
Accuracy of FDG-PET to Diagnose Lung Cancer in a Region of Endemic Granulomatous Disease
6
ORIGINAL ARTICLES: GENERAL THORACIC GENERAL THORACIC SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://cme.ctsnetjournals.org. To take the CME activity related to this article, you must have either an STS member or an individual non-member subscription to the journal. Accuracy of FDG-PET to Diagnose Lung Cancer in a Region of Endemic Granulomatous Disease Stephen Deppen, MA, MS, Joe B. Putnam, Jr, MD, Gabriela Andrade, MS, Theodore Speroff, PhD, Jonathan C. Nesbitt, MD, Eric S. Lambright, MD, Pierre P. Massion, MD, Ron Walker, MD, and Eric L. Grogan, MD, MPH Department of Thoracic Surgery, Vanderbilt-Ingram Cancer Center, Vanderbilt University School of Medicine, Institute for Medicine and Public Health, and Division of Pulmonary and Critical Care Medicine, Vanderbilt University Medical Center, Nashville; Department of Surgery, Departments of Radiology, Center for Health Services Research, Veterans Affairs Tennessee Valley Healthcare System, Nashville, Tennessee Background. The 18 F-fluorodeoxyglucose-positron emission tomography (FDG-PET) is used to evaluate suspicious pulmonary lesions due to its diagnostic accu- racy. The southeastern United States has a high preva- lence of infectious granulomatous lung disease, and the accuracy of FDG-PET may be reduced in this population. We examined the diagnostic accuracy of FDG-PET in patients with known or suspected non-small cell lung cancer treated at our institution. Methods. A total of 279 patients, identified through our prospective database, underwent an operation for known or suspected lung cancer. Preoperative FDG- PET in 211 eligible patients was defined by standard- ized uptake value greater than 2.5 or by description (“moderate” or “intense”) as avid. Sensitivity, specific- ity, positive and negative predictive values, likelihood ratios, and decision diagrams were calculated for FDG- PET in all patients and in patients with indeterminate nodules. Results. In all eligible patients (n 211), sensitivity and specificity of FDG-PET were 92% and 40%, respec- tively. Positive and negative predictive values were 86% and 55%. Overall FDG-PET accuracy to diagnose lung cancer was 81%. Preoperative positive likelihood ratio for FDG-PET diagnosis of lung cancer in this population was 1.5 compared with previously published values of 7.1. In 113 indeterminate lesions, 65% had lung cancer and the sensitivity and specificity were 89% and 40%, respectively. Twenty-four benign nodules (60%) had false positive FDG-PET scans. Twenty-two of 43 benign nodules (51%) were granulomas. Conclusions. In a region with endemic granulomatous diseases, the specificity of FDG-PET for diagnosis of lung cancer was 40%. Clinical decisions and future clinical predictive models for lung cancer must accommodate regional variation of FDG-PET scan results. (Ann Thorac Surg 2011;92:428 –33) © 2011 by The Society of Thoracic Surgeons T he proliferation of noninvasive imaging and interest in screening populations at high risk for non-small cell lung cancer with computed tomography has in- creased pulmonary nodule detection rates [1, 2]. Clini- cians rely heavily on available noninvasive diagnostic tools, and 18 F-fluorodeoxyglucose-positron emission to- mography (FDG-PET) has become widely accepted for the clinical diagnosis and staging of lung cancer in patients with suspicious pulmonary nodules [3, 4]. Recent studies of FDG-PET demonstrate a reduction in non- therapeutic resections (eg, resection for benign lesions or metastatic disease) by 17% to 20% [5– 8]. However, we questioned the accuracy of FDG-PET in diagnosing lung cancer in patients with pulmonary lesions in our region where histoplasmosis is endemic. A meta-analysis for FDG-PET accuracy to diagnose pulmonary lesions estimated a sensitivity of 94.2% and specificity of 83.3% [9]. Due to the suspected discrepancy between published specificity of FDG-PET and our clin- ical observations of poor specificity, we sought to deter- mine the accuracy of FDG-PET to diagnose lung cancer in our region of south-central United States, where high endemic rates of granulomatous disease occur primarily from Histoplasmosis sp. Material and Methods Population Using Vanderbilt University Medical Center’s Thoracic Surgery Quality Improvement database, we identified Accepted for publication Feb 14, 2011. Presented at the Fifty-seventh Annual Meeting of the Southern Thoracic Surgical Association, Orlando, FL, Nov 3– 6, 2010. Address correspondence to Dr Grogan, Department of Thoracic Surgery, Vanderbilt University Medical Center, 609 Oxford House, 1313 21st Ave, South Nashville, TN 37232; e-mail: [email protected]. © 2011 by The Society of Thoracic Surgeons 0003-4975/$36.00 Published by Elsevier Inc doi:10.1016/j.athoracsur.2011.02.052 GENERAL THORACIC
Transcript of Accuracy of FDG-PET to Diagnose Lung Cancer in a Region of Endemic Granulomatous Disease
GEN
ERA
LT
HO
RA
CIC
ORIGINAL ARTICLES: GENERAL THORACIC
GENERAL THORACIC SURGERY:The Annals of Thoracic Surgery CME Program is located online at http://cme.ctsnetjournals.org.To take the CME activity related to this article, you must have either an STS member or anindividual non-member subscription to the journal.
Accuracy of FDG-PET to Diagnose Lung Cancer ina Region of Endemic Granulomatous DiseaseStephen Deppen, MA, MS, Joe B. Putnam, Jr, MD, Gabriela Andrade, MS,Theodore Speroff, PhD, Jonathan C. Nesbitt, MD, Eric S. Lambright, MD,Pierre P. Massion, MD, Ron Walker, MD, and Eric L. Grogan, MD, MPHDepartment of Thoracic Surgery, Vanderbilt-Ingram Cancer Center, Vanderbilt University School of Medicine, Institute forMedicine and Public Health, and Division of Pulmonary and Critical Care Medicine, Vanderbilt University Medical Center,
Nashville; Department of Surgery, Departments of Radiology, Center for Health Services Research, Veterans Affairs TennesseeValley Healthcare System, Nashville, TennesseeBackground. The 18 F-fluorodeoxyglucose-positronemission tomography (FDG-PET) is used to evaluatesuspicious pulmonary lesions due to its diagnostic accu-racy. The southeastern United States has a high preva-lence of infectious granulomatous lung disease, and theaccuracy of FDG-PET may be reduced in this population.We examined the diagnostic accuracy of FDG-PET inpatients with known or suspected non-small cell lungcancer treated at our institution.
Methods. A total of 279 patients, identified throughour prospective database, underwent an operation forknown or suspected lung cancer. Preoperative FDG-PET in 211 eligible patients was defined by standard-ized uptake value greater than 2.5 or by description(“moderate” or “intense”) as avid. Sensitivity, specific-ity, positive and negative predictive values, likelihoodratios, and decision diagrams were calculated for FDG-PET in all patients and in patients with indeterminate
nodules.Vanderbilt University Medical Center, 609 Oxford House, 1313 21st Ave,South Nashville, TN 37232; e-mail: [email protected].
© 2011 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
Results. In all eligible patients (n � 211), sensitivityand specificity of FDG-PET were 92% and 40%, respec-tively. Positive and negative predictive values were 86%and 55%. Overall FDG-PET accuracy to diagnose lungcancer was 81%. Preoperative positive likelihood ratio forFDG-PET diagnosis of lung cancer in this populationwas 1.5 compared with previously published values of7.1. In 113 indeterminate lesions, 65% had lung cancerand the sensitivity and specificity were 89% and 40%,respectively. Twenty-four benign nodules (60%) hadfalse positive FDG-PET scans. Twenty-two of 43 benignnodules (51%) were granulomas.
Conclusions. In a region with endemic granulomatousdiseases, the specificity of FDG-PET for diagnosis of lungcancer was 40%. Clinical decisions and future clinicalpredictive models for lung cancer must accommodateregional variation of FDG-PET scan results.
(Ann Thorac Surg 2011;92:428–33)
© 2011 by The Society of Thoracic SurgeonsThe proliferation of noninvasive imaging and interestin screening populations at high risk for non-small
cell lung cancer with computed tomography has in-creased pulmonary nodule detection rates [1, 2]. Clini-cians rely heavily on available noninvasive diagnostictools, and 18 F-fluorodeoxyglucose-positron emission to-mography (FDG-PET) has become widely accepted forthe clinical diagnosis and staging of lung cancer inpatients with suspicious pulmonary nodules [3, 4]. Recentstudies of FDG-PET demonstrate a reduction in non-therapeutic resections (eg, resection for benign lesions ormetastatic disease) by 17% to 20% [5–8]. However, we
Accepted for publication Feb 14, 2011.
Presented at the Fifty-seventh Annual Meeting of the Southern ThoracicSurgical Association, Orlando, FL, Nov 3–6, 2010.
Address correspondence to Dr Grogan, Department of Thoracic Surgery,
questioned the accuracy of FDG-PET in diagnosing lungcancer in patients with pulmonary lesions in our regionwhere histoplasmosis is endemic.
A meta-analysis for FDG-PET accuracy to diagnosepulmonary lesions estimated a sensitivity of 94.2% andspecificity of 83.3% [9]. Due to the suspected discrepancybetween published specificity of FDG-PET and our clin-ical observations of poor specificity, we sought to deter-mine the accuracy of FDG-PET to diagnose lung cancerin our region of south-central United States, where highendemic rates of granulomatous disease occur primarilyfrom Histoplasmosis sp.
Material and Methods
PopulationUsing Vanderbilt University Medical Center’s Thoracic
Surgery Quality Improvement database, we identified0003-4975/$36.00doi:10.1016/j.athoracsur.2011.02.052
C
B
F
S
429Ann Thorac Surg DEPPEN ET AL2011;92:428–33 ACCURACY OF FDG-PET TO DIAGNOSE NSCLC
GEN
ERA
LT
HO
RA
CIC
279 patients who underwent a surgical procedure forknown or suspected lung cancer from January 1, 2005 toApril 30, 2009. The Vanderbilt University InstitutionalReview Board approved this study (IRB #081298) andwaived the need for individual informed consent. Clini-cal data elements were abstracted from the database andsupplemented by chart review. Individuals without areported lesion diameter were excluded from final anal-ysis. Each lesion was confirmed by pathologic examina-tion after thoracotomy, thoracoscopy, mediastinoscopy,or bronchoscopy with biopsy for known or suspectednon-small cell lung cancer (NSCLC). In patients withoutcancer, additional review was conducted to determine,where possible, the etiology of the benign lesion.
Preoperative FDG-PET was performed in 216 patients.Five patients were excluded. One underwent reoperationafter initial resection, 2 individuals had no reportedlesion size preoperatively in their medical record, and 2patients were excluded due to multiple nodules beingevaluated. A total of 211 patients were deemed eligibleand reviewed further. Imaging data specific to the pul-monary nodule were abstracted from radiological reportsfound in the electronic medical record. The FDG-PETresults were classified into avid (likely for lung cancer)and non-avid (not likely for lung cancer) based uponradiologist description, or standardized uptake value(SUV) of the pulmonary lesion. An avid FDG-PET resultwas defined by a SUV greater than 2.5 or by descriptionsuch as “likely” or “malignant” and “moderate” or “in-tense” uptake by the reading radiologist.
AnalysisContingency tables were created for the accuracy ofFDG-PET scan to diagnose lung cancer in all patients andin patients without a preoperative tissue diagnosis. Sen-sitivity, specificity, positive and negative predictive val-ues, and positive and negative likelihood ratios werecalculated for both groups. The observed values in ourpopulation were compared with results in the peer-reviewed literature. A test-treatment threshold graphwas calculated using observed sensitivity and specificityto estimate positive and negative likelihood ratios. Ob-served ratios were compared to reported likelihood ratios[10, 11]. Overall accuracy was estimated in 6 strata ofclinically determined tumor lesion sizes. Strata were 1 cmor less, greater than1 to 2 cm, greater than 2 to 3 cm,greater than 3 to 5 cm, greater than 5 to 7 cm, and greaterthan 7 cm. Sensitivity analysis of scans based upon yearof the scan and whether the test used combined FDG-PET-CT or isolated FDG-PET were conducted.
Results
In our population (n � 211), the prevalence of lung cancerwas 80%. Lesions ranged in size from 5 to 140 mm with amedian of 25 mm. One hundred-thirteen patients hadindeterminate nodules and their lung cancer prevalencewas 65% (Table 1). Adenocarcinoma was the most com-mon cancer histology (70 of 168, 42%), and granuloma
was the most common benign diagnosis (22 of 43, 51%)(Table 1). Of these 22 granulomas, 7 were histoplasmosisby cytologic staining or culture. Five of the 7 histoplas-mosis granulomas were FDG-PET positive. Other knowngranulomatous diseases observed were blastomycosis (2),sarcoidosis (1), cryptococcosis (1), and Mycobacterium avium(1). The etiologies of the remaining 10 granulomas wereindeterminate by initial pathologic staining.
The sensitivity of FDG-PET for diagnosis of cancer inall 211 cases was 92% (95% confidence interval [CI], 86%to 95%). The specificity was only 40% (95% CI, 25% to56%) (Table 2), far less than published data. Sensitivityand specificity in the 113 cases without a preoperativediagnosis was 89% (95% CI, 80% to 95%) and 40% (95%CI, 25% to 57%), respectively (Table 3). In our totalpopulation the positive likelihood ratio for an avid FDG-PET scan was 1.5, and negative likelihood ratio observedwas 0.2. A test-treatment plot of pre-test and post-test
Table 1. Patient Characteristics
CharacteristicsAll Patients
(n � 211)Indeterminate
(n � 113)
Gender: male 53% 47%Race: Caucasian 92% 93%Age (years) 64 63Smoking status
– Never 21% 19%– Ever 79% 81%
Pack-years 45 41Predicted FEV1 77% 78%Nodule Size (mm) 29 24FDG-PET SUV (SD)a 7.0 (5.6) 6.6 (6.1)
ancer diagnosis 168 (80%) 73 (65%)Adenocarcinoma 70 28Squamous 56 26NSCLC (not specified) 15 7Large cell 6 1Small cell 5 5Bronchoalveolar cell 5 2Other neuroendrocrine 5 0Carcinoid 3 2Melanoma 2 1Lymphoma 1 1
enign diagnosis 43 (20%) 40 (35%)Granuloma 22 21Fibrotic 7 7Inflammation 6 5Hamartoma 4 4Broncholith 1 1Other 3 2
Mean values are reported for age, pack years, FEV1, and nodule size.a Scans with a reported maximum mean standard uptake value (SUV) �60 (28%), 151 scans did not have a maximum SUV reported.
FDG-PET � 18 F-fluorodeoxyglucose-positron emission tomography;EV1 � forced expiratory volume in the first second of expiration;
NSCLC � non-small cell lung cancer; SD � standard deviation;UV � standardized uptake value.
probability of cancer compares the positive and negative

6bs
s
NSS
upl
Ctp
NSS
n
it
C
430 DEPPEN ET AL Ann Thorac SurgACCURACY OF FDG-PET TO DIAGNOSE NSCLC 2011;92:428–33
GEN
ERA
LT
HO
RA
CIC
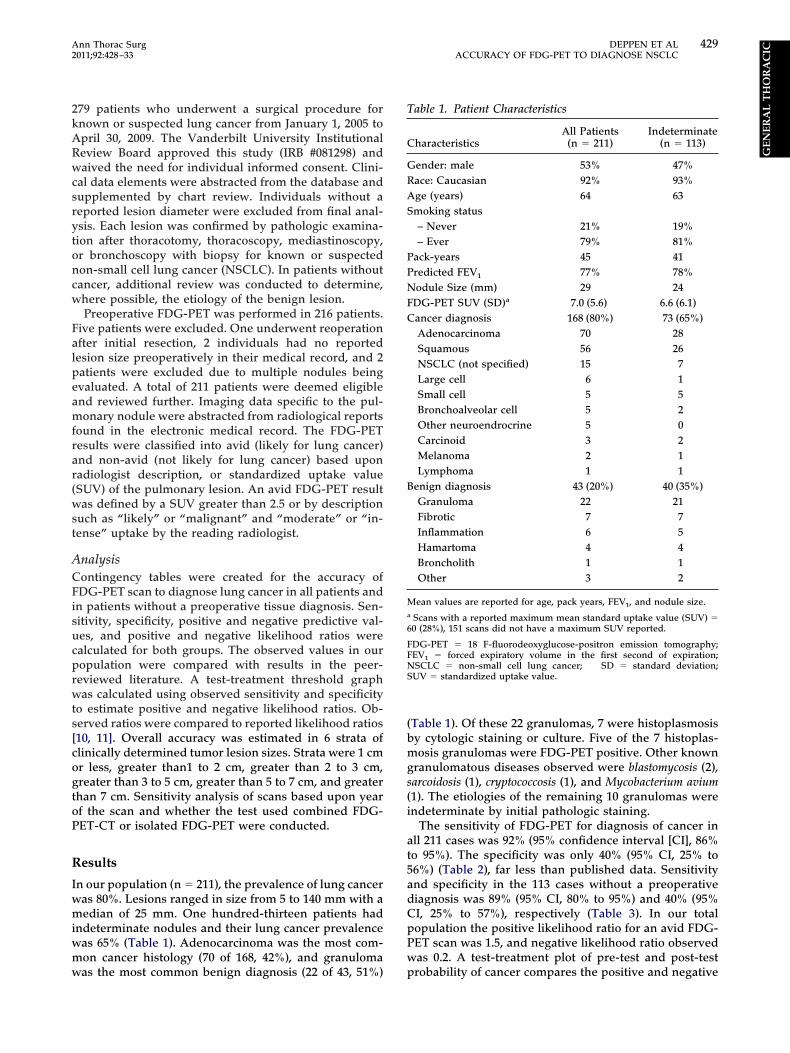
likelihood ratios observed in our cohort (Fig 1) to pub-lished likelihood ratios (positive likelihood ratio 7.1 andnegative likelihood ratio 0.06) for FDG-PET [9–11].
False positive FDG-PET results were identified in 26patients (26 of 43, 60.4%) with benign lesions: 12 granu-lomas, 6 fibrotic lesions, 3 inflammatory lesions, 1 bron-cholith, 1 hamartoma, and 3 of unknown etiology (Table1). Five of the 12 false positive granulomas were histo-plasmosis. False negative results occurred in 14 of 168(8.3%) patients with lung cancer: 6 occurred in adenocar-cinoma greater than 1 cm in maximum diameter; 1 eachin smaller (9 mm) lesions with adenocarcinoma andsquamous cell carcinoma; and 6 were bronchoalveolarcarcinoma or carcinoid tumors, histologies known toconfound FDG-PET.
Overall accuracy was 81%. Accuracy varied somewhatby lesion diameter (Fig 2). The lowest accuracy (56% 95%CI, 30% to 80%) occurred among 16 lesions with diame-ters �10 millimeters. The highest accuracy (95%; 95% CI,8% to 99%) was among 19 lesions whose diameter wasetween 5 and 7 cm. None of the groups by size wereignificantly different from the other 5 groups (p � 0.08).
Accuracy was less (72%) among those without a preop-erative diagnosis. Accuracy, sensitivity, and specificitydid not change among scans performed prior to 2008,when most FDG-PET without simultaneous CT scanoccurred. Scans performed outside our institution (n �87) were less sensitive (86%) and specific (25%) comparedwith those performed at our medical center (n � 123,ensitivity 97% and specificity 44%).
Comment
The FDG-PET was far less specific (40%) in its diagnosisof cancer in patients residing in a region of endemicgranulomatous disease when compared with previouslypublished meta-analysis (83%). Our observed specificitywas less than half that reported in meta-analysis or whichhas been used in most cost efficiency models [12–14]. Inour cohort, sensitivity and specificity of FDG-PET wassimilar whether it included or excluded patients with apreoperative diagnosis of lung cancer. Nor were differ-ences found between scans performed earlier in the
Table 2. Contingency Table for All Patients (n � 211)
FDG-PET Cancer Benign Values
Avida 154 26 PPV 86%, 95% CI 80%–90%ot-avidb 14 17 NPV 55%, 95% CI 36%–72%
ensitivity 92% 95% CI 86%–95% Prevalence 80%, 95%CI 74%–85%pecificity 40% 95% CI 25%–56%
The diagnosis was based upon pathological result of resected specimen.a FDG-PET avidity was defined by an SUV � 2.5 or moderate or intense
ptake. b Not-avid, cancerous lesions (n � 14) include 6 with areoperative tissue diagnosis, 6 with documented growth, 1 with spicu-
ated edge, and 1 larger than 4 cm in maximum diameter.
I � confidence interval; FDG-PET � 18 F-fluorodeoxyglucose-posi-ron emission tomography; NPV � negative predictive value; PPV �ositive predictive value; SUV � standardized uptake value.
study when compared with those performed more re-tp
cently. The FDG-PET scan was less sensitive to slowlygrowing carcinoid tumors and to lesions 10 mm or less indiameter. However, the sensitivity observed was similar(92%; 95% CI, 86% to 95%) to that found in the literature(94.2%) [9, 15].
Almost half (46%) of the false positive scans observedin our population were specifically due to granulomatousdisease. Croft and colleagues [16] reported similar resultsin their smaller, upper Midwestern (Iowa) cohort, with allimaging performed at a tertiary referral center, whereasour results are from the south-central US, from a varietyof regional imaging centers. Inflammation and granu-loma were the most common benign results in theirstudy as well. Fungal infections caused 66% false posi-tives in one study [17] using combined FDG-PET-CTimaging.
Lung nodules that are fungal in origin may be meta-bolically active and appear similar to malignancy on bothCT and FDG-PET scans. Regional endemic prevalence offungal disease confounds diagnosis of infection or cancerin asymptomatic individuals with pulmonary lesions.While our findings may be an extreme example of fungaldisease [18, 19], histoplasmosis is endemic throughoutmuch of the Mississippi, Ohio, and lower Missouri RiverValleys, while coccidioidomycosis is endemic in theSouthwest [20–22]. The efficacy of FDG-PET for thediagnosis of lung cancer in these regions of the countryappears very different from other regions (Fig 1).
Clinicians ordering a FDG-PET scan for diagnosis ofa pulmonary lesion must consider how the result of thescan will influence their decision making. This decisiondepends upon the surgeon’s pre-test estimate of thenodule’s malignancy, the patient’s operative risk, andtheir decision-to-operate threshold. For example, anFDG-PET scan in a patient with an estimated 40%pre-test probability for lung cancer and an FDG-PETnon-avid test result reduces the post-test probability ofcancer to 4%, using a published negative likelihoodratio of 0.06 (Fig 1). Using the FDG-PET scan likelihoodratio of 0.20 as found in our study, a non-avid FDG-PETscan identifies a 12% post-test probability of cancer. Inthis instance an FDG-PET scan whose accuracy reflects
Table 3. Contingency Table for Patients With IndeterminateLesions (n � 113)a
FDG-PET Cancer Benign Values
Avidb 65 24 PPV 73%, 95% CI 63%–82%ot-avidc 8 16 NPV 67%, 95% CI 45%–84%
ensitivity 89%, 95% CI 80%–95% Prevalence 65%, 95%CI 55%–73%pecificity 40%, 95% CI 25%–57%
The diagnosis was based upon pathological result of resected specimen.a Patients did not have a preoperative diagnosis or had a non-diagnostic
eedle biopsy. b FDG-PET avidity was defined by an SUV � 2.5 ormoderate or intense uptake. c Not-avid, cancerous lesions (n � 8)nclude 6 with documented growth, 1 with spiculated edge, and 1 largerhan 4 cm in maximum diameter.
I � confidence interval; FDG-PET � 18 F-fluorodeoxyglucose-posi-
ron emission tomography; NPV � negative predictive value; PPV �ositive predictive value; SUV � standardized uptake value.
431Ann Thorac Surg DEPPEN ET AL2011;92:428–33 ACCURACY OF FDG-PET TO DIAGNOSE NSCLC
GEN
ERA
LT
HO
RA
CIC
that found in the literature will change the surgeon’sdecision to a watch and wait strategy; however, an FDGPET scan with accuracy similar to our results, will havea post-test probability of cancer greater than 10%,irrespective of test outcome. These patients may re-ceive an FDG-PET scan for staging purposes but thescan’s information will not aid in diagnosis. Thus, theresults of the FDG-PET scan would not affect the
Fig 2. The 18F-fluorodeoxyglucose-positron emission tomography(FDG-PET) accuracy for diagnosis of lung cancer by lesion diameter.(*Accuracy � [true positives � true negatives]/N; **all diameters arepreoperative, clinical maximum diameters by computed tomography
[CT] or PET/CT.)surgeon’s decision to surgically obtain a tissue diagno-sis. In similar regions of the country, pre-test proba-bilities of cancer less than 6% or greater than 35% willnot change the decision to operate for surgeons with a10% post-test likelihood of cancer.
The utility of FDG-PET for baseline staging of lungcancer is well established [7, 15, 17, 23–26]. Our studyaddresses the accuracy of FDG-PET for the diagnosis ofindeterminate lung nodules or lung masses in a highendemic area for granulomatous diseases. Our resultswere very similar to series previously reported fromtertiary centers [16, 17]. Reporting of maximum SUV waslimited in our population (28% with SUV). Our institutionrarely reports SUV for various reasons [27–29]. However,the accuracy of FDG-PET scans performed at our insti-tution, all of which were fusion FDG-PET-CT scans, wasgreater than scans performed outside our institution. Thelack of SUV reporting eliminates the possibility of usingSUV as a continuous measurement of avidity and thusmanipulating the sensitivity and specificity of the testbased upon SUV.
Importantly, our study demonstrates the characteris-tics of FDG-PET scanning from a wide range of imagingcenters. Forty-two percent of the scans were performedoutside our institution. These scans used a variety of PETand PET-CT scanners, and were interpreted by localimaging physicians. Our results demonstrate the impor-tance of utilization of pre-test probabilities and likeli-hood ratios that are regionally appropriate for clinicaldecision making in the management of indeterminate
Fig 1. Operative test-treatment deci-sion diagram. Lines are the calcu-lated likelihood ratios (LR) for therespective 18F-fluorodeoxyglucose-positron emission tomography(FDG-PET) result based on the pre-test probability of cancer. Example:In a patient with a 40% pre-FDG-PET probability of cancer, an avidFDG-PET scan gives a 55% proba-bility of cancer in our observed pop-ulation (line A). A non-avid FDG-PET result yields a 12% likelihoodof cancer (line B). In this exampleusing our data, FDG-PET result,whether avid or non-avid, does notchange recommendation for resec-tion. However, in other areas of thecountry, a 40% pre-FDG-PET prob-ability of cancer results in a postFDG-PET probability of only 4%with a non-avid FDG-PET result(line C) and an 84% post-FDG-PETprobability of cancer in an avidFDG-PET (line D).
lung nodules or masses.

432 DEPPEN ET AL Ann Thorac SurgACCURACY OF FDG-PET TO DIAGNOSE NSCLC 2011;92:428–33
GEN
ERA
LT
HO
RA
CIC
In summary, our study highlights limitations ofFDG-PET to diagnose lung cancer in areas with en-demic infectious lung disease. While false-negativesoccurred in slowly growing carcinoid tumors, over 40%false negative scans occurred in tumors larger than 1cm with adenocarcinoma histology. Poor specificitydue to multiple false positives from endemic granulo-matous disease draws into question the cost effective-ness of FDG-PET for diagnosing lung cancer in ourregion of the United States. Future cancer predictionmodels must consider the regional variation that mayoccur with FDG-PET scans. In addition, clinicians mustbe aware of the limitations of FDG-PET to diagnoselung cancer and to determine whether a positive ornegative result will change the operative decision. Apersonalized diagnostic plan developed for patientswith suspected lung cancer depends upon the patient’srisk factors for developing cancer [30, 31] and theaccuracy of the diagnostic imaging that is specific tothe patient’s geographic location.
This research was supported by the following: Vanderbilt Phy-sician Scientist Development Award (E.L.G.), SPECS in lungcancer U01 CA114771 (P.P.M.), the lung SPORE CA90949(P.P.M.), Research Electronic Data Capture (REDCap) 1 UL1RR024975 from NCRR/NIH, and a Merit award from the Depart-ment of Veterans Affairs (P.P.M.).
References
1. Henschke CI, McCauley DI, Yankelevitz DF, et al. Early lungcancer action project: a summary of the findings on baselinescreening. Oncologist 2001;6:147–52.
2. Tan B, Flaherty K, Kazerooni E, Iannettoni M. The solitarypulmonary nodule. Chest 2003;123:89S–96S.
3. Wahidi MM, Govert JA, Goudar RK, Gould MK, McCroryDC. Evidence for the treatment of patients with pulmonarynodules: when is it lung cancer?: ACCP evidence-basedclinical practice guidelines (2nd edition). Chest 2007;132(3Suppl):94S–107S.
4. Rivera MP, Detterbeck F, Mehta AC. Diagnosis of lungcancer: the guidelines. Chest 2003;123(1 Suppl):129S–36S.
5. Silvestri GA, Gould MK, Margolis ML, et al. Noninvasivestaging of non-small cell lung cancer: ACCP evidenced-based clinical practice guidelines (2nd edition). Chest 2007;132(3 Suppl):178S–201S.
6. Herder GJ, Verboom P, Smit EF, et al. Practice, efficacy andcost of staging suspected non-small cell lung cancer: aretrospective study in two Dutch hospitals. Thorax 2002;57:11–4.
7. Cerfolio RJ, Ojha B, Bryant AS, Raghuveer V, Mountz JM,Bartolucci AA. The accuracy of integrated PET-CT comparedwith dedicated pet alone for the staging of patients withnonsmall cell lung cancer. Ann Thorac Surg 2004;78:1017–23.
8. Reed CE, Harpole DH, Posther KE, et al. Results of theAmerican College of Surgeons Oncology Group Z0050 trial:the utility of positron emission tomography in staging po-tentially operable non-small cell lung cancer. J Thorac Car-diovasc Surg 2003;126:1943–51.
9. Gould M, Maclean C, Kuschner W, Rydzak C, Owens D.Accuracy of positron emission tomography for diagnosis ofpulmonary nodules and mass lesions: a meta-analysis.JAMA 2001;285:914–24.
10. Dewan NA, Shehan CJ, Reeb SD, Gobar LS, Scott WJ,
Ryschon K. Likelihood of malignancy in a solitary pulmo-nary nodule: comparison of Bayesian analysis and results ofFDG-PET scan. Chest 1997;112:416–22.
11. Gurney JW, Lyddon DM, McKay JA. Determining the like-lihood of malignancy in solitary pulmonary nodules withBayesian analysis. Part II. Application. Radiology 1993;186:415–22.
12. Barnett PG, Ananth L ,Gould MK; Group VAPET. Cost andoutcomes of patients with solitary pulmonary nodules man-aged with PET scans. Chest 2010;137:53–9.
13. Gould M, Kuschner W, Rydzak C, et al. Test performance ofpositron emission tomography and computed tomographyfor mediastinal staging in patients with non small cell lungcancer: a meta analysis. Ann Intern Med 2003;139:879–92.
14. Lejeune C, Al Zahouri K, Woronoff-Lemsi M-C, et al. Use ofa decision analysis model to assess the medicoeconomicimplications of FDG PET imaging in diagnosing a solitarypulmonary nodule. Eur J Health Econ 2005;6:203–14.
15. Gould MK, Sanders GD, Barnett PG, et al. Cost-effectivenessof alternative management strategies for patients with soli-tary pulmonary nodules. Ann Intern Med 2003;138:724–35.
16. Croft DR, Trapp J, Kernstine K, et al. FDG-PET imaging andthe diagnosis of non-small cell lung cancer in a region ofhigh histoplasmosis prevalence. Lung Cancer 2002;36:297–301.
17. Bryant AS, Cerfolio RJ. The maximum standardized uptakevalues on integrated FDG-PET/CT is useful in differentiatingbenign from malignant pulmonary nodules. Ann ThoracSurg 2006;82:1016–20.
18. Leggiadro RJM, Luedtke GS, Convey AR, Gibson LL, BarrettFFM. Prevalence of histoplasmosis in a midsouthern popu-lation. Southern Med J 1991;84:1360–61.
19. CDC. Histoplasmosis map US. 2007; Available at: http://www.doctorfungus.org/Mycoses/images/North_Amer_Histo.gif. Last accessed March 12, 2011.
20. Gurney JW, Conces DJ. Pulmonary histoplasmosis. Radiol-ogy 1996;199:297–306.
21. Goodwin R, Loyd J, Des Prez R. Histoplasmosis in normalhosts. Medicine 1981;60:232–65.
22. Coccidioidmycosis. Red Book Online; Available at: http://aapredbook.aappublications.org/cgi/content/figsonly/2009/1/3.29. Last accessed March 12, 2011.
23. Gambhir SS, Hoh CK, Phelps ME, Madar I, Maddahi J.Decision tree sensitivity analysis for cost-effectiveness ofFDG-PET in the staging and management of non-small-celllung carcinoma. J Nucl Med 1996;37:1428–36.
24. Halpern B, Schiepers C, Weber W. Presurgical staging ofnon-small cell lung cancer: positron emission tomography,integrated positron emission tomography/CT, and softwareimage fusion. Chest 2005;128:2289–97.
25. Verhagen A, Bootsma G, Tjan-Heijnen V, et al. FDG-PET instaging lung cancer. How does it change the algorithm?Lung Cancer 2004;44:175–81.
26. Pieterman R, van Putten J, Meuzelaar J, et al. Preoperativestaging of non-small-cell lung cancer with positron-emissiontomography. N Engl J Med 2000;343:254–61.
27. Keyes JW Jr. SUV: standard uptake or silly useless value?J Nucl Med 1995;36:1836–9.
28. Delbeke D, Coleman RE, Guiberteau MJ, et al. Procedureguideline for tumor imaging with 18F-FDG PET/CT 1.0.J Nucl Med 2006;47:885–95.
29. Wahl RL, Jacene H, Kasamon Y, Lodge MA. From RECIST toPERCIST: evolving considerations for PET response criteriain solid tumors. J Nucl Med 2009;50(Suppl 1):122S–50S.
30. Gould MK, Fletcher J, Iannettoni MD, et al. Evaluation ofpatients with pulmonary nodules: when is it lung cancer?:ACCP evidence-based clinical practice guidelines (2nd ed).Chest 2007;132(3 Suppl):108S–30S.
31. Rivera MP, Mehta AC. Initial diagnosis of lung cancer:ACCP evidence-based clinical practice guidelines (2nd edi-
tion). Chest 2007;132(3 Suppl):131S–48S.
433Ann Thorac Surg DEPPEN ET AL2011;92:428–33 ACCURACY OF FDG-PET TO DIAGNOSE NSCLC
ERA
LT
HO
RA
CIC
DISCUSSION
opb
pl
yhtpi
DiSmf
DogpttWt
Dmohitus
GEN
DR WILLIAM F. SASSER (St. Louis, MO): Eric, Thank you verymuch for this presentation. I think it was very informative. In St.Louis, we experience many of the problems that you havebecause of the granulomatous nature of many of the pulmonarylesions. The Mississippi River area is very similar to the Cum-berland River area in this respect.
In the manuscript you indicate that the imaging data wereabstracted from dictated reports in the electronic medical re-cords. There was no consistency of the multiple radiologistsinvolved. Would it have been better and a stronger report if youhad retrieved the disc and one common reader interpret all ofthe data? The SUV [standard uptake value] that you mentionedthroughout the paper I assume was the max SUV. Dr Cerfoliohas pointed this out in the past that the max SUV is morereliable than just the mean SUV.
In one of your references, you used the meta-analysis from theJAMA in 2001. That was your standard for accuracy to diagnosepulmonary lesions. Most of these data that were published therewere established many years before. That was before there wasa combined PET-CAT [positron emission tomography-computed axial tomography] instrument. That came into beingin 2000. One of my other suggestions is that a more recentreference relating to the incidence of lung cancer involved withthis would be appropriate. I know this was a paper focused onpulmonary lesions. The PET does establish metastatic lesions aswell as nodal lesions, which frequently are much easier tobiopsy to get a diagnosis.
In closing, I would like to say that I appreciate the exercise yougave me in reviewing my statistical knowledge. Going back towords like sensitivity, specificity, accuracy, positive likelihood,negative likelihood, PPVs [positive predictive values] and NPVs[negative predictive values] has been very refreshing, and Iappreciate the opportunity to relearn those.
DR GROGAN: Thank you for your very insightful questions,and I think the audience would agree that they are right on.
Your first question was about the multiple radiologists read-ing the FDG-PET scans. I think that is both a strength and aweakness for this paper. This is a real world study. Many of thereports that have been done in the past have looked at singleinstitutions with single reviewers, single PET scans, and that hasbeen a strength of their paper. These are the patients that arereferred to us, which include radiology reads from really allthroughout the middle Tennessee, northern Alabama, southernKentucky regions, and so we are sort of left with the data that weare given, and that is the reality and the advantage and disad-vantage and limitations of this paper.
We went back and reviewed the reports and that was the datathat the surgeons had at the time that they made the operativedecision. So I think that is, as you mentioned, both a limitationbut also a strength.
With regard to max SUV, that is what we used, and wecategorized PET as avid if the SUV was dictated in the reportgreater than 2.5. If not, then we had to go with moderate tointense uptake as dictated by the radiologist that they weresuspicious for cancer, and, as before, that is a strength and alimitation for our paper.
As far as the meta-analysis question, I think that is a very good
point. However, even in the more current cost-effective model- Ping that Dr Gould has done for us, the specificity numbers thathe uses, which included even more current data, are very similarto what I have reported, which is around 80%. So although thatis an older reference, I think even most of the data which comesfrom regions outside of the southeast still report specificity inthe 80% range.
And with regard to metastatic and nodal disease, I think thatis something for future work and we are looking into that. I don’tcurrently have that data, but that is a very good point.
DR ROBERT J. CERFOLIO (Birmingham, AL): Congratulationson the paper. A few questions; first, you use an absolute value of2.5. You would agree that a 1 � 1 � 1 cm tumor with a max SUV
f 2.5 is very different than a 10 �10 � 10 cm tumor. Weublished about volume. If you haven’t done it, could you goack and look at the max SUV per cm2 or cm3 of volume of
tumor? That is number 1.Number 2. If I understood the slide correctly you are telling us
that a 12% difference versus a 50 or 60% difference doesn’t makea difference? In my life, if I can improve my odds from beingwrong or right from 12% to almost 60%, I would take it everyday.
DR GROGAN: Your point with max SUV per cm2 is a goodoint. We have not done that. I think that is something we can
ook at as we go forward.With regard to operative decision making, I don’t know about
ou, but I still would have a hard time watching a lesion in aealthy individual that has a 12% chance of malignancy, and I
hink comes down to a risk-benefit ratio for each individualatient. So we just have to be thoughtful with regard to the
ndividual patient coming in, what their risks are.
R CERFOLIO: I agree, but have you considered the differencen the risk of waiting of a patient with a mass that has a low maxUV, for example, say 2.6, the risk of waiting three months, sixonths, for him and getting nodal disease is less than waiting
or a patient with a max SUV of 12.
R MARK J. KRASNA (Towson, MD): Eric, great paper. An-ther real world question. If you are confronted now with a 2-cmround-glass opacity [GGO] but the PET shows you no uptake,lease tell us how you would use it in that situation as opposed
o a solid nodule where you have a high pretest probability thathere might be malignancy with a smoking history, et cetera?
hat would you do with a GGO now, that comes in and you didhe PET and the PET is negative?
R GROGAN: We had 14 false negatives, and a PET negativeeans that you are still going to have a greater than 10% chance
f malignancy, and I think that in our population the decisionas to be made based upon the CT [computed tomography] scan
n that particular patient depending on the pretest probabilityhat that patient brings, and I think that is the key. We have tonderstand what the pre-test probability is before we under-tand what the post-test probability with a positive or a negative
ET result will be.






![CYCLOTRON PRODUCED RADIONUCLIDES:GUIDANCE ON FACILITY DESIGN AND PRODUCTION OF [18F]FLUORODEOXYGLUCOSE (FDG)](https://static.fdokumen.com/doc/165x107/631647d8c32ab5e46f0db468/cyclotron-produced-radionuclidesguidance-on-facility-design-and-production-of-18ffluorodeoxyglucose.jpg)












