:46-50.2. Sutter PA, Gamulin Z, Forster A. Comparison of continuous spinal and
continuous epidural anesthesia for lower limb surgery in elderly patients. A retrospective study. Anesthesia 1989;44:47-50.
3. De Andres J, Bellver J, Bolincbes R. Comparison of continuous spinal anesthesia using a 32-gauge catheter with anesthesia using a single-dose 24-gauge atraumatic needle in young patients. Br J Anaesth 1994;73:747-50.
4. Denny N, Masters R, Pearson D, Read J, Sihota M, Selander D. Postdural puncture headache after continuous spinal anesthesia. Anesth Analg 1987;66:791-4.
5. Underwood RJ. Experiences with continuous spinal anesthesia in physical status group IV patients. Anesth Analg 1968;47:18-26.
6. Rabinowitz A, Bourdet B, Minville V, Chassery C, Pianezza A, Colombani A, et al. The paramedian technique: A superior initial approach to continuous spinal anesthesia in the elderly. Anesth Analg 2007;105:1855-7.
7. Ng A, Shah J, Smith G. Is continuous spinal analgesia via an epidural catheter appropriate after accidental subarachnoid administration of 15 mL of bupivacaine 0.1% containing fentanyl 2 μg/mL? Int J Obstet Anesth 2004;13:107-9.
8. Jadon A, Chakraborty S, Sinha N, Agrawal R. Intrathecal catheterization by epidural catheter: Management of accidental dural puncture and prophylaxis of PDPH. Indian J Anesthes 2009;53:30-4.
9. Denny NM, Selander DE. Continuous spinal anesthesia. Br J Anaesth 1998;81:590-7.
10. Shenkman Z, Eidelman LA, Cotev S. Continuous spinal anesthesia using a standard epidural set for extracorporeal shockwave lithotripsy. Can J Anaesth 1997;44:1042-6.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
190
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Original Article
Comparison of intrathecal bupivacaine-fentanyl and bupivacaine-butorphanol mixtures for lower limb orthopedic proceduresBinay Kumar, Aparna Williams, Dootika Liddle, Mary Verghese
Department of Anesthesia and Critical Care, Christian Medical College and Hospital, Ludhiana, Punjab, India
Corresponding author: Dr. Aparna Williams, Department of Anesthesiology and Critical Care, Christian Medical College and Hospital, Ludhiana - 141 008, Punjab, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_69_11R5 AP Done 27th Jan
AbstractContext: Intrathecal use of butorphanol is less explored in human subjects.Aims: To compare the safety and efficacy of anesthesia and analgesia of intrathecal bupivacaine-butorphanol mixture with intrathecal bupivacaine-fentanyl mixture.Settings and Design: Tertiary level, teaching hospital. Prospective, randomized, double-blind studyMaterials and Methods: Eighty patients aged above 18 years, of ASA physical status 1 or 2, undergoing lower limb orthopedic surgeries were randomly allocated to two groups of 40 patients each. Patients in group A and group B received intrathecal 2.5 ml of hyperbaric bupivacaine (0.5%), with 25 μg of fentanyl and 25 μg of butorphanol, respectively.Statistical Analysis Used: Fisher’s exact test and Chi square tests.Results: The times required for onset of sensory and motor blockade were comparable among the two groups. Significantly slower block regression to S2 level was observed in the group receiving intrathecal butorphanol as compared to intrathecal fentanyl (P=0.0230). A higher number of patients in group A requested for rescue analgesia during the postoperative period than in group B (9 versus 2; P=0.0238). The average times to first request for rescue analgesia were 308.6 ± 14.9 minutes and 365.9 ± 12.3 minutes in group A and B, respectively (P=0.0254).Conclusions: Both 25 μg fentanyl and 25 μg butorphanol given intrathecally along with 12.5 mg of hyperbaric bupivacaine provide effective anesthesia for lower limb surgeries. Intrathecal bupivacaine-butorphanol mixture provides longer duration of sensory blockade and superior analgesia than intrathecal fentanyl-bupivacaine mixture.
Key words: Analgesia, anesthesia, bupivacaine, butorphanol, fentanyl, spinal
INTRODUCTION
Neuraxial opioids are widely used in conjunction with local anesthetics (LA) as they permit the use of lower dose of LA while providing adequate anesthesia and analgesia. [1] Neuraxial opioids also allow prolonged analgesia in the postoperative period and faster recovery from spinal

191
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Kumar, et al.: Intrathecal bupivacaine-butorphanol versus intrathecal bupivacaine-fentanyl
anesthesia.[2] Antinociceptive synergism between LA and intrathecal opioids has been demonstrated in various animal studies.[3]
The present study was undertaken to compare the safety and efficacy of anesthesia and analgesia of intrathecal bupivacaine-butorphanol mixture with intrathecal bupivacaine-fentanyl mixture for lower limb orthopedic procedures. This study was conducted as only a limited number of studies have explored the use of intrathecal butorphanol in human subjects previously.
Butorphanol is a lipophilic opioid agonist-antagonist analgesic with a published affinity for opioid receptors in vitro of 1:4:25 (mu: delta: kappa).[4] Abboud et al. have reported a dose-dependent increase in the duration of analgesia provided by epidural butorphanol for relief of post-Cesarean section pain.[5] Fentanyl, a highly lipid soluble, pure μ-agonist opioid with rapid onset and short duration of action, has been used with various local anesthetics for a wide variety of surgical procedures.[6,7]
MATERIALS AND METHODS
This prospective, randomized, double blind study was conducted after approval from the institutional ethics committee and informed, written consent of patients. Eighty patients, aged 23-75 years, belonging to ASA physical status 1 or 2 and scheduled for elective, lower limb orthopedic surgeries were randomized into two groups using random numbers generated by the computer. Patients in group A (Gp A) received 2.5 ml of 0.5% hyperbaric bupivacaine (Sensorcaine,TM, Astra Zeneca, Bellary road, Karnataka, India) with 0.5 ml (containing 25 μg fentanyl) (Fendrop, TM, Sun Pharmaceuticals, Halol, Gujrat, India); a total volume of 3 ml intrathecally. The butorphanol (Butodol, TM, Neon, Andheri (E), Maharashtra, India) was diluted using distilled sterile water to obtain 25 μg in 0.5 ml. The 25 μg of butorphanol was then added to 2.5 ml of 0.5% hyperbaric bupivacaine to make a total volume of 3 ml to be given intrathecally to patients in group B (Gp B).
All patients underwent a complete general physical examination and systemic examination and were explained the linear visual analogue scale (LVAS) scoring system for pain during the pre anesthetic check-up. The LVAS used an 11-cm line where 0 denoted “no pain” while 10 denoted “worst pain imaginable”.
Patients in whom spinal anesthesia or the study drugs were contraindicated were excluded from the study. Patients with neurological disease, spinal deformities, local skin infection or mental disorders; those who were morbidly obese, hemodynamically unstable or had coagulation disorders, or patients with liver disease, impaired renal functions, ASA Physical status > 2 or a history of opioid dependence were also excluded from the study.
Patients were kept fasting for 6 hours to solids and 2 hours to clear fluids preoperatively and received no pre medication. In the operation theatre, an intravenous line was established. The intrathecal drugs were prepared by a trained anesthesia nurse beforehand to maintain the blinding process. Baseline heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), respiratory rate (RR) and peripheral arterial oxygen saturation (SpO2) were recorded for all subjects. All patients received 10 ml/kg of lactated ringer’s solution as preload within 20- 30 minutes. The primary investigator entered the operation theatre after this period and was therefore blinded to the patient allocation. All spinal blocks were given by the same anesthesiologist. Subarachnoid block was performed under strict aseptic conditions in the lateral position at the level of L 3-4 or L 4-5 inter vertebral space using 25 G Quincke’s spinal needles. The midline approach was used to perform the spinal blocks after infiltrating the skin with 1 ml of 2% Lidocaine. The test drug was injected over 15 seconds. Following the subarachnoid block, the patient was put in supine position.
Intraoperatively, HR, SBP, DBP, RR and SpO2 were recorded at 2 minutes (min) intervals for the first 20 min from the time of injection of spinal solution and there after every 15 min. for the complete period of surgery. This data was recorded by the attending anesthesiologist and the primary investigator, who were unaware of the patient allocation. Hypotension (MAP < 70 mmHg) was treated with fluid boluses and 6 mg intravenous (IV) boluses of ephedrine, while bradycardia (HR<50bpm) was treated with 0.6 mg IV atropine. Respiratory depression was defined as a respiratory rate < 8 breaths/min or a SpO2 of <90% on room air. All patients were given supplemental O2 via face mask at 6 l/min if the SpO2 decreased below 90%.
The highest level of sensory block was determined in the midclavicular line bilaterally, by pinprick test using a 20-G hypodermic needle every 2 min till the level had stabilized for four consecutive tests. The highest level of sensory block and the time taken to attain it from the time of the intrathecal injection were recorded. Further sensory testing was performed at 20-min intervals till the recovery of S2 dermatome. Motor block was assessed using the modified Bromage scale;[8] (grade 0 = no motor block; grade 1 = inability to raise extended legs, able to move knees and feet; grade 2 = inability to raise extended leg and move knee, able to move feet and grade 3 = complete motor block of the lower limbs) till achievement of the highest sensory level; at the end of the surgery and then at 30 min intervals till the patient had no motor blockade.
Side effects such as hypotension, bradycardia, nausea, vomiting, sedation, pruritis, shivering and respiratory depression were recorded. The time to voiding was also recorded. The quality of postoperative analgesia was

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
192
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Kumar, et al.: Intrathecal bupivacaine-butorphanol versus intrathecal bupivacaine-fentanyl
assessed using LVAS at 15 min, 30 min and thereafter every 30 min, till 2 hours postoperatively; and then every hour, till 4 hours postoperative duration. The time of first request of rescue analgesia was recorded. Patients reporting an LVAS score of ≥ 4 were treated with 75 mg diclofenac IV infusion in 100 ml of 0.9% saline, as rescue analgesic.
On the third postoperative day the patients were interviewed regarding complications of spinal e.g., backache, transient neurological symptoms (TNS) or postdural puncture headache (PDPH). PDPH was defined as headache that was mainly occipital or frontal, aggravated by erect or sitting posture, relieved on lying flat, and increased on coughing, sneezing or straining. TNS were defined as any pain or dysesthesia in the back, buttocks and legs or pain radiating to the lower limbs after recovery from spinal anesthesia, and which resolved within 72 hours. Thereafter, the patients were followed up daily till their discharge from the hospital to recognize any other complications of the subarachnoid block.
Using the Priori power analysis with α of 0.05, anticipated effect size of 0.8 and a desired statistical power level of 0.9, a minimum sample size of 34 subjects was required per group for a two tailed hypothesis. We decided to recruit 40 patients to each group to make up for any dropouts from the study groups.
The data were compiled using Microsoft excel (2007) and analyzed using paired/unpaired t tests and Fisher’s exact tests on the Epi Info software (version 8.0) to assess the statistical difference between the groups. A P value of <0.05 was accepted as statistically significant.
RESULTS
The two groups were comparable with regards to age, gender, weight, height and duration of surgery [Table 1].The mean baseline values of HR, SBP, DBP, RR and SpO2 were comparable among the groups.
The characteristics of sensory block in the two groups are depicted in Table 2. The median highest sensory level achieved and the times to reach peak sensory level were comparable among the two groups. Significantly slower block regression to S 2 level was observed in the group receiving butorphanol as compared to fentanyl (P=0.0230).
The characteristics of motor blockade achieved in the two groups are listed in Table 3. The time of onset of maximum motor blockade (P=0.1288) and time to reach grade 1 motor blockade (P=0.1080) were similar among the two groups.
The postoperative LVAS pain scores are presented in Table 4. Patients receiving butorphanol had lower LVAS pain scores at all observed times than patients who
received fentanyl, although this difference in LVAS scores reached a statistical significance only at 1-hour postoperative duration (P=0.0260). A higher number of patients in the fentanyl group requested for rescue analgesia during the postoperative study period than the butorphanol group (9 versus 2; P=0.0238) [Table 5]. The patients in the fentanyl group requested rescue analgesia earlier than patients in the butorphanol group as the average times to first request for rescue analgesia were 308.6 ± 14.9 and 365.9 ± 12.3 minutes, respectively (P=0.0254).
The complications observed during the study are listed in Table 5. Seven patients in the fentanyl-treated group and two patients in the butorphanol-treated group had
Table 1: Patient characteristicsParameter Group A Group B P valueAge (years) 45.2 ± 15.3 44.7 ± 14.1 0.8792
Height (cm) 166.9 ± 6.9 169.2 ± 4.6 0.0838
Weight (kg) 69.3 ± 7.7 68.1 ± 7.0 0.4660
Duration of surgery (min.) 134.6 ± 9.4 133.7 ± 7.4 0.6354Data is presented as mean ± SD
Table 2: Characteristics of sensory blockParameter Group A Group B P valueHighest sensory level [Median (range)]
T6 (6-9) T7 (7-10)
Time from injection to highest sensory level (min.)
8.0 ± 1.7 8.6 ± 1.4 0.0874
Time for sensory regression to S2 level (min.)
156.0 ± 18.4 167.0 ± 23.8 0.0230*
*P<0.05. Data is presented as mean ± SD, unless specified
Table 3: Characteristics of motor blockParameter Group A Group B P valueMaximum Bromage score achieved
Grade 2 [n (%)] 9 (22.5) 14 (35.0) 0.1616
Grade 3 [n (%)] 31 (77.5) 26 (65.0) 0.1616
Time to onset of maximum Bromage score (min.)
9.5 ± 1.8 10.1 ± 1.7 0.1288
Time to reach grade 1 Bromage score (min.)
176.4 ± 19.6 183.8 ± 21.2 0.1080
Data is presented as mean ± SD, unless specified
Table 4: Postoperative LVAS* scoreTime (min.) Group A Group B P value15 0 0 1
30 1.5 ± 0.3 1.1 ± 0.5 0
60 1.9 ± 0.2 1.6 ± 0.8 0.0260†
90 4.6 ± 0.1 2.9 ± 0.5 0
120 6.1 ± 0.3 4.2 ± 0.7 0
180 6.5 ± 0.5 5.1 ± 0.3 0
240 6.7 ± 0.2 6.0 ± 0.4 0*LVAS: Linear visual analogue scale. †P<0.05. Data is presented as mean ± SD

193
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Kumar, et al.: Intrathecal bupivacaine-butorphanol versus intrathecal bupivacaine-fentanyl
hypotension in the peri-operative period (P=0.0771). The intraoperative systolic blood pressures and diastolic blood pressures for the study groups are presented in Figures 1 and 2, respectively.
Bradycardia, responsive to a single dose of intravenous atropine was seen in two patients in the group receiving fentanyl as compared to none in the butorphanol group (P=0.2468). The intraoperative heart rates for the study groups are presented in Figure 3.
Pruritis was observed in five patients receiving fentanyl as compared to none of the patients who received butorphanol (P=0.0273). Although six patients in the butorphanol group had sedation compared to none in the fentanyl group (P=0.0127); none of the patients developed respiratory depression. Figure 4 depicts the intraoperative respiratory rates in the two study groups [Figure 4].
Comparable times to voiding were observed in both the groups (172.6 ± 4.5 min in group A and 188.7 ± 3.8 min in group B; [P=0]). Four patients in the fentanyl group and three in the butorphanol group required urinary catheterisation due to difficulty in voiding. Nausea; vomiting, PDPH and TNS were not reported by any of the patients.
DISCUSSION
The principal findings of this study are that intrathecal butorphanol-bupivacaine mixture provides longer duration of sensory blockade and superior analgesia (with lesser requirement for rescue analgesia) as compared to intrathecal fentanyl-bupivacaine mixture.
The use of opioids in conjunction with local anesthetic for spinal anesthesia has been associated with decreased pain scores and reduced analgesic requirement in the post-operative period.[6,9] Results of previous studies have
demonstrated that intrathecal opioids not only enhance analgesia when added to subtherapeutic doses of local anesthetics but also do not prolong recovery.[2,7,10]
In our study, both fentanyl and butorphanol along with bupivacaine, provided adequate anesthesia and analgesia; but significantly lesser analgesic requirement was observed in the group receiving intrathecal butorphanol and bupivacaine mixture compared to intrathecal fentanyl and bupivacaine mixture. The time for first request of analgesia with the use of intrathecal butorphanol and fentanyl, in conjunction with bupivacaine, in our study
Figure 3: Comparison of intraoperative heart rates among the study groups
60
65
70
75
80
85
0 5 10 15 20 35 50 65 80 95 110 125 140
TIME (minutes)
HE
AR
TR
AT
E(b
ea
ts/
min
ute
)
Group A
Group B
Table 5: Perioperative side effectsSide effect Group A
n (%)Group B
n (%)P value
Hypotension 7 (17.5) 2 (5) 0.0771
Pruritis 5 (12.5) 0 0.0273*
Sedation 0 6 (15) 0.0127*
Bradycardia 2 (5) 0 0.2468
Respiratory depression 0 0 1
Shivering 2 (5) 0 0.2468
Nausea 0 0 1
Vomiting 0 0 1
Urinary catheterization 4 (10) 3 (7.5) 1
PDPH† 0 0 1
TNS‡ 0 0 1
Request for analgesia 9 (22.5) 2 (5) 0.0238**P<0.05; †PDPH: Postdural puncture headache; ‡TNS: Transient neurological symptoms; Data is presented as number (%)
95
100
105
110
115
120
125
130
135
0 5 10 15 20 35 50 65 80 95 110 125 140
TIME (minutes)
SY
ST
OLI
C B
P (
mm
Hg
)
Group A
Group B
Figure 1: Comparison of intraoperative systolic blood pressures among the study groups
64
66
6870
72
74
7678
80
82
0 5 10 15 20 35 50 65 80 95 110 125 140
TIME (minutes)
DIA
ST
OL
ICB
P(m
mH
g)
Group A
Group B
Figure 2: Comparison of intraoperative diastolic blood pressures among the study groups
Figure 4: Comparison of intraoperative respiratory rates among the study groups
14
14.5
15
15.5
16
16.5
17
17.5
0 5 10 15 20 35 50 65 80 95 110 125 140
TIME (minutes)
RE
SP
IRA
TO
RY
RA
TE
(bre
ath
s/m
inu
te)
Group A
Group B

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
194
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Kumar, et al.: Intrathecal bupivacaine-butorphanol versus intrathecal bupivacaine-fentanyl
was about 6 hours and 5 hours respectively from the time of spinal injection. Kim et al. have reported the duration of analgesia of approximately 7 hours after the use of 4 mg bupivacaine with 25 μ fentanyl for TURP.[7] Earlier studies report the duration of analgesia with intrathecal fentanyl ranging from one to four hours.[11] Singh V et al., have also reported that lesser number of patients receiving intrathecal butorphanol requested for rescue analgesia as compared to those receiving intrathecal fentanyl.[12] Studies comparing intravenous butorphanol and fentanyl have reported the equianalgesic doses as 1 μg/kg and 20 μg/kg for fentanyl and butorphanol, respectively.[13] We studied the 25 μg dose of intrathecal fentanyl and butorphanol based on earlier studies.[12]
The results of our study are consistent with experimental evidence of synergistic interaction between spinal opioids and local anesthetics, which are characterized by enhanced somatic analgesia without effect on the degree or level of the local anesthetic induced sympathetic or motor blockade.[3,14] The synergism between intrathecal opioids in addition to local anesthetics is due to the drugs’ separate mechanism of action; blockade of Na+ channel by local anesthetics[15] and voltage-gated Ca++ channels with opioids.[16,17]
The combination of opioids with LA allows for a reduction in doses of the LA, thus lessening the likelihood of side effects.[18,19] A low incidence of side effects was observed in our study. Seven patients (17.5%) in the fentanyl treated group and two patients (5%) in the butorphanol-treated group had hypotension in our study requiring treatment with small doses of intravenous ephedrine (6 mg in 7 and 12 mg in 2 patients) in addition to crystalloid bolus. Neuraxial administration of opioids has been reported to be associated with hypotension.[20] Earlier studies comparing 25 μg intrathecal fentanyl and butorphanol with hyperbaric bupivacaine, have reported the instance of hypotension as 20% in the fentanyl group and 17% in the butorphanol group.[12]
However, animal studies have reported that fentanyl does not potentiate the effect of Bupivacaine on efferent sympathetic pathways.[3] Furthermore, the addition of fentanyl (20-25 μg) to low-dose bupivacaine (4 mg) has been reported to increase the perioperative quality of spinal blocks with fewer cardiovascular changes in elderly patients.[19]
Five patients (12.5%) in the group receiving fentanyl- bupivacaine had pruritis compared with none in the group receiving butorphanol-bupivacaine. The pruritis was mild in nature and did not require any treatment. Pruritis is the commonest side effect of intrathecal opioids. [21] In earlier studies on spinal anesthesia for ambulatory knee arthroscopy, the combination of
bupivacaine with fentanyl was associated with an instance of pruritis ranging from 48 to 75% compared with the groups receiving bupivacaine alone.[22] Ackerman et al.[23] have also reported that opioids that stimulated κ-receptors following epidural administration exhibited significantly less pruritis than pure μ-receptor opioids administered similarly. Furthermore, investigators have reported that continuous epidural butorphanol relieves pruritis associated with epidural morphine infusions in children.[24]
Although six patients had sedation in the group receiving butorphanol-bupivacaine, as compared with none in the group receiving fentanyl; none of them had respiratory depression. Sedation is a reported side effect of neuraxially administered butorphanol.[17] Varassi et al. have reported that bupivacaine 15 mg along with 25-μg fentanyl did not cause respiratory depression in elderly patients.[25]
Seven patients were catheterised during the postoperative period due to difficulty in voiding, although the average times to voiding were comparable among both the study groups. Previous studies have reported that intrathecal bupivacaine is associated with a clinically significant disturbance of bladder function and spontaneous voiding may not be expected until the sensory blockade has regressed to the S3 level.[26] None of the patients in the study experienced nausea or vomiting as we promptly treated all episodes of hypotension. None of the patients reported PDPH or TNS.
The obvious limitation of our study includes the absence of a control group (in which patients would have received 2.5 ml of hyperbaric bupivacaine along with 0.5 ml of saline intrathecally). The inclusion of a control group would have further supported our findings. We also recognize the fact that the wide variability in the age of the patients included in the study is a confounding factor in relation to perception of pain as pain perception varies for various age groups. We studied postoperative analgesia in the subjects for duration of 4 hours only and did not record the number of doses and the total dose of rescue analgesic required to relieve pain. Further investigation can be aimed at finding the minimal possible doses of intrathecal fentanyl and butorphanol in conjunction with hyperbaric bupivacaine that will provide adequate anesthesia and analgesia for lower limb surgeries.
In conclusion, both 25-μg fentanyl and 25-μg butorphanol given intrathecally with 12.5 mg of hyperbaric bupivacaine provide effective and safe anesthesia for lower limb surgeries with minor side effects. Intrathecal bupivacaine-butorphanol mixture provides longer duration of sensory blockade and better quality of analgesia than intrathecal fentanyl-bupivacaine mixture.

195
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Kumar, et al.: Intrathecal bupivacaine-butorphanol versus intrathecal bupivacaine-fentanyl
REFERENCES
1. Stocks GM, Hallworth SP, Fernando R, England AJ, Columb MO, Lyons G. Minimum local analgesic dose of intrathecal bupivacaine in labor and the effect of intrathecal fentanyl. Anesthesiology 2001;94:593-8; discussion 5A.
2. Kuusniemi KS, Pihlajamäki KK, Pitkänen MT, Helenius HY, Kirvelä OA. The use of bupivacaine and fentanyl for spinal anesthesia for urologic surgery. Anesth Analg 2000;91:1452-6.
3. Wang C, Chakrabarti MK, Whitwam JG. Specific enhancement by fentanyl of the effects of intrathecal Bupivacaine on nociceptive afferent but not on the sympathetic efferent pathways in dogs. Anesthesiology 1993;79:766-73; discussion 25A.
4. Commiskey S, Fan LW, Ho IK, Rockhold RW. Butorphanol: Effects of a prototypical agonist-antagonist analgesic on kappa-opioid receptors. J Pharmacol Sci 2005;98:109-16.
5. Abboud TK, Moore M, Zhu J, Murakawa K, Minehart M, Longhitano M, et al. Epidural butorphanol or morphine for the relief of post-caesarean section pain: Ventilatory responses to carbon dioxide. Anesth Analg 1987;66:887-93.
6. Ben-David B, Solomon E, Levin H, Admoni H, Goldik Z. Intrathecal fentanyl with small-dose dilute bupivacaine: Better anesthesia without prolonging recovery. Anesth Analg 1997;85:560-5.
7. Kim SY, Cho JE, Hong JY, Koo BN, Kim JM, Kil HK. Comparison of intrathecal fentanyl and sufentanil in low-dose dilute bupivacaine spinal anaesthesia for transurethral prostatectomy. Br J Anaesth 2009;103:750-4.
8. Bromage PR. Epidural Analgesia. Philadelphia: WB Saunders; 1978. p. 144.9. Demiraran Y, Yucel I, Akcali GE, Degirmenci E, Sezen G, Iskender A. Adding
intrathecal morphine to unilateral spinal anesthesia results in better pain relief following knee arthroscopy. J Anesth 2008;22:367-72.
10. Liu S, Chiu AA, Carpenter RL, Mulroy MF, Allen HW, Neal JM, et al. Fentanyl prolongs lidocaine spinal anesthesia without prolonging recovery. Anesth Analg 1995;80:730-4.
11. Hamber EA, Viscomi CM. Intrathecal lipophilic opioids as adjuncts to surgical spinal anesthesia. Reg Anesth Pain Med 1999;24:255-63.
12. Singh V, Gupta LK, Singh GP. Comparison among intrathecal fentanyl and butorphanol in combination with bupivacaine for lower limb surgeries. J Anesth Clin Pharmacol 2006;22:371-5.
13. Philip BK, Scott DA, Freiberger D, Gibbs RR, Hunt C, Murray E. Butorphanol compared with fentanyl in general anaesthesia for ambulatory laparoscopy. Can J Anaesth 1991;38:183-6.
14. Saito Y, Kaneko M, Kirihara Y, Sakura S, Kosaka Y. Interaction of intrathecally
infused morphine and lidocaine in rats (part I): Synergistic antinociceptive effects. Anesthesiology 1998;89:1455-63.
15. Butterworth JF 4th, Strichartz GR. Molecular mechanism of local anaesthesia: A review. Anesthesiology 1990;72:711-34.
16. Duggan AW, North RA. Electrophysiology of opioids. Pharmacol Rev 1983;35:219-81.
17. Zieglgänsberger W. Opioid action on mammalian spinal neurons. Int Rev Neurobiol 1984;25:243-75.
18. Ben-David B, Miller G, Gavriel R, Gurevitch A. Low-dose bupivacaine-fentanyl spinal anesthesia for cesarean delivery. Reg Anesth Pain Med 2000;25:235-9.
19. Kararmaz A, Kaya S, Turhanoglu S, Ozyilmaz MA. Low-dose bupivacaine-fentanyl spinal anaesthesia for transurethral prostatectomy. Anaesthesia 2003;58:526-30.
20. Singh H, Yang J, Thornton K, Giesecke AH. Intrathecal fentanyl prolongs sensory bupivacaine spinal block. Can J Anaesth 1995;42:987-91.
21. Chaney MA. Side effects of intrathecal and epidural opioids. Can J Anaesth 1995;42;891-903.
22. Nair GS, Abrishami A, Lermitte J, Chung F. Systematic review of spinal anaesthesia using bupivacaine for ambulatory knee arthroscopy. Br J Anaesth 2009;102:307-15.
23. Ackerman WE, Juneja MM, Kaczorowski DM, Colclough GW. A comparison of incidence of pruritis following epidural opioid administration in the parturient. Can J Anaesth 1989;36:388-91.
24. Gunter JB, McAuliffe J, Gregg T, Weidner N, Varughese AM, Sweeney DM. Continuous epidural butorphanol relieves pruritus associated with epidural morphine infusions in children. Paediatr Anaesth 2000;10:167-72.
25. Varrassi G, Celleno D, Capogna G, Costantino P, Emanuelli M, Sebastiani M, et al. Ventilatory effects of subarachnoid fentanyl in the elderly. Anaesthesia 1992;47:558-62.
26. Kamphuis ET, Ionescu TI, Kuipers PW, de Gier J, van Venrooij GE, Boon TA. Recovery of storage and emptying functions of the urinary bladder after spinal anesthesia with lidocaine and with bupivacaine in men. Anesthesiology 1998;88:310-6.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.

196
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Original Article
A comparison between intravenous paracetamol plus fentanyl and intravenous fentanyl alone for postoperative analgesia during laparoscopic cholecystectomyAnirban Hom Choudhuri, Rajeev Uppal
Department of Anesthesiology and Intensive Care, GB Pant Hospital, New Delhi, India
Corresponding author: Dr. Anirban Hom Choudhuri, 12/203, East End Apartments, Mayur Vihar I (extn), Delhi – 110 096, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_109_11R5
AbstractPurpose: our study compared the effect of fentanyl alone with fentanyl plus intravenous Paracetamol for analgesic efficacy, opioid sparing effects, and opioid-related side effects after laparoscopic cholecystectomy. Materials and Methods: eighty patients undergoing laparoscopic cholecystectomy were randomized into two groups, who were given either an IV placebo or an IV injection of 1g paracetamol just before induction. Both groups received fentanyl during induction and IM diclofenac for pain relief every 8 hourly for 24 h after surgery. The postoperative pain relief was evaluated by a visual analog scale (VAS) and consumption of fentanyl as rescue analgesic in the postoperative period for 24 h after surgery was measured. The incidence of PONV and sedation scores was also measured in the postoperative period. Results: the mean VAS score in first and second hour after surgery was less in the group receiving IV Paracetamol (3.3±0.4* vs. 5.2±0.9; 3.1±0.4* vs. 4.3±0.3); the fentanyl consumption over first 24 h was also less in the group receiving IV paracetamol (50±14.9 vs. 150±25.8). The time requirement of first dose of rescue analgesic in the postoperative period was also significantly prolonged in the group receiving IV paracetamol (76±24.7 vs. 48±15.8). There was no difference in the sedation scores and in the incidence of PONV in the two groups.Conclusion: the study demonstrates the usefulness of intravenous paracetamol as pre-emptive analgesic in the treatment of postoperative pain after laparoscopic cholecystectomy.
Key words: Intravenous paracetamol, pain after laparoscopic cholecystectomy, postoperative analgesia
INTRODUCTION
Pain is the most common complaint after laparoscopic cholecystectomy.[1,2] resulting in the use of rescue opioid analgesics in up to 80% patients.[3] Furthermore the pattern of pain after laparoscopic cholecystectomy is complex and unlikely to benefit always from identical analgesic treatment.[4]

197
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Choudhuri and Uppal: Pre-emptive analgesia with intravenous paracetamol in laparoscopic cholecystectomy
197
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Paracetamol (acetaminophen; N-acetyl-p-aminophenol) is an acetanilide derivative, safe, well-tolerated drug with proven efficacy as analgesic. Its clinical effects arise most likely from central action and intravenous administration provides rapid and predictable therapeutic plasma concentration. Paracetamol was introduced for intravenous administration in a unit-dose form, ready for infusion solution in 2002 (Perfalgan®; 1 g/100 mL). It has been available in India since the past one year.
The valuable analgesic properties of opioids viz. fentanyl in the treatment of acute, intense post-operative pain are well recognized.[5] It has been found that routine treatment of opioids at the beginning of operation conferred significantly better pain control than opioids given at the end of surgery.[6] However, to reduce the opioid-related side effects and hasten recovery, drugs such as NSAIDs, paracetamol, COX-2 inhibitors, local anesthetics, steroids etc. are often used for their opioid-sparing action.[7,8]
The aim of this randomized study was to compare the analgesic efficacy of intravenous fentanyl alone versus intravenous fentanyl plus paracetamol for postoperative pain relief after laparoscopic cholecystectomy
MaTeRIals aND MeThODs
The study was approved by our ethics committee. Written and informed consent was obtained from all. Patients aged 18–70 year scheduled for laparoscopic cholecystectomy, and classified as ASA physical status I or II were included. Patients with diagnostic laparoscopy, those having contraindications to paracetamol (allergy, liver disease) or to nonsteroidal anti-inflammatory drugs (NSAIDs) (esophagogastroduodenal disease, renal insufficiency, and abnormal coagulation) were excluded, as were those on treatment by steroids, NSAIDs, or opioids before surgery.
Patients received oral premedication, 5 mg Diazepam on the night before surgery.
The patients were randomly divided into two groups with 40 patients in each. The study design was randomized and unblinded. Patients were randomly allocated according to a randomization list.
In the operating room, all standard monitoring techniques were used and crystalloid infusion was started. Patients in the fentanyl group (Group F) received 100 mL of normal saline and those in the fentanyl plus paracetamol group (Group P) received 100 mL of Paracetamol IV (Perfalgan 1 gm) just before induction.
All drugs were available in the hospital pharmacy. They were administered to the patients by qualified resident doctors who were not involved in the study.
After the administration of oxygen, anesthesia was
induced in both the groups with IV propofol (2 mg/kg), fentanyl (2 µg/ kg), and rocuronium (0.6 mg/kg). Anesthesia was maintained by 1–2% isoflurane in nitrous oxide and oxygen (ratio 2:1). The lungs were mechanically ventilated, and ventilation was adjusted to maintain end-expiratory CO2 between 34–36 mm Hg depending on the different stages of laparoscopy. Fentanyl was repeated in the dose of 1 µg/kg intraoperatively if both HR and NIBP increased >20% from baseline despite maintaining adequate depth of anesthesia.
After tracheal extubation, patients were transferred to the PACU. Postoperative pain was assessed using a visual analog scale (VAS; 0_ “no pain” and 10_ “worst pain imaginable”). Postoperative analgesia was provided routinely to all patients by intramuscular diclofenac at 8 h interval and intravenous fentanyl 1 µg/kg was administered as rescue analgesic when the VAS score exceeded 3.
The degree of sedation was determined according to a sedation score ranging from 0 to 2 (0_ alert, 1_ drowsy but rousable to voice, and 2_ very drowsy, but rousable to shaking). The VAS scores and sedation scores were assessed at 1, 2, 4, 6, 8, 12, and 24 h after surgery. Total and incremental fentanyl consumption at these times for both the groups was also recorded. If nausea and/or vomiting occurred, the same was noted and 8 mg of ondansetron was given intravenously. The number of patients receiving antiemetics and their total dosages were noted. Patients were observed for the occurrence of any adverse effects during the first 24 h. After 24 h, patients were assessed for: (a) ability to mobilize and dress, (b) need for any analgesic, and (c) surgical complication, if any. When the patient scored yes on the former and no on the two latter questions, they were assessed ready for discharge from hospital. All measurements were recorded by the anesthesia resident who was blinded to the study drugs administered.
A sample size of 35 patients by group was calculated to detect a significant difference of 20% or more in opioid consumption with a power of 80% and a significance level of 5%. Data were reported as mean ± SD. Statistical assessment included analysis of variance (ANOVA) and student’s t-test for continuous data and VAS pain data. Fisher’s exact t-test and chi-square test was used to analyze nominal data; P<0.05 was considered to be significant.
ResUlTs
Both groups were similar in regard to age, weight, sex, ASA physical status, duration of anesthesia and surgery, intraoperative blood loss and the duration of hospital stay [Table 1]. None of the patients in either group required fentanyl intraoperatively [Table 2].
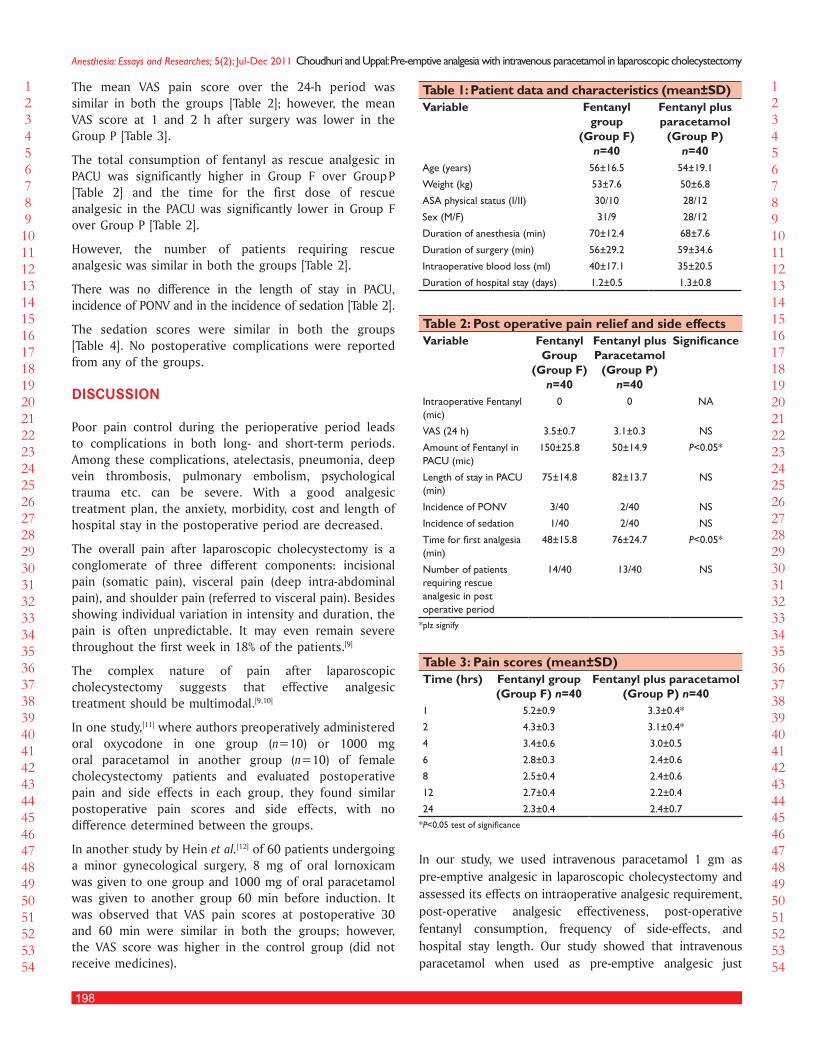
198
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Choudhuri and Uppal: Pre-emptive analgesia with intravenous paracetamol in laparoscopic cholecystectomy
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
The mean VAS pain score over the 24-h period was similar in both the groups [Table 2]; however, the mean VAS score at 1 and 2 h after surgery was lower in the Group P [Table 3].
The total consumption of fentanyl as rescue analgesic in PACU was significantly higher in Group F over Group P [Table 2] and the time for the first dose of rescue analgesic in the PACU was significantly lower in Group F over Group P [Table 2].
However, the number of patients requiring rescue analgesic was similar in both the groups [Table 2].
There was no difference in the length of stay in PACU, incidence of PONV and in the incidence of sedation [Table 2].
The sedation scores were similar in both the groups [Table 4]. No postoperative complications were reported from any of the groups.
DIsCUssION
Poor pain control during the perioperative period leads to complications in both long- and short-term periods. Among these complications, atelectasis, pneumonia, deep vein thrombosis, pulmonary embolism, psychological trauma etc. can be severe. With a good analgesic treatment plan, the anxiety, morbidity, cost and length of hospital stay in the postoperative period are decreased.
The overall pain after laparoscopic cholecystectomy is a conglomerate of three different components: incisional pain (somatic pain), visceral pain (deep intra-abdominal pain), and shoulder pain (referred to visceral pain). Besides showing individual variation in intensity and duration, the pain is often unpredictable. It may even remain severe throughout the first week in 18% of the patients.[9]
The complex nature of pain after laparoscopic cholecystectomy suggests that effective analgesic treatment should be multimodal.[9,10]
In one study,[11] where authors preoperatively administered oral oxycodone in one group (n=10) or 1000 mg oral paracetamol in another group (n=10) of female cholecystectomy patients and evaluated postoperative pain and side effects in each group, they found similar postoperative pain scores and side effects, with no difference determined between the groups.
In another study by Hein et al.[12] of 60 patients undergoing a minor gynecological surgery, 8 mg of oral lornoxicam was given to one group and 1000 mg of oral paracetamol was given to another group 60 min before induction. It was observed that VAS pain scores at postoperative 30 and 60 min were similar in both the groups; however, the VAS score was higher in the control group (did not receive medicines).
In our study, we used intravenous paracetamol 1 gm as pre-emptive analgesic in laparoscopic cholecystectomy and assessed its effects on intraoperative analgesic requirement, post-operative analgesic effectiveness, post-operative fentanyl consumption, frequency of side-effects, and hospital stay length. Our study showed that intravenous paracetamol when used as pre-emptive analgesic just
Table 1: Patient data and characteristics (mean±SD)Variable Fentanyl
group (Group F)
n=40
Fentanyl plus paracetamol
(Group P) n=40
Age (years) 56±16.5 54±19.1
Weight (kg) 53±7.6 50±6.8
ASA physical status (I/II) 30/10 28/12
Sex (M/F) 31/9 28/12
Duration of anesthesia (min) 70±12.4 68±7.6
Duration of surgery (min) 56±29.2 59±34.6
Intraoperative blood loss (ml) 40±17.1 35±20.5
Duration of hospital stay (days) 1.2±0.5 1.3±0.8
Table 2: Post operative pain relief and side effectsVariable Fentanyl
Group (Group F)
n=40
Fentanyl plus Paracetamol
(Group P) n=40
Significance
Intraoperative Fentanyl (mic)
0 0 NA
VAS (24 h) 3.5±0.7 3.1±0.3 NS
Amount of Fentanyl in PACU (mic)
150±25.8 50±14.9 P<0.05*
Length of stay in PACU (min)
75±14.8 82±13.7 NS
Incidence of PONV 3/40 2/40 NS
Incidence of sedation 1/40 2/40 NS
Time for first analgesia (min)
48±15.8 76±24.7 P<0.05*
Number of patients requiring rescue analgesic in post operative period
14/40 13/40 NS
*plz signify
Table 3: Pain scores (mean±SD)Time (hrs) Fentanyl group
(Group F) n=40Fentanyl plus paracetamol
(Group P) n=401 5.2±0.9 3.3±0.4*
2 4.3±0.3 3.1±0.4*
4 3.4±0.6 3.0±0.5
6 2.8±0.3 2.4±0.6
8 2.5±0.4 2.4±0.6
12 2.7±0.4 2.2±0.4
24 2.3±0.4 2.4±0.7*P<0.05 test of significance

199
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Choudhuri and Uppal: Pre-emptive analgesia with intravenous paracetamol in laparoscopic cholecystectomy
before induction as part of multimodal analgesic regime has significant opioid sparing effect. This is consistent with the findings in various studies where opioid-sparing effects of NSAIDs, COX-2 inhibitors, and paracetamol have been found to be in the range of 20–30%.[13,14]
There are evidences from other surgical procedures to support clinically relevant analgesic effect of paracetamol with additives (Opioids, NSAIDs etc.) in laparoscopic cholecystectomy.[15,16] It has been reported in previous studies that propacetamol behaves favorably with different ketorolac doses producing a 31–37% decrease in the morphine requirement during the first 24 h after surgery.[17,18] Our study results are consistent all previous findings in this regard.
In our study no differences were observed between the two groups in the adequacy of analgesia as assessed by VAS scores. However, the median pain scores were significantly lower in the paracetamol group (Group P) at two intervals and the time for first analgesic requirement was significantly lower in the fentanyl alone group (Group F). This may be because of the initial loading dose of paracetamol providing a higher plasma concentration. Piguet et al.[19]
had demonstrated the close correlation between plasma concentration and analgesic effect of paracetamol with intravenous doses of up to 2 gm in healthy volunteers. Juhl et al.[20] had demonstrated that the extent and duration of pain relief following third molar surgery was significantly improved after 2 g over 1 g of initial intravenous dose of paracetamol. Our results are consistent with these results.
Clinical studies have also found that 1 gm intravenous paracetamol employed alone is just as effective as 30 mg ketorolac, 75 mg diclofenac or 10 mg morphine.[21,22] Our study did not find any reduction in the opioid related side-effects (PONV, sedation etc.) in the paracetamol group (Group P) as might be expected because of the decrease in total fentanyl dose. This may be because of the lesser number of subjects in our study. Larger studies with adequate power to detect opioid-related side-effects would be able to demonstrate the reduction of dose-dependent side-effects of fentanyl, such as sedation, respiratory depression, urinary retention, or nausea.
Our study demonstrated the additive effect of combining intravenous paracetamol with fentanyl on postoperative analgesia resulting in decreased opioid amount and in slightly improved or similar pain relief. The different sites of action of these drugs in the nervous system may be the cause of better pain relief. Whereas the effect of Paracetamol is due to the inhibition of prostaglandins and activation of descending serotonergic inhibitory pathways[23,24] the analgesic effect of fentanyl is due to its agonist action in the opioid receptors of the central nervous system. The complimentary analgesic actions of the two drugs make them an important component of multimodal pain therapy.
However, our study had a few limitations. First, this was not a blind study and second, PCA pump was not used in the postoperative period. Both of these could have improved the results of our study but owing to technical reasons and limited availability it was not possible.
In conclusion, our study is the first such study conducted in Indian population. It demonstrates the usefulness of intravenous paracetamol for pre-emptive analgesia as adjunct to fentanyl for the postoperative pain after laparoscopic cholecystectomy. Intravenous paracetamol use is associated with a satisfactory analgesia and smaller opioid consumption. This may be beneficial in the management of pain after laparoscopic cholecystectomy in patients prone to opioid-related complications.
ReFeReNCes
1. McMohan AJ, Russel IT, Ramsay G, Sunderland G, Baxter JN, Anderson JR, et al. Laparoscopic and minilaparotomy cholecystectomy: A random-ized trial comparing postoperative pain and pulmonary function. Surgery 1994;115:533-9.
2. Troidl H, Spangenberger W, Langen R, al-Jaziri A, Eypasch E, Neugebauer E, et al. Laparoscopic cholecystectomy: technical performance, safety and patient’s benefit. Endoscopy 1992;24:252-61.
3. Madsen MR, Jensen KE. Postoperative pain and nausea after laparoscopic cholecystectomy. Surg Laparosc Endosc 1992;2:303-5.
4. Mouton WG, Bessell JR, Otten KT, Maddern GJ. Pain after laparoscopy. Surg Endosc 1999;13:445-8.
5. Practice guidelines for acute pain management in the perioperative setting: An updated report the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology 2004;100:1573-81.
6. Lane GE, Lathrop JC, Boysen DA, Lane RC. Effect of intramuscular intraop-erative pain medication on narcotic usage after laparoscopic cholecystec-tomy. Am Surg 1996;62:907-10.
7. Boccara G, Chaumeron A, Pouzeratte Y, Mann C. The preoperative admin-istration of ketoprofen improves analgesia after laparoscopic cholecystec-tomy in comparison with propacetamol or postoperative ketoprofen. Br J Anaesth 2005;94:347-51.
8. Marret E, Kurdi O, Zufferey P, Bonnet F. Effects of nonsteroidal anti-iflam-matory drugs on patient-controlled analgesia side-effects: Meta-analysis of randomized controlled trials. Anesthesiology 2005;102:1249-60.
9. Bisgaard T, Klarskov B, Kehlet H, Rosenberg J. Characteristics and prediction of early pain after laparoscopic cholecystectomy. Pain 2001;90:261-9.
10. Michaloliakou C, Chung F, Sharma S. Preoperative multimodal analgesia fa-cilitates recovery after ambulatory laparoscopic cholecystectomy. Anesth Analg 1996;82:44-51.
11. Speranza R, Martino R, Laveneziana D, Sala B. Oxycodone versus paracetamol in oral premedication in cholecystectomy. Minerva Anestesiol 1992;58:191-4.
12. Hein A, Norlander C, Blom L, Jakobsson J. Is pain prophylaxis in minor
Table 4: Sedation scoresTime (h) Fentanyl group
(Group F) n=40Fentanyl plus paracetamol
(Group P) n=401 1 (0–2) 1 (0–2)
2 1 (0–2) 1 (0–2)
4 1 (0–2) 1 (0–2)
6 1 (0–2) 0 (0–2)
8 hr 0 (0-2) 0 (0-2)
12hr 0 (0-2) 0 (0-2)
24 0 (0–2) 0 (0–2)

200
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Choudhuri and Uppal: Pre-emptive analgesia with intravenous paracetamol in laparoscopic cholecystectomy
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.
gynaecological surgery of clinical value? A double blind placebo controlled study of Paracetamol 1 gm versus lornoxicam 8 mg given orally. Ambul Surg 2001;9:91-4.
13. Fayaz MK, Abel RJ, Pugh SC, Hall JE, Djaiani G, Mecklenburgh JS. Opioid spar-ing effects of diclofenac and Paracetamol lead to improved outcomes after cardiac surgery. J Cardiothorac Vasc Anaesth 2004;18:742-7.
14. Hernández-Palazón J, Tortosa JA, Martínez-Lage JF, Pérez-Flores D. Intrave-nous administration of Propacetamol reduces morphine consumption alter spinal fusion surgery. Anesth Analg 2001;92:1473-6.
15. Hyllested M, Jones S, Pedersen JL, Kehlet H. Comparative effect of Paracetamol, NSAIDs or their combination in post-operative pain manage-ment. Br J Anaesth 2002;88:199-214.
16. Remy C, Marret E, Bonnet F. Effects of acetaminophen on morphine side-effects and consumption after major surgery: Meta-analysis of randomized controlled trials. Br J Anaesth 2005;94:505-13.
17. Reuben SS, Connelly NR, Steinberg R. Ketorolac as an adjunct to patient-controlled morphine in postoperative spine surgery patients. Reg Anesth 1997;22:343-6.
18. Reuben SS, Connelly NR, Lurie S, Klatt S, Gibson CS. Dose-response of Ketorolac as an adjunct to patient-controlled analgesia morphine in patients after spinal fusion surgery. Anesth Analg 1998;87:98-102.
19. Piguet V, Desmeules J, Dayer P. Lack of acetaminophen ceiling effect on R-III nociceptive flexion reflex. Eur J Clin Pharmacol 1998;53:321-4.
20. Juhl G, Norholt S, Tonnese E, Hiesse-Provost O, Jensen TS. Analgesic efficacy and safety of intravenous Paracetamol (acetaminophen) administered as a 2 g starting dose following 3rd molar surgery. Eur J Pain 2006;10:371-7.
21. Flower RJ, Vane JR. Inhibition of prostaglandin synthesis in brain ex-plains the anti-pyretic effect of Paracetamol (4-aminodophenol). Nature 1972;240:410-1.
22. Tjolsen A, Lund A, Hole K. Antinociceptive effect of Paracetamol in rats in partly dependent on spinal serotonergic systems. Eur J Pharmacol 1991;193:193-201.
23. Anderson BJ. Paracetamol (Acetaminophen): mechanisms of action. Paedi-atr Anaesth 2008;18:915-21.
24. Graham GG, Scott KF. Mechanism of action of paracetamol. Am J Ther 2005;12:46-55.
New features on the journal’s website
Optimized content for mobile and hand-held devicesHTML pages have been optimized of mobile and other hand-held devices (such as iPad, Kindle, iPod) for faster browsing speed.Click on [Mobile Full text] from Table of Contents page.This is simple HTML version for faster download on mobiles (if viewed on desktop, it will be automatically redirected to full HTML version)
E-Pub for hand-held devices EPUB is an open e-book standard recommended by The International Digital Publishing Forum which is designed for reflowable content i.e. the text display can be optimized for a particular display device.Click on [EPub] from Table of Contents page.There are various e-Pub readers such as for Windows: Digital Editions, OS X: Calibre/Bookworm, iPhone/iPod Touch/iPad: Stanza, and Linux: Calibre/Bookworm.
E-Book for desktopOne can also see the entire issue as printed here in a ‘flip book’ version on desktops.Links are available from Current Issue as well as Archives pages. Click on View as eBook

201
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Case Report
Heimlich’s maneuver-assisted bronchoscopic removal of airway foreign bodySohan Lal Solanki, Shivendu Bansal1, Arvind Khare1, Amit Jain2
Department of Anaesthesiology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, 1Department of Anaesthesia and Intensive Care, J. L. N. Medical College and Hospitals, Ajmer, Rajasthan, 2Department of Anesthesia and Intensive Care, Alchemist Hospitals Ltd., Panchkula, Haryana, India
Corresponding author: Dr Sohan Lal Solanki, Department of Anaesthesiology, SGPGIMS, Rae-Bareilly Road, Lucknow-226014, India. Email: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_48_11R5 AP Done 27th Jan
AbstractAspiration of foreign bodies (FBs) by children can lead to serious illness and sometimes even death. Bronchoscopic removal of the FB is necessary to prevent from any catastrophic event. Sometimes bronchoscopic removal is not possible due to the larger size of the FB, sharp FB, or long duration FB. Tracheostomy is normally used for the removal of such FBs. The aim of this case report is to highlight the use of Heimlich maneuver for the removal of such FBs before opting invasive procedures. In the present case, a 5-year-old child was presented with history of FB aspiration 5 h back. After multiple failed bronchoscopic attempts to remove the FB it was decided to use Heimlich maneuver in the supine position. A single attempt of Heimlich maneuver expelled the FB into the oral cavity, which was removed by Magill’s forceps. On repeated bronchoscope check, there was no remnant of FB. Child’s further course of stay in hospital was uneventful. In conclusion, Heimlich maneuver may be useful in patient with failed bronchoscope removal of airway FBs before proceeding for tracheotomy or other invasive procedures.
Key words: Bronchoscope, foreign body, Heimlich maneuver
INTRODUCTION
Foreign body (FB) aspiration has mainly been reported in children, but can occur in any age group, mostly while eating in intoxicated states. The course of illness after a FB lodges in the air passages depends upon the characteristics of the FB and its length of stay. Aspiration of FBs by children can lead to serious illness and sometimes even death.[1] On diagnosis, immediate
bronchoscope removal of FB is necessary to prevent any catastrophic event.
Heimlich maneuver is used to create pressure within the lungs which in turn helps to expel the lodged FB in the airway into the oral cavity which is further removed by hooking movement of fingers or by any instrument.[2] Here we present a case where a FB stuck at a level of subglottis during bronchoscopic extraction that was further removed with help of Heimlich maneuver while the patient was under general anesthesia in the supine position.
CASE REPORT
A 5-year-old, 18-kg male child was presented in the emergency department with a history of cough and labored breathing. Groundnut aspiration was suspected by his parents. Otorhinolaryngology consultation was

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
202
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Solanki, et al.: Heimlich’s maneuver assisted bronchoscopic removal of airway foreign body
obtained and it was planned for emergency bronchoscopic removal of the FB. He had taken breakfast 5 h back. His parents denied any other medical comorbidities or surgical treatment in the past. On examination, he was 107 cms in height, conscious, and well oriented. He was in labored breathing with the use of accessory muscles. Respiratory examination revealed decreased breath sounds on the right side of the chest along with wheezing. He was mallampati Class II with full range of neck movements. A preoperative chest radiograph showed obstructive emphysematous changes and electrocardiography (ECG) showed normal sinus rhythm. After explaining the procedure and risk involved, written informed consent was taken. In the operation room standard ECG, noninvasive blood pressure, and pulse oximetry were attached and baseline were parameters noted. A 22G cannula was secured and intravenous normal saline infusion was started. Patient was also given inj. Dexamethasone 2 mg i.v. The preoperative heart rate (HR) was 115/ min., blood pressure (BP) was 90/56 mmHg, respiratory rate was 26/ min, SpO2 (on room air) was 88% and arterial blood gases showed pH-7.32, pO2-61, pCO2-39, HCO3-15, BE = -5, and SO2-89. A 10 F Ryle’s tube was inserted to decompress the stomach. He was preoxygenated by the facemask with 100% oxygen. General anesthesia was induced by propofol 2.5 mg/kg and fentanyl 1.5 µg/kg. Intravenous succinylcholine 2 mg/ kg was given for muscle relaxation. The patient was positioned supine with a rolled towel across the back between the scapulae to extend the neck and to push the upper trachea forward. After direct laryngoscopy rigid bronchoscope was introduced under direct vision by surgeon. Anesthesia and ventilation was maintained with halothane in 100% oxygen through the side port of the bronchoscope by attaching a Jackson Rees T-piece. Repeat doses of succinylcholine were given as necessary. The FB was visualized in the right upper lobe bronchus and then serrated extraction forceps were used to retrieve it. The surgeon grasped the FB and tried to remove it but it stuck at the level of subglottis. Even after multiple attempts, the FB could not be extracted due to its larger size. Meanwhile all the vital parameters were carefully observed. An attempt of Heimlich maneuver was tried on patient in the supine position with performer’s hands positioned slightly above the naval and well below the xiphoid process and then pressed into the abdomen with quick a upward thrust. The maneuver led to the expulsion of the FB into the oropharynx that was immediately grasped and removed with the help of Magill’s forceps. Oral cavity was examined and the bronchoscope was reinserted to check for any possible remnant of FB and suction of secretions. After clearance by the surgeon, anesthesia was stopped and child was mask ventilated until he recovered fully. Post procedure he had a good cry, HR 80/ min, BP 100/60 mmHg, SpO2 97% on room air and arterial blood gases showed pH-7.42, pO2-72, pCO2-29,
HCO3-18, BE = -4 and SO2-97. Post-operatively the patient was given antibiotics and monitored carefully. His stay in hospital was uneventful and he was discharged on the next day.
DISCUSSION
FB aspiration is most often suffered by small children, who are unable to appreciate the hazards and have tendency of putting small objects in their mouth;[3] however, can occur in any age group. Groundnuts and peanuts are the most common cause of airway obstruction in children according to various studies.[4,5]
The FB aspiration in children usually presents with an initial episode of choking with subsequent respiratory symptoms. There may be cough, wheeze, or stridor with decreased or abnormal breath sounds on examination.[6]
Children with a triad of cough, wheezing, and decreased air entry should be suspected of FB in the tracheobronchial tree.[7] Fever and respiratory distress may be present in longstanding cases. The longstanding FB may also lead to complications such as recurrent pneumonia, bronchiectasis, atelectasis, and even death.[8] Therefore, immediate bronchoscopy should be done as soon as there is a suspicion of the FB. The rigid bronchoscope is mainly used for FB extraction and hemostasis from and in the bronchial tree.[9]
As in our case, rigid bronchoscopy was performed under general anesthesia with jet ventilation to maintain oxygenation and anesthesia. However, difficulty during extraction at the level of subglottis was observed possibly due to an increase in the size of the vegetative FB as it might have swollen over time due to water absorption.[10] Also, subglottic part is supposed to be the narrowest part of the airway in children.
Even experienced endoscopists sometimes fail to retrieve the FB. Open surgical procedures such as tracheostomy, thoracotomy, bronchotomy, and sometimes pulmonary resection are options and needed in 0.3-4% cases. [11,12] Singh et al.,[13] described the role of tracheostomy in the management of the FB airway obstruction in children. In their study, out of 342 patients who were studied for airway FB removal, four (1.2%) patients required tracheostomy. The indications for tracheostomy in the study by Singh et al. were subglottic FB of long duration, sharp subglottic FB, and FB that were larger than the glottis chink. Though the removal of the stucked vegetable FB can be done by fragmentation but this may cause further problems.[14]
In the present case, while the child was under general anesthesia and in the supine position, an attempt was made to remove the vegetative FB stucked at the

203
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Solanki, et al.: Heimlich’s maneuver assisted bronchoscopic removal of airway foreign body
subglottic level by Heimlich maneuver. The maneuver lifted the diaphragm and forced enough air from the lungs to create an artificial cough.[2] Cough was intended to move and expel the obstructing FB in upper airway. Though, such a maneuver when performed in supine position has shown to be effective in expelling water from the lung of drowning victims,[15] its use in managing a FB obstruction under general anesthesia has not been described. We speculate that the effectiveness of the Heimlich maneuver in removing the groundnut that impacted at the subglottic level was partly due to smooth and atraumatic margins of the FB.
Heimlich maneuver is not free from complications. Even if performed correctly, traumatic complications such as rib fractures, gastric, or esophagus perforations, pneumomediastinum, aortic valve cusp rupture, diaphragmatic herniation, jejunum perforation, hepatic rupture, splenic or mesenteric laceration, and acute pancreatitis have been described. However, the overall rate of complication is low. Further, the alternate technique such as tracheostomy is more invasive and not always free from complications,[16] but can be done if the Heimlich maneuver fails.
CONCLUSION
The case presents the successful use of the Heimlich maneuver in a pediatric patient for the retrieval of FB stucked at the subglottic level following failed attempts at rigid bronchoscopy under general anesthesia. Thus, we recommend that this lifesaving maneuver should always be attempted in such a situation before choosing surgical techniques like tracheostomy.
REFERENCES
1. Rovin JD, Rodgers BM. Pediatric Foreign Body Aspiration. Pediatr Rev 2000;21:86-90.
2. The Heimlich’s Institute Deaconess Foundation. How to do the Heimlich maneuver. Available from: http://www.heimlichinstitute.org/page.php?id = 34 [Last accessed on 2011 July 01].
3. “Choking Prevention” American Academy of Pediatrics. Available from: http://www.healthychildren.org. [Last accessed on 2010 June 14].
4. McGuirt WF, Holmes KD, Feehs R, Browne JD. Tracheobronchial foreign bodies. Laryngoscope 1988;98:615-8.
5. Sreenath J, Mahendrakar V. Management of tracheobronchial foreign bodies-a retrospective analysis. Indian J Otolaryngol Head Neck Surg 2002;54:127-31.
6. Hilliard T, Sim R, Saunders M, Hewer SL, Henderson J. Delayed diagnosis of foreign body aspiration in children. Emerg Med J 2003;20:100-1.
7. Kim IG, Brummitt WM, Humphry A, Siomra SW, Wallace WB. Foreign body in the airway: A review of 202 cases. Laryngoscope 1973;83:347-54.
8. Lakshmanan K, Santhanakrishnan BR. Foreign bodies in the tracheo-broncheal tree in children: Diagnostic problems and management. Indian J Pediatr 1987;54:765-8.
9. Weissberg D, Schwartz I. Foreign bodies in the tracheobronchial tree. Chest 1987;91:730-3.
10. Friedman EM. Tracheobronchial foreign bodies. Otolaryngol Clin North Am 2000;33:179-85.
11. Ulku R, Onen A, Onat S, Ozcelik C. The value of surgical approaches for aspirated pen caps. J Pediatr Surg 2005;40:1780-3.
12. Zhijun C, Fugao Z, Niankai Z, Jingjing C. Therapeutic experience from 1420 patients with pediatric tracheobronchial foreign body. J Pediatr Surg 2008;43:718-21.
13. Singh JK, Vasudevan V, Bhardwaj N, Narsimhan KL. Role of tracheostomy in the management of foreign body airway obstruction in children. Singapore Med J 2009;50:871-4.
14. Swensson EE, Rah KH, Kim MC, Brook JW, Salzberg AM. Extraction of large tracheal foreign bodies through a tracheostoma under bronchoscopic control. Ann Thorac Surg 1985;39:251-3.
15. Heimlich HJ, Patrick EA. Using the Heimlich maneuver to save near-drowning victims. Postgrad Med 1988;84:62-7, 71-3.
16. Cecchetto G, Viel G, Cecchetto A, Kusstatscher S, Montisci M. Fatal splenic rupture following Heimlich maneuver: Case report and literature review. Am J Forensic Med Pathol 2011;32:169-71.
How to cite this article: ???Source of Support: Nil, Conflict of Interest: None declared.

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
204
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Case Report
Giant cervical lipoma excision under cervical epidural anesthesia: A viable alternative to general anesthesiaRam Pal Singh, Aparna Shukla, Satyajeet Verma1
Departments of Anaesthesiology and Intensive Care, 1Surgery, Rohilkhand Medical College and Hospital, Bareilly, Uttar Pradesh, India
Corresponding author: Dr. Ram Pal Singh, Assistant Professor, Rohilkhand Medical College and Hospital, Bareilly, Uttar Pradesh - 243 006, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_46_11R4
AbstractThe technique of Cervical Epidural Anesthesia (CEA) was first described by Dogliotti in 1933 for upper thoracic procedures. Administration of local anesthetic into cervical epidural space results in anesthesia of the neck, upper extremity, and upper thoracic region. CEA provides high-quality analgesia and anesthesia of above dermatomes and, at the same time, it has favorable effect on hemodynamic variable by blocking sympathetic innervation of the heart. CEA is not practiced routinely because of its potential complications. We selected this technique of CEA for excision of giant cervical lipoma on the back of the neck in an adult patient, as the patient was unwilling for general anesthesia. CEA was induced with 10 ml of 1% lignocaine-adrenaline mixture administered into C7-T1 space through 18G Tuohy needle. Our patient maintained vital parameters throught the procedure. The added advantage of epidural anesthesia was that the patient was awake and comfortable throughout the procedure.
Key words: Cervical lipoma, epidural anesthesia, general anesthesia
INTRODUCTION
The technique of Cervical Epidural Anesthesia (CEA) can be used successfully for procedures involving the neck and upper thorax. This technique is less commonly practiced due to the concern of potential complications such as dural puncture and paralysis of respiratory muscles. However, in the hands of an expert anesthesiologist, the risks associated with these complications are low. A number of prospective and retrospective studies have compared the frequency of both perioperative
and postoperative complications of CEA. Results from some studies suggest that when CEA was used for procedures such as carotid endarterectomy, the morbidity and mortality rates were low and the hemodynamic variables better maintained.[1,2] This technique offers the advantage of better and early postoperative recovery and reduced incidence of postoperative cardio-respiratory complications. We successfully used technique of CEA for surgical excision of tumor on the back of neck.
CASE REPORT
After obtaining a written informed consent, a 40- year- old American Society of Anaesthesiologists (ASA) grade I male patient was posted for surgical excision of giant cervical lipoma, on the back of neck, measuring 12 × 10 × 4.5 cm. On preanesthetic check-up, all routine investigation results were within normal limit. The patient was kept nil orally after 12 midnight prior to surgery. He was premedicated with tablet alprazolam 0.5 mg half an

205
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Singh, et al.: Giant cervical lipoma excision under cervical epidural anesthesia
hour before dinner and at 6 o’clock in the morning of surgery to allay anxiety.
On arrival to the operation theater, an intravenous line was secured with 18G cannula and Lactated Ringer’s solution was started. All anesthetic equipment were checked and monitors attached to the patient. Electrocardiogram (ECG), Oxygen Saturation (SpO2), Noninvasive Blood Pressure (NIBP), and Heart Rate (HR) were monitored continuously throughout the intraoperative period. The patient was premedicated with injection ondansetron 6 mg and was properly briefed prior to the procedure. CEA was performed with the patient in a sitting position. With all aseptic precautions, the neck was flexed to make the cervical vertebrae prominent. The C7-T1 space was infiltrated with 3 ml of 2% lignocaine with adrenaline to provide local anesthesia. Thereafter, a wide-bore needle was inserted at the C7-T1 level to create a passage for epidural needle. An 18G Tuohy needle was inserted in the epidural space, which was identified using the ‘hanging drop’ technique. An 18G epidural catheter was then inserted in the space up to the depth of 3 cm [Figure 1]. The direction of catheter tip was kept cephalad. The catheter was fixed in position. Correct placement of the catheter was verified by negative aspiration for blood and CSF, followed by administration of a test dose of 3 ml of 2% lignocaine with adrenaline. The patient was positioned supine on the operating table and vital parameters were monitored with 5-lead ECG, SPO2, NIBP, and HR. After about 5 minutes, 10 ml of 1% lignocaine with adrenaline with 1 mg of butorphanol injected via epidural catheter. After assessing the level of sensory block, the patient’s position was changed to prone. A soft pillow was kept under his chest to make the surgical area prominent and one head ring under the forehead to keep the head in a fixed position. Oxygen was given by nasal cannula at the rate of 2 L/min. All emergency equipment were kept ready to handle any emergency. The surgery lasted for one hour and intraoperative period was uneventful. The patient’s vitals were maintained during the intraoperative period [Table 1]. The patient was awake
and comfortable during the entire intraoperative and postoperative period [Figure 2].
No significant decrease was observed in systolic and diastolic blood pressure from the baseline values. Although there was a slight decrease in systolic blood pressure, diastolic blood pressure, and heart rate, none of the patients required therapeutic intervention. The lowest mean blood pressure was 82 mm Hg at 5 minutes and the lowest heart was 62/ min at 60 minutes, which was acceptable. Oxygen saturation remained in the range of 95-99%.
DISCUSSION
The study found that CEA is a safe and effective alternative to general anesthesia during excision of tumors in the region of neck. Although we chose this technique due to the patient’s refusal to general anesthesia, our experience with this technique was encouraging. The patient not only remained awake and comfortable throughout the procedure, but also maintained vital parameters. There was no significant fall in systolic and diastolic blood pressure and heart rate so as to require therapeutic intervention. Our findings were comparable to those by Singh et al.,[3] who evaluated the safety and efficacy of CEA in 55 patients undergoing modified radical mastectomy. They found no clinically significant variations in per-operative pulse and respiratory rate; there was no fall in mean arterial blood pressure during the procedure. The authors concluded that CEA is a safe alternative to general anesthesia.
However, contradicting results were seen in the study of Domínguez et al.,[4] who reported three patients scheduled for shoulder surgery under CEA with 0.75% ropivacaine. They found that the extent of blockade to the upper thoracic sensory segments causes a total or partial sympathetic block with decreased HR, blood pressure, and cardiac output.
Figure 1: Cervical epidural catheter placement at the C7-T1 level Figure 2: Patient sitting comfortably in postoperative ward

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
206
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Singh, et al.: Giant cervical lipoma excision under cervical epidural anesthesia
Bonnet et al.[5] reported carotid surgery under CEA in 394 patients by using 15 ml of 0.5 per cent bupivacaine or 0.37-0.40 per cent bupivacaine plus fentanyl (50-100 µg).They found an effective sensory blockade from C2 to T4-T8. Patients were awake during the surgical procedure in comfortable condition. In their study, hypotension
and bradycardia were the most frequent side effects of CEA. They concluded that carotid artery surgery may be performed under CEA, but hemodynamic variables should be monitored and managed closely during the procedure.
In a retrospective study, Hakl et al.[6] compared the Cervical Plexus Block (CPB) and Cervical Epidural (CE) for carotid endarterectomy in 1,455 patients. They administered 20 ml drug consisting of 16 ml of bupivacaine 0.5% and 4 ml (20 µg) of sufentanil. They encountered 13 cases of accidental subarachnoid injection with CEA, but did not find any clinically significant respiratory distress.
From our study and other documentary evidences, we conclude that CEA is a safe and effective alternative to general anesthesia for neck surgery. The advantage of this technique is that it provides all benefits of regional anesthesia. Although in our study we did not encounter any episode of significant bradycardia or hypotension,
caution must be maintained while performing such block. We strongly recommend that the vitals of patients should be closely and continuously monitored throughout the intraoperative and postoperative period.
REFERENCES
1. Florani P, Sbarigia E, Speziale F, Antonini M, Fiorani B, Rizzo L, et al. General anaesthesia versus cervical block and peri-operative complications in carotid artery surgery. Eur J Vasc Endovasc Surg 1997;13:37-42.
2. McCleary AJ, Maritati G, Gough MJ. Carotid endartectomy: Local or general anaesthesia? Eur J Vasc Endovasc Surg 2001;22:1-12.
3. Singh AP, Tewari M, Singh DK, Shukla HS. Cervical epidural anesthesia: A safe alternative to general anesthesia for patients undergoing cancer Breast Surgery. World J Surg 2006;30:2043-7.
4. Domínguez F, Laso T, TijeroT, Ruiz-Moyano J, Hernández J, Puig A. Cervical epidural anesthesia with 0.75% ropivacaine in shoulder surgery. Rev Esp Anestesiol Reanim 2002;49:39-43.
5. Bonnet F, Derosier JP, Pluskwa F, Abhay K, Gaillard A. Cervical epidural anaesthesia for carotid artery surgery. Can J Anesth 1990;37:353-8.
6. Hakl M, Michalek P, Sevcík P, Pavlíková J, Stern M. Regional anaesthesia for carotid endarterectomy. An audit over 10 years. Br J Anaesth 2007;99:415-20.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.
Table 1: Intraoperative vital parameters of the patientTime interval (minutes)
Heart rate (/minute) NIBP (mm Hg) Oxygen saturation SpO2 (%)Systolic Diastolic Mean BP
Baseline 80 122 67 85 97
5 75 115 66 82 97
10 81 129 75 93 97
15 76 119 74 89 97
20 76 116 69 85 97
25 72 114 68 83 96
30 70 117 71 86 97
35 72 114 70 85 97
40 69 116 72 86 99
45 68 118 70 86 94
50 67 116 87 96 97
55 63 116 86 96 98
60 62 118 86 97 97

207
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Case Report
A very common case become rare: Anesthetic considerations of lepromatous leprosySandeep Sahu, Vipin Goyal, Sanjay Dhiraaj, Kamal Kishore, P. K. Singh
Department of Anaesthesiology and Intensive Care, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, Uttar Pradesh, India
Corresponding author: Dr. Sandeep Sahu, Assistant Professor, Department of Anaesthesiology and Intensive Care, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, Uttar Pradesh - 226 014, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_43_11R8AP Done 27th Jan
AbstractLeprosy or Hansen’s disease is very uncommon in developed countries. More than 80% of the world’s cases occurs and still reported from developing countries. But nowadays due to increase in international affairs, medical tourism, globalization and immigration, there is increasing possibility to find patients anywhere, which require anesthesia for surgical interventions. Leprosy is a chronic infectious disease caused by Mycobacterium leprae and involves mainly skin, peripheral nervous system, upper respiratory tract, eyes and testes. Anesthetic consideration is focused mainly on complications related to leprosy like cardiac or respiratory dysautonomia, autonomic dysfunctions and side effects which are related to drug therapy and are challenging. There can be drug-related hepatitis and renal insufficiency in these patients. We report the anesthetic management of a patient with lepromatous leprosy who had undergone laparoscopic radical nephrectomy for renal cell carcinoma under general anesthesia.
Key words: Complications, dysautonomia, lap-radical nephrectomy, lepromatous leprosy
INTRODUCTION
Leprosy was recognized in the ancient civilizations of China, Egypt and India. The first known written mention of leprosy is dated back to 600 B.C. According to recent key facts released about leprosy by WHO in 2010, based on official reports received during 2010 from 141 countries and territories, the global prevalence of leprosy registered at the beginning of 2010 stood at 211,903 cases, while the number of new cases detected during
2009 was 244,796 (excluding the small number of cases in Europe). Most previously highly endemic countries have now reached elimination. However, pockets of high endemicity still remain in some areas of Angola, Brazil, Central African Republic, Democratic Republic of Congo, India, Madagascar, Mozambique, Nepal and the United Republic of Tanzania. These countries remain highly committed in eliminating the disease, and hence continue to intensify their leprosy control activities.[1,2]
All South-eastern Asian region countries have now eliminated leprosy as a public health problem, which is defined as a registered prevalence rate lower than 1 case per 10,000 population at the national level. Till 2007, five countries including India contributed more than 80% of the newly detected cases worldwide. Multidrug therapy (MDT) was included in the National Leprosy Eradication Program (NLEP) of India in 1982 that decreases the prevalence rate (PR) from 5.7 cases per 10,000

208
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Sahu, et al.: Pearls for anaesthetic considerations in leprosy patient
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
populations (1983) to 0.74 (2008). As of 31st March 2009, 32 States in India have achieved the level of elimination and but still some states like Bihar and Chhattisgarh have PR between 2 and 3 per 10,000 population.[3] So still one can encounter leprosy patient as us, from nearby states or country, because India and some other Asian country was just about to declared leprosy free.
Leprosy is disease of developing countries and more prevalent in the people of lower socio-economic status. From the old world it is considered as social stigma. The causative agent for this disease is Mycobacterium leprae, an acid-fast bacilli. The routes of transmission of leprosy are mainly through nasal droplet infection, contact with infected soil or insect vectors. The Ridley-Jopling or the WHO classifications are often used to characterize the patient’s disease.[4] The spectrum of clinical presentation varies widely depending on the type of leprosy. A very important clinical setting is the presence of any leprous reactions, which are very serious complications consequence of dynamic changes in the immune status of the patient.[5] Clinical, bacteriological, pathological and immunological spectrum of leprosy varies between tuberculoid and lepromatous leprosy. In India around 90%, of cases are tuberculoid leprosy. In tuberculoid forms of leprosy clinical manifestations remain confined to the skin and peripheral nerves. The skin lesions consist of anhidrotic, hyperaesthetic, hypopigmented macules or plaques. Clinical manifestations of leprosy vary in accordance with the immune response of the host. Peripheral nerve involvement leads to their enlargement in thickness and neuropathy and commonly involves the ulnar, posterior auricular, peroneal and posterior tibial nerves. While lepromatous leprosy patient have clinical manifestations like skin nodule and plaque, they may also have peripheral neuropathy and involvement of other organs. Neuropathy leads to insensitivity and myopathy which in turn leads to planter ulceration, foot drop and joint deformities. In eyes there may be corneal ulceration and opacities, uveitis, cataract or glaucoma.[6,7] Other complications are orchitis, nerve abscess, amyloidosis, etc. Early diagnosis and treatment with MDT dapsone, rifampicin and clofazimine and this drug combination kills the pathogen and cures and remains the key elements in eliminating the disease as a public health concern. Chronic nature of disease and longer duration of treatment may lead to side effects and organs toxicity that complicates anesthetic management.[8]
CASE REPORT
We discuss a case of 65-year-old, ASA II, 63-kg male posted for left-sided laparoscopic radical nephrectomy due to renal cell carcinoma. Patient was a known case of lepromatous leprosy and was on medications rifampicin, dapsone and clofazimine since 7 months.
At first preanesthetic check-up (PAC) visit he was found to be a known case of chronic obstructive pulmonary disease on derriphyline and inhalers of budesonide and ipatropium bromide. Patient was also chronic smoker since 20 years. He was having bilateral basal coarse crepitations for which advised incentive spirometry, steam inhalation and prescribed antibiotics and nebulization with bronchodilator. He was examined to rule out cardiac dysautonomia (by normal 2D-Echo, Valsalva response, ECG changes to respiration and blood pressure changes related to posture and hyperventilation, all were within normal limits) and respiratory dysautonomia [by breath holding time 30 sec, pulmonary function test (PFT); values was showing obstructive pattern and sleep study were acceptable as per age]. Rest of his general examination and biochemical (liver and kidney functions test) investigations were within normal limits. On PAC review patient clinically improved and chest X-ray and PFT were acceptable. On night before surgery patient was given tablet rantidine 150 mg and lorazepam 1 mg perorally and advised to continue with respiratory medications.
In operation theatre monitoring was applied and large bore IV line was secured after local anesthetic application. Anesthesia was induced with propofol 150 mg after midazolam 2 mg and fentanyl 120 mcg and was intubated with size 8.5 cuffed endotracheal tube after administration of muscle relaxant; atracurium 50 mg. Anesthesia was maintained with oxygen, air (50:50) with sevoflurane, fentanyl, atracurium and propofol infusion. Central venous catheter was placed in right IJV for CVP monitoring and fluid management. Radial artery was cannulised to know beat to beat variability, invasive blood pressure monitoring and serial ABG analysis. Standard monitoring like ECG, SPO
2, ETCO2, temperature, urine output were done. While making left sided kidney positioning nerve and joints injury protection by adequate padding were done. All the universsal principals of anesthesia for laparoscopic surgery were followed. Patient remained hemodynamically stable intraoperatively. At the end of surgery anesthesia was reversed with neostigmine 2.5 mg and glycopyrrolate 0.4 mg. Extubation was smooth done after giving xylocard 60 mg. Post operative analgesia was maintained with IV paracetamol 1 gm\6 hrly and vitals monitored in postoperative care unit.
DISCUSSION
On review of literature not much references has been found regarding anesthetic management of leprosy patient in pubmed. Management of present case is important pearl to revisit leprosy patient in view of anesthetic considerations. Leprosy is a multisystem disease so anesthetic implication of leprosy needs particular attention toward the organs involved and a thorough PAC of patient is required. Patient may be posted for surgery either related to the

209
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Sahu, et al.: Pearls for anaesthetic considerations in leprosy patient
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
complication of leprosy like cataract, joint deformities, planter ulceration or elective and emergency surgical procedure related to systemic diseases.[9]
These are important anesthetic considerations that should be followed during laparoscopic urology surgery. Laparoscopic procedures in renal surgical patients are having similarity with abdominal surgical procedures. These include effects on the cardiovascular system, mechanical consequences due to pneumoperitoneum (raised intra-abdominal pressure), systemic absorption of carbon dioxide, neurohumoral responses and physiological changes associated with the positioning (near full lateral position, renal position) during surgery.[10,11] During laproscopic cholecystectomy renal cortex and medullary blood flow, glomerular filtration and creatinine clearance fall and urine production decreases. Handling the kidney increases plasma renin and antidiuretic hormone release. All these changes are more concerned in renal function deranged or damage patient undergoing renal laparascopic procedures.[12] Other important concerns in laparoscopic urology are these patients having renal dysfunction, due to diseases process leading impairment of drug metabolism and its variable systemic effects, fluid management, monitoring, complication of surgery and conversion to open procedure in these patients.[13]
Cardiovascular system involvement in leprosy characterized by cardiac dysautonomia leading bradycardia, hypotension, cardiac arrest, various arrhythmias and other ECG changes or absence of response to various perioperative manipulations such as intubation, extubation or anticholinergic drugs that need careful intraoperatively vigilance. All of these are more pronounced in patients with longer duration of leprosy. [14,15] Respiratory dysautonomia lead to decreased breath holding time, depressed cough reflex and alteration in PFT and risk of aspiration that may increase the incidence of postoperative complication or need for postoperative ventilation. Nasal obstruction and vocal cord involvement may occur in late stage of lepromatous leprosy, may leads to difficult airway.[16,17] Autonomic neuropathy may present and manifested as orthostatic hypotension, altered baroreceptor reflex and impaired response to valsalva manoeuvre. Luckily our patient PAC ruled out cardiac and respiratory dysautonomia and autonomic involvement but we were prepared with proper monitoring for possible complications and its management.
The effects of leprosy on haematological are as anemia, thrombocytopenia and agranulocytosis leading decrease in O2-carrying capacity, impaired coagulation and increase chances of postoperative infection. Increase bone resoption and osteomyelitis due to leprosy imposes for pathological fracture meanwhile positioning during surgery. Hepatitis due to leprae reaction or drug-related side effects may cause abnormal liver function tests (particularly increased aminotransferase level). The
specific granulomatous lesions suggestive of leprous hepatitis are mainly seen in lepromatous leprosy (40%), whereas, granulomata in the liver could be present in all types of leprosy (70%). Some of the hepatic lesions progressed to stellate fibrosis and early cirrhotic changes (40%).[18] Renal involvement in lepromatous leprosy may be manifested as glomerulonephritis and amyloidosis that causes renal failure. Hepatorenal derangements may cause delayed recovery from anesthesia due to impairment of drug metabolism and delayed clearance. Rifampicine is an inducer of hepatic cytochrome P450, so requirement of anesthetic drugs can be increased that are metabolized by it. Rifampicine may produce intermittent toxic syndromes (e.g., flu syndrome, shock syndrome, and rarely, thrombocytopenic purpura and acute renal failure) and hepatitis. Dapsone can produce haemolytic anemia, methaemoglobinaemia, agranulocytosis, hepatitis, peripheral neuropathy, psychosis and lepra reaction. [19] Spinal and epidural anesthesia should be used cautiously in patients with long-standing disease because hypotension and urinary retention are frequent problems. Neurological deficit can also follow after nerve blocks or regional anesthesia. As present case having normal biochemical parameters and was taking drugs for only one year still we chose atracurium as muscle relaxant and minimal doses of anesthetics due to all above issues.
As these patients are prone to nerve damage and neuropathies, that should be considered during regional blocks. These all above facts were considered while managing present case.
As leprosy patients may have cardiac, respiratory
dysautonomia and autonomic involvement. Due to drugs side effects and dysautonomia they are prone to multiple organ failure. Proper PAC assessment and optimisation with intraoperative period adequate monitoring and preparation is essential while managing leprosy patients.
WHO strategy for leprosy elimination (Key Facts report, 2010)The following actions are part of the ongoing leprosy elimination campaign, which should be strictly followed to eliminate and eradicate leprosy from universe.[2]
• Ensuring accessible and uninterrupted MDT servicesavailable to all patients through flexible and patient-friendly drug delivery systems;
• Ensuring the sustainability of MDT services byintegrating leprosy services into the general health services and building the ability of general health workers to treat leprosy;
• Encouraging self-reporting and early treatment bypromoting community awareness and changing the image of leprosy;
• MonitoringtheperformanceofMDTservices,thequalityof patients’ care and the progress being made toward elimination through national disease surveillance systems.

210
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Sahu, et al.: Pearls for anaesthetic considerations in leprosy patient
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
REFERENCES
1. WHO Leprosy forum report. Available from: http://www.WHO.int/lep/en. [Last accessed on May 2006].
2. WHO fact sheet about leprosy elimination. Available from: http://www.WHO.int/lep/en. [Last accessed on Feb 2010].
3. Gautam VP. Treatment of leprosy in India. J Postgrad Med 2009;55:220-4.4. Yens DA, Asters DJ, Teitel A. Subcutaneous nodules and joint deformity in
leprosy: Case report and review. J Clin Rheumatol 2003;9:181-6.5. Concha M, Cossio ML, Salazar I, Fich F, Perez C, Gonzalez S. [Hansen’s
disease: Case report and review of literature]. Rev Chil Infect 2008;25:64-9.6. Hernandez S, Jose Raman Ortiz-Gomez, Miguel Salvador, Julio Barrena, Ana
Carla Loban. Anesthesia implication of lepromatous leprosy in Europe, case report rare European experience. Anesthesiology and Rescue 2009;3:288-91.
7. Hempenstall K, Holland R. Regional anaesthesia for emergency caesarean section in a patient with lepromatous leprosy. Anaesth Intensive Care 1997;25:168-70.
8. Mitra S, Gombar KK, Gombar S. Anaesthetic considerations in a patient with lepromatous leprosy. Can J Anaesth 1998;45:1103-5.
9. Mitra S, Gombar KK. Leprosy and the anaesthesiologist. Can J Anaesth 2000:47;1001-7.
10. Leonard IE, Cunningham AJ. Anaesthetic considerations for laparoscopic cholecystectomy. Best Pract Res Clin Anaesthesiol 2002;16:1-20.
11. Lund C. Anaesthesia for minimally invasive gastric and bowel surgery. Best Pract Res Clin Anaesthesiol 2002;16:21-33.
12. Yokoyama M, Ueda W, Hirakawa M. Haemodynamic effects of the lateral decubitus position and the kidney rest lateral decubitus position during anaesthesia. Br J Anaesth 2000;84:753-7.
13. Conacher ID, Soomro NA, Rix D. Anaesthesia for laparoscopic urological surgery. Br J Anaesth 2004;93:859-64.
14. Kale HD, Zawar PC, Chawhan RN, Kulkarni GR. Cardiac dysautonomia in lepromatous leprosy. Indian J Lepr 1984;56:563-8.
15. Shah PK, Malhotra YK, Lakhotia M, Kothari A, Jain SK, Mehta S. Cardiovascular dysautonomia in patients with lepromatous leprosy. Indian J Lepr 1990;62:91-7.
16. Gupta OP, Jain AP, Jajoo UN, Kumar K, Parvez K. Respiratory dysautonomia in leprosy. Indian J Lepr 1984;56:844-6.
17. Grover S, Bobhate SK, Chaubey BS. Renal abnormality in leprosy. Lepr India 1983;55:286-91.
18. Cartel JL, Millan J, Guelpa-Lauras CC, Grosset JH. Hepatitis in leprosy patients treated by a daily combination of dapsone, rifampin, and a thioamide. Int J Lepr Other Mycobact Dis 1983;51:461-5.
19. Jacobson RR. Treatment of leprosy. In: Hastings RC, editor. Leprosy. 2nd ed. Edinburgh: Churchill Livingstone; 1994:328-98.
Announcement
Android App
A free application to browse and search the journal’s content is now available for Android based mobiles and devices. The application provides “Table of Contents” of the latest issues, which are stored on the device for future offline browsing. Internet connection is required to access the back issues and search facility. The application is compatible with all the versions of Android. The application can be downloaded from https://market.android.com/details?id=comm.app.medknow. For suggestions and comments do write back to us.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.

211
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Case Report
Bronchospasm following supraclavicular brachial plexus blockRohini V. Bhat Pai, Harihar V. Hegde, M. C. B. Santosh, S. Roopa
Department of Anaesthesiology, SDM College of Medical Sciences and Hospital, Dharwad, Karnataka, India
Corresponding author: Dr. Rohini V. Bhat Pai, Associate Professor, Department of Anaesthesiology, SDM College of Medical Sciences and Hospital, Dharwad, Karnataka - 580 009 India, E-mail: [email protected]
AER_45_11R5
AbstractSupraclavicular brachial plexus block is commonly performed for upper limb surgeries. In patients with compromised respiratory function or in the elderly it may be preferred over general anaesthesia. Bronchospasm, albeit a rare complication of this procedure, may turn the advantages of regional anaesthesia in these patients into a disadvantage. Bronchospasm following interscalene approach has been previously reported. However, the same following the supraclavicular approach has not yet been reported. A 70-year-old woman presented with cellulitis of the left upper limb. A successful left brachial plexus block was performed uneventfully via the supraclavicular approach for an emergency debridement. She developed bronchospasm in the post-operative care unit (1 hour after the performance of the block) which responded to the standard treatment and rest of her hospital stay was uneventful. Awareness of possibility of this less known complication is necessary, especially in patients of compromised respiratory function to initiate prompt treatment and avoid further complications.
Key words: Anaesthesia, bronchial spasm, complications, regional
INTRODUCTION
Performing regional anaesthetic techniques like plexus or nerve blocks is an integral part of the armamentarium of anaesthesiologists. Peripheral nerve blocks may be used alone or in conjunction with general anaesthesia. [1] Brachial plexus block by various approaches is the mainstay of anaesthesia and postoperative analgesia for upper limb surgical procedures. Bronchospasm following interscalene approach to brachial plexus block has been
reported.[2] Bronchospasm following supraclavicular approach has not yet been reported. We report a patient who developed bronchospasm following supraclavicular brachial plexus block.
CASE REPORT
A 70-year-old woman presented with cellulitis of the left upper limb. There was no other relevant medical or surgical history. The patient denied a previous history of bronchial asthma. On examination, she was febrile, her weight was 45 kg, heart rate was 110/ min and blood pressure in the right upper limb in supine position was 168/96 mmHg. Respiratory and cardiovascular systems were unremarkable. Laboratory investigations showed leucocytosis with neutrophilia and other parameters were within normal limits. ECG showed sinus tachycardia. Oxyhaemoglobin saturation (SpO2) on room air was 96%. She was scheduled to undergo an emergency debridement of the left upper limb.
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***

212
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Bhat, et al.: Bronchospasm: Supraclavicular brachial block
Regional anaesthesia was planned and left brachial plexus block was performed uneventfully via the supraclavicular approach. Lignocaine (2%) with adrenaline (5 μg/ml) 10 ml and bupivacaine (0.5%) 10 ml was injected after eliciting paresthesia and careful aspiration. The patient developed adequate anaesthesia of the left upper limb within 10 minutes and the heart rate decreased to 80/min. The surgery lasted for 20 minutes and the further intra-operative period was uneventful.
In the post-operative care unit, 30 minutes later, the patient complained of difficulty in breathing and the SpO2 decreased to 88% with O2 4 L/min by face mask. She was using accessory muscles of respiration. The heart rate increased to 120/min. On auscultation, there was reduced air entry bilaterally and rhonchi were heard all over the chest. She was treated with propped-up position, supplemental oxygen, salbutamol nebulization and intravenous hydrocortisone 100 mg. A chest screening done subsequently with a C-arm was normal. ECG showed no fresh changes. At this time, the right upper limb was also examined for any sensory/motor deficit which the patient could not differentiate due to the respiratory distress. A repeat examination of the right upper limb 1 hour later did not reveal any sensory/motor deficit while the left still had adequate anaesthesia. The patient improved with the above treatment and rest of her hospital stay was uneventful.
DISCUSSION
Brachial plexus block is one of the popular methods of anaesthetizing the upper limb. Various complications have been described. Common complications of interscalene approach include hemi-diaphragmatic paresis (100%), intra-arterial local anaesthetic injection, epidural or spinal anaesthesia, cervical sympathetic block (Horner’s syndrome) and recurrent laryngeal nerve block.[3] Common complications of supraclavicular approach include hemi-diaphragmatic paresis (50%), pneumothorax, intravascular injection, cervical sympathetic block (20-90%), and recurrent laryngeal nerve anaesthesia (1%).[3] Causes of respiratory distress following brachial plexus block using interscalene approach include unilateral/bilateral phrenic nerve paralysis, pneumothorax or bronchospasm. [2] The patient did not give any history or show any symptoms/signs suggestive of any respiratory compromise before the block. Since there was no contraindication to supraclavicular approach this method, which was a personal preference of the anesthesiologist, was selected Hemi-diaphragmatic paralysis is not as commonly seen after a supraclavicular approach as with the interscalene approach for brachial plexus block. The incidence of phrenic nerve paralysis has been reported to be 50% and paresis 17% following supraclavicular brachial plexus block in one series. All the patients in this series were asymptomatic with normal oxygen saturation on
room air.[4] The X-ray screening done postoperatively in our patient showed normal movement of the diaphragm, thus excluding this possibility.
Pneumothorax with a 25G needle, though less likely, could have occurred if a bulla was pricked during the performance of block, considering the patient’s age. This differential diagnosis was also ruled out with the chest X-ray. Recurrent laryngeal nerve paralysis as seen with interscalene approach can lead to upper airway obstruction and wheezing. These signs were absent in our patient. Pain, emotional and psychological factors may cause bronchospasm via the efferent pathway of vagus. The operative site was tested and found to be pain free.
The sympathetic nerve supply to the bronchi arises from T1-T4 segments of the sympathetic chain, while the dominant parasympathetic supply is from the vagus nerve. The integrity of normal airway is the result of the balance between the sympathetic (beta) bronchodilators and parasympathetic and sympathetic (alpha) constrictors. Sympathetic blockade associated with spinal and/or epidural anaesthesia produces constriction of the bowel due to unopposed vagal parasympathetic action. Similarly, blocking the sympathetic nerve supply to the bronchi must cause bronchoconstriction due to unopposed vagal parasympathetic action. Local anaesthetics, when injected in the interscalene groove, have been shown to spread to the opposite side if the midline septae are deficient and also spread as far as T4.
[5] The same mechanism may be the reason for bronchospasm in our patient. Only 2 cases have been described in the literature,[2] of bronchospasm following brachial plexus block using interscalene approach. To our knowledge, no case has yet been reported of this complication following supraclavicular approach.
Regional anaesthesia is usually preferred for patients with compromised respiratory function undergoing upper limb surgery. The number of elderly patients presenting for anaesthesia and surgery has increased in recent years. Although the type of anaesthesia (general versus regional) has no substantial effect on peri-operative morbidity or mortality in any age group, the elderly benefit from regional anaesthesia because of minimal sedation and excellent analgesia and faster recovery.[5] In our patient, the bronchospasm could have negated the beneficial effects of regional anaesthesia.
Regional anaesthesia does not necessitate instrumentation of the airway. Since elderly patients are more susceptible to hypoxaemic episodes in the post-operative recovery unit, patients who undergo regional anaesthesia may have a lower risk of hypoxaemia.[6] Similarly, the risk of aspiration due to the progressive decrease in the laryngo-pharyngeal sensory discrimination in the elderly can be lowered by the use of regional anaesthesia.[7]

213
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Bhat, et al.: Bronchospasm: Supraclavicular brachial block
CONCLUSION
Bronchospasm is a less known complication of the supraclavicular approach of the brachial plexus block. Anesthesiologists administering this block should be aware of this possible complication in susceptible patients and diagnose and treat it early and appropriately. Awareness of possibility of this less known complication is necessary, especially in patients of compromised respiratory function to initiate prompt treatment and avoid further complications.
REFERENCES
1. Morgan GE Jr 2nd, Mikhail MS, Murray MJ. Peripheral Nerve Blocks. In: Morgan GE, editor. Clinical Anesthesiology. 4th ed. New York: The McGraw-Hill Companies, Inc; 2009. p. 324-58.
2. Thiagarajah S, Lear E, Azar I, Salzer J, Zeiligsohn E. Bronchospasm following interscalene brachial plexus block. Anesthesiology 1984;61:759-61.
3. Neal JM. Upper Extremity Blocks. In: Rathmell JP, editor. Regional Anesthesia: The Requisites in Anesthesiology. 1st ed. Philadelphia: Elsevier Mobsy; 2004. p. 59-72.
4. Mak PH, Irwin MG, Ooi CG, Chow BF. Incidence of diaphragmatic paralysis following supraclavicular brachial plexus block and its effect on pulmonary function. Anaesthesia 2001;56:352-6.
5. Tsui BC, Wagner A, Finucane B. Regional anaesthesia in the elderly: A clinical guide. Drugs Aging 2004;21:895-910.
6. Moller JT, Wittrup M, Johansen SH. Hypoxemia in the postanesthesia care unit: An observer study. Anesthesiology 1990;73:890-5.
7. Aviv JE. Effects of aging on sensitivity of the pharyngeal and supraglottic areas. Am J Med 1997;103:74S-6.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.

214
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Case Report
Postoperative tension pneumocephalus following cerebral aneurysm surgery in supine position without prior lumbar drainageChaitali Biswas, Saswata Bharati, Anirban Pal
Department of Anaesthesiology, CNMC, Kolkata, India
Corresponding author: Dr. Chaitali Biswas, 135, P K Guha Lane, Jora-Pukur, Dum Dum Cantt, Kolkata - 700 028, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_74_11R6 AP Done 27th Jan
AbstractThe occurrence of tension pneumocephalus in neurosurgeries done in the supine position is scarcely reported. We present a case of 57-year-old man who developed tension pneumocephalus postoperatively, following cerebral aneurysm surgery, in supine position, where lumbar drainage before clipping surgery was not done. The patient’s neurological status deteriorated rapidly, characterized by convulsion and unresponsiveness to external stimuli, 1 h following the uneventful surgery. Immediate computed tomography scan revealed bi-frontal tension pneumocephalus. Long duration of surgery and cerebrospinal fluid loss were assumed to be the causative factors. The patient was treated immediately with frontal drill hole evacuation for intracranial air, which saved the patient from a life threatening complication.
Key words: Cerebral aneurysm surgery, cerebrospinal fluid loss, tension pneumocephalus
IntroductIon
Pneumocephalus, characterized by air in the cranial cavity, is a common occurrence following posterior fossa craniotomies performed in a sitting position,[1,2] but development of tension pneumocephalus is uncommon. This severe complication puts the patient’s life at risk, by producing a mass effect and abnormal neurological signs, which requires immediate treatment. Few cases have been reported as a complication of head trauma, trans-spheniodal, spinal, cranial (posterior fossa, supratentorial) surgeries, or even after accidental dural puncture.[1-3]
However, tension pneumocephalus after neurosurgical procedure in the supine position and without prior lumbar puncture has been very scarcely reported.[4,5] We report a case, where an adult patient developed tension pneumocephalus in an immediate postoperative period, after surgical clipping of anterior communicating artery aneurysm, in the supine position, without prior lumbar drainage.
case report
A 57-year-old male patient, weighing 60 kg and 165 cm in hight, was referred to our institute with a past history of sudden onset severe headache, nuchal rigidity, and diplopia 15 days back. At the time of presentation, central nervous system examination revealed a conscious, oriented patient with normal higher function, without diplopia or neck rigidity. There was no loss of power in all four limbs, 4/5 in both the upper limbs, and 4/5 in both the lower limbs as per Medical Research Council (MRC) rating. His sensory system, other cranial nerves,
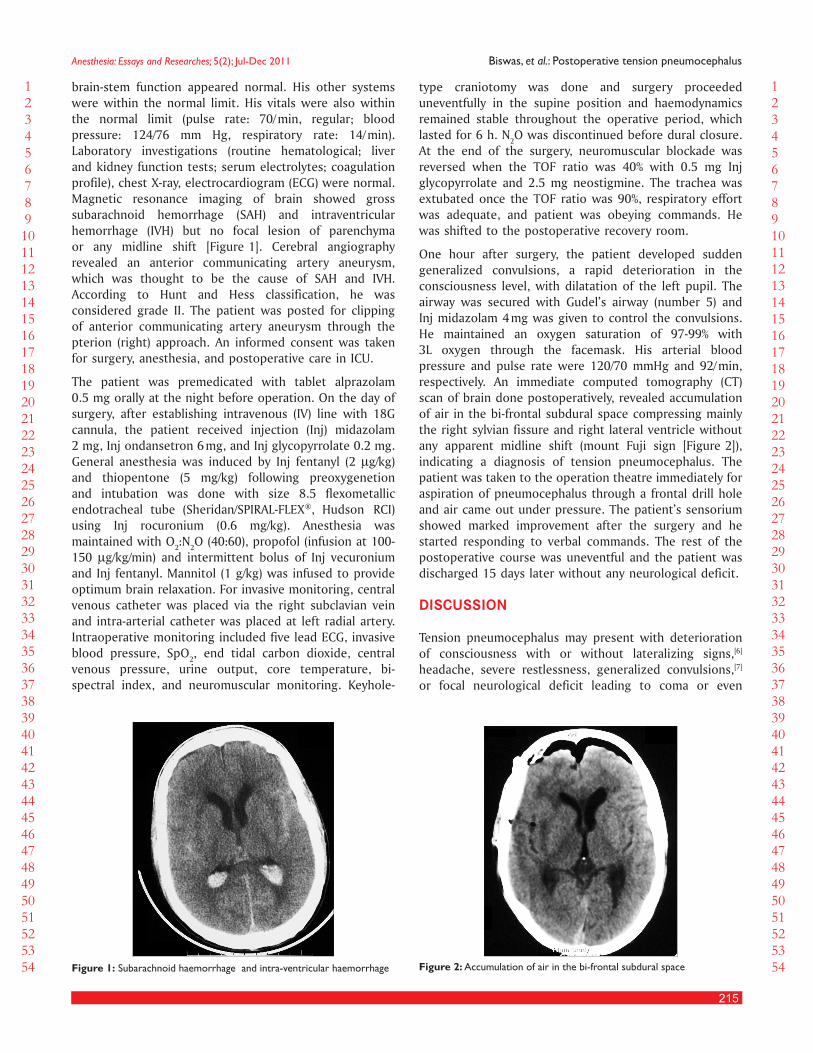
215
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Biswas, et al.: Postoperative tension pneumocephalus
brain-stem function appeared normal. His other systems were within the normal limit. His vitals were also within the normal limit (pulse rate: 70/ min, regular; blood pressure: 124/76 mm Hg, respiratory rate: 14/ min). Laboratory investigations (routine hematological; liver and kidney function tests; serum electrolytes; coagulation profile), chest X-ray, electrocardiogram (ECG) were normal. Magnetic resonance imaging of brain showed gross subarachnoid hemorrhage (SAH) and intraventricular hemorrhage (IVH) but no focal lesion of parenchyma or any midline shift [Figure 1]. Cerebral angiography revealed an anterior communicating artery aneurysm, which was thought to be the cause of SAH and IVH. According to Hunt and Hess classification, he was considered grade II. The patient was posted for clipping of anterior communicating artery aneurysm through the pterion (right) approach. An informed consent was taken for surgery, anesthesia, and postoperative care in ICU.
The patient was premedicated with tablet alprazolam 0.5 mg orally at the night before operation. On the day of surgery, after establishing intravenous (IV) line with 18G cannula, the patient received injection (Inj) midazolam 2 mg, Inj ondansetron 6 mg, and Inj glycopyrrolate 0.2 mg. General anesthesia was induced by Inj fentanyl (2 µg/ kg) and thiopentone (5 mg/kg) following preoxygenetion and intubation was done with size 8.5 flexometallic endotracheal tube (Sheridan/SPIRAL-FLEX®, Hudson RCI) using Inj rocuronium (0.6 mg/kg). Anesthesia was maintained with O2:N2O (40:60), propofol (infusion at 100-150 µg/kg/min) and intermittent bolus of Inj vecuronium and Inj fentanyl. Mannitol (1 g/kg) was infused to provide optimum brain relaxation. For invasive monitoring, central venous catheter was placed via the right subclavian vein and intra-arterial catheter was placed at left radial artery. Intraoperative monitoring included five lead ECG, invasive blood pressure, SpO2, end tidal carbon dioxide, central venous pressure, urine output, core temperature, bi-spectral index, and neuromuscular monitoring. Keyhole-
type craniotomy was done and surgery proceeded uneventfully in the supine position and haemodynamics remained stable throughout the operative period, which lasted for 6 h. N2O was discontinued before dural closure. At the end of the surgery, neuromuscular blockade was reversed when the TOF ratio was 40% with 0.5 mg Inj glycopyrrolate and 2.5 mg neostigmine. The trachea was extubated once the TOF ratio was 90%, respiratory effort was adequate, and patient was obeying commands. He was shifted to the postoperative recovery room.
One hour after surgery, the patient developed sudden generalized convulsions, a rapid deterioration in the consciousness level, with dilatation of the left pupil. The airway was secured with Gudel’s airway (number 5) and Inj midazolam 4 mg was given to control the convulsions. He maintained an oxygen saturation of 97-99% with 3L oxygen through the facemask. His arterial blood pressure and pulse rate were 120/70 mmHg and 92/ min, respectively. An immediate computed tomography (CT) scan of brain done postoperatively, revealed accumulation of air in the bi-frontal subdural space compressing mainly the right sylvian fissure and right lateral ventricle without any apparent midline shift (mount Fuji sign [Figure 2]), indicating a diagnosis of tension pneumocephalus. The patient was taken to the operation theatre immediately for aspiration of pneumocephalus through a frontal drill hole and air came out under pressure. The patient’s sensorium showed marked improvement after the surgery and he started responding to verbal commands. The rest of the postoperative course was uneventful and the patient was discharged 15 days later without any neurological deficit.
dIscussIon
Tension pneumocephalus may present with deterioration of consciousness with or without lateralizing signs,[6] headache, severe restlessness, generalized convulsions,[7] or focal neurological deficit leading to coma or even
Figure 1: Subarachnoid haemorrhage and intra-ventricular haemorrhage Figure 2: Accumulation of air in the bi-frontal subdural space

216
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Biswas, et al.: Postoperative tension pneumocephalus
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
cardiac arrest. It is always a life threatening condition. Several hypotheses have been implicated in the pathogenesis of tension pneumocephalus: They include nitrous oxide (N2O) anesthesia,[6,8,9] gross hydrocephalus, a functional ventriculo-peritoneal shunt, cerebrospinal fluid (CSF) leakage due to lumbar drainage, or dural rent after epidural anesthesia, dural defect creating one-way valve, factors that decrease the brain volume such as surgical decompression, intracranial dehydration, hyperventilation, duration of surgery.
Nitrous oxide has been held responsible in the pathogenesis of tension pneumocephalus by several authors,[6,8] particularly during sitting posture; although, its role has been questioned by others.[10,9] We believe that N2O played no significant role in our patient, as the patient deteriorated 1 h after completion of surgery, which was done in the supine position and N2O was stopped well before dural closure.
In gross hydrocephalus, a proportionately greater volume of CSF can be drained during surgery and this may suck air inside and can produce pneumocephalus. A functioning ventriculo-peritoneal shunt helps in continuous drainage of CSF in the peritoneal cavity creating space for intracranial air. Both factors were absent in our patient.
Continuous CSF leakage from lumbar puncture or dural rent during epidural anesthesia causes significant CSF loss creating negative pressure space, where air from positive pressure atmosphere rushes into the intracranial space via the dural defect causing tension pneumocephalus. Saito et al.[11] reported a case where tension pneumocephalus developed following lumbar drainage for cerebral aneurysm surgery. Lumbar drainage to facilitate brain retraction is not done routinely for aneurysm surgery in our institution.
Intracranial dehydration or hyperventilation result in a slack brain with the subsequent enlargement of the subdural space and is apt to increase the volume of entrapped intracranial air. These were not used in our patient, in fact, hyper-volemia and high-normal range of blood pressure was maintained to prevent cerebral ischemia (protection against potential vasospasm).
Prolong duration of surgery may lead to continuous CSF loss intraoperatively, which may be a causative factor. The
duration of surgery in our case was 6 h, so we assumed it might be a causative factor.
An adult patient developing tension pneumocephalus as a postoperative complication after clipping surgery for ruptured anterior communicating artery aneurysm in supine position without prior lumbar drainage is very rare. The present case helps us to conclude that efforts must be directed to minimize CSF loss during intracranial surgery and dura should be sutured water-tight during craniotomy closure, to prevent the development of tension pneumocephalus and once it has developed, immediate diagnosis and treatment are required to save the life of these patients.
reFerences
1. Toung TJ, McPherson RW, Ahn H, Donham RT, Alano J, Long D. Pneumocephalus: Effects of patient position on the incidence and location of aerocele after posterior fossa and upper cervical cord surgery. Anesth Analg 1986;65:65-70.
2. Di Lorenzo N, Caruso R, Floris R, Guerrisi V, Bozzao L, Fortuna A. Pneumocephalus and tension pneumocephalus after posterior fossa surgery in the sitting position: A prospective study. Acta Neurochir (Wien) 1986;83:112-5.
3. Gönül E, Yetişer S, Sirin S, Coşar A, Tasar M, Birkent H. Intraventricular traumatic tension pneumocephalus: A case report. Kulak Burun Bogaz Ihtis Derg 2007;17:231-4.
4. Prabhakar H, Bithal PK, Garg A. Tension pneumocephalus after craniotomy in supine position. J Neurosurg Anesthesiol 2003;15:278-81.
5. Demetriades AK, Pretorius P, Stacey R. Progressive tension pneumocephalus as a delayed postoperative complication in the absence of any obvious CSF leak. J Neurosurg Sci 2010;54:109-11.
6. Kitahata LM, Katz JD. Tension pneumocephalus after posterior fossa craniotomy, a complication of the sitting position. Anesthesiology 1976;44:448-50.
7. Dash HH, Bithal PK, Muley S, Vishnoi N, Saini SS, Tandon PN. Tension pneumocephalus following posterior fossa surgery in sitting position. J Anaesth Clin Pharmacol 1990;6:207-12.
8. Artru AA. Nitrous oxide plays a direct role in the development of tension pneumocephalus intraoperatively. Anesthesiology 1982;57:59-61.
9. Hernández-Palazón J, Martínez-Lage JF, de la Rosa-Carrillo VN, Tortosa JA, López F, Poza M. Anesthetic technique and development of pneumocephalus after posterior fossa surgery in the sitting position. Neurocirugia (Astur) 2003;14:216-21.
10. Friedman GA, Norfleet EA, Bedford RF. Discontinuance of nitrous oxide does not prevent tension pneumocephalus. Anesth Analg 1981;60:57-8.
11. Saito K, Inamasu J, Kuramae T, Nakatsukasa M, Kawamura F. Tension pneumocephalus as a complication of lumbar drainage for cerebral aneurysm surgery–case report. Neurol Med Chir (Tokyo) 2009;49:252-4.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.
217
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Case Report
Adrenal incidentaloma: Anesthetic management, the challenge and the outcomeReema M. Al-Hadhrami, Nehal Gahndour, Sherine Qudeera, Maher Moazin, Razan Nafakh
Departments of Anesthesia and Operating Theatres, and Urology, King Fahad Medical City, Riyadh, Kingdom of Saudia Arabia
Corresponding author: Dr. Reema M. Al-Hadhrami, Department of Anesthesia, King Fahad Medical City, Riyadh, Kingdom of Saudia Arabia. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_65_11R3
AbstractAdrenal incidentalomas is a term increasingly used now and applied to any adrenal mass that is found incidentally on an imaging of a patient with complaints not related to adrenal pathology. This case report presents a patient with incidental adrenal mass that was evaluated according to proposed recommendations and planned for robotic-assisted laparoscopic adrenalectomy. There is increasing number of literatures on the advantages of robotic surgery for adrenal resection; however, there is controversy regarding the hemodynamic stability of patients during these procedures especially with patient suspected to have pheochromocytoma. We included literature reviews on the role of robotics and use of laparoscopy for adrenalectomy and the anesthetic considerations in these procedures aiming to raise awareness and draw attention to this increasingly emerging disease entity.
Key words: Adrenalectomy, incidentalomas, laparoscopic, pheochromocytoma, robotic
IntroductIon
Adrenal incidentaloma is a term applied to an incidentally discovered adrenal mass on imaging performed for reasons unrelated to adrenal pathology.[1] Its prevalence is rising because of the big volume of radiologic explorations that are done every day. Its frequency in United States is estimated to be 2-9% of autopsies and 1-10% of CT scans and MRIs detect masses of 5 mm or more.[2] It was reported in one study that the overall prevalence of adrenal lesions among the contemporary CT scans with high
resolution was 4.4%, and that of benign adrenal masses was 4.2%.[3] They are a cluster of different pathologies, the majority of which are benign and nonfunctioning adrenal adenomas. However, mild hormonal alterations as well as metabolic abnormalities may be present in patients with adrenal incidentalomas. Thus, multidisciplinary approach with biochemical and radiologic evaluation is needed to characterize lesions and identify patient at high risk for hormonal or malignant evolution.[4]
Laparoscopic adrenalectomy has become the standard approach in the management of adrenal mass. This technique is minimally invasive and has the advantage of decreasing convalesces, less postoperative pain, and blood loss with improved cosmesis. Robotic-assisted laparoscopic adrenalectomy has been emerging as another modality less than a decade ago, and it is gaining increased acceptance among urologic community but it has been questioned concerning increased morbidity and negative hemodynamic sequelae especially in the management of pheochromocytoma.

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
218
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Al-Hadhrami, et al.: Adrenal incidentaloma: Anesthetic management, the challenge and the outcome
In this case, patient presented with incidental adrenal mass that was considered nonfunctioning adrenal tumor and she was scheduled for Robotic adrenalectomy but she developed hypertensive crisis intraoperatively and surgery was converted into open adrenalectomy and patient was stabilized till end of operation. This case serves to emphasize the importance of being well prepared for such unexpected occurrences and the need for good communication and collaboration between urologic surgeons, endocrinologists, and the anesthesiologist in the management of adrenal incidentalomas. As well as to give highlights on the advantages and drawbacks of using robotic surgery.
case report
A female, 54 years of age, presented with complaint of vague abdominal pain with nausea and general fatigue, was found incidentally to have right adrenal mass on ultrasonography. CT scan of abdomen confirmed the presence of the mass and laboratory studies were done and it was normal as shown in Table 1 and 2. Patient had no history of hypertension, diabetes, or symptoms of catecholamine excess secretion and the mass considered nonfunctioning and patient was scheduled for robotic-assisted laparoscopic adrenalectomy.
PreoperativeHistoryShe had no history of hypertension, diabetes or cardiovascular disease, had no allergies and not taking any regular medications.
Physical examinationOn examination patient was conscious, comfortable, looks quite obese (body weight 91.3 kg, BMI: 36.5), vital signs were normal. Preoperative evaluation of ASA is classified as 1, airway assessment of Mallampati 2, and good mouth opening with appropriate neck motion. Cardiovascular and respiratory are clinically free and rest of examination is unremarkable.
ElectrocardiogramShowed evidence of RBBB that considered insignificant.
Laboratory investigationsIncluded biochemical and initial hormonal studies with complete blood count, results were within normal or not conclusive.
ImagingCT abdomen reported large poorly defined lesion, homogenous, enhanced on the right suprarenal gland measuring (8.9 × 7.4 × 6 cm), compressing inferior surface of liver and upper pole of right kidney [Figure 1].
Reviewing the preoperative vital signs chart of the patient since admission confirmed that the patient had
Figure 1: CT abdomen reported large poorly defined lesion, homogenous, enhanced on the right suprarenal gland measuring (8.9 × 7.4 × 6 cm), compressing inferior surface of liver and upper pole of right kidney
Table 1: Preoperative biochemical and hormonal tests resultsBiochemistry tests Result Reference valuesSodium, plasma 139 mmol/L 135-145 mmol/L
Potassium, plasma 4.2 mmol/L 3.6-5.2 mmol/L
Chloride, plasma 106 mmol/L 98-107 mmol/L
Creatinine, plasma 71 umol/L 53-88 umol/L
Urea, plasma 3.8 mmol/L 2.5-6.4 mmol/L
Bicarbonate, plasma 31.1 mmol/L 21-32 mmol/L
Cortisol, serum 282.7 nmol/L 64-327 nmol/L
24 h urine cortisol 227 nmol/L 88-671 nmol/L
ACTH, plasma 8.9 pmol/L 0-13.3 pmol/L
Aldosterone, serum 73 pmol/L 105-861 pmol/L
DHEA-s, serum 1.17 umol/L 1-11.7 umol/L
Progesterone 17OH, serum 0.5 nmol/L 0-10 nmol/L
Normetanephrine, blood 24.14 nmol/L <0.44 nmol/L
Metanephrine, blood 0.25 nmol/L <0.37 nmol/L
24 h urine normetanephrine 34404 nmol/24 h 300-2200 nmol/24 h
24 h urine metanephrine 275 nmol/24 h 200-1500 nmol/24 h
24 h urine 3-ortho methyldopamine
728 nmol/24 h 200-1400 nmol/24 h
N.B: Tests of blood and total urine catecholamines were sent to laboratory outside the hospital due to unavailability of these tests in the hospital, and the results were not available till 19 days after sample sent and 12 days after the procedure. There was no request for repeating these investigations intraoperatively or postoperatively
Table 2: Complete blood count resultComplete blood count Result Reference valuesWBC 7.36 × 10.e9/L (4-11)
RBC 5.12 ×10.e12 (4.2-5.5)
HGB 15.4 g/dl (12-16)
HCT 45% (37-47)
MCV 87.9 fl (80-94)
MCH 30 pg (27-32)
MCHC 34 g/dl (32-36)
RDW 11.4 % (11.5-14.5)
Platelet count 183 × 10.e9/L (140-450)
MPV 9.43 fl (7.2-11.1) WBC: White blood cells, RBC: Red blood cells, HGB: Hemoglobin, HCT: Hematocrit, MCV: Mean corpuscular volume, MCH: Mean corpuscular hemoglobin, MCHC: Mean corpuscular hemoglobin concentration, RDW: Red cell distribution width, MPV: Mean plasma volume.
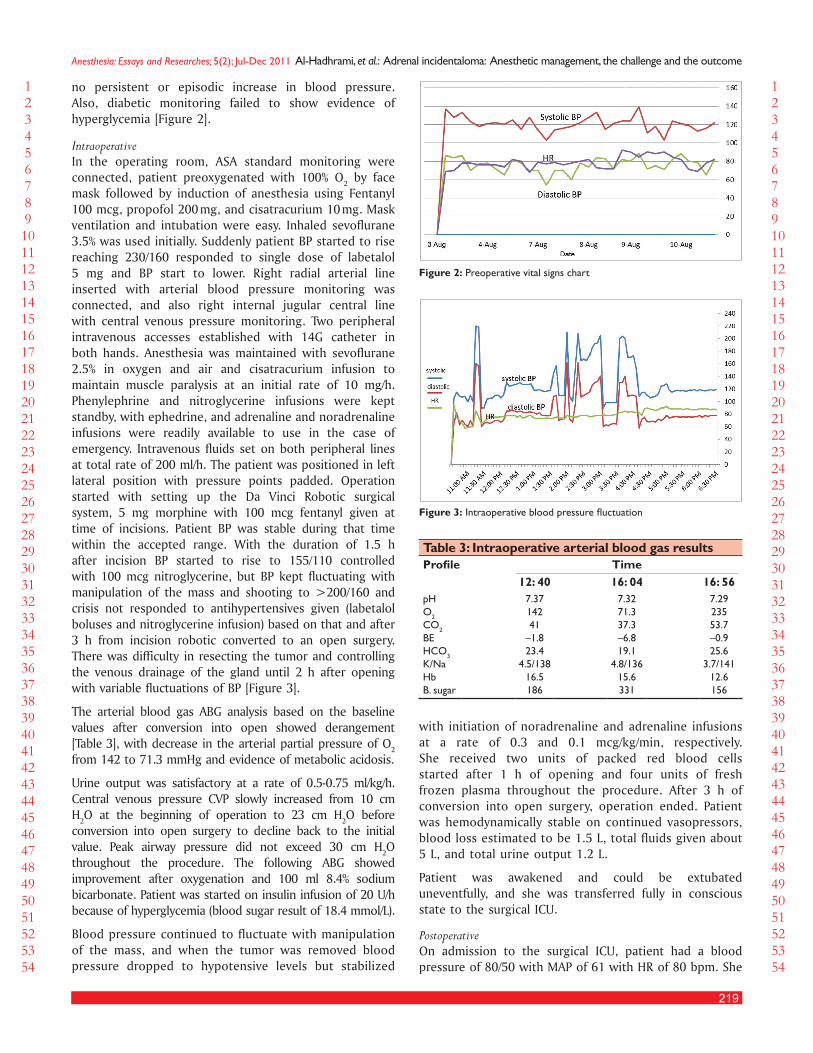
219
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Al-Hadhrami, et al.: Adrenal incidentaloma: Anesthetic management, the challenge and the outcome
no persistent or episodic increase in blood pressure. Also, diabetic monitoring failed to show evidence of hyperglycemia [Figure 2].
IntraoperativeIn the operating room, ASA standard monitoring were connected, patient preoxygenated with 100% O2 by face mask followed by induction of anesthesia using Fentanyl 100 mcg, propofol 200 mg, and cisatracurium 10 mg. Mask ventilation and intubation were easy. Inhaled sevoflurane 3.5% was used initially. Suddenly patient BP started to rise reaching 230/160 responded to single dose of labetalol 5 mg and BP start to lower. Right radial arterial line inserted with arterial blood pressure monitoring was connected, and also right internal jugular central line with central venous pressure monitoring. Two peripheral intravenous accesses established with 14G catheter in both hands. Anesthesia was maintained with sevoflurane 2.5% in oxygen and air and cisatracurium infusion to maintain muscle paralysis at an initial rate of 10 mg/h. Phenylephrine and nitroglycerine infusions were kept standby, with ephedrine, and adrenaline and noradrenaline infusions were readily available to use in the case of emergency. Intravenous fluids set on both peripheral lines at total rate of 200 ml/h. The patient was positioned in left lateral position with pressure points padded. Operation started with setting up the Da Vinci Robotic surgical system, 5 mg morphine with 100 mcg fentanyl given at time of incisions. Patient BP was stable during that time within the accepted range. With the duration of 1.5 h after incision BP started to rise to 155/110 controlled with 100 mcg nitroglycerine, but BP kept fluctuating with manipulation of the mass and shooting to >200/160 and crisis not responded to antihypertensives given (labetalol boluses and nitroglycerine infusion) based on that and after 3 h from incision robotic converted to an open surgery. There was difficulty in resecting the tumor and controlling the venous drainage of the gland until 2 h after opening with variable fluctuations of BP [Figure 3].
The arterial blood gas ABG analysis based on the baseline values after conversion into open showed derangement [Table 3], with decrease in the arterial partial pressure of O2 from 142 to 71.3 mmHg and evidence of metabolic acidosis.
Urine output was satisfactory at a rate of 0.5-0.75 ml/kg/h. Central venous pressure CVP slowly increased from 10 cm H2O at the beginning of operation to 23 cm H2O before conversion into open surgery to decline back to the initial value. Peak airway pressure did not exceed 30 cm H2O throughout the procedure. The following ABG showed improvement after oxygenation and 100 ml 8.4% sodium bicarbonate. Patient was started on insulin infusion of 20 U/h because of hyperglycemia (blood sugar result of 18.4 mmol/L).
Blood pressure continued to fluctuate with manipulation of the mass, and when the tumor was removed blood pressure dropped to hypotensive levels but stabilized
Figure 3: Intraoperative blood pressure fluctuation
Table 3: Intraoperative arterial blood gas resultsTimeProfile
16: 5616: 0412: 407.2923553.7–0.925.6
3.7/14112.6156
7.3271.337.3–6.819.1
4.8/13615.6331
7.3714241
–1.823.4
4.5/13816.5186
pHO2
CO2
BEHCO3
K/NaHbB. sugar
Figure 2: Preoperative vital signs chart
with initiation of noradrenaline and adrenaline infusions at a rate of 0.3 and 0.1 mcg/kg/min, respectively. She received two units of packed red blood cells started after 1 h of opening and four units of fresh frozen plasma throughout the procedure. After 3 h of conversion into open surgery, operation ended. Patient was hemodynamically stable on continued vasopressors, blood loss estimated to be 1.5 L, total fluids given about 5 L, and total urine output 1.2 L.
Patient was awakened and could be extubated uneventfully, and she was transferred fully in conscious state to the surgical ICU.
PostoperativeOn admission to the surgical ICU, patient had a blood pressure of 80/50 with MAP of 61 with HR of 80 bpm. She

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
220
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Al-Hadhrami, et al.: Adrenal incidentaloma: Anesthetic management, the challenge and the outcome
was kept on vasopressors (noradrenaline and adrenaline 0.2-0.15 mcg/kg/min, respectively). In addition, her blood pressure was maintained on the acceptable range. Eight hours later, she developed hypotension with BP of 70/50 and vasopressor doses doubled but BP not raised. It was noted that patient had bleeding in the drain estimated about 715 mL, with drop in the Hb of patient to 5.07 g/ dl, and decrease in the platelet count and prolonged coagulation profile, so resuscitation was started with blood transfusion (six units PRBC, six units platelets, ten units FFP). Intrabdominal bleeding was suspected but could not be confirmed due to unstable general condition of the patient. Patient’s general condition was stabilized with these conservative measures. Vasopressors could be withdrawn after 2 days and she was discharged from the ICU to the ward on fifth day postoperatively with good general condition.
The pathology report of the mass came back with a result confirming the mass as benign adrenocortical adenoma. Patient was discharged after 1 week of the procedure to be followed at the outpatient clinic.
dIscussIon
Adrenal incidentalomas are clinically silent adrenal masses that are discovered incidentally during diagnostic testing for clinical conditions unrelated to suspicion of adrenal disease.[5] Adrenal incidentalomas constitute an emerging clinical entity due to the increased use of abdominal imaging for diagnostic purposes. Most often, it consists of benign-nonfunctioning lesions. The two main concerns with regard to an adrenal incidentalomas are whether it is hormonally active or malignant.[6] These questions must be addressed when evaluating adrenal incidentalomas.
Although, in general, the majority of adrenal incidentalomas are nonhypersecretory adenomas, hormonal screening evaluation can reveal a significant number of cases of clinically unsuspected hormone-secreting adrenal tumors.[7] So a careful personal and family history, review of systems, and physical examination should be performed in all patients.
Screening for pheochromocytoma is mandatory in all cases because of this condition’s high rates of morbidity and mortality, as well as because of its unpredictable course. It is completely asymptomatic in up to 15% of cases.[8]
The adrenal tumor size has been used to differentiate between benign and malignant adrenal masses. Risk of malignancy increases with the adrenal tumor size, cutoff values ranging from 4 to 6 cm have been proposed by different clinicians for surgical resection of adrenal masses.[9]
Nowadays, the role of surgery in the treatment of adrenal incidentalomas, considering their biologic behavior, is still debated. Surgery is mandatory in cases
of hyperfunctioning adrenal masses, in the presence of suspect radiological malignancy, and when the maximum diameter is 4 cm or more.[10]
Laparoscopic adrenal surgery has significantly improved during the last years. Thus, at the moment it is possible to define such technique as the therapeutic “gold standard” option in the treatment of the adrenal tumors. However, some doubts are still remaining concerning the feasibility of laparoscopic adrenalectomy in the case of malignant adrenal tumors, hyper-vascular tumors (pheochromocytoma), and indeterminate incidentaloma.[11]
In recent years, as robotic surgery has become more prevalent, the indications for its use have come to encompass a wider variety of procedures, including adrenalectomy. The first robotic adrenalectomy in a human was reported in 2001 by Horgan and Vanuno among series of 34 robotic-assisted general surgery procedures.[12]
Opera tive time is commonly longer in robotic trials due to being performed prior understanding the efficient sys-tem setup. System docking times have been reported to be up to 35 min, but with experienced teams, docking should be completed in about 5 min .[13]
Surveys of robotic general surgeons are limited due to the small numbers of high volume users, but most surgeons feel that the learning curve of surgical robotics in general surgery is mainly due to the setup and docking of the system.
The reported conversion rates of robotic surgery to standard laparoscopy in most of the studies reviewed is very low or absent.
Brunaud et al.,[14] suggest that robotic adrenalectomy evaluation should be performed to minimize learning curve effects. Even when using a robotic system, several factors remain important in determining operative time (side, experience, and assistant’s skill). Difficult patients (obese patients and/or those with large tumor) seem to be good candidates of unilateral robotic adrenalectomy. Other potential advantages that still need to be evaluated are perioperative hemodynamic modifications in patients with pheochromocytoma and ergonomics for the surgeon.
The use of robots in surgery is likely to increase because of enhanced precision and control. Anesthesiologists need to be aware of this fast-changing field and how it affects anesthetic techniques and their delivery. As surgeons gain expertise with robotically assisted surgery, operative times are expected to decrease dramatically to the point of traditional open surgery. The inability to move the patient while the robot is engaged with the patient is a challenge when attempting to alter cardiac filling pressures by gravity, causing pharmacologic agents to be used more often. Anesthesiologists have experienced working in locations that are remote from the patient’s airway. It should come as no surprise that robotically

221
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Al-Hadhrami, et al.: Adrenal incidentaloma: Anesthetic management, the challenge and the outcome
assisted surgery of the upper body also presents that challenge. Improved monitoring methods are needed to make remote anesthesia safe and practical. Perhaps the “minimally invasive” revolution will advocate earlier patient recovery and the increased implementation of regional anesthetic techniques. The extent of the surgical stress response may be attenuated, ultimately minimizing the inflammatory response.[15]
Robotics is increasingly used in the urological procedure; as adrenal masses findings are raising with increasing volume of radiological imaging there is raising orientation toward treating these tumors with the robotic approach. It is considered that adrenal surgery should be performed by the urologist, because it is the medical specialty that knows the best this anatomical region.[16]
The anesthetic considerations applied for laparoscopic surgery are also applied for robotic-assisted cases with added special consideration to the use of robotic during procedure. There is no certain published anesthetic approach in managing patients with adrenal incidentalomas that can be applied to all patient, most of the patients have clinical pictures that cannot be attributed solely to the adrenal pathology until imaging findings suggest the mass to be the cause for the presentation of the patient.
With the age range patients present with adrenal incidentalomas, it is not unusual for these patients to have co-morbidities such as hypertension and/or diabetes mellitus. This usually presents a challenge to the anesthetist regarding how to best manage these patients preoperatively and perioperatively, and the conflicting issue is when some patients are totally asymptomatic and have no symptoms or signs of adrenal dysfunction whether to manage them as nonfunctioning tumor especially with normal biochemical studies or to manage them as probable suspected pathology such as Cushing’s disease or pheochromocytoma.
The preoperative assessment is usually the standard assessment with special attention to the history and physical signs of the patient regarding symptoms and signs of cortisol or catecholamines excess secretion. The biochemical studies are of paramount importance to decide if the tumor is functioning or not that has an implication on the anesthetic plan of the patient. Endocrinologists must be incorporated in the management of these patients. Patients with hypertension suspected to be secondary to pheochromocytoma should be treated and premedicated with alpha blockers.
The conduct of anesthesia in robotic surgery is with standard induction and airway control with the tracheal tube. Full routine monitoring including core temperature measurement should be applied. The arterial line or central access is not mandatory, unless patient has co-
morbidities. A large bore cannula is usual as establishing further i.v. access once the procedure has started is difficult. As the procedure may be prolonged, it is sensible to use a volatile agent for maintenance with a favorable recovery profile, for example, desflurane or sevoflurane. Many institutions choose to run a background infusion of remifentanil. The patient must remain paralyzed until the robot is undocked at the end of the procedure, usually with a continuous infusion of a nondepolarizing neuromuscular blocking agent. It is important that the anesthetist is especially rigorous in ensuring that there is no pressure in vulnerable areas, especially the elbows, axilla, back, and shoulders.[17]
The position of the tracheal tube should be checked regularly. There are reports of airway obstruction during insufflation of the pneumoperitoneum, secondary to tracheal tube migration resulting from physical movement of the diaphragm and mediastinum by the pneumoperitoneum. The physiological effects of pneumoperitoneum are numerous and can be severe. It is not uncommon for the patient to experience cardiovascular instability and hypoxaemia on carbon dioxide insufflation of the peritoneum and it is important to exclude other causes such as tracheal tube migration. If the patient remains haemodynamically unstable or hypoxaemia is resistant to application of PEEP, the operation may have to be abandoned or converted to an open procedure. End-tidal carbon dioxide should be maintained at normal levels to reduce the risk of further potentially catastrophic increases in cerebral blood volume and intracranial pressure.[17]
The robot itself introduces complexities that must be considered. It is an extremely heavy and bulky piece of equipment. The theatre can become very cramped with the addition of the surgical console, video tower, and robot cart. The arrangement of the equipment should be established and practiced in advance at institutions using a robot for the first time.[17]
When the robot is docked in position and the instrument and camera inserted through the laparoscopic ports, the robotic arms have little natural elasticity. Therefore, it is critical that the patient remains absolutely still, otherwise tearing could occur at the laparoscopic port sites. The table position must not be moved under any circumstances unless the surgical instruments are disengaged. In addition, patient coughing could cause serious injury and must be avoided with continuous muscle relaxation.[17]
Finally, the bulk of the robot is positioned over the abdomen and chest. Although the incidence of airway or serious cardiovascular events are no greater in robot-assisted surgery, if they do occur, the position of the robot will interfere with effective cardiopulmonary resuscitation and airway interventions. The theatre team

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
222
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Al-Hadhrami, et al.: Adrenal incidentaloma: Anesthetic management, the challenge and the outcome
should practice and be familiar with an emergency drill for the removal of the robotic cart.[17]
The successful use of the robot to assist in surgery depends upon excellent communication between all members of the theatre team. The surgeon sits behind a console, away from the site of operation, but must communicate effectively with both anesthetic staff and his operative assistant at the patients’ bedside. The loss of eye contact can have a dramatic effect on the quality of communication and special care must be taken to ensure that transfer of information is precise and clear. This is aided by the addition of audio speakers to the video tower that transmit the operating surgeon’s voice.[17]
When the robot’s arms have been removed from the patient, neuromuscular block may be reversed.
The postoperative course is usually uneventful. The incidence of complications is low. Blood transfusion is not normally required as intraoperative blood loss is very low, but significant hemorrhage may be insidious and the patient should be carefully monitored in the immediate postoperative period. Multimodal analgesic agents including acetaminophen and nonsteroidal antiinflammatory drugs (if there are no contraindications) should be administered. A small percentage of patients require opioids.[17]
The patient presentation reported in this case can serve as template for the scheme of management of patients with adrenal incidentalomas. She was incidentally found to have adrenal mass and was asymptomatic with near normal biochemical and hormonal studies; her age is typical for the presentation of adrenal mass. Patient was considered obese with BMI of 36, the association between obesity and nonsecreting adrenal incidentalomas has never been proven, but it is demonstrated in one study[18] a strong association between obesity and incidentally discovered nonfunctioning adrenal masses.
Although a study reported that patients with nonfunctioning adrenal incidentalomas exhibit higher fasting glucose with insulin resistance and dyslipidemia as part of the metabolic syndrome,[19] this patient had nearly normal blood glucose and diabetic monitoring did not show results of high blood sugar necessitating insulin administration. However, intraoperatively she developed hyperglycemia and needed insulin infusion to control it and this could be part of stress response and glycogenolysis or due to release of cortisol hormones from the mass during manipulation.
This patient did not receive any antihypertensives as preoperative medications because she had no hypertension or symptoms of catecholamine secretion, and her biochemical tests and hormonal results did not give any clue that this patient could have secreting mass. In spite of that the intraoperative plan takes into account
the high possibility of occurrence of hypertensive crisis and other events. For these reasons patient had the arterial and central line in place with emergency drugs ready and handy.
Patient with adrenal masses suspected to be pheochromocytoma represent the greatest challenge for the anesthetist in the perioperative management. There have been several studies on how to best manage these patients with various anesthetic techniques. However, manipulation of the tumor during open surgery, with its hemodynamic responses, may be inevitable but can usually be of short duration. Laparoscopic excision of pheochromocytoma requires persistent tissue traction and diathermy or ultrasound coagulation that may cause sustained hemodynamic consequences of at least the same severity as may be expected during open surgery, but for a rather longer period of time. Laparoscopic surgery may prove too difficult, requiring open surgery on the same occasion or subsequent.[20] Patient reported in this case showed severe hemodynamic instability with hypertensive crisis that risk the whole outcome of the procedure and increased its risk of morbidity. The decision to convert the robotic surgery into open was taken in this case to minimize the adverse outcome that could result from the prolonged operative time with the robotic manipulation and resection of the mass with the anticipated difficulty to ligate the venous drainage of the big adrenal mass. Patient was adversely affected hemodynamically and metabolically with the time consumed and the nature of the surgery adding to that the effect of hormones released with manipulation of the mass.
With vigilant efforts and vigorous attempts patient could be stabilized till end of procedure and successfully extubated and shifted on inotropes to the surgical ICU.
Although this patient’s tumor behaved as intraoperative pheochromocytoma excision, the preoperative laboratory studies did not give that impression with clinical presentation, the pitfall was the late catecholamine studies results that was sent outside the laboratory; based only on clinical presentation it was decided to proceed with the procedure. The results of catecholamines came late supporting the diagnosis of secreting adrenal mass that could be a pheochromocytoma, but the postoperative pathological diagnosis supports the finding of adrenocortical adenoma that is the most common pathological finding among adrenal incidentalomas.
In conclusion, incidental adrenal masses will continue to rise demanding the need to establish a protocol approaching these patients to reach the optimum outcome in managing adrenal incidentalomas. It is mandatory that the endocrinologist as well as the urologist and anesthesiologist reach an understanding of the nature and pathophysiology of the adrenal incidentalomas and be incorporated in taking the decisions as how best to

223
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Al-Hadhrami, et al.: Adrenal incidentaloma: Anesthetic management, the challenge and the outcome
manage such patients and tailored the plan according to the patient’s situation. It can be implied here in this case report that the tumor size should not be the primary factor in determining the adrenalectomy approach with robotic assistance. In this case, robotic surgery appeared to be unsafe for the patient individual situation and ineffective in resecting the mass with increase in the operative time and risk of the mortality and morbidity. We suggest further prospective or case control studies regarding the use of robotics in urological or other specialized procedures and to monitor the hemodynamic response during these procedures.
reFerences
1. Singh PK, Buch HN. Adrenal incidentaloma: Evaluation and management. J Clin Pathol - 2008;61:1168-73.
2. Griffing GT, Adrenal adenoma, St Louis School od Medicine, emedicine endocrinology, medscape [116587] Aug 17, 2009. Available from: http://emedicine.medscape.com (Last updated on 2011 Sep 22, Cited on 2011 Aug).
3. Bovio S, Cataldi A, Reimondo G, Sperone P, Novello S, Berruti A, et al. Prevalence of adrenal incidentalomas in a contemporary computerized tomography series. J Endocrinol Invest 2006;29:298-302.
4. Anagnostis P, Karagiannis A, Tziomalos K, Kakafika AI, Athyros VG, Mikhailidis DP. Adrenal incidentaloma: A diagnostic challenge, Hormones (Athens) 2009;8:163-84.
5. Moreno-Fernández J, García-Manzanares A, Sánchez-Covisa MA, García EI. Clinical management of adrenal incidentalomas: Results of a survey, Endocrinol Nutr 2009;56:447-51.
6. Rosoff JS, Otto BJ, Del Pizzo JJ. The emerging role of robotics in adrenal surgery, Curr Urol Rep 2010;11:38-43.
7. Arnaldi G, Masini AM, Giacchetti G, Taccaliti A, Faloia E, Mantero F . Adrenal incidentalomas. Braz J Med Biol Res 2000;33:1177-89.
8. Gopan T, Remer E, Hamrahian AH. Evaluating and managing adrenal incidentalomas. Cleve Clin J Med 2006;73:561-8.
9. Ioachimescu AG, Hamrahian AH. Diseases of the Adrenal Gland-Syndromes of adrenal hyperfunction, Adrenal Incidentaloma, Cleveland Clinic: Current Clinical Medicine, 2nd ed, New York: Elsevier; 2010. p. 338-48.
10. Guerrieri M, De Sanctis A, Crosta F, Arnaldi G, Boscaro M, Lezoche G, et al. Adrenal incidentaloma: Surgical update, J Endocrinol Invest 2007;30:200-4.
11. Bergamini C, Prosperi P, Bruscino A, Leahu A, Bargellini T, Poma A, et al. Update on the laparoscopic adrenal surgery in the second decade of the century: Doubts no more?, G Chir 2010;31:328-31.
12. Horgan S, Vanuno D. Robots in laparoscopic surgery. J Laparoendosc Adv Surg Tech A 2001;11:415-9.
13. Wilson EB. Evolution of robotic general surgery. Scand J Surg 2009;98:125-9.14. Brunaud L, Bresler L, Ayav A, Zarnegar R, Raphoz AL, Levan T, et al.,
Robotic-assisted adrenalectomy: What advantages compared to lateral transperitoneal laparoscopic adrenalectomy? Am J Surg 2008;195:433-8.
15. Goswami S, Nishanian E, Mets B. Anesthesia for robotic surgery. 7th ed. Chapter 76. Miller's Anesthesia. NewYork: Churchil Livingstone; 2009.
16. Hevia Suárez M, Abascal Junquera JM, Boix P, Dieguez M, Delgado E, Abascal García JM, et al. Management of adrenal mass: What urologists should know?, Actas Urol Esp 2010;34:586-91.
17. Irvine M, Patil V. Anesthesia for robot assisted laparoscopic surgery, continuing education in anaesthesia. Critical Care and Pain Advance Access, London Oxford University Press; 2009.
18. Kolańska K, Owecki M, Nikisch E, Sowinski J. High prevalence of obesity in patients with non-functioning adrenal incidentalomas. Neuro Endocrinol Lett 2010;31:418-22.
19. Peppa M, Boutati E, Koliaki C, Papaefstathiou N, Garoflos E, Economopoulos T, et al., Insulin resistance and metabolic syndrome in patients with nonfunctioning adrenal incidentalomas: A cause-effect relationship? Metabolism 2010;59:1435-41.
20. Prys-Roberts C. pheochromocytoma: recent progress in its management. Br J Anesth 2000;85:44-57.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
224
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Case Report
Dexmedetomidine and fentanyl combination for procedural sedation in a case of Duchenne muscular dystrophyAshish Kulshrestha, Sukhminder Jit Singh Bajwa, Amarjit Singh, Vinod Kapoor1
Department of Anaesthesiology and Intensive Care, GianSagar Medical College and Hospital, Ram Nagar, Banur, 1Department of Oral and Maxillo-facial Surgery, Gian Sagar Dental College and Hospital, Ram Nagar, Banur, Punjab, India
Corresponding author: Dr. Sukhminder Jit Singh Bajwa, Department of Anaesthesiology and Intensive Care, Gian Sagar Medical College and Hospital, Ram Nagar, Banur, Punjab, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_96_11R7 They are fine please go ahead with printing.
AbstractDuchenne muscular dystrophy, an X-linked disorder characterized by progressive muscle weakness, is the most common muscular dystrophy among children leading to death before the end of third decade. Anesthesia in such patients pose a great challenge due to various complications associated with it. The dreaded metabolic and clinical complications occur due to various inhalational anesthetics and succinylcholine in this subset of patients. We are reporting a child with diagnosed Duchenne muscular dystrophy who underwent excision of dentigerous cyst in oral cavity under procedural sedation with combination of dexmedetomidine and fentanyl and thus administration of general anesthesia was avoided.
Key words: Anesthesia, dexmedetomidine, duchenne muscular dystrophy, procedural sedation
IntroductIon
Neuromuscular diseases and muscular dystrophies have always been challenging to the attending anesthesiologist whenever such patients present for surgery. These disorders are invariably associated with various co-morbid diseases that further heighten the degree of difficulty for the concerned anesthesiologist. Duchenne muscular dystrophy is one of the most common muscular dystrophy in children with an incidence of 1 in 3500 live births and is transmitted by X-linked inheritance.[1] The patients
invariably develop cardio respiratory complications during growth that can ultimately prove to be fatal. The affected children start developing the progressive degeneration of skeletal, cardiac, and smooth muscles as early as third year of life. Administration of anesthesia in such patients is associated with numerous challenges and can result in varied spectrum of metabolic and clinical complications such as rhabdomyolysis, metabolic derangements, malignant hyperthermia, cardiac arrhythmia and death. These adverse effects are usually associated with general anesthesia and the implicated pharmacological agents being succinylcholine and inhalational anesthetic agents. We are reporting a 12-year-old male child suffering from Duchenne muscular dystrophy who presented to the oral and maxillofacial department for possible excision of symptomatic and painful dentigerous cyst. The case was managed with a combination of dexmedetomidine and fentanyl for procedural sedation and thus avoided the need for general anesthesia by a thorough pre-operative counseling of the mother and the child.

225
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Kulshrestha, et al.: Dexmedetomidine-fentanyl in duchenne muscular dystrophy
case report
A 12-year-old boy presented to the oral and maxillofacial surgery department of our institution with swelling in lower jaw since 6 months, which progressively increased in size and was painful. It was diagnosed to be dentigerous cyst that required excision due to its painful symptomatology. He was an established case of Duchenne muscular dystrophy since childhood and was confined to wheel chair since then. The child had no history of recent upper respiratory tract infection or previous anesthetic exposures. On physical examination, the weight of the child was measured to be 48 kg and he had wasting of muscles in both the lower limbs with motor power of grade II. Airway examination revealed mouth opening of >3 cm with modified Mallampati grade of II, normal thyromental and mento-hyoid distance and normal range of neck movements [Figure 1]. Examination of the back revealed a mild scoliosis involving the thoraco-lumbar region with convexity toward the right side. Cardiovascular and respiratory system examination was unremarkable. The laboratory investigations were all within normal limits except for raised creatine kinase levels of 1823 IU/L (normal 75–230). The electrocardiography showed sinus tachycardia and biventricular hypertrophy and findings of echocardiography revealed an ejection fraction of 32% with moderate depression of the left ventricular systolic function. The child was planned for excision of dentigerous cyst. During the preoperative visit, the child and the parents were highly anxious about the procedure but after careful counseling and discussion of various implications and the risks associated with general anesthesia, the parents and the child agreed to undergo the procedure under procedural sedation. The child was given nil per oral instructions according to the standard protocol and was advised tab. ranitidine 150 mg PO and tab. metoclopramide 10 mg PO in the night and in the morning 2 h before the planned procedure. On the day of procedure, the anesthesia machine was properly
checked and flushed to remove any traces of inhalational agents and all vaporizers were removed. The child was shifted to the operating room and an intravenous line was secured and preloading done with 400 mL of the normal saline solution. The monitoring included five lead electrocardiography, noninvasive blood pressure (NIBP) and pulse oximetry. The child was then premedicated with glycopyrrolate 0.2 mg intravenously (IV) and fentanyl 1 µg/kg was given IV to achieve analgesia. Dexmedetomidine was administered slowly with a loading dose of 1 µg/kg over 15 min followed by a continuous infusion at 0.5 µg/kg/h throughout the surgical procedure. Lignocaine with 1 in 2 lakh adrenaline was used for local infiltration and the child was given supplemental oxygen through nasal prongs at 3 L/min. The child remained calm and comfortable throughout the procedure which lasted for 40 min and did not complain of any pain. At the end of procedure, the dexmedetomidine infusion was discontinued and the child remained sedated but arousable to verbal commands. Postoperatively, the child was observed in a high dependency unit for 2 h. The recovery period was uneventful and the child was discharged after 6 h when fully awake and responding.
dIscussIon
Duchenne Muscular Dystrophy is an X-linked, progressive neuromuscular disease affecting 1in 3500 live male births.[1] It is thought to occur due to mutation in dystrophin gene located on X chromosome leading to formation of abnormal or low levels of dystrophin protein that is an integral part of skeletal muscles, thus causing muscular weakness. Those affected usually dies before the end of third decade due to widespread involvement of respiratory and cardiac muscles.[2] These patients develop multisystem involvement leading to cardiomyopathy, decreased lung volumes, sleep apnoea, weak pharyngeal muscles, gastric hypo-motility, kyphoscoliosis and muscle contractures. These patients are highly prone to perioperative metabolic reactions and complications when they are exposed to nondepolarising muscle relaxants and/or inhalational anesthetic agents leading to rhabdo-myolysis and hyper-metabolic reactions resembling malignant hyperthermia.[3,4] In addition, these patients are also vulnerable to adverse effects of general anesthesia and procedural sedation for example upper airway obstruction due to macroglossia and weak upper airway dilator muscles, inability in maintaining patency of upper airway due to limited mobility of mandible and cervical spine and postoperative atelectasis and hypoxemia due to reduced functional residual capacity. Our patient had an established diagnosis of Duchenne muscular dystrophy since childhood and was restricted to wheel chair with the involvement of the cardiovascular system. As the procedure involved a common area for surgeons and anesthesiologist, that is, oral cavity, there was a dilemma so as how to administer general anesthesia and to secure the airway to Figure 1: Frontal view of the face showing the mouth opening and oral cavity

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
226
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Kulshrestha, et al.: Dexmedetomidine-fentanyl in duchenne muscular dystrophy
prevent complications associated with loss of airway and a possible risk of aspiration of blood. Considering the fatal complications of general anesthesia in such patients and after thorough discussion with the surgeons and the parents of the child, it was decided to perform the procedure under sedation. The requirements were calm and comfortable, spontaneously breathing patient who can maintain upper airway patency as well as preserved airway reflexes. Thus, dexmedetomidine and fentanyl were selected as preferred agents. There have been several reports in literature about successful use of dexmedetomidine in conjunction with ketamine, benzodiazepines and opioids.[5-8] However, there are no reports of any oral cavity procedures done under procedural sedation using dexmedetomidine. As co-operative and awake state was desired during surgical procedure, so ketamine was not chosen for this procedure as it would have diminished the consciousness level and an ability to maintain a continuous verbal contact with the patient. Moreover, administration of ketamine is associated with copious oral secretions and it would have interfered with a smooth surgical procedure. Dexmedetomidine, a potent α2-agonist, does not cause any respiratory depression, maintains airway reflexes, potentiates analgesia by other agents and induces arousable sleep thus invasive procedures can easily be performed even inside oral cavity. The sole use of dexmedetomidine have been found to have limited utility in procedural sedation in patients with Duchenne muscular dystrophy for painful invasive procedures and is recommended to use in conjunction with other drugs like benzodiazepines, opioids and ketamine.[9]
The surgical procedure was performed in this patient in accordance with the guidelines formulated by American College of Chest Physicians for successful management of patients with Duchenne muscular dystrophy undergoing general anesthesia or procedural sedation with the back-up facility of intensive care unit.[10]
In conclusion, this case report suggests that
dexmedetomidine can successfully be used for sedation in invasive procedures involving oral cavity due to its minimal respiratory depression, ability to maintain airway reflexes and stable hemodynamic parameters. However, a good preoperative consultation with the surgeon and proper counseling of patient and the parents is essential for a better co-operation of patient intraoperatively.
reFerences
1. Morris P. Duchenne muscular dystrophy: a challenge for the anaesthetist. Paediatr Anaesth1997;7:1-4.
2. Eagle M, Baudouin SV, Chandler C, Giddings DR, Bullock R, Bushby K. Survival in Duchenne muscular dystrophy: improvements in life expectancy since 1967 and the impact of home nocturnal ventilation.NeuromusculDisord 2002;12:926-9.
3. Keifer HM, Singer WD, Reynolds RN. Malignant hyperthermia in a child with Duchenne muscular dystrophy. Pediatrics 1983;71:118-9.
4. Kleopa KA, Rosenberg H, Heiman-Patterson T. Malignant hyperthermia-like episode in Becker muscular dystrophy. Anesthesiology 2000;93:1535-7.
5. Rozmiarek A, Corridore M, Tobias JD. Dexmedetomidine-ketamine sedation during bone marrow aspirate and biopsy in a patient with Duchenne muscular dystrophy. Saudi J Anaesth 2011;5:219-22.
6. McVey JD, Tobias JD. Dexmedetomidine and ketamine for sedation during spinal anesthesia in children. J ClinAnesth 2010;22:538-45.
7. Barton KP, Munoz R, Morell VO, Chrysostomou C. Dexmedetomidine as the primary sedative during invasive procedures in infants and toddlers with congenital heart disease. Pediatr Crit Care Med 2008;9:612-5.
8. Luscri N, Tobias JD. Monitored anesthesia care with a combination of ketamine and dexmedetomidine during magnetic resonance imaging in three children with trisomy 21 and obstructive sleep apnea. PediatrAnesth 2006;16:782-6.
9. Jalowiecki P, Rudner R, Gonciarz M, Kawecki P, Petelenz M, Dziurdzik P. Sole use of dexmedetomidine has limited utility for conscious sedation during outpatient colonoscopy. Anesthesiology 2005;103:269-73.
10. Brinkrant DJ, Panitch HB, Benditt JO, Boitano LJ, Carter ER, Cwik VA, et al. American College of Chest Physicians consensus statement on the respiratory and related management of patients with Duchenne muscular dystrophy undergoing anesthesia or sedation. Chest 2007;132:1977-86.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.

227
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Case Report
Amniotic fluid embolism: A diagnostic dilemmaAshish Kulshrestha, Megha Mathur1
Department of Anaesthesia and Intensive Care GianSagar Medical College and Hospital, Ram Nagar, Banur, Patiala, Punjab, 1Department of Obstetrics and Gynecology, Govt. Medical College and Hospital, Chandigarh, India
Corresponding author: Dr. Ashish Kulshrestha, H.No.401/GH-18, Sector-5, Mansa Devi Complex, Panchkula, Haryana, India. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_82_11R4
AbstractAmniotic fluid embolism (AFE) is a rare obstetric catastrophe with an incidence of 7.7 per 100 000 deliveries and mortality as high as 60% to 80%. We describe a case of perioperative cardiac arrest in a young parturient undergoing an emergent cesarean section. Just after delivery of live healthy male baby, patient developed disseminated intravascular coagulation not responding to resuscitation with fluids and blood products. Her autopsy revealed edematous lungs with amniotic fluid debris within pulmonary vessels thus establishing the diagnosis of AFE. Amniotic fluid embolism is life threatening and difficult to predict or prevent condition, which should be always be kept in mind in a parturient with sudden cardiovascular collapse, so that resuscitation commences immediately, as early intervention is essential for a positive outcome.
Key words: Amniotic fluid embolism, asystole, cesarean section, disseminated intravascular coagulation, fibrin-degradation products
INTRODUCTION
Amniotic fluid embolism (AFE) is a rare catastrophe with an estimated frequency of approximately 7.7 per 100 000 deliveries.[1] This condition was originally described in 1941 by Steiner and Luschbaugh with evidence of fetal debris in pulmonary circulation in pregnant women.[2] Recently, a more descriptive term was suggested as “the anaphylactoid syndrome of pregnancy.”[3,4] This is a rare but important cause of peripartum death in the United States making up for 10% of all maternal deaths with an overall mortality rate as high as 60% to 80%.[1] More than 50% of patients die within first hour and about two-third
within 5 hour of the event with high incidence of severe and permanent neurological damage among survivors. We report a parturient who had cardiac arrest during emergency cesarean section culminating in disseminated intravascular coagulation (DIC).
Case RepORT
A 37-years old third gravida female presented with history of leaking per vaginum since 1 day and was admitted for further observation and management. She had regular antenatal checkups in the institution with no history of raised blood pressure anytime in the antenatal period and had uneventful previous two normal deliveries. She denied associated co-morbid illnesses or any allergies. Her obstetrical examination revealed a gestation period of 37 weeks and 3 days with vertex presentation and premature rupture of membranes. The patient was hospitalized and fetal monitoring established. She started having true labor pains 3h after admission along with the development of tachypnea and audible wheeze for which she was given
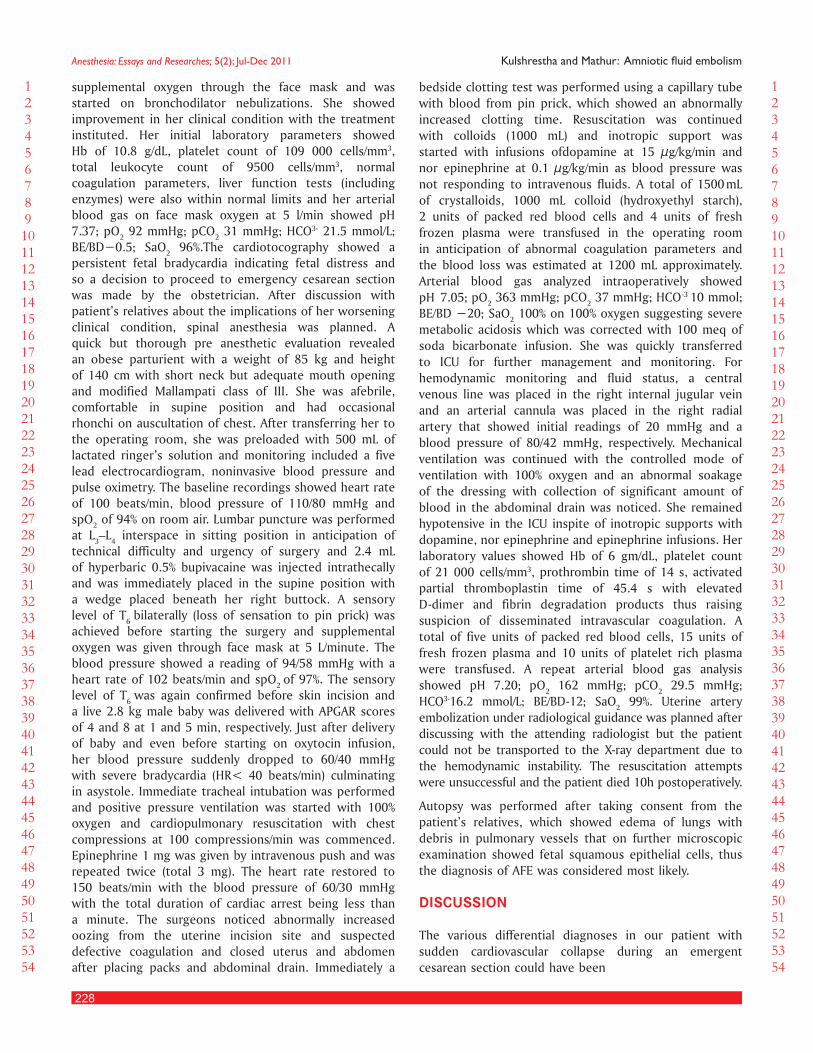
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
228
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 KulshresthaandMathur:Amnioticfluidembolism
supplemental oxygen through the face mask and was started on bronchodilator nebulizations. She showed improvement in her clinical condition with the treatment instituted. Her initial laboratory parameters showed Hb of 10.8 g/dL, platelet count of 109 000 cells/mm3, total leukocyte count of 9500 cells/mm3, normal coagulation parameters, liver function tests (including enzymes) were also within normal limits and her arterial blood gas on face mask oxygen at 5 l/min showed pH 7.37; pO2 92 mmHg; pCO2 31 mmHg; HCO3- 21.5 mmol/L; BE/BD−0.5; SaO2 96%.The cardiotocography showed a persistent fetal bradycardia indicating fetal distress and so a decision to proceed to emergency cesarean section was made by the obstetrician. After discussion with patient’s relatives about the implications of her worsening clinical condition, spinal anesthesia was planned. A quick but thorough pre anesthetic evaluation revealed an obese parturient with a weight of 85 kg and height of 140 cm with short neck but adequate mouth opening and modified Mallampati class of III. She was afebrile, comfortable in supine position and had occasional rhonchi on auscultation of chest. After transferring her to the operating room, she was preloaded with 500 mL of lactated ringer’s solution and monitoring included a five lead electrocardiogram, noninvasive blood pressure and pulse oximetry. The baseline recordings showed heart rate of 100 beats/min, blood pressure of 110/80 mmHg and spO2 of 94% on room air. Lumbar puncture was performed at L3–L4 interspace in sitting position in anticipation of technical difficulty and urgency of surgery and 2.4 mL of hyperbaric 0.5% bupivacaine was injected intrathecally and was immediately placed in the supine position with a wedge placed beneath her right buttock. A sensory level of T6 bilaterally (loss of sensation to pin prick) was achieved before starting the surgery and supplemental oxygen was given through face mask at 5 L/minute. The blood pressure showed a reading of 94/58 mmHg with a heart rate of 102 beats/min and spO2 of 97%. The sensory level of T6 was again confirmed before skin incision and a live 2.8 kg male baby was delivered with APGAR scores of 4 and 8 at 1 and 5 min, respectively. Just after delivery of baby and even before starting on oxytocin infusion, her blood pressure suddenly dropped to 60/40 mmHg with severe bradycardia (HR< 40 beats/min) culminating in asystole. Immediate tracheal intubation was performed and positive pressure ventilation was started with 100% oxygen and cardiopulmonary resuscitation with chest compressions at 100 compressions/min was commenced. Epinephrine 1 mg was given by intravenous push and was repeated twice (total 3 mg). The heart rate restored to 150 beats/min with the blood pressure of 60/30 mmHg with the total duration of cardiac arrest being less than a minute. The surgeons noticed abnormally increased oozing from the uterine incision site and suspected defective coagulation and closed uterus and abdomen after placing packs and abdominal drain. Immediately a
bedside clotting test was performed using a capillary tube with blood from pin prick, which showed an abnormally increased clotting time. Resuscitation was continued with colloids (1000 mL) and inotropic support was started with infusions ofdopamine at 15 µg/kg/min and nor epinephrine at 0.1 µg/kg/min as blood pressure was not responding to intravenous fluids. A total of 1500 mL of crystalloids, 1000 mL colloid (hydroxyethyl starch), 2 units of packed red blood cells and 4 units of fresh frozen plasma were transfused in the operating room in anticipation of abnormal coagulation parameters and the blood loss was estimated at 1200 mL approximately. Arterial blood gas analyzed intraoperatively showed pH 7.05; pO2 363 mmHg; pCO2 37 mmHg; HCO-3 10 mmol; BE/BD −20; SaO2 100% on 100% oxygen suggesting severe metabolic acidosis which was corrected with 100 meq of soda bicarbonate infusion. She was quickly transferred to ICU for further management and monitoring. For hemodynamic monitoring and fluid status, a central venous line was placed in the right internal jugular vein and an arterial cannula was placed in the right radial artery that showed initial readings of 20 mmHg and a blood pressure of 80/42 mmHg, respectively. Mechanical ventilation was continued with the controlled mode of ventilation with 100% oxygen and an abnormal soakage of the dressing with collection of significant amount of blood in the abdominal drain was noticed. She remained hypotensive in the ICU inspite of inotropic supports with dopamine, nor epinephrine and epinephrine infusions. Her laboratory values showed Hb of 6 gm/dL, platelet count of 21 000 cells/mm3, prothrombin time of 14 s, activated partial thromboplastin time of 45.4 s with elevated D-dimer and fibrin degradation products thus raising suspicion of disseminated intravascular coagulation. A total of five units of packed red blood cells, 15 units of fresh frozen plasma and 10 units of platelet rich plasma were transfused. A repeat arterial blood gas analysis showed pH 7.20; pO2 162 mmHg; pCO2 29.5 mmHg; HCO3-16.2 mmol/L; BE/BD-12; SaO2 99%. Uterine artery embolization under radiological guidance was planned after discussing with the attending radiologist but the patient could not be transported to the x-ray department due to the hemodynamic instability. The resuscitation attempts were unsuccessful and the patient died 10h postoperatively.
Autopsy was performed after taking consent from the patient’s relatives, which showed edema of lungs with debris in pulmonary vessels that on further microscopic examination showed fetal squamous epithelial cells, thus the diagnosis of AFE was considered most likely.
DIsCUssION
The various differential diagnoses in our patient with sudden cardiovascular collapse during an emergent cesarean section could have been

229
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 KulshresthaandMathur:Amnioticfluidembolism
• Total spinal coinciding with administration of oxytocics.
• Drug anaphylaxis.• Venous air embolism.• Subclinical sepsis (chorioamnionitis) with Acute lung
injury going in for systemic inflammatory response syndrome exaggerated with peak spinal effect.
• Amniotic fluid embolism.
Our patient developed cardiovascular collapse during cesarean section and also had few premonitory symptoms like tachypnea, audible wheeze and fetal bradycardia that could have pointed towards the possibility of AFE, but were not considered due to rarity of this condition and moreover the urgency of surgery was given more priority. Total spinal coinciding with administration of oxytocin was unlikely as the event occurred almost 15–20 min after intrathecal injection and also the sensory level was stable at T6 (checked twice) with stable hemodynamics and the oxytocics were not transfused till the episode occurred. Drug induced anaphylaxis was also unlikely as no antibiotic was given before the episode and local anesthetic was given intrathecally after ruling out any intravascular placement. Venous air embolism can occur in cesarean section under general anesthesia[5] and has also been reported with both epidural[6] and spinal anesthesia.[7] This diagnosis was also less likely as no air was detected in intravenous line and also at autopsy no evidence of air was found in pulmonary vessels. Subclinical sepsis due to chorioamnionitis usually has a history of premature rupture of membranes of longer duration and moreover patient had no fever preoperatively with a normal total leukocyte count and a normal arterial blood gas, so this possibility was also considered less likely. Our patient developed cardiovascular collapse during cesarean section and also had few symptoms preoperatively such as tachypnea, audible wheeze and fetal bradycardia that could have pointed toward the possibility of amniotic fluid embolism. The presence of hypoxia, cardiovascular collapse, high central venous pressure and severe metabolic acidosis in blood gas analysis pointed toward the diagnosis of pulmonary embolism and in our case as patient was pregnant and since venous air embolism was unlikely, possibility of AFE was considered as the likely diagnosis retrospectively. Transesophageal echocardiography can help in the diagnosis of AFE showing acute right ventricular strain with under filling of left ventricle but we were not able to perform it as bedside availability was not there and also the patient could not be shifted for same.[8,9]
Amniotic fluid embolism, a rare obstetrical catastrophe, can present with constellation of signs and symptoms such as respiratory distress (57%), sudden hypotension (37%), coagulopathy (13%), and seizures (10%). More atypical presentations include abdominal pain, chest pain, and arrhythmias.[10] Most cases occur during
labor (70%), during cesarean section (19%), or following vaginal delivery (11%). It has also been reported during early pregnancy, during second trimester abortions, amniocentesis or following abdominal injury.[11] The most recent CEMACH report shows an increase in number of deaths due to AFE (9 in 1985–1987 to 17 in 2003–2005).[12] Although the pathophysiology of AFE is poorly understood, a biphasic response to amniotic fluid emboli has been suggested.[13,14] An initial transient phase, due to a reaction to vasoactive substances in amniotic fluid primarily arachidonic acid metabolites, causes intense pulmonary vasospasm, pulmonary hypertension and hypoxia leading to cardiovascular collapse. This stage usually lasts for 30 min and is responsible for about 50% of the mortality due to AFE within the first hour. The second phase then comprise of left ventricular failure, DIC and acute respiratory distress syndrome. Both the phases were probably present in our patient but due to rapid development of events, these were difficult to differentiate.[15] The definitive diagnosis is mostly histological on autopsy with demonstration of squamous cells, mucin and other fetal debris in pulmonary microvasculature of deceased women; however, fetal squamous cells have been found in the blood of laboring women aspirated from pulmonary artery due to other reasons also, thus reducing the diagnosing accuracy of this test.[16,17]
The management of AFE comprises of prompt cardiopulmonary resuscitation without delay to achieve higher survival rate.[18] It is based on attempts at (a) maintaining maternal oxygenation, (b) optimizing the hemodynamic status, and (c) correcting the coagulopathy.[19]
Newer modalities of management include selective pulmonary vasodilators in the setting of acute pulmonary hypertension seen in amniotic embolism.[20] If AFE is suspected at an early stage, measures that should be undertaken to prevent further cardiovascular collapse include maintaining maternal oxygenation by oxygen supplementation, prompt inotropic support if the hypotension persists and preparation of blood and blood products in anticipation of development of DIC. In the scenario of cardiovascular collapse due to suspected amniotic fluid embolism, successful use of hemodialysis with plasmapheresis and extracorporeal membrane oxygenation with intraaortic balloon counter pulsations have also been described in the literature.[21,22]
In conclusion, AFE is a life threatening and difficult to predict or prevent condition that should be kept in mind in a parturient especially having risk factors such as known history of atopy or anaphylaxis, advanced gestational age at termination of pregnancy, rupture of membranes, or meconium staining of amniotic fluid.[23]
The main aim to report this case is to stress on the difficulty in predicting and preventing this rare but fatal complication of pregnancy especially in centers with

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
230
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 KulshresthaandMathur:Amnioticfluidembolism
limited resources where an algorithm for suspicion can be really helpful, as immediate resuscitation is essential for a positive outcome. It also stresses the importance of intensive care backup facilities for such cases.
ReFeReNCes
1. Abenhaim HA, Azoulay L, Kramer MS, Ledue L. Incidence and risk factors of amniotic fluid embolisms: A population- based study on 3 million births in United States. Am J Obstet Gynecol 2008;199:49.el-8.
2. Steiner PE, Luschbaugh CC. Maternal Pulmonary Embolism by amniotic fluid as a cause of obstetric shock and unexpected deaths in obstetrics. JAMA 1941;117:1341-5.
3. Clark SL, Hankins GD, Dudley DA, Dildy GA, Porter TF. Amniotic fluid em-bolism: analysis of the national registry. In: Transactions of the Thirteenth Annual Meeting of the American Gynecological and Obstetrical Society. Am J Obstet Gynecol 1995;172:1158-69.
4. Visconi CM, Clark SL. Amniotic fluid embolism. In: Norris MC, editor. Ob-stetric Anaesthesia 2nd ed. Philadelphia: Lippincott Williams and Wilkins; 1999. p. 579-91.
5. Lew TW, Tay DH, Thomas E. Venous air embolism during Cesarean section more common than previously thought. Anesth Analg 1993;77:448-52.
6. Fong J, Gadalla F, Gimbel AA. Precordial Doppler diagnosis of haemodynami-cally compromising air embolism during caesarean section. Can J Anaesth 1990;37:262-4.
7. Nims M, Hallonquist H, Camann W. Coronary arterial air embolism occur-ring during cesarean delivery. Int J Obstet Anesth 2006;15:166-9.
8. James CF, Feinglass NG, Menke DM, Grinton SF, Papadimos TJ. Massive am-niotic fluid embolism: Diagnosis aided by emergency transesophageal echo-cardiography. Int J Obstet Anesth 2004;13:279-83.
9. McDonnell NJ, Chan BO, Frengley RW. Rapid reversal of critical haemo-dynamic compromise with nitric oxide in a parturient with amniotic fluid embolism. Int JObstet Anesth 2007;16:269-73.
10. Visconi CM, Clark SL. Amniotic fluid embolism. In: Norris MC, editor. Ob-stetric Anaesthesia 2nd ed. Philadelphia: Lippincott Williams and Wilkins;
1999. p. 579-91.11. Dedhia JD, Mushambi MC. Amniotic fluid embolism. Br J Anaesth
2007;7:152-612. Confidential Enquiry into Maternal and Child Health (CEMACH). Saving
mother’s lives 2003-2005 Report: A Report of UK confidential enquiries into maternal deaths. London: RCOG Press; 2007.
13. Clark SL, Montz FJ, Phelan JP. Hemodynamic alterations associated with am-niotic fluid embolism: A reappraisal. Am J Obstet Gynecol 1985;151:617-21.
14. Clark SL. Amniotic fluid embolism. Crit Care Clin 1991;7:877-82.15. Howes LJ. Anaphylactoid reaction possibly caused by amniotic fluid embo-
lism. Intl J Obstet Anesth 1995;4:51-4.16. Aguilera LG, Fermandez D, Plaza A, Gracia J, Gomar C. Fatal amniotic fluid
embolism diagnosed histologically. Acta Anaesthesiol Scand 2002;46:334-7.17. Plauche WC. Amniotic fluid embolism. Am J Obstet Gynecol 1983;147:982.18. Aziz ES. A successfully resuscitated case of amniotic fluid embolism. Eur J
Anaesthesiol 2000;17:712-3.19. Rodgers L, Dangel-Palmer MO, Berner N. Acute circulatory and respira-
tory collapse in obstetrical patients: A case report and review of literature. AANA J 2000;68:444-50.
20. Conde-Agudelo A, Romero R. Amniotic fluid embolism: An evidence- based review. Am J Obstet Gynecol 2010;202:92.
21. Kaneko Y, Ogihara T, Tajima H, Mochimaru F. Continuous hemodiafiltration for disseminated intravascular coagulation and shock due to amniotic fluid embolism: report of a dramatic response. Intern Med 2001;40:945-7.
22. Hsieh YY, Chang CC, Li PC, Tsai HD, Tsai CH. Successful application of ex-tracorporeal membrane oxygenation and intra-aortic balloon counterpul-sation as lifesaving therapy for a patient with amniotic fluid embolism. Am J Obstet Gynecol 2000;183:496-7.
23. Edwards GJ, Davies NJ. Amniotic fluid embolism following feticide- a cau-tionary tale. J Obstet Gynaecol 2000;20:191.
Commentary
Amniotic fluid embolism: A catastrophic problem in need of a prepared team with a planThere are few things more tragic than the death of a new mother – particularly one who was previously healthy and the cause of death is sudden and unpredictable. Amniotic fluid embolism (AFE) is one case catastrophic problem – as illustrated in the case and review by Kulshrestha and Mathur.[1] AFE is rare, occurring in less than 10 per 100 000 deliveries, but it has a mortality rate of 60–80% and accounts for 10% of maternal deaths.[2] Furthermore, it affects mothers worldwide and spares no culture, no demographic group, no society, and no corner of the world
– it affects the rich, as well as the poor. Fortunately, this problem is rare and few clinicians – even in busy delivery suites – will encounter this horrible problem. However, this very fact illustrates the challenges in diagnosis and management, particularly when even the slightest delay can mean the difference between life and death. With such a high mortality and the patient’s demise occurring suddenly, often within a few hours after delivery, Reviews such as this one presented by Kulshrestha, become critical in raising the level of awareness by helping clinicians recognize the signs and symptoms of AFE and provide adequate resuscitation. To improve survival, the clinical team must have a high suspicion and quickly work through a differential diagnoses in which many problems can be confused with AFE. But, more importantly, the team needs to be prepared. Even if the problem is recognized immediately, as with most disasters – medical and otherwise – if everyone is prepared and if there are
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_110_11R3
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.

231
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 KulshresthaandMathur:Amnioticfluidembolism
checklists and protocols in place, then the chances for success increase dramatically.[3] Such concepts are not new to medicine. Even disease-specific check-lists exist with malignant hyperthermia being the prototypical example. Many operating rooms, even in the disadvantaged areas have checklists, emergency Dantroline kits, and easy to follow instructions that facilitate care in unusual areas and unexpected situations.[4,5] AFE can and should follow a similar model.
Unfortunately, again with most catastrophes throughout the world, preparation and anticipation of a problem rarely occurs until there is a disaster that raises the level of awareness and concern. However, there is no reason why obstetric and critical care teams across the world should not anticipate, prepare, and maybe even practice for the worse. The key is to do this before a death occurs. Hopefully this review, as so many other discussions on this topic, can precipitate a wake-up call.[6] While specific guidelines and protocols do not exists and treatment options can vary with the resources available in each center, clearly the topic is worthy of discussion. The question of “how do we respond to peri-partum cardiovascular collapse” needs to be asked. There might not be a simple answer to this problem since each center might answer the question differently based upon resources and expertise. Such a fact does not excuse the fact that such a question needs to be asked and discussed before it happens – and it will happen.
In such situations, while recognition is critical and a definitive diagnosis might come later, the responses need to be the same. Attention to the basics are obviously the first steps – establish an airway, ensure breathing, maintain and support the circulation should be practiced to the point in which they are routine and second nature. Then comes the more difficult part. If the baby has not been delivery then that must be the priority of one team, but just as importantly, there needs to be a second team solely dedicated to the acute needs of the mother. Such a protocol must incorporate a cry for help, and that help must be available in some form or another. One team cannot serve the complex needs of two lives in such situations. Such teams need to be defined in advance and roles assigned such that when the time comes, there is order rather than chaos. As importantly, the two teams must work side-by-side despite somewhat different priorities. Again, practice and review is critical. This is why elementary schools have fire drills, why airplanes instruct passengers on what to do in the event of loss of cabin pressure, and why even the best trained rescue teams spend most of the time practicing. A key is also that rules are followed with little question. The process is tried and true.[7]
No one would refute that algorithms such as those
used in basic life support (BLS), advanced cardiac life support (ACLS), or even advanced trauma life support (ATLS) courses improve patient outcomes, especially when used regularly by healthcare teams. What about an inexperienced team or one which does not encounter such situations or one that does not have access to the training, resources, and expertise necessary to develop skills? Algorithms can still improve standardization and overall performance in stressful, time-critical situations. Algorithms used in a crisis scenario have shown that participants thought that they would provide safer care using the algorithms in real life situations. Teams managing simulated crises exhibited an overall failure rate of 1 in 4 when working from memory alone, compared with a 96% success rate when using a checklist.[8] In fact, initiating an algorithm in a crisis situation allows time to recruit members to assist, notifiy more experienced team members, or contact facilities with more resources to stabilize the patient. It is important to remember that one algorithm is not ideal of every environment. What might work in a major medical center in a developed country with immediate access to technology such as extra-corporeal membrane oxygenation (ECMO), trauma surgery, computed tomography (CT scans), transesophageal echocardiography, and even advanced critical care might not work in a small village in Africa. Hence, it is imperitive that such “Code Teams” realize the extent of their resources when developing and implementing such protocols and algorithms. In fact, it is not unreasonable to believe that those with limited resources, if better prepared, might have better outcomes that those with unlimited technology but no plan for use or availability in the time of an emergency. But, the key first step is to get people together to talk before a catstrophie occurs and so a plan can be outlined.
Maternal amniotic fluid embolism is and will, most likely, unfortunately for years to come, remain a major cause of peri-partrum mortality in an otherwise healthy mother. There are no clues to prevention and treatment success, even in ideal situations, is rare. However, the keys to success are awareness, immediate recognition of a problem (even if the exact cause is undefined), and rapid implementation of a disaster plan for dealing with such problems. Such a plan needs to be developed, rehersed, recognizing the patterns of failure and correcting these, and having these plans readily accessable before it is needed. Unfortunately, despite what might be an obvious way to potentially save a life, few centers undertake such steps. Nevertheless, excellent reviews and discussions, such as the one by Kulshrestha, need to raise the awareness of all of those who might someday be faced with such a horrible problem.
Hopefully those reading this will agree and act. If one additional life gets saved because of these efforts, then

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
232
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 KulshresthaandMathur:Amnioticfluidembolism
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.
we all can claim a small victory in a battle that might never be won.
Karen Nelson DO, Michael S. FirstenbergDepartment of Surgery, Division of Cardiac Surgery,
The Ohio State University Medical Center, Columbus, Ohio, USA
Corresponding author: Dr. Michael S. Firstenberg, Division of Cardiac Surgery, N817 Doan Hall, 410 W 10th Avenue, Columbus, Ohio 43210, USA.
E-mail: [email protected]
ReFeReNCes
1. Kulshrestha A, Mathur M. Amniotic fluid embolism: A diagnostic dilemma. Anesth Essays Res 2011;5:227-30.
2. Clark SL, Hankins GD, Dudley DA, Dildy GA, Porter TF. Amniotic Flu-id Embolism: analysis of the national registry. Am J Obstet Gynecol 1995;172:1158-67.
3. Ziewacz JE, Arriaga AF, Bader AM, Berry WR, Edmondson L, Wong JM, et al. Crisis checklists for the operating room: development and pilot testing. J Am Coll Surg 2011;213:212-7.
4. Firstenberg M, Abel E, Blais D, Andritsos M. Delayed malignant hyperthermia after routine coronary artery bypass. Ann Thorac Surg 2010;89:947-8.
5. Miranda AD, Donovan LA, Schuster LL, Gerber DR. Malignant hyperthermia. Am J Crit Care 1997;6:368-74.
6. Firstenberg MS, Abel E, Blais D, Turner K, Halim-Armanios M, Dimitrova G, et al. Temporary extracorporeal circulatory support and pulmonary em-bolectomy for catastrophic amniotic fluid embolism. Heart Surg Forum 2011;14:E157-9.
7. Holzman RS, Cooper JB, Gaba DM, Philip JH, Small SD, Feinstein D. Anes-thesia crisis resource management: real-life simulation training in operating room crises. J Clin Anesth 1995;7:675-87.
8. Lingard L, Espin S, Whyte S, Regehr G, Baker GR, Reznick R, et al. Com-munication failures in the operating room: An observational classification of recurrent types and effects. Qual Saf Health Care 2004;13:330-4.
233
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Case Report
Hemoglobin drop after anesthesia in craniosynstosis: Dilemma of operate or not to operateNihal El-Ghandour, Salah Kassem, Abdelrahman J. Al Sabbagh1, Ayman Al-Banyan1, Firas A. Shubbak, Ahmad Hassib, Hazem Zaki
Departments of Anesthesia and 1Neuroscience, King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia
Corresponding author: Prof. Nihal El-Ghandour, Department of Anesthesia, King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_66_11R9
AbstractAn infant with craniosynostosis for craniectomy and cranial-vault remodelling was detected to have very low hemoglobin (6.8 gm%) after induction of anesthesia. This posed a dilemma whether to proceed with or abandon the surgical procedure. The case was postponed and was rescheduled for surgery one week later with hope that his hemoglobin would rise during this period. However, even before second anesthesia his hemoglobin level was found to be unchanged. Meticulous anesthesia management resulted in uneventful surgical procedure.
Key words: Prematurity, cytomegalo virus, homoglobin drop, craniosynostosis
IntroductIon
Craniosynostosis occurs as a result of premature fusion of one or more fibrous sutures of the skull. This results in skull deformity because of restricted skull growth.Elevated intracranial pressure secondary to rapid brain growth within the rigid skull results if multiple sutures are fused. Hydrocephalus is present in 5% to 10% of them with craniofacial sutures fusion. [1] It is estimated the condition affects 1 in 2000 live births. Parents usually bring the infant to clinician for the cosmetic considerations. Surgical correction of the skull deformity is the only option. An early surgical intervention results in cosmetic improvement and also allows adequate brain development. In presence of craniofacial deformities,such as Crouzen’s syndrome, facial sutures are also involved, which presents with additional
problems of airway management.[1] Because the infant scalp is highly vascular, the open surgical procedure often results in massive blood loss and may need transfusion of 20% to 500% of infant’s blood volume.[2,3] In view of anticipated massive blood loss during surgery it is imperative that the patients do not have pre-existing anemia. Occasionally though patient is admitted in the hospital in good physical condition and normal haemoglobin level, may develop anemia due to various reasons while waiting for corrective surgical procedure. Any improper anesthetic management during major surgery on such anemic infant may result in a catastrophe. Thus low haemoglobin missed during preanesthesia examination and detected only on the operation table poses a dilemma of whether to operate or postpone the procedure. Here, we present a case of craniosynostosis for craniectomy and fronto-orbital advancement, who was detected to be severely anemic after induction of anesthesia.
case report
An 8 months old male infant, weighing 6 kg, was admitted in the neurosurgical ward for correction of craniosynostosis along with fronto-orbital advancement. On examination, he had microcephaly, osteopectosis,

234
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 El-Ghandour, et al.: Haemoglobin drop after anesthesia in craniosynstosis
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Figure 1: Pre and post operative 3 dimensionally reconstructed CT scans of the patient, depicting pan sutural craniosynostosis and most significantly shallow retracted orbital rims. 2 days postoperatively, Orbital bar advancement is evident in addition to frontal bone remodelling. 3 months post operatively futher bone growth and progressive closure of the bony defects have occurred faster than expected due to the child's condition (Osteopetrosis).
AQ1
bilateral optic nerve atrophy, and hydrocephalus. Mother gave history of infant developing post traumatic seizures for which he was on anti convulsants; phenytoin and levatrocetam. His preoperative investigations (hemoglobin, complete blood count and serum biochemistry) were within normal limits. He underwent general anesthesia for insertion of ventriculo-peritoneal shunt for hydrocephalus. His airway management was difficult, and because of high location of larynx, tracheal intuabation was also difficult. Anesthesia course during the surgical procedure was uneventful. He desaturated after extubation and therefore, was reintubated and transferred to pediatric intensive care unit (PICU) for further management. In the PICU the infant developed septicemia for which he received appropriate treatment and made full recovery.
A week after his recovery from septicemia he was scheduled for correction of craniosynostosis and frontal bone advancement. On examination the infant was fully conscious with normal systemic examination. Apart from low haemoglobin (9.7 gm%), his all other investigations were in normal range. In the operation room after attaching routine monitors (ECG, pulse oximetr, and non invasive blood pressure), anesthesia was induced with fentanyl, propofol and tracheal intubation facilitated with rocuronium. After anesthesia induction two peripheral venous lines (each 20G) were secured. Right radial artery and right internal jugular vein was cannulated for invasive arterial pressure and CVP monitoring, respectively. A blood sample was drawn from arterial line to measure baseline blood gases and hemoglobin level. The blood sample showed a hemoglobin of 6.8 gm%. Suspecting an error in sampling or laboratory error,another blood sample was taken and this too showed the same hemoglobin level.The situation was informed to the chief surgeon who in turn discussed the risks of major surgery associated with low hemoglobin with the infant’s father. The later decided against the surgery and the operation was deferred.
One week later the case was discussed by the surgeon and anesthesiologist and it was decided to perform the procedure with the same haemoglobin level. Intraopearative monitoring consisted of continuous ECG, pulse oximetry, invasive arterial blood pressure, CVP, end tidal carbon dioxide, temperature and urine output, in addition to blood loss estimation. Patient’s temperature was maintained with forced warm air blanket. Patient lost approximatel 400 ml of blood and was transfused three units, each of 150cc of whole blood, during the operation. Total surgical duration was 10 hours. Patient was not extubated and transferred to PICU for further management. In the PICU his pulse rate was 190 beats per minute (BPM) and blood pressure of 130/70 mmHg. He was given fentanyl and midazolam which decreased his heart rate to 160 BPM. His coagulation profile was found to be deranged which was corrected with fresh frozen plasma.
During the PICU stay the infant developed bilateral lung wheeze with suspicion of tracheal tube block/atelectasis (90% oxygen saturation on 100% oxygen) for which flexible bronchscopy was conducted and tracheal tube was replaced with a new one. Mechanical ventilation was continued and broad spectrum antibiotics administered to treat underlying infection. Mechanical ventilation was discontinued after two weeks and trachea extubated.He was discharged home in good physical condition.
dIscussIon
Dysmorphic features of craniosynostosis,if left untreated,may impact brain growth and cause cognitive impairment. Peroperative concerns in craniosynostosis chiefly center around massive blood loss, and abnormal surgical position for surgery, though many authors have cautioned of venous air embolism also.[4] Amount of blood loss dependes on number of sutures involved and extent of surigacl repair. Massive blood loss usually results during cranio-vault remodelling procedures. Blood loss as high as 55 ml/kg was reported by van Uiterta and colleagues[5] in a retrospective analysis. They also observed that long duration of surgery and lower body weight were associated with significantly more blood loss and red cell transfusion. Our patient too lost approximately 70ml/kg of blood over 10 hours duration of the procedure Dahmani and colleagues[4] found continuous autologous transfusion very effective in these surgical procedures. Massive transfusions have their own share of complications including, dilutional coagulopathies,[6] and even cardiac arrest from transfusion related hyperkalemia.[7]
235
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 El-Ghandour, et al.: Haemoglobin drop after anesthesia in craniosynstosis
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
A massive blood loss assume more significance in presence of pre-existing anemia, as in our patient. To reduce the quanity of blood loss and transfusion, various authors have employed different strategies including, preoperative acute hemodilution,[8] hypotensive anesthesia,[9] intraoperative continuous infusion of tranexamic acid,[10] fibrinogen adminstiration,[11] etc. Administration of tranexamic acid and fibrinogen would have benefitted our anemicr patient but they were not available, while hypotensive anesthesia or hemodilution have potentials to increase morbidity in presence of anemia. Recent introduction of endoscopically assisted craniectomy technique which is less invasive and decreases time patients spend under anesthesia, the need for blood transfusion, and length of hospital stay, will prove a boon for this procedure.[12]
The major mistakes in our management of case were we relied on laboratory investigations which were one week old, more so since this patient was subjected to ventriculo-peritoneal shunt about one week ago. Furthermore, infant’s hemoglobin was not raised to an acceptable level by preoperative transfusion while waiting for surgery subsequent to previous cancellation of the surgical procedure.
In conclusion, we recommend that during pre anesthesia check up anesthesiologists should not rely on old laboratory reports especially, if the patient had undergone a surgical procedure, howsoever minor, before a major surgery.
acknowledgement
Authors wish to thank Prof. P. Bithal for his suggestions and review and editing the manuscript’s text.
reFerences
1. Velardi F, Di Chirico A, Di Rocco C. Blood salvage in craniosynostosis surgery. Childs Nerv Syst 1999;15:695-710.
2. Bonhomme V, Damas F, Born JD, Hans P. Perioperative management of blood loss during surgical treatment for craniosynostosis. Ann Fr Anesth Reanim 2002;21:119-25.
3. Meyer P, Renier D, Arnaud E, Jarreau MM, Charron B, Buy E, et al. Blood loss during repair ofcraniosynostosis. Br J Anaesth 1993;71:854-7.
4. Dahmani S, Orliaguet GA, Meyer PG, Blanot S, Renier D, Carli PA. Perioperative blood salvage during surgical correction of craniosynostosis in infants. Br J Anaesth 2000;85:550-5
5. Kearney RA, Rosales JK, Howes WJ. Craniosynostosis: An assessment of blood loss and transfusion practices. Can J Anaesth 1989;36:473-7.
6. Walters JH, Lee JS, Klein E, O’Hara J, Zippe C, Potter PS. Preoperative autologous donation versus cell salvage in the avoidancof allogeneic transfusion in patients undergoing radical retropubicprostatectomy. AnesthAnalg 2004;98:537-42.
7. Akingbola OA, Singh D, Srivastav SK, Walsh JW, Jansen DA, Frieberg EM. Intensive care unit course of infants and children after cranial vault reconstruction for craniosynostosis. BMC Res Notes 2011;4:347.
8. Kanev PM. Congenital malformations of the skull and meninges. Otolaryngol Clin North Am. 2007;40:9-26.
9. De Jong T, et al. Long-term functional outcome in 167 patients with syndromic craniosynostosis; dening a syndrome-specic risk role. J Plast Reconstr Aesthetic Surg 2010;63:163.
10. White N, Marcus R, Dover S, Solanki G, Nishikawa H, Millar C, et al. Predictors of blood loss in fronto-orbital advancement and remodeling. J Craniofac Surg 2009;20:378-81.
11. Ririe DG, David LR, Glazier SS, Smith TE, Argenta LC. Surgical Advancement Influences Perioperative Care: A Comparison of Two Surgical Techniques for Sagittal Craniosynostosis Repair. Anesth Analg 2003; 97:699-703.
12. Meier PM, Goobie SM, DiNardo JA, Proctor MR, Zurakowski D, Soriano SG. Endoscopic Strip Craniectomy in Early Infancy: The Initial Five Years of Anesthesia Experience. Anesth Analg 2011;112:407-14.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.
Author Queries?????AQ1: Fig 1 not cited in text???

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
236
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Historical Report
Historical report account on the development of anesthesiology and medical services in Kingdom Saudi Arabia 1956–1987: M. I. Al-Khawashki’s letter dated April 25th 1997Mohamad Said Maani Takrouri, Farah Maani Takrouri1
Department of Anesthesia, King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia, 1Department of Medical Students Affair, Medical School (Jordan University of Science and Technology, JUST), Irbid, Hashemite Kingdom of Jordan
Corresponding author: Dr. Mohamad Said Maani Takrouri, Department of Anesthesia, King Fahad Medical City, Riyadh, Saudi Arabia. E-mail: [email protected]
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
AER_107_11R3
AbstractIn this historical report, a new light is spotting new details of the development of anesthesiology and medical services in Kingdom Saudi Arabia 1956–1987. The value of this letter written in Arabic language and cannot be accessible to non-Arabic speakers. The translation and verification of author publications to support its evidence would augment the current of scientific history writing. The time covered was since 1952 to the eighties. It reflects the ambition of various ministers of health in Saudi Arabia and international health body WHO that allowed many health care providers to build the services. It is first-hand experience of the writer Al Khawashki. The picture would be more complete when more research would follow this paper publication.
Key words: Anesthesia in the sixties of the last century. Saudi Arabia. The development of anes-thesiology. Kingdom Saudi Arabia 1956-1987, I. Al-Khawashki, GalalAref, Saed Al Rays, Mohamad Rifaat, Fouad Hamdi, Rachad Faroon, Jameel Al Hujelan. HussainAbd Al Razak Al Jazaery Bashir Al Roumi, Hassan Al Nassif, Mohamad Kamal Ghalb Alexandria University, Kasr Al Einy Medical School in Cairo Universityregional, Office of (WHO) in the east Mediterraneanarea
INTRODUCTION
In response to a recently published article on services rendered by two Saudi Anesthesiologists in the last century.[1] The senior author of this report proposed
to publish a historical paper send to him by late MI Al Khawashki as it is a relevant historical document of our departed college. So the junior author (F. T.) put an intellectual effort in translating the Arabic letter and researched the names and data.
Mohamed Seraj[1] in his article indicated “He is considered to be the first qualified Saudi anesthetist in the Kingdom.” He graduated in 1958 from Cairo Medical College and worked for a few years in Riyadh Hospital.
In 1960, the first two Saudi graduate doctors, Abdullah Al-Enazy and Ishaq Al Khawashki were sent to Denmark on scholarship to obtain their diploma degrees in anesthesia. Both graduated successfully in 1962.

237
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Takrouri and Takrouri: Anesthesia services, KSA, mid 20th century
Only Dr. Ishaq Al Khawashki returned and worked in Riyadh Central Hospital, Ministry of Health. At that time there were very few expatriate anesthetists who covered several operating theatres and nights on call. Sometimes they even covered more than one hospital within the city. Dr. Ishaq Al Khawashki started to build the department of anesthesia and participated actively in supervising and updating the curriculum for the diploma of anesthesia for technicians, which had started earlier. The program consisted of a 3 year training program. This period was called the technician's era. The main objective was to produce anesthesia technicians to overcome the shortage of specialist manpower and provide a reasonable service at that time. He was highly respected as a commander with dedication and leadership in his field. He was loved by everyone. His leadership was extended to manage the main hospital in Riyadh. During his successful practice as consultant anesthetist and general director of Riyadh Central Hospital he managed to obtain his medical doctorate in anesthesia from Cairo Medical College in 1977. He continued as general director of the anesthesia department and director of the hospital until 1982. He served as Consultant to the WHO from 1982 until he died. He has several publications on safety of intravenous agents in anesthesia, road traffic accidents, spinal cord injury, and body cooling unit.[2-5]
One of the most important developing points in his life was being the principle inventor of the “body cooling unit” that became the standard of care for heat stroke management since the eighties and until now in numerous hospitals during Hajj seasons [affirmed in the pages of Figure 1 the covering letter]. He was selected Member of the Editorial Board of the Saudi Medical Journal, Middle East Journal of Anesthesia, and the Medical Journal issued by the Ministry of Health. He departed on August 12 2006.
By Presenting the personal account of Dr MI Al-Khawashki as it was dated April 25th 1997 [Figure 2]. This account is having same title published in 1989, but information update was noticed. This letter was written on the invitation of (M. S. T.) to document the history of anesthesia in Middle East with names and stages of anesthesia (a book edited by M. T. al Jassir in Araabic). Although Professor Seraj had an excellent effort to enlighten the readers about this issue still many loose ends were not presented yet. In this letter he ascertained all facts documented by Professor Seraj and he outlined the role of WHO in initiation of training in Denmark for local anesthesiologists, it showed as an effort to propagate anesthesia services mainly in ministry of health some help in recruiting practitioners and teachers from Egypt. The limitation of posthumously publishing would carry certain defect in perusing all mentioned data, but even the late Dr M. I. Al-Khawashki ended his document that Professor Seraj is instrusted to report the rest of the story [Figure 1].
• In the Aeabic document [Figure 2] M. I. Khawashkiwrote: We can consider the year 1956 the start point of anesthesiology and its development as one of the basic supporting medical sciences for the modern medical services in the Kingdom of Saudi Arabia [Figure 2]. There were no apparent evidence for the existing of this branch before that year. To show the stages of development of that brand over 40 years, it is appropriate to divide those stages into four decades as follows.
1. Initiation and foundation decade 1956–1965: This started when the late Dr. Rachad Faroon was appointed the minister of health. When the debut development of anesthesia, the late Dr. Bashir Al Roumi and Dr. Hassan Al Nassif, the director general, who introduced the anesthesia service into its major health care
As the contracted Egyptian anesthesiologist Dr. Saed Al Rays and Dr. Mohamad Rifaat, the first Doctor worked in Bab Shareef hospital and the women hospital then in King Saud Hospital. The second doctor worked in Ajeyad hospital along with the women hospital in Mekkah. Also the ministry contracted two anesthesia assistant technicians from English Hospital in Ghaza who worked in Riyadh city and other in Taayef. Thus, the Kingdom had only two anesthesiologists and two anesthesia assistant technicians working for it. Also, in the military hospital in Riyadh there was Dr. Fouad Hamdi who worked as anesthesiologist.
Avoiding this deficiency, the ministry of health requested from the WHO Mediterranean area office to send an expert anesthesiologist, Dr. Mohamad Kamal Ghalb, to work in King Saud hospital (Riyadh Central Hospital that was opened in 1956) so that he could initiate the training program for anesthesia in the anesthesia technician institute. Dr. Ghalb could not attract any physician to this anesthesia specialty but
Figure 1: : (a) second page Arabic letter and (b) first page Arabic letter [Arabic is read from right to left]
a b

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
238
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Takrouri and Takrouri: Anesthesia services, KSA, mid 20th century
only he laid the foundation of the program of assistant physician in the health technical institute.
In October 1957 after my graduation from Kasr Al Einy Medical School in Cairo University, I was appointed as general practitioner in King Saud Hospital. Then I took the post of anesthesia physician after consultations with Dr. Ghalb and Dr. Romy. Later on, I was naturalized as Saudi and was sent to Copenhagen, Denmarkto study anesthesia for 2 years. I returned back in 1962 to Riyadh, assumed the responsibility in the same department. Our ministry of health contracted later on that year with many anesthesiologists from Egypt and Britain who participated in the effort of serving the surgical patients and establishing the tradition of anesthesia in kingdom hospitals.[2-5]
The ministry of health institute for anesthesia technician qualified six anesthesia technician every year. Then they were distributed over the
hospitals in kingdom to work under supervision of anesthesiologists. In that year when late Dr. Youssef Al Hagery was minister of health, administrative decision was taken to put the entire anesthesia department in the central Riyadh hospital to coordinate the service and staff effort.
Increased number of surgery under the anesthesia led to the appearance of a new problem. When we have complication or postoperative death, people tended to sue the whole surgical team including the anesthesiologist or sue the anesthesia team alone when some surgeons put the complications or postoperative death blame on the anesthesiologist. That led to a Royal Decree to form medical and clerical jury committee to look into these cases. And that was a new advance in the medical environment. In that it re-assured the practitioners and the patient relatives of the fair judgment of this legal body.
2. Settlement and advances decade 1966–1975: In 1976, many development and expansions in the field of anesthesiology and the increasing number of anesthesiologist led to the fair distribution of man power on major hospital in the kingdom. On the other hand, the project of building intensive care unit in King Saud Hospital was allocated to German company that later on built an intensive care unit with eight beds. In 1969, it was operated under directorship of Professor Mohamad Bdoor from Alexandria University.
Later on in 1972, the minister of health Dr. Jameel Al Hujelan commissioned me to build five units of intensive care in Bab Shareef hospital in Mekkah, jedah, tayef, madina al mounwaram and Damam, under the directorship of Professor Jalal Aarf. Riyadh central Hospital (King Saud Hospital) provided the training for other staff such as physicians and nurses to this satellite units. In that era Professor Seraj was sent to Britain by Riyadh University, today King Saud University, to get the highest qualification of anesthesia and to be the first anesthesia professor in the kingdom. Due to low numbers of physicians working in anesthesia fields I was unable to follow up with external examination but I was able to go to QasrAyni Medical School in Cairo University in 1973 to present my PHD in anesthesia in 1976.
3. Growth and spread decades 1976–1985: New blood came to the scene like Dr. HussainAbd Al Razak Al Jazaery who was the founder dean of faculty of medicine in King Saud University and later the minister of health. He assigned me to be the director of Riyadh Center hospital as well as the director of anesthesia department and an advisor for anesthesia affair in the ministry.
After this I managed to put a development plan for human resources needs for all anesthesia services
Figure 2: (a) History report p. 1, (b) history report p.2, (c) history report p. 3 and (d) history report p.4
b
d
a
c
ED Please check Fig 2 changes OK???

239
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Takrouri and Takrouri: Anesthesia services, KSA, mid 20th century
in the ministry of health. Also starting the applied science institute in the late seventies, under the deanship of Dr. Ibrahim Al Swagh. I was hired as member in its board after a decision that was taken in that anesthesia will be one of its sciences majors.
Then the practical and academic activity augmented in the kingdom either in government hospitals or in private hospitals. In this era, the Saudi anesthesia association was founded under Professor Seraj presidency who created as well the anesthesia club of Riyadh, which is monthly meeting in Riyadh were a paper will be presented and dinner will be served for the attended members. In this time period and explosion in the development of anesthesia was established with modern hospitals and highly advanced surgeries.
4. Academic and scientific advances in anesthesia decade 1987–1997 I leave that on Professor Seraj to describe.
RefeReNCes
1. Seraj MA. Two Saudi anesthesiologists who served anesthesia in KSA in the last century. Anesth Essays Res [serial online] 2011;5:3-4. Available from: http://www.aeronline.org/text.asp? 2011/5/1/3/84170 [Last cited on 2011 Nov 11].
2. Al-Khawashki MI, Ghaleb HA, El-Gawhary N, Madkour MK, Radwan AM, El-Sherbiny AM. Pharmacological effects of althesin and its steroidal components on the cardiovascular system. Middle East J Anaesthesiol 1980;5:457-69.
3. Al-Khawashki MI. Anaesthesia in Saudi Arabia: Development, problems, present status. Middle East J Anaesthesiol 1979;5:149-54.
4. Al-Khawashki MI, Ghaleb HA, el-Gawhary N, Madkour MK, Radwan AM, el-Sherbiny AM. Effects of althesin and its steroidal components on a variety of excised smooth muscle preparations. J Egypt Med Assoc 1979;62:209-23.
5. Al-Khawashki MI, Ghaleb HA, el-Gawhary N, Madkour MK, Radwan AM, el-Sherbiny AM. Pharmacological assessment of the anaesthetic potency and acute toxicity of althesin and its steroidal components in laboratory animals. J Egypt Med Assoc 1979;62:191-208.
How to cite this article: ???
Source of Support: Nil, Conflict of Interest: None declared.
Announcement
iPhone App
A free application to browse and search the journal’s content is now available for iPhone/iPad. The application provides “Table of Contents” of the latest issues, which are stored on the device for future offline browsing. Internet connection is required to access the back issues and search facility. The application is Compatible with iPhone, iPod touch, and iPad and Requires iOS 3.1 or later. The application can be downloaded from http://itunes.apple.com/us/app/medknow-journals/id458064375?ls=1&mt=8. For suggestions and comments do write back to us.

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
240
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches
Editor-in-Chief : Mohamad Said Maani Takrouri
(KSA)
Open Access HTML Format
For entire Editorial Board visit : http://www.aeronline.org/editorialboard.asp
A E R
Letters to Editor
Bone cement implantation syndrome: A rare catastrophe
AER_61_11R9 AP Done 28th Jan
Sir,Bone cement implantation syndrome (BCIS) is characterized by hypoxia, hypotension or both and/or unexpected loss of consciousness occurring around the time of cementation, prosthesis insertion, reduction of the joint or, occasionally, limb tourniquet deflation in a patient undergoing cemented bone surgery.[1]
The following case report describes a cardiac arrest in a patient undergoing a cemented hemiarthroplasty. This report provides further clinical evidence of the risks and consequences of fat embolization during hip arthroplasty surgery. Data concerning the fatalities of BCIS is sporadic and rare, so more and more reporting of data may help in understanding the condition better.
A 68-year-old male patient was admitted to our hospital with history of fracture neck of femur left. He had history of fall one day ago. Patient was dyspnoeic at rest (Grade IV) on admission. On evaluation, he was found to have fibrosis of the left upper lung with collapse of the left lower zone. He was a chronic smoker. Other medical history included hypertension since six years and bronchial asthma since six years, on irregular medication; old Pulmonary Koch’s which was irregularly treated 20 years ago. ECG Electrocardiogram showed premature ventricular ectopics. On admission, patient was stabilized with anti-hypertensive medications, anti-asthma medications and oxygen. Active Koch’s was ruled out. After five days of treatment the patient felt symptomatically better, and it was decided to operate the patient for Austin Moore prosthesis (hemiarthroplasty).
On the day of surgery, the patient was conscious and coherent, with a pulse rate of 92/ min, blood pressure of 150/90 mm hg in supine position, respiratory rate was 22 and patient was not dyspnoeic. His cardiac examination was normal while respiratory examination showed decreased breath sounds on the left side; there were no adventitious sounds on either side. His investigation revealed hemoglobin of 9.8 g%, blood sugar of 117 mg/dl, blood urea of 50 mg/dl and serum creatinine of 1.9 mg/dl.
Patient was taken onto the operation table and monitors
(pulse oximetry, NIBP non invasive blood pressure and electrocardiogram monitors) were applied. In view of the respiratory condition of the patient, it was decided to proceed with regional anesthesia (epidural). Under all aseptic precautions, epidural space was identified with loss of resistance technique with 16-gauge tuhoy needle at 6 cm from the skin, 18-gauge epidural catheters were inserted and fixed at 9 cm from the skin at the L2-L3 level. Injection Ropivacaine 0.75% 10 ml was given in titrated doses. After 15 min, adequate anesthesia (T10) level was obtained. The patient’s blood pressure dropped to 130/80 mm of hg with NIBP and pulse rate was 84/ min and respiratory rate was 20/min. Patient was put on oxygen supplementation of 5 lit/min with face mask. Lateral position was given. Blood pressure was 130/84 mm hg and pulse rate 82/ min, respiratory rate was 20/ min after painting and draping procedure was started. The hemodynamics and respiration was normal during the procedure. After 45 min of surgery, medullary reaming was completed and bone cement (surgical simplex P, stryker) was applied. On application of bone cement, patient developed sudden bradycardia, with a heart rate of 20/ min, peripheral pulses were not felt, blood pressure was not recordable with NIBP. Patient became apnoeic and unconscious. Immediately, endotracheal intubation was done in lateral position with 7.5-mm portex endotracheal tube. Wound was packed and patient was shifted to supine position. Patient was ventilated with 100% oxygen, and effective cardiac compression started. Intravenousfluids were started; injection adrenaline 1 mg (1:1000) was given Intravenous, injection atropine 0.6 mg (1:1000) given and external cardiac compression started. After five cycles of cardiopulmonary resuscitation pulses were palpable and heart rate was 130/min, it was a sinus rhythm. Systolic blood pressure was recorded as 90 mm Hg. Intravenous fluids were continued to maintain preload along with inj dopamine 10 mcg/kg/min. Surgical closure was done and patient was shifted to acute medical care unit with life support.
In AMC, patient was put on ventilator, with dopamine support (10 mcg/kg/min) to maintain blood pressure around 100 mm Hg systolic and internal jugular catheterization was done to assess central venous

241
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Letters
pressure (CVP), which was around 12 cm throughout the period. Fluids were guided by CVP. Arterial blood gases and chest X-ray revealed no additional findings. Patient did not regain consciousness.
After eight hours of surgery, patient developed sudden pulseless electric activity, CPR was initiated including external cardiac compressions and injection atropine 0.6 mg IV and injection adrenaline 1 mg (1:1000); they were repeated every 3 min till three doses. Patient could not be revived after one hour of resuscitation.
Patient’s relatives did not consent for necropsy.
DISCUSSION
Bone cement is an acrylic substance used to secure implants to bone or to fill joint cavity. Bone cement is a filler and not an adhesive. The contents include methylmethacrylate monomer, a colorless flammable liquid, barium sulphate added to make cement radio-opaque, and polymer component – a white powder and benzyl peroxide.
Bone cement implantation syndrome is now an established entity, though there is no widely accepted definition to it. The cases range from a mild form like transient hypoxemia to a fatal form including death.
Severity classification of BCIS is as under:[1]
Grade 1: moderate hypoxia (SpO2 <94%) or hypotension [fall in systolic blood pressure (SBP) >20%]Grade 2: severe hypoxia (SpO2 < 88%) or hypotension (fall in SBP >40%) or unexpected loss of consciousness.Grade 3: cardiovascular collapse requiring CPR.
The incidence of BCIS varies widely in the literature and fatalities have been rare. In India two fatalities have been reported from Max Hospital, Delhi.[2] The etiology and pathophysiology of BCIS has not been completely understood. Various theories have been proposed including release of polymethyl methacrylate monomer into circulation during cementation.; recent studies focus on emboli formed during cementation and resultant right ventricular failure.
Embolization occurs as a result of high intramedullary pressures developing between cement and prosthesis insertion. The cement undergoes an exothermic reaction and expands between the space of the bone and prosthesis trapping air and medullary contents under pressure. The temperature of cement can increase up to 96 degrees centigrade. When prosthesis is put, the contents escape into the interstices of bone because of already developed intramedullary hypertension. This leads to embolization. Knowing that the extent of embolization is proportional to the intramedullary pressure.
The debris from the medulla can embolize to the lungs and heart. It is the shower of pulmonary emboli that result in characteristic circulatory changes leading to hypoxia and right ventricular dysfunction, though the degree of cardiovascular collapse is not proportional to the degree of embolization.
Numerous patient-related risk factors have been implicated in the genesis of BCIS including old age, poor preexisting physical reserve, impaired cardiopulmonary function, preexisting pulmonary hypertension, osteoporosis, bony metastases, and concomitant hip fractures, particularly pathological or intertrochanteric fractures.[1]
Surgical risk factors include previous uninstrumented femoral canal, and use of long-stem femoral component.[1]
Anesthetic risk for BCIS can be reduced by meticulous preoperative examination to rule out significant cardiac, pulmonary or metastatic bone diseases, complete investigation of the patient’s co-morbid diseases and careful pre-optimization of the patients. Increasing the inspired concentration of oxygen should be considered at the time of cementation.[3] Hemodynamic monitoring should be considered for all cases that are particularly at risk for BCIS.[3]
Surgical risk reduction strategies for BCIS include medullary lavage, good hemostasis before cement insertion, minimizing length of prosthesis, using non-cemented prosthesis and venting the medulla.[4] Venting the medulla permits air to escape from the end of the cement plug and reduces the air embolus.
A fall in end-tidal carbon dioxide concentration can be the first sign of the embolism and should alert the anesthesiologist. In awake patients, first symptoms may include dyspnoea and altered sensorium.[5]
If there is an evidence of BCIS, inspired oxygen concentration should be 100%, and it should be continued in the postoperative period. The hemodynamic collapse of the BCIS should be treated on the lines of right ventricular failure.[6] Aggressive resuscitation with IV fluids has been recommended.[2]
Choice of vasopressor is generally sympathetic alpha 1 agonist in view of the right heart failure and vasodilatation.
In our case as mentioned above, the patient was a high-risk candidate for BCIS as he was an elderly patient having severe cardiopulmonary disease with decreased functional reserve (age 68 years, pulmonary fibrosis, bronchial asthma and systemic hypertension, old pulmonary Koch’s). Immediately after putting bone cement, patient developed sudden bradycardia hypotension, and unconsciousness. Patient was resuscitated with endotracheal intubation and ventilation with 100% oxygen supplementation, effective cardiac compression, and injection adrenaline. Patient revived after five cycles of CPR, fluids were loaded and

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
242
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Letters
patient was treated on the lines of right ventricular failure. Patient developed pulseless electric activity after eight hours of surgery and could not be revived. This was Grade III bone cement implantation syndrome, despite our best efforts we could not revive the patient.
So, in conclusion, we should take extra precaution while using bone cement in patients with co-morbid diseases, increase inspired oxygen concentration while using bone cement, and keep a close vigil on the patient’s hemodynamic status during and after use of bone cement to prevent unexpected fatalities; “detect early and act fast” to save the patient.
Nikhil Mudgalkar, K. V. RameshDepartment of Anesthesia, Prathima Institute of Medical Sciences,
Karimnagar, Andhra Pradesh, India
Corresponding author:
Dr. Nikhil Mudgalkar, D 101,
PIMS Campus, Nugnur, Karimnagar,
Andhra Pradesh, India.
E-mail: [email protected]
REFERENCES
1. Donaldson AJ, Thomson HE, Harper NJ and Kenny NW. Bone cement implantation syndrome. Br J Anaesth 2009;102:18.
2. Govil P, Kakar PN, Arora D, Das S, Gupta N, Govil D, et al. Bone cement implantation syndrome: A report of four cases. Indian J Anaesth 2009;53:214-8.
3. Byrick RJ, Forbes D, Waddell JP. A monitored cardiovascular collapse during cemented total knee replacement. Anesthesiology 1986;65:213-6.
4. British Orthopaedic Associations. Primary total hip replacement: A guide to good practice. 2006. Available from: http://www.boa.ac.uk/site/showpublications.aspx?ID=59 [Last accessed on 2011 June 30].
5. Duncan JA. Intra-operative collapse or death related to the use of acrylic cement in hip surgery. Anaesthesia 1989;44:149-53
6. Byrick RJ. Cement implantation syndrome: A time limited embolic phenomenon. Can J Anaesth 1997;44:107-11.
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
guide mark of CVC was at skin level. The guide wire was then withdrawn through the catheter until a mark on guide wire indicated the tip to be exactly positioned at the tip of catheter. Then alligator was clip attached to guide
Sir,A use of central venous catheters (CVCs) is increasing day by day. Guidelines for CVCs positioning by FDA and other experts suggest that CVCs tip should not be placed in right atrium in order to avoid complications.[1,2] ECG guided CVCs insertion is done with the help of ECG adapter (Certodyn®, B.Braun Medical). But this adapter is expensive and not easily available in developing countries.
Present innovation is an alternative to Certodyn® which is very simple to make and very cost effective to correctly identify CVC tip position during its insertion. Changes in ‘P’ wave amplitude is used as a guide to position CVCs.1. Two ECG Electrodes [Figure 1a]2. One ‘U’ shaped steel paper clip [Figure 1c]3. Certofix® (B.Braun.Medical, Bethlehem, PA)4. ECG monitor [Figures 2a and b]
Two ECG electrodes were stick together by central sticky portion [Figures 1c and 3]. Right Arm lead of ECG monitor was attached to one side of ECG electrode assembly and other leads of ECG monitor were attached to surface electrodes in usual manner. A paper clip was attached to other side on metallic tip of ECG electrode assembly [Figures 1d and 3].
CVC was inserted by usual Seldinger technique. A CVC (20 cm) was inserted over guide wire (50 cm) until 20 cm
Central venous catheter placement: An alternative of Certodyn® (Universal Adapter)
AER_62_11R8
Figure 1: (a) Two ECG electrode. (b) One non plastic coated steel ‘U’ paper clip. (c) Adhered two ECG electrode (vertical view). (d) Adhered two ECG electrode with paper clip (horizontal view)
a
c
b
d

243
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Letters
Figure 2a: Showing normal ECG recording on standard monitor
Figure 2b: Showing peaked ‘P’ wave on ECG while putting CVC
Figure 3: Whole assembly on patient
wire at indicated position. The other end of cable was attached to ‘U’ shaped paper clip [Figure 3]. The catheter with guide wire was slowly adjusted according to ECG guidance. ‘P’ wave on lead II was observed on ECG monitor [Figure 2a]. Peaked ‘P’ wave [Figure 2b] indicates CVCs position in RA (right atrium), then CVC with guide wire was withdrawn until ‘P’ wave return to normal configuration. After further withdrawal of CVC for another 2 cm, CVC was
secured with skin sutures and dressing was done.
It is very important to confirm the correct position of CVCs tip. It should never be placed in right atrium. [1,2] Improper placement of CVCs tip can result into many complications like pleural effusion, hydrothorax, hemothorax, hydromediastinum, pneumothorax, and pneumomediastinum.[3] Radiological method (X-Ray, Image intensifier, computed tomography) are practical and reliable tools for confirmation of depth of CVCs tips. However confirmation by this method is usually done several hours after the insertion of CVCs with extra financial burden on patients or hospital and radiation hazard to patient. Ultrasound have very limited role for aiding confirmation of tip placement. However it is very much useful to find-out correct puncture site.
We have developed a very simple and cost effective technique for correct placement of CVCs tip. Principle of our technique is same as that of Certodyn®. Materials used in our technique are easily available and simple to assemble on spot. Its performance is equivalent to Certodyn®. It has no side effects. Safety of patient is ensured and avoids unnecessary exposure to radiation. Hence we conclude that this simple, safe and easy to assemble alternative can be used for accurate positioning of CVCs, thus avoiding complications which are not only difficult to manage but also a financial burden on patient and hospital.
Manish Jain, Bhavana Rastogi, V. P. Singh, Kumkum Gupta
Department of Anaesthesiology and Critical Care,N.S.C.B.Subharti Medical College
NH-58, Meerut, India
Corresponding author: Dr. Manish Jain,
A-5, Padam Kunj, Kishan Flour Mill, Railway Road, Meerut - 25005, India. E-mail: [email protected]
REFERENCES
1. Scott WL. Central venous catheters: And overview of food and drug administration activities. Surg Oncol Clin N Am 1995;4:377-93.
2. Bowdle TA. Complications of invasive monitoring. Anestheisol Clin North America 2002;20:571-88.
3. Duntley P, Siever J, Korwes ML, Harpel K, Heffner JE. Vascular erosion by central venous catheters. Chest 1993;104:1633-8.
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
244
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Letters
Rare artifacts mimicking sinus tachycardia in a case of vaginal hysterectomy with situs inversus totalisSir,The introduction of modern monitoring gadgets based on ever improving technology has made the life of the anesthesiologist and intensivist fairly easy and comfortable. But the rare pitfalls and shortcomings due to the inherent electronic limitations of these monitors can sometimes prove hazardous in the interpretation of the various vital parameters.[1] The most commonly observed artifacts are of electrocardiogram (ECG) interpretation which can exhibit any type of arrhythmia or ST-T wave changes and the source of these artifacts can be internal (physiological) or external (non-physiological).[2-4] The interpretation can be so difficult sometimes that even an experienced anesthesiologist has to apply all his clinical knowledge and acumen to correctly identify the type of artifact as happened in the present case.[5]
A 49-year-old postmenopausal female with an established diagnosis of third-degree uterine prolapse and situsinversuswas posted for trans-abdominal hysterectomy and was administered epidural anesthesia with 17 ml of 0.75% ropivacaine and 60 μg of dexmedetomidine. Surgery was initiated after complete establishment of sensory block up to T-5 level. In the midst of the surgical procedure, the heart rate of the patient decreased to 46/ min. Simultaneously, the non-invasive blood pressure (BP) measured was 130/88 mmHg and we administered 0.3 mg of atropine as a prophylactic measure to rectify the bradycardia. We suddenly observed a display of sinus tachycardia on the monitor’s ECG waveform which correlated well with the pulse oximetry waveform (SpO2) but not with the digital readings [Figure 1]. As the patient had situsinversus with dextrocardia, we got concerned about all the potential cardiac complications. Both the peripheral pulses and heart rate correlated with the digital readings of the monitor and the patient was asymptomatic. Thereafter, on careful analysis of the parameters on the monitor once again, we observed a slightly slower sweep cycle of the waveform of both ECG and SpO2 as the waveform speed was changed automatically from 25 ms to 12.5 ms [Figure 2]. Most probably this must have occurred when we pressed the blood pressure knob to measure the stat BP. After this initial rectification, the artifact waveform could not be reproduced on repeated attempts and the entire surgical period remained uneventful.
The electronic devices for continuous monitoring are liable to get damaged by the moisture, dust, fluctuation of the voltages, indiscriminate use and irregular servicing which can alter the values of the parameters
and put the patient at risk of unwanted and unnecessary interventions. Though these monitors become available for safe use after passing so many astringent industrial tests such incidents are liable to push the naive anesthesiologist and the intensivist to press the panic button.[6,7] These therapeutic interventions can unnecessarily enhance the risks for developing complications, especially in patients suffering from various other pre-op co-morbidities.[2]
Situs inversus totalis and dextrocardia can be associated with congenital cardiac lesions such as ventricular septal defect, atrial septal defect, pulmonary stenosis, tetralogy of Fallot, tricuspid atresia and single ventricle, which can have various anesthetic implications. The risks of developing arrhythmias and cardiovascular complications
AER_64_11R7
Figure 1: The false picture of sinus tachycardia on the ECG and SpO2 waveform not correlating with the digital reading
Figure 2: The real corrected ECG and SpO2 waveform matching with the digital reading

245
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Letters
are quite high in this subset of patients as compared to the general population.[8-10]
In the literature there are numerous reported artifacts during monitoring, resulting from offset potential, poor polarization, amplitude variations, differences in the impedance, stray currents through cables, voltage fluctuations and filtering defects in the monitor, frequency mismatching of the various devices, and so on.[2,11-13] The artifacts we encountered occurred solely due to some electronic snag in the monitor which must have been activated during the pressing of the blood pressure knob. Later on, it was found that the monitor was due for service since seven months and was withdrawn from the operation theatre and a complete check-up was done the next day by the engineer along with the servicing Till now, we had not faced any such problem in any of the operation theatres and intensive care unit and a team of biomedical engineer and a senior anesthesia technician has now been assigned the responsibility of getting the service done for all the electronic gadgets at least 15-30 days earlier than the recommended date.
To conclude, it is recommended that the anesthesiologist and the intensivist should always rely on their personal experience, knowledge and clinical acumen to counter any real or pseudo complications. They should make use of all their vital senses which can make them alert and vigilant in the operation theatre and intensive care unit to deal with any potential complication instead of relying solely on the electronic monitoring gadgets. The age-old proverb stands so true even in the modern electronic times i.e. ‘Treat the patient and not the monitor’.
Sukhminder Jit Singh Bajwa, Sukhwinder Kaur Bajwa1, Jasbir Kaur, Amarjit Singh1
Departments of Anesthesiology and Intensive Care, 1Obstetrics and Gynecology, GianSagar Medical College and Hospital,
Banur, Patiala, Punjab, India
Corresponding author: Dr. Sukhminder Jit Singh Bajwa,
Department of Anaesthesiology and Intensive Care, GianSagar Medical College
and Hospital, Ram Nagar, Banur, Punjab, India.
E-mail: [email protected]
REFERENCES
1. Drew BJ. Pitfalls and artifacts in electrocardiography. CardiolClin 2006;24:309-15.
2. Chase C, Brady WJ. Artifactual electrocardiographic change mimicking clinical abnormality on the ECG. Am J Emerg Med 2000;18:312-6.
3. Srikureja W, Darbar D, Reeder GS. Tremor induced ECG artifact mimicking ventricular tachycardia. Circulation 2000;102:1337-8.
4. Garvey JL.ECG techniques and technologies. Emerg Med Clin North Am 2006;24:209-25.
5. Knight BP, Pelosi F, Michaud GF, Strickberger SA, Morady F. Physician interpretation of electrocardiographic artifact that mimics ventricular tachycardia. Am J Med 2001;110:335-8.
6. Knight BP, Pelosi F, Michaud GF, Strickberger SA, Morady F. Clinical consequences of electrocardiographic artifact mimicking ventricular tachycardia. N Engl J Med 1999;341:1270-4.
7. Bronzetti G, Canzi A, Picchio FM, Boriani G. Fluttering waves in electrocardiograms recorded in neonatal intensive care unit. Int J Cardiol 2003;92:299-301.
8. Song JY, Rana N, Rottman CA. Laparoscopic appendicectomy in a female patient with situsinversus: Case report and literature review. JSLS 2004;8:175-7.
9. Anoop P, Kumar V, Sasidharan CK. Situs inverses totalis with complex cardiac malformations in GoldenharSyndrome. Kuwait Med J 2004;36:212-3.
10. Mathew PJ, Sadera GS, Sharafuddin S, Pandit B. Anaesthetic considerations in Kartagener’s syndrome - a case report. Acta Anaesthesiol Scand 2004;48:518-20.
11. Brande FV, Martens P. A false positive arrhythmia on electrocardiogram induced by a cell phone. Eur J Emerg Med 2003;10:357-60.
12. Marples IL. Transcutaneous electrical nerve stimulation (TENS): An unusual source of electrocardiogram artifact. Anaesthesia 2000;55:719-20.
13. Bonvini RF, Camenzind E. Electrocardiogram artifacts caused by an abdominal electro stimulator. Med J Aust 2004;181:455.
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***
maintenance. Unfortunately, failure to perform a proper check before use is common in practice.[2]
A 45-year-old, 55 kg, ASA physical status I male patients was scheduled for emergency exploratory laparotomy. After preoxygenation (target end-tidal oxygen >90%) with 100% oxygen, standard rapid sequence anesthesia was induced. Volume-controlled ventilation was started. Intraoperatively 5 leads ECG, heart rate, NIBP, oxygen saturation, end-
Sir,It is a well-known fact that failure in properly checking equipment is the main factor in many critical incidents. Disastrous consequences are possible when an anesthetic breathing circuit is obstructed by a foreign body.[1] Proper preuse checking of equipment can help prevent equipment-related morbidity and mortality, educate anesthesiologist about equipment and improve
An unusual foreign body in breathing circuit detected by capnography
AER_80_11R6

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
246
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Letters
Figure 1: Circuit adaptor showing wet cotton
tidal carbon dioxide (EtCO2), inspiratory and expiratory tidal volumes and airway pressures were monitored. After 45 minutes, during the course of an otherwise uneventful anesthesia, a sudden fall in the EtCO2 and final drop of the capnogram reading to zero was observed. There were no disconnections of the breathing circuit or capnography and no malfunctioning of ventilator was there. Hemodynamic parameters showed no significant variations. The peak inspiratory pressure and the plateau pressure remained unaltered. The tidal volume delivered to the patient was unchanged as indicated by movement of the bellows, peak inspiratory pressure and chest movement. Kinking or water banking in sample line tubing of capnography was also excluded. The inspection of the circuit adapter of capnograph showed a small plug of wet cotton stuck at the centre of the sampling port [Figure 1]. The problem was rectified immediately. The capnograph adapter and the tubing were replaced, following which the reading and waveform returned to normal. Subsequent anesthesia proceeded uneventfully.
Various types of foreign bodies have been reported in breathing circuits, having a great potential for serious outcomes.[1,3] Proper pre use checking of equipment and unusual changes in ventilator settings (airway pressures and volumes), capnography and patient vitals during the course of anesthesia can detect such foreign bodies. In our case, we discuss how the isolated changes in the capnography helped us detect an unusual foreign body in the breathing circuit. Above-mentioned findings in our case prompted us to look for kinking, water vapour or liquid water in the sample tube and water trap which can lead to gross inaccuracies in readings.[4] Contaminants may partially obstruct the sampling tubes of sidestream capnometers and increase resistance to flow thus affecting the response time and accuracy of the CO2 measurement. In more severe cases, the sampling tube may be occluded.[5]
Furthermore, thorough inspection of the circuit adapter showed a plug of wet cotton stuck at the sampling port placed in the centre of the circuit. This might have been missed during the routine inspection of the circuit due to the white colour of cotton. The initial normal capnography waveforms dampening to zero may be explained by the fact
that on examination the cotton plug was wet, which might be due to the moisture of the expired gases of the patient. The wetting of cotton plug led to complete obstruction of the centrally placed sidestream sampling port. It has been reported that leaks and obstructions can occur at any of the numerous connection points and tubes within the sidestream sampling system, the resulting distorted waveforms and the end-tidal values can be significantly different from actual, may not be detectable by normal calibration procedures[6] and pose a potential hazard to the patient monitoring.
The exact cause of this unusual incident could not be concluded. One hypothesis is that nontechnical staff, while cleaning the nondisposable circuits and machine, might have left a piece of cotton in the adapter. Thorough inspection of the circuits and machine and proper training of nontechnical staff of operation theatre can prevent equipment related mortalities and morbidities.
Shivendu Bansal, Sohan Lal Solanki1, Rupesh Yadav2
Department of Anaesthesiology and Intensive Care, Maulana Azad Medical College and Lok Nayak Hospital, New Delhi, 1Anaesthesiology, Sanjay Gandhi Postgraduate Institute of Medical
Sciences, Lucknow, 2Anaesthesiology and Intensive Care, Vardhaman Mahaveer Medical College and Safdarjung Hospital, New Delhi, India
Corresponding author: Dr. Shivendu Bansal,
5, Saraswati Enclave, Plot No - 26/3, Sector - 9, Rohini, New Delhi - 110 085, India.
E-mail: [email protected]
REFERENCES
1. Foreman MJ, Moyes DG. Anaesthetic breathing circuit obstruction due to blockage of tracheal tube connector by a foreign body- two cases. Anaesth Intensive Care 1999;27:73-5.
2. Dorsch JA, Dorsch SE. Equipment checking and maintenance. In: Dorsch JA, Dorsch SE, editors. Understanding anaesthesia equipment. 5th ed. New Delhi: Lippincott Williams and Wilkins, a Wolters Kluwer business; 2008. p. 931-54
3. Singh B, Bhardwaj M. A live foreign body in the breathing circuit. Anesth Analg 2006;102:1293.
4. Raemer DB, Calalang I. Accuracy of end-tidal carbon dioxide tension analyzers. J Clin Monit 1991;7:195-208.
5. Jaffe MB. Mainstream or Sidestream Capnography? Available from URL: http://oem.respironics.com/Downloads/Main%20vs%20Side.pdf. [Last accessed on 2011 Sept 4].
6. Healzer JM, Spiegelman WG, Jaffe RA. Internal gas analyzer leak resulting in an abnormal capnogram and incorrect calibration. Anesth Analg 1995;81:202-3.
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***

247
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Letters
alteration in electrolyte balance, and transient hematuria.[5] Recently it is reported that processing of cardiotomy blood with a cell saver in patients undergoing cardiac surgery resulted in an increase in postoperative bleeding and greater use of allogeneic blood products.[6]
We present a case of transient a symptomatic hematuria following cell saver use in scoliosis surgery. A 14-years-old female patient presented with the scoliosis (t4-l3) level. She was booked for scoliosis correction orthopedic spine surgery.
The patient was healthy with normal preoperative lab results (blood work up and urine). Her medical history, as well as family history was unremarkable. She has neither history of medication nor hospitalization. She is not known diabetic, hypertensive, or allergic to any substances.
After IV induction of general anesthesia, invasive monitors were inserted include arterial line, central venous line, and urinary catheter. As well as 2 (16G) peripheral cannulas, and body warmer. All procedures were smooth without any injuries or excessive bleeding. Cell saver were used during the surgery and 300 mL of blood filtered through cell saver given back to the patient; followed by another 100 mL of blood was given. One unit of packed red blood corpuscles (PRBCS) was cross matched and transfused to the patient by the end of the procedure. Throughout the operation the vital signs remained stable, but gradual change of the urine color in the urine bag to pink; darker pink then to red was noticed. No bleeding or petechial hemorrhages were noticed. Close monitoring was performed, the patient remains vitally stable and she recovered smoothly from anesthesia without any complications. The patient was shifted to the post anesthesia care unit (PACU) then to word. Few hours later the urine became clear spontaneously. The patient developed transient asymptomatic hematuria after infusion of filtered blood and PRBCS. The hematuria disappeared spontaneously after few hours. Review of the preoperative causes of hematuria in nonurological cases reveals no interference with the urinary system. Moreover, there was no urethral trauma during catheter insertion. Blood pressure was stable all through the operative course that rules out the possibility of shock and eventual hematuria.
Hemolysis of the filtered blood may contribute to the development of hematuria. Hemolysis during collection with cell saver use may be caused by several mechanisms that may include the smaller diameter suction device that is used to “skim” blood from a large surface in
Sir,Surgical correction of scoliosis involving metallic fixation of the vertebral bodies is associated with extensive blood loss. Cell saver is commonly used in scoliosis surgery as a mean of salvaging and returning the patient’s red blood cells. We present a case of transient a symptomatic hematuria following cell saver use in scoliosis surgery. A 14-year-old female patient presented with scoliosis (t4-l3) level. She was booked for scoliosis correction.
The patient was healthy with normal preoperative lab results (blood work up and urine). Her medical history, as well as family history, was unremarkable.
After IV induction of general anesthesia, invasive monitors were smoothly and safely inserted without any injuries or excessive bleeding. Cell saver was used during the surgery and 300 mL of blood filtered through cell saver given back to the patient; followed by another 100 mL of blood was given as well as one unit of packed red blood corpuscles (PRBCS) was cross matched and transfused to the patient by the end of the procedure. Throughout the operation, the vital signs remain stable, but gradual change of the urine color to pink, darker pink than to red was noticed in the urine bag. Close monitoring was performed, the patient remains vitally stable and she recovered smoothly from anesthesia without any complications.
Even though it is a safe procedure to use cell saver devices, we recommend a special caution to be taken as it has the potential for a transient hematuria that may not alarm the doctors or nurses.
Substantial blood loss and the requirement for blood transfusion remain major considerations for prolonged spinal surgeries. Surgical correction of scoliosis involving metallic fixation of the vertebral bodies is associated with extensive blood loss.[1] Excessive blood loss not only increases the operative time but also increases the risks of allogeneic blood transfusion. The extensive use of pre, intra- and postoperative red blood cell salvage and autologous blood transfusion has been highly effective in reducing blood loss and transfusion requirements.[2]
Cell saver is commonly used in scoliosis surgery as a mean of salvaging and returning the patient’s red blood cells.[3] The major advantages of cell saverinclude rapid availability, reduction of exposure to infectious agents transmitted by homologous blood transfusion, and a decrease in immune modulation.[4] However, the efficacy of cell saver use in pediatric spinal deformity surgery is unclear. In addition, there are reported complications with cell saver usage in pediatric patients, including concern for reinfusion of heparin zed blood leading to altered homeostasis, and
Anesthesia view of hematuria associated with cell saver use during scoliosis surgery
AER_101_11R3

123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
248
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
Anesthesia: Essays and Researches; 5(2); Jul-Dec 2011 Letters
spine surgery. This technique causes more mechanical trauma and aspirates air, increasing the amount of blood-air interface that promotes cell rupture.[7] Furthermore, hemolysis can be induced by irrigation with hypotonic fluid, excessive suction pressure > 100 mm Hg, aspiration of clotted blood, and cell rupture can be caused by the collection of blood with povidine iodine, alcohol, hydrogen peroxide, and bone cement. All can lead to hemolysis.[8,9]
In spite of the safe use wide of cell saver in scoliosis surgery complications that ranges from mild to severe or life threatening have occurred.[10] Hematuria is rare complication but not uncommon in 1997 a case of the patient who had life-threatening disseminated intravascular coagulation (DIC) was reported, in spite of the multiplicity of the predisposing factors, but the use of the Intraoperative blood salvage was among the major ones.[11]
Keverline and Sanders reported earlier three patients with transient hematuria associated with the use of intraoperative salvage and reinfusion in different pediatric orthopedic operations. It was thought to be caused by a direct insult to the kidneys by the return of poorly washed blood.[12] In a study of five intraoperative autologous transfusions (IAT) devices when used in cardiac surgery, free hemoglobin in the collection reservoir ranged between 49.9 and 4689.9 mg/L (mean of 651 mg/L, demonstrating hemolysis with the collection process indicating that the centrifugal processing, and washing does not remove all stoma-free hemoglobin.[9]
A recent study reported the usefulness of used of cell saver in significantly decreasing postoperativeneed for blood transfusion. Furthermore, they described number of factors to be considered as significant parameters in predicting intraoperative blood loss.[13]
Even though it is a safe procedure we recommend special caution must be taken while using cell saver devices in patients as it has the potential for light transient and asymptomatic complication.
Manal Bakhsh, Muaz Al Ghadir1, Razan Naffakh, Nahid El-Bakri2
Department of Anesthesia, Administration of Operating Rooms and Anesthesia, Medical City, 1Department of Orthopedic,
2Department of Research, Research and Scientific Publication Center, Riyadh, Kingdom of Saudi Arabia
Corresponding author: Dr. Manal Bakhsh,
KFMC, Main Hospital Riyadh, KSA P.O. Box 46059, Riyadh, Kingdom of Saudi Arabia.
E-mail:[email protected]
REFERENCES
1. Shapiro F, Sethna N. Blood loss in pediatric spine surgery. Neuro Spine J 2004;13(Suppl. 1):S6-17.
2. Karapurkar A, Kudalkar A, NaikL. Apportioning, to reduce preoperative blood loss in scoliosis surgery. Indian J anaesth 2002;46:378-80.
3. Weiss JM, Skaggs D, Tanner J, Tolo V. Cell Saver: Is it beneficial in scoliosis surgery? J Child Orthop 2007;1:221-7.
4. Bowen RE, Gardner S, Scaduto AA, Eagan M, Beckstead J. Efficacy of in-traoperative cell salvage systems in pediatric idiopathic scoliosis patients undergoing posterior spinal fusion with segmental spinal instrumentation.Spine (Phila Pa 1976) 2010;35:246-51.
5. Copley LA, Richards BS, Safavi FZ, Newton PO. Hem dilution as a method to reduce transfusion requirements in adolescent spine fusion surgery. Spine (Phila Pa 1976) 1999;24:219-22.
6. Freischlag JA. Intraoperative blood salvage in vascular surgery – worth the effort? Crit Care 2004;8(Supply 2):S53-6.
7. Waters JH, Williams B, Yazer MH, Kameneva MV. Modification of suction-induced hemolysis during cell salvage. Anesth Analg 2007;104:684-7.
8. Kim-Shapiro DB, Schechter AN, Gladwin MT. Unraveling the reactions of nitric oxide, nitrite, and hemoglobin in physiology and therapeutics. Arte-rioscler Thromb Vasc Biol 2006;26:697-705
9. Sloan TB, Myers G, Janik DJ, Burger EM, Patel VV, Jameson LC. Intraoperative Autologous Transfusion of Hemolyzed Blood.AnesthAnalg 2009;109:38-42.
10. Weiss HR, Goodall D. Rate of complications in scoliosis surgery – a system-atic review of the Pub Med literature. Scoliosis 2008;3:9.
11. Mckie JS, Herzenberg JE. Coagulopathy complicating intraoperative blood salvage in a patient who had idiopathic scoliosis. A case report. J bone Joint Surg Am 1997;79:1391-4.
12. Keverline JP, Sanders JO. Hematuria associated with low-volume cell saver in pediatric orthopedics. J Pediatric Ortho 1998;18:594-7.
13. Swamy G, Crosby J, Calthorpe D, Klezl Z, Bommireddy R. Use of cell saver in instrumented thoraco-lumbar spinal fusion surgery: Should we use it rou-tinely? Journal of Bone Joint Surg. [British Volume,93-B,I27].
Access this article onlineWebsite DOI Quick Response Code
www.aeronline.org ***