Analysis of Treatment Methods for Victims of Torture in Kenya ...
11
Traumatology 19(2) 107–117 © The Author(s) 2012 Reprints and permissions: sagepub.com/journalsPermissions.nav DOI: 10.1177/1534765612451341 tmt.sagepub.com Article Introduction Several descriptions of torture have been provided by differ- ent organizations and scholars. This study adopted the definition of torture contained in the General Assembly Resolution, released by the UN Convention Against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment (1984). In Kenya, torture was widespread particularly in the 1970s and 1980s when a large number of citizens were arrested, detained, and tortured for political activism or sus- picion of commitment to a political cause or group. Torture is a standard procedure in police investigations, according to People Against Torture (PAT), 2001. The government has been reluctant to prosecute the perpetrators, even where the evidence of torture is overwhelming. This is considered to be one of the most important factors in the prevalence of torture in Kenya. Over the past two decades, inhabitants of East and Central Africa have experienced various ethnic and political con- flicts. These conflicts entail violence and torture causing injury, death, and trauma, in order to survive. The worst con- sequences of torture for the survivors are the mental effects, with a majority suffering from what is referred to as post- traumatic stress disorder (PTSD), a disorder first diagnosed among Vietnam veterans in the United states. Victims of torture suffer from destructive psychological and physical symptoms that tend to be either ignored, misdiagnosed, undocumented, or denied. It is difficult to know the exact number of people tortured, detained, or at risk in a certain country due to secrecy, underreporting, and other varying factors. The feasible alternative, which is commonly used under such circumstances, is to estimate the number of tor- ture survivors in the refugee population from the respective countries (Baker, 1992). The findings of a study among refugees attending an out- patient psychiatric clinic in Oslo (Lavik, Hauff, Skrondal, & Solberg, 1996) revealed that the prevalence of torture was 70% in males and 31% in females. The prevalence of torture among asylum seekers was found to be 20% in Denmark (Jepsen, 1988), 23% in Sweden (Horvath- Lindberg, 1988), and 30% from those arrived from the Middle East to Denmark (Montgomery & Foldspang, 1994). The overall prevalence 451341TMT XX X 10.1177/15347656 12451341Pokhariyal et alTraumatology 1 University of Nairobi, Nairobi, Kenya 2 United States International University-Africa, Nairobi, Kenya Corresponding Author: Ganesh P. Pokhariyal, University of Nairobi, P. O. Box 30197, GPO, Nairobi, 30197, Kenya. Email: [email protected] Analysis of Treatment Methods for Victims of Torture in Kenya and East Africa Region Ganesh P. Pokhariyal 1 , Ruthie Rono 2 , and Samson Munywoki 2 Abstract In this article, a comparative study of multisensory trauma processing (MTP) and conventional treatment (CT) on victims of torture/trauma (VOTs) for Kenyan citizens and refugees from East African Region has been undertaken. Kenyan VOTs were selected from the rosters of People Against Torture (PAT) and Release Political Prisoners (RPP). Refugee VOTs were selected from the United Nations High Commission for Refugees (UNHCR) and Urban Refugee Program implemented by GOAL, Kenya. Participants were randomly assigned to the two (MTP and CT) conditions, and the Stress State Inventory (SSI) scores were used to measure changes in posttraumatic stress disorder (PTSD) symptoms. Data values for 34 Kenyan and 35 refugee VOTs were recorded and analyzed. The study confirms the occurrence of PTSD in both samples. The results revealed that PTSD prevalence was 56% among Kenyan and 77% among refugee VOTs. Both treatments reduced SSI scores and PTSD symptoms in the participants. The study provides preliminary evidence that MTP and CT are almost equally effective for Kenyan sample, whereas CT appears to be more effective for refugee sample in PTSD treatment. The paired t test was conducted to check the significance of the difference in the two treatment methods. Keywords multisensory trauma processing, conventional treatment at United States International University on June 24, 2015 tmt.sagepub.com Downloaded from
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Analysis of Treatment Methods for Victims of Torture in Kenya ...

Traumatology19(2) 107 –117© The Author(s) 2012Reprints and permissions: sagepub.com/journalsPermissions.navDOI: 10.1177/1534765612451341tmt.sagepub.com
Article
Introduction
Several descriptions of torture have been provided by differ-ent organizations and scholars. This study adopted the definition of torture contained in the General Assembly Resolution, released by the UN Convention Against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment (1984).
In Kenya, torture was widespread particularly in the 1970s and 1980s when a large number of citizens were arrested, detained, and tortured for political activism or sus-picion of commitment to a political cause or group. Torture is a standard procedure in police investigations, according to People Against Torture (PAT), 2001. The government has been reluctant to prosecute the perpetrators, even where the evidence of torture is overwhelming. This is considered to be one of the most important factors in the prevalence of torture in Kenya.
Over the past two decades, inhabitants of East and Central Africa have experienced various ethnic and political con-flicts. These conflicts entail violence and torture causing injury, death, and trauma, in order to survive. The worst con-sequences of torture for the survivors are the mental effects, with a majority suffering from what is referred to as post-traumatic stress disorder (PTSD), a disorder first diagnosed
among Vietnam veterans in the United states. Victims of torture suffer from destructive psychological and physical symptoms that tend to be either ignored, misdiagnosed, undocumented, or denied. It is difficult to know the exact number of people tortured, detained, or at risk in a certain country due to secrecy, underreporting, and other varying factors. The feasible alternative, which is commonly used under such circumstances, is to estimate the number of tor-ture survivors in the refugee population from the respective countries (Baker, 1992).
The findings of a study among refugees attending an out-patient psychiatric clinic in Oslo (Lavik, Hauff, Skrondal, & Solberg, 1996) revealed that the prevalence of torture was 70% in males and 31% in females. The prevalence of torture among asylum seekers was found to be 20% in Denmark (Jepsen, 1988), 23% in Sweden (Horvath- Lindberg, 1988), and 30% from those arrived from the Middle East to Denmark (Montgomery & Foldspang, 1994). The overall prevalence
451341 TMTXXX10.1177/1534765612451341Pokhariyal et alTraumatology
1University of Nairobi, Nairobi, Kenya2United States International University-Africa, Nairobi, Kenya
Corresponding Author:Ganesh P. Pokhariyal, University of Nairobi, P. O. Box 30197, GPO, Nairobi, 30197, Kenya. Email: [email protected]
Analysis of Treatment Methods for Victims of Torture in Kenya and East Africa Region
Ganesh P. Pokhariyal1, Ruthie Rono2, and Samson Munywoki2
Abstract
In this article, a comparative study of multisensory trauma processing (MTP) and conventional treatment (CT) on victims of torture/trauma (VOTs) for Kenyan citizens and refugees from East African Region has been undertaken. Kenyan VOTs were selected from the rosters of People Against Torture (PAT) and Release Political Prisoners (RPP). Refugee VOTs were selected from the United Nations High Commission for Refugees (UNHCR) and Urban Refugee Program implemented by GOAL, Kenya. Participants were randomly assigned to the two (MTP and CT) conditions, and the Stress State Inventory (SSI) scores were used to measure changes in posttraumatic stress disorder (PTSD) symptoms. Data values for 34 Kenyan and 35 refugee VOTs were recorded and analyzed. The study confirms the occurrence of PTSD in both samples. The results revealed that PTSD prevalence was 56% among Kenyan and 77% among refugee VOTs. Both treatments reduced SSI scores and PTSD symptoms in the participants. The study provides preliminary evidence that MTP and CT are almost equally effective for Kenyan sample, whereas CT appears to be more effective for refugee sample in PTSD treatment. The paired t test was conducted to check the significance of the difference in the two treatment methods.
Keywords
multisensory trauma processing, conventional treatment
at United States International University on June 24, 2015tmt.sagepub.comDownloaded from

108 Traumatology 19(2)
of torture among refugees has been estimated to range between 5% and 35% (Baker, 1992). The rates generally depend on the composition of the sample in relation to age, gender, nationality, and point of time. A cross-sectional study carried out in Kenya on 264 motor vehicle survivors attending the orthopedic and trauma clinic of Kenyatta National Hospital (KNH) found the prevalence of PTSD to be 13.3% (Ongecha-Owuor, 2003).
Posttraumatic Stress DisorderThe defining characteristic of a traumatic event is its capac-ity to provoke fear, helplessness, or horror in response to the threat of injury or death. People who are exposed to such events are at increased risk for developing PTSD as well as for major depression, panic disorder, generalized anxiety disorder, and substance abuse, as compared to those who have not experienced traumatic events (Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995).
Although psychological suffering in response to trau-matic events has always occurred in response to human trag-edy, it was not until 1980 that the term PTSD was officially introduced into psychiatric literature. Before 1980, posttrau-matic syndromes were recognized by a variety of names, including railway spine, shell shock, traumatic (war) neuro-sis, concentration camp syndrome, and rape trauma. It has been reported that “According to the DSM-IV, PTSD is caused by traumatic events that are outside the range of usual human experiences including (but not limited to) military com-bat, violent personal assault and rape, being kidnapped or taken hostage, terrorist attacks and automobile accidents” (Yeh et al., 2009; also, American Psychiatric Association, 2000).
A number of epidemiological surveys have shown that exposure to trauma with subsequent development of PTSD is not uncommon. A study carried out in a sample of 2,493 people living in St. Louis found a lifetime PTSD rate of 0.5% among men and 1.3% among women (Helzer, Robins, & McEvoy, 1987). The PTSD rate also varies due to exposure to specific stressors, as observed in two different samples in the St. Louis study. The first group that consisted of civilians exposed to physical attack had a PTSD prevalence rate of 3.5%, and the second group consisting of Vietnam veterans had a 6.3% prevalence rate. The study also found that the number of people who experienced some symptoms after trauma was found to be substantially higher, 15% among men and 16% among women. In the National Comorbidity Survey (Kessler et al., 1995) the rate of comorbidity with other psychiatric disorders (i.e., obsessive-compulsive disor-ders, dysthymia, and manic depressive disorder) was also high. It was observed that approximately 80% of patients with PTSD meet criteria for at least one other mental disorder.
One important limitation in the PTSD literature is that many of the traumatized populations have not been studied, and the relevance of much of the available information to
these populations is unclear. It is noticed that out of numer-ous PTSD studies only 6% have been carried out in develop-ing countries (De Girolamo & McFarlane, 1996). Moreover, as the review of traumatic events demonstrates, developing countries are far more commonly the sites of natural disas-ters, wars, crimes, and other large- or small-scale disasters—the events that typically trigger PTSD. Thus, there is clear need for research on PTSD in developing countries, which this study attempts to fulfill. It is being realized that the dif-ference between cultural patterns, social structures, and cop-ing behaviors of developed and developing countries may significantly influence the incidence, severity, and psycho-social outcome of PTSD.
Treatments for Posttraumatic Stress DisorderThe most common treatments offered to trauma victims include pharmacotherapy and psychotherapy. The psycho-dynamic therapies and cognitive behavioral therapy (which can be divided into two categories: exposure therapy and anxiety management treatment [AMT]) are also applicable to PTSD.
Eye movement desensitization and reprocessing (EMDR) is one of the techniques used in the treatment of PTSD (Sapiro,1995), which is a form of exposure desensitization accompanied by saccadic eye movements. It emphasizes patient focusing on a disturbing memory or image while the therapist waves a finger across the patient’s visual field with the patient tracking the finger.
Multisensory trauma processing (MTP) is a short-term treatment program evolved through treating hundreds of U.S. officers traumatized by exposure to multiple critical incidents (Davis, 2002, private communications). The MTP follows the model of short-term counseling offered by many law enforcement agencies in the United States, which merges with and expands on various existing therapeutic models found effective in reducing or eliminating the symptoms of PTSD. MTP evolved through treating hundreds of officers traumatized by exposure to multiple critical incidents. EMDR is a critical element in MTP. The foundation of both MTP and EMDR is based on Milton Erickson’s belief that an individual has all resources needed to effect change (Haley, 1993; Shapiro, 1995). Both MTP and EMDR cause trau-matic events from being “stuck” in the present to becoming past memory and thus leading to the reduction of symptoms. The MTP simultaneously uses three alternating stimulations, consisting of varying sounds and tapping as well as eye movement. One theory that has been advanced to explain the positive change brought about by MTP is that the stress hor-mones released during exposure to a traumatic incident cause the memory of the incident to become frozen or unprocessed in the right brain, particularly the hippocampus (Van der Kolk, 1995). This frozen memory apparently leads to the symptoms of PTSD. Alternating stimulation may enable both hemispheres of the brain to process the traumatic memory,
at United States International University on June 24, 2015tmt.sagepub.comDownloaded from

Pokhariyal et al. 109
moving it from “stuck” to an appropriate memory of the past. It has also been noted that the eye movement commonly used in EMDR is similar to the back and forth movement of eyes in paradoxical or rapid eye movement (REM) sleep. One symptom of PTSD is disturbed REM sleep and a change in eye movement accompanying this type of sleep. By repli-cating what the brain does naturally in REM sleep, the natu-ral ability of the brain to process a memory may be reactivated (Mellmann, Kulick-Bell, Ashlock, & Nolan, 1995).
Neurolinguistic programming (Bandler & Grinder, 1979), Gestalt therapy (Yontef, 1993), cognitive therapy (Beck, 1995), rational-emotive therapy (Ellis & Harper, 1974), and imagery based on Ericksonian principles (Hammond, 1990) are also components of MTP, added to increase the process-ing of traumatic incidents, to replace negative or traumatic images and belief systems with more positive ones, and to provide a way of altering a manner (AWK) in which a past loss is experienced. The MTP has been designed with the understanding that PTSD is a biologically based disorder, caused by stress hormones released during exposure of trauma incidents and defined by previous experiences and belief systems (Van der Kolk, 1997). Somewhat similar to MTP, the use of music such as drumming are becoming important therapeutic tools. It has been demonstrated that drumming greatly reduced stress among Vietnam veterans and other victims of trauma, apparently by altering their brain wave patterns (Akombo, 2003).
In recent years, due to conflicts in Iraq and Afghanistan, military personnel from the United States, the United Kingdom, and other countries have been deployed into combat duties. The unknown battlefronts and war tactics, uncertain enemy identification, and long-term deployments have produced the symptoms of PTSD and other mental dis-orders in a significant number of returning American ser-vice members. Multiple deployments of personnel on the combat front put them at higher risk of PTSD. In a study of mental health problems due to these conflicts, it was reported that “The percentage of study subjects whose responses met the screening criteria for major depression, generalized anxiety, or PTSD was significantly higher after duty in Iraq (15.6 to 17.1 percent) than after duty in Afghanistan (11.2 percent) or before deployment to Iraq (9.3 percent)” (Hoge et al., 2004). These estimates were made from the studies that were conducted before further escalation of violence at these places.
Exposure therapy is considered to be a behavioral treat-ment for PTSD, as it targets learned behaviors that people engage in response to situations or thoughts and memories that are considered as frightening or anxiety provoking. Telehealth is the delivery of health services through telecom-munication technology such as the internet, telephone, or videoconferencing. Gros and colleagues (Gros, Yoder, Tuerk, Lozano, & Acierno, 2011) looked at 62 veterans who took part in individual exposure therapy through telehealth tech-nology at a local community clinic. In addition, 27 veterans
received in-person exposure therapy. The exposure therapy was for 12 sessions. It was found that exposure therapy was successful in reducing PTSD symptoms, depression, anxi-ety, and stress. Patients who took part in the in-person ther-apy showed greater reduction in their PTSD symptoms and depression, as compared to those who were subjected to tele-health technology.
Alfredson (2002) explained the practice of using children as soldiers and the phenomenon of displacement within the context of human security and explored some links between these. It was concluded that displacement of these children results in increased insecurity and lack of access to choice, resource, and adequate opportunities. As a majority of the child soldiers are not likely to return to their homes, it results in the risk of death, disability, and serious psychological trauma. Thus, restoring human security and building a sound future for such communities and societies becomes much more difficult.
Verhey (2001) has tried to provide lessons and guidance for future programs of prevention, demobilization, and rein-tegration of child soldiers, drawn mainly from in-depth case studies on Angola and El Salvador. Though prevention has been considered as the best option, efforts of working to demobilize and reintegrate requires full support of all con-cerned parties.
Hughes (2006) in her research report on child soldiers in the U.S. military described, “The impact of child soldiers on the effectiveness of combat forces, the potential for negative mental health consequences, the role media and public sup-port may contribute to that outcome and the effect on mili-tary populations beyond combat forces.” Potts (2007) looked into major areas in the issue of child soldiers: the age of the children forced into the harsh way of life, the situation of rebels themselves, and conditions of villages and the chil-dren. The cases of children being taken away from families by rebels in Sri Lanka and Uganda, as well as their torture, are discussed.
Various studies on child soldiers revealed that these chil-dren were forced out from their respective environments by rebels to join combat duties. Harsh conditions away from home and the challenges of war and torture by rebels them-selves, caused death and disabilities to some and traumatic conditions for others.
Researchers have recently turned to the use of virtual reality (VR), where simulation of the situation of the deploy-ment environment is created, to deliver exposure therapy by the clinicians (Yeh et al., 2009). Difede and Hoffman (2002) reported positive results for PTSD that was caused from the attack on the World Trade Center, by using virtual reality exposure therapy (VRET) for a patient who was unable to improve with traditional exposure therapy. In a further study with World Trade Center victims, Difede et al. (2007) reported that the VR group showed statistically and clini-cally significant decreases on the Clinician-Administered PTSD Scale (CAPS).
at United States International University on June 24, 2015tmt.sagepub.comDownloaded from

110 Traumatology 19(2)
Conventional treatments (CT) are relatively longer in duration compared to MTP in treating PTSD and utilize the following approaches as and when needed: cognitive-behavioral therapy, gestalt therapy, stress management, grief therapy, rational emotive therapy, and client-centered ther-apy. Some these therapies were used to treat the patients depending on the cause of trauma in them.
MTP and CT are the two main techniques used to treat VOTs in Kenya, which is surrounded by countries that are either in crisis or emerging from crisis. Wars between Kenya’s neighbors or rebellions from within neighboring countries have resulted, over the years, in Kenya receiving refugees from Sudan, Somalia, Congo, Ethiopia, Rwanda, and Burundi. A significant number of these refugees have been victims of torture who are highly traumatized and require rehabilitation services to enable them to become pro-ductive members of their communities. In addition, the 1991-1996 period in Kenya was characterized by ethnic and tribal clashes. These conflicts affected several communities, resulting in deaths, injuries, displacement, loss of property, and loss of self-sufficiency. Although these clashes have subsided, violence and trauma continue to occur through assaults such as rape or mugging, car-jacking, accidents (including motor vehicle accidents [MVA]), and police tor-ture. The 1998 bombing of the U.S. embassy in Nairobi also contributed to some persons being traumatized in the coun-try. Postelection violence during January 2008 has resulted in deaths, loss of property, and displacement of many Kenyans that would have long-term effects on the society (as these internally displaced people are yet to be settled).
A large percentage of victims of torture in Kenya (Kenya citizens and refugees) continue to suffer psychological effects from their experiences. A number of these victims of torture can be expected to develop PTSD. Although PTSD has been acknowledged as a diagnosis for mental disorder in developing countries, there has been no systematic research in the area of epidemiology and treatment outcomes for this disorder in these countries. Treatment modalities for psycho-logical problems including PTSD are limited and are based on the Western model of counseling. There are only a few trained counselors to deliver these services. The standard psychotherapy and drug treatments involve numerous coun-seling sessions and use of expensive drugs (which are some-times difficult to get in developing countries, like Kenya). Given the high rates of both traumatic events and their sequelae, PTSD combined with ever-increasing population of those with PTSD because of the chronicity of the disorder, it is imperative to be able to identify, immediately following trauma, those who are likely to develop chronic PTSD and to develop efficacious and cost-effective treatment for these individuals. Most of the programs are supported by donor agencies, with limited as well as targeted funding, and the victims also go for other forms of treatments, which in some cases is likely to be the reason for the variations in the ses-sions as well as shifting of the treatment options. Some of the
victims continue with the treatment sessions so that they are allowed to stay in the camps; otherwise they are likely to be sent back to their homes.
The aims of this preliminary study were to test the appli-cability of MTP for treating torture/trauma victims cross-culturally in Kenya and to compare the efficacy and cost-effectiveness of MTP with CT in ameliorating the symptoms of PTSD among traumatized individuals in Kenya. Thus, we test the hypothesis that there is no signifi-cant difference between MTP and CT for treating VOTs from both samples. However, the difference in age and gen-der were not tested in the samples.
Materials and MethodsThe study participants were drawn from three sources: (1) the population of refugees undergoing assessment at United Nations High Commission for Refugees (UNHCR) Urban Refugee program implemented by GOAL Kenya, (2) a population of Kenyan torture survivors enlisted with PAT, and (3) Release Political Prisoners (RPP). The randomly selected participants were 17 years to 65 years of age, who had been victims of torture, and who needed counseling, because they were experiencing symptoms related to trauma. A list with names of 53 refugee VOTs from UNHCR and 43 Kenyan VOTs from PAT and RPP was obtained. The names were then converted to a number for confidentiality. The selected participants were then ran-domly assigned to the respective treatment conditions as described below.
Refugee VOT sample: Participants were assigned to two treatment groups:
1. Group 1, received MTP2. Group 2, received eclectic CT methods of psycho-
therapy.
Kenyan VOT sample: Participants were randomly assigned to two treatment conditions:
1. Group 1, received MTP treatment2. Group 2, received CT as did Group 2 of the refugee
sample.
The design utilized a series of interviews and inventories inclusive of observer participation in the form of tapping, retelling trauma stories, and presenting participants with healing images for the MTP and CT treatment groups. In addition, for the CT group the combination of the above-mentioned approaches was utilized. Twenty-seven partici-pants (9 Kenyan and 18 refugees) were excluded due to various reasons, which left 69 VOTs (34 Kenyan and 35 refugees) for the final study.
It was noticed that among the Kenyan participants, 91.2% were male and 8.2% female. For the refugee sample, 57.1%
at United States International University on June 24, 2015tmt.sagepub.comDownloaded from

Pokhariyal et al. 111
were male and 42.9% were female. The mean (standard deviation) age for the Kenyan participants for combined MTP and CT group was 36.36 years (10.39), and the refugee participants for CT and MTP groups were 28.52 (6.94) years and 25.64 (4.41) years, respectively. This showed that refugee participants were relatively younger than Kenyan participants.
All the recruited Kenyan VOTs were citizens, the major-ity of whom were Kikuyu, and the rest belonged to other ethnic groups (Luhya, Luo, Kamba, Meru, Borana, and Somali). Among the refugee participants, Ethiopian Oromos were in the majority, and the remaining refugees were from other ethnic groups in Ethiopia and other countries in the region, namely Rwanda, Burundi, Congo, Southern Sudan, and Somalia.
The permission to conduct research was granted by the Ministry of Education Science and Technology. Members of USIU (for Kenyan) and GOAL (for Refugee) victims of tor-ture research team gave all interviews and treatment. The interviewers were master degree holders in counseling psy-chology and had 3 years of experience in counseling. In addition, the interviewers received formal training to admin-ister the instruments and conduct MTP as per the treatment manual developed for MTP counselors, following the spe-cific treatment protocol.
In order to determine the level of the participants’ feel-ings, fears, behaviors, and thoughts, the Stress State Inventory (SSI) was administered. Diagnostic information was obtained for at least six psychiatric disorders: PTSD, acute stress disorders (ASD), depression, ASD with depres-sion, psychosomatic with depression, and schizoaffective
disorder with reactive depression. The instrument has 20 items symptomatic of trauma as follows: intrusive (8 items), arousal (7 items), and avoidance (5 items). For Kenyan victims, the process was conducted in Kiswahili and Kikuyu languages for better understanding and adequate responses. The SSI was used in this study to indicate the effi-cacy of counseling treatment and was administered to each participant twice: before treatment (for pretreatment SSI score) and after treatment (for posttreatment SSI score; Davis, 2002, private communications).
Data AnalysisDescriptive statistics, including frequencies and percentages on categorical data, were generated for participant demo-graphics, participant diagnoses, SSI scores (before and after the treatment), and treatment outcomes. Differences in sociodemographic characteristics were noted. Associations between categorical variables were explored. Demographic and biographical data of the study participants, which included age, sex, marital status, religion, educational level, financial status, area of residence, profession, tribe, and nationality, were recorded. Paired t tests for different param-eters were conducted.
ResultsOf the 34 Kenyan participants 17 received MTP treatment and 17 received treatment consisting of a combination of CTs (Table 1). The pretreatment SSI scores of the Kenyan MTP group ranged from 42 (signifying high stress levels) to
Table 1. Vot Kenyan MTP and Conventional Treatment.
ID AgeMTP
sessionsPre-SSI score
Post-SSI score Diagnosis ID Age
Conventional sessions Pre-SSI Post-SSI Diagnosis
0014 34 M 4 20 3 PTSD 002 37M 4 29 16 Stress0060 40M 6 40 17 PTSD 006 24M 3 23 16 Mild depression0062 53M 5 41 6 PTSD 007 55M 4 16 15 Stress0063 39M 6 36 14 PTSD 008 34M 4 22 18 Stress0064 37M 6 41 33 PTSD 009 28M 3 24 10 Stress0065 38M 6 38 20 PTSD 0010 28M 4 29 13 Depression0066 44M 5 24 13 PTSD 0017 32F 4 31 16 Depression0067 65M 7 42 24 PTSD 0021 51M 3 27 20 PTSD0068 45M 7 20 3 PTSD 0082 37M 6 32 6 Stress0069 19M 4 23 13 PTSD 0083 24M 3 25 4 Mild depression0070 22M 4 23 18 PTSD 0084 51M 4 30 6 PTSD0071 25F 6 32 14 PTSD 0085 34M 5 28 3 Stress0072 39M 2 38 6 PTSD 0088 28M 5 24 13 Depression0073 40M 9 25 18 PTSD 0089 -M 5 30 14 Depression0074 26M 4 38 24 PTSD 0090 32F 5 25 9 Psychosomatic depression0080 42M 5 24 7 PTSD 0091 40M 4 25 8 PTSD0087 27M 4 18 27 Stress 0092 30F 5 18 5 Stress
Note: In the column titled Age, M and F following number of years indicate M = male and F = female, respectively; ASD = acute stress disorder; PTSD = posttraumatic stress disorder; SSI = Stress State Inventory; MTP = multisensory trauma processing.
at United States International University on June 24, 2015tmt.sagepub.comDownloaded from

112 Traumatology 19(2)
18 (signifying mild stress). Within this MTP group pretreat-ment SSI scores revealed that eight individuals were highly stressed, one was moderately stressed, and eight were mildly stressed. All the participants with the highest SSI scores (42-36), with the exception of one, were able to significantly reduce their stress by two or three categories to mild or nor-mal stress through five to seven sessions of MTP treatment. Those individuals mildly stressed, with the exception of one, either reduced their stress (but stayed in the same stress cat-egory) or dropped down one category to achieve normal stress-level scores after two to nine sessions of MTP treat-ment. One client with moderate stress was able to achieve a normal stress level in six MTP sessions.
From Table 1 it is seen that the pretreatment scores (ranging from 16 mild to 31 moderate) for the 17 Kenyan VOTs receiving CT were lower than the Kenyan MTP group. The majority (n = 10) obtained SSI scores revealing mild stress, and the remaining indicated moderate stress. Subsequently, they received fewer counseling sessions (three to five, and four to six sessions, respectively), and most were able to obtain normal stress scores on their post-treatment SSIs. On testing the hypothesis, it was found that there is no significant difference between MTP and CT in treating Kenyan VOTs.
Of the 35 refugee participants, 14 received MTP treat-ment in combination with CTs. The remaining 21 refugees who were given only CTs (Table 2) had scores ranging from 41 (signifying high stress) to 20 (signifying mild stress). Six
individuals were highly stressed, 14 were moderately stressed, and 1 was mildly stressed. After 9 to 18 sessions of CT, 3 of the highly stressed refugees scored two categories lower (mild stress) and the other three achieved scores signi-fying moderate stress. Of the 14 refugees originally showing moderate stress levels, one brought his stress level down to normal after 11 sessions of CT, 9 reduced their stress to mild levels after 7 to 30 sessions of CT, 3 remained in the same stress category but reduced their stress scores after 7 to 25 sessions of CT, and one increased his score by one point, but remained in the moderate category after 11 sessions of CT. The refugee RW fled during genocide and it seems that he was permanently scarred and, as a consequence, even after 25 sessions showed a decline of only 4 points .The refugee who scored in the mild category on the pretreatment SSI achieved the higher category of moderate stress after receiv-ing six sessions of CT.
Pretreatment scores of the MTP refugee group (Table 3) ranged from 41 (signifying high stress) to 25 (signifying mild stress). Within the MTP group pretreatment SSI scores revealed five individuals with high stress, eight with moder-ate stress, and one with mild stress. After MTP treatment most refugees achieved lower scores on the post-SSIs. Of the five individuals who had shown high stress levels, one went down to a normal level of stress, one went to a mild level of stress, and three reduced to moderate levels of stress. One of the eight moderately stressed was able to achieve normal stress levels, three scored one category lower (mild stress),
Table 2. Vot Refugee Conventional Treatment.
ID Age Conventional sessions Pre-SSI score Post-SSI score Diagnosis Interpreter used
0001ET 28M 10 27 21 Reactive depression Yes0002ET 26F 8 38 21 ASD Yes0003ET 27M 6 36 20 PTSD Yes0004ET 23F 14 41 30 PTSD Yes0005ET 27M 30 33 20 PTSD Yes0006ET 40M 13 35 17 PTSD Yes0007ET 49M 12 28 17 PTSD Yes0008ET 17F 10 34 31 PTSD Yes0009ET 17M 14 37 34 PTSD Yes00010RW 25M 25 34 30 PTSD Yes00011ET 26M 6 20 26 ASD with depression Yes00012ET 27M 11 35 36 PTSD Yes00013ET 28M 9 31 23 ASD Yes00014ET 27M 9 27 23 PTSD Yes00015ET 31M 7 33 28 PTSD Yes00016ET 34M 18 37 23 PTSD Yes00017ET 29M 9 36 34 PTSD Yes00018ET 32M 11 34 11 ASD with anxiety Yes00019ET 28M 15 31 24 PTSD No00020ET 25M 10 31 24 PTSD No00021ET 33M 10 29 24 PTSD Yes
Note: In the column titled Age, M and F following number of years indicate M = male and F = female, respectively; ASD = acute stress disorder; PTSD = posttraumatic stress disorder; SSI = Stress State Inventory.
at United States International University on June 24, 2015tmt.sagepub.comDownloaded from
Pokhariyal et al. 113
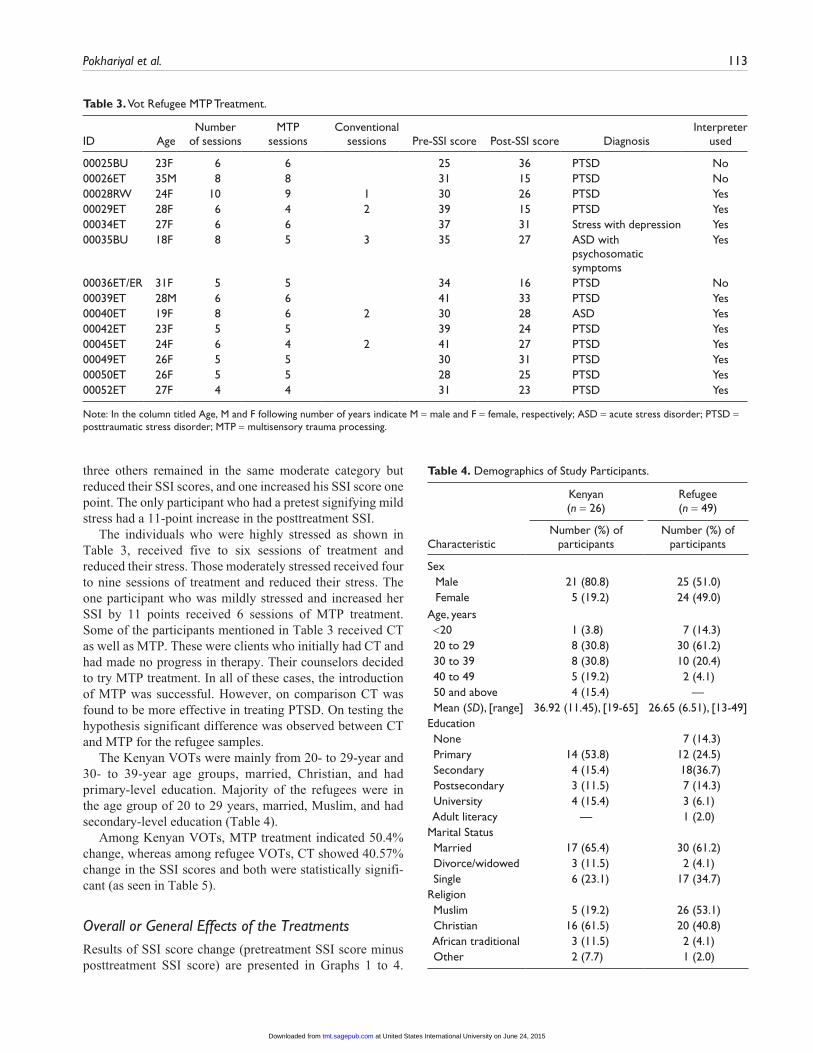
three others remained in the same moderate category but reduced their SSI scores, and one increased his SSI score one point. The only participant who had a pretest signifying mild stress had a 11-point increase in the posttreatment SSI.
The individuals who were highly stressed as shown in Table 3, received five to six sessions of treatment and reduced their stress. Those moderately stressed received four to nine sessions of treatment and reduced their stress. The one participant who was mildly stressed and increased her SSI by 11 points received 6 sessions of MTP treatment. Some of the participants mentioned in Table 3 received CT as well as MTP. These were clients who initially had CT and had made no progress in therapy. Their counselors decided to try MTP treatment. In all of these cases, the introduction of MTP was successful. However, on comparison CT was found to be more effective in treating PTSD. On testing the hypothesis significant difference was observed between CT and MTP for the refugee samples.
The Kenyan VOTs were mainly from 20- to 29-year and 30- to 39-year age groups, married, Christian, and had primary-level education. Majority of the refugees were in the age group of 20 to 29 years, married, Muslim, and had secondary-level education (Table 4).
Among Kenyan VOTs, MTP treatment indicated 50.4% change, whereas among refugee VOTs, CT showed 40.57% change in the SSI scores and both were statistically signifi-cant (as seen in Table 5).
Overall or General Effects of the TreatmentsResults of SSI score change (pretreatment SSI score minus posttreatment SSI score) are presented in Graphs 1 to 4.
Table 3. Vot Refugee MTP Treatment.
ID AgeNumber
of sessionsMTP
sessionsConventional
sessions Pre-SSI score Post-SSI score DiagnosisInterpreter
used
00025BU 23F 6 6 25 36 PTSD No00026ET 35M 8 8 31 15 PTSD No00028RW 24F 10 9 1 30 26 PTSD Yes00029ET 28F 6 4 2 39 15 PTSD Yes00034ET 27F 6 6 37 31 Stress with depression Yes00035BU 18F 8 5 3 35 27 ASD with
psychosomatic symptoms
Yes
00036ET/ER 31F 5 5 34 16 PTSD No00039ET 28M 6 6 41 33 PTSD Yes00040ET 19F 8 6 2 30 28 ASD Yes00042ET 23F 5 5 39 24 PTSD Yes00045ET 24F 6 4 2 41 27 PTSD Yes00049ET 26F 5 5 30 31 PTSD Yes00050ET 26F 5 5 28 25 PTSD Yes00052ET 27F 4 4 31 23 PTSD Yes
Note: In the column titled Age, M and F following number of years indicate M = male and F = female, respectively; ASD = acute stress disorder; PTSD = posttraumatic stress disorder; MTP = multisensory trauma processing.
Table 4. Demographics of Study Participants.
Kenyan (n = 26)
Refugee (n = 49)
CharacteristicNumber (%) of
participantsNumber (%) of
participants
SexMale 21 (80.8) 25 (51.0)Female 5 (19.2) 24 (49.0)
Age, years <20 1 (3.8) 7 (14.3) 20 to 29 8 (30.8) 30 (61.2) 30 to 39 8 (30.8) 10 (20.4) 40 to 49 5 (19.2) 2 (4.1) 50 and above 4 (15.4) — Mean (SD), [range] 36.92 (11.45), [19-65] 26.65 (6.51), [13-49]Education None 7 (14.3) Primary 14 (53.8) 12 (24.5) Secondary 4 (15.4) 18(36.7) Postsecondary 3 (11.5) 7 (14.3) University 4 (15.4) 3 (6.1) Adult literacy — 1 (2.0)Marital Status Married 17 (65.4) 30 (61.2) Divorce/widowed 3 (11.5) 2 (4.1) Single 6 (23.1) 17 (34.7)Religion Muslim 5 (19.2) 26 (53.1) Christian 16 (61.5) 20 (40.8) African traditional 3 (11.5) 2 (4.1) Other 2 (7.7) 1 (2.0)
at United States International University on June 24, 2015tmt.sagepub.comDownloaded from

114 Traumatology 19(2)
Both psychosocial treatments utilized produced a decrease in the stress level in both Kenyan and refugee participants. MTP treatment resulted in greater SSI score change in Kenyan VOTs compared to MTP-treated refugees’ SSI score
change. The CTs, on the other hand, emerged to be more effective in reducing the stress levels in refugees than in the Kenyan VOTs. Thus, CT treatment resulted in relatively larger SSI score change. There was a significant decrease in stress in both samples.
Table 6 presents the major psychiatric disorders diagnosed from the VOTs. The prevalence of PTSD among the Kenyan sample was 56% compared to 77% among the refugee sample.
Table 5. Paired t Test of Mean SSI Score Change Among Treatment Modalities.
Kenyan Refugees
Measures CT MTP CT MTP MTP + CT
Pretreatment SSI score (SD) 24.36 ± (4.50) 33.07 ± (7.57) 38.70 ± (5.41) 32.50 ± (5.63) 32.71 ± (5.51)Posttreatment SSI score (SD) 18.91 ± (2.51) 16.40 ± (8.52) 23.00 ± (6.48) 27.38 ± (4.69) 25.43 ± (5.61)Mean SSI score change (SD) 5.45 ± (4.20) 16.67 ± (9.26) 15.70 ± (8.76) 5.13 ± (7.72) 7.29 ± (7.10)% change 22.37 50.4 40.57 15.78 19.33p value (two-tailed) 0.002 0.000 0.000 0.102 0.002Correlation (significance) 0.39 (0.23) 0.34 (0.21) –0.08 (0.72) –0.11 (0.79) 0.19 (0.53)t value (df) 4.30 (10) 6.97 (14) 8.59 (22) 1.88 (7) 3.84 (13)
Note: CT = conventional treatment; MTP = multisensory trauma processing; SSI = Stress State Inventory.
Kenyan MTP Treatment Difference between Pre and Post-SSI Scores
(Signifying Improvement)
-15-10-505
10152025303540
14 60 62 63 64 65 66 67 68 69 70 71 72 73 74 80 87
Participant ID Numbers
SSI
Diffe
rence
s
Pre minus postSSI Score
Graph 1. SSI change in Kenyan VOTs as a result of MTP.Note: SSI = Stress State Inventory; VOT = victims of torture/trauma; MTP = multisensory trauma processing.
Kenyan Conventional Treatment Difference between pre and post SSI Scores
(signifying improvement)
0
5
10
15
20
25
30
2 6 7 8 9 10 17 21 82 83 84 85 88 89 90 91 92Participant ID Numbers
SSI
Diffe
rence
s
Pre minus postSSI Score
Graph 2. SSI change in Kenyan VOTs as a result of conventional treatment.Note: SSI = Stress State Inventory; VOT = victims of torture/trauma; MTP = multisensory trauma processing.
Refugee Conventional Treatment Difference between pre and post SSI Scores
(signifying improvement)
-10-505
10152025
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
Participant ID Numbers
SSI
Diffe
rence
s
Pre minus postSSI Score
Graph 3. SSI change in refugee VOTs as a result of conventional treatment.Note: VOT = victims of torture/trauma.
Refugee MTP Treatment Difference between pre and post SSI Scores
(signifying improvement)
-15-10
-505
1015202530
25 26 28 29 34 35 36 39 40 42 45 49 50 52
Participant ID Numbers
SSI
Diffe
rence
s
Pre minus postSSI Score
…………
Graph 4. SSI change in refugee VOTs as a result of MTP.Note: VOT = victims of torture/trauma; MTP = multisensory trauma processing.
at United States International University on June 24, 2015tmt.sagepub.comDownloaded from

Pokhariyal et al. 115
Table 6. Major Diagnostic Categories.
Major psychiatric disordersKenyan VOTs:
n = 34 (%)Refugee VOTs:
n = 35 (%)
Stress 8 (23.53) 1 (2.86)Depression 7 (20.59) 1 (2.86)Acute stress 0 (0) 6 (17.14)Posttraumatic stress disorder 19 (55.88) 27 (77.14)
Note: VOT = victims of torture/trauma.
PTSD comorbid psychiatric disorders diagnosed include acute stress disorder (ASD), which did not occur among the Kenyan VOTs but was seen among 17% of the refugee sample; depres-sion, which occurred in 21% of the Kenyan sample and in 3% of the refugee sample; and stress, which did appear in 24% of the Kenyan sample and 3% of the refugee sample.
DiscussionWe tested the hypothesis that there is no significant difference between MTP and CT for treating VOTs. It was found that there is no significant difference between MTP and CT for treating Kenyan VOTs. However, CT was found to be signifi-cantly better than MTP for treating the refugee group. In real-ity, MTP is an extension of CT. Most aspects of CT can be found in MTP. What is innovative about MTP is the additional use of drumming and tapping to unfreeze and shift trauma memory from the right side of the brain to the left, so that it can be put into perspective and stored and can be recollected as a management memory of the past. Preliminary findings indi-cate that MTP was more effective in treating the Kenyan sample participants, most of whom had been tortured by police. For the refugee sample participants, most of whom had been severely tortured by soldiers or government agents, CT appeared to be more effective. The paired t test indicated that SSI percentage changes were found to be statistically signifi-cant for both samples, using corresponding treatment options.
The prevalence of torture among Kenyan males was found to be higher, whereas for refugee males it was lower than that reported in the findings of Lavik and colleagues (1996). The overall prevalence of torture in our study was higher as com-pared to the results for Vietnam veterans in the United States (Baker, 1992), asylum seekers in Denmark (Jepsen, 1988), asylum seekers in Sweden (Horvath-Lindberg, 1988), and persons arrived from Middle East to Denmark (Montgomery & Foldspang, 1994). The relatively higher prevalence of tor-ture reported in our study can be attributed to the shortcom-ings in the available treatment facilities and other related factors. The incubation period from the time of traumatic event(s) to PTSD was not taken into account in this study.
Losses and FearsA major difference between the two populations is the fact that the Kenyan VOTs had not experienced loss on the same
level as the refugee VOTs. Kenyan participants know where their families are and they feel safe from most things as compared to the refugees. Refugees have had to flee from their countries and are usually without support systems. In transit there is likelihood of increased trauma for the refu-gees. They often continue to fear for their safety and usually have difficulty in having their basic needs met. The condi-tions of transiency in the camps as a consequence of not belonging to a permanent home could be considered as one factor for relatively higher trauma among refugees as com-pared to Kenyan clients. Findings in this study confirm a previous conclusion that one can get rid of more traumatic symptoms provided the client feels safe and the majority of their life issues have been addressed (Davis, 2002, private communications). This is clearly evident when comparing Graphs 1 and 2 with Graphs 3 and 4.
Counselors treating the refugees noted that the refugees had a strong desire to belong to the aid agency assisting them, probably since this was their only support system. Counselors experienced that treating victims of torture through interpreters was difficult due to their tone of voice, poor language skills, lack of sensitivity to body language, and a low level of professionalism. The counselors also faced difficulty translating from English into dialects. In some cases, there were no corresponding words, which could have a negative impact on a treatment session. The transla-tors and counselors were from both genders and were assigned to the clients of the same gender, in most of the cases. Majority of the females among the refugee sample (especially in the MTP group) had been raped and, as a con-sequence, were concerned of becoming HIV positive, which might account for MTP not appearing to be as successful a treatment for trauma among the refugees.
MTP as a Treatment for TortureAll the counselors believed that experienced therapists, trained in psychodynamics, should practice MTP and acknowledged that it worked well, often giving dramatic results. It was appreciated for the imagery work, which makes it easier for clients to let go of their conflicts, breaks defense mechanisms, and deals with material at an uncon-scious level. Some counselors recommended that the MTP protocol be reviewed and shortened, so that counselor and client could complete a session with relative ease. Different responses were reported by counselors during MTP drum tapping. Some VOTs had problem with closing their eyes possibly due to not being “in control” or an inability to trust, both probable consequences of torture.
In African societies drums can be used as warnings of impending danger or to provide joy during ceremonies. In Kenya drums usually signify happiness and joy within the community. People dance to the beat of drums. Some com-munities use drumming in rain-making rituals. It is a form of art associated with positive feelings and ecstasy. Counselors reported that some clients related to the drum sounds as
at United States International University on June 24, 2015tmt.sagepub.comDownloaded from

116 Traumatology 19(2)
music and found it soothing. When drums are used for warning, the sounds come unexpectedly, employing sharper beats, whereas drums for joy are more rhythmic. The MTP alternating drum sounds that the clients listen to during tap-ping are rhythmic. Clients from cultures where drums are associated with music and joy are more likely to benefit from MTP than are individuals who associate the drum sounds with danger or sadness.
MTP and Client Level of EducationTreating Kenyan VOTs through MTP, some counselors reported that better results were obtained for participants with higher educational background as compared to those from lower educational background (as reflected in the change of SSI scores). It would appear that Africans could generally relate better to MTP than CT, especially when the counselor and client could communicate in the same lan-guage. MTP, in general, is a transcultural therapy that emphasizes personal expectations and experiences rather than the differences between cultures and nations. MTP is action oriented, clear, and concise. In this study it was found to be a relatively provocative technique that gets directly to the problem and with some adjustments to the treatment protocol. It is likely to be a valuable therapy to use when treating traumatized individuals in Kenya and region. However, relatively larger study samples need to be under-taken for future investigations, covering various regions and cultures, in order to draw definite conclusions regarding the superiority of the treatment therapies. Regression analysis and factor analysis are planned for future studies with a larger sample.
Acknowledgments
The authors thank Dr. Nancy Davis for study material through private communication and USAID and USIU for sponsoring the study. Authors also thank the reviewers for suggestions to improve the article and Mr. C. Achola for going through the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received partial financial support from USAID and USIU for the research involved in the publication of this article.
References
Akombo, D. O. (2003) The use of drumming as cure for children with posttraumatic stress disorder (PTSD). Bowling Green, OH: Music Therapy International, Inc.
Alfredson, L. (2002, June). Child soldiers displacement and human security. Child Soldiers News Letter, pp. 17-27.
American Psychiatric Association. (2000). Diagnostic and statisti-cal manual of mental disorders (text rev.). Washington, DC: Author.
Baker, R. (1992). Psychosocial consequences for tortured refugees seeking asylum and refugee status in Europe. In. M. Basoglu (Ed.), Torture and its consequences: Current treatment approaches (pp. 83-106). Cambridge, UK: Cambridge University Press.
Bandler, R., & Grinder, J. (1979) Frogs into princes: Neuro-lingustic programming. Moab, UT: Real People Press.
Beck, J. (1995). Cognitive therapy: Basics and beyond. New York, NY: Guilford.
Verhey, B. (2001, November). Child soldiers: Preventing, demoblizing and reintegrating (Africa Region Working Paper Series No. 23). Washington, DC: World Bank.
De Girolamo, G., & McFarlane, A. C. (1996). The epidemiology of PTSD: A comprehensive review of international literature. In A. J. Marsella, M. J. Friedman, E. T. Gerrity, & R. M. Scurfield (Eds.), Ethnocultural aspects of posttraumatic stress disorder: Issues, research, and clinical applications (pp. 33-85). Wash-ington, DC: American Psychological Association.
Difede, J., Cukor, J., Jayasinghe, N., Hoffman, H. et. al. (2007). Virtual reality exposure therapy for the treatment of posttrau-matic stress disorder following September 11, 2001. Journal of Clinical Psychiatry, 68, 1639-1647.
Difede, J., & Hoffman, H. (2002). Virtual reality exposure for World Trade Center post traumatic stress disorder. Cyberpsy-chology and Behavior, 5(6), 529-535.
Ellis, A., & Harper, R. (1974). A guide to rational living. Los Angeles, CA: Wilshire Book Company.
Gros, D. F., Yoder, M., Tuerk, P. W., Lozano, B. E., & Acierno, R. (2011). Exposure therapy for PTSD delivered to Veterans via telehealth: Predictors of treatment completion and outcome and comparison to treatment delivered in person. Behavior Ther-apy, 42, 276-283.
Haley, J. (1993). Uncommon therapy: The psychiatric techniques of Milton H. Erickson. New York, NY: Norton.
Hammond, D. C. (1990). Handbook of hypnotic suggestions and metaphors. New York, NY: Norton.
Helzer, J. E., Robins, L. N., & McEvoy, L. (1987). Post-traumatic stress disorder in the general population: Findings of the epi-demiologic catchment area survey. New England Journal of Medicine, 317, 1630-1634.
Hoge, C. W., Castro, C. A., Messer, S. C., Mc Gurk, D., Cotting, D. I., & Koffman, R. L. (2004). Combat duty in Iraq and Afghani-stan, mental health problems and barriers to care. New England Journal of Medicine, 351(1), 13-22.
Horvath-Lindberg, J. (1988). Victims of torture: the Swedish expe-rience. In D. Meserez (Ed.), Refugees: The trauma of exile: The humanitarian role of the Red Cross and Red Crescent (pp. 49-52). Dordrecht, Netherlands: Martinus Nijhoff.
Hughes, J. (2006, February 15). Research report. Montgomery, AL: Air war college, Air University.
at United States International University on June 24, 2015tmt.sagepub.comDownloaded from

Pokhariyal et al. 117
Jepsen, S. (1988). The general health of asylum seekers: the Danish experience. In D. Meserez (Ed.), Refugees: The trauma of exile: The humanitarian role of the Red Cross and Red Crescent (pp. 80-86). Dordrecht, Netherlands: Martinus Nijhoff Publishers.
Kessler, R. C., Sonnega, A., Bromet, E., Hughes, M., & Nelson, C. (1995). Posttraumatic stress disorder in the National Comor-bidity Survey. Archives of General Psychiatry, 52, 1048-1060.
Lavik, N. J., Hauff, E., Skrondal, A., & Solberg, O. (1996). Mental disorder among refugees and impact of persecution and exile: Some findings from an out-patient population. British Journal of Psychiatry, 169, 726-732.
Mellmann, T. A., Kulick-Bell, R., Ashlock, L. E., & Nolan, B. (1995). Sleep events among Veterans with combat-related post-traumatic stress disorder. American Journal of Psychiatry, 152, 110-116.
Montgomery, E., & Foldspang, A. (1994). Criterion-related validity of screening for exposure to torture. Danish Medical Bulletin, 41, 588-591.
Ongecha-Owuor, F. A. (2003). Posttraumatic stress disorder among motor vehicle accident survivors attending the ortho-pedic trauma clinic at K N H. Master of medicine (psychiatry) dissertation, Department of Psychiatry, University of Nairobi, Nairobi, Kenya.
People Against Torture. (2001). Your aid against torture. Nairobi, Kenya: Author.
Potts, S. (2007, July 19). Child soldier research paper. Child Sol-dier’s Blog. Retrieved from http://www.myspace.com/child_ soldiers/blog/289638419
Shapiro, F.(1995). Eye movement desensitization and process-ing: Basic principles, protocols and procedures. New York, NY: Guilford.
United Nations Convention Against Torture and Other Cruel, Inhu-man or Degrading Treatment or Punishment. (1984). General assembly resolution (39/46). Retrieved from http://www.un.org
Van Der Kolk, B. (April, 1995). Posttraumatic stress disorder. Workshop Presented at a meeting of the Third World Congress on Stress, Trauma and Coping. Baltimore, MD.
Van Der Kolk, B. (1997). The psychobiology of posttraumatic stress disorder. Journal of Clinical Psychiatry, 58, 6-24.
Yeh, S. C., Newman, B., Liewer, M., Rizzo, A. A. et al. (2009). Application Development and Clinical Results from a Virtual Iraq System for the Treatment of Iraq War PTSD. Proceedings of the IEEE VR2009 Conference. Retrieved from http://www .Multy-Sensory Trauma Processing treatment for Trauma.
Yontef, G. (1993). Awareness, dialogue and process. New York, NY: The Gestalt Journal Press.
at United States International University on June 24, 2015tmt.sagepub.comDownloaded from