SWFT Board of Directors Agenda
352
SWFT Board of Directors Wed 06 July 2022, 14:00 - 16:00 Agenda 1. Length of Service Recognition Mr Ahmed Filali Naji, Technician 2. Apologies for Absence Charles Ashton, Chief Medical Officer (Scott Sanders deputising), Fiona Burton, Chief Nursing Officer (Ellie Ward deputising), Sarah Collett, Trust Secretary, David Spraggett (NED) 3. Declarations of Interest 4. Minutes of the Meeting held on 1 June 2022 2.00 pm - 2.05 pm Agenda Item 4 - Public Board Minutes 1 June 2022 - Final.pdf (11 pages) 5. Minutes of the Extraordinary Meeting held on 15 June 2022 2.05 pm - 2.10 pm Agenda Item 5 - Extraordinary Public Board Minutes 15 June 2022 - Final.pdf (4 pages) 6. Matters Arising and Actions Update Report 2.10 pm - 2.15 pm Agenda Item 6 - Public Board Actions Update 6 July 2022 - Final.pdf (2 pages) 7. ITEMS FOR APPROVAL 2.15 pm - 2.20 pm 7.1. Annual Review of the Standing Financial Instructions and Scheme of Delegation Kim Li Agenda Item 7.1 - Annual Review of SFIs and SOD June 22 v1 Final.pdf (73 pages) 8. PERFORMANCE REVIEW AND ASSURANCE
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of SWFT Board of Directors Agenda

SWFT Board of DirectorsWed 06 July 2022, 14:00 - 16:00
Agenda
1. Length of Service Recognition
Mr Ahmed Filali Naji, Technician
2. Apologies for Absence
Charles Ashton, Chief Medical Officer (Scott Sanders deputising), Fiona Burton, Chief Nursing Officer (Ellie Ward deputising),Sarah Collett, Trust Secretary, David Spraggett (NED)
3. Declarations of Interest
4. Minutes of the Meeting held on 1 June 2022
2.00 pm - 2.05 pm
Agenda Item 4 - Public Board Minutes 1 June 2022 - Final.pdf (11 pages)
5. Minutes of the Extraordinary Meeting held on 15 June 2022
2.05 pm - 2.10 pm
Agenda Item 5 - Extraordinary Public Board Minutes 15 June 2022 - Final.pdf (4 pages)
6. Matters Arising and Actions Update Report
2.10 pm - 2.15 pm
Agenda Item 6 - Public Board Actions Update 6 July 2022 - Final.pdf (2 pages)
7. ITEMS FOR APPROVAL
2.15 pm - 2.20 pm
7.1. Annual Review of the Standing Financial Instructions and Scheme of Delegation
Kim Li
Agenda Item 7.1 - Annual Review of SFIs and SOD June 22 v1 Final.pdf (73 pages)
8. PERFORMANCE REVIEW AND ASSURANCE

2.20 pm - 2.50 pm
8.1. Chief Executive's Report
Glen Burley
Agenda Item 8.1 - Chief Executive's Report.pdf (10 pages)
8.2. Integrated Performance Report
Anne Coyle
Agenda Item 8.2 - Integrated Performance Report May 2022 - Final.pdf (23 pages)
8.3. Monthly Safe Staffing Report
Ellie Ward
Agenda Item 8.3 - Safe Staffing Report June 2022 - Final.pdf (23 pages)
8.4. Capital Programme Quarterly Update Report
Sophie Gilkes
Agenda Item 8.4 - Capital Programme Quarterly Update Report-June 2022 - Final.pdf (15 pages)
8.5. Digital Health Board Quarterly Update
Adam Carson
Agenda Item 8.5 - Digital Health Board Update July 22 - Final.pdf (5 pages)
8.6. Audit Committee Report for 1 June 2022 and 15 June 2022
Rosemary Hyde
Agenda item 8.6 - Audit Committee Report for 1 June 2022 and 15 June 2022 - Final.pdf (53 pages)
8.7. Clinical Governance Committee Report for 8 June 2022
David Spraggett
Agenda item 8.7 - Clinical Governance Committee Report for June 2022 - Final.pdf (5 pages)
8.8. Foundation Group Strategy Committee Report for 31 May 2022
Simon Page
Agenda Item 8.8 - Foundation Group Strategy Committee Report for 31 May 2022 v1 - Final.pdf (8 pages)
9. RISK MANAGEMENT
2.50 pm - 3.00 pm
9.1. Board Assurance Framework and Risk Quarterly Report
Anne Coyle
Agenda item 9.1 - BAF and Risk Quarterly Report - Final.pdf (48 pages)
10. ITEMS FOR NOTING AND INFORMATION
3.00 pm - 3.20 pm

10.1. Summary of Ratified Policies
Anne Coyle
Agenda Item 10.1 - Summary of Ratified Policies - Final.pdf (2 pages)
10.2. Summary of Reports for Noting and Information
Health and Safety Annual Report - Harkamal HeranSecurity Annual Report - Harkamal HeranSecurity Standards Report - Harkamal Heran
Agenda item 10.2.1 - H&S Annual Report 2021-22 - Final.pdf (5 pages) Agenda Item 10.2.2 - Security Annual Report 1 April 2021 31 March 2022 (002).pdf (15 pages) Agenda item 10.2.3 - Security Standards Report - final.pdf (15 pages)
11. BOARD COMMITTEE MINUTES
3.20 pm - 3.30 pm
Agenda Item 11 - Board Committee Minutes (front sheet) - Final.pdf (1 pages)
11.1. Audit Committee Meeting held on 13 April 2022
Rosemary Hyde
Agenda item 11.1 - Audit Committee Minutes - Open Meeting - 13.04.2022.pdf (10 pages)
11.2. Audit Committee Meeting held on the 1 June 2022
Rosemary Hyde
Agenda item 11.2 - Audit Committee Minutes - Open Meeting - 01.06.22.pdf (8 pages)
11.3. Clinical Governance Committee Meeting held on 13 April 2022
Paramjit Gill
Agenda Item 11.3 - Clinical Governance Committee Minutes 11 May 2022.pdf (11 pages)
12. Any Other Business
3.30 pm - 3.35 pm
13. Questions from Governors and Members of the Public
Adjournment to discuss Matters of a Confidential Nature
CONFIDENTIAL AGENDA
14. Apologies for Absence
Charles Ashton, Chief Medical Officer, Fiona Burton, Chief Nursing Officer (Ellie Ward deputising), Sarah Collett, TrustSecretary, David Spraggett (NED)

15. Declarations of Interest
16. Minutes of the Meeting held on 1 June 2022
3.45 pm - 3.50 pm
17. Minutes of the Extraordinary Meeting held on 15 June 2022
3.50 pm - 3.55 pm
18. Matters Arising and Actions Update Report
3.55 pm - 4.00 pm
19. ITEMS FOR APPROVAL
19.1. Cardiac Catheterisation Laboratory (Cath Lab) Core Infrastructure Case
Sophie Gilkes
20. PERFORMANCE REVIEW AND ASSURANCE
4.00 pm - 4.05 pm
20.1. Appointments and Remuneration Committee Report 8 June 2022
Russell Hardy
21. ITEMS FOR NOTING AND INFORMATION
4.05 pm - 4.20 pm
21.1. Host Provider Verbal Update
Becky Hale
21.2. Audit Committee Closed Meeting held on 13 April 2022
Rosemary Hyde
21.3. Audit Committee Closed Meeting held on 1 June 2022
Rosemary Hyde
22. Board Committee Confidential / Closed Minutes
4.20 pm - 4.25 pm

22.1. Foundation Group Strategy Committee Meeting held on 22 February 2022
Simon Page
23. Any Other Confidential Business
4.25 pm - 4.30 pm
24. Date and Time of Next Meeting
The next SWFT Public Board meeting will be held on the 7 September 2022
Please note that there is not a SWFT Board Meeting in August 2022 meeting due to the Foundation Group Boards Meeting.

Agenda item 4SOUTH WARWICKSHIRE NHS FOUNDATION TRUST
Minutes of the Board of Directors Meeting Held onWednesday 1 June 2022 at 2.00pm via Microsoft Teams
Present:Russell HardyCharles AshtonYasmin BeckerParamjit Gill
(RH)(CA)(YB)(PG)
Chairman Chief Medical OfficerNon-Executive Director (NED)Nominated NED
Rosemary Hyde (RHy) NED Kim Li (KL) Chief Finance OfficerSimon PageDavid SpraggettSue Whelan Tracy
(SP)(DS)(SWT)
NEDNED NED
In attendance: Sarah CollettRichard ColleyAnjali DavePhil Gilbert
(SC)(RC)(AD)(PGb)
Trust SecretaryNED (Non-Voting)Associate Director of Operations for Family Health NED (Non-Voting)
Sophie GilkesClaire Hinds
(SG)(CH)
Chief Strategy OfficerAssociate Director of Operations for Support Services (deputising for Chief Operating Officer)
Gertie Nic PhilibMaria PearmanRadhae Raghavan
(GP)(MP)(RR)
Chief People OfficerDeputy Head of MidwiferyAssociate Medical Director
Dawn SpencerEllie Ward
(DSp)(EW)
Board AdministratorDeputy Head of Nursing (deputising for Chief Nursing Officer)
There were two Governors and two members of the public also in attendance.
MINUTE ACTION22.160
22.161
22.162
APOLOGIES FOR ABSENCE
Apologies for absence were received from the Managing Director, Chief Nursing Officer; and Chief Operating Officer.
Resolved – that the position be noted
DECLARATIONS OF INTEREST
Dr Spraggett , NED, declared that he had been appointed as an expert advisor on the guidelines panel for The National Institute for Health and Care Excellence (NICE).
Resolved – that the position be noted.
MINUTES OF THE MEETING HELD ON 4 MAY 2022
Resolved – that the Minutes of the meeting held on 4 May 2022 be confirmed as an accurate record of the meeting and signed by the Chairman.
1/11 1/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUSTMinutes of the Board of Directors Meeting Held Wednesday 1 June 2022
MINUTE ACTION22.163
22.163.01
22.163.02
22.164
22.165
MATTERS ARISING AND ACTIONS UPDATE REPORT
Actions Listed as Complete
The actions listed as complete in the Actions Update Report were noted and would now be removed from the report.
Resolved – that the position be noted.
Integrated Performance Dashboard (Minute 22.133 refers)
The Chief People Officer advised that Menopause had been identified as one of the five priorities for wellbeing and would be actioned throughout the year.
The Chief Finance Officer circulated a breakdown of agency analysis by staff type and division to review the mitigation for using agency staff.
Resolved – that the position be noted.
TRUST NAME CHANGE – ENGAGEMENT RESPONSES
The Chief Executive presented the report and advised that the report set out the responses from the engagement process. As an outcome of the engagement process the decision was made to move forward with the plan to change the Trust’s name to ‘South Warwickshire University NHS Foundation Trust’. The change would be implemented from 1 August 2022 and a working group had been set up to start the process of implementation.
The Chief Executive explained that investment had been made into the Research Strategy plan with the appointment of leadership roles.
The Chief Executive advised that, alongside the name change, the Chief People Officer had been revisiting the Trust Values to ensure that they were still appropriate and relevant to the Trust’s workforce. Staff had asked that the Trust was more overt in representing their commitment to equality, diversity and inclusion, therefore inclusive had now been added to the Trust Values.
The Chairman thanked the Managing Director, Foundation Trust Advisor and Professor Simon Brake, Warwick Medical School, for enabling the partnership with the University of Warwick’s Medical School.
The Chairman invited questions and perspectives, but there were no further comments.
Resolved – that the Trust Name Change and Engagement Reponses be received and noted.
REVIEW OF THE TRUST’S CONSTITUTION (INCLUDING ANNUAL REVIEW OF BOARD STANDING ORDERS)
The Trust Secretary presented the Review of the Trust’s Constitution and advised that the Constitution had been reviewed and amended to reflect the
2/11 2/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUSTMinutes of the Board of Directors Meeting Held Wednesday 1 June 2022
MINUTE ACTION
22.166
22.167
proposed name change. The review had been considered and approved at the Council of Governors meeting on 12 May 2022. The Board Standing Orders had also been reviewed and amended. A more detailed review of the Trust’s Constitution would be completed in due course.
The Chairman invited questions and perspectives, but there were no further comments.
Resolved – that:(A) the proposed amendments to the Trust’s Constitution associated
with the organisation’s name change be approved and ratified, and
(B) the Annual Review of the Board of Directors’ Standing Orders be approved and ratified.
DATA SECURITY AND PROTECTION TOOLKIT (DSPT) ASSESSMENT
The Chief Medical Officer presented the Data Security and Protection Toolkit (DSPT) Assessment and advised that the final submission of the 2021/22 DSPT would achieve a ‘Standards Met’ result.
The Chairman asked if there were other Trusts who had achieved all standards met in their DSPT assessments. The Chief Medical Officer commented that it was his understanding that not all Trusts were in this same position.
The Chairman invited questions and perspectives, and of particular note was the following point:
Mr Gilbert (NED) asked when the last Penetration Test was undertaken and the Chief Medical Officer confirmed that it had been completed at the end of May 2022.
Resolved – that (A) the position of the final submission of the 2021/22 Data Security
and Protection Toolkit (DSPT), which would achieve a ‘Standards Met’ result, be approved and ratified, and
(B) assurance that the Information Governance and Security Steering Group would continue to review, monitor and ensure continual improvements in Information Governance throughout the Trust, be received and noted.
CHIEF EXECUTIVE’S REPORT
The Chief Executive presented this report and highlighted that the Health and Care Bill, which formally established Integrated Care Systems had been granted Royal Assent and would be implemented from 1 July 2022. A press release that accompanied the Bill referenced work that had been completed by South Warwickshire NHS Foundation Trust (SWFT) and local authority colleagues concerning Discharge to Assess (D2A). The Chief Executive spoke about standing down from a National Level 4 Incident to a Level 3, Elective Recovery Plan, Infection Prevention and Control relaxation of guidelines, Quarterly Parallel Board meetings, agile working and the impact of inflation on
3/11 3/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUSTMinutes of the Board of Directors Meeting Held Wednesday 1 June 2022
MINUTE ACTION
22.168
the NHS. Also highlighted was the Nurse Led Outreach Team section within the report.
The Chairman invited questions and perspectives, and of particular note was the following point:
Mr Page (NED) spoke about the step down from a level 4 incident to a level 3 and sought clarification around whether this was an additional loosening of protocols to assist with flow. The Chief Executive responded that the Trust was now moving from a situation where the organisation was advised on actions from a national perspective to a more localised regional control basis.
Resolved – that the Chief Executive’s Report be received and noted.
INTEGRATED PERFORMANCE DASHBOARD (INCLUDING MORTALITY UPDATE)
The Chief Finance Officer presented this report on behalf of the Managing Director and in turn the Deputy Head of Nursing, Associate Director of Operations for Support Services, Chief People Officer and Chief Finance Officer gave updates on their respective areas.
The Chief Medical Officer advised that the Elective Recovery Targets for 2022-23 were targets that had been set using the financial value of the activity of the corresponding month in 2019-20. In 2019, the organisation was extremely busy as it had an additional operating theatre which was staffed. Current constraints included lack of theatre staff and to achieve 90% (target 104%) was a great effort. The Chief Executive advised that the methodology of the calculation of the elective recovery fund was complex and discussions were being had with the national team to look at the baseline. A high baseline had been set due to the organisation’s high level of activity. Outpatient activity was capped at 85% for follow-up activity which would not generate a level of income as the Trust had a low ‘new to follow-up’ ratio.
The Chairman invited questions and perspectives, and of particular note were the following points:
Mrs Whelan Tracy (NED) commented that it was pleasing to note that the Recommended Summary Plan for Emergency Care and Treatment (ReSPECT) form incidents were down in the quarter and enquired if this was a continuing trend. The Deputy Head of Nursing advised that the completion of the form was part of staff training with follow-up processes in place if the form did not accompany the patient. The resuscitation officer had assured the Deputy Head of Nursing that this was an improving and sustained situation.
The Chief Strategy Officer commented that the Trust had been given the opportunity to feedback on the Partnership Trust Strategy for the Children and Young People in Crisis and this would definitely take place.
The Chief Medical Officer advised that there was a continuous push with the medical staff to ensure that the ReSPECT forms were completed but that it
4/11 4/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUSTMinutes of the Board of Directors Meeting Held Wednesday 1 June 2022
MINUTE ACTIONwas a work in progress to make sure that discussions and the quality of information were incorporated into the forms.
Mrs Hyde (NED) sought clarification that, arrivals in A&E who were not from South Warwickshire (mainly from Birmingham and Solihull) this activity would be paid to the Trust and were there processes in place to ensure this was monitored and recorded. The Chief Executive responded that there was an increase in activity of 65% year on year for out of area patients and at the moment the Trust was not being paid for it and the Chief Finance Officer and her team were pushing for this activity to be recognised.
The Chairman thanked the Deputy Head of Nursing for supporting the Nursing team whilst the Chief Nursing Officer was absent due to sickness.
The Chief Executive congratulated the team for the Cancer performance figures and a huge thank you to the Orthopaedic team for their mutual aid offer to the system with very positive feedback received from Wye Valley Trust (WVT).
Dr Spraggett (NED) questioned whether there was an improvement in ambulance handover delays and that the Trust was managing the risks. The Chief Executive responded that each Chief Executive received an hourly report which was closely monitored and the Trust never appeared on the list for the longest delays; there were some delays over 60 minutes but these were low in numbers. The organisation was one of the best performing Trusts in the Midlands for ambulance handovers. The Associate Director of Operations for Support Services advised that she would provide figures for Dr Spraggett (NED) for assurance.
Mrs Whelan Tracy (NED) commented on the stranded patient figures, which had an upward national trend, and sought clarification around whether the same practices would be used for out of area patients as those currently in place for the Trust. The Chief Executive advised that patients who were out of area were harder to discharge and that closer links were to be made with Discharge to Assess (D2A) out of area teams in order to facilitate patients returning more rapidly to their homes.
The Chief Executive spoke about the positive position of recruitment and that work was ongoing to ensure that the nurse bank was working effectively in order to reduce agency spend. Another focus was supporting staff in hardship who were having financial distress.
Dr Spraggett (NED) asked about retention and the number of leavers and what percentage of those staff were retiring early. The Chief People Officer advised that she had commissioned a deep dive into understanding the turnover of staff and would report later in the year on the outcomes of the deep dive. The Chief People Officer advised that early retirement reasons were not significant but that it was important to understand and help retain the knowledge within the organisation. Further work was being undertaken for the retention of staff through all the spectrums.
CH
5/11 5/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUSTMinutes of the Board of Directors Meeting Held Wednesday 1 June 2022
MINUTE ACTIONMrs Hyde (NED) advised that NHS England / NHS Improvement (NHSE/I) issued requirements for organisations to reduce agency as well as bank spend and to make sure that all the work being done regarding bank was aligned to NHSE/I requirements as recruitment of substantive staff was absolutely key. The Chief People Officer advised that work was being undertaken with the bank to work with the approach taken by NHSE/I. The Chief Executive advised that additional hours were paid through bank and not through payroll. The bank was used whereby staff could be flexible and work additional hours. The Deputy Head of Nursing advised that discussions were being held with the Chief People Officer to look at easier ways where retired nurses were able to return to work part-time and examining ways where staff who were working on bank could be added to flexible working contracts.
The Chief Finance Officer asked for approval for a change in the plan. An allocation of £3m had been received for inflationary cost pressures and that brought the system to a closer break-even plan. As a result, organisations had been asked to resubmit their plans before the end of June 2022 with the Trust delivering a £3m surplus. The Chief Finance Officer highlighted that the allocation was not submitted on a fair share basis but they were based on individual organisations’ estimation of their inflationary cost pressures.
The Chairman sought clarification on the amount the Trust would have received if the inflationary cost pressures had been allocated on a fair share basis. The Chief Finance Officer could not confirm the value but advised that it would have been in excess of £3m.
Mrs Hyde (NED) sought clarification that the Trust had been given the inflationary amount but that the original budget did not include the inflation amount. Also whether it would be correct that the Trust would be signing off a £3m surplus given that the organisation’s costs would likely be higher. The Chief Finance Officer advised that the original plan absorbed the inflationary cost pressures and to break-even the organisation set a higher cost improvement plan (CIP) target in order to close the gap.
Following consideration, the Board approved the proposal to submit a revised Financial Plan for inflation and the additional income which would take the Trust closer to a break even submission.
22.169
Resolved – that (A) the Integrated Performance Dashboard (including Mortality
Report) be received and noted;(B) the Associated Director of Operations for Support Services to
provide data on ambulance handovers for Dr Spraggett (NED), and
(C) the adjustment to the Financial Plan for inflation and the additional income received be approved and ratified.
MONTHLY SAFE STAFFING REPORT
The Deputy Head of Nursing presented the report which was taken as read.
CH
6/11 6/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUSTMinutes of the Board of Directors Meeting Held Wednesday 1 June 2022
MINUTE ACTION
22.170
The Chairman invited questions and perspectives, and of particular note were the following points:
Mrs Whelan Tracy (NED) noticed that in maternity, both midwives and Special Care Baby Unit (SCBU) nurses, there was a change month on month and sought clarification around whether this was expected or planned for within the workforce plan. The Deputy Head of Nursing advised that these were existing vacancies and there would be additional vacancies highlighted within the previous business case. Mrs Whelan Tracy (NED) commented that the speed that the business cases could come through and the roles filled was important. The Deputy Head of Midwifery commented that interviews had taken place for midwives and clinical support workers (CSW) and posts filled with further interviews arranged for maternity support workers and midwives.
The Chairman asked the Deputy Head of Nursing if there were any particular areas of worry. The Deputy Head of Nursing advised that there was a focus on unregistered staff being difficult to recruit and retain. CSW recruitment days were face to face and had proved successful but monitoring would still take place. Resolved – that the Monthly Safe Staffing Report be received and noted
MATERNITY ASSURANCE QUARTERLY REPORT
The Deputy Head of Nursing presented this report and highlighted the assurance visit from the regional midwifery team which was very positive about the Trust’s leadership and open culture in maternity. There was a lot of detail in the action plans for the Ockenden Report and Saving Babies Lives. In the absence of the Chief Nursing Officer, the Deputy Head of Nursing, the Deputy Head of Midwifery and the Associate Director of Operations for Family Health would be meeting on a fortnightly basis to ensure the actions were completed and mitigations put in place. The Chairman invited questions and perspectives, and of particular note were the following points:
The Chief Executive congratulated the team on the Insights Visit with a positive feedback received on the quality of the services.
Dr Spraggett (NED) advised that the SCBU team had been awarded a gold accreditation by BLISS. BLISS was a national organisation dedicated to premature or sick babies and only ten units in the country had been awarded this accreditation and Warwick SCBU was the first unit in the West Midlands to receive it.
The Chief Medical Officer commented that transparency was at the heart of the Ockenden Report on previous enquiries and would be for future ones. It had been organisations that had Boards who had not been enquiring, not taking into account questions from relatives, recognition of problems and addressing them. The Deputy Head of Midwifery advised that she thought the Board had good oversight of the service and responded to any requests and support
7/11 7/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUSTMinutes of the Board of Directors Meeting Held Wednesday 1 June 2022
MINUTE ACTION
22.171
22.172
required from maternity and advised that all requests were in response to the measures that needed to be put in place.
Mrs Hyde (NED) concurred with the openness and transparency around Ockenden. There was a challenge on the Clinical Negligence Scheme for Trusts (CNST) and that the Trust was being penalised compared to other Trusts for monies not coming back into the Trust. The Deputy Head of Midwifery advised that the scoring for the submission would include the evidence for meeting standards and that the Trust was always working towards standards on the Maternity Incentive Scheme (MIS).
The Chairman commented that a third of mothers were on an antidepressant drug when pregnant and gave birth and that it would be useful for primary colleagues to be able to assist mothers to handle their medication at the end of pregnancy. There was an increase in BMI amongst pregnant women which was not good for the health and wellbeing of mother and baby. The Deputy Head of Nursing commented that diabetes was also an issue for pregnant mothers and that they would need a high level of care and work would be undertaken to work with partners to look at health and wellbeing interventions to reduce the numbers.
Resolved – that the Maternity Assurance Quarterly Report be received and noted.
CLINICAL GOVERNANCE COMMITTEE REPORT FOR 11 MAY 2022
Dr Spraggett (NED) presented the report which was taken as read.
The Chairman invited questions and perspectives, but there were no further comments.
Resolved – that the Clinical Governance Committee Report for 11 May 2022 be received and noted.
PATIENT EXPERIENCE ANNUAL REPORT (INCLUDING QUARTER 4)
The Deputy Head of Nursing presented the report and advised that the Learning and Disability Support Worker had commenced working in the wards and had provided valuable feedback. The Patient Advice and Liaison Service (PALS) referrals had risen but that was not a negative as the more people who contacted them for advice and support was for the better as it helped to make improvements.
The Chairman invited questions and perspectives, but there were no further comments.
Resolved – that the Patient Experience Annual Report (Including Quarter 4) be received and noted.
8/11 8/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUSTMinutes of the Board of Directors Meeting Held Wednesday 1 June 2022
MINUTE ACTION22.173
22.174
22.175
22.176
6 MONTHLY UPDATE ON TRUST’S PERFORMANCE AGAINST NATIONAL GUIDANCE ON LEARNING FROM DEATHS
The Chief Medical Officer presented the report and highlighted that the mortality indicators remained within control limits, the medical examiner function was working well and there was some variability in the Hospital Standardised Mortality Ratio (HSMR) but no underlying clinical trend had been identified.
The Chairman invited questions and perspectives, but there were no further comments.
Resolved – that the 6 Monthly Update on Trust’s Performance against National Guidance on Learning from Deaths report be received and noted.
CARE QUALITY COMMISSION (CQC) UPDATE INCLUDING INSIGHTS REPORT
The Deputy Head of Nursing presented the report which was taken as read.
The Chairman invited questions and perspectives, but there were no further comments.
Resolved – that the Care Quality Commission (CQC) Update including Insights Report be received and noted.
REPORT FROM THE COUNCIL OF GOVERNORS MEETING HELD ON 12 MAY 2022
The Chairman presented the report which was taken as read.
The Chairman invited questions and perspectives, but there were no further comments.
Resolved – that the Report from the Council of Governors Meeting held on 12 May 2022 be received and noted.
SUMMARY OF RATIFIED POLICIES
The Trust Secretary presented the report which included the summary of SWH 01783 – Managing Conflicts of Interest Policy, SWH 01656 – Gifts, Hospitality and Sponsorship Policy and SWH 00878 Mental Capacity Act.
The Chairman invited questions and perspectives, but there were no further comments.
Resolved – that the Summary of Ratified Policies report be received and noted.
9/11 9/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUSTMinutes of the Board of Directors Meeting Held Wednesday 1 June 2022
MINUTE ACTION22.177
22.178
22.179
22.180
22.181
22.182
SUMMARY OF REPORTS FOR NOTING AND INFORMATION
The Board received and noted the summary of the Senior Information Risk Owner (SIRO) Annual Report and the Health and Wellbeing Report.
The Chairman invited questions and perspectives, and of particular note were the following points:
The Chief Executive advised that as the Trust was supporting staff with hardship it would be useful to explore strengthening links with the Citizens Advice Bureau and to receive some direct contact for staff. The Chief People Officer advised that this was already in progress including contacting financial institutions to provide advice and support for staff. There would also be a report being presented to the Charity Trustee to develop an internal hardship fund.
The Chief Strategy Officer advised that she would add a link in for environmental areas as that was a concern for staff.
Resolved – that the Summary of Reports for Noting and Information be received and noted.
UPDATED REGISTER OF DIRECTOR’S INTERESTS
The Trust Secretary presented the report which was taken as read. She noted that Dr Spraggett (NED) had provided an update as declared earlier in the meeting (Minute 22.161 refers) which was highlighted on the Register.
The Chairman invited questions and perspectives, but there were no further comments.
Resolved – that the Updated Register of Director’s Interests be received and noted.
BOARD COMMITTEE MINUTES – OPEN MEETINGS
Resolved – that the Board Committee Minutes – Open Meetings for the Clinical Governance Committee meeting held on 13 April 2022 be received and noted.
ANY OTHER BUSINESS
There was no further business raised.
Resolved – that the position be noted.
QUESTIONS FROM GOVERNORS AND MEMBERS OF THE PUBLIC
There were no questions raised.
Resolved – that the position be noted.
ADJOURNMENT TO DISCUSS MATTERS OF A CONFIDENTIAL NATURE
10/11 10/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUSTMinutes of the Board of Directors Meeting Held Wednesday 1 June 2022
MINUTE ACTION
22.183
22.184
22.185
22.186
22.187
22.188
22.189
22.190
22.191
22.192
22.193
22.194
22.195
APOLOGIES FOR ABSENCE
DECLARATIONS OF INTEREST
CONFIDENTIAL MINUTES OF THE MEETING HELD ON 4 MAY 2022
CONFIDENTIAL MATTERS ARISING AND ACTIONS UPDATE REPORT
ISS CONTRACT EXTENSION
FORESCOUT BUSINESS CASE
ELLEN BADGER BUSINESS CASE
HOST PROVIDER UPDATE
SWFT CLINICAL SERVICES LTD UPDATE REPORT
LILLINGTON DEVELOPMENT – UPDATE REPORT
BOARD COMMITTEE MINUTES – CONFIDENTIAL/CLOSED MEETING
ANY OTHER CONFIDENTIAL BUSINESS
DATE AND TIME OF NEXT MEETING
The next meeting would be held virtually on Wednesday 6 July 2022 at 2.00pm.
Unfortunately, due to national guidance around the COVID-19 pandemic, members of the public would be unable to attend in person but would be able to register to join virtually and would be invited to submit questions in advance. The meeting would be recorded and published on the Trust’s website following the meeting.
Signed ______________________________ (Chairman) Date _______________Russell Hardy
11/11 11/347

Agenda item 5SOUTH WARWICKSHIRE NHS FOUNDATION TRUST
Minutes of the Extraordinary Board of Directors Meeting Held onWednesday 15 June 2022 at 2.00pm via Microsoft Teams
Present:David Spraggett Charles AshtonYasmin BeckerGlen BurleyAnne CoyleHarkamal Heran
(DS)(CA)(YB)(GB)(AC)(HH)
NED (Chair) Chief Medical OfficerNon-Executive Director (NED)Chief ExecutiveManaging Director Chief Operating Officer
Rosemary Hyde (RHy) NED Kim Li (KL) Chief Finance Officer
In attendance: Joanne BealesSarah CollettRichard ColleyPhil GilbertSophie Gilkes
(JB)(SC)(RC)(PGb)(SG)
Lead Risk, Health and Safety AdvisorTrust SecretaryNED (Non-Voting)NED (Non-Voting)Chief Strategy Officer
Dawn SpencerEllie Ward
(DSp)(EW)
Board AdministratorDeputy Director of Nursing (deputising for Chief Nursing Officer)
There were four Governors also in attendance.
MINUTE ACTION22.196
22.197
22.198
APOLOGIES FOR ABSENCE
Apologies for absence were received from the Chairman, Chief Nursing Officer, Mr Page (NED), Mrs Whelan Tracy (NED), Paramjit Gill (NED) and Chief People Officer.
The Extraordinary Meeting was declared quorate.
Resolved – that the position be noted
DECLARATIONS OF INTEREST
There were no declarations of interest.
Resolved – that the position be noted.
2021/22 ANNUAL ACCOUNTS
The Chief Finance Officer presented the report and advised that that it had been presented to the Audit Committee twice. A draft had been presented to the Audit Committee on the 1 June 2022 and again presented earlier that day.
The Chief Finance Officer highlighted that the Trust had delivered a control total surplus excluding technical accounting adjustment of £22k against a break-even plan. The External Auditors had suggested a few adjustments to be made and these were detailed in Appendix One. The delay to the completion of the Audit had been caused by the Auditors having staffing issues
1/4 12/347
SOUTH WARWICKSHIRE NHS FOUNDATION TRUSTMinutes of the Extraordinary Board of Directors Meeting Held Wednesday 15 June 2022
MINUTE ACTION
22.199
due to sickness. The Auditors recommended that the Audit Committee signed off the Annual Accounts.
Dr Spraggett (Chair) asked Mrs Hyde (NED) as the Audit Committee Chair if there were further comments to add. Mrs Hyde (NED) explained that the Audit was not completed but would be completed in time for the Accounts to be filed by the 22 June 2022 submission date. The Auditors have given assurance that no material adjustments would be made that would affect the bottom line. There was one technical area relating to staff costs which has taken significantly longer to complete due to a change in the accounting manual in the financial year.
Dr Spraggett (Chair) invited questions and perspectives, and of particular note was the following point:
The Chief Executive confirmed that the change that Mrs Hyde (NED) referred to had caused a delay in the completion of audits elsewhere. The Chief Executive advised that if there were any accounting changes to the Accounts then they would have to be resubmitted for Board approval but the view from the Auditors was that there was nothing material that would happen before the closure of the Accounts.
Resolved – that the final Annual Accounts 2021/22 be approved and ratified prior to submission to the Department of Health and Social Care (DHSC).
ANNUAL GOVERNANCE STATEMENT 2021/22
The Chief Executive advised that the Annual Governance Statement for 2021/22 had been presented to the Audit committee earlier that day and the following amendments had been agreed:
Page 1: The Chief Executive had been referred to as the ‘Accountable Officer’ and would be amended to read as ‘Accounting Officer.’
Page 10:’As at 31 March 2022 the Trust had completed 93 of the 110 mandatory evidence items and is on track to achieve a ‘Standard Met’ compliance statement by the 30 June 2022’ be amended to read’ As of 31 March 2022, 93 of the 109 mandatory evidence items were completed, since this date the Trust has now completed 109 requirements and will submit a “Standards Met” compliance statement by the 30 June 2022’.
The Audit Committee have asked for a review of the statement when compiled for the following year 2022/23 as it has increased in volume year on year.
Dr Spraggett (Chair) invited questions and perspectives, but there were no further comments.
Resolved – that, subject to the above amendments, the Annual Governance Statement 2021/22 be approved and ratified.
2/4 13/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUSTMinutes of the Extraordinary Board of Directors Meeting Held Wednesday 15 June 2022
MINUTE ACTION22.200
22.201
22.202
22.202.01
22.202.02
22.203
22.204
22.205
JOINT AUDIT COMMITTEE AND CLINICAL GOVERNANCE ASSURANCE STATEMENT
Mrs Hyde (NED) and Dr Spraggett (NED) presented this report which was taken as read. The statement was assurance on the operation of the organisation through the Audit Committee and the Clinical Governance Committee.
The Chairman invited questions and perspectives, but there were no further comments.
Resolved – that the Joint Audit Committee and Clinical Governance Committee Assurance Statement be received and noted.
ANY OTHER BUSINESS
There was no further business raised.
Resolved – that the position be noted.
QUESTIONS FROM GOVERNORS AND MEMBERS OF THE PUBLIC
Question from a Public Governor (Warwick and Leamington Towns)
‘With regard to the Accounts would it be possible to have one sentence that summarised the final financial position for easier understanding as they were complex for those who did not have an accounting background’.
This question was responded to by the Chief Executive who advised that when the Accounts were presented at the Annual General Meeting (AGM) there would be a summary of the financial position which would outline that the Trust did meet its financial duties. The External Auditors gave the technical judgement on the Trust’s Accounts in ensuring that they were accurately reported which they confirmed as part of the audit process.
Resolved – that the position be noted.
Question from a Public Governor (West Stratford and Borders)
‘The movement of assets and workforce to Innovate – did that amount to a significant transaction within the definition of the constitution or was the value of it below the threshold?
The Chief Finance Officer advised that the movement was below the threshold.
Resolved – that the position be noted.
ADJOURNMENT TO DISCUSS MATTERS OF A CONFIDENTIAL NATURE
APOLOGIES FOR ABSENCE
DECLARATIONS OF INTEREST
3/4 14/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUSTMinutes of the Extraordinary Board of Directors Meeting Held Wednesday 15 June 2022
MINUTE ACTION
22.206
22.207
22.208
22.209
FINAL APPROVAL OF 2021/22 ANNUAL REPORT
FINAL APPROVAL OF 2021/22 QUALITY REPORT
ANY OTHER CONFIDENTIAL BUSINESS
DATE AND TIME OF NEXT MEETING
The next meeting would be held virtually on Wednesday 6 July 2022 at 2.00pm.
Unfortunately, due to national guidance around the COVID-19 pandemic, members of the public would be unable to attend in person but would be able to register to join virtually and would be invited to submit questions in advance. The meeting would be recorded and published on the Trust’s website following the meeting.
Signed ______________________________ (Chair) Date _______________Dr David Spraggett
4/4 15/347

Agenda Item 6
1
SOUTH WARWICKSHIRE NHS FOUNDATION TRUST
ACTIONS UPDATE: PUBLIC BOARD OF DIRECTORS MEETING – 6 JULY 2022
AGENDA ITEM ACTION LEAD COMMENT
ACTIONS COMPLETE22.133Integrated Performance Dashboard(04.05.2022)
To ensure Womens’ Menopausal Network information be provided when available.
To ensure a breakdown of agency staff into professional groups in order to review the mitigation for using agency staff and the detail be considered at a future Board Workshop session
To ensure a deep dive on the reasons for staff leaving and to amend the method of workforce measures to annualised rather than monthly for easier understanding.
GP
KL
GP
Menopause identified as one of the 5 priorities for wellbeing and will be actioned through the year. Complete
Information circulated to Board members. Complete
Annualised turnover to be included in the Finance & Performance reporting. Deep dive of reasons for leaving to be actioned as part of Retention activity. Complete.
22.133Integrated Performance Dashboard(04.05.2022)
The Chief Nursing Officer to provide a reflection on the reason for the reduction of births at the Midwifery Led Unit setting since June 2021. Also to provide an update on the longer term plans for the Unit from a safety and financial sustainability perspective to be provided
FB Deferred until September 2022 Board
1/2 16/347

2
AGENDA ITEM ACTION LEAD COMMENT22.168Integrated Performance Dashboard(01.06.2022)
The Associate Director of Operations for Support Services to provide figures for ambulance handovers.
CH Work in progress
REPORTS SCHEDULED FOR FUTURE MEETINGS
ACTIONS REFERRED TO BOARD OF DIRECTORS SUB-COMMITTEES
2/2 17/347

Report Summary Report to Board of Directors Date of
Meeting 6 July 2022
Report Title Annual Review of Standing Financial Instructions and Scheme of Delegation
Agenda Item 7.1
Executive/ Non-Executive Lead
Kim Li, Chief Finance Officer Report Author(s)
Mick Sargent, Associate Director of Finance
Report Previously Discussed at
Purpose of the Report Annual review of the Trust’s Standing Financial Instructions and Scheme of Delegation.
For Approval For Discussion For Information
Recommendations and Action Required The Board of Directors is asked to approve the amendments and changes to the Trust’s Standing Financial Instructions and Scheme of Delegation as recommended by the Audit Committee.
Impact (is there any impact arising from the report on the following?) Quality Equality Finance Risk Performance Compliance Workforce Legal
Applicable Quality Improvement Priorities Elective Hub Health Inequalities Electronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety Compassionate Effectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk Register Are any existing risks on the BAF/Risk Register affected? No Identify the BAF/Risk Register risk ID and description – explain how the risk has been affected – reduced or increased as a consequence of the evidence within the report. Do you recommend a new entry to the BAF and/or Risk Register is made as a result of this report? If yes, describe the new risk.
No
1/73 18/347

South Warwickshire NHS Foundation Trust
Board of Directors – 6 July 2022
Annual Review of Standing Financial Instructions and Scheme of Delegation
1. Introduction
The Trust’s Standing Financial Instructions (SFIs) and Scheme of Delegation (SOD) have been through an annual review exercise which has included review by: Sarah Collett, Trust Secretary Ruth Allen, Associate Director of Procurement Kim Li, Chief Finance Officer Ravi Basi, Deputy Chief Finance Officer Mick Sargent, Associate Director of Finance-Strategy and Financial Services Other senior finance and non-finance staff have also been consulted as part of this review. The Audit Committee have reviewed the SFIs and Scheme of Delegation and have noted the changes below. The Audit Committee have recommended the SFIs and Scheme of Delegation for approval.
2. Key Changes
2.1 SFIs
To help identify changes and amendments, the SFIs submitted to Audit Committee have tracked changes identified within them. Please note any current formatting issues will be corrected once tracked changes have been accepted for the final published version. Key changes are:
• Charges to job titles • 9.3.2 Asset disposals- assets being disposed of with a remaining net book value
over £5k require CFO sign off. [page 31] • 9.4.1 Formal Competitive tendering- SFI waivers over £100k signed off by both
Chief Finance Officer and Managing Director. [page 36]. Formal tendering procedures may only be waived in the limited circumstances listed a) to l) on pages 34-35.
2.2 Scheme of Delegation (and Financial Limits)
Key changes to the Scheme of Delegation (Appendix A) and the Financial Limits (Appendix B) are:
• Innovate Healthcare Services Ltd Share Purchase added into SOD- The purchase of additional shares in Innovate Healthcare Services Ltd up to the value of £500k has been delegated by the Board of Directors to the Chief Executive and Chief Finance Officer. [see page 59]
2/73 19/347

• Financial limits: Non-Pay expenditure and capital expenditure delegated levels have been reviewed to align with the rest of the Foundation Group. [see pages 62 & 67] Key changes are:
o Level 2 Officers (Chief Officers) now maximum £50k (was £100k). o Deputy Chief Finance Officer and Deputy Chief Operating Officer
added into level 2 (£50k limit). o Capital aligns to non-pay expenditure, so Chief Strategy Officer as
Level 2 is £50k maximum (was £250k).
• Financial Limits: Charitable Funds expenditure for Fund Manager approvals 0-£5k. In periods of absence the Fund Manager’s line manager will provide alternative authorisation. [see page 67]
• Financial limits: Investments delegated financial limits added in for
investments with approved financial institutions for investments under £5m and investments over £5m. [see page 68]
It should also be noted that a review of the Trust’s policy for approval of temporary workforce usage is currently underway which, when concluded, will be included in the next SFI/SOD review.
3. Recommendation
The Board of Directors is asked to approve the amendments and changes to the Trust’s Standing Financial Instructions and Scheme of Delegation as recommended by the Audit Committee.
Kim Li Chief Finance Officer
3/73 20/347
Version 3.32 Job Title of Responsible Manager
Associate Director of Finance – Strategy & Financial Services
Replacing Document SWH 00942 Standing Financial Instructions & Scheme of Delegation Version 3.21
Ratifying ‘Body’ Board of Directors Date Ratified 11th March 2020 Date for Review February20221 February 2023 Relevant Standards:
Finance
SWH 00942 Standing Financial Instructions
And Scheme of Delegation
The Trust’s Intranet holds the current approved guidance documents. Notice to staff using a paper copy of this document. Staff must ensure that they are using the most up-to-date document to guide their practice and must check that the version number of the paper copy matches that of the one on the Intranet.
4/73 21/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 2 of 70
Document History Issue Status e.g. Draft or Final
Catalogue and Version Number
Document Title Date Actioned by: (Job Title or Name of Approving/ Ratifying Body)
Page/ Section/ Paragraph
Comments
Final SWH 00942 Version 2.0
Standing Financial Instructions And Scheme of Delegation
30 October 2013
Board of Directors Whole Document
Approved and ratified document.
Final SWH 00942 Version 3.0
Standing Financial Instructions And Scheme of Delegation
1 November 2017
Board of Directors Whole Document
Approved and ratified document.
Final SWH 00942 Version 3.1
Standing Financial Instructions And Scheme of Delegation
3 October 2018
Board of Directors
MD role incorporated and references to BPIC & Finance & Performance Executive removed.
Approved and ratified
Final SWH 00942 Version 3.2
Standing Financial Instructions And Scheme of Delegation
11 March 2020
Board of Directors Whole Document
Approved and ratified document.
Draft SWH 00942 Version 3.3
Standing Financial Instructions And Scheme of Delegation
May 2022 Associate Director of Finance
Whole Document
General review and update throughout as document had expired.
1 June 2022 Audit Committee Whole Document
Approved document
5/73 22/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 3 of 70
Final SWH 00942 Version 3.3
Standing Financial Instructions And Scheme of Delegation
6 July 2022 Board of Directors Whole Document
Approved and ratified document
6/73 23/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 4 of 70
Table of Contents To access a section directly from the Table of Contents – ‘hover’ the mouse over the section you require and then press Ctrl and click the mouse. DOCUMENT HISTORY ........................................................................................................................................ 2
1 INTRODUCTION .......................................................................................................................................... 6
2 PURPOSE .................................................................................................................................................... 6
3 AUDIENCE ................................................................................................................................................... 6
4 ASSOCIATED TRUST DOCUMENTS ....................................................................................................... 6
5 RESPONSIBILITIES/DUTIES ..................................................................................................................... 6
5.1 BOARD OF DIRECTORS .................................................................................................................................... 6 5.2 THE COUNCIL OF GOVERNORS ........................................................................................................................ 7 5.3 CHIEF EXECUTIVE ............................................................................................................................................ 7 5.4 CHIEF FINANCE OFFICER DIRECTOR OF FINANCE .......................................................................................... 8 5.5 ALL STAFF ........................................................................................................................................................ 8 5.6 CONTRACTORS AND THEIR EMPLOYEES........................................................................................................ 10
6 AUDIT ......................................................................................................................................................... 10
6.1 AUDIT COMMITTEE ......................................................................................................................................... 10 6.2 INTERNAL AUDIT ............................................................................................................................................. 11 6.3 EXTERNAL AUDIT ........................................................................................................................................... 12 6.4 FRAUD AND CORRUPTION .............................................................................................................................. 12 6.5 SECURITY MANAGEMENT ............................................................................................................................... 13 6.6 ACCESS TO RECORDS ................................................................................................................................... 14
7 THE TRUST’S OBJECTIVES AND THE ANNUAL PLANNING CYCLE ............................................. 14
8 BUDGETS .................................................................................................................................................. 14
8.1 BUDGET SETTING ........................................................................................................................................... 14 8.2 BUDGET DELEGATION .................................................................................................................................... 15 8.3 BUDGETARY CONTROL AND REPORTING ...................................................................................................... 16
9 AREAS SUBJECT TO FINANCIAL CONTROL ..................................................................................... 17
9.1 REVENUE INCOME .......................................................................................................................................... 17 9.1.1 Contracts with Commissioners/Service Level Agreements........................................................................... 18 9.1.2 Fees & Charges .................................................................................................................................................. 18 9.1.3 Credit Control/ Debt recovery ............................................................................................................................ 19 9.1.4 Security of Cash, Cheques and other Negotiable Instruments ..................................................................... 19 9.1.5 Injury Costs Recovery Scheme ......................................................................................................................... 19 9.1.6 Private Patients ................................................................................................................................................... 20 9.1.7 Overseas Visitors ................................................................................................................................................ 20
9.2 REVENUE EXPENDITURE ................................................................................................................................ 20 9.2.1 Pay ........................................................................................................................................................................ 20 9.2.2 Approved Staffing Levels (ASL) ........................................................................................................................ 21 9.2.3 Contracts of Employment ................................................................................................................................... 22 9.2.4 Non Pay Expenditure .......................................................................................................................................... 22 9.2.5 Expenditure Process ........................................................................................................................................... 23 9.2.6 Prepayments ........................................................................................................................................................ 24 9.2.7 Official Orders ...................................................................................................................................................... 24 9.2.8 Stores Stock and Receipt of Goods ................................................................................................................. 26
9.3 CAPITAL INVESTMENT AND EXPENDITURE ..................................................................................................... 27 9.3.1 Asset Registers & Security of Assets ............................................................................................................... 29 9.3.2 Asset Disposals ................................................................................................................................................... 31 9.4.1 Formal Competitive Tendering ................................................................................................................................ 33 9.4.2 Invitation to Tender ................................................................................................................................................... 36 9.4.3 Procedure for Managing Tenders ........................................................................................................................... 36
7/73 24/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 5 of 70
9.4.4 Acceptance of Formal Tenders ............................................................................................................................... 37 9.4.5 Quotations: Competitive and Non-Competitive ..................................................................................................... 38
9.5 OTHER – PATIENT PROPERTY .......................................................................................................................... 41 9.6 OTHER – CHARITABLE FUNDS ....................................................................................................................... 42 9.7 LOSSES & SPECIAL PAYMENTS ..................................................................................................................... 42
10 EXTERNAL BORROWING & INVESTMENTS ....................................................................................... 43
11 BANKING ARRANGEMENTS .................................................................................................................. 44
12 ANNUAL ACCOUNTS .............................................................................................................................. 44
13 WHOLLY OWNED SUBSIDIARIES ......................................................................................................... 45
14 MONITORING COMPLIANCE .................................................................................................................. 45
15 EQUALITY IMPACT ASSESSMENT ....................................................................................................... 45
16 AUTHORS .................................................................................................................................................. 45
17 CONTRIBUTORS ...................................................................................................................................... 45
18 REFERENCES ........................................................................................................................................... 46
19 APPENDICES ............................................................................................................................................ 46
20 APPENDIX A: SCHEME OF DELEGATION ........................................................................................... 47
21 APPENDIX B: FINANCIAL LIMITS .......................................................................................................... 62
22 APPENDIX C: MONITORING COMPLIANCE FORM ............................................................................ 69
23 APPENDIX D: EQUALITY IMPACT ASSESSMENT FORM ................................................................. 70
8/73 25/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 6 of 70
1 Introduction These Standing Financial Instructions (SFIs) are issued in accordance with the Trust (Functions) Directions 2000 issued by the Secretary of State which require that each Trust shall agree Standing Financial Instructions for the regulation of the conduct of its staff, Chief Executive, Managing Director and Chief Officers Directors in relation to all financial matters with which they are concerned. 2 Purpose These SFIs detail the financial responsibilities, policies and procedures adopted by the Trust. They are designed to ensure that the Trust's financial transactions are carried out in accordance with the law and with Government policy in order to achieve probity, accuracy, economy, efficiency and effectiveness. They should be used in conjunction with the Constitution and the Scheme of Delegation adopted by the Trust. 3 Audience These SFIs identify the financial responsibilities which apply to everyone working for the Trust and its constituent organisations including Trading Units. They do not provide detailed procedural advice and should be read in conjunction with the detailed departmental and financial procedure notes. These are available on the Trust internal website or from the Finance Department. All financial procedures must be approved by the Chief Finance Officer.Director of Finance Should any difficulties arise regarding the interpretation or application of any of the SFIs then the advice of the Chief Finance Officer Director of Finance must be sought before acting. The user of these SFIs should also be familiar with and comply with the provisions of the Trust’s Constitution. The failure to comply with SFIs can in certain circumstances be regarded as a disciplinary matter that could result in dismissal. 4 Associated Trust Documents
Budget Holder Manual – available on Trust’s intranet The Constitution – available on Trust’s website
5 Responsibilities/Duties 5.1 Board of Directors The Board of Directors exercises financial supervision and control by:
(a) formulating the financial strategy;
(b) requiring the submission and approval of budgets within approved allocations/overall income;
(c) defining and approving essential features in respect of important procedures and financial systems (including the need to obtain value for money);
Formatted Table
9/73 26/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 7 of 70
(d) Defining specific responsibilities placed on members of the Board and
employees as indicated in the Scheme of Delegation.
(e) The Board of Directors has retained sole rights to approve all financial transactions with a value in excess of the level specified for this purpose in the Scheme of Delegation, subject to the exclusion of any item covered by specific delegated authority. This applies to individual transactions and to term contracts for the provision of goods, services or capital works over a period of time.
(f) The Board of Directors acts as corporate trustee for all charitable funds.
(g) The Board of Directors is responsible for ensuring appropriate governance
arrangements are in place for the Trust’s wholly owned subsidiary company, SWFT Clinical Services Limited and the joint venture Innovate Healthcare Services Limited (which is jointly controlled between the Trust and George Eliot Hospital NHS Trust).
(h) The Board of Directors will maintain adequate policies and safeguards to prevent bribery and ensure compliance with the requirements of the Bribery Act 2010. (nb. The key policies affected are those relating to gifts/hospitality/sponsorship; staff recruitment and disciplinary; managing conflict of interests and declaration of interests).
The Board has resolved that certain powers and decisions may only be exercised by the Board in formal session. These are set out in the Constitution. All other powers have been delegated to such other Directors/Officers or Committees as the Trust has established. 5.2 The Council of Governors Under the provisions of the Health and Social Care Act 2012 the approval of the Council of Governors has to be sought for mergers, acquisitions, separations, dissolutions, and significant transactions, as follows:
(a) The Trust may only apply for a merger, acquisition, separation or dissolution with the approval of more than half of the members of the Council of Governors, and
(b) The Trust may enter into significant transactions only if more than half of the members of the Council of Governors of the Trust voting approve entering into the transaction.
The definition of a significant transaction is contained in the Constitution. 5.3 Chief Executive The Chief Executive, as far as possible, delegates their detailed responsibilities, but they remain accountable for financial control.
Within the SFIs, it is acknowledged that the Chief Executive is ultimately accountable to the Board, and as Accounting Officer, to Parliament, for ensuring that the Board meets its
Formatted Table
10/73 27/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 8 of 70
obligation to perform its functions within the available financial resources. The Chief Executive has overall executive responsibility for the Trust’s activities; is responsible to the Chairperson and the Board for ensuring that its financial obligations and targets are met and has overall responsibility for the Trust’s system of internal control. It is a duty of the Chief Executive to ensure that Members of the Board and, employees and all new appointees are notified of, and put in a position to understand their responsibilities within these Instructions. 5.4 Managing Director The Managing Director will support the Chief Executive to fulfil their role of Accounting Officer for the Trust by leading the Trust on a day to day basis. The Managing Director will ensure that there is constant and visible Trust wide leadership to direct and lead the Executive team, to ensure delivery of its performance, financial and governance requirements. 5.5 Chief Finance Officer Director of Finance The Chief Executive delegates powers to the Chief Finance Officer Director of Finance in their role as a first line budget holder responsible for the Finance, Information and Procurement Directorate. In addition to these, the Chief Finance Officer Director of Finance is provided with further powers to manage the approval of financial transactions initiated by other departments across the Trust, and other financial transactions on behalf of the Trust. The Board of Directors instruct that the Chief Finance Officer Director of Finance is required to implement the Trust’s financial policies, ensure that detailed financial procedures and systems are established and ensure that sufficient records are maintained to show and explain the Trust’s transactions, in order to disclose the financial position of the Trust at any time. The Chief Finance Officer Director of Finance shall prepare, document and maintain detailed financial policies, processes, procedures and systems incorporating the principles of separation of duties and internal control to supplement these instructions. In relation to any officer who is involved in a financial or procurement process or function, the Chief Finance Officer Director of Finance shall set out the requirements, the manner in which the officer discharges his/her duties and the form in which financial records are kept. All finance and procurement processes must be to the standard and satisfaction of the Chief Finance Officer Director of Finance. In addition to these, the Chief Finance Officer Director of Finance is provided with further powers to control the approval of financial transactions relating to the Trust capital programmes, in accordance with the Scheme of Delegation. 5.6 All Staff All members of the Board and employees, severally and collectively, are responsible for:
(a) the security of the property of the Trust; (b) avoiding loss;
11/73 28/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 9 of 70
(c) exercising economy and efficiency in the use of resources; (d) conforming with the requirements of the Constitution, SFIs, Financial
Procedures and the Scheme of Delegation.
All employees are reminded that absolute authority governing all actions within the Trust rests with the Board of Directors and that this authority is exercised through the Scheme of Delegation. All employees are bound through their contracts of employment to follow the instructions of the Board of Directors and to comply with the policies and procedures that are developed and authorised in their name. These SFIs set out specific Trust policies and procedures across a number of areas. All employees must comply with these requirements in all cases. Where exceptions are deemed necessary, prior approval from the Chief Finance Officer Director of Finance must be obtained, as guided in these SFIs. However, it is neither possible nor desirable to govern all the financial affairs of the entire Trust through a single set of instructions. Therefore, these Instructions make reference in a number of areas where it is considered appropriate for the Chief Executive, Managing Director, or the Chief Finance Officer Director of Finance to develop, on behalf of the Trust, a series of detailed policies, procedures and processes, which are not included in these Instructions. In such cases it is the responsibility of all employees of the Trust to ensure they understand fully the existence, contents and requirements of all such policies and procedures and to comply with them on the basis that they have received full authority from the Board of Directors. Guidance on the existence and relevance of policies and procedures to specific situations will be available in all cases from the Chief Executive, Managing Director, the Chief Finance Officer Director of Finance or the Associate Directors of Finance. All employees are urged to consult with one of these Executive officers in situations where they are unsure as to the most appropriate course of action. Such consultation must be sought in advance of making any financial commitment on behalf of the Trust. The Board of Directors will expect all employees of the Trust to comply with these requirements and will regard a breach as a disciplinary offence. All employees of the Trust have an individual and collective responsibility for safeguarding the interests of the Trust at all times. The public sector values section of these Instructions explains the general requirement of all staff to protect the reputation of the Trust as a public benefit organisation. This section is intended to remind Trust employees of the requirement to safeguard the financial resources of the Trust. These resources may take the obvious tangible form of fixed assets, cash or negotiable instruments, as well as less clear, or possibly intangible items such as lost or foregone income through failure to notify income sources or lost opportunities to earn or recover income due to the Trust. In addition all employees are responsible for avoiding unauthorised acts that may result in the Trust incurring liabilities (directly or indirectly) or which may diminish the value of any of the Trust’s assets (including the Trust’s brand or reputation). All employees are expected to report all income sources immediately to the Chief Finance Officer Director of Finance.
12/73 29/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 10 of 70
5.7 Contractors and their Employees Any contractor or employee of a contractor who is empowered by the Trust to commit the Trust to expenditure or who is authorised to obtain income shall be covered by these instructions. It is the responsibility of the Chief Executive, and Managing Director and Chief Finance Officer to ensure that such persons are made aware of this. For all members of the Board and any employees who carry out a financial function, the form in which financial records are kept and the manner in which members of the Board and employees discharge their duties must be to the satisfaction of the Chief Finance Officer Director of Finance. 6 Audit 6.1 Audit Committee In accordance with the Standing Orders, within the Constitution, the Board shall formally establish an Audit Committee, with clearly defined terms of reference and following guidance from the NHS Audit Committee Handbook which will provide an independent and objective view of internal control by: (a) overseeing Internal and External Audit services;
(b) reviewing financial and information systems and monitoring the integrity of
the financial statements and reviewing significant financial reporting judgments;
(c) reviewing the establishment and maintenance of an effective system of integrated governance, risk management and internal control, across the whole of the organisation’s activities (both clinical and non-clinical), that supports the achievement of the organisation’s objectives;
(d) monitoring compliance with Standing Orders and SFIs; (e) reviewing schedules of losses and compensations and making
recommendations to the Board;
(f) reviewing schedules of debtors/creditors balances over 6 months old and explanations/action plans;
(g) approving bad debt write offs, and (h) Reviewing the arrangements in place to support the Assurance Framework
process prepared on behalf of the Board and advising the Board accordingly.
Where the Audit Committee considers there is evidence of ultra vires transactions, evidence of improper acts, or if there are other important matters that the Committee wishes to raise, the Chair of the Audit Committee should raise the matter at a full meeting of the Board. Exceptionally, the matter may need to be referred to NHS England and NHS Improvement/Department of Health and Social Care. (To the Chief Finance Officer Director of Finance in the first instance.)
13/73 30/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 11 of 70
It is the responsibility of the Chief Finance Officer Director of Finance to ensure an adequate Internal Audit service is provided and the Audit Committee shall be involved in the selection process when/if an Internal Audit service provider is changed. 6.2 Internal Audit Internal Audit will review, appraise and report upon:
(a) the extent of compliance with, and the financial effect of, relevant established policies, plans and procedures;
(b) the adequacy and application of financial and other related management
controls; (c) the suitability of financial and other related management data; (d) the extent to which the Trust’s assets and interests are accounted for and
safeguarded from loss of any kind, arising from:
(i) fraud and other offences; (ii) waste, extravagance, inefficient administration; (iii) poor value for money or other causes.
(e) Internal Audit shall also independently verify the Assurance Statements in
accordance with guidance from NHS England and NHS Improvement/Department of Health and Social Care.
Whenever any matter arises which involves, or is thought to involve, irregularities concerning cash, stores, or other property or any suspected irregularity in the exercise of any function of a pecuniary nature, the Chief Finance Officer Director of Finance must be notified immediately. The Head of Internal Audit, or their representative, will normally attend Audit Committee meetings and has a right of access to all Audit Committee members, the Chairperson, Chief Executive and Managing Director of the Trust. The Head of Internal Audit shall be accountable to the Chief Finance Officer Director of Finance. The reporting system for internal audit shall be agreed between the Chief Finance Officer Director of Finance, the Audit Committee and the Head of Internal Audit. The agreement shall be in writing and shall comply with the guidance on reporting contained in the NHS Internal Audit Standards. The reporting system shall be reviewed at least every three years. The Chief Finance Officer Director of Finance is responsible for:
(a) ensuring there are arrangements to review, evaluate and report on the effectiveness of internal financial control including the establishment of an effective Internal Audit function;
14/73 31/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 12 of 70
(b) ensuring that Internal Audit is adequate and meets the NHS mandatory audit standards;
(c) deciding at what stage to involve the police in cases of misappropriation and
other irregularities not involving fraud or corruption;
(d) ensuring that an annual internal audit report is prepared by the Head of Internal Audit for the consideration of the Audit Committee. The report must cover:
• a clear opinion on the effectiveness of internal control in accordance
with current assurance framework guidance issued by the Department of Health and Social Care including for example compliance with control criteria and standards;
• major internal financial control weaknesses discovered; • progress on the implementation of internal audit recommendations; • progress against plan over the previous year; • strategic audit plan covering the coming three years; • a detailed plan for the coming year.
6.3 External Audit The External Auditor is appointed and removed by the Council of Governors and paid for by the Trust. The Audit Committee must ensure a cost-efficient service. If there are any problems relating to the service provided by the External Auditor, then this should be raised with the External Auditor. 6.4 Fraud and Corruption In line with their responsibilities, the Chief Executive, Managing Director and Chief Finance Officer Director of Finance shall monitor and ensure compliance with the relevant requirements of the NHS Standard Contract, which require providers of NHS services to put in place and maintain appropriate arrangements to address security management and counter fraud issues, and meet NHS Counter Fraud Authority Standards. The Trust shall nominate a suitable person to carry out the duties of the Local Counter Fraud Specialist (LCFS) as specified by the NHS CounterAnti-Fraud Manual and related guidance. Details of the Trust’s LCFS can be found in the Budget Holder Manual or on the intranet. Any employee discovering or suspecting a loss of any kind must immediately inform either the Chief Finance Officer Director of Finance or the LCFS. Where a criminal offence is suspected, the Chief Finance Officer Director of Finance will arrange for the LCFS to investigate or inform the police as appropriate. For losses apparently caused by theft, arson, neglect of duty or gross carelessness, except if trivial, the Chief Finance Officer Director of Finance will notify the Board of Directors. The Board of Directors recognises that in extreme cases financial loss may be the result of fraud (i.e. making an intentional deception to secure unlawful gain) or corruption. While the Board of Directors has every confidence in the integrity of Trust employees, it has a duty to put in place controls to minimise the opportunity for illegal appropriation of Trust
15/73 32/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 13 of 70
resources. Accordingly, the Chief Finance Officer Director of Finance shall ensure appropriate compliance with national standards and guidance regarding counter-fraud measures, which are referred to in these instructions. All employees of the Trust are required to ensure they fully understand the Trust’s Fraud, Bribery and Corruption Policy and the procedure for reporting suspicions or matters of possible concern. The Trust’s Fraud, Bribery and Corruption Policy will be updated regularly by the Chief Finance Officer. Director of Finance. The LCFS shall report to the Chief Finance Officer Director of Finance and shall work with staff in the NHS Counter Fraud Authority in accordance with the NHS CounterAnti-Fraud Manual. The LCFS will provide a written report, at least annually, on counter fraud work within the Trust. Please refer to the Trust Fraud and Corruption Policy SWH 00327 Furthermore the Trust has a whistle-blowing mechanism to report any suspected or actual fraud, bribery or corruption matters and internally publicise this, together with the national fraud and corruption reporting line provided by NHS Counter Fraud Authority (formerly NHS Protect). Please refer to ‘Whistle Blowing’ policy SWH 00310. 6.5 Security Management In line with their responsibilities, the Chief Executive will monitor and ensure compliance with Directions issued by the Secretary of State for Health on NHS security management. The Trust shall nominate a suitable person to carry out the duties of the Local Security Management Specialist (LSMS) as specified by the Secretary of State for Health guidance on NHS security management. The Chief Executive, in consultation with the Chief Finance Officer Director of Finance will develop, maintain and monitor detailed policies, procedures and instructions covering all aspects of the security of money, assets and other Trust resources. All employees of the Trust are expected to comply fully with these requirements and to take any and all corrective action as instructed by appropriate officers of the Trust. Further to this requirement, each employee has an individual and collective responsibility for the security of property and other resources of the Trust. All issues of concern or potential risk must be reported immediately to the Chief Finance OfficerDirector of Finance, including any concerns employees may have where existing practices may represent a risk to the assets or other resources of the Trust. Any damage to or losses of the Trust’s premises, assets, supplies or other resources must be reported to the Chief Finance OfficerDirector of Finance immediately in accordance with procedures of Losses and Special Payments, which shall be established by the Chief Finance OfficerDirector of Finance. The Trust shall nominate an Executive Director to be responsible to the Board for NHS security management. The Chief Executive has overall responsibility for controlling and coordinating security. However, key tasks are delegated to the Associate Director of Operations - Support Services and the appointed LSMS.
16/73 33/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 14 of 70
6.6 Access to Records The Chief Finance OfficerDirector of Finance or designated auditors are entitled without necessarily giving prior notice to require and receive:
(a) access to all records, documents and correspondence relating to any financial or other relevant transactions, including documents of a confidential nature;
(b) access at all reasonable times to any land, premises or members of the
Board or employee of the Trust;
(c) the production of any cash, stores or other property of the Trust under a member of the Board or an employee's control, and
(d) explanations concerning any matter under investigation.
7 The Trust’s Objectives and the Annual Planning Cycle Every year the Trust sets a number of key objectives. These key objectives are based on local and national priorities and are developed in association with the Trust’s Council of Governors. They are promoted internally so that all staff are aware of the Trust’s focus for the year. The Chief Executive, with the assistance of the Managing Director, Chief Strategy Officer Director of Development and Chief Finance OfficerDirector of Finance, shall compile and submit to the Board of Directors strategic plans and operational plans as required by the Board of Directors, which deliver these objectives as well as meet the requirements of the Independent Regulator (as described in NHS England and NHS Improvement’s published Guidance, Directions and Compliance Framework). Plans shall be reconcilable with the annual submission of NHS England and NHS Improvement’s Financial proformas in its Annual Plan Review. The Chief Executive shall require the Chief Finance Officer Director of Finance to report to the Board of Directors any significant in-year variance from the business plan and to advise the Board of Directors on action to be taken. Throughout the year, business cases are submitted to the Board of Directors for consideration. More detailed guidance on the Annual Planning Cycle and process for business cases can be found in the Budget Holder’s Manual. 8 Budgets 8.1 Budget Setting The Chief Finance Officer Director of Finance shall also be required to compile and submit to the Board of Directors, any and all such financial estimates and forecasts, of both revenue and capital nature as may be required from time to time. As a consequence, the Chief Finance Officer Director of Finance shall have full and complete right of access to all budget holders on financial related matters.
17/73 34/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 15 of 70
All Officers shall provide the Chief Finance Officer Director of Finance with all financial, statistical and other relevant information as necessary for the compilation of such business plans, estimates and forecasts, in accordance with the timetable required by the Chief Finance Officer. Director of Finance. More information on the budget setting process is set out in the Budget Holder Manual and in the Budget Setting Guidance which is issued annually. 8.2 Budget Delegation The Chief Executive may delegate management of a budget or part of a budget to officers to permit the performance of defined activities. The Scheme of Delegation shall include a clear definition of individual and group responsibilities for control of expenditure, exercise of virement, achievement of planned levels of services and the provision of regular reports upon the discharge of those delegated functions to the Chief Executive. In carrying out their duties no officers shall exceed the budgetary limits set them by the Chief Executive. Except where otherwise approved by the Chief Executive, taking account of advice of the Chief Finance OfficerDirector of Finance, budgets shall be used only for the purpose for which they were provided and any budgeted funds not required for their designated purpose shall revert to the immediate control of the Trust. Expenditure for which no provision has been made in an approved budget and which is not subject to funding under the delegated powers of virement shall only be incurred after authorisation by the Chief Executive, or Managing Director, and Chief Finance Officer Director of Finance or the Board of Directors as appropriate. All budget holders will sign up to their allocated budgets at the commencement of each financial year. The Chief Finance Officer Director of Finance has a responsibility to ensure that adequate training is delivered on an on-going basis to budget holders to help them manage their budgets successfully. The Chief Executive may delegate the management of a budget to permit the performance of a defined range of activities. This delegation must be in writing and be accompanied by a clear definition of:
(a) the amount of the budget; (b) the purpose(s) of each budget heading; (c) individual and group responsibilities; (d) authority to exercise virement; (e) achievement of planned levels of service; (f) the provision of regular reports.
The Chief Executive and delegated budget holders must not exceed the budgetary total or virement limits set by the Board. Any budgeted funds not required for their designated purpose(s) revert to the immediate control of the Chief Executive, subject to any authorised use of virement.
18/73 35/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 16 of 70
Non-recurring budgets should not be used to finance recurring expenditure without the authority in writing of the Chief Executive, as advised by the Chief Finance Officer. Director of Finance. 8.3 Budgetary Control and Reporting The Chief Finance Officer Director of Finance will devise and maintain systems of budgetary control. These will include:
(a) monthly financial reports to the Board in a form approved by the Board
containing:
• income and expenditure to date and forecast year-end position; • movements in working capital; • movements in cash and capital; • capital spend and projected outturn against plan; • explanations of any material variances from plan; • details of any corrective action where necessary and the Chief
Executive's and/or Chief Finance Officer’s Director of Finance's view of whether such actions are sufficient to correct the situation;
(b) the issue of timely, accurate and comprehensible advice and financial
reports to each budget holder, covering the areas for which they are responsible;
(c) investigation and reporting of variances from financial, workload and
manpower budgets; (d) monitoring of management action to correct variances; and (e) arrangements for the authorisation of budget transfers.
Each Budget Holder is responsible for ensuring that: (a) any likely overspending or reduction of income which cannot be met by
virement is not incurred without the prior consent of the Board;
(b) the amount provided in the approved budget is not used in whole or in part for any purpose other than that specifically authorised subject to the rules of virement;
(c) no permanent employees are appointed without the approval of the Chief
Executive other than those provided for within the available resources and manpower establishment as approved by the Board.
19/73 36/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 17 of 70
Budget holders are responsible for identifying and implementing cost improvements and income generation initiatives in accordance with the requirements of the Strategic and Operational Plans. 9 Areas Subject to Financial Control There are a number of areas that are subject to financial control. These are:
• Revenue Income • Revenue Expenditure • Capital Expenditure • Tendering and Contracting • Patient Property • Charitable Funds
9.1 Revenue Income
Revenue income is made up from several sources: • Contracts with our Commissioners • Service Level Agreements with other parties • Fees and Charges from Income Generation • Income from Private Patients and Overseas Visitors; and • Income from the Injury Cost Recovery Scheme
The flowchart below shows the financial process of how this income is collected by the Trust and turned into cash. Each of these income sources and the processes involved are subject to financial controls as set out below.
20/73 37/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 18 of 70
9.1.1 Contracts with Commissioners/Service Level Agreements The Board of Directors will approve standard terms and conditions for legally binding contracts, on the basis of which the Trust will provide healthcare services. Any variations to the standard terms and conditions will be approved in accordance with the Scheme of Delegation. The Chief Executive is responsible for ensuring the Trust enters into suitable contracts with service commissioners for the provision of NHS services to patients in accordance with the Annual Plan. The Chief Executive delegates the negotiation of contracts for the provision of services to the Chief Finance Officer Director of Finance and the Deputy Chief Finance OfficerAssociate Director of Finance - Income, Contracting & Financial Management with support from the Executive Directors. The Chief Finance Officer Director of Finance and Deputy Chief Finance OfficerAssociate Director of Finance - Income, Contracting & Financial Management will provide advice regarding costing and pricing of services, payment terms and conditions of service agreements. Contracts should be devised so as to achieve activity and performance targets, minimise risk, and to maximise the Trust's opportunity to generate income. The Trust will produce a reference cost tariff in accordance with NHS guidelines. The Trust will comply with national guidance on setting prices for the provision of NHS healthcare (i.e National Tariff Payment System Guidance) as far as this allows. Other prices and tariffs must be approved by the Chief Finance Officer Director of Finance and Deputy Chief Finance OfficerAssociate Director of Finance - Income, Contracting & Financial Management. The Chief Finance Officer Director of Finance shall ensure that a summary of the Trust’s contract income is reported annually to the Board of Directors. The Chief Finance Officer Director of Finance shall also produce regular reports detailing actual and forecast contract income with a detailed assessment of the impact of the variable elements of income. Any pricing of contracts at marginal cost should be undertaken by the Chief Finance Officer Director of Finance and Deputy Chief Finance OfficerAssociate Director of Finance - Income, Contracting & Financial Management in accordance with a policy and tariff reported to the Board of Directors. All copies of signed contracts will be retained by the Deputy Chief Finance OfficerAssociate Director of Finance - Income, Contracting & Financial Management. 9.1.2 Fees & Charges The Chief Finance Officer Director of Finance is responsible for designing, maintaining and ensuring compliance with systems for the proper recording, invoicing, collection and income coding of all monies due. The Chief Finance Officer Director of Finance is also responsible for ensuring the prompt banking of all monies received. The Trust shall follow the Department of Health and Social Care's advice in the "Costing" Manual in setting prices for NHS service agreements.
21/73 38/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 19 of 70
The Chief Finance Officer Director of Finance is responsible for approving and regularly reviewing the level of all fees and charges other than those determined by the Department of Health and Social Care or by Statute. Independent professional advice on matters of valuation shall be taken as necessary. Where sponsorship income (including items in kind such as subsidised goods or loans of equipment) is considered, the guidance in the Department of Health and Social Care’s Commercial Sponsorship – Ethical standards in the NHS shall be followed. All employees must inform the Chief Finance Officer Director of Finance promptly of money due arising from transactions which they initiate/deal with, including all contracts, leases, tenancy agreements, private patient undertakings and other transactions. 9.1.3 Credit Control/ Debt recovery The Chief Finance Officer Director of Finance is responsible for the appropriate recovery action on all outstanding debts. Income not received should be dealt with in accordance with losses procedures. Overpayments should be detected (or preferably prevented) and recovery initiated. 9.1.4 Security of Cash, Cheques and other Negotiable Instruments The Chief Finance Officer Director of Finance is responsible for approving the form of all receipt documents, agreement forms, or other means of officially acknowledging or recording monies received or receivable. The Chief Finance Officer Director of Finance is responsible for the provision of adequate facilities and systems for officers, whose duties include collecting and holding cash, including the provision of safes or lockable cash boxes, the procedures for keys and for coin operated machines. The Chief Finance Officer Director of Finance is responsible for prescribing systems and procedures for handling cash and negotiable securities on behalf of the Trust. All sites that handle cash must adhere to local cash handling arrangements as determined by the Finance Department. Official money shall not under any circumstances be used for the encashment of private cheques. All cheques, postal orders, cash etc., shall be banked intact. Disbursements shall not be made from cash received, except under arrangements approved by the Chief Finance OfficerDirector of Finance. The holders of safe keys shall not accept unofficial funds for depositing in their safes unless such deposits are in special sealed envelopes or locked containers. It shall be made clear to the depositors that the Trust is not to be held liable for any loss, and written indemnities must be obtained from the organisation or individuals absolving the Trust from responsibility for any loss. 9.1.5 Injury Costs Recovery Scheme The NHS Injury Costs Recovery (ICR) scheme aims to recover the cost of NHS treatment where personal injury compensation is paid, for example after a road traffic accident. The Department of Health and Social Care publishes monthly updates on the amount of money recovered under the ICR.
22/73 39/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 20 of 70
Funds are primarily recovered from insurance companies and then paid to the NHS hospital or ambulance trust that provided the treatment. The Chief Finance Officer Director of Finance shall ensure that there are processes in place to identify patients that have been treated where personal injury compensation is eligible and ensure that costs are recovered. 9.1.6 Private Patients The Chief Finance Officer Director of Finance shall ensure that the proportion of the Trust’s total income derived from private patient charges is not greater than allowed for under the Health and Social Care Act 2012. The Chief Finance Officer Director of Finance shall ensure that there is a process and guidance on the treatment of private patients that applies to all staff with responsibility for charging and collecting funds from private patients. It relates in particular to private patients’ officers, cashiers and the accounts receivable department. The process and guidance also applies to all staff responsible for the treatment and care of private patients. This process and guidance has been developed to include all relevant legal requirements relating to private patient treatment, national best practice and to reduce risks to the Trust of not recovering income when private patients are treated. 9.1.7 Overseas Visitors The Chief Finance Officer Director of Finance shall ensure that there are systems in place to identify overseas visitors requiring treatment and to ensure that any income due can be collected. The Chief Finance Officer Director of Finance shall ensure that there is a process and guidance on the treatment of overseas patients that applies to all staff with responsibility for charging and collecting funds from private patients. It relates in particular to private patients’ officers, cashiers and the accounts receivable department. The process and guidance also applies to all staff responsible for the treatment and care of patients from overseas. This process and guidance has been developed to include all relevant legal requirements relating to overseas visitor treatment, national best practice and to reduce risks to the Trust of not recovering income when patients from overseas are treated. Please refer to the Overseas visitors guidance available via the intranet. 9.2 Revenue Expenditure 9.2.1 Pay The Chief Finance OfficerDirector of Finance, with the Chief People OfficerDirector of Human Resources, shall make arrangements for the provision of payroll services to the Trust, to ensure the accurate determination of pay entitlement and to enable prompt and accurate payment to employees. The Chief Finance OfficerDirector of Finance, with the Chief People OfficerDirector of Human Resources, shall be responsible for establishing procedures covering advice to
23/73 40/347
SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 21 of 70
managers on the prompt and accurate submission of payroll data to support the determination of pay including, where appropriate, timetables and specifications for submission of properly authorised notification of new employees, amendments to standing pay data and terminations. The Chief Finance OfficerDirector of Finance will issue detailed procedures covering payments to staff including rules on handling and security of bank credit payments. There may be times when an overpayment of salary or other payment occurs. It is in the Trust’s interests to recover such overpayments as soon as is practicably possible, and the Trust’s procedure relating to overpayments will be used. When an overpayment is discovered, immediate action must be taken to ensure the overpayment is ended and future payment is made at the correct rate. In the same way that underpayments may be corrected up to 1 year, so will overpayments be recovered for the same period. 9.2.2 Approved Staffing Levels (ASL) The manpower plans incorporated within the annual budget will form the ASL or funded establishment. No Oofficer or Member of the Board of Directors or employee may engage, re-engage, or re-grade employees, either on a permanent or temporary nature, or hire agency staff, or agree to changes in any aspect of remuneration outside the limit of their approved budget and funded establishment. Certain posts are recruited through a central recruitment programme managed by Employment Services. Authority to rRecruit (ATR) is required for all other engagement, re-engagement, re-grading or increase in hours of substantive employees, whether fixed term or permanent. The electronic ATR process and associated ATR form is set out in the Trust’s Recruitment and Selection Policy SWH 00188. Occasionally, due to vacancies, peak in workload, short notice sickness, for example, it is necessary to engage with temporary workforce such as bank or agency, whilst remaining within the approved budget, which are outlined further in the policies referenced below:
• SWH 00504 Bank, Agency and Temporary Workers Procedure for Non-medical staff. This policy also contains further guidance on off payroll engagements following the April 2017 changes in relation to the tax legislation IR35 and Public Sector off payroll workers; and
• SWH 00093 Bank, Agency and Temporary Workers Procedure for Medical staff- which set out the authority required to engage with temporary workers and processes that must be followed.
Appropriately nominated managers have delegated responsibility for:
(a) submitting time records, and other notifications in accordance with agreed timetables via Healthroster. For further details on the entry of information into Healthroster please refer to the Staff Rostering Policy SWH 00634;
Formatted: Justified
24/73 41/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 22 of 70
(b) completing time records and other notifications in accordance with the Chief
Finance Officer’s Director of Finance's instructions and in the form prescribed by the Chief Finance Officer Director of Finance;
(c) submitting termination forms in the prescribed form immediately upon
knowing the effective date of an employee's or officer’s resignation, termination or retirement. Where an employee fails to report for duty or to fulfil obligations in circumstances that suggest they have left without notice, the Chief Finance Officer Director of Finance must be informed immediately.
Regardless of the arrangements for providing the payroll service, the Chief Finance Officer Director of Finance shall ensure that the chosen method is supported by appropriate (contracted) terms and conditions, adequate internal controls and audit review procedures and that suitable arrangements are made for the collection of payroll deductions and payment of these to appropriate bodies. 9.2.3 Contracts of Employment The Board shall delegate responsibility to the Chief People Officer Director of Human
Resources for: (a) ensuring that all employees are issued with a Contract of Employment in a
form approved by the Board and which complies with employment legislation;
(b) dealing with variations to, or termination of, contracts of employment. 9.2.4 Non Pay Expenditure
The Board will approve the level of non-pay expenditure on an annual basis and the Chief Executive, or Managing Director, will determine the level of delegation to budget managers. The Chief Executive will set out: (a) the list of managers who are authorised to place requisitions for the
supply of goods and services; (b) the maximum level of each requisition and the system for
authorisation above that level. The Chief Executive, or Managing Director, shall set out procedures on the seeking of professional advice regarding the supply of goods and services. Both the NHS Supply Chain (NHSSC) online ordering system and the Trust’s official E-procurement system are available to designated staff subject to the controls inherent within each system. These and other non pay purchases are subject to the controls and procedures as determined by the Chief Finance OfficerDirector of Finance. Please refer to Appendix B for the non pay authorisation summary table.
25/73 42/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 23 of 70
9.2.5 Expenditure Process The requisitioner, in choosing the item to be supplied (or the service to be performed) shall always obtain the best value for money for the Trust. In so doing, the advice of the Trust’s adviser on supply shall be sought. Where this advice is not acceptable to the requisitioner, the Chief Finance Officer, Director of Finance,and/or the Managing Director, and/or the Chief Executive shall be consulted. An official purchase order must then be raised to the supplier, which in turn must be quoted on supplier invoices. Further details are set out below. The Chief Finance Officer Director of Finance shall be responsible for the prompt payment of accounts and claims. Payment of contract invoices shall be in accordance with contract terms, or otherwise, in accordance with national guidance. The Chief Finance Officer Director of Finance will:
(a) advise the Board regarding the setting of thresholds above which
quotations (competitive or otherwise) or formal tenders must be obtained; and, once approved, the thresholds should be incorporated in SFIs and regularly reviewed;
(b) prepare procedural instructions or guidance within the Scheme of
Delegation on the obtaining of goods, works and services incorporating the thresholds;
(c) be responsible for the prompt payment of all properly authorised
accounts and claims; (d) be responsible for designing and maintaining a system of verification,
recording and payment of all amounts payable. The system shall provide for:
(i) A list of Board employees (including specimens of their signatures) authorised to certify invoices.
(ii) Certification that:
• goods have been duly received, examined and are in accordance with specification and the prices are correct;
• work done or services rendered have been satisfactorily
carried out in accordance with the order, and, where applicable, the materials used are of the requisite standard and the charges are correct;
• in the case of contracts based on the measurement of time,
materials or expenses, the time charged is in accordance with the time sheets, the rates of labour are in accordance with the appropriate rates, the materials have been checked as regards
Formatted: Font: Bold, Underline
26/73 43/347
SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 24 of 70
quantity, quality, and price and the charges for the use of vehicles, plant and machinery have been examined;
• where appropriate, the expenditure is in accordance with
regulations and all necessary authorisations have been obtained;
• the account is arithmetically correct;
• the account is in order for payment.
• Instructions to employees regarding the handling and payment
of accounts within the Finance Department.
• be responsible for ensuring that payment for goods and services is only made once the goods and services are received.
9.2.6 Prepayments Prepayments are only permitted where exceptional circumstances apply. In such instances: (a) Prepayments are only permitted where the financial advantages outweigh
the disadvantages (i.e. cash flows must be discounted to NPV using a rate which incorporates the National Loans Fund (NLF) rate+ 3.5% Public Dividend Capital rate + an appropriate percentage rate as advised from time to time by the Chief Finance OfficerDirector of Finance);
(b) The appropriate officer must provide, in the form of a written report, a case
setting out all relevant circumstances of the purchase. The report must set out the effects on the Trust if the supplier is at some time during the course of the prepayment agreement unable to meet his commitments;
(c) The Chief Finance Officer Director of Finance will need to be satisfied with
the proposed arrangements before contractual arrangements proceed (taking into account the Public Contracts Regulations 2015 EU public procurement rules where the contract is above a stipulated financial threshold), and
(d) The budget holder is responsible for ensuring that all items due under a
prepayment contract are received and they must immediately inform the appropriate Chief Officer Director or Chief Executive if problems are encountered.
9.2.7 Official Purchase Orders Official Purchase Orders must:
(a) be consecutively numbered;
27/73 44/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 25 of 70
(b) be in a form approved by the Chief Finance OfficerDirector of Finance; (c) state the Trust’s terms and conditions of trade; (d) only be issued to, and used by, those duly authorised by the Chief Executive.
(e) May be transmitted by a system of Electronic Data Interchange
Managers and officers must ensure that they comply fully with the guidance and limits specified by the Chief Finance OfficerDirector of Finance and that:
(a) all contracts (except as otherwise provided for in the Scheme of Delegation), leases, tenancy agreements and other commitments which may result in a liability are notified to the Chief Finance Officer Director of Finance in advance of any commitment being made;
(b) contracts above specified thresholds are advertised and awarded in
accordance with EU rules on Public Contracts public procurementRegulations 2015 and via the Find a Tender System;
(c) where consultancy advice is being obtained, the procurement of such advice
must be in accordance with guidance issued by the Department of Health and Social Care;
(d) no order shall be issued for any item or items to any firm which has made
an offer of gifts, reward or benefit to directors or employees, other than isolated gifts of a trivial character or inexpensive seasonal gifts, such as calendars; conventional hospitality, such as lunches in the course of working visits;
(e) no requisition/order is placed for any item or items for which there is no
budget provision unless authorised by the Chief Finance Officer Director of Finance on behalf of the Chief Executive;
(f) all goods, services, or works are ordered on an official purchase order
except works and services executed in accordance with a contract and purchases from petty cash; in line with the Trust adherence to No Purchase Order, No Pay procedures.
(g) verbal orders must only be issued very exceptionally - by an employee
designated by the Chief Executive and only in cases of emergency or urgent necessity. These must be confirmed by an official order and clearly marked "Confirmation Order";
(h) orders are not split or otherwise placed in a manner devised so as to avoid
the financial thresholds; (i) goods are not taken on trial or loan in circumstances that could commit the
Trust to a future uncompetitive purchase;
Commented [AR(ADoPSF1]:
Formatted: Underline
28/73 45/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 26 of 70
(j) Where goods are being trialled on a free of charge agreement, Procurement must be informed in order to advise on all relevant DoHDHSC indemnity documentation. must be completed and returned to Procurement, with the Ward or Department conducting the evaluation retaining one copy.
(j) changes to the list of employees and officers authorised to certify invoices
are notified to the Chief Finance OfficerDirector of Finance; (k) purchases from petty cash are restricted in value and by type of purchase in
accordance with instructions issued by the Chief Finance OfficerDirector of Finance;
(l) petty cash records are maintained in a form as determined by the Chief
Finance OfficerDirector of Finance.
The Chief Executive and Chief Finance OfficerDirector of Finance shall ensure that the arrangements for financial control and financial audit of building and engineering contracts and property transactions comply with the national guidance. The technical audit of these contracts shall be the responsibility of the relevant Chief OfficerDirector. Payments to local authorities and voluntary organisations made under the powers of section 28A of the NHS Act shall comply with procedures laid down by the Chief Finance Officer Director of Finance which shall be in accordance with these Acts. 9.2.8 Stores Stock and Receipt of Goods Stock , defined in terms of controlled stock and departmental stock (for immediate use) should be:
(a) kept to a minimum; (b) Must be rotated to take account of obsolescence; (b) (b)
subjected to annual stock take; (c)
(d) (c) valued at the lower of cost and net realisable value.
Subject to the responsibility of the Chief Finance OfficerDirector of Finance for the systems of control, overall responsibility for the control of stores shall be delegated to an employee by the Chief Executive. The day-to-day responsibility may be delegated to departmental employees and stores managers/keepers, subject to such delegation being entered in a record available to the Chief Finance OfficerDirector of Finance. The control of any Pharmaceutical stocks shall be the responsibility of a designated Pharmaceutical Officer; the control of any fuel oil and coal of a designated Estates Manager. The responsibility for security arrangements and the custody of keys for any stores and locations shall be clearly defined in writing by the designated manager/Pharmaceutical Officer. Wherever practicable, stocks should be marked as health service property.
Formatted: List Paragraph, Numbered + Level: 1 +Numbering Style: a, b, c, … + Start at: 1 + Alignment: Left+ Aligned at: 0.64" + Indent at: 1"
Formatted: List Paragraph, Numbered + Level: 1 +Numbering Style: a, b, c, … + Start at: 1 + Alignment: Left+ Aligned at: 0.64" + Indent at: 1"
Formatted: List Paragraph, Indent: Left: 0.26", Numbered+ Level: 1 + Numbering Style: a, b, c, … + Start at: 1 +Alignment: Left + Aligned at: 0.64" + Indent at: 1"
Formatted: List Paragraph, Indent: Left: 0.62", First line: 0", Tab stops: Not at 0.6" + 1"
29/73 46/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 27 of 70
The Chief Finance Officer Director of Finance shall set out procedures and systems to regulate the stores including records for receipt of goods, issues, and returns to stores, and losses. Stocktaking arrangements shall be agreed with the Chief Finance OfficerDirector of Finance and there shall be a physical check covering all items in store at least once a year. Where a complete system of stores control is not justified, alternative arrangements shall require the approval of the Chief Finance OfficerDirector of Finance. The designated Manager/Pharmaceutical Officer shall be responsible for a system approved by the Chief Finance Officer Director of Finance for a review of slow moving and obsolete items and for condemnation, disposal, and replacement of all unserviceable articles. The designated Officer shall report to the Chief Finance Officer Director of Finance any evidence of significant overstocking and of any negligence or malpractice. Procedures for the disposal of obsolete stock shall follow the procedures set out for disposal of all surplus and obsolete goods. For goods supplied via the NHSSC central warehouses, the Chief Executive shall identify those authorised to requisition and accept goods from the store. The authorised person shall check receipt against the delivery note before forwarding this to the Procurement Department. Any discrepancies will be notified to NHS Supply Chain within 3 days. Any unresolved discrepancy shall be notified to the Finance Department who will ensure that any discrepancy reflected in the settlement of any recharge. 9.3 Capital Investment and Expenditure
The Chief Executive, through the Capital and Estates Committee:
(a) shall ensure that there is an adequate appraisal and approval process in place for determining capital expenditure priorities and the effect of each proposal upon business plans;
(b) is responsible for the management of all stages of capital schemes
and for ensuring that schemes are delivered on time and to cost; (c) shall ensure that the capital investment is not undertaken without
confirmation of commissioner(s) support and the availability of resources to finance all revenue consequences, including capital charges:
(d) shall ensure that a business case is produced for all developments
that require capital investment. Please see Scheme of Delegation for limits. This must include an option appraisal of potential benefits compared with known costs to determine the option with the highest ratio of benefits to costs and include the involvement of appropriate Trust personnel and external agencies and refer to the Business Case checklist;
30/73 47/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 28 of 70
(e) shall ensure that the Chief Finance Officer Director of Finance has certified professionally the costs and revenue consequences detailed in the business case;
(f) shall ensure that there are procedures for the management of capital
schemes where the contracts stipulate stage payments,
The Chief Executive will issue a scheme of delegation for capital investment management and shall issue to the manager responsible for any scheme:
(a) specific authority to commit expenditure; (b) authority to proceed to tender (c) approval to accept a successful tender
The Chief Finance Officer Director of Finance shall issue procedures governing the financial management, including variations to contract, of capital investment projects and valuation for accounting purposes. These procedures shall fully take into account the delegated limits for capital scheme. The Chief Finance Officer Director of Finance shall issue procedures for the regular reporting of expenditure and commitment against authorised expenditure.
31/73 48/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 29 of 70
9.3.1 Asset Registers & Security of Assets
The Chief Executive is responsible for the maintenance of registers of assets, taking account of the advice of the Chief Finance Officer Director of Finance concerning the form of any register and the method of updating, and arranging for a physical check of assets against the asset register to be conducted once a year. The Trust will maintain an asset register recording fixed assets. The minimum data set to be held within these registers shall be as specified in the accounting instructions issued by HM Treasury and/or the Department of Health and Social Care. Additions to the fixed asset register must be clearly identified to an appropriate budget holder and be validated by reference to:
(a) properly authorised and approved agreements, architects’ certificates, suppliers’ invoices and other documentary evidence in respect of purchases from third parties;
(b) stores, requisitions and wages records for own materials and labour
including appropriate overheads; (c) lease agreements in respect of assets held under a finance lease and
capitalised. Where capital assets are sold, scrapped, lost or otherwise disposed of, their value must be removed from the accounting records and each disposal must be validated by reference to authorisation documents and invoices (where appropriate). The Chief Finance OfficerDirector of Finance shall approve procedures for reconciling balances on fixed assets accounts in ledgers against balances on fixed asset registers.
Up to max £25k
Up to max £250k
Up to max £500k
Over £500k
Designated Budget Managers
Chief Executive, or Managing Director, and Director of Finance
Director of Development
New Replacement New New New Replacement Replacement Replacement
Chief Executive, or Managing Director and Director of Finance
Management Board
Capital & Estates Committee
Management Board
Capital & Estates Committee
Management Board
Management Board
Capital & Estates Committee
Capital & Estates Committee
Capital Chart
Board of Directors
32/73 49/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 30 of 70
The value of each asset shall be indexed to current values in accordance with International Financial Reporting Standards (IFRS). The value of each asset shall be depreciated using methods and rates as specified in the IFRS. The Chief Finance Officer Director of Finance of the Trust shall calculate and pay capital charges as specified in guidance as issued by the Department of Health and Social Care. The overall control of fixed assets is the responsibility of the Chief Executive. Asset control procedures (including fixed assets, cash, cheques and negotiable instruments, and also including donated assets) must be approved by the Chief Finance officerDirector of Finance. This procedure shall make provision for:
(a) recording managerial responsibility for each asset; (b) identification of additions and disposals; (c) identification of all repairs and maintenance expenses; (d) physical security of assets; (e) periodic verification of the existence of, condition of, and title to, assets
recorded; (f) identification and reporting of all costs associated with the retention of an
asset; (g) reporting, recording and safekeeping of cash, cheques, and negotiable
instruments. All discrepancies revealed by verification of physical assets to the fixed asset register shall be notified to the Chief Finance OfficerDirector of Finance. Whilst each employee and officer has a responsibility for the security of property of the Trust, it is the responsibility of Board members and senior employees in all disciplines to apply such appropriate routine security practices in relation to NHS property as may be determined by the Board. Any breach of agreed security practices must be reported in accordance with agreed procedures. Any damage to the Trust’s premises, vehicles and equipment, or any loss of equipment, stores or supplies must be reported by Board members and employees in accordance with the procedure for reporting losses. Where practical, assets should be marked as Trust property.
33/73 50/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 31 of 70
9.3.2 Asset Disposals The Chief Finance Officer Director of Finance must prepare detailed procedures for the disposal of assets including condemnations, and ensure that these are notified to managers. When it is decided to dispose of an asset, the Head of Department or authorised deputy will determine and advise the Chief Finance Officer Director of Finance of the estimated market value of the item, taking account of professional advice where appropriate. All unserviceable articles shall be:
(a) condemned or otherwise disposed of by an employee authorised for that purpose by the Chief Finance OfficerDirector of Finance;
(b) recorded by the Condemning Officer in a form approved by the Chief
Finance OfficerDirector of Finance which will indicate whether the articles are to be converted, destroyed or otherwise disposed of. All entries shall be confirmed by the countersignature of a second employee authorised for the purpose by the Chief Finance OfficerDirector of Finance.
The Condemning Officer shall satisfy himself as to whether or not there is evidence of negligence in use and shall report any such evidence to the Chief Finance OfficerDirector of Finance who will take the appropriate action. Asset disposals with a remaining net book value of over £5,000 must be approved by the Chief Finance Officer. 9.4 Tendering and Contract Procedure
Minor changes to the Procurement Contracts Regulation 2015 have been brought in by the Public Procurement Regulations 2020, removing all reference to the European Union and requirements to publish OJEU notices. These regulations EU Directives Governing Public Procurement and Directives by the Council of the European Union promulgated by the Department of Health and Social Care (DoHDHSC) prescribeing procedures for awarding all forms of contracts shall have effect as if incorporated in these SFI’s. The procedure for making all contracts by or on behalf of the Trust shall comply with these SFIs. These instructions shall not only apply to expenditure from Exchequer funds but also to works, services and goods purchased from the Trust’s Charitable Funds and other resources. The diagram below summarises the most appropriate process before an order is placed.
34/73 51/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 32 of 70
Need Identified
Contract Value
New Expenditure?
<£10,000 £50k – OJEU OJEU Limit
Raise Requisition
Purchase Order
Formal Tender
Detailed Analysis and Procurement Strategy, including but not limited to, procurement frameworks, route to market, contract term, demand, market engagement
EU Tender
Advertise on Contracts Finder >25k
Signed Contract on NHS Terms & Conditions
Business Case
Contract Award Approval based on
Scheme of
>OJEU Limit
Tender Evaluation and Contract Award Recommendation
£10-50k
3 Formal Quotations
Approval by Board (> £500k)
Signed Contract on NHS Terms & Conditions
SFI Waiver
Must go to Audit Committee
No
35/73 52/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 33 of 70
N.B Find a Tender Service (FTS) refers to the UK Procurement advertising system (replacing the Official Journal of the European Union) for all procurement needs over the Public Contracts Regulations 2015 (PCR2015) threshold. Find A Tender Service (FTS) is the UK compliance portal and home to higher value, public contract opportunities within the UK.
9.4.1 Formal Competitive Tendering The Chief Executive or nominated member of staff shall ensure that competitive tenders are invited for the supply of goods, materials and manufactured articles. For the rendering of services including all forms of management consultancy services (other specialised services sought from or by the DoHDHSC): for the design, construction and maintenance of building and engineering works (including construction and maintenance of grounds and gardens); and for disposal. The Trust shall ensure that competitive tenders are invited for:
(a) the supply of goods, materials and manufactured articles;
Formatted: List Paragraph
36/73 53/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 34 of 70
(b) the rendering of services including all forms of management consultancy services (other than specialised services sought from or provided by the Department of Health and Social Care);
(c) the design, construction and maintenance of building and engineering works
(including construction and maintenance of grounds and gardens). Where the Trust elects to invite tenders for the supply of healthcare services these SFIs shall apply as far as they are applicable to the tendering procedure. Formal procedures need not be applied where:
(a) the estimated expenditure or income does not, or is not reasonably expected to exceed £10,000;
(b) the supply is proposed under special arrangements negotiated by the
DHSC in which event the said special arrangements must be complied with, and
(c) disposals are concerned.
Formal tendering procedures may only be waived in the following limited circumstances:
(a) in very exceptional circumstances where the Chief Executive, or Managing Director decides that formal tendering procedures would not be practicable or the estimated expenditure or income would not warrant formal tendering procedures, and the circumstances are detailed in an appropriate Trust record;
(b) where the requirement is covered by an existing contract;
(c) where a consortium arrangement is in place and a lead organisation
has been appointed to carry out tendering activity on behalf of the consortium members;
(d) where the timescale genuinely precludes competitive tendering but
failure to plan the work properly would not be regarded as a justification for a single tender;
(e) where specialist expertise is required and is available from only one
source; (f) when the task is essential to complete the project, and arises as a
consequence of a recently completed assignment and engaging different consultants for the new task would be inappropriate;
(g) there is a clear benefit to be gained from maintaining continuity with
an earlier project. However in such cases the benefits of such
Formatted: Indent: Left: 0.89", Hanging: 0.61"
37/73 54/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 35 of 70
continuity must outweigh any potential financial advantage to be gained by competitive tendering;
(h) for the provision of legal advice and services providing that any legal
firm or partnership commissioned by the Trust holds a current certificate of Authorisation issued by the Solicitors Regulation Authority (or by the Bar Council for England and Wales in relation to the obtaining of Counsel’s opinion) and are generally recognised as having sufficient expertise in the area of work for which they are commissioned.
(i) Where the requirement is ordered under existing contracts and where,
in the case of building and engineering works, they cannot be technically or financially separated from the existing contract without great inconvenience or where they are strictly necessary to its later stages;
(j) For disposals of land and/or buildings where regard shall b to advice laid
down in the National Health Service ESTATE CODE series on Property Transactions in the NHS (1993 and amendments).
(k) Items arising from works of construction, demolition or site clearance,
which should be dealt with in accordance with the relevant contract; (l) Where an authorised member of staff considers it would be
advantageous for financial or quality reasons, to negotiate the terms of a proposed contract with the manufacturers or suppliers direct. Negotiated procedure requires submission to Management Board with the reasons why competition has not been sought. If a decision not to invite a competitive tender or quotation is reached by Management Board then it should be formally reached and minuted. Negotiation may take place with one or more manufacturers or suppliers, who in the opinion of the authorised member of staff, have the necessary facilities for fulfilling the proposed contract, provided that:-
where tenders are subsequently invited, the authorised member of staff shall not
• use his/her powers of negotiation to discuss with any individual or body, which has submitted a tender, any part of the contract if tenders are not invited,
• then before a contract is entered into, evidence shall be made available to the Board of Directors to show that each of the manufacturers or suppliers so approached has been given equal opportunity of procuring the contract.
• tThe offer, which the authorised member of staff recommends to the Board of Directors for approval, where necessary, shall be clearly evidenced in writing when submitted for such approval.
• wWhether using formal tender/quotation procedures or negotiation the Legal onus is on the trust to demonstrate that
Formatted: Bulleted + Level: 1 + Aligned at: 1.73" +Indent at: 1.98"
Formatted: Bulleted + Level: 1 + Aligned at: 1.73" +Indent at: 1.98"
38/73 55/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 36 of 70
fair and equitable process has been undertaken that can stand up to scrutiny.
The waiving of competitive tendering procedures should not be used to avoid competition or for administrative convenience or to award further work to a consultant originally appointed through a competitive procedure. Where it is decided that competitive tendering is not applicable and should be waived, the fact of the waiver and the reasons should be documented and recorded in the agreed Single Tender Waiver Document, managed by the Procurement Department, and reported to the Audit Committee. Waivered spend <£100,000 requires approval by the Chief Finance Officer. Waivered spend >£100,000 requires approval from both the Chief Finance Officer and the Managing Director. The Trust shall ensure that invitations to bid are sent to a sufficient number of firms/individuals to provide fair and adequate competition as appropriate, and in no case less than 3 firms/individuals, having regard to their capacity to supply the goods or materials or to undertake the services or works required. All contract spend over £25,000 must be advertised via Contracts Finder. This procedure is managed by Procurement using the Trust e-tendering portal of choice. Competitive Tendering cannot be waived for building and engineering construction works and maintenance without Board approval. Items estimated to be below the limits set in this SFIs for which formal tendering procedures are not used which subsequently prove to have a value above such limits shall be reported to the Chief Executive, and be recorded in an appropriate Trust record.
9.4.2 Invitation to Tender All invitations to tender shall be directed through the Trust official E-tendering platform.
9.4.3 Procedure for Managing Tenders All official Trust tenders are published, managed and awarded through the Trust approved electronic e-tendering portal. The e-tendering provider will publish all proposed tender values over £25,000 via Contracts Finder and all proposed tender spend greater than the prevailing Public Contracts Regulation 2015 thresholds OJEU levels will be advertised via the Find a Tender Service portal.Official Journal of the European Union. System security is managed in accordance with Information Security Policy ISO 27001 and the Data protection Act 1998. The system is fully auditable with strict date and time opening procedure carried out within the Procurement Department. Every action taken within the tendering portal is recorded for audit purposes. All the information previously held within a Tender Register now sits centrally on a securedl online portal.
Formatted: Underline
39/73 56/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 37 of 70
Tenders received after the due time and date, but prior to the electronic opening of the other tenders, may be considered only if the Chief Executive or his nominated officer decides that there are exceptional circumstances i.e. submitted in good time but delayed through no fault of the tenderer. Only in the most exceptional circumstances will a tender be considered which is received after the opening of the other tenders While decisions as to the admissibility of late, incomplete or amended tenders are under consideration, evaluation of all other tender documents must not commence.
9.4.4 Acceptance of Formal Tenders Any discussions with a tenderer which are deemed necessary to clarify technical aspects of the tender before the award of a contract will not disqualify the tender. All clarification communication must be recorded using the trust official e- tendering system via the secure messaging portal. It is accepted that the lowest price does not always represent the best value for money. Evaluation criteria must be clearly presented within the tender documentation so that potential bidders can see the level of importance placed on specific criteria. An identified project evaluation panel will then score the tender submissions against the agreed criteria and associated weighting. An overall score, taking into account the technical and commercial criteria will be issued. A recommendation to award will be based on the supplier with the highest overall score. No tender shall be accepted which will commit expenditure in excess of that which has been allocated by the Trust and which is not in accordance with these Instructions except with the authorisation of the Chief Executive, or Managing Director
The use of these procedures must demonstrate that the award of the contract was:
(a) not in excess of the going market rate / price current at the time the contract was awarded;
(b) that best value for money was achieved. (c) All tenders should be treated as confidential and should be retained for
inspection. The Trust reserves the right not to award a tender.
Reports to the Board of Directors will be made on tenders over the prevailing OJEU threshold for Goods and Services. If in the opinion of the Chief Executive, or Managing Director, and the Chief Finance Officer Director of FinanceChief Finance Officer, or the Chief Officer Director with lead responsibility for clinical governance, it is impractical to use a potential contractor from the list of approved firms/individuals (for example where specialist services or skills are required and there are insufficient suitable potential
40/73 57/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 38 of 70
contractors on the list), or where a list for whatever reason has not been prepared, the Chief Executive should ensure that appropriate checks are carried out as to the technical and financial capability of those firms that are invited to tender or quote. All tender evaluations exceeding £0.5 million will require approval by the Board of Directors. Contracts above specified thresholds are advertised and awarded in accordance with EU rules on public contracts procurementregulations 2015 unless a specific exemption can be claimed under the regulations.
9.4.5 Quotations: Competitive and Non-Competitive Quotations are required where formal tendering procedures are not adopted and where the intended expenditure or income exceeds, or is reasonably expected to exceed £10,000 but not exceed £50,000.
(i) Quotations should be obtained from at least 3 firms/individuals based on specifications or terms of reference prepared by, or on behalf of, the Trust.
(ii) Quotations should be in writing unless the Chief Executive or nominated
officer determines that it is impractical to do so in which case quotations may be obtained by telephone. Confirmation of telephone quotations should be obtained as soon as possible and the reasons why the telephone quotation was obtained should be set out in a permanent record.
(iii) All quotations should be treated as confidential and should be retained for
inspection. (iv) The Chief Executive or nominated officer should evaluate the quotation and
select the quote which gives the best value for money. If this is not the lowest quotation if payment is to be made by the Trust, or the highest if payment is to be received by the Trust, then the choice made and the reasons why should be recorded in a permanent record.
Non-competitive quotations in writing may be obtained in the following circumstances:
(i) the supply of proprietary or other goods of a special character and the rendering of services of a special character, for which it is not, in the opinion of the responsible officer, possible or desirable to obtain competitive quotations;
(ii) the supply of goods or manufactured articles of any kind which are
required quickly and are not obtainable under existing contracts; (iii) miscellaneous services, supplies and disposals;
Providing all the conditions and circumstances set out in these SFIs have been fully complied with, formal authorisation and awarding of a contract may be decided to the value of the contract as per the Authorised Signatory List.
41/73 58/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 39 of 70
Where it is decided that competitive quotations is not applicable and should be waived, the fact of the waiver and the reasons should be documented and recorded in the agreed Single Quotation Waiver Document and reported to the Audit Committee. These levels of authorisation may be varied or changed. Formal authorisation must be put in writing. In the case of authorisation by the Board of Directors this shall be recorded in its minutes. Where competitive tendering or a competitive quotation is not required the Trust should adopt one of the following alternatives:
(a) the Trust shall use the NHSSC for procurement of all goods and services unless the Chief Executive or nominated officers deem it inappropriate. The decision to use alternative sources must be documented.
(b) If the Trust does not use the NHSSC - where tenders or quotations
are not required, because expenditure is below £10,000, the Trust shall procure goods and services in accordance with procurement procedures approved by the Chief Finance OfficerDirector of Finance.
Competitive Tendering or Quotation procedures shall not apply to the disposal of:
(a) any matter in respect of which a fair price can be obtained only by negotiation or sale by auction as determined (or pre-determined in a reserve) by the Chief Executive or nominated officer;
(b) obsolete or condemned articles and stores, which may be disposed
of in accordance with the supplies policy of the Trust; (c) items to be disposed of with an estimated sale value of less than
£10,000, this figure to be reviewed on a periodic basis; (d) items arising from works of construction, demolition or site clearance,
which should be dealt with in accordance with the relevant contract; (e) land or buildings concerning which DoHDHSC guidance has been
issued but subject to compliance with such guidance.
The Chief Executive shall be responsible for ensuring that best value for money can be demonstrated for all services provided on an in-house basis. The Trust may also determine from time to time that in-house services should be market tested by competitive tendering. In all cases where the Board determines that in-house services should be subject to competitive tendering the following groups shall be set up:
(a) Specification group, comprising the Chief Executive or nominated officer/s and specialist.
42/73 59/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 40 of 70
(b) In-house tender group, comprising a nominee of the Chief Executive, or Managing Director, and technical support.
(c) Evaluation team, comprising normally a specialist officer, a supplies
officer and a Chief Finance Officer Director of Finance representative. For services having a likely annual expenditure exceeding £1 million, a Non-Executive Director should be a member of the evaluation team.
All groups should work independently of each other and individual officers may be a member of more than one group but no member of the in-house tender group may participate in the evaluation of tenders. The evaluation team shall make recommendations to the Board. The Chief Executive shall nominate an officer to oversee and manage the contract on behalf of the Trust. Measured Term Contracts A measure term contract is a contract against which the requirements of the Trust may be ordered from time to time during the period covered by the contract. Measured term contracts shall be subject to quotation/tendering procedure and to the approval by the Chief Executive, or Managing Director, and once such approval has been given, the appropriate members of staff may place individual orders for the requirements within the terms of the contract based on the schedule of financial limits outlined in Appendix B. Extension of Existing Supplies and/or Service Purchase Contracts The authorised member of staff may from time to time negotiate with a contractor for an extension of the original supplied and/or services contract at the current price and no less than the current quality. Entering into such extension on behalf of the Trust without inviting quotations or tenders from any other individuals or body, but only where the authorised members of staff consider that such an extension would be greater financial advantage to the Trust than inviting quotations and tenders. No extension shall be entered into, by the authorised members of staff, if effect would result in the current price being increased, (subject to inflationary increases) quality being reduced or the original contract being extended by more than once its initial direction or 2 years whichever is the lesser. No extension can be granted if by doing so would affect or exceed the Public Contracts Regulation 2015 EU thresholds or timeframes detailed in the original OJEU advertisement. Managing Conflicts of Interest Any person whose place of work is within the Trust (whether employed by the Trust or any other body) who has a personal interest in any company being asked to provide a tender or quotation, which could influence a decision of the Trust in any way, should declare that interest and not take any part in the any decision of the Trust. Staff whose relatives are known to have similar interest in a company must also declare that interest. Please refer to SWH 01783 Managing Conflicts of Interest Policy for further detail and complete the Declarations of Interest form attached at Appendix A of the policy. Contact the Trust Secretary if you have any queries.
43/73 60/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 41 of 70
9.5 Other – Patient Property The Trust has a responsibility to provide safe custody for money and other personal property (hereafter referred to as "property") handed in by patients, in the possession of unconscious or confused patients, or found in the possession of patients dying in hospital or dead on arrival. The Chief Executive is responsible for ensuring that patients or their guardians, as appropriate, are informed before or at admission by:
o notices and information booklets; (notices are subject to sensitivity guidance)
o hospital admission documentation and property records; o the oral advice of administrative and nursing staff responsible for
admissions, The Trust will not accept responsibility or liability for patients' property brought into Health Service premises, unless it is handed in for safe custody and a copy of an official patients' property record is obtained as a receipt. The Chief Finance Officer Director of Finance must provide detailed written instructions on the collection, custody, investment, recording, safekeeping, and disposal of patients' property (including instructions on the disposal of the property of deceased patients and of patients transferred to other premises) for all staff whose duty is to administer, in any way, the property of patients. Due care should be exercised in the management of a patient's money in order to maximise the benefits to the patient. Detailed procedures can be found on the intranet. Where DoHDHSC instructions require the opening of separate accounts for patients' moneys, these shall be opened and operated under arrangements agreed by the Chief Finance OfficerDirector of Finance. In all cases where property of a deceased patient is of a total value in excess of £5,000 (or such other amount as may be prescribed by any amendment to the Administration of Estates, Small Payments, Act 1965), the production of Probate or Letters of Administration shall be required before any of the property is released. Where the total value of property is £5,000 or less, forms of identity shall be obtained. Staff should be informed, on appointment, by the appropriate departmental or senior manager of their responsibilities and duties for the administration of the property of patients. Where patients' property or income is received for specific purposes and held for safekeeping the property or income shall be used only for that purpose, unless any variation is approved by the donor or patient in writing.
Formatted: Indent: Left: 0", First line: 0"
44/73 61/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 42 of 70
9.6 Other – Charitable Funds The Trust’s Board of Directors is a corporate trustee for the management of funds it holds on Trust, and needs to comply with the latest guidance and best practice from the Charities Commission. The discharge of the Trust’s corporate trustee responsibilities are distinct from its responsibilities for exchequer funds and may not necessarily be discharged in the same manner, but there must still be adherence to the overriding general principles of financial regularity, prudence and propriety. Trustee responsibilities cover both charitable and non-charitable purposes. The Chief Finance Officer Director of Finance shall ensure that each trust fund which the Trust is responsible for managing is managed appropriately, with regard to its purpose and to its requirements. The trustee responsibilities must be discharged separately and full recognition given to the Trust’s dual accountabilities to the Charity Commission for charitable funds held on trust and to Parliament for exchequer funds. In so far as it is possible to do so, most of the sections of these SFIs will apply to the management of funds held on trust. The over-riding principle is that the integrity of each Trust must be maintained and statutory and Trust obligations met. Materiality must be assessed separately from Exchequer activities and funds. 9.7 Losses & Special Payments
The Chief Finance Officer Director of Finance must prepare procedural instructions on the recording of and accounting for condemnations, losses, and special payments. Any employee or officer discovering or suspecting a loss of any kind must either immediately inform their head of department, who must immediately inform the Chief Executive, Managing Director and the Chief Finance Officer Director of Finance or inform an officer charged with responsibility for responding to concerns involving loss. This officer will then appropriately inform the Chief Finance OfficerDirector of Finance, Managing Director and/or Chief Executive. Where a criminal offence is suspected, the Chief Finance Officer Director of Finance must immediately inform the police if theft or arson is involved. In cases of fraud and corruption or of anomalies which may indicate fraud or corruption, the Chief Finance Officer Director of Finance must inform the relevant LCFS and CFSMS regional team in accordance with Secretary of State for Health’s Directions. The Chief Finance Officer Director of Finance must notify the CFSMS and the External Auditor of all frauds. For losses apparently caused by theft, arson, neglect of duty or gross carelessness, except if trivial, the Chief Finance Officer Director of Finance must immediately notify:
(a) the Board;
45/73 62/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 43 of 70
(b) the External Auditor. Within limits delegated to it by the Chief Executive, the Audit Committee shall approve the writing-off of losses. All losses and special payments must be reported to the Audit Committee.
The Chief Finance Officer Director of Finance shall be authorised to take any necessary steps to safeguard the Trust’s interests in bankruptcies and company liquidations. For any loss, the Chief Finance Officer Director of Finance should consider whether any insurance claim can be made. The Chief Finance Officer Director of Finance shall maintain a Losses and Special Payments Register in which write-off action is recorded. No special payments exceeding delegated limits shall be made without the prior approval of the DoHDHSC. 10 External Borrowing & Investments
The Chief Finance Officer Director of Finance will advise the Board concerning the Trust’s ability to pay dividend on, and repay Public Dividend Capital (PDC) and any proposed new borrowing, within the limits set by the Department of Health and Social Care/NHS England and NHS Improvement. The Chief Finance Officer Director of Finance is also responsible for reporting periodically to the Board concerning the PDC debt and all loans and overdrafts. The Board will agree the list of employees (including specimens of their signatures) who are authorised to make short term borrowings on behalf of the Trust. This must contain the Chief Executive, Managing Director and the Chief Finance OfficerDirector of Finance. The Chief Finance Officer Director of Finance must prepare detailed procedural instructions concerning applications for loans and overdrafts. All short-term borrowings should be kept to the minimum period of time possible, consistent with the overall cash flow position, represent good value for money, and comply with the latest guidance from the Department of Health and Social Care/NHS England and NHS Improvement. Any short-term borrowing must be with the authority of two members of an authorised panel, one of which must be the Chief Executive, Managing Director, or the Chief Finance OfficerDirector of Finance. The Board must be made aware of all short term borrowings at the next Board meeting. All long-term borrowing must be consistent with the plans outlined in the current Annual Plan and Long Term Financial Model and be approved by the Board of Directors. Temporary cash surpluses must be held only in such public or private sector investments as authorised by the Board as set out in the Investment Policy. The Chief Finance Officer Director of Finance is responsible for advising the Board on investments and shall report periodically to the Board concerning the performance of any investments held.
46/73 63/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 44 of 70
The Chief Finance Officer Director of Finance will prepare detailed procedural instructions on the operation of investment accounts and on the records to be maintained. 11 Banking Arrangements
The Chief Finance Officer Director of Finance is responsible for managing the Trust’s banking arrangements, which should be approved by the Board, and for advising the Trust on the provision of banking services and operation of accounts. This advice will take into account guidance/ Directions issued from time to time by the DoHDHSC/NHS England and NHS Improvement. The Chief Finance Officer Director of Finance is responsible for:
(a) bank accounts and Government Banking Service (GBS) accounts; (b) establishing separate bank accounts for the Trust’s non-exchequer funds; (c) ensuring payments made from bank or GBS accounts do not exceed the
amount credited to the account except where arrangements have been made;
(d) reporting to the Board all arrangements made with the Trust’s bankers for
accounts to be overdrawn.
The Chief Finance Officer Director of Finance will prepare detailed instructions on the operation of bank and GBS accounts which must include:
(a) the conditions under which each bank and GBS account is to be operated; (b) those authorised to sign cheques or other orders drawn on the Trust’s
accounts.
The Chief Finance Officer Director of Finance must advise the Trust’s bankers in writing of the conditions under which each account will be operated. The Chief Finance Officer Director of Finance will review the commercial banking arrangements of the Trust at regular intervals to ensure they reflect best practice and represent best value for money by periodically seeking competitive tenders for the Trust’s commercial banking business. Competitive tenders should be sought at least every five years. The results of the tendering exercise should be reported to the Board. 12 Annual Accounts
The Chief Finance Officer Director of Finance, on behalf of the Trust, will:
(a) prepare financial returns in accordance with the accounting policies and guidance given by the DoHDHSC and the Treasury, NHS England and NHS Improvement, the Trust’s accounting policies, and generally accepted accounting practice;
47/73 64/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 45 of 70
(b) prepare and submit annual financial reports to NHS England and NHS Improvement certified in accordance with current guidelines;
(c) submit financial returns to the NHS Improvement for each financial year in
accordance with the timetable prescribed by NHS England and NHS Improvement.
The Trust’s annual accounts must be audited by an auditor appointed by the Council of Governors. The Trust’s audited annual accounts must be laid before Parliament and be made available to the public at the Annual Members’ Meeting. The Trust will publish an annual report, in accordance with guidelines on local accountability, and present it at the Annual Members’ Meeting. The document will comply with the DoHDHSC Financial Reporting Manual for Accounts. 13 Wholly Owned Subsidiaries Subsidiary SFIs must be aligned to these Group SFIs, with any proposed departures being reported to the Group Audit Committee.
14 Monitoring Compliance The Chief Finance Officer Director of Finance will ensure that the key processes set out in this document are audited. The results will be fed back to the Audit Committee. Where monitoring has identified deficiencies, recommendations and an action plan will be developed to improve compliance with the document. See Appendix C for specific details. 15 Equality Impact Assessment All Trust documents are required to have a preliminary Equality Impact assessment (EIA) performed on them in order to establish whether any group of people will be impacted on unfairly by the document. An EIA has been performed on this document and the outcome is shown in Appendix D. 16 Authors Kim Li, Chief Finance Officer Director of Finance Mick Sargent, Associate Director of Finance-Strategy and Financial Services 17 Contributors Audit Committee Sarah Collett, Acting Trust Secretary Ruth Allen, Associate DirectorHead of Procurement Sharon Dosanjh, Deputy Finance Manager
48/73 65/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 46 of 70
18 References Bribery Act 2010 SWH 01656 Gifts, Hospitality and Sponsorship Policy SWH 01783 Managing Conflicts of Interest Policy SWH 00188 Recruitment and Selection Policy SWH 00504 Bank, Agency and Temporary Workers Procedure for Non-medical staff SWH 00093 Bank, Agency and Temporary Workers Procedure for Medical staff 19 Appendices Appendix A: Appendix B
Scheme of Delegation Schedule of Financial Limits
Appendix C: Monitoring Compliance Form Appendix D: Equality Impact Assessment
49/73 66/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 47 of 70
20 Appendix A: Scheme of Delegation
Area Detail Delegated Responsible Officer Delegated To: Board/Committee Approval
Annual Accounts
Preparation of annual accounts and reports. Board of Directors Chief Finance Officer DIRECTOR OF FINANCE
Recommended by Audit Committee Approved by the Board of Directors
Assets register and security of assets
Approval of fixed asset control procedures.
Chief Executive Chief Finance Officer Director of Finance
Approve procedures for reconciling balances on fixed assets accounts in ledgers against balances on fixed asset registers. Calculate and pay capital charges in accordance with NHS England and NHS Improvement/ Department of Health and Social Care requirements.
Maintenance of asset registers (on advice from CFO DoF).
Prepare detailed procedures for disposal of assets including condemnations and ensure that these are notified to managers.
Banking Arrangements
Approval of Fees and Charges Chief Finance Officer Director of Finance Associate Director of Finance- Strategy and Financial Services
Opening of Bank Account Chief Finance Officer Director of Finance Associate Director of Finance- Strategy and Financial Services Board of Directors
Signing of cheques, BACS schedules and GBS authorisation Chief Finance Officer Director of Finance
Deputy Chief Finance Officer/Associate Directors of Finance & Senior Finance Managers
Budgetary Control
Delegation of Budgets Managing Director & Chief Finance Officer Director of Finance Designated Budget Managers
Devise and maintain systems of budgetary control. Board of Directors
Chief Finance Officer Director of Finance
Ensure adequate training is delivered on an ongoing basis to budget holders.
50/73 67/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 48 of 70
Overall Trust Budget Planning Process Chief Finance Officer Director of Finance Deputy Chief Finance Officer and Associate Directors of Finance Board of Directors
Area Detail Delegated Responsible Officer Delegated To: Board/Committee
Approval
Capital Investment
Certify professionally the costs and revenue consequences detailed in the business case for capital investment.
Chief Executive Chief Finance Officer DIRECTOR OF FINANCE
Issue procedures for the regular reporting of expenditure and commitment against authorised capital expenditure.
Issue procedures governing financial management, including variation to contract, of capital investment projects and valuation for accounting purposes.
Ensure adequate appraisal and approval process for determining capital expenditure priorities and the effect that each has on plans
Chief Executive Chief Strategy Officer Director of Development
Ensure that a business case is produced for each proposal. Issue manager responsible for any capital scheme with authority to commit expenditure, authority to proceed to tender and approval to accept a successful tender. Management of capital schemes and for ensuring that they are delivered on time and within cost;
51/73 68/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 49 of 70
Area Detail Delegated Responsible Officer Delegated To: Board/Committee Approval
Preparation of Annual Report and Accounts for funds held on Trust Charity Trustee Chief Finance Officer Director of Finance Charity Trustee
Charitable Funds Shall ensure that each trust fund which the Trust is responsible for managing is managed appropriately Chief Executive Chief Finance Officer DIRECTOR OF FINANCE
Cost Improvement Plans
Identify and implement cost improvements and income generation activities in line with the Annual Plan Board of Directors
Chief Executive Designated budget holders
External Audit Ensure cost-effective External Audit. Board of Directors Audit Committee
External Borrowing
Approve a list of employees authorised to make short term borrowings on behalf of the Trust. (This must include the CEO and CFO DoF.) Board of Directors Chief Finance Officer DIRECTOR OF FINANCE Ensure that Board members are aware of the Financial Framework and ensure compliance Board of Directors Chief Finance Officer DIRECTOR OF FINANCE Prepare detailed procedural instructions concerning applications for loans and overdrafts.
Board of Directors Chief Finance Officer DIRECTOR OF FINANCE
Board of Directors
Prepare detailed procedural instructions on the operation of investments held. The CFO DoF will advise the Board on the Trust’s ability to pay dividend on PDC and report, periodically, concerning the PDC debt and all loans and overdrafts. Will advise the Board on investments and report, periodically, on performance of same. Investment Decisions
Chief Finance Officer Director of Finance Associate Director of Finance- Strategy and
Financial Services Board of Directors Investment Policy
Loans and Loan Facilities including Working Capital Facility
Managing Director/Chief Executive/ Chief Finance Officer Director of Finance
Associate Director of Finance- Strategy and Financial Services Board of Directors
Treasury Management Policy Chief Finance Officer Director of Finance Associate Director of Finance- Strategy and Financial Services Board of Directors
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
52/73 69/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 50 of 70
Area Detail Delegated Responsible Officer Delegated To: Board/Committee Approval
Fraud and irregularity
Counter Fraud & Corruption Work Chief Finance Officer Director of Finance Local Counter Fraud Specialist
Decide at what stage to involve police in cases of misappropriation and other irregularities not involving fraud or corruption.
Chief Finance Officer DIRECTOR OF FINANCE Local Counter Fraud Specialist
Notify Board and External Auditor of losses caused theft, arson, neglect of duty or gross carelessness (unless trivial). Notify CFSMS and External Audit of all frauds. Where a criminal offence is suspected, CFO DoF must inform the police if theft or arson is involved. In cases of fraud and corruption CFO DoF must inform the relevant LCFS and CFSMS Regional Team in line with national guidance and standards. Monitor and ensure compliance with NHS Standard of Conduct Contract on fraud and corruption including the appointment of the Local Counter Fraud Specialist. Chief Executive Chief Finance Officer Director of Finance
Advice on interpretation or application of SFIs. Chief Executive Chief Finance Officer DIRECTOR OF FINANCE
General
Approval of all financial procedures. Chief Executive Chief Finance Officer DIRECTOR OF FINANCE Raise the matter at the Board meeting where Audit Committee considers there is evidence of ultra vires transactions or improper acts.
Audit Committee Audit Committee Chair
Responsible as the Accounting Officer to ensure financial targets and obligations are met and have overall responsibility for the System of Internal Control. Chief Executive Chief Executive and Managing Director
Have a duty to disclose any non-compliance with these Standing Financial Instructions to the Director of Finance as soon as possible. Board of Directors All members of the Board and employees
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps
Formatted: Not Small caps, Not Expanded by / Condensedby
53/73 70/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 51 of 70
Area Detail Delegated Responsible Officer Delegated To: Board/Committee Approval
General
Responsible for security of the Trust's property, avoiding loss, exercising economy and efficiency in using resources and conforming to the Trust’s Constitution, Standing Orders, Financial Instructions and financial procedures. Board of Directors All members of the Board and employees To ensure all Board members, officers and employees, present and future, are notified of and understand Standing Financial Instructions. Board of Directors Managing dDirector
Gifts & Hospitality
Ensure all staff are made aware of the Trust policy on the acceptance of gifts and other benefits in kind by staff Chief Executive Chief Finance Officer DIRECTOR OF FINANCE Maintenance of gifts and hospitality registers Chief Executive Trust Secretary
Income
Authorisation of discounts, credit notes Chief Finance Officer Director of Finance Associate Director of Finance (IC&FM) Authorisation of Individual Debt write off Audit Committee Credit Control- Collection of Debts and use of Debt Collection Agencies Chief Finance Officer Director of Finance
Associate Director of Finance for Strategy and Financial Services
Compile and submit to the Board an Annual Plan which takes into account financial targets and forecast limits of available resources. Chief Executive
Managing dDirector/ Chief Finance Officer DIRECTOR OF FINANCE/
Duty to inform CFO DoF of money due from transactions which they initiate/deal with. Board of Directors All Eemployees
Injury Costs Recovery Scheme Chief Finance Director of Finance Deputy Chief Finance Officer and Associate Directors of Finance
As the Accounting Officer, ensure that regular reports are provided to the Board detailing actual and forecast income from the Contract
Chief Executive Chief Finance Officer Director of Finance
The Chief Executive shall nominate an officer to oversee and manage the contract on behalf of the Trust. Chief Executive
Chief Finance Officer Director of Finance or Deputy Chief Finance OfficerAssociate Director of Finance (IC&FM)
Must ensure the Trust enters into suitable Contract with service commissioners for the provision of NHS services
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
54/73 71/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 52 of 70
Income
Overseas Visitors Policy Chief Finance Officer Director of Finance Associate Director Associate Director of Finance (IC&FM) Deputy Chief Finance Officer
Finance & Performance Committee
Private Patient Policy Finance & Performance Committee
Raising Debtor Requisitions Chief Finance Officer Director of Finance Budget holders and Finance Staff
Raising Invoices ( Debtor staff to raise) Chief Finance Officer Director of Finance
Debtors staff as managed by Associate Director of Finance for Strategy and Financial Services
Insurance Arrangements
Insurance (overall excluding Clinical negligence) Chief Executive Chief Finance Officer Director of Finance Board of Directors
Insurance for Clinical Negligence Chief Executive Director of Nursing Board of Directors
Internal Audit
Ensure an adequate internal audit service, for which he/she is accountable, is provided (and involve the Audit Committee in the selection process when/if an internal audit service provider is changed.)
Board of Directors Chief Finance Officer DIRECTOR OF FINANCE
Audit Committee recommends and Board approves appointment and removal of Internal Auditors
Provide independent and objective view on internal control and probity. Board of Directors Audit Committee
Review, appraise and report in accordance with NHS Internal Audit Manual and best practice.
Chief Finance Officer Director of Finance Head of Internal Audit
Area Detail Delegated Responsible Officer Delegated To: Board/Committee Approval
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
55/73 72/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 53 of 70
Area Detail Delegated Responsible Officer Delegated To: Board/Committee Approval
Losses and special payments
Authorisation of early retirement, redundancy and other termination payments - Board Level Chief Executive & Chief Finance Officer
Director of Finance Chief People Officer Director of Human Resources
Appointments and Remuneration Committee
Authorisation of early retirement, redundancy and other termination payments - Other Staff
Monitoring of Losses and Special Payments Chief Finance Officer Director of Finance Associate Director of Finance-Strategy and Financial Services Audit Committee
Authorisation of Individual Losses and Special Payments
Chief Executive Chief Finance Officer DIRECTOR OF FINANCE
Prepare procedures for recording and accounting for losses, special payments and informing police in cases of suspected arson or theft.
Discovery or suspicion of any kind of loss must be reported immediately to either head of department or nominated officer. The head of department / nominated officer must then inform the MD and CFO DoF.
Managing Director All Staff
Formatted: Not Small caps, Not Expanded by / Condensedby
56/73 73/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 54 of 70
Area Detail Delegated Responsible Officer Delegated To: Board/Committee Approval
Management Consultancy
Management Consultancy /Project Management Contracts/ Agency Over £50,000 exc. VAT Board of Directors
Managing Director and Chief Finance Officer Director of Finance
Management Consultancy and Project Management Contracts Up to £50,000 exc. VAT
Managing Director and Chief Finance Officer Director of Finance
Managing Director and Chief Director of Finance
Mergers, Acquisitions, Separations and Dissolutions
Application for a merger, acquisition, separation or dissolution requires the approval of more than half of the members of the Council of Governors
Board of Directors/Council of Governors Board of Directors/Council of Governors
Non Pay
Authorisation of expenses claims Chief Executive/Managing Director Budget holders as per Authorised Signatory
List
Authorisation of study leave requests
Hospitality Requests Purchase Cards - Up to Purchase Card Limit – Other Designated Supervisors Chief Finance Officer Director of Finance Designated Budget Managers
Official Orders
Authorise who may use and be issued with official orders.
Chief Executive Chief Finance Officer Director of Finance
Patient Property
To inform staff of their responsibilities and duties for the administration of the patient property and refer to instructions provided by CFO DOF (as above).
Chief Executive Departmental mManagers
Provision of clear and detailed written instructions for all staff involved/administering the collection, custody, investment, documentation, administration, safekeeping, and disposal of patients' property (including the property of deceased patients and of patients transferred to other premises.
Chief Executive Chief Finance Officer Director of Finance
Responsible for ensuring patients and guardians are informed about patients' money and property procedures on admission.
Chief Executive Director of Nursing
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
57/73 74/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 55 of 70
Area Detail Delegated Responsible Officer Delegated To: Board/Committee Approval
PAY
Advise the Board on and make recommendations on the remuneration and terms of service of the CE, other Directors and senior employees to ensure they are fairly rewarded having proper regard to the Trust’s circumstances and any national agreements;
Board of Directors
Appointments and Remuneration Committee
Report in writing to the Board its advice and its bases about remuneration and terms of service of directors and senior employees.
Establish a Remuneration & Terms of Service Committee (known as the Appointments and Remuneration Committee)
Board of Directors Board of Directors
Approve proposals presented by the Chief Executive for setting of remuneration and conditions of service for those employees and officers not covered by the Appointments and Remuneration Committee.
Authorisation for Urgent Payment Vouchers/Pay Advances Chief People Officer Director of Human
Resources & Chief Finance Officer Director of Finance
Deputy Chief Finance Officer/Associate Directors of Finance/Senior Finance Managers
Ensure that all employees are issued with a Contract of Employment in a form approved by the Board and which complies with employment legislation; and
Chief Executive Chief People Officer Director of Human Resources
58/73 75/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 56 of 70
Area Detail Delegated Responsible Officer Delegated To: Board/Committee Approval
PAY The Chief Executive shall nominate officers with delegated authority to enter into contracts of employment, regarding staff, agency staff or temporary staff service contracts.
Chief Executive
Chief People Officer Director of Human Resources
Ensure that any contractor or employees of a contractor who is empowered by the Trust to commit the Trust to expenditure or who is authorised to obtain income are made aware of these instructions and their requirement to comply.
Board of Directors Chief Executive
Petty Cash Chief Executive Chief Executive Budget holders as per Financial Limits Appendix B
Prepayment
Approve proposed prepayment arrangements. Chief Executive Chief Finance Officer Director of Finance
Ensure that all items due under a prepayment contract are received and any problems/issues must be immediately communicated to CFO DOF.
Chief Executive Budget holders
Approve proposed prepayment arrangements.
Chief Executive Chief Finance Officer Director of Finance
Make a written case to support the need for a prepayment.
Chief Executive APPROPRIATE CHIEF OFFICER EXECUTIVE DIRECTOR
59/73 76/347
SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 57 of 70
Area Detail Delegated Responsible Officer Delegated To: Board/Committee Approval
Sealing and Signing
Where a document shall be sealed the seal shall be affixed in the presence of :
- The Chief Executive and 1 other Chief Officer Executive Director, or
- 2 Chief OfficersExecutive Directors duly authorised by the Chief Executive and not from the originating department
The Trust Secretary will count as a Chief Officer an Executive Director for this purpose.
Chief Executive Chief Executive/CHIEF OFFICERS EXECUTIVE DIRECTORS/Trust Secretary
Where any document will be a necessary step in legal proceedings on behalf of the Trust, it shall, unless any enactment otherwise requires or authorises, be signed by:
- The Chief Executive or - Any Chief Officer Executive
Director The Trust Secretary will count as an Chief Officer Executive Director for this purpose
Chief Executive Chief Executive/CHIEF OFFICERS EXECUTIVE DIRECTORS/Trust Secretary
The Chief Executive shall keep a Register in which they or another manager of the Trust authorised by him/her shall enter a record of the sealing of every document
Chief Executive Trust Secretary
The common seal of the Trust shall be kept by the Chief Executive or a nominated Officer in a secure place
Chief Executive Trust Secretary
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
60/73 77/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 58 of 70
Area Detail Delegated Responsible Officer Delegated To: Board/Committee Approval
Sealing and Signing
The registration of leases at the Land Registry and the swearing of statutory declarations. Chief Executive Trust Secretary
Delegated by the Board 29 Feb 2012 (Minute 12.058.01 refers)
In land transactions, the signing of certain supporting documents will be delegated to officers and set out clearly in the Scheme of Delegation, but will NOT include the main or principal documents effecting the transfer
Chief Executive CHIEF OFFICERS EXECUTIVE DIRECTORS/TRUST Secretary
Security
Monitor and ensure compliance with Directions issued by the Secretary of State for Health on NHS security management including appointment of the Local Security Management Specialist.
Chief Executive Associate Director of operations - Support Services
Significant Transactions
The Trust may enter into a significant transaction only if more than half of the members of the Council of Governors of the Trust voting approve entering into the transaction
Board/Council of Governors Board/Council of Governors
Standards of Business Conduct Maintenance of register of interests for Board and Council of Governors and undertake an annual review
Chief Executive Trust Secretary
Stores & Stocks
Agree stocktaking arrangements.
Chief Executive Chief Finance Officer Director of Finance
Approve alternative arrangements where a complete system of stores control is not justified.
Approve system for review of slow moving and obsolete items and for condemnation, disposal and replacement of all unserviceable items.
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
61/73 78/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 59 of 70
Area Detail Delegated Responsible Officer Delegated To: Board/Committee Approval
Stores & Stocks
Set out procedures and systems to regulate the stores.
Chief Executive Chief Finance Officer DIRECTOR OF FINANCE
Responsible for systems of control over stores and receipt of goods Delegate overall responsibility for control of stores (subject to CFO DoF responsibility for systems of control). Further delegation for day-to-day responsibility subject to such delegation being recorded. (Good practice to append to the scheme of delegation document.) Identify persons authorised to requisition and accept goods from NHS Supplies stores. Chief Executive Managing Director
Management of Stock control for Stores and stocks Chief Finance Officer Director of Finance Head of Purchasing & Supplies
Responsibility for security of Trust assets including notifying discrepancies to CFO DoF, and reporting losses in accordance with Trust procedure.
Board of Directors Board, Executive Members and All senior staff
Responsible for control of stocks of fuel oil and coal. Chief Executive Designated Estates Officer
Responsible for controls of pharmaceutical stocks Chief Executive Designated Pharmaceutical officer
Security arrangements and custody of keys Chief Executive Nominated Officers
Share Purchase
The purchase of additional shares in Innovate Healthcare Services Ltd up to the value of £500k has been delegated by the Board of Directors to the Chief Executive and Chief Finance Officer Board of Directors Chief Executive AND Chief Finance Officer
Tendering
No quotation shall be accepted which will commit expenditure in excess of that which has been allocated by the Trust and which is not in accordance with these Instructions except with the authorisation of the Chief Executive. Chief Executive
Managing Ddirector orOR Chief Executive or Chief Finance Officer DIRECTOR OF FINANCE
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
Formatted: Not Small caps, Not Expanded by / Condensedby
62/73 79/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 60 of 70
No tender shall be accepted which will commit expenditure in excess of that which has been allocated by the Trust and which is not in accordance with these Instructions except with the authorisation of the Chief Executive. Chief Executive Chief Finance Officer DIRECTOR OF FINANCE
Area Detail Delegated Responsible Officer Delegated To: Board/Committee Approval
Tendering
Responsible for the receipt, endorsement and safe custody of tenders received.
Chief Executive Chief Strategy Officer Director of Development
Shall maintain a register to show each set of competitive tender invitations dispatched.
Chief Executive Chief Strategy Officer Director of Development
Report waivers of tendering procedures to the Audit Committee.
Chief Executive Chief Finance Officer Director of Finance
Shall ensure that appropriate checks are carried out as to the technical and financial capability of those firms that are invited to tender or quote.
Tendering and contract procedure.
Chief Executive Chief Finance Officer Director of Finance
The Chief Executive or his nominated officer should evaluate the quotation and select the quote which gives the best value for money.
63/73 80/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 61 of 70
The Chief Executive shall be responsible for ensuring that best value for money can be demonstrated for all services provided on an in-house basis.
Area Detail Delegated Responsible Officer Delegated To: Board/Committee Approval
Tendering
Waive formal tendering procedures.
Chief Executive Chief Finance Officer Director of Finance
Where one tender is received will assess for value for money and fair price.
To appoint a manager to maintain a list of approved firms.
64/73 81/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 62 of 70
21 Appendix B: Financial Limits
*Delegated Levels for Non Pay Expenditure
Delegated levels
List of Officers Delegated levels
List of Officers
Level 54 Officers
Budget Manager; Assistant Service Managers
Level 32 Officers
Clinical Directors; Associate Directors- Operational Division leads; Associate Directors Finance; Head of Corporate departments; Chief Operating Officer Director of Operations
Level 43 Officers
Budget Managers (Matrons, Head/Deputy Head of Departments); General Managers; Service Managers
Level 21 Officers
Chief Officers Executive directors for their own departments/areas; Managing Director Managing Director (OOH); Chief Technology Officer. Deputy Chief Finance Officer Deputy Chief Operating Officer
Level 1 Officers Chief Executive; Managing Director; Chief Finance Officer
Area/SFI Reference Delegation* Financial Limit
Non Pay Expenditure (SFI 9.2.4)
These limits represent the maximum limits to be applied to Groups of Officers. Actual limits applied to individual officers may be set at a lower level to reflect the level of delegated budgetary authority. The Chief Finance Officer will maintain an Authorised Signatory List specifying individual officer limits – this list shall have effect as if incorporated in this Scheme of Delegation.
Level 54
Level 43
Level 32
Level 21
Level 1
Chief Executive or Managing Director and Chief Finance OfficerDirector of Finance
Over £0 up toless than £5,000
Over £5,000 and up toless than £10,000
Over £10,000 and up toless than £25,000
Over £25,000 and up toless than £50100,000
Over £50,000 and up to £100,000 Over £100,000
Area/SFI Reference Delegation Additional notes
Pay Expenditure (SFI 9.2.1)
The Chief Finance Officer will maintain an Authorised Signatory List specifying rights for the areas delegated as shown on the right – this list shall have effect as if incorporated in this Scheme of Delegation.
Staff Appointments/ Change Forms Authorisation of Overtime and additional hours/duties
Officers must follow the Authority to Recruit procedures to engage, re-engage, or re-grade employees. As specified in the User Responsibility List maintained by Employment Services specifically for Electronic timesheets. Otherwise, as specified in the Authorised Signatory list maintained by the Chief Finance Officer.
Formatted: Underline
Formatted: Space Before: 12 pt, Don't adjust spacebetween Latin and Asian text, Don't adjust space betweenAsian text and numbers, Tab stops: 5.43", Left
Formatted: Font color: Black
Formatted: Font color: Black
Formatted Table
65/73 82/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 63 of 70
Authorisation of time sheets Engagement of temporary workers, regardless of engagement method. Approval of tax/NIC payments to HMRC; and pension payments to NHS Business Services Authority
As specified in the User Responsibility List maintained by Employment Services specifically for Electronic timesheets. Otherwise, as specified in the Authorised Signatory list maintained by the Chief Finance Officer. Additional authority must be obtained when engaging with temporary workers, for example agency or bank. See tables 1 and 2 below. Chief Finance Officer Director of Finance, Deputy Chief Finance Officer, or Associate Director of Finance
66/73 83/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 64 of 70
Table 1-Engagement of temporary workers, regardless– Non Medical
Method of engagement Within price cap/ standard AfC rates on bank
Above price cap/non-standard AfC rate (but for under £100/hr)
Above £100/hr (excl VAT) and shifts 50% above cap
From agency on approved framework
General Manager / Senior Manager/ Matron for engaging Department.
Nursing: Chief Finance Officer Director of Nursing Allied Health Professionals: Director of Nursing Other non medics: Relevant Director for service e.g. Chief Finance Officer Director of Finance, Chief Technology Officer. Out of hours: On-call Director
- MD sign-off required In advance of shift: At least Two Chief Officers Executive Directors or Executive Team Meeting. Retrospective MD sign-off required if not obtained prior to shift.
From an agency NOT on approved framework
Nursing: Chief Nursing Officer Director of Nursing Allied Health Professionals: Director of Nursing Other non medics: Relevant Director for service e.g. Chief Finance Officer Director of Finance, Chief Technology Officer. Out of hours: On-call Director
- MD sign-off required In advance of shift: At least Two Chief Officers Executive Directors or Executive Team Meeting. Out of hours: On-call Director Retrospective MD sign-off required if not obtained prior to shift.
- MD sign-off required In advance of shift: At least Two Chief Officers Executive Directors or Executive Team Meeting. Retrospective MD sign-off required if not obtained prior to shift.
Agency for a period over 3 months Purchase order must be raised
- MD sign-off required In advance of shift: MD (or CEO), Chief Nursing Officer Director of Nursing and Chief Finance Officer Finance Director or Executive Team Meeting.
- MD sign-off required In advance of shift: MD (or CEO), Chief Nursing Officer Director of Nursing and Chief Finance Officer Finance Director or Executive Team Meeting.
In advance of shift: MD (or CEO), Chief Nursing Officer Director of Nursing and Chief Finance Officer d Finance Director or Executive Team Meeting.
Trust bank or locum engaged through payroll
Budget-holder or roster approver from engaging department.
Nursing: Chief Nursing Officer Director of Nursing Allied Health Professionals: Chief Nursing Officer Director of Nursing Other non medics: Relevant DirectorDirector for service e.g. Chief Finance Officer Director of Finance, Chief Technology Officer. Out of hours: On-call Director
In advance of shift: At least Two Chief Officers Executive Directors or Executive Team Meeting.
Other methods of engagement
Authorisation limits as for non-pay. Purchase orders must be raised. The Corporate Financial Information Department must be contacted to ensure that appropriate checks are undertaken and engagement method is appropriate.
Formatted: Font: 10 pt
Formatted: Font: Not Bold, Font color: Auto
67/73 84/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 65 of 70
NHSEI Agency Rules Agency use is not permitted for admin and clerical workers without permission from NHSEI. Agency rules must be followed: https://www.england.nhs.uk/reducing-expenditure-on-nhs-agency-staff-rules-and-price-caps/
Formatted Table
68/73 85/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 66 of 70
Table 2- Engagement of temporary workers,–Medical
Method of Engagement Within price cap/Standard locum rate Above price cap/ non-standard locum rate (but under £100/hr)
Above £100/hr (excl VAT) and shifts 50% above cap/standard locum rate
From agency on approved framework
General Manager for engaging Department. Out of hours: On-call manager
Chief Medical Officer Medical Director Out of hours: On-call Director (to be ratified by Medical Director post shift)
- MD sign-off required In advance of shift: At least Two Chief Officers Executive Directors including Chief Medical Officer Medical Director or Executive Team Meeting. Retrospective MD sign-off required if not obtained prior to shift.
From an agency NOT on approved framework
Chief Medical OfficerMedical Director Out of hours: On-call Director (to be ratified by Chief Medical OfficerMedical Director post shift)
- MD sign-off required In advance of shift: Chief Medical Officer Medical Director + one other Director or Executive Team Meeting. Out of hours: On-call Director Retrospective MD sign-off required if not obtained prior to shift.
- MD sign-off required In advance of shift: At least Two Chief Officers Executive Directors including Chief Medical Officer Medical Director or Executive Team Meeting. Retrospective MD sign-off required if not obtained prior to shift.
Agency for a period over 3 months
- MD sign-off required In advance of shift: MD (or CEO), Chief Medical Director Medical Director and Chief Finance Officer Finance Director or Executive Team Meeting.
- MD sign-off required In advance of shift: MD (or CEO), Chief Medical Director Medical Director and Chief Finance Officer Finance Director or Executive Team Meeting.
In advance of shift: MD (or CEO), Chief Medical Officer Medical Director and Chief Finance Officer Finance Director or Executive Team Meeting.
Trust bank or locum engaged through payroll
Budget-holder or roster approver from engaging department.
In advance of shift: Chief Medical Officer Medical Director + one other Chief Officer Director or Executive Team Meeting. Out of hours: On-call Director (to be ratified by Medical Director post shift)
In advance of shift: Chief Medical Officer Medical Director + At least one other Chief Officer Executive Director or Executive Team Meeting.
Other methods of engagement
Authorisation limits as for non-pay. Purchase orders must be raised. The Corporate Financial Information Department must be contacted to ensure that appropriate checks are undertaken and engagement method is appropriate.
69/73 86/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 67 of 70
Area/SFI Reference
Capital Scheme Committee Approval
Order Sign off Financial Limit
Capital Expenditure (SFI 9.3 Replacement equipment/ maintaining core infrastructure)
Capital and Estates Committee
Designated Budget Managers per authorised signatory list
Up to Maximum of £25,000 (level 3)
Capital and Estates Committee
Chief Strategy Officer Director of Development
Up to maximum of £250,000 (level 2)
Capital and Estates Committee
Chief Executive or Managing Director and Chief Finance Officer Director of Finance
Up to Maximum of £500,000
Board of Directors Chief Executive or Managing Director and Chief Finance Officer Director of Finance
Above £500,000
Area/SFI Reference
Capital Scheme Committee Approval
Order Sign off Financial Limit
Capital Expenditure (SFI 9.3 New Strategic investments) For new IT systems Digital Health BoardEPR Programme Board approval will be sought prior to Management Board.
Management Board & Capital and Estates Committee
Designated Budget Managers per authorised signatory list
Up to Maximum of £25,000 (level 3)
Management Board & Capital and Estates Committee
Chief Strategy Officer Director of Development
Up to maximum of £250,000 (level 2)
Management Board & Capital and Estates Committee
Chief Executive or Managing Director and Chief Finance Officer Director of Finance
Up to Maximum of £500,000
Board of Directors Chief Executive or Managing Director and Chief Finance Officer Director of Finance
Above £500,000
Area/SFI Reference
Approval Financial Limit
Charitable Funds Expenditure (SFI 9.6)
Fund Manager [In periods of absence the Fund Manager’s line manager will provide alternative authorisation]
£0-£5k
Fund Manager and Chief Executive or Managing Director £5k-£15k
Fund Manager and Chief Executive or Managing Director and Charity Trustee.
[Note for exceptional expenditure requests over £15k and below £50k which are made between Trustee meetings that cannot wait for the Trustees to meet, the Charity Trustee will later ratify the expenditure. There remains a risk to the Trust for expenditure approved through this method as the Trustee approval is still needed and if not given the expenditure will be charged back to the Trust.]
Over £15k
Area/ SFI Reference
Authorised Officers
Delegation Financial Limit
Petty Cash Chief Executive Budget Holder Limit £30
70/73 87/347

SWH 00942
Standing Financial Instructions and Scheme of Delegation
Version 3.32 AprilFebruary 20220 Page 68 of 70
Area/ SFI Reference
Approval Financial Limit (based on contract life total costs)
Business Cases (NEW SPEND)
Management Board Up to 500k
Board of Directors Over 500k
Area/SFI Reference
Delegation Financial Limit
Investments (SFI 10)
Limits for authorisation of investments with approved institutions First line signatories:
One first and one second line signatory Two second line signatories Chief Executive Officer Managing Director Chief Finance Officer Deputy Chief finance Officer
Up to £5,000,000 Over £5,000,000
Second line signatories:
Associate Director of Finance Finance Manager- Financial Reporting
Staff authorised to enact investments with approved institutions after approval by authorised signatories.
Formatted Table
Formatted: Font: 10 pt, Bold, Italic
Formatted: Left
71/73 88/347

Version 3.32 April 2022February 2020 Page 69 of 70
22 Appendix C: Monitoring Compliance Form Title of Document Standing Financial Instructions, Scheme of Delegation and Financial Limits
Relevant Standards Health & Social Care Act Other e.g. West Midlands Quality Review Service, Peer Reviews etc
Monitoring/Audit Plan Process / minimum requirement to be audited / monitored
Lead Tool/How Written Reporting Frequency
Written Reporting Arrangements
Reports to Audit Committee
Chief Finance Officer Director of Finance
Compliance reporting
As agreed/required by Audit Committee
As agreed/required by Audit Committee
The above Table outlines the minimum requirements to be audited/monitored; additional audits will be commissioned in response to deficiencies identified within the service through morbidity and mortality reviews/benchmark data provided by CHKS or in response to national initiatives e.g. NICE, RCOG guidelines and CNST standards. Lessons learnt and action plans will be shared with all the relevant stakeholders.
Name: Kim Li Job Title: Chief Finance Officer Director of Finance Date: June February 20220
72/73 89/347

Version 3.32 April 2022February 2020 Page 70 of 70
23 Appendix D: Equality Impact Assessment Form
Has an Equality Impact Assessment been carried out? YES
Preliminary Stage 1 Equality Impact Assessment (must be completed if required*)
What date was Stage 1 completed and published? Input Date
Has a Full Assessment Stage 2 Equality Impact Assessment Tool been undertaken*? YES/NO/NO-NA
If yes, what was the date of assessment and publication of Stage 2 and action plan? Input Date or type NO
73/73 90/347

Report SummaryReport to Board of Directors Date of
Meeting6 July 2022
Report Title Chief Executive’s Report Agenda Item 8.1
Executive/Non-Executive Lead
Glen Burley, Chief Executive Report Author(s)
Glen Burley, Chief Executive
Report Previously Discussed at N/A
Purpose of the Report For ApprovalFor Discussion
To highlight to the Board of Directors important local and national developments.
For Information ✓
Recommendations and Action Required The Board of Directors is asked to receive and note this report.
Impact (is there any impact arising from the report on the following?) Quality EqualityFinance ResearchPerformance ComplianceWorkforce Legal
Applicable Quality Improvement Priorities Elective Hub Health InequalitiesElectronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety CompassionateEffectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk RegisterAre any existing risks on the BAF/Risk Register affected? N/AIdentify the BAF/Risk Register risk ID and description – explain how the risk has been affected – reduced or increased as a consequence of the evidence within the report. N/A
Do you recommend a new entry to the BAF and/or Risk Register is made as a result of this report? If yes, describe the new risk.
No
1/10 91/347

South Warwickshire NHS Foundation Trust
Report to Board of Directors – 6 July 2022
Chief Executive’s Report
South Warwickshire NHS Foundation Trust (SWFT) Special Care Baby Unit (SCBU) Achieves Bliss Gold Accreditation and Nurse Recognised for Outstanding Family-Centred Care
Emma-Louise Evans, Nursery Nurse, has been awarded the prestigious Nursing and Midwifery Award in the Regional Parliamentary Awards for the Midlands. NHS Midlands announced on Tuesday 14 June 2022 the ten individuals and teams chosen as regional champions to mark the NHS’s 74th birthday. MPs and NHS leaders in the region joined forces to honour health and care staff who have helped to improve treatment for patients. The judges, drawn from across the NHS, selected Emma-Louise alongside nine other winners (one in each of the 10 categories) from over 120 nominations.
Emma-Louise has been a key driver behind our Special Care Baby Unit (SCBU), delivering high-quality family-centred care as standard. This means involving the family as much as possible in their baby’s care. For the past four years, Emma-Louise has worked extremely hard as the Trust’s lead for the Bliss Baby Charter. This charter is a framework for neonatal units to assess the quality of the family-centred care they deliver. In May 2022, the unit achieved the full gold Baby Bliss Charter Accreditation, which has so far been achieved by only 10 SCBUs in the country. The following enhancements have been made in SCBU:
• Free parking for parents. • Development of notice boards to signpost support groups and provide key information
that families can digest at a time suitable to them. • Revised admission and discharge packs – to support and comfort families.• An admission checklist and improved discharge checklist – to ensure a consistent
approach to admitting / welcoming and discharging babies and their families.• Improved access to psychological support.• Introduction of Bliss’ milestone cards – encouraging parents to document their baby’s
key activities.• Folder created containing key information about other hospitals for parents whose
baby was transferred to another Trust.• Planning activities around the parent’s routine to provide individualised care.• QR codes introduced so parents can easily access informative videos.• Developmental and Family Integrated Care (FiCare) Lead Nurses roles introduced –
two volunteers to champion / promote family-centred care.
To further enhance the care the unit provides, Emma-Louise organised a fundraising event on World Prematurity Day and raised an impressive £1,445.00. During the day, she also arranged purple clothes and gifts for all the babies on the unit – helping to spread joy during what can be a stressful time for parents.
Messenger Review of NHS Leadership
This much anticipated review of NHS Leadership was published in June 2022. The report’s author, General Sir Gordon Messenger, is an ex-British Army General and was supported
2/10 92/347
in his work by Dame Linda Pollard, Chair of Leeds Teaching Hospitals NHS Trust. The report was commissioned last year by Secretary of State Sajid Javid.
The report makes a number of recommendations but has been met with disappointment by many internal stakeholders. In particular, the absence of recognition that the NHS operates with the lowest management costs compared to other sectors and compared to other healthcare systems in the developed world.
1. Targeted interventions on collaborative leadership and organisational values• A new, national entry-level induction for health and social care.• A new, national mid-career programme for managers.
2. Positive Equality, Diversity, and Inclusion (EDI) action• Embed inclusive leadership practice as the responsibility of all leaders.• Commit to promoting equal opportunity and fairness standards.• More stringently enforce existing measures to improve equal opportunities and
fairness.• Enhance CQC role in ensuring improvement in EDI outcomes.
3. Consistent management standards delivered through accredited training• A single set of unified, core leadership and management standards.• Training and development bundles to meet these standards.
4. A simplified, standard appraisal system for the NHS• A more effective, consistent, and behaviour-based appraisal system.
5. A new career and talent management function for managers• Creation of a new career and talent management function at regional level.
6. More effective recruitment and development of Non-Executive Directors (NED)• Establishment of an expanded, specialist NED talent and appointments team.
7. Encouraging top talent into challenged parts of the system• Improve the package of support and incentives in place to enable the best
leaders to take on some of the most difficult roles.
The Fuller Stocktake of Primary Care
The CEO of NHS England (NHSE) commissioned a review last year of the role and function of Primary Care in the new Integrated Care System (ICS) operating framework. The review was led by Dr Clare Fuller, a practicing GP and ICS lead from Surrey. It was a great privilege to chair one of the three main ‘life phase’ workstreams which contributed to the report. The final report and recommendations were published in May 2022. At the heart of the report is a new vision for integrating Primary Care, improving the access, experience, and outcomes for our communities, which centres around three essential offers:
• Streamlining access to care and advice for people who get ill but only use health services infrequently: providing them with much more choice about how they access care and ensuring care is always available in their community when they need it.
3/10 93/347

• Providing more proactive, personalised care with support from a multidisciplinary team of professionals to people with more complex needs, including, but not limited to, those with multiple long-term conditions.
• Helping people to stay well for longer as part of a more ambitious and joined-up approach to prevention.
I have summarised the main recommendations with the responsible bodies identified for each:
1. Develop a single system-wide approach to managing integrated urgent care including a more sustainable model for practices. - (ICSs)
2. Assist systems with integration of primary and urgent care access, looking at the role of NHS 111, and considering new metrics and standards - (NHSE)
3. Enable all PCNs to evolve into integrated neighbourhood teams, supporting better continuity and preventive healthcare as well as access, with a blended generalist and specialist workforce drawn from all sectors including Secondary care consultants and community and mental health teams. At place level, bring together teams on admissions avoidance, discharge and flow and focus on community engagement and outreach, across the life course. - (ICSs)
4. Put in place the appropriate infrastructure and support for all PCNs, across their functions including digital, data, intelligence and quality improvement, HR, finance, workforce plans and models, and estates. - (ICSs)
5. Develop a primary care forum or network at system level. Ensure primary care is represented on all place-based boards. - (ICSs)
6. Embed primary care workforce as an integral part of system thinking, planning and delivery. Improve workforce data and support mechanisms. Support innovative employment models and adoption of NHS terms and conditions. - (ICSs)
7. Include primary care as a focus in the national workforce strategy and rollout of the NHS Staff Survey in primary care. Examine further flexibilities in the Additional Roles Reimbursement Scheme. Review the GPs Performers List to include other appropriately qualified clinicians. - (Department of Health and Social Care with NHSE and Health Education England)
8. Focus system leadership as the primary driver of primary care improvement and development of neighbourhood teams. - (NHSE)
9. Improve data flows including by solving the problem of data-sharing liability, working
with system suppliers on extract functionality; improving data to support access and helping to identify population cohorts to be targeted by neighbourhood teams. - (NHSE)
10.Develop system-wide estates plans to support fit-for-purpose buildings for PCNs taking a ‘one public estate’ approach, maximising the use of community assets and spaces. - (ICSs)
11.Provide additional, expert support to help offer solutions to the most intractable estates (DHSC and NHSE)
4/10 94/347

In my work on the Stocktake I was keen to ensure that there were areas where organisations like ours could take action. These are predominantly annotated above as ICS issues, recognising that the ICS is made up of its constituent parts. In my view them most important areas for the Trust to become involved in are 1, 3, 4, 5, 6, 9 and 10 above.
NHS England Consultations on Provider Governance
NHS England has commenced an important consultation exercise on significant updates to Provider Governance. A draft Code of Governance for NHS providers was issued by NHSE on 27 May 2022 and is out for consultation until 8 July 2022. The new code will replace the NHS Foundation Trust Code of Governance which was last updated in 2014. For the first time, the code will apply to all Trusts. Alongside this code, consultation has also commenced on supporting draft documents, a draft document entitled ‘Guidance on Good Governance and Collaboration’ and a draft guide on the role of Foundation Trust Governors, and I have included these below for information.
Draft ‘Code of Governance for NHS providers ‘
Code-based governance has been adopted across many sectors in the UK and was first introduced to the NHS when foundation trusts were created. The NHS foundation trust code provided guiding principles with the flexibility for foundation trusts to adopt alternative practices where it was right for them providing that they could explain how they were meeting the core principles of good governance (often referred to as ‘comply or explain’). The revised code takes the same approach making it clear the obligations of statute.
The code has been updated to reflect:• its application to NHS trusts, following the extension of the NHS Provider licence to them• changes to the UK Corporate Governance Code in 2018• the legal establishment of integrated care systems (ICSs) under the Health and Care
Act 2022• the evolving NHS System Oversight Framework, under which trusts will be treated
similarly regardless of their constitution as a trust or foundation trust.
Disclosures to NHSE in relation to the ‘governance condition’ (Condition 4) of the Provider licence and to the code itself will be used by them to make determinations about adherence to the provider licence in terms of having safe, effective, outcomes-focused governance arrangements.
The provisions of the code do not greatly differ from the original version as the Health and Care Act 2022 does not change the statutory role, responsibilities, and liabilities of provider trust boards of directors. It does however bring incorporation of the requirement for boards of directors to assess the trust’s “contribution to the objectives of the Integrated Care Partnership (ICP) and Integrated Care Board (ICB), and place-based partnerships” as part of its assessment of its performance, and “system and place-based partners” are highlighted as key stakeholders throughout. There is also inclusion of the board’s role in assessing and monitoring the culture of the organisation and taking corrective action as required, alongside “investing in, rewarding and promoting the wellbeing of its workforce”. The previous code only mentioned wellbeing in the context of the finances of the organisation. There is also a new focus on equality, diversity and inclusion among board members including providing EDI training for those undertaking
5/10 95/347

director-level recruitment. The board should have a plan in place for the board and senior management of the organisation to reflect the diversity of the local community or workforce, whichever is richer.
For Foundation Trusts, the code brings potentially greater involvement for NHSE in recruitment and appointment processes. This includes utilising NHSE’s Non-Executive (NED) Talent and Appointments team in preference to external recruitment consultancies and having representation from NHSE on NED recruitment panels. When setting remuneration for NEDs, including the chair, foundation trusts should use the Chair and Non-executive director remuneration structure.
References to Monitor and other terminology has been updated and there are links to other relevant frameworks, manuals, and guidance (such as the Well-led framework).
The code stresses the importance of having an effective, diverse and entrepreneurial board which sets the trust’s vision, values and strategy. It should do so with regard to the triple aim duty of better health and wellbeing for everyone, better quality services, and the sustainable use of resources. There is now also specific reference to the trust’s role in reducing health inequalities, assessing, and monitoring culture, and investing in, rewarding, and promoting the wellbeing of its workforce.
Ensuring effective management of resources, risk management through internal controls, and stakeholder engagement (which now includes system partners) are identified as part of the role of the board. The provisions now include that boards should have systems and processes in place to assess the contribution of the trust to the objectives of the ICS as well as assessing the performance of the trust in relation to effectiveness, efficiency and economy and focusing on quality, risk management, clinical governance, and stakeholder engagement, making use of independent advice as required. The trust’s vision and values should now include the trust’s role “with reference to the ICP’s integrated care strategy and the trust’s role within system and place-based partnerships, and provider collaboratives.”
The metrics and measures used to assess performance should now be disaggregated by ethnicity and deprivation where relevant. The new code is more specific that while the chair should ensure the board as a whole has a clear understanding of the views of stakeholders (including system partners), the committee chairs now have particular responsibility for stakeholder engagement on significant matters within their purview. When the chair undertakes their own engagement with stakeholders, they should now do this in a “culturally competent” way. The annual report should describe how the interests of system and place-based partners have been considered in decisions and set out key “partnerships for collaboration” that the trust is part of.
The new code sets out the role of the chair and notes the need for clear division between the leadership of the board and executive leadership of the trust’s operations. The board’s collective responsibility for the performance of the trust and infrastructure and resources needed to function is specified, along with the role of the non-executives and their need for sufficient time to meet their board responsibilities. The provisions remain almost unchanged from the previous code; however, the appointment and removal of the company secretary becomes a matter for the board as a whole, rather than the chair and chief executive jointly.
6/10 96/347

The code sets out the need for formal, rigorous and transparent procedures for making board appointments. The board should be constituted, in terms of size, diversity of skills etc. to undertake its duties, and undertaken an annual evaluation of its effectiveness. Consideration of diversity is now included within the annual board evaluation.
The disclosures pull together the provisions from the code, setting out the provisions that trusts should comply with or explain how alternative arrangements comply. The disclosures are broken down into sections depending on what trusts should do. The alternative requirements are:
• provide a supporting explanation of compliance or explain non-compliance in the annual report
• “basic” comply or explain – where trusts are welcome but not required to provide statements of compliance but should explain where they have deviated from the code (most provisions fall into this category)
• provide information to the governors or make information available to members (FTs only)
• make information publicly available.
The role and responsibilities of Councils of Governors in law does not change with the new act, but the description of councils of governors’ duty to represent the interests of the “public at large” is a new focus. This includes the population of the local system of which the trust is part and the “whole population of England as served by the wider NHS”. There is also a new suggestion that the council may look at the nature of the trust’s “collaboration with system partners” as an indicator of organisational performance. There is also clarification of the council’s role in relation to approving significant transactions, mergers and acquisitions so that “to withhold its consent, the council of governors would need to provide evidence that due diligence was not undertaken.”
The code’s disclosure requirements sit alongside the corporate governance statement required in the annual plan (a forward-looking statement of arrangements for the coming year) and the annual governance statement required in the annual report (a backward look over the past year). These are both distinct requirements, not related to the code. The code disclosures provide an additional evaluation of corporate governance arrangements over the preceding year and are included within a trust’s annual report.
Draft ‘Guidance on good governance and collaboration’
This guidance sets a clear expectation that providers will collaborate with partners to agree shared objectives through ICPs and collaborate on delivery of the five-year joint plan and annual capital plan through system and place-based arrangements, and provider collaboratives. It states that effective collaboration requires system-minded leadership – recognising that trusts and other health and care organisations together are the system – and strong working relationships between partners to develop shared objectives and ensure their delivery. This must be underpinned by organisational and individual behaviours which create the right environment for collaborative change. Providers can put in place governance arrangements to help to ensure that these essential ingredients are in place and are used to deliver system improvements. The main requirements are that.
7/10 97/347

• Providers will engage consistently in shared planning and decision-making – participating consistently and constructively with partners in system and place-based partnerships and provider collaboratives and ensuring open sharing of information and appropriate delegations are in place to develop shared plans and priorities and reach shared decisions.
• Providers will consistently take collective responsibility with partners for delivery of services across various footprints including system and place. This may include place-based partnerships, provider collaboratives or other clinical networks. Guidance on good governance and collaboration helping to enable a shared understanding of performance, supporting arrangements for working together to manage any risks to delivery, and contributing to a culture which supports continuous system improvement.
• Providers will consistently take responsibility for delivery of improvements and decisions agreed through system and place-based partnerships, provider collaboratives, or any other relevant forums – ensuring that: organisational plans are integrated with the five-year joint system plan; annual capital plan is agreed with the ICB and its partners; and that the organisation implements shared decisions and plans agreed through all relevant forums in a timely manner.
Draft ‘Addendum to Your statutory duties’ – reference guide for NHS foundation trust governors
This addendum is based on the existing statutory duties in the 2006 Act, and the principles regarding collaboration and system working set out above and in ICS legislation. Updated considerations are set out in respect to the legal duties of councils of governors, which are: holding the Non-executive directors to account, representing the interests of trust members and the public, and approving significant transactions, mergers, acquisitions, separations or dissolutions. This addendum only applies to a council of governors’ statutory role within its own foundation trust’s governance.
While the meaning of ‘the public’ is not specified in legislation, councils of governors are not restricted to representing the interests of a narrow section of the public served by the NHS foundation trust – that is, patients and the public within the vicinity of the trust or those who form governors’ own electorates. To support collaboration between organisations and the delivery of better, joined up care, councils of governors are required to form a rounded view of the interests of the ‘public at large’. This includes the population of the local system of which the NHS foundation trust is part. It states that no organisation can operate in isolation, and each is dependent on the efforts of others. While staff governors and patient, carer and service user governors represent specific constituencies, they are also expected to represent the interests of the members of the trust as a whole and the public. Therefore, they are required to seek and form a view of the interests of the ‘public at large’.
More from Our Great Teams – Integrated Single Point of Access (iSPA) and Integrated Care Co-ordination (ICC)
The Integrated Single Point of Access (iSPA) receives referrals from the following:• GP’S• Community health and social care services• WMAS• Acute hospitals – consultants, ward referrals into OOHCC• Nursing and residential care homes• Patients, relatives and carers.
8/10 98/347

All routine referrals are sent directly through to the appropriate team within the Out of Hospital Care Collaborative (OOHCC) team. All potentially urgent calls received within the iSPA, will be transferred to the iSPA Integrated Care Co-ordination (ICC) Team for triage by a clinician.
The ICC was created in 2019 and consists of a group of clinicians, both nurses and allied health professionals (AHPs). The role of the team is to clinically triage all calls from iSPA to determine whether an urgent/same day response from nurses, therapists and/or clinical practitioners/advanced clinical practitioners is required, or whether signposting to an alternative service or clinical provider is more appropriate. The referrals are increasingly complex, and ICC is constantly monitoring and evaluating the service that we provide to ensure that we are able to keep pace with the increasing demand and complexity and to maintain that the service is safe and effective at all times.
ICC are at the forefront of technology within OOHCC and continue to explore interactive resources and systems to provide a smart and efficient service. We are currently working with Telehealth Systems such as Docobo and My Sense for a cohort of patients that fall under community services within SWFT. These patients may have long term conditions such as chronic obstructive pulmonary disease (COPD), heart failure, dementia, or may be clinically vulnerable. Patients living within care homes in Warwickshire are monitored via Docobo with the support of care home staff to enable the early identification and management of deteriorating patients. The ICC are responsible for clinically triaging all Docobo patient alerts as well as for completing all regular monitoring, and the team work to ensure that patients receive a safe and appropriate level of intervention by offering trusted clinical advice. They will also where necessary, allocate directly to a clinician to complete a visit in the timeliest manner.
Both teams combined complete on average approximately 13,000 calls per month with a rapid response time. Alongside these calls, the teams deal with email interactions and Telehealth alerts totalling an additional 2,000 contacts per month.
0
10
20
30
40
50
60
70
80
90
100
Mar-18
May-18Jul-1
8
Sep-18
Nov-18Jan-19
Mar-19
May-19Jul-1
9
Sep-19
Nov-19Jan-20
Mar-20
May-20Jul-2
0
Sep-20
Nov-20Jan-21
Mar-21
May-21Jul-2
1
Sep-21
Nov-21Jan-22
Mar-22
May-22
iSPA Service Level Mar 2018 - May 2022
9/10 99/347

0
50
100
150
200
250
300
75%
80%
85%
90%
95%
100%
Sep-21 Oct-21 Nov-21 Dec-21 Jan-22 Feb-22 Mar-22 Apr-22 May-22
No of Alerts Average Time Response within 2hrs
Docobo Care Home Resident Unwell - ICC Alerts & Time Taken
4281
30962830 2703
2528
167
0
500
1000
1500
2000
2500
3000
3500
4000
4500
Jan-22 Feb-22 Mar-22 Apr-22 May-22
COPD Alerts Heart Failure Alerts
Docobo at Home Patients - ICC Alerts Completed 2022
Glen Burley Chief Executive
050
100150200250300350400450500
Jan-21
Feb-21
Mar-21
Apr-21
May-21
Jun-21Jul-2
1
Aug-21
Sep-21
Oct-21
Nov-21
Dec-21
Jan-22
Feb-22
Mar-22
Apr-22
May-22
ICC 2021-22 Average Response Time in Seconds Se
cond
s
10/10 100/347

Report Summary Report to Board of Directors Date of
Meeting 6 July 2022
Report Title Integrated Performance Report
Agenda Item
8.2
Executive/ Non-Executive Lead
Anne Coyle, Managing Director
Report Author(s)
Anne Coyle, Managing Director Ellie Ward, Acting Chief Nursing Officer Harkamal Heran, Chief Operating Officer Gertie Nic Philib, Chief People Officer Kim Li, Chief Finance Officer
Report Previously Discussed at N/A
Purpose of the Report To provide the Board of Directors with oversight of the key issues, updates and assurance on operational and financial performance across the Trust.
For Approval For Discussion For Information
Recommendations and Action Required The Board of Directors is asked to receive this report and note delivery of the month 1 position for 2022/23.
Impact (is there any impact arising from the report on the following?) Quality Equality Finance Research Performance Compliance Workforce Legal
Applicable Quality Improvement Priorities Elective Hub Health Inequalities Electronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety Compassionate Effectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk Register Are any existing risks on the BAF/Risk Register affected? Identify the BAF/Risk Register risk ID and description – explain how the risk has been affected – reduced or increased as a consequence of the evidence within the report. Do you recommend a new entry to the BAF and/or Risk Register is made as a result of this report?
No
1/23 101/347

Integrated Performance Report May 2022 Integrated Performance Report: Public Guidance Pack
2/23 102/347

Managing Director – Executive Summary
In relation to the Chief Nursing Officer’s report, it is pleasing to see the majority of quality and safety Key Performance Indicators (KPIs) are within normal control limits. It is assuring to note that the number of inpatient falls with harm remains low and we can continue to demonstrate a positive reporting culture and learning from incidents. The falls prevention campaign in July 2022 is a good opportunity to reflect on learning from incidents and disseminate the principles of falls prevention. May 2022 saw its highest response rate for “I Want Great Care” patient feedback for the Emergency Department due to the implementation of the SMS text messaging service. This has allowed instant feedback for the team to respond to including introducing volunteers to support the waiting room during peak times. This provides regular communication on expected waiting times, refreshments and escalation of concerns to the triage nurse. The Chief Operating Officer’s commentary noted an excellent diagnostic performance and that the Diagnostic performance in Coventry and Warwickshire is the best in the UK. Performance against the 4 Hour standard in Accident and Emergency improved slightly in May 2022 to 68.6%, though remaining below the Lower Control Limit. There were high attendance numbers in May 2022, making the month the busiest recorded at SWFT (7,691). The numbers of people in beds with COVID-19 reduced significantly, starting the month with mid 20’s in beds, dropping to average around 10 at month end. Cancer performance remains stable but achieving compliance is a challenge. The main areas of concern remain Urology, Gynaecology and Colorectal. The Chief People Officer provides an overview of recruitment, sickness absence, appraisals and mandatory training compliance, with a particular focus on the wellbeing initiatives available to support the reduction in staff sickness absence. The Chief Finance Officer advised that at month 2 the Trust has delivered a £2.18m deficit against the break-even plan. This includes the part year impact of an assumed 2% pay award which has been funded but national discussions continue so this may be a further risk for the Trust. Mitigations are in place to manage this position and the Trust is forecast to achieve break even in 2022/23 in line with the initial plan submission. The key drivers of this position is high agency expenditure and non-delivery of Cost and Productivity Improvement Programmes (CPIPs). Workforce and CPIPs are the main focus for the Finance & Performance Executive meetings with Divisions and these remain as risks. The Trust has been notified that a further allocation in relation to Excess Inflation costs will be funded and the Trust has now submitted a revised £3m surplus plan. Progress against this revised plan will be reported from Month 3.
Anne Coyle Managing Director
3/23 103/347

Our Quality & Safety – Executive Narrative
There were 4 Serious Incidences (SIs) reported in May 2022 (2 of which occurred late in April 2022 and 2 occurred in May 2022); one retained item never event, one medication error, one fracture and one unexpected community death. All SIs undergo a full investigation to identify the root cause(s) as well as any potential learning opportunities. The incidents are discussed at the Clinical Governance Committee. In terms of patient experience, the total number of reviews received through the Friend and Family Test (FFT) in May 2022 was 1059 which is lower than April 2022 when 1558 reviews were received. Across all services the response rates were below target, this can be attributed to several packages containing our reviews that were not processed by our patient experience supplier, and a number of forms were held until contract renewal confirmation had been received, therefore they were also not processed in time. Both problems have now been resolved and the team are assured that all reviews will be recorded from now on. A&E Patient SMS alerts have increased the response rate from 1.2% in March 2022 to 6.1% in May 2022. We expect to see a continued improvement in the response rate over the coming months. Many of the patients who left reviews, gave lower scores for “the length of time they waited before they were seen”. These lower scores had a negative impact on the score with only 77.7% of A&E patients reporting that they had a positive experience. There was a further improvement for Acute In-Patients with 94.7% stating they had a positive experience. Despite a slight increase in falls from 55 in April 2022 to 59 in May 2022, there is a continued decreasing trend of falls and harm over the past few months. No falls with fractures or serious harm had been reported (up to 26 May 2022). The injury rate per 1000 bed days continues to remain below the threshold of 1.14 at 1.09. During May 2022 Nurses Day was celebrated with high performing Wards for 2021/22. There was also volunteer jubilance at being able to reengage again with falls prevention and provide support to increase safe set up of falls prevention alarms. In May 2022 we saw 38 incidents relating to discharges, 36 with no harm, 1 with low harm and one with moderate harm. This is the highest number of discharge incidents we have seen since September 2021. 17 incidents related To Take Out (TTOs), all at no harm with no stand out themes or areas for concern. The incident reported as moderate harm is under investigation to understand the actual harm level and any learning identified. The low harm incident related to a patient being discharged with an incorrect medication belonging to another patient which they proceeded to take; patient was reporting fatigue but no other symptoms, this is under investigation. The Safer Discharge Group is leading a trial on Avon Ward; during a week in May 2022 a medicines management technician supported the ward to check the (TTOs) were correct and council the patient at the point of discharge and ensure appropriate equipment and referral were in place. This supports the registered nurse, reduces the risk of errors and potential harm to patients and improves the patient’s experience at discharge. This is due to be evaluated in June 2022.
A summary of the Trust’s mortality position is shown below, however, the Summary Hospital-level Mortality Indicator position for the period January – December 2021 was 97.9 and well within acceptable limits.
Dr Charles Ashton Chief Medical Officer
Ellie Ward Acting Chief Nursing Officer
4/23 104/347

We are driving this measure because: Medication Error Incidences - Medication errors are any Patient Safety Incident where there has been an error in the process of prescribing, preparing, dispensing, administering, monitoring or providing advice on medicines. NHS organisations should ensure that a robust process is in place for identifying, reporting, reviewing and learning from medicines errors involving residents.
Assurance Variation Data Quality Mark
WIP
The system may achieve or fail the target subject to
random variation Common cause
variation
Performance and Actions
There were 132 incidents reported in May 2022 which is an increase from the 113 in April 2022. There were 5 harm incidents putting the trust ratio of harm to no harm 3.79% below the threshold target of 4 and national benchmark of 10. There were 13 insulin incidents, 11 of these in the community sector and a rise from previous months. A large proportion of the community incidents are around confusion with paperwork and locating the most recent directive to administer and responding to dosage changes. An electronic directive that show historical doses and when updates have occurred, available all on one document is being developed at the moment to help prevent this type of incident. There were 32 ‘controlled drug (CD)’ incidents in May 2022 a big increase from the 16 in April 2022. This is largely accounted for by an unusually high number of palliative care incidents in the community as 19 of the incidents occurred in the community sector; 17 of those “patient related”, in other words being about the clinical care as opposed to CD legislation or governance issues. These will be discussed in more detail at the palliative care incident meeting later in the month. Risks:
What the chart tells us: In terms of the number of medication incidents the numbers have always been fairly stable with common cause variation being seen, over the past four months the number of incidents has been over the average number. For the medication incidents with harm we see that the number of cases has reduced since the end of 2018, with there being only a small amount of variation since then.
5/23 105/347

6/23 106/347

7/23 107/347

Our Performance – Executive Narrative
Radiology continues to perform very well against the diagnostic (DM01) standard, meeting the standard despite a sustained increase in demand. 99.9% of imaging diagnostics were completed within 6 weeks from request, but we saw an increase in the number of patients on the waiting list and so this is something for us to monitor going forward. Diagnostic performance in Coventry and Warwickshire is the best in the UK.
Performance against the 4 Hour standard in Accident and Emergency (A&E) improved slightly in May 2022 to 69%. We saw very high attendance numbers in May 2022, making the month the busiest recorded at SWFT (7,691) and the number of admissions from Emergency Department (ED) was also high but lower than March 2022. In comparison with other Type 1 A&E departments in England, SWFT had the 25th best performance, with the average 4-hour performance across the top 10 Acute Trusts was 77.6% with the top performing General Trust performing at 85.8%. In May 2022 there were opportunities to bring Ambulatory areas back into full use and this shows in the figures with 38.6% of all emergency admissions having a 0 day Length of Stay (LoS). Bed occupancy remained high, with medical bed occupancy averaging 98%. The numbers of people in beds with COVID-19 reduced significantly, starting the month with mid 20’s in beds, dropping to average around 10 at month end. The new Elective Recovery Fund (ERF) targets for 2022-23 is that the financial value of our activity should reach 104% of the corresponding month of 2019-20 with working day adjustments being applied. The recovery of the in-patient elective work reached over 100% of May 2019 and the related estimated financial value is around 109%. Day case activity improved in May 2022 and was the highest figure recorded since October 2021. Referral to Treatment (RTT) performance improved slightly to 77.2%; with a substantial increase in the number of people on open pathways to 26,128 (+1,494). In terms of long waiters, currently there are 0 at 104 weeks, 19 at 78 weeks and 394 over 52 weeks. Two week wait performance remains stable and 28 day faster diagnostic standard was at 66.7% which was slightly below what we achieved in the previous quarter. The main areas of concern remain Urology, Gynaecology and Colorectal.
In May 2022 there were 265 deliveries: Vaginal births – 49.6%, Emergency C sections – 20.7% and Elective C sections – 20.3%. In Out of Hospital, the Admit, Discharge Transfer rate for the reporting period increased very significantly to 97.2% from 80% returning to be above the target of 95%
Harkamal Heran Chief Operating
Officer
8/23 108/347

We are driving this measure because: The National 4 Hour Standard requires all patients to be seen, treated and either admitted or discharged within four hours of presentation at the Emergency Department (ED) where clinically appropriate. Performance has been adversely affected by year on year increases in emergency presentation to our ED.
Sep-21
Oct-21
Nov-21
Dec-21
Jan-22
Feb-22
Mar-22
Apr-22
May-22
73.7% 58.5% 66.3% 72.3% 69.8% 68.1% 68.6% 67.3% 68.6%
Assurance Variation Data Quality Mark
WIP
The system is expected to consistently Fail the target
Special cause variation – cause for concern
(indicator where LOW is a concern)
Performance and Actions
Attends in May 2022 increased to a new high for SWFT and each of the 4 full weeks in May 2022 were in the top 5 across time. This brought the average number of arrivals up to 249 per day, still skewed towards Monday (265) & Tues (258) with Weds (247) also increasing. 4 Hour performance improved slightly in May 2022 to 68.6%, though remaining below the Lower Control Limit. High attendance numbers in May 2022, making the month the busiest recorded at SWFT (7,691); the number of admissions from ED was high but lower than March 2022. In May 2022 18.9% of arrivals to ED were not registered with a South Warwickshire GP, with Birmingham and Solihull registered patients driving some of the increase in attends and admissions. There were sustained issues with admitted patient performance, though a slight improvement when compared to April (May 4 Hour: 36.4%); furthermore, despite the marked increase in attends, non-admitted performance was maintained (79.4%). Risks: • Sustained pressure in ED • Flow challenges as demand for medical beds remains high,
(occupancy averaged 98% in May 2022) and a high volume of stranded patients.
• What the chart tells us: ED performance between the summer of 2018 and the onset of the pandemic had little variation and the Trust’s performance was consistently around the 95% mark. Performance initially dropped with the onset of the pandemic and the challenges that brought. Following the end of the first lockdown performance recovered to pre-pandemic level, but since the end of the second lock-down performance has consistently reduced as the number of ED attendances increased.
9/23 109/347

Our Workforce – Executive Narrative
Gertie NicPhilib Chief People Officer
The data shows that recruitment is very healthy to the Trust, although there has been a slight increase in Nursing vacancies this month. International Nurse recruitment continues with a steady flow of overseas nurses arriving each month, enabling us to be on track to achieve our target of 50 international nurse recruits by April 2023. There were 89 new substantive starters in May 2022, including 26 Registered Nurses, 4 Registered Midwives, 25 Clinical Support Workers (CSWs) and 2 Allied Health Professionals (AHPs). A task and finish group has been established to focus on recruitment and retention in Theatres, which has been identified as a key area of risk for the Trust. This has identified some “quick wins”, e.g. lunch vouchers, together with some long-term plans, e.g. ODP apprenticeship academy. Sickness absence increased slightly in April 2022, with the biggest increase being in the Elective Division (from 5.80% in March 2022 to 6.45% in April 2022). Out of Hospital remains the highest area of concern with sickness absence of 8.76% in April 2022. The highest reason for sickness absence within Out of Hospital is anxiety/stress/depression, accounting for nearly a third of all absence from work. Staff health and wellbeing remains a key priority for the People team, with the new My SWFT staff app launched this month giving access to a range of health and wellbeing support. Appraisal compliance has improved this month, although admin & clerical and medical staff have not achieved the target of 85% compliance. Core Skills Training Framework (CSTF) compliance is also good with all Divisions achieving the target of 85%, although compliance amongst medics remains low. These positions are monitored through Finance and Performance Executive (FPE) and the Divisions are developing trajectories to maintain and improve their compliance.
10/23 110/347

We are driving this measure because: Sickness absence affects availability of staff to deliver services, which could impact quality, safety, operational performance and result in increased temporary staffing costs. Understanding sickness levels and the underlying causes also enables us to provide the appropriate support to staff.
May 21
June 21
July 21
Aug 21
Sep 21
Oct 21
Nov 21
Dec 21
Jan 22
Feb 22
Mar 22
Apr 22
4.11 4.69 5.74 5.35 5.54 5.66 5.61 5.76 6.57 5.79 6.00 6.06
Assurance
Variation
Data Quality Mark
WIP
The system is expected to consistently Fail the target
Special cause variation - cause for concern (indicator where HIGH is a concern)
Performance and Actions
• The overall Trust sickness figure for April 2022 was 6.06%, a slight increase from the previous months figure of 6%, and still above Trust target of 3.8%.
• Anxiety/stress/depression is consistently the highest reason for sickness absence
• Continued support is offered to staff through Occupational Health, Staff Support, Employee Assistance Programme (EAP) and Wellbeing interventions.
• Targeted interventions in areas of highest sickness absence levels, with support from the People and Workforce team.
• Identifying hotspot areas and getting back to basics to ensure processes are in place to manage absence effectively within a timely manner.
• Health and Wellbeing support for staff including physical health, mental health and financial wellbeing
• Charitable hardship fund established to offer financial support
Risks: • The highest sickness levels remain in Out of Hospital
(OOH) • Overall the sickness absence levels divisionally remain
high, with most divisions seeing an increase compared to last month.
• The highest sickness absence is amongst Clinical Support Workers which has a significant operational impact.
What the chart tells us: Sickness absence levels were historically low, remaining under 5% until the end of 2018. Since then sickness levels have been extremely variable, peaking at over 7% during the pandemic. Over the last two years this extreme variation has continued, but over the past 12 months there has been a steady increase where the Trust has remained at over 5.5%.
11/23 111/347

Our Finance – Executive Narrative
In March 2022 in agreement with National Health Service England / Improvement (NHSE/I) the system submitted a deficit plan of £32m, as part of this first submission the Trust submitted a draft break even plan. Further work has been ongoing with NHSE/I regarding excess inflation costs higher than the planning assumptions in the planning guidance which has now been confirmed. This means that the System has now re-submitted an overall break-even plan during June 2022. The Trust is now required to deliver a £3m surplus and progress against this revised plan will be reported from Month 3. Systems will continue to be paid through the Elective Recovery Fund (ERF) scheme for activity delivered above nationally set thresholds compared to 2019/20 activity levels. The system ERF indicative value is £35.7m of which the Trust’s value is £8.286m Cost and Productivity Improvement Programmes (CPIPs) of circa £10m have been included in the plan, equating to 3% of operating expenditure. Work is on-going to develop detailed project plans to support delivery of these savings. At month 2 the Trust has delivered a £2.18m deficit against the break-even plan. This includes the part year impact of an assumed 2% pay award which has been funded but national discussions continue so this may be a further risk for the Trust. Mitigations are in place to manage this position and the Trust is forecast to achieve break even in 2022/23 in line with the initial plan submission. Delivery of Cost and Productivity Improvement Plans is in progress as the divisions with work on-going to develop detailed project plans to support delivery of these savings. Indicatively ERF achievement at month 1 is 90% which is below the 104% required however we have assumed that we will receive the ERF income in full for month 1 and month 2 as there is an expectation that national funding will still be distributed for Q1 due to the challenges of recovery when COVID is still prevalent. However, this is a risk. Total agency expenditure (excluding medics engaged through direct engagement) was high again in April 2022 and May 2022 with spend being more than double the in-month agency ceiling. There have been significant operational pressures due partly to COVID (self-isolation and increase in COVID patients). Nursing, theatres, clinical coding are the main staff groups using agency. This is an area of focus for the Trust to manage expenditure and the Trust has re-instated Temporary Workforce Groups for Nursing and Non-Nursing, as well as reconfirm the importance of adhering to Temporary Workforce controls. The cash balance at the end of May was £44.597m for the Group. The Board of Directors is asked to note the month 2 position for 2022/23 and the risks identified.
Kim Li Chief Finance Officer
12/23 112/347
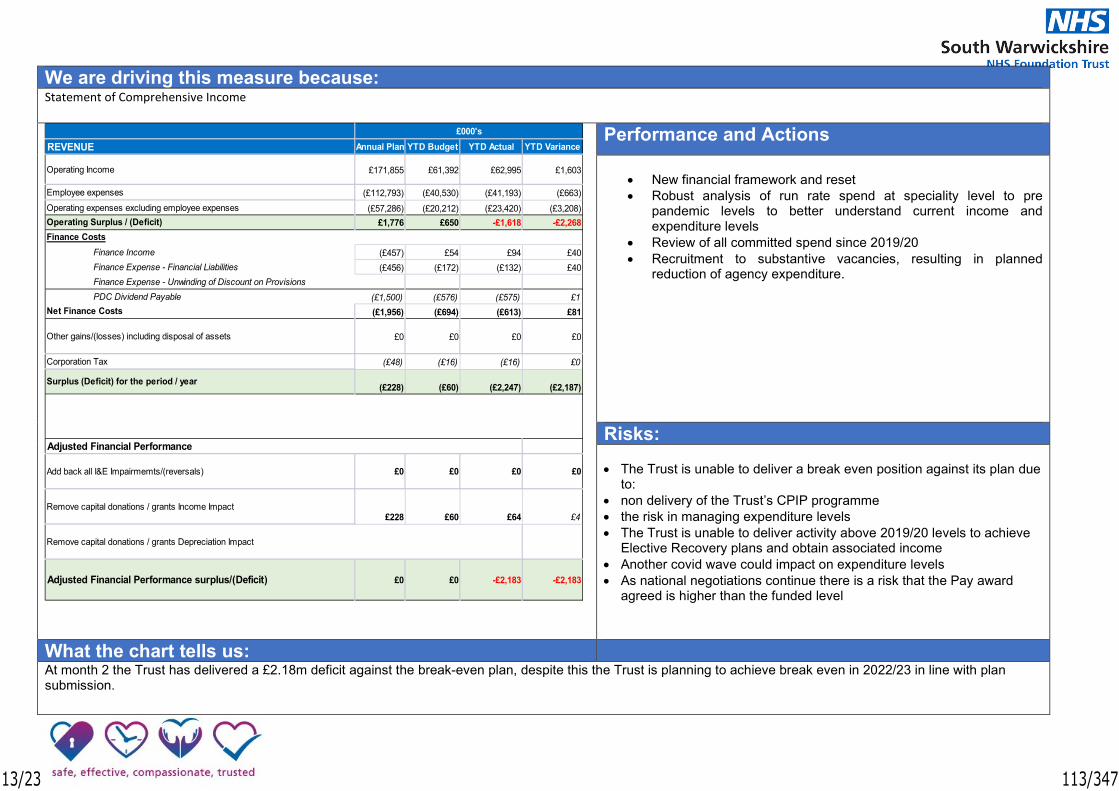
We are driving this measure because: Statement of Comprehensive Income
Performance and Actions
• New financial framework and reset • Robust analysis of run rate spend at speciality level to pre
pandemic levels to better understand current income and expenditure levels
• Review of all committed spend since 2019/20 • Recruitment to substantive vacancies, resulting in planned
reduction of agency expenditure.
Risks:
• The Trust is unable to deliver a break even position against its plan due
to: • non delivery of the Trust’s CPIP programme • the risk in managing expenditure levels • The Trust is unable to deliver activity above 2019/20 levels to achieve
Elective Recovery plans and obtain associated income • Another covid wave could impact on expenditure levels • As national negotiations continue there is a risk that the Pay award
agreed is higher than the funded level
What the chart tells us: At month 2 the Trust has delivered a £2.18m deficit against the break-even plan, despite this the Trust is planning to achieve break even in 2022/23 in line with plan submission.
Annual Plan YTD Budget YTD Actual YTD Variance
£171,855 £61,392 £62,995 £1,603
(£112,793) (£40,530) (£41,193) (£663)(£57,286) (£20,212) (£23,420) (£3,208)
£1,776 £650 -£1,618 -£2,268
Finance Income (£457) £54 £94 £40Finance Expense - Financial Liabilities (£456) (£172) (£132) £40Finance Expense - Unwinding of Discount on ProvisionsPDC Dividend Payable (£1,500) (£576) (£575) £1
(£1,956) (£694) (£613) £81
£0 £0 £0 £0
(£48) (£16) (£16) £0
(£228) (£60) (£2,247) (£2,187)
£0 £0 £0 £0
£228 £60 £64 £4
£0 £0 -£2,183 -£2,183
Employee expenses
£000'sREVENUE
Operating Income
Other gains/(losses) including disposal of assets
Operating expenses excluding employee expensesOperating Surplus / (Deficit)Finance Costs
Net Finance Costs
Remove capital donations / grants Depreciation Impact
Adjusted Financial Performance surplus/(Deficit)
Corporation Tax
Surplus (Deficit) for the period / year
Adjusted Financial Performance
Add back all I&E Impairmemts/(reversals)
Remove capital donations / grants Income Impact
13/23 113/347

We are driving this measure because: Cost and Productivity Improvement Plan (Efficiency)
Performance and Actions
• The target for 2022/23 has been set at £10m, or 3% of baseline budgets. The table on the right shows the breakdown of the target by Division.
• Divisions have been asked to present outline plans to the Trust’s
Finance & Performance Committee and are working to scope out and quantify savings.
• No schemes have yet progressed through the Quality Impact
Assessment stage and been signed off by the Trust’s Management Board.
• Support to divisions with CPIP programme using benchmarking data including GiRFT, Model Hospital, Peer Group etc
Risks:
If the Trust is unable to deliver the required levels of recurrent CPIP this will impact on the Trust’s ability to deliver a break even position
What the chart tells us: At present, approximately £2.2m of in year savings have been identified and are ready for approval, of which £1.7m are fully developed and £0.5m are in progress.
10 1,666 557 7,824
0 2,000 4,000 6,000 8,000 10,000 12,000
1
Budget Reduction CPIPs vs Target £000
Approved Fully Developed - Ready for Management Board
Plan in progress/ being worked up Gap to target
14/23 114/347

We are driving this measure because:
Agency Expenditure
Performance and Actions
• The Trust was issued with an agency spend ceiling value of £6.018m for 2022/23, which was consistent with previous years.
• Total agency expenditure in both April 2022 and May 2022 was £1.1m which is more than double the in-month agency ceiling.
• There have been significant operational pressures due to extra capacity being opened – not closed until May 2022, assessment areas being kept open overnight and high levels of vacancies. Sickness due to COVID has eased but agency usage remains at unprecedented levels.
Actions
• Investment in recruitment, retention, rostering and staff support (business case)
• Temporary Workforce Group meetings reinstated – nursing and non-nursing • Review weekly agency shift trend dashboards • Reinforcement of procedures
Risks: • Agency spend continues at this rate for the rest of the year, impacting on the
financial position
What the chart tells us: The 2021/22 agency spend was significantly above the NHSE/I ceiling, this trend has continued into months 1 & 2 2022/23. There has been a steady increase in the total agency costs as a percentage of the total staff costs during the year, and a steady increase in the monthly agency spend.
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
1,600,000
1,800,000
2,000,000
1 3 5 7 9 11 1 3 5 7 9 11 1 3 5 7 9 11 1 3 5 7 9 11 1
1819 1920 2021 2122 2223
Monthly Cost trend by staff type (Agency & Direct Engagement) - 2018 - 2022/23
15/23 115/347

We are driving this measure because:
Capital Programme
Performance and Actions The Trust’s planned capital programme spend for 2022/23 is £19.802m. The Coventry and Warwickshire Integrated Care System (ICS) was issued a total business as usual operational capital limit of only £39.434m for all four providers for 2022/23. This has resulted in the Trust having to agree to a £12.253m share of this allocation, of which £404k will be kept back until quarter 2 and is dependent on other capital slippage in the ICS. In addition to this the Trust also has £2.909m of OOH STP wave 2 PDC funding for the Ellen Badger Hospital development, £2.7m Capital Infrastructure Levy grant funding, £1.066m return of shareholder funding from Innovate Healthcare Services Ltd, £0.428m PDC for Community Diagnostic Centre funding and £0.425m donated funding planned for the MacGregor Ward scheme and £0.021m internally generated charitable funding for Theatres Welfare. Actual spend in May 2022 was £0.151m, year to date £0.692m. Risks:
• Slippage against planned schemes
What the chart tells us: The Trust forecast outturn on the capital programme is consistent with original plan submitted in April 2022
16/23 116/347

South Warwickshire Foundation Trust
Trust Key Performance Indicators (KPIs)-2022/23
Performance Against Target (Status)
Meeting Target Over 5% above Target
Not Meeting Target 5% above to 2% below target
More than 2% below Target to 5% below Target
Over 5% below Target
Regulatory Performance Measures CQC Domain Responsible Director Standard Mar-22 Apr-22 May-22 Numerator Denominator YTD 22/23
A&E max wait time 4hrs from arrival to departure Responsive Chief Operating Officer 95% 68.6% 67.3% 68.6% 5279 7691 68.0%
A&E minors max wait time 4hrs from arrival to departure Responsive Chief Operating Officer 95% 61.2% 61.4% 62.9% 3818 6071 62.2%
Stranded Patients - average numbers of patients in bed >21 days Effective Chief Operating Officer 109 95.0 103.4 99.3 99.3 0 101.35
Waiting Times - Diagnostic Waits <6 weeks Responsive Chief Operating Officer 99% 95.1% 93.2% 94.4% 6372 6752
Referral to Treatment Times - Open Pathways (92% within 18 weeks) Responsive Chief Operating Officer 92% 78.2% 76.2% 76.6% 20047 26128
Referral to Treatment Volume of Patients on Incomplete Pathways Waiting List Responsive Chief Operating Officer 16234 24207 24596 25897 25897 0
Referral to Treatment Number of Patients over 52 weeks on Incomplete Pathways Waiting List Responsive Chief Operating Officer 0 373 357 359 359 0
Referral to Treatment Number of Patients over 78 weeks on Incomplete Pathways Waiting List Responsive Chief Operating Officer 0 31 32 27 27 0
Referral to Treatment Number of Patients over 104 weeks on Incomplete Pathways Waiting List Responsive Chief Operating Officer 0 0 0 0 0 0
Referral to Treatment - Patients over 52 weeks on Incomplete Pathways Waiting List - Admitted Responsive Chief Operating Officer 0 154 156 150 151 0
Referral to Treatment - Patients over 52 weeks on Incomplete Pathways Waiting List - Non Admitted Responsive Chief Operating Officer 0 219 201 209 208 0
Referral to Treatment - Clock Stops Responsive Chief Operating Officer 120% 2019/20 130.2% 86.3% 100.0% 5180 5181
Patient Initiated Follow-Ups Effective Chief Operating Officer 5% of OPA Plan 2.1% 2.1% 1.7% 513 31029
Cancer 62-Day 2WW Ref to treat, all cancers Responsive Chief Operating Officer 85% 54.2% 49.7% 42 84 49.7%
Cancer 62-Day 2WW Ref to treat, all cancers patients waiting Responsive Chief Operating Officer 0 71.0 83.5 84 0
28 day referral to diagnosis confirmation to patients Responsive Chief Operating Officer 70% 70.8% 66.7% 808 1212 66.7%
Effective Occupancy rates Effective Chief Operating Officer 92% 92.4% 96.9% 94.3% 9693 10277 95.6%
Latest Period
Responsiveness
17/23 117/347

Financial Compliance CQC Domain Responsible Director Standard Mar-22 Apr-22 May-22 Numerator Denominator YTD 22/23
Liquidity (Days) Well Led Chief Finance Officer 1 C-19 C-19 C-19
Capital Service Capacity (Times) Well Led Chief Finance Officer 1 C-19 C-19 C-19
Overall Financial Sustainability Risk Rating Well Led Chief Finance Officer 1 C-19 C-19 C-19
I&E Margin % Well Led Chief Finance Officer 1 C-19 C-19 C-19
Variance in I&E Margin % Well Led Chief Finance Officer 1 C-19 C-19 C-19
Agency Ceiling % Well Led Chief Finance Officer 1 C-19 C-19 C-19
Latest Period
Financial efficiency
Financial Controls
Financial sustainability
18/23 118/347

Activity CQC Domain Responsible Director Mar-22 Apr-22 May-22 Numerator Denominator YTD 22/23
A&E Activity Responsive Chief Operating Officer PLAN 145.7% 103.7% 109.6% 7666 6994 106.7%
Same Day Emergency Care (SDEC) Responsive Chief Operating Officer PLAN 167.9% 93.8% 120.4% 442 367 106.5%
Emergency Ambulatory Pathways - Follow Up Attendances Responsive Chief Operating Officer PLAN 302.2% 172.0% 182.5% 219 120 177.3%
Non Elective Activity - Adult Acute Responsive Chief Operating Officer PLAN 149.1% 110.4% 131.7% 2466 1873 121.0%
Non Elective Activity - Paediatric Acute Responsive Chief Operating Officer PLAN 148.2% 117.6% 110.9% 387 349 114.2%
Maternity Activity (Deliveries) Responsive Chief Operating Officer PLAN 94.8% 88.5% 103.9% 265 255 96.1%
Maternity Activity (Non Deliveries) Responsive Chief Operating Officer PLAN 153.7% 89.9% 52.7% 39 74 71.9%
Total Non Elective Activity (Exc A&E) 150.6% 109.0% 125.7% 11484 10032 117.3%
Elective Activity - IP Responsive Chief Operating Officer 104% 2019/20 Outturn
118.1% 97.8% 90.5% 305 337 93.8%
Elective Activity - DC Responsive Chief Operating Officer 104% 2019/20 Outturn
125.3% 87.6% 102.5% 2772 2704 95.2%
Elective Activity - Total 124.6% 88.6% 101.2% 3077 3041 95.1%
Outpatient Activity - New OP F2F & Virtual (excl AHP & AEC) Responsive Chief Operating Officer 104% 2019/20 Outturn
155.2% 107.3% 119.0% 7483 6290 113.2%
Outpatient Activity - New OPP (excl AHP & AEC) Responsive Chief Operating Officer 104% 2019/20 Outturn
149.1% 74.7% 88.6% 1352 1526 81.7%
Outpatient Activity - Follow Up OP F2F & Virtual (excl AHP, incl AEC) Responsive Chief Operating Officer 85% 2019/20 Outturn
133.1% 98.0% 111.0% 13919 12535 104.63%
Outpatient Activity - Follow Up OPP (excl AHP, incl AEC) Responsive Chief Operating Officer 85% 2019/20 Outturn
122.9% 76.3% 95.3% 3337 3501 85.55%
Outpatient Activity - AHP Responsive Chief Operating Officer PLAN 90.0% 66.8% 81.1% 7289 8984 74.04%
Outpatient Activity - Total 124.4% 87.6% 101.7% 33380 32836 96.6%
Outpatient Activity - New Virtual Responsive Chief Operating Officer Virtual vs Total 23.9% 26.9% 25.0% 1868 7483 25.87%
Outpatient Activity - Follow Up Virtual Responsive Chief Operating Officer Virtual vs Total 29.5% 28.2% 27.6% 3839 13919 27.85%
Outpatients Activity - Virtual Total 27.5% 27.7% 26.7% 5707 21402 27.2%
Diagnostic Activity - Computerised Tomography Responsive Chief Operating Officer 120% 2019/20 Outturn
239.7% 113.4% 104.2% 560 494 138.0%
Diagnostic Activity - Magnetic Resonance Imaging Responsive Chief Operating Officer 120% 2019/20 Outturn
138.5% 173.8% 194.6% 975 501 184.1%
Diagnostic Activity - Endoscopy Responsive Chief Operating Officer 120% 2019/20 Outturn
145.2% 128.9% 124.4% 709 571 126.4%
Diagnostics Activity - Total 159.4% 139.0% 137.1% 2361 1722 138.0%
Community Service Contacts - OOH&CC Responsive Chief Operating Officer 2019/2020 Outturn
115.0% 101.3% 113.3% 45549 40197 107.3%
Community Service Inpatients - Support Services Responsive Chief Operating Officer 2019/2020 Outturn
119.3% 103.7% 110.9% 10122 9126 107.4%
Community Service Contacts - Family Health Responsive Chief Operating Officer 2019/2020 Outturn
144.8% 150.8% 160.9% 29169 18129 156.1%
Community Service Contacts - Support Services Responsive Chief Operating Officer 2019/2020 Outturn
184.1% 182.3% 184.0% 5428 2950 183.2%
Community Service Contacts - Elective Responsive Chief Operating Officer 2019/2020 Outturn
2800.0% 957.9% 1872.7% 206 11 1293.3%
Community Service Contacts - Emergency Responsive Chief Operating Officer 2019/2020 Outturn
905.9% 513.0% 309.0% 309 0 411.0%
Community Service Contacts - Total 127.6% 117.2% 128.7% 90783 70413 123.0%
Latest Period
Urgent Care
19/23 119/347

Access CQC Domain Responsible Director Standard Mar-22 Apr-22 May-22 Numerator Denominator YTD 22/23
A&E - Ambulance handover within 15 minutes Responsive Chief Operating Officer 65% 17.6% 16.5% 22.5% 395 1759 19.6%
A&E - Ambulance handover within 30 minutes Responsive Chief Operating Officer 95% 73.9% 68.9% 75.7% 1331 1759 72.4%
A&E - Ambulance handover over 60 minutes Responsive Chief Operating Officer 0.0% 9.5% 10.7% 6.8% 120 1759 8.7%
A&E - Time to Initial Assessment Responsive Chief Operating Officer - 32 28 27 27 0 275
A&E - Time to treatment (median) Responsive Chief Operating Officer - 81 80 80 80 0 80
A&E - Mean Time in Department for non-admitted patients Responsive Chief Operating Officer - 176 175 174 174 0 175
A&E - Total time in A&E (median) Responsive Chief Operating Officer - 200 197 196 196 0 197
A&E - Percentage of patients spending more than 12 hours in A&E Responsive Chief Operating Officer - 2.7% 2.8% 1.8% 142 7691 2.3%
A&E - Left department before being seen for treatment Responsive Chief Operating Officer - 4.9% 4.6% 5.2% 400 7691 4.9%
A&E - Unplanned Re-attendance with 7 days rate Responsive Chief Operating Officer - 3.4% 3.5% 4.3% 320 7456 3.9%
A&E Quality Indicator - 12 Hour Trolley Waits Responsive Chief Operating Officer 0 0 0 0 0 0 0
A&E - % of admitted patients who are admitted within 4 hours Responsive Chief Operating Officer 90% 37.4% 34.2% 36.4% 703 1930 35.3%
Cancer 62-Day National Screening Programme Responsive Chief Operating Officer 90% 78.6% 50.0% 5 9 50.0%
Cancer 31-Day Surgery, subsequent treatments Responsive Chief Operating Officer 94% 80.0% 75.0% 6 8 75.0%
Cancer 31-Day Drugs, subsequent treatments Responsive Chief Operating Officer 98% 100.0% 100.0% 1 1 100.0%
Cancer 31-Day Diag to treat, all new cancers Responsive Chief Operating Officer 96% 88.1% 90.3% 102 113 90.3%
Cancer 2WW all cancers, Urgent GP Referral Responsive Chief Operating Officer 93% 92.2% 90.0% 1101 1223 90.0%
Cancer 2WW Symptomatic Breast Responsive Chief Operating Officer 93% 93.6% 93.9% 62 66 93.9%
Cancelled Operations on day of Surgery Responsive Chief Operating Officer 0.8% 0.0% 0.0% 0.0% 0 95387 0.00%
Over 28 Day readmission following short notice cancelled operation Effective Chief Operating Officer 0 0 0 0 0 0 0
Outpatient - Short Notice Cancelled Clinics Effective Chief Operating Officer 2% 0.0% 0.7% 0.4% 69 16778 0.5%
Outpatient Hospital Reschedules Effective Chief Operating Officer 6% 6.5% 6.1% 5.1% 1191 23404 5.6%
Stroke Indicator 80% patients = 90% stroke ward Caring Chief Operating Officer 80% 36.4% 35.5% 52.2% 12 23 42.6%
Stroke Admissions - Admitted to stroke ward within 4 hours of presentation Caring Chief Operating Officer 65% 0.0% 0.0% 0.0% 0 20 0.0%
Stroke Admissions - CT Scan within 24 hours Caring Chief Operating Officer 80% 100.0% 96.6% 100.0% 20 20 98.0%
iSPA call response rate within one minute Effective Chief Operating Officer 80% 89.7% 92.7% 90.4% 9473 10477 91.5%
iSPA call abandoned rate Effective Chief Operating Officer 5% 1.4% 1.7% 2.5% 273 10800 2.1%
Main call centre response rate within one minute Effective Chief Operating Officer 95% 67.1% 70.1% 78.5% 12044 15350 73.8%
Urgent Response > 1st Assessment completed on same day (facilitated discharge & other) Responsive Chief Operating Officer 80% 89.3% 88.5% 90.2% 2165 2401 89.4%
Urgent Response > 1st Assessment completed within 2 hours (admission prevention) Responsive Chief Operating Officer 70% 67.5% 68.9% 69.4% 906 1306 69.1%
Trust Admissions - % recorded within 2 hours Effective Chief Operating Officer 95% 93.8% 93.1% 93.2% 5939 6373 93.2%
Trust Discharges - % recorded within 2 hours Effective Chief Operating Officer 95% 76.3% 76.4% 78.2% 2189 2799 77.3%
Trust Transfers - % recorded within 2 hours Effective Chief Operating Officer 95% 86.9% 84.4% 83.7% 1564 1868 84.1%
Latest Period
A&E Quality Indicators
Cancer
Cancelled Operations
Responsiveness
20/23 120/347

Local Performance Targets and Measures CQC Domain Responsible Director Standard Mar-22 Apr-22 May-22 Numerator Denominator YTD 22/23
Emergency Ambulatory Care - % of total adult emergencies (Ambulatory or 0 LOS) Responsive Chief Operating Officer 35% 38.7% 37.8% 41.2% 794 1925 39.6%
ALoS - Adult Emergency Inpatients Effective Chief Operating Officer 6.0 6.3 7.0 7.4 7594 1031 7.2
ALoS – Elective Inpatients Effective Chief Operating Officer 2.5 2.1 2.1 2.7 753 279 2.4
ALoS – D2A Pathway 2 Effective Chief Operating Officer >28 days 26 29 27 41 1125 0
Elective - Theatre Productivity Effective Chief Operating Officer 75% 85.8% 88.6% 90.1% 79075 87790 89.4%
Elective - Theatre utilisation Effective Chief Operating Officer 85% 86.0% 88.2% 89.1% 78214 87790 88.7%
Elective - Daycase rate Effective Chief Operating Officer 85% 89.9% 81.9% 87.4% 263 301 84.8%
BPT - Fracture Neck of Femur Effective Chief Operating Officer 75% 63.9% 67.7% 21 31 67.7%
BPT - Laparoscopic Cholecystectomies Effective Chief Operating Officer 60% 52.4% 33.3% 64.3% 9 14 52.2%
Occupancy Acute Wards Only Effective Chief Operating Officer 90% 92.2% 96.6% 94.6% 9960 10525 95.6%
Outpatient - DNA rate (consultant led) - First Effective Chief Operating Officer 3.35% 6.8% 6.8% 6.2% 406 6522 6.5%
Outpatient - DNA rate (consultant led) - Follow-Up Effective Chief Operating Officer 6% 7.5% 7.5% 7.8% 880 11346 7.6%
Outpatient - % OPD Slot Utilisation (All slot types) Effective Chief Operating Officer 95% 78.9% 78.1% 80.4% 15725 19558 79.4%
Outpatient - % of patients waiting over 6 weeks without a date Effective Chief Operating Officer 30% 66.4% 74.4% 69.9% 2692 3853 72.1%
Outpatient - % of patients waiting longer than 16 weeks over their due appointment date Effective Chief Operating Officer 9% 47.2% 48.0% 47.7% 6859 14388 47.8%
Outpatient - Advance Booking (new patients only - excluding patients seen within 3 weeks) Responsive Chief Operating Officer 80% 64.0% 69.4% 67.4% 2058 3054 68.3%
Maternity - Smoking at Delivery Effective Chief Nursing Officer 8% 3.7% 4.5% 2.8% 8 281 3.6%
Maternity - % of women who have seen a midwife by 12 weeks and 6 days of pregnancy Effective Chief Operating Officer 90% 90.0% 88.9% 82.8% 198 239 85.9%
Maternity - Elective Caesarean Section rate Effective Chief Nursing Officer - 15.0% 15.6% 20.4% 54 265 18.1%
Maternity -Emergency Caesarean Section rate Effective Chief Nursing Officer - 19.3% 20.8% 20.8% 55 265 20.8%
Increase the number of women birthing in a Midwifery Led Unit setting Effective Chief Nursing Officer - 26 25 29 29 0 54
Maternity - Vaginal Birth Rate Effective Chief Nursing Officer - 54.7% 55.7% 49.6% 132 266 52.4%
Community Family Services - Family Nurse Partnerships - Activity during pregnancy achieving plan Caring Chief Nursing Officer 70% 72.2% 82.6% 77.2% 146 189 79.9%
Health Visitor - Birth to first visit within 14 days - Latest Quarter - Warwickshire (Q4) Safe Chief Nursing Officer 90% 678 1372 52.7%
Health Visitor - Birth to first visit within 14 days - Latest Quarter - Coventry (Q4) Safe Chief Nursing Officer 90% 761 992 79.9%
Health Visitor - Birth to first visit within 14 days - Latest Quarter - Solihull (Q4) Safe Chief Nursing Officer 90% 443 471 72.9%
School Nursing - National Child Measurement Program (Reception aged pupils) Responsive Chief Operating Officer 90% 43.6% 53.1% 69.0% 2898 4203 69.0%
School Nursing - National Child Measurement Program (Year 6) Responsive Chief Operating Officer 90% 46.4% 55.3% 71.5% 3227 4513 71.5%
Latest Period
Maternity
Out of Hospitals (OOH)
Inpatients
Outpatients
21/23 121/347

Workforce Measures CQC Domain Responsible Director Standard Mar-22 Apr-22 May-22 Numerator Denominator YTD 22/23
Midwife to birth ratio Well Led Director of Nursing 1:27 1:29 1:28 1:27 1:27 1:27
Overall Sickness Well Led Chief HR Officer 3.8% 6.0% 6.1% 7807 128911 6.1%
Staff Turnover Rate Well Led Chief HR Officer 10% 2.1% 1.6% 1.1% 56 5056 1.3%
Temporary Staffing Rate Well Led Director of HR 0% TBC TBC TBC TBC TBC TBC
Appraisals - Latest Quarter (Q4) Well Led Chief HR Officer 85% 3730 4662 72.6%
Qualified Nursing Vacancies - percentage of unfilled posts against budget Well Led Chief HR Officer 8% 16.3% 16.7% 16.9% 276 1634 16.8%
Clinical Outcomes CQC Domain Responsible Director Standard Mar-22 Apr-22 May-22 Numerator Denominator YTD 22/23
HSMR - Rolling 12 months Feb 21 - Jan 22 Effective Chief Medical Officer 100 104.8 0 104.8
Mortality RAMI (2019) - Rolling 12 months Mar 21 - Feb 22 Effective Chief Medical Officer 100 93.3 0 93.3
Mortality SHMI - Rolling 12 months Nov 20 - Oct 21 Effective Chief Medical Officer 89-112 97.6 0 97.6
Avoidable Deaths - Rolling 12 months YTD: April 2021 (July 21 MSC) Safe Chief Medical Officer 0 0 0 0
Serious Incidents Safe Chief Nursing Officer - 5 2 2 2 0
Never Events Safe Chief Nursing Officer - 0 1 0 0 0
Sepsis screening - A&E (% screened) - Latest Quarter (Q3) Caring Chief Medical Officer 90% 50 50 100.0%
Sepsis screening - Inpatients (% screened) - Latest Quarter (Q3) Caring Chief Medical Officer 90% 50 50 100.0%
MRSA Bacteraemia Safe Chief Nursing Officer 0 0 0 0 0 0 0
MSSA Bacteraemia Safe Director of Nursing 0 2 4 3 3 0 7
BSI Bacteraemia bloodstream infection Safe Director of Nursing 0 8 4 4 4 0 8
C Diff Hospital Acquired, Avoidable (Target for Full Year) Safe Chief Nursing Officer 5 3 0 0
Hand Hygiene Safe Chief Nursing Officer 80% 98.8% 99.1% 99.0% 858 867 99.0%
Combined MRSA Screening Safe Chief Nursing Officer 95% 95.0% 95.1% 95.0% 1588 1671 95.0%
Maternity - Breast Feeding Initiation Rate (Warwick Hospital) Effective Chief Nursing Officer 81% 89.8% 88.8% 87.1% 230 264 87.9%
Maternity - Breast Feeding at 6 - 8 weeks (Community Midwives & Health Visitors) - Latest Quarter-Warwickshire Effective Chief Nursing Officer 46% 462 1454 39.9%
Maternity - Breast Feeding at 6 - 8 weeks (Community Midwives & Health Visitors) - Latest Quarter-Coventry (Q3) Effective Chief Nursing Officer 46% 466 943 50.7%
Maternity - Breast Feeding at 6 - 8 weeks (Community Midwives & Health Visitors) - Latest Quarter-Solihull (Q3) Effective Chief Nursing Officer 46% 288 489 46.7%
Maternity - Continuity of Care Effective Chief Nursing Officer 51% 42.9% 34.8% 26.6% 77 290
Latest Period
Latest Period
Quality - reduce avoidable death rates
Sepsis
Reduce Infection Rates
Maternity
Workforce
22/23 122/347

Patient Experience CQC Domain Responsible Director Standard Mar-22 Apr-22 May-22 Numerator Denominator YTD 22/23
Friends and Family Test Score: A&E% Recommended/Experience by Patients Caring Chief Nursing Officer >96% 75.6% 71.3% 77.7% 195 251 75.6%
Friends and Family Test: Response rate (A&E) Caring Chief Nursing Officer >12.8% 1.2% 3.3% 6.1% 251 4136 4.8%
Friends and Family Test Score: Acute % Recommended/Experience by Patients Caring Chief Nursing Officer >96% 93.4% 94.4% 94.7% 3906 4123 94.5%
Friends and Family Test: Response rate (Acute inpatients) Caring Chief Nursing Officer >25% 13.4% 28.5% 7.5% 135 1794 17.8%
Friends and Family Test Score: Maternity % Recommended/Experience by Patients Caring Chief Nursing Officer >96% 96.9% 98.1% 88.9% 24 27 95.1%
Friends and Family Test: Response rate (Maternity) Caring Chief Nursing Officer >23.4% 24.7% 22.4% 9.7% 27 278 15.7%
Friends and Family Test Score: Community % Recommended/Experience by Patients Caring Chief Nursing Officer >96% 95.4% 97.0% 94.9% 206 217 96.0%
Written complaints rate Caring Director of Nursing 0% - - - - - -
Catering Surveys (Patients rating food as Good or Excellent) Caring Chief Nursing Officer 90% 100.0% 100.0% 100.0% 209 209 100.0%
Mixed Sex Accommodation Breaches - Confirmed Caring Chief Nursing Officer 0 0 1 0 0 0 1
Patient ward moves emergency admissions (acute) Caring Chief Operating Officer 2% 0.9% 1.1% 1.1% 28 2633 1.1%
Reducing Harm CQC Domain Responsible Director Standard Mar-22 Apr-22 May-22 Numerator Denominator YTD 22/23
Falls with harm (per 1000 bed days) Safe Director of Nursing 1.14 1.34 0.62 1.09 14 12899 0.90
Medication Error Incidences Safe Chief Nursing Officer <6% 7.1% 5.3% 3.8% 5 132 4.5%
Pressure sores (Confirmed avoidable Grade 3,4) Caring Chief Nursing Officer 0 1 0 0 0 0 0
Dementia - Find : Patients 75 or over Admitted as an Emergency Caring Chief Nursing Officer 90% C-19 C-19 C-19 C-19 0 C-19
Dementia - Assess/Investigate : Patients 75 or over Admitted as an Emergency Caring Chief Nursing Officer 90% C-19 C-19 C-19 C-19 0 C-19
Dementia - Refer : Patients 75 or over Admitted as an Emergency Caring Chief Nursing Officer 90% C-19 C-19 C-19 C-19 0 C-19
VTE Risk Assessments Safe Chief Nursing Officer 95% 96.3% 97.9% 96.9% 1011 1043 97.4%
WHO Checklist Safe Chief Nursing Officer 100% 98.5% 98.1% 0.0% 0 0 98.1%
Patient Safety Alerts not completed by deadline Safe Chief Nursing Officer 0 0 0 0 0 0 0
Nurse Care /Community Care Indicators Caring Chief Nursing Officer 95% 95.2% 92.9% 90.2% 15017 16647 91.8%
Hygiene Cleaning Standards: Acute (Very High Risk) Safe Chief Nursing Officer 95% 98.3% 98.3% 98.2% 76 77 98.2%
Cleaning Standards: Community (Very High Risk) Safe Chief Nursing Officer 95% 98.3% 98.4% 98.2% 27 28 98.3%
Latest Period
Latest Period
Safety
Reduce the proportion of non value added time when patients are in hospital
Experience
23/23 123/347

Report SummaryReport to Board of Directors Date of Meeting 6 July 2022
Report Title Monthly Safe Staffing Report Agenda Item 8.3
Executive/Non-Executive Lead
Ellie Ward, Deputy Chief Nursing Officer
Report Author(s)
Rebecca Moore, Head of Nursing
Report Previously Discussed at N/A
Purpose of the Report For ApprovalFor Discussion
This report is an update to the Board of Directors regarding safe staffing in relation to Nursing, Maternity and Allied Health Professionals. For Information
Recommendations and Action Required The Board of Directors is asked to receive and note this report.
Impact (is there any impact arising from the report on the following?) Quality EqualityFinance ResearchPerformance Compliance Workforce Legal
Applicable Quality Improvement Priorities Elective Hub Health InequalitiesElectronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety Compassionate Effectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk RegisterAre any existing risks on the BAF/Risk Register affected? YesIdentify the BAF/Risk Register risk ID and description – explain how the risk has been affected – reduced or increased as a consequence of the evidence within the report – Risk ID 1639 Maternity services: Midwife vacancies resulting in lack of capacity to adequately support studentsRisk ID 1660 CERU: Trained nurse vacancy and high sickness rate Risk ID 1692 UCR South Place: Vacancies across all bands nursing and therapies
1/23 124/347

Risk ID 1738 HomeFirst South Nursing and Therapy: Reduced and revised staffing levels resulting in vacancyRisk ID 1739 Complex Discharge Team: Vacancy and maternity leave leading to delay in patient discharge and impact on organisational capacity and flowRisk ID 1737 Campion Ward: Increased bed base to support extra capacity leading to unfunded and unfilled shifts with potential for patient harmRisk ID 1684 County wide routine Therapy: Therapy waiting list - Community therapy were now required to support a range of urgent and routine pathways and services, increased waiting times for routine therapy, patients could be delayed in being seen promptly impacting on their recovery and potentially leading to a deterioration in clinical presentation.Risk ID 1598 CCNT band 6 recruitment: Vacancy in the band 6 line leading to gaps in senior nurse cover and increase in temporary workforce costsRisk ID 1664 Adult Occupational Therapy hand therapy: Lack of Band 5 Occupational Therapy staff due to inability to recruit to these vacancies resulting in patients not receiving treatment in a timely manner which could lead to patient harm and to remaining staff suffering from stress and sickness as a result of covering vacancies on top of existing caseloads
Do you recommend a new entry to the BAF and/or Risk Register is made as a result of this report? If yes, describe the new risk.
No
2/23 125/347

South Warwickshire NHS Foundation Trust
Report to Board of Directors – 6 July 2022
Monthly Safe Staffing Report
Executive Opinion
This report is an update to the Board of Directors regarding safe staffing in relation to Nursing, Maternity and Allied Health Professionals (AHP). Assurance remains that the organisation has clear oversight of these different disciplines and specialities, and this is monitored on a regular basis at Divisional and Service level with mitigating actions being taken when gaps exist. Ellie WardDeputy Chief Nursing Officer
Executive Summary
This report provides information related to the safe staffing across Emergency and Elective inpatient, Out of Hospital Care Collaborative (OOHCC), Family Health (Including Health Visiting and Childrens nursing), Maternity and Allied Health Professional (AHP) services. It provides information about gaps against planned rosters, incidents, sickness, vacancy, and parental leave and mitigating actions being taken to address any risks. It provides a summary of recruitment activity for these groups.
Recommendations
• Continue senior Corporate Nursing monitoring of Nurse Staffing (Corporate Nurse of the day Rota) as an assurance, supporting anticipated challenges and keeping oversight of risks to quality, safety and wellbeing and the mitigations in place.
• Human Resources to ensure managers are supported to manage sickness and absence in all areas to facilitate return to work in a timely and supportive manner.
• Continue recruitment activity including the restart of face-to-face recruitment sessions, prioritising those teams with the highest vacancy risk.
• Continue the recruitment, arrival and induction of international recruits including good pastoral care.
• Operational and clinical managers to ensure they work to rostering principles and Key Performance Indicators (KPIs) to staff their area safely and effectively with available resources. Roster reviews to continue with Corporate, Financial and Operational engagement.
• Divisions to continue to monitor Staffing Risks on their registers, review mitigation measures and update regularly.
• Continue to promote career development for our workforce, supporting opportunities for talent management as part of a retention strategy.
• Continue Clinical Retention Group work, supporting local retention plans that reflect our Values.
• Repeat inpatient Acuity audits in July 2022 using Safer Nursing Care Tool with an aspiration to fully automate this process by 2024.
3/23 126/347

1.0 Introduction
This report is an update to the Board of Directors regarding safe staffing in relation to Nurse and AHP workforce in the Emergency, Elective and Support Services Divisions, Maternity Service, Family Health Division, and the Out of Hospital Care Collaborative (OOHCC) based on the whole month data for May 2022.
2.0 Inpatient Ward Nurse Staffing
Graph 1 indicates the overall gap in relation to planned nurse staffing levels versus actual nurse staffing levels in inpatient areas for May 2022.
Graph 1
As an average figure, this should be viewed in context. The inpatient staffing levels during the day in May 2022 demonstrated 2% above planned for registered staff and 8% gap for unregistered staff, an improvement on previous months. The night staffing was 16% above planned for registered staff and 5% above planned for unregistered in May 2022.
Whilst the cover for registered staff remains stable and within usual parameters, in some instances we are utilising above planned registered staffing to compensate for the care support worker vacancy. The gap in unregistered care support workers remains a cause for concern. Senior staff are sighted on this and there is focus on the recruitment and retention of these staff across workforce, corporate and clinical teams. In May 2022 there were 645 unfilled care support worker shifts on the Acute Hospital site.
-3%
-30%
-20%
-10%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Sum of % actual Sum of % gap
All staff during both shifts staff levels %May 22
4/23 127/347

Graph 2
Further breakdown in month by Ward area is provided in Graph 3 with associated narrative for wards above or below planned staffing levels.
Graph 3 and 3a indicate areas shown in red, where there is a difference in percentage of either being staffed above or under the planned template for May 2022. Staffing above the expected template is apparent in those wards that have needed to provide one to one care for patients with high risk of falls or self-harm. This is done in conjunction with a patient risk assessment and is monitored by the Matrons and General Managers (GMs).
Graph 3
-40%-30%-20%-10%
0%10%20%30%40%50%60%70%80%90%
100%
Alls
opp
AMU
/Oke
n
Avon
Beau
cham
p
Beau
mon
t
Cam
pion
Card
iolo
gy
Cast
le
Chad
wic
k
Char
leco
te
FAA
Fairf
ax
Farr
ies
Feld
on
Gre
ville ITU
Mac
Gre
gor
Mar
y
Mat
erni
ty
Nic
hola
s
Nic
ol
SCBU
Surg
ical
Uni
t
Thom
asSum of % actual Sum of % gap
All staff during both shifts Staff levels % by all Wards May 2022
5/23 128/347

Graph 3a
Squire Ward staffing template allows for opening up to 21 beds; however, over this period there were times when there were fewer patients and therefore rostered staff were redeployed to other areas. As these shifts are not optional, this will show as a gap and influence the overall figure reported.
The staffing demand has continued in May 2022 due to the continued use of extra capacity. The use of our assessment areas overnight (Frailty Assessment and Acute Decisions Unit /Surgical Assessment Unit) also increased shifts required.
The increase in expected staffing Charlecote Ward, Frailty Wards, Beauchamp Ward and Macgregor Ward can be attributed to patients requiring 1:1 care or increased acuity levels.
Avon Ward appear under planned levels, however they are now trialling using those hours to have a coordinator on the late shift to improve flow and support timely and safe discharges, admissions and transfers.
Maternity Services saw a 6.9% gap in May 2022 which relates to parental and sickness leave in both the registered and unregistered staff leaving unfilled duties. Further detail is in Section 7.0.
Macgregor Ward continues to need additional resources to provide enhanced care to those children and young people in crisis on occasion. Staffing above a template would always be done in agreement with the GM and in discussion with the Matron or Head of Nursing.
The Corporate Nursing Team continue to work closely with the wards, Operational Managers and Site Capacity team to manage staffing safely in accordance with the agreed Procedure for Nurse Staffing Escalation. This includes the Corporate Nurse of the Day for Staffing rota to provide senior nursing oversight and support to the Site Capacity Team and Wards.
0%
20%
40%
60%
80%
100%
Short Stay Squire
Sum of % actual Sum of % gap
All staff during both shifts Staff Levels % Extra Capacity May 22
6/23 129/347

The Clinical Lead for Provisional Nursing and AHP Staffing is assisting on a daily basis particularly in areas with high levels of temporary staff or extra capacity. The Chief Nursing Officer (CNO) remains confident in the ongoing scrutiny and responsiveness to maintain safe staffing.
3.0 Staffing Related Incidents
Graph 4 shows the spread of the incidents by area for May 2022.
In May 2022 there were 45 incidents reported in regards to inadequate staffing levels and or skill mix, this is an decrease on previous months – April 2022 being 52 and March 2022 being high at 83. This includes incidents relating to non-clinical and medical staff.
Maternity services including Special Care Baby Unit (SCBU), Bluebell, Swan, Labour and antenatal assessment unit combined accounted for 53% of all staffing incidents (24). This reflects the high acuity and gaps due to parental leave and sickness. This is also indicative of a positive reporting culture. Further detail of mitigations are in the Maternity Services report in section 7.0.
All of the incidents were categorised as no harm however, it is accepted that some are likely to have impacted on both patient and staff experience. Examples cited included delays in administering care.
The consistant theme was that of unplanned sickness absence against high patient attendances plus the complexity of those patients and challenges in filling some bank and agency shifts.
Graph 4
13
4 43 3 3
2 2 2 21 1 1 1 1 1 1
0
2
4
6
8
10
12
14
Labour W
ard
Cance
r - Ayle
sford Unit
Swan
Ward
Bluebell Birt
h Centre
Beaumont W
ard
Antenatal A
ssessm
ent Unit
Community Child
ren's Nursi
ng
Macgre
gor W
ard
Campion W
ard -
(EBH)
Antenatal C
linic
Intensive Care
Unit
Accident &
Emergency
Allsopp W
ard
Specia
l Care
Baby U
nit (SC
BU)
Greville W
ard
Beauch
amp W
ard
Day Su
rgery
Unit
(blank)
Staffing Incidents by Ward/Site (May 2022)
7/23 130/347

Graph 5
Graph 5 describes the category of incident, the most common reporting being amongst Nursing and medical staff. There were 12 incidents reported of inpatient Nurse and Healthcare Assistant (HCA) staffing below the establishment or acuity level. There were 11 incidents reported for medical staff shortage which is a significant increase on the normal levels of reporting. This has primarily been an increase in sickness in this staff group and difficulties with covering the gaps.
Incidents relating to safe staffing, themes and risks are reviewed by the Head of Nursing and Matrons in Maternity and Nursing and support and feedback is offered to staff as appropriate.
11
5
3
4
1 1
2
12
6
0
2
4
6
8
10
12
14
Inadequate staffing levels/skills mix
(blank)
Medical staff (Doctor) shortage
Delayed or cancelled time critical maternal/neonatal activity
Delay in 1.1 care in established labour in any setting
(blank)
Delay in performing both maternal/neonatal observations
Delay in contact in maternity assessment suite for > 30 minutes
Delay of 2 hours between admission/induction of labour/beginning processCommunity Team staff shortage
Inpatient Nurse/HCA staffing below establishment/acuity level
Staffing Incidents by Category & Sub-category (May 2022)
Category
8/23 131/347

4.0 Breaches in 1:8 Registered Nurse to Patient Staffing Ratio
Once validated with the Matrons and the rosters, data which compares unplanned breaches in the 1:8 registered nurse to patient ratio, indicated a total of 49 shifts in May 2022. This is a significant decrease on previous months (64 in April 2022 and 82 in March 2022). This drop is as a result of the reduction in registered nurse vacancy.
Where most breaches have occurred, it is often by a narrow margin i.e., 1:9 or 1:10 and on analysis there are usually other staff present on a ward that mitigate any risk. Matrons have advised that some of these breaches were planned staffing levels of 1:9 and deemed to be safe by the Ward Managers but are still counted for transparency.
Greville Ward had a number of days where they closed half way through the day at the weekends and had rostered appropriately for low patient numbers or staff were then redeployed elsewhere for the remainder of the shift.
Allsopp Ward had band 4 Associate Practitioners and Registered Nursing Degree Apprentices on those shifts that breached to support the registered nurses at a rate of 1:9.5 which mitigated the risk. The Ward manager is a physiotherapist which will not be reflected in the skill mix when she completes a clinical shift due to not being a registered nurse, although provides excellent clinical skills and leadership to a shift.
Graphs 6a and 6b show the levels of registered nurses during the day and the night continues to improve. The key recruitment and retention focus is on unregistered workforce.
Graph 6a
Graph6b
0%
20%
40%
60%
80%
100%
120%
31/0
1/19
28/0
2/19
31/0
3/19
30/0
4/19
31/0
5/19
30/0
6/19
31/0
7/19
31/0
8/19
30/0
9/19
31/1
0/19
30/1
1/19
31/1
2/19
31/0
1/20
29/0
2/20
31/0
3/20
30/0
4/20
31/0
5/20
30/0
6/20
31/0
7/20
31/0
8/20
30/0
9/20
31/1
0/20
30/1
1/20
31/1
2/20
31/0
1/21
28/0
2/21
31/0
3/21
30/0
4/21
31/0
5/21
30/0
6/21
31/0
7/21
31/0
8/21
30/0
9/21
31/1
0/21
30/1
1/21
31/1
2/21
31/0
1/22
28/0
2/22
31/0
3/22
30/0
4/22
31/0
5/22
Sum of Actual Registered day
0%20%40%60%80%
100%120%140%
31/0
1/19
28/0
2/19
31/0
3/19
30/0
4/19
31/0
5/19
30/0
6/19
31/0
7/19
31/0
8/19
30/0
9/19
31/1
0/19
30/1
1/19
31/1
2/19
31/0
1/20
29/0
2/20
31/0
3/20
30/0
4/20
31/0
5/20
30/0
6/20
31/0
7/20
31/0
8/20
30/0
9/20
31/1
0/20
30/1
1/20
31/1
2/20
31/0
1/21
28/0
2/21
31/0
3/21
31/0
4/21
30/0
6/21
31/0
7/21
31/0
8/21
30/0
9/21
31/1
0/21
30/1
1/21
31/1
2/21
31/0
1/22
28/0
2/22
31/0
3/22
30/0
4/22
31/0
5/22
Sum of Actual Registered night
9/23 132/347
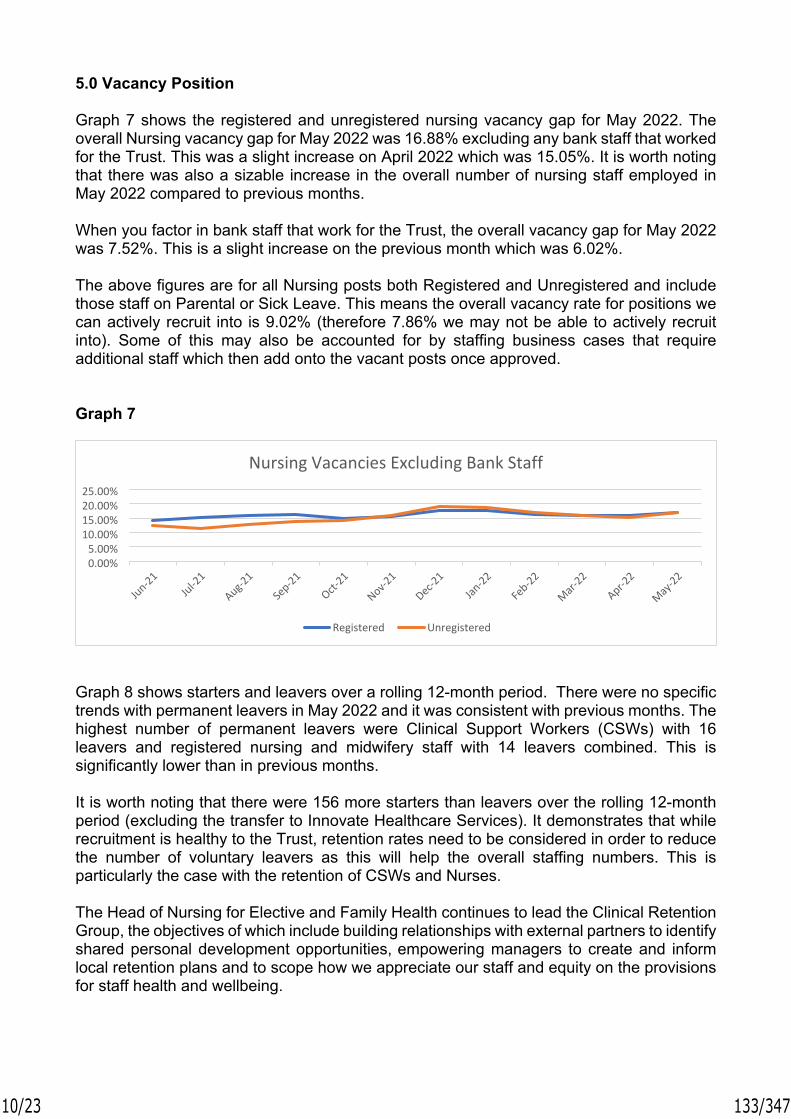
5.0 Vacancy Position
Graph 7 shows the registered and unregistered nursing vacancy gap for May 2022. The overall Nursing vacancy gap for May 2022 was 16.88% excluding any bank staff that worked for the Trust. This was a slight increase on April 2022 which was 15.05%. It is worth noting that there was also a sizable increase in the overall number of nursing staff employed in May 2022 compared to previous months.
When you factor in bank staff that work for the Trust, the overall vacancy gap for May 2022 was 7.52%. This is a slight increase on the previous month which was 6.02%.
The above figures are for all Nursing posts both Registered and Unregistered and include those staff on Parental or Sick Leave. This means the overall vacancy rate for positions we can actively recruit into is 9.02% (therefore 7.86% we may not be able to actively recruit into). Some of this may also be accounted for by staffing business cases that require additional staff which then add onto the vacant posts once approved.
Graph 7
Graph 8 shows starters and leavers over a rolling 12-month period. There were no specific trends with permanent leavers in May 2022 and it was consistent with previous months. The highest number of permanent leavers were Clinical Support Workers (CSWs) with 16 leavers and registered nursing and midwifery staff with 14 leavers combined. This is significantly lower than in previous months.
It is worth noting that there were 156 more starters than leavers over the rolling 12-month period (excluding the transfer to Innovate Healthcare Services). It demonstrates that while recruitment is healthy to the Trust, retention rates need to be considered in order to reduce the number of voluntary leavers as this will help the overall staffing numbers. This is particularly the case with the retention of CSWs and Nurses.
The Head of Nursing for Elective and Family Health continues to lead the Clinical Retention Group, the objectives of which include building relationships with external partners to identify shared personal development opportunities, empowering managers to create and inform local retention plans and to scope how we appreciate our staff and equity on the provisions for staff health and wellbeing.
0.00%5.00%
10.00%15.00%20.00%25.00%
Jun-21Jul-2
1
Aug-21
Sep-21
Oct-21
Nov-21
Dec-21
Jan-22
Feb-22
Mar-22
Apr-22
May-22
Registered Unregistered
Nursing Vacancies Excluding Bank Staff
10/23 133/347

Graph 8
Total Number of New Starters in May 2022
Of Which:
89 Permanent new starters in May 202238 Bank new starters in March 2022
Registered Nurses:• Acute• Community• Bank only
40 Registered Nurses in Total20 Acute5 Community14 Bank Only
Registered Other:• AHP
2 AHP’s started in total
Clinical Support Worker’s(CSWs):• Acute• Community• Bank only
38 Clinical Support Worker’s in Total20 Acute5 Community13 Bank Only
Registered Midwives: 4 Registered Midwives started
Others not included above 36 other Permanent roles including Medical, Admin, Estates etc. in Total11 other Bank roles including Medical, Admin, Estates etc. in Total
As part of the Trust’s attraction strategy for the recruitment of new staff, recruitment have started to carry out 6 face-to-face recruitment events between April 2022 and November 2022 in order to attract more applicants to CSW and Nursing roles. The first in April 2022 was very positive with many attenders, a lot of whom moved into applicants through the capture of pre-employment information, enabling interested and motivated new starters into post as quickly as possible..The proposal for the events is to promote the variety of Registered and Unregistered Nursing roles available at the Trust. There will be representation from Nursing teams to provide the
050
100150200250
Jun-21Jul-2
1
Aug-21
Sep-21
Oct-21
Nov-21
Dec-21
Jan-22
Feb-22
Mar-22
Apr-22
May-22
Starters Leavers
Permanent Starters and Leavers
11/23 134/347

practical clinical perspective on the roles and talk about what makes South Warwickshire NHS Foundation Trust (SWFT) a great place to work for.
In addition to the above Trust wide events, there are plans for individual events in specific Community locations. Recruitment will liaise with individual Locality Managers regarding these events and set up a separate schedule for these according to vacancy levels in each geographical location.
We have representation from our Learning and Development Team to promote the various training, development, and support available.
Areas at risk such as Theatre services are having a targeted recruitment campaign and retention strategies to try to reduce their vacancy gap, they have an open day for apprentices in June 2022 where they can look around theatre and meet staff and this has had a high level of positive response.
The Recruitment and Retention Lead Nurse continues to work closely with recruitment and department managers to facilitate processes and focus on recruitment hot spots.
The Trust remains an Employer of choice across the Coventry and Warwickshire region, the employment market is extremely competitive with high number of job vacancies across multiple sectors.
6.0 International Recruitment
The Trust has been carrying out International Recruitment primarily for Nursing roles but also for other staff groups including Qualified Radiographers for a number of years. There has been discussions this month with Allied Health Professionals (AHPs) and Therapy leaders to explore international recruitment for Occupational and Physiotherapists. This will continue into 2022/23 with the plan to recruit an additional 40-50 Registered Nurses throughout this financial year, working in partnership with George Eliot Hospital NHS Trust (GEH) in order to share best practice and recruit for both Trusts.
Recruitment will be primarily from India and the Philippines as these are designated as ethical recruitment locations by NHS England. There is funding from NHS England to support this.
39 International Nursing recruits have started since May 2021 with 4 recruited in May 2022. The Trust has a robust induction and support process for these candidates and will continue to offer the high standard of pastoral care and support all new starters need to settle.
We have seen some of our international nurses successful in more senior nursing roles within the wards which demonstrates how successful the programme is and the opportunities to grow and develop our workforce for the future.
12/23 135/347

7.0 Maternity Services
Vacancy Position
Vacancy WTE %
March 2022Midwives 8 7%
CSW’s 5 15%
SCBU Nurse 1.52 2 Overseas nurses not in numbers
SCBU Support staff Band 20.72
Recruited to will commence post 5th June
April 2022
Midwives 9.62 9%
CSW’s 4.9 18%
SCBU Nurse 4.8 22% - Overseas nurses included
SCBU Support Staff 0.72 14%
May 2022Midwives 7.82 6.9%
CSW’s 11.2 30%
SCBU Nurse 2 (2 overseas nurses recruited to these posts)
SCBU Support Staff 0.6 Recruited to
Safe staffing is being maintained through the use of bank staff and the redeployment of midwives to different clinical areas and use of specialist midwives if required. The Midwifery Manager on call is no longer providing clinical support during night shifts as the staffing numbers are no longer requiring this which is an improvement.
Sickness rates/Parenting Leave/Maternity
May 2022 WTE %
Sickness MW Registered 119.53
3.59 2.83%
MW Unregistered 39.47
2.71 6.8%
SCBU Registered 2.4 6.47%
SCBU Unregistered 1.8 4.54%
13/23 136/347

MW Registered 8.92 7%Parenting Leave
MW Unregistered 1.77 4.48%
SCBU Registered 2.61 13.3%
SCBU Unregistered 0 0
MW Registered 0.6 0.4%Long term sick
MW Unregistered 0.6 1.5%
SCBU registered 0.52 2.5%
SCBU Unregistered 0 0
Top 3 reasons for sickness; • Gastro 19%• Colds/Flu 14% • Anxiety 10%• Covid 8%
Our one-to-one care in labour:March 22 98.4%
April 22 98.7%
May 22 100%
Birth to Midwife Ratio: <1:26 >1:32
March 22 1:29
April 22 1:27
May 22 1:27
Recruitment and Retention Plan
Development and Workforce (DW) team are now in position with DW Lead now in post and 2 Retention and Well-being midwives also in post. They will be working with our new Band 5s and new to the Trust Midwives to support them in practice and to work alongside our newly appointed Band 3 Maternity Support Workers (MSWs). They will also be looking at innovation and transformation of our services to ensure safety and to also ensure that we are able to provide a strong team with shared vision and values.
A new Lead Matron for Inpatients is now in post and is being supported by the outgoing Matron to ensure a smooth transition period.
14/23 137/347

As of the end of May 2022 following the successful recruitment of 8 band 5 midwives the vacancy gap was only 0.96 WTE midwives. The team were then successful in the approval of a business case to increase the staffing numbers in the maternity assessment suite and swan wards night shift. This now gives them a vacancy of 7.82 WTE midwives and 11.0 maternity support workers which the team are confident they will recruit into successfully over the coming months. This will enable us to keep our women and babies safe.
Special Care Baby Unit (SCBU)
2 overseas nurses have now started in SCBU and are not currently counted in the nursing numbers. The first one started in February 2022 and is working towards completing Objective Standard Clinical Examination (OSCE) in May 2022, the second has started on 28 March 2022. The Band 3 post recruited to and to commence in post 5 June 2022.
Risk Register
The staffing risk has now been added to the Maternity Risk Register. There are now three incidents relating to SCBU, Locum Doctors and Obstetric Theatres with robust mitigations in place.
No reported harm has been related to the staffing incidents reported.
The team have put the following measures in place.
1. The sickness is being managed proactively by the Maternity Managers with the support of Human Resources and in liaison with Occupational Health.
2. Escalated to the Chief Nursing Officer for additional support who is also our Maternity Safety Champion.
3. Recruitment to SWFT bank pool from local maternity services.4. Utilisation of independent agency staff SCBU.5. Redeploying specialised midwives to cover essential clinical shifts.6. Reducing the number of management hours of Midwives in managerial positions.7. Non-essential training cancelled – Clinical Negligence Scheme for Trusts (CNST) risk
to the organisation. 8. Daily staffing meeting with the ward managers to review staffing, vacant shifts and
identification of flexibility within the rosters e.g. training, management time.9. Bank staff requested for support roles e.g. CSW, Ward Clerks and administrative staff.10.Sharing and communication of the actions being taken with the senior team to support
and address the concerns raised from the clinical area.14. Use of the Maternity Escalation Policy, suspending Bluebell Birth Centre and Homebirth Service.
Points for Celebration
The teams had a wonderful celebration on 5 May 2022 for the International Day of the Midwife.
SCBU has been awarded gold accreditation from Bliss for our baby charter. The visiting team were very impressed with what they saw and we scored 97.7%. The Team have made
15/23 138/347
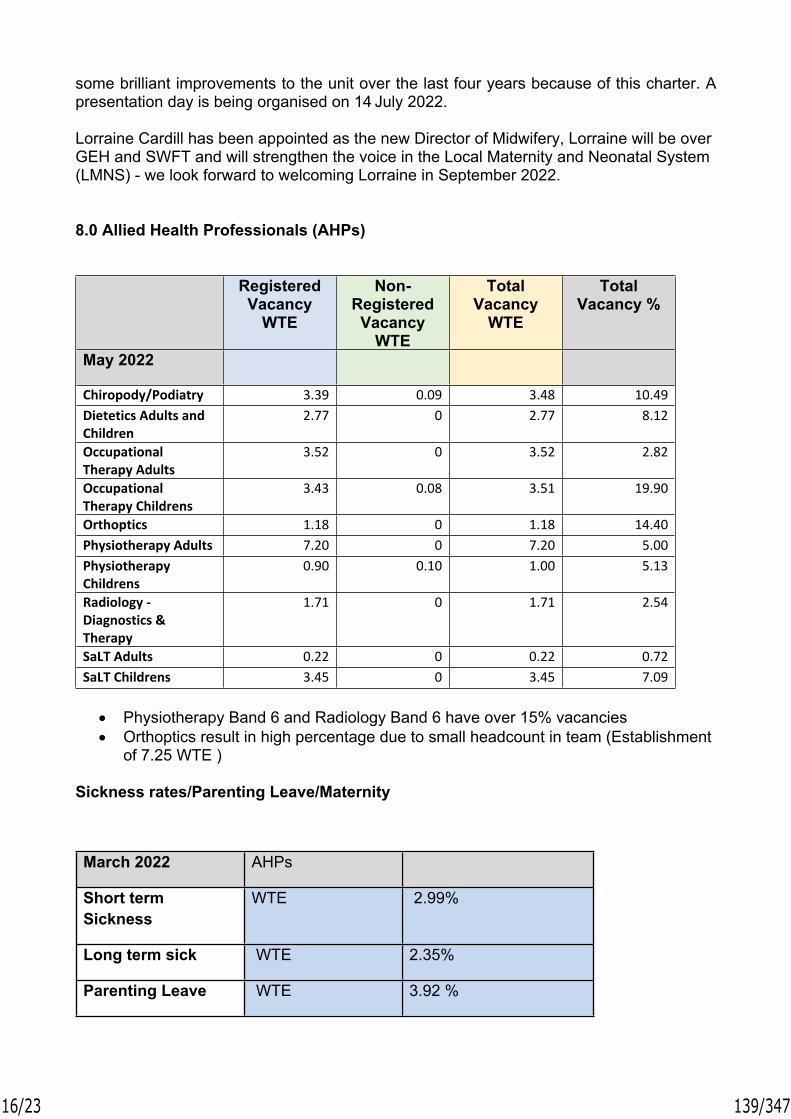
some brilliant improvements to the unit over the last four years because of this charter. A presentation day is being organised on 14 July 2022.
Lorraine Cardill has been appointed as the new Director of Midwifery, Lorraine will be over GEH and SWFT and will strengthen the voice in the Local Maternity and Neonatal System (LMNS) - we look forward to welcoming Lorraine in September 2022.
8.0 Allied Health Professionals (AHPs)
Registered Vacancy
WTE
Non-Registered Vacancy
WTE
Total Vacancy
WTE
Total Vacancy %
May 2022
Chiropody/Podiatry 3.39 0.09 3.48 10.49Dietetics Adults and Children
2.77 0 2.77 8.12
Occupational Therapy Adults
3.52 0 3.52 2.82
Occupational Therapy Childrens
3.43 0.08 3.51 19.90
Orthoptics 1.18 0 1.18 14.40Physiotherapy Adults 7.20 0 7.20 5.00Physiotherapy Childrens
0.90 0.10 1.00 5.13
Radiology - Diagnostics & Therapy
1.71 0 1.71 2.54
SaLT Adults 0.22 0 0.22 0.72SaLT Childrens 3.45 0 3.45 7.09
• Physiotherapy Band 6 and Radiology Band 6 have over 15% vacancies• Orthoptics result in high percentage due to small headcount in team (Establishment
of 7.25 WTE )
Sickness rates/Parenting Leave/Maternity
March 2022 AHPs
Short term Sickness
WTE 2.99%
Long term sick WTE 2.35%
Parenting Leave WTE 3.92 %
16/23 139/347

April 2022 AHPs
Short term Sickness
WTE 3.10%
Long term sick WTE 1.82 %
Parenting Leave WTE 4.19 %
May 2022 AHPs
Short term Sickness
WTE 1.88%
Long term sick WTE 1.49%
Parenting Leave WTE 4.44%
Recruitment and Retention Plan
• Planning on creating more consistency with our AHP adverts and recruitment processes across all the divisions- will be discussed in the AHP workforce meetings
• Improving oversite of AHP establishment and vacancy rate is being achieved through ongoing joint working with ESR, Finance and AHP workforce development lead. Further improvements to be made.
• Exploring options for international recruitment
Risk Register
Adult Occupational Therapy (OT):• Hand Therapy - Hand Therapy is a very small team of 2.16 WTE OTs. Ongoing
recruitment difficulties due to national shortage of trained Hand Therapists. Ongoing mitigations and active recruitment in place.
Good News Stories
• Funding for x2 band 7 dietetic posts has been agreed by Macmillan• New 8a Out of Hospital (OOH) therapy post has been created (due to be advertised
soon) to lead therapy services within OOH division. This is an exciting opportunity to create more AHP leadership within OOH division and ensure a progressive therapy community strategy is achieved
• Ongoing improvement noted in short term and long term sickness
9.0 Pharmacy
Vacancy Position and Recruitment
17/23 140/347

Pharmacy Grade Budget WTE
in post WTE
vacant WTE
appointed WTE
final vacancy WTE
Percentage vacancy
Pharmacists 36.12 22.12 14 6 8 22% Technicians 29.71 20.71 9 1 8 27% Assistants 18.03 13.43 4.6 1 3.6 20% Admin 3 2 1 0 1 33%Total 86.86 20.6 24%
The overall vacancy level of 24% is an improvement on last month’s figure of 36% but does continue to affect all aspects of service.
Pharmacy Staffing Risk Assessments are monitored on the local Risk Register and relate to service provision. The most significant risks identified are the provision of clinical pharmacy service to the wards and the provision of the pharmacy aseptic service (chemotherapy). There have been no reported clinical incidents directly related to this.
There will be a delay on seeing the benefits from the band 6 clinical pharmacist recruitment as has been mainly offered to pre-registration students due to come on the register and join the trust in August 2022 as our future workforce.
Pharmacy proactively book locums to fill gaps in the meantime.
10.0 OOHCC and Community Care
Vacancy position
Vacancy WTE
% Vacancy WTE
%
Month: April 2022 May 2022
North Place 14.19 8.20% 21.36 12.44%Rugby Place 17.19 13.37% 19.05 14.84%
South Place 36.45 12.07% 53.8 16.49%
The place-based teams are supporting Urgent response where they can and the staffing is reviewed daily across the division. Shifts go out to bank and agency to support gaps where possible. Sickness Rates/Parenting Leave/Maternity
The Out of Hospital Care Collaborative (OOHCC) Division have seen an increase in potential Urinary Tract Infection (UTI) sickness – advice around wellbeing, drinking plenty when on shift and agile working. Top 3 reasons for sickness:
• Anxiety/stress/depression/other psychiatric illnesses• Infectious Diseases • Genitourinary and Gynaecological disorders
18/23 141/347

March 2022 April 2022Sickness North PLACE 6.4% 8.85%
Rugby PLACE 8.95% 8.35%
South PLACE 8.9% 8.42%
Professional leads, Locality Managers, Quality Matron and General Managers work hard on supporting staff. Psychological support is also regularly accessed and HR support for Long Terms Sick (LTS) cases with alternative ways of managing and working to help support an earlier return to work.
Wellbeing and Self Care sessions are set for a rolling period open to all staff lead by SWFT Wellbeing Officer.. Roster Key Performance Indicators (KPIs) to Support Safe Staffing
Roster Key Performance Indicators (KPIs) for OOHCC continue to show small improvements following the work by the Quality Matrons and Locality Managers with Annual Leave target of below 14% with the exception of some specialist services over 20%, however these are smaller teams and so will hold a higher %. The Division continues to showcase compliance with the Working Day KPI of below 2% and successfully now achieving this within the majority of teams. Work continues with sum of Total Unavailability range of 22% displaying a significant improvement of compliance for Roster period 5 June – 2 July 2022 within teams from 27% - 35% now averaging between 20% - 26%.
Recruitment and Retention Plan
• Successfully appointed 3 District Nurse Students into Place Based Teams Alcester, Leamington North and Leamington South.
• Development post for Clinical Practitioner commenced in post.• Skill mix for Campion Ward and review of staffing skill set with a successful recruitment
of 1.0WTE Band 6 post. • Docobo Clinical Practitioner posts out to advert for Rugby and South.• Newly appointed ACP has commenced in post for North PLACE.
Risk Register
There are a number of teams and services on local and divisional risk registers these are all reviewed regularly, mitigated and downgraded when possible.
19/23 142/347

Warwickshire, Solihull and Coventry Family Health and Lifestyle
Vacancy position
Warwickshire and Solihull
Vacancy WTE
% Vacancy WTE
% Vacancy WTE
%
March 2022 April2022
May 2022 February 2022
Health Visitors Warwickshire
12.7 16%
8 10% 13.24 17%
Nursery Nurses Warwickshire
1.48 5%
0 01.37 5.3%
Health Visitors Solihull
5.3 16%
3.07 10%2.07 6.3%
School Nurses Solihull
0 0 0 0B5 1B6 2.2
15%57%
Nursery Nurses Solihull
0 0 0 01.15 14%
CoventryVacancy
WTE% Vacancy
WTE% Vacancy
WTE%
March 2022 April 2022 May 2022
Health Visitors (HV)
4.3 9% 5.4 11% 8.66 17%
Band 6 Vulnerable Families Health Visitor
1 100% 1 100% 1 100%
Band 5 Staff Nurse School Nurse
0.6 11% 0.6 11% 0.49 8%
Band 6 School nurses, brand new posts created.
2 New post
2 1.32 18.75%
Band 7 Family Nurse
0.9 18% 0.81 15%
20/23 143/347

Sickness /Other Leave
Top 3 reasons for sickness:
• Covid related illness/infectious diseases • Anxiety /stress• Coughs, colds, flu
May 2022 %Sickness Total
WarwickshireSolihullCoventry
4.71%2.82%6.39%
Parenting LeaveWarwickshireSolihullCoventry
000
Long term sickWarwickshireSolihullCoventry
WTE3.02.04.0
Recruitment and Retention Plan
• Band 6 posts converted to band 5 to encourage staff to train as health visitors and to increase capacity and demand.
• Health visitor and school nursing students increased by 100% on last year.• Warwickshire have recruited 5 students with 5 more going to advert.• Solihull recruited 4 health visiting students.• 75 % of students across the 3 areas have been secured employment with SWFT
from September 2022 as qualified health visitors.• Band 3 breast feeding support workers in Rugby to release some health visiting
sessions.
Risk Register
• All staffing risks monitored on local and Divisional registers.
Good News Stories
• Health visiting working with Warwick University regarding the Crying Infant research– staff being trained in Cognitive Behaviour Therapy
• Solihull to invest £300-£500K in 0-19 service for Covid recovery (non -recurrent)• 2 Psychology students (Warwick University) working with Solihull to look at parental
engagement and digital marketing. Reflection from hybrid working in Covid.• Coventry School Nursing and the Be Active, Be Healthy Team to participate in
research with Newcastle University around the National School Measurement Programme.
21/23 144/347

Community Childrens Nursing Team (CCNT)
CCNT remain on the risk register for staffing shortages, reviewed monthly at Family Health Division Health and Safety Meeting. The Team continue to run a social media campaign organised by recruitment for all bands of staff which has been much more successful than previous campaigns. Positively, our percentage of vacancies continues to reduce now the campaign continues. This risk is due to be reduced in June 2022.
Short term sickness has reduced significantly. There is still some long-term sickness which is proactively and supportively managed.
Main challenge remains recruiting band 6 nurses, there is still have 2 WTE vacancy at present. Encouragingly, the team have finally managed to recruit to all the band 5 vacancies.CSW posts will be fully recruited to and in post from June 2022.
The team have a partnership model working with Acacium Group agency to support a care package that we are really struggling to fulfil commissioned hours. This was approved at Finance and Performance Executive and was put in place to take some pressure from a very stressed team where sickness and absence was impacting on service delivery and has been extended to August 2022.
11.0 Nurse Staffing Acuity Update
The next full acuity review of inpatient staffing areas using the Safer Nursing Care Tool (SNCT) will be July 2022. The Clinical Lead for provisional Nursing and AHP Staff has been asked to continue to lead roster reviews across all areas and work with the Matrons and GMs to optimise existing staffing deployment through good rostering practice
The Clinical Lead for Provisional staffing is recruiting to additional posts in her team which will both support in depth roster reviews and also the roll out of Safecare over the next 18 months, enabling oversight of real time staffing and acuity.
The Emergency Department are conducting their very first acuity and dependency audit in June 2022 which will enable a thorough and accurate assessment of the nurse staffing requirements in ED, this will be coupled with a full roster review in July 2022 and a line by line budget review to better understand the position.
12.0 Conclusion
This report provides assurance that the organisation has good oversight as regards to safe staffing across all Divisions and the challenges and opportunities in those teams. Operational and Corporate staff are working together to prioritise patient safety and staff wellbeing with a good and transparent reporting culture.
The vacancy position is being proactively managed, and the Trust remains in a strong position to recruit and retain talented staff who believe in our values. With good career development opportunities for our workforce. Management of staff unavailability is carried out in a supportive manner.
Our quality and safety data consistently reports our patients to be safe and well cared for and that Divisions have good oversight of risks and so the Board of Directors should be
22/23 145/347

assured that scrutiny and oversight of safe staffing remains robust and responsive to patient needs.
13.0 Recommendations
• Continue senior Corporate Nursing monitoring of Nurse Staffing (Corporate Nurse of the day Rota) as an assurance, supporting anticipated challenges and keeping oversight of risks to quality, safety and wellbeing and the mitigations in place.
• Human Resources to ensure managers are supported to manage sickness and absence in all areas to facilitate return to work in a timely and supportive manner.
• Continue recruitment activity including the restart of face-to-face recruitment sessions, prioritising those teams with the highest vacancy risk.
• Continue the recruitment, arrival and induction of international recruits including good pastoral care.
• Operational and clinical managers to ensure they work to rostering principles and Key Performance Indicators (KPIs) to staff their area safely and effectively with available resources. Roster reviews to continue with Corporate, Financial and Operational engagement.
• Divisions to continue to monitor Staffing Risks on their registers, review mitigation measures and update regularly.
• Continue to promote career development for our workforce, supporting opportunities for talent management as part of a retention strategy.
• Continue Clinical Retention Group work, supporting local retention plans that reflect our Values.
Recommendation
The Board is asked to receive and note this report.
Ellie WardDeputy Chief Nursing Officer
23/23 146/347

Report SummaryReport to Board of Directors Date of
Meeting6 July 2022
Report Title Capital Programme Quarterly Update Report for 2022/23
Agenda Item
8.4
Executive/Non-Executive Lead
Sophie Gilkes, Chief Strategy Officer
Report Author(s)
Mark Jones, Associate Director of Strategic Estates and Capital FinanceMick Sargent, Associate Director of Finance
Report Previously Discussed at Capital and Estates Committee – 19 May 2022Management Board – 27 May 2022, 10 June 2022Board of Directors – 6 July 2022
Purpose of the Report For ApprovalFor Discussion
This paper reflects on the year to date position of the 2022/23 Capital Programme as the Trust finishes the first quarter of the financial year.
For Information
Recommendations and Action Required The Board of Directors is asked to note the update on the 2022/23 Capital Programme.
Impact (is there any impact arising from the report on the following?) Quality EqualityFinance ResearchPerformance ComplianceWorkforce Legal
Applicable Quality Improvement Priorities Elective Hub Health InequalitiesElectronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety CompassionateEffectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk RegisterAre any existing risks on the BAF/Risk Register affected? The 2022/23 Capital Programme addresses a range of risks associated within the Corporate Risk Register. There is also a risk being developed for the BAF linked to delivery of the programme due to increased market costs.
1/15 147/347

South Warwickshire NHS Foundation Trust
Report to Board of Directors – 8 July 2022
Capital Programme Quarterly Update Report for 2022/23
Executive Summary
Management Board have confirmed a final capital programme for 2022/23, detailed in this paper. This seeks to move forward with several projects within the community as well as replacement and refurbishment of essential infrastructure such as the Cath Lab.
There will be two key pieces of work this year that will focus on planning in Q2 and deliverables in Q3/4 and in 2023/24. These projects will be ‘Maternity Developments’ and ‘Urgent Care Developments’.
There is a high degree of risk around the delivery of this year’s capital programme due to the volatility of the market and increased costs associated with materials. Contractors are often only holding prices for 2 weeks and in some areas, we have seen costs double.
To mitigate this risk the Teams will also work up plans for business-as-usual items on the current unfunded list so that as we move through the financial year we can be as flexible as possible. This would be items such as replacement equipment. Please also note that a small % has also been added to the main scheme allocations to accommodate the expectation of increased costs.
Work has started to identify the 2023/24 programme and a prioritisation tool has been approved by Management Board. Teams will now start to populate this tool to help shape next year’s programme.
Recommendation
The Board of Directors is asked to note the update on the 2022/23 Capital Programme.
Sophie GilkesChief Strategy Officer
2/15 148/347
1. Summary
This paper reflects on the year-to-date position as the Trust finishes the first quarter of the financial year. It continues to be a changing capital year where access to additional funding, means that the Trust needs to be flexible in its approach to respond to the different demands.
It provides the Board with:
• an overview of the Trust’s 2022/23 Capital Programme, and • an update of progress against the major capital schemes.
1.1 Capital Programme for 2022/23 (Appendix 1)
A report is provided monthly to the Capital and Estates Committee meeting that reviews the Trust’s 2022/23 Capital Programme, attached in Appendix 1 for consideration by the Board.
Key areas to highlight:
• The Board should note the capital programme now stands at £19.802m and is comprised of:
- £12.253m internally generated funds- £1.066m IHCS share capital - £3.337m Public Dividend Capital (PDC).- £0.446m donations - £2.7m grants
1.2 Progress on Key Capital Schemes (Appendix 2)
A report is presented monthly to Management Board, providing an update on progress and issues on the key capital schemes. The report for June 2022 is attached in Appendix 2 for consideration by the Board. Key areas to highlight:
• Cath Lab – Equipment order placed last year in anticipation of replacement. Tenders returned and case developed for consideration to refurbish the area and replace the equipment. Joint work tendered with MacGregor Ward project and drainage for Elective Hub to maximise economies of scale.
• Elective Hub – Ongoing work to develop a decant plan for the development zone and exploration of new financial models to support this essential infrastructure.
• Acorn House – The community teams moved into the top floor of Acorn House in June 2022 and work due to be completed on ground floor in September 2022.
2. Recommendation
The Board of Directors is asked to note the update on the 2022/23 Capital Programme.
Sophie GilkesChief Strategy Officer
3/15 149/347

Capital Programme 2022/23 - Report to Capital and Estates Committee June 2022
Executive Summary
This report outlines the position of the 2022/23 capital programme.
The Trust’s planned capital programme spend for 2022/23 is £19.802m.
The Coventry and Warwickshire Integrated Care System (ICS) was issued a total business as usual operational capital limit of only £39.434m for all four providers for 2022/23. This has resulted in the Trust agreeing to a £12.253m share of this allocation, of which £404k will be kept back until quarter 2 and is dependent on other capital movement in the ICS. In addition to this the Trust also has £2.909m of Out Of Hospital STP wave 2 PDC funding for the Ellen Badger Hospital development, £0.428m PDC for Community Diagnostic Centre funding and £0.425m donated funding planned for the MacGregor Ward scheme and £0.021m internally generated charitable funding for a theatres welfare area.
Actual spend in May 2022 was £0.151m, year to date £0.692m.
The chart below shows the actual capital expenditure for the financial year, together with the monthly plan values submitted to NHS England/Improvement as part of the 28 April Capital plan submission and the latest forecast outturn.
Appendix 1
4/15 150/347

5
Funding
A breakdown of the funding of the Trust’s capital programme is detailed below:
Plan 2022/23
Apr 2022 May 2022 Jun 2022
£ 000's £ 000's £ 000's £ 000'sInternally funded 12,253 12,253 12,253 12,253Return of IHCS Share Funding 1,066 1,066 1,066 1,066PDC 3,337 3,337 3,337 3,337Charitable Funds ( External ) 425 425 425 425Charitable Funds (Internal) - - - 21Grants 2,700 2,700 2,700 2,700
19,781 19,781 19,781 19,802
Plan 2022/23
Apr 2022 May 2022 Jun 2022
£ 000's £ 000's £ 000's £ 000'sOOH STP -Ellen Badger Development 2,909 2,909 2,909 2,909CDC ( Comm Diagnostics Centre ) 428 428 428 428
3,337 3,337 3,337 3,337
Plan 2022/23
Apr 2022 May 2022 Jun 2022
£ 000's £ 000's £ 000's £ 000'sInternal Charitable FundsStaff Welfare Fund ( Theatres Welfare ) 0 0 0 21
0 0 0 21External Charitable FundsMacGregor Funding 425 425 425 425
425 425 425 425GrantsLillington CIL Grant 2,700 2,700 2,700 2,700
2,700 2,700 2,700 2,700
3,125 3,125 3,125 3,146
Total Capital Funding
PDC Funding
Charitable Funding /Grants
5/15 151/347

6
Expenditure:Details of allocations and actual expenditure to date are provided in the tables on pages 4 to 9, with changes in allocations highlighted in orange. The main changes in allocations are summarised in the table below:
SchemeMovement
£ 000Commentary
Equipment
T&O Treatment Room Enhancement C Arm Intensifier & Lead Lined Door for Fracture Clinic (TIF) -15 Moved to EMC - See Below
EMC
Lead Lined Door for Fracture Clinic (TIF) ** 15 See Above
SWFTCSIT Equipment ** 2 Additional Allocation
Generator ** -80 Risk to be assessed - Now on Unfunded List
Main Capital schemes
Feldon Staff Welfare Area Refurb ** 17 New Allocations Approved at May Capital Committee
SWIMS Clinical Area Ventilation ** 9 New Allocations Approved at May Capital Committee
Theatres Staff Welfare Area 21 New Allocations Approved at May Capital Committee
Theatres Staff Welfare Area ** 9 New Allocations Approved at May Capital Committee
Unallocated 42 Changes as a result of ** above
6/15 152/347

7
Capital Programme 2022/23
Cost Centre
Capital Reference Code
Scheme Description May-22
£ 000's £ 000's £ 000's £ 000's £ 000's
Various MED Schemes Medical Equipment Replacement 1,247 1,232 0 286 1,232Various EMC Schemes EMC 1,192 1,207 1 21 1,207Various SWFTCS Clinical Services Schemes 3,671 3,593 115 223 3,593Various SWFT/SWFTCS Community Diagnostics Centre ( CDC ) 451 451 0 2 451X29870 CAP DT Design Team 300 300 28 46 300X29817 CAP 08/18 Ellen Badger Development 4,500 4,500 -5 60 4,500X29929 CAP 14/19 Medical Gases 11 11 0 9 11X29651 CAP 02/21 Cath Lab 4,250 4,250 0 12 4,250X29691 CAP 07/21 Maternity Refurbishment Project 559 559 0 0 559
X29886CAP 10/21 MacGregor Ward ( Charitable ) 425 425 0 4 425
X29081 CAP 15/21 Elective Care Hub Programme Ph1 (TIF) 1,357 1,357 0 0 1,357X29243 CAP 03/22 Bulkington Community Centre 17 17 0 0 17X29245 CAP 04/22 Solihull Enterprise Centre 14 14 0 0 14X29246 CAP 05/22 Southam Clinic 7 7 0 0 7X29295 CAP 06/22 Emergency Front Door 500 500 0 0 500X29296 CAP 07/22 Feldon Staff Welfare Area Refurb 0 17 0 0 17
X29297 CAP 08/22 SWIMS Clinical Area Ventilation 0 9 0 0 9X29298 CAP 09/22 Theatres Staff Welfare Area 0 30 0 0 30X29280 EMC 10/22 HSDU 250 250 1 1 250
IT - Previous Year's Schemes 12 13 13
Over/ (Underspend) of Previous Year's Schemes 15 15 -0 15 15
Unallocated 1,014 1,057 0 1,057TOTALS 19,781 19,802 151 692 19,815
Approved Allocations May 2022
Proposed Allocations
Jun 2022
Actual Actual
Expenditure YTD
Forecast Spend
7/15 153/347

8
Medical Equipment
May-22£ 000's £ 000's £ 000's £ 000's £ 000's
X29073 MED 17/21 CT Scanner Software 20 20 0 0 20
X29075 MED 18/21T&O Treatment Room Enhancement C Arm Intensifier & Lead Lined Door for Fracture Clinic (TIF) 15 0 0 0 0
X29085 MED 20/21 Anaesthetic machine x 2 TIF 61 61 0 0 61
X29086 MED 21/21 Theatre Operating Trollies 42 42 0 0 42X29192 MED 28/21 Genesis Trays TIF 207 207 0 207 207
X29195 MED 29/21 Womens Unit Colposcopy 2nd rm TIF 22 22 0 0 22
X29196 MED 30/21 Mobile Xray Retrofit - Medray SCUBU 36 36 0 0 36
X29197 MED 31/21 Baby Incubator Draeger 34 34 0 0 34X29207 MED 33/21 Radiology Resus TIF 120 120 0 0 120X29211 MED 34/21 OCT Machine - Grafton Suite TIF 79 79 0 79 79
X29214 MED 35/21 Gynae Stacks - Accelerator Capital ( Elect Recov Sch TIFF) 192 192 0 0 192X29230 MED 38/21 Detectors Medray TIF 67 67 0 0 67X29271 MED 01/22 Hoists 45 45 0 0 45
X29276 MED 02/22 Breast Milk Recording System 25 25 0 0 25
X29277 MED 03/22 Wireless ECG Connection Cardiology EPR) 50 50 0 0 50X29278 MED 04/22 Defibs ( AED ) 90 90 0 0 90X29281 MED 05/22 ED Trollies 67 67 0 0 67X29282 MED 06/22 Paediatric Monitors 75 75 0 0 75
Over/ (Underspend) of Previous Year's Schemes 0 0 0 0
TOTAL 1,247 1,232 0 286 1,232
ActualApproved
Allocations May 2022
Proposed Allocations
Jun 2022Cost Centre
Capital Reference
CodeScheme Description
Forecast Spend
Actual Expenditure
YTD
8/15 154/347

9
Essential Maintenance
Scheme Description May-22 Forecast Spend
£ 000's £ 000's £ 000's £ 000's £ 000's
X29686 EMC 16/21 Mary Ward Refurb - Minor Works 1 1 0 1 1X29650 EMC 01/22 Green Lane Switch Gear 110 110 1 1 110X29232 EMC 02/22 Willoughby Roof Refurbishment 200 200 0 0 200X29673 EMC 03/22 Catering Equipment 50 50 0 0 50X29285 EMC 06/22 Fire Damper Remedials 15 15 0 0 15X29286 EMC 07/22 Block 14 - Dental Boiler Replacement 50 50 0 0 50X29247 EMC 08/22 Chillers Refurbishment 150 150 0 0 150X29661 EMC 11/22 CCTV Millers Road 37 37 0 19 37X29288 EMC 14/22 Block 23 - Physio Boiler Replacement 50 50 0 0 50X29290 EMC 15/22 Dilap Lifts 99 99 0 0 99X29291 EMC 16/22 Ventilation Improvements Waiting areas 15 15 0 0 15X29292 EMC 17/22 Clean AHU coils 30 30 0 0 30X29293 EMC 18/22 Hot water Generators 40 40 0 0 40X29296 EMC 19/22 Asbestos Survey Works 50 50 0 0 50X29289 EMC 20/22 LED Lighting Non patient areas 30 30 0 0 30X29248 EMC 21/22 Fire Alarm Upgrades 45 45 0 0 45X29251 EMC 22/22 Ph1 Tanks Pipework upgrade (Dead Legs) 55 55 0 0 55X29253 EMC 23/22 Water Softener system for HWS 25 25 0 0 25X29254 EMC 24/22 CarPark Drains Re-lining (PBartlett Quote) 10 10 0 0 10X29255 EMC 25/22 Access to Feldon Endo AHUs 15 15 0 0 15X29256 EMC 26/22 Nurse Call Installation Avon/Farries 15 15 0 0 15X29257 EMC 27/22 Flooring 30 30 0 0 30X29258 EMC 28/22 Solution Chadwick Windows 50 50 0 0 50X29259 EMC 29/22 Refurb toilets in bays B & C 20 20 0 0 20
X29075 EMC 30/22 Lead Lined Door for Fracture Clinic (TIF) 0 15 0 0 15
Over/ (Underspend) of Previous Year's Schemes 0 0 0 0
TOTAL 1,192 1,207 1 21 1,207
Proposed Allocations Jun
2022Cost CentreCapital
Reference Code
Approved Allocations May
2022
Actual Expenditure
YTD
Actual
9/15 155/347

10
Community Diagnostic Hub
May-22Forecast Spend
£ 000's £ 000's £ 000's £ 000's £ 000's
X29010 CAP 11/21 CDH Enabling Works 23 23 0 2 23
Z87037 FM CAP CDH Enabling Works 428 428 (0) 0 428
TOTAL 451 451 (0) 2 451
Actual Expenditure
YTD
ActualProposed Allocations
Jun 2022Cost CentreCapital
Reference Code
Scheme Description
Approved Allocations May 2022
10/15 156/347

11
SWFT Clinical Services Ltd
Scheme Description May-22Forecast Spend
£ 000's £ 000's £ 000's £ 000's £ 000's
Z87027 FM Cap Lillington and Cubbington 3,327 3,327 12 116 3,327
Z87009 Consultancy IT Equipment 0 2 1 2 2Z87033 FM Cap EV charging Points 10 10 - - 10Z87036 FM Cap Acorn House Development 254 254 102 104 254
Generator 80 0 - - -
TOTAL 3,671 3,593 115 223 3,593
Actual Expenditure
YTD
ActualProposed Allocations
Jun 2022Cost Centre
Capital Reference Code
Approved Allocations May 2022
11/15 157/347

Unfunded SchemesThe following schemes have previously been proposed for funding subject to agreement of a business case and a source of financing. Committee members are asked to please review the unfunded list and advise of any updates.
Mick Sargent: Associate Director of Finance – Strategy and Financial Services June 2022
Proposed SchemeProposed
Spend £'000Prioritise Scheme Status Business Case Dept Comments
Swipe Card Access 25 Ongoing Estates Part of ongoing site wide strategy to enhance access security
Trust wide review of accommodation/monitoring software 25 Ongoing CapitalPart of ongoing organisational wide asset utilisation strategy. Linked to ICS targets.
Walk in Freezer - Rehab Hospital 50 Estates Repair replacement
Respiratory Strategy TBCFeasibility - scope
tbaIs this associated with Victoria & Mary Ward plans? Conversion of wards into Respiratory Facility?
A&E Resuscitation Upgrade, provision of doors & ambulance bay works TBC
Project Team to be set up A&E Feasibility brief and scope to be advised.
Fire Compartmentation 1,239 Various Allocation drawn down annually.Refurbishment of Victoria Ward 200 Victoria Ward Ref Respiratory StrategyRefurbishment of Mary Ward 200 Mary Ward Ref Respiratory StrategyRefurbishment of McGregor ward bays and nurse bays 75 McGregor Status, feasibility and scope of works to be advised.Radiology Plain Film 2 - replace equipment TBC Radiology Was agreed as part of 3 machine purchase confirm with Steve ClarkeDay Surgery Chillers 350 High DSUNicol Unit - windows and extraction fans TBC Stratford Lack of ventilation, outcome of community bed review to be confirmedStratford Generator TBC Stratford SWFTCSNicol Unit - windows and extraction fans TBC Nicol Unit
2,164
Estates Strategy /Enabling Works
Booking Staff Relocation TBC Agreed locations Bookings etcReorganisation of office accommodation. Agreed Locations. Funding & refurb tba
Medical Measurement TBCMedical
Measurement Unsafe environment - SOA being preparedUrology Department TBC UrologyOutpatient Pharmacy TBC Pharmacy Additional capacity for TTOs Outpatients plus relocation as part of decant
Audiology TBC OPDCurrently part of ICS Pilot study. No fun ding identified. Scope of works developed.
0
Proposed EquipmentHi-low Alarm Beds x 8 55 high Charitable Funds?Hospital beds replacement at SWFT x 50 from 275 (year 3) 99 mediumHospital mattress replacement at SWFT x 50 from 200 (Year 4) 126 mediumFlexible Endoscopes (Olympus Keymed) 45 medium Need to reviewAudiology 5 Year Plan 2022-23 112 medium Review against 5 year planOphthalmology 5 Year Plan 2021-22 155 medium Review against 5 year planLight upgrade to 7 x Haag Streit Slit Lamps 45 lowMicroscope (Outpatients) 20 low Need to reviewFerno Trolley 22 lowUltrasound EBH 90 low Need to review - part of EBH developmentX-ray Unit Resus 45 tbc Further discussion Radiology 5 year replacement planX-Ray Unit CERU 300 tbc Further discussion Radiology 5 year replacement planMobile x-ray unit in ITU 35 tbc Further discussion Radiology 5 year replacement planPlain Film room 2 350 tbc Further discussion Radiology 5 year replacement planCT Scanner replacement- Warwick 950 tbc Further discussion Radiology 5 year replacement plan
2,449
Proposed ITPACS/RIS Voice Dictation TBCRobotic Process Automation 120New Ways of Working (Digital Meeting Rooms, 365, Hot desks) 100Cardiology EPR system 150Hardware for Sensyne R&D 180Anticoag Replacement IT System 16Ophthalmology Replacement System TBC Possibly 2022?
566
12/15 158/347

South Warwickshire NHS Foundation TrustReport to Management Board – 10 June 2022
Update on Key Capital Schemes
Progress RisksCap 08/18 Ellen Badger Development Allocation: (2022/23) £4.5m Completion date: September 2023 A• Appointment of Speller Metcalfe Ltd to provide pre-contract services approved by Board of Directors
on 6 October 2021.• Inpatient beds relocated to Campion Ward 5 January 2022 – no operational services remain on site –
decommissioning currently being undertaken• Bilateral agreement signed and sealed by all parties (SWFT/WCC/SDC) on 14 February 2022• Design Team and Speller Metcalfe currently finalising costs whilst undertaking VE exercise – target
outcome to be confirmed during week commencing 21 March 2022• EBH fully decommissioned and site boundaries secured – 31st March 2022.• Planning permission along with associated conditions granted by SDC on Thursday 17th March 2022• Approval to proceed with asbestos removal and purchase of boundary fencing to the rear of the
hospital secured at Capital and Estates Committee on the 19th of May 2022 (value 153K). Works scheduled to commence Monday 13th of June 2022.
• Update Report to Board of Directors 1st June 2022 secured approval to proceed and raise P/O with Speller Metcalfe for the main construction works subject to a number of financial and legal assurances being received from SMC in advance of the 10th of June 2022.
• Project estimated costs and current inflation issues impacting on the overall affordability of the project
• Fundraising Income• Community support in light of new pressure group formed
from the League of Friends.
Cap 02/21 Cath Lab Replacement Allocation: (2022/23) £4.25m Completion Date: January 2023 G• Proposed key dates to achieve costings and contractor appointment to be confirmed following tender
process• Clinical sign off for design agreed 11 February 2022 • The proposal to procure a modular building was discounted due to fabrication constraints and currently
exploring traditional construction method• Early purchase of Cath Lab equipment from Phillips Medical approved by Management Board and
Board of Directors. Procurement have obtained the URN from NHS Supply chain and order placed with Phillips 16 February 2022.
• Decision taken to proceed with joint tender process for Cath Lab, Drainage Works and MacGregor developments, which will attract potential cost and programme related efficiencies
• Tenders returned 23 May 2022 and currently being evaluated with report to be presented to Board of Directors 6 July 2022
• Capital availability• On commencement of the project, no longer able to place
a Vanguard on site.• Further investigation required on construction method• Current Cath Lab equipment reliability is causing concern• Infrastructure being reviewed in line with Trust Net Zero
Carbon targets• Operational risks due to extended tender period• Forecast programme may be extended due to material
supply and mobilisation related risks – precise impact will be confirmed following tender evaluation
Cap 15/21 Elective Care Hub Programme Allocation: (2022/23) £1.357m Completion: April 2024 A• Transformation Investment Fund application in progress and £1.6m granted in 2021/22 to commence
the projects.• Project Team established, outline brief has been developed for replacement of Hatton, 23 Hour Ward
and admissions, and Womens Treatment Unit• TIF Estates Bid submitted 17 February 2022 to the Midlands Elective Recovery Programme the value
of which equated to £48m split over three financial years. The Trust were unsuccessful in securing
• Expenditure risks associated with the £1.6m• Decant options associated with 23 Hour and Hatton
wards (Cost, capacity and programme)
Appendix 2
13/15 159/347

14
approval however the bid is currently first reserve to proceed in the event of unplanned slippage with the successful bids
• Continue to work with Archus to explore how the project can be delivered adapting different phasing scenarios to support affordability.
• Decant options being explored for Hatton / 23 Hour Wards, Catering and Pharmacy • Initial reviews of schedules of accommodation for DSU, Wards, and selected outpatient areas
currently being progressed with clinical leads• Inaugural meeting of Programme Board was held on 20th April 2022• Inaugural meeting of Site Enabling, Infrastructure and Demolition Workstream held on 4 May 2022• Feasibility work continues to be undertaken in respect of the required decant and infrastructure
requirements associated with phase 1 and 2 of the workstream.• Update report to be provided to Programme Board on the 15th of June 2022.SWFT/SWFTCS Acorn House Allocation: £260k Completion: tba G• Accommodation purchased by SWFT CS• Currently exploring utilisation and reconfiguration requirements• Scope of works for the ground and first floor completed. First floor works have recently been
tendered and preferred contractor identified. Report to be prepared for approval at Capital and Estates Committee. Corresponding work stream for ground floor works is currently being progressed
• Management Board approved the purchase of the F&E for the first floor on the 28 January 2022.• F & E requirements for first floor delivered pre 31 March 2022• Work commenced on first floor on 19 April 2022 with completion scheduled Tuesday 31 May 2022,
commissioning 1 – 17 June 2022 and operational from Monday 20 June 2022.• Scope of works for the ground floor agreed. Currently progressing tender documentation• Ground Floor – Schedule of works out to tender 17 May 2022 with tenders returns scheduled for the
8th of July 2022. Works are planned to commence on the 25 July 2022 with completion scheduled for the end of September 2022.
• Timescales• Utilisation – proposal to install sensors
SWFTCS Community Diagnostic Hub Allocation £4m Completion: 2023/24 A• Schedule of accommodation prepared to support the relocation of diagnostics, cardiology and
respiratory physiology from Building 2• Cost plan currently being prepared • Business case continues to be developed
• National funding not confirmed• Funding gap of £2m
SWFTCS/SWFT Lillington Development Allocation: (2022/23) £627k Completion: August 2023 G• Option supports integration of primary/community services and the disposal of Crown Way Clinic• CIL contribution secured for 22/23 and 23/24• Tenders period extended to 17 May 2022 - tender evaluation to be completed by 31 May 2022• Appoint Contractor June 2022 • Planned start on site 27 July 2022• Completion end of July 2023 - Operational August 2023 (precise date TBC)• Tenders received and evaluated. Two returns are very close at 5,108M and 5,140M. Agreed to
proceed with interview in order to select preferred bidder. Interviews scheduled for w/c 20 June 2022.• Existing garage facility to be demolished w/c 6th June 2022.
• Lag following planning approval on 7 June 2022 to allow for pre commencement conditions to be submitted and agreed
• Electrical infrastructure under review by Greenways due to impact of ventilation requirements on electrical loadings by Greenways
• Biodiversity assessment now required by Ecology which will now impact on the programme for securing planning approval.
14/15 160/347
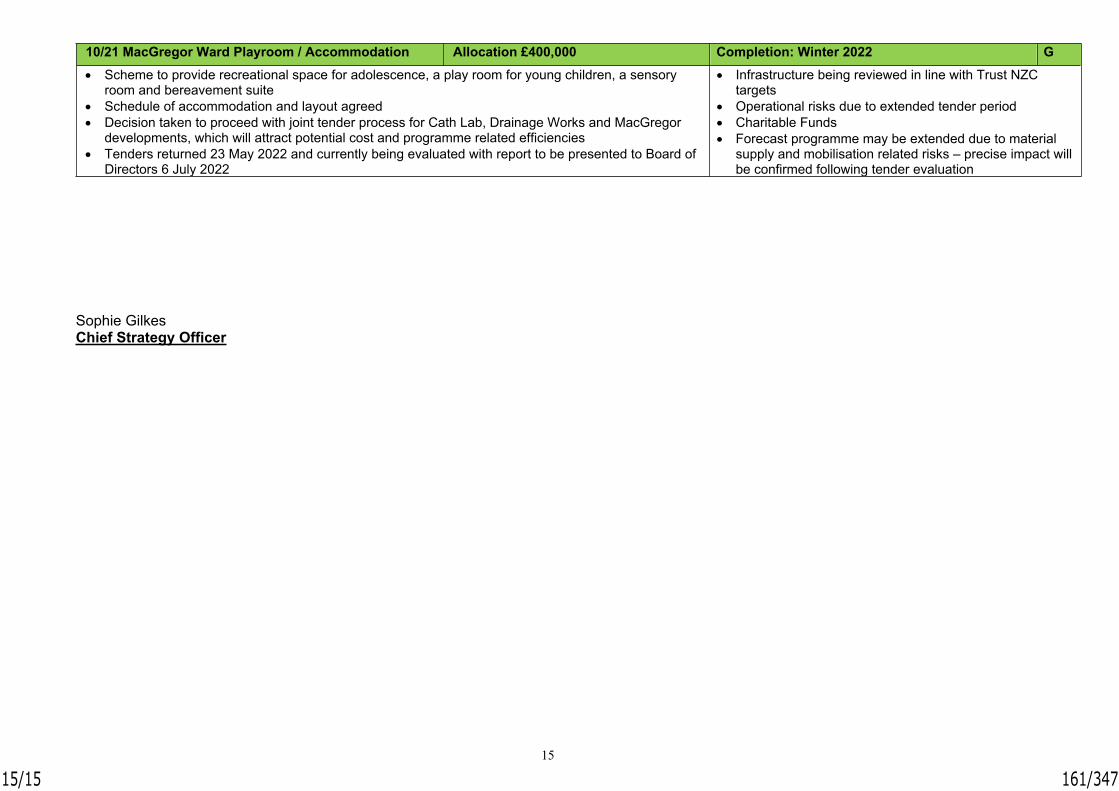
15
Sophie GilkesChief Strategy Officer
10/21 MacGregor Ward Playroom / Accommodation Allocation £400,000 Completion: Winter 2022 G• Scheme to provide recreational space for adolescence, a play room for young children, a sensory
room and bereavement suite• Schedule of accommodation and layout agreed• Decision taken to proceed with joint tender process for Cath Lab, Drainage Works and MacGregor
developments, which will attract potential cost and programme related efficiencies• Tenders returned 23 May 2022 and currently being evaluated with report to be presented to Board of
Directors 6 July 2022
• Infrastructure being reviewed in line with Trust NZC targets
• Operational risks due to extended tender period• Charitable Funds• Forecast programme may be extended due to material
supply and mobilisation related risks – precise impact will be confirmed following tender evaluation
15/15 161/347

Report SummaryReport to Board of Directors Date of
Meeting6 July 2022
Report Title Digital Heath Board Quarterly Update
Agenda Item 8.5
Executive/Non-Executive Lead
Adam Carson, Chief Executive -Innovate Healthcare Services
Report Author(s)
Adam Carson, Chief Executive
Report Previously Discussed at Digital Health Board
Purpose of the Report For ApprovalFor Discussion
To provide a summary of the key areas of work led by the Trust’s Digital Health Board during the last quarter.
For Information
Recommendations and Action Required The Board of Directors is asked to receive and note the report
Impact (is there any impact arising from the report on the following?) Quality EqualityFinance ResearchPerformance ComplianceWorkforce Legal
Applicable Quality Improvement Priorities Elective Hub Health InequalitiesElectronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety Compassionate Effectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk RegisterAre any existing risks on the BAF/Risk Register affected? NoIdentify the BAF/Risk Register risk ID and description – explain how the risk has been affected – reduced or increased as a consequence of the evidence within the report.
Do you recommend a new entry to the BAF and/or Risk Register is made as a result of this report? If yes, describe the new risk.
No
1/5 162/347

South Warwickshire NHS Foundation Trust
Report to Board of Directors – 6 July 2022
Digital Health Board Quarterly Update
Executive Opinion and Assurance
The focus of the Trust’s digital work over the last 6 months has shifted to more closely align with readiness to implement a replacement Electronic Patient Records (EPR) system. This has included the successful delivery of several initiatives that contribute to ensuring that the Trust has robust digital foundations in place.
The EPR programme has continued on plan, overseen by Digital Health Board and a Joint EPR Programme Board with George Eliot Hospital NHS Trust (GEH). Some risks exist to the timeline for the new EPR owing to a longer than expected period for regulatory approval of the Outline Business Case, caused by the number of cases being received nationally. As far as possible this risk has been mitigated through parallel development of the Full Business Case, which is scheduled to be received by Board of Directors in September 2022.
Recommendation
The Board of Directors is asked to receive and note the report.
Adam CarsonChief Executive – Innovate Healthcare Services Ltd.
2/5 163/347

South Warwickshire NHS Foundation Trust
Digital Healthcare Board – Quarterly Update
Executive Summary
During the last quarter work has focussed on the development of the Trust’s Full Business case for a replacement Electronic Patient Records system which will be completed over the coming month. Alongside this, digital work has focussed on several projects which put the Trust in a good position to implement the new EPR system, through the development of electronic processes and records management which will support a more rapid transition to the new system.
The Trust has also continued to work with system partners to support the delivery of several sharing and digital enablement initiatives. This has included work to implement electronic shared records for hospices, and the continued work to implement an integrated care record for Coventry & Warwickshire.
Headline Updates
Some of the significant areas of work during the last quarter are highlighted below:-
Electronic Patient records (EPR) Business Case
The Outline Business Case (OBC) for the Trust’s replacement Electronic Records System was submitted to NHS Digital in February 2022, following approval at both South Warwickshire NHS Foundation Trust and George Eliot Hospital NHS Trust Boards of Directors. Approval was originally anticipated within 3 months but owing to the number of cases being submitted nationally, regulatory approval has taken longer than expected. Comments and queries from the regulator have now been received and responded to, with no material issues identified. Final sign-off is anticipated by August.
Work on the Full Business Case (FBC) has continued, including finalising costs, benefits and resourcing models and well as completing the contractual schedules with the preferred supplier for inclusion as appendices to the case. Pending regulatory approval of the OBC, we expect the FBC to be received by Boards at both Trusts in September 2022. The FBC will again have to approved by regulators, but the Trust has been informed that this will be quicker given the amount of detail already in the OBC. Contractual sign-off with the preferred supplier is therefore anticipated this year, with implementation commencing early next summer.
Innovate Healthcare Services Ltd. has recently recruited Dan Milman as Director of Programmes & Digital Transformation, who will act as Programme Director for the new EPR.
Hospices Electronic Patient Record
Over the last year the Trust has supported the implementation of the EMIS EPR system at hospices across Warwickshire. Shipston Home Nursing, Shakespeare Hospice and Mary Anne Evans Hospice are now using EMIS as a full electronic record. The Trust have also
3/5 164/347

supported Myton hospice (who have a pre-existing EPR system) to be able to access a readable EMIS shared record. This completes the originally planned hospices work.
Following discussion with Myton, they are keen to replace their existing EPR system with EMIS and we have commenced work to scope this transition.
Patient Portal
The Trust’s patient portal has now been live for a year, and continues to receive positive feedback from patients, with over 60,000 users. Work is underway to further develop the portal to provide more access to clinical information. Between July and August 2022 access to discharge summaries and other clinical letters is being activated by speciality. Trials in using clinical patient forms have also been completed to support Patient initiated Follow-Ups (PIFUs).
Integrated Care Record
On behalf of Coventry and Warwickshire, SWFT hold a contract with Birmingham and Solihull (BSol) to deliver a managed solution for an Integrated Care Record (ICR) viewer covering both health and social care. During the last quarter work progressed with SWFT, George Eliot Hospital and Coventry and Warwickshire Councils now contributing data to the platform.
Challenges have remained around the technical provision and viewing of data from primary care, which Coventry & Warwickshire system partners continue to work through with BSol. It is planned that all partners are contributing and viewing data from the system by September, pending resolution of the current technical issues.
Other points to note
• A replacement system to manage the Trusts Intensive Therapy Unit (ITU) went live during May 2022 enabling a significantly more integrated way of working in the ITU, with real-time access to monitoring.
• A replacement endoscopy system was implemented during April 2022, allowing improved scheduling and clinical reporting, and allowing data sharing with partners across Coventry & Warwickshire.
Forward look
Some key highlights for the coming months include:
• The Full Business Case for the Trust replacement EPR system is due to be received by Board of Directors in September 2022.
• The Patient portal will be enhanced to include significantly more clinical patient information between July and October 2022.
• Electronic Prescribing is due to go live in the Trusts AMU• A clinically led project to develop a new policy for results acknowledgments, enabled
by electronic acknowledgement will go live over the summer. • Enhancements to the Trusts DIGIT ward management system will go live during the
summer, enabling greater electronic real-time ward management.
4/5 165/347

Recommendation
The Board is asked to receive and note this report.
Adam CarsonExecutive Director – Innovate Healthcare Services Ltd
5/5 166/347

Report Summary Report to Board of Directors Date of
Meeting 6 July 2022
Report Title Audit Committee Report for 1 June 2022 – Open Meeting
Agenda Item 8.6
Executive/ Non-Executive Lead
Kim Li, Chief Finance Officer / Rosemary Hyde, Non-Executive Director
Report Author(s)
Rosemary Hyde, Non-Executive Director
Report Previously Discussed at
Purpose of the Report To provide the Board with a summary of the key issues discussed by the Audit Committee
For Approval For Discussion For Information
Recommendations and Action Required The Board is asked to receive and note the key issues raised at the Audit Committee open meeting held on 1 June 2022
Impact (is there any impact arising from the report on the following?) Quality Equality Finance Risk Performance Compliance Workforce Legal
Applicable Quality Improvement Priorities Elective Hub Health Inequalities Electronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety Compassionate Effectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk Register Are any existing risks on the BAF/Risk Register affected? Identify the BAF/Risk Register risk ID and description – explain how the risk has been affected – reduced or increased as a consequence of the evidence within the report. Do you recommend a new entry to the BAF and/or Risk Register is made as a result of this report? If yes, describe the new risk.
1/53 167/347

South Warwickshire NHS Foundation Trust
Report to Board of Directors – 6 July 2022
Audit Committee Chair’s Report for 1 June 2022 – Open Meeting
Executive Opinion and Assurance The Board should be assured by the work of the Audit Committee and that there is a strong focus on audit and governance across the organisation. Kim Li Chief Finance Officer Reports/Items Considered by the Committee Internal Audit Reports (Coventry and Warwickshire (CW) Audit) Internal Audit Progress Report Internal audit work is on schedule for 2022/23, although a number of changes have been proposed to the audit plan. This includes a nationally mandated review of financial governance, which applies to all systems and individual NHS organisations. The review will be based on a Board level self-assessment tool recently published by HFMA “Improving NHS financial sustainability: Are you getting the basics right?” In addition, there will be a second follow up review of Patient Access Plans, following audit committee concern over the limited implementation of previous internal audit recommendations. Pathway to Delivering Zero The Internal auditors carried out a review of the pathway that the Trust is on towards delivering net zero. The Trust scored “1” on a Scale of 0-3 (where 0 is No Plan in Place, 1 is Plan in place but could be enhanced and 3 reflects a Robust Plan in Place and robust actions achieving outcomes). This reflects the early stage of the journey that the Trust is on. Notable recommendations (many of which are underway) include the need to refresh the Strategy to reflect NHS Net Zero ambitions, offer sustainability training to all staff, environmental impact assessment to be included in all tenders, and nominate “Carbon champions” across all sites. There was a need to move “Net Zero” to a similar place in the organization as “health and safety”, in that it needs to underpin everything the Trust does. Scanning Bureau Business Standards Institute (BSI) Standard Compliance The report provided only Moderate Assurance that the Trust would meet the BSI standard when the scanning bureau is next assessed in 2023. Progress in implementing recommendations from the last inspection in 2020 has been slower than expected, with 5 out of eight recommendations raised at the last review still outstanding. The auditors also noted that the scanning bureau was still working against the old 2014 version of the standard and needs to demonstrate compliance with the 2020 standard. Further recommendations were made around the completion of a business continuity plan and ratification of the information security policy for the scanning bureau. The CFO, as Deputy SIRO assured the Audit Committee that the Information Governance and Security Steering Group (IGSSG) would take responsibility for oversight of implementation of these recommendations.
2/53 168/347

Annual Report and Account Items External Audit Update (Deloitte, LLP) Sickness within the Deloitte, LLP team has caused some delays to the audit, which means they may not be able to achieve full sign off on 15 June 2022 and may issue the Auditor’s Annual report in draft but will be able to complete their work to meet the final submission date of 22 June 2022. However, the partner, Deloitte, noted that no material issues had been identified to date, and he was not anticipating any significant concerns. Draft Annual Accounts and Commentary 2021/22 The consolidated accounts show a deficit of £4,270k. After adjusting for technical accounting items (primarily £3,500k one off allowable adjustment for the derecognition of cloud based software intangible assets), the results reconcile to a £22k surplus reported in the year end Control Total. Other smaller adjustments relate to fixed asset impairments and donated assets. Overall, the Statement of Financial Position shows a reduction in Total Assets/Taxpayer’s Equity of £0.4m to £129.5m. Key changes include:
- Fixed asset additions of £21m - Investment in Innovate Healthcare Services of £8.0m - Reduction in value of shareholding in Sensyne Health Plc £5.6m - Increase in accruals and provisions £10.9m
Draft Annual Report 2021/22 The Annual Report is largely complete. The audit committee provided feedback and requested additional focus to be given to the Trust’s response to the Ockenden report. Draft Quality Report 2021/22 This report is no longer mandated and does not form part of the external auditor’s opinion. However, the Trust have decided, for transparency, to continue to publish the report as part of the Annual Report. Draft Annual Governance Statement 2021/22 The statement was approved by the Audit Committee, subject to inclusion of reference to the Ockenden report. Joint Audit and Clinical Governance Assurance Statement The statement was approved by the Audit Committee. National Cost Collections 2021/22 The Audit Committee considered and approved the process for producing the annual National Cost Collection data for the Trust. It was noted that the reference costs for 2020/21 have still not been published by NHSE/I. Annual Review of Trust’s Standing Financial Instructions (SFIs) and Scheme of Delegation
3/53 169/347

The Committee approved the changes, which have been made primarily to bring the instructions in line with other members of the Foundation Group. Areas of Concern for the Board’s Attention See comments in the Internal Audit section on concerns with the Scanning Bureau’s compliance with BSI standards. Decisions Made and Actions to be Taken The Audit Committee approved the Trust’s methodology for National Cost Collections, as well as changes to the Trust’s Standing Financial Instructions (SFI) and Scheme of Delegation, for ratification by the Board. Committee’s Level of Assurance The Board should be assured that the Audit Committee has good oversight of the governance arrangements of the Trust and is assured that these arrangements are operating satisfactorily. The Audit Committee has received assurance from the external auditor on the progress of the financial audit, and no concerns were noted. Rosemary Hyde Audit Committee Chair
4/53 170/347

Report Summary Report to Board of Directors Date of
Meeting 6 July 2022
Report Title Audit Committee Report for 15 June 2022 – Open Meeting
Agenda Item 8.6
Executive/ Non-Executive Lead
Kim Li, Chief Finance Officer / Rosemary Hyde, Non-Executive Director
Report Author(s)
Rosemary Hyde, Non-Executive Director
Report Previously Discussed at
Purpose of the Report To provide the Board with a summary of the key issues discussed by the Audit Committee
For Approval For Discussion For Information
Recommendations and Action Required The Board is asked to receive and note the key issues raised at the Audit Committee open meeting held on 15 June 2022
Impact (is there any impact arising from the report on the following?) Quality Equality Finance Risk Performance Compliance Workforce Legal
Applicable Quality Improvement Priorities Elective Hub Health Inequalities Electronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety Compassionate Effectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk Register Are any existing risks on the BAF/Risk Register affected? No Identify the BAF/Risk Register risk ID and description – explain how the risk has been affected – reduced or increased as a consequence of the evidence within the report. Do you recommend a new entry to the BAF and/or Risk Register is made as a result of this report? If yes, describe the new risk.
No
5/53 171/347

South Warwickshire NHS Foundation Trust
Report to Board of Directors – 6 July 2022
Audit Committee Chair’s Report for 15 June 2022 – Open Meeting
Executive Opinion and Assurance The Board should be assured by the work of the Audit Committee and that there is a strong focus on audit and governance across the organisation. Kim Li Chief Finance Officer Reports/Items Considered by the Committee Internal Audit Reports (CW Audit) Data Security and Protection Toolkit (DSPT) Compliance Review The DSPT is an annual mandatory self-assessment which allows the Trust to measure performance against the National Data Guardian’s ten data security standards. The toolkit is evolving each year, reflecting emerging risks in data security. For 2022, all NHS Trusts are required to submit the toolkit by 30 June 2022. This year Internal Audit carried out a limited scope review of 25 out of the 38 assertions that the Trust are required to confirm. This review was mandated, for the first time, by NHS Digital. These assertions are supported by 110 mandatory evidence items. The review took place before all the evidence work had been completed, and hence the overall report rating of “Moderate Assurance” reflected a point in time when certain work was incomplete. The Audit Committee were assured that since the completion of the audit all outstanding evidence had been gathered to enable the Trust to sign off the toolkit as “Standards Met”. The auditors identified a small number of recommendations for improvement, but these did not impact the sign off. It was noted that NHS Digital had changed its requirements for 2022/23 and Trusts would not be required to obtain compliance with Cyber Essentials Plus. However, the DSPT would be aligned to the Cyber Essentials framework. In addition, Innovate Healthcare Services (as a Company) intends to obtain Cyber Essentials Plus accreditation in the current year. Annual Report and Account Items External Audit Report on the Financial Statements (ISA 260) The Partner, Deloitte, stated that the external audit was very close to completion. The following areas still had to be finalised:
a) Finalisation of testing on the journals, revenue, credit note provision, accruals, deferred income, provisions, remuneration report, related party disclosures, agreement of balances and other disclosures;
b) Completion of internal quality procedures; c) Reconciliation of the final Trust Accounts Consolidation (TAC) schedules to the final
6/53 172/347

Accounts; d) Review of events since 31 March 2022 e) Review of final versions of the Accounts and the Annual Report; f) Receipt of the signed management representation letter.
The Value for Money work was also due to be finished in the day or so, and there were no significant control deficiencies to report. It was noted that the auditors were no longer required to review the Quality Report. The Partner, Deloitte recommended, that whilst the audit was not finalised, he was sufficiently confident about the status of the audit that it was suitable for the Board to approve the year end accounts. The Final Report to the Audit Committee on the 2021/22 Audit for the Audit Committee – 15 June 2022 has been appended to this report for your information. Annual Accounts and Commentary 2021/22 The Audit Committee reviewed and recommended the Annual Accounts 2021/22 to the Board for approval. Annual Governance Statement 2021/22 The statement was approved by the Audit Committee, subject two amendments: correction of title of Chief Executive from Accountable Officer to Accounting Officer; amend statement regarding the Data Security Protection Toolkit to state that the Trust was fully compliant. Annual Report 2021/22 The Audit Committee requested that further corrections to the Annual Report be made in respect of staff costs, Directors’ remuneration, and income, so that figures were consistent with the Annual Accounts. Subject to these changes, the Audit Committee recommended to the Board for approval. Quality Report 2021/22 The Audit Committee reviewed and recommended the Quality Report 2021/22 to the Board for approval. Areas of Concern for the Board’s Attention None noted Decisions Made and Actions to be Taken The Audit Committee recommended for Board approval the Annual Report and Accounts, including Quality Report and Governance statement. Committee’s Level of Assurance The Audit Committee has received assurance from the external auditor that they anticipate issuing an unmodified audit opinion on the Annual Report and Accounts, including Value for Money statement.
7/53 173/347

Rosemary Hyde Audit Committee Chair
8/53 174/347

Final Report to the Audit Committee on the 2021/22 audit Issued on 10 June for the meeting on 15 June 2022
South Warwickshire NHS FT
Deloitte Confidential: Government and Public Services
9/53 175/347

Deloitte Confidential: Government and Public Services
2
Contents
01 Final report 02 Appendices
Introduction 3
Quality indicators – impact on the execution of our audit
5
Our audit explained 6
Significant risks 7
Other areas of focus 13
Covid-19 15
Value for Money 16
Your control environment and findings 17
Other significant findings 19
Our audit report 20
Purpose of our report and
responsibility statement21
Audit adjustments 23
Fraud responsibilities and representations
27
Independence and fees 29
Draft management representation letter
30
Sector developments - Code of Governance for NHS provider trusts
36
Sector Benchmarking and risk assessment
37
10/53 176/347

Deloitte Confidential: Government and Public Services
3
Introduction
The key messages in this reportI have pleasure in presenting our final report to the Audit Committee for the 2021/22 audit. I would like to draw your attention to the key messages within this paper:
Status of our
financial
statement
audit
Our financial statement audit is in progress subject to completion of the following principal matters:
• Finalisation of testing on the journals, revenue, credit note provision, accruals, deferredincome, provisions, remuneration report, related party disclosures, agreement ofbalances, other disclosures and tie through;
• Completion of our internal quality assurance procedures;
• Reconciliation of the final Trust Accounts Consolidation schedules (TAC) to the FinalAccounts;
• Our review of events since 31 March 2022;
• Review of final versions of the Accounts and the Annual Report; and
• Receipt of the signed management representation letter.
We will certify our audit following completion of NAO group reporting in June.
Status of our
Value for
Money work
We have completed our Value for Money work. Our Value for Money commentary is included in
the accompanying Auditor’s Annual Report.
We have not identified any risks of significant weakness in arrangements to secure economy,
efficiency and effectiveness in the use of resources.
We have no matters to report by exception in our financial statement audit opinion.
Conclusions
from our
testing
• The key judgements in the audit process related to:
• Classification of capital expenditure;
• Validity of accruals, provisions and deferred income and;
• Agreement of balances with commissioners.
• To date, we have not identified any significant audit adjustments or disclosure deficiencies.
• Based on the current status of our audit work, we envisage issuing an unmodified audit
opinion, with no reference to any matters in respect of the Trust’s arrangements to secure
economy, efficiency and effectiveness in the use of resources, or the Annual Governance
Statement.
• To date we have not identified any inconsistencies between the financial statements and the
TACs.
Audit quality is our number one priority. We plan our audit to focus on audit quality and have set the following audit quality objectives for this audit:
• A robust challenge of the key judgements taken in the preparation of the financial statements.
• A strong understanding of your internal control environment.
• A well planned and delivered audit that raises findings early with those charged with governance.
11/53 177/347

Deloitte Confidential: Government and Public Services
4
Going concern In accordance with the requirements of the Department of Health and Social Care Group Accounting Manual
(GAM), the Trust has prepared its accounts on a going concern basis, applying the ‘continuing provision of
services’ approach, reflecting the anticipated continued provision of the Trust’s services (rather than necessarily
the financial position of the Trust as a legal entity). Under Practice Note 10 ‘Audit of Financial Statements of
Public Sector Bodies in the United Kingdom’, our work has therefore focused upon confirming the use of the
‘continued provision of service’ approach is appropriate. We have no matters to report in respect of this.
The Trust’s arrangements to secure financial sustainability are considered as part of our Value for Money work
rather than our financial statement audit and is included in the accompanying Auditor’s Annual Report.
Annual Report &
Annual Governance
Statement
We have reviewed the Trust’s Annual Report & Annual Governance Statement to consider whether it is
misleading or inconsistent with other information known to us from our audit work. Based on our review, we
consider that the Trust has followed the format prescribed by the FT ARM. We have suggested a number of
minor changes to management for consideration.
Impact of Covid-19 The Trust’s operations continued to be impacted by Covid-19, as throughout the NHS, the Trust continued to
operate within a block contract regime to achieve a £3.5m adjusted deficit against a breakeven plan, due to the
write off of previously capitalised intangible assets in year. Allowing for this right off the Trust has a surplus of
£22k. The cash balance at year end was £41.7m (2020/21 £44.2m).
Auditor
Independence
We consider that we comply with FRC Revised Ethical Standards for Auditors and that, in our professional
judgement, we are independent and the objectivity of the audit engagement partner and audit staff is not
compromised.
Accounting
performance
The Finance team have been proactive in raising matters for audit consideration and the quality of working
papers has been good. We would like to take this opportunity to thank management for their assistance during
the audit.
Ian HowseAudit lead
Introduction
The key messages in this report (continued)
12/53 178/347

Deloitte Confidential: Government and Public Services
5
Area Grading ReasonFurther
detail
Timing of key accounting judgements
Some key judgements, particularly provisions, were received later in the audit process than I expected. We would expect to review and agree a position ahead of the year end.
Page 17
Adherence to deliverables timetable
Overall performance has been good. Some areas required additional work to reconcile to the financial information and some resubmission of information to the audit team provide further detail. We will perform a lessons learnt review with management upon completion of the audit.
Page 17
Access to finance team and other key personnel
Quality and accuracy of management accounting papers
We would expect management to provide more detail for key judgements to support conclusions made with reference to accounting standards to support conclusions made.
Page 17
Quality and timing of audit committee papers
Quality of draft financial statements
Response to control deficiencies identified
Volume and magnitude of identified errors
Quality indicators
Impact on the execution of our audit
Management and those charged with governance are in a position to influence the effectiveness of our audit, through timely formulation of judgements, provision of accurate information, and responsiveness to issues identified in the course of the audit. This slide summarises some key metrics related to your control environment which can significantly impact the execution of the audit. We consider these metrics important in assessing the reliability of your financial reporting and provide context for other messages in this report.
!
Lagging Developing Mature! !
!
!
13/53 179/347

Deloitte Confidential: Government and Public Services
6
Our audit explained
We tailor our audit to your organisation and your strategy
Identify
changes
in your
business and
environment
Determine
materialityScoping
Significant
risk
assessment
Conclude on
significant
risk areas
Other
findings
Our audit
report
Identify changes in your business and environment
In our planning report we identified the key changes in your business and articulated how these impacted our audit approach.
Scoping
We performed our risk assessment in line with current NHSI requirements. We are completing our audit in line with our audit plan.
Significant risk assessment
In our planning report we explained our risk assessment process and detailed the significant risks we have identified on this engagement. We report our findings and conclusions on these risks in this report.
In our audit plan we stated we would complete ourrisk assessment over NHS revenue at the year end.We concluded that the recognition of NHS clinicalincome remains a significant risk for the purpose ofour audit and have pinpointed this risk to the mis-matches in the agreement of balances exercise as setout in the “risk identified” section on page 8.
Determine materiality
When planning our audit we set our materiality at £7.6m based on 2% of forecast income. Materiality has changed since our planning report to £8.0m as total income for the year increased against plan. We report to you in this paper all misstatements above £300k in line with our plan.
Other findings
As well as our conclusions on the significant risks we are required to report to you our observations on the internal control environment as well as any other findings from the audit. These are set out from page 17 of this report.
Our audit report
Based on the current status of our audit work, we envisage issuing an unmodified audit report.
Conclude on significant risk areas
We draw to the Audit Committee’s attention our progress to date on the significant audit risks on pages 7-12. In particular the Audit Committee must satisfy themselves that management’s judgements in relation to going concern are appropriate.
14/53 180/347

Deloitte Confidential: Government and Public Services
7
Significant audit risksManagement override of controlsRisk identified
In accordance with ISA 240 (UK) management override is a significant risk. This risk area includes the potential for management to use their judgement to influence the financial statements as well as the potential to override the Trust’s controls for specific transactions.
Key judgements
The key judgments in the financial statements are those which we have selected to be the significant audit risks revenue recognition, validity of accruals, provisions and deferred income, capitalisation of expenditure and valuation of the Trust’sestate. These are inherently the areas in which management has the potential to use their judgment to influence the financialstatements.
Deloitteresponse
We have considered the overall sensitivity of judgements made in preparation of the financial statements, and note that in the current year there are not direct financial incentives for achieving particular results. We have considered these factors and other potential sensitivities in evaluating the judgements made in the preparation of the financial statements. Specific areas of workare:
• We considered the overall control environment and ‘tone at the top’.
Journals
• We tested the design and implementation of controls in relation to journals.
• We have made inquiries of individuals involved in the financial reporting process about inappropriate or unusual activity relating to the processing of journal entries and other adjustments.
• We have selected a sample of journals using data analytics to focus on higher risk journals and tested them for reasonableness.
Accounting estimates
• We tested the design and implementation of controls in relation to accounting estimates.
• We performed testing on key accounting estimates as discussed above, and considered other accounting judgment areas.
• We have confirmed that the Trust has adopted consistent assumptions on asset lives for the purposes of depreciation and valuation.
• We are performing a retrospective review of management’s judgements and assumptions relating to significant estimates reflected in last year’s financial statements in line with ISA540.
• In addition to our work on key accounting estimates discussed above, our work included considering key areas of judgement for NHS providers (including those previously highlighted by NHS Improvement). In testing the principal accounting estimates, engagement team members were directed to consider their findings in the context of the identified fraud risk. Where relevant, the recognition and valuation criteria used were compared to the specific requirements of IFRS.
Significant transactions
• We did not identify any material unusual transactions to date outside the normal course of business.
Conclusion We have not identified any significant bias to date in the key judgements or estimates made by management. We will provide a verbal update to the committee on progress.
15/53 181/347

Deloitte Confidential: Government and Public Services
8
Significant audit risks
Recognition of NHS clinical revenueRisk identified The risk of fraud in revenue recognition is a presumed risk under International Standards on Auditing. We have identified
as a key risk the risk of revenue not being recognised at fair value due to adjustments agreed in settling current year disputes.
Key judgements
The Agreement of Balances (AoB) exercise has resulted in a number of differences between the Trust and a number of NHS bodies as set out below and on the next page.
Deloitteresponse
We have reviewed the Trust’s position with regard to the differences highlighted in the Agreement of Balances exercise and whilst we are satisfied that the Trust is able to support the positions it has taken, there is a risk that future negotiations may result in the Trust not fully recovering the income balances recognised. The Trust has confirmed that it has taken its positions based on known disputed balances and we will be seeking further assurances from the Trust in the letter of management representations in this regard. Further procedures performed included:
• We tested the design and implementation of controls in relation to the recognition of NHS clinical revenue;
• Testing the recognition of income through the period and evaluating the results of the agreement of balances exercise;
• Obtaining an understanding of the nature of each provision, the basis for the position adopted, and evidence of the historical accuracy of provisions made for disputes with commissioners;
• Considering the Trust’s track record in evaluating period-end provisions;
• Assessing the appropriateness of the judgements made in recognising revenue and providing for disputes on the basis of discussion with staff involved, and reviewing correspondence with commissioners and other relevant documentation; and
• Consideration of benchmark information from our knowledge of the local health economy.
The following is the agreement of balance differences with other NHS bodies which exceeds our clearly trivial threshold of £300k: Income & Expenditure Mis-matches
• Midlands regional office- £1,156k – Trust income is lower by this amount
• Central specialised commissioning - £735k – Trust income is higher by this amount
• Coventry & Warwickshire CCG - £1,419k – Trust income is lower by this amount
• Health Education England - £454k – Trust income is lower by this amount
• NHS Property Services - £462k – Trust expenditure is lower by this amount
16/53 182/347

Deloitte Confidential: Government and Public Services
9
Significant audit risks
Recognition of NHS clinical revenue (continued)
Deloitteresponse (continued)
Receivables & Creditors Mis-matches
• Central specialised commissioning - £302k – Trust receivable is lower by this amount.
• South west regional office - £741k – Trust receivable is lower by this amount
• George Eliot Hospital NHS Trust - £925k – Trust receivable is higher by this amount
• Coventry & Warwickshire CCG - £502k – Trust payable is lower by this amount
At the date of our report the net AoB differences across all counterparties are as follows:
• SWFT income is £2,502k lower than counterparty NHS bodies
• SWFT expenditure is £1,035k lower than counterparty NHS bodies
• SWFT receivables are £1,060k lower than counterparty NHS bodies
• SWFT payables are £912k lower than counterparty NHS bodies
Conclusion No significant issues have been identified as a result of the testing performed to date and we have concluded that income has been appropriately recognised.
17/53 183/347

Deloitte Confidential: Government and Public Services
10
Significant audit riskClassification of Capital Expenditure
Risk identified The Trust had £21.1m of capital expenditure in the year. There is a risk that capitalisation of this expenditure isinappropriate under accounting standards or recognised in an incorrect financial period.
Key judgement
Determining whether expenditure should be capitalised can involve significant judgement as to whether costs should becapitalised under International Financial Reporting Standards, and when to commence depreciation. In addition,previously capitalised works that are being replaced or refurbished need to be appropriately disposed of.
Deloitteresponse
• We tested the design and implementation of controls around the capitalisation of costs, and test spending on a samplebasis to confirm that it complies with the relevant accounting requirements;
• We have reviewed the projects ledger and the status of individual projects to evaluate whether they have beendepreciated from the appropriate point;
• We have reviewed a sample of capital payables at year end to confirm they are recognised appropriately;
• We challenged management’s assessment whether any impairment arises in respect of newly capitalised expenditure,
• We are checking whether any adjustments to the value of previously capitalised works are required and how thesehave been calculated; and
• We tested the Group and Trust presentation of capital items, and challenge whether these have been appropriatelytreated.
Conclusion As a result of the level of spending around the year-end, we have performed additional testing on year-end capitalcreditors. No significant issues have been identified to date as a result of the testing performed to date.
18/53 184/347

Deloitte Confidential: Government and Public Services
11
Significant audit riskValidity of accruals, provisions and deferred incomeRisk identified The changes to the NHS funding and monitoring regime
in the prior and current year have meant that there hasbeen a significant increase in the overall level of revenue and capital funding available to NHS providers, and a reduction in the overall pressure to achieve specific control
totals.
This may reduce the scrutiny of the validity of liabilities recognised at year-end and/or create an incentive to make overly prudent estimates and judgements so as to recognise expenditure in the current year and make future targets easier to achieve.
For the Trust this is especially the case given there were significant increases in these balances in the prior year as well. Over the last two years there has been an overall increase of £29.5m or 129.3%.
Key judgements
The recognition of accruals, provisions and deferred income include management judgement relating to the cut-off of the
expenditure / income to which it relates as well as often being manual calculations which increases the risk of
misstatement and requires additional judgement to identify an appropriate basis for the calculation. These therefore also
form part of our management override of controls consideration as outlined on page 7.
Deloitteresponse -Accruals
We are performing testing of the design and implementation of controls around the recognition of accruals at the balance
sheet date.
We are testing a sample of accruals to supporting documentation to check whether they were valid liabilities, that the
amount accrued was appropriately supported, and that the liability had been incurred as at 31 March 2022.
We re-performed the calculation for the annual leave accrual on a sample basis and agreed sufficient information used in
the calculation to supporting reports and documentation.
19/53 185/347

Deloitte Confidential: Government and Public Services
12
Significant audit riskValidity of accruals, provisions and deferred incomeDeloitteresponse -Provisions
We are performing testing of the design and implementation of controls around the recognition of provisions at the
balance sheet date.
We have applied professional scepticism in considering the completeness of actuals and provisions based on our
knowledge of the Trust and in comparison with other NHS bodies.
In addition to the legal claims and pension liability provisions, the Trust has included a number of significant ‘other’
provisions which can be described as follows:
• Annual leave accrual additional provision - £2,594k
• Flowers provision - £958k
• SSC EPR- £882k
• Staff car park VAT recovery- £350k
• Risk of consultancy - £335k
• Paediatric cover rota- £280k
• VAT provisions - £283k
We are reviewing the calculations of these provisions in year and assessing the reasonableness of the items included at
the balance sheet date.
Deloitteresponse -Deferred Income
We are performing testing of the design and implementation of controls around the recognition of deferred income at the
balance sheet date.
We are testing a sample of deferred income items to supporting documentation and evaluating management’s
assessment as to whether the criteria for revenue recognition has not been met as to 31 March 2022 and therefore the
value should be deferred.
Conclusions Our work in these areas is progressing. We will provide a verbal update to the committee on progress.
20/53 186/347

Deloitte Confidential: Government and Public Services
13
Other areas of focus
Property valuations and Innovate
Property Valuations
The Trust is required to hold property assets within Property, Plant and Equipment at a modern equivalent use valuation. The valuations are by nature significant estimates which are based on specialist and management assumptions and which can be subject to material changes in value.
In the prior year the Trust engaged Avison Young (AY) who undertook a full valuation of the estate at 31 March 2020 with an interim roll forward to 31 March 2022. The roll forward exercise does not pose a significant audit risk although this will continue to be monitored. The valuation of assets held by SWFT CS are valued by the District Valuers Service (DVS).
We performed the following audit work in this area:• We reviewed and challenged the appropriateness of the assumptions used in the year-end valuation of the Trust’s
properties and test the inputs to the year-end valuation. This will include the gross internal areas provided to the valuer. We tested a sample of measurements to check the accuracy of data through agreement to underlying data from the Trust’s estates team.
• We have engaged our Deloitte Real Estate specialists to review and challenge the appropriateness of the assumptions used in the year-end valuation of the Trust’s and SWFT CS’s estate and to review accuracy of underlying workings/calculations including the disclosures included in the financial statements.
• We have assessed the presentation of revaluation movements and impairments, taking into account revaluation reservesfor individual assets, and
• We have reviewed the Valuer’s report and assess management’s disclosure of key sources of estimation uncertainty.
No significant issues have been identified as a result of the testing performed to date.
Innovate Healthcare Services
We have confirmed that Innovate Healthcare Services (IHCS) was incorporated in June 2020 as Pursue Healthcare Limited. However, the entity did not start trading until December 2021. The Trust held an investment in their financial statements of £0.1m for this entity at 31 March 2021 which has risen to £7.7m at 31 March 2022.
• We have reviewed the arrangements in place and determine whether the appropriate accounting treatment and disclosures are in place at the Trust. This includes the signed contractual documentations for the sharing of control with other members of the Foundation Group and the recognition as a joint venture. The arrangement has been reviewed by our technical team and the recognition as a joint venture is appropriate.
• We have reviewed the additional investment into the joint venture by the Trust and confirmed this to signed agreements.
• We considered whether we required our Financial Instrument specialists to review and challenge the appropriateness of the assumptions used in the funding model entered into between the Trust and IHCS and concluded this was not required due to the lack of complexity. This has included the sale of IT assets and intangible assets which are recognised as disposals in the financial statements.
• We have reviewed the disclosure of the arrangement in the financial statements. Minor improvements have been suggested to the disclosure of the arrangement within the financial statements. These will be addressed through our review of the final accounts.
No significant issues have been identified as a result of the testing performed to date.
21/53 187/347

Deloitte Confidential: Government and Public Services
14
Other areas of focus
Cloud Computing
Derecognition of cloud computing intangible assets
The Trust have entered into cloud computing arrangements with a number of suppliers in recent years. In some cases the services provided have had to be configured to meet the Trust’s individual needs. The configuration of these services have historically been capitalised as an intangible asset under IAS 38. There has been clarification of guidance issued by the IFRS Interpretations Committee in March 2021 which confirmed that customisation costs for such assets can only be capitalised where an entity can demonstrate the item is controlled by the entity, i.e. that they have ‘the power to obtain the future economic benefits flowing from the underlying resource and to restrict the access of others to those benefits’.
In light of the clarification the Trust have performed a review of the assets previously capitalised and, in collaboration with IT colleagues, identified that a significant portion of these assets the Trust could not demonstrate ownership of the assets.Therefore, the Trust proposed to derecognise these assets to comply with the guidance.
We performed the following audit work in response to this derecognition:
• Reviewing the rationale set out by management assessing individual elements of the intangible assets held on balance sheet
• We have concluded, with help from our technical team, that we agree with management’s assessment that a prior year restatement is not required on the grounds of materiality of the assets identified. Note that a clarification of guidance would normally require restatement as it is deemed to have already been in place.
• We are discussing the assessment process with the Trust IT colleagues to understand the assessments made.
• We have reviewed the disclosure of the derecognition within the financial statements.
Regulatory developments
• The Trust is subject to, amongst others, the regulatory requirements and performance targets of the Care Quality Commission (CQC) and NHS England and NHS Improvement.
• The Trust received a “Outstanding” rating in its last CQC report, dated December 2019, with all areas receiving “Outstanding” or “Good” ratings.
• We will continue to monitor and consider the implications of any feedback received and any concerns that may be raised by external regulators.
22/53 188/347

Deloitte Confidential: Government and Public Services
15
Coronavirus (Covid-19) outbreak
Impact on reporting and our audit
Impact on annual report and financial statements
Impact on property, plant and equipment
Our work on property valuations (page 13) included challenging whether the Trust had appropriately considered theimpact on the valuation of the pandemic (including any changes as a result of the pandemic and consequent serviceand organisational changes in the NHS on the “modern equivalent asset” assumed in valuations).
Expected credit losses
While most debtors of NHS bodies are with public sector entities, where significant changes in recoverability are not
expected, for non-public sector debtors consideration is needed of the impact on the required level of provision for
expected credit losses under IFRS 9. The Trust has decreased its provision for non-NHS debtors from £6.7m of £14.6m
of debts at 31 March 2021 (45.9%) to £3.9m of £15.8m (24.7%) at 31 March 2022.
Accounting for Covid-19 response measures
There are a number of elements of the Department and NHS’s response to Covid-19 which have specific accounting
treatments which have been directed by amendments to the Group Accounting Manual. The principal impacts upon the
Trust are:
• Centrally procured Personal Protective Equipment – the Trust has recognised £1,090k of notional income, £1,381k
of notional expense which reflects the brought forward balance of inventory from the prior year for centrally
procured Personal Protective Equipment.
Narrative and other reporting issues
We have considered how the Trust has reflected the impact of the pandemic in its reporting, including:
• Annual report discussion of the impact on services, operations, performance, strategic direction, resources and
financial sustainability.
• Accounts disclosures on the impact on estimates and judgements, as well as disclosure of specific transactions such
as centrally provided Personal Protective Equipment.
We do not have any matters to report in respect of these disclosures.
Events after the reporting period and relevant disclosures
Events are likely to continue to move swiftly, and the Trust will need to consider the events after the Reporting Period
and whether these events will be adjusting or non-adjusting and make decisions on a transaction by transaction basis.
23/53 189/347

Deloitte Confidential: Government and Public Services
16
Value for money
Value for Money requirementsWe are required to consider the arrangements that the Trust has made securing financial resilience and economy, efficiency and effectiveness in its use of resources, if we identify any significant weaknesses to make recommendations, and to provide a narrative commentary on arrangements. To perform this work, we are required to:• Obtain an understanding of the Trust’s arrangements sufficient to support our risk assessment and commentary;• Assess whether there are risks of a significant weakness in the Trust’s arrangements, and perform additional procedures if a risk is identified.
If a significant weakness is identified, we report this and an accompanying recommendation;• Report in our audit opinion if we have reported any significant weaknesses by the time of the issue of our opinion;• Issue a narrative commentary in our Annual Auditor’s Report on the arrangements in place; • If our Value for Money work was not complete at the time of our audit opinion, report any additional significant weaknesses identified in
completing our work when certifying completion of the audit.
Work performed to obtain an understanding of the Trust’s arrangements to secure economy, efficiency and effectiveness in the useof resourcesAs part of our risk assessment, we have reviewed the summary of VfM arrangements prepared by the Trust, reviewed supporting documentation on arrangements, and held follow-up interviews on areas where additional information was required.
In addition, we have:
• reviewed of the Trust’s draft Annual Governance Statement; • reviewed internal audit reports through the year and the Head of
Internal Audit Opinion;• considered issues identified through our other audit work;• considered the Trust’s results, including observations from our
benchmarking of actual performance;
• reviewed the Care Quality Commission’s report on the Trust dated December 2019;
• reviewed of NHSI’s risk ratings;• considered the Trust’s NHS Resolution risk rating;• considered the Trust’s Information Governance toolkit score.
Findings of our work
We have not identified any risks of significant weakness in arrangements to secure economy, efficiency and effectiveness in the use of resources.
We have no matters to report by exception in our financial statement audit opinion.
Our work is complete and reported in our separate Auditor’s Annual Report
24/53 190/347

Deloitte Confidential: Government and Public Services
17
Control deficiencies and areas for management focus
Your control environment and findings
AreaPriority and year identified
Observation Trust Response
Segregation of Duties
2019/20
Our IT specialists identified that, until September 2021, four users have the ability to add and remove users on the Integra application, as well as carry out transactional duties on the application for financial purposes. Where users have these abilities, they may be able to circumvent configured application controls, either by amending their own access or by creating "dummy users”.
Access was removed in September 2021,
the Trust will run exception reports for
the users identified.
Revaluation reserve calculation
2021/22
We would expect that new assets are included as a separate line within a revaluation calculation as while they are included within the existing site there is no revaluation reserve brought forward for these assets. This would apply for new assets added since the move from DVs to AY as they will be separate lines within the valuers report.
The Trust will include new additions as
separate lines in future.
Accounting memorandums
2021/22
The Trust should prepare memorandums explaining the rationale and calculation behind significant judgements held at the balance sheet date with specific reference to applicable accounting standards, for example significant provisions or transactions that take place in the year. Where practical potentially significant judgements should be made available before the year end so a position can be agreed in advance.
The Trust did seek early engagement in
respect of two potentially significant
judgment areas prior to yearend, namely
the Innovate transaction and also the
derecognition of cloud software and will
endeavour to do this going forwards for
other potentially significant judgement
areas too
Inclusion of agency staff in the fair pay multiple calculation
2021/22
There is a requirement for NHS bodies to include agency
staff in the calculation of the fair pay multiple disclosed in
the annual report. This has not been included in the Trust’s
calculation due to the availability of the data so we
recommend that the Trust reviews its processes to include
this information in future periods.
Agreed the Trust will review the agency
data and processes.
During the course of our audit work to date we have identified internal control and risk management findings, which we have included below for information.
25/53 191/347

Deloitte Confidential: Government and Public Services
18
Your control environment and findings
Update on recommendations from previous years
Area Observation and recommendationProgress in the year to 31 March 2022
Conclusion
Segregation of Duties
Our IT specialists identified that four users have the ability to add and remove users on the Integra application, as well as carry out transactional duties on the application for financial purposes. Where users have these abilities, they may be able to circumvent configured application controls, either by amending their own access or by creating "dummy users”. We note that a mitigating control has been implemented to review any transaction postings by identified individuals. In addition, the finance controller has had their access revoked so all staff remaining are part of the financial systems team. We perform additional procedures around transactions posted by these individuals as part of our journals testing.
This has been addressed part way
through 2021/22 with the
revocation of access for the users
identified in September 2021.
Re-raised.
IAS 16 Compliance
In accordance with the requirements of IAS 16 all assets within a single class should be revalued at the same time. The valuation performed by the District valuer did not include a land asset acquired during Month 12 by SWFT Clinical Services. Further review and discussion identified that the Trust requested the land to be revalued at the 31 March 2021 although this was not performed due to capacity at the DV. The Trust propose to revalue this land ahead of the SWFT Clinical Services audit during the summer.
The Trust should ensure entire classes of assets are revalued in accordance with the requirements of IAS 16.
Agreed. This has been updated in
the current valuation at 31 March
2022.
Noted and
accepted.
In the previous audit we identified a number of recommendations for improvement. An update on these recommendations is given below:
ISA 610 and 315 require that the use of internal audit must not be excessive in the circumstances of the engagement and overshadow work of the external auditor as it is the external auditor’s sole responsibility for the provision of the audit opinion. We have conducted a review of the work performed by internal audit and assessed any impact on our audit scope. However, we have taken no reliance on work performed by internal audit.
The purpose of the audit was for us to express an opinion on the financial statements. The audit included consideration of internal control relevant to the preparation of the financial statements in order to design audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of internal control. The matters being reported are limited to those deficiencies that we have identified during the audit and that we have concluded are of sufficient importance to merit being reported to you.
Low Priority
Medium Priority
High Priority
26/53 192/347

Deloitte Confidential: Government and Public Services
19
Fraud and non-compliance with laws and regulations
We will explain in our audit report how we considered the audit capable of detecting irregularities, including fraud. In doing so, we will describe the procedures we performed in understanding the legal and regulatory framework and assessing compliance with relevant laws and regulations.
Whilst this requirement has been in place for a few years for public interest entities (as defined by the EU Audit Regulation), recent changes to ISAs (UK) mean it will apply to all entities for periods commencing on or after 15 December 2019.
Significant difficulties encountered:
None
Other matters:
None
External and internal factors impacting the Trust
Other significant findings
Qualitative aspects of your accounting practices:
None
Other matters relevant to financial reporting:
As outlined on page 17 the Trust should prepare memorandums explaining the rationale and calculation behind significant judgements held at the balance sheet date with specific reference to applicable accounting standards. Where practical potentially significant judgements should be made available before the year end so a position can be agreed in advance.
Significant matters discussed with management:
None
27/53 193/347

Deloitte Confidential: Government and Public Services
20
Our opinion on the financial statements
Based on the current status of our work our opinion on the financial statements is expected to be unmodified.
We will highlight that the going concern assessment is on the basis of the ‘continuing provision of service’ approach, and will report that we concur with management’s use of the going concern basis of accounting.
Emphasis of matter and other matter paragraphs
There are no matters we judge to be of fundamental importance in the financial statements that we consider it necessary to draw attention to in an emphasis of matter paragraph.
There are no matters relevant to users’ understanding of the audit that we consider necessary to communicate in an other matter paragraph.
Value for Money reporting by
exception
We have no matters to date to
report by exception in our
financial statement audit opinion.
Irregularities and fraud
We will explain the extent to which we considered the audit to be capable of detecting irregularities, including fraud.
In doing so, we will describe the procedures we performed in understanding the legal and regulatory framework and assessing compliance with relevant laws and regulations. We will discuss the areas identified where fraud may occur and any identified key audit matters relating to fraud.
Recent changes to ISAs (UK) mean this requirement will apply to all entities for periods commencing on or after 15 December 2019.
The form and content of our report
Our audit report
Here we discuss how the results of the audit impact on our audit report. Under the 2020 Code of Audit Practice and Auditor Guidance Note 7, Audit Reporting, Foundation Trusts are not required to have an ‘enhanced’ audit report. An overview of our financial statement audit work will be included in our Auditor’s Annual Report.
28/53 194/347

Deloitte Confidential: Government and Public Services
21
Purpose of our report and responsibility statement
Our report is designed to help you meet your governance duties
What we report
Our report is designed to help the Audit Committee and the Board discharge their governance duties. It also represents one way in which we fulfil our obligations under ISA (UK) 260 to communicate with you regarding your oversight of the financial reporting process and your governance requirements. Our report includes:
• Results of our work on key audit judgements and our observations on the quality of your Annual Report.
• Our internal control observations.
• Other insights we have identified from our audit.
What we don’t report
As you will be aware, our audit was not designed to identify all matters that may be relevant to the board.
Also, there will be further information you need to discharge your governance responsibilities, such as matters reported on by management or by other specialist advisers.
Finally, our views on internal controls and business risk assessment should not be taken as comprehensive or as an opinion on effectiveness since they have been based solely on the audit procedures performed in the audit of the financial statements and the other procedures performed in fulfilling our audit plan.
The scope of our work
Our observations are developed in the context of our audit of the financial statements.
We described the scope of our work in our audit plan.
We welcome the opportunity to discuss our report with you and receive your feedback.
Use of this report
This report has been prepared for the Board of Directors, as a body, and we therefore accept responsibility to you alone for its contents. We accept no duty, responsibility or liability to any other parties, since this report has not been prepared, and is not intended, for any other purpose. Except where required by law or regulation, it should not be made available to any other parties without our prior written consent.
Deloitte LLP
Birmingham | 10 June 2022
29/53 195/347

Deloitte Confidential: Government and Public Services
Appendices
30/53 196/347

Deloitte Confidential: Government and Public Services
23
Audit adjustments
Unadjusted misstatements
The following uncorrected misstatements have been identified up to the date of this report which we request that you ask management to correct as required by ISAs (UK).
Debit/(credit) income
statement£m
Debit/(credit) in net assets
£m
Debit/(credit) taxpayers and
other equity£m
If applicable, control
deficiency identified
Misstatements identified in current year
Sensyne Income Deferral [1] (2.3) 2.3
Sensyne Valuation of Shares [1]0.4
(0.4)
Total - - - -
Disclosure misstatements
The critical accounting estimates state that the income recognised upon receipt of the Sensyne shares is outside the scope of IFRS 15. Consistent with our findings in previous years, this is not in line with our understanding of the arrangement and therefore recommend that this be removed.
During our review of the consistency between the IFRS 16 workings and those used for the operating lease commitments we identified that the lease commitments note did not include leases with NHS property services which are included in the IFRS16 workings. The Trust are reviewing the disclosure. We will provide the committee with an update on progress.
The Trust has opted to include the adjusted financial performance figures on the face of the statement of comprehensive income (SOCI). While this is in the NHS template accounts it is deemed to be an alternative performance measure and therefore would be more appropriately disclosed in the notes to the accounts.
The trust has not included agency staff in the calculation of its fair pay multiple calculation in the current or prior year. Additional narrative will also be required in the remuneration report to draw attention to its exclusion.
[1] These errors have rolled forward from previous years in relation to the investment in Sensyne Plc and were first raised in 2018/19. note that in the prior year no data was shared and therefore there is no release to the income statement.
31/53 197/347

Deloitte Confidential: Government and Public Services
24
Audit adjustments
Corrected misstatements
The following misstatements have been identified up to the date of this report which have been corrected by management. We nonetheless communicate them to you to assist you in fulfilling your governance responsibilities, including reviewing the effectiveness of the system of internal control.
Debit/ (credit) income
statement£m
Debit/ (credit) in net assets
£m
Debit/ (credit) OCI/Equity
£m
If applicable, control
deficiency identified
Annual leave additional provision [1]
2.6
(2.6)
2.6
(2.6)
Total - - -
[1] The Trust had recognised a provision against the return of funds in relation to the unutilised central funding for the cost of additional annual leave entitlements. Discussions with the Trust identified that they are obligated to return the funds and thereforethis balance should shown within trade and other payables.
32/53 198/347

Deloitte Confidential: Government and Public Services
25
Prior year unadjusted misstatements
The following uncorrected misstatements have been identified which we request that you ask management to correct as required by ISAs (UK). We will follow up on these items throughout our audit.
Debit/ (credit) income statement
£m
Debit/ (credit) in net assets
£m
Debit/ (credit) taxpayers and other equity
£m
Misstatements identified in 2020/21
Sensyne Income Deferral [1] (2.3) 2.3
Sensyne Valuation of Shares [1]0.4
(0.4)
NHS income provisions held against cleared debt [2] (3.1) 3.1
Incorrect recognition of Deferred Income (Factual) [3]1.5
(1.5)
Incorrect recognition of Deferred Income (Extrapolated) [3]1.4
(1.4)
Notional Income for Donated PPE (Extrapolated) [4]1.7
(1.7)
Total 2020/21 (3.1) 0.8 2.3
33/53 199/347

Deloitte Confidential: Government and Public Services
26
Prior year unadjusted misstatements (continued)
1. These errors have rolled forward from previous years in relation to the investment in Sensyne Plc and were first raised in 2018/19. note that in the prior year no data was shared and therefore there is no release to the income statement.
2. This misstatement related to the provision for NHS receivables which are not expected to be received. We have reviewed the workings for 20/21 and identified that the majority of the historic debts and disputes have been settled in year. We would expect that this provision would be released in the year.
3. This misstatement is made up of the factual amount of £1.5m incorrectly recognised as deferred income, due to the cash not being receipted in advance, at the year end. The correcting entry is Dr Deferred Income £1.5m and Cr Receivable £1.5m.As our testing is based on a sample, the error rate has been extrapolated over the population to calculate a total projected error of £2.9m and therefore a further extrapolation of £1.4m has been raised.
4. The Trust were unable to provide evidence for the full amount of covid related personal protective equipment that agrees to the receipts recognised by NHSI. The Trust have recognised notional donated income of £5.4m and cost of £5.0m with the balance being in inventory. For a sample selected NHSI recognised 40,000 units while the Trust showed 24,600 unit. Based on the difference in the quantities recognised by NHSI and the Trust procurement and the agreed prices we have extrapolated a worst case difference on the balance giving £1.7m.
Disclosure misstatements
1. The critical accounting estimates state that the income recognised upon receipt of the Sensyne shares is outside the scope of IFRS 15. Consistent with our findings in previous years, this is not in line with our understanding of the arrangement and therefore recommend that this be removed.
2. The Trust have not included the tables included in the NHSI template in relation to staff exit packages in their annual report. These are included as part of the TAC consolidation schedules and we note the amounts are not material.
34/53 200/347

Deloitte Confidential: Government and Public Services
27
Responsibilities:
The primary responsibility for the prevention and detection of fraud rests with management and those charged with governance, including establishing and maintaining internal controls over the reliability of financial reporting, effectiveness and efficiency of operations and compliance with applicable laws and regulations. As auditors, we obtain reasonable, but not absolute, assurance that the financial statements as a whole are free from material misstatement, whether caused by fraud or error.
Required representations:
We have asked the Accounting Officer on behalf of the Board to confirm in writing that you have disclosed to us the results of your own assessment of the risk that the financial statements may be materially misstated as a result of fraud and that you are not aware of any fraud or suspected fraud that affects the Foundation Trust and Group.
We have also asked the Accounting Officer on behalf of the Board to confirm in writing their responsibility for the design, implementation and maintenance of internal control to prevent and detect fraud and error.
Audit work performed:
In our planning we identified the risk of fraud in revenue recognition and management override of controls as a key audit risk.
During course of our audit, we have had discussions with management and those charged with governance as well as Local Counter Fraud and Internal Audit. There were no known cases of fraud other than the findings in the Counter Fraud Progress Report which was sent to the Audit Committee.
In addition, we have reviewed management’s own documented procedures regarding fraud and error in the financial statements.
We will explain in our audit report how we considered the audit capable of detecting irregularities, including fraud. In doing so, we will describe the procedures we performed in understanding the legal and regulatory framework and assessing compliance with relevant laws and regulations.
Fraud responsibilities and representations
Our other responsibilities explained
Concerns:
No concerns have been brought to attention.
35/53 201/347

28
The performance report and accountability report
Our work includes:
• Reading these reports and assessing whether they comply with the applicable requirements of the NHS FT ARM for NHS Trusts;
• Considering whether the information presented is consistent with the financial statements, including cross-checking figures to the audited financial statements;
• Assessing whether, in light of our knowledge and understanding obtained during the audit, these reports contain any material misstatements.
In our audit report we will give positive statements regarding the preparation of the reports in accordance with legal and regulatory requirements and consistency with the financial statements.
If we find material misstatements, we will require that these be corrected, otherwise we will have to report these.
Annual Governance Statement
We read the Annual Governance Statement and assess whether it meets the disclosure requirements of the NHS FT ARM, and whether it is misleading or inconsistent with information of which we are aware from our audit.
In our audit report, we report any exceptions identified in respect of these responsibilities.
Remuneration report and staff report
We audit the part of the remuneration report and staff report subject to audit, and state in our audit report whether it has been properly prepared in accordance with the NHS Act 2006.
Examples of matters that would cause us to report
• The Annual Governance Statement doesn’t disclose significant control weaknesses identified in internal audit reviews.
• Risks to financial sustainability are not adequately disclosed in the Annual Report.
• Significant weaknesses in Value for Money arrangements are not appropriately disclosed in the Annual Governance Statement.
Information in your annual report
Our other responsibilities explained
Your annual report contains detailed financial and non-financial information including discussion of the Trust’s strategy, business model, risks and prospects. This provides stakeholders with a holistic view of the performance of the Trust and provides context for the Trust’s financial results and position as set out in the financial statements. We set out on this slide the work we perform in respect of this information and the matters we will report.
Deloitte Confidential: Government and Public Services36/53 202/347

Deloitte Confidential: Government and Public Services
29
Independence and feesAs part of our obligations under International Standards on Auditing (UK), we are required to report to you on the matters listed below:
Independence confirmation
We confirm the audit engagement team, and others in the firm as appropriate, Deloitte LLP and, where applicable, all Deloitte network firms are independent of the Trust and our objectivity is not compromised.
Fees Details of the fees proposed for the period are presented below. Non-audit fees are being incurred as below: - Coventry and Warwickshire Integrated Care System Digital Transformation Board (Part of STP governance, hosted by
South Warwickshire NHS Foundation Trust) – c. £40k per STP partner- Coventry and Warwickshire Integrated Care System Leadership Development Programme – c. £6k per STP partner
Non-audit services
In our opinion there are no inconsistencies between FRC’s Ethical Standard and the Trust’s policy for the supply of non-audit services or of any apparent breach of that policy We continue to review our independence and ensure that appropriate safeguards are in place including, but not limited to, the rotation of senior partners and professional staff and the involvement of additional partners and professional staff to carry out reviews of the work performed and to otherwise advise as necessary.
Relationships We have no other relationships with the Trust, its directors, senior managers and affiliates, and have not supplied any services to other known connected parties.
The professional fees earned by Deloitte in the period from 1 April 2021 to 31 March 2022 are as follows:
2021/22 (£) 2020/21 (£)
Audit of Trust (including Value for Money) 97,631 63,000
Audit of Charitable Funds 7,600 3,500
Audit of SWFT Subsidiaries 29,200 24,000
Targeted Audit Work* TBC 22,000
Total audit fees 134,431 112,500
Audit related assurance services ** - -
Total fees 134,431 112,500
* In 2021/22 we anticipate additional audit work will be required relating to the implementation of IFRS 16 (estimated fee £5,000 - £8,000). In addition, we have incurred additional cost for use of specialists and one of aspects of the current year audit. We will keep the Trust informed of any fee implications
** We do not expect to undertake external assurance work in respect of the Quality Accounts in 2021/22 and therefore no fee would be payable.
*** The audit fee may be impacted by practical considerations as a result of ongoing COVID-19 related measures. Should this be the case we will keep the Trust informed of any fee implications.
37/53 203/347

Deloitte Confidential: Government and Public Services
30
Draft management representation letter
Deloitte LLP
4 Brindley place
Birmingham
B1 2HZ
United Kingdom
XX June 2022
Our Ref:
Dear Engagement Leader
This representation letter is provided in connection with your audit of the annual financial statements of South Warwickshire NHS Foundation
Trust and its financial statements for the year ended 31 March 2022 for the purpose of expressing an opinion as to whether the financial
statements give a true and fair view of the financial position of South Warwickshire NHS Foundation Trust as of 31 March 2022 and of the results
of its operations, other recognised gains and losses and its cash flows for the year then ended in accordance with the directions given by NHS
Improvement - Independent Regulator of NHS Foundation Trusts in accordance with paragraph 25 of Schedule 7 of the National Health Service
Act 2006.
As Accounting Officer and on behalf of the board of directors, I confirm, to the best of my knowledge and belief, the following representations.
Financial Statement
1. I understand and have fulfilled our responsibilities for the preparation of the financial statements in accordance with the directions given by
NHS Improvement - Independent Regulator of NHS Foundation Trusts in accordance with paragraph 25 of Schedule 7 of the National Health
Service Act 2006 which give a true and fair view, as set out in the terms of the audit engagement letter.
2. The methods, the data, and the significant assumptions used by us in making accounting estimates and their related disclosures, including
those assessing the impact of Covid-19 on the Trust, are appropriate to achieve recognition, measurement or disclosure that is reasonable
in the context of the applicable financial reporting framework. In particular, when assessing the impact of Covid-19 on the Trust and Group
we have considered the following:
• Key assumptions adopted by the directors;
• Principal risk disclosures;
• Change in the funding regime for NHS bodies; and.
• Specific representations regarding any relevant disclosures in the financial statements.
30
38/53 204/347

Deloitte Confidential: Government and Public Services
31
Draft management representation letter
Financial statements
3. Related party relationships and transactions have been appropriately accounted for and disclosed in accordance with the requirements of
IAS24 “Related party disclosures”.
4. All events subsequent to the date of the financial statements and for which the applicable financial reporting framework requires
adjustment of or disclosure have been adjusted or disclosed.
5. We confirm that the financial statements have been prepared on the going concern basis and disclose in accordance with IAS 1 all matters
of which we are aware that are relevant to the Trust’s ability to continue as a going concern, including principal conditions or events and
our plans. In making our going concern assessment we have adopted the ‘continuing provision of service’ approach and accordingly we
are not aware of any material uncertainties related to events or conditions that may cast significant doubt upon the Trust’s ability to
continue as a going concern. There are no circumstances that we are aware of that would affect the appropriateness of the ‘continuing
provision of service’ approach. We confirm the completeness of the information provided regarding events and conditions relating to going
concern at the date of approval of the financial statements, including our plans for future actions.
6. We confirm that following discussions with our commissioners in respect of the period-end activity position and final income settlements,
these have been appropriately reflected in the 2021/22 financial statements.
7. We have considered the value of the tangible assets recorded in the Statement of Financial Position at 31 March 2022. We confirm that
this is best valuation available at this date.
8. We confirm that all deferred income balances have been appropriately deferred in line with intentions of the funding body.
9. We acknowledge our responsibility for ensuring the Trust has put in place arrangements for securing economy, efficiency and
effectiveness in its use of resources.
10. We are not aware of any deficiencies in the Trust’s arrangements to secure economy, efficiency and effectiveness in its use of resources.
11. All grants or donations, the receipt of which is subject to specific restrictions, terms or conditions, have been notified to you. We have
evaluated whether the restrictions, terms or conditions on grants or donations have been fulfilled with and deferred income to the extent
that they have not.
31
39/53 205/347

Deloitte Confidential: Government and Public Services
32
Draft management representation letter12. We confirm that we have accounted for all income streams from commissioners in accordance with the requirements of IFRS 15, Revenue
from Contracts with Customers, assessing each arrangement under the IFRS 15 five step model to determine when revenue should be
recognised. We confirm that all deferred and accrued income balances in respect of transactions accounted for under IFRS 15 have been
accounted for in line with our documented assessment of the IFRS 15 five step model (which we have shared with you for all transactions
with other NHS bodies).
13. We have no plans or intentions that may materially affect the carrying value or classification of assets and liabilities reflected in the
financial statements.
14. We confirm that we are not aware of any regulatory action being taken by NHS Improvement or the Care Quality Commission against the
Trust.
15. We confirm that we do not consider there to be any material judgements in applying IFRS 15 that require disclosure in the financial
statements.
16. We confirm that we consider all debtors recognised under IFRS 15 to be “contract receivables” and that there are no “contract assets” as
at the year end, as there are no debtors for which the Trust’s right to consideration is conditioned on something other than the passage of
time (including future performance).
17. The Trust is due payments relating to Section 106 and Community Infrastructure Levy income from Warwickshire District Council and
Stratford District Council at the year-end. We confirm that there are no issues around recoverability and are in receipt of these monies for
forwarding onto the Trust
18. We confirm that we have disclosed to you the details of all vesting certificates with suppliers used during the year, and that were in place
at the year-end, and confirm that the accounting treatment adopted for each reflects our assessment of the facts and circumstances for
each arrangement.
19. Based on discussions with other NHS bodies, we consider that the resolution of disputed balances and accrued income will not result in a
material adverse effect on the reported financial position. We have reviewed the basis of mis-matches for differences with other NHS
bodies and consider that the balances included in provisions and liabilities are a reasonable estimate of the disputed balances which are
not expected to be recovered. This includes the following:
Income & Expenditure Mis-matches
• Midlands regional office- £1,156k – Trust income is lower by this amount
• Central specialised commissioning - £735k – Trust income is higher by this amount
• Coventry & Warwickshire CCG - £1,419k – Trust income is lower by this amount
• Health Education England - £454k – Trust income is lower by this amount
• NHS Property Services - £462k – Trust expenditure is lower by this amount 32
40/53 206/347

Deloitte Confidential: Government and Public Services
33
Draft management representation letter19. Receivable and credtors mis-matches
• Central specialised commissioning - £302k – Trust receivable is lower by this amount.
• South west regional office - £741k – Trust receivable is lower by this amount
• George Eliot Hospital NHS Trust - £925k – Trust receivable is higher by this amount
• Coventry & Warwickshire CCG - £502k – Trust payable is lower by this amount
20. With respect to the revaluation of properties in accordance with the Group Accounting Manual:
i. the measurement processes used are appropriate and have been applied consistently, including related assumptions and models;
ii. ii. the assumptions appropriately reflect our intent and ability to carry out specific courses of action on behalf of the entity where
relevant to the accounting estimates and disclosures;
iii. we have considered whether any changes are required to the Modern Equivalent Asset assumed in the valuation for the impact of
increased infection control requirements following the experience of the Covid-19 pandemic, and following consultation with our
valuation experts do not consider any changes are required to assumptions at this time
iv. we have considered whether any changes are required to the Modern Equivalent Asset assumed in the valuation to reflect changes to
requirements as a result of climate change, and [following consultation with our valuation experts do not consider any changes are
required to assumptions at this time;
v. the disclosures are complete and appropriate; and
vi. there have been no subsequent events that require adjustment to the valuations and disclosures included in the financial
statements.
21. We confirm that we consider that depreciated historic cost is an appropriate proxy for the fair value of non-property assets and are not
aware of any circumstances that would indicate that these assets require revaluation.
22. We confirm that we consider the allocation of brought forward revaluation reserve against individual fixed assets to be appropriate and
that this allocation has been based on available information where possible.
23. We confirm we have included temporary used in the year, on a full time equivalent, annualised basis, in our calculation of the fair pay
disclosures in the remuneration report, for both the current and prior years.
33
41/53 207/347

Deloitte Confidential: Government and Public Services
34
Draft management representation letter
Information provided:
23. We have provided you with all relevant information and access as agreed in the terms of the audit engagement letter and required by the
National Health Service Act 2006.
24. All transactions have been recorded and are reflected in the financial statements and the underlying accounting records.
25. We acknowledge our responsibilities for the design, implementation and maintenance of internal control to prevent and detect fraud and
error.
26. We have disclosed to you the results of our assessment of the risk that the financial statements may be materially misstated as a result of
fraud.
27. We are not aware of any fraud or suspected fraud that affects the entity and involves:
(i) Management
(ii) employees who have significant roles in internal control; or
(iii) others where the fraud could have a material effect on the financial statements
28. We have disclosed to you all information in relation to allegations of fraud, or suspected fraud, affecting the entity’s financial statements
communicated by employees, former employees, analysts, regulators or others.
29. We are not aware of any instances of non-compliance, or suspected non-compliance, with laws, regulations and contractual agreements
whose effects should be considered when preparing financial statements.
30. We confirm that we have disclosed to you the details of all vesting certificates with suppliers used during the year, and that were in place
at the year-end, and confirm that the accounting treatment adopted for each reflects our assessment of the facts and circumstances for
each arrangement.
31. We confirm that we have disclosed to the Trust all matters as may be necessary for the purpose of making the directors’ remuneration
disclosures required by the National Health Service Act 2006.
32. We confirm that there are no directors who were opted out members of NHS pension arrangements for part of the financial year.
33. All known actual or possible litigation and claims whose effects should be considered when preparing the financial statements have been
disclosed to you and accounted for and disclosed in accordance with the applicable financial reporting framework. No other claims in
connection with litigation have been or are expected to be received.
34
42/53 208/347

Deloitte Confidential: Government and Public Services
35
Draft management representation letter
34. We confirm that:
• we consider that the Trust has appropriate processes to prevent and identify any cyber breaches other than those that are clearly
inconsequential; and
• we have disclosed to you all cyber breaches of which we are aware that have resulted in more than inconsequential unauthorised
access of data, applications, services, networks and/or devices
35. We acknowledge our responsibility for ensuring the Trust has put in place arrangements for securing economy, efficiency and
effectiveness in its use of resources.
36. We are not aware of any deficiencies in the Trust’s arrangements to secure economy, efficiency and effectiveness in its use of resources.
37. The Trust has used Mills & Reeve LLP during the period as legal advisors. No further legal advisors have been used during the period. We
confirm that we have made you aware of all ongoing litigation involving the Trust.
38. There are no loans, liabilities or other financial instruments associated with the Government Banking Service bank account which have not
been appropriately recorded in the financial.
39. We have performed an assessment of the impact on the financial statements of events in Russia and Ukraine including consideration of the
impact of sanctions and have concluded that no material impact exists.
We confirm that the above representations are made on the basis of adequate enquiries of management and staff (and where appropriate,
inspection of evidence) sufficient to satisfy ourselves that we can properly make each of the above representations to you.
Yours faithfully
Signed as Accounting Officer on behalf of the Board of Directors
35
43/53 209/347

Deloitte Confidential: Government and Public Services
36
NHS England is consulting on a revised Code for all providers, reflecting UK Corporate Governance Code changes and the move to Integrated Care Systems
Code of Governance for NHS provider trusts
Next steps
• We recommend the Trust consider whether to respond to the consultation.• Our experience is that companies needed significant discussion and analysis at board or committee level, usually led by the chair supported
by a well-informed company secretary, to consider how the Principles of the UK Code applied to them. The final approach in the new code to how the Principles and Provisions interact will be critical to understanding what boards need to do.
• We recommend starting planning for updated governance processes and controls based on the draft code.
Issue
The existing NHS Foundation Trust Code of Governance was issued in 2014, reflecting the UK Corporate Governance Code at that time.
There have since been significant changes to the UK Corporate Governance Code in 2018, and an increased focus on system and partnership working and governance models going beyond individual providers.
On 27 May 2022, NHS England issued three consultations, running to 8 July 2022.
The new Code of Governance for NHS provider trusts
NHS England propose for the first time applying the same requirements to NHS Trusts as to Foundation Trusts.
The draft code is a significant rewrite, reflecting the substantial changes in UK Corporate Governance Code (adapted for an NHS context). This
includes setting out new code Principles, and introducing new Provisions in the draft code including:
• The board’s role in monitoring and assessing culture;
• Mechanisms for gathering the views of the workforce;
• Reporting on how stakeholder interests have influenced the board’s decision-making;
• Succession planning and board member contribution;
• Diversity and inclusion; and.
• Board responsibility for identifying and assessing emerging risks (in addition to the principal risks).
We note that the UK Corporate Governance Code is based around both applying the Principles of the UK Code, and complying or clearly
explaining non-compliance with the Provisions of the UK Code. The consideration of the application of the Principles is key for the application of the UK Code. The draft code does not currently explain the role of the Principles, and clarification of this will be critical to understanding the
impact of the new code on organisations.
An addendum to “Your statutory duties – reference guide for NHS foundation trust governors”
This provides guidance to governors on how to consider system issues in fulfilling their duties.
Draft guidance on good governance and collaboration under the NHS provider licence
This sets out expectations on governance arrangements to support working with other organisations and in ICSs, emphasising the importance of
providers’ contributions to the success of ICSs. This includes engaging consistently in shared planning and decision-making; consistently taking collective responsibility for delivery of services; and consistently taking responsibility for delivery of agreed system improvements and decisions.
44/53 210/347

Deloitte Confidential: Government and Public Services
Sector benchmarking & risk assessment
45/53 211/347
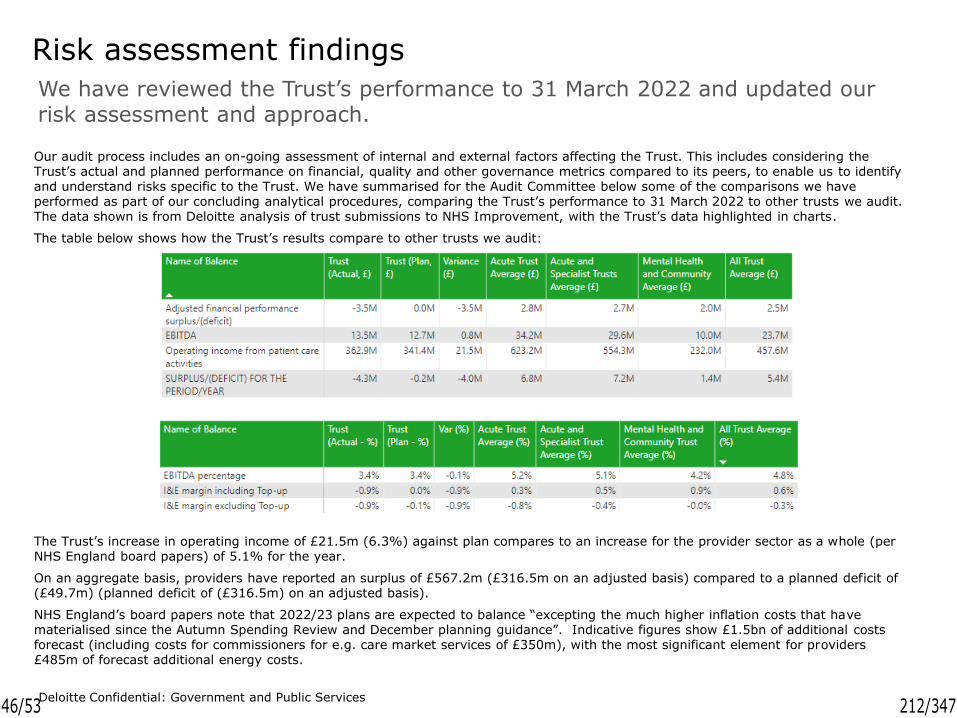
Deloitte Confidential: Government and Public Services
We have reviewed the Trust’s performance to 31 March 2022 and updated our risk assessment and approach.
Risk assessment findings
Our audit process includes an on-going assessment of internal and external factors affecting the Trust. This includes considering the Trust’s actual and planned performance on financial, quality and other governance metrics compared to its peers, to enable us to identify and understand risks specific to the Trust. We have summarised for the Audit Committee below some of the comparisons we have performed as part of our concluding analytical procedures, comparing the Trust’s performance to 31 March 2022 to other trusts we audit. The data shown is from Deloitte analysis of trust submissions to NHS Improvement, with the Trust’s data highlighted in charts.
The table below shows how the Trust’s results compare to other trusts we audit:
The Trust’s increase in operating income of £21.5m (6.3%) against plan compares to an increase for the provider sector as a whole (per NHS England board papers) of 5.1% for the year.
On an aggregate basis, providers have reported an surplus of £567.2m (£316.5m on an adjusted basis) compared to a planned deficit of (£49.7m) (planned deficit of (£316.5m) on an adjusted basis).
NHS England’s board papers note that 2022/23 plans are expected to balance “excepting the much higher inflation costs that have materialised since the Autumn Spending Review and December planning guidance”. Indicative figures show £1.5bn of additional costs forecast (including costs for commissioners for e.g. care market services of £350m), with the most significant element for providers £485m of forecast additional energy costs.
46/53 212/347

Deloitte Confidential: Government and Public Services
Risk assessment findings
The chart below shows EBITDA margin for trusts we audit, compared to plan. The Trust’s EBITDA of £13.5m compared to plan of £12.7m gives an EBITDA margin of 3.4%. This compares to an average margin for acute trusts of 5.2% and all types of trust of 4.8% (an increase from 4.4% for 2020/21).
The Trust’s overall income and expenditure margin (including top-up) of -0.9% compares to an average margin for acute trusts of 0.3% and all types of trust of 0.6%, as shown in the chart below. This reflects the write off of intangible assets in year.
Margins have improved slightly compared to prior year.
47/53 213/347

Deloitte Confidential: Government and Public Services
Risk assessment findings
The Trust has received a total of £0.2m of COVID-19 reimbursement income (0% of operating income). This compares to anaverage for acute trusts of £8.0m (1.3% of operating income).
Although generally lower than 2020/21, trusts have received significant reimbursement for Covid-19 related expenses
48/53 214/347

Deloitte Confidential: Government and Public Services
The national NHS provider capital budget of £6.9bn compares to £7.2bn in 2020/21 and £4.6bn for 2019/20. Reported spend was £6.8bn.
Risk assessment findings
The Trust's capital programme was behind plan at 31 March 2022, with spend against the “C-DEL” capital budget of £21.1m, compared to plan of £21.8m (97% of plan). (“C-DEL” excludes donated assets and is reduced by disposals).
Most trusts we audit were slightly ahead of plan, with average spend of £27.0m compared to plan of £26.7m (99% of plan), reflecting significant movement in the final month of the year with on average 37.5% (£10.1m) of capital expenditure recognised in the final month of the year.
This pattern of spending concentrated in the final quarter and indeed final month has been seen across the sector and also occurred last year. This is affected both by the timing of award of additional capital funding during the year, and the pressures to use capital budgets available as these do not carry over.
As discussed on page 9, we have assessed capital expenditure as a significant risk at year-end as a result of the high level of expenditure.
As a result of the level of spending around the year-end, we have performed additional testing on year-end capital creditors.
49/53 215/347

Deloitte Confidential: Government and Public Services
The additional funding in year has seen increasing trust cash balances.
Risk assessment findings
The Trust's 31 March 2022 cash balance was £41.7m, £2.5m below the 31 March 2021 balance of £44.2m.
On average acute trusts were £22.7m ahead of plan and all trusts we audit were £16.3m ahead of prior year.
The Trust debtor days at 31 March 2022 were 15.9 days compared to an average for acute trusts of 17.1 days and for all trusts of 17.3 days.
The Trust creditor days at 31 March 2022 were 135.3 days compared to an average for acute trusts of 171.0 days and for all trusts reviewed of 176.4 days.
Debtor and creditor days figures are using NHS Improvement’s calculation methodology.
50/53 216/347

Deloitte Confidential: Government and Public Services
On average, trusts have seen a significant increase in creditors, in particular capital creditors, accruals, deferred income and provisions.
Risk assessment findings
On average, trusts showed a significant increase in credit balances in 2021/22 compared to previous years. This trend has continued in the current year, albeit with a smaller average increase.
The Trust's trade and other payables have increased by £3.3m from £45.0m at 31 March 2021 to £48.3m at 31 March 2022 (a £7.3% increase. This compares to an average increase of 15.9% for acute trusts, and 14.8% for all trusts.
There are a number of factors affecting this. The main common element is the increased level of capital payables (due to the profile of capital expenditure discussed on page 9), whereas the trust have decreased by £4.5m, to £2.1m, a 68.2% decrease (compared to an average increase of 6.94% for acute trusts and an average increase of 4.6% for all trusts).
However, focussing on “revenue” items, trade payables has seen an increase of £0.5m to £7.5m, a 6.9% increase (compared to an average increase of 16.9% for all trusts), and “revenue” (non-capital) accruals has seen an increase of £6.9m to £30.2m, a 29.6% increase (compared to an average increase of 23.1% for all trusts).
Another contributing factor for the Trust is an increase in deferred income balances of £6.5m to £14m, a 46.4% increase (compared to an average increase of 25.0% for acute trusts and an average increase of 30.0% for all trusts).
51/53 217/347

Deloitte Confidential: Government and Public Services
Disclosures of estimated IFRS 16 impact show a significant range of impact between trusts
Risk assessment findings
Trusts have disclosed the expected impact of IFRS 16 on transition at 1 April 2022, and the expected impact on 2022/23. The current disclosures do not include the impact of application of IFRS 16 to PFI balances, pending guidance from DHSC.
On average, there is a forecast impact on net assets, as some bodies have “peppercorn” leases with assets being recognised without corresponding liabilities. The implementation of IFRS 16 is expected to on average be a net charge to the income statement, and to increase capital additions from new leases entered into, or extended, each year.
We have compared the ratio of expected lease liabilities to recognise under IFRS 16 (which is effectively measured at discounted lease payments) to the disclosed lease commitments under IAS 17. In principle, the IFRS 16 liability will be lower than IAS 17 if considering the same leases. In some cases, particularly for Mental Health and Community Trusts, there are arrangements which meet the definition of a lease under IFRS 16 as adapted for the public sector (in particular for assets owned by NHS Property Services without written agreements), but which are not included in the IAS 17 commitment disclosures, and so for some trusts the expected IFRS 16 additional liabilities are higher than the IAS 17 lease commitment.
TrustAcute Trusts] average
Acute and Specialist Trusts average
All Trusts average
(£m) Actual Actual Actual Actual
Right of use assets recognised at 1 April 2022 8.3 30.4 29.8 32.5
Lease liabilities recognised at 1 April 2022 (8.3) (16.5) (15.8) (21.1)
Other changes at 1 April 2022 0.0 0.0 0.0 0.0
Estimated impact on net assets at 1 April 2022 0.0 13.9 14.0 11.4
Estimated impact on surplus/deficit in 2022/23 0.0 (1.4) (1.2) (0.9)
Estimated increase in capital additions in 2022/23 0.0 8.2 6.6 4.8
Lease commitments at 31 March 2022 disclosed under IAS 17 0.7 20.0 19.9 24.3
Ratio of lease liabilities to recognise to lease commitments Note 1 83% 79% 87%
Note 1: During our review of the consistency between the IFRS 16 workings and those used for the operating lease commitments we identified that the lease commitments note did not include leases with NHS property services which are included in the IFRS16 workings. The Trust are reviewing the disclosure. We will provide the committee with an update on progress.
52/53 218/347

This document is confidential and it is not to be copied or made available to any other party. Deloitte LLP does not accept any liability for use of or reliance on the contents of this document by any person save by the intended recipient(s) to the extent agreed in a Deloitte LLP engagement contract.
Deloitte LLP is a limited liability partnership registered in England and Wales with registered number OC303675 and its registered office at 1 New Street Square, London, EC4A 3HQ, United Kingdom.
Deloitte LLP is the United Kingdom affiliate of Deloitte NSE LLP, a member firm of Deloitte Touche Tohmatsu Limited, a UK private company limited by guarantee (“DTTL”). DTTL and each of its member firms are legally separate and independent entities. DTTL and Deloitte NSE LLP do not provide services to clients. Please see www.deloitte.com/about to learn more about our global network of member firms.
© 2022 Deloitte LLP. All rights reserved.
53/53 219/347

Report SummaryReport to Board of Directors Date of
Meeting6 July 2022
Report Title Clinical Governance Committee Report for 8 June 2022
Agenda Item
8.7
Executive/Non-Executive Lead
Fiona Burton, Chief Nursing Officer/David Spraggett, Non-Executive Director and Chair of the Clinical Governance Committee
Report Author(s)
Dr David Spraggett, Non-Executive Director and Chair of the Clinical Governance Committee
Report Previously Discussed at N/A
Purpose of the Report For ApprovalFor Discussion
To provide the Board with a summary of the key issues discussed by the Clinical Governance Committee on 8 June 2022.
For Information
Recommendations and Action Required The Board of Directors is asked to receive and note the report.
Impact (is there any impact arising from the report on the following?) Quality EqualityFinance ResearchPerformance Compliance Workforce Legal
Applicable Quality Improvement Priorities Elective Hub Health InequalitiesElectronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety Compassionate Effectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk RegisterAre any existing risks on the BAF/Risk Register affected? NoIdentify the BAF/Risk Register risk ID and description – explain how the risk has been affected – reduced or increased as a consequence of the evidence within the report – No
Do you recommend a new entry to the BAF and/or Risk Register is made as a result of this report?
No
1/5 220/347

South Warwickshire NHS Foundation Trust
Report to Board of Directors – 6 July 2022
Clinical Governance Committee Report for 8 June 2022
Executive Opinion and Assurance
The Deputy Chief Nursing Officer agreed that this was an accurate summary of the agenda and discussion at the Clinical Governance Committee held on the 8 June 2022 and concurs with the areas for the Board’s attention.
Ellie WardDeputy Chief Nursing Officer
Reports/Items Considered by the Committee
1. Matters of Note from Action Log
All other outstanding actions noted as complete.
2. Drugs and Therapeutics Quarterly Report
It was noted that June 2022 is Medication Safety month. It was also noted that a controlled drug investigation had taken place regarding 3 ampoules of fentanyl that had gone missing. The Committee was assured that the investigation found no themes or trends that suggested the investigation needed to be escalated further.
The Committee raised questions regarding learning from common mistakes and were assured a process was in place for this to happen. It also raised concern regarding how allergies are recorded in Lorenzo system. The Chief Medical Officer advised that Cerner, the new electronic patient record system, would address this issue.
3. Looked After Children Report
The Named Nurse for Children in Care presented a comprehensive report which highlighted how difficult the past year had been due to a complete turnover of staff. The backlog of assessments this caused was a registered risk. The Committee was assured that a recovery plan was in place to address the backlog.
The Committee enquired as to how health inequalities and non-clinical issues were addressed by the team. The Committee was assured that there was close working between the team and local authority colleagues.
4. Patient Safety Monthly Report
This report remained assuring in that there continues to be a high number of incidents reported that is evidence of the open culture of the Trust.
The Committee made a number of observations regarding how positive it was that venous thromboembolism (VTE) assessments remain 97.9% compliant given how
2/5 221/347

extremely busy the Trust had been over the past few months. It also acknowledged that falls causing harm numbers were low again despite this high activity.
Concern was raised regarding high number labelling errors on samples. The Committee was assured that this was being addressed and training of staff is being reviewed.
5. Audit and Operational Governance Group (AOGG) Support Services Quarterly Report
A broadly assuring report was presented by the Podiatry Service Manager. In particular, assurance was given that risk has been minimised for those patients awaiting treatment.
She also acknowledged that the additional question posed regarding: What is the service doing in relation to prevention of ill health within the service to reduce future demand? had not been answered in this report but would be included in all future reports.
The Committee noted the marked increase in paediatric diabetes and enquired as to any reasons that have been noted. It was informed that it was likely to be associated with lifestyle and rising obesity in children and more information would be included in the next report.
6. Audit and Operational Governance Group (AOGG) Family Health Quarterly Report
A comprehensive report presented but particular attention was raised regarding the foetal medicine pathway which has made little progress due to issues with University Hospitals Coventry & Warwickshire (UHCW).
The Committee asked regarding the colposcopy waiting times as last year they were excessive. The AOGG Chair assured that with additional support to clear the backlog the intention was to see all new referrals within 6 weeks.
Children in Crisis on Macgregor Ward was also discussed and the AOGG C hair informed that the high numbers seen during lockdown had now reduced. There still remain some admissions particularly relating to eating disorders, the Committee was informed it being a national issue.
7. Commissioning for Quality and Innovation (CQUIN) Quarterly Exception Report
The Committee was informed that CQUIN had been reintroduced for 2022 with 15 Commissioning Care Group (CCG) set targets. 5 CQUIN were proposed to be adopted by the Trust, The Committee agreed this proposal.
8. Infection Prevention Board Quarterly Report
This report showed an increase in C Difficile as well as MRSA in the past Quarter, this being in line with the national picture. There has also been a norovirus outbreak on Chadwick Ward, however no staff were infected suggesting infection prevention and control measures in place are effective.
3/5 222/347

The Committee also sought assurance that ED staff were aware of monkeypox. This assurance was given with a microbiology consultant leading this work.
9. Serious Incident Monitoring Report
It was good to note that of the 68 new actions since the previous report, 44 had already been closed. It was noted the amount of work that was needed to achieve this.
An additional element to the report related to Ockenden and this will appear in future presentations.
It was also assuring to note that overdue risks and actions have been escalated to Management Board to ensure they are dealt with as promptly as possible.
The Committee made comment about chasing audit actions and was assured by the Patient Safety Manager that they are all tracked by the Patient Safety Team.
The Committee also raised specific concern over actions that are long overdue. It was agreed that the Chief Operating Officer and Chief Medical Officer will explore ways to address them.
10.Records Acknowledgement Update
The Committee was informed that the draft policy had been delayed due to clinical discussions that had taken place. It was planned that this will be resolved by end of June 2022 and will appear in the next report to this Committee.
The Head of Governance made Committee members aware that he was responsible for managing alerts and the Healthcare Records Policy. It was agreed that the senior manager for this project ensures the Head of Governance is informed of any changes that may impact his role.
11.Haemostasis and Thrombosis Committee Report
This was a comprehensive report that made clear the service remains significantly challenged due to staffing causing increased waiting times.
The Committee raised a number of questions and suggestions relating to staffing issues. These included outcomes from exit interviews and addressing issues raised and possible joint roles within the Foundation Group which may make jobs more attractive. In answer to another point raised, the Committee was informed that Haematology and Anticoagulation Teams will come together by September 2022.
A further concern was raised regarding long waiters and mitigations were in place to avoid harm. The Haematology Consultant assured that they were small numbers and there was no evidence that the patients had come to any harm due to delay.
12.Hospital Transfusion Committee Report
A very assuring report was received and the Committee raised no questions.
13.Joint Audit Committee and Clinical Governance Committee Assurance Statement
4/5 223/347
This statement was received by the Committee and no questions were raised.
14.Healthcare Recordkeeping Procedure for Maintaining Quality Records
This policy has been updated to reflect the more digitally focused elements of record keeping that will be the future. The Committee was asked by the Head of Governance to approve the policy.
The Committee raised no concerns and duly approved the amended policy.
15.Any Other Business (AOB)
There were no issues raised in AOB.
Areas of Concern for the Board’s Attention
The Board should note pathway issues with joint working in item 6 and staffing issues in item 11.
Decisions Made and Actions to be Taken
Item 7 and 14.
Committee’s Level of Assurance
The Committee was significantly assured.
Dr David SpraggettNon-Executive Director and Chair of the Clinical Governance Committee
5/5 224/347

Report Summary Report to Board of Directors Date of
Meeting 6 July 2022
Report Title Foundation Group Strategy Committee Report for 31 May 2022
Agenda Item 8.8
Executive/ Non-Executive Lead
Simon Page, Deputy Chairman and Non-Executive Director
Report Author(s)
Chelsea Ireland, Foundation Group EA
Report Previously Discussed at 1. George Eliot Hospital NHS Trust – Board Meeting – 5 July 2022
2. Wye Valley NHS Trust – Board Meeting – 7 July 2022
Purpose of the Report To provide the Board of Directors with an update on the dicussions at the last Foundation Group Strategy Committee meeting.
For Approval For Discussion For Information
Recommendations and Action Required The Board of Directors are asked to receive and note this report.
Impact (is there any impact arising from the report on the following?) Quality Equality Finance Research Performance Compliance Workforce Legal
Applicable Quality Improvement Priorities Elective Hub Health Inequalities Electronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety Compassionate Effectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk Register Are any existing risks on the BAF/Risk Register affected? N/A N/A Do you recommend a new entry to the BAF and/or Risk Register is made as a result of this report? If yes, describe the new risk.
No
1/8 225/347

South Warwickshire NHS Foundation Trust
Report to Board of Directors – 6 July 2022
Foundation Group Strategy Committee Report 31 May 2022
Executive Opinion The agenda for this meeting was focused on the following key items: 1. Group Strategy Update The Group Chief Executive provided an update on work which had commenced to refresh the Strategic ‘Wheel’ which represented the strategy of all three Trusts in the Group. He explained that he and the Group Chairman had met with the Group Chief Strategy Officers as part of the Strategy Refresh work, which was to realign and move forward the Group Strategy. The new focus points, as part of the Group Strategy, are outlined below and these will be discussed further at the individual Trust Boards face-to-face Strategy Refresh sessions in September 2022.
- Partnerships - Population Health Management - Sustainability - People - Elective Care - Digital - Health Inequalities - Prevention - Domiciliary Care Market Challenge
The Chief Strategy Officer at South Warwickshire Foundation Trust (SWFT) added that more work around Place and Research was also being added as a priority in the Strategy Refresh work and that assessing the must do’s around quality, compliance, finance, and sustainability would be addressed.
2. Worcestershire Acute Hospitals NHS Trust (WAHT) Update The Deputy Chief Nursing Officer at WAHT provided an update on the International Nurse Recruitment programme at WAHT which had been in place since 2018. She explained that the programme was initially introduced to help reduce bank and agency spends and the large number of nursing vacancies. She added that in April 2019 the Trust’s vacancy rate was 286 whole time equivalent (WTE) with a turnover of 12.1%. Through the recruitment drives and the partnerships that were in place, the Trust recruited 135 international nurses in 2019/20 which so far had a retention rate of 95.7%. In 2021, WAHT had already saved £975k of the £2.5million savings plan across the three-year plan. As of May 2022, the Trust only had 95 vacancies which was a significant reduction from 286. A discussion was had regarding key worker accommodation, and it was recommended that this be included in each Trusts’ Estates Strategy moving forward.
3. Digital Update The Group Digital Strategic Advisor provided an update on the digital work taking place across the Foundation Group. He provided a presentation on Scan4Safety, which was a programme focused on improving patient safety, improving clinical productivity and driving
2/8 226/347

operational efficiency. The system uses a barcode and scanning technology to ensure ‘right patient, right product, right treatment’. He explained three key things to focus on if we decided to adopt GS1 and Scan4Safety standards would be people, process, and systems. More information, including figures, was needed before a decision on Scan4Safety could be made, but it was felt it would most likely work for certain areas rather than a complete Trust or Group roll out. He explained the Digital Triage in A&E system being trialled at GEH, eTriage, which provided a digital check-in, history take, ECDS Capture and triage. The system would also automatically rate the risk and advise the best route to appropriate care. There had been mixed reviews on eTriage, Queen Mary’s Hospital at Sidcup rated it quite highly, however the clinical team at George Eliot Hospital NHS Trust (GEH) had different views so far. Discussion around the need for a Digital Strategy across the group were had to follow a logical pattern and drive improvement.
4. Improvement Update The Group Associate Director of Improvement updated on QSIR. She explained that 93 SWFT Staff, 73 GEH Staff and 89 WVT Staff had attended QSIR training. She explained that QSIR was being delivered at Place across Hereford and Worcester and this would be rolled out across SWFT and GEH. She added that 11 staff members across the Foundation Group had now also been trained as faculty members. QSIR Virtual at Silver Level had been retained, QSIR Practitioner at Gold Level would recommence in September 2022. She explained outside of the usual QSIR programme within the Trust, QSIR Express had been trailed with Healthwatch, Warwick University and Worcestershire University. The National Team had also expressed interest in QSIR Express. She informed the Committee that SWFT had just introduced its improvement forum, Open to Change, GEH had introduced Fab Friday and Wye Valley NHS Trust (WVT) already had Transformation Tuesday. GEH and WVT’s improvement forums also have twitter feeds which had been quite successful and would be introduced for SWFT. 5. Progress Towards the First Foundation Group Boards The Group Chief Executive provided an update on the progress of the first Foundation Group Boards meeting due to be held in August 2022. He explained that the plan for the first meeting was that it would be a confidential meeting, with future meetings moving to public if appropriate. The Foundation Group Boards meeting would be split into three sections, the first would be the Group Integrated Performance Report which the Group Analytics Board had been pulling together the data, and he highlighted that the individual Trusts Boards would see this for the first time at their July 2022 meetings. The Foundation Group Boards meeting would then also include a section on Productivity and Clinical Effectiveness (PACE), and the final section would be a ‘Drill Down’ to focus on important topics at that time. The first ‘Drill Down’ would focus on cancelled operations figures and new to follow-up ratios.
6. Foundation Group Strategy Self-Assessment of Effectiveness (Appendix A) The Group Chairman took the Foundation Group Strategy Self-Assessment of Effectiveness as read; however he highlighted a comment that the Committee being unclear on its purpose, which he addressed. He explained that the Committee should be used to drive improvement forward by identifying best practice across the Foundation Group and ensuring that this was shared to make change happen. Chelsea Ireland Foundation Group EA
3/8 227/347

2
SOUTH WARWICKSHIRE NHS FOUNDATION TRUST WYE VALLEY NHS FOUNDATION TRUST GEORGE ELIOT HOSPITAL NHS TRUST
Report to Foundation Group Strategy Committee – 31 May 2022
Annual Review of Self-Assessment of Effectiveness
1. Introduction
The inaugural meeting of the Foundation Group Strategy Committee (FGSC) was held on 23 January 2018. It is good governance for the Committee to undertake an Annual Self-Assessment to assess its effectiveness which will be presented to the Board of each respective organisation, along with an Annual Report. The Committee’s 2021/22 Annual Report will be considered by the Committee under a separate agenda item at the next meeting (August 2022). 2. Effectiveness Self-Assessment Tool The Committee Administrator circulated the self-assessment tool on 25 March 2022 with a return date of 2 May 2022. As of 23 May 2022, 6 responses were received which have been captured in the self-assessment tool attached (appendix a). It is worth noting that 2 forms were only partially completed. All narrative contributions have also been included. 3. Recommendation The Committee is asked to consider the responses received for its Annual Effectiveness Self-Assessment for 2022 which will subsequently be submitted to the three Boards in July 2022 for information. Chelsea Ireland Foundation Group EA and Committee Administrator
4/8 228/347

South Warwickshire NHS Foundation Trust, Wye Valley NHS Trust and George Eliot Hospital NHS Trust FOUNDATION GROUP STRATEGY COMMITTEE
EFFECTIVENESS SELF-ASSESSMENT TOOL 2022
Page 1 of 4
Please tick to indicate your level of agreement with the following statements. Please add any comments or actions required in the relevant column. If you have rated any of the statements as a 1 or a 2 (strongly disagree or disagree), please provide your reasons in the relevant section below.
Statement Strongly Agree (4)
Agree (3) Disagree (2)
Strongly Disagree (1)
Unable to Answer
Comments / Action
Theme 1 – Committee Focus The Committee is clear on its core purpose and objectives.
The Committee’s business covers matters of importance relevant to its Terms of Reference.
- Just recently joined
The Committee reviews its activities against those delegated to it in the Terms of Reference
- Just recently joined
The Committee has made a conscious decision about how it wants to operate in terms of the level of information it would like to receive for each of the items on its cycle of business.
- Just recently joined
There is appropriate detailed discussion focused on decisions required and decision making is clear and transparent.
- Just recently joined
The frequency of meetings is appropriate and enables the Committee to effectively carry out all of its duties.
If you have rated any of the above aspects as a 1 or a 2, please give your reasons below: - I have only recently just joined this meeting so there are some elements that at this stage is difficult to comment on
5/8 229/347

South Warwickshire NHS Foundation Trust, Wye Valley NHS Trust and George Eliot Hospital NHS Trust FOUNDATION GROUP STRATEGY COMMITTEE
EFFECTIVENESS SELF-ASSESSMENT TOOL 2022
Page 2 of 4
Statement Strongly Agree (4)
Agree (3) Disagree (2)
Strongly Disagree (1)
Unable to Answer
Comments / Action
Theme 2 – Committee Team Working The Committee has the right balance of experience, knowledge and skills.
The membership and attendance of the Committee as set out in the Terms of Reference is appropriate.
- Would like to see more from our 3 Directors of Strategy in this space.
The Committee ensures that the relevant director /manager attends meetings to enable it to secure the required level of understanding of the reports and information it receives.
Members are properly prepared for the meetings.
All members of the Committee behave with courtesy and respect, and views of others are respected and heard non-judgementally.
If you have rated any of the above aspects as a 1 or a 2, please give your reasons below:
6/8 230/347

South Warwickshire NHS Foundation Trust, Wye Valley NHS Trust and George Eliot Hospital NHS Trust FOUNDATION GROUP STRATEGY COMMITTEE
EFFECTIVENESS SELF-ASSESSMENT TOOL 2022
Page 3 of 4
Statement Strongly Agree (4)
Agree (3)
Disagree (2)
Strongly Disagree (1)
Unable to Answer
Comments / Action
Theme 3 – Committee Effectiveness Papers are received in sufficient time to allow proper consideration and understanding.
The quality of Committee papers received allows me to perform my role effectively.
Sufficient time is given to the proper debate and understanding of business items.
Members provide real and genuine challenge – they do not just seek clarification and/or reassurance.
The business is appropriately prioritised and debate is allowed to flow and conclusions reached without being cut short or stifled due to time constraints etc.
Each agenda item is ‘closed off’ appropriately so that I am clear the conclusion, who is doing what, when and how and how it is being monitored.
The Committee has a tracker system to ensure others are acting on and completing actions allocated to them and I feel confident that it will be implemented as agreed and in line with the timescale set down.
Assess the impact of the Foundation Group arrangement and overall performance of the three Trusts.
7/8 231/347

South Warwickshire NHS Foundation Trust, Wye Valley NHS Trust and George Eliot Hospital NHS Trust FOUNDATION GROUP STRATEGY COMMITTEE
EFFECTIVENESS SELF-ASSESSMENT TOOL 2022
Page 4 of 4
If you have rated any of the above aspects as a 1 or a 2, please give your reasons below:
Statement Strongly Agree (4)
Agree (3)
Disagree (2)
Strongly Disagree (1)
Unable to Answer
Comments / Action
Theme 4 – Committee Leadership and Administration The Committee Chair has a positive impact on the performance of the Committee.
Committee meetings are chaired effectively and with clarity of purpose and outcome (e.g. keeping agenda on time, checking for consensus between members before decisions are made)
The Committee has adequate administrative support.
Minutes clearly identify debate, actions and who is responsible for them.
If you have rated any of the above aspects as a 1 or a 2, please give your reasons below:
8/8 232/347

Report Summary Report to Board of Directors Date of
Meeting 6 July 2022
Report Title Board Assurance Framework and Risk Quarterly Report
Agenda Item 9.1
Executive/ Non-Executive Lead
Anne Coyle, Managing Director Report Author(s)
Joanne Beales, Lead Risk, Health & Safety Adviser
Report Previously Discussed at Risk Management Board – 13 June 2022
Purpose of the Report To provide an update on the Board Assurance Framework 2021-22 and 2022-23 and assurance for the Red (15-25) risks on the Divisional risk registers
For Approval For Discussion For Information
Recommendations and Action Required The Board of Directors is asked to: 1. receive and note the end of year Board Assurance Framework for 2021-22, 2. receive and note the Board Assurance Framework for 2022-23, and 3. receive and note the Red (15-25) risks on the Divisional Risk Register.
Impact (is there any impact arising from the report on the following?) Quality Equality Finance Research Performance Compliance Workforce Legal
Applicable Quality Improvement Priorities Elective Hub Health Inequalities Electronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety Compassionate Effectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk Register Are any existing risks on the BAF/Risk Register affected? No Do you recommend a new entry to the BAF and/or Risk Register is made as a result of this report? If yes, describe the new risk.
No
1/48 233/347

South Warwickshire NHS Foundation Trust
Report to Board of Directors – 6 July 2022
Board Assurance Framework and Risk Quarterly Report
1. Executive Opinion This report provides an overview of our risk profile and approach to risk management as part of our cycle of quarterly assurance to the Board. Our approach to risk has evolved over the past few years and as a consequence we have been able to identify business and operational risks, implement mitigation strategies and have generally delivered well against our plans, contractual and statutory duties. This report does not highlight any particular concerns about our ability to continue to do so but does flag our highest current risks including the financial challenge faced by SWFT and by other organisations in the local health economy. 2. Board Assurance Framework (BAF)
The end of year Board Assurance Framework (BAF) 2021-22 is presented for the Executive Team to agree the end of year position (Appendix A). The Chief Officers with open risks, Executive, Operating, Finance, Strategy and the Managing Director – SWFT, on the BAF 2021-22 were emailed and asked to advise whether the open risk should be, see table below for detail:
• Retained and carried forward onto the BAF 2022-23 • Moved onto a Divisional risk register • Closed
Risk Decision 1b. Relative financial positions of SWFT and the CCG result in a nil resource transfer to the Trust creating a financial pressure associated with resourcing lead provider responsibilities
Chief Executive Officer – Risk to be closed due to the new financial framework.
4. Staffing shortages within care, residential and domiciliary services may directly impact on care, residential home and domiciliary capacity affecting operating models resulting in additional community hospital and OOH services capacity requirements and delayed discharges from the acute hospitals
Chief Operating Officer – Risk to be transferred to the Out of Hospital Care Collaborative divisional risk register.
7a. There is a risk that the population health management system will not be fully operational by the end of the financial year, and therefore unable to easily provide the relevant PCN level data automatically.
Chief Finance Officer – Risk to be transferred to the Corporate divisional risk register.
8a. There are 3 issues that will slow down or stop this happening: a) The South Warwickshire PLACE financial position doesn't enable incentivisation/pump priming
Chief Finance Officer – Risk to be transferred to the BAF 2022-23 and linked to Objective 9c.
2/48 234/347

b) The C&W ICS decides to devolve budgets to a higher level e.g. linked to local authority boundaries c) National guidance/rules around ICS financial management 10. Impact development of ICS a key interdependency of success in management of Lead Provider contract for PLACE and implementation of new National reforms
Managing Director – SWFT – Risk to be re-worded and transferred to the BAF 2022-23.
10a. The Trust will not achieve a reduction in the carbon footprint in 2021-22 due to the increasing Estate and ventilation requirements for the COVID-19 Pandemic
Chief Strategy Officer – Risk to be closed, if needed a new risk will be opened during 2022-23 and will be linked to this year’s objectives on sustainability.
The Trust’s objectives were approved at Public Board on 2 March 2022. The Council of Governors contribute to the Trusts Objectives at Roundtable meetings with the Board of Directors. The 2022-23 BAF is presented in its entirety following agreement at Risk Management Board on 13 June 2022 (Appendix B). The Chief Executive assigned a lead Executive to each for objective and also identified more than one Executive who will be responsible for relevant support initiatives. The Risk Manager then contacted the Executive lead to identify risks to achieving their objectives and to agree the wording of the risk. Risk scores are agreed using the risk matrix identified in the Risk Management Strategy 2022-27. The controls and assurances were also identified and where necessary an action plan developed. The 2022-23 BAF will be reviewed on a quarterly basis by the Executive Team and presented to the Risk Management Board in its entirety. Only risks with a current risk score of 15-25 (Red) and 8-12 (Dark Amber) will be presented to the Board of Directors for information. Those risks below 8 will be managed locally by the Executive Team. The Chief Nursing Officer is currently on sick leave and her objectives have not formally been re-allocated, any risks identified to the achievement of her objectives will be highlighted in the BAF 2022-23 Quarter 2 update. The Chief Medical Officer has advised that it is too early to define a risk around the Research Strategy as people are only just being appointed. It is likely that risks will appear when the new team is established and a stocktake and action plan is in place. The People Officer has advised that there are currently no risks to the achievement of her objectives, however a number of red (15-25) risks have recently been added to the Corporate risk register and it may be appropriate for these to be transferred to the BAF.
3/48 235/347

Concerning Objective 9c: Develop a financial framework that incentivises changes in behaviours within Place, the Chief Finance Officer has advised there is a risk as the Financial Framework has not been developed. There are 3 issues that will slow down or stop this happening:
a) The South Warwickshire PLACE financial position doesn’t enable incentivisation/pump priming
b) The C&W ICS decides to devolve budgets to a higher level c) National guidance/rules around ICS financial management
The Chief Strategy Officer has highlighted that there may be risks concerning the deliverability of new environments due to affordability linked to current market pressures and achievement of the fundraising target in the current economic position. There may be risks to the achievement of the milestones to achieve net zero by 2040 and the Elective Hubs, investigations and planning is underway and if new risks are required they will be added to the BAF in the Quarter 2 update. The Managing Director – Innovate has yet to confirm whether there are any risks associated with the achievement of his objectives. 3. Red (15-25) Risks on the Divisional Risk Registers Risk Management Board (RMB) met on Monday 13 June 2022 and continues to meet quarterly. The Associate Directors of Operations (ADOs) for each Division are required to attend the RMB meetings and submit a report highlighting any significant 8-12 (dark amber) and 15-25 (red) risks on their divisional risk registers. The Red (15-25) risks on the Divisional risk registers are attached for information (Appendix C). In addition an Extra-Ordinary Risk Management Board was held on Tuesday 17 May 2022, to review all of the Red (15-25) risks on the Divisional risk registers. Emergency Care will be holding a separate meeting to review all of the ED risks. 4. Internal Audit – Assurance Framework Review 2021-22 Internal Audit have undertaken a Final Review of the BAF 2021-22, which reported that the Trust has a BAF in place, has been established which is designed and operating to meet the requirements of the Annual Governance Statement, and provides reasonable assurance that there is an effective system of internal control in place to manage the principal risks identified by the organisation. The audit made three minor recommendations concerning the Risk Management Board minutes, risk description wording and gaps in control, assurances and action plans. In response to Internal Audits review of the BAF 2021-22, risk descriptions will be worded in the Trusts x,y,z format and the controls and assurances were also identified and where necessary an action plan developed.
4/48 236/347

5. Risk Management Process The Risk Management Strategy 2022-27 was ratified by Board of Directors in April 2022. At the Board Workshop, in May 2022, the Interim Consortium Director from CW Audit and Lead Risk, Health & Safety Adviser launched the Risk Management Strategy, Trust Senior Managers were also invited to the workshop. Recommendation The Board of Directors is asked to: 1. receive and note the end of year Board Assurance Framework for 2021-22, 2. receive and note the Board Assurance Framework for 2022-23, and 3. receive and note the Red (15-25) risks on the Divisional Risk Register. Joanne Beales Lead Risk, Health & Safety Adviser
5/48 237/347

Enc 9b South Warwickshire NHS Foundation TrustBoard Assurance Framework 2021-22
Appendix A - Objectives 2021-22
Measures Executive Lead Quality Priorities
3Work with local providers to improve access to tertiary services locally, these highly specialised treatments such as transplants
Baseline assessment of relevant Tertiary Services and Benchmarking Agree plan with Tertiary providers to address variance
Chief Medical Officer
3aReview of Provider Collaborative Terms of Reference and agree work plan
Work plan agreed by Provider Collaborative (at May 2021 meeting), ToR review after Regional review concludes (August 2021)
Chief Executive
3bAgree Place Clinical Strategy and liaise with UHCW to review and deliver tertiary services specification
Place Clinical Strategy agreed by stakeholder governing bodies Chief Medical Officer 1
4Safely and efficiently recover services following impact of Covid-19, maintaining innovative working and a continuous improvement approach
Ensure KPIs are met for recovery of services and income opportunities are maximised. Using model of best practice to deliver transformation and efficiency gains
Chief Operating Officer
4a Undertake Trust and STP level capacity and demand analysisChair Elective Hub and ensure Trust and system demand and capacity is carried out to support delivery of recovery objectives and clinical prioritisation, maximising ERF opportunities
Chief Operating Officer
4b Deliver agreed activity planDevelop plans to deliver agreed activity to ensure national and Trust priorities are met. Ensure monthly reporting in place
Chief Operating Officer
4c Manage Clinical safety risks alongside treatment prioritisationLead a quality improvement project to minimise the risks of patients diagnosis being delayed or mistaken due to internal process errors.
Chief Medical OfficerChief Nursing Officer
2; 8
4dFacilitate the delivery of productivity gains through training more staff in continuous improvement and facilitating Group-wide sharing
Chief Strategy Officer 6
Objectives 2021-22
Quality
Updated: 01/01/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 1
6/48 238/347

Enc 9b South Warwickshire NHS Foundation TrustBoard Assurance Framework 2021-22
Appendix A - Objectives 2021-22
2Work with partners to develop future model to deliver urgent care across south Warwickshire
Establish work program to review current model and identify best practice
Chief Operating Officer
2aContinue to roll out A&E111 First, maximizing non-conveyance opportunities
Monitor 111 Numbers and activity. Identify opportunities to increase numbers. Work with partners to identify different models of care to reduce conveyancing to hospital
Chief Operating Officer 4
2b Agree future operating model for Stratford MIUWork with CCG partners to identify model of care and then develop delivery plan
Chief Operating Officer
2c Undertake any engagement and involvement required Work with local population to inform future models of care Chief Strategy Officer
7Bring together capacity and capability across group for informatics to contribute to place and system informatics and Intelligence cells*
Group wide Information ReviewInformation team resource & skill mix requirement assessment
Chief Finance Officer
7aEnsure that reporting arrangements are in place to provide PCNs with population health and demand management data
Implement data feeds with intelligence cell for PHM systemPHM analysis outputs with Commissioners and PCNContribute to developing PCN reporting as required
Chief Finance Officer
7bImprove finance and activity reporting to operational staff across Place and Board/Committees
New format Finance Report for Board of Directors, Management Board and Finance & Performance CommitteeFinancial Framework for pathways at PlaceIntroduce restoration reporting tools for operational teamsDevelop a local BI action plan to support management and operational agendasEnhance business information support to divisional staff with routine regular "intelligence" sessions
Chief Finance Officer
8Establish the infrastructure and governance required to manage a lead provider contract for Place and work with partners to implement new national reforms*
Clarity on structure and delivery functions specifically sub-contractual requirements for Warwickshire PLACE and building an infrastructure for SW PLACE that delivers a Population Health approach to address known health inequality
Managing Director
8aDevelop new Financial models to incentivize the delivery of Place priorities by partner providers
Financial Framework at Place Chief Finance Officer
8bReview the revisions to Trust and ICS Governance frameworks as part of the readiness exercise to implement the ICS White Paper
New Governance Framework in place and approved by Board and partners for assumed start of ICS body (01/04/2022)
Chief Executive
9Embed an intelligence driven service planning and delivery approach that responds to the health and care needs of our local communities, addressing health inequalities*
Chief Strategy Officer
9a Develop and Place-based planning model within the ICSDecision making that considers wider involvement of partners and ability to invest in the areas that have most impact
Chief Strategy Officer
9bReview Trust clinical policies to ensure inclusivity and a narrowing of health inequalities
Review practice and policy associated with prevent neonatal and maternal death to ensure health inequalities are addressed.Review our approach to 'every contact counts', think family and health inequalities in OOHCC practices to ensure staff have the skills and competence to proactively address health inequalities.Review and improve our cultural awareness training.
Chief Nursing Officer 7
Integration
Sustainability
Updated: 01/01/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 2
7/48 239/347

Enc 9b South Warwickshire NHS Foundation TrustBoard Assurance Framework 2021-22
Appendix A - Objectives 2021-22
1
Develop management and leadership capabilities, using systems to support care pathways. For example supporting frailty services within the community, primary care and hospital setting
Undertake a review of Executive portfolios in defining in-sourcing and out-sourcing functions to address known gaps
Managing Director
1a Review of Executive Portfolios Capacity and capability to ensure retain Outstanding well led rating Managing Director
1b Agree transfer of resources from CCG Transfer of resources Chief Executive
1c Review of Operational leadership roles
Conduct skill review and develop gap analysis. Work with providers such as Warwick Business School to develop operational business development programme. Embed plan in operational managers appraisals
Chief Operating Officer
1d Revision of Medical Leadership structure Plan agreed at Management Board and SIB Chief Medical Officer
6Continue to develop and implement support for staff health and wellbeing, particularly recognising the impact of covid-19*
Work with Foundation Group colleagues to support staff to stay well through prevention measures, training and awareness raising, including helping staff to recover well through effective interventions and supportWell-being & Mental wellbeing through recovery and beyondDevelopment of Health & Wellbeing promotions
Chief People Officer
6a Review professional support and development arrangements
Undertake staff engagement events to identify staffs thoughts on the trusts support and development opportunities. Implement a shared decision making model in maternity services. Implement a recruitment and retention clinical lead post to improve clinical engagement in recruitment and retention activities. Review the learning from COVID and implement a revised workforce strategy that supports staff to retain the new skills learnt.
Chief Nursing Officer
10Work with partners to deliver against anchor organisation commitments*
Completion of scoping exercise of deliver progress against Anchor Organisation commitments with gap analysis, mitigations and resources identified in their delivery specifically carbon footprint reduction and progress in delivery of headline ambition on Health Inequalities
Managing Director
10a Achieve a 5% year on year reduction in our carbon footprint 5% reduction in carbon footprint and green plan in place Chief Strategy Officer
10bDeliver key development projects with partners identified through place estate planning
Ellen Badger, Lillington and Cubbington developments started and agreed focus for South Warwickshire Place Estates
Chief Strategy Officer
Workforce
Updated: 01/01/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 3
8/48 240/347

Enc 9b South Warwickshire NHS Foundation TrustBoard Assurance Framework 2021-22
Appendix A - Objectives 2021-22
5Establish the digital hub to maximise the use of new technology to transform the way care is delivered
Develop links between the Research Department, Digital Hub, Warwick University and Business School to generate clinical engagement and development of initiatives
Chief Operating Officer
5a Ensure that the Digital Forum connect into the Hub programmeStrengthen links between clinical and operational teams, by creating standing item on agenda and 2 way sharing of ideas demonstrated by regular updates of activities
Chief Operating Officer
5b Ensure clinical engagement and ideas generationEvidence of new clinical ideas generated at SIB and the Group productivity program
Chief Medical Officer 9
11Continue to implement the Digital Strategy with a focus on mobilising and embedding Electronic Patient Record Systems*
Refresh IT Strategy and develop objectives for this year.Ensure ongoing projects are linked to transformation and supporting EPR mobilisation
Chief Operating Officer 3
11aComplete financial evaluation and resourcing of EPR Business Case
Production of 5 case model business case by SWFTCS Ltd.EPR costs and benefits to be identified and developed at EPR working group meetings supported by nominated SWFT and GEH finance leads. Case to be developed and finalised for the autumn
Chief Finance Officer
11b Oversee the EPR mobilization strategyDevelop StrategyProvide updates against milestones
Chief Operating Officer
11cEnsure appropriate clinical engagement to maximise system benefits and clinical productivity
Evidence of engagement in system clinical forum Chief Medical Officer
Digital
Updated: 01/01/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 4
9/48 241/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2021-22
Appendix A - Quality Improvement Priorities
Quality Priorities (QP) 2021-22
1 Agree Place Clinical Strategy and liaise with UHCW to review and deliver tertiary services specification
2 Manage Clinical safety risks alongside treatment prioritisation
3 Oversee the Electronic Patient Records (EPR) mobilisation strategy
4 Continue to roll out A&E111 First, maximising non-conveyance opportunities
5 Improve the quality and patient experience of hospital discharge processes
6Facilitate the delivery of productivity gains through training more staff in continuous improvement and facilitating Group-wide sharing
7 Review Trust clinical policies to ensure inclusivity and a narrowing of health inequalities
8 Reduce the incidence of delayed or missed diagnosis
9 Ensure clinical engagement and ideas generation
Patient Safety
Patient Experience
Patient Outcomes
Prepared: 01/06/2021 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 5
10/48 242/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2021-22
Appendix A - Abbreviations
BAF 2021-22 - Abbreviations
Board of Directors BoD Chief Executive CE
Finance & Performance Executive F&P Managing Director MD
Group Strategy Board GSB Chief Finance Officer CFO
Management Board MB Chief Medical Officer CMO
Strategic Innovation Board SIB Chief Nursing Officer CNO
Chief Operating Officer COO
South Warwickshire NHS Foundation Trust SWFT Chief People Officer CPO
George Eliot Hospital GEH Chief Strategic Officer CSO
Coventry & Warwickshire Partnership Trust CWPT Managing Director - Innovate MD - Innovate
Clinical Commissioning Group CCG
Coventry & Warwickshire Sustainability and Transformation Partnerships
C&W STP
Updated: 01/12/2021 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 6
11/48 243/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2021-22
Appendix A - Risk Appetite
Appetite Descriptor Risk Level
Open
Eager to be innovative and to choose options based on those that offer the highest probability of productive outcomes. Prepared to accept high and even extreme rated risks in pursuit of our objectives in this area to realise potential rewards
15-25
Moderate
Willing to consider all potential delivery options and choose based on delivery of an acceptable level of reward (and VfM). Prepared to accept that risks are likely to occur in the pursuit of our objectives in this area and that we will need to tolerate risks up to a rating of 'high' to realise potential rewards
8-12
Cautious
Preference for safe delivery options that have a low degree of inherent risk and may have more limited potential for reward. Willing to expend some time and resources to mitigate risks but accepting that some risks in this will not, or cannot, be mitigated below a moderate level
4-6
Averse
Preference for ultra safe delivery options that have a low degree of inherent risk and only limited reward potential. Prepared to expend significant time and resource to mitigate risk in this area to a minimal level
1-3
AvoidNo appetite, not prepared to tolerate risk above a negligible level 0
Prepared: 01/06/2021 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 7
12/48 244/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2021-22
Appendix A - Key to Assurance Levels
Level of AssuranceDefinition(Three Lines of Defence Model)
Level 1Operational
The lowest level of assurance and relates to local assurances provided by operational management, self assessment
Level 2Executive
Moderate level of assurance and relates to assurances provided by executive management/Board of Directors, independent assessment [internal] e.g. clinical audit
Level 3External
The strongest level of assurance and relates to e.g. external reviews, CQC, external/internal audit, external inspections etc.
Prepared: 01/06/2021 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 8
13/48 245/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2021-22
Objective 1b
Lead Director Links to Corporate Risk Register
Chief Executive
Quarter Consequence Likelihood Score Target Score Risk Appetite
Inherent Risk Score 2 5 10 8 10
Residual Risk Score Qtr. 1 2 5 10 8 10
Residual Risk Score Qtr. 2 1 5 5 8 10
Residual Risk Score Qtr. 3 1 5 5 8 10
Residual Risk Score Qtr. 4
Level of Control: 1 = Operational2 = Executive3 = External
2
2
Description of what is required to address gap in control / assurance Original Due Date
Board of Directors
Risk Strategic Objectives/Quality Priority/Partnership/Group working
Relative financial positions of SWFT and the CCG result in a nil resource transfer to the Trust creating a financial pressure associated with resourcing lead provider responsibilities
1. Develop management and leadership capabilities, using systems to support care pathways. For example supporting frailty services within the community, primary care and hospital setting1b. Agree transfer of resources from CCG
Responsible Committee
Rationale for Score
Q1 - The support structure does not pose a material risk to the Trust's financial position but the absence of a structure to control the lead provider contract would.Q2 - With the Trust's financial position now more stable, the support structure does not pose a material risk to the Trust's financial position but the absence of a structure to control the lead provider contract would.Q3 - Funding transfer situation unchanged although Trust forecast outturn now less pressured.End of Year: Risk to be closed due to the new financial framework
Controls AssuranceThe control measures or systems in place to assist and secure delivery of the objective(s) Contemporary Reports considered by Board/Committee that demonstrate control effectiveness
Discussion at Executive Away Day to agree broad structure Report to BoD (04/06/2021) setting out broad proposals on Executive portfolio changes
Meeting with MD, DOps and DD Changes agree at Remuneration Committee 09/09/2021
Gaps in Control / Assurance Action to Address Gap in Control / Assurance & Lead for Action
Controls or assurances that have been identified as required but are not yet in place Revised Due Date
Discussions to continue with CCG on potential resource transfer
Updated: 30/05/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 9
14/48 246/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2021-22
Objective 4
Lead Director Links to Corporate Risk Register
Chief Operating Officer
Quarter Consequence Likelihood Score Target Score Risk Appetite
Inherent Risk Score 3 3 9 6 6
Residual Risk Score Qtr. 1 3 2 6 6 6
Residual Risk Score Qtr. 2 4 5 20 6 6
Residual Risk Score Qtr. 3 4 5 20 6 6
Residual Risk Score Qtr. 4 4 5 20 6 6
Level of Control: 1 = Operational2 = Executive3 = External
2
2
3
1
3
1
3
1
Description of what is required to address gap in control / assurance Original Due Date
Board of Directors
Risk Strategic Objectives/Quality Priority/Partnership/Group working
Staffing shortages within care, residential and domiciliary services may directly impact on care, residential home and domiciliary capacity affecting operating models resulting in additional community hospital and OOH services capacity requirements and delayed discharges from the acute hospitals
Safely and efficiently recover services following impact of Covid-19, maintaining innovative working and a continuous improvement approach
Responsible Committee
Rationale for Score
Q2 - All in-patient beds opened, including winter capacity. Increased length of stay >15 days. Increased stranded patient numbers in 7, 14 & 21 days. Significant A&E breaches due to poor flow through the organisation.Q3 - As above and reflected in deterioration of the 4 hour standardQ4 - The Omicron variant, which is prevalent in the Community, has caused outbreaks in Care Homes and in Trust in-patient areas, which has made the placement of in-patients more challengingEnd of Year: Risk to be transferred to the Out of Hospital Care Collaborative Divisional Risk Register
Controls AssuranceThe control measures or systems in place to assist and secure delivery of the objective(s) Contemporary Reports considered by Board/Committee that demonstrate control effectiveness
Discharge Work stream Managing Flow - Winter Plan via the ADO OOHCC Report to Exec F&P
Daily Discharge PlanningCriteria to reside in place and on Digit for patients medically fit for dischargeWeekly stranded patient reviews
Escalation via Trust Bronze
Close collaboration with Social Care and Local AuthoritiesWeekly accommodation & support meetingsWeekly Care Expert Advisory BoardMonthly Joint Commissioning Board with Partners across the STP
Escalation into System Silver
Discharge Task & Finish Group Escalation into System Silver
OOHCC Teams bridging the gap between Acute and domiciliary care packages
Swabbing in place for patients as per national guidance
System Care & Residential Care Home Work stream Escalation into System Silver
Ageing Well Programme Governance & Structure approved - Provider Collaborative Group feed into A&E System Delivery Board
Gaps in Control / Assurance Action to Address Gap in Control / Assurance & Lead for Action
Controls or assurances that have been identified as required but are not yet in place Revised Due Date
Updated: 09/06/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 10
15/48 247/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2021-22
Objective 7a
Lead Director Links to Corporate Risk Register
Chief Finance Officer
Quarter Consequence Likelihood Score Target Score Risk Appetite
Inherent Risk Score 3 4 12 9 10
Residual Risk Score Qtr 1
Residual Risk Score Qtr 2
Residual Risk Score Qtr 33 4 12 9 9
Residual Risk Score Qtr 4 3 5 15 9 9
Level of Control: 1 = Operational2 = Executive3 = External
1
1
Description of what is required to address gap in control / assurance Original Due Date
Implementation delayed. Revised Project Plan now in place managed through Cerner PHM Project Board
01/03/2022
Board of Directors
Risk Strategic Objectives/Quality Priority/Partnership/Group working
There is a risk that the population health management system will not be fully operational by the end of the financial year, and therefore unable to easily provide the relevant PCN level data automatically.
7a - Ensure that reporting arrangements are in place to provide PCNs with population health and demand management data Measure: Implement data feeds with intelligence cell for PHM systemPHM analysis outputs with Commissioners and PCNContribute to developing PCN reporting as required
Responsible Committee
Rationale for ScoreQ3 - Population Health Management is being managed at system level. The Cerner platform has been procured, a regional project board and associated groups have been set up and a detailed approach and plan are being finalised. While initial conversations have been held with organisations, including SWFT, about the extraction of data to support PHM it is not likely that the data feed will be fully in place by the end of the financial year. Action learning sets are taking place to support organisations to make use of PHM approaches.Q4 - This project has been resourced by the CCG who have agreed funding (Feb 2022) so the project has not progressed as planned. There has also been some Information Governance concerns raised by the GPs so no data has been provided. The project cannot progress until LMC has made a decision about sharing data. This risk now needs to be transferred to the Corporate Risk Register 2022/23.End of Year: Risk to be transferred to the Corporate risk register
Controls AssuranceThe control measures or systems in place to assist and secure delivery of the objective(s) Contemporary Reports considered by Board/Committee that demonstrate control effectiveness
Gaps in Control / Assurance Action to Address Gap in Control / Assurance & Lead for Action
CTO Attendance at PHM Delivery Board PHM Project Plan is being developed for approval by PHM Board in December
Readiness activities to load data to the PHM platform completed as part of ICR programme Initial proposed target dates in the draft project plan are April 2022 to complete the on boarding of GP data, and July 2022 for acute data.
Controls or assurances that have been identified as required but are not yet in place Revised Due Date
01/08/2022
Opened: 04/03/2022 Collated By: Joanne Beales, Risk, Health and Safety Team 11
16/48 248/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2021-22
Objective 8a
Lead Director Links to Corporate Risk Register
Chief Finance Officer
Quarter Consequence Likelihood Score Target Score Risk Appetite
Inherent Risk Score
Residual Risk Score Qtr. 1
Residual Risk Score Qtr. 2 3 4 12 6 6
Residual Risk Score Qtr. 3 3 4 12 6 6
Residual Risk Score Qtr. 4 3 4 12 6 6
Level of Control: 1 = Operational2 = Executive3 = External
3
1
Description of what is required to address gap in control / assurance Original Due Date
Discussion with CCG planned for 06/09/2021 06/09/2021
Workshop should identify timelines 29/11/2021
Board of Directors
Risk Strategic Objectives/Quality Priority/Partnership/Group working
There are 3 issues that will slow down or stop this happening:a) The South Warwickshire PLACE financial position doesn't enable incentivisation/pump primingb) The C&W ICS decides to devolve budgets to a higher level e.g. linked to local authority boundariesc) National guidance/rules around ICS financial management
8a - Develop new Financial models to incentivise the delivery of Place priorities by partner providers
Responsible Committee
Rationale for Score
Q2 - Currently Lead Provider contracts/ownership of PLACE funding has not been agreed. This is impacting on the delivery of incentivesQ3 - no change in Q3, work is progressing.Q4 - A first draft of the SW Place financial position has been shared. Discussions on Due Diligence work is underway. End of Year: Risk to be transferred to BAF 2022-23 (Objective 9c)
Controls AssuranceThe control measures or systems in place to assist and secure delivery of the objective(s) Contemporary Reports considered by Board/Committee that demonstrate control effectiveness
Gaps in Control / Assurance Action to Address Gap in Control / Assurance & Lead for Action
Group Strategic Financial Advisor has opened discussion with CCG FD on mechanics around devolution of PLACE Finances. Regular updates on progress will be provided to CFO on progress.
Quarterly update on progress via BaF on discussions with CCG/ICS and mechanism to take this forward.
Finance Workshop undertaken on 29 November 2021 to progress discussions
Host Provider Finance meetings set up to develop work programme. Discussions held to ring fence an Investment Fund at ICS level.
Controls or assurances that have been identified as required but are not yet in place Revised Due Date
Timescale and mechanism for devolution of PLACE allocations still to be determined
Updated: 04/07/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 12
17/48 249/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2021-22
Objective 10
Lead Director Links to Corporate Risk Register
Managing Director
Quarter Consequence Likelihood Score Target Score Risk Appetite
Inherent Risk Score 3 4 12 8 15
Residual Risk Score Qtr 1 3 4 12 8 15
Residual Risk Score Qtr 2 3 4 12 8 15
Residual Risk Score Qtr 3 3 3 9 8 15
Residual Risk Score Qtr 4 3 3 9 8 15
Level of Control: 1 = Operational2 = Executive3 = External
1
1
3
3
2, 3
Description of what is required to address gap in control / assurance Original Due Date
Quantify resource gap 01/05/2021
Progress MOU with WCC 01/06/2021
Board of Directors
Risk Strategic Objectives/Quality Priority/Partnership/Group working
Impact development of ICS a key interdependency of success in management of Lead Provider contract for PLACE and implementation of new National reforms
10. Work with partners to deliver against anchor organisation commitments
Responsible Committee
Rationale for Score
Q1 - Currently decisions on Lead Provider contracts and PLACE are outside direct control. The most important outcome is one that delivers for populations served and strengthens partnerships.Q2- South Warwickshire NHS Foundation Trust Board of Directors approved setting up of workstream to progress Host Provider. PMO commenced in post, conversation held with wider stakeholders. Progress made but constrained due to lack of CCG resource allocation to the Trust. Capability and Capacity gaps identified and draft structure being considered by Remuneration Committee September 2021.Q3 - Work gathering momentum with publication of Thriving Places in September 2021; Warwickshire Care Collaborative Delivery Group established following ratification of Host Provider by Partnership Executive Group; awaiting ICS designate approval. Monthly updates on progress scheduled for monthly updates to Confidential Board of Directors.Q4 - Established Warwickshire Care Collaborative Delivery Board. Nationally date for legislation changes has been delayed to July 2022. The white paper ‘Joining up care for people, places and populations’ (February 2022) further supports this direction including the creation of ‘place boards’. In Warwickshire subject to confirmation by shadow Coventry and Warwickshire ICS it is anticipated this will be the Warwickshire Care Collaborative in March 2022. Due to uncertainty Nationally on passing legislation, due dates have not been achieved nonetheless we are working to ensure readiness.End of Year: Risk to be re-worded and transferred to BAF 2022-23
Controls AssuranceThe control measures or systems in place to assist and secure delivery of the objective(s) Contemporary Reports considered by Board/Committee that demonstrate control effectiveness
Internal preparedness Workshop scheduled with NED in May 2021
Paper to Confidential Board of Directors June 2021
Warwickshire Learning Event August 2021
Board of Directors workshop September 2021
Gaps in Control / Assurance Action to Address Gap in Control / Assurance & Lead for Action
Controls or assurances that have been identified as required but are not yet in place Revised Due Date
Recommended to Appointment and Remuneration Committee appointment of Chief Commissioning Officer with WCC to commence in April 2022.
Monthly updates in Confidential Board are shared on Host Provider, with risks captured and reported to Corporate Risk Group
Additional resources secured from CCG 01/10/2021
Confirmation of sub-contracting Commissioning functions to WCC 01/11/2021
Updated: 08/06/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 13
18/48 250/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2021-22
Objective 10a
Lead Director Links to Corporate Risk Register
Chief Strategy Officer
Quarter Consequence Likelihood Score Target Score Risk Appetite
Inherent Risk Score Low High
Residual Risk Score Qtr 1
Residual Risk Score Qtr 2 2 5 10 5 8
Residual Risk Score Qtr 3 2 5 10 5 8
Residual Risk Score Qtr 4 2 5 10 5 8
Level of Control: 1 = Operational2 = Executive3 = External
1
1 and 2
1 and 2
Description of what is required to address gap in control / assurance Original Due Date
Review the Sustainability Strategy to address new Guidelines to meet 2040 net zero targets
31/03/2022The current Sustainability Strategy does not include the requirements of the new Guidelines to meet 2040 net zero targets
Gaps in Control / Assurance Action to Address Gap in Control / Assurance & Lead for Action
Controls or assurances that have been identified as required but are not yet in place Revised Due Date
Sustainability Group in place to monitor progress Bi-monthly meetings to review plan
Reporting of carbon footprint and energy figures Sustainability Group - Bi-monthlyManagement Board & Trust Board - Annually
Electricity and gas data analysis Sustainability Group - Bi-monthlyManagement Board & Trust Board - Annually
Rationale for Score
The reduction achieved by March 21 was 10% of the 2013.14 baseline, despite the addition of Stratford Hospital to our footprint. Electricity and gas emissions have remained stable, despite multiple expansions, thanks to the installation of energy efficiency measures such as LED lighting, increased BMS controls and more efficient boilers. A notable reduction in business mileage occurred during the pandemic which has led to a significant reduction in the carbon footprint. The expansion of our estate (such as PAGU, the pre-operative assessment unit and the addition of new buildings: Thrifty, Dawsons and Canley Fieldworks) is like to lead to an increase our total carbon footprint. In addition the increased requirement for ventilation following COVID-19 guidelines is believed to be the cause for an increase in electricity and gas consumption (the lack of submetering data does not allow to state this for certain). These factors are combined with limited investment in sustainability projects in 2021-22. The Sustainability Team and Steering Group are working on a long term strategy to achieve the new 2040 net zero targets, changing the focus from a year on year reduction to a longer term strategic vision tied into the Estates Strategy. A new Green Plan will be presented to the ICS on 14th January that will put us in line with the NHS net zero target by 2040. Management Board have approved the kick-start of an integrated energy solution project that will aim to provide net zero estates related emissions for Warwick, Leamington and Stratford Hospital. End of Year: Risk Closed as ventalition works ongoing
Controls AssuranceThe control measures or systems in place to assist and secure delivery of the objective(s) Contemporary Reports considered by Board/Committee that demonstrate control effectiveness
Board of Directors
Risk Strategic Objectives/Quality Priority/Partnership/Group working
The Trust will not achieve a reduction in the carbon footprint in 2021-22 due to the increasing Estate and ventilation requirements for the COVID-19 Pandemic
10a. Achieve a 5% year on year reduction in our carbon footprint
Responsible Committee
Updated: 09/06/2022 Collated By: Joanne Beales, Lead Risk, Health and Safety Adviser 14
19/48 251/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2022-23
Appendix B - Objectives 2022-23
Measures Executive Lead Appetite Quality Priorities
1aFully implement Living Well with cancer agenda across all cancer sites
Chief Nursing OfficerChief Operating Officer
1bWork with partners to implement the recommendations of National Autism Strategy
Chief Nursing OfficerChief Operating Officer
1c Embed improvement methodologies with partners at PlaceChief Strategy OfficerChief Operating Officer
2aCreate an environment to support children and young people in a mental health crisis accessing our services
Chief Strategy OfficerChief Nursing Officer
2bImplement recommendations from Special Educational Needs (SEND) Ofsted and CQC assessment
Chief Operating OfficerChief Nursing Officer
3aDevelop a Green Plan with a commitment to achieving net zero carbon by 2040 with a specific focus in 2022/23 on local purchasing
Chief Strategy OfficerChief Finance Officer
3bInvestigate and develop financing for an integrated energy solution project that details how we will reach net zero for our estates related emissions by 2040
Chief Strategy OfficerChief Finance Officer
4Embed the Productivity and Clinical Efficiency programme
Establish the Group Board structure to share best practice across the Foundation Group (Wye Valley NHS Trust, George Eliot Hospital NHS Trust and Worcester Acute Hospitals NHS Trust, our associate member) and utilise benchmarking data through the programme to drive best practice at pace
Chief Finance OfficerChief Medical Officer
Open
5aFinalise plans for an Elective Hub at Warwick Hospital and strengthen plans to protect elective capacity
Chief Operating OfficerChief Strategy Officer
1
5bUtilise digital solutions to support the redesign of outpatient’s appointments
Chief Operating OfficerManaging Director - Innovate
5cFull implementation of patient initiated follow-ups across all services
Chief Operating OfficerChief Medical Officer
6a Deliver ambitions as set out in University Trust applicationChief Medical OfficerManaging Director
6b Develop research programme with Warwick Business SchoolChief Medical OfficerManaging Director
Open
Moderate
Moderate
Moderate
Moderate
Realise ambitions set out in the Group Research Strategy
Objectives 2022-23
Quality
Sustainability
Improve the experience, outcomes and safety of patients accessing our services
Improve the experience and mental wellbeing of children and young people
Progress plans to reach net zero by 2040
Implement the Elective Care Strategy
Prepared: 01/04/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 1
20/48 252/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2022-23
Appendix B - Objectives 2022-23
7 Embed a prevention mindset across all staff groupsUse population health data to drive planning and decision making to move resources that help keep people well for longer and reduce inequalities
Chief Commissioning Officer (Health and Care)Chief Strategy Officer
OpenModerate
8aEmbed a workforce approach to ensure staff recognise and address health inequalities in their service areas
Chief Medical OfficerChief Nursing Officer
8bEnsure there is Board visibility of inequalities and actions to address them
Managing Director
8c Implement the actions from the ‘Levelling Up’ ReportManaging DirectorChief Operating Officer
9aCreate capacity and capability to act as prime integrator and facilitator of Warwickshire Care Collaborative
Chief Commissioning Officer (Health and Care)Managing Director
9b Develop Lead Provider ModelChief Strategy OfficerManaging Director
9cDevelop a financial framework that incentivises changes in behaviours within Place
Chielf Finance Officer
10aDevelop colleague experience, leadership and talent management through inclusion and empowerment
Chief People Officer
10bDevelop our leaders’ capabilities to work collaboratively with partners to deliver better outcomes for our population
Chief Operating OfficerChief Medical OfficerChief Nursing Officer
10c Enhance inclusion, diversity and equity Chief People Officer
11aSupport Recovery and Restoration post Covid-19 to ensure that there is a retained focus on staff wellbeing, staff experience and staff voice
Chief Operating OfficerChief Medical OfficerChief Nursing Officer
11b Wellbeing and Mental Wellbeing promotions and supportChief People OfficerChief Strategy Officer
11c Respond to the National staff survey Chief People Officer
12a Enabling new ways of working and planning for the future Chief People Officer
12bWork with partners to develop new enhanced blended roles across health and social care
Chief People OfficerChief Commissioning Officer (Health and Care)
Open
Moderate
Open
Open
Open
Integration
Workforce
Continue to develop and implement support for staff health and wellbeing, particularly recognising the impact of Covid-19
Mobilise the new National Workforce Strategy
Create a workforce culture that empowers colleagues to contribute to compassionate care and deliver improved outcomes for our population
Reduce health inequalities for our local populations
Implement the National Strategy of operating at Place
Prepared: 01/04/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 2
21/48 253/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2022-23
Appendix B - Objectives 2022-23
12c Develop an implement a workforce strategy for maternity Chief Nursing Officer 5
Prepared: 01/04/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 3
22/48 254/347
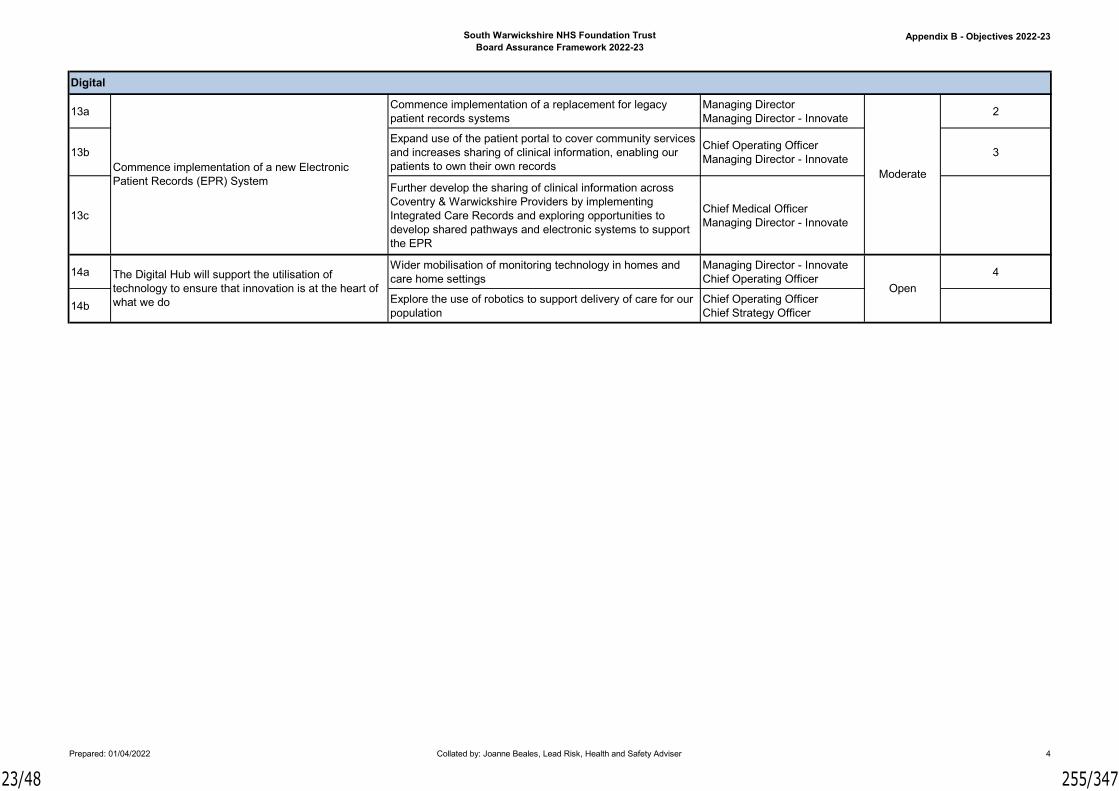
South Warwickshire NHS Foundation TrustBoard Assurance Framework 2022-23
Appendix B - Objectives 2022-23
13aCommence implementation of a replacement for legacy patient records systems
Managing DirectorManaging Director - Innovate
2
13bExpand use of the patient portal to cover community services and increases sharing of clinical information, enabling our patients to own their own records
Chief Operating OfficerManaging Director - Innovate
3
13c
Further develop the sharing of clinical information across Coventry & Warwickshire Providers by implementing Integrated Care Records and exploring opportunities to develop shared pathways and electronic systems to support the EPR
Chief Medical OfficerManaging Director - Innovate
14aWider mobilisation of monitoring technology in homes and care home settings
Managing Director - InnovateChief Operating Officer
4
14bExplore the use of robotics to support delivery of care for our population
Chief Operating OfficerChief Strategy Officer
Moderate
Open
Commence implementation of a new Electronic Patient Records (EPR) System
The Digital Hub will support the utilisation of technology to ensure that innovation is at the heart of what we do
Digital
Prepared: 01/04/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 4
23/48 255/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2022-23
Appendix B - Quality Improvement Priorities
Quality Priorities (QP) 2022-23
1 Finalise plans for an elective hub at Warwick Hospital and strengthen plans to protect elective capacity
2 Commence implementation of a replacement for legacy patient records systems
3Expand use of the patient portal to cover community services and increased sharing of clinical information, enabling our patients to own their own records
4 Wider mobilisation of monitoring technology in homes and care home settings
5 Develop and implement a workforce strategy for maternity
Patient Safety
Patient Experience
Patient Outcomes
Prepared: 27/05/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 5
24/48 256/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2022-23
Appendix B - Abbreviations
BAF 2022-23 - Abbreviations
Board of Directors BoD Chief Executive Officer CEO
Finance & Performance Executive F&P Managing Director - SWFT MD - SWFT
Group Strategy Board GSB Chief Finance Officer CFO
Management Board MB Chief Medical Officer CMO
Strategic Innovation Board SIB Chief Nursing Officer CNO
Chief Operating Officer COO
South Warwickshire NHS Foundation Trust SWFT Chief People Officer CPO
George Eliot Hospital GEH Chief Strategic Officer CSO
Coventry & Warwickshire Partnership Trust CWPT Managing Director - Innovate MD - Innovate
Clinical Commissioning Group CCGChief Commissioning Officer (Health and Care)
CCO (H&C)
Coventry & Warwickshire Sustainability and Transformation Partnerships
C&W STP
Prepared: 27/05/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 6
25/48 257/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2022-23
Appendix B - Risk Appetite
Appetite Descriptor
Open
Eager to be innovative and to choose options based on those that offer the highest probability of productive outcomes. Prepared to accept high and even extreme rated risks in pursuit of our objectives in this area to realise potential rewards
Moderate
Willing to consider all potential delivery options and choose based on delivery of an acceptable level of reward (and VfM). Prepared to accept that risks are likely to occur in the pursuit of our objectives in this area and that we will need to tolerate risks up to a rating of 'high' to realise potential rewards
Cautious
Preference for safe delivery options that have a low degree of inherent risk and may have more limited potential for reward. Willing to expend some time and resources to mitigate risks but accepting that some risks in this will not, or cannot, be mitigated below a moderate level
Averse
Preference for ultra safe delivery options that have a low degree of inherent risk and only limited reward potential. Prepared to expend significant time and resource to mitigate risk in this area to a minimal level
AvoidNo appetite, not prepared to tolerate risk above a negligible level
Prepared: 27/05/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 7
26/48 258/347

South Warwickshire NHS Foundation TrustBoard Assurance Framework 2022-23
Appendix B - Key to Assurance Levels
Level of AssuranceDefinition(Three Lines of Defence Model)
Level 1Operational
The lowest level of assurance and relates to local assurances provided by operational management, self assessment
Level 2Executive
Moderate level of assurance and relates to assurances provided by executive management/Board of Directors, independent assessment [internal] e.g. clinical audit
Level 3External
The strongest level of assurance and relates to e.g. external reviews, CQC, external/internal audit, external inspections etc.
Prepared: 27/05/2022 Collated by: Joanne Beales, Lead Risk, Health and Safety Adviser 8
27/48 259/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Gen
eral
Man
ager
- E
D 1. Recruitment of Middle Grades2. Recruitment of ED Nurses (B7)
1. Clinical Lead2. Deputy Director of Nursing
1-2. On-going 05/07/2022
Em
erge
ncy
Maj
or
(4)
Alm
ost
Cer
tain
(5
) 20
Un
like
ly (
2) 8 20
Lik
elih
oo
d (
curr
ent)
1. ED/Acute Medics to agree smoother pathways out of ED. Currently delays due to need to be clerked by medical SHO and post taked by SpR/Consultant if any suspicion of COVID-19 or if patient is from a residential or nursing home, or has a shielding requirement. To improve flow out of ED.2. To work with speciality teams to get agreement to stop GP expected patients coming into ED and to be able to directly attend ADU, SAU, PAU and FAA3. Waiting areas limited to patient only (visitors are asked to wait outside, except when they are needed for patient assistance)4. Change ED staffing model to better cope with peak times 5. Nurse in Charge in ED to be situationally aware and escalate issues relating to capacity in a
06/07/2021 (EmergencyRHSG) - Workforce review completed shows incorrect staffing levels. Risk remains the same07/09/2021 (EmergencyRHSG) - Over crowding a daily event with the potential for deteriorating patients. Risk score increased to 4:505/10/2021 (EmergencyRHSG) - Corridor care not available during COVID. All assessment areas will need to be staffed to aid flow. Risk remains the same02/11/2021 (EmergencyRHSG) - Further mitigation implemented. Risk remains the same07/12/2021 (EmergencyRHSG) - Issues remain overnight, twilight
Clin
ical
, H
ealth
& S
afet
y
23 N
ovem
ber
2017 1198 Crowding of the ED due to
large influxes of patients, the reduced waiting capacity due to the need to socially distance, and lack of flow out of the ED may result in increased mortality, increased clinical incidents/errors, increased complaints, decreased patient and staff satisfaction, and increased sickness.
Ch
ief
Ope
ratin
g O
ffic
er
Maj
or (
4)
Ra
tin
g (
cu
rren
t)
2021-22
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
RISK REGISTER 2022-23 Open Risks with a Current Score of 15-25 (not included on BAF)
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 1
28/48 260/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
relating to capacity in a timely manner to ED management in hours and site capacity/on call managers out of hours6. Workforce review completed7. Assessment areas open & staffed Mon-Fri8. Streamers at the Front Door9. Fit to sit to allow ambulances to unload10. Provide 2nd triage nurse each day
overnight, twilight shift finishes at 01:30. 3 SIs under investigation. Risk remains the same11/01/2022 (EmergencyRHSG) - GM to review & update01/02/2022 (EmergencyRHSG) - Clinical Lead to start 14/02/2022. Risk remains the same01/03/2022 (EmergencyRHSG) - Risk remains the same05/04/2022 (EmergencyRHSG) - Risk remains the same03/05/2022 (EmergencyRHSG) - Social distancing still in place. Risk remains the same16/06/2022 (EmergencyRHSG) - Separate meeting to take place to review all of ED risks
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 2
29/48 261/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
1-2. 30/04/2022 05/07/2022
Maj
or
(4)
Alm
ost
Cer
tain
(5
) 20 1. Organisational bed flow2. External services providing patient assessment GP appointments
1-2. GM - ED1. Utilising bank and agency staff – unknown entities at times 2. Nurse staffing proposal submitted3. Locum Consultant sought4. Proposed change in shift patterns for administrative staff 5. Provide 2nd triage nurse if staffing allows for waiting room/patients in car management6. Substantive staff recruitment agreed7. Streamers at the Front Door8. B7 Leadership9. Prompt review of speciality patients in ED – Internal Professional Standards re-issued
Em
erge
ncy
Ch
ief
Ope
ratin
g O
ffic
er
Gen
eral
Man
ager
- E
D
Maj
or (
4)
Alm
ost
Cer
tain
(5) 20 20 05/10/2021 - Added
to the risk register, agreed by EmergencyRHSG02/11/2021 (EmergencyRHSG) - Further mitigation implemented. Risk remains the same07/12/2021 (EmergencyRHSG) - Unpredictable attendance, issues remain at night. Current SHOs not worked in an Acute hospital. Risk remains the same11/01/2022 (EmergencyRHSG) - GM to review & update01/02/2022 (EmergencyRHSG) - Internal Professional Standards re-issued. Risk remains the same01/03/2022 (EmergencyRHSG) - Analyse hourly attendances. Senior Registrar 18:00-02:00. Risk remains the same05/04/2022 (EmergencyRHSG) - Draft Business Case for Medical Staffing to be finalised. Risk remains the same03/05/2022 (EmeregncyRHSG) - Business Case on hold. Attendances increased by 20%. Ongoing recruitment. Bank & agency staff utilised. Risk remains the same16/06/2022 (EmergencyRHSG) - Separate meeting to take place to review all of ED risks
Clin
ical
, P
erfo
rman
ce
05 O
ctob
er 2
021 1658 Emergency Department
(ED) average daily patient attendances have increased (from pre-pandemic numbers), in addition the COVID pathways for safe patient management which increases the length of time patients spend in ED, departmental staffing numbers (Administrative/Nursing/Medical/Support Service personnel) are currently not matching the increase workload leading to the inability to provide a consistently safe Emergency Care service; failure to deliver sustained performance across key performance and quality indicators
Key performance and quality indicators:• Triage• Delayed ambulance off loads• Initial Assessment • Identification of the deteriorating patient• Sepsis management• Poor patient satisfaction • Potential increase in complaints / concerns from patients and carers
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 3
30/48 262/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
Clin
ical
, C
ontr
act
ual
01 M
arc
h 20
22 1697 Heralded (specialty expected) patients attending the ED instead of appropriate clinical assessment units due to inappropriate referral pathways being used resulting in increased triage times and long waits; unachievement of targets; potential delays to treatment
Ch
ief
Ope
ratin
g O
ffic
er
Gen
eral
Man
ager
- E
D
Maj
or (
4)
Alm
ost
Cer
tain
(5) 20 20 1. Second triage room at
peak times when staffing numbers and skillset allows (This cannot always occur).2. Waiting room overview/checks during busy periods• RN observations• Safety check/pain management3. Streamlined access to GAU post triage4. Utilise ED staff to help support initial investigations and assessments5. Organisational management of Internal Professional standards (IPS)6. Organisational bed flow in place
Em
erge
ncy 01/03/2022 - Added
to the risk register, agreed by EmergencyRHSG05/04/2022 (EmergencyRHSG) - Risk remains the same03/05/2022 (EmergencyRHSG) - Streamers to commence. Internal Professional standards (IPS) launched, audit to be undertaken. Risk remains the same16/06/2022 (EmergencyRHSG) - Separate meeting to take place to review all of ED risks
Maj
or
(4)
Alm
ost
Cer
tain
(5
) 20 1. Access to 7/7 SDEC services 12-14 hours a day – to match demand2. Improved communications from GP’s to patients informing them of potential delay in assessment due to joining ED queue
1-2. Specialty Service Leads; Trust Exec Team
1-2. TBC 05/07/2022
Clin
ical
, H
ealth
& S
afet
y, R
eput
atio
nal
04 A
pril
2022 1701 The maternity unit does not
fully meet the 15 Immediate and Essential Safety Actions of the Ockenden report meaning there are standards of safety that are not met within the service. This has the potential to impact:• Care provided to women, babies and families• Awareness of the board and the ICS on activities and risks, incidents and complaints within the service• The working environment and the wellbeing of staff within the service• The reputational standing of the service and the trust
Ch
ief
Nur
sing
Off
icer
Ass
ocia
te D
irect
or o
f M
idw
ifery
Maj
or (
4)
Alm
ost
Cer
tain
(5) 20 20 1. GAP analysis of
compliance to the standards and an action plan to outline steps to meet the standards in full2. Monthly MDT meetings to ensure progress against the action plan3. Action plan shared at board4. Action plan shared with and monitored by the Maternity and Neonatal safety champions5. Support from NHSI6. Support from the regional maternity team. 7. Explore and participate in all opportunities to access funding to support progress against action plan
Mat
erni
ty 04/04/2022 - Added to the risk register, agreed by MNSG09/05/2022 (MNSG) - Action plan to be implemented. Risk remains the same06/06/2022 (MNSG) - Action plan being implemented, regular meetings taking place. Risk remains the same
Maj
or
(4)
Alm
ost
Cer
tain
(5
) 20 1. Complete actions on the action plan2. LMNS funding to be agreed
1. Action Owners2. Associate Director of Midwifery
1&2. 31/12/2022 04/07/2022
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 4
31/48 263/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
Clin
ical
, E
mpl
oym
ent
Rel
ated
Iss
ues
, P
erfo
rman
ce,
Rep
utat
iona
l
05 A
pril
2022 1704 Inadequate trained
Paediatric Nurse staffing levels and no dedicated Paediatric Emergency Medicine (PEM) Consultant within ED due to nurse vacancies and difficulty to recruit leading to potential late recognition of detoriating child and non-compliance with the Royal College of Paediatric and Child Health and Royal College of Emergency Medicine – Recommendation 10: every Emergency Department treating children must be staffed by 2 registered children’s nurses on each shift
Current staffing levels: 4 WTE Paediatric Nurses
Ch
ief
Peo
ple
Off
icer
Gen
eral
Man
ager
- E
D
Maj
or (
4)
Alm
ost
Cer
tain
(5) 20 20 1. All ED nurses have
Paediatric basic life support training2. Consultant on every day with advanced life support skills3. On-going recruitment for paediatric nurse staffing4. Shared paediatric SIM training for ED nurses and doctors5. Access to paediatric team (MacGregor Ward) to support nurses6. Four Paediatric trained nurses in post for day to day management of the area
Em
erge
ncy 05/04/2022 - Added
to the risk register, agreed by EmergencyRHSG03/05/2022 (EmergencyRHSG) - B7 ACP Trainee post. 3x B5; 1x B6 & 1x B7 dual trained appointed. Risk remains the same16/06/2022 (EmergencyRHSG) - Separate meeting to take place to review all of ED risks
Maj
or
(4)
Alm
ost
Cer
tain
(5
) 20 1. Training programme for Adult Nurses to gain focused knowledge, skills and competencies for children’s care2. Develop rolling programme for shared paediatric SIM training for ED nurses and doctors3. Write a business care to recruit play specialist to support care4. Write business case to recruit Paediatric Emergency Medicine Consultant (recruited into position 2021 – appointment fell through)
1. Clinical Lead Nurse2. Clinical Lead Nurse; Clinical Director3. General Manager4. Clinical Director; General Manager
1&2. Rolling Programme3. 30/06/20224. 30/06/2022
05/07/2022
Clin
ical
, In
fra
stru
ctur
e
05 A
pril
2022 1705 Paediatric Clinical Area
within ED is not sufficient to meet current demands due to having 4 paediatric cubicles with small corridor type waiting room, leading to delays with assessment and subsequent treatment
Paediatric Assessment Unit (PAU) impacts on flow out of ED due to limitations and adhoc closures
Ch
ief
Ope
ratin
g O
ffic
er
Gen
eral
Man
ager
- E
D
Maj
or (
4)
Alm
ost
Cer
tain
(5) 20 20 1. PAU opening is
discussed at 3 x per day Site Meetings2. Consultant & Nurse in charge who manage flow through ED3. Nurse station within Paediatric Area redesigned, to allow greater site
Em
erge
ncy 05/04/2022 - Added
to the risk register, agreed by EmergencyRHSG03/05/2022 (EmergencyRHSG) - Risk remains the same16/06/2022 (EmergencyRHSG) - Separate meeting to take place to review all of ED risks
Maj
or
(4)
Alm
ost
Cer
tain
(5
) 20 1. Redesign of Children’s area to manage 25% of ED attendances with suitable separated waiting area2. Re-location paediatric resus area to specific paediatric only resus room – adjacent to existing Children’s area
1&2. Consultant; General Manager; Clinical Nurse Lead
1. 30/09/20222. 30/06/2022
05/07/2022
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 5
32/48 264/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
Clin
ical
, E
mpl
oym
ent
Rel
ated
Iss
ues
, H
ealth
& S
afe
ty,
Rep
utat
ion
al
26 A
pril
2022 1710 Limited availability of
Paediatric Radiology service due to the Paediatric Radiologist only working two days a week and the replacement outsourcing company not always having a Paediatric Radiologist available resulting in delays in patient care, delayed discharges and delayed skeletal surveys for child protection cases.
Radiology have introduced and outsourcing company called Medica to review Paediatric Scans however Medica does not always have a paediatric radiologist available either. Over a weekend on call there tends to be delays of at least an 8 hour wait before the scan could be reported. This includes urgent scans. Skeletal surveys for child protection cases can wait up to 2 weeks to be reported if Dr Williams (Paediatric Radiologist) is on leave. Acute Paediatrics have received a patient compliant due to a 2-day delay. Delays in Skeletal Survey’s can cause a lot of anxiety and agony to parents, also causing a delay in issuing the full medical report form the Paediatrician.
Ch
ief
Ope
ratin
g O
ffic
er
Ope
ratio
nal M
anag
er -
Rad
iolo
gy
Ca
tast
roph
ic (
5)
Like
ly (
4) 20 - Work around in place by Radiology Department:7 days a week, out of hours and also including ‘in-hours’ when in-house Radiology support is unavailable – so long as it is possible for the scan to be performed – Radiology are able to outsource reporting on scans to Medica. - The team may require some support from the Paediatric Team to administer contract as they cannot cannulate anyone under 16.
1.Paediatric Team to attend and administer the contrast if Radiographers unable.- Radiographer would need to be there to complete the scan – lack of Radiologist would result in delay as they need to report on it.No mitigation in place – scan would be delayed. - Wye Valley support in reviewing Skeletal Surveys.
Sup
port
Ser
vice
s 26/05/2022 (SSAOGG) - Risk discussed; agreed to add to register.24/05/2022 (SSAOGG) - No change. Member of staff due to qualify as Paediatric Radiologist in November 2022 & it is hoped they will take on role. External company provides some support but it is hit and miss. Risk remains the same.
Ca
tast
rop
hic
(5
)
Lik
ely
(4) 20 From the 17th May, we
will have Everlight teleradiology company on board who will be able to report the skeletal surveys.
General Manager, Radiology
31/05/2022 28/06/2022
Em
ploy
men
t R
elat
ed
Issu
es,
Per
form
ance
, R
epu
tatio
nal
09 M
ay
2022 1724 If the Trust is not able to
recruit to key vacancies across all staff groups, the aspiration to have an engaged, passionate and capable workforce who are trusted to provide safe, effective, compassionate care will not be achieved
Ch
ief
Peo
ple
Off
icer
Ch
ief
Peo
ple
Off
icer
Maj
or (
4)
Alm
ost
Cer
tain
(5
) 20 20 1. Recruitment actively pursued through NHS Jobs, Trac, local recruitment options, apprenticeships etc.2. Where necessary, partnership with recruitment agencies to support International Recruitment.3. Rolling adverts for hard to recruit posts4. Use of Bank/agency staff to fill vacant shifts5. CSW recruitment open days6. New roles introduced, e.g. NAs, Aps & RNDAs7. Successful implementation of ACP roles
Co
rpor
ate 09/05/2022 - Added
to the risk register, agreed by CRG
Maj
or
(4)
Alm
ost
Cer
tain
(5
) 20 1. Improved data quality by ensuring establishment data is held in ESR to enable improved reporting2. Better understanding and closer scrutiny of vacancy positions at F&P3. Review of recruitment processes to identify areas to improve efficiency4. Investment secured through Management Board to improve recruitment processes and increase substantive staffing numbers5. Specific staffing risks identified on Divisional risk registers for areas of high vacancies/turnover
1-5. Operational Director of People & Workforce
1-5. 31/03/2023 13/06/2022
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 6
33/48 265/347
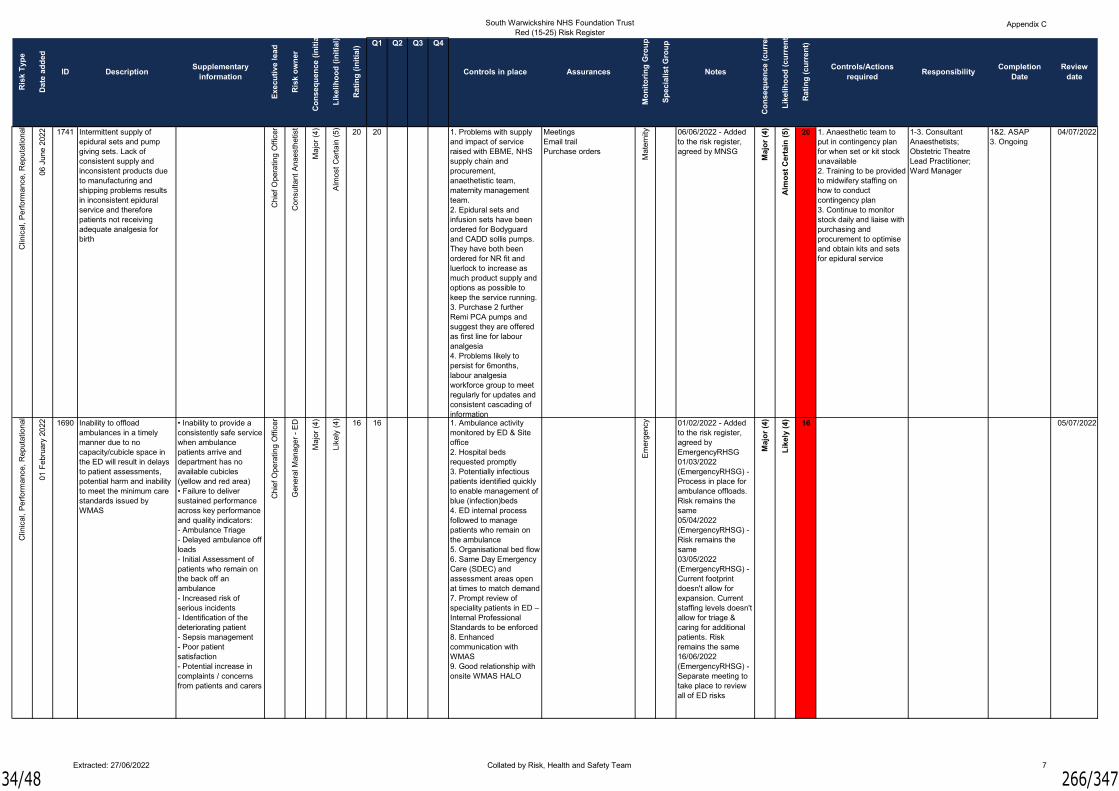
South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
Clin
ical
, P
erfo
rman
ce,
Rep
utat
iona
l
06 J
une
2022 1741 Intermittent supply of
epidural sets and pump giving sets. Lack of consistent supply and inconsistent products due to manufacturing and shipping problems results in inconsistent epidural service and therefore patients not receiving adequate analgesia for birth
Ch
ief
Ope
ratin
g O
ffic
er
Co
nsul
tant
Ana
esth
etis
t
Maj
or (
4)
Alm
ost
Cer
tain
(5) 20 20 1. Problems with supply
and impact of service raised with EBME, NHS supply chain and procurement, anaethetistic team, maternity management team.2. Epidural sets and infusion sets have been ordered for Bodyguard and CADD sollis pumps. They have both been ordered for NR fit and luerlock to increase as much product supply and options as possible to keep the service running. 3. Purchase 2 further Remi PCA pumps and suggest they are offered as first line for labour analgesia4. Problems likely to persist for 6months, labour analgesia workforce group to meet regularly for updates and consistent cascading of information
MeetingsEmail trailPurchase orders
Mat
erni
ty 06/06/2022 - Added to the risk register, agreed by MNSG
Maj
or
(4)
Alm
ost
Cer
tain
(5
) 20 1. Anaesthetic team to put in contingency plan for when set or kit stock unavailable2. Training to be provided to midwifery staffing on how to conduct contingency plan3. Continue to monitor stock daily and liaise with purchasing and procurement to optimise and obtain kits and sets for epidural service
1-3. Consultant Anaesthetists; Obstetric Theatre Lead Practitioner; Ward Manager
1&2. ASAP3. Ongoing
04/07/2022
Clin
ical
, P
erfo
rman
ce,
Rep
utat
iona
l
01 F
ebru
ary
2022 1690 Inability to offload
ambulances in a timely manner due to no capacity/cubicle space in the ED will result in delays to patient assessments, potential harm and inability to meet the minimum care standards issued by WMAS
• Inability to provide a consistently safe service when ambulance patients arrive and department has no available cubicles (yellow and red area)• Failure to deliver sustained performance across key performance and quality indicators:- Ambulance Triage- Delayed ambulance off loads- Initial Assessment of patients who remain on the back off an ambulance- Increased risk of serious incidents- Identification of the deteriorating patient- Sepsis management- Poor patient satisfaction - Potential increase in complaints / concerns from patients and carers
Ch
ief
Ope
ratin
g O
ffic
er
Gen
eral
Man
ager
- E
D
Maj
or (
4)
Like
ly (
4) 16 16 1. Ambulance activity monitored by ED & Site office2. Hospital beds requested promptly3. Potentially infectious patients identified quickly to enable management of blue (infection)beds4. ED internal process followed to manage patients who remain on the ambulance5. Organisational bed flow6. Same Day Emergency Care (SDEC) and assessment areas open at times to match demand7. Prompt review of speciality patients in ED – Internal Professional Standards to be enforced8. Enhanced communication with WMAS9. Good relationship with onsite WMAS HALO
Em
erge
ncy 01/02/2022 - Added
to the risk register, agreed by EmergencyRHSG01/03/2022 (EmergencyRHSG) - Process in place for ambulance offloads. Risk remains the same05/04/2022 (EmergencyRHSG) - Risk remains the same03/05/2022 (EmergencyRHSG) - Current footprint doesn't allow for expansion. Current staffing levels doesn't allow for triage & caring for additional patients. Risk remains the same16/06/2022 (EmergencyRHSG) - Separate meeting to take place to review all of ED risks
Maj
or
(4)
Lik
ely
(4) 16 05/07/2022
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 7
34/48 266/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
Clin
ical
, F
ina
ncia
l, R
epu
tatio
nal
04 A
pril
2022 1700 Potential that Trust will not
achieve BFI Stage 3 Accreditation (reassessment in July 2022) due to a lack of staffing resource within the BFI Team to carry out recommendations from original assessment especially with providing Parent Education and staff training resulting in the potential loss of BFI Level 2 Accreditation leading to reputational and financial damage
Reassessment required following original Unicef BFI Stage 3 Assessment in October 2021 when several of the BFI standards for Maternity Units were not met C
hie
f N
ursi
ng O
ffic
er
Ass
oci
ate
Dire
ctor
of
Mid
wife
ry
Maj
or (
4)
Like
ly (
4) 16 16 1. Action Plan developed to meet recommendations. 2. Funding requested for BFI resources through LMNS3. Small Feeding Team in place working towards Action Plan goals with extra staff being released from other areas on short term basis to assist with application process4. Face to face Parent Education sessions are to be resumed in April/May 2022
Mat
erni
ty 04/04/2022 - Added to the risk register, agreed by MNSG09/05/2022 - Potential that the antenatal education element may not be achieved. Risk remains the same06/06/2022 (MNSG) - Assessment scheduled for July 2022. Not meeting 80% of the assessments required by UNICEF. Risk remains the same
Maj
or
(4)
Lik
ely
(4) 16 1. More resource within
Infant Feeding Team to ensure standards are improving and to carry out audits of this to show a minimum level has been achieved in order for Unicef to agree to carry out the Re-assessment2. Staff needed to carry out training and provide specialist Infant Feeding support in line with BFI requirements3. Sufficient staff needed throughout the Maternity Unit in order for them to be able to be released for training
1-3. Associate Director of Midwifery
1-3. 31/07/2022 04/07/2022
Per
form
ance
, R
eput
atio
nal
05 A
pril
2022 1703 Inability to utilise ED
observation unit for ED patients after an extended period of care (> 4hours) due to the Observation Unit being used for patients who require a side room on an in-patient ward when non available and for those patients with no allocated bed when pending a 12 hour breach resulting in ED not having the ability to proactively manage and meet the 4 hour standard
Ch
ief
Ope
ratin
g O
ffic
er
Gen
eral
Man
ager
- E
D
Maj
or (
4)
Like
ly (
4) 16 16 1. Hospital beds requested promptly2. Site Team and ED working together to manage area proactively3. Site meeting 3-4 times daily, to facilitate discharges
Em
erge
ncy 05/04/2022 - Added
to the risk register, agreed by EmergencyRHSG03/05/2022 (EmergencyRHSG) - Non ED patients in ED Obs overnight leading to daytime capacity issues. Risk remains the same16/06/2022 (EmergencyRHSG) - Separate meeting to take place to review all of ED risks
Maj
or
(4)
Lik
ely
(4) 16 1. Organisational bed
flow to support the above2. Assessment areas open at times to match service demand.3. Prompt review of speciality patients in ED – Internal Professional Standards to be enforced4. Fully operational 24/7 ED Obs unit managed by ED
1-3. Organisational4. ED
1-4. 30/06/2022 05/07/2022
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 8
35/48 267/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
04/07/2022
Maj
or
(4)
Lik
ely
(4) 16 1. Series of business
cases to be submitted over the next two years to bolster the clinical establishment (midwifery workforce only) of the Maternity Department
1. Associate Director of Midwifery
1. 31/03/2024
Mat
erni
ty 09/05/2022 - Added to the risk register, agreed by MNSG06/06/2022 (MNSG) - 1 Business Case approved. Risk remains the same
Ass
oci
ate
Dire
ctor
of
Mid
wife
ry
Maj
or (
4)
Like
ly (
4) 16 16 1. Business case to be submitted to The Board of Directors this financial year to improve the staffing of obstetric theatres2. Business case to be submitted to The Board of Directors this financial year to improve the staffing of obstetric theatres3. Business case to be submitted to Management Board this financial year to ensure a dedicated midwife oversees MAS/Triage 24 hours a day, 7 days a week4. Business cases to be submitted to Management Board and The Board of Directors to bolster clinical establishment5. Business cases to be submitted to Management Board and The Board of Directors to bolster clinical establishment6. Business case to be submitted to bolster staffing of CoC Teams7. Use of escalation policy8. PMA and retention and wellbeing support for staff9. Escalated to safety champions and NEDs10. Daily web ex with the LMNS11. Regional sit reps
Clin
ical
, E
mpl
oym
ent
Rel
ated
Iss
ues
, H
ealth
& S
afet
y
09 M
ay
2022 1722 The Maternity workforce
does not meet the required establishment due to an increase in women who are deemed to be intermediate or high risk at booking resulting in potential poor outcomes for the women and babies and poor patient experience
Current clinical establishment in post 106.20wteOverall clinical establishment (registered midwifery workforce) should be 125.01wte
Ch
ief
Peo
ple
Off
icer
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 9
36/48 268/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
Em
ploy
men
t R
elat
ed
Issu
es,
Per
form
ance
, R
epu
tatio
nal
09 M
ay
2022 1723 The Trust absence rates
are above the target set. The lack of availability of appropriately trained and engaged staff will result in poorer patient experience and care, and will also impact staff experience (both in terms of their ability to deliver care and the resulting impact on their morale).Staff Survey results indicate that Health & Wellbeing is an area that the Trust needs to place specific focus.
Ch
ief
Peo
ple
Off
icer
Ch
ief
Peo
ple
Off
icer
Maj
or (
4)
Like
ly (
4) 16 16 1. Sickness Absence Management Policy developed and implemented in conjunction with Staff Side2. Attendance reviewed monthly via F&P3. Sickness absence management training available for all managers (although low take up)4. Action plan to respond to Staff Survey results5. Disability Policy & Passport of Reasonable Adjustments developed and implemented
Co
rpor
ate 09/05/2022 - Added
to the risk register, agreed by CRG
Maj
or
(4)
Lik
ely
(4) 16 1. Staff absence levels to
be monitored through monthly F&P with trajectories for improvement2. Staff absence to be included on local risk registers for areas of specific concern3. Absence management training to be incorporated into the Managers Development Toolkit with emphasis placed on early intervention4. Roll-out of the Carers Passport to identify flexible working requirements to support staff to meet caring responsibilities
1-4. Operational Director of People & Workforce
1-4. 31/12/2022 13/06/2022
16 1. To gather staff health and wellbeing feedback in relation to the support offered to facilitate continuous improvement2. To review staff wellbeing offers to identify high impact actions and measures of success3. Business Case to be developed and submitted for consideration of the introduction of a Staff Wellbeing Physiotherapist
1-3. Health & Wellbeing Lead
1-3. 31/12/2022 13/06/2022
Co
rpor
ate 09/05/2022 - Added
to the risk register, agreed by CRG
Maj
or
(4)
Lik
ely
(4)
Like
ly (
4) 16 16 1. Health & Wellbeing Group chaired by Head of Health & Wellbeing, including a range of colleagues from across the organisation. This group coordinates the wellbeing and welfare support offer to staff2. Health Needs Assessment questionnaire undertaken3. Winter Resilience Wellbeing pack launched November 20214. Covid and flu vaccinations available for all staff5. Occupational Health support via self-referral or management referral6. Employee Assistance Programme offering 24/7 telephone help, advice and counselling together with online resources7. Staff Support Service offered through Clinical Health Psychology8. With Staff in Mind (tertiary level support) offered through CWPT9. Mental Health First
Em
ploy
men
t R
elat
ed
Issu
es
09 M
ay
202
2 1725 There is a risk of the increased workload combined with the Covid-19 recovery plan impacting on individual staff welfare, including mental health, which could lead to adverse effects on individual, team and Trust resilience. Includes high risk areas and for those staff working from home
Ch
ief
Peo
ple
Off
icer
Ch
ief
Peo
ple
Off
icer
Maj
or (
4)
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 10
37/48 269/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
Clin
ical
, In
form
atio
n G
over
nanc
e,
Per
form
ance
, R
eput
atio
nal
06 J
une
2022 1740 Care to mothers and
babies does not meet national standards due to the Trust not being compliant with the Saving Babies Lives Care bundle, elements of the care bundle require implementation and others require evidence of embedded practice, resulting in a potential an adverse outcome
Ch
ief
Ope
ratin
g O
ffic
er
Ass
oci
ate
Dire
ctor
of
Mid
wife
ry
Maj
or (
4)
Like
ly (
4) 16 16 1. Gap analysis and ongoing action plan to meet compliance2. Regular meetings with NHSE/I to track progress and support actions3. Meetings with maternity safety champions to provide an update on progress and escalate concerns/barriers early
1. Regular updates to the MDT and service2. Compliance tracker 3. Safety champion meetings
Mat
erni
ty 06/06/2022 - Added to the risk register, agreed by MNSG
Maj
or
(4)
Lik
ely
(4) 16 04/07/2022
Em
ploy
men
t R
elat
ed I
ssue
s, P
erfo
rman
ce,
Rep
uta
tiona
l
16 J
une
2022 1746 Lack of management
capacity within the Emergency Division which is at a level that operational management is compromised. This affects delivery of Divisional objectives, HR management, Governance, Contractual performance and other KPIs
Ch
ief
Ope
ratin
g O
ffic
er
AD
O -
Em
erge
ncy
Car
e
Maj
or (
4)
Like
ly (
4) 16 16 1. Leadership focus on Divisional objectives 2. Move to self-managed/self-directed teams3. Refocus/prioritisation Management time on day to day operations4. Communication of management capacity across Trust and management of expectations5. Sustainable solutions delivered through Budget setting6. Review of structure and introduction of junior roles
Em
erge
ncy 16/06/2022 - Added
to the risk register, agreed by EmergencyRHSG M
ajo
r (4
)
Lik
ely
(4) 16 1. Recruit into vacant
posts 2. Structured induction3. Management Pastoral support
1-3. ADO - Emergency Care
1. ASAP2. On commencement3. Ongoing
05/07/2022
9. Mental Health First Aiders (limited availability)10. Team Time sessions11. Covid-19 & us team sessions12. Stress Resilience training13. Staff Pulse Checks undertaken quarterly14. Staff Covid-19 risk assessments reviewed on 6-monthly basis15. Self-isolation guidance reviewed on a regular basis in line with changes to national guidance taking a risk-assessment based approach
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 11
38/48 270/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
1-3. Head of Estates 1-3. 31/03/2023 08/08/20221. Weekly checking of generator systems. 2. Monthly operating/testing of the generator in mains failure mode with hourly monitoring. 3. Contractor placed on standby to supply a temporary generator within 4 hours.4. Un-interruptible Power Supplies (UPS) installed in some known critical patient areas supplying power via batteries to blue sockets.5. UPS availability is not guaranteed for a set period of time due to what is potentially plugged into it.6. Review of critical areas for installation of UPSs and IPSs
Co
rpor
ate
Ele
ctric
al S
afet
y
He
ad o
f E
stat
es
Maj
or (
4)
Un
like
ly (
2) 8 15
Clin
ical
, H
ealth
& S
afet
y, I
nfra
stru
ctur
e,
Rep
utat
iona
l
11 J
une
2019 1358 In the event of an external
loss of electrical power supply to the Warwick Hospital site, there is a risk of failure of the “Dale” back-up generator supplying electrical power(covering blocks 30, 31, 32, 45, 46 and 80) due to its age and the automatic changeover controls monitoring the incoming supply failing. This would have a detrimental effect on the Trust’s ability to provide services and care to patients, could result in loss of IT systems and some infrastructure, such as heating, air conditioning and lifts.
There is the potential risk to business continuity and loss of electrical supply to large sections of the hospital including DSU, Radiology, Aylesford, Bluebell, Helen Clarke, Mortuary, Castle, Macgregor, Mary & Victoria Wards, lifts W4 and W5 Parts of the IT network would also be affected possibly causing Trust wide disruption with significant “knock on” effects across local health economy.
Ch
ief
Str
ate
gy O
ffic
er 13/07/2021
(SSAOGG) - No Change. Risk remains the same10/08/2021 (SSAOGG) - No change; risk remains the same14/09/2021 (SSAOGG) - No change; risk remains the same12/10/2021 (SSAOGG) - Awaiting Estates strategy. No change; risk remains the same.09/11/2021 (SSAOGG) - No change; risk remains the same14/12/2021 (SSAOGG) - No change; risk remains the same. Estates transfers to Corporate division from 01/01/2022 so monitoring group changed to Corporate Risk Group18/01/2022 (ESG) - Engine past serviceable age, maintained & tested. Risk remains the same14/02/2022 (CRG) - To be addressed as part of the Estates and Net Zero Carbon Strategies. Risk remains the same09/05/2022 (CRG) -
Ca
tast
rop
hic
(5
)
Po
ssib
le (
3) 15 1. Replacement of the
generator, control systems and associated LV switch panels.2. Long term research and possibly change the philosophy in how the Trust’s backup electrical systems operate if/when a power cut occurs. 3. UPS/IPS to be installed as part of departmental infrastructure upgrades.
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 12
39/48 271/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
08/08/2022
Ca
tast
rop
hic
(5
)
Po
ssib
le (
3) 15 1. Replacement of the
generator, control systems and associated LV switch panels.2. Long term research and possibly change the philosophy in how the Trust’s backup electrical systems operate if/when a power cut occurs. 3. Green Lane sub-station: Review of critical areas for installation of UPSs and IPSs
1-3. Head of Estates 1-3. 31/03/20231. Weekly checking of generator systems. 2. Monthly operating/testing of the generator in mains failure mode with hourly monitoring. 3. Contractor placed on standby to supply a temporary generator within 4 hours.4. Un-interruptible Power Supplies (UPS) installed in some known critical patient areas supplying power via batteries to blue sockets. 5. UPS availability is not guaranteed for a set period of time due to what is potentially plugged into it.6. Some portable suction units are available.7. PPM increased on all generators throughout the Trust.- Replaced batteries.- Researched & written SOPs.- Training given
Co
rpor
ate
Ele
ctric
al S
afet
y
He
ad o
f E
stat
es
Ca
tast
roph
ic (
5)
Pos
sibl
e (3
) 15 15 13/07/2021 (SSAOGG) - No Change. Risk remains the same10/08/2021 (SSAOGG) - No change; risk remains the same14/09/2021 (SSAOGG) - No change; risk remains the same12/10/2021 (SSAOGG) - Awaiting Estates Strategy. No change; risk remains the same09/11/2021 (SSAOGG) - No change; risk remains the same14/12/2021 (SSAOGG) - No change; risk remains the same. Estates transfers to Corporate division from 01/01/2022 so monitoring group changed to Corporate Risk Group18/01/2022 (ESG) - Engine past serviceable age, maintained & tested. Risk remains the same14/02/2022 (CRG) - To be addressed as part of the Estates and Net Zero Carbon Strategies. Risk remains the same09/05/2022 (CRG) -
Clin
ical
, H
ealth
& S
afet
y, I
nfra
stru
ctur
e,
Per
form
ance
11 J
une
2019 1363 In the event of an external
loss of electrical power supply to the Warwick Hospital site, there is a risk of failure of the “Wilson” back-up generator supplying electrical power(covering blocks 4,10,11,12,13,14,18,19,20,21,22,23,30,45 and 85) due to its age and the automatic changeover controls monitoring the incoming supply failing. This would have a detrimental effect on the Trust’s ability to provide services and care to patients, could result in loss of IT systems and some infrastructure, such as heating, air conditioning and lifts.
There is the potential risk to business continuity and loss of electrical supply to large sections of the hospital including part of Radiology, Endoscopy, Switchboard, Security, Machen, M.R.I, Catheter Lab, Avon and Farries Wards. The vacuum plant failure would cause all suction systems to stop working in the above areas plus Malins, Squire, Castle, Macgregor, Mary and Victoria Wards, C.C.U and Charlecote Ward. This would have a major impact on patient care. Parts of the IT network would also be affected possibly causing Trust wide disruption with significant “knock on” effects across local health economy.
Ch
ief
Str
ate
gy O
ffic
er
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 13
40/48 272/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
Alm
ost
Cer
tain
(5
) 15 29/07/20221. PIP Guidelines available on the Intranet2. Escalated with Pharmacy dept.3. Regular meetings with Pharmacy representative4. Raised at divisional level (AOGG, Risk, H&S Committee and Clinical Practices Group) 5. Guidelines returned from Pharmacy are prioritised6. Paediatric representative available to attend all monthly Drugs & Therapeutic Committee meetings7. Concern raised at Drugs & Therapeutic Committee (26/01/2021)8. Admin support provided to update guidelines
Fam
ily H
ealth
Mo
der
ate
(3)
Min
or (
2)
Un
like
ly (
2) 4 15 05/08/2021 (FHRHSG) - No update from risk owner01/09/2021 (FHRHSG) - No communication from Pharmacy yet. PIP Guidelines available on the intranet - some clarification from DTC awaited. Risk remains the same07/10/2021 (FHRHSG) - Number of out of date guidelines increasing. Agreed to match the Maternity Guideline risk score 3:5 (Risk ID 1559) and escalate to SSAOGG04/11/2021 (FHRHSG) - Dr Amadu to liaise with Pharmacy. Risk remains the same09/12/2021 (FHRHSG) - Work ongoing with Pharmacy. Links to Risk ID 1559 Maternity Guidelines.
Clin
ical
04 F
ebru
ary
2021 1574 Out-of-date Paediatrics
guidelines due to a delay in reviewing and approving documents by pharmacy and ratification by Drugs & Therapeutics Committee resulting in the potential of inappropriate care and treatment
Ch
ief
Ope
ratin
g O
ffic
er
Gen
eral
Man
ager
- A
cute
Pae
diat
ric &
Wom
en’s
Ser
vice
s
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 14
41/48 273/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
Maternity Guidelines. Risk remains the same06/01/2022 (FHRHSG) - Admin support provided to update guidelines. Risk remains the same03/02/2022 (FHRHSG) - Working through the guidelines. New PIP Guidelines issued which require reviewing. Risk remains the same03/03/2022 (FHRHSG) - Guidelines being transferred to new format. Risk remains the same07/04/2022 (FHRHSG) - Admin required to transfer PIP Guidelines to be transferred to SWFT templates. Risk remains the same05/05/2022 (FHRHSG) - No update from Pharmacy. Admin support identified. Risk remains the same20/06/2022 (FHRHSG) -
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 15
42/48 274/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
15 04/07/20221. Use of bank staff to bring shifts up to 3 qualified staff2. Send out WhatsApp to staff for shifts not covered and any urgent/short notice shifts3. On-going recruitment4. Use of Thornbury Agency if essential5. Communication to Labour Ward, Senior Paediatrician & Registrar when less than 3 qualified members of staff on duty to advise re: difficulties with attending emergencies6. Ward Manager covering clinical shifts
Mat
erni
ty
Mo
der
ate
(3)
Alm
ost
Cer
tain
(5
)
Like
ly (
4) 12 15 05/07/2021 - Added to the risk register, agreed by MNPSG04/10/2021 (MNPSG) - 1 x 22 hrs recruited. Awaiting start of International nurses. Staff retiring early 2022. Bank & agency utilised where possible. Risk score increased to 3:501/11/2021 (MNPSG) - 1x new starter; 1x resignation; 1x maternity leave. Risk remains the same16/12/2021 (MNPSG) - Meeting Cancelled. Virtual update - adverts out for B5&6 nurses: no applicants. Recruited 2 WTE from overseas – waiting for them to arrive. Currently 2 WTE posts vacant. A further 2.5 WTE leaving or retired by May 2022. Risk remains the same10/01/2022 (MNSG) -
Clin
ical
, E
mpl
oym
ent
Rel
ated
Iss
ues
, H
ealth
& S
afet
y
05 J
uly
2021 1625 Difficulty in providing 3
qualified nurses on all shifts within SCBU due to 3 WTE on maternity leave from September 2021 and difficulties in recruiting (due to length of the recruitment process and limited applications) resulting in potential harm to babies, delayed care/treatment and staff fatigue/burnout.
The environment of 4 separate rooms increases the risk as it is impossible for nurses to continually observe all babies. Requirement to cover emergencies on Labour Ward; Bluebell Birthing Suite; A&E leads to qualified nurses being taken off the unit.
Ch
ief
Nur
sing
Off
icer
Ass
oci
ate
Dire
ctor
of
Mid
wife
ry
Mod
erat
e (3
)
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 16
43/48 275/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
10/01/2022 (MNSG) - Interviews scheduled for w/b 17/01/2022. Risk remains the same07/02/2022 (MNPG) - Staffing improving, 2 overseas nurses recruited; 1x maternity leave returning; 0.5 B6 recruited. 4x new maternity leave; 1x re-location. Risk remains the same07/03/2022 (MNSG) - 2x WTE vacancies. One staff member on maternity due to return in May, another one about to go on maternity leave. Risk remains the same.04/04/2022 (MNSG) - Overseas nurses commenced, but in training. Long-term sickness and maternity leave. New starter June 2022. Further interviews scheduled 07/04/2022. Risk remains the same09/05/2022 (MNSG) - Awaiting new starters, 1 starts in June 2022, other awaiting clearance. Risk remains the same06/06/2022 (MNSG) - New starters to commence: 2x B5 June/July 2022 & 1x B6 part-time June 2022. 3x sick leave &
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 17
44/48 276/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
Clin
ical
09 A
ugus
t 20
21 1631 No clear and coherent process for staff to follow when acknowledging patient investigations/results due the capabilities of the current system leading to the potential for abnormal results not being acted upon resulting in delayed or no treatment
UHCW Risk Assessment: BS RA41
SWFT Audit data:During the year 2020, 500,289 pathology requests were made for Warwick.• 166,553 of these were electronic order comms requests (33%)• 333,799 paper requests (66%)
Ch
ief
Nur
sing
Off
icer
Ch
ief
Nur
sing
Off
icer
Ca
tast
roph
ic (
5)
Pos
sibl
e (3
) 15 15 1. Clinical staff using manual processes to ensure that results are acknowledged/seen and acted upon2. Patients are often seen as Outpatients to ensure that results are not missed
Co
rpor
ate 09/08/2021 - Added
to the risk register, agreed by CRG. Replacing Risk ID 137908/11/2021 (CRG) - To be monitored via Digital Board. Risk ownership transferred to Chief Technology Officer. Risk remains the same14/02/2022 (CRG) - Number of incidents reduced. Risk ownership transferred to Chief Nursing Officer. Risk remains the same09/05/2022 (CRG) - New system for results acknowledgement due to go live in June 2022. Once the system was operational the risk may be downgraded or closed. Risk remains the same
Ca
tast
rop
hic
(5
)
Po
ssib
le (
3) 15 1. Clinically led Task &
Finish Group to be formed to decide further mitigation
1. Director of Nursing 1. 30/06/2022 08/08/2022
Clin
ical
, In
fras
truc
ture
, R
eput
atio
nal
10 J
anua
ry 2
022 1680 Emergency Theatre Team
are being utilised to complete Elective Caesarean Sections, due to an increase in acuity and complexity of women coming to the service resulting in potential poor outcome for either mother and/or baby
Ch
ief
Ope
ratin
g O
ffic
er
Ass
ocia
te D
irect
or o
f M
idw
ifery
Mod
erat
e (3
)
Alm
ost
Cer
tain
(5) 15 15 1. Requests overseen by
Theatre Lead and Consultant2. High Risk women given double slot3. Limit number of electives4. Quick turnaround between cases5. Delaying Elective Cases6. Audit of Theatre time completed7. Prompt start time, posters displayed advising MDT 08:40
Mat
erni
ty 10/01/2022 - Added to the risk register, agreed by MNSG07/02/2022 (MHSG) - Data proves extra sessions required. Business case to be developed. Risk remains the same07/03/2022 (MNSG) - No change; risk remains the same04/04/2022 (MNSG) - Risk remains the same09/05/2022 (MNSG) - Risk remains the same06/06/2022 (MNSG) - Business case to go to BoD July/Aug 2022. Risk remains the same
Mo
der
ate
(3)
Alm
ost
Cer
tain
(5
) 15 1. Consider long lists 2. Business case to be developed
1&2. Associate Director of Midwifery
1. As & when required2. 31/08/2022
04/07/2022
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 18
45/48 277/347
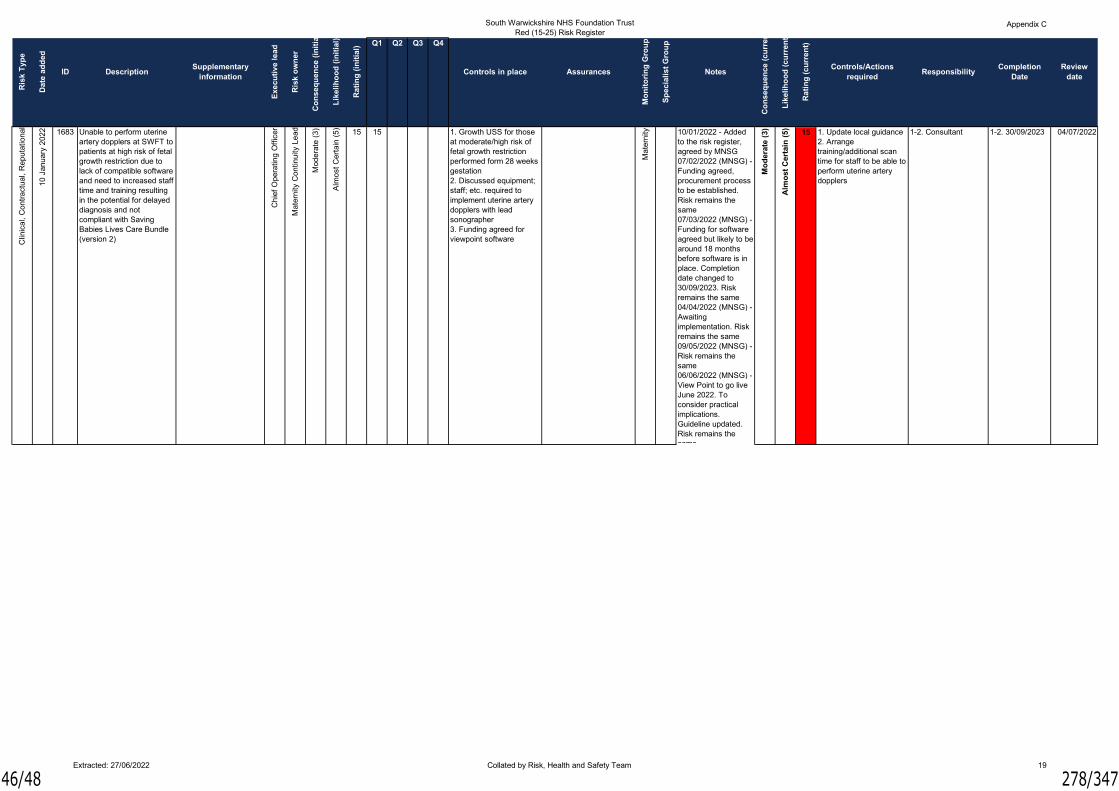
South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
Clin
ical
, C
ontr
act
ual,
Rep
utat
iona
l
10 J
anua
ry 2
022 1683 Unable to perform uterine
artery dopplers at SWFT to patients at high risk of fetal growth restriction due to lack of compatible software and need to increased staff time and training resulting in the potential for delayed diagnosis and not compliant with Saving Babies Lives Care Bundle (version 2)
Ch
ief
Ope
ratin
g O
ffic
er
Mat
erni
ty C
ontin
uity
Le
ad
Mod
erat
e (3
)
Alm
ost
Cer
tain
(5) 15 15 1. Growth USS for those
at moderate/high risk of fetal growth restriction performed form 28 weeks gestation2. Discussed equipment; staff; etc. required to implement uterine artery dopplers with lead sonographer3. Funding agreed for viewpoint software
Mat
erni
ty 10/01/2022 - Added to the risk register, agreed by MNSG07/02/2022 (MNSG) - Funding agreed, procurement process to be established. Risk remains the same07/03/2022 (MNSG) - Funding for software agreed but likely to be around 18 months before software is in place. Completion date changed to 30/09/2023. Risk remains the same04/04/2022 (MNSG) - Awaiting implementation. Risk remains the same09/05/2022 (MNSG) - Risk remains the same06/06/2022 (MNSG) - View Point to go live June 2022. To consider practical implications. Guideline updated. Risk remains the same
Mo
der
ate
(3)
Alm
ost
Cer
tain
(5
) 15 1. Update local guidance 2. Arrange training/additional scan time for staff to be able to perform uterine artery dopplers
1-2. Consultant 1-2. 30/09/2023 04/07/2022
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 19
46/48 278/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
Clin
ical
, E
mpl
oym
ent
Rel
ated
Iss
ues
, F
inan
cial
, R
eput
atio
nal
05 A
pril
2022 1706 The Acute Decisions Unit
(ADU) usual operating hours are 08:00 to 00:00, ADU has been bedded 24/7 for over 6 months due to capacity and flow issues leading to financial overspend and potential patient safety & experience issues.
The risk is that the clinical area is not designed to support patients to be accommodated for extended periods of time• No natural daylight or ventilation• No equipment to support longer length of stay• Workforce impact – reliant on agency staff to deliver the overnight care
Ch
ief
Ope
ratin
g O
ffic
er
Gen
eral
Man
ager
- A
cute
Med
icin
e
Mod
erat
e (3
)
Alm
ost
Cer
tain
(5) 15 15 1. Equipment purchased
to support the staff working within the unit and to offer the patients the best experience 2. Incidents completed when quality of care is not as expected 3. Any patient safety issues are actively followed up through existing process which includes following up with the agency4. Nurse in Charge on AMU to address any concerns which are raised5. Medical staffing levels increased to ensure that there is sufficient cover across all areas6. All efforts made to review and respond to overspends in the budget whilst patient safety prioritised7. AMU/ADU have developed a staff wellbeing plan which is monitored via the divisional governance meeting
Em
erge
ncy 05/04/2022 - Added
to the risk register, agreed by EmergencyRHSG03/05/2022 - Risk remains the same16/06/2022 (EmergencyRHSG) - Squire Ward has been opened temporarily for step-down patients to allow organisational flow. Risk remains the same
Mo
der
ate
(3)
Alm
ost
Cer
tain
(5
) 15 1. Bed capacity to be increased short term to support ADU to be unbedded. In order to facilitate this an overall agreed strategy will be required which inherently will mean increased pressure across the system short term, which will require a consistent and maintained response
1. ADOs - Emergency Care
1. TBC 05/07/2022
Clin
ical
03 M
ay
2022 1720 The internal size of the
temporary pods installed in AMU present a resus and patient transfer risk resulting in patients having to be moved from the pods to the main bay to enable patient transfers and/or resuscitation to take place
Ch
ief
Str
ate
gy O
ffic
er
Gen
eral
Man
ager
- A
cute
Med
icin
e
Ca
tast
roph
ic (
5)
Pos
sibl
e (3
) 15 15 1. Patients are removed from the pods and treated in the bay2. Patients are to be transferred within the bay to ensure that there is sufficient space to enable safe transfer
Em
erge
ncy 03/05/2022 - Added
to the risk register, agreed by EmeregncyRHSG16/06/2022 (EmergencyRHSG) - Resus Report has highlighted the size of the Pods are a concern, agreed to undertake a simulation exercise. IPC, H&S & Estates to visit. Risk remains the same
Ca
tast
rop
hic
(5
)
Po
ssib
le (
3) 15 1. Request review by the
Crash Team to look at alternate options2. Request review by the Moving and Handling Team3. Ongoing monitoring of frequency of incidents of CPR/Resus incidents in the pods through the Acute Medicine Governance Meetings
1. GM - Acute Medicine; Resus Lead2. GM - Acute Medicine; Moving and Handling Lead 3. Consultant; Ward Manager
1-3. TBC 05/07/2022
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 20
47/48 279/347

South Warwickshire NHS Foundation TrustRed (15-25) Risk Register
Appendix C
Q1 Q2 Q3 Q4
Lik
elih
oo
d (
curr
ent)
Ra
tin
g (
cu
rren
t)
Supplementary information
Co
nse
qu
ence
(in
itia
l)
Assurances
Exe
cuti
ve l
ead
ID
Ris
k o
wn
er
Mo
nit
ori
ng
Gro
up
Notes
Ris
k T
ype
ResponsibilityReview
date
Lik
elih
oo
d (
init
ial)
Ra
tin
g (
init
ial)
Controls in place
Sp
ecia
list
Gro
up
Co
nse
qu
ence
(cu
rren
t)
Da
te a
dd
ed
Controls/Actions required
DescriptionCompletion
Date
Clin
ical
, R
eput
atio
nal
09 M
ay
2022 1721 Insufficient assessment
areas within the maternity footprint to clinically assess in a timely fashion, women attending the Maternity Assessment Suite (Maternity Triage) resulting in delayed care/treatment leading to potential poor outcome for mother and baby.
Only one designated room to assess women attending with emergent issues in their pregnancy. This leads to women having to wait longer than the nationally accepted timeframes (15 minutes) which may result in their care being delayed and outcomes for them or their baby being affected adversely
Ch
ief
Str
ate
gy O
ffic
er
Mat
erni
ty L
ead
for
Hos
pita
l Ser
vice
s
Mod
erat
e (3
)
Alm
ost
Cer
tain
(5) 15 15 1. Use of bereavement
room or labour rooms when available
Mat
erni
ty 09/05/2022 - Added to the risk register, agreed by MNSG06/06/2022 (MNSG) - Risk remains the same
Mo
der
ate
(3)
Alm
ost
Cer
tain
(5
) 15 1. Capital funding to redesign and develop MAS waiting area to create more capacity
1. Chief Strategy Officer
1. TBC 04/07/2022
Em
ploy
men
t R
elat
ed I
ssue
s, F
inan
cial
16 J
une
2022 1747 Due to the lack of
candidates for the two substantive Respiratory Consultant posts, there is a risk that to maintain the current service provision the department will need to retain the use of the current expensive agency locum. This will therefore retain the current overspend within the Respiratory Consultant cost centre
Ch
ief
Fin
ance
Off
icer
Gen
eral
Man
ager
- R
espi
rato
ry a
nd R
heu
mat
olog
y
Mod
erat
e (3
)
Alm
ost
Cer
tain
(5) 15 15 1. ATR completed for 12
month NHS Locum2. 12 month NHS Locum post to be advertised including support for CESR3. Substantive post to be re-advertised4. Work with BPAPIO for recruitment5. Head hunter agencies advised of post6. Networking with international contacts7. Request for RCP, MTI registration and review of ability to recruit8. ACP to undertake clinics
Em
erge
ncy 16/06/2022 - Added
to the risk register, agreed by EmergencyRHSG
Mo
der
ate
(3)
Alm
ost
Cer
tain
(5
) 15 1. Interviews for vacancies
1. GM - Respiratory and Rheumatology
1. 31/10/2022 05/07/2022
Extracted: 27/06/2022 Collated by Risk, Health and Safety Team 21
48/48 280/347

Report SummaryReport to Board of Directors Date of
Meeting6 July 2022
Report Title Summary of Ratified Policies
Agenda Item
10.1
Executive/Non-Executive Lead
Anne Coyle,Managing Director
Report Author(s)
1. Phil Johns, Chief Technology Officer
2. Phil Johns, Chief Technology Officer
Report Previously Discussed at N/A
Purpose of the Report For ApprovalFor Discussion
To provide the Board of Directors with oversight and assurance of the policies that have been ratified by the Policy Review Group.
For Information
Recommendations and Action Required The Board is asked to receive and note the summary of the policies ratified by the Policy Review Group on 20 June 2022:
1. SWH 00530 Information Security Policy 2. SWH 01626 Internet Usage Policy
Impact (is there any impact arising from the report on the following?) Quality Equality Finance Research Performance Compliance Workforce Legal
Applicable Quality Improvement Priorities Elective Hub Health InequalitiesElectronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety Compassionate Effectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk RegisterAre any existing risks on the BAF/Risk Register affected? N/AIdentify the BAF/Risk Register risk ID and description – explain how the risk has been affected – reduced or increased as a consequence of the evidence within the report. N/ADo you recommend a new entry to the BAF and/or Risk Register is made as a result of this report?
N/A
1/2 281/347

South Warwickshire NHS Foundation Trust
Report to Board of Directors – 6 July 2022
Summary of Ratified Policies
The following policies were ratified by the Policy Review Group on 20 June 2022.
SWH 00530 Information Security Policy
The policy has been updated as it has reached its five year review date. Changes made take into account changes in the technology landscape including additional requirements of the Data Security and Protection Toolkit.The purpose of the policy was to establish and maintain the security and confidentiality of information, information systems, applications and networks owned or held by the Trust. It ensures that Trust data was kept confidential, maintains integrity and was available when required for business use.
The Trust has a legal obligation to ensure that there was adequate provision for the security management of the information assets the organisation own, control, or use.
The policy sets out a consistent approach to the security management of information throughout the Trust and will aim to deliver continuous business capability and minimise both the likelihood of occurrence and the impacts of information security incidents.
Main changes to note were:
• Change from 6 character password to minimum 20 character passphrase (e.g. IDriveABlueMercedesBenz)
o Passphrase to be changed annually
• Introduction of a Privileged Access Management process and supporting technology for staff with Administrative access to systems and services
• Policy for the collection and retention of system log files included
SWH 01626 Internet Usage Policy
The policy has been updated as it had reached its five year review date. The policy gives guidance to staff on acceptable usage of the internet. The only change was the removal of reference to Internet Explorer and the addition of Microsoft Edge.
2/2 282/347

Report Summary Report to Board of Directors Date of
Meeting 6 July 2022
Report Title Health & Safety Annual Report 2021-22 Summary
Agenda Item 10.2
Executive/ Non-Executive Lead
Harkamal Heran, Chief Operating Officer
Report Author(s)
Joanne Beales, Lead Risk, Health & Safety Adviser
Report Previously Discussed at Health & Safety Committee Monday 6 June 2022
Purpose of the Report To provide the Board of Directors with a summary of the Health & Safety Annual Report 2021-22
For Approval For Discussion For Information
Recommendations and Action Required The Board of Directors is asked to receive and note the Health & Safety Report 2021-22 summary
Impact (is there any impact arising from the report on the following?) Quality Equality Finance Research Performance Compliance Workforce Legal
Applicable Quality Improvement Priorities Elective Hub Health Inequalities Electronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety Compassionate Effectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk Register Are any existing risks on the BAF/Risk Register affected? N/A Identify the BAF/Risk Register risk ID and description – explain how the risk has been affected – reduced or increased as a consequence of the evidence within the report. Do you recommend a new entry to the BAF and/or Risk Register is made as a result of this report? If yes, describe the new risk.
N/A
1/5 283/347

South Warwickshire NHS Foundation Trust
Report to Board of Directors – 6 July 2022
Health & Safety Annual Report 2021-22 Summary
Executive Opinion and Assurance Whilst management of health and safety is a continuous process, South Warwickshire NHS Foundation Trust (SWFT) has a robust health and safety culture and processes embedded in our risk management approach. Levels of compliance with departmental audits are extremely high and the Board can be assured that the risk of non-compliance with health and safety legislation is low. Recommendation The Board of Directors is asked to receive and note the Health & Safety Report 2021-22 summary. Harkamal Heran Chief Operating Officer
2/5 284/347

Summary of Health and Safety Annual Report 2021-22 1. Executive Opinion
Whilst management of health and safety is a continuous process, SWFT has a robust health and safety culture and processes embedded in our risk management approach. Levels of compliance with departmental audits are extremely high and the Board can be assured that the risk of non-compliance with health and safety legislation is low. 2. Introduction
Health and Safety legislation requires employers to have a robust health and safety management system. Within the Trust responsibility for health and safety is discharged through the Health and Safety Committee with the Chief Operating Officer appointed as Lead Executive on behalf of the Chief Executive Officer. Associate Directors of Operations have responsibility within their Divisions for implementing the requirements of Trust health and safety policies in their areas and submit bi-annual reports to the Health and Safety Committee to provide appropriate governance and assurance to the Trust Board that legal requirements are implemented and control measures effective. Throughout 2021-22 the Coronavirus Pandemic (COVID-19) continued, although the Country was being urged to return to normal and national requirements were eased. Healthcare organisations were required to provide all services and implement recovery schemes. Many of the national measures introduced to ensure both staff and patients were kept safe continued until the beginning of April 2022. The Health and Safety Team along with colleagues in Infection, Prevention & Control reviewed national guidance as it was issued and where required local guidance was amended. Throughout the year clinical and non-clinical workplaces were required to remain COVID secure, to achieve this staff were encouraged to work from home where possible; when on site all staff needed to adhere to social distancing; good ventilation, barriers/Perspex screens, one-way flows and cleaning frequently touched surfaces remained in place. Guidance remained in place for Community staff who need to travel, in cars, as part of their role, which included mandating staff should travel alone, unless there was a lone working reason that they could not do so. If staff needed to travel together guidance was issued to minimise the risk of spreading the virus between staff members. As the Trust is actively promoting agile working, the Health and Safety Team issued regular guidance and reminders of good practice whilst working from home, which includes a Working from Home Checklist to promote good posture, regular breaks and exercise. In 2021-22, as with the previous year, COVID-19 has been the main area of focus for the Health and Safety Team, which has continued to act as a source of advice and information to staff from all departments. Assistance has been given for a wide variety of safety topics that have ranged from issues such as the hazards associated with using chemicals, office size and layout to minimise musculoskeletal injuries, including display screen equipment advice and FFP3 face fit testing. Information sharing continues with colleagues across the Foundation Trust Group is taking place to ensure a consistent approach.
3/5 285/347

3. Health and Safety Interventions 3.1 Health and Safety Executive (HSE) During 2021-22, the Trust reported 17 staff and 4 patient incidents to the Health & Safety Executive, under RIDDOR, none of which have resulted in further action or investigation. The RIDDOR Regulations require notification to the Health and Safety Executive within specific time frames. Failure to report on time leaves the Trust in breach of these requirements and liable to fines of up to £20,000 per occasion. The table below shows an analysis of RIDDOR reportable incidents during 2020-21.
Within HSE Timescale Outside HSE Timescale Staff 7 10 Patient 0 4 Total 7 14
Of the 21 incidents reported 7 (33%) were reported within the legal time frame. The late reporting of 10 staff incidents was due to either the timeliness of reporting the incident and further information being provided by the Line Manager. Line Managers have been reminded of the need for timely incident reporting. The late reporting of the 4 patient incidents is attributed to the length of time taken to gather enough information, on which to base a decision and undertake the initial investigation. For further detail refer to Tables 1 & 2 (Appendix 1). 4. Health and Safety Legislation
During 2021-22, there was very little Health and Safety Legislation issued, which would impact on the Trust, other than the introduction and subsequent relaxation of Coronavirus Pandemic guidelines. As the Government has moved into the living with COVID-19 phase, emphasis will now be on the continuation of working from home and stress and mental health issues. The COVID-19 Public Enquiry will be chaired by Dame Heather Hallett, there has been a consultation of the draft Terms of Reference (ToR), and the final ToR are awaited. It is anticipated that the evidence collection will start in 2022 with hearing taking place in 2023. The Personal Protective Equipment at Work (Amendment) Regulations 2022 were issued on 6 April 2022, under these Regulations, the types of duties and responsibilities on employers and employees under the 1992 Regulations remain unchanged but are extended to limb (b) workers, defined as workers who generally have a more casual employment relationship and work under a contract for service. A limb (b) worker now has a duty to use the PPE in accordance with their training and instruction, and ensure it is returned to the storage area provided by their employer. Although not having a direct impact on the Trust two pieces of legislation have been introduced in response to the Grenfell Tower enquiry. The Fire Safety Act 2021 came into force on 20 April 2021, this legislation amends the Regulatory Reform (Fire Safety) Order 2005. The Building Safety Bill has just been through the third reading in the House of Lords. These pieces of legislation aim to deliver the biggest changes to building safety for nearly 40 years and to make residents safer in their homes.
4/5 286/347

5. Health and Safety Strategy Objectives The Health and Safety Strategy 2019-2024 (SWH 01080) was reviewed, updated and ratified in August 2019. The strategy details three objectives for the Trust to work towards. Objective 1 – To maintain and monitor the effectiveness of the Health and Safety Management System across all areas, which will improve the practice and standards of health and safety management. This objective is monitored by undertaking a self-assessment against the Workplace Health and Safety standards, with gaps being reported to the Health and Safety Committee on a bi-annual basis. Objective 2 – Assurance that the organisation is operating to current legislative standards (minimum), Department of Health regulatory requirements and industry 'best practice'. This objective is achieved by ensuring the Board is kept up to date with legislative changes and the submission of divisional bi-annual health and safety reports to the Health and Safety Committee. Objective 3 – Coordination of Statutory and Occupational Health and Safety requirements across the Trust to provide adequate assurance of legal compliance to the Board of Directors. This objective is achieved by ensuring the reports detailed within the Health and Safety Committee’s schedule of business are presented to and discussed at the Committee. The Lead Risk, Health and Safety Adviser monitors compliance with the schedule of business and highlights any issues of concern to the Committee. 6. Policies
The following Policies and Standing Operating Procedures (SOPs) were reviewed, updated where necessary, and ratified. Document Number Ratified First Aid Provision A Managers Guide SWH 00855 June 2021 Mercury Spillage Procedure SWH 01419 April 2022
In addition to the above the Health & Safety Team have supported the development and updating of COVID-19 SOPs. 7. Summary
The Health & Safety Teams main focus was to assist the Trust in complying with the Government COVID-19 guidelines and issuing guidance as and when measures are eased/changed. The Team endeavoured to return to business as usual with regard to the IOSH Managing Safely courses and the Health & Safety inspections. The Health & Safety Team and Procurement will continue to focus on ensuring the Trust is compliant with the Health & Safety (Sharp Instruments in Healthcare) Regulations 2013, by reviewing the use of non-safety sharps; reviewing alternatives and where needed ensuring risk assessments are in place. Health & Safety Committee have not set priorities for 2021-22 due to the current focus on the Coronavirus Pandemic. Joanne Beales Lead Risk, Health & Safety Adviser
5/5 287/347

Report SummaryReport to Board of Directors Date of Meeting 6 July 2022Report Title Annual Security Report
1 April 2021 - 31 March 2022 Agenda Item 10.2
Executive/Non-Executive Lead
Harkamal Heran – Chief Operating Officer
Report Author Sean Mitchell, Security and Parking Manager
Report Previously Discussed at Health and Safety Committee 6.6.2022
Purpose of the Report For ApprovalFor Discussion
The purpose of this report is to provide the Board of Directors with the LSMS Annual Security Report 1 April 2021 - 31 March 2022
For Information x
Recommendations and Action Required The Board of Directors /Board Committee is asked to: e.g receive and note, approve
Impact (is there any impact arising from the report on the following?) Quality EqualityFinance ResearchPerformance ComplianceWorkforce Legal
Applicable Quality Improvement Priorities Elective Hub Health InequalitiesElectronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety CompassionateEffectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk RegisterAre any existing risks on the BAF/Risk Register affected? NoIdentify the BAF/Risk Register risk ID and description – explain how the risk has been affected – reduced or increased as a consequence of the evidence within the report.
Do you recommend a new entry to the BAF and/or Risk Register is made as a result of this report? If yes, describe the new risk.
No
1/15 288/347

South Warwickshire NHS Foundation Trust
Report to Board of Directors - 6 July 2022
Summary of Reports for Noting and Information
Security Annual Report
Executive Opinion
Significant work has been on-going over the year to address security issues as they arise. The Board should take assurance front the report that mechanisms that are in place are robust to support a safe environment across the Trusts and are supporting those who are subjected to violence, abuse and aggression.
Harkamal HeranChief Operating Officer
2/15 289/347

1. Executive Summary
The purpose of this report is to provide the Board of Directors with the 1 April 2021 – 31 March 2022 Local Security Management Specialist (LSMS) Annual Report.
Violence and aggressive behaviour against NHS staff have a serious impact on its ability to deliver the best possible care and patient experience. By preventing and tackling these incidents, the Trust helps to save valuable NHS resources.
The aim is to actively prevent and deter crime from occurring in the first place. When crime does occur, the Trust can respond to and investigate it. The completion of these investigations gives out a strong deterrent message to would be offenders and also promote to all staff that the Trust will support them and take an interest in their personal safety and security. It is important to ensure that learning outcomes are reviewed and communicated out across the Trust.
As a Trust we have over the last year again seen an increase in mental health issues increasingly in children, on ward areas and across all the Divisions. This adds additional pressure to the staff and their ability to treat and care for these patients by providing a safe and secure environment whilst remaining safe themselves.
We have also seen a rise of incidents being reported in the Community setting these being physical abuse verbal abuse and unfortunately racial and sexual abuse.
2. Background
The Trust operates from numerous sites and locations across Warwickshire and the West Midlands and employs approximately 4000+ staff, providing a full range of services. Security issues primarily consist of:
• Physical assaults against staff.• Racial and Sexual assaults.• Non physical assaults.• Damage to Trust property.• Theft/damage of NHS property.• Theft of staff & patient property.
The costs of these incidents are more than financial as they affect patients too, stolen or damaged equipment and staff off sick can mean delays in treatment and patient experience.
There has been a total of 531 (+163) incidents of Violence, Abuse and Harassment from 1 April 2021 - 31 March 2022 across the Trust, compared to 368 in 2020/21
3/15 290/347

Graph 1: Violence, Abuse & Harassment Incidents 1 April 2021 - 31 March 2022
Whilst the graph above shows that the two main areas as expected are Actual Physical Assault on Staff and Verbal Abuse on Staff, the graph bellows shows a comparison on 1 April 2020 - 31 March 2021 and 1 April 2021 - 31 March 2022
Graph 2: Trends on 1 April 2020 - 31 March 2021 and 1 April 2021 – 31 March 2022 Physical Assaults and Verbal Aggression
Incidents of Actual Physical Assault on staff saw an increase +46Incidents of Verbal Abuse on Staff saw an increase + 64
I have looked at the split between other incidents reported compared to verbal abuse, as shown in the table below:
4/15 291/347

The table below indicates other incidents that have been reported from 1 April 2021 - 31 March 2022
Incident 01.04.20 31.03.21 01.04.21 31.03.22 + /-Sexual Incidents 11 12 +1Staff on Staff 23 30 +07Physical Assaults Dementia/ Clinical Reasons 23 45 +22Racial Incidents 06 17 +11Lone Worker Issues 11 06 - 05
South Warwickshire NHS Foundation Trust with the support from BAME, Communications and Warwickshire Police have undertaken a campaign against racial abuse other discriminatory behaviour these have been sent out to all areas working for South Warwickshire NHS Foundation Trust and the Foundation group.
An area that I intend to continue focussing on is offering support to staff by encouraging them to Datix incidents, so we capture the true picture, and then be able to put appropriate sanctions in place. If the racial incidents are related to Hate Crime, staff supported by the Trust are encouraged to report it to the Police for them to investigate. We have added new guidance staff to use, these guidelines have been included in the SWH 00097 Violence Prevention and Reduction Policy
We have seen some success with Warwickshire Police and South Warwickshire NHS Foundation Trust working together regarding patients and relatives being prosecuted using the Assaults on Emergency Workers
5/15 292/347

Act 2018.
Name Department Incident arrested for Update /Conviction Mr D G Accident and
Emergency 5 or 6 separate offences, nearly all appear to relate to domestics with his partner
Has been charged to Warwick Crown Court - but no dates set as yet.
Mr M and Mrs LM
Accident and Emergency
Criminal damage (fire) breaking parole conditions
£100 fine - 2 Year Community Order - £95 Victim surcharge - Alcohol Treatment Order
Mr DH Stratford Hospital
Criminal damage (fire) breaking parole conditions
Found Guilty - Currently locked up in HMP Hewell, Redditch.
Mr RO Accident and Emergency
Racial Abuse Remanded on bail on the 22.05.21 at Coventry and Warwickshire Magistrates bail agreements - not to contact directly or indirect security officer RS - WO and staff member SB - Exclusion not to enter Warwick Hospital Lakin Road unless he has a pre booked appointment or there is an emergency.
Mr J M Accident and Emergency
Criminal damage - hand gel dispenser
Community Resolution Order - payed SWFT £80 to repair the broken hand gel dispenser.
Mr CR Accident and Emergency
Violence and Aggression Prison sentence received 13 weeks has recently been released and is staying at a half-way house. He appears to be engaging well with the support that has been offered to him.
Mr RC Place Based Team Bedworth
Racial Abuse - Sexual; Assault
Mr RC - 01.03.22 in separate visits by PBT Bedworth this patient was Racially abusive toward a member of staff sexually assaulted another staff member the incidents were raised to Warwickshire Police - Police log number 135 and they visited the patient at his home address and issued him with a caution.
Graph 3: The top hot spots of where incidents occurred 1 April 2021 – 31 March 2022
The number one hot spot area again this year was Accident and Emergency Department (Warwick Hopspital 52 ) this was more than double any other area reporting, followed by Mary Ward (25) and Magregor Ward (22) this is not unexpected owing to the increase theTrust has seen with children presenting with Mental Health concerns (CAMHS) and behaviour problems. (National shortage of beds and areas to admit these patients) The LSMS is currently working with Magregor Ward and the Family Health Division looking at security recommendations to try and put solutions in place to prevent the incidents escalating to violence and aggression e.g CCTV cameras - Pinpoint alarm system - Training. Violence and Aggression Risk Assessment
6/15 293/347

Tool.
In last years report three of the top four hot spots are located at Leamington Rehab Hospital, this years report we there are no wards from the Leamington Rehab Hospital in the top four.
The LSMS has been working across all areas at Leamington Rehab Hospital to look at staff being encouraged to complete Datix forms for all incidents and through these Datixs being completed we have when required supported the risk idenitifed with additional security being deployed at the Hospital.The Manager or Nurse in charge will try to speak to the alleged aggressor to try and resolve the concern raised.( zero tolerance)
Following this arranged meeting the incident could be resolved either by verbal communication or a letter being sent to the person outlining the meeting and actions agreed. (possibly a sanction letter or expectation letter) The LSMS will offer advise and support to prevent or reduce further incidents occuring.
Since January 2022 We have put in place a nightly presence by a security service, across the site, this would include ensuring the premises are secure for example : Heathcote House - IT Building -Whitnash Lodge, also included in the visit is a site visit to the wards to check in with staff - Chadwick Ward - Allsop Ward - Feldon Ward - Campion Ward.It is important for staff to remember, that if a member of the public, patient, visitor, relative, is being verbally abusive towards them they do have the right to ask them to stop being abusive, and if it continues to warn the other person that they will end the conversation and that the Trust has a zero tolerance policy regarding verbal and physical aggression against staff members.and if necssary to call for Police assistance via 999 call
Graph 4 : Violence, Abuse & Harassment Incidents by Division 1 April 2021 - 31 March 2022
3
64
191
64
151
54
20
50
100
150
200
250
Corporate Elective Care EmergencyCare
Family Health Out of HospitalCare
Collaborative
SupportServices
SWFTCS Ltd
Violence & Aggression by Division 1st Apr 2021 to 31st March 2022
The Emergency Care Division had 191 incidents in total this is not unexpected owing to the nature of the wards and departments in this Division. There has been a considerable rise in incidents being reported from OOHCC last year they reported 117 incidents this year’s report has seen this rise to 151.
7/15 294/347

ActionThe LSMS is currently working with the Warwickshire Community Stroke Team (OOHCC) trialling a lone worker device to see if this would be an option to be used in the Community setting.
Graph 5: Security Incidents 1 April 2021 – 31 December 2021.
There have been a total of 106 Security incidents in 1 April 2021 – 31 March 2022 across the Trust, compared to 151 in last year’s report. This is a positive step forward regarding security incidents occurring on SWFT sites As you can see from the graph above, the top four categories are categorised as - Intrusion 20 - Lost found missing keys (18) - Premises land and Real Estate - Lost Property(16)
Lost Property The LSMS has been working with Sarah Reynolds - Patient Experience Manager looking at introducing a new patient property bag for the wards and departments use to reduce the loss of patients property when they are admitted into the Hospital. The bags have been distributed and each ward has a supply of them with instructions on how to use. All the Wards and Departments have been issued with guidance on how to use the new property bags.
Lost found missing keys:A majority of these are the ward /department CD keys and the medicine cupboard keys going missing, the LSMS has discussed these concerns at the Health and Safety Committee the Divisional Health and Safety meetings. I plan in the new financial year (April) to restart the Medicine Management Audits across the Trust, the main emphasis of the audit will be the agreed 6 areas that MUST be compliant. I will be undertaking two audits one in the day and one at night these will be completed over a two month period to enable me to be able to report back at the Health and Safety Committee and the other Divisional Health and Safety Committees.
Graph 6 Security Incidents by Ward/Team 01st April 2021 - 31st December 2021
8/15 295/347

Action:The aim of the LSMS this year is to look at the incidents and identified problems in Graph 5 and 6 and to look at educating staff to be more proactive and security minded.
Graph 7: Total Absconded / Missing Persons Incidents by Ward/Site 01st April 2021 - 31st March 2022
The Number one hot spot area was Acute Medical Unit (13) (Emergency Care) followed by Accident and Emergency Department (07) (Emergency Care) Malins Ward (07) (Emergency Care)
We have partnership meetings with Warwickshire Police and Mental Health Committee to look more closely at all areas, looking for lessons learnt and how we can work better together.
The main purpose of these meetings is to be able to locate missing/vulnerable patients/people making sure we locate them as soon as possible and return then safely back to either the hospital or a designated safe environment.
9/15 296/347

The LSMS currently in the process of working alongside Warwickshire County Council looking at installing additional CCTV cameras along Millers road (4) to protect and give reassurance to staff members They can also be adapted viewed to contact the Hospital or Warwickshire Police in the cases of absconding patients. The CCTV cameras will be feedback /Warwickshire County Council control room.
3. RolesThe following roles are in place:
• A Security Management Director - SMD (Heron Harkamal Director of Operations) - to take overall responsibility for security management work at Board level and to support the Local Security Management Specialist (LSMS) in their role so they can fulfil their duties and statutory requirements.
• A Local Security Management Specialist - LSMS (Mark Rowlands and Sean Mitchell) - to work on behalf of the Trust to deliver an environment that is safe and secure so that the highest standards of care can be made available to patients. The LSMS will undertake their duties to tackle violence and general security management.
4. Areas of Activity
Under the new NHS Standard Contract for 2021/22, all organisations providing NHS services should have regards to the Violence Prevention and Reduction Standards and are required to review their status against it and provide Board assurance that they have been met twice a year.
This section provides information on the Trust’s work towards four key areas for action:• Strategic Governance• Inform and Involve• Prevent and Deter• Hold to Account
1. Policies All safety and security policies follow the process of consultation, approval and ratification:
• SWH00097 Conflict Resolution Policy ratified April 2022 - Now Violence Prevention and Reduction Policy SWH 00097
• SWH00455 Lone Working Policy ratified July 2018 • SWH00456 Lone Working Guidance ratified July 2018 • SWH00042 Safe & Secure Environment ratified 07.02.2019 • SWH0652 Security Strategy ratified October 2020 • SWH 00086 Searching Patients’ Belongings Procedure ratified July 2018
2. Datix The Trust is committed to an open reporting and learning process for all
security incidents and near misses that occur. Staffs have been made aware the importance of incident reporting
3. Security Bi-monthly News Bulletin. The bulletin is presented at Trust Health & Safety meeting.
4. it highlights current incidents, future projects
10/15 297/347
5. Capital New Builds and Improvement Projects The LSMS continue to attend project meetings, to look at ensuring buildings are safe and secure environments for staff, patients and visitors. E.g. New theatre extension – Ellen Badger Hospital
Prevent and DeterBi-annual Health and Safety Audit are completed twice a year by all services / departments managers. Sections 14 and 15 look at Security and Violence and Aggression,
Closed Circuit Television system CCTV. The Trust currently incorporates fixed and rotational cameras for the use in the prevention and detection of crime. In 2021 we reviewed the current CCTV system and the infrastructure. We set up a programme to look at upgrading the Closed Circuit Television system with Digital recording
Training. All SWFT staff receives Conflict Resolution training every three years.
Hold to Account
The LSMS is working with the external security operator ISS to promote a proactive security service incorporating the following:
• We are continuing visiting and checking all internal ward and department doors challenging staff when doors are found insecure or wedged open.
• We are more proactive on staff swipe card audits and raising awareness of the importance of wearing them. The LSMS and security officers have undertaken face to face audits in the main hospital corridors stopping staff/agency/contractors and requesting to be shown their swipe card/ID. Staff/agency/contractors who are continually non-compliant with wearing their swipe card/ID will be forwarded to the relevant manager for action to be undertaken. Regular meeting are held with the Estates Department, Medical Workforce and Innovate HS to look at improving the Locum packs and Medical Students ID.
• The LSMS is working with all areas within the Trust to promote a proactive security service incorporating the following: The LSMS has worked with the wards and departments undertaking proactive visits to wards and departments completing pharmacy audits, these audits were put on hold during the pandemic – start date in April 2022. The purpose of the audits has been discussed at the Health and Safety Committee, and the Patient Safety Surveillance Committee. - See graph 5 (lost keys).The finding from the audits are discussed at the Divisional AOGG and Health and Safety Meetings the Matrons are notified of all areas that are non-compliant and they then discus the findings with the ward managers to action /improve.
• The LSMS is continuing work with Family Health, Warwickshire Police reviewing security in the Maternity building. • 1st phase - As agreed following a meeting with Warwickshire Police a low level audit to be undertaken (December 2021) to see if the nominated person (Arranged by the Clinical Governance Midwife) could gain access. Actions put in place following the audit to reduce/prevent access onto the wards • 2nd phase -Meet with Warwickshire Police to arrange the running of a live drill with
11/15 298/347

the relevant emergency services involved. (To be undertaken 2022 - 2023)
• The LSMS has worked with the Manager for Macgregor Ward to look at introducing Violence and Aggression Risk Assessment Tool to assist staff and security to follow when requesting security assistance - This is now being completed on the ward.
• The LSMS is continuing work with the Governance Team and IT undertaking a conscientious approach to smartcard security raising awareness of the importance of smartcard security.
• The LSMS has been working with the security CCTV provider looking at existing CCTV camera and hot spot areas across the Trust that could leave the Trust vulnerable.
CCTV cameras installations 01st April 2021 - 31st March 2022.
• Two new Digital cameras to be installed Paediatric Assessment Unit corridor and main department entrance.
• Two new Panavision cameras installed visitor’s car park B. (Upgrade)
• Two new Panavision cameras installed visitor’s car park J. (Upgrade)
• One new Panavision camera installed staff car park F. (Upgrade)
• One new Panavision camera installed Aylesford Unit reception area. (Upgrade)
• One new Digital camera installed looking at the main entrance to the Endoscopy Department. (Upgrade)
• One new Digital CCTV camera installed covering the main kitchen areas waste compound and kitchen area back door.
• Four new Digital CCTV cameras installed in then Mortuary Department 2 internal and 2 externals covering the passageway and main doors. (Internal cameras Upgrade)
• Two new Digital cameras installed in the Fracture Clinic covering the main reception desk and the patient waiting area. (1 x Upgrade)
• Two new Digital cameras installed in the Pharmacy Department covering the main area and CD cupboard.
• We had upgraded the current software installed for the security cameras within the security office have installed four new monitors to improve the monitoring of the additional cameras in the MSCP.
• We have installed 44 new cameras in the staff carpark K (MSCP) these are relayed back to the security office.
Sanctions:
12/15 299/347

The Trust has continued to issue Caution, Yellow and Red cards to patients/relatives, where the individual’s behaviour towards a member of our staff is unacceptable.
The LSMS has introduced three new sanctions this year to support staff who have been subjected to incidents of aggression, verbal abuse, disorder of intimidation racial abuse sexual assaults or criminal damage.
Expectation letter - This letter will be issued when a need for treatment is still required and it’s not an option to cancel the service being provided. The manager of the area will visit the patient/relative with the staff member or LSMS and go through the concerns raised by the staff the letter will highlight the actions the patient/relative would be expected to follow to enable the service to maintain a safe and caring environment for you and the staff in attendance. This would be signed by the patient/relative if the expectation letter is not followed further sanctions will be issued. (yellow or red card sanction)
Script - The script will be issued to areas that have difficult or aggressive conversations with patients, relatives or staff, the purpose of the script is that all staff will follow the same response and answers providing evidence that we were not the aggressor and tried to help and advice the caller before we terminated the call.
Action Plans (March 2022) - The action plan will be initiated when a person will be attending an appointment /meeting onsite and has been categorised as high risk (potentially physical aggression, verbal abuse etc.) towards staff
We have also reviewed the how a red card sanction is issued we now organise an MDT meeting and the incident is reviewed the MDT meeting will be undertaken before withdrawal of treatment is considered. The meeting must ensure that request to Issue a Red Card form has been completed. The reasons why the withdrawal of treatment is to be considered the best option should also be documented.The meeting will consider alternative options about treatment delivery which may include different provider organisations.
Sanctions 01st April 2021 - 31st December 2021
01st April 2021 - 31st March 2022
Caution letters 25 42Yellow card sanction issued 2 3Red card sanction issued 1 4Expectation letters issued N/A 11
Scripts N/A 6Action plans N/A 1
I have been looking at the trends of when sanctions have been issued over the last 12 months
Green - Caution letter Yellow - Yellow card sanction Red - Red card sanction Blue - Expectation letter
Orange - Scripts Purple - Action plans
13/15 300/347

Following a meeting with a staff member who had been subject to an incident it was discussed that theletter was a very good idea to help support staff but for more serious incidents could we look at either a face toface (Team meeting or Verbal response from the LSMS) these have new being completed.
Support Letters The LSMS sent out 346 support letters to staff.
Elective Care 43Emergency Care 122Woman and Children/Family Health 41Support Services 51OOHCC 88Corporate 01
Update support email sent out to staff members - 168 (The LSMS sends these update support emails to staff as a final response to close the Datix following the unacceptable incident that they witnessed)
Staff responding to the update support emails - Positive responses - 43 We have received positive from staff following them receiving the update support emails.Examples:
• Thank you for your concern, I am fine thank you• Thank you for your support! I am all good• Thanks for the email I appreciate it.• Thank you for asking Sean, I am completely fine.• I am fine thank you. I haven’t had any other issues so far thank you for your support.• Thanks for your email. I am well thank you and have had no lasting effects from the
incident.• I am well thank you and there is no lasting effects. It was just a shock as I haven’t
14/15 301/347

been in that situation before but I was fine and back working normally after a break• Thank you, I’m OK. I spoke to occupational psychology because I was having panic
attacks but I’m much better now, thank you. I know I was unnecessarily spiralling but the human brain is a funny thing.
• I am fine and keeping well. I have no concerns at all since the incident. I have been back to KC to provide care and accompanying other staff members without any issues
• Thanks Sean. I am fine.• We are all fine now thank you. Sadly, it is one of those things we get subjected to fairly
regularly but we learn to brush it off! Most patients are only every "snappy" because they are afraid. I only took this one further because the Nurse in questions was reduced to tears. I understand the person in question has been seen since by the member of staff and all is well. Thank you for coming back to us.
Conclusion
For this year The LSMS’s main aim will be to continue to promote the following:
• To encourage staff to become more proactive in their response to reporting and dealing with incidents of physical and verbal abuse (including racial and sexual abuse) and promoting to staff that the Trust will support them in incidents of aggression and verbal abuse and through sanctions and prosecutions.
• To encourage staff to report all incidents of criminal damage to the LSMS or the Police. Owing to an increase in Datix’ s being submitted following patients becoming aggressive and causing criminal damage, the LSMS has been working with Warwickshire Police to look at Police support and assistance. We will now be asking all areas to report all incidents of criminal damage (Where the aggressor had been deemed to have capacity) to Warwickshire Police as an incident. We would look at the following to be considered The purpose of this action is so that South Warwickshire NHS Foundation Trust can send out a message that this behaviour is not accepted and will not be tolerated and will look at reporting any incidents of criminal damage to Warwick Police with the view to prosecute.
• Promoting staff to actively challenge people in their areas and on all Trust site (Swipe cards, security of ward and department doors, smart cards.
• To encourage staff to become more proactive in the security of medical drugs in the ward and departments
• Promote and look at improving working partnership with all external agencies.
Sean MitchellSecurity and Parking Manager
15/15 302/347

Report SummaryReport to Board of Directors Date of
Meeting6 July 2022
Report Title Security Standards Agenda Item 10.2
Executive/Non-Executive Lead
Harkamal Heran – Chief Operating Officer / SMD
Report Author(s)
Sean Mitchell Security and Parking Manager
Report Previously Discussed at
Purpose of the Report For ApprovalFor Discussion
The purpose of this report is to provide the Board of Directors /Board Committee, with the LSMS Security Standards
For Information
Recommendations and Action Required The Board of Directors /Board Committee is asked to: e.g receive and note, approve
Impact (is there any impact arising from the report on the following?) Quality EqualityFinance ResearchPerformance ComplianceWorkforce Legal
Applicable Quality Improvement Priorities Elective Hub Health InequalitiesElectronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety CompassionateEffectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk RegisterAre any existing risks on the BAF/Risk Register affected? NoIdentify the BAF/Risk Register risk ID and description – explain how the risk has been affected – reduced or increased as a consequence of the evidence within the report.
Do you recommend a new entry to the BAF and/or Risk Register is made as a result of this report? If yes, describe the new risk.
No
1/15 303/347

South Warwickshire NHS Foundation Trust
Report to Board of Directors - 6 July 2022
Summary of Reports for Noting and Information
Security Standards 2022 – 2023
Executive Opinion and AssuranceUnder the NHS Standard Contract for 2021/22, all organisations providing NHS services should have regard to the Violence Prevention and Reduction Standard (General Condition 5) and are required to review their current status against it and provide Board assurance.
The Standards will be presented to the Board of Directors to measure competence twice a year.
We have reviewed the current security provisions against the Violence Prevention and Reduction Standard (General Condition 5) and we have:
Fully Compliant
Partially Compliant
Not Compliant
21 11 0
These Security Standard work plans have been created to address the areas that are partially compliant to make them fully compliant.
Recommendation
The Board of Directors/Board Committee is asked to note the report.
Harkamal HeranChief Operating Officer
2/15 304/347

Violence Prevention and Reduction Standard – Gap Analysis Report [Work plan]
Date: June 2022Prepared By:
Sean Mitchell, Security and Parking Services Manager
Overview: Gap Analysis exercise (including a proposed Trust work plan) relating to the new national Violence Prevention and Reduction Standard, which has been developed in partnership with the Social Partnership Forum and its subgroups, including trade unions and the Workforce Issues and Violence Reduction Groups.
This report was endorsed by the Chief Operating Officer on 21 June 2022 and will be incorporated in the 2022/23 NHS Standard Contract from June 2022
This report is presented to the Board of Directors for consideration and discussion.
GAP ANALYSIS REPORTIntroduction and Background
Under the NHS Standard Contract for 2021/22, all organisations providing NHS services should have regard to the Violence Prevention and Reduction Standard (General Condition 5) and are required to review their status against it and provide Board assurance that the standards have been met on a six monthly basis.
The new contract removes all reference to ‘Security Management’ and replaces it with a risk-based framework that follows the Plan, Do Check, Act (PDCA) approach, an iterative four-step management method to validate, control and achieve continuous improvement of processes.
Providers need to demonstrate compliance in all four areas.
Commissioners are also expected to undertake compliance assessments as part of their regular contract reviews with the Provider, twice a year as a minimum or quarterly if significant concerns are identified and raised.
Scope and Objectives
The scope of this exercise is to ensure that appropriate consideration has been given to the organisations level of compliance against the new standard. In order to achieve this the Trust’s Security and Parking Services Manager has undertaken an initial ‘snapshot’ gap analysis to provide assurance to the organization as to the current level of conformity and to identify areas where arrangements could be further strengthened to improve standard compliance.
It should be noted that this analysis is a preliminary assessment, rather than as a result of detailed reviews and analysis.
Findings The Security and Parking Services Manager has undertaken a gap analysis against the standard contained within each of the areas of responsibility and has made the following observations:
3/15 305/347

Assessed compliance against these specific standards are follows:
Area Total No. of Standards
Fully Compliant
Partially Compliant
Not Compliant
Plan 11 07 04 0Do 8 06 02 0Check 9 06 03 0Act 4 02 02 0
Total 32 21 11 0
Conclusion Considering this preliminary assessment of these ratings the Security and Parking Services Manager believes that the organisation has several work streams to follow through in order to display a high level of compliance against the requirements set out in the new violence prevention and reduction standard.
The key areas of attention and development are:• Rename The Violence Prevention and Reduction Policy will (including
new Expectation Agreements), underpinned by the Trust’s Violence Reduction and Security Management Strategy and related policies.
• Clearly defined Violence Reduction and Security Management Work Plan (approved at Senior level);
• Ensure there is a clear and effective training programme in place for all staff in relation to violence and aggression, which is supported by Trust policies.
• Implement a robust auditing and review process to ensure all policies, procedures, incident reporting and management decision making is measurable, effective and sustainable.
The focus for the coming year will be to address the agreed areas for improvement that have been identified Trust wide and to provide regular updates on progress to the Security Director (Chief Operating Officer) and through the Health & Safety Committee.
Consideration of the resource requirements needed to enhance standard compliance will form part of the 2022/23 Security Work plan [Appendix B]. The Security and Parking Services Manager will ensure that the requirements set out in the standard is achieved and that appropriate evidence is collated to support this level of attainment that can be reviewed as part of any national and/or Organisational assessment process.
Appendices Appendix A - Trust Gap Analysis Appendix B - Security Work Plan 2022 - 2023
4/15 306/347

Appendix A – Trust Gap AnalysisRef Standard Comment CompliancePLAN - Violence Prevention and Reduction1 The Board have approved the Conflict Resolution
Policy within the last twelve months.The Trust is reviewing the current Conflict Resolution Policy to address violent and aggressive behaviour; this includes a full review of the existing Behavioural Agreements. The Policy will reflect the new standard (change of Policy name to the Violence Prevention and Reduction Policy) as well as considering clinical and mental health requirements in both an acute setting and a community environment.
Compliant
2 The Violence Prevention and Reduction Policy details compliance with legal or statutory requirements.
The Trust currently operates under a Policy for violent and aggressive behaviour and is supported by Trust wide policies
• Maternity Abduction Policy SWH 00553• Searching patients Belongings Procedure SWH
00886• Safeguarding Children Policy SWH 00623• Safe and Security Environment Policy SWH 00042• Lone Working Guidance SWH 00456• Security Strategy SWH 00652
As well as Mental Health and Security related legal and statutory requirements.The reviewed policy will incorporate all new requirements both legally and statutory.
Compliant
5/15 307/347

3 The Violence Prevention and Reduction Policy enable specific objectives, performance measures and mitigation requirements.
The current Violence Prevention and Reduction Policy sets out clear objectives and introduce specific performance measures and mitigation requirements which will be monitored and reviewed by Security and Parking Services Manager
Compliant
4 The Violence Prevention and Reduction Policy has been developed from the comprehensive risk assessments (workforce and workplace).
The Violence Prevention and Reduction Policy will consider intelligence and reported incidents relating to violence and aggression. A review of the Trust’s risk assessments both at a strategic and operational level will be undertaken and liaison with key personnel including Risk Management and Workforce.
Partially Compliant
5 The Violence Prevention and Reduction Policy is maintained and updated annually with Senior Management oversight and approval.
The Trust’s Local Management Specialists will review the scope of the Policy following Datix incidents reported, new procedures and guidelines initiated by NHS IE, the Government or through Warwickshire Police initiatives The Violence Prevention and Reduction Policy and reviewed annually by Security and Car Parking Services Manager with oversight through the Health and Safety Committee and Policy review group.
Compliant
6 The Violence Prevention and Reduction Policy objectives and targets are communicated to all staff.
Legacy policies are in situ and communicated to staff through existing methods such as E-Pulse /Intranet pages and Bimonthly reports through the Divisional Health and Safety meetingsSWFT has an awareness programme implemented and a robust training pathway through new e-learning and face to face training for Conflict Resolution and Security related matters, Security awareness is also imbedded in the Trusts Corporate Induction training through face-to-face training and informational leaflets and posters (market place initiatives)
Compliant
6/15 308/347
7 A comprehensive risk assessment (workforce and workplace) is undertaken to consider the associated factors (i.e. protected characteristics) of violence within the organisation.
In accordance with the Trust’s existing Security Policy, and Yearly Health & Safety Audit Guidelines SWH 03086 risk assessments on a site and departmental level will be undertaken and security intelligence and guidance provided on a local and national level from Police and Counter Terrorism will be incorporated: for example, guidance on ‘Crowded Places’ and mitigating risks.
A site and departmental level-based risk assessment will allow the Security Team to consider associated factors and work closely with our Mental Health colleagues and Police representatives to ensure all steps are taken to mitigate the level of risks.
Partially Compliant
8 The outputs from the Violence Prevention and Reduction Policy risk assessments informs the mitigation strategies and operational processes.
Existing policies and operational procedures are based on legacy risk assessments still covering the fundamental requirements of managing violence and aggression. Under the Violence Prevention and Reduction Policy new measures will be introduced and revised strategies and processes implemented to address new and emerging risks in accordance with each hospital site and Community settings.
Partially Compliant
9 The Violence Prevention and Reduction Policy plans for achieving the objectives and targets are implemented and maintained.
All violence and aggression related matters will be overseen by Trusts Local Security Management Specialist and the Security Director (Head of Operations) and through the Health & Safety Committee. Progress reports will monitor delivery against the agreed Violence Reduction and Security Management Work Plan and target achievement.
Compliant
7/15 309/347

10 All processes and procedures set out in the Violence Prevention and Reduction Policy have clearly defined performance measures.
The Violence Prevention and Reduction Policy, sets out clear performance measures which are monitored and reviewed by the Local Security Management Specialist. This will include lost property patient and staff and swipe cards audits
Any issues or concerns identified will be reported via the Annual Security report and through the Health and Safety Committee
Compliant
11 The violence performance measures are specific, measurable, achievable and relevant.
All performance measures will ensure they are sensible and significant; relevant to the Trust but reflective of different operational measures at each hospital site including the Community provide meaningful input and support for staff which is agreed and attainable. Ensuring that the measures in place are reasonable and realistic is key to ensure we have an embedded process in place and an effective policy. Including Policy performance Measure’s
Partially Compliant
8/15 310/347

Ref Standard Comment ComplianceDO - Violence Prevention and Reduction1 A designated Executive Level Violence Prevention and
Reduction Lead ensures that appropriate financial resources are available to support the organisations delivery of violence prevention and reduction programme, the appropriate level of resourcing will be determined locally and should be aligned to the organisational violence risk assessments.
The Trust’s nominated Executive Lead for Security, including violence and aggression is Director of Operations. Supported by the ADO for Support Services. Reporting on progress against the Violence Reduction and Security Management Work Plan and delivery of the Security agenda will be monitored and reported through the Health and Safety Committee and Divisional Health and Safety meetings
Compliant
2 A designated Operational Violence Prevention and Reduction Lead is formally accountable for the design, maintenance, documentation and improvement of the organisational violence prevention and reduction systems and processes.
The Trust’s Local Security Management Specialists who are the Security and Car Parking Services Manager and the General Manager for Hotel Services will oversee the Violence Reduction and Security Management Work Plan and update the Violence Prevention and Reduction Policy when required. Systems and processes implemented to reduce violence and aggression across the Trust will be reviewed, monitored and audited to ensure it is effective in its delivery and any improvements required addressed.
Compliant
3 The violence prevention and reduction process, plans and systematic approach are reviewed and updated in relation to any significant organisational changes, serious incident and undertaken in consultation with the Trusts Risk Management Team
The Health and Safety Committee and Divisional Health and Safety meetings, reviews, evaluates incidents and captures lessons learnt to ensure appropriate mitigation has been put in place following a serious incident. The Trust’s Local Security Management Specialists liaises with the Trust’s Emergency Planning Team in relation to business continuity plans and major incident planning; plus evaluates all security related incidents as part of an ongoing process reporting through the Security Bimonthly Security reports presenting information and intelligence at the Health & Safety Committee on a bi monthly basis.
Compliant
9/15 311/347

4 Changes to the organisation are documented and reflected as part of the violence prevention and reduction risk assessment process.
Existing legacy policies are place and appropriate risk assessments undertaken and reviewed in accordance with reported security incidents. The Violence Prevention and Reduction Policy will continue with this arrangement and any organisational changes will be reflected in the policy as well as documented within updated risks.
Compliant
5 Clear roles and responsibilities are defined in relation to the violence prevention and reduction strategy and policies throughout the organisation.
The Violence Prevention and Reduction Policy underpins the Trust’s Violence Reduction & Security Management Strategy and includes clear and defined roles and responsibilities, linking to other related policies and procedures.
Compliant
6 Organisational functions and support mechanisms that are necessary for achieving the delivery of the Violence Prevention and Reduction Strategy, associated policies, objectives and plans have been clearly identified.
Existing legacy policies do contain organisational functions and support mechanisms; the reviewed Violence Prevention and Reduction Policy will include the work plans and security objectives.
Partially Compliant
7 A documentation system has been established and is maintained to incorporate the Violence Prevention and Reduction Policy, risk management assessments, performance records and associated policies and plans.
A clear system will be introduced as part of the Trust’s Violence Reduction and Security Management Work Plan ensuring a clear process is in place to ensure the Violence Prevention and Reduction Policy, risk management assessments, performance records and related policies have regard for the new standard and maintained and up to date throughout the year.
Compliant
8 The Violence Prevention and Reduction Strategy and policy are communicated to all staff, including incident reporting mechanisms.
Existing communication methods staff intranet - E-pulse communications, will be used to ensure all staff are informed of the updated Violence Prevention and Reduction Policy title change and related strategies. Incident reporting mechanisms will be promoted in line with existing policies.
Partially Compliant
10/15 312/347

Ref Standard Comment Compliance
CHECK - Violence Prevention and Reduction
1 Procedures to monitor and measure organisational performance pertaining to violence prevention and reduction are established or maintained.
The Trust has an existing organisational policy and procedure relating to violence and aggression (underpinned by legacy policies). The Bi monthly Security reports captures data which can be monitored, reviewed, evaluated and reported on to key personnel. Incident reporting will continue and identified risks evaluated and reported through the Divisional AOGG and Health and Safety Meetings and the Health and Safety Committee.
Compliant
2 The frequency for measuring and monitoring the performance measures is proportional to the risks noted in the violence risk assessments and analysis of incident management data.
Current reporting and monitoring is in accordance with legacy policies. The Violence Prevention and Reduction Policy outlines a clear programme for monitoring and measuring the identified risks relating to violence and aggression. New Risk Assessments identified through Divisional AOGG and Health and Safety Meetings will be incorporated, and a clear audit process implemented.
Partially Compliant
3 Performance monitoring and measurement is suitable and sufficient to facilitate subsequent corrective and preventative action analysis.
The Violence Prevention and Reduction Policy will outline departmental and hospital site risk assessments with clear monitoring in place. Monthly reporting through the Security Dashboard will ensure incidents and risks are reviewed and evaluated. Any corrective and/or preventative action required will be documented through this process and a clear audit in place to monitor continued progress.
Partially Compliant
11/15 313/347

4 Data pertaining to violent incidents are traceable retrievable and accessible on the risk management system.
The Trust’s existing Incident Reporting system Datix ensures that all violent and aggressive incidents are monitored, reviewed and investigated. The Trust’s Local Security Management Specialists monitors the incidents through the Security incidents and data readily available from the Datix system
Compliant
5 There are controls in place to ensure the quality of the performance data is assured.
The Trust’s Internal Audit reviewed undertaken periodically ensures that there are robust controls in place.
Compliant
6 There is an established audit process to help ensure that violence prevention and reduction is efficient and effective.
A full audit process is incorporated within the Trust’s Violence Reduction and Security Management Work Plan on an annual basis; action plans are designed to ensure identified issues are reviewed and corrective action taken where necessary.
Partially Compliant
7 All incident data pertaining to violence, nonconformities and audit findings are reviewed in a timely manner and shared with relevant groups within governance structure (e.g. health and safety committee).
Existing reporting is incorporated within the action plans provided from the Divisional AOGG and Health and Safety Meetings and the Health and Safety Committee.
Compliant
8 Departmental or corporate risk registers which note risks pertaining to violence are reviewed and updated following any nonconformities incidents or audit findings.
Violence and aggression risks incorporated within departmental risk registers are reviewed by Divisional leads and reported upon at the Divisional AOGG and Health and Safety Meetings and the Health and Safety Committee
Compliant
9 Proposed corrective and preventative actions are assessed and implemented in a timely fashion.
The Trusts existing procedures and incident reporting in place monitors and measures violent and aggressive behaviour. Health and Safety/ Governance ensure any corrective and preventative actions are taken at the time of the incidents and reported through progress reports to Divisional AOGG and Health and Safety Meetings and the Health and Safety Committee. The Local Security Management Specialists has a oversight through the Divisional AOGG and Health and Safety Meetings a monthly basis and undertakes biannual reporting to Health & Safety Committee.
Compliant
12/15 314/347

Ref Standard Comment Compliance
ACT - Violence Prevention and Reduction
1 A designated Executive Violence Prevention and Reduction Lead has a defined role and accountability for reviewing and approving the organisations Violence Prevention and Reduction Policy and supporting framework at regular defined intervals.
The Trust’s nominated Executive Lead for Security, including violence and aggression is the Director of Operations /Security DirectorThe Security and Car Parking Services Manager has strategic and operational responsibility for reviewing the policy and implementing any necessary processes and procedures; Approval of related policies are through the Divisional Risk/ Health & Safety Committees and where necessary the Policy review grope and JNCC.
Compliant
2 Records of senior management reviews are retained as part of the violence prevention and reduction framework documentation system.
All policy reviews, including consultation with key personnel will be maintained and recorded providing a clear audit trail of feedback, comments and any corrective action taken on related policies. Through the Divisional Risk/ Health & Safety Committees and where necessary the Policy review grope and JNCC.
Partially Compliant
3 Any lessons learned are captured and considered by the organisation and subsequent changes are made to the Violence Prevention and Reduction Policy and supporting framework, as required.
Incidents are continually reviewed both at a departmental and organisational level. Lessons learnt and best practice will influence policy and procedure going forward.
Partially Compliant
4 The senior management has all the relevant information required to make informed decisions regarding the Violence Prevention and Reduction Policy and supporting framework.
Clear briefing mechanisms are in place to ensure Senior Management have a clear and concise outline with regards to policy decision making and any related matters.
Compliant
13/15 315/347

Appendix B – Violence Reduction & Security Management Work Plan for 1st April 2022 to 31st March 2023Overall Objective: Implement the Trust’s strategy for violence reduction and security management for 2022-2023, aimed at protecting patients, staff and visitors and promoting a pro-security culture across South Warwickshire NHS Foundation Trust.
Organisational CoverageObjectiveGroup Hospital
Site CommunityResponsibility
PLAN – Violence Prevention and Reduction 1) Review the Conflict Resolution Policy – The Policy will reflect the new
standards (change of Policy name to the Violence Prevention and Reduction Policy) as well as considering clinical and mental health requirements in both an acute setting and a community environment. This has been approved and ratified May 2022
Strategic
4) The Violence Prevention and Reduction Policy to be developed from the comprehensive risk assessments (workforce and workplace). Strategic
7) A comprehensive risk assessment (workforce and workplace) to be undertaken to consider the associated factors (i.e.protected characteristics) of violence within the organisation.
Strategic
8) The results from the Violence Prevention and Reduction Policy risk assessments will inform what the mitigation strategies and operational processes are.
Strategic
11) The violence performance measures are specific, measurable, achievable and relevant Strategic
DO - Violence Prevention and Reduction6) Organisational functions and support mechanisms that are necessary for
achieving the delivery of the Violence Prevention and Reduction Strategy, associated policies, objectives and plans are clearly identified.
Strategic
8) The Violence Prevention and Reduction Strategy and policy are communicated to all staff, including incident reporting mechanisms. Strategic
14/15 316/347

Organisational CoverageObjectiveGroup Hospital
Site CommunityResponsibility
CHECK - Violence Prevention and Reduction2) The frequency for measuring and monitoring the performance measures
is proportional to the risks noted in the violence risk assessments and analysis of incident management data.
Strategic & Operational
3) Performance monitoring and measurement is suitable and sufficient to facilitate subsequent corrective and preventative action analysis.
Strategic & Operational
ACT - Violence Prevention and Reduction1) Records of senior management reviews will be retained as part of the
violence prevention and reduction framework documentation system. Strategic & Operational
2) All lessons learnt are captured and considered by the organisation and subsequent changes are made to the Violence Prevention and Reduction Policy and supporting framework, as required.
Strategic & Operational
6) A established audit process to help ensure that violence prevention and reduction is efficient and effective
Strategic & Operational
15/15 317/347

Report SummaryReport to Board of Directors Date of
Meeting6 July 2022
Report Title Board Committee Minutes – Open Meetings
Agenda Item
11
Executive/Non-Executive Lead
1. Kim Li, Chief Finance Officer2. Kim Li, Chief Finance 3. Fiona Burton, Chief Nursing
Officer
Report Author(s)
1.Colleen Tooze, Committee Administrator2.Colleen Tooze, Committee Administrator3.Zoe Cox, Committee Administrator
Report Previously Discussed at Audit Committee on 1 June and 15 June 2022Clinical Governance Committee on 11 May 2022
Purpose of the Report For ApprovalFor Discussion
To provide the Board with oversight and assurance of the matters discussed at the Clinical Governance Committee meeting.
For Information
Recommendations and Action Required The Board of Directors is asked to receive and note the open Minutes of the Audit Committee Meeting on 13 April 2022 and 1 June 2022 and Clinical Governance Committee held on 13 April 2022.
Impact (is there any impact arising from the report on the following?) Quality Equality Finance Research Performance Compliance Workforce Legal
Applicable Quality Improvement Priorities Elective Hub Health InequalitiesElectronic Patient Record (EPR) Mobilisation
Patient Portal
Children and Young People in Crisis Remote Monitoring Technology Maternity Workforce Living Well with Cancer Autism Strategy
Trust Values (which of the Trust Values is the report helping to deliver?) Safety Compassionate Effectiveness Trusted
Relationship to the Board Assurance Framework (BAF) and Risk RegisterAre any existing risks on the BAF/Risk Register affected? N/AIdentify the BAF/Risk Register risk ID and description – explain how the risk has been affected – reduced or increased as a consequence of the evidence within the report. N/ADo you recommend a new entry to the BAF and/or Risk Register is made as a result of this report?
N/A
1/1 318/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST
Open Minutes of the Audit Committee Meeting
held on Wednesday 13 April 2022 at 9.00am Via Microsoft Teams Present: Rosemary Hyde (RH) Non-Executive Director (NED) and Committee Chair Richard Colley (RC) NED Simon Page (SP) NED
In attendance: Joanne Beales (JB) Lead Risk, Health and Safety Adviser (present for Minute
22.051 only) Sarah Collett (SC) Trust Secretary Vicky Dumigan (VD) Information Governance Manager (present for Minute 22.052
only) Fiona Dwyer (FD) Counter Fraud Specialist, CW Audit Services (absent from
Minute 22.053 to 22.057) Kim Li (KL) Chief Finance Officer Sumara Parvez (SP) Head Pharmacist (present for Minute 22.055 only) Ruth Mawby (RM) Manager, CW Audit Services Mo Ramzan (MR) Director, Deloitte, LLP Mick Sargent (MS) Associate Director of Finance (present until Minute 22.059) Sarah Swan (SS) Assistant Director, CW Audit Services Colleen Tooze (CT) Executive Assistant / Committee Administrator
MINUTE ACTION 22.044 INTRODUCTIONS AND APOLOGIES FOR ABSENCE The Committee Chair introduced the new NED, Mr Richard Colley, who
would be taking over the Chair of the Audit Committee in the coming months. The Committee Chair explained that the April meeting was the wrap up meeting before the Annual Report and Annual Accounts were finalised. An apology for absence was received for Ms Becker, NED. Resolved – that the position be noted.
22.045
DECLARATIONS OF INTEREST
There were no declarations of interest. Resolved – that the position be noted.
22.046
MINUTES OF THE OPEN MEETING HELD ON 9 FEBRUARY 2022 – OPEN MEETING
Resolved – that the Minutes of the Open meeting held on 9 February
2022 be confirmed as an accurate record of the meeting and signed by the Committee Chair.
1/10 319/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 13 April 2022
MINUTE ACTION 22.047 22.047.01
MATTERS ARISING AND PROGRESS MONITORING REPORT The Committee Chair asked for congratulations to be noted for the Chief Executive as he was recognised by the Health Service Journal (HSJ) as one of the top 6 Chief Executive Officers in the whole of the NHS. Resolved – that the position be noted.
22.047.02 Actions Listed as Complete The items listed as complete in the actions update report be noted and removed from the report. Resolved – that the position be noted.
22.047.03 Internal Audit Report – Review of Patient Access Plans – Follow Up (Minute 22.008 refers) That a further update to the Internal Audit Report – Review of Patient Access Plans – Follow Up be amended from April 2023 to February 2023. Resolved – that the position be noted.
22.048 2022/23 SCHEDULE OF BUSINESS (UPDATE) The Committee noted the 2022/23 Schedule of Business (Update). Resolved – that the 2022/23 Schedule of Business (Update) be received and noted.
22.049 EXTERNAL AUDIT PROGRESS UPDATE REPORT The Director, Deloitte, LLP commented that ongoing discussions were taking place with the Finance Team and there were no significant changes or risks identified. The Chief Finance Officer commented that the Finance Team had been working with Deloitte, LLP during the year and were just finalising the Trust’s outturn position. Resolved – that the verbal External Audit Progress Update Report be received and noted.
22.050
ANNUAL INTERNAL AUDIT REPORT 2021/22 INCLUDING HEAD OF AUDIT OPINION (DRAFT) The Manager, CW Audit Services presented the Internal Audit Annual Report 2021/22 and Head of Internal Audit Opinion (Draft) and provided Significant Assurance.
2/10 320/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 13 April 2022
MINUTE ACTION
Within the Opinion, it was noted that:
a) the Trust had an effective Assurance Framework; b) during the year, all reviews received Significant Assurance, with
the exception of Moderate Assurance for our Pathway to Net Zero review which was currently draft;
c) the Trust needed to continue with its focus on all outstanding actions to ensure it maintained a good record of effective implementation of agreed actions.
It was suggested that consideration was given in the Annual Governance Statement to reflect on the challenges that the Trust had continued to experience as a consequence of the COVID-19 pandemic in relation to service delivery and its wider impact across the organisation. Concerns around the delays in the implementation of the internal audit recommendations relating to Patient Access Plans was discussed, and it was requested that this should be brought to the attention of the Managing Director, and raised at Finance and Performance Executive meeting. Resolved – that:
(A) the Annual Internal Audit Report 2021/22 including Head of Audit Opinion (Draft) be received and noted, and
(B) the Chief Finance Officer raise the issue of Patient Access Plans as a consequence of the COVID-19 pandemic in relation to service delivery and its impact across the organisation at a future Finance and Performance Executive meeting. Also to ensure this was brought to the Managing Director’s attention.
KL KL
22.051 INTERNAL AUDIT REPORT – BOARD ASSURANCE FRAMEWORK (BAF) YEAR END The Manager, CW Audit Services presented the Internal Audit Report – Board Assurance Framework (BAF) Year End and completed Level A Assurance. The Committee Chair queried what other BAFs were like in other Trusts. It was explained that the Trust’s BAF focused on the strategic plan, however what it did not show was the whole strategic purpose. The Manager, CW Audit Services added that other Trusts had risks in their BAFs, however the BAF should not be a risk register. The Assistant Manager, CW Audit Services commented that the Trust did link their BAF to their strategic plan for the year. The Lead Risk, Health and Safety Adviser explained that the Chief Executive wanted the BAF to be a 12 month document as risks would be added and closed throughout the year, all others were held on a local risk register. The Board of Directors was sighted on red risks on a quarterly basis. The Chief Finance Officer commented that introducing local risk registers had made people think more closely about the risks
3/10 321/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 13 April 2022
MINUTE ACTION
in their area. Training sessions were now being provided. Resolved – that the Internal Audit Report – BAF Year End report be received and noted.
22.052 INFORMATION GOVERNANCE AND SECURITY QUARTERLY ASSURANCE REPORT The Information Governance Manager presented the Information Governance and Security Quarterly Assurance Report. The Committee Chair queried the work done so far on the Data Security and Protection Toolkit (DSPT). It was agreed that the Information Governance Manager would provide a DSPT Workshop prior to the Audit Committee meeting on 1 June 2022. The Information Governance Manager also confirmed that Innovate Healthcare Services Ltd was now the lead for implementation of the Cyber Essentials Plus standards. This was required for 2022/23 DSPT. The NEDs found the report very encouraging and assuring and were pleased that the Information Governance Team had real grip on the issues. Mr Page, NED queried medical devices connectivity remotely and if older hardware was a challenge to provide cyber security. The Information Governance Manager commented that the Chief Technology Officer would have to respond to that query. The Information Governance Manager explained that she would ask the Chief Technology Officer to respond to Mr Page, NED on his query. Resolved – that:
(A) the Information Governance and Security Quarterly Assurance Report be received and noted;
(B) the Information Governance Manager provide a DSPT Workshop on 1 June 2022 prior to the Audit Committee meeting;
(C) the Information Governance Manager liaise with the Chief Technology Officer to respond to Mr Page, NED on his query relating to medical devices connectivity remotely and whether older hardware was a challenge for cyber security.
VD VD VD VD
22.053 LOSSES AND COMPENSATION PAYMENTS The Associate Director of Finance presented the Losses and Compensation Payments report. Discussion took place on Flowers Payments. The Chief Finance Officer commented that she would liaise with the Senior Finance Manager in regards to the calculation of the ongoing holiday payments when working overtime. Mr Colley, NED commented that it would be advantageous for
KL
4/10 322/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 13 April 2022
MINUTE ACTION
it be accounted for in the year, rather than as a year-end adjustment. Resolved – that:
(A) the Losses and Compensation Payments be received and noted, and
(B) the Chief Finance Officer to ensure the ongoing holiday payments when working overtime were clarified in future reports and to be accounted for in the year, rather than as a year-end adjustment.
KL
22.054 ANNUAL REPORT OF BOARD OF DIRECTORS’ STANDING ORDER WAIVERS The Trust Secretary presented the Annual Report of Board of Directors’ Standing Order Waivers. The Committee noted the report. Resolved – that the Annual Report of Board of Directors’ Standing Order Waivers be received and noted.
22.055 INTERNAL AUDIT REPORT – PHARMACY WHOLESALE AND DEALERS LICENSE COMPLIANCE FOLLOW UP The Head of Pharmacy explained that the Pharmacy Team had done a lot of work on the Pharmacy Wholesale and Dealers License Compliance and that there was a new Pharmacy Lead who had a lot of experience related to this. Regular meetings took place and an action plan had been made. There were still some issues with transportation of medicines between sites but these issues were near resolution. At the initial internal audit review, the Head of Pharmacy was concerned but she was quite assured of the processes in place. They were all low-level manageable risks. The Committee Chair commented that she was pleased to hear of the progress made. The Chief Finance Officer commented that she would like to see the reduction of risks relating to the Pharmacy Wholesale Dealers License be recorded at Risk Management Board. Resolved – that:
(A) the Internal Audit Report – Pharmacy Wholesale and Dealers License Compliance Follow Up report be received and noted, and
(B) the Head of Pharmacy and Chief Finance Officer ensure the reduction of risks relating to the Pharmacy Wholesale Dealers License be recorded at Risk Management Board.
SP/KL SP/KL
5/10 323/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 13 April 2022
MINUTE ACTION 22.056 ACCOUNTING POLICIES 2021/22
The Chief Officer Finance presented the Accounting Policies 2021/22 report. The report highlighted the necessary changes that were required to the Trust’s accounting policies in relation to the change in accounting treatment for cloud software implementation and customisation costs and any new disclosures on accounting policies for the 2021/22 Annual Accounts. Resolved – that the change in accounting treatment for cloud software implementation and customisation costs and the proposed additional disclosures to the Trust’s Accounting Policies 2021/22 be approved.
22.057 DECLARATION OF GOING CONCERN The Chief Finance Officer presented the Declaration of Going Concern. The Chief Finance Officer highlighted the Trust’s Going Concern status and that based on the anticipated future provision of services by the Trust in the public sector, that it be satisfied to make the recommendation to the Board of Directors to endorse the declaration to External Audit that the Trust is a Going Concern as at 31 March 2022. The Committee approved the Declaration of Going Concern. Resolved – that the Audit Committee recommends to the Board of Directors the endorsement of the declaration to the Trust’s External Auditors that the Trust was a Going Concern as at 31 March 2022.
22.058 SWH 01783 MANAGING CONFLICTS OF INTEREST POLICY The Trust Secretary presented SWH 01783 Managing Conflicts of Interest Policy and SWH 01656 Gifts, Hospitality, and Sponsorship Policy which were up for a five-year review. The proposed amendments were shown as tracked changes. Both policies were reviewed prior to the Audit Committee meeting by the Executive Team. Changes were made to the policies to provide examples and provide clearer instructions to staff. Mr Page, NED sought assurance on whether staff were clear on who their line manager was. The Trust Secretary clarified that staff should be aware of who their line manager was and when an Associate Director of Operations (ADO) or Associate Medical Director made a declaration, that the appropriate Chief Officer was made aware. The Committee approved both policies. Resolved – that SWH 01783 Managing Conflicts of Interest Policy and SWH 01656 Gifts, Hospitality, and Sponsorship Policy be approved prior to submission to the Policy Review Group for
6/10 324/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 13 April 2022
MINUTE ACTION
ratification.
22.059 SWH 01656 GIFTS, HOSPITALITY, AND SPONSORSHIP POLICY This agenda item was discussed under the previous item (Minute 22.058 refers). Resolved – that the position be noted.
22.060 ANNUAL BOARD SELF CERTIFICATION FOR G6 LICENCE CONDITION The Trust Secretary presented the Annual Board Self-Certification for G6 Licence Condition and Annual Board Self Certification for Corporate Governance Statement and other Declarations. The Trust Secretary explained that it was the first occasion for the reports to come to the Audit Committee for scrutiny prior to submission to the Board of Directors for approval. For future meetings, these reports would be on the Schedule of Business for April meetings. The Committee approved both reports. Resolved – that the Annual Board Self Certification for G6 Licence Condition and Annual Board Self Certification for Corporate Governance Statement and Other Declarations be considered prior to submission to the Board of Directors for approval.
22.061 ANNUAL BOARD SELF CERTIFICATION FOR CORPORATE GOVERNANCE STATEMENT AND OTHER DECLARATIONS This agenda item was discussed under the previous item (Minute 22.060 refers). Resolved – that the position be noted.
22.062 AUDIT COMMITTEE EFFECTIVENESS SELF-ASSESSMENT FOR 2021/22 The Committee Chair presented the Audit Committee Effectiveness Self-Assessment for 2021/22 and thanked Paul Capener, Director, CW Audit Services for facilitating the process this year. The Committee Chair raised her concern on the feedback in relation to assurance providers to account for late or missing assurances. It was suggested that the feedback was in relation to the payroll audit reports, as the reporting timetable was usually later than the Trust’s annual accounts timetable. Mr Page, NED commented that the report was a good report and that there was no dissent of any value.
7/10 325/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 13 April 2022
MINUTE ACTION
Resolved – that the Audit Committee Effectiveness Self-Assessment for 2021/22 be considered prior to submission to Board of Directors on 4 May 2022 for information.
22.063 ANY OTHER BUSINESS There was no further business.
22.064 REFLECTION ON THE MEETING FOR THE OPEN SECTION
22.064.01 New NED The Committee Chair sought Mr Colley, NED reflections as it was his first meeting. Mr Colley, NED commented that he was trying to understand the issues and get up to speed with the meeting. Resolved – that the position be noted.
22.064.02 6 Monthly Report for Third Party Providers Further to the issues raised under the Audit Committee Effectiveness Self-Assessment for 2021/22 (Minute 22.062 refers), the Trust Secretary proposed a 6 monthly report on third party provider assurances to ensure the Committee was getting the update it required. The Trust Secretary agreed to share the report used at George Eliot Hospital NHS Trust with the Chief Finance Officer to see what would work for South Warwickshire NHS Foundation Trust (SWFT). Resolved - that the Trust Secretary share the GEH Audit Committee report on third party provider assurances with the Chief Finance Officer.
SC SC
22.064.03 Patient Access Plans Further to the discussion under the Annual Internal Audit Report 2021/22 including Head Of Audit Opinion (Draft) item (Minute 22.050 refers), Mr Page, NED raised the importance of Patient Access Plans and for the Chief Finance Officer to raise the issue at a future Finance and Performance Executive meeting to ensure management could make necessary improvements. Resolved - that the Chief Finance Officer raise the issue at a future Finance and Performance Executive meeting to ensure management could make the necessary improvements.
KL KL
22.065
SWFT CLINICAL SERVICES APOLOGIES FOR ABSENCE
8/10 326/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 13 April 2022
MINUTE ACTION 22.066 22.067 22.068
DECLARATIONS OF INTEREST MINUTES OF SWFT CLINICAL SERVCIES HELD ON THE 9 FEBRUARY 2022 SWFT CLINICAL SERVICES MATTERS ARISING AND PROGRESS MONITORING REPORT
22.069 INTERNAL AUDIT WORKPLAN 2022/23
22.070 INTERNAL AUDIT REPORT – 2021/22 PAYROLL PROVIDER
22.071 INTERNAL AUDIT ANNUAL REPORT 2021/22 AND HEAD OF INTERNAL AUDIT OPINION (DRAFT)
22.072 COUNTER FRAUD ANNUAL REPORT 2021/22 AND COUNTER FRAUD WORKPLAN 2022/23
22.073 ANY OTHER BUSINESS
CLOSED MEETING
22.074 22.075 22.076 22.077 22.078 22.079 22.080 22.081 22.082 22.083 22.084 22.085
APOLOGIES FOR ABSENCE DECLARATIONS OF INTEREST MINUTES OF THE CLOSED MEETING HELD ON 9 FEBRUARY 2022 MATTERS ARISING AND PROGRESS MONITORING REPORT BAD DEBT WRITE OFFS COUNTER FRAUD PROGRESS REPORT COUNTER FRAUD STAFF SURVEY RESULTS 2021/22 COUNTER FRAUD ANNUAL REPORT 2021/22 COUNTER FRAUD COMPLETE FRAUD RISK ASSESSMENT 2022/23 COUNTER FRAUD WORKPLAN 2022/23 WITH RISK ASSESSMENT ANY OTHER CONFIDENTIAL BUSINESS REFLECTION ON THE MEETING FOR THE CLOSED SECTION
9/10 327/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 13 April 2022
MINUTE ACTION 22.086 DATE AND TIME OF NEXT MEETING
The next meeting will be held on Wednesday 1 June 2022 at 9.30 am via Microsoft Teams. The time of the meeting was subsequently changed to 10.00 am.
Signed___________________________ (Committee Chair) Date 1 June 2022
10/10 328/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST
Open Minutes of the Audit Committee Meeting
held on Wednesday 1 June 2022 at 10.00am Via Microsoft Teams Present: Rosemary Hyde (RH) Non-Executive Director (NED) and Committee Chair Yasmin Becker (YB) NED Richard Colley (RC) NED Simon Page (SP) NED
In attendance: Joanne Beales (JB) Lead Risk, Health and Safety Adviser (present until Minute
22.100) Nigel Corcoran (NC) Head of Estates (present until Minute 22.094) Sarah Collett (SC) Trust Secretary Sophie Gilkes (SG) Chief Strategy Officer (present until Minute 22.094) Ian Howse (IH) Partner, Deloitte, LLP Kim Li (KL) Chief Finance Officer Ruth Mawby (RM) Manager, CW Audit Services Emma Ratley (ER) Assurance and Quality Manager (present from Minute 22.096
to 22.099) Mick Sargent (MS) Associate Director of Finance Sarah Swan (SS) Assistant Director, CW Audit Services Colleen Tooze (CT) Executive Assistant / Committee Administrator
MINUTE ACTION 22.087 APOLOGIES FOR ABSENCE Apologies for absence were received from the Counter Fraud Specialist.
Resolved – that the position be noted.
22.088
DECLARATIONS OF INTEREST
There were no declarations of interest. Resolved – that the position be noted.
22.089
MINUTES OF THE OPEN MEETING HELD ON 13 APRIL 2022 – OPEN MEETING
Resolved – that the Minutes of the Open meeting held on 13 April
2022 be confirmed as an accurate record of the meeting and signed by the Committee Chair.
22.090
MATTERS ARISING AND PROGRESS MONITORING REPORT
22.090.01 Actions Listed as Complete The items listed as complete in the actions update be noted and removed from the report. Resolved – that the position be noted.
1/8 329/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 1 June 2022
MINUTE ACTION
22.090.02 6 Monthly Report for Third Party Providers (Minute 22.064.03 refers)
The Chief Finance Officers across the Foundation Group had agreed to draft a standard template / report across the Group to present to the summer (September 2022) Audit Committee. The reporting schedule to be added to the Committee’s Schedule of Business. Resolved – that the Committee Administrator ensure the 6 Monthly Report for Third Party Providers be added to the Committee’s Schedule of Business.
CT
22.091 2022/23 SCHEDULE OF BUSINESS (UPDATE) The Committee noted the 2022/23 Schedule of Business (Update). Resolved – that the 2022/23 Schedule of Business (Update) be received and noted.
22.092 INTERNAL AUDIT PROGRESS REPORT The Assistant Manager, CW Audit Services presented the Internal Audit Progress Report and highlighted that there were four proposed changes to the audit plan. This included a nationally mandated review of financial governance, which applied to all systems and individual NHS organisations. The review would be based on a Board level self–assessment tool recently published by the Healthcare Financial Management Association (HFMA) Internal Audit would reassess the need for the reviews which had been removed as part of the planning for 2023/24. In addition, there would be a second follow up review of Patient Access Plans, following Audit Committee’s concern over the limited implementation of previous internal audit recommendations. Resolved – that the Internal Audit Progress Report be received and noted.
22.093 INTERNAL AUDIT REPORT – PATHWAY TOWARDS DELIVERING ZERO The Manager, CW Audit Services presented the Internal Audit Report – Pathway towards Delivering Zero and provided Moderate Assurance. The key issues that management must address were as follows:
• Refresh the Strategy to ensure it more accurately reflected the national changes, i.e. the move from the Sustainable Development Unit to the NHS Net Zero ambitions
• Offer Sustainability training to all staff • Environmental Impact Assessment to be included in tenders
2/8 330/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 1 June 2022
MINUTE ACTION
• Nominate ‘carbon champions’ to work across all sites • All actions in the green plan to show a timebound target
completion date • Operational leads to be identified on action plans • Include milestone dates for longer term actions.
The Chief Strategy Officer called for more corporate support so that it would become business as usual. She also commented that the Sustainability Manager was fundamental in delivering this plan. Mr Page, NED that the Chief Strategy Officer’s role was around policing and making sure things happened but the only way this plan was to be met was with the expectation of it being everyone’s job and responsibility. Resolved – that the Internal Audit Report – Pathway towards Delivering Zero be received and noted.
22.094 INTERNAL AUDIT REPORT 2021/22 – BS 10008-2014 COMPLIANCE (EVIDENTIAL WEIGHT AND LEGAL ADMISSIBILITY OF ELECTRONIC INFORMATION) The Manager, CW Audit Services presented the Internal Audit Report – Scanning Review Compliance – BS 10008 and provided Moderate Assurance. The key issues that management must address were as follows:
• Ratify the revised Information Security Policy and Scanning Bureau Policy as a matter of urgency
• Complete the Business Case Continuity Plan for the Scanning Bureau and test its effectiveness
• Revise processes for the sharing of patient notes with external bodies making requests via email
• Complete the workbook associated with the 2020 Standard and collate evidence to demonstrate compliance.
Progress in implementing recommendations from the last inspection of 2020 was slower than expected with 5 out of 8 recommendations raised at the last review still outstanding. The auditors also noted that the Scanning Bureau was still working against the old 2014 version of the standard and needed to demonstrate compliance with the 2020 standard. Further recommendations were made around the completion of a Business Continuity plan and ratification of the Information Security Policy for the Scanning Bureau. The Chief Finance Officer as Deputy Senior Information Risk Owner (SIRO) assured the Audit Committee that the Information Governance Security Steering Group (IGSSG) would take responsibility for oversight of implementation of these recommendations. Resolved – that:
(A) the Internal Audit Report – Scanning Review Compliance –
KL
3/8 331/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 1 June 2022
MINUTE ACTION
BS 10008 be received and noted; (B) the Chief Finance Officer see that the Information
Governance and Security Steering Group take responsibility for oversight of the implementation of the recommendations from the Internal Audit Report 2021/22 – BS 10008-2014 Compliance (Evidential Weight and Legal Admissibility of Electronic Information).
KL
22.095 EXTERNAL AUDIT UPDATE The Partner, Deloitte, LLP provided a verbal update and highlighted that Deloitte, LLP was deep into the audit. It was a slow start due to illness, however Deloitte, LLP was working with the Finance Team on any issues. Deloitte, LLP would be working to the tight deadline and the Finance Team were being responsive. The Committee Chair commented that she understood the resourcing constraints and the Partner, Deloitte, LLP confirmed that there was nothing of materiality to report. Resolved – that the External Audit Update be received and noted.
22.096 DRAFT ANNUAL ACCOUNTS AND COMMENTARY 2021/22 (PRE-AUDIT SIGN OFF) The Chief Finance Officer presented the Draft Annual Accounts and Commentary for 2021/22. The consolidated accounts showed a deficit of £4,270k. After adjusting for technical accounting items (primarily £3,500k one off allowable adjustment for the de-recognition of cloud based software intangible assets), the results reconcile to a £22k surplus reported in the year end control total. Other smaller adjustments relate to fixed asset impairments and donated assets. Overall, the Statement of Financial Position showed a reduction in Total Assets/Taxpayer’s Equity of £0.4m to £129.5m. Key changes included:
• Fixed asset additions of £21m • Investment in Innovate Healthcare Services of £8.0m • Reduction in value of shareholding in Sensyne Health Plc of
£5.6m • Increase in accruals and provisions of £10.9m.
Resolved – that the Draft Annual Accounts and Commentary 2021/22 (pre-audit sign off) be approved and noted.
22.097 DRAFT ANNUAL REPORT 2021/22 The Trust Secretary presented the Draft Annual Report for 2021/22 on behalf of the FT Adviser and noted that this version did not include the comments shared by members of the Audit Committee. The Committee
4/8 332/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 1 June 2022
MINUTE ACTION
Chair suggested that any further comments be made to the Trust Secretary or FT Adviser. Mr Page, NED provided the following comments and amendments to the Draft Annual Report 2021/22:
• Provide an important statement of intent in relation to the Ockenden Report
• Overly wordy • Punctuation errors • Use of jargon that required clarification • Inconsistent use of titles and abbreviations.
The Partner, Deloitte, LLP suggested to amend the wording in relation to Innovate Healthcare Services Ltd for consistency with the treatment of the Accounts. Subject to comments on the Ockenden Report and further comments made by Audit Committee members outside the meeting, it was agreed that the performance report included was a fair report of the Trust’s business. Resolved – that:
(A) subject to the amendments made above and provided outside the meeting, the content of the Draft Annual Report 2021/22 be considered and commented on, and
(B) the Performance Report be considered to ensure it contained a fair review of the Trust’s business and agreed.
22.098 DRAFT QUALITY REPORT 2021/22 It was explained that the Draft Quality Report for 2021/22 was no longer mandated and did not form part of the External Auditor’s opinion. However, the Trust decided, for transparency, to continue to publish the report as part of the Annual Report. The Assurance and Quality Manager presented the Draft Quality Report for 2021/22 and explained that the Quality Report would be an appendix to the Annual Report. The Assurance and Quality Manager confirmed that she would ensure there was consistency between the Annual Report and the Quality Report. The Committee Chair suggested that the Clinical Governance Committee Chair reviewed the report as his oversight would be valuable. Resolved – that subject to the amendments made above, the content of the Draft Quality Report 2021/22 be considered and commented on.
5/8 333/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 1 June 2022
MINUTE ACTION 22.099 DRAFT ANNUAL GOVERNANCE STATEMENT 2021/22
The Lead Risk, Health and Safety Adviser presented the Draft Annual Governance Statement for 2021/22 and explained that the yellow highlighted text was mandatory text and could not be changed or amended. From page 17 onwards, the Divisions were asked to include what changes took place due to COVID and how the Divisions were getting back to business as usual. The Committee Chair queried the final paragraph on page 10 as Equiniti was mentioned as the payroll provider but the current payroll provider was Civica. The Chief Finance Officer commented that Civica bought Equiniti. It was suggested that the Lead Risk, Health and Safety Adviser liaise with the Head of Employment Services for accuracy on the name of the current payroll provider. The Committee Chair commented that the document was very long and had very little to no focus on the Ockenden Report. The Committee Chair suggested that the Annual Governance Statement made some reference to the report as the Trust was acting on the recommendations from the Ockenden Report. The Committee Chair suggested for Audit Committee members to email the Lead Risk, Health and Safety Adviser if there were any other detailed comments. Resolved – that:
(A) subject to the amendments made above, the content of the Draft Annual Governance Statement 2021/22 be considered and commented on, and
(B) the Lead Risk, Health and Safety Adviser liaise with the Head of Employment Services for accuracy of the current payroll provider.
JB JB
22.100 JOINT AUDIT AND CLINICAL GOVERNANCE ASSURANCE STATEMENT The Committee Chair presented the Joint Audit and Clinical Governance Assurance Statement from the two Chairs which gave overall assurance on the Trust’s control environment. Resolved – that the Joint Audit and Clinical Governance Assurance Statement be received and noted, prior to submission to the Board of Directors for information.
22.101 NATIONAL COST COLLECTIONS 2021/22 – PRE-SUBMISSION REPORT The Chief Finance Officer explained that the Trust had to abide by a set
6/8 334/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 1 June 2022
MINUTE ACTION
of methodologies and national standards in relation to costs. Two reports each year were presented to the Audit Committee in relation to National Cost Collections. A costing exercise took place in the summer and then an index score was given based on a national average. The Finance Department was yet to receive published figures for 2020/21. The National Cost Collections 2021/22 – Pre-Submission Report sets out the approach and the background information. The Committee Chair expressed her disappointment on the length of time it was taking for NHS England / NHS Improvement (NHSE/I) to publish the information. The Committee approved the methods and agreed on the method of approach laid out in the report. Resolved – that the National Cost Collections 2021/22 – Pre-Submission Report be approved and noted on progress made.
22.102 ANNUAL REVIEW OF STANDING FINANCIAL INSTRUCTIONS (SFI) AND SCHEME OF DELEGATION The Associate Director of Finance presented the Annual Review of Standing Financial Instructions (SFI) and Scheme of Delegation and highlighted the following key changes:
• Changes of job titles • Scheme of Delegation financial limits
The Chief Finance Officer commented that there was a Temporary Workforce Group which reviewed internal controls for agency spend. Mr Page, NED queried the practice of No Purchase Order (PO) / No Pay in reality and if there was a mechanism to ensure compliance. He also suggested strengthening the wording on expenditures and what was acceptable. Ms Becker, NED queried that no risks were on the risk register and advised that there were identifiable risks in all that the Trust does. Mr Colley, NED suggested that a quotation should be required in order to raise a PO with no value. POs should have a secondary review before approval to ensure no segregation of duties or no collusion. The Committee Chair concluded that there were a few points of clarification. The key focus on No PO / No Pay should be on day to day controls and oversight on implementing new systems. Resolved – that subject to the amendments above, the Annual Review of Standing Financial Instructions (SFI) and Scheme of Delegation be approved and submitted to the Board of Directors for ratification.
7/8 335/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Open Minutes of the Audit Committee Held on 1 June 2022
MINUTE ACTION 22.103 ANY OTHER BUSINESS
22.103.01 Shared Financial Services – Problems with Resourcing The Committee Chair was made aware of problems with resourcing within the Shared Financial Services and thought it should be given important focus later in the year. The Committee Chair also wanted to ensure that recovery of money from staff overpayments was being expedited as she was aware of an ongoing issue around a former NED which indicated follow up was far too slow. The Assistant Director, CW Audit Services commented that it was noted for the future audit and they would pay particular attention to any staff overpayments. Resolved – that the position be noted.
22.104 REFLECTION ON THE MEETING FOR THE OPEN SECTION There were no reflections on the meeting for the open section. Resolved – that the position be noted.
CLOSED MEETING
22.105 22.106 22.107 22.108 22.109 22.110 22.111
APOLOGIES FOR ABSENCE DECLARATIONS OF INTEREST MINUTES OF THE CLOSED MEETING HELD ON 13 APRIL 2022 MATTERS ARISING AND PROGRESS MONITORING REPORT ANY OTHER CONFIDENTIAL BUSINESS REFLECTION ON THE MEETING FOR THE CLOSED SECTION DATE AND TIME OF NEXT MEETING The next meeting will be held on Wednesday 15 June 2022 at 9.30 am via Microsoft Teams.
Signed___________________________ (Committee Chair) Date 15 June 2022
8/8 336/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Minutes of the Clinical Governance Committee Meeting held on
Wednesday 11 May 2022 at 13.00 hours via Microsoft Teams
Present:
Dr David Spraggett (DS) Non-Executive Director (NED) (Committee Chair)
Dr Charles Ashton (CA) Chief Medical Officer
Chris Day (CD) Head of Governance Pablo Garcia de Paso (PGP) Associate Medical Director – Governance
Phil Gilbert (PG) Non-Executive Director
Harkamal Heran (HH) Chief Operating Officer
Ann Hutton (AH) Deputy Head of Pharmacy
Sue Whelan Tracy (SWT) NED
Ellie Ward (EW) Deputy Director of Nursing (Deputising for the Chief Nursing Officer)
In Attendance:
Adam Carson (ACa) Managing Director, Innovate Healthcare Services (IHS) (present from Minute 21.103)
Anna Crane (AC) Quality Lead for Patient Safety, Coventry & Warwickshire Clinical Commissioning Group (CWCCG) (Deputising for the Acting Director of Nursing and Quality CWCCG)
Mary Molloy (MM) Governor (Observer) Ruth Gibson (RG) Patient Safety and Quality Manager Sara Lee (SL) Associate Director of Operations (ADO) – Elective Division Sarah Mitchell (SM) Clinical Audit Manager (present from Minute 22.100 until
22.102) Sam Owen (SO) Head of Nursing, Out of Hospital Care Collaborative (OOHCC) Tracey Sheridan (TS) ADO – OOHCC Linda Ward (LW) Associate Director of Midwifery Hannah Webber (HW) Clinical Education Fellow Zoe Cox (ZC) Committee Administrator
MINUTE ACTION
22.095 APOLOGIES FOR ABSENCE Apologies were received from the Chief Nursing Officer, the Managing Director, the ADO – Family Health, the Acting Director of Nursing and Quality (CWCCG) and Mr Gill NED. Resolved – that the position be noted.
22.096 DECLARATIONS OF INTEREST The ADO OOHCC declared an interest in that she was leaving the organisation at the end of July 2022 to take up the post of Chief Executive Officer at the Shakespeare Hospice in South Warwickshire. The Committee Chair also declared an interest in that he had been appointed to the Expert Advisory Panel for NICE.
1/11 337/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Minutes of the Clinical Governance Committee Meeting held on
Wednesday 11 May 2022
Page 2 of 11
MINUTE ACTION
Resolved – that the position be noted.
22.097 MINUTES OF THE PREVIOUS MEETING HELD ON 13 APRIL 2022 Resolved – that the Minutes of the meeting held on 13 April 2022 be confirmed as an accurate record of the meeting and signed by the Committee Chair.
22.098
MATTERS ARISING AND ACTIONS UPDATE REPORT (INCLUDING OUTSTANDING CLINICAL QUALITY REVIEW GROUP (CQRG) ACTIONS)
22.098.01 22.098.02 22.098.03
Patient Safety Monthly Report (Minute 22.020.01 refers) It was advised that there was still no final plan around the Medical Examiner System as this was still being worked through and this action was to remain on the Action Log. Resolved - that as there was still no final plan around the Medical Examiner System as this was still being worked through this should remain on the Action Log. ICT Incident and Risk Management Bi-Annual Report (Minute 22.020.04 refers) It was advised that the action around the data sharing agreement would be addressed under Minute 22.104 as an update was included within the report. Resolved – that the position be noted. Coventry & Warwickshire Pathology Service Governance Bi-Annual Report (Minute 22.073.04 refers) The Chief Operating Officer advised that this action would be addressed as part of the agenda under Minute 22.106. Resolved – that the position be noted.
ACa
22.099 PATIENT SAFETY MONTHLY REPORT The Patient Safety and Quality Manager highlighted there had been 1095 incidents reported in total across the Trust between 1 - 30 April 2022 (excluding 30 rejected incidents). The top three categories of incidents reported in April 2022 related to pressure ulcers, medication and slip, trip and falls. It was advised that there had been one avoidable death identified in April 2022, but this had not made it through to this report as yet due to the
2/11 338/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Minutes of the Clinical Governance Committee Meeting held on
Wednesday 11 May 2022
Page 3 of 11
MINUTE ACTION
timings, however this would be incorporated in the information that went to the next Board of Directors. The Committee Chair invited questions. The Committee Chair commented that it was good to see falls had reduced and asked about the Zone Tagging. The Deputy Director of Nursing advised that this referred to ‘stay in the bay tagging’ and had been trialled in Frailty and Nicholas and had worked really well. It meant that those members of staff given a red tag were to stay in the bay with those vulnerable patients and did not leave them unattended due to them being at risk of falling. The Deputy Director of Nursing advised that the Falls Prevention Lead had been asked to evaluate the impact of this and produce some concrete data to show that this method worked in reducing falls. Mrs Whelan Tracy (NED) commented that there was a lot of good practice shown within the report and asked about medication incidents and that the Board to Ward in June 2022 was Medication Safety Month and whether this would be focussed on those areas where there were higher medication incidents. The Deputy Head of Pharmacy advised that there was a specific plan mapped out for the Board to Ward in June 2022 and the campaign would be centred around learning from incidents and would be an interactive campaign with some simple thought provoking messaging. The Deputy Director of Nursing commented that it was important to reach all Prescribers for example the End of Life Care Team and Dr Hoddell, Palliative Care Consultant attended the Grand Round and used that as an opportunity to do some learning from medication incidents and this had been well received. The Deputy Head of Pharmacy commented that the medication training package had also been updated for Junior Doctors around EPMA and that would be delivered in their induction sessions. The Deputy Head of Pharmacy agreed to contact the Patient Safety Team around using the Grand Round to help with learning from incidents. The AMD Governance commented that it was important to mention that when choosing the areas to prioritise, it may be worth taking into consideration that the number of incidents does not always relate to the safety issues in that particular area as not all the wards report their safety incidents. Resolved – that:
(A) the Patient Safety Monthly Report be received and noted, and (B) the Deputy Head of Pharmacy contact the Patient Safety
Team with a view to using the Grand Round to help promote learning from incidents.
AH AH
3/11 339/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Minutes of the Clinical Governance Committee Meeting held on
Wednesday 11 May 2022
Page 4 of 11
MINUTE ACTION
22.100 AUDIT AND OPERATIONAL GROUP GOVERNANCE (AOGG) OOHCC QUARTERLY REPORT The Head of Nursing OOHCC presented the report and summarised the key areas. The Committee Chair invited questions. Mrs Whelan Tracy (NED) commented that it was a very assuring report and asked about the wellbeing conversations being brought into appraisals and noted that it was hoped that the appraisal position would be better in the next quarterly update and asked if an update could be included in the next report about the appraisal position and how those wellbeing conversations were going and how many appraisals had included those conversations, as it was appreciated it was a little early to do evidence based reporting on this. The Professional Nurse Advocate (PNA) was going to be a national reporting element with a set of standards that has to be reported on with regard to upskilling the workforce and the OOHCC were lucky enough to have a PNA within their team. The Deputy Director of Nursing commented that it was great to see those Gold Standard Band 6 visits had started again and they would make a difference and commented on the staffing risks which were sighted by the Board of Directors through the Staffing Paper, so it was good to see that in terms of quality of care and patient experience that these had been maintained despite those staffing risks. The Committee Chair asked about those staffing risks being flagged around the urgent response work and was interested as to what impact that had on the service in South Warwickshire because if they were to use the proxy of those outcomes this had been managed really well but whether there was any other evidence that there had been issues as a result of this. The Head of Nursing OOHCC commented that the normal business continuity would be to stand down some of the routine work and then the organisation could see more pressure ulcers etc. as a result of that, but there had been nothing like that flagged. There had been a meeting about trying to use the current workforce in a different way. The ADO OOHCC commented that one of the biggest measures that could be used was the target of 70% for all urgent referrals and some of that impact seen was that the team were not quite hitting that target and therefore services were being tweaked to be able to manage that risk. Mrs Whelan Tracy (NED) asked about where Sexual Health Clinics fell and the ADO OOHCC advised that this service came under George Eliot Hospital NHS Trust (GEH). Resolved – that:
(A) the AOGG OOHCC Quarterly Report be received and noted,
SO
4/11 340/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Minutes of the Clinical Governance Committee Meeting held on
Wednesday 11 May 2022
Page 5 of 11
MINUTE ACTION
and (B) The Head of Nursing OOHCC bring an update back on the
appraisal position and an update on how many of those wellbeing conversations had taken place and how they were going as part of the next quarterly report.
SO
22.101 CLINICAL AUDIT ANNUAL REPORT 2021-22 (INCLUDING QUARTER 4) The Clincial Audit Manager presented the report and summarised the key areas. The Committee Chair invited questions. The Committee Chair shared his concerns around the 25% compliance rate of NICE Guidance as detailed on Page 9 of the report. The Clinical Audit Manager advised that work was underway to address that, and an exercise was being carried out to see whether they were still non-compliant. The Clinical Audit Manager assured the Committee that this was discussed at the Divisional AOGG’s and agreed to bring an update of that work back through the next report and update on the backlog to give the Committee more assurance. The Chief Medical Officer commented that the AOGG’s did need to work through this and sometimes the decision was around practice and largely there was no reason if it was only a change in practice that they couldn’t follow NICE Guidance, but sometimes it was about resource and equipment which may not be funded, but it was important to understand the difference. Mrs Whelan Tracy (NED) commented that she really appreciated the section around process change to be able to see how things had moved on. With regard to cancelled audits, Mrs Whelan Tracy (NED) shared her concerns around the Clinician in charge advising they were not going ahead with an audit and asked whether this was an adequate reason or whether it should be the speciality deciding whether the audit went ahead or not. The Clinical Audit Manager advised that this did go to the AOGG for a decision as to whether this audit when ahead or not and the Chief Medical Officer responded that there were sometimes just practical reasons as to why they couldn’t be done. Resolved – that:
(A) the Clinical Audit Annual Report 2021-22 (including Quarter 4) be received and noted, and
(B) the Clincial Audit Manager bring an update on where the Trust was against the backlog of NICE Guidance compliance and highlight those specific areas that were non-compliant for full transparency.
SM SM
22.102 MORTALITY SURVEILLANCE COMMITTEE QUARTERLY REPORT
5/11 341/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Minutes of the Clinical Governance Committee Meeting held on
Wednesday 11 May 2022
Page 6 of 11
MINUTE ACTION
The AMD Governance presented the report and drew out the key areas to note. Progress had been made in terms of the mortality review system in adapting the system being used at Wye Valley NHS Trust (WVT) and would be adapted by the Foundation Group. The testing element had already been rolled out and the next stage would be the implementation and completion was expected in Quarter 3 of 2022. It was highlighted that the Mortality Surveillance Committee had commissioned some in-depth reviews of several areas in the last 12 months looking for reassurance as the Hospital Standardised Mortality Ratio (HSMR) data had risen and all those reports had been very reassuring. The Committee Chair invited questions. The Chief Medical Officer commented that this was not an exact science and one of the problems with HSMR was that the diagnosis was taken when the patient was first admitted and may not be their diagnosis further down the line. The model would then look at that diagnosis first taken and predict their mortality average on that basis and that was always a confounding issue. Resolved – that the Mortality Surveillance Committee Quarterly Report be received and noted.
22.103 PATIENT ACCESS IMPROVEMENT AND BEST PRACTICE PROJECT UPDATE AND ACTION PLAN The ADO Elective Division presented the report and highlighted the progress made to date. It was advised that both action plans had been merged into one to make this easier for the Division to track. It was confirmed that there were currently 3 teams who did not put their access plans onto the system and they were very small teams, however these would be audited to see what process would work best for them in terms of those plans and being consistent with what other teams were doing. A Patient Access Manager was now in post and there had been another management tier introduced with a Senior Manager placed in post to help review the quality of patient care in this complex area which will ensure this area was more robust. The question around centralising all areas and standardising the process and having clear Key Performance Indicators (KPIs) would give the teams structure, however some services would need to be reviewed as certain areas such as Trauma and Orthopaedic worked really well at managing their own patients and waiting lists.
6/11 342/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Minutes of the Clinical Governance Committee Meeting held on
Wednesday 11 May 2022
Page 7 of 11
MINUTE ACTION
The Committee Chair invited questions. The Chief Medical Officer commented that centralising everything for patient access was a complex and difficult task as some Clinicians liked to have 1-1 input with their Bookers and have good outcomes as a result of that process. Mrs Whelan Tracy (NED) commented that this had been a long standing area of discussion at the Trust and these issues had been faced before, so it was about setting something up and making sure it stuck and getting the culture right and reporting against those KPIs. It was understood about the issues around centralising all services, but it was about having serious conversations with those areas that were not using standard practices. It was key to remember that the patient was at the heart of those decisions that were being made and the organisation was asking a lot of the patient when it came to navigating their way around the various departments on the telephone. The ADO Elective Division commented that there was a project underway around the telephone system to make this simpler so that patients could be directed to the right team within minimum effort, and this was being worked through. It was agreed it would be important to get those service users involved in this piece of work. The ADO Elective Division further advised that she felt one of the best ways of monitoring the patient access service and making sure any changes that were implemented were managed by way of setting up a Patient Access Board similar to the Cancer Board that was in place as this worked successfully in holding people to account and was very well attend and Chaired by the Chief Operating Officer. The Chief Operating Officer commented that centralisation had been a regular conversation and that this area was a very hard to recruit to area and if you decentralised this you would have no staff and it was very hard to cover staff sickness and annual leave. Those booking roles had changed a lot over time and they had to deal with a lot of difficult conversations with patients, some who may have been waiting for an appointment for a long time and those roles were only Band 2/3. The Chief Operating Officer stated that her personal preference would be to centralise that team all be it with specialist knowledge with Navigators to help assist patients to the right place. Resolved – that the Patient Access Improvement and Best Practice Project Update and Action Plan be received and noted.
22.104
ICT INCIDENT AND RISK MANAGEMENT BI-ANNUAL UPDATE The Managing Director IHS presented the report and drew out the key highlights and drew the Committee’s attention to the risk around the Acute Medical Unit (AMU).
7/11 343/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Minutes of the Clinical Governance Committee Meeting held on
Wednesday 11 May 2022
Page 8 of 11
MINUTE ACTION
The managing Director IHS shared the good news around the Integrated Care Record (ICR) which had been talked about for some time in that SWFT were about to go live with this as the number of GP Practices had now passed the threshold so the organisation could now go ahead and use this. There had been excellent progress in relation to Results Acknowledgement with work going on in the background. There had been a lot of work developing practices and should be able to launch later in the month. The Committee Chair invited questions. Mrs Whelan Tracy (NED) advised that she was meeting with the person who had been appointed to the Integrated Care Board and would be responsible for Digital and advised that she would contact the Managing Director IHS outside of this meeting with a view to him joining the meeting. Resolved – that:
(A) the ICT Incident and Risk Management Bi-Annual Update be received and noted, and
(B) Mrs Whelan Tracy (NED) contact the Managing Director IHS outside of the meeting with a view to him joining a meeting with the person appointed to the Integrated Care Board who would be responsible for Digital.
SWT SWT
22.105 LOOKED AFTER CHILDREN (LAC) ANNUAL REPORT The Committee Chair advised that as there was no one available to present this report that it be deferred to the next meeting. Resolved – that the LAC Annual Report be deferred to the next meeting.
ZC ZC
22.106 UROLOGY AND COLORECTAL CANCER STRATEGY UPDATE PRESENTATION The ADO Elective Division shared a presentation on Urology and Colorectal Cancer Strategy Update which was included within the papers. The Committee Chair invited questions. The Chief Medical Officer made an observation that with Urology there were 3 Urologists that were very established with no Urology on call and that things had moved on since then especially around Prostate Cancer. A much more modern guidance driven service had been implemented which included Urology on call and some of that work had been carried out by other people would then go to the on call team and that had taken a big chunk of efficiencies out. It had been agreed to invite Getting it Right First Time (GIRFT) to the Trust again to look at productivity as the
8/11 344/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Minutes of the Clinical Governance Committee Meeting held on
Wednesday 11 May 2022
Page 9 of 11
MINUTE ACTION
service were putting in more resource but having less productivity despite the capacity being the same. The Deputy Director Nursing asked whether there was a plan to look at using this recovery strategy with other areas using the same approach as this focused on Colorectal and Urology. The ADO Elective Division said that there was a plan to look at other areas and she regularly met with other services to look at improvements. The Committee Chair asked about other areas and the ADO Elective Division advised they were working through Radiology and Pathology which would all benefit. Navigator roles would be put into Radiology so it was not just aimed at Cancer and was looking at the bigger picture Trust wide. Resolved – that the Urology and Colorectal Cancer Strategy Update Presentation be received and noted.
22.107 MATERNITY ASSURANCE QUARTERLY REPORT AND OCKENDEN UPDATE The Associate Director of Midwifery presented the report and drew out the key areas to note. Staffing remained a risk due with a large staffing deficit to increased activity and acuity over the last two years, however several business cases had been worked up totalling around £1.4m to help support those staffing levels. The first two business cases were approved at Planning Group and will go to Management Board at the end of May 2022. The team were also awaiting information on additional funds applied for through the LMNS Board to help with the Ockenden recommendations. The Ockenden Insight visit which was held at the Trust on 5 April 2022 was very successful and the team were complimented on their safe service offered. There were some recommendations made as a result of the insight visit and they were included in the action plan. The Committee Chair invited questions. The Deputy Director of Nursing thanked the Associate Director of Midwifery for the comprehensive report and for being so open and transparent about the service. The report showed real aspirations to improve compliance and patient care. Mrs Whelan Tracey (NED) also thanked the Associate Director of Midwfery for her fantastic leadership and asked about what proportion of the £1.4m had been agreed as part of those two business cases and when would they expect to see that new resource to hit maternity. The Associate Director of Midwifery advised that the first two 2 business cases were around staffing the triage area and also ensuring the post natal ward
9/11 345/347

SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Minutes of the Clinical Governance Committee Meeting held on
Wednesday 11 May 2022
Page 10 of 11
MINUTE ACTION
had safe staffing at night which equalled around 30% of the overall ask and would be looking to recruit straight away once approved at Management Board and that even that 30% would make a significant difference. Mrs Whelan Tracey (NED) asked about the other 70% and the Associate Director of Midwifery advised that the other two business cases were around Theatres and Continuity of Carer and are a lot more about the future, but the Theatres case would be the next priority as one of the biggest risks was that it took two Midwives to go into Theatre at night and that left a significant deficit in the night workforce. The Chief Medical Officer commented that he had been very pleased to advise NHSE/I during their visit on the 5 April 2022, that the Trust’s NED’s had visited the Labour Ward at night and this was extremely helpful as it meant everyone was on board with the same goal. Resolved – that the Maternity Assurance Quarterly Report and Ockenden Update be received and noted.
22.108
ANY OTHER BUSINESS There was no further business raised. Resolved – that the position be noted.
22.109 ADJOURNMENT TO DISCUSS MATTERS OF A CONFIDENTIAL NATURE
22.110 APOLOGIES FOR ABSENCE
22.111 DECLARATIONS OF INTEREST
22.112 CONFIDENTIAL MINUTES FROM THE MEETING HELD ON 13 APRIL 2022
22.113 CONFIDENTIAL MATTERS ARISING AND ACTIONS UPDATE REPORT
22.114 SERIOUS INCIDENTS
22.115 PRESSURE ULCERS FOR NOTING
22.116 ANY OTHER CONFIDENTIAL BUSINESS
22.117 DATE AND TIME OF NEXT MEETING
The next meeting will be held on Wednesday 8 June 2022, via Microsoft Teams.
10/11 346/347
SOUTH WARWICKSHIRE NHS FOUNDATION TRUST Minutes of the Clinical Governance Committee Meeting held on
Wednesday 11 May 2022
Page 11 of 11
Signed ______________________________ Date 8 June 2022 (Chair of the Clinical Governance Committee)
11/11 347/347