Additive Interactions of Maternal Prepregnancy BMI and Breast-feeding on Childhood Overweight
10
Additive Interactions of Maternal Prepregnancy BMI and Breast-feeding on Childhood Overweight Chaoyang Li,*† Harsohena Kaur,*†‡ Won S. Choi,*† Terry T.-K. Huang,§ Rebecca E. Lee,** and Jasjit S. Ahluwalia*†‡¶ Abstract LI, CHAOYANG, HARSOHENA KAUR, WON S. CHOI, TERRY T.-K. HUANG, REBECCA E. LEE, AND JASJIT S. AHLUWALIA. Additive interactions of maternal prepregnancy BMI and breast-feeding on childhood overweight risk. Obes Res. 2005;13:362–371. Objective: To examine the interactions of maternal prepreg- nancy BMI and breast-feeding on the risk of overweight among children 2 to 14 years of age. Research Methods and Procedures: The 1996 National Longitudinal Survey of Youth, Child and Young Adult data in the United States were analyzed (n 2636). The weighted sample represented 51.3% boys, 78.0% whites, 15.0% blacks, and 7.0% Hispanics. Childhood overweight was defined as BMI 95th percentile for age and sex. Maternal prepregnancy obesity was determined as BMI 30 kg/m 2 . The duration of breast-feeding was measured as the weeks of age from birth when breast-feeding ended. Results: After adjusting for potential confounders, children whose mothers were obese before pregnancy were at a greater risk of becoming overweight [adjusted odds ratio (OR), 4.1; 95% confidence interval (CI), 2.6, 6.4] than children whose mothers had normal BMI (25 kg/m 2 ; p 0.001 for linear trend). Breast-feeding for 4 months was associated with a lower risk of childhood overweight (OR, 0.6; 95% CI, 0.4, 1.0; p 0.06 for linear trend). The additive interaction between maternal prepregnancy obesity and lack of breast-feeding was detected (p 0.05), such that children whose mothers were obese and who were never breast-fed had the greatest risk of becoming over- weight (OR, 6.1; 95% CI, 2.9, 13.1). Discussion: The combination of maternal prepregnancy obesity and lack of breast-feeding may be associated with a greater risk of childhood overweight. Special attention may be needed for children with obese mothers and lack of breast-feeding in developing childhood obesity intervention programs. Key words: interaction, prenatal exposure, nutrition, breast-feeding, BMI Introduction Prevalence of obesity among children and adults in the United States has increased rapidly during the past decade (1,2). According to the most recent data from 1999 to 2000 in the United States, one-third of adults, 15.3% of children 6 to 11 years of age, and 15.5% of adolescents 12 to 19 years of age were obese (1,2). Childhood overweight is a strong predictor of adult obesity (3) and other adverse health consequences, especially type 2 diabetes and cardiovascular disease in adolescence and adult life (4,5). It has been proposed that fetal life, adiposity rebound, and adolescence are three critical periods for the development of obesity (6). Previous studies have shown that maternal gestational dia- betes (7), birth weight (7,8), breast-feeding, and early child- hood growth (9 –11) have been associated with the devel- opment of overweight in childhood and adolescence. Associations of prenatal and early childhood influences with obesity later in life have led to the hypothesis of “fetal origins of obesity” (12,13). Maternal prepregnancy obesity is associated with an in- creased risk of adverse pregnancy-related outcomes such as Received for review May 13, 2004. Accepted in final form December 15, 2004. The costs of publication of this article were defrayed, in part, by the payment of page charges. This article must, therefore, be hereby marked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. *Department of Preventive Medicine and Public Health, †Kansas Cancer Institute, ‡Depart- ment of Pediatrics, and ¶Department of Internal Medicine, University of Kansas School of Medicine, Kansas City, Kansas and §Gerald J. and Dorothy R. Friedman School of Nutrition Science and Policy, Tufts University, Boston, Massachusetts; **Department of Health and Human Performance, University of Houston, Houston, TX 77204. Address correspondence to Chaoyang Li, Department of Preventive Medicine and Public Health, University of Kansas Medical Center, 3901 Rainbow Blvd., Mail-Stop 1008, Kansas City, KS 66160. E-mail: [email protected] Copyright © 2005 NAASO 362 OBESITY RESEARCH Vol. 13 No. 2 February 2005
Transcript of Additive Interactions of Maternal Prepregnancy BMI and Breast-feeding on Childhood Overweight

Additive Interactions of Maternal PrepregnancyBMI and Breast-feeding on ChildhoodOverweightChaoyang Li,*† Harsohena Kaur,*†‡ Won S. Choi,*† Terry T.-K. Huang,§ Rebecca E. Lee,** andJasjit S. Ahluwalia*†‡¶
AbstractLI, CHAOYANG, HARSOHENA KAUR, WON S. CHOI,TERRY T.-K. HUANG, REBECCA E. LEE, AND JASJITS. AHLUWALIA. Additive interactions of maternalprepregnancy BMI and breast-feeding on childhoodoverweight risk. Obes Res. 2005;13:362–371.Objective: To examine the interactions of maternal prepreg-nancy BMI and breast-feeding on the risk of overweightamong children 2 to 14 years of age.Research Methods and Procedures: The 1996 NationalLongitudinal Survey of Youth, Child and Young Adult datain the United States were analyzed (n � 2636). Theweighted sample represented 51.3% boys, 78.0% whites,15.0% blacks, and 7.0% Hispanics. Childhood overweightwas defined as BMI �95th percentile for age and sex.Maternal prepregnancy obesity was determined as BMI�30 kg/m2. The duration of breast-feeding was measured asthe weeks of age from birth when breast-feeding ended.Results: After adjusting for potential confounders, childrenwhose mothers were obese before pregnancy were at agreater risk of becoming overweight [adjusted odds ratio(OR), 4.1; 95% confidence interval (CI), 2.6, 6.4] thanchildren whose mothers had normal BMI (�25 kg/m2; p �0.001 for linear trend). Breast-feeding for �4 months wasassociated with a lower risk of childhood overweight (OR,
0.6; 95% CI, 0.4, 1.0; p � 0.06 for linear trend). Theadditive interaction between maternal prepregnancy obesityand lack of breast-feeding was detected (p � 0.05), suchthat children whose mothers were obese and who werenever breast-fed had the greatest risk of becoming over-weight (OR, 6.1; 95% CI, 2.9, 13.1).Discussion: The combination of maternal prepregnancyobesity and lack of breast-feeding may be associated with agreater risk of childhood overweight. Special attention maybe needed for children with obese mothers and lack ofbreast-feeding in developing childhood obesity interventionprograms.
Key words: interaction, prenatal exposure, nutrition,breast-feeding, BMI
IntroductionPrevalence of obesity among children and adults in the
United States has increased rapidly during the past decade(1,2). According to the most recent data from 1999 to 2000in the United States, one-third of adults, 15.3% of children6 to 11 years of age, and 15.5% of adolescents 12 to 19years of age were obese (1,2). Childhood overweight is astrong predictor of adult obesity (3) and other adverse healthconsequences, especially type 2 diabetes and cardiovasculardisease in adolescence and adult life (4,5). It has beenproposed that fetal life, adiposity rebound, and adolescenceare three critical periods for the development of obesity (6).Previous studies have shown that maternal gestational dia-betes (7), birth weight (7,8), breast-feeding, and early child-hood growth (9–11) have been associated with the devel-opment of overweight in childhood and adolescence.Associations of prenatal and early childhood influenceswith obesity later in life have led to the hypothesis of “fetalorigins of obesity” (12,13).
Maternal prepregnancy obesity is associated with an in-creased risk of adverse pregnancy-related outcomes such as
Received for review May 13, 2004.Accepted in final form December 15, 2004.The costs of publication of this article were defrayed, in part, by the payment of pagecharges. This article must, therefore, be hereby marked “advertisement” in accordance with18 U.S.C. Section 1734 solely to indicate this fact.*Department of Preventive Medicine and Public Health, †Kansas Cancer Institute, ‡Depart-ment of Pediatrics, and ¶Department of Internal Medicine, University of Kansas Schoolof Medicine, Kansas City, Kansas and §Gerald J. and Dorothy R. Friedman School ofNutrition Science and Policy, Tufts University, Boston, Massachusetts; **Department ofHealth and Human Performance, University of Houston, Houston, TX 77204.Address correspondence to Chaoyang Li, Department of Preventive Medicine and PublicHealth, University of Kansas Medical Center, 3901 Rainbow Blvd., Mail-Stop 1008, KansasCity, KS 66160.E-mail: [email protected] © 2005 NAASO
362 OBESITY RESEARCH Vol. 13 No. 2 February 2005

late fetal death and birth defects (14). Few studies haveexamined maternal prepregnancy obesity as a long-term riskfactor for childhood overweight among their offspring. In aprevious study, mothers of obese children tended to beobese before their pregnancy (15). Recent studies haveshown that maternal concurrent obesity is more highlycorrelated with childhood obesity than prenatal factors suchas birth weight (3,16). A recent study has shown that ma-ternal obesity in early pregnancy more than doubles the riskof obesity at 2 to 4 years of age (17). Nevertheless, mostprevious studies focused on maternal obesity during or afterpregnancy rather than maternal prepregnancy obesity,which may be a more reliable indicator of maternal impacton offspring overweight status, representing both sharedgenes and shared prenatal and postnatal environmental fac-tors within families (3,12,13).
Current literature on the impact of breast-feeding onoverweight in childhood is inconclusive. Some studies haveshown a significant protective effect (9,10,18–20), whereasothers have shown a weak effect or no effect (21–23). Theinconsistent results in previous studies suggest that theassociation between breast-feeding and childhood over-weight may be modified by one or more extraneous vari-ables. It is unclear whether breast-feeding predicts child-hood overweight independently of maternal prepregnancyobesity. In addition, it is not known whether the actual jointeffects of maternal prepregnancy obesity and lack of breast-feeding may exceed their combined independent effects onchildhood overweight.
Therefore, the objective of this study was to assess theindependent effects of maternal prepregnancy obesity andbreast-feeding, as well as their additive and multiplicativeinteractions on childhood overweight, by using the 1996child data of the National Longitudinal Survey of Youth(NLSY79)1 in the United States. We hypothesized thatmaternal prepregnancy obesity would be associated with anincreased risk, whereas breast-feeding would be associatedwith a decreased risk, of childhood overweight. We furtherhypothesized that the presence of both maternal prepreg-nancy obesity and lack of breast-feeding would exert agreater effect on childhood overweight than the combinedindependent effect of each single factor alone.
Research Methods and ProceduresDesign and Sample
The NLSY79 is a nationally representative sample of12,686 young men and women who were 14 to 22 years ofage when first surveyed in 1979. Beginning in 1986, allchildren of NLSY79 women were surveyed with supple-mental information on physical and behavioral development
and health status collected biennially through 2000 (24).Sampling weights were constructed to adjust for differentialnon-response and oversampling of blacks, Hispanics, andeconomically disadvantaged non-black/non-Hispanicwhites.
In this study, a sample of children 2 to 14 years of age in1996 was analyzed. We excluded the following childrenfrom the original sample: �2 years of age (n � 433), withgestational age �32 weeks or with extreme birth weights(�0.5 or �6 kg) (n � 587), with incomplete data for heightor weight (n � 149), and whose height or weight wasreported by their mothers (n � 1626). Compared withchildren included in these analyses (n � 2636), those ex-cluded from the analyses were similar in sex and ethnicity.The average number of siblings per household in the currentsample was 1.6. Therefore, the non-independence of obser-vations was unlikely to affect results in this study becausethe average household size of children was small.
ProceduresComputer-assisted personal interviewing, a research
technique that uses portable computers or unmanned termi-nals to conduct personal interviews, was used to collectinformation from NLSY79 women and their children (24).Mother-child assessments were conducted at the same timeat the main NLSY79 interview of each mother. Mothers’height, weight just before pregnancy, and weight just beforethe delivery of child were obtained by self-report at the firstinstance when their children were investigated. Informationabout the mother’s health and prenatal care, including tim-ing of first prenatal examination, extent of alcohol use, andsmoking during pregnancy, was assessed. Children’s char-acteristics at birth, such as birth weight, birth length, ges-tational age, and birth order, were reported by mothers. Theduration of breast-feeding, measured as the weeks of ageafter birth when breast-feeding ended, was determined at thefirst interview when the children were investigated. Foreach child in the study, demographic information such asdate of birth, age, sex, and race/ethnicity and characteristicsof the child’s immediate family, such as mother’s age andhighest education levels at childbirth, as well as annualfamily net income, were assessed. The overall response ratein the 1996 survey was �90%. Details of the various pre-and postnatal measures have been reported previously (25).
Definition of Childhood Overweight and MaternalPrepregnancy Obesity
Children’s height and weight were measured by inter-viewers using a portable scale and a tape measure. Details ofthe protocol for the weight and height measures have beenreported previously (26). BMI was calculated based onmeasured weight (kilograms) and height (meters) using thefollowing formula: BMI � weight divided by heightsquared. BMI percentile for age and sex was derived using
1 Nonstandard abbreviations: NLSY79, National Longitudinal Survey of Youth 1979; OR,odds ratio; CI, confidence interval.
Additive Interactions on Childhood Overweight, Li et al.
OBESITY RESEARCH Vol. 13 No. 2 February 2005 363

the Centers for Disease Control growth charts (27). Child-hood overweight was defined as BMI �95th percentile.Maternal prepregnancy BMI was calculated based on self-reported height and weight just before pregnancy. Maternalobesity was defined as a BMI �30 kg/m2, and overweightwas defined as 25 � BMI � 30 kg/m2 (28).
Statistical AnalysesThe primary outcome variable in this study was child-
hood overweight, which was dichotomized as 0 (nonover-weight, BMI � 95th percentile) and 1 (overweight, BMI �95th percentile). In the multiple logistic regression analysesof main effects, maternal prepregnancy BMI was catego-rized into three levels: 1 � normal (BMI � 25 kg/m2), 2 �overweight (25 � BMI � 30 kg/m2), and 3 � obese(BMI � 30 kg/m2). Breast-feeding was categorized intothree levels: 1 � never breast-fed, 2 � breast-fed 1–3months, and 3 � breast-fed �4 months. Maternal weightgain during pregnancy was calculated as the differencebetween mothers’ weight just before the delivery of childand weight just before pregnancy. The SUDAAN, a statis-tical package designed specifically to analyze data fromcomplex surveys that incorporate multistage sampling andunequally weighted designs (29), and SAS (30) were usedfor all analyses in this study.
The prevalence rates of childhood overweight stratifiedby each level of maternal prepregnancy BMI and breast-feeding duration were estimated for the total sample and bythree age groups (2 to 6, 7 to 10, and 11 to 14 years of age,with an approximate tertile split for age). The odds ratios(ORs) and 95% confidence intervals (CIs) for the maineffects of maternal prepregnancy BMI and breast-feedingon childhood overweight were assessed using multiple lo-gistic regression models adjusted for the effects of potentialconfounding factors such as age, sex, ethnicity, gestationalage, birth weight, birth order, maternal age at childbirth,maternal smoking, alcohol use, weight gain during preg-nancy, maternal highest educational levels, and annual fam-ily net income. Linear (�1, 0, 1) and quadratic (1, �2, 1)trends of ORs for each categorical variable were assessedwith the Wald F tests in the multiple logistic regressionmodels by specifying the EFFECTS statements (29).
Interaction between two or more exposures implies thatthe observed joint effect on disease risk when the two ormore exposures are present is greater (synergy) or smaller(antagonism) than the expected joint effect based on theirindependent effects alone (31–37). On the additive scale,the expected joint effect of two exposures is the addition ofthe independent effects of two exposures minus the baselineeffect of exposure to neither, and on the multiplicative scale,the expected joint effect is the multiplication of the twoindependent effects divided by the baseline effect (32–35).If no interaction is present, the observed joint effect of twoexposures on disease risk is equivalent to the expected joint
effect. In contrast, if the observed joint effect of two expo-sures is significantly greater or smaller than the expectedjoint effect on the additive scale, an additive interaction isassumed. Similarly, if the observed joint effect of twoexposures is significantly greater or smaller than the ex-pected joint effect on the multiplicative scale, a multiplica-tive interaction is assumed (32–35). The Wald statistics (For �2 test), likelihood-ratio statistics, and score (Rao) sta-tistics have been proposed to test for interaction on eitheradditive or multiplicative scale (31,34,37). We used theWald F tests available in SUDAAN to assess the interac-tions on both the additive and multiplicative scales in ourstudy (29).
The reference group for OR estimations was determinedas children whose mothers had normal prepregnancy BMIand who were breast-fed for �4 months. The analyses formain effects were performed for the total sample and thethree age-specific subsamples (2 to 6, 7 to 10, and 11 to 14years of age) separately. Because similar patterns in theassociations between the major predictors and the outcomevariable were observed, we combined all age groups toestimate and assess the interaction between maternalprepregnancy BMI and lack of breast-feeding on childhoodoverweight to ensure adequate statistical power (37).
ResultsDemographic, Maternal, and Early InfancyCharacteristics of the Sample
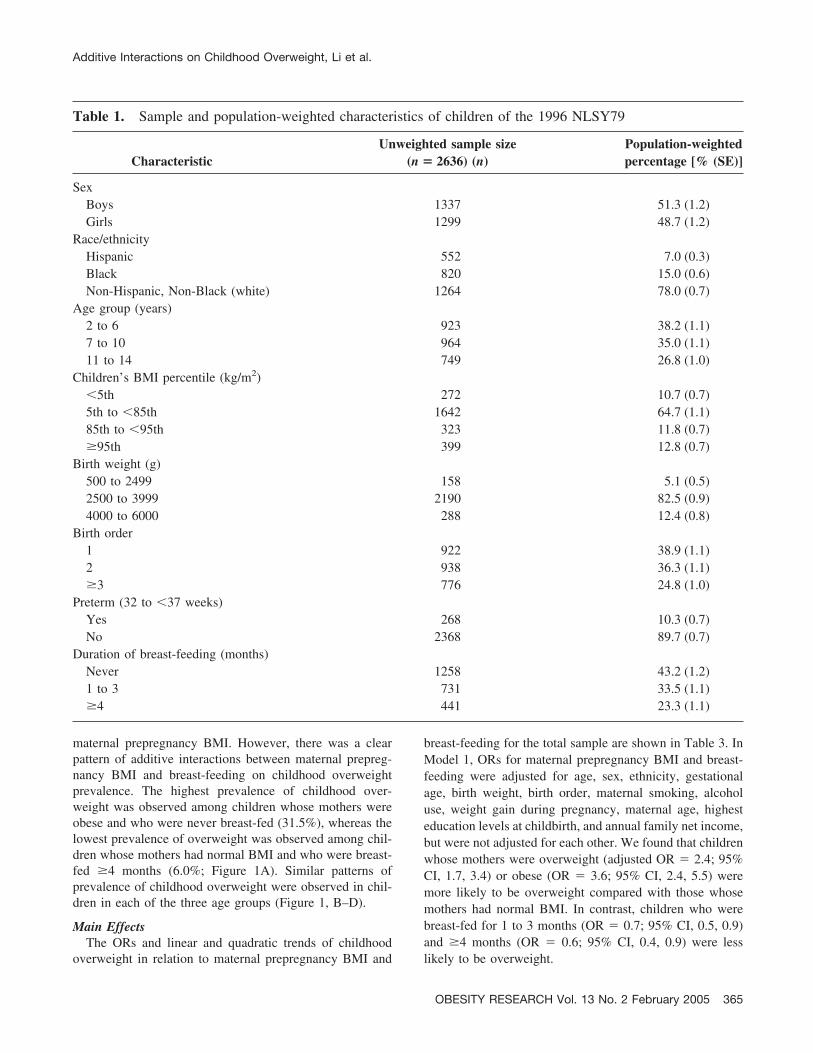
The unweighted sample size and weighted percentages ofthe sample for each characteristic of children are shown inTable 1. The weighted sample represented 51.3% boys,78.0% white, 15.0% black, and 7.0% Hispanic children.Nearly 12% of children were at risk of overweight (85th �BMI � 95th percentile), and 13% were overweight (BMI �95th percentile). In addition, 43.2% of children were neverbreast-fed, 33.5% were breast-fed for 1–3 months, and only23.3% were breast-fed for �4 months.
The unweighted sample size and weighted percentages ofthe sample for each characteristic of mothers are shown inTable 2. Among mothers, 17.6% were overweight (25 �BMI � 30 kg/m2) and 9.4% were obese (BMI � 30 kg/m2)just before pregnancy. Nearly 30% of mothers reported eversmoking, and 40% reported ever using alcohol during preg-nancy. Mean maternal weight gain during pregnancy was14.5 � 7.6 kg (SD).
Prevalence of OverweightThe weighted prevalence of childhood overweight was
higher among children whose mothers were overweight orobese before pregnancy than among those whose mothershad normal BMI (Figure 1). The prevalence of overweightwas lower among children who were ever breast-fed thanamong those who were never breast-fed at each level of
Additive Interactions on Childhood Overweight, Li et al.
364 OBESITY RESEARCH Vol. 13 No. 2 February 2005
maternal prepregnancy BMI. However, there was a clearpattern of additive interactions between maternal prepreg-nancy BMI and breast-feeding on childhood overweightprevalence. The highest prevalence of childhood over-weight was observed among children whose mothers wereobese and who were never breast-fed (31.5%), whereas thelowest prevalence of overweight was observed among chil-dren whose mothers had normal BMI and who were breast-fed �4 months (6.0%; Figure 1A). Similar patterns ofprevalence of childhood overweight were observed in chil-dren in each of the three age groups (Figure 1, B–D).
Main EffectsThe ORs and linear and quadratic trends of childhood
overweight in relation to maternal prepregnancy BMI and
breast-feeding for the total sample are shown in Table 3. InModel 1, ORs for maternal prepregnancy BMI and breast-feeding were adjusted for age, sex, ethnicity, gestationalage, birth weight, birth order, maternal smoking, alcoholuse, weight gain during pregnancy, maternal age, highesteducation levels at childbirth, and annual family net income,but were not adjusted for each other. We found that childrenwhose mothers were overweight (adjusted OR � 2.4; 95%CI, 1.7, 3.4) or obese (OR � 3.6; 95% CI, 2.4, 5.5) weremore likely to be overweight compared with those whosemothers had normal BMI. In contrast, children who werebreast-fed for 1 to 3 months (OR � 0.7; 95% CI, 0.5, 0.9)and �4 months (OR � 0.6; 95% CI, 0.4, 0.9) were lesslikely to be overweight.
Table 1. Sample and population-weighted characteristics of children of the 1996 NLSY79
CharacteristicUnweighted sample size
(n � 2636) (n)Population-weightedpercentage [% (SE)]
SexBoys 1337 51.3 (1.2)Girls 1299 48.7 (1.2)
Race/ethnicityHispanic 552 7.0 (0.3)Black 820 15.0 (0.6)Non-Hispanic, Non-Black (white) 1264 78.0 (0.7)
Age group (years)2 to 6 923 38.2 (1.1)7 to 10 964 35.0 (1.1)11 to 14 749 26.8 (1.0)
Children’s BMI percentile (kg/m2)�5th 272 10.7 (0.7)5th to �85th 1642 64.7 (1.1)85th to �95th 323 11.8 (0.7)�95th 399 12.8 (0.7)
Birth weight (g)500 to 2499 158 5.1 (0.5)2500 to 3999 2190 82.5 (0.9)4000 to 6000 288 12.4 (0.8)
Birth order1 922 38.9 (1.1)2 938 36.3 (1.1)�3 776 24.8 (1.0)
Preterm (32 to �37 weeks)Yes 268 10.3 (0.7)No 2368 89.7 (0.7)
Duration of breast-feeding (months)Never 1258 43.2 (1.2)1 to 3 731 33.5 (1.1)�4 441 23.3 (1.1)
Additive Interactions on Childhood Overweight, Li et al.
OBESITY RESEARCH Vol. 13 No. 2 February 2005 365

Thereafter, in Model 2, we further adjusted the ORs formaternal prepregnancy BMI and breast-feeding simulta-neously in addition to the covariates in Model 1. After theadditional adjustment, the effect of maternal prepregnancyBMI was slightly increased, whereas the effect of breast-feeding was slightly attenuated. The changes in the magni-tude of the effects of maternal prepregnancy BMI or breast-feeding on childhood overweight risk indicated that theassociation of breast-feeding and childhood overweight maybe partially confounded by maternal prepregnancy BMI and
vice versa. However, the persistent significance of bothmaternal prepregnancy BMI and breast-feeding furthershowed their independent effects on childhood overweight.
Model 2 was repeated for the three age-specific sub-samples, and similar patterns of ORs were yielded (Table 4)compared with the total sample. It seemed that the associ-ation between maternal prepregnancy obesity (BMI � 30kg/m2) and childhood overweight was slightly stronger inolder children (7 to 10 years of age: OR, 5.7; 95% CI, 2.9,11.7; 11 to 14 years of age: OR, 4.3; 95% CI, 1.7, 10.8)
Table 2. Sample and population-weighted characteristics of mothers of the 1996 NLSY79
CharacteristicUnweighted sample size
(n � 2636)Population-weightedpercentage [% (SE)]
Maternal prepregnancy BMI�18 128 5.1 (0.5)18 to 24.9 1688 67.9 (1.1)25 to 29.9 468 17.6 (0.9)�30 246 9.4 (0.7)
Maternal smoking during pregnancyNo 1895 73.1 (1.1)Yes 633 26.9 (1.1)
Maternal alcohol use during pregnancyNever 1452 59.0 (1.3)Less than once a month 386 20.1 (1.0)Once a month 198 10.5 (0.8)Once a week 197 9.5 (0.8)More than once a week 27 0.9 (0.2)
Maternal weight gain during pregnancy (kg, quartile)Quartile 1 (mean: 6.4 kg) 644 22.5 (1.0)Quartile 2 (mean: 12.1 kg) 755 30.0 (1.1)Quartile 3 (mean: 15.9 kg) 496 19.9 (0.9)Quartile 4 (mean: 22.5 kg) 699 27.7 (1.1)
Maternal age at childbirth (years)�23 476 15.2 (0.8)23 to 28 1456 53.9 (1.2)�29 704 30.9 (1.1)
Maternal education level (years)�11th 564 16.0 (0.8)12th 949 36.9 (1.1)Some college (13 to 15 years) 687 26.2 (1.0)College and higher (�16 years) 429 20.9 (0.9)
Annual family net income (US $)�$15,000 867 27.1 (1.0)
$15,000 to $24,999 361 11.2 (0.7)$25,000 to $49,999 720 29.0 (1.1)$50,000 to $74,999 404 18.7 (0.9)�$75,000 284 13.9 (0.9)
Additive Interactions on Childhood Overweight, Li et al.
366 OBESITY RESEARCH Vol. 13 No. 2 February 2005

compared with younger children (2 to 6 years of age: OR,2.8; 95% CI, 1.3, 6.0). The association between breast-feeding and childhood overweight was similar across thethree age groups. Because of reduced sample size for eachage group, the 95% CIs of ORs for both maternal prepreg-nancy BMI and breast-feeding were wider than those for thetotal sample (Table 3).
Linear and Quadratic TrendsFor the total sample, there was a significant linear trend
(or dose-response relationship) for the effects of maternalprepregnancy BMI on childhood overweight (p � 0.001),indicating that a higher level of maternal prepregnancy BMIwas associated with an increased risk of childhood over-weight (Table 3). In addition, there was a significant lineartrend for the effect of breast-feeding on childhood over-weight (p � 0.02), indicating that a longer duration ofbreast-feeding was associated with a reduced risk of child-hood overweight. The linear trend for the effect of breast-feeding on childhood overweight seemed to be slightly
attenuated after adjusting for maternal prepregnancy BMI(p � 0.02 vs. p � 0.06). No quadratic trends of maternalprepregnancy BMI and breast-feeding were detected in thisstudy.
Additive and Multiplicative InteractionsThe adjusted ORs of childhood overweight stratified by
the levels of maternal prepregnancy BMI and breast-feedingare shown in Table 5. According to the independent effectof maternal prepregnancy obesity (OR, 3.5; 95% CI, 1.2,10.0) and the independent effect of never being breast-fed(OR, 1.7; 95% CI, 0.9, 3.2) on childhood overweight, theexpected joint effect of maternal prepregnancy BMI andlack of breast-feeding was 4.2 (3.5 � 1.7 –1 � 4.2) on theadditive scale and 6.0 (3.5 � 1.7 � 1 � 6.0) on themultiplicative scale. Therefore, the observed joint effectwhen both exposures were present (OR, 6.1; 95% CI, 2.9,13.1) was greater than the expected joint effect on theadditive scale (OR, 4.2) but equivalent to the expected jointeffect on the multiplicative scale (OR, 6.0), indicating a
Figure 1: Prevalence of childhood overweight (BMI � 95th percentile) by maternal prepregnancy BMI and breast-feeding for the totalsample (A: 2 to 14 years of age) and by three age groups (B: 2 to 6 years of age; C: 7 to 10 years of age; D: 11 to 14 years of age). 1996NLSY79 Child and Young Adult Survey, United States.
Additive Interactions on Childhood Overweight, Li et al.
OBESITY RESEARCH Vol. 13 No. 2 February 2005 367

possible interaction between maternal prepregnancy BMIand lack of breast-feeding on the additive scale and noevidence of interaction on the multiplicative scale. TheWald F test further showed that the additive interactionbetween maternal prepregnancy BMI and lack of breast-feeding was statistically significant (Wald F, 3.1; df, 4; p �0.05), but the multiplicative interaction was not statisticallysignificant (Wald F, 0.31; df, 4; p � 0.87).
DiscussionFindings from our study indicated that higher maternal
prepregnancy BMI was strongly associated with an in-creased risk, whereas breast-feeding was associated with adecreased risk of childhood overweight. The effect ofbreast-feeding on childhood overweight was slightly atten-uated after adjusting for maternal prepregnancy BMI. Asignificant additive interaction between maternal prepreg-nancy BMI and lack of breast-feeding was identified in ourstudy, such that children whose mothers were obese beforepregnancy and who were never breast-fed were at a 6-foldgreater risk of being overweight during childhood comparedwith children whose mother had normal BMI before preg-nancy and who were breast-fed for at least 4 months. Themagnitude of risk for childhood overweight seemed to de-
cline with increasing duration of breast-feeding, indepen-dently of maternal prepregnancy BMI, but the protectiveeffect of breast-feeding seemed, in this study, to be mostsignificant among children whose mothers had normalprepregnancy BMI.
Maternal prepregnancy obesity was the strongest predic-tor of childhood overweight, which is consistent with pre-vious studies (3,17,38). It seems that this risk associationmay emerge at an early age and persist in the older agegroups, as shown in our study. The effect of maternalprepregnancy obesity on childhood overweight may be me-diated through maternal glucose intolerance or gestationaldiabetes (7,39). On the other hand, maternal prepregnancyobesity has been associated with increased birth weights ofchildren (14,40), which may, in turn, lead to childhoodoverweight. However, this mediated effect seems to beweak (7,40). Thus, it is likely that maternal prepregnancyobesity affects childhood overweight through shared genet-ics or pre- and postnatal environmental factors, as shown inprospective and twin studies (3,13,17,41).
One of the important findings in our study was that theprotective effect of breast-feeding against childhood over-weight seemed to be consistent regardless of maternalprepregnancy BMI. In particular, a significant protective
Table 3. Linear and quadratic effects of maternal prepregnancy BMI and breast-feeding on overweight (BMI �95th percentile) for children 2 to 14 years of age, the 1996 NLSY79, total sample
Characteristic
Model 1¶ Model 2¶¶
OR 95% CI OR 95% CI
Maternal prepregnancy BMI (kg/m2)�25 1.0 Referent 1.0 Referent25 to 29.9 2.4§ 1.7, 3.4 2.5§ 1.8, 3.6�30 3.6§ 2.4, 5.5 4.1§ 2.6, 6.4
p value for linear trend†† p � 0.001 p � 0.001p value for quadratic trend P � 0.08 P � 0.12Breast-feeding (months)
Never 1.0 Referent 1.0 Referent1 to 3 0.7† 0.5, 0.9 0.7* 0.5, 1.0�4 0.6† 0.4, 0.9 0.6† 0.4, 1.0
p value for linear trend P � 0.02 P � 0.06p value for quadratic trend P � 0.80 P � 0.76
* p � 0.10, † p � 0.05, § p � 0.001.¶ In Model 1, OR and 95% CI were adjusted for sex, ethnicity, age, gestational age, birth order, birth weight, maternal smoking, alcoholuse, weight gain during pregnancy, maternal age, highest education levels at childbirth, and annual family net income only.¶¶ In Model 2, OR and 95% CI were obtained by including both maternal prepregnancy BMI and breast-feeding simultaneously in additionto the covariates in Model 1.†† p values for linear and quadratic trends were estimated by using contrasts (�1, 0, 1 for linear trend and 1, �2, 1 for quadratic trend)in multiple logistic models.
Additive Interactions on Childhood Overweight, Li et al.
368 OBESITY RESEARCH Vol. 13 No. 2 February 2005
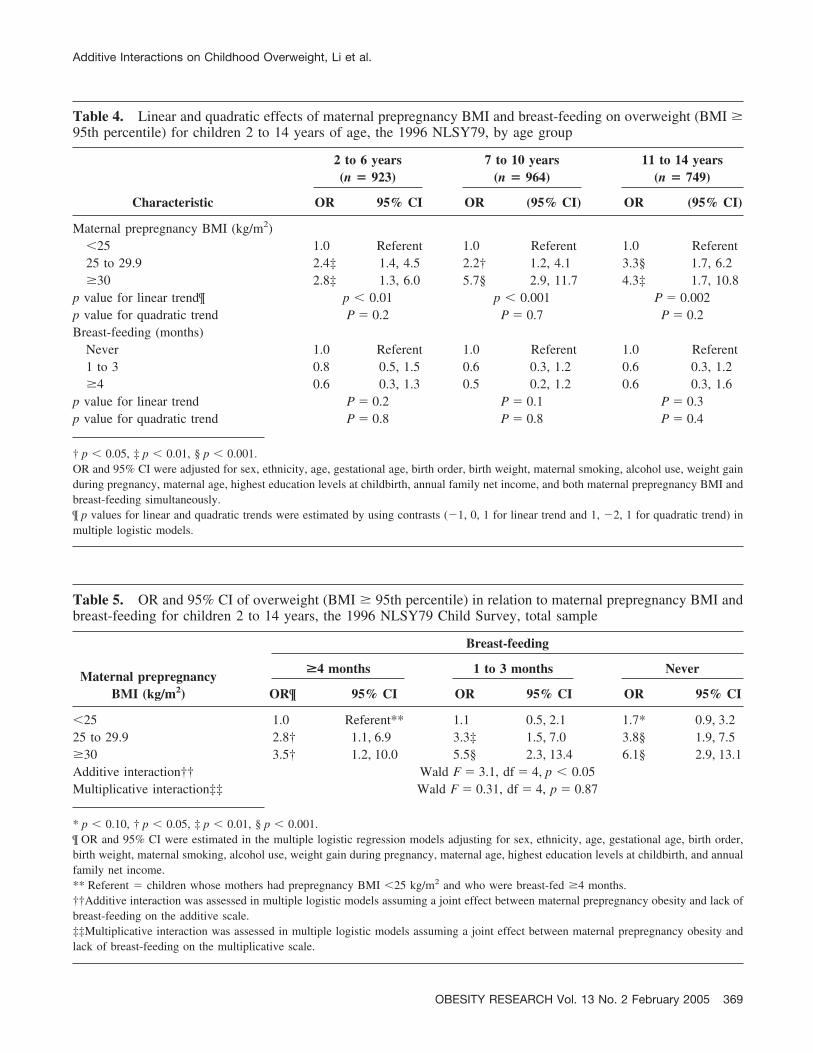
Table 4. Linear and quadratic effects of maternal prepregnancy BMI and breast-feeding on overweight (BMI �95th percentile) for children 2 to 14 years of age, the 1996 NLSY79, by age group
Characteristic
2 to 6 years(n � 923)
7 to 10 years(n � 964)
11 to 14 years(n � 749)
OR 95% CI OR (95% CI) OR (95% CI)
Maternal prepregnancy BMI (kg/m2)�25 1.0 Referent 1.0 Referent 1.0 Referent25 to 29.9 2.4‡ 1.4, 4.5 2.2† 1.2, 4.1 3.3§ 1.7, 6.2�30 2.8‡ 1.3, 6.0 5.7§ 2.9, 11.7 4.3‡ 1.7, 10.8
p value for linear trend¶ p � 0.01 p � 0.001 P � 0.002p value for quadratic trend P � 0.2 P � 0.7 P � 0.2Breast-feeding (months)
Never 1.0 Referent 1.0 Referent 1.0 Referent1 to 3 0.8 0.5, 1.5 0.6 0.3, 1.2 0.6 0.3, 1.2�4 0.6 0.3, 1.3 0.5 0.2, 1.2 0.6 0.3, 1.6
p value for linear trend P � 0.2 P � 0.1 P � 0.3p value for quadratic trend P � 0.8 P � 0.8 P � 0.4
† p � 0.05, ‡ p � 0.01, § p � 0.001.OR and 95% CI were adjusted for sex, ethnicity, age, gestational age, birth order, birth weight, maternal smoking, alcohol use, weight gainduring pregnancy, maternal age, highest education levels at childbirth, annual family net income, and both maternal prepregnancy BMI andbreast-feeding simultaneously.¶ p values for linear and quadratic trends were estimated by using contrasts (�1, 0, 1 for linear trend and 1, �2, 1 for quadratic trend) inmultiple logistic models.
Table 5. OR and 95% CI of overweight (BMI � 95th percentile) in relation to maternal prepregnancy BMI andbreast-feeding for children 2 to 14 years, the 1996 NLSY79 Child Survey, total sample
Maternal prepregnancyBMI (kg/m2)
Breast-feeding
>4 months 1 to 3 months Never
OR¶ 95% CI OR 95% CI OR 95% CI
�25 1.0 Referent** 1.1 0.5, 2.1 1.7* 0.9, 3.225 to 29.9 2.8† 1.1, 6.9 3.3‡ 1.5, 7.0 3.8§ 1.9, 7.5�30 3.5† 1.2, 10.0 5.5§ 2.3, 13.4 6.1§ 2.9, 13.1Additive interaction†† Wald F � 3.1, df � 4, p � 0.05Multiplicative interaction‡‡ Wald F � 0.31, df � 4, p � 0.87
* p � 0.10, † p � 0.05, ‡ p � 0.01, § p � 0.001.¶ OR and 95% CI were estimated in the multiple logistic regression models adjusting for sex, ethnicity, age, gestational age, birth order,birth weight, maternal smoking, alcohol use, weight gain during pregnancy, maternal age, highest education levels at childbirth, and annualfamily net income.** Referent � children whose mothers had prepregnancy BMI �25 kg/m2 and who were breast-fed �4 months.††Additive interaction was assessed in multiple logistic models assuming a joint effect between maternal prepregnancy obesity and lack ofbreast-feeding on the additive scale.‡‡Multiplicative interaction was assessed in multiple logistic models assuming a joint effect between maternal prepregnancy obesity andlack of breast-feeding on the multiplicative scale.
Additive Interactions on Childhood Overweight, Li et al.
OBESITY RESEARCH Vol. 13 No. 2 February 2005 369

effect of breast-feeding was detected among children whosemothers had normal prepregnancy BMI. Although the over-all risk of being overweight was high among children whosemothers were overweight or obese, breast-feeding seemedto reduce the magnitude of risk of being overweight duringchildhood. In previous studies, the protective effect ofbreast-feeding against childhood obesity has been inconsis-tent (9,10,18,19,21–23). The disagreement in previous re-search may be a consequence of several limitations such asvarying definition of breast-feeding, different age periods oflife course, and lack of adjustment for additional possibleconfounders. Most importantly, the association betweenbreast-feeding and childhood overweight may be modifiedby other prenatal factors. Maternal prepregnancy obesityseems to be a significant effect modifier in the associationbetween breast-feeding and childhood overweight on theadditive scale, as shown in this study.
Our study and previous studies suggest that the effect ofbreast-feeding may be more obvious in combination withmaternal nutritional, behavioral, and physical status beforeor during pregnancy. Nevertheless, the effect of breast-feeding on childhood overweight needs to be further studiedbecause little is known about the significance of exclusivityand duration of breast-feeding in different children. There-fore, while some breast-feeding seems to be protective, thecrafting of accurate health policies will require more sub-stantive research in this area. Our findings have significantimplications in clinical practice and prevention. As shownin a recent study (42), women who were obese beforepregnancy were less likely to initiate and maintain breast-feeding. Because there seems to be a significant additiveinteraction between maternal obesity before pregnancy andlack of breast-feeding on childhood overweight in the longrun, intervention may be needed among women who areobese before pregnancy to facilitate initiation and mainte-nance of breast-feeding to reduce offspring’s risk of over-weight during childhood.
It is noteworthy that the popularity of multiple regressionmethods based on multiplicative models has frequently ledto equating interaction exclusively with multiplicative in-teraction. However, additive interaction may be of greaterinterest if the prevention of health events (e.g., childhoodoverweight) is being considered. From the viewpoint oftranslating epidemiological findings into clinical and publichealth practice, presence of additive interaction is impera-tive, even if multiplicative interaction is absent (32,33).
There are several strengths in this study. First, we used anationally representative cohort to test our hypothesis, thusincreasing the external validity of our findings. Second,maternal prepregnancy BMI was used as a potential predic-tor for childhood overweight because it was a more validand reliable indicator of maternal influences in the prenatalenvironment. Finally, we used an innovative approach toexamine the additive interaction of maternal prepregnancy
BMI and breast-feeding on childhood overweight, whileadjusting for the possible confounding effects of maternalweight gain and smoking during pregnancy, gestational age,birth weight, and many other potentially important biolog-ical and socio-demographic factors.
Two limitations are present in this study. First, we did nothave information on diet or physical activity in childhood,which could possibly confound or moderate the relationshipbetween early life influences and childhood overweight.Second, maternal weight and height were self-reported.However, self-reported measures of height and weight inadults have been shown to be valid and reliable for identi-fying associations in epidemiological studies (43,44). Inaddition, maternally reported birth weights, gestational age,and other neonatal events have been shown to be suffi-ciently accurate for clinical and epidemiological research(45).
In conclusion, the findings from our research suggest thata combination of early life risk factors, such as maternalprepregnancy overweight or obesity and lack of breast-feeding, may significantly contribute to the increased risk ofchildhood overweight. These are potentially modifiable riskfactors that could be targeted in the prevention of childhoodoverweight. Future research is needed to help us understandthe mechanisms by which these early life factors affectsubsequent risk for childhood overweight.
AcknowledgmentsWe thank Dr. Michael I. Goran for constructive com-
ments on the first version of this paper. Dr. Li is partiallysupported by research grants from the American HeartAssociation (AHA 0460043Z) and the National Institute ofHealth/National Cancer Institute (R24 CA95835–01).
References1. Flegal KM, Carroll MD, Ogden CL, Johnson CL. Preva-
lence and trends in obesity among US adults, 1999–2000.JAMA. 2002;288:1723–7.
2. Ogden CL, Flegal KM, Carroll MD, Johnson CL. Preva-lence and trends in overweight among US children and ado-lescents, 1999–2000. JAMA. 2002;288:1728–32.
3. Whitaker RC, Wright JA, Pepe MS, Seidel KD, Dietz WH.Predicting obesity in young adulthood from childhood andparental obesity. N Engl J Med. 1997;337:869–73.
4. Must A, Strauss RS. Risks and consequences of childhoodand adolescent obesity. Int J Obes Relat Metab Disord 1999;23(Suppl 2):S2–11.
5. Goran MI, Ball GD, Cruz ML. Obesity and risk of type 2diabetes and cardiovascular disease in children and adoles-cents. J Clin Endocrinol Metab. 2003;88:1417–27.
6. Dietz WH. Critical periods in childhood for the developmentof obesity. Am J Clin Nutr. 1994;59:955–9.
7. Gillman MW, Rifas-Shiman S, Berkey CS, Field AE, Cold-itz GA. Maternal gestational diabetes, birth weight, and ado-lescent obesity. Pediatrics. 2003;111:e221–6.
Additive Interactions on Childhood Overweight, Li et al.
370 OBESITY RESEARCH Vol. 13 No. 2 February 2005
8. Li C, Johnson MS, Goran MI. Effects of low birth weight oninsulin resistance syndrome in Caucasian and African-Amer-ican children. Diabetes Care. 2001;24:2035–42.
9. Gillman MW, Rifas-Shiman SL, Camargo CA Jr, et al.Risk of overweight among adolescents who were breastfed asinfants. JAMA. 2001;285:2461–7.
10. Kramer MS. Do breast-feeding and delayed introduction ofsolid foods protect against subsequent obesity? J Pediatr.1981;98:883–7.
11. Ong KK, Ahmed ML, Emmett PM, Preece MA, DungerDB. Association between postnatal catch-up growth and obe-sity in childhood: prospective cohort study. BMJ. 2000;320:967–71.
12. Barker DJP. Mothers, Babies, and Health in Later Life.Edinburgh: Harcourt Brace; 1998.
13. Oken E, Gillman MW. Fetal origins of obesity. Obes Res.2003;11:496–506.
14. Cnattingius S, Bergstrom R, Lipworth L, Kramer MS.Prepregnancy weight and the risk of adverse pregnancy out-comes. N Engl J Med. 1998;338:147–52.
15. Fisch RO, Bilek MK, Ulstrom R. Obesity and leanness atbirth and their relationship to body habitus in later childhood.Pediatrics. 1975;56:521–8.
16. Frisancho AR. Prenatal compared with parental origins ofadolescent fatness. Am J Clin Nutr. 2000;72:1186–90.
17. Whitaker RC. Predicting preschooler obesity at birth: the roleof maternal obesity in early pregnancy. Pediatrics. 2004;114:e29–36.
18. Armstrong J, Reilly JJ. Breast-feeding and lowering the riskof childhood obesity. Lancet. 2002;359:2003–4.
19. Bergmann KE, Bergmann RL, Von Kries R, et al. Earlydeterminants of childhood overweight and adiposity in a birthcohort study: role of breast-feeding. Int J Obes Relat MetabDisord. 2003;27:162–72.
20. Grummer-Strawn LM, Mei Z. Does breast-feeding protectagainst pediatric overweight? Analysis of longitudinal datafrom the Centers for Disease Control and Prevention PediatricNutrition Surveillance System. Pediatrics. 2004;113:e81–6.
21. Hediger ML, Overpeck MD, Kuczmarski RJ, Ruan WJ.Association between infant breast-feeding and overweight inyoung children. JAMA. 2001;285:2453–60.
22. Parsons TJ, Power C, Manor O. Infant feeding and obesitythrough the lifecourse. Arch Dis Child. 2003;88:793–4.
23. Victora CG, Barros F, Lima RC, Horta BL, Wells J.Anthropometry and body composition of 18 year old menaccording to duration of breast feeding: birth cohort studyfrom Brazil. BMJ. 2003;327:901.
24. Center for Human Resource Research. Child and YoungAdult Data: User’s Guide. Columbus, OH: Ohio State Uni-versity; 2000.
25. Homer CJ, James SA, Siegel E. Work-related psychosocialstress and risk of preterm, low birthweight delivery. Am JPublic Health. 1990;80:173–7.
26. Strauss RS, Pollack HA. Epidemic increase in childhoodoverweight, 1986–1998. JAMA. 2001;286:2845–8.
27. Kuczmarski RJ, Ogden CL, Guo SS, et al. CDC GrowthCharts for the United States: methods and development. VitalHealth Stat 11. 2000;2002:1–190.
28. World Health Organization. Physical Status: The Use andInterpretation of Anthropometry. Report of a WHO ExpertCommittee. Geneva, Switzerland: World Health Organization;1995.
29. Research Triangle Institute. SUDDAN User’s Manual, Re-lease 8.0. Research Triangle Park, NC: Research TriangleInstitute; 2001.
30. SAS Institute. SAS/C Online Doc TM, Release 8.1. Cary, NC:SAS Institute; 2000.
31. Breslow NE, Storer BE. General relative risk functions forcase-control studies. Am J Epidemiol. 1985;122:149–62.
32. Rothman KJ, Greenland S, Waller AM. Concepts of inter-action. Am J Epidemiol. 1980;112:467–70.
33. Szklo M, Nieto J. Epidemiology: Beyond the Basics. Gaith-ersburg, MD: Aspen Publishers; 2000.
34. Rothman KJ. The estimation of synergy or antagonism. Am JEpidemiol. 1976;103:506–11.
35. Walter SD, Holford TR. Additive, multiplicative, and othermodels for disease risks. Am J Epidemiol. 1978;108:341–6.
36. Kupper LL, Hogan MD. Interaction in epidemiologic stud-ies. Am J Epidemiol. 1978;108:447–53.
37. Greenland S. Tests for interaction in epidemiologic studies: areview and a study of power. Stat Med. 1983;2:243–51.
38. Parsons TJ, Power C, Logan S, Summerbell CD. Child-hood predictors of adult obesity: a systematic review. Int JObes Relat Metab Disord. 1999;23:S1–107.
39. Dabelea D, Pettitt DJ. Intrauterine diabetic environment con-fers risks for type 2 diabetes mellitus and obesity in theoffspring, in addition to genetic susceptibility. J Pediatr En-docrinol Metab. 2001;14:1085–91.
40. Li C, Huang TTK, Ahluwalia HK, et al. Mediating effect ofbirth weight between maternal and childhood obesity. Am JEpidemiol. 2003;157:S5–18.
41. Loos RJ, Beunen G, Fagard R, Derom C, Vlietinck R. Birthweight and body composition in young adult men—a prospec-tive twin study. Int J Obes Relat Metab Disord. 2001;25:1537–45.
42. Li R, Jewell S, Grummer-Strawn L. Maternal obesity andbreast-feeding practices. Am J Clin Nutr. 2003;77:931–6.
43. Spencer EA, Appleby PN, Davey GK, Key TJ. Validity ofself-reported height and weight in 4808 EPIC-Oxford partic-ipants. Public Health Nutr. 2002;5:561–5.
44. Yu SM, Nagey DA. Validity of self-reported pregravidweight. Ann Epidemiol. 1992;2:715–21.
45. McCormick MC, Brooks-Gunn J. Concurrent child healthstatus and maternal recall of events in infancy. Pediatrics.1999;104:1176–81.
Additive Interactions on Childhood Overweight, Li et al.
OBESITY RESEARCH Vol. 13 No. 2 February 2005 371