lain Carlyle Cooke Supervisor: A Scarr - Cranfield University
A TLD STUDY OF ACUROS XB FOR LUNG SBRT USING A LUNG SUBSTITUTE MATERIAL
SUBMITTED
BY
Roger Soh Cai Xiang (U0940009B)
SUPERVISOR: Assoc Prof Lee Cheow Lei James
CO-‐SUPERVISOR:
Assoc Prof Phan Anh Tuan
DIVISION OF PHYSICS & APPLIED PHYSICS SCHOOL OF PHYSICAL AND MATHEMATICAL SCIENCES
A final year project report presented to
Nanyang Technological University in partial fulfilment of the requirements for the
Bachelor of Science (Hons) in Physics / Applied Physics Nanyang Technological University
May 2013
2
Abstract
Purpose: The recent development of a new photon transport algorithm, Acuros XB,
has shown good potential to be an alternative to the benchmark, Monte Carlo
method. The advantage of Acuros XB (AXB) is in regions of significant heterogeneity
where it has been shown to be almost equivalent to Monte Carlo and generally
better than other advanced model-‐based algorithms. This project focuses on the use
of Thermoluminesence Dosimeters (TLDs) for the validation of AXB on Lung SBRT.
A comparison between AXB, AAA (Anisotropic Analytical Algorithm, Varian Medical
Systems, USA), and physical TLD measurements in a lung substitute material
(composition cork) will be studied.
Methods: A thorough study was first done to prepare and calibrate TLDs for
measurement. Next, a study of clinical cases was done to determine the treatment
parameters and phantom dimensions for Lung Stereotactic Body Radiation Therapy
(SBRT) cases. Two multilayered slab phantom, consisting of combinations of Plastic
WaterTM (CIRS, Norfolk, VA) and composition cork was then built for TLD
measurement. A corresponding virtual phantom was created in the clinical
treatment planning system. Presence of bone is not considered in this study. The
phantom dose distributions of field sizes 2x2, 5x5, and 10x10 cm2 for 6 MV photon
beams were then analysed by comparison of TLD measurements on the phantom
against AXB and AAA calculations on the virtual phantom.
3
Results: TLDs were carefully calibrated and the best linear dose response range
was found to be between 0.1-‐1.0 Gy. All Lung SBRT treatments were delivered at
6MV with field sizes ranging from 5x5 to 10x10 cm2. 2x2 cm2 field size was included
to study small stereotactic field effects in lung medium. Overall TLD results show
that AXB was better than AAA in the lung medium and the lung to tissue interfaces.
Conclusion: AXB was found to be an accurate algorithm for lung correction. Based
on TLD measurements, it is accurate for AXB dose calculation in Lung SBRT, on
areas where smaller field sizes (< 10x10 cm2) are normally used.
Keywords: Acuros, TLD, Lung SBRT, composition cork
4
Acknowlegments When I was young, I loved superheroes from DC and Marvel comics (well, I still do). As
most superheroes have a certain involvement in the sciences, it inspired me to have this
thirst for scientific knowledge, in the hope that I might be a superhero too. One of them is
Dr. Bruce Banner, or commonly known as the Incredible Hulk. He was an extremely
intelligent radiation physicist, who was later irradiated accidentally with gamma
irradiation, transforming him into a big, green Goliath with incredible strength. Needless
to say, the Incredible Hulk uses his powers to fight crime, protect the innocent and save
the world. Being a medical physics student, I handle high doses of radiation everyday, so
as to contribute my research to help benefit the life of a cancer patient. It made me realize
that I am as close as I can get to be Bruce Banner. I am living my dream. I will like to use
this opportunity to thank the people who have helped me achieve this dream.
First of all, I will like to thank my supervisor Professor James Lee Cheow Lei, for being a
very supportive mentor to me. He is gentle, generous and patient, yet authoritative, driven
and just. He has done beyond his call as a supervisor, and even created an opportunity for
me to present my work in a Master’s Level medical physics conference as an
undergraduate. I was full of gratitude the moment I heard I won the award as one of the
best presenters. Without his guidance, this FYP will not be possible.
I will like to thank my co-supervisor Professor Phan Anh Tuan, who was also very
supportive of my work. Despite his busy schedule, he took the time to guide and show me
on how I should present my work, especially to those in the academia who are not in the
medical field. On top of that, he also showed his great support in sending me to the
medical physics conference.
I will like to thank Professor Yigal Horowitz, from Ben Gurion University, Beersheva,
Israel. He is a world-reknown expert in thermoluminesence dosimetry and author of three
volume books. Our paths crossed when I was stuck at my project and decided to e-mail
5
my problems to the authors of several publications I have cited. To my surprise, Professor
Horowitz replied by giving several pointers on how I should carry on with my project.
His pointers were right-on and the project was resumed. We maintained an e-mail
conversation until he saw the end of my project. I was really blessed and wish that I could
thank him personally someday.
I will like to thank Mr. Ang Khong Wei, Mr. Jerome Yap Haw Hwong and Ms. Wendy
Chow Wan Li. They are the medical physicists in National Cancer Centre Singapore
(NCCS), who have guided and mentored me in a fatherly and motherly manner. Many
times they have went beyond the call of duty by staying back after working hours, so as
to ensure our safety in handling the radiotherapy equipment.
I also like to thank my course mates, Mr. Melvin Chew Ming Long, Mr. Phua Jun Hao
and Mr. Tay Guan Heng, for all the fun times, the bad times, the happy times and the
busy times we had in NCCS. We have grown a lot by learning from one another through
this period.
I also will like to acknowledge my parents and my beloved girlfriend Ms. Chua Joo Leng,
who although have no idea what my project is about, showed continuous prayers, support
and encouragement to me. Without their emotional support, this would not have been
possible.
Lastly, I will like to thank God for being sovereign, by guiding me like “a lamp to my
feet and a light to my path” (Psa 119:105). To God be the glory.
6
Contents ABSTRACT ................................................................................................................................................ 2 ACKNOWLEGMENTS .............................................................................................................................. 4 CONTENTS ................................................................................................................................................ 6 1 INTRODUCTION ............................................................................................................................... 8 1.1 MOTIVATION ................................................................................................................................................... 8 1.2 OBJECTIVE ....................................................................................................................................................... 9 1.3 SCOPE OF THE PROJECT .............................................................................................................................. 10
2 THE PHYSICS OF RADIOTHERAPY .......................................................................................... 11 2.1 INTRODUCTION TO RADIOTHERAPY ........................................................................................................ 11 2.2 RADIATION DOSIMETRY ............................................................................................................................ 13 2.2.1 Absorbed Dose ...................................................................................................................................... 13 2.2.2 Linear Accelerators ............................................................................................................................ 14
2.3 RADIATION TREATMENT SETUPS ............................................................................................................. 18 2.3.1 Source Surface Distance (SSD) Setup ......................................................................................... 18 2.3.2 Source Axis Distance (SAD) Setup ............................................................................................... 19
2.4 PHOTON BEAMS .......................................................................................................................................... 21 2.5 SUMMARY ..................................................................................................................................................... 24
3 THERMOLUMINESENCE DOSIMETERS .................................................................................. 25 3.1 INTRODUCTION TO TLDS .......................................................................................................................... 25 3.1.1 A General Model of Thermoluminesence Dosimetry ........................................................... 27 3.1.2 Characteristics of TLDs .................................................................................................................... 29 3.1.3 TLD Reader ............................................................................................................................................ 30 3.1.4 TLD Glow Curve ................................................................................................................................... 32 3.1.5 TLD setup for radiotherapy ............................................................................................................ 34
3.2 TLD MEASUREMENT METHODS ................................................................................................................ 38 3.2.1 Element Correction Coefficient ..................................................................................................... 38 3.2.2 Reader Calibration Factor and Absorbed Dose ..................................................................... 42 3.2.3 Selection of Calibration and Field Dosimeters ....................................................................... 44 3.2.4 Linearity of TLD readings ............................................................................................................... 45
3.3 SUMMARY ..................................................................................................................................................... 47 4 DOSE CALCULATION ALGORITHMS ........................................................................................ 49 4.1 ANISOTROPIC ANALYTICAL ALGORITHMS (AAA) ................................................................................ 51 4.2 ACUROS EXTERNAL BEAM (AXB) ........................................................................................................... 53 4.2.1 Computed Tomography (CT) number – mass density relationship .............................. 54
4.3 LUNG STEREOTACTIC BODY RADIATION THERAPY (SBRT) .............................................................. 57 4.4 SUMMARY ..................................................................................................................................................... 62
7
5 APPLICATION OF TLD TO VALIDATE ACUROS XB FOR LUNG SBRT ............................ 64 5.1 BACKGROUND OF STUDY ........................................................................................................................... 64 5.2 METHODOLOGY ........................................................................................................................................... 67 5.2.1 Dose Calculation .................................................................................................................................. 67 5.2.2 Setup of the Lung Phantom ............................................................................................................ 68 5.2.3 TLD Calibration and measurement positions ........................................................................ 70
5.3 RESULTS AND DISCUSSIONS ...................................................................................................................... 72 5.3.1 Challenge encountered in preliminary TLD study ................................................................ 72 5.3.2 Perturbation Factors for TLDs ...................................................................................................... 72 5.3.3 Verification of AXB and AAA with TLD measurements ...................................................... 76 5.3.4 Discussions ............................................................................................................................................. 77
5.4 SUMMARY ..................................................................................................................................................... 82 6 CONCLUSION .................................................................................................................................. 84 6.1 SUMMARY ..................................................................................................................................................... 84 6.2 FUTURE WORKS .......................................................................................................................................... 87
7 REFERENCES .................................................................................................................................. 88 APPENDIX .............................................................................................................................................. 91 I. CAVITY THEORY ............................................................................................................................................... 91 II. ACUROS XB SOLUTION METHODS ............................................................................................................... 93 III. APPENDIX REFERENCES ............................................................................................................................... 105
8
1 Introduction 1.1 Motivation Medical Physics is the broad application of physics in medicine. Clinical Medical
Physics generally concerns physics being applied in medical imaging and
radiotherapy. This paper serves partially as a brief introduction on the physics of
radiotherapy, so as to assist the reader to understand better the study of
Thermoluminesence Dosimeters (TLDs) on dose calculation algorithms.
Radiation dosimeters, such as TLDs, are detectors that can be used to measure the
absorbed dose in biological medium of interests during or after irradiation. TLDs
are chosen for this study as they are one of the most flexible dosimetric systems and
can be used in various radiation dose measurement applications.
Dose calculation algorithms for radiation therapy in clinical Treatment planning
Systems (TPS) are used to simulate optimal dose distributions on the target volume
before the actual treatment. Dose calculation algorithms have improved profoundly
over the last few decades, creating higher demands on dose calculation algorithms
in terms of accuracy in heterogeneous medium and computation speed. Some
examples of dose calculation algorithms are the Anisotropic Analytical Algorithm
(AAA) and Monte Carlo (MC) calculations. Recently, a novel deterministic method,
Acuros XB (AXB), became commercially available for external photon beam dose
calculations. The AXB’s fundamental radiation transport theory is based on the grid-‐
based Boltzmann solver (GBBS), commonly known as discrete ordinates. The linear
9
Boltzmann transport equation (LBTE) is the equation that describes the distribution
of radiation particles resulting from their interactions with matter.
Many studies have shown that AXB is more accurate than the clinically widely used
AAA convolution method1. However, most studies found are normally benchmarked
against MC methods1-‐3. MC method solves the LBTE stochastically but they are time
consuming, hence few clinical systems use MC today. A few papers also validated
AXB with TLD measurements to further show the superiority of AXB in
heterogeneous medium2, 4. Furthermore, there is also some concerns regarding the
use of small fields on the accuracy of AXB and AAA for stereotactic treatments5.
In this study, the accuracy of AXB for Lung Stereotactic Body Radiotherapy (SBRT) is
validated using TLDs. TLDs will have to be carefully selected and calibrated. The
study will also check the TLD and AXB results against the AAA convolution method
as done in other studies5, 6. In order to simulate lung tissues, composite cork was
chosen as it was found that it has similar radiological properties as lung tissue7.
Field sizes of 2x2, 5x5, and 10x10cm2 were used.
1.2 Objective The objective of this work is to conduct a careful calibration of TLDs and to apply it
for the validation of a new dose calculation algorithm, Acuros XB. This validation of
the dose calculation algorithm was done for Lung Stereotactic Body Radiation
Therapy cases. The result in this study will have clinical implications on the choice
of dose calculation algorithm for Lung SBRT planning.
10
1.3 Scope of the project The physics of radiotherapy will be briefly covered in Chapter 2 of this paper. This
will include radiation dosimetry such as the concept of absorbed dose, the usage of
linear accelerators and the characteristics of photon beams.
An introduction of Thermoluminesence Dosimetry will be covered in Chapter 3.
The characteristics of TLDs, TLD reading equipment and TLD measurement
methods will be covered. A short study on the calibration of the TLDs will also be
presented.
Dose calculation algorithms such as AAA and AXB will be covered in Chapter 4. The
focus in this chapter is on the clinical use and implications of the dose calculation
algorithm. Note that the mechanics of the dose calculation algorithms is not within
the scope of this paper, however, details of AXB is covered in Appendix II. The
creation of the Lung SBRT phantom, including the virtual phantom, will also be
covered in this chapter.
Lastly, Chapter 5 will cover the validation of AXB and AAA using TLDs. Through this
validation, the implications of using different algorithms in a Lung SBRT treatment
will be evaluated. Perturbation factors for of TLDs for lung medium will also be
explained and applied to the measurement.
11
2 The Physics of Radiotherapy 2.1 Introduction to Radiotherapy Physics is extremely essential in cancer therapy. For example, radiotherapy was first
used to treat breast cancer patients shortly after the discovery of X-‐rays by German
physicist, Wilhelm Röntgen. Currently, radiotherapy is a common form of cancer
treatment for most cancer cases. Basically, it involves having a high-‐energy photon
beam directed towards a cancer patient’s tumor.
Cells are damaged when irradiated as radiation forms extremely reactive radicals
within the cell. These radicals cause the DNA bonds to be chemically broken down,
resulting in the cell’s inability to reproduce. With increased dosage, the probability
of sterilizing cells increases. However, both the malignant cells and the healthy cells
will experience the same damage when irradiated. Thus, there is a need to spare the
healthy cells during irradiation.
Thankfully, there is a minor contrast in the radiation response of malignant cells and
healthy cells. This difference in radiation response prevents the healthy cells within
the target volume, and the nearby tissues, from being destroyed. This phenomenon
is probably due to several reasons such as the cell’s radiosensitivity and differences
in the genetic mechanism that is affected by radiation8. In order to magnify this
radiation response, radiation is delivered in small doses per treatment, termed as
12
fractions. Such an approach generally allows therapeutic advantage as compared to
a single radiation treatment.
In a normal radiotherapy treatment, usually 30 fractions of around 2 Grays (Gy)i are
used. A usual treatment last approximately 5 to 8 weeks where each fraction is
treated once a day. Frequency of the treatment may be increased
(hyperfractionated), by delivering the fractions twice daily, or decreased by
delivering higher doses in lesser fractions (hypofractionated).
The second approach for reducing radiation damage is to decrease the dose
delivered to healthy tissues. This can be done by proper radiation treatment
planning and shaping of the radiation beam as discussed in 2.2.2.
i Radiation absorbed dose is defined as the energy imparted per unit mass of the irradiated
13
2.2 Radiation Dosimetry Radiation dosimetry generally involves finding out how much energy is deposited in a
given medium due to ionizing radiation. In this section we will define some dosimetric
quantities below.
2.2.1 Absorbed Dose
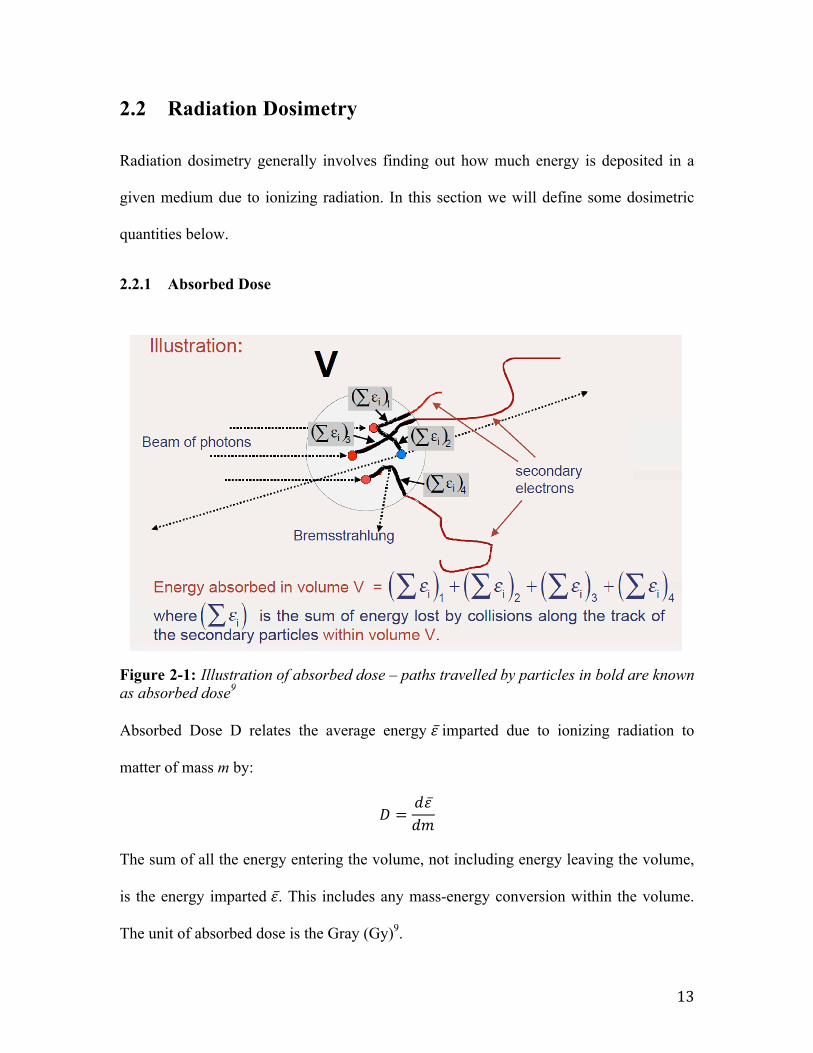
Figure 2-1: Illustration of absorbed dose – paths travelled by particles in bold are known as absorbed dose9 Absorbed Dose D relates the average energy 𝜀 imparted due to ionizing radiation to
matter of mass m by:
𝐷 =𝑑𝜀𝑑𝑚
The sum of all the energy entering the volume, not including energy leaving the volume,
is the energy imparted 𝜀. This includes any mass-energy conversion within the volume.
The unit of absorbed dose is the Gray (Gy)9.
DOSIMETRIC QUANTITIESAbsorbed dose
14
2.2.2 Linear Accelerators
Modern radiation therapy machines are known as medical linear accelerators (LINACS).
X-rays (bremsstrahlung) are produced when the linear accelerator accelerates electrons to
strike a high atomic number target. The bremsstrahlung produced is a forward-peaked X-
ray flux. A contoured flattening filter is used later to make the beam profile uniform.
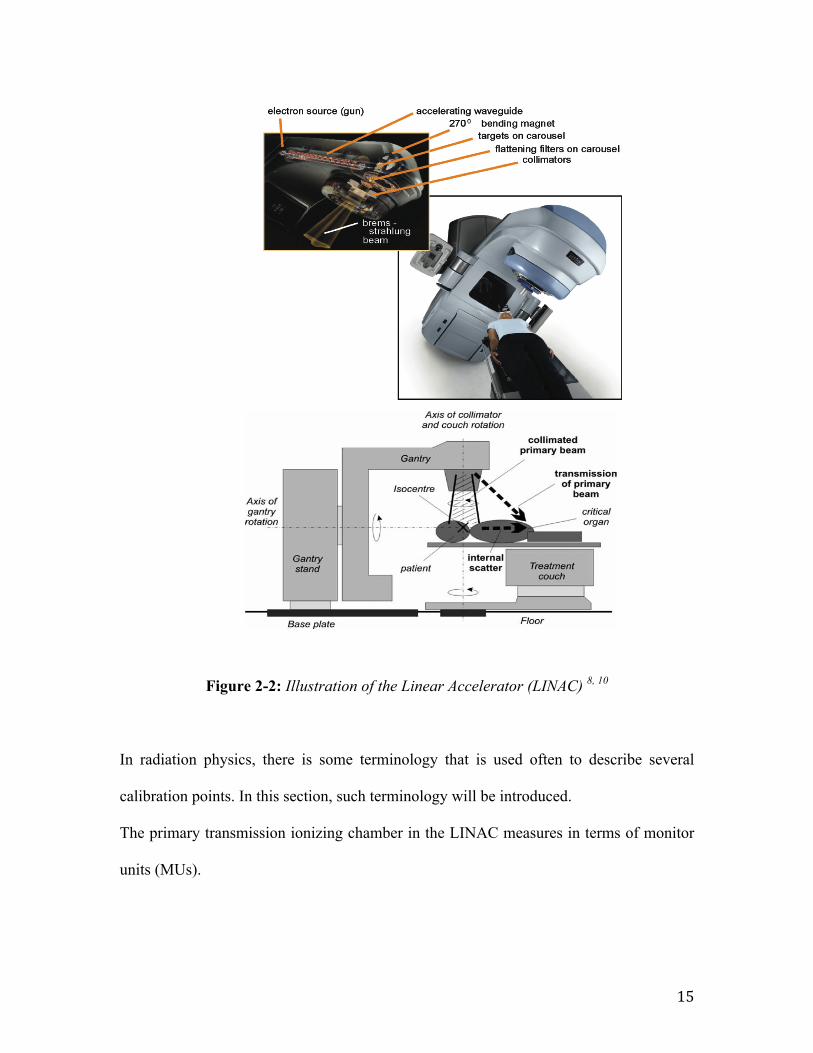
The gantry of the LINAC holds the beam transport system, accelerator, and the beam-
shaping devices. The gantry can also revolve 360° around the patient to allow treatment
in multiple directions. Figure 2-2 shows a patient lying on the couch and the shaped X-
ray beams are directed toward the patient. Photon beams deposit doses along its path as it
passes through the patient. The term X-ray beam and photon beam will be used
interchangeably in this study.
15
Figure 2-2: Illustration of the Linear Accelerator (LINAC) 8, 10
In radiation physics, there is some terminology that is used often to describe several
calibration points. In this section, such terminology will be introduced.
The primary transmission ionizing chamber in the LINAC measures in terms of monitor
units (MUs).
Applications of Thermoluminescent Dosimeters in Medicine 433
Fig. 11. Illustration of dose to normal tissues outside of the actual treatment field during the radiotherapy deliveryto a head and neck cancer patient.
problems taking into account individual variations in body shape and size. It is importantto caution that positional uncertainties in the placement of the TLDs in regions of highdose gradient may lead to inaccurate interpretation of the results.
Quality assurance for individual patients. With the advent of very complex radiotherapytechniques such as Intensity Modulated Radiation Therapy (IMRT) it has become com-mon practice to verify the treatment delivery sequence for individual patients. In IMRT theradiation treatment is delivered using multiple radiation fields each segmented into manysub-fields. As such, a total target dose may be delivered using many small abutting fieldsegments with an overall incident dose that is an order of magnitude larger than the result-ing dose. The ‘mix and match’ is complex and the fluency distribution in individual fieldscannot intuitively verified. Therefore, it is common practice to accurately verify the dosein IMRT treatment using a dosimeter that can determine the dose at one or more points(typically including the prescription point). Ionization chambers are usually used in thesemeasurements but they are bulky and fragile. TLDs can be appropriate especially for smallvolumes with homogeneous dose distributions. In these circumstances which may arise insimultaneous in-field boost scenarios (Fogliata et al., 2003) small detectors such as TLDsmay be the detector of choice. The measurements can be performed on a flat solid waterphantom or on an anthropomorphic phantom as previously described.In addition to point dose measurements, the dose distribution in one or more planes
through the target region can be of interest. An alternative to film may be sheets of TLdosimeters as shown in Figure 12 (courtesy of Keithley Instruments) (Iwata et al., 1995).Although not yet in common practice, medical physicists are searching for a replacementfor radiographic film in these applications since film processing has become less widelyavailable due to the increasing use of digital radiography.
16
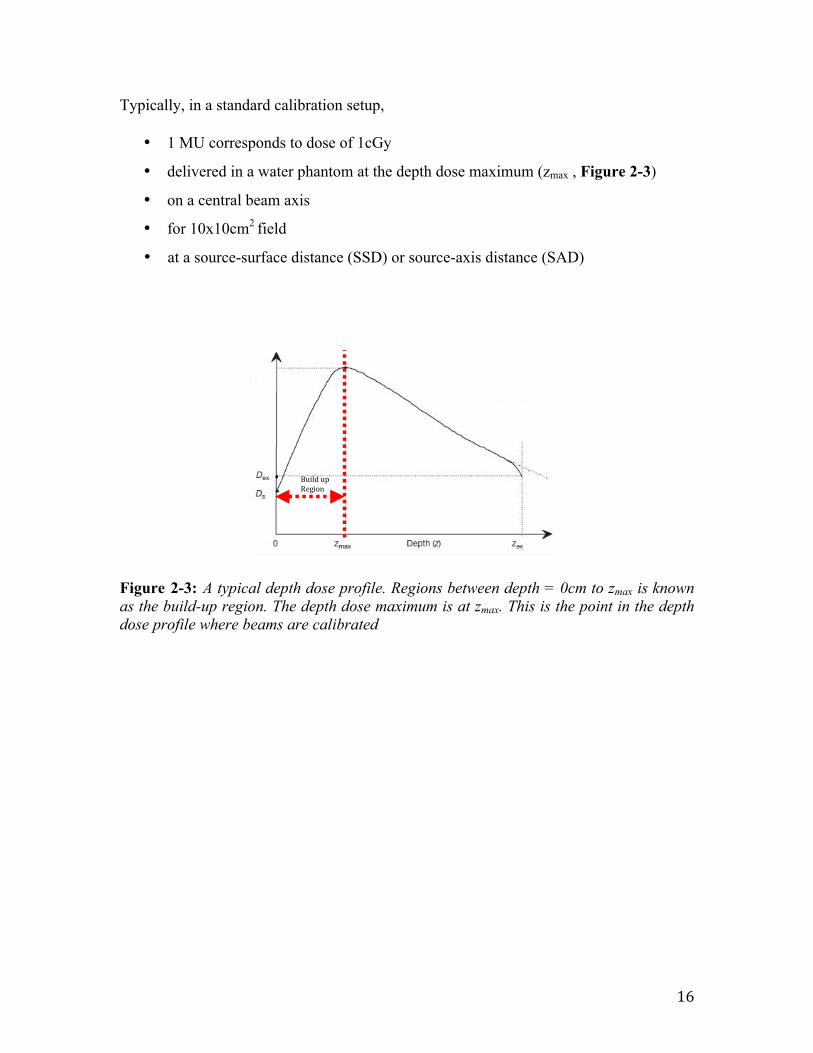
Typically, in a standard calibration setup,
• 1 MU corresponds to dose of 1cGy
• delivered in a water phantom at the depth dose maximum (zmax , Figure 2-3)
• on a central beam axis
• for 10x10cm2 field
• at a source-surface distance (SSD) or source-axis distance (SAD)
Figure 2-3: A typical depth dose profile. Regions between depth = 0cm to zmax is known as the build-up region. The depth dose maximum is at zmax. This is the point in the depth dose profile where beams are calibrated
PENETRATION OF PHOTON BEAMS INTO PATIENTBuildup region
Build up Region
17
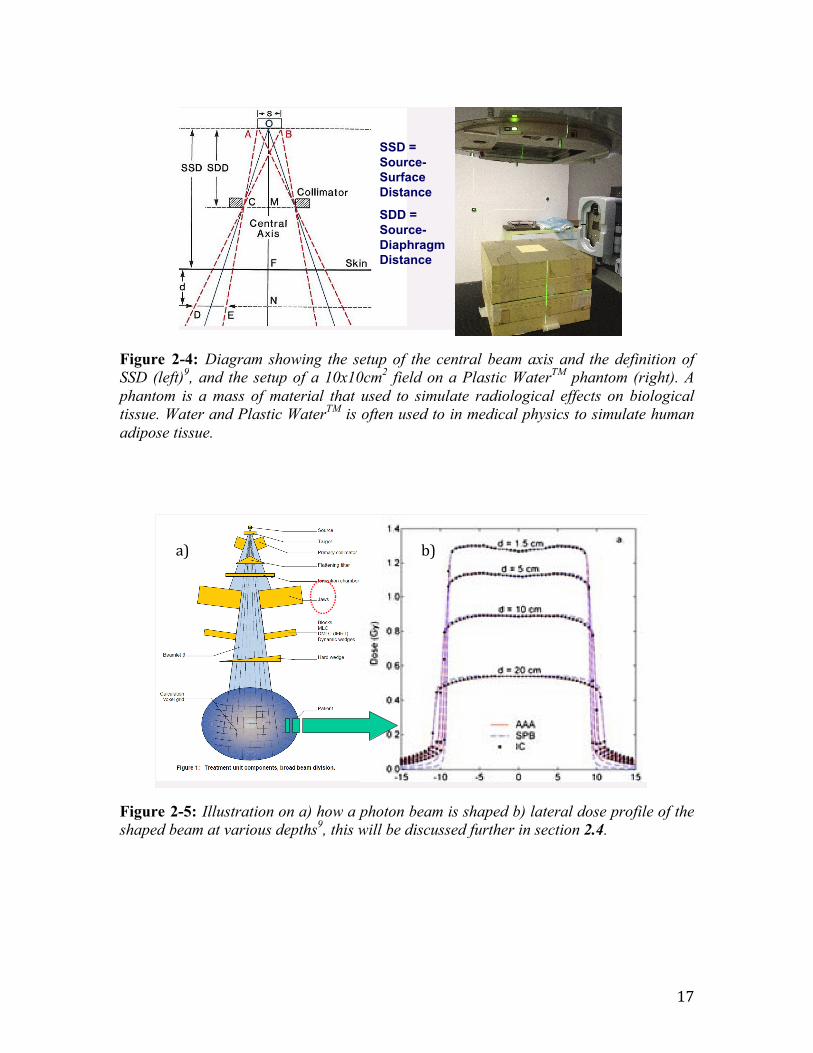
Figure 2-4: Diagram showing the setup of the central beam axis and the definition of SSD (left)9, and the setup of a 10x10cm2 field on a Plastic WaterTM phantom (right). A phantom is a mass of material that used to simulate radiological effects on biological tissue. Water and Plastic WaterTM is often used to in medical physics to simulate human adipose tissue.
Figure 2-5: Illustration on a) how a photon beam is shaped b) lateral dose profile of the shaped beam at various depths9, this will be discussed further in section 2.4.
GAMMA RAY BEAMS AND GAMMA RAY UNITSDose delivery with teletherapy machines
(80cm for Co60 machines)
SSD = Source-Surface Distance
SDD = Source-Diaphragm Distance
Beam collimationLINACS
(Assuming a flat surface on water)
b) a)
18
2.3 Radiation treatment setups
2.3.1 Source Surface Distance (SSD) Setup
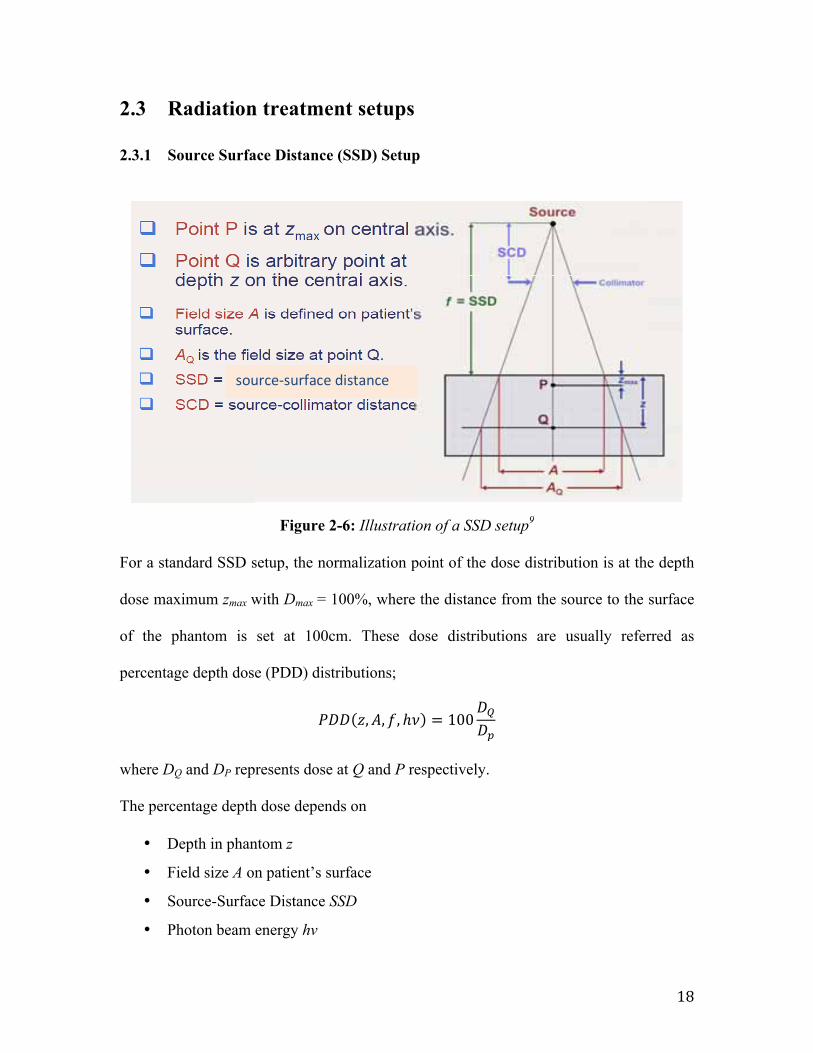
Figure 2-6: Illustration of a SSD setup9 For a standard SSD setup, the normalization point of the dose distribution is at the depth
dose maximum zmax with Dmax = 100%, where the distance from the source to the surface
of the phantom is set at 100cm. These dose distributions are usually referred as
percentage depth dose (PDD) distributions;
𝑃𝐷𝐷 𝑧,𝐴, 𝑓, ℎ𝜈 = 100𝐷!𝐷!
where DQ and DP represents dose at Q and P respectively.
The percentage depth dose depends on
• Depth in phantom z
• Field size A on patient’s surface
• Source-Surface Distance SSD
• Photon beam energy hν
RADIATION TREATMENT PARAMETERS
source-‐surface distance
19
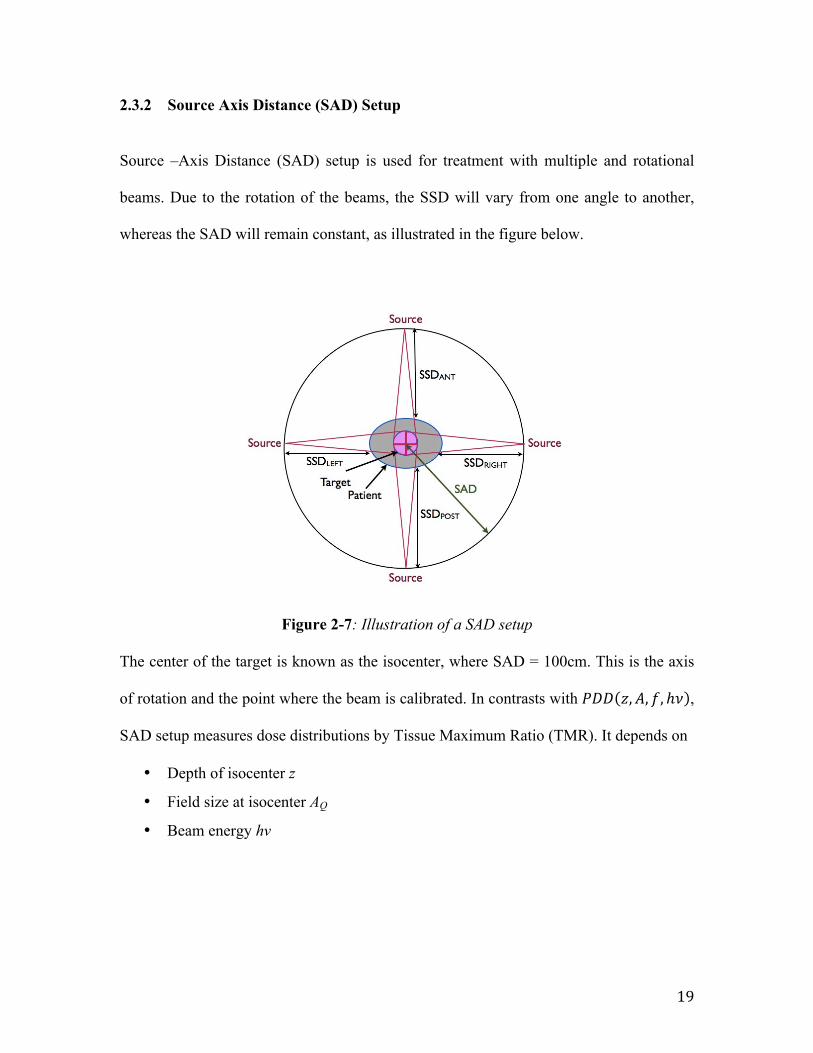
2.3.2 Source Axis Distance (SAD) Setup
Source –Axis Distance (SAD) setup is used for treatment with multiple and rotational
beams. Due to the rotation of the beams, the SSD will vary from one angle to another,
whereas the SAD will remain constant, as illustrated in the figure below.
Figure 2-7: Illustration of a SAD setup The center of the target is known as the isocenter, where SAD = 100cm. This is the axis
of rotation and the point where the beam is calibrated. In contrasts with 𝑃𝐷𝐷 𝑧,𝐴, 𝑓, ℎ𝜈 ,
SAD setup measures dose distributions by Tissue Maximum Ratio (TMR). It depends on
• Depth of isocenter z
• Field size at isocenter AQ
• Beam energy hν
20
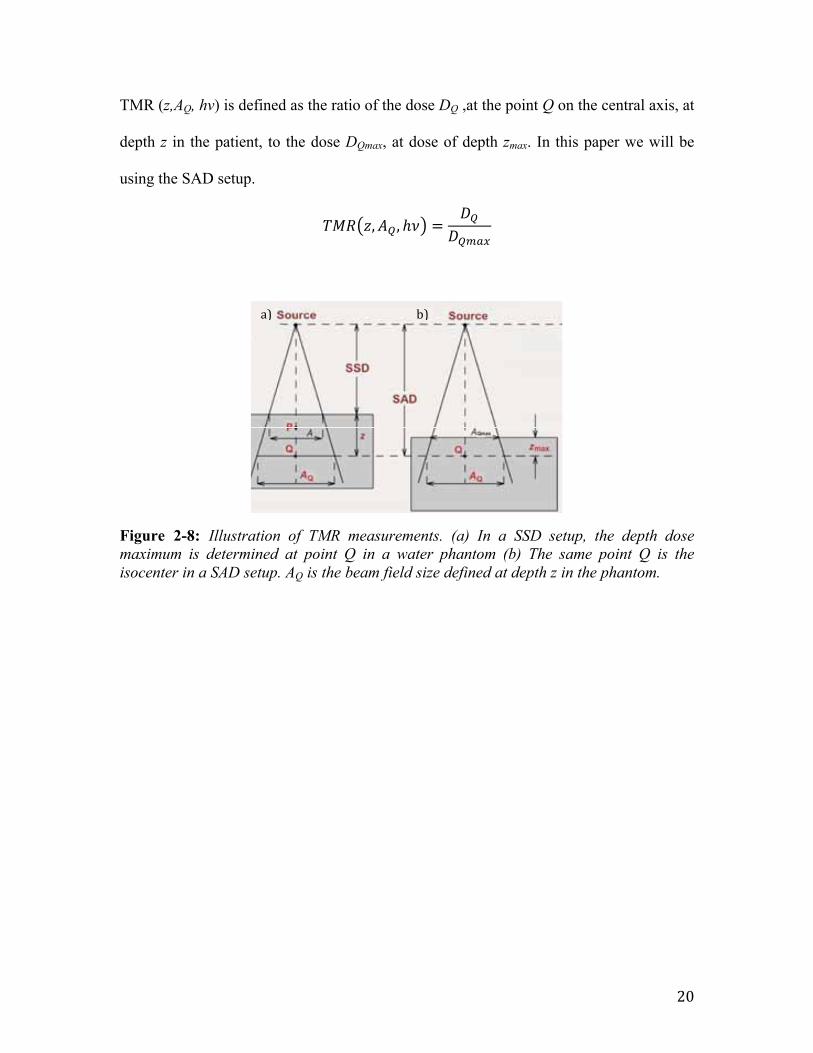
TMR (z,AQ, hν) is defined as the ratio of the dose DQ ,at the point Q on the central axis, at
depth z in the patient, to the dose DQmax, at dose of depth zmax. In this paper we will be
using the SAD setup.
𝑇𝑀𝑅 𝑧,𝐴! , ℎ𝜈 =𝐷!
𝐷!"#$
Figure 2-8: Illustration of TMR measurements. (a) In a SSD setup, the depth dose maximum is determined at point Q in a water phantom (b) The same point Q is the isocenter in a SAD setup. AQ is the beam field size defined at depth z in the phantom.
CENTRAL AXIS DEPTH DOSES IN WATER: SAD SETUPTissue-phantom ratio TPR and Tissue-maximum ratio TMR
a) b)
21
2.4 Photon Beams Factors that affect a single photon beam are:
1. beam energy (photon energy)
2. beam direction (beam angle with respect to a point within the patient)
3. beam intensityii
4. shape of the fieldiii
5. beam profileiv
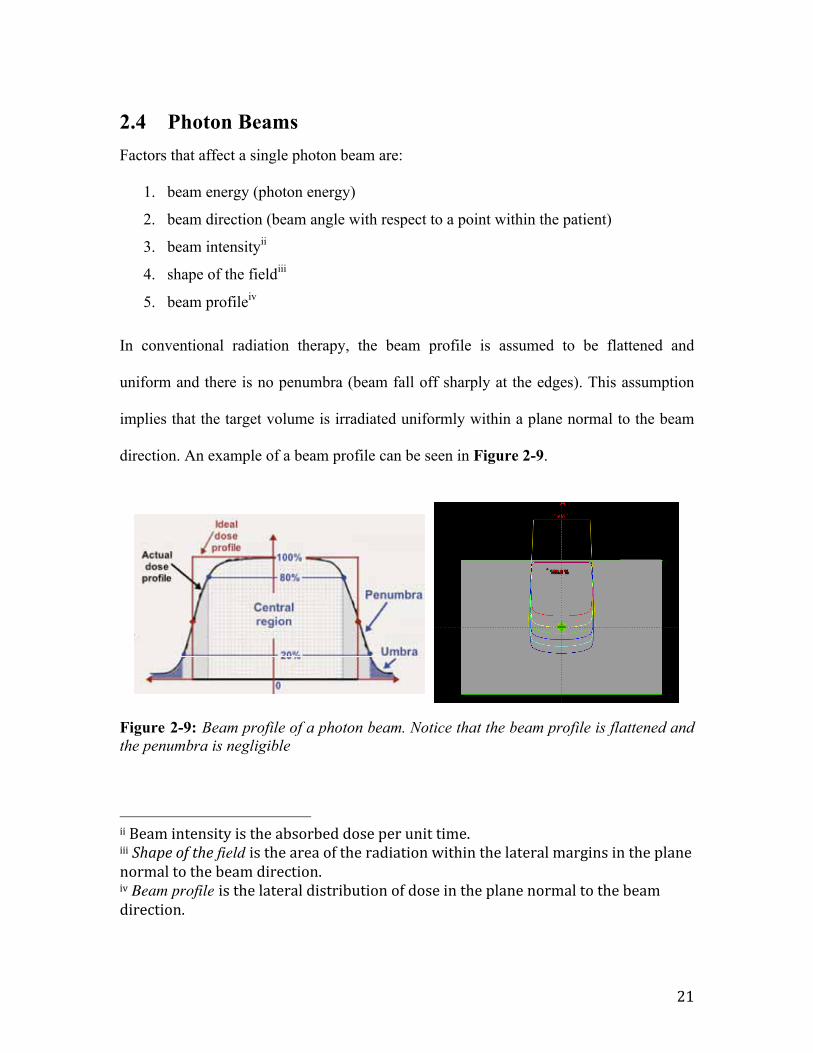
In conventional radiation therapy, the beam profile is assumed to be flattened and
uniform and there is no penumbra (beam fall off sharply at the edges). This assumption
implies that the target volume is irradiated uniformly within a plane normal to the beam
direction. An example of a beam profile can be seen in Figure 2-9.
Figure 2-9: Beam profile of a photon beam. Notice that the beam profile is flattened and the penumbra is negligible
ii Beam intensity is the absorbed dose per unit time. iii Shape of the field is the area of the radiation within the lateral margins in the plane normal to the beam direction. iv Beam profile is the lateral distribution of dose in the plane normal to the beam direction.
OFF-AXIS RATIOS AND BEAM PROFILES
22
In medical physics, the photon beam energy is measured in terms of megavolts, with
units MV. 1MV of a photon beam will produce about 1MeV of photons. This is not to be
confused with the unit mega electron volts, MeV used in conventional nomenclature in
physics.
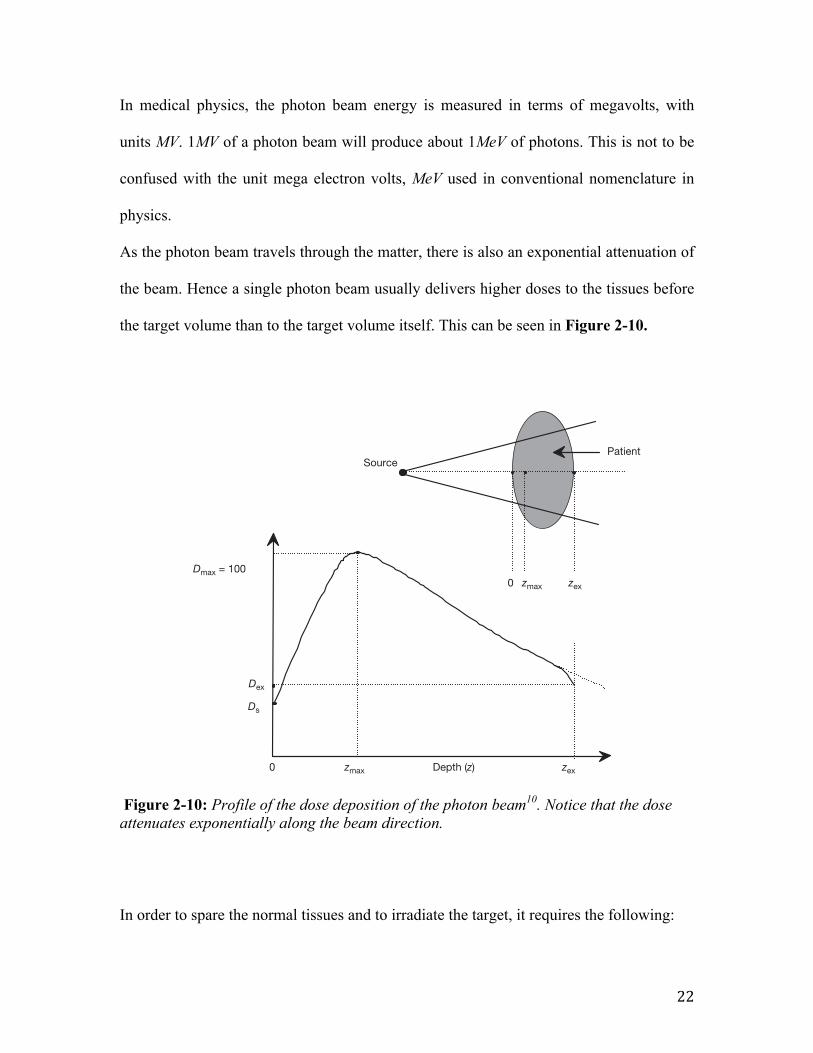
As the photon beam travels through the matter, there is also an exponential attenuation of
the beam. Hence a single photon beam usually delivers higher doses to the tissues before
the target volume than to the target volume itself. This can be seen in Figure 2-10.
Figure 2-10: Profile of the dose deposition of the photon beam10. Notice that the dose attenuates exponentially along the beam direction.
In order to spare the normal tissues and to irradiate the target, it requires the following:
CHAPTER 6
170
The functions are usually measured with suitable radiation detectors in tissue equivalent phantoms, and the dose or dose rate at the reference point is determined for, or in, water phantoms for a specific set of reference conditions, such as depth, field size and source to surface distance (SSD), as discussed in detail in Section 9.1.
A typical dose distribution on the central axis of a megavoltage photon beam striking a patient is shown in Fig. 6.3. Several important points and regions may be identified. The beam enters the patient on the surface, where it delivers a certain surface dose Ds. Beneath the surface the dose first rises rapidly, reaches a maximum value at depth zmax and then decreases almost exponentially until it reaches a value Dex at the patient’s exit point. The techniques for relative dose measurements are discussed in detail in Section 6.13.
0
Ds
Source
0
Patient
Dmax = 100zmax zex
Dex
zmax Depth (z) zex
FIG. 6.3. Dose deposition from a megavoltage photon beam in a patient. Ds is the surface dose at the beam entrance side, Dex is the surface dose at the beam exit side. Dmax is the dose maximum often normalized to 100, resulting in a depth dose curve referred to as the percentage depth dose (PDD) distribution. The region between z = 0 and z = zmax is referred to as the dose buildup region.
23
• Medical images to indicate the margins of the tumor and affected critical organs
• Patient positioning and immobilization
• Treatment planning – determination of the procedures in delivering the dose to the
tumor and shielding critical organs and healthy tissues. A computer simulation of
the treatment will be done to simulate the treatment procedures and fractionation
schemes
Treatment planning and evaluation is done virtually as it is able to simulate:
• Output of the LINAC
• interaction of radiation with matter - absorbed dose
• patient geometry
• the required number of beams from desired direction(s)
• dose distribution in the patient.
In summary, the planning process is the task of determining the method to treat a patient
with a virtual therapy machine, with the assumption that it is a good simulation of the
actual treatment. The treatment planning process will be discussed further in later
chapters.
24
2.5 Summary The end goal in radiation physics is to create an optimum situation where the radiation
dose is targeted at a target volume, with the appropriate amount of dose, and yet
minimizing dose to critical organs and healthy tissues.
The concept of absorbed dose is introduced as the relationship between the average
energy 𝜀 imparted by ionizing radiation to matter of mass m.
Modern radiotherapy machines are known as Linear Accelerators. LINAC creates the
high energy X-ray beam for radiotherapy. Several parameters of the photon beams are
introduced such as depth dose maximum and monitor units.
Lastly, there are two different radiation treatment setups, source-surface distance (SSD)
and source-axis distance (SAD). In this paper, we will use the SAD setup.
25
3 Thermoluminesence Dosimeters 3.1 Introduction to TLDs Radiation dosimeters are used to measure absorbed dose in a medium of interest during
or after irradiation. Absorbed dose is determined by the radiation dosimeter response. The
average absorbed dose in the medium can be related to the absorbed dose in the
dosimeter sensitive volume, by using several theoretical considerations, such as cavity
theory (Appendix I). Ionization chambers, films, MOSFET detectors, semiconductor
diodes, and thermoluminescent dosimeters (TLDs) are some examples of radiation
dosimeters.
Thermoluminescence dosimetry is one of the most flexible dosimetric systems and can be
used in various radiation dose measurement applications. It was reported that the first
medical use of TLD was in 1953 by Daniels et al.11
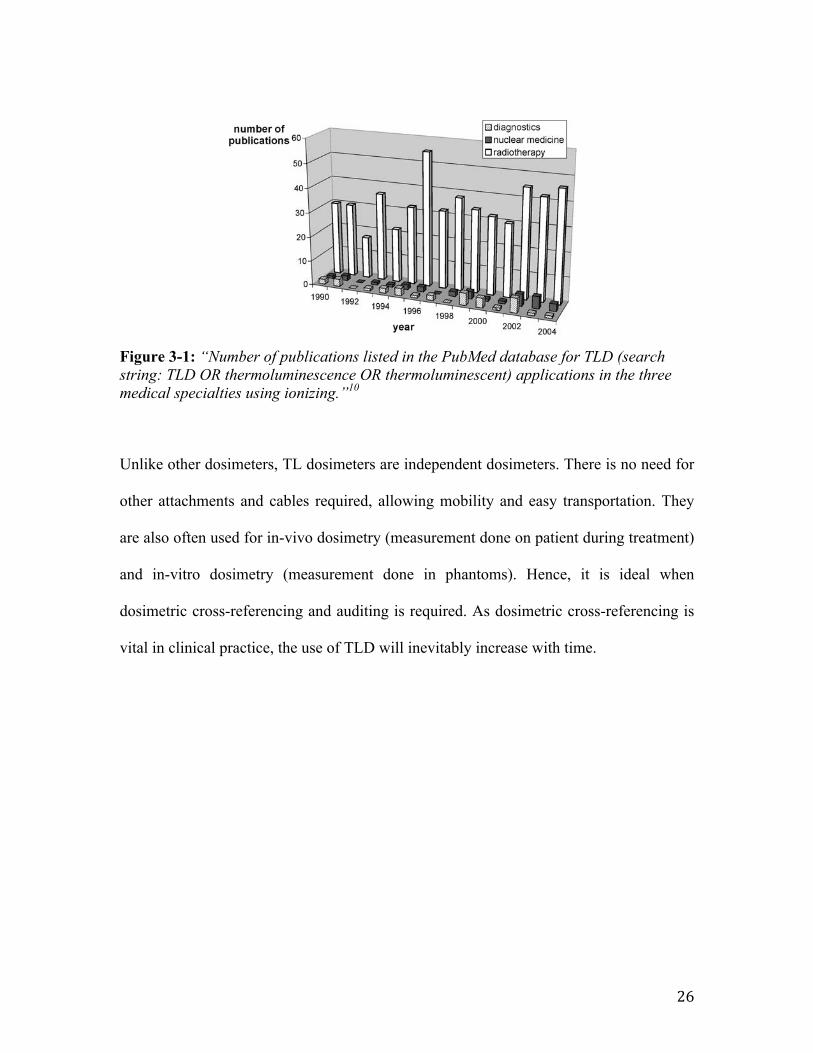
Mobit et al10 did a study and indicated that “radiotherapy is by far the most important
area in medicine where TLD is used”. It was shown in the study that “about 10 times
more papers are published annually concerning the use of TLD in radiotherapy
applications in comparison to using TLD for diagnostic procedures” 10 (Figure 3-1).
These include in-vivo dosimetry, which involve dose measurements done on patients and
in phantoms.
26
Figure 3-1: “Number of publications listed in the PubMed database for TLD (search string: TLD OR thermoluminescence OR thermoluminescent) applications in the three medical specialties using ionizing.”10
Unlike other dosimeters, TL dosimeters are independent dosimeters. There is no need for
other attachments and cables required, allowing mobility and easy transportation. They
are also often used for in-vivo dosimetry (measurement done on patient during treatment)
and in-vitro dosimetry (measurement done in phantoms). Hence, it is ideal when
dosimetric cross-referencing and auditing is required. As dosimetric cross-referencing is
vital in clinical practice, the use of TLD will inevitably increase with time.
Applications of Thermoluminescent Dosimeters in Medicine 413
1. Introduction
Thermoluminescence dosimetry (TLD) has a long history in medicine. Daniels (Danielset al., 1953), one of the pioneers of TLD, reported the first ‘medical’ application of TLDover half a century ago: “The crystals were swallowed by the patient (who had receivedan injection containing radioactive isotopes), recovered one or two days later, and the ac-cumulated dosage in roentgens was measured by matching thermoluminescence intensitywith that produced in crystals by a known roentgen dosage”.However, despite its many advantages, the use of TLD in medical applications has stag-
nated over the last few decades. Figure 1 shows the number of publications on TLD in threemedical subspecialties. The figure shows the publications listed with the keywords “TLD”,“thermoluminescent” or “thermoluminescence dosimetry” and a reference to radiotherapy,diagnostic radiology or nuclear medicine as listed in the PubMed database. The number ofpublications on the use of TLD in the medical field has stayed more or less constant overthe last 15 years (and beyond) despite increasingly complex irradiation geometries and anincreasing need for quality assurance and treatment dose verification.Figure 1 also indicates that radiotherapy is by far the most important area in medicine
where TLD is used. About 10 times more papers are published annually concerning theuse of TLD in radiotherapy applications than in diagnostic procedures. While most ofthe applications in diagnostic procedures are concerned with radiation protection in oneform or another, there are many more applications in radiotherapy. These include dosemeasurements in phantoms and directly on patients (“in vivo” dosimetry).The structure of the present chapter reflects this to a certain degree: after a very con-
cise discussion of some of the theoretical features of TLD relevant to medical applications,a brief overview of TLD applications in radiation protection is presented. This is followedby sections on the three most important areas of application in radiation medicine: radio-therapy, diagnostic radiology and nuclear medicine. The section on dosimetric intercom-
Fig. 1. Number of publications listed in the PubMed database for TLD (search string: TLD OR thermolumines-cence OR thermoluminescent) applications in the three medical specialties using ionizing.
27
3.1.1 A General Model of Thermoluminesence Dosimetry
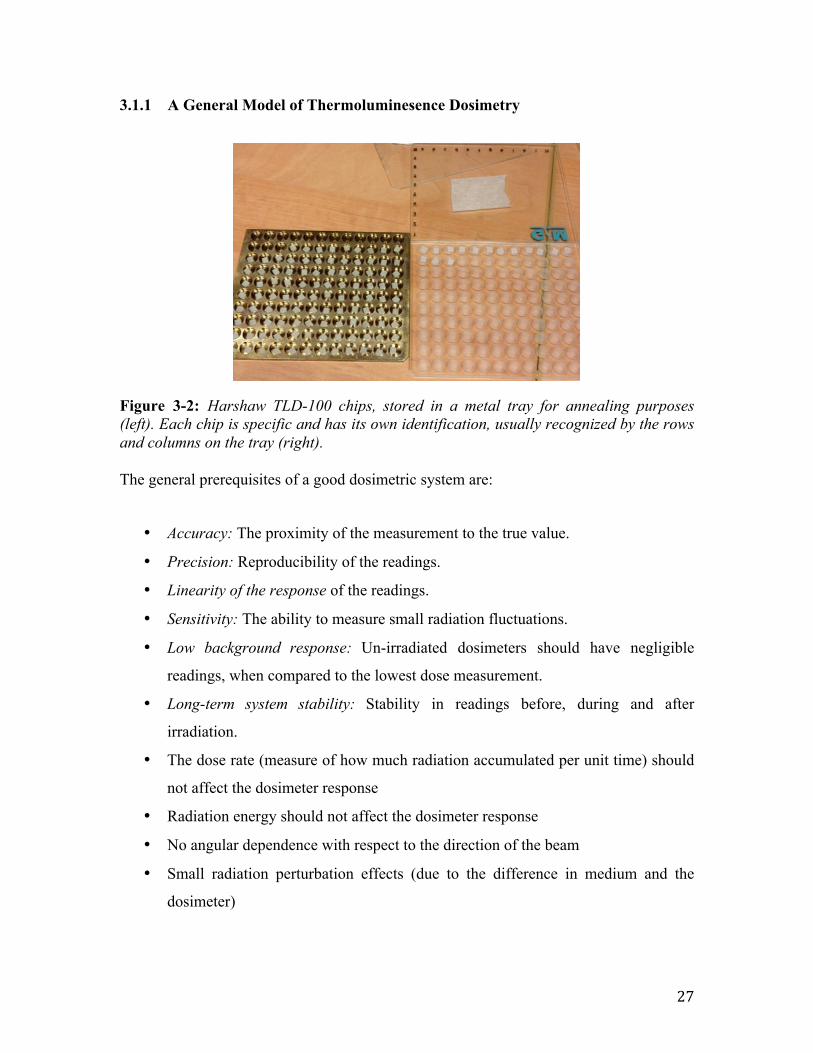
Figure 3-2: Harshaw TLD-100 chips, stored in a metal tray for annealing purposes (left). Each chip is specific and has its own identification, usually recognized by the rows and columns on the tray (right). The general prerequisites of a good dosimetric system are:
• Accuracy: The proximity of the measurement to the true value.
• Precision: Reproducibility of the readings.
• Linearity of the response of the readings.
• Sensitivity: The ability to measure small radiation fluctuations.
• Low background response: Un-irradiated dosimeters should have negligible
readings, when compared to the lowest dose measurement.
• Long-term system stability: Stability in readings before, during and after
irradiation.
• The dose rate (measure of how much radiation accumulated per unit time) should
not affect the dosimeter response
• Radiation energy should not affect the dosimeter response
• No angular dependence with respect to the direction of the beam
• Small radiation perturbation effects (due to the difference in medium and the
dosimeter)
28
There are other important factors such as cost, easy usage and the ability of the dosimeter
to provide an instant reading. It is indeed difficult for dosimetric systems to meet all of
the above requirements. However, depending on the dosimetric application, optimum
measurement capability can be achieved by balancing the advantages and disadvantages
of the chosen dosimetric system.
Advantages of thermoluminescence dosimetry
• Relatively cheap and easy to use
• Able to reuse
• Versatile – Depending on the radiation therapy dose measurement
applications, TLDs are available in many forms such as rods, chips, powder,
cards and discs to suit the situation
• Small perturbation of the radiation field due to its small size. Perturbation
effects can be corrected (Chapter 5.4.1)
• High spatial resolution
• No angular dependence
• No dependence on temperature and pressure of the environment
• TLDs are stand alone detectors and require no electrical connections
Disadvantages of thermoluminesence dosimetry systems
• For accurate dosimetry, significant effort is required for calibration
• Fading of the radiation induced signal will increase with time
• Fragile, care is needed in handling TLDs
• Precision of the measurements require strict operational procedures
• TLDs must be annealed and re-calibrated
• Long annealing process (~4 hours)
• Readings will be lost after readout
29
3.1.2 Characteristics of TLDs
In this paper, the TLDs used were Harshaw TLD-100 chips, which are Lithium Fluoride
crystals doped with Magnesium and Titanium ( LiF:Mg,Ti ). TLD-100 are often used
clinically for measurements of radiation dose as it has an effective atomic number of 8.2,
which is close to that of water or biological tissue10.
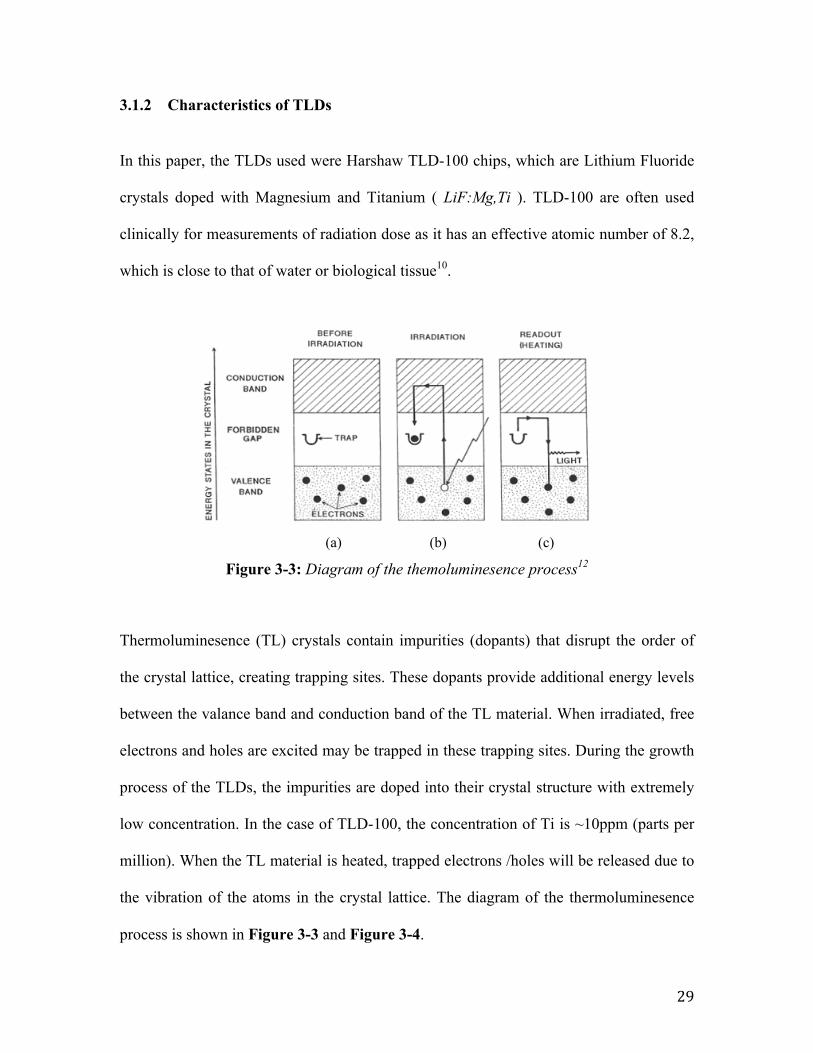
Figure 3-3: Diagram of the themoluminesence process12
Thermoluminesence (TL) crystals contain impurities (dopants) that disrupt the order of
the crystal lattice, creating trapping sites. These dopants provide additional energy levels
between the valance band and conduction band of the TL material. When irradiated, free
electrons and holes are excited may be trapped in these trapping sites. During the growth
process of the TLDs, the impurities are doped into their crystal structure with extremely
low concentration. In the case of TLD-100, the concentration of Ti is ~10ppm (parts per
million). When the TL material is heated, trapped electrons /holes will be released due to
the vibration of the atoms in the crystal lattice. The diagram of the thermoluminesence
process is shown in Figure 3-3 and Figure 3-4.
2. Theory
2.1. Thermoluminescence Dosimetry - A general model
Luminescence is a process in which, a material that is irradiated, absorbs
energy which is then emitted as a photon in the visible region of the electromagnetic
spectrum. Thermoluminescence is a form of luminescence in which heat is given to
the material which results in light emission [4].
In a crystal, electrons (e-) are found in the valence band (see figure 2.1.1a).
When the material is irradiated, e- move from the valence to the conduction band
where they move freely. Therefore, a hole (h) remains in the valence band (absence of
electron) which can also move inside the crystal. Due to impurities and doping of the
crystal, e- and h traps are created in the band gap between the valence and the
conduction band. Thus e- and h are trapped at defects (figure 2.1.1b). If these traps are
deep, the electrons and holes will not have enough energy to escape. By heating the
crystal their energy is increased, they leave the traps and recombine at luminescence
centers. As a result light is then emitted (figure 2.1.1c) [4-5].
(a) (b) (c)
Figure 2.1.1: The mechanism of TL dosimetry [5].
A TLD can be considered as an integrating detector in which the number of e-
and h, which are trapped, is the number of the e-/h pairs which are produced during
the exposure. Preferably, every trapped e-/h emits one photon. Consequently, the
number of emitted photons is equal to the number of charge pairs, which are also
proportional to the dose which is absorbed by the crystal [6].
3
30
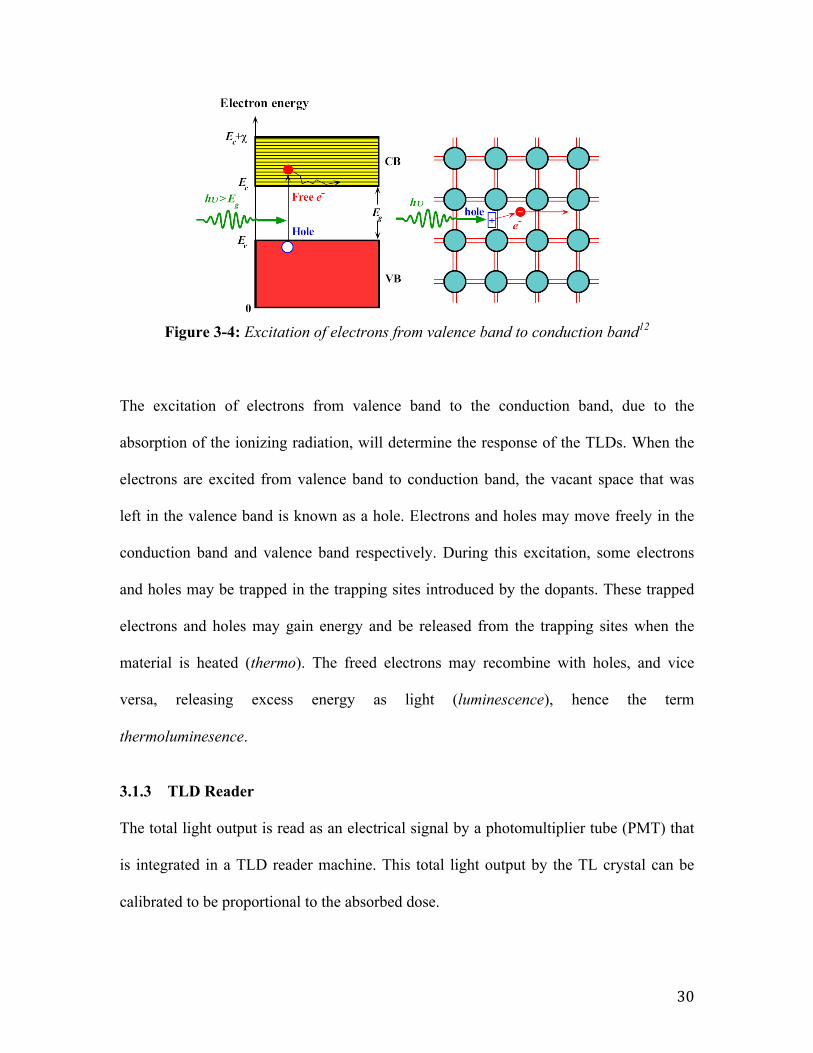
Figure 3-4: Excitation of electrons from valence band to conduction band12
The excitation of electrons from valence band to the conduction band, due to the
absorption of the ionizing radiation, will determine the response of the TLDs. When the
electrons are excited from valence band to conduction band, the vacant space that was
left in the valence band is known as a hole. Electrons and holes may move freely in the
conduction band and valence band respectively. During this excitation, some electrons
and holes may be trapped in the trapping sites introduced by the dopants. These trapped
electrons and holes may gain energy and be released from the trapping sites when the
material is heated (thermo). The freed electrons may recombine with holes, and vice
versa, releasing excess energy as light (luminescence), hence the term
thermoluminesence.
3.1.3 TLD Reader
The total light output is read as an electrical signal by a photomultiplier tube (PMT) that
is integrated in a TLD reader machine. This total light output by the TL crystal can be
calibrated to be proportional to the absorbed dose.
Electrons and holes in silicon crystalElectrons and holes in silicon crystal
• WhenȱaȱphotonȱbreaksȱaȱSiȬSiȱ bond,ȱaȱfreeȱelectronȱandȱaȱ
holeȱinȱtheȱSiȬSiȱbondȱisȱ created.
• Aȱphotonȱwithȱanȱenergyȱgreaterȱ thanȱbandgapȱenegyȱ(Eg
)ȱcanȱ exciteȱanȱelectronȱfromȱtheȱ
valenceȱbandȱtoȱtheȱconductionȱ band.
26
31
In this study, the TLD reader used is Harshaw Model 3500 Manual TLD Reader as
shown in Figure 3-5 below. The TLD reader machine uses contact heating that produces
linearly ramped temperatures accurate to within ±1°C to 400°C.
Figure 3-5: Harshaw Model 3500 Manual TLD Reader
To improve the accuracy of low-exposure readings, nitrogen gas is injected to flow
around the planchet (metal plate holding the TLD in place). The nitrogen gas eliminates
oxygen in the planchet area, which will eliminate unwanted oxygen-induced TL signals.
Nitrogen is also routed through the photomultiplier tube chamber to eliminate moisture
caused by condensation.
An electronic Reference Light is built into the PMT chamber for monitoring the
performance of the instrument. It is used for quality assurance check during the readout
process.
Model 3500 Manual TLD Reader with WinREMS3500-W-O-0805 Page 1-1
Operator’s Manual
Figure 1.1 Model 3500 Manual TLD Reader
1.0 System OverviewThe Harshaw Model 3500 Manual TLD
Reader is a PC-driven, manually-operated,tabletop instrument for thermoluminescentdosimetry (TLD) measurement. Iteconomically provides both high performanceand high reliability, and it complies with thelatest International Standards Organization(ISO) requirements. The 3500 reads onedosimeter per loading and accommodates avariety of TL configurations, including chips,disks, rods, and powder.
The system consists of two majorcomponents: the TLD Reader and theWindows Radiation Evaluation and Manage-ment System (WinREMS) software residenton a personal computer (PC), which isconnected to the Reader via a serialcommunications port .
1.1 TLD ReaderThe Reader's basic external components
include a front control panel consisting ofthree LED status lights and a Readpushbutton, a sample drawer assembly thatfeatures an interchangeable planchet and abuilt-in Reference Light for periodicmonitoring of Reader performance, and adrawer for neutral density filters. The rearpanel houses a voltage-selectable power inputmodule with fuse access, an instrument Resetbutton, a fitting for nitrogen gas tubing, anRS-232-C serial communication port, and arecessed pressure sensor adjusting screw.
The Reader uses contact heating with aclosed loop feedback system that produceslinearly ramped temperatures accurate towithin ±1o C to 400o C in the standard Reader,or 600o C with the High Temperature option.The Time Temperature Profile (TTP) is user-1.0 System Overview (cont’d)
32
3.1.4 TLD Glow Curve
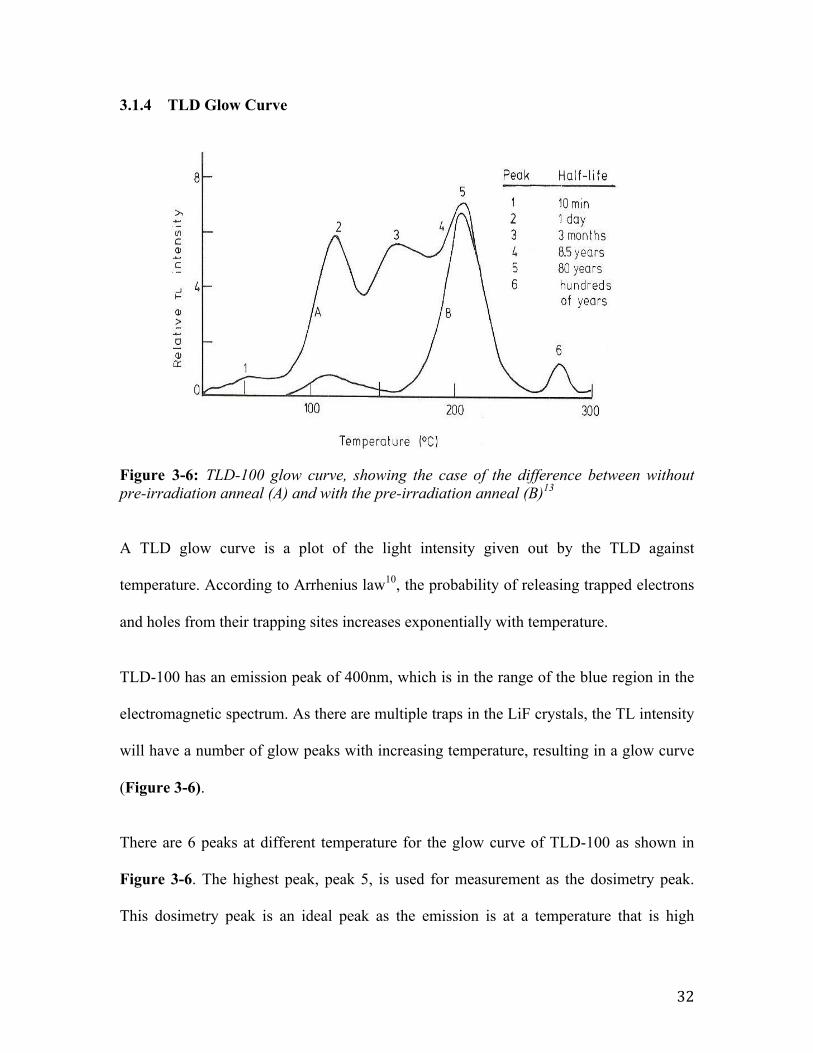
Figure 3-6: TLD-100 glow curve, showing the case of the difference between without pre-irradiation anneal (A) and with the pre-irradiation anneal (B)13
A TLD glow curve is a plot of the light intensity given out by the TLD against
temperature. According to Arrhenius law10, the probability of releasing trapped electrons
and holes from their trapping sites increases exponentially with temperature.
TLD-100 has an emission peak of 400nm, which is in the range of the blue region in the
electromagnetic spectrum. As there are multiple traps in the LiF crystals, the TL intensity
will have a number of glow peaks with increasing temperature, resulting in a glow curve
(Figure 3-6).
There are 6 peaks at different temperature for the glow curve of TLD-100 as shown in
Figure 3-6. The highest peak, peak 5, is used for measurement as the dosimetry peak.
This dosimetry peak is an ideal peak as the emission is at a temperature that is high
dose is the 5th peak. The dosimetry peak should have large enough temperature in
order not to be affected by the room temperature but also not to high in order not to be
affected by the black body emission of the TLD disc. The half-life of each peak is also
shown on figure 2.4.1.
Figure 2.4.1: Glow curve of TLD100 (A) – after pre-heating procedure (B) The half-lives of each
peak can also be seen. [4]
The problem is that at low temperatures the fading is high. Thus electrons
have enough energy to leave the traps and de-excite without the need of heat. That
affects the sensitivity of the dosimeter. It is possible to transfer the TL sensitivity of
low temperatures to the dosimetry peak by pre-heating just before the read-out. Thus
the background signal is removed and therefore, the dosimetry peak is much more
distinct (figure 2.4.1-curve B).
After the TLDs are read-out, they are annealed in order to ensure the signal
has been completely removed and the TLD is again ready for use. For the TLD100
the annealing is not as simple, as it is first heated at 4000C for an hour and then at
800C for 16 to 24 hours. If the used annealing temperature is more than 4000C the
sensitivity of the material is reduced [4].
The area under the glow curve, after the appropriate calibration, corresponds
to the absorbed dose which is measured using the TLD reader. If the rate of the
9
33
enough, so that it is not affected by room temperatures, and low enough, so that it is not
influenced by the TLD’s black body emission. Unlike the other peaks, fading of peak 5 is
slow as it has a long half-life, which is ideal for measurement, as shown in Figure 3-6.
At low temperatures, electrons may gain enough energy to escape the trapping sites and
de-excite without much increase in temperature. This causes a problem, as it will affect
the sensitivity of the dosimeter. The solution is to remove the peaks at low temperatures
by pre-heating the TLDs before readout. This pre-heating also removes the background
signal, resulting the dosimetry peak (peak 5) to be much more distinct as shown in
Figure 3-6 (curve B)
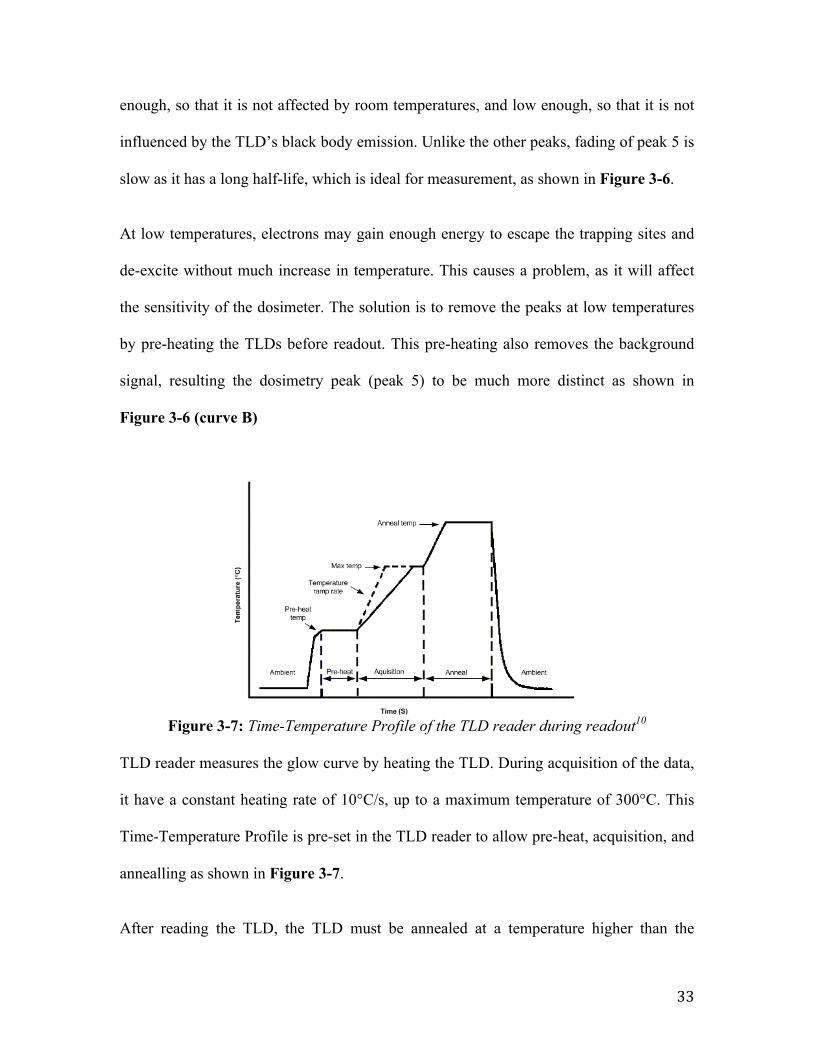
Figure 3-7: Time-Temperature Profile of the TLD reader during readout10 TLD reader measures the glow curve by heating the TLD. During acquisition of the data,
it have a constant heating rate of 10°C/s, up to a maximum temperature of 300°C. This
Time-Temperature Profile is pre-set in the TLD reader to allow pre-heat, acquisition, and
annealling as shown in Figure 3-7.
After reading the TLD, the TLD must be annealed at a temperature higher than the
TLD MaterialDOSM-0-N-1202-001 Page 1
Standard TTP Recommendations1 IntroductionThis technical notice consists ofHarshaw standard Time TemperatureProfile Recommendation tables for thefollowing TLD materials:
TLD Material See TableTLD-100; LiF:Mg,Ti 1TLD-100H; LiF:Mg,Cu, P 2TLD-200; CaF2:Dy 3TLD-300; CaF2:Tm 4TLD-400; CaF2:Mn 5TLD-500; Al2O3:C 6TLD-600; 6LiF:Mg,Ti 7TLD-600H; 6LiF:Mg,Cu, P 8TLD-700; 7LiF:Mg,Ti 9TLD-700H; 7LiF:Mg,Cu, P 10TLD-800; Li2B4O7:Mn 11TLD-900; CaSO4:Dy 12
Use these tables when setting up yourTime Temperature profile for yourappropriate TLD material and Reader.
The typical Time-Temperature Profile(TTP) diagram is shown in Figure 1. Theheating cycle normally consists ofPreheat, Acquisition, Anneal, and Coolsegments. Preheat is applied to segregatethe light generated from low-energytraps to minimize fade effect.Dosimetrically significant data aregenerated and stored during theAcquisition segment. To ensure currentexposures do not contribute tosubsequent measurements, the Annealcycle is applied. This has the effect ofremoving signal residual. The heatingcycle applied helps to establish thereproducibility of the dosimeter.
Figure 1 Typical Time-Temperature Profile (TTP) Diagram
34
readout temperature (400°C for 1 hour and 100°C for 3 hours for TLD-100). This
annealing process releases any trapped electrons and holes that are not released during
readout so that the TLD could be reused for subsequent measurements.
3.1.5 TLD setup for radiotherapy
In radiotherapy applications, TLDs are often calibrated to a lower megavoltage X-ray
beam. In this paper, the TLDs are calibrated to a 6 MV X-ray beam. If a photon or
electron beam of different energy is used, the readings by the TLDs can be corrected by
applying energy correction factors, as investigated by Mobit et al14, 15.
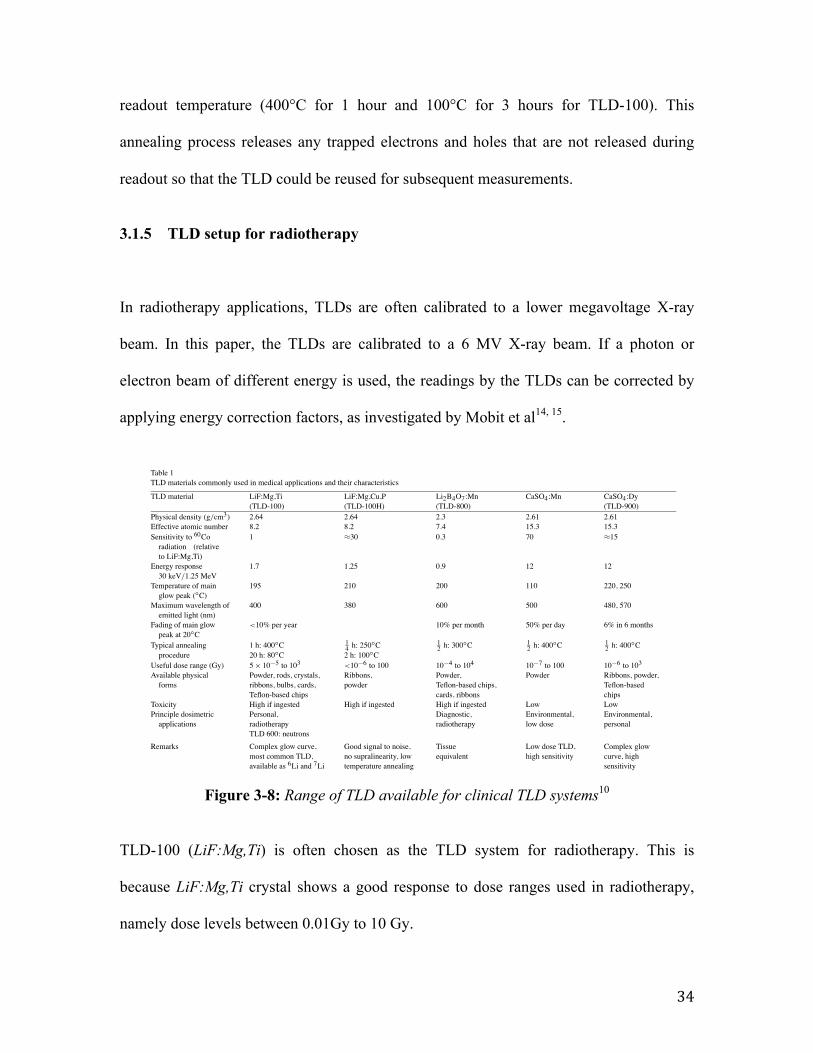
Figure 3-8: Range of TLD available for clinical TLD systems10
TLD-100 (LiF:Mg,Ti) is often chosen as the TLD system for radiotherapy. This is
because LiF:Mg,Ti crystal shows a good response to dose ranges used in radiotherapy,
namely dose levels between 0.01Gy to 10 Gy.
ApplicationsofThermolum
inescentDosim
etersinMedicine
417
Table 1TLD materials commonly used in medical applications and their characteristics
TLD material LiF:Mg,Ti LiF:Mg,Cu,P Li2B4O7:Mn CaSO4:Mn CaSO4:Dy(TLD-100) (TLD-100H) (TLD-800) (TLD-900)
Physical density (g/cm3) 2.64 2.64 2.3 2.61 2.61Effective atomic number 8.2 8.2 7.4 15.3 15.3Sensitivity to 60Coradiation (relativeto LiF:Mg,Ti)
1 !30 0.3 70 !15
Energy response30 keV/1.25 MeV
1.7 1.25 0.9 12 12
Temperature of mainglow peak ("C)
195 210 200 110 220, 250
Maximum wavelength ofemitted light (nm)
400 380 600 500 480, 570
Fading of main glowpeak at 20"C
<10% per year 10% per month 50% per day 6% in 6 months
Typical annealing 1 h: 400"C 14 h: 250
"C 12 h: 300
"C 12 h: 400
"C 12 h: 400
"Cprocedure 20 h: 80"C 2 h: 100"C
Useful dose range (Gy) 5# 10$5 to 103 <10$6 to 100 10$4 to 104 10$7 to 100 10$6 to 103Available physicalforms
Powder, rods, crystals,ribbons, bulbs, cards,Teflon-based chips
Ribbons,powder
Powder,Teflon-based chips,cards, ribbons
Powder Ribbons, powder,Teflon-basedchips
Toxicity High if ingested High if ingested High if ingested Low LowPrinciple dosimetricapplications
Personal,radiotherapyTLD 600: neutrons
Diagnostic,radiotherapy
Environmental,low dose
Environmental,personal
Remarks Complex glow curve,most common TLD,available as 6Li and 7Li
Good signal to noise,no supralinearity, lowtemperature annealing
Tissueequivalent
Low dose TLD,high sensitivity
Complex glowcurve, highsensitivity
Selected references Cameron et al., 1961;Mansfield, 1976;Horowitz, 1990, 1993;Kron et al., 1993
Zha et al., 1993;Horowitz, 1993
Horowitz et al., 1980;Horowitz, 1981, 1984
Bjarngard et al.,1976
Yamashita et al., 1971;Horowitz, 1984
35
As shown in Figure 3-2, each TLD is specific and is issued an identification, which is
marked by an alphabet (e.g. A,B,C,D,…) and a number (1 to 10), indicated on the
aluminum or plastic tray.
Quality assurance checks are done for the TLDs in order to select the reliable TLDs for
dosimetric experiments. These initial checks includes the following considerations:
• Visual check of any TLDs with chipped corners and discolouration
• TLD response uniformity
• TLD glow curves
• TLD reading reproducibility
• TLD linearity and supralinearity readings
It is important to examine the dose response for TLDs in radiation therapy applications.
In high precision applications, it is necessary to recalibrate the TLD before each
measurement. The operation procedure in handling the TLDs is shown in the diagram
below.
36
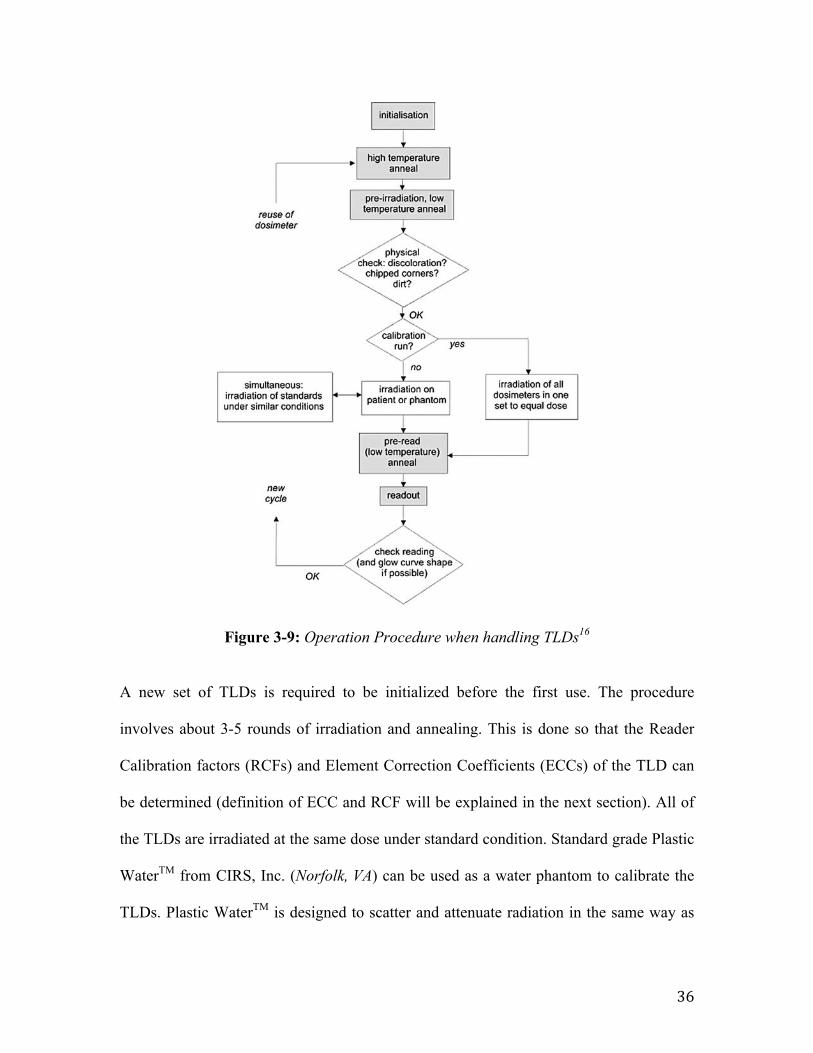
Figure 3-9: Operation Procedure when handling TLDs16
A new set of TLDs is required to be initialized before the first use. The procedure
involves about 3-5 rounds of irradiation and annealing. This is done so that the Reader
Calibration factors (RCFs) and Element Correction Coefficients (ECCs) of the TLD can
be determined (definition of ECC and RCF will be explained in the next section). All of
the TLDs are irradiated at the same dose under standard condition. Standard grade Plastic
WaterTM from CIRS, Inc. (Norfolk, VA) can be used as a water phantom to calibrate the
TLDs. Plastic WaterTM is designed to scatter and attenuate radiation in the same way as
422 P.N. Mobit and T. Kron
Fig. 5. Flow diagram illustrating the use of TL dosimeters.
The typical read-out procedure involves a pre-read anneal, which empties low energytraps, thereby reducing errors introduced by the fading of the TL signal. For LiF:Mg,Ti atypical pre-read anneal involves heating the detector to a temperature of 150!C and main-taining this temperature for 10 s. The details of the read-out procedure are somewhat arbi-trary and depend on the parameters of TL signal to be evaluated. In general, it is sufficientto determine the area under glow peaks IV and V of LiF:Mg,Ti to achieve the accuracy andreliability required for clinical dosimetry. In this case a stepped heating process is adequatein which the dosimeters are heated to 270!C for at least 10 s. It is worthwhile mentioningthat the heating rate employed to heat the samples to 270!C can affect the summed lightintensity of peaks IV and V due to a process called thermal quenching.
37
water and is often used for radiation beam calibration. Water is the standard medium in
radiotherapy because it is radiologically similar to human adipose tissue.
Figure 3-10: Plastic WaterTM Phantom by CIRS,Inc.
Once the ECCs and RCFs are calibrated, the TLDs will be used for measurements and
verifications. In this paper, TLDs are used for the verification of depth dose profiles of
clinical treatment plans using different dose calculation algorithms. This will be
discussed further in the later chapters.
38
3.2 TLD measurement methods
3.2.1 Element Correction Coefficient
TLDs may differ from one another in terms of Thermoluminesence Efficiency (where
Thermoluminenesce Efficiency (TLE) is defined as the emitted TL light intensity per unit
of absorbed dose). This can be corrected by calculating the individual Element
Correction Coefficients (ECCs) for each TLD. By applying ECCs, the spread of TLE will
be reduced from 10-15% to a low percentage of 1-2%.17
The ECC could be calculated by relating the TLE of each TLD of the sample TLD
population (called Field Dosimeters) to the average TLE of a small subset of the sample
TLD population that is used for calibration (called Calibration Dosimeters). The ECC
will correct the TLE of the Field Dosimeters to the mean value of the Calibration
Dosimeters group, accounting for any response difference between TLDs.
39
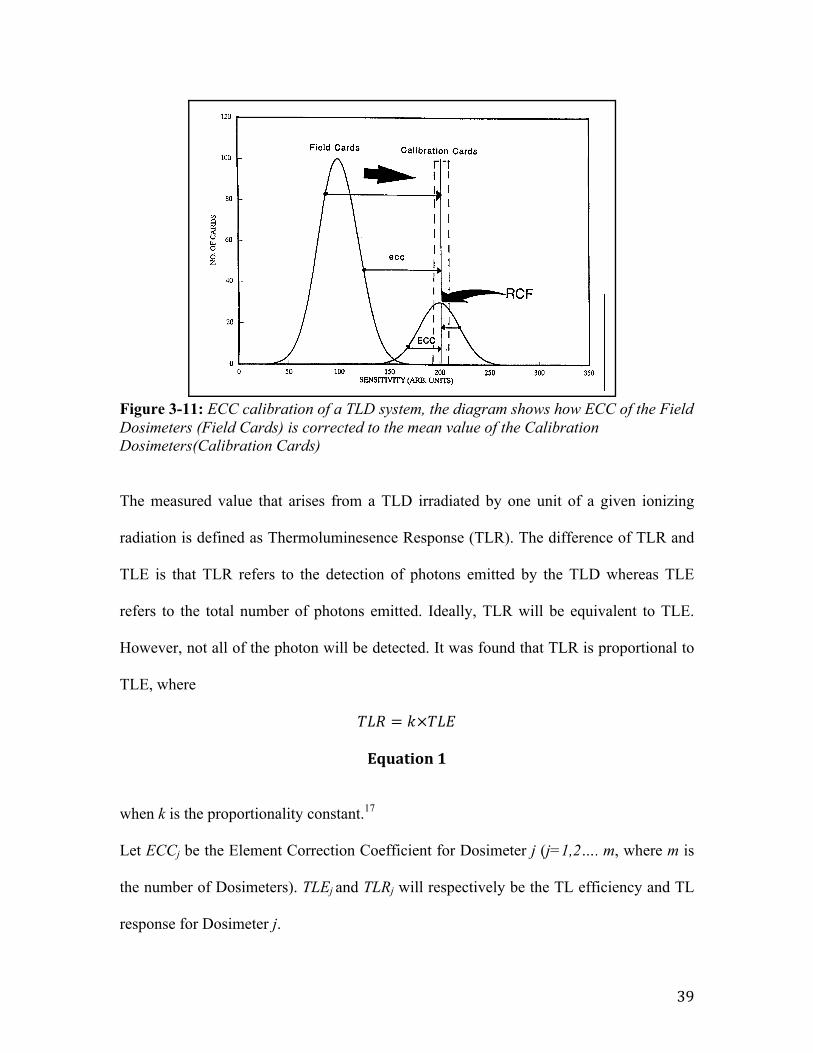
Figure 3-11: ECC calibration of a TLD system, the diagram shows how ECC of the Field Dosimeters (Field Cards) is corrected to the mean value of the Calibration Dosimeters(Calibration Cards)
The measured value that arises from a TLD irradiated by one unit of a given ionizing
radiation is defined as Thermoluminesence Response (TLR). The difference of TLR and
TLE is that TLR refers to the detection of photons emitted by the TLD whereas TLE
refers to the total number of photons emitted. Ideally, TLR will be equivalent to TLE.
However, not all of the photon will be detected. It was found that TLR is proportional to
TLE, where
𝑇𝐿𝑅 = 𝑘×𝑇𝐿𝐸
Equation 1
when k is the proportionality constant.17
Let ECCj be the Element Correction Coefficient for Dosimeter j (j=1,2…. m, where m is
the number of Dosimeters). TLEj and TLRj will respectively be the TL efficiency and TL
response for Dosimeter j.
Harshaw Dosimetry SystemALGM-0-C-0398 Page 29
System Calibration Procedure
Figure 9Internal Calibration of a TLD System
7.0 Calibration Methodology (cont'd)7.1 Element Correction Coefficients(cont'd)
Note that the ECC values for the FieldDosimeters would have been the same hadthey been generated at the same time as theCalibration Dosimeters' ECCs or at any othertime since the C values from (10) and (11)would have been canceled out in (12).
Once ECCs for the Field Dosimeters havebeen generated and applied, their TL efficiency(sensitivity) is virtually equal to the mean TLefficiency of the Calibration Dosimeters, and,as a result, all the dosimeter population willhave virtually the same TL efficiency, asshown in Figure 9. When new dosimeters areadded to the population, their TL efficiencycan be set to be virtually equal to the existingdosimeter population by generating ECCs forthe new dosimeters. The only parameterwhich must remain constant is the inherentsensitivity of the Calibration Dosimeters that
are being used. Extensive testing by BICRONand by our customers has shown, however,that the TL dosimeters used here can besubjected to hundreds of reuse cycles withoutany noticeable change in their TL efficiency.
Note that the radiation source used forgenerating the ECCs for the Field Dosimetersdoes not have to be the same one used forgenerating the ECCs for the CalibrationDosimeters, provided that a subset ofCalibration Dosimeters is exposed to the sameradiation field as the Field Dosimeters whoseECCs are being generated. Also note thatthere is no need for the dosimeters to bemounted in their holders during irradiation,since the only purpose of this irradiation is toinduce an excitation in the TL material, whichwill result in a measurable TL signal that isproportional to the TL efficiency of the TLdosimeter. Furthermore, no attempt has beenmade yet to correlate this TL response to anykind of "real" dose units.
40
𝐸𝐶𝐶! =< 𝑇𝐿𝐸 >𝑇𝐿𝐸!
Equation 2
where:
< 𝑇𝐿𝐸 >=1𝑚× 𝑇𝐿𝐸!
!!!
!!!
Equation 3
Substituting Equation 1 into Equation 2,
𝐸𝐶𝐶! =< 𝑇𝐿𝑅 >𝑇𝐿𝑅!
Equation 4
where:
< 𝑇𝐿𝑅 >=1𝑚× 𝑇𝐿𝑅!
!!!
!!!
Equation 5
The response of the TLD depends heavily on the TLD reader response. Experimentally,
the reader response with respect to the stability of the light detection and the heating
systems do not stay constant. The TLD reader report the TL response of the TLD in terms
of charge, where we define Qj as the charge reported for Calibration Dosimeter j
irradiated with n irradiation units. TLRj and <TLR> is then defines as:
41
𝑇𝐿𝑅! =𝑄!𝑛
Equation 6
< 𝑇𝐿𝑅 >=< 𝑄 >𝑛
Equation 7
where
< 𝑄 >=1𝑚× 𝑄!
!!!
!!!
Equation 8
Hence by substituting Equation 6 and Equation 7 into Equation 4 we get
𝐸𝐶𝐶! =< 𝑄 >𝑄!
Equation 9
Assuming that Calibration Dosimeters and Field Dosimeters are both exposed and read at
the same time, the charge reported by the TLD reader for Field Dosimeter j when
irradiated to n irradiation units is defined as qj´. During the readout of <Q>, the TLD
reader may have varied in response to the TL photons as there is a possibility that there
might be an accidental or intentional change in the experimental settings, which is
beyond experimental control. Assuming the response of the TLD reader is changed by a
factor C,
42
< 𝑄 > ´ = C × < 𝑄 >
Equation 10
and
𝑞!´ = C × 𝑞!
Equation 11
where qj is the unchanged charge of Field Dosimeter j and <Q>´ is the average reported
charge of the Calibrated Dosimeters under the new changed environmental settings.
Hence, by substituting Equation 10 and Equation 11 we see that
𝐸𝐶𝐶! =< 𝑄 > ´𝑞´!
Equation 12
3.2.2 Reader Calibration Factor and Absorbed Dose
In order to convert TL photons to measurable electric signals (in terms of charge), the
ratio between the average TL response of the Calibration Dosimeters and the irradiated
radiation quantity L can be found. This ratio is defined as Reader Calibration Factor
(RCF). It will account for the conditions of the experimental settings during
measurement, correcting for any stochastic changes in the experiment. It also acts as the
main link between the TL response in terms of charge and the absorbed dose, D, in terms
of Gray.
43
𝑅𝐶𝐹 =< 𝑄 >𝐷
Equation 13
To accurately obtain the RCF, it is important to reproduce the readings of the Calibration
Dosimeters by periodically calibrating it to sources that are traceable to recognized
absorbed dose standards. By substituting Equation 13 into Equation 12
𝐸𝐶𝐶! =𝑅𝐶𝐹×𝐿𝑞!
Equation 14 And hence, the dose response for Dosimeter j will be
𝐷! =𝑞!×𝐸𝐶𝐶!𝑅𝐶𝐹
Equation 15
44
3.2.3 Selection of Calibration and Field Dosimeters
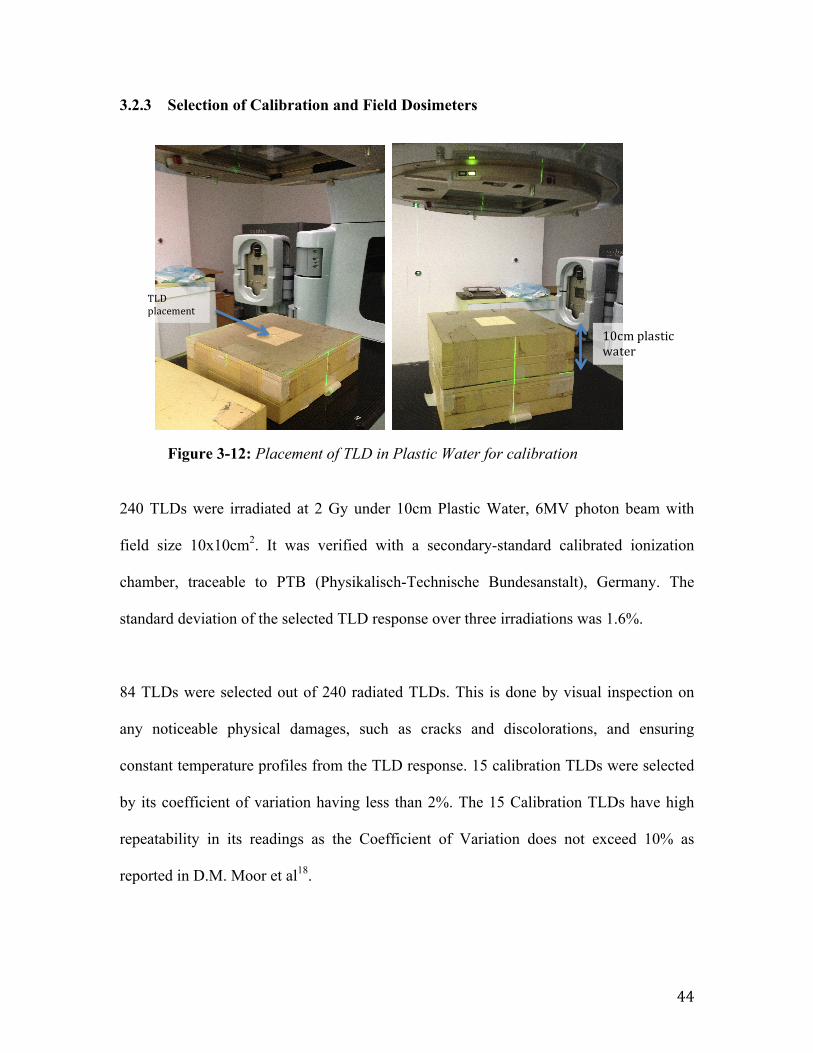
Figure 3-12: Placement of TLD in Plastic Water for calibration
240 TLDs were irradiated at 2 Gy under 10cm Plastic Water, 6MV photon beam with
field size 10x10cm2. It was verified with a secondary-standard calibrated ionization
chamber, traceable to PTB (Physikalisch-Technische Bundesanstalt), Germany. The
standard deviation of the selected TLD response over three irradiations was 1.6%.
84 TLDs were selected out of 240 radiated TLDs. This is done by visual inspection on
any noticeable physical damages, such as cracks and discolorations, and ensuring
constant temperature profiles from the TLD response. 15 calibration TLDs were selected
by its coefficient of variation having less than 2%. The 15 Calibration TLDs have high
repeatability in its readings as the Coefficient of Variation does not exceed 10% as
reported in D.M. Moor et al18.
TLD placement
10cm plastic water
45
3.2.4 Linearity of TLD readings
TLD readings may not be directly proportional to the irradiated dose. It was found that
TLD readings tend to be supralinear at high doses. TLD readings must not fluctuate by
more than 3% (1 SD) from 0.5 mGy to 1 Gy for clinical dosimetry applications19, 20. As
far as possible, a linear relationship between the TLD measured dose and the theoretical
dose is desired. However, when TLDs are not used in the linear region, a linearity
correction is required. The linearity correction is calculated from the TLD measured dose
to theoretical absorbed dose relationship.
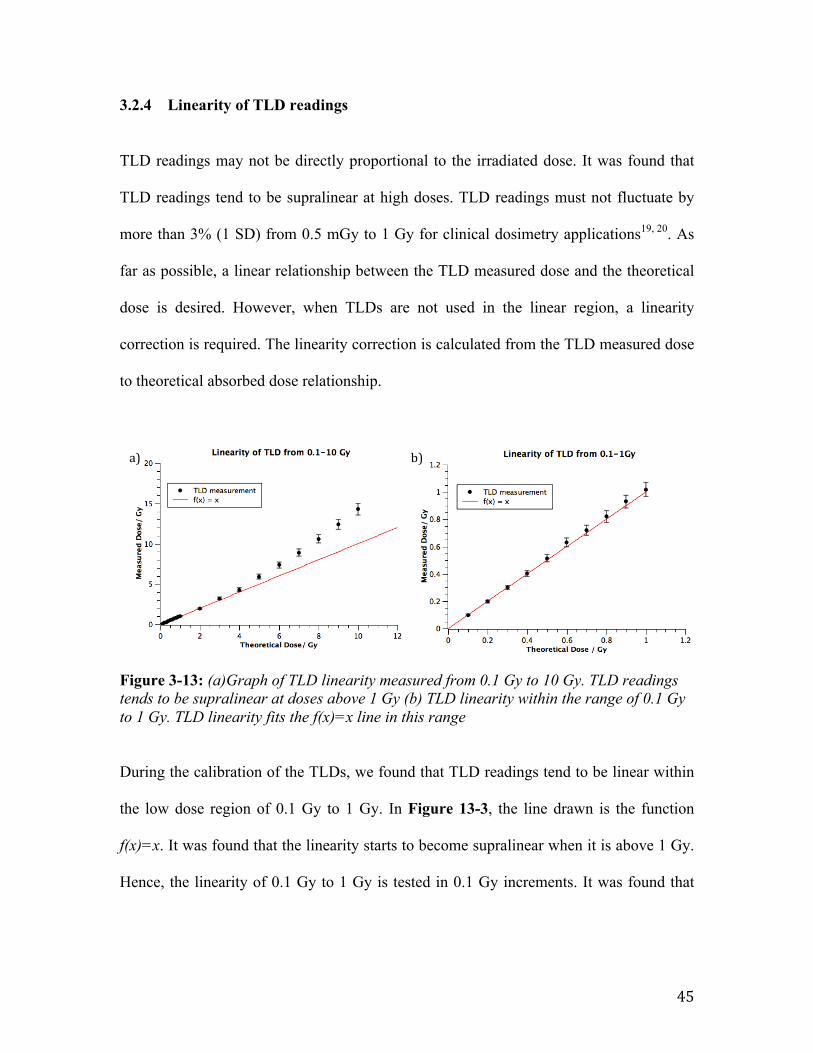
Figure 3-13: (a)Graph of TLD linearity measured from 0.1 Gy to 10 Gy. TLD readings tends to be supralinear at doses above 1 Gy (b) TLD linearity within the range of 0.1 Gy to 1 Gy. TLD linearity fits the f(x)=x line in this range
During the calibration of the TLDs, we found that TLD readings tend to be linear within
the low dose region of 0.1 Gy to 1 Gy. In Figure 13-3, the line drawn is the function
f(x)=x. It was found that the linearity starts to become supralinear when it is above 1 Gy.
Hence, the linearity of 0.1 Gy to 1 Gy is tested in 0.1 Gy increments. It was found that
a) b)

46
TLD measurements deviated from linearity by less than 3%. The results found are
consistent as reported in several studies19-21.
47
3.3 Summary
To summarize the theoretical framework of TLDs, we will need to have several
considerations.
Firstly, we have to recognize the advantages and disadvantages of having a TLD
dosimetric system. It is possible to obtain optimum measurement capability when TLDs
are applied for the appropriate dosimetric application.
TLDs are lithium fluoride crystals that are doped, in the case of TLD-100, with
magnesium and titanium. This creates trapping sites for excited electrons when TLD is
irradiated. During readout, these electrons de-excite and releases excess energy as light.
This response of the TLD is proportional to the dose absorbed and can be read using a
TLD reader.
TLD reader reads the TLD measurements in a plot of TL intensity against temperature,
which is known as the glow curve. The dosimetry peak of the glow curve will be the TL
response.
Calibration and Field dosimeters were chosen by visual inspection, their response values
and temperature profiles. The selection of TLDs allows proper calibration for high
precision measurement.

48
During calibration, the ECCs and the RCFs of the TLDs are determined. ECC corrects
the Thermoluminesence Efficiency differences between TLDs, where as RCF corrects
stochastic errors between each round of measurement.
Lastly, it was found that TL response is linear at dose region 0.1Gy to 1 Gy. Above 1 Gy,
linearity correction is required.
49
4 Dose Calculation Algorithms
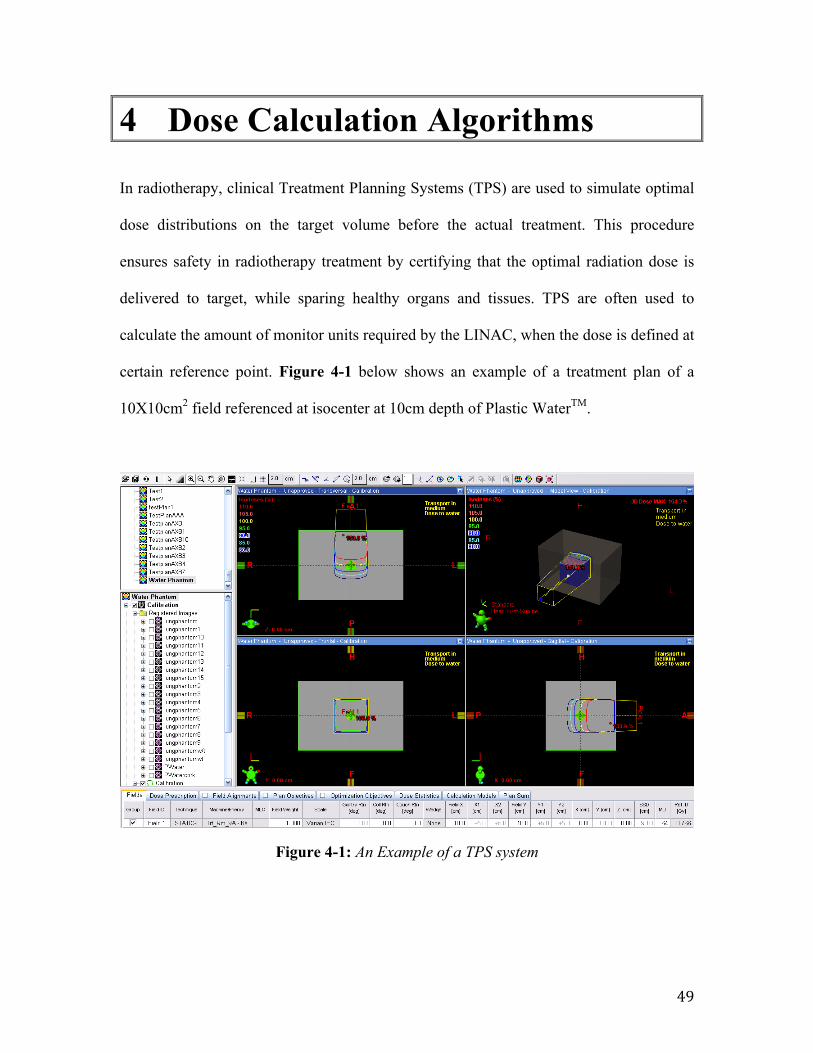
In radiotherapy, clinical Treatment Planning Systems (TPS) are used to simulate optimal
dose distributions on the target volume before the actual treatment. This procedure
ensures safety in radiotherapy treatment by certifying that the optimal radiation dose is
delivered to target, while sparing healthy organs and tissues. TPS are often used to
calculate the amount of monitor units required by the LINAC, when the dose is defined at
certain reference point. Figure 4-1 below shows an example of a treatment plan of a
10X10cm2 field referenced at isocenter at 10cm depth of Plastic WaterTM.
Figure 4-1: An Example of a TPS system
50
Modern TPS uses advanced dose calculation algorithms to calculate the dose
distributions in heterogeneous medium. Based on the calculation algorithm used, the
accuracy and the amount of time taken to generate the dose distribution will vary.
Currently, the golden standard for dose calculation algorithm is by Monte Carlo (MC)
calculations1, 3-5, 22. However, due to the complexity of modern radiotherapy, the
calculation time required by MC is significant and thus may not be suitable for clinical
use.
There is an increasing demand on dose calculation accuracy for treatment planning
optimization for heterogeneous medium. Hence, one of the current clinical dose
calculation algorithm is the Anistropic Analytical Algorithm (AAA)5, 23-27, which is
efficient and sufficiently accurate to be used clinically.
Since 2008, Transpire Inc. wrote a new dose calculation algorithm known as Acuros
XBTM, to improve the efficiency and accuracy for radiotherapy applications1, 2, 5, 28-30. We
will further investigate both AAA and Acuros XB further below. The validation of both
algorithms with TLDs will be done in the subsequent chapter.
51
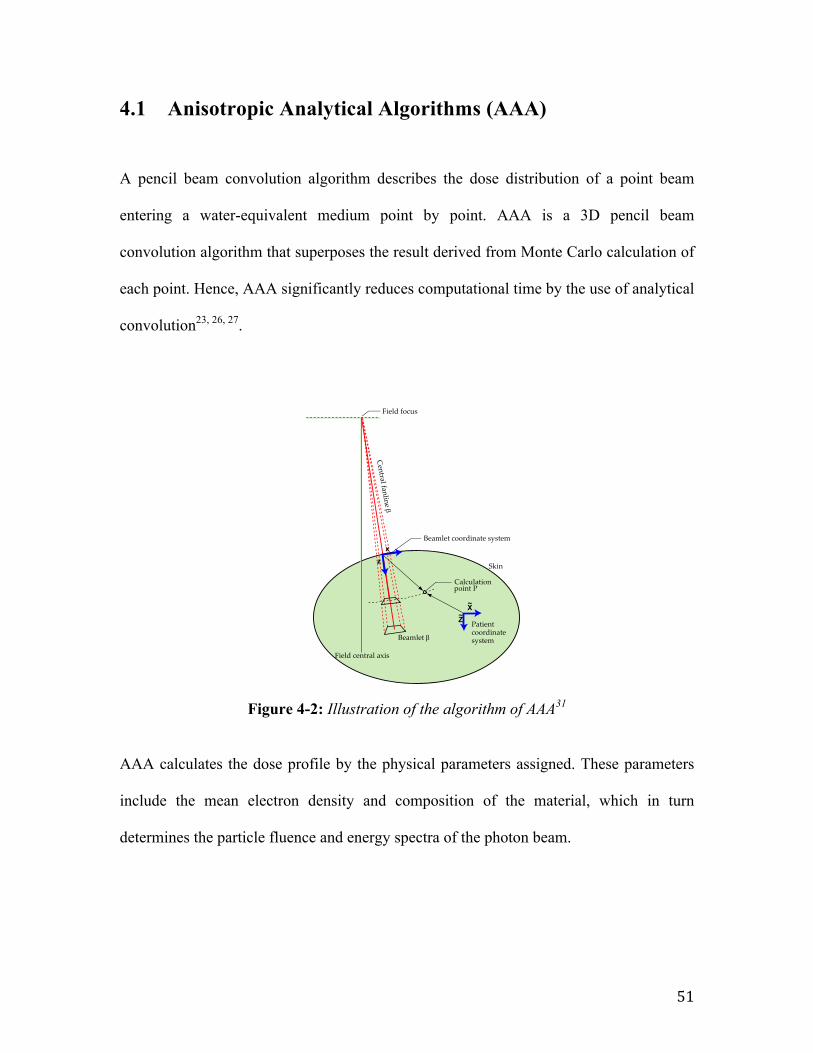
4.1 Anisotropic Analytical Algorithms (AAA)
A pencil beam convolution algorithm describes the dose distribution of a point beam
entering a water-equivalent medium point by point. AAA is a 3D pencil beam
convolution algorithm that superposes the result derived from Monte Carlo calculation of
each point. Hence, AAA significantly reduces computational time by the use of analytical
convolution23, 26, 27.
Figure 4-2: Illustration of the algorithm of AAA31
AAA calculates the dose profile by the physical parameters assigned. These parameters
include the mean electron density and composition of the material, which in turn
determines the particle fluence and energy spectra of the photon beam.
100 Eclipse Algorithms Reference Guide
Figure 13 Coordinates in Patient Coordinate System and Beamlet Coordinate System on X–Z Plane
TheȱbroadȱclinicalȱbeamȱisȱdividedȱintoȱfiniteȬsizeȱbeamletsȱE.ȱTheȱsideȱlengthȱofȱtheȱbeamletȱcorrespondsȱtoȱtheȱresolutionȱofȱtheȱcalculationȱgridȱonȱtheȱisocenterȱplane.
TheȱdoseȱcalculationȱisȱbasedȱonȱtheȱconvolutionsȱoverȱtheȱbeamletȱcrossȬsectionsȱseparatelyȱforȱtheȱprimaryȱphotons,ȱextraȬfocalȱphotonsȱ(secondȱsource),ȱscatterȱfromȱhardȱwedges,ȱandȱforȱelectronsȱcontaminatingȱtheȱprimaryȱbeam.ȱTheȱdoseȱisȱconvolvedȱbyȱusingȱtheȱphysicalȱparametersȱdefinedȱforȱeveryȱbeamletȱE.
AllȱdepthȬdependentȱfunctionsȱusedȱinȱtheȱbeamletȱconvolutionsȱareȱcomputedȱalongȱtheȱcentralȱfanlineȱofȱtheȱbeamletȱusingȱtheȱdepthȱcoordinateȱz.ȱLateralȱdoseȱscatteringȱdueȱtoȱphotonsȱandȱelectronsȱisȱdefinedȱonȱtheȱsphericalȱshellȱperpendicularȱtoȱtheȱcentralȱfanlineȱofȱtheȱbeamlet.ȱTheȱAAAȱmakesȱtheȱassumptionȱthatȱtheȱdoseȱresultingȱ
Fieldȱfocus
Skin
BeamletȱE
Fieldȱcentralȱaxis
Beamletȱcoordinateȱsystem
Patientcoordinatesystem
Centralȱfanline�E
x
Z
X
z
~
~
CalculationpointȱP
52
AAA approximates the broad clinical beam by dividing it into finite‐size beamlets as
shown in Figure 4-2. The length of the beamlet is determined by the resolution of the
calculation grid on the isocenter plane.
Therefore, the calculation is determined by the convolution of the interaction for every
beamlet. The central fanline of the beamlet is the source where all depth‐dependent
functions are computed. A modeled spherical shell perpendicular to the central fanline of
the beamlet approximates lateral dose scattering due to photons.31
Currently, AAA is used as the clinical dose calculation algorithm in National Cancer
Center Singapore. This dose algorithm has been validated and concluded that it has good
agreement between calculated and measured dose data with deviations smaller than 1%
for standard field sizes (10x10cm2)24.
53
4.2 Acuros External Beam (AXB)
Radiotherapy dose calculations can also be determined accurately using deterministic
solutions to the coupled system of linear Boltzmann transport equations (LBTEs)32-35.
The coupled system of LBTEs can be solved stochastically by Monte Carlo methods
using information from its particle histories. The second method is to use grid-based
LBTE solution methods by implementing discretization of photon and electron fluences
in space, energy, and angle so as to allow a deterministic solution of the transport of
radiation through matter. Through this second method, Attila® (Transpire Inc.) have
developed a new dose calculation algorithm so as to achieve both efficiency and
accuracy, and modify it specifically for radiotherapy applications. Acuros XBTM
algorithm (Transpire Inc.) has recently been implemented by Varian Medical Systems in
the Eclipse Treatment Planning Systems and was recently released for clinical dose
calculations.
Vassiliev et al35 investigated the accuracy of the AXB by comparing it with Monte Carlo
calculations36. Their study found an excellent ±2% agreement in depth dose profiles
through a heterogeneous unit density phantom and ±2% agreement in 99.9% of voxels.
Bush et al30 have concluded that AXB algorithm is capable of modeling radiotherapy
dose deposition with accuracy that is comparable to Monte Carlo.
In external photon beam radiotherapy, AXB is able to accurately account for the effects
of heterogeneities such as lung tissue, air, bone and other implants may significantly
54
influence the dose distribution in the patient, especially in the presence of small or
irregular fields.
4.2.1 Computed Tomography (CT) number – mass density relationship
The fundamental data used by AXB are macroscopic atomic cross sections. A
macroscopic cross section is the probability that an interaction will occur per unit path
length of particle travel. Macroscopic cross sections are composed from two values: the
interaction’s microscopic cross section and the mass density of the material.
In order to perform a calculation, AXB must know the macroscopic cross section of each
element in its computational grid. The treatment planning system provides AXB with a
mass density and material type in each voxel of the image grid by referring to a CT
Calibration Curve. A CT calibration curve relates the CT number of the material with the
material’s density. Hence, it is essential to calibrate and derive a CT calibration curve
accurately for AXB dose calculation.
X-ray Computed Tomography measures the attenuation of x-ray beams passing through
sections of a body through different angles. By having these measurements, the CT is
able to reconstruct the body virtually. For each given pixel, the CT determines a relative
linear attenuation coefficient, µeff (r), for each spatial coordinate. It is then normalized to
the linear attenuation coefficient of the reference material, water37-39.
55
𝐻𝑈 𝒓 =𝜇!"" 𝒓 − 𝜇!""
!!!
𝜇!""!!! − 𝜇!""!"#
Equation 16
CT numbers are known as Hounsfield Units (HU) 37 as shown in Equation 16 above. By
obtaining the HU of different materials of known densities and chemical compositions,
the CT calibration curve can be determined.
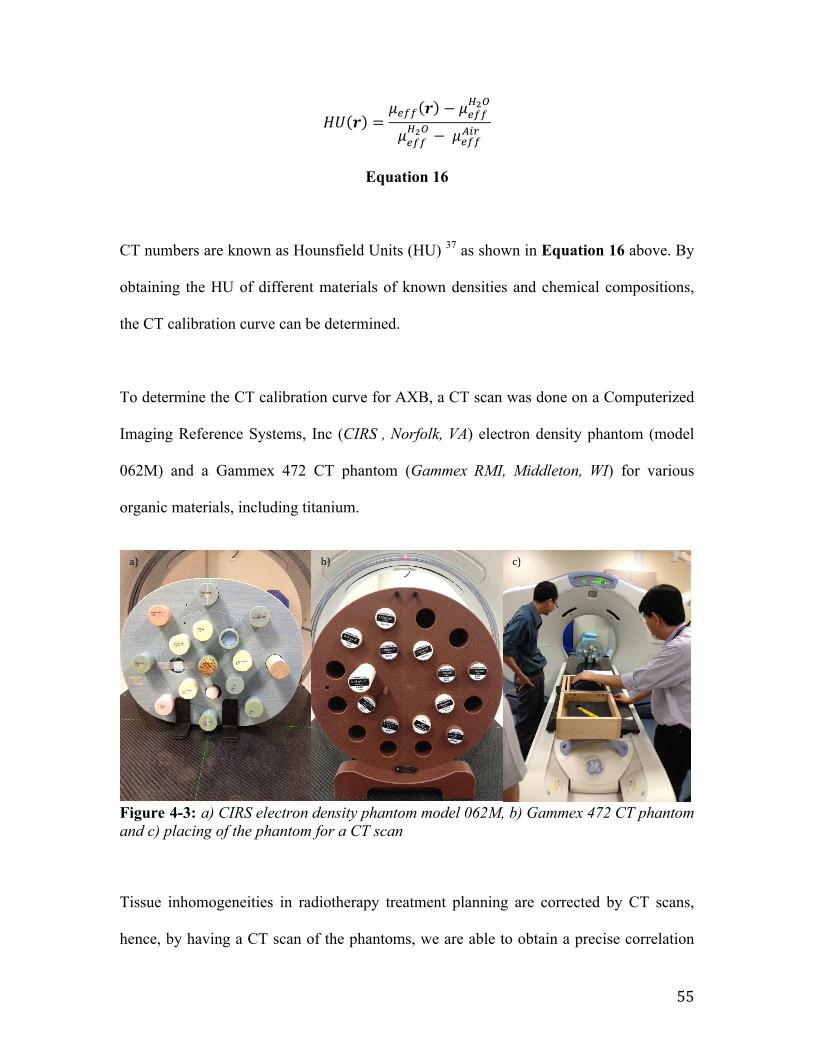
To determine the CT calibration curve for AXB, a CT scan was done on a Computerized
Imaging Reference Systems, Inc (CIRS , Norfolk, VA) electron density phantom (model
062M) and a Gammex 472 CT phantom (Gammex RMI, Middleton, WI) for various
organic materials, including titanium.
Figure 4-3: a) CIRS electron density phantom model 062M, b) Gammex 472 CT phantom and c) placing of the phantom for a CT scan
Tissue inhomogeneities in radiotherapy treatment planning are corrected by CT scans,
hence, by having a CT scan of the phantoms, we are able to obtain a precise correlation
a) b) c)
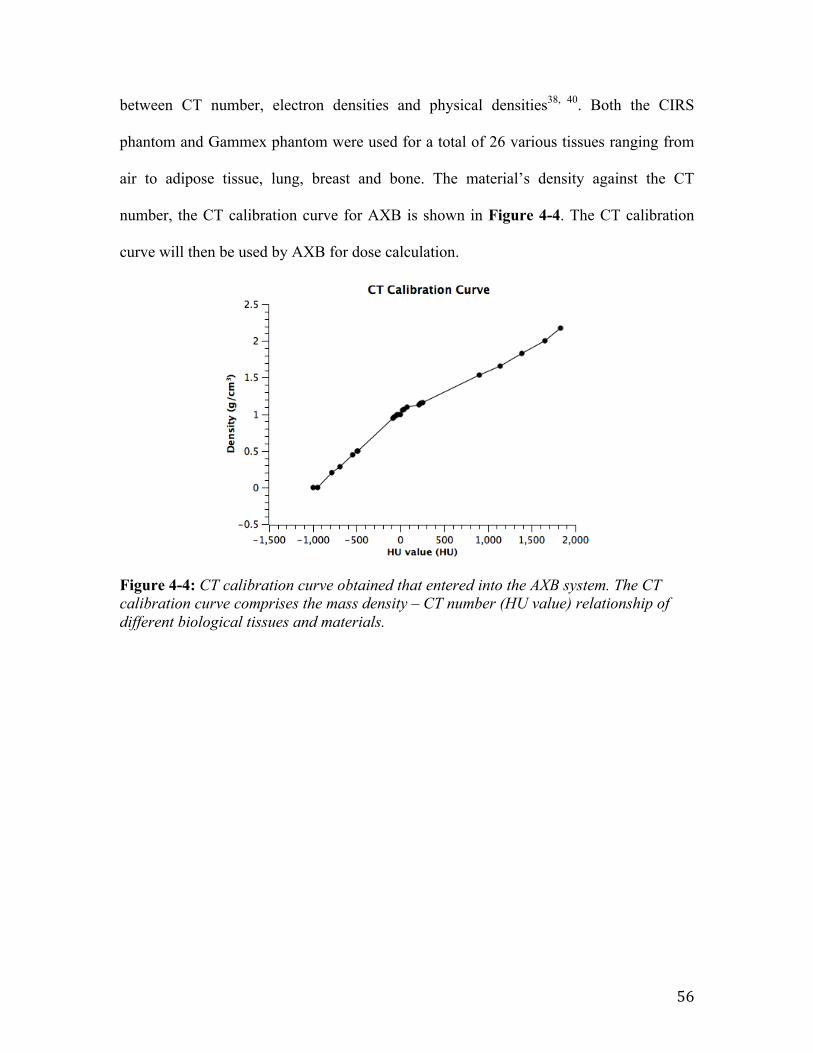
56
between CT number, electron densities and physical densities38, 40. Both the CIRS
phantom and Gammex phantom were used for a total of 26 various tissues ranging from
air to adipose tissue, lung, breast and bone. The material’s density against the CT
number, the CT calibration curve for AXB is shown in Figure 4-4. The CT calibration
curve will then be used by AXB for dose calculation.
Figure 4-4: CT calibration curve obtained that entered into the AXB system. The CT calibration curve comprises the mass density – CT number (HU value) relationship of different biological tissues and materials.
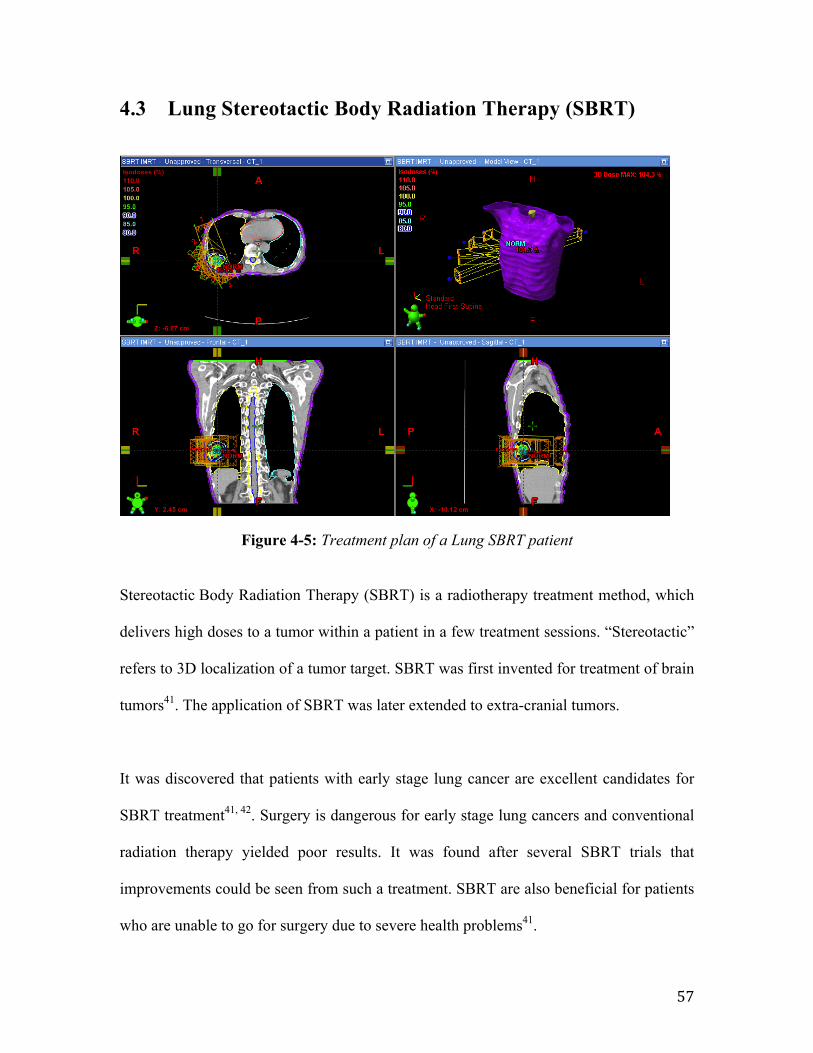
57
4.3 Lung Stereotactic Body Radiation Therapy (SBRT)
Figure 4-5: Treatment plan of a Lung SBRT patient
Stereotactic Body Radiation Therapy (SBRT) is a radiotherapy treatment method, which
delivers high doses to a tumor within a patient in a few treatment sessions. “Stereotactic”
refers to 3D localization of a tumor target. SBRT was first invented for treatment of brain
tumors41. The application of SBRT was later extended to extra-cranial tumors.
It was discovered that patients with early stage lung cancer are excellent candidates for
SBRT treatment41, 42. Surgery is dangerous for early stage lung cancers and conventional
radiation therapy yielded poor results. It was found after several SBRT trials that
improvements could be seen from such a treatment. SBRT are also beneficial for patients
who are unable to go for surgery due to severe health problems41.
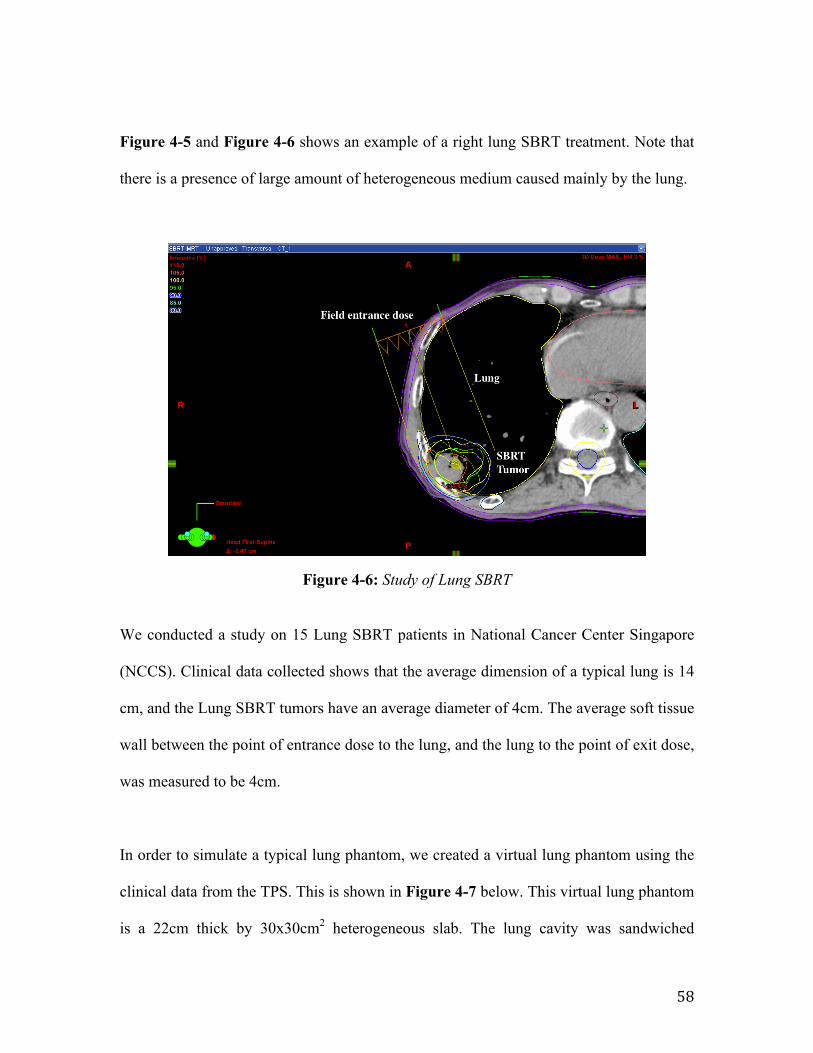
58
Figure 4-5 and Figure 4-6 shows an example of a right lung SBRT treatment. Note that
there is a presence of large amount of heterogeneous medium caused mainly by the lung.
Figure 4-6: Study of Lung SBRT
We conducted a study on 15 Lung SBRT patients in National Cancer Center Singapore
(NCCS). Clinical data collected shows that the average dimension of a typical lung is 14
cm, and the Lung SBRT tumors have an average diameter of 4cm. The average soft tissue
wall between the point of entrance dose to the lung, and the lung to the point of exit dose,
was measured to be 4cm.
In order to simulate a typical lung phantom, we created a virtual lung phantom using the
clinical data from the TPS. This is shown in Figure 4-7 below. This virtual lung phantom
is a 22cm thick by 30x30cm2 heterogeneous slab. The lung cavity was sandwiched
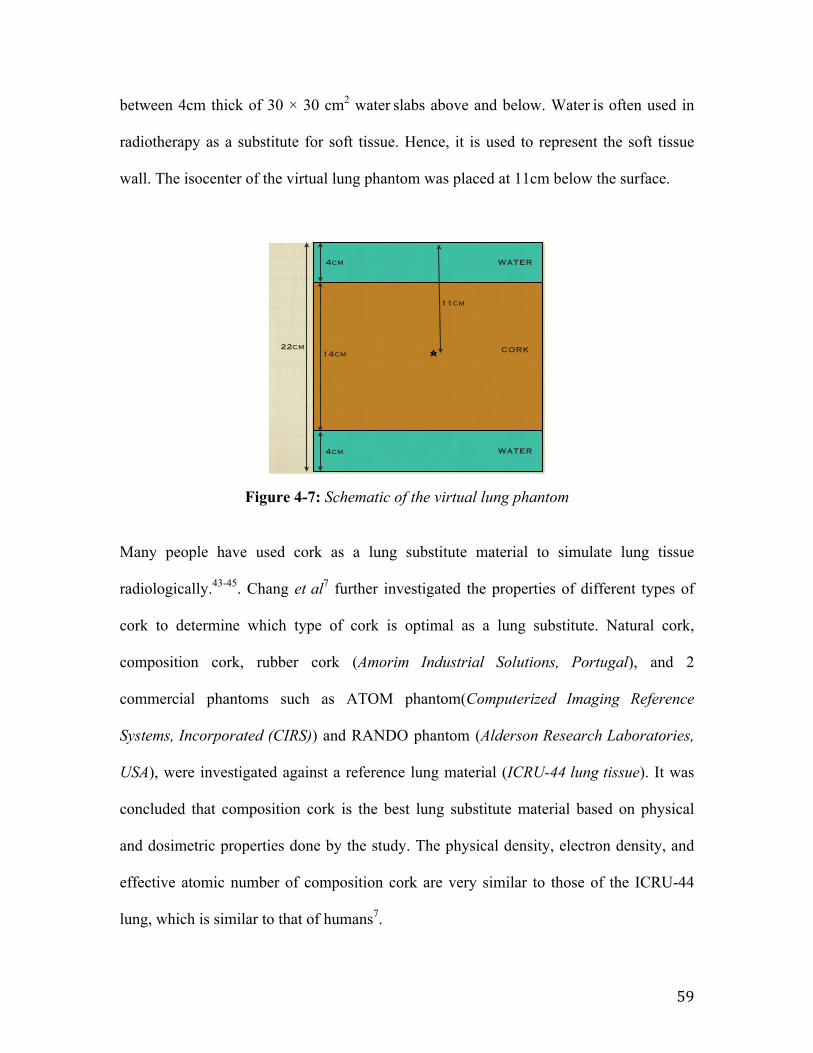
59
between 4cm thick of 30 × 30 cm2 water slabs above and below. Water is often used in
radiotherapy as a substitute for soft tissue. Hence, it is used to represent the soft tissue
wall. The isocenter of the virtual lung phantom was placed at 11cm below the surface.
Figure 4-7: Schematic of the virtual lung phantom
Many people have used cork as a lung substitute material to simulate lung tissue
radiologically.43-45. Chang et al7 further investigated the properties of different types of
cork to determine which type of cork is optimal as a lung substitute. Natural cork,
composition cork, rubber cork (Amorim Industrial Solutions, Portugal), and 2
commercial phantoms such as ATOM phantom(Computerized Imaging Reference
Systems, Incorporated (CIRS)) and RANDO phantom (Alderson Research Laboratories,
USA), were investigated against a reference lung material (ICRU-44 lung tissue). It was
concluded that composition cork is the best lung substitute material based on physical
and dosimetric properties done by the study. The physical density, electron density, and
effective atomic number of composition cork are very similar to those of the ICRU-44
lung, which is similar to that of humans7.
Isocenter set at 11cm below Surface
lung - 14cm Water - 4cm
PDD measurment:2cm before interfaceat interface2cm after interfaceIsocenter
0.01cm3 water
MEASUREMENTS
22cm
4cm
4cm
14cm
11cm
WATER
WATER
CORK
Wednesday, March 6, 13
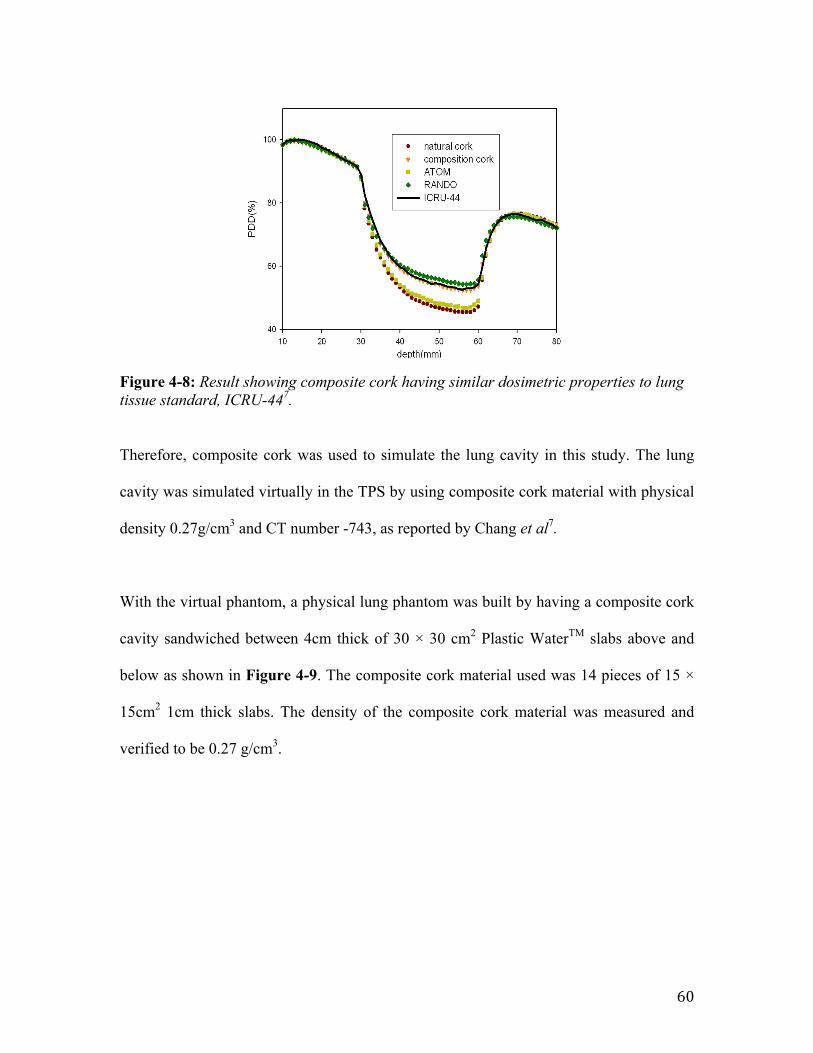
60
Figure 4-8: Result showing composite cork having similar dosimetric properties to lung tissue standard, ICRU-447.
Therefore, composite cork was used to simulate the lung cavity in this study. The lung
cavity was simulated virtually in the TPS by using composite cork material with physical
density 0.27g/cm3 and CT number -743, as reported by Chang et al7.
With the virtual phantom, a physical lung phantom was built by having a composite cork
cavity sandwiched between 4cm thick of 30 × 30 cm2 Plastic WaterTM slabs above and
below as shown in Figure 4-9. The composite cork material used was 14 pieces of 15 ×
15cm2 1cm thick slabs. The density of the composite cork material was measured and
verified to be 0.27 g/cm3.
composition cork results are used here to represent a known(C%, H%, O%) of lung material. Other lung simulationmaterials may be used to compare other factors (e.g., EDG)and how they will alter the dosimetric characteristics. This
will be further explained in Sec. IV. In Fig. 3(b), it is explicitthat there is negligible effect from physical density on thelarger field size. Other lung materials exhibited an analogoustrend. In an effort to determine if factors other than the phys-ical density affected the dosimetric characteristics, we fixedthe physical density value at 0.26 g/cm3 (identical to ICRU-44 lung) for each of the test materials; the results are shownin Fig. 4. The PDD curve of all materials for all field sizeswere lower than ICRU-44 lung; however, the RANDO lungwas the lowest. By comparing physical properties fromTable I, it is concluded that this is due to the lower EDG ofthe test materials (3.18! 1023 electrons/g for RANDO, and3.23–3.25! 1023 electrons/g for others) than that of theICRU-44 lung (3.35! 1023 electrons/g).
The hydrogen atom has an electron density nearly twicethat of other atoms. As seen in Table I, the weight fraction ofthe hydrogen of the ICRU-44 is 10.3% compared to 5.74%of RANDO and 7.69%–8.45% of the other materials. We
FIG. 2. Percentage depth dose (PDD) of the water-lung materials-water con-figuration per Fig. 1; Field sizes for (a) 1! 1 cm2 (b) 10! 10 cm2, and (c)dose differences (%) of lung substitutes (compared to ICRU-44 lung) atZ" 5 cm for various field sizes.
FIG. 3. PDD curves for various simulated physical densities (0.15–0.3 g =cm3)of the composition cork, for field sizes (a) 1! 1cm2 and (b) 10! 10 cm2.
2017 Chang et al.: Comparison of cork and others as lung substitutes 2017
Medical Physics, Vol. 39, No. 4, April 2012

61
Figure 4-9: Physical Lung Phantom with isocenter marked at 11cm below surface
62
4.4 Summary
In summary, several dose calculation algorithms and its concepts are highlighted in this
chapter. Treatment planning systems are used clinically to simulate the radiation dose
within a body before treatment. This procedure is essential as it ensures the safety and
efficiency of radiotherapy. Currently the algorithm benchmark in the TPS is the Monte
Carlo algorithm. However, Monte Carlo requires significant computation time and is not
readily available clinically.
Anistropic Analytical Algorithm is a clinical algorithm that is widely used today due to
its short computation time. It is an algorithm that superposes the result derived from
Monte Carlo calculation of each point beam dose distribution entering a water-equivalent
medium.
Another algorithm similar in accuracy to Monte Carlo is the Acuros External Beam
algorithm, which calculates the dose distribution by solving the Linear Boltzmann
Transport Equation via a deterministic solution of the transport of radiation through
matter.
The fundamental data used by AXB are dependent on the CT number and mass density of
the material irradiated. Hence, the CT calibration curve of the AXB algorithm in this
study was calibrated by using the CIRS electron density phantom (model 062M) and a
63
Gammex 472 CT phantom. The phantom carries a variety of tissue equivalent materials
with known physical densities. The CT calibration curve was obtained by CT scan.
Lastly, in order to have a study on lung stereotactic body radiotherapy, a simple phantom
was constructed in the TPS. Water was used to simulate the soft tissue wall before and
after the lung cavity, whereas composite cork was chosen to be the lung substitute
material. A physical lung phantom was built with Plastic WaterTM and composite cork to
allow the study of dose distribution with TLDs in the subsequent chapter.
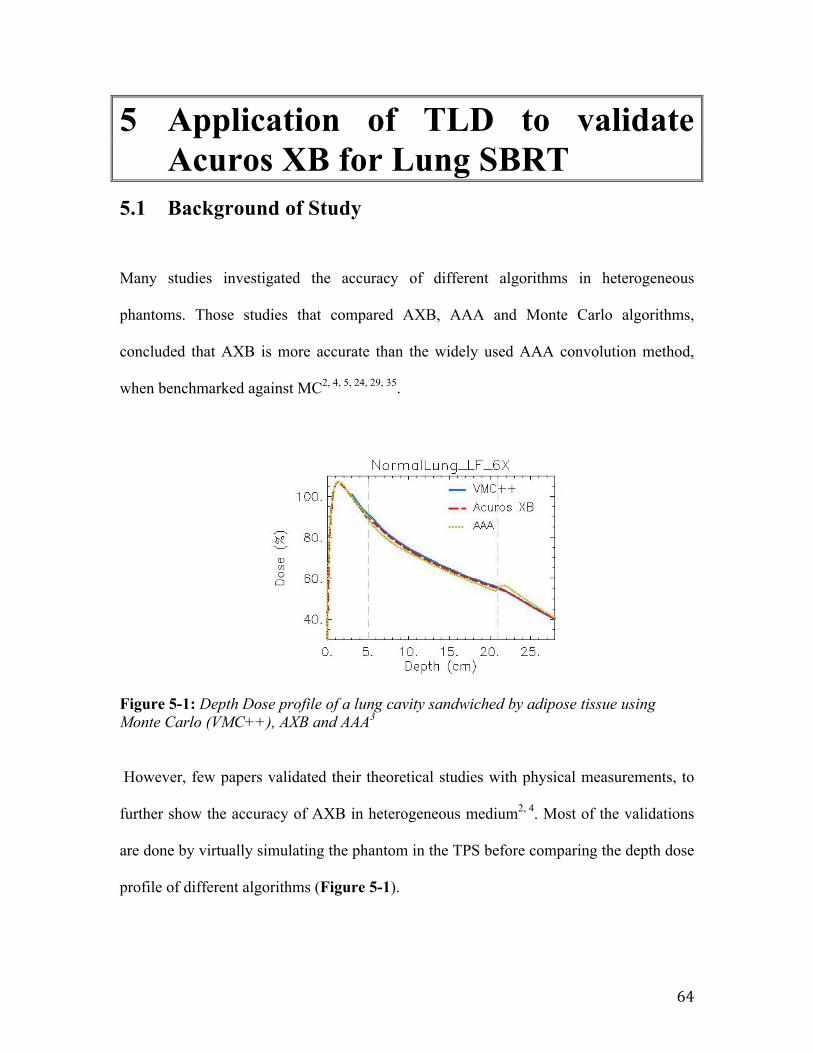
64
5 Application of TLD to validate Acuros XB for Lung SBRT
5.1 Background of Study
Many studies investigated the accuracy of different algorithms in heterogeneous
phantoms. Those studies that compared AXB, AAA and Monte Carlo algorithms,
concluded that AXB is more accurate than the widely used AAA convolution method,
when benchmarked against MC2, 4, 5, 24, 29, 35.
Figure 5-1: Depth Dose profile of a lung cavity sandwiched by adipose tissue using Monte Carlo (VMC++), AXB and AAA3
However, few papers validated their theoretical studies with physical measurements, to
further show the accuracy of AXB in heterogeneous medium2, 4. Most of the validations
are done by virtually simulating the phantom in the TPS before comparing the depth dose
profile of different algorithms (Figure 5-1).
Figure 3 EGSnrc and VMC++ comparison. Depth dose curves (DD) at -4 cm off-axis for the SF, 6X case in Normal Lung, Light Lung and Bonefor EGSnrc and VMC++.
Figure 4 Depth dose curves (DD) at -4 cm off-axis. Dose to medium calculations for VMC++, Acuros XB version 10, and AAA in phantom A. Incolumns: Normal Lung, Light Lung, Bone; in rows: SF and LF for 6X, SF and LF for 15X.
Fogliata et al. Radiation Oncology 2011, 6:82http://www.ro-journal.com/content/6/1/82
Page 7 of 15
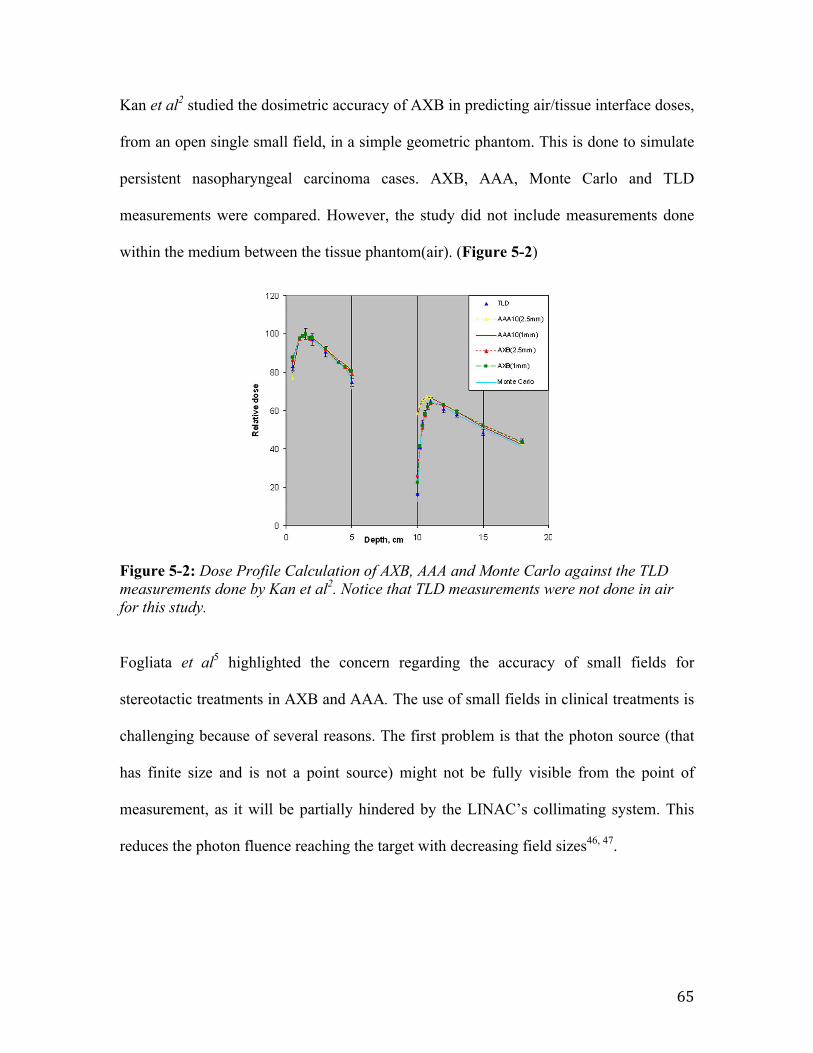
65
Kan et al2 studied the dosimetric accuracy of AXB in predicting air/tissue interface doses,
from an open single small field, in a simple geometric phantom. This is done to simulate
persistent nasopharyngeal carcinoma cases. AXB, AAA, Monte Carlo and TLD
measurements were compared. However, the study did not include measurements done
within the medium between the tissue phantom(air). (Figure 5-2)
Figure 5-2: Dose Profile Calculation of AXB, AAA and Monte Carlo against the TLD measurements done by Kan et al2. Notice that TLD measurements were not done in air for this study.
Fogliata et al5 highlighted the concern regarding the accuracy of small fields for
stereotactic treatments in AXB and AAA. The use of small fields in clinical treatments is
challenging because of several reasons. The first problem is that the photon source (that
has finite size and is not a point source) might not be fully visible from the point of
measurement, as it will be partially hindered by the LINAC’s collimating system. This
reduces the photon fluence reaching the target with decreasing field sizes46, 47.
4709 Kan, Leung, and Yu: Impact of Acuros XB on IMSRT for NPC 4709
infrared optical system. IMSRT planning was performed withthe Eclipse planning system using sliding window technique.
The final dose calculations of the original patient planswere performed by AAA with inhomogeneity correction us-ing 1.0 mm grid resolution. AXB dose calculation using 1.0mm grid resolution of each plan was performed retrospec-tively using exactly the same monitor units and MLC leafmovement setting as the corresponding AAA plan. Dose–volume histograms (DVHs) were produced for all plans sothat the doses to the PTV and OARs could be analyzed. Forthe PTV, the maximum dose, minimum dose, the coveragerepresented by V>95% (the volume receiving more than 95%of the reference dose), V>100% and the hot areas representedby V>110% were reported and compared between the predic-tion from the two algorithms. For the OARs, the dose encom-passing 1% (D1%) and 5% (D5%) of the volumes for brainstem, spinal cord, optic chiasm, optic nerve, and the meandoses to lens were also reported and compared. The plan con-formity was evaluated through comparisons using the con-formation number, CN, which was defined as the product ofVT,ref/VT and VT,ref/Vref, where VT,ref represents the volumeof the target receiving a dose equal to or greater than the ref-erence dose; VT represents the physical volume of the target,and Vref represents the total tissue volume receiving a doseequal to or greater than the reference dose.15 The referencedose used to compute the CN is the prescription dose. Thefirst ratio assesses quality of target coverage, and the secondratio assesses the amount of healthy tissue being involved inthe reference dose. The higher the CN values, the better theconformity. A CN value of 1 represents perfect conformity.
III. RESULTS
III.A. Verification of PDD in the rectangular phantomwith air cavity
It is seen from Figs. 3(a) to 3(c) that the Monte Carlo sim-ulated PDD data matched quite closely to the TLD measuredPDD. The results from the calculations using AAA are in-adequate to predict accurately the secondary build-up at andalso the first 1 cm beyond the distal interface between air andsolid water from 2 ! 2 to 5 ! 5 cm2 fields. If taking the mea-sured data by TLD as the reference (the accuracy of the TLDmeasurement was about 3%), the PDD measured at the dis-tal air/solid water interface was 16.3%, 23.3%, and 38.2% forthe 2 ! 2, 3 ! 3, and 5 ! 5 cm2 field, respectively, whilethose predicted by AAA using 1.0 mm grid size (AAA1.0 mm)were 57.1%, 60.0%, and 64.0%, respectively. The overesti-mation of PDD at the distal interface by AAA1.0 mm was upto 41% when 2 ! 2 cm2 field was used. On the other hand,significant improvement in predicting the secondary build-upcurves by AXB was observed. Overestimations of PDD byAXB were still observed at the distal air/solid water inter-face. The predicted PDD was 22.5%, 26.7%, and 45.5%, re-spectively, when using 1.0 mm grid size. The distal interfacePDD was overestimated by about 6% for 2 ! 2 cm2 by AXBusing 1.0 mm grid size (AXB1.0 mm). However, at depths 2mm or more beyond the distal interface, the predicted PDD
FIG. 3. The predicted percentage depth dose curves predicted by AAA andAXB compared to the measured and Monte Carlo simulated data using therectangular phantom for (a) 2 ! 2 cm2, (b) 3 ! 3 cm2, and (c) 5 ! 5 cm2
fields. The measured data and Monte Carlo simulated data were from Kanet al. (Ref. 7).
Medical Physics, Vol. 39, No. 8, August 2012
66
The second problem is that the fields might be small when compared to the maximum
lateral range of secondary electrons. This will result in a high dependence of the
computed and delivered dose on the density of the irradiated media48, 49.
Lastly, according to Bragg-Gray Cavity theory15, 50, an ideal dosimeter must be small
when compared to the field size of the beam, so that the dosimeter will not perturb the
fluence of the particles in the medium. However, at small fields, such ideal dosimeters
does not exist51.
Hence, in this study, the motivation is to validate the accuracy of AXB for Lung
Stereotactic Body Radiotherapy, in small, medium and standard field sizes, using TLDs.
This study will also check the results obtained against the AAA convolution method as
done in previous studies2, 4, 5, 24, 29, 35. The lung dose is of particular interest because it
relates to complications arising from high dose treatment to the tumor52.
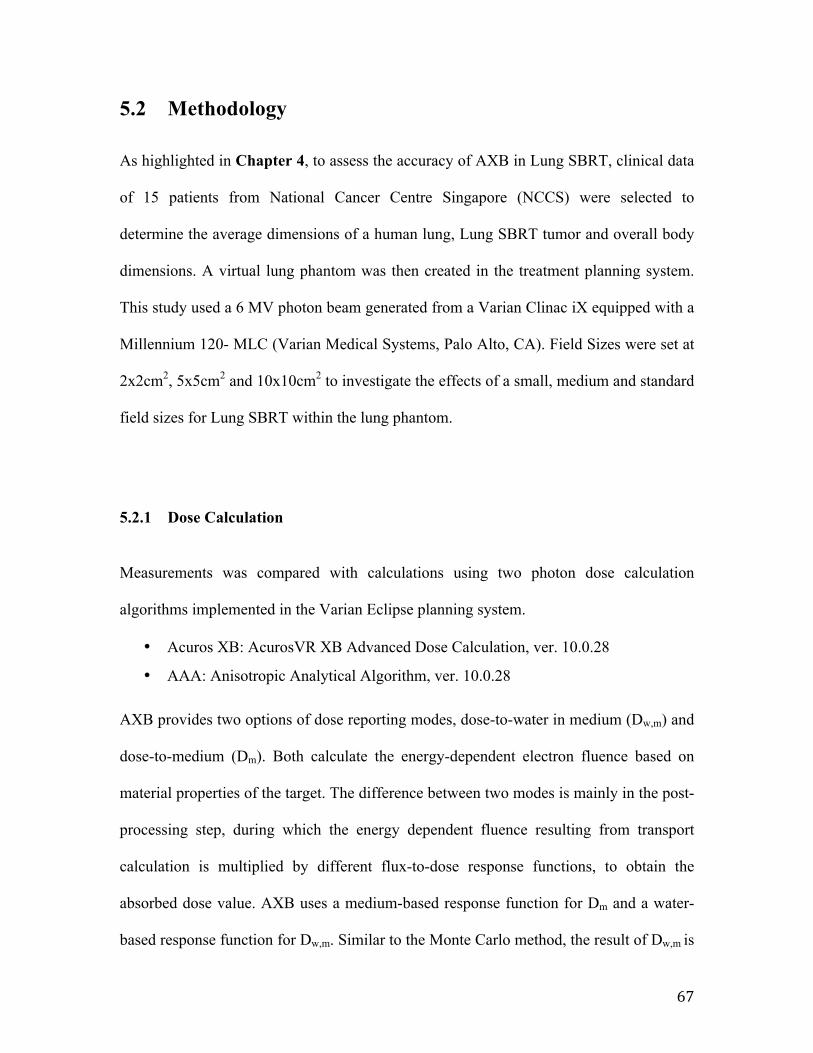
67
5.2 Methodology As highlighted in Chapter 4, to assess the accuracy of AXB in Lung SBRT, clinical data
of 15 patients from National Cancer Centre Singapore (NCCS) were selected to
determine the average dimensions of a human lung, Lung SBRT tumor and overall body
dimensions. A virtual lung phantom was then created in the treatment planning system.
This study used a 6 MV photon beam generated from a Varian Clinac iX equipped with a
Millennium 120- MLC (Varian Medical Systems, Palo Alto, CA). Field Sizes were set at
2x2cm2, 5x5cm2 and 10x10cm2 to investigate the effects of a small, medium and standard
field sizes for Lung SBRT within the lung phantom.
5.2.1 Dose Calculation
Measurements was compared with calculations using two photon dose calculation
algorithms implemented in the Varian Eclipse planning system.
• Acuros XB: AcurosVR XB Advanced Dose Calculation, ver. 10.0.28
• AAA: Anisotropic Analytical Algorithm, ver. 10.0.28
AXB provides two options of dose reporting modes, dose-to-water in medium (Dw,m) and
dose-to-medium (Dm). Both calculate the energy-dependent electron fluence based on
material properties of the target. The difference between two modes is mainly in the post-
processing step, during which the energy dependent fluence resulting from transport
calculation is multiplied by different flux-to-dose response functions, to obtain the
absorbed dose value. AXB uses a medium-based response function for Dm and a water-
based response function for Dw,m. Similar to the Monte Carlo method, the result of Dw,m is
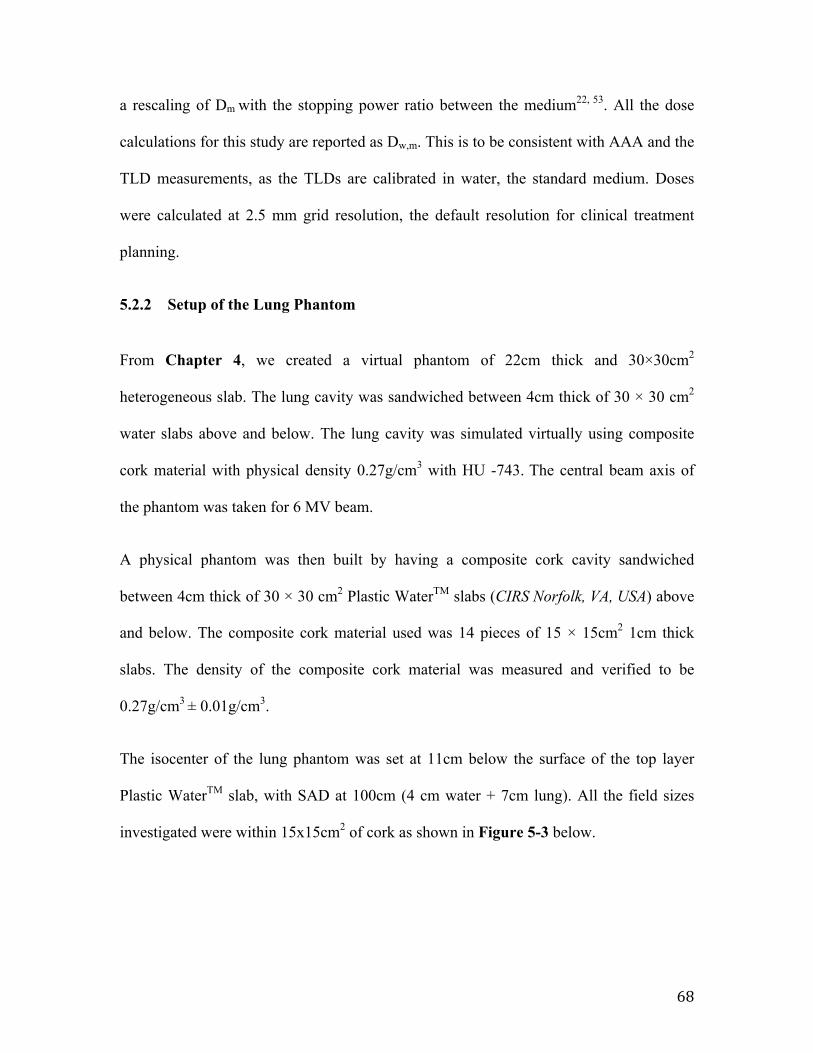
68
a rescaling of Dm with the stopping power ratio between the medium22, 53. All the dose
calculations for this study are reported as Dw,m. This is to be consistent with AAA and the
TLD measurements, as the TLDs are calibrated in water, the standard medium. Doses
were calculated at 2.5 mm grid resolution, the default resolution for clinical treatment
planning.
5.2.2 Setup of the Lung Phantom
From Chapter 4, we created a virtual phantom of 22cm thick and 30×30cm2
heterogeneous slab. The lung cavity was sandwiched between 4cm thick of 30 × 30 cm2
water slabs above and below. The lung cavity was simulated virtually using composite
cork material with physical density 0.27g/cm3 with HU -743. The central beam axis of
the phantom was taken for 6 MV beam.
A physical phantom was then built by having a composite cork cavity sandwiched
between 4cm thick of 30 × 30 cm2 Plastic WaterTM slabs (CIRS Norfolk, VA, USA) above
and below. The composite cork material used was 14 pieces of 15 × 15cm2 1cm thick
slabs. The density of the composite cork material was measured and verified to be
0.27g/cm3 ± 0.01g/cm3.
The isocenter of the lung phantom was set at 11cm below the surface of the top layer
Plastic WaterTM slab, with SAD at 100cm (4 cm water + 7cm lung). All the field sizes
investigated were within 15x15cm2 of cork as shown in Figure 5-3 below.
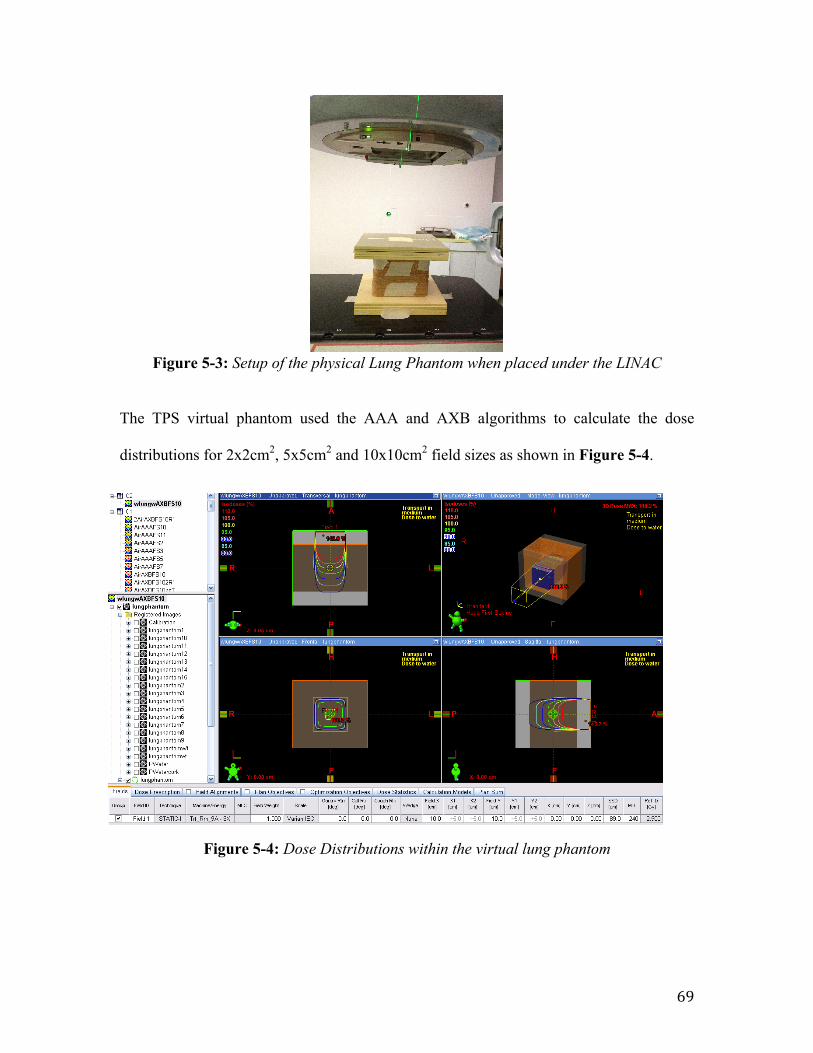
69
Figure 5-3: Setup of the physical Lung Phantom when placed under the LINAC
The TPS virtual phantom used the AAA and AXB algorithms to calculate the dose
distributions for 2x2cm2, 5x5cm2 and 10x10cm2 field sizes as shown in Figure 5-4.
Figure 5-4: Dose Distributions within the virtual lung phantom
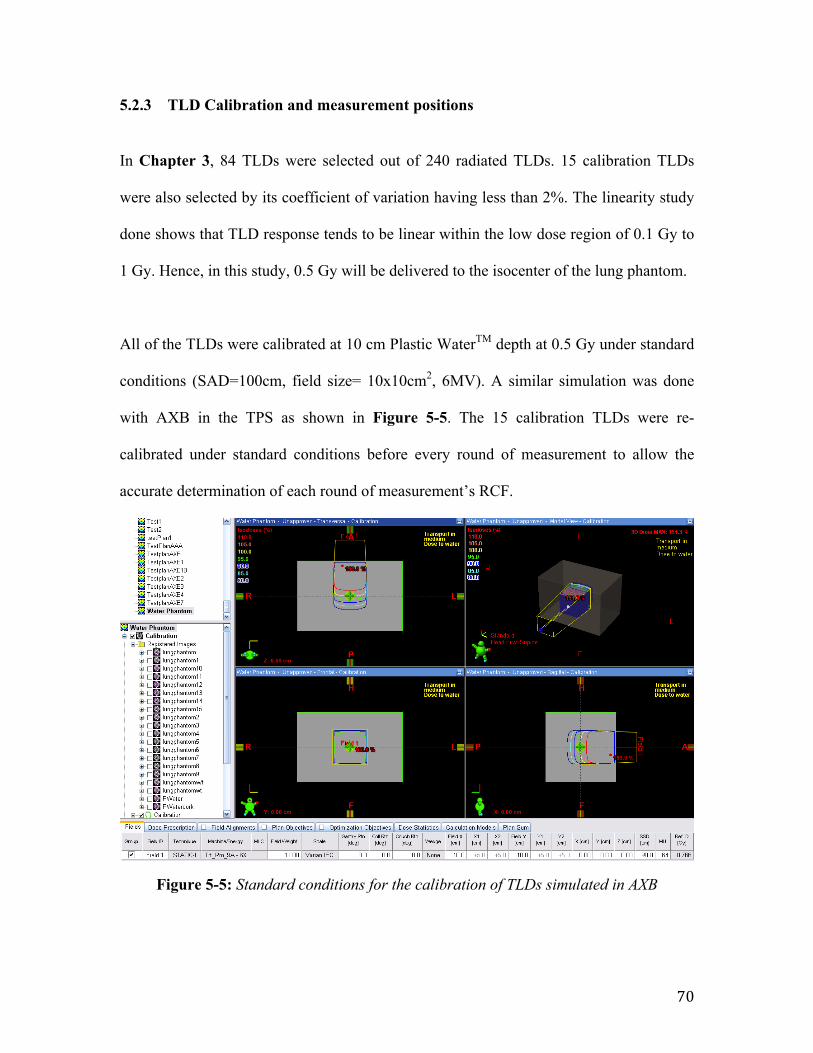
70
5.2.3 TLD Calibration and measurement positions
In Chapter 3, 84 TLDs were selected out of 240 radiated TLDs. 15 calibration TLDs
were also selected by its coefficient of variation having less than 2%. The linearity study
done shows that TLD response tends to be linear within the low dose region of 0.1 Gy to
1 Gy. Hence, in this study, 0.5 Gy will be delivered to the isocenter of the lung phantom.
All of the TLDs were calibrated at 10 cm Plastic WaterTM depth at 0.5 Gy under standard
conditions (SAD=100cm, field size= 10x10cm2, 6MV). A similar simulation was done
with AXB in the TPS as shown in Figure 5-5. The 15 calibration TLDs were re-
calibrated under standard conditions before every round of measurement to allow the
accurate determination of each round of measurement’s RCF.
Figure 5-5: Standard conditions for the calibration of TLDs simulated in AXB
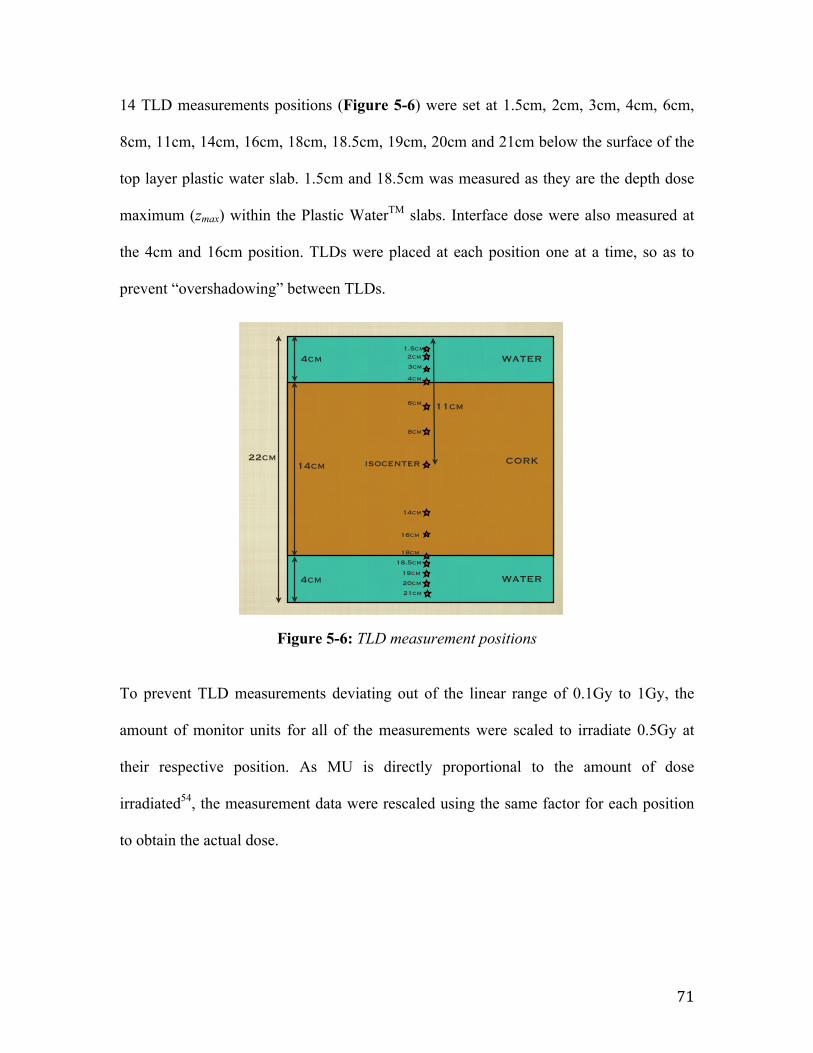
71
14 TLD measurements positions (Figure 5-6) were set at 1.5cm, 2cm, 3cm, 4cm, 6cm,
8cm, 11cm, 14cm, 16cm, 18cm, 18.5cm, 19cm, 20cm and 21cm below the surface of the
top layer plastic water slab. 1.5cm and 18.5cm was measured as they are the depth dose
maximum (zmax) within the Plastic WaterTM slabs. Interface dose were also measured at
the 4cm and 16cm position. TLDs were placed at each position one at a time, so as to
prevent “overshadowing” between TLDs.
Figure 5-6: TLD measurement positions
To prevent TLD measurements deviating out of the linear range of 0.1Gy to 1Gy, the
amount of monitor units for all of the measurements were scaled to irradiate 0.5Gy at
their respective position. As MU is directly proportional to the amount of dose
irradiated54, the measurement data were rescaled using the same factor for each position
to obtain the actual dose.
Isocenter set at 11cm below Surface
lung - 14cm Water - 4cm
PDD measurement:2cm before interfaceat interface2cm after interfaceIsocenter
0.01cm3 water volume of density 2.64g/cm3 as simulated TLD
MEASUREMENTS
22cm
4cm
4cm
14cm
11cm
isocenter
1.5cm
WATER
WATER
CORK
2cm
3cm
4cm
6cm
8cm
14cm
16cm
18cm
18.5cm
19cm
20cm
21cm
Wednesday, March 13, 13
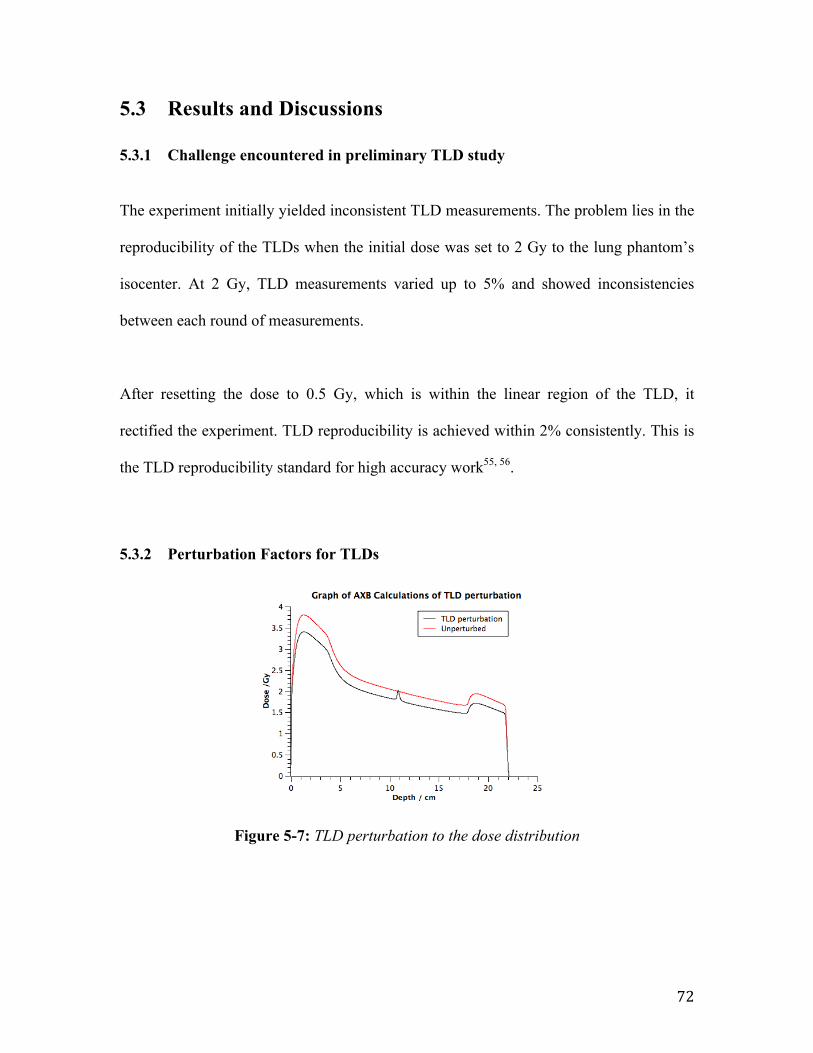
72
5.3 Results and Discussions
5.3.1 Challenge encountered in preliminary TLD study
The experiment initially yielded inconsistent TLD measurements. The problem lies in the
reproducibility of the TLDs when the initial dose was set to 2 Gy to the lung phantom’s
isocenter. At 2 Gy, TLD measurements varied up to 5% and showed inconsistencies
between each round of measurements.
After resetting the dose to 0.5 Gy, which is within the linear region of the TLD, it
rectified the experiment. TLD reproducibility is achieved within 2% consistently. This is
the TLD reproducibility standard for high accuracy work55, 56.
5.3.2 Perturbation Factors for TLDs
Figure 5-7: TLD perturbation to the dose distribution
factor[9] and reader calibration factor (RCF).[11,12] Following da Rosa et al. [9] who used Monte Carlo simulation, the TLD perturbation factors in lung were calculated with AXB by inserting a small water volume of 0.01cm3 drawn in the dimension of the TLD and positioned in composite cork. The density of the water volume was taken to be 2.64 g/cm3, which is the density of TLD-100. The TLD-100 is assumed to be radiological water equivalent as its effective atomic number (8.14) is sufficiently close to biological tissues.[13] The grid resolution used was 1.0 mm given the small volume. The corrected TLD doses were then compared with the predicted dose by AXB and AAA. All dose calculations were performed to deliver 2 Gy to the isocenter.
III. RESULTS
A. Perturbation factor caused by TLD in lung (AXB)
Fig.3: TLD PDD perturbation in AXB
Table 1 Perturbation Factors from AXB
Material Depth/cm Perturbation factor
Plastic Water 2 None
Plastic Water 4 None
Composite Cork 6 1.077
Composite Cork 11 1.102
Composite Cork 16 1.084
Composite Cork 18 1.086
Plastic Water 20 None
It was found that the AXB predicted perturbation factor was 1.102 at isocentre as shown in Fig.3. This perturbation factor was calculated by the shift in PDD predicted in AXB. In order to calculate the factor in the other positions within composite cork, the normalization point was fixed at isocentre and the difference in the peak reading and the unperturbed PDD was calculated. Results are shown in Table 1. Perturbations within composite cork ranges from 1.077-1.102.
B. Verification of PDD in the lung substitute phantom
Fig.4: TLD PDD comparison of 2×2cm2 field size
It is seen from Fig.4 that the AXB data matches closely to the TLD measured PDD to within an average of 2.2%. The results from the calculations using AAA are generally good (to within 2.4%) but the greatest deviation is 7% (as compared to 2.5% in AXB) occured at 2cm after the water/cork interface. Uncertainties associated with the TLD measurement was estimated at 5%, which is due largely to the repeatability of the measured dose per cycle relative to dose measured in first cycle.[14]
IV. DISSCUSSIONS
Some previous investigations showed that AXB was capable of accounting for specific material composition of the media, which would result in improved accuracy of dose calculation in heterogeneous media, as compared to the commonly used AAA.[3,15] The TLD verification of AXB using a lung substitute material is an important step to determine the reliability of AXB for small field Lung SBRT. However, TLD-100, with its finite dimensions and relatively higher density, causes significant perturbation in a low-density lung medium. This has to be accounted for. AXB proved to be self consistent as shown in the accuracy of the corrected TLD readings. Final results from the lung
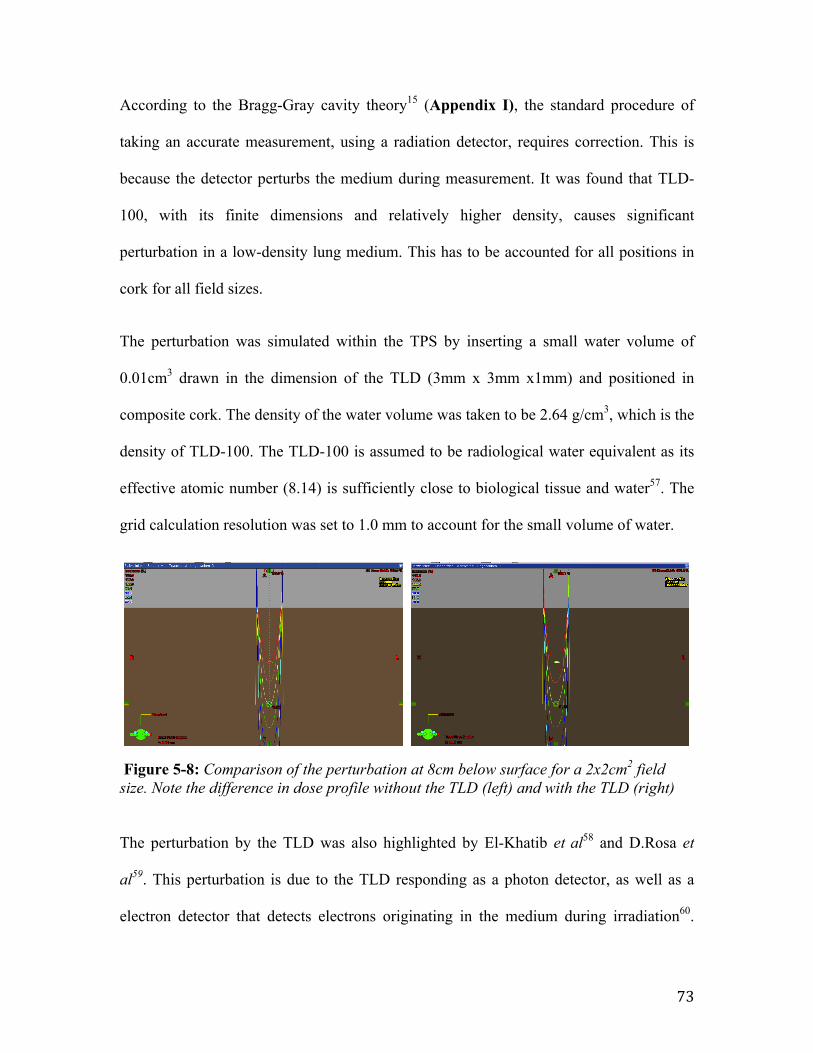
73
According to the Bragg-Gray cavity theory15 (Appendix I), the standard procedure of
taking an accurate measurement, using a radiation detector, requires correction. This is
because the detector perturbs the medium during measurement. It was found that TLD-
100, with its finite dimensions and relatively higher density, causes significant
perturbation in a low-density lung medium. This has to be accounted for all positions in
cork for all field sizes.
The perturbation was simulated within the TPS by inserting a small water volume of
0.01cm3 drawn in the dimension of the TLD (3mm x 3mm x1mm) and positioned in
composite cork. The density of the water volume was taken to be 2.64 g/cm3, which is the
density of TLD-100. The TLD-100 is assumed to be radiological water equivalent as its
effective atomic number (8.14) is sufficiently close to biological tissue and water57. The
grid calculation resolution was set to 1.0 mm to account for the small volume of water.
Figure 5-8: Comparison of the perturbation at 8cm below surface for a 2x2cm2 field size. Note the difference in dose profile without the TLD (left) and with the TLD (right)
The perturbation by the TLD was also highlighted by El-Khatib et al58 and D.Rosa et
al59. This perturbation is due to the TLD responding as a photon detector, as well as a
electron detector that detects electrons originating in the medium during irradiation60.
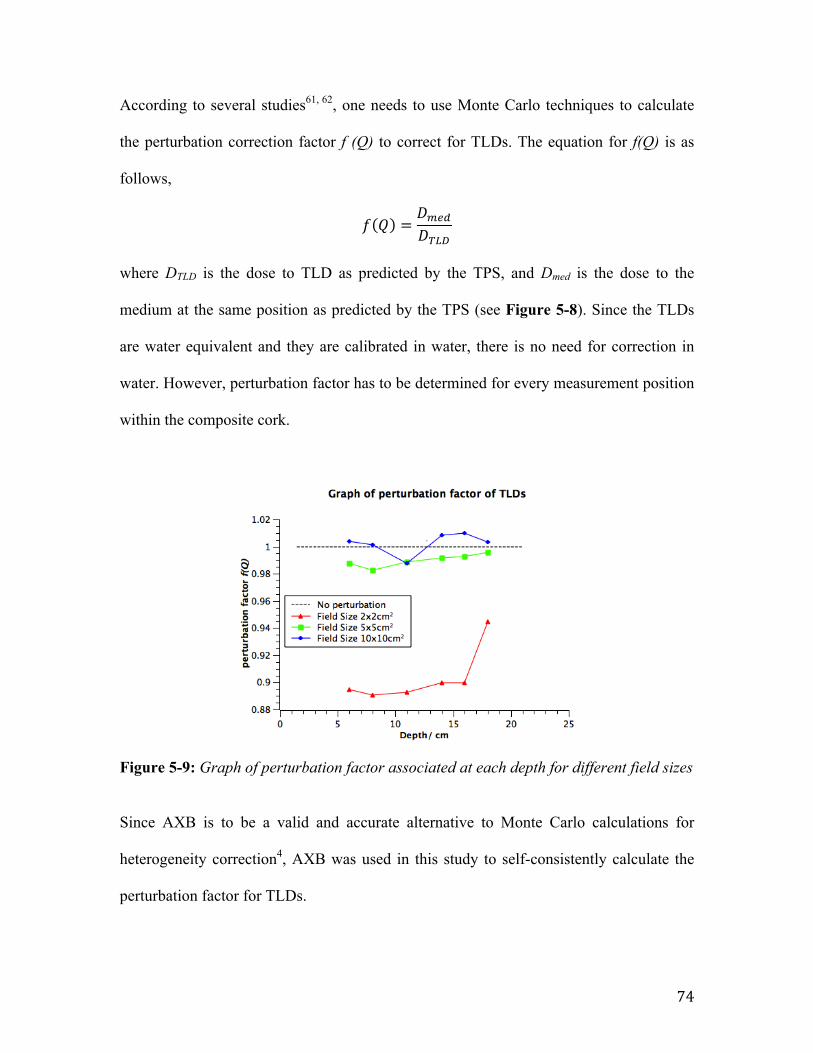
74
According to several studies61, 62, one needs to use Monte Carlo techniques to calculate
the perturbation correction factor f (Q) to correct for TLDs. The equation for f(Q) is as
follows,
𝑓 𝑄 =𝐷!"#𝐷!"#
where DTLD is the dose to TLD as predicted by the TPS, and Dmed is the dose to the
medium at the same position as predicted by the TPS (see Figure 5-8). Since the TLDs
are water equivalent and they are calibrated in water, there is no need for correction in
water. However, perturbation factor has to be determined for every measurement position
within the composite cork.
Figure 5-9: Graph of perturbation factor associated at each depth for different field sizes
Since AXB is to be a valid and accurate alternative to Monte Carlo calculations for
heterogeneity correction4, AXB was used in this study to self-consistently calculate the
perturbation factor for TLDs.
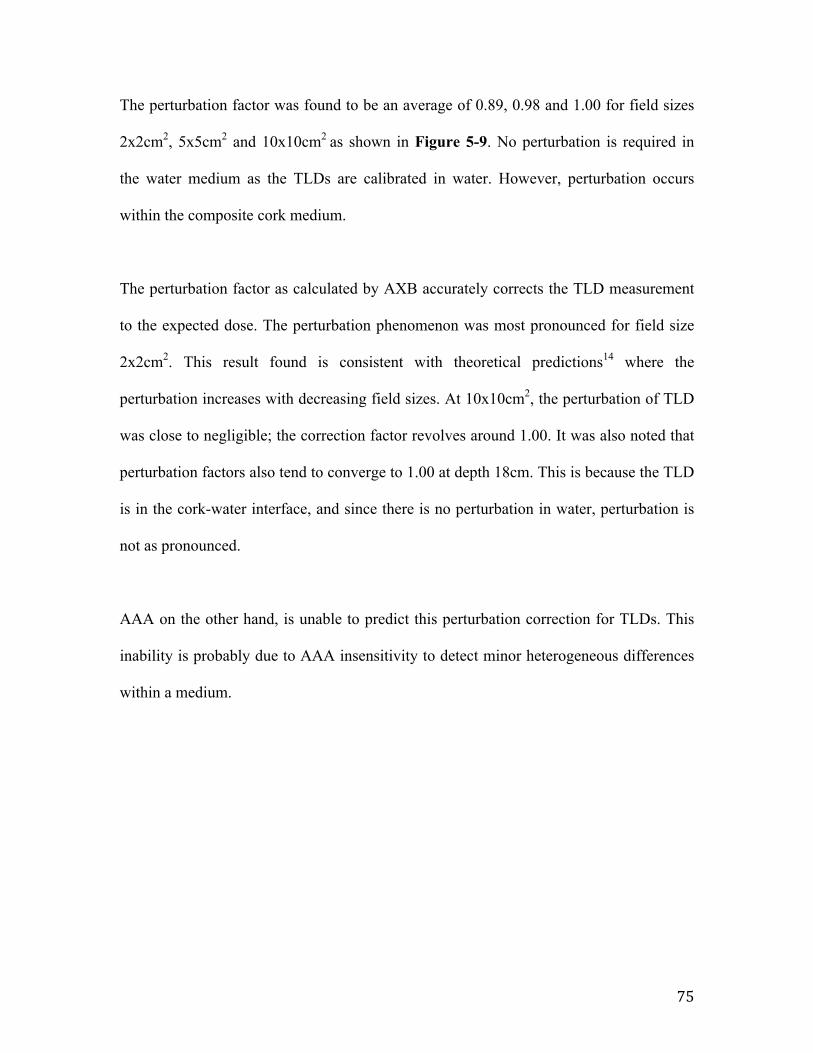
75
The perturbation factor was found to be an average of 0.89, 0.98 and 1.00 for field sizes
2x2cm2, 5x5cm2 and 10x10cm2 as shown in Figure 5-9. No perturbation is required in
the water medium as the TLDs are calibrated in water. However, perturbation occurs
within the composite cork medium.
The perturbation factor as calculated by AXB accurately corrects the TLD measurement
to the expected dose. The perturbation phenomenon was most pronounced for field size
2x2cm2. This result found is consistent with theoretical predictions14 where the
perturbation increases with decreasing field sizes. At 10x10cm2, the perturbation of TLD
was close to negligible; the correction factor revolves around 1.00. It was also noted that
perturbation factors also tend to converge to 1.00 at depth 18cm. This is because the TLD
is in the cork-water interface, and since there is no perturbation in water, perturbation is
not as pronounced.
AAA on the other hand, is unable to predict this perturbation correction for TLDs. This
inability is probably due to AAA insensitivity to detect minor heterogeneous differences
within a medium.
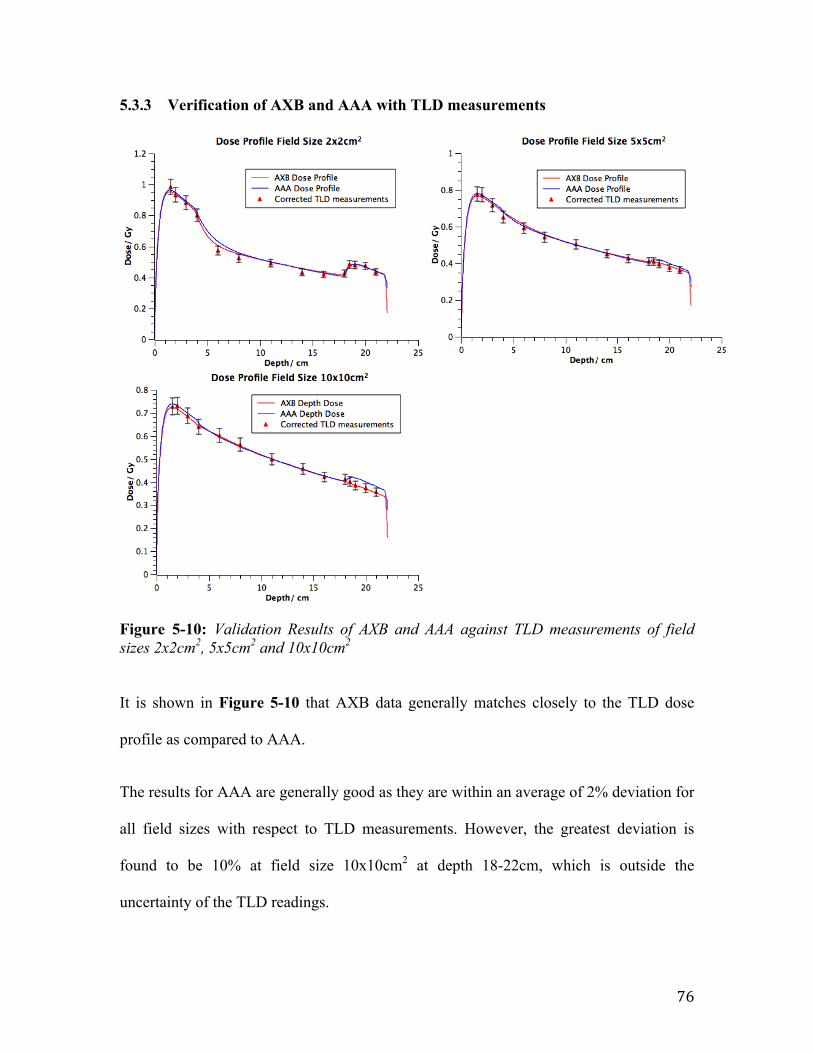
76
5.3.3 Verification of AXB and AAA with TLD measurements
Figure 5-10: Validation Results of AXB and AAA against TLD measurements of field sizes 2x2cm2, 5x5cm2 and 10x10cm2
It is shown in Figure 5-10 that AXB data generally matches closely to the TLD dose
profile as compared to AAA.
The results for AAA are generally good as they are within an average of 2% deviation for
all field sizes with respect to TLD measurements. However, the greatest deviation is
found to be 10% at field size 10x10cm2 at depth 18-22cm, which is outside the
uncertainty of the TLD readings.
77
AXB dose in lung phantom is better than AAA as its deviation have an average of 1% for
all field sizes with respect to the TLD measurements. Its greatest deviation is 5% at field
size 2x2cm2 at depth 8cm, but it is still within the uncertainty of TLD measurement. This
result found is consistent with theoretical validation of AXB with Monte Carlo
simulations1, 4, 30.
Uncertainties associated with the TLD measurement was estimated at 5%. Besides the
reproducibility of ±2%3, 63, factors that affect this uncertainty are errors associated when
determining the perturbation factor of the TLD, variation of TLD density, variation in
density of different slices of composite cork, and the placement of TLDs on the planchet
in the TLD reader during readout. An estimation of overall 5% uncertainty is therefore
reported in this study. This will be discussed further in the next section.
5.3.4 Discussions
Some previous investigations showed that AXB, accounting for specific material
composition of the medium, have improved accuracy of dose calculation in
heterogeneous media, as compared to the widely used AAA3, 30. The TLD verification of
AXB is an important step to determine the reliability of AXB for small field Lung SBRT.
Since AXB is a simulation of the dose distribution, it must be benchmarked against the
physical dose measurement of a radiation dosimeter.
The TLD dosimetric system has been calibrated for high precision measurements as far
as possible to be the benchmark for this validation. However, TLD-100, with its finite
78
dimensions and relatively higher density, causes significant perturbation in a low-density
lung medium, which is especially so in small fields. The determination of the
perturbation factors may incur some errors to the TLD measurements.
Table 5-1: Percentage error in calculating TLD perturbation factor
Density g/cc
% diff density
Perturbation Factor % error
2.638 0% 0.901 0.004 2.506 95% 0.904 -0.6 2.374 90% 0.910 -0.05 2.771 105% 0.897 -1.39 2.903 110% 0.894 -1.77
TLDs may differ in density from one another due to manufacturing fault as there is ±15%
sample-to-sample uniformity as reported by Radiation Products Design, Inc64. By
assuming that TLDs may have a 10% density variation from its default density
2.64g/cm3, there may be a percentage error of the perturbation factor up to 1.7% as
shown in Table 1 above.
The composite cork chosen may also differ in density between slices. Even though that
15 slices of composite cork have an average density of 0.27g/cm3, density of each
individual slices calculated may vary up to 3%. The density was calculated by measuring
the mass and volume of each slice of composite cork individually.
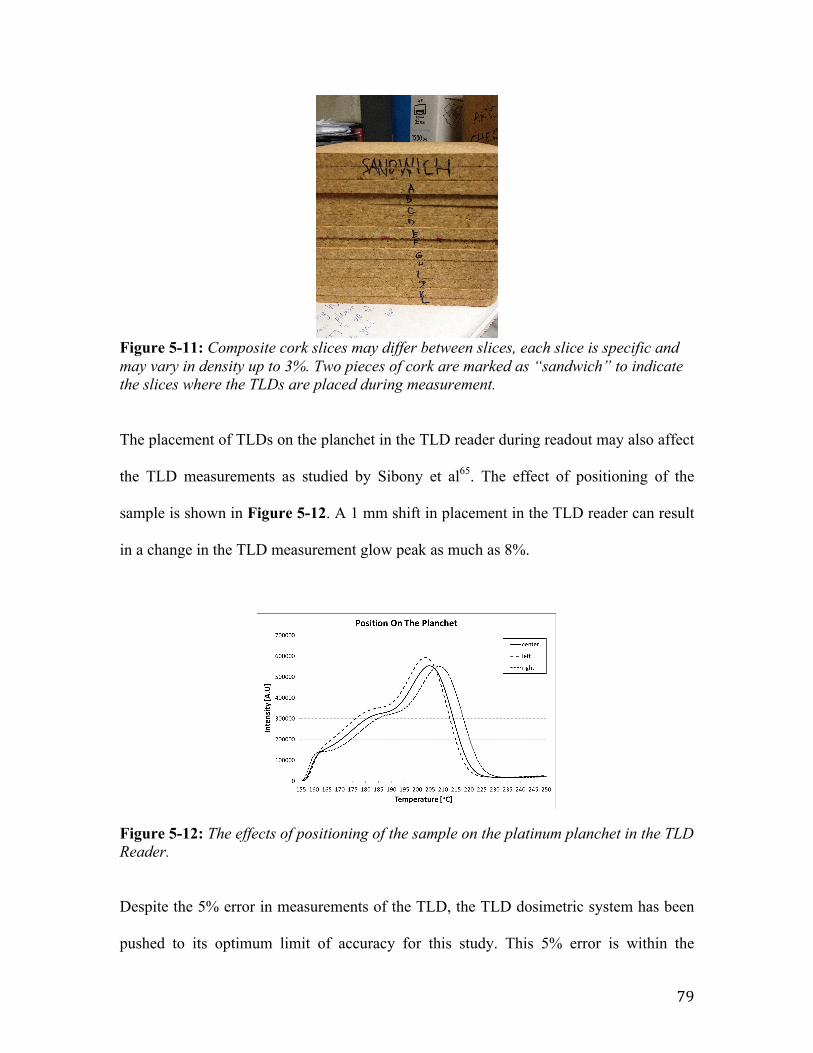
79
Figure 5-11: Composite cork slices may differ between slices, each slice is specific and may vary in density up to 3%. Two pieces of cork are marked as “sandwich” to indicate the slices where the TLDs are placed during measurement.
The placement of TLDs on the planchet in the TLD reader during readout may also affect
the TLD measurements as studied by Sibony et al65. The effect of positioning of the
sample is shown in Figure 5-12. A 1 mm shift in placement in the TLD reader can result
in a change in the TLD measurement glow peak as much as 8%.
Figure 5-12: The effects of positioning of the sample on the platinum planchet in the TLD Reader.
Despite the 5% error in measurements of the TLD, the TLD dosimetric system has been
pushed to its optimum limit of accuracy for this study. This 5% error is within the
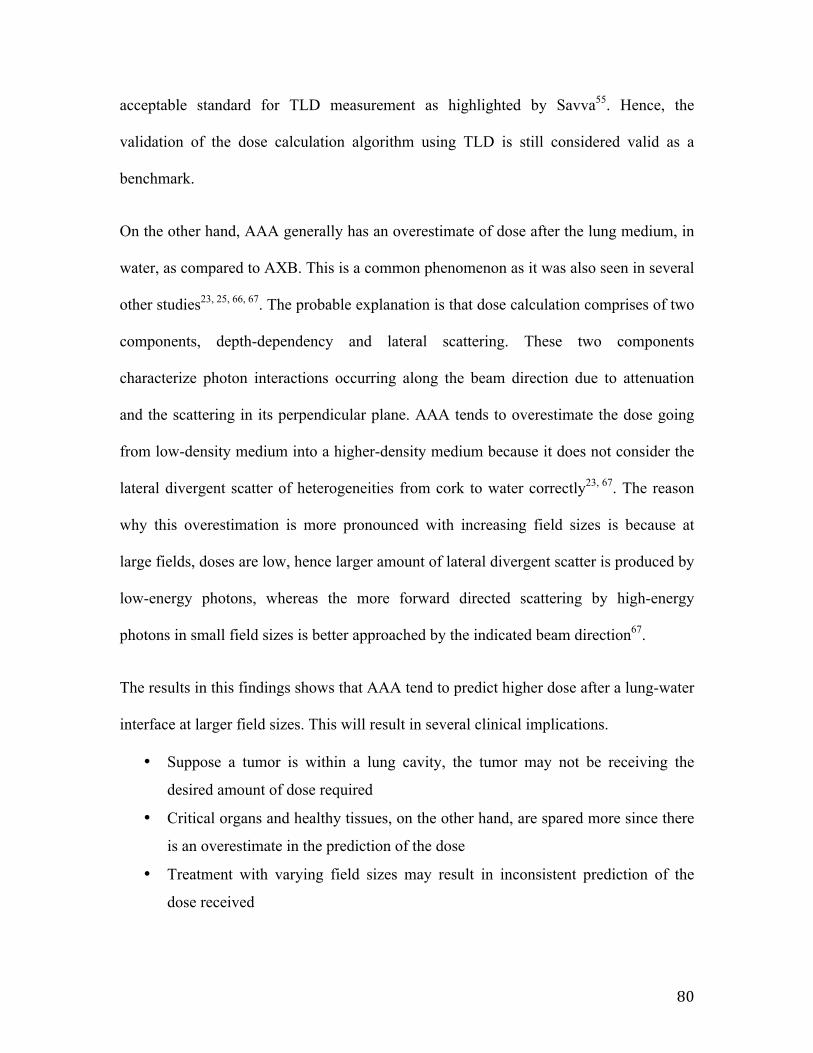
80
acceptable standard for TLD measurement as highlighted by Savva55. Hence, the
validation of the dose calculation algorithm using TLD is still considered valid as a
benchmark.
On the other hand, AAA generally has an overestimate of dose after the lung medium, in
water, as compared to AXB. This is a common phenomenon as it was also seen in several
other studies23, 25, 66, 67. The probable explanation is that dose calculation comprises of two
components, depth-dependency and lateral scattering. These two components
characterize photon interactions occurring along the beam direction due to attenuation
and the scattering in its perpendicular plane. AAA tends to overestimate the dose going
from low-density medium into a higher-density medium because it does not consider the
lateral divergent scatter of heterogeneities from cork to water correctly23, 67. The reason
why this overestimation is more pronounced with increasing field sizes is because at
large fields, doses are low, hence larger amount of lateral divergent scatter is produced by
low-energy photons, whereas the more forward directed scattering by high-energy
photons in small field sizes is better approached by the indicated beam direction67.
The results in this findings shows that AAA tend to predict higher dose after a lung-water
interface at larger field sizes. This will result in several clinical implications.
• Suppose a tumor is within a lung cavity, the tumor may not be receiving the
desired amount of dose required
• Critical organs and healthy tissues, on the other hand, are spared more since there
is an overestimate in the prediction of the dose
• Treatment with varying field sizes may result in inconsistent prediction of the
dose received
81
However, Lung SBRT cases are delivered with multiple beams from many directions
(Figure 4-5). This may cause the dose differences to be averaged out when using
conventional AAA algorithm. This is a subject of further study.
AXB has proven to be accurate and self-consistent as shown in our TLD measurements.
Final results from the lung substitute phantom shows that AXB’s accuracy under
electronic disequilibrium condition for small field size (2x2cm2) is better than AAA. This
validates the theory that AXB is an accurate dose algorithm as reported in several
studies3, 28. It should be considered for clinical application for Lung SBRT.
82
5.4 Summary
In this chapter, AXB was validated for Lung SBRT using TLD-100 and checked against
AAA, in a lung substitute phantom. The motivation for this study was that many papers
have validated AXB by simulating the dose in the TPS without physical measurements.
The lung phantom was built by having a slab of 14cm composite cork sandwiched by
4cm slabs of Plastic Water. The dimensions of the phantom were obtained by taking the
average dimensions of 15 Lung SBRT patients treated in National Cancer Center
Singapore. Composite cork was chosen as a lung substitute material, as it was found to
have similar radiological properties as lung tissue.
TLDs were calibrated at 0.5Gy under standard condition in 10cm Plastic Water. 0.5Gy
was then delivered to lung isocenter as it was found to be within the linear range of the
TLD response. 14 TLD measurement positions were placed within the lung phantom,
including the water-cork (lung) interfaces and the lung isocenter.
It was found that TLD-100, with its finite dimensions and relatively higher density,
causes significant perturbation in a low-density lung medium. This has to be accounted
for each of the field sizes. AXB was used to calculate the perturbation factor for TLDs in
this study. As field sizes decreases, the perturbation of the TLD increases. The AXB
perturbation factors also validates its accuracy to correct the TLD readings and hence its
self-consistency.
83
AXB data generally matches closely to the TLD dose profile as compared to AAA. The
perturbation factor as calculated by AXB accurately corrects for the TLD measurement
back to the expected dose. Uncertainties associated with the TLD measurement was
estimated at 5%. These errors include the ±2% reproducibility, the variation of density in
TLDs, variation in density of different slices of composite cork, and also the placement of
TLDs on the planchet in the TLD reader during readout.
AAA generally has an overestimate of dose after lung medium in water and this becomes
more pronounced with increasing field sizes. This is due to divergent scatter between
heterogeneous interfaces that is not accounted for in the AAA model.
TLD measurements have shown that the AXB results are more accurate than AAA in
lung. Results obtained imply that AXB should be considered for clinical application in
Lung SBRT treatment.
84
6 Conclusion 6.1 Summary
The end goal of physics in radiotherapy is to treat a target volume with the appropriate
amount of dose and yet minimizing dose to healthy tissues and critical organs. A brief
introduction of the physics of radiotherapy was done in Chapter 2, to help readers
understand some key concepts pertaining to radiation physics.
The objective of this work is to study thermoluminesence dosimeters and apply them to
validate a new the dose calculation algorithm, Acuros XB. This validation of the dose
calculation algorithm was done for Lung Stereotactic Body Radiation Therapy cases. The
result in this study will have clinical implications on the use of the appropriate algorithms
for Lung SBRT cases.
In Chapter 3, a study was done on thermoluminence dosimetry. Through the calibration
and selection of TLDs, we determined several correction factors such as Reader
Correction Factor and Element Correction Coefficient. These are essential to obtain an
accurate measurement using TLDs. The linearity response of the TLDs was also
investigated.
Dose calculation algorithms were introduced in Chapter 4. Two dose calculation
algorithms, Anistropic Analytical Algorithm and Acuros XB, was studied. AAA is a
clinical algorithm that is widely used today. AXB is a new dose calculation algorithm,
85
and was reported that it has excellent agreement with the gold standard for dose
calculation today, which is Monte Carlo calculation. AXB depends on the CT number –
mass density relationship to account for heterogeneities within a medium. A CT
calibration curve was obtained by having a CT scan of 2 different electron density
phantoms.
A lung phantom was built to simulate Lung SBRT cases. In earlier studies, composite
cork was found to be the best lung substitute material. Plastic WaterTM was used to
simulate soft tissue wall before and after the lung cavity.
Lastly, we validated AXB and AAA by taking 14 TLD measurements within the lung
phantom in Chapter 5. It was found that the high-density TLD cause significant
perturbation within the low-density lung medium. Hence, the TLD measurements have to
be corrected by a perturbation factor calculated using AXB. AAA, on the other hand, is
unable to determine this factor due to limitations in the algorithm.
It was found that AXB agrees with TLD measurements better than AAA. AAA tends to
have an overestimation in water after the low-density lung medium, and this phenomenon
was more pronounced with increasing field sizes. This is due to lateral divergent
scattering at low photon doses at large field sizes, as compared to forward directed
scattering in high photon doses at small field sizes. By such an overestimation, there will
be clinical implications when using AAA for Lung SBRT. For example, a tumor may not
be receiving the desired dose as there is an overestimation using AAA. However,
86
conventional Lung SBRT is delivered with multiple beams from many directions. This
might have caused the dose differences to be averaged out, self- correcting it to the
desired dose. Further studies could be done to investigate this implication.
87
6.2 Future Works
In this study, AAA overestimated the doses after the low-density lung medium at large
field sizes. However, this prediction was after a 14cm lung cavity. Most Lung SBRT
cases have a tumor at intermediate depths, such as after 5cm of lung cavity. Investigation
can be done to study the overestimation of AAA in a small tumor inserted at a mid-lung
position.
Most Lung SBRT cases are done using 4D-CT scans. Conventional CT scans simulate
the patient’s lung volume by compiling several image slices of the lung volume.
However, due to the respiratory motion of the patient, it is impossible to determine the
position of the tumor. A 4D-CT scan comprises of a large number of individual CT scans
obtained at various phases of the respiratory cycle68. This approach images the movement
of the tumor with respiration and it helps to determine an accurate internal margin for the
tumor. Hence, future works could create a lung phantom that is able to simulate the
respiratory movement of a patient. Further validation of AXB and AAA could be done
using TLDs on 4D-CT Lung SBRT.
A new version of AXB (ver. 11) will also be ready in the future. A comparison of AXB
and AAA from version 11 with AXB and AAA from version 10 can be done to
investigate the improvements in lung cases.
88
7 References 1. T. Han, F. Mourtada, K. Kisling, J. Mikell, D. Followill and R. Howell, Med. Phys.
38, 2651–2664 (2011). 2. M. W. K. Kan, L. H. T. Leung and P. K. N. Yu, Med. Phys. 39 (8) (August 2012). 3. A. Fogliata, G. Nicolini, A. Clivio, E. Vanetti and L. Cozzi, Radiation Oncology 6
(82) (2011). 4. A. Fogliata, G. Nicolini, A. Clivio, E. Vanetti, P. Mancosu and L. Cozzi, Phys.
Med. Biol. 56, 1879-‐1904 (2011). 5. A. Fogliata, G. Nicolini, A. Clivio, E. Vanetti and L. Cozzi, Am. Assoc. Phys. Med.
38 (11) (2011). 6. Tao Han, Firas Mourtada, Kelly Kisling, Justin Mikell, David Followill, Rebecca
Howell, Med. Phys. 39 (4) (2012). 7. K.-‐P. Chang, S.-‐H. Hung, Y.-‐H. Chie, A.-‐C. Shiau and R.-‐J. Huang, Med. Phys. 39
(4) (2012). 8. M. Goitein, Radiation Oncology: A Physicist's-‐Eye View. (Springer, 2008). 9. E. B. Podgorsak, Radiation Oncology Physics: A Handbook for Teachers and
Students. (IAEA, 2005). 10. Paul N. Mobit , Great Lakes Cancer Institute ,McLaren Regional Medical
Center and Tomas Kron, Peter MacCallum Cancer Centre, Department of Physical Sciences, in MICRODOSIMETRIC RESPONSE OF PHYSICAL AND BIOLOGICAL SYSTEMS TO LOW-‐ AND HIGH-‐LET RADIATIONS: THEORY AND APPLICATIONS TO DOSIMETRY, edited by Y. Horowitz (Elsevier B.V, 2006).
11. F. Daniels, Boyd, C. and Saunders, Science 117, 343–349 (1953). 12. J. V. Dam and G. Marinello, in ESTRO (ESTRO, Mounierlaan 83/12 – 1200
Brussels (Belgium), 2006). 13. McKinlay, Thermoluminescence dosimetry-‐Medical Physics Handbooks 5.
(Bristol: Adam Hilger Ltd, 1981). 14. P. N. Mobit, A. E. Nahum, Philip Mayles, Joint Department of Physics, Institute
of Cancer Research and Royal Marsden NHS Trust, and U. Sutton SM2 5PT, Phys. Med. Biol. 41, 979-‐993 (1996).
15. P. N. Mobit, P. Mayles, Alan E Nahum, Joint Department of Physics, Institute of Cancer Research and Royal Marsden NHS Trust, Sutton and U. SM2 5PT, Phys. Med. Biol. 41, 387-‐398 (1996).
16. T. Kron, Australas. Phys. Eng. Sci. Med. 18, 1-‐25 (1994). 17. Saint-‐Gobain Industrial Ceramics, Inc., Harshaw Dosimetry System, (TLD
Reader, REMS, and Dose Computation Algorithm), System Calibration Procedure, USA (1998).
18. D. M. Moor, B. Horspool and R. P. Stokes, Radiation Measurements 43, 533–537 (2008).
19. International Commission on Radiological Protection. Radiological Protection and Safety in Medicine, ICRP Publication 73 (Annals of ICRP 26 (2).) (1996).
20. T. Rivera, Applied Radiation and Isotopes 10, 1016 (2012).
89
21. Y. S. Horowitz and H. Datz, presented at the American Institute of Physics conference Proceedings, 2011 (unpublished).
22. L. A. R. d. Rosa, S. C. Cardoso, L. T. Campos, V. G. L. Alves, D. V. S. Batista and A. .Facure, Journal Of Applied Clinical Medical Physics 11 (1) (2010).
23. E. Sterpin, M. Tomsej, B. De Smedt, N. Reynaert and S. Vynckier, Medical Physics 34, 1665 (2007).
24. A. Fogliata, G. Nicolini, E. Vanetti, A. Clivio and L. Cozzi, Physics in Medicine and Biology, 51, 1421–1438 (2006).
25. C. M. Bragg and J. Conway, Radiotherapy and Oncology 81 (3), 315-‐323 (2006).
26. K. Breitman, S. Rathee, C. Newcomb, B. Murray, D. Robinson, C. Field, H. Warkentin, S. Connors, M. Mackenzie, P. Dunscombe and G. Fallone, Journal Of Applied Clinical Medical Physics 8 (2) (2007).
27. H. S. Rønde and L. Hoffmann, Acta Oncologica 48, 209-‐215 (2009). 28. S. Rana and K. Rogers, Journal of Medical Physics 38 (1), 9-‐14 (2013). 29. T. Han, F. Mourtada, K. Kisling, J. Mikell, D. Followill and R. Howell, Med. Phys.
39 (4) (2012). 30. K. Bush, M. Gagne, S. Zavgorodni, W. Ansbacher and W. Beckham, Med. Phys.
38 (4) (April 2011). 31. Varian Medical Systems, Inc., Eclipse Algorithms Reference Guide (P/N
B502679R01B, document version 2.0), Finland (2010). 32. K. A. Gifford, J. Horton, T. Wareing, G. Failla and F. Mourtada, Phys. Med. Biol.
51, 2253-‐2265 (2006). 33. K. A. Gifford, M. Price, J. Horton, T. Wareing and F. Mourtada, Phys. Med. Biol.
35, 2279-‐2285 (2008). 34. O. N. Vassiliev, T. Wareing, I. M. Davis, J. McGhee, D. Barnett, J. Horton, K. A.
Gifford, G. Failla, U. Titt and F. Mourtada, Int. J. Radiat. Oncol., Biol., Phys. 72, 220-‐227 (2008).
35. O. N. Vassiliev, T. Wareing, J. McGhee, G. Failla, M. R. Salehpour and F. Mourtada, Phys. Med. Biol. 55, 581-‐598 (2010).
36. B. R. Walters, I. Kawrakow and D. Rogers, 2005. 37. G. N. Hounsfield, Med. Phys. 7 (4) (1980). 38. U. Schneider, E. Pedroni and A. Lomax, Phys. Med. Biol. 41, 111-‐124 (1996). 39. H. Bornefalk, Phys. Med. Biol. 57, N83-‐N87 (2012). 40. C. Constantinou, J. C. Harrington and L. A. DeWed, Med. Phys. 19, 325-‐327
(1992). 41. D. Loiselle, (Global Resource for Advancing Cancer Education, 2012). 42. S. M. Carey, A. Katz and L. S. Constine., in Seminars in radiation oncology
(2006), Vol. 16. 43. M. J. P. Brugmans, A. v. d. Horst, J. V. Lebesque and B. J. Mijnheer, Int. J. Radiat.
Oncol., Biol.,Phys. 43, 893-‐904 (1999). 44. A. Mesbahi, Iran. J. Radiat. Res. 6, 70-‐76 (2008). 45. E. K. Osei, J. Darko, A. Mosseri and J. Jezioranski, Med. Phys. 30, 2706-‐2714
(2003). 46. E. Sham, J. Seuntjens, S. Devic and E. B. Podgorsak, Med. Phys. 35, 3317-‐3330
(2008).
90
47. I. J. Das, G. X. Ding and A. Ahnesjö, Med. Phys. 35 (1) (2007). 48. J. C. Chow, M. Seguin and A. Alexander, Med. Phys. 32, 759-‐765 (2005). 49. J. Dutreix, A. Dutreix and M. Tubiana, Phys. Med. Biol. 10, 177-‐190 (1965). 50. O. T. Ogunleye, F. H. Attix and B. R. Paliwal, Phys. Med. Biol. 25 (2), 203-‐213
(1980). 51. M. Bucciolini, F. B. Buonamici, S. Mazzocchi, C. D. Angelis, S. Onori and G. A. P.
Cirrone, Med. Phys. 30 (8) (2003). 52. P. A. Kupelian, R. Komaki and P. Allen, International Journal of Radiation
Oncology,Biology and Physics 36 (3) (1996). 53. V. Siebers, P. J. Keall, A. E. Nahum and R. Mohan, 45 983-‐995 (2000). 54. Swiss Society of Radiobiology and Medical Physics, in Recommendations No.
11 (Schweizerische Gesellschaft für Strahlenbiologie und Medizinische Physik, 2003).
55. A. Savva, Master of Science in Radiation Detection and Instrumentation Thesis: Personnel TLD monitors, their calibration and response, University of Surrey, Department of Physics, 2010.
56. B. Rathbone, Hanford External Dosimetry Technical Basis Manual PNL-‐ MA-‐842, US: Pacific Northwest National Laboratory, 2007.
57. C. Furetta, Handbook of Thermoluminescence: Second Edition,(World Scientific Publishing Co. Pte. Ltd., 2010).
58. E. El-‐Khatib, J. Antolak and J. Scimger, Med. Phys. 19 (2) (1992). 59. S. C. C. L.A.R. da Rosa, L.T. Campos, V.G.L. Alves, and A. F. D.V.S. Batista,
Journal Of Applied Clinical Medical Physics 11 (1) (2010). 60. J. G. Holt, G. R. Edelstein and T. E. Clark, Phys. Med. Biol. 20 (4) (1975). 61. D. W. O. Rogers, in Clinical Dosimetry Measurements in Radiotherapy, edited
by D. W. O. Rogers and J. E. Cygler (Medical Physics Publishing, 2009). 62. B. Reniers, F. Verhaegen and S. Vynckier, Phys. Med. Biol. 49 (8) (2004). 63. R. L. Hill and B. A. Rathbone, (US: Pacific Northwest National Laboratory,
2010). 64. Radiation Products Design Inc., Harshaw TLD-‐100 Chips Online Catalogue,
accessed 19 Mar 2013 65. D. Sibony, Y. S. Horowitz and L. Oster, 2013 (unpublished). 66. M. R. Arnfield, C. H. Siantar, J. Siebers, P. Garmon, L. Cox and R. Mohan, Med.
Phys. 27 (6) (2000). 67. A. V. Esch, L. Tillikainen, J. Pyykkonen, M. Tenhunen, H. Helminen, S.
Siljamäki, J. Alakuijala, M. Paiusco, M. Iori and D. P. Huyskens1, Med. Phys. 33, 4130-‐4148 (2006).
68. T. Pan, T.-‐Y. Lee, E. Rietzel and G. T. Y. Chen, Med. Phys. 31 (2) (2004).
91
Appendix I. Cavity theory Taken from “The quality dependence of LiF TLD in megavoltage photon beams: Monte Carlo simulation and experiments” by Mobit et al1 A cavity is formed when a radiation detector is placed in a medium, and is exposed to
irradiation. The detector will most likely have a different density and atomic number
from the medium. Hence, cavity theory relates the dose absorbed in a medium (Dmed ) and
the average dose absorbed in the cavity (Dcav):
𝐷!"# = 𝐷!"#𝑓!"#,!"#
where fmed,cav is a perturbation factor that is determined by the beam energy, radiation
response, medium, size and composition of the cavity. For a cavity that is relatively
small, when compared to the field size of the photon beams, the Bragg–Gray relation
states that:
𝑓!"#,!"# = 𝑠!"#,!"#
where smed,cav is the average mass stopping-power ratio of the medium to the cavity, as
studied by Spencer and Attix2. For a cavity that is large compared to the field size of a
photon beam, the dose in the medium can be obtained from the mass energy-absorption
coefficient ratio of the medium to the cavity material:
𝑓!"#,!"# = (𝜇!"𝜌 )!"#,!"#
where (µen/ρ)med,cav is the ratio of the mass energy-absorption coefficients, from the
medium to cavity, averaged over the photon energy fluence spectrum present in the
92
medium. This expression ignores the perturbation effects or interface effects that may
occur by the introduction of the detector material into a different medium as it then
becomes heterogeneous medium insert3, 4.
Burlin5 theorized a general cavity theory for photons for all sizes, which approaches the
Spencer–Attix theory in the small-size limit and the ratio of the mass energy-absorption
coefficient for very large cavities. According to this theory
𝑓!"#,!"# = 𝑑𝑠!"#,!"# + (1− 𝑑)(𝜇!"𝜌 )!"#,!"#
where d is a weighting factor which gives (1−d) the contribution to the total dose from
electrons generated by photon interaction in the cavity. Burlin’s cavity equation has been
critically examined and modified by Horowitz et al6 and Almond and McCray7. These
theoretical predictions may vary considerably as they are based on empirical fits to
experimental findings.
93
II. Acuros XB solution methods Taken from Varian Medical Systems, Acuros® XB advanced dose calculation for the EclipseTM treatment planning system manual by Failla et al8 The Acuros XB algorithm consists of four steps, which are performed in the following
order:
Transport of source model fluence into the patient.
Calculation of scattered photon fluence in the patient.
Calculation of scattered electron fluence in the patient.
Dose calculation
Steps 1- 3 are performed to calculate the electron fluence in every voxel of the patient.
Once the energy dependent electron fluence is solved, the desired dose quantity (dose-to-
medium or dose-to-water) is computed in Step 4. Step 1 is the only step repeated for each
field direction, and Steps 2 through 4 are performed once, regardless of the number of
fields.
Material specification
Before the first step, Acuros XB must have a material map of the imaged patient. Unlike
AAA, where heterogeneities are generally handled as density-based corrections applied
to dose kernels calculated in water, Acuros XB simulates the physical interaction of
radiation with matter. Therefore, Acuros XB requires the chemical composition and the
density of each material in which particles are transported through. To enable this, the
Eclipse Treatment Planning System provides Acuros XB with a mass density and
material type in each voxel of the image grid. The Acuros XB material library includes
94
five biological materials (lung, adipose tissue, muscle, cartilage, and bone) and 16 non-
biological materials, with a maximum supported density of 8.0 g/cc (steel).
The fundamental material data used by Acuros XB are known as macroscopic atomic
cross sections. A macroscopic cross section (cm-1) is the probability that a particular
reaction will occur per unit path length of particle travel taking into account the angular
and energy behavior probabilities associated. Macroscopic cross sections are derived
from these two factors: the microscopic cross section for a given reaction (barns/atom =
10-24 cm2/atom, 𝜎) and the mass density of the material ( ρ , g/cm3). The expression for
the macroscopic cross section, σ, is:
𝜎 =𝑁!𝜌𝑀 𝜎
where
M = Mass of the atom in atomic mass units
Na = Avogardo’s Number
Acuros XB uses coupled photon-electron cross sections produced by Coupled Electron-
Photon Cross Section Generating Code (CEPXS)9. For photon interactions, CEPXS
includes Compton scattering, the photoelectric effect, and pair production. CEPXS does
not account for Rayleigh scattering, because the effect of Rayleigh scattering is
insignificant for dose distributions at energies in photon beam radiotherapies.
The LBTE
In Steps 1-3, Acuros XB solves the time-independent three-dimensional system of
coupled Boltzmann transport equations (LBTE) shown below
(For brevity the dependent variables have been suppressed in the equations):

95
Eq. 1
Eq.2
where
Ψ!= Angular photon fluence as a function of position, energy and direction
Ψ! = Angular electron fluence
𝑞!!= Photon-to-photon scattering source, which is the photon
source resulting from photon interactions
𝑞!!= Electron-to-electron scattering source, which is the electron
source resulting from electron interactions
𝑞!"= Photon-to-electron scattering source, which is the electron
source resulting from photon interactions
𝑞!= Extraneous photon source for a point source at an arbitrary position. This source
represents all photons coming from the machine source model.
𝑞!= Extraneous electron source for a point source at an arbitrary position. This source
represents all electrons coming from the machine source model.
𝜎!!= Macroscopic photon total cross section
𝜎!!= Macroscopic electron total cross section
𝜎!= Macroscopic total cross section
SR= Restricted collisional plus radiative stopping power
2 0 | V A R I A N M E D I C A L S Y S T E M S
Acuros XB uses coupled photon-electron cross sections produced by CEPXS [ref.
4]. For photon interactions, CEPXS includes Compton scatter (also known as inco-
herent scatter), the photo-electric effect, and pair production. CEPXS does not
account for Rayleigh scatter (also known as coherent scatter), the effect of which is
insignificant for dose distributions at energies typical in photon beam radiotherapies.
The LBTE
In Steps 1 through 3, Acuros XB solves the time-independent three-dimensional
system of coupled Boltzmann transport equations (LBTE) shown below (for brevi-
ty the dependent variables have been suppressed in the equations):
Eq. 1
Eq. 2
where
= Angular photon fluence (or fluence if not time integrated), ,
as a function of position, , energy, E, and direction,
= Angular electron fluence,
= Photon-to-photon scattering source, , which is the photon
source resulting from photon interactions
= Electron-to-electron scattering source, , which is the electron
source resulting from electron interactions
= Photon-to-electron scattering source, , which is the electron
source resulting from photon interactions
= Extraneous photon source, , for point source ,
at position
This source represents all photons coming from the machine source model.
= Extraneous electron source, , for point source ,
at position
This source represents all electrons coming from the machine source model.
= Macroscopic photon total cross section, , units of cm-1
= Macroscopic electron total cross section, , units of cm-1
= Macroscopic total cross section, , units of cm-1
= Restricted collisional plus radiative stopping power, ),( ErSR!
RS
),( Ert!"t"
),( Eret
!"et"
),( Eryt
!"yt"
pr!
p)ˆ,( #Eqeeq
pr!
p)ˆ,( #Eq yyq
)ˆ,,( #Erq ye !yeq
)ˆ,,( #Erqee !eeq
)ˆ,,( #Erq yy !yyq
)ˆ,,( #$ Ere !e$
),,(ˆ %&'=#
),,( zyxr =!)ˆ,,( #$ Ery !($
( ) ,ˆ eeeeeR
eet
e qqqSE
++=$))
*$+$+,# ("!
, ˆ (((((( " qqt +=$+$+,#!
2 0 | V A R I A N M E D I C A L S Y S T E M S
Acuros XB uses coupled photon-electron cross sections produced by CEPXS [ref.
4]. For photon interactions, CEPXS includes Compton scatter (also known as inco-
herent scatter), the photo-electric effect, and pair production. CEPXS does not
account for Rayleigh scatter (also known as coherent scatter), the effect of which is
insignificant for dose distributions at energies typical in photon beam radiotherapies.
The LBTE
In Steps 1 through 3, Acuros XB solves the time-independent three-dimensional
system of coupled Boltzmann transport equations (LBTE) shown below (for brevi-
ty the dependent variables have been suppressed in the equations):
Eq. 1
Eq. 2
where
= Angular photon fluence (or fluence if not time integrated), ,
as a function of position, , energy, E, and direction,
= Angular electron fluence,
= Photon-to-photon scattering source, , which is the photon
source resulting from photon interactions
= Electron-to-electron scattering source, , which is the electron
source resulting from electron interactions
= Photon-to-electron scattering source, , which is the electron
source resulting from photon interactions
= Extraneous photon source, , for point source ,
at position
This source represents all photons coming from the machine source model.
= Extraneous electron source, , for point source ,
at position
This source represents all electrons coming from the machine source model.
= Macroscopic photon total cross section, , units of cm-1
= Macroscopic electron total cross section, , units of cm-1
= Macroscopic total cross section, , units of cm-1
= Restricted collisional plus radiative stopping power, ),( ErSR!
RS
),( Ert!"t"
),( Eret
!"et"
),( Eryt
!"yt"
pr!
p)ˆ,( #Eqeeq
pr!
p)ˆ,( #Eq yyq
)ˆ,,( #Erq ye !yeq
)ˆ,,( #Erqee !eeq
)ˆ,,( #Erq yy !yyq
)ˆ,,( #$ Ere !e$
),,(ˆ %&'=#
),,( zyxr =!)ˆ,,( #$ Ery !($
( ) ,ˆ eeeeeR
eet
e qqqSE
++=$))
*$+$+,# ("!
, ˆ (((((( " qqt +=$+$+,#!

96
The first term on the left hand side of Equations 1 and 2 is the streaming operator. The
second term on the left hand side of Equations 1 and 2 is the collision or removal
operator. Equation 2 is the Boltzmann Fokker-Planck transport equation, which is solved
for the electron transport. In Equation 2, the third term on the left represents the
continuous slowing down (CSD) operator, which accounts for Coulomb ‘soft’ electron
collisions. The right hand side of Equations 1 and 2 include the scattering, production,
and the external source terms from the AAA source module ( qγ and qe ).
The scattering and production sources are defined by:
Eq. 3
Eq. 4
Eq. 5
where
𝜎!!!= Macroscopic photon-to-photon differential scattering cross section
𝜎!!"= Macroscopic photon-to-electron differential production cross section
𝜎!!!= Macroscopic electron-to-electron differential scattering cross section
2 1 | V A R I A N M E D I C A L S Y S T E M S
The first term on the left hand side of Equations 1 and 2 is the streaming oper-
ator. The second term on the left hand side of Equations 1 and 2 is the collision or
removal operator. Equation 2 is the Boltzmann Fokker-Planck transport equation,
which is solved for the electron transport. In Equation 2, the third term on the left
represents the continuous slowing down (CSD) operator, which accounts for
Coulomb ‘soft’ electron collisions. The right hand side of Equations 1 and 2
include the scattering, production, and the external source terms from the AAA
source module ( and ).
The scattering and production sources are defined by:
Eq. 3
’
Eq. 4
Eq. 5
where
= Macroscopic photon-to-photon differential scattering cross section
= Macroscopic photon-to-electron differential production cross section
= Macroscopic electron-to-electron differential scattering cross section
The basic assumptions used in Equations 1 and 2 are briefly summarized as fol-
lows: Both charged pair production secondary particles are assumed to be elec-
trons instead of one electron and one positron. Also, the partial coupling technique
is assumed, whereby photons can produce electrons, but electrons do not produce
photons. Regarding the latter, the energy from Bremsstrahlung photons is
assumed to be negligible and is discarded.
These assumptions have only a minor effect on the energy deposition field, and
are similar to those employed in clinical Monte Carlo codes. A primary assumption
of Equation 2 is that the Fokker-Planck operator (of which the CSD operator is
the first order term), is used for Coulomb, or “soft”, interactions that result in
small energy losses. Catastrophic interactions that result in large energy losses are
represented with the standard Boltzmann scattering. This can be seen as the deter-
ministic equivalent to electron condensed history models in Monte Carlo.
ees!
es"!
""! s
) ,ˆ,,()ˆˆ,,( )ˆ,,(40
#$$%#$&#'$#$$=# !!(
ErEErdEdErq eees
ee '''
)
!
) ,ˆ,,()ˆˆ,,( )ˆ,,(40
#$$%#$&#'$#$$=# !!(
ErEErdEdErq es
e ''' "
)
"" !
)ˆ,,()ˆˆ,,( )ˆ,,(40
#$$%#$&#'$#$$=# !!(
ErEErdEdErq s
''' "
)
"""" !
eq"q
2 1 | V A R I A N M E D I C A L S Y S T E M S
The first term on the left hand side of Equations 1 and 2 is the streaming oper-
ator. The second term on the left hand side of Equations 1 and 2 is the collision or
removal operator. Equation 2 is the Boltzmann Fokker-Planck transport equation,
which is solved for the electron transport. In Equation 2, the third term on the left
represents the continuous slowing down (CSD) operator, which accounts for
Coulomb ‘soft’ electron collisions. The right hand side of Equations 1 and 2
include the scattering, production, and the external source terms from the AAA
source module ( and ).
The scattering and production sources are defined by:
Eq. 3
’
Eq. 4
Eq. 5
where
= Macroscopic photon-to-photon differential scattering cross section
= Macroscopic photon-to-electron differential production cross section
= Macroscopic electron-to-electron differential scattering cross section
The basic assumptions used in Equations 1 and 2 are briefly summarized as fol-
lows: Both charged pair production secondary particles are assumed to be elec-
trons instead of one electron and one positron. Also, the partial coupling technique
is assumed, whereby photons can produce electrons, but electrons do not produce
photons. Regarding the latter, the energy from Bremsstrahlung photons is
assumed to be negligible and is discarded.
These assumptions have only a minor effect on the energy deposition field, and
are similar to those employed in clinical Monte Carlo codes. A primary assumption
of Equation 2 is that the Fokker-Planck operator (of which the CSD operator is
the first order term), is used for Coulomb, or “soft”, interactions that result in
small energy losses. Catastrophic interactions that result in large energy losses are
represented with the standard Boltzmann scattering. This can be seen as the deter-
ministic equivalent to electron condensed history models in Monte Carlo.
ees!
es"!
""! s
) ,ˆ,,()ˆˆ,,( )ˆ,,(40
#$$%#$&#'$#$$=# !!(
ErEErdEdErq eees
ee '''
)
!
) ,ˆ,,()ˆˆ,,( )ˆ,,(40
#$$%#$&#'$#$$=# !!(
ErEErdEdErq es
e ''' "
)
"" !
)ˆ,,()ˆˆ,,( )ˆ,,(40
#$$%#$&#'$#$$=# !!(
ErEErdEdErq s
''' "
)
"""" !
eq"q
2 1 | V A R I A N M E D I C A L S Y S T E M S
The first term on the left hand side of Equations 1 and 2 is the streaming oper-
ator. The second term on the left hand side of Equations 1 and 2 is the collision or
removal operator. Equation 2 is the Boltzmann Fokker-Planck transport equation,
which is solved for the electron transport. In Equation 2, the third term on the left
represents the continuous slowing down (CSD) operator, which accounts for
Coulomb ‘soft’ electron collisions. The right hand side of Equations 1 and 2
include the scattering, production, and the external source terms from the AAA
source module ( and ).
The scattering and production sources are defined by:
Eq. 3
’
Eq. 4
Eq. 5
where
= Macroscopic photon-to-photon differential scattering cross section
= Macroscopic photon-to-electron differential production cross section
= Macroscopic electron-to-electron differential scattering cross section
The basic assumptions used in Equations 1 and 2 are briefly summarized as fol-
lows: Both charged pair production secondary particles are assumed to be elec-
trons instead of one electron and one positron. Also, the partial coupling technique
is assumed, whereby photons can produce electrons, but electrons do not produce
photons. Regarding the latter, the energy from Bremsstrahlung photons is
assumed to be negligible and is discarded.
These assumptions have only a minor effect on the energy deposition field, and
are similar to those employed in clinical Monte Carlo codes. A primary assumption
of Equation 2 is that the Fokker-Planck operator (of which the CSD operator is
the first order term), is used for Coulomb, or “soft”, interactions that result in
small energy losses. Catastrophic interactions that result in large energy losses are
represented with the standard Boltzmann scattering. This can be seen as the deter-
ministic equivalent to electron condensed history models in Monte Carlo.
ees!
es"!
""! s
) ,ˆ,,()ˆˆ,,( )ˆ,,(40
#$$%#$&#'$#$$=# !!(
ErEErdEdErq eees
ee '''
)
!
) ,ˆ,,()ˆˆ,,( )ˆ,,(40
#$$%#$&#'$#$$=# !!(
ErEErdEdErq es
e ''' "
)
"" !
)ˆ,,()ˆˆ,,( )ˆ,,(40
#$$%#$&#'$#$$=# !!(
ErEErdEdErq s
''' "
)
"""" !
eq"q

97
The basic assumptions used in Equations 1 and 2 are:
• Both charged pair production secondary particles are assumed to be electrons
instead of one electron and one positron.
• The partial coupling technique is assumed, whereby photons can produce
electrons, but electrons do not produce photons.
• The energy from Bremsstrahlung photons is assumed to be negligible and is
discarded.
These assumptions have only a minor effect on the energy deposition field, and are
similar to those used in clinical Monte Carlo codes. A primary assumption of Equation 2
is that the Fokker-Planck operator (of which the CSD operator is the first order term), is
used for Coulomb interactions that result in small energy losses. Catastrophic interactions
that result in large energy losses are represented in the standard Boltzmann scattering.
This can be seen as the deterministic equivalent to electron condensed history models in
Monte Carlo.
To represent the anisotropic behavior of the differential scattering and
production sources, the macroscopic differential scattering cross sections are expanded
into Legendre polynomials, Pl (µ0), where µ0 = 𝛺 ⋅ 𝛺ʹ. This expansion allows the
differential scattering or production cross section(s) to be expressed as:
Eq. 6
Similarly, the angular fluence appearing in the scattering source is expanded
into spherical harmonics moments:
2 2 | V A R I A N M E D I C A L S Y S T E M S
To represent the anisotropic behavior of the differential scattering and
production sources, in a mathematically practical manner, the macroscopic
differential scattering cross sections are expanded into Legendre polynomials,
, where . This expansion allows the differential scattering
or production cross section(s) to be expressed as:
Eq. 6
,
Similarly, the angular fluence appearing in the scattering source is expanded
into spherical harmonics moments:
Eq. 7
where
= Spherical harmonic functions
= Angular indices
= Spherical harmonics moments of the angular fluence, calculated as:
where * denotes the complex conjugate
= Macroscopic electron-to-electron differential scattering cross section
Equations 6 and 7 are exact. Additionally, for purely isotropic scattering, l = 0
is also exact. However, Acuros XB sets a limit on the scattering order, l !7, and
hence the number of spherical harmonic moments kept in the scattering/produc-
tion source. Using the Legendre addition theorem, the scattering and production
sources become:
Eq. 8
! ! "= !=
"
#$=
#7
0 0,,
//,
//
).ˆ('),()',('
)ˆ,,(
l
l
lmmlml
eeels
eee
YErEErdE
Erq
$$
$
%& '''
'''
ees&
),'ˆ,()ˆ('4
*," #(#)#
*
,ErYd ml$
),(, Erml )$%
ml,
)ˆ(, #mlY
)ˆ(),()ˆ,,( ,0
, #))=#))( ! !"
= !=ml
l
l
lmml YErEr
$$% ,
)(),(4
12
)ˆˆ,,(
0//
0
//
+&*
&
'''
'''
leee
s,ll
eees
PEErl
EEr
$)+
=
#),#$)
!"
=
$
$
#),#= ˆ0+)( 0+lP

98
Eq. 7
where
𝑌!,!(Ω)= Spherical harmonics moments of the angular fluence
l, m = Angular indices
𝜙!,!(𝑟,Ω!,E!)= Macroscopic electron-to-electron differential scattering cross section
Equations 6 and 7 are exact. Additionally, for purely isotropic scattering, l = 0 is also
exact. However, Acuros XB sets a limit on the scattering order, l ≤7, and hence the
number of spherical harmonic moments kept in the scattering source. Using the Legendre
addition theorem, the scattering and production sources become:
Eq. 8
Step 1: Transport of source model fluence into the patient
The external photon and electron sources, qγ and qe , are modeled as anisotropic
point sources in Acuros XB. At each static beam phase space, a
point source exists for each of the AAA sources. For the primary source, qγ, is described
through a 2D fluence grid, in which both the particle fluence and energy spectra are the
spatial variables. For the extra-focal and wedge scatter sources, the anisotropy of grid qγ,
is described through a 3D fluence grid, and the energy spectra is spatially constant. For
2 2 | V A R I A N M E D I C A L S Y S T E M S
To represent the anisotropic behavior of the differential scattering and
production sources, in a mathematically practical manner, the macroscopic
differential scattering cross sections are expanded into Legendre polynomials,
, where . This expansion allows the differential scattering
or production cross section(s) to be expressed as:
Eq. 6
,
Similarly, the angular fluence appearing in the scattering source is expanded
into spherical harmonics moments:
Eq. 7
where
= Spherical harmonic functions
= Angular indices
= Spherical harmonics moments of the angular fluence, calculated as:
where * denotes the complex conjugate
= Macroscopic electron-to-electron differential scattering cross section
Equations 6 and 7 are exact. Additionally, for purely isotropic scattering, l = 0
is also exact. However, Acuros XB sets a limit on the scattering order, l !7, and
hence the number of spherical harmonic moments kept in the scattering/produc-
tion source. Using the Legendre addition theorem, the scattering and production
sources become:
Eq. 8
! ! "= !=
"
#$=
#7
0 0,,
//,
//
).ˆ('),()',('
)ˆ,,(
l
l
lmmlml
eeels
eee
YErEErdE
Erq
$$
$
%& '''
'''
ees&
),'ˆ,()ˆ('4
*," #(#)#
*
,ErYd ml$
),(, Erml )$%
ml,
)ˆ(, #mlY
)ˆ(),()ˆ,,( ,0
, #))=#))( ! !"
= !=ml
l
l
lmml YErEr
$$% ,
)(),(4
12
)ˆˆ,,(
0//
0
//
+&*
&
'''
'''
leee
s,ll
eees
PEErl
EEr
$)+
=
#),#$)
!"
=
$
$
#),#= ˆ0+)( 0+lP
2 2 | V A R I A N M E D I C A L S Y S T E M S
To represent the anisotropic behavior of the differential scattering and
production sources, in a mathematically practical manner, the macroscopic
differential scattering cross sections are expanded into Legendre polynomials,
, where . This expansion allows the differential scattering
or production cross section(s) to be expressed as:
Eq. 6
,
Similarly, the angular fluence appearing in the scattering source is expanded
into spherical harmonics moments:
Eq. 7
where
= Spherical harmonic functions
= Angular indices
= Spherical harmonics moments of the angular fluence, calculated as:
where * denotes the complex conjugate
= Macroscopic electron-to-electron differential scattering cross section
Equations 6 and 7 are exact. Additionally, for purely isotropic scattering, l = 0
is also exact. However, Acuros XB sets a limit on the scattering order, l !7, and
hence the number of spherical harmonic moments kept in the scattering/produc-
tion source. Using the Legendre addition theorem, the scattering and production
sources become:
Eq. 8
! ! "= !=
"
#$=
#7
0 0,,
//,
//
).ˆ('),()',('
)ˆ,,(
l
l
lmmlml
eeels
eee
YErEErdE
Erq
$$
$
%& '''
'''
ees&
),'ˆ,()ˆ('4
*," #(#)#
*
,ErYd ml$
),(, Erml )$%
ml,
)ˆ(, #mlY
)ˆ(),()ˆ,,( ,0
, #))=#))( ! !"
= !=ml
l
l
lmml YErEr
$$% ,
)(),(4
12
)ˆˆ,,(
0//
0
//
+&*
&
'''
'''
leee
s,ll
eees
PEErl
EEr
$)+
=
#),#$)
!"
=
$
$
#),#= ˆ0+)( 0+lP

99
the electron contamination source, the anisotropy of qe is described through a 3D fluence
grid, and the energy spectra are spatially constant.
For a photon point source, 𝑞! 𝐸,Ω with position 𝑟!, Equation 1 becomes
Eq. 9
where
δ = Dirac-delta function
The principle of linear superposition may be used to define the photon angular
fluence as the summation of uncollided and collided fluence components,
Eq. 10
𝛹!"#! = Uncollided, or unscattered, photon angular fluence. Refers to photons
which have not yet interacted with the patient.
𝛹!"##! = Collided, or scattered, photon angular fluence. Refers to photons which were
produced or scattered by a photon interaction in the patient.
Substituting Equation 10 into Equation 9, leads to the following equation for the
uncollided photon fluence:
Eq. 11
2 3 | V A R I A N M E D I C A L S Y S T E M S
Step 1: Transport of source model fluence into the patient
The external photon and electron sources, and , are modeled as anisotropic
point sources in Acuros XB. At each static beam phase space (i.e. control point), a
separate point source exists for each of the AAA sources. For the primary source,
the anisotropy of is described through a 2D fluence grid, in which both the
particle fluence and energy spectra are spatially variable. For the extra-focal and
wedge scatter sources, the anisotropy of is described through a 3D fluence
grid, and the energy spectra is spatially constant. For the electron contamination
source, the anisotropy of is described through a 3D fluence grid, and the ener-
gy spectra is spatially constant. All point sources are located at the target for the
respective control point.
For a photon point source, located at position, , Equation 1
becomes:
Eq. 9
where
= Dirac-delta function
The principle of linear superposition may be used to define the photon angular
fluence as the summation of uncollided and collided fluence components,
Eq. 10
,
where
= Uncollided, or unscattered, photon angular fluence. Refers to photons
which have not yet interacted with the patient/phantom.
= Collided, or scattered, photon angular fluence. Refers to photons which
were produced or scattered by a photon interaction in the patient/
phantom.
Substituting Equation 10 into Equation 9, leads to the following equation for
the uncollided photon fluence:
Eq. 11
)ˆ(E,ˆ!
"# $$$$ %=&+&'(% qunctunc , rp!
r!
( ))
$coll&
$unc&
$$$collunc &+&*&
"
,r)ˆ(E,ˆp!!
"# $$$$$$ %+=&+&'(% qqt r!
( ))
pr!
ˆ,( %)Eq$
eq
yq
yq
eqyq
2 3 | V A R I A N M E D I C A L S Y S T E M S
Step 1: Transport of source model fluence into the patient
The external photon and electron sources, and , are modeled as anisotropic
point sources in Acuros XB. At each static beam phase space (i.e. control point), a
separate point source exists for each of the AAA sources. For the primary source,
the anisotropy of is described through a 2D fluence grid, in which both the
particle fluence and energy spectra are spatially variable. For the extra-focal and
wedge scatter sources, the anisotropy of is described through a 3D fluence
grid, and the energy spectra is spatially constant. For the electron contamination
source, the anisotropy of is described through a 3D fluence grid, and the ener-
gy spectra is spatially constant. All point sources are located at the target for the
respective control point.
For a photon point source, located at position, , Equation 1
becomes:
Eq. 9
where
= Dirac-delta function
The principle of linear superposition may be used to define the photon angular
fluence as the summation of uncollided and collided fluence components,
Eq. 10
,
where
= Uncollided, or unscattered, photon angular fluence. Refers to photons
which have not yet interacted with the patient/phantom.
= Collided, or scattered, photon angular fluence. Refers to photons which
were produced or scattered by a photon interaction in the patient/
phantom.
Substituting Equation 10 into Equation 9, leads to the following equation for
the uncollided photon fluence:
Eq. 11
)ˆ(E,ˆ!
"# $$$$ %=&+&'(% qunctunc , rp!
r!
( ))
$coll&
$unc&
$$$collunc &+&*&
"
,r)ˆ(E,ˆp!!
"# $$$$$$ %+=&+&'(% qqt r!
( ))
pr!
ˆ,( %)Eq$
eq
yq
yq
eqyq
2 3 | V A R I A N M E D I C A L S Y S T E M S
Step 1: Transport of source model fluence into the patient
The external photon and electron sources, and , are modeled as anisotropic
point sources in Acuros XB. At each static beam phase space (i.e. control point), a
separate point source exists for each of the AAA sources. For the primary source,
the anisotropy of is described through a 2D fluence grid, in which both the
particle fluence and energy spectra are spatially variable. For the extra-focal and
wedge scatter sources, the anisotropy of is described through a 3D fluence
grid, and the energy spectra is spatially constant. For the electron contamination
source, the anisotropy of is described through a 3D fluence grid, and the ener-
gy spectra is spatially constant. All point sources are located at the target for the
respective control point.
For a photon point source, located at position, , Equation 1
becomes:
Eq. 9
where
= Dirac-delta function
The principle of linear superposition may be used to define the photon angular
fluence as the summation of uncollided and collided fluence components,
Eq. 10
,
where
= Uncollided, or unscattered, photon angular fluence. Refers to photons
which have not yet interacted with the patient/phantom.
= Collided, or scattered, photon angular fluence. Refers to photons which
were produced or scattered by a photon interaction in the patient/
phantom.
Substituting Equation 10 into Equation 9, leads to the following equation for
the uncollided photon fluence:
Eq. 11
)ˆ(E,ˆ!
"# $$$$ %=&+&'(% qunctunc , rp!
r!
( ))
$coll&
$unc&
$$$collunc &+&*&
"
,r)ˆ(E,ˆp!!
"# $$$$$$ %+=&+&'(% qqt r!
( ))
pr!
ˆ,( %)Eq$
eq
yq
yq
eqyq
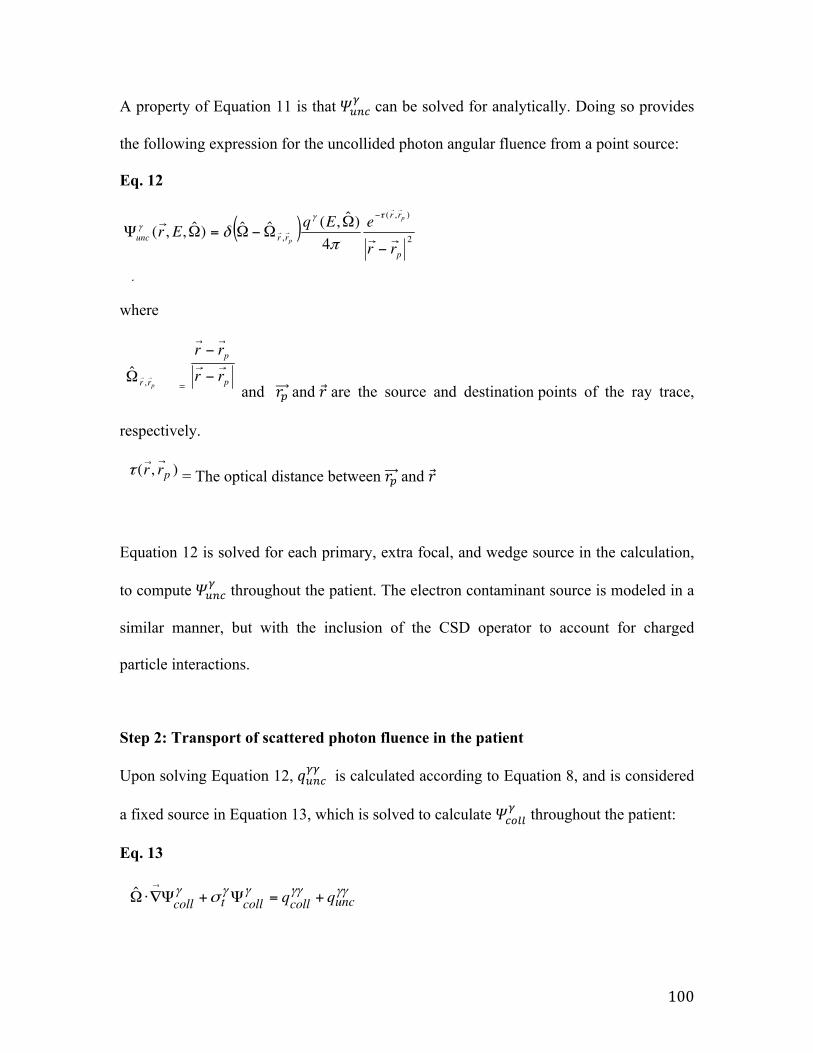
100
A property of Equation 11 is that 𝛹!"#! can be solved for analytically. Doing so provides
the following expression for the uncollided photon angular fluence from a point source:
Eq. 12
where
and 𝑟! and 𝑟 are the source and destination points of the ray trace,
respectively.
= The optical distance between 𝑟! and 𝑟
Equation 12 is solved for each primary, extra focal, and wedge source in the calculation,
to compute 𝛹!"#! throughout the patient. The electron contaminant source is modeled in a
similar manner, but with the inclusion of the CSD operator to account for charged
particle interactions.
Step 2: Transport of scattered photon fluence in the patient
Upon solving Equation 12, 𝑞!"#!! is calculated according to Equation 8, and is considered
a fixed source in Equation 13, which is solved to calculate 𝛹!"##! throughout the patient:
Eq. 13
2 4 | V A R I A N M E D I C A L S Y S T E M S
A property of Equation 11 is that can be solved for analytically. Doing
so provides the following expression for the uncollided photon angular fluence
from a point source:
Eq. 12
,
where
= , where and are the source and destination
points of the ray trace, respectively.
= The optical distance (measured in mean-free-paths) between and .
Equation 12 is solved for each primary, extra focal, and wedge source in the cal-
culation, to compute throughout the patient. The electron contaminant
source is modeled in a similar manner, but with the inclusion of the CSD operator
to account for charged particle interactions.
Step 2: Transport of scattered photon fluence in the patient
Once Equation 12 is solved, is calculated according to Equation 8, and is
considered a fixed source in Equation 13, which is solved to compute
throughout the patient:
Eq. 13
where
= First scattered photon source. Refers to photons which are created or scat-
tered from the first photon interaction inside the patient/phantom.
= Secondary scattered photon source. Refers to photons which are created or
scattered from secondary photon interactions inside the patient/phantom.
yycollq
yyuncq
, ˆ !!!!!!! " unccollcolltcoll qq +=#+#$%&'
!coll#
!!uncq
!unc#
pr'
r'),( prr
''(
r'
pr'
p
p
rr
rr''
''
)
)
prr''
,&̂
( )2
),(
, 4)ˆ,(ˆˆ)ˆ,,(
p
rr
rruncrr
eEqEr
p
p ''
'
''
''
)
&&)&=&#
)(!!
*+
!unc#
2 4 | V A R I A N M E D I C A L S Y S T E M S
A property of Equation 11 is that can be solved for analytically. Doing
so provides the following expression for the uncollided photon angular fluence
from a point source:
Eq. 12
,
where
= , where and are the source and destination
points of the ray trace, respectively.
= The optical distance (measured in mean-free-paths) between and .
Equation 12 is solved for each primary, extra focal, and wedge source in the cal-
culation, to compute throughout the patient. The electron contaminant
source is modeled in a similar manner, but with the inclusion of the CSD operator
to account for charged particle interactions.
Step 2: Transport of scattered photon fluence in the patient
Once Equation 12 is solved, is calculated according to Equation 8, and is
considered a fixed source in Equation 13, which is solved to compute
throughout the patient:
Eq. 13
where
= First scattered photon source. Refers to photons which are created or scat-
tered from the first photon interaction inside the patient/phantom.
= Secondary scattered photon source. Refers to photons which are created or
scattered from secondary photon interactions inside the patient/phantom.
yycollq
yyuncq
, ˆ !!!!!!! " unccollcolltcoll qq +=#+#$%&'
!coll#
!!uncq
!unc#
pr'
r'),( prr
''(
r'
pr'
p
p
rr
rr''
''
)
)
prr''
,&̂
( )2
),(
, 4)ˆ,(ˆˆ)ˆ,,(
p
rr
rruncrr
eEqEr
p
p ''
'
''
''
)
&&)&=&#
)(!!
*+
!unc#
2 4 | V A R I A N M E D I C A L S Y S T E M S
A property of Equation 11 is that can be solved for analytically. Doing
so provides the following expression for the uncollided photon angular fluence
from a point source:
Eq. 12
,
where
= , where and are the source and destination
points of the ray trace, respectively.
= The optical distance (measured in mean-free-paths) between and .
Equation 12 is solved for each primary, extra focal, and wedge source in the cal-
culation, to compute throughout the patient. The electron contaminant
source is modeled in a similar manner, but with the inclusion of the CSD operator
to account for charged particle interactions.
Step 2: Transport of scattered photon fluence in the patient
Once Equation 12 is solved, is calculated according to Equation 8, and is
considered a fixed source in Equation 13, which is solved to compute
throughout the patient:
Eq. 13
where
= First scattered photon source. Refers to photons which are created or scat-
tered from the first photon interaction inside the patient/phantom.
= Secondary scattered photon source. Refers to photons which are created or
scattered from secondary photon interactions inside the patient/phantom.
yycollq
yyuncq
, ˆ !!!!!!! " unccollcolltcoll qq +=#+#$%&'
!coll#
!!uncq
!unc#
pr'
r'),( prr
''(
r'
pr'
p
p
rr
rr''
''
)
)
prr''
,&̂
( )2
),(
, 4)ˆ,(ˆˆ)ˆ,,(
p
rr
rruncrr
eEqEr
p
p ''
'
''
''
)
&&)&=&#
)(!!
*+
!unc#
2 4 | V A R I A N M E D I C A L S Y S T E M S
A property of Equation 11 is that can be solved for analytically. Doing
so provides the following expression for the uncollided photon angular fluence
from a point source:
Eq. 12
,
where
= , where and are the source and destination
points of the ray trace, respectively.
= The optical distance (measured in mean-free-paths) between and .
Equation 12 is solved for each primary, extra focal, and wedge source in the cal-
culation, to compute throughout the patient. The electron contaminant
source is modeled in a similar manner, but with the inclusion of the CSD operator
to account for charged particle interactions.
Step 2: Transport of scattered photon fluence in the patient
Once Equation 12 is solved, is calculated according to Equation 8, and is
considered a fixed source in Equation 13, which is solved to compute
throughout the patient:
Eq. 13
where
= First scattered photon source. Refers to photons which are created or scat-
tered from the first photon interaction inside the patient/phantom.
= Secondary scattered photon source. Refers to photons which are created or
scattered from secondary photon interactions inside the patient/phantom.
yycollq
yyuncq
, ˆ !!!!!!! " unccollcolltcoll qq +=#+#$%&'
!coll#
!!uncq
!unc#
pr'
r'),( prr
''(
r'
pr'
p
p
rr
rr''
''
)
)
prr''
,&̂
( )2
),(
, 4)ˆ,(ˆˆ)ˆ,,(
p
rr
rruncrr
eEqEr
p
p ''
'
''
''
)
&&)&=&#
)(!!
*+
!unc#

101
where
𝑞!"#!! = First scattered photon source. Refers to photons, which are created or scattered
from the first photon interaction inside the patient.
𝑞!"##!! = Secondary scattered photon source. Refers to photons, which are created or
scattered from secondary photon interactions inside the patient.
Step 3: Transport of scattered electron fluence in the patient
Upon solving Equation 13, 𝑞!"##!" is calculated according to Equation 8, and is considered
a fixed source in Equation 14. Similarly, from the solution to Equation 12, 𝑞!"#!" is
calculated according to Equation 8, and is also considered a fixed source in Equation 14.
Equation 14 is solved to calculate Ψe throughout the patient:

102
Eq. 14
where
𝑞!"#!" = First scattered electron source. Refers to electrons, which are created or scattered
from the first photon interaction inside the patient.
𝑞!"##!" = Secondary scattered electrons source. Refers to electrons, which are created or
scattered from secondary photon interactions inside the patient.
Discretization methods
Acuros XB discretizes in space, angle, and energy iteratively to solve Equations 12-14.
Spatial discretization
The computational grid in Acuros XB consists of spatially variable Cartesian elements,
where the local element size is adapted to achieve a higher spatial resolution inside the
beam fields, with reduced resolution in lower dose, lower gradient regions outside the
beam penumbra. Commonly referred to as adaptive mesh refinement (AMR), the mesh is
limited to refinement in factors of 2 (from one level to the next) in any direction,
allowing for localized refinement to resolve areas of sharp gradients. Spatial
discretization is performed through using a linear discontinuous Galerkin finite-element
method10, providing a linear solution variation throughout each element, with
discontinuities permitted across element faces. The first scattered photon and first
produced electron sources, obtained from solving Equation 12, are also represented as
linear varying functions in each element, since these sources are used for the linear
discontinuous discretization of Equations 13 and 14. To accurately integrate these first
2 5 | V A R I A N M E D I C A L S Y S T E M S
Step 3: Transport of scattered electron fluence in the patient
Once Equation 13 is solved, is calculated according to Equation 8, and is
considered a fixed source in Equation 14. Similarly, from the solution to Equation
12, is calculated according to Equation 8, and is also considered a fixed
source in Equation 14. Equation 14 is solved to compute throughout the
patient:
Eq. 14
where
= First scattered electron source. Refers to electrons which are created or scat-
tered from the first photon interaction inside the patient/phantom.
= Secondary scattered electrons source. Refers to electrons which are created
or scattered from secondary photon interactions inside the patient/phan-
tom.
Discretization methods
Acuros XB discretizes in space, angle, and energy to iteratively solve Equations 12
through 14, the methods of which are discussed below.
Spatial discretization
The computational grid in Acuros XB consists of spatially variable Cartesian ele-
ments, where the local element size is adapted to achieve a higher spatial resolution
inside the beam fields, with reduced resolution in lower dose, lower gradient
regions outside the beam penumbra. Commonly referred to as adaptive mesh
refinement (AMR), the mesh is limited to refinement in factors of 2 (from one
level to the next) in any direction, allowing for localized refinement to resolve areas
of sharp gradients. Spatial discretization is performed through using a linear dis-
continuous Galerkin finite-element method [ref. 1], providing a linear solution
variation throughout each element, with discontinuities permitted across element
faces. The first scattered photon and first produced electron sources, obtained from
solving Equation 12, are also represented as linear varying functions in each ele-
ment, since these sources are used for the linear discontinuous discretization of
Equations 13 and 14. To accurately integrate these first scattered sources, the ana-
lytic solution is computed at a density inside the primary beam and penumbras of
at least 8 ray traces per output grid voxel.
yecollq
yeuncq
, ˆ eeunc
ecoll
eeeR
eet
e qqqqSE
+++=!""
#!+!$%& ''()
e!
yeuncq
yecollq
103
scattered sources, the analytic solution is computed at a density inside the primary beam
and penumbras of at least 8 ray traces per output grid voxel.
Energy discretization
Energy discretization is performed through the standard multigroup method10, which is
used in both the energy dependence of Equations 12 and 13 and the Boltzmann scattering
in Equation 14. In energy, the energy derivative of the continuous slowing down (CSD)
operator in Equation 14 is discretized using the linear discontinuous finite-element
method11. The Acuros XB cross section library includes 25 photon energy groups and 49
electron energy groups, although not all groups are used for energies lower than 20 MV.
Angular discretization
For the spatial transport of the scattered particle field, the discrete ordinates method is
used to discretize in angle10. The discrete ordinates method consists of requiring
Equations 13 and 14 to hold for a fixed number of directions, Ω! . These discrete
directions are chosen from an angular quadrature set that also serves to compute the
angular integrals in Equation 5 for the generation of the scattering source. Square-
Tchebyshev legendre quadrature sets are used and the quadrature order ranges from N=4
(32 discrete angles) to N=16 (512 discrete angles). The angular quadrature order varies
both by particle type and energy. Higher energy particles have longer mean free paths, or
ranges for electrons, and thus for each particle type, the angular quadrature order is
increased with the particle energy.
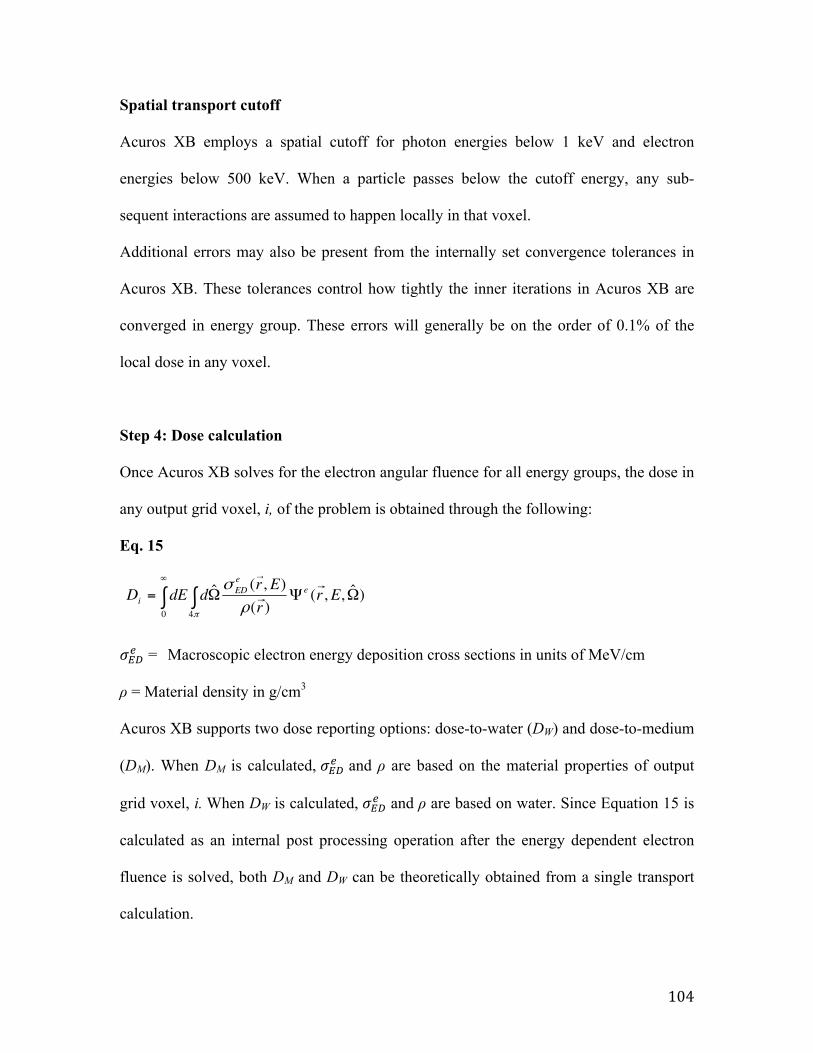
104
Spatial transport cutoff
Acuros XB employs a spatial cutoff for photon energies below 1 keV and electron
energies below 500 keV. When a particle passes below the cutoff energy, any sub-
sequent interactions are assumed to happen locally in that voxel.
Additional errors may also be present from the internally set convergence tolerances in
Acuros XB. These tolerances control how tightly the inner iterations in Acuros XB are
converged in energy group. These errors will generally be on the order of 0.1% of the
local dose in any voxel.
Step 4: Dose calculation
Once Acuros XB solves for the electron angular fluence for all energy groups, the dose in
any output grid voxel, i, of the problem is obtained through the following:
Eq. 15
𝜎!"! = Macroscopic electron energy deposition cross sections in units of MeV/cm
ρ = Material density in g/cm3
Acuros XB supports two dose reporting options: dose-to-water (DW) and dose-to-medium
(DM). When DM is calculated, 𝜎!"! and ρ are based on the material properties of output
grid voxel, i. When DW is calculated, 𝜎!"! and ρ are based on water. Since Equation 15 is
calculated as an internal post processing operation after the energy dependent electron
fluence is solved, both DM and DW can be theoretically obtained from a single transport
calculation.
2 7 | V A R I A N M E D I C A L S Y S T E M S
Step 4: Dose calculation
Once Acuros XB solves for the electron angular fluence for all energy groups, the
dose in any output grid voxel, i, of the problem is obtained through the following:
Eq. 15
,
where
= Macroscopic electron energy deposition cross sections in units of MeV/cm
= Material density in g/cm3
Acuros XB supports two dose reporting options: dose-to-water (DW) and dose-
to-medium (DM). When DM is calculated, and are based on the materi-
al properties of output grid voxel, i. When DW is calculated, and are
based on water. Since Equation 15 is calculated as an internal post processing oper-
ation after the energy dependent electron fluence is solved, both DM and DW can
be theoretically obtained from a single transport calculation.
!eED"
!eED"
!
eED"
)ˆ,,()(
),(ˆ40
#$#= !!%
Err
ErddED e
eED
i
&
&
&
!"
'
105
III. Appendix References 1. P. N. Mobit, P. Mayles, Alan E Nahum, Joint Department of Physics, Institute of
Cancer Research and Royal Marsden NHS Trust, Sutton and U. SM2 5PT, Phys. Med. Biol. 41, 387-‐398 (1996).
2. L. V. Spencer and F. H. Attix, Radiat. Res. 3, 239-‐254 (1955). 3. A. G. Carlsson, Acta Radiol. Suppl. (332) (1973). 4. G. Bertilsson, University of Lund, 1975. 5. T. E. Burlin, Br. J. Radiol. 39, 727-‐734 (1966). 6. Y. S. Horowitz, M. Moscovith and A. Dubi, Phys. Med. Biol. 28, 829-‐840
(1983). 7. P. R. Almond and K. McCray, Phys. Med. Biol. 15, 355-‐342 (1970). 8. G. A. Failla, T. Wareing, Y. Archambault and S. Thompson, California, USA. 9. L. Lorence, J. Morel and G. Valdez, SAND89-‐1685,Sandia National Laboratory
(1989). 10. E. E. Lewis and W. F. Miller, Wiley, New York (1984). 11. T. A. Wareing, J. E. Morel and J. M. McGhee, Trans Am. Nucl. Soc., Washington
D.C. 83 (2000).
Copyright © 2022 FDOKUMEN