
AGENDA - Hutt Valley District Health Board
201
Hutt Valley District Health Board MAY 2014 AGENDA Held on Friday 2 May 2014 Boardroom, Pilmuir House, Hutt Hospital Commencing at 9.00am BOARD PUBLIC SESSION Item Action Presenter Min Time Pg 1. PROCEDURAL 5 9.00 am 1.1 Karakia Peter Douglas 1.2 Apologies RECORD Virginia Hope 1.3 Continuous Disclosure - Interest Register - Conflict of Interest CONFIRM Virginia Hope 2 1.4 Minutes of previous meeting ADOPT Virginia Hope 7 1.5 Matters arising from previous meetings ACCEPT Graham Dyer 15 2. PRESENTATION 2.1 Primary Care RECEIVE Bridget Allen 20 9:05 am 16 2.2 Regional Public Health RECEIVE Peter Gush 15 9:25 am 25 3. DISCUSSION PAPERS 3.1 Chair Verbal Report RECEIVE Virginia Hope 5 9:40 am - 3.2 Chief Executive Report NOTE Graham Dyer 15 9:45 am 29 4. COMMITTEE VERBAL REPORT BACKS 4.1 CPHAC NOTE Virginia Hope 5 10:00 am 40 5. OTHER 5.1 General 5 10:05 am 5.2 Resolutions to Exclude the Public APPROVE Virginia Hope 5 10:10 am 46 CLOSE 10:15 am ADDENDUMS 2.1.1 PHO Funding Streams 47 2.1.2 PHO Performance 52 2.1.3 TeAHN Annual Report 54 2.1.4 TeAHN and DHB 6 month report 72 2.2.1 CvD Diabetes CPHAC Paper 151 2.2.2 RPH Presentation 158 3.2.1 Hutt Balanced Scorecard 166 3.2.2 Operating Report 167 3.2.3 3D Programme Update 179 3.2.4 Communications Update 181 3.2.5 OIAs 185 Hutt Valley PUBLIC 2 May 2014 - Agenda 1
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of AGENDA - Hutt Valley District Health Board
Hutt Valley District Health Board MAY 2014
AGENDAHeld on Friday 2 May 2014 Boardroom, Pilmuir House, Hutt Hospital
Commencing at 9.00am
BOARD PUBLIC SESSION
Item Action Presenter Min Time Pg
1. PROCEDURAL 5 9.00 am
1.1 Karakia Peter Douglas
1.2 Apologies RECORD Virginia Hope
1.3 Continuous Disclosure- Interest Register- Conflict of Interest
CONFIRM Virginia Hope 2
1.4 Minutes of previous meeting ADOPT Virginia Hope 7
1.5 Matters arising from previous meetings ACCEPT Graham Dyer 15
2. PRESENTATION
2.1 Primary Care RECEIVE Bridget Allen 20 9:05 am 16
2.2 Regional Public Health RECEIVE Peter Gush 15 9:25 am 25
3. DISCUSSION PAPERS
3.1 Chair Verbal Report RECEIVE Virginia Hope 5 9:40 am -
3.2 Chief Executive Report NOTE Graham Dyer 15 9:45 am 29
4. COMMITTEE VERBAL REPORT BACKS
4.1 CPHAC NOTE Virginia Hope 5 10:00 am 40
5. OTHER
5.1 General 5 10:05 am
5.2 Resolutions to Exclude the Public APPROVE Virginia Hope 5 10:10 am 46
CLOSE 10:15 am
ADDENDUMS
2.1.1 PHO Funding Streams 47
2.1.2 PHO Performance 52
2.1.3 TeAHN Annual Report 54
2.1.4 TeAHN and DHB 6 month report 72
2.2.1 CvD Diabetes CPHAC Paper 151
2.2.2 RPH Presentation 158
3.2.1 Hutt Balanced Scorecard 166
3.2.2 Operating Report 167
3.2.3 3D Programme Update 179
3.2.4 Communications Update 181
3.2.5 OIAs 185
Hutt Valley PUBLIC 2 May 2014 - Agenda
1
HUTT VALLEY DISTRICT HEALTH BOARD
Hutt Valley Board INTEREST REGISTER9 MARCH 2014
Name InterestDr Virginia HopeChair
∑ Chair, Hutt Valley District Health Board∑ Chair, Capital & Coast District Health Board∑ Chair, Wairarapa, Hutt Valley and CCDHB Hospital Advisory Committees∑ Deputy Chair, Wairarapa, Hutt Valley and CCDHB Community Public Health Advisory
Committee and Disability Support Advisory Committees∑ Member, Wairarapa, Hutt Valley and CCDHB Finance Risk & Audit Committee∑ Member, Hutt Valley, Finance Risk & Audit Committee∑ Member, Capital & Coast District Health Board, Finance Risk & Audit Committee∑ Health Programme Leader, Institute of Environmental Science & Research∑ Director & Shareholder, Jacaranda Limited∑ Fellow, Royal Australasian College of Medical Administration∑ Fellow and New Zealand Committee Member, Australasian Faculty of Public Health
Medicine∑ Fellow, New Zealand College of Public Health Medicine∑ Member, Territorial Forces Employer Support Council∑ Member, CRISP Governance Board∑ Member, Laboratory Round Table∑ Brother and Sister work in Health Sector in the Wairarapa Disability Support and
LaboratoriesWayne GuppyDeputy Chair
∑ Chair, Wairarapa, Hutt Valley and CCDHB Finance Risk & Audit Committee∑ Chair, Hutt Valley District Health Board, Finance Risk & Audit Committee∑ Deputy Chair, Hutt Valley District Health Board∑ Member, Capital & Coast, Hutt Valley and Wairarapa DHBs Community Public Health Advisory
Committee and Disability Support Advisory Committee∑ Member, Capital & Coast District Health Board, Finance Risk & Audit Committee∑ Wife employed by various community pharmacies in the Hutt Valley∑ Trustee - Orongomai Marae∑ Upper Hutt City Council Mayor∑ Director MedicAlert
Katy AustinMember
∑ Member, Hutt Valley District Health Board∑ Member, Wairarapa, Hutt Valley and CCDHB Hospital Advisory Committees∑ Fergusson Home (Upper Hutt) – Voluntary input
David BassettMember
∑ Deputy Chair, Hutt Valley District Health Board, Finance Risk & Audit Committee∑ Member, Hutt Valley District Health Board∑ Member, Wairarapa, Hutt Valley and CCDHB Finance Risk & Audit Committee∑ Deputy Mayor Hutt City Council∑ Son owns Hutt City Auto Services, which has an automotive contract for the DHB∑ Director, Capacity Infrastructure Services Ltd
Peter DouglasMember
∑ Chair, Capital & Coast District Health Board, Finance Risk & Audit Committee∑ Chair, Hato Paora College Board of Trustees∑ Chair, Hato Paora College Proprietors Trust Board∑ Deputy Chair, Wairarapa, Hutt Valley & CCDHB Finance Risk & Audit Committee∑ Member, Hutt Valley District Health Board∑ Member, Capital & Coast District Health Board
Hutt Valley PUBLIC 2 May 2014 - Procedural Business
2
∑ Member, Wairarapa, Hutt Valley and CCDHB Hospital Advisory Committees∑ Member, Capital & Coast District Health Board, Finance Risk & Audit Committee∑ Member, Hutt Valley, Finance Risk & Audit Committee∑ Member, Wairarapa, Hutt Valley and CCDHB Community Public Health Advisory Committee
and Disability Support Advisory Committees∑ Director, Te Ohu Kaimoana Custodian Limited∑ Director, Charisma Developments Limited∑ Chief Executive, Te Ohu Kaimoana, Māori Fisheries Trust∑ Member, Age Concern Board
Jaimes WoodMember
∑ Member, Hutt Valley District Health Board∑ Member, Wairarapa, Hutt Valley and CCDHB Finance Risk & Audit Committee∑ Member, Hutt Valley District Health Board, Finance Risk & Audit Committee∑ Principal Advisor; Melbourne Business School-Mt Eliza∑ Strategic Advisor; Lightfoot Solutions (UK) Limited∑ Son-in-Law works for a supplier of HVDHB – and is the son of the principle shareholder
WM Bamford & Co Limited∑ Part time member – Local Government Commission
Ron MarkMember
∑ Member, Hutt Valley District Health Board∑ Member, Wairarapa District Health Board∑ Member, Wairarapa, Hutt Valley and CCDHB Community Public Health Advisory Committee
and Disability Support Advisory Committees∑ Member, Wairarapa Iwi Kainga Committee∑ Mayor for Carterton District Council∑ Patron, Te Awa Ora a Maori Mental Health Service Provider in Christchurch∑ Trustee & Lead Negotiator, Ngati Kanhungunu ki Wairarapa Tamaki Nui A Rua (Treaty
Settlement) TrustKen LabanMember
∑ Member, Hutt Valley District Health Board∑ Member, Hutt Valley District Health Board, Finance Risk & Audit Committee∑ Member, Wairarapa, Hutt Valley and CCDHB Finance Risk & Audit Committee∑ Trustee, Hutt Mana Charitable Trust∑ Member, Ulalei Wellington∑ Member, Hutt City Sports Awards Committee∑ Member, Greater Wellington Regional Council∑ Commentator, Sky Television∑ Broadcaster, Numerous Radio Stations∑ Member, Christmas in the Hutt Committee∑ Member, Hurricanes Rugby Board∑ Member, Wellington Rugby Football Union∑ Trustee, Tana Umaga Foundation
David OgdenMember
∑ Member, Hutt Valley District Health Board∑ Member, Hutt Valley District Health Board, Finance Risk & Audit Committee∑ Member, Wairarapa, Hutt Valley and CCDHB Finance Risk & Audit Committee∑ Principal, Oak Chartered Accountants Limited∑ Accountant, affiliated, with Simple Accounting Services Limited, and indirectly its
subsidiary, Five Plus Accounting Limited. Both companies have various clients involved in the Health Sector
∑ Presiding Member – Lotteries Commission Wellington and Wairarapa Communities Committee. The Funding Committee shares some applicants with regional health board providers
∑ My daughter is an Intern Psychologist with a Health Board outside this regionJohn TerrisMember
∑ Member, Hutt Valley District Health Board∑ Member, Wairarapa, Hutt Valley and CCDHB Hospital Advisory Committees
Sandra GreigMember
∑ Member, Hutt Valley District Health Board∑ Member, Wairarapa, Hutt Valley and CCDHB Community Public Health Advisory Committee
and Disability Support Advisory Committees∑ President Woburn Probus∑ Member Greater Wellington Regional Council∑ Cousin is a midwife in Napier
Hutt Valley PUBLIC 2 May 2014 - Procedural Business
3

Hutt Valley PUBLIC 2 May 2014 - Procedural Business
4
Updated April 2014
Wairarapa and Hutt Valley DHB Executive Leadership Team
Interest register April 2014
Name Interest
Graham DyerChief ExecutiveWairarapa and Hutt Valley DHBs
∑ Trustee, Bossley Dyer Family Trust∑ Wife is a Director of i-Management which does consulting and
audit work in the Health Sector∑ Member, Crisp Interim Governance Board∑ Member, Health Workforce New Zealand
Bridget AllanChief Executive, Te Awakairaongi Health Network (PHO)
∑ Chief Executive, Te Awakairangi Health Network (PHO)∑ Board member of Vibe
Ashley BloomfieldDirector Service Integration and Development
∑ Trustee, AR and EL Bloomfield Trusts ∑ Fellow, NZ College of Public Health Medicine ∑ Board Member, Action on Smoking and Health (ASH) NZ ∑ Member NZ College of Public Health Medicine Finance and Risk
Committee∑ Sister is a nurse at Hutt DHB∑ Wife was employed at Hutt Family Planning Association clinic
during 2009-10Pete ChandlerChief Operating Officer
∑ Chair – Central Region Chief Operating Officers Group∑ Chair – National Laboratory Engagement Group
Carolyn CooperExecutive Director, people and Culture
∑ Sister in law is an independent member of the Community Labs Group
Judith ParkinsonFinance Manager
No interests declared.
Helen PocknallExecutive Director Nursing and Midwifery
∑ Board Member, Health Workforce New Zealand
Nadine MackintoshBoard Secretary
No interests declared.
Hutt Valley PUBLIC 2 May 2014 - Procedural Business
5

Updated April 2014
Richard SchmidtExecutive Officer
∑ Member of the Hutt Foundation
Russell SimpsonExecutive Director Allied Health, Scientific and Technical
∑ Chair, Central Region Directors of Allied Health∑ Member, Regional Leadership Committee
Jill StringerCommunications Manager
∑ Trustee, Wairarapa Regional All Weather Track Trust∑ Husband works for Rigg Zschokke Ltd
Iwona StolarekChief Medical Officer
∑ Member, ASMS JCC∑ Husband Andrew Simpson:
- Executive Director for Medicine Cancer & Community CCDHB
- Executive Member of the Cancer Society Wellington Division
- National Clinical Director Cancer Programme – Ministry of Health
Justine Thorpe ∑ Tihei Wairarapa Programme Director, employed by Compass Health
∑ A member of the Wairarapa Campaign Committee for the NZ Labour Party
Cate TyrerGeneral Manager Quality and Risk
∑ Shareholder and Director of Framework For Compliance Ltd (FFC)
∑ Husband is an employee of Hutt Valley DHB
Stephanie TurnerDirector Maori Health
∑ Represent Rangitane Iwi on the Wairarapa Cultural Trust (Aratoi)
∑ Establishing member of Pasifika Wairarapa Trust∑ Director Waingawa Ltd∑ Director Aroha Ki Te Whanau Trust∑ Member Cameron Community House Governance Group
Tofa Suafole GushDirector Pacific Peoples Health
∑ Member of the Te Awakairangi Health Board∑ Husband is an employee of Hutt Valley DHB
Kuini PuketapuManager Maori Health Advisor
∑ Chair of Board of Trustees, Pukeatua Te Kohanga Reo∑ Board Member, Te Runanganui o Taranaki Whanui ki te Upoko
o te Ika a Maui who has contracts with Hutt Valley DHB to provide health services in the Hutt Valley area and is an approved Whanau Ora provider
∑ Member, Wainuiomata Community Governance Group∑ Chair, Waiwhetu Medical Group which is a limited liability
company affiliated to Te Awakairangi Health PHO
John Ryan3DHB Executive Director, Corporate Services
∑ Son works for Spotless Services.∑ Cousin works as Orthopaedic Nurse at Capital and Coast DHB
Hutt Valley PUBLIC 2 May 2014 - Procedural Business
6
PUBLIC
Hutt Valley District Health Board MARCH 2014 Page 1
MINUTES Held on Friday 21 March 2014 Board Room, Pilmuir House, Hutt Hospital, Lower Hutt
Commencing at 9.10am
BOARD PUBLIC SECTION
HUTT VALLEY DISTRICT HEALTH BOARD
PRESENTVirginia Hope ChairWayne Guppy Deputy ChairKaty Austin MemberDavid Bassett MemberPeter Douglas MemberSandra Grieg MemberRon Mark MemberDavid Ogden MemberJohn Terris MemberJaimes Wood Member
IN ATTENDANCEGraham Dyer Chief ExecutiveNadine Mackintosh Board SecretaryAshley Bloomfield Director Service Integration Development UnitJill Stringer Communications ManagerBridget Allen Chief Executive Te Awakairangi Network
PUBLICTwo members of the press
PRESENTERSTofa Gush 2DHB Director of Pacific HealthSharon Ritchie Hutt Valley Emergency Management ManagerCate Tyrer General Manager Quality and Safety
1.0 PROCEDURAL BUSINESS1.1 KARAKIA
The meeting was opened with a Karakia by Mr P Douglas.
1.2 APOLOGIESNo apologies were required for the meeting.
1.3 CONTINUOUS DISCLOSURE
1.3.1 INTEREST REGISTERAmendments to the interest register were received from Sandra Greig, David Ogden, Ken Laban and Ron Mark as follows:
Hutt Valley PUBLIC 2 May 2014 - Procedural Business
7

PUBLIC
Hutt Valley District Health Board MARCH 2014 Page 2
Sandra Greig - President Woburn Probus, Member Greater Wellington Regional Council and Cousin is a Midwife in Napier
David Ogden – Daughter is an Intern Psychologist with a Health Board outside this region
Ken Laban – Member Greater Wellington Regional Council, Commentator for Sky Television, Broadcaster for numerous Radio Stations, member of Christmas in the Hutt Committee, member of Hurricanes Rugby Board, member of Wellington Rugby Football Union and Trustee for Tana Umaga Foundation.
Ron Mark - Trustee & Lead Negotiator, Ngati Kanhungunu ki Wairarapa Tamaki Nui A Rua (Treaty Settlement) Trust
The Board RESOLVED to ADOPT the amendments to the interest register.
MOVED David Bassett SECONDED James Wood CARRIED
1.3.2 CONFLICTS RELATED TO AGENDA ITEMSSandra Greig and David Bassett declared a potential conflict of interest with respect to agenda item 3.3 on the DHB position statement for community water fluoridation with the Chair advising the Board would consider how we address the conflicts when the item is discussed.
CONFIRMED The Board confirmed that it was not aware of any other matters (including matters reported to, and decisions made, by the Board at this meeting) which require disclosure.
MOVED David Bassett SECONDED James Wood CARRIED
1.4 CONFIRMATION OF MINUTESRESOLVED to ADOPT the minutes of the members’ (Public) meeting held on 11 February 2013 as a true and accurate record of the meeting.
MOVED David Bassett SECONDED James Wood CARRIED
1.5 MATTERS ARISINGAmendment: The Board requested that AP74 be broadened to organisational service visits.
2.0 PRESENTATION
2.1 PACIFIC HEALTHPresenter: Director of Pacific Health
Tofa Gush presented a detailed update on the Pacific Health Sector:- The establishment of Pacific Health sector- Population of the community and leadership- Engagement with key contacts in the community- Health improvement results- Health condition concerns.- Workforce development
Hutt Valley PUBLIC 2 May 2014 - Procedural Business
8

PUBLIC
Hutt Valley District Health Board MARCH 2014 Page 3
The Board discussed- that DNA had been a concern with this group and were content with the significance of the
reporting and engagement with the people- the measurement and evaluation of the impacts of the work- the importance of quality experiences for people attending the appointments - their support for the plan- acknowledgment of the experience that Director of Pacific Health’s brings to the DHB.
ACTIONB08 The Communication Manager is to provide a positive media story on the joint Wairarapa and Hutt
Valley Pacific Health Director appointment.
The Board NOTED the contents of the presentation.
3.0 DECISION PAPERS
3.1 GOVERNANCE MANUALPresenter: Chair
The paper was taken as read. The Board supported for the 3DHB Governance Manual noting its that the manual will be regularly reviewed and the next version will address any comments raised adopt this as a working document.
The Board RESOLVED to ADOPT the attached Board manual as being applicable for Wairarapa DHB, Hutt Valley DHB and Capital & Coast DHB.
MOVED Jaimes Wood SECONDED David Bassett CARRIEDAGAINST David Ogden and John Terris
ACTIONB06 Develop an Engagement Plan for the DHB including the 3DHB work.B05 Review Institute of Directors practice on the technical matters of meeting procedures and test with
legal Counsel.
3.2 BOARD COMMITTEE MEMBERSHIPS WITHIN THE LOWER NORTH ISLAND (LNI)Presenter: Chair
The paper was taken as read acknowledging the movements of Capital & Coast member representives:Board CPHAC HACCCDHB David Choat
Chris LaidlawHelene RitchiePeter Douglas (FRAC Chair)
Sue KedgleyNick LeggettDerek Milne
HVDHB Virginia Hope Wayne Guppy (FRAC Chair)Sandra GreigRon Mark
Virginia Hope John TerrisKaty Austin
WDHB Derek Milne (Chair)Leanne Southey (FRAC Chair)Helen KjestrupJanine VollebregtLiz Falkner
Rob IrwinFiona SamuelAlan Shirley
Hutt Valley PUBLIC 2 May 2014 - Procedural Business
9

PUBLIC
Hutt Valley District Health Board MARCH 2014 Page 4
* CPHAC and HAC will retain the Maori representation and HAC a PHO representative.
Wairarapa Hutt Valley Capital & CoastLeanne Southey (Chair)Rob IrwinRon KaraitianaRick LongDerek Milne
Wayne Guppy (Chair)David BassettPeter DouglasVirginia HopeKen LabanDavid OgdenJaimes Wood
Peter Douglas (Chair)Judith AitkenRoger JarroldDarrin SykesDerek MilneVirginia Hope
The Board RESOLVED to:
a. AGREE to co-opt members from either Wairarapa, Hutt Valley and/or Capital & Coast as set out in this paper for the CPHAC/DSAC and HAC committees, as applicable.
b. NOTE the membership change for the Capital & Coast FRAC committee.
MOVED Wayne Guppy SECONDED David Bassett CARRIED
3.3 POSITION STATEMENT - COMMUNITY WATER FLUORIDATIONPresenter: 3DHB Director of SIDU
The Board discussed fluoridation of the council water supply. The Board members agreed that the matter of fluoridation was treated as a “concience vote” at council meetings and Board members who were also council members were at liberty the exercise their votes independently of council decisions.
The Deputy Mayor of Hutt City Council reported that this has been an issue for a number of years and that there has been a small increase in support for removal of fluoridation amongst the councillors. Hutt City Council has a provision of two aquifer taps in the City and installation of two additional taps for those members of the community that are against fluoridation.
The Board members views on the subject of fluoridation or non-fluoridation policy discussed were:- Benefits to dental care- Consumption of tap water- Fluoride in toothpaste- Upper Hutt City Council endorsement of fluoridation of water- Anti-fluoridation evidence- Aquifer water supplies non fluoridated water in the Hutt City Council region providing opportunity
for those who don’t wish to use fluoridated water in Petone and Dowse.
It was noted that anti-fluoridation groups are well prepared for meetings of discussion groups and that these meetings need to include the contradicting view in order to allow sound decision making.
The Director of SIDU advised this paper provides a position statement for a District Health Board from a public health perspective. The last paragraph reports that the Council receive good balanced evidence on the matter in order to support their vote.
There was a request to add an amendment to move the decision of water fluoridation to National policy.
MOVED David Ogden SECONDED John Terris NOT CARRIED
Hutt Valley PUBLIC 2 May 2014 - Procedural Business
10

PUBLIC
Hutt Valley District Health Board MARCH 2014 Page 5
The Chair confirmed that there had been value in having a free and frank discussion on this item with all Board members noting the potential conflict of some members and that discussion was from a personal perspective.
The Board RESOLVED to:a. NOTE the endorsement from the Community and Public Health Advisory Committee and Disability
Support Advisory Committee for the Position Statement regarding Community Water Fluoridationb. ADOPT the Position Statement regarding Community Water Fluoridation
MOVED Wayne Guppy SECONDED Sandra Grieg CARRIED
Dr Hope noted a linkage between RPH and her workplace in relation to gathering evidence on the impacts of fluoridation and indicated a wish to abstain.
ABSTAINED Virginia HopeAGAINST David Ogden and John Terris
4.0 DISCUSSION PAPERS
4.1 CHAIR UDPATEThe Chair provided a verbal reporting on key discussions attributed to recent meetings.
- Board Induction processes with a number of planned information sessions to be held throughout the year
- The Minister opening the new dialysis unit located at Kenepuru Hospital which services the region. The facilities are among the best in the country and will service our communities well.
ACTIONB04 Arrange a tour of the dialysis unit at Kenepuru Hospital when practicable.
The Board RECEIVED the update.
4.2 CHIEF EXECUTIVE’S REPORT – MARCH 2014 Presenter: Chief Executive
The report was taken as read with the Chief Executive discussing key highlights of the report.- The DHB is continuing to make good gains on the Health Targets- The key issues reported in the Balanced Scorecard: Theatre Utilisation and DNAs- Appointment to the role of Executive Director of Maori Health across the 3DHBs- Improved vertical health integration in particular health pathways and ALT frameworks - High levels of hepatitis A in the Hutt Valley- Quality of drinking water and role of public health for health protection- Financial pressures
Board member discussion ensued on: - The current over delivery of elective targets being required to compliment the move to a four month
elective wait time target, acknowledging there is still further work required to achieve the four month requirement. The financial impacts of over delivery were also noted.
- The Cardio Vascular Disease indicators and processes should further improve results in primary care.- Support for the 3DHB programme at Committee meetings.
The Board NOTED the information contained in this report.
Hutt Valley PUBLIC 2 May 2014 - Procedural Business
11

PUBLIC
Hutt Valley District Health Board MARCH 2014 Page 6
5.0 INFORMATION PAPER
5.1 EMERGENCY MANAGEMENT UPDATEPresenter: Quality and Risk Manager and Emergency Preparedness Manager
A detailed update on plans was presented highlighting the DHB are working toward a coordinated approach for integrated health responses across the sub-region in preparation of an adverse event. A trial exercise will take place in October 2014.
Board discussions ensued on- workforce management across the sub-region for an adverse event- the national health emergency plan that feeds to the regional and local plans, particularly
communications- lessons learnt from last years severe weather conditions and earthquakes
The Board RESOLVED to:
a. RECEIVED the report
b. SUPPORT the heightened level of activity in the plan
c. NOTED that there are contingency plans in place in the event of a major incident
d. NOTED that there are improvements in resilience being achieved through a 2D and 3D approach
MOVED Virginia Hope SECONDED Sandra Grieg CARRIED
6.0 COMMITTEE VERBAL REPORT BACKS
6.1 CHPAC-DSAC REPORT BACKThe paper was taken as read. It was noted that this committee is working effectively after a year of establishment.
The Board NOTED the contents of this report.
6.2 HAC VERBALThe Chair reported the meeting had a particular focus on the areas of- Health of Older People- Presentations at the Provider Arm
Future reporting will work toward the alignment of reporting across the committees to the Boards with an emphasis of performance based reporting.
The Board NOTED the verbal reporting.
7.0 OTHER
7.1 GENERALNil
Hutt Valley PUBLIC 2 May 2014 - Procedural Business
12

PUBLIC
Hutt Valley District Health Board MARCH 2014 Page 7
7.2 RESOLUTIONS TO EXLUDE THE PUBLICRESOLVED: The Board resolved to agree that as provided by Clause 32(a), of Schedule 3 of the New Zealand Public Health and Disability Act 2000, the public are excluded from the meeting for the following reasons:
Agenda Item Reason Reference
Chief Executive ReportProject the privacy of the naturals persons and to enable a Minister of the Crown or any department or organisation holding the information to carry out, without prejudice or disadvantage, commercial activities
Section 9(2)(a) (i)
Sustainability Plan
Board RepresentationOpportunity to discuss availability including personal commitments Section 9(2)(a)
Governance ManualPaper contains information and advice that is likely to prejudice or disadvantage negotiations
Section 9(2)(j)
Lab Information Systems (LIS)
Draft Annual Plan
Subject to ministerial Approval Section 9(2)(f) (iv)
Draft RSP
Draft 2014/15 Budget
To enable a Minister of the Crown or any department or organisation holding the information to carry out, without prejudice or disadvantage, commercial activities
Section 9(2)(i)
Funder Commitment List 2014/15
Loan Rollover
Insurance Premium
PHO Funder Delegation
CRISP Paper contains information and advice that is likely to prejudice or disadvantage negotiations Section 9(2)(j)
Board Work Plan
MOVED David Bassett SECONDED Wayne Guppy CARRIED
THE MEETING CLOSED AT 11.11 AM
Hutt Valley PUBLIC 2 May 2014 - Procedural Business
13
PUBLIC
Hutt Valley District Health Board MARCH 2014 Page 8
8. DATE OF NEXT MEETING
Friday 2 May 2014, Boardroom, Pilmuir House, Lower Hutt
CONFIRMED that these minutes constitute a true and correct record of the proceedings of the meeting.DATED this day of 2014
VIRGINIA HOPECHAIR
Hutt Valley PUBLIC 2 May 2014 - Procedural Business
14

PUBLIC
Hutt Valley District Health Board Page 1 MAY 2014
SCHEDULE OF ACTION POINTS FOR PUBLIC BOARDOriginal Meeting Date
Ref Topic Action Resp How Dealt with Delivery date Completed Date
21 March 2014 B08 Pacific Health The Communication Manager is to provide a positive media story on the joint Wairarapa & Hutt Valley Pacific Health Director appointment .
Jill Stringer Local Paper March Completed
B06 Governance Manual Engagement Plan to include 3DHB work Board Secretary and Legal
Update Paper 1 March 2015
B05 Review Institute of Directors practice on the technical matters of meeting procedures & test with the legal council.
B04 Chair Update Arrange a tour of the dialysis unit at Kenepuru Hospital Board Secretary Future HAC or next Board workshop
July or later
B03 Overview of Heart Disease and Diabetes
Management to request that the PHO report back on the cardio vascular disease and risk programme as part of their bi-annual reports to the Board.
Bridget Allan & Justine Thorpe
Presentation May In presentation
1 November 2012 AP74 Organisational Service Visits
Management to review the annual work plan and integrate organisational service visits when when agenda is light.
Board Secretary Annual Work plan Ongoing
4 October 2013
AP69
Maori Health Targets
Management to request TeAHN to provide an update at their next presentation on the strategy for addressing Maori health targets. Maori Health Service could be requested to assist with this strategy.
CE TeAHN Presentation May
In presentation
Hutt Valley PUBLIC 2 May 2014 - Procedural Business
15

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Boards Page 1 MAY 2014
BOARD INFORMATION PAPER
Date: 28 April 2014
Author Sandra Williams, Group Manager, Service Integration: Population Health, Mental Health and Addiction
Endorsed By Ashley Bloomfield, Director Service Integration and Development
Subject Wairarapa, Hutt Valley and Capital & Coast DHBs Primary Care Update
RECOMMENDATION
It is recommended that the Boards
a. Receive & Note the contents of this update report on Primary Care and the work programme of the Alliance Leadership Teams (ALTs)
b. Note Primary Health Organisation (PHO) and ALT representatives will be in attendance at the meeting to discuss this paper and respond to any questions.
ADDENDA
2.1.1 PHO Funding Streams (additional information)2.1.2 PHO Performance2.1.3 TeAHN Annual Report2.1.4 TeAHN Board and DHB 6 month Report
1 PURPOSE
The purpose of this paper is to provide an overview to the Boards about primary care and the work of the Alliance Leadership Teams (ALTs) across the sub-region of Wairarapa District Health Board(Wairarapa DHB), Hutt Valley District Health Board (Hutt Valley DHB) and Capital & Coast District Health Board (CCDHB). This report includes:
ß An overview of Primary Health Organisations (PHOs) and their performance (section 3 and Appendix 1 and 2)
ß An overview of the sub regional enablers common to each of the ALTs including (section 4):o HealthPathwayso Shared care records (Manage My Health (MMH))o E referralso Common Primary Options for Acute Care (POAC) activity across the three
DHBs.ß An update on the work programme and activity of each ALT (section 5).
2 BACKGROUND
PHOs were established as the vehicle for implementing the Government’s Primary Health Care Strategy 2001. This strategy focussed on six key directions:
ß To work with local communities and enrolled populations; ß Identify and remove health inequalities; ß Offer access to comprehensive services to improve, maintain, and restore people’s health;
Hutt Valley PUBLIC 2 May 2014 - PRESENTATION
16
PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board Page 2 MAY 2014
ß Co-ordinate care across service areas; ß Develop the primary health care workforce; and ß Continuously improve quality, using good information.
Wairarapa DHB has a single PHO managed by Compass Health (Compass). Hutt Valley DHB has one PHO, Te Awakairangi Health Trust (TAH) and a practice participating in Cosine Primary Health Network (Cosine), a cross boundary PHO. Capital & Coast DHB has four PHOs: Compass , Well Health Trust (WellHealth), Ora Toa PHO (Ora Toa), and Cosine.
In 2008, the National-led Government introduced its health manifesto of “Better, Sooner, More Convenient” (BSMC). For primary care, this was intended to accelerate delivery of the previous Government’s primary health care strategy, with a focus on delivering a more personalised primary health care system that provides services closer to home, makes Kiwis healthier and reduces pressure on hospitals. The “how” included Integrated Family Health Centres, services shifted out of hospitals, increased focus on long-term conditions management in the community, increased clinical engagement and leadership, and reduced management bureaucracy (fewer PHOs).
A new national PHO Agreement developed collaboratively with Primary Care was implemented 1 July 2013. This Agreement better reflects the role of primary care in an integrated health system. The changes are designed to improve people's health and individual patient experience, while supporting the clinical and financial sustainability of the health system. The Agreement includes a new introductory section providing background and context to the relationship between PHOs and DHBs, and sets out the policy objectives for health care and primary health care services. It details the objective that health services should be provided on a “best for patient” and "best for system" basis.
It also describes the parties' respective roles and responsibilities, including reinforcing the requirement of DHBs and PHOs to work together in Alliancing arrangements, developing the DHB Annual Plan and agreeing the explicit contributions the PHO will make to the successful delivery of the plan.
The Agreement sets out the new minimum requirements that all PHOs will meet, the functions of the PHO and the outcomes that the PHO will endeavour to achieve, including facilitating and promoting service development, co-ordination and integration. It also provides a transition process into the new Flexible Funding Pool arrangements associated with Alliancing which were agreed by Cabinet earlier in 2013.
Each of the three District Health Boards now have Alliance Leadership Teams (ALTs) that are tasked with providing a whole-of-system view across the health system, while looking for opportunities for greater integration. The Wairarapa was one of the nine original BSMC business cases and has had an Alliance Agreement and an ALT since 2010. This programme of work is called Tihei Wairarapa. Hutt Valley DHB and CCDHB established their ALTs in July 2013. The HVDHB ALT is called Hutt Inc and was developed out of the Primary Secondary Strategy Group (PSSG), while at CCDHB the Integrated Care Collaborative (ICC) has evolved into the ALT.
3 PRIMARY HEALTH ORGANISATIONS
3.1 Demographic Information
Wairarapa DHB
There are seven general practices in the Wairarapa. Over half the population is enrolled with the largest practice, Masterton Medical. There are two other small practices in Masterton, one of which is a VLCApractice and one practice in each of the four South Wairarapa towns.
Hutt Valley DHB
There are currently 24 General Practices in the Hutt Valley. Of these 24 practices, 23 are members of Te Awakairangi Health Network and one, Ropata Medical Centre, is a member of Cosine.
Hutt Valley PUBLIC 2 May 2014 - PRESENTATION
17

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board Page 3 MAY 2014
Capital and Coast DHB
There are currently 61 funded General Practices in the Capital & Coast District with 338 GPs including locums. Of these 61 practices,
∑ 52 are members of Compass Health, ∑ Four are members of Well Health Trust, ∑ Four are members of Ora Toa PHO, and ∑ One is a member of the Cosine Primary Care Network.
Sustainability of solo (or very small) general practice providers in this funding, and broader primary care, environment is a challenge for PHOs. Although the majority of practices in CCDHB are classified as medium (four to six working GPs) or large (6+), there are 20 practices that have one to three GPs working currently.
PHO/Primary Care Core Services Funding
PHO core funding covers first contact care (standard visits to general practice), very low cost access, free under-sixes visits, services to improve access (SIA) and health promotion. In addition, they receive PHO quality performance payments throught the PHO performance progamme (PPP), funding for managing patients with long-term conditions (Care Plus), and funding for primary care mental health services.
Table 1: Sub-regional PHO information, Jan-Mar 2014 registers
DHB Area PHONo. of
practices
No. of VLCA#
practices
Total enrolled
populationHigh needs population
% high need
patients
Capital & Coast
Compass Health 53 6 247,842 48,682 20%
WellHealth 3 3 12,791 9,326 73%
Ora Toa 4 4 12,587 10,117 80%Cosine -Karori MC 1 0 14,319 1,508 11%
Hutt Valley
Cosine -Ropata MC 1 0 18,997 3,513 18%Te Awakairangi 24 6 116,537 43,161 37%
WairarapaCompass Health 7 1 41,884 11,590 28%
Source: MOH PHO Enrolment Datamart
# VLCA = Very Low Cost AccessVLCA is based on practices receiving very low cost access capitation payments for the January 2014quarter.High needs is defined as Maori, Pacific and non-Maori non-Pacific living in quintile 5HUCHS in Te Awakairangi has two sites and has been counted twice as per the MOH register
Hutt Valley PUBLIC 2 May 2014 - PRESENTATION
18
PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Boards Page 4 MAY 2014
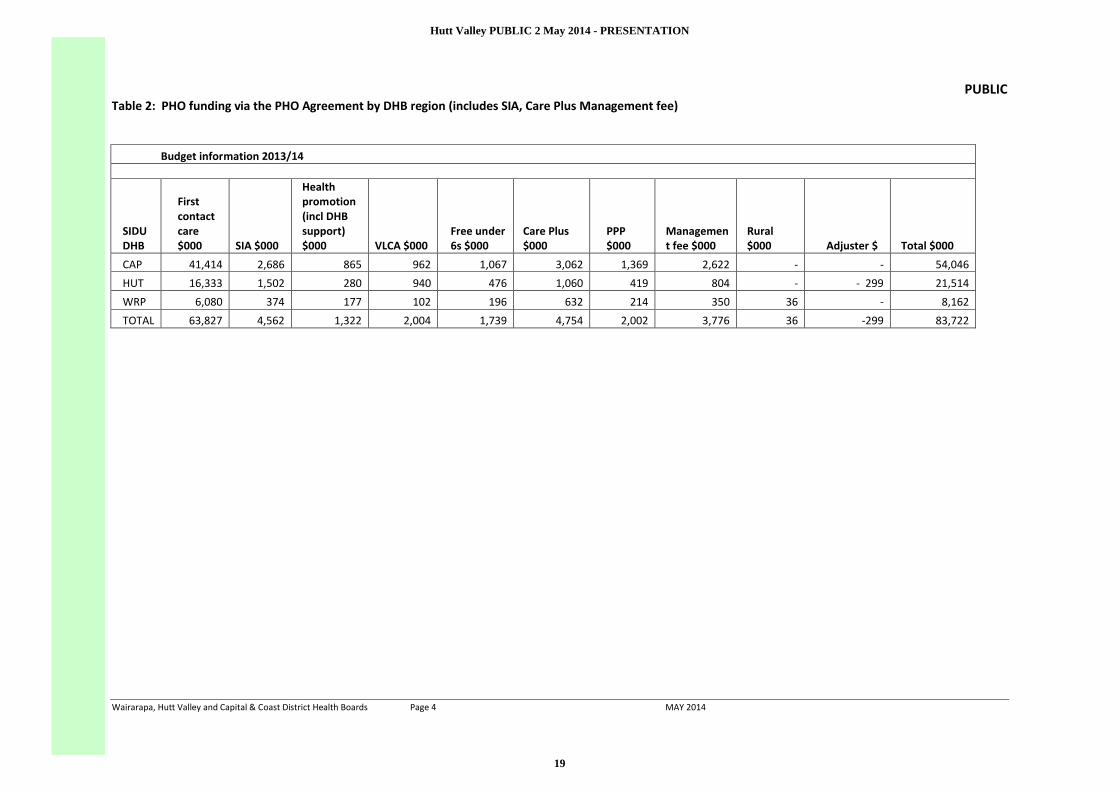
Table 2: PHO funding via the PHO Agreement by DHB region (includes SIA, Care Plus Management fee)
Budget information 2013/14
SIDU DHB
First contact care$000 SIA $000
Health promotion (incl DHB support)$000 VLCA $000
Free under 6s $000
Care Plus$000
PPP$000
Management fee $000
Rural$000 Adjuster $ Total $000
CAP 41,414 2,686 865 962 1,067 3,062 1,369 2,622 - - 54,046
HUT 16,333 1,502 280 940 476 1,060 419 804 - - 299 21,514
WRP 6,080 374 177 102 196 632 214 350 36 - 8,162
TOTAL 63,827 4,562 1,322 2,004 1,739 4,754 2,002 3,776 36 -299 83,722
Hutt Valley PUBLIC 2 May 2014 - PRESENTATION
19

PUBLIC
Page 5 of 9
All three DHBs contract for a range of additional services over and above these eight key funding streams:
∑ Wairarapa DHB: $1.6m for services including rural primary care, after hours, Primary care sustainability, B4School Checks, Sexual Abuse Assessment and Treatment (SAATs), diabetes, Cardiovascular Disease Risk Assessment (CVDRA), Immunisation, Tobacco Control, Sexual Health, and Primary Mental Health.
∑ Hutt Valley DHB: $4m for services such as VLCA, Community Radiology, Primary Mental Health, after hours and free under 6, reducing inequalities, Primary Care Sustainability, Tobacco Control, CVDRA and Diabetes.
∑ Capital & Coast DHB: $14.9m for services such as Retinopathy screening (3 DHB), Specialist Sexual Health (Hutt and CCDHB), Community Radiology, CVDRA, VLCA, Diabetes, Podiatry, SAATs, primary sexual health, smoking cessation, refugee health, after hours and free under 6, and improving access.
Further information on PHO funding streams are contained in Appendix 1.
Information on PHO performance is contained in Appendix 2.
4 COMMON SUB-REGIONAL ENABLERS
4.1 3D HealthPathways
HealthPathways is a clinically-driven progamme of work that provides guidance to clinicians on managing over 500 clinical conditions. The pathways, available through a website, contain medical guidance on the assessment and management of clinical conditions, and administrative information on access to diagnostics, specialist opinion, specialist treatment services, and other supports. On 20 February around 170 clinicians and managers from across the sub-region attended a planning seminar with the Canterbury Health Pathways team to introduce the Health Pathways process to the three DHBs.
Initial priority has been given to reviewing existing clinical pathways in use in one or more of the 3 DHBs and completing and publishing pathways that are priorities for the ALTs. Currently 15 pathways have been finalised and are on the 3D Health pathways site, while a further 14 are in the process of being translated from individual DHBs to the 3D site. A further four are currently in development as they are priorities for the ALT’s.
4.2 Shared Care Records (Manage My Health)
ManageMyHealth (MMH) is a secure website that receives an individual’s personal health information uploaded from their doctor, or health practitioner’s practice management system. It can allow access to this personal health record summary to other authorised clinicians, such as hospital clinicians, removing the boundaries of patient health information silos. Privacy issues have been well canvassed at a national level, including an opinion from the Privacy Commissioner. The key benefits include:ß reducing delays and time to diagnose patients by having access to patient’s medical information ß enabling safe and secure sharing of patient medical information outside normal GP clinic times
with after hours and emergency cliniciansß advancing the delivery of care by making it easy to access patient information at the point of care ß enhancing patient experience and continuity of care
The provider portal has been in use at Wairarapa DHBsince 2011, where six of the seven practices are participating in ManageMyHealth covering 95% of the enrolled population. All six participating practices are live with the shared care record module which provides key health information to hospital staff and pharmacies. Masterton Medical Limited and Carterton Medical Centre are currently trialling the provider
Hutt Valley PUBLIC 2 May 2014 - PRESENTATION
20

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board Page 6 MAY 2014
portal module which allows health professionals from rest homes to access patient notes for palliative care patients. This portal can also be expanded to other community health providers. Both Masterton Medical Ltd and Carterton Medical Centre have commenced enrolling patients to use the patient portal, which at this stage is being used to make appointments, order repeat prescriptions and check lab results.
In CCDHB primary care, most practices are participating in ManageMyHealth covering over 80% of the enrolled CCDHB population. The Shared Care Record went live in the hospital in April 2014 and can be accessed by selected senior clinicians, nurses and pharmacists in the hospital. The shared care record has been well received and there is consideration being made about widening access in the hospital, which should create further improvements in information flow and therefore patient care.
The Hutt Valley is planning to implement Manage My Health and build on the successful implementation in both Wellington and the Wairarapa. The timing of contract renewals with the software vendor at the other two DHBs may extend the timelines for implementation in the Hutt Valley. One large local practice intends (subject to negotiation) to go live with the MMH patient portal in advance of any wider arrangement.
4.3 E referrals
Electronic ‘E’ referrals allow GPs to electronically submit outpatient referrals to the DHB Booking Centre from within ractice software, rather than by fax or post. There are benefits to both primary and secondary care including time efficiency, cost reductions and accuracy.
In WDHB, e-referrals are working well and medical practices also find the e-advice function valuable. GPs have requested improvements to the e-advice function as currently it only allows for an initial response not a secure conversation if required. The top priority for further development in the Wairarapa is to the FOCUS (NASC) service.
In the Hutt Valley, e-referrals have been in place for several years with an on-going process of improvement and development.
In CCDHB a generic e-referrals was initially rolled out in 2011. Since then more service specific referrals have been developed and the platform has been upgraded in 2014.
4.4 Activities to reduce acute demand for hospital level care
Reducing acute demand is one of top three top priorities for 2013/14 for all three DHBs and features in the work programme of all three Alliance Leadership Teams (ALTs). To support this, a ‘Primary Options for Acute Care’ (POAC) process is being put in place to support delivery of and payment for services delivered in primary care that would previously have been delivered in a hospital setting.
In Wairarapa, Compass Health has funded intravenous (IV) treatment of cellulitis in the community since 2010 as part of the BSMC business case initiative. In 2013 this was extended to treatment of deep vein thrombosis (DVT) in the community. These two initiatives have made a significant contribution to the reduction of triage 4 and 5 (low acuity) attendances at the Emergency Department. Discussion has commenced on how to make these services sustainable and develop a more formalised POAC structure.
The CCDHB ICC Acute Demand workstream has explored alternative options to ED attendance and avoidance of unnecessary admissions for people presenting with urgent or unplanned care needs. To date, clinical pathways for management of adult cellulitis and acute DVT have been completed (with input from clinicians at Wairarapa and Hutt Valley where pathways were already in place). HVDHB currently funds IV therapy for cellulitis via Ropata Medical Centre following a successful trial at Silverstream Medical Centre.
Hutt Valley PUBLIC 2 May 2014 - PRESENTATION
21
PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board Page 7 MAY 2014
A POAC programme has been developed in both DHBs to ensure that primary care has the capacity to deliver the treatment as per the pathway. The programme includes an agreed funding mechanism as well as audit capacity to ensure providers are working within the scope of clinical pathways and also audit of claiming practices.
5 SERVICE INTEGRATION WORK PROGRAMMES
SIDU plays a key role in ensuring links across the three ALT work programmes and other subregional initiatives. By identifying workstreams and project areas across the region that align, resources and learning’s can then be shared to enhance outcomes for populations across the region. As an initial start in this area sub regional service level alliances on Youth and Health of Older People are currently being scoped.
5.1 Tihei Wairarapa
The Tihei Wairarapa Integration Programme was established as one of the nine BSMC business cases in 2010. As an Alliance, Tihei Wairarapa aims to provide increasingly integrated and co-ordinated health services through whole of system service improvement that is clinically-led. The approach that the alliance takes to service improvement is underpinned by the triple aim and ensures that improvement initiatives improve the patient experience (quality and safety), improve the health of the Wairarapa population overall (equity) and make best use of health resources (effectiveness and efficiency).
The Alliance Leadership Team consists of hospital and community based clinicians, Iwi and community representatives and both the PHO and DHB CEO’s. Current work streams are Integrated Care, Technology, Maternal and Child Health, Youth and Mental Health.
Tihei Wairarapa has had many successes since its inception including:
• Reduced triage 4s and 5s at the emergency department
• Mental Health Service Integration - in particular the two PHO employed mental health nurses now work in practices and part of the secondary care crisis team afterhours
• Integration of the National Immunisation Register Administration/District Immunisation Facilitator roles within the PHO, supporting improved childhood immunisation rates for Wairarapa children
• B4 School Check coordination integrated into the PHO team and clinics held at the practices has been key to Wairarapa’s success in this area
• The implementation of the shared care record, which includes hospital and pharmacy access
• E-Referral and E-Advice implementation
• A successful RFP for two IFHC Business Cases within the context of a Wairarapa Integrated Family Health Network
More recently, a key focus of Tihei Wairarapa has been on further developing the concept of an Integrated Family Health Network for the Wairarapa. As part of the RFP to develop the IFHC business cases an extensive consultation process with hospital and community based health professionals has been undertaken. The process has included 16 patient journey mapping exercises to identify key themes for service improvement, a variety of meetings with community health providers and hospital services, and three overarching workshops to bring it all together.
A series of seven proposals for improving the model of care have emerged from this process and are grouped into two categories (1) Improving integration between services and (2) Integrating care (see diagram below). Some of these proposals are not new and have been discussed for a number of years and already some progress has been made. During April and May 2014 the ALT will be undertaking a process of prioritisation which will inform the integration work programme for the next three years.
Hutt Valley PUBLIC 2 May 2014 - PRESENTATION
22

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board Page 8 MAY 2014
5.2 Hutt INC
The Hutt INC work programme is grouped into the following areas:1. Enablers2. Acute Demand3. Clinical Pathways4. Long Terms Conditions5. Quality.
Key achievements of Hutt INC include:
ß Implementation of initiatives within the Ambulatory Sensitive Hospitalisations (ASH) program to reduce the number of bed days in Cellulitis, Gastroenteritis and Chronic Obstructive Pulmonary Disease (COPD) has lead to the following reductions in hospital bed days:o Cellulitis discharges have reduced with a target of less than 56 per month the monthly average
over the life of the project is 54.7 o Gastroenteritis bed days target of 10 per month has been achieved with a monthly average
9.7 bed days over the life of the projecto COPD monthly bed days has reduced to 100.8 from 132 per month.
Other achievements include:ß A Primary Care Sustainability project in progress: engagement with primary and secondary care
has commenced with co-design workshops planned for May and June ß An Afterhours Working Group has been established to provide options to Hutt INC on future
provision of after hours services in the region;ß this is especially important to the Hutt Valley given the current issues facing primary care sustainability and increasing utilisation of after hours in the Under 6 age group.
ß Community Pharmacists now have access to the Hutt Hospital Concerto system
Improving integration between services
Systems, infrastructure and culture
3. Active communication; enhance existing communication channels, and consider establishing new ones
1. Managing change: capacity, capabilityand a structure for on-going system improvement
2. Use technology to make it easier to communicate and improve services
6. Extend Guided Care services for high risk/use patients – such as frail elderly, and/or those with complex long term conditions
5. Integrate (virtual or otherwise) services that visit or work with people in their own home and
Integrating careServices, and the way they are organised
7. Move towards a patient-centred health home model
4. Provide clinicians with information about available services and pathways
Hutt Valley PUBLIC 2 May 2014 - PRESENTATION
23

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board Page 9 MAY 2014
Hutt INC is looking at establishing a flexible services pool for 2014/15 to further support greater integration, and work is underway to identify services to be included within the pool.
5.3 CCDHB Integrated Care Collaborative (ICC)
The aim of the ICC Programme is to provide the best health care for our patients and population through improved experience, safety and quality of care with easy access and equity to all populations. The effect of the approach is to remove barriers between the hospital and community to create a single health service.
The Programme Sponsor for the ICC Programme is the CEO of CCDHB, Debbie Chin and the ICC overall management and clinical leadership of the Programme is provided through the ICC Alliance Leadership Team.
The ICC has five work streams identified to determine the work to be completed in integrated care over the next few years as follows:
These work streams were designed to cover key areas of interest from the Collaborative and the areas that could be significantly improved. A standard process is to be practiced to determine issues and initiatives. These work streams will involve key clinicians, managers and support from primary and secondary care.
Within each work stream, specific projects have been developed and implemented through the integrated collaborative approach. Projects that have been completed in the first stages of the programme were:ß Free Under Sixesß Diabetes Care Improvement Planß Shared Care Record in primary careß Oxycodone Prescribingß Advance Care Planning
More recently projects that have been developed and completed include: ß Implementation of the Shared Care Record (Manage My Health) in the hospital (as above)ß Primary Options for Acute Care (as above)ß Clinical pathways for cellulitis, lower limb Deep Vein Thrombosis (DVT), frail older person,
dementia, diabetes nutrition and childhood obesity
These pathways have been developed through the Acute Demand, Health of Older People and Child Health work streams. As with all ICC developments they have been developed through collaboration of clinicians from across the DHB. These pathways have been forwarded to the wider 3DHB Clinical Pathway programme for localisation across the sub region.
Enablers
ICC Programme
Living Well with Long-Term Conditions
After Hours and Acute Demand
Health of Older People
Child Health
Hutt Valley PUBLIC 2 May 2014 - PRESENTATION
24

PUBLIC
Hutt Valley District Health Board Page1 MAY 2014
BOARD INFORMATION PAPER
Date: April 2014
Author Peter Gush, Service Manager, Regional Public Health
Endorsed By Debbie Chin, Interim CEO, CCDHB & Acting CEO HVDHB
Subject Regional Public Health Update
RECOMMENDATION
It is recommended that the Board NOTE this report.
ADDENDUMS
2.2.1 March 2013 CPHAC Information paper and 2.2.2 RPH presentation
1 WHAT IS PUBLIC HEALTH?
1.1 A definition
“The science and art of promoting health, preventing disease and prolonging life through organised efforts of society.”
C E Winslow, American Bacteriologist
As someone who came into the management role within Regional Public Health (RPH) with no public health background this appeals as it encapsulates the different dimensions within which we aim to work.
“The science…” Holding onto an evidence base for our actions and interventions.“…and art…” The ability to be innovative, adapt and be responsive, particularly
when working in community settings.“…through organised efforts of society.”If we are to make a difference to the lives (health outcomes) of those in our communities RPH has to work well with many organisations, some within the health sector, but also other sectors which affect the wider determinants of health for our communities.
1.2 So what’s ‘hot’ at the moment?
o Alcohol – The Sale and Supply of Alcohol Act 2012 with a particular emphasis on reducing alcohol related harm.
o Housing – and all that can be achieved through the provision of warm, secure housing (disease prevention and improved social outcomes).
o Nutrition and physical activity; obesity, diabetes and cardiovascular disease.o Tobacco – continuing the battle towards “Smokefree Aotearoa 2025”o Community Water Fluoridation
Hutt Valley PUBLIC 2 May 2014 - PRESENTATION
25

PUBLIC
Hutt Valley District Health Board Page2 MAY 2014
These are just five of the many areas that the team at RPH are involved with and I provide a brief snapshot of some others at the end of the paper.
2 THE TOP FIVE
2.1 The Sale and Supply of Alcohol Act 2012
This piece of legislation amongst other provisions requires each Territorial Local Authority to develop a Local Alcohol Policy (LAP) for their area, and increases the responsibilities of the Medical Officers of Health and public health units in this setting. The legislation includes in its ‘Object’:(a) The sale, supply, and consumption of alcohol should be undertaken safely and responsibly; and(b) The harm caused by the excessive or inappropriate consumption of alcohol should be minimised.
In the Hutt Valley, Hutt City has developed its provisional LAP which is subject to a number of appeals which will not now be heard until November by the Alcohol Regulatory and Licensing Authority. The DHB has appealed the Hutt City LAP in particular seeking a reduction in the off-license hours for supermarkets and large food stores. Upper Hutt City will be considering their draft LAP in June.
In March RPH took the lead in a new off-license application in Upper Hutt where we opposed a new licence because the location was known to be a popular “hang out” for young people in the vicinity of McDonald’s family restaurant and a major bus stop. Our opposition was supported by the police and by key community leaders. The Authority refused the application and this illustrates how when we have strong support from the community it is possible to achieve decisions on alcohol that in the past were unthinkable.
2.2 Housing
Our Housing Assessment and Advice Service offers a home visit by a public health (housing) nurse, links clients with housing interventions that make a home warmer and drier, provides education about healthy housing, and follows up each family to check on completion of the referrals made.
The service can be referred to through both primary and secondary care pathways – criteria is financial (Community Service Card, or financial hardship), and one of the following health conditions -Rheumatic Fever (acute or past history), communicable disease (Meningococcal disease), respiratory conditions (Asthma, COPD, Bronchiolitis, Pneumonia, Bronchiectasis), and skin infections. In particular the programme is focussed on:
• new cases of Rheumatic Fever (sub-regional), • cases on the Bicillin register (sub-regional), • Hutt Valley DHB Paediatrics, and Community Paediatrics,• Hutt Valley DHB Respiratory Service,• Hutt Valley DHB Social Work team.
Referrals identified by RPH at secondary care will be linked back to their primary care provider and in the first instance a joint visit will be offered (Primary care and RPH). If a joint visit is not possible, RPH will complete the referral and an update on the client will be provided to the primary care provider.
Sub-regionally our Housing Public Health Nurses also offer an Advice Service to support the health sector address housing need with their clients. This service is available via phone and email.
We are currently working towards this service being extended to CCDHB Secondary care by integrating this work with the agreed actions in the Integrated Care Collaborative Housing subgroup.
Hutt Valley PUBLIC 2 May 2014 - PRESENTATION
26

PUBLIC
Hutt Valley District Health Board Page3 MAY 2014
2.3 Nutrition and Physical Activity
Please note the Addendum on this topic which was considered by CPHAC at their meeting on 7 April 2014.
Our efforts in this space are well documented in the Addendum and I draw your attention to the ‘Maternal and Infant Physical Activity and Nutrition’ description (paragraph 4.1 of the Addendum) as this partnership is a great example of both the art of public health, as well as the organised efforts of society with many providers coming together to influence improved health outcomes. This is a sub-regional initiative.
On 14 March 2014 the Minister announced another initiative under the Healthy Families banner seeking Registrations of Interest (by 14 May) from a locally-based lead provider responsible for bringing together a partnership of key organisations in the community, and a dedicated health promotion workforce. These health promoters will work across schools, early childhood education centres, workplaces, and sports clubs, supporting New Zealanders to make healthy living choices. They will also work with other key organisations to implement initiatives supporting healthy living.
Hutt City is one of the ten communities selected nationwide to be part of this new initiative. In partnership with Te Awakairangi Health Network RPH hosted a meeting of interested organisations on 15 April to facilitate initial conversations around identifying a lead provider and seeking expressions of interest about what role they saw themselves playing in this initiative. A follow up meeting is scheduled for Tuesday 29 April.
At the CPHAC meeting members sought clarification regarding the DHB policies on the sale of ‘fizzy’ drinks in particular; referencing the comment in paragraph 2.1 of the Addendum regarding a ‘food environment paper’ that is to be presented to the two Executive Teams for the DHB’s. The policies or guidelines between each of the DHB’s are different and the paper mentioned above seeks to introduce a sub-regional approach to nutrition at DHB sites.
2.4 Tobacco
As part of the Central Region Services Plan an initiative has been developed involving all those in the tobacco control and smokefree spaces looking to develop a Central Region Tobacco Control Plan. This initiative involved the three public health units, six District Health Boards, primary care organisations, non-government organisations and others coming together to share resources, agree best practiseand make the most of the collective experiences and learnings. RPH took a lead in bringing this group together. An example of this sharing is that the RPH produced quarterly ‘Tobacco Retailers Newsletter’ which would normally be circulated to 700 retailers sub-regionally will now be circulated to all retailers in the Central Region.
The Health Select Committee recently called for submissions on the ‘Smoke-free Environments (Tobacco Plain Packaging) Bill, which RPH submitted on in March and an oral submission was made to Select Committee on 16 April. Amongst the recommendations in our submission was support for the passage and full implementation of the Bill without any delay.
2.5 Community Water Fluoridation (CWF)
Since the Board approved the CWF Position Statement at your last meeting we have circulated it to the Mayors and Chief Executives for the two TLA’s in the valley.
Sub regionally the Kapiti Coast District Council has circulated statements from CCDHB and those opposed to CWF with their Annual Plan asking their residents to answer the following question:
Hutt Valley PUBLIC 2 May 2014 - PRESENTATION
27

PUBLIC
Hutt Valley District Health Board Page4 MAY 2014
“Do you think we should keep adding fluoride to the drinking water in Waikanae, Paraparaumu and Raumati? Yes / No “
3 OTHER
3.1 School Based Public Health Nursing
With the development of a computerised Patient Management System for the school nurses last year we are now starting to see good data regarding activity levels and referral areas. Additionally the care being provided by our nurses is now ‘visible’ to both primary and secondary care clinicians, and we already seen stories of improved joined up care as a result of this visibility.
School Health and Immunisation Group
Capital and Coast
Hutt Valley Wairarapa
Total629 466 77 1,172866 630 88 1,584
1,274 1,211 131 2,61640 52 12 104
565 478 48 1,09128 28 8 64
3.43 5.18 3.46
1.56 1.86 1.57
Top 5 Referrals for Open Referrals by DHBDHB Condition Rank NumberCCDHB Vision 1 143CCDHB Behavioural 2 93CCDHB Hearing Concerns 3 83CCDHB Developmental 4 61CCDHB Eczema 5 55HVDHB Behavioural 1 136HVDHB Developmental 2 78HVDHB Hearing Concerns 3 73HVDHB Vision 4 72HVDHB Learning difficulties 5 51Wairarapa Dental 1 12Wairarapa Sexual Health and Puberty 1 12Wairarapa Eczema 3 11Wairarapa Head lice 4 9Wairarapa Hygiene 4 9
Average Contacts per Open Referral
Average Time Spent per Open Referral (hrs)
Highest Time Spent for an Open Referral (hrs)
Highest Number of Contacts for an Open Referral
Number of Closed Referrals
Number of Open Referrals
Number of Conditions Associated with Open Referrals
Statistics Report - by DHB
Number of New Referrals
From 01-Oct-2013 to 31 Mar2014
3.2 Webpage
Our webpage has many resources including our submissions – www.rph.org.nz
Hutt Valley PUBLIC 2 May 2014 - PRESENTATION
28

PUBLIC
Wairarapa and Hutt Valley District Health Board
BOARD INFORMATION PAPER
Date: 22 April 2014
Author Pete Chandler, Chief Operating Officer
Endorsed By Debbie Chin, Acting Chief Executive Wairarapa and Hutt Valley DHBs
Subject Chief Executive’s Report – May 2014
RECOMMENDATION
It is recommended that the Boards
a. Note the information contained in this report.
ADDENDUMS
1. Balanced Scorecard
2. Finance Report
3. 3DHB Health Services Development Programme Update
4. Communications Update
5. Official Information Act Requests
1 GOVERNMENT PRIORITIES AND HEALTH TARGETS
1.1 Hospital Health Targets
Wairarapa and Hutt Valley DHBs are continuing to perform well in all hospital health targets.
Both DHBs are:
∑ Meeting or exceeding the national ED 6 hour wait time target – this position has now been held for four successive quarters at Hutt for the first time ever. Wairarapa remains one of the top performers in the sector
∑ Exceeding the elective surgery volume targets for the year to date – for both DHBs this is the best year of elective surgery performance achievement so far. Surgical pathway efficiency improvements are beginning to yield productivity benefits in both DHBs. Work to reduce cancelled operations by over 50% at Hutt has been successful, with similar effort now being applied at Wairarapa
∑ Exceeding the hospital smoking cessation advice target.
Both DHBs have a plan to achieve the new four month waiting time target by the end of the year. Reduced numbers of anaesthetists at Hutt, and last year’s fire at Wairarapa, have presented considerable challenges in this to date. However, recruitment has been successful in both DHBs and a number of new anaesthetic Senior Medical Officers (SMOs) have now joined our services which will considerably support the four month wait plan - a key priority for the rest of 2014.
Hutt Valley PUBLIC 2 May 2014 - DISCUSSION PAPERS
29
PUBLIC
Wairarapa and Hutt Valley District Health Board
1.2 PHO Health Targets
Te Awakairangi Health Network (TeAHN)
Practices across the Network have been working hard over the last year and have achieved good results. Since April 2013, there have been significant improvements in “More Heart and Diabetes Checks”, where CVD risk assessments have gone from 38.4% to 69.4% (almost 10,800 checks) and in “Help for Smokers to Quit” where the brief advice indicator has doubled (from 32.2% to 65.5%). These are excellent results.
A growing number of practices have achieved the target percentage for some or many of the indicators. TeAHN will continue to support the practice teams to make the next improvement step.
1.3 Balanced Scorecard (BSC)Please find attached as Appendix One the BSC.
2 IMPROVING PROCESS AND CULTURE
2.1 Distributive Clinical Leadership
Last month, the Association of Salaried Medical Specialists (ASMS) published their Specialist newsletter which contained a synopsis of results from one of their more recent surveys of Senior Medical Officers (SMOs) on the subject of distributive clinical leadership. This term describes the involvement of the wider SMO workforce at grass roots level, in organisational development and clinical service changes rather than simply involving formal clinical leaders. The expertise of our SMO workforce is a critical component in shaping our organisation to meet the changing demands within healthcare such as meeting the needs of the ageing population and improving models of care.
ASMS comment that one of the greatest barriers to distributive clinical leadership is the availability of non-clinical time, and to assess this across the sector the previous survey (2011, which was re-published in December 2013) looked at this aspect of clinician resources in some detail. Wairarapa and Hutt Valley DHBs did not fare well, however in the three years since then considerable improvements have been made.
The most recent survey (undertaken in the latter part of 2013 and published in February) assessed SMOs perceptions of the genuine level of commitment to progressing distributive clinical leadership across the DHBs. Whilst there was a relatively low sector response rate of 30% of DHB employed SMOs, and the results present some mixed messages, we see the survey as an opportunity for improvement and have committed to making significant improvements in this area over the coming year.
At our Joint Consultation Committee (the formal, quarterly ASMS-DHB engagement forum) meetings over the last six months this has been a significant topic of discussion and we are working with ASMS, our Clinical Directors and our clinical teams to determine effective means to improved organisational involvement of our medical workforce.
In addition, we are taking advice from Professor Robin Gauld at the University of Otago, an acknowledged New Zealand expert on the topic. Robin was involved in the original ASMS clinical engagement survey and has been very helpful in providing a steer, along with some complimentary feedback on our current approach. It is becoming clear that the very specific ASMS survey questions do not provide us with enough local perspective on wider SMO workforce opinion and therefore we are considering undertaking our own clinical engagement survey later this year at both Wairarapa and Hutt DHBs.
Hutt Valley PUBLIC 2 May 2014 - DISCUSSION PAPERS
30

PUBLIC
Wairarapa and Hutt Valley District Health Board
2.2 Healthy Workplace initiative
The recent Kings Fund summary of the Francis enquiry into the UK Mid Staffordshire NHS Trust re-emphasises the importance of organisational culture in ensuring excellent and safe care delivery, and provides useful prompts to us.
Starting in April, we will be working through an ‘organisational culture refresh’ series of activities which will continue for the rest of the year. This will involve a more focussed approach to engaging the whole organisation, with unions, in working together to improve workforce morale, improve communication and transparency, and galvanise strong collective effort to enhance quality, safety and efficiency. This stream of work links wholly to the envisioning activities which have been underway for some months, involving our union partners, facilitated by Tom Schneider.
Our first action was a trial, to see if we could shift organisational thinking to focus on our ‘Healthy Workplace’ areas, where morale and team spirit were especially high, celebrate these and use as models of excellence to inspire other areas. This has created considerable postings on our intranet blog, a competitive spirit between departments and been very well received by staff and unions. The final results of the nominations were as follows:
Hutt Valley PUBLIC 2 May 2014 - DISCUSSION PAPERS
31

PUBLIC
Wairarapa and Hutt Valley District Health Board
We’ll be celebrating the winner (our Endoscopy service) and asking staff from the top voted three services to share with the organisation what’s great about working in their departments. In summary, staff comments about their department were:
∑ They have a great manager
∑ Everyone works hard, and really well together as a team
∑ Workplace relationships between staff are excellent
∑ The team are proud of the service they offer and they believe they provide a very efficient model of care based on the ‘Valuing the Patient’s Time’ principle adopted from Canterbury DHB
∑ Patient feedback on the service, it’s efficiency and the outstanding level of patient care by the staff is consistently excellent.
This is an exciting focus and has stirred up considerable discussion within the DHB, with more celebratory opportunities being planned for the rest of the year. A similar activity will be launched at Wairarapa in May.
3 FINANCIAL SUSTAINABILITY
3.1 Financial Result Wairarapa
The DHB is currently $115k unfavourable to budget year to date, (Funder $249k unfavourable, Governance $168k favourable, Provider $34k unfavourable). Savings not being achieved year to date are mostly being offset by other underspends however this is not expected to continue for the remaining months of this financial year.
Further information can be found in the Wairarapa DHB Financial Report attached as Appendix Two.
3.2 Financial Result Hutt Valley DHB
The Hutt Valley DHB is currently $799k behind plan year-to-date, original plan lines are $2,871k behindtarget and are partially offset by other underspends and new initiatives. There remains a significant challenge for the last quarter of the year. The year-to-date total financial position for the DHB is anunfavourable variance to budget of $1,572k, (year-end forecast deficit $1,546k).
Further details can be found in the Hutt Valley DHB Finance Report attached as Appendix Two.
Hutt Valley PUBLIC 2 May 2014 - DISCUSSION PAPERS
32
PUBLIC
Wairarapa and Hutt Valley District Health Board
4 WORKING WITH OUR NEIGHBOURS
4.1 3DHB Health Services Development (HSD) Programme
Attached as Appendix Three is an update on work undertaken under the 3DHB Health Services Development (HSD) Programme to the end of March 2014, outlining programme highlights, key planned activities and emerging priorities.
5. INTEGRATING HEALTH SERVICES INTO A MORE UNIFIED SYSTEM
5.1 Hutt INC
Hutt INC had its regular monthly meeting on Thursday 17 April 2014. The main items of discussion are set out below:
∑ An approach to POAC (Primary Options for Acute Care) in the Hutt Valley continues to develop. The focus of this work is improved pathways around cellulitis and DVT, and the possibility of adopting co-ordination functions for community based care. Any such co-ordination function would best be considered part of a sub-regional approach to get the best value for any investment.
∑ ENT pathways developed sub-regionally are now available to GPs on the HuttHealthPathways website, with communication and training for primary clinicians being organised.
∑ A workgroup has started developing a clinical governance approach that brings primary and secondary care together to consider the journey of patients across different aspects of the health system. Clinical Governance is already strongly embedded in both secondary and primary care, but there are opportunities to improve visibility of patients that move through both parts of the system.
∑ Advice was sought and provided in relation to several workstreams, including radiology criteria, the best way for Hutt INC to contribute to sub-regional work, and the use of “Yellow Card” medicines lists.
∑ Hutt INC is considering whether there is any opportunity to think in a more collaborative way about how the Hutt health system works to deliver care in the community. The DHB, PHOs, and primary practices all provide services in the community, but it is not clear how well these services are aligned, and whether greater linkages between staff would assist in supporting and driving earlier care in the community.
∑ Te Awakairangi Health Network, under the sponsorship of Hutt INC, is working on finding ways to improve the sustainability of primary care in the Hutt Valley into the medium and long term. A brief presentation was received from Synergia on the general approach and the importance of addressing sustainability as a “whole of system” issue, and on developing options that support services increasingly being provided to patients closer to their homes.
∑ Additional resource for workstreams has been provided by SIDU, which was welcomed by the Group. Sarah Eames, who has previously worked in primary care in the Hutt Valley, was welcomed to
Hutt INC as programme manager.
5.2 Hutt Valley DHB Laboratory Information System
Hutt Valley DHB has successfully implemented Sysmex Delphic, the new Laboratory Information System (LIS). Over the next few weeks the focus will be on supporting the Hutt Lab and bedding in the system and process changes. Post go-live support arrangements are in place to ensure any issues are identified and resolved in a timely manner.
The team work and commitment across Labs and ICT for this project has been fantastic and I’d like to acknowledge all those involved.
Hutt Valley PUBLIC 2 May 2014 - DISCUSSION PAPERS
33

PUBLIC
Wairarapa and Hutt Valley District Health Board
5.3 New Finance System
Hutt Valley DHB was the first DHB in New Zealand to transition to a new shared service being put in place by Health Benefits Ltd on behalf of all DHBs. Essentially the aim of this project is to streamline finance, procurement and supply chain processes so that all DHBs are speaking a common language when it comes to how goods and services get ordered, delivered, paid for and stored.
The Hutt Valley Phase 1 Implementation went live on 1 April 2014, with the cut down version of the finance system including; accounts receivable, accounts payable, general ledger and cash management. There were some minor issues to resolve but in general the go live went to plan. This is a significant milestone and its success is a credit to the team at Hutt and in ICT who worked on this project, often in very difficult circumstances. Work continues on streamlining processes and completing some minor issues unable to be resolved in time for go live. The month end process is yet to be fully tested with the first MoH reporting due from the new system on 12 May.
Hutt Valley PUBLIC 2 May 2014 - DISCUSSION PAPERS
34

PUBLIC
Wairarapa and Hutt Valley District Health Board
6. OTHER MATTERS OF INTEREST TO THE BOARD
6.1 Wairarapa Clinical Board
The Wairarapa Clinical Board met on Wednesday 16 April. The format of the meetings has changed to including summary reports from the Allied Health, Nursing and Medical representatives.
The main focus for the meeting was a discussion on the Terms of Reference which are in need of review. Further discussion will take place at the next meeting.
6.2 College Accreditation Visits
Australian & New Zealand College of Anaesthetists (ANZCA)
The Chair and two representatives of the ANZCA accreditation committee visited Hutt Hospital on 28 March as a formal follow up to their visit in December 2012. Many changes have occurred since then. The visit went well and informal feedback was positive. Formal feedback is awaited.
Royal Australian & New Zealand College of Obstetricians & Gynaecologists (RANZCOG)
The Hutt Hospital was accredited as a training site in the College’s Integrated Training Program (now known as the Core Training Program) in 2011 for a period of four years, following a recommendation by the RANZCOG New Zealand Training Accreditation Committee. In accordance with College process, a team from the RANZCOG visited the hospital approximately one year after the first trainees were appointed to review the site’s performance as a newly accredited unit.
This review was conducted on 18 February 2014 by a team from the RANZCOG including the Chair of the New Zealand Training Accreditation Committee. The Hutt Hospital is a Level 2 site and is a peripheral rotation for the Wellington Hospital.
The Hutt Hospital was granted an initial four-year accreditation period in July 2011 (expiring July 2015). The current progress review, which would normally have taken place approximately 12 months afterwards (late 2012), was delayed so that sufficient trainees had rotated to the site to provide adequate feedback. Because of this delay, the current accreditation rating is extended to the end of January 2016. The next re-accreditation visit will fall due in February 2016.
Royal Australian & New Zealand College of Radiologists (RANZCR)
The college undertook an accreditation visit in October 2013. Hutt is linked to Wellington for training and currently has one trainee on rotation. Hutt was noted to be a valuable and complementary rotation to the Wellington training program but the training opportunities were not being fully utilised at present. Good teaching and supervision was available despite workload pressures on SMOs but could be improved significantly with increased SMO staffing. The presence of a solo trainee and the rotation duration of 6 months resulted in the trainee missing out on teaching and education opportunities, formal or otherwise. RANZCR felt this would be alleviated by the addition of a second trainee and/or an increased rotation length however increased staffing would be required to support this. In view of this Hutt was downgraded from a ‘A’ unit to a ‘B’ training unit pending the recruitment of an additional full time equivalent SMO. Therefore Hutt Hospital was granted Level B Linked accreditation, valid to 31 December 2018 and for a maximum of one trainee.
6.3 Wairarapa Hospital Maintenance and Storage Facility
With the sod turning earlier in March 2014, the Holmes Construction Group led construction of the storage facility is in full swing.
The construction is expected to take between four to five months and is well underway with forestation removed and the ground prepared for foundations with sub base compaction completed.
Hutt Valley PUBLIC 2 May 2014 - DISCUSSION PAPERS
35

PUBLIC
Wairarapa and Hutt Valley District Health Board
6.4 Elective Services Patient Flow Indicators (ESPIs)
We are currently working towards the next milestone goal of achieving a maximum four month waiting time for first specialist assessment (FSA) and elective treatment by the end of December 2014. Below is an update on the national and local picture against elective waiting time goals.
National performance improved in February. There are, however, very few DHBs across the country who are managing to sustain performance against the maximum five month waiting time expectation on a consistent basis, with only two DHBs having met the five month expectation for both FSAs and treatment (ESPI 2 and ESPI 5) in February. The Ministry will expect to see waiting time performance managed more tightly, with good improvement achieved by the end of this financial year. Both Wairarapa and Hutt Valley DHBs have plans in place to support reductions.
The following graphs show last year's improvement against the five month goal (dotted lines), and current progress towards four months (solid lines) for Wairarapa and Hutt DHBs, and at a national level. The blue lines relate to the number of patients waiting over the respective time frame for first specialist assessment, and the red lines relate to elective treatment. The most recent data is for February 2014, extracted from National Collections on 7 April 2014.
Hutt Valley PUBLIC 2 May 2014 - DISCUSSION PAPERS
36
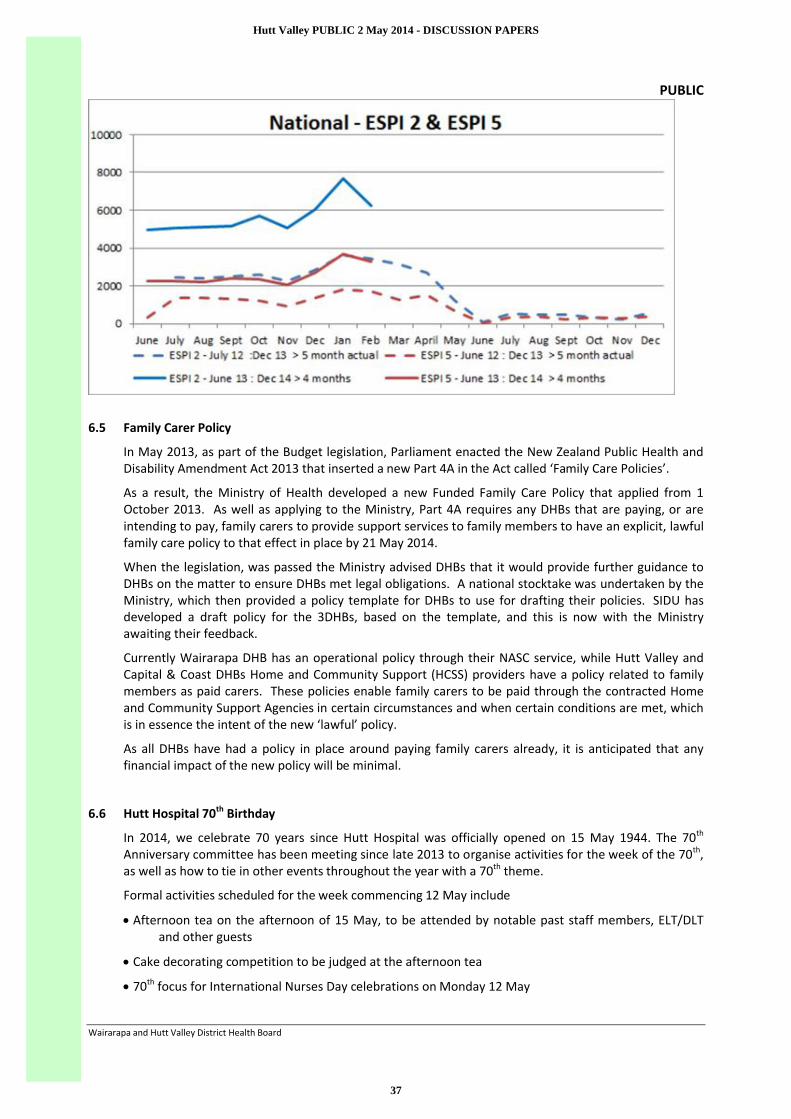
PUBLIC
Wairarapa and Hutt Valley District Health Board
6.5 Family Carer Policy
In May 2013, as part of the Budget legislation, Parliament enacted the New Zealand Public Health and Disability Amendment Act 2013 that inserted a new Part 4A in the Act called ‘Family Care Policies’.
As a result, the Ministry of Health developed a new Funded Family Care Policy that applied from 1 October 2013. As well as applying to the Ministry, Part 4A requires any DHBs that are paying, or are intending to pay, family carers to provide support services to family members to have an explicit, lawful family care policy to that effect in place by 21 May 2014.
When the legislation, was passed the Ministry advised DHBs that it would provide further guidance to DHBs on the matter to ensure DHBs met legal obligations. A national stocktake was undertaken by the Ministry, which then provided a policy template for DHBs to use for drafting their policies. SIDU has developed a draft policy for the 3DHBs, based on the template, and this is now with the Ministry awaiting their feedback.
Currently Wairarapa DHB has an operational policy through their NASC service, while Hutt Valley and Capital & Coast DHBs Home and Community Support (HCSS) providers have a policy related to family members as paid carers. These policies enable family carers to be paid through the contracted Home and Community Support Agencies in certain circumstances and when certain conditions are met, which is in essence the intent of the new ‘lawful’ policy.
As all DHBs have had a policy in place around paying family carers already, it is anticipated that any financial impact of the new policy will be minimal.
6.6 Hutt Hospital 70th Birthday
In 2014, we celebrate 70 years since Hutt Hospital was officially opened on 15 May 1944. The 70th
Anniversary committee has been meeting since late 2013 to organise activities for the week of the 70th, as well as how to tie in other events throughout the year with a 70th theme.
Formal activities scheduled for the week commencing 12 May include
∑ Afternoon tea on the afternoon of 15 May, to be attended by notable past staff members, ELT/DLT and other guests
∑ Cake decorating competition to be judged at the afternoon tea
∑ 70th focus for International Nurses Day celebrations on Monday 12 May
Hutt Valley PUBLIC 2 May 2014 - DISCUSSION PAPERS
37
PUBLIC
Wairarapa and Hutt Valley District Health Board
∑ Exhibition display of history boards/uniforms and other memorabilia to be situated in the corridor by the auditorium for the week of the 15 May
∑ Plastics reunion dinner on Friday 16 May
∑ Nurses reunion dinner on Saturday 17 May
Other activities include
∑ Three large A0 size canvases featuring photos of the hospital taken by the clinical photographer Ric Croasdale (canvases donated by Pixelpaint) – these will be placed in high traffic areas and the caption will acknowledge that they were donated for the 70th
∑ Special grand round featuring 70th memories (organised by Peter Barnes) scheduled for June/July
∑ Wearable art competition around September
∑ Ongoing digitisation of historical assets (photos, videos and stories) to preserve them for the future
∑ Follow-up photo essay by Eunice Mowles profiling members of staff who were originally photographed for the series of portraits in the Learning Centre corridor.
An article appeared in the Hutt News asking for help in identifying a group of student nurses, this was successful and a follow up has been published on our public internet page. A feature article will be pitched to Hutt News and we will also use Health Highlights to cover. Facebook/Twitter/Intranet/Internet coverage will intensify in the week before the 70th.
6.7 Pacific Health Scholarship Awards
The Pacific Health Awards were held on 22 April 2014. As background the Awards started in 2004 as a way of Hutt Valley DHB’s “growing your own initiative”. Pacific young people looking for careers in the health sector. The DHB in partnership with the Hospital Foundation Trust has provided support to enable this initiative to continue to date.
We have assisted and supported up to 23 Pacific young people from the Hutt Valley in their tertiary studies during the last ten years, all have graduated and are either serving here in the Hospital and or in the community setting or working in the sector in other centres.
This year we have 19 recipients of the Awards, which range from $1,000 to $5,000, most are in their final year of studies and some in their first year. The range of studies are from nursing/medicine/policy analyst/social work/physiotherapy/Master of Physics (in imaging) Health management/environment officer.
A panel made up of a Community clinician, nursing development unit and member of Hutt Foundation deliberated on the final decision. This initiative is well known in the Hutt Valley Pacific community as we market this very well with information provided to churches and Pacific leaders to encourage their young people to look to health as a career option.
The celebration of the Awards was well attended by many including the Minister of Pacific Island Affairs, Hon Peseta Sam Lotu-Iiga, who was our guest speaker, Board members, Interim Chief Executive of CCDHB, Pacific Community Leaders, Award recipients and their families.
Hutt Valley PUBLIC 2 May 2014 - DISCUSSION PAPERS
38

PUBLIC
Wairarapa and Hutt Valley District Health Board
Hon Peseta Sam Lotu-Iiga, centre, congratulates recipients of the Pacific Health Scholarship6.8 Communications Update
I have included as Appendix Four the projects and initiatives the DHBs’ Communications Team have been working on locally and in the 2DHB and 3DHB space.
6.9 Official Information Act Requests
Attached as Appendix Five are details of requests for information the DHB has received under the Official Information Act since the last Board meeting and our responses.
Hutt Valley PUBLIC 2 May 2014 - DISCUSSION PAPERS
39

Public
Wairarapa, Hutt Valley and Capital & Coast District Health Boards
WAIRARAPA, HUTT VALLEY AND CAPITAL & COAST DISTRICT HEALTH BOARDSCOMMUNITY PUBLIC HEALTH ADVISORY AND DISABILITY SUPPORT ADVISORY COMMITTEES
9.35am Monday 07 April 2014
PRESENT: IN ATTENDANCE:
Committee Management & Externals
Derek Milne (Chair)Virginia Hope (Deputy Chair) - lateWayne Guppy (Member)David Choat (Member)Chris Laidlaw (Member)Helene Ritchie (Member)Helen Kjestrup (Member)Janine Vollebregt (Member)Sandra Greig (Member)Liz Falkner (Member)Peter Douglas (Member)
Debbie Chin (Interim CEO, CCDHB) - lateSandra Williams (Group Manager, Service Integration)Dr Pauline Boyles (Senior Disability Advisor)Nicola Ryan (Minute Secretary, SIDU)Peter Gush (RPH Service Manager, SIDU)Joanne Reid (RPH Group Manager, SIDU)
APOLOGIES:
Committee Management & Externals
Ron Mark (Member)Leanne Southey (Member)
Carolyn Cooper (Director, People & Culture)Dr Ashley Bloomfield (Director OF SIDU)
Peter Douglas opened with a Maori Prayer
Wayne Guppy advised he will leaving at 11am for Royal introduction.
Interest register – one change from Derek. Brother in Law on Health Care NZ ltd. Daughter working at Auckland Hospital.
1.0 CONFIRMATION OF MINUTES
The Committees
Agreed that the minutes of the meeting held on 24 February 2014 are a true and correct record of the proceedings
Moved: Derek Milne Seconded: Peter Douglas CARRIED
The Committees noted the apologies.
2.0 ACTION POINT UPDATE:
∑ PHO presentations need some thought and priority – staff with discussion with CEO’s and Chairsto consider in light of the presentations to the Boards at May 14 meetings.
Hutt Valley PUBLIC 2 May 2014 - COMMITTEE VERBAL REPORT BACKS
40

Public
Wairarapa, Hutt Valley and Capital & Coast District Health Boards
∑ RPH information on Fluoridation handed out. Check with Ashley as to whether the link in the action point has been covered off.
3.0 CPHAC-DSAC TERMS OF REFERENCE
Terms of Reference noted. These were covered off last meeting, but will remain on the agenda for the future as a reminder for people.
4.0 DIRECTOR, SIDU REPORT
9:45am Janine Vollebregt arrived
Receipt of report.
Moved: Derek Milne Seconded: Helene Ritchie
Discussion Points:
∑ P20. Pathways care – were discussed. It was noted that some GPs had presented a counter view as to the usefulness of Pathways.
∑ Pathways are enablers not prescriptive pathways. It’s a very useful enabling tool for health professionals to see what choices they have.
9:49am Peter Gush and Joanne Reid arrived
∑ Sub regional Community Pharmacy Forum - further work to be done in terms of GPs and Pharmacists working together more closely and in an integrated way. A comment was made thatthere was a lot of information in the papers and too little time to discuss and make the points each member wanted.
∑ Health of Older People. Interest expressed in the work being done. Noted it was working well in the Wairarapa and that work is underway in the other two DHBs. Noted that monthly there would be an update on the work with a full briefing to come to CPHAC-DSAC in due course.
10:10am Sue Kedgley arrived
Action Points:
∑ Report back on discharge care planning for vulnerable and frail elderly. Identify a date for havinga discharge policy in place with tight rules.
The Committees noted the contents of the paper.
4.0 Annual Plans 2013 / 14 – Six Month Report & Performance Reporting
Discussion Points:
∑ The work on a sub-regional mental health advocacy service is behind schedule due to other work having been prioritized first. However it is expected that this work will be back on track before the end of the year..
∑ P41 and 42. A member raised the recollection that there is another mental health performance measure. Used to be proportion of people with crisis management plans in place. Clarificationrequired about the measure and whether the information was still being collected and could be reported.
Hutt Valley PUBLIC 2 May 2014 - COMMITTEE VERBAL REPORT BACKS
41

Public
Wairarapa, Hutt Valley and Capital & Coast District Health Boards
Action Point:
∑ Report back on whether the Mental Health Performance Measure – proportion of people with crisis management plans in place is still reported.
It is recommended that the Committees:
Note the six-month report against the Annual Plans for Wairarapa, Hutt Valley and Capital & Coast DHBs;
Note the most recent results against Government Health Targets and other key performance measures for 2013/14.
Note the actions being taken to improve performance across the sub-region on the two primary care targets – heart and diabetes checks and smoking cessation.
Derek Milne moved that the recommendations are noted.
5.0 Nutrition and Physical Activity Initiatives including those to prevent Cardiovascular disease and Diabetes
Discussion Points:
∑ Peter Gush and Joanne Reid (Regional Public Health) were in attendance to answer any questions around this paper.
∑ Clarification was sought about the work RPH did in schools in terms of prevention and promotion particularly nutrition. Work in some individual schools such as the Health Promoting Schools programme. Work is more about wellbeing, social and physical health. Also public health nurses in schools around the region. Working with about 32 schools across the Hutt and Capital & Coastareas. Health Promoting Schools is more of a framework, focus on lower decile schools. Nutrition is a common topic and teaching on healthy food options. Looking at school lunch packs sold in schools around the region and looking at how we can promote the sale of healthy food nearby.
∑ It was raised that the DHBs should be starting with their own hospitals. Fizzy drinks, cafeteria foods were two areas staff were advised to consider develop a sub-regional policy for.
∑ Staff advised that a sub-regional policy is being worked on for the Executive Leadership Teams.Further information to come back to CPHAC-DSAC. It was drawn to staff’s attention that some years ago there was a report identifying that the leading cause of health issues is a poor diet and the cause of obesity issues particularly in children.
∑ It was noted that guidelines are available, although voluntary. As there was no baseline, it is not possible to comment on whether schools have maintained at the guidelines.
∑ There was a request from members of the Regional Council to work closely with that entity and also local councils given the agreement of the Committees was that good nutrition was important and impacted significantly on the health system.
10:36 – Virginia Hope arrived.
The Committees recommended to the working group developing a sub-regional DHB food policy that all fizzy drinks should be excluded and that there be reporting back to individual Boards.
Action Points:
∑ Sue Kedgley to receive a copy of Capital & Coast food policy.
Hutt Valley PUBLIC 2 May 2014 - COMMITTEE VERBAL REPORT BACKS
42

Public
Wairarapa, Hutt Valley and Capital & Coast District Health Boards
It is recommended that the Committees:
Note the range of activities underway to improve nutrition, promote physical activity and prevent cardiovascular disease and diabetes across the sub-region.
Recommendation noted.
6.0 PROGRESS ON SUB-REGIONAL DISABILITY PLANNING referred to Pauline Boyles
Discussion Points:
11:05 Debbie Chin arrived
∑ Report taken as read.
∑ There is a need for data to measure inequalities for people with disabilities. By June 2015 there will be baseline data although we cannot yet do that in the Wairarapa. We can measure health passport uptake in the Wairarapa.
∑ Icon - implementation of icon on track with the first set of baseline data to be produced for CCDHB June 14 and for Hutt Valley June 15. At this stage Wairarapa does not have appropriate software to use the icon.
∑ Passport - It was noted that the passport in the Wairarapa is invisible at present. In response itwas noted that the DHB buys them, does the communication, trains staff and works with communities. The Passport is the patient’s tool and it’s their responsibility to use it.
∑ The move of the Masterton Medical Centre has affected the leadership from Primary Care.
∑ It is clear project management is required on the ground as well as community buy in.
∑ Sub-regional Forum May 2014 – planning is going well. All members are encouraged to engage.
∑ P76 3.31 – the indicator access improved and monitored across all 3D sites is currently red, and why is this? Reds are not a worry in themselves as this is 13/14. Hutt Valley and Wairarapa access for people with a disability needs to be addressed. There are also issues with car parks but there should be a simple solution.
∑ Sandra Greig is on the Regional Council’s disability committee and wondered how she could assist. Engagement is more than an accessibility committee.
Action Points:
∑ Review the one sentence statement on the Regional Council’s Disability Committee, to provide more context.
It is recommended that the Committees:
a) Note the progress against Sub-Regional NZDS Implementation Plan for 2013/14;
b) Note the Sub-Regional Disability Advisory Group (SRDAG) report back;
c) Note the plan for a Sub-Regional Disability Forum May 2014.
Noted: Derek Milne. Seconded: Virginia Hope.
Hutt Valley PUBLIC 2 May 2014 - COMMITTEE VERBAL REPORT BACKS
43
Public
Wairarapa, Hutt Valley and Capital & Coast District Health Boards
7.0 3D WORK PROGRAMME FEBRUARY UPDATE
Discussion Points:
∑ The Committee noted there was a lot of information contained in the appendix to the paper.
∑ There was a query as to the sub-regional work and where it fitted within the regional work. It was clarified that the sub-regional work is part of the regional plan. Although a lot of sub-regional work is occurring in this region there was less sub-regional work occurring in other areas due to either geographical or infrastructural differences.
∑ Clarification was sought form the CEO about the children’s hospital p174. In response, paediatricians have been discussing how to best service children. Paediatric services and resources are scare resources but the future model will be a more community-based model that a hospital model around inpatient beds. There is not a sufficient-sized population to support another Starship hospital.
It is recommended that the committees:
∑ Note and provide feedback on the 3DHB HSD report as attached and progress against the work programme for February 2014;
∑ Note the attached 3DHB Project Register.
Moved: Derek Milne. Seconded: Helene Ritchie.
10 GENERAL BUSINESS
10.1 Ethics
Discussion Points:
∑ It was suggested that it may be useful to have a presentation at some stage on ethical issues that clinicians face, noting that many clinicians need training.
Action Point:
∑ Invite CEs to consider how they could most appropriately get onto the work plan a presentation on concept of ethics.
10.2 Legal Highs
Discussion Points:
∑ Legal highs were discussed – it was acknowledged that considerable work had been done in this area by other parties who were better placed to do this analysis and consideration.
∑ Chair noted that there is an issue but it is the Government’s role to regulate.
11 RESOLUTION TO EXCLUDE THE PUBLIC
It is recommended that the Community & Public Health and Disability Advisory Services Committees:
(a) Agree that as provided by Clause 32(a), of Schedule 3 of the New Zealand Public Health and Disability Act 2000, the public are excluded from the meeting for the following reasons:
Hutt Valley PUBLIC 2 May 2014 - COMMITTEE VERBAL REPORT BACKS
44

Public
Wairarapa, Hutt Valley and Capital & Coast District Health Boards
Subject Reason Reference*
Community & Public Health and Disability Services Advisory Committees Public Excluded Minutes
For the reasons set out in the 2 September 2011 Board Agenda
DIRECTOR OF SIDU REPORT Enable a Minister of the Crown or any department or organisation holding the information to carry out, without prejudice or disadvantage, commercial activities
Enable a Minister …, negotiations (including commercial and industrial negotiations)
Section 9(2)(I);
Section 9(2)(j)
DHB ANNUAL PLANNING AND REGIONAL SERVICES PLANNING UPDATE
Enable a Minister of the Crown or any department or organisation holding the information to carry out, without prejudice or disadvantage, commercial activities
Enable a Minister …, negotiations (including commercial and industrial negotiations)
Section 9(2)(I);
Section 9(2)(j)
* Official Information Act 1982.
Moved: Derek Milne Seconded: Virginia Hope
The meeting finished at 12:10pm
CONFIRMED that these minutes constitute a true and correct record of the proceedings of the meeting.
DATED this day of 2014
Derek MilneCHAIR
Hutt Valley PUBLIC 2 May 2014 - COMMITTEE VERBAL REPORT BACKS
45
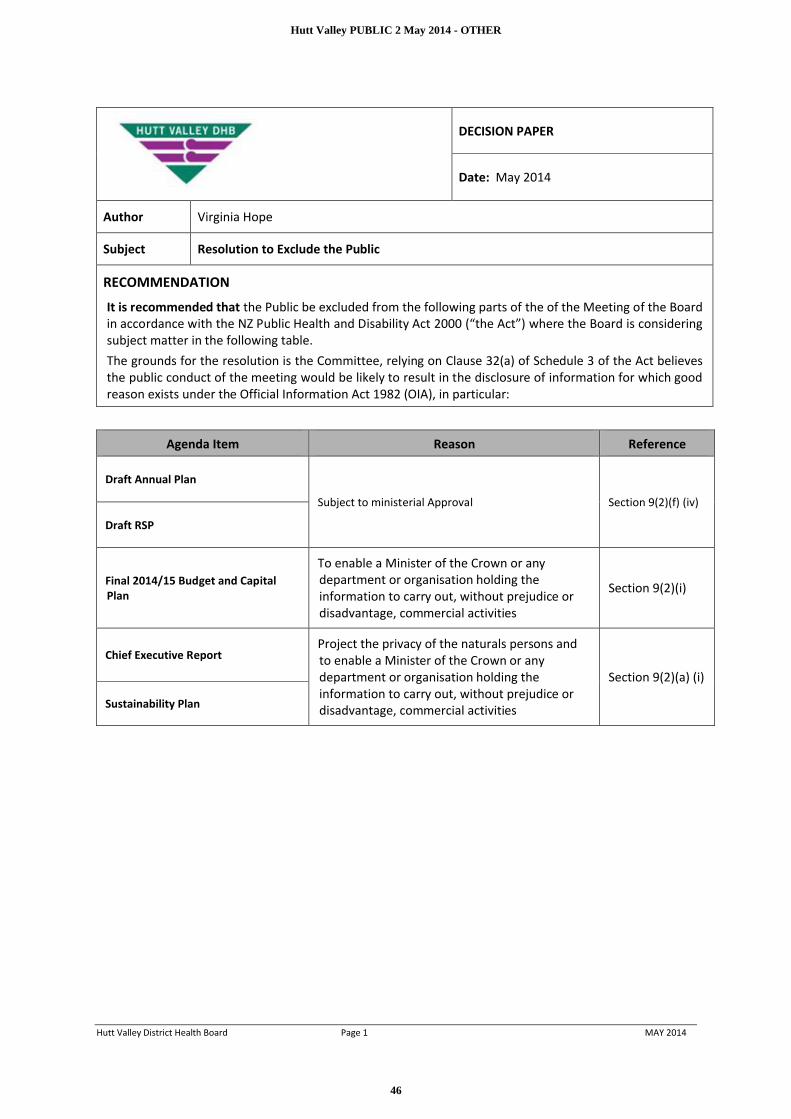
Hutt Valley District Health Board Page 1 MAY 2014
DECISION PAPER
Date: May 2014
Author Virginia Hope
Subject Resolution to Exclude the Public
RECOMMENDATION
It is recommended that the Public be excluded from the following parts of the of the Meeting of the Board in accordance with the NZ Public Health and Disability Act 2000 (“the Act”) where the Board is considering subject matter in the following table.The grounds for the resolution is the Committee, relying on Clause 32(a) of Schedule 3 of the Act believes the public conduct of the meeting would be likely to result in the disclosure of information for which good reason exists under the Official Information Act 1982 (OIA), in particular:
Agenda Item Reason Reference
Draft Annual Plan
Subject to ministerial Approval Section 9(2)(f) (iv)
Draft RSP
Final 2014/15 Budget and Capital Plan
To enable a Minister of the Crown or any department or organisation holding the information to carry out, without prejudice or disadvantage, commercial activities
Section 9(2)(i)
Chief Executive ReportProject the privacy of the naturals persons and to enable a Minister of the Crown or any department or organisation holding the information to carry out, without prejudice or disadvantage, commercial activities
Section 9(2)(a) (i)
Sustainability Plan
Hutt Valley PUBLIC 2 May 2014 - OTHER
46

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board
APPENDIX One: PHO funding Streams (additional information)
1. Very Low Cost Access & Free under Sixes funding
Eligibility for the Very Low Cost Access payment is limited to PHOs/practices currently charging or prepared to reduce their fees for standard consultations to the thresholds specified below:
ß Zero fees for children 0 - 5 years.
ß $11.50 maximum for children 6 - 17 years.
ß $17.50 maximum for all adults 18 years and over.
ß New practices to the programme must meet the eligibility criteria of 50% high needs population (defined as Māori, Pacific or New Zealand Deprivation Index quintile 5).
As of 1 July 2012, all CCDHB practices offer zero fees for under sixes. In CCDHB, 13 practices offer very low cost access fees. Similarly all HVDHB practices offer zero fess for under sixes while six practices offer very low cost access fees. All Wairarapa practices offer zero fees for under sixes and one practice offers very low cost access fees.
Additional funding has been released for VLCA practices in 2013/14. Two pools were made available:
∑ VLCA sustainability funding (multi year)
∑ VLCA Nurse funds (this is one off for 13/14).
2. Co-payments: PHO general practice providers are able to charge a co-payment for their services.
Table 1: Co-payments currently charged by practices in Wairarapa DHB as at May 2013
Under 6 6-17 yrs 18-24yrs 25-44 yrs 45-64 yrs Over 65
Lowest to Highest $0.00 $11.50 - $29 $17 - $33 $17 - $36.50$17 -
$36.50 $17 - $32.50
Average Co-payment $0.00 $25.57 $28.71 $30.90 $31.57 $29.20
Table 2: Co-payments currently charged by practices in Hutt Valley DHB as at February 2013
Range $ Under 6 6-17 yrs 18-24yrs 25-44 yrs 45-64 yrs Over 65
Lowest to Highest $0.00 $5-$45 $15-$45 $15-$45 $15-$45 $5-$40
Average Co-payment $0.00 $23.60 $30.14 $31.77 $31.81 $28.98
Table 3: Co-payments currently charged by practices in CCDHB as at April 2013
Range $ Under 6 6-17 yrs 18-24yrs 25-44 yrs 45-64 yrs Over 65
Lowest to Highest $0.00 $0-$53 $0-$57 $10-$63 $10-$63 $5-$58
Average Co-payment $0.00 $27.48 $34.64 $37.83 $38.68 $36.74
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
47

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board
3. General Practice Fee (co-payment) Increases
General Practices are able to increase their fees based by a nationally determined allowable percentage each year. This percentage is based on an analysis of cost pressures carried out independently and set at a national level. Practices are also able to carry forward any unused percentage from previous years. PHOs are required to notify their DHB of any fees increases, and these are approved if they are equal to or less than the allowable percentages. Fee increases can be approved or sent to a Regional Fees Review Committee to review.
In 2013/2014, all GP fee increases received by HVDHB have been within the reasonable increase as defined by the annual statement therefore no increases have been referred to the Central Region Fees Review Committee.
In 2012/13 CCDHB has received three proposed GP fee increases above the allowable increases. These have been referred to the Central Region Fees Review Committee (CRFRC). Two fee increases were accepted by the committee and the third was initially rejected by the committee. Following discussion with the PHO and resubmission of a lower percentage increase this has also been accepted. SIDU staff have been working with the PHO to minimise fee increases, particularly for young people.
A full list of GP fees as at 2012/2013 is attached as Appendix 4.
4. After Hours
All children under the age of six years have access to free after-hours care for acute presentations. CCDHB is currently undertaking a survey on the impact the under sixes project has had on the region and data to date suggest a reduction in the number of six year olds presenting at the Wellington Hospital Emergency Department and that GPs are comfortable with the level of presentations they are receiving.
Wairarapa, Hutt Valley, and Capital & Coast DHBs all receive additional funding from the Ministry of Health for a range of afte-hours services. The Ministry of Health has devolved this funding to DHBs for the 2014/5 year.
Wairarapa DHB uses the funding to reduce after-hours fees for children and young people and all those with a Community Services Card. Some of the funding is also used to communicate primary care arrangements (including after-hours) to Wairarapa residents and visitors to the region.
Currently, Hutt Valley DHB invests in a Telephone Nurse Triage service. Patients are able to access advice twenty four hours a day by ringing their own general practice. The total funding for Telephone Nurse Triage service in 2013/2014 is $197k. The balance of the funding is utilised to support Free Under Sixes access to after-hours care. The Telephone Nurse Triage service is currently being reviewed under the Hutt Inc After-Hours work stream.
CCDHB invests the additional funding ($502,500) in subsidies for high needs after-hours patients at Wellington After Hours Medical Centre, Kenepuru Accident and Medical Centre, extended hours for Newtown Union Health Service, and a discharge planning service in Kapiti. A review of after-hours spending is planned during 2014.
5. Services to Improve Access Funding
Services to Improve Access (SIA) are core PHO services designed to reduce health inequalities by improving access to primary care services for high need groups in the enrolled population (i.e. Maori, Pacific peoples and those living in NZDep 9 and 10 decile areas). PHOs obtain approval for their SIA spending from the DHB as part of their annual business planning processes.
Wairarapa
Wairarapa SIA funding is now part of the flexible funding pool with delegation for its use devolved to the Alliance Leadership Team. Currently the amount of funding used to reduce access barriers is the same as that determined through the funding formula. A small proportion of the funding is used for pharmacy vouchers and the Red Cross transport services and the balance is distributed to the practices to use as they see fit to ensure their high needs population is able to access care. The practices are using the funding in a variety of ways including a Marae-based drop in clinic (for enrolled patients) and Whanau funds.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
48

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board
Hutt Valley DHB
Te Awakairangi Health Network utilise their Services to Improve Access (SIA) funding to provide programmes outlined below:
∑ Outreach nursing ∑ Community Health Workers ∑ CVD risk assessment subsidy for high needs population ∑ Dietetic services∑ Transport (so patients can access services)∑ Language Line (interpreters).
Capital and Coast DHB
Compass Health utilise their funding to employ a Whanau Navigation team (Clinical leads, Nurses, community health workers, project managers) to work across programmes contributing to their identified strategic directions, as well as applying funding to specific programmes. The other PHOs invest in a number of activities.
1. Care Plus
Care Plus provides additional funding to PHOs for people who have to visit a GP or nurse more frequently because of a chronic condition, such as diabetes or heart disease, acute medical or mental health needs, or a terminal illness. A total of $244.09 (GST Excl) annually is available for each Care Plus Client.
As of 1 July 2012, 98% of the Care Plus eligible population in CCDHB was enrolled.
Te Awakairangi Health Network’s Care Plus programme enables patients to receive four Care Plus sessions. The first and the fourth Care Plus session are face-to-face contact with either the GP or Practice Nurse. Sessions two and three may vary depending on the practice, however these sessions can be face-to-face or in some cases phone consultations.
Wairarapa Care Plus funding is included in the Flexible Funding Pool and is being used to fund Guided Care. Over 100% of the eligible population was enrolled into Care Plus prior to the establishment of the Alliance, and a similar number of people are now enrolled in the Guided care programme. Under Guided Care, practices are bulk funded to assess the needs and plan for the care of their LTC population, with increased discretion about how they use the funding allocated.
2. Primary Mental Health Services
The Ministry of Health funded these services separately in 2013/14 and has indicated that this funding will be devolved in 2014/15 to DHBs. The Minister has announced that new investment will be put into extending the primary mental health initiative to all youth including un-enrolled youth (i.e. non-Maori, non- Pacific and non-High needs youth who are already covered by the existing funding). There is also an expectation that 18% of existing funding will already be targeted at Maori, Pacific and high needs youth (12-19 years).
Wairarapa DHB
In Wairarapa, Compass Health employs two mental health nurses who work in the practices, closely linked to the DHB mental health services. One of these positions was devolved from the DHB as part of the Tihei Wairarapa integration initiatives. The PHO also coordinates additional primary mental health services, including packages of care and extended consultations with GPs and practice nurses.
Hutt Valley DHB
Te Awakairangi Health Network provides the Wellbeing Primary Mental Health Service. This service is based on a model that is both centralised and community based. Te Awakairangi Health Network has formed formal partnerships with community providers to deliver services in agreed community locations. Patients can access
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
49

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board
the service from a centralised location based within Te Awakairangi Health Network, and also via an outreach service, based in the network but delivered in community setting. Community based services are embedded within agreed community settings i.e. General Practices, or NGOs.
HVDHB utilises the youth non-high need funding to fund Hutt Valley Youth Health Trust (VIBE) to provide services to ensure all youth 12-19 years within the DHB are able to access youth mental health and AOD services.
Capital & Coast DHB
All four CCDHB PHOs deliver Ministry of Health funded Primary Mental Health services for clients with mild to moderate mental illness. Each PHO employs a number of mental health practitioners to provide assessment and treatment for clients using evidence based therapies, provide education for practitioners and manage the referral process. PHOs also contract for packages of care and brief interventions, which can include counselling sessions, medication management reviews, psychological therapy and behavioural therapy.
Table 4: Primary Mental Health funding 2013/14
Total PMHI
funding$000
Subset targeted at
12-19 years high need $000
New youth non-high
need funding
$000
Total funding 2013/14
$000
Capital & Coast DHB
$1,851 $333 $166 $2,017
Hutt Valley DHB $1,018 $183 $71 $1,089
Wairarapa $344 $43 $26 $370
3. More Health and Diabetes Checks
On 13 May 2013, the Minister of Health announced that additional funding would be made availableover four years for the health target and DCIP implementation. The national funding allocation is:∑ $35.5m extra nationally for diabetes and heart disease prevention and management∑ $15.9m for more heart and diabetes checks (the national target)∑ $12.4m for diabetes care improvement package∑ $7.2m for green prescriptions
New investments were made available to the three DHBs as outlined below:
1. More Heart and Diabetes Checks (2 September 2013 to 30 September 2017). The expectation is that the national target will be achieved and maintained and the following funds were allocated to PHOs:
a. Wairarapa DHB $43.4k pab. Hutt Valley DHB $126.5k pac. CCDHB $233.5k pa
2. Diabetes Care Improvement Plans 2013/14 (October 13 CFA). Table 5 outlines the following amounts have been allocated for 2013/14 for activities agreed with the Ministry.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
50
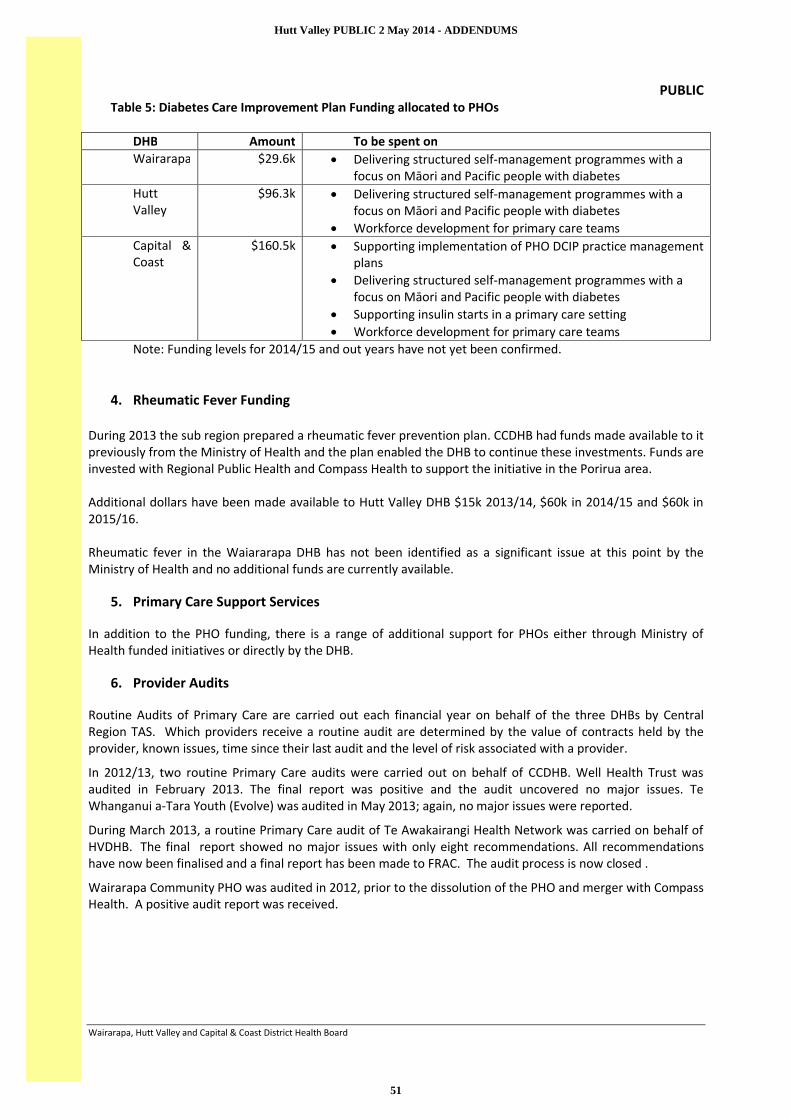
PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board
Table 5: Diabetes Care Improvement Plan Funding allocated to PHOs
DHB Amount To be spent onWairarapa $29.6k ∑ Delivering structured self-management programmes with a
focus on Māori and Pacific people with diabetesHutt Valley
$96.3k ∑ Delivering structured self-management programmes with a focus on Māori and Pacific people with diabetes
∑ Workforce development for primary care teamsCapital & Coast
$160.5k ∑ Supporting implementation of PHO DCIP practice management plans
∑ Delivering structured self-management programmes with a focus on Māori and Pacific people with diabetes
∑ Supporting insulin starts in a primary care setting∑ Workforce development for primary care teams
Note: Funding levels for 2014/15 and out years have not yet been confirmed.
4. Rheumatic Fever Funding
During 2013 the sub region prepared a rheumatic fever prevention plan. CCDHB had funds made available to it previously from the Ministry of Health and the plan enabled the DHB to continue these investments. Funds are invested with Regional Public Health and Compass Health to support the initiative in the Porirua area.
Additional dollars have been made available to Hutt Valley DHB $15k 2013/14, $60k in 2014/15 and $60k in 2015/16.
Rheumatic fever in the Waiararapa DHB has not been identified as a significant issue at this point by the Ministry of Health and no additional funds are currently available.
5. Primary Care Support Services
In addition to the PHO funding, there is a range of additional support for PHOs either through Ministry of Health funded initiatives or directly by the DHB.
6. Provider Audits
Routine Audits of Primary Care are carried out each financial year on behalf of the three DHBs by Central Region TAS. Which providers receive a routine audit are determined by the value of contracts held by the provider, known issues, time since their last audit and the level of risk associated with a provider.
In 2012/13, two routine Primary Care audits were carried out on behalf of CCDHB. Well Health Trust was audited in February 2013. The final report was positive and the audit uncovered no major issues. Te Whanganui a-Tara Youth (Evolve) was audited in May 2013; again, no major issues were reported.
During March 2013, a routine Primary Care audit of Te Awakairangi Health Network was carried on behalf of HVDHB. The final report showed no major issues with only eight recommendations. All recommendationshave now been finalised and a final report has been made to FRAC. The audit process is now closed .
Wairarapa Community PHO was audited in 2012, prior to the dissolution of the PHO and merger with Compass Health. A positive audit report was received.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
51

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board Page 1 MAY 2014
APPENDIX TWO: PHO PERFORMANCE
1. Information on the three primary care heath targets is presented in the PHO league table attached.
1.1. Increased Immunisation: The target is 90% of 8 month olds will have their primary course of immunisation at on time by July 2014. All 3 DHBs are doing well in the overall target. The national performance average for the 8 month target is 92%. Compass Waiararapa, Cosine and Well Health all achieved the target as at the end of Quarter 2. Compass CCDHB at 94% and Te Awakairangi at 93% are close to the target and expected to reach the target by 30 June 2014. Ora Toa is sitting at 82% and is ranked at 35th out of 36 PHOs. This is an uncharacteristic result for Ora Toa which has previously maintained performance within the top 10 PHOs (last quarter they were at 95%). Ora Toa has already reviewed its systems and processes and is tracking to restore its previous achievement.
1.2.Better Help for Smokers to Quit: The target is 90% of patients who smoke and are seen by a health practitioner in primary care are offered brief advice and support to quit smoking. The national performance is 66% at the end of quarter 2 2013/14. Compass Wairarapa has achieved the health target and is number one on the league table. Compass CCDHB at 81% is above the national average performance. The other four PHOs are below the national performance level. Progress is slow but a steady improvement is seen each quarter.
1.3.More Heart and Diabetes Checks: This target is that 90% of the eligible population will have had their cardiovascular risk assessments in the last five years by July 2014. The national average performance is 73%. Compass Wairarapa is at number 5 on the league table at 84%. Compass CCDHB (81%), Cosine (81%), Ora Toa (74%) are all above the national average while Well Health at 70% is not far behind. Te Awakairangi is number 34 on the league table at 58%. The PHO has developed a recovery plan at the request of the Ministry of Health and the PHO has further improved its result in the 3rd quarter ended 31 March and is sitting at 69.4%.
2. Additional relevant information was presented in the CPHAC-DSAC February Equity report on ASH, primary care access and Diabetes.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
52

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
53

1 | P a g e
Te Awakairangi Health Network
2012/13 Annual Report
September 2013
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
54

2 | P a g e
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
55

3 | P a g e
Contents
Chair’s Report Page 4
Management Report Page 5
The People We Serve Page 6
Our Provider Members Page 7
Our Community Services Page 8
Community Services Page 9
Service Highlights Page 10
Looking Ahead Page 16
Audited Financial Statements Page 18
Our Vision
A healthy Hutt Valley for all
Our Mission
To be a community leader for
health in the Hutt Valley
Our Values
People centred
Aiming for equity
Excellence in all we do
Working co-operatively
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
56

4 | P a g e
Chair’s Report It is with pleasure that the Board of Trustees of
Te Awakairangi Health Network (TeAHN) submits
its 2012/13 Annual Report.
As Board Chair, I look back on the past year with
a sense of real achievement and progress. It has
been a year of consolidation and coming
together for our governance Board, our TeAHN
team and our different provider members.
During 2012/13, we have brought together the
programmes, activities and provider members
from five former organisations: Piki te Ora ki te
Awakairangi PHO; Valley PHO; Family Care PHO;
Tamaiti Whangai PHO; and Kōwhai Health Trust.
The reshaped Board of Trustees reflects our
history and the diversity in the Hutt Valley.
Working with the community representatives we
have on our Board - Teresea Olsen, Brendon
Baker, Tofa Suafole Gush and Muriel Tunoho –
our Board is helping to ensure our organisation
has a positive impact on the health and wellbeing
of the people of the Hutt Valley. I also want to
acknowledge the contribution of the new
primary care physician representatives who have
joined Dr David Young on our Board – Dr Lise
Kljakovic, Dr Hans Snoek and Barry Cooper.
As a Board, we have developed a common vision,
mission and strategic direction. In reshaping our
mission and vision, we have maintained our focus
on the needs of our population, providing
excellent services for all our patients, and
targeting additional services to those with the
highest health needs and poorest access to care.
We have strengthened our Clinical Governance
Committee to better enable it to advise the
Board on clinical matters.
We have also been fortunate to appoint a new
Chief Executive, Bridget Allan, who brings
considerable knowledge and health experience
to this important role.
The past year has seen us maintain our focus on
intervening early. Our health promotion
programmes are helping people quit smoking,
our population is having more heart checks, and
we have a real focus on promoting better
nutrition and physical activity, and reducing
obesity.
We have better integrated and consolidated our
our community health worker teams, our
outreach nursing activity, our transport
programmes and our different models of primary
mental health service delivery.
We have reshaped some programmes, and have
seen a significant improvement in the number of
people being enrolled into Care Plus. Looking
forward, we will better align our various long
term conditions programmes.
Without question, we recognise and
acknowledge the importance of our Network
general practices. In 2012/13, the TeAHN team
has actively supported practices with
Cornerstone accreditation, staff recruitment,
training and education, and enhancement of
their information systems. The Network has also
worked on behalf of our primary care provider
members to strengthen the primary care voice at
local, sub-regional and national levels.
Finally, we are working more closely with our
PHO neighbours in Wellington and Wairarapa.
Our relationship with Hutt Valley DHB continues
to strengthen, with primary care clinicians and
managers participating strongly in Hutt INC, the
new Alliance Leadership Team.
M N (Joe) Asghar Board Chair
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
57

5 | P a g e
Management Report
From the Chief Executive’s Desk As the new CE of Te Awakairangi Health Network
(TeAHN), I welcome this opportunity to reflect on
the year that has been. It has been a busy year
but also a year in which I believe we have made
good progress. I would like to thank my Board
and the team at TeAHN for their support and
dedication during my first year in the role.
Our 2012/13 Annual Plan committed Te
Awakairangi Health Network to bring together
the programmes, activities and provider
members of five previous organisations.
It committed us to makes these changes whilst
living within budget.
Our 2012/13 Annual Plan also had a strong focus
on how we can best support those in our
community who have the greatest health need.
We have remained true to this focus.
Highlights Looking back over the year, we can see progress
in a number of areas:
Health targets – excellent child immunisation
rates have been maintained and we have
made good progress with smoking cessation.
Some progress has been made against the
health targets for heart and diabetes checks
but further improvement is required
Strengthened our Clinical Governance
Committee, with additional general
practitioner, practice nurse, practice
manager and community pharmacy
representation on this independent clinical
grouping, ensuring we have stronger links
with our front line provider members
Maintained our support to practice members
Better integrated our PHO programmes for
high needs populations
Strengthened our working relationships with
Hutt Valley DHB and other providers
Successfully managed additional DHB
funding for service programmes.
Our Focus Looking ahead, we want to:
Provide affordable health care to our
populations with the greatest need
Work more closely with our Māori and
Pacific communities
Encourage more people to make healthy
choices
Support people with long term conditions to
pro-actively manage their condition and gain
greater independence
Continue to build primary care’s financial
sustainability, capacity and capability
Advocate for change on behalf of our
population and practice members
Continue to reshape local health services
through our work with Hutt Valley DHB as
part of the local Alliance Leadership Team
known as Hutt INC (Hutt Integrated Network
of Care)
Work more at a sub-regional level with
neighbouring DHBs and PHOs
Live within our means.
“By working with our general
practices to secure a strong and
sustainable future, we can better
support the people within our
community who have the poorest
health outcomes.”
Bridget Allan Chief Executive Office
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
58

6 | P a g e
The People We Serve
Te Awakairangi Health Network (TeAHN) has
an enrolled population of 117,200.
The population we serve is slightly younger and
we have slightly more Māori and Pacific people
than the national average. In total, TeAHN has
almost 20,000 Māori and over 10,000 Pacific
people enrolled across its practice members.
From a deprivation perspective, 43,000 people
or over a third of our population is considered
to be high needs – either Māori, Pacific or living
in high deprivation areas.
Many of our high needs populations are
clustered in Pomare, Taita, Naenae, Stokes
Valley, Moera and Wainuiomata. This creates
particular challenges for the general practices
located in these areas.
Typically, people with high needs are more
likely to:
Be admitted to hospital for an avoidable
hospital admission
Have a long term condition such as
diabetes, heart or respiratory disease
Have less ability to pay for medical care
We respond to our high needs populations in
three different ways:
We support practices, particularly those
operating in high needs areas, as they
respond to the health needs of their
populations on a day-to-day basis.
We support high needs populations
directly through the programmes we
deliver. Our outreach nurses, community
health workers, dietitians, primary mental
health workers and our health promotion
and healthy lifestyle coaches deliver face-
to-face services to people most in need.
We advocate at a local, sub regional and
national level on behalf of our population.
This includes working with the DHB
through Hutt INC and with other local
providers, working with neighbouring
PHOs, working with the local whanau ora
collectives, Te Runanga O Taranaki Whanui
and Takiri Mai Te Ata, to support the
implementation of whanau ora
programmes, and enhancing our networks
within the Pacific community.
“As a Network, we must focus on
what it means to deliver health
services which are both affordable
and accessible to people who are
more likely to have significant
health issues, for the financial
viability of these practices, and for
the staff working within them.”
17%
9%
11%63%
Te Awakairangi Network Patient Profile
Maori Pacific Non-Maori Pacific Non-LCAF
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
59

7 | P a g e
Our Provider Members
In 2012/13, Te Awakairangi Health’s enrolled
population was spread across our 24 practice
members1 in the Hutt Valley:
Avalon Medical Centre
Dr Dunn’s Surgery
Dr Hans Snoek
Epuni Medical Centre
Fergusson Drive Surgery
Fitzherbert Road Medical
Gain Health
Hutt Union and Community Health Services
(HUCHS) – Petone and Pomare sites
Hutt City Health Centre (HCHC)
Kopata Medical Centre
Main Street Surgery
Manuka Medical Centre
Muritai Health Centre
Naenae Medical Centre
Petone Medical Centre
Pretoria Street Surgery
Silverstream Health Centre
Soma Medical Centre
Stokes Valley Medical Centre
Strand Care (now HCHC Wainuiomata)
Taita Medical Centre
Upper Hutt Health Centre
Waiwhetu Medical Centre
Whai Oranga O Te Iwi
Our practice members provide comprehensive,
accessible, culturally appropriate, high quality
primary healthcare services to Te Awakairangi
Health’s enrolled population.
Together, our practices have 68.9 FTE general
practitioners (including locums) and 53.1 FTE
practice nurses as well as other health workers
and administrative staff.
These health professionals provided a total of
423,000 patient contacts in 2012/13, with
145,000 of these being for high need clients.
Eight practices have a high needs population
percentage of greater than 40% and one practice
has 87% of its enrolled population falling into the
high needs category.
“Our goals are to be a strong
Network, with sustainable practices
and providers, a culture of innovation
and integration, comprehensive and
connected services, and wise use of
funds.”
Te Awakairangi Health has continued to work
with practice members to improve performance
and sustainability. Of our 24 practices, 11 have
fewer than 2 FTE general practitioners.
In 2012/13, our practice liaison and support
activity included:
Supporting practices to make progress
against the PHO health targets
Supporting practices to achieve Cornerstone
and Te Wana accreditation
Facilitating professional education and
workforce development
Assisting practices with business and
information system issues
Specific project work supported by Hutt INC
looking at practice sustainability.
1 Up until 6 June 2013, there were 24 practices making up the Network. From June 2013, the Hutt City Health Centre began running the established Strand Care
practice as a satellite practice, reducing the number of practices down to 23.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
60

8 | P a g e
Our Community Services Te Awakairangi Health Network offers a wide
range of community based services and
programmes. These are in addition to the
regular visits people make to GPs and practice
nurses in our Network.
These include programmes focused on
improving the health of the whole population
while at the other end of the continuum, other
activity focuses on working with particular high
need families and individuals:
Population education and prevention
services: Services to promote healthier
lifestyles
Screening, diagnostic and early
intervention services: Early disease
identification and intervention
Long term conditions: Services to help
people better manage conditions such as
heart disease, diabetes and respiratory
conditions
Primary Mental Health: Services to treat
people with mild to moderate mental
illness, and foster better mental health and
wellbeing within our community
Wrap around services: Services to improve
the health of people with the highest
needs and to assist them better access
existing services.
Feedback from our community shows strong
support for these services.
These services also help our general practice
network and the Hutt Valley DHB’s hospital
based services by reducing the potential
demand for acute care and by supporting
people to live healthier and more independent
lives in the community.
Taken together, our outreach nurses,
community health workers, primary mental
health teams, dietician service and healthy
families coach delivered a total of 35,526
patient contacts in 2012/13.
These contacts included a mixture of face-to-
face client contacts, phone calls, follow-up
visits including home visits, group sessions and
client referrals to other agencies.
“I cannot ever underestimate the
difference this has made to our lives.
Sarah (our Healthy Families Coach)
and dietitian Jan have been very
encouraging and have gently
pushed us into losing weight.
My confidence and self esteem, well
being and sense of purpose has
changed dramatically. I feel my life
has changed and I find myself
wanting to shout to other people that
they need to be aware of this
fantastic community support network,
so we can help ourselves, improve
ourselves, so we can be better
people.”
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
61

9 | P a g e
Community Services
Leve
l o
f n
ee
d a
nd
in
ten
sity
of se
rvic
e e
ffo
rt w
ith
in
div
idu
al c
lie
nts
Wrap around
services for
people with high
needs
Helping people
access services
Primary mental
health services
Helping people
with diagnosed
long term
conditions such
as heart disease
and diabetes
Screening,
diagnostic and
early intervention
services
Population
education and
prevention
services
Outreach Nurses
Work with at risk patients in the community providing advice, health
education, advocacy and support
Community Health Workers
Facilitate access to primary care services and to community organisations
and social support agencies such as WINZ and Housing NZ
Wellbeing Service, HUCHs and Whai Oranga
Primary mental health and addiction services to people living in the Hutt Valley,
with a focus on high needs populations with mild to moderate mental illness
Hutt Valley Youth Health Service (Vibe) and Lower Hutt Women’s Centre
Specialised primary mental health service providers for specific population groups people and women
living in the Hutt Valley
Healthy Family Coach
Physical activity and lifestyle
programmes for at risk
populations
Dietitians
Provide dietary information and
advice to at risk populations,
including individual patient
interventions
Pacific Healthy
Lifestyles
Focuses on healthy lifestyle
activities for Pacific
Sexual Health
Educating and providing
free sexual health
services to under 20 yrs
Skin Lesions
Funds GPs to remove
skin lesions for high
needs patients
Community
Radiology
Access to imaging services
in the community
Cervical Screening
Encourages high needs
women to have a cervical
smear
Immunisation Support
Supports practices to maintain
high immunisation levels and
prevent diseases (e.g. measles)
Transport Services
Free transport to primary and secondary
services for high needs patients
Language Line
Telephone interpreting service for people who
do not speak English
CVD Risk Screening
and Education
Assessing at risk population for
heart disease
Care Plus
Helps people better manage a long
term condition, an acute medical
need or terminal illness
Cardiac Continuum Helps people with a cardiac condition better manage
their situation by offering free GP visit and nurse
education sessions following a hospital admission
Diabetes Care
Helps high needs people with diabetes
better manage their condition, with a
focus on those newly diagnosed
Respiratory Services
Helps high needs people with asthma or
respiratory disease better manage their
condition, with a focus on those newly diagnosed
Rheumatic Fever Reduce the incidence of
rheumatic fever and
prevent reoccurrences
Medicines Management
Facilitators provide support and
advice to prescribers
Warfarin
Monitoring
Helps people use warfarin
Podiatry
Free foot care for
high needs people
with diabetes
Smokefree
Supports practices to use
the ABC approach to
encourage smokers to quit
Health Promotion
Healthy lifestyle events, promote healthy
lifestyles and help population reduce risk of
developing chronic diseases
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
62

10 | P a g e
Our Service Highlights
Our Practice Member Services In 2012/13, the 24 practice members within Te
Awakairangi Health Network (TeAHN)
provided a total of 423,000 patient contacts.
This included a total of 307,000 GP visits and
116,000 practice nurse visits.
Of these visits, 35% of the visits to nurses and
34% of the visits to GPs involved people with
high needs.
TeAHN supported the practices as they
delivered these front line services, including
making our clinical programme facilitation,
immunisation support and medicines
management services available to practices.
TeAHN also offered assistance with
information technology issues such as the
better use of decision support tools, PHO
performance targets, register management,
and claims management.
In the early part of 2013/14, all practices will
have Patient Dashboard installed. This will
provide them with information from their
patient management systems about each
patient as the consultation takes place. It
offers the opportunity to address outstanding
health screening or follow-up issues and to
make progress against the PHO performance
targets.
“We continue to perform well with
childhood immunisations, being
amongst the top in the country.”
Looking to the future, use of the Dashboard
should also assist practices make
improvements with our smoking cessation
efforts and the number of cardiovascular
disease (CVD) risk assessments we are
providing.
73%
27%
Nurse and GP Visits 2012/2013
GP Visits Nurse Visits
GP Visits Nurse Visits
Other 203025 74928
High Needs 104471 40903
0%
20%
40%
60%
80%
100%
Nurse and GP Visits 2012/2013
0%
20%
40%
60%
80%
100%
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
2011/12 2012/13 2013/14
CVD Risk Assessments(Total Population)
Programme Target
TeAHN Target (CVD Plan)
Actual
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
63

11 | P a g e
“Whilst we are improving our CVD and
smoking cessation performance, we
need to do much better in 2013/14.”
We have also been able to help some of our
practice members consider practice
sustainability issues and assist them address
their workforce development and education
needs. This will remain a priority focus in
2013/14.
Changing People’s Lifestyles During 2012/13, Te Awakairangi Health
Network’s Health Promotion Team was very
active in the community. It worked with
practice members and community groups to
deliver heart checks in community settings and
to encourage people to have heart checks at
their medical practice.
The Health Promotion Team assisted local
communities to run “Good Food Programmes”
in Petone, Pomare, Wainuiomata, Taita and
Stokes Valley.
The Team helped a variety of organisations to
deliver a range of community health
promotion projects including heart checks at
Te Ra o Te Raukura and Tumeke Taita, Chinese
Health and Wellbeing Day, WelTec Health
Promotion events, Pacific Kirikiti Tournament,
Refugee Health and Safety Day, Upper Hutt
Teen Unit’s healthy eating programme, and
World Smokefree Day Quit stall at Queensgate
Shopping Centre.
In 2012/13, the Team also worked with existing
support groups focused on long term
conditions such as diabetes, and was involved
in the development of new groups such as the
gout leadership group.
0%
50%
100%
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
2011/12 2012/13 2013/14
Brief Advice to Quit Smoking(Total Population)
Programme Target TeAHN Target
Actual
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
64

12 | P a g e
The Team expanded the Valley Fit gym
programme to Wainuiomata and was also
instrumental in making the Te Awakairangi
TRYathlon happen.
This saw 126 people complete the event, with
many of those attending health education
sessions prior to the event.
The Pacific Health Lifestyles Programme sits
alongside the work of the Health Promotion
Team, the Healthy Families Coach and the
dieticians. This programme, run by the Pacific
Health Service, involves daily Pasifika style
aerobic exercise classes.
In 2012/13, our Healthy Families Coach
delivered a total of 2,221 patient contacts and
our dietitians delivered 3,113 patient contacts.
People were seen in their own home, at their
GP practice or in the gym. For many people,
this contact can be the start of a life changing
journey.
Long Term Conditions In 2012/13, many of our programmes and
funding streams focused on supporting people
with a long term condition, some of these
directly funded by the Hutt Valley DHB.
These “long term conditions programmes”
included Care Plus and our specific disease
management programmes which have been
separately focused on diabetes, heart disease
and respiratory disease. For people with heart
disease, these programmes have been
supported by initiatives such as warfarin
management.
These different programmes have helped
many people better manage their condition.
However, we have come to recognise that this
siloed approach to different long term
conditions has led to fragmentation and is not
necessarily best meeting the needs of our
patients. We need to be able to respond to
patient needs in more flexible ways rather than
focus on individual disease programmes.
National changes to diabetes programmes
have seen local efforts refocus on the needs of
Māori, Pacific and people living in high needs
areas who have diabetes. Whilst there is an
underlying expectation that all people with
diabetes should receive an annual clinical
review, this is no longer funded for people
outside the target group. There has been a
drop in the number of annual reviews being
provided.
This is of concern as it is possible that health
outcomes will deteriorate for people with
diabetes who are outside the target
population. In 2013/14, together with our
practice members, we will address this
situation.
Meanwhile, there continues to be good access
to podiatry sessions in the community. Te
Awakairangi Health manages the payment for
these sessions which are funded by Hutt Valley
DHB.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
65
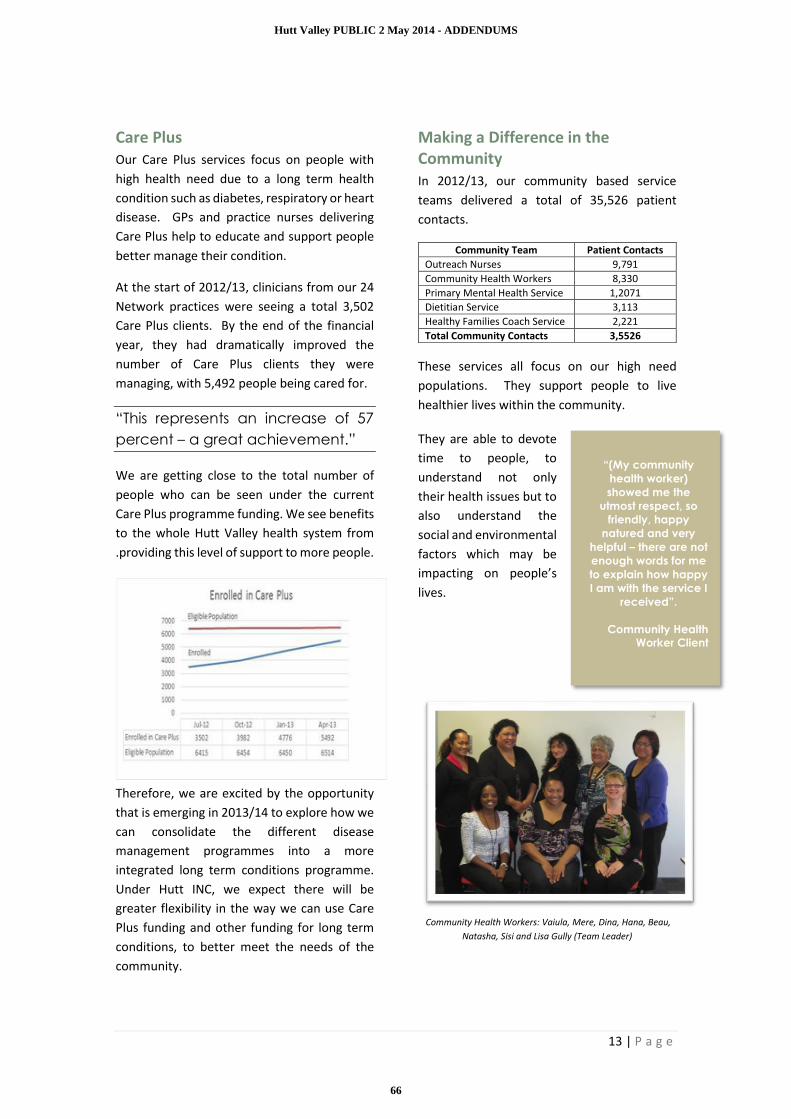
13 | P a g e
Care Plus Our Care Plus services focus on people with
high health need due to a long term health
condition such as diabetes, respiratory or heart
disease. GPs and practice nurses delivering
Care Plus help to educate and support people
better manage their condition.
At the start of 2012/13, clinicians from our 24
Network practices were seeing a total 3,502
Care Plus clients. By the end of the financial
year, they had dramatically improved the
number of Care Plus clients they were
managing, with 5,492 people being cared for.
“This represents an increase of 57
percent – a great achievement.”
We are getting close to the total number of
people who can be seen under the current
Care Plus programme funding. We see benefits
to the whole Hutt Valley health system from
.providing this level of support to more people.
Therefore, we are excited by the opportunity
that is emerging in 2013/14 to explore how we
can consolidate the different disease
management programmes into a more
integrated long term conditions programme.
Under Hutt INC, we expect there will be
greater flexibility in the way we can use Care
Plus funding and other funding for long term
conditions, to better meet the needs of the
community.
Making a Difference in the Community In 2012/13, our community based service
teams delivered a total of 35,526 patient
contacts.
Community Team Patient Contacts
Outreach Nurses 9,791
Community Health Workers 8,330
Primary Mental Health Service 1,2071
Dietitian Service 3,113
Healthy Families Coach Service 2,221
Total Community Contacts 3,5526
These services all focus on our high need
populations. They support people to live
healthier lives within the community.
They are able to devote
time to people, to
understand not only
their health issues but to
also understand the
social and environmental
factors which may be
impacting on people’s
lives.
Community Health Workers: Vaiula, Mere, Dina, Hana, Beau,
Natasha, Sisi and Lisa Gully (Team Leader)
“(My community
health worker)
showed me the
utmost respect, so
friendly, happy
natured and very
helpful – there are not
enough words for me
to explain how happy
I am with the service I
received”.
Community Health
Worker Client
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
66

14 | P a g e
For instance, our
community health
workers help
people with social
and housing issues
and advocate with
Work and Income
on their behalf.
These community
and outreach
services
complement the
services which our
practice members
deliver. They also
work with general
practice to better co-ordinate people’s health
needs, connecting people with programmes
such as Care Plus where this is appropriate.
Better Mental Health and Wellbeing In 2012/13, Te Awakairangi Health Network’s
various primary mental health and addiction
service providers collectively delivered a total
of 12,071 contacts to people living in the Hutt
Valley, with a focus on high needs populations
with a mild to
moderate
mental illness.
The primary
mental health
service is valued
by service users
and by local GPs
who make
referrals to the
service.
The Wellbeing
Service provides
primary mental
health services
to the population enrolled
with Te Awakairangi
Health Network’s 24
practice members and the
population enrolled with
Ropata Medical Centre.
Vibe and the Lower Hutt
Women’s Centre provide
primary mental health
and wellbeing services to
specific population groups
including young people.
The service responds to
the primary mental health
needs of Māori, Pacific,
young people and those in
high deprivation areas.
However, there is also
demand from the wider
Hutt Valley population.
Te Awakairangi Health will
continue to target
resources at priority population groups. This
will require close monitoring as the number of
referrals can exceed service capacity.
We will continue to identify and explore
opportunities for how our primary mental
health services can better integrate with
services provided by Hutt Valley DHB’s Social
Work Department and its more specialised
mental health services.
Medicines Management On average, each practice received three visits
from the clinical pharmacist team during
2012/13 with all practices receiving at least
one visit.
These visits give the clinical pharmacists an
opportunity to share clinical information and
advice with practice staff, and to sort through
any medication queries.
“Our PHO patients
have access to a
professional and
financially
accessible service
and I have only had
positive feedback
from patients. The
main response has
been that someone
took the time to
listen to them and
offer options to
cope. In this current
health arena of
"Better, Faster,
Sooner" the pressure
to attempt to
address patients
mental health needs
are limited in 15 min
consult time slots.
The Wellbeing
Service is an
invaluable service”.
Local GP
“I found [therapist] to
be a life line when I
was at my lowest over
a situation I found
myself in. Although the
situation is still on-
going I probably
would have still been
in my bed if not for
therapist … I cannot
say how much I
appreciate my time
with her. Thank you so
very much”.
Wellbeing Service
Client
“I have been listened
to and been made
aware of what is
happening inside of
me. The doctor has
never told me about
my medical
conditions - they just
tell me what to do.
The outreach nurse
took the time and
explained it to me
and now I am aware
of my illnesses and
what can happen to
me”.
Outreach Nurse Client
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
67

15 | P a g e
Feedback surveys indicate this support is
valued by the Network’s practice members.
“The Clinical Advisory Pharmacists are
making a significant and positive
impact on the prescribing of
medicines in general practice.”
Comment from GP survey
During 2012/13, the clinical pharmacists also
delivered a range of education sessions to local
pharmacists, practice nurses and the local
diabetes support group.
Sexual Health Services This programme, previously funded by the
Hutt Valley DHB, allows young people to access
free sexual health consultations. The service
continues to be well utilised, with
approximately two thirds of the 4000
consultations provided in 2012/13 being
delivered by GPs. However, this service will be
funded at a lower level in 2013/14 and will be
available to a smaller age range (12 to 19 years
inclusive).
Language Line and Transport These two relatively small programmes make a
big difference in some people’s lives.
In 2012/13, the transport service made a total
of 1097 trips involving 339 unique patients.
More than half these trips were to secondary
health care appointments while most of the
balance was to primary health care
appointments.
As the transport service is meant to improve
access to primary care, the use of the service
to access secondary healthcare appointments
remains an on-going concern, particularly as
this is putting pressure on the relatively small
budget available for the service.
In 2012/13, 237 calls were made to Language
Line, giving patients and GPs access to an
interpreter during the patient consultation. 15
of the Network’s 24 practices used Language
Line over this period.
Partnering with Hutt Valley DHB In 2012/13, we have made significant advances
in our partnering work with Hutt Valley DHB.
Over the past two years, primary and
secondary clinicians supported by senior
management, have met regularly to improve
services and integration across the Hutt Valley.
This group (previously called the Primary
Secondary Strategy Group) is now called the
Hutt Integrated Network of Care (Hutt INC).
In 2012/13, this joint work has involved a focus
on reducing avoidable hospitalisations, with
activity to address skin infections,
gastroenteritis, and respiratory conditions in
our community; improving access to diagnostic
services; reducing pressure on specific
services; and improving enablers, such as
pathways development, and improved
information systems to support shared care.
8691
71
86
106
87
75
96 95 94
122
89
405060708090
100110120130
Number of Transport Service TripsJuly 2012 - June 2013
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
68

16 | P a g e
Looking Ahead
Quality Systems and Processes In 2013/14, Te Awakairangi Health Network
will continue to support quality initiatives
which benefit our practice members and
enhance the services they deliver.
We will continue to encourage the use of
information systems and information tools
that support good clinical practice. The Patient
Dashboard which is being made available free
to all Network members is one such tool.
The new Clinical Governance Committee will
play a crucial role in identifying and addressing
clinical quality and patient safety issues across
the Network, drawing on the skills of the
diverse multidisciplinary membership of the
committee.
We will continue to support the Network
members seeking to achieve practice
accreditation.
Through our on-going commitment to training
and workforce development, we will ensure
our practice members can access the support
they need to get the maximum benefit from
these decision support tools.
Te Awakairangi practices continue to have
higher patient to GP ratios than the national
average, and slightly higher patient to practice
nurse ratios than the national average.
We will support practices wanting to expand
the number of general practitioners and/or
nurses they have. In the first instance, we will
do this by promoting the Hutt Valley as a good
place to live and work.
In 2013/14, we will continue to work with
practice members who want our assistance to
address sustainability issues. This may include
advice on business planning and potential
practice consolidation.
Our practice support will also continue involve
advocating on our Network members behalf at
a local, regional and national level.
Long Term Conditions In 2013/14, we will work with Hutt Valley DHB
and our practice members to explore how the
various funding streams available to support
the management of long term conditions and
Care Plus can be used more flexibly.
This will be a critical piece of work for the
future given our ageing population,
particularly those aged 75 years and over, and
the need to manage increasingly complex and
unwell people in the community.
This will involve work with Hutt INC on patient
pathways and the most appropriate way of
delivering care to people, including how we
support people to manage their own health
better. It will also involve more emphasis on
prevention and early intervention.
In exploring how we can make a positive
difference in people’s lives, we will be
improving our CVD risk assessment rates, our
diabetes care, and the number of smoking
cessation interventions being delivered across
our Network.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
69

17 | P a g e
“We want to support our Network
members to achieve our PHO
performance targets in 2013/14.”
Our Strategic Relationships We already have a strong working relationship
with Hutt Valley DHB and with other PHOs in
the Greater Wellington region.
In 2013/14, we will continue to reshape local
health services through our participation in the
local Alliance Leadership Team known as Hutt
INC (Hutt Integrated Network of Care) .
Hutt INC is focused on better integration using
a whole-of-system approach. This involves
work on new ways of delivering value: new
models of care; more wrap-around services;
new use of workforce; more services in
community settings; shifts in the funding for
long term conditions; new information
systems with clinicians accessing shared views
of patient information; and continuing the
emphasis on value-for-money and achieving
efficiencies.
We expect this work will deliver better
outcomes for the Hutt Valley population, with
fewer hospitalisations for preventable
conditions such as cellulitis, gastroenteritis,
and respiratory conditions; improving access
to elective surgery and diagnostic services; and
more integrated services for people with
complex conditions. We also expect that this
work will improve the systems that support
clinicians (e.g clinical pathways and and
information systems) and make better use of
the resources available within the Hutt Valley.
In 2013/14, we will build further on these
strategic relationships. In prioritising what
joint activity we will become involved in, we
will be guided by what will most benefit the
health and wellbeing of our population and
what will best assist our Network members to
succeed.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
70

18 | P a g e
Financial Statements
(available on request)
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
71
1 | P a g e
Te Awakairangi Health Network
Six Monthly Report to Hutt Valley DHB
(Period: 1 July 2013 to 31 December 2013)
January 2014
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
72

2 | P a g e
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
73

3 | P a g e
TABLE OF CONTENTS
1. Executive Summary ......................................................................................................................... 4
2. Our Context ..................................................................................................................................... 7
3. Programmes................................................................................................................................... 11
Long Term Conditions Coordination ........................................................................................... 11
Cardiovascular Risk Assessment Programme ............................................................................. 11
Diabetes Care Improvement Programme (DCIP) ........................................................................ 16
Tu Kotahi Asthma Service ........................................................................................................... 19
Abc Smoking Cessation Programme ........................................................................................... 21
Cervical Screening Programme ................................................................................................... 23
Immunisation Support ................................................................................................................ 24
Care Plus ..................................................................................................................................... 26
Clinical Pharmacy Services .......................................................................................................... 27
PHO Performance Programme ................................................................................................... 31
4. Services .......................................................................................................................................... 33
Outreach Nursing ................................................................................................................................... 33
Community Health Workers ................................................................................................................. 43
Primary Mental Health .......................................................................................................................... 52
Health Promotion ................................................................................................................................... 58
Dietitians .................................................................................................................................................. 65
Healthy Families Coach .......................................................................................................................... 69
Transport Service .................................................................................................................................... 73
Language Line.......................................................................................................................................... 75
5. Practice Support ............................................................................................................................ 76
Practice Liaison And Support ................................................................................................................ 76
Quality Improvement ............................................................................................................................. 77
Workforce Development And Liaison.................................................................................................. 78
Primary Nurses Reference Group ........................................................................................................ 79
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
74

4 | P a g e
EXECUTIVE SUMMARY
This report outlines the activities of Te Awakairangi Health Network for the July to December 2013 period. It
reports on achievements and service provision, and outlines key issues and risks, across the services and
programmes delivered by Te Awakairangi staff and contracted practices and providers. It has been prepared to
provide information to the Board of Te Awakairangi Health Network (TeAHN) and Hutt Valley DHB.
This six month period has been one of growth and development, with skilled and experienced teams now in
place across the organisation with a consolidated strategy to guide their work arising from work by the Board to
confirm its strategic direction. The alliancing approach is building momentum with Hutt INC providing a key
forum for shared planning, the development of a consolidated work programme and establishment of a number
of key projects. These include a Primary Care Sustainability initiative, an Information Systems (shared electronic
health record) project, an Acute Demand workstream and a unified planning process to support the
development of the annual plans. Hutt INC is also linked into a number of 3D initiatives including Health
Pathways which is expected to lead to a number of clinically focussed projects aimed at streamlining the referral
and management of people with common conditions. TeAHN is actively engaged in these projects, working
closely with counterparts in other PHOs with the aim of developing a locally relevant but regionally consistent
approach to service delivery.
ACHIEVEMENTS
Some notable outcomes for the July to December 2013 period include:
TeAHN staff are now actively involved in a number of the work streams flowing out from Hutt INC,
including the new Primary Care Sustainability Initiative, Information Systems, Medications
Management, Acute Demand and Health Pathways;
TeAHN continues to perform well with childhood immunisations, being amongst the top in the
country for both the 8 month and 2 year old targets;
There have been significant improvements in performance against the other two health targets, with
CVD risk assessments rising from 44 % at June 2013 to 58% at December 2013, and brief advice for
smoking cessation rising from 50% at June 2013 to 63% at December 2014;
TeAHN’s programme team, working with DHB and SIDU partners, have prepared and agreed a service
implementation plan outlining the approach to investing the additional MoH funding (close to
$500,000 over four years) made available for “More Heart and Diabetes Checks”. The plan includes
business proposals being developed for every practice, based on the number of people still to be
screened. This has been well received by practices;
Utilising some of the funding made available through the “More Heart and Diabetes Checks” we have
commenced an evaluation of BPAC’s decision support tools. These will provide timely data feeds to
practices and TeAHN on a range of the health indicators as well as offering a range of clinical
templates to facilitate diabetes checks and long term condition management;
Our Clinical Advisory Pharmacists have completed a round of visits to practices delivering topics on
non-steroidal anti-inflammatories and a number of new therapeutic agents;
Our Care Plus enrolments have dropped off slightly toward the end of the period after a surge earlier
in the year. We are expecting to undertake a review of our long term conditions management during
2014 that will include the allocation of Care Plus funding.
The outreach nursing team were joined by another experienced team member. Talesha Sculley brings
a wealth of acute and community skills to the team, fresh from a period working with boat people
being housed on Christmas Island. Across the Network, the Outreach Nurses and Integrated Case
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
75

5 | P a g e
Management Nurses carried a caseload of at least 130 patients per month, and provided over 1250
contacts and 3400 services in the six month period;
Across the Network, Community Health Workers carried an average caseload of 134 patients per
month, and provided a total of 1562 contacts and 5140 services covering a wide range of services
(including case management, education and support, phone calls, follow up visits and contacting
other agencies);
The primary mental health team provided 6343 services to more than 1000 unique individuals in this
period (including client sessions and face-to-face contacts) , slightly up on the last period;
The dietician service looked after an average caseload of 116 patients per month and provided 1535
contacts in the period, up around 500 on the last period with a significant number of these over the
July to August period. The team engaged in specialised training to improve their expertise in dealing
with “food addiction” and in cognitive behaviour therapy to assist people in modifying their lifestyles;
Over July to December period, the Healthy Families Coach service made 1496 contacts with patients,
seeing them in their homes, at Te Awakairangi Health Network, at their GP practice or in the gym.
Patient caseloads have continued to increase , this period up to an average of 130 patients at any one
time, reflecting the increased capacity in the team;
The health promotion team have continued to run programmes (Heart Check health promotion, the
Good Food Programme, the Valley Fit Programme) and support groups, and participate in many
community projects and events;
The health promotion team has worked closely with the clinical facilitation team over the past 6
months on raising the profile of cardiovascular risk assessments and heart health. See the
Cardiovascular Risk Assessment section of the report for information about the various community
and practice based activities. They completed three Good Food programmes during the period.
TeAHN are a partner in Health 4 Life, a joint project of Regional Public Health (RPH), Service Integration
and Development Unit (SIDU) of Capital and Coast DHB, Hutt Valley DHB and Wairarapa DHB; Te
Awakairangi Health Network; and Compass Health. Health 4 Life is an early intervention programme
aimed at improving nutrition and physical activity in the pre-school population starting in pregnancy. It
requires participation across a wide range of providers who deliver services to women during pregnancy
and infants in their first year of life;
During the July to December period, the transport service funded 741 trips by 280 unique patients. The
proportion of trips to secondary care rose to 60% (443) with the remaining 40% (298) to primary care
appointments;
Workforce Development has continued with TeAHN formally taking over the role of CME provider
from GP Services. A CME committee has been established to oversee this work, and a framework
established for the activities in 2014. An interim nurse professional education calendar has been
released which has a stronger emphasis on the use of online learning and topics that have been
requested by practices nurses or been identified through a needs assessment/gap analysis.
ISSUES AND RISKS
We are concerned that:
Care Plus is not being well targeted and requires review but we are recognise this needs to be done in
the context of a wider review of long term condition management. We have been constrained by
limited staff resources but expect to be able to address this in the first half of 2014;
The uptake of Diabetes Care Improvement Plan (DCIP) has remained a challenge and the MOH have
now announced more funding to support the extension of self-management programmes and
professional education. Although there been improvements in our systems to make it easier to record
assessments as they occur, we are still not seeing a systematic embedding of diabetes annual reviews
across our network;
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
76

6 | P a g e
We remain concerned at the gaps in community mental health services for people discharged from
secondary care and we are continuing to work with our DHB colleagues to identify solutions. The
primary mental health service continues to target the priority referral groups, but there have been
challenges in establishing contact, impacts on volumes of contacts and an increase in the DNA rates for
a group of clients with multiple stresses and more chaotic lives. The situation is being monitored and
we are proactively working to reduce barriers to high needs clients.
NEXT STEPS
The Network is rising to the challenge and the opportunity of demonstrating to its key stakeholders (our
population, our practices and providers, and Hutt Valley DHB and other funders) how we add value in all our
activities. The priorities for 2013/14 are:
Building capacity and capability in primary care, with a special focus on practice sustainability, business
models, and workforce development;
Performing well, continuing to deliver excellent services across the Network and achieving Health
Targets and PPP indicators. While we are making good progress on the CVDRA and Smoking Cessation
targets, it is proving an ongoing challenge to lift the number of diabetes reviews and overall uptake of
the DCIP. We recognise this may require a shift in mindset and to this end, we are working to introduce
training aimed at encouraging nurses to work to the top of their scope, and empowering them to take
a greater lead in managing people with diabetes. At the same time, the new funding from the MOH is
seen as a potential game changer, to support practices to cross the threshold of 90% CVDRA,
embedding these assessments as part of their day to day work;
Innovating, with a special focus on integrating the wide range of services and programmes within the
current TeAHN responsibilities and in conjunction with more DHB services. We will continue to be very
actively involved with the new alliance leadership team, Hutt INC, exploring new opportunities
especially for managing Long Term Conditions, reducing avoidable hospitalisations and addressing
acute care;
Enabling, working to equip our clinicians with skills, tools and systems that help them manage their
risks, deliver better care and keep a track of people in their practice who are at greater risk. Examples
include implementing new decision support tools aimed at making it easy to do the right thing at the
right time.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
77

7 | P a g e
OUR CONTEXT
WHO WE ARE
Te Awakairangi Health Network (TeAHN) was established on 1 July 2012 bringing together the programmes,
activities and provider members of four former Primary Health Organisations (PHOs): Piki te Ora ki te
Awakairangi, Valley PHO, Family Care PHO and Tamaiti Whangai PHO, and the management services
organisation, Kowhai Health Trust. It has an enrolled population of more than 117,000 people and includes 23
member practices within the Hutt Valley.
The practices are based in communities across the Valley and include some serving high needs areas, along with
other city based practices with less high need populations. We have three large multi partner/doctor practices,
a number of solo doctor practices and most with 3-5 doctors. There are a number of business models operating
within this cluster of practices ranging from not-for-profit Trust based entities through to large commercially
focussed, shareholder owned practices.
One of our key challenges for 2013/14 is supporting the positive development of these practices, aiming to
strengthen and extend their capacity as the system increasingly looks to primary care for an expanding range of
services. A key contribution is likely to be around helping them explore new models of care, providing stability
and certainty of revenue (as far as this is possible) and investing in clinical leadership that is sensitive to the
pressures these teams face yet able to inspire and support change.
OUR PEOPLE
The Network works with its 23 member practices and a range of community provider organisations across the
Hutt Valley. On a daily basis TeAHN is working with practice teams to both support their delivery of front line
services as well as providing a number of direct patient services ourselves in areas such as our Wellbeing Service
(primary mental health), Outreach Nursing and Community Health Worker Services.
OUR REGION
A series of changes occurred in 2012/13 within the sub-region with the establishment of the Service Integration
and Development Unit (SIDU) across three DHBs, and the merger of the Executive teams of Wairarapa and Hutt
Valley DHBs. These changes have affected a number of the DHB teams we interact with, but the new teams are
now settling down and engagement is improving.
TeAHN practices have been generally stable within the July to December 2013 period. Hutt City Health Centre is
now running one practice across their two sites (in central Hutt and Wainuiomata) and will be moving to new
premises early in 2014. Three practices prepared proposals to access additional Very Low Cost Access (VLCA)
funding. One (HUCHS) was successful in attracting funding for a New Entrant to Practice (NETP) nurse under the
VLCA scheme. We expect all three to receive the additional ongoing funding, as agreed with Hutt Valley DHB in
the proposals.
The primary care sustainability project (mandated by Hutt INC and funded by the MoH) is now underway. This
project will support a range of discussions between primary and secondary clinicians re sustainability, and will
support practices exploring opportunities around co-location and establishing closer working arrangements.
TeAHN has continued building its linkages with local government in the Hutt Valley, supporting new migrant
seminars run by Hutt City Council, and participating in regular meetings of health and community agencies,
hosted by the Upper Hutt City Council. TeAHN has maintained its connections with the two Whanau Ora
providers within the Hutt Valley and the Maori Health Service Development Group of Hutt Valley DHB.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
78
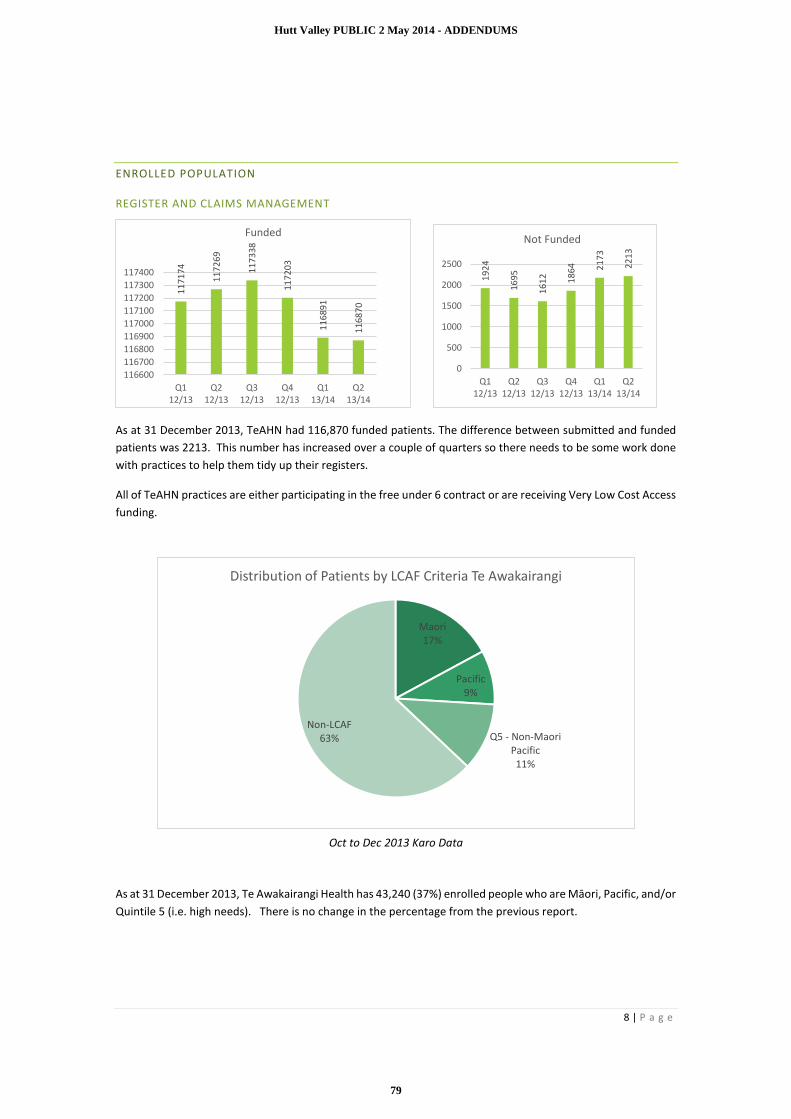
8 | P a g e
ENROLLED POPULATION
REGISTER AND CLAIMS MANAGEMENT
As at 31 December 2013, TeAHN had 116,870 funded patients. The difference between submitted and funded
patients was 2213. This number has increased over a couple of quarters so there needs to be some work done
with practices to help them tidy up their registers.
All of TeAHN practices are either participating in the free under 6 contract or are receiving Very Low Cost Access
funding.
Oct to Dec 2013 Karo Data
As at 31 December 2013, Te Awakairangi Health has 43,240 (37%) enrolled people who are Māori, Pacific, and/or
Quintile 5 (i.e. high needs). There is no change in the percentage from the previous report.
11
71
74
11
72
69
11
73
38
11
72
03
11
68
91
11
68
70
116600
116700
116800
116900
117000
117100
117200
117300
117400
Q112/13
Q212/13
Q312/13
Q412/13
Q113/14
Q213/14
Funded
19
24
16
95
16
12 18
64 21
73
22
13
0
500
1000
1500
2000
2500
Q112/13
Q212/13
Q312/13
Q412/13
Q113/14
Q213/14
Not Funded
Maori17%
Pacific9%
Q5 - Non-Maori Pacific11%
Non-LCAF63%
Distribution of Patients by LCAF Criteria Te Awakairangi
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
79

9 | P a g e
Oct to Dec 13 Karo data
Eight practices have a high needs population percentage of greater than 40% and one practice has 87% of its
enrolled population falling into the high needs category.
GENERAL PRACTICE WORKFORCE
FTE figures from TeAHN Provider Lists as at 20 November 2013. National averages are taken from
www.healthypractice.co.nz correct as at January 2013.
Period Enrolled
Population
GP FTE Nurse FTE
1 Jul to 31 Dec 116,870 63.9 59.4
Period Ratio of GPs to Enrolled
Population
Ratio of Nurses to Enrolled Population
1 Jul to 31 Dec 1:1829 1:1967
Te Awakairangi practices continue to have significantly higher patient to GP ratios (with 1828 patients per GP
FTE) than the national average (1708 patients per GP FTE). Note: As part of our work on practice sustainability,
we have reviewed the data collection for workforce numbers. Previous analyses may have underestimated the
number of GP FTEs in the Hutt Valley.
Te Awakairangi practices have increased the number of nursing FTE over the last six months, leading to a
decrease in the patient to practice nurse ratios. TeAHN now has a lower patient to nurse ratio than the national
average.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
m t v n x o c p d q j k e r h s a l b g w y u f
Percentage of High Needs Patients across Te Awakairangi HealthGeneral Practices Oct to Dec 13
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
80
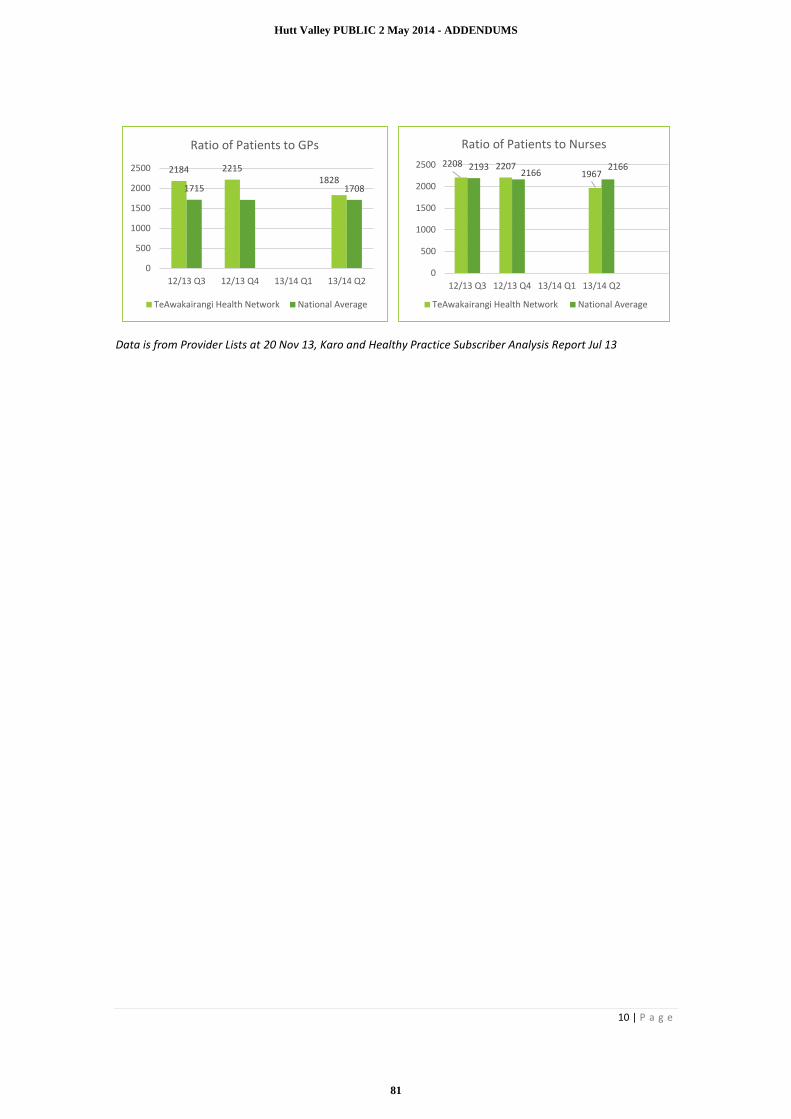
10 | P a g e
Data is from Provider Lists at 20 Nov 13, Karo and Healthy Practice Subscriber Analysis Report Jul 13
2184 22151828
1715 1708
0
500
1000
1500
2000
2500
12/13 Q3 12/13 Q4 13/14 Q1 13/14 Q2
Ratio of Patients to GPs
TeAwakairangi Health Network National Average
2208 22071967
21932166
2166
0
500
1000
1500
2000
2500
12/13 Q3 12/13 Q4 13/14 Q1 13/14 Q2
Ratio of Patients to Nurses
TeAwakairangi Health Network National Average
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
81

11 | P a g e
PROGRAMMES
LONG TERM CONDITIONS COORDINATION
To provide and facilitate a coordinated approach to long term condition management to the enrolled population
of Te Awakairangi Health Network with a focus on preventing additional co-morbidities.
To assist practices to support their high need populations with long term conditions within the primary care
setting and assist the uptake and coordination of existing programmes.
KEY ACTIVITIES
TeAHN has commenced work to identify a preferred provider for clinical decision support tools.
BPAC has been identified and we have started to pilot their systems in a number of practices. This is
intended to provide practices with a new set of tools to assist in the management of long term
conditions.
A revised advanced form has been installed in all TeAHN practices to support the Diabetes Care
Improvement Programme (DCIP) and enable more streamlined data capture, reporting and payments.
TeAHN attended a National Diabetes strategy workshop in Auckland in early December at which the
concept of a revised approach to long term conditions, commencing with a revised DCIP was
discussed.
We have agreed a new data template to underpin the agreement we have with Tu Kotahi for work on
respiratory conditions. They have embarked on a major upgrade of their data systems to enable this
and other reporting.
Work in the dementia pathway is now well underway.
TeAHN has completed a review of its Continuing Medical Education (CME) strategy and appointed a
CME Advisory Group to oversee the selection, development and delivery of topics. We expect to see
a number of LTC related topics presented during 2014.
The work of our Clinical Advisory Pharmacists continues to focus on Long Term Condition
management as they visit practices and work with pharmacy teams to promote best practice.
CARDIOVASCULAR RISK ASSESSMENT PROGRAMME
The aim of the TeAHN Cardiovascular Disease Risk Assessment (CVDRA) Programme is to increase the rates of
cardiovascular risk screening and management for Hutt Valley people, particularly those identified as being at
higher risk ( Māori, Pacific, Indo-Asian people and/or people living in Quintile 5 areas, referred to as “high
needs”).
PROGRESS THIS PERIOD
The overall eligible total population for the CVDRA programme is 34,072 (composed of High Needs population
of 12,227 and ‘Other’ population of 21,845). Provisional data indicates that cumulatively (to the end of
December 2013) 58.3 % of the Total Population of TeAHN who are eligible have received a CVR assessment.
This means that TeAHN has met the MOH target of 58% for December 2013.
TeAHN has done even better for the High Needs population, achieving 65.2% uptake. TeAHN has therefore met
its PPP targets for the High Needs (62.9%) and Total Population (53.9%) indicator for the 2013 year.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
82

12 | P a g e
There have been some significant highlights in this reporting period:
In December the Network achieved a record 494 target CVDRAs in one week
Soma Medical Centre became the first TeAHN practice to screen 90% of its eligible population for
CVDRA
Patient Dashboard was introduced to TeAHN practices in June 2013, and was fully implemented in the
first quarter of 2013/14. The tool has helped to increase the number of opportunistic CVDRAs and
ensure that they are recorded correctly.
There has been a significant increase in CVDRAs in all TeAHN practices in the last six months which is attributed
to initiatives in the Indicator Improvement Plan and a customised approach with each of the practices. The key
initiatives in the last six months have included:
1. In August TeAHN hosted Buck Shelford (Patron of the ‘More Heart and Diabetes Checks’ national
programme) for a day to promote CVDRA to the Hutt Valley community, workplaces and medical
practices. This helped raise the profile of the importance of CVDRA and received significant media
coverage including an article on Maori TV. Many of our larger workplaces held their own heart health
promotional events. A follow up visit from Buck is being planned for early 2014.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
83

13 | P a g e
Buck Shelford visits the workers at Pak’n’Save Petone as part of their workplace heart promotion week
2. TeAHN has invested considerable time and energy into the marketing and promotion of the importance
of CVDRA for health and well-being. This includes press releases, Facebook promotions, local radio,
workplace promotions and community events. The whole of July/August 2013 was dedicated to CVDRA
promotions in the community and promotions were set up in all TeAHN practices. TeAHN also worked
closely with the Health Promotion Agency and used their resources in local promotions.
Mayor Ray Wallace and Scribe get their hearts checked by Harley Rogers at the Taita Polynesian festival
3. TeAHN has made significant improvements to the training of staff in TeAHN practices around CVDRA.
In conjunction with the Heart Foundation, TeAHN developed and ran both basic and advanced training
for nurses on CVDRA. This included improving skills in using the Predict decision support tool to
accurately record and manage CVDRA. Advanced training has been provided on giving lifestyle advice
and education in a CVDRA consultation as well as referring patients to TeAHN wellness programmes.
4. Each week the practice with the most CVDRAs completed that week has received an award and
recognition as the leading practice. This has created a competitive spirit amongst the practices and has
been a very effective incentive to improve and maintain performance.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
84

14 | P a g e
The staff at Stokes Valley Medical Centre receive the weekly CVDRA award
5. TeAHN has continued a customised approach with all TeAHN medical practices to meet the specific
needs of the practice population and health providers. Practices in the past which have had little
increase in CVDRA are now beginning to catch up to their peers with close support from the Clinical
Programme Facilitators.
Kopata Medical Centre staff and their CVDRA practice promotion during the Christmas period
6. TeAHN has created a voucher for high needs people eligible for a free CVDRA and promoted these
vouchers widely via workplaces, health professionals and community events. This voucher has helped
to reach significant numbers of high needs patients and raised awareness in the Hutt Valley.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
85
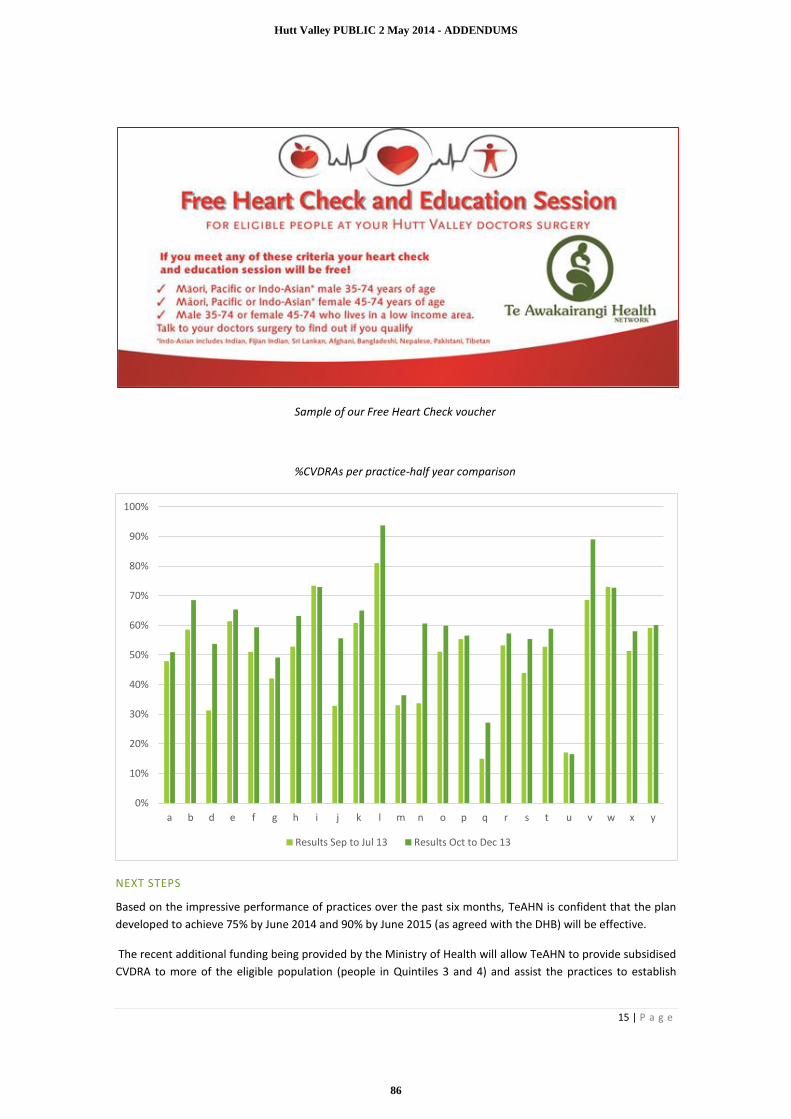
15 | P a g e
Sample of our Free Heart Check voucher
%CVDRAs per practice-half year comparison
NEXT STEPS
Based on the impressive performance of practices over the past six months, TeAHN is confident that the plan
developed to achieve 75% by June 2014 and 90% by June 2015 (as agreed with the DHB) will be effective.
The recent additional funding being provided by the Ministry of Health will allow TeAHN to provide subsidised
CVDRA to more of the eligible population (people in Quintiles 3 and 4) and assist the practices to establish
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
a b d e f g h i j k l m n o p q r s t u v w x y
Results Sep to Jul 13 Results Oct to Dec 13
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
86

16 | P a g e
systems that will enable them to both reach and sustain the gains being made. TeAHN has developed a new
service delivery model to guide the use of the additional Ministry funding and achieve the agreed targets in
2014/15. There are six key strategies within this model:
1 .Improved access to testing equipment
2. Building strategic partnerships and capacity with other providers of CVDRA
3. Continuing to develop the workforce providing CVDRA
4. Supporting practices with resources such as additional nursing
5. Building a sustainable business case for each practice to be involved in CVD risk assessment and
management
6. Creating effective partnerships with secondary health care
The ultimate aim is still to embed CVDRA into all of the practices as an established programme with a reducing
reliance on additional funding over the next four years.
Taking every opportunity to promote heart checks we have decorated our floor windows for all to see
DIABETES CARE IMPROVEMENT PROGRAMME (DCIP)
The Diabetes Care Improvement Programme has a particular focus on high need population groups
including Maori, Pacific and people living in Quintile Four and Five areas. This programme commenced
on 1 October 2012 at all Te Awakairangi Health Network practices.
PROGRESS THIS PERIOD
Under the Diabetes Care Improvement Plan, TeAHN has undertaken a range of initiatives in the July
to December 2013 period:
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
87

17 | P a g e
In December TeAHN reviewed and reconfigured its nurse professional development courses
and set a new programme and timetable for 2014. Significant changes have been made to
diabetes training with the introduction of advanced workshops to increase skill level. These
include retinopathy, pharmacy and insulin initiation, foot screening, early nephropathy, care
for Maori and Pacific peoples and health promotion. An advanced half day workshop for cardiac
condition management has also been created.
Plans are in place to increase the use of online training in the Network with the introduction of
the diabetes online training module. All Network nurses will be encouraged to complete this
training to supplement a one day diabetes introductory course.
The Patient Dashboard Tool was introduced to practices in June 2013. Dashboard prompts the
practice team to complete the diabetes review, makes it easy to complete opportunistically
and then automatically files the data in the correct screening table. This will help provide a
more accurate picture of how many reviews are occurring and ensure the work practices
complete is reflected in their records.
A new Medtech based Diabetes Annual Review form was introduced into practices in
November and provides a much more comprehensive record and review process. The new
review form contains a full cardiovascular risk assessment, automated linked referrals for
health services and expanded examination sections including a more comprehensive foot
assessment. The previous review form will be removed from Medtech in February 2014 as user
training is completed and the form is adopted by the Network.
Together with the HVDHB Diabetes Team, we have identified and mentored four nurses in the
Network who have a high level of diabetes knowledge, skills and experience. TeAHN plans to
expand this number of highly skilled nurses to 12 by the end of the year through training,
mentoring and support.
Diabetes Annual Reviews
The number of Diabetes Annual Reviews in the last two quarters has remained fairly consistent. At
December 2013, TeAHN had not achieved its PPP target for the total population group (with 71.1%
achieved compared to a target of 84.3%). TeAHN also did not achieve its PPP target for the high needs
group although the gap was much smaller (with 76% achieved compared to a target of 79.4%).
TeAHN will continue to promote diabetes annual reviews (as per our Practice Indicator Improvement
Plan) and practices are now well aware of their targets and progress. In addition we plan to undertake
the following activities in 2014 to increase the number of annual reviews:
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
88

18 | P a g e
There will be a special focus on the practices which are not meeting their targets for diabetes
annual reviews and we will customize an improvement plan together with each practice and
its clinicians.
We will provide practices with assistance to invite patients overdue for an annual review
including a text reminder campaign. Strategies such as booking the patient for their next annual
review at the end of their current review may be effective.
We are developing a programme to improve the self–management of diabetes by our network
patients. This strategy will help to engage our patients with diabetes about the importance of
annual reviews and encourage them to be proactive so that they drive demand themselves.
We will develop an education programme for General Practitioners to reinforce the importance
of diabetes annual reviews.
Alongside the introduction of the Patient Dashboard Tool to practices in June 2013, TeAHN is now
planning to implement the BPAC Best Practice Intelligence system to improve the delivery, recording
and reporting of clinical programmes. These tools, along with other activities outlined above, will
assist us to increase the number of Diabetes Annual reviews in 2014.
Nurse education sessions
Nurse education sessions continue to increase compared to the same period last year but are still
below the target level. TeAHN will be providing new advanced skills workshops for Network nurses to
improve their confidence and ability to provide more nurse education sessions in the future.
Podiatry
Podiatry services remain unchanged from those previously provided in the Hutt Valley. This service
is however volume constrained and there is evidence of unmet need in this area, partly due to the
fact that many patients require ongoing podiatry input and so tend to remain on the programme.
A new Comprehensive Foot Assessment and an At Risk Foot Care Pathway has been developed which
will see improved screening provided in primary care.
In conjunction with the DHB Podiatry Services team a plan is being created to streamline the referral
process for podiatry, aiming to reduce the waiting time for patients and freeing up the HVDHB podiatry
service to focus on more serious podiatry cases.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
89

19 | P a g e
NEXT STEPS
New funding recently announced by the Minister will provide some transitional support to assist with
the establishment of more nurse-led diabetes clinics within practices, with a key focus around
enhanced patient self-management within a sustainable model of care. Part of this funding will go
towards improving the skills and training of practice nurses over and above what is already provided,
including the new training programme of advanced diabetes skills modules.
These include:
Insulin Initiation
The new foot care pathway
Retinopathy
Nephropathy
Engaging high risk populations
Promoting health in a primary care setting
There should be a corresponding increase in both the number of annual reviews and nurse education
sessions following this training programme.
TU KOTAHI ASTHMA SERVICE
Tu Kotahi Maori Asthma Trust aims to improve the quality of life of those with asthma through improved
understanding of respiratory illnesses, management, education and support. Tu Kotahi focuses specifically on
the PHO populations with asthma and respiratory conditions and their whanau including those with a new
diagnosis of asthma and those with poor asthma control, primarily Maori, Pacific Island and low income whanau.
Clients can be visited at home to help manage their asthma until they have developed independence in their own
asthma management. Management plans are personalised to each client.
This section relates to a service that is contracted by Te Awakairangi Health Network for the provision of asthma
services to our high need population. This section is drawn from a detailed quarterly report provided by the
team at Tu Kotahi Asthma Trust.
Following detailed discussions between TeAHN and Tu Kotahi Asthma Trust, agreement has been reached on
the implementation of a new data reporting capability aimed at improving the level of data related to activities
they undertake under this agreement. The implementation of these changes has meant the quantitative data
is not available for this report, at this time. As part of these negotiations Tu Kotahi has developed and very
recently implemented a research quality database written in Microsoft Access specific to Tu Kotahi’s data
capture requirements. We expect to see a much more accurate set of data reported from this provider going
forward as they refocus the data collection to better report on the contract obligations.
KEY ACTIVITIES
WAINUIOMATA HIGH SCHOOL CLINIC
The school clinic has successfully been running once a month during the school year. Students are able to book
an appointment at the student services. Education is provided to students individually or in groups. Feedback
from staff, teachers and parents of the students continues to be very positive.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
90
20 | P a g e
Because of the complex needs of teenagers an asthma kit has been developed aimed specifically for teens.
Students participated in the development of the teen kits. The education booklet includes whanau goals that
will complement the other resources given to the student at each monthly appointment.
Benefits of the school based asthma clinic and teen asthma pack:
The clinic is based where the students are.
Supports students by providing a safe place to talk about sensitive issues that may be interfering with their ability to take care of their health.
Supports the school environment by helping student’s attendance and by identifying and addressing health problems that may intervene in the learning process.
Since there are less sick days it supports families by allowing parents to stay at work.
Saves money by keeping children out of hospitals and emergency rooms
If asthma is well managed it is more likely that students will be able to take part in physical activities.
Teaches students to be better health care consumers. Parents are informed of their child’s progress. A consent form must be signed by a parent or guardian if
Rangatahi are under the age of 18.
WAINUIOMATA COMMUNITY CENTRE CLINIC
The free monthly asthma clinic at Wainuiomata Community Centre continues to operate. Wainuiomata
Community Centre has a variety of services available free to their community, including internet and computer
services, Y-Nui youth group, Nui FM, budget advice and Kokiri Marae health and social services. Clients can
access spirometry tests, asthma management plans, asthma education, healthy housing home visits, advocacy
support letters to WINZ and GPs and accompany whanau to appointments. Whanau can either book an
appointment at the community centre or walk in. Clinic services are advertised on the local radio station and in
the local newspaper.
HEALTH SKIN PROGRAMME MEMBERSHIP
A Healthy Skin Focus Group meets every three months. These meetings include a variety of topics around skin
disorders, medications, guest speakers and case studies. As a member, Tu Kotahi Maori Asthma Trust receives
weekly healthy skin updates from Regional Public Health.
There is a lot of research that links asthma and eczema. Both are inflammatory disorders, an allergic reaction
occurring when the body's immune system overreacts to substances that are usually not harmful. These include
allergens that are the same as asthma allergens such as dust mites, pollen, animal dander and certain foods.
Our clients with asthma usually also have eczema and atopic dermatitis. Being part of this focus group enabled
the service to link up with agencies such as Work and Income who provide additional support in relation to skin
disorders e.g. financial support around:
Household items (bedding, towels, bleach, washing machine, vacuum cleaner)
Living environment (pet treatments, pest services)
Medical supplies (skin care products, dressings, prescription costs).
PRESENTATION TO OSCAR HOUSE
Oscar House provide after school and before school care for children ages 5-13 years old. They have 6 providers
in the Lower Hutt area. Oscar House invited Tu Kotahi to do a two hour presentation to their staff and parents.
22 staff and parents attended the presentation.
Topics presented included:
Asthma
Triggers
Signs and symptoms
Asthma medication.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
91

21 | P a g e
A question and answer session was included as well as instruction on using emergency asthma kits with a role
play.
TU KOTAHI PEER NURSE HUI
Continued attendance at a monthly hui to share and discuss research articles and debrief about nursing matters
with in our service.
STATISTICS
As outlined although the service is operating as usual the statistics have not been reported. The data is being
collected through a new programme and is only just being implemented
ABC SMOKING CESSATION PROGRAMME
TeAHN is committed to helping make New Zealand smokefree by 2025. The TeAHN ABC Smoking Cessation Programme aims to decrease smoking prevalence in the Hutt Valley, by encouraging all primary health practitioners to offer brief advice and cessation support to smokers at every consultation.
PROGRESS THIS PERIOD
Supporting the delivery and recording of brief advice and cessation support has been a key focus for TeAHN over the previous six months. This focus has resulted in a significant improvement in the brief advice indicator as illustrated below. TeAHN has improved its placing from 32nd place (of 35 PHOs) at September 2012 to 17th place at September 2013.
Karo data
Provisional results for Quarter 2 2013/14 have just been received. Smoking status ever recorded for the Total Population was 84% at September 2013 and 86% at December 2013, an improvement from the same time last year. The delivery and recording of brief advice for the Total Population was at 64% at September 2013 and is estimated to be at a similar level (63%) at December 2013. This is a significant improvement (greater than 30%) from the same time last year.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
92

22 | P a g e
While the improvement over the past year is pleasing, TeAHN recognises that continued effort and innovation is needed to reach the national Health Target of 90% for brief advice. The Indicator Strategy Group (comprising key Te Awakairangi staff and the DHB Smokefree Coordinator) continues to meet fortnightly to progress work detailed in the ABC Smoking Cessation Plan. In early 2014, work is focussing on a new initiative where practices with high numbers of smokers offer patients cessation support over the New Year period by sending text messages to current smokers.
SYSTEM IMPROVEMENTS
The installation off Patient Dashboard in all practices has supported practice staff to obtain smoking status for more patients and prompted the delivery and recording of more brief advice conversations. Additional nurse resource was provided to many practices to identify patients with no smoking status recorded
but who had mention of smoking in the PMS. Lists were generated and updated in several practices.
BRIEF ADVICE
A key focus in the reporting period has been the completion of the ABC Brief Advice Project. This project aimed to highlight the importance of increasing the delivery and recording of brief advice as part of everyday general practice. In acknowledgement of the brief advice ‘catch up’ required to progress towards meeting the primary care tobacco target, TeAHN supported practices to contact a large number of smokers and offer brief advice and cessation support over the telephone. Practices chose whether to contact smokers by phone or to work with Quitline who contacted smokers on behalf of practices. Seven practices opted for the Quitline provision, one practice worked with Aukati Kaipaipa to contact smokers and all other practices contacted smokers themselves. Quitline contacted 684 smokers as part of the Brief Advice project, and of these, 107 have been referred on to cessation support. Also as a result of this project, TeAHN had its first practice reach the 90% target for Brief Advice. Over December 2013, TeAHN worked with nine practices who have the highest proportion of smokers in their practice population. In recognition of the greater challenge faced by these practices to reach the 90% target, TeAHN will work these practices to offer patients cessation support over the New Year period by sending text messages to current smokers.
A poster resource was developed to show the financial benefits of quitting smoking and to highlight the 2014 tobacco price increases. The poster which has been shared with all practices with the wider Smokefree Network around New Zealand has received a lot of positive feedback.
ABC TRAINING
Nineteen of the total 25 practice sites have at least one nurse who is ABC trained. In the instance where a practice does not have any Quit Card providers, this issue is given priority in discussions with practices.
Ongoing ABC updates and training opportunities have been well promoted. Training options include monthly training held at the DHB, in-practice updates and online e-training.
TeAHN worked with the Heart Foundation and DHB Smokefree Coordinator to run two ‘Lighting the Fire’ training sessions, one in the afternoon, and one in the evening, to optimise access. The training was offered to all nurses and midwives in the Hutt Valley. The sessions aimed to motivate staff to intervene with every smoker with enthusiasm and conviction, and to ensure staff were confident with the provision of NRT and referring to support provider/s. Lighting the Fire training was attended by 12 nurses, 4 midwives and 2 community health workers.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
93
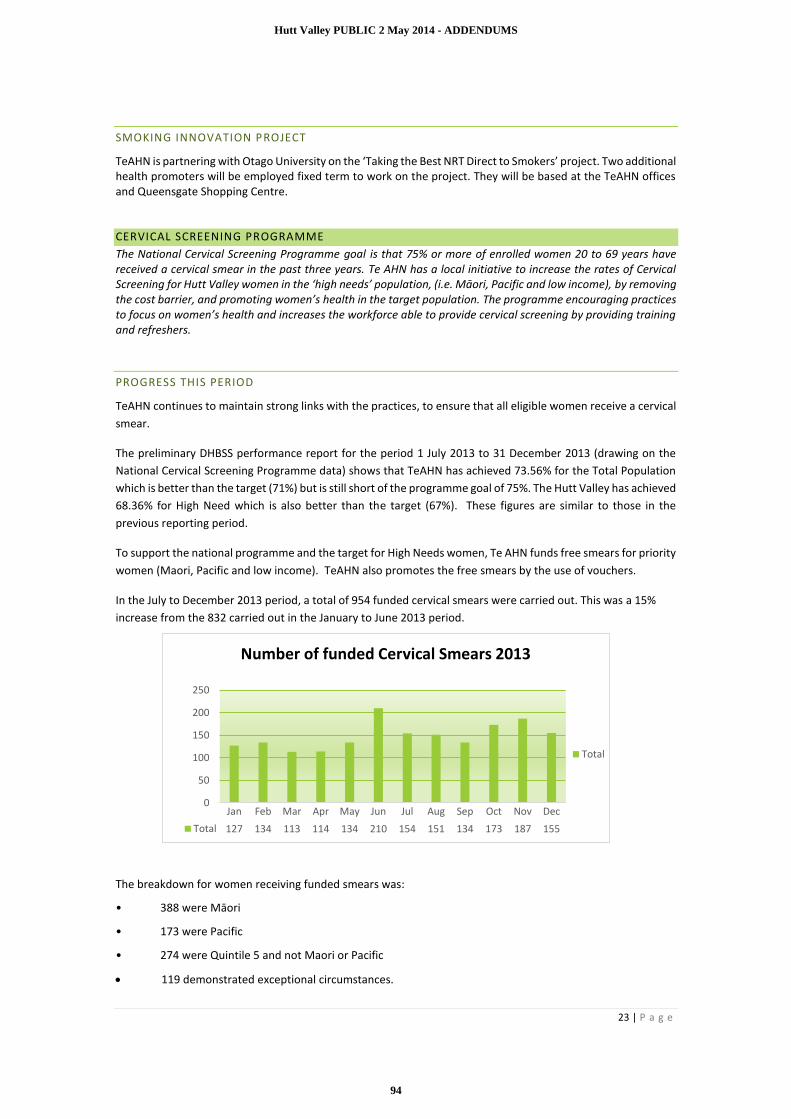
23 | P a g e
SMOKING INNOVATION PROJECT
TeAHN is partnering with Otago University on the ‘Taking the Best NRT Direct to Smokers’ project. Two additional health promoters will be employed fixed term to work on the project. They will be based at the TeAHN offices and Queensgate Shopping Centre.
CERVICAL SCREENING PROGRAMME
The National Cervical Screening Programme goal is that 75% or more of enrolled women 20 to 69 years have received a cervical smear in the past three years. Te AHN has a local initiative to increase the rates of Cervical Screening for Hutt Valley women in the ‘high needs’ population, (i.e. Māori, Pacific and low income), by removing the cost barrier, and promoting women’s health in the target population. The programme encouraging practices to focus on women’s health and increases the workforce able to provide cervical screening by providing training and refreshers.
PROGRESS THIS PERIOD
TeAHN continues to maintain strong links with the practices, to ensure that all eligible women receive a cervical
smear.
The preliminary DHBSS performance report for the period 1 July 2013 to 31 December 2013 (drawing on the
National Cervical Screening Programme data) shows that TeAHN has achieved 73.56% for the Total Population
which is better than the target (71%) but is still short of the programme goal of 75%. The Hutt Valley has achieved
68.36% for High Need which is also better than the target (67%). These figures are similar to those in the
previous reporting period.
To support the national programme and the target for High Needs women, Te AHN funds free smears for priority
women (Maori, Pacific and low income). TeAHN also promotes the free smears by the use of vouchers.
In the July to December 2013 period, a total of 954 funded cervical smears were carried out. This was a 15%
increase from the 832 carried out in the January to June 2013 period.
The breakdown for women receiving funded smears was:
• 388 were Māori
• 173 were Pacific
• 274 were Quintile 5 and not Maori or Pacific
119 demonstrated exceptional circumstances.
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Total 127 134 113 114 134 210 154 151 134 173 187 155
0
50
100
150
200
250
Number of funded Cervical Smears 2013
Total
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
94
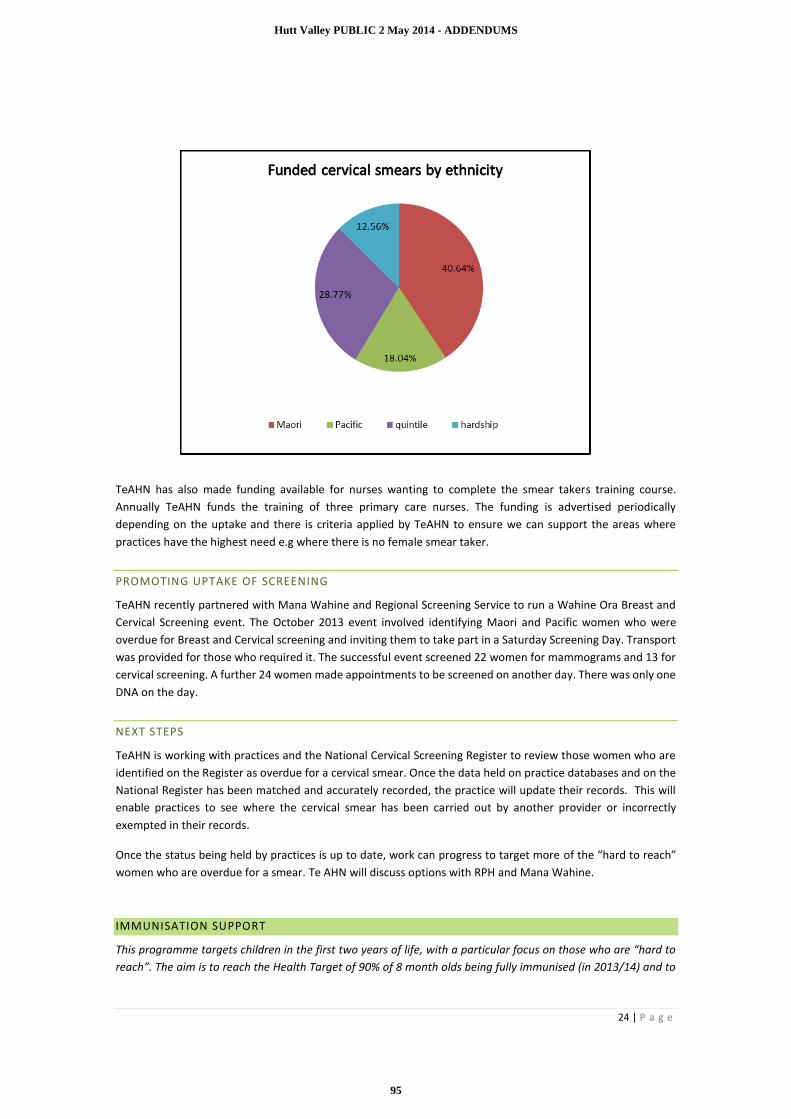
24 | P a g e
TeAHN has also made funding available for nurses wanting to complete the smear takers training course.
Annually TeAHN funds the training of three primary care nurses. The funding is advertised periodically
depending on the uptake and there is criteria applied by TeAHN to ensure we can support the areas where
practices have the highest need e.g where there is no female smear taker.
PROMOTING UPTAKE OF SCREENING
TeAHN recently partnered with Mana Wahine and Regional Screening Service to run a Wahine Ora Breast and
Cervical Screening event. The October 2013 event involved identifying Maori and Pacific women who were
overdue for Breast and Cervical screening and inviting them to take part in a Saturday Screening Day. Transport
was provided for those who required it. The successful event screened 22 women for mammograms and 13 for
cervical screening. A further 24 women made appointments to be screened on another day. There was only one
DNA on the day.
NEXT STEPS
TeAHN is working with practices and the National Cervical Screening Register to review those women who are
identified on the Register as overdue for a cervical smear. Once the data held on practice databases and on the
National Register has been matched and accurately recorded, the practice will update their records. This will
enable practices to see where the cervical smear has been carried out by another provider or incorrectly
exempted in their records.
Once the status being held by practices is up to date, work can progress to target more of the “hard to reach”
women who are overdue for a smear. Te AHN will discuss options with RPH and Mana Wahine.
IMMUNISATION SUPPORT
This programme targets children in the first two years of life, with a particular focus on those who are “hard to
reach”. The aim is to reach the Health Target of 90% of 8 month olds being fully immunised (in 2013/14) and to
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
95
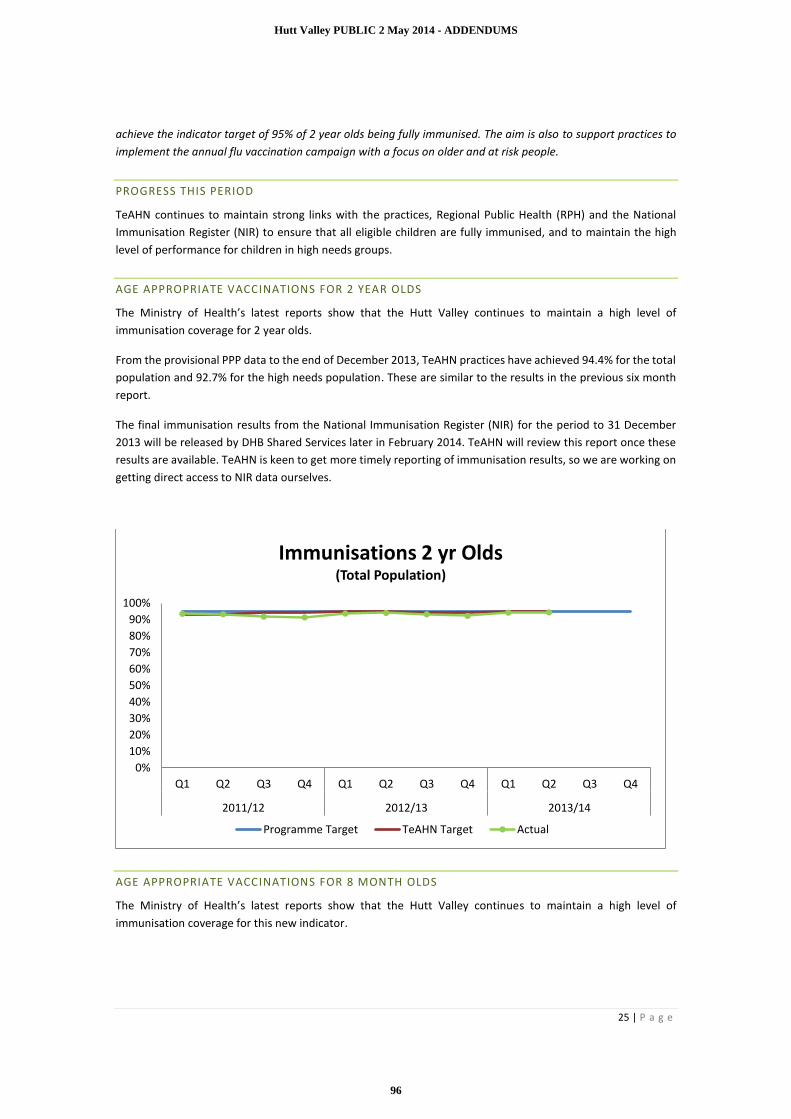
25 | P a g e
achieve the indicator target of 95% of 2 year olds being fully immunised. The aim is also to support practices to
implement the annual flu vaccination campaign with a focus on older and at risk people.
PROGRESS THIS PERIOD
TeAHN continues to maintain strong links with the practices, Regional Public Health (RPH) and the National
Immunisation Register (NIR) to ensure that all eligible children are fully immunised, and to maintain the high
level of performance for children in high needs groups.
AGE APPROPRIATE VACCINATIONS FOR 2 YEAR OLDS
The Ministry of Health’s latest reports show that the Hutt Valley continues to maintain a high level of
immunisation coverage for 2 year olds.
From the provisional PPP data to the end of December 2013, TeAHN practices have achieved 94.4% for the total
population and 92.7% for the high needs population. These are similar to the results in the previous six month
report.
The final immunisation results from the National Immunisation Register (NIR) for the period to 31 December
2013 will be released by DHB Shared Services later in February 2014. TeAHN will review this report once these
results are available. TeAHN is keen to get more timely reporting of immunisation results, so we are working on
getting direct access to NIR data ourselves.
AGE APPROPRIATE VACCINATIONS FOR 8 MONTH OLDS
The Ministry of Health’s latest reports show that the Hutt Valley continues to maintain a high level of
immunisation coverage for this new indicator.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
2011/12 2012/13 2013/14
Immunisations 2 yr Olds(Total Population)
Programme Target TeAHN Target Actual
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
96

26 | P a g e
From the provisional PPP data to the end of December 2013, TeAHN practices have achieved 92.9% for the total
population and 94.6% for the high needs population. These results remain above the 90% target for this indicator
and show a small improvement on the previous six month period.
65 YEARS AND OVER FLU VACCINE COVERAGE
Based on the provisional PPP results to the end of December 2013, TeAHN has achieved the PHO Performance
Programme target for 2013 comfortably, achieving 68.9% for total population and 67.9% for high needs.
NEXT STEPS
We plan to obtain NIR access to enable easier and more timely monitoring of progress. We will also review
instructions for practice nurses on recording immunisations in practice management systems to ensure practices
have the most up to date information available to them.
CARE PLUS
Care Plus aims to improve chronic care management, reduce inequalities, improve primary health care teamwork
and reduce the cost of services for high-need primary health user, by:
• improving access to care for people with long term conditions
• improving patient self-management.
CURRENT SITUATION
The graph below identifies the enrolments and the assessments carried out in the year January 2013 to
December 2013.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
2011/12 2012/13 2013/14
Immunisations 8 month Olds(Total Population)
Programme Target Actual TP
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
97

27 | P a g e
Overall the enrolments are sitting at 100% (6559 patients) 1at the end of the last quarter. We note there are
still significant variations across our practices in terms on their enrolments and some high enrollers have
continued despite our advice. We will be looking to provide these practices with more specific advice, likely
managing a cap on their enrolments as we seek to address some of the underlying issues.
KEY ISSUES
Due to staff changes and the unexpected departure of some key people, we have been unable to advance the
issues underpinning the Care Plus programme. We remain concerned that some practices have high enrolments
and may not have sufficiently robust systems to manage the assessment prior to re-enrolment. We have begun
to meet with these practices and to work through their processes aiming to lead a change in behaviour.
Te Awakairangi Health network sent a representative to the recent long term condition forum and also to the
diabetes forum where the role of Care Plus was discussed. There are a number of new models emerging around
the care of people with long term conditions that uses the Care Plus funding differently We are expecting to be
in a position be able to engage with our practices to explore these options from March when we are back up to
full staffing and have capacity to advance this work.
CLINICAL PHARMACY SERVICES
The clinical pharmacy facilitation activities focus on working with practices and other primary care professionals
to optimise medicines related health outcomes for patients in the Hutt Valley. The services offered work within
the Triple Aim approach.
ACHIEVEMENTS
The following is a summary of the clinical pharmacy facilitation activities undertaken within Te Awakairangi
Health Network (TeAHN) practices by the pharmacy team in the July - December 2013 period.
1 Karo_Reg_AnalysisPHO_TeAHN Oct 13 Report.
0
100
200
300
400
500
600
Number of enrolments and C+ assessments Jan 13 to Dec 13
Enrol and C+1 C+2 C+3 C+4
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
98

28 | P a g e
PHARMACY FACILITATION VISITS TO PRACTICES AND COMMUNITY PHARMACIES
During this period, all TeAHN practices (23 practices over 25 sites) were visited by a clinical pharmacist as part
of the scheduled pharmacy practice visits. In addition, all (30) community pharmacies were visited or the
community pharmacists attended the scheduled visit at the neighbouring practice. The clinical information
package has been well received by general practice teams and community pharmacists. TeAHN is confident that
the inclusion of community pharmacists in these visits is contributing to strengthening the linkages between
general practice and community pharmacy in the Hutt Valley.
The following information was developed by the pharmacy team or sourced for inclusion in the clinical
information package taken to practices and pharmacies:
Clinical Update on NSAIDs – with a focus on recent concern over the increased cardiovascular risk
associated with diclofenac use
Medicines Update on benzbromarone - a newly funded medication for the chronic treatment of gout
when allopurinol and/or probenecid are not tolerated, contraindicated or ineffective despite optimal
treatment doses
Medicines Update on ticagrelor – a newly funded oral antiplatelet agent that is indicated (in combination
with aspirin) for the prevention of atherothrombotic events in adults with acute coronary syndromes
(ACS). The medication is now being prescribed more frequently in secondary care.
A SaferX bulletin on melatonin (newly funded) – sourced from Waitemata DHB.
Health Quality and Safety Commission (HQSC) patient information leaflet “Taking your medicine safely”
(for community pharmacies only)
BPAC Antibiotic Guide (2013 Edition) – a consensus guide to help assist in the appropriate selection of
antibiotics for infections commonly seen in general practice.
A query build to assist with the bpacNZ audit: Renal function testing in patients on dabigatran (see below)
CLINICAL AUDITS
Renal Function testing in People Taking Dabigatran
bpacNZ data indicated that only 28% of patients started on dabigatran in TeAHN had their renal function
tested prior to starting the medication (a recommended requirement). This was lower compared to
the national data of 58%. The limitation of the bpacNZ data was that it did not include hospital lab
testing data.
In response to this data, bpacNZ has produced a MOPs accredited audit for identifying patients on
dabigatran who require an annual renal function test. The TeAHN clinical pharmacy supported GPs with
participating in this audit by developing a query build to assist with identifying patients suitable for
inclusion in the audit. Practices were also offered the option of assistance from a TeAHN pharmacist
to run the audit.
The dabigatran audit was specifically offered in the July – Dec period with 3 practices requesting
clinical pharmacist input into running the audit and other practices choosing to run the audit
themselves.
In total the pharmacy team responded to 10 requests (by practices) to run a number of available in-house clinical
audits i.e. dabigatran, gout and appropriate prescribing of self-monitoring blood glucose strips.
A clinical audit tool for benzodiazepine use in the elderly has also been developed and has gained MOPs
accreditation in preparation for the next round of visits (in 2014).
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
99

29 | P a g e
Onsite Pharmacist Facilitator Feedback
A member of the pharmacy team spent a day a week at one of the VLCA practices for a period of 6 weeks during
August –September. The intention was to explore the value added to services provided by the practice with the
addition of an onsite clinical advisory pharmacist. Very positive feedback has been received and to quote from
a GP “It was great having you here, quite helpful. It makes our lives way easier with your meds interactions checks
and safer for older patients. I think it would extremely helpful if we could have you here maybe once weekly or
so on a permanent basis.”
PRACTICE CONTACTS OVERALL
The number of direct contacts made between each practice and the pharmacy team over the 6 month Jul-Dec
2013 period ranged from 1 to 12 contacts (average = 2.7 ).
0
2
4
6
8
10
12
q i g n w d t x m b u e a j c k r p v s f y l h o
Practices
0
5
10
15
20
25
30
Clinical Audit Clinical Visit MedicationQuery
Peer Review Other
Key Reason for Clinical Pharmacist contact with Practices1 July – 31 Dec 2013
No of Clinical Pharmacist Contacts with Practices
1 July – 31 Dec 2013
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
100
30 | P a g e
PRESCRIBER TIPS
Prescribing (Rx) Tips are produced to complement Continuing Medical Education (CME) sessions. While no new
bulletins were prepared within the July to December 2013 reporting period, the clinical pharmacy team reviewed
existing resources relevant to the topic that was provided to participants. Community pharmacists have been
invited and have attended the CME sessions for collaborative learning with GPs.
MEDICATION QUERIES
During the July – Dec 2013 period, 34 medication queries were researched and answered. Medication enquires
undertaken by the team varied in their complexity and research requirements. Enquires took from 15 minutes
to up to 3 hours to complete.
EDUCATION SESSIONS
TeAHN clinical pharmacists continue to make a significant contribution to helping patients understand their
medicines better, and assisting practice nurses with their continuing professional development. Five education
presentations were given in the period between July-Dec 2013:
Patient Education Session to Kaumatua Group (Wainuiomata Marae) on general medication use
Patient Education Session on use of respiratory medicines at Pacific Health Services
Two Respiratory education sessions for practice nurses
One Cardiac Continuum education session for practice nurses.
PRESCRIBING ANALYSIS
In October 2013 a report was prepared to inform members of the Hutt INC’s Medicines Management
workstream of TeAHN’s pharmacy-related facilitation activities for January to December 2013. This report
included an analysis of patterns/trends identified from BPAC practice-level data and the MOH Cube Tool
prescriber-level data. The prescribing analysis confirmed that the 2013 pharmacy facilitation activities
undertaken were relevant to prescribers. The analysis also identified areas of deviance from national prescribing
trends that were more relevant to secondary care prescribing. The 2012/13 practice-level reports (BPAC) are
now available and will be analysed in a similar way to identify future topics for facilitation activities. It is
anticipated that local prescribing patterns could be incorporated (where relevant) into the GP/Pharmacy CME
sessions.
HUTT INC MEDICINES MANAGEMENT WORKSTREAM
TeAHN has made a significant contribution in supporting Hutt INC’s Medicines Management workstream since
August 2013. TeAHN has provided meeting support and staff from its senior management and pharmacy team
as members of the workstream. Representatives from hospital pharmacy, SIDU and community pharmacy are
included. The group has met twice. The first project aimed at improving the accuracy of medication lists will be
looking at the implementation the commonly known “yellow card”. Hospital pharmacy, community pharmacy
and TeAHN pharmacy facilitators will work across the interface to promote this. The workstream is chaired by
a GP, Dr Lise Kljakovic. Lise is also a member of the Board of TeAHN and the Chair of Hutt INC.
HVDHB HEALTH PATHWAYS
A workshop on the care of frail older person with complex needs was organised by TeAHN in November. The
TeAHN pharmacy team made a significant contribution at this workshop by presenting on medicines utilisation
data and organising the evening. Feedback from the workshop clearly indicated the need for a tiered Medicines
Management Service that frail older people could be referred into when an issue with medications was
identified. Referrals would be as part of a Comprehensive Geriatric Assessment which is a best practice approach
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
101

31 | P a g e
to improving the quality of care provided to these patients. Hutt INC has endorsed the establishment of a
workstream on the Care of Frail Older People and the workstream will require ongoing involvement and
resources from the TeAHN pharmacy team.
STRENGTHENING LINKAGES BETWEEN GENERAL PRACTICE AND COMMUNITY PHARMACY
CARDIOVASCULAR DISEASE RISK ASSESSMENT (CVDRA)
A proposal for an integrated provider model aimed at increasing the HVDHB’s CVDRA performance was
made to HVDHB in this period. The model proposed would see a community pharmacy offering/undertaking
CVDRAs at the pharmacy. The community pharmacy would work in collaboration with the local medical
centre to identify eligible people who have not yet had a CVDRA. The model offers choice and greater access
to people who may not otherwise present at their general practice for a CVDRA. CVDRA data from the
community pharmacy will be entered into the practice PMS. A pilot of this model in intended to be trialed
in 2014.
RHEUMATIC FEVER SCREENING AND TREATMENT
Another example of an integrated model of care involving community pharmacy is being developed to help
identify and treat children at risk of rheumatic fever in the Hutt Valley area. In collaboration with their
general practices, three community pharmacies will be trialing the feasibility of community pharmacists
assessing and treating (as enabled by PHARMAC’s recent PSO changes). The feasibility trial will occur in
early 2014.
PHO PERFORMANCE PROGRAMME
The PHO Performance Programme (PPP) is a quality programme which aims to support improvements in the
health of enrolled populations and reduce inequalities through supportive clinical governance and continuous
quality improvement processes.
KEY ACTIVITIES
TeAHN has given priority to working with practices to achieve a significant improvement in the numbers of
patients who have received smoking brief advice/cessation referral and/or CVD risk assessment. We are very
close to reaching the programme goal of 95% for the number of childhood immunisations given. See the relevant
sections of the report for more details.
ACHIEVEMENTS
This report refers to preliminary data from the DHBSS performance report for the period 1 July to 31 December
2013. During this period Te Awakairangi Health Network achieved 15 of the 21 funded indicators (against the
targets set for our Network).
The funded indicators achieved were:
cardiovascular risk detection for both total and high need populations
cardiovascular risk assessment for the total and high need population
diabetes detection for both total and high need populations
smoking status ever recorded for the high need and ‘other’ populations
flu vaccine coverage both total and high need population
breast screening high need population
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
102

32 | P a g e
age appropriate vaccinations 8 months total and high need
cervical screening for both total and high need populations.
Funded indicators not achieved
brief advice and/or smoking cessation support high need and other
age appropriate vaccinations 2yr total and high need
diabetes annual review for both total and high need populations
Childhood immunisations for 8 month olds and for two year olds remain high. As immunisations tend to decline
in December and over the holiday period, this result is better than expected. There has been significant
improvement in the CVD risk assessment results, with the Total Population result increasing significantly from
44% at the end of June 2013 to 58% at the end of December 2013. There has also been a significant improvement
in the brief advice for smoking cessation indicator, which has increased from 50% to 63%.
The DHBSS data indicating the definitive results and the national data for comparison will not be available until
February 2014.
KEY ISSUES AND IDENTIFIED RISKS
1. Cardiovascular risk assessment: The CVD risk assessment programme has had a significant increase in the
number of people who have had an assessment but considerable work is still required to achieve the
programme goal. Additional strategies are being put in place to assist with this work (see 3.2 for further
detail).
2. Smoking cessation: the programme has had a significant increase in the number of people who have
received brief advice but considerable work is still required to achieve the programme goal. Additional
strategies are being put in place to assist with this work (see 3.5 for further detail).
3. Childhood Immunisations: TeAHN is keen to get more timely reporting of immunisation results, so we are
working on getting direct access to NIR data ourselves. This should assist us to reach the programme goal
(see 3.7 for further detail).
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
103

33 | P a g e
SERVICES
OUTREACH NURSING
To reduce health inequalities and improve health outcomes by improving access to primary care services for high
need groups within the PHO, who are not currently accessing care or accessing it in a limited way proportional
to their health needs in particular.
KEY ACTIVITIES
Work across the Network’s 23 Practices (over 25 sites) to identify people who are not accessing primary
care or requiring education and support to work with their primary care provider.
Work collaboratively with wider community organisations; Pharmacies and NGOs, to identify people who
are not accessing primary care or who are requiring education and support to work with their primary care
provider.
Work in close collaboration across the wider Network team such as the Wellbeing Service, Community
Health Workers and Health Promotion to identify people who are not accessing primary care or who are
requiring education and support to work with their primary care provider.
Provision of assessment, follow-up, health education and promotion, community liaison, advocacy services
and disease-management visits for identified individuals and their whānau.
ACHIEVEMENTS
A major achievement during this reporting period was successfully recruiting a third experienced Outreach Nurse
into TeAHN central team, which brought us up to a full complement of staff.
Work is continuing around linkages and reporting templates for the Integrated Case Management Nursing
(ICMN) services within the Network, with further discussions having been held with clinical leaders, Outreach
Nurses (ONs), Integrated Case Management Nurses (ICMNs) and managers at Whai Oranga and Hutt Union and
Community Health Services (HUCHS).
The team are maintaining close contact with practices as part of their day-to-day activities. This includes liaising
with staff for specific patient issues and updates, meet-and-greets for new staff, supporting patients with
transport to and during appointments, and delivering providing information such as brochures. One ON has
developed a system with one of her allocated practices for regular referrals to help locate patients for urgent
DNA recall appointments such as cervical smears and mammograms.
In addition to accompanying patients to practice based consultations, the ONs also receive many requests from
patients to accompany them to various secondary care appointments e.g. podiatry, breast screening,
paediatrics, respiratory, diabetes, audiology, sleep tech, renal, plastics, ENT, OPRS, OT and ACCESS. As part of
patients’ care plan discussions, staff ensure their roles (e.g. advocate, adviser or facilitator) at these
appointments are carefully defined and agreed upon beforehand, so as to make best use of the time.
Our ON team have assisted the Health Promotion team on the Pacific Wellbeing Day, and provided Island food
for their ‘fat kit’ photo shoot.
The ON team continue to participate in the Hutt Valley Primary Health Nurse Reference Group, Samoan Nurses
Association, Vibe, and contact with the Pacific Health Service nurses. These contacts improve working
relationships, share information and training opportunities, and assist with peer reviews of practice. Training is
an ongoing requirement for our nurses’ role to ensure they practice competently, both independently and in
collaboration with other health professionals. Some of the training they have undertaken during this reporting
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
104
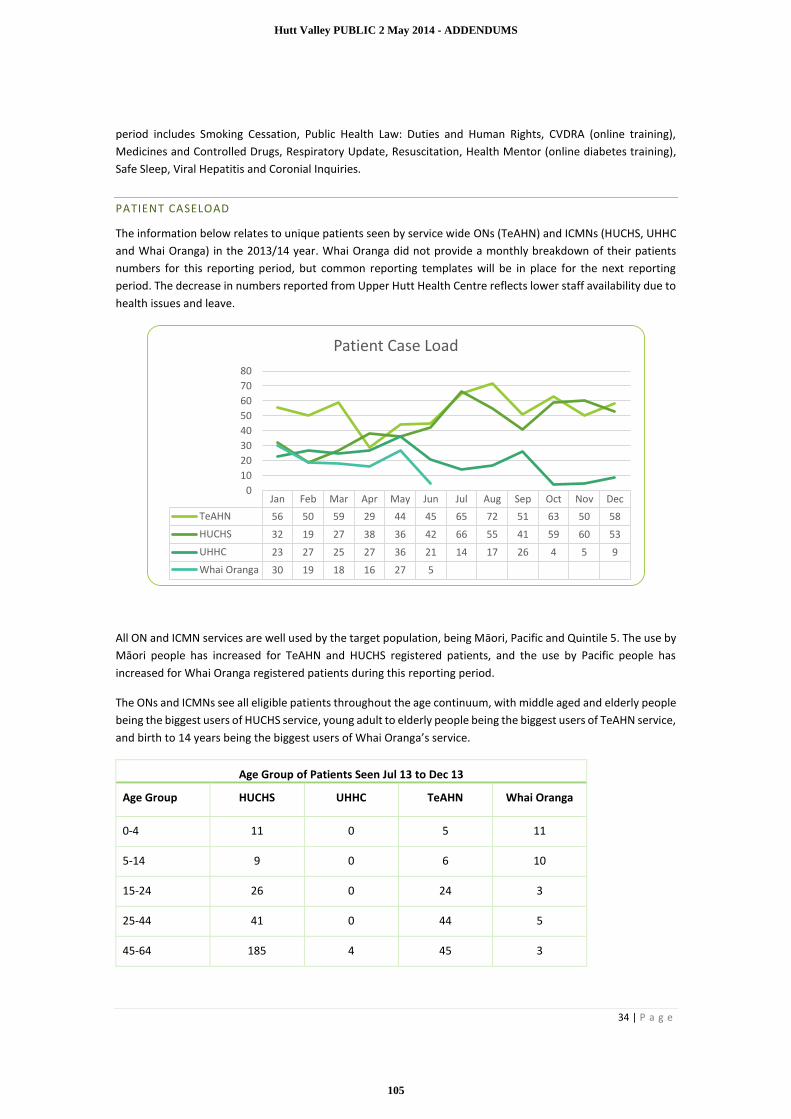
34 | P a g e
period includes Smoking Cessation, Public Health Law: Duties and Human Rights, CVDRA (online training),
Medicines and Controlled Drugs, Respiratory Update, Resuscitation, Health Mentor (online diabetes training),
Safe Sleep, Viral Hepatitis and Coronial Inquiries.
PATIENT CASELOAD
The information below relates to unique patients seen by service wide ONs (TeAHN) and ICMNs (HUCHS, UHHC
and Whai Oranga) in the 2013/14 year. Whai Oranga did not provide a monthly breakdown of their patients
numbers for this reporting period, but common reporting templates will be in place for the next reporting
period. The decrease in numbers reported from Upper Hutt Health Centre reflects lower staff availability due to
health issues and leave.
All ON and ICMN services are well used by the target population, being Māori, Pacific and Quintile 5. The use by
Māori people has increased for TeAHN and HUCHS registered patients, and the use by Pacific people has
increased for Whai Oranga registered patients during this reporting period.
The ONs and ICMNs see all eligible patients throughout the age continuum, with middle aged and elderly people
being the biggest users of HUCHS service, young adult to elderly people being the biggest users of TeAHN service,
and birth to 14 years being the biggest users of Whai Oranga’s service.
Age Group of Patients Seen Jul 13 to Dec 13
Age Group HUCHS UHHC TeAHN Whai Oranga
0-4 11 0 5 11
5-14 9 0 6 10
15-24 26 0 24 3
25-44 41 0 44 5
45-64 185 4 45 3
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
TeAHN 56 50 59 29 44 45 65 72 51 63 50 58
HUCHS 32 19 27 38 36 42 66 55 41 59 60 53
UHHC 23 27 25 27 36 21 14 17 26 4 5 9
Whai Oranga 30 19 18 16 27 5
0
10
20
30
40
50
60
70
80
Patient Case Load
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
105

35 | P a g e
65+ 62 5 33 0
Unknown 0 57 2 5
PATIENT CONTACTS AND SERVICES
The table below shows the number of ON and ICMN patient contacts and services provided in this period, with
numbers from TeAHN and UHHC pertaining to outreach services, and HUCHS and Whai Oranga numbers based
on nurse-led projects undertaken within practices (Cervical Smear and Skin Clinic projects respectively).
Provider Patient Contacts Services
Te Awakairangi Health Network 734 2963
Upper Hutt Health Centre 119 119
HUCHS 334 334
Whai Oranga O Te Iwi 66 66
Service Wide 1253 3482
TEAHN OUTREACH NURSING
In the July to December 2013 period, TeAHN ON service provided a total of 734 patient contacts, and 2,963
services (on average, 494 services each month) to patients who accessed the service.
Their work covered home and clinic visits, telephone calls, and meetings with practice staff to discuss patient
health issues and barriers. They also provided support and information on disease and medication education,
organised visits to podiatry services, arranged smoking cessation support and organised transport to various
168134 136
70
14991
133 143104 123 119 112
673
608
529
193
494
407
501
608
485449
581
339
0
100
200
300
400
500
600
700
800
Jan Feb Mar Apr May Jun July Aug Sept Oct Nov Dec
Volume of Work - TeAHN Outreach Nurses1 Jan to 31 Dec 13
Patient Contacts Services Provided
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
106

36 | P a g e
appointments which have possibly not been attended previously. As most patients who are referred to the
service have one or more long-term conditions, the nurses carried out basic measurements, blood pressure,
blood sugar levels, and diabetes assessments as routine tasks.
TeAHN Outreach Nurses
Service Type
Jan to Jun 13 Jul to Dec 13
Patient Contact 1103 1084
Facilitation Service 1006 901
Liaising Agencies 456 811
Measurements 122 149
Referrals 213 18
Unknown 4 0
TOTAL 2904 2963
WHAI ORANGA O TE IWI HEALTH CENTRE
The ICMN contract has allowed Whai Oranga O Te Iwi HC to continue supporting their nurse-led Skin Clinic and
services, as well as the mobile nursing services/home visits. The ICMNs are helping to make improvements with
PPP targets, including vaccinations, cervical screening, mammograms and CVD assessments.
The Skin Nurse continues to run Skin Clinics during weekly set sessions as well as running a late Wednesday
evening Clinic. This allows a more convenient time for patients to visit her, and also the evening is the best time
for her to call patients when follow up is required. The service is specialised, accessible and affordable, with
patients aged 6 years or older only being charged a nurse consult fee of $5.00.
The Skin Nurse has been very involved with intense dressing changes and education to whānau groups. She
liaises closely with District Health and Public Health Nurses to assess home situations that involve flea infections,
dampness, and overcrowding that cause skin infections and asthma. She also helps to prepare Work and Income
application forms for patients to assist with the financial cost of dressings.
The Skin Nurse is very proactive with the GPs and encourages them to refer all patients with skin conditions to
her for education and wrap around support for the patient/whanau. She continues to educate new clinical staff
and has gained the respect and acknowledgement of her peers, other health providers and our patients for her
extensive knowledge and skills. Recent referrals have been received from the Hospital’s Paediatric Team and
Plunket, with excellent relationships having been established with key staff.
Often referrals are sent to the Skin Nurse from a GP to follow up a baby with a related skin problem. The nurse
will find that other family members are also experiencing the same problems in the home, so all can be treated
at the same time. Patients and their whānau are provided with a Care Plan. They also receive information on the
creams and treatments, how they work, the benefits and when to use them. Skin packs are also provided, which
includes information on care for covering open sores and advice on when further treatment may be required.
The nurse provides education and support, and follows up with a recall system, which reduces the risk of further
infection, spread or recurrence of the problem and avoids hospitalisation.
The nurse is now using the new screening/auditing tool that has been set up and installed by TeAHN, which will
help keep a record of patients’ seen in the Skin Clinic and will enable provision of more in-depth reporting.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
107
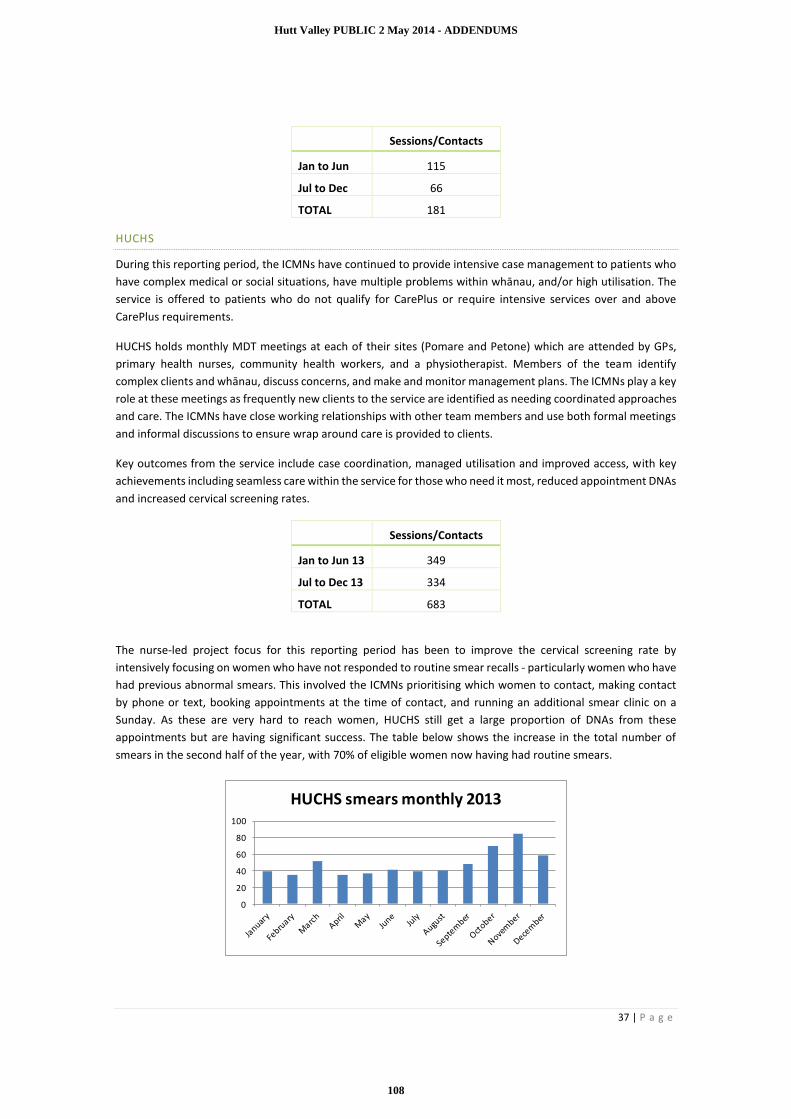
37 | P a g e
Sessions/Contacts
Jan to Jun 115
Jul to Dec 66
TOTAL 181
HUCHS
During this reporting period, the ICMNs have continued to provide intensive case management to patients who
have complex medical or social situations, have multiple problems within whānau, and/or high utilisation. The
service is offered to patients who do not qualify for CarePlus or require intensive services over and above
CarePlus requirements.
HUCHS holds monthly MDT meetings at each of their sites (Pomare and Petone) which are attended by GPs,
primary health nurses, community health workers, and a physiotherapist. Members of the team identify
complex clients and whānau, discuss concerns, and make and monitor management plans. The ICMNs play a key
role at these meetings as frequently new clients to the service are identified as needing coordinated approaches
and care. The ICMNs have close working relationships with other team members and use both formal meetings
and informal discussions to ensure wrap around care is provided to clients.
Key outcomes from the service include case coordination, managed utilisation and improved access, with key
achievements including seamless care within the service for those who need it most, reduced appointment DNAs
and increased cervical screening rates.
Sessions/Contacts
Jan to Jun 13 349
Jul to Dec 13 334
TOTAL 683
The nurse-led project focus for this reporting period has been to improve the cervical screening rate by
intensively focusing on women who have not responded to routine smear recalls - particularly women who have
had previous abnormal smears. This involved the ICMNs prioritising which women to contact, making contact
by phone or text, booking appointments at the time of contact, and running an additional smear clinic on a
Sunday. As these are very hard to reach women, HUCHS still get a large proportion of DNAs from these
appointments but are having significant success. The table below shows the increase in the total number of
smears in the second half of the year, with 70% of eligible women now having had routine smears.
0
20
40
60
80
100
HUCHS smears monthly 2013
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
108

38 | P a g e
Relationship with key nurses leads to better compliance, coordination of care and access to appropriate services.
Education and support is a key focus of the service along with effective integration within the HUCHS team of
doctors, nurses, community health workers, physiotherapists, primary mental health and family violence
worker.
UPPER HUTT HEALTH CENTRE
Upper Hutt Health Centre ONs continue to provide nursing care to enrolled patients with complex health needs
e.g. patients with physical, psychological and/or social issues, or those requiring end-stage care have been
recipients of our outreach service this reporting period.
Health care for these patients has been enhanced by the ONs facilitating interdisciplinary and family meetings
to minimise clinical risk and maintain patient safety. With the appropriate support services put in place by the
outreach service, patients have been able to continue living independently in the community.
The ONs also respond to situations more acute in nature, and liaise with both primary and secondary care
providers to ensure patients are receiving the best health care. Various funded services are utilised to enhance
patient care and promote good outcomes e.g. TeAHNs: Transport, Dietitian and Healthy Family Coach Services.
The ONs have been involved in cases where patients needed to go to hospital or hospice and this process was
facilitated by them through liaising with the patient’s GP.
The ON service at UHHC is pivotal in providing health care to patients who have high clinical and social needs.
They play a significant role in linking patients with the services they need and this has subsequently resulted in
patients receiving appropriate interventions and a reduction in complications and hospitalisations
Sessions/Contacts
Jan to Jun 13 251
Jul to Dec 13 119
TOTAL 370
RHEUMATIC FEVER
From 1 July 2013, the ON service has been fulfilling a SIDU contract for follow-up of clients aged 16 to 21years
residing in the HVDHB area with rheumatic fever (RF), who need support to ensure they receive their monthly
prophylactic antibiotic.
Patients have responded well to the change from Hutt Paediatrics to TeAHN’s service, with the ON having
formed great working relationships with her 17 RF patients and whānau to date. The ON has met monthly with
Shennan Brown (Compass Health Rheumatic Fever Mobile Nurse) and Barbara Eddie (RPH) as a regular forum
for ongoing support and review of this programme.
TeAHN wishes to thank all the staff at Hutt City Health Centre, for their medical oversight of the service, for the
use of the vaccine fridge for the bicillin injections, and being so accommodating toward our nurse (who will rush
in at times to grab an injection after confirming the whereabouts of her elusive RF patients).
PACKAGES OF CARE
This programme is used to reduce the financial barrier to access health services for our high-needs enrolled
population. It is managed by the Outreach Nurse service.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
109
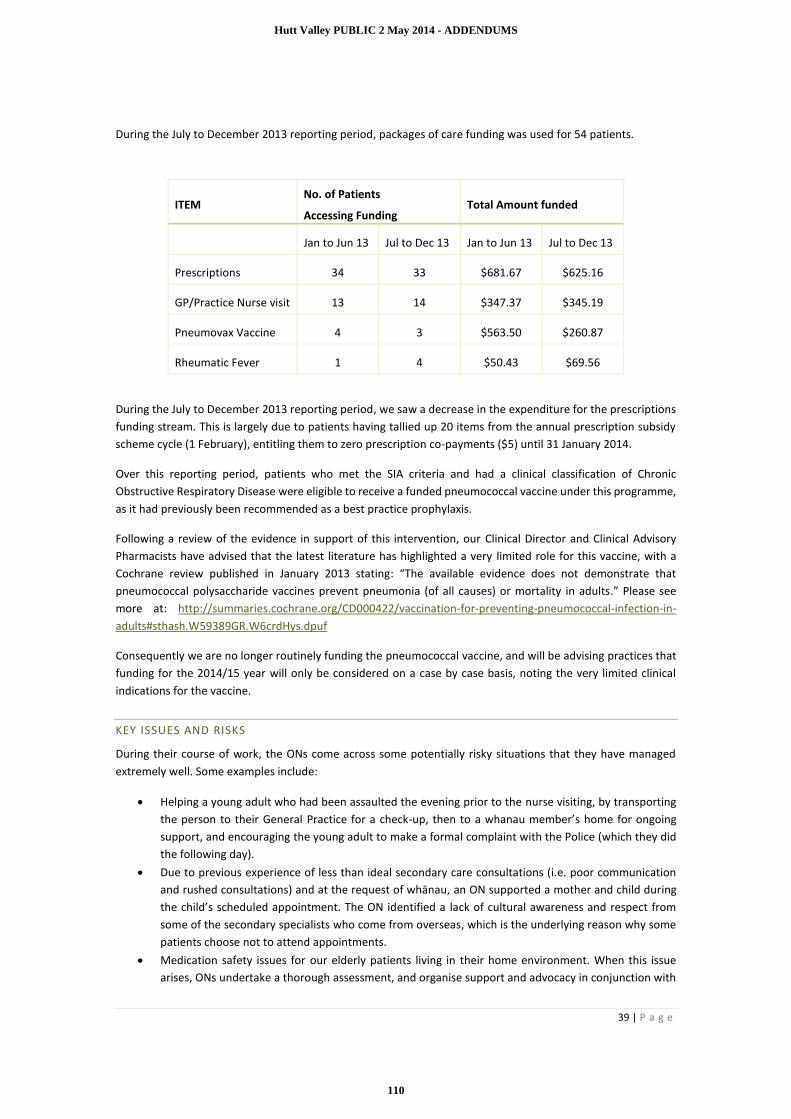
39 | P a g e
During the July to December 2013 reporting period, packages of care funding was used for 54 patients.
During the July to December 2013 reporting period, we saw a decrease in the expenditure for the prescriptions
funding stream. This is largely due to patients having tallied up 20 items from the annual prescription subsidy
scheme cycle (1 February), entitling them to zero prescription co-payments ($5) until 31 January 2014.
Over this reporting period, patients who met the SIA criteria and had a clinical classification of Chronic
Obstructive Respiratory Disease were eligible to receive a funded pneumococcal vaccine under this programme,
as it had previously been recommended as a best practice prophylaxis.
Following a review of the evidence in support of this intervention, our Clinical Director and Clinical Advisory
Pharmacists have advised that the latest literature has highlighted a very limited role for this vaccine, with a
Cochrane review published in January 2013 stating: “The available evidence does not demonstrate that
pneumococcal polysaccharide vaccines prevent pneumonia (of all causes) or mortality in adults.” Please see
more at: http://summaries.cochrane.org/CD000422/vaccination-for-preventing-pneumococcal-infection-in-
adults#sthash.W59389GR.W6crdHys.dpuf
Consequently we are no longer routinely funding the pneumococcal vaccine, and will be advising practices that
funding for the 2014/15 year will only be considered on a case by case basis, noting the very limited clinical
indications for the vaccine.
KEY ISSUES AND RISKS
During their course of work, the ONs come across some potentially risky situations that they have managed
extremely well. Some examples include:
Helping a young adult who had been assaulted the evening prior to the nurse visiting, by transporting
the person to their General Practice for a check-up, then to a whanau member’s home for ongoing
support, and encouraging the young adult to make a formal complaint with the Police (which they did
the following day).
Due to previous experience of less than ideal secondary care consultations (i.e. poor communication
and rushed consultations) and at the request of whānau, an ON supported a mother and child during
the child’s scheduled appointment. The ON identified a lack of cultural awareness and respect from
some of the secondary specialists who come from overseas, which is the underlying reason why some
patients choose not to attend appointments.
Medication safety issues for our elderly patients living in their home environment. When this issue
arises, ONs undertake a thorough assessment, and organise support and advocacy in conjunction with
ITEM No. of Patients
Accessing Funding Total Amount funded
Jan to Jun 13 Jul to Dec 13 Jan to Jun 13 Jul to Dec 13
Prescriptions 34 33 $681.67 $625.16
GP/Practice Nurse visit 13 14 $347.37 $345.19
Pneumovax Vaccine 4 3 $563.50 $260.87
Rheumatic Fever 1 4 $50.43 $69.56
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
110

40 | P a g e
alternate service providers and whānau. With a large percentage of our target population being in the
65+ age bracket, we are now updating our current nursing assessment tool for new patients.
CASE STUDY 1
Client
86 years old, of European decent and Quintile 5. Residing alone in a Housing NZ home with minimal family
support in Wellington, referral received from the client’s Practice Nurse outlining concerns regarding medication
management.
Current health issues
Insulin dependent diabetes mellitus type II
Essential hypertension
Vascular dementia
Osteoarthritis
Recent fracture NOF Left 2012 Right 2013
x 3 amputated toes 2013
Acute renal failure
Outreach Nurse Assessment and Role:
Client’s short term memory loss is largely impacting upon her ability to manage independently at home,
especially her medication management. Client claims to administer her insulin each morning and record her BSLs
prior, however on weekly monitoring the ON noted that the patient has not been taking BSL recording prior to
insulin administration. On discussion, it becomes evident that the patient is unaware how to treat hypoglycaemic
episodes.
Her three children live in the upper North Island and client is adamant she will not leave the home at any point
to move into a rest-home. The family have Enduring Power Of Attorney and at this stage respect her wishes,
hoping for all to be done to ensure she can stay at home for as long as possible.
Actions
On discussion with and consent given by family, referral made to Mission for Seniors for further
support networks within the home
Fortnightly visits to assess BSL recordings and provide education regarding insulin administration
Contact made with Enlivens’ Care Coordinator to query regarding re-assessment of current care plan
Further discussion had with Enliven Coordinator to change the timing of personal care to include
medication prompt early morning
Liaison with nephew who lives locally and is also an insulin dependent diabetic, to assist with support
of his Aunt
Regular visits and liaison with Practice Nurse and GP regarding care
Transport to pathology.
Service Input
Number of phone calls to client: 4
Number of home visits to client: 6
Number of practice visits and liaisons: 5
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
111

41 | P a g e
Number of liaisons with NOK: 5
Number of liaisons with alternate service: 3
Number of referrals: 1 (Wellington City Mission’s, Mission for Senior’s programme)
Providers Involved:
GP - Regular visits and liaison regarding care
Practice Nurse - Regular visits and liaison regarding care
Enliven - Personal care daily visit to assist with showering and dressing, and domestic assistance fortnightly
District Nursing- Fortnightly visits to dress toes
Outcomes:
Client continues to manage independently at home with the input of several stakeholders. Her monitoring and
management of her diabetes has improved. Her family are fully aware of the risk, concerns and current services
that are made available to her. The client is happy with how the services are running currently and wishes for
no further changes to this. Ongoing monitoring by all stakeholders will continue on a regular basis.
CASE STUDY 2
Client
A referral was received from the Practice Nurse at Hutt City Health Centre (HCHC). The client was a 48 year old
Māori woman who had been bitten by her neighbour’s dog on 28 August 2013. She had initially presented to
the Emergency Department, where the wound was sutured. She did not attend any follow up appointments at
the Dressing Clinic at HVDHB due to lack of transport and financial difficulties.
Current health issues:
She presented to HCHC on 19 September 2013 to get the sutures removed from the wound. The wound was
infected and she could not afford to pay for her script for antibiotics at the time, so she was referred to our
Service for assistance to pay for antibiotics via Packages of Care Prescription Subsidy.
Outreach Nurse Assessment and Role:
Visited at home, wound assessed. As client lives with her 3 pre-school mokopuna, ON educated her
on how to keep wound clean and dry, and how to dress it properly, to avoid cross infection.
Packages of Care Prescription Subsidy issued x 2 for her to get her antibiotics.
Regular home visits to ensure medication compliance and education to client and whānau as client
not 100% compliant with taking antibiotics as directed and had missed a few doses. Client also has
some alcohol abuse issues.
Client required follow-up with GP for review after finishing first course of antibiotics. Wound still not
resolved.
Regular monitoring via home visits to ensure completion and correct compliance of taking antibiotics
and care of wound.
Referral made to CHW to follow up with any financial and alcohol issues.
Final visit made when wound was fully healed up. Educated regarding getting prompt treatment in the future
for any health issues for her or whānau.
Service Input
Number of home visits to client: 9
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
112

42 | P a g e
Number of phone calls to client: 4
Number of Packages of Care Prescription Subsidy: 2
Number of referrals: 1 (Community Health Worker, TeAHN)
Providers Involved
GP
Practice Nurse
Pharmacy
Community Health Worker
Outcomes
The work alongside this client highlighted the need for some clients and whānau to be closely followed up and
supported, even though the initial referral was just for financial assistance regarding collecting script. The client
was under the ON service for a period of 3 months, from referral to discharge. A very good result was achieved,
as the patient did not end up having to be admitted to hospital for infected wound, debridement and possible
plastic surgery.
CASE STUDY 3
Client
Patient is a 61 year old woman with diabetes, hypothyroidism, lipid disorder and somatisation disorder. She is a
highly anxious lady who requires a lot of input from health services. She has a history of extremely high ED
attendance (1-2 times weekly), and frequent specialist outpatients appointments and inpatient admissions. She
has poor stress management strategies and has in the past thrown things at visiting DHB nurses, and shouted
and hit other patients with her stick in hospital and GP waiting rooms.
ICMN Nurse Assessment and Role
ICMN has focused on building a relationship of trust which is reassuring and allays anxiety, managing ongoing
health issues, and having a planned and agreed programme of general practice contacts. The current contact
plan is two phone calls per week with the nurse, fortnightly appointments with nurse case manager, and six
weekly appointments with the doctor. The plan is developed and shared in monthly MDT meeting, and agreed
with patient.
Outcomes
This is a significant reduction in contacts compared to previously. The arrangement has helped to monitor and
manage the patient’s long-term conditions, reduced the number of hospital presentations and admissions,
reduced the number of primary care presentations and helped promote more appropriate behaviour. Recently
the patient has started to discuss childhood traumas as well as her ongoing somatic conditions, which is the first
time she has discussed these with anyone.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
113

43 | P a g e
COMMUNITY HEALTH WORKERS
The purpose of this service is to develop and maintain collaborative relationships with Te Awakairangi Health
Network practices and other health providers to enable the facilitation of appropriate access to primary health
care for at risk patients.
KEY ACTIVITIES
• Patient Care e.g. advocating with Work and Income and other Government agencies.
• Community Development and Health Promotion e.g. assessing current social problems and difficulties
and helping to address these needs through agreed individual Care Plans.
• Working with General Practice e.g. coordinating health needs.
• Working alongside other Service Providers, for example, referring to appropriate health providers,
community groups and organisations.
ACHIEVEMENTS
The CHW team has successfully kept the service running smoothly despite a couple of members from the team
requiring extended leave (one each at HUCHS Petone and TeAHN). This was made possible by TeAHN managing
to quickly acquire a skilled person to fill in for three months.
The virtual CHW team continues to meet regularly (15 July, 19 August, 16 September, 21 October, 18 November
2013) with venues being rotated between work sites (HUCHS Pomare, Whai Oranga and TeAHN). Guest speakers
are invited and provide pertinent presentations to enhance the work the CHWs undertake with patients.
Examples include:
TeAHN Health Promoter and Clinical Programmes Facilitator presenting on Smoking Cessation ABC
Project and Free Heart and Diabetes Checks and the role the CHWs play in supporting our target
population to take these up (15 July).
The Naenae Work and Income Service Centre Manager presenting on the significant changes to
the benefit system from July 2013 (19 August).
Ministry of Education’s Early Childhood Education & Early Learning Taskforce team speaking about
CHWs assisting vulnerable children and parents to participate in some sort of ECE learning to
prepare them for school (16 September).
These meetings continue to prove invaluable for discussing and agreeing on expected activities, outputs, activity
reporting, referral and discharge criteria and processes, and an opportunity for staff to share modalities used in
day-to-day practice. The reporting systems have been fine-tuned over the last few months, with two common
reporting templates being installed in TeAHN, HUCHS and Whai Oranga patient management systems. This has
enabled easier manipulation and compilation of reporting requirements.
With every meeting held, the CHWs gain significant traction on working collectively as one cohesive service,
including recognising team member’s strengths e.g. local networking knowledge, work interests and passions,
fluency in Te Reo or Pacific languages and being well versed in Māori and Pacific cultures.
The Outreach Team Leader and TeAHN CHWs have made various service presentations at the request of the
following groups: Upper Hutt Health Centre, HVDHB Social Work, Alzheimer’s Carers, Te Umiumiga Parents As
First Teachers and Valley Fit Exercise Group. These presentations were well received with respective audiences
asking many questions, resulting in referrals to the service.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
114

44 | P a g e
The experienced team of CHWs continue to actively participate in many different intersectoral groups, networks
and forums e.g. Suicide Intervention, Cohesive Communities Working Together - Upper Hutt, Hutt Valley
Community Response, HVDHB Violence Intervention Programme Steering Group, HVDHB Māori Health Services
Development Group, HVDHB Maternity Clinical Governance Group, Naku Enei Tamariki, Āhuru Mōwai O Te
Awakairangi (Family Violence), Northern Community Committee Hutt City Council, Rimutaka Māori Women’s
Welfare League, Taita Community Trust, White Ribbon Day and Tumeke Taita. When CHWs share their
experiences and stories of work with patients, the groups can identify trends and recommend appropriate
pathways.
The Outreach Team Leader has been actively involved in Manderson Grove’s community residents’ hui regarding
housing and health concerns e.g. gas leaks, street clean up, upgrade of playground, earthquake assessment,
insulation, pest eradication, fencing, flood and drainage, health and safety audits. Other partners involved in the
project include Waka Moemoea Trust, Housing NZ, Hutt City Council (HCC), ACC, Kokiri Marae, and Epuni Primary
School (venue for hui). Over the past four months, a great deal of work has been achieved collectively e.g. HCC
and ACC developed and undertook health and safety audits, HCC erected a ‘No Exit’ sign and cleared blocked
drains, Housing NZ addressed some housing concerns, and residents were given gift packs made up of donations
from partners (slip mats, energy efficient light bulbs, Healthlink fridge magnets, brochures for self-referring to
services, lip balms, bottles of water and balloons).
A regional home insulation programme targeting low-income households is currently being rolled out,
particularly for those who experience health challenges such as respiratory conditions, asthma, skin infections
and rheumatic fever which are exacerbated by living in damp and cold housing. CHWs are actively seeking those
who meet the financial and health criteria as they recognise that by improving the warmth of housing, we
improve peoples’ health and wellbeing.
A blessing of Pomare land being redeveloped was carried out by local iwi. In attendance were local community,
organisations and schools, HVDHB staff, Minister of Housing, Real Estate Agents, Building Contractors, Social
Housing Providers and the Property Developers. The redevelopment project has begun with the show home
being ready for viewing by beginning of March.
The community around the Jackson Street Flats in Petone has had difficult times in recent months. There have
been two tragic deaths in the community, and HUCHS Petone Clinic has been under threat of closure. A
community meeting hosted by Mayor Ray Wallace passed two unanimous resolutions. The first was to keep the
HUCHS Petone Clinic open, and the second was to start a “Positive Petone” group similar to the successful
Positive Pomare group. The aim of this group is to bring community members, community groups and health
and social service agencies together to respond to community issues and to work with the community on
projects which will have a positive impact on the local area.
HUCHS CHWs met with a local lawyer who specialises in Family Law, CYFS and Domestic Violence. He is
interested in running clinics at Petone and Pomare Clinics for people from the local communities who need
assistance with anything to do with family law. CHWs recognise that our communities do not always have easy
access to a service like this, so bringing it to our community provides access and builds positive relationships and
trust.
Whai Oranga CHWs have five families using the community garden, with a bumper crop this year of vegetables
varying from corn, potatoes, rhubarb, bok choy, carrots, beans, tomatoes, strawberries, broccoli, zucchini, salad
greens, herbs, chives, parsley and celery. It has been particularly exciting for one family as this is their first ever
attempt to grow vegetables, facilitated by a ‘one on one’ education session, including planting, with the CHW.
Another family with a garden bed have been garden volunteers since the very beginning of the project. They
have helped on all working bees, planting sessions and general tidy up chores. The youngest member of this
family - a 10 year old boy – is showing a keen interest in gardening. He is able to explain and demonstrate to his
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
115

45 | P a g e
siblings the planting process and the best way and time of day to water plants, and to describe the different
materials needed for composting. He credits his knowledge to time spent with CHWs in the garden.
The CHW has also utilised opportune moments via organising a seedling workshop with a group of youth, which
was a great success. They were shown how to plant seeds by recycling and reusing everyday containers like egg
cartons, yogurt and butter containers. The CHW also organised an informative organic gardening education
session with a kuia, who shared a wealth of knowledge that has been instilled in her from birth.
Following Whai Oranga’s Smoke Free Cars Campaign launch in February, there has been another study to 'count'
the smokers in cars. This count found that just under six months after the launch and after counting over 5700
vehicles, smoking in cars in Wainuiomata decreased from 11% to 6%. This is a great result, and comes from being
out in the community and helping to make small but significant changes to the local smoking culture. The CHWs
invested time preparing for a day to celebrate this success. Plans are now in place to help those still smoking in
cars (the 6%) to change, to give the tamariki a better start to life, and to give the matua longer and better quality
lives.
This year’s local White Ribbon Day (WRD) was attended by the WRD Chairperson, Judge Peter Boshier. WRD is
a great way to reinforce the messages that “Family Violence Is Not OK” and it was great to hear what was being
done in our communities to keep families safe. There were speeches from Dr Mathew Shaw who is part of the
Family Violence Death Review Committee, and a performance by youth group, Taiohi Morehu, who deliver
messages around family violence through dance, drama and kapahaka.
The team have been assisting DHB and RPH staff with appointments to key positions. The Outreach Team Leader
assisted HVDHB’s Māori Health Advisor with interviews for their new Family Support Coordinator - Acute role.
A HUCHS CHW was asked to be part of the interview panel for Regional Public Health’s new Public Health Advisor
- Community Liaison role. HVDHB and RPH recognise our team’s knowledge of the community and value our
input into how potential candidates will fit into their respective roles and ensure appointees have the right skills
and fit within a community setting.
SERVICES PROVIDED
Over the reporting period July to December 2013, the CHWs carried an average caseload of 134 patients each
month.
Provider Caseload / Unique Patients
Jul to Dec 13
Average Patients per month
Te Awakairangi Health Network 151 63
HUCHS 182 40
Whai Oranga 137 46
Service Wide 470 134
The following graph outlines the caseload of unique patients each month in the July to December 2013 period.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
116

46 | P a g e
For the patients cared for in the reporting period, 54% were Maori, and 25% were Pacific. Most patients seen
were Quintile 5 (53%) or Quintile 4 (29%), with the remaining patients (18%) spread across Quintiles 1to 3.
In the July to December 2013 period, the virtual team of CHWs provided a total of 1,562 patient contacts, and
5,140 services to patients. The lower numbers in September and December were due to a couple of members
from the team requiring extended leave, and the resignation of one CHW and the recruitment of a new CHW in
December.
Provider Patient Contacts
Jul to Dec 13
Services (includes advocacy)
Jul to Dec 13
Te Awakairangi Health Network 989 3151
HUCHS 307 769
Whai Oranga 266 1220
Service Wide 1562 5140
6165
48
7165
70
36
47
19 2129 32
54
38
17
48 51
29
0
10
20
30
40
50
60
70
80
July August September October November December
Caseload / Unique Patients
TeAHN Whai Oranga O Te Iwi HUCHS
Māori 54%
Pacific25%
Other21%
Ethnicity Service Wide1 Jul to Dec 13
Q13% Q
Q311%
Q429%
Q553%
unknown
0%
Quintile Service Wide1 Jul to 31 Dec 13
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
117

47 | P a g e
The following table shows the number of advocacy services undertaken with specific organisations this reporting
period, with the majority of outreach activities involving advocacy alongside primary and secondary care
practitioners, and Work and Income staff.
The graph below breaks down the various services provided to patients who accessed the service. Phone calls,
home based visits, education and support, contacting other agencies, and referring on to other services were
the five most frequent services provided this reporting period.
291 263168
287 327226
1002867
592
819
1130
730
0
200
400
600
800
1000
1200
Jul Aug Sep Oct Nov Dec
Volume of Work Service Wide1 Jul to 31 Dec 2013
Patient Contacts Services Provided
Advocacy Services TeAHN HUCHS Whai Oranga O Te Iwi
Service Wide
Government Organisations 48 0 0 48
Housing NZ 15 30 5 50
NGO (Non-Government Organisations) 71 21 5 97
Other Advocacy 102 28 38 168
Primary Care 84 62 74 220
Secondary Care 56 76 34 166
Work and Income 100 40 31 171
Service Wide 477 257 187 920
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
118

48 | P a g e
KEY ISSUES AND RISKS
As the new welfare reforms are implemented, the impact of the new Work and Income processes has become
more apparent. Many of the CHW clients need education on the changes and the implications for them.
The cost of prescription co-payments (the $5 per item charge) continues to be an issue for many patients. This
is particularly evident every February, when the counting of prescription numbers starts again, as many families
struggle to find the $100 needed before the cap comes into play.
BRIEF INTERVENTION 1
A client rings, as she needs to sort some business out with Work and Income and also tend to some personal
issues. She is unable to get a caregiver in to look after her husband who is currently having cancer treatments
and is unable to leave him alone. CHW assists by looking after husband while she tends to her business. Client is
grateful for help as she would have had to rebook her appointments which would have meant a week or two
wait.
BRIEF INTERVENTION 2
A female patient who suffers from multiple health issues and is on an Invalids Benefit made contact with the
CHW seeking help to get a food parcel. She did not have enough money left over after bills to buy enough food
for her and her two children. After a discussion with this patient, she disclosed to the CHW that she had not
picked up her prescription either, due to not having enough money.
The CHW identified that it was a priority for patient to get her medication due to severe health conditions. The
CHW had to find a way to fund the patient’s prescription. She spoke to one of TeAHN’s Outreach Nurses, who
was able to access the Packages of Care funding to pay this prescription charge.
24 31 55 59 72 75 97136 149 151 166
289
647
858
1186
0
200
400
600
800
1000
1200
1400Fa
xes
Wh
anau
/Aig
a M
eeti
ng
Emai
ls
Lett
ers
Inte
rpre
tin
g
Pat
ien
t V
isit
- P
ract
ice
Tran
spo
rt P
rovi
ded
(n
ot
WFA
)
Pat
ien
t V
isit
- O
ther
Ven
ue
Cu
ltu
ral S
up
po
rt
Text
Mes
sage
s
Int/
Ext
Ref
err
als
Co
nta
ct O
ther
Age
ncy
Edu
cati
on
an
d S
up
po
rt
Pat
ien
t V
isit
- H
om
e
Ph
on
e C
alls
Services Provided This Period1 Jul to 31 Dec 13
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
119

49 | P a g e
CHW then organised a food parcel. She is now working with the Outreach Nurse to support this patient and her
kids to get a budget sorted. She is investigating whether this patient is entitled to a Work and Income Disability
Allowance that can help cover the costs of medication.
CASE MANAGEMENT 1
Client
A referral was received from a GP at Stokes Valley Medical Centre for an inpatient at Te Whare Ahuru. Support
and advocacy were required to assist the client upon discharge.
CHW Assessment and Role
There was a delay in gaining first contact, due to the client’s suicide attempts and lack of response to the initial
contacts. First home visit was made at the client’s mother’s home, where the client was visiting. The CHW was
advised that the client had Te Paepae Arahi already assisting her, so the CHW gained consent to meet with her
support person from Te Paepae Arahi to ensure we would not be doubling up on resources. At the meeting, it
was discovered that the client had a great deal of support already in place, and was going to be provided ongoing
support through supported living arrangements.
The CHW identified that much more support was needed, though, for the client’s children and their
grandmother. All the children were living with their grandmother in her overcrowded 2-bedroom flat. She had
no support or assistance for the care she was giving to the children, and her own health issues were escalating
due to all the stress. All family members were aware of the suicide attempts, with two of the teenage children
experiencing their own issues resulting in truancy, angry behaviour and ongoing issues at school and at home.
The client was spending some time with her mother and her children. However, because she was heavily
medicated, she was unable to deal with her own, her children’s or her family’s issues. This then created more
work and stress for the grandmother. The doctors, the school and the grandmother had also identified that the
children were feeling responsible for their mother’s ongoing mental health illness.
Actions
Once the support person at Te Paepae Arahi gained the grandmother’s consent to refer to our service, the CHW
talked to the grandmother about getting Strengthening Families on board to provide a coordinated response
and ensure ongoing wraparound supports were put in place for the whole whānau.
The referral for Strengthening Families was then completed and accepted, with the following issues and
concerns needing to be addressed:
Parenting
Child Management
Child/Young person’s literacy/numeracy
Behaviour at school
Stand down/suspension
Housing issues
Benefit entitlement
Accommodation for whānau as grandmother’s flat was overcrowded.
Health
Parents/Caregivers physical health/disability
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
120

50 | P a g e
Young person mental health
Safety/Justice
Child’s behaviour
Young Person’s behaviour
Concerns
Children taking on the parenting role
Children’s safety (i.e. possible additional guardianship needed)
Service Input:
Number of visits to the client (mother): 14
Number of phone contact to client (mother): 13
Number of visits to the client (grandmother): 9
Number of phone calls to the client (grandmother): 5
Number of contacts and phone calls to organisations: 37
Number of referrals: 2 (Strengthening Families and Grandparents Raising Grandchildren)
Number of liaisons with alternate service: 28
Providers Involved:
General Practice staff
Work and Income
Housing NZ
X3 Schools
Strengthening Families
Birthright
Community Mental Health
Te Paepae Arahi
Grandparents Raising Grandchildren
Outcomes:
The mother of the 3 children is now taking an active role in her children’s lives. Housing NZ has placed the family
on a priority list for a 3 bedroom home just around the corner from the grandmother. The home will be allocated
to the mother, and resources have been provided for the mother to set up her new home. The two older children
will live with their mother in the new home, and the youngest will stay living with the grandmother. There will
be no overcrowding.
Ongoing appropriate supports are now in place for individual family members, and all Work and Income
entitlements are in place. Support for the grandmother is now in place and her health is improving.
The mother and grandmother have a coordinated approach with all the schools to monitor the children and
assist where needed. The schools are looking at ongoing options for the children. The children are more settled
at school and at home, and are all excited with the new plans.
The above work has been achieved in only 2½ months, and with the family having appropriate ongoing supports
in place, they have been discharged from the CHW service.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
121

51 | P a g e
CASE MANAGEMENT 2
Client
A referral was received from an independent Pacific consultant working in Pacific communities. She made a
phone call to one of our CHWs, regarding a 40 year old Samoan sole-parent father of two sons aged 13 and 15
years. Their mother had moved away and left the family in crisis. The father was about to lose his job, Housing
NZ were looking at terminating his tenancy, Inland Revenue had sent him a $3,000 debt notice, and his estranged
wife was still claiming for child support despite the children now being in his care.
CHW Assessment and Role
Provision of transportation and advocacy to a Housing NZ mediation meeting, where the CHW
successfully negotiated maintaining the client’s tenancy. A payment plan was put in place at $70 per
week for debt.
CHW arranged a Work and Income appointment were they approved a $150 food grant for some
much needed groceries for the aiga.
CHW organised a meeting with the client’s work supervisor to update them on his circumstances,
including being overwhelmed with personal issues which were preventing him from working and
making contact with them. The meeting was held at his place of work, with his boss proving very
supportive of his situation.
After numerous phone calls to Inland Revenue and assisting the client to fill out various forms, the
$3,000 debt was waived.
As English is the client’s second language, all communication to various departments involved were
arranged and translated by the CHW in the client’s presence.
Service Input
Number of home visits to client: 13
Number of liaisons with other professionals: 25
Number of transports provided to appointments: 4 (Housing NZ, Work and Income, Inland Revenue
and the patient’s place of employment)
Outcomes
A great deal of encouragement and empowerment based work was used for the client to gain the confidence
needed to move forward. He is now back at work and his arrears with Housing NZ have been paid in full.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
122

52 | P a g e
PRIMARY MENTAL HEALTH
The Primary Mental Health Service aims to improve health outcomes for people with a mild to moderate mental
illness and addictions. The primary mental health incorporates two Te Awakairangi Health Network (TeAHN)
providers (Wellbeing Service and Hutt Union and Community Health Service (HUCHS)) as well as Vibe (for youth)
and the Lower Hutt Women’s Centre, which offers groups and support for women.
TARGET GROUPS
People aged 13 and older affected by a mild to moderate mental illness or addictions. People who are Maori,
Pacific, from Quintile 5 areas or aged under 25 years are prioritised in accordance with the 2013-14 service
specifications. Referrals are also accepted where there is evidence of barriers to accessing suitable services,
such as low income and a Community Services Card. Where low income people who do not fall within these
groups are referred, they may be assisted to access alternative low cost services or accepted for services
depending on the referred person’s needs and resources and the capacity of the primary mental health service.
KEY ACTIVITIES
Assessment, brief talk therapy, information and resources, support, monitoring and group programmes are
available for clients while practice staff are supported to assist in their work with people affected by mental
illness and addictions.
The Wellbeing Service’s centralised multidisciplinary mental health team in Lower Hutt serves most TeAHN
practices plus Ropata Medical Centre. Wellbeing outreach clinics are available in Upper Hutt and Wainuiomata.
Whai Oranga O Te Iwi Medical Centre hosts the Wainuiomata clinics; these are available for all Wainuiomata
residents. In November, TeAHN also began offering appointments in Stokes Valley hosted by Koraunui Marae at
its Tui Glen School clinic. HUCHS embedded services are available for HUCHS enrolled patients. Vibe’s services
are primarily available at its Lower Hutt and Upper Hutt sites with some nurse appointments offered via Vibe’s
school clinics.
ACHIEVEMENTS
Delivering high quality primary mental health assessment, therapies and supports to referred clients and their
families/whanau continued to be the focus. Data showing referral numbers and characteristics, and services
provided, is presented later in this section.
Following feedback from a TAS audit earlier in 2013, a comprehensive informed consent form has been
introduced and processes for recording informed consent have been improved.
The team strengthened its capacity to work effectively with Maori and with people affected by addictions
through recruitment of two part–time staff with specific skills and experience in these respective areas, and by
contracting a DAPAANZ registered counsellor who had previously worked with Whai Oranga O Te Iwi Health
Centre.
The new premises for the Wellbeing Service’s Upper Hutt clinics secured in late June became operational in July.
Having sole use of these premises has enabled the Wellbeing Service to increase its Upper Hutt presence from
three to four days per week.
Through an agreement reached with Whai Oranga O Te Iwi Health Centre, the Wellbeing Service also took over
responsibility for delivery of primary mental health service to the Health Centre’s enrolled patients and through
agreement with Whai Oranga. The existing DAPAANZ counsellor was contracted to continue working one a day
per week, and a Wellbeing Service nurse has been based in the medical centre half a day a week for most of the
reporting period. Appointments from these Wainuiomata premises are now available to all residents of
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
123

53 | P a g e
Wainuiomata. Establishing the service in Wainuiomata has improved access to primary mental health services
for people who faced transport barriers and cost barriers in getting to a Central Hutt location for appointments.
In November, a pilot clinic started operating in Stokes Valley. This was made possible through strengthening
our links with staff at Koraunui Marae who host our clinics in the Tui Glen School clinic rooms. The clinic itself is
in its early stages of establishment; however an immediate positive outcome has been regular opportunities to
link with Koraunui in ongoing collaboration regarding shared clients, community needs and increase mutual
understanding of what each agency can offer.
The July to December 2013 reporting period was marked by a higher than average rate of suspected suicides in
the Hutt Valley area through winter and spring. More intensive suicide prevention efforts were activated by
Regional Public Health and primary mental health representatives became core postvention group members
along with the police, DHB mental health services, city council and Koraunui Marae (as a small cluster of deaths
were in the Stokes Valley area). Key outcomes to date have been strengthening relationships among agencies,
and educating community representatives about agency roles and key suicide prevention messages which can
then be disseminated more widely into the community. Representatives from the Wellbeing team and our
primary mental health partner Vibe took part in a panel answering questions about suicide and access to support
services at a Stokes Valley Community meeting at Koraunui Marae in October.
In October 2013, practices were encouraged to promote Mental Health Awareness week and promotional
materials were provided to assist with this. The Wellbeing Service also partnered with the Health Promotion
team to hold a Mental Health Awareness day at WelTech, promoting the theme of building connections with
others as one way to build resilience and encourage positive mental health.
CLIENT NUMBERS AND NEW REFERRALS
The table below shows total client numbers and new referral numbers for each provider agency and totalled for
the primary mental health service as a whole. Figures from the previous six months are provided for comparison,
where available. Wellbeing figures include Whai Oranga numbers for both periods.
Overall service users decreased by 7% and referral numbers by 10% in the Jul to Dec 2013 period, when
compared to the previous six months, with variability between the providers. The reduction at TeAHN is an
expected result of the Wellbeing Service continuing to communicate with practices about referral criteria and
priority groups over the year. Non-priority group referrals have steadily reduced, except those with evidence of
other barriers to accessing services, such as a low income qualifying for a Community Services Card. The
144
612
88
244
1088
150
519
110229
1008
0
200
400
600
800
1000
1200
HUCHS WellbeingServiceTeAHN
and WhaiOranga
Vibe Lower HuttWomen's
Centre
ServiceWide
Unique Service Users
Jan to Jun 13 Jul to Dec 13
55
457
49148
709
75
387
58118
638
0
200
400
600
800
HUCHS WellbeingService
TeAHN andWhai
Oranga
Vibe Lower HuttWomen's
Centre
ServiceWide
New Referrals
Jan to Jun 13 Jul to Dec 13
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
124

54 | P a g e
reduction in inappropriate referrals has reduced the workload involved with the intake process, freeing up
clinical time for client support and therapy.
Referrals are broken down by practice below.
New Referrals
Referral Practice Jan to Jun 13 Jul to Dec 13
Avalon Medical Centre 8 4
Dr Dunns Surgery 6 6
Dr Hans Snoek 12 5
Epuni Medical Centre 10 5
Fergusson Drive Surgery 7 3
Fitzherbert Road Medical 2 4
Gain Health Centre 7 12
HUCHS - Petone 2 2
HUCHS - Pomare 58 75
Hutt City Health Centre (incl. Wainuiomata site) 50 26
Kopata Medical Centre 26 22
Main Street Surgery 7 4
Manuka 4 3
Muritai Health Centre 11 7
Naenae Medical Centre 46 27
Petone Medical Centre 17 18
Pretoria St 10 5
Ropata Medical Centre 69 43
Silverstream Medical Centre 31 15
Soma Medical Centre 5 11
Stokes Valley Medical Centre 43 38
Taita Medical Centre 2 1
Upper Hutt Health Centre 44 54
Vibe Youth Health Service 47 54
Waiwhetu Medical Centre 8 22
Whai Oranga Health Centre 27 46
Unknown 2 1
SERVICE WIDE 561 513
After a significant rise in Maori accessing the Wellbeing Service since July-December 2012 the percentage has
remained consistent at 23% for the last 12 months. 41% of HUCHS and 28% of Vibe’s service users identified as
Maori, with13% at the Lower Hutt Women’s Centre. Primary mental health service specifications for 2013/14
include young people under 25 years of age as a priority target group. This age group made up just over 30% of
all service users, including all from Vibe, 29% of those accessing the Wellbeing Service, 18% from HUCHS and 9%
using the Lower Hutt Women’s Centre. A more detailed breakdown by ethnicity and age are provided in the
figures below:
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
125

55 | P a g e
Of those who accessed the Wellbeing Service, HUCHS or Vibe, 76% of those referred or accessing primary mental
health care met priority access criteria (Maori, Pacific, Q5 or 13-24 years of age). Lower Hutt Women’s Centre
data is not included as quintile is not available.
SERVICES PROVIDED
The table below shows a summary of services and contacts across the primary mental health service for the
current reporting period. From July to December 2013, there were 1930 scheduled (including DNAs) and
unscheduled client sessions and face-to-face contacts via the Wellbeing Service, Vibe and HUCHS, compared to
2291 for the previous six months. Average number of sessions per client varied between 2.2 and 5.3 depending
upon provider agency. There were 1645 attendances at Lower Hutt Women’s Centre for group programmes
and individual support in the current reporting period, compared with 1546 in the previous six months. Overall
sessions and contacts were slightly higher (6343) than in the previous period (6171) however the Wellbeing
figures in particular included increased missed appointments and phone contacts. A detailed breakdown by
service and contact type will be provided in the Primary Mental Health Service six monthly report to the DHB in
February 2014.
Service Wide Total: 6343 Jul to Dec 13
Sessions (incl. DNAs and rescheduled)
1930
Intake Screening 282
Phone calls 1832
Letters 573
Referrals Made 55
Other Meetings 26
LHWC Group Session Attendances 993
LHWC Drop In & individual support 652
Māori, 24.0%
Pacific, 5.0%Other,
72.0%
Ethnicity of All Service UsersJul to Dec 13
0 to 11yrs0.2%
12 to 19yrs14.5%
20 to 24yrs16.0%
25 to 44yrs35.3%
45 to 64yrs28.2%
65+5.6%
unknown0.3%
Age Groups of All Service UsersJul to Dec 13
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
126

56 | P a g e
KEY ISSUES AND RISKS
The Wellbeing Service has worked to become increasingly targeted on priority referral groups over the last 12
months. There have been positive outcomes for many people as a result of having their mental health needs
addressed. However there have also been challenges in establishing contact, impacts on volumes of contacts
and an increase in DNA rates particularly for those with multiple stresses and more chaotic lives. For example,
the Wellbeing Service received 70 referrals in this period where no contact could be established with the client,
compared with 46 in the previous six months. The situation is being monitored and we are proactively working
to reduce barriers to higher needs clients. Included here are now being able to offer a choice of part-time
therapists who identify as Maori and Pacific; increasing capacity to work with those with addictions through
employing and contracting appropriately qualified and experienced clinicians; offering appointments in
Wainuiomata and Stokes Valley, and increasing to four days per week in Upper Hutt; increased capacity for home
visits. We continue to work closely with other TeAHN teams and have strengthened our relationship with
Koraunui Marae’s social services.
Work is currently underway within the DHBS on developing a 3DHB Mental Health and Addictions Strategic
Framework for the Wellington Region. It is expected that the resulting strategic framework will inform the
2014/15 Primary Mental Health Service Specifications. The Wellbeing team leader has represented Te
Awakairangi Health Network at two workshops which sought provider and consumer views and ideas on what
services should incorporate and potential models that could form the basis for the framework. A separate
process began in December with regard to youth health including youth mental health, with TeAHN and Vibe
representatives included.
In December Hutt Inc. approved a collaborative project between the Hutt DHB Mental Health Directorate and
TeAHN that aims to smooth transitions and improve outcomes for adolescents and adults discharged form DHB
mental health services to primary care. Scoping and project planning is expected to begin shortly.
CASE STUDY: MR A
A Wellbeing Service mental health nurse first saw Mr A. two years ago when he was referred by his GP for help
with his health anxiety and panic attacks. Mr A had used mental health services extensively in the past but for
many years his condition had been reasonably well controlled under the watchful eye of his GP. However Mr A
finds it hard to cope with stress and is particularly vulnerable when his wife’s own much less stable mental health
deteriorates significantly. When she has an admission to hospital or other crisis intervention Mr A is left at home
alone. He gets worrying chest pains triggering calls to the ambulance and visits to the emergency department.
He feels overwhelmed by concerns about his wide, his own health and feels unsupported despite reassurances
that he is physically ok.
Using a cognitive behavioural therapy approach the Wellbeing Service nurse helped Mr A understand the links
between his thoughts about stressful situations, his emotions, physical sensations and behaviour. They tracked
his cycle of the anxiety and Mr A learned to take a different perspective on his symptom, such as considering
the probability that his chest pain might be a heart attack pain, indigestion or anxiety-related. He developed
more helpful ways of responding to the sensations he experienced. Mr A formed a good rapport with the nurse
and found the sessions helpful. When he’d felt back in control of his anxiety and his life for some time he was
discharged.
Mr A self- referred back to the Wellbeing Service a year later after another very stressful time triggered by his
wife’s health. This led to an increase in calls to the ambulance and visits to ED again. Fortunately the same
nurse was able to see him again. First they revised the CBT work to ensure Mr A remembered what he’d learned
and he began to use the strategies that he remembered had helped. Then they wrote down his typical cycle and
a management plan in a way that made sense to Mr A. This included what helps, what doesn’t and steps to try
himself before deceiding if he needs to call an ambulance, seek extra help or support. He keeps copies on his
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
127

57 | P a g e
fridge and in his wallet to be an ongoing reminder to himself, for times when he finds it hard to recall what to
do. Mr A and the nurse also shared the plan with his GP, practice nurse, ambulance service and emergency
department.
Mr A has found writing and sharing the plan validating and empowering. Feedback from other services is that
the plan is helpful for them too. Everyone understands the cycle better, so can remind him of what might help
and reinforce him in a consistant and respectful way. Mr A also finds his pain and suffering is decreasing as he
feels more in control and able to cope.
Even though his wife’s health remains of concern Mr A. is happy he doesn’t need to go to ED as frequently. He
hasn’t needed further appointments with the Wellbeing Service nurse but has been offered phone support as
he gains confidence to implement the plan for himself. Time on these calls is reducing and the emphasis is on
celebrating Mr A’s anxiety management successes.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
128

58 | P a g e
HEALTH PROMOTION
The health promotion team aims to develop and implement a range of health promotion initiatives to support
individuals, families and target populations to stay healthy and well. The initiatives emphasise healthy eating,
physical activity, being smokefree, and overall wellbeing, as well as encouraging people to get health checks.
The main programmes include:
Cardiovascular disease health promotion
Good Food Programme
Community health promotion events and presentations
Polyfest / Pacific Wellbeing Day
Communications and Media
Health 4 Life Project
Pasifika Choice Project
Support Groups including Valley Fit Programme
Pacific Healthy Lifestyle Programme
Provision of the Healthy Families Coach Service
CARDIOVASCULAR DISEASE HEALTH PROMOTION
The health promotion team has worked closely with the clinical facilitation team over the past 6 months on
raising the profile of cardiovascular risk assessments and heart health. See the Cardiovascular Risk Assessment
section of the report for information about the various community and practice based activities.
GOOD FOOD PROGRAMME
Three Good Food Programmes have been completed over this reporting period. The four week programmes
were run at the Te Aroha Complex in Waiwhetu (as part of the training programme for the Te Awakairangi
TRYathlon), at Orongomai Marae and at Trentham Community House. All three programmes were popular and
well attended with an average of 13 people per session.
Evaluation of the programme indicates that attending the
programme results in participants reporting increased
confidence and knowledge around preparing healthy meals for
their family. Evaluation also shows that participants report
increased understanding of key nutrition concepts such as
understanding of fat, fibre, salt and sugar in their diet and how
these impact on
our bodies.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
129

59 | P a g e
COMMUNITY HEALTH PROMOTION EVENTS AND PRESENTATIONS
TE AWAKAIRANGI TRYATHLON
The Te Awakairangi TRYathlon was held in September 2013. The event is aimed at encouraging inactive people
to ‘get off the couch’ and was completed by 100 people. The TeAHN health promotion team supported event
organisers (Te Aroha Trust) by facilitating weekly morning training sessions, supporting promotion and
enrolment, offering the Valley Fit Naenae and Wainuiomata sessions to participants, facilitating the Tane Hauora
Health evening and running a 4-week Good Food nutrition programme to complement the physical training.
GAMBLE FREE DAY
The team represented TeAHN at the Gamble Free Day celebrations (run by the Health Promotion Agency) at
Walter Nash Stadium in September.
STROKE AWARENESS WEEK
TeAHN worked with Rotary and Stroke Foundation to set up a
blood pressure testing stall at the Saturday River Bank Markets in
October. Over 200 people were tested over the morning. Thirty-
eight of those tested had stage 2 hypertension (blood pressure of
160+/100+). These patients were encouraged to contact their
general practices for an appointment, and TeAHN also passed
their names back to their general practice for follow-up.
WAHINE ORA DAY
TeAHN partnered with Mana Wahine and Regional Screening Service to run a Wahine Ora Breast and Cervical
Screening event in October. The event involved identifying Maori and Pacific women who were overdue for
Breast and Cervical screening and inviting them to take part in a Saturday Screening Day. Transport was provided
for those who required it. The successful event screened 22 women for mammograms and 13 for cervical
screening. A further 24 women made appointments to be screened on another day. There was only one DNA on
the day.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
130

60 | P a g e
HEALTHY LUNCH PROMOTION TRENTHAM SCHOOL
The health promotion team worked with Trentham School on a
healthy lunch promotion in November. The entire school was
focusing on healthy eating and completing a number of activities to
increase healthy lunches. Health promotion team members attended
‘Sandwich Day’ where each class made a salad sandwich and took
part in other activities such as Jump Rope for Heart.
WORKPLACE WELLNESS FORUM
TeAHN attended the Workplace Wellness Forum run by Health
Promotion Agency and Regional Public Health in November. The
forum was well attended by many Wellington and Hutt Valley
workplaces. Attending the event was a great opportunity to link with
local employers and explore ways that TeAHN could support their
workplace heath initiatives.
KAUMATUA DAY
The health promotion team attended the annual Kaumatua Health Day organised by Kokiri Health and Social
services at Wainuiomata Marae. The team focused on educating kaumatua about healthy eating.
MENTAL HEALTH AWARENSS WEEK AT WELTEC
CAMPUS
The health promotion and wellbeing teams set up a
‘Winning Ways to Wellbeing’ stall at Weltec to mark
Mental Health Awareness Week. Hundreds of staff and
students engaged in conversations about positive
mental health and were invited to spin the ‘Wellbeing
Wheel’ to win prizes donated by local cafes.
NAENAE FESTIVAL
Members from several TeAHN teams partnered with
the Pacific Health Service staff to promote heart checks and other services at the Naenae Festival in November.
RIMUTAKA PRISON HEALTH EXPO
The health promotion team attended the Rimutaka Staff Health Expo in December. TeAHN provided a healthy
lunch option for staff and spent the day talking about healthy lifestyles and performing blood pressure checks.
PUBLIC HEALTH CONFERENCE
Two members of the health promotion team presented at the Public Health Conference in Taranaki in
September. The presentation about TeAHN’s work on community based CVD risk testing was well received.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
131

61 | P a g e
POLYFEST/ PACIFIC WELLBEING DAY
The health promotion team
supported local primary and
intermediate schools to run a
Polynesian festival over two
evenings in July. TeAHN provided
financial support, and influenced
the event to ensure it was
promoted health messages such
as fizzyfree and smokefree. Over
the two evenings, TeAHN staff
talked to parents/audience prior
to the performances about
healthy snacks for children. Our
staff also provided free Heart
Health Check vouchers to people who meet the criteria.
COMMUNICATIONS AND MEDIA
The health promotion team is playing a key role in the development of the TeAHN communication plan which
aims to increase awareness of TeAHN and its services, celebrate organisational success and increase access to
healthy lifestyle messages and services.
HEALTHY MESSAGING ON ATIAWA TOA FM
The health promotion team has been increasing its presence on the local iwi radio Atiawa Toa FM. The team
worked with Vibe to script and record two advertisements on heart checks and youth mental health which have
featured regularly on the radio over recent months.
Planning has been completed for a six month health promotion programme which will run from January to June
2014. Each month will feature two health themes which will be profiled via advertisements and interviews.
FACEBOOK PAGE
TeAHN has launched its Facebook page which aims to increase awareness and access to healthy lifestyle services
and events in the Hutt Valley.
HEALTH 4 LIFE
Health 4 Life is a joint project by Regional Public Health (RPH), Service Integration and Development Unit (SIDU)
of Capital and Coast DHB, Hutt Valley DHB and Wairarapa DHB; Te Awakairangi Health Network; and Compass
Health.
This project is one of seven projects the Ministry of Health has funded to focus on improving nutrition and
physical activity in the pre-school population starting in pregnancy.
Health 4 Life is an early intervention programme that requires participation across a wide range of providers
who deliver services to women during pregnancy and infants in their first year of life.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
132

62 | P a g e
The aim of this project is to improve the quality and uptake of nutrition and physical activity advice given to
pregnant women, mothers of infants in the first year of life and their whanau. This will be achieved through the
development and delivery of simple common messages on maternal and child nutrition and physical activity.
The project is currently in development stage with several members of TeAHN’s health promotion and dietitian
teams contributing to the project working groups, and TeAHN senior management participating in project
governance.
PASIFIKA CHOICE
Pasifika Choice is a joint project by TeAHN, Pacific Health Services and Family Centre. Pasifika Choice is an early
intervention programme that will work with Pacific children and their families to lay the foundations for healthy
lives. This project is one of several projects the Ministry of Health has funded through the Pacific Innovation
Fund to focus on reducing the prevalence of risk factors affecting Pacific people’s health.
The project is currently in development stage. TeAHN’s Candice Apelu has been seconded to Pacific Health
Service to provide project management, and the project is also supported by the health promotion team.
SUPPORT GROUPS
MĀORI PACIFIC HEALTH SUPPORT GROUP
The Valley Health Support Group held three final meetings over July, August and September. Meetings were
attended by members of the outreach and wellbeing teams who discussed various health issues. The Group has
since been discontinued while the health promotion team works with other network staff to evaluate the
group’s format and to explore how resources may be better utilised to help more patients with, or at risk of
developing chronic disease. It is hoped that by working with practice staff and by aligning more closely with
existing primary care programmes such as Heart and Diabetes checks that we can develop a programme which
meets the education needs of patients and practices.
REGIONAL WELLINGTON DIABETES SUPPORT GROUPS
Coordination support continues for the Upper Hutt, Lower Hutt and Wainuiomata Diabetes groups. Activities
arranged for these groups in the last six months included:
Dietitian presentation
Optometrist presentation
Communication and education about new Diabetes meters
Late in 2013, the health promotion team worked with Sport Wellington to submit a Request for Proposal to
provide innovative Green Prescription (GRX) services to diabetic and pre-diabetic patients. If successful, the
team will work with Sport Wellington and targeted practices to deliver group education to patients newly
diagnosed with diabetes or pre-diabetes.
VALLEY FIT
The Healthy Families Coaches continue to run group exercise classes at Naenae Leisure Active Fitness Suite
(twice a week) and in Wainuiomata Way of Life gym (once a week). Valley Fit supports people who are
overweight and who do not feel comfortable working out in the gym on their own.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
133

63 | P a g e
Sessions are well attended. Over the past six month period the Naenae group has been attended 345 times by
38 individuals and the Wainuiomata class has been attended 115 times by 20 people.
TeAHN is in the process of expanding the Valley Fit exercise class to Upper Hutt. We expect to run the group in
collaboration with Sport Wellington with the support of Activation Upper Hutt. Planning is currently underway
with a venue provider and we plan to get this class underway in February 2014.
In December Valley Fit members from the Wainuiomata and Naenae groups completed the TeAHN TRYnui
triathlon. The event is an annual event for the Valley Fit attendees designed by the Healthy Families Coaches to
be a challenging yet achievable goal for the group. This year 15 people participated.
CONNECTIONS NETWORKS AND FORUMS
The health promotion team collaborates with many other agencies and organisations and regularly attends the
relevant meetings. Of particular note this reporting period has been strengthened relationships with the Health
Promotion Agency, Te Aroha Trust, Trentham Community House, Pacific Health Service, Koraunui School,
Trentham School, Vibe, Sport Wellington, Heart Foundation, Regional Screening Services, Upper Hutt City
Council, Arthritis Foundation, Otago University, Regional Public Health and Quitline.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
134

64 | P a g e
The health promotion team participates in a number of networks including Workplace Health and Wellness
Stakeholder Group, Regional Screening Coordination Group, Wellington Nutrition and Physical Activity Network,
Wellington Regional Smokefree Network, Primary Care Tobacco Teleconference and the Regional Smokefree
Hui.
Members of the Health Promotion team sit on steering groups for the Health 4 Life, Pasifika Choice and Alive
(Upper Hutt physical activity initiative) projects.
PRACTICE EDUCATION AND CONNECTIONS
Increasing practice connections is one of the team’s key goals over 2013/14. Currently each TeAHN practice is
visited by the healthy families coach or dietitians every six weeks.
The dietitian and healthy family coach team presented to practice nurses as part of the CVD education
programme. The talk focused on improving the nutrition and physical activity component of the CVD education
sessions.
PACIFIC HEALTHY LIFESTYLES PROGRAMME
This programme is facilitated and delivered by Pacific Health Service Hutt Valley based in Naenae and is open to
everyone in the Hutt Valley. It delivers healthy
lifestyle activities that are responsive and
accessible to the Pacific communities.
KEY ACTIVITIES
Daily Pasifika style aerobic exercise at Naenae
Community Hall. (Zumba, Contra-band,
Pacific style aerobics), with six-weekly Health
Education Group Sessions run in conjunction
with the exercise programme.
ACHIEVEMENTS IN JUNE TO DECEMBER
2013 PERIOD
31 New clients joined the programme during the period
120 1 hour exercise sessions
50 average attendants per day
Hosted 10 health education sessions were well attended by an average of 25 participants per
session
20% increase in number of completed health screening
Increase in middle aged participants.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
135

65 | P a g e
ETHNICITY BREAKDOWN
DIETITIANS
The Dietitians work alongside patients, health professionals, individuals, families and communities to provide
tailored interventions to resolve nutrition problems with the purpose of supporting lifestyle change and
preventing chronic illness.
ACHIEVEMENTS
The Dietitian service has been able to strengthen links with the Maori community through our Maori Dietitian.
Her ability to speak Te Reo has increased engagement with Kaumatua groups at Kokiri and Wainuiomata marae
and with individual patients. The Maori Dietitian and Healthy Family Coach ran a successful healthy lifestyle
session with a traditionally hard to reach group of Maori males. The group was respectful and very appreciative
of the interactive talk where they asked about artificial sweeteners, alcohol and carbohydrates.
One of the Dietitians contributed to research by the Health Promotion Agency to develop five behavioural
profiles for low income Maori, Pacific and NZ European families so that attitudes, needs and characteristics of
these audiences can be understood. This has a close synergy with the Health 4 Life project which has enabled
the Dietitians to provide input into nutrition and physical activity messaging for pre-pregnant, pregnant and
lactating mothers and infants in their first year of life.
In the July to December 2013 period, the Dietitian Service experienced an 18 percent reduction in DNAs when
compared to the January to June period. This can mainly be attributed to the text-to-remind messages that are
sent to patients the day before their appointment.
83%
6%
3%
1%1%
5%
1%
Ethnicity of attendees at Pacific Healthy Lifestyle Programme
Pacific
European
African
Indian
Latin American
Maori
Other
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
136

66 | P a g e
Over the last six months (July to December 2013), the average caseload was 116 per month compared with 106
in the previous period reflecting the continuity of the service in this period.
REFERRAL SOURCES
A total of 203 referrals were received and of these, only 7 did not meet the eligibility criteria. Patients were from
21 of the 23 TeAHN General Practices. Eighty six percent of the referrals were from practices, 7% from other
TeAHN services, 3% from HVHDB, 2% were self- referrals and 2% were from NGOs (Tamariki Ora). The
predominant reasons for referral were weight management, followed by Type 2 Diabetes, then cardiovascular
disease and hypertension.
Of the 137 patients who were discharged in the period, 7% declined the service when contacted for the first
time. For those patients who accessed the service, 192 nutrition problems were diagnosed and 86% of these
were resolved or are resolving. Of the 54% of patients who aimed to lose weight, 12% lost greater than 5% of
body weight (clinically significant) and 41% lost less than 5% of body weight. A further 36% remained within 1kg
of their initial weight and 11% gained weight.
SERVICES PROVIDED
There were 1535 patient contacts recorded in the July to December period which is almost 500 more that the
same period last year. A further 704 contacts (almost a third of total contacts) were made with health
professionals, family members and other agencies related to the patient. This meant that a team of people
worked together to support the patient and in particular provided motivation and positive reinforcement.
98 102
68
98 97
125 124115 114
125136
117
0
20
40
60
80
100
120
140
Jan 13 Feb 13 Mar 13 Apr 13 May 13 Jun 13 Jul 13 Aug 13 Sep 13 Oct 13 Nov 13 Dec 13
Patient Case Load
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
137

67 | P a g e
The graph below summarises the range of interventions that were provided by dietitians after assessing and
diagnosing nutrition issues. Food behaviour strategies such as motivational interviewing, problem solving and
contingency management were the most common interventions. During this period, the Dietitians received
training in ‘food addiction’ and cognitive behaviour therapy to improve their expertise in assisting people to
modify lifestyles. In addition to exercise education, goal setting and review was a common intervention and
assisted patients to make a series of achievable changes and self-monitor progress. The Dietitians made 10
referrals to other health professionals or agencies, both internal and external.
In addition to working with individuals, the Dietitians contributed to many of the Health Promotion Team
community events including the TryNui triathalon, the Naenae Festival, diabetes support groups and advising
on Nutrition Books for the Hutt City Library. Te Awakairangi staff requested an interactive session on healthy
eating which helped to provide a supportive healthy work environment for the staff.
231
189
98
201
259279
295
344
277262
237
12098 102
6898 97
125139
11397
129 126100
0
50
100
150
200
250
300
350
400
Jan 13 Feb 13 Mar 13 Apr 13 May 13 Jun 13 Jul 13 Aug 13 Sep 13 Oct 13 Nov 13 Dec 13
Volume of Work
Patient Contacts Liaising Services
45 34 28
144 150
370397
360
103
287
244
141
274
167
0
50
100
150
200
250
300
350
400
450
Facilitation Services Provided this Period
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
138

68 | P a g e
KEY ISSUES AND RISKS
As a result of performing increased numbers of cardiovascular disease risk assessments, practices found that
they needed more visual tools to illustrate the fat content of foods to Pacific people. In consultation with the
Pacific Health service and with the help of the Health Promotion team, the Dietitians have been developing a fat
resource for practices.
Patient Satisfaction surveys were not sent for several months while discussing a preferred method for gathering
information. The reception staff have now started sending surveys monthly and entering them into an online
database. Early feedback received from patients seen in the last 6 months (n=13) shows high scores for
satisfaction with the service and reported positive changes in lifestyle. A more detailed report will be presented
in the next period.
The dietitians have offered to assist practice nurses or GPs with nutrition consultations by offering to sit
alongside during lifestyle education sessions, run group sessions or help in any other way. More time will be
invested in the next period to work positively with practices in ways that provide the most benefit.
CASE STUDY
SB is a 22 year old, Maori, Quintile 5, female. She was referred to the Dietitian service for lifestyle advice by her
Practice Nurse who reported she was worried about her weight and out of control eating. She is obese with BMI
of 34.5.
On assessment SB reported a regular meal pattern of three meals and three to four large snacks daily. She
was meeting Ministry of Health (MoH) fruit recommendations. She was not meeting MoH recommendations
for milk and milk products and vegetables. SB was consuming in excess of the breads and cereals and meat and
meat alternatives to MoH recommendations. She often chose high saturated fat and high simple carbohydrate
food options, with high levels of butter and eating takeaways one or two times a week. SB did not have any
planned exercise, however, in the past she used to go for 6km walks, which had previously helped her lose 5-
6kg. She enjoys walking and will walk to drop and pick up her daughter from daycare.
The interventions that were used to resolve these problems were primarily motivational interviewing and self-
monitoring (8 contact hours). This enabled SB to discuss what triggered her to consume excess food and helped
her develop strategies for avoiding these triggers and problem solving what to do when she was faced with the
triggers. The Dietitian provided SB with nutrition information (salt, fat, sugar, snacks, portion sizes and meal
pattern), skills (label reading, meal planning) and exercise education (timing, intensity, types, importance) that
she could use. Goal setting and review enabled SB to monitor her progress and at the same time discuss areas
she was having difficulty with and/or did not understand. During the intervention the Dietitian gave her a lot of
encouragement, which helped to keep her focussed and ensured she realised the importance of these healthy
lifestyle changes for herself and her young family.
After intervention SB has lost 14.5kg or 12.7% of her body weight. She is very happy with her progress so far and
would like to continue to lose weight towards her goal weight of 85kg. She realised that this was a long way from
her original weight and knew it was important to take it in small steps. SB is now eating a regular meal pattern
of three meals and will only have snacks if she feeling especially hungry. She has talked openly with the Dietitian,
her friends and family about the skills, knowledge and strategies she had learned through TeAHN’s service and
feels confident in managing on her own. SB has treated herself to some of the higher fat, higher simple
carbohydrate snacks she used to indulge in, however she has limited these and works extra hard on her exercises
if she felt she had overindulged. She found the exercise easier than the food and will workout on her hired
machines for 50 minutes at night time.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
139
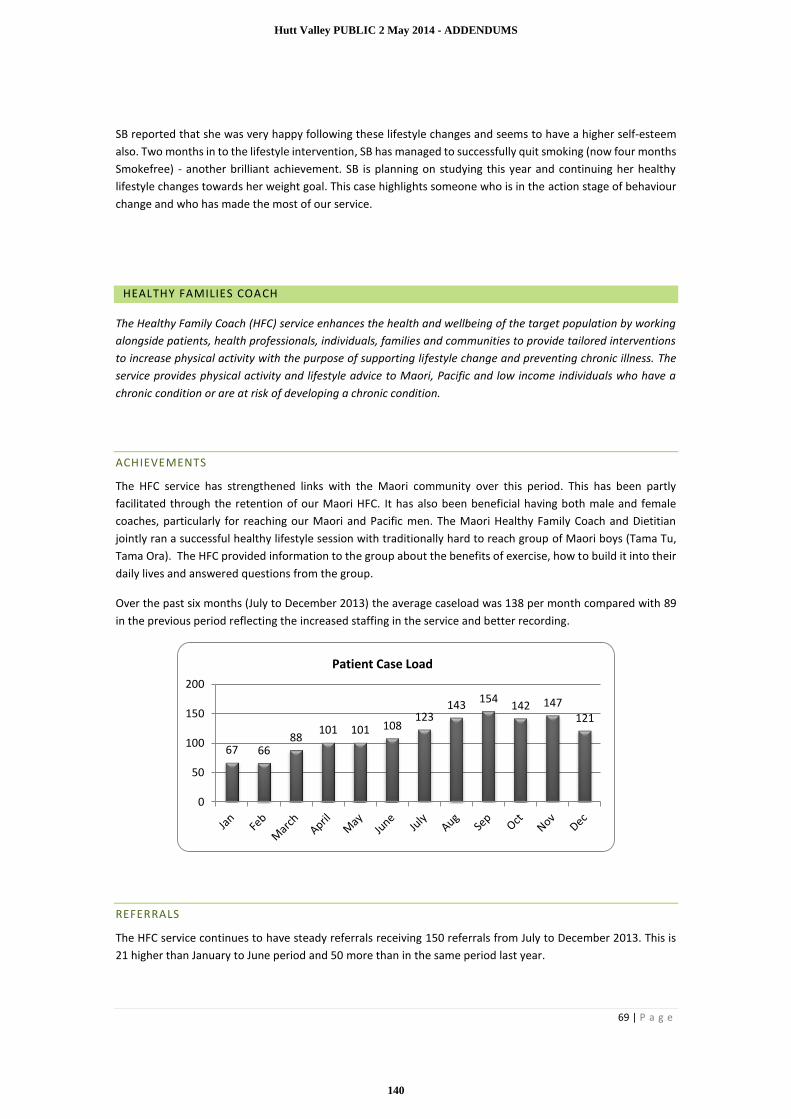
69 | P a g e
SB reported that she was very happy following these lifestyle changes and seems to have a higher self-esteem
also. Two months in to the lifestyle intervention, SB has managed to successfully quit smoking (now four months
Smokefree) - another brilliant achievement. SB is planning on studying this year and continuing her healthy
lifestyle changes towards her weight goal. This case highlights someone who is in the action stage of behaviour
change and who has made the most of our service.
HEALTHY FAMILIES COACH
The Healthy Family Coach (HFC) service enhances the health and wellbeing of the target population by working
alongside patients, health professionals, individuals, families and communities to provide tailored interventions
to increase physical activity with the purpose of supporting lifestyle change and preventing chronic illness. The
service provides physical activity and lifestyle advice to Maori, Pacific and low income individuals who have a
chronic condition or are at risk of developing a chronic condition.
ACHIEVEMENTS
The HFC service has strengthened links with the Maori community over this period. This has been partly
facilitated through the retention of our Maori HFC. It has also been beneficial having both male and female
coaches, particularly for reaching our Maori and Pacific men. The Maori Healthy Family Coach and Dietitian
jointly ran a successful healthy lifestyle session with traditionally hard to reach group of Maori boys (Tama Tu,
Tama Ora). The HFC provided information to the group about the benefits of exercise, how to build it into their
daily lives and answered questions from the group.
Over the past six months (July to December 2013) the average caseload was 138 per month compared with 89
in the previous period reflecting the increased staffing in the service and better recording.
REFERRALS
The HFC service continues to have steady referrals receiving 150 referrals from July to December 2013. This is
21 higher than January to June period and 50 more than in the same period last year.
67 6688
101 101 108123
143154
142 147121
0
50
100
150
200
Patient Case Load
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
140

70 | P a g e
Of the 150 referrals received this period 71% came from 19 TeAHN general practices (up from 61% last 6month
period), 6% from other Te AHN services, 3% self-referrals, 15% from HVHDB (Community Dietitians and Public
Health Nurses, Occupational therapists, Physiotherapist and Maori Health unit) and 5% from NGOs including
Kokiri Marae and Sport Wellington.
Of note this period is the increase in referrals from HVDHB which have increased threefold compared to January
to June period, indicating the good reputation the HFC service has with a number of DHB services. An example
of the increased HFC-DHB collaboration is the coordinated joint appointments with a patient and her Specialist
Consultant Dr Carol. This approach has been very successful as the patient values both the HFC and specialist
assistance. It meant that the three of us were all on the same page and able to work together to provide the
appropriate advice and use that to set goals. Dr Carol also reported that he found this very beneficial and has
asked that the HFC attend the quarterly appointments with this patient.
Of the 128 patients who were discharged in the period, half are doing well (30% are able to continue without
support, 16% have achieved their goals, and 3% are getting alternative support). The remainder did not engage
with the service (with 25% not attending appointments, 12% not ready to make changes and 11% declining the
service).
SERVICES PROVIDED
There were 1,496 patient contacts recorded in the July to December period, and a further 314 contacts were
made with health professionals, family members and other agencies related to the patient. This meant that a
team of people worked together to support the patient and in particular provided motivation and positive
reinforcement.
The table below shows an increase in the number of unique patients receiving services, and an increase in the
total and average contacts per month. This partly reflects the increased HFC staffing as well as better recording
of services delivered. On average, 250 patient contacts were made each month, an increase of 20 contacts per
month on the previous period.
2013 Total Contacts Average no. of Contacts per
month
Unique Patients this period
Average no. of patients at any
one time
January to June 1380 230 215 89
July to December 1496 250 271 130
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
141

71 | P a g e
The above graph details volume of work over the past year. The drop in volume over August and September are
due to the full time HFC staff member taking annual leave.
After assessing the patient’s life history (to gauge readiness for change, current activity levels, past weight loss
attempts and challenges, diet history, medication and medical history) the HFCs provide a range of interventions
as illustrated in the ‘Services Provided’ graph.
Fifty one satisfaction surveys were completed this period and the service received some very positive feedback.
“Home visits took a great deal of stress out of having to seek advice. My coach could not have been more
encouraging and I appreciate my coach listening without judging”
“They came to my home, were prompt, good communication and good rapport”
“The commitment in not giving up on me when some days I had totally given up on myself”
“I was so very grateful for the referral to this wonderful service”
The HFC Service has been working on ways to better evaluate the service by revising its measures of success. By
working with similar services in other regions the evaluation measures have been improved in an effort to show
159 150
239 248
282302
335
158173
292 280258
174209
318
293
380
322 336
233
191
339310
233
0
50
100
150
200
250
300
350
400
Jan Feb Mar Apr May Jun July Aug Sep Oct Nov Dec
Volume of Work
Patient Contacts Services provided
57 39
131189
88
201
290337
419
050
100150200250300350400450
Ind
ivid
ual
exe
rcis
ese
ssio
ns
Med
icat
ion
ed
uca
tio
n
Cas
e m
anag
eme
nt
Nu
trit
ion
Ed
uca
tio
n
Edu
cati
on
on
me
dic
alco
nd
itio
ns
Hea
lth
y W
eig
ht
An
al
Go
al s
ett
ing
and
revi
ews
Exer
cise
Ed
uca
tio
n
Gro
up
gym
se
ssio
n
Services Provided July - December 2013
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
142

72 | P a g e
more accurately where patients have or have not changed their physical activity levels. New MedTech assessment
forms will be implemented from 1 January 2014.
In addition to working with individuals, the HFC contributed to many of the Health Promotion Team community
events including TryNui triathalon, diabetes groups, Stroke Awareness Week, Kaumatua day, Pacific Wellbeing
Day, Healthy Messaging on Atiawa Toa FM and presentations. Te Awakairangi staff requested a work place
wellness initiative to provide a supportive healthy work environment for the staff, and the HFC staff organised
the speakers and events.
KEY ISSUES AND RISKS
Patient Satisfaction surveys were not sent for several months while discussing a preferred method for gathering
information. The administration staff have started sending surveys monthly and entering them into an online
database. Early feedback received from patients seen in the last 6 months (n=31) shows high scores for
satisfaction with the service and reported positive changes in lifestyle. A more detailed report for 2013 is
currently being composed by our administration team and will be available once all surveys have been returned.
The HFCs and Dietitians have offered to assist practice nurses or GPs with nutrition and physical activity
consultations by offering to sit alongside them during lifestyle education sessions, run group sessions or help in
any other way. More time will be invested in the next period to work positively with practices in ways that
provide the most benefit.
CASE STUDY
The following case study is based on a letter received from a patient who has made many changes to her life since receiving support from both the HFC Service and the Wellbeing Service. “I have had many challenges to overcome in my life. I was born with Congenital Dislocation of both hips as well
as dealing with the injuries from being hit by a motorbike when I was 10 years old. This has resulted in many
surgeries and head injury resulting in Epilepsy and Bipolar II.
I realised in late 2012, I found myself losing what control I had over my Bipolar. I spoke to my GP in late February
2013 and was referred to [a primary mental health clinician] at Te Awakairangi Health in March 2013. What has
happened since that referral has been amazing. The skills that I have learnt from [the clinician] have given me a
life that once I only dreamed about.
[The clinician] suggested that I attend [HFC staff member’s] Valley Fit programme as I might find exercise of
value in controlling my anxiety levels as this activated my bipolar symptoms. Going to the classes twice a week
has been fantastic. I have gained confidence, my anxiety levels have dropped to pretty well non-existent. I even
completed a Tryathlon on 8 September 2013. This was amazing for me as I had always hated exercise and had
trouble with due to a hip replacement and prolapsed disk in my back.
In early December 2013, I was told I have Breast Cancer. The mastectomy and lymph node surgery was done in
early December. I am now awaiting Chemotherapy and Radiation to complete my treatment. With the skills
that I have learnt from [the clinician] and attending Valley Fit have meant that I have been able to deal with a
very emotional and frightening period in my life. I have good control over my bipolar symptoms. This is what
my attitude is to dealing with my cancer: “Cancer touched my breast so I kicked its butt!!!!!”.
My relationship with my family has changed. We have all become much closer. My family say how proud they
are of me with how far I have moved forward with my life. Before my breast cancer diagnosis, I had found part
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
143

73 | P a g e
time employment. My family have also said how amazed they are at my positive attitude to dealing with my
breast cancer.
My life before being referred to [TeAHN staff] was spent waiting for life to come to me. I now have goals that I
set and attain. So now I grab life and run. Life is fantastic.
I still have up and down periods, but they are nothing now compared to what they were, as I now have the skills
to deal with them. Thank you [TeAHN staff] for showing me how wonderful and beautiful life can be.”
TRANSPORT SERVICE
The purpose of the transport service is to improve access to primary health services for the enrolled population
of Te Awakairangi Health Network by providing free transport to patients for whom lack of transport is a barrier
to attending primary health services.
SERVICES PROVIDED AND REFERRALS
Wellington Free Ambulance (WFA) is contracted to transport patients to and from health appointments.
For July to December 2013, a total of 741 trips were made, by 280 unique patients. This is a 29% increase on the
number of trips (571) made in the January to June 2013 period, when a total of 571 trips were made, by 230
unique patients.
TeAHN is aware that the transport service contract is now over budget and is looking at ways to reduce the
number of trips being delivered. Utilisation of the service to access secondary healthcare appointments has
increased disproportionately, remains high and is an ongoing concern.
248279 266
305
368 373
0
50
100
150
200
250
300
350
400
Q1 12/13 Q2 12/13 Q3 12/13 Q4 12/13 Q1 13/14 Q2 13/14 Q3 13/14 Q4 13/14
Number of Transport Service TripsJuly 2012 - June 2014
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
144

74 | P a g e
We have had discussions recently with the WFA and they are still working on improving the data collection. Data
recording of patient eligibility continues to be an issue but has improved with help of TeAHN developing a data
systems for WFA to adhere to.
DESTINATIONS
During the July to December 2013 period, 298 trips (40%) were made to primary health appointments. 60% of
the trips (443) were to secondary health care appointments with 193 trips to Hutt Hospital, 223 to Wellington
Hospital, 11 to Kenepuru Hospital, 8 to Bowen Hospital, 7 to Boulcott Hospital, and 1 to Southern Cross Hospital.
Further investigation of the trips to private hospitals has shown that patients going to Bowen Hospital were
attending publically funded sleep apnoea clinics, and patients going to Boulcott Hospital were there for radiology
appointments at Pacific Radiology. There was a one-off transport to Southern Cross hospital for a client of Te
Awakairangi Outreach Nurse team. Careful consideration was given to transporting this patient due to
unforeseen circumstances.
The graph below shows the figures for the July to December 2013 period.
21%
9%
21%25%
24%
Ethnicity/Quintile of Transport Service Users
Maori Pacific Q5 not M or P Unknown Non Target
7 8
193
11
173
5367
5
223
1
BoulcottHospital
BowenHospital
HuttHospital
KenepuruHospital
MedicalCentre
other Podiatrist Radiology WellingtonPublic
Hospital
SouthernCross
Transport Trips by Destination July-December 2013
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
145
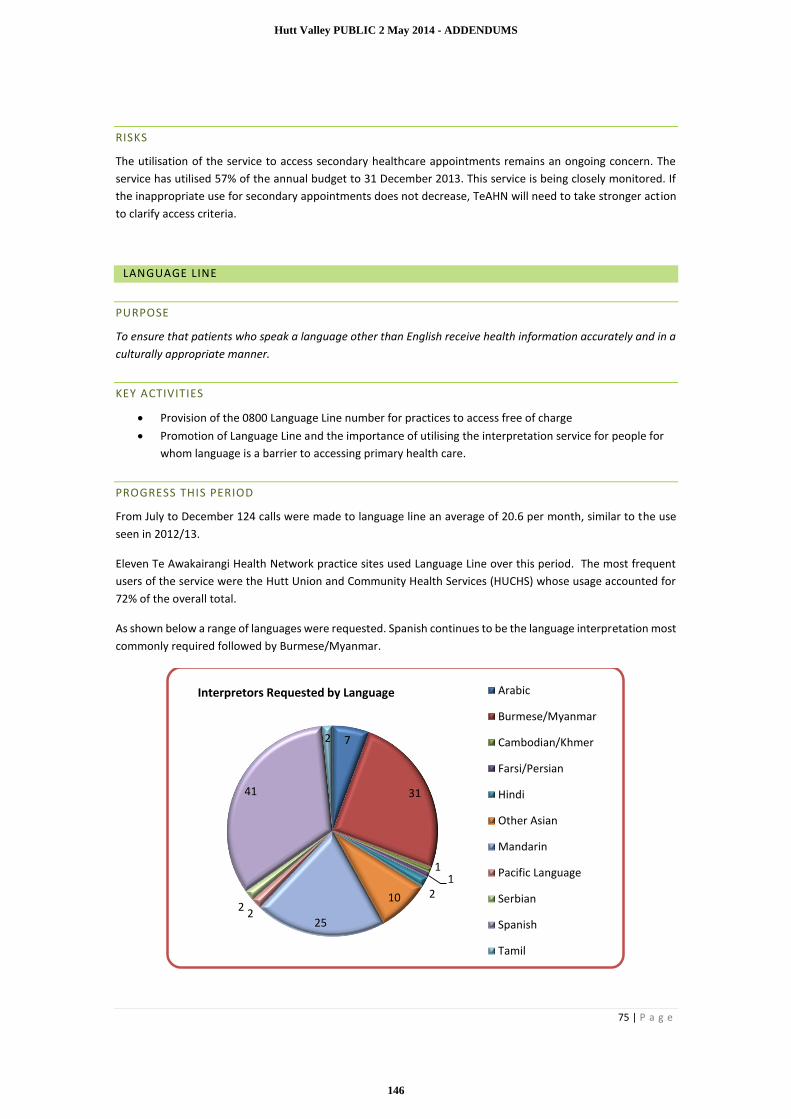
75 | P a g e
RISKS
The utilisation of the service to access secondary healthcare appointments remains an ongoing concern. The
service has utilised 57% of the annual budget to 31 December 2013. This service is being closely monitored. If
the inappropriate use for secondary appointments does not decrease, TeAHN will need to take stronger action
to clarify access criteria.
LANGUAGE LINE
PURPOSE
To ensure that patients who speak a language other than English receive health information accurately and in a
culturally appropriate manner.
KEY ACTIVITIES
Provision of the 0800 Language Line number for practices to access free of charge
Promotion of Language Line and the importance of utilising the interpretation service for people for
whom language is a barrier to accessing primary health care.
PROGRESS THIS PERIOD
From July to December 124 calls were made to language line an average of 20.6 per month, similar to the use
seen in 2012/13.
Eleven Te Awakairangi Health Network practice sites used Language Line over this period. The most frequent
users of the service were the Hutt Union and Community Health Services (HUCHS) whose usage accounted for
72% of the overall total.
As shown below a range of languages were requested. Spanish continues to be the language interpretation most
commonly required followed by Burmese/Myanmar.
7
31
11
210
252
2
41
2
Interpretors Requested by Language Arabic
Burmese/Myanmar
Cambodian/Khmer
Farsi/Persian
Hindi
Other Asian
Mandarin
Pacific Language
Serbian
Spanish
Tamil
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
146

76 | P a g e
PRACTICE SUPPORT
PRACTICE LIAISON AND SUPPORT
Practice liaison covers a number of areas providing frontline support to all Te Awakairangi Health Network
practices that wish to receive this support.
Practice Liaison and Support involves supporting practices with the implementation of new services, and a range
of business advice applicable to general practices. During this period this has included:
Supporting Practices with the installation and use of Patient Dashboard.
Working with the team at Karo Data Management to improve diabetes review recording and
installing the new Diabetes/CVD advanced form into the Practices and working with the Nurses and
GP’s to encourage the use of this form.
Inviting our Practices to potentially help fund them to attend a PMAANZ and APPM combined
Education training weekend.
Working with Hutt City Health Centre and Manuka Health Centre with the change to a new PMS
(My Practice) and working with Karo Data Management and our IT team to enable them to be able
to send their monthly claims to TeAHN in the same way as they did in Medtech.
There are several components of practice liaison and support which operate as core functions and have been
carried out this quarter. These include:
Preparation for register uploads each quarter and register cleansing tools for practice staff, and
one-on-one support for practices as requested
Collation and submission of quarterly lists of practices opting in for Under 6 and Very Low Cost
Access funding
Reminding and supporting practices to download/upload patient registers within required
deadlines
Providing practices with information, support, advice and resources to enable them to make
informed decisions on:
o Very Low Cost Access or Under Six Funding
o Utilisation of TeAHN services
o Management of patient registers
o Claiming systems and processes
o Enrolment processes and eligibility
Assistance with day to day issues and troubleshooting.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
147

77 | P a g e
QUALITY IMPROVEMENT
PROGRESS THIS PERIOD
TeAHN is committed to the fulfilment of its strategic vision, mission and objectives through the provision of high
quality, patient-centred, primary health care services with minimal risk to the population it serves. The quality
and safety of services delivered by TeAHN and its contracted providers are overseen by the Clinical Governance
Committee.
IMPLEMENT AND EVALUATE SYSTEMS AND PROCESSES
The Network has prepared a draft Clinical Quality Plan in a new format identifying a three year cycle of
development. The plan will be presented to the February 2014 TeAHN board meeting. This plan acknowledges
Te Awakairangi Health’s contractual requirements with Hutt Valley District Health Board to ensure the enrolled
population and casual users will receive a service that uses quality management principles through a framework
that incorporates the key dimensions of quality in the health and disability system. A three year Quality Action
Plan is included as an appendix.
CLINICAL FACILITATION SUPPORT FOR PRACTICES
Support to practices has included further implementation and education on the Patient Dashboard system to
assist practices to improve their performance against the Health Targets and other indicators. A new diabetes
advanced form has been implemented to assist with recording of diabetes reviews. Particular emphasis has been
provided to assist practices to work towards increasing their CVD risk assessments, providing smoking brief
advice/cessation referral and to reach the Health Target for immunisations.
A wide range of education and information sessions have been held for practice staff including Treaty of
Waitangi, Health and Disability Commission and Privacy Commission sessions.
SUPPORT FOR CORNERSTONE ACCREDITATION
Regular support meetings are being held to assist the seven practices who have registered for the Cornerstone
accreditation programme. Evening education and information sessions have been well attended. Individual
practice support has also been given as well as assistance with problem solving. Some practices have chosen to
implement the Healthy Practice system developed by the Medical Assurance Society (MAS) to assist with the
development of policies and guidelines, along with information provided by TeAHN.
TAS AUDIT OF CONTRACTUAL COMPLIANCE
TeAHN has met with Hutt Valley DHB to sign off all recommendations identified from the audit. One of the areas
of development included having all TeAHN staff vetted by Police, and this has now been implemented.
CLINICAL GOVERNANCE COMMITTEE (CGC)
The new Clinical Governance Committee is now well established and continues to provide expert clinical advice
to the TeAHN Board and management team. It oversees the quality and safety of the organisation, including
contracted practices and providers, and provides relevant reports to the Board of TeAHN. Guiding principles
include a Triple Aim approach.
The committee will continue to oversee the PHO Performance Programme including the changes that will occur
with the development of the new national Integrated Performance and Incentive Framework (IPIF). The
committee meets six weekly. In the six months to December 2013, the committee has discussed a number of
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
148

78 | P a g e
clinical pathways, including the subregional ENT pathways, the local dementia pathway and the local COPD
pathway.
EMERGENCY MANAGEMENT
TeAHN has continued to make significant progress over the last six months with Emergency Management. The
newly developed Emergency and Business Continuity Plan has been completed and presented to the Board of
TeAHN.
All the Local Emergency Management Groups (LEGs) have now been established, with most having had their
second meeting. Barry Simpson, MoH-funded Emergency Planner, continues to work with practices in the
development or updating of their BCPs and to provide support to the TeAHN Emergency Managers. An emphasis
is being placed on the completion of practice BCPs by 30 June 2014. Regular stakeholder meetings were put on
hold in the middle of the year but were reactivated at the end of 2013. These will now be held three monthly.
TeAHN staff members have attended an EOC training exercise in the Wairarapa and an emergency management
exercise was held for all TeAHN staff in December 2013. With the assistance of the Emergency Planner, TeAHN
has scheduled the commencement of emergency management training for practice staff and LEG groups. The
goal is to complete this training by December 2014.
RISK MANAGEMENT AND ISSUES REGISTER
TeAHN maintains a risk register which is presented to the TeAHN Board quarterly. Items are updated and new
items identified as required.
TeAHN also presents its Issues Register to both the CGC committee and TeAHN six monthly (or more frequently
as required). The issues register records all health and safety incidents, complaints and other incidents as they
arise.
There is also a schedule for the review of all policies, procedures and guidelines.
WORKFORCE DEVELOPMENT AND LIAISON
Over the July to December 2013 period, TeAHN has continued to facilitate both nurse professional development
topics and Continuing Medical Education (CME) topics.
CME topics included Understanding Insomnia: Diagnosis and management of a common sleep disorder; Pain
Management; ACC – Fitness to Work - clinically determining safe levels of activity; Inflammatory Arthritis in
primary care and pearls in management of Gout; Decision Tools: Shared care records, practice sustainability,
clinical pathways; Orthopaedics – back and shoulder pain investigation and management in primary care
These sessions attracted a number of podiatrists and community pharmacists as well as the usual general
practitioner audience. Audiences ranked these sessions at between 4.21 and 4.65 out of a possible 5 with very
positive feedback in the comments.
In October General Practice Services Trust (Hutt Valley) formally handed over accountability for the running of
CME to TeAHN. This involved a transition agreement with the transfer of resources to enable us to continue
this work.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
149

79 | P a g e
More than 29 GPs, practice nurses and managers attended a session in 18 November to discuss a range of topics
including the way in which CME would be offered going forward. An invitation was extended to GPs present to
join a CME Advisory group which held its first meeting 17 December. This group will provide clinical oversight
of the programme going forward.
A revised nurse education calendar has now been published after some ongoing discussions and negotiations
with various hospital services that have traditionally provided input. We have significantly refocused our
Diabetes education, to align this with the requirement to have our nurses meet the required standards, while
taking advantage of the on line course material now available. We are in discussion with other services around
further refinements to their courses and continue to work closely with our nurses and practice teams to ensure
the content is relevant and valued.
Our work with the group of practices on the journey to Cornerstone accreditation continues and we have been
pleased with the attendance at the meetings arranged to assist with this.
We also continue to support our practice teams through the development of emergency plans and facilitating
the establishment of local emergency groups.
PRIMARY NURSES REFERENCE GROUP
Representatives from TeAHN have continued to contribute to this forum over the past six months.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
150

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board
CPHAC INFORMATION PAPER
Date: 31 March 2014
Authors Regional Public Health and Shayne Nahu, Group Manager, SIDU
Endorsed By Dr Ashley Bloomfield, Director SIDU
Subject Nutrition and Physical Activity Initiatives including those to prevent cardiovascular disease and diabetes
The purpose of this paper is to provide the Boards with an overview of current activities undertaken by Regional Public Health (RPH) to improve nutrition and promote physical activity that will contribute to preventing heart disease and diabetes.
It responds to the February 2014 Action Point (4.1) of the Capital Coast DHB Board: A summary sheet outlining RPH involvement in sub regional nutrition and physical activity initiatives will be distributed to the Board for feedback to the Director SIDU.
Additional information on preventative activity within Primary Care to address cardiovascular disease and diabetes has also been included.
RECOMMENDATION
It is recommended that the Committees:
Note the range of activities underway to improve nutrition, promote physical activity and prevent cardiovascular disease and diabetes across the sub-region.
ADDENDA N/A
1 THE PROBLEM AND APPROACHES TO THE PROBLEM – BACKGROUND
Globally, non-communicable diseases (NCDs), mainly cardiovascular diseases (CVD), cancers, chronic respiratory diseases and diabetes, represent a leading threat to human health and development. The most prominent non-communicable diseases are linked to a common set of risk factors, namely tobacco use, harmful use of alcohol, an unhealthy diet and lack of physical activity. They are largely preventable by means of effective interventions that tackle these shared risk factors. Prevention of poor health and early deaths from these diseases is crucial to achieve the triple aim of improved population health (including reduced inequalities), a better patient journey and clinical, and financial sustainability.
Regional Public Health (RPH) takes a multi level approach to tackling risk factors based on the Ottawa Charter: building healthy public policy; creating supportive environments; strengthening community action; developing personal skills; and reorienting the health (and social) sectors. Where possible, RPH links its work on the major risk factors relating to tobacco, alcohol, and nutrition and physical activity. This paper outlines nutrition and physical activity preventive actions.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
151
PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board
The Government has recently announced the establishment of the Healthy Families NZ programme,based on the Australian ‘Healthy Together Victoria’ model to support reducing childhood obesity. Lower Hutt has been identified as one of the initial pilot sites and RPH and Te Awakairangi PHO are convening a meeting of interested groups in early April to initiate the development of a proposal for Lower Hutt.
Early identification of CVD and diabetes, is a key factor in better managing and delaying negative health impacts upon individuals. Primary Care is best placed to pick up these issues earlier with their patients to assist them with better management of their health.
Below are examples of public health activity undertaken by RPH and activity within primary care.
REGIONAL PUBLIC HEALTH (RPH)
2 POLICY LEVEL ACTIONS (BUILDING HEALTHY PUBLIC POLICY)
2.1 Nutrition and physical activity
Policy approaches have been identified internationally as the most cost effective, equitable and sustainable means of impacting population health. Healthy food procurement policies and environmental change are key strategies in obesity prevention. RPH’s actions at a policy level include:
∑ Submissions on food and nutrition documents:o Submissions in 2012 to sub-regional Territorial Local Authority Long Term Plans to highlight
ways to improve access to healthy food including zoning policies. We will continue to promote this approach with local authorities.
o Written and oral submissions in 2013 presented on the Wellington City Councils ‘Our Capital Spaces’ document (see also transport).
o Findings of the Food Environment in Eastern Porirua paper 2009 by RPH were presented to Porirua City Council, highlighting the lack of locally available healthy food.
∑ A food environment paper will soon be presented to the Executive Teams of the DHBs to engage their support for a food environment policy for all three DHBs.
∑ Work with Early Childhood Centres on the provision of healthy food for children under five and the development of food safety policies in their centres to meet the 2008 early childhood centre regulations.
∑ A food stall guideline/policy recently supported a ‘sugar free’ Te Ra o Te Raukura festival in Lower Hutt and a ‘fizz-free’ Creekfest festival in Porirua
∑ Future work includes looking at strategies to promote and influence improvements in the food environments. We are considering the development of a toolkit for writing and implementing food policy in a range of settings.
2.2 Urban environments including transport
RPH aims to influence regional transport and urban planning processes, which impact on active and public transport. RPH provides practical feedback on policies making the transition from walking and cycling to public transport more attractive and accessible. Submissions on transport and other urban environment policies include:
∑ New Zealand Transport Authority Basin Bridge Proposal: RPH recommended offsetting potential long-term traffic congestion with increased investment in active and public transport.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
152

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board
∑ RPH is providing public health advice on detailed landscape management plans for the area below the Basin Bridge flyover which will impact on the walking and cycling environment.
∑ Public Transport Spine Study: RPH recommended that the Wellington public transport system is integrated with active modes such as walking and cycling.
∑ Contributing to the Porirua City Council Road Safety Plan, which has the potential to improve local neighbourhood environments for walking and cycling. We will continue to work with authorities to ensure that potential health and social impacts from the future Link Road from Transmission Gully into Waitangirua are addressed during planning.
∑ In 2013, written and oral submissions were presented on the Wellington City Councils ‘Our Capital Spaces’ discussion document (see also Nutrition section).
∑ RPH continues to advocate for lower speed limits in high pedestrian areas, through opportunities such as the Wellington Central City Safer Speed Limit Proposal.
∑ Submissions on Hutt City Council Draft Urban Growth Strategy 2013 and on Kapiti Coast District Council proposed District Plan 2013.
∑ RPH will provide feedback on the Hutt City Council Walking and Cycling Strategy.
∑ RPH is the only health organisation represented at the Regional Active Transport quarterly forums and provides a public health perspective to the group.
3 INFORMATION BASED ACTIONS (INFORMING AND CREATING SUPPORTIVE ENVIRONMENTS)
3.1 Nutrition and physical activity
Information based actions include developing information and sharing this with others. RPH has undertaken the following;
∑ A number of papers have been developed by RPH to support working on the wider physical, economic, socio-cultural and political factors that impact food choices:
Food Desert or Food Swamp? 2009: An in-depth exploration of neighbourhood food environments in Eastern Porirua and Whitby
Discussion Paper | Disability Allowance 2014: Opportunities to improve access to Work and Income’s Disability Allowance (for food)
Identifying Ways to Impact Food Insecurity in the Wellington Region 2013: An analysis of potential actions on food insecurity
Factors Influencing the Stocking, Promotion and Pricing of Healthy Foods in Small Stores 2011: barriers and promoters of stocking, pricing and promoting healthy food by small store owners in Eastern Porirua
Food Costs for Families 2011: Analysis of the proportion of the minimum wage and benefit entitlements that families need to purchase a healthy diet
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
153

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board
Guide to promoting health and wellness in the workplace 2011: Healthy employees are productive employees – support for workplaces to implement health and wellness initiatives
Impact of Open Spaces on Health and Wellbeing 2010: Outlines the connections between health and wellbeing, and urban open spaces. In addition, it summarises the relationship between open space in relation to physical and mental health, and environmental, economic, social and cultural wellbeing.
∑ In 2013, along with the Health Promotion Agency; Accident Compensation Corporation; Wellington City Council and the Health and Productivity Institute of New Zealand, we ran a regional workshop for employers, Create a healthy workplace on a budget.
∑ The RPH website aims to empower communities in the Wellington region to make healthier and affordable food choices more readily available and accessible.
∑ We produce an electronic communication ‘Nutrition and Physical Update’ to inform stakeholders of key work, research and events in the region.
∑ We are working, along with other organisations, with the Office of the Commissioner for Children on a review of Food in Schools guidelines.
3.2 Urban environments including transport
The Healthy Open Spaces Paper: A summary of the impact of open spaces on health and wellbeing(2010) provided urban decision makers with a summary of the impacts of open spaces on health and wellbeing, including the physical environment’s role in creating active lifestyles.
Work is ongoing with local authorities to provide public health information that supports healthy urban planning. Papers in development include: ∑ the relationship between health promoting urban environments and economic development∑ supporting Maori worldviews of the natural and built environment∑ child friendly and accessible environments
Local action on important urban design and housing matters include:∑ Pomare Draft Redevelopment – RPH Feedback Report (2012)∑ Pomare Redevelopment Project – RPH Response (2013)∑ Castor Loop Redevelopment Feedback Report (2102)
We also promote the use of existing frameworks to support healthy urban planning such as:∑ the New Zealand Urban Design Protocol∑ Health Promotion and Sustainability through Environmental Design Guide (HPSTED)∑ New South Wales Healthy Urban Development Checklist∑ Crime Prevention through Environmental Design (CPTED) and Maori Urban Design principles.
4 ACTIVITY BASED ACTIONS (COMMUNITY ACTION, PERSONAL SKILLS, REORIENTING HEALTH SECTOR)
4.1 Nutrition and physical activity
RPH works in four broad settings to promote good nutrition and physical activity: community programmes and events; education based activities; workplace health and wellness; and maternal and infant nutrition and physical activity (Health 4 Life).
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
154
PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board
Community Programmes∑ Support for communities to develop initiatives such as community gardens, markets and food
cooperatives that empower and strengthen ownership and responses to food security challenges, for example. o Food co-operative in Naenae (low cost accessible food)o Breakfast co-operative in Naenae school (low cost food)o A fruit and vegetable co-operative is to commence in May 2014 in Eastern Porirua in
partnership with Wesley Food Pantry, Corinna School and the Salvation Army.
∑ Support for a range of community events such as Creekfast and Te Ra o Te Raukura. A food guideline/policy recently supported a ‘fizz-free’ Creekfest and sugar free drinks at Te Ra o Te Raukura. RPH also funded a water tank at Te Ra o Te Raukura as a way of promoting ‘water as free and as the first choice of drink’ at the event.
∑ Workshops for store owners to support better chip frying practises.
∑ Increasing participation in recreation and physical activity includes contributing to: o Wellington City Council’s Ki o Rahi Poneke Project with the aim of increasing participation
in sport and recreationo HEHA Porirua’s ‘Pound the Pavement’ family evento Hutt City Council’s Connex project for 16 - 20 year oldso Te Awakairangi TRYathlon
∑ The Wairarapa Baby Friendly Community Initiative aims to increase breastfeeding rates in vulnerable families and in the wider community
Education based activities∑ We run training for cooks in early childhood education centres alongside food policy training for
Managers of these organisations
∑ We provide after hours workshops for Pacific Early Childhood Centre staff on nutrition, illness management and skin infections (one per DHB district)
∑ We are supporting Pasifika early childhood community leaders to hold a combined health and education conference during March 2014. This is a community led initiative.
∑ We worked with Ora Toa Health Services and the Heart Foundation to set up health focussed activities at Titahi Bay North Annual Gala.
∑ Our Health Promoting Schools staff members support schools that choose nutrition and physical activity as one of their health topics. Nutrition education sessions are held in Wairarapa on a request basis.
∑ The Early Childhood Health Bus in Wairarapa aims to improve health literacy through increasing health knowledge and interpretation skills at an early childhood level for children, parents and teachers
∑ With the Heart Foundation, we have supported Porirua College students in identifying the need to improve food consumed at their school. They are to present a paper to their School Board.
Workplace
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
155

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board
∑ In 2009, we worked with the Corrections service to assess if their menus were in line with the Ministry of Health nutritional guidelines. This process is likely to be undertaken again in 2014 and reaches vulnerable communities.
∑ Following on from the regional workshop for employers, Create a health workplace on a budgetwe will engage with and support workplaces with high Pacific, Maori and low income employees to initiate workplace programmes.
∑ We have recently worked with Rimutaka and Arohata prisons to provide workplace health and wellbeing programmes for their staff (which include physical activity and nutrition components).
∑ We participate in the local Workplace Health Forum.
Maternal and Infant Physical Activity and Nutrition
The Health 4 Life programme of work aims to improve maternal and child nutrition and physical activity through development and delivery of simple common messages for pregnant women, infants and their mothers (including support for breastfeeding) and their surrounding whānau as part of currently delivered antenatal and well child services, primary care and other health and social services. It will focus initially on pregnant women and mothers and infants in vulnerable families and in later years could extend to all pregnant women and infants.
This project is delivered by a partnership comprising RPH, SIDU, Te Awakairangi Health Network and Compass Health. The project was announced in October 2013 by Minister Ryall under the banner “Healthy Families NZ: $810,000 healthy start for greater Wellington families”.
General∑ We participate in a range of local and regional stakeholder meetings to widen the scope of
influence on physical activity and nutrition outcomes including:o Childhood Obesity and Type 2 Diabetes Prevention network o Integrated Care Collaborative Pathways for childhood obesity and type 2 diabetes o Public health dietitians meetingso Upper Hutt Councils ALIVE project, which aims to engage non active people in recreational
activities.
4.2 Urban environments including transport
RPH provides ongoing advice regarding the natural and built environment in high priority areas, for example:
∑ Pomare is undergoing significant neighbourhood change. We are working with the community, Hutt City Council, social housing providers, Housing New Zealand, developers and urban designers to influence ongoing redevelopment processes. This work has included recommendations to: improve the environment for walking and cycling, enhance connections and access ways to public transport, recreation and community areas, and the development of high quality ‘multi-use’ public spaces.
∑ Work with the Wellington Regional Council on the Genuine Progress Index, which has a focus on health promoting environments and can act as a proxy for well-being. Relevant indicators for the Wellington region include: ease of walking and cycling; active transport uptake; access to open spaces; air quality; obesity; physical activity; and smoking.
∑ We work with agencies involved in safety including Safer Hutt Valley and Safe As Porirua
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
156

PUBLIC
Wairarapa, Hutt Valley and Capital & Coast District Health Board
∑ We work with Hutt City Council on place-based projects such as ‘Our Place Naenae’ to improve the local environment based on feedback from the local community,
∑ We participate in a range of local and regional stakeholder meetings to widen the scope of influence on urban environments and transport including:o Regional Active Transport Forumo Walk to Work day (12 March 2014)o Active a2b – a sustainable transport programme for workplaceso Safe and Sustainable Transport Reference Group.
4.3 Primary care
As noted in the Board paper on CVD and diabetes in February 2014, the primary care team has a key role in providing advice and support for patients to modify their lifestyles to prevent disease and/or reduce the risk of developing complications. At the same time there is an increasing recognition that patients can have a major part in self-managing their own conditions when provided with good information to make decisions.
Primary care teams can also prescribe their patients a Green prescription, which is supported by good evidence. There are two components to the GRx initiative one service for adults and another service for children and their families (known as GRx Active Families).
Through the GRx adult service, adults who are currently considered by their Primary Health Care providers to be physically “inactive” (that is less than two and a half hours of physical activity per week), are able to access physical activity opportunities and receive support for lifestyle changes from trained professionals.
The Green Prescription (GRx) initiative was established in 1998 Budget 2013 allocated new funding of $7.2 million over the next four years to support GRx adult patients referred because of pre-diabetes or type 2 diabetes conditions.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
157

Hutt ValleyDistrict Health Board
Peter Gush
Service Manager 2 May 2014
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
158

What is Public Health?
“The science and art of promoting health, preventing disease and prolonging life through organised efforts of society.”
C E Winslow
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
159

The Determinants of Health
Dahlgren & Whitehead
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
160
What do we do?
o Health Protection
o Health Promotion
o Healthy Public Policy
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
161

Our strategic priorities are:
- working with Maori- engagement with primary care- focus on children
What is our focus?
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
162

Who are we?
Wairarapa DHBHutt ValleyDHB
Capital andCoast DHB
MidCentral DHB
MidCentral DHBpublic health regulatoryservices contracted to
Hutt Valley DHB
Masterton
• Serve populations of 3 DHBs• 143.9 FTE (doctors/nurses/HPOs/PH advisors/admin/analysts/support staff)• From communicable disease investigation to influencing planning decisions by TLAs• From seeing young children in the ear van to working with youth at risk around alcohol
and drug use/abuse• Annual revenue of $14.5m
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
163

Ministry - Core53%
Other11%
District Health Boards36%
Expenditure –Personnel Costs $11m or 76% and Operating Costs $3.5m or 24%
RPH Revenue by Source
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
164
Bold Goal
“Halving the rate of avoidable hospital admissions for Maori, Pacific and children, by 2021.”
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
165

Target Month YTD QTR3 Target Month Target YTD
Shorter Stays in Emergency Departments 95% 95% 95% 95% Inpatient Acute Readmission Rate Feb-14 8.0% 8.8% 8.0% 8.7%
Improved Access to Elective Surgery 100% 92% 106% 101% Mental Health Readmission Rate Feb-14 8.0% 12.2% 8.0% 10.6%
Better Help for Smokers to Quit 95% 94% 97% 96% Acute Inpatient Length of Stay 3.9 4.0 3.9 4.0
Target Month Target YTD Elective Inpatient Length of Stay (Surgical) 3.2 3.0 3.2 3.0
Mental Health Relapse Prevention Plans 95% 92% 95% 91% Elective/Arranged Day of Surgery Admission 95% 96% 95% 96%
HONOS Compliance - Inpatient 80% 97% 80% 84% Ward Bed Utilisation - Daily (Incl Weekends) 85% 89% 85% 89%
HONOS Compliance - Community 80% 84% 80% 71% Ward Bed Utilisation - Weekdays Only 85% 91% 85% 90%
Bed Days due to Cellulitis (Avg LOS) 3.0 4.5 3.0 2.8 Funded Theatre Sessions Utilised 95% 96% 95% 88%
Surgical Site Infections Reported 1 2 9 7 Theatre Session Utilisation (Time in Theatre) 85% 81% 85% 79%
Patient Falls Causing Harm 12 11 108 129 Theatre Sessions Starting on Time 90% 86% 90% 89%
Medication Errors 20 23 180 198 Acute Patients impacting on Elective Sessions 43 38 387 333
Pressure Injuries 3 1 27 14 Cancelled on Day of Surgery - Patient 12 10 106 87
Cancelled on Day of Surgery - Hospital 15 7 124 7
WAITLISTSWAITLISTSWAITLISTSWAITLISTS Cancelled on Day of Surgery - Percentage 5.0% 3.5% 5.0% 4.4%
Target Month Booked Outpatient DNA (FSA & Followup) 359 460 3110 4598
Waiting >150 days for Treatment (ESPI5) 0 7 5 2 Outpatient DNA (FSA & Followup) - DNA Rate 6.0% 7.7% 6.0% 8.9%
Waiting >150 Days for Outpatient FSA (ESPI2) 0 3 0 3 Ward Utilisation is General Wards Only: Surgical, Medical, Rehab, Orthapaedic, Plastics Wards
HEALTHY WORKPLACEHEALTHY WORKPLACEHEALTHY WORKPLACEHEALTHY WORKPLACE Target Month Target YTD
Target Month Target YTD Total Caseweight 1781 1859 15657 16446
Hospital Staff Turnover % (Headcount) 10% 7.4% 10% 9.8% Elective Caseweights 551 619 4755 5130
Sickness Absence - % Paid Hours Worked 2.3% 2.9% 2.3% 2.6% Acute Caseweights 1230 1239 10902 11316
Number of Staff having >24 Mths O/S Leave 180 209 Outpatient FSA Volumes 1340 1290 12436 11031
Physical Assaults U/D 9 U/D 56 Outpatient FU Volumes 2980 3464 27578 30199
Blood and Body Fluid Exposure U/D 1 U/D 13 Hospital FTEs inc overtime 1572 1582 1572 1559
Slips, Trips and Falls U/D 8 U/D 27 Hospital Operating Costs ($'000) 15,264 15,601 140,251 142,565
Hospital Personnel inc outsourced ($'000) 11,107 11,197 103,119 104,257
MOH Performance Measures KEY: N/A = Not available U/D = Under Development Alert MOH Health Targets
Waitlist Patients (ESPI5 and ESPI2)
Mar-14
Hutt Hospital Operational Services
Monthly Balanced Scorecard March 2014KEY PERFORMANCE INDICATORS 2013/2014
PATIENT EXPERIENCE PATIENT EXPERIENCE PATIENT EXPERIENCE PATIENT EXPERIENCE Period Mar-14
Good News
Mar-14 Period
PeriodPROCESS & EFFICIENCYPROCESS & EFFICIENCYPROCESS & EFFICIENCYPROCESS & EFFICIENCY
VALUE FOR MONEYVALUE FOR MONEYVALUE FOR MONEYVALUE FOR MONEYMar-14 Period
Unbooked
Key Issue
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
166

HVDHB Monthly Operating Report Page 1 24 April 2014
Finance Report
March 2014
Graham Dyer Judith ParkinsonChief Executive Finance Manager
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
167

HVDHB Monthly Operating Report Page 2 24 April 2014
FINANCIAL PERFORMANCE OVERVIEW
Unfavourable variance to budget year to date of ($1,572k) has been reported. The bottom line result at the end of March was a deficit of ($2,733k) compared to a budget deficit of ($1,162k).
Key results year to date were: ∑ Funder ($1,666k) unfavourable (Feb ($1,510k))∑ Governance $17k favourable (Feb $42k)∑ Provider $78k favourable (Feb ($81k))
Material Variances Year to Date to March 2014
The key variances to budget were:
ß Interest income: favourable $629k due to higher cash balance than expected in the budget.
ß IDF inflows: ($1,203k), Acute ($911k) 196 less CWD than budgeted. Acute ED and dental are slightly up but acute plastic surgery is down by 185 CWD.
ß Infrastructure Depreciation: favourable $1,337k site improvements were valued downwards partly offset by building revaluations upwards.
ß Pharmaceuticals: ($466k) the financial Impact of Pharmac’s Hospital Medicines List (HML) national decision to provide equity of medicines across all DHBs.
ß Blood: ($786k) savings target not met however the Ministry of Health has indicated this will be seen as savings in community pharmaceuticals which will be realised in the funder arm by June.
ß IDF outflows: ($2,826k), Acute ($1,674k) 359 more CWD than budget. This result includes some specialties which are significantly over budget because of high volumes in particular cardiology, oncology and specialist neonates. There have been 22 cases so far this year attracting more than 15 CWD.
ß Personnel: Nursing ($2,371k): savings initiatives not achieved due to higher occupancy, particularly in general medical and reduced Christmas shutdown. Forecast to continue until year end. Management and Admin ($159k) the FPSC project is running behind the scheduled.
Year end forecastThe year end forecast deficit of $1.5m is a most likely position with a risk that it could be as high as $3.4m. The significant area of risk relates to Acute IDF outflow.
The following table provides a summary of the financial performance of the DHB at the end of March 2014.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
168
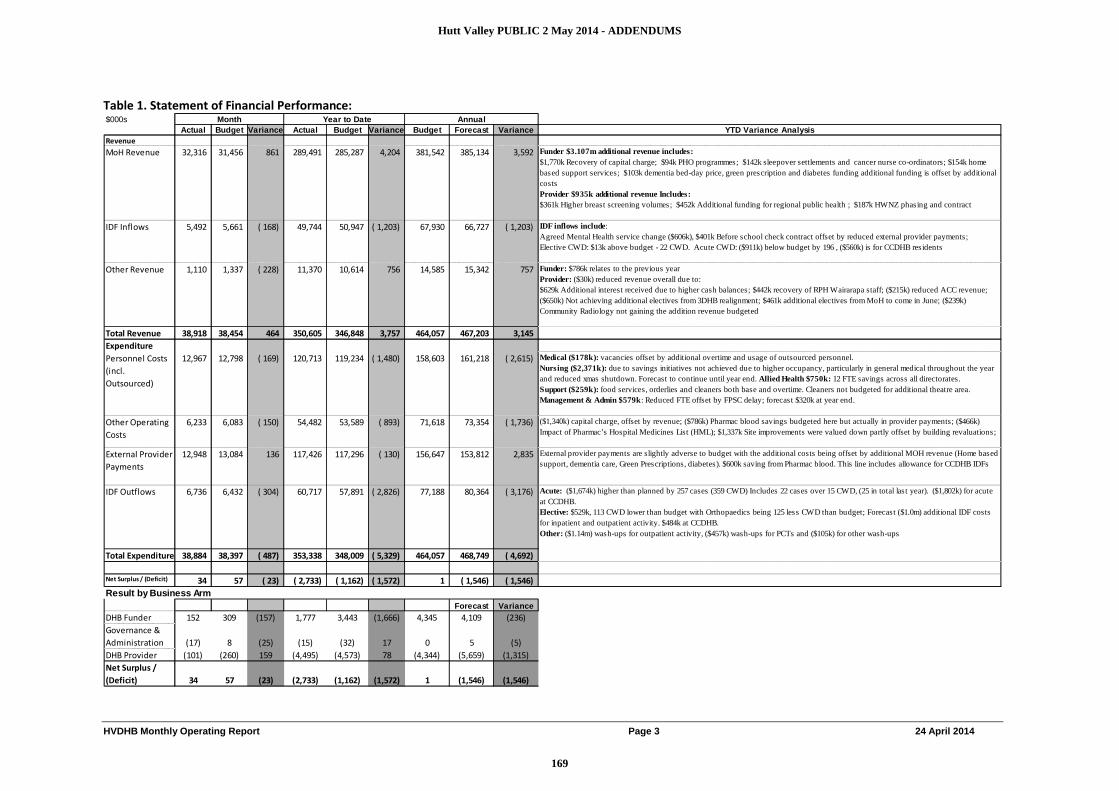
HVDHB Monthly Operating Report Page 3 24 April 2014
Table 1. Statement of Financial Performance: $000s Month Year to Date
Actual Budget Variance Actual Budget Variance Budget Forecast Variance YTD Variance AnalysisRevenueMoH Revenue 32,316 31,456 861 289,491 285,287 4,204 381,542 385,134 3,592 Funder $3.107m additional revenue includes:
$1,770k Recovery of capital charge; $94k PHO programmes; $142k sleepover settlements and cancer nurse co-ordinators; $154k home based support services; $103k dementia bed-day price, green prescription and diabetes funding additional funding is offset by additional costsProvider $935k additional revenue Includes:$361k Higher breast screening volumes; $452k Additional funding for regional public health ; $187k HWNZ phasing and contract
IDF Inflows 5,492 5,661 ( 168) 49,744 50,947 ( 1,203) 67,930 66,727 ( 1,203) IDF inflows include:Agreed Mental Health service change ($606k), $401k Before school check contract offset by reduced external provider payments; Elective CWD: $13k above budget - 22 CWD. Acute CWD: ($911k) below budget by 196 , ($560k) is for CCDHB residents
Other Revenue 1,110 1,337 ( 228) 11,370 10,614 756 14,585 15,342 757 Funder: $786k relates to the previous year Provider: ($30k) reduced revenue overall due to: $629k Additional interest received due to higher cash balances; $442k recovery of RPH Wairarapa staff; ($215k) reduced ACC revenue; ($650k) Not achieving additional electives from 3DHB realignment; $461k additional electives from MoH to come in June; ($239k) Community Radiology not gaining the addition revenue budgeted
Total Revenue 38,918 38,454 464 350,605 346,848 3,757 464,057 467,203 3,145ExpenditurePersonnel Costs (incl. Outsourced)
12,967 12,798 ( 169) 120,713 119,234 ( 1,480) 158,603 161,218 ( 2,615) Medical ($178k): vacancies offset by additional overtime and usage of outsourced personnel. Nursing ($2,371k): due to savings initiatives not achieved due to higher occupancy, particularly in general medical throughout the year and reduced xmas shutdown. Forecast to continue until year end. Allied Health $750k: 12 FTE savings across all directorates. Support ($259k): food services, orderlies and cleaners both base and overtime. Cleaners not budgeted for additional theatre area. Management & Admin $579k: Reduced FTE offset by FPSC delay; forecast $320k at year end.
Other Operating Costs
6,233 6,083 ( 150) 54,482 53,589 ( 893) 71,618 73,354 ( 1,736) ($1,340k) capital charge, offset by revenue; ($786k) Pharmac blood savings budgeted here but actually in provider payments; ($466k) Impact of Pharmac’s Hospital Medicines List (HML); $1,337k Site improvements were valued down partly offset by building revaluations;
External Provider Payments
12,948 13,084 136 117,426 117,296 ( 130) 156,647 153,812 2,835 External provider payments are slightly adverse to budget with the additional costs being offset by additional MOH revenue (Home based support, dementia care, Green Prescriptions, diabetes). $600k saving from Pharmac blood. This line includes allowance for CCDHB IDFs
IDF Outflows 6,736 6,432 ( 304) 60,717 57,891 ( 2,826) 77,188 80,364 ( 3,176) Acute: ($1,674k) higher than planned by 257 cases (359 CWD) Includes 22 cases over 15 CWD, (25 in total last year). ($1,802k) for acute at CCDHB. Elective: $529k, 113 CWD lower than budget with Orthopaedics being 125 less CWD than budget; Forecast ($1.0m) additional IDF costs for inpatient and outpatient activity. $484k at CCDHB. Other: ($1.14m) wash-ups for outpatient activity, ($457k) wash-ups for PCTs and ($105k) for other wash-ups
Total Expenditure 38,884 38,397 ( 487) 353,338 348,009 ( 5,329) 464,057 468,749 ( 4,692)
Net Surplus / (Deficit) 34 57 ( 23) ( 2,733) ( 1,162) ( 1,572) 1 ( 1,546) ( 1,546)Result by Business Arm
Forecast Variance
DHB Funder 152 309 (157) 1,777 3,443 (1,666) 4,345 4,109 (236)Governance & Administration (17) 8 (25) (15) (32) 17 0 5 (5)DHB Provider (101) (260) 159 (4,495) (4,573) 78 (4,344) (5,659) (1,315)Net Surplus / (Deficit) 34 57 (23) (2,733) (1,162) (1,572) 1 (1,546) (1,546)
Annual
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
169

HVDHB Monthly Operating Report Page 4 24 April 2014
Table 2. Statement of Financial Performance – by Area (current month)$000s DHB Funder Governance & Administration DHB Provider Hutt Valley DHB
Actual Budget Var Last Yr Actual Budget Var Last Yr Actual Budget Var Last Yr Actual Budget Var Last YrRevenue Govt & Crown Agency 35,941 35,692 249 35,363 272 272 - 256 2,589 2,320 268 2,276 38,540 38,022 518 37,645 Other 46 - 46 10 - - - - 333 432 ( 99) 417 378 432 ( 53) 427 Internal - - 15,888 15,604 284 15,759 -Total Revenue 35,987 35,692 295 35,374 272 272 - 256 18,809 18,357 453 18,452 38,918 38,454 464 38,072Expenditure Personnel Costs - - - - 5 6 1 46 12,584 12,647 63 12,641 12,589 12,653 63 12,687 Outsourced Staff - - - - 18 378 145 ( 233) 343 378 145 ( 233) 361 Outsourced Services 552 263 ( 289) 251 168 167 ( 0) 82 690 506 ( 184) 335 858 673 ( 184) 417 Clinical Supplies - 10 0 ( 10) - 2,296 2,266 ( 30) 1,977 2,306 2,266 ( 40) 1,977 Infrastructure - - - - 52 34 ( 18) 35 3,018 3,109 92 2,409 3,069 3,144 74 2,445 Provider Payments 35,283 35,120 ( 163) 35,786 - - - - - 19,684 19,516 ( 168) 20,027 Internal Allocations - 15 17 2 15 ( 15) ( 17) ( 2) ( 15) - 0 0 -Total Expenditure 35,835 35,383 ( 452) 36,037 249 224 ( 25) 196 18,951 18,657 ( 294) 17,690 38,884 38,397 ( 487) 37,914
Surplus/(Deficit)Before Overheads 152 309 ( 157) ( 663) 23 48 ( 25) 60 ( 142) ( 300) 159 762 34 57 ( 23) 158
Corporate Overheads - 41 41 - 34 ( 41) ( 41) ( 0) ( 34) - ( 0) ( 0) -
Surplus/(Deficit) 152 309 ( 157) ( 663) ( 17) 8 ( 25) 26 ( 101) ( 260) 159 796 34 57 ( 23) 158
Table 3. Statement of Financial Performance – by Area (YTD)$000s DHB Funder Governance & Administration DHB Provider Hutt Valley DHB
Actual Budget Var Last Yr Actual Budget Var Last Yr Actual Budget Var Last Yr Actual Budget Var Last YrRevenue Govt & Crown Agency 323,866 321,655 2,211 316,406 2,452 2,452 - 2,346 21,707 21,218 489 20,651 345,662 342,961 2,700 337,147 Other 641 - 641 460 - - - 12 4,303 3,886 416 4,418 4,943 3,886 1,057 4,889 Internal - - 142,224 140,662 1,562 138,768 -Total Revenue 324,507 321,655 2,852 316,866 2,452 2,452 - 2,358 168,233 165,766 2,467 163,836 350,605 346,848 3,757 342,036Expenditure Personnel Costs - - - - 45 56 10 1,001 117,408 117,841 433 114,522 117,453 117,896 443 115,523 Outsourced Staff - 12 - ( 12) 34 3,249 1,337 ( 1,911) 2,492 3,260 1,337 ( 1,923) 2,526 Outsourced Services 4,222 2,363 ( 1,859) 2,256 1,508 1,505 ( 3) 315 4,768 3,719 ( 1,049) 3,453 6,276 5,224 ( 1,052) 3,768 Clinical Supplies - 10 0 ( 10) 5 20,916 19,975 ( 942) 20,368 20,927 19,975 ( 952) 20,373 Infrastructure - - - - 419 448 29 338 26,860 27,943 1,083 26,535 27,280 28,391 1,111 26,873 Provider Payments 318,508 315,849 ( 2,659) 314,621 - - - - - 178,143 175,187 ( 2,956) 175,853 Internal Allocations - 148 150 3 146 ( 148) ( 150) ( 3) ( 164) - 0 0 ( 18)Total Expenditure 322,730 318,212 ( 4,518) 316,877 2,142 2,159 17 1,839 173,053 170,664 ( 2,389) 167,206 353,338 348,009 ( 5,329) 344,897
Surplus/(Deficit)Before Overheads 1,777 3,443 ( 1,666) ( 11) 310 293 17 519 ( 4,820) ( 4,898) 78 ( 3,369) ( 2,733) ( 1,162) ( 1,572) ( 2,861)
Corporate Overheads - 325 325 - 300 ( 325) ( 325) ( 0) ( 300) - ( 0) ( 0) -
Surplus/(Deficit) 1,777 3,443 ( 1,666) ( 11) ( 15) ( 32) 17 219 ( 4,495) ( 4,573) 78 ( 3,069) ( 2,733) ( 1,162) ( 1,572) ( 2,861)
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
170

HVDHB Monthly Operating Report Page 5 24 April 2014
Table 4. IDF Inflows Variance SummaryIDF Inflows
Variance
$000s YTD Variance Analysis
Elective Inpatients 13Elective caseweights (CWD) are down by 40. Higher CWD for plastics offset by lower CWD in rheumatology, orthopaedics and general surgery.
Acute Inpatients* (912)For the year acute CWD are down by 195. Emergency medical services and dental are slightly up but acute plastics surgery is down by 185 caseweights.
Regional Mental Health Contracts (606) Contract changes - offset by reduced external provider payments.
Plunket contract 401 Additional funding which is offset by external provider payments
Agreed changes and wash-ups (100)
Total Variance in IDF Inflows (1,203) Note: 54% of IDFs originate from CCDHB*IDF acute inflows are below plan for: Midcentral (down 30%), Capital & Coast (down 9%) and Whanganui (down 37%)
Table 5. IDF Outflow Variance SummaryIDF Outflows
Variance
$000s YTD Variance Analysis
Elective Inpatients 529
Elective IDF outflows are under budget by 114 CWD. Orthopaedics and Cardiothoracic are under budget offset by Ophthalmology, Urology, Vascular surgery and General surgery.
Acute Inpatients* (1,674)
Acute IDF outflows are over budget by 359 CWD. This result includes some specialties which are significantly over budget because of high volumes in particular cardiology, oncology and specialist neonates. There have been 22 cases so far this year attracting more than 15 CWD, there were a total of 25 in the whole of last year.The only significant flow is to Counties Manukau for a single burns case which is 46 CWD ($212k).
Other (1,682) ($1.114m) wash-ups for outpatient activity, ($475k) wash-ups for PCTs and ($105k) for other wash-ups
Total Variance in IDF Outflows (2,826) Note: 93% of IDFs are to CCDHB*IDF acute outflows are above plan for: Counties Manukau (up 64%), Capital & Coast (up 12%)
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
171
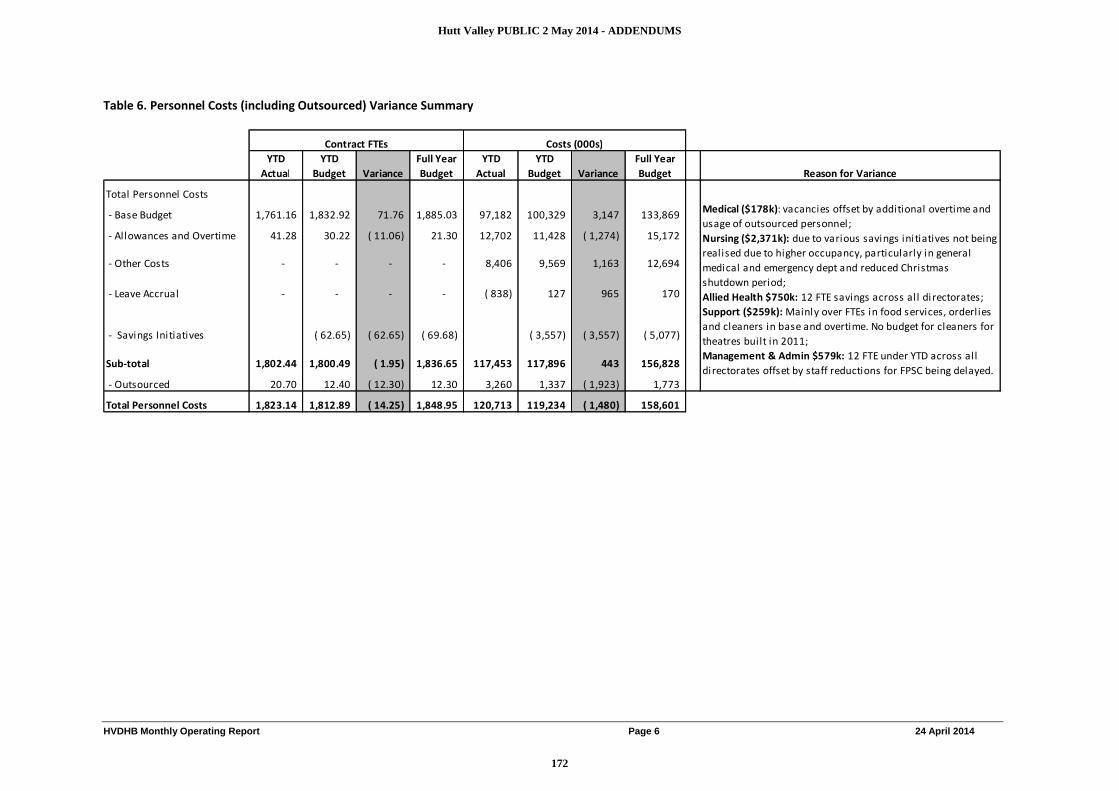
HVDHB Monthly Operating Report Page 6 24 April 2014
Table 6. Personnel Costs (including Outsourced) Variance Summary
YTD Actual
YTD Budget Variance
Full Year Budget
YTD Actual
YTD Budget Variance
Full Year Budget Reason for Variance
Total Personnel Costs
- Base Budget 1,761.16 1,832.92 71.76 1,885.03 97,182 100,329 3,147 133,869
- Allowances and Overtime 41.28 30.22 ( 11.06) 21.30 12,702 11,428 ( 1,274) 15,172
- Other Costs - - - - 8,406 9,569 1,163 12,694
- Leave Accrual - - - - ( 838) 127 965 170
- Savings Initiatives ( 62.65) ( 62.65) ( 69.68) ( 3,557) ( 3,557) ( 5,077)
Sub-total 1,802.44 1,800.49 ( 1.95) 1,836.65 117,453 117,896 443 156,828
- Outsourced 20.70 12.40 ( 12.30) 12.30 3,260 1,337 ( 1,923) 1,773
Total Personnel Costs 1,823.14 1,812.89 ( 14.25) 1,848.95 120,713 119,234 ( 1,480) 158,601
Medical ($178k): vacancies offset by additional overtime and usage of outsourced personnel; Nursing ($2,371k): due to various savings initiatives not being realised due to higher occupancy, particularly in general medical and emergency dept and reduced Christmas shutdown period; Allied Health $750k: 12 FTE savings across all directorates; Support ($259k): Mainly over FTEs in food services, orderlies and cleaners in base and overtime. No budget for cleaners for theatres built in 2011; Management & Admin $579k: 12 FTE under YTD across all directorates offset by staff reductions for FPSC being delayed.
Contract FTEs Costs (000s)
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
172

HVDHB Monthly Operating Report Page 7 24 April 2014
Annual LeaveThe following graph shows the historical trends in annual leave for the last two years. The reduction in the accrual is close to budget and reflects the amount of annual leave taken over the summer period.
Accrued Annual leave $000
13,000
13,500
14,000
14,500
15,000
15,500
Jul -11
Sep-11
Nov-11
Jan-12
Mar-12
May-12
Jul -12
Sep-12
Nov-12
Ja n-13
Mar-13
May-13
Jul -13
Sep-13
Nov-13
Jan-14
Mar-14
May-14
Thou
sand
s
Actua l Budget
Note the reduction in budget in January which is incorporated into the sustainability plan
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
173

HVDHB Monthly Operating Report Page 8 24 April 2014
Chart: FTE Trends by Professional category
FTEs per month by Professional Category
-
200
400
600
800
1,000
1,200
1,400
1,600
1,800
2,000
Mar-13 Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14Actual Medical Actual Nursing Actual Allied Health
Actual Non Health Support Actual Managemt/Admin Total Budget
Mar-13 Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14Medical 229 230 228 228 226 226 225 226 228 230 231 232 231Nursing 706 692 701 700 699 702 702 702 705 707 707 711 714Allied Health 435 430 433 433 418 419 419 420 422 422 423 423 424Non Health Support 139 135 138 138 134 134 135 136 136 136 134 134 134Managemt/Admin 327 294 320 316 278 288 294 295 298 299 298 298 298Actual FTE 1,835 1,781 1,821 1,815 1,754 1,769 1,776 1,778 1,789 1,794 1,792 1,799 1,802Budget 1,841 1,824 1,838 1,837 1,802 1,805 1,806 1,808 1,818 1,807 1,803 1,802 1,800
Act
ual
Tota
l
Note : SIDU 22FTE moved to CCDHB July 2013: Public Health 5.59 FTE from Wairarapa transferred to Hutt payroll from Nov 2013.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
174
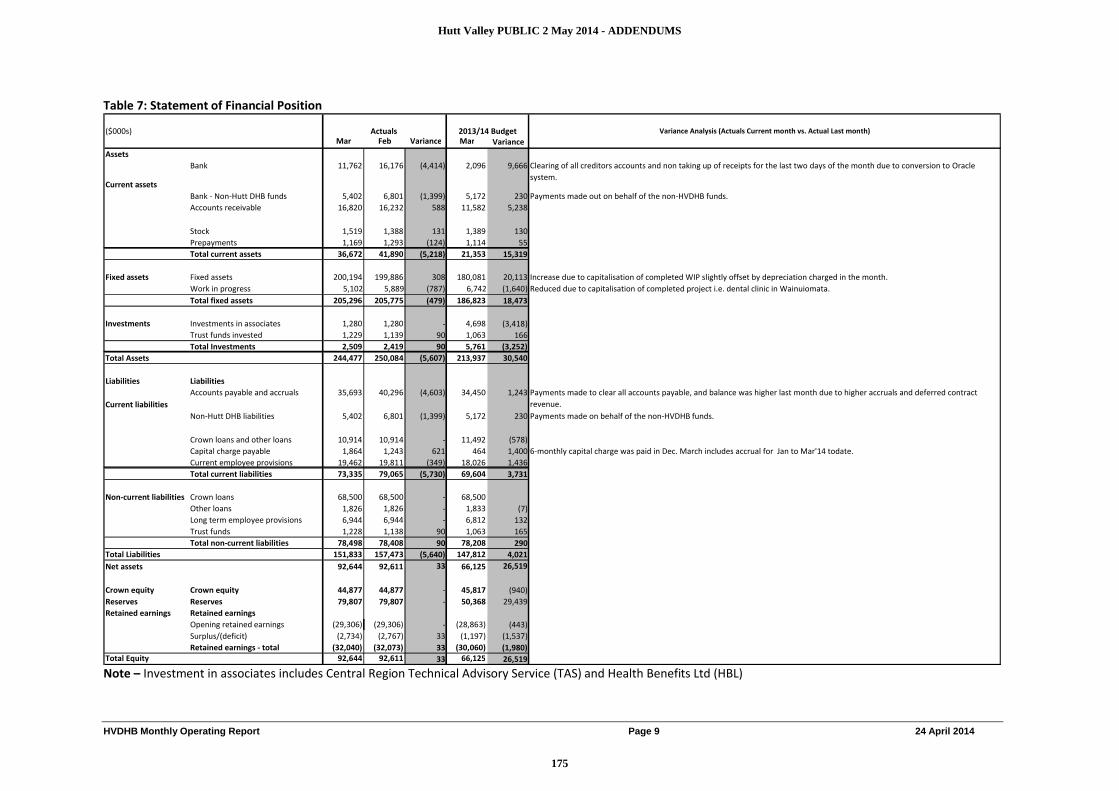
HVDHB Monthly Operating Report Page 9 24 April 2014
Table 7: Statement of Financial Position
($000s) Variance Analysis (Actuals Current month vs. Actual Last month)Mar Feb Variance Mar Variance
Assets
Current assets
Bank 11,762 16,176 (4,414) 2,096 9,666 Clearing of all creditors accounts and non taking up of receipts for the last two days of the month due to conversion to Oracle system.
Bank - Non-Hutt DHB funds 5,402 6,801 (1,399) 5,172 230 Payments made out on behalf of the non-HVDHB funds.Accounts receivable 16,820 16,232 588 11,582 5,238
Stock 1,519 1,388 131 1,389 130Prepayments 1,169 1,293 (124) 1,114 55Total current assets 36,672 41,890 (5,218) 21,353 15,319
Fixed assets Fixed assets 200,194 199,886 308 180,081 20,113 Increase due to capitalisation of completed WIP slightly offset by depreciation charged in the month.Work in progress 5,102 5,889 (787) 6,742 (1,640) Reduced due to capitalisation of completed project i.e. dental clinic in Wainuiomata.Total fixed assets 205,296 205,775 (479) 186,823 18,473
Investments Investments in associates 1,280 1,280 - 4,698 (3,418)Trust funds invested 1,229 1,139 90 1,063 166Total Investments 2,509 2,419 90 5,761 (3,252)
Total Assets 244,477 250,084 (5,607) 213,937 30,540
Liabilities Liabilities
Current liabilitiesAccounts payable and accruals 35,693 40,296 (4,603) 34,450 1,243 Payments made to clear all accounts payable, and balance was higher last month due to higher accruals and deferred contract
revenue.Non-Hutt DHB liabilities 5,402 6,801 (1,399) 5,172 230 Payments made on behalf of the non-HVDHB funds.
Crown loans and other loans 10,914 10,914 - 11,492 (578)Capital charge payable 1,864 1,243 621 464 1,400 6-monthly capital charge was paid in Dec. March includes accrual for Jan to Mar'14 todate.Current employee provisions 19,462 19,811 (349) 18,026 1,436Total current liabilities 73,335 79,065 (5,730) 69,604 3,731
Non-current liabilities Crown loans 68,500 68,500 - 68,500Other loans 1,826 1,826 - 1,833 (7)Long term employee provisions 6,944 6,944 - 6,812 132Trust funds 1,228 1,138 90 1,063 165Total non-current liabilities 78,498 78,408 90 78,208 290
Total Liabilities 151,833 157,473 (5,640) 147,812 4,021Net assets 92,644 92,611 33 66,125 26,519
Crown equity Crown equity 44,877 44,877 - 45,817 (940)Reserves Reserves 79,807 79,807 - 50,368 29,439Retained earnings Retained earnings
Opening retained earnings (29,306) (29,306) - (28,863) (443)Surplus/(deficit) (2,734) (2,767) 33 (1,197) (1,537)Retained earnings - total (32,040) (32,073) 33 (30,060) (1,980)
Total Equity 92,644 92,611 33 66,125 26,519
2013/14 BudgetActuals
Note – Investment in associates includes Central Region Technical Advisory Service (TAS) and Health Benefits Ltd (HBL)
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
175

HVDHB Monthly Operating Report Page 10 24 April 2014
Table 8: Statement of Cash flows
Description
Year to date actual ($000)
Year to date budget ($000)
Variance-Over/(under) budget ($000) Notes - Explanation for major variances
Operating activitiesReceipts 345,153 347,524 (2,371) Higher budgeted revenue from Crown and other DHBs.PaymentsPayments to employees 113,528 117,707 (4,179) Payments to suppliers 216,156 212,656 3,500 Capital charge paid 3,765 4,122 (357) GST (Net) 137 - 137 Payments - total 333,586 334,485 (899) Net cash flow from operating activities 11,567 13,039 (1,472) Investing activitiesReceiptsProceeds from Asset sales (3) - (3) PaymentsInvestment in associates - 2,178 (2,178) Budgeted payment for CRISP project is delayed.Purchase of fixed assets 5,635 9,569 (3,934) Delay in the purchase of MRI scanner and Citrix Farm & LIS projects.Net cash flow from investing activities (5,638) (11,747) 3,931 Financing activitiesReceiptsLoans - - - Equity injection 800 - 800 Equity injection for COH (Child Oral Health) project, not budgeted for.Receipts - total 800 - 800 PaymentsRepayment of loans 294 - 294 Capital repayments of financing leases for MRI scanner and ultrasound.Equity repayments - - Interest payments 1,638 3,006 (1,368) Lower interest for finance leases & Crown(CHFA) loans. Payments - total 1,932 3,006 (1,074) Net cash flow from financing activities (1,132) (3,006) 1,874 Net Inflow/(outflow) of Hutt Valley DHB funds 4,797 (1,714) 6,511
Opening cash 24,650 8,982 15,668 Movement in Non-Hutt Valley DHB funds:Primary Healthcare IT Grants fund (2,923) - (2,923) National Haemaphiliac Management Group Fund (2,977) - (2,977) NZ Universal List of Medicine Fund 170 - 170 Net cash flow of Non-Hutt Valley DHB funds (5,731) - (5,731) Payments made on behalf of other Funds not budgeted for.Ending cash 23,716 7,268 16,448
Summary ending cash positionHutt DHB funds 18,314 7,268 11,046 Non-Hutt Valley DHB funds 5,402 - 5,402 Total 23,716 7,268 16,448
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
176

HVDHB Monthly Operating Report Page 11 24 April 2014
Table 9. Capital Expenditure (Asset) summary report 2014-15
Capital Plan 2012-13
carry forward
Full year capital plan
YTD approved capex
YTD Actual Spent
(invoiced)
Capital budget
unspent
Remaining budget
available to be allocated
Strategic Capex ($000) ($000) ($000) ($000) ($000)
Emergency Department & Theatre (ED&T) - 156 156 156 60 97 -Digital Mammography - 1,294 1,294 1,294 351 942 -Finance & Procurement Supply Chain (FPSC) System 736 - 736 736 377 359 -Novell Netware to MS Exchange - 168 168 168 172 (4) -Laboratory Information Systems ($1,000k from Prior Year) 747 275 1,022 1,022 1,008 14 -Child Oral Health (externally funded initiatives) - 3,466 3,466 3,466 82 3,384 -Central Region Information Systems Plan (PMS, EMR, PACS, RIS, ED, eReferrals, WhiteBoard) Programme
2,168 - 2,168 - - 2,168 2,168
Citrix Farm 1,000 - 1,000 1,000 731 269 -e-Pharmacy 500 - 500 - - 500 500MRI Scanner 2,300 - 2,300 468 - 2,300 1,832Non specified 1 - 1 - - 1 1
7,452 5,360 12,812 8,311 2,781 10,031 4,501
Baseline Capex Buildings & Plant 3,000 1,282 4,282 1,495 322 3,960 2,787Clinical Equipment 2,000 660 2,660 1,939 1,005 1,654 720Other Equipment 100 - 100 6 5 95 94Information Technology 850 780 1,630 1,535 1,059 571 95Intangible Assets (Software) 1,000 - 1,000 469 232 768 531
6,950 2,722 9,672 5,445 2,624 7,048 4,227
Total Capex 22,484 13,755 5,405 17,079 8,728
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
177

HVDHB Monthly Operating Report Page 12 24 April 2014
Table 10. Treasury Summary Report
Year Amount 2013/14 $10,500
Current month Last month 2014/15 $4,0002015/16 $14,450
Average balance for the month $30,476 $27,200 2017/18 $19,000Lowest balance for the month $13,467 $9,450 2018/19 $20,950
2019/20 $5,000Average interest rate 4.00% 3.89% 2020/21 $5,100
Total $79,000Net interest earned for the month $102,832 $80,996
4) Hedges2) Debt
Term debt - Crown (formerly CHFA) loans Repayment date Amount Interest rateCore loan 15-Dec-17 $19,000 6.535% 5) Foreign exchange transactions for the monthLoan 1 15-Apr-14 $4,500 5.490% No. of transactions involving foreign currency 5Loan 2 15-Dec-18 $4,500 5.970% Total value of transactions $26,672 NZDLoan 4 15-Apr-16 $2,000 5.520% Largest transaction $15,280 NZDLoan 5 15-Apr-16 $5,000 5.020%Loan 6 15-Mar-19 $5,000 5.685% No. of Equivalent Exchange ratesLoan 7 15-Apr-15 $4,000 4.500% AUD 5 $26,672 0.927Loan 8 15-Dec-18 $5,450 5.090%Loan 9 15-Dec-15 $5,450 4.240%Loan 10 15-Dec-18 $6,000 3.710%Loan 11 15-Apr-14 $6,000 2.915%Loan 12 15-Jun-20 $5,000 3.355% Total 5 $26,672Loan 13 15-May-21 $5,100 3.450%Loan 14 30-Jun-16 $2,000 2.750%
Total $79,000
Weighted cost of funds 4.921%
1) Short term funds / investment
No hedging contracts have been entered into for the year to date.
HBL banking activities for the month
3) Debt repayment profile
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
178

Appendix Three - 3DHB Health Service Development Programme Report 23 April 2014
March / April Programme Highlights;
Single Service Project Report In February 2014 the Sub Regional Clinical Leadership Group (SRCLG) received the first draft of the 3DHB Sub-regional Single Service Report. The development of this report had been guided by a Project Steering Group sponsored by the Chief Operating Officers (COOs). The objective of this project was to define what is meant by a sub-regional single service for the purpose of 3D HSD programme and list all the issue and requirements that need to be considered to support the development of sub-regional single services. The report outlined a number of actions that could be progressed to align services in the sub-region without significant service change.
Orthopaedics Concept Paper In February 2014 an Orthopaedics concept paper was presented to SRCLG by the Clinical Leader for this project. The recommendations in this concept paper were phased into short, medium and longer term considerations. The short term recommendations included addressing the acute and elective surgical service capacity and analysis on the viability of increasing orthopaedic surgical capacity at Kenepuru to provide elective orthopaedic surgery. Also being considered is the potential opportunity of theatre utilisation in the Hutt Valley to meet the same demand for the sub-region. A sub-regional approach to Orthopaedic Clinical Pathways is also under consideration. Any clinical pathway development will be directly linked to the regional elective project currently underway with TAS.
Single Integrated Child Health ServiceFollowing the approved mandate to progress an integrated child and youth health service for the sub-region, a project brief and comprehensive work plan has been established to co-ordinate the key activities that are required to progress a single service design. The work has been divided into three categories of Acute and Inpatient Care, Primary/Secondary Integration looking at Outpatients, models of care for children with chronic conditions, child development and services to provide care for children with disability. The third work stream is tasked with developing a Regional Paediatric Tertiary plan. Membership of each work stream includes clinicians involved in service delivery across the sub-region from medial, nursing and allied health. February and March have been spent consolidating the work into clear project briefs with defined objectives and deliverables. Each ‘work package’ has a clinical lead from the sub-region with wider membership identified to support service design. As part of this project, the 10 most common used paediatric clinical pathways have been selected for priority editing for the sub-region. We are now at a phase where we will be seeking primary care support in individual aspects of service design along with nominations for the project governance steering group. The Steering Group will be tasked with providing the strategic oversight to the project, the child health expertise will be provided through the three work streams. Vaughan Richardson remains the clinical lead for this project.Non Melanoma Skin Cancer
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
179

This project is looking at the design of a sub-regional non melanoma skin cancer (NMSC) service that would provide equity of care and access to all patients across the sub-region for the diagnosis and treatment of non melanoma skin cancer. The 3D NMSC Working Group is chaired by Mr Chris Adams and includes operational and clinical membership from Plastics, Dermatology, and Radiology Oncology along with nominated representative from each of the Alliance Leadership Team (ALTs). The group recently held their second meeting where they reviewed available skin lesion removal data across the 3DHBs. The Group discussed different models of care for a sub regional NMSC service. Chris Masters, clinical lead for HealthPathways will also attend the next meeting, to update the group on the opportunity the new HealthPathways platform provides for the sub-region.
ENTThe sub-regional ENT Steering Group who developed 14 ENT clinical pathways are the fist clinical pathways to be loaded onto the soon to be launched 3D HealthPathways website. These have been adapted into the format for the HealthPathways website and are the foundation sub-regional pathways to be implemented. This has enabled a much quicker ‘go live’ date for the primary care role out of the new pathway tool. The ENT Clinical Leaders supported have presented to primary care teams in Wellington and Kapiti about the pathways, Hutt Valley and Wairarapa dates are being confirmed. Feedback from primary care has been very positive. A sub-regional ENT operational group has replaced the Project Steering Group.
Gastroenterology A sub regional project steering group have been meeting for over the past year with a key objective of agreeing a sub-regional approach to the management of colonoscopy. The results from this and the ENT Project Steering group provided the impetus for the Single Service Project. The working group has evolved to a point where the agreed emphasis that would provide the most benefit for the sub-region is the development of a single Gastroenterology Service which will be progressed through the COOs and Clinical Leader for this work.
Key Planned Activities/Emerging Priorities;o Single Service project to develop guidance and a tool kit to support clinical services designo HealthPathways implementation group working closely with the sub-regional clinical groups noted in this report.
New Risks/Concerns and Mitigation;N/A
Communication;
∑ The single service project will develop a communication tool kit to compliment the service design information and recommendations.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
180

Page 1 of 4
Appendix Four - Wairarapa and Hutt Valley Communications Update April 2014
1 External communications / Media
Health Highlights
Now published post-Board meeting, with Board line-up and Chair’s column featured.
Both March pages focused on Pacific Health, affirmation of 3DHB direction, endorsing the Board’s pro-fluoride stance, flu vaccination and Emergency Planning. (Hutt) Evacuation training using new evac-chairs, 70th anniversary, children’s ward refurbishment. (Wairarapa) Masterton Medical Practice now on site, Deaf Interpreter service.
Media releases/enquiries 8 March – 17 April 2014
2 Primary Care, including Tihei Wairarapa and Hutt Inc
∑ Monthly advertising of the ‘ED or GP’ message, listing after-hours services and Healthline.
∑ Wairarapa – requirement for MML support now minimal, successful transition onto the hospital site.
3 Working with our neighbours
Sub-Regional (3DHB)
∑ Consultation paper proposing a 3DHB Communications function still being developed in HR
∑ Communications re: FPSC – including special edition of e-Link for new finance system, intranet pages and links to resources
∑ Single print room service project – site visits to two sites to evaluate providers in action
∑ Flu vaccination campaign underway
Wairarapa
Emergency Management
Health Targets
Coroner’s report
Patient condition updates
Breastfeeding awareness
Hutt Valley
Health Targets
Coroners report
Patient condition updatesAlcohol and ED
Antidepressants
New bladder scanner
Stolen gowns and towels
17yo pedestrian struck by vehicle on SH2
Dog attack victim
Hutt City Sports Awards
Health Highlights March
Long-serving midwives retire
Young smokers
Skill saw accident victim
Under-15 Alcohol & ED
Nurses in old photo (70th)
Too many hospital beds
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
181

Page 2 of 4
∑ Further workshop regarding labour/management partnership, now working on strategy of convergence with other initiatives in the sub-region including the Values Based Behaviours work done by the Organisational Development officer in CCDHB, organisational culture work underway within HR in Hutt, and a number of profession-based initiatives.
∑ Attended National Communications Managers conference which included presentations from Prof Swee Tan, a CCDHB Internal medicine specialist on ED wait times, Minister of Health, Director General of Health, HQSC, and a variety of national project managers.
∑ Radiology and Lab projects.
∑ Aligning the Early Warning Score initiatives.
2DHB
∑ Shared website successfully launched 2 March. Positive feedback. Stats tracking well.
5 Jan – 1 Feb 2 Feb – 1 Mar 2 Mar – 29 Mar
Users total 8,604 8,954 10,467
Pageviews total 30,678 31,455 41,357
Average duration of visit
00:01:46 00:01:35 00:01:52
Bounce rate (visited home page only)
63.97% 64.26% 55.13%
% Returning visitors
58.4% 59.3% 54.5%
% New visitors 41.6% 40.7% 45.5%
∑ Facebook presence updated on both sites. Twitter monitored
∑ User testing environment established for Shared workspaces. Need for webmeister/portal administrator role reaffirmed
∑ Response to Ministers office – emergency preparedness
∑ Version 7.2 Organisation charts published.
4 Internal communications
All staff memos
Shared
Mental Health Leadership Approach
Sub-regional mental health
Update for Perioperative Department
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
182

Page 3 of 4
Wairarapa
Advance Care Planning
Chaplain's leave
Masterton Medical invite
Wairarapa Alcohol survey
Flu vaccination for staff
Safe services the priority
Insite online
Farewell for Diane Brewster
Hutt Valley
Weekly staff eLink (emailed/printable newsletter)
Support Hutt Hospital Foundation Trust by shopping at Z-Vic Corner (good in the hood campaign - Hutt) Occupational Health – change to the case management process for non-work injuries – Hutt
Special edition of Staff News for the rollout of new Finance System - Hutt
Intranet stories 7 March - 16 April 2014
Shared
Confirmation of Perioperative Services Leadership Structure
3DHB Mental Health Proposal
Minister announces new DHB appointments
3DHB Radiology Service
National Administration Professionals Day
Flu vacc free for DHB staff
End of life care survey: Your views welcomed ‘Sign Up’ for better service
Sub regional Mental Health Services
Minister launches flu immunisation campaign Political affiliations register inappropriate
Wairarapa
National April Falls Quiz 2014
Flu vacc free for DHB staff
Health records champion
Coroner's Recommendations
Nurturing Baby - breastfeeding awareness
Safe services the priority
Going, going, gone.
'Health Pathways' project launched
Welcome to MML
Wairarapa Help Desk Calls being answered by Capital Coast Team
We welcome three new doctors
Latest results for health targets out
Community alcohol survey
Hutt Valley
Mystery nurses identified
New electronic ordering – Radiology requests
Election guidance for public servants from SSC
Easter payroll deadlines
New Finance System goes live
Conversations that Count Day –Advance Care Planning
Board members getting their flu shots
Microsoft home use program
Clown Doctors visit Hutt Hospital
New pricing agreement with Active Healthcare saves $110,000
Fire alarm trial evacuation
Midwives farewelled after 40 years of service
Coronial recommendations recap
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
183

Page 4 of 4
New Hutt Hospital Chaplain starts
February Balanced Scorecard (how we’re doing)
Health Pathways project launch
Pregnancy and yoghurt study – call for participants
Liz Sargeant visit – Allied Health
Healthy Workplace Awards – team morale/spirit
Freemasons donate bladder scanners to hospital
Betty Poot becomes Nurse Practitioner
7 Other Communications projects
Wairarapa
Influenza vaccination
Palliative Care – Kahukura/Hospice Wairarapa partnership – patient documentation
Shared intranet/workspaces
Patient information and brochure development
Launch of 5 things in the first 10 weeks of pregnancy campaign
Shared intranet/workspaces
Displays in foyer of Hospital: Stroke Awareness, falls, flu and Admin Appreciation
Patient information and brochure development
Redo site maps
Hutt Valley
70th anniversary of Hutt Hospital, including digitising several hundred archive photos
Updating image libraries
Patient information and brochure development
Pacific Health Scholarships
Annual report planning
Healthy Families initiative – how to support
Employee Recognition initiatives
Allied Health Intranet page reorganisation
Theatre Algorithms – loading onto intranet
Art Canvas project for hospital walls
Establishment of studio for clinical and corporate photographer in old ICU
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
184

Page 1 of 17
Appendix Four - Official Information Act Requests – Hutt Valley DHB
OIA 117
Andrea O’NealDom Post
11.02.2014 I'm seeking information on how many hospital gowns and towels have been taken home by patients and not returned, in each of the last 5 years. If we could categorise this by Hutt & Wairarapa DHBs that would be great.The total number of gowns and towels in circulation in the DHBs would be helpful to put it in context.I would also like to know the cost to replace a gown and a towel, and how much the DHBs spend on those items a year.Response:We cannot identify numbers of gowns and towels taken home by patients and not returned. All losses are classified as “unidentified”.Our Laundry/Linen service is provided by Allied Laundry for five District Health Boards. The stock is pooled and generic across all five District Health Boards and we do not have “loss” numbers separated out for MidCentral.The average losses per year over the last five years across all five District Health Boards are :2,622 gowns (average cost $18.56 per gown)6,800 standard bath towels (average cost $5.24 each)
Completed 06.03.2014
OIA 118
David Clark MP Dunedin North
13.02.2014 Request:1. The amount of mental health funding that was retained for provision delivered by DHB directly, for 2009/10, 2010/11, 2011/12 & 2012/13 financial years.ResponsePlease refer to Appendix 1 for details.2. A list of all the changes made by your DHB to the community provision of mental health since 2009. The information sought on the identity of the provider has been withheld. The information withheld is in accordance with section 9(2)(b)(ii), 9(2)(i) and 9(2)(j).
ResponsePlease refer to Appendix 2 for details.The information sought on the identity of the provider has been withheld. The information withheld is in accordance with section 9(2)(b)(ii), 9(2)(i) and 9(2)(j).3. Is the DHB required to ring-fence mental health funding now? If so, please provide a breakdown showing the way in which mental health funding is spent.Response
Completed 13.03.2014
OIA Requestor Received Request/Response Status
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
185

Page 2 of 17
Please refer to Appendix 3 for details.4. For the community organisations that have received mental health funding from your DHB, please provide a breakdown of spending by organisation and by type of provision for the 2009/10, 2010/11, 2011/12 & 2012/13 financial years.
ResponsePlease refer to Appendix 2 for details.
The information sought on the identity of the provider has been withheld. The information withheld is in accordance with section 9(2)(b)(ii), 9(2)(i) and 9(2)(j).
You have a right to seek a review, under section 28(3) of the Official Information Act by way of a complaint to the Ombudsman(The Board is welcome to request the appendices)
OIA 119
Rebecca StevensonFairfax
17.02.2014 RequestI am seeking information about New Zealand hospitals and issues with sub-standard fire safety systems under the Official Information Act 1982.Is Hutt Valley DHB aware of any issues with sub-standard fire safety systems including passive fire protection systems at any of its sites?What sort of defects/faults have been found?Where/which facilities have been found to have sub-standard fire safety systems including compromised passive fire protection systems?What is being done about these sub-standard systems?What is the estimated cost to fix the systems?When did Hutt Valley DHB become aware of the first hospital with issues with its fire safety systems?When did the DHB become aware of further hospitals/sites with sub-standard fire safety systems? Dates and all detail available please.Is there a danger to the public using these hospitals in case of fire?Can the DHB b release all correspondence between it and contractors/fire engineers/certifiers related to sub-standard systems?Has the DHB commissioned any reports/enquiries/inspections into fire safety at its hospitals? If so, what are they, can I please see them.What emergency planning has been done in relation to these sub-standard fire safety systems, including passive fire protection, and the evacuation of patients in case of fire?Is any action - including seeking compensation/remedial work - being taken against contractors/fire engineers/certifiers for sub-standard fire safety systems in the DHB's hospitals?Response:Hutt Valley and Capital and Coast DHBs maintain their facilities, including fire protection and detection
Completed13.03.2014
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
186
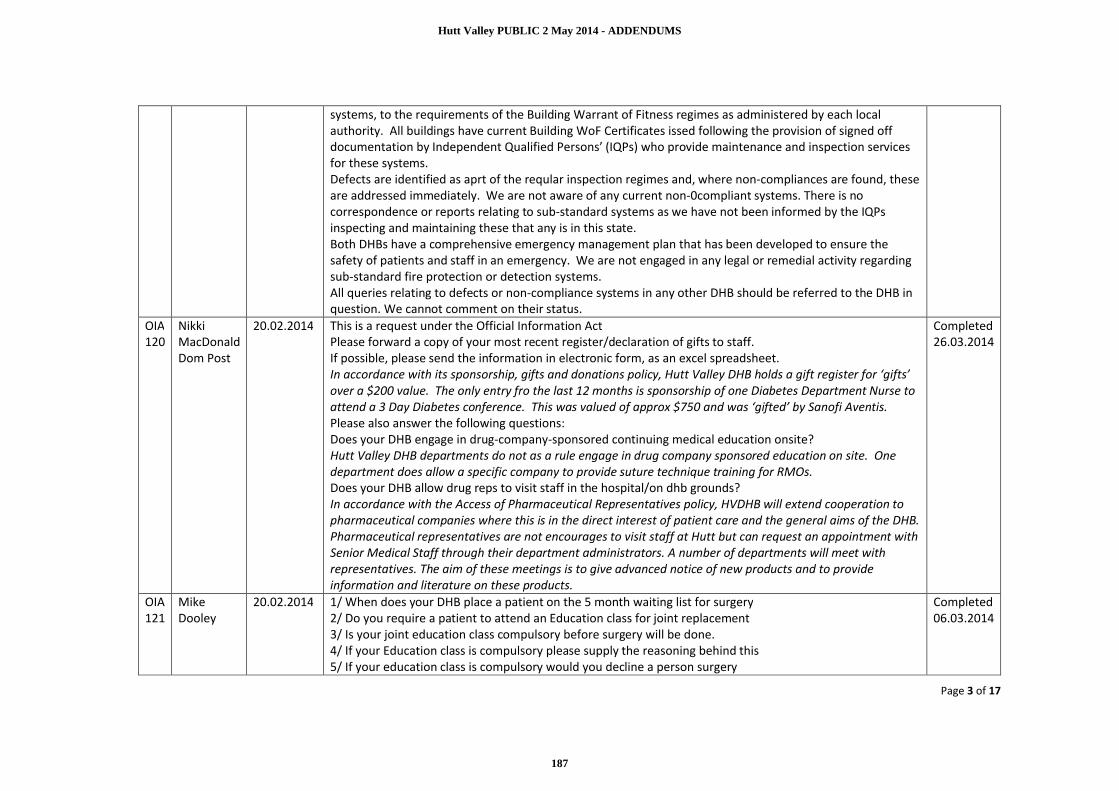
Page 3 of 17
systems, to the requirements of the Building Warrant of Fitness regimes as administered by each local authority. All buildings have current Building WoF Certificates issed following the provision of signed off documentation by Independent Qualified Persons’ (IQPs) who provide maintenance and inspection services for these systems.Defects are identified as aprt of the reqular inspection regimes and, where non-compliances are found, these are addressed immediately. We are not aware of any current non-0compliant systems. There is no correspondence or reports relating to sub-standard systems as we have not been informed by the IQPs inspecting and maintaining these that any is in this state.Both DHBs have a comprehensive emergency management plan that has been developed to ensure the safety of patients and staff in an emergency. We are not engaged in any legal or remedial activity regarding sub-standard fire protection or detection systems.All queries relating to defects or non-compliance systems in any other DHB should be referred to the DHB in question. We cannot comment on their status.
OIA120
Nikki MacDonaldDom Post
20.02.2014 This is a request under the Official Information ActPlease forward a copy of your most recent register/declaration of gifts to staff.If possible, please send the information in electronic form, as an excel spreadsheet.In accordance with its sponsorship, gifts and donations policy, Hutt Valley DHB holds a gift register for ‘gifts’ over a $200 value. The only entry fro the last 12 months is sponsorship of one Diabetes Department Nurse to attend a 3 Day Diabetes conference. This was valued of approx $750 and was ‘gifted’ by Sanofi Aventis.Please also answer the following questions:Does your DHB engage in drug-company-sponsored continuing medical education onsite?Hutt Valley DHB departments do not as a rule engage in drug company sponsored education on site. One department does allow a specific company to provide suture technique training for RMOs.Does your DHB allow drug reps to visit staff in the hospital/on dhb grounds?In accordance with the Access of Pharmaceutical Representatives policy, HVDHB will extend cooperation to pharmaceutical companies where this is in the direct interest of patient care and the general aims of the DHB.Pharmaceutical representatives are not encourages to visit staff at Hutt but can request an appointment with Senior Medical Staff through their department administrators. A number of departments will meet with representatives. The aim of these meetings is to give advanced notice of new products and to provide information and literature on these products.
Completed 26.03.2014
OIA 121
Mike Dooley
20.02.2014 1/ When does your DHB place a patient on the 5 month waiting list for surgery2/ Do you require a patient to attend an Education class for joint replacement3/ Is your joint education class compulsory before surgery will be done.4/ If your Education class is compulsory please supply the reasoning behind this5/ If your education class is compulsory would you decline a person surgery
Completed 06.03.2014
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
187

Page 4 of 17
Response:1. Currently this is when the patient is listed for surgery following the First Specialist Appointment (FSA)
and a discussion with the Consultant. We are in the process of considering changes to the model of care with the clear intention to move to a "fit for surgery" before placing the patient on the wait list.
2. Yes we do.3. No. However there is a high expectation that all primary joints patients attend. Those that are having
a revision are advised of the class and are able to attend if they wish to do so.4. N/A.5. N/A.
OIA 122
Annette KingMP
24.02.2014 How many patients are currently waiting for ultrasound and how long are patients waiting?Response:Hutt Valley District Health Board currently has 11 patients waiting for an ultrasound. The average waiting time for these patients is between two days and one week.
Completed 12.03.2014
OIA 123
Annette King MP
24.02.2014 The number of nursing vacancies as of 28 February 2014?The number of senior medical officer vacancies as of 28 February 2014?Details of the length of time it is taking to fill vacancies?Response:On 28 February 2014 there were four Nursing vacancies and no SMO vacancies. The length of time it has taken to fill the vacancies (from the date the Authority to Appoint form is received by Human Resources up to and including 28 February) for Nursing vacancies is one to two months. Mental Health Nursing vacancies can take longer to fill.
Completed 21.03.2014
OIA 124
Annette KingMP
25.02.2014 Request : All Mix and match Part II reports of ‘Trend Care’ from January 2013Response:
1. Has the DHB performed any mix and match part 2 calculations?No.2. And;
a. Which wards and department have had the part 2 calculations done ?None as yet.b. How long the DHB has been implementing CCDM?Hutt Valley DHB is participating in the CCDM process. A Letter of Agreement was signed with the SSHW Unit and NZNO and PSA in August 2013 to undertake the programme.c. Explanation of why the calculations have been done in only some wards / departments (depending how long they have been on the programme).Hutt Valley DHB has completed the Mix & Match part 1 two week data collection phase in a pilot
Completed21.03.2014
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
188
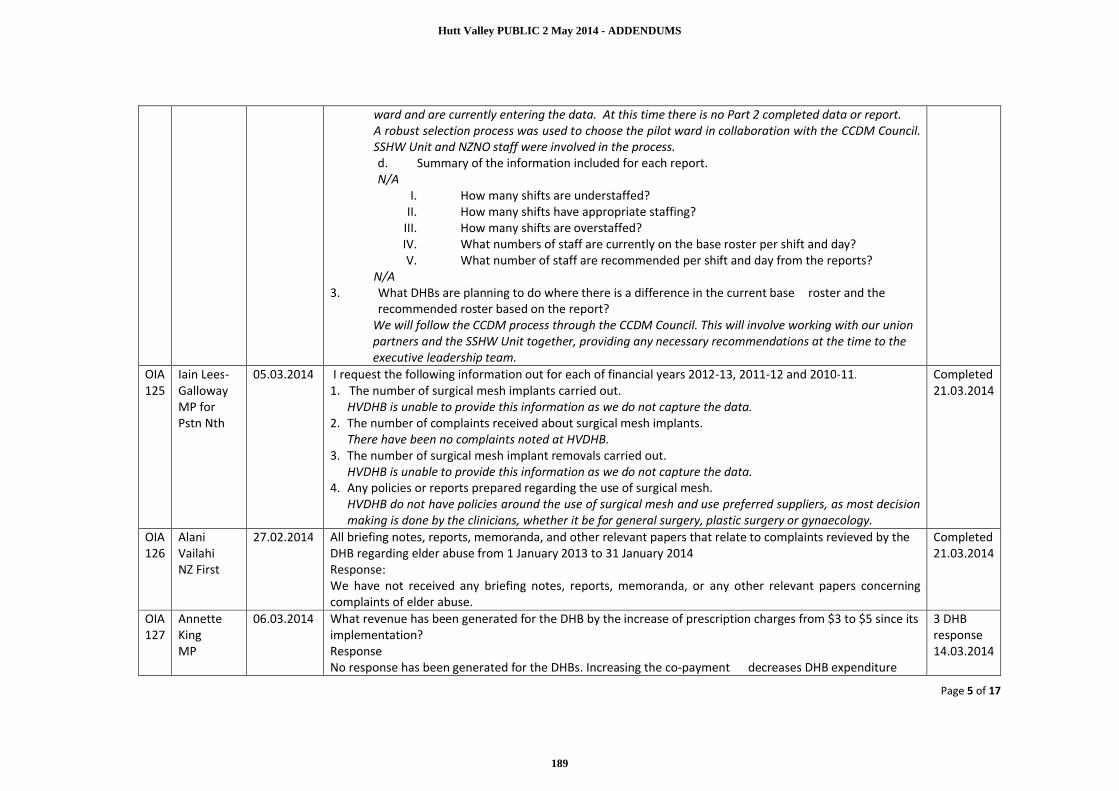
Page 5 of 17
ward and are currently entering the data. At this time there is no Part 2 completed data or report.A robust selection process was used to choose the pilot ward in collaboration with the CCDM Council. SSHW Unit and NZNO staff were involved in the process.d. Summary of the information included for each report.N/A
I. How many shifts are understaffed?II. How many shifts have appropriate staffing?
III. How many shifts are overstaffed?IV. What numbers of staff are currently on the base roster per shift and day?V. What number of staff are recommended per shift and day from the reports?
N/A3. What DHBs are planning to do where there is a difference in the current base roster and the
recommended roster based on the report?We will follow the CCDM process through the CCDM Council. This will involve working with our union partners and the SSHW Unit together, providing any necessary recommendations at the time to the executive leadership team.
OIA 125
Iain Lees-GallowayMP for Pstn Nth
05.03.2014 I request the following information out for each of financial years 2012-13, 2011-12 and 2010-11.1. The number of surgical mesh implants carried out.
HVDHB is unable to provide this information as we do not capture the data.2. The number of complaints received about surgical mesh implants.
There have been no complaints noted at HVDHB.3. The number of surgical mesh implant removals carried out.
HVDHB is unable to provide this information as we do not capture the data.4. Any policies or reports prepared regarding the use of surgical mesh.
HVDHB do not have policies around the use of surgical mesh and use preferred suppliers, as most decision making is done by the clinicians, whether it be for general surgery, plastic surgery or gynaecology.
Completed21.03.2014
OIA 126
Alani VailahiNZ First
27.02.2014 All briefing notes, reports, memoranda, and other relevant papers that relate to complaints revieved by the DHB regarding elder abuse from 1 January 2013 to 31 January 2014 Response:We have not received any briefing notes, reports, memoranda, or any other relevant papers concerning complaints of elder abuse.
Completed 21.03.2014
OIA 127
Annette KingMP
06.03.2014 What revenue has been generated for the DHB by the increase of prescription charges from $3 to $5 since its implementation?ResponseNo response has been generated for the DHBs. Increasing the co-payment decreases DHB expenditure
3 DHB response 14.03.2014
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
189

Page 6 of 17
rather than increasing DHB revenue.In Budget 2012, the Government re-priortised DHB funding ($20 million in 2012/13 and $40 million per annum from 2013/14) in line with the forecast reduction in DHB expenditure on pharmaceutical claims caused by increasing the patient co-payment to $5. Official information was released on this as part of the Treasury-led information release process for the budget. The information is already publically available on the Treasury website. www.treasury.govt.nz/publications/informationreleases/budget/2012
OIA 128
Annette KingMP
06.03.2014 The number of colposcopies undertaken from 2009/10 to 2013/14Response:
2009/10 2010/11 2011/12 2012/13 2013/ 14Wairarapa DHB
349 324 341 343 287 YTD
Hutt Valley DHB
475 560 644 640 426 YTD
Completed 27.03.2014
OIA 129
Annette KingMP
06.03.2014 The Number of varicose veins treated by non-surgical methods eg UGS or EVLA from 2009/10 to 2013/14Response:Neither Wairarapa or Hutt Valley DHB carry out these types of procedures.
Completed 03.04.2014
OIA 130
Clare SziranyiRadio NZ
07.03.2014 Request∑ How many pediatric oncology patients from Hutt Valley DHB have been diagnosed and sent to Auckland or Christchurch since Wellington ceased its service?
Answer: 26 patients∑ What has been the cost to Hutt Valley DHB in transporting these patients and their family members out of Wellington in order to receive oncology treatment in the other centres?∑ Answer: Total costs between July 2009 to December 2013 totals $250,885.90∑ What has been the cost to Hutt Valley DHB of accommodating family members in Auckland or Christchurch?∑ Answer: Total costs between July 2009 to December 2013 totals $146,014.86
Completed 08.04.2014
OIA 131
Jared NicolHutt News
12.03.2014 How many people went to the Hutt Hospital's ED while intoxicated in 2008 and in 2013?How old were they?Were they male or female?How many people went to the ED for alcohol-related problems in 2008 and 2013? And how many were admitted?Board can request a copy of response as is a large spreadsheet.
Completed 07.04.2014
OIA Iain Lees- 12.03.2014 I request the following information for each of financial years 2012-13, 2011-12 and 2010-11. Completed
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
190

Page 7 of 17
132 GallowayMP
1. The number of people with mental illness living in supported accommodation funded by the DHB.
2. The amount spent by the DHB on supported accommodation for people with mental illness.
3. The number people with mental illness assessed as able to transition from acute care to supported accommodation who have remained in acute care for any period of time due to unavailability of supported accommodation. This data is not readily available locally as the information is not part of any existing DHB reporting. To extract the information the DHB will need to review individual case files which will require additional capacity (time and personnel) including individual consumer approval and NGO providers input.As there would be considerable time involved by DHB and NGO staff to provide this information we would need to charge for the supply of this information. If you are able to refine your request we may be able to reduce any costs to you. Once you have confirmed your requirements we can advise the expected costs. 4. The average waiting time from referral to entering supported accommodation for people with mental illness.This data is not readily available locally as the information is not part of any existing DHB reporting. To extract the information the DHB will need to review individual case files which will require additional capacity (time and personnel) including seeking individual consumer approval and NGO providers input.
As there would be considerable time involved by DHB and NGO staff to provide this information we
15.04.2014
Hutt Valley DHB Residential Services:Comments
Provider PU service 2010/11 2011/12 2012/13 2010/11 2011/12 2012/13Provider 1 MHA24 residential beds 8 8 6 4.9 4.8 4.8Provider 2 MHA24 residential beds 10 12 9 7.5 7.8 9.6
Provider 3 MHA25 residential beds 17 18 9 9.6 9.8 6.4
reallocation of beds to CSW Transition service occurred in 2012/13
Provider 4 MHA07 residential beds 7 7 8 6.4 6.9 5.1Total 42 45 32 28.4 29.2 25.9
unique clients beds used
PU code PU description $ 2010/11 $ 2011/12 $ 2012/13MHA24 Housing and Recovery Services Day time/ Awake Night support 657,000 402,072 407,340MHA25 Housing and Recovery Services Day time/Responsive Night support 764,688 519,000 526,236Total 1,421,688 921,072 933,576
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
191

Page 8 of 17
would need to charge for the supply of this information. If you are able to refine your request we may be able to reduce any costs to you. Once you have confirmed your requirements we can advise the expected costs. 5. Any reports prepared regarding the availability of supported accommodation for people with mental illness.
There are no such reports
You have the right to seek a review, under Section 28(3) of the Official Information Act by way of a complaint to the Ombudsman.
OIA 133
Megan SmithBeat Bowel Cancer
10.03.2014 The portion of Patients diagnosed with bowel cancer who are discussed at a multidisciplinary team meeting.(NB: this is a transfer from MoH)Response:Hutt Hospital have a Colo-rectal MDM here, but some cases could be discussed through the Wellington Hospital MDM. We are unable to supply the proportionate number of patients discussed, as we do not record this information.
Completed 27.03.2014
OIA 134
Annette KingMP
12.03.2014 How many complaints has the DHB, through any mechanism, received relating to health and safety concerns in the last 12 months?Response:Wairarapa and Hutt Valley DHB have not received any complaints relating to health and safety concerns.
Completed 27.03.2014
OIA 135
Mike Dooley
17.03.2014 In 2011 the Auditor general’s office released a performance audit report titled “ Progress in delivering funded scheduled services to patients”In this report it highlighted the following:The priority areas that we recommend they focus on are ensuring that:• patients are more consistently selected for first specialist assessments;• patients are more consistently prioritised for treatment;• a greater proportion of patients receive scheduled services within the expectedtime limits;• a greater proportion of patients are treated in priority order; and• progress is made in quantifying the level of unmet need for scheduled services.1/ Patients are more consistently selected for first specialist assessments. The report highlights:We found that patients are selected for an FSA using three main methods. Two of these methods are likely to achieve consistency within the DHB even if selection tools are not used.The three methods are:a) The first method involves a single individual, such as a GP liaison12 or semi-retiredsurgeon, who assesses all referrals received by a specialty. This individual accepts or declines patients for an
Completed 10.04.2014
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
192
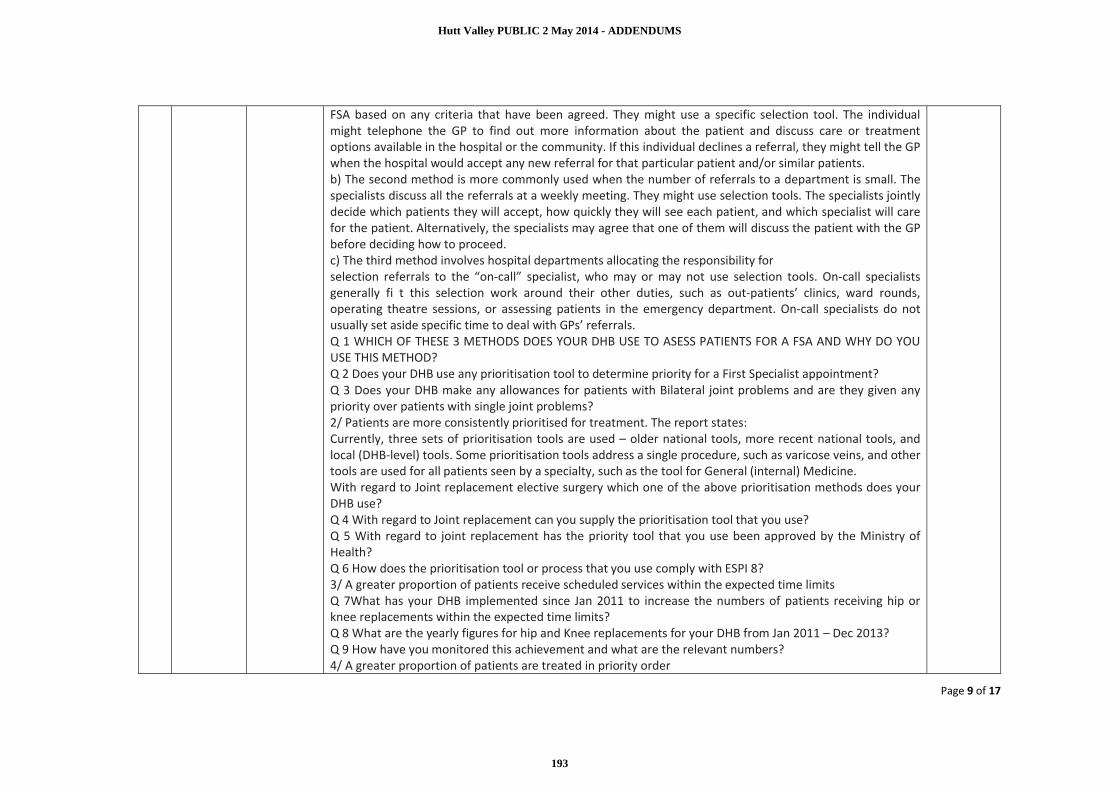
Page 9 of 17
FSA based on any criteria that have been agreed. They might use a specific selection tool. The individual might telephone the GP to find out more information about the patient and discuss care or treatment options available in the hospital or the community. If this individual declines a referral, they might tell the GP when the hospital would accept any new referral for that particular patient and/or similar patients.b) The second method is more commonly used when the number of referrals to a department is small. The specialists discuss all the referrals at a weekly meeting. They might use selection tools. The specialists jointly decide which patients they will accept, how quickly they will see each patient, and which specialist will carefor the patient. Alternatively, the specialists may agree that one of them will discuss the patient with the GP before deciding how to proceed.c) The third method involves hospital departments allocating the responsibility forselection referrals to the “on-call” specialist, who may or may not use selection tools. On-call specialists generally fi t this selection work around their other duties, such as out-patients’ clinics, ward rounds, operating theatre sessions, or assessing patients in the emergency department. On-call specialists do not usually set aside specific time to deal with GPs’ referrals. Q 1 WHICH OF THESE 3 METHODS DOES YOUR DHB USE TO ASESS PATIENTS FOR A FSA AND WHY DO YOU USE THIS METHOD?Q 2 Does your DHB use any prioritisation tool to determine priority for a First Specialist appointment?Q 3 Does your DHB make any allowances for patients with Bilateral joint problems and are they given any priority over patients with single joint problems?2/ Patients are more consistently prioritised for treatment. The report states:Currently, three sets of prioritisation tools are used – older national tools, more recent national tools, and local (DHB-level) tools. Some prioritisation tools address a single procedure, such as varicose veins, and other tools are used for all patients seen by a specialty, such as the tool for General (internal) Medicine.With regard to Joint replacement elective surgery which one of the above prioritisation methods does your DHB use?Q 4 With regard to Joint replacement can you supply the prioritisation tool that you use?Q 5 With regard to joint replacement has the priority tool that you use been approved by the Ministry of Health?Q 6 How does the prioritisation tool or process that you use comply with ESPI 8?3/ A greater proportion of patients receive scheduled services within the expected time limitsQ 7What has your DHB implemented since Jan 2011 to increase the numbers of patients receiving hip orknee replacements within the expected time limits?Q 8 What are the yearly figures for hip and Knee replacements for your DHB from Jan 2011 – Dec 2013?Q 9 How have you monitored this achievement and what are the relevant numbers?4/ A greater proportion of patients are treated in priority order
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
193

Page 10 of 17
Q 10 How does your DHB decide on priority order for Hip and Knee replacement and how accurate is it?5/ Progress is made in quantifying the level of unmet need for scheduled servicesQ 11 Unmet need has been a point of concern recently with announcements being made that these figures are not kept. Q 12 Does your DHB know what the unmet need for Hip and Knee replacement is?Q 13 If your DHB does not keep these figures why is this?ResponseIn Wairarapa and Hutt Valley DHB’s a mix of one individual or on call specialists triaging referrals is used. National tools are used for all triaging. Some are older, some are under review such as the orthopaedic tool (which includes all orthopaedic procedures) and some are new and are just being introduced – ENT and Gynaecology. National tools are approved by the Ministry of Health so ESPI 8 is compliant.Patients being referred for all joint replacements are triaged against the same criteria. Please see attachment.In regards to orthopaedic service delivery an additional FTE has been employed and additional theatre time provided for surgery. This is for elective surgery but hip and knee replacements are only part of this. We look at standard intervention rates per 10,000 population and this report was last done in December 2013. At that time the findings were:Wairarapa DHB’s standardised discharge rate is 24.75 and this ranks them 5 in New Zealand.Hutt Valley DHB’s standardised discharge rate is 23.15 and this ranks them 7 in New Zealand.Hip and Knee replacement at Wairarapa and Hutt Valley DHBs
Hip and Knee Joint replacements (including revisions)
2011 2012 2013
Wairarapa DHB 123 115 125Hutt Valley DHB 274 321 309
All patients on all elective waiting lists are treated in priority order looking at priority (urgent, semi urgent) and time waiting on the list. Patients are treated within the Ministry waiting times in both DHB’s.In regards to unmet need we have by specialty the volumes declined for an FSA. Hip and Knee referrals cannot be singled out of this volume as the information is generated from the comments of the GP on the referral – e.g. sore knee, OA knee, pain knee, ? knee replacement required, bilateral knees and a variety of other descriptors. Some referrals will be requests for advice for patients. We do not keep specific figures for hip and knee, as this is irrelevant. All those who meet the triaging criteria are seen. Those that do not meet the criteria regardless of their presenting complaint, are declined. In both DHB’s you can only see what you have capacity to see and treat so this is reliant on manpower, theatre access and beds
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
194

Page 11 of 17
all being available.
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
195

Page 12 of 17
OIA 136
Denise TairuaAPEX
17.03.2014 Pursuant to section 12 of the Official Information Act 1982, APEX requests the data and/or information held by Hutt Valley District Health Board, with regards to Clinical Physiologists. In particular, could you please provide the following information: a. The current numbers of Clinical physiology staff with a breakdown by specialty i.e. – Sleep, Cardiac, Respiratory and Renal, of Physiologists, Physiology Technicians and ECG Technicians and the number on each salary, this includes Renal Physiologists – formerly known as Dialysis Technicians.
Head CountEmployee Status
MECA Specialty Salary FULL PART CASUALGrand Total
APEX Clinical Physiologist $49,272 1 1Clinical Physiology Technician $49,272 1 1Clinical Physiologist Provisional $46,536 1 1
Grand Total 2 1 0 3
b. The number of Clinical Physiologists, including Renal Physiologists, formerly known as Dialysis technicians, who have successfully used merit progression. With a breakdown by specialty – Sleep, Cardiac, Respiratory, Renal, and by years i.e. the number in 2011, 2012 and 2013.
Merit Progression 2011 2012 2013
Head Count 0 0 0
c. The Continuing Medical Education/Continuing Professional Development budget for Physiology Staff as well as the actual amount used in 2011, 2012, and 2013 and excluding the amount used for training for Physiology related qualifications.
2011 2012 2013
CPD 943 2,191 4,442Educational Leave 1,022 3,527 1,103Total Spent 1,965 5,718 5,545
Completed 15.04.2014
OIA 137
Denise TairuaNZ Med Lab Workers Union
18.03.2014 Pursuant to section 12 of the Official Information Act 1982, The New Zealand Medical Laboratory Workers Union (NZMLWU) requests the data and/or information held by Hutt Valley District Health Board, with regards to Laboratory Workers, including Medical Laboratory Scientist, Medical Laboratory Technicians, Specimen Services Technicians QSST, Phlebotomists, Mortuary Technicians and Medical Laboratory Assistants. In particular, could you please provide the following information:a. The current numbers of Laboratory staff on each step of the salary scale with a breakdown by Scientists,
In Progress
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
196
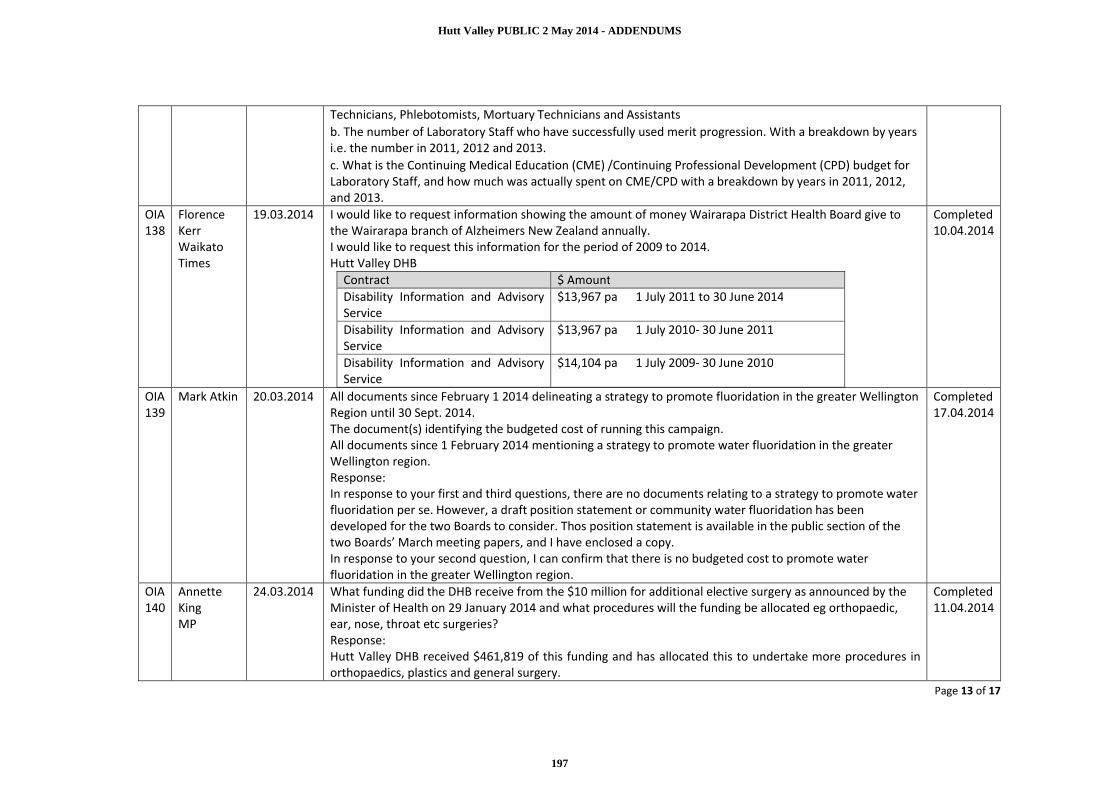
Page 13 of 17
Technicians, Phlebotomists, Mortuary Technicians and Assistants b. The number of Laboratory Staff who have successfully used merit progression. With a breakdown by years i.e. the number in 2011, 2012 and 2013. c. What is the Continuing Medical Education (CME) /Continuing Professional Development (CPD) budget for Laboratory Staff, and how much was actually spent on CME/CPD with a breakdown by years in 2011, 2012, and 2013.
OIA 138
Florence KerrWaikato Times
19.03.2014 I would like to request information showing the amount of money Wairarapa District Health Board give to the Wairarapa branch of Alzheimers New Zealand annually.I would like to request this information for the period of 2009 to 2014.Hutt Valley DHB
Contract $ AmountDisability Information and Advisory Service
$13,967 pa 1 July 2011 to 30 June 2014
Disability Information and Advisory Service
$13,967 pa 1 July 2010- 30 June 2011
Disability Information and Advisory Service
$14,104 pa 1 July 2009- 30 June 2010
Completed 10.04.2014
OIA 139
Mark Atkin 20.03.2014 All documents since February 1 2014 delineating a strategy to promote fluoridation in the greater Wellington Region until 30 Sept. 2014. The document(s) identifying the budgeted cost of running this campaign.All documents since 1 February 2014 mentioning a strategy to promote water fluoridation in the greater Wellington region.Response:In response to your first and third questions, there are no documents relating to a strategy to promote water fluoridation per se. However, a draft position statement or community water fluoridation has been developed for the two Boards to consider. Thos position statement is available in the public section of the two Boards’ March meeting papers, and I have enclosed a copy.In response to your second question, I can confirm that there is no budgeted cost to promote water fluoridation in the greater Wellington region.
Completed 17.04.2014
OIA 140
Annette KingMP
24.03.2014 What funding did the DHB receive from the $10 million for additional elective surgery as announced by the Minister of Health on 29 January 2014 and what procedures will the funding be allocated eg orthopaedic, ear, nose, throat etc surgeries?Response:Hutt Valley DHB received $461,819 of this funding and has allocated this to undertake more procedures in orthopaedics, plastics and general surgery.
Completed 11.04.2014
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
197

Page 14 of 17
OIA 141
Jo CoffeyNZNO
25.03.2014 I am hereby requesting under the Official Information Act 1982, any information held by the DHB that is relevant to the recent Part 2 Calculations done on Hutt Medical Ward and decisions around the FTE calculations be shared with myself as the members representative. This request is made pursuant to and in reliance upon the provisions of the Privacy Act 1993.In addition to the above the ED Department have been reviewing an escalation model that affects the hospital, with no NZNO consultation or NZNO delegate involvement in that process, which has also been raised with the CNM. This is an important process and has wider hospital implications for our membership. NZNO is also requesting that under clause 24.0 to be involved in this work through a proper co-operation, consultation and management of change process.
In Progress
OIA 142
Mary Bryne
26.03.2014 Please provide a copy of the Report on fluoridation that was given to the Hutt Valley DHB members last week.I am requesting this under the official Information Act.Response:Under Section 18(d) of the Official Information Act 1982, this information is publicly available on the Hutt Valley District Health Board website.http://www.huttvalleydhb.org.nz/contentClick on ‘Who we are’.Then ‘Board and Governance’, then ‘view meeting times and papers’.
Completed 27.03.2014
OIA 143
Michelle DuffFairfax
26.03.2014 This is an Official Information Act request for a copy of your district health board's last ACC audit report, as detailed below."As Accredited Employers DHBs are required to have an approved independent auditor undertake an annual audit against ACC audit standards for Safety Management Practices and Injury Management."
In Progress
OIA 144
Janine Ryder
27.03.2014 • How many and which DHB's currently fund Practice Nurse Subsidiary for their Accidentand Medical Clinic(s);
• Which DHB's currently fund Practice Nurse Subsidiary for their Emergency Departments .
In Progress
OIA 145
Jonathon BrownNZ Taxpayers Union
01.04.2014 1. Has the Ministry/DHB adopted a standard definition of ‘front line staff’? If so, provide details2. Does the Ministry/DHB collect data on the number of staff that are/aren’t front line staff? If so we request that information3. What is the amount spent in the last financial year on employment of front line staff as a percentage of the total employee expenses of the Ministry/DHB?
Withdrawn 10.04.2014
OIA 146
Mary BullApex
01.04.2014 Requests a copy of all written documentation and communication relating to the 3DHB Radiology Project –including all notes, emails, letters, minutes, workshop material, proposals and any other documentation from: The 3DHB Plan, The 3DHB Radiology Project, The Radiology Working Group, and The 3DHB Radiology
In progress
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
198

Page 15 of 17
Steering Group.OIA 147
Chris Waggstaff
Request1. Any legislative changes to the "Smoke Free Environmental Act 1990", that has occurred from 2008 till the present2. Any and all public complaints,Any and all visits from the 'Public Health Service',Any and all outcomes that has affected Fidel's Cafe,Any other information that the "Public Health service" has on file3. a copy of the "Ministry of Health Smoke-Free Compliance and Enforcement Manual"
Response:1. There have been a number of changes to the Smokefree Environments Act. A copy of the Act can be found here: http://www.legislation.govt.nz/act/public/1990/0108/latest/DLM223191.html
A copy of the High Court ruling between the Cancer Society of New Zealand v The Ministry of Health is attached.
2. We have identified a number of documents as being within your request. This information, and my decision in respect of it, is set out in the table below:
Number Document Description Action2-8 Emails/ correspondence / letters
various dates between RPH and Fidels
Released
9 Pam Smith email from MoH Released with parts withheld under s9(2)(g)(i) to maintain the effective conduct of public affairs through the free and frank expression of opinions
10 - 15 Emails between WCC and RPH Released with parts withheld under s9(2)(a) to protect the privacy of natural persons.
17 - 26 DomPost article/ summary of facts Released27 -56 Complaints form Released with parts withheld under
s9(2)(a) to protect the privacy of natural persons.
Completed 10.04.2014
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
199

Page 16 of 17
57 - 63 Diary pages Released with parts withheld which address appointments not related to Fidels. These are outside the scope of your request.
64 - 66 Letters/ fax correspondence (Fidels/RPH and RPH/MoH)
Released
67 Email between Cindy Crampton-Cains and Pam Smith
Released with parts withheld under s9(2)(g)(i) to maintain the effective conduct of public affairs through the free and frank expression of opinions
68 - 86 Calculator/ photos/ letters/ fax correspondence/ emails/ companies office information/ liquor license/ opening drawings/ notes
Released
87 Complaint form Released with parts withheld under s9(2)(a) to protect the privacy of natural persons.
88 - 102 Emails/ letters/ notes/ photos Released103 Complaints data entry form Released with parts withheld under
s9(2)(a) to protect the privacy of natural persons.
104 to 163
Various items of correspondence between Regional Public Health, Ministry of Health legal team and solicitors
Withheld to maintain legal privilege (s9(2)(h)).
Where I have decided to withhold, I have reached the view that the withholding of that information is not outweighed by other considerations rendering it desirable, in the public interest, to make that information available.
3. The Smoke-free Compliance and Enforcement Manual is a Ministry of Health document. I have accordingly transferred this request under s14(b)(c)) of the Act to the Ministry of Health on 7 April 2014. (See document 1)
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
200

Page 17 of 17
You have the right, under section 28(3) of the Official Information Act, to ask the Ombudsman to investigate and review my decisions in this matter.
OIA 148
Jared NicollHutt News
08/04/2014 The stats show that about six intoxicated kids under-15 are treated and discharged each year.What extra difficulty is involved with treating a drunk patient under-15 as opposed to a sober patient?Does it tend to take more time to treat an intoxicated under-15 than sober? Is this okay?Do hospital staff contact the kids' parents or family if they aren't around?May I ask if there are any sort of injuries that intoxicated under-15s are prone to?
In Progress
Hutt Valley PUBLIC 2 May 2014 - ADDENDUMS
201




















