
AGENDA – PUBLIC - Canterbury District Health Board
58
01/04/2021 AGENDA – PUBLIC HOSPITAL ADVISORY COMMITTEE MEETING to be held in the Board Room, Level 1, 32 Oxford Terrace, Christchurch Thursday, 1 April 2021 commencing at 9:00am Administration Apologies 9.00am 1. Conflict of Interest Register 2. Confirmation of Minutes – 28 January 2021 3. Carried Forward / Action List Items Presentations 4. Mental Health: The Acute Adult Pathway Dr Greg Hamilton General Manager Specialist Mental Health Service 9.05-9.35am Reports for Noting 5. Hospital Service Monitoring Report: Medical/Surgical; Women’s & Children’s Health; & Orthopaedics ESPIs Older Persons Health & Rehabilitation Specialist Mental Health Service Hospital Laboratories Rural Health Services Pauline Clark General Manager, Medical/Surgical; Women’s & Children’s Health; & Orthopaedics Dr Helen Skinner General Manager & Chief of Service, Older Persons Health & Rehabilitation Dr Greg Hamilton General Manager, Specialist Mental Health Services Kirsten Beynon General Manager, Laboratories Win McDonald Transition Programme Manager Rural Health Services Berni Marra Manager, Ashburton Health Services 9.35-10.20am 6. Clinical Advisor Update (Oral) Allied Health Dr Jacqui Lunday-Johnstone Executive Director of Allied Health, Scientific & Technical 10.20-10.30am HAC - 01 April 2021 - P - Agenda 1
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of AGENDA – PUBLIC - Canterbury District Health Board

HAC-01apr21-agenda Page 1 of 2 01042021
AGENDA ndash PUBLIC
HOSPITAL ADVISORY COMMITTEE MEETING
to be held in the Board Room Level 1 32 Oxford Terrace Christchurch Thursday 1 April 2021 commencing at 900am
Administration
Apologies 900am
1 Conflict of Interest Register
2 Confirmation of Minutes ndash 28 January 2021
3 Carried Forward Action List Items
Presentations
4 Mental Health The Acute Adult Pathway Dr Greg Hamilton General Manager
Specialist Mental Health Service
905-935am
Reports for Noting
5 Hospital Service Monitoring Report
MedicalSurgical Womenrsquos amp Childrenrsquos Health amp Orthopaedics
ESPIs
Older Persons Health amp Rehabilitation
Specialist Mental Health Service
Hospital Laboratories
Rural Health Services
Pauline Clark General Manager MedicalSurgical Womenrsquos amp Childrenrsquos Health amp
Orthopaedics
Dr Helen Skinner General Manager amp Chief of Service
Older Persons Health amp Rehabilitation
Dr Greg Hamilton
General Manager Specialist Mental Health Services
Kirsten Beynon
General Manager Laboratories
Win McDonald Transition Programme Manager
Rural Health Services Berni Marra
Manager Ashburton Health Services
935-1020am
6 Clinical Advisor Update (Oral)
Allied Health
Dr Jacqui Lunday-Johnstone Executive Director of Allied Health
Scientific amp Technical
1020-1030am
HAC - 01 April 2021 - P - Agenda
1
HAC-01apr21-agenda Page 2 of 2 01042021
7 Resolution to Exclude the Public 1030am
Estimated Finish Time 1030am
NEXT MEETING Thursday 3 June 2021 at 900am
HAC - 01 April 2021 - P - Agenda
2
HAC-01apr21-BCL900DE46F Page 1 of 2 01042021
ATTENDANCE
HOSPITAL ADVISORY COMMITTEE MEMBERS Andrew Dickerson (Chair) Naomi Marshall (Deputy Chair) Barry Bragg Catherine Chu James Gough Jo Kane Ingrid Taylor Jan Edwards Dr Rochelle Phipps Michelle Turrall Sir John Hansen (Ex-officio) Gabrielle Huria (Ex-officio)
Executive Support (as required as per agenda) Dr Peter Bramley ndash Chief Executive Evon Currie ndash General Manager Community amp Public Health Savita Devi ndash Acting Chief Digital Officer Dr Richard French ndash Acting Chief Medical Officer David Green ndash Acting Executive Director Finance amp Corporate Services Becky Hickmott ndash Executive Director of Nursing Mary Johnston ndash Chief People Officer Ralph La Salle ndash Acting Executive Director Planning Funding amp Decision Support Dr Jacqui Lunday-Johnstone ndash Executive Director of Allied Health Scientific amp Technical Hector Matthews ndash Executive Director Maori amp Pacific Health Dr Rob Ojala ndash Executive Director for Facilities Karalyn Van Deursen ndash Executive Director of Communications Anna Craw ndash Board Secretariat Kay Jenkins ndash Executive Assistant Governance Support
HAC - 01 April 2021 - P - Attendance
3
HAC-01apr21-BCL900DE46F Page 2 of 2 01042021
COMMITTEE ATTENDANCE SCHEDULE 2020
NAME
280121
010421
030621
050821
071021
021221
Andrew Dickerson (Chair) radic
Naomi Marshall (Deputy Chair) radic
Barry Bragg
Catherine Chu x
James Gough ^
Jo Kane radic
(Zoom)
Ingrid Taylor radic
Jan Edwards radic
Dr Rochelle Phipps
Michelle Turrall x
Sir John Hansen (ex-officio) radic
Gabrielle Huria (ex-officio) x
radic Attended
x Absent Absent with apology ^ Attended part of meeting ~ Leave of absence Appointed effective No longer on the Committee effective
HAC - 01 April 2021 - P - Attendance
4
HAC-01apr21-interest register Page 1 of 5 01042021
(As disclosed on appointment to the BoardCommittee and updated from time-to-time as necessary)
Andrew Dickerson Chair ndash HAC Board Member
Canterbury Health Care of the Elderly Education Trust - Chair Promotes and supports teaching and research in the care of older people Recipients of financial assistance for research education or training could include employees of the CDHB
Canterbury Medical Research Foundation - Member Provides financial assistance for medical research in Canterbury Recipients of financial assistance for research education or training could include employees of the CDHB
Heritage NZ - Member Heritage NZrsquos mission is to promote the identification protection preservation and conservation of the historical and cultural heritage of New Zealand It identifies records and acts in respect of significant ancestral sites and buildings CDHB owns buildings that may be considered to have historical significance and Heritage NZ has already been involved with CDHB buildings Maia Health Foundation - Trustee Is a charitable trust established to support health care in the CDHB area Current projects include fundraising for a rooftop helipad and enhancements to the childrenrsquos wards at Christchurch Hospital NZ Association of Gerontology - Member
Professional association that promotes the interests of older people and an understanding of ageing
Naomi Marshall Deputy Chair - HAC Board Member
College of Nurses Aotearoa NZ ndash Member Riccarton Clinic amp After Hours ndash Employee Employed as a Nurse Riccarton Clinic amp After Hours provides general practice and after-hours care It is part privately and PHO funded The PHO receives funding from the CDHB
Barry Bragg Board Member
Air Rescue Services Limited - Director Subsidiary of the Canterbury West Coast Air Rescue Trust Has gaming licenses with specified purpose of fundraising for air rescue services Canterbury West Coast Air Rescue Trust ndash Trustee The Trust has a services agreement with Garden City Helicopters for the provision of air rescue and air ambulance services Garden City Helicopters has a long-term air ambulance contract with the CDHB CMUA Project Delivery Limited - Director 100 owned by the Christchurch City Council and is responsible for the delivery of the Canterbury Multi-Use Arena project within agreed parameters Farrell Construction Limited - Shareholder Farrellrsquos Construction Limited is a commercial and light commercial construction company based in Christchurch
CONFLICTS OF INTEREST REGISTER HOSPITAL ADVISORY COMMITTEE (HAC)
HAC - 01 April 2021 - P - Conflict of Interest Register
5
HAC-01apr21-interest register Page 2 of 5 01042021
New Zealand Flying Doctor Service Trust ndash Trustee The Trust has a services agreement with Garden City Helicopters for the provision of air ambulance services Garden City Helicopters has a long-term air ambulance contract with the CDHB Ngai Tahu Farming ndash Chairman Farming interests in North Canterbury and Queenstown Lakes District and Forestry interests in Canterbury West Coast and Otago regions Paenga Kupenga Limited ndash Chair Commercial arm of Ngai Tuahuriri Runanga Quarry Capital Limited ndash Director Property syndication company based in Christchurch Stevenson Group Limited ndash Deputy Chairman Property interests in Auckland and mining interests on the West Coast Verum Group Limited ndash Director Verum Group Limited provides air quality testing and asbestos sampling and analysis services methamphetamine contamination testing dust gas and noise workplace monitoring services in New Zealand There is the potential for future work with the CDHB
Catherine Chu Board Member
Christchurch City Council ndash Councillor Local Territorial Authority Riccarton Rotary Club ndash Member The Canterbury Club ndash Member
Jan Edwards Age Concern Canterbury ndash Member Anglican Care ndash Volunteer Neurological Foundation of NZ - Member
James Gough Board Member
Amyes Road Limited ndash Shareholder Formally Gough GroupGough Holdings Limited Currently liquidating Christchurch City Council ndash Councillor Local Territorial Authority Includes appointment to FendaltonWaimairi Harewood Community Board Christchurch City Holdings Limited (CCHL) ndash Director Holds and manages the Councilrsquos commercial interest in subsidiary companies Civic Building Limited ndash Chairman Council Property Interests JV with Ngai Tahu Property Limited Gough Corporation Holdings Limited ndash DirectorShareholder Holdings company Gough Property Corporation Limited ndash DirectorShareholder Manages property interests
HAC - 01 April 2021 - P - Conflict of Interest Register
6
HAC-01apr21-interest register Page 3 of 5 01042021
Medical Kiwi Limited ndash Independent Director Research and distribution company of medicinal cannabis and other health related products In process of listing on NZX The Antony Gough Trust ndash Trustee Trust for Antony Thomas Gough The Russley Village Limited ndash Shareholder Retirement Village Via the Antony Gough Trust The Terrace Car Park Limited ndash (Alternate) Director Property company ndash manages The Terrace car park (under construction) The Terrace On Avon Limited ndash (Alternate) Director Property company ndash manages The Terrace
Jo Kane Board Member
Christchurch Resettlement Services - Member Christchurch Resettlement Services provides a range of services to people from refugee and migrant backgrounds It works alongside refugee communities in delivering services that aim to achieve positive resettlement outcomes HurriKane Consulting ndash Project Management PartnerConsultant A private consultancy in management communication and project management Any conflicts of interest that arise will be disclosedadvised Latimer Community Housing Trust ndash Project Manager Delivers social housing in Christchurch for the vulnerable and elderly in the community
NZ Royal Humane Society ndash Director Provides an awards system for acts of bravery in New Zealand It is not anticipated any conflicts of interest will arise
Dr Rochelle Phipps Accident Compensation Corporation ndash Medical Advisor ACC is a Crown entity responsible for administering NZrsquos universal no-fault accidental injury scheme As a Medical Advisor I analyse and interpret medical information and make recommendations to improve rehabilitation outcomes for ACC customers OraTaiao New Zealand Climate amp Health Council ndash Founding Executive Board Member (no longer on executive) The Council is a not-for-profit politically non-partisan incorporated society and comprises health professionals in AotearoaNew Zealand concerned with the negative impacts of climate change on health the health gains possible through strong health-centred climate action highlighting the impacts of climate change on those who already experience
disadvantage or ill health (equity impacts) and reducing the health sectors contribution to climate change Royal New Zealand College of General Practitioners ndash Christchurch Fellow and Former Board Member The RNZCGP is the professional body and postgraduate educational institute for general practitioners
HAC - 01 April 2021 - P - Conflict of Interest Register
7
HAC-01apr21-interest register Page 4 of 5 01042021
Ingrid Taylor Board Member
Loyal Canterbury Lodge (LCL) ndash Manchester Unity ndash Trustee LCL is a friendly society administering funds for the benefit of members and often makes charitable donations One of the recipients of such a donation may have an association with the CDHB Manchester Unity Welfare Homes Trust Board (MUWHTB) ndash Trustee MUWHTB is a charitable Trust providing financial assistance to organisations in Canterbury associated with the care and assistance of older persons Recipients of financial assistance may have an association with the CDHB Sir John and Ann Hansenrsquos Family Trust ndash Independent Trustee Taylor Shaw ndash Partner Taylor Shaw has clients that are employed by the CDHB or may have contracts for services with the CDHB that may mean a conflict or potential conflict may arise from time to time Such conflicts of interest will need to be addressed at the appropriate time
I Taylor Shaw have acted as solicitor for Bill Tate and family The Youth Hub ndash Trustee The Youth Hub is a charitable Trust established to provide residential and social services for the Youth of Canterbury including services for mental health and medical care that may include involvement with the CDHB
Michelle Turrall Manawhenua
Canterbury Clinical Network (CCN) Maori Caucus - Member Canterbury District Health Board - Daughter employed as registered nurse Christchurch PHO Ltd ndash Director Christchurch PHO Trust - Trustee
Manawhenua ki Waitaha ndash Board Member and Chair Oranga Tamariki ndash Iwi and Maori ndash Senior Advisor Papakainga Hauora Komiti ndash Te Ngai Tuahuriri ndash Co-Chair
Sir John Hansen Ex-Officio ndash HAC Chair CDHB
Bone Marrow Cancer Trust ndash Trustee Canterbury Cricket Trust - Member Christchurch Casino Charitable Trust - Trustee Court of Appeal Solomon Islands Samoa and Vanuatu Dot Kiwi ndash Director and Shareholder Judicial Control Authority (JCA) for Racing ndash Appeals Tribunal Member The JCA is an independent statutory authority constituted under the Racing Act The JCA ensures that judicial and appeal proceedings in thoroughbred and harness racing are heard and decided fairly professionally efficiently and in a consistent and cost effective manner Ministry Primary Industries Costs Review Independent Panel
HAC - 01 April 2021 - P - Conflict of Interest Register
8
HAC-01apr21-interest register Page 5 of 5 01042021
Rulings Panel Gas Industry Co Ltd Sir John and Ann Hansenrsquos Family Trust ndash Ingrid Taylor sits as independent Trustee and provides legal services to the Trust and to Sir John and Ann Hansen
Gabrielle Huria Ex-Officio ndash HAC Deputy Chair CDHB
Pegasus Health Limited ndash Sister is a Director Primary Health Organisation (PHO) Rawa Hohepa Limited ndash Director Family property company Sumner Health Centre ndash Daughter is a General Practitioner (GP) Doctorrsquos clinic Te Kura Taka Pini Limited ndash General Manager The Royal New Zealand College of GPs ndash Sister is an ldquoappointed independent Directorrdquo College of GPs Upoko Rawiri Te Maire Tau of Ngai Tuahuriri - Husband
HAC - 01 April 2021 - P - Conflict of Interest Register
9
HAC-28jan21ndashminutesndashdraft Page 1 of 6 01042021
MINUTES ndash PUBLIC
DRAFT MINUTES OF THE HOSPITAL ADVISORY COMMITTEE MEETING
held in the Board Room Level 1 32 Oxford Terrace Christchurch on Thursday 28 January 2021 commencing at 900am
PRESENT Andrew Dickerson (Chair) Jan Edwards James Gough Jo Kane (via Zoom) Naomi Marshall Ingrid Taylor and Sir John Hansen (Ex-Officio) APOLOGIES Apologies for absence were received and accepted from Barry Bragg and Dr Rochelle Phipps An apology for early departure was received and accepted from James Gough (1010am) EXECUTIVE SUPPORT Dr Andrew Brant (Acting Chief Executive) Becky Hickmott (Acting Executive Director of Nursing) Ralph La Salle (Acting Executive Director Planning Funding amp Decision Support) Dr Jacqui Lunday-Johnstone (Executive Director Allied Health Scientific amp Technical) Kay Jenkins (Executive Assistant Governance Support) and Anna Craw (Board Secretariat)
APOLOGIES Kirsten Beynon (General Manager Laboratories) Dr Richard French (Acting Chief Medical Officer) Berni Marra (Manager Ashburton Health Services) and Win McDonald (Transition Programme Manager Rural Health Services) IN ATTENDANCE
Full Meeting
Pauline Clark General Manager MedicalSurgical Womenrsquos amp Childrenrsquos Health amp Orthopaedics Dr Helen Skinner General Manager amp Chief of Service Older Persons Health amp Rehabilitation Dr Greg Hamilton General Manager Specialist Mental Health Services 1 INTEREST REGISTER
AdditionsAlterations to the Interest Register Naomi Marshall ndash Addition ndash NZ Nurses College Aotearoa - Member There were no other additionsalterations Declarations of Interest for Items on Todayrsquos Agenda There were no declarations of interest for items on todayrsquos agenda Perceived Conflicts of Interest There were no perceived conflicts of interest
2 CONFIRMATION OF PREVIOUS MEETING MINUTES
Resolution (0121) (Moved Ingrid TaylorSeconded Jan Edwards ndash carried) ldquoThat the minutes of the Hospital Advisory Committee meeting held on 3 December 2020 be approved and adopted as a true and correct recordrdquo
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
10
HAC-28jan21ndashminutesndashdraft Page 2 of 6 01042021
3 CARRIED FORWARD ACTION ITEMS
The carried forward action items were noted
4 HampSS MONITORING REPORT
The Committee considered the Hospital and Specialist Services Monitoring Report for December 2020 The report was taken as read General Managers introduced their respective divisions and spoke to their areas as follows Specialist Mental Health Services (SMHS) ndash Dr Greg Hamilton General Manager
Report focuses on SMHS Intellectual Disability Services to provide a greater depth of understanding Services are provided to inpatients in two different units o PSAID Unit This falls under our population-based funding and is for those
people with an intellectual disability and a mental health diagnosis o Whaikaha (ATampR ndash Assessment Treatment and Rehabilitation) This is funded
by Ministry of Health Disability Support Services with whom we have two contracts and is for people who are under Court order under two different Acts It is a secure unit Generally this cohort of people have relatively poor health both physical and mental health Some people have been there for a long period with the longest standing consumer having been there since 2003 This is an institutional type approach for a group of people who are highly vulnerable
There are a lot of incidents some of which are assaults ndash injury to staff and assaults between consumers
Staff are amazing in their commitment to this cohort of people People who work here are values driven and come to work to make a difference for this vulnerable population which includes taking on some of that risk we are trying to mitigate
Considerable frustration for ATampR with Disability Support Services in terms of how they fund that and the ability to provide a really good service Dr Hamilton thanked the Board for its investment The four new pods on the new facility are hoped to be occupied by the end of March 2021 He noted that this will significantly change the living standards and lives of some of the more complex long-term consumers
Older Persons Health amp Rehabilitation (OPHampR) Service ndash Dr Helen Skinner General Manager amp Chief of Service
Pressure Injury Prevention Project update The validated figures for the last four months of the 2020 year show 48 patients with pressure injuries versus 73 for the year prior so a reduction of 25 in terms of pressure injuries Staff are now very enthusiastic at looking at skin and ensuring they are picking up every possible blemish There is still further work to be done to get down to the aim of 95 avoidable pressure injuries knowing that 5 are unavoidable in terms of international best practice
Vestibular Screening Tool Pilot There is evidence for using vestibular screening which involves a series of four questions when patients come in to assess whether they have a risk of vestibular problems and what to do about it This is a piece of work the Allied Health Team is leading on and is being rolled out across the Older Persons Health amp Rehabilitation Service and will be rolled out into the community as well ED is interested also There is good evidence in terms of the validation of the tool in ED and the Acute setting so is something that could be used across the DHB in terms or reducing the risk of falls and identifying what the risks are
ERAS Highlighted OPHampRrsquos 2020 results from the national hip fracture registry database
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
11
HAC-28jan21ndashminutesndashdraft Page 3 of 6 01042021
There was discussion around needs assessments for patients particularly at Burwood for Aged Residential Care (ARC) Dr Skinner advised that times are monitored and data is kept to ensure there are no delays In terms of initial assessments there has been no delay There has been some delay in terms of community re-assessments Timeframes for assessment take anywhere between one to two working days
Queried whether there was too much demand versus supply with regards to ARC Dr Skinner advised we are running high occupancy levels in terms of dementia hospital elder care This is the one area where we run high compared to the rest of the country in terms of the capacity we have
There was discussion around the number of over 75s coming from rest homes and being admitted through ED and what is or could be done to address this Dr Skinner spoke of Advance Care Planning and Shared Goals of Care as well as what can be done differently in the community Becky Hickmott Acting Executive Director of Nursing noted that Ashburton has its own unique challenges in this space part of which is the primary health sector understanding its role She advised of a lot of changes and turnover in staff in Ashburton and this impacting the flow through to ED There is a significant piece of work underway to address this but it is not quite at the implementation stage
MedicalSurgical amp Womenrsquos amp Childrenrsquos Health amp Orthopaedics ndash Pauline Clark General Manager
Increase in acute presentations to Christchurch Hospital It is not just ED experiencing this but also the Acute Medical Assessment Unit the ldquoBone Shoprdquo the Surgical Assessment Unit and the Childrenrsquos Acute Assessment o ED experienced a sharp uplift in presentations that occurred in late September
prior to the transition to Waipapa Between January and the end of September 2020 there were an average 1830 presentations to ED per week Since then this has risen to an average of 2163 per week ndash an increase of 48 per day or 18
o This cannot be explained by population pressures ndash the rate of ED attendances per 10000 population increases sharply at the same time
o Within this we have seen an increase in self-referrals to the ED of around 2 - or 250 presentations per week
o Conversely there has been a slight decrease in GP referrals People are presenting directly but their reasons for being there are in alignment with their health needs Overall people presenting need to be assessed in an ED environment in a tertiary centre
o 24 hour medical centres both Riccarton and Moorhouse are also experiencing increased presentations so not just the ED
Medical Oncology As previously advised additional project support has been invested in to assist with a revision to the model of care This is in place and work is starting to pay dividends Two new medical oncologists have been appointed and discussions continue around a third appointment
High neo-natal occupancy This is a phenomenon being seen around New Zealand possibly not helped by the MoH lead in the space Andrew Simpson having left his role So again work in the neo-natal cot space has stalled CDHBrsquos neo-natal service is designed to take 40 to 45 Currently it is sitting at 54 Another four are being cared for as part of the paediatric ward which is putting additional pressure on paediatrics who are already experiencing demand issues We also have some women and babies out in other parts of NZ Very tight nationally when it comes to neo-natal bedscots
Return of surgery and progress against plan The opening of Waipapa provided a significant increase in acute theater capacity on the Christchurch Campus Will be in a position to report on this in more detail at the Committeersquos next meeting
Have seen significant gains in terms of the pre-operative stay in inpatients
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
12
HAC-28jan21ndashminutesndashdraft Page 4 of 6 01042021
Planned on having outplaced surgery back by Christmas with the exception of paediatric dental (which is planned for March due to availability of workforce and appropriate facilities) Outplacing has ceased
The plan around returning outsourced surgery is currently being tweaked to accommodate some unexpected sickness which will result in key people being away for a period of time
Recruitment of Anesthetic Technicians is an issue Have two staff coming from the UK in the next quarter and the search continues
Been working very closely with Sterile Supply They are a keen enabler
ESPIs CDHB and MoH have agreed an ESPI improvement plan which sees the DHB achieve compliance in ESPI 2 and 5 by 30 June 2021 A wobble was experienced in late Decemberearly January but are now on track to achieve this Specific actions that services are undertaking to enable us to deliver include o Orthopaedics have taken 64 long waiting electiveplanned patients requiring hand
surgery from the Plastic Service waitlist and put it into their own waitlist They are able to do this without needing to use anesthesia and are utilising theatre space at Burwood for this
o Vascular Surgery have been able to utilise funding that the MoH provided for additional clinics Have repatriated ambulatory treatment of varicose veins to the Outpatient Department
o Ear Nose and Throat Parental leave has affected capacity in the rhinology subspecialty however the full team is now back on board
o General Surgery A number of SMO staff have recently returned from extended sick and annual leave and a new fellow has started this week
o Some services are already green and will remain there
Discussion took place around
Issues with neo-natal cot capacity from both a regional and national perspective
Clinical safety in light of increased acute presentations
Fee structure for afterhours care The HampSS Monitoring report was noted
5 CLINICAL ADVISOR UPDATE (ORAL)
Becky Hickmott Acting Executive Director of Nursing provided the following updates
Acknowledged NICUrsquos capacity issues noting there have been a large number of extreme preterm as well as preterm births with babies who have high need and long stay The long stay has an ongoing impact Many came spontaneously in labour or with membranes ruptured Across the nation similar things are happening
Maternity is under pressure from a staffing point of view From a safety angle we are working to divert some of our nursing teams to help support
Christchurch and Burwood Hospitals were very full over the Christmas period What would normally be a quieter period was not Staff have been under significant pressure but have done a stellar job
Recently visited the SMHS site at Hillmorton to see the built environment and the constraints impacting on patients and staff Acknowledged the challenges that staff are working under They are dealing with complex patients in very challenging conditions yet the professionalism in care was clearly evident with constant reassessing triaging and attention to safety Progress with new facilities cannot come quick enough for staff
Burwood has a key quality focus on medication administration at the moment This involves a cross disciplinary approach
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
13
HAC-28jan21ndashminutesndashdraft Page 5 of 6 01042021
Looking across the board at how to mobilise and utilise nursing resources A current focus is on outpatient services ndash how we use that workforce in a different way and also advancing working at top of scope
Trendcare implementation and CCDM is progressing well in spite of some hiccups within the system These have largely been rectified ICU goes live with Trendcare mid-February and Surgery will be underway soon as well CCDM teams have been described as ldquobull doggishrdquo in their approach which will continue to ensure accurate and reliable data
COVID readiness planning is well underway working closely with Allied Health to ensure we are taking a cross disciplinary approach
MIQ nursing staff and the welfare teams have been under significant pressure during the holiday period but have delivered a high standard of care and support They perform a vital role in keeping NZ safe Mindful that staff have times where they feel stigmatised in the community and their wider family are impacted on by the role that they hold
Commend primary health who keep mobilising to support Whole system approach is working well
In spite of the pressure on staff across the system we continue to receive numerous letters and emails on the care provided and the willingness of nurses to go the extra mile
6 SERVICES SUPPORTING OLDER PEOPLE LIVING IN RURAL COMMUNITIES
Ralph La Salle Acting Executive Director Planning Funding amp Decision Support introduced the report noting it was in response to a request from the Committee last year to better understand initiativesservices in place currently and those that are planned to support our rural older population to remain in their own homescommunities and into the future Greta Bond Service Development Manager Older Persons Health (OPH) and Andrea Davidson OPH Portfolio Manager were in attendance The report was taken as read Discussion took place around the following
Strengths of the rural community as well as challenges presented by distance
Ageing population ndash in terms of this community it is not only about the clients of the services but also the people who are delivering the services Rurally we have an ageing workforce and in addition particularly with nursing a workforce where this is not their only job
The increase in demand for dementia care Rurally this can be difficult to deliver so new models of care are being looked at
Resources being deployed to rural areas and ensuring they are being utilised in the best possible way Working with the community to make sure that services are developing to meet the current needs of people as opposed to the traditional way that services have always been delivered
Falls prevention referral programme and uptake in the rural community
The availability of consumables particularly in terms of those which are meant to be provided on discharge from hospital and the impact this has on providing nursing rurally
An electronic referral form is being implemented within secondary care so someone referring for services in the community will be able to do this electronically This will be a big benefit to providing rural services
The Services Supporting Older People Living in Rural Communities report was noted
7 2021 WORKPLAN
The Committee received the 2021 Workplan noting that this is a working document
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
14
HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-01apr21-agenda Page 2 of 2 01042021
7 Resolution to Exclude the Public 1030am
Estimated Finish Time 1030am
NEXT MEETING Thursday 3 June 2021 at 900am
HAC - 01 April 2021 - P - Agenda
2
HAC-01apr21-BCL900DE46F Page 1 of 2 01042021
ATTENDANCE
HOSPITAL ADVISORY COMMITTEE MEMBERS Andrew Dickerson (Chair) Naomi Marshall (Deputy Chair) Barry Bragg Catherine Chu James Gough Jo Kane Ingrid Taylor Jan Edwards Dr Rochelle Phipps Michelle Turrall Sir John Hansen (Ex-officio) Gabrielle Huria (Ex-officio)
Executive Support (as required as per agenda) Dr Peter Bramley ndash Chief Executive Evon Currie ndash General Manager Community amp Public Health Savita Devi ndash Acting Chief Digital Officer Dr Richard French ndash Acting Chief Medical Officer David Green ndash Acting Executive Director Finance amp Corporate Services Becky Hickmott ndash Executive Director of Nursing Mary Johnston ndash Chief People Officer Ralph La Salle ndash Acting Executive Director Planning Funding amp Decision Support Dr Jacqui Lunday-Johnstone ndash Executive Director of Allied Health Scientific amp Technical Hector Matthews ndash Executive Director Maori amp Pacific Health Dr Rob Ojala ndash Executive Director for Facilities Karalyn Van Deursen ndash Executive Director of Communications Anna Craw ndash Board Secretariat Kay Jenkins ndash Executive Assistant Governance Support
HAC - 01 April 2021 - P - Attendance
3
HAC-01apr21-BCL900DE46F Page 2 of 2 01042021
COMMITTEE ATTENDANCE SCHEDULE 2020
NAME
280121
010421
030621
050821
071021
021221
Andrew Dickerson (Chair) radic
Naomi Marshall (Deputy Chair) radic
Barry Bragg
Catherine Chu x
James Gough ^
Jo Kane radic
(Zoom)
Ingrid Taylor radic
Jan Edwards radic
Dr Rochelle Phipps
Michelle Turrall x
Sir John Hansen (ex-officio) radic
Gabrielle Huria (ex-officio) x
radic Attended
x Absent Absent with apology ^ Attended part of meeting ~ Leave of absence Appointed effective No longer on the Committee effective
HAC - 01 April 2021 - P - Attendance
4
HAC-01apr21-interest register Page 1 of 5 01042021
(As disclosed on appointment to the BoardCommittee and updated from time-to-time as necessary)
Andrew Dickerson Chair ndash HAC Board Member
Canterbury Health Care of the Elderly Education Trust - Chair Promotes and supports teaching and research in the care of older people Recipients of financial assistance for research education or training could include employees of the CDHB
Canterbury Medical Research Foundation - Member Provides financial assistance for medical research in Canterbury Recipients of financial assistance for research education or training could include employees of the CDHB
Heritage NZ - Member Heritage NZrsquos mission is to promote the identification protection preservation and conservation of the historical and cultural heritage of New Zealand It identifies records and acts in respect of significant ancestral sites and buildings CDHB owns buildings that may be considered to have historical significance and Heritage NZ has already been involved with CDHB buildings Maia Health Foundation - Trustee Is a charitable trust established to support health care in the CDHB area Current projects include fundraising for a rooftop helipad and enhancements to the childrenrsquos wards at Christchurch Hospital NZ Association of Gerontology - Member
Professional association that promotes the interests of older people and an understanding of ageing
Naomi Marshall Deputy Chair - HAC Board Member
College of Nurses Aotearoa NZ ndash Member Riccarton Clinic amp After Hours ndash Employee Employed as a Nurse Riccarton Clinic amp After Hours provides general practice and after-hours care It is part privately and PHO funded The PHO receives funding from the CDHB
Barry Bragg Board Member
Air Rescue Services Limited - Director Subsidiary of the Canterbury West Coast Air Rescue Trust Has gaming licenses with specified purpose of fundraising for air rescue services Canterbury West Coast Air Rescue Trust ndash Trustee The Trust has a services agreement with Garden City Helicopters for the provision of air rescue and air ambulance services Garden City Helicopters has a long-term air ambulance contract with the CDHB CMUA Project Delivery Limited - Director 100 owned by the Christchurch City Council and is responsible for the delivery of the Canterbury Multi-Use Arena project within agreed parameters Farrell Construction Limited - Shareholder Farrellrsquos Construction Limited is a commercial and light commercial construction company based in Christchurch
CONFLICTS OF INTEREST REGISTER HOSPITAL ADVISORY COMMITTEE (HAC)
HAC - 01 April 2021 - P - Conflict of Interest Register
5
HAC-01apr21-interest register Page 2 of 5 01042021
New Zealand Flying Doctor Service Trust ndash Trustee The Trust has a services agreement with Garden City Helicopters for the provision of air ambulance services Garden City Helicopters has a long-term air ambulance contract with the CDHB Ngai Tahu Farming ndash Chairman Farming interests in North Canterbury and Queenstown Lakes District and Forestry interests in Canterbury West Coast and Otago regions Paenga Kupenga Limited ndash Chair Commercial arm of Ngai Tuahuriri Runanga Quarry Capital Limited ndash Director Property syndication company based in Christchurch Stevenson Group Limited ndash Deputy Chairman Property interests in Auckland and mining interests on the West Coast Verum Group Limited ndash Director Verum Group Limited provides air quality testing and asbestos sampling and analysis services methamphetamine contamination testing dust gas and noise workplace monitoring services in New Zealand There is the potential for future work with the CDHB
Catherine Chu Board Member
Christchurch City Council ndash Councillor Local Territorial Authority Riccarton Rotary Club ndash Member The Canterbury Club ndash Member
Jan Edwards Age Concern Canterbury ndash Member Anglican Care ndash Volunteer Neurological Foundation of NZ - Member
James Gough Board Member
Amyes Road Limited ndash Shareholder Formally Gough GroupGough Holdings Limited Currently liquidating Christchurch City Council ndash Councillor Local Territorial Authority Includes appointment to FendaltonWaimairi Harewood Community Board Christchurch City Holdings Limited (CCHL) ndash Director Holds and manages the Councilrsquos commercial interest in subsidiary companies Civic Building Limited ndash Chairman Council Property Interests JV with Ngai Tahu Property Limited Gough Corporation Holdings Limited ndash DirectorShareholder Holdings company Gough Property Corporation Limited ndash DirectorShareholder Manages property interests
HAC - 01 April 2021 - P - Conflict of Interest Register
6
HAC-01apr21-interest register Page 3 of 5 01042021
Medical Kiwi Limited ndash Independent Director Research and distribution company of medicinal cannabis and other health related products In process of listing on NZX The Antony Gough Trust ndash Trustee Trust for Antony Thomas Gough The Russley Village Limited ndash Shareholder Retirement Village Via the Antony Gough Trust The Terrace Car Park Limited ndash (Alternate) Director Property company ndash manages The Terrace car park (under construction) The Terrace On Avon Limited ndash (Alternate) Director Property company ndash manages The Terrace
Jo Kane Board Member
Christchurch Resettlement Services - Member Christchurch Resettlement Services provides a range of services to people from refugee and migrant backgrounds It works alongside refugee communities in delivering services that aim to achieve positive resettlement outcomes HurriKane Consulting ndash Project Management PartnerConsultant A private consultancy in management communication and project management Any conflicts of interest that arise will be disclosedadvised Latimer Community Housing Trust ndash Project Manager Delivers social housing in Christchurch for the vulnerable and elderly in the community
NZ Royal Humane Society ndash Director Provides an awards system for acts of bravery in New Zealand It is not anticipated any conflicts of interest will arise
Dr Rochelle Phipps Accident Compensation Corporation ndash Medical Advisor ACC is a Crown entity responsible for administering NZrsquos universal no-fault accidental injury scheme As a Medical Advisor I analyse and interpret medical information and make recommendations to improve rehabilitation outcomes for ACC customers OraTaiao New Zealand Climate amp Health Council ndash Founding Executive Board Member (no longer on executive) The Council is a not-for-profit politically non-partisan incorporated society and comprises health professionals in AotearoaNew Zealand concerned with the negative impacts of climate change on health the health gains possible through strong health-centred climate action highlighting the impacts of climate change on those who already experience
disadvantage or ill health (equity impacts) and reducing the health sectors contribution to climate change Royal New Zealand College of General Practitioners ndash Christchurch Fellow and Former Board Member The RNZCGP is the professional body and postgraduate educational institute for general practitioners
HAC - 01 April 2021 - P - Conflict of Interest Register
7
HAC-01apr21-interest register Page 4 of 5 01042021
Ingrid Taylor Board Member
Loyal Canterbury Lodge (LCL) ndash Manchester Unity ndash Trustee LCL is a friendly society administering funds for the benefit of members and often makes charitable donations One of the recipients of such a donation may have an association with the CDHB Manchester Unity Welfare Homes Trust Board (MUWHTB) ndash Trustee MUWHTB is a charitable Trust providing financial assistance to organisations in Canterbury associated with the care and assistance of older persons Recipients of financial assistance may have an association with the CDHB Sir John and Ann Hansenrsquos Family Trust ndash Independent Trustee Taylor Shaw ndash Partner Taylor Shaw has clients that are employed by the CDHB or may have contracts for services with the CDHB that may mean a conflict or potential conflict may arise from time to time Such conflicts of interest will need to be addressed at the appropriate time
I Taylor Shaw have acted as solicitor for Bill Tate and family The Youth Hub ndash Trustee The Youth Hub is a charitable Trust established to provide residential and social services for the Youth of Canterbury including services for mental health and medical care that may include involvement with the CDHB
Michelle Turrall Manawhenua
Canterbury Clinical Network (CCN) Maori Caucus - Member Canterbury District Health Board - Daughter employed as registered nurse Christchurch PHO Ltd ndash Director Christchurch PHO Trust - Trustee
Manawhenua ki Waitaha ndash Board Member and Chair Oranga Tamariki ndash Iwi and Maori ndash Senior Advisor Papakainga Hauora Komiti ndash Te Ngai Tuahuriri ndash Co-Chair
Sir John Hansen Ex-Officio ndash HAC Chair CDHB
Bone Marrow Cancer Trust ndash Trustee Canterbury Cricket Trust - Member Christchurch Casino Charitable Trust - Trustee Court of Appeal Solomon Islands Samoa and Vanuatu Dot Kiwi ndash Director and Shareholder Judicial Control Authority (JCA) for Racing ndash Appeals Tribunal Member The JCA is an independent statutory authority constituted under the Racing Act The JCA ensures that judicial and appeal proceedings in thoroughbred and harness racing are heard and decided fairly professionally efficiently and in a consistent and cost effective manner Ministry Primary Industries Costs Review Independent Panel
HAC - 01 April 2021 - P - Conflict of Interest Register
8
HAC-01apr21-interest register Page 5 of 5 01042021
Rulings Panel Gas Industry Co Ltd Sir John and Ann Hansenrsquos Family Trust ndash Ingrid Taylor sits as independent Trustee and provides legal services to the Trust and to Sir John and Ann Hansen
Gabrielle Huria Ex-Officio ndash HAC Deputy Chair CDHB
Pegasus Health Limited ndash Sister is a Director Primary Health Organisation (PHO) Rawa Hohepa Limited ndash Director Family property company Sumner Health Centre ndash Daughter is a General Practitioner (GP) Doctorrsquos clinic Te Kura Taka Pini Limited ndash General Manager The Royal New Zealand College of GPs ndash Sister is an ldquoappointed independent Directorrdquo College of GPs Upoko Rawiri Te Maire Tau of Ngai Tuahuriri - Husband
HAC - 01 April 2021 - P - Conflict of Interest Register
9
HAC-28jan21ndashminutesndashdraft Page 1 of 6 01042021
MINUTES ndash PUBLIC
DRAFT MINUTES OF THE HOSPITAL ADVISORY COMMITTEE MEETING
held in the Board Room Level 1 32 Oxford Terrace Christchurch on Thursday 28 January 2021 commencing at 900am
PRESENT Andrew Dickerson (Chair) Jan Edwards James Gough Jo Kane (via Zoom) Naomi Marshall Ingrid Taylor and Sir John Hansen (Ex-Officio) APOLOGIES Apologies for absence were received and accepted from Barry Bragg and Dr Rochelle Phipps An apology for early departure was received and accepted from James Gough (1010am) EXECUTIVE SUPPORT Dr Andrew Brant (Acting Chief Executive) Becky Hickmott (Acting Executive Director of Nursing) Ralph La Salle (Acting Executive Director Planning Funding amp Decision Support) Dr Jacqui Lunday-Johnstone (Executive Director Allied Health Scientific amp Technical) Kay Jenkins (Executive Assistant Governance Support) and Anna Craw (Board Secretariat)
APOLOGIES Kirsten Beynon (General Manager Laboratories) Dr Richard French (Acting Chief Medical Officer) Berni Marra (Manager Ashburton Health Services) and Win McDonald (Transition Programme Manager Rural Health Services) IN ATTENDANCE
Full Meeting
Pauline Clark General Manager MedicalSurgical Womenrsquos amp Childrenrsquos Health amp Orthopaedics Dr Helen Skinner General Manager amp Chief of Service Older Persons Health amp Rehabilitation Dr Greg Hamilton General Manager Specialist Mental Health Services 1 INTEREST REGISTER
AdditionsAlterations to the Interest Register Naomi Marshall ndash Addition ndash NZ Nurses College Aotearoa - Member There were no other additionsalterations Declarations of Interest for Items on Todayrsquos Agenda There were no declarations of interest for items on todayrsquos agenda Perceived Conflicts of Interest There were no perceived conflicts of interest
2 CONFIRMATION OF PREVIOUS MEETING MINUTES
Resolution (0121) (Moved Ingrid TaylorSeconded Jan Edwards ndash carried) ldquoThat the minutes of the Hospital Advisory Committee meeting held on 3 December 2020 be approved and adopted as a true and correct recordrdquo
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
10
HAC-28jan21ndashminutesndashdraft Page 2 of 6 01042021
3 CARRIED FORWARD ACTION ITEMS
The carried forward action items were noted
4 HampSS MONITORING REPORT
The Committee considered the Hospital and Specialist Services Monitoring Report for December 2020 The report was taken as read General Managers introduced their respective divisions and spoke to their areas as follows Specialist Mental Health Services (SMHS) ndash Dr Greg Hamilton General Manager
Report focuses on SMHS Intellectual Disability Services to provide a greater depth of understanding Services are provided to inpatients in two different units o PSAID Unit This falls under our population-based funding and is for those
people with an intellectual disability and a mental health diagnosis o Whaikaha (ATampR ndash Assessment Treatment and Rehabilitation) This is funded
by Ministry of Health Disability Support Services with whom we have two contracts and is for people who are under Court order under two different Acts It is a secure unit Generally this cohort of people have relatively poor health both physical and mental health Some people have been there for a long period with the longest standing consumer having been there since 2003 This is an institutional type approach for a group of people who are highly vulnerable
There are a lot of incidents some of which are assaults ndash injury to staff and assaults between consumers
Staff are amazing in their commitment to this cohort of people People who work here are values driven and come to work to make a difference for this vulnerable population which includes taking on some of that risk we are trying to mitigate
Considerable frustration for ATampR with Disability Support Services in terms of how they fund that and the ability to provide a really good service Dr Hamilton thanked the Board for its investment The four new pods on the new facility are hoped to be occupied by the end of March 2021 He noted that this will significantly change the living standards and lives of some of the more complex long-term consumers
Older Persons Health amp Rehabilitation (OPHampR) Service ndash Dr Helen Skinner General Manager amp Chief of Service
Pressure Injury Prevention Project update The validated figures for the last four months of the 2020 year show 48 patients with pressure injuries versus 73 for the year prior so a reduction of 25 in terms of pressure injuries Staff are now very enthusiastic at looking at skin and ensuring they are picking up every possible blemish There is still further work to be done to get down to the aim of 95 avoidable pressure injuries knowing that 5 are unavoidable in terms of international best practice
Vestibular Screening Tool Pilot There is evidence for using vestibular screening which involves a series of four questions when patients come in to assess whether they have a risk of vestibular problems and what to do about it This is a piece of work the Allied Health Team is leading on and is being rolled out across the Older Persons Health amp Rehabilitation Service and will be rolled out into the community as well ED is interested also There is good evidence in terms of the validation of the tool in ED and the Acute setting so is something that could be used across the DHB in terms or reducing the risk of falls and identifying what the risks are
ERAS Highlighted OPHampRrsquos 2020 results from the national hip fracture registry database
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
11
HAC-28jan21ndashminutesndashdraft Page 3 of 6 01042021
There was discussion around needs assessments for patients particularly at Burwood for Aged Residential Care (ARC) Dr Skinner advised that times are monitored and data is kept to ensure there are no delays In terms of initial assessments there has been no delay There has been some delay in terms of community re-assessments Timeframes for assessment take anywhere between one to two working days
Queried whether there was too much demand versus supply with regards to ARC Dr Skinner advised we are running high occupancy levels in terms of dementia hospital elder care This is the one area where we run high compared to the rest of the country in terms of the capacity we have
There was discussion around the number of over 75s coming from rest homes and being admitted through ED and what is or could be done to address this Dr Skinner spoke of Advance Care Planning and Shared Goals of Care as well as what can be done differently in the community Becky Hickmott Acting Executive Director of Nursing noted that Ashburton has its own unique challenges in this space part of which is the primary health sector understanding its role She advised of a lot of changes and turnover in staff in Ashburton and this impacting the flow through to ED There is a significant piece of work underway to address this but it is not quite at the implementation stage
MedicalSurgical amp Womenrsquos amp Childrenrsquos Health amp Orthopaedics ndash Pauline Clark General Manager
Increase in acute presentations to Christchurch Hospital It is not just ED experiencing this but also the Acute Medical Assessment Unit the ldquoBone Shoprdquo the Surgical Assessment Unit and the Childrenrsquos Acute Assessment o ED experienced a sharp uplift in presentations that occurred in late September
prior to the transition to Waipapa Between January and the end of September 2020 there were an average 1830 presentations to ED per week Since then this has risen to an average of 2163 per week ndash an increase of 48 per day or 18
o This cannot be explained by population pressures ndash the rate of ED attendances per 10000 population increases sharply at the same time
o Within this we have seen an increase in self-referrals to the ED of around 2 - or 250 presentations per week
o Conversely there has been a slight decrease in GP referrals People are presenting directly but their reasons for being there are in alignment with their health needs Overall people presenting need to be assessed in an ED environment in a tertiary centre
o 24 hour medical centres both Riccarton and Moorhouse are also experiencing increased presentations so not just the ED
Medical Oncology As previously advised additional project support has been invested in to assist with a revision to the model of care This is in place and work is starting to pay dividends Two new medical oncologists have been appointed and discussions continue around a third appointment
High neo-natal occupancy This is a phenomenon being seen around New Zealand possibly not helped by the MoH lead in the space Andrew Simpson having left his role So again work in the neo-natal cot space has stalled CDHBrsquos neo-natal service is designed to take 40 to 45 Currently it is sitting at 54 Another four are being cared for as part of the paediatric ward which is putting additional pressure on paediatrics who are already experiencing demand issues We also have some women and babies out in other parts of NZ Very tight nationally when it comes to neo-natal bedscots
Return of surgery and progress against plan The opening of Waipapa provided a significant increase in acute theater capacity on the Christchurch Campus Will be in a position to report on this in more detail at the Committeersquos next meeting
Have seen significant gains in terms of the pre-operative stay in inpatients
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
12
HAC-28jan21ndashminutesndashdraft Page 4 of 6 01042021
Planned on having outplaced surgery back by Christmas with the exception of paediatric dental (which is planned for March due to availability of workforce and appropriate facilities) Outplacing has ceased
The plan around returning outsourced surgery is currently being tweaked to accommodate some unexpected sickness which will result in key people being away for a period of time
Recruitment of Anesthetic Technicians is an issue Have two staff coming from the UK in the next quarter and the search continues
Been working very closely with Sterile Supply They are a keen enabler
ESPIs CDHB and MoH have agreed an ESPI improvement plan which sees the DHB achieve compliance in ESPI 2 and 5 by 30 June 2021 A wobble was experienced in late Decemberearly January but are now on track to achieve this Specific actions that services are undertaking to enable us to deliver include o Orthopaedics have taken 64 long waiting electiveplanned patients requiring hand
surgery from the Plastic Service waitlist and put it into their own waitlist They are able to do this without needing to use anesthesia and are utilising theatre space at Burwood for this
o Vascular Surgery have been able to utilise funding that the MoH provided for additional clinics Have repatriated ambulatory treatment of varicose veins to the Outpatient Department
o Ear Nose and Throat Parental leave has affected capacity in the rhinology subspecialty however the full team is now back on board
o General Surgery A number of SMO staff have recently returned from extended sick and annual leave and a new fellow has started this week
o Some services are already green and will remain there
Discussion took place around
Issues with neo-natal cot capacity from both a regional and national perspective
Clinical safety in light of increased acute presentations
Fee structure for afterhours care The HampSS Monitoring report was noted
5 CLINICAL ADVISOR UPDATE (ORAL)
Becky Hickmott Acting Executive Director of Nursing provided the following updates
Acknowledged NICUrsquos capacity issues noting there have been a large number of extreme preterm as well as preterm births with babies who have high need and long stay The long stay has an ongoing impact Many came spontaneously in labour or with membranes ruptured Across the nation similar things are happening
Maternity is under pressure from a staffing point of view From a safety angle we are working to divert some of our nursing teams to help support
Christchurch and Burwood Hospitals were very full over the Christmas period What would normally be a quieter period was not Staff have been under significant pressure but have done a stellar job
Recently visited the SMHS site at Hillmorton to see the built environment and the constraints impacting on patients and staff Acknowledged the challenges that staff are working under They are dealing with complex patients in very challenging conditions yet the professionalism in care was clearly evident with constant reassessing triaging and attention to safety Progress with new facilities cannot come quick enough for staff
Burwood has a key quality focus on medication administration at the moment This involves a cross disciplinary approach
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
13
HAC-28jan21ndashminutesndashdraft Page 5 of 6 01042021
Looking across the board at how to mobilise and utilise nursing resources A current focus is on outpatient services ndash how we use that workforce in a different way and also advancing working at top of scope
Trendcare implementation and CCDM is progressing well in spite of some hiccups within the system These have largely been rectified ICU goes live with Trendcare mid-February and Surgery will be underway soon as well CCDM teams have been described as ldquobull doggishrdquo in their approach which will continue to ensure accurate and reliable data
COVID readiness planning is well underway working closely with Allied Health to ensure we are taking a cross disciplinary approach
MIQ nursing staff and the welfare teams have been under significant pressure during the holiday period but have delivered a high standard of care and support They perform a vital role in keeping NZ safe Mindful that staff have times where they feel stigmatised in the community and their wider family are impacted on by the role that they hold
Commend primary health who keep mobilising to support Whole system approach is working well
In spite of the pressure on staff across the system we continue to receive numerous letters and emails on the care provided and the willingness of nurses to go the extra mile
6 SERVICES SUPPORTING OLDER PEOPLE LIVING IN RURAL COMMUNITIES
Ralph La Salle Acting Executive Director Planning Funding amp Decision Support introduced the report noting it was in response to a request from the Committee last year to better understand initiativesservices in place currently and those that are planned to support our rural older population to remain in their own homescommunities and into the future Greta Bond Service Development Manager Older Persons Health (OPH) and Andrea Davidson OPH Portfolio Manager were in attendance The report was taken as read Discussion took place around the following
Strengths of the rural community as well as challenges presented by distance
Ageing population ndash in terms of this community it is not only about the clients of the services but also the people who are delivering the services Rurally we have an ageing workforce and in addition particularly with nursing a workforce where this is not their only job
The increase in demand for dementia care Rurally this can be difficult to deliver so new models of care are being looked at
Resources being deployed to rural areas and ensuring they are being utilised in the best possible way Working with the community to make sure that services are developing to meet the current needs of people as opposed to the traditional way that services have always been delivered
Falls prevention referral programme and uptake in the rural community
The availability of consumables particularly in terms of those which are meant to be provided on discharge from hospital and the impact this has on providing nursing rurally
An electronic referral form is being implemented within secondary care so someone referring for services in the community will be able to do this electronically This will be a big benefit to providing rural services
The Services Supporting Older People Living in Rural Communities report was noted
7 2021 WORKPLAN
The Committee received the 2021 Workplan noting that this is a working document
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
14
HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-01apr21-BCL900DE46F Page 1 of 2 01042021
ATTENDANCE
HOSPITAL ADVISORY COMMITTEE MEMBERS Andrew Dickerson (Chair) Naomi Marshall (Deputy Chair) Barry Bragg Catherine Chu James Gough Jo Kane Ingrid Taylor Jan Edwards Dr Rochelle Phipps Michelle Turrall Sir John Hansen (Ex-officio) Gabrielle Huria (Ex-officio)
Executive Support (as required as per agenda) Dr Peter Bramley ndash Chief Executive Evon Currie ndash General Manager Community amp Public Health Savita Devi ndash Acting Chief Digital Officer Dr Richard French ndash Acting Chief Medical Officer David Green ndash Acting Executive Director Finance amp Corporate Services Becky Hickmott ndash Executive Director of Nursing Mary Johnston ndash Chief People Officer Ralph La Salle ndash Acting Executive Director Planning Funding amp Decision Support Dr Jacqui Lunday-Johnstone ndash Executive Director of Allied Health Scientific amp Technical Hector Matthews ndash Executive Director Maori amp Pacific Health Dr Rob Ojala ndash Executive Director for Facilities Karalyn Van Deursen ndash Executive Director of Communications Anna Craw ndash Board Secretariat Kay Jenkins ndash Executive Assistant Governance Support
HAC - 01 April 2021 - P - Attendance
3
HAC-01apr21-BCL900DE46F Page 2 of 2 01042021
COMMITTEE ATTENDANCE SCHEDULE 2020
NAME
280121
010421
030621
050821
071021
021221
Andrew Dickerson (Chair) radic
Naomi Marshall (Deputy Chair) radic
Barry Bragg
Catherine Chu x
James Gough ^
Jo Kane radic
(Zoom)
Ingrid Taylor radic
Jan Edwards radic
Dr Rochelle Phipps
Michelle Turrall x
Sir John Hansen (ex-officio) radic
Gabrielle Huria (ex-officio) x
radic Attended
x Absent Absent with apology ^ Attended part of meeting ~ Leave of absence Appointed effective No longer on the Committee effective
HAC - 01 April 2021 - P - Attendance
4
HAC-01apr21-interest register Page 1 of 5 01042021
(As disclosed on appointment to the BoardCommittee and updated from time-to-time as necessary)
Andrew Dickerson Chair ndash HAC Board Member
Canterbury Health Care of the Elderly Education Trust - Chair Promotes and supports teaching and research in the care of older people Recipients of financial assistance for research education or training could include employees of the CDHB
Canterbury Medical Research Foundation - Member Provides financial assistance for medical research in Canterbury Recipients of financial assistance for research education or training could include employees of the CDHB
Heritage NZ - Member Heritage NZrsquos mission is to promote the identification protection preservation and conservation of the historical and cultural heritage of New Zealand It identifies records and acts in respect of significant ancestral sites and buildings CDHB owns buildings that may be considered to have historical significance and Heritage NZ has already been involved with CDHB buildings Maia Health Foundation - Trustee Is a charitable trust established to support health care in the CDHB area Current projects include fundraising for a rooftop helipad and enhancements to the childrenrsquos wards at Christchurch Hospital NZ Association of Gerontology - Member
Professional association that promotes the interests of older people and an understanding of ageing
Naomi Marshall Deputy Chair - HAC Board Member
College of Nurses Aotearoa NZ ndash Member Riccarton Clinic amp After Hours ndash Employee Employed as a Nurse Riccarton Clinic amp After Hours provides general practice and after-hours care It is part privately and PHO funded The PHO receives funding from the CDHB
Barry Bragg Board Member
Air Rescue Services Limited - Director Subsidiary of the Canterbury West Coast Air Rescue Trust Has gaming licenses with specified purpose of fundraising for air rescue services Canterbury West Coast Air Rescue Trust ndash Trustee The Trust has a services agreement with Garden City Helicopters for the provision of air rescue and air ambulance services Garden City Helicopters has a long-term air ambulance contract with the CDHB CMUA Project Delivery Limited - Director 100 owned by the Christchurch City Council and is responsible for the delivery of the Canterbury Multi-Use Arena project within agreed parameters Farrell Construction Limited - Shareholder Farrellrsquos Construction Limited is a commercial and light commercial construction company based in Christchurch
CONFLICTS OF INTEREST REGISTER HOSPITAL ADVISORY COMMITTEE (HAC)
HAC - 01 April 2021 - P - Conflict of Interest Register
5
HAC-01apr21-interest register Page 2 of 5 01042021
New Zealand Flying Doctor Service Trust ndash Trustee The Trust has a services agreement with Garden City Helicopters for the provision of air ambulance services Garden City Helicopters has a long-term air ambulance contract with the CDHB Ngai Tahu Farming ndash Chairman Farming interests in North Canterbury and Queenstown Lakes District and Forestry interests in Canterbury West Coast and Otago regions Paenga Kupenga Limited ndash Chair Commercial arm of Ngai Tuahuriri Runanga Quarry Capital Limited ndash Director Property syndication company based in Christchurch Stevenson Group Limited ndash Deputy Chairman Property interests in Auckland and mining interests on the West Coast Verum Group Limited ndash Director Verum Group Limited provides air quality testing and asbestos sampling and analysis services methamphetamine contamination testing dust gas and noise workplace monitoring services in New Zealand There is the potential for future work with the CDHB
Catherine Chu Board Member
Christchurch City Council ndash Councillor Local Territorial Authority Riccarton Rotary Club ndash Member The Canterbury Club ndash Member
Jan Edwards Age Concern Canterbury ndash Member Anglican Care ndash Volunteer Neurological Foundation of NZ - Member
James Gough Board Member
Amyes Road Limited ndash Shareholder Formally Gough GroupGough Holdings Limited Currently liquidating Christchurch City Council ndash Councillor Local Territorial Authority Includes appointment to FendaltonWaimairi Harewood Community Board Christchurch City Holdings Limited (CCHL) ndash Director Holds and manages the Councilrsquos commercial interest in subsidiary companies Civic Building Limited ndash Chairman Council Property Interests JV with Ngai Tahu Property Limited Gough Corporation Holdings Limited ndash DirectorShareholder Holdings company Gough Property Corporation Limited ndash DirectorShareholder Manages property interests
HAC - 01 April 2021 - P - Conflict of Interest Register
6
HAC-01apr21-interest register Page 3 of 5 01042021
Medical Kiwi Limited ndash Independent Director Research and distribution company of medicinal cannabis and other health related products In process of listing on NZX The Antony Gough Trust ndash Trustee Trust for Antony Thomas Gough The Russley Village Limited ndash Shareholder Retirement Village Via the Antony Gough Trust The Terrace Car Park Limited ndash (Alternate) Director Property company ndash manages The Terrace car park (under construction) The Terrace On Avon Limited ndash (Alternate) Director Property company ndash manages The Terrace
Jo Kane Board Member
Christchurch Resettlement Services - Member Christchurch Resettlement Services provides a range of services to people from refugee and migrant backgrounds It works alongside refugee communities in delivering services that aim to achieve positive resettlement outcomes HurriKane Consulting ndash Project Management PartnerConsultant A private consultancy in management communication and project management Any conflicts of interest that arise will be disclosedadvised Latimer Community Housing Trust ndash Project Manager Delivers social housing in Christchurch for the vulnerable and elderly in the community
NZ Royal Humane Society ndash Director Provides an awards system for acts of bravery in New Zealand It is not anticipated any conflicts of interest will arise
Dr Rochelle Phipps Accident Compensation Corporation ndash Medical Advisor ACC is a Crown entity responsible for administering NZrsquos universal no-fault accidental injury scheme As a Medical Advisor I analyse and interpret medical information and make recommendations to improve rehabilitation outcomes for ACC customers OraTaiao New Zealand Climate amp Health Council ndash Founding Executive Board Member (no longer on executive) The Council is a not-for-profit politically non-partisan incorporated society and comprises health professionals in AotearoaNew Zealand concerned with the negative impacts of climate change on health the health gains possible through strong health-centred climate action highlighting the impacts of climate change on those who already experience
disadvantage or ill health (equity impacts) and reducing the health sectors contribution to climate change Royal New Zealand College of General Practitioners ndash Christchurch Fellow and Former Board Member The RNZCGP is the professional body and postgraduate educational institute for general practitioners
HAC - 01 April 2021 - P - Conflict of Interest Register
7
HAC-01apr21-interest register Page 4 of 5 01042021
Ingrid Taylor Board Member
Loyal Canterbury Lodge (LCL) ndash Manchester Unity ndash Trustee LCL is a friendly society administering funds for the benefit of members and often makes charitable donations One of the recipients of such a donation may have an association with the CDHB Manchester Unity Welfare Homes Trust Board (MUWHTB) ndash Trustee MUWHTB is a charitable Trust providing financial assistance to organisations in Canterbury associated with the care and assistance of older persons Recipients of financial assistance may have an association with the CDHB Sir John and Ann Hansenrsquos Family Trust ndash Independent Trustee Taylor Shaw ndash Partner Taylor Shaw has clients that are employed by the CDHB or may have contracts for services with the CDHB that may mean a conflict or potential conflict may arise from time to time Such conflicts of interest will need to be addressed at the appropriate time
I Taylor Shaw have acted as solicitor for Bill Tate and family The Youth Hub ndash Trustee The Youth Hub is a charitable Trust established to provide residential and social services for the Youth of Canterbury including services for mental health and medical care that may include involvement with the CDHB
Michelle Turrall Manawhenua
Canterbury Clinical Network (CCN) Maori Caucus - Member Canterbury District Health Board - Daughter employed as registered nurse Christchurch PHO Ltd ndash Director Christchurch PHO Trust - Trustee
Manawhenua ki Waitaha ndash Board Member and Chair Oranga Tamariki ndash Iwi and Maori ndash Senior Advisor Papakainga Hauora Komiti ndash Te Ngai Tuahuriri ndash Co-Chair
Sir John Hansen Ex-Officio ndash HAC Chair CDHB
Bone Marrow Cancer Trust ndash Trustee Canterbury Cricket Trust - Member Christchurch Casino Charitable Trust - Trustee Court of Appeal Solomon Islands Samoa and Vanuatu Dot Kiwi ndash Director and Shareholder Judicial Control Authority (JCA) for Racing ndash Appeals Tribunal Member The JCA is an independent statutory authority constituted under the Racing Act The JCA ensures that judicial and appeal proceedings in thoroughbred and harness racing are heard and decided fairly professionally efficiently and in a consistent and cost effective manner Ministry Primary Industries Costs Review Independent Panel
HAC - 01 April 2021 - P - Conflict of Interest Register
8
HAC-01apr21-interest register Page 5 of 5 01042021
Rulings Panel Gas Industry Co Ltd Sir John and Ann Hansenrsquos Family Trust ndash Ingrid Taylor sits as independent Trustee and provides legal services to the Trust and to Sir John and Ann Hansen
Gabrielle Huria Ex-Officio ndash HAC Deputy Chair CDHB
Pegasus Health Limited ndash Sister is a Director Primary Health Organisation (PHO) Rawa Hohepa Limited ndash Director Family property company Sumner Health Centre ndash Daughter is a General Practitioner (GP) Doctorrsquos clinic Te Kura Taka Pini Limited ndash General Manager The Royal New Zealand College of GPs ndash Sister is an ldquoappointed independent Directorrdquo College of GPs Upoko Rawiri Te Maire Tau of Ngai Tuahuriri - Husband
HAC - 01 April 2021 - P - Conflict of Interest Register
9
HAC-28jan21ndashminutesndashdraft Page 1 of 6 01042021
MINUTES ndash PUBLIC
DRAFT MINUTES OF THE HOSPITAL ADVISORY COMMITTEE MEETING
held in the Board Room Level 1 32 Oxford Terrace Christchurch on Thursday 28 January 2021 commencing at 900am
PRESENT Andrew Dickerson (Chair) Jan Edwards James Gough Jo Kane (via Zoom) Naomi Marshall Ingrid Taylor and Sir John Hansen (Ex-Officio) APOLOGIES Apologies for absence were received and accepted from Barry Bragg and Dr Rochelle Phipps An apology for early departure was received and accepted from James Gough (1010am) EXECUTIVE SUPPORT Dr Andrew Brant (Acting Chief Executive) Becky Hickmott (Acting Executive Director of Nursing) Ralph La Salle (Acting Executive Director Planning Funding amp Decision Support) Dr Jacqui Lunday-Johnstone (Executive Director Allied Health Scientific amp Technical) Kay Jenkins (Executive Assistant Governance Support) and Anna Craw (Board Secretariat)
APOLOGIES Kirsten Beynon (General Manager Laboratories) Dr Richard French (Acting Chief Medical Officer) Berni Marra (Manager Ashburton Health Services) and Win McDonald (Transition Programme Manager Rural Health Services) IN ATTENDANCE
Full Meeting
Pauline Clark General Manager MedicalSurgical Womenrsquos amp Childrenrsquos Health amp Orthopaedics Dr Helen Skinner General Manager amp Chief of Service Older Persons Health amp Rehabilitation Dr Greg Hamilton General Manager Specialist Mental Health Services 1 INTEREST REGISTER
AdditionsAlterations to the Interest Register Naomi Marshall ndash Addition ndash NZ Nurses College Aotearoa - Member There were no other additionsalterations Declarations of Interest for Items on Todayrsquos Agenda There were no declarations of interest for items on todayrsquos agenda Perceived Conflicts of Interest There were no perceived conflicts of interest
2 CONFIRMATION OF PREVIOUS MEETING MINUTES
Resolution (0121) (Moved Ingrid TaylorSeconded Jan Edwards ndash carried) ldquoThat the minutes of the Hospital Advisory Committee meeting held on 3 December 2020 be approved and adopted as a true and correct recordrdquo
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
10
HAC-28jan21ndashminutesndashdraft Page 2 of 6 01042021
3 CARRIED FORWARD ACTION ITEMS
The carried forward action items were noted
4 HampSS MONITORING REPORT
The Committee considered the Hospital and Specialist Services Monitoring Report for December 2020 The report was taken as read General Managers introduced their respective divisions and spoke to their areas as follows Specialist Mental Health Services (SMHS) ndash Dr Greg Hamilton General Manager
Report focuses on SMHS Intellectual Disability Services to provide a greater depth of understanding Services are provided to inpatients in two different units o PSAID Unit This falls under our population-based funding and is for those
people with an intellectual disability and a mental health diagnosis o Whaikaha (ATampR ndash Assessment Treatment and Rehabilitation) This is funded
by Ministry of Health Disability Support Services with whom we have two contracts and is for people who are under Court order under two different Acts It is a secure unit Generally this cohort of people have relatively poor health both physical and mental health Some people have been there for a long period with the longest standing consumer having been there since 2003 This is an institutional type approach for a group of people who are highly vulnerable
There are a lot of incidents some of which are assaults ndash injury to staff and assaults between consumers
Staff are amazing in their commitment to this cohort of people People who work here are values driven and come to work to make a difference for this vulnerable population which includes taking on some of that risk we are trying to mitigate
Considerable frustration for ATampR with Disability Support Services in terms of how they fund that and the ability to provide a really good service Dr Hamilton thanked the Board for its investment The four new pods on the new facility are hoped to be occupied by the end of March 2021 He noted that this will significantly change the living standards and lives of some of the more complex long-term consumers
Older Persons Health amp Rehabilitation (OPHampR) Service ndash Dr Helen Skinner General Manager amp Chief of Service
Pressure Injury Prevention Project update The validated figures for the last four months of the 2020 year show 48 patients with pressure injuries versus 73 for the year prior so a reduction of 25 in terms of pressure injuries Staff are now very enthusiastic at looking at skin and ensuring they are picking up every possible blemish There is still further work to be done to get down to the aim of 95 avoidable pressure injuries knowing that 5 are unavoidable in terms of international best practice
Vestibular Screening Tool Pilot There is evidence for using vestibular screening which involves a series of four questions when patients come in to assess whether they have a risk of vestibular problems and what to do about it This is a piece of work the Allied Health Team is leading on and is being rolled out across the Older Persons Health amp Rehabilitation Service and will be rolled out into the community as well ED is interested also There is good evidence in terms of the validation of the tool in ED and the Acute setting so is something that could be used across the DHB in terms or reducing the risk of falls and identifying what the risks are
ERAS Highlighted OPHampRrsquos 2020 results from the national hip fracture registry database
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
11
HAC-28jan21ndashminutesndashdraft Page 3 of 6 01042021
There was discussion around needs assessments for patients particularly at Burwood for Aged Residential Care (ARC) Dr Skinner advised that times are monitored and data is kept to ensure there are no delays In terms of initial assessments there has been no delay There has been some delay in terms of community re-assessments Timeframes for assessment take anywhere between one to two working days
Queried whether there was too much demand versus supply with regards to ARC Dr Skinner advised we are running high occupancy levels in terms of dementia hospital elder care This is the one area where we run high compared to the rest of the country in terms of the capacity we have
There was discussion around the number of over 75s coming from rest homes and being admitted through ED and what is or could be done to address this Dr Skinner spoke of Advance Care Planning and Shared Goals of Care as well as what can be done differently in the community Becky Hickmott Acting Executive Director of Nursing noted that Ashburton has its own unique challenges in this space part of which is the primary health sector understanding its role She advised of a lot of changes and turnover in staff in Ashburton and this impacting the flow through to ED There is a significant piece of work underway to address this but it is not quite at the implementation stage
MedicalSurgical amp Womenrsquos amp Childrenrsquos Health amp Orthopaedics ndash Pauline Clark General Manager
Increase in acute presentations to Christchurch Hospital It is not just ED experiencing this but also the Acute Medical Assessment Unit the ldquoBone Shoprdquo the Surgical Assessment Unit and the Childrenrsquos Acute Assessment o ED experienced a sharp uplift in presentations that occurred in late September
prior to the transition to Waipapa Between January and the end of September 2020 there were an average 1830 presentations to ED per week Since then this has risen to an average of 2163 per week ndash an increase of 48 per day or 18
o This cannot be explained by population pressures ndash the rate of ED attendances per 10000 population increases sharply at the same time
o Within this we have seen an increase in self-referrals to the ED of around 2 - or 250 presentations per week
o Conversely there has been a slight decrease in GP referrals People are presenting directly but their reasons for being there are in alignment with their health needs Overall people presenting need to be assessed in an ED environment in a tertiary centre
o 24 hour medical centres both Riccarton and Moorhouse are also experiencing increased presentations so not just the ED
Medical Oncology As previously advised additional project support has been invested in to assist with a revision to the model of care This is in place and work is starting to pay dividends Two new medical oncologists have been appointed and discussions continue around a third appointment
High neo-natal occupancy This is a phenomenon being seen around New Zealand possibly not helped by the MoH lead in the space Andrew Simpson having left his role So again work in the neo-natal cot space has stalled CDHBrsquos neo-natal service is designed to take 40 to 45 Currently it is sitting at 54 Another four are being cared for as part of the paediatric ward which is putting additional pressure on paediatrics who are already experiencing demand issues We also have some women and babies out in other parts of NZ Very tight nationally when it comes to neo-natal bedscots
Return of surgery and progress against plan The opening of Waipapa provided a significant increase in acute theater capacity on the Christchurch Campus Will be in a position to report on this in more detail at the Committeersquos next meeting
Have seen significant gains in terms of the pre-operative stay in inpatients
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
12
HAC-28jan21ndashminutesndashdraft Page 4 of 6 01042021
Planned on having outplaced surgery back by Christmas with the exception of paediatric dental (which is planned for March due to availability of workforce and appropriate facilities) Outplacing has ceased
The plan around returning outsourced surgery is currently being tweaked to accommodate some unexpected sickness which will result in key people being away for a period of time
Recruitment of Anesthetic Technicians is an issue Have two staff coming from the UK in the next quarter and the search continues
Been working very closely with Sterile Supply They are a keen enabler
ESPIs CDHB and MoH have agreed an ESPI improvement plan which sees the DHB achieve compliance in ESPI 2 and 5 by 30 June 2021 A wobble was experienced in late Decemberearly January but are now on track to achieve this Specific actions that services are undertaking to enable us to deliver include o Orthopaedics have taken 64 long waiting electiveplanned patients requiring hand
surgery from the Plastic Service waitlist and put it into their own waitlist They are able to do this without needing to use anesthesia and are utilising theatre space at Burwood for this
o Vascular Surgery have been able to utilise funding that the MoH provided for additional clinics Have repatriated ambulatory treatment of varicose veins to the Outpatient Department
o Ear Nose and Throat Parental leave has affected capacity in the rhinology subspecialty however the full team is now back on board
o General Surgery A number of SMO staff have recently returned from extended sick and annual leave and a new fellow has started this week
o Some services are already green and will remain there
Discussion took place around
Issues with neo-natal cot capacity from both a regional and national perspective
Clinical safety in light of increased acute presentations
Fee structure for afterhours care The HampSS Monitoring report was noted
5 CLINICAL ADVISOR UPDATE (ORAL)
Becky Hickmott Acting Executive Director of Nursing provided the following updates
Acknowledged NICUrsquos capacity issues noting there have been a large number of extreme preterm as well as preterm births with babies who have high need and long stay The long stay has an ongoing impact Many came spontaneously in labour or with membranes ruptured Across the nation similar things are happening
Maternity is under pressure from a staffing point of view From a safety angle we are working to divert some of our nursing teams to help support
Christchurch and Burwood Hospitals were very full over the Christmas period What would normally be a quieter period was not Staff have been under significant pressure but have done a stellar job
Recently visited the SMHS site at Hillmorton to see the built environment and the constraints impacting on patients and staff Acknowledged the challenges that staff are working under They are dealing with complex patients in very challenging conditions yet the professionalism in care was clearly evident with constant reassessing triaging and attention to safety Progress with new facilities cannot come quick enough for staff
Burwood has a key quality focus on medication administration at the moment This involves a cross disciplinary approach
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
13
HAC-28jan21ndashminutesndashdraft Page 5 of 6 01042021
Looking across the board at how to mobilise and utilise nursing resources A current focus is on outpatient services ndash how we use that workforce in a different way and also advancing working at top of scope
Trendcare implementation and CCDM is progressing well in spite of some hiccups within the system These have largely been rectified ICU goes live with Trendcare mid-February and Surgery will be underway soon as well CCDM teams have been described as ldquobull doggishrdquo in their approach which will continue to ensure accurate and reliable data
COVID readiness planning is well underway working closely with Allied Health to ensure we are taking a cross disciplinary approach
MIQ nursing staff and the welfare teams have been under significant pressure during the holiday period but have delivered a high standard of care and support They perform a vital role in keeping NZ safe Mindful that staff have times where they feel stigmatised in the community and their wider family are impacted on by the role that they hold
Commend primary health who keep mobilising to support Whole system approach is working well
In spite of the pressure on staff across the system we continue to receive numerous letters and emails on the care provided and the willingness of nurses to go the extra mile
6 SERVICES SUPPORTING OLDER PEOPLE LIVING IN RURAL COMMUNITIES
Ralph La Salle Acting Executive Director Planning Funding amp Decision Support introduced the report noting it was in response to a request from the Committee last year to better understand initiativesservices in place currently and those that are planned to support our rural older population to remain in their own homescommunities and into the future Greta Bond Service Development Manager Older Persons Health (OPH) and Andrea Davidson OPH Portfolio Manager were in attendance The report was taken as read Discussion took place around the following
Strengths of the rural community as well as challenges presented by distance
Ageing population ndash in terms of this community it is not only about the clients of the services but also the people who are delivering the services Rurally we have an ageing workforce and in addition particularly with nursing a workforce where this is not their only job
The increase in demand for dementia care Rurally this can be difficult to deliver so new models of care are being looked at
Resources being deployed to rural areas and ensuring they are being utilised in the best possible way Working with the community to make sure that services are developing to meet the current needs of people as opposed to the traditional way that services have always been delivered
Falls prevention referral programme and uptake in the rural community
The availability of consumables particularly in terms of those which are meant to be provided on discharge from hospital and the impact this has on providing nursing rurally
An electronic referral form is being implemented within secondary care so someone referring for services in the community will be able to do this electronically This will be a big benefit to providing rural services
The Services Supporting Older People Living in Rural Communities report was noted
7 2021 WORKPLAN
The Committee received the 2021 Workplan noting that this is a working document
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
14
HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-01apr21-BCL900DE46F Page 2 of 2 01042021
COMMITTEE ATTENDANCE SCHEDULE 2020
NAME
280121
010421
030621
050821
071021
021221
Andrew Dickerson (Chair) radic
Naomi Marshall (Deputy Chair) radic
Barry Bragg
Catherine Chu x
James Gough ^
Jo Kane radic
(Zoom)
Ingrid Taylor radic
Jan Edwards radic
Dr Rochelle Phipps
Michelle Turrall x
Sir John Hansen (ex-officio) radic
Gabrielle Huria (ex-officio) x
radic Attended
x Absent Absent with apology ^ Attended part of meeting ~ Leave of absence Appointed effective No longer on the Committee effective
HAC - 01 April 2021 - P - Attendance
4
HAC-01apr21-interest register Page 1 of 5 01042021
(As disclosed on appointment to the BoardCommittee and updated from time-to-time as necessary)
Andrew Dickerson Chair ndash HAC Board Member
Canterbury Health Care of the Elderly Education Trust - Chair Promotes and supports teaching and research in the care of older people Recipients of financial assistance for research education or training could include employees of the CDHB
Canterbury Medical Research Foundation - Member Provides financial assistance for medical research in Canterbury Recipients of financial assistance for research education or training could include employees of the CDHB
Heritage NZ - Member Heritage NZrsquos mission is to promote the identification protection preservation and conservation of the historical and cultural heritage of New Zealand It identifies records and acts in respect of significant ancestral sites and buildings CDHB owns buildings that may be considered to have historical significance and Heritage NZ has already been involved with CDHB buildings Maia Health Foundation - Trustee Is a charitable trust established to support health care in the CDHB area Current projects include fundraising for a rooftop helipad and enhancements to the childrenrsquos wards at Christchurch Hospital NZ Association of Gerontology - Member
Professional association that promotes the interests of older people and an understanding of ageing
Naomi Marshall Deputy Chair - HAC Board Member
College of Nurses Aotearoa NZ ndash Member Riccarton Clinic amp After Hours ndash Employee Employed as a Nurse Riccarton Clinic amp After Hours provides general practice and after-hours care It is part privately and PHO funded The PHO receives funding from the CDHB
Barry Bragg Board Member
Air Rescue Services Limited - Director Subsidiary of the Canterbury West Coast Air Rescue Trust Has gaming licenses with specified purpose of fundraising for air rescue services Canterbury West Coast Air Rescue Trust ndash Trustee The Trust has a services agreement with Garden City Helicopters for the provision of air rescue and air ambulance services Garden City Helicopters has a long-term air ambulance contract with the CDHB CMUA Project Delivery Limited - Director 100 owned by the Christchurch City Council and is responsible for the delivery of the Canterbury Multi-Use Arena project within agreed parameters Farrell Construction Limited - Shareholder Farrellrsquos Construction Limited is a commercial and light commercial construction company based in Christchurch
CONFLICTS OF INTEREST REGISTER HOSPITAL ADVISORY COMMITTEE (HAC)
HAC - 01 April 2021 - P - Conflict of Interest Register
5
HAC-01apr21-interest register Page 2 of 5 01042021
New Zealand Flying Doctor Service Trust ndash Trustee The Trust has a services agreement with Garden City Helicopters for the provision of air ambulance services Garden City Helicopters has a long-term air ambulance contract with the CDHB Ngai Tahu Farming ndash Chairman Farming interests in North Canterbury and Queenstown Lakes District and Forestry interests in Canterbury West Coast and Otago regions Paenga Kupenga Limited ndash Chair Commercial arm of Ngai Tuahuriri Runanga Quarry Capital Limited ndash Director Property syndication company based in Christchurch Stevenson Group Limited ndash Deputy Chairman Property interests in Auckland and mining interests on the West Coast Verum Group Limited ndash Director Verum Group Limited provides air quality testing and asbestos sampling and analysis services methamphetamine contamination testing dust gas and noise workplace monitoring services in New Zealand There is the potential for future work with the CDHB
Catherine Chu Board Member
Christchurch City Council ndash Councillor Local Territorial Authority Riccarton Rotary Club ndash Member The Canterbury Club ndash Member
Jan Edwards Age Concern Canterbury ndash Member Anglican Care ndash Volunteer Neurological Foundation of NZ - Member
James Gough Board Member
Amyes Road Limited ndash Shareholder Formally Gough GroupGough Holdings Limited Currently liquidating Christchurch City Council ndash Councillor Local Territorial Authority Includes appointment to FendaltonWaimairi Harewood Community Board Christchurch City Holdings Limited (CCHL) ndash Director Holds and manages the Councilrsquos commercial interest in subsidiary companies Civic Building Limited ndash Chairman Council Property Interests JV with Ngai Tahu Property Limited Gough Corporation Holdings Limited ndash DirectorShareholder Holdings company Gough Property Corporation Limited ndash DirectorShareholder Manages property interests
HAC - 01 April 2021 - P - Conflict of Interest Register
6
HAC-01apr21-interest register Page 3 of 5 01042021
Medical Kiwi Limited ndash Independent Director Research and distribution company of medicinal cannabis and other health related products In process of listing on NZX The Antony Gough Trust ndash Trustee Trust for Antony Thomas Gough The Russley Village Limited ndash Shareholder Retirement Village Via the Antony Gough Trust The Terrace Car Park Limited ndash (Alternate) Director Property company ndash manages The Terrace car park (under construction) The Terrace On Avon Limited ndash (Alternate) Director Property company ndash manages The Terrace
Jo Kane Board Member
Christchurch Resettlement Services - Member Christchurch Resettlement Services provides a range of services to people from refugee and migrant backgrounds It works alongside refugee communities in delivering services that aim to achieve positive resettlement outcomes HurriKane Consulting ndash Project Management PartnerConsultant A private consultancy in management communication and project management Any conflicts of interest that arise will be disclosedadvised Latimer Community Housing Trust ndash Project Manager Delivers social housing in Christchurch for the vulnerable and elderly in the community
NZ Royal Humane Society ndash Director Provides an awards system for acts of bravery in New Zealand It is not anticipated any conflicts of interest will arise
Dr Rochelle Phipps Accident Compensation Corporation ndash Medical Advisor ACC is a Crown entity responsible for administering NZrsquos universal no-fault accidental injury scheme As a Medical Advisor I analyse and interpret medical information and make recommendations to improve rehabilitation outcomes for ACC customers OraTaiao New Zealand Climate amp Health Council ndash Founding Executive Board Member (no longer on executive) The Council is a not-for-profit politically non-partisan incorporated society and comprises health professionals in AotearoaNew Zealand concerned with the negative impacts of climate change on health the health gains possible through strong health-centred climate action highlighting the impacts of climate change on those who already experience
disadvantage or ill health (equity impacts) and reducing the health sectors contribution to climate change Royal New Zealand College of General Practitioners ndash Christchurch Fellow and Former Board Member The RNZCGP is the professional body and postgraduate educational institute for general practitioners
HAC - 01 April 2021 - P - Conflict of Interest Register
7
HAC-01apr21-interest register Page 4 of 5 01042021
Ingrid Taylor Board Member
Loyal Canterbury Lodge (LCL) ndash Manchester Unity ndash Trustee LCL is a friendly society administering funds for the benefit of members and often makes charitable donations One of the recipients of such a donation may have an association with the CDHB Manchester Unity Welfare Homes Trust Board (MUWHTB) ndash Trustee MUWHTB is a charitable Trust providing financial assistance to organisations in Canterbury associated with the care and assistance of older persons Recipients of financial assistance may have an association with the CDHB Sir John and Ann Hansenrsquos Family Trust ndash Independent Trustee Taylor Shaw ndash Partner Taylor Shaw has clients that are employed by the CDHB or may have contracts for services with the CDHB that may mean a conflict or potential conflict may arise from time to time Such conflicts of interest will need to be addressed at the appropriate time
I Taylor Shaw have acted as solicitor for Bill Tate and family The Youth Hub ndash Trustee The Youth Hub is a charitable Trust established to provide residential and social services for the Youth of Canterbury including services for mental health and medical care that may include involvement with the CDHB
Michelle Turrall Manawhenua
Canterbury Clinical Network (CCN) Maori Caucus - Member Canterbury District Health Board - Daughter employed as registered nurse Christchurch PHO Ltd ndash Director Christchurch PHO Trust - Trustee
Manawhenua ki Waitaha ndash Board Member and Chair Oranga Tamariki ndash Iwi and Maori ndash Senior Advisor Papakainga Hauora Komiti ndash Te Ngai Tuahuriri ndash Co-Chair
Sir John Hansen Ex-Officio ndash HAC Chair CDHB
Bone Marrow Cancer Trust ndash Trustee Canterbury Cricket Trust - Member Christchurch Casino Charitable Trust - Trustee Court of Appeal Solomon Islands Samoa and Vanuatu Dot Kiwi ndash Director and Shareholder Judicial Control Authority (JCA) for Racing ndash Appeals Tribunal Member The JCA is an independent statutory authority constituted under the Racing Act The JCA ensures that judicial and appeal proceedings in thoroughbred and harness racing are heard and decided fairly professionally efficiently and in a consistent and cost effective manner Ministry Primary Industries Costs Review Independent Panel
HAC - 01 April 2021 - P - Conflict of Interest Register
8
HAC-01apr21-interest register Page 5 of 5 01042021
Rulings Panel Gas Industry Co Ltd Sir John and Ann Hansenrsquos Family Trust ndash Ingrid Taylor sits as independent Trustee and provides legal services to the Trust and to Sir John and Ann Hansen
Gabrielle Huria Ex-Officio ndash HAC Deputy Chair CDHB
Pegasus Health Limited ndash Sister is a Director Primary Health Organisation (PHO) Rawa Hohepa Limited ndash Director Family property company Sumner Health Centre ndash Daughter is a General Practitioner (GP) Doctorrsquos clinic Te Kura Taka Pini Limited ndash General Manager The Royal New Zealand College of GPs ndash Sister is an ldquoappointed independent Directorrdquo College of GPs Upoko Rawiri Te Maire Tau of Ngai Tuahuriri - Husband
HAC - 01 April 2021 - P - Conflict of Interest Register
9
HAC-28jan21ndashminutesndashdraft Page 1 of 6 01042021
MINUTES ndash PUBLIC
DRAFT MINUTES OF THE HOSPITAL ADVISORY COMMITTEE MEETING
held in the Board Room Level 1 32 Oxford Terrace Christchurch on Thursday 28 January 2021 commencing at 900am
PRESENT Andrew Dickerson (Chair) Jan Edwards James Gough Jo Kane (via Zoom) Naomi Marshall Ingrid Taylor and Sir John Hansen (Ex-Officio) APOLOGIES Apologies for absence were received and accepted from Barry Bragg and Dr Rochelle Phipps An apology for early departure was received and accepted from James Gough (1010am) EXECUTIVE SUPPORT Dr Andrew Brant (Acting Chief Executive) Becky Hickmott (Acting Executive Director of Nursing) Ralph La Salle (Acting Executive Director Planning Funding amp Decision Support) Dr Jacqui Lunday-Johnstone (Executive Director Allied Health Scientific amp Technical) Kay Jenkins (Executive Assistant Governance Support) and Anna Craw (Board Secretariat)
APOLOGIES Kirsten Beynon (General Manager Laboratories) Dr Richard French (Acting Chief Medical Officer) Berni Marra (Manager Ashburton Health Services) and Win McDonald (Transition Programme Manager Rural Health Services) IN ATTENDANCE
Full Meeting
Pauline Clark General Manager MedicalSurgical Womenrsquos amp Childrenrsquos Health amp Orthopaedics Dr Helen Skinner General Manager amp Chief of Service Older Persons Health amp Rehabilitation Dr Greg Hamilton General Manager Specialist Mental Health Services 1 INTEREST REGISTER
AdditionsAlterations to the Interest Register Naomi Marshall ndash Addition ndash NZ Nurses College Aotearoa - Member There were no other additionsalterations Declarations of Interest for Items on Todayrsquos Agenda There were no declarations of interest for items on todayrsquos agenda Perceived Conflicts of Interest There were no perceived conflicts of interest
2 CONFIRMATION OF PREVIOUS MEETING MINUTES
Resolution (0121) (Moved Ingrid TaylorSeconded Jan Edwards ndash carried) ldquoThat the minutes of the Hospital Advisory Committee meeting held on 3 December 2020 be approved and adopted as a true and correct recordrdquo
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
10
HAC-28jan21ndashminutesndashdraft Page 2 of 6 01042021
3 CARRIED FORWARD ACTION ITEMS
The carried forward action items were noted
4 HampSS MONITORING REPORT
The Committee considered the Hospital and Specialist Services Monitoring Report for December 2020 The report was taken as read General Managers introduced their respective divisions and spoke to their areas as follows Specialist Mental Health Services (SMHS) ndash Dr Greg Hamilton General Manager
Report focuses on SMHS Intellectual Disability Services to provide a greater depth of understanding Services are provided to inpatients in two different units o PSAID Unit This falls under our population-based funding and is for those
people with an intellectual disability and a mental health diagnosis o Whaikaha (ATampR ndash Assessment Treatment and Rehabilitation) This is funded
by Ministry of Health Disability Support Services with whom we have two contracts and is for people who are under Court order under two different Acts It is a secure unit Generally this cohort of people have relatively poor health both physical and mental health Some people have been there for a long period with the longest standing consumer having been there since 2003 This is an institutional type approach for a group of people who are highly vulnerable
There are a lot of incidents some of which are assaults ndash injury to staff and assaults between consumers
Staff are amazing in their commitment to this cohort of people People who work here are values driven and come to work to make a difference for this vulnerable population which includes taking on some of that risk we are trying to mitigate
Considerable frustration for ATampR with Disability Support Services in terms of how they fund that and the ability to provide a really good service Dr Hamilton thanked the Board for its investment The four new pods on the new facility are hoped to be occupied by the end of March 2021 He noted that this will significantly change the living standards and lives of some of the more complex long-term consumers
Older Persons Health amp Rehabilitation (OPHampR) Service ndash Dr Helen Skinner General Manager amp Chief of Service
Pressure Injury Prevention Project update The validated figures for the last four months of the 2020 year show 48 patients with pressure injuries versus 73 for the year prior so a reduction of 25 in terms of pressure injuries Staff are now very enthusiastic at looking at skin and ensuring they are picking up every possible blemish There is still further work to be done to get down to the aim of 95 avoidable pressure injuries knowing that 5 are unavoidable in terms of international best practice
Vestibular Screening Tool Pilot There is evidence for using vestibular screening which involves a series of four questions when patients come in to assess whether they have a risk of vestibular problems and what to do about it This is a piece of work the Allied Health Team is leading on and is being rolled out across the Older Persons Health amp Rehabilitation Service and will be rolled out into the community as well ED is interested also There is good evidence in terms of the validation of the tool in ED and the Acute setting so is something that could be used across the DHB in terms or reducing the risk of falls and identifying what the risks are
ERAS Highlighted OPHampRrsquos 2020 results from the national hip fracture registry database
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
11
HAC-28jan21ndashminutesndashdraft Page 3 of 6 01042021
There was discussion around needs assessments for patients particularly at Burwood for Aged Residential Care (ARC) Dr Skinner advised that times are monitored and data is kept to ensure there are no delays In terms of initial assessments there has been no delay There has been some delay in terms of community re-assessments Timeframes for assessment take anywhere between one to two working days
Queried whether there was too much demand versus supply with regards to ARC Dr Skinner advised we are running high occupancy levels in terms of dementia hospital elder care This is the one area where we run high compared to the rest of the country in terms of the capacity we have
There was discussion around the number of over 75s coming from rest homes and being admitted through ED and what is or could be done to address this Dr Skinner spoke of Advance Care Planning and Shared Goals of Care as well as what can be done differently in the community Becky Hickmott Acting Executive Director of Nursing noted that Ashburton has its own unique challenges in this space part of which is the primary health sector understanding its role She advised of a lot of changes and turnover in staff in Ashburton and this impacting the flow through to ED There is a significant piece of work underway to address this but it is not quite at the implementation stage
MedicalSurgical amp Womenrsquos amp Childrenrsquos Health amp Orthopaedics ndash Pauline Clark General Manager
Increase in acute presentations to Christchurch Hospital It is not just ED experiencing this but also the Acute Medical Assessment Unit the ldquoBone Shoprdquo the Surgical Assessment Unit and the Childrenrsquos Acute Assessment o ED experienced a sharp uplift in presentations that occurred in late September
prior to the transition to Waipapa Between January and the end of September 2020 there were an average 1830 presentations to ED per week Since then this has risen to an average of 2163 per week ndash an increase of 48 per day or 18
o This cannot be explained by population pressures ndash the rate of ED attendances per 10000 population increases sharply at the same time
o Within this we have seen an increase in self-referrals to the ED of around 2 - or 250 presentations per week
o Conversely there has been a slight decrease in GP referrals People are presenting directly but their reasons for being there are in alignment with their health needs Overall people presenting need to be assessed in an ED environment in a tertiary centre
o 24 hour medical centres both Riccarton and Moorhouse are also experiencing increased presentations so not just the ED
Medical Oncology As previously advised additional project support has been invested in to assist with a revision to the model of care This is in place and work is starting to pay dividends Two new medical oncologists have been appointed and discussions continue around a third appointment
High neo-natal occupancy This is a phenomenon being seen around New Zealand possibly not helped by the MoH lead in the space Andrew Simpson having left his role So again work in the neo-natal cot space has stalled CDHBrsquos neo-natal service is designed to take 40 to 45 Currently it is sitting at 54 Another four are being cared for as part of the paediatric ward which is putting additional pressure on paediatrics who are already experiencing demand issues We also have some women and babies out in other parts of NZ Very tight nationally when it comes to neo-natal bedscots
Return of surgery and progress against plan The opening of Waipapa provided a significant increase in acute theater capacity on the Christchurch Campus Will be in a position to report on this in more detail at the Committeersquos next meeting
Have seen significant gains in terms of the pre-operative stay in inpatients
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
12
HAC-28jan21ndashminutesndashdraft Page 4 of 6 01042021
Planned on having outplaced surgery back by Christmas with the exception of paediatric dental (which is planned for March due to availability of workforce and appropriate facilities) Outplacing has ceased
The plan around returning outsourced surgery is currently being tweaked to accommodate some unexpected sickness which will result in key people being away for a period of time
Recruitment of Anesthetic Technicians is an issue Have two staff coming from the UK in the next quarter and the search continues
Been working very closely with Sterile Supply They are a keen enabler
ESPIs CDHB and MoH have agreed an ESPI improvement plan which sees the DHB achieve compliance in ESPI 2 and 5 by 30 June 2021 A wobble was experienced in late Decemberearly January but are now on track to achieve this Specific actions that services are undertaking to enable us to deliver include o Orthopaedics have taken 64 long waiting electiveplanned patients requiring hand
surgery from the Plastic Service waitlist and put it into their own waitlist They are able to do this without needing to use anesthesia and are utilising theatre space at Burwood for this
o Vascular Surgery have been able to utilise funding that the MoH provided for additional clinics Have repatriated ambulatory treatment of varicose veins to the Outpatient Department
o Ear Nose and Throat Parental leave has affected capacity in the rhinology subspecialty however the full team is now back on board
o General Surgery A number of SMO staff have recently returned from extended sick and annual leave and a new fellow has started this week
o Some services are already green and will remain there
Discussion took place around
Issues with neo-natal cot capacity from both a regional and national perspective
Clinical safety in light of increased acute presentations
Fee structure for afterhours care The HampSS Monitoring report was noted
5 CLINICAL ADVISOR UPDATE (ORAL)
Becky Hickmott Acting Executive Director of Nursing provided the following updates
Acknowledged NICUrsquos capacity issues noting there have been a large number of extreme preterm as well as preterm births with babies who have high need and long stay The long stay has an ongoing impact Many came spontaneously in labour or with membranes ruptured Across the nation similar things are happening
Maternity is under pressure from a staffing point of view From a safety angle we are working to divert some of our nursing teams to help support
Christchurch and Burwood Hospitals were very full over the Christmas period What would normally be a quieter period was not Staff have been under significant pressure but have done a stellar job
Recently visited the SMHS site at Hillmorton to see the built environment and the constraints impacting on patients and staff Acknowledged the challenges that staff are working under They are dealing with complex patients in very challenging conditions yet the professionalism in care was clearly evident with constant reassessing triaging and attention to safety Progress with new facilities cannot come quick enough for staff
Burwood has a key quality focus on medication administration at the moment This involves a cross disciplinary approach
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
13
HAC-28jan21ndashminutesndashdraft Page 5 of 6 01042021
Looking across the board at how to mobilise and utilise nursing resources A current focus is on outpatient services ndash how we use that workforce in a different way and also advancing working at top of scope
Trendcare implementation and CCDM is progressing well in spite of some hiccups within the system These have largely been rectified ICU goes live with Trendcare mid-February and Surgery will be underway soon as well CCDM teams have been described as ldquobull doggishrdquo in their approach which will continue to ensure accurate and reliable data
COVID readiness planning is well underway working closely with Allied Health to ensure we are taking a cross disciplinary approach
MIQ nursing staff and the welfare teams have been under significant pressure during the holiday period but have delivered a high standard of care and support They perform a vital role in keeping NZ safe Mindful that staff have times where they feel stigmatised in the community and their wider family are impacted on by the role that they hold
Commend primary health who keep mobilising to support Whole system approach is working well
In spite of the pressure on staff across the system we continue to receive numerous letters and emails on the care provided and the willingness of nurses to go the extra mile
6 SERVICES SUPPORTING OLDER PEOPLE LIVING IN RURAL COMMUNITIES
Ralph La Salle Acting Executive Director Planning Funding amp Decision Support introduced the report noting it was in response to a request from the Committee last year to better understand initiativesservices in place currently and those that are planned to support our rural older population to remain in their own homescommunities and into the future Greta Bond Service Development Manager Older Persons Health (OPH) and Andrea Davidson OPH Portfolio Manager were in attendance The report was taken as read Discussion took place around the following
Strengths of the rural community as well as challenges presented by distance
Ageing population ndash in terms of this community it is not only about the clients of the services but also the people who are delivering the services Rurally we have an ageing workforce and in addition particularly with nursing a workforce where this is not their only job
The increase in demand for dementia care Rurally this can be difficult to deliver so new models of care are being looked at
Resources being deployed to rural areas and ensuring they are being utilised in the best possible way Working with the community to make sure that services are developing to meet the current needs of people as opposed to the traditional way that services have always been delivered
Falls prevention referral programme and uptake in the rural community
The availability of consumables particularly in terms of those which are meant to be provided on discharge from hospital and the impact this has on providing nursing rurally
An electronic referral form is being implemented within secondary care so someone referring for services in the community will be able to do this electronically This will be a big benefit to providing rural services
The Services Supporting Older People Living in Rural Communities report was noted
7 2021 WORKPLAN
The Committee received the 2021 Workplan noting that this is a working document
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
14
HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-01apr21-interest register Page 1 of 5 01042021
(As disclosed on appointment to the BoardCommittee and updated from time-to-time as necessary)
Andrew Dickerson Chair ndash HAC Board Member
Canterbury Health Care of the Elderly Education Trust - Chair Promotes and supports teaching and research in the care of older people Recipients of financial assistance for research education or training could include employees of the CDHB
Canterbury Medical Research Foundation - Member Provides financial assistance for medical research in Canterbury Recipients of financial assistance for research education or training could include employees of the CDHB
Heritage NZ - Member Heritage NZrsquos mission is to promote the identification protection preservation and conservation of the historical and cultural heritage of New Zealand It identifies records and acts in respect of significant ancestral sites and buildings CDHB owns buildings that may be considered to have historical significance and Heritage NZ has already been involved with CDHB buildings Maia Health Foundation - Trustee Is a charitable trust established to support health care in the CDHB area Current projects include fundraising for a rooftop helipad and enhancements to the childrenrsquos wards at Christchurch Hospital NZ Association of Gerontology - Member
Professional association that promotes the interests of older people and an understanding of ageing
Naomi Marshall Deputy Chair - HAC Board Member
College of Nurses Aotearoa NZ ndash Member Riccarton Clinic amp After Hours ndash Employee Employed as a Nurse Riccarton Clinic amp After Hours provides general practice and after-hours care It is part privately and PHO funded The PHO receives funding from the CDHB
Barry Bragg Board Member
Air Rescue Services Limited - Director Subsidiary of the Canterbury West Coast Air Rescue Trust Has gaming licenses with specified purpose of fundraising for air rescue services Canterbury West Coast Air Rescue Trust ndash Trustee The Trust has a services agreement with Garden City Helicopters for the provision of air rescue and air ambulance services Garden City Helicopters has a long-term air ambulance contract with the CDHB CMUA Project Delivery Limited - Director 100 owned by the Christchurch City Council and is responsible for the delivery of the Canterbury Multi-Use Arena project within agreed parameters Farrell Construction Limited - Shareholder Farrellrsquos Construction Limited is a commercial and light commercial construction company based in Christchurch
CONFLICTS OF INTEREST REGISTER HOSPITAL ADVISORY COMMITTEE (HAC)
HAC - 01 April 2021 - P - Conflict of Interest Register
5
HAC-01apr21-interest register Page 2 of 5 01042021
New Zealand Flying Doctor Service Trust ndash Trustee The Trust has a services agreement with Garden City Helicopters for the provision of air ambulance services Garden City Helicopters has a long-term air ambulance contract with the CDHB Ngai Tahu Farming ndash Chairman Farming interests in North Canterbury and Queenstown Lakes District and Forestry interests in Canterbury West Coast and Otago regions Paenga Kupenga Limited ndash Chair Commercial arm of Ngai Tuahuriri Runanga Quarry Capital Limited ndash Director Property syndication company based in Christchurch Stevenson Group Limited ndash Deputy Chairman Property interests in Auckland and mining interests on the West Coast Verum Group Limited ndash Director Verum Group Limited provides air quality testing and asbestos sampling and analysis services methamphetamine contamination testing dust gas and noise workplace monitoring services in New Zealand There is the potential for future work with the CDHB
Catherine Chu Board Member
Christchurch City Council ndash Councillor Local Territorial Authority Riccarton Rotary Club ndash Member The Canterbury Club ndash Member
Jan Edwards Age Concern Canterbury ndash Member Anglican Care ndash Volunteer Neurological Foundation of NZ - Member
James Gough Board Member
Amyes Road Limited ndash Shareholder Formally Gough GroupGough Holdings Limited Currently liquidating Christchurch City Council ndash Councillor Local Territorial Authority Includes appointment to FendaltonWaimairi Harewood Community Board Christchurch City Holdings Limited (CCHL) ndash Director Holds and manages the Councilrsquos commercial interest in subsidiary companies Civic Building Limited ndash Chairman Council Property Interests JV with Ngai Tahu Property Limited Gough Corporation Holdings Limited ndash DirectorShareholder Holdings company Gough Property Corporation Limited ndash DirectorShareholder Manages property interests
HAC - 01 April 2021 - P - Conflict of Interest Register
6
HAC-01apr21-interest register Page 3 of 5 01042021
Medical Kiwi Limited ndash Independent Director Research and distribution company of medicinal cannabis and other health related products In process of listing on NZX The Antony Gough Trust ndash Trustee Trust for Antony Thomas Gough The Russley Village Limited ndash Shareholder Retirement Village Via the Antony Gough Trust The Terrace Car Park Limited ndash (Alternate) Director Property company ndash manages The Terrace car park (under construction) The Terrace On Avon Limited ndash (Alternate) Director Property company ndash manages The Terrace
Jo Kane Board Member
Christchurch Resettlement Services - Member Christchurch Resettlement Services provides a range of services to people from refugee and migrant backgrounds It works alongside refugee communities in delivering services that aim to achieve positive resettlement outcomes HurriKane Consulting ndash Project Management PartnerConsultant A private consultancy in management communication and project management Any conflicts of interest that arise will be disclosedadvised Latimer Community Housing Trust ndash Project Manager Delivers social housing in Christchurch for the vulnerable and elderly in the community
NZ Royal Humane Society ndash Director Provides an awards system for acts of bravery in New Zealand It is not anticipated any conflicts of interest will arise
Dr Rochelle Phipps Accident Compensation Corporation ndash Medical Advisor ACC is a Crown entity responsible for administering NZrsquos universal no-fault accidental injury scheme As a Medical Advisor I analyse and interpret medical information and make recommendations to improve rehabilitation outcomes for ACC customers OraTaiao New Zealand Climate amp Health Council ndash Founding Executive Board Member (no longer on executive) The Council is a not-for-profit politically non-partisan incorporated society and comprises health professionals in AotearoaNew Zealand concerned with the negative impacts of climate change on health the health gains possible through strong health-centred climate action highlighting the impacts of climate change on those who already experience
disadvantage or ill health (equity impacts) and reducing the health sectors contribution to climate change Royal New Zealand College of General Practitioners ndash Christchurch Fellow and Former Board Member The RNZCGP is the professional body and postgraduate educational institute for general practitioners
HAC - 01 April 2021 - P - Conflict of Interest Register
7
HAC-01apr21-interest register Page 4 of 5 01042021
Ingrid Taylor Board Member
Loyal Canterbury Lodge (LCL) ndash Manchester Unity ndash Trustee LCL is a friendly society administering funds for the benefit of members and often makes charitable donations One of the recipients of such a donation may have an association with the CDHB Manchester Unity Welfare Homes Trust Board (MUWHTB) ndash Trustee MUWHTB is a charitable Trust providing financial assistance to organisations in Canterbury associated with the care and assistance of older persons Recipients of financial assistance may have an association with the CDHB Sir John and Ann Hansenrsquos Family Trust ndash Independent Trustee Taylor Shaw ndash Partner Taylor Shaw has clients that are employed by the CDHB or may have contracts for services with the CDHB that may mean a conflict or potential conflict may arise from time to time Such conflicts of interest will need to be addressed at the appropriate time
I Taylor Shaw have acted as solicitor for Bill Tate and family The Youth Hub ndash Trustee The Youth Hub is a charitable Trust established to provide residential and social services for the Youth of Canterbury including services for mental health and medical care that may include involvement with the CDHB
Michelle Turrall Manawhenua
Canterbury Clinical Network (CCN) Maori Caucus - Member Canterbury District Health Board - Daughter employed as registered nurse Christchurch PHO Ltd ndash Director Christchurch PHO Trust - Trustee
Manawhenua ki Waitaha ndash Board Member and Chair Oranga Tamariki ndash Iwi and Maori ndash Senior Advisor Papakainga Hauora Komiti ndash Te Ngai Tuahuriri ndash Co-Chair
Sir John Hansen Ex-Officio ndash HAC Chair CDHB
Bone Marrow Cancer Trust ndash Trustee Canterbury Cricket Trust - Member Christchurch Casino Charitable Trust - Trustee Court of Appeal Solomon Islands Samoa and Vanuatu Dot Kiwi ndash Director and Shareholder Judicial Control Authority (JCA) for Racing ndash Appeals Tribunal Member The JCA is an independent statutory authority constituted under the Racing Act The JCA ensures that judicial and appeal proceedings in thoroughbred and harness racing are heard and decided fairly professionally efficiently and in a consistent and cost effective manner Ministry Primary Industries Costs Review Independent Panel
HAC - 01 April 2021 - P - Conflict of Interest Register
8
HAC-01apr21-interest register Page 5 of 5 01042021
Rulings Panel Gas Industry Co Ltd Sir John and Ann Hansenrsquos Family Trust ndash Ingrid Taylor sits as independent Trustee and provides legal services to the Trust and to Sir John and Ann Hansen
Gabrielle Huria Ex-Officio ndash HAC Deputy Chair CDHB
Pegasus Health Limited ndash Sister is a Director Primary Health Organisation (PHO) Rawa Hohepa Limited ndash Director Family property company Sumner Health Centre ndash Daughter is a General Practitioner (GP) Doctorrsquos clinic Te Kura Taka Pini Limited ndash General Manager The Royal New Zealand College of GPs ndash Sister is an ldquoappointed independent Directorrdquo College of GPs Upoko Rawiri Te Maire Tau of Ngai Tuahuriri - Husband
HAC - 01 April 2021 - P - Conflict of Interest Register
9
HAC-28jan21ndashminutesndashdraft Page 1 of 6 01042021
MINUTES ndash PUBLIC
DRAFT MINUTES OF THE HOSPITAL ADVISORY COMMITTEE MEETING
held in the Board Room Level 1 32 Oxford Terrace Christchurch on Thursday 28 January 2021 commencing at 900am
PRESENT Andrew Dickerson (Chair) Jan Edwards James Gough Jo Kane (via Zoom) Naomi Marshall Ingrid Taylor and Sir John Hansen (Ex-Officio) APOLOGIES Apologies for absence were received and accepted from Barry Bragg and Dr Rochelle Phipps An apology for early departure was received and accepted from James Gough (1010am) EXECUTIVE SUPPORT Dr Andrew Brant (Acting Chief Executive) Becky Hickmott (Acting Executive Director of Nursing) Ralph La Salle (Acting Executive Director Planning Funding amp Decision Support) Dr Jacqui Lunday-Johnstone (Executive Director Allied Health Scientific amp Technical) Kay Jenkins (Executive Assistant Governance Support) and Anna Craw (Board Secretariat)
APOLOGIES Kirsten Beynon (General Manager Laboratories) Dr Richard French (Acting Chief Medical Officer) Berni Marra (Manager Ashburton Health Services) and Win McDonald (Transition Programme Manager Rural Health Services) IN ATTENDANCE
Full Meeting
Pauline Clark General Manager MedicalSurgical Womenrsquos amp Childrenrsquos Health amp Orthopaedics Dr Helen Skinner General Manager amp Chief of Service Older Persons Health amp Rehabilitation Dr Greg Hamilton General Manager Specialist Mental Health Services 1 INTEREST REGISTER
AdditionsAlterations to the Interest Register Naomi Marshall ndash Addition ndash NZ Nurses College Aotearoa - Member There were no other additionsalterations Declarations of Interest for Items on Todayrsquos Agenda There were no declarations of interest for items on todayrsquos agenda Perceived Conflicts of Interest There were no perceived conflicts of interest
2 CONFIRMATION OF PREVIOUS MEETING MINUTES
Resolution (0121) (Moved Ingrid TaylorSeconded Jan Edwards ndash carried) ldquoThat the minutes of the Hospital Advisory Committee meeting held on 3 December 2020 be approved and adopted as a true and correct recordrdquo
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
10
HAC-28jan21ndashminutesndashdraft Page 2 of 6 01042021
3 CARRIED FORWARD ACTION ITEMS
The carried forward action items were noted
4 HampSS MONITORING REPORT
The Committee considered the Hospital and Specialist Services Monitoring Report for December 2020 The report was taken as read General Managers introduced their respective divisions and spoke to their areas as follows Specialist Mental Health Services (SMHS) ndash Dr Greg Hamilton General Manager
Report focuses on SMHS Intellectual Disability Services to provide a greater depth of understanding Services are provided to inpatients in two different units o PSAID Unit This falls under our population-based funding and is for those
people with an intellectual disability and a mental health diagnosis o Whaikaha (ATampR ndash Assessment Treatment and Rehabilitation) This is funded
by Ministry of Health Disability Support Services with whom we have two contracts and is for people who are under Court order under two different Acts It is a secure unit Generally this cohort of people have relatively poor health both physical and mental health Some people have been there for a long period with the longest standing consumer having been there since 2003 This is an institutional type approach for a group of people who are highly vulnerable
There are a lot of incidents some of which are assaults ndash injury to staff and assaults between consumers
Staff are amazing in their commitment to this cohort of people People who work here are values driven and come to work to make a difference for this vulnerable population which includes taking on some of that risk we are trying to mitigate
Considerable frustration for ATampR with Disability Support Services in terms of how they fund that and the ability to provide a really good service Dr Hamilton thanked the Board for its investment The four new pods on the new facility are hoped to be occupied by the end of March 2021 He noted that this will significantly change the living standards and lives of some of the more complex long-term consumers
Older Persons Health amp Rehabilitation (OPHampR) Service ndash Dr Helen Skinner General Manager amp Chief of Service
Pressure Injury Prevention Project update The validated figures for the last four months of the 2020 year show 48 patients with pressure injuries versus 73 for the year prior so a reduction of 25 in terms of pressure injuries Staff are now very enthusiastic at looking at skin and ensuring they are picking up every possible blemish There is still further work to be done to get down to the aim of 95 avoidable pressure injuries knowing that 5 are unavoidable in terms of international best practice
Vestibular Screening Tool Pilot There is evidence for using vestibular screening which involves a series of four questions when patients come in to assess whether they have a risk of vestibular problems and what to do about it This is a piece of work the Allied Health Team is leading on and is being rolled out across the Older Persons Health amp Rehabilitation Service and will be rolled out into the community as well ED is interested also There is good evidence in terms of the validation of the tool in ED and the Acute setting so is something that could be used across the DHB in terms or reducing the risk of falls and identifying what the risks are
ERAS Highlighted OPHampRrsquos 2020 results from the national hip fracture registry database
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
11
HAC-28jan21ndashminutesndashdraft Page 3 of 6 01042021
There was discussion around needs assessments for patients particularly at Burwood for Aged Residential Care (ARC) Dr Skinner advised that times are monitored and data is kept to ensure there are no delays In terms of initial assessments there has been no delay There has been some delay in terms of community re-assessments Timeframes for assessment take anywhere between one to two working days
Queried whether there was too much demand versus supply with regards to ARC Dr Skinner advised we are running high occupancy levels in terms of dementia hospital elder care This is the one area where we run high compared to the rest of the country in terms of the capacity we have
There was discussion around the number of over 75s coming from rest homes and being admitted through ED and what is or could be done to address this Dr Skinner spoke of Advance Care Planning and Shared Goals of Care as well as what can be done differently in the community Becky Hickmott Acting Executive Director of Nursing noted that Ashburton has its own unique challenges in this space part of which is the primary health sector understanding its role She advised of a lot of changes and turnover in staff in Ashburton and this impacting the flow through to ED There is a significant piece of work underway to address this but it is not quite at the implementation stage
MedicalSurgical amp Womenrsquos amp Childrenrsquos Health amp Orthopaedics ndash Pauline Clark General Manager
Increase in acute presentations to Christchurch Hospital It is not just ED experiencing this but also the Acute Medical Assessment Unit the ldquoBone Shoprdquo the Surgical Assessment Unit and the Childrenrsquos Acute Assessment o ED experienced a sharp uplift in presentations that occurred in late September
prior to the transition to Waipapa Between January and the end of September 2020 there were an average 1830 presentations to ED per week Since then this has risen to an average of 2163 per week ndash an increase of 48 per day or 18
o This cannot be explained by population pressures ndash the rate of ED attendances per 10000 population increases sharply at the same time
o Within this we have seen an increase in self-referrals to the ED of around 2 - or 250 presentations per week
o Conversely there has been a slight decrease in GP referrals People are presenting directly but their reasons for being there are in alignment with their health needs Overall people presenting need to be assessed in an ED environment in a tertiary centre
o 24 hour medical centres both Riccarton and Moorhouse are also experiencing increased presentations so not just the ED
Medical Oncology As previously advised additional project support has been invested in to assist with a revision to the model of care This is in place and work is starting to pay dividends Two new medical oncologists have been appointed and discussions continue around a third appointment
High neo-natal occupancy This is a phenomenon being seen around New Zealand possibly not helped by the MoH lead in the space Andrew Simpson having left his role So again work in the neo-natal cot space has stalled CDHBrsquos neo-natal service is designed to take 40 to 45 Currently it is sitting at 54 Another four are being cared for as part of the paediatric ward which is putting additional pressure on paediatrics who are already experiencing demand issues We also have some women and babies out in other parts of NZ Very tight nationally when it comes to neo-natal bedscots
Return of surgery and progress against plan The opening of Waipapa provided a significant increase in acute theater capacity on the Christchurch Campus Will be in a position to report on this in more detail at the Committeersquos next meeting
Have seen significant gains in terms of the pre-operative stay in inpatients
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
12
HAC-28jan21ndashminutesndashdraft Page 4 of 6 01042021
Planned on having outplaced surgery back by Christmas with the exception of paediatric dental (which is planned for March due to availability of workforce and appropriate facilities) Outplacing has ceased
The plan around returning outsourced surgery is currently being tweaked to accommodate some unexpected sickness which will result in key people being away for a period of time
Recruitment of Anesthetic Technicians is an issue Have two staff coming from the UK in the next quarter and the search continues
Been working very closely with Sterile Supply They are a keen enabler
ESPIs CDHB and MoH have agreed an ESPI improvement plan which sees the DHB achieve compliance in ESPI 2 and 5 by 30 June 2021 A wobble was experienced in late Decemberearly January but are now on track to achieve this Specific actions that services are undertaking to enable us to deliver include o Orthopaedics have taken 64 long waiting electiveplanned patients requiring hand
surgery from the Plastic Service waitlist and put it into their own waitlist They are able to do this without needing to use anesthesia and are utilising theatre space at Burwood for this
o Vascular Surgery have been able to utilise funding that the MoH provided for additional clinics Have repatriated ambulatory treatment of varicose veins to the Outpatient Department
o Ear Nose and Throat Parental leave has affected capacity in the rhinology subspecialty however the full team is now back on board
o General Surgery A number of SMO staff have recently returned from extended sick and annual leave and a new fellow has started this week
o Some services are already green and will remain there
Discussion took place around
Issues with neo-natal cot capacity from both a regional and national perspective
Clinical safety in light of increased acute presentations
Fee structure for afterhours care The HampSS Monitoring report was noted
5 CLINICAL ADVISOR UPDATE (ORAL)
Becky Hickmott Acting Executive Director of Nursing provided the following updates
Acknowledged NICUrsquos capacity issues noting there have been a large number of extreme preterm as well as preterm births with babies who have high need and long stay The long stay has an ongoing impact Many came spontaneously in labour or with membranes ruptured Across the nation similar things are happening
Maternity is under pressure from a staffing point of view From a safety angle we are working to divert some of our nursing teams to help support
Christchurch and Burwood Hospitals were very full over the Christmas period What would normally be a quieter period was not Staff have been under significant pressure but have done a stellar job
Recently visited the SMHS site at Hillmorton to see the built environment and the constraints impacting on patients and staff Acknowledged the challenges that staff are working under They are dealing with complex patients in very challenging conditions yet the professionalism in care was clearly evident with constant reassessing triaging and attention to safety Progress with new facilities cannot come quick enough for staff
Burwood has a key quality focus on medication administration at the moment This involves a cross disciplinary approach
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
13
HAC-28jan21ndashminutesndashdraft Page 5 of 6 01042021
Looking across the board at how to mobilise and utilise nursing resources A current focus is on outpatient services ndash how we use that workforce in a different way and also advancing working at top of scope
Trendcare implementation and CCDM is progressing well in spite of some hiccups within the system These have largely been rectified ICU goes live with Trendcare mid-February and Surgery will be underway soon as well CCDM teams have been described as ldquobull doggishrdquo in their approach which will continue to ensure accurate and reliable data
COVID readiness planning is well underway working closely with Allied Health to ensure we are taking a cross disciplinary approach
MIQ nursing staff and the welfare teams have been under significant pressure during the holiday period but have delivered a high standard of care and support They perform a vital role in keeping NZ safe Mindful that staff have times where they feel stigmatised in the community and their wider family are impacted on by the role that they hold
Commend primary health who keep mobilising to support Whole system approach is working well
In spite of the pressure on staff across the system we continue to receive numerous letters and emails on the care provided and the willingness of nurses to go the extra mile
6 SERVICES SUPPORTING OLDER PEOPLE LIVING IN RURAL COMMUNITIES
Ralph La Salle Acting Executive Director Planning Funding amp Decision Support introduced the report noting it was in response to a request from the Committee last year to better understand initiativesservices in place currently and those that are planned to support our rural older population to remain in their own homescommunities and into the future Greta Bond Service Development Manager Older Persons Health (OPH) and Andrea Davidson OPH Portfolio Manager were in attendance The report was taken as read Discussion took place around the following
Strengths of the rural community as well as challenges presented by distance
Ageing population ndash in terms of this community it is not only about the clients of the services but also the people who are delivering the services Rurally we have an ageing workforce and in addition particularly with nursing a workforce where this is not their only job
The increase in demand for dementia care Rurally this can be difficult to deliver so new models of care are being looked at
Resources being deployed to rural areas and ensuring they are being utilised in the best possible way Working with the community to make sure that services are developing to meet the current needs of people as opposed to the traditional way that services have always been delivered
Falls prevention referral programme and uptake in the rural community
The availability of consumables particularly in terms of those which are meant to be provided on discharge from hospital and the impact this has on providing nursing rurally
An electronic referral form is being implemented within secondary care so someone referring for services in the community will be able to do this electronically This will be a big benefit to providing rural services
The Services Supporting Older People Living in Rural Communities report was noted
7 2021 WORKPLAN
The Committee received the 2021 Workplan noting that this is a working document
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
14
HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-01apr21-interest register Page 2 of 5 01042021
New Zealand Flying Doctor Service Trust ndash Trustee The Trust has a services agreement with Garden City Helicopters for the provision of air ambulance services Garden City Helicopters has a long-term air ambulance contract with the CDHB Ngai Tahu Farming ndash Chairman Farming interests in North Canterbury and Queenstown Lakes District and Forestry interests in Canterbury West Coast and Otago regions Paenga Kupenga Limited ndash Chair Commercial arm of Ngai Tuahuriri Runanga Quarry Capital Limited ndash Director Property syndication company based in Christchurch Stevenson Group Limited ndash Deputy Chairman Property interests in Auckland and mining interests on the West Coast Verum Group Limited ndash Director Verum Group Limited provides air quality testing and asbestos sampling and analysis services methamphetamine contamination testing dust gas and noise workplace monitoring services in New Zealand There is the potential for future work with the CDHB
Catherine Chu Board Member
Christchurch City Council ndash Councillor Local Territorial Authority Riccarton Rotary Club ndash Member The Canterbury Club ndash Member
Jan Edwards Age Concern Canterbury ndash Member Anglican Care ndash Volunteer Neurological Foundation of NZ - Member
James Gough Board Member
Amyes Road Limited ndash Shareholder Formally Gough GroupGough Holdings Limited Currently liquidating Christchurch City Council ndash Councillor Local Territorial Authority Includes appointment to FendaltonWaimairi Harewood Community Board Christchurch City Holdings Limited (CCHL) ndash Director Holds and manages the Councilrsquos commercial interest in subsidiary companies Civic Building Limited ndash Chairman Council Property Interests JV with Ngai Tahu Property Limited Gough Corporation Holdings Limited ndash DirectorShareholder Holdings company Gough Property Corporation Limited ndash DirectorShareholder Manages property interests
HAC - 01 April 2021 - P - Conflict of Interest Register
6
HAC-01apr21-interest register Page 3 of 5 01042021
Medical Kiwi Limited ndash Independent Director Research and distribution company of medicinal cannabis and other health related products In process of listing on NZX The Antony Gough Trust ndash Trustee Trust for Antony Thomas Gough The Russley Village Limited ndash Shareholder Retirement Village Via the Antony Gough Trust The Terrace Car Park Limited ndash (Alternate) Director Property company ndash manages The Terrace car park (under construction) The Terrace On Avon Limited ndash (Alternate) Director Property company ndash manages The Terrace
Jo Kane Board Member
Christchurch Resettlement Services - Member Christchurch Resettlement Services provides a range of services to people from refugee and migrant backgrounds It works alongside refugee communities in delivering services that aim to achieve positive resettlement outcomes HurriKane Consulting ndash Project Management PartnerConsultant A private consultancy in management communication and project management Any conflicts of interest that arise will be disclosedadvised Latimer Community Housing Trust ndash Project Manager Delivers social housing in Christchurch for the vulnerable and elderly in the community
NZ Royal Humane Society ndash Director Provides an awards system for acts of bravery in New Zealand It is not anticipated any conflicts of interest will arise
Dr Rochelle Phipps Accident Compensation Corporation ndash Medical Advisor ACC is a Crown entity responsible for administering NZrsquos universal no-fault accidental injury scheme As a Medical Advisor I analyse and interpret medical information and make recommendations to improve rehabilitation outcomes for ACC customers OraTaiao New Zealand Climate amp Health Council ndash Founding Executive Board Member (no longer on executive) The Council is a not-for-profit politically non-partisan incorporated society and comprises health professionals in AotearoaNew Zealand concerned with the negative impacts of climate change on health the health gains possible through strong health-centred climate action highlighting the impacts of climate change on those who already experience
disadvantage or ill health (equity impacts) and reducing the health sectors contribution to climate change Royal New Zealand College of General Practitioners ndash Christchurch Fellow and Former Board Member The RNZCGP is the professional body and postgraduate educational institute for general practitioners
HAC - 01 April 2021 - P - Conflict of Interest Register
7
HAC-01apr21-interest register Page 4 of 5 01042021
Ingrid Taylor Board Member
Loyal Canterbury Lodge (LCL) ndash Manchester Unity ndash Trustee LCL is a friendly society administering funds for the benefit of members and often makes charitable donations One of the recipients of such a donation may have an association with the CDHB Manchester Unity Welfare Homes Trust Board (MUWHTB) ndash Trustee MUWHTB is a charitable Trust providing financial assistance to organisations in Canterbury associated with the care and assistance of older persons Recipients of financial assistance may have an association with the CDHB Sir John and Ann Hansenrsquos Family Trust ndash Independent Trustee Taylor Shaw ndash Partner Taylor Shaw has clients that are employed by the CDHB or may have contracts for services with the CDHB that may mean a conflict or potential conflict may arise from time to time Such conflicts of interest will need to be addressed at the appropriate time
I Taylor Shaw have acted as solicitor for Bill Tate and family The Youth Hub ndash Trustee The Youth Hub is a charitable Trust established to provide residential and social services for the Youth of Canterbury including services for mental health and medical care that may include involvement with the CDHB
Michelle Turrall Manawhenua
Canterbury Clinical Network (CCN) Maori Caucus - Member Canterbury District Health Board - Daughter employed as registered nurse Christchurch PHO Ltd ndash Director Christchurch PHO Trust - Trustee
Manawhenua ki Waitaha ndash Board Member and Chair Oranga Tamariki ndash Iwi and Maori ndash Senior Advisor Papakainga Hauora Komiti ndash Te Ngai Tuahuriri ndash Co-Chair
Sir John Hansen Ex-Officio ndash HAC Chair CDHB
Bone Marrow Cancer Trust ndash Trustee Canterbury Cricket Trust - Member Christchurch Casino Charitable Trust - Trustee Court of Appeal Solomon Islands Samoa and Vanuatu Dot Kiwi ndash Director and Shareholder Judicial Control Authority (JCA) for Racing ndash Appeals Tribunal Member The JCA is an independent statutory authority constituted under the Racing Act The JCA ensures that judicial and appeal proceedings in thoroughbred and harness racing are heard and decided fairly professionally efficiently and in a consistent and cost effective manner Ministry Primary Industries Costs Review Independent Panel
HAC - 01 April 2021 - P - Conflict of Interest Register
8
HAC-01apr21-interest register Page 5 of 5 01042021
Rulings Panel Gas Industry Co Ltd Sir John and Ann Hansenrsquos Family Trust ndash Ingrid Taylor sits as independent Trustee and provides legal services to the Trust and to Sir John and Ann Hansen
Gabrielle Huria Ex-Officio ndash HAC Deputy Chair CDHB
Pegasus Health Limited ndash Sister is a Director Primary Health Organisation (PHO) Rawa Hohepa Limited ndash Director Family property company Sumner Health Centre ndash Daughter is a General Practitioner (GP) Doctorrsquos clinic Te Kura Taka Pini Limited ndash General Manager The Royal New Zealand College of GPs ndash Sister is an ldquoappointed independent Directorrdquo College of GPs Upoko Rawiri Te Maire Tau of Ngai Tuahuriri - Husband
HAC - 01 April 2021 - P - Conflict of Interest Register
9
HAC-28jan21ndashminutesndashdraft Page 1 of 6 01042021
MINUTES ndash PUBLIC
DRAFT MINUTES OF THE HOSPITAL ADVISORY COMMITTEE MEETING
held in the Board Room Level 1 32 Oxford Terrace Christchurch on Thursday 28 January 2021 commencing at 900am
PRESENT Andrew Dickerson (Chair) Jan Edwards James Gough Jo Kane (via Zoom) Naomi Marshall Ingrid Taylor and Sir John Hansen (Ex-Officio) APOLOGIES Apologies for absence were received and accepted from Barry Bragg and Dr Rochelle Phipps An apology for early departure was received and accepted from James Gough (1010am) EXECUTIVE SUPPORT Dr Andrew Brant (Acting Chief Executive) Becky Hickmott (Acting Executive Director of Nursing) Ralph La Salle (Acting Executive Director Planning Funding amp Decision Support) Dr Jacqui Lunday-Johnstone (Executive Director Allied Health Scientific amp Technical) Kay Jenkins (Executive Assistant Governance Support) and Anna Craw (Board Secretariat)
APOLOGIES Kirsten Beynon (General Manager Laboratories) Dr Richard French (Acting Chief Medical Officer) Berni Marra (Manager Ashburton Health Services) and Win McDonald (Transition Programme Manager Rural Health Services) IN ATTENDANCE
Full Meeting
Pauline Clark General Manager MedicalSurgical Womenrsquos amp Childrenrsquos Health amp Orthopaedics Dr Helen Skinner General Manager amp Chief of Service Older Persons Health amp Rehabilitation Dr Greg Hamilton General Manager Specialist Mental Health Services 1 INTEREST REGISTER
AdditionsAlterations to the Interest Register Naomi Marshall ndash Addition ndash NZ Nurses College Aotearoa - Member There were no other additionsalterations Declarations of Interest for Items on Todayrsquos Agenda There were no declarations of interest for items on todayrsquos agenda Perceived Conflicts of Interest There were no perceived conflicts of interest
2 CONFIRMATION OF PREVIOUS MEETING MINUTES
Resolution (0121) (Moved Ingrid TaylorSeconded Jan Edwards ndash carried) ldquoThat the minutes of the Hospital Advisory Committee meeting held on 3 December 2020 be approved and adopted as a true and correct recordrdquo
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
10
HAC-28jan21ndashminutesndashdraft Page 2 of 6 01042021
3 CARRIED FORWARD ACTION ITEMS
The carried forward action items were noted
4 HampSS MONITORING REPORT
The Committee considered the Hospital and Specialist Services Monitoring Report for December 2020 The report was taken as read General Managers introduced their respective divisions and spoke to their areas as follows Specialist Mental Health Services (SMHS) ndash Dr Greg Hamilton General Manager
Report focuses on SMHS Intellectual Disability Services to provide a greater depth of understanding Services are provided to inpatients in two different units o PSAID Unit This falls under our population-based funding and is for those
people with an intellectual disability and a mental health diagnosis o Whaikaha (ATampR ndash Assessment Treatment and Rehabilitation) This is funded
by Ministry of Health Disability Support Services with whom we have two contracts and is for people who are under Court order under two different Acts It is a secure unit Generally this cohort of people have relatively poor health both physical and mental health Some people have been there for a long period with the longest standing consumer having been there since 2003 This is an institutional type approach for a group of people who are highly vulnerable
There are a lot of incidents some of which are assaults ndash injury to staff and assaults between consumers
Staff are amazing in their commitment to this cohort of people People who work here are values driven and come to work to make a difference for this vulnerable population which includes taking on some of that risk we are trying to mitigate
Considerable frustration for ATampR with Disability Support Services in terms of how they fund that and the ability to provide a really good service Dr Hamilton thanked the Board for its investment The four new pods on the new facility are hoped to be occupied by the end of March 2021 He noted that this will significantly change the living standards and lives of some of the more complex long-term consumers
Older Persons Health amp Rehabilitation (OPHampR) Service ndash Dr Helen Skinner General Manager amp Chief of Service
Pressure Injury Prevention Project update The validated figures for the last four months of the 2020 year show 48 patients with pressure injuries versus 73 for the year prior so a reduction of 25 in terms of pressure injuries Staff are now very enthusiastic at looking at skin and ensuring they are picking up every possible blemish There is still further work to be done to get down to the aim of 95 avoidable pressure injuries knowing that 5 are unavoidable in terms of international best practice
Vestibular Screening Tool Pilot There is evidence for using vestibular screening which involves a series of four questions when patients come in to assess whether they have a risk of vestibular problems and what to do about it This is a piece of work the Allied Health Team is leading on and is being rolled out across the Older Persons Health amp Rehabilitation Service and will be rolled out into the community as well ED is interested also There is good evidence in terms of the validation of the tool in ED and the Acute setting so is something that could be used across the DHB in terms or reducing the risk of falls and identifying what the risks are
ERAS Highlighted OPHampRrsquos 2020 results from the national hip fracture registry database
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
11
HAC-28jan21ndashminutesndashdraft Page 3 of 6 01042021
There was discussion around needs assessments for patients particularly at Burwood for Aged Residential Care (ARC) Dr Skinner advised that times are monitored and data is kept to ensure there are no delays In terms of initial assessments there has been no delay There has been some delay in terms of community re-assessments Timeframes for assessment take anywhere between one to two working days
Queried whether there was too much demand versus supply with regards to ARC Dr Skinner advised we are running high occupancy levels in terms of dementia hospital elder care This is the one area where we run high compared to the rest of the country in terms of the capacity we have
There was discussion around the number of over 75s coming from rest homes and being admitted through ED and what is or could be done to address this Dr Skinner spoke of Advance Care Planning and Shared Goals of Care as well as what can be done differently in the community Becky Hickmott Acting Executive Director of Nursing noted that Ashburton has its own unique challenges in this space part of which is the primary health sector understanding its role She advised of a lot of changes and turnover in staff in Ashburton and this impacting the flow through to ED There is a significant piece of work underway to address this but it is not quite at the implementation stage
MedicalSurgical amp Womenrsquos amp Childrenrsquos Health amp Orthopaedics ndash Pauline Clark General Manager
Increase in acute presentations to Christchurch Hospital It is not just ED experiencing this but also the Acute Medical Assessment Unit the ldquoBone Shoprdquo the Surgical Assessment Unit and the Childrenrsquos Acute Assessment o ED experienced a sharp uplift in presentations that occurred in late September
prior to the transition to Waipapa Between January and the end of September 2020 there were an average 1830 presentations to ED per week Since then this has risen to an average of 2163 per week ndash an increase of 48 per day or 18
o This cannot be explained by population pressures ndash the rate of ED attendances per 10000 population increases sharply at the same time
o Within this we have seen an increase in self-referrals to the ED of around 2 - or 250 presentations per week
o Conversely there has been a slight decrease in GP referrals People are presenting directly but their reasons for being there are in alignment with their health needs Overall people presenting need to be assessed in an ED environment in a tertiary centre
o 24 hour medical centres both Riccarton and Moorhouse are also experiencing increased presentations so not just the ED
Medical Oncology As previously advised additional project support has been invested in to assist with a revision to the model of care This is in place and work is starting to pay dividends Two new medical oncologists have been appointed and discussions continue around a third appointment
High neo-natal occupancy This is a phenomenon being seen around New Zealand possibly not helped by the MoH lead in the space Andrew Simpson having left his role So again work in the neo-natal cot space has stalled CDHBrsquos neo-natal service is designed to take 40 to 45 Currently it is sitting at 54 Another four are being cared for as part of the paediatric ward which is putting additional pressure on paediatrics who are already experiencing demand issues We also have some women and babies out in other parts of NZ Very tight nationally when it comes to neo-natal bedscots
Return of surgery and progress against plan The opening of Waipapa provided a significant increase in acute theater capacity on the Christchurch Campus Will be in a position to report on this in more detail at the Committeersquos next meeting
Have seen significant gains in terms of the pre-operative stay in inpatients
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
12
HAC-28jan21ndashminutesndashdraft Page 4 of 6 01042021
Planned on having outplaced surgery back by Christmas with the exception of paediatric dental (which is planned for March due to availability of workforce and appropriate facilities) Outplacing has ceased
The plan around returning outsourced surgery is currently being tweaked to accommodate some unexpected sickness which will result in key people being away for a period of time
Recruitment of Anesthetic Technicians is an issue Have two staff coming from the UK in the next quarter and the search continues
Been working very closely with Sterile Supply They are a keen enabler
ESPIs CDHB and MoH have agreed an ESPI improvement plan which sees the DHB achieve compliance in ESPI 2 and 5 by 30 June 2021 A wobble was experienced in late Decemberearly January but are now on track to achieve this Specific actions that services are undertaking to enable us to deliver include o Orthopaedics have taken 64 long waiting electiveplanned patients requiring hand
surgery from the Plastic Service waitlist and put it into their own waitlist They are able to do this without needing to use anesthesia and are utilising theatre space at Burwood for this
o Vascular Surgery have been able to utilise funding that the MoH provided for additional clinics Have repatriated ambulatory treatment of varicose veins to the Outpatient Department
o Ear Nose and Throat Parental leave has affected capacity in the rhinology subspecialty however the full team is now back on board
o General Surgery A number of SMO staff have recently returned from extended sick and annual leave and a new fellow has started this week
o Some services are already green and will remain there
Discussion took place around
Issues with neo-natal cot capacity from both a regional and national perspective
Clinical safety in light of increased acute presentations
Fee structure for afterhours care The HampSS Monitoring report was noted
5 CLINICAL ADVISOR UPDATE (ORAL)
Becky Hickmott Acting Executive Director of Nursing provided the following updates
Acknowledged NICUrsquos capacity issues noting there have been a large number of extreme preterm as well as preterm births with babies who have high need and long stay The long stay has an ongoing impact Many came spontaneously in labour or with membranes ruptured Across the nation similar things are happening
Maternity is under pressure from a staffing point of view From a safety angle we are working to divert some of our nursing teams to help support
Christchurch and Burwood Hospitals were very full over the Christmas period What would normally be a quieter period was not Staff have been under significant pressure but have done a stellar job
Recently visited the SMHS site at Hillmorton to see the built environment and the constraints impacting on patients and staff Acknowledged the challenges that staff are working under They are dealing with complex patients in very challenging conditions yet the professionalism in care was clearly evident with constant reassessing triaging and attention to safety Progress with new facilities cannot come quick enough for staff
Burwood has a key quality focus on medication administration at the moment This involves a cross disciplinary approach
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
13
HAC-28jan21ndashminutesndashdraft Page 5 of 6 01042021
Looking across the board at how to mobilise and utilise nursing resources A current focus is on outpatient services ndash how we use that workforce in a different way and also advancing working at top of scope
Trendcare implementation and CCDM is progressing well in spite of some hiccups within the system These have largely been rectified ICU goes live with Trendcare mid-February and Surgery will be underway soon as well CCDM teams have been described as ldquobull doggishrdquo in their approach which will continue to ensure accurate and reliable data
COVID readiness planning is well underway working closely with Allied Health to ensure we are taking a cross disciplinary approach
MIQ nursing staff and the welfare teams have been under significant pressure during the holiday period but have delivered a high standard of care and support They perform a vital role in keeping NZ safe Mindful that staff have times where they feel stigmatised in the community and their wider family are impacted on by the role that they hold
Commend primary health who keep mobilising to support Whole system approach is working well
In spite of the pressure on staff across the system we continue to receive numerous letters and emails on the care provided and the willingness of nurses to go the extra mile
6 SERVICES SUPPORTING OLDER PEOPLE LIVING IN RURAL COMMUNITIES
Ralph La Salle Acting Executive Director Planning Funding amp Decision Support introduced the report noting it was in response to a request from the Committee last year to better understand initiativesservices in place currently and those that are planned to support our rural older population to remain in their own homescommunities and into the future Greta Bond Service Development Manager Older Persons Health (OPH) and Andrea Davidson OPH Portfolio Manager were in attendance The report was taken as read Discussion took place around the following
Strengths of the rural community as well as challenges presented by distance
Ageing population ndash in terms of this community it is not only about the clients of the services but also the people who are delivering the services Rurally we have an ageing workforce and in addition particularly with nursing a workforce where this is not their only job
The increase in demand for dementia care Rurally this can be difficult to deliver so new models of care are being looked at
Resources being deployed to rural areas and ensuring they are being utilised in the best possible way Working with the community to make sure that services are developing to meet the current needs of people as opposed to the traditional way that services have always been delivered
Falls prevention referral programme and uptake in the rural community
The availability of consumables particularly in terms of those which are meant to be provided on discharge from hospital and the impact this has on providing nursing rurally
An electronic referral form is being implemented within secondary care so someone referring for services in the community will be able to do this electronically This will be a big benefit to providing rural services
The Services Supporting Older People Living in Rural Communities report was noted
7 2021 WORKPLAN
The Committee received the 2021 Workplan noting that this is a working document
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
14
HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-01apr21-interest register Page 3 of 5 01042021
Medical Kiwi Limited ndash Independent Director Research and distribution company of medicinal cannabis and other health related products In process of listing on NZX The Antony Gough Trust ndash Trustee Trust for Antony Thomas Gough The Russley Village Limited ndash Shareholder Retirement Village Via the Antony Gough Trust The Terrace Car Park Limited ndash (Alternate) Director Property company ndash manages The Terrace car park (under construction) The Terrace On Avon Limited ndash (Alternate) Director Property company ndash manages The Terrace
Jo Kane Board Member
Christchurch Resettlement Services - Member Christchurch Resettlement Services provides a range of services to people from refugee and migrant backgrounds It works alongside refugee communities in delivering services that aim to achieve positive resettlement outcomes HurriKane Consulting ndash Project Management PartnerConsultant A private consultancy in management communication and project management Any conflicts of interest that arise will be disclosedadvised Latimer Community Housing Trust ndash Project Manager Delivers social housing in Christchurch for the vulnerable and elderly in the community
NZ Royal Humane Society ndash Director Provides an awards system for acts of bravery in New Zealand It is not anticipated any conflicts of interest will arise
Dr Rochelle Phipps Accident Compensation Corporation ndash Medical Advisor ACC is a Crown entity responsible for administering NZrsquos universal no-fault accidental injury scheme As a Medical Advisor I analyse and interpret medical information and make recommendations to improve rehabilitation outcomes for ACC customers OraTaiao New Zealand Climate amp Health Council ndash Founding Executive Board Member (no longer on executive) The Council is a not-for-profit politically non-partisan incorporated society and comprises health professionals in AotearoaNew Zealand concerned with the negative impacts of climate change on health the health gains possible through strong health-centred climate action highlighting the impacts of climate change on those who already experience
disadvantage or ill health (equity impacts) and reducing the health sectors contribution to climate change Royal New Zealand College of General Practitioners ndash Christchurch Fellow and Former Board Member The RNZCGP is the professional body and postgraduate educational institute for general practitioners
HAC - 01 April 2021 - P - Conflict of Interest Register
7
HAC-01apr21-interest register Page 4 of 5 01042021
Ingrid Taylor Board Member
Loyal Canterbury Lodge (LCL) ndash Manchester Unity ndash Trustee LCL is a friendly society administering funds for the benefit of members and often makes charitable donations One of the recipients of such a donation may have an association with the CDHB Manchester Unity Welfare Homes Trust Board (MUWHTB) ndash Trustee MUWHTB is a charitable Trust providing financial assistance to organisations in Canterbury associated with the care and assistance of older persons Recipients of financial assistance may have an association with the CDHB Sir John and Ann Hansenrsquos Family Trust ndash Independent Trustee Taylor Shaw ndash Partner Taylor Shaw has clients that are employed by the CDHB or may have contracts for services with the CDHB that may mean a conflict or potential conflict may arise from time to time Such conflicts of interest will need to be addressed at the appropriate time
I Taylor Shaw have acted as solicitor for Bill Tate and family The Youth Hub ndash Trustee The Youth Hub is a charitable Trust established to provide residential and social services for the Youth of Canterbury including services for mental health and medical care that may include involvement with the CDHB
Michelle Turrall Manawhenua
Canterbury Clinical Network (CCN) Maori Caucus - Member Canterbury District Health Board - Daughter employed as registered nurse Christchurch PHO Ltd ndash Director Christchurch PHO Trust - Trustee
Manawhenua ki Waitaha ndash Board Member and Chair Oranga Tamariki ndash Iwi and Maori ndash Senior Advisor Papakainga Hauora Komiti ndash Te Ngai Tuahuriri ndash Co-Chair
Sir John Hansen Ex-Officio ndash HAC Chair CDHB
Bone Marrow Cancer Trust ndash Trustee Canterbury Cricket Trust - Member Christchurch Casino Charitable Trust - Trustee Court of Appeal Solomon Islands Samoa and Vanuatu Dot Kiwi ndash Director and Shareholder Judicial Control Authority (JCA) for Racing ndash Appeals Tribunal Member The JCA is an independent statutory authority constituted under the Racing Act The JCA ensures that judicial and appeal proceedings in thoroughbred and harness racing are heard and decided fairly professionally efficiently and in a consistent and cost effective manner Ministry Primary Industries Costs Review Independent Panel
HAC - 01 April 2021 - P - Conflict of Interest Register
8
HAC-01apr21-interest register Page 5 of 5 01042021
Rulings Panel Gas Industry Co Ltd Sir John and Ann Hansenrsquos Family Trust ndash Ingrid Taylor sits as independent Trustee and provides legal services to the Trust and to Sir John and Ann Hansen
Gabrielle Huria Ex-Officio ndash HAC Deputy Chair CDHB
Pegasus Health Limited ndash Sister is a Director Primary Health Organisation (PHO) Rawa Hohepa Limited ndash Director Family property company Sumner Health Centre ndash Daughter is a General Practitioner (GP) Doctorrsquos clinic Te Kura Taka Pini Limited ndash General Manager The Royal New Zealand College of GPs ndash Sister is an ldquoappointed independent Directorrdquo College of GPs Upoko Rawiri Te Maire Tau of Ngai Tuahuriri - Husband
HAC - 01 April 2021 - P - Conflict of Interest Register
9
HAC-28jan21ndashminutesndashdraft Page 1 of 6 01042021
MINUTES ndash PUBLIC
DRAFT MINUTES OF THE HOSPITAL ADVISORY COMMITTEE MEETING
held in the Board Room Level 1 32 Oxford Terrace Christchurch on Thursday 28 January 2021 commencing at 900am
PRESENT Andrew Dickerson (Chair) Jan Edwards James Gough Jo Kane (via Zoom) Naomi Marshall Ingrid Taylor and Sir John Hansen (Ex-Officio) APOLOGIES Apologies for absence were received and accepted from Barry Bragg and Dr Rochelle Phipps An apology for early departure was received and accepted from James Gough (1010am) EXECUTIVE SUPPORT Dr Andrew Brant (Acting Chief Executive) Becky Hickmott (Acting Executive Director of Nursing) Ralph La Salle (Acting Executive Director Planning Funding amp Decision Support) Dr Jacqui Lunday-Johnstone (Executive Director Allied Health Scientific amp Technical) Kay Jenkins (Executive Assistant Governance Support) and Anna Craw (Board Secretariat)
APOLOGIES Kirsten Beynon (General Manager Laboratories) Dr Richard French (Acting Chief Medical Officer) Berni Marra (Manager Ashburton Health Services) and Win McDonald (Transition Programme Manager Rural Health Services) IN ATTENDANCE
Full Meeting
Pauline Clark General Manager MedicalSurgical Womenrsquos amp Childrenrsquos Health amp Orthopaedics Dr Helen Skinner General Manager amp Chief of Service Older Persons Health amp Rehabilitation Dr Greg Hamilton General Manager Specialist Mental Health Services 1 INTEREST REGISTER
AdditionsAlterations to the Interest Register Naomi Marshall ndash Addition ndash NZ Nurses College Aotearoa - Member There were no other additionsalterations Declarations of Interest for Items on Todayrsquos Agenda There were no declarations of interest for items on todayrsquos agenda Perceived Conflicts of Interest There were no perceived conflicts of interest
2 CONFIRMATION OF PREVIOUS MEETING MINUTES
Resolution (0121) (Moved Ingrid TaylorSeconded Jan Edwards ndash carried) ldquoThat the minutes of the Hospital Advisory Committee meeting held on 3 December 2020 be approved and adopted as a true and correct recordrdquo
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
10
HAC-28jan21ndashminutesndashdraft Page 2 of 6 01042021
3 CARRIED FORWARD ACTION ITEMS
The carried forward action items were noted
4 HampSS MONITORING REPORT
The Committee considered the Hospital and Specialist Services Monitoring Report for December 2020 The report was taken as read General Managers introduced their respective divisions and spoke to their areas as follows Specialist Mental Health Services (SMHS) ndash Dr Greg Hamilton General Manager
Report focuses on SMHS Intellectual Disability Services to provide a greater depth of understanding Services are provided to inpatients in two different units o PSAID Unit This falls under our population-based funding and is for those
people with an intellectual disability and a mental health diagnosis o Whaikaha (ATampR ndash Assessment Treatment and Rehabilitation) This is funded
by Ministry of Health Disability Support Services with whom we have two contracts and is for people who are under Court order under two different Acts It is a secure unit Generally this cohort of people have relatively poor health both physical and mental health Some people have been there for a long period with the longest standing consumer having been there since 2003 This is an institutional type approach for a group of people who are highly vulnerable
There are a lot of incidents some of which are assaults ndash injury to staff and assaults between consumers
Staff are amazing in their commitment to this cohort of people People who work here are values driven and come to work to make a difference for this vulnerable population which includes taking on some of that risk we are trying to mitigate
Considerable frustration for ATampR with Disability Support Services in terms of how they fund that and the ability to provide a really good service Dr Hamilton thanked the Board for its investment The four new pods on the new facility are hoped to be occupied by the end of March 2021 He noted that this will significantly change the living standards and lives of some of the more complex long-term consumers
Older Persons Health amp Rehabilitation (OPHampR) Service ndash Dr Helen Skinner General Manager amp Chief of Service
Pressure Injury Prevention Project update The validated figures for the last four months of the 2020 year show 48 patients with pressure injuries versus 73 for the year prior so a reduction of 25 in terms of pressure injuries Staff are now very enthusiastic at looking at skin and ensuring they are picking up every possible blemish There is still further work to be done to get down to the aim of 95 avoidable pressure injuries knowing that 5 are unavoidable in terms of international best practice
Vestibular Screening Tool Pilot There is evidence for using vestibular screening which involves a series of four questions when patients come in to assess whether they have a risk of vestibular problems and what to do about it This is a piece of work the Allied Health Team is leading on and is being rolled out across the Older Persons Health amp Rehabilitation Service and will be rolled out into the community as well ED is interested also There is good evidence in terms of the validation of the tool in ED and the Acute setting so is something that could be used across the DHB in terms or reducing the risk of falls and identifying what the risks are
ERAS Highlighted OPHampRrsquos 2020 results from the national hip fracture registry database
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
11
HAC-28jan21ndashminutesndashdraft Page 3 of 6 01042021
There was discussion around needs assessments for patients particularly at Burwood for Aged Residential Care (ARC) Dr Skinner advised that times are monitored and data is kept to ensure there are no delays In terms of initial assessments there has been no delay There has been some delay in terms of community re-assessments Timeframes for assessment take anywhere between one to two working days
Queried whether there was too much demand versus supply with regards to ARC Dr Skinner advised we are running high occupancy levels in terms of dementia hospital elder care This is the one area where we run high compared to the rest of the country in terms of the capacity we have
There was discussion around the number of over 75s coming from rest homes and being admitted through ED and what is or could be done to address this Dr Skinner spoke of Advance Care Planning and Shared Goals of Care as well as what can be done differently in the community Becky Hickmott Acting Executive Director of Nursing noted that Ashburton has its own unique challenges in this space part of which is the primary health sector understanding its role She advised of a lot of changes and turnover in staff in Ashburton and this impacting the flow through to ED There is a significant piece of work underway to address this but it is not quite at the implementation stage
MedicalSurgical amp Womenrsquos amp Childrenrsquos Health amp Orthopaedics ndash Pauline Clark General Manager
Increase in acute presentations to Christchurch Hospital It is not just ED experiencing this but also the Acute Medical Assessment Unit the ldquoBone Shoprdquo the Surgical Assessment Unit and the Childrenrsquos Acute Assessment o ED experienced a sharp uplift in presentations that occurred in late September
prior to the transition to Waipapa Between January and the end of September 2020 there were an average 1830 presentations to ED per week Since then this has risen to an average of 2163 per week ndash an increase of 48 per day or 18
o This cannot be explained by population pressures ndash the rate of ED attendances per 10000 population increases sharply at the same time
o Within this we have seen an increase in self-referrals to the ED of around 2 - or 250 presentations per week
o Conversely there has been a slight decrease in GP referrals People are presenting directly but their reasons for being there are in alignment with their health needs Overall people presenting need to be assessed in an ED environment in a tertiary centre
o 24 hour medical centres both Riccarton and Moorhouse are also experiencing increased presentations so not just the ED
Medical Oncology As previously advised additional project support has been invested in to assist with a revision to the model of care This is in place and work is starting to pay dividends Two new medical oncologists have been appointed and discussions continue around a third appointment
High neo-natal occupancy This is a phenomenon being seen around New Zealand possibly not helped by the MoH lead in the space Andrew Simpson having left his role So again work in the neo-natal cot space has stalled CDHBrsquos neo-natal service is designed to take 40 to 45 Currently it is sitting at 54 Another four are being cared for as part of the paediatric ward which is putting additional pressure on paediatrics who are already experiencing demand issues We also have some women and babies out in other parts of NZ Very tight nationally when it comes to neo-natal bedscots
Return of surgery and progress against plan The opening of Waipapa provided a significant increase in acute theater capacity on the Christchurch Campus Will be in a position to report on this in more detail at the Committeersquos next meeting
Have seen significant gains in terms of the pre-operative stay in inpatients
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
12
HAC-28jan21ndashminutesndashdraft Page 4 of 6 01042021
Planned on having outplaced surgery back by Christmas with the exception of paediatric dental (which is planned for March due to availability of workforce and appropriate facilities) Outplacing has ceased
The plan around returning outsourced surgery is currently being tweaked to accommodate some unexpected sickness which will result in key people being away for a period of time
Recruitment of Anesthetic Technicians is an issue Have two staff coming from the UK in the next quarter and the search continues
Been working very closely with Sterile Supply They are a keen enabler
ESPIs CDHB and MoH have agreed an ESPI improvement plan which sees the DHB achieve compliance in ESPI 2 and 5 by 30 June 2021 A wobble was experienced in late Decemberearly January but are now on track to achieve this Specific actions that services are undertaking to enable us to deliver include o Orthopaedics have taken 64 long waiting electiveplanned patients requiring hand
surgery from the Plastic Service waitlist and put it into their own waitlist They are able to do this without needing to use anesthesia and are utilising theatre space at Burwood for this
o Vascular Surgery have been able to utilise funding that the MoH provided for additional clinics Have repatriated ambulatory treatment of varicose veins to the Outpatient Department
o Ear Nose and Throat Parental leave has affected capacity in the rhinology subspecialty however the full team is now back on board
o General Surgery A number of SMO staff have recently returned from extended sick and annual leave and a new fellow has started this week
o Some services are already green and will remain there
Discussion took place around
Issues with neo-natal cot capacity from both a regional and national perspective
Clinical safety in light of increased acute presentations
Fee structure for afterhours care The HampSS Monitoring report was noted
5 CLINICAL ADVISOR UPDATE (ORAL)
Becky Hickmott Acting Executive Director of Nursing provided the following updates
Acknowledged NICUrsquos capacity issues noting there have been a large number of extreme preterm as well as preterm births with babies who have high need and long stay The long stay has an ongoing impact Many came spontaneously in labour or with membranes ruptured Across the nation similar things are happening
Maternity is under pressure from a staffing point of view From a safety angle we are working to divert some of our nursing teams to help support
Christchurch and Burwood Hospitals were very full over the Christmas period What would normally be a quieter period was not Staff have been under significant pressure but have done a stellar job
Recently visited the SMHS site at Hillmorton to see the built environment and the constraints impacting on patients and staff Acknowledged the challenges that staff are working under They are dealing with complex patients in very challenging conditions yet the professionalism in care was clearly evident with constant reassessing triaging and attention to safety Progress with new facilities cannot come quick enough for staff
Burwood has a key quality focus on medication administration at the moment This involves a cross disciplinary approach
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
13
HAC-28jan21ndashminutesndashdraft Page 5 of 6 01042021
Looking across the board at how to mobilise and utilise nursing resources A current focus is on outpatient services ndash how we use that workforce in a different way and also advancing working at top of scope
Trendcare implementation and CCDM is progressing well in spite of some hiccups within the system These have largely been rectified ICU goes live with Trendcare mid-February and Surgery will be underway soon as well CCDM teams have been described as ldquobull doggishrdquo in their approach which will continue to ensure accurate and reliable data
COVID readiness planning is well underway working closely with Allied Health to ensure we are taking a cross disciplinary approach
MIQ nursing staff and the welfare teams have been under significant pressure during the holiday period but have delivered a high standard of care and support They perform a vital role in keeping NZ safe Mindful that staff have times where they feel stigmatised in the community and their wider family are impacted on by the role that they hold
Commend primary health who keep mobilising to support Whole system approach is working well
In spite of the pressure on staff across the system we continue to receive numerous letters and emails on the care provided and the willingness of nurses to go the extra mile
6 SERVICES SUPPORTING OLDER PEOPLE LIVING IN RURAL COMMUNITIES
Ralph La Salle Acting Executive Director Planning Funding amp Decision Support introduced the report noting it was in response to a request from the Committee last year to better understand initiativesservices in place currently and those that are planned to support our rural older population to remain in their own homescommunities and into the future Greta Bond Service Development Manager Older Persons Health (OPH) and Andrea Davidson OPH Portfolio Manager were in attendance The report was taken as read Discussion took place around the following
Strengths of the rural community as well as challenges presented by distance
Ageing population ndash in terms of this community it is not only about the clients of the services but also the people who are delivering the services Rurally we have an ageing workforce and in addition particularly with nursing a workforce where this is not their only job
The increase in demand for dementia care Rurally this can be difficult to deliver so new models of care are being looked at
Resources being deployed to rural areas and ensuring they are being utilised in the best possible way Working with the community to make sure that services are developing to meet the current needs of people as opposed to the traditional way that services have always been delivered
Falls prevention referral programme and uptake in the rural community
The availability of consumables particularly in terms of those which are meant to be provided on discharge from hospital and the impact this has on providing nursing rurally
An electronic referral form is being implemented within secondary care so someone referring for services in the community will be able to do this electronically This will be a big benefit to providing rural services
The Services Supporting Older People Living in Rural Communities report was noted
7 2021 WORKPLAN
The Committee received the 2021 Workplan noting that this is a working document
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
14
HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-01apr21-interest register Page 4 of 5 01042021
Ingrid Taylor Board Member
Loyal Canterbury Lodge (LCL) ndash Manchester Unity ndash Trustee LCL is a friendly society administering funds for the benefit of members and often makes charitable donations One of the recipients of such a donation may have an association with the CDHB Manchester Unity Welfare Homes Trust Board (MUWHTB) ndash Trustee MUWHTB is a charitable Trust providing financial assistance to organisations in Canterbury associated with the care and assistance of older persons Recipients of financial assistance may have an association with the CDHB Sir John and Ann Hansenrsquos Family Trust ndash Independent Trustee Taylor Shaw ndash Partner Taylor Shaw has clients that are employed by the CDHB or may have contracts for services with the CDHB that may mean a conflict or potential conflict may arise from time to time Such conflicts of interest will need to be addressed at the appropriate time
I Taylor Shaw have acted as solicitor for Bill Tate and family The Youth Hub ndash Trustee The Youth Hub is a charitable Trust established to provide residential and social services for the Youth of Canterbury including services for mental health and medical care that may include involvement with the CDHB
Michelle Turrall Manawhenua
Canterbury Clinical Network (CCN) Maori Caucus - Member Canterbury District Health Board - Daughter employed as registered nurse Christchurch PHO Ltd ndash Director Christchurch PHO Trust - Trustee
Manawhenua ki Waitaha ndash Board Member and Chair Oranga Tamariki ndash Iwi and Maori ndash Senior Advisor Papakainga Hauora Komiti ndash Te Ngai Tuahuriri ndash Co-Chair
Sir John Hansen Ex-Officio ndash HAC Chair CDHB
Bone Marrow Cancer Trust ndash Trustee Canterbury Cricket Trust - Member Christchurch Casino Charitable Trust - Trustee Court of Appeal Solomon Islands Samoa and Vanuatu Dot Kiwi ndash Director and Shareholder Judicial Control Authority (JCA) for Racing ndash Appeals Tribunal Member The JCA is an independent statutory authority constituted under the Racing Act The JCA ensures that judicial and appeal proceedings in thoroughbred and harness racing are heard and decided fairly professionally efficiently and in a consistent and cost effective manner Ministry Primary Industries Costs Review Independent Panel
HAC - 01 April 2021 - P - Conflict of Interest Register
8
HAC-01apr21-interest register Page 5 of 5 01042021
Rulings Panel Gas Industry Co Ltd Sir John and Ann Hansenrsquos Family Trust ndash Ingrid Taylor sits as independent Trustee and provides legal services to the Trust and to Sir John and Ann Hansen
Gabrielle Huria Ex-Officio ndash HAC Deputy Chair CDHB
Pegasus Health Limited ndash Sister is a Director Primary Health Organisation (PHO) Rawa Hohepa Limited ndash Director Family property company Sumner Health Centre ndash Daughter is a General Practitioner (GP) Doctorrsquos clinic Te Kura Taka Pini Limited ndash General Manager The Royal New Zealand College of GPs ndash Sister is an ldquoappointed independent Directorrdquo College of GPs Upoko Rawiri Te Maire Tau of Ngai Tuahuriri - Husband
HAC - 01 April 2021 - P - Conflict of Interest Register
9
HAC-28jan21ndashminutesndashdraft Page 1 of 6 01042021
MINUTES ndash PUBLIC
DRAFT MINUTES OF THE HOSPITAL ADVISORY COMMITTEE MEETING
held in the Board Room Level 1 32 Oxford Terrace Christchurch on Thursday 28 January 2021 commencing at 900am
PRESENT Andrew Dickerson (Chair) Jan Edwards James Gough Jo Kane (via Zoom) Naomi Marshall Ingrid Taylor and Sir John Hansen (Ex-Officio) APOLOGIES Apologies for absence were received and accepted from Barry Bragg and Dr Rochelle Phipps An apology for early departure was received and accepted from James Gough (1010am) EXECUTIVE SUPPORT Dr Andrew Brant (Acting Chief Executive) Becky Hickmott (Acting Executive Director of Nursing) Ralph La Salle (Acting Executive Director Planning Funding amp Decision Support) Dr Jacqui Lunday-Johnstone (Executive Director Allied Health Scientific amp Technical) Kay Jenkins (Executive Assistant Governance Support) and Anna Craw (Board Secretariat)
APOLOGIES Kirsten Beynon (General Manager Laboratories) Dr Richard French (Acting Chief Medical Officer) Berni Marra (Manager Ashburton Health Services) and Win McDonald (Transition Programme Manager Rural Health Services) IN ATTENDANCE
Full Meeting
Pauline Clark General Manager MedicalSurgical Womenrsquos amp Childrenrsquos Health amp Orthopaedics Dr Helen Skinner General Manager amp Chief of Service Older Persons Health amp Rehabilitation Dr Greg Hamilton General Manager Specialist Mental Health Services 1 INTEREST REGISTER
AdditionsAlterations to the Interest Register Naomi Marshall ndash Addition ndash NZ Nurses College Aotearoa - Member There were no other additionsalterations Declarations of Interest for Items on Todayrsquos Agenda There were no declarations of interest for items on todayrsquos agenda Perceived Conflicts of Interest There were no perceived conflicts of interest
2 CONFIRMATION OF PREVIOUS MEETING MINUTES
Resolution (0121) (Moved Ingrid TaylorSeconded Jan Edwards ndash carried) ldquoThat the minutes of the Hospital Advisory Committee meeting held on 3 December 2020 be approved and adopted as a true and correct recordrdquo
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
10
HAC-28jan21ndashminutesndashdraft Page 2 of 6 01042021
3 CARRIED FORWARD ACTION ITEMS
The carried forward action items were noted
4 HampSS MONITORING REPORT
The Committee considered the Hospital and Specialist Services Monitoring Report for December 2020 The report was taken as read General Managers introduced their respective divisions and spoke to their areas as follows Specialist Mental Health Services (SMHS) ndash Dr Greg Hamilton General Manager
Report focuses on SMHS Intellectual Disability Services to provide a greater depth of understanding Services are provided to inpatients in two different units o PSAID Unit This falls under our population-based funding and is for those
people with an intellectual disability and a mental health diagnosis o Whaikaha (ATampR ndash Assessment Treatment and Rehabilitation) This is funded
by Ministry of Health Disability Support Services with whom we have two contracts and is for people who are under Court order under two different Acts It is a secure unit Generally this cohort of people have relatively poor health both physical and mental health Some people have been there for a long period with the longest standing consumer having been there since 2003 This is an institutional type approach for a group of people who are highly vulnerable
There are a lot of incidents some of which are assaults ndash injury to staff and assaults between consumers
Staff are amazing in their commitment to this cohort of people People who work here are values driven and come to work to make a difference for this vulnerable population which includes taking on some of that risk we are trying to mitigate
Considerable frustration for ATampR with Disability Support Services in terms of how they fund that and the ability to provide a really good service Dr Hamilton thanked the Board for its investment The four new pods on the new facility are hoped to be occupied by the end of March 2021 He noted that this will significantly change the living standards and lives of some of the more complex long-term consumers
Older Persons Health amp Rehabilitation (OPHampR) Service ndash Dr Helen Skinner General Manager amp Chief of Service
Pressure Injury Prevention Project update The validated figures for the last four months of the 2020 year show 48 patients with pressure injuries versus 73 for the year prior so a reduction of 25 in terms of pressure injuries Staff are now very enthusiastic at looking at skin and ensuring they are picking up every possible blemish There is still further work to be done to get down to the aim of 95 avoidable pressure injuries knowing that 5 are unavoidable in terms of international best practice
Vestibular Screening Tool Pilot There is evidence for using vestibular screening which involves a series of four questions when patients come in to assess whether they have a risk of vestibular problems and what to do about it This is a piece of work the Allied Health Team is leading on and is being rolled out across the Older Persons Health amp Rehabilitation Service and will be rolled out into the community as well ED is interested also There is good evidence in terms of the validation of the tool in ED and the Acute setting so is something that could be used across the DHB in terms or reducing the risk of falls and identifying what the risks are
ERAS Highlighted OPHampRrsquos 2020 results from the national hip fracture registry database
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
11
HAC-28jan21ndashminutesndashdraft Page 3 of 6 01042021
There was discussion around needs assessments for patients particularly at Burwood for Aged Residential Care (ARC) Dr Skinner advised that times are monitored and data is kept to ensure there are no delays In terms of initial assessments there has been no delay There has been some delay in terms of community re-assessments Timeframes for assessment take anywhere between one to two working days
Queried whether there was too much demand versus supply with regards to ARC Dr Skinner advised we are running high occupancy levels in terms of dementia hospital elder care This is the one area where we run high compared to the rest of the country in terms of the capacity we have
There was discussion around the number of over 75s coming from rest homes and being admitted through ED and what is or could be done to address this Dr Skinner spoke of Advance Care Planning and Shared Goals of Care as well as what can be done differently in the community Becky Hickmott Acting Executive Director of Nursing noted that Ashburton has its own unique challenges in this space part of which is the primary health sector understanding its role She advised of a lot of changes and turnover in staff in Ashburton and this impacting the flow through to ED There is a significant piece of work underway to address this but it is not quite at the implementation stage
MedicalSurgical amp Womenrsquos amp Childrenrsquos Health amp Orthopaedics ndash Pauline Clark General Manager
Increase in acute presentations to Christchurch Hospital It is not just ED experiencing this but also the Acute Medical Assessment Unit the ldquoBone Shoprdquo the Surgical Assessment Unit and the Childrenrsquos Acute Assessment o ED experienced a sharp uplift in presentations that occurred in late September
prior to the transition to Waipapa Between January and the end of September 2020 there were an average 1830 presentations to ED per week Since then this has risen to an average of 2163 per week ndash an increase of 48 per day or 18
o This cannot be explained by population pressures ndash the rate of ED attendances per 10000 population increases sharply at the same time
o Within this we have seen an increase in self-referrals to the ED of around 2 - or 250 presentations per week
o Conversely there has been a slight decrease in GP referrals People are presenting directly but their reasons for being there are in alignment with their health needs Overall people presenting need to be assessed in an ED environment in a tertiary centre
o 24 hour medical centres both Riccarton and Moorhouse are also experiencing increased presentations so not just the ED
Medical Oncology As previously advised additional project support has been invested in to assist with a revision to the model of care This is in place and work is starting to pay dividends Two new medical oncologists have been appointed and discussions continue around a third appointment
High neo-natal occupancy This is a phenomenon being seen around New Zealand possibly not helped by the MoH lead in the space Andrew Simpson having left his role So again work in the neo-natal cot space has stalled CDHBrsquos neo-natal service is designed to take 40 to 45 Currently it is sitting at 54 Another four are being cared for as part of the paediatric ward which is putting additional pressure on paediatrics who are already experiencing demand issues We also have some women and babies out in other parts of NZ Very tight nationally when it comes to neo-natal bedscots
Return of surgery and progress against plan The opening of Waipapa provided a significant increase in acute theater capacity on the Christchurch Campus Will be in a position to report on this in more detail at the Committeersquos next meeting
Have seen significant gains in terms of the pre-operative stay in inpatients
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
12
HAC-28jan21ndashminutesndashdraft Page 4 of 6 01042021
Planned on having outplaced surgery back by Christmas with the exception of paediatric dental (which is planned for March due to availability of workforce and appropriate facilities) Outplacing has ceased
The plan around returning outsourced surgery is currently being tweaked to accommodate some unexpected sickness which will result in key people being away for a period of time
Recruitment of Anesthetic Technicians is an issue Have two staff coming from the UK in the next quarter and the search continues
Been working very closely with Sterile Supply They are a keen enabler
ESPIs CDHB and MoH have agreed an ESPI improvement plan which sees the DHB achieve compliance in ESPI 2 and 5 by 30 June 2021 A wobble was experienced in late Decemberearly January but are now on track to achieve this Specific actions that services are undertaking to enable us to deliver include o Orthopaedics have taken 64 long waiting electiveplanned patients requiring hand
surgery from the Plastic Service waitlist and put it into their own waitlist They are able to do this without needing to use anesthesia and are utilising theatre space at Burwood for this
o Vascular Surgery have been able to utilise funding that the MoH provided for additional clinics Have repatriated ambulatory treatment of varicose veins to the Outpatient Department
o Ear Nose and Throat Parental leave has affected capacity in the rhinology subspecialty however the full team is now back on board
o General Surgery A number of SMO staff have recently returned from extended sick and annual leave and a new fellow has started this week
o Some services are already green and will remain there
Discussion took place around
Issues with neo-natal cot capacity from both a regional and national perspective
Clinical safety in light of increased acute presentations
Fee structure for afterhours care The HampSS Monitoring report was noted
5 CLINICAL ADVISOR UPDATE (ORAL)
Becky Hickmott Acting Executive Director of Nursing provided the following updates
Acknowledged NICUrsquos capacity issues noting there have been a large number of extreme preterm as well as preterm births with babies who have high need and long stay The long stay has an ongoing impact Many came spontaneously in labour or with membranes ruptured Across the nation similar things are happening
Maternity is under pressure from a staffing point of view From a safety angle we are working to divert some of our nursing teams to help support
Christchurch and Burwood Hospitals were very full over the Christmas period What would normally be a quieter period was not Staff have been under significant pressure but have done a stellar job
Recently visited the SMHS site at Hillmorton to see the built environment and the constraints impacting on patients and staff Acknowledged the challenges that staff are working under They are dealing with complex patients in very challenging conditions yet the professionalism in care was clearly evident with constant reassessing triaging and attention to safety Progress with new facilities cannot come quick enough for staff
Burwood has a key quality focus on medication administration at the moment This involves a cross disciplinary approach
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
13
HAC-28jan21ndashminutesndashdraft Page 5 of 6 01042021
Looking across the board at how to mobilise and utilise nursing resources A current focus is on outpatient services ndash how we use that workforce in a different way and also advancing working at top of scope
Trendcare implementation and CCDM is progressing well in spite of some hiccups within the system These have largely been rectified ICU goes live with Trendcare mid-February and Surgery will be underway soon as well CCDM teams have been described as ldquobull doggishrdquo in their approach which will continue to ensure accurate and reliable data
COVID readiness planning is well underway working closely with Allied Health to ensure we are taking a cross disciplinary approach
MIQ nursing staff and the welfare teams have been under significant pressure during the holiday period but have delivered a high standard of care and support They perform a vital role in keeping NZ safe Mindful that staff have times where they feel stigmatised in the community and their wider family are impacted on by the role that they hold
Commend primary health who keep mobilising to support Whole system approach is working well
In spite of the pressure on staff across the system we continue to receive numerous letters and emails on the care provided and the willingness of nurses to go the extra mile
6 SERVICES SUPPORTING OLDER PEOPLE LIVING IN RURAL COMMUNITIES
Ralph La Salle Acting Executive Director Planning Funding amp Decision Support introduced the report noting it was in response to a request from the Committee last year to better understand initiativesservices in place currently and those that are planned to support our rural older population to remain in their own homescommunities and into the future Greta Bond Service Development Manager Older Persons Health (OPH) and Andrea Davidson OPH Portfolio Manager were in attendance The report was taken as read Discussion took place around the following
Strengths of the rural community as well as challenges presented by distance
Ageing population ndash in terms of this community it is not only about the clients of the services but also the people who are delivering the services Rurally we have an ageing workforce and in addition particularly with nursing a workforce where this is not their only job
The increase in demand for dementia care Rurally this can be difficult to deliver so new models of care are being looked at
Resources being deployed to rural areas and ensuring they are being utilised in the best possible way Working with the community to make sure that services are developing to meet the current needs of people as opposed to the traditional way that services have always been delivered
Falls prevention referral programme and uptake in the rural community
The availability of consumables particularly in terms of those which are meant to be provided on discharge from hospital and the impact this has on providing nursing rurally
An electronic referral form is being implemented within secondary care so someone referring for services in the community will be able to do this electronically This will be a big benefit to providing rural services
The Services Supporting Older People Living in Rural Communities report was noted
7 2021 WORKPLAN
The Committee received the 2021 Workplan noting that this is a working document
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
14
HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-01apr21-interest register Page 5 of 5 01042021
Rulings Panel Gas Industry Co Ltd Sir John and Ann Hansenrsquos Family Trust ndash Ingrid Taylor sits as independent Trustee and provides legal services to the Trust and to Sir John and Ann Hansen
Gabrielle Huria Ex-Officio ndash HAC Deputy Chair CDHB
Pegasus Health Limited ndash Sister is a Director Primary Health Organisation (PHO) Rawa Hohepa Limited ndash Director Family property company Sumner Health Centre ndash Daughter is a General Practitioner (GP) Doctorrsquos clinic Te Kura Taka Pini Limited ndash General Manager The Royal New Zealand College of GPs ndash Sister is an ldquoappointed independent Directorrdquo College of GPs Upoko Rawiri Te Maire Tau of Ngai Tuahuriri - Husband
HAC - 01 April 2021 - P - Conflict of Interest Register
9
HAC-28jan21ndashminutesndashdraft Page 1 of 6 01042021
MINUTES ndash PUBLIC
DRAFT MINUTES OF THE HOSPITAL ADVISORY COMMITTEE MEETING
held in the Board Room Level 1 32 Oxford Terrace Christchurch on Thursday 28 January 2021 commencing at 900am
PRESENT Andrew Dickerson (Chair) Jan Edwards James Gough Jo Kane (via Zoom) Naomi Marshall Ingrid Taylor and Sir John Hansen (Ex-Officio) APOLOGIES Apologies for absence were received and accepted from Barry Bragg and Dr Rochelle Phipps An apology for early departure was received and accepted from James Gough (1010am) EXECUTIVE SUPPORT Dr Andrew Brant (Acting Chief Executive) Becky Hickmott (Acting Executive Director of Nursing) Ralph La Salle (Acting Executive Director Planning Funding amp Decision Support) Dr Jacqui Lunday-Johnstone (Executive Director Allied Health Scientific amp Technical) Kay Jenkins (Executive Assistant Governance Support) and Anna Craw (Board Secretariat)
APOLOGIES Kirsten Beynon (General Manager Laboratories) Dr Richard French (Acting Chief Medical Officer) Berni Marra (Manager Ashburton Health Services) and Win McDonald (Transition Programme Manager Rural Health Services) IN ATTENDANCE
Full Meeting
Pauline Clark General Manager MedicalSurgical Womenrsquos amp Childrenrsquos Health amp Orthopaedics Dr Helen Skinner General Manager amp Chief of Service Older Persons Health amp Rehabilitation Dr Greg Hamilton General Manager Specialist Mental Health Services 1 INTEREST REGISTER
AdditionsAlterations to the Interest Register Naomi Marshall ndash Addition ndash NZ Nurses College Aotearoa - Member There were no other additionsalterations Declarations of Interest for Items on Todayrsquos Agenda There were no declarations of interest for items on todayrsquos agenda Perceived Conflicts of Interest There were no perceived conflicts of interest
2 CONFIRMATION OF PREVIOUS MEETING MINUTES
Resolution (0121) (Moved Ingrid TaylorSeconded Jan Edwards ndash carried) ldquoThat the minutes of the Hospital Advisory Committee meeting held on 3 December 2020 be approved and adopted as a true and correct recordrdquo
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
10
HAC-28jan21ndashminutesndashdraft Page 2 of 6 01042021
3 CARRIED FORWARD ACTION ITEMS
The carried forward action items were noted
4 HampSS MONITORING REPORT
The Committee considered the Hospital and Specialist Services Monitoring Report for December 2020 The report was taken as read General Managers introduced their respective divisions and spoke to their areas as follows Specialist Mental Health Services (SMHS) ndash Dr Greg Hamilton General Manager
Report focuses on SMHS Intellectual Disability Services to provide a greater depth of understanding Services are provided to inpatients in two different units o PSAID Unit This falls under our population-based funding and is for those
people with an intellectual disability and a mental health diagnosis o Whaikaha (ATampR ndash Assessment Treatment and Rehabilitation) This is funded
by Ministry of Health Disability Support Services with whom we have two contracts and is for people who are under Court order under two different Acts It is a secure unit Generally this cohort of people have relatively poor health both physical and mental health Some people have been there for a long period with the longest standing consumer having been there since 2003 This is an institutional type approach for a group of people who are highly vulnerable
There are a lot of incidents some of which are assaults ndash injury to staff and assaults between consumers
Staff are amazing in their commitment to this cohort of people People who work here are values driven and come to work to make a difference for this vulnerable population which includes taking on some of that risk we are trying to mitigate
Considerable frustration for ATampR with Disability Support Services in terms of how they fund that and the ability to provide a really good service Dr Hamilton thanked the Board for its investment The four new pods on the new facility are hoped to be occupied by the end of March 2021 He noted that this will significantly change the living standards and lives of some of the more complex long-term consumers
Older Persons Health amp Rehabilitation (OPHampR) Service ndash Dr Helen Skinner General Manager amp Chief of Service
Pressure Injury Prevention Project update The validated figures for the last four months of the 2020 year show 48 patients with pressure injuries versus 73 for the year prior so a reduction of 25 in terms of pressure injuries Staff are now very enthusiastic at looking at skin and ensuring they are picking up every possible blemish There is still further work to be done to get down to the aim of 95 avoidable pressure injuries knowing that 5 are unavoidable in terms of international best practice
Vestibular Screening Tool Pilot There is evidence for using vestibular screening which involves a series of four questions when patients come in to assess whether they have a risk of vestibular problems and what to do about it This is a piece of work the Allied Health Team is leading on and is being rolled out across the Older Persons Health amp Rehabilitation Service and will be rolled out into the community as well ED is interested also There is good evidence in terms of the validation of the tool in ED and the Acute setting so is something that could be used across the DHB in terms or reducing the risk of falls and identifying what the risks are
ERAS Highlighted OPHampRrsquos 2020 results from the national hip fracture registry database
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
11
HAC-28jan21ndashminutesndashdraft Page 3 of 6 01042021
There was discussion around needs assessments for patients particularly at Burwood for Aged Residential Care (ARC) Dr Skinner advised that times are monitored and data is kept to ensure there are no delays In terms of initial assessments there has been no delay There has been some delay in terms of community re-assessments Timeframes for assessment take anywhere between one to two working days
Queried whether there was too much demand versus supply with regards to ARC Dr Skinner advised we are running high occupancy levels in terms of dementia hospital elder care This is the one area where we run high compared to the rest of the country in terms of the capacity we have
There was discussion around the number of over 75s coming from rest homes and being admitted through ED and what is or could be done to address this Dr Skinner spoke of Advance Care Planning and Shared Goals of Care as well as what can be done differently in the community Becky Hickmott Acting Executive Director of Nursing noted that Ashburton has its own unique challenges in this space part of which is the primary health sector understanding its role She advised of a lot of changes and turnover in staff in Ashburton and this impacting the flow through to ED There is a significant piece of work underway to address this but it is not quite at the implementation stage
MedicalSurgical amp Womenrsquos amp Childrenrsquos Health amp Orthopaedics ndash Pauline Clark General Manager
Increase in acute presentations to Christchurch Hospital It is not just ED experiencing this but also the Acute Medical Assessment Unit the ldquoBone Shoprdquo the Surgical Assessment Unit and the Childrenrsquos Acute Assessment o ED experienced a sharp uplift in presentations that occurred in late September
prior to the transition to Waipapa Between January and the end of September 2020 there were an average 1830 presentations to ED per week Since then this has risen to an average of 2163 per week ndash an increase of 48 per day or 18
o This cannot be explained by population pressures ndash the rate of ED attendances per 10000 population increases sharply at the same time
o Within this we have seen an increase in self-referrals to the ED of around 2 - or 250 presentations per week
o Conversely there has been a slight decrease in GP referrals People are presenting directly but their reasons for being there are in alignment with their health needs Overall people presenting need to be assessed in an ED environment in a tertiary centre
o 24 hour medical centres both Riccarton and Moorhouse are also experiencing increased presentations so not just the ED
Medical Oncology As previously advised additional project support has been invested in to assist with a revision to the model of care This is in place and work is starting to pay dividends Two new medical oncologists have been appointed and discussions continue around a third appointment
High neo-natal occupancy This is a phenomenon being seen around New Zealand possibly not helped by the MoH lead in the space Andrew Simpson having left his role So again work in the neo-natal cot space has stalled CDHBrsquos neo-natal service is designed to take 40 to 45 Currently it is sitting at 54 Another four are being cared for as part of the paediatric ward which is putting additional pressure on paediatrics who are already experiencing demand issues We also have some women and babies out in other parts of NZ Very tight nationally when it comes to neo-natal bedscots
Return of surgery and progress against plan The opening of Waipapa provided a significant increase in acute theater capacity on the Christchurch Campus Will be in a position to report on this in more detail at the Committeersquos next meeting
Have seen significant gains in terms of the pre-operative stay in inpatients
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
12
HAC-28jan21ndashminutesndashdraft Page 4 of 6 01042021
Planned on having outplaced surgery back by Christmas with the exception of paediatric dental (which is planned for March due to availability of workforce and appropriate facilities) Outplacing has ceased
The plan around returning outsourced surgery is currently being tweaked to accommodate some unexpected sickness which will result in key people being away for a period of time
Recruitment of Anesthetic Technicians is an issue Have two staff coming from the UK in the next quarter and the search continues
Been working very closely with Sterile Supply They are a keen enabler
ESPIs CDHB and MoH have agreed an ESPI improvement plan which sees the DHB achieve compliance in ESPI 2 and 5 by 30 June 2021 A wobble was experienced in late Decemberearly January but are now on track to achieve this Specific actions that services are undertaking to enable us to deliver include o Orthopaedics have taken 64 long waiting electiveplanned patients requiring hand
surgery from the Plastic Service waitlist and put it into their own waitlist They are able to do this without needing to use anesthesia and are utilising theatre space at Burwood for this
o Vascular Surgery have been able to utilise funding that the MoH provided for additional clinics Have repatriated ambulatory treatment of varicose veins to the Outpatient Department
o Ear Nose and Throat Parental leave has affected capacity in the rhinology subspecialty however the full team is now back on board
o General Surgery A number of SMO staff have recently returned from extended sick and annual leave and a new fellow has started this week
o Some services are already green and will remain there
Discussion took place around
Issues with neo-natal cot capacity from both a regional and national perspective
Clinical safety in light of increased acute presentations
Fee structure for afterhours care The HampSS Monitoring report was noted
5 CLINICAL ADVISOR UPDATE (ORAL)
Becky Hickmott Acting Executive Director of Nursing provided the following updates
Acknowledged NICUrsquos capacity issues noting there have been a large number of extreme preterm as well as preterm births with babies who have high need and long stay The long stay has an ongoing impact Many came spontaneously in labour or with membranes ruptured Across the nation similar things are happening
Maternity is under pressure from a staffing point of view From a safety angle we are working to divert some of our nursing teams to help support
Christchurch and Burwood Hospitals were very full over the Christmas period What would normally be a quieter period was not Staff have been under significant pressure but have done a stellar job
Recently visited the SMHS site at Hillmorton to see the built environment and the constraints impacting on patients and staff Acknowledged the challenges that staff are working under They are dealing with complex patients in very challenging conditions yet the professionalism in care was clearly evident with constant reassessing triaging and attention to safety Progress with new facilities cannot come quick enough for staff
Burwood has a key quality focus on medication administration at the moment This involves a cross disciplinary approach
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
13
HAC-28jan21ndashminutesndashdraft Page 5 of 6 01042021
Looking across the board at how to mobilise and utilise nursing resources A current focus is on outpatient services ndash how we use that workforce in a different way and also advancing working at top of scope
Trendcare implementation and CCDM is progressing well in spite of some hiccups within the system These have largely been rectified ICU goes live with Trendcare mid-February and Surgery will be underway soon as well CCDM teams have been described as ldquobull doggishrdquo in their approach which will continue to ensure accurate and reliable data
COVID readiness planning is well underway working closely with Allied Health to ensure we are taking a cross disciplinary approach
MIQ nursing staff and the welfare teams have been under significant pressure during the holiday period but have delivered a high standard of care and support They perform a vital role in keeping NZ safe Mindful that staff have times where they feel stigmatised in the community and their wider family are impacted on by the role that they hold
Commend primary health who keep mobilising to support Whole system approach is working well
In spite of the pressure on staff across the system we continue to receive numerous letters and emails on the care provided and the willingness of nurses to go the extra mile
6 SERVICES SUPPORTING OLDER PEOPLE LIVING IN RURAL COMMUNITIES
Ralph La Salle Acting Executive Director Planning Funding amp Decision Support introduced the report noting it was in response to a request from the Committee last year to better understand initiativesservices in place currently and those that are planned to support our rural older population to remain in their own homescommunities and into the future Greta Bond Service Development Manager Older Persons Health (OPH) and Andrea Davidson OPH Portfolio Manager were in attendance The report was taken as read Discussion took place around the following
Strengths of the rural community as well as challenges presented by distance
Ageing population ndash in terms of this community it is not only about the clients of the services but also the people who are delivering the services Rurally we have an ageing workforce and in addition particularly with nursing a workforce where this is not their only job
The increase in demand for dementia care Rurally this can be difficult to deliver so new models of care are being looked at
Resources being deployed to rural areas and ensuring they are being utilised in the best possible way Working with the community to make sure that services are developing to meet the current needs of people as opposed to the traditional way that services have always been delivered
Falls prevention referral programme and uptake in the rural community
The availability of consumables particularly in terms of those which are meant to be provided on discharge from hospital and the impact this has on providing nursing rurally
An electronic referral form is being implemented within secondary care so someone referring for services in the community will be able to do this electronically This will be a big benefit to providing rural services
The Services Supporting Older People Living in Rural Communities report was noted
7 2021 WORKPLAN
The Committee received the 2021 Workplan noting that this is a working document
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
14
HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-28jan21ndashminutesndashdraft Page 1 of 6 01042021
MINUTES ndash PUBLIC
DRAFT MINUTES OF THE HOSPITAL ADVISORY COMMITTEE MEETING
held in the Board Room Level 1 32 Oxford Terrace Christchurch on Thursday 28 January 2021 commencing at 900am
PRESENT Andrew Dickerson (Chair) Jan Edwards James Gough Jo Kane (via Zoom) Naomi Marshall Ingrid Taylor and Sir John Hansen (Ex-Officio) APOLOGIES Apologies for absence were received and accepted from Barry Bragg and Dr Rochelle Phipps An apology for early departure was received and accepted from James Gough (1010am) EXECUTIVE SUPPORT Dr Andrew Brant (Acting Chief Executive) Becky Hickmott (Acting Executive Director of Nursing) Ralph La Salle (Acting Executive Director Planning Funding amp Decision Support) Dr Jacqui Lunday-Johnstone (Executive Director Allied Health Scientific amp Technical) Kay Jenkins (Executive Assistant Governance Support) and Anna Craw (Board Secretariat)
APOLOGIES Kirsten Beynon (General Manager Laboratories) Dr Richard French (Acting Chief Medical Officer) Berni Marra (Manager Ashburton Health Services) and Win McDonald (Transition Programme Manager Rural Health Services) IN ATTENDANCE
Full Meeting
Pauline Clark General Manager MedicalSurgical Womenrsquos amp Childrenrsquos Health amp Orthopaedics Dr Helen Skinner General Manager amp Chief of Service Older Persons Health amp Rehabilitation Dr Greg Hamilton General Manager Specialist Mental Health Services 1 INTEREST REGISTER
AdditionsAlterations to the Interest Register Naomi Marshall ndash Addition ndash NZ Nurses College Aotearoa - Member There were no other additionsalterations Declarations of Interest for Items on Todayrsquos Agenda There were no declarations of interest for items on todayrsquos agenda Perceived Conflicts of Interest There were no perceived conflicts of interest
2 CONFIRMATION OF PREVIOUS MEETING MINUTES
Resolution (0121) (Moved Ingrid TaylorSeconded Jan Edwards ndash carried) ldquoThat the minutes of the Hospital Advisory Committee meeting held on 3 December 2020 be approved and adopted as a true and correct recordrdquo
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
10
HAC-28jan21ndashminutesndashdraft Page 2 of 6 01042021
3 CARRIED FORWARD ACTION ITEMS
The carried forward action items were noted
4 HampSS MONITORING REPORT
The Committee considered the Hospital and Specialist Services Monitoring Report for December 2020 The report was taken as read General Managers introduced their respective divisions and spoke to their areas as follows Specialist Mental Health Services (SMHS) ndash Dr Greg Hamilton General Manager
Report focuses on SMHS Intellectual Disability Services to provide a greater depth of understanding Services are provided to inpatients in two different units o PSAID Unit This falls under our population-based funding and is for those
people with an intellectual disability and a mental health diagnosis o Whaikaha (ATampR ndash Assessment Treatment and Rehabilitation) This is funded
by Ministry of Health Disability Support Services with whom we have two contracts and is for people who are under Court order under two different Acts It is a secure unit Generally this cohort of people have relatively poor health both physical and mental health Some people have been there for a long period with the longest standing consumer having been there since 2003 This is an institutional type approach for a group of people who are highly vulnerable
There are a lot of incidents some of which are assaults ndash injury to staff and assaults between consumers
Staff are amazing in their commitment to this cohort of people People who work here are values driven and come to work to make a difference for this vulnerable population which includes taking on some of that risk we are trying to mitigate
Considerable frustration for ATampR with Disability Support Services in terms of how they fund that and the ability to provide a really good service Dr Hamilton thanked the Board for its investment The four new pods on the new facility are hoped to be occupied by the end of March 2021 He noted that this will significantly change the living standards and lives of some of the more complex long-term consumers
Older Persons Health amp Rehabilitation (OPHampR) Service ndash Dr Helen Skinner General Manager amp Chief of Service
Pressure Injury Prevention Project update The validated figures for the last four months of the 2020 year show 48 patients with pressure injuries versus 73 for the year prior so a reduction of 25 in terms of pressure injuries Staff are now very enthusiastic at looking at skin and ensuring they are picking up every possible blemish There is still further work to be done to get down to the aim of 95 avoidable pressure injuries knowing that 5 are unavoidable in terms of international best practice
Vestibular Screening Tool Pilot There is evidence for using vestibular screening which involves a series of four questions when patients come in to assess whether they have a risk of vestibular problems and what to do about it This is a piece of work the Allied Health Team is leading on and is being rolled out across the Older Persons Health amp Rehabilitation Service and will be rolled out into the community as well ED is interested also There is good evidence in terms of the validation of the tool in ED and the Acute setting so is something that could be used across the DHB in terms or reducing the risk of falls and identifying what the risks are
ERAS Highlighted OPHampRrsquos 2020 results from the national hip fracture registry database
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
11
HAC-28jan21ndashminutesndashdraft Page 3 of 6 01042021
There was discussion around needs assessments for patients particularly at Burwood for Aged Residential Care (ARC) Dr Skinner advised that times are monitored and data is kept to ensure there are no delays In terms of initial assessments there has been no delay There has been some delay in terms of community re-assessments Timeframes for assessment take anywhere between one to two working days
Queried whether there was too much demand versus supply with regards to ARC Dr Skinner advised we are running high occupancy levels in terms of dementia hospital elder care This is the one area where we run high compared to the rest of the country in terms of the capacity we have
There was discussion around the number of over 75s coming from rest homes and being admitted through ED and what is or could be done to address this Dr Skinner spoke of Advance Care Planning and Shared Goals of Care as well as what can be done differently in the community Becky Hickmott Acting Executive Director of Nursing noted that Ashburton has its own unique challenges in this space part of which is the primary health sector understanding its role She advised of a lot of changes and turnover in staff in Ashburton and this impacting the flow through to ED There is a significant piece of work underway to address this but it is not quite at the implementation stage
MedicalSurgical amp Womenrsquos amp Childrenrsquos Health amp Orthopaedics ndash Pauline Clark General Manager
Increase in acute presentations to Christchurch Hospital It is not just ED experiencing this but also the Acute Medical Assessment Unit the ldquoBone Shoprdquo the Surgical Assessment Unit and the Childrenrsquos Acute Assessment o ED experienced a sharp uplift in presentations that occurred in late September
prior to the transition to Waipapa Between January and the end of September 2020 there were an average 1830 presentations to ED per week Since then this has risen to an average of 2163 per week ndash an increase of 48 per day or 18
o This cannot be explained by population pressures ndash the rate of ED attendances per 10000 population increases sharply at the same time
o Within this we have seen an increase in self-referrals to the ED of around 2 - or 250 presentations per week
o Conversely there has been a slight decrease in GP referrals People are presenting directly but their reasons for being there are in alignment with their health needs Overall people presenting need to be assessed in an ED environment in a tertiary centre
o 24 hour medical centres both Riccarton and Moorhouse are also experiencing increased presentations so not just the ED
Medical Oncology As previously advised additional project support has been invested in to assist with a revision to the model of care This is in place and work is starting to pay dividends Two new medical oncologists have been appointed and discussions continue around a third appointment
High neo-natal occupancy This is a phenomenon being seen around New Zealand possibly not helped by the MoH lead in the space Andrew Simpson having left his role So again work in the neo-natal cot space has stalled CDHBrsquos neo-natal service is designed to take 40 to 45 Currently it is sitting at 54 Another four are being cared for as part of the paediatric ward which is putting additional pressure on paediatrics who are already experiencing demand issues We also have some women and babies out in other parts of NZ Very tight nationally when it comes to neo-natal bedscots
Return of surgery and progress against plan The opening of Waipapa provided a significant increase in acute theater capacity on the Christchurch Campus Will be in a position to report on this in more detail at the Committeersquos next meeting
Have seen significant gains in terms of the pre-operative stay in inpatients
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
12
HAC-28jan21ndashminutesndashdraft Page 4 of 6 01042021
Planned on having outplaced surgery back by Christmas with the exception of paediatric dental (which is planned for March due to availability of workforce and appropriate facilities) Outplacing has ceased
The plan around returning outsourced surgery is currently being tweaked to accommodate some unexpected sickness which will result in key people being away for a period of time
Recruitment of Anesthetic Technicians is an issue Have two staff coming from the UK in the next quarter and the search continues
Been working very closely with Sterile Supply They are a keen enabler
ESPIs CDHB and MoH have agreed an ESPI improvement plan which sees the DHB achieve compliance in ESPI 2 and 5 by 30 June 2021 A wobble was experienced in late Decemberearly January but are now on track to achieve this Specific actions that services are undertaking to enable us to deliver include o Orthopaedics have taken 64 long waiting electiveplanned patients requiring hand
surgery from the Plastic Service waitlist and put it into their own waitlist They are able to do this without needing to use anesthesia and are utilising theatre space at Burwood for this
o Vascular Surgery have been able to utilise funding that the MoH provided for additional clinics Have repatriated ambulatory treatment of varicose veins to the Outpatient Department
o Ear Nose and Throat Parental leave has affected capacity in the rhinology subspecialty however the full team is now back on board
o General Surgery A number of SMO staff have recently returned from extended sick and annual leave and a new fellow has started this week
o Some services are already green and will remain there
Discussion took place around
Issues with neo-natal cot capacity from both a regional and national perspective
Clinical safety in light of increased acute presentations
Fee structure for afterhours care The HampSS Monitoring report was noted
5 CLINICAL ADVISOR UPDATE (ORAL)
Becky Hickmott Acting Executive Director of Nursing provided the following updates
Acknowledged NICUrsquos capacity issues noting there have been a large number of extreme preterm as well as preterm births with babies who have high need and long stay The long stay has an ongoing impact Many came spontaneously in labour or with membranes ruptured Across the nation similar things are happening
Maternity is under pressure from a staffing point of view From a safety angle we are working to divert some of our nursing teams to help support
Christchurch and Burwood Hospitals were very full over the Christmas period What would normally be a quieter period was not Staff have been under significant pressure but have done a stellar job
Recently visited the SMHS site at Hillmorton to see the built environment and the constraints impacting on patients and staff Acknowledged the challenges that staff are working under They are dealing with complex patients in very challenging conditions yet the professionalism in care was clearly evident with constant reassessing triaging and attention to safety Progress with new facilities cannot come quick enough for staff
Burwood has a key quality focus on medication administration at the moment This involves a cross disciplinary approach
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
13
HAC-28jan21ndashminutesndashdraft Page 5 of 6 01042021
Looking across the board at how to mobilise and utilise nursing resources A current focus is on outpatient services ndash how we use that workforce in a different way and also advancing working at top of scope
Trendcare implementation and CCDM is progressing well in spite of some hiccups within the system These have largely been rectified ICU goes live with Trendcare mid-February and Surgery will be underway soon as well CCDM teams have been described as ldquobull doggishrdquo in their approach which will continue to ensure accurate and reliable data
COVID readiness planning is well underway working closely with Allied Health to ensure we are taking a cross disciplinary approach
MIQ nursing staff and the welfare teams have been under significant pressure during the holiday period but have delivered a high standard of care and support They perform a vital role in keeping NZ safe Mindful that staff have times where they feel stigmatised in the community and their wider family are impacted on by the role that they hold
Commend primary health who keep mobilising to support Whole system approach is working well
In spite of the pressure on staff across the system we continue to receive numerous letters and emails on the care provided and the willingness of nurses to go the extra mile
6 SERVICES SUPPORTING OLDER PEOPLE LIVING IN RURAL COMMUNITIES
Ralph La Salle Acting Executive Director Planning Funding amp Decision Support introduced the report noting it was in response to a request from the Committee last year to better understand initiativesservices in place currently and those that are planned to support our rural older population to remain in their own homescommunities and into the future Greta Bond Service Development Manager Older Persons Health (OPH) and Andrea Davidson OPH Portfolio Manager were in attendance The report was taken as read Discussion took place around the following
Strengths of the rural community as well as challenges presented by distance
Ageing population ndash in terms of this community it is not only about the clients of the services but also the people who are delivering the services Rurally we have an ageing workforce and in addition particularly with nursing a workforce where this is not their only job
The increase in demand for dementia care Rurally this can be difficult to deliver so new models of care are being looked at
Resources being deployed to rural areas and ensuring they are being utilised in the best possible way Working with the community to make sure that services are developing to meet the current needs of people as opposed to the traditional way that services have always been delivered
Falls prevention referral programme and uptake in the rural community
The availability of consumables particularly in terms of those which are meant to be provided on discharge from hospital and the impact this has on providing nursing rurally
An electronic referral form is being implemented within secondary care so someone referring for services in the community will be able to do this electronically This will be a big benefit to providing rural services
The Services Supporting Older People Living in Rural Communities report was noted
7 2021 WORKPLAN
The Committee received the 2021 Workplan noting that this is a working document
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
14
HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-
HAC-28jan21ndashminutesndashdraft Page 2 of 6 01042021
3 CARRIED FORWARD ACTION ITEMS
The carried forward action items were noted
4 HampSS MONITORING REPORT
The Committee considered the Hospital and Specialist Services Monitoring Report for December 2020 The report was taken as read General Managers introduced their respective divisions and spoke to their areas as follows Specialist Mental Health Services (SMHS) ndash Dr Greg Hamilton General Manager
Report focuses on SMHS Intellectual Disability Services to provide a greater depth of understanding Services are provided to inpatients in two different units o PSAID Unit This falls under our population-based funding and is for those
people with an intellectual disability and a mental health diagnosis o Whaikaha (ATampR ndash Assessment Treatment and Rehabilitation) This is funded
by Ministry of Health Disability Support Services with whom we have two contracts and is for people who are under Court order under two different Acts It is a secure unit Generally this cohort of people have relatively poor health both physical and mental health Some people have been there for a long period with the longest standing consumer having been there since 2003 This is an institutional type approach for a group of people who are highly vulnerable
There are a lot of incidents some of which are assaults ndash injury to staff and assaults between consumers
Staff are amazing in their commitment to this cohort of people People who work here are values driven and come to work to make a difference for this vulnerable population which includes taking on some of that risk we are trying to mitigate
Considerable frustration for ATampR with Disability Support Services in terms of how they fund that and the ability to provide a really good service Dr Hamilton thanked the Board for its investment The four new pods on the new facility are hoped to be occupied by the end of March 2021 He noted that this will significantly change the living standards and lives of some of the more complex long-term consumers
Older Persons Health amp Rehabilitation (OPHampR) Service ndash Dr Helen Skinner General Manager amp Chief of Service
Pressure Injury Prevention Project update The validated figures for the last four months of the 2020 year show 48 patients with pressure injuries versus 73 for the year prior so a reduction of 25 in terms of pressure injuries Staff are now very enthusiastic at looking at skin and ensuring they are picking up every possible blemish There is still further work to be done to get down to the aim of 95 avoidable pressure injuries knowing that 5 are unavoidable in terms of international best practice
Vestibular Screening Tool Pilot There is evidence for using vestibular screening which involves a series of four questions when patients come in to assess whether they have a risk of vestibular problems and what to do about it This is a piece of work the Allied Health Team is leading on and is being rolled out across the Older Persons Health amp Rehabilitation Service and will be rolled out into the community as well ED is interested also There is good evidence in terms of the validation of the tool in ED and the Acute setting so is something that could be used across the DHB in terms or reducing the risk of falls and identifying what the risks are
ERAS Highlighted OPHampRrsquos 2020 results from the national hip fracture registry database
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
11
HAC-28jan21ndashminutesndashdraft Page 3 of 6 01042021
There was discussion around needs assessments for patients particularly at Burwood for Aged Residential Care (ARC) Dr Skinner advised that times are monitored and data is kept to ensure there are no delays In terms of initial assessments there has been no delay There has been some delay in terms of community re-assessments Timeframes for assessment take anywhere between one to two working days
Queried whether there was too much demand versus supply with regards to ARC Dr Skinner advised we are running high occupancy levels in terms of dementia hospital elder care This is the one area where we run high compared to the rest of the country in terms of the capacity we have
There was discussion around the number of over 75s coming from rest homes and being admitted through ED and what is or could be done to address this Dr Skinner spoke of Advance Care Planning and Shared Goals of Care as well as what can be done differently in the community Becky Hickmott Acting Executive Director of Nursing noted that Ashburton has its own unique challenges in this space part of which is the primary health sector understanding its role She advised of a lot of changes and turnover in staff in Ashburton and this impacting the flow through to ED There is a significant piece of work underway to address this but it is not quite at the implementation stage
MedicalSurgical amp Womenrsquos amp Childrenrsquos Health amp Orthopaedics ndash Pauline Clark General Manager
Increase in acute presentations to Christchurch Hospital It is not just ED experiencing this but also the Acute Medical Assessment Unit the ldquoBone Shoprdquo the Surgical Assessment Unit and the Childrenrsquos Acute Assessment o ED experienced a sharp uplift in presentations that occurred in late September
prior to the transition to Waipapa Between January and the end of September 2020 there were an average 1830 presentations to ED per week Since then this has risen to an average of 2163 per week ndash an increase of 48 per day or 18
o This cannot be explained by population pressures ndash the rate of ED attendances per 10000 population increases sharply at the same time
o Within this we have seen an increase in self-referrals to the ED of around 2 - or 250 presentations per week
o Conversely there has been a slight decrease in GP referrals People are presenting directly but their reasons for being there are in alignment with their health needs Overall people presenting need to be assessed in an ED environment in a tertiary centre
o 24 hour medical centres both Riccarton and Moorhouse are also experiencing increased presentations so not just the ED
Medical Oncology As previously advised additional project support has been invested in to assist with a revision to the model of care This is in place and work is starting to pay dividends Two new medical oncologists have been appointed and discussions continue around a third appointment
High neo-natal occupancy This is a phenomenon being seen around New Zealand possibly not helped by the MoH lead in the space Andrew Simpson having left his role So again work in the neo-natal cot space has stalled CDHBrsquos neo-natal service is designed to take 40 to 45 Currently it is sitting at 54 Another four are being cared for as part of the paediatric ward which is putting additional pressure on paediatrics who are already experiencing demand issues We also have some women and babies out in other parts of NZ Very tight nationally when it comes to neo-natal bedscots
Return of surgery and progress against plan The opening of Waipapa provided a significant increase in acute theater capacity on the Christchurch Campus Will be in a position to report on this in more detail at the Committeersquos next meeting
Have seen significant gains in terms of the pre-operative stay in inpatients
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
12
HAC-28jan21ndashminutesndashdraft Page 4 of 6 01042021
Planned on having outplaced surgery back by Christmas with the exception of paediatric dental (which is planned for March due to availability of workforce and appropriate facilities) Outplacing has ceased
The plan around returning outsourced surgery is currently being tweaked to accommodate some unexpected sickness which will result in key people being away for a period of time
Recruitment of Anesthetic Technicians is an issue Have two staff coming from the UK in the next quarter and the search continues
Been working very closely with Sterile Supply They are a keen enabler
ESPIs CDHB and MoH have agreed an ESPI improvement plan which sees the DHB achieve compliance in ESPI 2 and 5 by 30 June 2021 A wobble was experienced in late Decemberearly January but are now on track to achieve this Specific actions that services are undertaking to enable us to deliver include o Orthopaedics have taken 64 long waiting electiveplanned patients requiring hand
surgery from the Plastic Service waitlist and put it into their own waitlist They are able to do this without needing to use anesthesia and are utilising theatre space at Burwood for this
o Vascular Surgery have been able to utilise funding that the MoH provided for additional clinics Have repatriated ambulatory treatment of varicose veins to the Outpatient Department
o Ear Nose and Throat Parental leave has affected capacity in the rhinology subspecialty however the full team is now back on board
o General Surgery A number of SMO staff have recently returned from extended sick and annual leave and a new fellow has started this week
o Some services are already green and will remain there
Discussion took place around
Issues with neo-natal cot capacity from both a regional and national perspective
Clinical safety in light of increased acute presentations
Fee structure for afterhours care The HampSS Monitoring report was noted
5 CLINICAL ADVISOR UPDATE (ORAL)
Becky Hickmott Acting Executive Director of Nursing provided the following updates
Acknowledged NICUrsquos capacity issues noting there have been a large number of extreme preterm as well as preterm births with babies who have high need and long stay The long stay has an ongoing impact Many came spontaneously in labour or with membranes ruptured Across the nation similar things are happening
Maternity is under pressure from a staffing point of view From a safety angle we are working to divert some of our nursing teams to help support
Christchurch and Burwood Hospitals were very full over the Christmas period What would normally be a quieter period was not Staff have been under significant pressure but have done a stellar job
Recently visited the SMHS site at Hillmorton to see the built environment and the constraints impacting on patients and staff Acknowledged the challenges that staff are working under They are dealing with complex patients in very challenging conditions yet the professionalism in care was clearly evident with constant reassessing triaging and attention to safety Progress with new facilities cannot come quick enough for staff
Burwood has a key quality focus on medication administration at the moment This involves a cross disciplinary approach
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
13
HAC-28jan21ndashminutesndashdraft Page 5 of 6 01042021
Looking across the board at how to mobilise and utilise nursing resources A current focus is on outpatient services ndash how we use that workforce in a different way and also advancing working at top of scope
Trendcare implementation and CCDM is progressing well in spite of some hiccups within the system These have largely been rectified ICU goes live with Trendcare mid-February and Surgery will be underway soon as well CCDM teams have been described as ldquobull doggishrdquo in their approach which will continue to ensure accurate and reliable data
COVID readiness planning is well underway working closely with Allied Health to ensure we are taking a cross disciplinary approach
MIQ nursing staff and the welfare teams have been under significant pressure during the holiday period but have delivered a high standard of care and support They perform a vital role in keeping NZ safe Mindful that staff have times where they feel stigmatised in the community and their wider family are impacted on by the role that they hold
Commend primary health who keep mobilising to support Whole system approach is working well
In spite of the pressure on staff across the system we continue to receive numerous letters and emails on the care provided and the willingness of nurses to go the extra mile
6 SERVICES SUPPORTING OLDER PEOPLE LIVING IN RURAL COMMUNITIES
Ralph La Salle Acting Executive Director Planning Funding amp Decision Support introduced the report noting it was in response to a request from the Committee last year to better understand initiativesservices in place currently and those that are planned to support our rural older population to remain in their own homescommunities and into the future Greta Bond Service Development Manager Older Persons Health (OPH) and Andrea Davidson OPH Portfolio Manager were in attendance The report was taken as read Discussion took place around the following
Strengths of the rural community as well as challenges presented by distance
Ageing population ndash in terms of this community it is not only about the clients of the services but also the people who are delivering the services Rurally we have an ageing workforce and in addition particularly with nursing a workforce where this is not their only job
The increase in demand for dementia care Rurally this can be difficult to deliver so new models of care are being looked at
Resources being deployed to rural areas and ensuring they are being utilised in the best possible way Working with the community to make sure that services are developing to meet the current needs of people as opposed to the traditional way that services have always been delivered
Falls prevention referral programme and uptake in the rural community
The availability of consumables particularly in terms of those which are meant to be provided on discharge from hospital and the impact this has on providing nursing rurally
An electronic referral form is being implemented within secondary care so someone referring for services in the community will be able to do this electronically This will be a big benefit to providing rural services
The Services Supporting Older People Living in Rural Communities report was noted
7 2021 WORKPLAN
The Committee received the 2021 Workplan noting that this is a working document
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
14
HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-28jan21ndashminutesndashdraft Page 3 of 6 01042021
There was discussion around needs assessments for patients particularly at Burwood for Aged Residential Care (ARC) Dr Skinner advised that times are monitored and data is kept to ensure there are no delays In terms of initial assessments there has been no delay There has been some delay in terms of community re-assessments Timeframes for assessment take anywhere between one to two working days
Queried whether there was too much demand versus supply with regards to ARC Dr Skinner advised we are running high occupancy levels in terms of dementia hospital elder care This is the one area where we run high compared to the rest of the country in terms of the capacity we have
There was discussion around the number of over 75s coming from rest homes and being admitted through ED and what is or could be done to address this Dr Skinner spoke of Advance Care Planning and Shared Goals of Care as well as what can be done differently in the community Becky Hickmott Acting Executive Director of Nursing noted that Ashburton has its own unique challenges in this space part of which is the primary health sector understanding its role She advised of a lot of changes and turnover in staff in Ashburton and this impacting the flow through to ED There is a significant piece of work underway to address this but it is not quite at the implementation stage
MedicalSurgical amp Womenrsquos amp Childrenrsquos Health amp Orthopaedics ndash Pauline Clark General Manager
Increase in acute presentations to Christchurch Hospital It is not just ED experiencing this but also the Acute Medical Assessment Unit the ldquoBone Shoprdquo the Surgical Assessment Unit and the Childrenrsquos Acute Assessment o ED experienced a sharp uplift in presentations that occurred in late September
prior to the transition to Waipapa Between January and the end of September 2020 there were an average 1830 presentations to ED per week Since then this has risen to an average of 2163 per week ndash an increase of 48 per day or 18
o This cannot be explained by population pressures ndash the rate of ED attendances per 10000 population increases sharply at the same time
o Within this we have seen an increase in self-referrals to the ED of around 2 - or 250 presentations per week
o Conversely there has been a slight decrease in GP referrals People are presenting directly but their reasons for being there are in alignment with their health needs Overall people presenting need to be assessed in an ED environment in a tertiary centre
o 24 hour medical centres both Riccarton and Moorhouse are also experiencing increased presentations so not just the ED
Medical Oncology As previously advised additional project support has been invested in to assist with a revision to the model of care This is in place and work is starting to pay dividends Two new medical oncologists have been appointed and discussions continue around a third appointment
High neo-natal occupancy This is a phenomenon being seen around New Zealand possibly not helped by the MoH lead in the space Andrew Simpson having left his role So again work in the neo-natal cot space has stalled CDHBrsquos neo-natal service is designed to take 40 to 45 Currently it is sitting at 54 Another four are being cared for as part of the paediatric ward which is putting additional pressure on paediatrics who are already experiencing demand issues We also have some women and babies out in other parts of NZ Very tight nationally when it comes to neo-natal bedscots
Return of surgery and progress against plan The opening of Waipapa provided a significant increase in acute theater capacity on the Christchurch Campus Will be in a position to report on this in more detail at the Committeersquos next meeting
Have seen significant gains in terms of the pre-operative stay in inpatients
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
12
HAC-28jan21ndashminutesndashdraft Page 4 of 6 01042021
Planned on having outplaced surgery back by Christmas with the exception of paediatric dental (which is planned for March due to availability of workforce and appropriate facilities) Outplacing has ceased
The plan around returning outsourced surgery is currently being tweaked to accommodate some unexpected sickness which will result in key people being away for a period of time
Recruitment of Anesthetic Technicians is an issue Have two staff coming from the UK in the next quarter and the search continues
Been working very closely with Sterile Supply They are a keen enabler
ESPIs CDHB and MoH have agreed an ESPI improvement plan which sees the DHB achieve compliance in ESPI 2 and 5 by 30 June 2021 A wobble was experienced in late Decemberearly January but are now on track to achieve this Specific actions that services are undertaking to enable us to deliver include o Orthopaedics have taken 64 long waiting electiveplanned patients requiring hand
surgery from the Plastic Service waitlist and put it into their own waitlist They are able to do this without needing to use anesthesia and are utilising theatre space at Burwood for this
o Vascular Surgery have been able to utilise funding that the MoH provided for additional clinics Have repatriated ambulatory treatment of varicose veins to the Outpatient Department
o Ear Nose and Throat Parental leave has affected capacity in the rhinology subspecialty however the full team is now back on board
o General Surgery A number of SMO staff have recently returned from extended sick and annual leave and a new fellow has started this week
o Some services are already green and will remain there
Discussion took place around
Issues with neo-natal cot capacity from both a regional and national perspective
Clinical safety in light of increased acute presentations
Fee structure for afterhours care The HampSS Monitoring report was noted
5 CLINICAL ADVISOR UPDATE (ORAL)
Becky Hickmott Acting Executive Director of Nursing provided the following updates
Acknowledged NICUrsquos capacity issues noting there have been a large number of extreme preterm as well as preterm births with babies who have high need and long stay The long stay has an ongoing impact Many came spontaneously in labour or with membranes ruptured Across the nation similar things are happening
Maternity is under pressure from a staffing point of view From a safety angle we are working to divert some of our nursing teams to help support
Christchurch and Burwood Hospitals were very full over the Christmas period What would normally be a quieter period was not Staff have been under significant pressure but have done a stellar job
Recently visited the SMHS site at Hillmorton to see the built environment and the constraints impacting on patients and staff Acknowledged the challenges that staff are working under They are dealing with complex patients in very challenging conditions yet the professionalism in care was clearly evident with constant reassessing triaging and attention to safety Progress with new facilities cannot come quick enough for staff
Burwood has a key quality focus on medication administration at the moment This involves a cross disciplinary approach
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
13
HAC-28jan21ndashminutesndashdraft Page 5 of 6 01042021
Looking across the board at how to mobilise and utilise nursing resources A current focus is on outpatient services ndash how we use that workforce in a different way and also advancing working at top of scope
Trendcare implementation and CCDM is progressing well in spite of some hiccups within the system These have largely been rectified ICU goes live with Trendcare mid-February and Surgery will be underway soon as well CCDM teams have been described as ldquobull doggishrdquo in their approach which will continue to ensure accurate and reliable data
COVID readiness planning is well underway working closely with Allied Health to ensure we are taking a cross disciplinary approach
MIQ nursing staff and the welfare teams have been under significant pressure during the holiday period but have delivered a high standard of care and support They perform a vital role in keeping NZ safe Mindful that staff have times where they feel stigmatised in the community and their wider family are impacted on by the role that they hold
Commend primary health who keep mobilising to support Whole system approach is working well
In spite of the pressure on staff across the system we continue to receive numerous letters and emails on the care provided and the willingness of nurses to go the extra mile
6 SERVICES SUPPORTING OLDER PEOPLE LIVING IN RURAL COMMUNITIES
Ralph La Salle Acting Executive Director Planning Funding amp Decision Support introduced the report noting it was in response to a request from the Committee last year to better understand initiativesservices in place currently and those that are planned to support our rural older population to remain in their own homescommunities and into the future Greta Bond Service Development Manager Older Persons Health (OPH) and Andrea Davidson OPH Portfolio Manager were in attendance The report was taken as read Discussion took place around the following
Strengths of the rural community as well as challenges presented by distance
Ageing population ndash in terms of this community it is not only about the clients of the services but also the people who are delivering the services Rurally we have an ageing workforce and in addition particularly with nursing a workforce where this is not their only job
The increase in demand for dementia care Rurally this can be difficult to deliver so new models of care are being looked at
Resources being deployed to rural areas and ensuring they are being utilised in the best possible way Working with the community to make sure that services are developing to meet the current needs of people as opposed to the traditional way that services have always been delivered
Falls prevention referral programme and uptake in the rural community
The availability of consumables particularly in terms of those which are meant to be provided on discharge from hospital and the impact this has on providing nursing rurally
An electronic referral form is being implemented within secondary care so someone referring for services in the community will be able to do this electronically This will be a big benefit to providing rural services
The Services Supporting Older People Living in Rural Communities report was noted
7 2021 WORKPLAN
The Committee received the 2021 Workplan noting that this is a working document
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
14
HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-
HAC-28jan21ndashminutesndashdraft Page 4 of 6 01042021
Planned on having outplaced surgery back by Christmas with the exception of paediatric dental (which is planned for March due to availability of workforce and appropriate facilities) Outplacing has ceased
The plan around returning outsourced surgery is currently being tweaked to accommodate some unexpected sickness which will result in key people being away for a period of time
Recruitment of Anesthetic Technicians is an issue Have two staff coming from the UK in the next quarter and the search continues
Been working very closely with Sterile Supply They are a keen enabler
ESPIs CDHB and MoH have agreed an ESPI improvement plan which sees the DHB achieve compliance in ESPI 2 and 5 by 30 June 2021 A wobble was experienced in late Decemberearly January but are now on track to achieve this Specific actions that services are undertaking to enable us to deliver include o Orthopaedics have taken 64 long waiting electiveplanned patients requiring hand
surgery from the Plastic Service waitlist and put it into their own waitlist They are able to do this without needing to use anesthesia and are utilising theatre space at Burwood for this
o Vascular Surgery have been able to utilise funding that the MoH provided for additional clinics Have repatriated ambulatory treatment of varicose veins to the Outpatient Department
o Ear Nose and Throat Parental leave has affected capacity in the rhinology subspecialty however the full team is now back on board
o General Surgery A number of SMO staff have recently returned from extended sick and annual leave and a new fellow has started this week
o Some services are already green and will remain there
Discussion took place around
Issues with neo-natal cot capacity from both a regional and national perspective
Clinical safety in light of increased acute presentations
Fee structure for afterhours care The HampSS Monitoring report was noted
5 CLINICAL ADVISOR UPDATE (ORAL)
Becky Hickmott Acting Executive Director of Nursing provided the following updates
Acknowledged NICUrsquos capacity issues noting there have been a large number of extreme preterm as well as preterm births with babies who have high need and long stay The long stay has an ongoing impact Many came spontaneously in labour or with membranes ruptured Across the nation similar things are happening
Maternity is under pressure from a staffing point of view From a safety angle we are working to divert some of our nursing teams to help support
Christchurch and Burwood Hospitals were very full over the Christmas period What would normally be a quieter period was not Staff have been under significant pressure but have done a stellar job
Recently visited the SMHS site at Hillmorton to see the built environment and the constraints impacting on patients and staff Acknowledged the challenges that staff are working under They are dealing with complex patients in very challenging conditions yet the professionalism in care was clearly evident with constant reassessing triaging and attention to safety Progress with new facilities cannot come quick enough for staff
Burwood has a key quality focus on medication administration at the moment This involves a cross disciplinary approach
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
13
HAC-28jan21ndashminutesndashdraft Page 5 of 6 01042021
Looking across the board at how to mobilise and utilise nursing resources A current focus is on outpatient services ndash how we use that workforce in a different way and also advancing working at top of scope
Trendcare implementation and CCDM is progressing well in spite of some hiccups within the system These have largely been rectified ICU goes live with Trendcare mid-February and Surgery will be underway soon as well CCDM teams have been described as ldquobull doggishrdquo in their approach which will continue to ensure accurate and reliable data
COVID readiness planning is well underway working closely with Allied Health to ensure we are taking a cross disciplinary approach
MIQ nursing staff and the welfare teams have been under significant pressure during the holiday period but have delivered a high standard of care and support They perform a vital role in keeping NZ safe Mindful that staff have times where they feel stigmatised in the community and their wider family are impacted on by the role that they hold
Commend primary health who keep mobilising to support Whole system approach is working well
In spite of the pressure on staff across the system we continue to receive numerous letters and emails on the care provided and the willingness of nurses to go the extra mile
6 SERVICES SUPPORTING OLDER PEOPLE LIVING IN RURAL COMMUNITIES
Ralph La Salle Acting Executive Director Planning Funding amp Decision Support introduced the report noting it was in response to a request from the Committee last year to better understand initiativesservices in place currently and those that are planned to support our rural older population to remain in their own homescommunities and into the future Greta Bond Service Development Manager Older Persons Health (OPH) and Andrea Davidson OPH Portfolio Manager were in attendance The report was taken as read Discussion took place around the following
Strengths of the rural community as well as challenges presented by distance
Ageing population ndash in terms of this community it is not only about the clients of the services but also the people who are delivering the services Rurally we have an ageing workforce and in addition particularly with nursing a workforce where this is not their only job
The increase in demand for dementia care Rurally this can be difficult to deliver so new models of care are being looked at
Resources being deployed to rural areas and ensuring they are being utilised in the best possible way Working with the community to make sure that services are developing to meet the current needs of people as opposed to the traditional way that services have always been delivered
Falls prevention referral programme and uptake in the rural community
The availability of consumables particularly in terms of those which are meant to be provided on discharge from hospital and the impact this has on providing nursing rurally
An electronic referral form is being implemented within secondary care so someone referring for services in the community will be able to do this electronically This will be a big benefit to providing rural services
The Services Supporting Older People Living in Rural Communities report was noted
7 2021 WORKPLAN
The Committee received the 2021 Workplan noting that this is a working document
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
14
HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-28jan21ndashminutesndashdraft Page 5 of 6 01042021
Looking across the board at how to mobilise and utilise nursing resources A current focus is on outpatient services ndash how we use that workforce in a different way and also advancing working at top of scope
Trendcare implementation and CCDM is progressing well in spite of some hiccups within the system These have largely been rectified ICU goes live with Trendcare mid-February and Surgery will be underway soon as well CCDM teams have been described as ldquobull doggishrdquo in their approach which will continue to ensure accurate and reliable data
COVID readiness planning is well underway working closely with Allied Health to ensure we are taking a cross disciplinary approach
MIQ nursing staff and the welfare teams have been under significant pressure during the holiday period but have delivered a high standard of care and support They perform a vital role in keeping NZ safe Mindful that staff have times where they feel stigmatised in the community and their wider family are impacted on by the role that they hold
Commend primary health who keep mobilising to support Whole system approach is working well
In spite of the pressure on staff across the system we continue to receive numerous letters and emails on the care provided and the willingness of nurses to go the extra mile
6 SERVICES SUPPORTING OLDER PEOPLE LIVING IN RURAL COMMUNITIES
Ralph La Salle Acting Executive Director Planning Funding amp Decision Support introduced the report noting it was in response to a request from the Committee last year to better understand initiativesservices in place currently and those that are planned to support our rural older population to remain in their own homescommunities and into the future Greta Bond Service Development Manager Older Persons Health (OPH) and Andrea Davidson OPH Portfolio Manager were in attendance The report was taken as read Discussion took place around the following
Strengths of the rural community as well as challenges presented by distance
Ageing population ndash in terms of this community it is not only about the clients of the services but also the people who are delivering the services Rurally we have an ageing workforce and in addition particularly with nursing a workforce where this is not their only job
The increase in demand for dementia care Rurally this can be difficult to deliver so new models of care are being looked at
Resources being deployed to rural areas and ensuring they are being utilised in the best possible way Working with the community to make sure that services are developing to meet the current needs of people as opposed to the traditional way that services have always been delivered
Falls prevention referral programme and uptake in the rural community
The availability of consumables particularly in terms of those which are meant to be provided on discharge from hospital and the impact this has on providing nursing rurally
An electronic referral form is being implemented within secondary care so someone referring for services in the community will be able to do this electronically This will be a big benefit to providing rural services
The Services Supporting Older People Living in Rural Communities report was noted
7 2021 WORKPLAN
The Committee received the 2021 Workplan noting that this is a working document
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
14
HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-28jan21ndashminutesndashdraft Page 6 of 6 01042021
8 RESOLUTION TO EXCLUDE THE PUBLIC
Resolution (0221) (Moved Naomi MarshallSeconded Jan Edwards ndash carried)
ldquoThat the Committee
i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 3 December 2020
For the reasons set out in the previous Committee agenda
2 CEO Update (if required) Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that
the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982rdquo
There being no further business the public section of the Hospital Advisory Committee meeting was closed at 1030am Approved and adopted as a true and correct record __________________________ ____________________ Andrew Dickerson Date of approval Chairperson
HAC - 01 April 2021 - P - Confirmation of Minutes - 28 January 2021
15
HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-01apr21-carried forward action list Page 1 of 1 01042021
CARRIED FORWARDACTION ITEMS
HOSPITAL ADVISORY COMMITTEE CARRIED FORWARD ITEMS AS AT 1 APRIL 2021
DATE RAISED ACTION REFERRED TO STATUS
1 01 Oct 2020 HampSS Monitoring Report ndash development of ldquoLiving Within Our Meansrdquo section
Dr Peter Bramley David Green
Under action
HAC - 01 April 2021 - P - Carried Forward Action List Items
16
Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

Mental HealthThe Acute
Adult Pathway
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
17
Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

Person centred response to people with acute mental health needs
bull Outline adult acute pathways
bull Demonstrate the services available
bull Understand how assessment (need) drives service responses
bull Provide context of responses within an integrated system
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
18
Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

Ministry of Health
bull Mental Wellbeing Framework
bull Kia Kaha Kia Māia Kia Ora Aotearoa COVID-19 Psychosocial and Mental Wellbeing Plan
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
19
What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

What happens when a person has a mental health problem
Person has mental health
problem
Community Response
Whanau
Community
General practice
NGO
Homecare medical
Specialist Assessment (real time referral)
Single point of Entry (SPOE)
Crisis resolution
Psych consult liaison
Watch house
Homecare medical
Specialist Response
Crisis Resolution (5d-6wk)
Community Service (outpatient) ndash case management (short-long term)
Inpatient ndash adult acute rehab
Acute community inpatient alternative
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
21
From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

From a service provision perspective
Specialist Mental Health Services
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
22
First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

First steps
bull When people are unwell and canrsquot be managed in the community with natural supports general practice and community resourceshellip
bull Referral
bull Phone
bull Turn up
bull Identified by other services
bull Triage ndash screening ndash assessment
bull Liaison ndash problem solving ndash supports ndash case management ndash high risk admission
bull Return people home with right supports
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
23
Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

Adult community servicesIn 2020
122000 contacts
6500 people
20
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
24
Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

Community Service Contacts
bull Multiple service responses
bull Support people to live and succeed in the community
Service 2020
Ashburton (including crisis) 4967
Crisis Resolution 878
Adult (East North South West) 90452
Hereford 7735
Psych Consult Liaison 4433
Rural 3129
Totara 5786
Watch house 2255
Clozapine clinic 102
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
25
Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

Adult inpatient services
In 2020
1356 admissions
Seagar 38 admissions
Tupuna 13 admissions
227 crisis admissions
24
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
26
Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

Key measures for inpatients
Good performance
0
20
40
60
80
100
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Au
g-1
7
No
v-1
7
Feb
-18
May
-18
Au
g-1
8
No
v-1
8
Feb
-19
May
-19
Au
g-1
9
No
v-1
9
Feb
-20
May
-20
Au
g-2
0
No
v-2
0
Feb
-21
Avg
No
of
Pat
ien
ts
Average Number of Te Awakura Patients Under Care and Sleeping at Midnight
Under care
TA Sleeping at midnight
40
50
60
70
80
90
100
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
Aphellip
Juhellip
Auhellip
Ochellip
Dehellip
Fehellip
o
f ca
ses
wh
ich
met
KP
I 19
Te Awakura Discharges which met KPI 19 (community care in the 7 days following the day of discharge)
40
45
50
55
60
65
70
75
80
85
Feb
-16
May-1
6
Au
g-16
No
v-16
Feb
-17
May-1
7
Au
g-17
No
v-17
Feb
-18
May-1
8
Au
g-18
No
v-18
Feb
-19
May-1
9
Au
g-19
No
v-19
Feb
-20
May-2
0
Au
g-20
No
v-20
Feb
-21
o
f ca
ses
wh
ich
met
KP
I 18
Te Awakura Admissions which met KPI 18 (community care in the 7 days prior to the day of admission)
0
5
10
15
20
25
30
35
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
Mahellip
Mahellip
Jul-hellip
Sehellip
Nohellip
Janhellip
R
ead
mit
ted
wit
hin
28
day
s
KPI 2 Te Awakura Patients Readmitted within 28 days of Discharge
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
27
Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

Impact of COVID-19
bull Significant decrease in admissions ndash but no decrease in community contacts
bull Innovative virtual services ndash not embedded
bull Facilities ndash inability to house Covid-positive inpatients (recycled air)
Admissions and Discharges
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
28
Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

Challenges
Community (outpatient)
bull Volumes
bull Complexity
bull Communication and planning
bull Housing and social supports
Inpatient
bull Environment ndash not fit for purpose
bull Seagar ndash bed reduction
bull Seclusion
System responses pathways and
communication
Facility redevelopment and programme
business case
HAC - 01 April 2021 - P - Mental HealthThe Acute Adult Pathway - Presentation
29
HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HampSS MONITORING REPORT
HAC-01apr21-HampSS monitoring report Page 1 of 1 01042021
TO Chair amp Members Hospital Advisory Committee
PREPARED BY General Managers Hospital Specialist Services
APPROVED BY Ralph La Salle Acting Executive Director Planning Funding amp Decision SupportDavid Green Acting Executive Director Finance amp Corporate Services
DATE 1 April 2021
Report Status ndash For Decision o Noting ˛ Information o
1 ORIGIN OF THE REPORT
This report is a standing agenda item highlighting the Hospital Specialist Services activity on the improvement themes and priorities
2 RECOMMENDATION
That the Committee
i notes the Hospital Advisory Committee Activity Report
3 APPENDICES
Appendix 1 Hospital Advisory Committee Activity Report ndashMarch 2021
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
30
HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 1 of 25
Hospital Advisory CommitteeHospital Activity Report
March 2021
Index Based on the CDHB Outcomes Framework and Five Focus areas plus Specialist Mental Health
Page 2 Frail Older Personsrsquo Pathway
Authors Helen Skinner General Manager amp Chief of Service OPHampR
Bernice Marra Manager Ashburton health Services
Page 7 Faster Cancer Treatment
Author Pauline Clark General Manager Christchurch Campus
Page 11 Enhanced Recovery After Surgery
Author Helen Skinner General Manager amp Chief of Service OPHampR
Page 13 Elective Surgery Performance Indicators
Author Pauline Clark General Manager Christchurch Campus
Page 16 Theatre Capacity and Theatre Utilisation
Author Pauline Clark General Manager Christchurch Campus
Page18 Mental Health Services
Author Greg Hamilton General Manager Specialist Mental Health Services
Page 23 Living within Our Means
Authors David Green Acting Executive Director Finance and Corporate Services and Pauline Clark General Manager Christchurch Campus
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
31
HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 2 of 25
Outcome and Strategy IndicatorsFigure 11
Covid 19 Alert Level restrictions led to a reduced number of ED attendances by people over 75 years in March and April 2020 with a subsequent return to forecast levels of attendances by that group
Figure12
Since mid-October total ED visits have increased by around 30 people a day predominantly by those under 30 years old This mostly involves triage levels 4 and 5 and thus places demand within the ED as these patients are not generally admitted
This along with the team working in a new and larger unit is providing challenges that contribute to patients spending a longer time in EDPlanning and Funding ED the Communication teamHealthline and Urgent Care providers are working together to put in place plans to improve the systemrsquos ability to provide the care required by the population Key hospital services including General Medicine Cardiology Orthopaedics and General Surgery are also working with the Emergency Department to optimise timeliness of flow through the department for people requiring specialist service care
Frail Older Personsrsquo Pathway
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
32
HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 3 of 25
Figure 13
The number admitted has returned to the forecast range following the COVID lockdown period
Figure 14
During the last nine months the number and rate of in hospital deaths against admissions has been within forecast range which reflects an underlying reducing trend in the rate
Figure 15
Readmissions remain within the expected range
Figure 16
Ashburton rate of attendances75+ age group has been running in line with expected attendance means
AchievementsIssues of Note
Ashburton Health Services Noting Figure 11 and Figure 12 is an extract of total ED data reporting we are mindful to provide clarity that this data set also includes presentations through Ashburton Acute Assessment Unit (AAU) The AAU data flow is rolled up and reported within the CDHB ED data extract set to the Ministry of Health The commentary however relates the type of growth experienced in ED Christchurch
Whilst AAU has experienced a growth in presentations this is not consistent daily but described as clumpy our admission rate of 30 remains constant and our presentation growth is in Triage 3 On average the occupancy of the wards remains high but this is currently influenced by the increased pressure from non-weight bearing patients from across Canterbury These patients are accepted into both wards and transferred once confirmation of bed availability This process may take place over several days A steady cohort of these patients require close observation that is ldquoone to onerdquo cares based on clinical assessment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
33
HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 4 of 25
Without access to pool resources of HCA and nursing alongside the fact that our staff is predominantly part time workers when we experience a spike in staff on leave via ACC injury it is a challenge to roster to any standard pattern In the first two months of the year this challenge has provided the team the environment of thinking outside the box and considering what is essential on the day
AAU presentationsThe graph below demonstrates the distribution of presentations to AAU across our three main cohorts The core information in the graph below is the variability Whilst we consistently look for trend data that can be interpreted to inform roster or resource distribution the volume on any given day is not consistent enough to create a succinct pattern This means our resourcing is consistent to the average but must also respond to surge In March we are commencing a weekend shift pattern of ED Registrars We will regularly reviewthe flow and test the impact this resource has on managing the consistently increased weekend surge on AAU ED Registrars are required to complete a community run as part of their training this provides the community run for this specialist service and a deployable resource for demand via the AAU
Occupancyinpatient trendsThe following table reports the length of stay by clinical cohort As a generalist service progressing towards a consolidation of wards (two physical wards will remain but the objective is to operate as one ldquovirtual wardrdquo) the length of stay is identified as a key monitor of integrated service delivery Any variance on occupancy of same clinical cohort between wards will be closely monitored to identify interventions that can connect ensure there is consistency for the patient experience
Integration influenceAlongside the review of acute flow and occupancy the integration cluster incorporating NASC district nursing and clinical nurse specialists have been detailing the flow of referral management and service response to primary care with an intent to create a more proactive responsive community service
The journey from health pathway information ERMS referral management through to service response has identified a number of areas for improvement We are working toward a target of 1 decline rate for referrals
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
34
HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 5 of 25
We are supporting the introduction of STRATA for inpatients led by Planning and Funding and are upliftingour information on patient care directly into the HealthOne platform This will enable primary care to have a distinct patient ldquocontactresponserdquo record as opposed to searching through Health Connect South for the progress note
Older Persons Health and Rehabilitation
Dementia-Friendly HospitalAlzheimers NZrsquos Accreditation Committee has now completed its assessment of Burwood Hospital againsttheir Dementia Friendly Recognition Programme standards and criteria Based on this Burwood Hospital hasbeen recognised as NZrsquos first hospital to be lsquoWorking to be Dementia Friendlyrsquo
To apply for this status the division provided a comprehensive self-assessment and the feedback receivedstated that this told ldquoa story of an organisation committed to working to be dementia friendly to seeking tounderstand the needs of people with dementia and to raising awareness and understanding across your staffand organisation The Committee were very impressed with the work you have described and also noted thecommitment you have shown in progressing work related to standards not required for this level ofrecognition Our review of your self-assessment concluded that Burwood Hospital meets the requirementsfor Working to be Dementia Friendlyrdquo
Burwood Hospital is now recognised as Working to be Dementia Friendly for two years from 10th March2021 In acknowledgement of this achievement Alzheimerrsquos NZ will visit the site to present a certificate andtake the opportunity to publicly promote Burwood Hospitalrsquos achievement and the dementia friendlyconcept together
As part of our journey towards being certified as being a lsquodementia friendlyrsquo hospital OPHampR are promoting the online training available at httpswwwalzheimersorgnzget-involvedbecome-a-dementia-friendwith the aim of engaging as many of our staff as possible from across all workforces to support dementia awareness provide excellent services for people with dementia and become a recognised lsquodementia friendrsquo
Safe medication administrationThe OPHampR senior clinical leadership team have commenced an interdisciplinary working group looking at safe medication administration practice aimed at reducing medication errors within the division
Initial work was focused around gaining a better understanding of current practice relating to administration of medication and the group are now seeking input from all nursing staff working in the hospital to better understand barriers to best practice and how the working environment can support safe medication administration To ensure learnings across the DHB this group is working alongside union partners and nursing leads across CDHB
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
35
HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 6 of 25
Outcome and Strategy Indicators
Key Outcomes - Faster Cancer Treatment Targets (FCT)
62 Day Target In the three months to the end of January 2021 there were 167 records submitted by Canterbury District Health Board ndash slightly down just on the 172 submitted for the three months to the end of December 32 patients missed the 62 days target 25 did so through patient choice or clinical reasons and are therefore excluded from consideration With 7 of the 142 patients missing the 62 days target through capacity issues our compliance rate was 951 once again meeting the 90 target
31 Day Performance Measure Of 327 records submitted towards the 31-day measure 294 (899) eligible patients received their first treatment within 31 days from a decision to treat the CDHB continues to meet the 85 target A total of 33 patients did not meet the 31 days target but it is worth noting that 11 missed it by 5 days or less and 7 through patient choice or clinical considerations
FCT performance in CDHB
The dip in numbers in the last month of every report (January in this case) reflects the timing of when the report is compiled which is governed by the reporting requirements of the Ministry A significant number of the patients who have a 1st treatment date in the period this report covers will be awaiting coding and will be picked up in the following monthrsquos extract
Faster Cancer Treatment
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
36
HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 7 of 25
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
37
HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 8 of 25
Patients who miss the targets
The MoH requires DHBs to allocate a code (referred to as a delay code) to all patients who miss the 62 days target There are three codes but only one can be submitted even if the delay is due to a combination of circumstances which is often the case When this happens the reason that caused the greatest delay is the one chosenThe codes are
1 Patient choice eg the patient requested treatment to start after a vacation or wanted more time to consider options
2 Clinical considerations includes delays due to extra tests being required for a definitive diagnosis or a patient has significant co-morbidities that delay the start of their treatment
3 Capacity this covers all other delays such as lack of theatre space unavailability of key staff or process issues
Each patient that does not meet the target is reviewed to see why This is necessary in order to determine and assign a delay code but where the delay seems unduly long a more in-depth check is performed These cases are usually discussed with the tumour stream Service Manager(s) to check whether any corrective action is requiredThe graph below shows the days waiting for each patient who met the 62 days criteria
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
38
HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 9 of 25
AchievementsIssues of Note
National Bowel Screening Updatesum Although the National Bowel Screening programme had a relatively soft launch in Canterbury and is still
in its early stages participation is nearing 56 - close to the target of 60 sum Equity for target groups is improving a weekly basis sum As at the beginning of March 2021 101 diagnostic procedures had been carried out as a result of positive
screening tests leading to the diagnosis of eight cancers that would have otherwise not been identified until after they became symptomatic This earlier diagnosis and treatment of bowel cancer will contribute to reducing the mortality associated with bowel cancer in Canterbury It will also result in less complex surgery being required and reduce demand on other services including Oncology
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
39
HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 10 of 25
Outcome and Strategy Indicators ndash Fractured Neck of Femur (NoF)Figure 31
Admissions are generally following the expected mean count Coding delay impacts the latest data point
Figure 32
The time spent in the ED by people with a fracturedneck of femur has increased This is in line with thedegradation in the proportion of people leaving EDwithin six hours of arrival that is commented on aboveIt is associated with a step change in the number ofpeople attending ED that occurred in October 2020 andthe shift to a new building Review of work practicesand resource levels against demand and therequirements of the environment is underway
Figure 33
The Functional Independence Measure (FIM) is a basic indicator of severity of disability
Figure 34
Readmissions continue to remain within expected mean values
Enhanced Recovery After Surgery (ERAS)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
40
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-
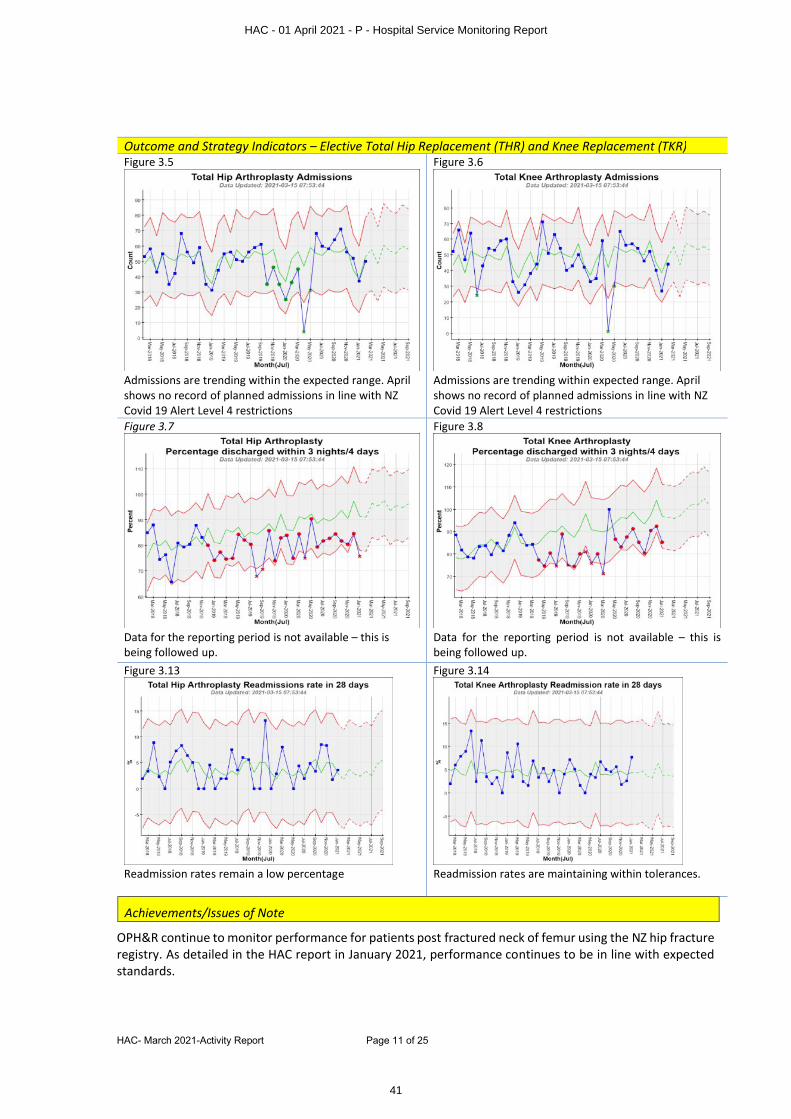
HAC- March 2021-Activity Report Page 11 of 25
Outcome and Strategy Indicators ndash Elective Total Hip Replacement (THR) and Knee Replacement (TKR)Figure 35
Admissions are trending within the expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 36
Admissions are trending within expected range April shows no record of planned admissions in line with NZ Covid 19 Alert Level 4 restrictions
Figure 37
Data for the reporting period is not available ndash this is being followed up
Figure 38
Data for the reporting period is not available ndash this is being followed up
Figure 313
Readmission rates remain a low percentage
Figure 314
Readmission rates are maintaining within tolerances
AchievementsIssues of Note
OPHampR continue to monitor performance for patients post fractured neck of femur using the NZ hip fracture registry As detailed in the HAC report in January 2021 performance continues to be in line with expected standards
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
41
HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 12 of 25
Elective Services Performance Indicators
Summary of ESPI 2 Performance - From MoH Final Summary January 2021 (published on 3 March)
Nov-20 Dec-20 Jan-21
ESPI 2 (FSA) Improvement required Status
Improvement required Status
Improvement required Status
Cardiothoracic Surgery 0 00 0 00 0 00Ear Nose and Throat 65 64 98 98 120 116General Surgery 18 14 43 37 192 160Gynaecology 4 13 4 12 14 34Neurosurgery 1 07 0 00 3 19Ophthalmology 112 92 160 116 324 221Orthopaedics 83 87 125 124 171 164Paediatric Surgery 7 64 6 53 6 47Plastics 164 309 191 375 253 442Thoracic 0 00 0 00 0 00Urology 0 00 2 300 8 12Vascular 65 348 81 370 86 387
Elective Surgery Performance Indicators100 Days
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
42
HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 13 of 25
Cardiology 17 42 10 24 31 67Dermatology 1 15 1 15 3 41Diabetes 13 76 20 118 37 213Endocrinology 9 34 16 57 27 89Endoscopy 292 210 297 207 298 207Gastroenterology 16 51 21 74 29 102General Medicine 4 29 1 06 2 10Haematology 0 00 1 16 1 14Infectious Diseases 1 100 0 00 0 00Neurology 13 37 26 77 53 139Oncology 8 29 5 16 17 53Paediatric Medicine 159 308 178 318 158 283Pain 0 00 0 00 14 452Renal Medicine 2 51 0 00 0 00Respiratory 22 73 26 86 25 77Rheumatology 0 00 1 03 5 15Total 1076 98 1313 116 1877 157ESPI 5 (Treatment)Cardiothoracic Surgery 0 00 0 00 0 00Dental 77 266 79 316 78 236Ear Nose and Throat 145 218 189 268 249 338General Surgery 223 342 254 334 277 351Gynaecology 37 121 32 105 50 144Neurosurgery 0 00 0 00 0 00Ophthalmology 31 82 33 82 68 147Orthopaedics 60 97 75 125 111 188Paediatric Surgery 18 149 25 223 24 212Plastics 79 82 169 163 247 214Urology 5 15 18 49 42 108Vascular 5 65 4 38 12 110Cardiology 81 229 92 284 124 355Total 761 158 970 193 1282 236
Note - ESPI 5 figures and ESPI2 figures are taken from the MoH ESPI Finals report for January 2021 published 3 March 2021
The CDHB Improvement Action Plan 2021 is in place and focusses on CDHB achieving ESPIPlanned Care compliance in the majority of services by the end of June Prior to the Christmas holidays CDHB was meeting the planrsquos overall target for the number of patients waiting for First Specialist Assessment however reduced capacity over the holiday period has been difficult to reverse As at 12th March the overall target is no longer being met 2028 people have waited longer than 120 days for their appointment Seven specialty areas have no patients waiting for First Specialist Assessment for longer than 120 days seven are meeting their recovery plan target and 32 are not
When considering patients waiting times for admission and treatment as at 12th March CDHB is not meeting the planrsquos targets 1338 people have waited longer than 120 days Three specialty areas are meeting their recovery plan target and ten are not
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
43
HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 14 of 25
Campus clinicians supported by operational teams are optimising the provision of clinic and theatre activity rigorously managing acceptance of referrals against HealthPathways criteria
Maternity Assessment Unit
The Maternity Assessment unit that was introduced in 2019 as a part of the Canterbury Maternity Strategy continues to achieve its goal of ensuring that pregnant women receive the right care at the right time
251 women presented at the unit in January and 249 in February with around one fifth of those going on to be transferred to the birthing suite for further treatment or consultation The average length of stay from the time of presentation to leaving the unit is around two hours
The unit continues to ensure that women are rapidly assessed those that need complex care are transferred immediately and those that do not are able to quickly return home It has reduced queues in the birthing suite and maternity unit and eliminated the long waiting times previously experienced in those settings
Telehealth Rheumatology care for Kaikourasum Some patients requiring long term care from the Rheumatology service require regular three or six
monthly follow up sum A Rheumatology clinic was been put in place in Kaikoura that had grown to two days every three
months however this clinic had become over-subscribedsum In order to address this a telemedicine clinic has been put in place in Kaikoura that enables
patients to receive on site care from a specifically trained registered nurse in Kaikoura while medical or CNS review is provided from Christchurch via telemedicine
sum The first telemedicine clinic will be provided in April and will enable on-site clinics in Kaikoura to be prioritised for those who most require face to face care while avoiding the need for stable patients requiring review to travel to Christchurch
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
44
HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 15 of 25
sumPlanned care targets have been provided to the Ministry of Health As per last year they incorporate
planned inpatient operations as well as range of procedures provided to hospital inpatients outpatients and patients in community settings
sum As at year end our target is to deliver a total of 31359 planned care interventions made up of 19614 surgical discharges 11409 minor procedures and 336 non-surgical interventions This is 2 higher than the 201920 target of 30675
sum Reporting from the Ministry of Health to the end of January shows that Canterbury District Health Board is exceeding its overall planned care targets by 38 however within this inpatient surgical discharges have fallen behind target
sum Internal reporting to the week ending 12 March shows that 29126 planned care events have been provided ndash this is 7911 ahead of the target of 21215
sum Within this 12981 planned inpatient surgical discharges were provided ndash 59 below the phased target of 13040 Planning and Funding Operational and Production Planning teams are working together to forecast capacity over the remainder of the year as a part of planning to ensure that we successfully deliver against these targets
sum 16071 Minor procedures have been provided 8127 ahead of the target of 7944 Inpatient outpatient and community provision are all ahead of target
Current theatre volumes sum Overall when all operating by or on behalf of Canterbury DHB is considered (in house outplaced and
outsourced) fewer operations were provided in theatres in January 2021 than in January 2020 (2019 compared with 2350) and more in February 2021 than February 2020 (2415 compared with 2366) despite a significant reduction in the use of outplaced and outsourced surgery following transition to Waipapa Further detail follows
sum Demand for arranged and acute surgery during January and February was 7 higher than in 2020 with 1110 theatre events in January 2021 and 1031 in February Initial analysis indicates that patients spent less time waiting for surgery following acute and arranged admission due to the improved availability of acute surgical capacity ndash however there are some specific periods when waiting times for acute surgery
Theatre Capacity and Theatre Utilisation
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
45
HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 16 of 25
remains a challenge As is our usual practice analysis of demand will inform planning of theatre capacity required during future public holidays
sum The number of planned operations carried out at Burwood Hospital was 22 lower in January and 1 higher in February than the same months the previous year with 154 planned events in January 2021and 258 in February
sum The number of outsourced and outplaced events has been reduced with increased in-house capacity enabling much of this work to be repatriated The final tranche of outplaced surgery being repatriated occurred in the last week of February when dental operating returned to Christchurch campus During January 93 outplaced or outsourced theatre events were provided ndash 31 of January 2020 there were 163 such events in February ndash 41 of the previous February
sum More elective surgery was provided at Christchurch Hospital during both January and February than in those months in 2020 with 687 elective theatre events in January 2021 and 977 in February 2021 compared with 679 and 660 in 2020
Waste minimisation grant application
Provision of cataract operating by the eye service has previously generated significant waste associated with the sterile packaging of surgical instruments It is estimated that cataract operations would generate 624 bags of steripeel waste and 312 bags of blue paper wrap in a year
The eye service has obtained a grant from the Christchurch City Council waste minimisation fund that has enabled it to purchase 13 stainless-steel cases and instrument sets enabling it to eliminate the requirement for disposable sterile packaging for its intraocular sets
An earlier pilot proved that as well as achieving the goal of eliminating consumable packaging but that it enables safe efficient management of fragile instruments It is hoped that modelling this approach will encourage broader adoption across other high-volume areas of surgery
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
46
HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 17 of 25
Recent reports from Specialist Mental Health Services to the Hospital Advisory Committee have focused on the adult child and youth forensic and intellectual disabilities This report focuses on the specialist services
The Anxiety Disorders Service
The Anxiety Disorders Service is a community-based team that provides treatment for people with moderate to severe anxiety disorders This service supports adult community services for people who respond to a more tailored service response The work includes a contribution to the broader mosque response
New cases for the Anxiety Disorders Service
Average waiting time to first face to face contact for the Anxiety Disorders Service
Outpatient face-to-face contacts for the Anxiety Disorders Service
Note the impact of Covid 19 the decrease in face-to-face contacts was replaced by large increases in phone and audio-visual contacts
Mental Health Services
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
47
HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 18 of 25
Eating Disorders amp Mothers amp Babies
The South Island Eating Disorders Service (SIEDS) is the tertiary level provider of eating disorders treatment for the five DHBs in the South Island It provides specialist inpatient beds for the South Island alongside specialist outpatient treatment training supervision and consultation This service considers the needs of consumers and their familywhanau across the age span whilst working at each level of the health care sector ie primary and secondary care
The South Island Mothers amp Babies Service provides a specialist perinatal mental health service for perinatal mental health care to the South Island incorporating inpatient and outpatient care education training and consult liaison for the treatment of mothers who are pregnant or have babies up to one year old The service operates as a hub and spoke model with the Mothers and Babies Service acting as a centre of expertise providing treatment supervision clinical consultation and input into workforce development to allow care to be provided in other DHBs the South Island where possible The goal is that every mother with severe mental health problems in the South Island has access to appropriate specialised care
New outpatient cases for the outpatient Eating Disorders and Mothers amp Babies teams
Average waiting time to first face to face contact for the outpatient Eating Disorders and Mothers amp Babies teams
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
48
HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 19 of 25
Outpatient contacts for the outpatient Eating Disorders and Mothers amp Babies teams
C Ward is the inpatient unit based at Princess Margaret Hospital which takes Eating Disorders and Mothers amp Babies patients in need of an admission C Ward has six beds for mothers six beds for babies and seven Eating Disorders beds which are used flexibly Adolescents with eating disorders are usually admitted to C Ward whereas children with eating disorders tend to be admitted to the 16 bed Child and Adolescent Unit
Admissions to C Ward
Note CWE = Eating Disorders CWM=Mothers amp Babies
Length of stay for C Ward
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
49
HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 20 of 25
Addictions Services
In Canterbury the co-ordination of addictions services is managed by the Christchurch Central Service (CCS) led by Odyssey House (a non-Government Organisation [NGO]) in partnership with other NGOs and Specialist Services Two outpatient addictions services are provided by Specialist Mental Health Services the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service CADS provides assessments and outpatient treatment for people that need assistance with co-existing moderate to severe alcohol or other drug dependence and mental illness The Christchurch Opioid Recovery Service is a harm reduction programme that leads opioid substitution treatment (methadone or suboxone) for people who have opioid dependence This service works in partnership with general practice and community pharmacy to provide community-based services for people who are stable
New outpatient cases for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
Average waiting time to first face to face contact for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
50
HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 21 of 25
Outpatient contacts for the Community Alcohol and Drug Service (CADS) and the Christchurch Opioid Recovery Service (CMP)
The Kennedy Detox Unit is based at Hillmorton Hospital The Kennedy Detox Unit is a six-bed regional inpatient unit which provides specialist medical withdrawal management and stabilisation from alcohol and other drugs for those with alcohol andor other drug dependence Patients usually commence NGO-run community-based addictions treatment programmes immediately upon discharge People commencing on opioid substitution also typically spend a half day at the Kennedy Detox Unit for establishment before moving onto treatment in the community
Admissions to the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
51
HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 22 of 25
Length of stay for the Kennedy Detox Unit
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
52
HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 23 of 25
The CDHB Statement of Financial Performance covers the following Hospital ServicesOlder Persons Health amp Rehab Medical amp SurgicalWomenrsquos amp Childrenrsquos Health Hospital Support amp LabsMental Health Facilities Management
2021 2021 2021 2021 2021 2021
Actual Budget Variance Actual Budget Variance
$000 $000 $000 $000 $000 $000
Operating Revenue
302 266 36 From Funder Arm 2177 2120 57
1689 1538 151 MOH Revenue 13019 12595 424
4700 4435 265 Patient Related Revenue 37520 35154 2366
2644 1704 940 Other Revenue 22455 13673 8782
9335 7943 1392 TOTAL OPERATING REVENUE 75171 63542 11629
Operating Expenditure
Personnel Costs
65445 64473 (972) Personnel Costs - CDHB Staff 542868 547445 4577
1833 1948 115 Personnel Costs - Bureau amp Contractors 16553 15838 (715)
67278 66421 (857) Total Personnel Costs 559421 563283 3862
12286 13988 1702 Treatment Related Costs 108045 111060 3015
3746 4037 291 Non Treatment Related Costs 32182 32262 80
83310 84446 1136 TOTAL OPERATING EXPENDITURE 699648 706605 6957
OPERATING RESULTS BEFORE
(73975) (76503) 2528 INTEREST AND DEPRECIATION (624477) (643063) 18586
Indirect Income
- 1 (1) Donations amp Trust Funds 98 10 88
- 1 (1) TOTAL INDIRECT INCOME 98 10 88
Indirect Expenses
2994 2413 (581) Depreciation 22233 19700 (2533)
- - - Loss on Disposal of AssetsNet (Gain) Loss on Disposal of Fixed assets (330) - 330
2994 2413 (581) TOTAL INDIRECT EXPENSES 21903 19700 (2203)
(76969) (78915) 1946 TOTAL SURPLUS (DEFICIT) (646282) (662753) 16471
Canterbury District Health Board
Statement of Financial Performance
Hospital amp Specialist Service Statement of Comprehensive Revenue and ExpenseFor the 8 Months Ended 28 February 2021
MONTH $000 YEAR TO DATE $000
Living within our means
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
53
HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 24 of 25
Waipapa Stock Levels
Transition to Waipapa has provide an opportunity to rationalise some of our approaches to ward suppliessum The physical structure of Waipapa has enabled reduced stock holding Store areas in Waipapa are shared
between two wards ndash halving the value of stock on hand for those areassum All Waipapa areas have gone on to scanning ensuring stock is ordered and delivered when it is neededsum The stock that was bought over from the wards was too much to hold in the shared rooms this surplus
is now being used as the first source of stock to top up ward store areas Items not being used quickly enough to avoid expiry is being directed elsewhere
sum There is active communication between wards and coordinators about stock that is no longer required or where minimummaximum values can be reduced ndash further trimming the value of holdings
Paediatric Medical Day Ward Trial of Play Therapy
The Paediatric Medical Day ward cares for 300-500 patients per month Tamariki attending the day ward often have complex and long-term health issues and benefit from building trust with the day ward team who support them and their whānau over their ongoing psychosocial and medical needs
Prior to Play Therapy being available on the Day Ward sedation was being used to enable anxious children to undergo various procedures The team was concerned about this and keen to provide a more tamarikiwhānau friendly option in partnership with the whānau to help increase coping skills
An audit of this service for cost effectiveness and improving health literacy coping skills and medication taking skills of the tamariki and their whānau to prevent inpatient admission This has improved adherence to the medication and ongoing treatment plans contributing to reduced admissions and timely discharge
Savings of $4700000 have been identified over this 12-month period viasum decrease in sedations for procedures $1780000 savingsum Tamariki now able to swallow tablets avoiding infusions $1029600 savingsum Improved management of constipation avoiding admission for dis impaction $464000 savingsum Improved management of constipation meaning one tamariki could be removed from the surgical
waitlist $1445000 saving
Whānau satisfaction with the service is high
Just in time supplies for whānau - Paediatric Outreach
Several whānau receive ongoing supplies via the Paediatric Outreach Nurses which enable their tamariki to stay at home attend school or early childhood education thus maintaining their wellbeing The type of supplies involved includes those required to assist with breathing or feeding for tamariki that have difficulties with these most fundamental human functions
In the past supplies were packaged up on a two monthly basis and delivered to the patientrsquos home However changes in the whānaursquos requirements meant that that supplies were sometimes wasted
The system has been changed Whānau now phone the Paediatric Outpatientrsquos aide ordering their requirements from a template The supplies are left at the orderlyrsquos lodge meaning that a family member can retrieve it with no parking costs
The small adjustments ensure that whānau feel more in control and order only what they can need ndash this has saved approx $1000 in the last month
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
54
HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC- March 2021-Activity Report Page 25 of 25
AchievementsIssues of Note
HAC - 01 April 2021 - P - Hospital Service Monitoring Report
55
HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-01apr21-clinical advisor update-allied health Page 1 of 1 01042021
CLINICAL ADVISOR UPDATE ndash ALLIED HEALTH
NOTES ONLY PAGE
HAC - 01 April 2021 - P - Clinical Advisor Update - Allied Health
56
HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-01apr21-resolution to exclude public Page 1 of 2 01042021
RESOLUTION TO EXCLUDE THE PUBLIC TO Chair amp Members Hospital Advisory Committee PREPARED BY Anna Craw Board Secretariat APPROVIED BY David Green Acting Executive Director Finance amp Corporate Services DATE 1 April 2021
Report Status ndash For Decision Noting Information
1 ORIGIN OF THE REPORT
The following agenda items for the meeting are to be held with the public excluded This section contains items for discussion that require the public to be excluded for the reasons set out below The New Zealand Public Health and Disability Act 2000 (the Act) Schedule 3 Clause 32 and 33 and the Canterbury District Health Board (CDHB) Standing Orders (which replicate the Act) set out the requirements for excluding the public
2 RECOMMENDATION
That the Committee i resolves that the public be excluded from the following part of the proceedings of this
meeting namely items 1 and 2 ii notes that the general subject of each matter to be considered while the public is excluded
and the reason for passing this resolution in relation to each matter and the specific grounds under Schedule 3 Clause 32 of the Act in respect to these items are as follows
GENERAL SUBJECT OF EACH MATTER TO BE CONSIDERED
GROUND(S) FOR THE PASSING OF THIS RESOLUTION
REFERENCE ndash OFFICIAL INFORMATION ACT 1982 (Section 9)
1 Confirmation of the minutes of the public excluded meeting of 28 January 2021
For the reasons set out in the previous Committee agenda
2 CEO Update (if required)
Protect information which is subject to an obligation of confidence To carry on without prejudice or disadvantage negotiations (including commercial and industrial negotiations) Maintain legal professional privilege
s 9(2)(ba)(i) s 9(2)(j) s 9(2)(h)
iii notes that this resolution is made in reliance on the Act Schedule 3 Clause 32 and that the
public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6 7 or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
HAC - 01 April 2021 - P - Resolution to Exclude the Public
57
HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-

HAC-01apr21-resolution to exclude public Page 2 of 2 01042021
3 SUMMARY
The Act Schedule 3 Clause 32 provides
ldquoA Board may by resolution exclude the public from the whole or any part of any meeting of the Board on the grounds that (a) the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of
information for which good reason for withholding would exist under any of sections 67 or 9 (except section 9(2)(g)(i) of the Official Information Act 1982rdquo
In addition Clauses (b) (c) (d) and (e) of Clause 32 provide further grounds on which a Board may exclude members of the public from a meeting which are not considered relevant in this instance
Clause 33 of the Act also further provides
ldquo(1) Every resolution to exclude the public from any meeting of a Board must state
(a) the general subject of each matter to be considered while the public is excluded and
(b) the reason for the passing of that resolution in relation to that matter including where that resolution
is passed in reliance on Clause 32(a) the particular interest or interests protected by section 6 or 7 or section 9 of the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the meeting in public and
(c) the grounds on which that resolution is based(being one or more of the grounds stated in Clause 32)
(2) Every resolution to exclude the public must be put at a time when the meeting is open to the public and the text of that resolution must be available to any member of the public who is present and form part of the minutes of the Boardrdquo
HAC - 01 April 2021 - P - Resolution to Exclude the Public
58
- Agenda
- Attendance
- Conflict of Interest Register
- Confirmation of Minutes - 28 January 2021
- Carried Forward Action List Items
- Mental HealthThe Acute Adult Pathway - Presentation
- Hospital Service Monitoring Report
- Clinical Advisor Update - Allied Health
- Resolution to Exclude the Public
-




















