(to be filled by the Nodal Officer or Principal Chief Conservator ...
Upload
independentCategory
view
0download
0
REVIEW ARTICLE – GASTROINTESTINAL ONCOLOGY
Accuracy of Endoscopic Ultrasound to Diagnose Nodal Invasionby Rectal Cancers: A Meta-Analysis and Systematic Review
Srinivas R. Puli, MD1, Jyotsna B.K. Reddy1, Matthew L. Bechtold1, Abhishek Choudhary1,
Mainor R. Antillon1, and William R. Brugge2
1Division of Gastroenterology and Hepatology, University of Missouri-Columbia, Columbia, MO; 2GI Unit, Massachusetts
General Hospital, Boston, MA
ABSTRACT
Background. Nodal staging in patients with rectal cancer
predicts prognosis and directs therapy. Published data on
the accuracy of endoscopic ultrasound (EUS) for diag-
nosing nodal invasion in patients with rectal cancer has
been inconsistent.
Aim. To evaluate the accuracy of EUS in diagnosing nodal
metastasis of rectal cancers.
Method. Study Selection Criteria: Only EUS studies
confirmed by surgical histology were selected. Data Col-
lection and Extraction: Articles were searched in Medline,
Pubmed, and CENTRAL. Statistical Method: Pooling was
conducted by both fixed-effects model and random-effects
model.
Results. The initial search identified 3610 reference arti-
cles in which 352 relevant articles were selected and
reviewed. Data were extracted from 35 studies (N = 2732)
that met the inclusion criteria. Pooled sensitivity of EUS in
diagnosing nodal involvement by rectal cancers was 73.2%
(95% confidence interval [95% CI] 70.6–75.6). EUS had a
pooled specificity of 75.8% (95% CI 73.5–78.0). The
positive likelihood ratio of EUS was 2.84 (95% CI 2.16–
3.72), and negative likelihood ratio was 0.42 (95% CI
0.33–0.52). All the pooled estimates, calculated by fixed-
and random-effect models, were similar. SROC curves
showed an area under the curve of 0.79. The P for chi-
squared heterogeneity for all the pooled accuracy estimates
was [.10.
Conclusions. EUS is an important and accurate diagnostic
tool for evaluating nodal metastasis of rectal cancers. This
meta-analysis shows that the sensitivity and specificity of
EUS is moderate. Further refinement in EUS technologies
and diagnostic criteria are needed to improve the diagnostic
accuracy.
Rectal cancer is a serious disease affecting many
patients worldwide, especially in Western Europe and
North America. In the United States in 2004, invasive
rectal cancer was found in 13.1 patients per 100,000.1,2
Rectal cancer is diagnosed in *41,000 Americans annu-
ally.1,2 Although *45% of rectal cancers are localized,
*15% have distant metastasis and *6% are not staged for
various reasons.2 Risk factors for rectal cancer include
familial polyposis syndromes (FAP, HNPCC), history of
adenomatous polyps, diabetes mellitus, obesity, excessive
alcohol, and cigarette smoking.3–7 With an increased par-
ticipation in risk factors (alcohol, smoking) and obesity in
combination with overall incidence, timely diagnosis and
adequate treatment are crucial. However, before treatment,
it is imperative to evaluate the extent of the disease with
TNM staging.
In rectal cancer, the TNM staging is usually performed
to guide treatment decisions and prognosis.8 The TNM
staging for rectal cancer is dependent on the depth of
invasion of the lesion (T), regional lymph node invasion
(N), and the presence of distant metastasis (M). N staging
depends on regional lymph node involvement. NX and N0
represent nodes that cannot be assessed or no regional
lymph node metastases, respectively. Nodal invasion by
rectal cancer is considered locally advanced disease.9
Stage 0 disease represents Tis without lymph node
involvement (N0) or distant metastasis (M0), which has the
best prognosis. Stage I disease represents T1N0M0 and
T2M0N0 lesions and correlates to a 5-year survival rate of
*85–90%.2,10–12 Stage II disease represents T3N0M0 and
� Society of Surgical Oncology 2009
First Received: 25 October 2008;
Published Online: 14 February 2009
S. R. Puli, MD
e-mail: [email protected]
Ann Surg Oncol (2009) 16:1255–1265
DOI 10.1245/s10434-009-0337-4

T4N0M0 lesions and exhibit a 5-year survival rate of
*60–65%.2,10–12 Stage III disease represents any T level
with one or two lymph nodes invaded but no distant
metastasis (T1-4N1-2M0). Stage III disease correlates with
a 5-year survival rate of *30–40%.10–12 There is a marked
decrease in survival with nodal invasion by rectal cancer.
The optimal treatment of rectal cancer varies with the
stage of disease. This difference in treatment regimens
emphasizes the importance of accurate staging. All patients
with locally advanced rectal cancer without metastasis are
treated with multimodality treatment. Surgery alone, in the
form of total pelvic exenteration, is associated with high
morbidity.13,14 Treatment with radiation followed by sur-
gery is associated with complete response in two-thirds, but
recurrence occurs in one-third of these patients.15–18
Improved rates of resectability, enhanced local control, and
increased survival can be achieved by combining moderate-
to high-dose preoperative radiation therapy with concurrent
5-FU based chemotherapy.2,20–24 Therefore, appropriate
treatment is guided by the stage of rectal cancer.
In an attempt to accurately stage rectal cancer, many
modalities have been used, from computed tomography
(CT) of the abdomen, magnetic resonance imaging (MRI)
of the abdomen, and endoscopic ultrasound (EUS).
Regarding nodal invasion, CT has a accuracy of 55–65%
and MRI has accuracy of 60–65%.25,26
With such an important difference in treatment and
prognosis between early and locally advanced disease, the
accuracy of N staging is pivotal. The reports of the accu-
racy of N staging of rectal cancers by EUS vary in the
literature. Due to this inconsistency and the clinical
importance of correct staging for treatment and prognosis,
we performed a meta-analysis to evaluate the accuracy of
EUS in staging nodal disease in rectal cancer.
METHODS
Study Selection Criteria
Only EUS studies confirmed by surgical histology were
selected. Nodal invasion of rectal cancers was defined as
invasion to perirectal lymph nodes. From this pool, only
studies from which a 2 9 2 table could be constructed for
true positive, false negative, false positive, and true nega-
tive values were included.
Data Collection and Extraction
Articles were searched in MEDLINE (through PubMed,
an electronic search engine for published articles, and
Ovid) for the years 1966 to January 2008, PubMed, Ovid
journals, EMBASE, Cumulative Index for Nursing &
Allied Health Literature, ACP journal club, DARE,
International Pharmaceutical Abstracts, old Medline,
Medline nonindexed citations, OVID Healthstar, and
Cochrane Central Register of Controlled Trials (CEN-
TRAL). The terms used for search were endoscopic
ultrasound, EUS, ultrasound, endosonography, rectal can-
cer, tumor staging, nodal invasion, staging, surgery,
sensitivity, specificity, positive predictive value, and neg-
ative predictive value. Study authors were contacted when
the required data could not be determined from the publi-
cations. The data extracted from each study were used to
construct 2 9 2 tables. Two authors (SP and JR) inde-
pendently searched and extracted the data into an
abstraction form. Any differences were resolved by mutual
agreement. The agreement between reviewers for the col-
lected data was quantified using the Cohen’s j.27
Quality of Studies
Clinical trials designed with control and treatment arms
can be assessed for quality of the study. A number of cri-
teria have been used to assess the quality of a study (e.g.,
randomization, selection bias of the arms in the study,
concealment of allocation, and blinding of outcome).28,29
There is no consensus on how to assess studies designed
without a control arm. Hence, these criteria do not apply to
studies without a control arm.29 Therefore, for this meta-
analysis and systematic review, studies were selected based
on completeness of the data and inclusion criteria. Com-
pleteness was defined as data available for true positive,
false negative, false positive, and true negative values of
the diagnostic test (EUS). Quality Assessment of Studies of
Diagnostic Accuracy Included in Systematic Reviews
(QUADAS) criteria has been proposed to evaluate quality
of diagnostic studies.30,31 This was used to evaluate the
studies on 14 items described in the QUADAS criteria.
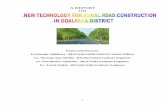
Refining search gave352 relevant articles
35 studies met theinclusion criteria
Initial search gave3,610 potential articles
2,808 articles did notlook at rectal cancer
• 283 did not meet inclusion criteria• 14 studies did not have full data to construct 2x2 table• 20 studies were in other languages
FIG. 1 Search results
1256 S. R. Puli et al.

Statistical Methods
Meta-analysis for the accuracy of EUS in diagnosing
nodal staging of rectal cancers was performed by calcu-
lating pooled estimates of sensitivity, specificity,
likelihood ratios, and diagnostic odds ratios. EUS studies
were grouped into periods of time to standardize the
change in EUS technology, experience of endoscopist,
and EUS criteria for lymph node involvement.32 These
periods of time were 1986–1994, 1995–2000, and 2001–
2008. Pooling was conducted using both Mantel-Haenszel
Method (fixed-effects model) and DerSimonian Laird
Method (random-effects model). The confidence intervals
were calculated using the F distribution method.33 Forrest
plots were drawn to show the point estimates in each
study in relation to the summary pooled estimate. The
width of the point estimates in the Forrest plots indicates
the assigned weight to that study. For 0 value cells, a 0.5
was added as described by Cox.34 The heterogeneity of
the sensitivities and specificities were tested by applying
the likelihood ratio test.35 The heterogeneity of likelihood
ratios and diagnostic odds ratios were tested using
Cochran Q test based on inverse variance weights.36
Heterogeneity among studies was also tested using sum-
mary receiver operating characteristic (SROC) curves.
SROC curves were used to calculate the area under the
curve (AUC). The effect of publication and selection bias
on the summary estimates was tested by Egger bias
indicator and Begg-Mazumdar bias indicator.37,38 Also,
funnel plots were constructed to evaluate potential
0.60.20 0.8 1.00.4
Saitoh, et al. 1986
Pappalardo, et al. 1990
Boyce, et al. 1991
Glaser, et al. 1992
Herzong, et al. 1993
Thaler, et al. 1994
Kaneko, et al. 1995
Nielsen, et al. 1996
Sailer, et al. 1997
Osti, et al. 1997
Ramana, et al. 1997
Caseiro-Alves, et al. 1998
Massari, et al. 1998
Adams, et al. 1998
Norton, et al. 1999
Norton, et al. 1999
Spinelli, et al. 1999
Akasu, et al. 2000
Akasu, et al. 2000
Gualdi, et al 2000
Kim, et al. 2001
Garcia-Aguilar, et al. 2002
Mackay, et al. 2003
Hsieh, et al. 2003
Vanagunas, et al. 2003
Zbar, et al. 2004
Bali, et al. 2004
Rifking, et al. 2004
Manger, et al. 2004
Shami, et al. 2004
Meyenberger, et al. 2005
Maor, et al. 2006
Bianchi, et al. 2006
Kim, et al. 2006
Giovannini, et al. 2006
Pooled sensitivity = 0.73 (0.71 to 0.76)
Sensitivity
0.79
0.88
0.61
0.80
0.89
0.64
0.81
0.79
0.56
0.68
0.83
0.29
0.70
0.17
0.83
0.83
0.68
1.00
0.79
0.73
0.17
0.33
0.67
0.70
0.97
0.75
0.50
0.50
0.88
0.94
0.67
0.57
0.75
0.51
0.80
(0.67 – 0.88)
(0.47 – 1.00)
(0.39 – 0.80)
(0.68 – 0.89)
(0.79 – 0.96)
(0.35 – 0.87)
(0.63 – 0.93)
(0.63 – 0.90)
(0.21 – 0.86)
(0.46 – 0.85)
(0.36 – 1.00)
(0.04 – 0.71)
(0.54 – 0.83)
(0.02 – 0.48)
(0.52 – 0.98)
(0.52 – 0.98)
(0.48 – 0.84)
(0.69 – 1.00)
(0.69 – 0.87)
(0.39 – 0.94)
(0.00 – 0.64)
(0.24 – 0.44)
(0.57 – 0.77)
(0.51 – 0.84)
(0.84 – 1.00)
(0.53 – 0.90)
(0.21 – 0.79)
(0.30 – 0.70)
(0.83 – 0.92)
(0.70 – 1.00)
(0.09 – 0.99)
(0.29 – 0.82)
(0.35 – 0.97)
(0.34 – 0.68)
(0.63 – 0.92)
Sensitivity (95% CI)
FIG. 2 Forrest plot showing sensitivity of EUS to diagnose nodal invasion of rectal cancer
Accuracy of EUS in N Staging of Rectal Cancers: A Meta-Analysis 1257

publication bias using the standard error and diagnostic
odds ratio.39,40
RESULTS
The initial search identified 3610 reference articles.
Among these, 352 relevant articles were selected and
reviewed. Data were extracted from 35 studies (N = 2732)
that met the inclusion criteria.26,41–73 Figure 1 shows the
search results. The included 35 selected studies were
published as full-text articles in peer-reviewed journals. All
the pooled estimates given are estimates calculated by the
fixed-effect model. The change adjusted agreement analy-
sis between the reviewers for data collected separately gave
a kappa value of 1.0. QUADAS criteria to evaluate the
quality of studies showed that all the studies fulfilled 4 to 5
out of 14 described criteria.
Accuracy of EUS to N stage Rectal Cancers
Pooled sensitivity of EUS in diagnosing nodal involve-
ment by rectal cancers was 73.2% (95% CI 70.6–75.6).
Figure 2 depicts the pooled sensitivity as a Forrest plot.
EUS had a pooled specificity of 75.8% (95% CI 73.5–
78.0). Forrest plot in Fig. 3 depicts specificity from indi-
vidual studies. The positive likelihood ratio of EUS was
2.84 (95% CI 2.16–3.72), and negative likelihood ratio was
0.42 (95% CI 0.33–0.52). Figures 4 and 5 depict the pooled
positive and negative likelihood ratios as a Forrest plot.
The diagnostic odds ratio, the odds of having nodal
0.60.20 0.8 1.00.4
Saitoh, et al. 1986
Pappalardo, et al. 1990
Boyce, et al. 1991
Glaser, et al. 1992
Herzong, et al. 1993
Thaler, et al. 1994
Kaneko, et al. 1995
Nielsen, et al. 1996
Sailer, et al. 1997
Osti, et al. 1997
Ramana, et al. 1997
Caseiro-Alves, et al. 1998
Massari, et al. 1998
Adams, et al. 1998
Norton, et al. 1999
Norton, et al. 1999
Spinelli, et al. 1999
Akasu, et al. 2000
Akasu, et al. 2000
Gualdi, et al 2000
Kim, et al. 2001
Garcia-Aguilar, et al. 2002
Mackay, et al. 2003
Hsieh, et al. 2003
Vanagunas, et al. 2003
Zbar, et al. 2004
Bali, et al. 2004
Rifking, et al. 2004
Manger, et al. 2004
Shami, et al. 2004
Meyenberger, et al. 2005
Maor, et al. 2006
Bianchi, et al. 2006
Kim, et al. 2006
Giovannini, et al. 2006
Pooled specificity = 0.76 (0.74 to 0.78)
Specificity
0.14
0.83
0.91
0.83
0.27
1.00
0.89
0.56
0.91
0.64
1.00
1.00
0.84
0.97
0.68
0.53
0.79
0.60
0.72
0.80
0.33
0.82
0.90
0.77
0.94
0.67
0.65
0.92
0.65
0.32
1.00
0.80
0.81
0.61
1.00
(0.03 – 0.35)
(0.36 – 1.00)
(0.71 – 0.99)
(0.72 – 0.90)
(0.15 – 0.42)
(0.72 – 1.00)
(0.80 – 0.95)
(0.40 – 0.71)
(0.77 – 0.98)
(0.44 – 0.81)
(0.40 – 1.00)
(0.69 – 1.00)
(0.67 – 0.95)
(0.88 – 1.00)
(0.48 – 0.84)
(0.29 – 0.76)
(0.64 – 0.90)
(0.47 – 0.71)
(0.60 – 0.82)
(0.52 – 0.96)
(0.04 – 0.78)
(0.75 – 0.88)
(0.84 – 0.94)
(0.56 – 0.91)
(0.83 – 0.99)
(0.35 – 0.90)
(0.38 – 0.86)
(0.84 – 0.97)
(0.53 – 0.75)
(0.19 – 0.48)
(0.29 – 1.00)
(0.66 – 0.90)
(0.58 – 0.95)
(0.45 – 0.76)
(0.69 – 1.00)
Specificity (95% CI)
FIG. 3 Forrest plot showing specificity of EUS to diagnose nodal invasion of rectal cancer
1258 S. R. Puli et al.

metastasis in positive compared with negative EUS studies,
was 7.9 (95% CI 5.3–11.7). Forrest plot in Fig. 6 shows the
diagnostic odds ratios from various studies included in this
analysis. All the pooled estimates, calculated by fixed- and
random-effect models, were similar. SROC curves showed
an area under the curve of 0.79. Figure 7 shows the SROC
curve and the area under the curve. The P for chi-squared
heterogeneity for all the pooled accuracy estimates was
[0.10.
Effect of Technology over Time
EUS studies were grouped into three time periods to
standardize criteria for EUS imaging of lymph node
involvement, improvement in endoscopists experience, and
change in technology over the past 2 decades. These time
periods were 1984–1994, 1995–2000, and 2001–2008.
During these time periods, the number of studies that met
the inclusion criteria for EUS as an imaging modality only
were 6, 14, and 15, respectively. For the most recent time
period, EUS alone had a sensitivity of 70.9% (95% CI
67.3–74.3) and specificity of 78.6% (95% CI 75.5–81.5).
All pooled estimates during the three time periods are
given in Table 1. The P for chi-squared heterogeneity for
all the pooled accuracy estimates was [.10.
Bias Estimates
Publication bias calculated using Harbord-Egger bias
indicator gave a value of -0.47 (95% CI -1.79 to 0.85,
P = .52), indicating that there was no publication bias. The
Begg-Mazumdar indicator gave a Kendall tau b value of
0.01 1001
Saitoh, et al. 1986
Pappalardo, et al. 1990
Boyce, et al. 1991
Glaser, et al. 1992
Herzong, et al. 1993
Thaler, et al. 1994
Kaneko, et al. 1995
Nielsen, et al. 1996
Sailer, et al. 1997
Osti, et al. 1997
Ramana, et al. 1997
Caseiro-Alves, et al. 1998
Massari, et al. 1998
Adams, et al. 1998
Norton, et al. 1999
Norton, et al. 1999
Spinelli, et al. 1999
Akasu, et al. 2000
Akasu, et al. 2000
Gualdi, et al 2000
Kim, et al. 2001
Garcia-Aguilar, et al. 2002
Mackay, et al. 2003
Hsieh, et al. 2003
Vanagunas, et al. 2003
Zbar, et al. 2004
Bali, et al. 2004
Rifking, et al. 2004
Manger, et al. 2004
Shami, et al. 2004
Meyenberger, et al. 2005
Maor, et al. 2006
Bianchi, et al. 2006
Kim, et al. 2006
Giovannini, et al. 2006
Pooled positive LR = 2.84 (2.16 to 3.72)
Positive LR
0.91
5.25
6.70
4.55
1.22
15.20
7.17
1.79
6.48
1.90
7.86
6.88
4.47
4.83
2.59
1.76
3.24
2.36
2.81
3.64
0.25
1.86
6.66
3.02
15.84
2.25
1.42
6.33
2.48
1.38
5.00
2.80
3.94
1.32
17.42
(0.74 – 1.12)
(0.86 – 32.02)
(1.72 – 26.12)
(2.79 – 7.44)
(1.00 – 1.48)
(0.98 – 235.55)
(3.78 – 13.58)
(1.23 – 2.60)
(1.90 – 22.17)
(1.08 – 3.35)
(0.55 – 112.09)
(0.38 – 124.52)
(1.95 – 10.23)
(0.75 – 31.01)
(1.43 – 4.70)
(1.03 – 3.01)
(1.72 – 6.11)
(1.74 – 3.21)
(1.92 – 4.10)
(1.24 – 10.65)
(0.04 –1.63)
(1.19 – 2.93)
(4.15 – 10.67)
(1.45 – 6.31)
(5.28 – 47.49)
(0.98 – 5.17)
(0.60 – 3.34)
(2.68 – 14.95)
(1.84 – 3.36)
(1.08 – 1.74)
(0.34 – 74.52)
(1.37 – 5.73)
(1.50 – 10.37)
(0.80 – 2.16)
(1.16 – 262.62)
Positive LR (95% CI)
FIG. 4 Forrest plot showing positive likelihood ratio of EUS to diagnose nodal invasion of rectal cancer
Accuracy of EUS in N Staging of Rectal Cancers: A Meta-Analysis 1259

0.06 (P = .62), suggesting no publication bias. The funnel
plots in Fig. 8 show no publication bias for EUS studies
estimating nodal invasion of rectal cancers.
DISCUSSION
Nodal invasion by rectal cancer is considered locore-
gional spread. Locoregional spread plays a pivotal role in
estimating survival and determining the appropriate treat-
ment. The survival is lower with locoregional spread. In
these patients, giving preoperative high-dose radiation and
chemotherapy with 5-FU-based chemotherapy improves
rates of resectability with possibly local control and
improved survival.
Apart from predicting nodal invasion, EUS also pro-
vides the ability to perform fine needle aspiration (FNA)
during the procedure. Several EUS studies report very low
(0.5–2.5%) to no complications in performing FNA.74–76
In this meta-analysis and systematic review, sensitivity
and specificity of EUS to diagnose nodal invasion by rectal
cancers was approximately 75%. On the other hand, CT
has an accuracy of 55–65% and MRI has accuracy of 60–
65%.25,26
Positive likelihood ratio of a diagnostic test is a measure
of how well the test correctly identifies a disease stage. The
higher the positive likelihood ratio, the better the diag-
nostic test performs in correctly identifying the true disease
state. On the flip side, negative likelihood ratio of a
0.01 1001
Saitoh, et al. 1986
Pappalardo, et al. 1990
Boyce, et al. 1991
Glaser, et al. 1992
Herzong, et al. 1993
Thaler, et al. 1994
Kaneko, et al. 1995
Nielsen, et al. 1996
Sailer, et al. 1997
Osti, et al. 1997
Ramana, et al. 1997
Caseiro-Alves, et al. 1998
Massari, et al. 1998
Adams, et al. 1998
Norton, et al. 1999
Norton, et al. 1999
Spinelli, et al. 1999
Akasu, et al. 2000
Akasu, et al. 2000
Gualdi, et al 2000
Kim, et al. 2001
Garcia-Aguilar, et al. 2002
Mackay, et al. 2003
Hsieh, et al. 2003
Vanagunas, et al. 2003
Zbar, et al. 2004
Bali, et al. 2004
Rifking, et al. 2004
Manger, et al. 2004
Shami, et al. 2004
Meyenberger, et al. 2005
Maor, et al. 2006
Bianchi, et al. 2006
Kim, et al. 2006
Giovannini, et al. 2006
Pooled negative LR = 0.42 (0.33 to 0.52)
Negative LR
1.56
0.15
0.43
0.25
0.40
0.38
0.22
0.38
0.49
0.50
0.24
0.72
0.36
0.86
0.25
0.32
0.41
0.08
0.30
0.34
2.50
0.81
0.36
0.39
0.03
0.38
0.77
0.54
0.19
0.20
0.43
0.54
0.31
0.80
0.22
(0.49 – 4.91)
(0.02 – 0.97)
(0.25 – 0.73)
(0.15 – 0.40)
(0.17 – 0.93)
(0.19 – 0.75)
(0.11 – 0.45)
(0.19 – 0.74)
(0.23 – 1.02)
(0.26 – 0.94)
(0.06 – 1.01)
(0.44 – 1.17)
(0.22 – 0.58)
(0.67 – 1.12)
(0.07 – 0.89)
(0.08 – 1.20)
(0.23 – 0.71)
(0.01 – 1.15)
(0.19 – 0.45)
(0.13 – 0.92)
(0.76 – 8.19)
(0.69 – 0.96)
(0.27 – 0.49)
(0.23 – 0.69)
(0.00 – 0.22)
(0.17 – 0.83)
(0.40 – 1.50)
(0.37 – 0.80)
(0.13 – 0.27)
(0.03 – 1.38)
(0.11 – 1.60)
(0.29 – 1.00)
(0.09 – 1.04)
(0.53 – 1.20)
(0.11 – 0.42)
Negative LR (95% CI)
FIG. 5 Forrest plot showing negative likelihood ratio of EUS to diagnose nodal invasion of rectal cancer
1260 S. R. Puli et al.

diagnostic test is a measure of how well the test correctly
excludes a disease stage. The lower the negative likelihood
ratio, the better the diagnostic test’s ability to exclude a
disease stage. EUS has a low negative likelihood ratio, but
the positive likelihood ratio is modest. So, EUS performs
better to exclude nodal invasion by rectal cancer when
compared with the ability to confirm nodal invasion. In
other words, if EUS reveals that there is no nodal invasion,
then one could be more confident in the diagnosis than if
EUS reveals there was nodal involvement.
The diagnostic odds ratio of EUS to diagnose nodal
invasion by rectal cancer is high (*8). Diagnostic odds
ratio is defined as the odds of having a positive test in
patients with true anatomic stage of the disease when
compared with patients who do not have the disease.
Clinically, if EUS demonstrates a patient with rectal cancer
has nodal metastasis, the odds of having the correct ana-
tomic stage of disease is 8 times.
The effect of FNA on the accuracy estimates could not
be evaluated as there were not enough studies with accu-
racy estimated for EUS with FNA. This is one of the
limitations of this analysis.
In all the studies included, the authors mention that the
EUS was performed by an experienced endosonographer.
EUS technologies, quality of nodal imaging, and endos-
copists’ experience have improved over the past 2 decades.
To assess the effect of these changes, studies were grouped
into periods of time. The hypothesis is that during a period
of time, the technology of EUS used might be the same. A
weakness of this kind of pooling is that some of the studies
might use older equipment, even though the paper was
published in the most recent time period. However,
0.01 1001
Saitoh, et al. 1986
Pappalardo, et al. 1990
Boyce, et al. 1991
Glaser, et al. 1992
Herzong, et al. 1993
Thaler, et al. 1994
Kaneko, et al. 1995
Nielsen, et al. 1996
Sailer, et al. 1997
Osti, et al. 1997
Ramana, et al. 1997
Caseiro-Alves, et al. 1998
Massari, et al. 1998
Adams, et al. 1998
Norton, et al. 1999
Norton, et al. 1999
Spinelli, et al. 1999
Akasu, et al. 2000
Akasu, et al. 2000
Gualdi, et al 2000
Kim, et al. 2001
Garcia-Aguilar, et al. 2002
Mackay, et al. 2003
Hsieh, et al. 2003
Vanagunas, et al. 2003
Zbar, et al. 2004
Bali, et al. 2004
Rifking, et al. 2004
Manger, et al. 2004
Shami, et al. 2004
Meyenberger, et al. 2005
Maor, et al. 2006
Bianchi, et al. 2006
Kim, et al. 2006
Giovannini, et al. 2006
Pooled diagnostic odds ratio = 7.87 (5.31 to 11.66)
Diagnostic Odds Ratio
0.59
35.00
15.56
18.49
3.06
39.73
32.87
4.74
13.33
3.83
33.00
9.55
12.46
5.60
10.56
5.56
7.98
30.97
9.47
10.67
0.10
2.30
18.34
7.67
490.67
6.00
1.83
11.67
13.40
7.00
11.67
5.20
12.75
1.65
79.80
(0.15 – 2.27)
(1.74 – 703.00)
(2.91 – 83.26)
(7.99 – 42.78)
(1.10 – 8.54)
(1.94 – 813.99)
(10.63 – 101.66)
(1.77 – 12.69)
(2.27 – 78.20)
(1.22 – 11.98)
(1.06 – 1,023.57)
(0.39 – 235.78)
(3.93 – 39.55)
(0.71 – 44.48)
(1.90 – 58.53)
(0.95 – 32.46)
(2.71 – 23.51)
(1.75 – 549.05)
(4.63 – 19.36)
(1.71 – 66.72)
(0.01 – 1.54)
(1.25 – 4.23)
(9.48 – 35.47)
(2.36 – 24.86)
(48.82 – 4,931.89)
(1.32 – 27.29)
(0.41 – 8.27)
(3.75 – 36.26)
(7.30 – 24.59)
(0.84 – 58.40)
(0.32 – 422.14)
(1.47 – 18.44)
(1.84 – 88.35)
(0.67 – 4.06)
(4.18 – 1,522.93)
Diagnostic Odds Ratio (95% CI)
FIG. 6 Forrest plot showing diagnostic odds ratio of EUS to diagnose Nodal invasion of rectal cancer
Accuracy of EUS in N Staging of Rectal Cancers: A Meta-Analysis 1261

statistically, there is no alternative way of looking at this
effect, and this seems to be an accepted method of looking
at the effect of technology.32 The criteria for nodal invasion
used during the most recent time period were: larger than
1 cm, hypoechoic, or round instead of elliptical. Over the
past 2 decades, the specificity of EUS to diagnose nodal
invasion has improved, which may represent improvement
in the imaging technology, experience, or criteria. The
sensitivity of EUS to nodal invasion remains the same over
the past 2 decades.
Heterogeneity among different studies was evaluated by
the test of heterogeneity and by drawing SROC curves and
finding the AUC, since different studies might use slightly
different criteria for staging. An AUC of 1 for any diag-
nostic test indicates that the test is excellent. SROC curves
for EUS showed that the value of AUC was very close to 1,
indicating that EUS is an excellent diagnostic test for
staging nodal invasion by rectal cancers.
EUS studies with statistically significant results tend to
be published and cited. Smaller studies may show larger
treatment effects because there are fewer case-mix differ-
ences (e.g., patients with only early or late disease) than
larger trials. This publication and selection bias may affect
the summary estimates. This bias can be estimated by bias
indicators and construction of Funnel plots. Bias among
studies can affect the shape of the funnel plot. In this meta-
analysis and systematic review, bias calculations using
Egger bias indicator and Begg-Mazumdar bias indicator
showed no statistically significant bias.37,38 Furthermore,
analysis using funnel plot showed no significant publica-
tion among the studies included in this analysis.
All the studies included in this analysis were either
retrospective or consecutive. A limitation of this meta-
analysis is that there were no prospective studies in the
literature that could be included in this analysis. QUA-
DAS criteria for the quality of studies showed that the
studies fulfilled 30–35% of the 14 criteria. Some of the
criteria cannot be applied to EUS studies, so there are
some inherent weaknesses of using this kind of scoring
system to evaluate EUS studies. Though the quality of
included studies was low, all the studies in literature
evaluating nodal staging of rectal cancers had similar
scores.
This meta-analysis and systematic review was written in
accordance with the proposal for reporting by the Quality
of Reporting of Meta-analyses (QUOROM) statement.77
Since this manuscript looks at diagnostic accuracy of a test,
the study design for this meta-analysis and systematic
review conformed to the guidelines of Standards for
Reporting of Diagnostic Accuracy (STARD) initiative.78
1.0Sensitivity
0.8
0.6
0.4
0.2
0 1.00.4 0.6 0.8
Symmetric SROCAUC = 0.7985SE(AUC) = 0.0225Q* = 0.7348SE(Q*) = 0.0197
1 - Specificity0.2
FIG. 7 Forrest plot showing SROC of EUS to diagnose nodal
invasion of rectal cancer
TABLE 1 Pooled diagnostic accuracy estimates of EUS for different time periods with 95% confidence intervals
Time period No. of studies Pooled sensitivity Pooled specificity Pooled LR? Pooled LR- Pooled DOR
1984–1994 6 79.7% (74.0–84.6) 62.9% (55.5–69.9) 2.6 (1.2–5.7) 0.39 (0.25–0.610) 7.4 (1.9–28.1)
1995–2000 13 73.0% (67.9–77.7) 76.4% (72.6–79.9) 2.8 (2.2–3.6) 0.39 (0.28–0.57) 9.2 (6.5–13.1)
2001–2008 15 70.9% (67.3–74.3) 78.6% (75.5–81.5) 2.8 (1.8–4.2) 0.44 (0.30–0.64) 7.1 (3.6–14.1)
LR? positive likelihood ratio, LR- negative likelihood ratio, DOR diagnostic odds ratio
0.00
StandardError
0.75
1.50
-4 60 2 4Log(Odds Ratio)
-2
FIG. 8 Funnel plots looking at publication bias in EUS studies
looking at rectal cancer invasion of locoregional lymph nodes
1262 S. R. Puli et al.

CONCLUSIONS
EUS is an important and accurate diagnostic tool for
evaluating nodal metastasis of rectal cancers. This meta-
analysis shows that the sensitivity and specificity of EUS is
moderate. EUS performs better if there is no anatomic
nodal invasion than if there is anatomic nodal invasion.
Further refinement in EUS technologies and diagnostic
criteria are needed to improve the diagnostic accuracy.
REFERENCES
1. Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer
statistics, 2007. CA Cancer J Clin. 2007;57:43–66.
2. National Cancer Institute. Surveillance epidemiology and end results
(SEER). U.S. National Institutes of Health. http://seer.cancer.gov/
csr/1975_2004/results_merged/ sect_06_colon_rectum.pdf.
3. Atkin WS, Morson BC, Cuzick J. Long-term risk of colorectal
cancer after excision of rectosigmoid adenomas. N Engl J Med.1992;326:658–62.
4. Larsson SC, Orsini N, Wolk A. Diabetes mellitus and risk of
colorectal cancer: a meta-analysis. J Natl Cancer Inst.2005;97:1679–87.
5. Cho E, Smith-Warner SA, Ritz J, van den Brandt PA, Colditz
GA, Folsom AR, et al. Alcohol intake and colorectal cancer: a
pooled analysis of 8 cohort studies. Ann Intern Med.2004;140:603–13.
6. Giovannucci E, Ascherio A, Rimm EB, Colditz GA, Stampfer
MJ, Willett WC. Physical activity, obesity, and risk for colon
cancer and adenoma in men. Ann Intern Med. 1995;122:327–34.
7. Paskett ED, Reeves KW, Rohan TE, Allison MA, Williams CD,
Messina CR, et al. Association between cigarette smoking and
colorectal cancer in the Women’s Health Initiative. J Natl CancerInst. 2007;99:1729–35.
8. Greene FL, Page DL, Fleming ID, Fritz A, Balch CM, Haller DG,
et al. AJCC cancer staging manual. 6th ed. New York: Springer-
Verlag, 2002.
9. Guillem JG, Chessin DB, Cohen AM, Shia J, Mazumdar M,
Enker W, et al. Long-term oncologic outcome following preop-
erative combined modality therapy and total mesorectal excision
of locally advanced rectal cancer. Ann Surg. 2005;241:829–36.
10. Rich T, Gunderson LL, Lew R, Galdibini JJ, Cohen AM, Don-
aldson G. Patterns of recurrence of rectal cancer after potentially
curative surgery. Cancer. 1983;52:1317–29.
11. Minsky BD, Mies C, Recht A, Rich TA, Chaffey JT. Resectable
adenocarcinoma of the rectosigmoid and rectum: patterns of
failure and survival. Cancer. 1988;61:1408–16.
12. Willett CG, Lewandrowski K, Donelly S, Shellito PC, Convery
K, Eliseo R, et al. Are there patients with stage I rectal carcinoma
at risk for failure after abdominoperineal resection? Cancer.1992;69:1651–5.
13. Law WL, Chu KW, Choi HK. Total pelvic exenteration for
locally advanced rectal cancer. J Am Coll Surg. 2000;190:78–83.
14. Hafner GH, Herrera L, Petrelli NJ. Morbidity and mortality after
pelvic exenteration for colorectal adenocarcinoma. Ann Surg.1992;215:63–7.
15. Emami B, Pilepich M, Willett C, Munzenrider JE, Miller HH.
Effect of preoperative irradiation on resectability of colorectal
carcinomas. Int J Radiat Oncol Biol Phys. 1982;8:1295–9.
16. Dosoretz DE, Gunderson LL, Hedberg S, Hoskins B, Blitzer PH,
Shipley W, et al. Preoperative irradiation for unresectable rectal
and rectosigmoid carcinomas. Cancer. 1983;52:814–8.
17. Mendenhall WM, Million RR, Bland KI, Pfaff WW, Copeland
3rd EM. Initially unresectable rectal adenocarcinoma treated
with preoperative irradiation and surgery. Ann Surg. 1987;205:
41–4.
18. Stevens KR, Fletcher WS. High dose preoperative pelvic irradi-
ation for unresectable adenocarcinoma of the rectum or sigmoid.
Int J Radiat Oncol Biol Phys. 1983;9:148.
19. Mohiuddin M, Regine WF, John WJ, Hagihara PF, McGrath PC,
Kenady DE, et al. Preoperative chemoradiation in fixed distal
rectal cancer: dose time factors for pathological complete
response. Int J Radiat Oncol Biol Phys. 2000;46:883–8.
20. Janjan NA, Khoo VS, Abbruzzese J, Pazdur R, Dubrow R, Cleary
KR, et al. Tumor downstaging and sphincter preservation with
preoperative chemoradiation in locally advanced rectal cancer:
the M. D. Anderson Cancer Center experience. Int J Radiat OncolBiol Phys. 1999;44:1027–38.
21. Videtic GM, Fisher BJ, Perera FE, Bauman GS, Kocha WI,
Taylor M, et al. Preoperative radiation with concurrent 5-fluo-
rouracil continuous infusion for locally advanced unresectable
rectal cancer. Int J Radiat Oncol Biol Phys. 1998;42:319–24.
22. Chen ET, Mohiuddin M, Brodovsky H, Fishbein G, Marks G.
Downstaging of advanced rectal cancer following combined
preoperative chemotherapy and high dose radiation. Int J RadiatOncol Biol Phys. 1994;30:169–175.
23. Janjan NA, Crane CN, Feig BW, Cleary K, Dubrow R, Curley
SA, et al. Prospective trial of preoperative concomitant boost
radiotherapy with continuous infusion 5-fluorouracil for locally
advanced rectal cancer. Int J Radiat Oncol Biol Phys.2000;47:713–8.
24. Kwok H, Bissett IP, Hill GL. Preoperative staging of rectal
cancer. Int J Colorectal Dis. 2000;15:9–20.
25. Guinet C, Buy JN, Ghossain MA, Sezeur A, Mallet A, Bigot J-M,
et al. Comparison of magnetic resonance imaging and computed
tomography in the preoperative staging of rectal cancer. ArchSurg. 1990;125:385–8.
26. Rifkin MD, Ehrlich SM, Marks G. Staging of rectal carcinoma:
prospective comparison of endorectal US and CT. Radiology.1989;170:319–22.
27. Brennan P, Silman A. Statistical methods for assessing observer
variability in clinical measures. BMJ. 1992;304:1491–4.
28. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJM,
Gavaghan DJ, et al. Assessing the quality of reports of random-
ized clinical trials: is blinding necessary? Controlled Clin Trials.1996;17:1–12.
29. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD,
Rennie D, et al. Meta-analysis of observational studies in epi-
demiology: a proposal for reporting. Meta-analysis of
observational studies in Epidemiology (MOOSE) group. JAMA.2000;283:2008–12.
30. Whiting P, Rutjes AW, Reitsma JB, Bossuyt PMM, Kleijnen J.
The development of QUADAS: a tool for the quality assessment
of studies of diagnostic accuracy included in systematic reviews.
BMC Med Res Methodol. 2003;3:25.
31. Whiting PF, Weswood ME, Rutjes AW, Reitsma JB, Bossuyt
PMM, Kleijnen J. Evaluation of QUADAS, a tool for the quality
assessment of diagnostic accuracy studies. BMC Med ResMethodol. 2006;6:9.
32. Puli SR, Singh S, Hagedorn CH, Reddy J, Olyaee M. Diagnostic
accuracy of EUS for vascular invasion in pancreatic and pe-
riampullary cancers: a meta-analysis and systematic review.
Gastrointest Endosc. 2007;65:788–97.
33. Leemis LM, Trivedi KS. A comparison of approximate interval
estimators for the Bernoulli parameter. Am Stat. 1996;50:63–8.
34. Cox DR. The analysis of binary data. London: Methuen, 1970.
35. Agresti A. Analysis of ordinal categorical data. New York: John
Wiley & Sons, 1984.
Accuracy of EUS in N Staging of Rectal Cancers: A Meta-Analysis 1263

36. Deeks JJ. Systematic reviews of evaluations of diagnostic and
screening tests. In Egger M, Smith GD, Altman DG (eds). Sys-
tematic reviews in health care. Meta-analysis in context. London:
BMJ Books, 2001.
37. Harbord RM, Egger M, Sterne JAC. A modified test for small-
study effects in meta-analyses of controlled trials with binary
endpoints. Stat Med. 2005;25:3443–57.
38. Begg CB, Mazumdar M. Operating characteristics of a rank
correlation test for publication bias. Biometrics. 1994;50:1088–
1101.
39. Sterne JAC, Egger M, Davey-Smith G. Investigating and dealing
with publication and other biases in meta-analysis. Br Med J.2001;323:101–5.
40. Sterne JAC, Egger M. Funnel plots for detecting bias in meta-
analysis: guidelines on choice of axis. J Clin Epidemiol.2001;54:1046–55.
41. Adams DR, Blatchford GJ, Lin KM, Ternent CA, Thorson AG,
Christensen MA. Use of preoperative ultrasound staging for
treatment of rectal cancer. Dis Colon Rectum. 1999;42: 159–66.
42. Akasu T, Kondo H, Moriya Y, Sugihara K, Gotoda T, Fujita S,
et al. Endorectal ultrasonography and treatment of early stage
rectal cancer. World J Surg. 2000;24:1061–8.
43. Akasu T, Sugihara K, Moriya Y, Fujita S. Limitations and pitfalls
of transrectal ultrasonography for staging of rectal cancer. DisColon Rectum. 1997;40:S10–5.
44. AP Zbar. Endorectal ultrasonography in rectal cancer: a preliminary
Barbadian experience. West Indian Med J. 2006;55:313–8.
45. Vanagunas A, Lin DE, Stryker SJ. Accuracy of endoscopic
ultrasound for restaging rectal cancer following neoadjuvant
chemoradiation therapy. Am J Gastroenterol 99:109–12.
46. Bali C, Nousias V, Fatouros M, Stefanou D, Kappas AM.
Assessment of local stage in rectal cancer using endorectal
ultrasonography (EUS). Tech Coloproctol. 2004;8:S170–3.
47. Bianchi P, Ceriani C, Palmisano A, Pompili G, Passoni GR,
Rottoli M, et al. A prospective comparison of endorectal ultra-
sound and pelvic magnetic resonance in the preoperative staging
of rectal cancer. Ann Ital Chir. 2006;77:41–6.
48. Boyce GA, Sivak MV Jr, Lavery IC, Fazio VW, Church JM,
Milsom J, et al. Endoscopic ultrasound in the pre-operative
staging of rectal carcinoma. Gastrointest Endosc. 1992;38:468–
71.
49. Giovannini M, Bories E, Pesenti C, Moutardier V, Moutardier V,
Lelong B, Delpero JR. Three-dimensional endorectal ultrasound
using a new freehand software program: results in 35 patients
with rectal cancer. Endoscopy. 2006;38:339–43.
50. Glaser F, Kuntz C, Schlag P, Herfarth C. Endorectal ultrasound
for control of preoperative radiotherapy of rectal cancer. AnnSurg. 1993;217:64–71.
51. Gualdi GF, Casciani E, Guadalaxara A, d’Orta C, Polettini E,
Pappalardo G. Local staging of rectal cancer with transrectal
ultrasound and endorectal magnetic resonance imaging: com-
parison with histologic findings. Dis Colon Rectum.2000;43:338–45.
52. Herzog U, von FM, Tondelli P, Schuppisser JP. How accurate is
endorectal ultrasound in the preoperative staging of rectal cancer?
Dis Colon Rectum. 1993;36:127–34.
53. Hsieh PS, Changchien CR, Chen JS, Tang R, Chiang JM, Yeh
CY, et al. Comparing results of preoperative staging of rectal
tumor using endorectal ultrasonography and histopathology.
Chang Gung Med J. 2003;26:474–8.
54. Kaneko K, Boku N, Hosokawa K, Ohtsu A, Fujii T, Koba I, et al.
Diagnostic utility of endoscopic ultrasonography for preoperative
rectal cancer staging estimation. Jpn J Clin Oncol. 1996;26:30–5.
55. Kim JC, Kim HC, Yu CS, Han KR, Kim JR, Lee KH, et al.
Efficacy of 3-dimensional endorectal ultrasonography compared
with conventional ultrasonography and computed tomography in
preoperative rectal cancer staging. Am J Surg. 2006;192:89–97.
56. Mackay SG, Pager CK, Joseph D, Stewart PJ, Solomon MJ.
Assessment of the accuracy of transrectal ultrasonography in
anorectal neoplasia. Br J Surg. 2003;90:346–50.
57. Maor Y, Nadler M, Barshack I, Zmora O, Koller M, Kundel Y,
et al. Endoscopic ultrasound staging of rectal cancer: diagnostic
value before and following chemoradiation. J GastroenterolHepatol. 2006;21:454–8.
58. Massari M, De Simone M, Cioffi U, Gabrielli F, Boccasanta P,
Bonavina L. Value and limits of endorectal ultrasonography for
preoperative staging of rectal carcinoma. Surg Laparosc Endosc.1998;8:438–44.
59. Meyenberger C, Huch Boni RA, Bertschinger P, Zala GF, Klotz
HP, Krestin GP. Endoscopic ultrasound and endorectal magnetic
resonance imaging: a prospective, comparative study for preop-
erative staging and follow-up of rectal cancer. Endoscopy.1995;27:469–79.
60. Nielsen MB, Qvitzau S, Pedersen JF, Christiansen J. Endoson-
ography for preoperative staging of rectal tumours. Acta Radiol.1996;37:799–803.
61. Pappalardo G, Reggio D, Frattaroli FM, Oddi A, Mascagni D,
Urciuoli P, et al. The value of endoluminal ultrasonography and
computed tomography in the staging of rectal cancer: a pre-
liminary study. J Surg Oncol. 1990;43:219–22.
62. Norton SA, Thomas MG. Staging of rectosigmoid neoplasia with
colonoscopic endoluminal ultrasonography. Br J Surg.1999;86:942–6.
63. Sailer M, Leppert R, Kraemer M, Fuchs KH, Thiede A. The value
of endorectal ultrasound in the assessment of adenomas, T1- and
T2-carcinomas. Int J Colorectal Dis. 1997;12:214–9; DOI:
10.1007/s003840050092.
64. Saitoh N, Okui K, Sarashina H, Suzuki M, Arai T, Nunomura M.
Evaluation of echographic diagnosis of rectal cancer using
intrarectal ultrasonic examination. Dis Colon Rectum.1986;29:234–42.
65. Shami VM, Parmar KS, Waxman I. Clinical impact of endo-
scopic ultrasound and endoscopic ultrasound-guided fine-needle
aspiration in the management of rectal carcinoma. Dis ColonRectum. 2004;47:59–65.
66. Spinelli P, Schiavo M, Meroni E, Di Felice G, Andreola S,
Gallino G, et al. Results of EUS in detecting perirectal lymph
node metastases of rectal cancer: the pathologist makes the dif-
ference. Gastrointest Endosc. 1999;49:754–8.
67. Thaler W, Watzka S, Martin F, La Guardia G, Psenner K, Bonatti
G, et al. Preoperative staging of rectal cancer by endoluminal
ultrasound vs. magnetic resonance imaging. Preliminary results
of a prospective, comparative study. Dis Colon Rectum.1994;37:1189–93.
68. Ramana KN, Murthy PV, Rao KP, Bhagawanulu, Mandapal T,
Pratap B. Transrectal ultrasonography versus computed tomog-
raphy in staging rectal carcinoma. Indian J Gastroenterol.1997;16:142–3.
69. Garcia-Aguilar J, Pollack J, Lee SH, Hernandez de Anda E,
Mellgren A, Wong WD, et al. Accuracy of endorectal ultraso-
nography in preoperative staging of rectal tumors. Dis ColonRectum. 2002;45:10–5.
70. Manger T, Stroh C. Accuracy of endorectal ultrasonography in
the preoperative staging of rectal cancer. Tech Coloproctol.2004;8:s14–5.
71. Kim JC, Yu CS, Jung HY, Kim HC, Kim SY, Park SK, et al.
Source of errors in the evaluation of early rectal cancer by end-
oluminal ultrasonography. Dis Colon Rectum. 2001;44:1302–9.
72. Osti MF, Padovan FS, Pirolli C, Sbarbati S, Tombolini V, Meli C,
et al. Comparison between transrectal ultrasonography and
1264 S. R. Puli et al.

computed tomography with rectal inflation of gas in preoperative
staging of lower rectal cancer. Eur Radiol. 1997;7:26–30.
73. Caseiro-Alves F, Goncalo M, Cruz L, Ilharco J, Leite J, Agost-
inho A, et al. Water enema computed tomography (WE-CT) in
the local staging of low colorectal neoplasms: comparison with
transrectal ultrasound. Abdom Imaging. 1998;23:370–4.
74. Wiersema MJ, Vazquez-Sequeiros E, Wiersema LM. Evaluation
of mediastinal lymphadenopathy with endoscopic US-guided
fine-needle aspiration biopsy. Radiology. 2001;219:252–7.
75. Vilmann P. Endoscopic ultrasonography-guided fine-needle
aspiration biopsy of lymph nodes. Gastrointest Endoscopy.1996;43:S24–9.
76. Silvestri GA, Hoffman BJ, Bhutani MS, Hawes RH, Coppage L,
Sanders-Cliette A, et al. Endoscopic ultrasound with fine-needle
aspiration in the diagnosis and staging of lung cancer. AnnThorac Surg. 1996;61:1441–5; discussion 1445–6.
77. Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF.
Improving the quality of reports of meta-analyses of randomised
controlled trials: the QUOROM statement, Lancet. 1999;354:
1896–900.
78. Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP,
et al. Standards for Reporting of Diagnostic Accuracy Group.
Towards complete and accurate reporting of studies of diagnostic
accuracy: the STARD initiative. The Standards for Reporting of
Diagnostic Accuracy Group. Croat Med J. 2003;44:635–8.
Accuracy of EUS in N Staging of Rectal Cancers: A Meta-Analysis 1265
Copyright © 2022 FDOKUMEN