
A web-based self-monitoring system for people living with HIV/AIDS
12
Computer Methods and Programs in Biomedicine 69 (2002) 75 – 86 A web-based self-monitoring system for people living with HIV/AIDS E.J. Go ´ mez *, C. Ca ´ceres, D. Lo ´pez, F. Del Pozo ETSI Telecomunicacio ´n, Grupo de Bioingenierı ´a y Telemedicina, Uniersidad Polite ´cnica de Madrid, 28040 Madrid, Spain Received 16 February 2001; received in revised form 11 June 2001; accepted 14 June 2001 Abstract Available evidence indicates that the internet is becoming the main source for delivering information on the prevention, control and treatment of HIV/AIDS. This paper presents a further step in the use of the internet to meet the new challenge of managing HIV as a chronic illness. It describes a work carried out under the SEAHORSE EU project to build and test a Web-based self-monitoring system for HIV/AIDS patient care. The user interface has been carefully designed to provide a high-level of interaction and therefore improve some of the current limitations of Web applications. The system comprises three modules: (1) a patient self-monitoring personal diary, to create a follow-up patient record; (2) a data analysis and visualisation tool; and (3) a section to allow patients to ask for advising and remote doctor support. One of the crucial system design issues has been the system security and users anonymity features required in this clinical domain. A feasibility pilot has been carried out to test the system in three organisations involved in the research project: the Immune Development Trust (London), the Lambeth, Southwark and Lewisham Health Authority (London) and Apoyo Positivo in Madrid. The preliminary results of the system evaluation show the potential validity and usefulness of the tool for helping people living with HIV/AIDS to promote and manage their health and for providing health professionals with new means for tele-monitoring and tele-caring patients. © 2002 Elsevier Science Ireland Ltd. All rights reserved. Keywords: HIV; AIDS; Internet; Self-monitoring; Chronic care management www.elsevier.com/locate/cmpb 1. Introduction The internet is having a tremendous radical impact on healthcare models and in particular on how healthcare is currently delivered. It is trans- forming the relationships between healthcare ad- ministrations and companies, professionals and patients. Furthermore, patients are using the in- ternet to gather information about diseases and drugs and to communicate directly with their physicians. In fact health-related sites are among the most frequently accessed information re- sources on the Web [1]. The impact of this internet revolution is also affecting newly discovered diseases that have poorer forecasts, where prevention (i.e. informa- tion) is vital. This is the case of the HIV/AIDS. This epidemic was first discovered in the 1980s and today more than 21.8 million people have * Corresponding author. Tel.: +349-1549-5700x332. E-mail address: [email protected] (E.J. Go ´ mez). 0169-2607/02/$ - see front matter © 2002 Elsevier Science Ireland Ltd. All rights reserved. PII:S0169-2607(01)00182-1
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of A web-based self-monitoring system for people living with HIV/AIDS
Computer Methods and Programs in Biomedicine 69 (2002) 75–86
A web-based self-monitoring system for people living withHIV/AIDS
E.J. Gomez *, C. Caceres, D. Lopez, F. Del PozoETSI Telecomunicacion, Grupo de Bioingenierıa y Telemedicina, Uni�ersidad Politecnica de Madrid, 28040 Madrid, Spain
Received 16 February 2001; received in revised form 11 June 2001; accepted 14 June 2001
Abstract
Available evidence indicates that the internet is becoming the main source for delivering information on theprevention, control and treatment of HIV/AIDS. This paper presents a further step in the use of the internet to meetthe new challenge of managing HIV as a chronic illness. It describes a work carried out under the SEAHORSE EUproject to build and test a Web-based self-monitoring system for HIV/AIDS patient care. The user interface has beencarefully designed to provide a high-level of interaction and therefore improve some of the current limitations of Webapplications. The system comprises three modules: (1) a patient self-monitoring personal diary, to create a follow-uppatient record; (2) a data analysis and visualisation tool; and (3) a section to allow patients to ask for advising andremote doctor support. One of the crucial system design issues has been the system security and users anonymityfeatures required in this clinical domain. A feasibility pilot has been carried out to test the system in threeorganisations involved in the research project: the Immune Development Trust (London), the Lambeth, Southwarkand Lewisham Health Authority (London) and Apoyo Positivo in Madrid. The preliminary results of the systemevaluation show the potential validity and usefulness of the tool for helping people living with HIV/AIDS to promoteand manage their health and for providing health professionals with new means for tele-monitoring and tele-caringpatients. © 2002 Elsevier Science Ireland Ltd. All rights reserved.
Keywords: HIV; AIDS; Internet; Self-monitoring; Chronic care management
www.elsevier.com/locate/cmpb
1. Introduction
The internet is having a tremendous radicalimpact on healthcare models and in particular onhow healthcare is currently delivered. It is trans-forming the relationships between healthcare ad-ministrations and companies, professionals andpatients. Furthermore, patients are using the in-
ternet to gather information about diseases anddrugs and to communicate directly with theirphysicians. In fact health-related sites are amongthe most frequently accessed information re-sources on the Web [1].
The impact of this internet revolution is alsoaffecting newly discovered diseases that havepoorer forecasts, where prevention (i.e. informa-tion) is vital. This is the case of the HIV/AIDS.This epidemic was first discovered in the 1980sand today more than 21.8 million people have
* Corresponding author. Tel.: +349-1549-5700x332.E-mail address: [email protected] (E.J. Gomez).
0169-2607/02/$ - see front matter © 2002 Elsevier Science Ireland Ltd. All rights reserved.
PII: S0 169 -2607 (01 )00182 -1
E.J. Gomez et al. / Computer Methods and Programs in Biomedicine 69 (2002) 75–8676
died from it, and there is an estimated 36.1 mil-lion people living with HIV/AIDS in the world[2]. The general public is becoming increasinglyaware of how HIV is transmitted and how toavoid the infection, but this information has to bebroadcast to the greatest number of people possi-ble and in every possible media [3,4]. The best andmore universal media used now in the industri-alised world is the internet, and in the HIV/AIDShealth care domain, there is a wealth of valuableinformation.
In any case, the main problem now is that theinternet hosts thousands of Web pages referringto HIV/AIDS, brimming with information andmisinformation [5]. The SEAHORSE II Europeanproject [6] aims to provide solutions in this direc-tion by defining and developing a Web site thatselects, classifies and validates (with an expertreviewers group) the most interesting HIV/AIDSWeb sites. It also allows users to post commentsand articles to rate the existing resources.
The work presented in this paper has beendeveloped within the SEAHORSE II project, toextend the possibilities of the internet health careinformation services, to transmit information onprevention to the community (which is the mostcommon use nowadays in the field of HIV/AIDS)and to provide, both health professionals andpatients with tools to improve the illness monitor-ing [7].
Potent combination antiretroviral therapy hasled to steep declines in AIDS-related deaths andopportunistic diseases. AIDS health care profes-sionals have begun to openly share a perceptionthat they have held privately for some time: HIVinfection can be transformed from a uniformlyfatal disease into a long-term illness [8].
Therefore, HIV infection is becoming chronicbut only for those patients who tolerate or haveaccess to those potent treatments. Quality of life isanother issue to be tackled, because the power ofthese drugs involves new side effects, and thenewness of the treatments makes it impossible topredict the long-term effects.
As people living with HIV/AIDS become awareof their new health status, they have to learn howto manage their chronic disease. This new situa-tion leads to the incorporation of the self-moni-
toring concept HIV/AIDS in the domain in orderto improve health status and reduce hospitalisa-tions [9]. Within the home care monitoring pro-grammes [10], this is now one of the leadingproducts in the medical industry.
The combination of self-diagnostics, homemonitoring and the internet is being demonstratedas a really powerful product for attending chronicpatients [11]. This paper describes a new self-mon-itoring web-based system for HIV/AIDS patients.
2. System design and development
The main objective of this system is supplyingpeople living with HIV/AIDS with a new tool toachieve the follow up of the evolution of theirhealth status. Furthermore, the system allowshealth care professionals to assess the effect ofseveral therapeutic strategies on the illnessevolution.
2.1. User requirements
The first stage of the system design was to carryout a comprehensive analysis of user requirementsusing a user-centred methodology developed byauthors in earlier research work [12]. The userrequirements collection was realised by a struc-tured questionnaire provided to users, patientsand professionals, from the seven pilot sites of theSEAHORSE project, although the main contribu-tion came from the Apoyo Positivo NGO (NonGovernmental Organisation) set up in Madrid,Spain. The structured information was furtheranalysed by informal interviews with some clinicalexperts in Spain to gather their opinion on theintegration of these requirements within their ownhospital organisations, to achieve the final goal toimprove the HIV/AIDS patients treatment.
A summary of the user requirements documentis depicted as follows:� Anonymity: although people are more and
more aware of the meaning of HIV/AIDS,there is still a lot of social exclusion, stigmati-sation and discrimination on people living withHIV/AIDS. In some countries where informa-tion is easily and rapidly broadcasted through
E.J. Gomez et al. / Computer Methods and Programs in Biomedicine 69 (2002) 75–86 77
the media (and here the internet has an impor-tant role) most people now do not hold stigma-tisation views about persons with HIVinfection or AIDS. However, a substantial mi-nority still holds that discriminatory attitudes[13] and in other countries this minority be-comes the majority [14]. All these lead us to ausual wish of every person living with HIV/AIDS: their anonymity on using and accessingto information systems.
� Easy-to-use: the user interface is one of themost critical components that determine theultimate success of an interactive end-user sys-tem. In our case, most patients have no com-puter skills at all, so in order to make it easy tolearn how to introduce, visualise and managedata, the system must have a very easy-to-useinterface that hides the technological complex-ity as much as possible.
� Impact of the therapies: both patients andhealth professionals are interested to visualisethe impact their therapies have on the healthstatus of the person living with HIV/AIDS.
� Evaluation of the treatment adherence: theHIV treatment compliance is one of the moststudied issues nowadays in the field of HIV/AIDS [15]. The biopsychosocial approach [16]is a clear need to improve monitoring proce-dures of patients. The measurement of thetreatment adherence is done by simple ques-tions, displaying graphically the answer results.
� Management of complementary therapies: useof these therapies to complement the tradi-tional treatment is becoming a common habit[17]. One of the SEAHORSE II project pilotsites (Immune Development Trust, London) isspecialised in such therapies, so it was decidedto include this information on the patient datarecord.
� Quality of life: patient monitoring requires tocollect a short diary, consume profiles (to-bacco, alcohol and recreational drugs) andsome subjective parameters to be collected. Toachieve this task the Visual Analogue Scale(VAS) is commonly used to evaluate the qual-ity of life of the patient [18]. This method isused in hospitals, mainly in oncology to regis-ter pain, and is easy to introduce and tovisualise.
� Communication with experts: HIV/AIDS pa-tients are increasing their role to manage theillness complications, but at the same time theyneed better means to increase the frequencyand quality of support for health care profes-sionals. Their knowledge of HIV/AIDS issuesand the influence that this terrible illness has intheir life, foster them to ask for a secondopinion [19]. This process of patient empower-ment is being supported by new communica-tion channels of doctors and patients throughthe web [20] and the e-mail is the most usedmethod of information exchange.
� System performance: the system must be asefficient as possible, managing all data andfunctionalities fast, accurate and properly. Per-formance is measured mainly with the timeresponse, but interactivity, security and volumeof data have also to be considered.
� Costs: minimising costs is one of the objectivesof the system [21]. Minimising extraordinaryvisits to the doctor for asking doubts thatcould be solved by a telemedicine procedurecan be a mean to reduce patient care costs.
� Language: users that will evaluate the systemwill be English and Spanish, so the tool mustbe translated into these two languages.
� Technical maintenance: users are mainly work-ing with NGOs, so they usually have few tech-nical maintenance resources. This means thatthe tool has to be very easy to install andstable.
2.2. System design
The user requirements analysis led to definethree application scenarios to be supported by thesystem: the first one in which the patients carryout the self-monitoring process collecting andconsulting personal and clinical data, to continu-ously update the patient monitoring record; thesecond one, that provides patients and health careprofessionals a set of data analysis and visualisa-tion tools to compare and study the evolution ofall those follow-up parameters based on the dif-ferent therapeutic goals; and the third scenario inwhich the patients can ask for advising to aHIV/AIDS expert on related issues of their illness
E.J. Gomez et al. / Computer Methods and Programs in Biomedicine 69 (2002) 75–8678
process, based on the available information onthe patient record.
At any of these scenarios a hierarchical taskanalysis was performed, following the user-cen-tred methodology mentioned above, to specifythe user interface components and structured di-alogues. The usage scenario, simplicity and easy-to-use of the tool, the required universal accessand interactivity, and a preliminary cost-benefitanalysis were absolute priorities both in the de-sign and further implementation of the system.On that purpose, the most suitable technicalplatform for developing and delivering the sys-tem that fulfil the user needs was a highly inter-active web-based system. The newest internetprogramming techniques have been employedwith the outcome of a web site hosting the wholesystem.
2.3. Security and anonymity
To cope with the anonymity requirement, theaccess to the system is controlled by an alias orusername and a password. In order to getting atotally anonymous registration, there will not ap-pear any name, address, telephone number, oreven e-mail address. This anonymity is the firstlevel of security, meaning that from the storeddata it is not possible to get the real name of theuser. Other levels of security deal with the accessto the database and the illegal access to differentweb pages (all this is transparent for the ‘legal’user).
Access to the database is protected by pass-word and data are encrypted, so that raw datacan not be accessed editing the data file.
To prevent someone accessing to pages ‘jump-ing’ over the control page where the alias andpassword are asked, session variables were used.This means that, when a correct user is iden-tified, a variable is created and it is destroyedwhen he/she closes his/her session on the system.So all the pages ask for this variable before re-turning information to the user and, if the vari-able does not exist, the server returns an errorpage.
Protecting the server and the client are impor-tant tasks in any web application. The browser
cache on the client must be managed carefullysince all the web pages the user visits are storedin the user PC, where they could be accessible toother users of that particular PC. The web pagesof this system are defined as ‘non-cacheable’ inorder to solve this problem.
2.4. Self-monitoring personal diary
The self-monitoring process implies to registera set of health status data that conforms thepatient monitoring record:� Personal data, such as the birth date, gender,
city, country, marital status, studies, profession,NGO, sexual preference, HIV detection date,infection date (if known) and risk practice.
� Clinical data: the level of the immune system(CD4) and the viral load (VL), as well as theopportunistic infections the patient has hadduring the infection (with starting and finishingdates and days being hospitalised). It is recom-mended that the patient has the complete med-ical record to fill out all these data, althoughAIDS patients are very concerned regardingtheir illness and they usually know all the data.
� Life style data, it implies a short diary for thepatient to describe the feelings, and consumeprofiles of tobacco, alcohol and recreationaldrugs. The Visual Analogue Scales (VAS) isused for entering and visualising subjective datalike pain, fatigue, sleepiness, nausea, interest,appetite, nervousness, breathing, hope, sadnessand general feeling.
� Treatment data referring to antiretroviral orother drugs designed to combat infection, andto complementary therapies (like yoga,acupuncture, vitamins, herbs, …). To evaluatethe adherence to that therapy, short and simplequestions are used, as for example ‘‘do I haveany problem with taking this drug?’’, ‘‘howmany times last week did I miss a dose?’’,‘‘when I don’t take this drug, this is usuallybecause of… oblivion, timetable difficulty,afraid of side effects, holiday or weekend, con-fused doctor instructions, …’’. The goal is toget an independent self-monitoring record ofevery therapy annotating the changes of doses,adherence, side effects and subjective benefit.
E.J. Gomez et al. / Computer Methods and Programs in Biomedicine 69 (2002) 75–86 79
It is important to remark that all the data thepatient has introduced about the evolution of thetherapy can be visualised immediately in a sim-ple and complete way, being able to move alongthe whole record in order to see both thechanges of drugs in the therapy and the evolu-tion of every drug.
2.5. Web-based user interface design
The user interface of the system is fully Web-based but as far as possible hides the Webbrowser to simplify the interaction for peoplewho are not used to computers. The appearanceof a folder with different tags, using a real-worldmetaphor has been selected to increase systemusability.
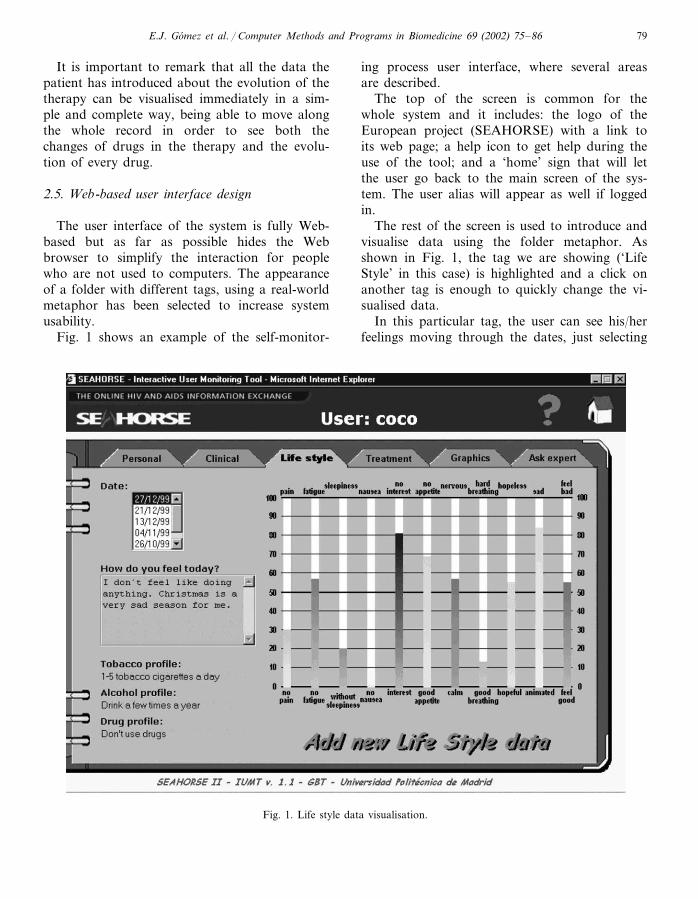
Fig. 1 shows an example of the self-monitor-
ing process user interface, where several areasare described.
The top of the screen is common for thewhole system and it includes: the logo of theEuropean project (SEAHORSE) with a link toits web page; a help icon to get help during theuse of the tool; and a ‘home’ sign that will letthe user go back to the main screen of the sys-tem. The user alias will appear as well if loggedin.
The rest of the screen is used to introduce andvisualise data using the folder metaphor. Asshown in Fig. 1, the tag we are showing (‘LifeStyle’ in this case) is highlighted and a click onanother tag is enough to quickly change the vi-sualised data.
In this particular tag, the user can see his/herfeelings moving through the dates, just selecting
Fig. 1. Life style data visualisation.
E.J. Gomez et al. / Computer Methods and Programs in Biomedicine 69 (2002) 75–8680
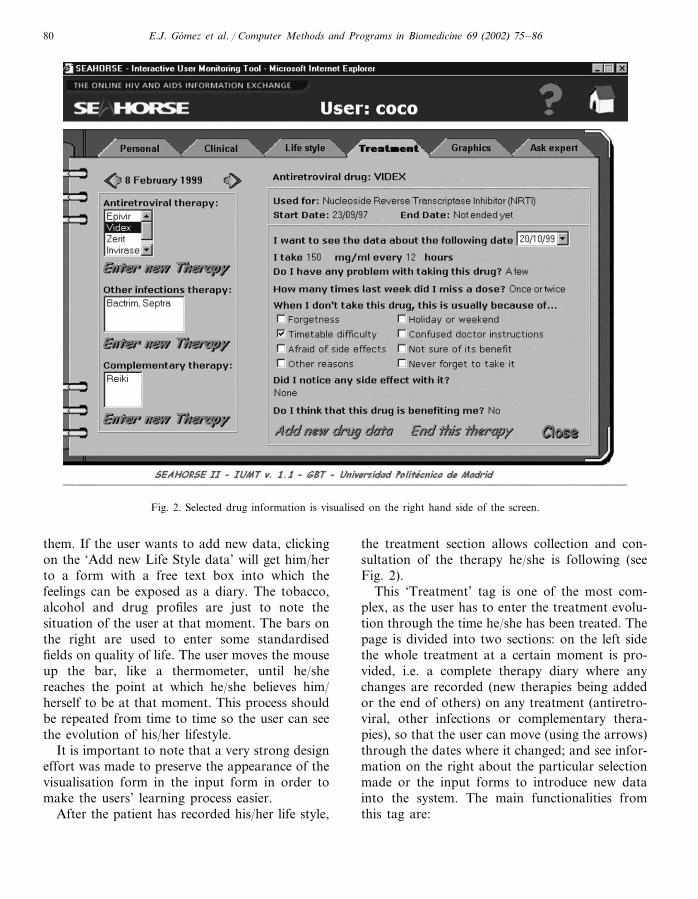
Fig. 2. Selected drug information is visualised on the right hand side of the screen.
them. If the user wants to add new data, clickingon the ‘Add new Life Style data’ will get him/herto a form with a free text box into which thefeelings can be exposed as a diary. The tobacco,alcohol and drug profiles are just to note thesituation of the user at that moment. The bars onthe right are used to enter some standardisedfields on quality of life. The user moves the mouseup the bar, like a thermometer, until he/shereaches the point at which he/she believes him/herself to be at that moment. This process shouldbe repeated from time to time so the user can seethe evolution of his/her lifestyle.
It is important to note that a very strong designeffort was made to preserve the appearance of thevisualisation form in the input form in order tomake the users’ learning process easier.
After the patient has recorded his/her life style,
the treatment section allows collection and con-sultation of the therapy he/she is following (seeFig. 2).
This ‘Treatment’ tag is one of the most com-plex, as the user has to enter the treatment evolu-tion through the time he/she has been treated. Thepage is divided into two sections: on the left sidethe whole treatment at a certain moment is pro-vided, i.e. a complete therapy diary where anychanges are recorded (new therapies being addedor the end of others) on any treatment (antiretro-viral, other infections or complementary thera-pies), so that the user can move (using the arrows)through the dates where it changed; and see infor-mation on the right about the particular selectionmade or the input forms to introduce new datainto the system. The main functionalities fromthis tag are:
E.J. Gomez et al. / Computer Methods and Programs in Biomedicine 69 (2002) 75–86 81
� Enter new therapy: depending on the kind oftherapy (antiretroviral, for other infections orcomplementary) the user wants to enter, he/shewill get different forms. With these forms,when the user enters the drug name, the toolautomatically shows the common use of thatdrug (which may not match with the particularuse): the starting date, the quantity and fre-quency of the dose, the problems that appear,the times and reasons for missing doses, sideeffects and benefits.It is important to note that the user must fill in
these fields. So, to enter a new therapy, the usermust have taken the drug for at least a week.
To see the details of a specific therapy, userssimply have to click on it from the list. Then theuser will get that particular information onthe right hand side of the window, as shown inFig. 2 for VIDEX (a particular antiretroviraldrug).From these new windows, the user can:� View the evolution of that particular therapy:
as the user changes the date, the doses, prob-lems, side effects, … change to the values ofthe selected date.
� Add new drug data: the evolution of a particu-lar therapy can be registered by clicking hereand filling the form on other date. Every timethe user notices any change regarding a ther-apy he/she is taking, it must be registered here.
� End this therapy: clicking here will register theending date of that particular therapy, so itwill no longer appear from that date on.
2.6. Data analysis and �isualisation
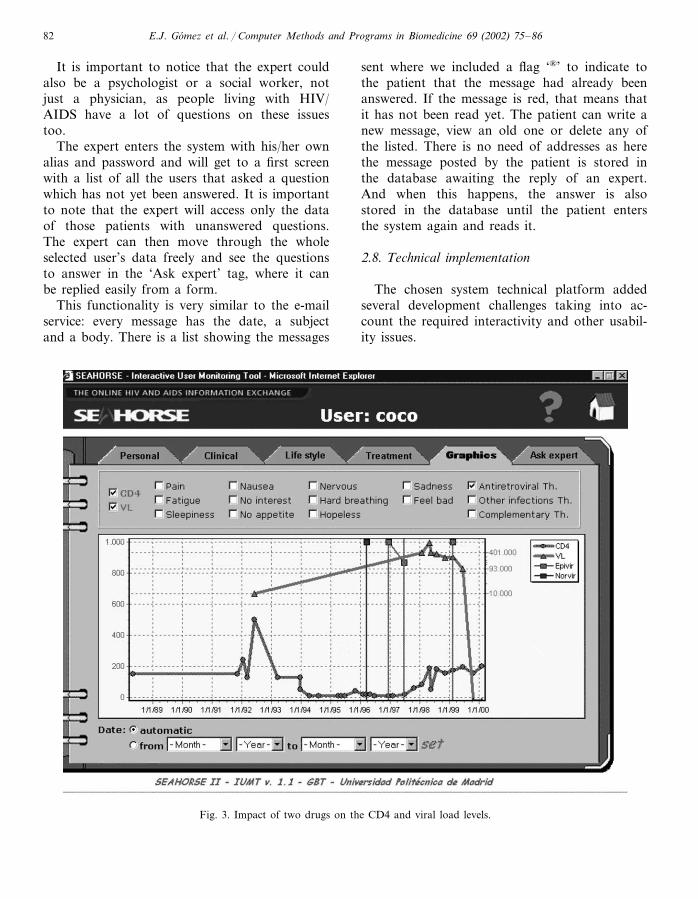
In this module the user can visualise all theparameters introduced earlier in order to studythe evolution of the infection and the impact thedifferent therapies have on it with the possibilityof over striking all the parameters in the samegraph. An example showing the features of thisfunction is displayed in Fig. 3, the visualisation ofthe impact that a certain therapy has on the viralload or on the defence level.
Clicking on the boxes that appear in the upperpart of the screen will represent the parametersselected by the user. Another menu will appearwith all the therapies the user has had through
the whole of the infection’s life, and from themthe user selects those that will be representedaccording to the following notation: a vertical linewill note the start and end of a therapy and inbetween them, the line will represent the compli-ance the user had on that particular treatment.This adherence representation helps the user tosee the real impact of the treatment on theparameters shown. If the adherence is low on aparticular drug, it cannot influence the parame-ters as much as it could if the compliance washigh. If there is no end line (as the second timethe user ‘Coco’ took Epivir or with Norvir) itmeans that the therapy is still being taken. Wecan see in the example of Fig. 3 with real data,that the second time ‘Coco’ took Epivir the viralload (VL) dropped to undetectable levels in 8months time and that this drug has a real impacton the parameter because the adherence to it hasbeen kept high.
The user can also use the zoom or decide thetimeline range in order to see the details of thegraphic. Compliance and all the life style data willuse the left vertical axis (from 0 to 1.000) as areference, although these values are from 0 to100.
2.7. Communication with expert utility
Communication with the expert is provided tothe patient for him or her to make any consulta-tion or ask any question. This means that a groupof experts, having all the data on the screencollected by the patient, could advise and helpwith the questions the patient has.
The main advantages this system of ask-an-ex-pert has over the usual system on the internet are:(a) on the e-mail there is complete anonymity(there is no name or e-mail address) and thepersonalisation of the answer is much better. Theexperts that usually respond to these questions onthe internet tend to give vague or too generaladvice as they do not have sufficient knowledgeof the patient’s situation. By visualising the pa-tient data, the expert can make more specificanswers as well as evaluating the effect that dif-ferent therapeutic strategies have on differentpeople living with HIV/AIDS.
E.J. Gomez et al. / Computer Methods and Programs in Biomedicine 69 (2002) 75–8682
It is important to notice that the expert couldalso be a psychologist or a social worker, notjust a physician, as people living with HIV/AIDS have a lot of questions on these issuestoo.
The expert enters the system with his/her ownalias and password and will get to a first screenwith a list of all the users that asked a questionwhich has not yet been answered. It is importantto note that the expert will access only the dataof those patients with unanswered questions.The expert can then move through the wholeselected user’s data freely and see the questionsto answer in the ‘Ask expert’ tag, where it canbe replied easily from a form.
This functionality is very similar to the e-mailservice: every message has the date, a subjectand a body. There is a list showing the messages
sent where we included a flag ‘®’ to indicate tothe patient that the message had already beenanswered. If the message is red, that means thatit has not been read yet. The patient can write anew message, view an old one or delete any ofthe listed. There is no need of addresses as herethe message posted by the patient is stored inthe database awaiting the reply of an expert.And when this happens, the answer is alsostored in the database until the patient entersthe system again and reads it.
2.8. Technical implementation
The chosen system technical platform addedseveral development challenges taking into ac-count the required interactivity and other usabil-ity issues.
Fig. 3. Impact of two drugs on the CD4 and viral load levels.
E.J. Gomez et al. / Computer Methods and Programs in Biomedicine 69 (2002) 75–86 83
Providing this interactivity and usabilitythrough the internet was an important challengeand we coped with it by developing the systemusing the Microsoft Notepad. That simple pro-gram gave us entire control of the code we wrote,meaning that we knew that the code we wrote wasthe code the users would get on their computers(for example other development tools such asMicrosoft FrontPage, Microsoft Visual Interdevor Netscape Composer wouldn’t guarantee that).On the other hand, this meant that writing anddebugging the code was very much more tediousand complex.
A base screen resolution of 800×600 was usedduring the design of the system, which is the mostcommonly used resolution nowadays, althoughhigher resolutions are supported.
DHTML (Dynamic HTML) was used for theanimation of the system, writing the functions inJavaScript language and using different layers.The tool is developed mainly for the MicrosoftInternet Explorer browser and the system is com-patible from its version 4.0 on.
Active Server Pages (ASP) were used for thedatabase connection with Microsoft Access. Us-ing VisualBasicScript language and SQL sentencesthrough ODBC facilitated the access to every datastored in the database. As explained before, thisdatabase is encrypted to prevent someone access-ing the data by simply editing the file. It is alsoprotected with a password, to prevent accessingwith Microsoft Access. Note that using ASPforces the server to be a Microsoft Internet Infor-mation Server.
For the graphical analysis, we needed morefunctionalities than HTML, or even DHTML,can give. Therefore an ActiveX component wasdesigned and developed with Borland Delphi inorder to embed it into the web page and use it toshow graphical data, so that unlimited differentlines could be displayed at the same time.
3. Status report
Since July 2000, the self-monitoring system hasbeen installed in several trial sites of the SEA-HORSE II project to carry out a feasibility pilot
study. Three AIDS organisations participated inthe system evaluation: Lambeth, Southwark andLewisham Health Authority, Immune Develop-ment Trust and Apoyo Positivo.
Lambeth, Southwark and Lewisham HealthAuthority is one of London’s largest Health Au-thorities, with responsibility for the healthcareneeds of a significant proportion of the UK capi-tal’s population. The authority provides health-care for the second largest concentration ofpeople living with HIV/AIDS in the UK. To thisend, it is actively pursuing policies and experi-ments aimed at developing home-based telecarefor people living with HIV/AIDS. Ten ‘homealone’ HIV patients, with donated computers con-nected to the internet, and two health profession-als (physician and nurse) have evaluated thesystem.
Immune Development Trust is a London-basedNon Governmental Organisation (NGO) forHIV/AIDS, attending 200 patients with HIV/AIDS, specialising in complementary therapies(13 complementary therapists in 13 hospital sites).Ten HIV patients using the system from a PCwith internet connection in the NGO, and twocomplementary health advisers made theevaluation.
Apoyo Positivo is a Madrid-based NGO,providing support and information services forHIV/AIDS, with a particular targeting strategytowards families affected by HIV, and intra-venous drug users. More than 300 patients andtheir families are attended by this organisationthat participated in the evaluation of the system.Ten HIV patients used the system from a PC withinternet connection in the NGO and three healthprofessionals (physician, psychologist and socialworker) made the evaluation.
The evaluation was carried out by subjectivemethods based on two questionnaires: a pre-testand a post-test, completed by thirty seven users.Questions achieved aspects like personal data,knowledge of HIV/AIDS issues, health status,usage of the system and rating of its services.Furthermore, we also used a direct observationevaluation method for the users and focus groupsfor patients and professionals separately [22].
E.J. Gomez et al. / Computer Methods and Programs in Biomedicine 69 (2002) 75–8684
This preliminary evaluation has provided someencouraging results. Users felt that the tool wasvaluable and that it could provide a useful guideto managing unpredictable and rapidly changingcircumstances. It was also agreed that it was easyto use and the graphics could be easily under-stood. The feedback provided by the system,even with limited inputs, shows a clear picture ofthe effects of different interventions. Serviceusers also felt that they were in greater controlof their situation and could recognise which in-terventions had assisted in promoting or main-taining their health.
4. Discussion
There are many issues to be taken into ac-count in the development of a web-based self-monitoring system for people living withHIV/AIDS.
First of all, being a web-based system involvesuniversal access to it. This has pros and cons asthe wider access implies lower security and, aswe are dealing with clinical data, which are verysensitive, the security issue was one of the mostimportant in the development of the system.First solution was not to include the name, ad-dress, telephone number or even e-mail addressin the system. This solves the problem ofanonymity and the security was then taken tothe already solved field of mere access to pageswithout permission.
Using the internet as the framework of thedevelopment is also time and money consuming.As the amount of data grows, the size of the filesto transfer gets bigger, and although we tried toreduce size as much as possible, it can be re-duced even more by developing the web pagesdirectly this size. The amount of time the userhad to be online to fill in the data was alsocriticised, but costs have changed nowadays withthe flat rates that the Internet Service Providersare offering.
There is another interesting issue about theusers group of the system. As this system wascreated to be implemented within an Europeanproject, the cultural and social divergences of the
users had to be taken into account. For example,in Spain there is a very different HIV/AIDS pa-tients profile (most of them are intravenous drugusers) than the rest of the EU. Furthermore,patients and health professionals want to moni-tor different parameters depending on the ‘coun-try profile’. For example, in England comple-mentary therapies are used more frequently thanin other countries, so users are more interested inthis aspect of the system.
Finally, the Spanish profile shows poor com-puter awareness, so the easy-to-use quality of thesystem is really crucial in this country. Feedbackfrom users from the evaluation results indicatethat the system interface is comprehensiveenough and easy-to-use.
The socio-economic profile of the user and thecountry also influences the implementation, asaccess to the internet is not as universal aspretended.
4.1. Future work
Although most of the system functionalitieshave been evaluated with very good results, morefunctionalities have been suggested, after theevaluation of the system, that could be addedand we are working in that direction. The fol-lowing suggestions are:� New functionalities: (1) to improve the graphi-
cal representation and the expert user interface;(2) to provide automatic advice assessed bydata mining tools that classify users with profi-les personalising the system. (3) Saving to diskall the data in order to take it to other healthprofessional without internet access. (4) To ex-tract all the anonymous data from the serverfor statistical analysis purposes and for qualityassurance purposes. (5) To add more questionsto collect more medical, psychological and so-cial data, getting a complete anonymous clini-cal record of the patient.
� Introduce new technologies to facilitate theuniversal access to the system, incorporatingexisting solutions to transform the system intoa multi-access architecture system [23] (Com-puter-Telephony Integration, WebTV, WAP/UMTS, …).
E.J. Gomez et al. / Computer Methods and Programs in Biomedicine 69 (2002) 75–86 85
4.2. Clinical benefits
The system is envisaged to offer many benefits,depending on the user, related to the improve-ment of health and quality of life through the useof the internet.� For patients, friends and families: to have their
own clinical record with the possibility of asecond opinion from different experts, optimis-ing the time and money spent on the careservice. The internet also removes discriminat-ing factors in the access to services such asdistance, getting better advice from severalsources anywhere, getting the right knowledgeat the right time.
� For health care providers: to enrich theirknowledge on the HIV/AIDS disease and onthe patients management process through theaccess to the information they collected. Theycan also disseminate good clinical practice thatenables the availability of guidelines and ofsecond opinion consultation services. This canimprove co-operation between different organi-sations (hospitals, community health managersand NGOs) working on HIV/AIDS.
5. Conclusion
This paper has addressed the development, im-plementation and evaluation of a new web-basedself-monitoring system for people living withHIV/AIDS.
There are many difficulties in the follow-up ofHIV/AIDS patients and one of the aims of thissystem is to facilitate this monitoring through theuse of the internet technologies. The developedsystem has been adapted to the user requirementsand provides both patients and professionals withan easy-to-use tool to measure the impact of theirhealth strategies and a complementary communi-cation to enable a second opinion.
The SEAHORSE European project has been aperfect framework for this development because itgave us the opportunity of getting requirementsfrom a larger number of users and making theevaluation in three different scenarios.
As exposed earlier, the evaluation results are
encouraging. New functionalities, parameters andtechnologies will be addressed in the near futureto improve the system and a further evaluation isalready scheduled to cope with the final goal toprovide a better support for patients and healthprofessionals on the new approaches to manageHIV/AIDS as a chronic illness.
Acknowledgements
This research has been partially funded by theEuropean Project SEAHORSE II (HC-4019) andthe Spanish Research Council grant (TEL1999-1724-CE). We would like to thank all the SEA-HORSE partners, especially Dr Joseph Cullenfrom the Tavistock Institute (London, UK) andJohn Boyle from the Oxford Computer Consul-tants (Oxford, UK) for their support and contri-bution on this research. We would like to give ourspecial thanks to Chris Long from the Lambeth,Southwark and Lewisham Health Authority(London), Dr Simon Hincks from the ImmuneDevelopment Trust (London) and Dr MonicaYanes from Apoyo Positivo (Madrid, Spain) fortheir work and collaboration during the evalua-tion of the system, extending this gratitude to allthe users that participated with them. We alsowant to mention here our colleagues of the Bio-engineering and Telemedicine Group from thePolytechnic University of Madrid (Spain) for theirsupport to this work.
References
[1] E.H. Shortliffe, Health care and the next generationInternet, Annals of Internal Medicine 129 (1998) 138–140.
[2] Joint United Nations Programme on HIV/AIDS (UN-AIDS) and World Health Organization (WHO), AIDSEpidemic Update, December 2000, http://www.unaids.org.
[3] G. Perry, Web sites as weapons in the war on HIV:education and prevention geared to the new at-risk popu-lations, Health care on the Internet. The Haworth Press,Inc. Vol. 2, No. 2/3, 1998, pp. 39–51.
[4] T. Tan-Torres, Disseminating health information in de-veloping countries: the role of the Internet, British Medi-cal Journal 321 (2000) 797–800.
E.J. Gomez et al. / Computer Methods and Programs in Biomedicine 69 (2002) 75–8686
[5] A. Zuger, A sampling of HIV/AIDS information on theWeb, AIDS Clinical Care, 2000, Massachusetts MedicalSociety.
[6] SEAHORSE European Project Home Page, http://www.seahorse.oxi.net.
[7] P.M. Reeves, Coping in cyberspace: the impact of Inter-net use on the ability of HIV-Positive individuals to dealwith their illness, Journal of Health Communication 5(2000) 47–59.
[8] G.S. Reiter, Comprehensive clinical care: Managing HIVas a chronic illness, AIDS Clinical Care, 2000, Massachu-setts Medical Society.
[9] K.R. Lorig, D.S. Sobel, A.L. Steward, et al., Evidencesuggesting that a chronic disease self-management pro-gram can improve health status while reducing hospital-ization: a randomized trial, Medical Care 37 (1999) 5–14.
[10] P. Flatley-Brennan, Computer network home caredemonstration: a randomized trial in persons living withAIDS, Computers in Biology and Medicine 28 (1998)489–508.
[11] E.J. Gomez, F. Del Pozo, M.E. Hernando, Telemedicinefor diabetes care: the DIABTel approach towards dia-betes telecare, Medical Informatics 21 (1996) 283–295.
[12] E.J. Gomez, J.A. Quiles, M.F. Sanz, F. Del Pozo, Auser-centered co-operative information system for medicalimaging diagnosis, Journal of the American Society forInformation Science 49 (1998) 810–816.
[13] Centers for Disease Control and Prevention, HIV-relatedknowledge and stigma—United States, Morbidity andMortality Weekly Report 49 (2000) 1062–1064.
[14] Joint United Nations Programme on HIV/AIDS (UN-AIDS), HIV and AIDS-related stigmatisation, discrimina-tion and denial: forms, contexts and determinants.
Research studies from Uganda and India, June 2000.[15] D.L. Paterson, S. Swindells, J. Mohr, et al., Adherence to
protease inhibitor therapy and outcomes in patients withHIV infection, Annals of Internal Medicine 133 (2000)21–30.
[16] B. Soloway, G. Friedland, Antiretroviral failure: abiopsychosocial approach, AIDS Clinical Care, 2000,Massachusetts Medical Society.
[17] C. Calabrese, L. Standish, Alternative medical care out-comes in AIDS, Alternative Therapies in Health andMedicine 3 (1997) 93–94.
[18] R.C. Aitken, Measurement of feelings using visual ana-logue scales, Proceedings of the Royal Society ofMedicine 62 (1969) 989–993.
[19] G.C. Scott, D.J. Cher, L.A. Lenert, Second Opinion:Interactive Web-Based Access to a Decision Model, ProcAMIA Annual Fall Symposium 1997, pp. 1004.
[20] B. Pal, Internet helps communication between doctorsand patients, British Medical Journal 320 (2000) 59.
[21] D.E. Goodman, B. Kendall, Supported Self Care: Inte-grated Technological Solution to Cost-Effectively Man-age the Chronically Ill, Proc AMIA Annual FallSymposium 1997, pp. 941.
[22] E.J. Gomez, F. Del Pozo, E.J. Ortiz et al., A broadbandmultimedia collaborative system for advanced teleradiol-ogy and medical imaging diagnosis, IEEE Trans on InfoTech in Biomedicine 2 (1998) pp. 146–156.
[23] M.E. Hernando, E.J. Gomez, A. Garcia and F. Del Pozo,A multi-access server for the virtual management of dia-betes, Libro de actas del ESEM 99 (Fifth conference ofthe European Society for Engineering and Medicine)1999, pp. 309–310.




















