The free movement of persons living with HIV/AIDS - Sida Studi
322
The free movement of persons living with HIV/AIDS Jean-Yves Carlier, in association with Graciela Schiffino Edited by Dr Lieve Fransen EU HIV/AIDS PROGRAMME IN DEVELOPING COUNTRIES Produced by the European Commission Editor: Lieve Fransen
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of The free movement of persons living with HIV/AIDS - Sida Studi
The free movement ofpersons living with HIV/AIDSJean-Yves Carlier, in association with Graciela SchiffinoEdited by Dr Lieve Fransen
EUHIV/AIDSPROGRAMMEINDEVELOPINGCOUNTRIES
Pro
duce
d by
the
Eur
opea
n C
omm
issi
on
Ed
itor:
Lie
ve F
rans
en
Luxembourg: Office for Official Publications of the European Communities, 1999© European Communities, 1999European CommissionDirectorate-General for DevelopmentRue de la Loi, 200B-1049 BrusselsWorld Wide Web: http://europa.eu.int/comm/dg08/eu_hiv_aids/index.htm
Order number: 451/506E
ISBN 92-828-7126-6
Ce livre est également publié en français. English translation from the French original by Michael Lomax.
The present volume is the result of a study requested by the Commission of the EuropeanCommunities (Contract nr. B7.6211/96/029). The findings, interpretations, and conclusions are those of the authors and do not necessarily reflect the views of the European Union, European Commission or EU HIV/AIDS programme in developing countries.
Reproduction is authorised, provided the source is acknowledged.
Printed in the United Kingdom

The free movement ofpersons living with HIV/AIDSProfessor Jean-Yves Carlierin association with Graciela Schiffino
Edited by Dr Lieve Fransen
‘Le choléra fini, il restera les miroirs à affronter’Jean Giono, Le Hussard sur le toit, ch. XII.

ForewordThe twentieth century will be recorded by history as an era when considerable progress was
made in the field of human development, both on political and moral levels. States have
adopted more democratic forms of government, citizens’ rights have been recognised, and
societies have developed along more compassionate and humane lines. For the last half-
century the Universal Declaration of Human Rights has extended its protection to all
human beings, regardless of an individual’s nationality, race, sex or religion, considering
them equal in dignity and rights.
The European Union has incorporated these universal rights and humanistic values
into all the treaties and basic instruments that guide its relations with third nations. These
same values also constitute the guiding principles of European Union strategies and form the
touchstone of the Union’s overall policies.
Progress in the field of science and technology has been equally remarkable this century,
leading to the improved quality and duration of life for many through the reduction of child
mortality, by the control of epidemics and the treatment of diseases, and by improving public
health and general well-being.
However, in the mid-eighties the international community realised that the inexorable
progress of the HIV/AIDS pandemic could reverse much of the progress that has been made
on these fronts. It became apparent that in the wake of persistent social and economic
inequalities in the poorest regions of the world, an additional and particularly cruel
inequality was developing. The HIV/AIDS pandemic was accentuating the development
gap, increasing disparities between nations and adding to the already heavy burden of the
least privileged.
In response, the European Union immediately launched an extensive intervention and
assistance programme for the developing countries most severely threatened by HIV/AIDS,
while at the same time facilitating the coordination of some preventive HIV/AIDS strategies
and research in its own Member States.
The European Union’s HIV/AIDS programme in developing countries not only
undertook to address basic issues of public health and well-being of societies and individuals
stricken by the HIV/AIDS pandemic, but to embrace matters concerning the legal status and
human rights of people living with HIV/AIDS. This was in response to a change triggered off
2 The free movement of persons living with HIV/AIDS – Foreword
by the pandemic in which public and private attitudes began to harden against individuals
and groups affected by the disease. Ancient beliefs, prejudices and suspicions began to re-
surface and re-establish themselves, manifesting as fear, social disapproval and ostracism.
The present study, commissioned by the European Union’s HIV/AIDS programme in
developing countries, responds to a request from the European Parliament, the EU–ACP
Joint Assembly and from European Union Member States to address the overlapping issues
of HIV/AIDS, the free movement of people and human rights in the context of our
partnership with developing countries.
The study analyses laws and rules governing the free movement within the European
Union and within third states of persons, whether tourists, travellers, refugees, immigrants,
students or professionals, in relation to HIV/AIDS.
The study examines hundreds of national and international laws, including those
of the Member States of the European Union, in an effort to pinpoint areas where action
taken in relation to the HIV/AIDS pandemic may impact on a person’s basic human rights
and freedoms.
The author points out that some laws, rules and administrative measures that limit
an individual’s rights by restraining his or her freedom of movement are ineffective strategies
to contain the spread of HIV/AIDS. Despite a great deal of convergence on many levels,
the author also argues that some laws are still in need of refinement to further the rights
of the individual.
The European Union’s strategy to confront HIV/AIDS in developing countries is
underscored by the need to face up to the pandemic without discriminating against or
compromising a person’s freedoms and rights. These same principles have guided European
Union free movement policies.
The study clarifies issues for decision-makers, to guide legislators and assist governments
in elaborating efficient and adequate policies towards HIV/AIDS.
It is hoped that in the future we will be able to look back on the European Union’s
leadership and response to the HIV/AIDS pandemic as having made a major contribution
to overall progress in the field of human rights.
Dr Lieve Fransen, MD, PhD
Principal Administrator, EU HIV/AIDS programme in developing countries
Social, Human and Cultural Development; Gender Unit VIII/A2
The free movement of persons living with HIV/AIDS – Foreword 3

4 The free movement of persons living with HIV/AIDS
The free movement of persons living with HIV/AIDS – Summary of contents 5
Summary of contents
List of abbreviations 6
Table of contents 7
General introduction 17
Part I: International and European law 21
Part II: European Union Member States (15 States) 53
Part III: Third Countries (91 States) 121
General conclusions 207
Annexes: Legislative texts and case law 221
Bibliography 312
6 The free movement of persons living with HIV/AIDS – List of abbreviations
List of abbreviationsA. AustriaAIDS Acquired Immuno-Deficiency SyndromeAm. J. Int’l L. American Journal of International LawAnn.dr. Annales de droit de LouvainB. BelgiumBGBl BundesgesetzblattBull. Quest. et Rép. Sénat Bulletin des questions et réponses du Sénat (Belgium)C.E. Conseil d’État (Belgium, France)Com. L. Yearbook Comparative Law YearbookCom.M.L.R. Common Market Law ReviewCRA Compte-rendu analytique (analytical account)D. GermanyDK. DenmarkD.P. Débats parlementaires (parliamentary debates)E. SpainEC European CommunityECHR European Convention for the Protection of Human Rights and Fundamental FreedomsECJ European Court of JusticeECR European Court ReportsEJIL European Journal of International LawF. FranceFasc. fasciculeFIN. FinlandGaz. Pal. Gazette du palais (Court Gazette, France)GR. GreeceHIV Human Immuno-Deficiency VirusI. ItalyICCPR International Covenant on Civil and Political RightsIDHL International digest of health legislationI.O.M. International Organization for MigrationIRL. IrelandJ.T.D.E. Journal des Tribunaux-droit européen (Court Gazette – European Law)L. LuxembourgL.G.D.J. Libraire générale de droit et de jurisprudenceM.B. Moniteur belgeNL. Netherlandso.c. Opus citatumOJ Official Journal of the European CommunitiesP. Portugalp. PagePNUD Programme des Nations Unies pour le DéveloppementR.A.C.E. Recueil des arrêts et avis du Conseil d’État (Belgique) (Collection of Decrees and
Opinions of the Council of State) (Belgium)Rev. belge dr. int. Revue belge de droit international (Belgian International Law)S. SwedenSida Syndrome d’immunodéficience acquiseSIS Schengen Information SystemTEU Treaty on European UnionUK. United KingdomUNDP United Nations Development ProgrammeUNHCR United Nations High Commissioner for RefugeesVIH Virus de l’immunodéficience humaineWHO World Health Organization
SourcesIn drafting the present report, in addition to journals and nationals sources, the following main sources were used:International Digest of Health Legislation (I.D.L.H.), Geneva, WHOUNHCR Refworld, Geneva, UNHCR, January 1998 (CD-ROM)
Table of contentsSummary of contents 5
List of abbreviations 6
Table of contents 7
General introduction 17
Part I: International and European lawI. Presentation 22
A. Description 22B. Main conclusions from Part I 22
II. The free movement of persons and international law: scope of the principle of non-discrimination 24A. General remarks 24B. Fundamental rights 26C. Non-discrimination 28
III. The free movement of persons and European law: scope of the limit of public health 32A. General remarks 32
1. Movement of persons 322. Public health 34
B. Access (crossing external borders and short stays) 351. Union citizens 352. Third country nationals 35
C. Travel (crossing internal borders, the right to travel) 371. Union citizens 372. Third country nationals 38
D. Residence 391. Union citizens 392. Third country nationals 45
IV. First conclusions (international and European law) 49
Part II: European Union Member StatesI. Presentation 54
A. Description 54B. Main conclusions from Part II 55
The free movement of persons living with HIV/AIDS – Table of contents 7
II. General examination of legislation in European Union Member States 57A. Entry 57
1. Union citizens 572. Third country nationals 57
B. Residence 581. Union citizens 582. Third country nationals 58
C. Expulsion 62
D. Human rights: inhuman and degrading treatment (Strasbourg) 62
E. Free movement: proportionality (Luxembourg) 66
III. Second conclusions (national laws in the union) 68
IV. Country-by-country examination of the legislation in EuropeanUnion Member States 71
Introduction 711. (A) Austria 72
1. Foreigners in general 722. Special categories 73
2. (B) Belgium 731. Foreigners in general 732. Special categories 78
3 (D) Germany 821. Foreigners in general 822. Special categories 84
4. (DK) Denmark 861. Foreigners in general 862. Special categories 88
5. (E) Spain 881. Foreigners in general 882. Special categories 91
6. (F) France 921. Foreigners in general 922. Special categories 100
7. (FIN) Finland 1011. Foreigners in general 1012. Special categories 102
8. (GR) Greece 1031. Foreigners in general 1032. Special categories 104
8 The free movement of persons living with HIV/AIDS – Table of contents
9. (I) Italy 1051. Foreigners in general 1052. Special categories 106
10. (IRL) Ireland 1071. Foreigners in general 1072. Special categories 107
11. (L) Luxembourg 1081. Foreigners in general 1082. Special categories 110
12. (NL) Netherlands 1111. Foreigners in general 1112. Special categories 112
13. (P) Portugal 1131. Foreigners in general 1132. Special categories 113
14. (S) Sweden 1141. Foreigners in general 1142. Special categories 115
15. (UK) United Kingdom 1161. Foreigners in general 1162. Special categories 120
Part III: Third countriesI. Presentation 122
A. Description 122
B. Main conclusions from Part III 122
II. General examination of legislation in third countries 124A. Entry 124
1. Public policy 1242. Public health 1243. Financial means 126
B. Residence 1271. Residence in general 1272. Particular categories 130
C. Expulsion 1311. Public policy 1312. Public health 131
III. Third conclusions (third countries’ national laws) 134
The free movement of persons living with HIV/AIDS – Table of contents 9
IV. Country-by-country examination of legislation in third countries 136A. Africa 136
1. South Africa 1362. Angola 1383. Botswana 1394. Burkina Faso 1395. Burundi 1406. Cameroon 1417. Ethiopia 1418. Gabon 1419. Gambia 14210. Equatorial Guinea 14311. Kenya 14312. Lesotho 14413. Madagascar 14414. Malawi 14515. Mali 14616. Namibia 14617. Nigeria 14718. Oman 14819. Uganda 14920. Rwanda 14921. Senegal 15022. Seychelles 15123. Swaziland 15224. Tanzania 15325. Tunisia 15326. Zambia 15427. Zimbabwe 154
B. Asia 15528. Cambodia 15529. China 15630. India 15831. Indonesia 15932. Malaysia 16033. Nepal 16134. Pakistan 16135. Philippines 16236. Sri Lanka 16337. Syria 163
10 The free movement of persons living with HIV/AIDS – Table of contents
38. Thailand 16439. Turkey 16540. Vietnam 166
C. Central and South America 16741. Argentina 16742. Bahamas 16843. Barbados 16944. Belize 16945. Bolivia 17046. Brazil 17047. Chile 17148. Colombia 17149. Costa Rica 17250. Cuba 17351. Dominican Republic 17452. Ecuador 17453. Jamaica 17554. Mexico 17555. Nicaragua 17656. Panama 17757. Peru 17758. El Salvador 17859. Trinidad and Tobago 17960. Venezuela 179
D. South Sea Islands 18061. Fiji 18062. Papua New Guinea 18063. Western Samoa 18164. Tonga 182
E. Central Europe 18365. Albania 18366. Bulgaria 18367. Hungary 18568. Poland 18569. Romania 18670. Slovakia 18771. Czech Republic 188
F. Former Yugoslavia 18972. Former Federal Socialist Republic of Yugoslavia 189
The free movement of persons living with HIV/AIDS – Table of contents 11

73. Croatia 18974. Macedonia 19075. Slovenia 191
G. Community of Independent States 19276. The former Union of Soviet Socialist Republics 19277. Armenia 19378. Belarus 19379. Estonia 19480. Georgia 19481. Kazakhstan 19682. Kyrghyzistan 19783. Latvia 19784. Lithuania 19885. Moldova 19986. Mongolia 20087. Uzbekistan 20088. Russia 20189. Tajikistan 20290. Turkmenistan 20391. Ukraine 204
General conclusions1. The Main Facts 208
A. National law 208B. European law 210C. International law 210
2. Conclusions 2163. Proposals 217
Annexes: Legislative texts and case lawAnnexe I. International and European law 222
(1) International protection of human rights 222(2) Secondary community legislation (EC) 223(3) Non-binding community texts 224
Annexe II. European Union Member States 230(1) National texts 231
1. (A) Austria 2312. (B) Belgium 2313. (D) Germany 2324. (DK) Denmark 233
12 The free movement of persons living with HIV/AIDS – Table of contents
5. (E) Spain 2336. (F) France 2367. (FIN) Finland 2388. (GR) Greece 2389. (I) Italy 24010. (IRL) Ireland 24011. (L) Luxembourg 24212. (NL) Netherlands 24413. (P) Portugal 24514. (S) Sweden 24615. (UK) United Kingdom 246
(2) Case law: European Court of Human Rights, 2 May 1997, D. v. United Kingdom 249(3) Summary table 274
Annexe III. Third countries 276(1) National texts 276
A. Africa 2761. South Africa 2762. Angola 2763. Botswana 2774. Burkina Faso 2775. Burundi 2777. Ethiopia 2789. Gambia 27810. Equatorial Guinea 27811. Kenya 27912. Lesotho 27913. Madagascar 28014. Malawi 28016. Namibia 28117. Nigeria 28118. Oman 28119. Uganda 28120. Rwanda 28221. Senegal 28222. Seychelles 28223. Swaziland 28324. Tanzania 28325. Tunisia 28326. Zambia 28427. Zimbabwe 284
The free movement of persons living with HIV/AIDS – Table of contents 13
B. Asia 28428. Cambodia 28429. China 28530. India 28531. Indonesia 28632. Malaysia 28633. Nepal 28634. Pakistan 28635. Philippines 28736. Sri Lanka 28737. Syria 28738. Thailand 28839. Turkey 28840. Vietnam 288
C. Central and South America 28941. Argentina 28942. Bahamas 29043. Barbados 29044. Belize 29045. Bolivia 29147. Chile 29148. Colombia 29149. Costa Rica 29250. Cuba 29251. Dominican Republic 29252. Ecuador 29253. Jamaica 29354. Mexico 29355. Nicaragua 29456. Panama 29458. El Salvador 29559. Trinidad and Tobago 295
D. South Sea Islands 29562. Papua New Guinea 29563. Western Samoa 29664. Tonga 296
E. Central Europe 29765. Albania 29766. Bulgaria 297
14 The free movement of persons living with HIV/AIDS – Table of contents
67. Hungary 29768. Poland 29870–71. Czech Republic and Slovakia 298
F. Former Yugoslavia 29973. Croatia 29974. Macedonia 30075. Slovenia 300
G. Community of Independent States 30078. Belarus 30079. Estonia 30180. Georgia 30181. Kazakhstan 30282. Kyrghyzistan 30283. Latvia 30284. Lithuania 30385. Moldova 30386. Mongolia 30487. Uzbekistan 30588. Russia 30589. Tajikistan 30690. Turkmenistan 30691. Ukraine 306
(2) Summary Table 307
Annexe IV. Basic bibliography 312(1) On AIDS 312(2) On free movement of persons, migrations and human rights 317
The free movement of persons living with HIV/AIDS – Table of contents 15

Generalintroduction

The free movement of persons living with HIV/AIDS– General introduction 19
General introduction1. The study concerns the movement of persons living with HIV/AIDS. It falls within
the context of relationships between developing countries and European Union Member
States 1. Although this study develops general principles, the examination is mainly
concerned with persons circulating between the European Union and developing
countries, as well as within those specific areas.
2. The issue involved in the free movement of persons with respect to HIV/AIDS is the
following: should measures be taken with regard to international travellers and migrants?
Before assessing legislation or national practices, it is necessary to determine what
restrictions on the free movement of persons are authorised or forbidden by international
and European law. This is the subject of the first part of the study. The second part of the
study examines the legislation of the various European Union Member States. The third
part of the study concerns other countries that are not members of the European Union
(third countries). The third countries examined by this study are principally developing
countries concerning which it was possible to collect legislative or reglementary
information (a total of 64 countries). Countries with which the Union has relations of
cooperation or of association, or for which this kind of relation is envisaged in the future,
principally in the Central and Eastern Europe countries (CEEC), are also studied insofar
as it has been possible to collect legislative or reglementary information concerning them
(27 countries).
A total amount of 106 states were included in the study.
The study was conducted in 1997. When it was possible, updating was added for
1998. Examination of these laws and practices allows us to summarise the facts in general
conclusions and to make suggestions (§§ 539 et seq.). These are centred on the necessary
respect of the principle of proportionality between the objective pursued, which is
combating the AIDS pandemic, and the means employed. Where these means affect
fundamental human rights such as freedom of movement, they must be replaced, as much
as possible, by other efficient means of combating AIDS.
1 The European Commission also implemented a ‘Europe against AIDS’ plan of action, COM(95) 521 final, 7November 1995. See also the communication ‘for increased solidarity to confront AIDS in developingcountries’, COM(98)407 final, 3 July 1998.

International andEuropean law
Part 1

22 The free movement of persons living with HIV/AIDS – Part 1: International and European law
I PresentationA. Description3. This first part concerns international and European data. It analyses international law
and the texts which, in the context of Community and governmental cooperation
(between the fifteen or a limited number of Union countries), directly or indirectly affect
the movement of persons with HIV/AIDS, and in particular the entry into the Union of
people from developing countries.
4. After briefly considering international law on the free movement of persons (II), we
shall successively examine under European law (III) the issues of (B) access to the
territory, (C) travel and (D) residence for people with HIV/AIDS before coming to first
conclusions (IV).
B. Main conclusions from Part I5. The concept of movement includes three elements: entry into European Union
territory, travel within the Union and residence on the territory of Union Member States.
6. A priori, there is no justification for a distinction between travel (tourism, business,
etc.) and migration (work, study, asylum, etc.) with respect to protection against AIDS.
Migrants who set up residence and are joined by their families will often have less ‘at risk’
sexual relations than an occasional traveller on holiday or on a business trip.
Therefore, every time people cross borders, for whatever reason, there is a question of
principle that must be answered: is it necessary to restrict or prohibit people carrying
HIV/AIDS from crossing borders?
7. Neither international nor European law contains an absolute obligation ‘prohibiting
prohibition’. As a result, measures restricting the free movement of persons carrying
HIV/AIDS, insofar as they are expressly stipulated by a legal text, are not as such in
absolute contradiction with either international or European law.
8. Nevertheless, indirectly, in their effects, measures restricting the free movement of
persons carrying HIV/AIDS or likely to do so, may under international law contravene
the principle of non-discrimination along with other fundamental rights (protection of

The free movement of persons living with HIV/AIDS – Part 1: International and European law 23
privacy and family life, prohibition of inhuman and degrading treatment) and, under
European law, the principle of the free movement of persons.
9. Under European law, the dominant fact is that, to date, no restrictive text has been
issued stating that AIDS or HIV-positivity justify exceptions to the free movement of
persons. On the contrary, conclusions, resolutions and communications stress that free
movement should be guaranteed for persons living with HIV/AIDS. Since no text
permits controls, such controls should at present be ruled out.
24 The free movement of persons living with HIV/AIDS – Part 1: International and European law
II The free movement of persons andinternational law: scope of the principleof non-discriminationA. General remarks10. The movement of persons may be sub-divided into short-term travel covering a
journey with a short stay for tourism or business reasons, and medium- or long-term
residence including migration for reasons of work, study or asylum. Although it appears to
be legally possible to make a distinction between the right to travel and the right to
migrate, the former being broader and more open than the latter, such a distinction is
avoided in this report for two reasons. The first reason is linked to the subject of the
study, people carrying HIV/AIDS. Given the way in which the virus is transmitted, the
duration of a trip, journey or migration has no significant impact. Where countries take
measures to permit only access to their territory to people not carrying HIV/AIDS and
limit such measures to migrations rather than short stay travel, it is not based on a
concern for public health and the dangers of an epidemic, but on economic grounds to
limit migration in general, particularly limiting migrants that might place a burden on
the social security system due to the health care to which they will be entitled. Indeed,
with regard to the risk of an epidemic, risk behaviour is probably more pronounced
amongst tourists – including sexual tourism – and business travellers than amongst long-
term migrants setting up with their families or creating families within the country.
11. The second reason that justifies making no distinction in the present study between
the right to travel and the right to migrate is that neither of these two rights exists
absolutely under international law. At the present time there is no international law
giving the right to freedom of movement, in the general sense of freedom to cross borders.
However, it should be noted that international law contains a remarkable paradox on this
point which results from the cold war, during which the main texts for the protection of
fundamental rights were drafted. International law recognises the right to cross a border,
but in one direction only – leaving a territory, but not entering another one 2. Even
though logically the world is divided into states and it does not seem possible to leave one

The free movement of persons living with HIV/AIDS – Part 1: International and European law 25
country without entering the territory of another 3, such is the case under international
law: each country is sovereign in determining the conditions of access to its territory.
Visas to leave a territory have therefore been eliminated in almost all countries, but entry
visas have been retained. In principle, each state determines the conditions for issuing a
visa for access to its territory. However, a common standard visa and a common list of
third countries whose nationals need a visa to enter the European Union has become,
since the Treaty of Maastricht, a European competence (article 100C E.C.; infra, § 27).
Would it be possible for a state to make proof that the traveller is not carrying HIV/AIDS
one of the required conditions for public health reasons? Is such a condition legally
possible and does it happen in practice? This is the subject of the present study.
12. The issue of the free movement of persons with regard to epidemics was raised in the
middle of the 19th century at international conferences, the first of which took place in
Paris in 1851 with a view to combating cholera, plague and yellow fever epidemics 4.
Subsequently, in a health convention in 1903, signatory states agreed to reject excessive
and arbitrary controls at borders 5. In 1951 the World Health Organization (WHO) drew
up international regulations stipulating quarantine measures that countries could employ
to combat cholera, plague, yellow fever and smallpox, setting out restrictions that could
be applied to international traffic to control other diseases. The aim was to ensure
maximum security against diseases but cause the least possible inconvenience to
international traffic. There was no provision for issuing certificates guaranteeing that a
person did not carry a certain disease 6.
2 International Covenant on Civil and Political Rights (CCPR) article 12.2: ‘Everyone shall be free to leave anycountry, including his own’. The same text appears in Protocol 4, article 2 of the European Convention onHuman Rights (ECHR). Note that this right to leave is not absolute since it may be ‘subject to any restrictions... provided by law [that are] necessary to protect national security, public order, public health or morals ...’.
3 This nonsense is illustrated by a movie by the Greek Angelopoulos, Le pas suspendu de la cigogne, the stork is amigratory bird and the suspended step is a step over the border line.
4 A. HENDRIKS, ‘The right to freedom of movement and the (un)lawfulness of AIDS/HIV specific travelrestrictions from a European perspective’, Nordic journal of international law, 1990, p. 189; L.J. NELSON,‘International travel restrictions and the AIDS epidemic’, American journal of international law, 1987, p. 233.
5 A. HENDRIKS, o.c., p. 190-191.6 L.J. NELSON, o.c., p. 234; A. HENDRIKS, o.c., p. 191.

26 The free movement of persons living with HIV/AIDS – Part 1: International and European law
Countries come up against two limitations on the conditions for issuing
authorisation to enter their territories: firstly, the limitations of fundamental rights
underpinned by the principle of non-discrimination (see below §§ 14 et seq., §§ 16 et
seq.) and secondly the limitations of international agreements with other states,
particularly in the case of Europe (see below §§ 20 et seq.).
B. Fundamental rights13. Although under international law freedom of movement is not a recognised
fundamental right for all, the limits to freedom of movement may nevertheless not affect
other fundamental individual rights recognised under international law. This is the crux
of the issue which requires a balance to be found between the interests involved. On the
one hand we have the interests of the state which enable it to restrict access to its
territory. This interest is further reinforced by an obligation on countries to take ‘the
necessary steps for ... the prevention, treatment and control of epidemic diseases’ 7. On
the other hand, we have the interests of the individual, some of whose fundamental rights
may be violated by the application of compulsory testing or a requirement to prove that
one is not a carrier of HIV/AIDS. The major fundamental rights concerned are respect
for privacy and family life 8 and the prohibition of inhuman and degrading treatment 9.
On the subject of an indirect test for HIV, the European Court of Justice judged that since
such a test was carried out against the wishes of the person concerned, it was a violation
of his privacy 10. This reasoning could be applied to a test imposed when crossing borders.
Certainly, the decision does not expressly forbid the refusal to recruit an individual who
declines to submit to a test, but reminds that this concerns only a test ‘that the medical
officer considers necessary in order to evaluate his suitability for the post for which he has
applied’, and in so doing the Court recalls the general principle of proportionality
according to which ‘restrictions may be applied to fundamental rights 11, provided that
7 International Covenant on Economic, Social and Cultural Rights, article 12, 2, c.8 ICCPR, article 17; ECHR, article 8.9 ICCPR, article 7; ECHR, article 3.10 ECJ, 5 October 1994, X v. Commission of the E.C., C-404/92, ECR, 1994, I-4737.11 In fact, it would be better to write ‘to certain fundamental rights’ such as, in this case, the protection of privacy
and family life, since others, such as the prohibition of inhuman and degrading treatment, are subject toabsolute and unconditional protection.

The free movement of persons living with HIV/AIDS – Part 1: International and European law 27
they in fact correspond to objectives of general public interest and do not constitute, with
regard to the objectives pursued, a disproportionate and intolerable interference which
infringes upon the very substance of the right protected’. The example is all the more
remarkable because in this case it is the European Court of Justice (Luxembourg) and not
the European Court of Human Rights (Strasbourg) which came out against an HIV test
on recruitment of a European official, basing its decision on article 8 of the European
Convention on Human Rights. This means that such protection of fundamental rights by
the European Convention on Human Rights has been added to the other protections
based on the principle of free movement of persons in the broader sense, even in the
Community body of law (see below §§ 20 et seq.) 12.
14. It remains that the balance between the interests of the state and those of the
individual would be difficult to establish within the framework of measures limiting the
free movement of persons because of HIV/AIDS. It would probably be necessary to stress
that the public interest and the protection of public health, which countries put forward
to justify measures restricting the free movement of persons, are not properly safeguarded
and that, on the contrary, measures such as compulsory screening are counter-productive
and exclude people carrying HIV/AIDS from health care systems and possible frameworks
for dealing with them. This has been declared on several occasions in resolutions and
recommendations from international organisations such as the World Health
Organization and the World Health Assembly, as well as regional organisations such as
the Council of Europe and the constitutions of the Member States of the European Union.
15. As one example from the many texts, let us take Recommendation no. R (89)14 of 24
October 1989 by the Ministerial Committee of the Council of Europe on the ethical
implications of HIV infection in its health and social aspects, in which points 29 and 33 declare
that routine compulsory screening is ‘unethical, ineffective, fails to respect privacy, is
discriminatory and ultimately harmful’. Points 46 to 48 of the same text read as follows:
12 Which is in line with articles F2 and K2 of the Treaty on European Union (TEU - Maastricht) restating thatthe Union respects fundamental rights, article 6 of the TEU, consolidated (Amsterdam).
28 The free movement of persons living with HIV/AIDS – Part 1: International and European law
‘46. It is recommended that public health authorities should:
47. Refrain from introducing restrictions on freedom of movement by means
of costly and ineffective border controls for all categories of travellers,
including migrant workers;
48. Not employ coercive measures such as quarantine and isolation for
individuals infected with HIV or patients with AIDS.’
The reasons given in explanation of the Recommendation stress that ‘a conflict between
individual and collective interests could arise in the choice of methods used to detect
HIV infection’ and that ‘in compliance with the principles prescribed in this
Recommendation, the decision on whether or not to proceed with a test is, in the last
resort, the responsibility of the individual and not of society’ (points 155 and 156).
Although it is the responsibility of doctors and medical experts to decide whether
such measures are ineffective, or even harmful 13, examining here whether or not they
conform with the principle of non-discrimination is a matter for legal experts.
C. Non-discrimination16. Jurisprudence of the European Court of Human Rights, followed by national
jurisprudence, stipulates that differential treatment for two categories of persons is not
discriminatory if it is based on objective criteria and is proportional, that is to say there is
proportionality between the objective pursued and the means employed 14. Once again we
see that the question of proportionality is central and that it involves a balancing test
13 Report of the Secretary General of the United Nations for the 51st session (1995) on international andnational measures taken to protect human rights and to prevent discrimination with regard to HIV/AIDS: the‘WHO has stated that since HIV infection is already in every region and virtually every major city in theworld, even total exclusion of all travellers (foreigners and citizens travelling abroad) cannot prevent theintroduction and spread of HIV’. E. LAWSON, Encyclopedia of Human Rights, Washington, Taylor & Francis,2nd edition, 1996, p. 33.
14 The principle of non-discrimination is covered by article 14 of the ECHR and articles 2 and 26 of the ICCPR.The latter article is the broadest in that it affirms not only the principle of non-discrimination as beingsubsidiary to the fundamental rights referred to in the text, such as article 14 of the ECHR, but in general, theequality of every person ‘before the law’.
The free movement of persons living with HIV/AIDS – Part 1: International and European law 29
between the objective pursued (combating AIDS) and the effectiveness of the means
employed, that being compulsory screening prior to access to the territory. Effectiveness
has to be judged both from an objective point of view (medical studies, statistics) and
from a subjective point of view with regard to the infringement of democratic values.
However, such examinations are not precisely the same. The threshold at which
fundamental individual rights are violated is in effect lowered. On the other hand,
protection of such rights is increased. It may happen that treatment that is not in itself
judged to conflict with a fundamental right, such as protection of privacy and family life
or the prohibition of inhuman or degrading treatment, could become so where it is
directed only at one category of people, even if this category could be ‘objectively’
distinguished from another, and the means employed, because of the fact that it is
aimed solely at this category of people, would not necessarily be proportional to the
objective pursued.
17. Where freedom of movement of persons living with HIV/AIDS is concerned,
‘objective’ criteria are used as a basis for differential treatment.
The first criterion for differential treatment is nationality.
Although foreigners do not have a right to access to a territory, nationals do. ‘No one
shall be arbitrarily deprived of the right to enter his own country’ 15. As a result,
international law prohibits depriving a national of the right to enter his country because
he is an HIV carrier. This does not expressly state that screening is forbidden. However,
testing carried out only on nationals who travel and not on those who remain in the
country could be considered as discriminatory because the objective factor on which it is
based, travel, is a poor reason for justifying such major differences in means with regard to
the objective of public health. Nationality is also used as a basis for differentiating
between certain categories of foreigners. By virtue of international treaties, certain
foreigners benefit from a right to enter a territory without prior authorisation (visa). This
15 ICCPR, article 12.4 and the almost identical ECHR, Protocol no. 4, article 3.2. The ECHR does not use thesame adverb ‘arbitrarily’ which could allow certain exceptions. It does give an unconditional right to nationals.Conversely, the Convention is broader in scope when it speaks of ‘his own country’ which does not necessarilylimit it strictly to nationals.

30 The free movement of persons living with HIV/AIDS – Part 1: International and European law
is the case for refugees by virtue of the principle of non-refoulement which is extended to
asylum seekers 16. It is also the case for citizens of the European Union and members of
their families on the territory of all Member States (see below §§ 20 et seq.).
The second criterion for differential treatment is HIV/AIDS.
On whom can one impose a test followed by refusal of access to the territory?
18. The combination of the two criteria – nationality and AIDS – becomes complex. In
the case of nationality, either the test is imposed on everyone, despite the consequence of
not being able to deny access to the territory to nationals and certain privileged
categories of foreigners; or the test is only imposed on certain categories of foreigners to
whom the objective case of public health does not seem to be pursued by an appropriate
means: a migrant setting up with his family probably represents a lesser risk than a
national returning from a sex tourism trip. The measure is not proportionate and
therefore violates the principle of non-discrimination.
In the case of AIDS, either the test is imposed on everyone or on all persons of a
certain nationality, depending on the choice for the first criterion, or the test is only
imposed on groups deemed to be ‘at risk’ (homosexuals, drug addicts). In the second case,
the criterion for differential treatment cannot be judged to be objective in that it is based
solely on the private lives of those concerned. In the first case, the test could be envisaged
if it were imposed on everyone, regardless of nationality, given the remarks made
concerning this criterion. If a measure to refuse access to the territory results from a test,
AIDS becomes the ‘objective’ criterion for differential treatment. The principle of
proportionality is then based on whether the refusal of access to the territory (the means
employed) is proportional to the objective pursued (to combat AIDS).
19. The same question of proportionality with regard to fundamental rights (B) reappears.
This is bolstered by the obstacles that it has to overcome to avoid infringing the principle
of non-discrimination (C). More generally, the criterion of nationality and, to an even
greater extent, the criterion of AIDS, are not necessarily ‘objective’ criteria for
differential treatment because, even if they are objectively identifiable, trends in
fundamental rights will tend to consider that they no longer constitute an objective basis
for differential treatment as was once the case for trends in discrimination on grounds of
16 Geneva Convention of 28 July 1951 relating to the status of refugee, article 33. This article does not providefor any exception on the grounds of public health, only for ‘national security’.

The free movement of persons living with HIV/AIDS – Part 1: International and European law 31
race or gender, which were also regarded as objective criteria.
Whatever comes about, in the current situation of protection of fundamental rights,
although the imposition of limits on the free movement of persons because of HIV/AIDS
is not expressly forbidden, it remains that implementing such restrictions is difficult to
reconcile with the principle of non-discrimination. Finally, such restrictions certainly
could only be implemented by virtue of a law in the broad sense, that is to say a legal text
brought to the knowledge of the general public, justifying the legitimate goal pursued 17.
17 Article 8 of the ECHR stipulates that intrusion into private or family life must be covered by a law. Moreover,article 6 of the Convention of 28 January 1981 of the Council of Europe for the Protection of Individuals withregard to Automatic Processing of Personal Data, stipulates that ‘personal data concerning health or sexualactivities may not be automatically processed unless internal laws provide appropriate guarantees’.
32 The free movement of persons living with HIV/AIDS – Part 1: International and European law
III The free movement of persons and European law: scope of the limit of public healthA. General remarks20. The protection of fundamental rights analysed above (II) is also provided for under
Community law. In the case of the free movement of persons – in the broad sense of
freedom to move, not in the strict Community sense of the right of residence –
Community law includes provisions beyond those promoting freedom of movement based
on an extension of the initial concept of the free movement of workers. The two
protections – of fundamental rights and freedom of movement – are sometimes combined.
In 1975 the ECJ judged restrictions on the free movement of workers by a state for
reasons of public policy to contravene articles 8 and 11 of the ECHR and article 2 of
Protocol no. 4 (the right within the territory of a state to liberty of movement and
freedom to choose his residence) 18. Restrictions on the grounds of public health could be
subject to the same type of condemnation.
21. Given the substantial evolution of Community law, we need to recall some of the
issues concerning (1) the free movement of persons and (2) public health before
examining in detail the conditions of (B) access, (C) travel and (D) residence within the
Union with respect to public health.
1. Movement of personsEach component of the concept of movement (entry, travel, residence) may be examined
making a distinction between Union nationals and nationals of third countries.
22. For entry, that is to say crossing external borders, Union nationals are subject only to
a visual control 19. For nationals of other countries, there is a common European visa
policy, whilst the rest of the migration policy is covered by intergovernmental
18 ECJ, 28 October 1975, Rutili, C-36/75, ECR, p. 1219.19 ECJ, 27 April 1989, Commission v. Belgium, C-321/87, ECR, p. 997.
The free movement of persons living with HIV/AIDS – Part 1: International and European law 33
cooperation. Within this framework, a draft agreement on crossing external borders was
presented by the Commission on 10 December 1993 20. All those questions entered into
European Community law with the ratification of the Treaty of Amsterdam signed on 2
October 1997. The new consolidated version of the EC Treaty would have a new Title IV:
‘Visas, asylum, immigration and other policies related to free movement of persons’.
As for travel, that is to say crossing internal borders, all controls must be eliminated
both for nationals of third countries and for Union nationals. In fact it is impossible to
control third country nationals without also controlling Union nationals. The
elimination of internal border controls would lose any useful effect unless it was applied
to everyone, regardless of nationality. The Convention implementing the Schengen
agreements nevertheless stipulates that a non-citizen of the Union must make a
declaration (article 22) 20b.
23. The right of residence for European nationals, known technically as ‘free movement of
workers’ and ‘establishment’ for self-employed workers, is based on articles 48 and 52 of
the Treaty of Rome. These articles enshrine three main principles: the rule of treatment
equal to that of a national, free access to the territory and the right of residence, as well as
the right to exercise a professional activity in any Member State. As free movement
constitutes a fundamental principle, secondary legislation can only promote this principle 21;
exceptions must be interpreted restrictively 22. The principle of free movement has been
extended to job seekers (article 48-3), students (Directive 93/96), graduates (Kraus case 23),
retired people (Directive 90/365) and the unemployed (article 7 of Directive 68/360).
Freedom of movement is, however, subject to certain limitations, including the
20 COM(93) 684. This draft contains, with some differences, a text signed in Brussels on 20 June 1991.20b The Amsterdam Treaty confirms the progressive implementation of an ‘area of freedom, security and justice’ (new
Title IV, article 61, consolidated EC Treaty) in which, among others, ‘the absence of any control on persons, bethey citizens of the Union or nationals of third countries, when crossing internal borders’ (article 62,1) isguaranteed. It is noted that the protocols annexed to the Treaty allow three countries to remain outside thiscommon space: the United Kingdom, Ireland and Denmark.
21 ECJ, 5 March 1991, Giagounidis, C-376/89, ECR, p. 1069; ECJ, 23 February 1994, Scholz, C-419/92, ECR, p. 505.22 ECJ, 13 July 1983, Forcheri, C-152/82, ECR, p. 2323; ECJ, 3 July 1986, Kempf, C-139/85, ECR, p. 1741; ECJ, 26
February 1991, Antonissen, C-292/89, ECR, p. 745.23 ECJ, 31 March 1993, Kraus, C-19/92, ECR, p. 1663.
34 The free movement of persons living with HIV/AIDS – Part 1: International and European law
reservation of public policy, public safety and public health (article 48-3). The right of
residence for third country nationals is based on the following elements: family reunion,
agreements between the Community and third countries, refugee status or favor of
residence as a worker. The last two fall under the responsibility of the Member States.
2. Public health24. What about public health within the Union? Article 3 (o) of the EC Treaty stipulates
that Community action must contribute to the attainment of a high level of health
protection. Article 129 (under Title X ‘Public Health’) stipulates that the Community
shall contribute towards ensuring a high level of human health protection by encouraging
cooperation between the Member States and, if necessary, lending support to their action.
The Community’s action is limited to coordinating national policies, the adoption of
encouraging measures by decisions from the Parliament or the Council, and the adoption
of recommendations by the Council. Harmonisation of Member States’ laws falls outside
the remit of the Council. Health protection policy has frequently been developed in line
with other Community policies (consumer protection, environmental protection, etc.),
but in the case of combating AIDS it is independent because the resolutions taken by the
Council only concern public health 24.
In one of its judgements which concerns the free movement of goods, but which could
be transposed to the free movement of persons, the Court deemed that restrictions on free
movement were only legitimate where they were necessary for safeguarding public health 25.
24 L. DUBOUIS, ‘L’Europe de la santé’, Ann. Dr., 1993, p. 163. article 129 E.C., amended by the Treaty ofAmsterdam (new article 152 of the consolidated version) make clear that the community action shallcomplement national policies.
25 ECJ, 20 February 1979, Rewe Zentral A.G., case 120/78, ECR, p. 6490. article 36 EC reads as follows:‘The provisions of articles 30 to 34 shall not preclude prohibitions or restrictions on imports, exports or goodsin transit justified on grounds of public morality, public policy, public security, the protection of health andlife of humans, animals or plants; the protection of national treasures possessing artistic, historic orarchaeological value; or the protection of industrial and commercial property. Such prohibitions orrestrictions shall not, however, constitute a means of arbitrary discrimination or a disguised restriction ontrade between Member States.’
The free movement of persons living with HIV/AIDS – Part 1: International and European law 35
25. Generally speaking, it can be stated that restrictions on freedom of movement in
the territory of the Union, which are based on AIDS and the protection of public health,
are possible for access to the territory of the Union, that is to say crossing external
borders, and impossible for travel within the Union, that is to say crossing internal
borders, and that they would be difficult to envisage for residence within the Union,
except for nationals of third countries which then involves the first hypothesis of access
to common territory.
B. Access (crossing external borders and short stays)1. Union citizens26. Union citizens are subject only to visual control on entry. This principle, stated in a
judgement from the Court on 27 April 1989 26, is found in article 5-1 of the draft
agreement on crossing external borders. This principle is already in force for the external
borders of the Schengen area (Benelux, France, Germany, Spain, Portugal, Italy, Austria,
Greece) by virtue of article 6 of the convention implementing the Schengen agreements.
2. Third country nationals27. A common European policy exists on visas (article 100 C of the EC Treaty). The
Council adopted a regulation setting out the third countries whose nationals should carry
a visa on entry to the Union 27. Furthermore, the Council has proposed a regulation
establishing a standard visa 28. However, each country remains responsible for deciding
the conditions for issuing visas. Article 100 C-5 is worded as follows: ‘This article shall be
without prejudice to the exercise of the responsibilities incumbent upon the Member
States with regard to the maintenance of public policy and the safeguarding of internal
security’. One might question whether the fact of being infected with HIV/AIDS could
justify refusal of a visa on grounds of public policy. If necessary, the question could be put
to the Court. The absence of any reference to public health, in addition to public policy
and internal security, could make it possible to maintain that AIDS cannot in itself
provide grounds for refusing to issue a visa.
26 ECJ, 27 April 1989, Commission v. Belgium, C-321/87, ECR, p. 997.27 Regulation 2317/95, OJ, L 234, p. 1; its contents were maintained in spite of its cancellation by ECJ, 10 June
1997, European Parliament v. Council, C-392/95, ECR, 1997, I-3213.28 Regulation 1683/95, OJ, L 164, p. 1.

36 The free movement of persons living with HIV/AIDS – Part 1: International and European law
28. The draft agreement on crossing external borders stipulates that external borders must
be crossed at transit points and that nationals of third countries are subject to a thorough
control. According to the draft (article 7), nationals of third countries can obtain
authorisation to enter for a short stay under certain conditions, including the absence of a
threat to ‘public policy’ and ‘national security’. As for the common visa policy, the
question arises of whether HIV/AIDS could be considered to be a threat to public policy
resulting in a refusal of entry. As the new draft stipulates that the Court is competent by
virtue of article K3 (last sub-paragraph) of the Treaty, it could be required to decide on
the content of the reservation on public policy. Another condition is not to appear on a
common list. The fact that a person is carrying HIV/AIDS would not, in principle, justify
inclusion in this list given the stipulation contained in article 6 of the Convention of the
Council of Europe for the Protection of Individuals with Regard to Automatic Processing of
Personal Data 29. Nationals of third countries may also be refused entry ‘under all
circumstances in which a national of a Member State of the European Communities
could be refused entry into a Member State in compliance with Directive 64/221’ (article
7 of the draft). Directive 64/221 contains provisions concerning entry into the territory
taken by Member States for reasons of law and order, public security and public health. In
the field of public health, the only diseases that may be used to justify refusal of entry are
those figuring in the attached list. This list does not expressly mention AIDS (see § 36,
infra). If a question were brought before it concerning the interpretation of the directive,
the Court would base its reply on jurisprudence developed on the subject of Community
nationals. However, the Court has never pronounced on the reservation of public health
with respect to AIDS or HIV-positivity. Conversely, there is a large body of case law
concerning public policy, which the Court has made restrictive in character 30.
29. In the Convention implementing the Schengen agreements, third country nationals
are subject to a thorough control at external borders including seeking out and
preventing threats to ‘national security’ and ‘public policy’ (article 6). Could HIV/AIDS,
if it were deemed to be a threat to public policy, result in refusal to allow crossing of an
external border? The concepts of ‘public policy’ and ‘national security’, as conditions for
29 See above, footnote 17.30 ECJ, 26 February 1975, Bonsignore, 67/74, ECR, p. 297; ECJ, 8 April 1976, Royer, 48/75, ECR, 1976, p. 497.

The free movement of persons living with HIV/AIDS – Part 1: International and European law 37
the right of residence for a period of less than three months, are found in article 5, which
nevertheless stipulates that even if the required conditions are not fulfilled, countries may
grant the right to entry on ‘humanitarian grounds’. Finally, on the subject of the
Schengen information system, article 94 stipulates that data listed in the first sentence of
article 6 of the Convention of the Council of Europe of 28 January 1981 for the Protection
of Individuals with Regard to Automatic Processing of Personal Data, are not authorised. The
existence of AIDS or HIV-positivity do not form part of the authorised data since the
Convention of 28 January 1981 expressly mentions in article 6 ‘personal data concerning
health or sexual activities’.
29b. The Treaty of Amsterdam introduces these questions in Community law in a new
Title 30b and by a Protocol integrating the Schengen acquis into the framework of the
European Union. This integration, however, contains two important limitations.
Quantitatively, it does not concern the United Kingdom, Ireland and Denmark.
Qualitatively, it ‘shall not affect the exercise of responsibilities incumbent upon Member
States with regard to the maintenance of law and order and the safeguarding of internal
security’ (article 64, consolidated version). Therefore, the ECJ would become competent,
but could not decide on any measure or decision relating to the maintenance of law and
order and the safeguarding of internal security. This leaves open the question of public
health, which is not precisely affected. It would therefore be possible that the ECJ declare
itself competent for interpretation of controls or tests at the internal borders for reasons of
public health (see also infra, § 32b).
C. Travel (crossing internal borders, the right to travel)1. Union citizens30. Article 7A of the EC Treaty provides for the creation on 1 January 1993 of a single
market comprised of an area without internal frontiers in which the free movement of
persons is ensured. The position of the Commission, contrary to that of the states, is to
interpret article 7A as an obligation to ensure results that eliminate all internal border
controls as from 1 January 1993 31. In 1995 the Commission proposed a directive on the
30b Title IV: Visas, asylum, immigration and other policies related to free movement of persons. This title implements anarea of freedom, security and justice.
31 Communication from the Commission to the Council and the Parliament on the ‘abolition of border controls’,Brussels, 8 May 1992, SEC (92)877.

38 The free movement of persons living with HIV/AIDS – Part 1: International and European law
elimination of controls on people at internal borders 32. For European citizens, article 7A
is today reinforced by article 8A, introduced by the Maastricht Treaty.
31. By virtue of article 2-1 of the Convention implementing the Schengen agreement,
internal borders may be crossed at any point without controls. Article 2-2 however
envisages the possibility of re-establishing controls if required for reasons of ‘public policy’
or ‘national security’. Could AIDS or HIV-positivity be used to justify the application of
article 2-2 if they were classified as threats to ‘public policy’? The absence of any mention
of an exception based on public health and the restrictive interpretation of the concept
of public policy by the Court lead us to reply negatively.
2. Third country nationals32. The Commission considers that ‘any interpretation of article 8A (now 7A) which
might lead to limiting the effects solely to Community nationals would deprive this
provision of any useful effect’ 33. It would not then be possible to eliminate internal border
controls for the sole benefit of Community nationals. Accordingly on 24 August 1995 the
Commission proposed a directive concerning the right of nationals from third countries
to travel within the Community 34. This draft directive invited Member States to grant
nationals of third countries the right to travel, that is to say to cross internal Union
borders and reside for a maximum of three months in another Union country provided
that they hold a residence permit for a Member State and adequate means of subsistence.
An exception is made where a national of a third country ‘constitutes a threat to the
public policy, public security or international relations of the country’. Once again, no
exception is made on grounds of public health.
The same reasoning is applied with regard to the convention implementing the
Schengen agreements, which nevertheless contains certain specific provisions. Article 22
of the convention stipulates an obligation of declaration, whilst articles 19 to 21, which
concern the movement of third country nationals, make this subordinate to fulfilment of
the condition in article 5 (e) – the absence of a threat to public policy and national
security. The question of whether people living with HIV/AIDS could have their
movements limited in the name of public policy must, for the reasons given, be answered
32 COM(95) 347 final. See also about travel, Directive 64/221, infra, paragraph 35 about residence.33 Communication from the Commission to the Council and the Parliament on the ‘abolition of border controls’, o.c.34 COM(95) 346 final, OJ, C 306, 17 November 1995, p. 5.

The free movement of persons living with HIV/AIDS – Part 1: International and European law 39
negatively. Whilst the criterion of nationality can no longer be used to justify internal
border controls that have been eliminated for everyone, the construction of a single
internal market characterised by freedom for everyone to travel cannot be called in
question by introducing AIDS as a new criterion to replace nationality.
32b. The Treaty of Amsterdam, ratifying the states’ positions, postpones the obligation to
reach the absence of all controls, for all persons, at the internal borders, to five years after
its coming into force. The quantitative (United Kingdom, Ireland, Denmark) and
qualitative (public policy, internal security) limits already mentioned are also applicable
to the suppression of controls at the internal borders (supra, § 29b).
The exact possibility of control by the Court in these matters is not clear. New article
68 par. 2 EC in the consolidated version, states that ‘the Court of Justice shall not have
jurisdiction to rule on any measure or decision … relating to the maintenance of law and
order and the safeguarding of internal security’ in the crossing of the internal borders. Some
Commission representatives argue that this limitation of the competence of the Court would
only concern general decisions taken by a Member State in order to reinstore controls at the
internal borders, and not particular decisions in individual cases of violation of public policy.
Even so, a general measure of controls at the internal borders justified by public policy to
fight against AIDS could escape the control of the Court of Justice unless one considers that
a question of public health, that is not expressly mentioned in the Treaty, could not be
included in the concept of public policy. In this interpretation, we believe that the Court of
Justice would be competent.
D. Residence1. Union citizens33. Residence for Union citizens within the Union recognized to each Union citizen by
article 8A EC introduced by the Treaty of Maastricht is governed by articles 48 (workers),
52 (establishment) and 59 (provision of services) of the Treaty and by secondary legislation,
in particular Directive 68/360 of 15 October 1968 on the abolition of restrictions on movement
and residence within the Community for workers of Member States and their families 35. Article 10
35 OJ, L 257, 19 October 1968, p. 3. See for establishment and provision of services, Directive 73/148, Council,21 May 1973, on the abolition of restrictions on movement and residence within the community for nationals ofMember States with regard to establishment and the provision of services, OJ, L 172, 28 June 1973, p. 14. Article 8 issimilar to article 10 in Directive 68/360. Adde infra, § 40.

40 The free movement of persons living with HIV/AIDS – Part 1: International and European law
of this directive stipulates that Member States shall not derogate from the principle of free
movement save on grounds of public policy, public safety and public health. The
reservation concerning public health may be used in the context of article 3 (entry) and
article 4 (first residence permit) of the directive, but not with regard to article 6 (renewal of
residence permit). It makes granting a residence permit subject to taking a medical
examination certifying that the person is not affected by the diseases figuring in the annexe
to Directive 64/221. This annexe does not expressly mention AIDS (see infra, § 36).
The right of residence does not only concern workers. It also extends to students,
retired people and any European citizen with adequate financial resources. Directive
93/96 on the right of residence of students 36 recognises the right of residence for any student
who is a national of a Member State and who does not enjoy that right under other
provisions of Community law, and for the student’s spouse and children. Directive 90/365
on the right of residence for employees and self-employed persons who have ceased their
professional activities 37 grants the right of residence to nationals of Member States who
have pursued an activity as an employee or self-employed person, and to members of their
families. This is the directive covering retired people. Finally, Directive 90/364 on the right
of residence 38, the so-called ‘residual’ directive, recognises the right of residence for
nationals of Member States who do not enjoy this right under other provisions of
Community law, and to members of their families.
34. Two aspects need to be highlighted in the three residence directives. The first aspect
concerns health insurance coverage as a condition for the right of residence. For HIV-
positive people and those infected with AIDS, such insurance should cover the cost of
care, which could be very high. In the case of students, the condition concerning health
insurance poses no problem provided that they are insured in their country of origin as
dependants of the insurance policyholder. However, the situation will be different if they
have subscribed, in the country of origin, to a special insurance scheme for students,
which does not always provide cover in the host country, in which case major payments
will have to be made in the form of premiums. For retired people, the condition of being
36 OJ, L 317, 18 December 1993, p. 59.37 OJ, L 180, 13 July 1990, p. 28.38 OJ, L 180, 13 July 1990, p. 26.

The free movement of persons living with HIV/AIDS – Part 1: International and European law 41
covered by health insurance should not raise problems because such people were formerly
workers covered by a social security system. Difficulties may nevertheless arise for the host
country if the person returns to his country of origin to receive care (in this case articles
29 et seq of Regulation 1408/71 of 14 June 1971 concerning the application of social security
systems to employees and self-employed persons travelling within the Community 39 apply).
Within the framework of the residual directive, the condition concerning health
insurance limits freedom of movement because it presumes subscription to a private
insurance scheme, since Regulation 1408/71 on social security does not apply to people
who are not working.
The second aspect of note in the three residence directives is the possibility of
derogation from the provisions on grounds of public policy, public security and public
health. In this case residence directives refer to Directive 64/221.
35. Directive 64/221 of 25 February 1964 on the coordination of special measures
concerning the movement and residence of foreign nationals which are justified on
grounds of public policy, public security or public health 40 is aimed at nationals of a
Community Member State who reside or go to another Community Member State either
with a view to pursuing an activity as an employed or self-employed person, or as a
recipient of services. The directive also applies to spouses and members of the family
(article 1). The field of application of the directive has been extended to workers and
members of their families who remain on the territory of a Member State after having
held a job (Directive 72/194 of 18 May 1972 41) and to persons who remain on the
territory of a Member State after having exercised an activity as a self-employed person
(Directive 75/35 of 17 December 1974 42). The reference made to this by the three 1990
residence directives extends the field of application to all European nationals who reside
on the territory of another Union country.
Directive 64/221 relates to measures concerning entry into their territory, the issue
or renewal of residence permits, or expulsion from their territory, taken by Member States
on grounds of public policy, public security or public health (article 2).
39 OJ, L 149, 5 July 1971.40 OJ, L 56, 4 April 1964, p. 850.41 OJ J, L 121, 26 May 1972.42 OJ, L 14, 20 January 1975.
42 The free movement of persons living with HIV/AIDS – Part 1: International and European law
36. Article 4 of the directive states that the only diseases justifying refusal of entry or
refusal to issue a first residence permit are those listed in the Annexe to the directive.
This list does not include either AIDS or HIV-positivity but rather ‘other infectious
diseases or contagious parasites diseases if they are the subject of provisions for the
protections of nationals of the host country’ 43. Do AIDS and HIV-positivity fall into the
concept of ‘other infectious diseases or contagious parasitic diseases’? Certain authors are
against this idea. They invoke the fact that AIDS and the HIV virus are transmitted only
in very particular circumstances, and that the reservation of public health should be
interpreted restrictively 44. Others are of the opinion, to the contrary, that the expression
‘other infectious diseases or contagious parasitic diseases’ includes any contagious disease
not yet listed in the annexe. They base their arguments on the directive’s preamble which
states that it would be difficult to compile an exhaustive list and therefore, as a result, it is
sufficient to classify those diseases which could endanger public health into groups 45.
43 Annexe to Directive 64/221:A. Diseases which might endanger public health:
1. diseases subject to quarantine listed in International Health Regulation no. 2 of the World HealthOrganization of 25 May 1951;2. tuberculosis of the respiratory system in an active stage or showing a tendency to develop;3. syphilis;4. other infectious diseases or contagious parasitic diseases if they are the subject of provisions for theprotection of nationals of the host country.
B. Diseases and disabilities which might threaten public policy or public security:1. drug addiction;2. profound mental disturbance, manifest conditions of psychotic disturbance with agitation, delirium,hallucinations or confusion.
44 M. DISPERSYN, ‘Les personnes séropositives ou atteintes du sida et la libre circulation dans la Communauté’,in Le sida, un défi au droit: actes, Brussels, Bruylant, 1991; D. MARTIN and E. GUILD, Free Movement ofPersons in the European Union, London, Butterworths, 1996, p. 110: ‘When read together paragraphs 1 and 3make it clear that the fact of being infected with HIV virus cannot justify recourse by a Member State to thepublic health proviso of article 48(3)’.This idea is found in Resolution 255 (1994) ‘on local and regional authorities faced with AIDS and HIV-positivity’ of the Permanent Conference of Local and Regional Authorities of Europe, which observes that ‘AIDSis a disease which, generally, is transmitted by voluntary risk behaviour. The infection is not transferable in dailylife (...). The conventional public health measures are difficult to apply.’ (item 1). See also the explanatorymemorandum of Recommendation 94 (14) of the Council of Europe according to which ‘the reasoning whichjustifies restrictions on free movement, quarantine, and isolation is not applicable in the case of HIV infection, inthe absence of contagion in daily life, due to the long latency period and in the absence of curative treatment’(item 173).
45 J. VAN OVERBEEK, ‘AIDS/HIV infraction and the free movement of persons within the European EconomicCommunity’, Com.M.L.R. 1990, p. 91.
The free movement of persons living with HIV/AIDS – Part 1: International and European law 43
37. What is true is that the constant case law of the European Court of Justice has
established that the free movement of persons is a general and directly applicable
principle, which should be interpreted extensively, with any limitation to this principle
being necessarily interpreted in a restrictive manner 46. However, it appears difficult for us
to maintain that HIV/AIDS could not be included under the infectious or contagious
parasitic diseases referred to in item 4 of letter A of the Annexe, which was published at a
time (1964), where this disease was not yet known.
The fact remains that, in this case, if one upholds that AIDS is to be included in the
field of application of Directive 65/221, two conditions still need to be fulfilled for
limitations on residence founded on AIDS be in conformity with Community law.
38. First of all, based on the Annexe, it is necessary to prove the existence, in the state
invoking the public health reserve, of provisions to protect nationals.
39. Secondly, Article 4 of the directive includes a stand still clause which prevents
Member States from introducing ‘new provisions or practices which are more restrictive
than those in force at the date of notification of this Directive’.
The fact is that AIDS appeared only after this date. Three options are possible,
supposing that AIDS is targeted by the directive. The first option is to affirm that any
measure is more restrictive, as none existed at the date of notification of the directive,
and that consequently, AIDS cannot be the subject of any control 47. The second option
considers, on the contrary, that no measure is more restrictive, as no measure existed at
the date of the directive and, in consequence, AIDS can be controlled by every means.
Finally, a third option consists of accepting that, since this is a new disease, new measures
are possible, but that these may not be more restrictive than those which apply to the
other diseases mentioned in the Annexe. In other terms, the more restrictive measures
which are not permitted are those which were not applied previously, and which are
unjustified, discriminatory or disproportionate. This could be the case for systematic HIV
screening when crossing frontiers. We support this latter thesis, which falls under the
application of the principle of proportionality.
46 J.Y. CARLIER, ‘La circulation des personnes dans l’Union européenne’, J.T.D.E., 1995, p. 99; ECJ, 13 July 1983,Forcheri, C-152/82, ECR, p. 2327, point 11; ECJ, 3 July 1986, Kempf, C-139/85, ECR, p. 1741, point 13; ECJ, 26Feburary 1991, Antonissen, C-292/89, ECR, p. 745.
47 This is the implicit option of D. MARTIN and E. GUILD, o.c., note 44.
44 The free movement of persons living with HIV/AIDS – Part 1: International and European law
40. With regard to the right of establishment and provision of services, Directive 73/148
on the abolition of restrictions on movement and residence within the Community for nationals of
Member States with regard to establishment and the provision of services 48 makes provision for
Member States to abolish restrictions on movement and residence for nationals of
Member States who are established or wish to establish themselves in another Member
State in order to pursue activities as self-employed persons, or who wish to provide
services in that state, for nationals of Member States wishing to go to another Member
State as recipients of services, and these nationals’ family members. The Member States
may derogate from the provisions of this directive solely on grounds of public policy,
public security or public health. With regard to the public health reservation, reference
should be made to the list annexed to Directive 64/221 (see supra, § 36). Indeed, Article
10 of Directive 73/148 states that the Directive of 25 February 1964 on the abolition of
restrictions on movements and residence within the Community for nationals of Member
States with regard to establishment and the provision of services shall remain applicable
until Directive 73/148 is implemented by the Member States. However, with respect to
the above-quoted Directive of 25 February 1964, the Economic and Social Committee
has stated that, in the area of public health, reference should be made to the list annexed
to Directive 64/221 49.
41. For the principle of free movement of persons to be effectively secured to the benefit
of workers, Regulation 1408/71 makes provision for the preserving of social security
rights. This regulation contains provisions which could eventually apply to people
suffering from AIDS and to HIV virus carriers. In particular, we should look at articles 22
and 35-3 included in Chapter I entitled ‘Sickness and maternity’ of Title III of the
regulation.
Article 22 covers the following possibilities: stay outside the competent state –
return to or transfer of residence to another Member State during sickness, and the need
to go to another Member State in order to receive appropriate treatment. The regulation
provides for the right to benefits in kind provided on behalf of the competent institution
by the institution in the place of stay or residence in accordance with the legislation
which it administers, the length of the period during which benefits are provided being
48 OJ, L 172, 28 June 1973, p. 14.49 OJ, 4 April 1964, p. 850/64.

The free movement of persons living with HIV/AIDS – Part 1: International and European law 45
governed, however, by the legislation of the competent state. The regulation also makes
provision for the right to cash benefits provided by the competent institution in
accordance with the legislation which it administers. These benefits may be provided by
the institution of the place of stay or residence on behalf of the competent institution, in
accordance with the legislation of the competent state.
Article 35-3 of the regulation provides in turn that where, under the legislation of a
Member State, the granting of benefits is conditional upon the origin of the illness, that
condition shall apply neither to workers nor to the members of their families.
2. Third country nationals42. The secondary legislation as analysed above with regard to the right of residence of
Community nationals may also present an interest for third country nationals, in
particular those from developing countries. On the one hand, these provisions extend to
the families of Member State nationals, even when the family members (spouse, parents,
children) do not have the nationality of a Member State. A couple consisting of a
Belgian male and Rwandan female, or an English female and a Pakistani male will, for
example, be directly involved. On the other hand, the general principles in favour of
European citizens, including the principle of free movement and the interpretation of the
limits of public policy or public health, will guide the interpretation of the same concepts
when applied to access to the territory by third country nationals.
Third country nationals’ right of residence may result from family reunification
agreements concluded between the Community and third countries, or, for other
foreigners, from the privilege of residence as a worker.
43. With respect to family reunification, we need to distinguish between two categories.
The first category consists of family members (spouse, parent, dependent children and
children under the age of 21) of European citizens, who are assimilated as Union citizens 50.
For the delivery of a residence permit and access to the territory, a visa may first be
required, but Member States are required to grant ‘all facilities for obtaining visas’ 51. Both
these texts and jurisprudence show that no other condition, for example relating to
50 Regulation 1612/68 of 15 October 1968 concerning the free movement of workers within the Community.51 Directive 68/360 of 15 October 1968 concerning the abolition of restrictions on movement and residence within the
Community of workers from Member States and their families, article 3, paragraphs 2 and 3.

public health, or a fortiori attached to AIDS, can limit the right of access to the territory
of the Union for family members of a Union citizen 52. The same applies for the family
of a national, in those cases when national legislation assimilates this family to that
of a European 53.
The second category consists of the family members of third country nationals who
are regularly resident in the territory of a Union Member State. In principle, it is national
law which determines the conditions of residence attached to the family reunification of
such persons.
44. However, insofar as all Union Member States have this type of family reunification, it
has appeared useful to strive towards a certain harmonisation of legislation, within the
framework of inter-governmental cooperation. It is with this intention that ministers
responsible for immigration adopted, at the Copenhagen summit on 1 June 1993, a
resolution concerning the harmonisation of national policies on the subject of family
reunification. This resolution relates to third country nationals who are regularly resident
in the territory of a Member State, on a basis offering them the prospect of permanent or
long-term residence. Member States reserve the right to make entry and residence of
family members subject to their having health insurance coverage. For persons who are
HIV-positive or who have AIDS, this insurance needs to cover the cost of treatment,
which can require heavy contributions. Moreover, in this resolution, states reserve the
right to refuse entry and residence for public health reasons. This reservation ought to be
subject to identical interpretation to that of Directive 64/221, permitting a restriction
linked to AIDS only if this is based on a measure which is no more restrictive than that
previously existing for other sicknesses, and if the means used is proportionate to the
objective pursued, which, as we have seen, appears difficult.
45. With regard to agreements concluded between the Community and third countries,
certain provisions of the association agreements with Turkey, of the cooperation
agreements with the North African countries, and the Lomé agreements can concern the
free movement of persons living with HIV/AIDS.
46 The free movement of persons living with HIV/AIDS – Part 1: International and European law
52 ECJ, 31 May 1991, Communities v. Netherlands, C-68/89, ECR, 2637.53 Belgian law of 15 December 1980 concerning access to the territory, residence, establishment and the expulsion of
foreigners, article 40, paragraph 6; ECJ, 18 October 1990, Dzodzi, C-297/88 and 197/89, ECR, 3763.

46. Article 39 of the supplementary protocol to the EEC-Turkey association agreement of
20 November 1970 54 makes provision for aggregating insurance periods for, in particular,
health care for workers and their families. Moreover, article 6-2 of decision no. 1/80 of
the EEC – Turkey Association Council of 1 September 1980 55 states that absences for
reasons of long-term sickness do not affects rights acquired by virtue of the previous
period of employment, whilst article 14 states that the provisions of the decision are
applied subject to limitations justified by reasons of public policy, public security and
public health. Would Turkish workers benefit, with respect to this provision, from an
interpretation by analogy with Directive 64/221 and the Court’s interpretation with
regard to reservations of public policy and public health? Yes, if we consider that the
principle of non-discrimination ‘with regard to conditions of work and pay’ should be
extended to the right of residence linked to periods of employment. This is not certain 56.
47. The cooperation agreements concluded with Morocco, Algeria and Tunisia 57 make
provision for a system based on absence of discrimination in the field of social security as
well as the aggregation of periods of insurance when it comes to medical care.
48. With regard to the Lomé agreements signed between the EEC and the ACP
countries 58, article 5 provides that ‘the Member States of the Community (and/or where
appropriate, the Community itself) and the ACP States will continue to ensure, through
the legal or administrative measures which they have or will have adopted, that migrant
workers, students and other foreign nationals legally within their territory are not subject
to discrimination on the basis of racial, religious, cultural or social differences, notably in
respect of housing, education, health care, other social services and employment’. By
virtue of this provision, the principle of non-discrimination could be invoked by ACP or
Community nationals suffering from AIDS or who are carriers of the virus. However,
The free movement of persons living with HIV/AIDS – Part 1: International and European law 47
54 OJ, L 293/3/1972.55 OJ, C 110/6, 25 April 1983.56 Article 37 of the Supplementary Protocol, OJ, L 293, 29 December 1972, and article 6 of Decision no. 1/80 of the
Association Council.57 OJ, L 263, 264 and 265, 27 September 1978.58 Fourth Convention of 15 December 1989, OJ, 1991, L 229, p. 3.

Article 5 provides only limited protection as it covers only persons already legally inside
the territory of a contracting state. This article therefore does not cover access to the
territory of the Union, and can, with difficulty, cover movement or residence within the
Union in so far as are targeted ‘housing, education, health care, other social services and
employment’, preceded, it is true by the adverb ‘notably’. Moreover, article 5 has no
direct effect, given that it is couched in very general terms and is placed within the text
of the Agreement in Chapter I, ‘Objectives and principles of cooperation’, within the first
part of the Convention, entitled ‘General provisions of ACP-EEC cooperation’.
As a result, ACP nationals who benefit from the right of movement within the
Union, once they are regularly resident there, given the removal of internal frontiers
control of all people, remain subject to national legislation, within the limits set out
above, with regard to access to and residence in the Union.
49. Other foreigners who do not fall into a privileged category due to family reunification
or special agreements, are therefore dependent, when it comes to any rights of residence,
on the national legislation concerned. In general this legislation makes the right of
residence a privilege which each state may grant, subject to such conditions as it
considers appropriate.
48 The free movement of persons living with HIV/AIDS – Part 1: International and European law
IV First conclusions (international and European law)50. The Community institutions have, on several occasions, come out in favour of
safeguarding the free movement within the Union of people suffering from AIDS or carrying
the virus. In their conclusions of 15 May 1987 59 and of 31 May 1988 60, the Council and the
representatives of Member State governments condemned the systematic screening and
contradictory national policies with respect of third countries. Systematic screening was also
advised against in the resolution of the Council of Health Ministers of 22 December 1989 61.
The same principles were expressed in a European parliamentary resolution of 30 March
1989 62 which asks Member States to abolish tests at borders, and to stop expelling third
country nationals for reasons linked to HIV/AIDS. In this way, the Commission has
manifested its attachment to the principle of the free movement of persons 63.
Parallel with this, the European Community has constantly given absolute priority to
prevention through information and education, and particularly that aimed at target
groups, including migrants.
51. However, all these texts constitute declarations of intent, which are without binding
force, and which individuals cannot invoke before the Court, even if, as the case may be,
the Court could decide to interpret them based on Article 177 of the Treaty 64. Moreover,
Directive 64/221 on the coordination of special measures concerning the movement and
residence of foreign nationals which are justified on grounds of public policy, public
security or public health, does not contain any explicit reference to AIDS. As a result,
several options are theoretically possible.
The free movement of persons living with HIV/AIDS – Part 1: International and European law 49
59 OJ, C 178, 7 July 1987, p. 1.60 OJ, C 197, 27 July 1988, p. 8.61 OJ, C 10, 16 January 1990, p. 3.62 OJ, C 158, 26 June 1989, p. 477.63 COM(87) 63 final, 11 February 1987, p. 2, COM(88) 268 Final, 17 May 1988, p. 2. See all those texts in
Annexe I, 3, p. 224.64 J. VAN OVERBEEK, o.c., p. 191.
52. First of all, one could conclude that since controls are not forbidden by any binding act,
they are permitted, and that, on the other hand, there is no obstacle in Directive 64/221
preventing states from taking restrictive measures with regard to the free movement of
persons living with HIV/AIDS 65. However, this interpretation can pose a problem, as it is
not certain that AIDS counts among the ‘other infectious diseases or contagious parasitic
diseases’ targeted by Directive 64/221. And even if this is the case, two difficulties arise: first
of all, for this interpretation to be valid, provisions to protect nationals have to exist in the
state invoking the public health reservation. Finally, Article 4 of Directive 64/221 forbids
Member States from taking measures which are more restrictive than those in effect at the
date of notification of the directive (supra, §§ 36 to 39).
53. Secondly, one could propose adopting a directive forbidding obligatory screening at
frontiers. This would get round the difficulty linked to the absence of a binding text.
Certain authors have suggested a directive to ensure the free movement of homosexuals
who are HIV-positive or have AIDS 66, but the directive could be general and cover all
people affected by AIDS or carrying the virus. However, if this directive were to be based
on Article 100 of the Treaty, this would require a unanimous vote in the Council. Apart
from this obstacle, this solution would not put an end to indirect discrimination, for
example towards people considered as belonging to risk groups 67.
54. Thirdly, one could envisage modifying the annexe to Directive 64/221, either to
introduce AIDS, or, on the contrary, to prevent initiatives aimed at including AIDS in
the list of diseases in the annexe 68.
55. Fourthly, it could be argued that any infringement of the freedom of movement of
persons which is not explicitly authorized by the texts is contrary to Community law. This
position is based on the constant affirmation of case law according to which the free
movement of persons is the rule, and should be broadly interpreted, whereas any limitation
50 The free movement of persons living with HIV/AIDS – Part 1: International and European law
65 J. VAN OVERBEEK, o.c.66 F. SNYDER, ‘Subsidiarity: an aspect of European Community Law and its relevance to lesbians and gay men’,
in Homosexuality, a European issue, edited by Kees Waaldijk and Andrew Clapham, Doordrecht, MartinusNijhoff Publishers, 1993, p. 235.
67 J. VAN OVERBEEK, o.c.68 M. DISPERSYN, o.c.

of free movement is the exception and should be interpreted in a restrictive fashion. From
this viewpoint one should emphasize the fact that Directive 64/221 does not carry any
explicit reference to AIDS and that it forbids states from taking more restrictive measures
than those in effect at the time of notification of the directive (which can be interpreted as
meaning that states cannot adopt measures which were not applied previously and which
are unjustified, discriminatory and disproportionate). The fact remains that, within the
meaning of European law, free movement refers to residence within the territory of Europe,
not to access to this territory by the crossing of external borders, in particular for nationals
from developing countries. However, the free movement of persons, as a general and
broadly interpreted principle, appears to have necessarily to extend progressively to access
to the common territory, in so far as exceptions to the freedom of movement must be
proportional to the objective pursued. In this way, the successive acts adopted by the
Community institutions, even though not binding, testify to the desire of the Community
to secure the principle of free movement for people suffering from AIDS or carrying the
virus. When it comes more specifically to the texts adopted by Member States’
representatives within the Council, it would be contradictory for states to take action at
national level against the disease without respecting the principles to which they have
subscribed 69. In a decision relating to AIDS screening tests for officials, the Court of Justice
considers that ‘the right of respect of private life, enshrined in Article 8 of the European
Convention on Human Rights, and which derives from the constitutional traditions shared
by Member States, constitutes one of the fundamental rights protected by the Community
legal order’ and that ‘it includes in particular a person’s right to keep his state of health
secret’. The Court acknowledges that restrictions can be applied to fundamental rights, but
‘provided that they in fact correspond to objectives of general interest and do not
constitute, with regard to the objectives pursued, a disproportionate and intolerable
interference which infringes upon the very substance of the right protected’ 70. The fact is
that obligatory screening at borders could well constitute a ‘disproportionate interference’,
with regard to the objective of general interest being pursued.
The free movement of persons living with HIV/AIDS – Part 1: International and European law 51
69 P. KLEIN, ‘Les organisations internationales face au sida’, Rev. belge dr. int., 1990, p. 153.70 ECJ, 5 October 1994, X. v. Commission of the E.C., C-404/92P, ECR, 1994, I-4737.
56. By way of conclusion, by combining international or regional texts protecting
fundamental rights with the provisions relating to the movement of persons specific to
European law, we can outline, at least within the Community legal order, the following
principles:
1. It is absolutely contrary to international law to practice or demand an HIV/AIDS
test for persons crossing a border of any kind, without provision being made for this
practice in a published legislative text, setting out the legitimate objective which is
being pursued. No HIV/AIDS control without text.
2. Even where a text does exist, HIV/AIDS tests are:
a) out of the question for crossing internal borders within the Union, for everyone
(right to travel);
b) quasi-out of the question for the passing of external borders and for residence in
another Union country for citizens of the Union and certain privileged foreign
nationals (Directive 64/221 and proportionality principle);
c) difficult for the crossing of external borders for non-privileged foreign nationals,
in particular those coming from developing countries (proportionality in the
principle of non-discrimination).
52 The free movement of persons living with HIV/AIDS – Part 1: International and European law
European UnionMember States
Part 2

54 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
I PresentationA. Description57. The second part is divided into two sections.
The first section takes an across-the-board approach, examining the legislation of the
fifteen European Union Member States on the free movement of people living with
HIV/AIDS (II). This general examination of national legislation is sub-divided into three
parts, concerning (A) the entry, (B) the residence and (C) the expulsion of people
travelling to Europe who are living with HIV/AIDS. Two further sub-divisions examine
(D) the first ruling of the European Court of Human Rights on the expulsion of a
foreigner living with HIV/AIDS and (E) the principle of proportionality.
The second section gives the conclusions of this across-the-board approach (III).
The third section successively examines the laws, regulations, and where possible, the
practices of the fifteen European Union States with relation to the movement of
foreigners living with HIV/AIDS (IV). Mention of the countries is made by their official
initials and their study made in alphabetical order of the initials. This section of the study
is based mainly on an analysis of legislative and regulatory texts adopted by Member
States on the subject of immigration. This main source was supplemented by an analysis
of case law and doctrine relating to the issue of the free movement of people living with
HIV/AIDS, as well as practical information obtained from governmental and non-
governmental organisations 70b.
58. Thirty questionnaires were sent to the fifteen Union Member States. In each state the
questionnaire was sent to a governmental organisation (ministry) as well as to a non-
governmental organisation (association). Nineteen questionnaires were answered by the
following organisations:
■ Austria: Ministry of the Interior, Ministry of Labour, Health and Social Affairs and
AIDS-Hilfe Wien
■ Belgium: Foreigner’s Office and the Foreigners’ Social Service (Service social des
étrangers)
70b The initials can be found in the List of abbreviations at the beginning of the book. The legal texts are inAnnexe II, 1, at the end of the book.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 55
■ Denmark: E. Brinch Jorgensen
■ Finland: Ministry of Social Affairs and Health (Ombudsman for Foreigners) and the
Ministry of the Interior
■ Germany: Ministry of the Interior
■ Ireland: Irish Refugee Council
■ Italy: F. Trucillo (lawyer)
■ Luxembourg: Ministry of Health and the SESOPI – Inter-Community Centre
(SESOPI – Centre intercommunautaire)
■ Netherlands: Ministry of Justice and the Dutch HIV Association (HIV Vereniging
Nederland)
■ Spain: Ministry of Health and Consumer Affairs and the Spanish Commission for
Aid to Refugees (Comisión Española de Ayuda al Refugiado)
■ Sweden: National Immigration Board and the Noah’s Ark Red Cross Foundation
■ United Kingdom: Terence Higgins Trust and the Immigration and Nationality
Directorate.
B. Main conclusions from Part II59. The main restrictions observed in the countries of the European Union on the free
movement of people living with HIV/AIDS primarily relate to nationals from countries
other than the fifteen Union Member States, and sometimes to specific categories of third
country nationals such as students. This especially concerns nationals of developing
countries. Such restrictions usually relate to long-term residence. They can stem from legal
provisions stipulating the submission of a medical certificate for entitlement to a residence
permit and even from specific provisions excluding the right of residence for people living
with HIV/AIDS. In some cases these restrictions have no specific legal basis at all.
An examination of national legislation and practices in the various Union countries
reveals variations, mainly with respect to third country nationals. This would appear to
indicate a lack of harmonisation among European Union Member States in policies
regarding nationals from non-Union countries living with HIV/AIDS. Although this
issue chiefly concerns European Union health and immigration policies, it is also at the
heart of relations between the Union and developing countries.
From a human rights standpoint it is apparent that restricting the free movement of
people living with HIV/AIDS is an a priori disproportionate means for controlling this

56 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
pandemic. A European Court of Human Rights decision of 2 May 1997 ruled that the
expulsion by the United Kingdom of a foreigner in the terminal stages of AIDS, was
inhumane and degrading treatment which contravened article 3 of the European
Convention on Human Rights (infra, §§ 76 et seq.).
60. It is possible to classify European Union Member States into three main groups with
regard to entry to the territory and residence of third country nationals, particularly
developing countries, relating to HIV/AIDS.
The first group (five states: B, D, FIN, NL, P) does not expressly provide for public
health controls.
The second group (six states: DK, E, GR, I, IRL, UK) provides for public health
controls without expressly mentioning HIV/AIDS. In practice, some countries do not
practice HIV/AIDS testing whilst others practise ‘voluntary’ testing which may or may
not be followed by measures to refuse entry or residence.
The third group (four states: A, F, L, S) expressly excludes HIV/AIDS testing,
sometimes in legislation specifically concerning entry to and residence in the territory (L)
and sometimes in general legislation (law or decree: A and S), or limits the possibility of
controls (F: limited to ‘clinical signs’).
In the long-term, Member State obligations could evolve from a negative obligation
not to implement measures hindering the free movement of people living with
HIV/AIDS (standstill), towards a positive obligation expressly excluding HIV/AIDS
controls governing entry to the country and residence, following the example of
Luxembourg.
This raises the question of whether or not positive action is needed since, although it
protects a particular group (in this case people living with HIV/AIDS), it also stigmatises
this group in the eyes of the general public (infra, § 561).
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 57
II General examination of legislation in European Union Member StatesA. Entry1. Union citizens61. The legislation of several states stipulates that Union citizens may be refused entry on
public health grounds. Such legislation reproduces the list of diseases enumerated in
Directive 64/221 71 (B 72, IRL 73, NL 74, P 75) or part of this list (E 76, F 77). French legislation
only mentions drug addiction and blatant psychological or mental disorders, clear states of
excitative type psychosis, paranoid psychosis or hallucinations or mental confusion, which
excludes HIV/AIDS. Spanish legislation, like French legislation, only partially reproduces
the list of diseases annexed to Directive 64/221, but the illnesses included are those listed
in the International Health Regulations, drugs and other infectious diseases or contagious
parasitic diseases, if they are the subject of measures to protect Spanish nationals.
It should be noted that Member States which do not transpose the entire list annexed
to the directive are not infringing Community law. Since public health is an exception to
the principle of free movement, its interpretation is restrictive. The diseases mentioned in
the annexe to the directive are ‘the only ones … justifying refusal of entry into a territory’
(article 4). Consequently only states where legislation adds to the diseases on the list
would be infringing Community law, which is not the case for any Member State.
2. Third country nationals62. The legislation of several states does not expressly provide for refusal of entry to third
country nationals on public health grounds (B, D, FIN, NL, P, S).
71 See §§ 35 et seq. above for an analysis of the directive. 72 Article 43 of the law of 15 December 1980.
National legislation is referenced by the date of the basic legislation. Account has been taken of updates tosuch legislation (see Annexe II, 1, Member States, p. 230).
73 Article 4 of the European Communities (Aliens) Regulations of 1977.74 Article 91 of the decree of 19 September 1966.75 Article 12 of the statutory order of 3 March 1993.76 Article 15 of the decree of 26 June 1992.77 Article 6 of the decree 94/211 of 11 March 1994.

58 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
By contrast, several countries have legislation which instigates medical controls for
people entering the territory (DK 78, E 79, F 80, GR 81, I 82, IRL 83, L 84, UK 85). Luxembourg
legislation expressly excludes medical controls for HIV/AIDS 86.
Some states refuse to carry out systematic AIDS testing at borders, either by virtue of
a normative act (A 87), or of a general policy (e.g. DK, I, NL, S).
B. Residence1. Union citizens63. In some countries, national legislation provides for Union citizens to be refused
residence on public health grounds. Such legislation reproduces the list of diseases
figuring in the annexe to Directive 64/221 (B 88, IRL 89, NL 90, P 91) or part of this list (E 92,
F 93). The analysis of this national legislation is the same as for Directive 64/221 94.
2. Third country nationals2.1. Residence permits
64. Some Union Member States have adopted rules which allow for residence to be
refused on public health grounds and call for a compulsory medical certificate before a
residence permit can be granted (E 95, I 96, GR 97, L 98, P 99).
78 Article 28 of Act no. 894 of 27 October 1994.79 Article 11 of the law of 1 July 1985.80 Article 4 of the order of 7 November 1994.81 Article 6 of law 1975/91.82 Article 3 of the law of 28 February 1990.83 Article 3 of the 1975 Aliens Order.84 Article 2 of the law of 28 March 1972.85 Annexe 2, section 4, part I.2 of the 1971 Immigration Act.86 Article 5 of the Regulation of 17 October 1995.87 Decree of 25 February 1987.88 Article 43 of the law of 15 December 1980.89 Article 12 of the European Communities (Aliens) Regulations of 1977.90 Article 97 of the decree of 19 September 1966.91 Article 12 of the statutory order of 3 March 1993.92 Article 15 of the decree of 26 June 1992.93 Article 6 of decree 94/211 of 11 March 1994.94 See §§ 35 et seq above.95 Article 56 of the implementing Regulation of 23 February 1996.96 Article 4-12 of the law of 28 February 1990.97 Article 12 of law 1975/91.98 Article 2 of the law of 28 March 1972.99 Article 4 of the decree of 15 December 1993.

The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 59
In other states or regional sub-divisions of states, texts stipulate that an HIV test
has to be carried out and that residence should be refused to persons living with
HIV/AIDS (Bavaria 100). The European Commission has reacted against measures such
as these 101.
By contrast, some states have adopted regulations prohibiting refusal of the right of
residence on the grounds of being HIV positive, in the absence of clinical signs (F 102).
Nonetheless, an a contrario interpretation of French legislation indicates that the
presence of clinical signs can justify refusal of the right of residence. This raises the issue
of defining the concept of ‘clinical signs’ 103.
65. This being a public health issue, several countries make no distinction in their
legislation between access to the territory which includes both a short stay of under three
months and long-term residence. However, the above observations mainly concern long-
term stays. This is because the measures taken by certain states are motivated by
economic concerns. Indeed, high treatment costs for sufferers may make Member States
reluctant to defray the possible medical costs of persons living with HIV/AIDS in cases
where such persons do not have adequate financial resources. This concern emerged in
the replies to our questionnaires by various governmental organisations (infra III, ex. § 187).
It should be noted that article 2, paragraph 2 of Directive 64/221 on the coordination
of special measures concerning the movement and residence of foreign nationals which are
justified on the grounds of public policy, public security or public health stipulates that ‘such
grounds shall not be invoked to economic ends’. Even though the directive concerns only
Union citizens, it may, with regard to the principles of proportionality and non-
discrimination, be used to guide the interpretation of the same grounds given to justify
measures relating to third country nationals.
66. In some states it is possible for foreigners living with HIV/AIDS to be granted the
right of residence on humanitarian grounds. This is the practice in the United Kingdom
and the Netherlands in cases where the person has already been living in the country for
100 Notice no. 1A2-2081.10 of 19 May 1987 (Bekanntmachung des Bayerischen Staatsministeriums des Inneren).101 Le Courrier ACP-CEE, September-October 1987, no. 105, p. XII.102 Circular of 8 December 1987.103 P. VAN OVERBEEK, ‘AIDS/HIV infection and the free movement of persons within the European
Community’, Com.M.L.R., 1990, 91.
60 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
a certain time. It is also the case in Denmark, by virtue of paragraph 9.3 of the Aliens’
Act, where the foreigner has not been granted refugee status. In France, a foreigner
suffering from AIDS may, at the discretion of the authorities, be granted refugee status. In
France, a foreigner suffering from AIDS may, at the discretion of the authorities, be
granted (Autorisation provisoire de séjour – APS).
2.2. Work permits
67. In the legislation of some Member States, information regarding health (FIN 104) or a
medical certificate (B 105, P 106) may be required when a work permit is requested. In some
national legislation it is stipulated that authorisation to enter the country for work
reasons may be revoked on public health grounds (GR 107).
In some states the HIV test is compulsory for certain foreigners requesting a work
permit (GR 108).
2.3. Studies
68. Some Union Member States make a residence permit for studies conditional on the
applicant scholarship-holder not having the HIV virus or AIDS (B 109, GR) although it is
not necessarily possible to find a legal basis for the measure.
When testing is offered to – rather than imposed on – foreign students, this raises the
issue of whether testing is indeed practised systematically and whether foreign students
are really aware of their right to refuse it.
69. Again the measures adopted with regard to students reflect economic concerns
relating to the risk of bearing the financial cost of medical treatment. Furthermore, the
legislation of several countries stipulates that students must be covered by health
insurance. This condition corresponds to the condition contained in Directive 93/96 on
the right of residence for Community students 110.
104 Article 28 of the law of 22 February 1991.105 Article 2 of the Royal Decree of 6 November 1967 and article 6 of the Royal Decree of 2 August 1985.106 Article 4 of the decree of 15 December 1993.107 Article 22 of law 1975/91.108 P. CATTORINI, D. MORELLI and M. ZANCHETTI, AIDS: Comparison and analysis of European Legislation
on AIDS from an ethical and legal standpoint, Istituto Scientifico H. San Raffaele, Milan, 1996.109 In Belgium the initially compulsory test is now offered to students on their arrival.110 See § 33 above.

The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 61
70. In the Council resolution of 30 November 1994 on the admission of third-country nationals
to the territory of Member States for study purposes 111, the Council considers that Member
States should facilitate the admission and residence of third country nationals who have
come to study in Europe. Conversely, the measures taken by Member States to impose HIV
testing restrict the right of residence for students who are third country nationals. However,
the Council resolution is not binding and, moreover, it expressly stipulates that application
of the principles it contains should not override national provisions for protecting public
order, public security and public health. Nevertheless, such restrictions should be subject to
restrictive interpretation and ought to be exceptions to the rule.
2.4. Right of asylum
71. In general, the test is carried out on a voluntary basis (B, F, NL, S). Nevertheless, this
once again raises the problem of whether the asylum seeker is aware of his right to refuse
testing and whether testing is indeed carried out systematically. In the past, Belgium did
practise systematic testing although it no longer does so today.
Some texts provide for the right of asylum to be refused to persons living with
HIV/AIDS (Bavaria 112).
72. The systematic testing of asylum seekers raises problems of compatibility with the
Geneva Convention of 28 July 1951 relating to the Status of Refugees. Article 33 of this
convention includes the principle of not returning a refugee (non-refoulement), including
an asylum seeker according to all doctrine, to a country in which he fears for his life or
liberty. This principle of not turning away asylum seekers contains one exception where
there is a threat to the security of the host country. It includes no exceptions based on
public health. A Council resolution of 20 June 1995 113 on minimum guarantees for asylum
procedures does however stipulate that the authorities responsible for requests for asylum
have the right, where necessary, to request the opinion of experts on specific issues,
especially those of a medical nature. However, the ratio legis of this provision is to permit
the decision-making authorities to request information on medical aspects associated
with the fear of persecution claimed by the asylum seeker, and not to use such medical
111 OJ, C 274, 19 September 1996, p. 10.112 Bekanntmachung des Bayerischen Staatsministeriums des Inneren of 19.5.87, no. 1E/1A/1C-5280-8.2/7/87.113 OJ, C 274, 19 September 1996, p. 13.
62 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
information to refuse the asylum seeker either entry or residence.
73. Right of asylum can sometimes be granted on humanitarian grounds where an
individual has the HIV virus or AIDS (practices observed in B, E, FIN, NL, S).
C. Expulsion74. In their legislation, several states state that a foreigner may be expelled on the
grounds of public health (B 114, D 115, GR 116, L 117, with regard to people entitled to
residence on the basis of Community law, E 118, FIN 119, IRL 120).
Some express provisions were made for expelling persons living with HIV/AIDS
(Bavaria 121).
75. Expulsion can have serious consequences for people whose state of health requires a
level of medical care not certain to be provided in the country of origin, which is
particularly the case for nationals of developing countries. Furthermore, the execution of
the expulsion decision may in itself create risks for the person in question 122. Hence the
measure taken may sometimes be disproportionate to the fact which originally justified it.
Again, it is the criterion of proportionality which can be used to judge the legality of the
measure (supra, §§ 36 et seq).
D. Human rights: inhuman and degrading treatment (Strasbourg)76. The European Court of Human Rights ruled for the first time on the expulsion of a
foreigner living with HIV/ AIDS on 2 May 1997 in a case concerning the United
Kingdom 123. It concerned a national from St. Kitts and Nevis who had been sentenced to
prison for drug trafficking. After he was released from prison his request for permission to
114 Article 7 of the law of 15 December 1980.115 paragraph 46, sub-para. 1, no. 5 of the law of 9 July 1990. 116 Article 27 of law 1975/91.117 Article 9 of the law of 28 March 1972.118 Article 15 of the decree of 26 June 1992.119 Article 40 of the law of 22 February 1991.120 Article 14 of the European Communities (Aliens) Regulations 1977.121 Bekanntmachung des Bayerischen Staatsministeriums des Inneren of 19.5.87, B3.122 Conseil national du Sida (France), Rapport suivi d’un avis du Conseil national du Sida sur la situation des personnes
atteintes par le VIH, de nationalité étrangère et en irrégularité de séjour, [Report followed by an opinion from theNational AIDS Council on the situation of irregular foreign residents who are HIV positive], December 1995.
123 ECHR, D. v. the United Kingdom, 2 May 1997. See Annexe II, 2, p. 249.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 63
remain in the United Kingdom on humanitarian grounds was rejected. The person in
question was seriously ill with the disease and at the time of filing the application he was
not expected to survive more than one year. At the hearing before the Court, it was
declared that he was nearing the end of his life. He died after the Court’s decision.
77. The petitioner invoked the infringement of article 3 (prohibiting inhuman or
degrading treatment), article 8 (protecting privacy), article 2 (guaranteeing the right to
life) and article 13 (guaranteeing the right to a substantive appeal).
The British government did not dispute the fact that sending the person in question
back to his country of origin would reduce his life expectancy still further, but claimed
that it had never authorised the person in question to enter its territory and could
therefore not authorise him to remain there. The United Kingdom went on to argue that
the fact that the person in question had been imprisoned on its territory did not oblige it
to provide him with health care for the remainder of his life. The British government also
claimed that the life of the person in question was threatened by an incurable disease
from which he was suffering prior to being sentenced and not by the limited possibilities
of medical treatment in St. Kitts.
78. With regard to article 3 of the ECHR, the Court pointed out that, by virtue of a well-
established principle of international law and without prejudice to their undertakings in
international treaties, signatory states had the right to control the entry, residence and
removal of aliens. Nevertheless, the Court stated that ‘it is precisely for this reason that
the Court has repeatedly stressed in its line of authorities involving extradition, expulsion
or deportation of individuals to third countries that article 3 prohibits in absolute terms
torture or inhuman or degrading treatment or punishment and that its guarantees apply
irrespective of the reprehensible nature of the conduct of the person in question’ (pt. 47).
The Court notes that this principle was applied in cases where the risk of treatment in
contravention of article 3 was the result of intentional acts on the part of either the public
authorities of the country of destination or of organisations independent from the state
against which the authorities were not in a position to offer a person suitable protection.
Nevertheless, the Court deems that ‘it is not therefore prevented from scrutinising an
applicant’s claim under article 3 where the source of the risk of proscribed treatment in the
receiving country stems from factors which cannot engage either directly or indirectly the
responsibility of the public authorities of that country, or which, taken alone, do not in

64 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
themselves infringe the standards of that Article’ (pt. 49). The Court bases its argument on
the absolute nature of article 3 and states that it must rigorously examine all the
circumstances of the case, in particular the situation of the petitioner in the state expelling
him. The Court also states that it must ascertain if there is a real risk that the expulsion
infringes article 3 in view of the petitioner’s state of health at the time of its ruling.
The Court states that the petitioner was in the terminal phase of an incurable disease,
saying: ‘It is not disputed that his removal will hasten his death. There is a serious danger
that the conditions of adversity which await him in St. Kitts will further reduce his already
limited life expectancy and subject him to acute mental and physical suffering. Any medical
treatment which he might hope to receive there could not contend with the infections
which he may possibly contract on account of his lack of shelter and of a proper diet as well
as exposure to the health and sanitation problems which beset the population of St. Kitts.
While he may have a cousin in St. Kitts, no evidence has been adduced to show whether
this person would be willing to or capable of attending to the needs of a terminally ill man.
There is no evidence of any other form of moral or social support. Nor has it been shown
whether the applicant would be guaranteed a bed in either of the hospitals on the island
which, according to the Government, care for AIDS patients’ (pt. 52).
In view of the exceptional circumstances and the critical stage of the illness, the Court
concluded that article 3 had been infringed, even though, in principle, non-nationals who
have served a prison sentence and are subject to an expulsion order may not claim the right
to remain on the territory of a signatory state and benefit from medical care. The United
Kingdom’s argument that it was a case not of expulsion but of a refusal to grant residence, is
considered by the Court as an artificial construct because ‘Regardless of whether or not he
ever entered the United Kingdom in the technical sense, it is to be noted that he has been
physically present there and thus within the jurisdiction of the respondent state within the
meaning of article 1 of the Convention since 21 January 1993’.
79. The Court does not deem it necessary to examine whether article 2 was violated,
since the petitioner’s grievances based on article 2 cannot be fundamentally dissociated
from those based on article 3. When examining the violation of article 2, the
Commission stated in its report that ‘there is no precedent for treating the risk to life-
expectancy itself as falling within the scope of this provision’124.
80. With respect to article 8, which the petitioner claimed had been violated on the
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 65
grounds that the impact on his health was disproportionate to the legitimate aim being
pursued, i.e. to control immigration, the Court also concluded that the grievance did not
raise any separate issue.
81. Finally, after examining the grievance claiming a breach of article 13, the Court
decided that the English jurisdiction was competent to grant the petitioner the redress he
demanded and that ‘the fact that it had decided not to do so is not a pertinent
consideration since the substantive nature of the appeal stipulated in article 13 does not
depend on the certainty of a favourable result’. The Court pointed to its own
jurisprudence, in particular the Vilvarajah ruling.
Another action brought against France by a Congolese citizen living with AIDS was
submitted to the Court. Actually, in this case, the Court will consider that there is no
inhuman or degrading treatment if the exclusion order is not executed but is replaced by
a compulsory residence order. Here are the facts.
After being refused refugee status and after having been sentenced for drug trafficking,
the applicant was to be jailed and deported. After his liberation, he was subject to a
compulsory residence order because of his health, but the deportation order was not
formally cancelled. Carrying his plea to the European Court of Human Rights for inhuman
and degrading treatment, the applicant invoked that the fact that a compulsory residence
order had been made did not mean that he had lost the locus standi as a victim of inhuman
treatment, that the measure was not appropriate in view of the seriousness of his condition
as it necessitated reporting at regular intervals to the gendarmerie and the police and that
only a residence permit would give him full rights under the social welfare system.
The Court ‘accepts that the compulsory residence order […]does not signify that there
has been a change in the applicant’s situation since it merely rescinds a similar measure
imposed [before] in order to restore it with effect in a different département’ but ‘it
appears, however, that as regards article 3 of the Conventions the measure reflects,
through its continuity and duration, the French authorities’ intention to allow Mr BB to
receive the treatment his present condition requires and to guarantee him, for the time
being, the right to remain in France’125
. The Court notes that ‘the government indicated
124 European Commission of Human Rights, report of 15 October 1996, petition no. 30240/96, D. v. The UnitedKingdom.
125 ECHR, B.B. v. France, 7 September 1998, paragraph 37.

66 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
that they had not shown any intention of actually deporting Mr BB’. The Court sees that
‘as tantamount to an undertaking by the French Government not to expel the applicant
to his country of origin, the risk of potential violation therefore having ceased at least
until such time as any new factors emerge justifying a fresh examination of the case’.
Therefore the Court strikes the case out of the list but reserves the power to restore it to
the list if new circumstances arise justifying such a measure.
E. Free movement: proportionality (Luxembourg)82. The central criterion of proportionality can be applied to all three aspects of
movement (entry, residence, settlement). This criterion of proportionality has already
been widely introduced into the jurisprudence of the European Court of Justice in
relation to the free movement of people (article 48 EC, workers; article 52 EC,
settlement; article 59 EC, service provision). The main criteria defined in jurisprudence
to ascertain whether the means used are proportional to the aim being pursued are the
effectiveness and interchangeability of the said means. Are the means effective in
achieving the pursued aim and would it not be possible to substitute such means? In other
words, are there no alternative means for achieving the goal being pursued which are just
as effective as those used? Since this is a matter concerning persons living with
HIV/AIDS with relation to public health and their free movement, the issues it raises in
both national legislation and European law (supra, § 13) can be summarised as follows:
1. Are the means used (refusal of entry, refusal of residence, or expulsion) effective in
achieving the legitimate aim pursued (protecting public health)?
2. Even if the answer to the first question is affirmative, we need to examine whether
there are any alternative means for achieving the same aim without infringing, or
infringing to a lesser degree, one of the fundamental liberties of the people
concerned, in this case their freedom of movement.
The European Court of Justice has not yet been presented with a case concerning
the free movement of a person living with HIV/AIDS. However, it does have experience
of a case involving an HIV test in relation to employment (supra, § 13). The Court did in
fact use the criterion of proportionality between the legitimate aim pursued (effectiveness
in the job) and the means used (the HIV test) in relation to respect for privacy.
83. With regard to the movement of persons living with HIV/AIDS as it pertains to

The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 67
human rights, jurisprudence is available from another legal authority, that of Strasbourg.
Readers should refer to the commentary on the ruling D. vs. the United Kingdom (§ 76)
and to the analysis of article 3 contained therein.
It is true that the wording of article 3 of the ECHR does not include the principle of
proportionality since it is not limited by a qualifying clause, as are the majority of articles
safeguarding other fundamental rights and liberties. It is this which makes the nature of
protection against inhuman and degrading treatment both absolute and unconditional.
Nonetheless, this same principle of proportionality indirectly guides the interpretation of
article 3 of the ECHR. Control is in a way internal to the protected right itself and no
longer external, regarding the way in which it is protected. Indeed, in order to ascertain
whether there is inhuman or degrading treatment, in other words, to gauge the inhuman
or degrading nature of the treatment, the legitimate aim pursued by such treatment must
implicitly be weighed against the inhuman or degrading nature of the means used or of
the consequences of the measure taken. Hence the European Court of Human Rights has
always considered that controlling entry to their territory and the expulsion of foreigners
as one of the prerogatives of Member States which are thereby pursuing a legitimate aim.
Thus, refusal of entry, or expulsion, are not in themselves considered to be inhuman or
degrading treatment. However, the Court considers it necessary to ascertain whether the
consequences of refusal of entry or expulsion indirectly result in inhuman or degrading
treatment. This might be the case if the person concerned is liable to suffer inhuman or
degrading treatment in the country to which he would be expelled. According to the
above-mentioned ruling, this might also be the case where the physical or moral integrity
of the person concerned is seriously at risk 126.
In other cases where a petitioner living with HIV/AIDS was not effectively expelled,
the Commission considered the appeal as inadmissible on the grounds that the petitioner
could not be termed a victim 127.
126 In the Soering case, the Court took solemnly into consideration the serious harm to the mental integrity ondeath row in the United States of a person who had been sentenced to die. Soering case (1989), ECR, Series A,no. 161; Cruz Varas case (1991), ECR, Series A, no. 201; Vilvarajah case (1991), ECR, Series A, no. 215;Chahal case (1996).
127 Petition no. 30011/96, Lenga v. France and petition no. 15291/89, Belbachir v. Belgium, infra §§ 98 and 148. Seealso B.B. v. France, supra § 81.
III Second conclusions (national laws in the Union)84. From this across-the-board approach it is possible to identify three factors which
characterise the way in which European Union Member States approach the free
movement of persons living with HIV/AIDS:
1. Nationality of the person: citizens of third countries are subject to more severe
restrictions than citizens of the Union 128.
2. Length of stay: restrictions on free movement mainly concern long-term residence 129.
3. Type of stay: restrictions generally concern applications for a residence permit,
student residence permit, work permit or asylum.
85. Regulatory sources of restrictions on free movement in the case of HIV/AIDS vary
from one Member State to another. Nevertheless, in no Union country do immigration
laws expressly mention HIV/AIDS 130. By contrast, decrees, notices, circulars and
instructions sometimes expressly refer to HIV/AIDS. Such texts concern nationals of
third countries. More generally, national legislation often provides for a medical
examination or requires a medical certificate. Such provisions may be used to impose
indirect restrictions on the free movement of people who are HIV-positive or suffering
from AIDS. It should be noted that some national measures have no legal foundation.
This also applies to measures taken by some states with regard to students.
86. The grounds for refusing the right of residence to persons living with HIV/AIDS are
sometimes only indirectly related to AIDS. This is the case for people who are jobless
because of AIDS and do not have adequate financial resources. In England, the High
Court 131 ruled that persons living with HIV/AIDS who were nationals of a European
128 A. HENDRIKS, ‘The right to freedom of movement and the (un)lawfulness of AIDS/HIV specific travelrestrictions from a European perspective’, Nordic Journal of International Law, p. 200.
129 Idem.130 However, it should be noted that in Luxembourg, the rule concerning the medical inspection of foreigners
expressly mentions HIV/AIDS to exclude authorisation for medical inspection.131 English High Court; Times Law report, 20 October 1995.
68 The Free Movement of Persons Living With AIDS – Part 2 European Union Member States
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 69
Union Member State did not have the right to shelter as laid down in English law
because they were jobless and were not officially resident. The direct basis of this decision
was not the existence of the disease but the lack of financial resources. Since the matter
concerned Union citizens, this decision was nevertheless overturned by the Court of
Appeal, saying that the people concerned did not need to have authorisation to stay.
Later decisions of the High Court awarded shelter and medical help to third country
nationals residing illegally, suffering from AIDS (infra, § 216b).
87. Clearly there is a lack of uniformity in the policies of European Union Member States
with regard to third country nationals living with HIV/AIDS. This appears to run
counter to the admittedly non-binding acts promulgated by Community institutions
stressing the need for non-conflicting policies with regard to Community citizens 132.
The different policies of European Union Member States concerning the free
movement of persons living with HIV/AIDS, in view of national legislation and the
trend in jurisprudence, could gradually be harmonised in three stages extending from the
short- to the long-term:
1. Short-term: Member States abstain from introducing new measures to restrict the
free movement of persons living with HIV/AIDS (standstill).
2. Medium-term: the principle of proportionality is applied in evaluating existing
measures: do they pursue a legitimate aim using effective means in the absence of
alternative means which would achieve the same aim?
3. Long-term: restrictions on the free movement of persons living with HIV/AIDS are
gradually removed.
This, particularly the second point, would involve medical science and
epidemiological considerations which it is not within our remit to examine. Nevertheless,
we take the liberty of identifying one question which needs to be answered in order to
clarify the legal treatment of the free movement of persons living with HIV/AIDS and
permit the gradual harmonisation of the legislation and practices of Member States: is the
restriction on the physical movement of persons proportionate to combatting AIDS? This
means applying two classic criteria:
132 See supra, Part I and Annexe 1.

70 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
1. Is restricting the free movement of persons an effective means for combating AIDS?
2. Do other means exist that are just as effective or more effective and are less
detrimental to free movement?
The answers to these questions from experts can be used to guide concrete actions
which could be taken both at Community level and by individual Member States. Firstly,
based on the answers to these questions the national and European jurisdictions (in
Luxembourg and in Strasbourg) could ascertain to what degree the legal provisions or acts
limiting the free movement of persons living with HIV/AIDS are or are not
disproportionate. Secondly, these same answers could be used to guide the actions of
Community and national institutions in eliminating restrictions on the free movement of
persons living with HIV/AIDS by proposing to supplement these ‘negative’ actions,
which impose an obligation on Member States to abstain from introducing any new
measures limiting the free movement of persons living with HIV/AIDS, with ‘positive’
actions which propose other measures for combatting the disease that respect individual
liberties.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 71
IV Country-by-country examination of the legislation in European UnionMember StatesIntroduction88. This section IV details, on a country by country basis, the legislation, and where
possible the practices, relating to free movement which may concern persons living with
HIV/AIDS. The countries are listed in alphabetical order of their abbreviations. The
legislation is examined from two angles: firstly, the general legislation applying to all
foreigners, and secondly, the specific legislation applying to certain categories of
foreigners, in particular Union citizens, students and refugees. Nationals of developing
countries are concerned both by the measures applying to all foreigners and by measures
which specifically concern students or refugees.
Principal law texts are printed in Annexe II, 1 (p. 230) and a summary table is given
in Annexe II, 3 (p. 274).
Where possible a distinction is made, primarily for general legislation, between the
three stages of the free movement of people: entry, residence and expulsion.

72 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
1. (A) Austria1. Foreigners in general1.1. Entry
89. The authority responsible for issuing visas to third country nationals for entry to the
territory must take care to safeguard the public interests and public health (law of 17 June
1995 on foreigners, paragraph 7).
A visa must be refused if the person concerned has no health insurance or if his stay
would jeopardise public policy, order or safety (paragraph 10 of the law). This paragraph
does not expressly mention public health.
There is no screening upon entry to the territory (decree of 25 February 1987 by the
Ministry of Health and Environmental Protection concerning AIDS, the screening of
hospital patients, pre-recruitment screening by the local and regional authorities and the screening
of travellers on entry to Austria) 133.
The AIDS Committee of the Higher Board of Hygiene deemed that screening
travellers entering Austria was absurd and inadequate, stating that it should be rejected.
Consequently, the procedure in the aforementioned paragraph 7 of the Aliens’ Act
does not require any proof of not having contracted the virus, in compliance with the
provisions made at Community level 134.
1.2. Residence
90. Residence may be refused to a foreigner whose residence constitutes a threat to public
policy or public safety (paragraph 18 of the law). This provision covers people who are
already in Austria. Paragraph 18 of the law does not specifically mention public health.
Theoretically, this article could be used to refuse residence to persons living with
HIV/AIDS, but up to now it has not been used for this purpose 135.
Legislation concerning right of residence in Austria contains no provision for
refusing the right of residence to a foreigner who might constitute a threat to public
health as long as he fulfils all the other conditions required by law.
133 Information confirmed by the Ministry of Labour, Health and Social Affairs on 5 September 1997.134 Information provided by the Ministry of the Interior on 5 May 1997 and by the Ministry of Labour, Health and
Social Affairs on 5 September 1997.135 Information provided by AIDS -Hilfe Wien.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 73
The Ministry of Labour, Health and Social Affairs states that there are no reasons
fixed for refusing a work permit for people infected with AIDS/HIV in the Aliens
Employment Law 136.
2. Special categories2.1. Union citizens
91. Foreigners entitled to entry without a visa, which chiefly concerns Union citizens,
can be refused entry during a border control if their residence jeopardises public policy,
order or safety (paragraph 32).
Like paragraph 10, paragraph 32 of the law does not expressly mention public health.
The fact that they are HIV-positive or suffering from AIDS has no influence on the
conditions of entry and residence of European Union citizens 137.
2.2. Refugees
92. No HIV test is imposed on refugees 138. Aliens are only tested for some highly
infectious diseases, for example tuberculosis 139.
2. (B) Belgium1. Foreigners in general1.1. Entry
93. There are no specific provisions with regard to AIDS for the entry of third country
nationals to the territory. General legislation allows for non-EC foreigners to be refused
entry to the territory they are considered by the Minister [of the Interior] or his
representative to be likely to jeopardise the peace, public policy or national security 140.
Contrary to article 43 relating to nationals of a Union Member State, or their
equivalent, public health is not expressly mentioned in relation to foreigners from third
countries. In view of the interpretation upheld by doctrine regarding Union citizens, even
136 Information provided by the Ministry of Labour, Health and Social Affairs on 5 September 1997.137 Information provided by AIDS-Hilfe Wien.138 Information provided by the Ministry of the Interior on 5 May 1997.139 Information provided by the Ministry of Labour, Health and Social Affairs on 5 September 1997.140 Law of 15 December 1980, article 3, paragraph 7.

74 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
where public health is cited as the reason for refusing entry in accordance with Directive
64/221, AIDS cannot be used as legal grounds for refusing entry to Belgian territory.
Neither can AIDS be used as grounds for refusing entry to the territory to foreigners
under common law, even though this right does not mention the protection of public
health. Such is the position adopted by the Aliens’ Office 141.
Practice confirms that there is no HIV test before or during border crossings and that
HIV/AIDS is not used as a reason for refusing entry to the territory.
94. The same provision relating to entry to the territory also refers to foreigners who are
‘notified’ as non-admissible to signatory states to the Convention on the Application of
the Schengen Agreement, concluded on 19 June 1990, either because their presence
‘jeopardises public policy or national security, or because they [are] subject to an
expulsion order which has been neither revoked nor suspended, and which contains a
ban on entry due to a failure to comply with national regulations relating to the entry or
residence of foreigners’ (article 3, paragraph 5). Public health is not expressly mentioned
and could not be integrated into the notion of public policy according to prevailing
doctrine (supra, § 29). Nevertheless, a foreigner living with HIV/AIDS could indirectly
be refused entry to Belgium on the grounds of the second condition: in cases where he has
been subject to an expulsion order in another Member State because of HIV/AIDS,
where national legislation includes this possibility. So, could a Turk living with
HIV/AIDS who has been expelled from Bavaria on these grounds be refused entry to
Belgium on the basis of a ministerial notice? The case could be examined from two
aspects. Firstly, is it possible to speak of ‘national regulations’ in the case of Bavaria?
Secondly, do the Belgian authorities have the power to judge the grounds which led to
expulsion from Bavaria and hence the classification in the Schengen information system
(supra, § 29) as a non-admissible or undesirable foreigner? If it is possible to examine the
grounds (the grounds being AIDS), such grounds could be examined by applying the
principle of proportionality. In a matter which did not concern AIDS, in this case a
refusal to recognise refugee status in Germany, a French jurisdiction ruled that the
141 Information provided by the Aliens’ Office on 10 April 1997.

The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 75
classification in the Schengen information system (SIS) subsequent to a refusal should
not automatically lead to refusal of entry to French territory but that the grounds should
be examined 142.
1.2 Residence
95. Belgian law does not stipulate that the HIV test is necessary for nationals from third
countries to obtain a work or residence permit. However, article 2 of the Royal Decree of
6 November 1967 relating to the conditions for granting and withdrawing job authorisations and
work permits for workers of foreign nationality stipulates that where a worker does not
officially reside in Belgium or where he has been an official resident for less than two
years but is working there for the first time, the application for a work permit must be
accompanied by a medical certificate stating that, on the basis of a general check-up as
well as a serological examination and a lung X-ray, he is not suffering from any contagious
or communicable disease and that there is nothing to indicate that his state of health will
render him incapable of working in the near future.
The secretary of state for public health stated that screening for HIV antibodies was
not required for granting a work or residence permit 143. With regard to work permits, the
pre-printed medical form from the competent ministries includes a question relating to
the person’s serology, but this question normally refers to viral infections other than
HIV/AIDS. Nevertheless, general practitioners are not always familiar with legislation
regarding work permits and may include HIV screening in the serology. If the foreign
national is HIV-positive, the application is rejected by the administrative authorities on
the grounds that the person is ‘contagious’. With regard to residence permits, some third
country nationals would appear to have been subjected to a test through the Belgian
consulate after having applied for a visa or for family reunification, but this situation
would appear to be rare 144. According to the administrative authorities, where a medical
142 Tribunal administratif de Lyon, 6 May 1995, Journal des Procès, 1995, no. 293, p. 17, comment by A.M.SWARTENBROEKX, ‘Accords de Schengen, le juge doit garder un droit de contrôle’ [Schengen Agreements, thejudge must have a right of control].
143 J.P. LEGRAND, ‘Les personnes de nationalité étrangère et le sida’ [People of foreign nationality and AIDS], in: Lesida: un défi aux droits, actes [AIDS: a challenge to rights], Brussels, Bruylant, 1991, p. 759.
144 Information provided by the Foreigners’ Social Service (Service social des étrangers) on 3 April 1997.

76 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
certificate mentions the result of an HIV test, this is not a specific requirement from the
Aliens’ Office but stems from concurrent regulations, or even a spontaneous action. In a
situation such as this, the administrative authorities are content to verify compliance
with the requirements of the law of 15 December 1980 on Aliens’ residence. The use of
the test result as a criterion for examining the application for a visa or residence permit
would be patently illegal 145.
1.3. Expulsion
96. Article 7 of the Belgian Aliens’ Act states that the Minister can order a foreigner who
is not authorised or not allowed to reside more than three months or to settle in Belgium,
to leave the territory prior to a specified date if he is suffering from one of the illnesses or
infirmities listed in the annexe to the law (article 7, paragraph 7). The Minister of Justice
stated with regard to this provision that ‘if the illness or infirmity requires the foreigner to
be hospitalised, the latter will of course not be removed’ 146. Since the annexe to the law
makes no express mention of HIV/AIDS, the latter may not in principle be used as
grounds for removal 147. This is confirmed by the administrative authorities 148.
97. According to jurisprudence on safeguarding public policy which can be applied to
public health, an authority planning to expel or send back a foreigner who has clearly
settled in Belgium with his family, should ascertain whether, in a democratic society, the
necessity to safeguard public health through an expulsion order overrides the right to
family life guaranteed by article 8 of the ECHR 149. This is another application of the
principle of proportionality, in this case with regard to family life.
98. A Moroccan living with HIV/AIDS filed a procedure against Belgium in the
Strasbourg courts. In this case, the petitioner had been imprisoned in Belgium after
having been sentenced for drug trafficking and theft. Whilst he was in prison, he learned
that he had contracted the AIDS virus. Under a Royal Decree of 9 December 1986, the
petitioner was ordered to leave the territory within eight days of being released from
145 Information provided by the Aliens’ Office on 10 April 1997.146 D.P., Chambre, 1977-1978, no. 144/7, p. 74.147 M. TAVERNE, L’étranger et le droit belge [Foreigners and Belgian Law], 1991, p. 15.148 Information provided by the Aliens’ Office on 10 April 1997.149 C.E., 25 September 1986, RACE, 1986, nos. 26932 and 26933.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 77
prison. He appealed to the Council of State for this decision to be repealed. A stay of
execution was also requested due to the petitioner’s state of health. The Council of State
rejected the application for a stay of execution on the grounds that the basis for the
application was flawed. Nevertheless, the deadline for leaving the territory was extended.
Subsequently, although the person concerned was ordered to leave the territory, he
remained in Belgium. Meanwhile, the Council of State rejected the appeal for the
decision to be revoked. The petitioner was again sentenced to prison for possession of
drugs, rebellion and battery. After his release when he had been issued with various orders
to leave the territory, a Royal Decree was adopted on 23 April 1991. In accordance with
this Royal Decree, execution of the Decree of December 1986 was suspended for a period
of three years during which the Decree of 9 December 1986 would be definitively
repealed if the conduct of the person concerned was beyond reproach.
An appeal was lodged under application of the ECHR. The petitioner pleaded
violation of article 3 due to his uncertainty over whether or not he would be able to
remain in Belgium. It was also claimed that article 2 was being violated on the grounds
that expulsion would immediately deprive the petitioner of any kind of treatment and
would shortly lead to his death. The petitioner also pleaded violation of article 8, since if
he were expelled he would be separated from his family which had settled in Belgium. The
person concerned claimed that his family ties had been strengthened as a result of his
serious health problems. Finally, the petitioner pleaded violation of article 14 guaranteeing
the principle of non-discrimination with respect to fundamental rights protected by the
convention. In this case, the petitioner felt that he was being discriminated against, not
only because he was being obliged to leave the country solely on the grounds of his
nationality, but also because the fact that he was suffering from AIDS was considered to be
an aggravating factor making his expulsion all the more necessary.
The Commission judged the appeal to be inadmissible. It decided that ‘the condition
of irreproachable conduct imposed upon the petitioner for the ruling to be repealed could
not be considered inordinate’ and that ‘the petitioner has never in fact been expelled from
Belgium, has continued to benefit from the care which his state of health requires and his
family ties have never been affected’. The Commission concluded that the petitioner
could not be described as a victim 150. Nevertheless, if a national from a third country were
150 Petition no. 15291/89, Belbachir v. Belgium.

78 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
indeed subject to expulsion, the appeal could be declared admissible 151.
Expulsion would then be subject to a case-by-case examination following the
principle of proportionality. It was ruled by a Brussels court that, even if article 3 of the
European Convention on Human Rights and article 23, 2° of the Belgian Constitution
give a right to health protection, ‘those articles cannot lead to the conclusion that a state
may never expel a foreigner living with AIDS; it all depends on the stage of the illness,
on the requirement for treatment and on the possibility for the patient to receive that
treatment in the country of origin’ 151b.
Similarly the Council of State suspended the deportment order served on a Tunisian
who was in a ‘very advanced stage’ of AIDS, on the grounds that ‘the genuineness of the
illness from which the petitioner has suffered for a number of years and the serious nature
of his state are established by many medical reports and certificates in the administrative
file. The various items in the file show that it is highly improbable that the drugs that the
petitioner is receiving in Belgium and without which he would be unable to survive, are
available in Tunisia.’ 151c
2. Special categories2.1. Union citizens
2.1.1. Entry
99. Union citizens may be refused entry to Belgium on public health grounds (article 43
of the Aliens’ Act of 15 December 1980). Only the diseases included in the annexe to
the law may justify refusal of entry. The list of diseases, which incorporates the list in
European Directive 64/221, does not expressly mention HIV/AIDS, but it does mention
the quarantinable diseases listed in the international Regulation of 25 May 1951,
tuberculosis, syphilis, as well as ‘other infectious or contagious parasitic diseases if in the
host country they are the subject of provisions to protect nationals’. According to Belgian
doctrine, the fact of suffering from AIDS or being HIV-positive may not, in principle,
justify refusal of entry or residence since ‘AIDS is neither a quarantinable disease nor an
151 See E. Court H.R., 2 May 1997, D. v. The United Kingdom, supra, § 76.151b Civ. Bruxelles (réf.), 18 September 1997, no. 97/1057/C, Mosikwa v. Belgium, non published. Quoted in F.
MOTULSKY and M. BOBRUSHKIN, ‘Le séjour des étrangers en Belgique et le contentieux médical’ [Residenceof aliens in Belgium and medical conflicts], Journal des Tribunaux, 1998, p. 283.
151c Council of State, 19 Mei 1998, M. v. Belgian State, no. 73790, unpublished.

The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 79
infectious disease listed in paragraph 4 of the annexe. In fact, Belgian nationals suffering
from AIDS are not subject to protection measures’152. This conclusion is confirmed by the
administrative authorities 153.
With regard to article 43 of the Aliens’ Act covering Union citizens, it should be
noted that Belgian law considers the family of Union citizens as Union citizens, in
accordance with Community law, but also the family of a Belgian national, in accordance
with national law, in order to avoid reverse discrimination against the family of a Belgian
national. Consequently, the wife of a Belgian national from Togo benefits from the same
protection as Union citizens 154.
2.1.2. Residence
100. Article 43 of the Aliens’ Act applies to the residence of Union citizens in Belgium.
Refer to the comments on this provision regarding the entry of Community nationals (§ 99).
2.2. Students
101. By virtue of article 58 of the law of 15 December 1980, foreigners wishing to study in
Belgium must supply certain documents, including a medical certificate stating that they
are not suffering from any of the diseases or infirmities listed in the annexe. The annexe
does not expressly mention HIV/AIDS.
In June 1985, the Ministry of Foreign Affairs planned to subject applicant student
grant-holders from central Africa to a compulsory HIV test. The Belgian Medical
Association (Conseil national de l’ordre des médecins) considered that, in the absence of
compulsory legislation on the matter, such a test could only be carried out with the
consent of the people concerned. In July 1985, directives from the secretary of state for
Cooperation and Development were issued stating that the physical examination of
third-world applicant student grant-holders would include a blood analysis and screening
for HIV antibodies. On 24 October 1986, the Ministerial Committee for Foreign Affairs
stated that applicant student grant-holders should be submitted to this examination in
their country of origin. Should the result be positive or should they refuse to submit to
152 J. P. LEGRAND, ‘Les personnes de nationalité étrangère et le sida’, in Le sida: un défi aux droits, actes, Brussels,Bruylant, 1991 and M. TAVERNE, ‘Statut administratif’ [Administrative Status], in L’étranger et le droit belge,Bruges, La Charte, 1991, p. 15, footnote 74.
153 Information provided by the Aliens’ Office on 10 April 1997.154 ECJ, 18 October 1990, ECR, C-297/88 and 197/89, Dzodzi, ECR, 3763.
80 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
the test, students would not be granted authorisation. Student grant-holders who were
already resident in Belgium would also have to submit to an annual test. Seropositivity or
a refusal to submit to the test would result in the student being obliged to leave Belgium.
The withdrawal of the grant would be notified to the country of origin. At the end of
March 1987, the secretary of state for public health allowed student grant-holders to
remain in Belgium to continue their studies.
The measures taken by Belgium against certain categories of students have been the
subject of much criticism.
It was argued that the HIV/AIDS infection did not figure in the annexe to the
Aliens’ Act of 15 December 1980, with the result that the measures had no basis in law.
It was also maintained that disclosing the test result to the organisation awarding grants,
the General Development Cooperation Agency (Agence générale de coopération au
développement – A.G.C.D.), as well as to the country of origin, would be a violation of
medical confidentiality. Others held that the measure was tantamount to a forced medical
intervention and was an invasion of students’ privacy. Finally, it was claimed that the
obligation to submit to a test could be motivated by financial considerations, aimed at
avoiding having to pay medical costs, which made it an ineffective and discriminatory
measure 155.
According to the administrative authorities, no decision has ever been taken to
expel an HIV-positive student 156. The test is now voluntary, in that it is offered to
students upon their arrival 157.
2.3. Refugees
102. Legislation contains no specific provisions concerning public health with respect to
refugees. It appears that systematic screening was practised in the past but that this
measure is no longer in force. However, doctors in reception centres apparently
frequently carry out HIV screening on asylum seekers who are said to submit to it without
necessarily understanding the meaning of the terms ‘HIV’ or ‘AIDS’. The Public Social
155 See in particular: M. VINCINEAU (editor) Le sida, un défi aux droits, actes, Brussels, Bruylant, 1991, 766 and L.THIRY, ‘Les boursiers et le sida, accompagner ou punir?’ [Student grant-holders and AIDS, help and support orpunishment?] Journal des Procès, 1987, no. 103.
156 Information provided by the Foreigners’ Social Service on 8 April 1997.157 Information provided by the AGCD.

The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 81
Welfare Centre of the city of Liège demands that asylum-seekers receiving welfare benefit
should receive a full medical examination every six months, including HIV screening.
The implicit sanction should they refuse to submit to the medical examination is the
suspension of welfare benefits 158.
Some refugees, fearing that seropositivity will be used to refuse them the right of
residence, renounce medical care and welfare benefits 159.
Replying in the Parliament (Sénat) to an oral question on 20 February 1986, the
secretary of state for public health declared that ‘the authorities, in application of the law
of 15 December 1980, must check whether a political refugee is suffering from one of the
diseases listed in the annexe to the law. If the examination proves positive, the person
concerned must leave the territory’ 160. It was pointed out that article 32 of the Geneva
Convention stipulates that a refugee may only be expelled for reasons of national security
and public policy, not on the grounds of public health. Likewise, the Belgian Aliens’ Act
states that a refugee may be refused residence for reasons of public policy and national
security but not on the grounds of public health (article 52a).
In answer to a parliamentary question, it was said that ‘no measures apply to refugees
other than those which apply to any HIV-positive person residing in Belgium’ 161.
According to the Aliens’ Office, asylum-seekers are not refused entry or residence
because of HIV/AIDS. On the contrary, they claim that there is positive discrimination
towards certain patients in the terminal stages of their illness. In a very serious medical
situation, for instance, it would be possible for a person who was not in a state to be
moved to have his residence regularised. When an illegal foreigner or non-suited asylum
seeker is still in a state to be moved, he is normally repatriated but receives medicine to
take on his return 162.
158 Information provided by the Foreigners’ Social Service on 8 April 1997.159 M. LOUHENAPESSY, ‘Care issues and migrants’, in M. HAOUR-KNIPE and R. RECTOR (Eds.) Crossing
borders, migration, ethnicity and AIDS, Taylor & Francis, London, 1996.160 C.R.A., Senate, 1985-86, 20 February 1986, p. 177.161 Bull. Quest. et Rép. Senat, 1986-87, no. 25, 31 March 1987.162 Information provided by the Aliens’ Office on 10 April 1997.

82 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
3. (D) Germany1. Foreigners in general1.1. Entry
103. The Aliens’ Act (Auslandergesetz) of 9 July 1990 (BGBl, p. 1354) in its 28 October
1994 version (BGBl, I, p. 3186) contains no specific provision concerning a medical
examination prior to entry to the territory. This means that the federal authorities cannot
make authorisation to enter the territory conditional upon a medical examination.
A circular of 21 April 1987 from the Minister of the Interior of the FRG previously
authorised the border police to refuse entry to the territory to foreigners suspected of
suffering from AIDS 163. This circular is no longer in application 164.
1.2. Residence
104. By virtue of the Aliens’ Act of 9 July 1990 165, right of residence may only be granted
if the foreigner’s presence does not affect Germany’s interests. Some people infer from this
that the law prohibits granting an HIV-positive person the right of residence except
where this person has very strong ties with Germany 166. All aspects of public interest,
including public health, are considered as being interests of the Germany 167.
Residence permits may also be refused if the foreigner is suffering from a contagious
disease which has to be declared, in accordance with paragraph 3, sub-paragraphs 1 and 2
of the federal law on epidemics (Bundesseuchengesetz). If there is reason to believe that this
is the case, the authority must request a medical certificate, except where the foreigner is
entitled to receive a residence permit or have one extended. The HIV infection is not
included in paragraph 3 of the law on epidemics, but is considered as a contagious disease
under the terms of this law. There are no regulations for the application of HIV screening,
and in practice the delivery of a residence permit does not normally appear to depend on a
prior medical examination, except in the case of Bavaria 168.
163 Le Monde, 13 May 1987.164 Information provided by Assistant Public Prosecutor Bruns on 29 March 1997.165 Article 7, paragraph 2, paragraph 3.166 W. ZITZELSBERGER, ‘Ausländerrechtliche Aspekte der Aids-Problematik’ [Foreign law aspect of the AIDS
Problem], Aids-Forschung (AIFO), 1988, p. 49.167 Information provided by the Ministry of the Interior on 21 March 1997.168 Information provided by the Ministry of the Interior on 21 March 1997.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 83
105. It is the Länder that establish the conditions for the medical certificate to be
provided by foreigners requesting the right of residence. The Länder can decide whether
this certificate should contain information regarding possible seropositivity.
106. In a decision dated 30 July 1987, the higher administrative court of the Land of
Baden-Württemberg refused to consider that seropositivity could constitute a threat to
public health and serve as grounds for refusing to extend the right of residence 169.
107. The authorities of the Land of Bavaria have taken different measures against
foreigners living with HIV/AIDS, aimed at limiting their opportunity to reside
in Bavaria.
Foreigners requesting a permit to stay more than three months in Bavaria
are subjected to screening 170. There may be exceptions for people with special links
with Germany, such as those married to German nationals. In this case, a residence
permit is granted provided that the foreigners give an assurance that they will not
spread the disease.
Where an HIV-positive foreigner is in possession of a residence permit, this permit
may be rescinded at the discretion of the immigration authorities. They mainly take into
account the foreigner’s ties with Germany, family ties, and the period of residence.
The European Commission reacted to the measures taken by the Land of Bavaria
saying that they contravened the principle of the free movement of persons, as well as the
conclusions of the Council and Member States governments representatives at the
Council meeting of 15 May 1987. The Commission did not consider itself to have the
legal means to intervene directly with the Land of Bavaria 171. It nevertheless pointed out
that the ad hoc group was responsible for proposing a procedure for providing mutual
information at Community level concerning any administrative and legal initiatives
planned or adopted by Member States.
169 VGH Mannheim, 30.7.1987-11 S 805/87, Neue Juristische Wochenschrift, 1987, Heft 46, p. 2953-2954.170 Bekanntmachung des Bayerischen Staatsministeriums des Inneren, no. 1A2-2081.10 and no. 1E/1A/1C-5280-8.2/7/87
of 19 May 1987.171 Written question no. 708/87 from Mr Konstantinos Filinis to the Commission of the European Communities, OJ,
C 283, 7 November 1988; written question no. 663/87 from Mrs Raymonde Dury to the Commission of theEuropean Communities, OJ, C 195, 25 July 1988; ‘Réaction de la Commission aux menaces à la libre circulationdans la CEE’, The ACP-EEC Courrier, September-October, 1987, p. XII.

84 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
1.3. Expulsion
108. Paragraph 46, sub-paragraph 5 of the Aliens’ Act states that a person can be expelled
if he endangers public health through his conduct. Often the decision is based on the
personality and social life of the person concerned.
Expulsion does not depend solely on suffering from a contagious disease that must be
declared or on suffering from a venereal disease, under the terms of the federal law on
epidemics, but also on whether the foreigner’s conduct constitutes a threat to public
health, in that the person takes no precautions to avoid spreading the disease or fails to
respect the necessary protection measures. These grounds for expulsion are normally
examined after an explanatory memorandum has been issued by the Public Hygiene
Department 172.
109. In a judgment on 2 October 1985, the Saarland administrative court upheld
seropositivity as grounds for expulsion.
110. In Bavaria, the aforesaid notice expressly provides that persons living with
HIV/AIDS may be expelled. Holders of a residence permit who may be HIV-positive are
subjected to a test and should they prove to be HIV-positive their permission to stay may
be withdrawn 173. Furthermore, it provides that foreigners practising prostitution or taking
drugs may be expelled even if they are not HIV-positive 174.
2. Special categories2.1. Union citizens
111. The Aliens’ Act only applies to Union citizens if European law does not contain a
contrary provision.
In accordance with paragraph 12, sub-paragraph 6 of the law on EEC residence
(Aufenthaltsgesetz/EWG), the free movement of a Union citizen may only be restricted if
172 Information provided by the Ministry of the Interior on 21 March 1997.173 Bekanntmachung des Bayerischen Staatsministeriums des Inneren of 19.5.1987, B3.174 Bekanntmachung des Bayerischen Staatsministeriums des Inneren, 19.5.1987 no. IE/1A/1C-5280-8.2/7/87.

The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 85
he is suffering from a disease that must be declared by virtue of the federal law on
epidemics (Bundesseuchengesetz). This does not concern HIV/AIDS 175.
The issue of the entry and residence of Union citizens living with HIV/AIDS does
not appear to have arisen in practice, since no ruling has ever been made on the subject.
Even though article 4 of Directive 64/221 and paragraph 12, sub-paragraph 6 of the law
on EEC residence do in theory allow restrictions on free movement on public health
grounds, this does not apply to Union citizens who might be affected by the virus. In any
case, in accordance with the European directive, it is not permitted to refuse to extend, or
to withdraw a residence permit in cases where the virus appears after the person
concerned has received a first residence permit 176.
The obligation to undergo an HIV test imposed by Bavaria on foreigners requesting
a residence permit does not apply to Union citizens or nationals from the following
countries: Andorra, Iceland, Liechtenstein, Malta, Monaco, San Marino, Switzerland
and Norway.
2.3. Refugees
112. Paragraph 48 of the Aliens’ Act provides special protection against expulsion. Under
this provision, a foreigner holding a residence permit in accordance with paragraph 32
may be expelled only for serious reasons that jeopardise public security and public policy,
although public health is not mentioned. Paragraph 32 concerns refugees fleeing from war
or civil war.
113. On the basis of the aforementioned notice, in Bavaria, refugees who are living with
HIV/AIDS may be refused the right of asylum.
175 Information provided by Assistant Public Prosecutor Bruns on 29 March 1997.176 Information provided by the Ministry of the Interior on 27 May 1997.
86 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
4. (DK) Denmark1. Foreigners in general1.1. Entry
114. The Danish Aliens’ Act (Act no. 894 of 27 October 1994, amended in 1995)
provides that entry may be refused if health grounds indicate that the alien should not be
allowed to stay in Denmark (article 28).
Health inspections are authorised by virtue of the ‘Epidemiological Diseases Act’ and
of legislation on foreigners. However, there is widespread agreement that this type of
measure is not necessary in the case of HIV/AIDS because of the way the virus is
transmitted 177.
Generally speaking, nobody in Denmark can be obliged to undergo a test. In fact, the
Danish Parliament considered that the fight against AIDS should be based on an
individual’s right to make his own decisions.
1.2. Residence
115. Article 10 of the law states that in cases where a foreigner must be considered a
threat to his entourage due to a contagious disease, he may be issued with a residence
permit only if particular reasons make this appropriate.
There is no jurisprudence relating to the application of article 10 to persons living
with HIV/AIDS, which is logical since the HIV test is not compulsory and consequently
the authorities are unaware of any seropositivity. Even assuming that the authorities were
aware that the foreigner was suffering from HIV/AIDS, it is not very likely that he would
be refused a residence permit on the grounds that he would constitute a danger or a threat
to his entourage 178.
Article 9, paragraph 3 of the Aliens’ Act stipulates that a residence permit may be
granted for humanitarian reasons where the person is not recognised as a refugee. On this
basis, a residence permit may be granted to a person suffering from a serious disease such
as HIV/AIDS. This principle would appear to be illustrated by the Minister of the
Interior’s decision of 20 May 1993 179.
177 A. SNARE, ‘The legal treatment of AIDS in Denmark’, AIDS and Human rights, an international perspective,Copenhagen, Akademisk Forlag, 1988, p. 37.
178 Information provided by E. Brinch Jorgensen on 5 May 1997.179 Indenrigsministeriets Nyhedsvref, 20 May 1993; Vdlaendingeretten, DJØF-publishing, 1995, p. 107.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 87
A 28-year old Ugandan national who had requested refugee status, was refused in
March 1993. He then asked for a residence permit on humanitarian grounds based on
article 9 of the Aliens’ Act. A medical examination had revealed that the immune
defence system of the person concerned was moderately lowered without the appearance
of signs associated with the HIV/AIDS infection. However, the medical examination
showed that there was a risk that the symptoms of HIV and AIDS would appear in later
years. The foreigner’s request was rejected on the grounds that he displayed no symptoms
of HIV/AIDS and that only a moderate lowering of the immune system had been
detected. When this decision was announced, the Minister of the Interior stated that the
administrative practice should not be allowed to develop in such a way that any foreigner
suffering from the virus would be able to obtain a residence permit for humanitarian
reasons, adding that an individual assessment would be required on a case-by-case basis.
An analysis of this decision appears to indicate that foreigners presenting symptoms
of HIV or AIDS, who were refused refugee status on the basis of article 7, could be
granted a residence permit for humanitarian reasons.
1.3. Expulsion
116. The Aliens’ Act does not provide for expulsion on public health grounds. Expulsion
is only allowed in cases of a threat to national security, a criminal sentence, alcohol
abuse, drug taking or not having a residence permit.
Furthermore, article 26 of the law states that the expulsion decision must have
regard not only to ties with Denmark, but also other elements, including the state of
health of the person concerned.
With regard to the application of article 26, the foreigner’s state of health is given
special consideration if he is unable to obtain medical care in his country of origin 180.
Even where the foreigner is under an expulsion order because he has committed a
criminal offence, his situation may be re-examined if a new element arises, such as the
appearance of a serious illness (article 50 of the Aliens’ Act).
It was ruled that a person who had been sentenced to prison for one-and-a-half years
and had become depressive whilst in prison, should not be expelled. In fact, expulsion
180 Information provided by E. Brinch Jorgensen on 5 May 1997.

88 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
could have affected the person’s state of health, especially as a result of being separated
from the home environment 181.
It would therefore seem that HIV/AIDS can serve as grounds to justify the
application of articles 26 and 50 to avoid expulsion.
2. Special categories2.1. Refugees
117. There is no compulsory test for refugees. It is highly unlikely that right of asylum could
be refused for reasons associated with HIV/AIDS 182. A foreigner living with HIV/AIDS
who is refused refugee status can request the right of residence on humanitarian grounds 183.
5. (E) Spain1. Foreigners in general1.1. Entry
118. Article 11 of the law of 1 July 1985 on the rights and liberties of foreigners in Spain
stipulates that foreigners must submit to the tests demanded for public health reasons by
the health service at border crossing points. The Ministry of the Interior, in agreement
with the Ministry of Health and Consumer Affairs, decides which cases require a
certificate proving that the person is not suffering from a disease endangering public
health. The certificate is issued in the country of origin by the medical services appointed
under consular regulations. If this is not the case, the foreigner must undergo an
examination by the Spanish services on arrival 184.
119. Article 8 of the implementing Regulation of 23 February 1996 (concerning third
country nationals and applying to Union citizens only on a subsidiary basis) provides
that, in the case of an epidemic, borders may be closed at the request of the Minister of
the Interior and of Health.
120. No restriction on entry is expressly provided for persons living with HIV/AIDS 185.
181 Judgment in UfR 1990.719 H.182 Information provided by E. Brinch Jorgensen on 5 May 1997.183 Supra, § 115.184 Jose Maria ESPINAR VICENTE, La nacionalidad y la extranjeria en el sistema juridico español [Nationality and
immigration in the Spanish legal system], Madrid, Civitas, 1994, 251.185 Information provided by the Health Ministry on 19 February 1997.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 89
1.2. Residence
121. Article 27 of the Regulation of 23 February 1996 applying to third country nationals
provides that in order to obtain a residence permit a medical certificate must be presented
in compliance with article 37 of the regulation. Article 37 entitled ‘health requirements’
states that foreigners entering Spain must provide a medical certificate or submit to a
medical examination in order to check that they are not suffering from one of the following:
■ a quarantinable disease listed in the international health regulations
■ drug dependency or a mental illness endangering public policy or public safety
■ an infectious or parasitic disease indicated by the Health Minister.
A foreigner requesting a residence permit must prove that he possesses the financial
means, in particular to cover health care for himself and his family (article 28 of the
Regulation of 23 February 1996).
Article 32 of the regulation states that no residence permit will be granted if the
foreigner’s presence is a threat to public policy, public safety or public health.
A certificate of seronegativity is not required by the local authorities for obtaining a
residence permit 186.
The order of 11 April 1996 on exemptions regarding visas accepts as grounds for
exemption the fact that a foreigner is suffering from a disease requiring medical care and
preventing him from returning to his country to obtain a visa. This provision could be
applied to persons living with HIV/AIDS 187.
122. The implementing Regulation of 23 February 1996 states that a medical certificate
must be provided in order to obtain a residence or work permit (articles 56 and 87), in
compliance with the aforementioned article 37.
In principle a certificate of seronegativity is not necessary for obtaining a work
permit 188. Article 22 of Law 31/1995 of 8 November on the prevention of occupational risks
186 Information provided by the Health Ministry on 19 February 1997.187 Information provided by the Health Ministry on 19 February 1997.188 Information provided by the Health Ministry on 19 February 1997.

90 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
states that a medical examination requires the consent of the worker. Exceptions may be
made, provided that workers’ representatives are notified and that the means used are the
least prejudicial possible and proportionate to the risk. In any case, the right to privacy,
dignity and confidentiality must be respected.
123. Article 9 of the implementing Regulation of 23 February 1996 states that
foreigners are entitled to benefit from the services organised by the public authorities
for protecting health.
1.3. Expulsion
124. The Spanish Aliens’ Act does not provide for expulsion on public health grounds.
However, article 21, paragraph 4 of this law states that in exceptional cases, a reasoned
decision by the Minister of the Interior may prevent the foreigner from leaving the
country if this measure is required to protect national security, public policy or public
health. Article 121 of the implementing Regulation of 23 February 1996 relating to bans
on leaving the country, states that a foreigner who has a contagious disease may be
forbidden to leave the territory if, by virtue of Spanish legislation and international
conventions, this disease requires his immobilisation or confinement. The ban on leaving
the country on public health grounds is an international cooperation measure to prevent
disease spreading to other countries. This prohibition also reflects a concern to protect
the country itself, since it allows the necessary steps to be taken to control the spread of
the epidemic and analyse the situation 189. It would appear that there has never been an
expulsion on the grounds of HIV/AIDS and that this disease has never been used to
justify a ban on leaving the country 190.
189 Jose Maria ESPINAR VICENTE, op. cit., p. 300.190 Information provided by the Health Ministry on 19 February 1997.

The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 91
2. Special categories2.1. Union citizens
2.1.1. Entry
125. In the case of Union citizens, Royal Decree 766/1992 of 26 June on the entry and
residence in Spain of nationals from European Community Member States, amended by Royal
Decree 737/1995 of 5 May states that public health may be used as grounds for refusing
entry. The diseases mentioned are those listed in Directive 64/221 (article 15 of the
decree). The Royal Decree also applies, irrespective of nationality, to members of the
family of both Spanish nationals and Union citizens (article 2 of the decree).
2.1.2. Residence
126. Union citizens may be refused residence on public health grounds, by virtue of
article 15 of Royal Decree 766/1992. The diseases referred to in this article are based on
those in Directive 64/221.
2.1.3. Expulsion
127. Article 15 of Royal Decree 1992/766 states that Union citizens may be expelled if
they pose a threat to public health. The diseases mentioned are those figuring in the
annexe to Directive 64/221.
2.2. Students
128. There is no systematic screening of students 191. Nevertheless, African students at the
University of Madrid and Uruguayans have been obliged to submit to a screening test 192.
2.3. Refugees
129. A medical examination is carried out on refugees.
In 1991, the FASE (Spanish association) intervened in favour of asylum-seekers,
especially those from Africa, whom the authorities had asked to be screened for HIV. At a
meeting with this association, the Minister of the Interior declared that HIV tests were
191 Information provided by the Health Ministry on 19 February 1997.192 Comite ciudadano anti-sida (Anti-AIDS Citizens’ Committee), Informe sobre la problemática sanitaria del sida (Report
on the AIDS health problem), April 1991, in Étude comparative sur la discrimination à l’encontre des séropositifs etmalades du sida, Strasbourg, 1993, 108.

92 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
neither automatically offered nor carried out on potential refugees 193. This policy is
still in force 194.
The fact that treatment cannot be continued in the country of origin sometimes
serves as grounds for granting the right of asylum 195.
6. (F) France1. Foreigners in general1.1. Entry
130. Article 5 of the Order of 2 November 1945 relating to the conditions of entry and
residence of foreigners in France, as amended, states that entry to French territory may be
refused to any foreigner whose presence might pose a threat to public policy or who is
either under a ban on entering the territory or under an expulsion order. Article 5 does
not expressly mention public health. Nevertheless the wording of the provision relating
to Union citizens (infra, § 150) implies that certain diseases or infirmities may endanger
‘public policy’.
131. No screening is practised upon entry to France. In 1987, the President of the French
Republic declared that a sense of ethics should make it possible to preserve the humanist
values threatened by the determination of certain states to introduce systematic screening
and a border inspection 196.
132. The order on foreigners (article 22, II, letter a) states that a foreigner may be sent
back to the border if he fails to fulfil the conditions set out in article 5 of the Convention
on the Application of the Schengen Agreements or if he cannot prove that he entered
France in accordance with articles 19 and 20 of the Convention.
133. Screening is compulsory for French military personnel returning from certain
African countries and from French Guyana.
193 Idem.194 Information provided by the Health Ministry on 19 February 1997.195 Information provided by la Comisión Española de Ayuda al Refugiado [Spanish Commission for Aid to Refugees] on
22 January 1997.196 Le Monde, 11 June 1987.

The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 93
1.2. Residence
134. France’s policy with regard to residence is not to impose a health inspection for
tourist or business trips but only for foreigners staying for some time in France, i.e.
foreigners obtaining a permit to stay in France for more than three months. According to
G. Moreau, Director of the population and migration department, this medical
examination is used merely as a preventive measure. During this medical examination,
information is allegedly provided on the benefits of screening 197.
The delivery of a so-called ‘short stay’ tourist visa (less than three months) is not
subject to medical conditions and no screening is required 198.
135. Foreigners subject to the order of 2 November 1945, refugees and members of a
refugee’s family, and the family members of a stateless person requesting a French
residence permit must undergo a medical examination which is carried out abroad by a
doctor approved by the French Embassy. However, for certain categories of foreigners
(students or self-employed workers) the medical examination takes place in France. An
HIV screening test does not form part of compulsory examinations. Seropositivity is not
considered to be a sufficient medical reason for refusing a residence permit 199.
136. Decree no. 46-1574 of 30 June 1946 (amended by decree no. 94-768) calls for a
medical certificate in a number of cases.
Article 7 of the 1946 decree requires a medical certificate for a foreigner requesting a
temporary residence card. The requirement for a medical certificate also appears in article
11 of the decree for applying the provisions of article 15 (paragraph 1 to 5) of the order of
2 November 1945 on foreigners concerning the automatic delivery of residence cards. The
conditions for issuing a medical certificate were specified by ministerial order 200.
197 G. MOREAU, ‘La politique française en matière d’immigration et de sida’ [France’s policy regarding immigrationand AIDS], Sida, sociétés et populations, John Libbey Eurotext, Montrouge, 1996, p. 235.
198 Information extracted from the document published by Aides, entitled ‘L’entrée sur le territoire français’ [Entry intoFrench territory].
199 Information extracted from the document published by Aides, entitled ‘L’entrée sur le territoire français’ .200 A.M., 30 July 1986, J.O., 24 August 1986.
François JULIEN-LAFERRIÈRE, ‘Condition des étrangers en France’ [Condition of foreigners in France],Jurisclasseur Droit international, fasc. 524, no. 58.

94 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
137. By virtue of the order of 7 November 1994 concerning the health control of foreigners
authorised to stay in France, third country nationals must submit to a general clinical
examination carried out by a doctor. Article 4 of the order states that foreigners do not
fulfil the health conditions if they are suffering from plague, cholera, yellow fever, active
pulmonary tuberculosis, drug addiction or a mental disorder. Since HIV/AIDS is not
mentioned in the order of 7 November 1994, it should not constitute grounds for refusing
the right of residence 201.
138. The circular of 8 December 1987 concerning the health inspection of foreigners wishing to
stay in France does refer to HIV/AIDS. It stipulates that only the presence of clinical signs
or a request by the person concerned can lead to screening for HIV antibodies. The
existence of positive serology in the absence of clinical signs should not constitute
grounds for refusing authorisation to reside in France.
Some people claim that in this circular ‘freedom to come and go is respected, since
there is no screening at borders and the existence of positive serology does not constitute
grounds for refusing a residence permit’ 202. For others, the circular could create a false
impression of protection because an a contrario interpretation may mean that
seropositivity does constitute grounds for refusing the right of residence where clinical
signs are present. Could a simple fever be interpreted as a clinical sign justifying screening
and refusal of the right of residence 203?
139. With regard to family reunification, article 29 of the 1945 order states that this right
may be refused for public health reasons. Family members must not be suffering from a
disease or infirmity that is likely to jeopardise public health or safety; their presence must
not constitute a threat to public policy. These conditions are not required of certain
foreigners covered by a treaty: European citizens, Central Africa, Gabon, Burkina-Faso,
Mauritania and Togo 204.
140. It was decided that the refusal to issue a residence permit to a foreigner suffering
201 AIDES, Droit et sida Guide pratique, [Law and AIDS, Practical Guide], 3rd ed., Paris, LGDJ, 1996, p. 71.202 J. FOYER and L. KHAIAT, ‘Droit et sida: la situation française’ [Law and AIDS: the French Situation], Droit et
sida, comparaison internationale, Paris, CNRS Editions, 1994, p. 255.203 P. VAN OVERBEEK, ‘AIDS/HIV infection and the free movement of persons within the European Community’,
Comm.M.L.R., 1990, p. 91.204 P. MAYER, Droit international privé [International private law], 4th ed., Paris, Montchrestien, 1991, 578.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 95
from serious health problems could be flawed by a manifest error of judgment 205. This
case concerned a seriously ill foreign student who, because of his illness, had postponed
completing the formalities required to renew his residence card. This case did not directly
concern HIV/AIDS but the same reasoning could be applied to persons living with
HIV/AIDS.
141. Foreigners other than tourists residing in France have the same rights to health care
as French nationals.
A circular of 4 March 1997, drawn up by the General Health Directorate, the Social
Security Department, the Hospitals Department and the Social Services Department,
defines the prescription and treatment procedures for new AIDS therapies 206. This
circular states that ‘all patients must be taken in charge by public hospital service,
irrespective of their administrative situation’ (point 3.4).
The circular also contains the following provision: ‘medical care in a health care
institution is open in particular to foreign nationals residing in France without an official
residence permit. It allows for care dispensed by health care institutions, including
outpatient clinics, to be taken in charge. Also taken in charge are any medicinal products
prescribed on this occasion […]. Furthermore, foreign nationals who establish that they
have the required permit to reside officially in France (including cases where they have
been resident in France for less than three months), as well as any persons who can prove
their uninterrupted residence in mainland France for over three years (even without
a legal residence permit), may also be means-tested for receiving home health care’
(point 3.4.2.1.).
1.3. Expulsion
142. French legislation provides for expulsion, not on the grounds of public health, but ‘if
the presence of a foreigner on French territory poses a serious threat to public policy’ 207.
143. The medical situation does not in itself shield a foreigner from a measure to remove
205 C.E., 14 February 1996, D., 1997, Cahier 5, summaries commented by François JULIEN-LAFERRIÈRE, p. 38.206 Framework circular DGS/DSS/DH/DAS no. 97/166, relating to the new system for exemptions and people with the
antiretrovirus, introduced on 1 January 1997.207 Article 23 of the amended Order of 2 November 1945.
]
96 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
him from the territory. Nevertheless, a foreigner can invoke humanitarian grounds in
cases where expulsion would have exceptionally serious consequences on his state of
health or on his family life. Authorisation to reside in France may be granted under such
circumstances. This is based on article 25, paragraph 8 of the order of 2 November 1945
concerning ‘a foreigner habitually residing in France who is suffering from a serious illness
requiring medical treatment, the lack of which could result in exceptionally severe
consequences, provided that he cannot effectively pursue an appropriate course of
treatment in the country to which he is returned’.
144. In order to obtain provisional authorisation to stay in France for health care
(autorisation provisoire de séjour pour soins – APS), three documents are required: a doctor’s
recommendation, a valid passport and a sworn affidavit to leave the territory when the
treatment is finished. Generally speaking, an APS was granted for a renewable three-
month term. However, this procedure posed certain problems: the measure relies on
discretionary power, with variations from one prefecture to another; the authorisation is
only a precarious document; the APS is not valid as a work permit. These problems were
partially remedied by the circular of 24 June 1997 which provides for the delivery of a
temporary residence card, i.e. limited to three months, ‘if the report by the medical
health inspector of the département shows the necessity of long-term treatment for
foreigners in a situation such as this […], except in the case of a threat to public policy’.
Furthermore, it includes an authorisation to work, with ‘the wording “employee” if the
foreigner so requests and if the medical health inspector of the département deems that the
state of health of the person concerned is compatible with a professional activity’ 208.
145. In principle, Council of State jurisprudence obliges the administrative authorities to
make sure that the expulsion order does not contravene the provisions of article 8 of the
208 Ministry of the Interior, circular of 24 June 1997, relating to re-examining the situation of certain categories offoreigners in an irregular situation, NOR/INT/D/97/00104/C, point 1.7.; J.O., 26 June 1997, 9819. In order toavoid discretionary power, associations are asking for more precise wording in the circular. On the previousproblems raised, see Conseil national du sida [National AIDS Council]: Rapport suivi d’un avis sur la situation despersonnes atteintes par le VIH, de nationalité étrangère et en irrégularité de séjour [Follow-up report on an opinion of theNational AIDS Council on the situation of foreign nationals with the HIV virus residing unofficially in France],December 1995, p.29 . This category of ‘serious illness requiring medical treatment’ is confirmed by new article 29of the 1946 order, introduced by article 21 of the law of 11 May 1998; J.O., 12 May 1998, 7087.

The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 97
ECHR and that it is not likely to result in exceptionally severe consequences for the
person concerned.
It was judged that the expulsion of a person having undergone medical treatment did
not have exceptionally severe consequences for the personal situation of the petitioner,
even though the treatment had ceased on the date of the expulsion order and it had not
been established that the person’s state of health could be monitored under normal
conditions in the country of origin 209. By contrast, in the case of a person still undergoing
medical treatment, it was judged that returning the person to the border would have
severe consequences for the person concerned 210.
146. In an official statement on 12 July 1993, the National AIDS Council (Conseil
national du sida) recommended that ‘the authorities responsible for applying the law
should defer applying an expulsion in all cases where, due to a lack of proper health
resources and infrastructure, the patient would be unable to continue the medical
treatment which his state of health requires in the country to which he is returned. The
aim is to prevent expulsion resulting in consequences which are disproportionate to the
circumstances prompting the expulsion’.
147. One case raised the issue of France’s right to expel a Tunisian national undergoing
triple therapy 211. In this case, the person concerned, who was living with HIV/AIDS, was
expelled on 7 February 1997, despite the fact that he was in possession of a provisional
authorisation valid until 4 June 1997. This provisional authorisation was granted on the
grounds that there was no possibility of treatment in Tunisia. The person concerned had
lived in France since 1972 and been under an expulsion order since 1984. The Minister
of the Interior gave an assurance that this person would not be expelled without an
assessment by medical experts. Furthermore, during the forced evacuation of Africans
209 C.E., 28 December 1992, Gaz. Pal., 1993, Panorama de droit administratif [Overview of administrative law], 129.210 C.E., 19 June 1992, Gaz. Pal., 1993, Panorama de droit administratif, 27.211 Migration News Sheet, March 1997; Nouvel Observateur, 20-26 February 1997, p. 48; Libération, 25 March 1997, p. 14.
98 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
occupying the Saint Bernard church in Paris, the Prime Minister confirmed that ill
persons would not be expelled from France.
The Ministry of the Interior nevertheless decided to expel the Tunisian national on
the grounds that he represented ‘a serious threat to public policy’, even though his last
sentence, for theft, dated back to 1995 and the Isère prefecture had renewed his
residence permit. In its decision of 21 March 1997, the administrative court of Grenoble
ordered a stay of execution on the ruling endorsing the expulsion of the person
concerned, namely the ruling repealing the Tunisian national’s residency order. In fact
the court considered that the expulsion decision was likely to be quashed and that its
execution was severely prejudicial to the foreigner. The court held that the Minister of
the Interior had not examined all the consequences of his decision on the personal
situation of the person concerned.
148. Another case involving France, relating to an Angolan person suffering from AIDS,
was brought in Strasbourg but was thrown out by the Commission. The facts of the case are
as follows. Between 1986 and 1994, France granted several residence permits to the
petitioner and, as from 1991, he benefited from the provisions pertaining to non-suited
asylum-seekers. In 1995 the petitioner was sentenced by the Paris high court to one year in
prison and a ban on residing in French territory for three years for drug trafficking. After
serving his sentence, the petitioner was put under administrative detention with a view to
executing the Paris court’s decision to ban him from residing in the territory. In 1996, the
Paris court extended the administrative detention and ordered a medical examination, in
view of the fact that his very serious state of health prevented him from leaving France. The
Paris Court of Appeal confirmed this decision, saying firstly that the person concerned did
not fulfil the required conditions for obtaining a residency order and secondly that
according to the medical examination, his state of health was compatible with the
detention measure. Subsequently, the Paris prefectural police asked the doctor at the
detention centre to state whether detention was compatible with the petitioner’s state of
health. Following this the person concerned was released. The Minister of the Interior then
issued two orders. The first order was to expel the petitioner on the grounds that he posed a
threat to public policy. The second order stated that, due to the state of health of the person
concerned, he would be compelled to reside in Paris and must regularly report to the police.
The petitioner claimed that his expulsion from French territory would violate article 3

The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 99
of the ECHR because of his state of health. After the French government stated that the
petitioner would not be returned to his country unless his state of health improved or he
threatened public policy again, the Commission considered that the petitioner was no
longer a victim and that the dispute was resolved 212.
An action was also brought against France by a Congolese citizen living with AIDS.
As the expulsion was suspended, the Court said that there was no breach of article 3
ECHR 213. Two similar actions were brought by a Tunisian citizen and a Moroccan citizen 214.
149. In its report of December 1995, the National AIDS Council issued the following
conclusion: ‘the National AIDS Council considers the situation of foreign nationals
living with HIV/AIDS residing unofficially in France to be very worrying. Such persons
run the risk of being expelled to countries where they do not always have ties and where
they cannot always benefit from the medical follow-up required by their state of health.
In France, such persons suffer the dual problem of access to care and means of subsistence.
It would appear that in practice they are often deprived of their rights under the law’.
These various findings have led the National AIDS Council to make a number of
recommendations. These concern, in particular, the issuing of clear directives regarding:
the delivery of residence permits for health care; the submission of appraisals to
independent doctors specially trained in HIV pathology; and taking into consideration
the nature of the disease and the duration of treatment when fixing the duration of the
provisional residence authorisation 215. These recommendations are partially taken into
account in the circular of 24 June 1997 (supra, § 144).
2. Special categories2.1. Union citizens
150. With respect to the residence of Union citizens in France, decree no. 94/211 of 11
March 1994 regulating the conditions of entry and stay in France of citizens of the Member
States of the European Community benefiting from the free movement of persons states that a
212 Petition no. 30011/96, Lenga v. France.213 See supra, § 81214 Petitions nos 34794/97 and 37681/97.215 National AIDS Council, o.c., p. 27 et seq.

100 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
residence card may be refused if the applicant is suffering from one of the diseases or
infirmities figuring in the annexe (article 6) which might threaten public policy or public
safety. This annexe does not make reference to HIV/AIDS 216. Even though this provision
is intended to apply Directive 64/221, its wording is somewhat different, in that it
replaces the notion of ‘public health’ referred to in the directive by the notion of ‘disease
or infirmity which might threaten public policy or public safety’ . Even though this
wording cannot be interpreted differently from the notion of public health in the
directive, it does lead to the a contrario possibility that public health may be included in
the notion of public policy for foreigners in general.
2.2. Students
151. In order to obtain a ‘student’ residence permit a medical certificate must be
established by a doctor approved by the IMO in France.
2.3. Refugees
152. Article 12 of the 1946 decree provides that refugees and members of their family, as
well as the family members of stateless persons, must provide a medical certificate.
The HIV test is not compulsory for refugees. Asylum-seekers who enter the national
reception centre scheme are therefore not screened, except if they so request.
Nevertheless, some doctors systematically offer screening in which case it is generally
requested 217. The person’s state of health does not constitute legitimate grounds for
obtaining refugee status 218.
216 The annexe covers ‘1. Drug addiction. 2. Blatant psychological or mental disorders, clear states of excitative typepsychosis, paranoid psychosis or hallucinations or mental confusion’ .
217 Information provided by France Terre d’Asile on 8 April 1997.218 Information contained in the document published by Aides entitled ‘Les différents titres de séjour’ [Different types
of residence permit].

The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 101
7. (FIN) Finland1. Foreigners in general1.1. Entry
153. The Finnish Aliens’ Act of 22 February 1991 does not provide for refusal of entry to
foreigners on grounds of public health.
Article 37 mentions the general conditions of entry to Finland. Public health is not
mentioned, and neither is public policy in general. The law refers to more specific cases,
such as a criminal sentence.
HIV/AIDS is not used as grounds for refusing right of entry 219.
Article 12 of decree 14/94 on foreigners states that a visa must be granted if refusing
entry would be unreasonable in view of the state of health of the person concerned or of
that of related or closely associated persons.
1.2. Residence
154. The law provides that a residence permit can be rescinded if the foreigner misleads
the authorities as to his identity, gives false information or conceals certain information,
or for ‘other strong grounds’ (article 21). However, right of residence can neither be
refused nor revoked on the grounds of HIV/AIDS 220.
155. Article 28 of the Finnish Aliens’ Act stipulates that a foreigner requesting a work
permit may be required to supply certain information, particularly regarding his state of
health. Parallel with this, article 21 of decree 142/94 on foreigners states that the work
permit application must contain the information specified in article 28 of the Aliens’
Act, except in certain cases where such information is not necessary according to
instructions from the Ministry of Labour. A description of the foreign applicant’s state of
health is required in cases where it is required of a Finnish national applying for a similar
job. Article 28 is therefore not a provision allowing an HIV test to be imposed on
foreigners requesting a permit to work in Finland 221.
219 Information provided by the Ombudsman for Foreigners on 25 March 1997.220 Information provided by the Ministry of the Interior on 16 April 1997.221 Information provided by the Ombudsman for Foreigners on 25 March 1997.

102 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
1.3. Expulsion
156. Article 40 of the Aliens’ Act lists the grounds for expelling a foreigner. This article
states that a foreigner may be expelled if he has no residence permit, is unable to support
himself, commits an offence, or demonstrates by his behaviour that he is a danger to
others or is engaged in illegal activities, espionage or sabotage. There is no express
provision for the expulsion of a foreigner in general on public health grounds. HIV/AIDS
is not a reason for expulsion. On the contrary, it appears that expulsion can be ruled out
on the grounds of a foreigner’s state of health. The Finnish courts will have to take
cognisance of a lawsuit concerning the transmission of the virus by an American national
to a third party, even though he knew he was infected by the disease. If this person is
sentenced, he may be expelled because of the fact that he knowingly passed on the
disease and not merely on the grounds of HIV/AIDS 222.
2. Special categories2.1. Union citizens
157. Foreigners entitled to residence on the basis of Union law may only be expelled if
they pose a threat to public policy, public safety or public health (article 40 in fine). A
ministerial circular was issued concerning the application of general legislation relating to
foreigners to comply with Union law, in particular Directive 64/221 223. Article 40 does
not permit the expulsion of Union citizens living with HIV/AIDS 224.
2.2. Students
158. There is no compulsory screening for students 225. The test is carried out only on a
voluntary basis 226.
222 Information provided by the Ombudsman for Foreigners on 25 March 1997.223 Ministry of the Interior Circular of the 8/010/93 and Instruction 10/010/94 relating to the application of the
provisions of the Aliens’ Act in compliance with Community law (Regulations 1612/68 and 1251/70, Directives68/360, 64/221, 73/148, 73/34, 90/364, 90/365 and 93/96).
224 Information provided by the Ministry of the Interior on 16 April 1997.225 Information provided by the Ombudsman for Foreigners on 25 March 1997.226 Information provided by the Ministry of the Interior on 16 April 1997.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 103
2.3. Refugees
159. Article 40 provides for the expulsion of refugees if they threaten national security or
public policy, though not public health.
Asylum-seekers must undergo a physical examination but the decision relating to the
request for asylum is not influenced by whether or not the asylum-seeker is suffering from
HIV/AIDS. Nevertheless, if the asylum seeker is in a particularly poor state of health, he
may be granted right of residence even if he does not fulfil all the conditions 227. The HIV
test is performed on a voluntary basis 228.
8. (GR) Greece1. Foreigners in general1.1. Entry
160. The provisions relating to foreigners are found in law 1975/91 of 21 November 1991.
This law does not apply to people entitled to residence under Community law.
Article 6, paragraph 5, letter a, of law 1975/91 states that entry will be refused to any
foreigner suffering from a disease which, by virtue of a decision by the Minister
competent on subjects of health in accordance with international WHO rules, is deemed
as capable of constituting a danger to public health. Nevertheless, no ministerial decision
has ever been adopted with relation to HIV/AIDS.
161. Article 22-4 of the same law provides that authorisation to enter Greece for work
reasons may be revoked or suspended for public health reasons.
1.2. Residence
162. Article 12 of the Aliens’ Act states that public health is one of the elements which
should be taken into account when granting a short-term residence permit.
The HIV test is considered to be a prerequisite for extradited persons and for certain
foreigners requesting a work permit 229. Circular number 4548/90 states that the test must
be performed after the person has received proper information and given his consent.
This circular has no legal value but sets out guidelines.
227 Information provided by the Ombudsman for Foreigners on 25 March 1997.228 Information provided by the Ministry of the Interior on 16 April 1997.229 Circular 4548/90.

104 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
Performing artists requesting a work permit who are suspected of being ill are
subjected to a test 230.
163. Article 31, paragraph 2 of the Aliens’ Act states that the public services are obliged
to refuse to examine a request from a foreigner who is not in possession of the requisite
residence permit or who cannot prove that he is legally resident. It is stipulated that
hospitals are exempted from fulfilling this obligation if the foreigner has entered Greece
for emergency treatment.
1.3. Expulsion
164. One of the grounds for expulsion mentioned in article 27, paragraph 1, letter c, of
the Greek law is where the presence of the person concerned on Greek territory is
considered to be a danger to public health. There would appear to have been expulsions
for HIV/AIDS-related reasons 231.
1.4. Code
165. The Greek Centre for the Control of Infectious Diseases (Keel) has established a
code of basic principles for protecting persons living with HIV/AIDS. With regard to
foreigners, this code considers that screening should not be authorised upon entry to the
territory or for granting the right of residence. The code also considers that HIV/AIDS
should not be used to justify expulsion, that no test should be imposed on refugees and
students and that the presence of HIV/AIDS should not lead to refusal of the right
of asylum.
2. Special categories2.1. Union citizens
166. Entry to the territory and the right of residence of Union citizens is governed not by
general legislation but by special legislation 232. This special legislation transposes
230 Memorandum from the Ministry of Foreign Affairs of 8 August 1988.231 A. HENDRIKS, o.c., p. 197.232 Presidential decree no. 525 of 31 December 1983 transposing Directives 64/221, 73/148, 75/34 and 75/35
supplemented, for other directives, by presidential decrees 499/1987 and 278/1992.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 105
Community law. A medical certificate may be requested 233. Reference should be made
to Directive 64/221 234.
2.2. Students
167. Article 15 of the Aliens’ Act concerns student residence permits. Medical
and pharmaceutical expenses are taken into consideration when authorising the
renewal of residence permits, as is the absence of danger to public health.
The HIV test is imposed on students from countries where the epidemic is
very widespread 235.
2.3. Refugees
168. Article 24 of law 1975/91 relates to refugees. This article states that the conditions
and procedure for granting medical and pharmaceutical care are governed by a
presidential decree proposed by the competent ministers.
9. (I) Italy1. Foreigners in general1.1. Entry
169. Article 3 of the law of 28 February 1990 on foreigners, concerning the documents
required by third country nationals to enter Italy, states that before a visa may be issued,
the foreigner must be in compliance with health provisions. Nevertheless, there are no
health regulations which must be respected by third country nationals 236. Entry may be
refused in order to curb the spread of a contagious disease 237.
233 P. VERBIST, in Center for International Legal Studies, D. Campbell (Ed.), International Immigration and NationalityLaw, Greece, The Hague, Kluwer, 1994, III, 2, 3 and 4.
234 Supra, §§ 35 et seq.235 Circular 4548/90. See also, P. CATTORINI, D. MORELLI and M. ZANCHETTI, AIDS: comparison and analysis
of European legislation on AIDS from the ethical and legal standpoint, Istituto Scientifico H. San Raffaele, 1996, p. 75.236 Information provided by F. Trucillo on 2 May 1997. See also F. LEITA, in B. NASCIMBENE (E.), La condizione
giuridica dello straniero, Diritto vigente e prospettive di riforma, Padova, CEDAM, 1997, p. 176.237 A. CORRADO and R. TARDIOLI, in Center for International Legal Studies, D. Campbell (Ed.), International
Immigration and Nationality Law, Italy, The Hague, Kluwer, 1994, III, 2.
106 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
1.2. Residence
170. A residence permit for the purposes of tourism, studies or work for nationals from third
countries may be refused on health grounds. Article 4-12 of the law of 1990, regarding the
residence of third country nationals, provides for refusal to grant residence on grounds of
public health. Article 4 (2) of statutory order no. 489 of 18 November 1995 stipulated a
health inspection for immigrants. This inspection was also provided for in statutory order
no. 132 of 19 March 1996 and statutory order no. 269 of 17 May 1996. By contrast, in the
statutory order of 16 July 1996, no reference is made to a health inspection.
HIV screening was proposed for tourists and immigrants but it was judged to be futile
and discriminatory. The Italian government has rejected such practices.
Widespread compulsory screening is expressly prohibited by article 5 c.3 of law
no. 135 of 15 June 1990. According to this provision, ‘nobody may be subjected, without
their express consent, to tests aimed at establishing the presence of HIV infection, except
for reasons of clinical necessity or in the person’s own interest’ . Given that there is no
compulsory screening for foreigners, right of residence is not refused on the grounds of
HIV/AIDS 238.
The immigration legislation reforms examined by the Italian Parliament in May
1997 among others concern public health, but there is no provision to introduce a
compulsory HIV test.
1.3. Expulsion
171. Article 7 of the statutory order of 17 May 1996 239 provides for expulsion to be
decided on the grounds of public policy and state security. Public health is not expressly
mentioned.
Expulsion may not be justified by HIV/AIDS 240.
2. Special categories2.1. Union citizens
172. In Italy there are no special provisions governing the entry and residence of
Union citizens.
238 Information provided by F. Trucillo on 2 May 1997.239 Statutory order of 17 May 1996, no. 269, Gazzetta ufficiale della republica italiana, 18 May 1996, 21.240 Information provided by F. Trucillo on 2 May 1997.
2.2. Refugees
173. There is no compulsory screening for refugees. Consequently, HIV/AIDS is not used
as grounds for refusing the right of asylum 241.
10. (IRL) Ireland1. Foreigners in general1.1. Entry
174. The Aliens’ Act provides for a medical examination upon entry to the country 242.
The immigration officer may refuse authorisation to enter the country in cases where
a foreigner is suffering from a disease figuring in the annexe to the law 243. This annexe
reproduces the exact list of diseases mentioned in Directive 64/221.
At present there are no restrictions on the entry of persons living with HIV/AIDS 244.
1.2. Residence
175. A residence permit may not be refused for HIV/AIDS-related reasons 245.
1.3. Expulsion
176. In practice nobody would appear to have been expelled on the grounds of
HIV/AIDS 246.
2. Special categories2.1. Union citizens
177. Entry may be refused to Union citizens suffering from one of the diseases mentioned
in the annexe to the law on the entry and residence of Union citizens, which reproduces
Directive 64/221 247.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 107
241 Information provided by F. Trucillo on 2 May 1997.242 Aliens Order 1946, article 7 (1).243 Aliens Order 1975, article 5 (2).244 Information provided by The Irish Refugee Council on 18 April 1997.245 Information provided by The Irish Refugee Council on 18 April 1997.246 Information provided by The Irish Refugee Council on 18 April 1997.247 European Communities (Aliens) Regulations 1977, article 4 and European Communities (right of residence for non-
economically active persons) Regulations 1993, article 4.

A medical examination may be imposed on Union citizens to check whether they
are suffering from one of the diseases mentioned in the Schedule (European Communities
(Aliens) Regulations, article 10). If the person concerned does not submit to this
examination, delivery of the first residence permit may be refused (article 12). The only
diseases which may justify a refusal to deliver the first residence permit are those listed in
the Schedule (article 12). These principles are reiterated in the text relating to the right
of residence of non-economically active Union citizens (European Communities
Regulations 1993, article 6).
178. Union citizens may be expelled if a first residence permit has not yet been issued and
the person is suffering from one of the diseases mentioned in the annexe. These are the
diseases mentioned in Directive 64/221 248.
2.2. Refugees
179. There is no compulsory test for refugees and it would appear that HIV/AIDS is not
used as grounds for refusing the right of asylum 249.
11. (L) Luxembourg1. Foreigners in general1.1. Entry
180. A foreigner likely to jeopardise public health may be refused entry to Luxembourg 250.
Any foreigner entering the Grand Duchy may be obliged to undergo a medical
examination. The medical examination upon entry to the territory may not include
HIV/AIDS testing. Article 5 of the grand-ducal Regulation of 17 October 1995 relating to
the medical examination of foreigners, reproduces the classic list of the European Directive
64/221 but, after the ‘other infectious or parasitic illnesses mentioned in protective
provisions concerning national citizens’ adds the words ‘with the exception of
HIV/AIDS’.
108 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
248 European Communities (Aliens) Regulations 1977, articles 12 and 14 and European Communities (right of residence fornon-economically active persons) Regulations 1993, article 7.
249 Information provided by The Irish Refugee Council on 18 April 1997.250 Article 2 of the law of 28 March 1972 concerning the entry and residence of foreigners, the medical control of foreigners
and the employment of foreign workers.

1.2. Residence
181. A foreigner likely to jeopardise public health may be refused residence (article 2).
Any foreigner declining to undergo the medical examination specified in article 21
of the law, or one who knowingly misinforms the authority responsible for this
examination regarding his state of health, may be refused authorisation to settle in
Luxembourg (article 5, paragraph 6).
The foreigners’ identity card may be withdrawn or its renewal refused in cases where
a foreigner is likely to jeopardise public health (article 6).
Any foreigner, with the exception of Union citizens, who is planning to reside in
Luxembourg for longer than three months, must undergo a medical examination within
three days of entering the country (article 2 of the grand-ducal Regulation of 17 October
1995 relating to the medical examination of foreigners). A foreigner whose foreigners’ identity
card has expired and who wishes to re-establish his residence in Luxembourg must
undergo a further medical examination (article 3 of the regulation).
As in the case of entry to the country, the medical examination may not include
HIV/AIDS since this disease is expressly excluded by article 5 of the aforesaid regulations
(supra, § 180).
In its opinion on the draft of modification of the 28 March 1972 law (by the law of
18 August 1995), concerning the medical examination of foreigners, the Council of State
drew attention to the fact that article 21 theoretically allowed the possibility of
submitting certain foreigners to screening. Paragraph 1 of article 21 provides that ‘with
the exception of nationals from European Union Member States, but without prejudice
to the provisions of paragraph 2 of the present article, any foreigner entering the Grand
Duchy and any foreigner wishing to reside there may be obliged to undergo a medical
examination’. Paragraph 2 states ‘If during a border control, the officials in charge of
controlling persons have doubts as to a foreigner’s state of health, they may call for a
doctor and demand a medical examination of the person concerned’. The Council of
State deemed that instructions needed to be given to prevent any abuses, which has not
been done on 31 December 1997. Nevertheless, right of residence has never been refused
for HIV/AIDS-related reasons 251.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 109
251 Information provided by the SESOPI - Inter-Community Centre (SESOPI - Centre intercommunautaire) on 10 April 1997 and the Health Ministry on 18 April 1997.

1.3. Expulsion
182. Any foreigner likely to jeopardise public health may be expelled (article 9, paragraph
1). There are provisions for removal from the territory by the law enforcement authority,
especially for foreigners not authorised to reside in the country who have been refused
entry because they are likely to jeopardise public health or for foreigners not authorised to
reside in the country, who in the cases mentioned in article 2, paragraph 2 of the
Application Convention of the Schengen Agreement, are likely to jeopardise public
policy (article 12). There has never been an expulsion or removal on HIV/AIDS-related
grounds 252. Article 14 expressly states that no expulsion or deportation may be decided if
in the country of destination the foreigner is exposed to treatment contrary to article 3 of
the ECHR. In the case of persons living with HIV/AIDS, the fact that they have no
access to treatment for the disease in the country of destination could fall within the
scope of application of article 3 of the ECHR 253.
Where a foreigner cannot be expelled immediately and is made subject to a
placement order, he has the right to be examined by a doctor (article 15, paragraph 6).
2. Special categories2.1. Union citizens
183. Union citizens are not, in principle, required to undergo the medical examination for
foreigners under common law (article 21 of the law of 28 March 1972; article 1 of the grand-
ducal Regulation of 17 October 1995 relating to the medical examination of foreigners).
However, article 21, paragraph 1 of the law of 1972 does stipulate that it applies
without prejudice to the provisions of paragraph 2, which states that ‘if during a control,
the officials responsible for controlling persons have doubts as to a foreigner’s state of
health, they may call for a doctor and demand a medical examination of the person
concerned’.
110 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
252 Information provided by the Health Ministry on 18 April 1997.253 See supra, § 76.
12. (NL) Netherlands1. Foreigners in general1.1. Entry
184. Article 8 of the 3 January 1965 Aliens’ Act mentions public policy, the peace and
national security as general conditions for entering the territory. Public health is not
expressly mentioned.
Legislation on immigration does not provide for medical controls upon entry to the
territory.
185. There is no HIV test at borders and no seronegativity certificate is required for entry
to the territory 254.
186. Where an application for entry is made on medical grounds, an inquiry is carried out
by the Ministry of Justice Medical Inspector.
1.2. Residence
187. HIV/AIDS is not used as grounds for refusing the right of residence 255.
1.3. Expulsion
188. Dutch legislation does not provide for expulsion to be decided on public health
grounds. HIV/AIDS does not in principle serve as grounds for expulsion 256.
189. The Aliens’ Act states that a foreigner may not be expelled if his return is unjustified
in view of his state of health (Aliens’ Act of 13 January 1965, article 25).
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 111
254 D. ZEEGERS, ‘Droit et sida: perspectives aux Pays-Bas’ [Law and AIDS: perspectives in the Netherlands], Droit etsida: comparaison internationale, o.c., p. 339; information confirmed by the Ministry of Justice on 10 June 1997.
255 Information provided by the Ministry of Justice on 10 June 1997. It transpires from the documents forwarded bythe Dutch administration that, since 1994, the question of granting right of residence to persons living withHIV/AIDS has arisen in practice. It appears that the expulsion of foreigners suffering from the virus was rejected. Itthen remained to settle the question of whether HIV/AIDS could justify a residence authorisation. There iscontroversy over the issue of whether right of residence should be granted on the basis of article 25 of the Aliens’Act, explicitly mentioning the state of health, or on the basis of humanitarian grounds. The latter is preferredbecause it leaves greater latitude to decide on a case-by-case basis, especially with regard to the cost of health careto the state.
256 Idem.

190. Foreigners who are in the terminal stages of AIDS are not expelled from the
Netherlands 257.
2. Special categories2.1. Union citizens
191. Article 91, point 1, letter b of the decree of 19 September 1966 on foreigners states
that Union citizens suffering from one of the diseases listed in the annexe may be refused
entry. This provision does not apply to nationals of Belgium and Luxembourg. Even
though it is clearly based on the BENELUX Treaty of 3 February 1958, this exception is
not found expressis verbis in Belgian and Luxembourg legislation. The annexe, which
reproduces the list of diseases figuring in Directive 64/221, does not expressly mention
HIV/AIDS. This point is emphasised by doctrine 258. Unless it is expressly mentioned,
HIV/AIDS may not lead to a Union citizen being refused entry or expelled 259.
192. In accordance with article 97 of the decree, if a foreigner comes under any of the
categories mentioned in article 94 (persons entitled to residence on the basis of Directive
68/360, Regulation 1251/70, Directive 73/148, Directive 75/34, the three Directives on
the right of residence: 90/364, 90/365 and 93/96), a residence permit may be refused if the
foreigner is suffering from one of the diseases listed in the annexe.
2.2. Refugees
193. Refugees are only submitted to an HIV test on a voluntary basis and HIV/AIDS is
not used as grounds for refusing the right of asylum 260.
According to practitioners, recent jurisprudence shows that right of residence or
asylum is more freely granted where the requisite medical treatment is unavailable in the
country of origin 261.
112 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
257 Information provided by the Ministry of Justice on 10 June 1997.258 T.L. BADOUX, in Center for International Legal Studies, D. Campbell (Ed.), International Immigration and Nationality
Law, The Netherlands, The Hague, Kluwer, 1994, VII, 17.259 Information provided by the Ministry of Justice on 10 June 1997. See supra, §§ 35 seq.260 Information provided by the Ministry of Justice on 10 June 1997.261 Information provided by HIV Vereniging Nederland on 10 March 1997, by Vluchtelingen Werk on 3 April 1997 and
by the Ministry of Justice on 10 June 1997.

13. (P) Portugal1. Foreigners in general1.1. Entry
194. Article 10 of the 3 March 1993 Aliens’ Act 262 provides for entry to be prohibited in
cases where there is a threat to public policy or national security, but not on the grounds
of public health.
195. There is no systematic screening at borders.
1.2. Residence
196. In order to obtain a short-stay visa, the Aliens’ Act of 3 March 1993 stipulates that
the person concerned must not endanger public policy or national security (article 33-4),
although public health is not expressly mentioned in article 33 of the law of 3 March 1993.
197. Article 4-1 of the decree of 15 December 1993 263 applicable to third country
nationals calls for a medical certificate to accompany applications for residence, work and
study permits, which must be obtained prior to application for residence. This certificate
must prove that the person concerned is suffering from no infectious or contagious
disease. AIDS is included in the notion of infectious or contagious disease 264.
1.3. Expulsion
198. The Aliens’ Act of 3 March 1993 provides for expulsion to be decided on grounds of
national security, public policy and morals, but not for public health reasons (article 67).
2. Special categories2.1. Union citizens
199. Article 12 of the decree of 3 March 1993 (statutory order n° 60/93 of 3 March),
concerning Union citizens and their families, states that entry may be refused on the
grounds of public health. This decree reproduces the list of diseases mentioned in
Directive 64/221.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 113
262 Statutory order n° 59/93 of 3 March.263 Decreto regulamentar no. 43/93.264 Information provided by the Portuguese Embassy in Brussels on 17 January 1997.
200. Union citizens and their families may be refused residence on public health grounds
if the person is suffering from one of the diseases mentioned in decree 60/93 referring to
those listed in Directive 64/221. In compliance with the directive, if any of these diseases
occurs after right of residence is granted, an extension to the right of residence may not
be refused (statutory order 60/93, article 12).
201. Union citizens may only be expelled on public health grounds if they are suffering
from a disease mentioned in article 12 of statutory order 60/93.
14. (S) Sweden1. Foreigners in general1.1. Entry
202. The Aliens Act (1989:529) 265 with amendments October 1997, does not provide for
entry to be refused on the grounds of public health. Chapter 4 of this act list the grounds
for refusing entry to the territory. Public health is not one of these. Generally speaking,
although public policy does not figure on the list either, the law does state that entry may
be refused, for instance, in cases where the person concerned has received a criminal
sentence or is suspected of illegal activities.
203. Screening is sometimes offered to immigrants on a voluntary basis 266.
Swedish law allows compulsory screening only in association with body searches
(article 28:12 of the Code of Procedure). In fact, compulsory screening is contrary to the
constitution (article 6 of Chapter II) which affirms that all citizens are protected against
any forced physical violation at the hands of the public authorities. In the absence of
specific provisions, foreigners benefit from the same rights as Swedish citizens with regard
to protection against physical violation (article 2: 2; article 3:5).
114 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
265 As modified in October 1997.266 L. WESTERHALL and A. SALDEEN, ‘Réflexions sur le sida et le droit suédois’ [Remarks on AIDS and Swedish
law], Droit et sida, comparaison internationale, o.c., p. 393; information confirmed by the National Immigration Boardon 24 April 1997.
In Sweden it is thought that compulsory screening would not alter the epidemiology
of AIDS 267.
1.2. Residence
204. HIV/AIDS is not used as grounds for refusing the right of residence in Sweden 268.
Medical information is not one of the elements on which residence permit decisions are
based.
205. In the case of international child adoption, the adoptive parents may indicate their
agreement to a test being carried out 269.
1.3. Expulsion
206. Expulsion for public health reasons is not covered by legislation on foreigners.
Expulsion is possible where there is a threat to national security 270. However, it would
seem that in practice people cannot be expelled on the grounds of HIV/AIDS 271.
2. Special categories2.1. Refugees
207. Refugees are not subject to a compulsory HIV test 272. However, it is possible for
asylum-seekers not to be informed that the test is voluntary and can be refused 273.
There have been several cases of refugees being authorised to remain in Sweden even
when it was discovered that such persons were living with HIV/AIDS. It was considered
inhumane to expel them 274.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 115
267 M. SALOMONET and R. TOUBON, Sida, sociétés et populations, o.c., p. 238.268 Information provided by The Noah’s Ark-Red Cross Foundation on 25 April 1997 and by the National Immigration
Board on 24 April 1997.269 General recommendations no. 20 of 30 August 1989 from the Department of Health on the medical examination
of children adopted abroad.270 M. BRORSSON in Center for International Legal Studies, D. Campbell (Ed.), International Immigration and
Nationality Law, Sweden, The Hague, Kluwer, 1994, 0-1; section 11 of the Aliens Act (1989:529).271 Information provided by The Noah’s Ark-Red Cross Foundation on 25 April 1997 and the National Immigration
Board on 24 April 1997.272 Information provided by the National Immigration Board on 24 April 1997.273 M. HAOUR-KNIPE, Migrants and travellers group, final report, Lausanne, Institut universitaire de médecine sociale
et prévention, Cahiers de recherche et de documentation, 1991, p. 61; EUROCASO, Report of the first seminar on lawand HIV/AIDS, Amsterdam, 13-14 April 1991, p. 66.
274 EUROCASO, Report of the first seminar on law and HIV/AIDS, o.c., p. 66.

15. (UK) United Kingdom1. Foreigners in general1.1. Entry
208. Persons arriving in the United Kingdom may be examined by a medical inspector
(Schedule 2, Section 4, Part I, 2 of the 1971 Immigration Act, paragraph 8 of the
Regulation of 23 May 1994 275). The immigration officer may authorise entry but demand
a further medical examination in the interests of public health (Schedule 2, Section 4,
Part I, 7 of the Immigration Act). Where it is decided not to refuse entry on
humanitarian grounds, the immigration officer tells the foreigner to report to the medical
health inspector for a further examination and treatment (paragraph 38 of the 1994
regulation).
209. Article 36 of the Regulation of 23 May 1994 provides that persons arriving in the
United Kingdom to receive medical care should be referred to the medical inspector.
It has been judged that the argument that the disease can be treated in the country
of origin is not enough to refuse entry to the territory 276.
210. Formerly the Ministers of the Interior and of Health declared that entry would be
prohibited to people carrying the HIV virus, with application of the measure being left to
the discretion of port or airport officials 277. Immigration officers apparently frequently
detained visitors belonging to groups at risk, in order to ask them questions concerning
their state of health and financial situation, sometimes trying to intimidate them 278.
Furthermore, it would appear that the ‘Viral Infectivity Regulations’ applied in English
prisons (a policy favouring the segregation of HIV-positive prisoners and the imposition
116 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
275 HC 395.276 Immigration Appeal Board, Mohan, (1973) Immigration Appeal Reports 9.277 M. VINCINEAU (editor) Le sida, un défi aux droits, actes, 1991, p. 94.278 Information provided by Mr. D. Geer from the Immunity Legal Centre, during an interview on 16 May 1992, in
Etude comparative sur la discrimination à l’encontre des séropositifs et des malades du sida [Comparative study ondiscrimination against people who are HIV-positive or suffering from AIDS].
279 Information provided by Mrs K. Hutton from the National AIDS Trust during an interview on 15 May 1992, inEtude comparative sur la discrimination à l’encontre des séropositifs et des malades du sida.
of limitations on medical confidentiality) had been applied by immigration officers to
foreigners living with HIV/AIDS 279.
211. A Ministry of the Interior BDI general policy document explains to immigration
officials the directives they should follow for persons living with HIV/AIDS.
The provisions set out in the immigration rules are applied without derogation to
applications for entry to the country. Entry is refused where the person concerned is not
entitled under the immigration provisions 280. Where immigration officers are aware that a
foreigner requesting entry to the territory is suffering from AIDS, the foreigner must
prove that he has sufficient financial means to pay for his medical treatment.
The fact that someone has AIDS or is HIV positive is not in itself grounds for
refusing entry clearance. However, where in any case it appears that public health may be
at risk, advice would be sought from the Department of Health 281.
1.2. Residence
212. Any person intending to stay in the United Kingdom for more than six months
must normally report to the medical inspector (paragraph 36 of the Regulation of
23 May 1994).
If the inspector finds that the foreigner is suffering from an illness which might affect
his ability to support himself and his family, this factor will be taken into account when
granting right of residence (paragraph 37 of the Regulation of 23 May 1994).
The conditions of residence for medical reasons are set out in paragraph 51 of the
1994 Regulations. It is necessary for the foreigner:
■ to comply with paragraph 41 concerning entry to the territory
■ in the case of a communicable disease, to have satisfied the medical inspector that
there is no danger to public health
■ to show, if required, that the treatment is of finite duration
■ to have the intention of leaving the United Kingdom at the end of the treatment
■ to provide various forms of proof regarding the treatment, its costs and the person’s
financial ability to pay such costs.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 117
280 Information confirmed by the Immigration and Nationality Directorate on 8 September 1997.281 Information provided by the Immigration and Nationality Directorate on 8 September 1997.
Where the conditions of paragraph 51 are satisfied, right of residence is granted for a
renewable period of six months (§§ 52 et seq.).
213. By virtue of the directives contained in the aforementioned BDI document,
applications for a residence permit from persons living with HIV/AIDS must be dealt
with on the facts of the case in accordance with the rules in force. However, there is
scope for a derogation on serious humanitarian grounds. Point 3 states that, in certain
cases where there is clearly no means of treatment available in the applicant’s country of
origin and it is likely that this lack of treatment will significantly reduce the life
expectancy of the person concerned, a residence permit should normally be granted.
214. Instructions have been issued by the Home Office for granting a three-month
residence permit to a foreigner wishing to care for a member of his family. If it involves a
friend, the permit is in principle refused except in an emergency. The permit is granted
on a discretionary basis, independently of the rules on immigration.
215. In the case of work permits, an application may pose problems where the person is
living with HIV/AIDS 282.
216. The High Court judged that two European citizens suffering from HIV/AIDS had no
right to temporary shelter, as provided for under the law, on the grounds that they were
unemployed and were not officially resident in the United Kingdom 283. The Home Office
had informed one of the persons concerned that he was not officially resident but that no
measures would be taken to oblige him to leave the territory. The Home Office had taken
no position regarding the other person.
The Court of Appeal reversed the High Court’s decision 284 on the grounds that the
people concerned did not require a residence permit.
It can be inferred from the High Court decision that persons living with HIV/AIDS
may be considered as unlawfully resident, not because of the disease itself but because
they are not working or do not have sufficient resources. The point raised in such cases is
the lack of financial means and not the existence of HIV/AIDS but the result is the same,
118 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
282 D. HARRIS and R. HAIGH, AIDS , a guide to law, London, Routledge, 1990, p. 1170.283 English High Court; Times Law Report, 20 October 1995.284 Court of Appeal; Times Law Report, 27 February 1996.
namely that the presence of the person concerned on national territory is unlawful. It can
be inferred from the Court of Appeal decision reversing the High Court decision that
Union citizens are better protected in that they may not be refused right to temporary
shelter since they are not required to have prior authorisation to stay in the country.
216b. On 19 December 1997, a High Court judge ruled that a Brazilian illegal immigrant
suffering from AIDS was entitled to claim food, shelter and health care from the local
council until he became fit enough to travel home. The High Court pointed out that the
law of humanity was above all laws and that it was a ‘duty of all civilized nations to
safeguard life and health’ so that the assistance is needed as long as ‘he cannot undertake
the journey out of the UK without risk to his life or serious injuries to his health’ 285.
217. As a rule, English public hospitals are obliged to care for any person who is in the
country. However, the National Health Service provisions (Charges to overseas visitors)
1989 Regulations relating to hospital costs owed by foreigners are sometimes used to refuse
medical care to certain patients 285b. For instance, certain hospitals require persons of
African origin to produce a British passport or establish that they are solvent 286.
1.3. Expulsion
218. People may be expelled from the United Kingdom in two cases. The first is where
there is a criminal sentence. The second relates to a decision by the Home Secretary.
Section 3 of the Immigration Act establishes three grounds for expulsion in this respect:
1. Failure to comply with a condition relating to the residence permit.
2. Where it is in the public interest.
3. In the case of the spouse or child of a person who is to be expelled.
A person living with HIV/AIDS may be expelled in the second case 287.
219. In accordance with information provided by the Home Office, foreigners with no
right of residence have been expelled after receiving treatment for HIV/AIDS 288.
The free movement of persons living with HIV/AIDS – Part 2: European Union Member States 119
285 Migration News Sheet, October 1997 and January 1998, p. 6 and information from The Terrence Higgins Trust.285b Information provided by The Terrence Higgins Trust on 9 May 1997.286 Étude comparative sur la discrimination à l’encontre des séropositifs et malades du sida, o.c., p. 141.287 D. HARRIS and R. HAIGH, o.c., p. 120.288 Black HIV/AIDS Network, BHAN policy Report 1- AIDS and the black communities (London, 1991), p. 28, in
Étude comparative sur la discrimination à l’encontre des séropositifs et malades du sida.

220. The European Court of Human Rights ruled the expulsion by the United Kingdom
of a national from St. Kitts who was seriously ill with HIV/AIDS and had no possibility of
treatment in his country of origin, to be contrary to ECHR article 3 (see supra, § 76).
2. Special categories2.1. Union citizens
221. Union citizens are not, in principle, subject to the system of prior authorisation for
entry or residence in the territory 289. Neither are such persons subject to the aforesaid
health inspections (s. 7 (1)). First residence could therefore only be refused under the
provisions of Directive 64/221.
This explains why the Court of Appeal deemed that European nationals could not be
expelled on the grounds that they were not given a residence permit because they lacked
sufficient means of subsistence, since they do not need prior authorisation (supra, § 215).
222. Right of residence is granted to the family members of a Union citizen under certain
conditions, including the absence of a threat to public health (paragraph 259 of the
Regulation of 23 May 1994).
2.2. Refugees
223. According to practitioners, there is no compulsory test for asylum seekers, and right
of asylum may not be refused on the grounds of HIV/AIDS 290. Nevertheless, refugees are
subject to general legislation on foreigners under common law for entry to the territory
(supra, §§ 208 seq.).
120 The free movement of persons living with HIV/AIDS – Part 2: European Union Member States
289 Immigration Act 1988 (1988 C 14), Section 7, Persons exercising Community Rights and Nationals of MemberStates.
290 Information provided by The Terrence Higgins Trust on 9 May 1997 and confirmed by the Immigration andNationality Directorate on 8 September 1997.
Third CountriesPart 3
122 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
I PresentationA. Description224. The third part is devoted to the legislations and practices in countries outside the
European Union with which the Union has co-operation programmes. This part is
divided into three sections.
225. The first section is an across-the-board approach which summarizes the general
tendencies in all the countries examined (II). This general examination is sub-divided
into three subdivisions dealing with (A) the entry, (B) the residence and (C) the
expulsion of persons living with HIV/AIDS.
A second section gives the conclusions of this across-the-board approach (III).
The third section examines, for each of the third countries studied, the laws, the
regulations and, as far as possible, the practice concerning the movement of persons
living with HIV/AIDS (IV). This part of the study is based mainly on an analysis of
legislative and reglementary texts adopted by these states concerning immigration or
AIDS prevention. This main source was supplemented by an analysis of doctrine relating
to the issue of the free movement of persons living with HIV/AIDS, as well as practical
information obtained from governmental and non-governmental organizations.
B. Main conclusions from Part 3226. As regards the right of entry, express restrictions of the right of access to the
territory for foreigners living with HIV/AIDS are relatively rare in the countries studied.
However, in the numerous countries in which the legislation contains provisions
concerning access to the territory regarding public health or requirements for medical
controls, the possibility of limiting the right of access for HIV positive foreigners or those
who are suffering from AIDS is not excluded, even in the absence of express stipulations
to this effect.
As regards the right to residence, several states have adopted specific legislation
aiming at limiting the right to residence, generally for a long period, for foreigners living
with HIV/AIDS, and sometimes for certain categories of foreigners such as students or
workers. In other states, the provisions concerning public health which are frequently
incorporated into the legislation on foreigners could be used as grounds for establishing
limitations to the right to the free movement of persons living with HIV/AIDS.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 123
As regards expulsion, in certain states foreigners living with HIV/AIDS may be
expelled from the territory. In others, an expulsion order may be adopted more generally
in order to protect public health.
227. Once again, proportionality and non-discrimination are the leading principles to
interpret those texts and practices: are those means proportionate to the aim pursued,
that is the fight against AIDS? The general conclusions will come back to this question
(infra, § 554).
124 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
II General examination of legislation in third countries228. This part gives an across-the-board summary of the different countries studied.
The footnotes refer only to legislation connected with the problem of AIDS. For the
other references, the reader should refer to the country concerned in point IV (§ 257)
and in annexe III. The countries are mentioned in the order of the sub-groups defined in
point IV: Africa, Asia, South America, South Sea Islands, Central Europe, the former
Yugoslavia, and the Community of Independent States.
A. Entry1. Public policy229. Certain countries have legislated that entry may be refused with the aim of
protecting public policy or interests in general: Kyrghyzstan, Tajikistan, Turkmenistan
and Poland. This leads to the question of whether the notion of public health is
contained in the more general notion of public policy.
2. Public health2.1. Public health in general
230. Numerous countries have adopted legislation refusing access to the territory to
foreigners for reasons of health if they are suffering from an illness, particularly a
contagious illness. Sometimes this is legislation on public health (Dominican Republic).
However, the majority of the laws concerned involve immigration, especially for the
following countries: South Africa, Botswana, Burundi, Kenya, Lesotho, Malawi, Namibia,
Nigeria, Rwanda, Seychelles, Swaziland, Tanzania, Uganda, Zambia, Zimbabwe, India,
Malaysia, Pakistan, Sri Lanka, Thailand, Turkey, Argentina, Bahamas, Barbados, Belize,
Chile, Colombia, Ecuador, Mexico, Trinidad and Tobago, Papua New Guinea, Tonga,
Albania, Bulgaria, Hungary, Macedonia, Belarus, Georgia, Kazakhstan, Lithuania
and Ukraine.
Sometimes these laws envisage the possibility, despite the prohibition on principle,
of permitting the presence of such persons in the country on the basis of certain
conditions (Seychelles, Swaziland, Zambia, Zimbabwe, Belize, and Trinidad and Tobago).

The free movement of persons living with HIV/AIDS – Part 3: Third Countries 125
231. Among the countries that have adopted legislation to refuse entry to foreigners for
health reasons, few have defined the illnesses that might justify this refusal. In South
Africa, a notice of 1987 had included AIDS in this notion. In 1991, a notice struck AIDS
off the list of illnesses that might justify refusal of entry to the territory. In Malawi, the
regulation on immigration which lists the illnesses concerned does not mention AIDS.
The same holds true for Zimbabwe, but in this country the practice leads to considering
AIDS as an illness justifying refusal of access to the territory. In Malaysia, in a declaration
and a law on immigration, AIDS is considered to be an infectious illness that could lead
to refusal of authorization of the right of entry. In Thailand, an application Regulation of
1986 concerning immigration included AIDS in the list of illnesses justifying a refusal of
entry. This regulation was modified in 1992, and now no longer mentions AIDS.
2.2. Health Control and Medical Certificate
232. Very numerous countries have laws that require a medical control at the border.
These may be laws on public health, for example, in the Dominican Republic or in El
Salvador. In the majority of cases, this requirement is found in laws concerning aliens, for
example, in the following countries: South Africa, Botswana, Burkina Faso, Burundi,
Equatorial Guinea, Ethiopia, Gabon, Kenya, Madagascar, Namibia, Rwanda, Senegal,
Swaziland, Tanzania, Uganda, Zambia, Zimbabwe, India, Malaysia, Nepal, Pakistan,
Philippines, Sri Lanka, Thailand, Argentina, Bahamas, Barbados, Belize, Chile,
Colombia, Ecuador, Jamaica, Mexico, Nicaragua, Trinidad and Tobago, Papua New
Guinea, Tonga, Albania, Bulgaria, Hungary, Slovakia, Macedonia and Georgia. Certain
laws specifically require an AIDS test (infra § 234).
233. Certain laws on immigration permit refusal of access to the territory or require
presentation of a medical certificate from persons coming from a country where an
epidemic is in progress. Such laws obtain in the following countries: Philippines, Fiji,
Croatia and Slovenia.
126 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
2.3. AIDS
234. Few of the studied laws expressly refuse entry to persons living with HIV/AIDS.
Nevertheless, such laws have been adopted, for example, in China 291 and in Moldova 292.
Certain laws on AIDS oblige foreigners to declare whether they are HIV positive or to
undergo a test. This is the case in Vietnam, Mongolia and Uzbekistan.
235. Certain states declare that they follow the policy of the WHO concerning travelling
restrictions (Burkina Faso, Jamaica and Croatia) or that they apply the principle of
reciprocity by requiring a test if the foreigner’s country of origin requires it (Nigeria,
Sri Lanka).
236. Only rarely do laws expressly forbid testing at the border. This is the case in Bolivia 293.
Certain countries, such as Kenya, Namibia or Indonesia, have not passed laws to this
effect, but indicate in circulars or texts of general policy that they are opposed to
systematic testing and to restrictions in immigration for persons living with HIV/AIDS.
3. Financial means237. Several countries have laws that state expressly that entry can be refused to aliens
who, because of their illness, present a risk of becoming a public liability. This provision is
found in the laws of the following countries: South Africa, Botswana, Lesotho, Malawi,
Namibia, Rwanda, Seychelles, Swaziland and Zimbabwe.
The refusal of entry for foreigners living with HIV/AIDS for economic reasons,
namely, the cost of treatment, had already been highlighted in Part II, where it had been
emphasized in particular that certain European countries refused the presence of
foreigners living with HIV/AIDS on their territory in certain cases, not because of the
existence of the virus or the illness, but more indirectly because of their inability to work
and to cover their needs financially as a result of the illness (supra, § 216).
291 Regulation of 26 December 1987 on surveillance and control measures applicable to AIDS and specificregulations to implement the law of the Peoples' Republic of China concerning border health control andquarantine (6 March 1989).
292 Law of 25 May 1993 on prevention of the illness HIV/AIDS. 293 Resolution no. 0660 for the prevention and surveillance of HIV/AIDS.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 127
B. Residence1. Residence in general1.1. Public policy
238. Certain countries possess laws stating that the right to residence may be refused in
case of danger for public policy in general: Angola, Tunisia or Turkey. As for entry, this
leads to asking whether the concept of public health may be contained in the notion of
public policy permitting refusal of a residence permit for a foreigner.
1.2. Public health
1.2.1. Public health in general
239. The laws mentioned concerning entry which render undesirable foreigners suffering
from certain illnesses, especially contagious ones, also concern the residence of foreigners
since foreigners who are ill will be authorized neither to enter nor to reside in these
countries. Reference should be made for this point to the list of states mentioned above
in § 230.
240. Several laws examined permit refusal of the right to residence in case of threat to
public health: Lesotho, Nepal, Ecuador, Nicaragua, Albania, Slovakia, Czech Republic,
Macedonia, Latvia and Lithuania. On grounds of these general provisions, the right to
stay for persons living with HIV/AIDS could be restricted.
241. Other laws permit restriction of the right to free movement for foreigners, for various
reasons including health: Georgia, Kazakhstan, Kyrgyzstan, Tajikistan, Turkmenistan and
Ukraine. This type of legal provision would also permit limiting the freedom of
movement of persons living with HIV/AIDS.
1.2.2. Health control and medical certificates
242. The right of residence depends on delivery of a medical certificate in certain
countries: Equatorial Guinea, Madagascar, Uganda, Seychelles, Cambodia, Nepal,
Pakistan, Argentina, Colombia, Hungary, Croatia, Georgia. This measure can also limit
the right to residence for foreigners living with HIV/AIDS insofar as this certificate might
be required to state whether the applicant is HIV positive or not.

128 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
1.2.3. AIDS
243. The legislations of certain states expressly provide for refusal of the right of residence
for foreigners who are HIV positive or who are suffering from AIDS.
In the first place, these were laws adopted in the framework of the campaign against
AIDS: China 294 Vietnam 295, Syria 296, Argentina 297, Panama 298, Bulgaria 299, Georgia 300,
Kazakhstan 301, Ukraine 302
These may also be laws adopted concerning immigration: Philippines 303, Estonia 304,
Slovakia and the Czech Republic 305, Moldova 306, and Russia 307. There is not always a law
on this question. Resolutions, directives or declarations have been issued in certain
countries, with the same end of refusing residence to foreigners living with HIV/AIDS:
India, Belize, Bolivia 308, Cuba 309, and Uzbekistan 310. In the latter country, the resolution
does not forbid the presence of persons living with HIV/ AIDS, but of nationals of
294 Regulation of 26 December 1987 on surveillance and control measures applicable to AIDS.295 Governmental decree no. 16/CP of 18 December 1992 regulating certain aspects of the measures of prevention and
of the campaign against the infection by HIV and against AIDS: residence of over three months. 296 Decree no. 17/t of 30 March 1991. 297 Law 237/98 on the Campaign against AIDS, which included the AIDS test in the medical control for foreigners. 298 Law no. 26 of 17 December 1992 giving measures for the prophylaxis and control of the Acquired Immuno-
Deficiency Syndrome (AIDS) and the spread of the Human Immuno-Deficiency Virus (HIV): residence of over oneyear.
299 Decree no. 4 of 2 April 1992 on the conditions and the procedure applicable to the testing of the infection by theAcquired Immuno-Deficiency Syndrome Virus: residence of over one month for students and workers.
300 Law of 21 March 1995 on the prevention of HIV/AIDS: residence of over one month. 301 Law of 5 October 1994 on the prevention of AIDS: without specification of the period of residence. 302 Law of 12 December 1991on the Prevention of AIDS and the social protection of the population: without
specification of the period of residence. 303 Instruction no. 14 of 17 February 1988 with Regulation on Immigration and Instruction no. 21 of 13 April 1988
with Regulation on Immigration. 304 Regulation of 21 September 1993 for the issue and extension of residence permits and employment permits to aliens. 305 Act no. 123/1992 of 4 March 1992 governing the stay of and residence of foreigners in the Czech and Slovak
Republics.306 Law of 10 November 1994 on the Legal Status of Aliens and Stateless Persons. 307 Federal law of 15 August 1996 on the procedure for exit from the Russian Federation and entry into the Russian
Federation and Law no. 38 of 30 March 1995 on the prevention of the spread in the Federation of Russia of theaffection caused by the Human Immuno-Deficiency Virus (Infection by HIV).
308 Interministerial Resolution 0415/89. 309 Ministerial Resolution no. 144 of 11 June 1987. 310 Resolution no. 12 of 17 November 1992 introducing preventive measures against the introduction and spread of
quarantinable diseases and of AIDS into the Republic of Uzbekistan.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 129
countries where AIDS is rife if they cannot prove they have been tested. The list of
countries concerned mentions eight countries of the European Union, as well as
numerous countries of Africa and America.
For certain states, information has been collected according to which residence
could be refused to foreigners living with HIV/AIDS, without its being possible to
identify the legal or reglementary basis for this, presuming it exists. This is the case for the
following countries: Colombia, Chile, Dominican Republic, El Salvador, Mexico,
Trinidad and Tobago, Papua New Guinea, Samoa and Lithuania.
In certain countries, legislations to the end of refusing residence for foreigners living
with HIV/AIDS formerly existed but have since been modified or abolished, as in
Thailand 311 or Costa Rica 312.
244. It is important to emphasize that the residence restrictions applicable to foreigners
living with HIV/AIDS concern mainly the right to long-term residence and not short
stays. Thus, the restrictions concern only long periods of residence of over one year
(China, Panama, India, Trinidad and Tobago), of over three months (Korea, Vietnam,
Kazakhstan, Cuba, Russia) or for an unspecified period (Ukraine, Belize, Philippines,
Slovakia and the Czech Republic, Colombia, Dominican Republic, Mexico, Papua New
Guinea, Samoa, Lithuania, Chile: foreigners other than tourists). However, the test is
sometimes required even in the case of a short-term stay: Uzbekistan and Georgia (over
one month), Bulgaria (any length of stay), Bolivia and El Salvador.
245. As concerns the marriage of foreigners, it should be noted that in Syria 313 foreigners
wishing to marry a national must undergo an AIDS test, and that in Vietnam 314 it is
forbidden for an HIV positive foreigner to marry a national.
311 Regulation of 26 August 1986 issued for the application of the 1979 Immigration Act modified by the Ruling of 20February 1992 with the same title.
312 Decree no. 18781-S-G of 19 January 1989 abrogated by the decree no. 20202-S-G of 17 January 1991. 313 Decree no. 17/t of 30 March 1991. 314 Decree no. 16/CP of 18 December 1992 regulating certain aspects of the measures of prevention and of the campaign
against infection by the HIV virus and AIDS.

130 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
1.3. Financial means
246. Certain laws provide for refusal of the right to residence for foreigners who risk
becoming a public financial liability because of their illnesses. This is the case in Lesotho.
247. As concerns medical treatment, it should be noted that in certain countries such as
Sri Lanka, the hospitals refuse to admit HIV positive foreigners. By contrast in Georgia,
the application of the law on the Prevention of HIV/AIDS of 2 March 1995 should produce
the right to medical assistance for foreigners even if they are HIV positive.
2. Particular categories2.1. Workers
248. In several countries, foreigners are required to produce a certificate attesting they are
HIV negative in order to obtain a work permit: Angola, Oman, Seychelles, Malaysia,
Syria, Belize, Papua New Guinea, Bulgaria, Estonia, Ukraine. It has not always been
possible to identify the legal basis for this measure. In certain countries, this measure has
a clear basis in a legal text: Syria 315, Bulgaria 316, Estonia 317 and Ukraine 318.
2.2. Students
249. Testing is required from students by the legislations of several states: Syria 319,
Cuba 320, Bulgaria 321, and Ukraine 322.
315 Regulatory Decree no. 36T of 26 October 1987 of the Health Ministry. 316 Decree no. 4 of 2 April 1992 on the conditions and the procedure applicable to the testing of the infection by the
Acquired Immuno-Deficiency Syndrome virus.317 Regulation of 21 September 1993 for the issue and extension of residence permits and employment permits to aliens. 318 Law of 12 December 1991 on the prevention of AIDS and the social protection of the population. 319 Regulatory Decree no. 36/T of 26 October 1987 of the Health Ministry. 320 Ministerial Resolution no. 144 of 11 June 1987. 321 Decree no. 4 of 2 April 1992 on the conditions and the procedure applicable to the testing of the infection by the
Acquired Immuno-Deficiency Syndrome virus. 322 Law of 12 December 1991 on the prevention of AIDS and the social protection of the population.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 131
In certain states, it has not been possible to identify the legal basis for the testing
required of students, presuming it exists: for example, in Poland or in Hungary. Certain
countries require testing for their own national students who have received grants when
they return after having studied abroad (Syria).
2.3. Refugees
250. In several states, refugees may have to undergo a medical control. The texts do not
specify whether the AIDS test forms part of this examination. A medical control is
required for refugees in the following countries: Turkey, Bulgaria, Czech Republic,
Slovakia, Belarus, Lithuania, Tajikistan and Ukraine.
Generally, legislations on refugees provide for refusal of this status if the candidate
represents a threat for public policy in general and that the refugee may be expelled for
the same reason (Burundi, Senegal, Turkey, Bulgaria, Croatia and the Czech Republic).
By contrast, public health is rarely mentioned as a reason for refusing the right to asylum
or as justification for expulsion. However, in Lithuania the right to asylum may be legally
refused if the refugee is ill.
Sometimes, medical assistance is assured for refugees and candidates for refugee status:
Bulgaria, Czech Republic, Slovakia, Croatia, Macedonia, Slovenia, Russia, Tajikistan
and Ukraine.
C. Expulsion1. Public policy251. In very numerous states, the legislations on immigration provide for the possibility of
ordering expulsion, not specifically in case of threat to public health, but more generally
if the public policy or welfare are endangered. This is the case in the following countries:
Angola, Botswana, Burundi, Rwanda, Seychelles, Swaziland, Tunisia, Zambia, Zimbabwe,
Indonesia, Thailand, Bahamas, Jamaica, Venezuela, Samoa, Latvia. Although it is
couched in general terms, this kind of provision can be used as grounds for expulsion of
foreigners who are HIV positive or who suffer from AIDS. This has been observed to be
true as regards, for example, Indonesia or Samoa.
2. Public health2.1. Public health in general
252. In several states, legislations on immigration permit expulsion in case of danger to
132 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
public health. The following countries may be cited by way of examples: Madagascar,
Malawi, Malaysia, Sri Lanka, Vietnam, Bulgaria, Moldova, Belarus, Georgia, Kazakhstan,
Kyrgyzstan, Tajikistan, Turkmenistan, and Ukraine.
These provisions are used to justify expulsion orders for foreigners who are HIV
positive or who suffer from AIDS. This is the case in Bulgaria, where foreigners living
with HIV/AIDS have been expelled on these grounds.
253. Few states have legislations providing for taking into account the state of health of
the foreigner when considering an expulsion order. However, Polish legislation contains a
provision whereby a foreigner’s state of health must be taken into account when
considering whether he should be arrested prior to expulsion.
254. Some laws, such as those of Macedonia or of Slovenia, stipulate that expulsion must
be avoided if it will lead to a risk of inhuman treatment in the country of destination.
Expulsion of a foreigner who is HIV positive or suffering from AIDS may constitute
inhuman treatment inasmuch as the sick person might not benefit from the possibility of
receiving treatment in the country of destination, but might do so in the state in which
he is residing until the expulsion order is executed. In this connection, reference should
be made to the jurisprudence of the European Court of Human Rights, and more
particularly to the ruling D v. United Kingdom (supra, §§ 76 et seq.).
2.2. AIDS
255. A number of states have legislations that expressly provide for the expulsion of
foreigners living with HIV/AIDS. This is the case for the following countries: Oman (the
law concerns confirmed cases of AIDS) 323, China 324, Syria 325, Cuba 326, Kazakhstan 327,
323 Ministerial Resolution no. 1 of 19 January 1991 on the national programme for the prevention of the AcquiredImmuno-Deficiency Syndrome (AIDS).
324 Regulation of 26 December 1987 on surveillance and control measures applicable to AIDS. 325 Decree no. 17/t of 30 March 1991. 326 Ministerial Resolution no. 144 of 11 June 1987. 327 Law of 5 October 1994 on the prevention of AIDS.

The free movement of persons living with HIV/AIDS – Part 3: Third Countries 133
Moldova 328, Uzbekistan 329, Russia 330, Ukraine 331. Expulsion is sometimes provided for if
the foreigner refuses to undergo the AIDS test: Belarus 332, Kazakhstan 333, and Mongolia 334.
328 Law of 25 May 1993 on the prophylaxis of AIDS. 329 Resolution no. 12 of 17 November 1997 introducing preventive measures against the introduction and spread of
quarantinable diseases and of AIDS in the Republic of Uzbekistan. 330 Federal Law no. 38 of 30 March 1995 on the prevention of the propagation in the federation of Russia of the affection
caused by the Human Immuno-Deficiency Virus (Infection by HIV). 331 Law of 12 December 1991 on the prevention of AIDS and the social protection of the population. 332 Law of 18 June 1993 on public health. 333 Law of 5 October 1994 on the prevention of AIDS. 334 Law of 1 March 1994 on the prevention of the Acquired Immuno-Deficiency Syndrome.

134 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
III Third conclusions (third countries’national laws)256. As regards the provisions concerning the free movement of persons living with
HIV/AIDS, a distinction can be made between three types of measures.
The first category of measures is formed by provisions that are manifestly contrary to
the principles of international law. This includes measures adopted in order to forbid HIV
positive foreigners to marry a national (Syria, Vietnam). These provisions are in
contradiction to article 23.2 of the International Covenant on Civil and Political Rights
(1966), to article 17.2 of the American Convention on Human Rights (1969), to article
18.1 of the African Charter on Human Rights and Peoples’ Rights (1981) 335 and to
article 16 of the Universal Declaration of Human Rights (1948) 336.
The second category of measures contains those that are contrary to the principle of
proportionality. Several states have legislations expressly permitting measures limiting
access to their territory and residence for persons living with HIV/AIDS and expressly
permitting their expulsion (Oman, China, Philippines, Syria, Vietnam, Cuba, Panama,
Bulgaria, Czech Republic, Slovakia, Estonia, Georgia, Kazakhstan, Moldova, Uzbekistan,
Russia, Ukraine). Furthermore, the information obtained on practice shows that even
when legislations do not exist, persons living with HIV/AIDS are refused entry or
residence, and are expelled. In principle, such practices, which generally appeal to the
protection of public policy or of public health, can be judged to be contrary to the
principle of proportionality (supra §§ 13 to 19 and 87). Countries with restrictive measures
against free movement of persons living with HIV/AIDS, based on legislations or practice,
are mentioned in bold face in the summary table found in annexe III, 2 (p. 307).
The third category of measures are the positive measures adopted by states so as to
limit or prohibit offences to the free movement of persons living with HIV/AIDS.
Although they are rare, these provisions must be mentioned insofar as they show the will
335 However, this article does stipulate that the family shall be protected by the state ‘which shall take care of itsphysical health and moral [welfare]’.
336 Nevertheless, this declaration has no character of legal binding obligation.

The free movement of persons living with HIV/AIDS – Part 3: Third Countries 135
of certain states not only to abstain from any limitation of the free movement of persons
living with HIV/AIDS (negative action), but also to act concretely against such limitation
(affirmative action). This leads to the question of long-term action (infra, § 561).
These measures are particularly those forbidding the systematic testing of foreigners
at the border (Bolivia or, without laws, Kenya, Namibia and Indonesia), providing for
guaranteed medical assistance or intending generally to campaign against discrimination
with regard to vulnerable groups (Gabon). Countries that exclude restrictions, by means
of legislations or declarations that are put into practice, are mentioned in italics in the
summary table found in annexe III, 2 with the sign (+) indicating that these countries are
taking affirmative action against restrictions of the free movement of persons living with
HIV/AIDS.
It is sometimes difficult to define the complexity of the reality. Some countries may
be found in both the second and the third categories. Thus, the same country may adopt
anti-discriminatory measures that exclude systematic testing and hence the test at the
border, and also discriminatory measures that permit expulsion of persons living with
HIV/AIDS (Bolivia, Colombia, Indonesia).
136 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
IV Country-by-country examination of legislation in third countries257. This section lists in detail, country by country, the legislation and the practice
concerning free movement which may affect persons living with HIV/AIDS. The
countries are classed by geographical regions and within each region according to French
alphabetical order. (In this English-language translation the text has not been re-arranged
in accordance with English alphabetical order in order that the paragraph numbers and
notes might correspond to the French original.)
As far as possible, and according to the information it has been possible to collect, a
distinction will be made between entry to the territory on the one hand, and on the
other, residence and expulsion.
A. Africa 336b
1. South AfricaA. Entry
258. Article 7 (1) (IV) of the law on foreigners of 1991 states that if the immigration
officer suspects the foreigner to be suffering from an illness or infirmity which might
justify a refusal to admit him to the territory, he may be required to undergo a medical
examination.
Article 39 of this law lists the cases whereby foreigners may be refused entry to the
territory. This may occur if the foreigner may become a public charge on account of an
illness, or else if the person suffers from a contagious illness or is carrier of a virus.
On the basis of article 56 (c) of the law on foreigners, contagious illnesses and
viruses which may lead to refusal of entry to the territory may be dealt with by a decree
issued by the minister. A governmental opinion of 30 October 1987 337 included in the list
336b For an attempt to classify the attitude of African countries according their attachment to Civil law, Commonlaw or Muslim law, see ALKAS P.H. and SHANDERA W.X., ‘HIV and AIDS in Africa. African policies inresponse to AIDS in relation to various national legal traditions’, The Journal of Legal Medicine, 17, 527-546(1996).
337 IDLH, 1989, 40 (1), p. 59.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 137
of persons forbidden to enter the South African Republic persons living with HIV/AIDS.
It appears that this restriction was originally aimed at miners from Mozambique, Malawi
and Zimbabwe 338. However, an opinion of 13 September 1991 339 struck HIV/AIDS off
the list of illnesses barring a foreigner from the territory. Since this date, it would appear
that persons living with HIV/AIDS are no longer the object of discrimination for their
entry into the country 340.
Nevertheless, E. CAMERON observes that the rules on immigration, including the
announcement of 1987 which created a discrimination, were not applied, and that the
change in the ruling was thus not so much a victory for human rights as the realization on
the part of the government that coercive measures do not necessarily stop the
propagation of the illness. The same author states that other forms of discrimination
subsist against persons living with HIV/AIDS 341: refusal of treatment, abuse in insurance
and work. Actions and infomations are being developed against those discriminations 341b.
B. Residence and expulsion
259. The provisions cited above regarding entry also concern residence inasmuch as
undesirable foreigners may neither enter nor reside in the country.
C. Miscellaneous
260. The problem of the importation of illnesses is still alive to-day. This question is dealt
with by the International Health Regulations of 1969 and 1974, which contain no
reference to the HIV virus or AIDS, nor to other illnesses. This is why the health
authorities have established a policy concerning transport in South Africa of persons with
a contagious illness. This policy was examined from 1 April to 31 July 1997 342. It is
338 Information communicated by Lawyers for Human Rights on 27 May 1997; see also ZACKIE ACHMAT,‘Création d’un réseau sud-african’, in Réseau africain sur l’éthique, le droit et le VIH, actes de la consultationinterpays, Dakar, 27 June – 1 July 1994, p. 59.
339 IDLH, 1992, 43(1), p. 33.340 Information communicated by Lawyerss for Human Rights on 27 May 1997 and by Department of Health,
National HIV/AIDS and STD Directorate, on 20 January 1998.341 E. CAMERON, ‘Human Rights, Racism and AIDS: the New Discrimination’, in South African Journal on
Human Rights, Centre for Applied Legal Studies, University of the Witwatersrand, Johannesburg, 1993.341b D. FINE, M. HEYWOOD, A. STRODE: HIV/AIDS and the law, published by AIDS law project and Lawyers for
human rights, South Africa, 1997.342 Information communicated by the Embassy of South Africa in Brussels on 14 May 1997.
138 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
problematic and should be revised. The proposed text expressly states HIV/AIDS among
the illnesses concerned.
If the patient is considered as having a contagious illness, he may not, in principle,
be transported on a commercial flight with other passengers. It is stipulated that the crew
must inform the control tower at the airport of destination when they have a sick
passenger on board. Appropriate measures must be taken in order to avoid contact
between the sick person and the other passengers. On arrival, the health official will be
allowed to come on board and he must take the necessary measures in order to disinfect
the aeroplane.
It should be noted that the law on foreigners contains provisions that are applicable
to captains of ships, who may be required to provide a report mentioning the illnesses
which may have appeared during the voyage, suspected or confirmed cases of illnesses,
the names of the persons suffering from them, and the nature of the illnesses.
2. AngolaA. Entry
261. Law of 1994 on the Legal Status of Aliens does not provide for possible refusal of entry
for reasons of public health.
Decree 48/94 of 25 November 1994 stipulates that when application is made for a
visa for medical reasons, the applicant must produce proof of his admission to a hospital,
of the date of treatment and of sufficient financial means.
B. Residence and expulsion
262. The law of 1994 does not envisage refusal of residence for reasons of health.
Authorization of residence may be revoked if the foreigner offends public policy or
national security. By contrast, public health is not mentioned explicitly.
263. Since 31 January 1997, a certificate of HIV negative status must be presented in
order to obtain a residence visa for work 343.
264. In the law of 1994, expulsion is provided for in case of threat to national security
and to public policy, but not in case of threat to public health.
343 Information confirmed by the Embassy of Angola in Brussels on 8 July 1997.

The free movement of persons living with HIV/AIDS – Part 3: Third Countries 139
3. BotswanaA. Entry
265. Foreigners may be required to undergo a medical examination on the basis of article
7(b) of the Immimgration Act of 1966, which also states that entry and residence may be
refused to foreigners if they suffer from illnesses that may justify their exclusion from the
territory (unless they possess an authorization and comply with the conditions of this
authorization). Foreigners may also be refused access to the territory if they risk becoming
a public charge because of their illness (article 7(a) and (c)).
However, there are no specific provisions applicable to the entry and residence of
foreigners living with HIV/AIDS 344.
B. Residence and expulsion
266. The provisions affecting residence are the same as those concerning entry.
267. Expulsion is provided for by the legislation on foreigners in case of necessity for the
public good but not specifically in case of threat to public health.
4. Burkina FasoA. Entry
268. Law no. 23/94/ADP of 19 May 1994 promulgating the Code of Public Health 345
contains in its articles 123 to 125 provisions on health control at the border.
Article 123 states that ‘the international health regulations will be applied to any
aircraft or person in a situation of “international travel”. The same ruling shall be applied
to trains and road transport coming from abroad’. This article deals with so-called
quarantine illnesses (plague, cholera, yellow fever). In order to obtain an entry visa,
foreigners must be vaccinated against yellow fever, and vaccination against cholera is
recommended. By contrast, no information on HIV status is asked of foreigners entering
the country, in conformity with the recommendations of the WHO 346.
Article 125 states that any person refusing to comply with urgent demands made to
him by a health control service at the border may be fined or imprisoned.
344 Information communicated by the Embassy of Botswana in Brussels on 26 June 1997.345 IDLH, 1995, 46 (4), p. 449.346 Information communicated by the Embassy of Burkina Faso in Brussels on 12 September 1997.
140 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
269. Entry restrictions have not been expressly provided for for persons living with
HIV/AIDS 347.
B. Residence and expulsion
270. In order to obtain a residence permit, the medical requirements involve obligatory
vaccination against yellow fever and a recommendation to be vaccinated against cholera.
There is no requirement as regards testing for the HIV virus or AIDS.
5. BurundiA. Entry
271. The legislation on immigration contains restrictions concerning public health.
In order to obtain authorization to enter Burundi, foreigners must possess a medical
certificate established less than three months previously by a medical doctor, attesting
that the bearer is free of all contagious illnesses 348. Foreigners may be refused entry
if they do not produce the documents required and if they are suffering from a
contagious illness 349.
However, information received suggests that the Burundian government does not use
these general provisions as grounds for refusing access to the territory to persons living
with HIV/AIDS 350.
B. Residence and expulsion
272. Expulsion is provided for in general terms in case of danger for public policy and
national security 351. Public health is not cited expressly as grounds for expulsion.
273. Foreigners recognized as political refugees may be expelled from Burundi ‘only in
such cases in which they offend public order or national security’ 352.
347 This information is drawn from the list established by The Laboratory Center for Disease Control (Canada) in June 1997, and was confirmed by the Embassy of Burkina Faso in Brussels on 12 September 1997.
348 Decree-Law no. 1/23 of 9 July 1982 regulating the access, stay, establishment and removal of foreigners to, in andfrom Burundi.
349 Article 4 of the Decree-Law of 9 July 1982, o.c., and article 4 of the Decree-Law no. 1/007 of 20 March 1989regulating the access, stay, establishment and removal of foreigners to, in and from Burundi.
350 Information communicated by the Embassy of Burundi in Brussels on 26 March 1997.351 Article 26 of the Decree-Law of 20 March 1989 cited above.352 Article 31 of the Decree-Law of 9 July 1982 cited above.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 141
6. CameroonA. Entry
274. Law no. 90/043 of 19 December 1990 on immigration does not include a condition
concerning public health in the conditions of access.
B. Residence and expulsion
275. Nor does Law no. 90/043 contain provisions concerning public health as regards
residence and expulsion.
7. EthiopiaA. Entry
276. The legislation on immigration contains rules concerning public health.
Foreigners wishing to enter Ethiopia must produce a medical certificate showing they
have received the immunisations required by the minister 353.
‘Undesirable’ foreigners can be refused entry (article 8 of the law). This notion is
defined by article 3 (11), which does not mention offense to public health, but rather
offense to state security or becoming a public charge.
Nevertheless, the authorities have taken no specific measures concerning the
movement of persons living with HIV/AIDS 354 and no restrictions concerning entry have
been expressly provided for 355.
B. Residence and expulsion
277. Undesirable foreigners may be the object of an expulsion order.
8. GabonA. Entry
278. All travellers must hold a medical certificate in order to enter the country 356.
353 Article 6 c) of the proclamation no. 271 of 1969 regulating the issuance of travel documents and visas, andregistration of foreigners in Ethiopia.
354 Information communicated by the Department of Immigration in Ethiopia.355 Information drawn from the list established by The Laboratory Center for Disease Control in June 1997.356 Information drawn from the list established by The Laboratory Center for Disease Control in June 1997.
142 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
B. Residence and expulsion
279. A study published in 1991 speaks of there being no restrictions for persons living
with HIV/AIDS as concerns residence 357.
C. Miscellaneous
280. It must be emphasized that according to article 38 of the Order no. 1/95 Giving
Guidelines for Health Policy in the Gabonese Republic, the policy of protection of vulnerable
groups must ensure in particular a campaign against exclusion and discrimination. Insofar
as migrants and persons living with HIV/AIDS may be considered to constitute a
vulnerable group, this provision could concern them.
9. GambiaA. Entry
281. There is no legislation forbidding foreigners living with HIV/AIDS to enter the
country 358. The Public Health Act 359 does not contain provisions concerning HIV/AIDS.
Although there is no legislation in Gambia permitting discrimination against carriers
of the AIDS virus, the state officials must take into account the consequences of their
decisions for public health, including decisions concerning granting the right of entry to
the territory 360.
B. Residence and expulsion
282. Any person suffering from any communicable disease that may be prescribed as such
by the Minister shall be prohibited immigrant 361.
357 Restriction of entry and residence for people with HIV/AIDS, a global survey, Archiv für Sozialpolitik, ordered byDeutsche AIDS-Hilfe, Berlin, Frankfurt, 1991.
358 Information communicated by the Ministry of Health in Gambia on 12 May 1997.359 Public Health Act, ch. 535.360 Information communicated by the Embassy of Gambia in Brussels on 3 April 1997.361 Article 13b of the Immigration Act of 1990.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 143
10. Equatorial GuineaA. Entry
283. All foreigners entering the Republic of Guinea are required to present at their arrival
a valid international health record, recognized by international conventions or the
rulings in force 362. There is no specific restriction of entry for persons living with
HIV/AIDS 363.
B. Residence and expulsion
284. Applications for a resident’s card must be accompanied by a medical certificate
delivered by an approved doctor less than three months previously. The same condition
applies to applications for renewal of residents’ cards 364. It should be noted that foreigners
from countries that have signed conventions of reciprocity with the Republic of Guinea
are exempted from the requirement to hold residents’ cards.
285. Expulsion for reasons of public health is not expressly provided for. By contrast, this
measure is possible when the foreigner is declared to be personally undesirable 365 or when
he constitutes a threat for public policy 366.
11. KenyaA. Entry
286. On the basis of article 3 (1)(c) of the Immigration Act of 1967, foreigners may be
considered as being barred from the territory if they refuse to undergo a medical
examination. The same is the case for those who, after having been examined by a
medical inspector, are declared to be undesirable for medical reasons.
No entry restriction has been adopted specifically with regard to travellers living
with HIV/AIDS 367. Two elements permit deduction from the absence of specific
362 Article 14 of Law L/94/019/CTRN setting out the conditions for the entry and stay of foreigners in the Republic of Guinea.
363 Information drawn from the list established by The Laboratory Center for Disease Control in June 1997.364 Articles 38 and 39 of Law L/94019/CTRN cited above.365 Article 64 of Law L/94/019/CTRN cited above.366 Article 67 of Law L/94/019/CTRN cited above.367 This information is drawn from the list established by The Laboratory Center for Disease Control in June 1997.
144 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
legislation that this general legislation is not used to limit the free movement of persons
living with HIV/AIDS. On the one hand, article 81 (1) of the constitution guarantees
freedom of movement. This right may be suspended in the interests of public security or if
public policy demands it. On the other hand, Kenya considers that the measures
restricting travel adopted by certain states with regard to people who are HIV positive or
who are suffering from AIDS are contrary to the Universal Declaration of Human Rights
inasmuch as the simple presence of the person on the territory does not constitute a
danger. For this reason, Kenya condemns this type of measure 368.
B. Residence and expulsion
287. Refer to the provisions mentioned in § 286.
12. LesothoA. Entry
288. The immigration officer may, in order to authorize entry, demand the presentation of
a medical certificate proving the absence of illness 369. This general legislation could be
used concerning AIDS. However, this assertion is not confirmed in practice 370.
B. Residence and expulsion
289. Residence may be refused to foreigners who might compromise public health or
become a public charge on account of an illness from which they might be suffering 371.
13. MadagascarA. Entry
290. According to the legislation, an international vaccination card must be presented as
a condition for admission 372. There are no restrictions for entry for persons living with
HIV/AIDS 373.
368 AIDS in Kenya – Socioeconomic Impact and Policy Implications, US Agency for International Development,AIDSCAP/Family Health International, 1996, p. 152.
369 Article 13 (2) of the Aliens Act of 1968.370 Information provided by the Lesotho Embassy in Brussels on 4 December 1997.371 Annexe 1 of the Aliens Act.372 Article 9 for non-immigrants and article 13 for immigrants of Decree no. 94-652 of 1994, which establishes the
norms for applying Law no. 62-002 of 16 June 1962 establishing the organization and control of immigration toMadagascar.
373 This information is drawn from the list established by The Laboratory Center for Disease Control in June 1997.

The free movement of persons living with HIV/AIDS – Part 3: Third Countries 145
B. Residence and expulsion
291. Foreigners who wish to reside in Madagascar for over three months must possess a
resident’s card delivered by the Minister of the Interior 374. Among the conditions for
delivery of the resident’s card figures production of a medical certificate in the conditions
fixed by the Minister of Health 375.
292. Article 13 of the law of 1962 states that foreigners admitted for temporary residence
may be expelled if their presence on the territory constitutes a threat for the protection
of health.
14. MalawiA. Entry
293. Article 4 (1)(e) of the Immigration Act of 1964 states that foreigners may be refused
admittance to the territory if they are suffering from an illness that can justify refusal
unless they possess express authorization. In case of doubt, the immigration officer may
require a medical examination (article 13). The illnesses to which article 4 (1)(e) refers
are listed in article 11 of the immigration reglementation, which does not mention
HIV/AIDS. There does not seem to be any restriction of entry applicable to persons
living with HIV/AIDS 376.
Nevertheless, mention should be made of article 4 (1)(c) according to which
foreigners may also be refused entry to the territory if they might become a public charge
on account of the illness from which they are suffering. This provision does not apply to
nationals of neighbouring countries who have signed a convention with Malawi.
B. Residence and expulsion
294. Article 23 of the immigration Regulation states that foreigners applying for a
permanent residence permit must produce a medical certificate.
374 Article 6 of the Law of 1962.375 Article 22 of the Decree of 1994.376 This information was communicated by the Ministry of Health and Population of Malawi on 6 October 1997.
It corresponds to the list established by The Laboratory Center for Disease Control in June 1997.

146 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
295. An expulsion order may be established for reasons of public health on the basis of
article 39 (2)(b) of the Immigration Act. A study published in 1991 contains information
to the effect that persons living with HIV/AIDS are not expelled 377.
296. The legislation on refugees of 8 May 1989 provides for an exception to the
prohibition of expulsion of foreigners who have obtained refugee status in case of danger
for the security of Malawi or of penal condemnation; public health is not expressly
mentioned.
15. MaliA. Entry
297. There are no laws forbidding the entry of persons living with HIV/AIDS 378.
B. Residence and expulsion
298. In order to obtain a visa, vaccination against yellow fever is obligatory. As regards
the VIH virus or AIDS, it would seem there is no particular requirement, since there is
no law prohibiting the residence of persons living with HIV/AIDS 379.
16. NamibiaA. Entry
299. Foreigners wishing to enter the country must convince the immigration officer that
they do not form part of the category of foreigners prohibited access to the territory 380.
The law cites in the list of foreigners who may be barred from the territory those suffering
from contagious illnesses or carriers of a virus, as well as people who may become a public
charge because of their illness 381.
300. The minister may decree rulings concerning norms for the medical control of
foreigners and for the contagious illnesses that would bar foreigners from the territory 382.
377 Restrictions of entry and residence for people with HIV/AIDS, o.c.378 Information communicated by the Embassy of Mali in Brussels on 19 March 1997.379 Information communicated by the Embassy of Mali in Brussels on 19 March and 6 May 1997.380 Article 7 of the Immigration Control Act of 1994.381 Article 39.382 Article 58.

The free movement of persons living with HIV/AIDS – Part 3: Third Countries 147
301. Paragraph 4.8 of the National Policy on AIDS 383 states that the Namibian
authorities may not impose restrictions concerning immigration and must encourage the
other authorities to do the same. Paragraph 4.1.2.2 states in a general manner that the
systematic testing of certain groups is unjustified.
302. The modification in 1987 of the legislation on the admission of persons to the
Republic, which barred persons suffering from the HIV virus or AIDS from the territory,
does not apply in Namibia 384.
B. Residence and expulsion
303. The provisions permitting prohibition of access to the territory for sick foreigners
(supra point a) also concern the right to residence. If foreigners are suspected of suffering
from an illness that can bar them from the territory, they may be obliged to undergo
a medical control 385.
Article 21 (1) (g-i) of the Namibian Constitution states that everyone has the
right to free movement in Namibia, to reside and settle in the country and to return
to Namibia.
The national policy with regard to AIDS is opposed to restrictions.
C. Miscellaneous
304. Captains of ships must provide, if requested, a report listing the cases of illnesses that
have appeared during the voyage, the cases of illnesses suspected or known, the names of
the sick persons, and the nature of their illnesses (article 15 (1)(d)).
17. NigeriaA. Entry
305. Article 49 of the Immigration Act of 1963 states that the immigration officer may
refuse entry to foreigners who are undesirable for medical reasons.
383 Positive Responses and Choices: Policies and Guidelines for HIV/AIDS Prevention and Control, December 1991.384 M. FIGUERA, ‘AIDS, the Namibian Constitution and Human Rights – an Overview’, South African Journal
on Human Rights, Centre for Applied Legal Studies, University of the Witwatersrand, Johannesburg, 1993, p. 35.
385 Article 8, e) of the Law of 1994, cited above.

148 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
Restrictions of entry may be applied to foreigners living with HIV/AIDS on the basis
of the principle of reciprocity, if the foreigners’ states apply the same restrictions to
Nigerian nationals 386.
B. Residence and expulsion
306. Article 17 states that foreigners suffering from a mental illness may be the object of
an expulsion order. This provision does not allude to other types of illnesses.
307. The prohibition of expulsion of refugees may find an exception in case of danger for
the security of Nigeria 387. Public health is not expressly mentioned as an exception to the
principle of prohibition of expulsion of refugees.
18. OmanA. Entry
308. Foreigners intending to take up employment in the private sector must have an
AIDS test on their arrival. This test must be renewed every two years for the renewal of
their work permit 388.
B. Residence and expulsion
309. A resolution 389 states that the groups considered to be particularly at risk, according
to the criteria of the Technical Committee for the Campaign against AIDS, must be
made to undergo the tests that are necessary to prove the absence of infection. The same
resolution states that ‘foreigners resident in the country who are suffering from confirmed
AIDS must be expelled to their own countries in order to undergo medical treatment
with the help of specialized authorities’.
386 D.C. JAYASURIYA, AIDS, Health, policy and Legal Aspects. Commonwealth Secretariat, London, 1992, p. 29.387 Article 1 of the Decree of 1989 on Refugees.388 This information is drawn from the list established by The Laboratory Center for Disease Control in June 1997
and Le tableau récapitulatif des dispositions prises par certains pays envers les voyageurs internationaux concernant lestests de dépistage des anticorps anti-VIH (sida) [The summarizing table giving the provisions adopted by certaincountries with regard to international travellers concerning tests for antibodies against the HIV (AIDS)],established by the Federal Department of Foreign Affairs in Switzerland.
389 Ministerial resolution no. 1 of 19 January 1990 on the national programme for the prevention of the AcquiredImmuno-Deficiency Syndrome (AIDS), IDHL, 1992, 43(1), p. 37.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 149
19. UgandaA. Entry
310. Among the foreigners whose presence in Uganda is illegal are those who refuse to
undergo a medical examination and those who declare that they are suffering from a
contagious illness that renders their presence in Uganda dangerous 390.
Nevertheless, according to information received, there is no specific legislation
applicable to persons living with HIV/AIDS, and their freedom of movement is not
restricted 391. This information is confirmed by declarations made during a conference
(infra § 312).
B. Residence and expulsion
311. The ruling on applications for entry permits and residence permits states that
foreigners who have lived in the country for fifteen years may request a life residence
permit. It states further that such foreigners must produce a medical certificate proving
they are in good health.
C. Miscellaneous
312. A conference held on 18 May 1994 at Kampala on Juridical and Ethical Aspects of
the HIV/AIDS Epidemic in Uganda recommended that obligatory testing should not be
practiced generally. The Conference resolved that no AIDS test should be practiced
without the person’s prior informed consent 392.
20. RwandaA. Entry
313. The law contains provisions concerning health conditions required for entering the
territory 393. Foreigners must produce medical certificates of the vaccinations prescribed by
international conventions and established either according to the model adopted by the
World Health Organization or else according to the provisions decreed by the Minister of
390 Guidelines for Issuance of Entry Permits, Certificates of Residence and Other Passes, document communicated bythe Embassy of Uganda in Brussels.
391 Information communicated by the Embassy of Uganda in Brussels on 28 August 1997. 392 African network on ethics law and HIV, Proceedings of the intercountry consultation, Dakar, Senegal,
27 June – 1 July 1994, p. 75. 393 Article 2 of the Law of 1963 concerning the immigration police and the conditions of entry and stay.
150 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
public health. This rule does not concern persons living with HIV/AIDS, since it regards
vaccination certificates.
The law cites among undesirable foreigners who may not enter Rwanda foreigners
suffering from contagious illnesses specified by a ministerial decision. Foreigners are also
declared to be undesirable if, because of their illness, they cannot guarantee sufficient
normal means of subsistance, as well as their dependants 394. However, according to a study
made in 1997, there are no restrictions of entry for persons living with HIV/AIDS 395.
B. Residence and expulsion
314. Foreigners suffering from an illness or those who may become a public charge
because of their illness may be considered to be undesirable and be refused the right of
residence on these grounds 396. Undesirable foreigners or those who compromise public
peace or policy may be expelled 397.
21. SenegalA. Entry
315. There are restrictions of entry concerning public health 398. Nevertheless, these speak
of the requirement for international vaccination certificates and thus do not concern
HIV/AIDS. HIV testing performed without the consent of the individual is theoretically
forbidden. Indeed, the Senegalese Constitution, criminal law, the Declaration of Human
Rights, the African Charter on Human and People’s Rights ratified by Senegal, set down
the principle of physical integrity of the human being 399.
B. Residence and expulsion.
316. The provisions of the 1971 Decree on foreigners make no mention of public health.
317. It is stated that refugees may be expelled for reasons of national security or public
policy, but not expressly for reasons of public health 400.
394 Article 13 of the Law of 1963 cited above.395 This information is drawn from the list established by The Laboratory for Disease Control in June 1997.396 Article 13 cited above.397 Article 18 of the law of 1963 cited above.398 Decree no. 71-860 of 28 July 1971 concerning the conditions for the admission, stay and establishment of foreigners.399 A. SOW/SIDIBE, Le droit à l’épreuve du VIH, 1er colloque international Sida et religion, 31 octobre –
2 novembre 1997, p. 9.400 Law no. 68-27 of 24 July 1968 giving refugee status, article 4.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 151
22. SeychellesA. Entry
318. The law states that foreigners are undesirable if they are suffering from or are
carrying illnesses, and if they are capable of infecting other people with their illness 401.
Foreigners who might become a public charge because of the illness from which they are
suffering are also undesirable 402. Nevertheless, a provisional permit may be granted to
undesirable foreigners 403. Furthermore, the minister can exempt certain foreigners 404.
The immigration officer is empowered to require of any person suspected of being an
undesirable foreigner, on account of his physical condition, to undergo a medical
examination. The text states that if the foreigner refuses to undergo a medical
examination or to undergo any test connected with the medical examination he may be
fined or imprisoned 405.
B. Residence and expulsion
319. Applications for residence permits must be accompanied by a medical certificate
showing that the applicant and the members of his family are not suffering from
infectious and contagious illnesses and are in good health 406. The request for a permit in
order to exercise a lucrative profession is considered by the minister taking different
elements into account, including the applicant’s state of health and that of the members
of his family 407.
320. It would appear that this general legislation is used to impose restrictions on persons
living with HIV/AIDS. It seems that a distinction is made not only on the basis of the
length of stay but also of the type of work and of sector concerned (public or private).
Visitors who must work for the government or for a para-governmental body must
produce a certificate proving they are HIV negative. Those who intend working in the
401 Article 19 of the Immigration Decree of 1981.402 Idem.403 Article 18 of the Decree of 1981 cited above.404 Article 19 of the Decree of 1981 cited above.405 Article 28 of the Decree of 1981 cited above.406 First annexe to the Decree of 1981 cited above. 407 Article 17 of the Decree of 1981 cited above.

152 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
private sector, diplomatic staff and people applying for a residence permit for
a short stay are not required to produce this certificate 408.
321. Foreigners constituting a threat to the peace and order of the country may
be expelled 409.
C. Miscellaneous
322. Repayment of costs advanced by the state for undesirable foreigners, especially as
concerns medical treatment, may be ordered by a decision of justice (Decree on
Immigration, subsidiary legislation, section 6).
23. SwazilandA. Entry
323. The general legislation concerning immigration contains restrictions with regard to
public health. The law states that foreigners may be obliged to undergo a medical control.
They are considered to be undesirable if they are suffering from an illness which can
justify prohibition to be within the territory, except for express authorization, or if they
become a public charge because of the illness from which they are suffering. Undesirable
foreigners may neither enter the territory nor reside there 410.
However, there is no restriction to entry specifically provided for with regard to
persons living with HIV/AIDS 411.
B. Residence and expulsion
324. Undesirable foreigners may not reside within the territory: refer to the provisions
mentioned above in § 323 concerning entry. The Minister may sign an expulsion order if
he considers this to be necessary for the public good 412.
408 This information is drawn from the list established by The Laboratory Center for Disease Control in June 1997.409 Article 23 of the Decree of 1981 cited above.410 Immigration Act of 1965, articles 5, 9 and 11.411 This information is drawn from the list established by The Laboratory Center for Disease Control in June 1997.412 Article 25 of the Law of 1965 cited above.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 153
24. TanzaniaA. Entry
325. The law states that foreigners are undesirable particularly if they refuse to undergo a
medical examination or if they are declared to be suffering from a contagious illness
which would render their presence in Tanzania dangerous for the public 413.
Nevertheless, there is no specific legislation relative to the entry or the residence of
persons living with HIV/AIDS 414. According to the Minister of Justice and
Constitutional Affairs, the free movement of persons living with HIV/AIDS is not
limited, whether they be nationals or foreigners 415.
B. Residence and expulsion
326. Foreigners who are undesirable for reasons of health may be refused the right to
residence in the country 416.
C. Miscellaneous
327. The Resolutions of the National Workshop on Ethics, Law, Human Rights and the HIV
Virus or AIDS in Tanzania 417 contain a series of recommendations addressed to the
government. They affirm the principle of free consent to any procedure and process to
which persons living with HIV/AIDS might be submitted, and this could imply the
refusal of obligatory testing for foreigners.
25. TunisiaA. Entry
328. Tunisian legislation on health contains no restrictive measures concerning the free
movement of travellers, even if they are carriers of the AIDS virus 418.
B. Residence and expulsion
329. The law states that residents’ cards may be withdrawn for reasons of public policy.
Public health is not expressly mentioned as grounds for withdrawal 419.
413 Article 6 of the Immigration Act of 1972.414 Information communicated by the Embassy of Tanzania in Brussels on 27 March 1997.415 Information communicated by the Minister of Justice and Constitutional Affairs on 25 July 1997.416 Article 6 of the Immigration Act of 1972.417 13-15 January 1997, Bulletin du réseau africain sur l’éthique, le droit et le VIH, June 1997, no. 3, p. 7.418 Information communicated by the Embassy of Tunisia in Brussels on 26 August 1997.419 Law no. 66-7 of 8 March 1968 concerning the situation of foreigners in Tunisia.
154 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
330. Expulsion may occur for reasons of public policy. Public health is not specifically
mentioned by the law as grounds for expulsion 420.
26. ZambiaA. Entry
331. The Immigration Act contains a series of provisions concerning public health. The
law states that authorization for entry can be delivered only if the foreigner is not
undesirable 421. The notion of an undesirable foreigner is defined by the law 422. It covers
particularly persons ‘who are carriers of prescribed diseases and who may contaminate
other persons’ 423 It is not specified whether persons living with HIV/AIDS are included
in this definition. There is no express restriction with regard to persons living with
HIV/AIDS 424.
The law permits delivery of a temporary permit to undesirable foreigners 425.
Foreigners may be obliged to undergo an examination if the immigration officer suspects
them of being undesirable foreigners on account of their physical state 426.
B. Residence and expulsion
332. The legislative provisions with regard to undesirable foreigners concern both their
entry and their residence in the country.
333. Expulsion is provided for if foreigners constitute a danger for public policy 427.
27. ZimbabweA. Entry
334. The law states that foreigners may be obliged to undergo a medical control if the
authorities suspect them of suffering from an illness that could render them undesirable 428.
420 Law of 8 March 1968 cited above, article 18.421 Article 14 of the Immigration and Deportation Act of 1967.422 Article 22 of the Law of 1967 cited above.423 Annexe 2 of the Law of 1967 cited above.424 This information is drawn from the list established by The Laboratory for Disease Control in June 1997.425 Article 17 of the Law of 1967 cited above.426 Article 25 of the Law of 1967 cited above.427 Article 26 of the Law of 1967 cited above.428 Article 12 (3) of the 1979 Immigration Act.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 155
The law mentions in the category of undesirable foreigners persons suffering from
illnesses that may justify their prohibition from the territory, unless they possess an
authorization and respect its conditions 429. The law also declares foreigners to be
undesirable if the may become a public charge because of the illness from which they are
suffering 430. The illnesses concerned are cited by the law, which mentions particularly
tuberculosis and syphilis 431. The HIV virus and AIDS are not mentioned, but the
Department of Immigration does not exclude it from the field of application of this
provision 432. Nevertheless, restrictions of entry have not been expressly stipulated with
regard to persons who are HIV positive or those suffering from AIDS 433.
The law specifies that refugees cannot be considered as undesirable foreigners 434.
B. Residence and expulsion
335. Undesirable foreigners may not reside in the country and may be expelled 435.
336. Expulsion of refugees is provided for in express terms in case of threat for national
security or public policy, but not for public health 436.
B. Asia28. CambodiaA. Entry
337. The law on immigration contains no public health provision covering access to the
territory. It allows for a ban on entry to be ordered on grounds of national security, though
not on public health grounds 437.
429 Article 14 of the 1979 Immigration Act.430 Idem.431 Article 43 of the 1979 Immigration Act.432 Information contained in the study restrictions of entry and residence for people with HIV/AIDS, a global survey,
o.c., p. 69.433 This information is drawn from the list established by The Laboratory for Disease Control in June 1997.434 Article 15 of the Immigration Act.435 Article 17 of the Immigration Act.436 Article 15 of the Law of 1983 on Refugees.437 Article 9 of the Immigration law of 1994.
156 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
B. Residence and expulsion
338. In order to stay in the country, foreigners who come under the ‘immigrants’ category 438
must be physically able to exercise their profession and prove this by means of a medical
certificate issued by a doctor from the country of origin 439.
339. A foreigner can be expelled if he poses a threat to national security; public policy
and health are not mentioned as grounds for expulsion 440.
29. ChinaA. Entry
340. The health inspection services are required to control people entering the country in
order to detect infectious diseases and take any measure required to prevent or control
such diseases. The health inspection services are authorised to demand health
declarations or a medical certificate from people entering the country 441. Any person
arriving in China must accurately complete a health declaration and submit it for
verification to the border health control and quarantine service. Persons living with
AIDS and those infected by the virus are not authorised to enter the country. If a
foreigner is already on Chinese territory, he must leave the country as soon as possible or
be escorted back to the border. Before leaving the country, the foreigner is subject to
isolation measures 442.
341. The health and quarantine organisation must prohibit any foreigner living with
AIDS from entering the country. The health and quarantine organisation monitors
transmissible diseases among all persons entering or leaving the country, and staying in
hotels or establishments hosting foreigners in a border port, and must adopt all the
necessary prevention and control measures. The doctor in charge of quarantine measures
can issue any person coming from an area infected with a quarantinable or transmissible
438 These are foreigners who wish to set up a business or to carry out activities related to industry, services, trade oragriculture, and foreigners who are not covered by article 7 of the Immigration law defining non-immigrants.
439 Article 11c of the Immigration law of 1994.440 Article 36 of the Immigration law of 1994.441 Presidential decree no. 46 of 2 December 1986 promulgating the law of the People’s Republic of China relating to
border health controls and quarantine, articles 15 and 16, IDHL, 1987, 38(4), p. 816.442 Regulation of 26 December 1987 on surveillance and control measures applicable to AIDS, articles 4 and 6,
IDHL, 1989, 39 (3), p. 623.

The free movement of persons living with HIV/AIDS – Part 3: Third Countries 157
disease with a card bearing the wording ‘for your health’. When the holder of such a card
goes to a health organisation he must be dealt with urgently. If he turns out to be
suffering, or presumed to be suffering from a disease, the necessary health measures must
be adopted immediately and the service which issued the card must be notified 443.
Some foreigners have attempted to rebel against the screening test by claiming that
health rules in Chinese hospitals were not very reassuring and that they could contract
hepatitis or other diseases from unsterilised syringes 444.
342. Chinese citizens who have stayed abroad for more than one year must undergo an
AIDS screening test when they return 445.
B. Residence and expulsion
343. Any foreigner arriving in China with a view to residing there permanently or staying
their for over one year (or studying for a period exceeding one year) must, when making a
request for an entry visa, present a certificate issued by a hospital or organisation in his
own country testifying that he has undergone a serological AIDS detection test. This
certificate must have been approved by a diplomatic mission or a Chinese consulate and
is valid for six months from its date of issue. Foreigners who have not undergone a
serological AIDS detection test in their own country must go to a specialised health
organisation within twenty days in order to be tested 446.
344. Foreigners resident in China who prove to be living with AIDS or to be carrying the
virus may be ordered to leave the country immediately 447. Between 1985 and 1991, 92
non-Chinese seropositives were asked to return to their country of origin. Most of these
were African students; the other cases concerned Asians, Americans and Europeans, in
descending order of importance 448.
443 Special rules on the application of the law of the People’s Republic of China relating to border health controls andquarantine, articles 99 and 100.
444 J.S. ROTH, All about AIDS, London, Harwood Academic Publishers, 1989, p. 115.445 DC. JAYASURIYA, o.c., p. 31.446 Article 5 of the aforesaid Regulation of 26 December 1987.447 Article 7 of the aforesaid Regulation of 26 December 1987.448 J.P. CABESTAN, ‘Sida et droit en Chine populaire’, Droit et sida, comparaison internationale, Paris, CNRS,
1994, p. 108.

158 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
In 1987, a seropositive Irish national was isolated before being expelled. The Irish
Government reproached China for having taken this measure 449.
30. IndiaA. Entry
345. Authorisation to enter the country is refused if the authorities are convinced that
a foreigner is suffering from a contagious disease which, according to the medical
inspector in the port or border-crossing point, could make the foreigner’s entry a threat
to public health 450.
B. Residence and expulsion
346. By virtue of central government directives, foreigners wishing to reside in the
country for more than one year, adult members of their family and students are required
to undergo an AIDS test. An exception is made for foreign members of a foreign
diplomatic representation office or consulate or from the United Nations, whether or not
they have diplomatic status; for foreign journalists accredited by the government press
and information office; for clergymen; for foreigners under the age of 18; and for holders
of a seronegative certificate dating back at least one month. The test is carried out by a
monitoring centre within a period of one month following arrival 451. Foreigners who test
seropositive and those refusing to undergo the test are expelled 452.
C. Miscellaneous
347. With respect to the movement of persons living with HIV/AIDS, the regulations
stipulate that the railway authority should not carry people suffering from any of
the infectious or contagious diseases mentioned in the current regulations which
includes AIDS 453.
449 PANOS INSTITUTE, The Third Epidemic – Repercussions of the Fear of AIDS, London, 1990, p. 128.450 The Foreigners Order 1948, article 2.2.C.451 This information comes from the list established by the Federal Department of Foreign Affairs in Switzerland
in February 1997.452 Idem.453 The carriage of passengers suffering from infectious or contagious diseases, 1990, IDHL, 1993, 44 (1), p. 28.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 159
348. As regards foreigners, Doctor Paintal from the Indian Council for Medical Research
tabled a bill in June 1988 according to which sexual relations between Indians and
foreigners would be prohibited in order to prevent the spread of AIDS, on pain of
sanctions. The media criticised this idea whilst the bill was being considered by
Parliament. The Minister of Justice rejected the proposal, which would have contravened
the Indian Constitution 454.
31. IndonesiaA. Entry
349. On 3 January 1991, a circular was issued by a Ministry of Health department
affirming that HIV/AIDS should not interfere with tourism and international travel 455.
350. By virtue of the decree of 1994 concerning the national strategy for controlling AIDS in
Indonesia 456, any HIV/AIDS diagnostic test must be subject to the enlightened consent of
the person concerned, which should exclude the systematic screening of foreigners.
B. Residence and expulsion
351. According to a study dating from June 1997, there is no screening policy but if a
foreigner is found to be seropositive, he would not be granted an extension to his
residence permit 457.
352. Section 51 of law no. 9 of 1953 on the control of foreigners (Emergency Act) appears
to have been used to expel persons with HIV/AIDS. According to this provision,
foreigners considered to jeopardise the peace, public decency or public welfare may be
expelled from Indonesia 458.
Indonesia is rather an unusual case in that the country implements both anti-
discriminatory measures – by excluding systematic screening – and discriminatory
measures – leading to the expulsion of persons living with HIV/AIDS.
454 PANOS INSTITUTE, o.c., p. 29.455 DC. JAYASURIYA, HIV Law and Law Reform in Asia and the Pacific, New Delhi, UNDP regional project on
HIV and development, 1995, p. 224.456 IDHL, 1995, 46 (1), p. 25.457 This information comes from the list established by The Laboratory Centre for Disease Control in June 1997.458 Restrictions of entry and residence for people with HIV/AIDS, o.c., p. 37.

160 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
32. MalaysiaA. Entry
353. The law allows for the minister to pass a regulation relating to the entry of people
into Malaysia, their movements within the country and their departure from the
territory 459. By virtue of general legislation on immigration, the entry of foreigners
suffering form serious contagious diseases may be prohibited 460.
The law holds that foreigners suffering from a contagious or infectious disease which
makes their presence in Malaysia a danger to the community, are undesirable 461.
According to a declaration of 22 May 1985, AIDS is an infectious disease as defined in
the law on immigration 462. Moreover, the law lists the infectious diseases and mentions
HIV/AIDS 463. It is clear that, even in the absence of specific legislation relating to AIDS,
general legislation permits restrictions on the access of persons living with HIV/AIDS to
the territory.
Article 39 of the law on immigration stipulates that anyone wishing to enter
Malaysia or to obtain a permit can be made to undergo a medical examination. Any
foreigner refusing to undergo the medical examination may be declared undesirable by
virtue of article 8.
B. Residence and expulsion
354. Foreigners requesting a work permit to work in the construction sector, plantations
or as domestic staff must undergo an AIDS test 464.
355. The immigration department may order a foreigner living with HIV/AIDS to leave
the country on the grounds that he might contaminate other people 465.
459 Law no. 342 of 13 August 1988 modifying and updating legislation relating to measures for the prevention and controlof infectious diseases and for related purposes, article 31.2.
460 Information provided by the Malaysian Embassy in Brussels on 17 March 1997.461 Article 8 of the Immigration Act of 1959.462 Directory of legal instruments dealing with HIV infection and AIDS, Geneva, WHO, 1997, p. 121.463 Annexe 1 to the aforesaid law of 13 August 1988.464 This information comes from the list established by the US government in January 1996.465 This information comes from the list established by The Laboratory Centre for Disease Control in June 1997.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 161
C. Miscellaneous
356. Where a person is unable to provide for his needs as a result of the disease from
which he is suffering, he may ask to be repatriated at the government’s expense 466.
33. NepalA. Entry
357. Foreigners may be obliged to undergo a medical inspection 467. No specific provision
has been made for entry restrictions against foreigners with HIV/AIDS 468.
B. Residence and expulsion
358. A visa issued to a foreigner may be cancelled under various circumstances, in
particular where a foreigner fails to produce an international health certificate when this
is requested, or where a foreigner is suffering from a serious illness or contagious disease 469.
34. PakistanA. Entry
359. Legislation allows for a foreigner to be made to undergo a medical examination 470.
Any foreigner suffering from an infectious disease who, in the view of the medical
inspector of the port or border-crossing point, is liable to jeopardise public health may be
refused entry 471. However, there is no specific law applying to the movement of persons
living with HIV/AIDS and neither is any such law in the planning stage 472.
B. Residence and expulsion
360. Foreigners who wish to stay in the country for more than one year may be required
by the embassy issuing the visa to produce a certificate relating to various diseases. It has
not been possible to obtain any information on the consequences of a seropositivity 473.
466 Article 46 of the aforesaid Immigration Act.467 Article 3(2)(c) of the law of 1958 on foreigners.468 This information comes from the list established by The Laboratory Centre for Disease Control in June 1997.469 Article 28 of the 1994 Immigration Rules.470 Article 3(2)(e) of the law of 1946 on foreigners.471 Order of 1951 on foreigners.472 Information provided by the IOM head office in Pakistan on 13 March 1997 and by the Pakistani Embassy in
Brussels on 23 May 1997.473 Information provided by the IOM head office in Pakistan on 13 March 1997.

162 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
This medical requirement applies primarily to foreigners requesting a long-term residence
permit who come from countries where AIDS is widespread 474.
361. Persons living with HIV/AIDS can be expelled: one author cites the case of a
foreigner who was expelled whilst he was suffering from the disease and who died during
his return journey 475.
35. PhilippinesA. Entry
362. The law allows for the medical authorities to give an opinion to immigration officers
about the foreigner’s right to enter and to stay in the country 476. A medical examination
is carried out by government medical inspectors appointed on the order of the president
especially for carrying out such examinations and determining whether the foreigner is
suffering from any mental or physical illness. If no medical inspector is available, a private
doctor may carry out the examination 477. The categories of people who are not allowed to
enter the country include foreigners suffering from dangerous or contagious illnesses, such
as epilepsy 478.
363. The law also authorises the president to suspend the right of foreigners from
countries where cholera or another infectious or contagious disease is widespread, to
enter the country 479.
B. Residence and expulsion
364. The following people are subject to a screening test:
■ foreigners requesting a permanent visa
■ foreigners who are not legally resident
■ foreigners exchanging their temporary visa for a permanent visa
■ foreigners assigned to refugee centres 480.
474 This information comes from the list established by The Laboratory Centre for Disease Control in June 1997.475 DC. JAYASURIYA, HIV Law and Law Reform in Asia and the Pacific, o.c., p. 255.476 Section 6 of the Immigration Act of 1940.477 Section 28 of the aforesaid Act of 1940. 478 Section 29 of the aforesaid Act of 1940.479 Section 47 of the aforesaid Act of 1940.480 Immigration Regulation instructions no. 14 of 17 February 1988 and Immigration Regulation instructions no.
21 of 13 April 1988 (both issued by the Commission on Immigration and Deportation, Department of Justice)Directory of legal instruments dealing with HIV infection and AIDS, o.c., p. 143.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 163
36. Sri LankaA. Entry
365. The law stipulates that no entry visa may be issued to a foreigner who is declared
undesirable for medical reasons in the opinion of the medical inspector, except where this
concerns foreigners exempted by law 481. Entry may be refused to foreigners living with
HIV/AIDS on this basis 482. Sri Lanka stated that restrictions could be established based
on the principle of reciprocity 483.
The medical examination of foreigners provided for by law takes place upon arrival
or as early as possible after arrival 484.
B. Residence and expulsion
366. A foreigner who is declared undesirable for reasons of health may be order to leave
the territory 485. The provision does not apply to foreigners benefiting from an exemption
by virtue of the law 486.
C. Miscellaneous
367. Hospitals do not admit foreigners who are seropositive or living with AIDS 487.
37. SyriaA. Entry
368. Screening is compulsory upon entry for foreign students and upon return for Syrian
grant-holders who have studied abroad 488.
B. Residence and expulsion
369. Screening is compulsory for the following categories 489:
481 Article 11 of the Immigrants and Emigrants Act of 1949.482 This information comes from the list established by The Laboratory Centre for Disease Control in June 1997. 483 DC. JAYASURIYA, AIDS, Health, Policy and Legal Aspects, o.c., p. 29.484 Article 18 of the aforesaid Act of 1949.485 Article 31 of the aforesaid Act of 1949.486 Article 30 of the aforesaid Act of 1949.487 This information comes from the list established by the Federal Department of Foreign Affairs in Switzerland
in February 1997.488 Regulatory decree no. 36/T of 26 October 1987 of the Ministry of Health, IDHL, 1988, 39 (2), p. 369.489 Idem.
164 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
■ foreign nationals domiciled in the Syrian Arab Republic for professional purposes,
when they make their first request for a work permit (people domiciled in the Syrian
Arab Republic and not claiming any specific citizenship are exempted)
■ foreign students who come to follow a training course in a university or college, upon
their arrival and when they enrol in such training institutions
■ grant-holders studying abroad, when they return to the Syrian Arab Republic and
prior to their re-entry into the institution which awarded them the study grant.
Generally speaking it is permitted to carry out screening on foreigners residing in the
country for professional, study or other purposes. The said persons receive a residence
permit only when they prove that they are seronegative.
370. A foreigner wishing to marry a Syrian national must undergo the test 490.
371. The competent authorities and embassies concerned make provisions for repatriating
foreigners living with HIV/AIDS 491.
38. ThailandA. Entry
372. There is no law prohibiting the entry of foreigners living with HIV/AIDS into the
country 492. This is the situation in 1997. Formerly entry restrictions were applied before.
The general law on immigration allows for foreigners suffering from any of the
diseases listed in the ministerial regulation to be refused entry 493. The law makes the
medical inspector responsible for diagnosing the said diseases. The previous regulation
cited AIDS among the diseases for which entry could be prohibited 494. This regulation
reflected the belief that AIDS is an imported disease. It was criticised both nationally and
internationally since it aggravated discriminatory tendencies and violated the general
principle of the right to free movement 495. It seems that proof of seronegativity was not
490 Decree no. 17/T of 30 March 1991.491 Idem.492 Information provided by the Thai Embassy in Brussels on 18 March 1997.493 Immigration Act of 1979, section 12.494 Ministerial Regulation no. 11 (1986) issued under the Immigration Act, 1979 (dated 26 August 1986) IDHL,
1987, 38 (2), p. 252.495 V. MUNTARBHORN, ‘Le sida et la loi: le dilemme thaïlandais’, Droit et sida, comparaison internationale, o.c.,
p. 421.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 165
required with the result that in spite all this, seropositive people were able to enter the
country, whereas people who were carrying drugs for treating their disease could be
refused entry 496. The new regulation no longer includes AIDS among the diseases which
may lead to a refusal to grant right of entry 497.
B. Residence and expulsion
373. At present there is no law prohibiting the residence of foreigners living with
HIV/AIDS 498. In the previous regulation, AIDS was cited among the diseases which
could lead to a ban on settling in Thailand. The new regulation abolishes this restriction
since AIDS no longer figures on the list of diseases entailing such a ban.
374. There is no law specifying that persons living with HIV/AIDS can be expelled 499.
However, the law provides in general that expulsion may be ordered in cases where the
measure is required in the interests of peace, public policy and public decency 500.
39. TurkeyA. Entry
375. By virtue of the law, persons afflicted with contagious diseases may be refused entry 501.
However, persons whose condition does not pose a threat to public health and safety, who
arrive by their own means or with the pecuniary assistance of their guardian or curator, in
order to undergo medical or other treatment, may be exempted from this provision. There
is no restriction on the entry of foreigners living with HIV/AIDS. There is no law
prohibiting the entry of foreigners who are seropositive or living with AIDS 502. According
to the information received, there is no restriction on the entry of foreigners living with
HIV/AIDS which would allow the general law to be used for this purpose 503.
496 PANOS INSTITUTE, o.c., p. 128.497 Regulation no. 14 of 20 February 1992 of the Ministry of the Interior made for the implementation of the law of
1970 on immigration.498 Information provided by the Thai Embassy in Brussels on 18 March 1997.499 Idem.500 Section 5 of the law of 7 July 1964 on deportation.501 Article 8 of the Passport Act of 1950.502 Information provided by the Turkish Embassy in Brussels on 28 August 1997.503 Idem.
166 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
B. Residence and expulsion
376. The law stipulates in general that no residence permit shall be issued to foreigners
who disturb public policy 504. There is no law prohibiting foreigners living with
HIV/AIDS from staying in the country 505. There is no restriction applying to the right of
such people to stay in Turkey 506.
377. The law specifies that any foreigner who is a threat to public safety may be expelled.
Public health is not mentioned as a ground for expulsion 507. No law provides for the
expulsion of foreigners living with HIV/AIDS 508.
378. A medical inspection is stipulated for refugees 509. In the case of a contagious disease,
all the necessary measures are taken and the authorities informed. Foreigners suffering
from serious diseases are treated in state hospitals. The costs are covered, with certain
exceptions. A refugee may only be expelled in compliance with the Geneva Convention
and if the person concerned is a threat to national security or public policy 510.
40. VietnamA. Entry
379. The law provides for a request for an entry or exit visa to be refused with a view to
preventing and controlling an epidemic 511. Foreigners with HIV/AIDS must make a
declaration upon their arrival, with the procedure relating to this declaration being
determined by the government 512.
380. Vietnamese nationals returning to their home country have been subjected to a test 513.
504 Article 7 of the law of 1950 concerning the stay and travelling of foreigners in Turkey.505 Information provided by the Turkish Embassy in Brussels on 28 August 1997.506 Idem.507 Law of 1950, article 19.508 Information provided by the Turkish Embassy in Brussels on 28 August 1997.509 Decision no. 94/6169 of 30 November 1994, applying to refugees.510 Idem.511 Ordinance of 1992 on the exit, entry, residence and travel of foreigners in Vietnam, article 6.512 Ordinance of 31 May 1995 on the prevention and control of HIV/AIDS, article 19 and decree no. 34/CP of
1 June 1996. Also see the list established by the Federal Department of Foreign Affairs in Switzerland inFebruary 1997.
513 This information comes from the list established by The Laboratory Centre for Disease Control in June 1997.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 167
B. Residence and expulsion
381. Foreigners registered as residents in Vietnam for a period exceeding three months
must undergo a screening test 514.
382. A foreigner may be subject to an expulsion order if he poses a threat to the health of
other people living in Vietnam 515.
C. Miscellaneous
383. No foreigner infected by the HIV virus or living with AIDS is authorised to marry a
Vietnamese citizen 516.
C. Central and South America41. ArgentinaA. Entry
384. By virtue of the law, on no account may foreigners suffering from transmissible
diseases which present a risk to the community enter or stay in the country 517. The
national health authorities and authorities delegated by them are responsible for
determining the risk.
HIV screening is included in the health control of immigrants. The constitutional
validity of this provision is debatable. Indeed, article 14 of the Constitution recognises
that the rights of the nation’s inhabitants include the right to enter, stay, pass through and
leave Argentine territory. Furthermore, the preamble to the Constitution states that the
Grand Charter is aimed at ‘anyone in the world who wishes to live on Argentine soil’ 518.
B. Residence and expulsion
385. Foreigners suffering from diseases that reduce their ability to work are deemed
unsuitable for admittance as permanent or temporary residents 519. In order to obtain a
514 Governmental decree no. 16/CP of 18 December 1992 regulating certain aspects of the measures of prevention andof the campaign against the infection by HIV and against AIDS, IDHL, 1993, 44 (2), p. 230.
515 Article 14 of the aforesaid law of 1992.516 Article 15 of aforesaid decree no. 16/CP.517 Article 21(a) of decree 1023/94 of 29 June 1994 approving the immigration regulation.518 N. MINYERSKY, J. MONTI, M.E. VASQUEZ ACUNA, ‘La problématique du sida en Argentine’, Droit et
sida, comparaison internationale, o.c., p. 47.519 Article 22(a) of aforesaid decree 1023/94.
168 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
temporary or permanent residence permit, a foreigner must provide a medical certificate
established by a doctor or a health authority recognised for the purpose, describing his
physical state of health 520.
386. In certain cases of expulsion, health care may be provided as far as the place of
destination. Moreover, the national immigration department may request the
collaboration of the health authorities to ensure that foreigners who are subject to an
expulsion order and who are in need of medical care are detained in suitable official
health institutions where they are provided with medical care 521.
387. Asylum-seekers and refugees must respect public policy, the peace and public safety.
Refugees may be given temporary or permanent resident status. Their right of residence
may be terminated in compliance with the general rules mentioned above 522.
42. BahamasA. Entry
388. The law stipulates that a foreigner may only be allowed to enter and stay in the
country if he is not suffering from a contagious or infectious disease which, in the opinion
of the medical inspector, makes his presence a danger to the community 523. There is no
official legislation banning foreigners living with HIV/AIDS from entering the country.
However, by extending the application of general legislation to AIDS, the Ministry of
Health recommended that persons living with HIV/AIDS should not be authorised to
enter the country 524.
B. Residence and expulsion
389. Foreigners other than those benefiting from a permanent right of residence may be
ordered to leave the territory if this is in the public interest 525.
520 Articles 39 and 44 of aforesaid decree 1023/94.521 Articles 85 and 87 of aforesaid decree 1023/94.522 Reference should be made on this matter to articles 21 and 22 of aforesaid decree 1023/94. Nevertheless it
should be noted that by virtue of article 173, the provisions of article 22 do no apply to refugees. 523 Immigration Act of 1967, article 19.524 Restrictions of entry and residence for people with HIV/AIDS, o.c., p. 16.525 Article 36 of the Act of 1967 on immigration.

The free movement of persons living with HIV/AIDS – Part 3: Third Countries 169
43. BarbadosA. Entry
390. Foreigners arriving on the territory are subjected to a medical examination 526.
B. Residence and expulsion
391. The law lists the categories of foreigner considered to be undesirable 527. These
include foreigners suffering from contagious diseases as defined in the legislation on
health services, as well as foreigners who, due to a physical disability, are unable to
provide for their own needs or who become a public charge. AIDS is neither expressly
included nor excluded from these provisions. Foreigners entering the country for medical
treatment may, however, receive dispensation from these rules subject to authorisation
from the minister 528.
44. BelizeA. Entry
392. A medical examination for foreigners is provided for by law 529. Any foreigner
refusing to undergo a medical inspection may be refused entry.
Mentioned in the law as undesirable foreigners are foreigners suffering from
contagious diseases, making their entry a danger to the community, as well as foreigners
who are liable to become a public charge because of the disease from which they are
suffering 530. As a result of a government declaration relating to residence, the restrictive
measures of this general legislation were extended to AIDS. However the law does
authorise the Minister to exempt certain foreigners from the above-mentioned rules.
Furthermore, the law, without prejudice to the issue of whether or not a foreigner is
undesirable, allows any person to be granted a special permit authorising him to remain
temporarily in the country for medical treatment against any contagious disease. The
person concerned must nevertheless respect the conditions laid down by the government
medical inspector 531.
526 Article 12 of the Act of 1976 on immigration.527 Annexe 1 to the aforesaid Act of 1976.528 Article 8(2)(a) of the aforesaid Act of 1976.529 Article 22 of the Immigration Ordinance of 1958.530 Article 4 of the Immigration Ordinance of 1958.531 Article 16 of the Immigration Ordinance of 1958.
170 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
B. Residence and expulsion
393. According to a government declaration, foreigners wishing to settle, work or apply
for naturalisation must show proof of a negative test dating back a maximum of two
months. A dispensation is allowed for diplomatic staff 532.
45. BoliviaA. Entry
394. Generally speaking a person’s consent is required before carrying out AIDS screening.
The law expressly prohibits AIDS screening for foreigners and nationals entering Bolivia.
There are sanctions for failing to comply with the aforesaid provisions 533. Formerly there
were entry restrictions 534.
B. Residence and expulsion
395. People requesting temporary or permanent right of residence must undergo an AIDS
test within 48 hours of entering the country 535. An exception is made for diplomatic staff 536.
The obligation to undergo a screening test in order to obtain a residence or work permit
appears to be contrary to the texts adopted as part of the fight against AIDS which require
the individual’s consent before carrying out a screening test 537.
46. BrazilA. Entry
396. By decision of the National Commission for the Control and Prevention of AIDS, the
legislation in force in Brazil does not stipulate screening for foreigners travelling to Brazil 538.
532 This information comes from the list established by the Federal Department of Foreign Affairs in Switzerlandin February 1997.
533 Resolution no. 0660 of December 1996 on the prevention and surveillance of HIV/AIDS in Bolivia, articles 8, 45and 65.
534 Restrictions of entry and residence for people with HIV/AIDS, o.c., p. 18.535 Inter-ministerial resolution no. 0415/89, article 48 in H. FUENZALIDA PUELMA, A. LINARES PARADA
and D. SERRANO LA VERTU, Aportes de la ética y el derecho al estudio del sida, Pan-American HealthOrganization, 1991, p. 56.
536 This information comes from the list established by the Federal Department of Foreign Affairs in Switzerlandin February 1997.
537 Aforesaid resolution no. 0660.538 Information provided by the Brazilian Embassy in Brussels on 20 June 1997.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 171
B. Residence and expulsion
397. Brazilian immigration legislation does not require any type of certificate and requires
no medical examination in order to obtain a visa 539.
47. ChileA. Entry
398. Entry is refused to any foreigner suffering from a disease which, according to the
Chilean authorities, may constitute grounds for refusing the right to enter the country 540.
B. Residence and expulsion
399. Visitors other than tourists are required to present a medical certificate attesting that
they are in good health and are not suffering from any contagious disease. A foreigner
must also provide a certificate proving that he has undergone an AIDS screening test,
issued by the laboratory division of the Ministry of Health 541.
48. ColombiaA. Entry
400. The law states that immigration is governed by social, demographic, economic,
scientific, cultural, public policy and health requirements. No foreigner suffering from an
infectious/contagious disease may enter the country 542. There is no specific legislation
relating to the entry of foreigners suffering from HIV/AIDS 543. The information relating
to foreigners staying in the country tends to consider that the scope of general legislation
is sufficient to allow for restrictions on access to the territory on the grounds of AIDS.
However this interpretation is not hardly compatible with the decree on the prevention
of transmissible diseases which prohibits systematic screening (infra § 402).
539 Idem.540 Article 15 of statutory order no. 1094 of 1975 establishing the laws concerning foreigners in Chile.541 This information comes from the list established by The Laboratory Centre for Disease Control in June 1997.542 Articles 5 and 166 of decree no. 2731 of 27 December 1996.543 Information provided by the Colombian Embassy in Brussels on 1 September 1997.
172 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
B. Residence and expulsion
401. Before a visa can be granted the law requires foreigners to provide a medical
certificate in cases where this is stipulated by the ministry of foreign affairs for
health reasons 544.
Foreigners wishing to reside permanently must present a certificate proving the
absence of HIV infection 545. Certificates issued abroad are accepted 546.
The law allows a foreigner to obtain a one-year residence permit in order to receive
medical treatment. For this purpose the foreigner must present proof of the necessity
and duration of such treatment, as well as proof of adequate financial resources 547.
Failure to respect the provisions of the decree on immigration may result
in expulsion 548.
C. Miscellaneous
402. It is prohibited to demand certificates relating to sexually-transmitted diseases,
including HIV infection, which should exclude the systematic screening of foreigners.
Since this prohibition applies ‘without prejudice to any health measures of an individual
nature’, there is reason to question the interpretation of this phrasing and whether it
could include the possibility of carrying out systematic screening on foreigners 549.
49. Costa RicaA. Entry
403. Restrictions were applied in the past 550. The law provided that foreigners requesting
a permanent or temporary residence permit had to undergo an AIDS test, the test being
544 Article 19 paragraph 4 of aforesaid decree no. 2731.545 This information comes from the list established by the Federal Department of Foreign Affairs in Switzerland
in February 1997.546 This information comes from the list established by The Laboratory Centre for Disease Control in June 1997.547 Articles 101 et seq. of aforesaid decree no. 2731.548 Article 195 of aforesaid decree no. 2731.549 Decree no. 0559 of 22 February 1991 issuing regulation for the partial implementation of laws no. 09 of 1979 and
no. 19 of 1990, on the prevention, control and surveillance of communicable diseases, with particular reference toinfection by the human immunodeficiency virus (HIV) and the acquired immune deficiency syndrome (AIDS) andpromulgating other provisions on this subject, IDHL, 1992, 43(3), p. 508.
550 Decree no. 18781-S-G of 19 January 1989 containing provisions concerning the screening which certains categories offoreign nationals resident in Costa Rica must undergo, replacing the provisions of decree no. 18536-S-G of 6 October 1988 containing detailed provisions relating to treatment administered to persons living with AIDS.

The free movement of persons living with HIV/AIDS – Part 3: Third Countries 173
carried out at the ministry of health, and that a seropositive foreigner could be refused
entry 551. This legislation was repealed 552.
B. Residence and expulsion
404. Former legislation authorised the expulsion of any foreigner who was seropositive 553.
This legislation was repealed but the legislation on immigration allows for a foreigner to
be expelled if he threatens national security, the peace or public policy, or where special
circumstances so require 554.
50. CubaA. Entry
405. All foreign grant-holders or non-Cuban nationals who come to reside in Cuba for
periods exceeding three months must undergo an AIDS screening test upon arrival or on
the order of the health authorities 555. The test is carried out upon arrival or when the
health authorities deem it necessary. Diplomatic staff are exempted from application of
the law 556. Cuban authors have justified the measure by saying: ‘This health and
epidemiological control is all the more necessary since we are certain (with the support of
clinical statistics) that sexual relations are at the origin of the transmission of AIDS into
our country and, inevitably, sexual relations with foreigners constitute one of the
principal sources of contamination’ 557. If such is the justification for compulsory
screening, one might wonder why the measure is aimed only at foreigners requesting long-
term residence and not those requesting short stays, notably tourists, in particular when
one considers the existence of sex tourism in the Caribbean.
551 Aforesaid decree of 19 January 1989.552 Decree no. 20202-S-G of 17 January 1991, IDHL, 1991, 42(2), p. 242.553 Decree no. 18536-S-G of 6 October 1988 repealed by the decree of 19 January 1989, itself replaced by the
decree of 17 January 1991.554 Article 121 of the law of 1986 on immigration.555 Ministerial resolution no. 144 of 11 June 1987.556 O. MESA CASTILLO, R. FRANCO RIVERO, A. VASQUEZ SANCHEZ and A. MARTINEZ MARTIN,
‘La législation cubaine face au sida’, in Droit et sida, comparaison internationale, o.c., p. 144-145.557 Idem, p. 145.
174 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
406. A sero-epidemiological examination is required for Cuban nationals who have been
living permanently in Africa and who entered Cuba after 1975, as well as for Cubans
having lived on a permanent basis in Nicaragua 558.
B. Residence and expulsion
407. Any foreign national who tests seropositive must be sent back to his own country 559.
51. Dominican RepublicA. Entry
408. The only regulation relating to the health inspection of foreigners is contained in
the public health code 560. By virtue of this law, the secretary of state for public health
assists the executive authority on health aspects of the immigration policy and submits a
draft regulation to the President setting out the minimum health conditions required for
people wishing to enter the country. It also makes it compulsory for all foreigners to
undergo a medical examination in order to receive authorisation to enter the country.
The same legislation states that under no circumstances may people suffering from
transmissible diseases be allowed to stay in the country. There is no specific legislation on
the entry and residence of foreigners with HIV/AIDS 561.
B. Residence and expulsion
409. Foreigners wishing to settle in the country must provide proof of a negative test
when applying for permanent residence 562.
52. EcuadorA. Entry
410. Foreigners wishing to enter Ecuador must pass an examination carried out by the
health authorities 563.
558 Ministerial resolution no. 129/86 in H. FUENZALIDA PUELMA, A. LINARES PARADA and D.SERRANO LA VERTU, o.c., p. 77.
559 Article 2 of the aforesaid resolution of 11 June 1987.560 Law no. 4471 of 3 June 1956, public health code, book II, section III, chapter III, article 108.561 Information provided by the Embassy of the Dominican Republic in Brussels on 2 August 1997.562 This information comes from the list established by the Federal Department of Foreign Affairs in Switzerland
in February 1997.563 Article 7-II of law no. 1899 of 1972 on immigration.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 175
B. Residence and expulsion
411. Foreigners suffering from serious, chronic and contagious diseases, such as tuberculosis,
leprosy, trachoma and other similar diseases not subject to quarantine may not obtain a visa
to enter the country 564. Such foreigners are subject to an exclusion clause.
Furthermore, the law stipulates that where one of the above cases for exclusion
applies to a foreigner, his expulsion may be ordered 565. No express or implicit application
of these general provisions to AIDS has been reported.
53. JamaicaA. Entry
412. The law makes provision for a medical inspection upon entry to the territory. For a
foreigner to be authorised to enter the country, he must not be the subject of a certificate
sent by the medical inspector to the immigration officer stating that the foreigner is
undesirable for medical reasons 566. Jamaica has declared its support for the WHO policy
on travellers suffering from HIV/AIDS 567. From this it must be inferred that the general
provisions do not extend to AIDS.
B. Residence and expulsion
413. Expulsion may be ordered if the minister deems this measure to be in the
public interest 568.
54. MexicoA. Entry
414. The law states that any foreigner who, according to the health authority, is not in
good physical condition may be refused entry 569. A foreigner entering the country must
present an official certificate issued by the authorities in the country of origin, proving
564 Article 9-VII of aforesaid law no. 1899.565 Article 17 of aforesaid law no. 1899.566 Articles 9(1) and 6 of the Aliens Act of 1946.567 N. GILMORE, ‘Medical and Political Aspects of Travel for HIV Positives’, Travel Medicine 2, Proceedings of
the Second Conference on International Travel Medicine, Atlanta, Georgia, USA, May 9-12 1991, p. 208;Restrictions of Entry and Residence for People with HIV/AIDS, o.c., p. 40.
568 Article 15(6) of the Aliens Act of 1946.569 Article 37 of the general population Act of 1992.
176 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
that he is in good physical health, in the cases stipulated by the secretary of state. The
law also states that foreigners must pass the health authority examination 570. Any
foreigner suffering from an infectious or contagious disease constituting a risk to public
health may be refused entry to the territory 571. There is no legislation limiting the entry
of foreigners living with HIV/AIDS 572.
B. Residence and expulsion
415. There is no law which specifically restricts the right of foreigners with HIV/AIDS to
stay in the country 573. Nevertheless, in practice, foreigners wishing to reside permanently
in Mexico must present a certificate of seronegativity 574.
55. NicaraguaA. Entry
416. Foreigners wishing to enter the country with a view to residing there on a temporary or
permanent basis, together with the members of their families, must provide a medical
certificate issued by the health authorities of the country of origin 575. Foreigners who belong
to the category of non-residents (in particular tourists) must provide the same certificate 576.
B. Residence and expulsion
417. Foreigners suffering from contagious or infectious diseases constituting a danger to
public health are not admitted as permanent or temporary residents. An exception is
made in the case of family reunification 577. Non-resident foreigners are not admitted to
the country in cases where their entry constitutes a threat to the health of the nation 578.
Furthermore, the law allows for the residence permit to be revoked for reasons relating to
public policy 579.
570 Article 62 of the aforesaid law of 1992.571 Article 57 of the Regulation of 30 September 1992 implementing the General Population Act.572 Information provided by the Mexican Embassy in Brussels on 19 March 1997.573 Idem.574 This information comes from the list established by The Laboratory Centre for Disease Control in June 1997,
as well as the list established by the US government in December 1996.575 Immigration Act no. 153 of 1993, articles 11, 31 and 57.576 Aforesaid Act no. 153, article 60.577 Articles 4 and 5 of law no. 154 of 1993 on foreigners.578 Article 5 of aforesaid law no. 154.579 Article 29 of aforesaid law no. 154.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 177
56. PanamaA. Entry
418. There is no specific restriction on access to the territory for short stays.
B. Residence and expulsion
419. Foreign nationals entering Panama with the intention of settling there permanently
or for a period exceeding one year must hold a medical certificate issued in their country
of origin testifying that they have been screened for AIDS and tested seronegative. If a
foreigner tests seropositive, he is refused entry. The certificate, certified as accurate by the
competent diplomatic mission or consulate, is valid for only two months 580.
57. PeruA. Entry
420. There is no legal provision in Peru governing the movement of foreigners living with
HIV/AIDS 581. There does not appear to be any restriction on access to the territory 582.
B. Residence and expulsion
421. Compulsory screening was formerly imposed on people wishing to elect domicile in
Peru 583 but the legislation imposing this measure was repealed.
422. A law dating back to 1996 584 states that screening is voluntary (except for blood and
organ donors), which should now exclude any systematic screening of foreigners wishing
to stay in the country.
580 Law no. 26 of 17 December 1992 giving measures for the prophylaxis and control of the acquired immune deficiencysyndrome (AIDS) epidemic and the spread of the human immunodeficiency virus (HIV), IDHL, 1995, 46(4), p. 474.
581 Information provided by the Peruvian Embassy in Brussels on 14 October 1997.582 This information comes from the list established by The Laboratory Centre for Disease Control in June 1997.583 Law no. 25275 of 10 July 1990 declaring measures for the control of AIDS to be in the public interest and of priority
importance with regard to the national health policy, Directory of legal instruments dealing with HIV infection andAIDS, o.c., p. 142.
584 Law no. 26626 of 19 June 1996 assigning to the ministry of health the task of drawing up the national plan for thecontrol of the human immunodeficiency virus, AIDS and sexually transmitted diseases (CONTRASIDA), Directoryof legal instruments dealing with HIV infection and AIDS, o.c., p. 143.

178 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
C. Miscellaneous
423. A 1987 resolution relates the epidemiological situation in Peru. According to this
resolution, the first cases of AIDS concerned homosexuals who had travelled abroad;
next the disease was diagnosed in homosexuals who had not travelled but had engaged in
sexual relations with foreigners; finally, the disease was found in homosexuals and
heterosexuals who, despite not having travelled abroad nor having had sexual relations
with foreigners, had contracted the disease 585.
58. El SalvadorA. Entry
424. The health authorities are authorised to impose regular medical examinations on the
entire population, as well as medical examinations, either periodically or otherwise, for
certain population groups in the case of an epidemic or specific risk. Any traveller
entering Salvadorian territory must present to the appropriate health authority valid
international vaccination certificates or other certificates of serological examinations
concerning diseases specified by the ministry. In addition, travellers must undergo any
medical examination required by the competent health authority. Immigrants must undergo
a medical examination stipulated by the health authority, if it deems it necessary, in order
to confirm the medical certificates obtained in their countries of origin and duly certified
as accurate by the Salvadorian health authorities on the basis of clinical, radiological and
laboratory examinations testifying that the persons in question are neither suffering from
nor carrying transmissible diseases 586.
B. Residence and expulsion
425. An AIDS test is required for foreigners requesting temporary or permanent residence 587.
585 Resolution no. 011-87-SA of 2 April 1987 approving the multi-sector national programme for the prevention andcontrol of AIDS.
586 The Health Code (promulgated by decree no. 955 of 11 May 1988), IDHL, 1990, 41(1), p. 9.587 H. FUENZALIDA PUELMA, A. LINARES PARADA and D. SERRANO LA VERTU, o.c., p. 37; this
information also comes from the list established by the Federal Department of Foreign Affairs in Switzerland inFebruary 1997.

The free movement of persons living with HIV/AIDS – Part 3: Third Countries 179
59. Trinidad and TobagoA. Entry
426. The law allows for people suffering from contagious or infectious diseases to be
banned from entering the country, as defined in the public health order 588. Such people
are deemed to be undesirable. The minister may authorise such persons to enter or stay in
the country subject to certain conditions. The person concerned must not be liable to
become a public charge and must have relatives in the country. Moreover, the minister of
health must have given his agreement for treatment in a hospital or any other location in
the country 589. There is no law specifically limiting the entry and residence of foreigners
living with HIV/AIDS 590. According to information relating to residence, application of
the general law extends to AIDS.
B. Residence and expulsion
427. When considering a foreigner’s application for residence the minister must check
that he is not an undesirable alien 591. Foreigners requesting a residence permit or wishing
to remain in the country for more than one year must undergo an AIDS test. Foreigners
living with HIV/AIDS may be refused right of residence 592.
60. VenezuelaA. Entry
428. A resolution adopted in 1994 593 limits screening to various situations that do not
include mention of screening for foreigners with HIV/AIDS. In addition, this resolution
stipulates that tests to detect the HIV antibody may not be administered without the free,
express and manifest consent of the person undergoing such an examination, and that
such an examination may not be carried out in any situation likely to limit his freedom to
exercise individual, social, economic, political and cultural rights 594. This provision
588 Article 8(1)(b) of the 1980 Immigration Act.589 Article 10(3) of the 1980 Immigration Act.590 Information provided by the Embassy of Trinidad and Tobago in Brussels on 19 April 1997.591 Article 6(2) of the 1980 Immigration Act.592 This information comes from the list established by The Laboratory Centre for Disease Control in June 1997.593 Resolution no. SG-439 of 26 August 1994, IDHL, 1994, 45(4), p. 503.594 See An advocate’s guide to the international guidelines on HIV/AIDS and human rights, prepared by ICASO,
October 1997, p. 8.
180 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
should exclude the systematic screening of foreigners. Nevertheless, it would appear
that the test has been carried out, at least in the past, on foreign sailors 595.
B. Residence and expulsion
429. It would appear that the test may be required of foreigners requesting
a residence permit 596.
430. The expulsion of a foreigner may be ordered if he jeopardises public safety or policy 597.
D. South Sea Islands61. FijiA. Entry
431. There is no legislation aimed at restricting the free movement of persons with
HIV/AIDS 598.
B. Residence
432. No medical certificate is required in order to obtain a visa, except if a foreigner has
stayed in a country where ‘yellow fever, cholera, malaria, etc.’ are rampant 599.
62. Papua New GuineaA. Entry
433. The law states that a foreigner may be subjected to a medical examination 600. Any
foreigner suffering from a disease constituting a threat to the community or who refuses to
undergo a medical examination may be refused entry 601.
Visitors of good faith who enter the country for work or leisure reasons benefit from
laws guaranteeing the principle of non-discrimination. In exchange, the emphasis is
placed on the responsibility each visitor must assume. As a result of the efforts of the
595 Restrictions of entry and residence for people with HIV/AIDS, o.c., p. 68; see also N. GILMORE, o.c., p. 209.596 This information comes from the list established by the US government in January 1996. It has not been
possible to confirm it from other sources.597 Article 37 of the law on foreigners of 1997.598 Information provided by the Fijian Embassy in Brussels on 2 October 1997.599 Idem.600 Article 9(2) of the Migration Act of 1978.601 Article 9(1) of the aforesaid Act of 1978.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 181
World Trade Organisation to promote the free movement of people, the government
faces the dilemma of whether fundamental freedoms should be compromised in order
to control the disease. This is why Papua New Guinea is cautious about accepting
foreign travellers 602.
B. Residence and expulsion
434. The test is compulsory for foreigners applying to stay in the country 603. A work
permit is delivered only upon presentation of a certificate of seronegativity 604.
63. Western SamoaA. Entry
435. Visitors and tourists do not have to declare their seropositive status in order to
be allowed access to the territory. The same applies to returning Samoan nationals 605.
A contrario restrictions do apply to foreigners other than visitors and tourists.
B. Residence and expulsion
436. The law allows the minister to order a foreigner to leave the country if he considers
that the foreigner is rebellious or likely to pose a threat to the country’s peace, order or
proper administration or if the foreigner is undesirable 606. The decision of the minister is
final and may not be appealed against in the courts. This regulation has been used to
expel foreigners living with HIV/AIDS. Indeed the case of two tourists, one of whom was
seropositive, and to whom section 13(1)(a) was applied, was mentioned in doctrine 607. In
this case, immigration and health officers had questioned the two tourists and found them
to be carrying drugs. The persons concerned had claimed that the drugs were intended to
alleviate pain. The competent authorities then required the minister to exercise the
powers provided under section 13 of the law on immigration.
602 Information provided by the Embassy of Papua New Guinea in Brussels on 29 April 1997.603 This information comes from the list established by the US government in January 1996.604 This information comes from the list established by the Federal Department of Foreign Affairs in Switzerland
in February 1997.605 Information provided by the Samoan Embassy in Brussels on 2 April 1997.606 Section 13(1)(a) of the law of 1996 on immigration.607 DC. JAYASURIYA, HIV Law and Law Reform in Asia and the Pacific, o.c., p. 299.

182 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
437. In general, the policy applying to foreigners living with HIV/AIDS varies according
to whether this involves a short- or long-term stay. In cases where they are seropositive,
foreigners requesting a residence permit must declare this when requesting a permit 608.
C. Miscellaneous
438. The director-general for health may decide to detain a person and order him to
undergo further examination if the person concerned is suspected of suffering from an
infectious disease posing a threat to the general public. Furthermore, where a ship or air
passenger is suffering from a disease suspected of being infectious, the official in charge of
the ship or aeroplane must notify the director of the existence of such disease 609. The
order laying down these measures does not expressly include HIV/AIDS among the
infectious diseases. Nevertheless, the text does apply to this disease by virtue of a 1987
notice from the government 610.
64. TongaA. Entry
439. A foreigner may be obliged to undergo a medical examination 611.
B. Residence and expulsion
440. Any foreigner refusing to undergo a medical examination or to assist with a test
which the medical inspector might require is undesirable according to the law. Any
foreigner suffering from a contagious disease making his presence a danger to the
community is also considered to be undesirable 612. The express or tacit application of this
provision to AIDS has not been confirmed.
608 Information provided by the Samoan Embassy in Brussels on 2 April 1997. 609 Health Ordinance 1959, articles 29 and 33.610 DC. JAYASURIYA, HIV Law and Law Reform in Asia and the Pacific, o.c., p. 298.611 Article 5(d) of the law on immigration of 1969.612 Article 8(2)(d) of the aforesaid law.

The free movement of persons living with HIV/AIDS – Part 3: Third Countries 183
E. Central Europe65. AlbaniaA. Entry
441. The law specifies that entry may be refused on health grounds and that the list of
diseases justifying refusal of entry must be established in the implementing regulations 613.
The minister is responsible for organising and directing health and disease control
services at air, sea and land border-crossing points, depending on traffic and the
epidemiological situation, in order to prevent dangerous diseases from being imported,
in compliance with the international health regulation 614.
The reference to the international health regulation would imply that AIDS
is not included among the diseases that allow for restrictions, as defined in this
general legislation.
B. Residence and expulsion
442. As with access to the territory, the law states that the right of residence may be
refused on health grounds 615.
443. Foreigners expelled on health grounds have the right to lodge an appeal before the
Court of Appeal 616.
C. Miscellaneous
444. Anyone has the right to leave the country. Nevertheless, this right may be restricted,
in particular on the grounds of public health 617.
66. BulgariaA. Entry
445. People who are likely to transmit a contagious disease or do not have a vaccination
certificate may be refused entry if an epidemic is raging in the country of origin of the
person concerned 618.
613 Chapter III of Immigration law no. 7939 of 25 May 1995, article 10.614 Chapter II (articles 9 to 22) of law no. 7761 of 19 October 1993 on measures for the prevention and control of
communicable diseases, IDHL, 1995, 46(3), p. 310.615 Article 10 of the Immigration law of 25 May 1995.616 Idem.617 Article 6 of the aforesaid Immigration law.618 Article 7 of the law of 1972 on residence for foreigners.
184 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
B. Residence and expulsion
446. The law states that foreigners of Bulgarian origin, foreigners married to Bulgarian
nationals, their children and the children adopted by Bulgarian nationals may obtain a
permanent residence permit except under certain circumstances, including cases where a
foreigner is suffering from a contagious disease 619. Furthermore, legislation allows a
residence permit to be revoked on the same grounds 620.
447. The law on residence for foreigners allows foreigners working in Bulgaria the same
rights and obligations as Bulgarian citizens, particularly with regard to health care 621.
448. AIDS screening is compulsory both for Bulgarian citizens and for foreign nationals
and stateless persons living in Bulgaria 622. Foreign nationals and stateless persons who
come to stay in Bulgaria for over one month for study or professional purposes, as well as
immigrants, independently of the length of their stay, are subject to screening 623. The test
is carried out in a hospital or laboratory within 72 hours of arrival. Foreign diplomats are
not affected by the measure 624.
449. Foreigners liable to transmit serious contagious diseases may be subject to an
expulsion order 625. If a foreigner is refused by the destination country, he must be
admitted into a health care institution until the departure of this person becomes
possible. The measure has been applied to persons living with HIV/AIDS 626.
450. A medical examination is stipulated for asylum-seekers 627. Refugee status may be
refused on the basis of peace or public security, with public health not being expressly
mentioned 628. During the asylum procedure the asylum-seeker is entitled to medical care 629.
619 Article 8 of the aforesaid law of 1972.620 Article 31 of the aforesaid law of 1972.621 Article 22 of the aforesaid law of 1972.622 Article 36 of decree no. 1564 of 18 November 1988 amending the law on public health, IDHL, 1990, 41(2), p. 246.623 Order no. 4 of 2 April 1992 on the conditions and the procedure applicable to the testing of the infection by the
Acquired Immuno-Deficiency Syndrome virus, IDHL, 1994, 45(2), p. 169.624 This information comes from the list established by the Federal Department of Foreign Affairs in Switzerland
in February 1997.625 Article 32(4) of the aforesaid law of 1972.626 Restrictions of Entry and Residence for People with HIV/AIDS, o.c., p. 20.627 Article 9 of decree no. 208 of 4 October 1994 on refugees.628 Article 3 of aforesaid decree no. 208.629 Article 21 of aforesaid decree no. 208.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 185
67. HungaryA. Entry
451. The authorities may refuse right of entry or residence where there is a threat to
public health 630. A circular 631 stipulates various situations where screening is compulsory.
The screening of foreigners arriving in the country is not mentioned.
B. Residence and expulsion
452. An application for a residence permit must be accompanied by a certificate testifying
that the foreigner does not suffer from a disease which endangers public health 632. The
issue or renewal of a residence permit may be refused if a foreigner fails to respect
Hungarian public health regulations 633. A medical certificate must accompany the
application for an immigration permit (granted in cases where a foreigner has remained in
Hungary without interruption for at least three years) 634.
All foreigners wishing to obtain a residence permit enabling them to settle there
permanently (more than one year) must undergo an AIDS test, except for diplomatic and
consular staff. The AIDS test certificate must be authenticated by the competent
authority on the spot 635. Student grant-holders from Sub-Saharan Africa must also
undergo the test 636.
68. PolandA. Entry
453. In general the law provides that a visa may be refused if a person is undesirable with
regard to the public interest 637. No specific legislation has been passed with a view to
limiting the movement of foreigners living with HIV/AIDS 638.
630 Article 23 of the law of 14 September 1993 on the entry, residence and immigration of aliens.631 Circular no. 53636 of 28 December 1986 of the Ministry of health on the standardized procedure for the detection
of HIV, DIHL, 1988, 39(2), p. 367.632 Article 15 of the aforesaid law of 14 September 1993.633 Article 16 of the aforesaid law of 14 September 1993.634 Article 17 of the aforesaid law of 14 September 1993.635 This information comes from the list established by the Federal Department of Foreign Affairs in Switzerland
in February 1997.636 This information comes from the list established by The Laboratory Centre for Disease Control in June 1997.637 Article 5 of the law of 1963 on foreigners.638 Information provided by The National Office for AIDS Prevention in Poland on 13 June 1997.
186 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
B. Residence and expulsion
454. The law on employment includes the obligation to undergo a medical examination 639.
The law on the control of contagious diseases also allows for the possibility of any person
staying in Poland to undergo a medical examination 640. This law concerns AIDS which is
considered to be a contagious disease 641.
In 1987, the Ministry of Health proposed a regulation providing for compulsory
screening for foreigners who stay in Poland for a period of over one month. This idea has
remained at the draft stage but serves as the basis for the screening carried out on foreign
students 642. The screening of foreign students is still in application 643.
455. In considering an arrest measure prior to expulsion, the person’s state of health
must be taken into account 644. A 1993 order covers the detention of foreigners with a
view to their expulsion. Medical care is guaranteed. The order states that a foreigner
must undergo a medical examination. Persons undergoing treatment in hospital may not
be detained 645.
69. RomaniaA. Entry
456. Current Romanian legislation does not contain any specific regulation relating to
the movement of persons with HIV/AIDS 646. Nevertheless, a bill concerning the regime
of foreigners in Romania was put before Parliament in October 1997. It states that ‘a
Romanian visa may be refused to foreigners suffering from diseases which endanger
public health’ 647.
The visa obligation concerns nationals from Africa, Asia and South America 648.
639 Article 13 of the law of 1 January 1995 on employment, applicable to both Polish and foreign nationals.640 Law of 13 November 1963 on controlling contagious diseases.641 Restrictions of entry and residence for people with HIV/AIDS, o.c., p. 53.642 M. BREUM and A. HENDRIKS, AIDS and Human Rights: An International Perspective, Copenhagen,
Akademisk Forlag, 1988, p. 117.643 This information comes from the list established by the Federal Department of Foreign Affairs in Switzerland
in February 1997.644 Article 17 of the aforesaid law of 1963.645 Order from the Minister of the Interior of 9 July 1993.646 Information provided by the Romanian Embassy in Brussels on 20 October 1997.647 Idem.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 187
B. Residence and expulsion
457. The aforesaid bill which permits foreigners suffering from diseases which endanger
public health to be refused a visa, also concerns the residence of foreigners living with
HIV/AIDS.
70. SlovakiaA. Entry
458. The law permits entry to be refused with a view to protecting public health 649.
B. Residence and expulsion
459. Residence may be refused in order to protect public health 650. AIDS screening is
compulsory for foreigners wishing to reside in the country 651. The law on the stay and
residence of foreigners in the Czech Republic and Slovakia applies to both countries
(infra § 463).
460. The legislation on health care contains provisions relating to the treatment
of foreigners 652.
461. Provision is made for the medical examination of asylum-seekers in the law on
refugees. Refugee centres must provide basic medical care 653.
648 The countries concerned are: Afghanistan, Albania, Algeria, Angola, Bangladesh, Benin, Bhutan, BurkinaFaso, Burundi, Cameroon, Cambodia, Cape Verde, Central African Republic, China, Chad, the ComorosIslands, Congo, Ivory Coast, Cuba, Djibouti, Dominican Republic, Egypt, Ethiopia, Fiji, Philippines, Gabon,Gambia, Ghana, Guinea, Guinea Bissau, Equatorial Guinea, Guyana, Haiti, India, Jordan, Iraq, Iran, Kenya,Laos, Lebanon, Liberia, Libya, Madagascar, Maldives, Mali, Morocco, Mauritania, Mauritius, Mongolia,Mozambique, Nepal, Niger, Nigeria, Pakistan, Palestine, Papua New Guinea, Rwanda, Sao Tome and Principe,Senegal, Sierra Leone, Syria, Somalia, Sri Lanka, Sudan, Surinam, Tanzania, Thailand, Togo, Tunisia, Uganda,Vietnam, Yemen, Zaire and Zambia.
649 Article 12 of the law of 5 April 1995 on the residence of foreigners on the territory of Slovakia.650 Idem.651 This information comes from the list established by the Federal Department of Foreign Affairs in Switzerland
in February 1997.652 Law of 24 August 1994 on health care.653 Articles 5 and 24 of law no. 283 of 14 November 1995 on refugees.
188 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
71. Czech RepublicA. Entry
462. Directives adopted in 1988 provided for screening for foreign students, airline
personnel, and persons returning from stays of over six months in Africa, Western Europe
or the USA 654. This text was replaced in 1992 by a new text that provides that AIDS
testing is theoretically voluntary and anonymous, except for refugees and persons
travelling to states which require HIV testing at the border 654b.
B. Residence and expulsion
463. Foreigners requesting a long-term or permanent residence permit must provide proof
that they are not suffering from an infectious disease, the spreading of which is punishable
under the law 655. Notice no. 104/1987 from the Minister of Justice is based on penal code
no. 1/1991 in which AIDS is considered as a disease, the propagation of which is
punishable by law 656. In practice, it appears that immigration officers apply this medical
requirement only in specific cases, and that foreigners requesting short-term residence
permits are not asked to provide a medical certificate 657.
A foreigner may be refused a residence permit for a period exceeding one year if this
is necessary for the protection of health 658.
464. Persons living with HIV/AIDS have been expelled, notably Romanians and
Angolans 659.
465. Provision is made in the law on refugees for the medical inspection of foreigners
requesting refugee status 660. Refugee status may be refused in general where there is a
654 Methodological Directives of 1988 to ensure a uniform procedure for prevention of AIDS in the Czech SocialistRepublic.
654b New instructions in prevention and treatment of HIV infection, March 1992, articles 2 and 7, Directory of legalinstruments dealing with HIV infection and AIDS, o.c., p. 44.
655 Section 8 of law no. 123/1992 of 4 March 1992 governing the stay and residence of foreigners in the Czech andSlovak Republic.
656 Information provided by the Embassy of the Czech Republic in Brussels on 14 April 1997 and by theDepartment for Foreigners and Border Control in the Czech Republic on 17 April 1997.
657 Information provided by the Department for Foreigners and Border Control in the Czech Republic on 17 April1997.
658 Section 14 of the aforesaid law of 4 March 1992.659 EUROCASO, Report of the First Seminar on Law and HIV/AIDS, Amsterdam, 13-14 April 1991, p. 68.660 Section 7(2) of law no. 498 of 16 November 1990 on refugees.

The free movement of persons living with HIV/AIDS – Part 3: Third Countries 189
threat to public policy 661 and is specifically mandatory for refugees through the new 1992
instructions (supra, § 462). Medical care is provided for people having been given
provisional refugee status 662.
F. Former Yugoslavia72. Former Federal Socialist Republic of Yugoslavia466. In the former republic, conclusions provided particularly for measures to be taken so
as to guarantee the respect of human rights and of the dignity of persons living with
HIV/AIDS and so as to prevent any form of discrimination including travel in Yugoslavia
and abroad 663.
73. CroatiaA. Entry
467. The Law on the Movement and Residence of Foreigners in the Republic of Croatia 664 does
not provide for restricting the entry or the movement of persons living with HIV/AIDS 665.
It does provide for the possibility of refusing entry to foreigners who compromise public
policy in general 666.
B. Residence and expulsion
468. The law states that a visa application may be refused if the applicant comes from a
country in which an epidemic of a contagious disease is rife and if he has no vaccination
certificate 667. This provision would not seem to concern HIV/ AIDS directly as long as as
no vaccination exists against this illness.
469. The Law on the Protection of the Population against Infectious Diseases includes AIDS in
the list of diseases the prevention and control of which concern the interests of the
Republic, but does not restrict the liberty of movement of persons living with HIV/AIDS 668.
However, the Minister of Health may adopt special measures such as prohibition of travel to
661 Section 14 of aforesaid law no. 498.662 Resolution by the Czech government of 21 December 1994 relating to temporary recognition of the right of asylum.663 Conclusions no. 50-2/89 of 15 March 1989, IDHL, (1990), 41 (1), p. 66.664 Law of 1991.665 Information communicated by the Ministry of Health of Croatia on 27 May 1997.666 Article 3 of the Law of 1991 cited above.667 Article 18 of the Law of 1991 cited above.668 Information communicated by the Ministry of Health of Croatia on 27 May 1997.

190 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
certain countries and restrictions to the freedom of movement in infected or threatened
areas. There exists the possibility of restricting freedom of movement so as to protect the
population against transmitted diseases. The authorities may forbid the movement of
persons concerning whom it has been established or who are suspected of suffering from a
contagious disease 669.
470. According to the Ministry of Health, the policy is to follow the International Health
Regulation on Travel published in 1997, which contains no restrictions concerning AIDS 670.
471. A request for asylum may be refused for reasons of public policy in general 671; public
health is not expressly mentioned as grounds for refusal. Likewise, refugee status may be
withdrawn for reasons concerning public policy in general 672.
472. Medical protection is given to foreigners, but for a limited period 673. The law also
provides for rights to medical assistance for refugees 674.
74. MacedoniaA. Entry
473. Entry may be refused to foreigners if they come from an area that is infected by a
contagious disease and if they do not possess a vaccination certificate 675. This provision
could not be directly applied to AIDS, as long as no vaccination exists for this illness.
B. Residence and expulsion
474. The right to residence may be denied a foreigner for reasons of public health 676.
669 Presidential Decree no. PA 4-71/92 of 25 September 1992 promulgating the law concerning the protection of thepopulation against transmitted illnesses, articles 59, 60, 61 and 62.
670 Information communicated by the Ministry of Health of Croatia on 27 May 1997.671 Article 33 of the Law of 1991 cited above.672 Article 43 of the Law of 1991 cited above.673 Article 36 of the Law of 1991 cited above.674 Law of 1993 on the status of displaced persons and refugees.675 Article 17 of the Law of 1992 on the movement and residence of foreigners.676 Article 30 of the Law of 1992 cited above.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 191
475. The law prohibits expulsion if this would expose the foreigner to inhuman treatment 677.
According to the European Court of Human Rights, expulsion of foreigners living with
HIV/AIDS may, in certain circumstances, constitute inhuman treatment 678.
476. Refugee status may be refused in case of threat to the security and the defense of the
country 679 but not for reasons of health. The law provides for medical assistance to
refugees for a limited period 680.
75. SloveniaA. Entry
477. The law states that entry may be denied a foreigner coming from an infected area
and who does not produce a vaccination certificate 681. The same provision is found in the
legislations of Croatia and Macedonia examined above (§§ 468 and 473).
B. Residence and expulsion
478. The right to residence may be refused for the same reasons as those mentioned
in § 477 682.
With a view to protecting public health, the right to residence may be withdrawn
from a foreigner staying in the country on the basis of a foreign passport, an entry visa, an
international convention or a temporary residence permit 683.
479. Expulsion must be avoided if this would expose the foreigner to a risk of inhuman
treatment 684. Inasmuch as this provision resembles the one existing in the legislation of
Macedonia, the reader should refer to the commentary made about this country (§ 475).
480. Medical protection for a limited period is granted to foreigners having acquired
refugee status 685.
677 Article 39 of the Law of 1992 cited above.678 See. D. v. United Kingdom, supra §§ 76ff.679 Article 47 of the Law of 1992 cited above.680 Article 51 of the Law of 1992 cited above.681 Article 10 of the Foreigners’ Act of 1991.682 Article 19 of the Act cited above.683 Article 23 of the Act cited above.684 Article 33 of the Act cited above.685 Article 39 of the Act cited above.

192 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
C. Miscellaneous
481. The Office for Immigration and Refugees is entrusted with supervising procedures of
medical testing for those asking for asylum, refugees and other immigrants 686.
G. Community of Independent StatesThe majority of CIS States have adopted, more than others, specific provisions
concerning AIDS and in particular restricting the free movement of persons.
76. The Former Union of Soviet Socialist Republics482. At the time of the USSR, a regulation contained several provisions concerning the
free movement of persons living with HIV/AIDS 687. This ruling is still in force in the
Russian Federation (infra, § 520) 688. According to this regulation, the following persons
must undergo the AIDS test: Soviet citizens returning from missions or voyages abroad of
a duration of over three months, foreign nationals and stateless persons who have come
to the USSR for the purposes of study, work or other purposes, Soviet citizens travelling
abroad to countries that require this test, and Soviet citizens and foreign nationals who
have had sexual contacts with persons suffering from the HIV virus or AIDS.
The ruling provides for the right of foreign national to ask for a member of the medical
staff or an Embassy official to be present when the blood sample is taken (article 7), the
right to ask for a medical report concerning the results of the examination (article 8) and
the right to ask to undergo a second examination in another establishment (article 9).
Diplomatic staff are not required to undergo obligatory testing (article 10).
686 Decree of 1992 on the establishing of an office for immigration and refugees.687 Regulation of 4 October 1990 on medical testing for detection of the human immunodeficiency virus (AIDS), IDHL,
(1991), vol. 42 (1), p. 21.688 Directory of legal instruments dealing with HIV infection and AIDS, o.c., p. 149.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 193
77. ArmeniaA. Entry
483. The law does not envisage denial of the right of entry for reasons of public health 689.
The law states that entry may be denied the foreigner but does not stipulate the reasons
for this denial 690. Foreigners in the exercise of their freedom must respect public policy
in general 691.
B. Residence and expulsion
484. The law does not envisage the possibility of denial of the right of residence for
reasons of health 692. Danger to public policy is mentioned in the list of reasons for
expulsion, but not public health 693.
78. BelarusA. Entry
485. Foreigners and stateless persons may be refused the right of entry for reasons
of health 694.
B. Residence and expulsion
486. The law permits expulsion of a foreigner when this is necessary for public health 695.
Expulsion of foreign nationals and stateless persons who refuse to undergo an
examination in order to detect infection by the human immuno-deficiency virus is
authorized 696. It should be noted that diplomatic staff cannot be required to undergo a
test unless they have given their prior consent.
689 Law of 17 June 1994 on the Status of Foreigners.690 Article 9 of the Law of 17 June 1994 cited above.691 Article 25 of the Law of 17 June 1994 cited above.692 Law of 17 June 1994 cited above.693 Article 32 of the Law of 17 June 1994 cited above.694 Law of 3 June 1993 on the legal status of aliens and stateless persons in the Republic of Belarus, article 20.695 Article 25 of the Law of 3 June 1993 cited above.696 Law of 18 June 1993 on public health.
194 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
487. Refugees are required to undergo a medical examination and they have the right to
medical help 697. The rights of foreigners requesting refugee status may be restricted for
various reasons, particularly those of health 698. This provision raises questions of
compatibility with current international norms.
79. EstoniaA. Entry
488. The law does not provide for refusal of entry for reasons of public health 699.
B. Residence and expulsion
489. The law does not provide for the possibility of refusing the right to residence for
reasons of health 700. Nevertheless, in order to obtain a residence or work permit,
foreigners must produce a medical certificate 701, which must mention an AIDS test,
which must have been performed less than four months previously. This test must have
been performed in the foreigner’s home country or in one of the ‘AIDS’ centres existing
in Estonia 702.
80. GeorgiaA. Entry
490. Right of entry may be denied foreigners and stateless persons in order to protect
health 703. The law imposes on persons applying for the right of permanent residence the
obligation of undergoing a medical examination 704. Entry is denied if the person is
suffering from AIDS 705.
697 Article 8 of the Law of 22 February 1995 on Refugees.698 Article 12 of the Law on refugees cited above.699 Alien’s Act of 8 July 1993.700 Article 12 of the Law of 8 July 1993 cited above.701 Article 22 of the Regulation of 21 September 1993 for the issue and extension of residence permits and employment
permits to aliens.702 Information communicated by the Embassy of Estonia in Brussels on 24 April 1997.703 Law of 3 June 1993 on the legal status of aliens, article 23.704 Article 5 of the Immigration Act of 27 July 1993.705 Articles 4 and 5 of the Act of 27 July 1993 cited above.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 195
B. Residence and expulsion
491. The movement of foreigners and the choice of their residence may be limited when
this is necessary for the protection of national security, public policy, or public health 706.
492. Foreigners may be denied the right of permanent residence if they are suffering
from AIDS, from a venereal disease or from other diseases mentioned in the list defined
by the Minister of Health 707. Article 4, 4° speaks of AIDS and not of HIV positive status.
The law states that citizens and persons residing temporarily or permanently in the
country have the right to undergo the AIDS test 708. Foreigners who come to the country
for more than one month must possess a certificate proving that they have had the test.
An exception is the case of diplomatic staff for whom individual consent is required.
In the case of persons working in NGOs and other organizations, the question is resolved
on the basis of the existence of multilateral agreements 709. Citizens and foreigners
residing temporarily or permanently living with HIV/AIDS are obliged to submit to
preventive measures 710.
493. Foreigners have the right to medical assistance 711. Citizens and foreigners residing
temporarily or permanently in the country have the right to medical help even if they are
HIV positive or suffering from AIDS 712.
494. The legislation in force permits ordering the expulsion of a foreigner in order to
protect health 713.
706 Article 18 of the Law of 3 June 1993 cited above.707 Article 4 of the Act of 27 July 1993 cited above.708 Article 3 of the Law of 21 March 1995 on the Prevention of HIV/AIDS in Georgia.709 Article 4 of the Law of 21 March 1995 cited above.710 Article 6 of the Law of 21 March 1995 cited above.711 Article 9 of the Law of 3 June 1993 on the legal status of aliens.712 Article 8 of the Law of 21 March 1995 cited above.713 Article 29 of the Law of 3 June 1993 cited above.
196 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
81. KazakhstanA. Entry
495. Entry may be refused in the interests of security, public policy or of the health of
the population 714.
B. Residence and expulsion
496. Refusal of residence for reasons of public health is not expressly provided for by the
legislation on immigration. The law states that residence may be denied when the
foreigner has committed an offence or a crime against humanity or ‘other reasons’ 715.
497. The freedom of movement of foreigners may be limited for reasons of health 716.
498. Foreigners have the right to medical assistance 717.
499. A test is required of foreigners who wish to reside in the country 718. Citizens and
foreigners or stateless persons have the right to have an AIDS test 719. Citizens and
foreigners or stateless persons are required to undergo a test if there are sufficient reasons
to presume that they are infected by the AIDS virus 720. Diplomatic and consular staff may
be tested only if the person concerned gives his consent. Foreigners who wish to stay
more than three months in the country must present a certificate attesting their HIV
negative status 721.
500. Current legislation authorizes the expulsion of foreigners when this is necessary for
the protection of health 722. Foreigners residing on the territory who refuse to undergo an
714 Article 22 of the Law of 19 June 1995 on the legal status of aliens.715 Article 25 of the Law of 26 June 1992 on immigration.716 Article 16 of the Law of 19 June 1995 on the legal status of aliens.717 Article 7 of the Law of 19 June 1995 cited above.718 AIDS Surveillance in Europe, Quarterly Report no. 42, 30 June 1994, European Centre for the Epidemiological
Monitory of AIDS, St. Maurice, France, p. 26.719 Law of 5 October 1994 on the prevention of AIDS.720 Article 6 of the Law of 5 October 1994 cited above.721 This information is drawn from the list established by the Federal Department of Foreign Affairs in
Switzerland in February 1997.722 Article 28 of the Law of 19 June 1995 cited above.

The free movement of persons living with HIV/AIDS – Part 3: Third Countries 197
examination, who are infected by the HIV virus or who are suffering from AIDS, are
expelled from the territory 723. Foreigners whose spouse is a citizen of Kazakhstan are
not expelled 724.
82. KyrghyzistanA. Entry
501. Refusal of entry for reasons of health is not provided for expressly by the legislation
on immigration, which does permit refusal of entry in the interests of security or of the
protection of public policy, in the interests of the citizens of the Republic, when the
foreigner concerned has broken the law, when he has given false information or does not
produce certain documents, or else ‘for other reasons’ provided for by the national
legislation 725.
502. The law provides for the possibility of limiting the freedom of movement of
foreigners for various reasons, particularly those of health 726.
503. Foreigners have the right to medical assistance 727.
B. Residence and expulsion
504. Foreigners may be expelled if this is necessary for the protection of health 728.
83. LatviaA. Entry
505. The legislation on immigration does not envisage refusal of access to the territory for
reasons of public health 729.
723 Article 6 of the Law of 5 October 1994 cited above.724 Idem.725 Article 6 of the Law of 14 December 1993 on the order for residence of aliens.726 Article 18 of the Law of 14 December 1993 cited above.727 Article 9 of the Law of 14 December 1993 cited above.728 Article 24 of the Law of 14 December 1993 cited above.729 Law of 9 June 1992 on the Entry and Residence of Foreign Citizens and Stateless Persons in the Republic of Latvia.

198 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
B. Residence and expulsion
506. A residence permit may be denied to foreigners suffering from an illness or a physical
condition – the nature, gravity and potential duration of which constitute a threat for
public security and health or which requires the special surveillance of a health
institution, or from an illness or state of health mentioned in the list established by the
Minister 730. Foreigners applying for a work permit for over three months must prove their
negative HIV status 731.
507. Expulsion may be justified by reasons of public policy. Public health is not
mentioned by the law expressly as a reason for expulsion 732.
84. LithuaniaA. Entry
508. Access to the territory must be refused to foreigners if their entry constitutes a
danger for national security, public policy, health or morals 733. There is no specific
legislation applicable to the entry or residence of foreigners living with HIV/AIDS 734.
Nevertheless, it appears from information on practice concerning residence that the
health restrictions include AIDS.
B. Residence and expulsion
509. A permanent residence permit must be refused to foreigners suffering from serious
and contagious diseases 735. Foreigners requesting a permanent right of residence must
undergo the AIDS test 736.
510. Foreigners cannot obtain the right to asylum if they are suffering from a contagious
disease or refuse a medical control in case they are suspected of suffering from such a
730 Article 35 of the Law of 9 June 1992 cited above.731 This information is drawn from the list established by the Federal Department of Foreign Affairs in
Switzerland in February 1997.732 Article 53 of the Law of 9 June 1992 cited above.733 Article 27 of the Law on the Legal Status of Foreigners.734 Information communicated by the Embassy of Lithuania in Brussels on 28 August 1997.735 Article 5 of the Immigration Act of 4 September 1991.736 This information is drawn from the list established by The Laboratory Centre for Disease Control in June 1997.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 199
disease. This text raises problems of compatibility with international norms 737. Those
requesting asylum must undergo a medical examination 738.
85. MoldovaA. Entry
511. Access to the territory of Moldova is forbidden for foreign citizens and stateless
persons living with HIV/AIDS 739.
B. Residence and expulsion
512. The law does not mention public health among the reasons for refusal of the right of
entry 740. Nevertheless, foreigners and stateless persons must undergo an AIDS test 741.
Citizens and foreigners or stateless persons who live in the country or are temporarily
present there are obliged to undergo a medical examination if there are reasons for
suspecting such persons of having been infected with the AIDS virus 742. The right of
residence for over three months is conditional on the proof of a test showing HIV
negative status 743. All foreigners who do not possess such proof are obliged to present
themselves within 10 days at the competent institution in order to undergo the test.
Subsequently, this procedure will be repeated once a year.
513. Foreigners may be expelled for reasons of health 744. Foreign citizens and stateless
persons with temporary residence in Moldova who avoid the AIDS medical examination
are expelled in conformity with current legislation 745. Foreigners and stateless persons with
temporary residence in Moldova who are discovered to be carriers of the virus or to be
suffering from AIDS are expelled from the country 746. This measure seems to concern only
those foreigners benefitting from a right to temporary residence. Foreigners and stateless
persons with stable residence in Moldova have a right to medical and social insurance 747.
737 Article 4 of the Law of 4 July 1995 on the Status of Refugees in the Republic of Lithuania.738 Article 13 of the Law of 4 July 1995 cited above.739 Article 11 (1) of the Law of 25 May 1993 on prevention of the illness HIV/AIDS.740 Article 9 of the Law of 10 November 1994 on the legal status of aliens and stateless persons.741 Article 8 of the Law of 10 November 1994 cited above.742 Article 3 (1) of the Law of 25 May 1993 cited above.743 Article 11 of the Law of 25 May 1993 cited above.744 Article 23 of the Law of 10 November 1994 cited above.745 Article 5 of the Law of 25 May 1993 cited above.746 Article 12 of the Law of 25 May 1993 cited above.747 Article 8 of the Law of 25 May 1993 cited above.

200 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
86. MongoliaA. Entry
514. All citizens must undergo medical examinations and detection tests required by an
establishment of health care in order to determine whether they are infected by the HIV
virus. This provision is also applied to all foreigners or stateless persons in the country 748.
Foreign students must undergo a test 749.
B. Residence and expulsion
515. The law states that all foreign nationals or stateless persons infected by
HIV/AIDS who refuse to comply with instructions delivered by the competent health
organizations must become the object of an expulsion order in conformity with the
legislation of Mongolia 750.
87. UzbekistanA. Entry
516. A resolution makes the ministers and other authorities concerned responsible for
supplying in due time the territorial authorities of the State Health and Epidemiologic
Services with reliable data on groups or persons from countries in which quarantine
diseases and AIDS are rife, with the indication of their itinerary and the place and
duration of their stay in the country so as to be able to submit them, if required, to
medical observation 751. The same resolution makes the competent authorities responsible
for informing foreign representations of the modifications operated in the medical
requirements applicable to entry to the territory. The resolution states that the authorities
must forbid the presence on the territory of nationals from countries ‘where AIDS is rife’
if they do not possess a certificate proving that they have had the test. For Africa, the
countries concerned are Burundi, Congo, Ivory Coast, Ghana, Guinea-Bissau, Kenya,
Malawi, Mozambique, Rwanda, Sierra Leone, Tanzania, Zaire, Zambia and Zimbabwe.
748 Article 1 of Decree no. 103 of 26 June 1989 of the Presidium of the Great Khural of the Mongolian People’sRepublic on measures to prevent Acquired Immuno-Deficiency Syndrome, IDHL, 1989, 40 (4), p. 803.
749 This information is drawn from the list established by The Laboratory Centre for Disease Control in June1997.
750 Article 12 of the Law of 1 March 1994 on the prevention of the Acquired Immuno-Deficiency Syndrome (AIDS).751 Resolution no. 12 of 17 November 1992 introducing preventive measures against the introduction and the spread of
quarantinable diseases and of AIDS into the Republic of Uzbekistan, IDHL, 1994, 45 (1), p. 32.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 201
For America, the countries concerned are Brazil, Martinique, Mexico and the USA. In
Europe, the countries concerned are Belgium, France, Germany, Italy, Netherlands,
Spain, Sweden, Switzerland and the United Kingdom. Persons bearing a certificate on
their arrival but who remain for more than one month must undergo a new test at their
place of residence.
Similar provisions have been adopted to those in Russia 752.
B. Residence and expulsion
517. The above-mentioned resolution makes the authorities responsible for expelling
persons living with HIV/AIDS.
C. Miscellaneous
518. The authorities must require of all citizens going abroad to hold a medical
certificate. The Uzbek Tourist Organization must concert with the Minister of Health
on the possibility of travelling to certain countries on the basis of the epidemiological
situation of these countries and must organize medical follow-up of tourists who
travel abroad 753.
The Uzbek Tourist Organization must see to it that a medical service and isolation
rooms be available in hotels for foreign tourists.
88. RussiaA. Entry
519. Foreigners and stateless persons may be refused entry to Russia if they apply for a
right to residence for over three months and do not present the results of an HIV test 754.
Diplomatic representations or consular services deliver a Russian entry visa to foreign
nationals for a stay of more than three months on condition that the applicants present a
certificate showing that they are not infected by the HIV virus saving contrary provisions
of international agreements to which Russia is party 755.
752 Regulation of 1991 on the medical testing to detect the Human Immuno-Deficiency Virus (AIDS) and on preventivesurveillance which largely repeats the provisions of the Ruling of 4 October 1990 on the same subject adoptedin Russia.
753 Resolution no. 12 cited above.754 Article 27 of the Law of 15 August 1996 on the procedure for exit from the Russian Federation and entry into the
Russian Federation.755 Article 10 of Federal Law no. 38 of 30 March 1995 on the prevention of the spread in the Federation of Russia of the
affection caused by the Human Immuno-Deficiency Virus (HIV infection), IDHL, 1995, 46 (3), p. 318.
202 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
B. Residence and expulsion
520. The law states that foreigners and stateless persons living with HIV/AIDS must be
expelled 756. The previous provisions of the former USSR are still applicable (supra § 482).
521. Refugees have the right to access to medical assistance 757. Displaced persons also
have this right and must undergo a medical examination 758.
89. TajikistanA. Entry
522. Entry may be denied to foreigners in the interests of national security or of public
policy, in the interest of the citizens, if the foreigners have broken the law or given false
information or ‘for other reasons’ 759.
B. Residence and expulsion
523. The law permits restriction of the right to free movement for foreigners for reasons
of health 760.
524. Foreigners may be expelled for the protection of health 761. It has not been shown
whether this general legislation covers AIDS.
525. Foreigners have a right to medical assistance 762.
526. Candidates for refugee status must undergo medical testing and have the right of
access to health services 763. Candidates for the status of displaced persons must also
undergo a medical examination and they have the right to medical assistance 764.
756 Article 11 of the Law of 30 March 1995 cited above.757 Article 7 of the Law of 19 February 1993 on refugees.758 Article 4 of the Law of 20 December 1995 on displaced persons.759 Article 24 of the Law of 1 February 1996 on the legal status of aliens.760 Article 19 of the Law of 1 February 1996 cited above.761 Article 31 of the Law of 1 February 1996 cited above.762 Article 9 of the Law of 1 February 1996 cited above.763 Law of 20 July 1994 on Refugees.764 Law of 20 July 1994 on Displaced Persons.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 203
90. TurkmenistanA. Entry
527. The law disposes that entry may be denied to foreigners in the interests of national
security or of public policy, in order to protect the interests of the citizens, if the
foreigners have broken the law or given false information or ‘for other reasons’ established
by the national legislation 765.
B. Residence and expulsion
528. Restrictions may be applied to freedom of movement for foreigners for different
reasons, particularly those of health 766.
529. Foreigners have the right to medical assistance 767.
530. Testing is obligatory for foreign nationals and stateless persons requesting a medical
consultation, in conformity with the clinical signs 768. Diplomatic and consular staff may be
made to undergo testing only following individual consent. The testing is perfomed in the
state medical establishments. Foreign nationals and stateless persons, as well as citizens who
undergo the test, may ask for a second test to be performed in another establishment.
531. Foreigners may be expelled when this measure is necessary in order to protect
public health 769.
C. Miscellaneous
532. Citizens of Turkmenistan travelling abroad must undergo the test if the country of
destination requires a certificate of testing for infection by the HIV virus 770.
765 Article 24 of the Law of 8 September 1993 on the legal status of aliens.766 Article 19 of the Law of 8 September 1993 cited above.767 Article 9 of the Law of 8 September 1993 cited above.768 Regulation of 7 June 1995 on HIV/AIDS testing in Turkmenistan, IDHL, 1995, 46 (4), p. 475.769 Article 3 of the Law of 8 September 1993 cited above.770 Ruling of 7 June 1995 cited above.
204 The free movement of persons living with HIV/AIDS – Part 3: Third Countries
91. UkraineA. Entry
533. Current legislation permits refusal of access to the territory for foreigners when such
refusal is necessary in order to protect public health 771. As regards business or tourist visits
or short stays, no medical certificate is required of foreigners.
B. Residence and expulsion
534. Restrictions may be applied to the freedom of movement of foreigners, for reasons of
health, among others 772.
Foreigners have the right to medical assistance 773.
535. Foreigners and stateless persons residing or present on the territory have the right to
undergo testing and to be informed of the results 774. Foreigners and stateless persons
residing in the country in order to study or to exercise an activity must undergo testing.
The following categories of persons are dispensed from this requirement: persons
possessing the certificate provided for in a relevant agreement between the Ukraine and
another state, and diplomatic and consular staff 775. Foreigners applying for the right of
permanent residence must present, before they leave for Ukraine, a complete medical
certificate (including the results of the AIDS test). The Ukrainian authorities examine
the applications individually 776.
536. Expulsion for reasons of public health is provided for by the law 777. Foreigners and
stateless persons infected with the HIV virus undergo administrative expulsion in
conformity with the legal procedure 778. Foreign nationals and stateless persons whose
spouse is a Ukrainian citizen do not undergo expulsion.
771 Article 25 of the Law of 4 February 1994 on the legal status of aliens.772 Article 20 of the Law of 4 February 1994 cited above.773 Article 10 of the Law of 4 February 1994 cited above.774 Article 6 of the Law of 12 December 1991 on the prevention of AIDS and the social protection of the population,
IDHL, 1993, vol 44 (2), p. 223-228.775 Article 8 of the Law of 12 December 1991 cited above.776 Information communicated by the Embassy of Ukraine in Brussels on 2 April 1997.777 Article 32 of the Law of 4 February 1994 cited above.778 Article 12 of the Law of 12 December 1991 cited above.
The free movement of persons living with HIV/AIDS – Part 3: Third Countries 205
537. Candidates for refugee status must undergo medical testing at the request of the
authorities. Candidates for refugee status and those who have acquired it have the right
to medical assistance 779.
C. Miscellaneous
538. Citizens and foreigners or stateless persons infected by the HIV virus or suffering
from AIDS who are resident or present on the territory have the right:
■ to social relations characterized by respect and humanity, excluding all forms of
denigration of human dignity;
■ to demand confidentiality for the data concerning the state of their health, if the
conditions and characteristics of their life and their work do not represent a threat of
infection for other people;
■ to indemnization for prejudice connected with the restriction of their rights
following publishing of information to the effect that such people are infected by the
HIV virus;
■ to a professional activity in a profession of their choice with the exception of a
specialized activity or a post contained in a special list;
■ to a free supply of medicine necessary for the treatment of any illness they may
suffer from;
■ to transport to or from the place of their treatment at the expense of the
establishment of therapeutic care that delivered the order of treatment;
■ to dispose of an isolated habitable room 780.
It is most surprising to discover a list of ‘rights’ in a general context of discriminatory
treatment. More particularly, as regards foreigners, inasmuch as the expulsion of persons
living with HIV/AIDS can be ordered, the interest of these ‘rights’ is more than debatable.
779 Law of 24 December 1993 on refugees.780 Article 17 of the Law of 12 December 1991 cited above.


Generalconclusions
208 The Free Movement of Persons Living With AIDS – General conclusions
539. The book is divided into three parts. Part one examines the principles of international
and European law which apply to the problem of the free movement of persons living with
HIV/AIDS (paragraphs 1 to 56). Parts two and three examine the travel restrictions which
have been placed by European Union countries (paragraphs 57 to 223) and non-EU
countries (‘third countries’) (paragraphs 224 to 538) on persons living with HIV/AIDS.
The present general conclusions set out the main facts which are established by the
study as a whole (1), examine the conclusions which can be drawn from them (2), and
formulate certain proposals for both the short- and the long-term (3).
1. The main facts540. Facts can be established at three levels: those of national law (A), European law (B),
and international law (C).
A. National law541. The study has examined legislation and practice in 106 countries. Since the study
concerned the movement of persons living with HIV/AIDS in the frame of the
relationship between Europe and the developing countries, the 15 Member States of the
European Union and the states of Eastern Europe, Asia, Africa, South and Central
America have been studied.
542. Taking all the different countries together, we can distinguish four types of legislation:
■ legislation which does not place any limit on the movement of persons living with
HIV/AIDS or any restriction relating to public health in general;
■ legislation in the area of immigration, which permits general limits to be placed on
the principle of the free movement of persons, based on public health;
■ legislation which introduces limitations specific to AIDS, aimed at limiting the
movement of persons living with HIV/AIDS. These can be laws specific to AIDS or
laws covering immigration in general;
■ legislation outlawing limitations specific to AIDS, with a view to eliminating
restrictions on the free movement of persons living with HIV/AIDS. These can be
laws specific to AIDS or laws covering immigration in general.
The Free Movement of Persons Living With AIDS – General conclusions 209
543. Of these four categories of legislation, the second is the one most frequently
encountered.
It is in most cases general legislation covering immigration which is used as a means,
at the national level, of restricting the free movement of persons living with HIV/AIDS.
These restrictions generally derive from provisions which make it possible to refuse access
to the national territory or the right to stay in it to foreigners for reasons of public health.
Similar restrictions could also result from national legislation which encourages the use of
local labour in order to combat the epidemic 781.
544. Both in European Union Member States and in third countries, restrictions, where
they exist, relate generally to foreigners requesting permits for long-term visits, to the
exclusion of foreigners applying for short-term visits (§ 84 and § 244 supra).
This situation is explained mainly by economic reasons, with states not wanting to
pick up the cost of treatment and health care which the sickness can occasion (for the
WHO’s position on economic justifications, see § 550 infra).
Two items must be remembered here. First of all, Directive 64/221 states that limits
on the free movement of persons which are justified by reasons of public policy or public
health may not be used to pursue economic ends (§§ 35 et seq., supra). Although this rule
directly concerns only citizens of the European Union, it could also guide the
interpretation of the principles which apply to third country nationals. On the other
hand, the distinction between short- and long-term residence appears difficult to justify
in terms of protection against AIDS in so far as the migrant who settles permanently in a
country and is joined by his or her family will have less frequent ‘high risk’ sexual
relations than the occasional business or tourist traveller (including sex tourism).
545. In the case of European Union Member States, the restrictions which apply to
long-term visits are directed essentially at third country nationals and at times certain
categories of third country nationals such as students. We note a lack of uniformity
within Union countries with regard to the policy applied to third country nationals
(§ 59 supra).
781 This solution has for example been recommended in the work A. WHITESIDE, Integration of the HIV/AIDSproblematic in development assistance, A Toolkit.

210 The Free Movement of Persons Living With AIDS – General conclusions
B. European law546. Within European law, there is no binding text relating to the free movement of
persons living with HIV/AIDS. Should we deduce from this that limits to the free
movement of persons living with HIV/AIDS are authorized by European law? We should
answer negatively. According to case law and authors, restrictions to the principle of the
free movement of persons ought to be interpreted in a restrictive fashion. Directive 64/221,
which covers the limits applicable in the area of public health, does not expressly mention
HIV/AIDS. Some legal experts deduce from this that no restriction is possible (§ 50 supra).
There is reason to conclude that, at a minimum, AIDS screening is excluded when
crossing internal borders, quasi-excluded for Union citizens crossing the external borders
or having residence in another Union State, and difficult for developing country
nationals given the principles of proportionality and non-discrimination (§ 554 infra).
C. International law547. As in European law, there is no binding text (treaty, convention) in international
law relating specifically to the free movement of persons living with HIV/AIDS. The
main sources are the position of the WHO [item a] and various declarations or resolutions
concerning fundamental rights [item b]. These texts fall into the area of ‘soft law’, i.e.
non-binding law. Nonetheless, they can usefully guide the interpretation of a
fundamental human right, that of the principle of non-discrimination. This principle is
inscribed in the main texts protecting fundamental rights 782. These texts condemn, in a
general way, any discrimination based on membership of a particular social group, or more
widely, on ‘any situation’ 783. However, this principle of non-discrimination applies only to
human rights and to the fundamental freedoms guaranteed by the same texts. However,
whilst these texts recognize the right for every person to leave any country, they do not
recognize the right to enter another country 784. In other words, apart from certain
782 Article 2 of the Universal Declaration of Human Rights of 10 December 1948, article 14 of the EuropeanConvention for the Protection of Human Rights and Fundamental Freedoms of 4 November 1950, article 1 ofthe American Convention on Human Rights of 22 November 1969, article 2 of the African Charter ofHuman and Peoples’ Rights of 28 June 1981, article 3 of the Universal Islamic Declaration of Human Rights of19 September 1981.
783 Article 2 of the Universal Declaration of Human Rights.784 The Universal Islamic Declaration however states that ‘Given the fact that the Islam world is truly Ummah
Islamia, any Muslim must have the right to enter freely into and leave freely from any Muslim country’.
The Free Movement of Persons Living With AIDS – General conclusions 211
regional integrations like the European Union, there is no absolute right to free
movement, and hence no absolute condemnation of discrimination in these areas. The
fact remains that non-discrimination is tending to become a general principle having
autonomous force. Overtly discriminatory treatment of a particular category of persons, as
would be the case of persons living with HIV/AIDS, needs then to be examined with
regard to the proportionality between the legitimate objective which might be pursued
and the means used (§§ 13 to 19 and § 87 supra and § 554 infra).
a) The position taken by the WHO 785
548. The WHO is opposed to the imposing by states of restrictions in the area of travel,
at least on short stay visits. For longer visits, the WHO’s position is more nuancé.
WHO’s policy distinguishes between restrictions which are introduced by states for
reasons of public health, and restrictions introduced for economic reasons.
549. With regard to restrictions introduced by states with respect to persons living with
HIV/AIDS and which these states justify on grounds of public health, the WHO’s
position is to state that such measures are unfounded. In particular it argues that:
■ States cannot in any event prevent their nationals from travelling and so avoid
any risks attached to travel.
■ Screening is not perfectly reliable, as a person can test seronegative when in fact
he or she is in the process of developing the virus.
■ A false sense of security is created within the population, which comes to think
that AIDS is a ‘foreign’ problem which can be solved by border controls.
■ HIV/AIDS can be passed on only in specific circumstances and not by
day-to-day contact.
■ AIDS is already present in every country in the world.
785 See: Report of the consultation on international travel and HIV infection, Geneva, 2-3 March 1987; Backgroundpaper for a preparatory meeting for a consultation on long-term travel restrictions and HIV/AIDS, Geneva, 4-6 October 1994; Report of the preparatory meeting for a consultation on long-term travel restrictions andHIV/AIDS, Geneva, 4-6 October 1994; WHO policy of non-sponsorship of international conferences on AIDS incountries with HIV/AIDS-specific short-term travel restrictions, February 1993.
212 The Free Movement of Persons Living With AIDS – General conclusions
■ It is impossible to close frontiers effectively and permanently.
■ Restrictions may lead people to enter a country illegally and, because of their
clandestine status, not use preventive measures.
■ Restricting travel is expensive, and funds should be used instead for education and
promotion activities.
These various reasons led the WHO to adopt in 1987 a declaration on the screening
of international travellers for infection by the Human Immuno-Deficiency Virus, which
states that no programme of testing international travellers can avoid the introduction
and propagation of HIV infection.
550. With regard to restrictions on travel, for which the reasons put forward are the
economic costs in relation with long-term residence, the WHO has emphasized the
following principles which ought to be applied by states which impose such measures:
■ States must not forget that the movement of persons, and in particular of workers, is
economically beneficial.
■ Restrictions are justified only when one can effectively expect that a call for
financial assistance will present itself.
■ Restrictions are founded only if the costs linked to HIV/AIDS are equal to or higher
than those of other sicknesses for which similar measures apply.
■ The cost of the financial support exceeds the benefits which are expected from
admitting the traveller.
■ The principles of international law need to be respected.
■ Where screening is required, it is important to respect the principle of the consent of
the person and the principle of confidentiality.
Faithful to its policy, the WHO has refused to sponsor conferences in countries
which apply restrictions on short-stay visits by persons living with HIV/AIDS, motivating
its decision with the fact that discrimination based solely on seropositive status is not
justified at the level of public health, violates human rights and stigmatises persons living
with HIV/AIDS. On this occasion, the WHO reaffirmed its rejection of any form of
discrimination based solely on HIV/AIDS, including in this long stay visits.
The Free Movement of Persons Living With AIDS – General conclusions 213
b) Human rights declarations551. In various parts of the world declarations on AIDS have been adopted at the inter-
state level, frequently in the context of international conferences. These declarations are
of interest to the movement of persons living with HIV/AIDS, either because they
expressly guarantee the principle of free movement of these persons, or because, more
generally, they forbid discrimination against persons living with HIV/AIDS.
However, all these texts are declarations of principle, and lack any binding force per se.
552. By way of example we can mention the following declarations:
■ Recommendation no. R(89) 14, of 24 October 1989, of the Committee of Ministers
of the Council of Europe on the ethical effects of HIV infection in its health and social
aspects (§ 14 supra), items 46 and 47 of which state that: ‘It is recommended that
public health authorities should refrain from introducing restrictions on freedom of
movement by means of costly and ineffective border procedures for all categories of
travellers, including migrant workers’. It will be noted that this recommendation is
close to the policy adopted by the WHO, whilst being more extensive in that it
categorically excludes AIDS controls at borders, both for long and short stay
travellers, whereas the WHO’s policy towards long stay travel is more nuancé.
■ The South African AIDS Consortium’s Charter of Rights relating to AIDS and HIV
dd. 24 March 1992 786 states in article 1.1 that ‘persons living with HIV/AIDS enjoy
the same rights as the rest of the population with regard to the principles of liberty,
autonomy and freedom of movement’. Article 1.2 states that ‘restrictions based on
HIV/AIDS should not created with respect to the free movement of persons in and
between states’ 787.
■ The Cebu Declaration of 3 May 1993 788 states that persons living with HIV/AIDS
should be sheltered from any form of discrimination.
786 Approved by the representatives of 40 organisations.787 On this charter, see also: D. FINE, M. HEYWOOD and A. STRODE, HIV/AIDS and the law, published by the
AIDS Law Project and Lawyers for Human Rights, South Africa, May 1997, p. 275.788 Approved by participants at the Inter-Country Conference on Law, Ethics and HIV, which was held at Cebu
in the Philippines from 3 to 6 May 1993.
■ The Dakar Declaration of 1 July 1994 789 confirms the principle of non-
discrimination, stating that ‘any person directly affected by the epidemic must
remain an integral part of his or her community with the same rights (...) to freedom
of movement (...)’. The same declaration states that ‘any HIV screening without
prior informed consent must be proscribed’ and that ‘HIV screening must not be
demanded for access to work, travel or any other service’.
■ The New Delhi Declaration and Action Plan of December 1995 on HIV/AIDS 790
makes provision for different national legislative initiatives, and in particular a ban
on discrimination in various areas, including travel.
■ International directives on HIV/AIDS and human rights were prepared with a view
to the second international consultation on HIV/AIDS and human rights, which
was held in September 1996 at Geneva, where they were adopted 791. Directive no. 3
articulates in particular that states must ‘make sure that screening tests take place
with the informed consent of the person undergoing them’. According to Directive
no. 5, states also need to ‘promulgate anti-discriminatory laws or strengthen existing
laws to protect persons suffering from HIV/AIDS, whether or not they present
symptoms, persons suspected of being seropositive and groups rendered vulnerable
to infection due to the discrimination which they suffer’. The same directives assert
214 The Free Movement of Persons Living With AIDS – General conclusions
789 This declaration was drawn up and approved by participants at the inter-country consultation of the AfricanNetwork on Ethics, Law and HIV/AIDS organized at Dakar, Senegal, from 27 June to 1 July 1994, by theUNDP’s HIV and Development programme. Participants came from the following countries and organizations:South Africa, Côte d’Ivoire, Ghana, Kenya, Uganda, the Central African Republic, Rwanda, Senegal, Zambia,the WHO’s Global Programme on AIDS, the WHO’s African Regional Office, the UNDP’s ManagementDevelopment and Governance Division, the UNDP’s HIV and Development project for Asia and the Pacific,the Asian and Latin American networks on ethics, law and HIV, AFRICASO, the Association of AfricanLegal Experts, ENDA Third World, the pan-African AIDS Prevention organization, ORSTOM and theAfrican Network of Persons Living with HIV/AIDS.
790 Approved by participants at the International Conference held from 6 to 10 December 1995 at New Delhi onthe topic of ‘AIDS-law and humanity’.
791 On the subject of this directive, see: An advocate’s guide to the international guidelines on HIV/AIDS and humanrights, prepared by ICASO, October 1997 and the NGO Summary of the International Guidelines on HIV/AIDSand human rights, prepared by ICASO. The Geneva consultation was attended by 35 experts, includinggovernment representatives, human rights defenders, academics, representatives of regional and nationalexperts working in the areas of ethics, law and human rights, representatives of the United Nations, NGOsand AIDS prevention organizations. Since publication, the directives have been officially adopted by twoUnited Nations bodies: the Human Rights Commission and the Sub-Commission on Prevention ofDiscrimination and Protection of Minorities.
in particular that states should ‘abrogate laws, regulations and practices which
restrict the freedom of movement and association of members of vulnerable groups
within the context of HIV/AIDS’. Finally, according to Directive no. 8, states
should ‘support the setting up of HIV prevention programmes and of suitably
adapted care for persons who find it more difficult to access national programmes,
for linguistic or economic reasons, or because they are marginalized’. This includes
in particular migrants and refugees.
■ Many South American countries have adopted recommendations concerning
AIDS, as called for at the third Ibero-American conference of presidents and
governments in 1993. These recommendations provide among other things that
South American countries should scrap the requirement for AIDS screening as a
prerequisite for obtaining a visa. Our study shows that so far these recommendations
have been little applied 792.
553. All the facts that we have established show that neither international law, nor
European law nor national law, with a few rare exceptions, formally bans restrictions on
the free movement of persons living with HIV/AIDS. On the other hand, neither
international law, nor European law, nor national law, with a few rare exceptions,
expressly authorizes restrictions on the free movement of persons living with HIV/AIDS.
The question then becomes pretty simple. Is what is formally neither forbidden nor
authorized in fact forbidden or authorized? What is not forbidden is in principle
authorized. The only limit results from the effect of measures taken with respect to other
well-established rights. These limitations on the right to restrict free movement should
be interpreted with reference to a fundamental right, that of non-discrimination, and to
what has now become a general principle in the interpretation of fundamental rights,
that is the principle of proportionality. The many non-binding texts (‘soft law’)
mentioned in the establishment of facts ought to guide the interpretation of the
principle of non-discrimination and of the principle of proportionality in so far as they
represent general principle, if not of law, at least of ethics ‘recognized by civilized
nations’, paraphrasing article 38, paragraph 1, sub-paragraph C of the statutes of the
International Court of Justice.
The Free Movement of Persons Living With AIDS – General conclusions 215
792 See also: Report of the preparatory meeting for a consultation on long-term travel restrictions and HIV/AIDS, WHO,Geneva, 4-6 October 1994.

2. Conclusions554. The question of the free movement of persons living with HIV/AIDS must be
examined from the viewpoint of the principle of non-discrimination. This fundamental
principle needs to be measured with respect to the principle of proportionality: is the
damage to the fundamental principle of non-discrimination proportional to the objective
being pursued? This question contains two sub-questions:
1. Is a legitimate objective being pursued? In particular, one needs to see whether there is
another objective other than a purely economic one, in particular in the area of public
health. However, one should also bear in mind that these two objectives can be
interlinked. For example, the drawing power of a country which has advanced further
in developing AIDS care can impact both the public health budget (economic aspect)
and the health care granted to the population out of this budget (public health aspect).
2. Is the means used – viz. the infringement of freedom of movement by means of
refusals to grant access to the territory, or obligatory screening at the border, or
expulsion – proportional?
This second sub-question may itself be the subject of two tests:
a) The effectiveness test: is the method used effective in achieving the desired
objective?
b) The interchangeability test: does an equally effective method exist which would
make it possible to achieve the same objective?
555. The European Court of Justice (Luxembourg) has applied the principle of
proportionality in a case which concerned mandatory AIDS screening prior to
recruitment. On this occasion, the Court of Justice recalled that restrictions could be
made to fundamental rights, on condition that these respond effectively to objectives of
general interest and that they do not constitute, in the light of the objective being
pursued, a disproportionate and intolerable intervention which would violate the very
substance of the right which is protected (§ 13 supra) 793.
556. It is at another judicial order, that of the European Convention for the Protection of
216 The Free Movement of Persons Living With AIDS – General conclusions
793 ECJ, 5 October 1994, X. v. Commission of the E.C., C-404/92P, ECR, 1994, I-4737.
Human Rights and Fundamental Freedoms, that case law specifically relating to the free
movement of persons living with HIV/AIDS has been developed. The European Court of
Human Rights (Strasbourg) ruled that the expulsion by a state of a foreign national in the
terminal stage of AIDS and without means of treatment in his country of origin was
contrary to article 3 of the Convention (forbidding inhuman and degrading treatment),
even if, by virtue of a well-established principle of international law, states have the right
to control the entry, residence and expulsion of non-nationals (§ 76 supra).
557. Among all the legislations which have been examined, the number of legislations
which expressly limit the free movement of persons living with HIV/AIDS, even though
such legislation exists in many countries, are not in the majority. On the other hand,
most of the legislations which we studied made provision for restrictions in the area of
public health in general.
We need to deduce from the principle of proportionality that without legislation
which expressly permits restrictions on the free movement of persons due to AIDS,
general legislation which does not expressly make provision for restrictions linked to
AIDS may not be interpreted as authorizing them.
In this respect it can be noted that, for the WHO, including AIDS under the
concept of ‘infectious or contagious sicknesses’ which is contained in many national laws
and which permits the exclusion of travellers, causes a problem since this sickness can be
transmitted only in very specific ways, and may be avoided by any non-infected persons
by not adopting ‘high risk’ behaviour patterns 794.
3. Proposals558. The proposals which can be made with respect to the facts established and the
conclusions drawn above follow three lines, passing from the short- to the long-term.
559. In the short-term, states ought to abstain from taking in any new measure limiting
the free movement of persons living with HIV/AIDS. This ‘stand still’ position is
The Free Movement of Persons Living With AIDS – General conclusions 217
794 Background paper preparatory to a meeting for a consultation on long term travel restrictions and HIV/AIDS, WHO,Geneva, 4-6 October 1994. See, on genetic screening, the development of principles similar to the principle ofproportionality on the objective and the method: ‘Usually, an overall requirement is, that the advantages of ascreening programme – both for the target population as a whole and for the individual participants – prevailover the disadvantages’, S. GEVERS, ‘Population screening. The role of the law’, European Journal of HealthLaw, 1998, p. 7.
destined to avoid the introduction into the text of discriminatory restrictions which go
against the principles advanced in the declarations.
560. In the medium-term, states ought to evaluate the existing measures with reference
to the principle of proportionality. At this stage, states ought therefore to examine
whether the said measures pursue a legitimate objective. If the answer is yes, it is
important to verify whether the means used are effective (effectiveness test) and whether
there are not other means which make it possible to achieve this objective without
infringing the principle of free movement of persons, or to infringe this principle to a
lesser extent (interchangeability test). Answering these questions requires recourse to
medical and epidemiological studies, which will make it possible to adapt national and
even Community legislation as a function of the answers obtained. These answers will
also enable national or Community judges to assess the proportional nature of the
restrictions taken by states with regard to persons living with HIV/AIDS.
It should be borne in mind that the WHO examined the question of the
effectiveness of AIDS controls at borders and concluded that, from the public health
viewpoint, these measures lack foundation. If the objective pursued by states imposing
screening at borders is economic in nature, it is again important that the WHO’s
principles with regard to restrictions of a financial order be respected and that the
discrimination is not based solely on the existence of HIV/AIDS. To this extent only
could a distinction be made between short-term and long-term visits, with the latter
possibly being deemed more susceptible with regard to the principle of proportionality. In
this case, the method used – controls – could be considered as effective and difficult to
interchange in safeguarding a state’s public health system, which is considered as a
legitimate objective. It should be noted that, in order to achieve this, the legitimate
objective which is being pursued may not be purely economic, but also have a public
health aspect, and that the means used, that is controls on and restrictions to free
movement, may not strike solely persons living with HIV/AIDS. Similarly, the principle
of proportionality ought to distinguish between access to the territory and expulsion.
Expulsion represents a more serious infringement of fundamental rights than refusal of
access to a country’s territory.
561. In the long-term, limits to the freedom of movement ought to be progressively
eliminated. At least, states ought to be invited to take a position and to declare that they
218 The Free Movement of Persons Living With AIDS – General conclusions

will examine the proportional nature of measures taken with respect to the free
movement of persons living with HIV/AIDS.
Should legislation be promoted which bans restrictions on the free movement of
persons living with HIV/AIDS (positive actions)? Among the countries studied, few have
legislation which expressly bans AIDS controls at borders (for Europe, this is the case in
Luxembourg 795, and, outside Europe, in Bolivia 796) even if several human rights
declarations have enshrined this principle. Certain responses from the states show
hesitations resulting from the absence of positive legislation and the potential usefulness
of introducing positive legislation (see for example § 443 supra with regard to Papua New
Guinea) 797. On the other hand, introducing legislation to ban restrictions on the free
movement of persons specifically with respect to HIV/AIDS is tantamount to
stigmatizing this category of persons compared with others. In the long-term objective of
eradicating discrimination and promoting the free movement of every person, positive
action to support persons living with HIV/AIDS ought to constitute only a temporary
means, limited in time, so as to respond to the very principle of proportionality which is
defended here in the area of fundamental rights. The legitimate objective which is
pursued is non-discrimination in the area of freedom of movement. The means used is
positive discrimination through specific legislation to protect persons living with
HIV/AIDS. The means is proportional only if it is time-limited with a view to
establishing equality.
In the long-term, the extension of the more general principle of freedom of
movement within large regional groupings such as the European Union, as well as
between such groupings, should be promoted.
Specifically in the countries of the Union, the lack of uniformity which has been
observed in policies towards third countries nationals needs to be remedied, pursuant to
the texts adopted within the framework of European law.
The Free Movement of Persons Living With AIDS – General conclusions 219
795 See §§ 180 et seq.796 See § 394.797 In favour of positive antidiscriminatory law, see O. DE SCHUTTER, ‘Epidémie de sida et droits de l’homme’,
Revue trimestrielle des droits de l’homme, 1994, p. 86.

798 When national texts are translated, these are not official translations
Legislative textsand case law 798
Annexes
Annexe I. International and European law(1) International protection of human rights■ European Convention for the protection of human rights and fundamental
freedoms (4 November 1950)
Article 3
No-one shall be subjected to torture or to inhuman or degrading treatment or punishment.
Article 8
1. Everyone has the right to respect for his private and family life, his home and his
correspondence.
2. There shall be no interference by a public authority with the exercise of this right except
such as in accordance with the law and is necessary in a democratic society in the interests
of national security, public safety or the economic well-being of the country, for the
prevention of disorder or crime, for the protection of health or morals, or for the protection
of the rights and freedoms of others.
Article 14
The enjoyment of the rights and freedoms set forth in the Convention shall be secured
without discrimination on any ground such as sex, race, colour, language, religion, political
or other opinion, national or social origin, association with a national minority, property,
birth or other status.
■ International covenant on civil and political rights (19 December 1966)
Article 2
Each State party to the present Covenant undertakes to respect and to ensure to all
individuals within its territory and subject to its jurisdiction the rights recognized in the
present Covenant, without distinction of any kind, such as race, colour, sex, language,
religion, political or other opinion, national or social origin, property, birth or other status.
Article 17
1. No one shall be subjected to arbitrary or unlawful interference with his privacy, family,
222 The free movement of persons living with HIV/AIDS – Annexe I (1): Int’l and European law, Int’l protection of human rights
home or correspondence, nor to unlawful attacks on his honour and reputation.
2. Everyone has the right to the protection of the law against such interference or attacks.
Article 26
All persons are equal before the law and are entitled without any discrimination to the equal
protection of the law. In this respect, the law shall prohibit any discrimination and guarantee
to all persons equal and effective protection against discrimination on any ground such as
race, colour, sex, language, religion, political or other opinion, national or social origin,
property, birth or other status.
■ Council of Europe Convention for the protection of people with regard to the
automated processing of personal data (28 January 1981)
Article 6
Personal data concerning health or sexual life may not be processed automatically unless
domestic law provides appropriate safeguards.
(2) Secondary community legislation (EC)■ Council Directive 64/221 of 25 February 1964 on the coordination of special
measures concerning the movement and residence of foreign nationals which are
justified or grants of public policy, public security or public health.
Article 4
1. The only diseases or disabilities justifying refusal of entry into a territory or refusal to
issue a first residence permit shall be those listed in the Annexe to this Directive.
2. Diseases or disabilities justifying refusal of entry into a territory or refusal to issue a first
residence permit shall be those listed in the Annexe to this Directive.
3. Member States shall not introduce new provisions or practices which are more restrictive
than those in force at the date of notification of this Directive.
Annexe:
1. Diseases subject to quarantine listed in International Health Regulation No. 2 of the
World Health Organization of 25 May 1951;
2. Tuberculosis of the respiratory system in an active state or showing a tendency to develop;
3. Syphilis;
4. Other infectious diseases or contagious parasitic diseases if they are the subject of
provisions for the protection of nationals of the host country.
The free movement of persons living with HIV/AIDS – Annexe I (2): Int’l and European law, Secondary community legislation 223
(3) Non-binding community texts■ Resolution of the Council and of the representatives of the Governments of the
Member States, meeting within the Council, of 29 May 1986 concerning the
adoption of a European emergency health card 799
The Council and the representatives of the governments of Member States consider that, in
order further to protect the health of European citizens and to enhance their freedom of
movement it is desirable to provide for means whereby, in an emergency, their pre-existing or
present health problems can be identified. To this end, an appropriate means appears to be a
European emergency health card, clearly and succinctly setting out certain vital information.
■ Communication from the Commission of 11 February 1987 on the fight
against AIDS 800
The Commission believes that compulsory screening of certain groups should be rejected
on the basis of effectiveness, logistical problems, cost and consideration of civil liberties.
It calls for joint examination, with Member States’ representatives, of the possible
relevance of certain measures which could limit the freedom of movement of persons,
such as notification of cases of AIDS or systematic screening, in order to avoid the
development of contradictory national practices.
■ Conclusions of the Council of 15 May 1987 concerning AIDS 801
The Council and the representatives of the Governments of the Member States consider
that AIDS represents a ‘priority international cause in the field of public health’. They
confirm their commitment to full respect of the principle of freedom of movement of
persons and consider it necessary, by means of reciprocal information and appropriate
coordination, to prevent contradictory national policies from being developed in regard
to third-country nationals. The Council and the representatives of the Governments of
the Member States stress the ineffectiveness, in terms of prevention, of any policy of
systematic and compulsory screening, in particular during health checks at frontiers. They
also decide to introduce arrangements for systematically informing international
travellers about AIDS. The ad hoc working party is instructed to organize information on
technical, administrative and legal measures envisaged or adopted by the Member States.
224 The free movement of persons living with HIV/AIDS – Annexe I(3): Int’l and European law, Non-binding community texts
799 OJ, C 184, 23 July 1986, p. 4.800 COM (87) 63 Final, 11 February 1987.801 OJ, C 178, 7 July 1987, p. 1.
■ Conclusions of the Council of 31 May 1988 concerning AIDS 802
The Council and the representatives of the governments of the Member States note that
all the Member States are pursuing homogenous policies in the fight against AIDS, in
accordance with the common approach outlined in their conclusions of 15 May 1987.
They note in particular that all Member States are ensuring the freedom of movement of
persons. The commitment to certain principles is reaffirmed, in particular the
ineffectiveness of systematic and compulsory screening, the rejection of any
discrimination against or stigmatisation of persons affected by AIDS, and the giving of
absolute priority to prevention through health education and information.
■ Communication of the Commission of 17 May 1988 on Community action
against AIDS in 1987 803
The Commission records that, in its communication of 11 February 1987, it stressed the
need, among other things, for joint examination of the possible relevance of certain
measures relating, in one way or another, to migration policy, and the free movement of
persons. It notes that the work has been held up for various reasons. It proposes setting up
a simple and fast system of exchange of information on the public and private measures
adopted or envisaged in the Member States. With respect to systematic screening at
frontiers, the Commission reminds that it has systematically expressed its commitment to
respecting the principle of freedom of movement and it has stressed the need to prevent
contradictory national practices developing.
■ Resolution of the European Parliament of 30 March 1989 on the fight
against AIDS 804
Parliament judges that it is necessary for a Community system to be established for regular
and rapid exchanges of information on activities, measures and initiatives associated with
the fight against AIDS between Member States’ governments and between regional
services responsible for preventive measures, and for the care and supervision of patients.
The purpose of such exchanges should be to assist the Member States in the fight against
AIDS, to help to safeguard freedom of movement and to prevent the development of
contradictory or discriminatory national policy for citizens of third countries. Parliament
The free movement of persons living with HIV/AIDS – Annexe I(3): Int’l and European law, Non-binding community texts 225
802 OJ, C 197, 27 July 1988, p. 8.803 COM (88) 268 Final, 17 May 1988, p. 2.804 OJ, C 158, 26 June 1989, p. 477.
is of the opinion that systematic and compulsory screening is ineffective from the point of
view of prevention. It asks Member States to refrain from HIV testing at borders and the
expulsion or isolation of people from outside the Community because of HIV or AIDS. It
requests the Commission to create a central data bank to record cases of discrimination.
■ Resolution of the Council and the Ministers for Health of the Member States of
22 December 1989 on the fight against AIDS 805
In the fight against AIDS, top priority should, alongside research, continue to be given to
prevention by means of health information and health education. On the basis of the present
state of knowledge, no public health reason justifies the systematic and compulsory screening
of individuals. The free movement of persons is and must continue to be guaranteed.
■ Decision of the Council and the Ministers for Health of the Member States,
meeting within the Council on 4 June 1991, adopting a plan of action in the
framework of the 1991-1993 ‘Europe against AIDS’ programme 806
The plan of action makes provision for, in particular, informing and increasing the
awareness of the public and of certain target groups as well as measures to combat
discrimination against HIV-infected persons.
■ Resolution of the Council and the Ministers for Health of the Member States,
meeting within the Council of 13 November 1992 on the monitoring and
surveillance of communicable diseases 807
The Council considers that the mobility of people as a result of the development of the
internal market increases the importance of more comparable and more accessible data
and of timely exchanges of information collected by the Member States in order to
monitor outbreaks of communicable diseases. It invites the Commission to produce
reports on transnational surveillance networks and to submit proposals aimed at
improving and extending such networks.
226 The free movement of persons living with HIV/AIDS – Annexe I(3): Int’l and European law, Non-binding community texts
805 OJ, C 10, 16 January 1990, p. 3.806 OJ, L 175, 4 July 1991, p. 26.807 OJ, C 326, 11 December 1992, p. 1.
■ Report from the Commission on the implementation of the plan of action in
1991-1992 808
With regard to raising awareness on the problems of AIDS, the Commission considers
that Community action focused at specific target groups, in particular those crossing
national borders and migrants, are easy to implement and can have particularly useful
value. The Commission points out that projects have already been financed in these areas
and will be developed further.
■ Proposal for a decision of the Council and the Ministers of Health of the
Member States, meeting within the Council, concerning the extension to the
end of 1994 of the 1991-1993 plan of action in the framework of the ‘Europe
against AIDS’ programme 809
The Council stresses that increasing tourism and travel within the Community and to
and from the Community and to other states bring with them greater possibilities for the
spread of this disease. It considers that attempting to combat this by limiting free
movement between states would have unacceptable consequences and would be
ineffective. However, the Council believes that providing information and running
specific campaigns can have a considerable impact and that such activities can often most
easily and effectively be carried out at Community level. The 1994 plan of action
includes in particular: studies of the information campaigns for the general public and
target sections of the population, including migrants; studies and exchanges of
information and experience on problems related to tourism, people travelling within the
Community and to and from other countries, and combating discrimination against
people with HIV and AIDS.
■ Communication from the Commission concerning a Community action
programme on the prevention of AIDS and certain other communicable diseases
in the context of the framework for action in the field of public health 810
Discrimination against people with HIV and AIDS is condemned. The Commission
The free movement of persons living with HIV/AIDS – Annexe I(3): Int’l and European law, Non-binding community texts 227
808 COM (93) 42 Final, 10 March 1993.809 COM (93) 453 Final, 29 September 1993.810 COM (94) 413 Final, 9 November 1994, p. 5.
observes that when such discrimination is combined with prejudice against people in
marginalized groups and minorities, such as homosexuals and migrants, severe social
tensions can result. Among forms of discrimination, the Commission alludes to obligatory
screening for immigrants. The actions to be undertaken could include analysis of actual
and potential discriminatory situations in the Community, such as obligatory screening at
frontiers. On the other hand, the Commission points to a growing and increasing need
for information activities to respond to the growing mobility of the Community
population and proposes specific measures to be targeted at tourists, migrants, refugees
and occupational travellers.
■ Proposal for a European Parliament and Council decision adopting a programme
of Community action on the prevention of AIDS and certain other communicable
diseases within the framework for action in the field of public health 811
The programme envisages examination and exchange of information on problems linked
to risk situations. According to the problem, these include migrant populations and cross-
border areas.
■ Commission report on the implementation of the ‘Europe against AIDS’ action
plan in 1993 812
Activities are mentioned with regard to migrants (support for the establishment of an
information centre for certain immigrant communities, etc.). Mention is made of
Commission financing of a feasibility study concerning the establishment of coordinated,
Community-wide information and prevention campaigns for international tourists
travelling within the European Community.
■ Commission report on the implementation of the ‘Europe against AIDS’ action
in 1994 813
With regard to the fight against discrimination, the Commission points first of all to an
analysis of the status of implementation of the Council Resolution of 22 December 1989.
It also mentions an analysis carried out on the possibilities of drawing up a European code
relating to discrimination against those afflicted by HIV/AIDS. Questions relating to the
228 The free movement of persons living with HIV/AIDS – Annexe I(3): Int’l and European law, Non-binding community texts
811 COM (94) 413 Final, 9 November 1994, p. 39.812 COM (94) 525 Final, 25 November 1994, p. 2.813 COM (95) 521 Final, 7 November 1995, p. 2.
free movement of persons will be dealt with in the context of this project. The conclusions
of the report on the implementation of the plan stress in particular that increased tourism
has given rise to a sustained prevention, information and assistance campaign.
■ Commission communication of 7 March 1996 concerning communicable disease
surveillance networks in the European Community 814
The Commission observes that the more people travel about, the greater the risks of the
propagation of infectious diseases (the Commission specifically quotes AIDS as an
example). From this it draws as a conclusion the necessity to agree on measures for
communicable disease surveillance.
■ Proposal for a European Parliament and Council Decision of 7 March 1996
creating a network for the epidemiological surveillance and control of
communicable diseases in the European Community 815
The proposal seeks to establish a system of close cooperation between Member States in
the field of surveillance, with a view to controlling a certain number of serious
communicable diseases. The Decision contains specific provisions aimed at ensuring
cohesion with other relevant Community policies, including freedom of movement.
■ Decision N° 647/96/EC of the European Parliament and of the Council of
29 March 1996 adopting a programme of Community action on the prevention
of AIDS and certain other communicable diseases within the framework for
action in the field of public health (1996 to 2000) 816
A programme of community action on the prevention of AIDS and certain other
communicable diseases shall be adopted for the period 1 January 1996 to 31 December
2000. The following actions are mentioned: the coordination of studies and information
on the problems and situations of persons placed in particular situations (among others
travel); the encouragement of initiatives intended to inform and educate migrants, taking
particular account of cultural and linguistic differences, examination of actual or
potential discriminatory situations.
The free movement of persons living with HIV/AIDS – Annexe I(3): Int’l and European law, Non-binding community texts 229
814 COM (96) 78 Final, 7 March 1996, p. 2.815 COM (96) 78 Final, 7 March 1996, p. 45.816 JO, L 95, 16 April 1996, 16.
230 The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts
Annexe II. European Union Member States(1) National texts
1. (A) AustriaNo testing at the borders.
Public health is dealt with in the decisions concerning the granting of visas
(paragraph 7 of the law of 17 June 1995 on foreign citizens 817). The law states that entry
can be refused if the applicant represents a threat to public policy or security but it does
not make express mention of public health.
■ Osterreichisches Fremdengesetz, 17 June 1995
Article 7 (3)
In exercising the discretionary power granted under paragraph (1) for assessing the reason
for the intended residence of the visa applicant, the authority shall give due consideration not
only to his personal circumstances, in particular his family ties, his financial situation and
the duration of his residence to date, but also to the public interests, in particular security
policing and economic aspects, the state of the labour market and public health concerns.
Article 18 (1)
A residence ban shall be imposed on the alien if on the basis of certain facts it can justifiably
be assumed that his residence constitutes a threat to public policy (öffentliche Ruhe) or
public safety.
2. (B) BelgiumThe law of 15 December 1980 818 stipulates that entry and stay may be refused to Union
citizens for reasons of public health (article 43).
The same legislation states that a decision may be taken to expel the foreigner if
there is a threat to public health (article 7).
817 Österreichisches Fremdengesetz, modified on 17 June 1995. A new modification of this law is planned for early1998.
818 Loi du 15 décembre 1980 sur l’accès au territoire, le séjour, l’établissement et l’éloignement des étrangers,M.B., 31 XII 1980, modified on several occasions of which the last was 15 July 1996.
The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts 231
■ Law of 15 December 1980 on access to the territory, stay, residence and
expulsion of foreigners
Article 3
Apart from derogations applied by an international treaty or by the law, a foreigner may be
refused entry by the border control authorities if he corresponds to one of the following
cases:
(...)
5) if he is listed as not to be admitted to the States signatories to the Convention for the
Application of the Schengen Agreement, signed on 19 June 1990, either because his
presence constitutes a danger for public policy or national security, or because he has been
the object of an expulsion order which has neither been postponed nor suspended, containing
prohibition of entry, based on non-respect of the national rules concerning the entry or the
stay of foreigners;
7° if it is considered by the Minister or his delegate that he could trouble public peace, public
policy or national security.
Article 7
Without prejudice to more favourable dispositions contained in an international treaty, the
Minister or his delegate may give the order to leave the territory before a specific date to any
foreigner who is neither authorized nor admitted to stay more than three months or to take
up residence in the Kingdom (...) if he suffers from one of the illnesses or infirmities listed in
the annexe to the present law.
Article 43
Entry and stay may be refused to Union citizens only for reasons of public policy, public
security or public health (...). Only those illnesses and infirmities mentioned on the list
annexed to the present law may justify refusal of entry to the territory or of granting an
initial residence permit. No illness or infirmity can justify the renewal of a residence permit
or expulsion from the territory, once such a permit has already been delivered.
Annexe
A. Illnesses that may endanger public health:
1. quarantine illnesses mentioned in the international health regulation n° 2 of 25 May
1951 of the World Health Organization;
2. active or progressive tuberculosis of the respiratory system;
3. syphilis;

232 The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts
4. other infectious or parasitic contagious illnesses inasmuch as they constitute, in the host
country, the object of provisions for the protection of national citizens.
B. Illnesses and infirmities that may endanger public policy or public security:
1. drug addiction;
2. major psychic or mental alterations; manifest states of agitation psychosis, delirium or
hallucination and confusion psychosis.
3. (D) GermanyThe law on foreign citizens of 9 July 1990 819 does not require a medical examination on
entry. paragraph 46 states that expulsion may occur for reasons of public health.
■ Ausländergesetz of 9 July 1990
Article 46, 5°
A person may be deported, in particular if he endangers public health through his conduct.
■ Bavaria
Notice n° 1 A 2 – 2081.10 of 19 May 1987 of the Ministry of the Interior of
Bavaria: Legislation concerning foreigners; Medical examination as a condition for
delivering a residence permit 820
The present notice modifies anew a notice dated 19 June 1979 by introducing as a condition
for delivery of a residence permit the obligation to present to the authorities in charge of
foreigners a medical certificate attesting to the good state of health of the applicant, containing
especially the result of a test for detection of HIV infection and mentioning the laboratory
having performed the test. This obligation does not apply to foreigners whose stay abroad has
been only temporary nor to citizens of the Member States of the European Communities or
of the following countries: Andorra, Austria, Finland, Iceland, Liechtenstein, Malta,
Monaco, Norway, San Marino, the Vatican, Sweden and Switzerland.
819 Ausländergesetz of 9 July 1990, BGBl. I, p. 1354, modified on 28 October 1994, BGBl. I, p. 3186.820 Ministerialamtsblatt der Bayerischen Inneren Verwaltung, 25 May 1987, vol. 39, no. 10, p. 256 and International
Digest of Health Legislation, WHO, (Geneva, 1987), 38 (3), p. 510.
The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts 233
4. (DK) DenmarkThe Danish law on foreign citizens 821 states that entry may be refused for reasons of
public health (article 28).
Article 10 of this law states that the right of residence may be delivered only if
particular reasons justify this decision when because of a contagious illness the foreigner
must be considered to be dangerous for those in contact with him.
The law specifies that decisions of expulsion must take into account the state of
health of the person concerned (article 26).
■ Aliens Act no. 894 (Udlændingeloven), 27 October 1994
Article 10
(...) a residence permit may be issued only where particular reasons make it appropriate if
because of a communicable disease (...) the alien must be deemed to represent a threat or
cause substantial inconvenience to his surroundings.
Article 26
In deciding on expulsion, regard shall be had not only to the alien’s ties with the Danish
community, including the duration of his residence in Denmark, but also to the question
whether expulsion must be assumed to be particularly burdensome on him, in particular
because of (…) the alien’s age, health, and other personal circumstances (…).
Article 28
An alien not issued with a residence permit or a national of a Nordic country not
permanently resident in Denmark may (…) be denied entry on arrival if (…) other
reasons of public policy, security, or health indicate that the alien should not be allowed to
stay in Denmark.
5. (E) SpainThe law of 1 July 1985 822 organizes medical examinations at the frontiers (article 11).
The executive order of 23 February 1996 823 provides for the possibility of closing the
821 Consolidated Act no. 894 of 27 October 1994, udlændingeloven, j.nr. 1994-3701-649, modified on 14 June1995, on 24 April 1996, on 22 May 1996 and on 11 December 1996, Consolidated by ministerial decree, no.51 of 22 January 1997 (Indenrigsministeriet lov bekendt gorelse). The 1994 article numbers are used here.
822 Ley orgánica 7/1985, de 1 de julio, sobre derechos y libertades de los extranjeros en España, BOE, 3 júlio 1985,20825.
823 Reglamento de ejecución de la ley orgánica 7/1985 de 1 de julio sobre derechos y libertades de los extranjerosen España, BOE, 23 febrero 1996, 6951.
234 The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts
frontiers in the case of a threat to public health (article 18).
The same order provides for delivery of a medical certificate in order to obtain a
residence visa or a residence or work permit (articles 27, 56 and 85).
The real decreto 766/1992 of 26 June on the entry and stay in Spain of Union citizens 824
states that refusal of entry and stay as well as expulsion may be decided for reasons of
public health (article 15).
■ Ley orgánica 7/1985 of 1 July 1985, sobre derechos y libertades de los
extranjeros en España (on the rights and liberties of foreigners in Spain)
Article 11
At the entry points they must undergo the medical examinations and the measures of control
demanded by the Spanish health services for reasons of public health in the form of and
following the guarantees established by those international treaties of which Spain is a party,
and according to the dispositions in force.
■ Reglamento de ejecución de la ley orgánica 7/1985
Article 18
Closure, whether temporary or sine die, of the entry and exit points into and out of Spain
may be decided by the government whenever circumstances demand this. In practical terms
(...) following a proposal from the Minister of Justice and of the Interior preceded by a
report in favour of this measure from the Minister of Health and Consumption, in case of
epidemic (...).
Article 27
Residence visa applicants must present (...) a medical certificate in conformity with the
dispositions contained in article 37 of the present order.
Article 32
The visa will not be granted to a foreigner whose coming to Spain represents a danger for
public policy, national security, public health (...).
824 Reál decreto 737/1995 de 5 de mayo por el que se modifica el Reál Decreto 766/1992 de 26 de júnio sobreentrada y permanéncia en España de nacionales de Estados miembros de las Comunidades Europeas, BOE, 5junio 1995, 16547.
The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts 235
Article 37
When the Ministers of Justice and of the Interior so decide, in agreement with the Minister
of Health and of Consumption, all persons wishing to enter the Spanish territory must
present at the frontier points a health certificate delivered in their country of origin by the
medical services designated by the Spanish diplomatic or consular mission, or else must
undergo at their arrival a medical examination performed by the competent medical services
so as to prove that they are not suffering from the following disorders:
a) quarantine illnesses defined as such according to the International Health Regulations
adopted by the 22nd World Health Assembly in 1969, third edition, 1983, of the World
Health Organization;
b) drug addiction, major psychic disorders, manifest states of psychopathic illness
accompanied by agitation, delirium, hallucinations or confusion psychosis, when these
disorders endanger public policy or public security according to the dispositions of the
legislation in force;
c) infectious or parasitic illnesses designated by the Minister of Health and of Consumption.
Article 56
The application for a residence permit (...) will be accompanied by the following
documents: (...) an official medical certificate, according to article 37 of this order, if the
applicant had not supplied this for the delivery of the visa.
■ Reál decreto 766/1992 (modified by the Reál decreto 737/1995) sobre entrada y
permanéncia en España de nacionales de Estados miembros de las Comunidades
Europeas (Royal decree on the entry and stay in Spain of citizens of Member States
of the European Communities)
Article 15
When reasons of public policy, public security or public health require, the following
measures may be applied:
a) refusal of entry to Spain (...);
b) refusal of delivery or renewal of permits;
c) ordering expulsion from the Spanish territory;
(...)
Only the following illnesses and infirmities may justify adoption of one of the measures
provided for in paragraph 1 of the present article:
236 The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts
a) quarantine illnesses mentioned in the International Health Regulations n° 2 of 25 May
1951 of the World Health Organization;
b) drug addiction, when this constitutes a danger for public policy or public security in
conformity with the legislation in force;
c) other infectious or parasitic contagious illnesses inasmuch as they are the object of
dispositions of protection concerning Spanish citizens.
If these illnesses or infirmities have been contracted subsequent to the delivery of an initial
residence permit they may not justify a refusal to renew a permit nor expulsion from the
Spanish territory.
6. (F) FranceThe Order of 2 November 1945 does not provide for a refusal of entry to the territory for
reasons of health 825.
The decree n° 94/211 of 11 March 1994 826 states that the stay may be refused for
reasons of public health.
Foreigners who are not Union citizens must undergo a medical examination
according to the dispositions of the order of 7 November 1994 827.
An HIV positive result not accompanied by clinical signs does not constitute a
motive for refusal of the right of residence.
■ Order of 2 November 1945 relating to the conditions of entry and residence of
foreigners in France, as modified
Article 5
(...) Access to the French territory may be refused to any foreigner whose presence could
constitute a threat for public policy or who is concerned by an order banning him from the
territory or an expulsion order.
825 Ordonnance du 2 novembre 1945 relative aux conditions d’entrée et de séjour des étrangers en France,modified in particular by the law of 27 December 1994, Journal Officiel, 28 December 1994, 18536, Law no.97-396 of 24 April 1997, Journal Officiel, 25 June 1997, 8651 and the Law no. 98-349 of 11 May 1998, JournalOfficiel, 12 May 1998, 7087.
826 Décret n° 94-211 du 11 mars 1994 réglementant les conditions d’entrée et de séjour en France desressortissants des États membres de la Communauté européenne bénéficiaires de la libre circulation despersonnes, Journal Officiel, 13 March 1994.
827 Arrêté du 7 novembre 1994 relatif au contrôle sanitaire des étrangers autorisés à séjourner en France, JournalOfficiel, 9 November 1994.
The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts 237
■ Decree 94/221 of 11 March 1994 regulating the conditions for entry and stay in
France of citizens of the Member States of the European Community benefitting
from the free movement of persons
Article 6
(...) The resident’s card may be refused for reasons of public policy if it has been shown that
the applicant suffers from one of the illnesses or infirmities capable of endangering public
policy or public security and mentioned in the list given in annexe to the present decree.
Annexe
Illnesses and infirmities capable of endangering public order or public security:
1. drug addiction;
2. major psychic and mental troubles; manifest states of agitation psychosis, delirium or
hallucination psychosis or confusion psychosis.
■ Order of 7 November 1994 concerning health control of foreigners authorized to
stay in France
Article 4
A foreigner does not fulfil the health conditions if he is suffering from one of the illnesses
mentioned in section V of the international health regulations published by the above-
mentioned decree of 24 January 1989 or from progressive tuberculosis of the respiratory
system or from addiction to substances or plants classified as narcotics or from mental
troubles of a kind capable of disturbing public policy or the safety of persons.
■ Circular letter DGS/1C n° 784 of 8 December 1987 concerning the health
inspection of foreigners wishing to stay in France
(...) only the presence of clinical signs of AIDS or the request of the person concerned may
lead to performing clinical research for HIV antibodies; the existence of an HIV positive
result in the absence of clinical signs must not constitute grounds for refusal of authorization
to stay in France.
■ Circular letter NOR/INT/D/97/00104/C of 24 June 1997 concerning the re-
examination of certain categories of foreigners whose official papers are not in order 828
Point 1.7. Ill foreigners.
In application of article 25, 8° of the order of 2 November 1945, ‘a foreigner usually
828 Journal Officiel, 26 June 1997, 9819. Confirmed by law of 11 May 1998; supra, note 825.
238 The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts
residing in France who suffers from a serious illness requiring medical treatment and whose
departure could entail exceptionally grave consequences for him, provided that he cannot in
fact receive appropriate treatment in the country towards which he is expelled...’.
Foreigners who fulfil the conditions imposed by the law normally obtain a provisional
renewable residence authorization for three months or else they are placed under house
arrest if they are under an expulsion order. From now on, if the report established by the
Inspection Medical Officer of the Département mentions the need for long term medical
treatment for foreigners in this situation, you will deliver a temporary resident’s card unless
public policy is threatened.
This card will bear the mention ‘salaried employee’ if the foreigner requests this and if the
Inspection Medical Officer of the Département considers that the state of health of the
person in question is compatible with a professional activity.
7. (FIN) FinlandThe Finnish Aliens’ Act of 22 February 1991829 does not provide for refusal of entry for
reasons of public health.
In the context of foreigners benefiting from a right of residence on the basis of
European law, article 40 provides for expulsion in the case of a threat to public health.
■ Ulkomaalaisloki (Aliens Act) 378/91 of 22 February 1991, after modification
Article 40
(...) An alien who has the right of residence based on the Agreement on the European
Economic Area may be deported only on grounds of public policy, public security and public
health.
8. (GR) GreeceThe law 1975/91 830 on foreigners authorizes refusal of entry in case of threat to public
health (article 6, 5°).
Public health is taken into account in the process of granting a short-term residence
permit (article 12).
829 Aliens Act 378/91, modified 3 February 1995.830 Law 1975/91 of 21 November 1991 concerning acces to the territoy, exit, residence, employment, and the expulsion
of foreigners and concerning the procedure of recognition of refugee status and other disposition, Official Journal of theHellenic Republic, no 184/1991, 4 december 1991.
The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts 239
It is also taken into account in permission for renewal of the permit for studies
(article 15).
Revocation of the authorization of entry for reasons of work may be based on reasons
of public health (article 22-4).
Expulsion may be decided on in the case of threat for reasons of health (article 27, 1°).
■ Law 1975/91 of 21 November 1991 concerning access to the territory, exit,
residence, employment, and the expulsion of foreigners and concerning the
procedure for recognition of refugee status and other dispositions
Article 6, 5°
The entry of an alien in Greek territory is prohibited if (…) he suffers from a disease which,
by virtue of a decision of the Minister competent on matters of health, has been judged, in
accordance with international standards, and the World Health Organization, as capable of
constituting a danger for public health.
Article 12
For the granting or not of this [short-term] permit, consideration is given to (…) public
health and the social or public interest in general.
Article 15
(…) For granting the renewal of the residence permit for studies, consideration is given to
medical and pharmaceutical attendance expenditures and the non-existence of serious
reasons relating to public security and health.
Article 22
(…) The preliminary approval (of the entry of the foreign for work reasons) (…) can be
revoked or suspended decisively for reasons of public policy, public security, public health or
the protection of public interest.
Article 27
The administrative deportation of an alien, with the reservation of the international
obligations of our country, is feasible if (…) his presence on Greek territory is judged to be
dangerous for the public policy or security of the country or public health.
240 The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts
9. (I) ItalyForeigners who are not citizens of the European Union must conform to the health
conditions in order to enter the territory (article 3 of the law of 28 February 1990) 831.
The right to stay in Italy can be refused for reasons of public health (article 4, 12°).
■ Legge (law) n° 39/90 of 28 February 1990 conversione in legge con modificazioni
del decreto-legge 30 dicembre 1989 n° 416 recante norme urgenti in materia di
asilo politico, di ingresso e soggiorno dei cittadini extracomunitari e di
regolarizzazione dei cittadini extracomunitari ed apolidi già presenti nel territorio
dello stato (transformation into a law with modifications of the legal decree of 30
December 1989 no. 416 providing urgent norms concerning political asylum, entry
and stay of non-European citizens and regularization of non-European citizens and
stateless persons who are already present on the territory of the state), known as
‘legge Martelli’.
Article 3
A foreigner may enter the territory of the State if he presents himself at the frontier control
with a valid passport or an equivalent document recognized by the Italian authorities (...)
and which is in conformity with the dispositions in force as concerns administration, health
and social security (...).
Article 4, 12°
The residence permit may be refused if the conditions and dispositions contained in the law
are not satisfied and (...) motivated for reasons concerning State security and public policy
or public health.
10. (IRL) IrelandThe basic legislation is the Aliens Act 1935, which has been completed by
subsequent texts.
Entry to the territory can be refused for reasons involving public health (article 3,
Aliens Amendment Order 1975 832).
831 Legge 28 febbraio 1990, n° 39, conversione in legge con modificazioni del decreto-legge 30 dicembre 1989 n°416 recante norme urgenti in materia di asilo politico, di ingreso e soggiorno dei cittadini extracomunitari e diregolarizzazione dei cittadini extracomunitari ed apolidi gia presenti nel territorio dello stato, Gazzeta ufficialedella republica Italiana, 28 february 1990, serie generale, n° 49, as modified on 9 December 1996, Gazzettaufficiale della republica italiana, 9 decembre 1996.
832 Statutory instruments, SI N° 128 of 1975.
The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts 241
For European citizens, refusal of entry and stay or an expulsion may occur if
the foreigner has certain illnesses (European Communities Aliens Regulation 1977,
article 4, 12, 14 833).
■ Aliens (Amendment) Order 1975
Article 3
An immigration officer may refuse leave to land to an alien (…) where the immigration
officer is satisfied that the alien (…) is suffering from a disease or disability specified in the
Fifth Schedule to this Order.
Schedule 5
1) diseases subject to the International Health Regulations for the time being adopted by the
World Health Assembly of the World Health Organisation;
2) tuberculosis of the respiratory system in an active state or showing a tendency to develop;
3) syphilis;
4) other infectious or contagious parasitic diseases in respect of which special provisions are
in operation to prevent the spread of such diseases from abroad;
5) drug addiction;
6) profound mental disturbance; manifest symptoms of psychotic disturbance with
agitation, delirium, hallucinations or confusion.
■ European Communities (Aliens) Regulations 1977
Article 4
The person to whom these Regulations apply (…) may not be refused leave to land
unless he is suffering from a disease or disability specified in the Second Schedule to these
Regulations.
Article 12
(...) The only disease or disability in respect of which a decision to refuse to issue a first
residence permit may be based, or in respect of which a person may be required to leave the
State, shall be one specified in the Second Schedule to these Regulations.
833 Statutory Instruments, Sl N° 393 of 1977.
242 The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts
Article 14
A person (...) may be required by the Minister to leave the State (…) where the person has
not been given a first residence permit [and is] suffering from a disease or disability specified
in the Second Schedule to these Regulations..
Second schedule
A. Diseases which might endanger public health:
1) diseases subject to the International Health Regulations for the time being adopted by the
World Health Assembly of the World Health Organization;
2) tuberculosis of the respiratory system in an active state or showing a tendency to develop;
3) syphilis;
4) other infectious or contagious parasitic diseases in respect of which special provisions are
in operation to prevent the spread of such diseases from abroad.
B. Diseases and disabilities which might justify decisions on grounds of public policy or
which might endanger public security:
1) drug addiction;
2) profound mental disturbance, manifest conditions of psychotic disturbance with agitation,
delirium, hallucinations or confusion.
11. (L) LuxembourgOn the basis of the law of 28 March 1972 834, entry and stay may be refused for reasons of
public health. Public health may also be invoked to justify expulsion. The ruling on the
medical control excludes HIV/AIDS from the latter 835.
■ Law of 28 March 1972 concerning the entry and residence of foreigners, the
medical control of foreigners and the employment of foreign workers
Article 2
Entry and stay in the Grand Duchy may be refused to a foreigner (...) if he might trouble
public security, peace, order or health.
834 Loi du 28 mars concernant l’entrée et le séjour des étrangers, le contrôle médical des étrangers et l’emploi de lamain-d’œuvre étrangère, Mém. A 1972, p. 818 modified by the laws of 16 April 1975, p. 621; of 29 July 1977,Mém. 1977, p. 1345; of 8 April 1993, Mém. A 1993, p. 582; of 17 June 1994, Mém. A 1994, p. 1023; of 18August 1995, Mém. A 1995, p. 1908.
835 Règlement grand-ducal du 17 octobre 1995 relatif au contrôle médical des étrangers, Mém. A 1995, p. 2055.
The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts 243
Article 6
The foreigner’s identity card may be confiscated and its renewal refused if the foreigner (…)
3) might endanger public health.
Article 9
Even if they have been authorized to reside in the Grand Duchy, insofar as their extradition
is not requested, foreigners may be expelled from the Grand Duchy if (…) 1) they come
into the categories mentioned in article 6 of the present law.
Article 12
Foreigners who are not authorized to reside in the territory may be expelled by the public
forces with no form of procedure other than simple observation of the fact in the form of a
police report to be addressed to the Minister of Justice (...).
3) who have been refused entry to the country according to article 2 of the present law
(...).
5) who, according to the hypotheses mentioned in article 2, paragraph 2 of the Application
Convention of the Schengen Agreement (...) may trouble public security, peace or order.
Article 21
With the exception of citizens of Member States of the European Union, but without
prejudice to the dispositions of the paragraph 2 of the present article, all foreigners entering
the Grand Duchy and all foreigners wishing to reside therein may be obliged to undergo a
medical examination.
If during a frontier control the agents responsible for the control of persons are in doubt
concerning the state of health of a foreigner, they may call a doctor and demand a medical
examination of the person concerned.
■ Grand ducal Regulation of 17 October 1995 relating to the medical examination
of foreigners
Article 5
The medical examination, which must obligatorily include an X-ray of the lungs, shall
concern the following illnesses and infirmities: (...)
4) other infectious or parasitic contagious illnesses mentioned in protective provisions
concerning national citizens, with the exception of HIV/AIDS .
244 The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts
12. (NL) NetherlandsEntry and stay may be refused to Union citizens suffering from one of the illnesses mentioned
in the annexe to the ruling (articles 91 and 97 of the decree of 19 September 1966 836).
Expulsion of a foreigner may not take place if it is not justified taking into account
the state of his health (article 25 of the law on foreigners of 13 January 1965 837).
■ Vreemdelingenwet (Alien’s Act) of 13 January 1965, as amended
Article 25
An alien shall not be removed from the Netherlands if this is regarded as unreasonable in
view of his state of health or that of any of the members of his family.
■ Vreemdelingenbesluit (Alien’s Decree) of 19 September 1966, as amended
Article 91
Access may be refused to a foreigner who is a citizen of a member State of the European
Economic Community (...) only if he is suffering from one of the illnesses mentioned
in the schedule.
Article 97
If the foreigner falls into one of the categories of resident permits mentioned in article 94, an
authorization to stay may be refused only if he is suffering from one of the illnesses
mentioned in the schedule.
Schedule
A. Illnesses that may endanger public health.
1. quarantine illnesses mentioned in the international health regulation n° 2 of 25 May
1951 of the World Health Organization;
2. active or progressive tuberculosis of the respiratory system;
3. syphilis;
4. other infectious or parasitic contagious illness insofar as they are the object, in the host
country, of dispositions of protection concerning national citizens.
836 Vreemdelingenbesluit van 19 September 1966, Staatsblad, 387, amended on 10 July 1995, Staatsblad (O.J.), 356.837 Vreemdelingenwet, 13 Januari 1965, Staatsblad, 40 amended on 2 February 1995, Staatsblad (O.J.), 43.
The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts 245
B. Illnesses and infirmities that can endanger public order or security:
1. drug addiction;
2. major psychic and mental derangements; manifest states of agitation psychosis, delirium
or hallucinatory psychosis and confusion psychosis.
13. (P) PortugalThe decree-law 59/93 of 3 March 1993 838 does not mention the absence of danger for
public health in the general conditions for access.
Entry and residence may be refused Union citizens suffering from certain illnesses
(decreto-lei n° 60/93 of 3 March 1993, article 12 839).
For citizens of other countries, a medical certificate attesting that the person is
suffering from no infectious or contagious illness is necessary in order to obtain a visa for
residence, work or studies (decreto regulamentar n° 43/93, article 4 840).
■ Decreto-lei 59/93 of 3 March 1993 on the access, stay, exit and expulsion of
foreigners on the national territory
Article 10
Entry on national territory will be prohibited to foreigners (…) who constitute a menace for
public policy, national security or international relations (…)
■ Decreto-lei 60/93 of 3 March 1993
Article 12
(...) 2. Refusal of entry to the national territory or of delivery of an initial residence permit
may be justified by one of the following illnesses:
A. Illnesses that may endanger public health:
1. quarantine illnesses mentioned in the international health regulation no. 2 of 25 May
1951 of the World Health Organization;
2. active or progressive tuberculosis of the respiratory system;
3. syphilis;
4. other infectious or parasitic contagious illnesses insofar as in the host country they are the
838 Decreto-lei n° 59/93 de 3 de Marco, Diario Da Republica, I Serie A, 3-3-1993, 52.839 Decreto-lei n° 60/93 de 3 de Marco, Diario Da Republica, I Serie A, 3-3-1993, 52.840 Decreto regulamentar n° 43/93 de 15 de dezembro, Diario Da Republica, I Serie B, 15-12-1993, 291.
246 The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts
object of dispositions of protection concerning national citizens.
B. Illnesses and infirmities that may endanger public policy or security:
1. drug addiction;
2. major psychic and mental disorders; manifest states of agitation psychosis, delirium or
hallucinatory psychosis and confusion psychosis;
The appearance of one of the illnesses listed in the foregoing number after delivery of the
initial residence permit cannot justify refusal to renew this permit nor expulsion from the
national territory.
■ Decreto regulamentar 43/93 of 15 December 1993
Article 4
All visa applications must be accompanied by the following documents: (...) medical
certificate for applications for residence, work or study visas.
14. (S) SwedenThe general legislation concerning the access and stay of foreigners are the laws 841 and
the ordinance 842 of 1989, as amended.
Refusal of entry or stay and expulsion for reasons of public health are not provided
for in the Aliens Act.
15. (UK) United KingdomA medical examination is required by the legislation on foreigners 843 for persons entering
the territory.
Expulsion from the United Kingdom may occur in case of necessity for the public good.
Refusal of entry and expulsion of Union citizens may occur for reasons of public health.
Instructions have been issued concerning the entry and stay of persons living with
HIV/AIDS.
841 Utlänningslagen (Aliens Act) (SFS 1989: 529), modified on 19 January 1993.842 Utlänningsförordningen (Aliens Ordinance) (SFS 1989: 547; SFS 1995: 254).843 Immigration Act 1971 (1971 c 77), Immigration Act 1988 (1988 c 14), Immigration Order 1996 n° 2145.
The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts 247
■ Immigration Act 1971
Schedule 2, Section 4, Part I, 2
(...) Any such person, if he is seeking to enter the United Kingdom, may be examined also
by a medical inspector or by any qualified person carrying out a test or examination required
by a medical inspector.
Section 3, (5)
A person who is not a British citizen shall be liable to deportation from the United Kingdom
(…) if the Secretary of State deems his deportation to be conducive to the public good.
■ Regulation of 23 May 1994 (HC 395)
Article 36
A person who intends to remain in the United Kingdom for more than six months should
normally be referred to the Medical Inspector for examination (…). Any person seeking
entry who mentions health or medical treatment as a reason for his visit, or who appears not
to be in good mental or physical health, should be referred to the Medical Inspector (…).
Article 37
Where the Medical Inspector advises that a person seeking entry is suffering from a specified
disease or condition which may interfere with his ability to support himself or his dependants,
the Immigration Officer should take account of this, in conjunction with other factors, in
deciding whether to admit that person.
Article 259
The conditions for the issue of an EEA family permit are that (…)
(iii) the applicant is not a person who is liable to excluded on grounds of public policy, public
security or public health.
■ Instruction BDI
2.1. (…) The fact that an applicant has AIDS or is HIV positive is not grounds for
refusing leave to remain if the person concerned otherwise qualifies under the Immigration
Rules.
2.2. Equally the fact that an applicant has AIDS or is HIV positive is not in itself sufficient
to justify the exercise of discretion where the requirements of the Rules are not met. As a
general rule, AIDS cases requiring the exercise of discretion should be evaluated in the same
way as any other case where the applicant has a terminal illness e.g. cancer. Cases involving
persons certified as having AIDS should be distinguished from those where the person

248 The free movement of persons living with HIV/AIDS – Annexe II(1): European states, National texts
concerned has only been diagnosed as HIV positive. Such a person may still be well and a
serious case for exceptional treatment is unlikely to arise.
3. Removal
3.1. The general policy is that enforcement action may be pursued in relation to persons
with AIDS or who are HIV positive unless the medical evidence available is sufficient to
satisfy the Department that the person is not fit to travel and/or their life expectancy would
be substantially shortened if they were removed or deported. It follows that removal action,
where appropriate, should be undertaken as soon as possible.
3.2. In many cases the medical facilities and treatment available in the person’s country of
origin will be substantially less advanced than those available in the UK. This is likely to be
true as regards any serious illness and does not in itself constitute grounds for allowing
someone with AIDS/HIV to remain. It is, however, a factor which will have to be taken
into account in considering removal as enforcement action may be inappropriate in the case
of a terminally ill person where there are no facilities for treatment in the country to which
he would be removed.

The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK 249
(2) Case Law: case of D. v. United KingdomJudgment of the European Court of Human Rights of 2 May 1997(146/1996/767/964)
Summary
United Kingdom – proposed removal of an alien drug courier dying of AIDS to his
country of origin (St. Kitts) where he has no accommodation, family, moral or financial
support and no access to adequate medical treatment.
I. Article 3 of the Convention
Expulsion of alien drug couriers is a justified response to the scourge of drug trafficking –
right of contracting states to expel aliens is however subject to the need to respect the
absolute nature of the prohibition contained in article 3 – duty of respondent state to
secure to the applicant the guarantees contained in article 3 irrespective of the gravity of
the offence committed – applicant within the jurisdiction of the respondent state since
21 January 1993 even if he never entered in the technical sense.
Application of this principle is not confined to contexts in which the individual to
be expelled faces a real risk of being exposed to forms of treatment proscribed by article 3
which are intentionally inflicted by public authorities in receiving state or by non-state
bodies when the public authorities in that state are unable to afford him appropriate
protection – Court must be able to apply article 3 in other contexts so as to avoid
undermining the absolute character of the article’s protection.
Conditions which await applicant in St. Kitts do not in themselves breach standards
of article 3 – respondent state has assumed responsibility for treating applicant since
August 1994 – applicant now reliant on medical and palliative care provided to him –
applicant has entered final stages of fatal illness – removal at this stage would hasten his
death and expose him to a real risk of dying under most distressing circumstances and
thus to inhuman treatment – no adequate medical treatment, no shelter, no family
support in receiving country.
Aliens who have served their prison sentences and are subject to expulsion cannot in
principle claim any entitlement to remain on territory of Contracting state in order to
continue to benefit from medical, social or other forms of assistance provided by that
state during their stay in prison.
250 The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK
However, in view of the very exceptional circumstances of case and the compelling
humanitarian considerations at stake, removal of applicant would violate article 3.
Conclusion: violation if the applicant were to be removed (unanimously).
II. Article 2 of the Convention
Applicant’s contention that circumstances of case engaged responsibility of
Government under article 2 – having regard to finding under article 3 not necessary to
examine article 2 complaint.
Conclusion: not necessary to examine this complaint (unanimously).
III. Article 8 of the Convention
Applicant’s assertion that removal would amount to a disproportionate interference
with his right to respect for private life, in particular his physical integrity – having regard
to finding under article 3 complaint article 8 raises no separate issue.
Conclusion: no separate issue arises (unanimously).
IV. Article 13 of the Convention
Confirmation of conclusion reached in certain earlier judgments concerning the
respondent state that judicial review proceedings constitute an effective remedy –
domestic court subjected the applicant’s plight to a most anxious scrutiny and had the
power to grant relief sought – substance of complaints examined.
Conclusion: no violation (unanimously).
V. Article 50 of the Convention
A. Damages: none claimed.
B. Costs and expenses: partial reimbursement of amount claimed.
Conclusion: respondent state to pay a specified sum to applicant (unanimously).
Court’s case-law referred to
7.7.1989, Soering v. the United Kingdom; 30.10.1991, Vilvarajah and Others v. the United
Kingdom; 15.11.1996, Chahal v. the United Kingdom; 17.12.1996, Ahmed v. Austria.
Arrest
In the case of D. v. the United Kingdom 1 The European Court of Human Rights, sitting, in
accordance with article 43 of the Convention for the Protection of Human Rights and

The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK 251
Fundamental Freedoms (‘the Convention’) and the relevant provisions of Rules of Court
A 2 , as a Chamber composed of the following judges:
Mr R. Ryssdal, President, Mr C. Russo, Mr A. Spielmann, Mr J. De Meyer, Sir John
Freeland, Mr A.B. Baka, Mr P. Kuris, Mr U. Lohmus, Mr J. Casadevall, and also of Mr H.
Petzold, Registrar, and Mr P.J. Mahoney, Deputy Registrar,
Having deliberated in private on 20 February and 21 April 1997,
Delivers the following judgment, which was adopted on the last-mentioned date:
Procedure
1. The case was referred to the Court by the European Commission of Human Rights
(‘the Commission’) and by the Government of the United Kingdom of Great Britain and
Northern Ireland (‘the Government’) on 28 October 1996 and 14 November 1996
respectively, within the three-month period laid down by articles 32 paragraph 1 and
article 47 of the Convention. It originated in an application (no. 30240/96) against the
United Kingdom lodged with the Commission under article 25 on 15 February 1996 by
D., a national of St. Kitts. In the proceedings before the Commission the applicant was
identified only as ‘D.’. At the wish of the applicant this practice was maintained in the
proceedings before the Court.
The Government’s application referred to article 48 and the Commission’s request to
articles 44 and 48 and to the declaration whereby the United Kingdom recognised the
compulsory jurisdiction of the Court (article 46). The object of the application and the
request was to obtain a decision as to whether the facts of the case disclosed a breach by
the respondent state of its obligations under articles 2, 3, 8, and 13 of the Convention.
2. In response to the enquiry made in accordance with Rule 33 paragraph 3 (d) of Rules
of Court A, the applicant stated that he wished to take part in the proceedings and
designated the lawyer who would represent him (Rule 30).
1 The case is numbered 146/1996/767/964. The first number is the case’s position on the list of cases referred tothe Court in the relevant year (second number). The last two numbers indicate the case’s position on the listreferred to the Court since its creation and the list of the corresponding originating applications to theCommission.
2 Rules A apply to all cases referred to the Court before the entry into force of Protocol No. 9 (1 October 1994)and thereafter only to cases concerning States not bound by that Protocol. They correspond to the Rules thatcame into force on 1 January 1983, as amended several times subsequently.
252 The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK
3. The Chamber to be constituted included ex officio Sir John Freeland, the elected judge
of British nationality (article 43 of the Convention), and Mr R. Ryssdal, the President of
the Court (Rule 21 paragraph 4 (b)). On 29 October 1996 in the presence of the
Registrar, the President of the Court drew by lot the names of the other seven members,
namely Mr C. Russo, Mr A. Spielmann, Mr J. De Meyer, Mr A.B. Baka, Mr P. Kuris, Mr
U.Lohmus, and Mr J. Casadevall (article 43 in fine of the Convention and Rule 21
paragraph 5).
Pursuant to Rule 36 of its Rules of Procedure, the Commission had requested the
Government not to deport the applicant and the Government provided assurances to
that effect. The Government was informed by the Registrar on 29 October 1996 that
under Rule 36 of Rules of Court A the interim measure indicated by the Commission
remained recommended.
4. As President of the Chamber (Rule 21 paragraph 6), Mr Ryssdal, acting through the
Registrar, consulted the Agent of the Government, the applicant’s lawyer and the
Delegate of the Commission on the organisation of the proceedings (Rules 37 paragraph 1
and 38). Pursuant to the order made in consequence, the Registrar received the applicant’s
and the Government’s memorial on 9 January and 10 January 1997 respectively.
5. In accordance with the President’s decision, the hearing took place in public in the
Human Rights Building, Strasbourg, on 20 February 1997. The Court had held a
preparatory meeting beforehand.
There appeared before the Court:
(a) for the Government:
Mr M. Eaton, Deputy Legal Adviser, Foreign and Commonwealth Office Agent, Mr D.
Pannick Q.C., Mr N. Garnham, Counsel, Ms S. McClelland, Mr S. Hewett, Advisers;
(b) for the Commission:
Mr J.-C. Geus, Delegate;
(c) for the applicant:
Mr N. Blake Q.C., Mr L. Daniel, Counsel, Mr A. Simmons, Ms R. Francis,
Solicitors, Mrs N. Mole, Adviser.
The Court heard addresses by: Mr Geus, Mr Blake and Mr Pannick and also replies
to questions put by two of its members.
The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK 253
As to the fact
I. Particular circumstances of the case
The applicant
6. The applicant was born in St. Kitts and appears to have lived there most of his life. He
is one of seven children. One sister and one brother moved to the United States in the
1970s and the rest of the family appears to have followed at unspecified dates. The
applicant visited the United States in 1989 to try to join his family. During his stay there
he was arrested on 5 September 1991 for possession of cocaine and subsequently
sentenced to a three year term of imprisonment. After one year, he was paroled for good
behaviour and deported on 8 January 1993 to St. Kitts.
The applicant’s arrival in the United Kingdom and subsequent imprisonment
7. The applicant arrived at Gatwick Airport, London, on 21 January 1993 and sought
leave to enter the United Kingdom for two weeks as a visitor. He was found at the airport
terminal to be in possession of a substantial quantity of cocaine with a street value of
about £120,000. The Immigration Officer refused him leave to enter on the ground that
his exclusion was conducive to the public good and gave him notice that he would be
removed to St. Kitts within a matter of days.
However, after being arrested and charged, the applicant was remanded in custody
and subsequently prosecuted for being knowingly involved in the fraudulent evasion of
the prohibition on the importation of controlled drugs of Class A. He pleaded guilty at
Croydon Crown Court on 19 April 1993 and was sentenced on 10 May 1993 to six years’
imprisonment. He apparently behaved well while in H.M. Prison Wayland and was
released on licence on 24 January 1996. He was placed in immigration detention pending
his removal to St. Kitts. Bail was granted by an adjudicator on 31 October 1996 after the
Commission’s report had been made public.
Diagnosis of AIDS
8. In August 1994, while serving his prison sentence, the applicant suffered an attack of
pneumocystis carinii pneumonia (‘PCP’) and was diagnosed as HIV positive and as
suffering from AIDS. The infection appears to have occurred some time before his arrival
in the United Kingdom.
254 The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK
9. On 3 March 1995, the applicant was granted a period of compassionate leave to be
with his mother whose air fare to the United Kingdom to visit him had been covered by
charitable donations.
10. On 20 January 1996, immediately prior to his release on licence, the immigration
authorities gave directions for the applicant’s removal to St. Kitts.
The applicant’s request to remain in the United Kingdom
11. By letter dated 23 January 1996, the applicant’s solicitors requested that the secretary
of state grant the applicant leave to remain on compassionate grounds since his removal to
St. Kitts would entail the loss of the medical treatment which he was currently receiving
thereby shortening his life expectancy (see §§ 13 and 14 below). This request was refused
on 25 January 1996 by the Chief Immigration Officer. In his letter of refusal addressed to
the applicant’s solicitors the Chief Immigration Officer stated:
‘In reaching this decision full account was taken of paragraph 4 of the Immigration
and Nationality Department B Division Instructions regarding AIDS and HIV positive
cases. You will be aware that paragraph 4 of this instruction which relates to persons
whose applications are for leave to enter the United Kingdom states [see paragraph 27 of
the judgment below] ... While we are saddened to learn of Mr D[..]’s medical
circumstances we do not accept, in line with Departmental Policy, that it is right
generally or in the individual circumstances of this case, to allow an AIDS sufferer to
remain here exceptionally when, as here, treatment in this country is carried out at public
expense, under the National Health Service. Nor would it be fair to treat AIDS sufferers
any differently from others suffering medical conditions....’
Judicial review proceedings
12. On 2 February 1996, the applicant applied unsuccessfully to the High Court for leave
to apply for judicial review of the decision to refuse him leave to enter. On 15 February
1996, the Court of Appeal dismissed his renewed application. It found that section 3 of
the Immigration Act 1971 drew a distinction between leave to enter and leave to remain.
It held that the Chief Immigration Officer had correctly treated Mr D.’s application as an
application for leave to enter and was not required to take into account paragraph 5 of
the Home Office guidelines which applied to applications for leave to remain (see §§ 27
and 28 below). As to the applicant’s argument that the Home Office acted unreasonably
The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK 255
or irrationally in not acceding to the compassionate circumstances of his plea, Sir Iain
Glidewell stated in his judgment:
‘Nobody can but have great sympathy for this applicant in the plight in which he finds
himself. If he is to return to St. Kitts it seems that he will be unable to work because of his
illness. His expectation of life, if the medical evidence is correct, may well be shorter than it
would be if he remained under the treatment that he is receiving in the United Kingdom,
and in many ways his plight will be great. On the other hand he would not be here if he had
not come on a cocaine smuggling expedition in 1993; and if he had not been imprisoned he
would have gone back to St. Kitts, if he had ever come here at all, long before his AIDS was
diagnosed. Taking account of the fact that the court must give most anxious scrutiny to a
decision which involves questions particularly of life expectancy, as this one apparently
does, nevertheless I cannot find that an argument in this case that the decision of the Chief
Immigration Officer was irrational is one that has any hope of success at all. Putting it the
opposite way, it seems to me to be one which was well within the bounds of his discretion,
and thus is not one with which the court can properly interfere.’
Reports on the applicant’s medical condition, treatment and prognosis
13. Since August 1995, the applicant’s CD4 cell count has been below 10. He has been in
the advanced stages of the illness, suffering from recurrent anaemia, bacterial chest
infections, malaise, skin rashes, weight loss and periods of extreme fatigue.
14. By letter dated 15 January 1996, Dr Evans, a consultant doctor, stated:
‘His current treatment is AZT 250 mgs. b.d. and monthly nebulised pentamidine, he
occasionally takes mystatin pastilles and skin emollients.
In view of the fact that [the applicant] has now had AIDS for over 18 months and
because this is a relentlessly progressive disease his prognosis is extremely poor.
In my professional opinion [the applicant’s] life expectancy would be substantially
shortened if he were to return to St. Kitts where there is no medication; it is important
that he receives pentamidine treatment against PCP and that he receives prompt anti-
microbial therapy for any further infections which he is likely to develop...’
15. In a medical report provided on 13 June 1996, Professor Pinching, a professor of
immunology at a London hospital, stated that the applicant had suffered severe and
irreparable damage to his immune system and was extremely vulnerable to a wide range of
256 The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK
specific infections and to the development of tumours. The applicant was reaching the
end of the average durability of effectiveness of the drug therapy which he was receiving.
It was stated that the applicant’s prognosis was very poor and limited to 8-12 months on
present therapy. It was estimated that withdrawal of the proven effective therapies and of
proper medical care would reduce that prognosis to less than half of what would be
otherwise expected.
Medical facilities in St. Kitts
16. By letter dated 20 April 1995, the High Commission for the Eastern Caribbean States
informed the doctor treating the applicant in prison that the medical facilities in St. Kitts
did not have the capacity to provide the medical treatment that he would require. This
was in response to a faxed enquiry of the same date by Dr Hewitt, the managing medical
officer at H.M. Prison Wayland. By letter of 24 October 1995, Dr Hewitt informed the
Home Office of the contents of the letter from the High Commission, which had also been
sent to the Parole Unit on 1 May 1995. He stated that the necessary treatment was not
available in St. Kitts but was widely and freely available in the United Kingdom and
requested due consideration be given to lifting the deportation order in respect of the
applicant. By letter dated 1 August 1996, the High Commission for the Eastern Caribbean
States confirmed that the position in St. Kitts had not changed.
17. By letter dated 5 February 1996, the Antigua and Barbuda Red Cross informed the
applicant’s representatives that they had consulted their officer on St. Kitts who stated
that there was no health care providing for drugs treatment of AIDS.
Results of enquiries made by the Government of the authorities in St. Kitts suggest
that there are two hospitals in St. Kitts which care for AIDS patients by treating them for
opportunistic infections until they are well enough to be discharged, and that an
increasing number of AIDS sufferers there live with relatives.
The applicant’s family situation in St.Kitts
18. The applicant has no family home or close family in St. Kitts other than, according to
information provided by the Government, a cousin. His mother, who currently lives in
the United States, has declared that her age, bad health and lack of resources prevent her
from returning to St. Kitts to look after her son if he were to be returned there. She has
also stated that she knew of no relatives who would be able to care for him in St. Kitts.
The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK 257
The applicant’s situation since the adoption of the Commission’s report
19. When granted bail on 31 October 1996 (see § 7 above) the applicant was released
to reside in special sheltered accommodation for AIDS patients provided by a
charitable organisation working with homeless persons. Accommodation, food and
services are provided free of charge to the applicant. He also has the emotional
support and assistance of a trained volunteer provided by the Terrence Higgins
Trust, the leading Charity in the United Kingdom providing practical support, help,
counselling and legal and other advice for persons concerned about or having AIDS
or HIV infection.
20. In a medical report dated 9 December 1996 Dr J.M. Parkin, a consultant in clinical
immunology treating the applicant at a London Hospital, noted that he was at an
advanced stage of HIV infection and was severely immunosuppressed. His prognosis was
poor. The applicant was being given antiretroviral therapy with D4T and 3TC to reduce
the risk of opportunistic infection and was continuing to be prescribed Pentamidine
nebulisers to prevent a recurrence of PCP. Preventative treatment for other opportunistic
infections was also foreseen. Dr Parkin noted that the lack of treatment with anti-HIV
therapy and preventative measures for opportunistic disease would hasten his death if he
were to be returned to St. Kitts.
21. The applicant was transferred to an AIDS hospice around the middle of January 1997
for a period of respite care. At the beginning of February there was a sudden deterioration
in his condition and he had to be admitted to a hospital on 7 February for examination.
At the hearing before the Court on 20 February 1997, it was stated that the applicant’s
condition was causing concern and that the prognosis was uncertain. According to his
counsel, it would appear that the applicant’s life was drawing to a close much as the
experts had predicted (see § 15 above).
II. Relevant domestic law and practice
22. The regulation of entry into and stay in the United Kingdom is governed by Part 1 of
the Immigration Act 1971. The practice to be followed in the administration of the Act
for regulating entry and stay is contained in statements of the rules laid by the secretary of
state before Parliament (‘the Immigration Rules’).
258 The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK
23. Section 3(1) provides that a person who is not a British citizen shall not enter the
United Kingdom unless given leave to do so in accordance with the provisions of the
Act. Leave to enter may be granted for a limited or for an indefinite period.
24. Under section 4(1) of the Act the power to grant or refuse leave to enter is exercised
by immigration officers whereas the power to grant leave to remain in the United
Kingdom is exercised by the secretary of state. These powers are exercisable by notice in
writing given to the person affected.
25. A person, such as the applicant, who has been refused leave to enter but is physically
in the United Kingdom pending his removal, and seeks to be allowed to stay there does
not fall to be treated as applying for leave to remain. Since no leave to enter had been
granted to the applicant, it was right according to the judgment of Sir Iain Glidewell in R
v. Secretary for State for the Home Department ex parte D (Court of Appeal, 15 February
1996) for the Immigration Officer to treat his application as an application for leave to
enter rather than for leave to remain.
Policy guidelines on how to proceed in cases in which persons seeking to enter or
remain in the United Kingdom are suffering from AIDS or are HIV positive
26. The Immigration and Nationality Department of the Home Office issued a policy
document (BDI 3/95) on this subject in August 1995. Paragraph 2 of the guidelines
specifies that the fact that a person is suffering from AIDS or is HIV positive is not a
ground for refusing leave to enter or leave to remain if the person concerned otherwise
qualifies under the Immigration Rules. Equally this fact is not in itself a sufficient ground
to justify the exercise of discretion where the person concerned has not met the
requirements of the Rules.
The policy guidelines distinguish between applications for leave to enter and
applications for leave to remain.
27. On applications for leave to enter (paragraph 4 of the guidelines), where the person is
suffering from AIDS, the policy and practice is to adhere to the provisions of the
Immigration Rules in the normal way. Where such a person does not qualify under the
Rules, entry is refused.
The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK 259
28. On applications for leave to remain (paragraph 5 of the guidelines), the application
should be dealt with normally on its merits under the applicable Rules. However, there is
a discretion outside the Rules which can be exercised in strong compassionate
circumstances. Paragraph 5.4 states that ‘... there may be cases where it is apparent that
there are no facilities for treatment available in the applicant’s own country. Where
evidence suggests that this absence of treatment significantly shortens the life expectancy
of the applicant it will normally be appropriate to grant leave to remain.’
Other relevant materials
29. Among the documentary materials submitted by the applicant, are the following:
1. International policy statements on human rights and AIDS
30. International concern about AIDS has resulted in the adoption of several
international texts which have addressed inter alia the protection of the human rights of
the victims of the disease. Thus, the United Nations Commission on Human Rights
adopted a Resolution on 9 March 1993 on the protection of human rights in the context
of human immunodeficiency virus (HIV) or acquired immunodeficiency syndrome
(AIDS) in which it called upon:
‘all states to ensure that their laws, policies and practices introduced in the context
of AIDS respect human rights standards’.
31. At a Summit of Heads of Government or Representatives of forty-two states meeting
in Paris on 1 December 1994, a Declaration was adopted in which the participating states
solemnly declared their obligation:
‘to act with compassion for and in solidarity with those with HIV or at risk of becoming
infected, both within [their] societies and internationally’.
2. Extract of the WHO Report on ‘Health Conditions in the Americas’, 1994,
Volume II, concerning St. Kitts and Nevis
32. ‘Health and Living Conditions
‘...there are a number of serious environmental problems, such as inadequate disposal of
solid and liquid waste – especially untreated sewage – into coastal lands and waters,
260 The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK
resulting in coastal zone degradation, fish depletion and health problems (gastro-
enteritis)...’
33. According to this publication, there are two general hospitals in St. Kitts, one with
174 beds and the other with 38. There is also a ‘cottage’ hospital with 10 beds. There are
two homes providing geriatric care.
3. ‘Treatment issues – a basic guide to medical treatment options for people with
HIV and AIDS’ produced in April 1996 by the Terrence Higgins Trust
34. This guide describes the three medical strategies available for treating HIV and AIDS:
using anti-HIV drugs which attack HIV itself to delay or prevent damage to the immune
system, treating or preventing opportunistic infections which take advantage of damage
to the immune system and strengthening and restoring the immune system. Amongst the
first category, several drugs can be used, including AZT (also known as zidovudine or its
tradename retrovir). This belongs to a family of drugs called nucleoside analogues which
inhibit an enzyme produced by HIV called reverse transcriptase (RT). If RT is inhibited,
HIV cannot infect new cells and the build up of virus in the body is slowed down.
However, the existing drugs are only partially effective and at best can only delay the
worsening of HIV-related disease rather than prevent it.
35. As regards the second category, persons whose immune systems have been
significantly damaged are vulnerable to a range of infections and tumours known as
opportunistic infections. These commonly include cytomegalovirus (herpes virus),
kaposi’s sarcoma, anaemia, tuberculosis, toxiplasmosis and PCP. PCP is a form of
pneumonia which in people with HIV may affect the lymph nodes, bone marrow, spleen
and liver as well as the lungs. Steps to avoid such infections include taking care with food
and drink and prophylactic treatment by drugs. In the case of PCP which was a common
cause of death during the first years of the epidemic and is still one of the commonest
AIDS illnesses, options include the long-term taking of antibiotics such as co-trimoxazole
and the use of nebulised pentamidine which is intended to protect the lungs.
36. In relation to the third category, treatment which strengthens or restores the immune
system, research has yet to produce any clear results.

The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK 261
Proceeding before the Commission
37. The applicant lodged his application (no. 30240/96) with the Commission on 15
February 1996. He alleged that his proposed removal to St. Kitts would be in violation of
articles 2, 3 and 8 of the Convention and that he had been denied an effective remedy to
challenge the removal order in breach of article 13.
The Commission declared the application admissible on 26 June 1996. In its report
of 15 October 1996 (article 31), it expressed the opinion that article 3 would be violated
if the applicant were to be removed to St. Kitts (11 votes to 7); that it was unnecessary to
examine the complaint under article 2 (unanimously); that no separate issue arose under
article 8 (unanimously); and that there had been no violation of article 13 (13 votes to
5). The full text of the Commission’s opinion and of the two separate opinions contained
in the report are reproduced as an annexe to this judgment 3.
Final submissions to the Court
38. In their memorial and at the oral hearing the Government requested the Court to
decide and declare that the facts disclose no breach of the applicant’s rights under articles
2, 3, 8 or 13 of the Convention.
The applicant requested the Court in his memorial and at the oral hearing to find
that his proposed removal from the United Kingdom would, if implemented, constitute a
breach of articles 2, 3 and 8 of the Convention and that he had no effective remedy in
respect of those complaints in breach of article 13.
As to the law
I. Alleged violation of article 3 of the Convention
39. The applicant maintained that his removal to St. Kitts would expose him to inhuman
and degrading treatment in breach of article 3 of the Convention, which provides:
‘No one shall be subjected to torture or to inhuman or degrading treatment
or punishment.’
3 Note by the Registrar. For practical reasons this annexe will appear only with the printed version of thejudgment (in Reports of Judgments and Decisions - 1997), but a copy of the Commission’s report is obtainablefrom the registry.
262 The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK
A. Arguments of those appearing before the Court
The applicant
40. The applicant maintained that his removal to St. Kitts would condemn him to spend
his remaining days in pain and suffering in conditions of isolation, squalor and
destitution. He had no close relatives or friends in St. Kitts to attend to him as he
approached death. He had no accommodation, no financial resources and no access to
any means of social support. It was an established fact that the withdrawal of his current
medical treatment would hasten his death on account of the unavailability of similar
treatment in St. Kitts. His already weakened immune system would not be able to resist
the many opportunistic infections to which he would be exposed on account of his
homelessness, lack of proper diet and the poor sanitation on the island. The hospital
facilities were extremely limited and certainly not capable of arresting the development of
infections provoked by the harsh physical environment in which he would be obliged to
fend for himself. His death would thus not only be further accelerated, it would also come
about in conditions which would be inhuman and degrading.
41. In June 1996, his life expectancy was stated to be in the region of eight to twelve
months even if he continued to receive treatment in the United Kingdom. His health
had declined since then. As he was now clearly weak and close to death, his removal by
the respondent state at this late stage would certainly exacerbate his fate.
The Government
42. The Government requested the Court to find that the applicant had no valid claim
under article 3 in the circumstances of the case since he would not be exposed in the
receiving country to any form of treatment which breached the standards of article 3. His
hardship and reduced life expectancy would stem from his terminal and incurable illness
coupled with the deficiencies in the health and social welfare system of a poor,
developing country. He would find himself in the same situation as other AIDS victims in
St. Kitts. In fact he would have been returned in January 1993 to St. Kitts, where he had
spent most of his life, had it not been for his prosecution and conviction.
43. The Government also disputed the applicant’s claim that he would be left alone and
without access to treatment for his condition. They maintained that he had at least one
cousin living in St. Kitts and that there were hospitals caring for AIDS patients,
The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK 263
including those suffering from opportunistic infections (see § 17 above). Even if the
treatment and medication fell short of that currently administered to the applicant in the
United Kingdom, this in itself did not amount to a breach of article 3 standards.
44. Before the Court the Government observed that it was their policy not to remove a
person who was unfit to travel. They gave an undertaking to the Court not to remove the
applicant unless, in the light of an assessment of his medical condition after the Court
gives judgment, he is fit to travel.
The Commission
45. The Commission concluded that the removal of the applicant to St. Kitts would
engage the responsibility of the respondent state under article 3 even though the risk of
being subjected to inhuman and degrading treatment stemmed from factors for which the
authorities in that country could not be held responsible. The risk was substantiated and
real. If returned, he would be deprived of his current medical treatment and his already
weakened immune system would be exposed to untreatable opportunistic infections
which would reduce further his limited life expectancy and cause him severe pain and
mental suffering. He would be homeless and without any form of moral, social or family
support in the final stages of his deadly illness.
B. The Court’s assessment
46. The Court recalls at the outset that contracting states have the right, as a matter of
well-established international law and subject to their treaty obligations including the
Convention, to control the entry, residence and expulsion of aliens. It also notes the
gravity of the offence which was committed by the applicant and is acutely aware of the
problems confronting contracting states in their efforts to combat the harm caused to
their societies through the supply of drugs from abroad. The administration of severe
sanctions to persons involved in drug trafficking, including expulsion of alien drug
couriers like the applicant, is a justified response to this scourge.
47. However in exercising their right to expel such aliens contracting states must have
regard to article 3 of the Convention which enshrines one of the fundamental values of
democratic societies. It is precisely for this reason that the Court has repeatedly stressed
in its line of authorities involving extradition, expulsion or deportation of individuals to
third countries that article 3 prohibits in absolute terms torture or inhuman or degrading
264 The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK
treatment or punishment and that its guarantees apply irrespective of the reprehensible
nature of the conduct of the person in question (see, most recently, the Ahmed v. Austria
judgment of 17 December 1996, § 38; and the Chahal v. the United Kingdom judgment
of 15 November 1996, §§ 73-74).
48. The Court observes that the above principle is applicable to the applicant’s removal
under the Immigration Act 1971. Regardless of whether or not he ever entered the
United Kingdom in the technical sense (see § 25 above) it is to be noted that he has
been physically present there and thus within the jurisdiction of the respondent state
within the meaning of article 1 of the Convention since 21 January 1993. It is for the
respondent state therefore to secure to the applicant the rights guaranteed under article 3
irrespective of the gravity of the offence which he committed.
49. It is true that this principle has so far been applied by the Court in contexts in which
the risk to the individual of being subjected to any of the proscribed forms of treatment
emanates from intentionally inflicted acts of the public authorities in the receiving
country or from those of non-state bodies in that country when the authorities there are
unable to afford him appropriate protection (see, for example, the Ahmed v. Austria
judgment, § 44).
Aside from these situations and given the fundamental importance of article 3 in the
Convention system, the Court must reserve to itself sufficient flexibility to address the
application of that article in other contexts which might arise. It is not therefore
prevented from scrutinising an applicant’s claim under article 3 where the source of the
risk of proscribed treatment in the receiving country stems from factors which cannot
engage either directly or indirectly the responsibility of the public authorities of that
country, or which, taken alone, do not in themselves infringe the standards of that article.
To limit the application of article 3 in this manner would be to undermine the absolute
character of its protection. In any such contexts, however, the Court must subject all the
circumstances surrounding the case to a rigorous scrutiny, especially the applicant’s
personal situation in the expelling state.
50. Against this background the Court will determine whether there is a real risk that the
applicant’s removal would be contrary to the standards of article 3 in view of his present
medical condition. In so doing the Court will assess the risk in the light of the material
The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK 265
before it at the time of its consideration of the case, including the most recent information
on his state of health (see the Ahmed v. Austria judgment, § 43).
51. The Court notes that the applicant is in the advanced stages of a terminal and
incurable illness. At the date of the hearing, it was observed that there had been a
marked decline in his condition and he had to be transferred to a hospital. His condition
was giving rise to concern (see § 21 above). The limited quality of life he now enjoys
results from the availability of sophisticated treatment and medication in the United
Kingdom and the care and kindness administered by a charitable organisation. He has
been counselled on how to approach death and has formed bonds with his carers (see
§ 19 above).
52. The abrupt withdrawal of these facilities will entail the most dramatic consequences
for him. It is not disputed that his removal will hasten his death. There is a serious danger
that the conditions of adversity which await him in St. Kitts will further reduce his
already limited life expectancy and subject him to acute mental and physical suffering.
Any medical treatment which he might hope to receive there could not contend with the
infections which he may possibly contract on account of his lack of shelter and of a
proper diet as well as exposure to the health and sanitation problems which beset the
population of St. Kitts (see § 32 above). While he may have a cousin in St. Kitts (see §
18 above) no evidence has been adduced to show whether this person would be willing to
or capable of attending to the needs of a terminally ill man. There is no evidence of any
other form of moral or social support. Nor has it been shown whether the applicant would
be guaranteed a bed in either of the hospitals on the island which, according to the
Government, care for AIDS patients (see § 17 above).
53. In view of these exceptional circumstances and bearing in mind the critical stage now
reached in the applicant’s fatal illness, the implementation of the decision to remove him
to St. Kitts would amount to inhuman treatment by the respondent state in violation of
article 3.
The Court also notes in this respect that the respondent state has assumed
responsibility for treating the applicant’s condition since August 1994. He has become
reliant on the medical and palliative care which he is at present receiving and is no doubt
psychologically prepared for death in an environment which is both familiar and

266 The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK
compassionate. Although it cannot be said that the conditions which would confront
him in the receiving country are themselves a breach of the standards of article 3, his
removal would expose him to a real risk of dying under most distressing circumstances
and would thus amount to inhuman treatment.
Without calling into question the good faith of the undertaking given to the Court
by the Government (see § 44 above), it is to be noted that the above considerations must
be seen as wider in scope than the question whether or not the applicant is fit to travel
back to St. Kitts.
54. Against this background the Court emphasises that aliens who have served their
prison sentences and are subject to expulsion cannot in principle claim any entitlement
to remain on the territory of a Contracting state in order to continue to benefit from
medical, social or other forms of assistance provided by the expelling state during their
stay in prison.
However, in the very exceptional circumstances of this case and given the
compelling humanitarian considerations at stake, it must be concluded that the
implementation of the decision to remove the applicant would be a violation of article 3.
II. Alleged violation of article 2 of the Convention
55. The applicant further maintained that the implementation by the United Kingdom
authorities of the decision to remove him to St. Kitts would be in breach of article 2 of
the Convention, which provides:
‘1. Everyone’s right to life shall be protected by law. No one shall be deprived of his life
intentionally save in the execution of a sentence of a court following his conviction of a
crime for which this penalty is provided by law.
2. Deprivation of life shall not be regarded as inflicted in contravention of this article
when it results from the use of force which is no more than absolutely necessary.
(a) in defence of any person from unlawful violence;
(b) in order to effect a lawful arrest or to prevent the escape of a person
lawfully detained;
(c) in action lawfully taken for the purpose of quelling a riot or insurrection.’
The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK 267
56. The applicant contended that his removal to St. Kitts would engage the responsibility
of the respondent state under article 2. He is terminally ill, and the medical evidence
submitted to the Court (see §§ 14 and 15 and 20 and 21 above) confirmed that his
already reduced life expectancy would be further shortened if he were to be suddenly
deprived of his current medical treatment and sent back to St. Kitts. There would, he
argued, be a direct causal link between his expulsion and his accelerated death such as to
give rise to a violation of the right to life. He submitted that article 2 denoted a positive
obligation to safeguard life which in the circumstances at issue required the Government
not to take a measure which would further reduce his limited life expectancy.
57. The Government did not dispute the fact that the removal of the applicant to St.
Kitts and the consequential loss of the current medical treatment would hasten his death.
However the threat to his life expectancy stemmed not from factors for which the
Government could be held responsible but from his own fatal illness in conjunction
with the lack of adequate medical treatment in the receiving country. Article 2 was
therefore not applicable to the circumstances at issue. In any event the substance of
the applicant’s complaints could not be separated from the arguments he advanced in
furtherance of his allegation under article 3 and for that reason were best dealt with
under the latter provision.
58. The Commission did not find it necessary to decide whether the risk to the
applicant’s life expectancy created by his removal disclosed a breach of article 2. It
considered that it would be more appropriate to deal globally with this allegation when
examining his related complaints under article 3.
59. The Court for its part shares the views of the Government and the Commission that
the complaints raised by the applicant under article 2 are indissociable from the substance
of his complaint under article 3 in respect of the consequences of the impugned decision
for his life, health and welfare. It notes in this respect that the applicant stated before the
Court that he was content to base his case under article 3.
Having regard to its finding that the removal of the applicant to St. Kitts would give rise
to a violation of article 3 (see § 54 above), the Court considers that it is not necessary to
examine his complaint under article 2.
268 The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK
III. Alleged violation of article 8 of the Convention
60. The applicant also alleged that his proposed removal to St. Kitts would violate his
right to respect for his private life, as guaranteed by article 8 of the Convention.
Article 8 provides:
‘1. Everyone has the right to respect for his private and family life, his home and his
correspondence.
2. There shall be no interference by a public authority with the exercise of this right
except such as is in accordance with the law and is necessary in a democratic society in
the interests of national security, public safety or the economic well-being of the
country, for the prevention of disorder or crime, for the protection of health or morals,
or for the protection of the rights and freedoms of others.’
61. In support of this argument the applicant maintained that his removal would amount
to a disproportionate interference with his right to respect for his private life, and in
particular his right to respect for his physical integrity. While readily accepting that the
offence he had committed was a very serious one, he requested the Court to consider the
impact which his removal to St. Kitts would entail for him, a terminally ill person with
no family or close relatives in the receiving country, no moral or social support and no
adequate medical treatment to stave off infection to his already weakened immune
system. His continued presence in the United Kingdom could not be considered a burden
on the domestic health resources and, furthermore, there were no indications that he
would re-offend.
62. The Government maintained that the applicant could not rely on article 8 to
challenge the impact of the impugned decision on his right to private life since his private
life was constituted in the receiving country where he had lived most of his life. Any links
which the applicant had with the United Kingdom were the direct result of the offence for
which he had been sentenced. Even if article 8 were to be regarded as applicable, the
interference with his medical interests by removing him to St. Kitts was justified, given the
seriousness of the offence he had committed, for reasons of the prevention of crime and in
the interests of the economic well-being of the United Kingdom.
63. Although the Commission found that no separate issue arose under article 8 in view of
its findings under article 3, the Delegate invited the Court to find a violation of article 8
The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK 269
in the event of a conclusion that the applicant’s removal to St. Kitts would not violate
article 3.
64. Having regard to its finding under article 3 (see § 54 above), the Court concludes
that the applicant’s complaints under article 8 raise no separate issue.
IV. Alleged violation of article 13 of the Convention
65. The applicant complained that he had no effective remedy in English law in respect
of his complaints under articles 2, 3 and 8 of the Convention. He contended that this
gave rise to a breach of article 13 of the Convention, which provides:
‘Everyone whose rights and freedoms as set forth in [the] Convention are violated
shall have an effective remedy before a national authority notwithstanding that the
violation has been committed by persons acting in an official capacity.’
66. The applicant pointed to the limitations which circumscribed an effective review by
courts in the United Kingdom of the decisions reached by the authorities in expulsion
cases. When reviewing the legality of administrative decisions the courts did not treat the
Convention and the principles developed by the Court as a relevant consideration; nor
was the decision-maker obliged to take account of the Convention and the case-law of
the Convention institutions when exercising the powers conferred by legislation such as
the Immigration Act 1971. Admittedly the domestic courts will review decisions with
greater rigour when they have an impact on human rights, but even in such cases they do
not take a Convention-based approach. Thus, in the case at issue, the Court of Appeal
did not seek to satisfy itself whether the removal of the applicant would expose him to
inhuman and degrading treatment but merely examined whether the decision-maker had
taken this factor into account. This, he maintained, fell short of the test of ‘independent
scrutiny’ of a claim that there exist substantial grounds for fearing a real risk of treatment
proscribed by article 3 which the Court in its Chahal v. the United Kingdom judgment
(loc. cit., paragraph 151) had considered to be a crucial aspect of an effective remedy.
Furthermore the Court of Appeal had regarded the seriousness of the applicant’s offence
as a paramount consideration in deciding that the impugned decision was not an
irrational one and had failed also to take adequate account of the Convention’s
requirements when dealing with his complaints under articles 2 and 8. For these reasons
it could not be said that the judicial review proceedings afforded him an effective remedy
within the meaning of article 13.
270 The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK
67. The Government disputed this argument and invited the Court to confirm the
conclusion which it had reached in certain earlier judgments that judicial review
proceedings afforded an effective remedy to challenge the legality of a decision to expel or
deport an individual. The courts in the United Kingdom applied a ‘most anxious scrutiny’
test when reviewing administrative decisions which affect the fundamental rights of
individuals. The Court of Appeal applied such a test in this case when assessing the
merits of the decision to remove the applicant and took due account of the hardship
which the implementation of the decision would cause the applicant. The applicant
cannot therefore argue that he was denied an effective remedy.
68. The Commission agreed with the Government. The Court of Appeal examined the
substance of the applicant’s complaint, including the hardship which would result from his
removal. Although the Court of Appeal did not quash the decision to remove him it had
the power to do so. The remedy afforded by judicial review was therefore an effective one.
69. The Court observes that article 13 of the Convention guarantees the availability at
national level of a remedy to enforce the substance of the Convention rights and
freedoms in whatever form they might happen to be secured in the domestic legal order.
The effect of this article is thus to require the provision of a domestic remedy allowing
the competent national authority both to deal with the substance of the relevant
Convention complaint and to grant appropriate relief, although contracting states are
afforded some discretion as to the manner in which they conform to their obligations
under this provision (see, among other authorities, the Soering v. the United Kingdom
judgment of 7 July 1989, Series A no. 161, p. 47, paragraph 120; the Vilvarajah and
Others v. the United Kingdom judgment of 30 October 1991, Series A no. 215, p. 39
paragraph 122).
70. In its Vilvarajah and Others judgment (loc. cit., p. 39, paragraph 123) and its Soering
judgment (loc. cit., pp. 47-48, paragraphs 121-124) the Court considered judicial review
proceedings to be an effective remedy in relation to the complaints raised under article 3
in the contexts of deportation and extradition. It was satisfied that English courts could
effectively control the legality of executive discretion on substantive and procedural
grounds and quash decisions as appropriate. It was also accepted that a court in the
exercise of its powers of judicial review would have power to quash a decision to expel or

The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK 271
deport an individual to a country where it was established that there was a serious risk of
inhuman or degrading treatment, on the grounds that in all the circumstances of the case
the decision was one that no reasonable secretary of state could take.
71. While it is true that the source of the risk of the prohibited treatment to which the
applicant will be exposed and the impugned measure are different from those in the
above cases there is no reason to depart from the conclusion reached in those cases in
respect of the effectiveness of judicial review proceedings for the purposes of article 13.
Indeed the Court of Appeal had regard to domestic case-law which required it to submit
the applicant’s plight to the most anxious scrutiny on account of the established risk to
his life expectancy. It did so against the background of the criteria which need to be
satisfied before an administrative decision can be challenged on the grounds of its
irrationality. The substance of the applicant’s complaint was therefore examined by the
Court of Appeal. That court had the power to afford him the relief he sought. The fact
that it did not do so is not a material consideration since the effectiveness of a remedy for
the purposes of article 13 does not depend on the certainty of a favourable outcome for an
applicant (see the Vilvarajah and Others judgment, loc. cit., p. 39, paragraph 122).
72. The applicant maintained that the effectiveness of the remedy invoked first before the
High Court and subsequently before the Court of Appeal was undermined on account of
their failure to conduct an independent scrutiny of the facts in order to determine whether
they disclosed a real risk that he would be exposed to inhuman and degrading treatment.
He relied on the reasoning in the Chahal v. the United Kingdom judgment (paragraph
151). However the Court notes that in that case the domestic courts were precluded from
reviewing the factual basis underlying the national security considerations invoked by the
Home Secretary to justify the expulsion of Mr Chahal. No such considerations arise in the
case at issue.
73. The applicant thus had available to him an effective remedy in relation to his
complaints under articles 2, 3 and 8 of the Convention. Accordingly there has been no
breach of article 13.
272 The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK
V. Application of article 50 of the Convention
74. Article 50 of the Convention provides:
‘If the Court finds that a decision or a measure taken by a legal authority or
any other authority of a High Contracting Party is completely or partially in
conflict with the obligations arising from the ... Convention, and if the internal
law of the said Party allows only partial reparation to be made for the
consequences of this decision or measure, the decision of the Court shall, if
necessary, afford just satisfaction to the injured party.’
A. Costs and expenses
75. The applicant did not seek damages. He claimed reimbursement of £49,443 and
FF13,811 incurred by way of costs and expenses in respect of the proceedings brought
before the Convention institutions.
76. The Government requested the Court to reduce the amount, mainly because the time
billed in respect of the preparation of certain parts of the case was excessive and the
number of lawyers engaged to work on the case unreasonable. They proposed the sum of
£29,313.16 and FF9,194.
77. The applicant defended the amount claimed on account of inter alia the complexity
of the issues involved and the speed with which the case had been treated by both the
Commission and the Court.
78. Making an assessment on an equitable basis, the Court awards the applicant £35,000
plus any VAT that may be chargeable under this head, less the FF33,216 already paid in
legal aid by the Council of Europe.
B. Default interest
79. According to the information available to the Court, the statutory rate of interest
applicable in the United Kingdom at the date of adoption of the present judgment is 8%
per annum.
For these reasons, the Court unanimously
1. Holds that the implementation of the decision to remove the applicant to St. Kitts
would violate article 3 of the Convention;

The free movement of persons living with HIV/AIDS – Annexe II (2): European states, Case law, D. v. UK 273
2. Holds that having regard to its conclusion under article 3 it is not necessary to
examine the applicant’s complaint under article 2 of the Convention;
3. Holds that the applicant’s complaint under article 8 of the Convention gives rise to
no separate issue;
4. Holds that there has been no violation of article 13 of the Convention;
5. Holds
(a) that the respondent state is to pay the applicant, within three months, £35,000
(thirty-five thousand pounds sterling) in respect of costs and expenses less FF33,216
(thirty three thousand two hundred and sixteen francs) to be converted into pounds
sterling at the rate applicable at the date of delivery of the present judgment;
(b) that simple interest at an annual rate of 8% shall be payable from the expiry of
the above-mentioned three months until settlement.
Done in English and in French, and delivered at a public hearing in the Human Rights
Building, Strasbourg, on 2 May 1997.
For the President,
Jan De Meyer, Judge
For the Registrar,
Michael O’Boyle,
Head of Division in the registry of the Court
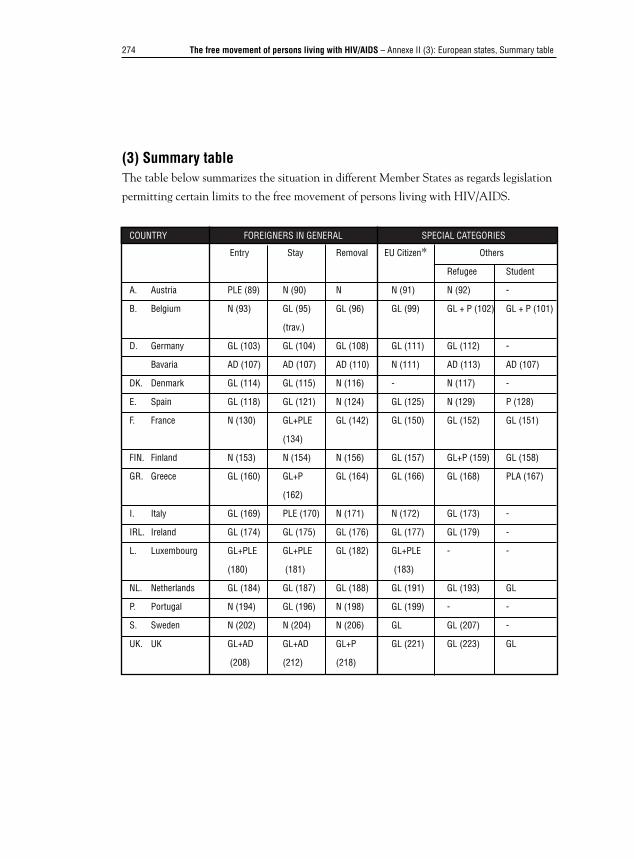
274 The free movement of persons living with HIV/AIDS – Annexe II (3): European states, Summary table
(3) Summary tableThe table below summarizes the situation in different Member States as regards legislation
permitting certain limits to the free movement of persons living with HIV/AIDS.
COUNTRY FOREIGNERS IN GENERAL SPECIAL CATEGORIES
Entry Stay Removal EU Citizen* Others
Refugee Student
A. Austria PLE (89) N (90) N N (91) N (92) -
B. Belgium N (93) GL (95) GL (96) GL (99) GL + P (102) GL + P (101)
(trav.)
D. Germany GL (103) GL (104) GL (108) GL (111) GL (112) -
Bavaria AD (107) AD (107) AD (110) N (111) AD (113) AD (107)
DK. Denmark GL (114) GL (115) N (116) - N (117) -
E. Spain GL (118) GL (121) N (124) GL (125) N (129) P (128)
F. France N (130) GL+PLE GL (142) GL (150) GL (152) GL (151)
(134)
FIN. Finland N (153) N (154) N (156) GL (157) GL+P (159) GL (158)
GR. Greece GL (160) GL+P GL (164) GL (166) GL (168) PLA (167)
(162)
I. Italy GL (169) PLE (170) N (171) N (172) GL (173) -
IRL. Ireland GL (174) GL (175) GL (176) GL (177) GL (179) -
L. Luxembourg GL+PLE GL+PLE GL (182) GL+PLE - -
(180) (181) (183)
NL. Netherlands GL (184) GL (187) GL (188) GL (191) GL (193) GL
P. Portugal N (194) GL (196) N (198) GL (199) - -
S. Sweden N (202) N (204) N (206) GL GL (207) -
UK. UK GL+AD GL+AD GL+P GL (221) GL (223) GL
(208) (212) (218)
The free movement of persons living with HIV/AIDS – Annexe II (3): European states, Summary table 275
Key
AD Administrative decision imposing HIV screening
GL General legislation permitting certain restrictions on public health grounds,
without specifically targeting HIV.
PLA Particular legislation authorizing HIV screening
PLE Particular legislation excluding HIV screening
N Nihil
P HIV screening practised
( ) The figures in parentheses refer to the paragraph numbers in the text.
* All national legislation makes reference, in respect of Union citizens, to European
law. Reference should therefore be made to the interpretation of Directive 64/221
(§§ 35 seq.).
276 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
Annexe III. Third countriesIn order to facilitate research, the reference numbers are the same as those in the text.
(1) National texts
A. Africa1. South Africa■ Law of 1991 on foreigners (entered into force on 1st October)
article 39 (2)
The persons referred to in sub-section 1 (prohibited persons) shall be the following, namely -
(a) any person who is likely to become a public charge by reason of infirmity of mind or
body (…)
(f) any person who is afflicted with any such contagious, communicable or other disease, or
who is a carrier of such a virus, as may be prescribed;
■ Governmental opinion no. R 2247 of 13 September 1991
The diseases and viruses specified under article 39 (f) are deemed to be the following:
a) cholera;
b) plague;
c) yellow fever.
2. Angola■ Law no 3/94 of 1994 on the legal status of Aliens (entered into force on
21st January)
Article 46
The residence authorization granted to foreigners is cancelled for ever as soon as (…) public
policy or national security are harmed.
Article 51
Notwithstanding international agreements and conventions to which the Republic of Angola
is party, foreigners who harm national security or public policy as expelled from the territory
(…)
The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 277
3. Botswana■ Immigration Act of 1996 (entered into force on 30th September)
Article 7
Subject to this Act, the following persons shall be prohibited immigrants and their entry into
or presence within Botswana is unlawful:
a) any person who, if he entered or remained in Botswana, would be likely to become a
public charge by reason of infirmity of mind or body (…) ;
b) any person who is infected or afflicted with or suffering from a prescribed disease unless
he has the written authority of an immigration officer to enter and remain in Botswana (…)
4. Burkina Faso■ Law no. 23/94/ADP promulgating the Code of Public Health
Article 123
The international health regulations will be applied to every aircraft and every person in an
‘international travel’ situation. (…) All the provisions of these regulations will apply in
particular with regard to the so-called quarantinable diseases: plague, cholera, yellow fever.
Article 124
Subject to possible subsequent modifications, the vaccination required upon arrival in
Burkina Faso, on a permanent basis, is vaccination against yellow fever for travellers aged
at least nine months with the exception of travellers from non-infected countries spending
less than fifteen days in the country. Vaccination must be certified by presentation of an
international vaccination certificate which is valid according to the definitions of the
international health regulations.
5. Burundi■ Decree-Law no 1/23 of 9 July 1982 regulating the access, stay, establishment and
removal of foreigners to, in and from Burundi
Article 2
In order to be authorized to enter the Republic of Burundi, the foreigner must fulfil the
following conditions:
(2) hold a medical certificate no more than three months old issued by a medical
practitioner, certifying that the holder is free of any contagious disease.
Article 4
Except for exceptions provided by an international treaty or by the law, access to the
278 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
territory is barred to any foreigner attempting to enter Burundi without carrying the required
documents or where the foreigner is in one of the following situations
(6) if he is afflicted by contagious diseases.
■ Decree-Law no. 1/007 of 20 March 1989 regulating the access, stay,
establishment and removal of foreigners to, in and from Burundi
Article 7
Subject to the provisions of chapter II of the present decree-law, access to Burundi is barred
in particular to foreigners who:
(4) are not in full possession of their mental faculties or who are afflicted by a contagious or
transmittable disease.
7. Ethiopia■ Proclamation no 271 of 1969 regulating the issuance of travel documents and visas,
and registration of foreigners in Ethiopia (entered into force on 22nd August)
Article 6
(1) No foreigner shall enter Ethiopia unless he is in possession of:
(c) a valid international health certificate demonstrating that he has received such
immunizations as our Minister of Public Health may from time to time prescribe.
9. Gambia■ Immigration Act Cap 16.02 of 1990
Article 13b
The following persons, not being citizens of Gambia, shall be prohibited immigrants […]:
any person suffering from any communicable disease that may be prescribed as such by the
Minister for the purposes of this Act.
10. Equatorial Guinea■ Law L/94/019/CTRN setting out the conditions for the entry and stay of
foreigners in the Republic of Guinea
Article 14
Any foreigner entering the Republic of Guinea is required to present, upon arrival, a valid
international health carnet which is recognized by international conventions or by the laws
and regulations in effect.
The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 279
Article 38
In order to obtain the residence card or the alien’s carnet every applicant must send the
department in charge of security an application setting out the reasons for his application.
This application must be accompanied by a medical certificate delivered by an approved
medical practitioner, an extract of legal record, both under three months’ old (…).
11. Kenya■ Immigration Act of 1967 (entered into force on 1st December)
Article 3
(1) In this Act, a prohibited immigrant means a person who is not a citizen of Kenya and
who is
(c) a person who
(i) refuses to submit to examination by a medical practitioner after being required to do so
under section 11 (1) (d) of this Act; or
(ii) is certified by a medical practitioner to be suffering from a disease which makes his
presence in Kenya undesirable for medical reasons.
12. Lesotho■ Aliens Act of 1968 (entered into force on 1st March)
Article 13
(…) an authorized officer may, if he considers it necessary, require such an alien entering
or landing, to produce a medical certificate showing him to be free from any disease or
affliction.
Annexe 1
(…) An alien shall not be permitted or allowed under any provision of this Act to enter,
land in, or sojourn in Lesotho, unless -
(2) he will be able to subsist without becoming a public charge by reason of infirmity of
mind or body (…)
(3) his actions will benefit, and will not adversely affect -
(iv) the interests of defence, public safety, public policy, public health (…)

280 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
13. Madagascar■ Law no. 62-006 of 1992 establishing the organization and control of immigration
(entered into force on 16th June)
Article 13
A foreigner who has been allowed to stay temporarily in the country may be expelled when
his presence in the territory constitutes a threat to the maintenance of public policy, to the
protecting of health (…)
■ Decree no. 94-652 of 1994 abrogating decree no. 66-101 of 2 March 1996 and
establishing new rules for the application of law no. 62-002 of 16 June 1962
establishing the organization and control of immigration (entered into force on
7th November)
Article 22
Applications for residence permits must be submitted by applicants of both sexes aged 21 or over
with the administrative authority of their place of residence and contain the following items:
(d) a medical certificate issued under conditions to be set by the Minister of Public Health
14. Malawi■ 1964 Immigration Act
Section 4
(1) Subject to this Act, the following persons shall be prohibited immigrants and their entry
into or presence within Malawi shall be unlawful
(c) any person who at the time of his entry is to become a public charge by reason of
infirmity of mind or body (…)
(e) any person who is infected, afflicted with or suffering from a prescribed disease, unless
he is in possession of a permit issued by the Minister (…)
■ 1968 Immigration Regulation, Part III
Prescribed diseases
The following diseases shall be the diseases prescribed for the purposes of section 4 (1) (e) of
the Act
a) tuberculosis;
b) trachoma;
c) favus;
d) framboesia or yaws;
The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 281
e) syphilis or gonorrhoea;
f) scabies; and
g) leprosy.
16. Namibia■ Immigration Control Act of 1994 (entered into force on 29th July)
Article 39
(2) A person referred to in subsection (1) shall be a prohibited immigrant in respect of
Namibia, if
(c) such a person is likely to become a public charge by reason of infirmity of mind or body
(…)
(e) such a person is infected or afflicted with a contagious disease or is a carrier of such a
virus or disease, as may be prescribed
17. Nigeria■ Immigration Act of 1963 (entered into force on 1st August)
Article 49
49. Special cases where entry may be refused
(d) on the advise of a medical inspector it is undesirable for medical reasons to admit
such a person.
18. Oman■ Ministerial resolution no. 1 of 19 January 1990 on the the national programme
for the prevention of acquired immuno-deficiency syndrome (AIDS)
Article 4
Foreigners resident in the country and afflicted by confirmed AIDS must be expelled
to their countries in order to undergo medical treatment there with the assistance of the
specialist authorities.
19. Uganda■ Statutory Instrument no. 29 of 1984
Section 19
No person shall be granted a Certificate of Residence unless he (…) has undergone a
medical examination to certify his mental and physical condition and obtained a certificate to
the effect that he is a normal and healthy person.

282 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
Section 8(1)
Prohibited Immigrants: (…)
(c) any person who
(i) refuses to submit to a medical examination after having been required so to do under the
provisions of Section 5 of the Immigration Act;
(ii) is certified by a medical practitioner appointed for the purpose by the Minister, to be
suffering from a contagious or infectious disease which makes his presence in Uganda
dangerous to the community.
20. Rwanda■ Law of 1963 concerning the immigration police and the conditions of entry and
stay (entered into force on 15th October)
Article 13
Any person, not being able to plead Rwandan citizenship and being in one of the situations
listed below, is considered as undesirable and may therefore not enter or reside in Rwanda;
(8) who is afflicted by one of the contagious diseases determined by ministerial decree.
21. Senegal■ Decree no 71-860 of 28 July 1971 concerning the conditions for the admission,
residence and establishment of foreigners
Article 1
In order to be allowed to enter Senegalese territory, every foreigner must present (…)
(c) the international vaccination certificates required by the health regulations.
22. Seychelles■ Immigration Decree of 1981, Chapter 93 (entered into force on 1st June)
Article 19
The following persons, not being citizens of Seychelles, are prohibited immigrants -
(a) any person who is infected or inflicted with or is a carrier of a prescribed disease and
who is capable or likely to become capable of infecting any other person with such disease or
of transmitting to him such disease.
First schedule
Section 15
5. The under-mentioned documents should be attached to this application (for a residence
The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 283
permit) (…) a medical certificate from a medical practitioner to the effect that he finds you,
your spouse, your children and members of your household who are to reside with you (…)
not suffering from any infectious or contagious diseases.
23. Swaziland■ Immigration Act of 1995 (entered into force on 1st February)
Article 9
(1) Subject to the other provisions of this Act, the following persons are hereby declared to
be prohibited immigrants -
(b) a person who, if he entered Swaziland, would be likely to become or, having entered
Swaziland, has become a public charge by reason of infirmity of mind or body (…)
(d) a person who is infected or afflicted with, or suffering from, a prescribed disease, or who
is not in possession of a prescribed certificate of inoculation or vaccination against a
prescribed disease and is not able to show sufficient evidence of protection against that
disease by reason of previous attack of that disease, unless he has the written authority of an
immigration officer to enter and remain in Swaziland (…).
24. Tanzania■ Immigration Act of 1972 (entered into force on 12th May)
Article 6
6. Meaning of ‘prohibited immigrant’ (…)
(c) a person
(i) who refuses to submit to examination by a medical practitioner after having been
required to do so under the provisions of paragraph (c) of subsection (1) or section 5;
(ii) who is certified by a medical practitioner to be suffering from a contagious or infectious
disease which makes or which would make his presence in Tanzania dangerous to the public.
25. Tunisia■ Law no 68-7 of 8 March 1968 concerning the situation of foreigners in Tunisia
Article 18
The Secretary of State for the Interior may issue an expulsion order for any foreigner whose
presence on Tunisian territory constitutes a threat to public policy.
284 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
26. Zambia■ Immigration and Deportation Act of 1967 (entered into force on 21st February)
Article 22
Prohibited immigrants
(1) any person who belongs to a class set out in the Second Schedule shall be a prohibited
immigrant in relation to Zambia.
Schedule 2
Classes of prohibited immigrants
Class A. Persons capable of transmitting a prescribed disease
Any person who is infected or inflicted with or is a carrier of a prescribed disease and who is
capable or likely to become capable of infecting any other person with such disease or of
transmitting to him such disease.
27. Zimbabwe■ 1979 Immigration Act
Article 14
(1) Subject to the provisions of this Act, the following persons are prohibited persons -
(c) any persons who at the time of his entry into Rhodesia is likely to become a public charge
by reason of infirmity of mind or body (…)
(e) any persons who is infected or afflicted with or suffering from a prescribed disease,
unless he is in possession of a permit to enter and remain in Rhodesia issued upon conditions
fixed in the permit and complies with such conditions.
B. Asia28. Cambodia■ Immigration Law of 1994 (entered into force on 26th August)
Article 11
Those immigrants who have fulfilled the conditions mentioned in article 8 of this law shall be
allowed to stay in the Kingdom of Cambodia, but beside this they shall have to fulfil also the
following conditions:
(c) to have sufficient physical aptitude for performing their own professions, which proved
by medical certificates issued by doctors of the countries from which the persons have
emigrated (…).
The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 285
29. China■ Specific regulations issued by the Minister of Public Health on 6 March 1989 to
implement the law of the People’s Republic of China concerning border health
controls and quarantine
Article 99
The health and quarantine organization must forbid any foreigner afflicted by AIDS, a
sexually transmittable disease, leprosy, psychiatric disturbances or pulmonary tuberculosis
from entering the country.
■ Regulation of 26 December 1987 on surveillance and control measures applicable
to AIDS
Article 5
Any foreigner travelling to China with a view to residing there permanently or staying there
for more than one year (or studying for more than one academic year) must, when applying
for an entry visa, present a certificate, delivered by a public hospital of his country or a
private hospital approved by an approved body in his country, certifying that he has
undergone serological screening for AIDS. This certificate must be approved by a Chinese
diplomatic mission or consulate and is valid for six months from the date of delivery. Where
applicable, foreigners who have not undergone serological AIDS screening in their own
country must, within 20 days of entering China, visit a specified specialist health institution
in order to undergo such testing.
Article 7
Foreigners resident in China may, if they turn out to belong to categories A or B as referred
to in article 2 of the present regulations (AIDS sufferers and persons infected by the AIDS
virus), receive orders from the public security department, based on a proposal by the local
health administration department, to leave the country immediately.
30. India■ The Foreigners Order 1948
Article 3
Leave to enter shall be refused if the civil authority is satisfied that:
(c) he (the foreigner) is suffering from a loathsome or infectious disease in consequence of
which, in the opinion of the Medical Officer of the port or the place of entry, as the case
may be, the entry of the foreigner is likely to prejudice public health.
286 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
31. Indonesia■ Presidential decree of 1994 concerning the national strategy for combating AIDS
in Indonesia
Article 7
Any HIV/AIDS diagnosis test must be preceded by an interview and the obtaining of the
enlightened consent of the party concerned (…)
32. Malaysia■ Immigration Act 959/63 of 1959 (entered into force on 1st May)
Article 8
(3) The following persons are members of the prohibited classes:
(b) any persons (…) suffering from a contagious or infectious disease which makes his
presence in Malaysia dangerous to the community;
(c) any person who refuses to submit to a medical examination after being required to do so
under section 39A(1).
33. Nepal■ Immigration rules, 1994
Article 28
(1) The Department may cancel visas issued to foreigners in the following circumstances:
(a) in the case (any foreigner) does not produce an international health certificate when
demanded (...)
(d) if he suffers from any serious or communicable disease.
34. Pakistan■ Foreigners Order of 1951 (entered into force on 26th October)
Article 3
Leave to enter shall be refused if the civil authority is satisfied that
(b) he is suffering from a loathsome or infectious disease in consequence of which, in the
opinion of the medical officer of the port or the place of entry, as the case may be, his entry
is likely to prejudice the public health.

The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 287
35. Philippines■ Immigration Act of 1940 (entered into force on 26th August)
Article 29
The following categories of aliens shall be excluded from entry into the Philippines:
(2) persons afflicted with a loathsome or dangerous and contagious disease, as epilepsy.
Article 47
Notwithstanding the provisions of this Act, the President is authorized:
(5) to suspend the entry of aliens into the Philippines from any country in which cholera or
another infectious or contagious disease is prevalent.
36. Sri Lanka■ Immigrants and Emigrants Act of 1949 (entered into force on 1st November)
Article 11
(…) no endorsement or visa shall be granted or issued to any person who:
(b) is declared by a prescribed medical officer to be a person whom, for medical reasons,
it is undesirable to admit into Sri Lanka.
Article 31
The Minister may in any of the following cases make an order requiring any person to
whom this Part applies to leave Sri Lanka and to remain thereafter out of Sri Lanka:
(a) where that person is shown, by evidence which the Minister may deem efficient,
to be (…)
(iii) a person whom, for medical reasons, it is undesirable to allow to remain in Sri Lanka.
37. Syria■ Regulatory decree of the Health Minister no. 36/T of 26 October 1987
Under the terms of article 1 of the present decree, the systematic blood testing in order to
detect persons who are seropositive to HIV are limited to the following categories: (…)
b) foreign nationals domiciled in the Syrian Arab Republic for professional purposes, when
they make their first application for a work permit (persons domiciled in the Syrian Arab
Republic and not claiming any particular citizenship are exempted)
c) students coming from abroad to follow a training programme in a university establishment
or a college upon their arrival and at the time of their enrolment in these establishments
d) students studying abroad under bursaries, upon their return to the Syrian Arab Republic
and prior to their re-enrolment in the organization which granted them the study bursary.
288 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
38. Thailand■ Immigration Act of 1979 (entered into force on 31st May)
Article 12
No alien under any of the following descriptions shall be admitted into the Kingdom:
(3) being a person (…) afflicted with any one of the diseases as prescribed by the
Ministerial Regulation.
39. Turkey■ Passport Act of 1950 (entered into force on 24th July)
Article 8
Persons whose entry into Turkey is forbidden:
(2) Persons suffering from mental illness or contagious diseases. Nonetheless exemptions
from the present article may be made for persons whose state does not constitute a danger
for public health and safety, who arrive under their own resources or with the financial
assistance of their tutor or guardian in order to undergo medical or other treatment.
■ Law of 1950 concerning the residence and travelling of foreigners in Turkey
(entered into force on 21st July)
Article 7
Residence permits are not granted to foreigners (…):
(e) who disturb the public policy whilst in Turkey.
40. Vietnam■ Ordinance of 1992 on the exit, entry, residence and travel of foreigners in
Vietnam (entered into force on 1st May)
Article 6
An application for an entry visa or entry-exit visa may be refused in the following cases:
(3) for reasons of (…) preventing and combating epidemic diseases.
Article 14
A foreigner may be expelled from Vietnam if he falls into one of the following categories:
(4) being himself a hazard to the life or health of others in Vietnam.
■ Ordinance of 31 May 1995 on the prevention and control of HIV/AIDS
Article 19
Foreigners infected by HIV/AIDS must declare themselves on entering Vietnam. The
declaration procedure will be stipulated by the government.
The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 289
■ Governmental decree no. 16/CP of 18 December 1992 regulating certain aspects
of the measures of prevention and of the campaigns against the infection by HIV
and against AIDS.
Article 9
Foreign nationals registered as residents in Vietnam for a period longer than three months
must in any event undergo serological testing in order to detect anti-HIV antibodies.
Article 15
Any foreign national who, upon entry into Vietnam, knows himself to be living with AIDS
must declare this. No foreign national infected with HIV or living with AIDS is authorized
to marry a Vietnamese citizen.
C. South and Central America41. Argentina■ Decree 1023/94 of 29 June 1994 approving the immigration regulation
Article 21
Foreigners belonging to one of the following categories are absolutely not eligible to be
admitted to and/or stay in the country in any category of migrants, except for those which
are expressly excepted:
(a) those who are affected by transmittable diseases in such a way as to be presumed to
represent a danger to the health of the community. The presumption of this danger will be
determined by the national health authorities or the authority to which it delegates.
Article 22
Foreigners belonging to one of the following categories are relatively not eligible to be
admitted as permanent or temporary residents:
(a) those having congenital or acquired physical or mental disability, or a chronic disease
which partially reduces their ability to work (…)
Article 39
(…) Foreigners who are granted permission to enter as permanent or temporary residents in
order to obtain the respective visa, must present themselves to the Argentine consular
authority (…)
(e) A certificate delivered by a medical practitioner or a health authority recognized to for
this purpose establishing his physical and mental condition;

290 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
Article 44
Foreigners who are in the national territory and who petition the immigration authority to be
admitted to the country as permanent or temporary residents must present (…)
(d) a medical certificate delivered by the immigration medical authority or another official
health authority giving the foreigner’s physical and mental condition.
42. Bahamas■ Immigration Act of 1967 (entered into force on 2nd November)
Article 19
(1) Subject to the provisions of this Act an Immigration Officer may grant leave to any
person to land and remain in the Colony for such period as he may determine in
accordance with the provisions of subsection (2) of this section, upon being satisfied that
that person:
(e) is not suffering from any contagious or infectious disease which, in the opinion of a
medical practitioner appointed in accordance with the provisions of paragraph (d) or section
6(1) makes his presence in the Colony dangerous to the community.
43. Barbados■ Immigration Act of 1976 (entered into force on 2nd February)
Schedule 1
Prohibited persons
1. Persons suffering from communicable diseases within the meaning of any regulations
relating to such diseases made under the Health Services Act.
44. Belize■ Immigration Ordinance of 1 January 1958
Article 4
Categories of prohibited immigrants (…):
(a) any person who is likely if he entered Belize to become a charge on public funds by
reason of infirmity of body or mind (…).
(b) any person certified by a medical practitioner to be suffering from a communicable
disease which makes his entry into Belize dangerous to the community.
The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 291
45. Bolivia■ Resolution no. 0660 of December 1996 for the prevention and surveillance of
HIV/AIDS in Bolivia
Article 45
It is forbidden to demand serological tests for determining HIV infection as a mandatory
prerequisite in the following circumstances (…)
d) the entry into the country of foreign and national citizens.
47. Chile■ Decree-law no. 1.094 of 1975 establishing the laws concerning foreigners in
Chile
Article 15
The following foreigners are forbidden to enter the country:
4) those suffering from diseases which the Chilean health authority considers as an
impediment to entering the national territory.
48. Colombia■ Decree no 2731 of 27 December 1996 governing in a general fashion the delivery
of visas, the control of foreigners and establishing other provisions in the matter
of immigration
Article 5
Immigration is regulated according to (…) health needs.
article 19, paragraph 4
Persons applying for a visa, except for the exceptions provided for in this Decree, must
attach (…)
(3) the items required for the visa being applied for
(4) a medical certificate where this is required for health reasons by the Ministry of
Foreign Affairs.
Article 166
No foreigner may enter the national territory if he is in one of the following situations:
(1) suffering from a infectious-contagious disease (…).
292 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
49. Costa Rica■ Decree no. 20202-S-G of 17 January 1991
The present decree expressly repeals Executive Decree no. 18452-S of 19 September 1988
containing detailed provisions relating to treatment administered to persons living with AIDS
and Executive Decree no. 18781-S-G of 19 January 1989 containing provisions
concerning the screening which certain categories of foreign nationals resident in Costa Rica
must undergo.
50. Cuba■ Ministerial resolution no. 144 of 11 June 1987
(1) All foreign bursary students or other non-Cuban personnel coming to reside in Cuba for
periods longer than three months must, upon arrival or upon the order of the health
authorities undergo serological testing for detecting HIV (the agent causing AIDS).
(2) Any foreign national who proves seropositive to said virus must be sent back to the place
he came from (country of origin or other country).
51. Dominican Republic■ Law 4471 of 3 June 1956, public health code
Article 108
Every immigrant will be required to undergo a full medical examination before being allowed
to enter the country. In no event will persons affected with transmittable diseases (…) be
allowed to remain in the country.
52. Ecuador■ Law no 1899 of 1972 on immigration (entered into force on 2nd March)
Article 9
Except where provision is made in other legal dispositions, foreigners outside the country
contained in the following categories are not eligible for visas and must be excluded if they
apply for admission to enter the country:
(VII) Those suffering from diseases qualified as serious, chronic and contagious, such as
tuberculosis, leprosy, tracoma and other similar diseases not subject to quarantine.
The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 293
53. Jamaica■ Aliens Act of 1946
Article 6
Leave shall not be given to an alien to land in the Island unless he complies with the
following conditions, that is to say:
(d) he is not the subject of a certificate given to the immigration officer by a Health Officer that
for medical reasons it is undesirable that the alien should be permitted to enter the country.
54. Mexico■ General Population Act of 1992
Article 37
The Government Secretary may refuse entry to the country or a change in immigrant status
for one of the following reasons:
(VII) the person in question in not physically or mentally healthy in the judgement of the
health authority.
Article 62
In order to enter the Republic, foreigners must meet for following conditions:
(I) Present an official certificate of good physical and mental health delivered by the
authorities of the countries from which they have come in the cases established by the
Government Secretary.
(II) Be approved in the examination undertaken by the health authorities
Regulation of 1992 implementing the General Population Act (entered into force on
30th September).
Article 57
The Secretary may, in the following circumstances, by virtue of particular elements, refuse
foreigners entry, return, or a change in immigrant status (…):
(IV) when the health authority informs the immigration authority that the foreigner is
suffering from any infectious-contagious disease which presents a danger to public health.
294 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
55. Nicaragua■ Immigration Act no. 153 of 1993 (entered into force on 30th May)
Article 57
In order to be admitted as a permanent or temporary resident, the foreigner, upon entry into
the country (…) must present:
(…) a medical certificate delivered by the health authority of the country of origin or the
country he has come from.
Article 60
In order to be admitted as non-residents, foreigners (…) must present, upon entry into the
country:
(…) a medical certificate delivered by the health authority of the country of origin or the
country he has come from.
■ Law no. 154 of 1993 on foreigners (entered into force on 2nd June)
Article 4
Foreigners in the following categories will not be admitted to the country as permanent or
temporary residents:
(a) those suffering from an infections-contagious or transmittable disease which presents a
danger to public health.
Article 5
Foreigners in the non-resident category will not be admitted to the country when their entry
constitutes a danger to public health (…).
56. Panama■ Law no. 26 of 17 December 1992 giving measures for the prophylaxis and
control of the acquired immuno-deficiency syndrome (AIDS) and the spread of
the human immuno-deficiency syndrome (HIV)
Article 20
Any foreigner intending to enter the Republic of Panama as a permanent resident or intending
to remain for more than one year should, upon, entry to the national territory, present along
with his visa a medical certificate delivered by a public or private hospital, approved by the
minister of health or a body charged with directing health policy in his country of origin, which
states that he has undergone screening for the antibodies of the human immuno-deficiency
virus with a negative outcome. If outcome is positive, entry to the country is refused.
The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 295
58. El Salvador■ The Health Code (promulgated by Decree no 955 of 11 May 1988)
Article 164 requires every traveller entering Salvadorian territory to present, to the
appropriate health authority, valid international vaccination certificates or other certificates
of serological examinations regarding the diseases specified by the ministry (…) Immigrants
are also required to submit to the medical examination as required by the health authority in
order to confirm, if the latter considers this useful, the medical certificates obtained in their
countries of origin, and duly certified as being in conformity by the Salvadorian consular
authorities, based on clinical, X-ray and laboratory examinations attesting that the persons
in question are not afflicted by or carriers of transmittable diseases.
59. Trinidad and Tobago■ 1980 Immigration Act
Article 8
Except as provided in subsection (2), entry into Trinidad and Tobago of the persons
described in this subsection, other than citizens and, subject to section 7(2), residents, is
prohibited, namely:
(c) persons afflicted with any infectious or dangerous infectious disease.
D. South Sea Islands62. Papua New Guinea■ Migration Act of 1978 (entered into force on 12th September)
Article 9
1. Notwithstanding the possession of an entry permit, a person, other than a citizen may,
on arrival at the country or on reporting to an officer in accordance with Section 10(1), be
refused entry if:
(b) he is, in the opinion of an officer, suffering
(ii) from a disease which would make his presence in the country a danger to the
community; or
(c) he refuses to submit to a medical examination after being required to do so under
Subsection (2).
2. An officer may, for the purposes of forming an opinion under Subsection (1)(b), require
a person seeking to enter the country to submit himself to a medical examination by a
medical practitioner, or may detain him for that purpose.

296 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
Article 22
Repatriation
If the Minister is satisfied that a person, other than a citizen:
a) is destitute, infirm or mentally incapable.
63. Western Samoa■ Health Ordinance 1959
Article 29
Special powers of Director – The Director may from time to time, if authorized in writing so
to do by the Minister, exercise the following special powers for the prupose of preventing the
outbreak or spread of any infectious disease:
e) He may require persons to report themselves or submit themselves for medical
examination at specified times and places.
64. Tonga■ Act no. 16 of 1969 on Immigration
Article 5
(…) any immigration officer may:
d) require any person who desires to enter the Kingdom to submit to be examined by a
Government medical officer, and to undergo, and to assist in the carrying out of, any test or
investigation which such Government medical officer may require.
Article 8
Prohibited immigrants:
d) any person
i) who refuses to submit to an examination by a Government medial officer after being
required to do so under the provisions of section 5(1)(d) of this Act, or to undergo, or to
assist in the carrying out of, any test or investigation which such medical officer may require;
ii) who at the time of his entry into the Kingdom is certified by a Government medical
officer to be suffering from a contagious or infectious disease which makes his presence in the
Kingdom dangerous to the community.
The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 297
E. Central Europe65. Albania■ Immigration Law no. 7939 of 25 May 1995
Article 10
To persons who request a permission to enter or stay in the Republic of Albania and who
meet the requirements defined in this law, this permission can be denied if the Minister of the
Interior, himself, decides that their exclusion is imperative for the sake of public policy,
public security or health security reasons.
(…) The list of diseases and other cases which legitimate the denial of entry permission, is
contained in the regulations established for the implementation of this law.
66. Bulgaria■ Decree no. 4 of 2 April 1992 on the conditions and the procedures applicable to
the testing of the infection by the Acquired Immuno-Deficiency Syndrome virus
Article 2
The following must undergo compulsory screening for infection by HIV:
(6) foreign nationals and stateless persons coming to stay for more than one month in
Bulgaria in order to study or for professional purposes, as well as immigrants, regardless of
the length of their stay.
67. Hungary■ Act LXXXVI of 14 September 1993 on the entry, residence, and immigration of
aliens to Hungary
Article 15
2. (…) and the application for a residence permit shall be supplemented by an official
medical certificate showing that the alien does not suffer from a disease endangering
public health.
Article 16
Issue of the residence permit or the extension of the period of residence may be denied if
the alien:
(c) during his residence in Hungary does not observe the rules of Hungarian public health
regulations in force.
298 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
Article 19
1. To the application (for an immigration permit) shall be appended:
(d) an official medical certificate issued not earlier than three months, certifying that the
alien does not have a disease dangerous to public health.
Article 23
Prohibitions from entry and stay may be ordered against the alien:
(e) whose entry and stay would in any other way violate or endanger national security,
public safety, the economic order, public health or the human environment.
68. Poland■ Law of 1963 on foreigners (entered into force on 29th March)
Article 17
When issuing a decision to place a foreigner under arrest before expulsion the foreigner’s
condition of health and family situation must be taken into consideration (…)
70-71. Czech Republic and Slovakia■ Act no. 123/1992 of 4 March 1992 governing the stay and residence of
foreigners in the Czech and Slovak Republic
Article 8
A foreigner is obliged, upon request, to enclose with his application for the granting of a long-
term residence permit or permanent residence permit, or with his application for an extension
of the period of time stated in his long-term residence permit (…) evidence (…) that he does
not suffer from any infectious disease, the spreading of which is punishable by law.
Article 14
A foreigner may be prohibited from residing in the CSFR for a period of no less than one
year in the following cases:
(e) if it is unavoidable for the protection of health.
Czech Republic
■ Guidelines of March 1992 and instructions on prevention and treatment
of HIV infection
Article 2
Testing for HIV is voluntary and, in the case that the person tested or his legal
representative (…) so desires, it is anonymous. Testing is not anonymous (…) in the case
The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 299
of refugees, when a condition of their placement in a refugee camp includes consent to an
examination and HIV testing upon arrival, or when persons travel to a State which requires
HIV testing before entering the territory.
Slovakia
■ Law of 5 April 1995 on the residence of foreigners on the territory of Slovakia
Article 12
A foreigner is denied permission to enter or stay in the territory of the Slovak Republic if:
(i) it is necessary for state security, keeping the public policy, protection of health (…).
F. Former Yugoslavia73. Croatia■ Act of 1991 on the movement and residence of foreigners (entered into force on
8th October)
Article 18
A request for issuing a visa to an alien will be rejected if:
8. he is coming from a territory where there is an epidemic of contagious disease, and with
no vaccination certificate.
■ Presidential decree no. PA4-71/92 of 25 September 1992 promulgating the law
concerning the protection of the population against transmittable diseases
Article 60
In order to protect the Croatian Republic against the introduction of contagious diseases,
when crossing the border Croatian nationals are subject to a medical control (…).
Article 62
(…) In the application of this control, the management bodies who are responsible for the
health inspection are authorized to:
1. forbid the circulation of persons who are known to be afflicted by, or who might possibly
be afflicted by particular contagious diseases.
300 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
74. Macedonia■ Law of 1992 on the movement and residence of foreigners (entered into force
on 8th June)
Article 17
An alien would be refused admission in the Republic of Macedonia, respectively the
issuance of a visa, should:
(…) he/she be coming from an area infected by contagious diseases and is not in possession
of a vaccination certificate.
Article 30
An alien residing on the territory of the Republic of Macedonia (…) or who has been
granted approval for temporary residence, may be denied the right to residence, should
(…) matters of public health protection be concerned.
75. Slovenia■ Alien’s Act of 1991 (entered into force on 25th June)
Article 10
Foreigners may be denied entry to the state – denied visas – for the following reasons;
(…) if he/she is coming from an infected area (danger of spreading infectious diseases) and
can present no vaccination certificate.
Article 23
Residence may be cancelled to any foreigner residing in the territory of the Republic of
Slovenia on the basis of a foreign passport, a valid visa/entry permit, or conforming with
international agreements or possessing a valid temporary residential permit for one of the
following reasons:
(…) securing people’s health.
G. Community of Independent States78. Belarus■ Law of 3 June 1993 on the legal status of aliens and stateless persons in the
Republic of Belarus
Article 20
Aliens and stateless persons may be denied entry to the Republic of Belarus:
(2) in the interest of (…) the health of inhabitants.
The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 301
Article 25
Aliens and stateless persons may be deported from the Republic of Belarus:
1) if it is necessary for the protection of health (…)
■ Law of 18 June 1993 on public health
Article 27
Foreign nationals and stateless persons who refuse an examination for the purpose of
detection by the human immuno-deficiency virus (AIDS) or prophylactic observation, may
be expelled from the Republic of Belarus, in accordance with the procedure provided for by
the legislation of the Republic of Belarus.
79. Estonia■ Regulation of 21 September 1993 for the issue and extension of residence permits
and employment permits to aliens
Article 22
The alien shall submit the following documents to the foreign representation to apply for
a residence and employment permit:
6) medical certificate, for which the standard shall be confirmed by the Ministry of
Social Affairs.
80. Georgia■ Law of 21 March 1995 on the prevention of HIV/AIDS
Article 4
Foreign citizens arriving in Georgia for more than one month (excluding those possessing
diplomatic privileges and immunities) should possess a certificate to certify HIV/AIDS
examination. In the case of not having such a certificate these persons should undergo
HIV/AIDS medical examination according to the established rules.
■ Immigration Act of 27 July 1993
Article 4
A foreigner may be denied immigration to the Republic of Georgia:
4) if he has AIDS (…).
302 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
■ Law of 3 June 1993 on the legal status of aliens in Georgia
Article 29
Aliens, as well as stateless persons, temporarily residing in the Republic of Georgia, may be
deported from the Republic of Georgia if (…):
d) this is necessary for the protection of health.
81. Kazakhstan■ Law of 5 October 1994 on the prevention of AIDS
Article 6
The citizens of the Republic of Kazakhstan, foreign nationals and stateless persons are
required to undergo a medical examination where sufficient reasons exist to presume that
they are infected by the human immuno-deficiency virus (…). Foreign nationals residing in
the territory of the Republic of Kazakhstan who refuse to undergo an examination or a
prophylactic observation or who are infected by HIV or are living with AIDS are expelled
outside the frontiers of the Republic of Kazakhstan. Foreign nationals whose spouse is a
citizen of the Republic of Kazakhstan are not expelled.
82. Kyrghyzistan■ Law of 14 December 1993 on the order for residence of aliens in the Kyrghyz
Republic
Article 24
An alien may be deported from the Kyrghyz Republic:
2) if it is necessary for the protection of health (…).
83. Latvia■ Law of 9 June 1992 on the entry and residence of foreign citizens and stateless
persons in the Republic of Latvia
Article 35
Residence permits shall not be issued if a person suffers from an illness or health conditions,
the nature, severity and potential duration of which threatens the security and health of
society or requires the special supervision of health institutions, and those illnesses and
health conditions which are mentioned in the list confirmed by the Republic of Latvia
Welfare Ministry.
The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 303
84. Lithuania■ Immigration Act of 4 September 1991
Article 5
A foreigner may not be issued a permit to immigrate into the Republic of Lithuania if he or she:
1. is afflicted with a dangerous contagious disease.
■ Law of the Republic of Lithuania on the legal status of foreigners in the Republic
of Lithuania
Article 27
A foreigner may not be permitted to enter the Republic of Lithuania if:
2) his entry poses a threat to (…) health (…).
85. Moldova■ Law of 10 November 1994 on the legal status of aliens and stateless persons in
the Republic of Moldova
Article 8
(…) 2. Aliens and stateless persons shall be obliged to undergo medical screening in order to
reveal HIV-infection or AIDS.
Article 23
Aliens and stateless persons may be deported from the Republic of Moldova if (…)
(2) the stay in the Republic damages (…) health.
■ Law of 25 May 1993 on the prevention of the illness HIV/AIDS
Article 3
Citizens of the Republic of Moldova, foreign citizens and stateless persons who reside or who
are staying temporarily in the territory of the Republic of Moldova are required, according to
a decision taken by the health organizations and the medical institutions, to pass a medical
examination, where there are well-founded reasons for suspecting these persons of having
been infected by the human immuno-deficiency virus.
Article 5
Foreign citizens and stateless persons having temporary residence in the Republic of
Moldova and who refuse to take the medical examination will be expelled from the Republic
in accordance with the legislation in effect.
304 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
Article 11
Access to the territory of the Republic of Moldova is forbidden to foreign citizens and
stateless persons coming from other countries and infected by the HIV virus or who are
living with AIDS. Access to the territory of the Republic of Moldova for more than three
months is permitted solely to persons presenting a medical certificate proving that they have
tested negative for AIDS. Persons not passing the above-mentioned test are required to
present themselves within 10 days of their arrival in the Republic of Moldova, to the
institution in question, in order to pass an AIDS screening examination. This procedure will
be repeated once a year thereafter.
Article 12
Foreign citizens and stateless persons having temporary residence in the Republic of
Moldova and who are found following medical examination to be carriers of the HIV virus
(AIDS disease) are expelled from the country.
86. Mongolia■ Decree no 103 of 26 June 1989 of the Presidium of the Grand Khural of the
Mongolian People’s Republic on measures to prevent Acquired Immuno-
Deficiency Syndrome
Article 1
Any citizen of the Mongolian People’s Republic must undergo medical examinations and
screening which are required by a health care establishment in order to determine whether he
is infected with HIV. This provision applies equally to any foreigner of stateless person who
is in the Mongolian People’s Republic.
Article 3
The provisions of article 29 of the law concerning the rights and duties of foreigners who are in
the Mongolian People’s Republic are applicable to foreigners who are in the Mongolian People’s
Republic and who refuse to undergo medical examination and screening intended to determine
whether they are infected by HIV or whose infection with HIV has been confirmed.
■ Law of 1 March 1994 on the prevention of the Acquired Immuno-Deficiency
Syndrome
Article 12
Any foreigner national or stateless person infected by HIV or living with AIDS and who
refuses to conform to the instructions of the responsible health authorities must be expelled in
accordance with Mongolian legislation.

The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts 305
87. Uzbekistan■ Resolution no. 12 of 17 November 1992 introducing preventive measures against
the introduction and the spread of quarantinable diseases and of AIDS into the
Republic of Uzbekistan.
Article 1 requires the ministers and other specified organizations:
(7) to forbid the presence in the territory of the Republic of Uzbekistan of persons from
countries where AIDS is widespread (Africa: Burundi, Congo, Ghana, Guinea Bissau,
Ivory Coast, Kenya, Malawi, Mozambique, Rwanda, Sierra Leone, United Republic of
Tanzania, Zaire, Zambia and Zimbabwe. America: Brazil, Martinique, Mexico and the
United States of America. Europe: Belgium, France, Germany, Great Britain, Italy,
Netherlands, Spain, Sweden and Switzerland, if they do not hold a certificate certifying that
they have undergone screening for the antibodies of the human immuno-deficiency virus
(HIV). Persons holding such a certificate at the time of their entry into the Republic of
Uzbekistan but who prolong their stay for more than one month from their arrival must
undergo a new AIDS screening test at the place of stay.
(8) to deport immediately foreign nationals who turn out to be living with AIDS or
HIV carriers.
88. Russia■ Federal Law of 15 August 1996 on the procedure for exit from the Russian
Federation and entry into the Russian Federation
Article 27
Foreign citizens or stateless persons shall be denied entry into the Russian Federation
where (…):
4) they apply for a Russian visa for more than a three-month period and did not present
a certificate on the lack of HIV-infection, until submission of such certificate.
■ Federal law no. 38 of 30 March 1995 on the prevention of the spread in the
Federation of Russia of the affection caused by the Human Immuno-deficiency
Virus (HIV infection)
Article 11
2. In the event that HIV infection is found in foreign nationals or stateless persons who are
in the territory of the Russian Federation, said persons must be expelled from the Russian
Federation in accordance with the procedure for which provision is made in the legislation of
the Russian Federation.
306 The free movement of persons living with HIV/AIDS – Annexe III (1): Third countries, national texts
89. Tajikistan■ Law of 1 February 1996 on the legal status of aliens in the Republic of Tajikistan
Article 31
An alien may be deported from the Republic of Tajikistan:
2) if it is necessary for the protection of health (…).
90. Turkmenistan■ Law of 8 September 1993 on the legal status of aliens in Turkmenistan
Article 31
An alien may be deported from Turkmenistan:
2) if it is necessary for the protection of health (…).
■ Regulation of 7 June 1995 on HIV/AIDS testing in Turkmenistan
Article 2 defines the categories of persons subject to HIV screening. These include (…) foreign
nationals and stateless persons requesting a medical consultation, in accordance with clinical
indications (…).
91. Ukraine■ Law of 4 February 1994 on the legal status of aliens
Article 25
(…) An alien shall not be allowed to enter the Ukraine
- if it is necessary for the protection of health (…).
Article 32
An alien may be deported from the Ukraine (…) if (…) it is necessary for the protection of
health (…).
■ Law of 12 December 1991 on the prevention of AIDS and the social protection
of the population
Article 8
Nationals of other States and stateless persons staying in Ukrainian territory to study or
exercise an activity are subject to a compulsory medical examination in order to detect HIV
infection. Persons in possession of the certificate for which provision is made by an appropriate
agreement between the Ukraine and other State are dispensed from the examination (…).
Article 12
Nationals of other States and stateless persons infected with HIV are subject to an
administrative expulsion in accordance with the fixed legal procedure. Foreign nationals and
stateless persons whose spouse is a Ukrainian citizen are not subject to expulsion.

The free movement of persons living with HIV/AIDS – Annexe III (2): Third countries, Summary table 307
(2) Summary table
KeyThe table summarizes the situation in various third countries studied from the viewpoint
of legislation allowing certain limits to the free movement of persons living with
HIV/AIDS.
The numbers in parentheses refer to the paragraph numbers in the text.
The countries and numbers in bold face indicate the existence of restrictions on the
free movement of persons living with HIV/AIDS.
A mention in italics followed by (+) to signify ‘affirmative action’ is given to those
countries which, by legislation, or more often by general policy declarations, have
indicated that they are opposed to screening at their borders and/or to restrictions on the
free movement of persons living with HIV/AIDS.
Some countries are in bold face and italics as they belong to the two categories.
Most of the countries are printed in normal roman type. This means that, for those
countries, no particular legislation or practise against or in favour of the free movement of
persons living with HIV/AIDS were reported. It is possible that some of those countries
use the general legislation relating to migration against persons living with HIV/AIDS.
Moreover, on the one hand it should not be excluded that other states practise
restrictions or, vice versa, adopt affirmative action which we have not become aware of,
and on the other hand it is not impossible that the states mentioned in bold face have
decided to remove the restrictions applied to the free movement of persons living with
HIV/AIDS.
The aim is not to condemn or stigmatize the states mentioned in bold face or to
congratulate those mentioned in italics. The aim is to draw attention to the situation of
persons living with HIV/AIDS, with regard to their freedom of movement.
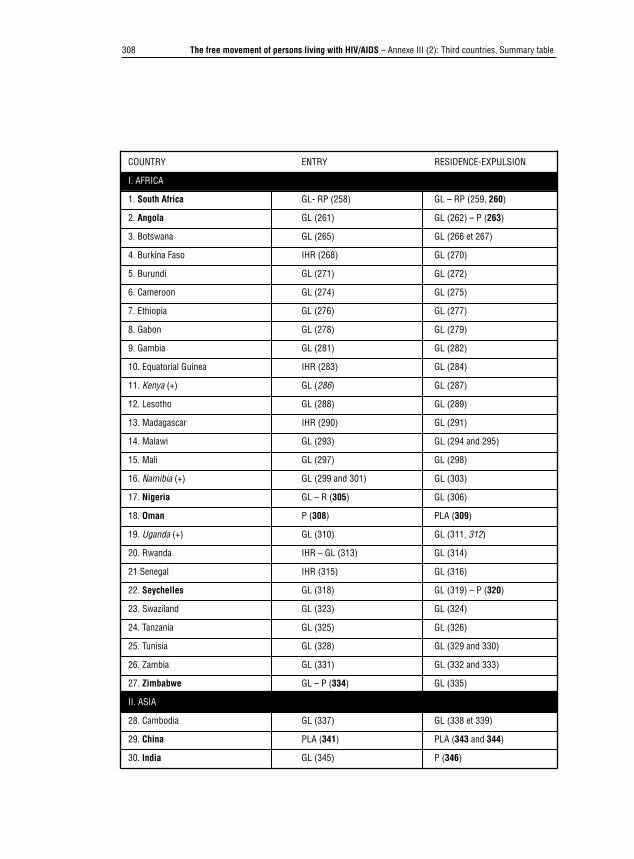
308 The free movement of persons living with HIV/AIDS – Annexe III (2): Third countries, Summary table
COUNTRY ENTRY RESIDENCE-EXPULSION
I. AFRICA
1. South Africa GL- RP (258) GL – RP (259, 260)
2. Angola GL (261) GL (262) – P (263)
3. Botswana GL (265) GL (266 et 267)
4. Burkina Faso IHR (268) GL (270)
5. Burundi GL (271) GL (272)
6. Cameroon GL (274) GL (275)
7. Ethiopia GL (276) GL (277)
8. Gabon GL (278) GL (279)
9. Gambia GL (281) GL (282)
10. Equatorial Guinea IHR (283) GL (284)
11. Kenya (+) GL (286) GL (287)
12. Lesotho GL (288) GL (289)
13. Madagascar IHR (290) GL (291)
14. Malawi GL (293) GL (294 and 295)
15. Mali GL (297) GL (298)
16. Namibia (+) GL (299 and 301) GL (303)
17. Nigeria GL – R (305) GL (306)
18. Oman P (308) PLA (309)
19. Uganda (+) GL (310) GL (311, 312)
20. Rwanda IHR – GL (313) GL (314)
21 Senegal IHR (315) GL (316)
22. Seychelles GL (318) GL (319) – P (320)
23. Swaziland GL (323) GL (324)
24. Tanzania GL (325) GL (326)
25. Tunisia GL (328) GL (329 and 330)
26. Zambia GL (331) GL (332 and 333)
27. Zimbabwe GL – P (334) GL (335)
II. ASIA
28. Cambodia GL (337) GL (338 et 339)
29. China PLA (341) PLA (343 and 344)
30. India GL (345) P (346)
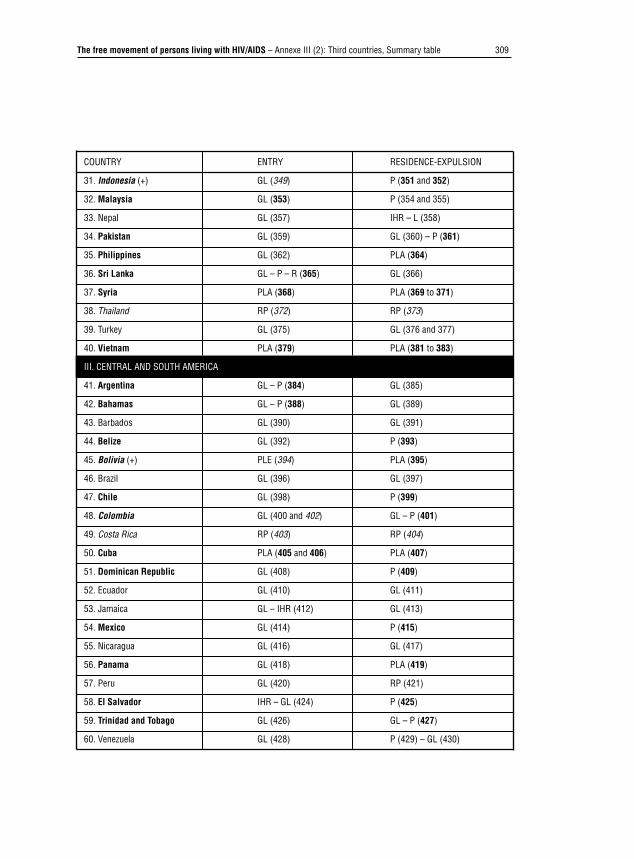
The free movement of persons living with HIV/AIDS – Annexe III (2): Third countries, Summary table 309
COUNTRY ENTRY RESIDENCE-EXPULSION
31. Indonesia (+) GL (349) P (351 and 352)
32. Malaysia GL (353) P (354 and 355)
33. Nepal GL (357) IHR – L (358)
34. Pakistan GL (359) GL (360) – P (361)
35. Philippines GL (362) PLA (364)
36. Sri Lanka GL – P – R (365) GL (366)
37. Syria PLA (368) PLA (369 to 371)
38. Thailand RP (372) RP (373)
39. Turkey GL (375) GL (376 and 377)
40. Vietnam PLA (379) PLA (381 to 383)
III. CENTRAL AND SOUTH AMERICA
41. Argentina GL – P (384) GL (385)
42. Bahamas GL – P (388) GL (389)
43. Barbados GL (390) GL (391)
44. Belize GL (392) P (393)
45. Bolivia (+) PLE (394) PLA (395)
46. Brazil GL (396) GL (397)
47. Chile GL (398) P (399)
48. Colombia GL (400 and 402) GL – P (401)
49. Costa Rica RP (403) RP (404)
50. Cuba PLA (405 and 406) PLA (407)
51. Dominican Republic GL (408) P (409)
52. Ecuador GL (410) GL (411)
53. Jamaica GL – IHR (412) GL (413)
54. Mexico GL (414) P (415)
55. Nicaragua GL (416) GL (417)
56. Panama GL (418) PLA (419)
57. Peru GL (420) RP (421)
58. El Salvador IHR – GL (424) P (425)
59. Trinidad and Tobago GL (426) GL – P (427)
60. Venezuela GL (428) P (429) – GL (430)

310 The free movement of persons living with HIV/AIDS – Annexe III (2): Third countries, Summary table
COUNTRY ENTRY RESIDENCE-EXPULSION
IV. SOUTH SEA ISLANDS
61. Fiji GL (431) GL (432)
62. Papua New Guinea GL (433) P (434)
63. Samoa P (435) GL (436) – P (437)
64. Tonga GL (439) GL (440)
V. CENTRAL EUROPE
65. Albania GL – IHR (441) GL (442)
66. Bulgaria GL (445) PLA (448) – GL (449)
67. Hungary GL (451) GL – P (452)
68. Poland GL (453) GL – P (454)
69. Romania GL (456) GL (457)
70. Slovakia GL (458) GL – P (459)
71. Czech Republic LPA (462) GL (463) – P (464)
VI. FORMER YUGOSLAVIA
73. Croatia GL (467) GL (468) – IHR (470)
74. Macedonia GL (473) GL (474)
75. Slovenia GL (477) GL (478)
VII. CIS
77. Armenia GL (483) GL (484)
78. Belarus GL (485) GL – PLA (486)
79. Estonia GL (488) GL – PLA (489)
80. Georgia PLA (490) PLA (492) – GL (494)
81. Kazakhstan GL (495) PLA (499 and 500)
82. Kyrghyzistan GL (501) GL (504)
83. Latvia GL (505) GL (506) – P (506)
84. Lithuania GL (508) GL – P (509)
85. Moldova PLA (511) PLA (512 and 513)
86. Mongolia PLA (514) PLA (515)
87. Uzbekistan PLA (516) PLA (517)
88. Russia PLA (519) PLA (520 and 482)
89. Tajikistan GL (522) GL (523 and 524)
90. Turkmenistan GL (527) PLA (530) – GL (531)
91. Ukraine GL (533) PLA (535 and 536)
The free movement of persons living with HIV/AIDS – Annexe III (2): Third countries, Summary table 311
Key
GL No particular legislation. Application of general immigration legislation which can
contain restrictions relating to public policy and public health.
PLA Particular legislation authorizing AIDS screening
PLE Particular legislation excluding AIDS screening
P AIDS screening practised
RP Special legislation authorizing AIDS screening has been repealed
IHR Application of international health regulations or WHO policy
R Restrictions may exist on a reciprocal basis
312 The free movement of persons living with HIV/AIDS – Annexe IV (1): Bibliography, AIDS
Annexe IV. Basic bibliographyOnly the works, studies and articles specifically used for this study are included in this
bibliography, because they concern AIDS and the right to free movement of persons.
To make things easier, the bibliography is divided between these two problems, even if
certain works concern both. For a more complete bibliography of every aspect of this
double problem – free movement and AIDS – the references in this bibliography can
be used.
Two basic references for health and migration legislations:
– WHO (World Health Organization), International Digest of Health Legislation,
Geneva.
– UNHCR (United Nations High Commissioner for Refugees), Refworld, CD Rom,
Geneva, January 1998 (also on Web: http://www.unhcr.ch).
(1) On AIDSAFRICAN NETWORK ON ETHICS, LAW AND HIV, Proceedings of the intercountry
consultation, Dakar, Senegal, 27 June-1st July 1994, UNDP, Dakar, 1996.
AGADZI, VK, AIDS-the African perspective of the killer disease, Ghana Universities, Press
Accra, 1989.
AIDES,
– Droit et sida, guide juridique, 3e édition, Paris, LGDJ, 1996.
– Dix ans d’existence, dix ans de résistance, 7es Assises nationales, Paris,
23-25 septembre 1994.
ALKAS, P.H. and SHANDERA, W.X, ‘HIV and AIDS in Africa, African policies in
response to AIDS in relation to various national legal traditions’, The Journal of Legal
Medicine, 1996, p. 527.
ARCAT, Sida, VIH et vacances, Paris, 1996.
BINDMAN, G., ‘Extending anti-discrimination law to AIDS and HIV’, N.L.J., 1996,
p. 62.
BREUM, M. and HENDRIKS, A., AIDS and human rights: an international perspective,
Copenhagen, Akademisk Forlag, 1988.
Bulletin du réseau africain sur l’éthique, le droit et le VIH, PNUD, Sénégal.
CAMERON, E., ‘Human rights, racism and AIDS: the new discrimination’, South African
Journal on human rights, 1993, p. 22.
The free movement of persons living with HIV/AIDS – Annexe IV (1): Bibliography, AIDS 313
CATTORNI, P., MORELLI, D., ZANCHETTI, M., AIDS, comparison and analysis of
European Legislation on AIDS from ethical and legal standpoint, Italy, Istituto Scientifico
H. San Raffaele, 1996.
COLLECTIVE,
– Sida’venture, sida, éthique, discriminations, Paris, Editions Syllepse, 1989.
– AIDS in Asia and the Pacific Conference, Canberra, Australia, official proceedings
document, 5-8 August 1990.
– HIV law, ethics and human rights, New-Delhi, UNDP, 1995.
CONSEIL NATIONAL DU SIDA (France), Rapport suivi d’un avis du conseil national du
sida sur la situation des personnes atteintes par le VIH de nationalité étrangère et en
irrégularité de séjour, Paris, décembre 1995.
DECOSAS, J., ‘Migration et sida en Afrique de l’Ouest’, Le journal du sida, juin-juillet
1996, n° 86-87.
DÉPARTEMENT FÉDÉRAL DES AFFAIRES ÉTRANGÈRES (Switzerland), Tableau
récapitulatif des dispositions prises par certains pays envers les voyageurs internationaux
concernant les tests de dépistage des anticorps anti-HIV (sida), Berne, 17 February 1997.
DEPARTMENT OF HEALTH (SOUTH AFRICA), Guidelines for the management of
patients/sick passengers with a (suspected) communicable disease entering South Africa,
March 1997.
DE SCHUTTER, O., ‘Épidémie de sida et droits de l’homme’, Revue trimestrielle des droits
de l’homme, 1994, p. 59.
EUROCASO, Report of the first seminar on law and HIV/AIDS, Amsterdam, 13-14 avril
1991.
EUROPEAN CENTRE FOR THE EPIDEMIOLOGICAL MONITORING OF AIDS,
HIV/AIDS surveillance in Europe: 1994-1996, Quarterly Report n° 42, 30 June 1994.
European Commission,
– The European Union in the global response to HIV/AIDS in developing countries.
– Les Européens et le sida, Enquête eurobaromètre 43.0 et 43.1, Luxembourg, 1996.
– Community action programme ‘Europe against AIDS’, Directory of the actions
implemented in 1995.
FEUILLET – LE MINTIER, B. (sous la direction de), Le sida, aspects juridiques, Paris,
Economica, 1995.
FIGUEIRA, M., ‘AIDS, the Namibian Constitution and human rights, an overview’,
South African Journal on human rights, 1993, p. 30.
314 The free movement of persons living with HIV/AIDS – Annexe IV (1): Bibliography, AIDS
FINE, D., HEYWOOD, M. and STRODE, A. (Ed.), HIV/AIDS and the law, published by
the AIDS law project and lawyers for human rights, South Africa, 1997.
FOYER, J. et KHAIAT, L., Droit et sida, comparaison internationale, Paris, CNRS Editions,
1994.
FRANSEN, L. and WHITESIDE, A. (Ed.), HIV/AIDS and development assistance,
Workshop proceedings, Brussels, 13 June 1996.
FUENZALIDA-PUELMA, H., LINARES PARADA, A. y SERRAMO LA VERTU, D.,
Aportes de la ética y el derecho al estudio del sida, Organizacion panamericana de la
salud, 1991.
GEVERS, S., ‘Population Screening: The role of the law’, European Journal of Health Law,
1998, p. 7.
GILMORE, N., ‘Medical and political aspects of travel for HIV-Positive’, in Travel
Medicine 2, proceedings of the second conference on international travel medicine, Atlanta,
Georgia, USA, May 9-12, 1991, p. 207.
GOSTIN, L. and PORTER L., International Law and AIDS, International responses, current
issues and future directions, International health law committee, USA, 1992.
HAOUR-KNIPE, M. and RECTOR, R., Crossing borders, migration, ethnicity and AIDS,
London, Taylor & Francis, 1996.
HAOUR-KNIPE, M., Migrants and travellers group, final report, Institut Universitaire de
médecine sociale et préventive, Lausanne, Cahiers de recherche et de
documentation, 1991.
HARRIS, D. and HAIGH, R., AIDS: a guide to law, Routledge, London, 1990.
HEILMANN, E., Sida et libertés, la régulation d’une épidémie dans un État de droit, Avignon,
Actes Sud, 1991.
HELLENIC CENTRE FOR THE CONTROL OF INFECTIOUS DISEASES (Keel),
AIDS, fundamental principles for the protection of human rights and civil liberties,
Ministry of health, Athens, 1996.
HENDRIKS, A.,
– The right to freedom of movement and the (un)lawfulness of AIDS/HIV specific
travel restrictions from a European perspective’, Nordic Journal of International
Law, 1990, p. 86.
– ‘AIDS-test, European Union, pre-employment medical examinations, right to
private life’, The European journal of health law, 1995, vol. 2, n° 2.

The free movement of persons living with HIV/AIDS – Annexe IV (1): Bibliography, AIDS 315
I.C.A.S.A., Xth international conference on AIDS and STD in Africa, ‘AIDS and
development’, abstracts book, Abidjan, Côte d’Ivoire, 7-11 December 1997.
ICASO (International Council of AIDS Service Organizations),
– An advocate’s guide to the international guidelines on HIV/AIDS and human rights,
Canada, 1997.
– NGO summary of the international guidelines on HIV/AIDS and human rights,
Canada, 1997.
INSTITUT SUISSE DE DROIT COMPARÉ, Étude comparative sur la discrimination à
l’encontre des séropositifs et des malades du sida, Étude réalisée sous l’égide du Conseil de
l’Europe, Strasbourg, 1993.
JAYASURIYA, D.C.,
– AIDS, public health and legal dimensions, Dordrecht, Martinus Nijhoff publishers,
1988.
– AIDS, health, policy and legal aspects, London, Commonwealth Secretariat, 1992.
– HIV law and law reform in Asia and the Pacific, New-Delhi, UNDP, 1995.
JAYLE, D. et PIALOUX, G. (Ed.), Le guide du sida, Paris, Crips-Vigot, 1996.
LABORATORY CENTRE FOR DISEASE CONTROL (Canada), Countries with HIV-
related entry restrictions, June 1997.
NATIONAL COUNCIL FOR INTERNATIONAL HEALTH HIV/AIDS
PROGRAMME, International perspectives on legal issues and human rights.
NATIONS-UNIES, Rapport d’une consultation internationale sur le sida et les droits de
l’homme, Geneva, 26-28 July 1989, New-York, 1991.
NELSON, ‘International travel restrictions and AIDS epidemic’, 81 Am. J. Int’l L.,
(1987) p. 230.
ODA (Overseas development administration),
– Sexual health and health care: HIV, AIDS and sexually transmitted infections, global
Epidemiology, impact and prevention, Health and population occasional paper,
London, 1996.
– Sexual health and care: sexually transmitted infections, guidelines for prevention and
treatment, Health and population occasional paper, London, 1996.
ODHIAMBO, D., ‘L’expérience du réseau éthique et juridique sur le VIH/sida du Kenya’,
Sociétés d’Afrique et sida, n° 15, January 1997, p. 10.
PANAMERICAN HEALTH ORGANIZATION, AIDS, profile of an epidemic,
Washington, 1989.
316 The free movement of persons living with HIV/AIDS – Annexe IV (1): Bibliography, AIDS
PANOS INSTITUTE, The third epidemic repercussions of the fear of AIDS, London, 1990.
PROCETTS, Contrasida informa, Boletin informativo, Ano 1, n° 1-2 (Peru).
ROTH, JAY S., All about AIDS, New-York, Harwood Academic Publishers, 1989.
SABATIER, R., Blaming others, London, Panos Institute, 1988.
SALOMON, M. and TOUBON, R, Sida, sociétés et populations, Montrouge, John Libbey
Eutotext, 1996.
Sociétés d’Afrique et sida, GRID, Université de Bordeaux.
SOW/SIDIBE, A., Le droit à l’épreuve du VIH, 1er Colloque international sida et religion,
31 October-2 November 1997.
Stop AIDS, HIV test, yes or no, Denmark, July 1992.
TERL, Allan H., AIDS and the law, a basic guide for the non lawyer, Washington,
Hemisphere Publishing Corporation, 1992.
TESSIER, D., FRÉCKETTE, G., ‘VIH et voyages, conseils relatifs aux immunisations et à
l’évaluation pré-voyage’, FMC, 1994, 40, p. 740.
THIRY, L., ‘Les boursiers et le sida: accompagner ou punir?’, Journal des procès, n° 103, 20
mars 1987, p. 8.
TOPAZE (Collective), Sida, structures d’accueil et d’hébergement, Brussels, October 1996.
TORRELLI, M ., ‘Le sida et la lutte anti épidémiologique’, Annuaire français de droit
international, XXXIII, 1987, CNRS, Paris.
US AGENCY FOR INTERNATIONAL DEVELOPMENT, AIDS in Kenya –
Socioeconomic impact and policy implications, Aidscap/Family health international,
1996.
VAN OVERBEEK, J., ‘AIDS/HIV infection and the free movement of persons within the
European Economic Community’, Common Law Market Review, 1990, p. 191.
VANSWEEVELT, T., Le sida et le droit, Une étude de droit de la responsabilité et de droit des
assurances, Bruxelles, Bruylant, 1990.
VINCINEAU, M. (Ed.), Le sida, un défi aux droits, actes, Bruxelles, Bruylant, 1991.
WAALDIJK, K. and CLAPHAM, A., Homosexuality: a European Community issue,
Dordrecht, Martinus Nijhoff Publishers, 1993.
WHITESIDE, A., Integration of the HIV/AIDS problematic in development assistance, A
Toolkit, European Commission.
WHO (World Health Organization),
– Background paper preparatory meeting for a consultation on long- term travel

The free movement of persons living with HIV/AIDS – Annexe IV (1): Bibliography, AIDS 317
restrictions and HIV/AIDS, Geneva, 4-6 October 1994.
– Directory of legal instruments dealing with HIV infection and AIDS, Geneva, 1997.
WORLD BANK, Confronting AIDS, public priorities in a global epidemic, Oxford University
Press, 1997.
X,
– Restrictions of entry and residence for people with HIV/AIDS, a global survey, Archiv
für sozialpolitik Aids-Archiv, ordered by Deutsche Aids-Hilfe, Berlin, Frankfurt
am Main, November 1991.
– Legislative Response to AIDS, Dordrecht, Martinus Nijhoff, 1989.
ZEEGERS, ‘AIDS and the law: a comparative overview’, Comp. L. Yearbook, 1992, p.195.
318 The free movement of persons living with HIV/AIDS – Annexe IV (2): Bibliography, free movement of persons
(2) On free movement of persons, migrations and human rightsBONNECHÈRE, M. (Ed.), Trente ans de libre circulation des travailleurs, Paris,
a documentation francaise, 1998.
BOSSUYT, M., L’interdiction de la discrimination dans le droit international des droits de
l’homme, Bruxelles, Bruylant, 1976.
CARLIER, J.-Y.,
– ‘Le droit d’entrée et de séjour des ressortissants des États membres’, in ‘1993, le
marché unique et l’Europe des personnes’, Actualité du droit, 1994/1, t. II.
– ‘L’Europe et les ressortissants des États tiers: de la coopération
intergouvernementale vers le droit communautaire’, Annales de droit de Louvain,
1993/2, p. 207.
– ‘La libre circulation des personnes dans l’Union européenne’, Journal des
tribunaux. Droit européen, 1995, p. 97, 1996, p. 63 and 1997, p. 193.
CARLIER, J.-Y. and VAN SIMAEYS, B., ‘Le nouvel espace de liberté, de sécurité et de
justice’, in Y. LEJEUNE (Ed.), Le Traité d’Amsterdam, Bruxelles, Bruylant, 1998,
pp.228–285.
CARLIER, J.-Y. and VERWILGHEN, M., Free Movement of Workers in the European
Community. Casebook of Judgment on the European Court of Justice, Brussels, Bruylant,
1998, 3 vol.
CENTRE FOR INTERNATIONAL LEGAL STUDIES, International immigration and
nationality law, The Hague, Kluwer, 1994.
Commentaire MEGRET, Le droit de la CEE, partic. t. I et t. III, 2e éd, Bruxelles, ULB,
1990 and 1992.
DRUESNE, G. (Ed), Code européen des personnes, 2e édition, Paris, Dalloz, 1996.
ESPINAR VICENTE, J. M., La nacionalidad y la extranjeria en el sistemo juridico espanol,
Madrid, Civitas, 1994.
EVANS, A., ‘Third country nationals and the Treaty of the European Union’, E.J.I.L.,
1994, p. 199.
FUND FOR INTEGRATION, How to establish residence in Austria, Vienna, 1996.
GISTI, Entrée et séjour des étrangers, la nouvelle loi Pasqua, 3e éd, Paris, décembre 1994.
GOODWIN-GILL, G.S., International law and the movement of persons between States,
Oxford Clarendon Press, 1978.
GUILD, E (Ed.), The legal framework and social consequences of free movement of persons in
The free movement of persons living with HIV/AIDS – Annexe IV (2): Bibliography, free movement of persons 319
the European Union, The Hague, Kluwer Law International, 1998.
IOM, Legislative acts of the CIS and the Baltic states on citizenship, migration, and related
matters, Moscow & Helsinki, 1996.
JORGENSEN, E., Union citizens, free movement and non discrimination, Denmark, Jurist-og
Okonomforbundets Forlag, 1996.
LAWSON, E., Encyclopedia of Human Rights, Washington, Taylor and Francis, 1996.
LOUSSOUARN, Y. and BOUREL, P., Droit international privé, 4e éd, Paris, Dalloz, 1993,
p. 636 ss.
MARTIN, D., and GUILD, E., Free movement of persons in the European Union, London,
Butterworths, 1996.
MAYER, P., Droit international privé, 4e éd, Paris, Montchrestien, 1991, p. 569.
MOTULSKY, F. et BOBRUSHKIN, M., ‘Le séjour des étrangers en Belgique et le
contentieux médical’, Journal des tribunaux, 1998, p. 281.
PLENDER, R.,
– International Migration Law, Dordrecht, Martinus Nijhoff, 1988.
– Legal documents on international migration law, The Hague, Kluwer Law
International, 1997.
RIGAUX, F., FALLON, M., Droit international privé, Bruxelles, Larcier, t. I et II, 1987,
1993.
SALINERO, G.B., ‘Analisis detallado del reglamento de extranjeria’, Economist and Jurist,
Mayo-Junio 1996, n° 19 (Spain).
TAVERNE, M., L’étranger et le droit belge, Statut administratif, La Charte.
TURPIN, D. (Ed.), Immigrés et réfugiés dans les démocraties occidentales-défis et solutions,
Paris, Economica, 1990.
VERWILGHEN, M. (Ed.), Droits humains fondamentaux, recueil de documents
internationaux et nationaux, Bruxelles, 1993.
X, ‘Aperçu législatif sur le ressortissant étranger dans l’organisation italienne’, Vie
italienne, 1985, October-December, n° 4, p. 55.
X. (Conference),
– ‘Les personnes: quelle place dans l’Europe de 1993?’, Annales de droit de Louvain,
1993/2.
– ‘1993, le marché unique et l’Europe des personnes’, Université de Liège, Actualités
du droit, 1994/2.
EUHIV/AIDSPROGRAMMEINDEVELOPINGCOUNTRIES
European Commission, Directorate-General for DevelopmentLuxembourg: Office for Official Publications of the European Communities
Do human rights charters or international and European lawsprohibit restrictions on the free movement of people living with HIVor AIDS? And can any such restrictions be considered a reasonableresponse to AIDS and its consequences? This book makes a majorcontribution to public policy by examining relevant international andnational law across 106 countries – focusing on the EuropeanUnion, its Member States, Eastern Europe and developing countriesin Asia, Africa, South and Central America.
It will be of interest to lawyers, policymakers, and all those whohave an interest in the human rights of people living with HIV/AIDS.
Dr Lieve Fransen is the Principal Administrator of the EU HIV/AIDS programme indeveloping countries at the European Commission, Brussels.
Jean-Yves Carlier is a barrister and Professor in International and European Law atthe Louvain Catholic University (Louvain-la-Neuve, Belgium), Visiting Professor atthe University of Paris II (France), and Visiting Professor at the University ofOuagadougou (Burkina Faso).
Graciela Schiffino is a barrister.
9 789282 871263
ISBN 92-828-7126-6