
identifying human trafficking victims in the emergency ...
35
IDENTIFYING HUMAN TRAFFICKING VICTIMS IN THE EMERGENCY DEPARTMENT: THE IMPORTANCE OF COMMUNITY PARTNERSHIPS Melissa Holland, MA KaitlinWeber RN, BSN
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of identifying human trafficking victims in the emergency ...

IDENTIFYING HUMAN TRAFFICKING VICTIMS IN THE
EMERGENCY DEPARTMENT: THE IMPORTANCE OF COMMUNITY
PARTNERSHIPS
Melissa Holland, MA Kaitlin Weber RN, BSN
WHY HEALTHCARE?
• Healthcare professionals frequently come into contact with human trafficking victims(McKinney, 2015)
• In a 2017 survey, over half of labor and sex trafficking victims went to a healthcare facility during their victimization
• 97% received no information about human trafficking (HT) or referrals for help
• Latest numbers are showing that up to 87% of victims today seek medical care, with over 60% of that number in emergency departments (Egyud, Stephens, Swanson-Bierman, DiCuccio,& Whiteman, 2017).
Healthcare systems can change the statistics!
HOW DO WE CHANGE THE STATISTICS?
The first step is education and training. Reading this PowerPoint and coming to HT classes is a big first step
The second step is to make a hospital-wide plan
The third and last step is to follow through with the plan set in place to ensure all patients are screened for HT victimization and given help, if requested

Fighting Commercial Sexual Exploitation

AWAKEN MISSION STATEMENT
We seek to increase awareness and education surrounding the issue of commercial sexual
exploitation and to provide housing and restoration for its victims.
Is Prostitution a Choice?
HUMAN SEX TRAFFICKING IS NOW CONSIDERED THE FASTEST GROWING ILLEGAL TRAFFICKING ACTIVITY IN
THE WORLD

ADJUSTED FOR POPULATION, NEVADA’S COMMERCIAL SEX MARKET
IS BY FAR THE LARGEST OF ANY STATE!
171
10589 89 86 84 82 78 78 77
Nevada New York Florida Rhode Island Delaware California North Carolina South Carolina North Dakota Georgia
Top states: Unique monthly sex providers per 100K residents
Ads market to the tastes of consumers. They provide insight into the sex buyers which create the demand for the market.
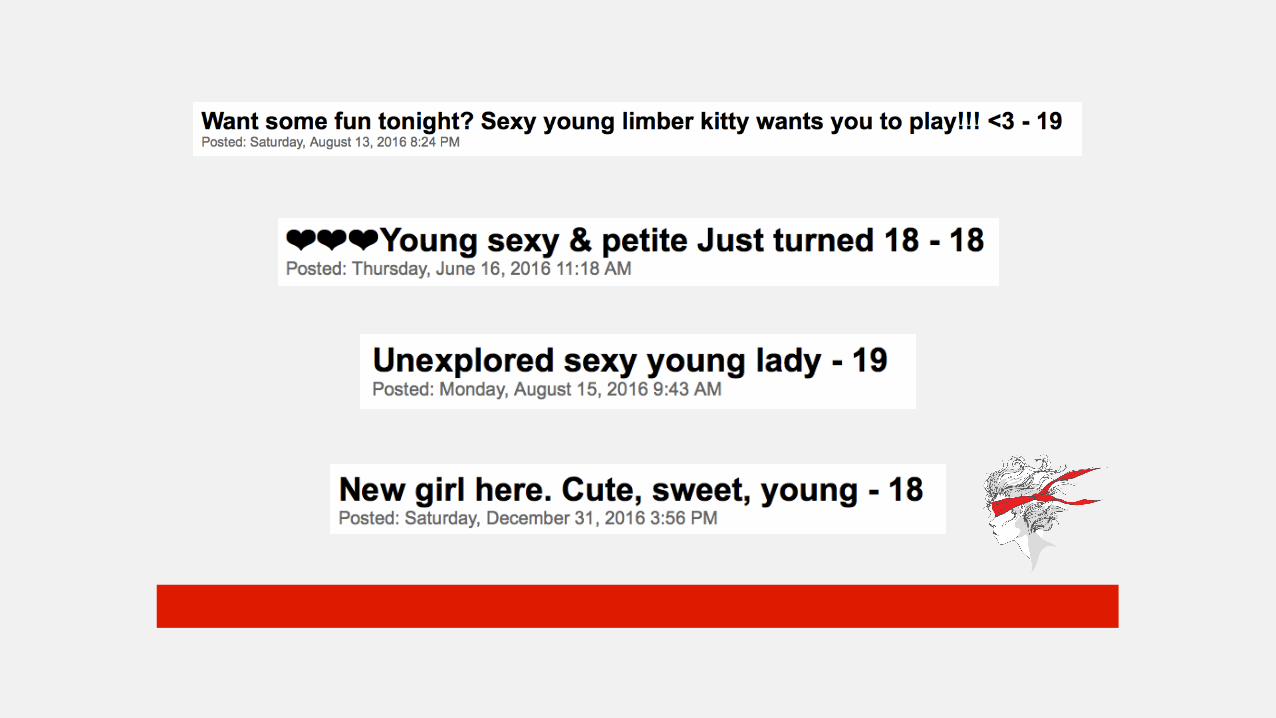
A full 72% have at least some indicator of being young, with the potential of being underage, or working in groups likely to have a trafficker.

#fight4someone
Reno/Sparks900-1000/month
Sexual Exploitation in Our Community
NEVADA/WC
• Nevada ranks 47th in overall child-well-being
• 16,554 children in Washoe County live below the poverty line
• Over 3,000 students in WC schools experienced homelessness;
• 300 lived on the streets or are couchsurfing
• WC had 492 substantiated cases of child abuse and neglect last year
Human Trafficking in a Hospital Setting
• Nearly all (92.2%) trafficked women in one study report being subjected to physical violence, such as:
• Many are victims of multiple forms of violence.
• Being shot • Strangled • Burned
• Beaten • Stabbed• Punched
• 55% Report suffering from post traumatic stress disorder
• 42% Had attempted suicide at least once
• 47% of young prostituted women reported being raped by pimps or buyers.
• 42% reported being first sold under the age of 18 and had been victims of customer-related or pimp-related violence and had been to the emergency room at least once as a result.
American Journal of Epidemiology
Women in prostitution have the highest rates of rape, physical assault, and homicide of any women ever studied.
Victims Often do NOT Self-Identify as Victims
Victims may not ask for help
• May blame themselves
• Youth may view commercial sex work as survivor to escape abuse/neglect in home
• Due to prior abuse, may not see difference between healthy and abusive/ exploitative relationship
Patient and client care staff should assess all vulnerable persons, for human trafficking concerns.
Assessing
• Children and youth • Commercial sex workers • Undocumented immigrants • Persons struggling with
homelessness
• Addiction• Persons lacking in family or
community support • Young mothers, • Foreign nationals
• Patients with controlling companions • A companion who refuses to leave the patient’s side • Patients not speaking for themselves• Patients with signs of medical/physical neglect• Patients who are submissive, fearful, hypervigilant,
and/or uncooperative.
Red Flags
The Journal of Emergency Nursing study developed these guidelines for
practice:
Major Indicators of Trauma Bonding
• Hyper vigilant to exploiter’s needs: seeks to keep exploiter happy to decrease violence
• Sees pimp as good guy, protector
• Sees world from exploiter’s perspective: may not have own perspective
• Negative feelings towards family, friends, or authorities trying to support them or help them exit the life or leave the trafficker
• Inability to engage in behaviors that may assist in their detachment
• Grateful pimp/trafficker has not killed them
Psychology of Trauma
• PTSD• Stockholm Syndrome• Complex Trauma• Trauma Bond
• “I Love Him”• “Screw You”• “He didn’t make me do it,
he just needs to get back on his feet”
• “I told him I was 18”• “I just want to go home, I’ll
be a good girl”
TWO STEP ASSESSMENT PROCESS
Red Flag Alert
• All staff from admitting, lab, radiology, ESI, and emergency services will receive education on red flags
• When red flags are identified that person will notify the ED charge RN or supervisor of a HT red flag alert
Silent Notification
• Posters will be displayed in all patient bathrooms in the emergency department (see next slide for display)
• Patients will place sticker on urine specimen cups if they answer yes to any of the questions on poster
• If any staff see blue sticker, notify ED charge RN or supervisor
SILENT NOTIFICATION POSTER
Were you (or anyone you work with) ever beaten, hit, yelled at, raped, threatened or made to feel physical pain for working slowly or trying to leave?
Are you not allowed come and go as you please?Is anyone forcing you do to anything you do not want to do?
Were you promised a job in the United States? Do you owe an individual money for transporting you?
Is someone holding documents for you? (ID, Passports, Green Card etc.) or were you promised these documents?
Are you being held against your will if you complain about conditions that you are living/working in? Are you getting paid for all hours and days you are working as well as
getting paid at least minimum wage?
If you said yes to any of these questions, please place a purple dot sticker on the bottom on your urine cup. You will be brought to a secure and safe location in the
hospital to talk with a nurse in private.
WHO TALKS DIRECTLY WITH THE PATIENT?
• It is recommended that those individuals responsible for coordinating and having conversations with be case management and specially trained RNs referred to as Nurse Advocates
• No more than two people should be having a conversation with these patients as they are large flight risks and a huge safety concern
• If you have interest in becoming a nurse advocate please see Kaitlin Weber. A 2 hour training session is required with one on one role play and case studies
The main objective for the majority of hospital staff is to be knowledgeable of the signs and know who to notify
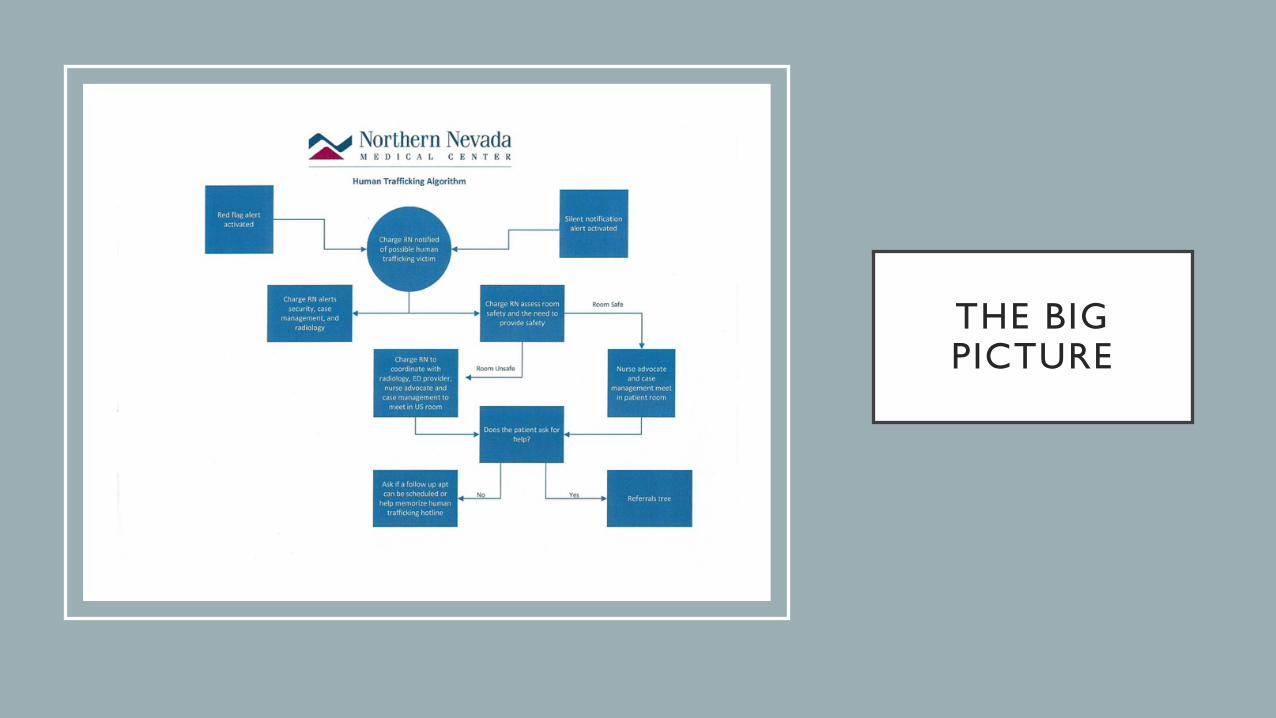
THE BIG PICTURE
REFERRAL TREE
Minors
• Follow mandated reporting protocol
• Ensure patients safety and make comfortable to decrease risk of elopement
Non Minors
• Ask patient for permission to alert local enforcement and human trafficking hotline
• If they decline then ask if we can make a follow up appointment or help to memorize hotline number
• If they accept follow tree with help of case management
REFERRAL TREE CONTINUED…
• Contact the HT hotline 1-888-373-7888
• Contact local law Enforcement
• Non emergent
• Sparks: 775-353-2231
• Reno: 775-334-2121
• Emergent call 911
• Sex trafficking
• Awaken (775) 393-9183
• Labor Trafficking
• Tu Casa (775) 432-9929
Figure 2. Referral tree adapted from the Coordinating Council, retrieved from http://www.tcccalhoun.org/referral-tree-2/

WHERE DO WE SEND THEM AFTER DISCHARGE?
• Gospel Mission, 24 hours, men and women
• (775) 329-0485
• Nevada Urban Indians 0600-1700, men and women
• (775) 788-7606
• Crisis Center, 24 hours, men and women
• (800) 273-8255
• Safe Embrace, 24 hours, women
• (775) 322-3466

THANK YOU FOR MAKING THE HOSPITAL
A SAFER PLACE FOR OUR COMMUNITY!
• Thank you for taking time out of your day to learn about human
trafficking and Northern Nevada’s plan for helping victims
• If you have any comments, questions, or concerns please don’t hesitate to reach out to
Kaitlin Weber at [email protected]
Figure 2. Pictured Barbara Amaya, human trafficking survivor. Adapted from ‘Survival Stories’ by Barbara Amaya, retrieved from http://richmondjusticeinitiative.com/human-trafficking/survival-stories/
REFERENCES
Egyud, A., Stephen, K., Swanson-Bierman, B., DiCuccio, & M., & Whiteman, K. (2017). Implementation of human trafficking education and treatment algorithm in the emergency department. Journal of Emergency Nursing, 43(6), 526-531. doi:10.1016/j.jen.2017.01.008
McKinney, M. (2015). Hospitals train staff to spot victims of human trafficking. Modern Health.Retrieved from http://www.modernhealthcare.com/article/20150620/magazine/306209987
Amaya, B. Survival stories. Richmond Justice Initiative. Retrieved from http://richmondjusticeinitiative.com/human-trafficking/survival-stories/

RESOURCES
Reporting Resources
• Federal Bureau Of Investigation
• Local Law Enforcement
Other Resources
• Awaken (775-393-9183) [email protected]