
Maternal or neonatal infection: association with neonatal encephalopathy outcomes
Upload
khangminh22Category
view
3download
0
Advances in Neonatal Acute KidneyInjuryMichelle C. Starr, MD, MPH,a Jennifer R. Charlton, MD, MSc,b Ronnie Guillet, MD, PhD,c Kimberly Reidy, MD,d
Trent E. Tipple, MD,e Jennifer G. Jetton, MD,f Alison L. Kent, BMBS, FRACP, MD,c,g Carolyn L. Abitbol, MD,h
Namasivayam Ambalavanan, MD,i Maroun J. Mhanna, MD, MPH, MBA,k David J. Askenazi, MD, MSPH,j
David T. Selewski, MD, MS,l Matthew W. Harer, MD, on behalf of the Neonatal Kidney Collaborative Boardm
In this state-of-the-art review, we highlight the major advances over the last 5years in neonatal acute kidney injury (AKI). Large multicenter studies revealthat neonatal AKI is common and independently associated with increasedmorbidity and mortality. The natural course of neonatal AKI, along with therisk factors, mitigation strategies, and the role of AKI on short- and long-termoutcomes, is becoming clearer. Specific progress has been made in identifyingpotential preventive strategies for AKI, such as the use of caffeine in prematureneonates, theophylline in neonates with hypoxic-ischemic encephalopathy, andnephrotoxic medication monitoring programs. New evidence highlights theimportance of the kidney in “crosstalk” between other organs and how AKIlikely plays a critical role in other organ development and injury, such asintraventricular hemorrhage and lung disease. New technology has resulted inadvancement in prevention and improvements in the current management inneonates with severe AKI. With specific continuous renal replacement therapymachines designed for neonates, this therapy is now available and is beingused with increasing frequency in NICUs. Moving forward, biomarkers, such asurinary neutrophil gelatinase–associated lipocalin, and other new technologies,such as monitoring of renal tissue oxygenation and nephron counting, willlikely play an increased role in identification of AKI and those most vulnerablefor chronic kidney disease. Future research needs to be focused ondetermining the optimal follow-up strategy for neonates with a history of AKIto detect chronic kidney disease.
Since the publication of the“Neonatal Acute Kidney Injury”review in 2015, our understanding ofthe epidemiology and impact ofneonatal acute kidney injury (AKI)has exponentially increased.1 Single-center and multicenter work hasclearly revealed that AKI occurscommonly in critically ill neonatesand adversely impacts outcomes.2–4
In parallel to these advancements,our ability to identify AKI early,mitigate AKI, and provide renalreplacement therapy (RRT) withdevices designed for neonates has
improved.5,6 In this state-of-the-artreview, we will review neonatalkidney physiology, provide an updateof neonatal AKI knowledge(definitions, prevalence, outcomes,and complications), discuss thecurrent state of research, andappraise cutting edge data ontherapeutics and devices that willimprove care in the coming decade.
NEONATAL KIDNEY PHYSIOLOGY ANDIMPLICATIONS FOR AKI
A basic understanding of kidneystructure and function during
abstract
aDivision of Pediatric Nephrology, Department ofPediatrics, School of Medicine, Indiana University,Indianapolis, Indiana; bDivision of Nephrology, Departmentof Pediatrics, University of Virginia, Charlottesville,Virginia; cDivision of Neonatology, Department ofPediatrics, Golisano Children’s Hospital, University ofRochester Medical Center, Rochester, New York; dDivisionof Pediatric Nephrology, Department of Pediatrics, AlbertEinstein College of Medicine, Bronx, New York; eSection ofNeonatal-Perinatal Medicine, Department of Pediatrics,College of Medicine, The University of Oklahoma, OklahomaCity, Oklahoma; fDivision of Nephrology, Dialysis, andTransplantation, Stead Family Department of Pediatrics,University of Iowa Stead Family Children’s Hospital, IowaCity, Iowa; gCollege of Health and Medicine, The AustralianNational University, Canberra, Australia Capitol Territory,Australia; hDivision of Pediatric Nephrology, Department ofPediatrics, Miller School of Medicine, University of Miamiand Holtz Children’s Hospital, Miami, Florida; iDivisions ofNeonatology and jNephrology, Department of Pediatrics,University of Alabama at Birmingham, Birmingham,Alabama; kDepartment of Pediatrics, Louisiana StateUniversity Shreveport, Shreveport, Louisiana; lDivision ofNephrology, Department of Pediatrics, Medical Universityof South Carolina, Charleston, South Carolina; andmDivision of Neonatology, Department of Pediatrics, Schoolof Medicine and Public Health, University ofWisconsin–Madison
Drs Starr and Harer conceptualized and designed thisreview, drafted the initial manuscript, and reviewed andrevised the manuscript; Drs Charlton and Selewskiconceptualized and designed this review, coordinatedand provided oversight, and reviewed and revised themanuscript; Drs Guillet, Reidy, Tipple, Jetton, Kent,Abitbol, Ambalavanan, Mhanna, and Askenazi providedsubstantial acquisition and assimilation of the data,drafted sections of the manuscript, and criticallyrevised the manuscript; and all authors approved thefinal manuscript as submitted and agree to beaccountable for all aspects of the work.
DOI: https://doi.org/10.1542/peds.2021-051220
Accepted for publication Aug 13, 2021
To cite: Starr M C, Charlton J R, Guillet R, et al.Advances in Neonatal Acute Kidney Injury.Pediatrics. 2021;148(5):e2021051220
PEDIATRICS Volume 148, number 5, November 2021:e2021051220 STATE OF THE ART REVIEW
development is essential tounderstand neonatal AKI and itsconsequences.1 Nephrogenesisbegins at 5 weeks’ gestation andcontinues until 34 to 36 weeks’gestation.7 The nephron number ishighly variable at birth, rangingfrom 200 000 to 2.7 million, and isimpacted by a multitude of factors,including prematurity.8,9
There are several core principles ofneonatal physiology that uniquelyimpact the diagnosis andmanagement of neonatal AKI. First,both renal blood flow and perfusionpressure increase over the firstweeks of life in neonates. Theproportion of cardiac outputdelivered to the kidneys increasesfrom 5% during fetal life to 20% by2 years.10 Much of this increasedblood flow occurs after birth, withrenal blood flow doubling in thefirst 2 postnatal weeks. After birth,the distribution of blood flowtransitions from deeper, moremature glomeruli to superficial,cortical glomeruli.11 This change inblood flow can be altered bymedications (such as indomethacin),perinatal asphyxia, and maternalhemorrhage, which all predisposeneonates to AKI. Second, congruentwith the increased blood flow, theglomerular filtration rate (GFR)increases dramatically after birthand reaches adult levels by 2 yearsof age.12 The GFR is low in infants,both in absolute value and whencorrected for body surface area(milliliters per minute per 1.73meters2). For example, prematureinfants born at 26 weeks have a GFRas low as 0.7 mL/minute per kg onday 1 of age, which improves onlyslightly during the first severalweeks of life.12 In neonates with aphysiologically low GFR, additionalstressors, such as sepsis, hypoxia,hypotension, or other clinicalconditions common in prematurity,may increase the risk AKI. Third,urinary concentrating ability is low
at birth and reaches adult levels by1 year of age.13 Poor urinaryconcentrating ability, particularly inneonates with high insensible lossesor critical illness, predisposesneonates to volume depletion andsubsequent prerenal azotemia.Finally, neonatal kidneys appear tobe particularly susceptible toischemic injury to the renal tubules,even after a mild and short-terminsult. This is further complicatedwhen nephrotoxic medications, suchas gentamicin and otheraminoglycosides, are commonlyprescribed to critically ill neonatesand result in tubular injury.
DEFINITIONS OF AKI
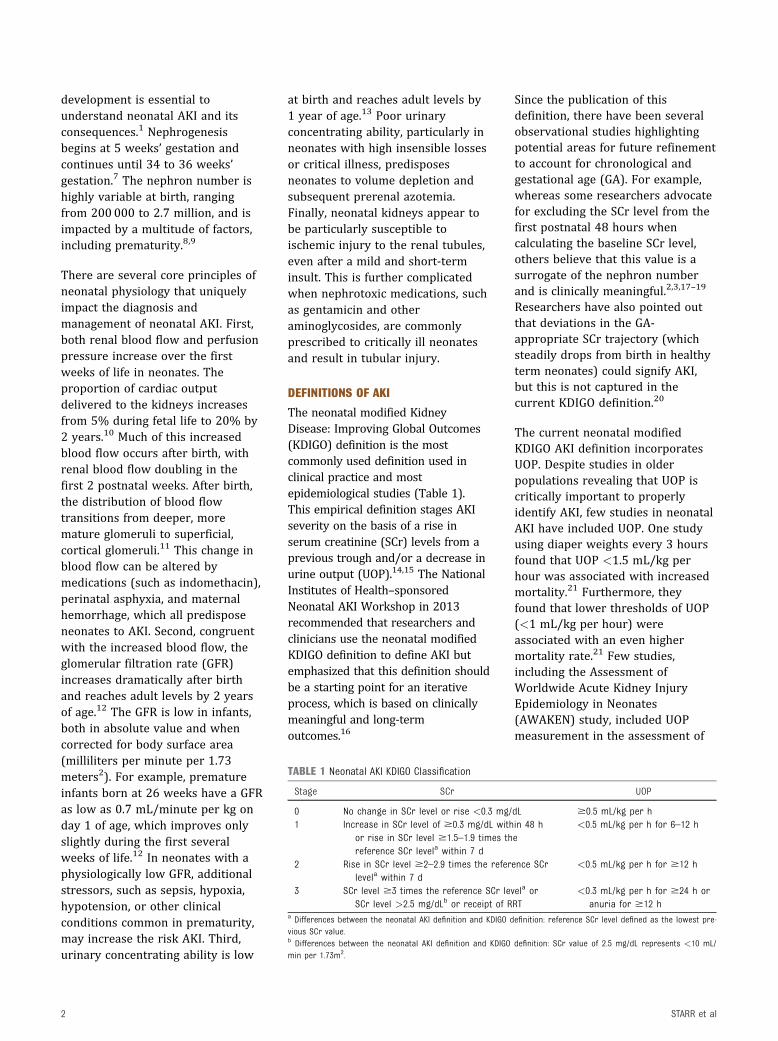
The neonatal modified KidneyDisease: Improving Global Outcomes(KDIGO) definition is the mostcommonly used definition used inclinical practice and mostepidemiological studies (Table 1).This empirical definition stages AKIseverity on the basis of a rise inserum creatinine (SCr) levels from aprevious trough and/or a decrease inurine output (UOP).14,15 The NationalInstitutes of Health–sponsoredNeonatal AKI Workshop in 2013recommended that researchers andclinicians use the neonatal modifiedKDIGO definition to define AKI butemphasized that this definition shouldbe a starting point for an iterativeprocess, which is based on clinicallymeaningful and long-termoutcomes.16
Since the publication of thisdefinition, there have been severalobservational studies highlightingpotential areas for future refinementto account for chronological andgestational age (GA). For example,whereas some researchers advocatefor excluding the SCr level from thefirst postnatal 48 hours whencalculating the baseline SCr level,others believe that this value is asurrogate of the nephron numberand is clinically meaningful.2,3,17–19
Researchers have also pointed outthat deviations in the GA-appropriate SCr trajectory (whichsteadily drops from birth in healthyterm neonates) could signify AKI,but this is not captured in thecurrent KDIGO definition.20
The current neonatal modifiedKDIGO AKI definition incorporatesUOP. Despite studies in olderpopulations revealing that UOP iscritically important to properlyidentify AKI, few studies in neonatalAKI have included UOP. One studyusing diaper weights every 3 hoursfound that UOP <1.5 mL/kg perhour was associated with increasedmortality.21 Furthermore, theyfound that lower thresholds of UOP(<1 mL/kg per hour) wereassociated with an even highermortality rate.21 Few studies,including the Assessment ofWorldwide Acute Kidney InjuryEpidemiology in Neonates(AWAKEN) study, included UOPmeasurement in the assessment of
TABLE 1 Neonatal AKI KDIGO Classification
Stage SCr UOP
0 No change in SCr level or rise <0.3 mg/dL $0.5 mL/kg per h1 Increase in SCr level of $0.3 mg/dL within 48 h
or rise in SCr level $1.5–1.9 times thereference SCr levela within 7 d
<0.5 mL/kg per h for 6–12 h
2 Rise in SCr level $2–2.9 times the reference SCrlevela within 7 d
<0.5 mL/kg per h for $12 h
3 SCr level $3 times the reference SCr levela orSCr level >2.5 mg/dLb or receipt of RRT
<0.3 mL/kg per h for $24 h oranuria for $12 h
a Differences between the neonatal AKI definition and KDIGO definition: reference SCr level defined as the lowest pre-vious SCr value.b Differences between the neonatal AKI definition and KDIGO definition: SCr value of 2.5 mg/dL represents <10 mL/min per 1.73m2.
2 STARR et al

AKI, thus limiting the available dataon which to base thresholds fordiagnosis and determination ofseverity of AKI. In future studies,researchers should carefullymeasure UOP to determine theimpact of UOP on AKI diagnosis inneonates.
Given the interest and focus on AKIdiagnostic thresholds, it is likely thata refined definition of neonatal AKIwill emerge. Two recentpublications, including an analysis ofthe AWAKEN study, suggest analternative definition for neonatalAKI.22,23 In this study, the authorsproposed different cutoffs for thefirst postnatal week by GA,compared with the subsequentweeks, and provided cutoffs by GAgroup.23 For example, in infants#29 weeks’ GA, a rise in the SCrlevel of 0.6 mg/dL confers thehighest prediction of mortality,whereas in infants >29 weeks’ GA, arise of 0.3 mg/dL is of highestmortality prediction.23 Furthermore,we anticipate that novel approachesof using urine biomarkers, SCrthresholds, UOP thresholds, andfluid balance metrics will be used toenhance the current neonatal KDIGOdefinition. In the interim, werecommend that the neonatalmodified KDIGO definition be usedas the standard until newerdefinitions are widely validated inlarge multisite trials and correlatedwith long-term outcomes.
EPIDEMIOLOGY, RISK FACTORS, ANDASSOCIATED FINDINGS WITH AKI
AKI is common in critically illneonates. We present a summary ofthe risk factors associated withneonatal AKI (Table 2) and the most
notable studies evaluating theepidemiology and impact ofneonatal AKI in the last 5 years(Table 3). Much of this increasedknowledge stems from the AWAKENstudy, which enrolled neonates atrisk for AKI (determined by >48hours of intravenous fluids). In thiscohort, the risk of AKI occurred in abimodal pattern, with extremely lowgestational age neonates (ELGANs)(<28 weeks) and term infants at thegreatest risk.4 The AWAKEN studyidentified a clear variation in SCrmonitoring practices across centers,with less than half of centerschecking $5 SCr levels duringhospital admission. Not surprisingly,the rates of AKI by center weredirectly correlated with the averagenumber of SCr samples ascertainedper subject.4 This practice variationis particularly notable in the contextof the recent Baby NephrotoxicInjury Negated by Just-in-TimeAction (NINJA) publication, whichrevealed that by monitoring SCrmore frequently in neonates withhigh nephrotoxic medicationexposure, there was an increasedawareness of the risk for AKI that,in turn, resulted in a lower rate andduration of AKI.17 These datasuggest that critically ill neonatesmay benefit from protocolized SCrmonitoring during high-risk events.
Preterm Neonates
The risk of AKI increases markedlywith decreasing GA.2,3 In cohorts ofvery low birth weight (VLBW)neonates, the incidence of AKI isreported between 18% and 40%.3,24
In ELGANs enrolled in the PretermErythropoietin NeuroprotectionTrial, 38% had at least 1 episode ofAKI.2 In the AWAKEN study, AKI
occurred in 45% of neonates <29weeks’ GA and in 14% of neonates 29to 36 weeks’ GA. In the AWAKENstudy, the potentially modifiable riskfactors for early AKI in ELGANs weremainly medication exposures.25 Givenimmature tubular function andresulting poor urinary concentrationability, along with the increasedinsensible losses common in pretermneonates, volume depletion leading toprerenal azotemia is a common factorpredisposing this population to AKI.
Patent ductus arteriosus (PDA) is animportant clinical issue for preterminfants and is associated with ahigher risk of AKI.26,27 PDArepresents a clinical challengebecause AKI may result if it is leftuntreated; however, classic PDAtherapies may also be associatedwith AKI. Although nonsteroidalantiinflammatory drug (NSAID)treatment of PDA added anadditional risk for mild AKI, severeAKI was less likely when NSAIDtreatment was effective.26
Term or Near-Term Critically IllNeonates
In the AWAKEN study, the incidenceof AKI in neonates born at $36weeks and admitted to a NICU was37%.4 The etiology of AKI in termneonates is often multifactorial andincludes risk factors related to theirillness and management(Table 2).25,28 Multiorgandysfunction is common and occursin up to 70% of neonates withAKI.29–31 Some of the major riskfactors for AKI include hypoxic-ischemic encephalopathy (HIE),cardiac disease, surgery, andnephrotoxic medications.
TABLE 2 Epidemiology, Risk Factors and Associated Findings with Neonatal AKI
Prenatal Perinatal Postnatal
Factors that increase risk of a preterm or LBWneonate, placental insufficiency
Exposure to nephrotoxic medications (ACEinhibitors, NSAIDs), delivery complicationsresulting in hypoxia and/or asphyxia, HIE
Prematurity, LBW, CHD, inborn errors ofmetabolism, sepsis, nephrotoxin exposure,PDA, extracorporeal therapies
ACE, angiotensin-converting enzyme; LBW, low birth weight.
PEDIATRICS Volume 148, number 5, November 2021 3

HIE
There is a general agreement thatthe presence of AKI in the setting ofHIE is associated with pooroutcomes (increased mortality, poorneurodevelopmental outcomes,longer hospital stay, and longerduration of mechanicalventilation).30,32,33 In addition, thereis a correlation between severity ofHIE and AKI, with 70% of those
with stage III HIE having AKI,compared with 7.4% of those withstage II HIE.32
Cardiac Disease and ExtracorporealMembrane Oxygenation
Infants who require cardiac surgeryand those who need extracorporealmembrane oxygenation (ECMO) areat high risk for AKI. AKI occurs in30% to 50% of patients undergoing
surgery for congenital heart disease(CHD).34–36 One single-centerretrospective study of neonates withsingle ventricle physiologyundergoing stage 1 Norwoodpalliation found that 21% developedAKI.36 A large Danish registry studyrevealed that 33% of neonates hadAKI within 5 days of surgery.35 In amulticenter retrospective cohortstudy of 832 pediatric patients on
TABLE 3 Summary of Neonatal AKI Studies Published Between 2015 and 2020
Author (Year), NStudy Design and Population
Details Main Findings
Jetton et al4 (2017),N 5 2162
Neonates requiring >48 h ofintravenous fluids in the NICU
AKI occurred in 45% of the infants at #28 wk GA and in 14% of infants at 29–36wk GA.
Charlton et al25,28
(2019), N 5 2162Secondary analysis of infants
from the AWAKEN studyAntimicrobial agents, methylxanthines, diuretics, NSAIDs, hypertensive disorders of
pregnancy, and hypoglycemia were associated with lower odds of early AKI. Ininfants at 29–25 wk GA, outborn status, saline bolus during resuscitation, andmore frequent SCr monitoring were associated with higher odds of early AKI.
Askenazi et al2
(2000), N 5 923Prospective study of ELGANs in
the PENUT trialThirty-eight percent had at least 1 episode of stage 1 or higher AKI, and 18.2%
had 1 episode of stage 2 or higher AKI.Selewski et al51
(2019), N 5 645Retrospective analysis of infants
at $36 wk GA from theAWAKEN study
Median peak fluid balance was 1.0% (IQR: �0.5 to 4.6) over the first postnatalweek and occurred on postnatal d 3 (IQR: 1 to 5). Mechanical ventilation onpostnatal d 7 was associated independently with the following measures offluid balance over the first postnatal week: peak fluid balance (aOR: 1.12; 95%CI: 1.08 to 1.17), lowest fluid balance in first postnatal week (aOR: 1.14; 95% CI:1.07 to 1.22), fluid balance on postnatal d 7 (aOR: 1.12; 95% CI: 1.07 to 1.17),and negative fluid balance at postnatal d 7 (aOR: 0.3; 95% CI: 0.16 to 0.67).
Selewski et al53
(2020), N 5 1007Retrospective analysis of infants
at <36 wk GA from theAWAKEN study
Median peak fluid balance was 0% (IQR:�2.9 to 2) and occurred on postnatal d 2 (IQR:1 to 5). Mechanical ventilation on postnatal d 7 was associated independently withthe following measures of fluid balance over the first postnatal week: peak fluidbalance (aOR: 1.14; 95% CI: 1.10 to 1.19), lowest fluid balance (aOR: 1.12; 95% CI: 1.07to 1.16), fluid balance on postnatal d 7 (aOR: 1.10; 95% CI: 1.06 to 1.13), and negativefluid balance at postnatal d 7 protected against the need for mechanical ventilationat postnatal d 7 (aOR: 0.21; 95% CI: 0.12 to 0.35).
Nour et al120 (2020),N 5 30
Retrospective analysis inneonates with HIE whounderwent cooling viaselective head cooling
No difference in AKI between the those receiving selective head cooling and thosenot. SCr levels and UOP were significantly improved on d 4 and d 10 samplescompared with baseline samples in both groups regardless of cooling. Therewas a difference in NGAL levels, but not CysC levels, on d 4 and 10.
Bellos et al90 (2019),N 5 458
Meta-analysis of effectiveness oftheophylline administration inneonates with perinatalasphyxia
Incidence of AKI significantly lower in neonates receiving theophylline (OR: 0.24;95% CI: 0.16 to 0.36), whereas mortality rates were similar between the 2groups (OR: 0.86; 95% CI: 0.46 to 1.62). Theophylline administration wasassociated with significantly decreased SCr levels (MD: �0.57 mg/dL; 95% CI:�0.68 to �0.46) in the third day of life.
Harer et al89 (2018),N 5 675
Retrospective analysis ofpremature infants at <33 wkGA from the AWAKEN study
AKI occurred less frequently in neonates who received caffeine in the first weekof life than in those who were not treated with caffeine (11.2% vs 31.6%; P <
.01). Neonates who received caffeine had more AKI risk factors, including loweraverage GA, lower birth wt, and high severity of illness scores, and were stillless likely to develop stage 2 or 3 AKI. The No. needed to treat with caffeine toprevent 1 episode of AKI was 4.3.
Stoops et al17
(2019)Prospective quality improvement
effort to reduce nephrotoxicmedication–associated AKI inthe NICU
Reduced high nephrotoxic medication exposures from 16.4 to 9.6 per 1000patient-days (P 5 .03), reduced nephrotoxic medication–associated AKI from30.9% to 11.0% (P < .001), and reduced AKI severity from 9.1 to 2.9 per 100susceptible patient-days (P < .001) prevented 100 AKI episodes during the 18-mo sustainability era.
Starr et al103 (2019),N 5 546
Retrospective analysis ofpremature infants at <32 wkGA from the AWAKEN study
Infants born between 29 and 32 wk GA with AKI had fourfold higher odds ofmoderate or severe BPD or death after controlling for multiple factors (aOR:4.21; 95% CI: 2.07 to 8.61).
aOR, adjusted odds ratio; BPD, bronchopulmonary dysplasia; IQR, interquartile range; MD, mean difference; PENUT, Preterm Erythropoietin Neuroprotection Trial.
4 STARR et al

ECMO, 74% had AKI.34 AKI waspresent at initiation of ECMO in themajority of cases and was associatedwith a longer ECMO duration andincreased mortality.34 The risk ofAKI in those on ECMO varies byunderlying diagnosis; those withcongenital diaphragmatic herniawere more likely to require RRT.37
Surgery
The incidence of AKI is high innoncardiac surgery; 34% of neonatesundergoing abdominal and thoracicsurgery have an episode of AKI.38
Infants with AKI after surgery weremore likely to have VLBW. They werealso more likely to have sepsis, alonger duration of mechanicalventilation, an operative time >120minutes, necrotizing enterocolitis(NEC), and a higher risk ofmortality.38 Among infants withsurgically managed NEC, almost 60%had severe AKI (stage 2 or 3).39
Nephrotoxic Medications
Many neonates are exposed tonephrotoxic medications in theNICU, which can contribute to AKI.Although there are manynephrotoxic medications, theseprimarily include antimicrobialagents (eg, acyclovir, amphotericinB, aminoglycosides,vancomycin).25,28 It was recentlyreported in Baby NINJA, a single-center quality improvementprogram focused on reducingnephrotoxic medication–associatedAKI, that attention to high-riskneonates, including daily SCrmonitoring, reduces nephrotoxicmedication exposures (P 5 .03),nephrotoxic medication–associatedAKI (P < .001), and AKI duration (P< .001).17 This suggests thatidentification and monitoring ofhigh-risk neonates, with a thoughtfulconsideration of nephrotoxicmedications, may minimize AKI andits consequences in critically illneonates.
FLUID BALANCE
The development of fluid overload isan independent predictor of adverseoutcomes across pediatric criticalcare populations.40–49 Thedevelopment of fluid overload isoften multifactorial, resulting fromAKI, iatrogenic fluid administration,capillary leak from systemicinflammation, and aberranthomeostatic mechanisms.41
Additionally, fluid overload canmake the diagnosis of AKI morechallenging because SCr is diluted inthe setting of a positive fluidbalance, resulting in a potentialunderdiagnosis of AKI.41 Precisedefinitions are essential tounderstanding the epidemiology andimpact of excessive fluidaccumulation on outcomes inneonates (Table 4).50 The 2 mostcommon methods used to calculatefluid balance are the cumulativefluid balance and weight-basedmethods. The weight-based methodto describe fluid balance is used tocalculate the degree of fluidoverload on the basis of a change inweight from a baseline weight (birthweight or determined dry weight)51:daily fluid balance 5 change in dailyweight day to day; cumulative fluidbalance 5 daily weight � baselineweight; percentage fluid overload44 5([daily weight � baseline weight]/baseline weight) � 100.
Although each method has beenused in older children, the weight-based methods represent thestandard in neonates because fluidbalances have been shown to beinaccurate.51–53 It is critical to use
standardized weight measurementprotocols to properly perform theweight-based technique.52,54
Fluid balance in the early postnatalperiod can be challenging tointerpret in the setting of normalpostnatal diuresis and expectednegative fluid balance. Although anaverage weight loss of 7% frombirth weight is described in termneonates, the normal fluid balancefor neonates of other GAs is lessclearly defined, particularly inextremely preterm neonates withexcessive skin permeability.55 Earlypositive postnatal fluid balance isassociated with adverse short-(death, mechanical ventilation onday 7) and long-term outcomes(bronchopulmonary dysplasia) inneonates.51,53,56–59 There remains apaucity of data defining thepathologic state of fluid overload incritically ill neonates, which in olderchildren, is commonly defined as acumulative positive fluid balance of$10% to 20%.48,60 Multiple criticalgaps exist in our understanding ofthe causes and impact of abnormalfluid balance in neonates. Thesegaps include interpreting fluidbalance in neonates, especially thosewho have spent a considerable timein the NICU. Research is greatlyneeded to understand the optimalthreshold to define appropriate fluidbalance and to understand thedetrimental effects of neonatal fluidoverload on extrarenal organsystems (eg, oxygenation index andcardiac dysfunction due to excessivefluid and reduced contractility).Understanding the role of fluid
TABLE 4 Definitions of Excessive Fluid Accumulation in Neonates
Term Definition
Daily fluid balance Daily difference between input and output or change in wt over a 24-h period
Cumulative fluid balance Change in fluid balance over a given durationFluid overload Cumulative fluid balance expressed as a percentage of body wt; used
to refer to the pathologic state of excessive fluid accumulationassociated with the development of sequelae attributable to fluidaccumulation and adverse outcomes
PEDIATRICS Volume 148, number 5, November 2021 5

balance in various neonatalpopulations (premature versus termneonates) at critical time points(perinatal versus postnatal versuspostsurgical) in the context ofunderlying disease process (NEC,lung disease, and sepsis) is a criticalknowledge gap. Answers to thesequestions will drive therapeuticinterventions designed to preventand mitigate harm from fluids.
NEW ADVANCES IN AKI RESEARCH
Biomarkers of AKI
Proteins and metabolites are 2examples of biomarkers that can bemeasured consistently and correlatewith the disease occurrence orprogression.61 Given the diversity ofGA and etiologies of AKI inneonates, 1 biomarker does notappear to reliably predict AKI.However, more reference ranges arebecoming available for novel urinarybiomarkers by GA and postnatalage.62 SCr represents the currentstandard for diagnosing neonatalAKI. However, it is critical tounderstand the shortcomings of SCrand develop novel biomarkers thatfill these gaps. A rise in the SCr levelindicates a loss of kidney function,reflecting injury that occurred up to48 to 72 hours before.63 As a result,biomarker studies, such as the onesbelow, have been focused onidentifying injury and functionalchanges before permanent damage(Table 5).
Cystatin C (CysC) is a cysteineprotease inhibitor that is freely
filtered by glomeruli and reabsorbedin the proximal tubule. Althoughboth serum and urinary CysC havebeen assessed as early markers ofAKI, a rise in the serum CysC levelreflects a change in kidney function,whereas an elevated urinary CysClevel is considered reflective oftubular injury.12,64–68 A recentsystematic review of neonatesacross all GA groups suggested thatserum CysC may be superior to SCrfor assessing the GFR.65
Furthermore, an elevated urinaryCysC level has been shown to havean area under the curve of 0.85(95% confidence interval [CI]: 0.81to 0.88) in predicting a rise in theSCr level 24 to 96 hours later inneonates post surgery or afterperinatal asphyxia.67
There are several other biomarkersthat may help identify injury andfunctional changes beforepermanent damage in neonates withAKI. Neutrophilgelatinase–associated lipocalin(NGAL) is a protein bound toneutrophil granules, filtered by theglomerulus, and reabsorbed by theproximal tubules.69 NGAL is highlysensitive (87%–93%) and specific(87%–93%) for AKI in neonateswith perinatal asphyxia.70 Thecombination of G1 cell cycle arrestbiomarkers urinary tissue inhibitorof metalloproteinase 2 (TIMP-2) andinsulinlike growth factor bindingprotein 7 (IGFBP-7) is promising fordetecting early AKI. It has beenshown to have a sensitivity of 89%and a specificity of 51% for
predicting AKI in critically illneonates.71 This combination hasbeen evaluated in pediatric andadult populations and has beenshown to perform well in predictingsubsequent severe AKI.63 Both NGALand TIMP-2 and IGFBP-7 arecurrently used off label in multiplepediatric and adult ICUs to evaluatefor AKI, and there are severalongoing studies assessing theirutility in pediatric AKI.72 Kidneyinjury molecule 1 is atransmembrane protein that isupregulated in kidney injury, andelevated levels have been shown topredict AKI.73 By using SCr as thegold standard, the areas under thecurve of several of these biomarkers(in particular, NGAL and TIMP-2and IGFBP-7) are highly predictivefor AKI.73 It is imperative that webegin to incorporate novelbiomarkers into future definitionsof neonatal AKI and into clinicalcare.
Nephron Number
In humans, there is wide variabilityin the nephron number present,even in the neonatal period becausethe completion of nephrogenesisoccurs at 26 to 34 weeks.8,9,74 Themechanisms (in utero and ex utero)that influence nephrogenesis, andultimately nephron endowment, andthe processes regulating nephronloss are poorly understood.7
Preclinical advancements have beenmade in measuring the whole-kidney functional nephron numberin vivo with a novel contrast agent.Cationic ferritin-enhanced MRI has
TABLE 5 Biomarkers in Use or Under Study to Assist With AKI Prediction and Diagnosis
Biomarker Location of Injury Notes
SCr Reflects kidney function, not injury; metabolic product ofskeletal muscle creatine
Delayed marker (48–72 h) of kidney function
CysC Reflects kidney function, not injury (serum); proximaltubule injury (urine)
Increase in the serum CysC level is thought to reflect a changein GFR or kidney function, whereas an elevated urinary CysClevel is considered reflective of tubular injury
NGAL Distal tubule and collecting duct Highly sensitive for ischemia and nephrotoxinsKidney injury molecule 1 Proximal tubule injury Regulates apoptosis, promotes epithelial regenerationTIMP-2 and IGFBP-7 Tubule cells Limits proliferation of damaged tubule cells; marker of early AKI
6 STARR et al

been used to measure theglomerular number and size inhealth and disease.75,76 The radialglomerular count, a surrogatemarker of glomerulogenesis,suggests that the nephron number isdecreased in both prematureneonates and in those with AKI.77
Further work is necessary totranslate this technique to humans,including neonates, to furtherunderstand those at risk for futurechronic kidney disease (CKD).78
Tissue Oxygenation
Noninvasive continuous monitoringof renal oxygen saturation withnear-infrared spectroscopy (NIRS) isa new diagnostic tool that may leadto earlier diagnosis of AKI.79 Renaltissue oxygenation (RrSO2)monitoring is a surrogate for localtissue oxygen use. In neonates withCHD, NIRS monitoring of the kidneypostoperatively can predict AKI.80 Inpremature neonates, those whosubsequently develop AKI havelower RrSO2 in the first postnatalday or week.81,82 In postoperativecardiac patients, NIRS detected adecline in RrSO2 before AKI wasdefined by SCr or UOP.83 In thoseundergoing therapeutic hypothermiafor HIE, neonates with AKI hadhigher RrSO2 values, likely pointingto a different cause or type of injury,than preterm infants or infants withCHD.84 Further work is needed toestablish normative RrSO2 values inneonatal populations and treatmentguidelines incorporating RrSO2
values.
EVALUATION OF NEONATAL AKI
Evaluating a neonate who developsAKI requires a systematic approach,which includes consideration ofcommon factors contributing to AKI.A detailed history should beobtained to assess for risk factorsfor AKI, including birth weight andGA, antenatal events (includingprenatal ultrasounds), pregnancycomplications, birth history
(interventions required at delivery),nephrotoxic medications exposure,and postnatal events. Physicalexamination should include anassessment of volume status, whichshould also include weight, dailyfluid balance, and cumulative fluidbalance. Fluid balance assessment isessential because volume depletionis a common cause of AKI andvolume overload is a commoncomplication of AKI. Positive fluidbalance still may mean poor renalperfusion if neonates have ongoingthird spacing due to capillary leak.Maintaining euvolemia is achallenging but essentialmanagement strategy in infants bothto prevent AKI and to mitigatesevere volume overload andcomplications. Focused laboratoryevaluation should be performed,including measurement of serumelectrolytes and serum ureanitrogen, as well as of SCr and/orCysC for GFR assessment.65 At thistime, there is not a definitive rolefor urine biomarker assessment inall neonates, but growing datasuggest that it may be useful incertain clinical settings to predictAKI.71 Fractional excretion ofsodium may be helpful in someinfants in differentiating volumedepletion from intrinsic causes ofAKI but can be challenging tointerpret in premature infantsbecause of tubular immaturity.12 Werecommend that an ultrasound beobtained to evaluate for evidence ofobstruction as well as congenitalabnormalities of the kidney. Anultrasound can also determinekidney size. However, more studiesare needed to know if kidney size ishelpful in understanding clinicallykidney-related meaningfuloutcomes.85
MANAGEMENT OF NEONATAL AKI
Although the search for treatmentsor interventions for establishedneonatal AKI has remained elusive,medications have been evaluated in
high-risk neonatal cohorts toprevent AKI. There have beenmultiple therapeutics evaluated forAKI prevention in neonates (withoutpositive results), includingerythropoietin, therapeutichypothermia, remote ischemicpreconditioning, andcorticosteroids.86–88
Methylxanthines have beenevaluated in multiple neonatalpopulations and have had promiseas a preventive treatment of AKI inhigh-risk populations.89,90
After diagnosis of AKI, carefulmanagement of fluid balance andmedications is essential topreventing the development ofcomplications. Strict documentationof all fluid input and output, alongwith daily weights, is essential tooptimizing fluid balance.Nephrotoxic medications should beassessed daily and reduced oreliminated whenever possible.17
Cumulative fluid balance should becarefully monitored to assess overallvolume status. Infants with volumedepletion may require additionalfluid in the form of either enteralfeeding, intravenous boluses, ordrips. In infants with volumeoverload, diuretics can be trialed tomaintain UOP.91 Response tofurosemide (furosemide stress test)has been used as a functionalbiomarker for predicting severeAKI.92 Although furosemide has notbeen evaluated in all neonatalpopulations, term infants with CHDwith a lower response to furosemide(median UOP at 2 hours afterfurosemide treatment 1.2 vs 3.4 mL/kg per hour; P 5 .01) have anincreased risk for persistent AKI.Although furosemide responsivenessis a potential functional marker ofkidney status, more studies inneonates are needed to standardizethe dose and definitions used.
Theophylline and its related salt,aminophylline, have had success inincreasing UOP and may prevent
PEDIATRICS Volume 148, number 5, November 2021 7

AKI in infants with HIE.Theophylline is an adenosinereceptor antagonist that preventsAKI by inhibiting adenosine-induced renal vasoconstriction. Arecent meta-analysis of 7randomized controlled trials (458neonates with asphyxia notreceiving therapeutichypothermia) found thattheophylline administration wasassociated with a significantlylower incidence of AKI (odds ratio[OR]: 0.24; 95% CI: 0.16 to 0.36).90
On the basis of this evidence, asingle dose of theophylline withinthe first 6 postnatal hours innewborns with HIE is endorsed inthe 2012 KDIGO guidelines toprevent AKI.15 Aminophylline hasalso had promise as a rescuetherapy in neonates with AKItreated with therapeutichypothermia.93
Caffeine is also an adenosinereceptor antagonist that has beenevaluated for renoprotective effectsin preterm cohorts. Two studiesrevealed that AKI occurred lessfrequently in VLBW infants andpreterm infants <33 weeks’ GA whoreceived caffeine within the firstpostnatal week. In a retrospectivestudy of 140 VLBW neonates,94 AKIoccurred less frequently in thosewho received caffeine (17.8% vs43.6%; P 5 .002). In a secondaryanalysis of the AWAKEN study, AKIoccurred less frequently in neonates<33 weeks GA who receivedcaffeine in the first postnatal week(11.2% vs 31.6%, P < .01).89 Onthe basis of these data, the numberthat needed to be exposed tocaffeine to prevent 1 episode ofAKI was 4.3.89
RRT
RRT remains the primary therapyfor the complications of severe AKI.The indications for RRT in neonatesinclude acidosis, fluid overload,electrolyte abnormalities, and
uremia refractory to medicalmanagement. The 2 most commonmodalities for RRT in neonates areperitoneal dialysis (PD) andcontinuous renal replacement therapy(CRRT). CRRT can be added to theextracorporeal circuit in infantsreceiving ECMO therapy. Between PDand CRRT, the choice often dependson the available resources, centerexperience, and patientcharacteristics.95 These therapies arecomplementary in that someneonates or situations will have ahigher chance of success with PD,whereas others will benefit fromCRRT. PD remains a common firstchoice for RRT in most institutionsbecause it does not require vascularaccess, is more available, and is oftentechnically easier in the smallestpatients.95 PD can be performed byusing a temporary catheter if the RRTrequirement is thought to be short-term. Depending on the catheter used,PD can be successful in neonates assmall as 830 g.96
CRRT may be preferred inhemodynamically unstable infants,those with a history of abdominalsurgery or NEC (which makes PDtechnically challenging), or those inwhom tight control of volume statusis necessary. In the past, the soleavailability of CRRT equipmentdesigned for adults and largerchildren presented a challenge toperform CRRT in neonates. Thisnecessitated the use for largercatheters, tubing, and filters, resultingin high extracorporeal volumes andgreater hemodynamic instability,often requiring either bloodtransfusions or blood priming witheach circuit change. Recent advanceshave made CRRT increasinglyaccessible and successful forneonates. Introduction of smallerfilters, such as the HF-20 (totalextracorporeal vol of 60 mL), whichwas recently approved by the USFood and Drug Administration for usein the United States, has improved
both the availability and acceptanceof therapies by decreasing theextracorporeal volume and improvingfluid removal precision.97
In recent years, industry has madesignificant innovations in neonatalRRT by developing neonatal-specificCRRT machines and repurposingmachines for neonatal use.98 TheCardio-Renal Pediatric DialysisEmergency Machine (Medtronic,Minneapolis, MN) was approved foruse in children between 2.5 and8 kg the United States in 2020 andhas been used in multiple countriesoutside the United States. Thismachine was developed specificallyfor neonates and small children.5 Incontrast, Aquadex (AquadexFlexFlow; CHF Solutions, EdenPrairie, MN) is an ultrafiltrationdevice designed for adults but withan extracorporeal vol of 33 mL,making it ideal to adapt to safelyprovide CRRT to infants.5 SuccessfulCRRT using Aquadex has beenreported in infants as small as 1.4kg.5 These machines and others,such as the Newcastle InfantDialysis and Ultrafiltration System(Newcastle National Health ServiceFoundation Trust, Newcastle, UnitedKingdom), have begun torevolutionize the field of CRRT forneonates by lowering the associatedrisks and will change theconversation about when and inwhom to initiate CRRT.6,99
COMPLICATIONS OF AKI
Cross Talk Between AKI and OtherOrgans
AKI has been shown to adverselyimpact other organs.100 Initiallythought to be only an association,studies suggest a causal relationshipin which AKI appears to drive otherorgan dysfunction and vice-versa,referred to as “crosstalk.”101
Experimental models describe alung-focused inflammatory process,driven in part by cytokines such as
8 STARR et al

interleukins after AKI, which aredeleterious to the lungs.102 Bothpreterm and term infants with AKIhave worse lung outcomes thantheir peers without AKI, includinglonger durations of mechanicalventilation and higher rates ofbronchopulmonarydysplasia.103,104 Neonatal AKI hasbeen shown to be an independentrisk factor for neurologiccomplications, such asintraventricular hemorrhage, poorlong-term neurocognitiveoutcomes, and cardiovasculardisease (hypertension).105,106
Risk of CKD After AKI
The risk of developing CKD or end-stage kidney disease after AKI iswell detailed in adults.107 Theevidence of progression from AKI toCKD is less established in childrenwith AKI. In a systematic review of346 children (mean follow-up 6.5years), the incidence of an abnormalGFR <90 mL/minute per 1.73 m2
was 6.3% (95% CI: 5.1 to 7.5).108
The mechanisms for progression toCKD are incompletely understoodbut likely are secondary tomaladaptive repair, ongoinginflammation, and disorderedregeneration.109,110 Histologicfindings of preterm neonates revealabnormal glomeruli likely to developsclerosis later, which could be theexplanation for later CKD in thosewith AKI.111 These changes may besuperimposed on a decreasednephron number and reduction infuture development of nephrons dueto prematurity.74
The evidence for progression fromAKI to CKD in neonates is less clear.Several studies have identifiedevidence of kidney abnormalities inpreterm infants with a history ofAKI.112,113 In contrast, other studieshave failed to identify differences inCKD or GFR in follow-up of preterminfants who had AKI as
neonates.86,114,115 The lack ofappropriately powered studies,consensus definitions for AKI andCKD, and a consistent follow-upperiod are barriers to clearlydefining the relationship betweenneonatal AKI and subsequent CKD.Although the Chronic KidneyDisease in Children study manageschildren with CKD and includesinformation on birth weight, it doesnot include detailed data onneonatal course and AKI. Largemulticenter long-term follow-upstudies of neonates after AKI areneeded to completely understandthe future risk of CKD.
CONCLUSIONS
Dramatic advances in the diagnosisand epidemiology of neonatal AKIand our ability to care for neonateswith kidney disease have occurredin the last decade.116 Newtechnologies and therapies designedto prevent and treat neonatal AKIaugment these findings. Futurework, including interventional trialsof therapeutics to treat AKI(methylxanthines, RRT with noveldevices), prospective long-termfollow-up studies to understand riskfactors for CKD development, andimproved definitions of fluidoverload, is needed. Additionally,continued integration of biomarkersinto routine clinical use, morewidespread availability and use ofneonatal-specific extracorporealdevices for kidney support therapy,and standardization of monitoringand follow-up of neonates with AKIwill continue to advance the field ofneonatal AKI.117,118 Ongoingcollaboration betweenneonatologists, pediatricians, andnephrologists (including theNeonatal Kidney Collaborative;www.babykidney.org) will helpdrive these research initiatives,mentor young faculty, educate clini-cians, inform families, and advocate
for neonates at risk for short- andlong-term kidney-related dis-ease.98,119
ABBREVIATIONS
AbbreviationsAKI: acute kidney injuryAWAKEN: Assessment of
Worldwide AcuteKidney InjuryEpidemiology inNeonates
CHD: congenital heart diseaseCI: confidence intervalCKD: chronic kidney diseaseCRRT: continuous renal
replacement therapyCysC: cystatin CECMO: extracorporeal membrane
oxygenationELGAN: extremely low
gestational age neonateGA: gestational ageGFR: glomerular filtration rateHIE: hypoxic-ischemic
encephalopathyIGFBP-7: insulinlike growth
factor binding protein 7KDIGO: Kidney Disease
Improving GlobalOutcomes
NEC: necrotizing enterocolitisNGAL: neutrophil
gelatinase–associatedlipocalin
NINJA: Nephrotoxic InjuryNegated by Just-in-TimeAction
NIRS: near-infrared spectroscopyNSAID: nonsteroidal
antiinflammatory drugOR: odds ratioPD: peritoneal dialysisPDA: patent ductus arteriosusRrSO2: Renal tissue oxygenationRRT: renal replacement therapySCr: serum creatinineTIMP-2: tissue inhibitor of
metalloproteinase 2UOP: urine outputVLBW: very low birth weight
PEDIATRICS Volume 148, number 5, November 2021 9

Address correspondence to Michelle C. Starr, MD, MPH, School of Medicine, Indiana University and Riley Hospital for Children, 699 Riley Hospital Dr, RR230, Indianapolis, IN 46202.E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2021 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: For full disclosure, we provide here an additional list of other authors’ commitments and funding sources that are not directly related to thisstudy: Dr Askenazi is a consultant for Baxter, Nuwellis, Medtronic Bioporto, the Acute Kidney Injury Foundation, and Seastar; he receives grant funding for studies not related tothis project from Baxter, Nuwellis, Medtronic, and the National Institutes of Health; the other authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Selewski DT, Charlton JR, Jetton JG, etal. Neonatal acute kidney injury. Pediat-rics. 2015;136(2). Available at: www.pediatrics.org/cgi/content/full/136/2/e463
2. Askenazi DJ, Heagerty PJ, Schmicker RH,et al; PENUT Trial Consortium. Preva-lence of acute kidney injury (AKI) inextremely low gestational age neonates(ELGAN). Pediatr Nephrol. 2020;35(9):1737–1748
3. Carmody JB, Swanson JR, Rhone ET,Charlton JR. Recognition and reportingof AKI in very low birth weight infants.Clin J Am Soc Nephrol. 2014;9(12):2036–2043
4. Jetton JG, Boohaker LJ, Sethi SK, et al;Neonatal Kidney Collaborative (NKC). Inci-dence and outcomes of neonatal acutekidney injury (AWAKEN): a multicentre,multinational, observational cohortstudy. Lancet Child Adolesc Health.2017;1(3):184–194
5. Menon S, Broderick J, Munshi R, et al.Kidney support in children using anultrafiltration device: a multicenter, ret-rospective study. Clin J Am Soc Nephrol.2019;14(10):1432–1440
6. Vidal E, Garzotto F, Parolin M, et al. Thera-peutic plasma exchange in neonates andinfants: successful use of a miniaturizedmachine. Blood Purif. 2017;44(2):100–105
7. Chambers JM, Wingert RA. Advances inunderstanding vertebrate nephrogene-sis. Tissue Barriers. 2020;8(4):1832844
8. Chevalier RL. Evolutionary nephrology.Kidney Int Rep. 2017;2(3):302–317
9. Straub RH, Schradin C. Chronic inflam-matory systemic diseases: an
evolutionary trade-off between acutelybeneficial but chronically harmful pro-grams. Evol Med Public Health. 2016;2016(1):37–51
10. Iacobelli S, Guignard JP. Maturation ofglomerular filtration rate in neonatesand infants: an overview. Pediatr Neph-rol. 2021;36(6):1439–1446
11. Hyink DP, Abrahamson DR. Origin of theglomerular vasculature in the develop-ing kidney. Semin Nephrol. 1995;15(4):300–314
12. Abitbol CL, Seeherunvong W, Galarza MG,et al. Neonatal kidney size and functionin preterm infants: what is a true esti-mate of glomerular filtration rate?J Pediatr. 2014;164(5):1026–1031.e2
13. Su SW, Stonestreet BS. Core concepts:neonatal glomerular filtration rate. Neo-reviews. 2010;11(12):e714–e721
14. Jetton JG, Guillet R, Askenazi DJ, et al;Neonatal Kidney Collaborative. Assess-ment of worldwide acute kidney injuryepidemiology in neonates: design of aretrospective cohort study. Front Pediatr.2016;4:68
15. Kellum JA, Lameire N; KDIGO AKI Guide-line Work Group. Diagnosis, evaluation,and management of acute kidney injury:a KDIGO summary (part 1). Crit Care.2013;17(1):204
16. Zappitelli M, Ambalavanan N, AskenaziDJ, et al. Developing a neonatal acutekidney injury research definition: areport from the NIDDK neonatal AKIworkshop. Pediatr Res. 2017;82(4):569–573
17. Stoops C, Stone S, Evans E, et al. BabyNINJA (Nephrotoxic Injury Negated byJust-in-Time Action): reduction of neph-rotoxic medication-associated acute
kidney injury in the neonatal intensivecare unit. J Pediatr. 2019;215:223–228.e6
18. Thayyil S, Sheik S, Kempley ST, Sinha A.A gestation- and postnatal age-basedreference chart for assessing renalfunction in extremely premature infants.J Perinatol. 2008;28(3):226–229
19. Askenazi DJ, Ambalavanan N, GoldsteinSL. Acute kidney injury in critically illnewborns: what do we know? What dowe need to learn? Pediatr Nephrol.2009;24(2):265–274
20. Gupta C, Massaro AN, Ray PE. A newapproach to define acute kidney injuryin term newborns with hypoxic ischemicencephalopathy. Pediatr Nephrol. 2016;31(7):1167–1178
21. Bezerra CT, Vaz Cunha LC, Lib�orio AB.Defining reduced urine output in neona-tal ICU: importance for mortality andacute kidney injury classification. Neph-rol Dial Transplant. 2013;28(4):901–909
22. Bruel A, Roz�e JC, Flamant C, Simeoni U,Roussey-Kesler G, Allain-Launay E. Criti-cal serum creatinine values in very pre-term newborns. PLoS One. 2013;8(12):e84892
23. Askenazi D, Abitbol C, Boohaker L, et al;Neonatal Kidney Collaborative. Optimiz-ing the AKI definition during first postna-tal week using assessment ofworldwide acute kidney injury epidemi-ology in neonates (AWAKEN) cohort.Pediatr Res. 2019;85(3):329–338
24. Koralkar R, Ambalavanan N, Levitan EB,McGwin G, Goldstein S, Askenazi D. Acutekidney injury reduces survival in verylow birth weight infants. Pediatr Res.2011;69(4):354–358
25. Charlton JR, Boohaker L, Askenazi D, etal; Neonatal Kidney Collaborative.
10 STARR et al

Incidence and risk factors of early onsetneonatal AKI. Clin J Am Soc Nephrol.2019;14(2):184–195
26. Majed B, Bateman DA, Uy N, Lin F. Patentductus arteriosus is associated withacute kidney injury in the preterminfant. Pediatr Nephrol. 2019;34(6):1129–1139
27. Guillet R, Selewski DT, Griffin R, RastogiS, Askenazi DJ, D’Angio CT; Neonatal Kid-ney Collaborative. Relationship of patentductus arteriosus management withneonatal AKI. J Perinatol. 2021;41(6):1441–1447
28. Charlton JR, Boohaker L, Askenazi D, etal; Neonatal Kidney Collaborative (NKC).Late onset neonatal acute kidney injury:results from the AWAKEN Study. PediatrRes. 2019;85(3):339–348
29. Polglase GR, Ong T, Hillman NH. Cardio-vascular alterations and multiorgan dys-function after birth asphyxia. ClinPerinatol. 2016;43(3):469–483
30. Bozkurt O, Yucesoy E. Acute kidney injuryin neonates with perinatal asphyxiareceiving therapeutic hypothermia. Am JPerinatol. 2021;38(9):922–929
31. Kirkley MJ, Boohaker L, Griffin R, et al;Neonatal Kidney Collaborative (NKC).Acute kidney injury in neonatal encepha-lopathy: an evaluation of the AWAKENdatabase. Pediatr Nephrol. 2019;34(1):169–176
32. Michniewicz B, Al Saad SR, KarbowskiLM, Gadzinowski J, Szymankiewicz M,Szpecht D. Organ complications ofinfants with hypoxic ischemic encepha-lopathy before therapeutic hypothermia.Ther Hypothermia Temp Manag.2021;11(1):58–63
33. Selewski DT, Jordan BK, Askenazi DJ,Dechert RE, Sarkar S. Acute kidneyinjury in asphyxiated newborns treatedwith therapeutic hypothermia. J Pediatr.2013;162(4):725–729.e1
34. Fleming GM, Sahay R, Zappitelli M, et al.The incidence of acute kidney injury andits effect on neonatal and pediatricextracorporeal membrane oxygenationoutcomes: a multicenter report fromthe kidney intervention during extracor-poreal membrane oxygenation studygroup. Pediatr Crit Care Med. 2016;17(12):1157–1169
35. Madsen NL, Goldstein SL, Frøslev T,Christiansen CF, Olsen M. Cardiac
surgery in patients with congenitalheart disease is associated with acutekidney injury and the risk of chronic kid-ney disease. Kidney Int.2017;92(3):751–756
36. Wong JH, Selewski DT, Yu S, et al. Severeacute kidney injury following stage 1Norwood palliation: effect on outcomesand risk of severe acute kidney injury atsubsequent surgical stages. Pediatr CritCare Med. 2016;17(7):615–623
37. Murphy HJ, Gien J, Sahay R, et al. Acutekidney injury, fluid overload, and renalreplacement therapy differ by underly-ing diagnosis in neonatal extracorporealsupport and impact mortality dispa-rately [published online ahead of printJanuary 18, 2021]. Blood Purif. doi:10.1159/000512538
38. Wu Y, Hua X, Yang G, Xiang B, Jiang X.Incidence, risk factors, and outcomes ofacute kidney injury in neonates aftersurgical procedures. Pediatr Nephrol.2020;35(7):1341–1346
39. Garg PM, Britt AB, Ansari MAY, et al.Severe acute kidney injury in neonateswith necrotizing enterocolitis: risk fac-tors and outcomes [published onlineahead of print January 14, 2021].Pediatr Res. doi: 10.1038/s41390-020-01320-6
40. Flori HR, Church G, Liu KD, GildengorinG, Matthay MA. Positive fluid balance isassociated with higher mortality andprolonged mechanical ventilation inpediatric patients with acute lung injury.Crit Care Res Pract. 2011;2011:854142
41. Gist KM, Selewski DT, Brinton J, MenonS, Goldstein SL, Basu RK. Assessment ofthe independent and synergistic effectsof fluid overload and acute kidney injuryon outcomes of critically ill children.Pediatr Crit Care Med. 2020;21(2):170–177
42. Goldstein SL, Currier H, Graf JM, CosioCC, Brewer ED, Sachdeva R. Outcome inchildren receiving continuous venove-nous hemofiltration. Pediatrics. 2001;107(6):1309–1312
43. Gorga SM, Sahay RD, Askenazi DJ, et al.Fluid overload and fluid removal in pedi-atric patients on extracorporeal mem-brane oxygenation requiring continuousrenal replacement therapy: a multicen-ter retrospective cohort study. PediatrNephrol. 2020;35(5):871–882
44. Hassinger AB, Wald EL, Goodman DM.Early postoperative fluid overload pre-cedes acute kidney injury and is associ-ated with higher morbidity in pediatriccardiac surgery patients. Pediatr CritCare Med. 2014;15(2):131–138
45. Li Y, Wang J, Bai Z, et al. Early fluid over-load is associated with acute kidneyinjury and PICU mortality in critically illchildren. Eur J Pediatr. 2016;175(1):39–48
46. Mah KE, Hao S, Sutherland SM, et al. Fluidoverload independent of acute kidneyinjury predicts poor outcomes in neo-nates following congenital heart surgery.Pediatr Nephrol. 2018;33(3):511–520
47. Selewski DT, Cornell TT, Lombel RM, etal. Weight-based determination of fluidoverload status and mortality in pediat-ric intensive care unit patients requiringcontinuous renal replacement therapy.Intensive Care Med. 2011;37(7):1166–1173
48. Sutherland SM, Zappitelli M, AlexanderSR, et al. Fluid overload and mortality inchildren receiving continuous renalreplacement therapy: the prospectivepediatric continuous renal replacementtherapy registry. Am J Kidney Dis.2010;55(2):316–325
49. Valentine SL, Sapru A, Higgerson RA, etal; Pediatric Acute Lung Injury and Sep-sis Investigator’s (PALISI) Network; AcuteRespiratory Distress Syndrome ClinicalResearch Network (ARDSNet). Fluid bal-ance in critically ill children with acutelung injury. Crit Care Med.2012;40(10):2883–2889
50. Hoste EA, Maitland K, Brudney CS, et al;ADQI XII Investigators Group. Fourphases of intravenous fluid therapy: aconceptual model. Br J Anaesth.2014;113(5):740–747
51. Selewski DT, Akcan-Arikan A, BonacheaEM, et al; Neonatal Kidney Collaborative.The impact of fluid balance on outcomesin critically ill near-term/term neonates:a report from the AWAKEN study group.Pediatr Res. 2019;85(1):79–85
52. van Asperen Y, Brand PL, Bekhof J. Reli-ability of the fluid balance in neonates.Acta Paediatr. 2012;101(5):479–483
53. Selewski DT, Gist KM, Nathan AT, et al;Neonatal Kidney Collaborative. Theimpact of fluid balance on outcomes in
PEDIATRICS Volume 148, number 5, November 2021 11
premature neonates: a report from theAWAKEN study group. Pediatr Res.2020;87(3):550–557
54. Bontant T, Matrot B, Abdoul H, et al.Assessing fluid balance in critically illpediatric patients. Eur J Pediatr. 2015;174(1):133–137
55. Paul IM, Schaefer EW, Miller JR, et al.Weight change nomograms for the firstmonth after birth. Pediatrics. 2016;138(6):e20162625
56. Wadhawan R, Oh W, Perritt R, et al. Asso-ciation between early postnatal weightloss and death or BPD in small andappropriate for gestational ageextremely low-birth-weight infants.J Perinatol. 2007;27(6):359–364
57. Schmidt B, Roberts RS, Fanaroff A, et al;TIPP Investigators. Indomethacin prophy-laxis, patent ductus arteriosus, and therisk of bronchopulmonary dysplasia: fur-ther analyses from the Trial of Indo-methacin Prophylaxis in Preterms(TIPP). J Pediatr. 2006;148(6):730–734
58. Oh W, Poindexter BB, Perritt R, et al; Neo-natal Research Network. Associationbetween fluid intake and weight lossduring the first ten days of life and riskof bronchopulmonary dysplasia inextremely low birth weight infants.J Pediatr. 2005;147(6):786–790
59. Askenazi DJ, Koralkar R, Hundley HE,Montesanti A, Patil N, Ambalavanan N.Fluid overload and mortality are associ-ated with acute kidney injury in sicknear-term/term neonate. Pediatr Neph-rol. 2013;28(4):661–666
60. Selewski DT, Goldstein SL. The role offluid overload in the prediction of out-come in acute kidney injury. PediatrNephrol. 2018;33(1):13–24
61. Askenazi DJ, Koralkar R, Patil N, HalloranB, Ambalavanan N, Griffin R. Acute kid-ney injury urine biomarkers in very low-birth-weight infants. Clin J Am Soc Neph-rol. 2016;11(9):1527–1535
62. DeFreitas MJ, Seeherunvong W, KatsoufisCP, et al. Longitudinal patterns of urine bio-markers in infants across gestational ages.Pediatr Nephrol. 2016;31(7):1179–1188
63. Wasung ME, Chawla LS, Madero M. Bio-markers of renal function, which andwhen? Clin Chim Acta. 2015;438:350–357
64. Chowdhary V, Vajpeyajula R, Jain M, etal. Comparison of different definitions of
acute kidney injury in extremely lowbirth weight infants. Clin Exp Nephrol.2018;22(1):117–125
65. Renganathan A, Warner BB, Tarr PI,Dharnidharka VR. The progression ofserum cystatin C concentrations withinthe first month of life after pretermbirth-a worldwide systematic review.Pediatr Nephrol. 2021;36(7):1709–1718
66. Yang Y, Li SJ, Pan JJ, et al. Reference val-ues for serum cystatin C in very low-birthweight infants: from two centres ofChina. J Paediatr Child Health. 2018;54(3):284–288
67. Nakashima T, Inoue H, Fujiyoshi J, Matsu-moto N. Longitudinal analysis of serumcystatin C for estimating the glomerularfiltration rate in preterm infants. PediatrNephrol. 2016;31(6):983–989
68. Treiber M, Pe�covnik Balon B, GorenjakM. A new serum cystatin C formula forestimating glomerular filtration rate innewborns. Pediatr Nephrol. 2015;30(8):1297–1305
69. Devarajan P. Neutrophil gelatinase-asso-ciated lipocalin: a promising biomarkerfor human acute kidney injury. Bio-markers Med. 2010;4(2):265–280
70. Tanigasalam V, Bhat V, Adhisivam B, Srid-har MG. Does therapeutic hypothermiareduce acute kidney injury among termneonates with perinatal asphyxia?–arandomized controlled trial. J MaternFetal Neonatal Med. 2016;29(15):2545–2548
71. Chen J, Sun Y, Wang S, et al. The effec-tiveness of urinary TIMP-2 and IGFBP-7in predicting acute kidney injury in criti-cally ill neonates. Pediatr Res. 2020;87(6):1052–1059
72. Fan W, Ankawi G, Zhang J, et al. Currentunderstanding and future directions inthe application of TIMP-2 and IGFBP7 inAKI clinical practice. Clin Chem Lab Med.2019;57(5):567–576
73. Stojanovi�c VD, Bari�si�c NA, Vu�ckovi�c NM,Doronjski AD, Peco Anti�c AE. Urinary kid-ney injury molecule-1 rapid test predictsacute kidney injury in extremely low-birth-weight neonates. Pediatr Res.2015;78(4):430–435
74. Charlton JR, Baldelomar EJ, Hyatt DM,Bennett KM. Nephron number and itsdeterminants: a 2020 update. PediatrNephrol. 2021;36(4):797–807
75. Baldelomar EJ, Charlton JR, deRonde KA,Bennett KM. In vivo measurements ofkidney glomerular number and size inhealthy and Os/1 mice using MRI. Am JPhysiol Renal Physiol. 2019;317(4):F865–F873
76. Baldelomar EJ, Charlton JR, Beeman SC,Bennett KM. Measuring rat kidney glo-merular number and size in vivo withMRI. Am J Physiol Renal Physiol.2018;314(3):F399–F406
77. Rodr�ıguez MM, G�omez AH, Abitbol CL,Chandar JJ, Duara S, Zilleruelo GE. Histo-morphometric analysis of postnatal glo-merulogenesis in extremely preterminfants. Pediatr Dev Pathol. 2004;7(1):17–25
78. Charlton JR, Baldelomar EJ, deRonde KA,et al. Nephron loss detected by MRIfollowing neonatal acute kidney injuryin rabbits. Pediatr Res. 2020;87(7):1185–1192
79. Harer MW, Chock VY. Renal tissue oxy-genation monitoring-an opportunity toimprove kidney outcomes in the vulnera-ble neonatal population. Front Pediatr.2020;8:241
80. Hazle MA, Gajarski RJ, Aiyagari R, et al.Urinary biomarkers and renal near-infrared spectroscopy predict intensivecare unit outcomes after cardiac sur-gery in infants younger than 6 monthsof age. J Thorac Cardiovasc Surg.2013;146(4):861–867.e1
81. Bonsante F, Ramful D, Binquet C, et al.Low renal oxygen saturation at near-infrared spectroscopy on the first day oflife is associated with developing acutekidney injury in very preterm infants.Neonatology. 2019;115(3):198–204
82. Dorum BA, Ozkan H, Cetinkaya M, KoksalN. Regional oxygen saturation and acutekidney injury in premature infants.Pediatr Int. 2021;63(3):290–294
83. Harer MW, Adegboro CO, Richard LJ,McAdams RM. Non-invasive continuousrenal tissue oxygenation monitoring toidentify preterm neonates at risk foracute kidney injury. Pediatr Nephrol.2021;36(6):1617–1625
84. Chock VY, Frymoyer A, Yeh CG, VanMeurs KP. Renal saturation and acutekidney injury in neonates with hypoxicischemic encephalopathy undergoingtherapeutic hypothermia. J Pediatr.2018;200:232–239.e1
12 STARR et al

85. Sanderson KR, Chang E, Bjornstad E, etal. Albuminuria, hypertension, andreduced kidney volumes in adolescentsborn extremely premature. FrontPediatr. 2020;8:230
86. Askenazi DJ, Heagerty PJ, Schmicker RH,et al. The impact of erythropoietin onshort- and long-term kidney-related out-comes in neonates of extremely low ges-tational age. Results of a multicenter,double-blind, placebo-controlled random-ized clinical trial. J Pediatr. 2021;232:65–72.e7
87. Pedersen KR, Ravn HB, Povlsen JV,Schmidt MR, Erlandsen EJ, Hjortdal VE.Failure of remote ischemic precondition-ing to reduce the risk of postoperativeacute kidney injury in children undergo-ing operation for complex congenitalheart disease: a randomized single-cen-ter study. J Thorac Cardiovasc Surg.2012;143(3):576–583
88. Lomivorotov V, Kornilov I, Boboshko V, etal. Effect of intraoperative dexametha-sone on major complications and mor-tality among infants undergoing cardiacsurgery: the DECISION randomized clini-cal trial. JAMA. 2020;323(24):2485–2492
89. Harer MW, Askenazi DJ, Boohaker LJ, etal; Neonatal Kidney Collaborative (NKC).Association between early caffeine cit-rate administration and risk of acutekidney injury in preterm neonates:results from the AWAKEN study. JAMAPediatr. 2018;172(6):e180322
90. Bellos I, Pandita A, Yachha M. Effective-ness of theophylline administration inneonates with perinatal asphyxia: ameta-analysis. J Matern Fetal NeonatalMed. 2019;34(18):3080–3088
91. Mohamed TH, Klamer B, Mahan JD,Spencer JD, Slaughter JL. Diuretic ther-apy and acute kidney injury in pretermneonates and infants [published onlineahead of print May 21, 2021]. PediatrNephrol. doi: 10.1007/s00467-021-05132-6
92. Kakajiwala A, Kim JY, Hughes JZ, et al.Lack of furosemide responsiveness pre-dicts acute kidney injury in infants aftercardiac surgery. Ann Thorac Surg.2017;104(4):1388–1394
93. Chock VY, Cho SH, Frymoyer A. Aminoph-ylline for renal protection in neonatalhypoxic-ischemic encephalopathy in theera of therapeutic hypothermia. PediatrRes. 2021;89(4):974–980
94. Carmody JB, Harer MW, Denotti AR,Swanson JR, Charlton JR. Caffeine expo-sure and risk of acute kidney injury in aretrospective cohort of very low birthweight neonates. J Pediatr. 2016;172:63–68.e1
95. Kaddourah A, Goldstein SL. Renalreplacement therapy in neonates. ClinPerinatol. 2014;41(3):517–527
96. Harshman LA, Muff-Luett M, NeubergerML, et al. Peritoneal dialysis in anextremely low-birth-weight infant withacute kidney injury. Clin Kidney J.2014;7(6):582–585
97. Munshi R, Lee-Son K, Hackbarth RM, etal. Clinical evaluation of the Prismaflex™HF 20 set and Prismaflex™ system 7.10for acute continuous kidney replace-ment therapy (CKRT) in children. PediatrNephrol. 2020;35(12):2345–2352
98. Askenazi DJ. AWAKEN-ing a new frontierin neonatal nephrology. Front Pediatr.2020;8:21
99. Garzotto F, Vidal E, Ricci Z, et al. Continu-ous kidney replacement therapy in criti-cally ill neonates and infants: aretrospective analysis of clinical resultswith a dedicated device. Pediatr Neph-rol. 2020;35(9):1699–1705
100. Faubel S, Shah PB. Immediate conse-quences of acute kidney injury: theimpact of traditional and nontraditionalcomplications on mortality in acute kid-ney injury. Adv Chronic Kidney Dis.2016;23(3):179–185
101. Basu RK, Wheeler DS. Kidney-lung cross-talk and acute kidney injury. PediatrNephrol. 2013;28(12):2239–2248
102. Grigoryev DN, Liu M, Hassoun HT, Chea-dle C, Barnes KC, Rabb H. The local andsystemic inflammatory transcriptomeafter acute kidney injury. J Am SocNephrol. 2008;19(3):547–558
103. Starr MC, Boohaker L, Eldredge LC, etal; Neonatal Kidney Collaborative. Acutekidney injury and bronchopulmonarydysplasia in premature neonates bornless than 32 weeks’ gestation. Am JPerinatol. 2020;37(3):341–348
104. Starr MC, Boohaker L, Eldredge LC, etal; Neonatal Kidney Collaborative. Acutekidney injury is associated with poorlung outcomes in infants born $32weeks of gestational age. Am J Perina-tol. 2020;37(2):231–240
105. Stoops C, Sims B, Griffin R, Askenazi DJ.Neonatal acute kidney injury and therisk of intraventricular hemorrhage inthe very low birth weight infant. Neona-tology. 2016;110(4):307–312
106. Kraut EJ, Boohaker LJ, Askenazi DJ,Fletcher J, Kent AL; Neonatal Kidney Col-laborative (NKC). Incidence of neonatalhypertension from a large multicenterstudy [Assessment of Worldwide AcuteKidney Injury Epidemiology in Neonates-AWAKEN]. Pediatr Res. 2018;84(2):279–289
107. Coca SG, Singanamala S, Parikh CR.Chronic kidney disease after acute kid-ney injury: a systematic review andmeta-analysis. Kidney Int. 2012;81(5):442–448
108. Greenberg JH, Coca S, Parikh CR. Long-term risk of chronic kidney disease andmortality in children after acute kidneyinjury: a systematic review. BMC Neph-rol. 2014;15:184
109. Chawla LS, Eggers PW, Star RA, KimmelPL. Acute kidney injury and chronic kid-ney disease as interconnected syn-dromes. N Engl J Med. 2014;371(1):58–66
110. Basile DP, Bonventre JV, Mehta R, et al;ADQI XIII Work Group. Progression afterAKI: understanding maladaptive repairprocesses to predict and identify thera-peutic treatments. J Am Soc Nephrol.2016;27(3):687–697
111. Sutherland MR, Gubhaju L, Moore L, etal. Accelerated maturation and abnor-mal morphology in the preterm neona-tal kidney. J Am Soc Nephrol.2011;22(7):1365–1374
112. Abitbol CL, Bauer CR, Montan�e B,Chandar J, Duara S, Zilleruelo G. Long-term follow-up of extremely low birthweight infants with neonatal renal fail-ure. Pediatr Nephrol. 2003;18(9):887–893
113. Harer MW, Pope CF, Conaway MR,Charlton JR. Follow-up of Acute KidneyInjury in Neonates During ChildhoodYears (FANCY): a prospective cohortstudy. Pediatr Nephrol. 2017;32(6):1067–1076
114. Bruel A, Roz�e JC, Quere MP, et al. Renaloutcome in children born preterm withneonatal acute renal failure: IRENEO-aprospective controlled study. PediatrNephrol. 2016;31(12):2365–2373
115. Maqsood S, Fung N, Chowdhary V, RainaR, Mhanna MJ. Outcome of extremely
PEDIATRICS Volume 148, number 5, November 2021 13

low birth weight infants with a historyof neonatal acute kidney injury. PediatrNephrol. 2017;32(6):1035–1043
116. Askenazi DJ, Morgan C, Goldstein SL, etal. Strategies to improve the understand-ing of long-term renal consequencesafter neonatal acute kidney injury. PediatrRes. 2016;79(3):502–508
117. Starr MC, Kula A, Lieberman J, et al. Theimpact of increased awareness of acutekidney injury in the neonatal intensivecare unit on acute kidney injury
incidence and reporting: results of aretrospective cohort study. J Perinatol.2020;40(9):1301–1307
118. Vincent K, Murphy HJ, Ross JR,Twombley KE. Acute kidney injury guide-lines are associated with improved rec-ognition and follow-up for neonatalpatients. Adv Neonatal Care. 2020;20(4):269–275
119. Kent AL, Charlton JR, Guillet R, et al.Neonatal acute kidney injury: a
survey of neonatologists’ and neph-rologists’ perceptions and practicemanagement. Am J Perinatol.2018;35(1):1–9
120. Nour I, Elmaghraby R, Shehata R, et al.Selective head cooling and acutekidney injury in neonates withhypoxic ischemic encephalopathy.J Neonatal Perinatal Med. 2020;13(1):21–30
14 STARR et al

originally published online October 1, 2021; Pediatrics Matthew W. Harer
Ambalavanan, Maroun J. Mhanna, David J. Askenazi, David T. Selewski andTipple, Jennifer G. Jetton, Alison L. Kent, Carolyn L. Abitbol, Namasivayam
Michelle C. Starr, Jennifer R. Charlton, Ronnie Guillet, Kimberly Reidy, Trent E.Advances in Neonatal Acute Kidney Injury
ServicesUpdated Information &
021-051220http://pediatrics.aappublications.org/content/early/2021/09/29/peds.2including high resolution figures, can be found at:
References
021-051220#BIBLhttp://pediatrics.aappublications.org/content/early/2021/09/29/peds.2This article cites 116 articles, 10 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/nephrology_subNephrologyhttp://www.aappublications.org/cgi/collection/neonatology_subNeonatologysubhttp://www.aappublications.org/cgi/collection/fetus:newborn_infant_Fetus/Newborn Infantfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
originally published online October 1, 2021; Pediatrics Matthew W. Harer
Ambalavanan, Maroun J. Mhanna, David J. Askenazi, David T. Selewski andTipple, Jennifer G. Jetton, Alison L. Kent, Carolyn L. Abitbol, Namasivayam
Michelle C. Starr, Jennifer R. Charlton, Ronnie Guillet, Kimberly Reidy, Trent E.Advances in Neonatal Acute Kidney Injury
http://pediatrics.aappublications.org/content/early/2021/09/29/peds.2021-051220located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2021has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
Copyright © 2022 FDOKUMEN




















