
a systematic review of the blood pressure lowering efficacy of
296
A SYSTEMATIC REVIEW OF THE BLOOD PRESSURE LOWERING EFFICACY OF CALCIUM CHANNEL BLOCKERS IN THE TREATMENT OF PRIMARY > HYPERTENSION by MICHELLE M O N Y E E W O N G A THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF SCIENCE in THE FACULTY OF GRADUATE STUDIES (Pharmacology and Therapeutics) THE UNIVERSITY OF BRITISH COLUMBIA March 2007 © Michelle Mon Yee Wong, 2007
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of a systematic review of the blood pressure lowering efficacy of

A S Y S T E M A T I C R E V I E W O F T H E B L O O D P R E S S U R E L O W E R I N G E F F I C A C Y O F C A L C I U M C H A N N E L B L O C K E R S I N T H E T R E A T M E N T O F P R I M A R Y >
H Y P E R T E N S I O N
by
M I C H E L L E M O N Y E E W O N G
A THESIS S U B M I T T E D IN P A R T I A L F U L F I L L M E N T OF T H E R E Q U I R E M E N T S F O R T H E D E G R E E OF
M A S T E R OF S C I E N C E
in
T H E F A C U L T Y OF G R A D U A T E S T U D I E S
(Pharmacology and Therapeutics)
T H E U N I V E R S I T Y OF BRIT ISH C O L U M B I A
March 2007
© Michelle Mon Yee Wong, 2007
A B S T R A C T
Context - Calcium channel blockers (CCBs) are widely used drugs to lower elevated blood
pressure and manage angina and arrhythmias. Although the goal of antihypertensive therapy
is to lower the risk of cardiovascular disease-related morbidity and mortality, efficacy is most
often gauged by blood pressure reduction.
Objectives — This systematic review of the blood pressure lowering efficacy of CCBs aims
to determine the dose-related changes in systolic blood pressure (SBP), diastolic blood
pressure (DBP), heart rate, and withdrawals due to adverse events (WDAE) with C C B
treatment compared with placebo for a duration of 3-12 weeks, in patients with primary
hypertension (SBP > 140 mm H g and/or D B P > 90 mm Hg).
Design — A systematic review, as per the methodology of the Cochrane Collaboration, of
randomized placebo-controlled trials.
Methods - Electronic databases were searched using a modified, expanded version of the
search strategy used by the Cochrane Hypertension Review Group. RevMan 4.2 software
was used to analyze data.
Participants — 106 trials were included and reported data on 13 878 patients with a mean
age of 55 years, mean baseline blood pressure of 158.2/101.6 mm Hg, mean pulse pressure
of 56.7 mm Hg, and mean treatment duration of 5.7 weeks.
Results — Maximal blood pressure lowering efficacy of CCBs is achieved at twice the
manufacturer's recommended starring doses. This maximal reduction is 10/7 mmHg for
dihydropyridines and 8/6 mmHg for non-dihydropyridines and likely represents an
overestimate of the true blood pressure lowering effect due to publication bias. Combined,
ii
dihydropyridines and non-dihydropyridines lower pulse pressure by 3 mm H g (95% CI: -4, -
2). Compared with placebo, W D A E increased in a dose-related fashion for dihydropyridines
[relative risk of 1.8 (95% CI 1.2, 2.6) at 2 times the starting dose compared with 3.9 (95% CI:
2.2, 7.0) at 4 times the starting dose]. There were insufficient data to make a conclusion
about the effect of non-dihydropyridines on W D A E .
Conclusion — Dihydropyridines reduce blood pressure to a greater degree than non-
dihydropyridines. Maximal blood pressure lowering for both subclasses occurs with twice
the manufacturer-recommended starring dose. Increasing the doses of dihydropyridines
above recommended starting doses increases withdrawals due to adverse effects.
iii
T A B L E O F C O N T E N T S
A B S T R A C T i i
T A B L E O F C O N T E N T S iv
LIST O F T A B L E S ix
LIST O F F I G U R E S xii
LIST O F A B B R E V I A T I O N S xiri
P R E F A C E xiv
A C K N O W L E D G E M E N T S xv
1. B A C K G R O U N D I N F O R M A T I O N 1
1.1 H Y P E R T E N S I O N 1 1.1.1 Definition of hypertension and its relation to cardiovascular morbidity and
mortality • 1 1.1.2 Blood pressure variability, pulse pressure and heart rate: relation to
cardiovascular outcomes 3 1.1.3 Types of chronic hypertension 4
1.1.3.1 Isolated systolic hypertension 4 1.1.3.2 Primary hypertension 5 1.1.3.3 Secondary hypertension 6
1.1.4 Management and treatment of chronic hypertension 6 1.1.4.1 Non-pharmacological treatment 6 1.1.4.2 Pharmacological treatment 7
1.1.5 Blood pressure reduction and cardiovascular events 9 1.1.6 Blood pressure measurement 1 0 1.1.7 Dose-response relationships 1 2
1.2 T H E R O L E O F C A L C I U M IN T H E C A R D I O V A S C U L A R S Y S T E M 1 2
1.2.1 Calcium 1 2 1.2.2 Calcium Channels in the cardiovascular system 1 3
1.3 C A L C I U M C H A N N E L B L O C K E R S 1 4
1.3.1 Historical Aspects 1 4 1.3.2 Classification .- 1 5 1.3.3 Pharmacodynamics of Calcium Channel Blockers 16
1.3.3.1 Molecular mechanism of action 1 6 1.3.3.2 Physiological effects 1 7 1.3.3.3 Phenylalkylamines 1 8 1.3.3.4 Benzothiazepines 1 8
iv

1.3.3.5 Dihydropyridines 19 1.3.3.6 Benzimidazolyls 19
1.3.4 Pharmacokinetics of calcium channel blockers 20 1.3.5 Clinical use of calcium channel blockers 21
1.4 S Y S T E M A T I C R E V I E W S 27
1.4.1 What are systematic reviews? 27 1.4.2 How does a systematic review differ from a narrative review? 29 1.4.3 The Cochrane Collaboration 30 1.4.4 Arm of this systematic review 30
2 . P R O T O C O L 32
2.1 O B J E C T I V E S 32 2.2 M E T H O D O L O G Y 32
2.2.1 Types of studies 32 2.2.1.1 Why are only randomized controlled trials included? 33 2.2.1.2 Why is a parallel placebo arm necessary? 33 2.2.1.3 Why is blinding (masking) necessary? 34 2.2.1.4 Why is a baseline measurement subsequent to or during a
washout/placebo run-in period important? 35 2.2.1.5 Why is the 3-12 week window selected? 35
2.2.2 Types of participants 35 2.2.3 Types of interventions '. 36 2.2.4 Types of outcome measures 36 2.2.5 Search strategy for identification of studies 37 2.2.6 Study selection 42 2.2.7 Data extraction 42 2.2.8 Quality assessment 44
2.2.8.1 The Cochrane approach for assessment of allocation concealment.. 45 2.2.8.2 Jadad method 46
2.2.9 Data analysis 46 2.2.10 Statistical considerations 49
2.2.10.1 Individual study data 49 2.2.10.2 Pooling trials 50
2.2.11 Starting doses 51 2.2.12 Direct and indirect comparisons between doses 52
3. R E S U L T S 54
3.1 S E A R C H F I N D I N G S 54 3.2 C H A R A C T E R I S T I C S O F I N C L U D E D S T U D I E S 55 3.3 C H A R A C T E R I S T I C S O F S T U D I E S A W A I T I N G D A T A F R O M A U T H O R S 134 3.4 C H A R A C T E R I S T I C S O F E X C L U D E D STUDIES 136 3.5 O V E R V I E W O F I N C L U D E D T R I A L S 146 3.6 V A L U E S U S E D T O I M P U T E M I S S I N G V A R I A N C E S 148
v

3.6.1 Standard deviation of blood pressure change 148 3.6.2 Standard deviation of heart rate change 149
3.7 D O S E - R E L A T E D B L O O D P R E S S U R E L O W E R f N G O F I N D I V I D U A L C C B D R U G S 149
3.7.1 Amlodipine vs. placebo 150 3.7.2 Barnidipine vs. placebo 153 3.7.3 Darodipine vs. placebo 154 3.7.4 Felodipine vs. placebo 155 3.7.5 Isradipine vs. placebo 159 3.7.6 Lacidipine vs. placebo 162 3.7.7 Lercamdipine vs. placebo 163 3.7.8 Manidipine vs. placebo '. 165 3.7.9 Nicardipine vs. placebo 166 3.7.10 Nifedipine vs. placebo 168 3.7.11 Nilvadipine vs. placebo 170 3.7.12 Nisoldipine vs. placebo 171 3.7.13 Nitrendipine vs. placebo 172 3.7.14 Prandipine vs. placebo 174 3.7.15 Summary of blood pressure lowering efficacy of dihydropyridines 175
3.7.15.1 Dihydropyridines - Assessment of publication bias 176 3.7.15.1.1 Dihydropyridines -subgroup analysis based on trial size 176 3.7.15.1.2 Dihydropyridines -trim and fill method 177
3.7.16 Diltiazem vs. placebo 180 3.7.17 Verapamil vs. placebo 182 3.7.18 Tiaparnil vs. placebo 184 3.7.19 Summary of blood pressure lowering efficacy of non-dihydropyridines 185
3.7.19.1 Non-dihydropyridines - Assessment of publication bias 186 3.7.19.1.1 Non-cuhydropyridines-subgroup analysis based on trial size... 186
3.7.20 Other CCBs 188 3.7.20.1 Lidoflazine vs. placebo 188 3.7.20.2 Mibefradil vs. placebo .189
3.8. B L O O D PRESSURE VARIABILITY 190 3.8.1 Systolic vs. diastolic blood pressure 190 3.8.2 Calcium channel blockers vs. placebo 191 3.8.3 Systolic vs. diastolic blood pressure entry criteria 191 3.8.4 Baseline vs. endpoint 192
3.9. P U L S E PRESSURE 193 3.10. D O S E - R E L A T E D C H A N G E IN HEART RATE OF INDIVIDUAL C C B DRUGS :.. 194
3.10.1 Dihydropyridines vs. placebo 194 3.10.1.1 Amlodipine vs. placebo 195 3.10.1.2 Darodipine vs. placebo 196 3.10.1.3 Felodipine vs. placebo 196 3.10.1.4 Isradipine vs. placebo 197 3.10.1.5 Lercanidipine vs. placebo 197 3.10.1.6 Manidipine vs. placebo 198 3.10.1.7 Nicardipine vs. placebo 198 3.10.1.8 Nifedipine vs. placebo 199 3.10.1.9 Nisoldipine vs. placebo 199
3.10.1.10 Nitrendipine vs. placebo 200 3.10.2 Non-dihydropyridines vs. placebo 200
3.10.2.1 Diltiazem vs. placebo 201 3.10.2.2 Verapamil vs. placebo 202 3.10.2.3 Tiapamil vs. placebo 202
3.10.3 Other calcium channel blockers 203 3.10.3.1 Lidoflazine vs. placebo , 203 3.10.3.2 Mibefradil vs. placebo 203
3.11 DOSE-RELATED WITHDRAWALS DUE TO ADVERSE EVENTS 205 3.11.1. Dihydropyridines vs. placebo 205
3.11.1.1 Amlodipine vs. placebo 206 3.11.1.2 Darodipine vs. placebo 206 3.11.1.3 Felodipine vs. placebo 207 3.11.1.4 Isradipine vs. placebo 207 3.11.1.5 Lercanidipine vs. placebo 208 3.11.1.6 Manidipme vs. placebo 208 3.11.1.7 Nicardipine vs. placebo 209 3.11.1.8 Nifedipine vs. placebo 210 3.11.1.9 Nilvadipine vs. placebo 210 3.11.1.10 Nisoldipme vs. placebo 211 3.11.1.11 Nitrendipine vs. placebo 211 3.11.1.12 Prandipine vs. placebo 212
3.11.2. Non-dihydropyridines vs. placebo 212 3.11.2.1 Diltiazem vs. placebo 213 3.11.2.2 Verapamil vs. placebo 214
3.11.3. Other calcium channel blockers 215 3.11.3.1 Mibefradil vs. placebo 215
. D I S C U S S I O N 216
4.1 WHAT METHODOLOGICAL ISSUES AND POTENTIAL SOURCES OF BIAS WERE ENCOUNTERED WHILE CONDUCTING THE SYSTEMATIC REVIEW? 216 4.1.1 Publication bias 218 4.1.2 Selection bias , 220
4.2 WHAT IS THE DOSE-RELATED BLOOD PRESSURE LOWERING EFFICACY OF EACH SUBCLASS? IS THERE A DIFFERENCE IN THE BEST ESTIMATE OF THE MAGNITUDE OF B P LOWERING EFFECT OF DIFFERENT SUBCLASSES OF CCBS? 221
4.3 IS THERE A DIFFERENCE IN THE BEST ESTIMATE OF THE MAGNITUDE OF BP LOWERING EFFECT OF DRUGS IN EACH SUBCLASS? 222
4.4 WHAT IS THE EFFECT ON BLOOD PRESSURE IN THE PLACEBO GROUP IN SHORT-TERM TRIALS? 222
4.5 DOES THE METHOD OF BLOOD PRESSURE MEASUREMENT AFFECT THE BLOOD PRESSURE LOWERING EFFICACY OF CCBS? 223
4.6 DOES TRIAL QUALITY AFFECT THE BLOOD PRESSURE-LOWERING EFFICACY OF CALCIUM CHANNEL BLOCKERS? 223
4.7 WAS THERE A DIFFERENCE IN BLOOD PRESSURE LOWERING EFFICACY AT TROUGH VS. PEAK? ...224
vii

4.8 D I D F U N D I N G S O U R C E A F F E C T T H E R E P O R T E D B L O O D P R E S S U R E L O W E R I N G
E F F I C A C Y O F C C B S ? 2 2 4
4.9 D O E S A G E A F F E C T T H E B L O O D P R E S S U R E L O W E R I N G E F F I C A C Y O F C C B S ? 2 2 5
4 . 1 0 D O E S C O - M O R B I D I T Y A L T E R T H E B L O O D P R E S S U R E L O W E R I N G E F F I C A C Y O F
CCBs? 2 2 6 4.11 D O E S B L O O D P R E S S U R E L O W E R I N G E F F I C A C Y O F CCBs D I F F E R F O R I S O L A T E D
SYSTOLIC H Y P E R T E N S I O N VS. D I A S T O L I C O R S Y S T O - D I A S T O L I C H Y P E R T E N S I O N ? . . . . 2 2 6
4 . 1 2 H o w D O T H E D I R E C T C O M P A R I S O N S B E T W E E N D O S E S D I F F E R F R O M T H E I N D I R E C T
C O M P A R I S O N S ? 2 2 7
4 . 1 3 F O R E A C H C C B D R U G , D O T H E M A N U F A C T U R E R ' S S T A R T I N G D O S E S C O I N C I D E W I T H
T H E L O W E S T E F F E C T I V E D O S E AS D E T E R M I N E D B Y THIS S Y S T E M A T I C R E V I E W ? 2 2 8
4 . 1 4 W H A T IS T H E E F F E C T O F CCBs O N B P VARIAB IL ITY? 2 2 9
4 . 1 5 W H A T IS T H E E F F E C T O F CCBs O N P U L S E PRESSURE? 231
4 . 1 6 Is TF IERE A N Y E V I D E N C E O F A D O S E - R E S P O N S E R E L A T I O N S H I P W I T H R E S P E C T T O
C H A N G E I N H E A R T R A T E ? 2 3 2
4 . 1 7 IS T H E R E A N Y E V I D E N C E O F A D O S E - R E P O N S E R E L A T I O N S H I P W I T H R E S P E C T T O
W I T H D R A W A L S D U E T O A D V E R S E E V E N T S ? 2 3 2 4 . 1 8 C A N T H E M A G N I T U D E O F B L O O D P R E S S U R E L O W E R I N G E F F I C A C Y O F C A L C I U M
C H A N N E L B L O C K E R S B E L I N K E D T O T H E I R M E C H A N I S M O F A C T I O N ? 2 3 3 4 . 1 9 H O W C A N TFIE B L O O D P R E S S U R E L O W E R I N G E F F I C A C Y O F C A L C I U M C H A N N E L
B L O C K E R S IN S H O R T - T E R M TRIALS B E R E L A T E D T O T H E I R E F F E C T S O N M O R T A L I T Y A N D M O R B I D I T Y O U T C O M E S IN L O N G - T E R M TRIALS? 2 3 4
5. C L I N I C A L I M P L I C A T I O N S 237
6. I M P L I C A T I O N S F O R F U T U R E R E S E A R C H 240
7. R E F E R E N C E S 243
8. A P P E N D I C E S 277 A P P E N D I X A - T R I A L S E L E C T I O N F O R M 2 7 7
A P P E N D I X B - S T A N D A R D D A T A E X T R A C T I O N F O R M F O R E A C H T R I A L 2 7 8
viii

L I S T O F T A B L E S
Table 1: Classes of current drugs used to treat hypertension 7 Table 2: Comparison of 3 hypertension guidelines 8 Table 3: Classification of group A calcium antagonists 16 Table 4: Group B calcium antagonists 16 Table 5: Pharmacokinetic parameters of CCBs 21 Table 6: Long term clinical trials of CCBs for treatment of hypertension 24 Table 7: Data input for continuous data in RevMan 49 Table 8: Data input for dichotomous data in RevMan 49 Table 9: Formulae for individual study responses for dichotomous data in RevMan 49 Table f 0: Starting doses of calcium channel blockers 52 Table 11: Results of search strategy 54 Table 12: Amlodipine — Characteristics of included studies 56 Table 13: Barnidipine — Characteristics of included studies 62 Table 14: Darodipine — Characteristics of included studies 63 Table 15: Diltiazem — Characteristics of included studies ; 64 Table 16: Felodipine — Characteristics of included studies 73 Table 17: Isradipine — Characteristics of included studies 81 Table 18: Lacidipine — Characteristics of included studies 89 Table 19: Lercanidipine — Characteristics of included studies 90 Table 20: Lidoflazine — Characteristics of included studies 94 Table 21: Manidipine — Characteristics of included studies 95 Table 22: Mibefradil - Characteristics of included studies 97 Table 23: Nicardipine— Characteristics of included studies 100 Table 24: Nifedipine — Characteristics of included studies 105 Table 25: Nilvadipine — Characteristics of included studies 113 Table 26: Nisoldipine — Characteristics of included studies 115 Table 27: Nitrendipine — Characteristics of included studies 116 Table 28: Pranidipine — Characteristics of included studies 123 Table 29: Tiapamil — Characteristics of included studies : 124 Table 30: Verapamil - Characteristics of included studies 125 Table 31: Characteristics of studies awaiting office blood pressure data from authors ... 134 Table 32: Reasons for exclusion of certain studies meeting inclusion criteria 136 Table 33: Overview of included trials using CCBs as monotherapy for primary
hypertension 146 Table 34: Blood pressure lowering efficacy of amlodipine 1.25-10 mg/day 150 Table 35: Blood pressure lowering efficacy of barnidipine 10-30 mg/day 153 Table 36: Blood pressure lowering efficacy of darodipine 100-300 mg/day 154 Table 37: Blood pressure lowering efficacy of felodipine 2.5-20 mg/day 155 Table 38: Blood pressure lowering efficacy of felodipine in older and younger subgroups. 156 Table 39: Blood pressure lowering efficacy of felodipine in trials with inclusion criteria of
systolic/systodiastolic hypertension vs. diastolic hypertension 157 Table 40: Blood pressure lowering efficacy of isradipine 1-20 mg/day 159 Table 41: Blood pressure lowering efficacy of isradipine according to formulation 160 Table 42: Blood pressure lowering efficacy of lacidipine 2-4 mg/day 162 Table 43: Blood pressure lowering efficacy of lercanidipine 2.5-20 mg/day 163 Table 44: Blood pressure lowering efficacy of manidipine 10-40 mg/day 165
ix

Table 45: Blood pressure lowering efficacy of nicardipine 40-120 mg/day 166 Table 46: Blood pressure lowering efficacy of nifedipine 20-100 mg/day 168 Table 47: Blood pressure lowering efficacy of nilvadipine 8-30 mg/day 170 Table 48: Blood pressure lowering efficacy of nisoldipine 10-30 mg/day 171 Table 49: Blood pressure lowering efficacy of nitrendipine 5-20 mg/day 172 Table 50: Blood pressure lowering efficacy of pranidipine 1-8 mg/day 174 Table 51: Summary of blood pressure lowering efficacy of dihydropyridines 175 Table 52: Blood pressure lowering efficacy of dihydropyridines combined according to
multiples of starting dose 176 Table 53: Dihydropyridines: post-hoc subgroup analysis of trough B P lowering based on trial
size 177 Table 54: Blood pressure lowering efficacy of diltiazem 90 - 540 mg/day 180 Table 55: Blood pressure lowering efficacy of verapamil 60 — 540 mg/day 182 Table 56: Blood pressure lowering efficacy of tiapamil 300-1200 mg/day 184 Table 57: Summary of blood pressure lowering efficacy of non-dihydropyridines 185 Table 58: Blood pressure lowering efficacy for non-chhydropyridines combined according to
multiples of starting dose 186 Table 59: Non-dihydropyridines: post-hoc subgroup analysis of trough blood pressure
lowering based on trial size 187 Table 60: Blood pressure lowering efficacy of lidoflazine 180 mg/day 188 Table 61: Blood pressure lowering efficacy of mibefradil 6.25-100 mg/day 189 Table 62: Variability of SBP and D B P at end of treatment '. 190 Table 63: Baseline standard deviations of blood pressure according to entry criteria 191 Table 64: Standard deviations of B P at baseline vs. endpoint in trials with D B P entry
criteria 192 Table 65: Change in pulse pressure 193 Table 66: Effect of dihydropyridines on heart rate 195 Table 67: Effect of amlodipine on heart rate 195 Table 68: Effect of darodipine on heart rate 196 Table 69: Effect of felodipine on heart rate 196 Table 70: Effect of isradipine on heart rate 197 Table 71: Effect of lercanidipine on heart rate 197 Table 72: Effect of manidipine on heart rate 198 Table 73: Effect of nicardipine on heart rate 198 Table 74: Effect of nifedipine on heart rate 199 Table 75: Effect of nisoldipine on heart rate 199 Table 76: Effect of nitrendipine on heart rate 200 Table 77: Effect of non-cuhydropyridines (diltiazem and verapamil) on heart rate 201 Table 78: Effect of diltiazem on heart rate 201 Table 79: Effect of verapamil on heart rate 202 Table 80: Effect of tiapamil on heart rate 202 Table 81: Effect of lidoflazine on heart rate 203 Table 82: Effect of mibefradil on heart rate 203 Table 83: Effect of dihydropyridines on withdrawals due to adverse events 205 Table 84: Effect of amlodipine on withdrawals due to adverse events 206 Table 85: Effect of darodipine on withdrawals due to adverse events 206 Table 86: Effect of felodipine on withdrawals due to adverse events 207 Table 87: Effect of isradipine on withdrawals due to adverse events 207

Table 88: Effect of lercarridipine on withdrawals due to adverse events 208 Table 89: Effect of manidipine on withdrawals due to adverse events 208 Table 90: Effect of nicardipine on withdrawals due to adverse events 209 Table 91: Effect of nifedipine on withdrawals due to adverse events 210 Table 92: Effect of nilvadipine on withdrawals due to adverse events 210 Table 93: Effect of nisoldipine on withdrawals due to adverse events 211 Table 94: Effect of nitrendipine on withdrawals due to adverse events 211 Table 95: Effect of pranidipine on withdrawals due to adverse events 212 Table 96: Effect of non-dihydropyridines on withdrawals due to adverse events 213 Table 97: Effect of diltiazem on withdrawals due to adverse events 213 Table 98: Effect of verapamil on withdrawals due to adverse events 214 Table 99: Effect of mibefradil on withdrawals due to adverse events 215 Table 100: Comparison of manufacturer's recommended starting doses and lowest effective
doses determined in this systematic review : 228
x i
LIST OF FIGURES
Figure 1: Binding sites of calcium channel blocker drugs 17 Figure 2: Example of a forest plot 47 Figure 3: Log dose-response curve for amlodipine 1.25-10 mg/day 152 Figure 4: Funnel plot of standard error against effect size of change in SBP for amlodipine
5 to 20 mg/day 152 Figure 5: Funnel plot of standard error against effect size of change in SBP for felodipine
5 to 20 mg/day 158 Figure 6: Funnel plot of change in SBP for dihydropyridines at maximal blood pressure
lowering 178 Figure 7: Funnel plot of change in D B P for dihydropyridines at maximal blood pressure
lowering 179
x i i
L I S T O F A B B R E V I A T I O N S
Ambulatory Blood Pressure Monitoring A B P M Blood Pressure B P Calcium Channel Blocker C C B Calcium ion C a 2 +
Cardiovascular C V Cochrane Collaboration C C Confidence Interval CI Congestive heart failure C H F Consolidated Standards of Reporting C O N S O R T Controlled Delivery C D Coronary heart disease CFID Diastolic Blood Pressure D B P Double-Blind D B Electrocardiogram E C G Female f Gastro-fntestinal Therapeutic System GfTS Hazard Ratio - HazR Heart Rate H R fsolated Systolic Hypertension 1 S H Joint National Committee J N C Male ' m Mean Arterial Pressure M A P Medical Subject Heading MeSH Mercury H g Milligram mg Millimetres of mercury mm H g Multicentre M C Odds Ratio O R Placebo-Controlled PC Randomized Controlled Trial R C T Randomized R Relative Risk (Risk Ratio) RR Review Manager RevMan Slow-Release SR Standard Deviation SD Standard Error of the Mean S E M Systolic Blood Pressure SBP Weighted Mean Difference W M D Withdrawals Due to Adverse Events W D A E World Flealth Organization - International Society of Hypertension W H O / f S H
P R E F A C E
"...evidence based medicine requires you not only to read papers but to read the right papers at the right time and then to alter your behaviour (and, what is often more difficult, the behaviour of other people) in the light of what you have found."
- Trisha Greenhalgh, 1997 (from: Flow to read a paper: the basics of evidence based medicine. London: B M J Publishing Group, p. 2)
xiv
A C K N O W L E D G E M E N T S
I wish to thank my supervisor, Dr. James M . Wright, for his patience and guidance.
His dedication to revealing the truth about drug efficacy and safety has inspired me to be
involved in evidence-based medicine research.
I would also like to thank my other supervisory committee members, Dr. David
Godin, Dr. Casey Van Breemen and Dr. Michael Walker, for their comments and expertise.
I wish to express my gratitude to all the members of the Therapeutics Initiative and
the Cochrane Hypertension Group for their support over the last few years. I wish to thank
Dr. Ken Bassett and Dr. Tom Perry, Jr. for their guidance on my critical appraisal projects
and Mr. Ciprian Jauca for his coordinating efforts for the TI and the Hypertension Group.
I would like to extend my appreciation to those who helped me execute this
systematic review. Especially, I am indebted to Dr. Vijaya Musini for her assistance and
direction throughout every stage of this review. I am grateful to Mr. Benji Heran for being
the second independent reviewer and for developing a new, high-yield search strategy. Mr.
Stephen Adams retrieved a myriad of articles for this systematic review, and his efficiency
was invaluable. I also wish to thank Dr. Sonia Franciosi, Ms. Laurence Jacquaz, Dr. Marco
Perez, Dr. Frederique Rodieux, Dr. Stephan Schwarz, Dr. Michelle Van den Engh, and Dr.
Alexander Zolotoy for translation of foreign language articles. I must also thank all of the
clinical trial authors who took the time and effort to correspond with me during the process
of developing this review.
I would like to thank my systematic review colleagues, of past and present, for their
camaraderie: Benji, Marco, Jenny, Vijaya, Cremona, Dal and Jose.
Last but not least, I thank my family for their unconditional support in all my
endeavors.
xv
1. B A C K G R O U N D I N F O R M A T I O N
1.1 Hypertension
Hypertension, or elevated blood pressure, depending on how it is denned, is present
in up to 20-30% of adults (1). Although often referred to as a "silent disease", hypertension
is actually a surrogate marker and major risk factor for cardiovascular disease (2), rather than
a disease itself. Elevated blood pressure is a risk factor for stroke, coronary artery disease
(CAD) and congestive heart failure (CHF), and these cardiovascular diseases are the most
common causes of morbidity and mortality in developed countries. Elevated blood pressure
has been estimated to cause 4.5% of global disease burden (3). However, developing
countries have a greater share of the global burden of cardiovascular disease mortality than
developed countries (4).
1.1.1. Def in i t ion of hypertension and its relation to cardiovascular morbidity and mortality
The Joint National Committee on Prevention, Detection, Evaluation and Treatment
of High Blood Pressure (JNC) describes the relationship between systolic blood pressure
and cardiac risk as "strong, continuous, graded, consistent, independent, predictive and
etiologically significant" (5). Rather • than using a strict numerical divide between
normotension and hypertension, it is more practical to define hypertension as "that level of
blood pressure above which investigation and treatment do more good than harm" (6), or
stated more precisely by Kaplan: "that level of blood pressure at which the benefits (minus
the risks and costs) of action exceed the risks and costs (minus the benefits) of inaction" (7).
With this pragmatic clinical approach, the definition is subject to change as new evidence
1

regarding the treatment of hypertension becomes available. This definition also underscores
the importance of individualizing the diagnosis and treatment of hypertension.
There are two views of the epidemiologic data relating B P to adverse cardiovascular
events. One view is that the risk is linear and continuous and the other is that there is a
threshold. The concept of individualizing the diagnosis of hypertension according to age
and sex was the focus of a recent reanalysis of epidemiological data from the Framingham
Heart study (8). Using a logistic spline model, they proposed that overall mortality is
unrelated to SBP at pressures below an age- and sex-dependent threshold (approximately at
the 70 t h percentile). However, above the 80 t h percentile, the mortality risk increases
logistically. The numerical criteria used to define normotension and hypertension are thus
arbitrary and subject to change. In another study involving a meta-analysis of observational
data from individual patients aged 40-89 years, they found a direct relationship between
vascular mortality (due to stroke, ischemic heart disease and other vascular casuses) and
blood pressure for each decade of age (9). For ages 40-69, each difference of 20 mm H g
from the "usual" SBP for each age group, or 10 mm H g from the "usual" D B P age was
associated with a two-fold difference in vascular mortality (9). However, there were no data
representing patients with blood pressures less than 115/75 mm Hg, and data on overall
mortality were also not reported.
Although elevated blood pressure itself is generally asymptomatic, the target organ
damage resulting from chronic hypertension is the antecedent to cardiovascular morbidity
and mortality. In hypertension, the increased afterload on the heart leads to diastolic and
systolic dysfunction, which can subsequently lead to heart failure. Combined with the
increase in myocardial oxygen demand, the decrease in coronary oxygen supply that results
from the hypertension-induced acceleration of atherosclerosis can lead to myocardial
2

infarction. Arterial damage from hypertension also contributes to the development of aortic
aneurysm/dissection, stroke, retinopathy, nephrosclerosis and renal failure.
According to 1999 Canadian Hypertension Guidelines, chronic hypertension is
diagnosed in 3 clinic visits i f resting BP exceeds the arbitrary threshold of 140/90 mm H g
and there is target organ damage or resting BP is over 180/105 mm Hg, and in 5 visits over
6 months i f these features are absent but the resting mean B P remains over 140/90 mm H g
(10).
1.1.2. Blood pressure variability, pulse pressure and heart rate: relation to cardiovascular outcomes
The degree of variation of blood pressure throughout a 24-hour period is important
clinically because it correlates with severity of target organ damage and contributes to the
risk of cardiovascular mortality in hypertensive patients (11). Blood pressure variability
tends to be increased in patients with primary hypertension (11). Furthermore, increased
systolic BP variability has been found to predict progression of carotid artery wall
atherosclerosis and rate of cardiovascular events independently of increased blood pressure
itself (12). More prospective studies utilizing continuous ambulatory blood pressure
monitoring are necessary to confirm the prognostic value of blood pressure variability.
Pulse pressure, calculated as the difference between systolic and diastolic blood
pressure, can be considered an element of blood pressure variability because it reflects the
blood pressure changes within the cardiac cycle (11). A marker of arterial stiffness, the
magnitude of the pulse pressure also depends on stroke volume and the speed of reflected
pressure waves. Pulse pressure correlates not only with surrogate outcomes such as carotid
artery damage, but also with major cardiovascular endpoints. For example, clinic-measured
pulse pressure has been linked to recurrent events after myocardial infarction in patients with
3

left ventricular dysfunction (13). The Progetto Ipertensione Umbria Monitoraggio
Ambulatoriale (PIUMA) registry of subjects with primary hypertension showed that
ambulatory pulse pressure was a strong independent predictor of total cardiovascular risk,
with better prognostic value than pulse pressure derived from conventional BP readings (14).
A n epidemiologic study showed that pulse pressure appeared to be the best blood pressure
parameter in predicting mortality in people > 65 years old (15).
Elevated resting heart rate is also considered an important predictor of hypertension
and a risk factor for cardiovascular and non-cardiovascular death. In the Frarningham study,
those with a baseline resting heart rate of greater than 84 beats per minute were shown to be
at significandy increased cardiovascular risk than those with lower heart rates (16).
Blood pressure parameters aside, many other risk factors that contribute to
cardiovascular disease have been identified through monitoring of the Frarningham study
population (17). These include non-modifiable factors such as male gender, increased age
(>55 years for men, > 65 years for women), positive family history of premature
cardiovascular disease, prior cerebrovascular accident or myocardial infarction, and
modifiable factors such as smoking, dyslipidemia, diabetes mellitus, increased weight, low
physical activity and left ventricular hypertrophy.
1.1.3. Types of chronic hypertension
1.1.3.1 Isolated systolic hypertension
The definition of isolated systolic hypertension (ISH) is in flux and varies from SBP
> 160 mm H g and D B P < 95 mm H g to SBP > 140 mm H g and D B P < 90 mm H g (17).
Since systolic blood pressure rises with age, ISH is the most common form in the elderly.
Pulse pressure is increased in this population as well. The main cause of an increase in SBP
4
(and concomitant decline in DBP) is thought to be tidckening and stiffening of conduit
arteries resulting from degeneration of the arterial wall after exposure to chronic cyclic stress
(18). This reduced arterial compliance enhances the amplitude and velocity of the pressure
wave originating from the heart. Hence, the pressure wave is reflected from peripheral to
central arteries earlier, thus increasing the pressure in late systole (18). The increases in
afterload and myocardial work can lead to left ventricular hypertrophy. Coupled with
diminished coronary perfusion pressure, these increased strains on the heart could
contribute to myocardial ischemia.
1.1.3.2. Primary hypertension
Primary hypertension, or so-called "essential" hypertension comprises over 90% of
hypertensive patients, and implies that there is no known cause. Vascular alterations in
hypertension include decreased lumen diameter, increased reactivity and stiffness, and
increased wall thickness-to-lumen ratio of resistance vessels (19). Rather than attributing
these alterations merely to vascular growth, some studies have shown that the same amount
of vascular material is restructured via a process termed "eutrophic remodelling" (20).
Hypertension is also associated with impairment of endothelial nitric oxide activity, though it
remains to be discovered i f nitric oxide dysfunction is a cause or consequence of
hypertension (21).
According to the mosaic theory of primary hypertension, the interplay of multiple
genetic and environmental factors contributes to elevated arterial pressure (22). Because of
this multifactorial nature, there is large heterogeneity in individual responses to any
antihypertensive medication. The ongoing Genetics of Hypertension Associated Treatment
(GenHAT) study is assessing how hypertension susceptibility genes interact with
antihypertensive drugs to modify blood pressure response and risk of coronary heart disease
5

(23). This pharmacogenetic study is analyzing various polymorphisms of genes regulating
the renin-angiotensin-aldosterone system, sodium-volume homeostasis, insulin resistance,
and sympathetic nervous system activation.
1.1.3.3. Secondary hypertension
Hypertension that arises secondary to some identifiable mechanism is less common.
Several secondary causes of hypertension have been identified, including renal (e.g. nephritis,
renal artery stenosis), endocrinological (e.g. Cushing's syndrome, phaeochromocytoma), and
neurological (e.g. encephalitis, porphyria). Other causes include coarctation of the aorta,
pregnancy, and alcohol or drug use.
1.1.4. Management and treatment of primary hypertension
1.1.4.1 Non-pharmacological treatment
A l l hypertension guidelines agree on the use of non-pharmacological control of
blood pressure as first-line treatment, including diet alteration (e.g. reduced intake of salt),
weight reduction, smoking cessation and dynamic exercise. A systematic review of short-
term sodium restriction in patients with elevated blood pressure demonstrated modest
decreases in SBP and D B P (by about 4 and 2 mm Hg, respectively) (24). Another Cochrane
review of long-term restriction in dietary salt found an even smaller effect size, with
decreases in SBP by 1.1 mm H g and in D B P by 0.6 mm H g (25). A n analysis of 44 trials
that assessed the effect of exercise on resting B P demonstrated that the average reductions
in SBP and D B P in hypertensive patients were 7.4 mm H g and 5.8 mm Hg, respectively,
compared to a reduction of 2.6 mm H g and 1.8 mm H g in normotensive patients (26).
Because of a lack of relationship between exercise frequency, time per session, or intensity
and the magnitude of blood pressure reduction, it is suggested that the dose-response curve
is flat (26).
6

1.1.4.2. Pharmacological treatment
From a historical perspective, pharmacological treatment of hypertension has
evolved from a few agents with many adverse effects that were reserved only for
severe/malignant hypertension, to a wide array of currendy available drugs with diverse
mechanisms of action (Table 1). During the 1940s, veratrum alkaloids, thiocyanates, and
ganglion blockers such as hexamethonium were some of the only pharmacological
alternatives to bilateral sympathectomy and rigid sodium restriction (27). From the 1950s
onwards, a better understanding of the pathogenesis of hypertension has led to the
development several new classes of antihypertensive drugs: rauwolfia alkaloids such as
reserpine, vasodilators such as hydralazine, peripheral sympathetic inhibitors such as
guanethidine, and thiazide diuretics such as chlorothiazide. In the 1960s, beta blockers and
centrally acting sympathetic inhibitors (e.g. alpha methyldopa) were introduced. In the
1970s, alpha adrenergic blockers and angiotensin converting enzyme inhibitors were made
available, followed by calcium channel blockers in the 1980s and angiotensin II receptor
blockers in the 1990s.
Table 1: Classes of current drugs used to treat hypertension Class Example Thiazide diuretics Hydrochlorothiazide Loop diuretics Furosemide Beta blockers Propranolol A C E Inhibitors Benazepril Alpha blockers Prazosin Calcium channel blockers Amlodipine, verapamil, diltiazem Autonomic agents Reserpine Angiotensin II receptor antagonists Losartan
Currendy, the most optimal management of hypertension is unclear. Supposedly
evidence-based guidelines are highly variable with respect to the thresholds for initiation of
anti-hypertensive therapies and the choice of initial drugs (Table 2) (28).
7
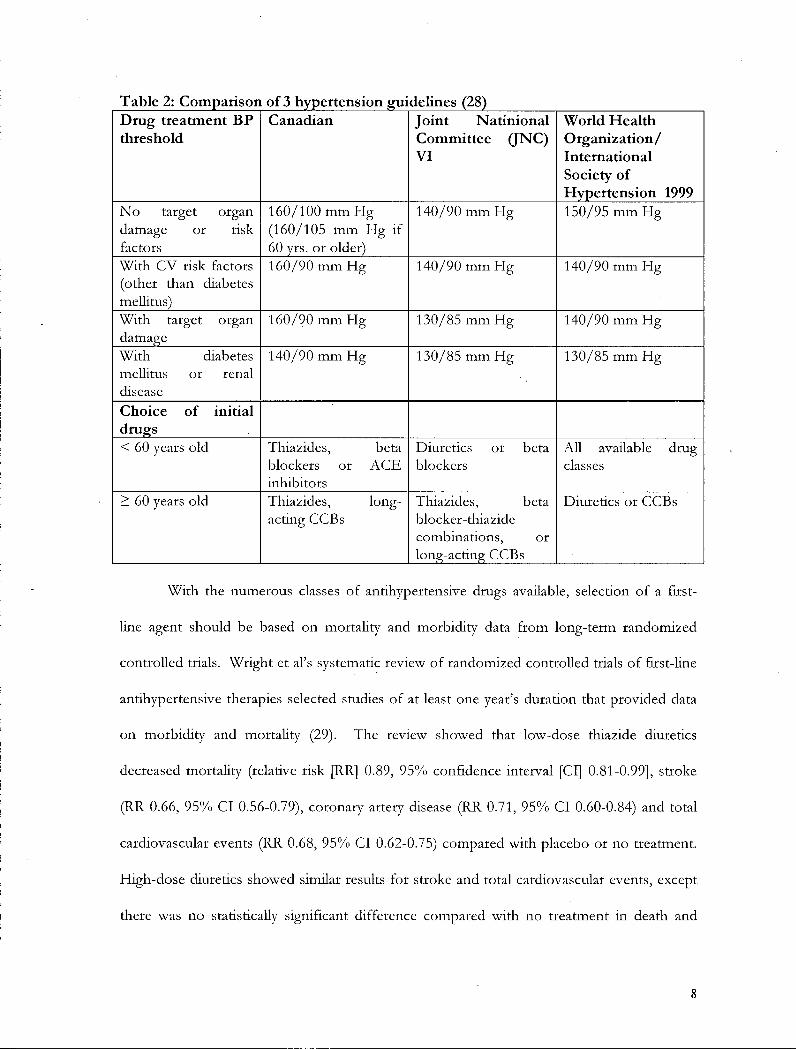
Table 2: Compar ison of 3 hypertension guidelines (28) D r u g treatment B P threshold
Canadian Joint Nat in iona l Committee (JNC) V I
Wor ld Hea l th Organ iza t ion / International Society of Hypertension 1 9 9 9
N o target organ damage or risk factors
160/100 m m H g (160/105 mm H g if 60 yrs. or older)
140/90 mm H g 150/95 m m H g
With C V risk factors (other than diabetes mellitus)
160/90 mm H g 140/90 mm H g 140/90 m m H g
With target organ damage
160/90 mm H g 130/85 m m H g 140/90 mm H g
With diabetes mellitus or renal disease
140/90 mm H g 130/85 mm H g 130/85 m m H g
Choice of ini t ial drugs < 60 years old Thiazides, beta
blockers or A C E inhibitors
Diuretics or beta blockers
A l l available drug classes
> 60 years old Thiazides, long-acting CCBs
Thiazides, beta blocker-thiazide combinations, or long-acting CCBs
Diuretics or CCBs
With the numerous classes of antihypertensive drugs available, selection of a first-
line agent should be based on mortality and morbidity data from long-term randomized
controlled trials. Wright et al's systematic review of randomized controlled trials of first-line
antihypertensive therapies selected studies of at least one year's duration that provided data
on morbidity and mortality (29). The review showed that low-dose thiazide diuretics
decreased mortality (relative risk [RR] 0.89, 95% confidence interval [CI] 0.81-0.99], stroke
(RR 0.66, 95% CI 0.56-0.79), coronary artery disease (RR 0.71, 95% CI 0.60-0.84) and total
cardiovascular events (RR 0.68, 95% CI 0.62-0.75) compared with placebo or no treatment.
Eligh-dose diuretics showed similar results for stroke and total cardiovascular events, except
there was no statistically significant difference compared with no treatment in death and
8
C A D . For first-line beta blockers there was no statistically significant difference compared
with placebo/no treatment for all four outcomes. For calcium channel blockers, one
placebo-controlled trial (SYST-EUR) showed a reduction in the risk of stroke (RR 0.61, 95%
CI 0.43-0.87) and cardiovascular events (RR 0.71, 95% CI 0.57-0.87) but not death and
C A D . In terms of blood pressure lowering efficacy, the drop in SBP was statistically
significandy greater with thiazides than with beta blockers or CCBs, while the drop in D B P
was similar among all three of these classes.
Using a technique called "network meta-analysis", Psaty et al. combined
cardiovascular endpoint data from both placebo-controlled and comparative trials of first-
line antihypertensive agents (30). For C A D , C H F , stroke, cardiovascular disease events,
cardiovascular mortality and total mortality, low-dose thiazide diuretics were superior to
placebo. None of the other classes of agents (beta blockers, A C E inhibitors, CCBs, alpha
blockers, angiotensin receptor blockers) were significantly better than low-dose diuretics in
any of the listed outcomes. In comparison with CCBs, low dose diuretics were associated
with a reduction in C H F (RR, 0.75; 95% CI, 0.67-0.81) and cardiovascular disease events
(RR, 0.94; 95% CI, 0.89-1.00).
Thus, results from both Wright et al. and Psaty et al.'s analyses support the use of
low-dose thiazide diuretics as first choice for first-line drug therapy for treatment of
hypertension. The J N C guidelines support this approach (17).
1.1.5. B lood pressure reduction and cardiovascular events
Meta-analyses of major clinical trials have demonstrated clear benefits of
antihypertensive therapy, including reductions in cardiac and cerebrovascular events.
Although the goal of any antihypertensive therapy is to lower the risk of cardiovascular
9

disease-related morbidity and mortality outcomes (5), efficacy is most often gauged by blood
pressure reduction, a validated surrogate outcome.
1.1.6. Methods of b lood pressure measurement
Blood pressure is a highly variable measurement that is modified by many unknown
and known factors, including circadian rhythm, seasonal variation, activity level and
emotional state. Despite this obstacle, blood pressure measurement is a universal tool in
medical practice. Since hypertension is generally clinically silent, accurate diagnosis and
treatment would not be possible without proper use of instruments to measure blood
pressure (31). There are two modalities of measuring blood pressure: 1) non-invasively,
using an indirect method by which pressure in an occlusive cuff is correlated with blood
flow phenomena, and 2) invasively, using a catheter to obtain a direct measure (32).
The indirect method of auscultation is the historical standard for recording clinic
blood pressure. The Korotkoff sounds involved in indirect blood pressure measurement
originate from the intra-vessel turbulence and vibrations during compression of the brachial
artery. The appearance of Korotkoff sounds (phase I) as the bladder cuff deflates correlates
with the systolic blood pressure, while the disappearance of these sounds (phase V) best
reflects the diastolic blood pressure. There are several factors that can interfere with
accurate blood pressure measurement — these arise from the patient, the measurer, the
instrument and the technique (33). Given the fluctuation of blood pressure during clinical
measurements, the average of two or more blood pressure measurements in a single arm is a
more reliable than a single reading. There are also substantial variations in blood pressure
throughout the day and with routine activities. Other patient factors such as bowel or
bladder distension, emotional extremes, recent ingestion of alcohol, and even talking can
10
elevate blood pressure. Measurer factors include the rate of cuff inflation and deflation,
hearing acuity, and expectation bias, including end-digit preference. Technique factors
include device calibration, cuff size, and arm position. The most common physician
mistakes in blood pressure measurement include using an inappropriately small cuff, failing
to allow a pre-measurement rest period of 5 minutes, deflating the cuff too fast, failing to
measure in both arms, and failing to palpate maximal systolic blood pressure before
auscultation (33).
Automated instruments utilize auscultatory, oscillometric or Doppler ultrasound
techniques. The most commonly used devices are oscillometric and employ proprietary
algorithms to determine blood pressures. Despite existing validation protocols that are used
to test these devices, the accuracy of available devices is highly variable (34). A small study
by Gerin et al found that office blood pressures measured with an automatic device in the
absence of a doctor or nurse were more representative of daily ambulatory pressure than
physician- or nurse- measurements (35). Studies have shown that automated pressures
tended to be lower than those recorded by a doctor or nurse. "White-coat hypertension"
refers to patients who are diagnosed with hypertension according to clinic pressures
measured by medical staff but who have normal ambulatory pressures. "White coat" effects
can increase blood pressure by more than 20 mm H g (SBP) and 10 mm H g (DBP) in up to
40% of patients (33).
The position of measurement impacts blood pressure readings. Blood pressures
measured in the supine position show an increase of 0-3 mm H g in SBP and a 2-5 mm H g
decrease in D B P compared to those measured in the sitting position (33). Expected
orthostatic changes upon standing consist of a decrease in SBP (5-10 mm Hg), a rise in D B P
(5 mm Hg), and an increase in heart rate by 5-10 beats per minute (33). It is not known if
11
position of measurement impacts the blood pressure lowering efficacy of antihypertensive
agents.
1.1.7. Dose-response relationships
The most fundamental concept in pharmacology and therapeutics is the log-linear
dose-response curve, which quantitatively describes drug actions, whether therapeutic or
toxic. In the past, several antihypertensive drugs were commonly prescribed at excessively
high doses due to a lack of formal dose-response studies (27). Dose-response analyses of
drugs are important in order to identify the lowest possible dose that is both efficacious and
safe. Several factors can affect the pharmacodynamic dose-response curves of
antihypertensive medications, including population variation and length of therapy (acute
versus chronic). Blood pressure decreases can be offset by counterregulatory mechanisms,
such as volume retention and reflex tachycardia. The pharmacokinetic properties of an
antihypertensive drug can also affect the magnitude of its effect depending on the time that
blood pressure is measured relative to drug administration. The trough-to-peak ratio is
calculated as the blood pressure decrease at the end of the dosage interval divided by the
largest blood pressure decrease during the dosage interval, which usually occurs at the time
of peak plasma drug concentration. As the trough-to-peak ratio gets closer to 1, the
antihypertensive effect is consistently maintained throughout the dosage interval and thus
the pharmacologically-generated blood pressure variability is reduced (36). According to the
Food and Drug Administration guidelines, a trough effect that is at least 50% of the peak
effect is desired (36).
12

1.2 The role of calcium in the cardiovascular system
1.2.1. C a l c i u m
Calcium ions (Ca 2 +) play significant regulatory roles in excitable tissue, from neuronal
transmitter release to muscle contraction. With respect to the cardiovascular system, entry
of external calcium through the L-type calcium channels plays a vital role in excitation-
contraction coupling in the heart and regulation of diameter in vascular smooth muscle. A
resting intracellular calcium concentration of about 150 n M and an extracellular calcium
concentration of about 1-2 m M create a large concentration gradient across the cell
membrane (37). Thus, calcium ions are sensitive signal transducers.
1.2.2. C a l c i u m channe l s i n the ca rd iovascu la r s ys tem
There are two distinct families of calcium channels: intracellular release channels,
which allow calcium ions to move into the cytosol from intracellular stores, and plasma
membrane calcium channels, which control the entry of calcium ions from the extracellular
space. A t the plasma membrane, there are three main types of channels which differ by their
regulatory mechanism: voltage-operated channels, store-operated channels and receptor-
operated channels (38). The voltage-gated calcium channels are further classified according
to their electrophysiological and pharmacological properties (L, N , P / Q , R and T types). In
the cardiovascular system, L - and T-type channels predominate.
The L-type ("long lasting") channel, which has a large conductance and slow
inactivation rate, is the major type of calcium channel in excitable cells and is composed of
five subunits. This type is also the main target of clinically available CCBs. In the heart, the
function of L-type channels at the sinoatrial and atrioventricular nodes is for pacemaker
activity and conduction of impulses, respectively. In cardiac muscle, action potentials
13

depolarize the plasma membrane which then triggers the opening of L-type calcium channels
in the plasma membrane. These localized increases in C a 2 + concentration then lead to release
of C a 2 + through ryanodine-receptor channels from the sarcoplasmic reticulum by a process
called "Ca 2 +-induced C a 2 + release" (39). The smooth muscle of the vasculature utilizes a
similar process to initiate contraction, except that the release of C a 2 + from intracellular stores
also occurs via inositol trisphosphate (IP3) receptors. The IP 3 receptors permit the alteration
of force production in the absence of a change in membrane potential because IP 3 acts as a
second messenger following binding of agonists to receptors at the plasma membrane
("pharmacomechanical coupling"). Hormones influence C a 2 + influx by acting on receptor-
operated C a 2 + channels. The diameter of the vasculature also depends on several local
factors, including perfusion pressure, p H , and p 0 2 .
T-type calcium channels are found on arterial vascular walls, myocardial conduction
tissue (atrioventricular node, sinoatrial node, Purkinje cells) and at neurohormonal release
sites (39). While the L-type channels play a major role in myocardial contraction, T-type
.channels instead exert their effects on pacemaker function and regulation of vascular smooth
muscle tone.
To maintain a low resting level of C a 2 + in the cytosol, C a 2 + is removed via C a 2 + -
ATPase pumps at the sarcoplasmic reticulum or plasma membrane, and also C a 2 + / N a +
exchangers.
1.3 Calcium channel blockers
1.3.1. H i s t o r i c a l aspects
In the 1960s, Fleckenstein et al. discovered the calcium antagonist properties of
verapamil and prenylamine in studies using isolated cardiac tissue (40). These and
subsequent studies elucidated important effects of calcium antagonists on the heart, namely
14

coronary artery dilation and negative inotropic effects that could be reversed by increasing
the extracellular C a 2 + concentration. Not until the 1970s were the peripheral vasodilator
properties of CCBs discovered. Since then, the array of therapeutic uses of CCBs has grown
from angina, hypertension and arrhythmias, to cerebral vasospasm, migraine and Raynaud's
phenomenon, among others.
1.3.2. Classif icat ion
In theory, calcium antagonists refer to all compounds that potentially inhibit calcium-
dependent processes. Calcium channel blocker drugs belong to a chemically heterogeneous
family. According to the W H O classification (41), Group A CCBs consist of agents that
have high affinity and specificity for the L-type calcium channel including the
phenylalkylamines, cUhydropyridines, benzothiazepines (Table 3). Group B CCBs (Table 4)
are less specific L-type channel blockers and they are much less widely used.
15
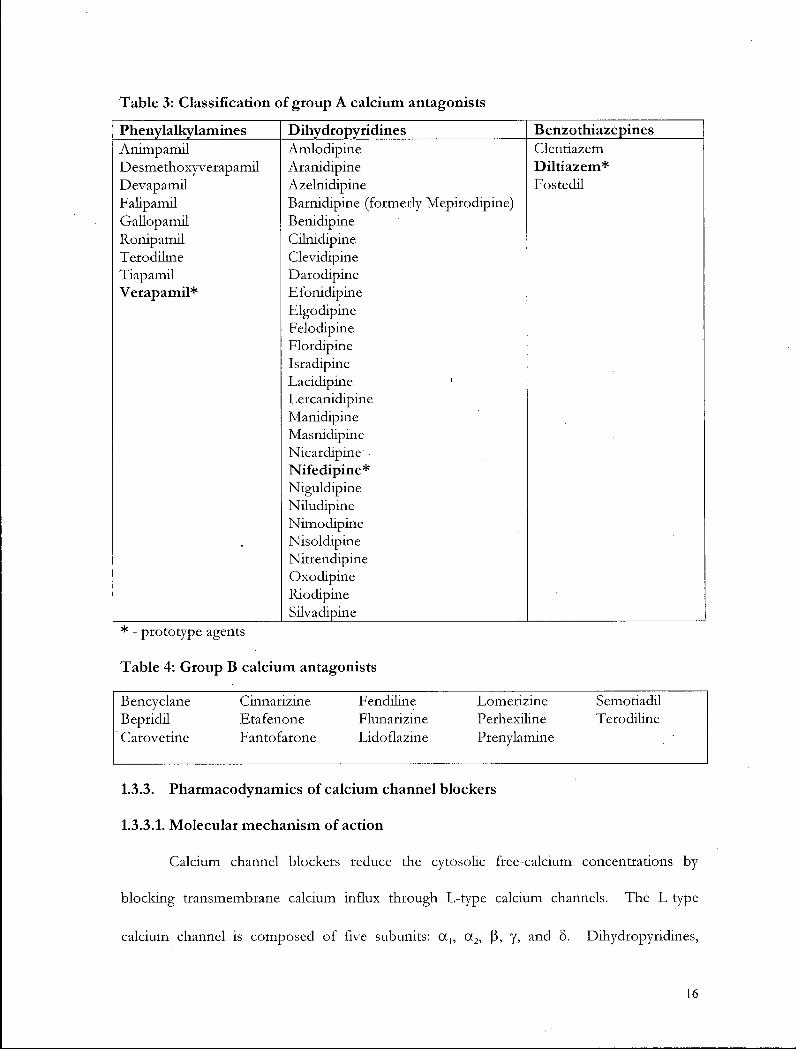
Table 3: Classif icat ion of group A calc ium antagonists
Phenylalkylamines Dihydropyridines Benzothiazepines Animparnil Amlodipine Clentiazem Desmethoxyverapamil Aranidipine Di l t i azem* Devapamil Azelnidipine Fostedil Falipamil Barnidipine (formerly Mepirodipine) Gallopamil Benidipine Rompamil Cilnidipine Terodiline Clevidipine Tiapamil Darodipine Verapami l * Efonidipine
Elgodipine Felodipine Flordipine Isradipine Lacidipine 1
Lercanidipine Manidipine Masnidipine Nicardipine • Ni fed ip ine* Niguldipine Niludipine Nimodipine Nisoldipine Nitrendipine Oxodipine Riodipine Silvadipine
- prototype agents
Table 4: Group B calc ium antagonists
Bencyclane Cinnarizine Fendiline Lomerizine Semotiadil Bepridil Etafenone Flunarizine Perhexiline TerocUline Caroverine Fantofarone Lidoflazine Prenylamine
1.3.3. Pharmacodynamics of calc ium channel blockers
1.3.3.1. Molecular mechanism of action
Calcium channel blockers reduce the cytosolic free-calcium concentrations by
blocking transmembrane calcium influx through L-type calcium channels. The L-type
calcium channel is composed of five subunits: a,, a 2 , [3, y, and 5. Dihydropyridines,
16

benzodiazepines and phenylalkylamines bind to the pore-containing a,-subunit of the L -
type calcium channel, the former two near the external face of the pore and the latter within
the pore. Ligand-binding sites on the L-type channel have several aflosteric interactions
between each other and with the gating machinery of the channel pore (Figure 1) (42).
CCBs are believed to induce a conformation change that influences gating of the in the L -
type calcium channel (43).
Figure 1. B ind ing sites of calc ium channel blocker drugs. (-) denotes a negative allosteric interaction. (+) denotes a positive allosteric interaction. Adapted from Triggle 1991 (42).
17

1.3.3.2. P h y s i o l o g i c a l effects
In general, calcium channel blockers relax arteriolar smooth muscle, resulting in
vasodilatation and decreased peripheral resistance. The decreased afterload therefore
decreases blood pressure. In addition to peripheral vasodilatation, CCBs increase coronary
blood flow. CCBs also have a negative inotropic effect on the myocardium. Agents that
slow the rate of recovery of L-type calcium channels (verapamil, diltiazem) have negative
chronotropic and dromotropic effects on the heart's conducting system. The natriuretic
effect of CCBs may contribute to their ability to lower blood pressure.
The most common side effects associated with CCBs stem from excessive
vasodilatation (40), and include hypotension, dizziness, headache, flushing and nausea.
Constipation (caused by decreased gut motility), peripheral edema (caused by redistribution
of extracellular fluid), coughing and wheezing also occur with CCBs. CCB-induced
vasodilatation also tends to trigger a reflex increase in sympathetic activity, producing the-
tachycardia commonly observed with dihydropyridines.
1.3.3.3. P h e n y l a l k y l a m i n e s
Verapamil, the prototype phenyalltylamine, is indicated for treatment of
hypertension, angina and arrhythmias (40). O f all the subclasses of CCBs, it has the most
cardiac effects. Verapamil's vasodilatory activity is less than that of dihydropyridines, but the
negative chronotropic effect of the drug mitigates any reflex tachycardia. The prolongation
of refractor)' periods in the cardiac conduction system can lead to heart block or sinus arrest
in some patients. Heart failure precipitated by the negative inotropic effect is another
potentially serious adverse effect associated with verapamil.
18
1.3.3.4. Benzothiazepines
The benzodiazepine prototype diltiazem is indicated as an antihypertensive and
antianginal agent. Diltiazem decreases blood pressure through arterial dilatation. It is less
cardiodepressant than verapamil but negative chronotropic effects usually cause a decrease in
heart rate (40). The most common side effects of diltiazem include headache,
swelling/edema, arrhythmias (first degree heart block), and asthenia (44).
1.3.3.5. Dihydropyridines
1,4-Dihydropyridines represent the largest subclass of CCBs. Nifedipine is the
prototype of this group of relatively vascular-selective CCBs. The fall in blood pressure and
relief of angina can be attributed to vasodilatation in peripheral arterioles and coronary
arteries, respectively (40). The negative inotropic effect of nifedipine is minor at therapeutic
doses and is usually overcome by the baroreceptor-mediated sympathetic reflexes.
Dihydropyridines are associated with exacerbation of myocardial ischemia due to several
possible mechanisms: excessive hypotension, coronary vasodilatation of nonischemic areas
("coronary steal"), and increased oxygen demand resulting from increased reflex sympathetic
activity. Common side effects of dihydropyridines in the hypertensive population include
edema, headache, fatigue, dizziness, constipation, nausea, flushing, palpitation and
tachycardia (44).
1.3.3.6. Benzimidazoly ls
While most calcium channel antagonists predominantly block the L-type calcium
channel, a newer class of benzimidazolyl tertraline derivatives inhibits both L - and T-type
channels (45). One drug from this class is mibefradil, which possesses higher selectivity for
T-type than L-type calcium channels. Mibefradil also binds to a unique site on the L-type
19
channel, with negative allosteric interactions with the verapamil, diltiazem and fantofarone
binding sites. Mibefradil reduces heart rate but lacks both the negative inotropic effects of
other cardio-selective calcium channel blockers and the reflex increases in sympathetic
activity associated with some dihydropyridines. Though initially approved in 1997 as a
treatment for hypertension and chronic stable angina, mibefradil (Posicor®) was removed
from the market in 1998 because of the incidence of serious drug interactions arising from
cytochrome P450 inhibition, leading to cardiogenic shock in a small number of patients (46).
1.3.4 Pharmacokinet ics of calc ium channel blockers
C C B drugs are well absorbed (>90%) from the gastrointestinal tract but undergo
first-pass hepatic metabolism resulting in low bioavailability (40). Drugs in the
dihydropyridine subclass are highly bound to plasma proteins (> 95%) while diltiazem and
verapamil are less so. Early calcium antagonists were all short-acting, with time to maximum
concentration occurring within about 2 hours. The rapid decreases in blood pressure gave
rise to many side effects, especially tachycardia from reflex sympathetic nervous system
activation, flushing, headache and dizziness. Newer CCBs such as amlodipine and slow-
release formulations of older CCBs were developed to produce a more gradual decrease in
blood pressure with a longer duration of BP control, increased safety, and less side effects.
Extensive metabolism of CCBs occurs via oxidative enzymes in the liver, primarily
the 3A4 isozyme of the cytochrome P450 family (47). Half-lives and clearance rates vary
considerably among CCBs (Table 5). Dihydropyridines are eliminated in the urine with the
majority in the form of inactive metabolites and small amounts in the unchanged form, ft is
important to note that pharmacokinetic parameters can vary according to length of
administration (acute vs. chronic) and that there is much interindividual variability.
20

Table 5: Pharmacokinet ic parameters of C C B s (44, 47)
Drug Absorption (%)
Bioavailability (%)
PPB (%) (hours)
tl/2 (hours)
Renal Unchanged %
Elim. Met. %
Amlodipine >95% 63 97.5 6-10 35-50 10 60 Diltiazem immediate release
80-90 40-67 70-80 2-4 3.5-6 5-8 (repetitive dosage)
2-4
sustained release
7-11 5-7
controlled deliver)'
10-14 5^8
Felodipine extended release
>95% 15 99 2.5-5 11-16 <0.5 70
Flunarizine Well-absorbed
99 2-4 19 days
Isradipine >90% ' 15-24 95 2-4 8.3 <1 65 Lacidipine >90% 14-19 98 3 7-18 >1 70 Nicardipine >90% 10-17 98 0.5-1 2 <1 60 Nifedipine immediate release
>90% 45-75 95 0.5-2 2-5 0.1 - 7 5
prolonged action
50-70 98 4
extended release
86 6 10
Nilvadipine >90% 14-19 99 2.15 7-18 <1 - 7 5 Nimodipine >90% 13 99 1-2 (early)
8-9 (terminal)
2 0 15 1-2 (early) 8-9 (terminal)
Nisoldipine >90% 8 99 1-2 10-12 <1 - 7 5 Nitrendipine >90% - 3 0 98 1-2 6-15 0.1 45 Verapamil immediate release
>90 10-20 >90 1-2 2.8-7.4 4.5-12 (repetitive dosage)
3 86
sustained release
20-35 4-8 5.3-9.6
P P B = percentage protein binding Renal unchanged % = % excreted renally as unchanged drug E l i m Met % = % eliminated as metabolites tmax = time to maximum plasma concentration t i / 2 = half life
1.3.5 C l in ica l use of calc ium channel blockers
Calcium channel blockers are used widely in clinical practice to lower elevated blood
pressures and manage angina and arrhythmias. Although CCBs are generally considered
21
second- or tliird-line therapies in the treatment of hypertension in subjects under 60 years of
age, CCBs have been recommended as first-line treatment for treatment of isolated systolic
hypertension in the elderly (10). In 2003, the C C B amlodipine (Norvasc®) was the fourth
top selling prescription drug in the world (48).
Nevertheless, controversy surrounds the use of CCBs in the treatment of chronic
hypertension, fn 1995, two retrospective studies showed increased risks of myocardial
infarction and mortality in those taking calcium channel blockers (49, 50). Psaty's case-
control study showed that among users of CCBs (with or without a diuretic) the risk ratio of
myocardial infarction was 1.62 (95% CI 1.11-2.34) compared with those taking a diuretic
alone, and 1.57 (95% CI 1.21-2.04) compared with users of beta-blockers (49). Pahor et
al's cohort study of elderly hypertensive patients showed that in comparison with beta-
blockers, the relative risks for mortality associated with use of verapamil, diltiazem, and
short-acting nifedipine were 0.8 (95% Cf 0.4-1.4), 1.3 (95% CI 0.8-2.1), and 1.7 (95% CI 1.1-
2.7), respectively (50). A meta-analysis by Furberg et al. showed that the use of short-acting
nifedipine was associated with increased mortality in patients with coronary heart disease
(overall RR 1.16, 95% CI 1.01-1.33) (51). A dose-response relationship was present, with the
risk rising sharply with doses above 80 mg/day of nifedipine (RR at 80 mg/day was 2.83;
95% Cf 1.35-5.93). The potential mechanisms by which calcium channel blockers may
increase mortality are varied, including pro-ischemic effects, marked hypotension, negative
inotropic effects, prohemorrhagic effects and activation of the sympathetic- and renin-
angiotensin systems, thereby predisposing to arrhythmias (51).
To assess whether similar effects were observed with long-acting CCBs, another
case-control study was performed (52). The study showed no difference in risk of
cardiovascular events between beta-blockers and long-acting CCBs, but there was a marked
22
increase in risk in patients who took short-acting CCBs compared with beta-blockers
(adjusted odds ratio 3.88, 95% CI 1.15-13.11) and long-acting CCBs (risk ratio 8.56, 95% CI
1.88-38.97). However, it is important to note that all observational studies are subject to
confounding since the patients may differ fundamentally between treatment groups. For
example, in the aforementioned studies, the prevalence of coronary heart disease was greater
in the groups taking short-acting CCBs (53).
Links between use of CCBs and increased risk of cancer, major hemorrhage and
suicide had been suggested initially from observational studies, although these associations
were contradicted in subsequent studies (53). The debate over calcium channel antagonist
safety was addressed further with respect to the potential conflict of interest arising from
authors' relationships with the pharmaceutical industry (54). This study of calcium-channel-
antagonist articles published between March 1995 and September 1996 found that 96% of
the authors who were supportive of the use of calcium channel blockers had financial
relationships with C C B manufacturers, compared to 60% of neutral authors and 37% of
critical authors (p<0.001).
Numerous large, long-term clinical trials of CCBs have been carried out (Table 6) but
the debate over the efficacy and safety of CCBs still rages. The findings of Pahor et al.'s
systematic review demonstrating that CCBs given as first-line antihypertensives are
associated with a higher incidence of major cardiovascular events compared with other drug
classes (55) have been tempered by the results of recent clinical trials (ASCOT [56], F E V E R
[57]) that show CCBs in combination with other antihypertensives may have benefits in
terms of cardiovascular events and mortality.
23
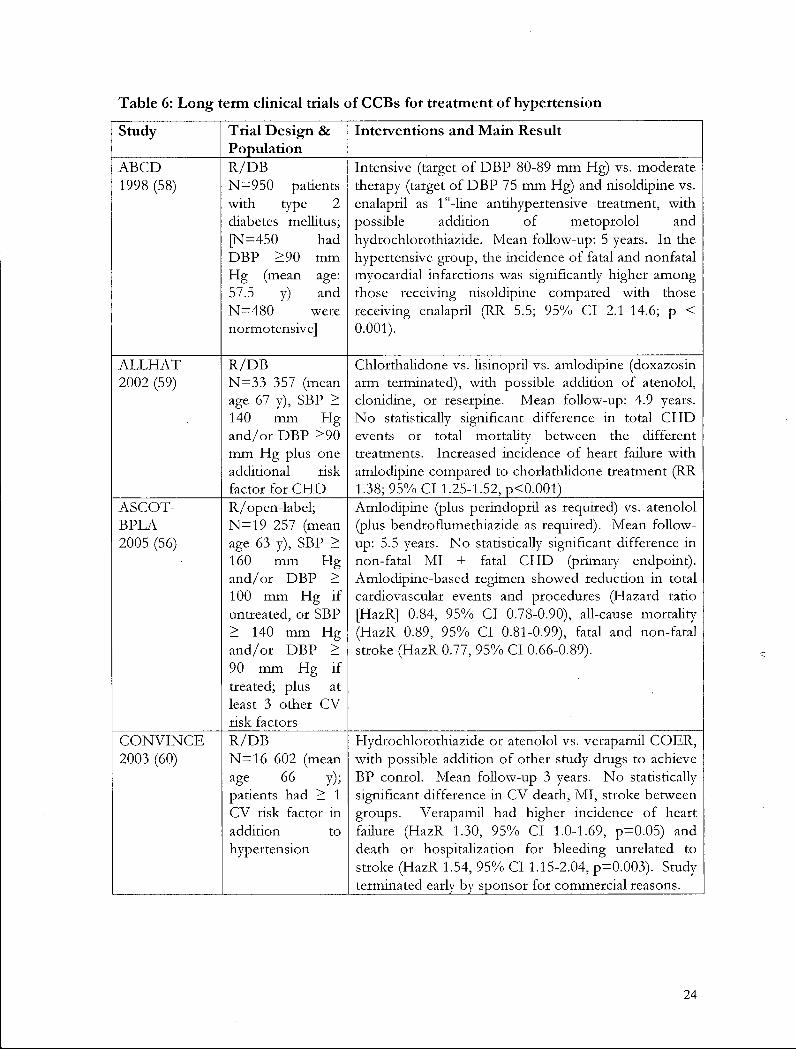
Table 6: L o n g term clinical trials of C C B s for treatment of hypertension
Study Tria l Design & Population
Interventions and M a i n Result
A B C D 1998 (58)
R / D B N=950 patients with type 2 diabetes mellitus; [N=450 had D B P >90 mm Elg (mean age: 57.5 y) and N=480 were normotensive]
fntensive (target of D B P 80-89 mm Hg) vs. moderate therapy (target of D B P 75 mm Hg) and nisoldipine vs. enalapril as l s t-Une antihypertensive treatment, with possible addition of metoprolol and hydrochlorothiazide. Mean follow-up: 5 years. In the hypertensive group, the incidence of fatal and nonfatal myocardial infarctions was significantly higher among those receiving nisoldipine compared with those receiving enalapril (RR 5.5; 95% CI 2.1-14.6; p < 0.001).
A L L H A T 2002 (59)
R / D B N=33 357 (mean age 67 y), SBP > 140 mm H g and/or D B P >90 mm H g plus one additional risk factor for C H D
Chlorthalidone vs. lisinopril vs. amlodipine (doxazosin arm terminated), with possible addition of atenolol, clonidine, or reserpine. Mean follow-up: 4.9 years. N o statistically significant difference in total C H D events or total mortality between the different treatments, fncreased incidence of heart failure with amlodipine compared to chorlathlidone treatment (RR 1.38; 95% CI 1.25-1.52, p<0.001)
A S C O T -B P L A 2005 (56)
R/open-label; N=19 257 (mean age 63 y), SBP > 160 mm H g and/or D B P > 100 mm H g if untreated, or SBP > 140 mm H g and/or D B P > 90 mm H g if treated; plus at least 3 other C V risk factors
Amlodipine (plus perindopril as required) vs. atenolol (plus bendro flume thiazide as required). Mean follow-up: 5.5 years. N o statistically significant difference in non-fatal M f + fatal C H D (primary endpoint). Amlodipine-based regimen showed reduction in total cardiovascular events and procedures (Hazard ratio [HazR] 0.84, 95% CI 0.78-0.90), all-cause mortality (HazR 0.89, 95% Cf 0.81-0.99), fatal and non-fatal stroke (HazR 0.77, 95% CI 0.66-0.89).
C O N V I N C E 2003 (60)
R / D B N=16 602 (mean age 66 y); patients had > 1 C V risk factor in addition to hypertension
Hydrochlorothiazide or atenolol vs. verapamil C O E R , with possible addition of other study drugs to achieve B P conrol. Mean follow-up 3 years. N o statistically significant difference in C V death, M I , stroke between groups. Verapamil had higher incidence of heart failure (HazR 1.30, 95% CI 1.0-1.69, p=0.05) and death or hospitahzation for bleeding unrelated to stroke (HazR 1.54, 95% CI 1.15-2.04, p=0.003). Study terminated early by sponsor for commercial reasons.
24
Study Tr ia l Des ign & Populat ion
Interventions and M a i n Result
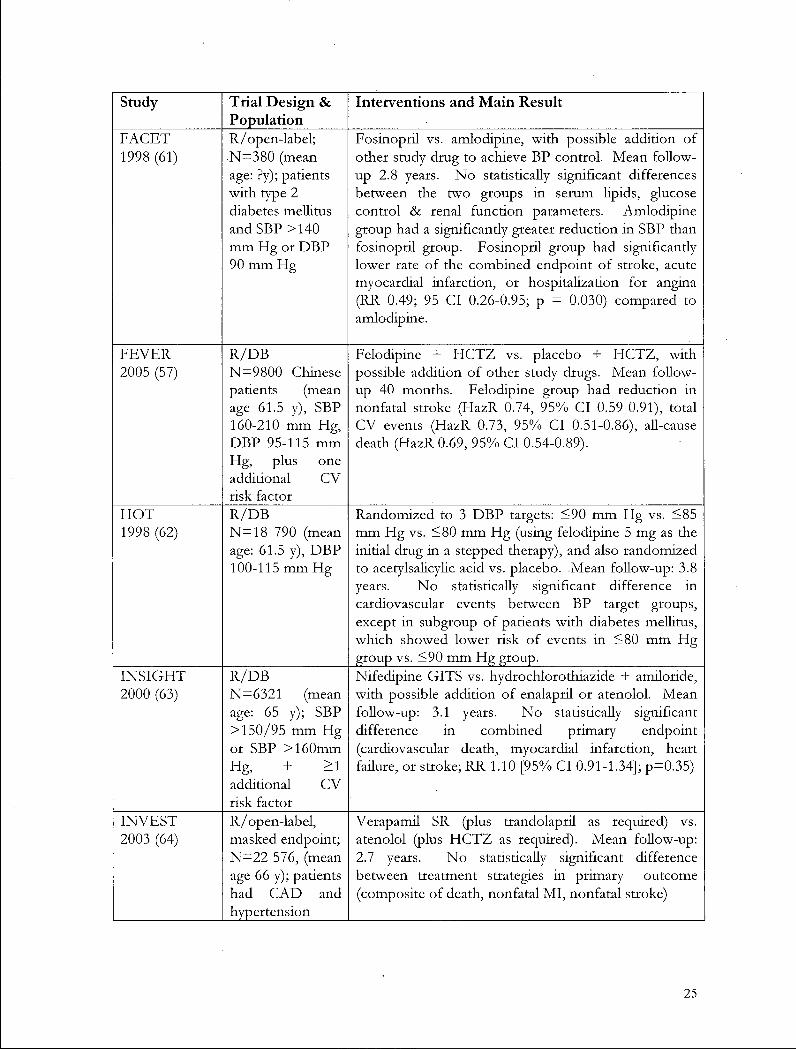
F A C E T 1998 (61)
R/open-label; N=380 (mean age: ?y); patients with type 2 diabetes mellitus and SBP >140 mm H g or D B P 90 mm H g
Fosinopril vs. amlodipine, with possible addition of other study drug to achieve BP control. Mean follow-up 2.8 years. N o statistically significant differences between the two groups in serum lipids, glucose control & renal function parameters. Amlodipine group had a significantiy greater reduction in SBP than fosinopril group. Fosinopril group had significandy lower rate of the combined endpoint of stroke, acute myocardial infarction, or hospitalization for angina (RR 0.49; 95 CI 0.26-0.95; p = 0.030) compared to amlodipine.
F E V E R 2005 (57)
R / D B N=9800 Chinese patients (mean age 61.5 y), SBP 160-210 mm Fig, D B P 95-115 mm Hg, plus one additional C V risk factor
Felodipine + H C T Z vs. placebo + H C T Z , with possible addition of other study drugs. Mean follow-up 40 months. Felodipine group had reduction in nonfatal stroke (HazR 0.74, 95% CI 0.59-0.91), total C V events (HazR 0.73, 95% CI 0.51-0.86), all-cause death (HazR 0.69, 95% CI 0.54-0.89).
H O T 1998 (62)
R / D B N=18 790 (mean age: 61.5 y), D B P 100-115 m m H g
Randomized to 3 D B P targets: <90 mm H g vs. <85 mm H g vs. <80 mm Fig (using felodipine 5 mg as the initial drug in a stepped therapy), and also randomized to acetylsalicylic acid vs. placebo. Mean follow-up: 3.8 years. N o statistically significant difference in cardiovascular events between BP target groups, except in subgroup of patients with diabetes mellitus, which showed lower risk of events in <80 mm H g group vs. <90 mm Fig group.
I N S I G H T 2000 (63)
R / D B N=6321 (mean age: 65 y); SBP > 150/95 mm H g or SBP > 160mm Hg, + >1 additional C V risk factor
Nifedipine GITS vs. hydrochlorothiazide + amiloride, with possible addition of enalapril or atenolol. Mean follow-up: 3.1 years. N o statistically significant difference in combined primary endpoint (cardiovascular death, myocardial infarction, heart failure, or stroke; R R 1.10 [95% CI 0.91-1.34]; p=0.35)
I N V E S T 2003 (64)
R/open-label, masked endpoint; N=22 576, (mean age 66 y); patients had C A D and hypertension
Verapamil SR (plus trandolapril as required) vs. atenolol (plus H C T Z as required). Mean follow-up: 2.7 years. N o statistically significant difference between treatment strategies in primary outcome (composite of death, nonfatal M I , nonfatal stroke)
25
Study Tr ia l Des ign & Populat ion
Interventions and M a i n Result
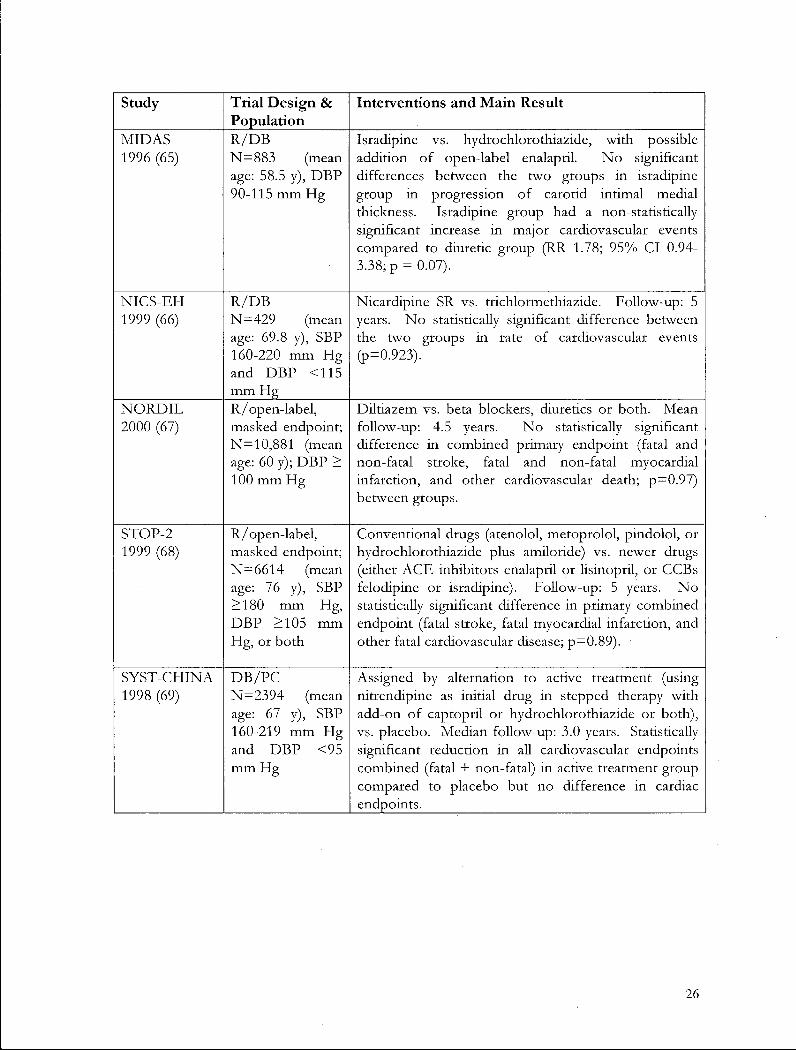
M I D A S 1996 (65)
R / D B N=883 (mean age: 58.5 y), D B P 90-115 m m H g
Isradipine vs. hydrochlorothiazide, with possible addition of open-label enalapril. N o significant differences between the two groups in isradipine group in progression of carotid mtimal medial thickness. Isradipine group had a non-statistically significant increase in major cardiovascular events compared to diuretic group (RR 1.78; 95% CI 0.94-3.38; p = 0.07).
N I C S - E H 1999 (66)
R / D B N=429 (mean age: 69.8 y), SBP 160-220 mm H g and D B P <115 mm H g
Nicardipine SR vs. trichlormethiazide. Follow-up: 5 years. N o statistically significant difference between the two groups in rate of cardiovascular events (p=0.923).
N O R D I L 2000 (67)
R/open-label, masked endpoint; N = 10,881 (mean age: 60 y); D B P > 100 mm H g
Diltiazem vs. beta blockers, diuretics or both. Mean follow-up: 4.5 years. N o statistically significant difference in combined primary endpoint (fatal and non-fatal stroke, fatal and non-fatal myocardial infarction, and other cardiovascular death; p=0.97) between groups.
S T O P - 2 1999 (68)
R/open-label, masked-endpoint; N=6614 (mean age: 76 y), SBP >180 mm Hg, D B P >105 mm Hg, or both
Conventional drugs (atenolol, metoprolol, pindolol, or hydrochlorothiazide plus amiloride) vs. newer drugs (either A C E inhibitors enalapril or lisinopril, or CCBs felodipine or isradipine). Follow-up: 5 years. N o statistically significant difference in primary combined endpoint (fatal stroke, fatal myocardial infarction, and other fatal cardiovascular disease; p=0.89).
S Y S T - C H I N A 1998 (69)
D B / P C N=2394 (mean age: 67 y), SBP 160-219 mm H g and D B P <95 mm H g
Assigned by alternation to active treatment (using nitrendipine as initial drug in stepped therapy with add-on of captopril or hydrochlorothiazide or both), vs. placebo. Median follow-up: 3.0 years. Statistically significant reduction in all cardiovascular endpoints combined (fatal + non-fatal) in active treatment group compared to placebo but no difference in cardiac endpoints.
26
Study T r ia l Des ign & Populat ion
Interventions and M a i n Result
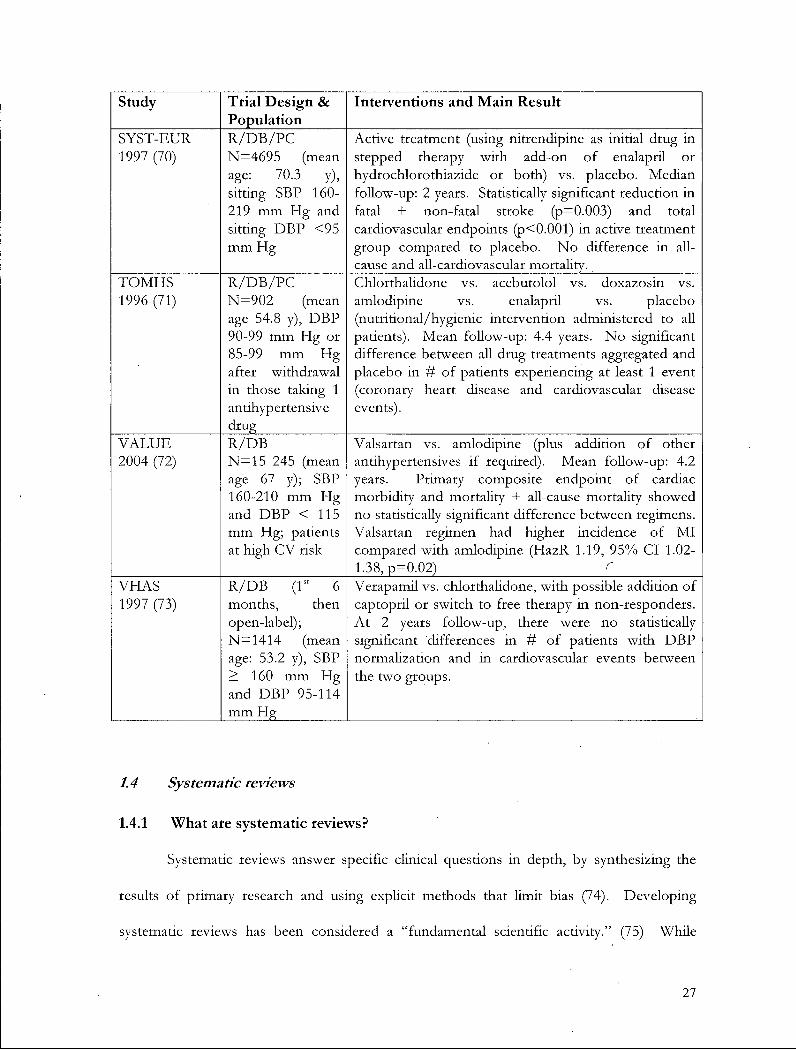
S Y S T - E U R 1997 (70)
R / D B / P C N=4695 (mean age: 70.3 y), sitting SBP 160-219 mm H g and sitting D B P <95 mm H g
Active treatment (using nitrendipine as initial drug in stepped therapy with add-on of enalapril or hydrochlorothiazide or both) vs. placebo. Median follow-up: 2 years. Statistically significant reduction in fatal + non-fatal stroke (p=0.003) and total cardiovascular endpoints (p<0.001) in active treatment group compared to placebo. N o difference in all-cause and all-cardiovascular mortality.
T O M H S 1996 (71)
R / D B / P C N=902 (mean age 54.8 y), D B P 90-99 mm H g or 85-99 mm H g after withdrawal in those taking 1 antihypertensive drug
Chlorthalidone vs. acebutolol vs. doxazosin vs. amlodipine vs. enalapril vs. placebo (nutritional/hygienic intervention administered to all patients). Mean follow-up: 4.4 years. N o significant difference between all drug treatments aggregated and placebo in # of patients experiencing at least 1 event (coronary heart disease and cardiovascular disease events).
V A L U E 2004 (72)
R / D B N=15 245 (mean age 67 y); SBP 160-210 mm H g and D B P < 115 mm Hg; patients at high C V risk
Valsartan vs. amlodipine (plus addition of other antihypertensives i f required). Mean follow-up: 4.2 years. Primary composite endpoint of cardiac morbidity and mortality + all-cause mortality showed no statistically significant difference between regimens. Valsartan regimen had higher incidence of M I compared with amlodipine (HazR 1.19, 95% CI 1.02-1.38,p=0.02) r
V H A S 1997 (73)
R / D B (1 s t 6 months, then open-label); N=1414 (mean age: 53.2 y), SBP > 160 mm H g and D B P 95-114 mm Tig
Verapamil vs. chlorthalidone, with possible addition of captopril or switch to free therapy in non-responders. A t 2 years follow-up, there were no statistically significant differences in # of patients with D B P normalization and in cardiovascular events between the two groups.
1.4 Systematic reviews
1.4.1 What are systematic reviews?
Systematic reviews answer specific clinical questions in depth, by synthesizing the
results of primary research and using explicit methods that limit bias (74). Developing
systematic reviews has been considered a "fundamental scientific activity." (75) While
27

researchers can use reviews to identify new hypotheses and to refine their approaches, health
care providers and policy makers can apply the results of such reviews towards rational
decision making (75). However, it is important to note that research evidence is only one of
many components that are involved in decision making in each patient-clinician encounter
(74).
A well-formulated question specifies the following five variables: 1) types of study
designs, 2) types of participants, 3) types of interventions, 4) types of outcomes, and 5) types
of control comparisons. For example, the question addressed in this review can be stated as:
In randomized controlled trials, how much do calcium channel blockers lower blood
pressure compared with placebo in patients with primary hypertension?
Systematic reviews can be categorized as qualitative or quantitative. In the latter
case, the review is referred to as a meta-analysis and involves quantitatively combining results
from individual studies. Using statistical methods to combine the data increases the power
and precision of the estimate of the effect size.
The other advantages of a systematic review are well established. Health care
workers, researchers and consumers are often deluged with unmanageable amounts of
information (76). Systematic reviews concisely and efficiently integrate up-to-date
information such that important effects of health care can be identified promptly (74). In
addition, systematic reviews can establish the degree of generalizabiHty and consistency of
the findings across populations and different treatments (76). Lastly, since systematic
reviews explicitly apply scientific principles that are designed to reduce random and
systematic errors, the results are more likely to be reliable and accurate than individual
studies or narrative reviews.
28
Like all secondary research, systematic reviews are retrospective studies and are
hence subject to bias. Meta-analyses can produce inflated effect sizes due to publication
bias, which describes a systematic error arising from the tendency of positive-result trials to
be more likely to be published. (and often numerous times) than negative-result trials.
Systematic reviews are designed to reduce bias by 1) including studies with multiple
publications only once; 2) using explicit, reproducible criteria for selecting studies and for
extracting data; and 3) having more than one independent reviewer to perform these tasks
(76).
1.4.2 How does a systematic review differ from a narrative review?
"Narrative" or "traditional" reviews of research have always been common in
medical literature. Frequently, these reviews have a broad scope and are written by experts
in the field who tend to focus only on studies that support their own view. As well, the
majority of narrative reviews lack explicit, systematic methods with respect to how studies
are selected and integrated. For these reasons, there is great likelihood of introducing bias.
Since the methodologic quality of medical review articles is quite variable, there are concerns
about the validity of their conclusions (77).
Conversely, a systematic review utilizes an explicit search strategy that is applied to
several sources. Systematic reviews are focused on a specific clinical question and studies are
selected using pre-specified inclusion criteria. This approach allows a more objective view
than traditional narrative reviews. Thus, a major advantage of a systematic review is that the
same rigor as that expected from primary research is applied. Consequently, carrying out a
systematic review requires much more time and effort than a narrative review.
29
1.4.3 The Cochrane Col laborat ion
The Cochrane Collaboration (CC) is an international organization that aims to
prepare, maintain and make accessible systematic reviews of the effects of health care.
Established in 1992, the organization was named after Archie Cochrane, a British
epidemiologist who recognized the importance of having reliable reviews of evidence to
make informed decisions about heath care. The C C espouses the following ten principles:
collaboration, building on the enthusiasm of individuals, avoiding duplication, minimizing
bias, keeping up to date, ensuring relevance, ensuring access, continually improving the
quality of its work, continuity and enabling wide participation (78). The systematic reviews
produced within the C C are published electronically in the Cochrane Library, which is
updated quarterly. The format of a Cochrane review allows readers to find the results
quickly and allows them to submit comments and criticisms. As well, the format facilitates
updating reviews with new or previously missing trials. A study that compared Cochrane
reviews with articles published in paper-based journals revealed that Cochrane reviews
tended to have greater methodological rigor and were more likely to be updated (79).
1.4.4 A i m of this systematic review
A t the present time, the blood pressure-lowering efficacy of the different subclasses
of calcium channel blockers and the individual drugs within each subclass is not known, and
a systematic review of the short-term dose-related blood pressure lowering effect of calcium
channel blocker drugs has not been previously performed. The aims of this systematic
review are to determine these dose-related effects in patients with primary hypertension and
to establish dose equivalencies of different drugs within the calcium channel blocker family.
The information derived from this review should facilitate future reviews of head-to-head
30

comparisons with other drug classes and assist clinicians in choosing optimal doses
calcium channel blockers.
2. P R O T O C O L
The protocol for this systematic review was finalized in March 2000 and first
published in Issue 2, 2002 of the Cochrane Library (80) to outline the scientific methods that
would be employed. The methodology was based on the Cochrane Reviewers' Handbook
(76) and on a previous systematic review that assessed the blood pressure lowering efficacy
of thiazide and loop diuretics (81).
2.1 Objectives
Primary objective:
To quantify the dose-related effects of various doses and types of calcium channel blockers
on systolic and diastolic blood pressure versus placebo in patients with primary hypertension.
Secondary objectives:
1. To determine the effects of calcium channel blockers on variability of blood pressure.
2. To determine the effects of calcium channel blockers on pulse pressure.
3. To quantify the dose-related effects of calcium channel blockers on heart rate.
4. To quantify the effects of calcium channel blockers in different doses on withdrawals
due to adverse events.
2.2 Methodology
2.2.1 Types of studies
Included studies must be randomized controlled trials (RCTs) and their design must
meet the following criteria:
32

• random allocation to calcium channel blocker monotherapy group (s) and a parallel
placebo control group
• double-blind
• duration of follow-up of at least three weeks
• office blood pressure measurements were made at baseline (following washout) and at
one or more time points between 3 to 12 weeks after starting treatment
2.2.1.1. Why are only randomized controlled trials included?
Randomized controlled trials are prospective, quantitative, comparative experiments
in which patients are allocated randomly to receive one of two or more interventions and the
ensuing clinical outcomes are compared. Since all patients have the same chance of being
assigned to each group, any baseline differences that arise between groups occur by chance.
Random allocation reduces the risk of imbalance of both known and unknown baseline
factors. In this way, the investigators can isolate the impact of the intervention being
studied, thereby rrunimizing the influence of other factors that could affect the outcome of
the study. Proper randomization can be achieved in many ways; usually random number
tables or computers are used to produce a pre-specified randomization list. Randomization
controls for selection bias (that is, systematic differences in the way comparison groups are
assembled), although efforts to randomize can be undermined i f allocation is not concealed.
2.2.1.2. Why is a parallel placebo arm necessary?
Included RCTs must have a parallel placebo arm as the control comparison since a
significant but variable placebo effect (in the range of 0 to 10 mm H g decrease in SBP and 0
to 8 mm H g in DBP) exists for antihypertensive drugs (82). Since the objective of this
33

review is to assess the dose-related blood pressure lowering efficacy of calcium channel
blockers compared to placebo, the overall effect of calcium antagonist treatment is obtained
by subtracting the effect in the placebo group from the effect in the active treatment group.
Having a placebo group not only controls for bias, but also minimizes the effect of
"regression to the mean", a statistical phenomenon that describes the spontaneous within-
patient variation and/or variation due to measurement errors. This effect has been
demonstrated in hypercholesterolemic and hypertensive patients by a shift from high to low
values with time, independent of treatment (83). Thus, regression to the mean is responsible
for many false positive results in experiments that involve before-after measurements of a
continuous variable (83).
For the purposes of this review, cross-over trials are only accepted if data are
reported for the first 3-12 week phase of treatment with active drug versus a placebo arm.
Thus, this is effectively the same as a parallel-design trial.
2.2.1.3. Why is blinding (masking) necessary?
Ascertainment bias involves systematic distortion of the results of the trial by
knowledge of group assignment, the source of which can be the observers, participants, or
assessors (84). Bknding, also known as masking, reduces the risk of this form of bias, fn a
double-blind R C T , both the participants and the investigators do not know the group
assignment of each participant. Proper blinding is achieved by testing an intervention
against a matched placebo, with identical taste, smell, and appearance as the active drug.
Methods for assessing the success of blinding are available. However, the success of
blinding in hypertension trials has rarely been tested.
34
2.2.1.4 Why is a baseUne measurement subsequent to or during a washout/placebo run-in period important?
The main purpose of a washout period is to eliminate carry-over effects from
previous drug administration prior to commencing the trial. Commonly, the washout period
is comprised of or is followed by a single-blind placebo "run-in" before randomization. The
most accurate estimates of the baseline blood pressure and heart rates are obtained at the
end of this period. This pre-study period also aids in the selection of participants who are
truly hypertensive, as those who do not meet the inclusion criteria cut-off after the
washout/run-in do not continue in the study. Repetitive measurements before study entry
allow blood pressures to stabilize, and thus, the problem of regression to the mean is
m i r L i m i z e d .
2.1.1.5. Why is the 3-12 week window selected?
Based on a previous systematic review (81), a follow-up of 3-12 weeks during
treatment represents an appropriate window of time from which to extract outcome data. A
rninimum of three weeks is usually necessary for the effect of therapy to become maximal
and stable. For practical reasons, the upper duration limit of 12 weeks was chosen since
many antihypertensive drug trials involve dose titration or addition of other drugs in those
who fail to achieve a target blood pressure after a certain length of time on treatment. As
well, a shorter duration allows the data to include the maximum number of patients, as
withdrawals and drop-outs, which can confound results, occur at higher rates in trials with
long duration.
2.2.2. Types of participants
Participants must have had a baseline systolic blood pressure > 140 mm H g and/or a
diastolic blood pressure > 90 mm Fig, measured in a standard way. Patients with creatinine
35

levels greater than 1.5 times the normal level were excluded. This criterion thereby excludes
patients with secondary hypertension due to renal failure. Patients who were pregnant
during the study were excluded since pre-eclampsia is considered a form of secondary
hypertension. Participants who took medications that affect blood pressure other than the
study medications were excluded. Participants were not restricted by age, gender, baseline
risk, or any other co-morbid conditions.
2.2.3. Types of interventions
The intervention of interest is monotherapy with any calcium channel blocker, as
listed in Table 4 and 5.
Trials in which titration to a higher dose is based on blood pressure response were
not eligible i f the titration occurred before three weeks of treatment. This restriction is in
place because dose-response relationships cannot be analyzed i f patients witiiin each
randomized group are taking different doses. However, trials in which a response-
dependent titration took place during or after the 3-f2 week interval were eligible i f pre-
titration data were given. In cases of forced (i.e., response-independent) titration, data from
the highest dose given for the specified duration of time, provided this duration was > 3
weeks, were extracted.
2.2.4. Types of outcome measures
Primary:
Change from baseline in trough and/or peak systolic and diastolic blood pressure at
3-12 weeks treatment, compared to placebo. If blood pressure measurements were available
at more than one time within the acceptable window, the weighted means of blood pressures
taken in the 3-12 week range were used.
36
Secondary:
1. Standard deviation of the change in blood pressure compared with placebo.
2. Change in standard deviation of blood pressure compared with placebo.
3. Change in pulse pressure compared with placebo.
4. Change in heart rate compared with placebo.
5. Number of patient withdrawals due to adverse events compared with placebo.
2.2.5. Search strategy for identif ication of studies
To identify randomized placebo-controlled trials of calcium channel blockers,
Medline (Jan. 1966-June 2003), E M B A S E (fan. 1988-June 2003), C I N A H L (Jan. 1982-June
2003), the Cochrane Controlled Clinical Trials Register, and bibliographic citations were
searched. Previously published meta-analyses on dose-response of calcium channel blockers
were used to help identify references to trials. N o language restrictions were applied.
The following search strategy was utilized to identify randomized, placebo-controlled
trials of calcium channel blockers for hypertension. This approach was a modified,
expanded version of the standard search strategy of the Hypertension Review Group, with
additional terms related to calcium channel blockers in general (85).
A " / " at the end of a term signifies a Medical Subject Heading (MeSH) term; "exp"
means the term is exploded (all MeSH terms nested under the exploded term are included);
"pt" denotes publication type; "mp" following a term will retrieve citations that contain the
term in the tide, abstract or key words; "or /" followed by a number range will retrieve the
group of citations that fall under any of the corresponding terms. The symbol "$"
represents a wildcard character used to search for multiple forms of a term. The search
37
modifier "adj" plus a number between two terms returns records that contain the two terms
within the specified number of words of each other.
1. randomized controlled trial.pt
2. randomized controlled trial$.mp
3. controlled clinical trial.pt
4. controlled clinical trial$.mp
5. random allocation.mp
6. exp double-blind method/
7. double-blind.mp
8. exp single-blind method/
9. single-blind.mp
10. or/1-9
11. exp animal/
12. 10 not 11
13. clinicaltrial.pt
14. clinical trialf.mp
15. exp clinical trials/
16. (clinf ad)25 trtal$).mp
17. ((singl$ or doubl$ or tripl$ or trebl$) adj25 (blind$ or mask$)).mp
18. randorn$.mp
19. exp research design/
20. research design.mp
21. or/13-20
38
22. 21 not 11
23. 22 not 12
24. comparative stud$.mp
25. exp evaluation studies/
26. evaluation studfi.mp
27. follow-up stud$.mp
28. prospective studf.mp
29. (control! or prospective or volunteer!).
30. or/24-29
31. 30 not 11
32. 31 not (12 or 23)
33. 12 or 23 or 32
34. exp calcium channel blockers/
35. calcium channel blocker$.mp
36. calcium channel antagonist$.mp
37. calcium antagonist!.mp
38. amlodipine.mp
39. anipamil.mp
40. aranidipine.mp
41. azelnidipine.mp
42. barnidipine.mp
43. bencyclane.mp

44. benidipine.mp
45. bepridil.mp
46. cilnickpine.mp
47. cinnarizine.mp
48. clentiazem.mp
49. clevidipine.mp
50. darodipine.mp
51. desmethoxyverapamil.mp
52. devapamil.mp
53. diltiazem.mp
54. dopropidil.mp
55. efonidipine.mp
56. elgodipine.mp
57. etafenone.mp
58. falipamil.mp
59. fanofarone.mp
60. felodipine.mp
61. fendiline.mp
62. flunarizine.mp
63. fostedil.mp
64. gallopamil.mp
65. isradipine.mp
66. lacidipine.mp
67. lercanidipine.mp
68. Hdoflazine.mp
69. lomerizine.mp
70. manidipine.mp
71. masnidipine.mp
72. mibefradil.mp
73. nicardipine.mp
74. nifedipine.mp
75. niguldipine.mp
76. nilvadipine.mp
77. niiriodipine.mp
78. nisoldipine.mp
79. nitrendipine.mp
80. perhexiline.mp
81. pranidipine.mp
82. prenylamine.mp
83. riodipine.mp
84. ronipamil.mp
85. semotiadil.mp
86. silvadipine.mp
87. terodiline.mp
88. dapamil.mp
89. verapamil.mp
90. or/34-89
91. exp hypertension/
92. hypertension.mp
93. exp blood pressure/
94. blood presure.mp
95. or/91-94
96. 90 and 95
97. 33 and 96
98. placebo$.mp
99. 97 and 98
2.2.6. Study Selection
The initial search of all the databases was performed to identify citations with
potential relevance. A l l citations were stored and categorized in the Reference Manager
program. The initial screen of these abstracts excluded articles whose tides and/or abstracts
were clearly irrelevant. The full texts of remaining articles were then retrieved (and
translated into English where required). The bibliographies of pertinent articles, reviews and
texts were searched for additional citations. Two independent reviewers assessed the
eligibility of the trials using a trial selection form (Appendix A) . A third reviewer resolved
discrepancies. Trials with more than one publication were counted only once.
2.2.7. Data Extract ion
Data were extracted independendy by two reviewers using a standard form
(Appendix B), and then cross-checked. If data were presented numerically (in tables or text)
and graphically (in figures), the numeric data were preferred because of possible
42

measurement error when estimating from graphs. A l l numeric calculations and extractions
from graphs or figures were confirmed by a second reviewer.
The position of the patient during blood pressure measurement may affect the blood
pressure lowering effect. However, in order not to lose valuable data, i f only one position
was reported, data from that position were extracted. When blood pressure measurement
data were available in more than one position, sitting blood pressure was the first preference.
If only standing and supine blood pressures are available, that of the standing position was
used. In case of missing information in the included studies, investigators were contacted
(using e-mail, letter and/or fax) to obtain the missing information. In the case of missing
standard deviation of the change in blood pressure or heart rate, the standard deviation was
imputed based on the information in the same trial or from other trials using the same drug
and dose. The following hierarchy (listed from high to low preference) was used to impute
standard deviation values:
1. pooled standard deviation calculated either from the t-statistic corresponding to an exact
p-value reported (86) or from the 95% confidence interval of the mean difference
between treatment group and placebo
2. standard deviation of change in blood pressure/heart rate from a different position than
that of the blood pressure/heart rate data used
3. standard deviation of blood pressure/heart rate at the end of treatment
4. standard deviation of blood pressure/heart rate at the end of treatment measured from a
different position than that of the blood pressure/heart rate data used
5. standard deviation of blood pressure/heart rate at baseline (except i f this measure is used
for entry criteria)
43
6. weighted mean standard deviation of change in blood pressure/heart rate calculated
from at least 3 other trials using the same drug and dose
7. weighted mean standard deviation of change in blood pressure/heart rate calculated
from other trials using the same drug
8. weighted mean standard deviation of change in blood pressure/heart rate calculated
from all other trials (any drug and dose)
2.2.8. Quality Assessment
Assessing the quality of trials in a systematic review is important in order to
determine the validity of its findings. The quality of reports of randomized trials can be
incorporated into a meta-analysis in a number of ways. In a sensitivity analysis, studies
below a certain quality threshold are removed to determine the effect on the overall estimate.
This approach can be used to attempt to explain heterogeneity between trial results. Studies
can also be weighted according to quality; with this approach, studies of lower quality have
less influence on the overall estimate (87). One of the difficulties with assessing trial quality
is that we must rely upon information provided in the written report. To address this issue,
the Consolidation of the Standards of Reporting Trials (CONSORT) statement issued by a
group of researchers and journal editors has aimed to improve the quality of reporting of
randomized controlled trials (87).
Two quality assessment scales are utilized commonly in systematic reviews: the
Cochrane Collaboration approach and the Jadad method. The quality of all included trials
was assessed by two independent reviewers using these two approaches.
44

2.2.8.1. The Cochrane approach for assessment of allocation concealment
When studies are entered into the RevMan program, the Cochrane quality
assessment scale based on allocation concealment is a default field for the "included trial
characteristics" table (76). Each trial in the systematic review is assigned a grade (A, B, C, or
D):
Grade A : Adequate concealment
Adequate concealment can be executed by the following methods: centralized
(central office unaware of subject characteristics) or pharmacy-controlled randomization;
pre-numbered or coded identical containers that are administered serially to patients; on-site
computer system with allocations kept in a locked computer file that can be accessed only
after patients enter; sequentially numbered, sealed, opaque envelopes.
Grade B: Uncertain
Grade B is assigned to trials in which the allocation concealment is not reported, or
despite a description that reports adequate concealment (the use of a list, table or sealed
envelopes), there are other features that lead the reviewer to be suspicious.
Grade C: Clearly inadequate concealment
Inadequte allocation concealment consists of the following methods: alternation; use
of case record numbers, dates of birth or date at which the patient is invited to participate in
the study; any procedure that is transparent before allocation, such as an open list of random
numbers. While these methods in theory produce random groups, knowledge of group
assignment before enrollment can affect the decision to enroll or not enroll the patient.
Grade D : N o t used
Allocation concealment was not used to assess validity.
45
2.2.8.2. Jadad Method
Jadad developed a validated tool to assess trial quality (88). This tool is easy to use
and gives consistent measurements. This five-point scoring system is outlined as follows:
1. Was the study described as randomised? (Yes=+1; No=0)
If "Yes", was the method of randomization well described and appropriate? (Yes =
+ 1, N o = -1, Method not reported = 0)
2. Was the study described as double-blind? (Yes= + 1; No=0)
If "Yes", was the method of double blmding well described and appropriate? (Yes =
+ 1, N o = -1, Method not reported = 0)
3. Was there a description of withdrawals and dropouts in each group and the reasons?
(Yes= + l ;No=0)
A score of 0-2 reflects low quality, while a score of 3-4 indicates moderate quality
and a score of 5 represents a high quality study.
2.2.9. Data Analysis
Data synthesis and analyses were done using the Cochrane Collaboration software,
Review Manager (RevMan) 4.2.8. This program allows reviewers to construct systematic
reviews according to the Cochrane publication format. RevMan also allows the data to be
displayed in a "forest plot".
46

Review: Blood pressure lowering efficacy of calcium channel blockers for "primary hypertension Comparison:. -01'Dose Amlodipine :ys. placebo Outcome: ;01 Change in Systolic Blood Pressure Study. . Amlodipine. Placebo VWD (fixed) Weight VVtyiD (fixed) on sub-category .,N ' hMeani;SD) N-: Mean (SD). ' • 95% CI '. .% 95% CI ' Year- Order 01 1.25 rrigVclay; Frick.1988 ^ 48 -5 60 di 70) *45 -6 10(14 10). '.6 ' 4 4 0. - 4 . 78, 5.78) "1988 0 Mehtal993 -7 80(14 40) :39 -3 70(13 60)- 4 ?2. -4 io • -10 28, Z. 081 "1993 0 Subtotal (95% CI)' -•88" 84 .11-16 -1 44,' -S: 46~;' 2.'57] " Test for heterogeneity: Chi = 1.23," 0.27) F" = 18.7%
Test for overall effect: Z = 0.71 (P = 0.48) 02 25 mg/day-• Trick 1988- 46' -8 7DJ11 70) 45 -6 10(14 10) 6 33. -2 say -'?- 93', 2. 73] 1988 'o 'Mehta1993 40 -7 30 (14 40) 39 -3 70(13 60) 4 72 -3 60 ' -9. 78, 2'. 58]' -1"? 0 "FrisKman 1995„ 1 72 -IO1 70(15 00) '•69 -i 00(18 70) 5 72 -9 70 -is 31 -4.09] 1995 0 Subtotal (95% CI) 158 1S3 • 16 7 7 -5 30 -8.58, -2.03)' Test tor heterogeneity: Chi = 3.64, = 2 (P = 0.16) r = 45. %
Test lor overall effect:'Z = 3.17 (P = 0.002) 03 5 mg/day Frick 1988 48 -18 70(10 40) 45 -6 10(14 10) •7 02: r12 60 ' -17 66 -7.54]' '1988 ,1 Mroczek1988. 10 -16 70 (i 1 70) 5 4 50 (2 a
-id) « 0 50 -21 20 -40 2S -2.IS]' 1988 2 Merita'1993 44 -8 60 (10 30) 39 -3 70(13 60)- -6 55 -4 90 -10 14 0-341 1993 3 Kuschnir. 1996 77 -17 SO (12 00) 76 -z 10(14 10) .10 44. -IS 40 -19 5S -11.-25] 1996 4 Farsarig' 2001 ;84 -is Z0 (13 50) 83 -0 90(14 10)- -* 10 ?6. -14 30 -18 49 . -rlO.il] 2001 5 Poor2001 110 -10 80 (10 40) -iis -3 00(14 ib) # 17 27 -7 80 -11 03 -4.57] .2001 6 ' Cnrysant 2003 183 -10 301(10 40) 6S -0 80(14 10) 12 83 -9 so -13 24 -5.76]. . 2003 i
Subtotal (95% CI) 556 428 .t 64 86 -10 72 -12 38 -9.OS]
Test for heterogeneity: Ch* =.17.67 df - 6 (P = 0.007), I1 = 6 6.0% Test for overall'effect: Z = 12.61 (P <"0.00001 ) 04 10 mg/day Licata1993 . is T20 '90'(17 .40) 15 r-i 00 (19 30) «• ; 1 01 -16 90' -30 24 -3.'S6] . i993 0 Mehta.1993' • 40" -13 40(10 60) 39 -3 70 (13 60) .6 20 -9 70.. -IS 09 -4.31] i993 "0 Subtotal (95% CI): •'ss:,. : ' s 4 • .7 21- -10 71 -is 70 -S.72]. Test for heterogeneity: Ch '« O.9E; if = 1 (P = 0.33) P = 0% Test for overall effect: Z » 4.20 (P < 0.0001) Total (95% CI) 85r 719 ,100 00 -8 77 -10 .11 -7.43] Test for heterogeneity: Ch = 46.42 df-13(P«0.0001),P 72.0% Test .for overall effect; Z « 12.82 (P. « 0.00001 )
-100. -50 ,0' 50 100 Favours Amlodipine Favours Placebo
Figure 2. Example of a forest plot.
In a forest plot, the outcome of interest is listed at the top. The vertical line
represents the line of no effect. Component studies are shown as squares (the size of which
represents the weight) and the horizontal line running through each square shows the 95%
confidence interval. The overall estimate is represented as a diamond; its centre represents
the point estimate and the horizontal tips represent the confidence interval. If the
confidence interval crosses the line of no effect, there is no statistically significant difference
between the intervention and the control.
Data for changes in blood pressure and heart rate were combined using a weighted
mean difference method. The withdrawals due to adverse events were analyzed using
relative risk, risk difference, and number needed to harm.
47

Tests for heterogeneity of treatment effect between the trials were performed using a
standard chi-square statistic for heterogeneity. The fixed effects model was applied to obtain
summary statistics of pooled trials, unless significant between-study heterogeneity was
present, in which case the random effects model was used.
Subgroup analyses were used to examine the results for specific categories of
participants. The number of subgroup analyses performed should be kept to a minimum,
since the greater number of hypotheses tested, the greater the number of differences one will
find by chance alone (76). Possible subgroup analyses included:
1) Calcium channel blocker subclass: dihydropyridines, non-dihydropyridines (including
benzothiazepines and phenylalkylamines) and others
2) Different formulations of the same active chemical entity
3) Age: children, adults, older people
4) Co-morbid conditions: ischemic heart disease, diabetes
5) Baseline severity of hypertension: mild, moderate, severe
6) Type of hypertension: elevated D B P , isolated systolic
Sensitivity analyses are performed to assess how sensitive the results are to changes
in the way the analyses were done (76). If these sensitivity analyses do not change the results
substantially, more confidence can be placed in the results. However, i f the results do
change, they must be interpreted with greater care. The robustness of the results of this
systematic review were tested using the following sensitivity analyses, including:
1) Trials of high quality vs. poor quality
2) Trials that are industry-sponsored vs. non-industry sponsored
3) Trials with blood pressure data measured in the sitting position vs. other measurement
positions
48
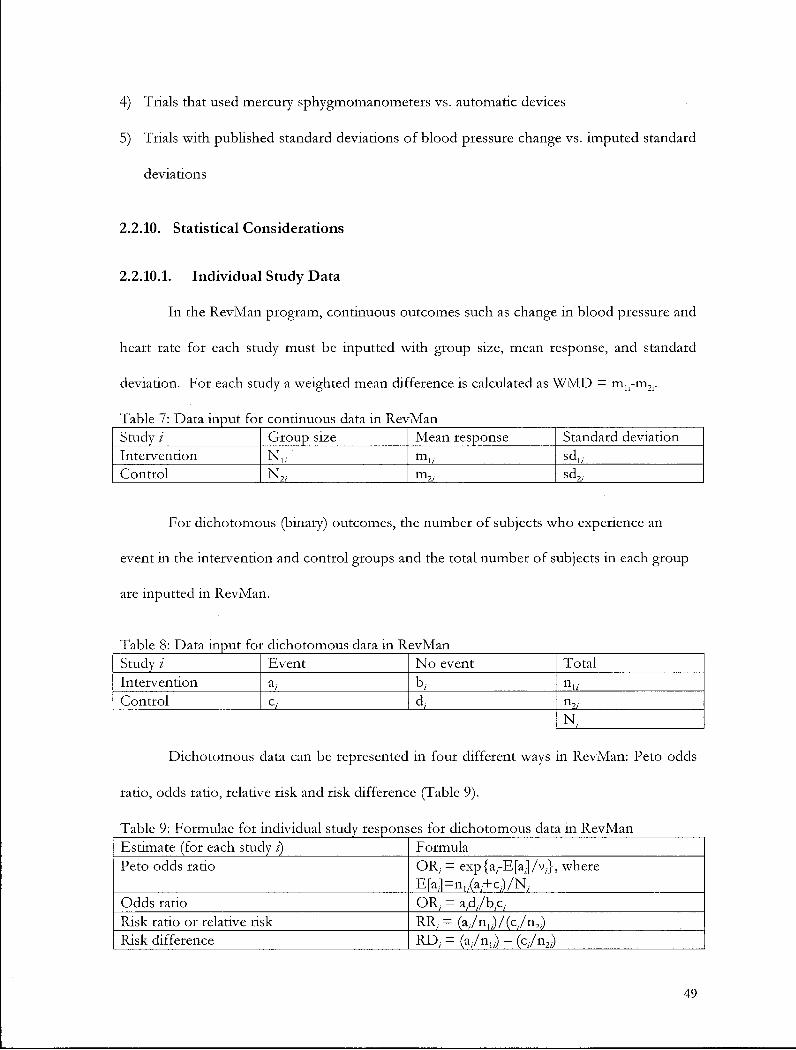
4 ) Trials that used mercury sphygmomanometers vs. automatic devices
5) Trials with published standard deviations of blood pressure change vs. imputed standard
deviations
2.2.10. Statistical Considerations
2.2.10.1. Individual Study Data
In the RevMan program, continuous outcomes such as change in blood pressure and
heart rate for each study must be inputted with group size, mean response, and standard
deviation. For each study a weighted mean difference is calculated as W M D = m i r m 2 i .
Table 7: Data input for continuous data in RevMan Study i Group size Mean response Standard deviation Intervention sd,,-Control N 2 , m 2 ; sd,,
For dichotomous (binary) outcomes, the number of subjects who experience an
event in the intervention and control groups and the total number of subjects in each group
are inputted in RevMan.
Table 8: Data input for dichotomous data in RevMan Study i Event N o event Total Intervention a, Control c; d, n 2,
N,.
Dichotomous data can be represented in four different ways in RevMan: Peto odds
ratio, odds ratio, relative risk and risk difference (Table 9).
Table 9: Formulae for individual study responses for dichotomous data in RevMan Estimate (for each study z) Formula Peto odds ratio OR, = exp{a,-E[a,]/v,}, where
Efa^n .^.+cVH-Odds ratio O R , = a,d,/b,c, Risk ratio or relative risk RR,.= (a,./n„)/(c,/n 2,) Risk difference R D , = (a,/n„) - (c,/n2,)
49
2.2.10.2. Pool ing trials
There are two main approaches for summarizing the results of studies in a meta
analysis: the "fixed effect" model and the "random effects" model. The fixed effect
approach assumes that the group of studies being analyzed is a distinct population (a "fixed"
set) and the aim is to estimate the mean effect size of these trials only. The fixed effect
model tests the significance of the null hypothesis (i.e., no overall difference between
treatment and control in the selected group of studies). Because the fixed effect approach
ignores between-study variation, it assumes the studies have homogeneous effect sizes. The
statistic jg is calculated to test for interstudy heterogeneity. ff statistically significant
heterogeneity is present, the fixed-effect estimate of the overall effect size may not be valid
(89). The inverse variance method is used to combine weighted mean differences for
continuous data. The effect size for each study is weighted by the reciprocal of the square of
the standard error. Thus, studies with large sample size are weighted more heavily than
smaller trials. Likewise, studies with smaller variances have greater influence on the overall
effect size than studies with large variances. For dichtomous data, the Mantel-Haenszel
method is used to produce odds ratio, relative risk, and risk difference estimates. The odds
ratio and relative risk are relative measures and their values are similar i f the outcome is rare
(76). However, the relative risk is recommended because the odds ratio is more difficult to
interpret. Risk difference expresses results in absolute terms.
The random effects model assumes that the set of studies being analyzed is a random
sample from a larger population of studies. The DerSimonian and Laird method is used to
combine continuous data or dichotomous data. The weight assigned to each study takes
into account both intra- and inter-study variances. This approach accounts for interstudy
50
heterogeneity and produces wider confidence intervals than the fixed effect approach. A n
advantage of the random effects approach is that it estimates the effect size for a
hypothetical population of studies, which may include future studies or previous studies that
may have been missed (89).
Which of the two competing models is used depends on whether or not we wish to
take into account between-study variation, f f there is no statistically significant heterogeneity
between studies, the fixed-effect and random-effects estimates will be similar. A
disadvantage of the random effects model is that more weight is assigned to smaller studies
compared to the fixed effect model. These small studies are more likely to be of poorer
quality and are more subject to publication bias (76).
2.2.11 S ta r t ing doses
fn order to combine trial data in the analyses, calcium channel blocker drugs were
analysed as increments of the recommended starting dose, as determined from reference
pharmacopeias (44, 90). ff a range was given, the lower dose was taken as the starting dose.
Table 10 lists starting doses of calcium channel blockers assessed in this review. This
approach is based upon the assumption that starting doses recommended by companies
must have evidence for blood pressure lowering efficacy and that the blood pressure
lowering efficacy of each of the starting doses is approximately the same.
51

Table 10: Starting doses of calc ium channel blockers (44, 90) D r u g Brand name (Company) Starting dose/day
for hypertension Available in Canada?
Amlodipine Norvasc® (Pfizer) Also available in combination with benazepril- Lotrel® (Novartis)
5 mg Yes
Barnidipine Hypoca®, Vasexten® (Yamanouchi)
10 mg N o
Darodipine n/a 100 mg* N o
Diltiazem Cardizem®, Tiazac® (Biovail) Generic available
120-240 mg Yes
Felodipine Plendil® (AstraZeneca) Renedil® (Sanofi-Aventis)
5 mg Yes
Isradipine DynaCirc® (ReHant), Lomir® 5 m g N o Lacidipine Lacipil® (GlaxoSiTUthKline),
Caldine®, Lacimen®, Lacipil®, Midotens®, Motens®
2-4mg N o
Lercanidipine Zanidip® (Recordati) 10 mg N o Lidoflazine Clinium® (Janssen) Angina only N o Manidipine Calslot® (Takeda) 10 mg N o Nicardipine Cardene® (Roche) 60 mg N o Nifedipine Adalat® (Bayer)
Generic available 20-30 mg Yes
Nilvadipine Escor®, Nivadil® (Fujisawa) 8 m g N o Nisoldipine Sular® (Bayer) 10 mg N o Nitrendipine Bayotensin®, Baypress®
(Bayer) 5-20 mg N o
Pranidipine n /a 2 mg* N o Tiapamil n/a N o doses were
statistically significantly different from placebo*
N o
Verapamil Isoptin® (Abbott) Generic available
180-240 mg Yes
* For darodipine, pranidipine and tiapamil, no dosing information was available in the monographs; therefore dose Listed is the lowest effective dose as determined by the systematic review
2.2.12. Direct and indirect comparisons between doses
When possible, direct and indirect comparisons of effect sizes between doses were
performed for each C C B drug. In the direct method, only trials that randomized
participants to different doses were included in the analysis. In the indirect method, an
52
"adjusted indirect comparison" and the associated standard error were calculated using the
method described by Bucher et al (91) and Song et al (92). Briefly, C C B drug doses were
compared from all the placebo-controlled trials, by adjusting for the common placebo
intervention. The difference between the indirect and direct estimates was then assessed.
53

3. R E S U L T S
3.1 Search findings
Table 11: Results of the search strategy
N u m b e r of publications
Publications identified by search strategy 4093
Trials excluded upon reading tides/abstracts 3076
Review articles identified by search strategy 563
Relevant review articles retrieved 138
Trials retrieved for detailed reading 454
Trials excluded upon detailed reading 217
Number of trials meeting inclusion criteria 237
O f the trials meeting the inclusion criteria:
Data available Included Studies
Data not available Excluded Studies
106
131
The search strategy was highly sensitive but lacked specificity since 75% of hits (not
including review articles) were excluded upon reading the tides or abstracts. There was an
overlap of 983 studies between Medline and E M B A S E databases. One hundred thirty-eight
relevant review articles identified by the search strategy were checked for references to trials.
102/106 (96%) of the included studies were found in the Cochrane Central Register of
Controlled Trials ( C E N T R A L ) . References that have not been indexed yet in C E N T R A L
have been sent to the Cochrane Hypertension Group for revision of the database. Two of
the missing studies (Circo 1997, Ninci 1997) were also not indexed in Medline or E M B A S E ,
but rather, were found from the reference list of a review article.
Four of the 106 included studies were originally excluded due to lack of reporting of
the number of patients in each arm; however these trials were included after obtaining the
54
missing values from Law et al's published meta-analysis of five classes of antihypertensives
(93).
3.2 Characteristics ofincluded studies
O f the 4093 citations identified by the search strategy, 106 trials (2.6%), published
between 1976 and 2003, met the inclusion criteria and contained extractable data for 19 C C B
drugs. O f these included trials, 99 (92%) of the studies were published in English, 3 (3%) in
French, 3 (3%) in German, and 2 (2%) in Italian. One hundred four (97%) of the included
studies had a parallel-group design, while only 3 (3%) were cross-over studies (only the pre-
cross-over data were used in this analysis).
Tables 12-30 summarize the characteristics of each included study. Each study was
assigned a unique identifier consisting of either the trial acronym or the surname of the first
author followed by the year of publication.
55
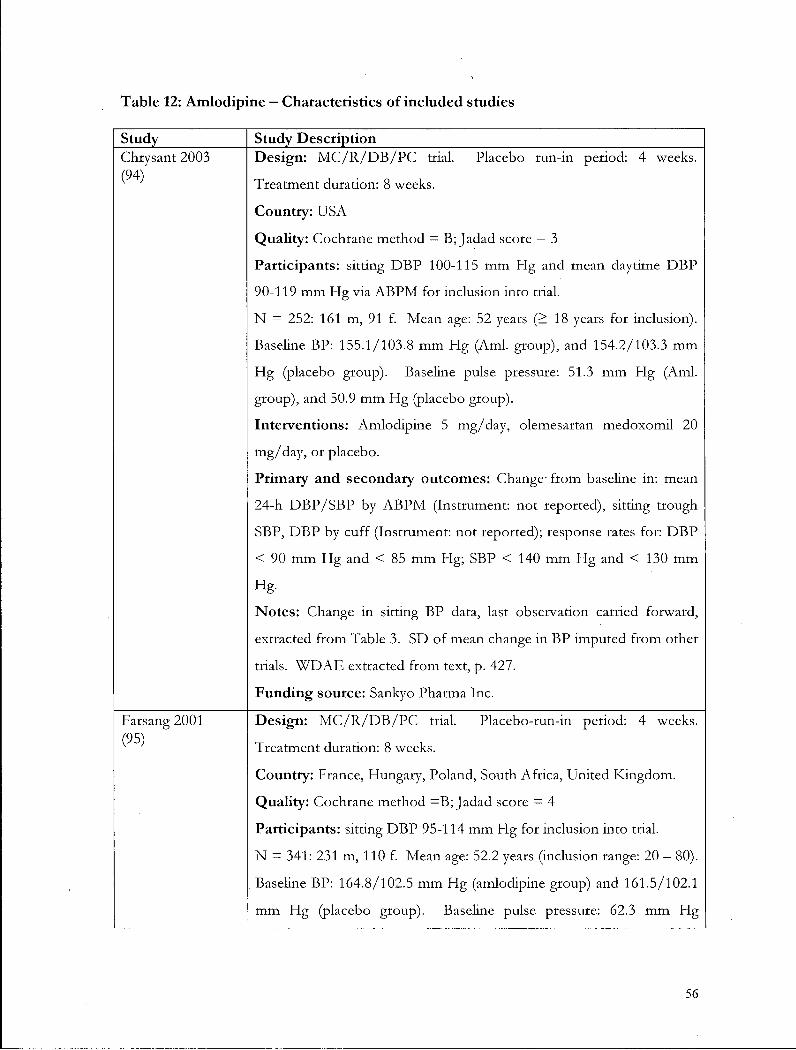
Table 12: Amlod ip ine - Characteristics of included studies
Study Study Descr ipt ion Chrysant 2003 (94)
Design: M C / R / D B / P C trial. Placebo run-in period: 4 weeks.
Treatment duration: 8 weeks.
Country: U S A
Quality: Cochrane method = B; jadad score = 3
Participants: sitting D B P 100-115 mm Hg and mean daytime D B P
90-119 mm H g via A B P M for inclusion into trial.
N = 252: 161 m, 91 f. Mean age: 52 years (> 18 years for inclusion).
Baseline BP: 155.1/103.8 mm Fig (Ami. group), and 154.2/103.3 mm
H g (placebo group). Baseline pulse pressure: 51.3 mm H g (Ami.
group), and 50.9 mm H g (placebo group).
Interventions: Amlodipine 5 mg/day, olemesartan medoxomil 20
mg/day, or placebo.
Primary and secondary outcomes: Change- from baseline in: mean
24-h D B P / S B P by A B P M (Instrument: not reported), sitting trough
SBP, D B P by cuff (Instrument: not reported); response rates for: D B P
< 90 mm H g and < 85 mm Hg; SBP < 140 mm H g and < 130 mm
Hg-
Notes: Change in sitting BP data, last observation carried forward,
extracted from Table 3. SD of mean change in BP imputed from other
trials. W D A E extracted from text, p. 427.
Fund ing source: Sankyo Pharma Inc.
Farsang 2001 (95)
Design: M C / R / D B / P C trial. Placebo-run-in period: 4 weeks.
Treatment duration: 8 weeks.
Country: France, Flungary, Poland, South Africa, United Kingdom.
Quality: Cochrane method =B; jadad score = 4
Participants: sitting D B P 95-114 mm Fig for inclusion into trial.
N = 341: 231 m, 110 f. Mean age: 52.2 years (inclusion range: 20 - 80).
Baseline BP: 164.8/102.5 mm H g (amlodipine group) and 161.5/102.1
mm H g (placebo group). Baseline pulse pressure: 62.3 mm H g
56
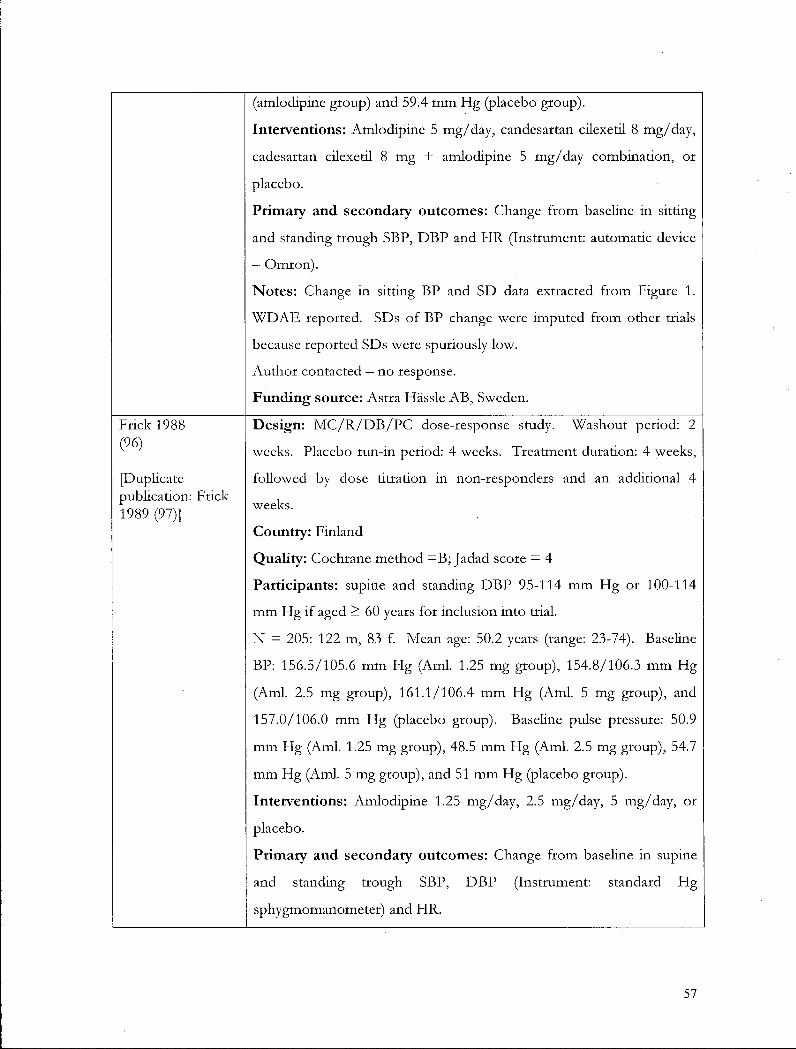
(amlodipine group) and 59.4 mm Fig (placebo group).
Interventions: Amlodipine 5 mg/day, candesartan cilexetil 8 mg/day,
cadesartan cilexetil 8 mg + amlodipine 5 mg/day combination, or
placebo.
Primary and secondary outcomes: Change from baseline in sitting
and standing trough SBP, D B P and H R (Instrument: automatic device
— Omron).
Notes: Change in sitting B P and SD data extracted from Figure 1.
W D A E reported. SDs of B P change were imputed from other trials
because reported SDs were spuriously low.
Author contacted — no response.
Fund ing source: Astra Hassle A B , Sweden.
Frick 1988 (96)
[Duplicate publication: Frick 1989 (97)]
Design: M C / R / D B / P C dose-response study. Washout period: 2
weeks. Placebo run-in period: 4 weeks. Treatment duration: 4 weeks,
followed by dose titration in non-responders and an additional 4
weeks.
Country: Finland
Quality: Cochrane method =B; Jadad score — 4
Participants: supine and standing D B P 95-114 mm H g or 100-114
mm H g if aged > 60 years for inclusion into trial.
N = 205: 122 m, 83 f. Mean age: 50.2 years (range: 23-74). Baseline
BP: 156.5/105.6 mm H g (Ami. 1.25 mg group), 154.8/106.3 mm H g
(Ami. 2.5 mg group), 161.1/106.4 mm H g (Ami. 5 mg group), and
157.0/106.0 mm H g (placebo group). Baseline pulse pressure: 50.9
mm H g (Ami. 1.25 mg group), 48.5 mm H g (Ami. 2.5 mg group), 54.7
mm H g (Ami. 5 mg group), and 51 mm H g (placebo group).
Interventions: Amlodipine 1.25 mg/day, 2.5 mg/day, 5 mg/day, or
placebo.
Primary and secondary outcomes: Change from baseline in supine
and standing trough SBP, D B P (Instrument: standard H g
sphygmomanometer) and HR.
57

Notes: Change in standing B P data at week 4 extracted from Table 3
(Frick 1989). SD of mean change in B P imputed from weighted mean
SD of other trials. W D A E reported but cannot determine i f they
occurred before or after titration in non-responders.
Pfizer (Kent, U K ) contacted — no data.
Funding source: Not reported.
Frishman 1995 (98)
Design: M C / R / D B / P C trial. Washout period: 2 weeks. Placebo
run-in period: 2-4 weeks. Treatment duration: 8 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 4
Participants: Sitting D B P 100-115 mm Fig for inclusion into trial.
N = 332: 209 m, 123 f. Mean age: 53.7 years (inclusion range: 21-80).
Baseline BP: 157.8/103.8 mm H g (amlodipine group) and 158.0/103.9
mm H g (placebo group). Baseline pulse pressure: 54.0 (amlodipine
group) and 54.1 (placebo group)
Interventions: Amlodipine 2.5 mg/day, benazepril 10 mg/day,
benazepril 10 mg + amlodipine 2.5 mg/day combination, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
and standing trough SBP, D B P (Instrument: standard H g
sphygmomanometer), and H R .
Notes: sitting BP data extracted from Figure 2. SD of mean change in
B P imputed from SDs of week-8 BPs. W D A E reported.
Author contacted -
Funding source: Ciba-Geigy Corp.
Kuschnir 1996 (99)
Design: M C / R / D B / P C trial. Washout period: 2 weeks. Placebo run-
in period: 2-4 weeks. Treatment duration: 8 weeks.
Country: Argentina
Quality: Cochrane method = B; Jadad score — 4
Participants: Sitting D B P 100-120 mm H g for inclusion into trial.
N = 308: 138 m, 170 f. Mean age: 56.5 years (inclusion range 21-80).
Baseline BP: 165.6/106.5 mm Fig (amlodipine group) and 166.4/106.9
58

mm H g (placebo group). Baseline pulse pressure: 59.1 mm H g
(amlodipine group) and 59.5 mm H g (placebo group).
Interventions: Amlodipine 5 mg/day, benazepril 20 mg/day,
amlodipine 5 mg + benazepril 20 mg/day combination, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
trough SBP, D B P (Instrument: H g manometer), and HR.
Notes: sitting B P data extracted from Table II. SD of mean change in
SBPs imputed from SD of baseline BPs and SD of mean change in
D B P imputed from other trials. W D A E reported.
Attempted to contact author — no response.
Funding source: Ciba Geigy Corp., USA.
Licata 1993 (100)
Design: R / D B / P C trial. Placebo run-in period: 2 weeks. Treatment
duration: 4 weeks.
Country: Italy
Quality: Cochrane method — B; Jadad score = 3
Participants: Supine D B P >90 mm H g for inclusion into trial.
N = 30: 14 m, 16 f. Mean age: 45.4 years (range: not reported).
Baseline BP: 165.9/100.0mm Hg (treatment group) and 163.1/101.0
mm H g (placebo group). Baseline pulse pressure: 65.9 (treatment
group) and 62.1 (placebo group).
Interventions: Amlodipine 10 mg/day or placebo.
Primary and secondary outcomes: Change from baseline in supine
trough SBP, D B P , (Instrment: H g sphygmomanometer), and H R ; renal
hemodynamic measurements.
Notes: Supine BP data extracted from Table 1. SD of mean change in
BPs imputed from SDs of week-4 BPs. W D A E not reported.
Funding source: Not reported.
Mehta 1993 (101)
Design: M C / R / D B / P C dose-finding study. Placebo run-in period: 4
weeks. Treatment duration: 4 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 4
59

Participants: Supine and standing D B P 95-114 mm H g for inclusion
into trial.
N = 210: 112 m, 98 f. Mean age: 52.8 years (inclusion range: 18-75).
Baseline BP: 147.3/101.6 mm H g (Ami. 1.25 mg group), 150.7/102.2
mm H g (Ami. 2.5 mg group), 151.0/101/6 mm H g (Ami. 5 mg group),
152.8/101.9 (Ami. 10 mg group), and 153.4/102.0 mm H g (placebo
group). Baseline pulse pressure: 45.7 mm H g (Ami. 1.25 mg group),
48.5 mm H g (Ami. 2.5 mg group), 49.4 (Ami. 5 mg group), 50.9 (Ami.
10 mg group), and 51.4 (placebo group).
Interventions: Amlodipine 1.25 mg/day, 2.5 mg/day, 5 mg/day, 10
mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in supine
and standing trough SBP, D B P (Instrument: standard H g
sphygmomanometer), and H R ; E C G ; body weight; biochemical,
hematologic, urinalysis lab tests.
Notes: Change in standing B P and S E M extracted from Figure 1.
W D A E reported.
Author contacted — no data available.
Fund ing source: Pfizer Research, USA.
Mroczek 1988 (102)
[Multiple publications: Mroczek 1991a (103), Mroczek 1991b (104), Burris 1994 (105)]
Des ign: R / D B / P C trial. Placebo run-in period: 4 weeks. Treatment
duration: 4 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 4
Participants: Standing and supine D B P 95-114 mm H g for inclusion
into trial.
N = 16: 11 m, 5 f. Mean age: 56.9 years (range: 37-75). Baseline
standing BP: 154.9/102.2 mm H g (amlodipine group) and 146.9/105.6
mm Fig (placebo group). Baseline pulse pressure: 52.7 (amlodipine
group) and 41.3 (placebo group).
Interventions: Amlodipine 5 mg/day or placebo.
Primary and secondary outcomes: Change from baseline in supine
60

and standing trough SBP, D B P (Instrument: standard H g
sphygmomanometer).
Notes: Mean change in standing B P extracted from Table 2 (Mroczek
1991a) and S E M extracted from Figure 1 (Mroczek 1991b). W D A E
reported.
Fund ing source: Pfizer Inc., USA.
Pool 2001
(106)
Design: M C / R / D B / P C trial. Washout period: 2 weeks. Placebo run-
in period: 2-4 weeks. Treatment duration: 8 weeks.
Country: U S A
Quality: Cochrane method =A; Jadad score — 5
Participants: sitting D B P 100-115 mm H g for inclusion into trial.
N = 454: 286 m, 168 f. Mean age: 53.8 years (inclusion range: 21-80).
Baseline BP: 154.4/104.2 mm H g (amlodipine group) and 156.1/105.1
mm H g (placebo group). Baseline pulse pressure: 50.2 (amlodipine
group) and 51 (placebo group).
Interventions: Amlodipine 5 mg/day, benazepril lOmg/day,
amlodipine 5 mg + benazepril 10 mg/day combination, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
trough SBP, D B P (Instrument: not reported) and HR.
Notes: Mean change in BP data extracted from Table 1. SD of mean
change in BPs imputed from SDs from other trials. W D A E reported.
Attempted to contact author — no response.
Fund ing source: Novartis Pharmaceuticals, USA.
61

Table 13: Barnidipine - Characteristics of included studies
Study Study Description Hart 1997 (107)
Design: M C / R / D B / P C trial. Placebo run-in period: 4 weeks.
Treatment duration: 6 weeks, followed by dose titration in non-
responders and an additional 6 weeks.
Country: Netherlands
Quality: Cochrane method = B; Jadad score = 4
Participants: Sitting D B P 95-114 mm H g for inclusion into trial.
N = 190 (intention-to-treat): 124 m, 66 f. Mean age: 55.8 years
(inclusion range: 18 -,75).
Baseline BP (sitting): 161.0/102.0 mm H g (Bar. 10 mg/day group),
163.6/102.9 mm H g (Bar. 20 mg/day group), 166.2/102.5 mm H g
(Bar. 30 mg/day group), and 165.2/102.5 mm H g (placebo group).
Baseline pulse pressure: 59 mm H g (Bar. 10 mg/day group), 60.7 mm
H g (Bar. 20 mg/day group), 63.7 mm H g (Bar. 30 mg/day group), and
62.7 mm H g (placebo group).
Interventions: Barnidipine 10 mg/day, 20 mg/day, 30 mg/day, or
placebo.
Primary and secondary outcomes: Change from baseline in sitting
and standing trough SBP, D B P (Instrument: sphygmomanometer) and
HR.
Notes: Change in sitting B P at week 6 extracted from Figure 1. SDs
of changes in B P imputed from other trials. N o significant change in
H R (no H R data provided at 6 weeks). W D A E not reported for each
group separately.
Attempted to contact author — no response.
Funding source: Yamanouchi Europe B.V. , Netherlands.
62

Table 14: Darodipine - Characteristics of included studies
Study Study Description Chrysant 1988 (108)
Design: R / D B / P C trial. Placebo run-in period: 3 weeks. Treatment
duration: 4 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 4
Participants: Supine D B P 100-115 mm H g for inclusion into trial.
N = 43: 26 m, 17 f. Mean age: 51.7 years (range: not reported).
Baseline BP (standing): 157/103 mm H g (Dar. 100 mg/day group),
160/104 mm H g (Dar. 200 mg/day group), 154/103 mm H g p a r . 300
mg/day group), and 157/102 mm H g (placebo group). Baseline pulse
pressure: 54 mm H g (Dar. 100 mg/day group), 56 mm H g (Dar. 200
mg/day group), 51 mm H g (Dar. 300 mg/day), and 55 mm H g
(placebo group).
Interventions: Darodipine 100 mg/day, 200 mg/day, 300 mg/day, or
placebo.
Primary and secondary outcomes: Change from baseline in supine
and standing SBP, D B P (Instrument: not reported) and H R ; metabolic
parameters ( B U N , glucose, electrolytes, Ever enzymes); E C G .
Notes: standing B P and H R data and associated SEMs extracted from
Figures 1-4. Changes in BP and H R calculated by subtracting baselines
from weighted means of week 3 and 4 data. SD of change in BP and
H R imputed from weighted mean SD of week 3 and 4 data. N o
patients withdrew due to adverse events.
Author contacted — data no longer available.
Funding source: Not reported.
63

Table 15: Diltiazem - Characteristics of included studies
Study Study Description Burris 1990 (109)
Design: M C / R / D B / P C , 5 x 4 multifactorial-design trial. Placebo
run-in: 4-6 weeks. Treatment duration: 6 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score — 3
Participants: Supine D B P 95-110 mm H g for inclusion into trial.
N = 297: 184 m, 113 f. Mean age: 52.1 years (range: not reported).
Baseline supine BP: 151.6/99.4 mm H g (all groups combined).
Baseline pulse pressure: 52.2 mm H g (all groups combined).
Interventions: Diltiazem SR 120 mg/day, 180 mg/day, 240 mg/day,
360 mg/day, hydrochlorothiazide 12.5 mg/day, 25 mg/day, 50
mg/day, all possible diltiazem SR-hydrochlorothiazide combinations
thereof, or placebo.
Primary and secondary outcomes: Change from baseline in supine
and standing SBP, D B P (Instrument: standard H g
sphygmomanometer) and H R ; % achieving goal B P (supine D B P < 90
mm H g at week 6); E C G ; lab tests.
Notes: Change in D B P data extracted from Figure 1. SD of B P
change imputed from other trials.
Author contacted — no access to data; attempts to contact other
authors/Biovail unsuccessful. Number of patients in each group was
not explicidy reported; this data was obtained from a published meta
analysis (93). W D A E not reported separately for each group.
Funding source: Marion Laboratories Inc.
Chan 1997 (110)
Design: M C / R / D B / P C , 3 x 2 multifactorial-design trial. Placebo
run-in: 4 weeks. Treatment duration: 12 weeks.
Country: Taiwan and Hong Kong
Quality: Cochrane method = B; Jadad score = 4
Participants: sitting D B P 95-114 mm H g for inclusion into trial. \
N = 156: 134 m, 52 f. Mean age: 72 years (range: 65 - 88).
64
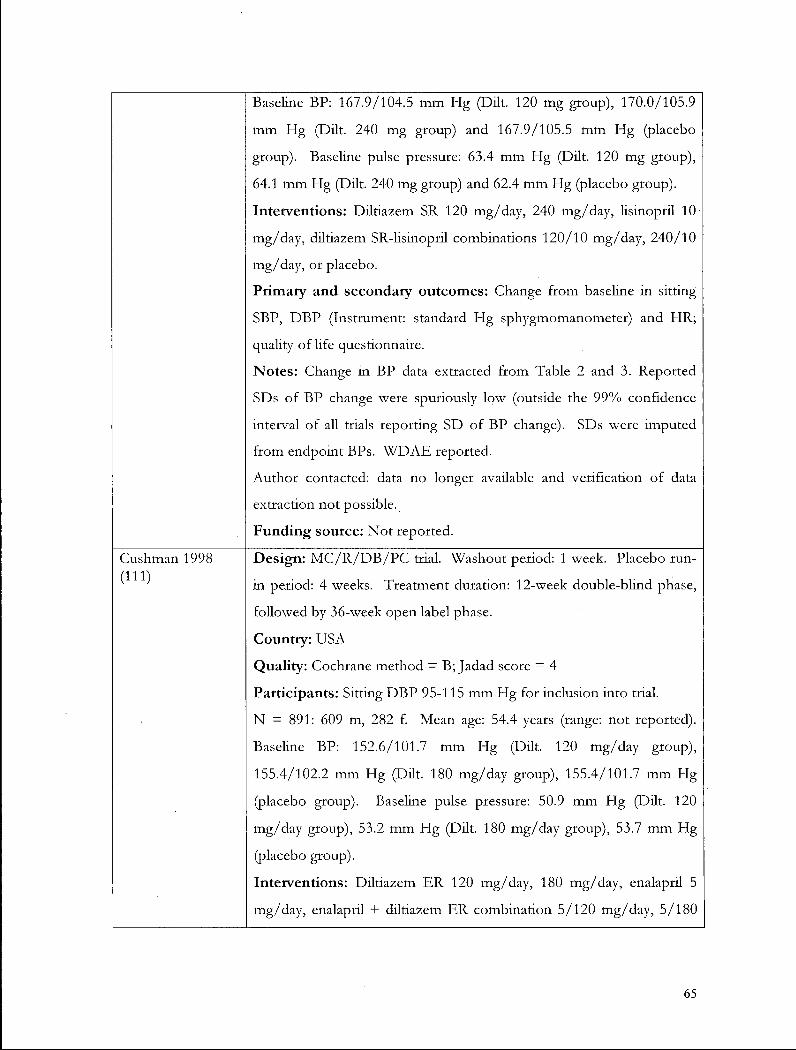
Baseline BP: 167.9/104.5 mm H g (Dilt. 120 mg group), 170.0/105.9
mm H g (Dilt. 240 mg group) and 167.9/105.5 mm H g (placebo
group). Baseline pulse pressure: 63.4 mm H g (Dilt. 120 mg group),
64.1 mm H g (Dilt. 240 mg group) and 62.4 mm H g (placebo group).
Interventions: Diltiazem SR 120 mg/day, 240 mg/day, lisinopril 10
mg/day, diltiazem SR-lisinopril combinations 120/10 mg/day, 240/10
mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
SBP, D B P (Instrument: standard H g sphygmomanometer) and H R ;
quality of life questionnaire.
Notes: Change in B P data extracted from Table 2 and 3. Reported
SDs of B P change were spuriously low (outside the 99% confidence
interval of all trials reporting SD of BP change). SDs were imputed
from endpoint BPs. W D A E reported.
Author contacted: data no longer available and verification of data
extraction not possible.
Funding source: Not reported.
Cushman 1998 (111)
Design: M C / R / D B / P C trial. Washout period: 1 week. Placebo run-
in period: 4 weeks. Treatment duration: 12-week double-blind phase,
followed by 36-week open label phase.
Country: U S A
Quality: Cochrane method — B; Jadad score = 4
Participants: Sitting D B P 95-115 mm H g for inclusion into trial.
N = 891: 609 m, 282 f. Mean age: 54.4 years (range: not reported).
Baseline BP: 152.6/101.7 mm H g (Dilt. 120 mg/day group),
155.4/102.2 mm H g (Dilt. 180 mg/day group), 155.4/101.7 mm H g
(placebo group). Baseline pulse pressure: 50.9 mm H g (Dilt. 120
mg/day group), 53.2 mm H g (Dilt. 180 mg/day group), 53.7 mm H g
(placebo group).
Interventions: Diltiazem E R 120 mg/day, 180 mg/day, enalapril 5
mg/day, enalapril + diltiazem E R combination 5/120 mg/day, 5/180
65
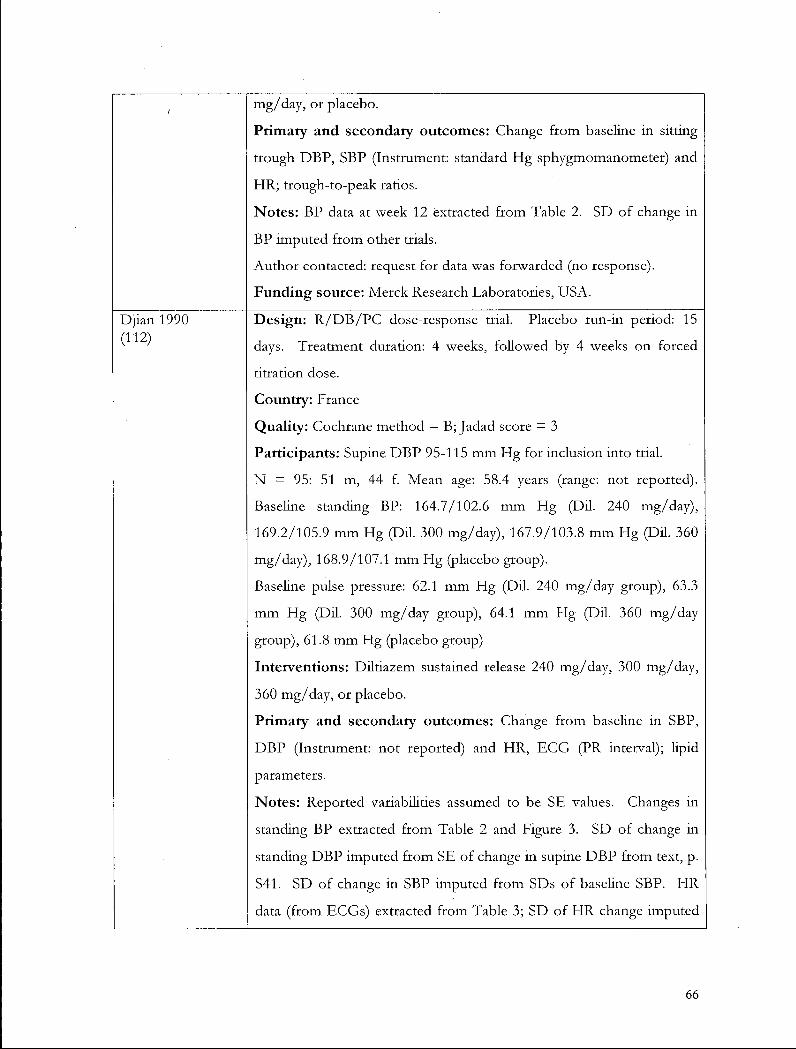
mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
trough D B P , SBP (Instrument: standard H g sphygmomanometer) and
H R ; trough-to-peak ratios.
Notes: B P data at week 12 extracted from Table 2. SD of change in
BP imputed from other trials.
Author contacted: request for data was forwarded (no response).
Funding source: Merck Research Laboratories, USA.
Djian 1990 (112)
Design: R / D B / P C dose-response trial. Placebo run-in period: 15
days. Treatment duration: 4 weeks, followed by 4 weeks on forced
titration dose.
Country: France
Quality: Cochrane method = B; Jadad score = 3
Participants: Supine D B P 95-115 mm H g for inclusion into trial.
N = 95: 51 m, 44 f. Mean age: 58.4 years (range: not reported).
Baseline standing BP: 164.7/102.6 mm H g (Dil. 240 mg/day),
169.2/105.9 mm Fig (Dil. 300 mg/day), 167.9/103.8 mm H g (Dil. 360
mg/day), 168.9/107.1 mm H g (placebo group).
Baseline pulse pressure: 62.1 mm H g (Dil. 240 mg/day group), 63.3
mm Fig (Dil. 300 mg/day group), 64.1 mm H g (Dil. 360 mg/day
group), 61.8 mm H g (placebo group)
Interventions: Diltiazem sustained release 240 mg/day, 300 mg/day,
360 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in SBP,
D B P (Instrument: not reported) and H R , E C G (PR interval); lipid
parameters.
Notes: Reported variabilities assumed to be SE values. Changes in
standing B P extracted from Table 2 and Figure 3. SD of change in
standing D B P imputed from SE of change in supine D B P from text, p.
S41. SD of change in SBP imputed from SDs of baseline SBP. H R
data (from ECGs) extracted from Table 3; SD of H R change imputed
66

from baseline SDs.
Funding source: Not reported.
Felicetta 1992 (113)
Design: M C / R / D B / P C dose-response trial. Placebo run-in period: 4-
6 weeks. Treatment duration: 4 weeks.
Country: USA
Quality: Cochrane method = B; Jadad score = 3
Participants: Supine D B P 95-110 mm H g for inclusion into trial.
N = 229: 162 m, 67 f. Mean age: 48.8 years (inclusion range: 18-60).
Baseline BP: 146.9/100.0 mm Fig (Dil. 90 mg/day group), 148.4/100.3
mm H g (Dil. 180 mg/day group), 150.9/99.9 mm H g (Dil. 360 mg/day
group), 152.0/101.0 mm H g (Dil. 540 mg/day group), 153.3/100.4
mm H g (placebo group). Baseline pulse pressure: 46.9 mm H g (Dil. 90
mg/day group), 48.1 mm H g (Dil. 180 mg/day group), 51.0 mm H g
(Dil. 360 mg/day group), 51 mm Fig (Dil. 540 mg/day group), 52.9
mm H g (placebo group).
Interventions: Diltiazem C D 90 mg/day, 180 mg/day, 360 mg/day,
540 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
and peak supine SBP, D B P (Instrument: not reported), and H R ; %
satisfactory B P response, defined as supine D B P < 90 mm H g or > 6
mm H g reduction; trough-peak ratios.
Notes: Change in B P and associated SD extracted from Table II.
W D A E reported.
Funding source: Not reported.
Fiddes1994 (114)
Design: M C / R / D B / P C trial. Placebo run-in period: 4 weeks.
Treatment duration: 4 weeks, followed by titration in non-responders
and an additional 8 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 3
Participants: Supine D B P 95-114 mm H g for inclusion into trial.
N = 350: 156 m, 194 f. Mean age: 64.7 years (> 55 for inclusion).
67

Baseline standing BP: 157.1/100 mm H g (diltiazem group) and
157.1/100 mm H g (placebo group). Baseline pulse pressure: 57.1 mm
H g (diltiazem group) and 57.1 mm H g (placebo group).
Interventions: Diltiazem (extended-release) 240 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
supine/standing D B P , SBP, and H R ; % achieving BP < 90 mm Hg;
lab tests.
Notes: Change in supine D B P data at week 4 extracted from Figure 1.
SD of D B P change imputed using pooled SD calculated from p value.
W D A E reported but cannot determine i f they occurred before or after
titration in non-responders.
Attempted to contact author: no response.
Fund ing source: Not reported.
Herpin 1990 (115)
Des ign: R / D B / P C trial. Placebo run-in period: 1 week. Treatment
duration: 3 weeks.
Country: France
Quality: Cochrane method = B; Jadad score — 3
Participants: Supine D B P 95-115 mm Fig for inclusion into trial.
N = 38 (efficacy analysis): 16 m, 22 f. Mean age: 51.4 years (inclusion
range: 18 - 75). Baseline BP: 164/101 mm H g (Dil. 240 mg/day
group), 163/102 mm Fig (Dil. 300 mg/day group), and 163/100 mm
Fig (placebo group).
Baseline pulse pressure: 63 mm H g (Dilt. 240 mg/day group), 61 mm
H g (Dilt. 300 mg/day group), and 63 mm H g (placebo group).
Interventions: Diltiazem SR 240 mg/day, 300 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in clinic
supine D B P , SBP (Instrument: H g manometer), and ambulatory
S B P / D B P (Instrument: Spacelab monitor).
Notes: Clinic B P data extracted from Table II. SDs of BP change
imputed from endpoint BPs. W D A E reported, but number of patients
initially randomized to each group is not reported.
68

Fund ing source: Not reported.
Meeves 1994 (116)
Des ign: M C / R / D B / P C trial. "Placebo run-in period: 4-6 weeks.
Treatment duration: 4 weeks (forced titration at week 1).
Country: U S A
Quality: Cochrane method = B; Jadad score = 3
Participants: Supine D B P 95-110 mm H g for inclusion into trial.
N = 111: 57 m, 54 f. Mean age: 53.3 years (> 18 for inclusion).
Baseline supine BP: 149.5/99.7 mm H g (Diltiazem group), and
149.3/99.6 mm H g (placebo group).
Baseline pulse pressure: 49.8 mm H g (Diltiazem group), and 49.7 mm
H g (placebo group).
Interventions: Diltiazem C D 180 mg/day (1 week) 300 mg/day (3
weeks), or placebo.
Primary and secondary outcomes: Change from baseline in SBP,
D B P (Instrument: standard H g sphygmomanometer), and H R ; trough-
peak ratios; E C G .
Notes: Change in BP , H R and associated SE data extracted from
Table II. W D A E extracted from text, p. 234.
Fund ing source: Marion Merrell Dow Inc., USA.
Pool 1993 (117)
Design: M C / R / D B / P C trial. Placebo run-in period: 4-6 weeks.
Treatment duration: 6 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 4
Participants: Supine D B P 95-110 mm H g for inclusion into trial.
N = 254: 168 m, 86 f. Mean age: 54.4 years (inclusion range: 18 -70).
Baseline BP: 152.7/99.4 mm H g (diltiazem group) and 152.9/99.9
(placebo group). Baseline pulse pressure: 53.3 (diltiazem group) and
53.0 (placebo group).
Interventions: Diltiazem SR 120 mg/day, hydrochlorthiazide 12.5 mg,
combination diltiazem SR-hydrochlorthiazide 120/12.5 mg/day, or
placebo.
69

Primary and secondary outcomes: Change from baseline in trough
supine/standing SBP, D B P (Instrument: H g sphygmomanometer) and
H R ; E C G ; fasting lab tests; 12-hour B P monitoring at baseline and
week 6.
Notes: Change in supine S B P / D B P and associated SE data extracted
from Table 2. W D A E for each group not reported.
Funding source: Marion Merrell Dow Inc., USA.
Prisant 2000 (119)
Design: M C / R / D B / P C trial with 3 x 4 factorial design. Placebo run-
in period: 4 weeks. Treatment duration: 6 weeks (forced titration at
week 1.)
Country: U S A
Quality: Cochrane method = B; Jadad score = 3
Participants: Supine D B P 95-114 mm H g for inclusion into trial.
N = 329: 198 m, 131 f Mean age: 51.6 years (range: 19 - 86).
Baseline BP: 153.4/99.7 mm Fig (Dilt. 120 mg/day group),
149.9/100.5 mm H g (Dilt. 180 mg/day group), 149.7/99.3 mm H g
(Dilt. 240 mg/day group), 153.3/99.6 mm H g (Dilt. 360 mg/day
group), and 150.7/99.8 mm H g (placebo group)
Baseline pulse pressure: 53.7 mm H g (Dilt. 120 mg/day group), 49.4
mm H g (Dilt. 180 mg/day group), 50.4 mm H g (Dilt. 240 mg/day
group), 53.7 mm Fig (Dilt. 360 mg/day group), and 50.9 mm H g
(placebo group).
Interventions: Diltiazem X R 120 mg/day, 180 mg/day, 240 mg/day,
360 mg/day, indapamide 1.25 mg/day, 2.5 mg/day, or diltiazem X R +
indapamide combination 120/1.25, 180/1.25, 240/1.25, 120/2.5,
180/2.5, 240/2.5 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in supine
clinic SBP, D B P (Instrument: not reported) and ambulatory BP
(Instrument: SpaceLabs); hematologic, serum chemistry and urinalysis
testing; E C G .
Notes: Change in supine SBP and D B P extracted from Table 3. SDs
70

of BP change imputed from other trials. W D A E from each group not
reported.
Fund ing source: Rhone-Poulenc Rorer, Inc., USA.
Weir 1992 (119)
Design: M C / R / D B / P C trial. Placebo run-in period: 4-6 weeks.
Treatment duration: 12 weeks (3 forced titration periods of 4 weeks
each.)
Country: U S A
Quality: Cochrane method = B; Jadad score = 3
Participants: Supine D B P 95-110 mm H g for inclusion into trial.
N - 298 (efficacy analysis N=274): 179 m, 95 f. Mean age: 53.5 years.
Baseline BP: 150.1/99.8 mm H g (diltiazem group) and 152.7/99.5 mm
H g (placebo group).
Baseline pulse pressure: 50.3 (diltiazem group) and 53.2 (placebo
group).
Interventions: Diltiazem SR 60 mg/day (4 weeks) 90 mg/day (4
weeks) -^120 mg/day (4 weeks); hydrochlorthiazide 6.25 (8 weeks)
12.5 mg/day (4 weeks); diltiazem SR/hydrochlorthiazide 60/6.25
mg/day (4 weeks) -> 90/6.25 mg/day (4 weeks) ~> 120/12.5 mg/day
(4 weeks), or placebo.
Primary and secondary outcomes: Change from baseline in
supine/standing SBP, D B P (Instrument: H g sphygmomanometer) and
H R ; % responders, defined as supine D B P < 90 mm H g and/or
decrease > 10 mm Hg.
Notes: Change in supine D B P and SBP and associated SE data were
extracted from Figure 3 and 4.
Fund ing source: Marion Merrell Dow Inc., USA.
Whelton 1992 (120)
Des ign: M C / R / D B / P C trial. Placebo run-in period: 4 weeks.
Treatment duration: 4 weeks.
Country: USA
Quali ty: Cochrane method = B; Jadad score = 3
Participants: Supine D B P 95-114 mm H g for inclusion into trial.
71
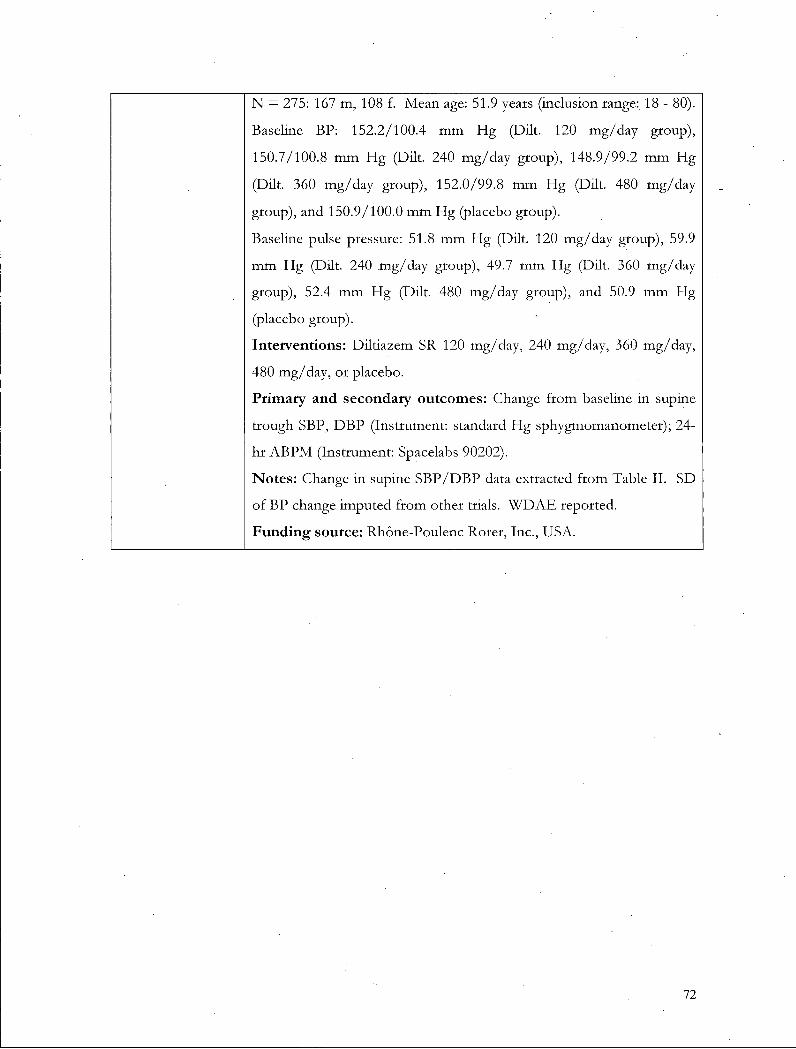
N = 275: 167 m, 108 f. Mean age: 51.9 years (inclusion range: 18 - 80).
Baseline BP: 152.2/100.4 mm H g (Dilt 120 mg/day group),
150.7/100.8 mm H g (Dilt. 240 mg/day group), 148.9/99.2 mm H g
(Dilt. 360 mg/day group), 152.0/99.8 mm H g (Dilt. 480 mg/day
group), and 150.9/100.0 mm H g (placebo group).
Baseline pulse pressure: 51.8 mm H g (Dilt. 120 mg/day group), 59.9
mm H g (Dilt. 240 mg/day group), 49.7 mm H g (Dilt. 360 mg/day
group), 52.4 mm H g (Dilt. 480 mg/day group), and 50.9 mm H g
(placebo group).
Interventions: Diltiazem SR 120 mg/day, 240 mg/day, 360 mg/day,
480 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in supine
trough SBP, D B P (Instrument: standard H g sphygmomanometer); 24-
hr A B P M (Instrument: Spacelabs 90202).
Notes: Change in supine S B P / D B P data extracted from Table II. SD
of B P change imputed from other trials. W D A E reported.
Funding source: Rhone-Poulenc Rorer, Inc., USA.
72

Table 16: Felodipine - Characteristics of included studies
Study Study Description
Black 2001 (121)
Design: M C / R / D B / P C trial. Washout period: < 8 weeks. Placebo
run-in period: 4 weeks. Treatment duration: 8 weeks, followed by
titration in non-responders -^ total duration of follow-up: 52 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 4
Participants: sitting SBP 140-159 mm H g and D B P < 90 mm Fig for
inclusion into trial (isolated systolic hypertension).
N = 171: 84 m, 87 f. Mean age: 66 years (> 55 for inclusion).
Baseline BP: 149/83 mm H g (Fel. group), and 150/84 mm H g
(placebo group). Baseline pulse pressure: 66 mm H g (Fel. group), and
66 mm H g (placebo group).
Interventions: Felodipine E R 2.5 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
sitting SBP at week 52 (last observation carried forward), D B P
(Instrument: H g sphygmomanometer), FIR, quality of life
measurements, weight, E C G measurements.
Notes: Change in SBP at week 8 data extracted from Figure 1. SD of
SBP change imputed from other trials. W D A E reported but cannot
determine i f they occurred before or after titration in non-responders.
Funding source: AstraZeneca, L P , USA.
Felodipine Co-op 1987 (122)
[Duplication publication: Hamilton 1987a (123)]
Design: M C / R / D B / P C trial. Washout period: 4 weeks. Placebo run-
in period: 2 weeks. Treatment duration: 8 weeks.
Country: U K
Quality: Cochrane method = B; Jadad score = 3
Participants: D B P 95-110 mm H g for inclusion into trial.
N = 109: 59 m, 50 f. Mean age: 52 years (range: 20-70 for inclusion).
Baseline BP: 166.8/104.4 mm H g (Fel. 5 mg/d group), 165.9/104.4
mm H g (Fel. 10 mg/d group), 171.2/105.4 mm H g (Fe. 20 mg/d
73

group), and 162.9/104.4 mm H g (placebo group). Baseline pulse
pressure: 62.4 mm H g (Fel. 5 mg/d group), 61.5 mm H g (Fel. 10 mg/d
group), 65.8 mm H g (Fel. 20 mg/d group), 58.5 mm H g (placebo
group).
Interventions: Felodipine 5 mg/day, 10 mg/day, 20 mg/day
(administered in two divided doses/day), or placebo.
Primary and secondary outcomes: Change from baseline in
supine/standing BP , H R (Instrument: Hawksley random zero
sphygmomanometer), ankle circumference, bodyweight.
Notes: standing B P / H R and SD data (12 hours postdose) from Week
8 extracted from Figure 4. W D A E extracted from Table V .
Funding source: Not reported.
Fagan 1997 (124)
Design: M C / R / D B / P C study. Placebo run-in period: 2-4 weeks.
Treatment duration: 9 weeks (dose titration at week 3 and 6 in non-
responders).
Country: U S A
Quality: Cochrane method = B; Jadad score = 4
Participants: Sitting D B P 95-115 mm H g for inclusion into trial.
N = 243: 163 m, 80 f. Mean age: 58.2 years (range: 26-83). Baseline
BP: 159/102 mm H g (Fel. group) and 159/101 mm H g (placebo
group). Baseline pulse pressure: 57 mm H g (Fel. group) and 58 mm
Fig (placebo group).
Interventions: Felodipine E R 2.5 mg/day or placebo.
Primary and secondary outcomes: Change from baseline in sitting
trough SBP, D B P (Instrument: standard H g sphygmomanometer), FIR,
body weight.
Notes: B P data at week 3 extracted from Table 2. SDs of BP change
were imputed from p values. Patients stratified by age: older (>65
years) vs. younger patients (< 60 years). W D A E reported but cannot
determine i f they occurred before or after titration in non-responders.
Funding source: Merck, Sharp and Dohme, USA.
74

Fetter 1994 (125)
Design: R / D B / P C trial. Placebo run-in period: 2 weeks. Treatment
duration: 12 weeks.
Country: Germany
Quality: Cochrane method = B; Jadad "score = 3
Participants: WFIO stage I-II hypertension (DBP > 115 mm H g for
inclusion into trial.
N = 71: m / f ratio not reported. Mean age: 47.5 years (range: 30 - 65).
Baseline BP: 164/97 mm Fig (Fel. group) and 161/98 mm Fig (placebo
group).
Baseline pulse pressure: 67 mm H g (Fel. group) and 63 mm H g
(placebo group).
Interventions: Felodipine 10 mg/day or placebo.
Primary and secondary outcomes: Blood flow velocity in extra- and
intracranial arteries, B P (Instrument: not reported).
Notes: Published in German. BPs extracted from Table 1. SDs of B P
change imputed from other trials. W D A E from each dosage group not
reported.
Funding source: Astra Chemicals GmbPI, Germany.
Gradman 1997 (126)
Design: M C / R / D B / P C factorial design study. Placebo run-in period:
4 weeks. Treatment duration: 8 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 3
Participants: Sitting D B P 95-115 mm H g for inclusion into trial.
N = 707: 457 m, 250 f. Mean age: 53.5 years. Baseline BP:
155.5/101.9 mm H g (all patients). Baseline pulse pressure: 53.6 mm
Hg-
Interventions: Felodipine E R 2.5 mg/day, 5 mg/day, 10 mg/day,
enalapril 5 mg/day, 20 mg/day, felodipine E R + enalapril combination
2.5/5, 2.5/20, 5/5, 5/20, 10/5, 10/20 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
sitting D B P , SBP (Instrument: not reported - auscultatory method),
75
and H R .
Notes: Change in B P data extracted from Figure 1 and 2. SDs of
change in SBP imputed from baseline SBP value; SD of change in
D B P imputed from other trials. W D A E from each dosage group not
reported.
Attempted to contact author — no response.
Funding source: Astra Merck, USA.
Kiesewetter 1994 (127)
Design: R / D B / P C trial. Placebo run-in period: 2 weeks. Treatment
duration: 4 weeks.
Country: Germany
Quality: Cochrane method = B; Jadad score — 4
Participants: D B P 90-120 mm H g and SBP > 140 mm H g for
inclusion into trial. N — 104: 74 m, 30 f. Mean age: 56.2 years (range:
45-65 for inclusion). Baseline BP: 154/94 mm H g (Fel. group) and
152/93 mm H g (placebo group). Baseline pulse pressure: 60 mm H g
(Fel. group) and 59 mm Fig (placebo group).
Interventions: Felodipine 10 mg/day or placebo.
Primary and secondary outcomes: Peak supine SBP, D B P
(Instrument: sphygmomanometer) and HR; haemorheological
parameters; urinalysis.
Notes: BPs and HRs extracted from text, page 361. SD of B P change
imputed from SD of week 4 BPs.
Author contacted — dose and W D A E information obtained.
Funding source: Not reported.
Liedholm 1989 (128)
Design: M C / R / D B / P C trial. Washout period: 4 weeks. Placebo run-
in period: 4 weeks. Treatment duration: 4 weeks.
Country: Sweden
Quality: Cochrane method — B; Jadad score = 4
Participants: Supine D B P 95-120 mm H g for inclusion into trial.
N = 151: 147 m, 4 f. Median age: 51.8 years (range: 38-68). Baseline
BP: 156.2/99.5 mm H g (Fel. 10 mg/day group), 157.6/101.4 mm H g
76

(Fel. 20 mg/day group), and 158.6/101.4 mm H g (placebo group).
Baseline pulse pressure: 56.7 mm H g (Fel. 10 mg/day group), 56.2 mm
H g (Fel. 20 mg/day group), and 57.2 mm H g (placebo group).
Interventions: Felodipine E R 10 mg/day, 20 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in peak
and trough supine/standing SBP, D B P (Instrument: H g
sphygmomanometer) and H R ; blood and urine lab tests.
Notes: Change in trough supine BP , H R data and associated SDs
extracted from Table 2. W D A E reported.
Fund ing source: A B Hassle (subsidiary of A S T R A Pharmaceuticals),
Sweden.
Scholze 1999 (129)
Design: M C / R / D B / P C 3 x 4 factorial design, combination dose-
finding study. Washout period: Not reported. Treatment duration: 6
weeks.
Country: Germany
Quality: Cochrane method = B; Jadad score = 4
Participants: W H O class f-II (mild-to-moderate hypertension) for
inclusion into trial. N = 507: 327 m, 180 £ Mean age: 50.2 years
(range: 18-73). Baseline BP: 165.4/106.7 mm H g (Fel. 5 mg/day
group), 166.0/107.0 mm Fig (Fel. 10 mg/day group), and 166.6/107.3
mm Fig (placebo group). Baseline pulse pressure: 58.7 mm H g (Fel. 5
mg/day group), 59 mm Fig (Fel. 10 mg/day group), and 59.3 mm H g
(placebo group).
Interventions: Felodipine E R 5mg/day, 10 mg/day, ramipril 2.5
mg/day, 5 mg/day, 10 mg/day, all ramipril-felodipine E R
combinations thereof, or placebo.
Primary and secondary outcomes: Change from baseline in trough
standing/supine SBP, D B P (Instrument: H g sphygmomanometer), and
a composite supine-standing mean arterial pressure.
Notes: Change in supine BPs and associated SEMs extracted from
Table 1.
77

Author contacted - baseline BPs, number of patients in intention-to-
treat population, W D A E in each group obtained from Aventis Pharma.
Fund ing source: Hoechst, Germany.
van Ree 1996 (130)
Design: M C / R / D B / P C study. Placebo run-in period: 4 weeks.
Treatment duration: 6 weeks.
Country: Netherlands
Quality: Cochrane method = B; Jadad score = 4
Participants: Sitting D B P 100-115 mm H g and SBP 140-200 mm H g
for inclusion into trial.
N = 129: 38 m, 91 f. Mean age: 63 years (range: 50 — 80 for inclusion).
Baseline BP: 175/104 mm H g (Fel. 2.5 mg/day group) mm Hg,
173/105 mm H g (Fel. 5 mg/day group), 177/105 mm H g (placebo
group).
Baseline pulse pressure: 71 mm H g (Fel. 2.5 mg/day group), 68 mm
H g (Fel. 5 mg/day group), 72 mm H g (placebo group).
Interventions: Felodipine E R 2.5 mg/day, 5 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
sitting B P (Instrument: random zero sphygmomanometer — Hawksley),
FIR; 24-hour A B P M .
Notes: Change in BP and associated SD (at week 6) data extracted
from Figure 1. W D A E extracted from text, p. 615.
Fund ing source: Astra Pharmaceutica B V , Netherlands.
Weber 1994 (131)
Design: M C / R / D B / P C study. Placebo run-in period: 4 weeks.
Treatment duration: 8 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 4
Participants: Sitting D B P 95-115 mm H g for inclusion into trial.
N = 286: 186 m, 100 f. Mean age: 54-55 years in all groups (range: 24-
75). Baseline BP: 151.4/100.6 mm H g (Fel. 2.5 mg/day group),
147.9/100.6 mm H g (Fel. 5 mg/day group), 153.8/101.2 mm H g (Fel.
10 mg/day group), and 154.4/101.0 mm H g (placebo group).
78

Baseline pulse pressure: 50.8 mm H g (Fel. 2.5 mg/day group), 47.3 mm
H g (Fel. 5 mg/day group), 52.6 mm H g (Fel. 10 mg/day), and 53.4 mm
H g (placebo group).
Interventions: Felodipine E R 2.5 mg/day, 5 mg/day, 10 mg/day, or
placebo.
Primary and secondary outcomes: Change from baseline in peak
and trough sitting D B P , SBP, (Instrument: standard Fig
sphygmomanometer), and HR.
Notes: Change in trough sitting BP extracted from Table 1. SD of BP
change calculated as weighted mean of SD of BP change at week 4 and
8 (extracted from Figure 1 and 2). W D A E extracted fom text, p.348.
Fund ing source: Merck Research Laboratories, USA.
Wester 1991 (132)
[Duplicate publication: Wester 1990-abstract only (133)]
Design: M C / R / D B / P C study. Placebo run-in period: 4 weeks.
Treatment duration: 4 weeks.
Country: U K and Netherlands
Quality: Cochrane method = B; Jadad score = 4
Participants: Supine D B P 95-120 mm H g for inclusion into trial.
N = 183: 88 m, 95 f. Mean age: 53 years (range: 28-65). Baseline
standing BP: 161/105 mm H g (Fel. 5 mg/day group), 158/103 mm H g
(Fel. 10 mg/day group), 164/106 mm H g (Fel. 20 mg/day group), and
165/103 mm Fig (placebo group).
Baseline pulse pressure: 56 mm H g (Fel. 5 mg/day group), 55 mm H g
(Fel. 10 mg/day group), 58 mm H g (Fel. 20 mg/day group), and 62
mm H g (placebo group).
Interventions: Felodipine E R 5 mg/day, 10 mg/day, 20 mg/day, or
placebo.
Primary and secondary outcomes: Change from baseline in trough
supine and standing SBP, D B P (Instrument: random zero
sphygmomanometer - Hawksley), and HR.
Notes: Standing BPs extracted from Table 1. SD of change in SBP
imputed from week 4 SBP values. SD of change in standing D B P
79
imputed from S D of change in supine D B P given in Figure 1. W D A E
extracted from text, p. 279.
Funding source: Not reported.
80

Table 17: Isradipine - Characteristics of inc luded studies
Arosio 1993 (134)
Design: R / D B / P C crossover study. Washout period: at least 3
weeks. Treatment duration: 2 months (each treatment period was 1
month).
Country: Italy
Quality: Cochrane method = B; Jadad score = 2
Participants: "mild to moderate essential hypertension" for inclusion
into trial. N =16: 12 m, 4f. Mean age: 41 years (range: 30-45).
Baseline BP: 157/102 mm H g (Israd. group) and 156/101 mm H g
(placebo group). Baseline pulse pressure: 55 (Israd. group) and 55
(placebo group).
Interventions: Isradipine SR 5 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in supine
SBP, D B P , H R (Instrument: automatic device - Dinamap); brachial
artery hemodynamics.
Notes: Pre-crossover data B P data (at week 4) extracted from Table 1.
SDs of change in BP imputed from week 4 SDs of B P values. H R data
and W D A E not reported.
Fund ing source: Not reported.
Burger 1993 (135)
Design: M C / R / D B / P C trial. Placebo run-in: 2 weeks. Treatment
duration: 3 weeks.
Country: Germany
Quality: Cochrane method — B; Jadad score = 3
Participants: D B P 100-115 mm H g for inclusion into trial.
N = 37: 11 m, 18 f. Mean age: 56 years (range: 42 - 75).
Baseline BP: 171/110 mm H g (Israd. group), 163/106 mm H g
(placebo group). Baseline pulse pressure: 61 mm H g (Israd. group),
and 57 mm H g (placebo group).
Interventions: Isradipine SRO 10 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in SBP,
D B P (Instrument: sphygmomanometer), H R ; A B P M (Instrument:
81

SpaceLabs).
Notes: Published in German. Office BPs and HRs extracted from
Table 2. SDs of B P / H R change imputed from other trials.
Fund ing source: Not reported.
Chyrsant 1995a (136)
[Duplicate publication: Chrysant 1995b (137)]
Design: M C / R / D B / P C trial. Placebo run-in period: 3 weeks.
Treatment duration: 6 weeks (weekly forced titration in 5 mg
increments to target dose in active treatment groups).
Country: U S A
Quality: Cochrane method = B; Jadad score = 3
Participants: Sitting D B P 100-114 mm H g for inclusion into trial.
N = 402 (384 Intent-to-treat): approx. 75% "white males". Mean age:
56 (range: not reported).
Baseline BP: 161/104 mm Fig (5 mg group), 158/104 mm H g (10 mg
group), 156/104 (15 mg group), 156/104 (20 mg group), 158/104 mm
H g (placebo group). Baseline pulse pressure: 57 (5 mg group), 54 (10
mg group), 52 (15 mg group), 52 (20 mg group), and 54 (placebo
group).
Interventions: Isradipine CR 5 mg/day (6 weeks), 10 mg/day (5
weeks), 15 mg/day (4 weeks), 20 mg/day (3 weeks), or placebo.
Primary and secondary outcomes: Change from baseline in
sitting/supine/standing SBP, D B P (Instrument: Not reported -
auscultatory method), and FIR.
Notes: Change in B P data extracted from Figure 1. SD of changes in
S B P / D B P not available and were imputed using data from other trials.
W D A E in each group not reported.
Author contacted: baseline BPs obtained.
Fund ing source: Sandoz Research Institute, USA.
Holmes 1993 (138)
Design: M C / R / D B / P C trial. Placebo run-in period: 3 weeks.
Treatment duration: 4 weeks.
Country: Not reported.
Quality: Cochrane method = B; Jadad score = 3
82

Participants: Supine D B P 100-120 mm H g for inclusion into trial.
N = 190: 84 m, 106 f. Mean age: 57 years (range: 21 - 89).
Baseline BP: 176/108 mm H g (Israd. 2.5 mg/day group), 171/107 mm
H g (Israd. 5 mg/day group), 172/107 mm H g (placebo group).
Baseline pulse pressure: 68 mm H g (Israd. 2.5 mg/day group), 64 mm
H g (Israd. 5 mg/day group) and 65 mm H g (placebo group).
Interventions: Isradipine SRO 2.5 mg/day, 5 mg/day, or placebo.
Primary and secondary outcomes: Change from, baseline in sitting
SBP, D B P (Instrument: H g sphymomanometer), and H R — trough.
Notes: unpublished B P / H R / W D A E data extracted from Sandoz
archive files.
Author contacted - B P / H R / W D A E data received.
Fund ing source: Sandoz Pharma, Switzerland.
Italian-Belgian Group 1989 (139)
Design: M C / R / D B / P C trial. Placebo run-in: 3 weeks. Treatment
duration: 5 weeks.
Country: Italy and Belgium
Quality: Cochrane method = B; Jadad score = 3
Participants: supine D B P 100-120 mm H g for inclusion into trial.
N = 178: 85 m, 93 f. Mean age: 60 years (inclusion range: 30 - 85).
Baseline BP: 171/104 mm H g (Israd. 1 mg/day group), 175/105 mm
Tig (Israd. 2.5 mg/day group), 175/105 mm Hg (Israd. 5 mg/day
group), 176/104 mm H g (placebo group). Baseline pulse pressure: 67
mm H g (Israd. 1 mg/day group), 70 mm H g (Israd 2.5 mg/day group),
70 mm H g (Israd. 5 mg/day group), and 72 mm H g (placebo group).
Interventions: Isradipine 1 mg/day, 2.5 mg/day, 5 mg/day, or
placebo.
Primary and secondary outcomes: Change from baseline in supine
and standing SBP, D B P (Instrument: Tig sphygmomanometer), H R ,
Notes: Trough B P s / H R s and associated SDs extracted from Table II.
SDs of SBP change and FIR change imputed from baseline SDs. SD
of D B P change imputed from other trials. W D A E extracted from text,
83
p. 97.
Fund ing source: Not reported.
Kirch 1990 (140)
Des ign: M C / R / D B / P C trial. Placebo run-in: 2 weeks. Treatment
duration: 4 weeks.
Country: Germany
Quality: Cochrane method = B; Jadad score — 4
Participants: Sitting D B P > 105 mm H g for inclusion into trial.
N = 86: 46 m, 37 f (3 patients unaccounted for in demographics table).
Mean age: 58.2 years (> 18 for inclusion).
Baseline BP: 174/109 mm H g (Israd. 2.5 mg/day group), 175/108 mm
H g (Israd. 5 mg/day group), 175/108 (Israd. 10 mg/day group),
176/108 mm H g (placebo group). Baseline pulse pressure: 65 mm H g
(Israd. 2.5 mg/day group), 67 mm H g (Israd. 5 mg/day group), 67 mm
H g (Israd. 10 mg/day group) and 68 mm H g (placebo group).
Interventions: Isradipine 2.5 mg/day, 5 mg/day, 10 mg/day, or
placebo.
Primary and secondary outcomes: Change from baseline in sitting
and standing SBP, D B P (Instrument: sphygmomanometer), and H R
(2-3 hours post-dose).
Notes: sitting BPs extracted from Table 2. SD of B P change imputed
from weighted mean SD of week 3 and 4 BPs. W D A E extracted from
text, p. S56.
Fund ing source: Not reported.
Man in't Veld 1991 (141)
Design: M C / R / D B / P C trial. Placebo run-in: 3-5 weeks. Treatment
duration: 6 weeks.
Country: Not reported. Author from Netherlands
Quality: Cochrane method = B ; Jadad score = 3
Participants: sitting D B P 95-1 f 5 mm Fig for inclusion into trial.
N = 187: 99 m, 88 f. 110 patients received isradipine in the 4-week
selection phase; the remaining 77 patients had received isradipine for
up to 127 weeks before entering study. Mean age: 49 years (range: 23 -
84
65).
Baseline BP: 158/102 mm H g (Israd. group), 160/102 mm H g
(placebo group). Baseline pulse pressure: 56 mm H g (Israd. group),
and 58 mm H g (placebo group).
Interventions: Isradipine 5 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
SBP, D B P (Instrument: H g sphygmomanometer), responder rate
(DBP < 90 mm H g or fall of > 10 mm Hg).
Notes: A l l patients had demonstrated prior reponse to isradipine
treatment prior to trial entry. BPs extracted from Table 1. SDs of B P
change imputed from weighted mean of SDs of week 4 and 6 BPs.
W D A E extracted from text, p. 133S.
Fund ing source: Not reported.
O'Grady 1997 (142)
Design: R / D B / P C trial. Placebo run-in: 2 weeks. Treatment
duration: 4 weeks.
Country: Austria
Quality: Cochrane method = B ; Jadad score = 3
Participants: "mild to moderate hypertension", scintigraphalfy-visible
atherosclerotic lesions of carotid vessels and platelet uptake ratio >1.15
for inclusion into trial.
N = 40: 25 m, 15 f. Mean age: 45 years (range: 28 - 68).
Baseline BP: 134/100 mm H g (group), 136/100 mm H g (placebo
group). Baseline pulse pressure: 34 mm H g (Israd. group), and 36 mm
Fig (placebo group).
Interventions: Isradipine SRO 5 mg/day, or placebo.
Primary and secondary outcomes: Platelet parameters (platelet
uptake ratio, platelet survival), change from baseline in SBP, D B P
(Instrument: not reported), and HR.
Notes: BPs extracted from Fig. 1. SDs of B P change imputed from
SDs of week 6 BPs. W D A E extracted from text, p. 367.
Fund ing source: Not reported.
"85
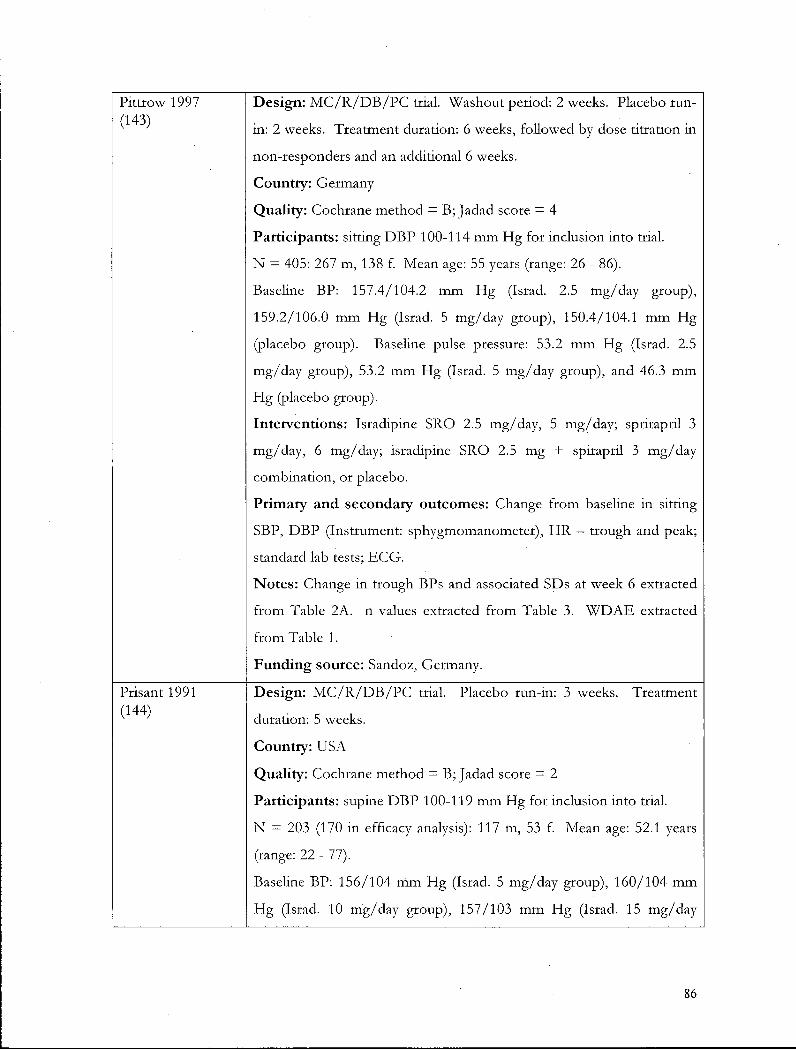
Pittrow 1997 (143)
Design: M C / R / D B / P C trial. Washout period: 2 weeks. Placebo run-
in: 2 weeks. Treatment duration: 6 weeks, followed by dose titration in
non-responders and an additional 6 weeks.
Country: Germany
Quality: Cochrane method = B; Jadad score = 4
Participants: sitting D B P 100-114 mm H g for inclusion into trial.
N = 405: 267 m, 138 f. Mean age: 55 years (range: 26 - 86).
Baseline BP: 157.4/104.2 mm H g (Israd. 2.5 mg/day group),
159.2/106.0 mm H g (Israd. 5 mg/day group), 150.4/104.1 mm Hg
(placebo group). Baseline pulse pressure: 53.2 mm H g (Israd. 2.5
mg/day group), 53.2 mm Pig (Israd. 5 mg/day group), and 46.3 mm
Pig (placebo group).
Interventions: Isradipine SRO 2.5 mg/day, 5 mg/day; sprirapril 3
mg/day, 6 mg/day; isradipine SRO 2.5 mg + spirapril 3 mg/day
combination, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
SBP, D B P (Instrument: sphygmomanometer), FIR — trough and peak;
standard lab tests; E C G .
Notes: Change in trough BPs and associated SDs at week 6 extracted
from Table 2A. n values extracted from Table 3. W D A E extracted
from Table 1.
Fund ing source: Sandoz, Germany.
Prisant 1991 (144)
Des ign: M C / R / D B / P C trial. Placebo run-in: 3 weeks. Treatment
duration: 5 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 2
Participants: supine D B P 100-119 mm H g for inclusion into trial.
N = 203 (170 in efficacy analysis): 117 m, 53 f. Mean age: 52.1 years
(range: 22 - 77).
Baseline BP: 156/104 trim Fig (Israd. 5 mg/day group), 160/104 mm
Fig (Israd. 10 mg/day group), 157/103 mm H g (Israd. 15 mg/day
86

group, 152/104 mm H g (Israd. 20 mg/day group), 150/104 mm H g
(placebo group). Baseline pulse pressure: 52 mm H g (Israd 5 mg/day
group), 56 mm H g (Israd. 10 mg/day group), 54 mm H g (Israd. 15
mg/day group), 49 mm H g (Israd. 20 mg/day group), and 47 mm H g
(placebo group).
Interventions: Isradipine 5 mg/day (5 weeks), 10 mg/day (1 week at 5
mg/day 4 weeks at 10 mg/day), 15 mg/day (1 week at 5mg/day
1 week at 10 mg/day 3 weeks at 15 mg/day), 20 mg/day (1 week at
10 mg/day 1 week at 15 mg/day 3 weeks at 20 mg/day), or
placebo.
Primary and secondary outcomes: Change from baseline in SBP,
D B P (Instrument: not reported); E C G markers of ischemia.
Notes: Peak BPs, HRs, and associated SDs extracted from Table II.
SDs of B P change and H R change imputed from, endpoint BPs /HRs .
Funding source: Not reported.
Youssef 1992 (145)
[Duplicate publication: Youssef 1993 (146)]
Design: R / D B / P C trial. Treatment duration: 8 weeks.
Country: Egypt
Quality: Cochrane method = B; Jadad score = 2
Participants: supine D B P 95-114 mm H g for inclusion into trial.
N = 90: 57 m, 33 f. Mean age: not reported (range: 44 - 68).
Baseline BP: 173/104 mm H g (Israd. group), 178/104 mm H g
(placebo group). Baseline pulse pressure: 69 mm H g (Israd. group),
and 74 mm H g (placebo group).
Interventions: Isradipine 5 mg/day, enalapril 20 mg/day, benazepril
10 mg/day, xipamide 10 mg + triamterine 30 mg/day combination, or
placebo.
Primary and secondary outcomes: Change from baseline in supine
SBP, D B P (Instrument: not reported); serum lipid profile.
Notes: BPs extracted from Table 1 of Youssef 1993 paper. SDs of B P
change imputed from other trials. Reported SDs of B P at baseline and
endpoint were spuriously low.
87

Attempts to contact author unsuccessful.
Fund ing source: Not reported.
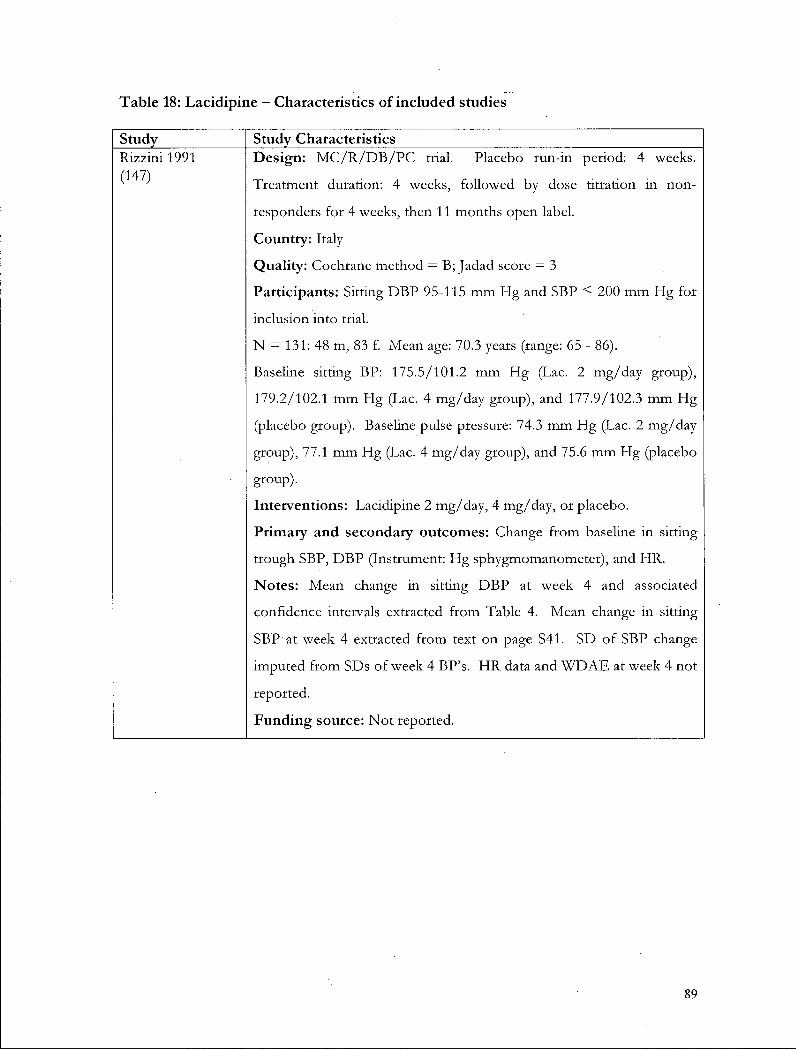
Table 18: Lac id ip ine - Characteristics of inc luded studies
Study Study Characteristics Rizzini 1991 (147)
Design: M C / R / D B / P C trial. Placebo run-in period: 4 weeks.
Treatment duration: 4 weeks, followed by dose titration in non-
responders for 4 weeks, then 11 months open-label.
Country: Italy
Quality: Cochrane method = B; Jadad score = 3
Participants: Sitting D B P 95-115 mm H g and SBP < 200 mm H g for
inclusion into trial.
N = 131: 48 m, 83 f. Mean age: 70.3 years (range: 65 - 86).
Baseline sitting BP: 175.5/101.2 mm H g (Lac. 2 mg/day group),
179.2/102.1 mm H g (Lac. 4 mg/day group), and 177.9/102.3 mm H g
(placebo group). Baseline pulse pressure: 74.3 mm H g (Lac. 2 mg/day
group), 77.1 mm H g (Lac. 4 mg/day group), and 75.6 mm H g (placebo
group).
Interventions: Lacidipine 2 mg/day, 4 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
trough SBP, D B P (Instrument: H g sphygmomanometer), and H R .
Notes: Mean change in sitting D B P at week 4 and associated
confidence intervals extracted from Table 4. Mean change in sitting
SBP at week 4 extracted from text on page S4f. SD of SBP change
imputed from SDs of week 4 BP's. H R data and W D A E at week 4 not
reported.
Fund ing source: Not reported.
89
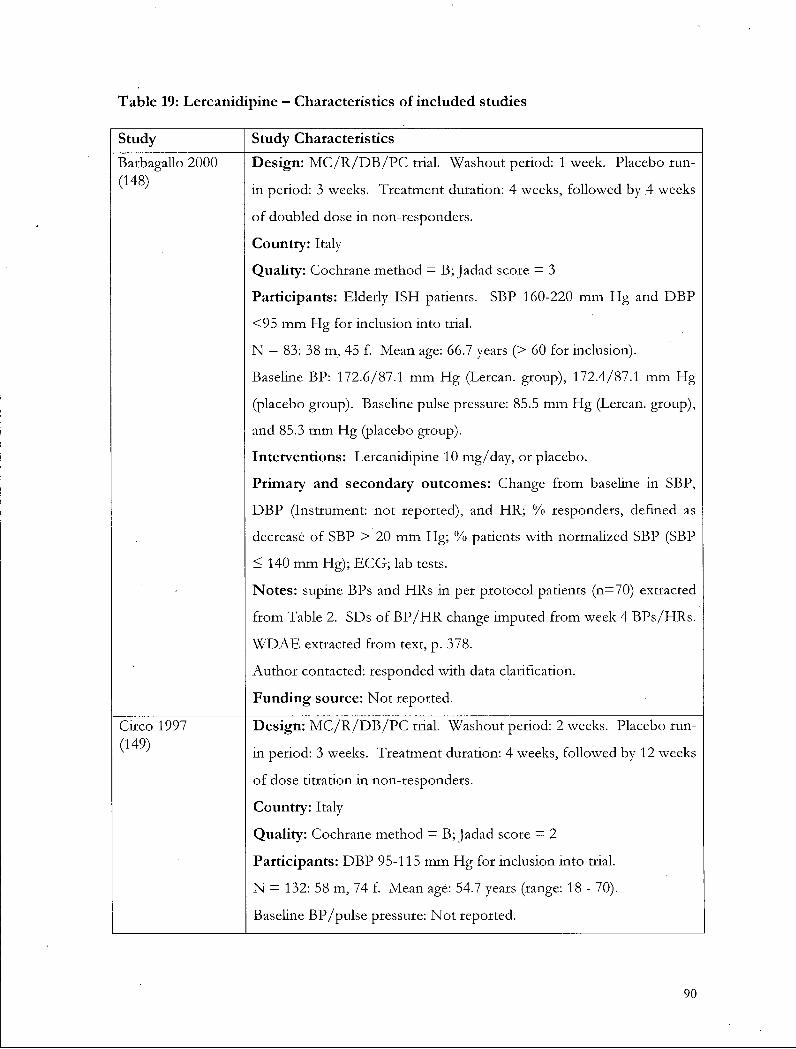
Table 19: Lercanidip ine - Chatacteristics of included studies
Study Study Characteristics
Barbagallo 2000 (148)
Design: M C / R / D B / P C trial. Washout period: 1 week. Placebo run-
in period: 3 weeks. Treatment duration: 4 weeks, followed by .4 weeks
of doubled dose in non-responders.
Country: Italy
Quality: Cochrane method = B ; Jadad score = 3
Participants: Elderly ISH patients. SBP 160-220 mm H g and D B P
<95 mm H g for inclusion into trial.
N = 83: 38 m, 45 f. Mean age: 66.7 years (> 60 for inclusion).
Baseline BP: 172.6/87.1 mm H g (Lercan. group), 172.4/87.1 mm H g
(placebo group). Baseline pulse pressure: 85.5 mm H g (Lercan. group),
and 85.3 mm H g (placebo group).
Interventions: Lercanidipine 10 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in SBP,
D B P (Instrument: not reported), and H R ; % responders, defined as
decrease of SBP > 20 mm Hg; % patients with normalized SBP (SBP
< 140 mm Hg); E C G ; lab tests.
Notes: supine BPs and HRs in per protocol patients (n=70) extracted
from Table 2. SDs of B P / H R change imputed from week 4 B P s / H R s .
W D A E extracted from text, p. 378.
Author contacted: responded with data clarification.
Fund ing source: Not reported.
Grco 1997 (149)
Design: M C / R / D B / P C trial. Washout period: 2 weeks. Placebo run-
in period: 3 weeks. Treatment duration: 4 weeks, followed by 12 weeks
of dose titration in non-responders.
Country: Italy
Quality: Cochrane method = B; Jadad score — 2
Participants: D B P 95-115 mm H g for inclusion into trial.
N = 132: 58 m, 74 f. Mean age: 54.7 years (range: 18-70).
Baseline BP/pulse pressure: Not reported.
90
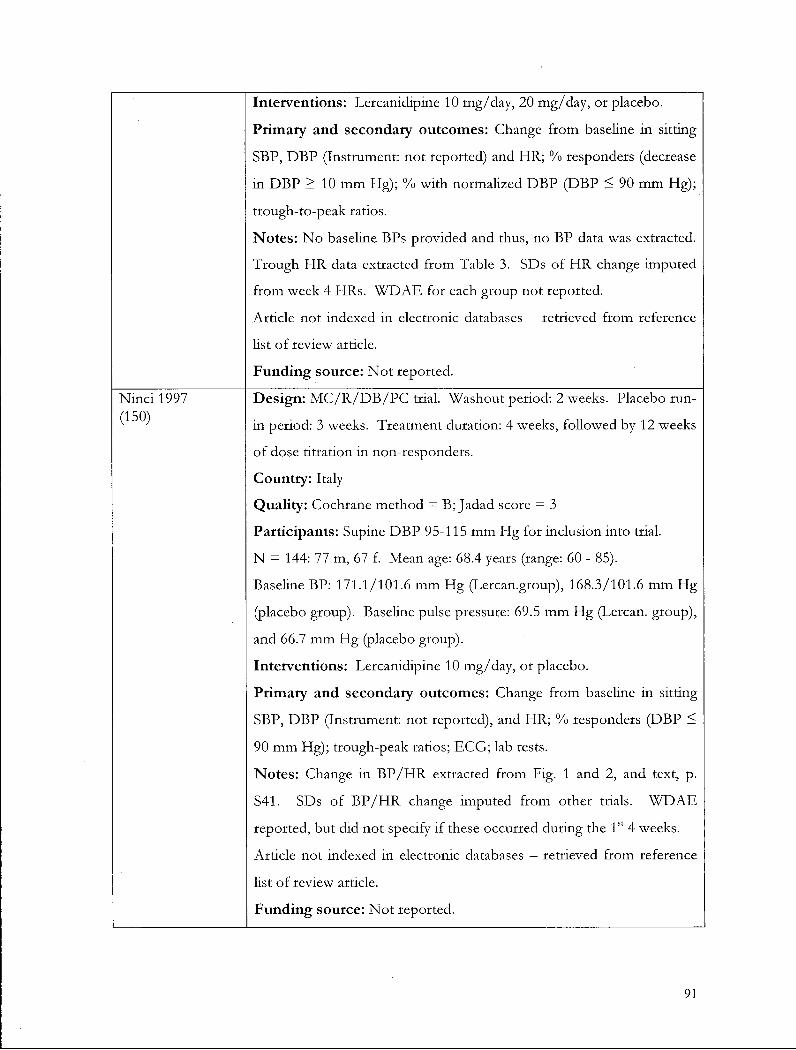
Interventions: Lercanidipine 10 mg/day, 20 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
SBP, D B P (Instrument: not reported) and H R ; % responders (decrease
in D B P > 10 mm Hg); % with normalized D B P (DBP < 90 mm Hg);
trough-to-peak ratios.
Notes: N o baseline BPs provided and thus, no B P data was extracted.
Trough H R data extracted from Table 3. SDs of H R change imputed
from week 4 HRs. W D A E for each group not reported.
Article not indexed in electronic databases — retrieved from reference
list of review article.
Fund ing source: Not reported.
Ninci 1997 (150)
Design: M C / R / D B / P C trial. Washout period: 2 weeks. Placebo run-
in period: 3 weeks. Treatment duration: 4 weeks, followed by 12 weeks
of dose titration in non-responders.
Country: ftaly
Quali ty: Cochrane method = B ; Jadad score = 3
Participants: Supine D B P 95-115 mm H g for inclusion into trial.
N = 144: 77 m, 67 f. Mean age: 68.4 years (range: 60 - 85).
Baseline BP: 171.1/101.6 mm H g g_ercan.group), 168.3/101.6 mm H g
(placebo group). Baseline pulse pressure: 69.5 mm H g (Lercan. group),
and 66.7 mm H g (placebo group).
Interventions: Lercanidipine tO mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
SBP, D B P (Instrument: not reported), and H R ; % responders (DBP <
90 mm Hg); trough-peak ratios; E C G ; lab tests.
Notes: Change in B P / H R extracted from Fig. f and 2, and text, p.
S41. SDs of BP /P fR change imputed from other trials. W D A E
reported, but did not specify i f these occurred during the 1" 4 weeks.
Article not indexed in electronic databases - retrieved from reference
list of review article.
Fund ing source: Not reported.
91

Omboni 1998 (151)
Des ign: M C / R / D B / P C trial. Washout period: 2 weeks. Placebo run-
in period: 3 weeks. Treatment duration: 4 weeks.
Country: Italy
Quality: Cochrane method = B; Jadad score = 3
Participants: Supine D B P 90-109 mm H g for inclusion into trial.
N = 243: 156 m, 87 f. Mean age: 51 years (range: not reported).
Baseline supine BP: 154/98 mm H g (Lercan. 2.5 mg/day group),
155/99 mm H g (Lercan. 5 mg/day group), 156/99 mm H g (Lercan. 10
mg/day group), 155/99 mm H g (placebo group). Baseline pulse
pressure: 56 mm H g (Lercan. 2.5 mg/day group), 56 mm H g (Lercan. 5
mg/day group), 57 mm H g (Lercan. 10 mg/day group), and 56 mm H g
(placebo group).
Interventions: Lercanidipine 2.5 mg/day, 5 mg/day, 10 mg/day, or
placebo.
Primary and secondary outcomes: Change from baseline in supine
SBP, D B P (Instrument: standard H g sphygmomanometer) and H R ; %
responders, defined as D B P < 85 mm H g or D B P reduction > 10 mm
Hg; 24-hr A B P M (Instrument: Spacelabs 90207).
Notes: Change in BP and associated SDs extracted from Fig. 1.
W D A E extracted from text, p. 1836.
Fund ing source: Recordati S.p.A., Italy.
Rimoldi 1993 (152)
Design: M C / R / D B / P C trial. Washout period: 1 week. Placebo run-
in period: 3 weeks. Treatment duration: 4 weeks.
Country: Italy
Quality: Cochrane method = B ; Jadad score = 1
Participants: Supine D B P 95-114 mm H g for inclusion into trial.
N = 152: 67 m, 85 f. Mean age: 56.3 years (range: 21 - 70).
Baseline D B P : 101.3 mm H g (Lercan. tab. group), 101.5 (Lercan.
capsule group), 101.3 mm H g (placebo group). Baseline SBP/pulse
pressure: not reported/cannot be calculated.
Interventions: Lercanidipine tablets 10 mg/day (1 week) 20
92
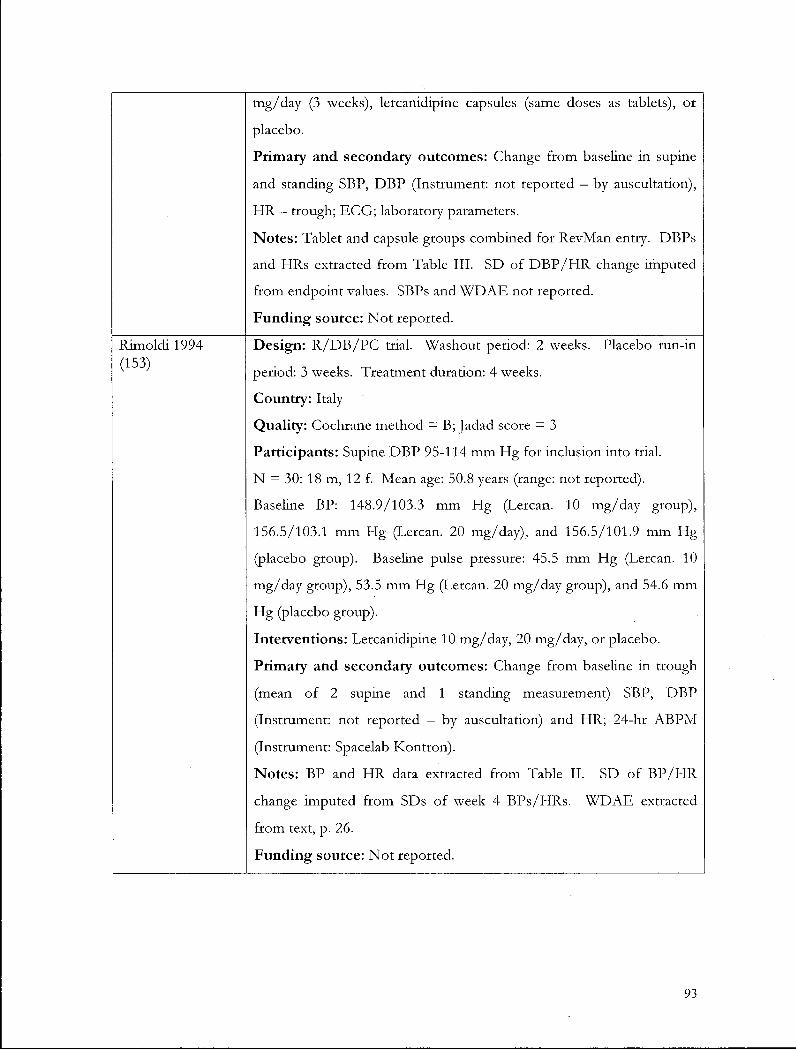
mg/day (3 weeks), lercanidipine capsules (same doses as tablets), or
placebo.
Primary and secondary outcomes: Change from baseline in supine
and standing SBP, D B P (Instrument: not reported — by auscultation),
H R — trough; E C G ; laboratory parameters.
Notes: Tablet and capsule groups combined for RevMan entry. DBPs
and HRs extracted from Table III. SD of D B P / H R change imputed
from endpoint values. SBPs and W D A E not reported.
Fund ing source: Not reported.
Rimoldi 1994 (153)
Design: R / D B / P C trial. Washout period: 2 weeks. Placebo run-in
period: 3 weeks. Treatment duradon: 4 weeks.
Country: Italy
Quality: Cochrane method = B; Jadad score = 3
Participants: Supine D B P 95-114 mm H g for inclusion into trial.
N = 30: 18 m, 12 f. Mean age: 50.8 years (range: not reported).
Baseline BP: 148.9/103.3 mm H g (Lercan. fO mg/day group),
156.5/103.1 mm H g (Lercan. 20 mg/day), and 156.5/101.9 mm H g
(placebo group). Baseline pulse pressure: 45.5 mm H g (Lercan. 10
mg/day group), 53.5 mm H g (Lercan. 20 mg/day group), and 54.6 mm
H g (placebo group).
Interventions: Lercanidipine 10 mg/day, 20 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
(mean of 2 supine and f standing measurement) SBP, D B P
(fnstrument: not reported — by auscultation) and FfR; 24-hr A B P M
(fnstrument: Spacelab Kontron).
Notes: BP and H R data extracted from Table II. SD of B P / H R
change imputed from SDs of week 4 BPs /HRs . W D A E extracted
from text, p. 26.
Fund ing source: Not reported.
93
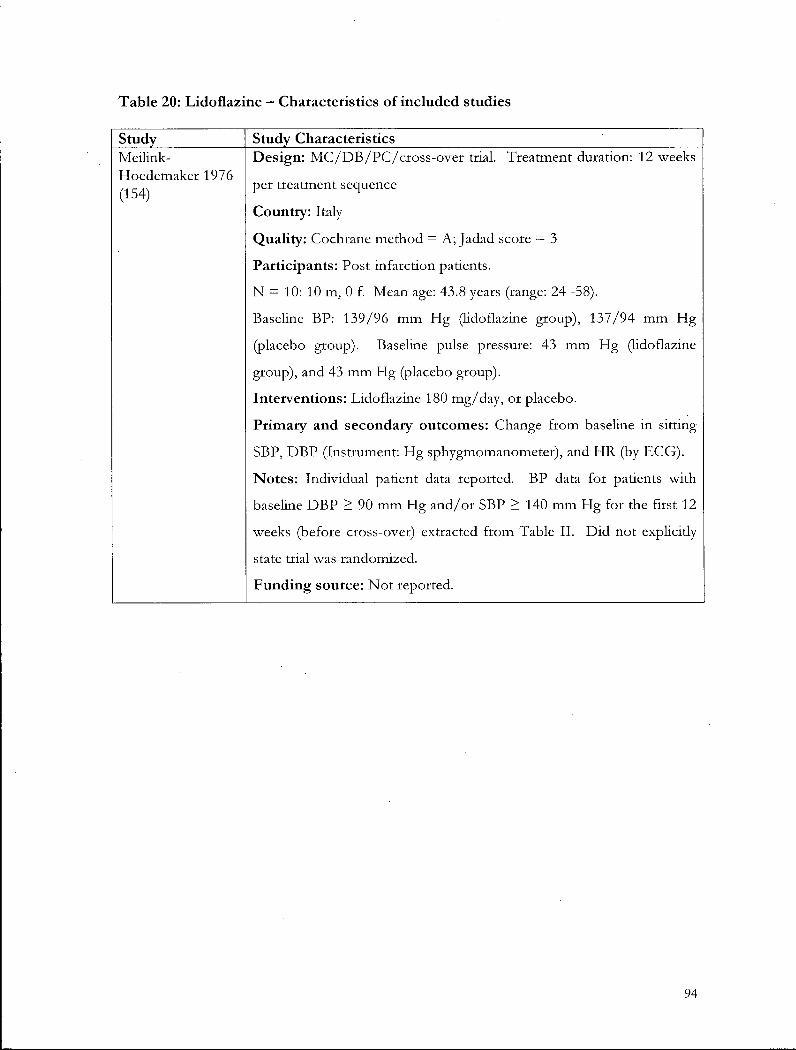
Table 20: L idof laz ine - Characteristics of included studies
Study Study Characteristics Meilink-Hoedemaker 1976 (154)
Design: M C / D B / P C / c r o s s - o v e r trial. Treatment duration: 12 weeks
per treatment sequence
Country: Italy
Quality: Cochrane method = A ; Jadad score = 3
Participants: Post-infarction patients.
N = 10: 10 m, 0 f. Mean age: 43.8 years (range: 24 -58).
Baseline BP: 139/96 mm H g (lidoflazine group), 137/94 mm H g
(placebo group). Baseline pulse pressure: 43 mm H g (lidoflazine
group), and 43 mm H g (placebo group).
Interventions: Lidoflazine 180 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
SBP, D B P (Instrument: H g sphygmomanometer), and H R (by E C G ) .
Notes: Individual patient data reported. B P data for patients with
baseline D B P > 90 mm H g and/or SBP > 140 mm H g for the first 12
weeks (before cross-over) extracted from Table II. D i d not explicitiy
state trial was randomized.
Fund ing source: Not reported.
94
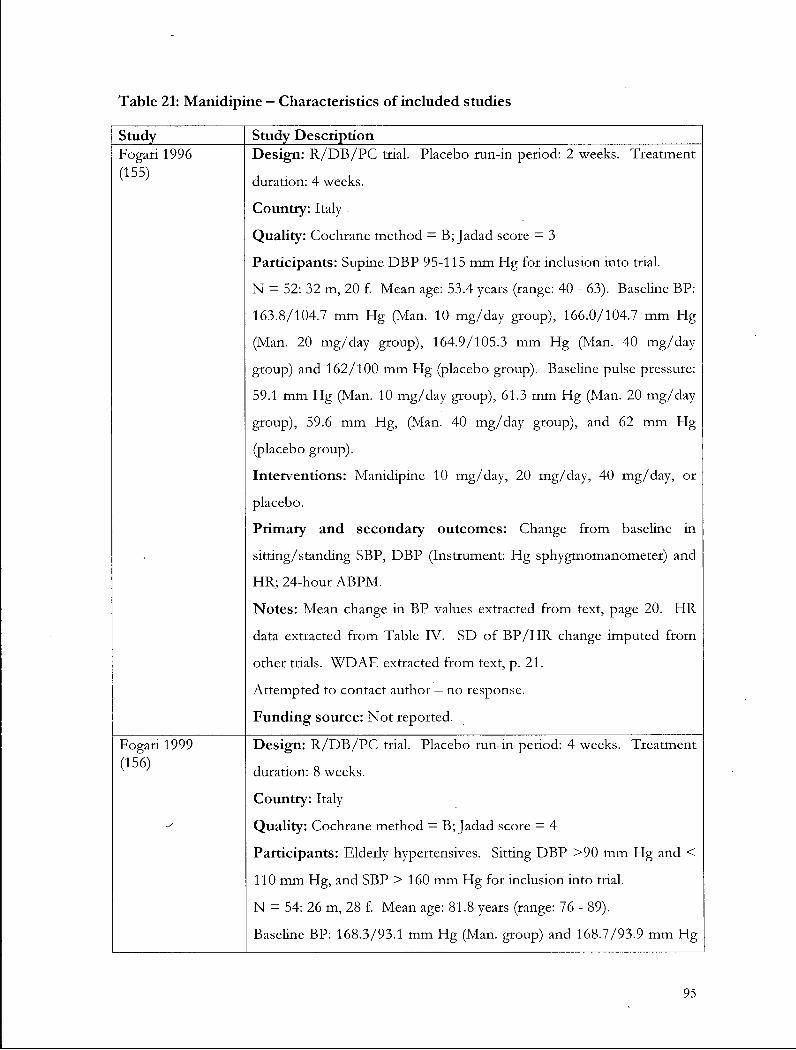
Table 21: Manid ip ine - Characteristics of inc luded studies
Study Study Descr ipt ion Fogari 1996 (155)
Design: R / D B / P C trial. Placebo run-in period: 2 weeks. Treatment
duration: 4 weeks.
Country: Italy .
Quality: Cochrane method = B; Jadad score = 3
Participants: Supine D B P 95-115 mm H g for inclusion into trial.
N = 52: 32 m, 20 f. Mean age: 53.4 years (range: 40 - 63). Baseline BP:
163.8/104.7 mm H g (Man. 10 mg/day group), 166.0/104.7 mm H g
(Man. 20 mg/day group), 164.9/105.3 mm H g (Man. 40 mg/day
group) and 162/100 mm Fig (placebo group). Baseline pulse pressure:
59.1 mm H g (Man. 10 mg/day group), 61.3 mm H g (Man. 20 mg/day
group), 59.6 mm Hg, (Man. 40 mg/day group), and 62 mm H g
(placebo group).
Interventions: Manidipine 10 mg/day, 20 mg/day, 40 mg/day, or
placebo.
Primary and secondary outcomes: Change from baseline in
sittmg/standing SBP, D B P (Instrument: H g sphygmomanometer) and
FIR; 24-hour A B P M .
Notes: Mean change in BP values extracted from text, page 20. H R
data extracted from Table IV. SD of B P / H R change imputed from
other trials. W D A E extracted from text, p. 21.
Attempted to contact author — no response.
Fund ing source: Not reported.
Fogari 1999 (156)
Des ign: R / D B / P C trial. Placebo run-in period: 4 weeks. Treatment
duration: 8 weeks.
Country: Italy
Quality: Cochrane method = B ; Jadad score = 4
Participants: Elderly hypertensives. Sitting D B P >90 mm Fig and <
110 mm Hg, and SBP > 160 mm H g for inclusion into trial.
N = 54: 26 m, 28 f. Mean age: 81.8 years (range: 76 - 89).
Baseline BP: 168.3/93.1 mm H g (Man. group) and 168.7/93.9 mm H g
95

(placebo group). Baseline pulse pressure: 55.2 (Man. group) and 74.8
(placebo group).
Interventions: Manidipine 10 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in
sitting/standing SBP, D B P (Instrument: standard H g
sphygmomanometer), and HR; 24-hour A B P M (Instrument: Spacelabs
90207); E C G ; body weight.
Notes: Sitting B P and H R data extracted from Table 2. Endpoint BPs
and HRs were calculated as the weighted mean of data from week 4
and 8. SD of B P change imputed from weighted mean of SD of BPs
at week 4 and 8. N o W D A E occurred.
Fund ing source: Not reported.
96

Table 22: Mibef rad i l - Characteristics of inc luded studies
Study Study Descr ipt ion
Bernink 1996 (157)
Design: M C / R / D B / P C trial. Placebo run-in period: 4 weeks.
Treatment duration: 4 weeks.
Country: Germany, Netherlands, Sweden, Finland, Austria, Denmark
Quality: Cochrane method = B; Jadad score = 3
Participants: Sitting D B P 95-114 mm H g for inclusion into trial.
N = 202: 122 m, 80 f. Mean age: 55.6 years (range: 1 8 - 7 0 for
inclusion).
Baseline sitting D B P : 105.5 mm H g (Mib. 25 mg/day group), 104.0
mm H g (Mib. 50 mg/day group), 104.4 mm H g (Mib. 100 mg/day
group), 103.9 mm H g (Mib. 150 mg/day group), 105.4 mm H g
(placebo group). Baseline pulse pressure: not reported and cannot be
calculated. r
Interventions: Mibefradil 25 mg/day, 50 mg/day, 100 mg/day, 150
mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
and standing SBP, D B P (Instrument: H g sphygmomanometer) and
HR.
Notes: Change in trough sitting D B P data and associated SDs
extracted from Table 2. Because baseline SBPs and HRs were not
reported, the corresponding data was not extracted. W D A E extracted
from text, p.429.
Author contacted - no additional data available.
Fund ing source: F. Hoffman-LaRoche Ltd., Switzerland. Bursztyn 1997 (158)
Design: M C / R / D B / P C trial. Placebo run-in period: 4 weeks.
Treatment duration: 4 weeks.
Country: Europe, Brazil, Israel
Quality: Cochrane method = A ; Jadad score = 3
Participants: Sitting SBP 160-220 mm H g and D B P 90-110 mm H g
for inclusion into trial.
97
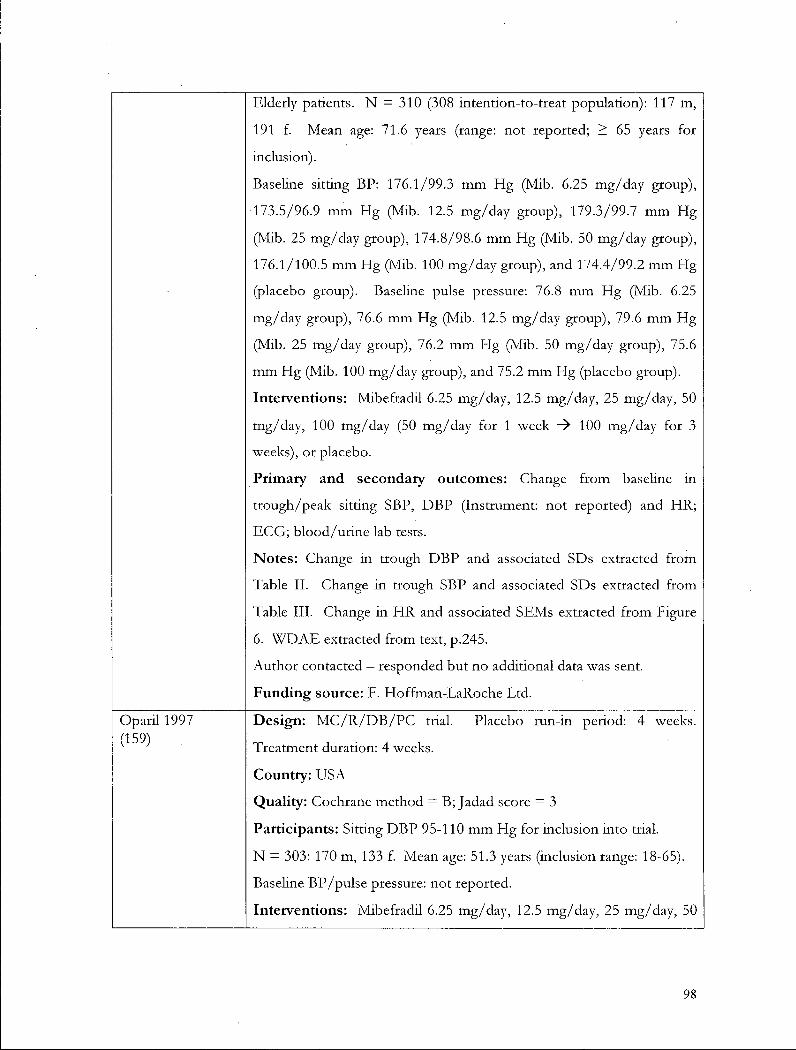
Elderly patients. N = 310 (308 intention-to-treat population): 117 m,
191 f. Mean age: 71.6 years (range: not reported; > 65 years for
inclusion).
Baseline sitting BP: 176.1/99.3 mm H g (Mib. 6.25 mg/day group),
173.5/96.9 mm H g (Mib. 12.5 mg/day group), 179.3/99.7 mm H g
(Mib. 25 mg/day group), 174.8/98.6 mm H g (Mib. 50 mg/day group),
176.1/100.5 mm H g (Mib. 100 mg/day group), and 174.4/99.2 mm H g
(placebo group). Baseline pulse pressure: 76.8 mm H g (Mib. 6.25
mg/day group), 76.6 mm H g (Mib. 12.5 mg/day group), 79.6 mm H g
(Mib. 25 mg/day group), 76.2 mm H g (Mib. 50 mg/day group), 75.6
mm H g (Mib. 100 mg/day group), and 75.2 mm H g (placebo group).
Interventions: Mibefradil 6.25 mg/day, 12.5 mg/day, 25 mg/day, 50
mg/day, 100 mg/day (50 mg/day for 1 week 100 mg/day for 3
weeks), or placebo.
Primary and secondary outcomes: Change from baseline in
trough/peak sitting SBP, D B P (Instrument: not reported) and H R ;
E C G ; blood/urine lab tests.
Notes: Change in trough D B P and associated SDs extracted from
Table II. Change in trough SBP and associated SDs extracted from
Table III. Change in H R and associated SEMs extracted from Figure
6. W D A E extracted from text, p.245.
Author contacted - responded but no additional data was sent.
Fund ing source: F. Hoffman-LaRoche Ltd.
Oparil 1997 (159)
Design: M C / R / D B / P C trial. Placebo run-in period: 4 weeks.
Treatment duration: 4 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 3
Participants: Sitting D B P 95-110 mm H g for inclusion into trial.
N = 303: 170 m, 133 f. Mean age: 51.3 years (inclusion range: 18-65).
Baseline BP/pulse pressure: not reported.
Interventions: Mibefradil 6.25 mg/day, 12.5 mg/day, 25 mg/day, 50
98

mg/day, 100 mg/day, 150 mg/day, 200 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in
trough/peak sitting SBP, D B P (Instrument: not reported) and H R ;
E C G , blood/urine lab tests.
Notes: Baseline B P s / H R s not reported, and thus, change in B P / H R
data could not be used. W D A E extracted from text, p. 739.
Author contacted: no data.
Fund ing source: F. Hoffman-LaRoche Ltd., Switzerland.
99

Table 23: N i ca rd ip ine - Characteristics of inc luded studies
Study Study Descr ipt ion
Asplund 1985 (160)
Design: R / D B / P C trial. Washout period: 4 weeks. Treatment
duration: 6 weeks.
Country: Sweden
Quality: Cochrane method = B; Jadad score — 4
Participants: Supine D B P 95-115 mm H g for inclusion into trial.
N = 50: 36 m, 14 f. Mean age: 46 years (range: 36 - 60).
Baseline BP: 161.4/113.9 mm H g (nicard. group), 154.6/112.9 mm H g
(placebo group). Baseline pulse pressure: 47.5 mm H g (nicard. group),
and 41.7 mm H g (placebo group).
Interventions: Nicardipine 90 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in
supine/standing SBP, D B P (Instrument: random zero H g
sphygmomanometer) and H R ; lab tests; E C G .
Notes: Change in standing B P extracted from text, p. 122S. HRs and
associated SDs extracted from Fig. 2. SDs of B P / H R change imputed
from weighted mean of week 4 and 6 data, extracted from Fig. 2.
Fund ing source: Not reported.
Bellet 1987a (161)
[Duplicate publication: Bellet 1987b (162)]
Design: R / D B / P C trial. Washout period: 2 weeks. Placebo run-in
period: 2 weeks. Treatment duration: 3 weeks.
Country: France
Quality: Cochrane method = A ; Jadad score = 3
Participants: Sitting D B P 95-120 mm H g for inclusion into trial.
N = 40: 27 m, 13 f. Mean age: 53 years (range: 27 - 72).
Baseline standing BP: 154/107 mm H g (nicard. group), and 148/103
mm H g (placebo group). Baseline pulse pressure: 47 mm H g (nicard.
group), and 45 mm H g (placebo group).
Interventions: Nicardipine 100 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
standing SBP, D B P , H R (Instrument: H g sphygmomanometer and
100
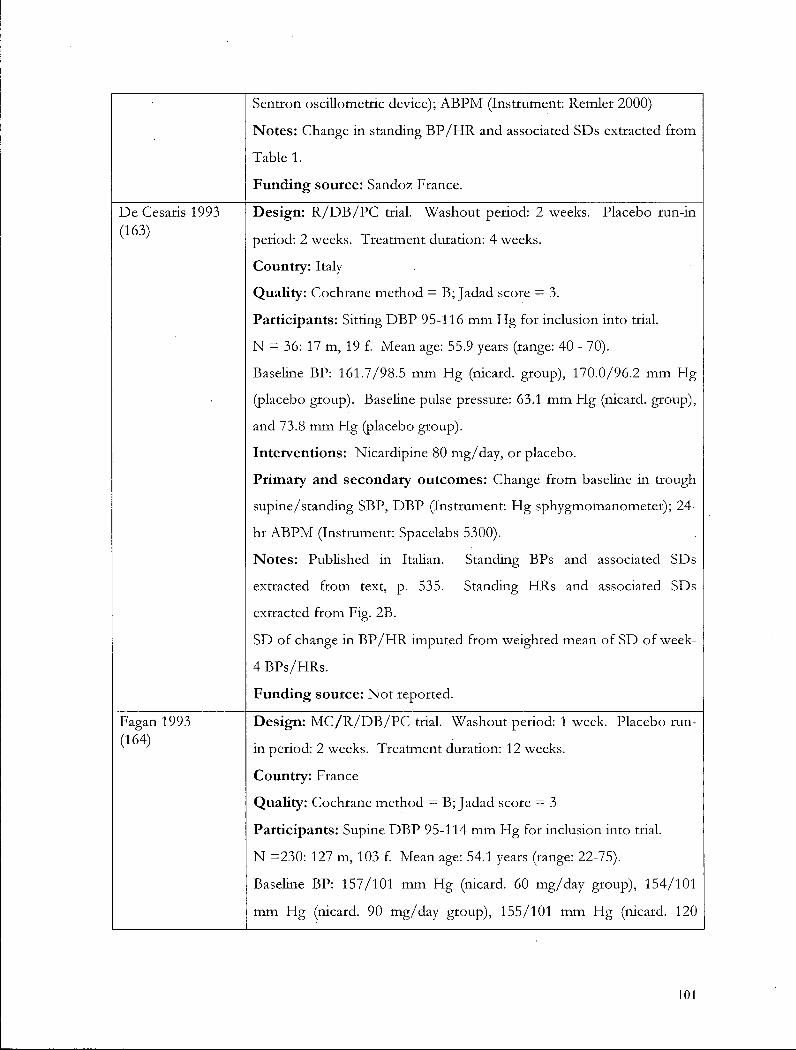
Sentron oscillometric device); A B P M (Instrument: Remler 2000)
Notes: Change in standing B P / H R and associated SDs extracted from
Table 1.
Funding source: Sandoz France.
De Cesaris 1993 (163)
Design: R / D B / P C trial. Washout period: 2 weeks. Placebo run-in
period: 2 weeks. Treatment duration: 4 weeks.
Country: Italy
Quality: Cochrane method — B; Jadad score — 3.
Participants: Sitting D B P 95-116 mm H g for inclusion into trial.
N = 36: 17 m, 19 f. Mean age: 55.9 years (range: 40 - 70).
Baseline BP: 161.7/98.5 mm H g (nicard. group), 170.0/96.2 mm H g
(placebo group). Baseline pulse pressure: 63.1 mm Fig (nicard. group),
and 73.8 mm Fig (placebo group).
Interventions: Nicardipine 80 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
supine/standing SBP, D B P (Instrument: H g sphygmomanometer); 24-
hr A B P M (Instrument: Spacelabs 5300).
Notes: Published in Italian. Standing BPs and associated SDs
extracted from text, p. 535. Standing HRs and associated SDs
extracted from Fig. 2B.
SD of change in B P / H R imputed from weighted mean of SD of week-
4 BPs /HRs .
Funding source: Not reported.
Fagan 1993 (164)
Design: M C / R / D B / P C trial. Washout period: 1 week. Placebo run-
in period: 2 weeks. Treatment duration: 12 weeks.
Country: France
Quality: Cochrane method = B; Jadad score = 3
Participants: Supine D B P 95-114 mm H g for inclusion into trial.
N =230: 127 m, 103 f. Mean age: 54.1 years (range: 22-75).
Baseline BP: 157/101 mm H g (nicard. 60 mg/day group), 154/101
mm H g (nicard. 90 mg/day group), 155/101 mm H g (nicard. 120
101

mg/day group), 155/100 mm H g (placebo group). Baseline pulse
pressure: 56 mm H g (nicard. 60 mg/day group), 53 mm H g (nicard. 90
mg/day group), 54 (nicar. 120 mg/day group), and 55 mm H g (placebo
group).
Interventions: Nicardipine SR 60 mg/day, 90 mg/day, 120 mg/day,
or placebo.
Primary and secondary outcomes: Change from baseline in trough
supine/standing SBP, D B P (Instrument: H g or aneroid
sphygmomanometer) and H R ; A B P M (Instrument: SpaceLabs 90202).
Notes: Change in BPs and associated SDs extracted from Fig. 1. H R
data reported only for nicar. 120 mg/day. W D A E extracted from
Table 4.
Attempted to contact author — no response.
Funding source: Syntex Research.
Marcadet 1991 (165)
Design: R / D B / P C trial. Washout period: 2 weeks. Placebo run-in
period: 15 days. Treatment duradon: 8 weeks.
Country: France
Quality: Cochrane method = B; Jadad score — 3
Participants: Male athletes. Sitting D B P 90-115 mm H g for inclusion
into trial.
N = 38: 38 m, 0 f. Mean age: 30.5 years (range: 18 — 50 for inclusion).
Baseline BP: 154/98 mm Fig (nicardipine group), 155/96 mm H g
(placebo group). Baseline pulse pressure: 56 mm H g (nicardipine
group), and 59 mm H g (placebo group).
Interventions: Nicardipine L P 100 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in supine
SBP, D B P (Instrument: Fig sphygmomanometer) and H R at rest and
on effort; maximum oxygen consumption and effort duration; weight.
Notes: Published in French. Change in BPs and associated SDs
extracted from Table III. H R data extracted from Fig. 2.
Funding source: Not reported.
102
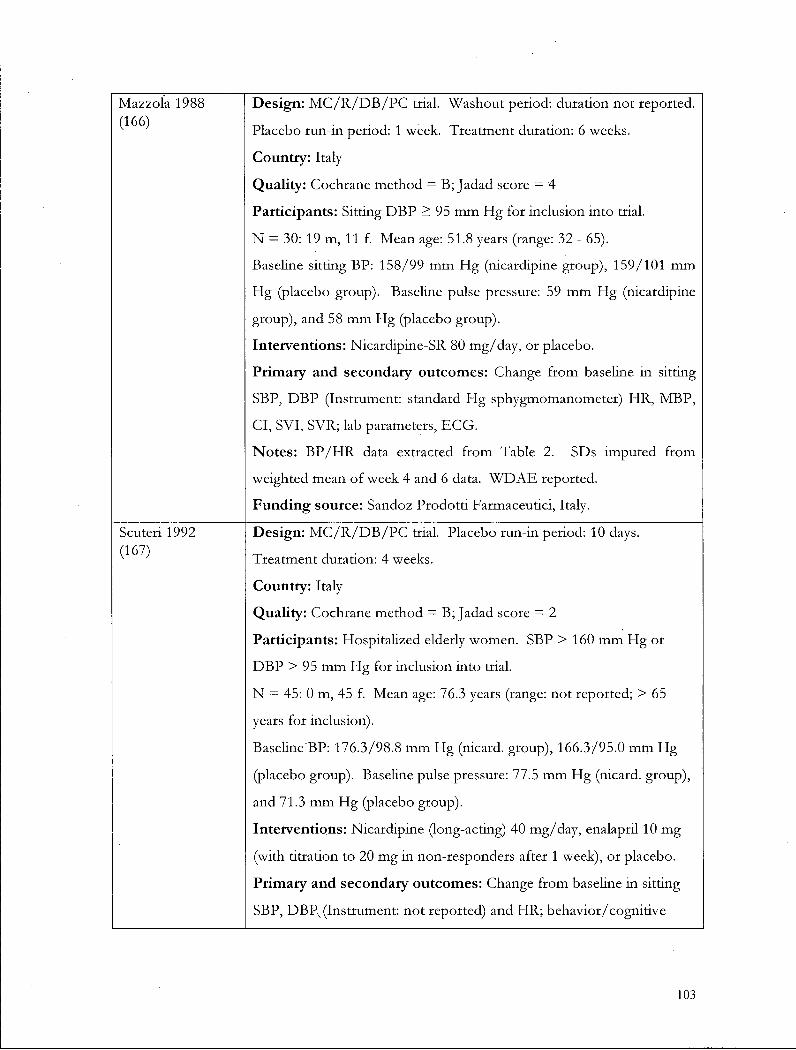
Mazzola 1988 (166)
Design: M C / R / D B / P C trial. Washout period: duration not reported.
Placebo run-in period: 1 week. Treatment duration: 6 weeks.
Country: Italy
Quality: Cochrane method = B; Jadad score = 4
Participants: Sitting D B P > 95 mm H g for inclusion into trial.
N = 30: 19 m, 11 f Mean age: 51.8 years (range: 32 - 65).
Baseline sitting BP: 158/99 mm H g (nicardipine group), 159/101 mm
H g (placebo group). Baseline pulse pressure: 59 mm H g (nicardipine
group), and 58 mm Fig (placebo group).
Interventions: Nicardipine-SR 80 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
SBP, D B P (Instrument: standard H g sphygmomanometer) H R , M B P ,
CI, SVI, SVR; lab parameters, E C G .
Notes: B P / H R data extracted from Table 2. SDs imputed from
weighted mean of week 4 and 6 data. W D A E reported.
Fund ing source: Sandoz Prodotti Farmaceutici, Italy.
Scuten 1992 (167)
Design: M C / R / D B / P C trial. Placebo run-in period: 10 days.
Treatment duration: 4 weeks.
Country: Italy
Quality: Cochrane method — B; Jadad score = 2
Participants: Hospitalized elderly women. SBP > 160 mm H g or
D B P > 95 mm H g for inclusion into trial.
N = 45: 0 m, 45 f. Mean age: 76.3 years (range: not reported; > 65
years for inclusion).
Baseline BP: 176.3/98.8 mm Fig (nicard. group), 166.3/95.0 mm H g
(placebo group). Baseline pulse pressure: 77.5 mm H g (nicard. group),
and 71.3 mm H g (placebo group).
Interventions: Nicardipine (long-acting) 40 mg/day, enalapril 10 mg
(with titration to 20 mg in non-responders after 1 week), or placebo.
Primary and secondary outcomes: Change from baseline in sitting
SBP, D B P X (Instrument: not reported) and FIR; behavior/cognitive
103

function tests: M M S E , GRS, S C A G .
Notes: B P and H R data extracted from Table 1. SDs imputed from
week 4 data. W D A E not reported.
Fund ing source: Sandoz Prodotti Farmaceutici, Italy.
Soro 1990 (168)
[Duplicate publication: De Simone 1989 (169)]
Des ign: R / D B / P C trial. Placebo run-in period: 2 weeks. Treatment
duration: 8 weeks.
Country: Italy
Quality: Cochrane method — B; Jadad score — 3
Participants: " M i l d to moderate primary arterial hypertension" for
inclusion into trial.
N = 18: 8 m, 10 f. Mean age: years (range: 27 - 65).
Baseline standing BP: 164/106 mm H g (Nicardipine group), and
167/105 mm Fig (placebo group). Baseline pulse pressure: 58 mm Fig
(Nicardipine group), and 62 mm H g (placebo group).
Interventions: Nicardipine 60 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in
supine/standing SBP, D B P and H R (Instrument: automatic device:
Sentron); body weight; serum electrolytes, renin, aldosterone, P T H ,
cholesterol, fasting blood glucose, L V function by echocardiography.
Notes: Standing office BPs and SDs extracted from text, p. 135 of
Soro f 990. SDs of BP change imputed from week 8 data. HRs and
W D A E s extracted from De Simone 1989.
Author (De Simone) contacted — clarified duplicate publication.
Fund ing source: Not reported.
104
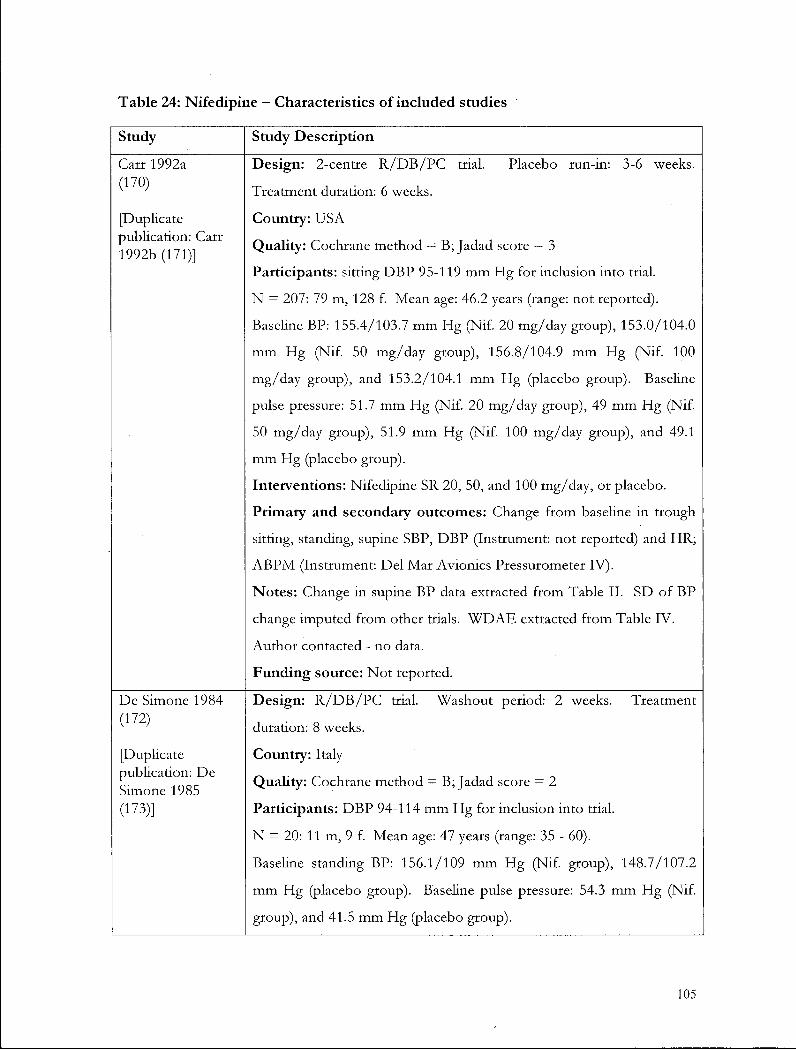
Table 24: Nifedipine - Characteristics of included studies
Study Study Description
Carr 1992a (170)
[Duplicate publication: Carr 1992b (171)]
Design: 2-centre R / D B / P C trial. Placebo run-in: 3-6 weeks.
Treatment duration: 6 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 3
Participants: sitting D B P 95-119 mm H g for inclusion into trial.
N = 207: 79 m, 128 f. Mean age: 46.2 years (range: not reported).
Baseline BP: 155.4/103.7 mm H g (Nif. 20 mg/day group), 153.0/104.0
mm H g (Nif. 50 mg/day group), 156.8/104.9 mm H g (Nif. 100
mg/day group), and 153.2/104.1 mm H g (placebo group). Baseline
pulse pressure: 51.7 mm H g (Nif. 20 mg/day group), 49 mm H g (Nif.
50 mg/day group), 51.9 mm H g (Nif. 100 mg/day group), and 49.1
mm H g (placebo group).
Interventions: Nifedipine SR 20, 50, and 100 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
sitting, standing, supine SBP, D B P (Instrument: not reported) and H R ;
A B P M (Instrument: De l Mar Avionics Pressurometer IV).
Notes: Change in supine B P data extracted from Table II. SD of B P
change imputed from other trials. W D A E extracted from Table IV.
Author contacted - no data.
Funding source: Not reported.
De Simone 1984 (172)
[Duplicate publication: De Simone 1985 (173)]
Design: R / D B / P C trial. Washout period: 2 weeks. Treatment
duration: 8 weeks.
Country: Italy
Quality: Cochrane method — B; Jadad score = 2
Participants: D B P 94-114 mm H g for inclusion into trial.
N = 20: 11 m, 9 f. Mean age: 47 years (range: 35 - 60).
Baseline standing BP: 156.1/109 mm H g (Nif. group), 148.7/107.2
mm Hg (placebo group). Baseline pulse pressure: 54.3 mm H g (Nif.
group), and 41.5 mm H g (placebo group).
105
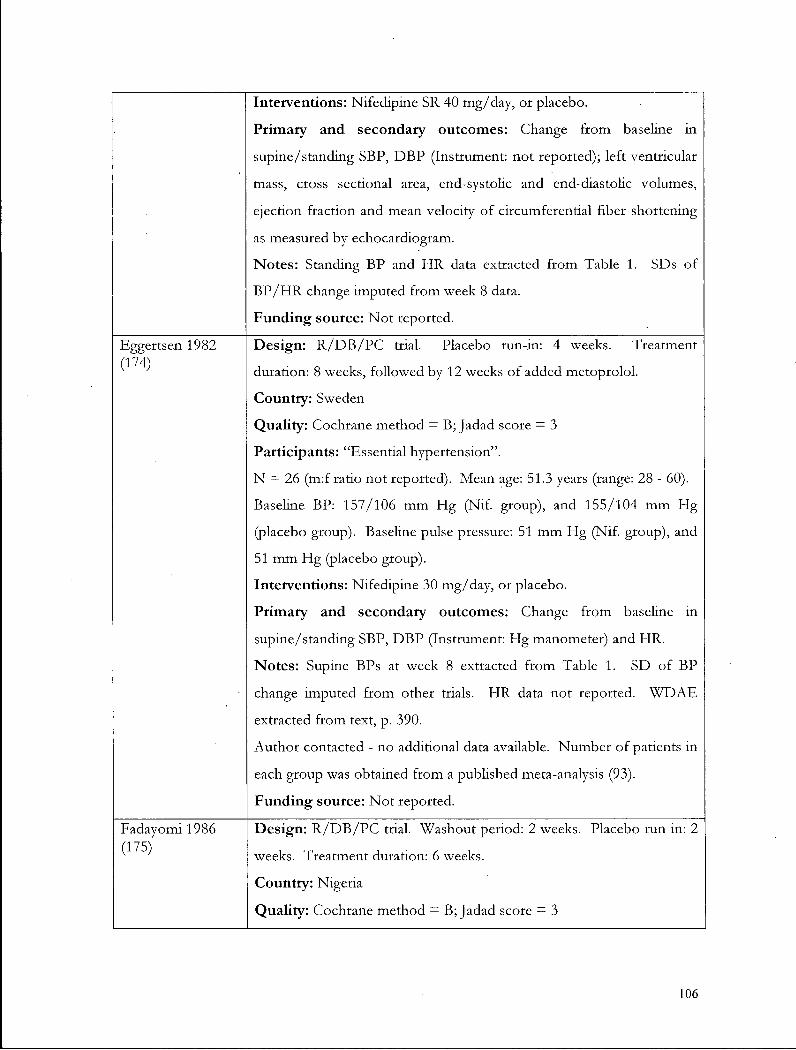
Interventions: Nifedipine SR 40 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in
supine/standing SBP, D B P (Instrument: not reported); left ventricular
mass, cross sectional area, end-systolic and end-diastolic volumes,
ejection fraction and mean velocity of circumferential fiber shortening
as measured by echocardiogram.
Notes: Standing B P and H R data extracted from Table 1. SDs of
B P / H R change imputed from week 8 data.
Fund ing source: Not reported.
Eggertsen 1982 (174)
Design: R / D B / P C trial. Placebo run-in: 4 weeks. Treatment
duration: 8 weeks, followed by 12 weeks of added metoprolol.
Country: Sweden
Quality: Cochrane metiiod = B; Jadad score = 3
Participants: "Essential hypertension".
N = 26 (m:f ratio not reported). Mean age: 51.3 years (range: 28 - 60).
Baseline BP: 157/106 mm H g (Nif. group), and 155/104 mm H g
(placebo group). Baseline pulse pressure: 51 mm H g (Nif. group), and
51 mm H g (placebo group).
Interventions: Nifedipine 30 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in
supine/standing SBP, D B P (Instrument: H g manometer) and H R .
Notes: Supine BPs at week 8 extracted from Table 1. SD of BP
change imputed from other trials. H R data not reported. W D A E
extracted from text, p. 390.
Author contacted - no additional data available. Number of patients in
each group was obtained from a published meta-analysis (93).
Fund ing source: Not reported.
Fadayomi 1986 (175)
Design: R / D B / P C trial. Washout period: 2 weeks. Placebo run-in: 2
weeks. Treatment duration: 6 weeks.
Country: Nigeria
Quality: Cochrane method = B; Jadad score = 3
106

Participants: supine D B P > 110 mm H g (newly diagnosed
hypertensives) or > 100 mm Fig (diagnosed 3-6 months earlier and
inadequately controlled) for inclusion into trial.
N = 32: 18 m, 14 f. Mean age: 48 years (range: 37 - 59).
Baseline BP: 181.3/114.7 mm H g (Nif. group), and 179.5/114.0 mm
H g (placebo group). Baseline pulse pressure: 66.6 mm H g (Nif.
group), and 65.5 mm H g (placebo group).
Interventions: Nifedipine (Adalat Retard) 40 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in
supine/standing SBP, D B P (Instrument: standard H g
sphygmomanometer) and H R ; body weight.
Notes: Individual patient BP data for 30 patients extracted from Table
1 and 2. SD of BP change calculated from this data. H R data not
extracted, as data was reported for nifedipine group only. W D A E
extracted from text, p. 468.
Author contacted - replied but no missing data was supplied.
Funding source: Bayer Pharmaceuticals Ltd., Nigeria.
Feig 1993 (176)
Design: M C / R / D B / P C trial. Placebo run-in: 4 weeks. Treatment
duration: 6 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 4
Participants: supine D B P 95-114 mm Fig for inclusion into trial.
N = 233: 130 m, 103 f. Mean age: 55 years (range: 19 - 75).
Baseline standing BP: 150/100 mm Fig (Nif. 30 mg/day group),
150/100 mm H g (Nif. 60 mg/day group), 153/101 mm H g (Nif. 90
mg/day group), and 149/100 mm Fig (placebo group). Baseline pulse
pressure: 50 mm H g (Nif. 30 mg/day group), 50 mm Hg (Nif. 60
mg/day group), 52 mm H g (Nif. 90 mg/day group), and 49 mm H g
(placebo group).
Interventions: Nifedipine coat-core 30 mg/day, 60 mg/day, 90
mg/day, or placebo.
107
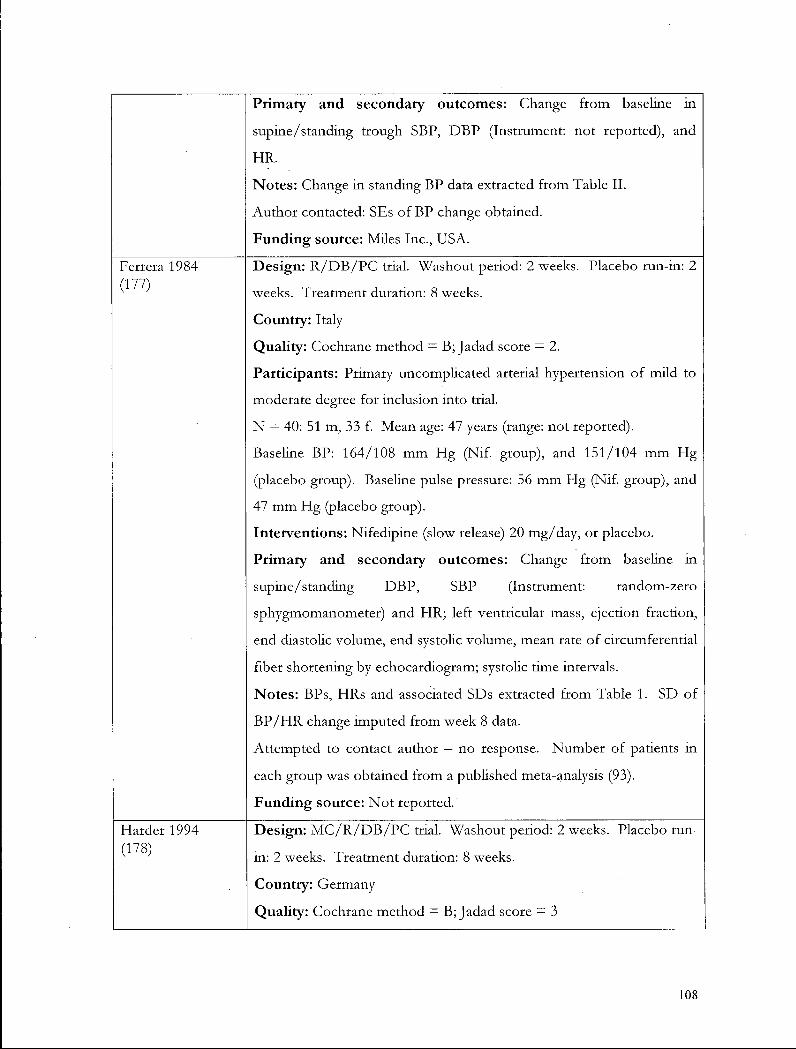
Primary and secondary outcomes: Change from baseline in
supine/standing trough SBP, D B P (Instrument: not reported), and
HR.
Notes: Change in standing B P data extracted from Table II.
Author contacted: SEs of B P change obtained.
Fund ing source: Miles Inc., USA.
Ferrera 1984 (177)
Design: R / D B / P C trial. Washout period: 2 weeks. Placebo run-in: 2
weeks. Treatment duration: 8 weeks.
Country: Italy
Quality: Cochrane method = B; Jadad score = 2.
Participants: Primary uncomplicated arterial hypertension of mild to
moderate degree for inclusion into trial.
N = 40: 51 m, 33 f. Mean age: 47 years (range: not reported).
Baseline BP: 164/108 mm Fig (Nif. group), and 151/104 mm H g
(placebo group). Baseline pulse pressure: 56 mm H g (Nif. group), and
47 mm Ffg (placebo group).
Interventions: Nifedipine (slow release) 20 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in
supine/standing D B P , SBP (Instrument: random-zero
sphygmomanometer) and H R ; left ventricular mass, ejection fraction,
end diastolic volume, end systolic volume, mean rate of circumferential
fiber shortening by echocardiogram; systolic time intervals.
Notes: BPs, HRs and associated SDs extracted from Table 1. SD of
B P / H R change imputed from week 8 data.
Attempted to contact author — no response. Number of patients in
each group was obtained from a published meta-analysis (93).
Fund ing source: Not reported.
Harder 1994 (178)
Design: M C / R / D B / P C trial. Washout period: 2 weeks. Placebo run-
in: 2 weeks. Treatment duration: 8 weeks.
Country: Germany
Quality: Cochrane method = B; Jadad score = 3
108

Participants: D B P 95-115 mm H g for inclusion into trial.
N — 88: 51 m, 33 f. Mean age: 54 years (range: not reported).
Baseline BP: 155/102 mm H g (Nif. group), and 155/102 mm H g
(placebo group). Baseline pulse pressure: 53 mm H g (Nif. group), and
53 mm H g (placebo group).
Interventions: Nifedipine (slow release) 60 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
trough D B P , SBP (Instrument: H g sphygmomanometer; semi
automatic auscultatory device - Tonoprint) and HR.
Notes: BPs (manual readings) and HRs extracted from Table I. SD of
B P / H R change imputed from week 8 data. W D A E extracted from
text, p. 135.
Fund ing source: Not reported.
Jueng 1987 (179)
Design: M C / R / D B / P C trial. Washout period: 1 week. Placebo run-
in: 3 weeks. Treatment duration: 2-week dose titration, followed by 8
weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 4
Participants: sitting D B P 95-110 mm H g for inclusion into trial.
N = 29: 22 m, 7 f. Mean age: 52.4 years (range: 27 - 83).
Baseline BP: 159/102 mm H g (nifed. group), 153/105 mm H g
(placebo group). Baseline pulse pressure: 57 mm Fig (nifed. group),
and 48 mm Hg (placebo group).
Interventions: Nifedipine GITS 30 mg/day (2 weeks)-^ 60 mg/day,
hydrochlorothiazide 25 mg/day (2 weeks) 50 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
trough SBP, D B P (Instrument: not reported), HR, metabolic
parameters.
Notes: B P s / H R s extracted from Table 2. SDs of change in B P s / H R s
imputed from week 8 values. W D A E extracted from text, p. 697.
Fund ing source: Pfizer Pharmaceuticals, USA.
109
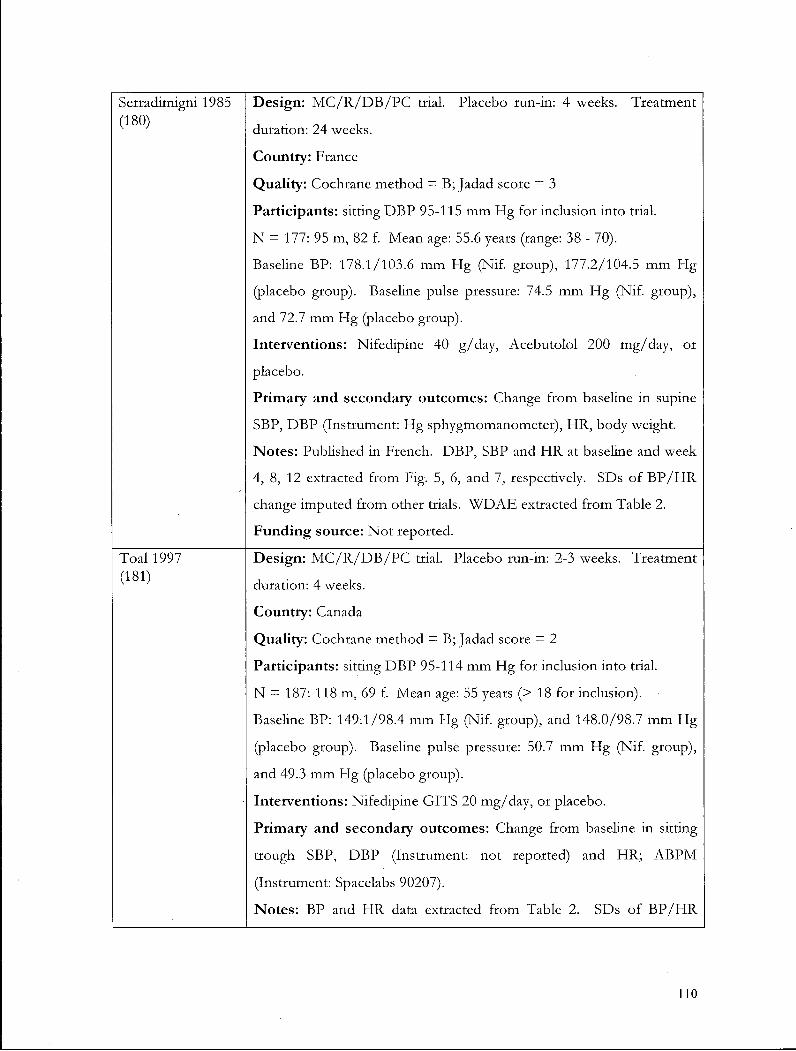
Serradimigni 1985 (180)
Design: M C / R / D B / P C trial. Placebo run-in: 4 weeks. Treatment
duration: 24 weeks.
Country: France
Quality: Cochrane method = B; Jadad score = 3
Participants: sitting D B P 95-115 mm H g for inclusion into trial.
N = 177: 95 m, 82 f. Mean age: 55.6 years (range: 38 - 70).
Baseline BP: 178.1/103.6 mm H g (Nif. group), 177.2/104.5 mm H g
(placebo group). Baseline pulse pressure: 74.5 mm Ffg (Nif. group),
and 72.7 mm H g (placebo group).
Interventions: Nifedipine 40 g/day, Acebutolol 200 mg/day, or
placebo.
Primary and secondary outcomes: Change from baseline in supine
SBP, D B P (Instrument: Fig sphygmomanometer), H R , body weight.
Notes: Published in French. D B P , SBP and H R at baseline and week
4, 8, 12 extracted from Fig. 5, 6, and 7, respectively. SDs of B P / F I R
change imputed from other trials. W D A E extracted from Table 2.
Fund ing source: Not reported.
Toal 1997 (181)
Design: M C / R / D B / P C trial. Placebo run-in: 2-3 weeks. Treatment
duration: 4 weeks.
Country: Canada
Quality: Cochrane method = B; Jadad score = 2
Participants: sitting D B P 95-114 mm Fig for inclusion into trial.
N - 187: 118 m, 69 f. Mean age: 55 years (> 18 for inclusion).
Baseline BP: 149.1/98.4 mm Fig (Nif. group), and 148.0/98.7 mm H g
(placebo group). Baseline pulse pressure: 50.7 mm H g (Nif. group),
and 49.3 mm Fig (placebo group).
Interventions: Nifedipine GfTS 20 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
trough SBP, D B P (Instrument: not reported) and HR; A B P M
(Instrument: Spacelabs 90207).
Notes: BP and H R data extracted from Table 2. SDs of B P / H R
110
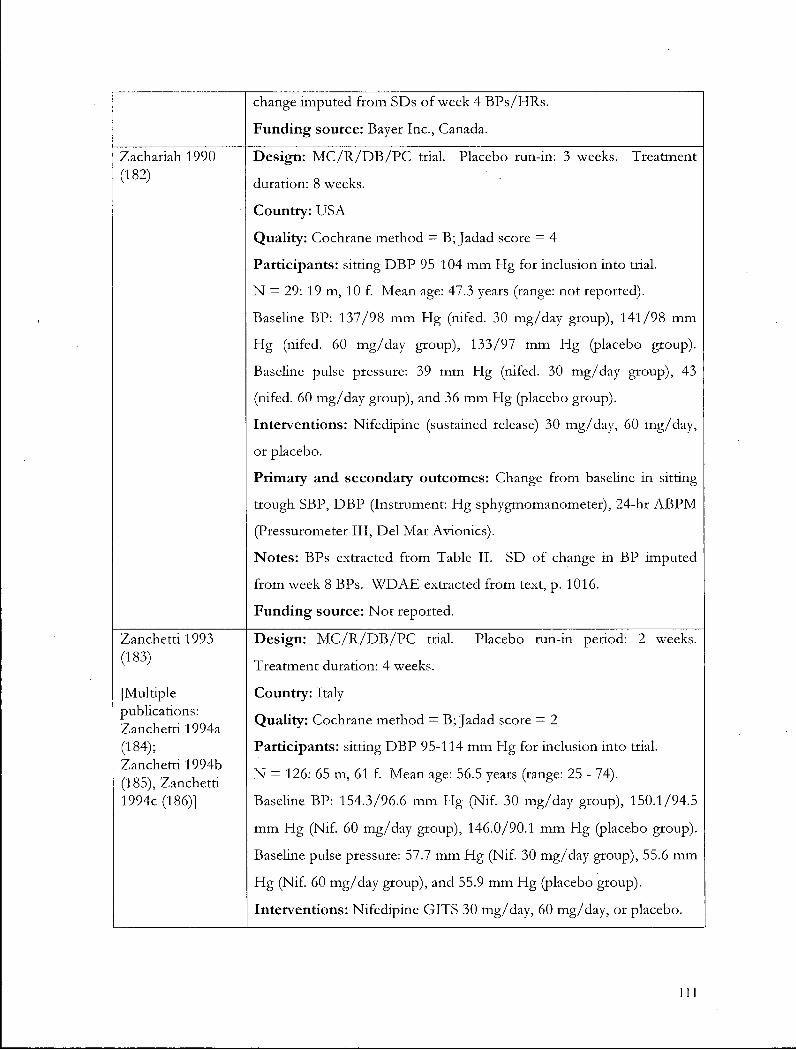
change imputed from SDs of week 4 BPs /HRs .
Funding source: Bayer Inc., Canada.
Zachariah 1990 (182)
Design: M C / R / D B / P C trial. Placebo run-in: 3 weeks. Treatment
duration: 8 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 4
Participants: sitting D B P 95-104 mm H g for inclusion into trial.
N = 29: 19 m, 10 f. Mean age: 47.3 years (range: not reported).
Baseline BP: 137/98 mm H g (nifed. 30 mg/day group), 141/98 mm
H g (nifed. 60 mg/day group), 133/97 mm H g (placebo group).
Baseline pulse pressure: 39 mm H g (nifed. 30 mg/day group), 43
(nifed. 60 mg/day group), and 36 mm H g (placebo group).
Interventions: Nifedipine (sustained release) 30 mg/day, 60 mg/day,
or placebo.
Primary and secondary outcomes: Change from baseline in sitting
trough SBP, D B P (Instrument: H g sphygmomanometer), 24-hr A B P M
(Pressurometer III, Del Mar Avionics).
Notes: BPs extracted from Table II. SD of change in B P imputed
from week 8 BPs. W D A E extracted from text, p. 1016.
Funding source: Not reported.
Zanchetti 1993 (183)
[Multiple publications: Zanchetti 1994a (184) ; Zanchetti 1994b (185) , Zanchetti 1994c (186)]
Design: M C / R / D B / P C trial. Placebo run-in period: 2 weeks.
Treatment duration: 4 weeks.
Country: Italy
Quality: Cochrane method = B; Jadad score = 2
Participants: sitting D B P 95-114 mm H g for inclusion into trial.
N = 126: 65 m, 61 f. Mean age: 56.5 years (range: 25 - 74).
Baseline BP: 154.3/96.6 mm H g (Nif. 30 mg/day group), 150.1/94.5
mm H g (Nif. 60 mg/day group), 146.0/90.1 mm H g (placebo group).
Baseline pulse pressure: 57.7 mm H g (Nif. 30 mg/day group), 55.6 mm
H g (Nif. 60 mg/day group), and 55.9 mm H g (placebo group).
Interventions: Nifedipine GITS 30 mg/day, 60 mg/day, or placebo.
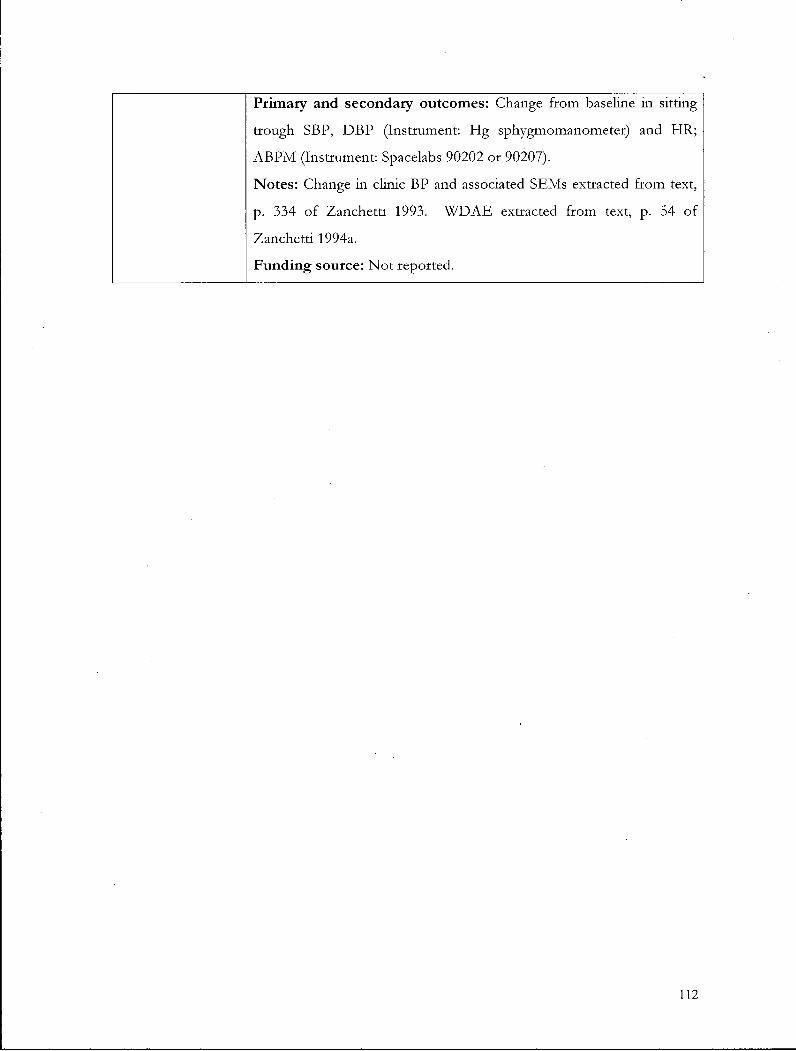
Primary and secondary outcomes: Change from baseline in sitting
trough SBP, D B P (Instrument: H g sphygmomanometer) and H R ;
A B P M (Instrument: Spacelabs 90202 or 90207).
Notes: Change in clinic BP and associated SEMs extracted from text,
p. 334 of Zanchetti 1993. W D A E extracted from text, p. 54 of
Zanchetti 1994a.
Fund ing source: Not reported.
112
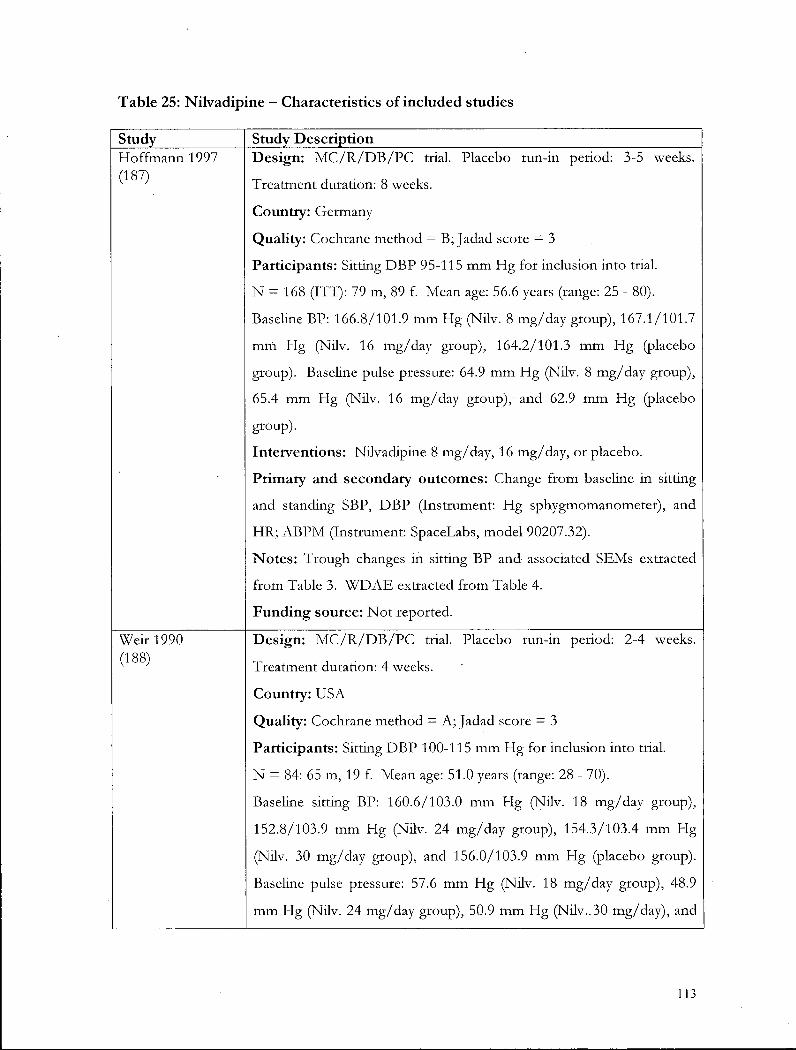
Table 25: Ni lvad ip ine - Characteristics of inc luded studies
Study Study Descr ipt ion Hoffmann 1997 (187)
Design: M C / R / D B / P C trial. Placebo run-in period: 3-5 weeks.
Treatment duration: 8 weeks.
Country: Germany
Quality: Cochrane method = B; Jadad score — 3
Participants: Sitting D B P 95-115 mm H g for inclusion into trial.
N = 168 (ITT): 79 m, 89 f. Mean age: 56.6 years (range: 25 - 80).
Baseline BP: 166.8/101.9 mm H g (Nilv. 8 mg/day group), 167.1/101.7
mm H g (Nilv. 16 mg/day group), 164.2/101.3 mm H g (placebo
group). Baseline pulse pressure: 64.9 mm H g (Nilv. 8 mg/day group),
65.4 mm Pig (Nilv. 16 mg/day group), and 62.9 mm H g (placebo
group).
Interventions: Nilvadipine 8 mg/day, 16 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
and standing SBP, D B P (Instrument: H g sphygmomanometer), and
HR; A B P M (Instrument: SpaceLabs, model 90207.32).
Notes: Trough changes in sitting B P and associated SEMs extracted
from Table 3. W D A E extracted from Table 4.
Fund ing source: Not reported.
Weir 1990 (188)
Design: M C / R / D B / P C trial. Placebo run-in period: 2-4 weeks.
Treatment duration: 4 weeks.
Country: USA
Quality: Cochrane method = A ; Jadad score = 3
Participants: Sitting D B P 100-115 mm H g for inclusion into trial.
N = 84: 65 m, 19 f. Mean age: 51.0 years (range: 28 - 70).
Baseline sitting BP: 160.6/103.0 mm H g (Nilv. 18 mg/day group),
152.8/103.9 mm H g (Nilv. 24 mg/day group), 154.3/103.4 mm H g
(Nilv. 30 mg/day group), and 156.0/103.9 mm H g (placebo group).
Baseline pulse pressure: 57.6 mm H g (Nilv. 18 mg/day group), 48.9
mm H g (Nilv. 24 mg/day group), 50.9 mm Fig (Nilv..30 mg/day), and
113
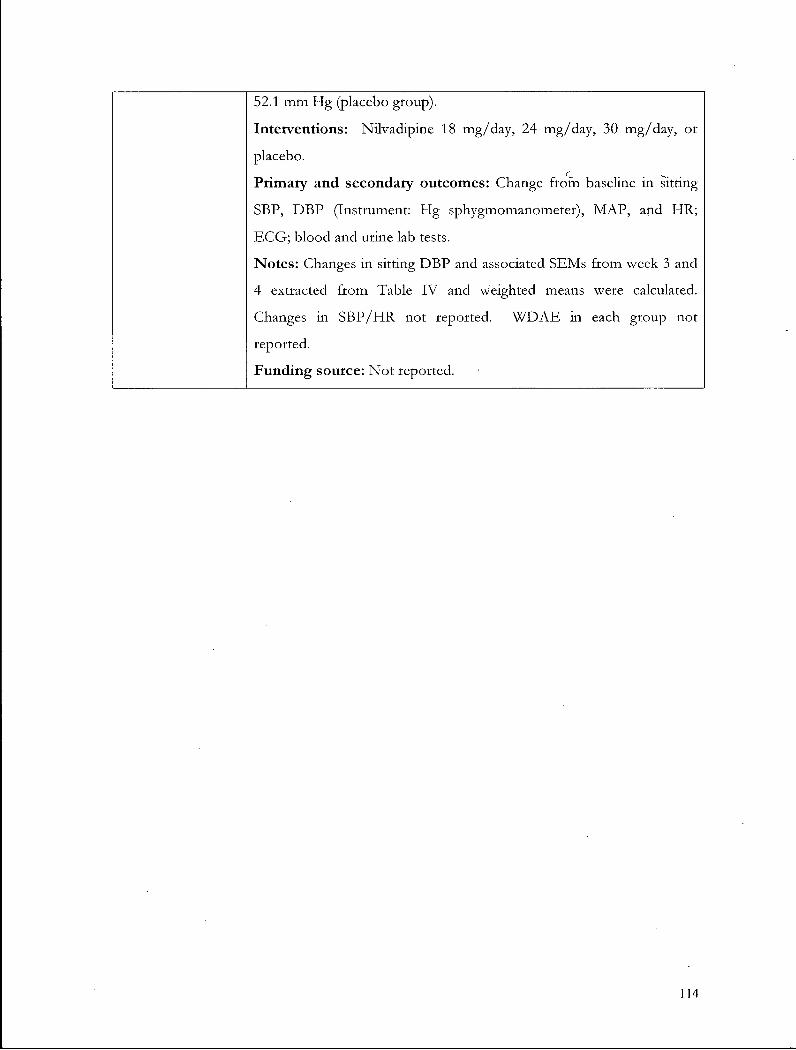
52.1 mm H g (placebo group).
Interventions: Nilvadipine 18 mg/day, 24 mg/day, 30 mg/day, or
placebo.
Primary and secondary outcomes: Change from baseline in sitting
SBP, D B P (fnstrument: H g sphygmomanometer), M A P , and H R ;
E C G ; blood and urine lab tests.
Notes: Changes in sitting D B P and associated SEMs from week 3 and
4 extracted from Table IV and weighted means were calculated.
Changes in S B P / H R not reported. W D A E in each group not
reported.
Fund ing source: Not reported.
114
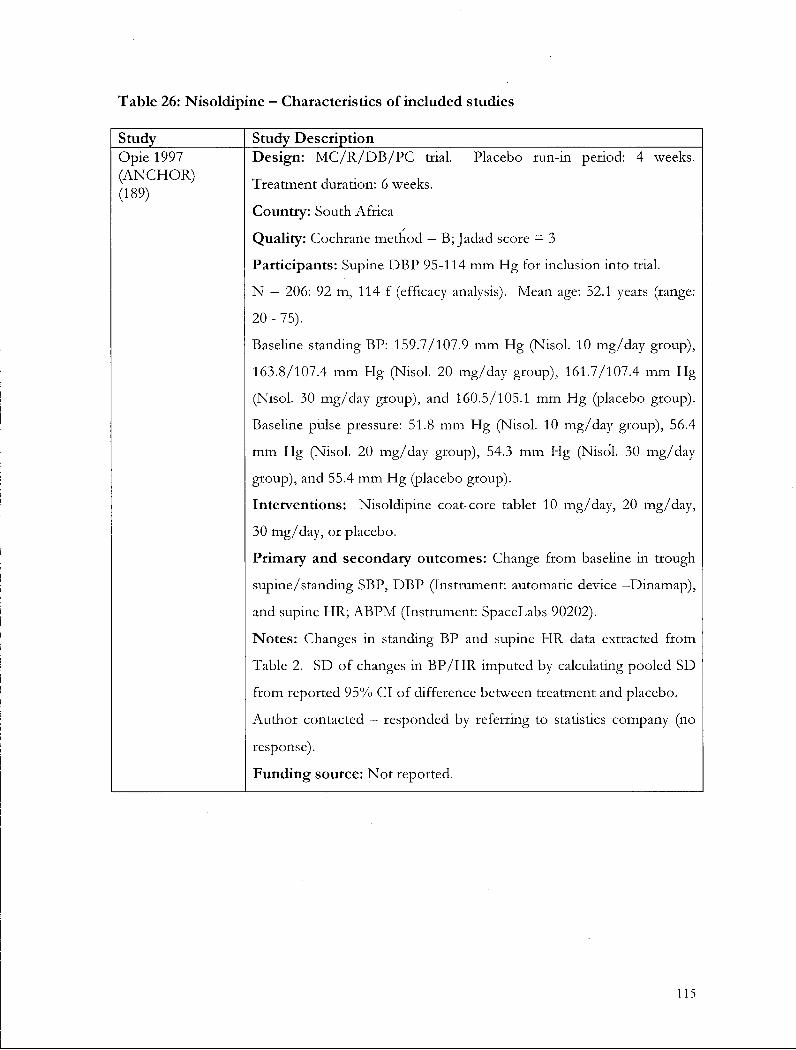
Table 26: N iso ld ip ine - Characteristics of included studies
Study Study Descr ipt ion Opie 1997 ( A N C H O R ) (189)
Design: M C / R / D B / P C trial. Placebo run-in period: 4 weeks.
Treatment duration: 6 weeks.
Country: South Africa
Quality: Cochrane method = B; Jadad score — 3
Participants: Supine D B P 95-114 mm H g for inclusion into trial.
N = 206: 92 m, 114 f (efficacy analysis). Mean age: 52.1 years (range:
20 - 75).
Baseline standing BP: 159.7/107.9 mm H g (Nisol. 10 mg/day group),
163.8/107.4 mm H g (Nisol. 20 mg/day group), 161.7/107.4 mm H g
(Nisol. 30 mg/day group), and 160.5/105.1 mm H g (placebo group).
Baseline pulse pressure: 51.8 mm H g (Nisol. 10 mg/day group), 56.4
mm H g (Nisol. 20 mg/day group), 54.3 mm H g (Nisol. 30 mg/day
group), and 55.4 mm H g (placebo group).
Interventions: Nisoldipine coat-core tablet 10 mg/day, 20 mg/day,
30 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
supine/standing SBP, D B P (Instrument: automatic device —Dinamap),
and supine H R ; A B P M (Instrument: SpaceLabs 90202).
Notes: Changes in standing BP and supine H R data extracted from
Table 2. SD of changes in B P / H R imputed by calculating pooled SD
from reported 95% CI of difference between treatment and placebo.
Author contacted — responded by referring to statistics company (no
response).
Fund ing source: Not reported.
115
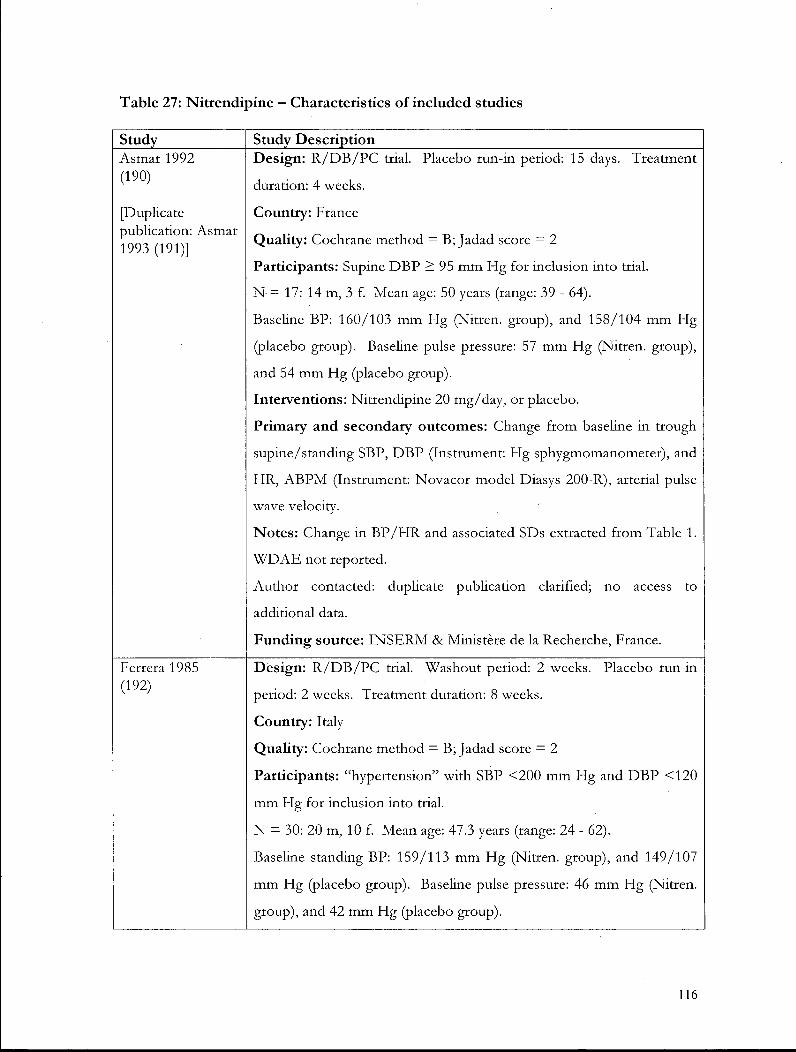
Table 27: Ni t rendip ine - Characteristics of included studies
Study Study Descr ipt ion Asmar 1992 (190)
[Duplicate publication: Asmar 1993 (191)]
Design: R / D B / P C trial. Placebo run-in period: 15 days. Treatment
duration: 4 weeks.
Country: France
Quality: Cochrane method = B; Jadad score = 2
Participants: Supine D B P > 95 mm Fig for inclusion into trial.
N- = 17: 14 m, 3 f. Mean age: 50 years (range: 39 - 64).
Baseline BP: 160/103 mm H g (Nitren. group), and 158/104 mm H g
(placebo group). Baseline pulse pressure: 57 mm H g (Nitren. group),
and 54 mm H g (placebo group).
Interventions: Nitrendipine 20 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
supine/standing SBP, D B P (Instrument: Fig sphygmomanometer), and
FIR, A B P M (Instrument: Novacor model Diasys 200-R), arterial pulse
wave velocity.
Notes: Change in B P / H R and associated SDs extracted from Table 1.
W D A E not reported.
Audior contacted: duplicate publication clarified; no access to
additional data.
Fund ing source: I N S E R M & Ministere de la Recherche, France.
Ferrera 1985 (192)
Design: R / D B / P C trial. Washout period: 2 weeks. Placebo run-in
period: 2 weeks. Treatment duration: 8 weeks.
Country: Italy
Quality: Cochrane method = B; Jadad score = 2
Participants: "hypertension" with SBP <200 mm H g and D B P <120
mm Fig for inclusion into trial.
N = 30: 20 m, 10 f. Mean age: 47.3 years (range: 24 - 62).
Baseline standing BP: 159/113 mm H g (Nitren. group), and 149/107
mm H g (placebo group). Baseline pulse pressure: 46 mm H g (Nitren.
group), and 42 mm Fig (placebo group).
116
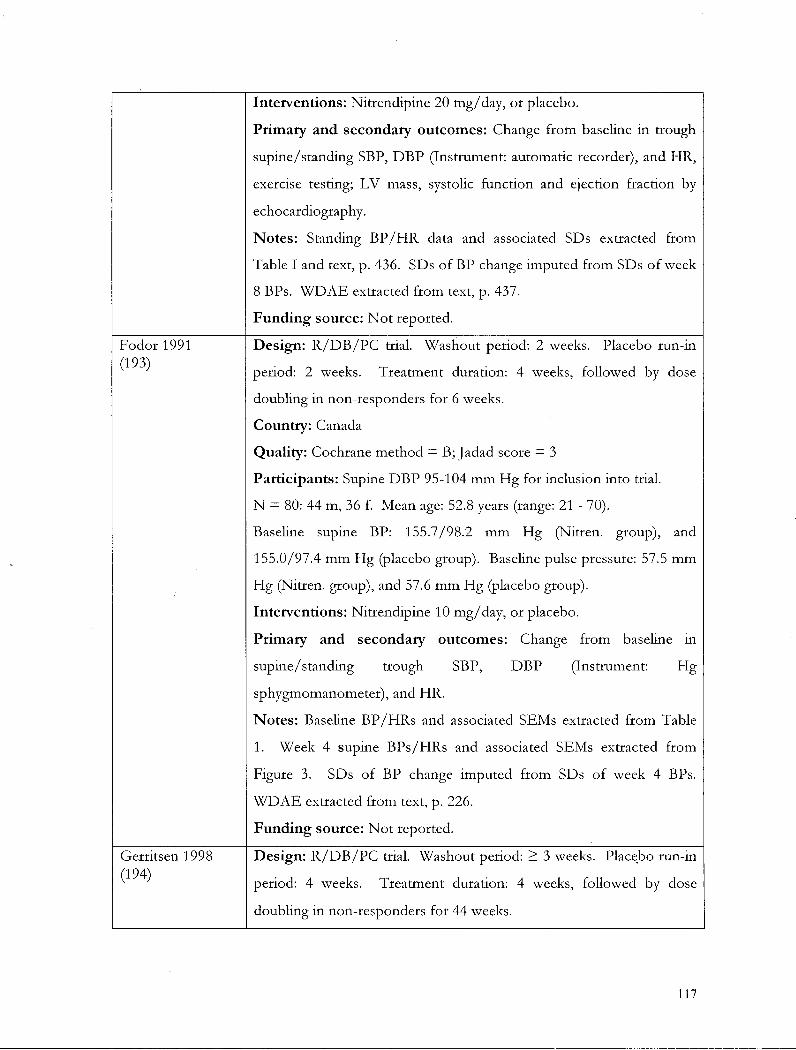
Interventions: Nitrendipine 20 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
supine/standing SBP, D B P (Instrument: automatic recorder), and H R ,
exercise testing; L V mass, systolic function and ejection fraction by
echocardiography.
Notes: Standing B P / F I R data and associated SDs extracted from
Table f and text, p. 436. SDs of B P change imputed from SDs of week
8 BPs. W D A E extracted from text, p. 437.
Fund ing source: Not reported.
Fodor1991 (193)
Design: R / D B / P C trial. Washout period: 2 weeks. Placebo run-in
period: 2 weeks. Treatment duration: 4 weeks, followed by dose
doubling in non-responders for 6 weeks.
Country: Canada
Quality: Cochrane method = B; Jadad score = 3
Participants: Supine D B P 95-104 mm H g for inclusion into trial.
N = 80: 44 m, 36 f. Mean age: 52.8 years (range: 21 - 70).
Baseline supine BP: 155.7/98.2 mm H g (Nitren. group), and
155.0/97.4 mm H g (placebo group). Baseline pulse pressure: 57.5 mm
Fig (Nitren. group), and 57.6 mm H g (placebo group).
Interventions: Nitrendipine 10 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in
supine/standing trough SBP, D B P (Instrument: H g
sphygmomanometer), and FIR.
Notes: Baseline BP/FIRs and associated SEMs extracted from Table
1. Week 4 supine BPs/FIRs and associated SEMs extracted from
Figure 3. SDs of BP change imputed from SDs of week 4 BPs.
W D A E extracted from text, p. 226.
Fund ing source: Not reported.
Gerntsen 1998 (194)
Design: R / D B / P C trial. Washout period: > 3 weeks. Placebo run-in
period: 4 weeks. Treatment duration: 4 weeks, followed by dose
doubling in non-responders for 44 weeks.
117
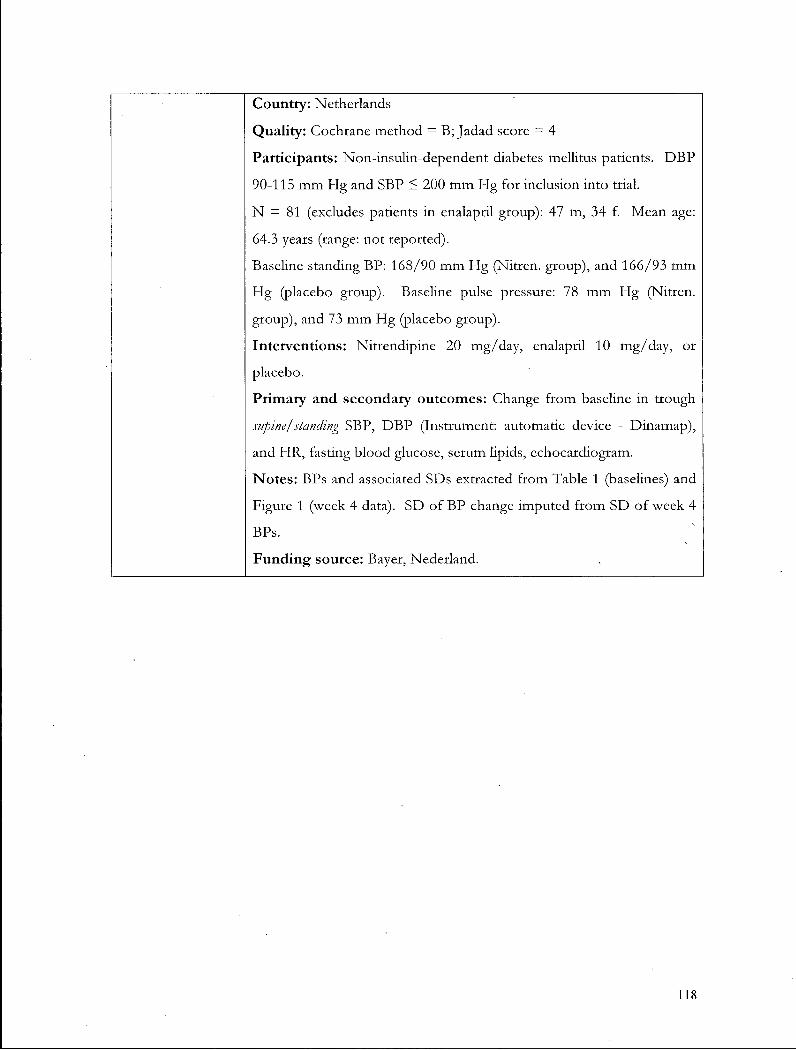
Country: Netherlands
Quality: Cochrane method = B; Jadad score = 4
Participants: Non-insulin-dependent diabetes mellitus patients. D B P
90-115 mm H g and SBP < 200 mm H g for inclusion into trial.
N = 81 (excludes patients in enalapril group): 47 m, 34 f. Mean age:
64.3 years (range: not reported).
Baseline standing BP: 168/90 mm Pig (Nitren. group), and 166/93 mm
Pig (placebo group). Baseline pulse pressure: 78 mm H g (Nitren.
group), and 73 mm Pig (placebo group).
Interventions: Nitrendipine 20 mg/day, enalapril 10 mg/day, or
placebo.
Primary and secondary outcomes: Change from baseline in trough
supine/standing SBP, D B P (fnstrument: automatic device - Dinamap),
and H R , fasting blood glucose, serum lipids, echocardiogram.
Notes: BPs and associated SDs extracted from Table 1 (baselines) and
Figure 1 (week 4 data). SD of BP change imputed from SD of week 4
BPs.
Funding source: Bayer, Nederland.
118
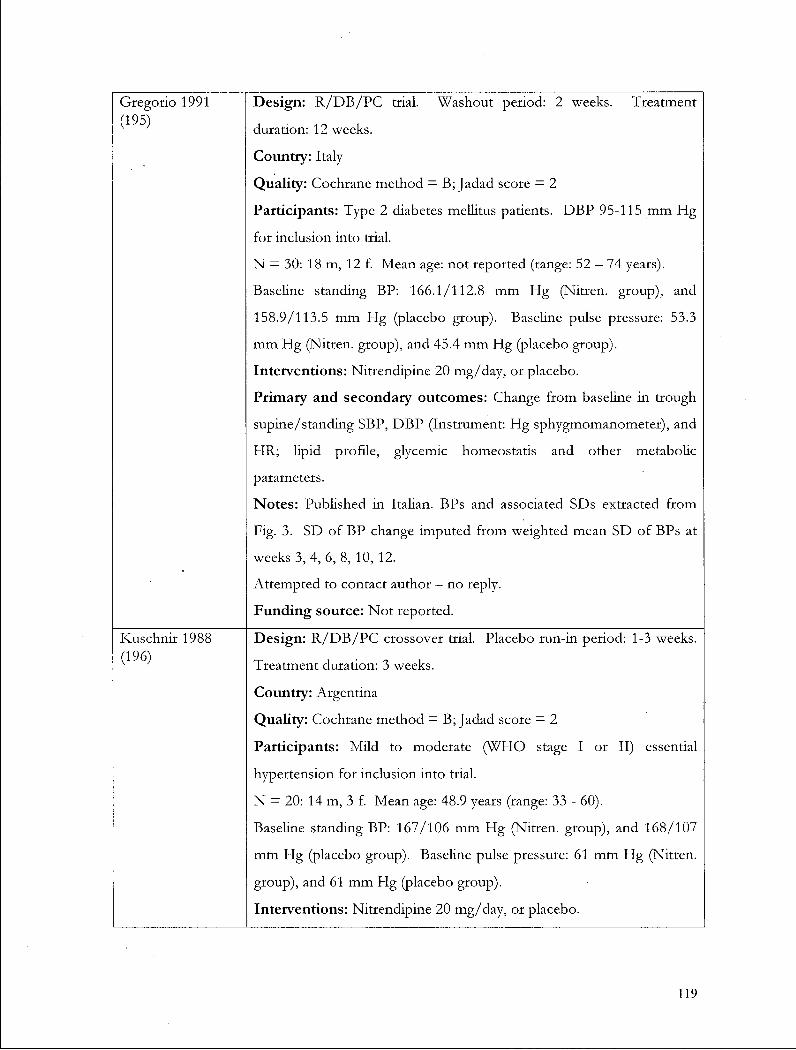
Gregorio 1991 (195)
Design: R / D B / P C trial. Washout period: 2 weeks. Treatment
duration: 12 weeks.
Country: Italy
Quality: Cochrane method = B; Jadad score = 2
Participants: Type 2 diabetes mellitus patients. D B P 95-115 mm H g
for inclusion into trial.
N = 30: 18 m, 12 f. Mean age: not reported (range: 52 — 74 years).
Baseline standing BP: 166.1/112.8 mm H g (Nitren. group), and
158.9/113.5 mm H g (placebo group). Baseline pulse pressure: 53.3
mm H g (Nitren. group), and 45.4 mm H g (placebo group).
Interventions: Nitrendipine 20 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
supine/standing SBP, D B P (Instrument: H g sphygmomanometer), and
H R ; lipid profile, glycemic homeostatis and other metabolic
parameters.
Notes: Published in Italian. BPs and associated SDs extracted from
Fig. 3. SD of B P change imputed from weighted mean SD of BPs at
weeks 3, 4, 6, 8,10,12.
Attempted to contact author — no reply.
Fund ing source: Not reported.
Kuschnir 1988 (196)
Design: R / D B / P C crossover trial. Placebo run-in period: 1-3 weeks.
Treatment duration: 3 weeks.
Country: Argentina
Quality: Cochrane method = B; Jadad score = 2
Participants: Mi ld to moderate ( W H O stage I or II) essential
hypertension for inclusion into trial.
N = 20: 14 m, 3 f. Mean age: 48.9 years (range: 33 - 60).
Baseline standing BP: 167/106 mm H g (Nitren. group), and 168/107
mm H g (placebo group). Baseline pulse pressure: 61 mm Fig (Nitren.
group), and 61 mm H g (placebo group).
Interventions: Nitrendipine 20 mg/day, or placebo.
119

Primary and secondary outcomes: Change from baseline in trough
supine/standing SBP, D B P (Instrument: H g sphygmomanometer), and
H R , peripheral hemodynamic parameters by radionuclide techniques.
Notes: B P s / H R s and associated SDs extracted from Table 2. SDs of
B P / H R change imputed from other trials.
Funding source: Not reported.
Lederle 1991 (197)
[Duplicate publication: Klaus 1990 (198)]
Design: M C / R / D B / P C trial. Placebo run-in period: 2 weeks.
Treatment duration: 6 weeks.
Country: Germany
Quality: Cochrane method = B; Jadad score = 3
Participants: WFIO stage f mild essential hypertension for inclusion
into trial.
N = 141: 88 m, 53 f. Mean age: 54.8 years (range: not reported).
Baseline sitting BP: 161.4/99.6 mm H g (Nitren. group), and 161.3/99.6
mm H g (placebo group). Baseline pulse pressure: 61.8 mm H g (Nitren.
group), and 61.7 mm Fig (placebo group).
Interventions: Nitrendipine 10 mg/day, or placebo.
Primary and secondary outcomes: Number of treatment responders
(DBP reduced by > 10 mm H g and/or to a value of < 90 mm Hg)
after 6 weeks of treatment. Change from baseline in sitting trough
SBP, D B P (Instrument: sphygmomanometer), and HR.
Notes: B P s / H R s and associated SDs extracted from text, p. S49 and
figure 1. SDs of S B P / H R change imputed from weighted mean of
week 4 and 6 SBPs/FIRs. W D A E extracted from text, p. S50.
Funding source: Not reported.
Maclean 1990 (199)
Design: M C / R / D B / P C trial. Washout period: 2-4 weeks. Placebo
run-in period: 3 weeks. Treatment duration: 6 weeks, followed by dose
doubling in nonresponders for 6 weeks.
Country: U K
Quality: Cochrane method = B; Jadad score = 3
Participants: Sitting D B P 95-115 mm H g for inclusion into trial.
120

N — 64 (excluding atenolol and combination groups): 29 m, 35 f.
Mean age: 51 years (range: 18-75).
Baseline sitting BP: 171/108 mm H g (Nitren. group), and 171/108 mm
H g (placebo group). Baseline pulse pressure: 63 mm H g (Nitren.
group), and 63 mm H g (placebo group).
Interventions: Nitrendipine 20 mg/day, atenolol 50 mg/day, atenolol
50 mg + nitrendipine 20 mg combination, or placebo.
Primary and secondary outcomes: Change from baseline in trough
sitting/standing SBP, D B P (Instrument: Hawkesley random-zero
sphygmomanometer), and HR.
Notes: Sitting B P s / H R s extracted from Table 4. SDs of baseline and
week 6 BPs extracted from Figure 2. SD of B P change imputed from
week 6 SD of BPs. (95% CI of differences between treatment and
placebo were reported but mean differences were not reported).
W D A E extracted from text, p. 457.
Fund ing source: Not reported.
PaoHsso 1991 (200)
Design: R / D B / P C trial. Washout period: > 3 weeks. Treatment
duration: 60 days.
Country: Italy
Quality: Cochrane method — B; Jadad score = 2
Participants: Elderly patients with ISH.
N = 20: 11 m, 9 f. Mean age: 76.8 years (range: not reported). -
Baseline BP: 180/92 mm H g (Nitren. group), and 178/91 mm H g
(placebo group). Baseline pulse pressure: 88 mm Fig (Nitren. group),
and 87 mm Fig (placebo group).
Interventions: Nitrendipine 20 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in SBP,
D B P (Instrument: not reported), and H R ; hemodynamic and
laboratory tests; oral glucose tolerance test.
Notes: B P s / H R s and associated SEMs extracted from table, p. 696.
SDs of BP change imputed from SDs of week 8 BPs.
121
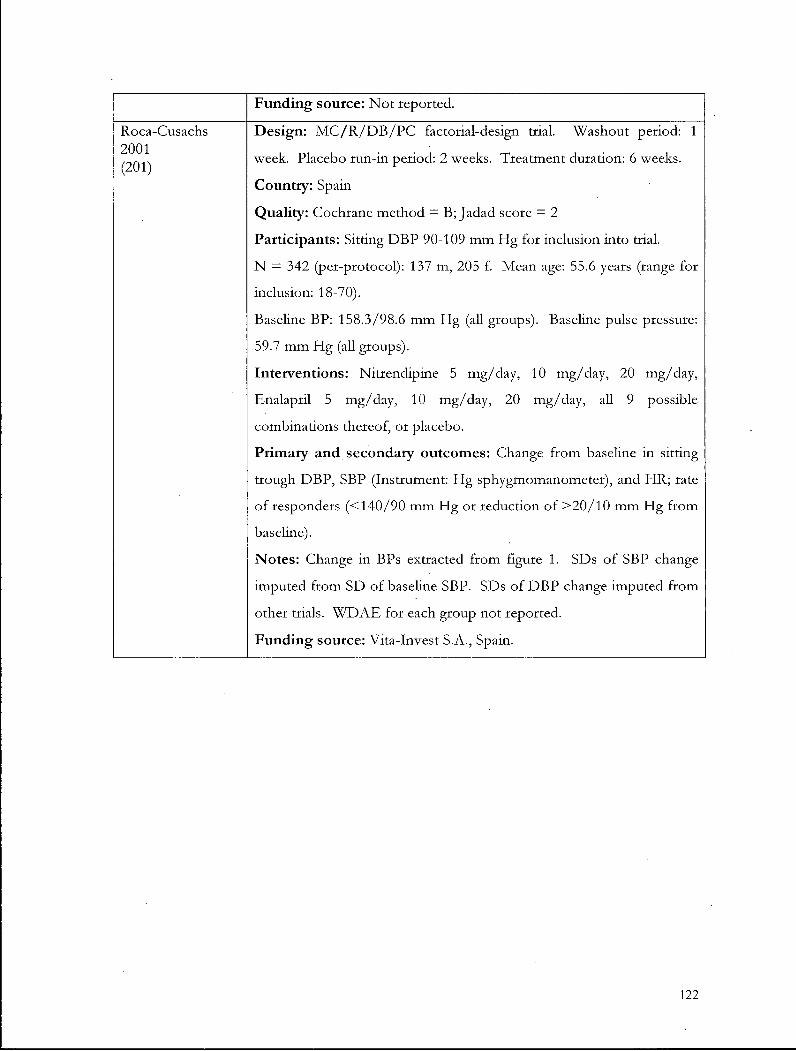
Funding source: Not reported.
Roca-Cusachs 2001 (201)
Design: M C / R / D B / P C factorial-design trial. Washout period: 1
week. Placebo run-in period: 2 weeks. Treatment duration: 6 weeks.
Country: Spain
Quality: Cochrane method = B; Jadad score = 2
Participants: Sitting D B P 90-109 mm H g for inclusion into trial.
N = 342 (per-protocol): 137 m, 205 f. Mean age: 55.6 years (range for
inclusion: 18-70).
Baseline BP: 158.3/98.6 mm H g (all groups). Baseline pulse pressure:
59.7 mm H g (all groups).
Interventions: Nitrendipine 5 mg/day, 10 mg/day, 20 mg/day,
Enalapril 5 mg/day, 10 mg/day, 20 mg/day, all 9 possible
combinations thereof, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
trough D B P , SBP (Instrument: Fig sphygmomanometer), and FIR; rate
of responders (< 140/90 mm H g or reduction of >20/10 mm Fig from
baseline).
Notes: Change in BPs extracted from figure 1. SDs of SBP change
imputed from SD of baseline SBP. SDs of D B P change imputed from
other trials. W D A E for each group not reported.
Funding source: Vita-Invest S.A., Spain.
122
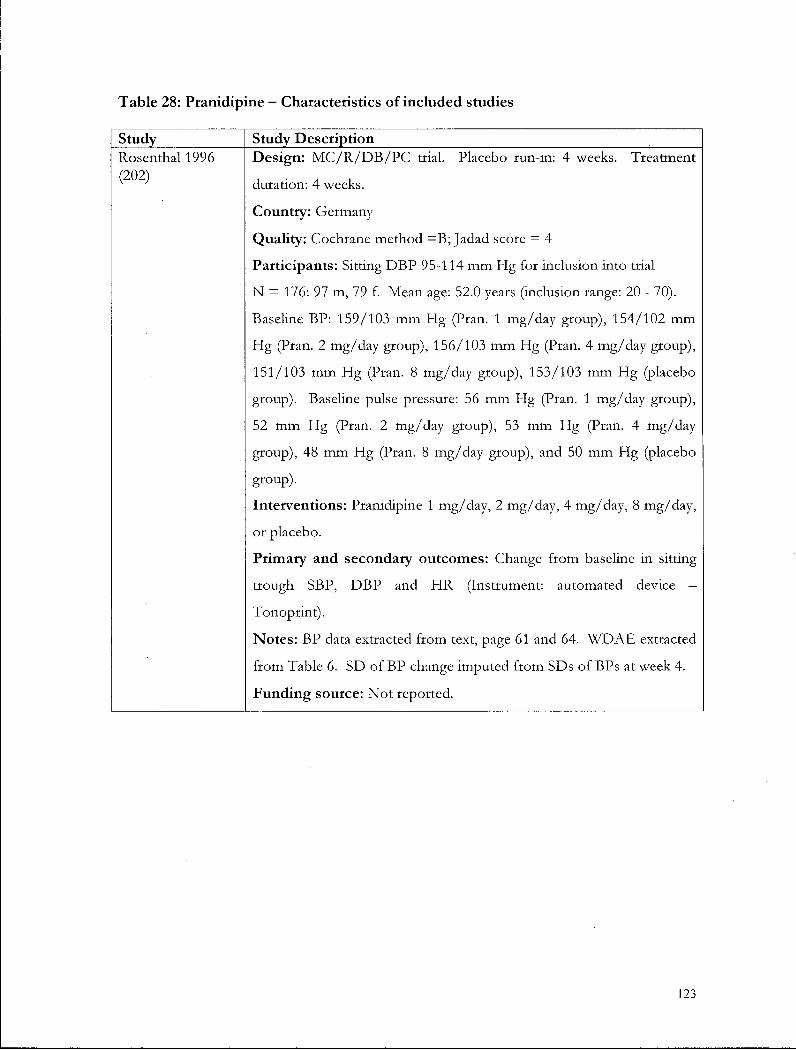
Table 28: Pranidipine - Characteristics of inc luded studies
Study Study Descr ipt ion Rosenthal 1996 (202)
Des ign: M C / R / D B / P C trial. Placebo run-in: 4 weeks. Treatment
duration: 4 weeks.
Country: Germany
Quali ty: Cochrane method =B; Jadad score = 4
Participants: Sitting D B P 95-114 mm H g for inclusion into trial
N = 176: 97 m, 79 f. Mean age: 52.0 years (inclusion range: 20 - 70).
Baseline BP: 159/103 mm H g (Pran. 1 mg/day group), 154/102 mm
H g (Pran. 2 mg/day group), 156/103 mm H g (Pran. 4 mg/day group),
151/103 mm H g (Pran. 8 mg/day group), 153/103 mm H g (placebo
group). Baseline pulse pressure: 56 mm H g (Pran. 1 mg/day group),
52 mm H g (Pran. 2 mg/day group), 53 mm H g (Pran. 4 mg/day
group), 48 mm Pig (Pran. 8 mg/day group), and 50 mm H g (placebo
group).
Interventions: Pranidipine 1 mg/day, 2 mg/day, 4 mg/day, 8 mg/day,
or placebo.
Primary and secondary outcomes: Change from baseline in sitting
trough SBP, D B P and PIR (Instrument: automated device —
Tonoprint).
Notes: B P data extracted from text, page 61 and 64. W D A E extracted
from Table 6. SD of B P change imputed from SDs of BPs at week 4.
Fund ing source: Not reported.
123

Table 29: Tiapamil - Characteristics of included studies
Study Study Description Blanchett 1991 (203)
Design: M C / R / D B / P C trial. Placebo run-in: 4 weeks. Treatment
duration: 6 weeks, followed by 1 week washout.
Country: USA
Quality: Cochrane method =B; Jadad score = 3
Participants: Sitting D B P 95-115 mm H g for inclusion into trial
N = 58: 36 m, 22 f. Mean age: 50.5 years (range: 24 - 67).
Baseline BP: 153/103 mm H g (Level. I group), 150/100 mm H g (Level
II group), 155/104 mm Fig (placebo group). Baseline pulse pressure:
50 mm H g (Level I group), 50 mm H g (Level II group), and 51 mm
H g (placebo group).
Interventions: Tiapamil 300 mg/day or 600 mg/day ("Level I"), 900
mg/day or 1200 mg/day ("Level II"), or placebo.
Primary and secondary outcomes: Change from baseline in
standing/sitting/supine trough SBP, D B P and FIR (Instrument:
sphygmomanometer, A B P M (Instrument: Spacelabs 5200)
Notes: BPs, HRs and associated SDs extracted from table 2 (reported
in dosage groups 300-600 mg/day and 900-1200 mg/day). W D A E
extracted from text, p. 61. SD of change in B P s / H R s imputed from
week 6 BPs.
Author contacted to obtain # of patients on each dose — no response.
Funding source: Hoffman La-Roche, Inc., USA.
124
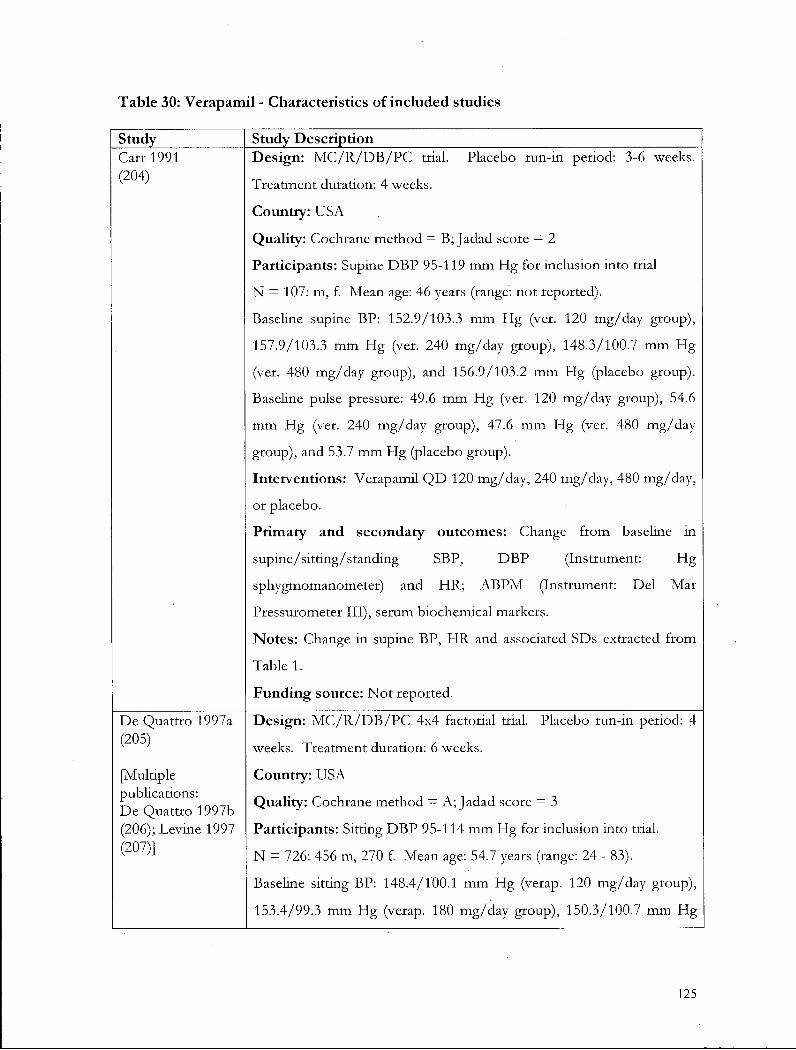
Table 30: Verapami l - Characteristics of inc luded studies
Study Study Descr ipt ion Carr 1991 (204)
Design: M C / R / D B / P C trial. Placebo run-in period: 3-6 weeks.
Treatment duration: 4 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 2
Participants: Supine D B P 95-119 mm H g for inclusion into trial
N = 107: m, f. Mean age: 46 years (range: not reported).
Baseline supine BP: 152.9/103.3 mm H g (ver. 120 mg/day group),
157.9/103.3 mm H g (ver. 240 mg/day group), 148.3/100.7 mm Pig
(ver. 480 mg/day group), and 156.9/103.2 mm H g (placebo group).
Baseline pulse pressure: 49.6 mm Pig (ver. 120 mg/day group), 54.6
mm H g (ver. 240 mg/day group), 47.6 mm H g (ver. 480 mg/day
group), and 53.7 mm H g (placebo group).
Interventions: Verapamil Q D 120 mg/day, 240 mg/day, 480 mg/day,
or placebo.
Primary and secondary outcomes: Change from baseline in
supine/sitting/standing SBP, D B P (Instrument: H g
sphygmomanometer) and PIR; A B P M (Instrument: Del Mar
Pressurometer III), serum biochemical markers.
Notes: Change in supine BP , PIR and associated SDs extracted from
Table f.
Fund ing source: Not reported.
De Quattro 1997a (205)
[Multiple publications: De Quattro 1997b (206) ;Levine 1997 (207) ]
Design: M C / R / D B / P C 4x4 factorial trial. Placebo run-in period: 4
weeks. Treatment duration: 6 weeks.
Country: U S A
Quality: Cochrane method = A ; Jadad score = 3
Participants: Sitting D B P 95-114 mm H g for inclusion into trial.
N = 726: 456 m, 270 f. Mean age: 54.7 years (range: 24 - 83).
Baseline sitting BP: 148.4/100.1 mm H g (verap. 120 mg/day group),
153.4/99.3 mm H g (verap. 180 mg/day group), 150.3/100.7 mm H g
125
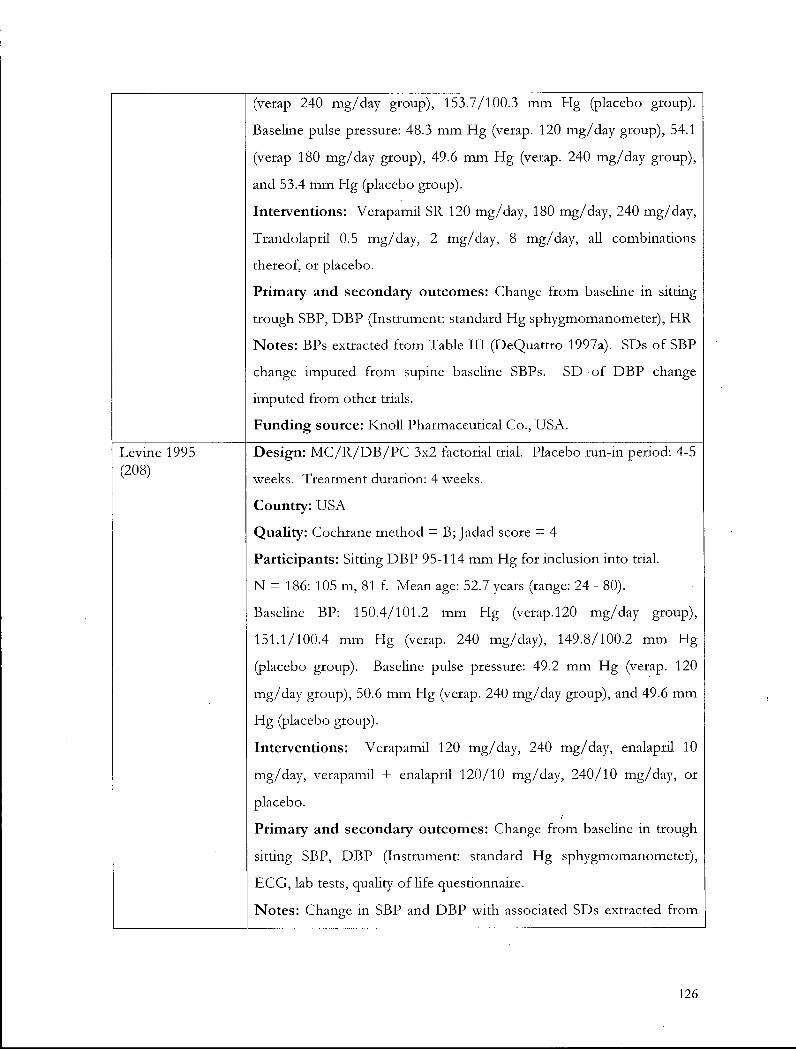
(verap 240 mg/day group), 153.7/100.3 mm H g (placebo group).
Baseline pulse pressure: 48.3 mm H g (verap. 120 mg/day group), 54.1
(verap 180 mg/day group), 49.6 mm H g (verap. 240 mg/day group),
and 53.4 mm H g (placebo group).
Interventions: Verapamil SR 120 mg/day, 180 mg/day, 240 mg/day,
Trandolapril 0.5 mg/day, 2 mg/day, 8 mg/day, all combinations
thereof, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
trough SBP, D B P (Instrument: standard H g sphygmomanometer), H R
Notes: BPs extracted from Table III (DeQuattro 1997a). SDs of SBP
change imputed from supine baseline SBPs. SD of D B P change
imputed from other trials.
Funding source: Kno l l Pharmaceutical Co., USA.
Levine 1995 (208)
Design: M C / R / D B / P C 3x2 factorial trial. Placebo run-in period: 4-5
weeks. Treatment duration: 4 weeks.
Country: USA
Quality: Cochrane method = B; Jadad score — 4
Participants: Sitting D B P 95-114 mm H g for inclusion into trial.
N = 186: 105 m, 81 f. Mean age: 52.7 years (range: 24 - 80).
Baseline BP: 150.4/101.2 mm H g (verap.120 mg/day group),
151.1/100.4 mm H g (verap. 240 mg/day), 149.8/100.2 mm H g
(placebo group). Baseline pulse pressure: 49.2 mm H g (verap. 120
mg/day group), 50.6 mm H g (verap. 240 mg/day group), and 49.6 mm
H g (placebo group).
Interventions: Verapamil 120 mg/day, 240 mg/day, enalapril 10
mg/day, verapamil + enalapril 120/10 mg/day, 240/10 mg/day, or
placebo.
Primary and secondary outcomes: Change from baseline in trough
sitting SBP, D B P (Instrument: standard H g sphygmomanometer),
E C G , lab tests, quality of life questionnaire.
Notes: Change in SBP and D B P with associated SDs extracted from
126

Table 2 and 3, respectively. W D A E extracted from text, p. 497.
Fund ing source: Lederle Laboratories, USA.
McMahon 1989 (209)
Design: M C / R / D B / P C trial. Placebo run-in period: 1-4 weeks.
Treatment duration: 6 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 3
Participants: Supine D B P 95-114 mm H g for inclusion into trial.
N = 221: 127 m, 94 f. Mean age: 54.8 years (>f 8 for inclusion).
Baseline supine BP: 159.6/101.8 mm Fig (verap. 60 mg/day group),
152.6/99.8 mm H g (verap. 120 mg/day group), 157.7/101.4 mm H g
(verap. 240 mg/day group), 151.8/99.6 mm H g (verap. 480 mg/day),
156.2/100.7 mm H g (placebo group). Baseline pulse pressure: 57.8
mm H g (verap. 60 mg/day group), 52.8 mm H g (verap. 120 mg/day
group), 56.3 mm H g (verap. 240 mg/day group), 52.2 mm H g (verap.
480 mg/day group), and 55.5 mm H g (placebo group).
Interventions: Verapamil-SR 60 mg/day, 120 mg/day, 240 mg/day,
480 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in supine
peak and trough SBP, D B P (Instrument: not reported; by auscultation),
FIR, E C G , lab tests.
Notes: Trough BPs and associated SEs extracted from Table II. SD
of B P change imputed from SD of endpoint BPs. Baseline HRs not
reported. W D A E extracted from Table 111.
Author deceased.
Fund ing source: Not reported.
Messerli 1998 (210)
Design: M C / R / D B / P C trial. Placebo run-in period: 4 weeks.
Treatment duration: 6 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 3
Participants: D B P 95-114 mm H g for inclusion into trial.
N = 631: 401 m, 230 f. Mean age: 54.5 years (range: 21-88).
127

Baseline sitting BP: 151.1/100.8 mm H g (verapamil group),
153.6/100.5 mm H g (placebo group). Baseline pulse pressure: 50.3
mm H g (verapamil group), and 53.1 mm H g (placebo group).
Interventions: Verapamil SR 240 mg/day, trandolopril 4 mg/day,
verapamil SR 240 mg/trandolopril 4 mg combination, or placebo.
Primary and secondary outcomes: Change from baseline in trough
sitting D B P , SBP (Instrument: standard H g sphygmomanometer), H R
at peak and trough; % responders (DBP < 90 mm H g or > 10 mm H g
decrease).
Notes: Change in BPs and associated SEs extracted from Table 2.
Changes in B P reported were already adjusted for placebo effect.
Therefore, SDs of change in BP for the placebo group were imputed
from other trials.
Fund ing source: Kno l l Pharmaceutical Company, New Jersey.
Neutel 1996 (211)
Design: M C / R / D B / P C trial. Washout period: 1-2 weeks. Placebo
run-in period: 2-4 weeks. Treatment duration: 4 weeks.
Country: U S A
Quality: Cochrane method = B ; Jadad score = 3
Participants: Sitting D B P 95-114 mm H g and mean daytime
ambulatory D B P >90 mm H g for inclusion into trial.
N = 95: 64m, 31 f. Mean age: 56.7 years (range: not reported).
Baseline BP: 158.6/99.9 mm H g (verapamil group), 157.5/101.2 mm
H g (placebo group). Baseline pulse pressure: 58.7 mm H g (verapamil
group), and 56.3 mm H g (placebo group).
Interventions: Verapamil COER-24 240 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
SBP, D B P (Instrument: H g sphygmomanometer), A B P M (Instrument:
SpaceLabs 90202).
Notes: Change in BPs and associated SDs, W D A E extracted from
text, p. 1203. Baseline HRs not reported.
Fund ing source: Not reported.
128
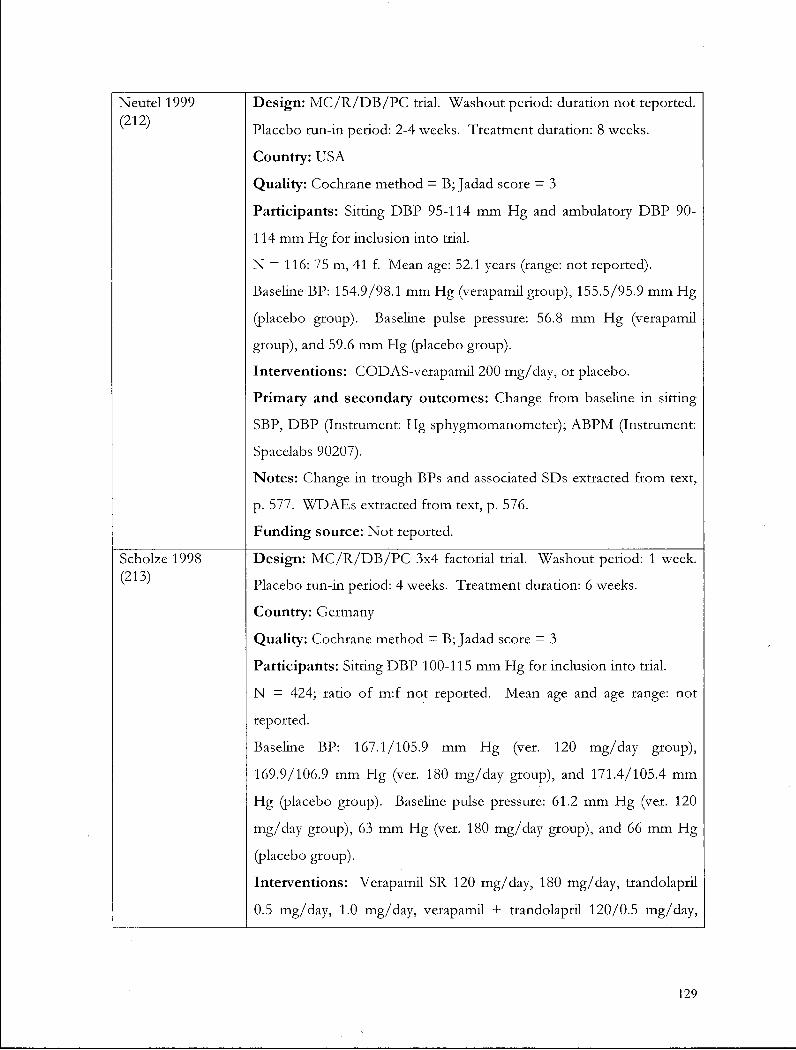
Neutel 1999 (212)
Design: M C / R / D B / P C trial. Washout period: duration not reported.
Placebo run-in period: 2-4 weeks. Treatment duration: 8 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 3
Participants: Sitting D B P 95-114 mm H g and ambulatory D B P 90-
114 mm H g for inclusion into trial.
N = 116: 75 m, 41 f. Mean age: 52.1 years (range: not reported).
Baseline BP: 154.9/98.1 mm H g (verapamil group), 155.5/95.9 mm H g
(placebo group). Baseline pulse pressure: 56.8 mm H g (verapamil
group), and 59.6 mm H g (placebo group).
Interventions: CODAS-verapamil 200 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
SBP, D B P (Instrument: H g sphygmomanometer); A B P M (Instrument:
Spacelabs 90207).
Notes: Change in trough BPs and associated SDs extracted from text,
p. 577. W D A E s extracted from text, p. 576.
Fund ing source: Not reported.
Scholze 1998 (213)
Design: M C / R / D B / P C 3x4 factorial trial. Washout period: 1 week.
Placebo run-in period: 4 weeks. Treatment duration: 6 weeks.
Country: Germany
Quality: Cochrane method — B; Jadad score = 3
Participants: Sitting D B P 100-115 mm H g for inclusion into trial.
N = 424; ratio of m:f not reported. Mean age and age range: not
reported.
Baseline BP: 167.1/105.9 mm H g (ver. 120 mg/day group),
169.9/106.9 mm Fig (ver. 180 mg/day group), and 171.4/105.4 mm
H g (placebo group). Baseline pulse pressure: 61.2 mm Fig (ver. 120
mg/day group), 63 mm Fig (ver. 180 mg/day group), and 66 mm Fig
(placebo group).
Interventions: Verapamil SR 120 mg/day, 180 mg/day, trandolapril
0.5 mg/day, 1.0 mg/day, verapamil + trandolapril 120/0.5 mg/day,
129
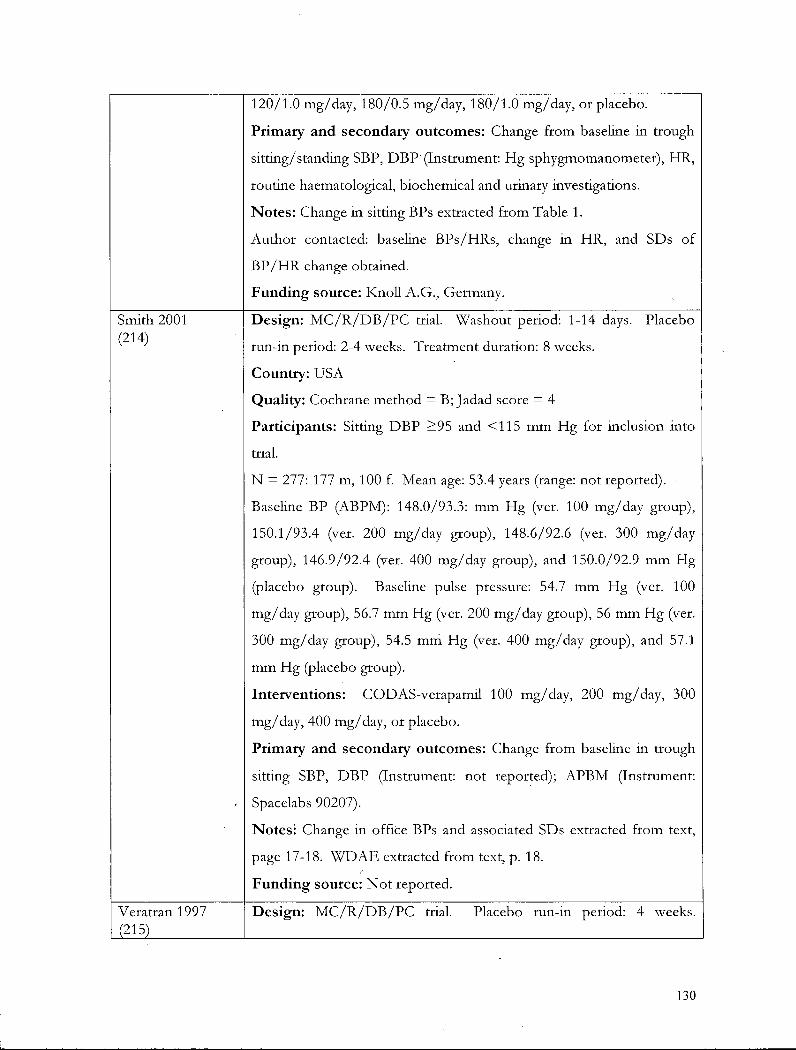
120/1.0 mg/day, 180/0.5 mg/day, 180/1.0 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
sitting/standing SBP, D B P (fnstrument: H g sphygmomanometer), H R ,
routine haematological, biochemical and urinary investigations.
Notes: Change in sitting BPs extracted from Table 1.
Author contacted: baseline B P s / H R s , change in HR, and SDs of
B P / H R change obtained.
Fund ing source: Kno l l A . G . , Germany.
Smith 2001 (214)
Design: M C / R / D B / P C trial. Washout period: 1-14 days. Placebo
run-in period: 2-4 weeks. Treatment duration: 8 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 4
Participants: Sitting D B P >95 and <115 mm H g for inclusion into
trial.
N = 277: 177 m, 100 f. Mean age: 53.4 years (range: not reported).
Baseline B P (ABPM): 148.0/93.3: mm H g (ver. 100 mg/day group),
150.1/93.4 (ver. 200 mg/day group), 148.6/92.6 (ver. 300 mg/day
group), 146.9/92.4 (ver. 400 mg/day group), and 150.0/92.9 mm H g
(placebo group). Baseline pulse pressure: 54.7 mm Fig (ver. 100
mg/day group), 56.7 mm H g (ver. 200 mg/day group), 56 mm H g (ver.
300 mg/day group), 54.5 mm H g (ver. 400 mg/day group), and 57.1
mm H g (placebo group).
Interventions: CODAS-veraparnil 100 mg/day, 200 mg/day, 300
mg/day, 400 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in trough
sitting SBP, D B P (Instrument: not reported); A P B M (fnstrument:
Spacelabs 90207).
Notes: Change in office BPs and associated SDs extracted from text,
page 17-18. W D A E extracted from text, p. 18.
Fund ing source: Not reported.
Veratran 1997 (215)
Design: M C / R / D B / P C trial. Placebo run-in period: 4 weeks.
130

Treatment duration: 8 weeks.
Country: Italy
Quality: Cochrane method = B; Jadad score = 3
Participants: Sitting D B P 100-110 mm H g for inclusion into trial
N = 272 (234 in efficacy analysis): 134 m, 100 f. Mean age: 49.9 years
(range: 18 — 65 for inclusion).
Baseline BP: 156.0/104.2 mm H g (verapamil group), 158.2/103.5 mm
H g (placebo group). Baseline pulse pressure: 51.8 mm H g (verapamil
group), and 54.7 mm H g (placebo group).
Interventions: Verapamil SR 180 mg/day, trandolapril 1 mg/day,
verapamil SR 180 mg/day + trandolapril 1 mg/day combination, or
placebo.
Primary and secondary outcomes: Change from baseline in sitting
SBP, D B P (Instrument: H g sphygmomanometer) and H R
Notes: Week 8 BPs, HRs and associated SDs extracted from Table 1.
SDs of B P / H R change imputed from week 8 BPs /HRs . # of patients
in each group reported for efficacy analysis only — cannot use W D A E
data since # of patients at randomization not reported.
Funding source: Not reported.
V o n Manteuffel 1995 (216)
Design: M C / R / D B / P C trial. Placebo run-in period: 4 weeks.
Treatment duration: 6 weeks.
Country: Germany and Austria
Quality: Cochrane method = B; Jadad score = 2
Participants: Sitting D B P 100-115 mm H g for inclusion into trial
N = 176: 91 m, 85 f. Mean age: 56.3 years (range: 1 8 - 7 0 for
inclusion).
Baseline BP: 173.7/106.7 mm H g (verapamil group), 168.2/105.6 mm
Fig (placebo group). Baseline pulse pressure: 67 mm H g (verpamail
group), and 62.6 mm Tig (placebo group).
Interventions: Verapamil SR 240 mg/day, hydrochlorothiazide 12.5
mg/day, verapamil SR 240 mg/day + H C T Z 12.5 mg/day
131

combination, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
SBP, D B P (Instrument: not reported), % responders (decrease in D B P
> 10 mm H g or normalization of D B P to < 90 mm Hg).
Notes: Published in German. Weighted mean SBPs at week 4 and 6
extracted from Figure 2. SD of change in SBP imputed from baseline
SBP. D B P at week 6 extracted from text, p. 375. SD of change in
D B P imputed from other trials.
Fund ing source: Not reported.
White 1995 (217)
Design: M C / R / D B / P C trial. Washout period: 1 week. Placebo run-
in period: 2-4 weeks. Treatment duration: 8 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 2
Participants: Sitting D B P 95-114 mm Fig and A B P M daytime D B P >
90 mm H g for inclusion into trial.
N = 287; ratio of m:f not reported. Mean age: 53.2 years (range: not
reported).
Baseline BP: 159/101 mm H g (ver. 120 mg/day group), 155/100 mm
H g (ver. 180 mg/day), 158/102 mm Fig (ver. 360 mg/day), 158/101
mm H g (ver. 540 mg/day), 156/101 mm H g (placebo group). Baseline
pulse pressure: 58 mm H g (ver. 120 mg/day group), 55 mm H g (ver.
180 mg/day group), 56 mm H g (ver. 360 mg/day group), 57 mm H g
(ver. 540 mg/day group), and 55 mm H g (placebo group).
Interventions: Physiologic pattern release (PPR)-verapamil 120
mg/day, 180 mg/day, 360 mg/day, 540 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in sitting
SBP, D B P (Instrument: H g sphygmomanometer), HR; A B P M
(Instrument: Spacelabs 90202).
Notes: Change in trough clinic B P s / H R s and SEs extracted from
Table II. W D A E data incompletely reported.
Fund ing source: Not reported.
132
\

White 2002 Des ign: M C / R / D B / P C trial. Washout period: 1-2 weeks. Placebo (218) run-in period: 2-4 weeks. Treatment duration: 8 weeks (forced titration
at week 4).
Country: U S A
Quality: Cochrane method = B; Jadad score — 3
Participants: Sitting D B P 95-114 mm H g and A B P M daytime D B P >
85 mm Pig for inclusion into trial.
N = 357: 219 m, 138 f. Mean age: 54.5 years (range: not reported).
Baseline sitting BP: 146/95 mm H g (verapamil group), 148/95 mm H g
(placebo group). Baseline pulse pressure: 51 mm Pig (verapamil
group), and 53 mm H g (placebo group).
Interventions: COER-verapamil 240 360 mg/day, enalapril l O - ^
20 mg/day, losartan 50~^ 100 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in
sitting/standing SBP, D B P (fnstrument: H g sphygmomanometer) &
H R ; A B P M (fnstrument: Spacelabs 90207).
Notes: Change in sitting B P and associated SDs at week 8 extracted
from Table IV. Clinic HRs not reported. W D A E ' reported but on
what dose these occurred is not specified.
Fund ing source: Not reported.
133

3.3 Characteristics of studies awaiting data from authors
Table 31: Characteristics of studies meeting inclusion criteria and await ing office blood pressure data from authors
Study Study Descr ipt ion Bakris 2002 (219)
Design: M C / R / D B / P C trial. Washout period: 1-2 weeks. Placebo
run-in period: 2-4 weeks. Treatment duration: 8 weeks (forced titration
at week 4)
Country: U S A and Canada
Quality: Cochrane method = B; Jadad score = 3
Participants: Sitting D B P 95-114 mm H g for inclusion into trial.
N = 405: 223 m, 182 f. Mean age: years (inclusion range: 21 — 80).
Baseline sitting BP: 145/95 mm H g (verap. group), and 146/96 mm H g
(placebo group). Baseline pulse pressure: 50 mm H g (verap. group),
and 50 mm H g (placebo group).
Interventions: COER-verapamil 240 360 mg/day, enalapril 10-^
20 mg/day, losartan 50 100 mg/day, or placebo.
Primary and secondary outcomes: Change from baseline in
sitting/standing office SBP, D B P (fnstrument: not reported), 24-hour
A B P M (fnstrument: Spacelabs 90207), rate of rise of B P / H R during
the morning acceleration phase.
Notes: Office B P s / H R s to be obtained from author.
Fund ing Source: Pharmacia Corp., USA.
Glasser 2003 (220)
Design: M C / R / D B / P C trial. Placebo run-in period: 3-4 weeks.
Treatment duration: 7 weeks.
Country: U S A
Quality: Cochrane method = B; Jadad score = 3
Participants: sitting D B P 100-114 mm H g for inclusion into trial.
N — 478: 303 m, 175 f. Mean age: 52 years (inclusion range: 18 — 70).
Baseline BP/pulse pressure: office values not reported.
Interventions: Diltizaem extended-release 120 mg/day, 240 mg/day,
360 mg/day, 540 mg/day, or placebo.
134

Primary and secondary outcomes: Change from baseline in
sitting/standing office SBP, D B P (Instrument: not reported) and H R ;
24-hour A B P M (Instrument: Spacelabs 90207).
Notes: Office B P s / H R s to be obtained from author.
Fund ing Source: Not reported.
135

3.4 Characteristics of excluded studies
Table 32 below documents the reasons why 134 studies that met the primary
inclusion criteria had to be excluded from the analysis. Several of these studies were either
cross-over trials that did not report pre-crossover data or parallel-group studies that allowed
dose titration in non-responders. Other common reasons for exclusion included failure to
report details such as number of patients in each arm, baseline blood pressures, or pre-
titration data.
Table 32: Reasons for exclusion of certain studies meeting inclusion criteria
Study I D Reason for exclusion Abadie 1985 (221)
R / D B / P C parallel group trial that assessed the effect of nifedipine 30 mg/day on carbohydrate metabolism — no blood pressures reported.
Ahmed 1992a (222)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1" four weeks of treatment (nicardipine 90 mg/day vs. placebo)
Allrkmets 1997 (223)
R / D B / P C parallel group trial with no data reported for the 1 s t four weeks of treatment prior to titration in non-responders (isradipine 5 mg/day vs. placebo)
Andersson 1989 (224)
[Duplicate publication: Andersson 1990 (225)1
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t nine weeks of treatment [isradipine 2.5 mg (3 weeks) 5 mg (3 weeks) 7.5 mg (3 weeks) vs: placebo]
Andren 1988 (226)
R / D B / P C cross-over trial with no data reported for the 1 s t three weeks of treatment, prior to cross-over and also prior to titration in non-responders (diltiazem 240 mg/day vs. placebo)
Arita 1999 (227)
R / D B / P C cross-over trial with no pre-crossover data for the 1 s t
four weeks of treatment (azelnidipine 8 mg vs. placebo) ArziUi 1993 (228)
R / D B / P C cross-over trial with no pre-crossover data for the 1 s t 4 weeks of treatment (isradipine SRO 5 mg vs. placebo)
Bainbridge 1993 (229)
R / D B / P C cross-over trial with no pre-crossover data for the 1 s t 4 weeks of treatment (felodipine E R 5 mg/day vs. ramipril 2.5 mg/day vs. felodipine E R 5 mg + ramipril 2.5 mg vs. placebo)
B aylac-D omengetroy 1990 (230)
R / D B / P C parallel group trial that studied nitrendipine 20 mg/day vs. placebo. N o data reported for the placebo group.
BeUet 1985 (231)
R / D B / P C parallel group trial. Dose titration in non-responders after 15 days of treatment (nicardipine 60 mg/day vs. placebo)
Bossini 1990 (232)
R / D B / P C cross-over trial with no pre-crossover data for the 1s t 4 weeks of treatment (felodipine E R 10 mg/day vs. placebo)
136

Study I D Reason for exclusion British Isradipine Hypertension Group 1989 (233)
R / D B / P C parallel group trial with no data reported for the 1 s t
three weeks of treatment prior to titration in non-responders [isradipine 2.5 mg/day (1.25 mg twice daily or 2.5 mg once daily) vs. placebo].
CampbeU 1990 (234)
R / D B / P C parallel group trial with no data reported for the 1 s t six weeks of treatment prior to titration in non-responders (felodipine E R 5 mg vs. placebo)
Capewell 1989 (235)
R / D B / P C cross-over trial with no pre-crossover data for the 1 s t 4 weeks of treatment (felodipine 10 mg/day vs. placebo). Titration in non-responders after 2 weeks treatment.
Carr 1990 (236)
R / D B / P C parallel group trial with initial dose titrated to response. Data from responders and non-responders reported separately, (isradipine 5, 10, 15, or 20 mg, depending on B P response vs. placebo).
Chalmers 1990 (237)
Reports on 3 studies. The 3 r d study was a R / D B / P C cross-over trial with no pre-crossover data for the 1 s t four weeks of treatment with diltiazem 240 mg/day
Clement 1987 (238)
R / D B / P C cross-over trial with no pre-crossover data for the 1 s t
three weeks of treatment (nifedipine SR 40 mg/day vs. atenolol 100 mg/day vs. placebo). N o baseline B P values given.
Cleroux 1992 (239)
R / D B / P C cross-over trial with no pre-crossover data for the 1 s t
four weeks of treatment (isradipine SR 5 mg vs. placebo) Cleroux 1994 (240)
R / D B / P C cross-over trial with no pre-crossover data for the 1 s t
four weeks of treatment. 8-week treatment periods but titration in non-responders after 4 weeks treatment, (verapamil 240mg/day vs. quniapril 10 mg/day vs. atenolol 50 mg/day)
Cox 1988 (241)
R / D B / P C cross-over trial with no pre-crossover data for the 1 s t six weeks of treatment (verapamil 40/80/120 mg/day vs. placebo). Open titration phase to determine dose before randomization.
Cox 1989 (242)
R / D B / P C cross-over trial with no pre-crossover data for the 1 s t
four weeks of treatment (nicardipine 120 mg/day vs. placebo) Crozier 1990 (243)
R / D B / P C cross-over trial with no pre-crossover data for the 1" five weeks of treatment (felodipine 20 mg/day vs. placebo)
De Brmjn 1988 (244)
R / D B / P C parallel group trial with 8-week treatment period. Dose titration in non-responders at 2-week intervals (starting dose: amlodipine 2.5 mg vs. atenolol 50 mg/day vs. placebo)
Diemont 1991 (245)
Reports on two studies: one single blind study and one cross-over trial with no pre-crossover data for the 1 s t four weeks of isradipine M R 5 mg/day vs. isradipine M R 10 mg/day vs. placebo
Dittrich 1992 (246)
R / D B / P C parallel group trial. Doses of 60 mg, 90 mg, or 120 mg/day of nicardipine were studied. Number of patients on each dose and titration schedule not reported.
Draaijer 1995 (247)
R / D B / P C parallel group trial. B P data reported only at the end of six months of treatment (felodipine 5 mg/day vs. enalapril 10 mg/day vs. placebo)

Study I D Reason for exclusion Dupont 1991 (248) .
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t three weeks of diltiazem L P 300 mg/day vs. placebo
Duprez 1991 (249)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t six weeks of isradipine 10 mg/day vs. placebo
Durel 1992 (250)
A study consisting of six 28-day cross-over trials in a quasi-random order. N o baseline B P data and no pre-crossover data reported for the 1 s t 4 weeks of verapamil 240 mg/day vs. placebo.
Faguer de Moustier 1989 (251)
[Duplicate publication: Faguer de Moustier 1990 (252)
R / D B / P C parallel group trial with titration in non-responders after 15 days of treatment with nicardipine 60 mg/day vs. placebo.
Ferreira-Filho 1995 (253)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of nifedipine SR 40 mg/day vs. placebo
Fogan 1993 (254)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of isradipine SRO 5 mg/day (administered morning or night) vs. placebo
Forette 1984 (255)
[Duplicate publication: Forette 1985 (256)]
R / D B / P C parallel group trial with titration in non-responders every 8 days during treatment, starting with nicardipine 30 mg/day vs. placebo.
Fnshman 1988 (257)
(Multiple publications: Frishman 1994 (258) , Johnson 1992 (259), Johnson 1995 (260)]
R / D B / P C parallel group trial with titration in non-responders every 2 weeks during treatment, starting with amlodipine 2.5 mg/day vs. atenolol 50 mg vs. placebo.
Gavras 1987 (261)
R / D B / P C parallel group trial with titration in non-responders after 1 week of treatment with nifedipine GITS 30 mg/day vs. placebo.
Gebera 1996 (262)
R / D B / P C cross-over trial with dose titration in non-responders after 2 weeks of treatment with verapamil 240 mg/day vs. placebo. Pre-crossover data not reported
Grimm 2002 (263)
R / D B / P C parallel group trial with no data reported for the 1 s t four weeks of treatment with amlodipine 5 mg/day vs. placebo prior to titration in non-responders.
Hamilton B 1987 (264)
Reports on several phase III studies, including a R / D B / P C parallel group trial of isradipine 5 mg/day, 10 mg/day, 15 mg/day, 20 mg/day, or placebo. B P data not reported.
Harrington 1987 (265)
Reports on 2 studies: a short-term single-blind study, and a R / D B / P C cross-over trial with dose titration in non-responders every 2 weeks of treatment, starting with felodipine 5 mg/day vs. placebo. Pre-crossover data not reported.
138

Study ID Reason for exclusion Hedback 1984 (266)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of verapamil 360 mg/day vs. placebo
Herrera 1997 (267)
R / D B / P C parallel group trial with titration in non-responders during weeks 2-4 of treatment, starting with diltiazem C D 180 mg/day vs. placebo.
Honorato 1989 (268)
R / D B / P C parallel group 6-week trial of nitrendipine 20 mg/day vs. placebo. N o "n" values reported. Author contacted — no response.
Hosie 1991 (269)
R / D B / P C parallel group trial with titration in non-responders after 2 week of treatment with felodipine E R 5 mg/day vs. placebo.
[Conference abstract: Hosie 1990 (270)] Jeffrey 1990 (271)
R / D B / P C cross-over trial with dose titration in non-responders after 2 weeks of treatment with felodipine 10 mg/day vs. placebo. N o pre-crossover data reported. Only mean arterial pressure reported.
Kelemen 1990 (272)
R / D B / P C parallel group trial with exercise co-intervention.
[Duplicate publication: Stewart 1990 (273)] Khalil-Manesh 1987 (274)
R / D B / P C parallel group trial with titration in non-responders every 2 weeks during treatment, starting with diltiazem 120 mg/day vs. placebo.
Kjellstrom 1994 (275)
R / D B / P C cross-over trial with dose titration in non-responders after 2 weeks of treatment with felodipine E R 10 mg/day vs. placebo. Baseline B P and pre-crossover data not reported
Klauser 1990 (276)
[Duplicate publication: Klauser 1991 (277)]
R / D B / P C cross-over trial with 4-week treatment periods. Forced titration with isradipine 10 mg/day (2 weeks) isradipine 20 mg/day (2 weeks) vs. placebo. N o pre-crossover data reported
Krakoff 1989 (278)
R / D B / P C parallel group trial with titration in non-responders after 2 weeks of treatment with nicardipine 60 mg/day vs. placebo.
Lacourciere 1995 (279)
R / D B / P C parallel group trial with an 8-week treatment period during which there was forced titration every 2 weeks, starting with diltiazem E R 120 mg/day.
Lacourciere 1998 (280)
R / D B / P C parallel group trial with no data reported for the 1 s t
eight weeks of treatment with amlodipine 5 mg/day vs. placebo prior to titration in non-responders.
Landmark 1985 (281)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t eight weeks of nifedipine 40 mg/day vs. placebo
Lessem 1990 (282)
R / D B / P C parallel group trial that studied nicardipine 30 mg/day, 60 mg/day, 90 mg/day, and 120 mg/day vs. placebo. N o baseline BPs reported.
139
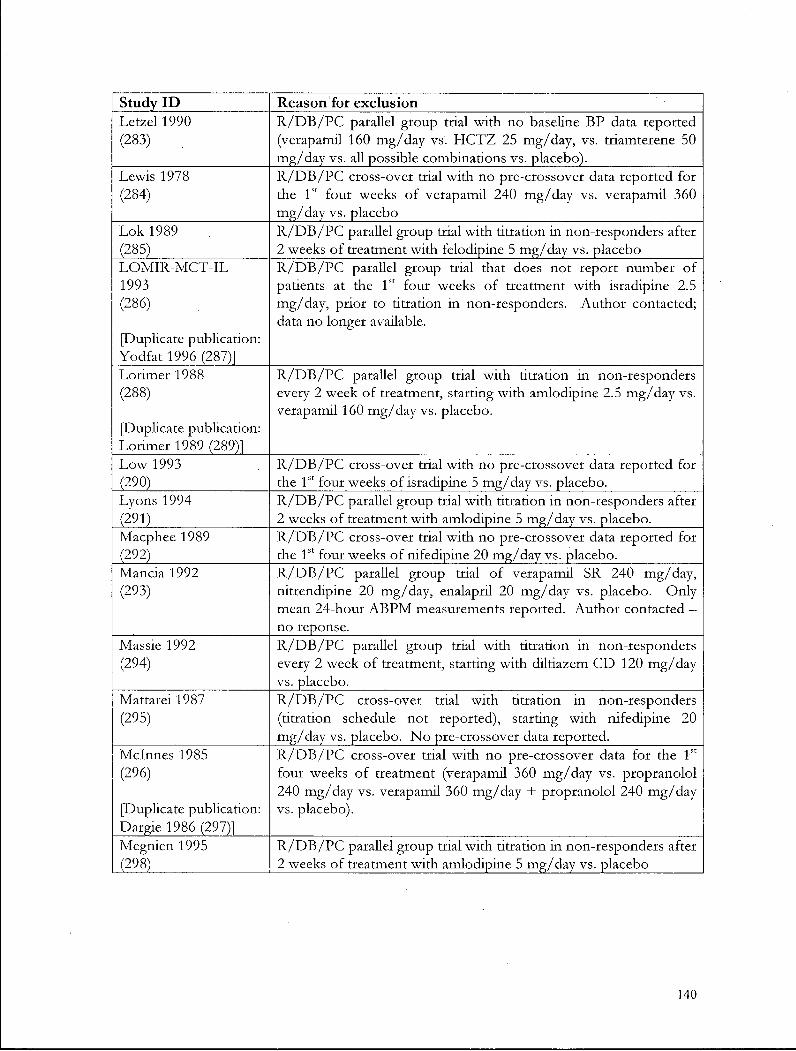
Study I D Reason for exclusion Letzel 1990 (283)
R / D B / P C parallel group trial with no baseline B P data reported (verapamil 160 mg/day vs. H C T Z 25 mg/day, vs. triamterene 50 mg/day vs. all possible combinations vs. placebo).
Lewis 1978 (284)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of verapamil 240 mg/day vs. verapamil 360 mg/day vs. placebo
Lok 1989 (285)
R / D B / P C parallel group trial with titration in non-responders after 2 weeks of treatment with felodipine 5 mg/day vs. placebo
L O M I R - M C T - I L 1993 (286)
[Duplicate publication: Yodfat 1996 (287)1
R / D B / P C parallel group trial that does not report number of patients at the 1 s t four weeks of treatment with isradipine 2.5 mg/day, prior to titration in non-responders. Author contacted; data no longer available.
Lorimer 1988 (288)
[Duplicate publication: Lorimer 1989 (289)1
R / D B / P C parallel group trial with titration in non-responders every 2 week of treatment, starting with amlodipine 2.5 mg/day vs. verapamil 160 mg/day vs. placebo.
Low 1993 (290)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of isradipine 5 mg/day vs. placebo.
Lyons 1994 (291)
R / D B / P C parallel group trial with titration in non-responders after 2 weeks of treatment with amlodipine 5 mg/day vs. placebo.
Macphee 1989 (292)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of nifedipine 20 mg/day vs. placebo.
Mancia 1992 (293)
R / D B / P C parallel group trial of verapamil SR 240 mg/day, nitrendipine 20 mg/day, enalapril 20 mg/day vs. placebo. Only mean 24-hour A B P M measurements reported. Author contacted — no reponse.
Massie 1992 (294)
R / D B / P C parallel group trial with titration in non-responders every 2 week of treatment, starting with diltiazem C D 120 mg/day vs. placebo.
Mattarei 1987 (295)
R / D B / P C cross-over trial with titration in non-responders (titration schedule not reported), starting with nifedipine 20 mg/day vs. placebo. N o pre-crossover data reported.
Mclnnes 1985 (296)
[Duplicate publication: Dargie 1986 (297)1
R / D B / P C cross-over trial with no pre-crossover data for the 1 s t
four weeks of treatment (verapamil 360 mg/day vs. propranolol 240 mg/day vs. verapamil 360 mg/day + propranolol 240 mg/day vs. placebo).
Megnien 1995 (298)
R / D B / P C parallel group trial with titration in non-responders after 2 weeks of treatment with amlodipine 5 mg/day vs. placebo
140

Study ID Reason for exclusion Midtbo 1980 (299)
[Duplicate publication: Storstein 1981 (300)1
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of verapamil 480 mg/day vs. placebo
Morgan 2001 (301)
R / D B / P C cross-over trial with forced titration after 1 month of treatment. N o pre-crossover data for the 1 s t 2 months of treatment with felodipine (dose not reported) vs. amlodipine 5 mg (1 month)
amlodipine 10 mg (1 month) vs. placebo. B P data from felodipine and amlodipine treatments lumped together.
Morgan 2002 (302)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1" four weeks of felodipine 5 mg/day vs. placebo.
Moser 1984 (303)
R / D B / P C parallel group trial with a weekly forced titration for 3 weeks, starting with nitrendipine 10 mg/day vs. placebo, followed by a 2-week maintenance period.
Nelson 1986 (304)
R / D B / P C parallel group trial with 3-week treatment period and weekly forced titration: isradipine 5 mg/day (1 week) - ^ 1 0 mg/day (1 week) 20 mg/day (1 week) vs. placebo.
Neutel 1995 (305)
R / D B / P C parallel group trial with no data reported for the 1 s t four weeks of treatment with verapamil 120 mg/day vs. placebo prior to titration in non-responders. Author contacted: no response?
Nikkila 1989 (306)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t three weeks of diltiazem 240 mg/day vs. placebo, prior to titration in non-reponsders.
Nikolova 1995 (307)
R / D B / P C parallel group trial comparing nifedipine 30 mg/day with placebo in treatment of hypertensive venous leg ulcers. Patients in both groups were allowed centrally acting antihypertensive drugs in addition to randomized treatment.
Nilsson 1996 (308)
R / D B / P C cross-over trial with single-blind diltiazem O D 300 mg/day run-in prior to randomization. N o pre-crossover data reported for the 1" six weeks of diltiazem O D 300 mg/day vs. placebo.
Ollivier 1995 (309)
R / D B / P C parallel group trial with titration in non-responders every 2 weeks, starting with diltiazem SR 200 mg/day vs. placebo.
Pacheco 1986 (310)
R / D B / P C parallel group trial with titration in non-responders during the 1 s t three weeks of treatment, starting with nifedipine 30 mg/day vs. placebo
Pandita-Gunawardena 1999 (311)
D B / P C parallel group trial. Allocation by minimization. N o data reported for the 1 s t four weeks of treatment with amlodipine 5 mg vs. placebo) prior to titration in non-responders
Pannarale 1996 (312)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of felodipine E R 10 mg/day vs. placebo
141

Study ID Reason for exclusion Persson 1989a (313)
[Multiple publications: Persson 1989b (314), Persson 1992 (315)]
R / D B / P C cross-over trial with no data reported for the 1 s t three weeks of treatment with isradipine 5 mg/day vs. placebo prior to titration in non-responders. N o pre-crossover data reported.
Pool 1985 (316)
R / D B / P C parallel group trial with titration in non-responders every 2 weeks of treatment, starting with diltiazem 120 mg/day vs. placebo.
Pool 1986 (317)
R / D B / P C parallel group trial with titration in non-responders every 2 weeks of treatment, starting with diltiazem 120 mg/day vs. placebo.
Pool 1988 (318)
[Duplicate publication: Pool 1989 (319)1
R / D B / P C parallel group trial with titration in non-responders every 2 weeks of treatment, starting with diltiazem 120 mg/day vs. placebo.
Pool 1990 (320)
Reports on 3 trials. Trial #2 was a R / D B / P C parallel group trial with no data reported in the 1 s t 4 weeks of treatment with diltiazem 240 mg/day vs. placebo prior to titration in non-responders .
Pnsant 1998 (321)
[Duplicate publication: Prisant 1999 (322)]
R / D B / P C parallel group trial with a 6-week titration period during which doses were titrated in non-responders every 2 weeks, starting with amlodipine 2.5 mg/day vs. placebo.
Ramirez 1992 (323)
R / D B / P C parallel group trial that studied nifedipine GfTS 60 mg/day vs. 90 mg/day vs. 120 mg/day vs. 180 mg/day vs. placebo. BPs from nifedipine arms were grouped together and not reported for each dose separately.
Ricciardelli 1997 (324)
R / D B / P C parallel group trial with no data reported for the 1 s t six weeks of treatment with nitrendipine 10 mg/day vs. placebo prior to titration in non-responders.
Romero-Vecchione 1995 (325)
D B / P C parallel group trial with titration in non-responders every week for 4 weeks, starting with nifedipine 10 mg/day.
Rossi 2002 (326)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t three weeks of lacidipine 4 mg/day vs. placebo.
Salvetti 1987 (327)
R / D B / P C cross-over trial with no baseline data and no pre-crossover data reported for the 1 s t four weeks of nifedipine 40 mg/day vs. placebo. Only mean arterial blood pressure values given.
Salvetti 1989a (328)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1s t four weeks of nicardipine SR 80 mg/day vs. placebo.
142

Study I D Reason for exclusion Salvetti 1989b (329)
[Duplicate publication: Salvetti 1991 (330)1
R / D B / P C cross-over trial with no baseline S B P / D B P data and no pre-crossover data reported for the 1 s t four weeks of nifedipine 40 mg/day vs. placebo.
Salvetti 1996 (331)
R / D B / P C cross-over trial with no pre-crossover data reported for the P ' four weeks of nifedipine GfTS 30 mg/day vs. nifedipine retard 40 mg/day vs. placebo.
Schuster 1998 (332)
R / D B / P C cross-over trial with dtradon in non-responders after 2 weeks of treatment with felodipine 5 mg/day vs. placebo. N o pre-crossover data reported.
Siche 2001 (333)
R / D B / P C parallel group trial with no data reported for the f s t four weeks of treatment with amlodipine 5 mg/day vs. placebo prior to titration in non-responders.
Simon 1984 (334)
R / D B / P C parallel group trial with titration in non-responders every week for 3 weeks, starting with nitrendipine fO mg/day vs. placebo.
Slomm 1991 (335)
R / D B / P C parallel group trial with titration in non-responders, starting with isradipine 2.5 mg/day vs. placebo. Timing of titration and number of patients on each dose are not reported.
Spence 2000 (336)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of amlodipine 5 mg/day titrated up to 10 mg/day vs. placebo.
Spieker 1998 (337)
[Duplicate publication: Smilde 2000 (338)]
Presents results of 4 studies, one of which was a R / D B / P C crossover trial with no pre-crossover data reported for barnidipine 20 mg vs. placebo.
Spritzer 1990 (339)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of nitrendipine 20 mg/day vs. placebo.
Staessen 1989 (340)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of isradipine 10 mg/day vs. placebo, prior to titration in non-responders.
Stornello 1989 (341)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of nicardipine 60 mg/day vs. placebo.
Stornello 1990 (342)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t six weeks of nicardipine-SR 80 mg/day vs. placebo.
Suzuki 1999 (343)
R / D B / P C parallel group trial with titration in non-responders, starting with benidipine 4 mg/day vs. placebo. Timing of titration and number of patients on each dose are not reported.
Szlachic 1989 (344)
R / D B / P C parallel group trial with an 8-week titration in non-responders, starting with diltiazem 120 mg/day vs. placebo
Tonkin 1990 (345)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of diltiazem 240 mg/day vs. placebo
143
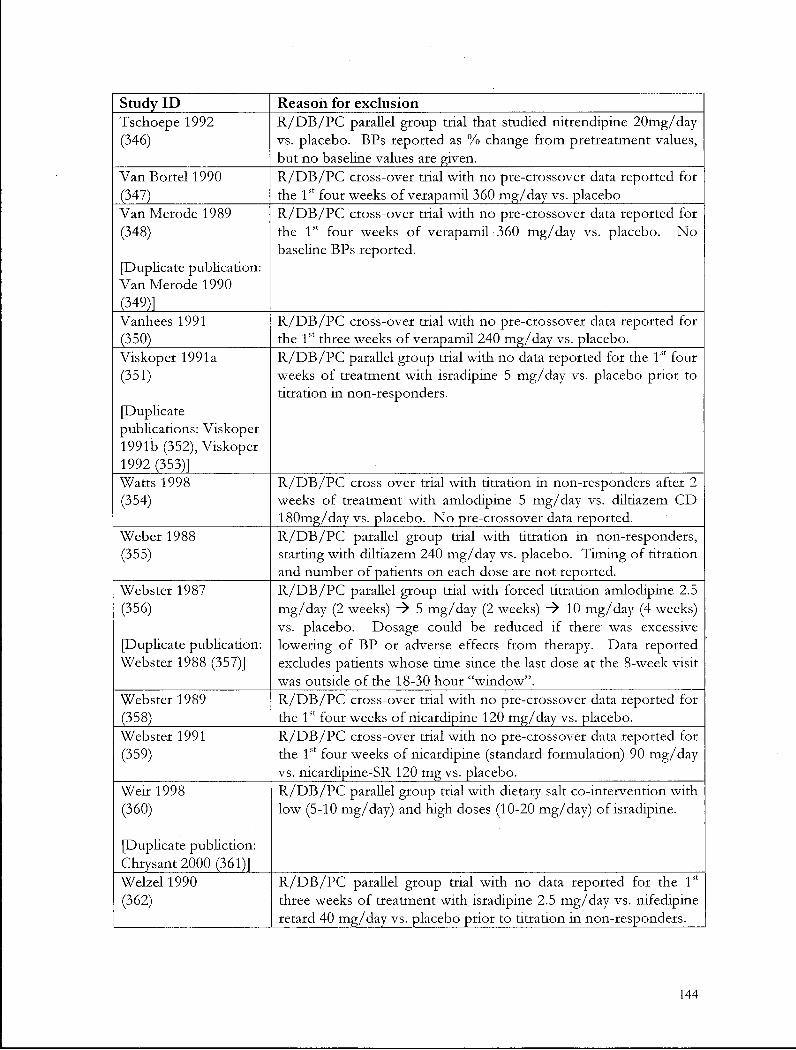
Study I D Reason for exclusion Tschoepe 1992 (346)
R / D B / P C parallel group trial that studied nitrendipine 20mg/day vs. placebo. BPs reported as % change from pretreatment values, but no baseline values are given.
Van Bortel 1990 (347)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of verapamil 360 mg/day vs. placebo
Van Merode 1989 (348)
[Duplicate publication: Van Merode 1990 (349)1
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of verapamil 360 mg/day vs. placebo. N o baseline BPs reported.
Vanhees1991 (350)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t three weeks of verapamil 240 mg/day vs. placebo.
Viskoper 1991a (351)
[Duplicate publications: Viskoper 1991b (352), Viskoper 1992 (353)1
R / D B / P C parallel group trial with no data reported for the 1 s t four weeks of treatment with isradipine 5 mg/day vs. placebo prior to titration in non-responders.
Watts 1998 (354)
R / D B / P C cross-over trial with titration in non-responders after 2 weeks of treatment with amlodipine 5 mg/day vs. diltiazem C D 180mg/day vs. placebo. N o pre-crossover data reported.
Weber 1988 (355)
R / D B / P C parallel group trial with titration in non-responders, starting with diltiazem 240 mg/day vs. placebo. Timing of titration and number of patients on each dose are not reported.
Webster 1987 (356)
[Duplicate publication: Webster 1988 (357)]
R / D B / P C parallel group trial with forced titration amlodipine 2.5 mg/day (2 weeks) 5 mg/day (2 weeks) - ^ 1 0 mg/day (4 weeks) vs. placebo. Dosage could be reduced if there was excessive lowering of BP or adverse effects from therapy. Data reported excludes patients whose time since the last dose at the 8-week visit was outside of the 18-30 hour "window".
Webster 1989 (358)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of nicardipine 120 mg/day vs. placebo.
Webster 1991 (359)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t four weeks of nicardipine (standard formulation) 90 mg/day vs. nicardipine-SR 120 mgvs. placebo.
Weir 1998 (360)
R / D B / P C parallel group trial with dietary salt co-intervention with low (5-10 mg/day) and high doses (10-20 mg/day) of isradipine.
[Duplicate publiction: Chrysant 2000 (361)] Welzel 1990 (362)
R / D B / P C parallel group trial with no data reported for the 1s t
three weeks of treatment with isradipine 2.5 mg/day vs. nifedipine retard 40 mg/day vs. placebo prior to titration in non-responders.
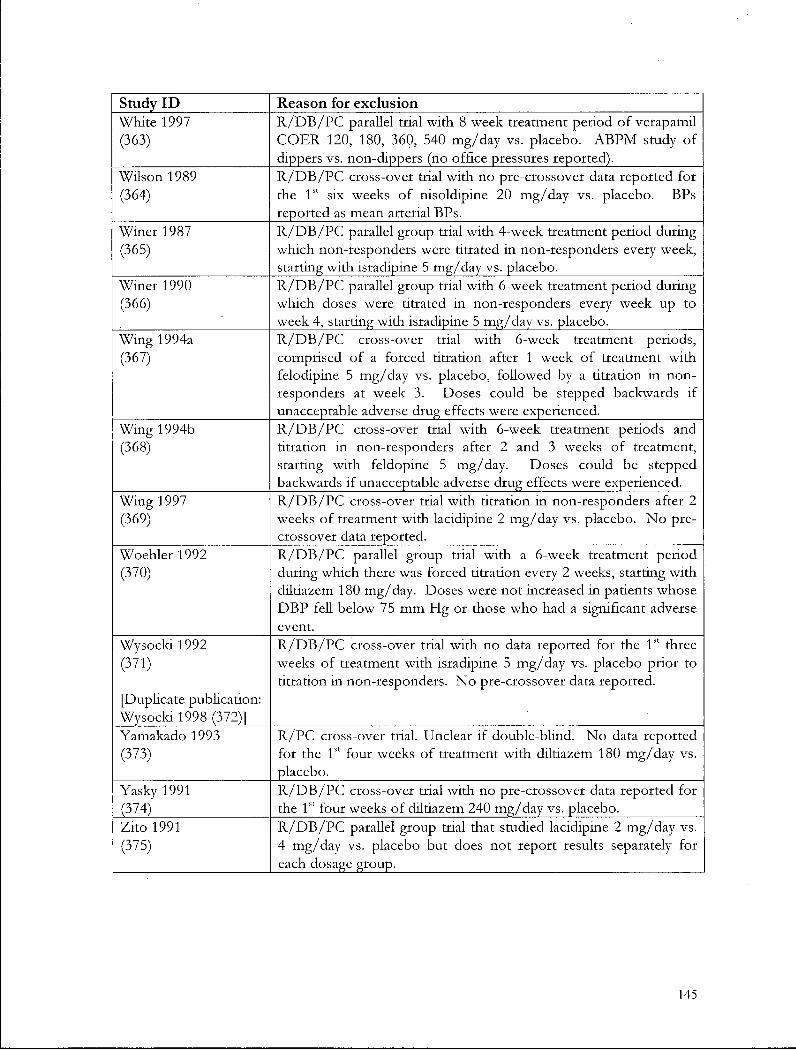
Study I D Reason for exclusion White 1997 (363)
R / D B / P C parallel trial with 8 week treatment period of verapamil C O E R 120, 180, 360, 540 mg/day vs. placebo. A B P M study of dippers vs. non-dippers (no office pressures reported).
Wilson 1989 (364)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1 s t six weeks of nisoldipine 20 mg/day vs. placebo. BPs reported as mean arterial BPs.
Winer 1987 (365)
R / D B / P C parallel group trial with 4-week treatment period during which non-responders were titrated in non-responders every week, starting with isradipine 5 mg/day vs. placebo.
Winer 1990 (366)
R / D B / P C parallel group trial with 6-week treatment period during which doses were titrated in non-responders every week up to week 4, starting with isradipine 5 mg/day vs. placebo.
Wing 1994a (367)
R / D B / P C cross-over trial with 6-week treatment periods, comprised of a forced titration after 1 week of treatment with felodipine 5 mg/day vs. placebo, followed by a titration in non-responders at week 3. Doses could be stepped backwards i f unacceptable adverse drug effects were experienced.
Wing 1994b (368)
R / D B / P C cross-over trial with 6-week treatment periods and titration in non-responders after 2 and 3 weeks of treatment, starting with feldopine 5 mg/day. Doses could be stepped backwards i f unacceptable adverse drug effects were experienced.
Wing 1997 (369)
R / D B / P C cross-over trial with titration in non-responders after 2 weeks of treatment with lacidipine 2 mg/day vs. placebo. N o pre-crossover data reported.
Woehler 1992 (370)
R / D B / P C parallel group trial with a 6-week treatment period during which there was forced titration every 2 weeks, starting with diltiazem 180 mg/day. Doses were not increased in patients whose D B P fell below 75 mm H g or those who had a significant adverse event.
Wysocki 1992 (371)
[Duplicate publication: Wysocki 1998 (372)]
R / D B / P C cross-over trial with no data reported for the 1 s t three weeks of treatment with isradipine 5 mg/day vs. placebo prior to titration in non-responders. N o pre-crossover data reported.
Yamakado 1993 (373)
R / P C cross-over trial. Unclear i f double-blind. N o data reported for the 1 s t four weeks of treatment with diltiazem 180 mg/day vs. placebo.
Yasky 1991 (374)
R / D B / P C cross-over trial with no pre-crossover data reported for the 1s t four weeks of diltiazem 240 mg/day vs. placebo.
Zito 1991 (375)
R / D B / P C parallel group trial that studied lacidipine 2 mg/day vs. 4 mg/day vs. placebo but does not report results separately for each dosage group.
145
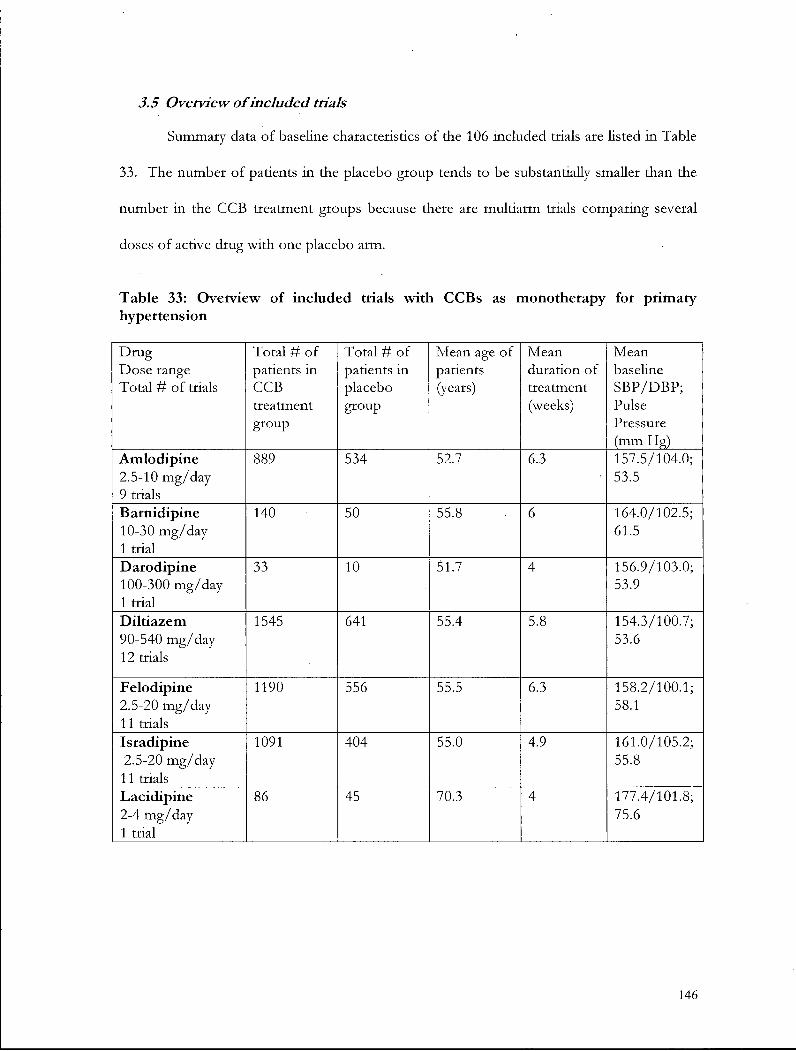
3.5 Overview of included trials
Summary data of baseline characteristics of the 106 included trials are listed in Table
33. The number of patients in the placebo group tends to be substantially smaller than the
number in the C C B treatment groups because there are multiarm trials comparing several
doses of active drug with one placebo arm.
Table 33: Overview of included trials wi th C C B s as monotherapy for primary hypertension
Drug Dose range Total # of trials
Total # of patients in C C B treatment group
Total # of patients in placebo group
Mean age of patients (years)
Mean duration of treatment (weeks)
Mean baseline S B P / D B P ; Pulse Pressure (mm Hg)
Amlodip ine 2.5-10 mg/day 9 trials
889 534 52.7 6.3 157.5/104.0; 53.5
Barnidipine 10-30 mg/day 1 trial
140 50 55.8 6 164.0/102.5; 61.5
Darodipine 100-300 mg/day 1 trial
33 10 51.7 4 156.9/103.0; 53.9
Di l t iazem 90-540 mg/day 12 trials
1545 641 55.4 5.8 154.3/100.7; 53.6
Felodipine 2.5-20 mg/day 11 trials
1190 556 55.5 6.3 158.2/100.1; 58.1
Isradipine 2.5-20 mg/day 11 trials
1091 404 55.0 4.9 161.0/105.2; 55.8
Lacid ip ine 2-4 mg/day 1 trial
86 45 70.3 4 177.4/101.8; 75.6
146

Drug Total # of Total # of Mean age of Mean Mean Dose range Total # of trials
patients in C C B
patients in placebo
patients (years)
duration of treatment
baseline S B P / D B P ;
treatment group (weeks) Pulse group Pressure
(mm Hg) Lercanidipine 532 252 57.7 3.8 161.9/98.9; 2.5-20 mg/day 63.1 6 trials Lidof laz ine 5 5 43.8 12 138.0/95.0; 180 mg/day 43.0 1 trial Manid ip ine 66 40 67.8 6 167.4/99.1; 10-40 mg/day 68.3 2 trials Mibefradi l 685 128 60.0 4 175.7/101.3; 6.25-200 mg/day 74.4 3 trials Nicard ip ine 303 169 52.3 6.4 157.4/101.6; 40-100 mg/day 55.9 8 trials Nifed ip ine 675 413 52.7 7.1 157.1/102.1; 20-100 mg/day 55.0 12 trials Ni lvadip ine 172 80 54.2 4 162.6/102.3; 8-30 mg/day 60.3 2 trials Niso ld ip ine 148 58 52.1 6 161.4/106.9; 10-30 mg/day 54.5 1 trial Nit rendip ine 310 255 55.7 6.2 162.5/100.4; 10-20 mg/day 62.1 10 trials Prandipine 144 32 52.0 4 154.6/102.8; 1-8 mg/day 51.8 1 trial T iapami l 49 9 50.5 6 152.0/101.9; 300-1200 mg/day 50.2 1 trial Verapami l 1450 684 53.4 6 154.6/99.8; 60-540 mg/day 54.8 13 trials T O T A L : 9513 4365 55.0 5.7 158.2/101.6; 106 trials, 56.7 13 878 patients
147
3.6 Values used to impute miss ing variances
3.6.1. Standard deviation of b lood pressure change
Thkty-seven (35%) of the trials included in this systematic review reported the
standard deviation of the change in SBP and/or D B P . These values were used to calculate
weighted means of the standard deviation of changes in SBP and D B P for both the C C B
treatment and placebo groups. For the CCB-treatment group, the weighted mean standard
deviations of the change in SBP and D B P were 13.3 mm H g (SD 2.1) and 7.7 mm Fig (SD
1.6), respectively. For the placebo group, the weighted mean SD of B P change was 13.0 mm
H g (SD 4.1) for SBP and 7.4 mm H g (SD 2.3) for D B P .
Those trials whose reported SD values were not witliLn three standard deviations of
the weighted mean SD of B P change were then excluded from the calcuation in order to
obtain an adjusted weighted mean SD of B P change. Three trials with outlier SDs were
excluded from the calculation (Chan 1997, Farsang 2001, Asmar 1992), resulting in an
adjusted weighted mean SD for C C B treatment of 13.5 mm H g and 7.8 mm H g for SBP and
D B P , respectively, and corresponding values for placebo of 14.1 mm H g and 7.9 mm Hg.
There was no statistically significant difference in SD of SBP change between placebo and
C C B treatment groups (p=0.15), nor in SD of D B P change (p=0.86). The adjusted values
were used to impute the SD of B P change in the trials with outlier SDs and for other trials as
per the protocol's imputation hierarchy.
The SD of B P change was imputed for 70 (67%) of the included trials with extracted
BP data. O f these, there were 3 trials (4%) in which variances were imputed by calculating
the pooled standard deviation from a reported p value; 1 (1%) was imputed using SD
reported from BP measured in a different position; 38 (56%) were imputed using endpoint
148

SDs; 6 (9%) were imputed using baseline SDs (for SBP only); 20 (30%) were imputed using
the mean SD data reported in other trials.
3.6. 2. Standard deviation of heart rate change
Twelve trials reported SD of the change in heart rate, resulting in a weighted mean
value of 8.8 beats/minute for C C B group and 8.4 beats/minute for placebo group. There
was no statistically significant difference between the SD of heart rate change in C C B - and
placebo-treated groups (p=0.4). These values were used to impute the standard deviations
according to the hierarchy outlined in the protocol.
3.7 Dose-related b lood pressure lowering of indiv idual C C B drugs
Effect sizes are expressed as the weighted mean difference (CCB treatment effect
minus placebo effect) followed by the 95% confidence interval in parentheses. In all
analyses, "statistical significance" refers to p < 0.05. For analyses for which there was
statistically significant interstudy heterogeneity, the random effects model was applied to
determine i f there was a statistically significant difference between C C B treatment and
placebo. If a statistically significant difference was present using the random effects model,
the effect size is reported using the fixed effect model because of the tendency of the former
to overweight smaller trials.
The weighted mean changes in SBP and D B P in placebo groups across all trials was
-3.5 mm H g (range -16.7 - 9) and -3.8 mm Fig (range -11.4 - 4.5), respectively.
149
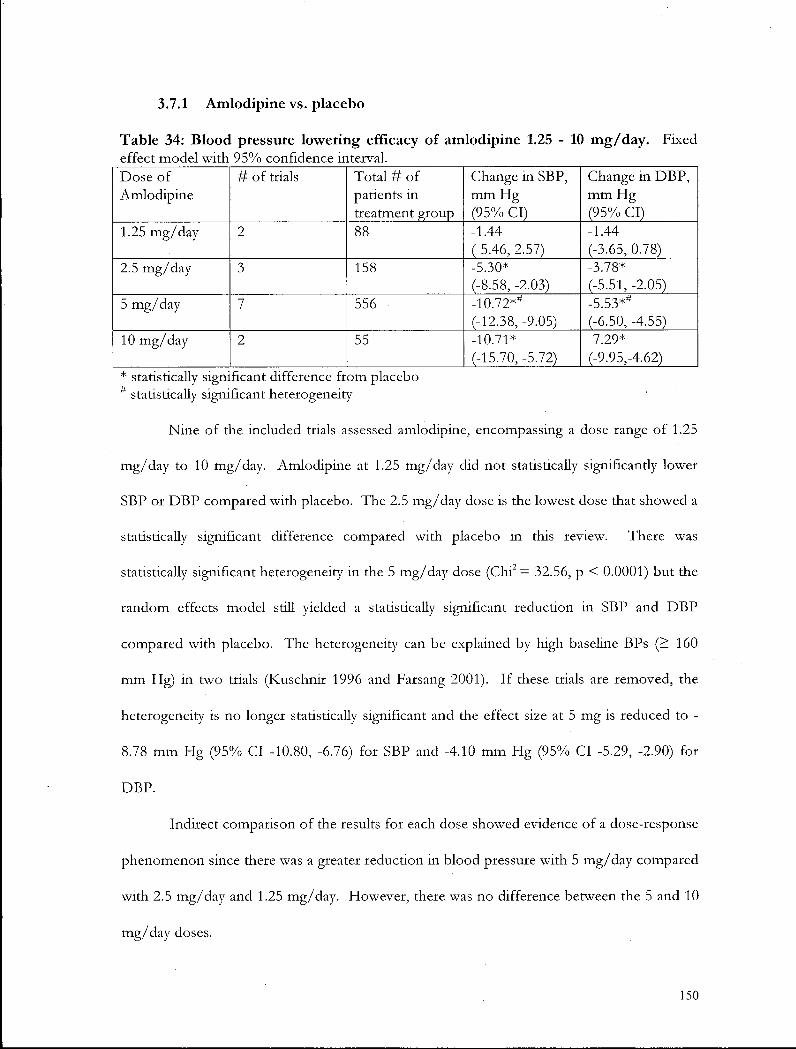
3.7.1 Amlod ip ine vs. placebo
Table 34: B lood pressure lowering efficacy of amlodipine 1.25 - 10 mg /day . Fixed effect model with 95% confidence interval. Dose of Amlodipine
# of trials Total # of patients in treatment group
Change in SBP, mm H g (95% CI)
Change in D B P , mm H g (95% CI)
1.25 mg/day 2 88 -1.44 (-5.46, 2.57)
-1.44 (-3.65, 0.78)
2.5 mg/day 3 158 -5.30* (-8.58, -2.03)
-3.78* (-5.51, -2.05)
5 mg/day 7 556 -10.72*#
(-12.38, -9.05) -5.53*#
(-6.50, -4.55) 10 mg/day 2 55 -10.71*
(-15.70, -5.72) -7.29* (-9.95,-4.62)
* statistically significant difference from placebo # statistically significant heterogeneity
Nine of the included trials assessed amlodipine, encompassing a dose range of 1.25
mg/day to 10 mg/day. Amlodipine at 1.25 mg/day did not statistically significandy lower
SBP or D B P compared with placebo. The 2.5 mg/day dose is the lowest dose that showed a
statistically significant difference compared with placebo in this review. There was
statistically significant heterogeneity in the 5 mg/day dose (Chi 2 = 32.56, p < 0.0001) but the
random effects model still yielded a statistically significant reduction in SBP and D B P
compared with placebo. The heterogeneity can be explained by high baseline BPs (> 160
mm Hg) in two trials (Kuschnir 1996 and Farsang 2001). If these trials are removed, the
heterogeneity is no longer statistically significant and the effect size at 5 mg is reduced to -
8.78 mm Fig (95% CI -10.80, -6.76) for SBP and -4.10 mm H g (95% CI -5.29, -2.90) for
D B P .
Indirect comparison of the results for each dose showed evidence of a dose-response
phenomenon since there was a greater reduction in blood pressure with 5 mg/day compared
with 2.5 mg/day and 1.25 mg/day. Flowever, there was no difference between the 5 and 10
mg/day doses.
150
In the direct comparison analysis, only two trials were included (Frick 1988, Mehta
1993). There was no statistically significant difference in the effect sizes between the direct
and indirect comparisons of amlodipine doses.
Since all amlodipine trials had a mean age of <60 years and inclusion criteria of
elevated D B P , subgroup analyses based on age and type of hypertension were not possible.
A l l trials were of moderate quality Qadad score 3 or 4 out of 5) except for one study which
had a Jadad score of 5/5 (Pool 2001). Sensitivity analyses of B P measurement position did
not change the results. In all trials BP measurements were taken in the trough period of the
dosing interval; thus an analysis of peak vs. trough effect was not possible. Only 2
amlodipine trials reported SD of B P change (Mehta 1992 and Mroczek 1988), while imputed
values were used for the rest of the trials. The results were insensitive to whether the values
were imputed according the hierarchy or directiy from the trials that did report the SD of B P
change.
From the included studies, the best estimate of the maximal B P lowering efficacy of
amlodipine occurring at 5 to 10 mg/day is -10.72 mm H g (95% CI: -12.30, -9.14) for SBP
and -5.73 mm H g (95% CI: -6.65, -4.82) for D B P . The log dose-response curve is displayed
in Figure 3. A funnel plot of the amlodipine studies at starting dose (5 mg) and above
showed an absence of small negative-result trials (Figure 4). Thus, publication bias is likely
and the best estimate of the blood pressure lowering efficacy of amlodipine is likely an
overestimate of the actual effect size.
151

5n
I
CL
m
<u G) C <o o -20J
0.25 Log Dose
0.50 0.75 Change in SBP Change in DBP
Figure 3. Log dose-response curve for amlodipine, 1.25-10 mg/day.
Review:. Blood pressure.lowering eff icacy of.caldium channel blockers for primary hypertension Comparison: 01 Dose Amlodipine vs . placebo :
Outcome: 0t change in-Systolic Blood Pressure
SE(WMD)
+4
-100 -50 50 100 WMD (fixed)
Figure 4. Funnel plot of standard error against effect size of change in SBP for amlodipine 5 to 20 mg/day. Each dot represents an active treatment group.
152
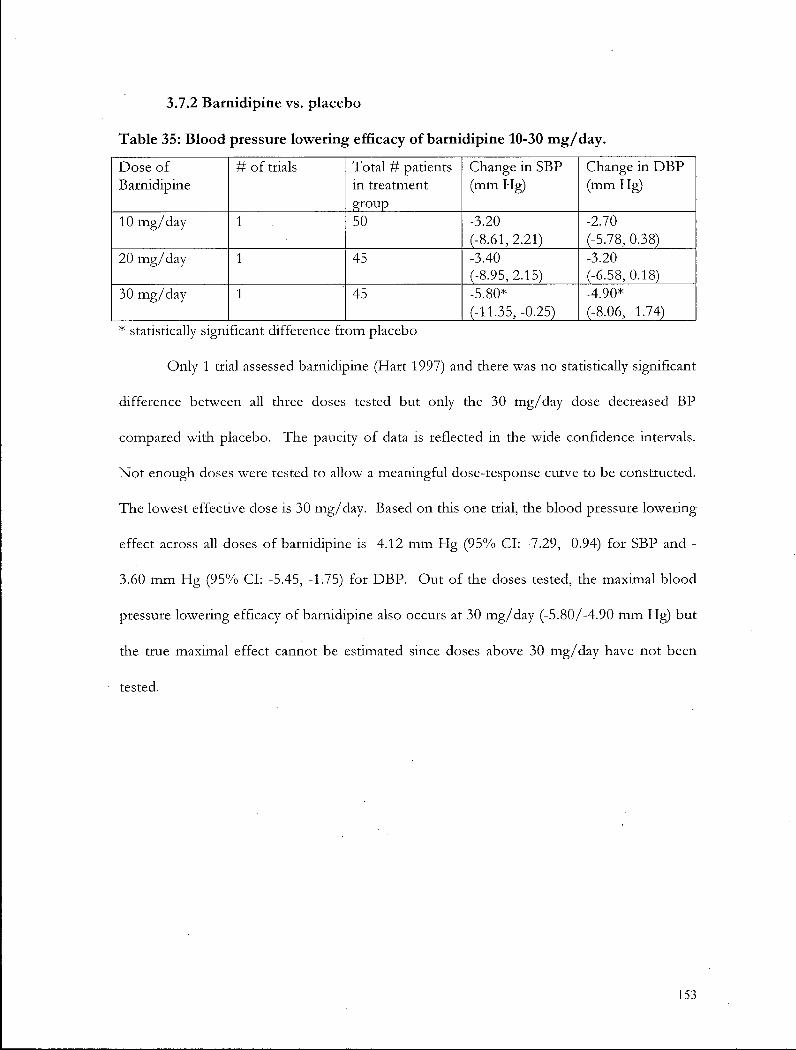
3.7.2 Barnidipine vs. placebo
Table 35: B lood pressure lowering efficacy of barnidipine 10-30 mg /day .
Dose of # of trials Total # patients Change in SBP Change in D B P Barnidipine in treatment (mm Hg) (mm Hg)
group 10 mg/day 1 50 -3.20 -2.70
(-8.61,2.21) (-5.78, 0.38) 20 mg/day 1 45 -3.40 -3.20
(-8.95, 2.15) (-6.58, 0.18) 30 mg/day 1 45 -5.80* -4.90*
(-11.35, -0.25) (-8.06, -1.74) statistically significant difference from placebo
Only 1 trial assessed barnidipine (Hart 1997) and there was no statistically significant
difference between all three doses tested but only the 30 mg/day dose decreased BP
compared with placebo. The paucity of data is reflected in the wide confidence intervals.
Not enough doses were tested to allow a meaningful dose-response curve to be constructed.
The lowest effective dose is 30 mg/day. Based on this one trial, the blood pressure lowering
effect across all doses of barnidipine is -4.12 mm H g (95% CI: -7.29, -0.94) for SBP and -
3.60 mm H g (95% CI: -5.45, -1.75) for D B P . Out of the doses tested, the maximal blood
pressure lowering efficacy of barnidipine also occurs at 30 mg/day (-5.80/-4.90 mm Hg) but
the true maximal effect cannot be estimated since doses above 30 mg/day have not been
tested.
153

3.7.3 Darodipine vs. placebo
Table 36: B lood pressure lowering efficacy of darodipine 100-300 mg /day .
Dose of # of trials Total # of Change in SBP, Change in D B P , Darodipine patients in mm H g mm H g
treatment group (95% CI) (95% CI) 100 mg/day 1 13 -16.70* -6.70
(-29.05, -4.35) (-14.48, 1.08) 200 mg/day 1 9 -24.80* -14.10*
(-39.88, -9.72) (-22.69, -5.51) 300 mg/ day 1 11 -15.70* -11.40*
(-28.30, -3.10) (-19.35, -3.45) * statistically significant difference from placebo
Only 1 trial assessed darodipine (Chrysant 1988) and there was no statistically
significant difference between any of the three doses tested. A l l doses had statistically
significant difference compared with placebo except for change in D B P in the 100 mg/day
group. From the available data, the lowest effective dose is 100 mg/day, but it may occur at
a lower dose for which there are no data. It is unclear i f the doses tested in this trial reflect
the plateau of the dose-response curve or i f doses above 300 mg/day have greater efficacy.
Thus the true maximal blood pressure lowering efficacy of darodipine cannot be estimated.
However, from the data that are available, it appears that the lowest dose with maximal
blood pressure lowering efficacy is 100 mg/day. Maximum efficacy may be achieved at
doses lower than 100 mg/day but again there are no available data. The overall blood
pressure lowering effect across all doses of darodipine is -18.40 mm H g (95% CI: -26.02, -
10.79) for SBP and -10.51 mm H g (95% CI: -15.17, -5.84) for D B P . However, since this
result is based on one trial in a small number of individuals, its uncertainty is reflected by the
wide confidence limits.
154

3.7.4 Felodipine vs. placebo
Table 37: B lood pressure lowering efficacy of felodipine 2.5-20 mg /day . Fixed effect model with 95% confidence interval. Dose of Felodipine
# of trials Total # of patients in treatment group
Change in SBP, mm H g (95% CI)
Change in D B P , mm H g (95% CI) .
2.5 mg/day 5 407 -5.02* (-7.25, -2.79)
-3.16* (-4.53,-1.79)
5 mg/day 6 293 -5.42* (-8.03, -2.81)
-5.12* (-6.39, -3.86)
10 mg/day 8 335 -10.10*#
(-11.95, -8.24) _7 79* #
(-8.75, -6.83) 20 mg/day 3 87 -6.26*
(-10.07, -2.44) -4.80* (-6.70, -2.90)
* statistically significant difference from placebo * statistically significant heterogeneity
A l l doses of felodipine resulted in statistically significant reduction in blood pressure
compared with placebo. Thus, the lowest effective dose is 2.5 mg/day. However, the true
lowest effective dose may be lower than 2.5 mg/day but there are no data available. The 10
mg/day dose had significant inter-study heterogeneity and had statistically significant
differences in effect size compared with all other doses tested, even 20 mg/day. However,
the result for 20 mg/day is based on only 87 patients, compared with 335 patients in the 10
mg/day category. Differences in baseline B P did not account for this result. The weighted
mean baseline BP was 158.3/101.0 mm H g in the 10 mg/day group and 162.7/103.8 mm
H g in the 20 mg/day group. The true lowest effective dose may be lower than 10 mg/day
but there are no data available
Differences in the time of B P measurement relative to dosing appear to account for
the superior response observed in the 10 mg/day group. In 9 out of 11 trials, the B P
measurements were taken at trough, whereas in one trial B P measurements were taken at 2-3
hours post-dose (Kiesewetter 1994) and in another trial the time of measurement was not
155
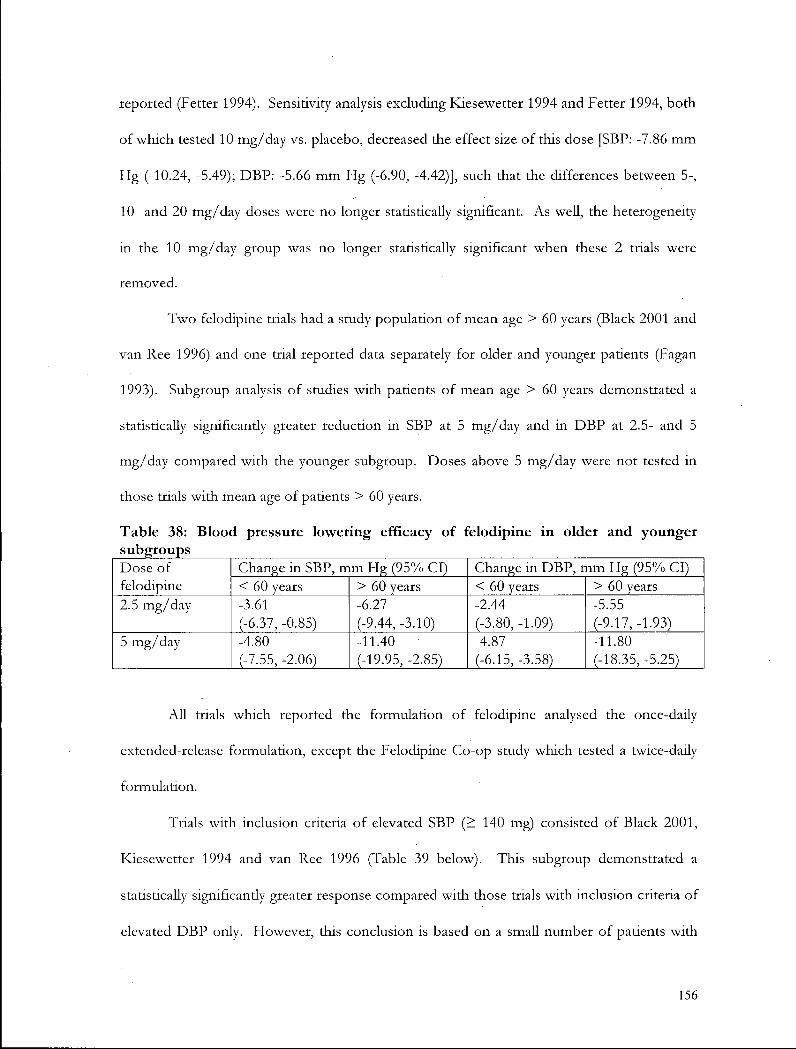
reported (Fetter 1994). Sensitivity analysis excluding Kiesewetter 1994 and Fetter 1994, both
of which tested 10 mg/day vs. placebo, decreased the effect size of this dose [SBP: -7.86 mm
H g (-10.24, -5.49); D B P : -5.66 mm H g (-6.90, -4.42)], such that the differences between 5-,
10- and 20 mg/day doses were no longer statistically significant. As well, the heterogeneity
in the 10 mg/day group was no longer statistically significant when these 2 trials were
removed.
Two felodipine trials had a study population of mean age > 60 years (Black 2001 and
van Ree 1996) and one trial reported data separately for older and younger patients (Fagan
1993). Subgroup analysis of studies with patients of mean age > 60 years demonstrated a
statistically significandy greater reduction in SBP at 5 mg/day and in D B P at 2.5- and 5
mg/day compared with the younger subgroup. Doses above 5 mg/day were not tested in
those trials with mean age of patients > 60 years.
Table 38: Blood pressure lowering efficacy of felodipine in older and younger subgroups Dose of Change i n SBP, mm H g (95% Cf) Change in D B P , mm H g (95% Cf) felodipine < 60 years > 60 years < 60 years > 60 years 2.5 mg/day -3.61 -6.27 -2.44 -5.55
(-6.37, -0.85) (-9.44, -3.10) (-3.80, -1.09) (-9.17,-1.93) 5 mg/day -4.80 -11.40 -4.87 -11.80
(-7.55, -2.06) (-19.95, -2.85) (-6.15, -3.58) (-18.35, -5.25)
A l l trials which reported the formulation of felodipine analysed the once-daily
extended-release formulation, except the Felodipine Co-op study which tested a twice-daily
formulation.
Trials with inclusion criteria of elevated SBP (> 140 mg) consisted of Black 2001,
Kiesewetter 1994 and van Ree 1996 (Table 39 below). This subgroup demonstrated a
statistically significandy greater response compared with those trials with inclusion criteria of
elevated D B P only. Flowever, this conclusion is based on a small number of patients with
156
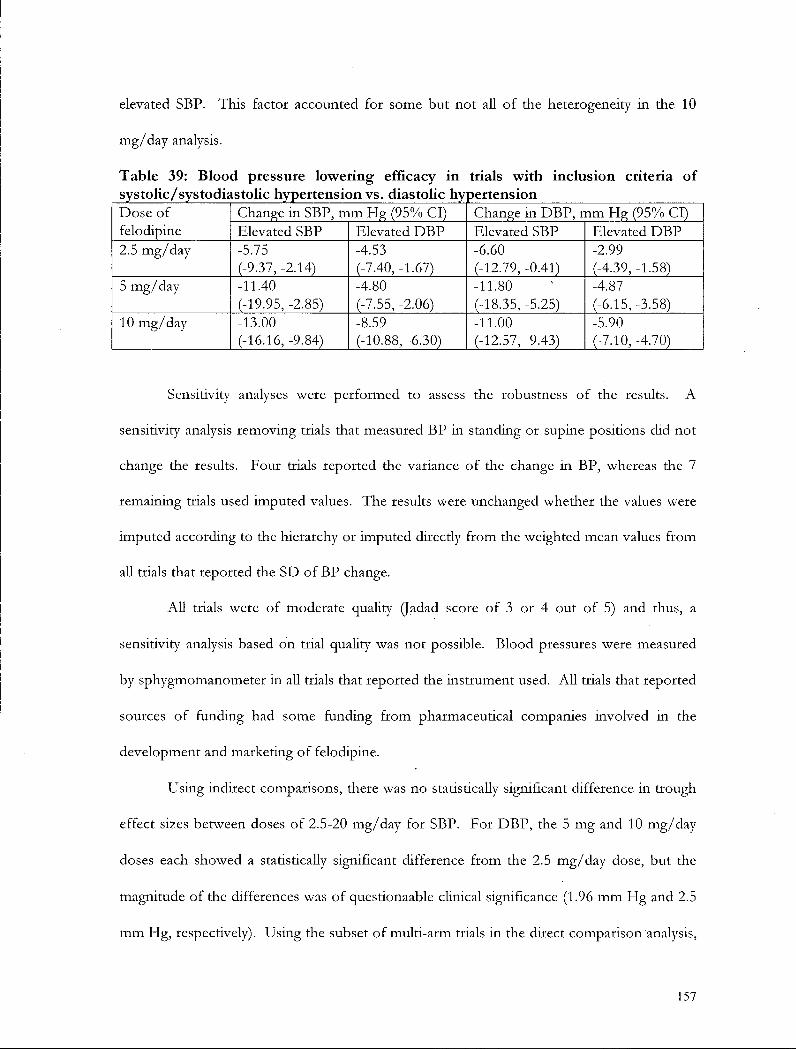
elevated SBP. This factor accounted for some but not all of the heterogeneity in the 10
mg/day analysis.
Table 3 9 : B lood pressure lowering efficacy i n trials wi th inc lus ion criteria of
Dose of Change in SBP, mm H g (95% CI) Change in D B P , mm H g (95% CI) felodipine Elevated SBP Elevated D B P Elevated SBP Elevated D B P 2.5 mg/day -5.75 -4.53 -6.60 -2.99
(-9.37, -2.14) (-7.40, -1.67) (-12.79, -0.41) (-4.39, -1.58) 5 mg/day -11.40 -4.80 -11.80 -4.87
(-19.95, -2.85) (-7.55, -2.06) (-18.35, -5.25) (-6.15, -3.58) 10 mg/ day -13.00 -8.59 -11.00 -5.90
(-16.16, -9.84) (-10.88, -6.30) (-12.57, -9.43) (-7.10, -4.70)
Sensitivity analyses were performed to assess the robustness of the results. A
sensitivity analysis removing trials that measured B P in standing or supine positions did not
change the results. Four trials reported the variance of the change in BP , whereas the 7
remaining trials used imputed values. The results were unchanged whether the values were
imputed according to the hierarchy or imputed direcdy from the weighted mean values from
all trials that reported the SD of B P change.
A l l trials were of moderate quality (Jadad score of 3 or 4 out of 5) and thus, a
sensitivity analysis based on trial quality was not possible. Blood pressures were measured
by sphygmomanometer in all trials that reported the instrument used. A l l trials that reported
sources of funding had some funding from pharmaceutical companies involved in the
development and marketing of felodipine.
Using indirect comparisons, there was no statistically significant difference in trough
effect sizes between doses of 2.5-20 mg/day for SBP. For D B P , the 5 mg and 10 mg/day
doses each showed a statistically significant difference from the 2.5 mg/day dose, but the
magnitude of the differences was of questionaable clinical significance (1.96 mm Fig and 2.5
mm Fig, respectively). Using the subset of multi-arm trials in the direct comparison analysis,
157
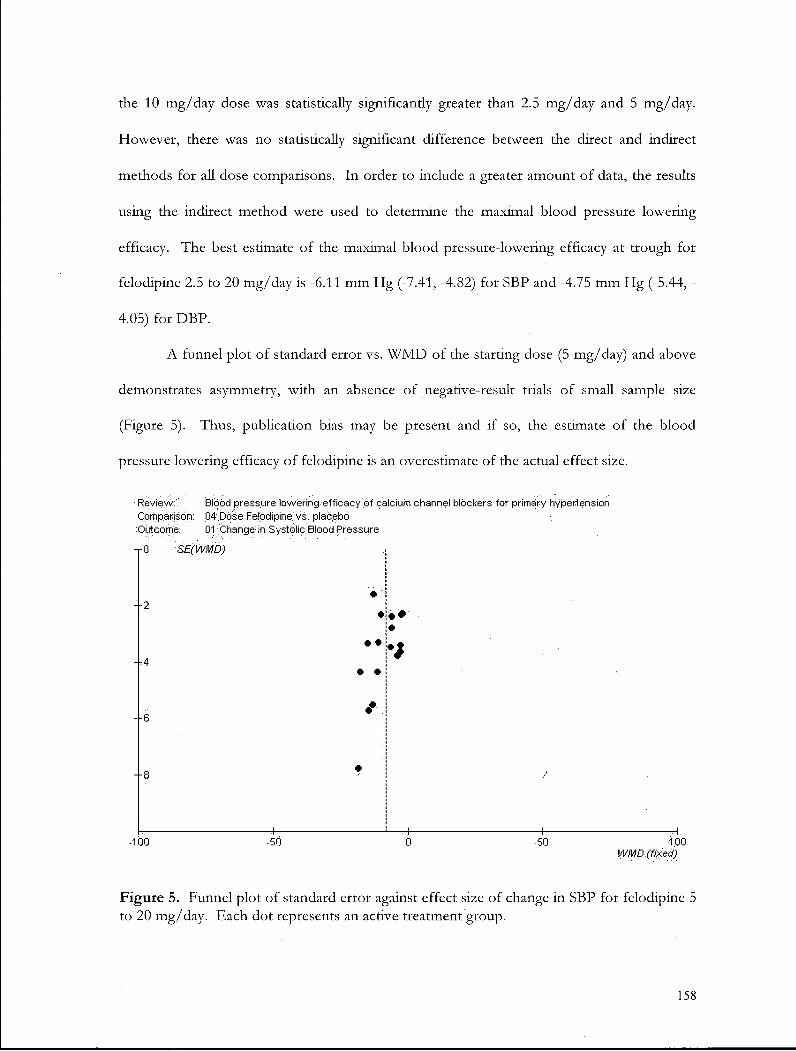
the 10 mg/day dose was statistically significantly greater than 2.5 mg/day and 5 mg/day.
However, there was no statistically significant difference between the direct and indirect
methods for all dose comparisons. In order to include a greater amount of data, the results
using the indirect method were used to determine the maximal blood pressure lowering
efficacy. The best estimate of the maximal blood pressure-lowering efficacy at trough for
felodipine 2.5 to 20 mg/day is -6.11 mm H g (-7.41, -4.82) for SBP and -4.75 mm H g (-5.44, -
4.05) for D B P .
A funnel plot of standard error vs. W M D of the starting dose (5 mg/day) and above
demonstrates asymmetry, with an absence of negative-result trials of small sample size
(Figure 5). Thus, publication bias may be present and i f so, the estimate of the blood
pressure lowering efficacy of felodipine is an overestimate of the actual effect size.
Revieyy:.' "Bipod pressure lowering eff icacy of calcium channel blockers' for primary-hypertension Comparison: 04 Dose Felodipine vs . placebo Outcome: 01 Change 1 in Systolic Blood Pressure
T 0 SE(WMD)
+3
•
-100 -50 50 100. WMD (fixed)
Figure 5. Funnel plot of standard error against effect size of change in SBP for felodipine 5 to 20 mg/day. Each dot represents an active treatment group.
158

3.7.5 Isradipine vs. placebo
Table 40: B lood pressure lowering efficacy of isradipine 1-20 mg /day . Fixed effect model with 95% confidence interval. Dose of # of trials Total # of Change in SBP, Change in D B P , Isradipine patients in
treatment group mm H g (95% CI)
mm H g (95% CI)
1 mg/day 1 . 44 -6.00* (-11.35, -0.65)
-1.00 (-4.70, 2.70)
2.5 mg/day 4 181 -8.44* (-11.73, -5.15)
-5.22* (-7.21, -3.23)
5 mg/day 10 484 -10.25*#
(-12.00, -8.50) -7.82*#
(-8.85, -6.79) 10 mg/day 4 143 -16.46*
(-19.75, -13.18) -11.55* (-13.49, -9.61)
15 mg/day 2 112 -17.00* (-20.79, -13.20)
-10.84* (-13.00, -8.69)
20 mg/day 2 107 -15.57* (-19.25, -11.89)
-11.48* (-13.80, -9.17)
* statistically significant difference from placebo statistically significant heterogeneity
A l l doses of isradipine showed a statistically significant reduction in BP compared
with placebo, except for change in D B P in the 1 mg/day group. Indirect comparisons
showed that the 10-, 15-, and 20 mg/day groups were not significandy different from each
other but all were statistically greater than the 1-, 2.5- and 5 mg/day groups. There was
statistically significant heterogeneity in the 5 mg/day analysis.
A subgroup analysis was performed on drug formulation (twice daily versus once-daily
sustained release). The twice-daily formulation at 5 mg showed a statistically significantly
greater blood pressure lowering as compared to the sustained-release formulation (Table 41).
159
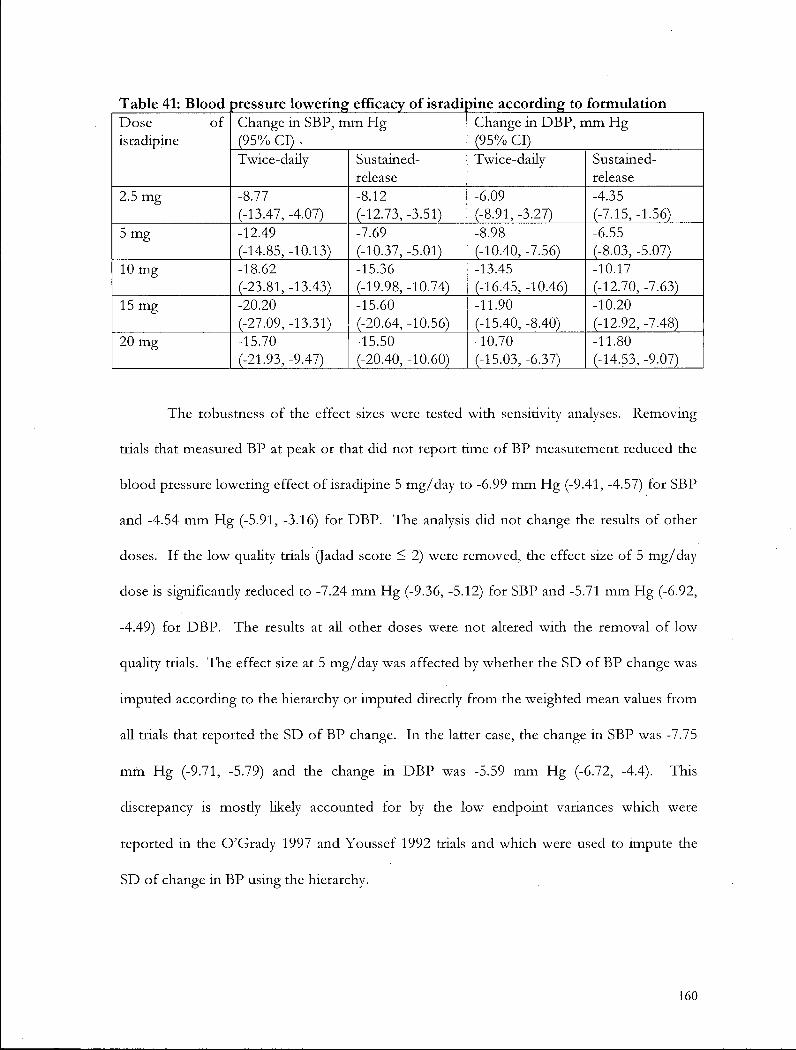
Table 41: B lood pressure lowering efficacy of isradi nne according to formulation Dose of isradipine
Change in SBP, mm H g (95% CI) .
Change in D B P , mm H g (95% CI)
Dose of isradipine
Twice-daily Sustained-release
Twice-daily Sustained-release
2.5 mg -8.77 (-13.47,-4.07)
-8.12 (-12.73, -3.51)
-6.09 (-8.91, -3.27)
-4.35 (-7.15,-1.56)
5 m g -12.49 (-14.85, -10.13)
-7.69 (-10.37, -5.01)
-8.98 (-10.40, -7.56)
-6.55 (-8.03, -5.07)
10 mg -18.62 (-23.81, -13.43).
-15.36 (-19.98, -10.74)
-13.45 (-16.45, -10.46)
-10.17 (-12.70, -7.63)
15 mg -20.20 (-27.09, -13.31)
-15.60 (-20.64, -10.56)
-11.90 (-15.40, -8.40)
-10.20 (-12.92, -7.48)
20 mg -15.70 (-21.93, -9.47)
-15.50 (-20.40, -10.60)
-10.70 (-15.03, -6.37)
-11.80 (-14.53, -9.07)
The robustness of the effect sizes were tested with sensitivity analyses. Removing
trials that measured B P at peak or that did not report time of BP measurement reduced the
blood pressure lowering effect of isradipine 5 mg/day to -6.99 mm H g (-9.41, -4.57) for SBP
and -4.54 mm H g (-5.91, -3.16) for D B P . The analysis did not change the results of other
doses, f f the low quality trials (Jadad score < 2) were removed, the effect size of 5 mg/day
dose is significandy reduced to -7.24 mm H g (-9.36, -5.12) for SBP and -5.71 mm Pig (-6.92,
-4.49) for D B P . The results at all other doses were not altered with the removal of low
quality trials. The effect size at 5 mg/day was affected by whether the SD of BP change was
imputed according to the hierarchy or imputed direcdy from the weighted mean values from
all trials that reported the SD of BP change, fn the latter case, the change in SBP was -7.75
mm H g (-9.71, -5.79) and the change in D B P was -5.59 mm H g (-6.72, -4.4). This
discrepancy is mosdy likely accounted for by the low endpoint variances which were
reported in the O'Grady 1997 and Youssef 1992 trials and which were used to impute the
SD of change in B P using the hierarchy.
160

Removing trials that did not measure B P in the sitting position or did not report
position of measurement only altered the effect size at 5 mg/day, with a change in SBP of -
5.21 mm H g (95% CI -8.13, -2.29) and a change in D B P of-4.61 mm H g (95% CI -6.19, -
3.03).
Only three trials reported funding sources, and all three had industry funding. Only
one small trial used an automatic device to measure BP (Arosio 1993), while the rest used
the auscultatory method with mercury sphygmomanometers. Removing this trial did not
alter the results. In one trial (O'Grady 1997) all patients had active atherosclerotic lesions.
Again, removing this trial did not change the effect size.
The lowest dose with maximal B P lowering occurs at 10 mg/day. A t trough, the
best estimate of the maximal blood pressure lowering effect at 10 to 20 mg/day is -14.84
mm H g (-17.47, -12.20) for SBP and -10.57 mm H g (-12.15, -8.98) for D B P . This estimate is
based on only one clinical trial (Chrysant 1995); thus, the confidence intervals are wide.
Funnel plots of the starting dose (5 mg/day) and above showed there was a
possibility of publication bias since there was some asymmetry in the shape of the plot.
161

3.7.6 Lac id ip ine vs. placebo
Table 42: B lood pressure lowering efficacy of lacidipine 2-4 mg /day .
Dose of # of trials Total # of Change in SBP, Change in D B P , Lacidipine patients in mm H g mm H g
treatment group (95% CI) (95% CI) 2 mg/day 1 46 -4.00 -3.10*
(-9.92, 1.92) (-6.10, -0.19) 4 mg/day 1 39 -7.00* -4.20*
(-13.17,-0.83) (-7.67, -0.73) * statistically significant difference from placebo
Only 1 included trial assessed lacidipine (Rizzini 1991). The study's population was
comprised of elderly hypertensives. Compared with placebo, the 2 mg/day group had a
statistically significant reduction in D B P but not SBP. The lowest effective dose is 4
mg/day, which showed a statistically significant difference from 2 mg/day.
Because there was no data for doses above 4 mg/day, the true maximal blood
pressure lowering efficacy cannot be estimated. However, based on the available data, blood
pressure lowering occurs at 4 mg/day has a magnitude of -7.00 mm H g (-13.17, -0.83) for
SBP and -4.20 mm H g (-7.67, -0.73) for D B P .
162
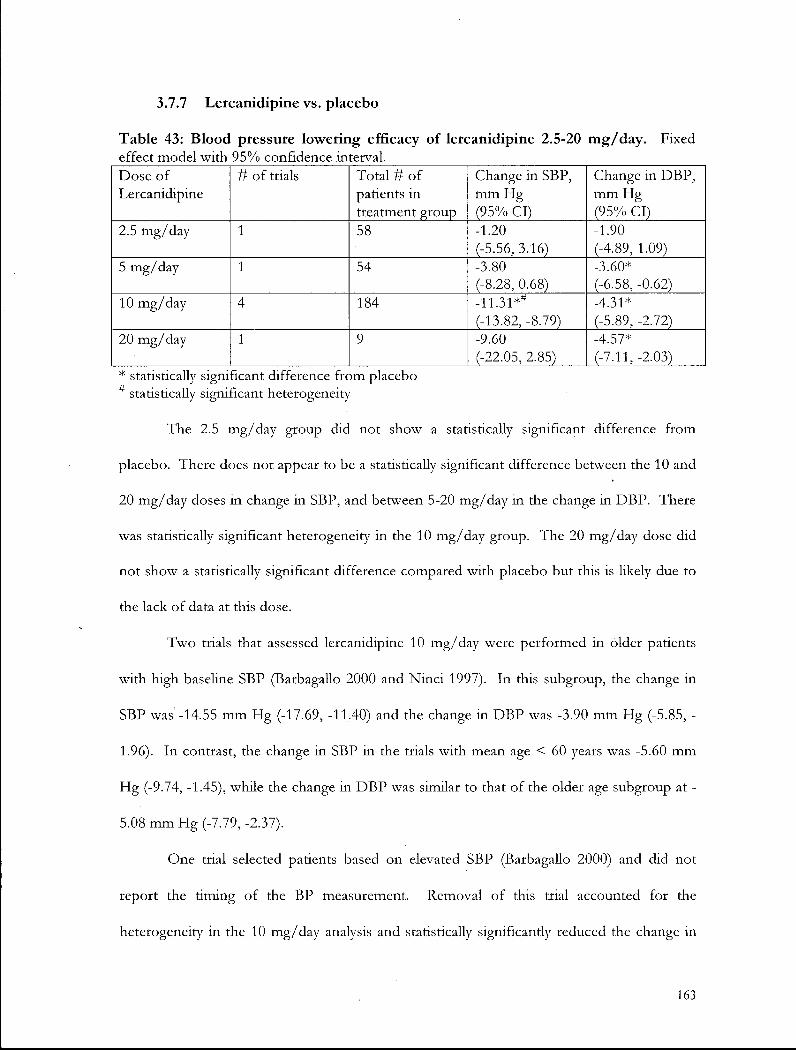
3.7.7 Lercanidipine vs. placebo
Table 43: B lood pressure lowering efficacy of lercanidipine 2.5-20 mg /day . Fixed effect model with 95% confidence interval. Dose of Lercanidipine
# of trials Total # of patients in treatment group
Change in SBP, mm H g (95% CI)
Change in D B P , mm H g (95% CI)
2.5 mg/day 1 58 -1.20 (-5.56, 3.16)
-1.90 (-4.89, 1.09)
5 mg/ day 1 54 -3.80 (-8.28, 0.68)
-3.60* (-6.58, -0.62)
10 mg/day 4 184 -11.31** (-13.82, -8.79)
-4.31* (-5.89, -2.72)
20 mg/day 1 9 -9.60 (-22.05, 2.85)
-4.57* (-7.11, -2.03)
* statistically significant difference from placebo # statistically significant heterogeneity
The 2.5 mg/day group did not show a statistically significant difference from
placebo. There does not appear to be a statistically significant difference between the 10 and
20 mg/day doses in change in SBP, and between 5-20 mg/day in the change in D B P . There
was statistically significant heterogeneity in the 10 mg/day group. The 20 mg/day dose did
not show a statistically significant difference compared with placebo but this is likely due to
the lack of data at this dose.
Two trials that assessed lercanidipine 10 mg/day were performed in older patients
with high baseline SBP (Barbagallo 2000 and Ninci 1997). In this subgroup, the change in
SBP was -14.55 mm Fig (-17.69, -11.40) and the change in D B P was -3.90 mm H g (-5.85, -
1.96). In contrast, the change in SBP in the trials with mean age < 60 years was -5.60 mm
H g (-9.74, -1.45), while the change in D B P was similar to that of the older age subgroup at -
5.08 mm H g (-7.79, -2.37).
One trial selected patients based on elevated SBP (Barbagallo 2000) and did not
report the timing of the BP measurement. Removal of this trial accounted for the
heterogeneity in the 10 mg/day analysis and statistically significantly reduced the change in
163
SBP to -6.60 mm H g (-9.71, -3.49) but did not alter the change in D B P , which was -4.65 mm
H g (-6.57, -2.72).
One of the included trials was of low quality (Rimoldi 1993). Removal of this trial
did not change the results in a statistically significant way. A l l trials that reported details
regarding the instrument and timing of measurement had trough BPs taken by auscultation.
Only one trial in the analysis measured B P in the sitting position (Ninci 1997). The SD of
the B P change was reported in only 1 trial (Omboni 1998) and imputed for the rest of the
trials, fmputing using the hierarchy or direcdy from all trials that reported SD of B P change
did not alter the results.
The best estimate of the maximal blood pressure lowering efficacy of lercanidipine at
10-20 mg/day is -11.24 mm H g (-13.71, -8.78) for SBP and -4.38 mm H g (-5.72, -3.03) for
D B P .
164

3.7.8 Manid ip ine vs. placebo
Table 44: B lood pressure lowering efficacy of manidipine 10-40 mg /day . Fixed effect model with 95% confidence interval. Dose of # of trials Total # of Change in SBP, Change in D B P , Manidipine patients in mm H g mm Fig
treatment group (95% CI) (95% CI) 10 mg/day 2 40 -10.37* -4.89*
(-15.31, -5.43) (-7.64, -2.13) 20 mg/day 1 12 -20.10* -11.00*
(-30.92, -9.28) (-17.16, -4.84) 40 mg/day 1 13 -23.50* -14.40*
(-34.11, -12.89) (-20.43, -8.37) * statistically significant difference from placebo
Two of the included trials evaluated manidipine. A l l manidipine doses demonstrated
a statistically significant reduction in BP compared with placebo. One trial (Fogari 1999)
was performed in elderly subjects (mean age of 81.8 years), and had a similar effect size
compared with the trial performed in younger patients (Fogari 1996, mean age of 53.4 years).
Considering all the doses tested, the lowest effective dose is 10 mg/day. The true lowest
effective dose may be lower than 10 mg/day but there are no data available. Indirect
comparisons showed that the effect sizes of the 20 and 40 mg/day doses were statistically
significantly different from that of the 10 mg/day dose. Based on the data from two trials,
the maximal blood pressure lowering efficacy of manidipine at 20-40 mg/day is -21.83 mm
H g (-29.33, -14.34) and -12.73 mm H g (-17.02, -8.45) for SBP and D B P , respectively;
however, because of the small number of patients, this is uncertain.
165
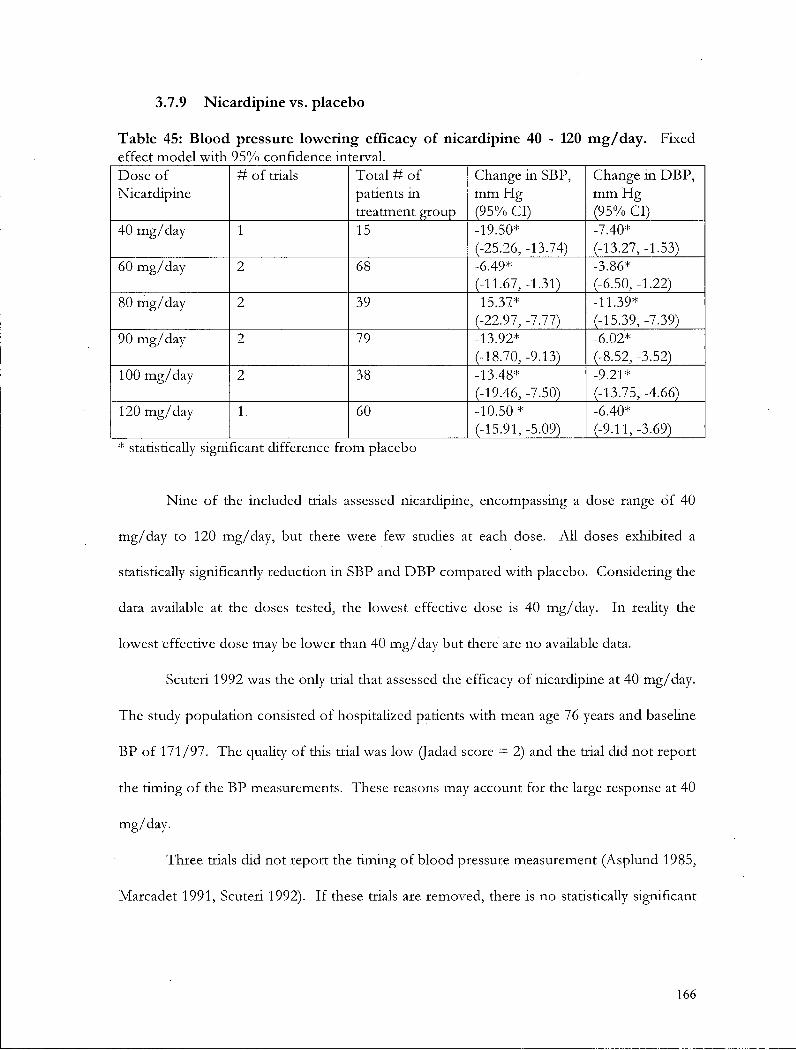
3.7.9 Nicard ip ine vs. placebo
Table 45: B lood pressure lowering efficacy of nicardipine 40 - 120 mg /day . Fixed effect model with 95% confidence interval. Dose of # of trials Total # of Change in SBP, Change in D B P , Nicardipine patients in
treatment group mm H g (95% CI)
mm H g (95% CI)
40 mg/day 1 15 -19.50* (-25.26,-13.74)
-7.40* (-13.27,-1.53)
60 mg/day 2 68 -6.49* -3.86* 60 mg/day (-11.67, -1.31) (-6.50, -1.22)
80 mg/day 2 39 -15.37* (-22.97, -7.77)
-11.39* (-15.39, -7.39)
90 mg/ day 2 79 -13.92* (-18.70, -9.13)
-6.02* (-8.52, -3.52)
100 mg/day 2 38 -13.48* (-19.46, -7.50)
-9.21* (-13.75, -4.66)
120 mg/day 1 60 -10.50 * (-15.91,-5.09)
-6.40* (-9.11,-3.69)
* statistically significant difference from placebo
Nine of the included trials assessed nicardipine, encompassing a dose range of 40
mg/day to 120 mg/day, but there were few studies at each dose. A l l doses exhibited a
statistically significandy reduction in SBP and D B P compared with placebo. Considering the
data available at the doses tested, the lowest effective dose is 40 mg/day. In reality the
lowest effective dose may be lower than 40 mg/day but there are no available data.
Scuteri 1992 was the only trial that assessed the efficacy of nicardipine at 40 mg/day.
The study population consisted of hospitalized patients with mean age 76 years and baseline
B P of 171/97. The quality of this trial was low (Jadad score = 2) and the trial did not report
the timing of the B P measurements. These reasons may account for the large response at 40
mg/day.
Three trials did not report the timing of blood pressure measurement (Asplund 1985,
Marcadet 1991, Scuteri 1992). If these trials are removed, there is no statistically significant
166
difference between any of the doses (60 mg/day-120 mg/day), using the indirect comparison
method.
Two of the eight included nicardipine trials tested a thrice-daily formulation (Soro
1990 and Asplund 1985), while the remainder tested a slow-release twice-daily formulation.
Subgroup analysis did not show a statistically significant difference in effect size between the
formulations.
The effect size was also insensitive to the instrument used for B P measurement and
strategy used to impute missing variances.
Considering only the trials that reported trough blood pressures, the best estimate of
the maximal B P lowering efficacy of nicardipine occurring at 60 to 120 mg/day is -10.49 mm
H g (95% CI: -13.20, -7.77) for SBP and -5.98 mm H g (95% Cf: -7.38, -4.57) for D B P .
167
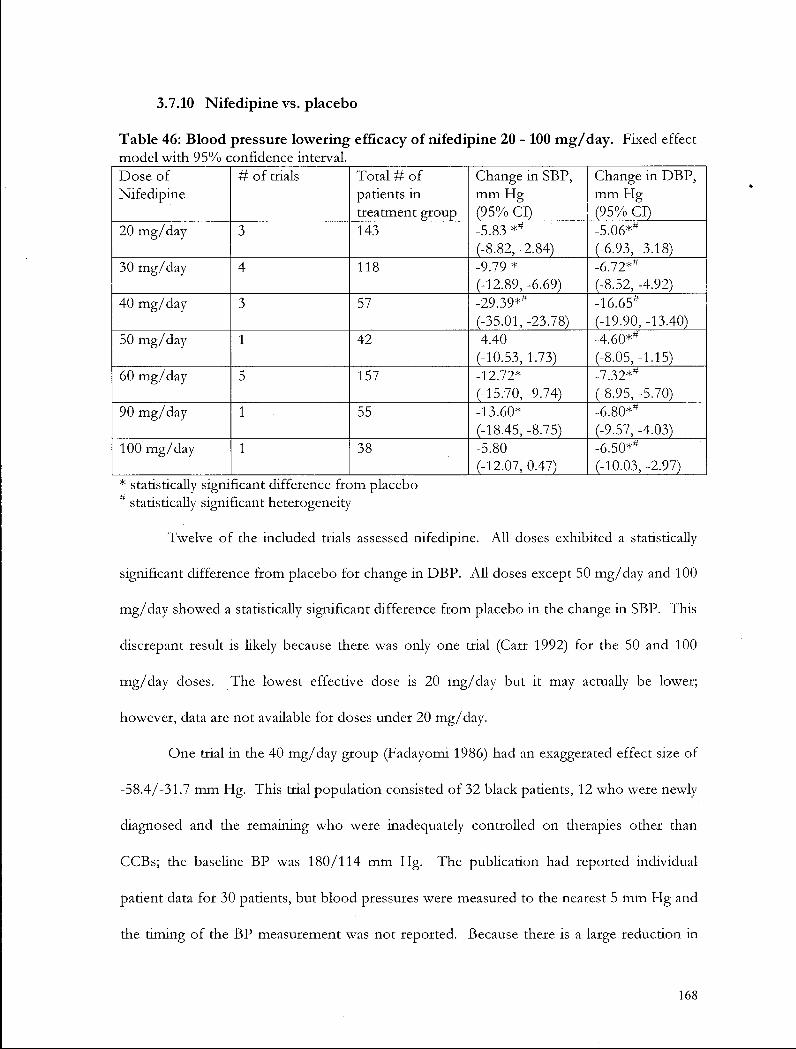
3.7.10 Ni fed ip ine vs. placebo
Table 46: B lood pressure lowering efficacy of nifedipine 20 - 100 mg /day . Fixed effect model with 95% confidence interval. Dose of Nifedipine
# of trials Total # of patients in treatment group
Change in SBP, mm H g (95% CI)
Change in D B P , mm H g (95% CI)
20 mg/day 3 143 -5.83 * #
(-8.82, -2.84) -5.06*#
(-6.93, -3.18) 30 mg/day 4 118 -9.79 *
(-12.89, -6.69) -6.72*#
(-8.52, -4.92) 40 mg/day 3 57 -29.39**
(-35.01, -23.78) -16.65#
(-19.90, -13.40) 50 mg/day 1 42 -4.40
(-10.53, 1.73) -4.60*#
(-8.05,-1.15) 60 mg/day 5 157 -12.72*
(-15.70, -9.74) -7.32*#
(-8.95, -5.70) 90 mg/day 1 55 -13.60*
(-18.45, -8.75) -6.80*#
(-9.57, -4.03) 100 mg/day 1 38 -5.80
(-12.07, 0.47) -6.50*#
(-10.03, -2.97) * statistically significant difference from placebo
statistically significant heterogeneity
Twelve of the included trials assessed nifedipine. A l l doses exhibited a statistically
significant difference from placebo for change in D B P . A l l doses except 50 mg/day and 100
mg/day showed a statistically significant difference from placebo in the change in SBP. This
discrepant result is likely because there was only one trial (Carr 1992) for the 50 and 100
mg/day doses. The lowest effective dose is 20 mg/day but it may actually be lower;
however, data are not available for doses under 20 mg/day.
One trial in the 40 mg/day group (Fadayomi 1986) had an exaggerated effect size of
-58.4/-31.7 mm Hg. This trial population consisted of 32 black patients, 12 who were newly
diagnosed and the remaining who were inadequately controlled on therapies other than
CCBs; the baseline BP was 180/114 mm Hg. The publication had reported individual
patient data for 30 patients, but blood pressures were measured to the nearest 5 mm H g and
the timing of the B P measurement was not reported. Because there is a large reduction in
the standard deviation of SBP from baseline (15.3 mm Hg) to endpoint (8.0 mm Hg) - a
pattern that is inconsistent with the pooled data of this systematic review - blinding may
have been compromised in this trial and data from this trial must be viewed with suspicion.
A sensitivity analysis was performed in which trials with trough measurements were
retained and trials that did not report timing of BP measurement were removed (de Simone
1985, Eggertsen 1982, Fadayomi 1986, Ferrera 1984, Serradimigni 1985). In this analysis,
there were no trials remaining in the 40 mg/day group, and there was no statistically
significant difference between the 30, 60 and 90 mg/day doses. There was a statistically
significant difference between 20 mg/day and 30 mg/day for reduction in SBP but not for
D B P .
There was statistically significant heterogeneity in every dose group in the change in
D B P . While the heterogeneity in the 20 mg/day group was resolved by removing trials that
did not report timing of the B P measurement, the heterogeneity in the other doses remained
and could not be explained by any of the predefined sensitivity/subgroup analyses.
The best estimate of the maximal blood pressure lowering efficacy at trough for 30
to 100 mg/day is -9.11 mm Fig (-10.69, -7.54) for SBP and -6.14 mm H g (-7.04, -5.23) for
D B P .
169

3.7.11. Ni lvad ip ine vs. placebo
Table 47: B lood pressure lowering efficacy of ni lvadipine 8-30 mg /day .
Dose of # of trials Total # of Change in SBP, Change in D B P , Nilvadipine padents in mm H g mm H g
treatment group (95% Cf) (95% CI) 8 rng/ day 1 60 -10.90*
(-16.58, -5.22) -5.50* (-8.82,-2.18)
16 mg/day 1 49 -11.00* (-17.10, -4.90)
-7.80* (-11.88, -3.72)
18 mg/day 1 17 Not reported -7.00* (-12.53,-1.47)
24 mg/day 1 19 Not reported -6.80* (-12.07,-1.53)
30 mg/day 1 20 Not reported -8.20* (-13.40, -3.00)
statistically significant difference from placebo
Only 2 included trials evaluated the blood pressure lowering efficacy of nilvadipine:
Hoffmann 1997 tested 8-16 mg/day and Weir 1990 tested 18-30 mg/day. Although all
nilvadipine groups had a statistsically significant difference from placebo, there was no
statistically significant difference between any of the doses assessed. The true maximum
blood pressure lowering efficacy of nilvadipine cannot be estimated since doses below 8
mg/day and above 30 mg/day were not tested. However, based on the available data, the
best estimate of the maximal B P lowering efficacy of nilvadipine at trough across all doses
tested (8-30 mg/day) is -10.95 mm H g (95% CI: -15.10, -6.79) for SBP and -6.80 mm H g
(95% Cf: -8.78, -4.83) for D B P . This result is based on data from very few patients, and
hence, the confidence intervals are wide.
170

3.7.12 Niso ld ip ine vs. placebo
Table 48: B lood pressure lowering efficacy of nisoldipine 10-30mg/day.
Dose of # of trials Total # of Change in SBP, Change in D B P , Nisoldipine patients in mm H g mm H g
treatment group (95% CI) (95% CI) 10 mg/ day 1 49 -9.50* -6.90*
(-15.43, -3.57) (-9.87, -3.93) 20 mg/day 1 51 -15.90* -9.20*
(-21.77, -10.03) (-12.10, -6.30) 30 mg/day 1 48 -16.20* -10.60*
(-22.09, -10.31) (-13.51, -7.69) statistically significant difference from placebo
One included trial assessed nisolidipine at doses of 10, 20 and 30 mg/day (Opie
1997). A l l doses demonstrated a statistically significant reduction in B P compared with
placebo. Using indirect comparisons there was no statistically significant difference between
any of the doses. Based on the results of this one small trial, the best estimate of maximal
blood pressure lowering efficacy for nisoldipine 10-30 mg/day is -13.89 mm H g (95% CI: -
17.30, -10.49) for SBP and -8.93 mm H g (95 % CI: -10.62, -7.24) for D B P . However,
because of the lack of data and doses tested, this result provides very limited information
regarding the dose-response of nisolidipine.
171

3.7.13 Ni t rendipine vs. placebo
Table 49: B lood pressure lowering efficacy of nitrendipine 5-20 mg /day . Fixed effect model with 95% confidence interval. Dose of # of trials Total # of Change in SBP, Change in D B P , Nitrendipine patients in mm H g mm H g
treatment group (95% CI) (95% CI) 5 mg/day 1 20 -2.00 -2.00
(-10.69, 6.69) (-7.88, 3.88) 10 mg/day 3 129 -8.34* -5.50*#
(-11.38, -5.30) (-7.00, -4.00) 20 mg/day 8 154 -13.80*# -9.46*#
(-17.12, -10.49) (-11.54, -7.38) * statistically significant difference from placebo # statistically significant heterogeneity
Nitrendipine at 5 mg/day did not statistically significantiy reduce blood pressure
compared with placebo. The lowest effective dose was 10 mg/day. Indirect comparisons
did not show a statistically significant difference between the 5 and 10 mg/day groups. The
20 mg/day group demonstrated a statistically significant difference from both the 5 and 10
mg/day groups.
There was statistically significant heterogeneity in the 20 mg/day group, most
notably in D B P (I2=88.9%). One trial had inclusion criteria of isolated systolic hypertension
(Paolisso 1991) and a concomitant high baseline SBP (> 170 mm Hg). Removing this trial
and another trial with high baseline (Maclean 1990) reduced the heterogeneity in the 20
mg/day group but it was still statistically significant. Six of the ten included studies were of
low quality (Jadad score of 2). If these trials are excluded, litde data remain in the analysis
but the heterogeneity is no longer statistically significant and the resultant effect size in the
20 mg/day group is -9.17 mm H g (-12.12, -6.21) for SBP and -6.06 mm H g (-7.47, -4.65) for
D B P .
172

Two studies had a mean age of participants > 60 years (Gerritsen 1998 and Paolisso
1991) but there were not enough data for a subgroup analysis based on age.
The best estimate of the maximal trough blood pressure lowering efficacy at 20
mg/day is -13.80 mm H g (-17.12, -10.49) for SBP and -9.46 (-11.54, -7.38) for D B P . The
heterogeneity observed in this dose could only be accounted for by removing low quality
studies.
173
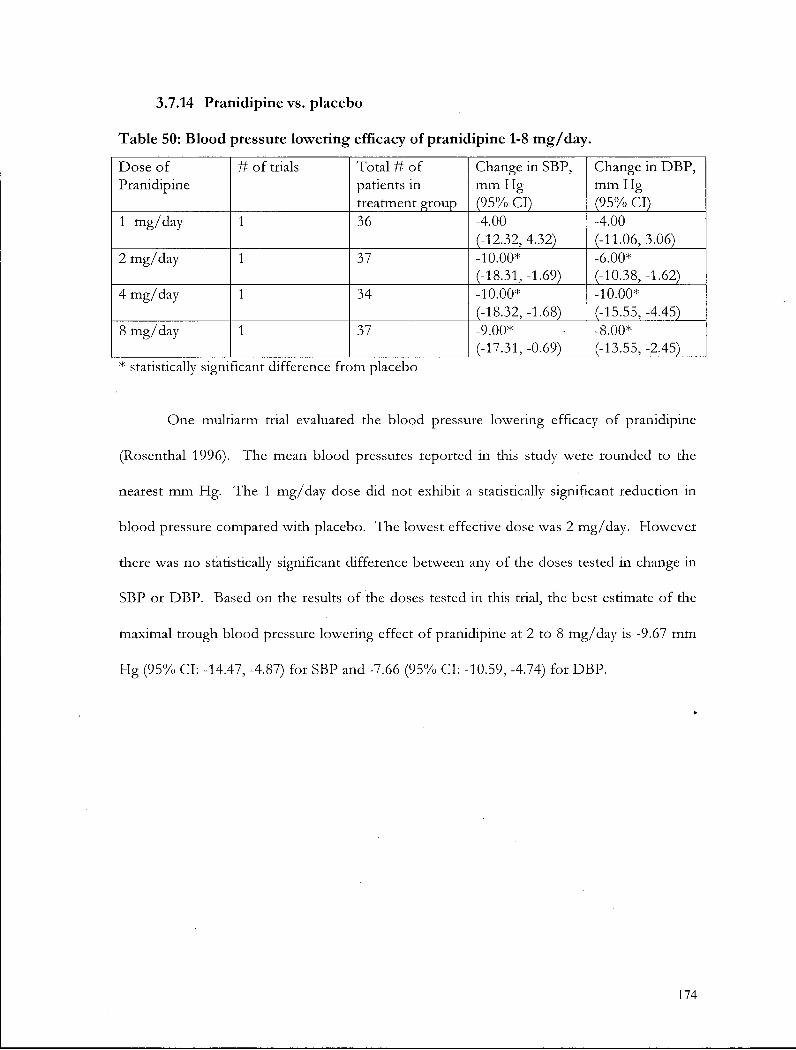
3.7.14 Ptanidipine vs. placebo
Table 50: B lood pressure lowering efficacy of pranidipine 1-8 mg /day .
Dose of # of trials Total # of Change in SBP, Change in D B P , Pranidipine patients in mm H g mm H g
treatment group (95% CI) (95% CI) 1 mg/day 1 36 -4.00 -4.00
(-12.32, 4.32) (-11.06, 3.06) 2 mg/day 1 37 -10.00* -6.00*
(-18.31, -1.69) (-10.38, -1.62) 4 mg/day 1 34 -10.00* -10.00*
(-18.32,-1.68) (-15.55, -4.45) 8 mg/day 1 37 -9.00* -8.00*
(-17.31, -0.69) (-13.55, -2.45) * statistically significant difference from placebo
One multiarm trial evaluated the blood pressure lowering efficacy of pranidipine
(Rosenthal 1996). The mean blood pressures reported in this study were rounded to the
nearest mm Fig. The 1 mg/day dose did not exhibit a statistically significant reduction in
blood pressure compared with placebo. The lowest effective dose was 2 mg/day. However
there was no statistically significant difference between any of the doses tested in change in
SBP or D B P . Based on the results of the doses tested in this trial, the best estimate of the
maximal trough blood pressure lowering effect of pranidipine at 2 to 8 mg/day is -9.67 mm
H g (95% CI: -14.47, -4.87) for SBP and -7.66 (95% CI: -10.59, -4.74) for D B P .
174

3.7.15 Summary of b lood pressure lowering efficacy of dihydropyridines
Table 51: Summary of b lood pressure lowering efficacy of dihydropyridines Dihydropyr idine drug
Lowest effective dose (mg /day ) * #
Lowest dose wi th maximal B P lowering ( m g / d a y ) A #
Magni tude of max imal trough B P lowering (mm H g ) , 95% CI
Dihydropyr idine drug
Lowest effective dose (mg /day ) * #
Lowest dose wi th maximal B P lowering ( m g / d a y ) A # S B P D B P
Amlodipine 2.5 mg 5 m g -10.72 (-12.30, -9.14)
-5.73 (-6.65, -4.82)
Barnidipine 30 mg 30 mg -5.80 (-11.35, -0.25)
-4.90 (-8.06,-1.74)
Darodipine fOOmg 100 mg -18.40 (-26.02, -10.79)
-10.51 (-15.17, -5.84)
Felodipine 2.5 mg 2.5 mg -6.11 (-7.41, -4.82)
-4.75 (-5.44, -4.05)
Isradipine 1 mg 10 mg -14.84 (-17.47, -12.20)
-10.57 (-12.15, -8.98)
Lacidipine 4 m g 4 m g -7.00 (-13.17, -0.83)
-4.20 (-7.67, -0.73)
Lercanidipine 10 mg 10 mg -11.24 (-13.71, -8.78)
-4.38 (-5.72, -3.03)
Manidipine fOmg 20 mg -21.83 (-29.33, -14.34)
-12.73 (-17.02, -8.45)
Nicardipine 40 mg 60 mg -10.49 (-13.20, -7.77)
-5.98 (-7.38, -4.57)
Nifedipine 20 mg 30 mg -9.11 (-10.69, -7.54)
-6.14 (-7.04, -5.23)
Nilvadipine 8 m g 8 m g -10.95 (-15.10, -6.79)
-6.80 (-8.78, -4.83)
Nisoldipine 10 mg 10 mg -13.89 (-17.30, -10.49)
-8.93 (-10.62, -7.24)
Nitrendipine 10 mg 20 mg -13.80 (-17.12, -10.49)
-9.46 (-11.54, -7.38)
Pranidipine 2 m g 2 mg -9.67 (-14.47, -4.87)
-7.66 (-10.59, -4.74)
* The lowest effective dose is the lowest dose for which t lere is a statistically significant difference vs. placebo A The lowest dose with maximal blood pressure lowering efficacy is achieved at the dose that exhibits a statistically significantly greater response than all other doses lower than it, whereas doses higher than it do not exhibit a statistically significant difference in effect size. # If there was a discrepancy between the determined dose for SBP and DBP, that of SBP is used.
Dihydropyridines were pooled from trials reporting trough blood pressures and were
grouped according to increments of the manufactuer's recommended starting dose (Table
175
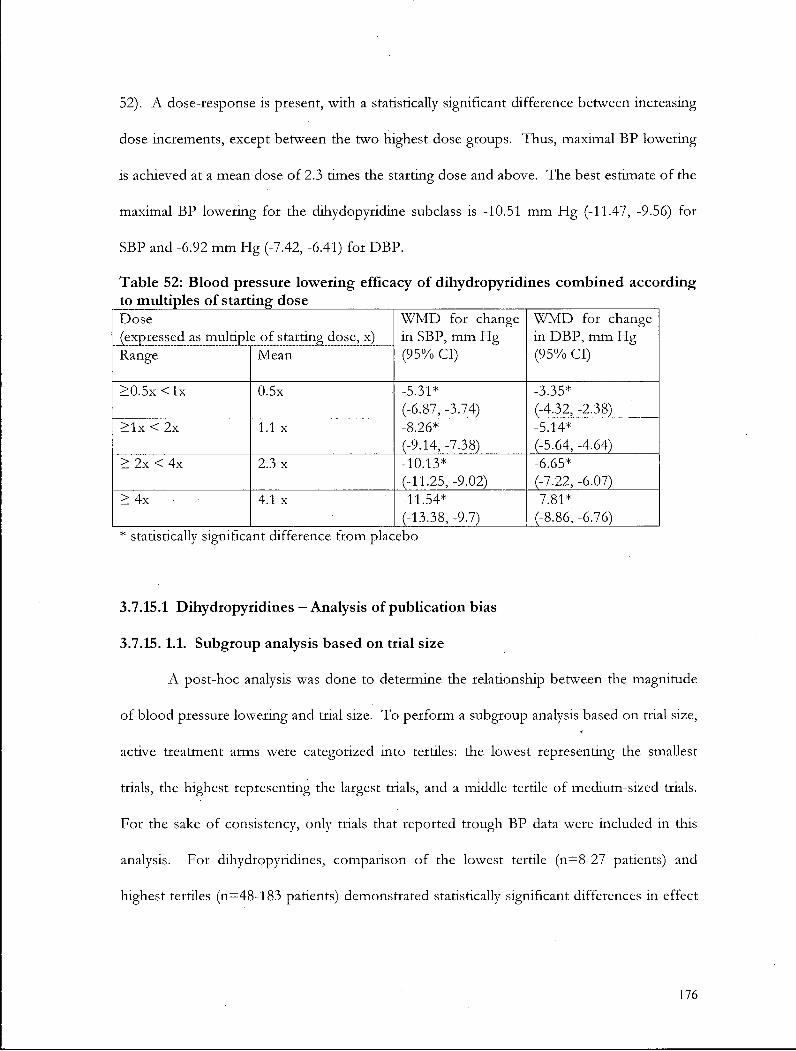
52). A dose-response is present, with a statistically significant difference between increasing
dose increments, except between the two highest dose groups. Thus, maximal B P lowering
is achieved at a mean dose of 2.3 times the starting dose and above. The best estimate of the
maximal B P lowering for the dihydopyridine subclass is -10.51 mm H g (-11.47, -9.56) for
SBP and -6.92 mm H g (-7.42, -6.41) for D B P .
Table 52: B lood pressure lowering efficacy of dihydropyridines combined according to multiples of starting dose Dose (expressed as multiple of starting dose, x)
W M D for change in SBP, mm H g (95% CI)
W M D for change in D B P , mm H g (95% CI) Range Mean
W M D for change in SBP, mm H g (95% CI)
W M D for change in D B P , mm H g (95% CI)
>0.5x < lx 0.5x -5.31* (-6.87, -3.74)
-3.35* (-4.32, -2.38)
> lx < 2x 1.1 X -8.26* (-9.14, -7.38)
-5.14* (-5.64, -4.64)
> 2x < 4x 2.3 x -10.13* (-11.25, -9.02)
-6.65* (-7.22, -6.07)
> 4x 4.1 x -11.54* (-13.38, -9.7)
-7.81* (-8.86, -6.76)
statistically significant difference from placebo
3.7.15.1 Dihydropyridines - Analysis of publ icat ion bias
3.7.15.1.1. Subgroup analysis based on trial size
A post-hoc analysis was done to determine the relationship between the magnitude
of blood pressure lowering and trial size. To perform a subgroup analysis based on trial size,
active treatment arms were categorized into tertiles: the lowest representing the smallest
trials, the highest representing the largest trials, and a middle tertile of medium-sized trials.
For the sake of consistency, only trials that reported trough BP data were included in this
analysis. For dihydropyridines, comparison of the lowest tertile (n=8-27 patients) and
highest tertiles (n=48-183 patients) demonstrated statistically significant differences in effect
176

size for both SBP and D B P , with larger and more variable effect sizes seen in the smaller
trials (Table 53).
Table 53: Dihydropyridines: post-hoc subgroup analysis of trough B P lowering based on trial size Dihydropyr idines, T rough measurements
Lowest tertile (8-27 patients)
H ighest tertile (48-183 patients)
Mean of W M D for change in -12.6 mm H g (6.4) -9.0 mm H g (4.1) SBP (SD) # of observations 25 27 t-test low vs. high tertile p = 0.02 Mean of W M D for change in -9.1 mm H g (5.2) -5.4 mm H g (2.2) D B P (SD) # of observations 28 28 t-test low vs. high tertile p = 0.001
To obtain another estimate of the maximal blood pressure lowering efficacy of
dihydropyridines, the tertile analysis was restricted to trials with doses greater than or equal
to twice the starting dose. Combined, the middle and highest tertiles give an estimate of -9.1
mm H g (95% CI: -10.8, -7.4) for maximal change in SBP and -6.0 mm H g (95% CI: -5.2, -
6.9) for maximal change in D B P .
3.7.15.1.2. Tr im-and-f i l l method of adjusting for publ icat ion bias
The nonparametric ttim-and-fill method was used to adjust the effect size for the
presence of publication bias (376). The funnel plot of the maximal blood pressure lowering
efficacy of dihydropyridines at greater than or equal to twice the starting dose showed
asymmetry, with an absence of negative-result trials (Figures 6 and 7). Data points were
filled in to make the funnel plot symmetrical and a new effect size was calculated. For
change in SBP, seven data points were filled in and the adjusted effect size was -10.15 mm
Fig (-11.08, -9.22). For change in D B P , five data points were filled in and the resulting
adjusted effect size was -6.67 mm H g (-7.17, -6.17). Thus, the original effect size was
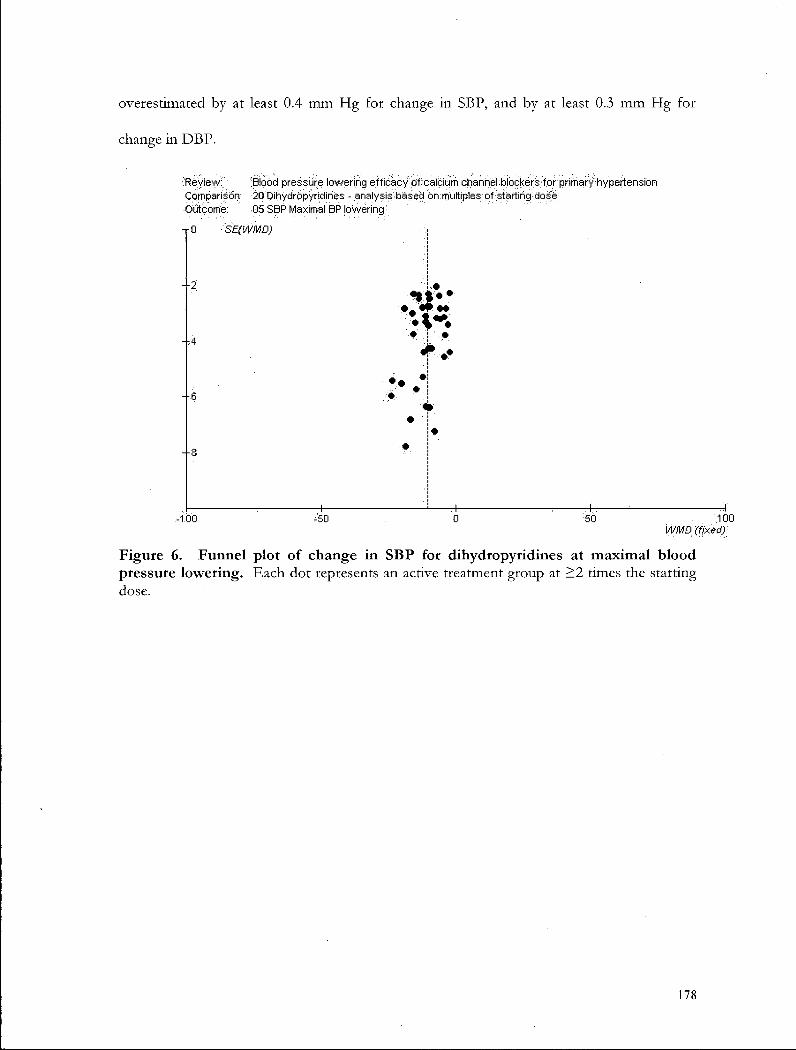
overestimated by at least 0.4 mm H g for change in SBP, and by at least 0.3 mm H g for
change in D B P .
'Review: ;Blo6d pressure lowering eff icacy of calcium channel blockers-for primary^hypertensibn Comparison: 20 Dihydropyridines - analysis based on multiples of starting dose -Outcome: 05 SBP Maximal BP lowering
0 SE(WMD)
+6
•
-100 ^50 50 .100 WMD (fixed)
Figure 6. Funnel plot of change in SBP for dihydropyridines at maximal blood pressure lowering. Each dot represents an active treatment group at >2 times the starting dose.
178

Review;. Blood pressure loweringefficacypt Comparison: 20 Dihydropyridines - analysis based on multiples of starting dose Outcome: 06 DBP Maximal BP lowering
-r0 SEiyVMD)
• A -•
+ 6
-too :50 1 0 0 WMO (fixed)
Figure 7. Funnel plot of change in D B P for dihydropyridines at maximal blood pressure lowering efficacy. Each dot represents an active treatment group at >2 times the
starting dose.
179
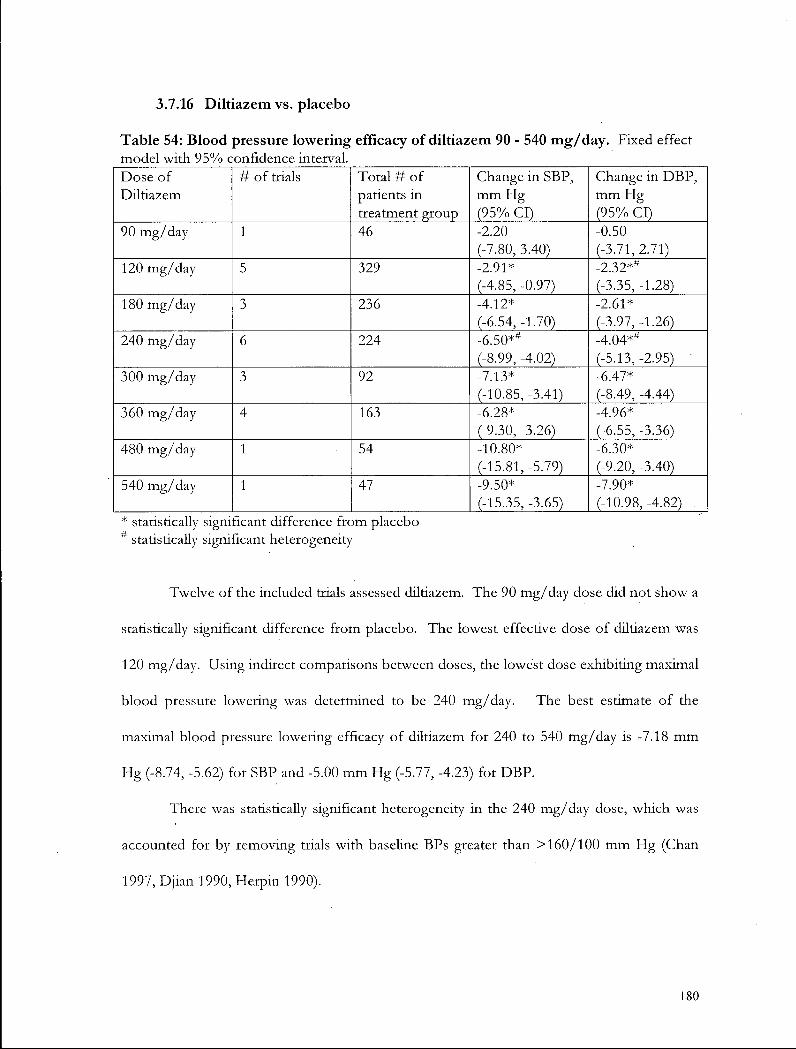
3.7.16 Di l t iazem vs. placebo
Table 54: B lood pressure lowering efficacy of di l t iazem 90 - 540 mg /day . Fixed effect model with 95% confidence interval. Dose of # of trials Total # of Change in SBP, Change in D B P , Diltiazem patients in mm H g mm H g
treatment group (95% Cf) (95% CI) 90 mg/day 1 46 -2.20
(-7.80, 3.40) -0.50 (-3.71, 2.71)
120 mg/day 5 329 -2.91* -2.32*# 120 mg/day (-4.85, -0.97) (-3.35,-1.28)
180 mg/day 3 236 -4.12* (-6.54, -1.70)
-2.61* (-3.97,-1.26)
240 mg/day 6 224 -6.50*#
(-8.99, -4.02) -4.04*#
(-5.13, -2.95) 300 mg/day 3 92 -7.13*
(-10.85, -3.41) -6.47* (-8.49, -4.44)
360 mg/day 4 163 -6.28* (-9.30, -3.26)
-4.96* (-6.55, -3.36)
480 mg/day 1 54 -10.80* (-15.81,-5.79)
-6.30* (-9.20, -3.40)
540 mg/day 1 47 -9.50* (-15.35, -3.65)
-7.90* (-10.98,-4.82)
y~ statistically significant difference from placebo * statistically significant heterogeneity
Twelve of the included trials assessed diltiazem. The 90 mg/day dose did not show a
statistically significant difference from placebo. The lowest effective dose of diltiazem was
120 mg/day. Using indirect comparisons between doses, the lowest dose exhibiting maximal
blood pressure lowering was determined to be 240 mg/day. The best estimate of the
maximal blood pressure lowering efficacy of diltiazem for 240 to 540 mg/day is -7.18 mm
H g (-8.74, -5.62) for SBP and -5.00 mm Fig (-5.77, -4.23) for D B P .
There was statistically significant heterogeneity in the 240 mg/day dose, which was
accounted for by removing trials with baseline BPs greater than > 160/100 mm H g (Chan
1997, Djian 1990, Herptn 1990).
180

Two trials were performed in older patients (Chan 1997 and Fiddes 1994). The
effect sizes were greater in this subgroup compared with younger patients (mean age < 60
years). Although there were not sufficient data for a subgroup analysis, removing these two
trials did account for the heterogeneity observed in the 240 mg/day group.
A l l trials evaluated sustained-release formulations; in 9 of the trials, dosing was once-
daily, while the other 3 trials used twice-daily regimens. There was no statistically significant
difference in effect size between these regimens.
A l l trials that reported timing of B P measurement in relation to the dosing interval
measured trough values. Seven trials reported funding sources and all of these had industry
funding. As well, all trials were of moderate quality and had inclusion criteria of elevated
D B P . Only 2 trials reported BPs measured in the sitting position, while the remaining 10
trials had supine blood pressures. Four of the diltiazem trials reported the SD of BP change,
f f trials that did not report the SD of change in B P were imputed direcdy with the weighted
mean from all trials that reported this value, the result is not different than using the
imputation hierarchy.
181
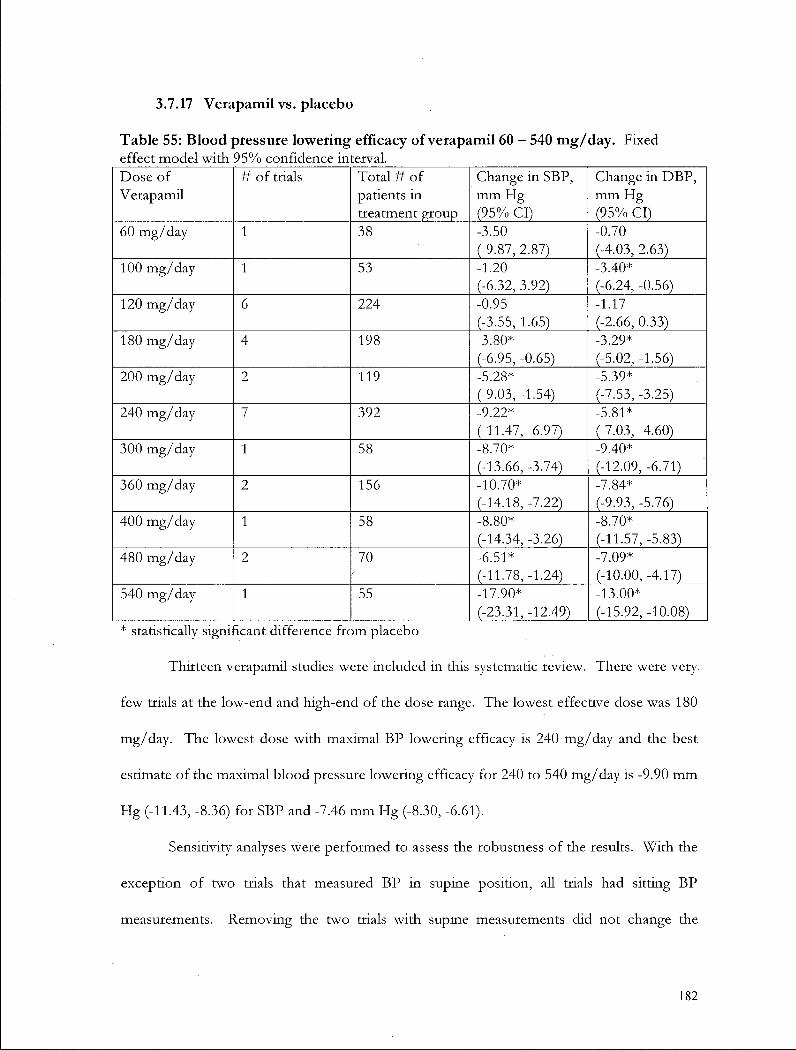
3.7.17 Verapamil vs. placebo
Table 55: Blood pressure lowering efficacy of verapamil 60 - 540 mg/day. Fixed effect model with 95% confidence interval. Dose of # of trials Total # of Change in SBP, Change in D B P , Verapamil patients in
treatment group mm H g (95% CI)
mm H g (95% CI)
60 mg/day 1 38 -3.50 (-9.87, 2.87)
-0.70 (-4.03, 2.63)
100 mg/day 1 53 -1.20 (-6.32, 3.92)
-3.40* (-6.24, -0.56)
120 mg/day 6 224 -0.95 (-3.55, 1.65)
-1.17 (-2.66, 0.33)
180 mg/day 4 198 -3.80* (-6.95, -0.65)
-3.29* (-5.02,-1.56)
200 mg/day 2 119 -5.28* (-9.03,-1.54)
-5.39* (-7.53, -3.25)
240 mg/day 7 392 -9.22* (-11.47, -6.97)
-5.81* (-7.03, -4.60)
300 mg/day 1 58 -8.70* (-13.66, -3.74)
-9.40* (-12.09, -6.71)
360 mg/day 2 156 -10.70* (-14.18, -7.22)
-7.84* (-9.93, -5.76)
400 mg/day 1 58 -8.80* (-14.34, -3.26)
-8.70* (-11.57,-5.83)
480 mg/day 2 70 -6.51* (-11.78, -1.24)
-7.09* (-10.00, -4.17)
540 mg/day 1 55 -17.90* (-23.31, -12.49)
-13.00* (-15.92,-10.08)
* statistically significant difference from placebo
Thirteen verapamil studies were included in this systematic review. There were very,
few trials at the low-end and high-end of the dose range. The lowest effective dose was 180
mg/day. The lowest dose with maximal B P lowering efficacy is 240 mg/day and the best
estimate of the maximal blood pressure lowering efficacy for 240 to 540 mg/day is -9.90 mm
H g (-11.43, -8.36) for SBP and -7.46 mm H g (-8.30, -6.61).
Sensitivity analyses were performed to assess the robustness of the results. With the
exception of two trials that measured B P in supine position, all trials had sitting B P
measurements. Removing the two trials with supine measurements did not change the
182
results. Nine trials reported the variance of the change in BP , whereas the 4 remaining trials
used imputed values. The results were insensitive to whether the values were imputed
according to the hierarchy or imputed direcdy from the weighted mean value from all trials
that reported the SD of BP change. One of the trials had a high baseline BP (Von
Manteuffel 1995) but excluding this trial did not alter the results, nor did removing trials with
low quality. A l l trials tested once-daily sustained-release forms of verpamil. Subgroup
analysis based on age was not possible since all trials had a mean age of < 60 years. A l l trials
had inclusion criteria of elevated diastolic blood pressure and used sphygmomanometers to
measure BP. The four trials that reported funding source were all industry-funded.
183

3.7.18 Tiapamil vs. placebo
Dose of # of trials Total # of Change in SBP, Change in D B P , Tiapamil patients in mm H g mm H g
treatment group (95% CI) (95% CI) 300-600 mg/day 1 24 -4.00 -1.00
(-12.90, 4.90) (-6.82, 4.82) 900-1200 1 25 -5.00 -4.00 mg/day (-13.47, 3.47) (-9.55, 1.55)
Data from the one included trial that evaluated tiapamil (Blanchett 1991) showed
that doses 300-1200 mg/day did not reduce blood pressure compared with placebo. Based
on this limited evidence, the lowest effective dose and the maximal blood pressure lowering
efficacy of tiapamil cannot be estimated.
184
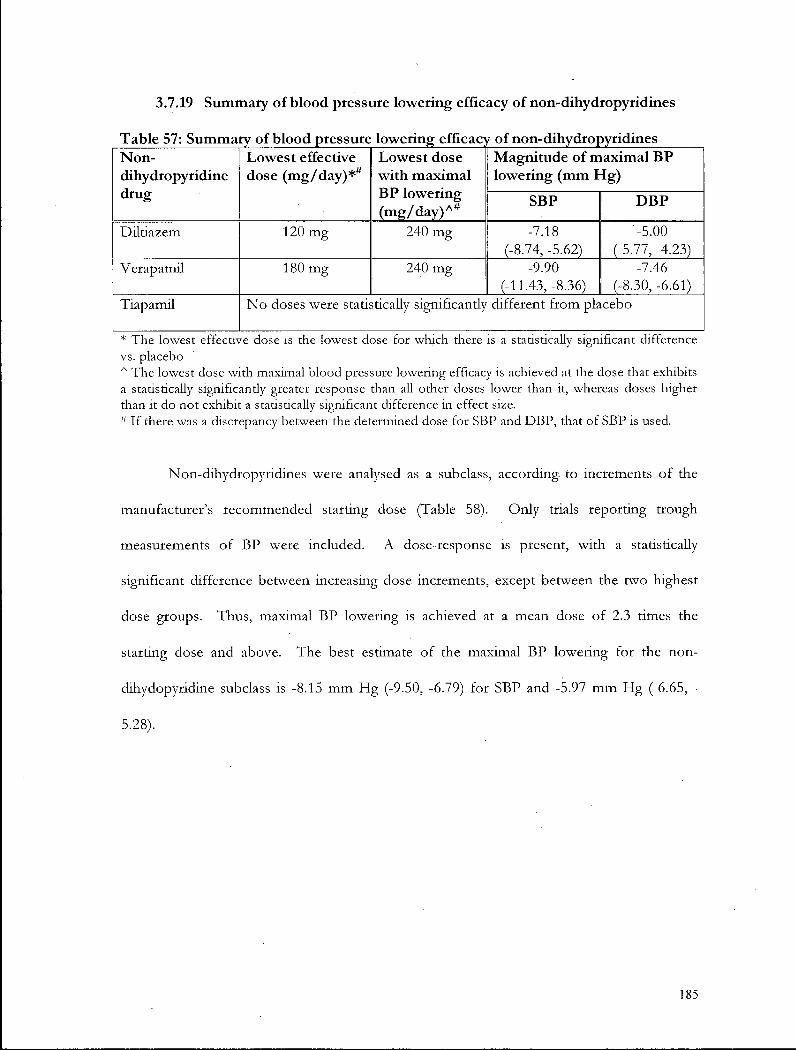
3.7.19 Summary of b lood pressure lowering efficacy of non-dihydropyridines
Table 57: Summary of b lood pressure lowering efficacy of non-dihydropyridines N o n -dihydropyridine drug
Lowest effective dose (mg/day)* *
Lowest dose with maximal B P lowering ( m g / d a y ) A #
Magni tude of max imal B P lowering (mm H g )
N o n -dihydropyridine drug
Lowest effective dose (mg/day)* *
Lowest dose with maximal B P lowering ( m g / d a y ) A #
S B P D B P
Diltiazem 120 mg 240 mg -7.18 (-8.74, -5.62)
-5.00 (-5.77, -4.23)
Verapamil 180 mg 240 mg -9.90 (-11.43, -8.36)
-7.46 (-8.30, -6.61)
Tiapamil N o doses were statistically significandy different from placebo
* The lowest effective dose is the lowest dose for which there is a statistically significant difference vs. placebo A The lowest dose with maximal blood pressure lowering efficacy is achieved at the dose that exhibits a statistically significantly greater response than all other doses lower than it, whereas doses higher than it do not exhibit a statistically significant difference in effect size. * If there was a discrepancy between the determined dose for SBP and DBP, that of SBP is used.
Non-dihydropyridines were analysed as a subclass, according, to increments of the
manufacturer's recommended starting dose (Table 58). Only trials reporting trough
measurements of BP were included. A dose-response is present, with a statistically
significant difference between increasing dose increments, except between the two highest
dose groups. Thus, maximal BP lowering is achieved at a mean dose of 2.3 times the
starting dose and above. The best estimate of the maximal B P lowering for the non-
dihydopyridine subclass is -8.15 mm H g (-9.50, -6.79) for SBP and -5.97 mm H g (-6.65, -
5.28).
185
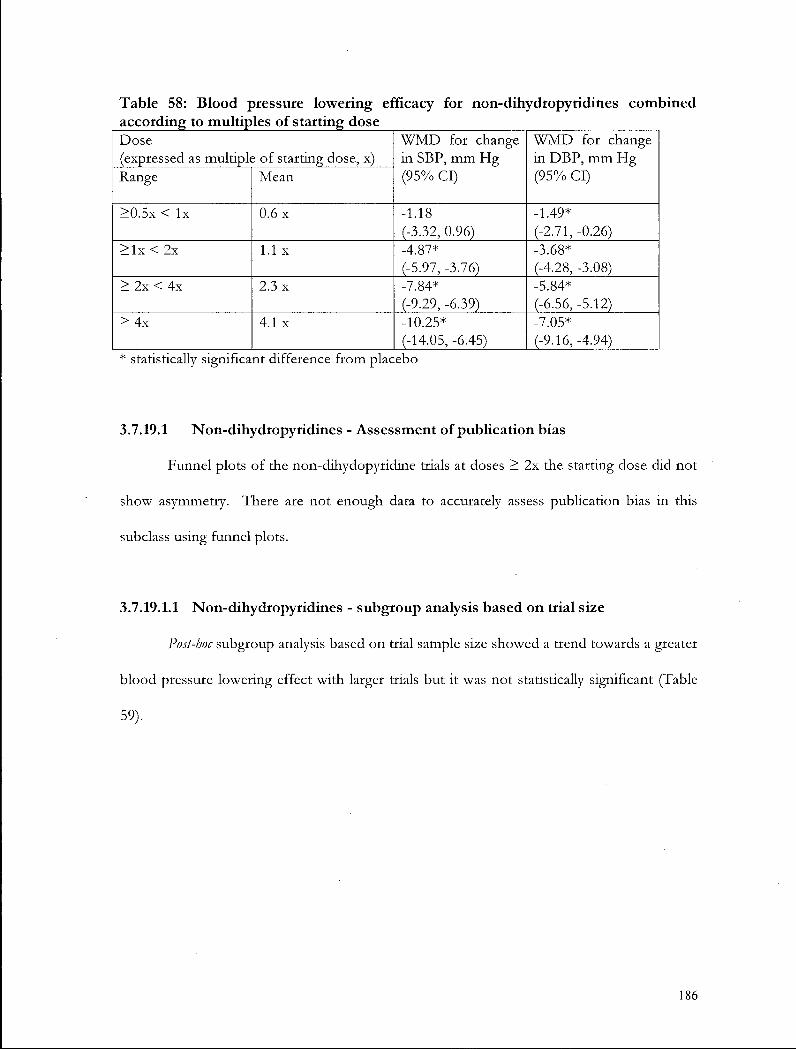
Table 58: B lood pressure lowering efficacy for non-dihydropyridines combined according to multiples of starting dose Dose (expressed as multiple of starting dose, x)
W M D for change in SBP, mm H g (95% CI)
W M D for change in D B P , mm H g (95% CI) Range Mean
W M D for change in SBP, mm H g (95% CI)
W M D for change in D B P , mm H g (95% CI)
>0.5x < l x 0.6 x -1.18 (-3.32, 0.96)
-1.49* (-2.71,-0.26)
> lx < 2x 1.1 X -4.87* (-5.97, -3.76)
-3.68* (-4.28, -3.08)
> 2x < 4x 2.3 x -7.84* (-9.29, -6.39)
-5.84* (-6.56, -5.12)
> 4x 4.1 x -10.25* (-14.05, -6.45)
-7.05* (-9.16, -4.94)
statistically significant difference from placebo
3.7.19.1 Non-dihydropyr id ines - Assessment of publ icat ion bias
Funnel plots of the non-dihydopyridine trials at doses > 2x the starting dose did not
show asymmetry. There are not enough data to accurately assess publication bias in this
subclass using funnel plots.
3.7.19.1.1 Non-dihydropyr idines - subgroup analysis based on trial size
Post-hoc subgroup analysis based on trial sample size showed a trend towards a greater
blood pressure lowering effect with larger trials but it was not statistically significant (Table
59).
186

Table 59: Non-dihydtopyr id ines: post-hoc subgroup analysis of trough blood pressure lowering based on trial size N o n - dihydropyridines, Lowest tertile Highest tertile trough measurements (15-43 patients) (56-238 patients) Mean of W M D for change in -6.9 mm H g (4.7) -5.8 mm H g (2.4) SBP (SD) # of observations 11 13 t-test lowest vs. highest p = 0.5 tertile Mean of W M D for change in -5.5 mm H g (3.0) -4.7 mm H g (2.4) D B P (SD) # of observations 13 14 t-test lowest vs. highest p = 0.4 tertile
Another estimate of the maximal blood pressure lowering efficacy of non-
dihydropyridines was obtained by restricting the tertile analysis to trials with doses greater
than or equal to twice the starting dose. Combined, the middle and highest tertiles give an
estimate of -8.1 mm H g (95% CI: -10.2, -6.1) for maximal change in SBP and -5.7 mm H g
(95% CI: -7.3, -4.1) for maximal change in D B P .
187

3.7.20 Other C C B s
3.7.20.1 Lidof lazine vs. placebo
Table 60: B lood pressure lowering efficacy of l idoflazine 180 mg /day . Dose of # of trials Total # of Change in SBP, Change in D B P , Lidoflazine padents in mm H g mm H g
treatment group (95% Cf) (95% CI) 180 mg/day 1 5 16.00 -5.00
(-4.34, 36.34) (-16.91,6.91)
One trial evaluated lidoflazine in post-infarcdon patients who were not selected on
the basis of elevated blood pressure. Since individual patient data were reported, data were
extracted for the 10 patients (5 in each of lidoflazine and placebo groups) who met the
criteria for hypertension at baseline. In this trial there was no statistically significant
difference between lidoflazine and placebo in change in blood pressure. Lidoflazine actually
exhibited an increase in SBP after 3 months treatment, but this result may be a chance effect
in a very small sample.
188
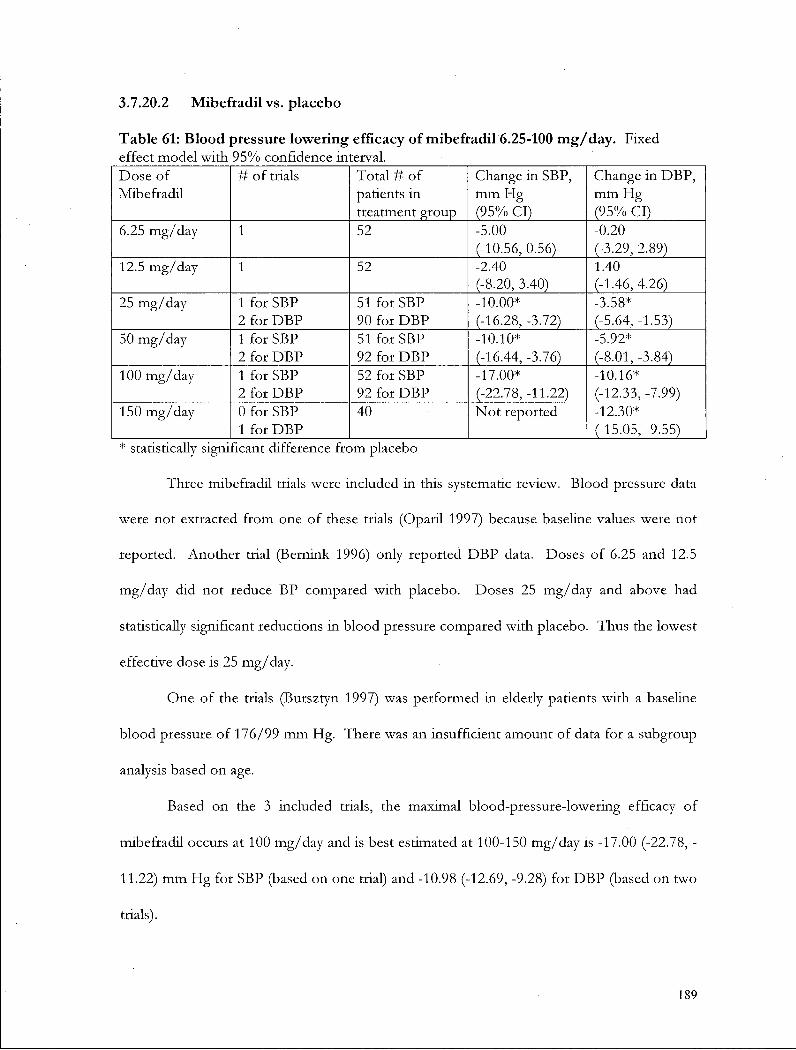
3.7.20.2 Mibef rad i l vs. placebo
Table 61: B lood pressure lowering efficacy of mibefradi l 6.25-100 mg /day . Fixed effect model with 95% confidence interval. Dose of # of trials Total # of Change in SBP, Change in D B P , Mibefradil patients in mm H g mm H g
treatment group (95% CI) (95% CI) 6.25 mg/day 1 52 -5.00 -0.20
(-10.56, 0.56) (-3.29, 2.89) 12.5 mg/day 1 52 -2.40 1.40
(-8.20, 3.40) (-1.46, 4.26) 25 mg/day 1 for SBP 51 for SBP -10.00* -3.58*
2 for D B P 90 for D B P (-16.28, -3.72) (-5.64, -1.53) 50 mg/day 1 for SBP 51 for SBP -10.10* -5.92*
2 for D B P 92 for D B P (-16.44, -3.76) (-8.01, -3.84) 100 mg/day 1 for SBP 52 for SBP -17.00* -10.16*
2 for D B P 92 for D B P (-22.78, -11.22) (-12.33, -7.99) 150 mg/day 0 for SBP 40 Not reported -12.30*
1 for D B P (-15.05, -9.55) * statistically significant difference from placebo
Three mibefradil trials were included in this systematic review. Blood pressure data
were not extracted from one of these trials (Oparil 1997) because baseline values were not
reported. Another trial (Bernink 1996) only reported D B P data. Doses of 6.25 and 12.5
mg/day did not reduce B P compared with placebo. Doses 25 mg/day and above had
statistically significant reductions in blood pressure compared with placebo. Thus the lowest
effective dose is 25 mg/day.
One of the trials (Bursztyn 1997) was performed in elderly patients with a baseline
blood pressure of 176/99 mm Fig. There was an insufficient amount of data for a subgroup
analysis based on age.
Based on the 3 included trials, the maximal blood-pressure-lowering efficacy of
mibefradil occurs at 100 mg/day and is best estimated at 100-150 mg/day is -17.00 (-22.78, -
11.22) mm H g for SBP (based on one trial) and -10.98 (-12.69, -9.28) for D B P (based on two
trials).
189
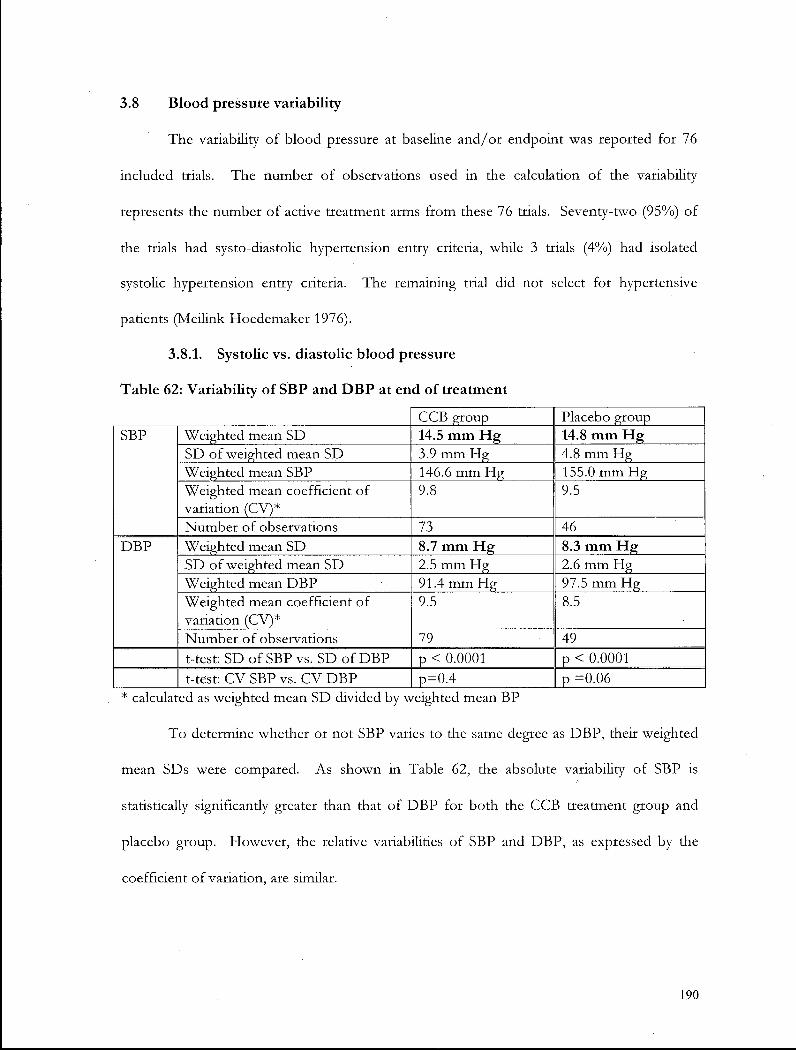
3.8 B lood pressure variabil ity
The variability of blood pressure at baseline and/or endpoint was reported for 76
included trials. The number of observations used in the calculation of the variability
represents the number of active treatment arms from these 76 trials. Seventy-two (95%) of
the trials had systo-diastolic hypertension entry criteria, while 3 trials (4%) had isolated
systolic hypertension entry criteria. The remaining trial did not select for hypertensive
patients (Meilink-Hoedemaker 1976).
3.8.1. Systolic vs. diastolic b lood pressure
Table 62: Variabi l i ty of S B P and D B P at end of treatment
C C B group Placebo group SBP Weighted mean SD 14.5 m m H g 14.8 m m H g
SD of weighted mean SD 3.9 mm H g 4.8 mm H g Weighted mean SBP 146.6 mm H g 155.0 mm H g Weighted mean coefficient of 9.8 9.5 variation (CV)* Number of observations 73 46
D B P Weighted mean SD 8.7 m m H g 8.3 m m H g SD of weighted mean SD 2.5 mm H g 2.6 mm Pig Weighted mean D B P 91.4 mm Pig 97.5 mm Pig Weighted mean coefficient of 9.5 8.5 variation (CV)* Number of observations 79 49 t-test: SD of SBP vs. SD of D B P p < 0.0001 p < 0.0001 t-test: C V SBP vs. C V D B P p=0.4 p =0.06
calculated as weighted mean SD divided by weighted mean BP
To determine whether or not SBP varies to the same degree as D B P , their weighted
mean SDs were compared. As shown in Table 62, the absolute variability of SBP is
statistically significandy greater than that of D B P for both the C C B treatment group and
placebo group. Pfowever, the relative variabilities of SBP and D B P , as expressed by the
coefficient of variation, are similar.
190

3.8.2. Ca lc ium channel blockers vs. placebo
As shown in Table 62, the weighted mean SD of SBP at the end of treatment was
14.5 mm H g for the C C B group, while the corresponding value for placebo was 14.8 mm
H g (p=0.6). For D B P , the weighted mean SD was 8.7 mm H g for C C B group and 8.3 mm
Fig for placebo group (p=0.4). Thus, there was no statistically significant difference in BP
variability between C C B and placebo treatment.
3.8.3. Systolic vs. diastolic b lood pressure entry criteria
To determine i f BP entry criteria affected baseline BP variability, comparisons were
made between the weighted mean baseline standard deviations of trials that used isolated
systolic hypertension as entry criteria, only D B P entry criteria, and trials with criteria of
elevated SBP and/or D B P (Table 63).
Table 63: Baseline standard deviations of b lood pressure according to entry criteria
A l l patients Trials with only D B P Trials with only SBP Trials with both SBP entry criteria entry criteria and/or D B P entry (61 trials) (3 trials) criteria* (11 trials)
Weighted mean SD 14.5 7.9 13.3 of SBP at baseline (mm Hg) SD of weighted 3.2 3.7 3.6 mean SD of SBP (mm Hg) Number of 165 6 28 observations t-test systo-diastolic hypertension vs. isolated s ystolic hypertension: p < 0.0001 Weighted mean SD 5.5 6.1 5.3 of D B P at baseline (mm Hg) SD of weighted 2.0 1.6 2.5 mean SD of D B P (mm Hg) Number of 176 6 28 observations t-test systo-diastolic hypertension vs. isolated s ystolic hypertension: p : = 0.4 * includes those trials using World Health Organization classification of hypertension
191
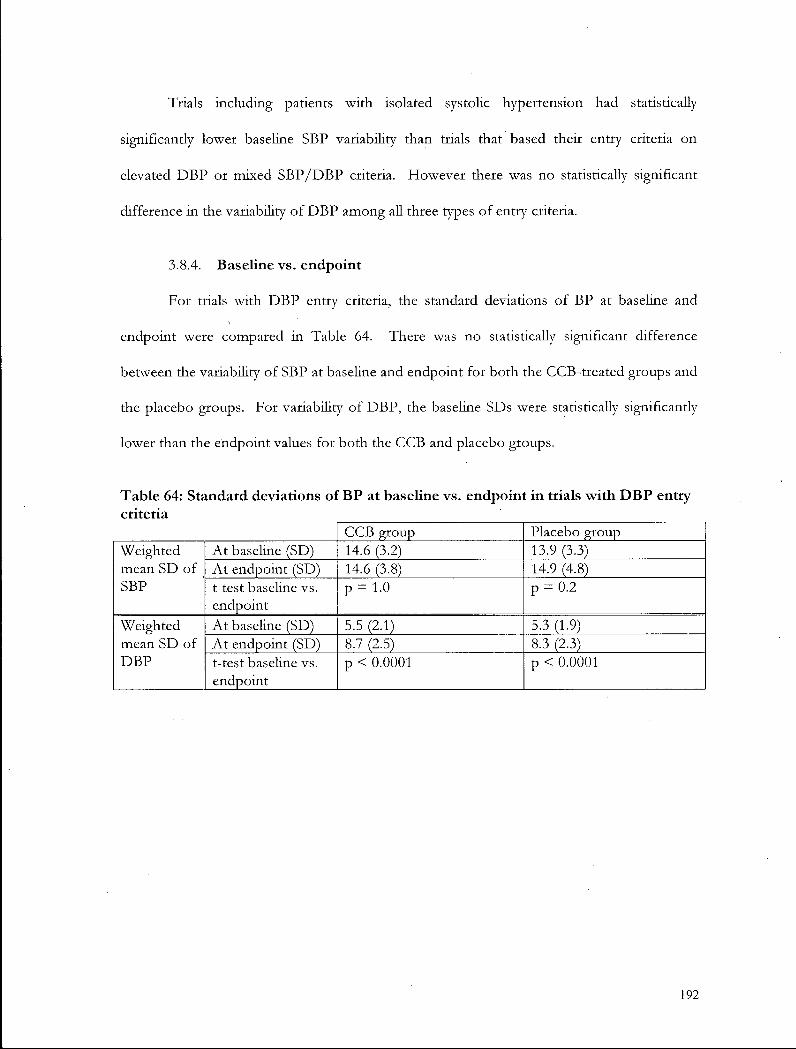
Trials including patients with isolated systolic hypertension had statistically
significantly lower baseline SBP variability than trials that based their entry criteria on
elevated D B P or mixed S B P / D B P criteria. However there was no statistically significant
difference in the variability of D B P among all three types of entry criteria.
3.8.4. Baseline vs. endpoint
For trials with D B P entry criteria, the standard deviations of B P at baseline and
endpoint were compared in Table 64. There was no statistically significant difference
between the variability of SBP at baseline and endpoint for both the CCB-treated groups and
the placebo groups. For variability of D B P , the baseline SDs were statistically significandy
lower than the endpoint values for both the C C B and placebo groups.
Table 64: Standard deviations of BP at baseline vs. endpoint in trials with DBP entry criteria
C C B group Placebo group Weighted mean SD of SBP
A t baseline (SD) 14.6 (3.2) 13.9 (3.3) Weighted mean SD of SBP
A t endpoint (SD) 14.6 (3.8) 14.9 (4.8) Weighted mean SD of SBP t-test baseline vs.
endpoint p = 1.0 p = 0.2
Weighted mean SD of D B P
A t baseline (SD) 5.5 (2.1) 5.3 (1.9) Weighted mean SD of D B P
A t endpoint (SD) 8.7 (2.5) 8.3 (2.3) Weighted mean SD of D B P t-test baseline vs.
endpoint p < 0.0001 p < 0.0001
192

3 . 9 Pulse Pressure
Although none of the included trials reported pulse pressure as a primary or
secondary outcome, the change in pulse pressure was calculated by subtracting the change in
D B P from the change in SBP for each trial that reported both parameters. A weighted mean
change in pulse pressure was then calculated, along with the associated standard deviation.
Table 65 below shows the change in pulse pressure at trough for dihydropyridines and non-
dihydropyridines at twice the starting dose and above (i.e., at maximal B P lowering). The
effect size of placebo was calculated from all trials reporting both SBP and D B P data.
Table 65: Change in pulse pressure
# of studies Weighted mean change in pulse pressure (95% CI)
Dihydropyridines 43 -3.4 (-4.3, -2.5)
Non-dihydropyridines 18 -2.4 (-3.7,-1.1)
Placebo 94 0.3 (-0.2, 0.8)
Dihydropyridines vs. non-dihydropyridines: p=0.2, NS Dihydropyridines vs. placebo: p < 0.001 Non-dihydropyridines vs. placebo: p < 0.001
Placebo treatment does not have a statistically significant effect on change in pulse
pressure, but both the dihydropyridines and non-dihydropyridines demonstrated statistically
significant reductions in pulse pressure. Because there is no statistically significant difference
between dihydropyridines and non-dihydropyridines, the results of both subclasses were
combined to give an overall change in pulse pressure of -3.1 mm H g (95% CI: -3.8, -2.3).
193

3.10 Dose-related change in heart rate of indiv idual C C B drugs
Forty-seven of the 106 included trials (44%) had heart rate data that either were
extractable from the publications or were obtained dtrectiy from authors. The results are
described for each individual drug as well as grouped into dmydropyridines and non-
dihydropyridines, categorized according to increments of the manufacturer's recommended
starting dose. Lidoflazine and mibefradil are considered separately.
3.10.1 Dihydropyridines vs. placebo
Thirty-eight dihydropyridine trials reported heart rate data (Table 66). In the group
of trials at 1-1.33 times the starting dose, there was no statistically significant difference in
heart rate compared with placebo. There was a statistically significant increase in heart rate
in the middle dose range of 1.5-3 times the starting dose. There was also statistically
significant heterogeneity in this group, stemming from one trial (Rimoldi 1994) that had a
very large increase in heart rate in the treatment group. The highest dosage range of > 3
times the starting dose had a non-statistically-significant increase in heart rate compared with
placebo; however only 8 studies were included in this category and thus the analysis lacked
power. A l l trials reported trough changes in heart rate except for two trials (Kiesewetter
1994, Prisant 1991), which reported peak values. Sensitivity analysis removing these 2 trials
did not alter the results.
194
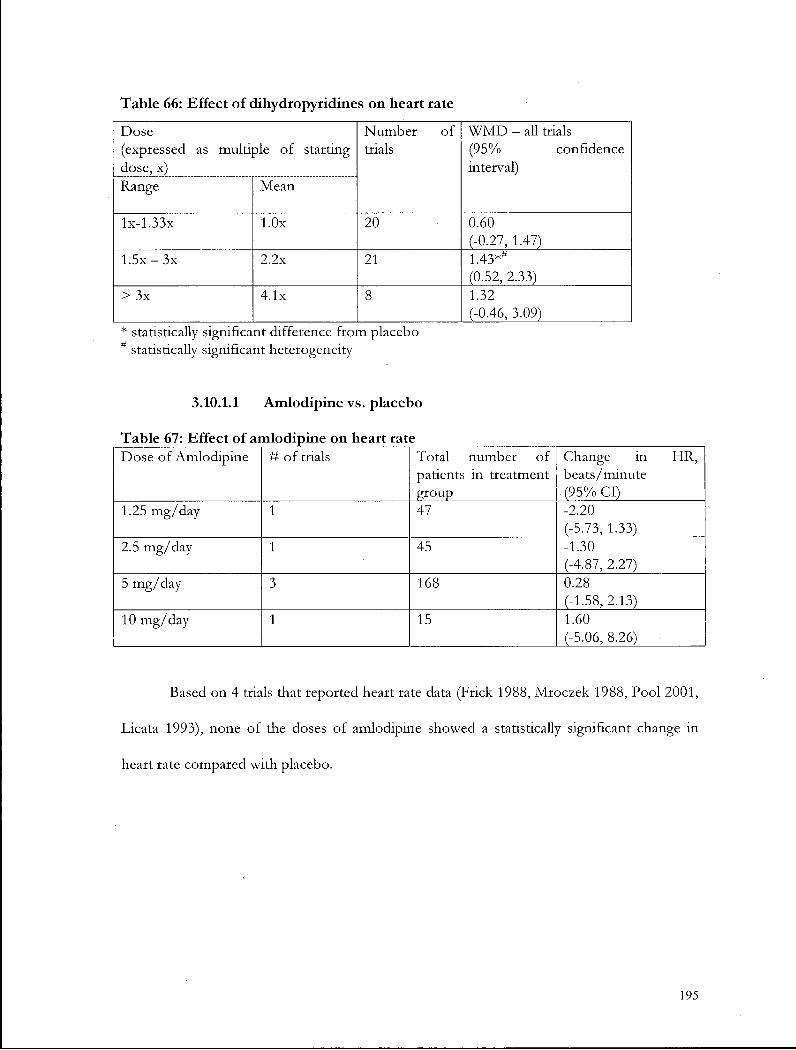
Table 66: Effect of dihydropyridines on heart rate
Dose (expressed as multiple of starting dose, x)
Number of trials
W M D - all trials (95% confidence interval)
Range Mean
Number of trials
W M D - all trials (95% confidence interval)
lx-1.33x l.Ox 20 0.60 (-0.27, 1.47)
1.5x-3x 2.2x 21 1.43*#
(0.52, 2.33) > 3x 4.1x 8 1.32
(-0.46, 3.09) * statistically significant difference from placebo # statistically significant heterogeneity
3.10.1.1 Amlod ip ine vs. placebo
Table 67: Effect of amlodipine on heart rate Dose of Amlodipine # of trials Total number of
patients in treatment group
Change in H R , beats/minute • (95%CI)
1.25 mg/day 1 47 -2.20 (-5.73, 1.33)
2.5 mg/day 1 45 -1.30 (-4.87, 2.27)
5 mg/day 3 168 0.28 (-1.58, 2.13)
10 mg/day 1 15 1.60 (-5.06, 8.26)
Based on 4 trials that reported heart rate data (Frick 1988, Mroczek 1988, Pool 2001,
Licata 1993), none of the doses of amlodipine showed a statistically significant change in
heart rate compared with placebo.
195
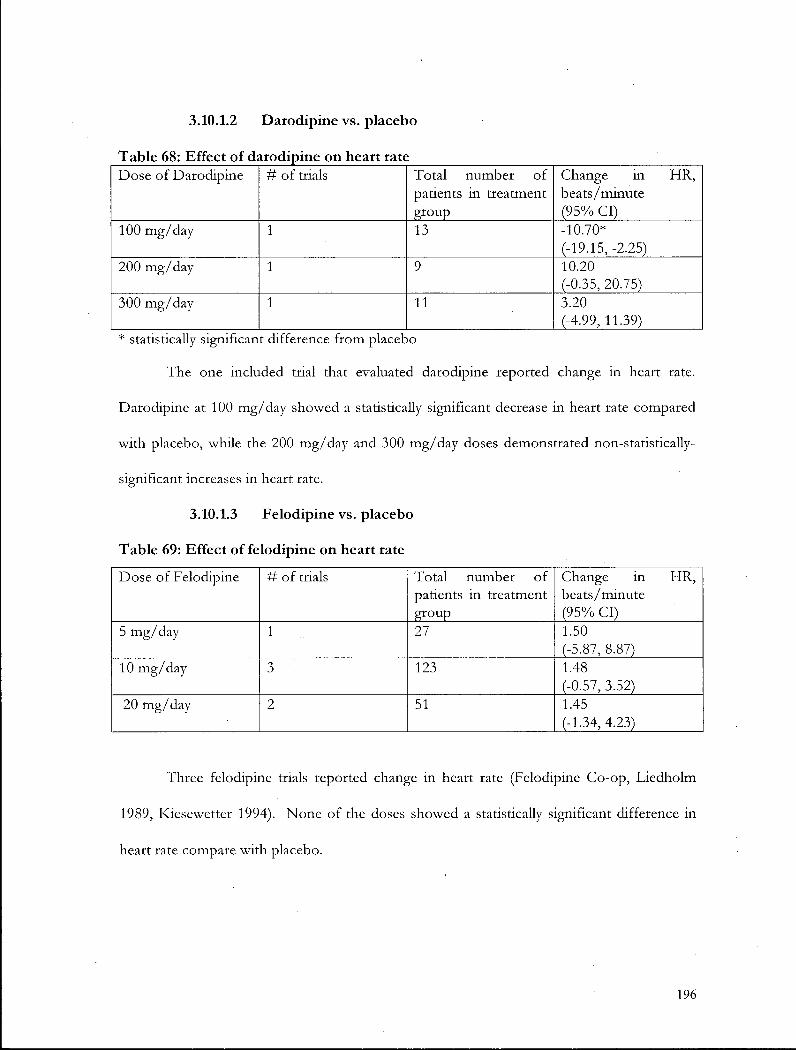
3.10.1.2 Darodipine vs. placebo
Table 68: Effect of darodipine on heart rate Dose of Darodipine # of trials Total number of
patients in treatment group
Change in H R , beats/minute (95% CI)
100 mg/day 1 13 -10.70* (-19.15, -2.25)
200 mg/day 1 9 10.20 (-0.35, 20.75)
300 mg/day 1 11 3.20 (-4.99, 11.39)
statistically significant difference from placebo
The one included trial that evaluated darodipine reported change in heart rate.
Darodipine at 100 mg/day showed a statistically significant decrease in heart rate compared
with placebo, while the 200 mg/day and 300 mg/day doses demonstrated non-statistically-
significant increases in heart rate.
3.10.1.3 Felodipine vs. placebo
Table 69: Effect of felodipine on heart rate
Dose of Felodipine # of trials Total number of patients in treatment group
Change in H R , beats/minute (95% CI)
5 mg/day 1 27 1.50 (-5.87, 8.87)
10 mg/day 3 123 1.48 (-0.57, 3.52)
20 mg/day 2 51 1.45 (-1.34, 4.23)
Three felodipine trials reported change in heart rate (Felodipine Co-op, Liedholm
1989, Kiesewetter 1994). None of the doses showed a statistically significant difference in
heart rate compare with placebo.
196
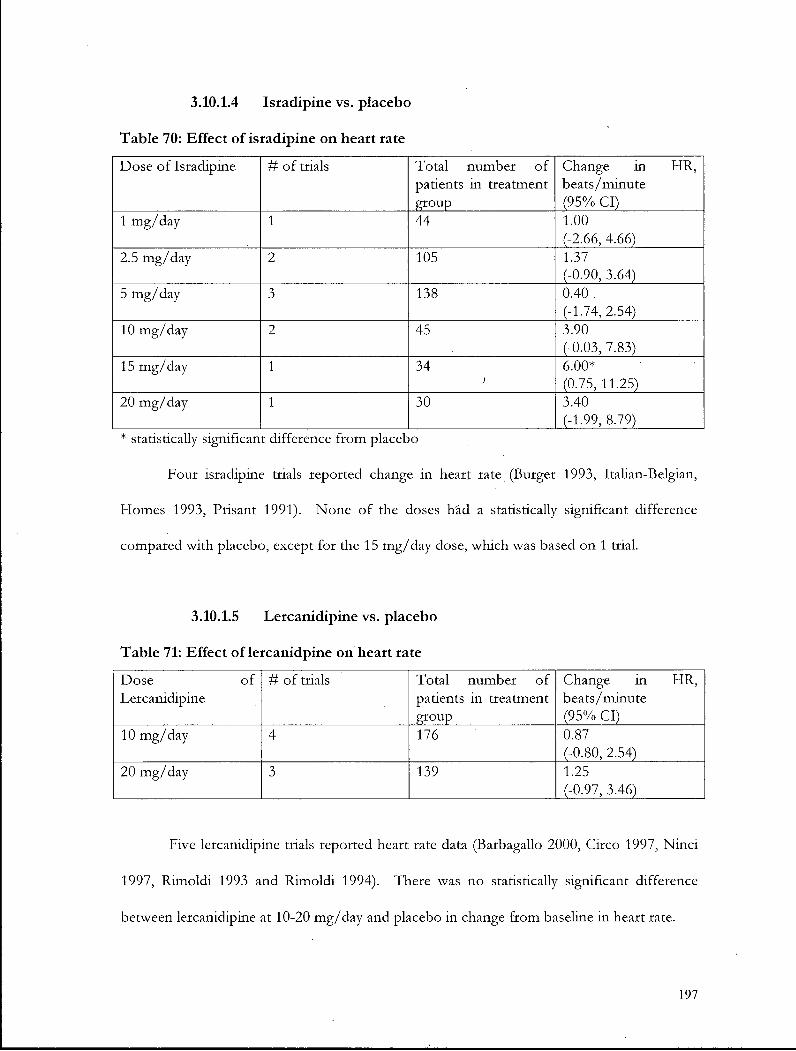
3.10.1.4 Isradipine vs. placebo
Table 70: Effect of isradipine on heart rate
Dose of Isradipine # of trials Total number of patients in treatment group
Change in HR, beats/minute (95% CI)
1 nig/day 1 44 1.00 (-2.66, 4.66)
2.5 mg/day 2 105 1.37 (-0.90, 3.64)
5 mg/day 3 138 0.40 (-1.74, 2.54)
10 mg/day 2 45 3.90 (-0.03, 7.83)
15 mg/day 1 34 >
6.00* (0.75, 11.25)
20 mg/day 1 30 3.40 (-1.99, 8.79)
* statistically significant difference from placebo
Four isradipine trials reported change in heart rate (Burger 1993, Italian-Belgian,
Homes 1993, Prisant 1991). None of the doses had a statistically significant difference
compared with placebo, except for the 15 mg/day dose, which was based on 1 trial.
3.10.1.5 Lercanidipine vs. placebo
Table 71: Effect of lercanidpine on heart rate
Dose of Lercanidipine
# of trials Total number of patients in treatment group
Change in HR, beats/ minute (95% CI)
10 mg/day 4 176 0.87 (-0.80, 2.54)
20 mg/day 3 139 1.25 (-0.97, 3.46)
Five lercanidipine trials reported heart rate data (Barbagallo 2000, Circo 1997, Ninci
1997, Rimoldi 1993 and Rimoldi 1994). There was no statistically significant difference
between lercanidipine at 10-20 mg/day and placebo in change from baseline in heart rate.
197
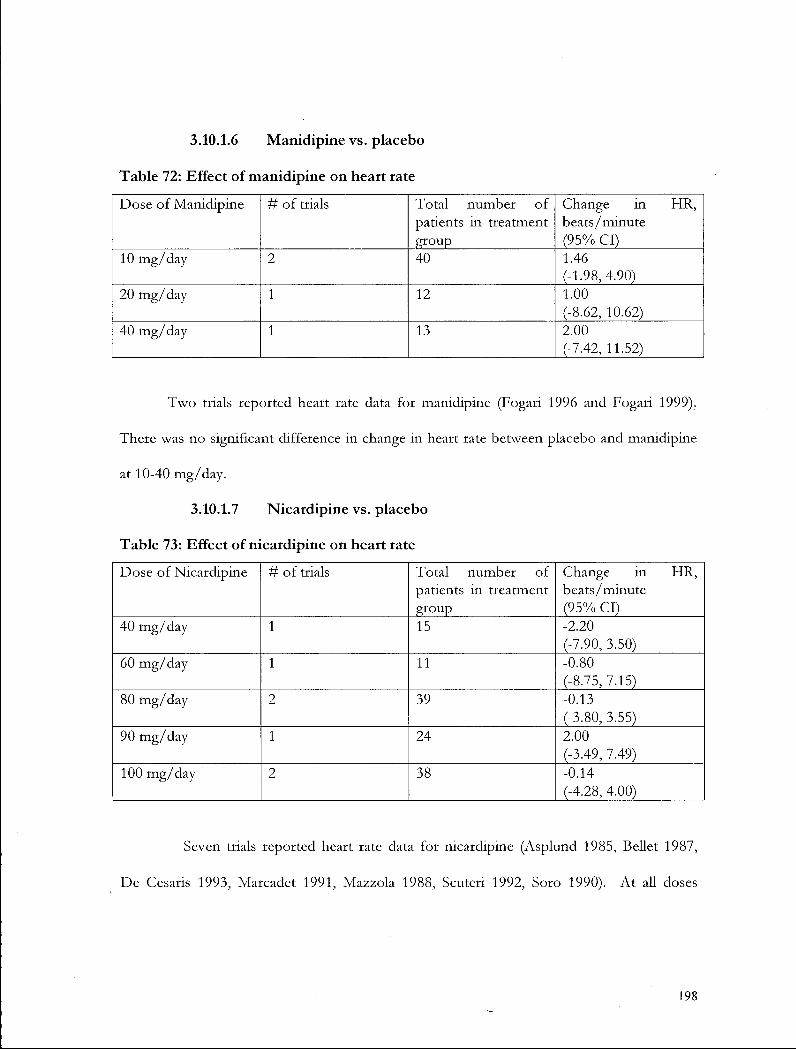
3.10.1.6 Manid ip ine vs. placebo
Table 72: Effect of manidipine on heart rate
Dose of Manidipine # of trials Total number of patients in treatment group
Change in H R , beats/minute (95% CI)
10 mg/day 2 40 1.46 (-1.98, 4.90)
20 mg/day 1 12 1.00 (-8.62, 10.62)
40 mg/ day 1 13 2.00 (-7.42, 11.52)
Two trials reported heart rate data for manidipine (Fogari 1996 and Fogari 1999).
There was no significant difference in change in heart rate between placebo and manidipine
at 10-40 mg/day.
3.10.1.7 Nicard ip ine vs. placebo
Table 73: Effect of nicardipine on heart rate
Dose of Nicardipine # of trials Total number of patients in treatment group
Change in H R , beats/minute (95% CI)
40 mg/day 1 15 -2.20 (-7.90, 3.50)
60 mg/day 1 11 -0.80 (-8.75, 7.15)
80 mg/day 2 39 -0.13 (-3.80, 3.55)
90 mg/day 1 24 2.00 (-3.49, 7.49)
100 mg/day 2 38 -0.14 (-4.28, 4.00)
Seven trials reported heart rate data for nicardipine (Asplund 1985, Bellet 1987,
De Cesaris 1993, Marcadet 1991, Mazzola 1988, Scuten 1992, Soro 1990). A t all doses
198

tested (40-100 mg/day), nicardipine was not associated with a statistically significant change
in heart rate compared with placebo.
3.10.1.8 Ni fed ip ine vs. placebo
Table 74: Effect of nifedipine on heart rate
Dose of Nifedipine # of trials Total number of patients in treatment group
Change in H R , beats/minute (95% CI)
20 mg/day 2 103 -0.61 (-1.77,2.99)
30 mg/day 1 62 -2.50 (-5.81, 0.81)
40 mg/day 2 42 -0.34 (-4.63, 3.96)
60 mg/day 3 112 -1.50 (-4.09, 1.09)
90 mg/day 1 59 -1.40 (-4.71, 1.91)
Seven trials reported heart rate data for nifedipine (DeSimone 1985, Feig 1993,
Ferrera 1984, Harder 1994, Jueng 1987, Serradimigni 1985, Toal 1997). Doses 20-90
mg/day did not exhibit statistically significant differences in heart rate compared with
placebo.
3.10.1.9 Niso ld ip ine vs. placebo
Table 75: Effect of nisoldipine on heart rate
Dose of Nisoldipine # of trials Total number of patients in treatment group
Change in H R , beats/minute (95% CI)
10 mg/day 1 49 2.90 (-1.02, 6.82)
20 mg/day 1 51 2.20 (-1.71,6.11)
30 mg/day 1 48 5.00* (1.06, 8.94)
* statistically significant difference from placebo
199
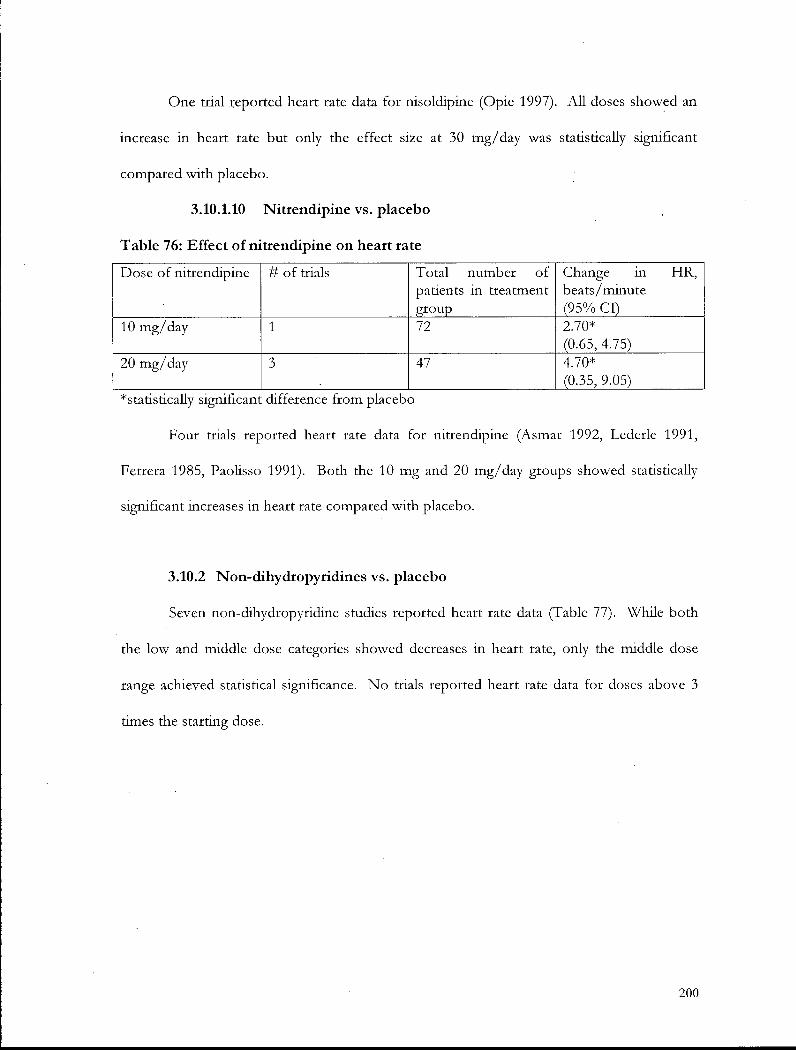
One trial reported heart rate data for nisoldipine (Opie 1997). A l l doses showed an
increase in heart rate but only the effect size at 30 mg/day was statistically significant
compared with placebo.
3.10.1.10 Ni t rendipine vs. placebo
Table 76: Effect of nitrendipine on heart rate
Dose of nitrendipine # of trials Total number of patients in treatment group
Change in HR, beats/minute (95% CI)
10 mg/day 1 72 2.70* (0.65, 4.75)
20 mg/day 3 47 4.70* (0.35, 9.05)
statistically significant difference from placebo
Four trials reported heart rate data for nitrendipine (Asmar 1992, Lederle 1991,
Ferrera 1985, Paolisso 1991). Both the 10 mg and 20 mg/day groups showed statistically
significant increases in heart rate compared with placebo.
3.10.2 Non-dihydropyr idines vs. placebo
Seven non-dihydropyridine studies reported heart rate data (Table 77). While both
the low and middle dose categories showed decreases in heart rate, only the middle dose
range achieved statistical significance. N o trials reported heart rate data for doses above 3
times the starting dose.
200
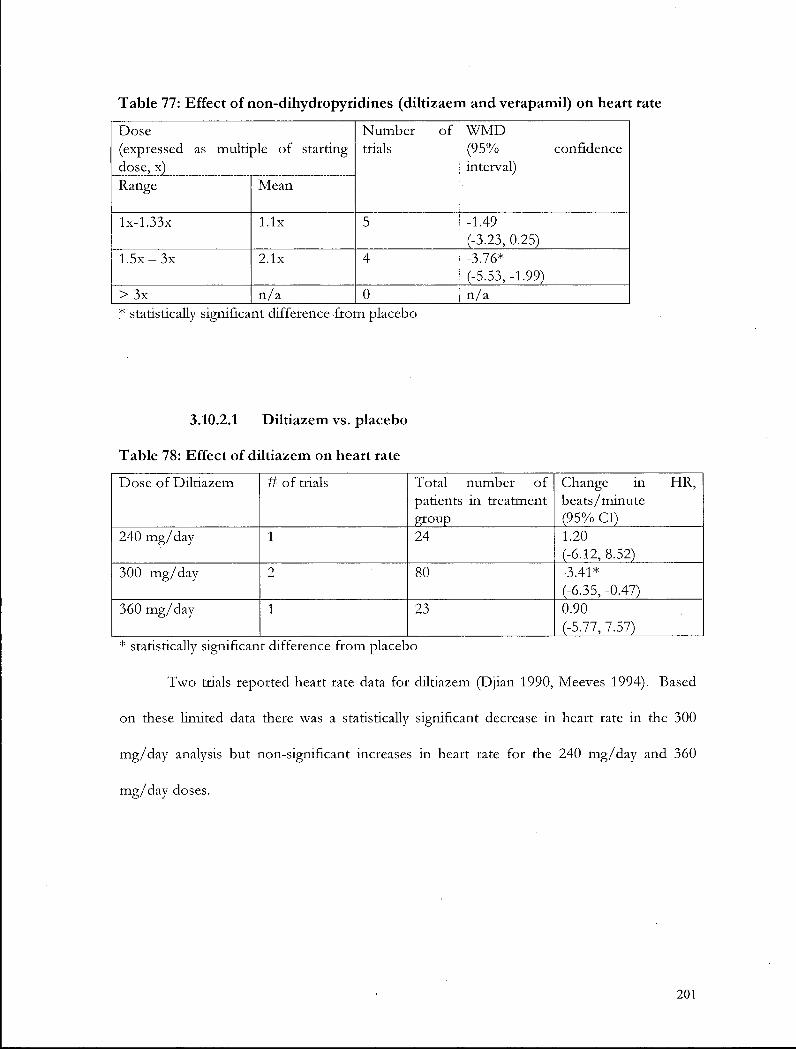
Table 77: Effect of non-dihydropyridines (di l t izaem and verapamil) on heart rate
Dose (expressed as multiple of starting dose, x)
Number of trials
W M D (95% confidence interval)
Range Mean
Number of trials
W M D (95% confidence interval)
lx-1.33x l . l x 5 -1.49 (-3.23, 0.25)
1.5x-3x 2.1x 4 -3.76* (-5.53, -1.99)
> 3x n/a 0 n/a * statistically significant difference from placebo
3.10.2.1 D i l t iazem vs. placebo
Table 78: Effect of di l t iazem on heart rate
Dose of Diltiazem # of trials Total number of patients in treatment group
Change in H R , beats/minute (95% CI)
240 mg/day 1 24 1.20 (-6.12, 8.52)
300 mg/day 2 80 -3.41* (-6.35, -0.47)
360 mg/day 1 23 0.90 (-5.77, 7.57)
* statistically significant difference from placebo
Two trials reported heart rate data for diltiazem (Djian 1990, Meeves 1994). Based
on these limited data there was a statistically significant decrease in heart rate in the 300
mg/day analysis but non-significant increases in heart rate for the 240 mg/day and 360
mg/day doses.
201

3.10.2.2 Verapamil vs. placebo
Table 79: Effect of verapamil on heart rate
Dose of Verapamil # of trials Total number of padents in treatment group
Change in H R , beats/minute (95% CI)
120 mg/day 3 117 -2.44* (-4.59, -0.28)
180 mg/day 3 141 -1.22 (-3.38, 0.94)
240 mg/day 1 27 -2.60 (-5.81, 0.61)
360 mg/day 1 59 -5.30* (-8.22, -2,38)
480 mg/day 1 26 -1.00 (-5.39, 3.39)
540 mg/day 1 55 -5.80* (-8.86, -2.74)
statistically significant difference from placebo
Four trials (Carr 1991, Scholze 1998, V E R A T R A N , White 1995) reported heart rate
data for verapamil over a dose range of 120 — 540 mg/day. The 120 mg/day, 360 mg/day
and 540 mg/day groups showed a statistically significant decrease in heart rate compared
with placebo, while the 180 mg/day, 240 mg/day, and 480 mg/day groups did not.
However, the results for 240-540 mg/day are based on only one trial at each dose.
3.10.2.3 Tiapamil vs. placebo
Table 80: Effect of tiapamil on heart rate
Dose of tiapamil # of trials Total number of patients in treatment group
Change in H R , beats/minute (95% CI)
300-600 mg/day 1 24 3.00 (-2.58, 8.58)
900-1200 mg/day 1 25 2.00 (-4.02, 8.02)
202

The effect of tiapamil on heart rate was examined in one included trial (Blanchett
1991). There was no statistically significant difference in heart rate at doses 300-1200
mg/day compared with placebo.
3.10.3 Other calc ium channel blockers
3.10.3.1 Lidof lazine vs. placebo
Table 81: Effect of l idoflazine on heart rate
Dose of lidoflazine # of trials Total number of patients in treatment group
Change in H R , beats/minute (95% CI)
180 mg/day 1 5 -15.20* (-24.99, -5.41)
*statistically significant difference from placebo
The one included trial assessing lidoflazine (Meilink-Hoedemaker 1976) reported
heart rate data. There was a statistically significant drop in heart rate with lidoflazine 180
mg/day compared with placebo.
3.10.3.2 Mibefradi l vs. placebo
Table 82: Effect of mibefradi l on heart rate
Dose of mibefradil # of trials Total number of patients in treatment group
Change in HR, beats/minute (95% CI)
6.25 mg/day 1 52 -0.80 (-4.17, 2.57)
12.5 mg/day 1 52 -0.40 (-4.03, 3.23)
25 mg/day 1 51 -2.00 (-5.53, 1.53)
50 mg/day 1 51 -5.20* (-9.01,-1.39)
100 mg/day 1 52 -6.60* (-10.13, -3.07)
* statistically significant difference from placebo
203

One included trial (Bursztyn 1997) reported heart rate data for mibefradil. The 50
and 100 mg/day doses had a statistically significant decrease in heart rate compared with
placebo, while the effect sizes at lower doses were not statistically significant.
204
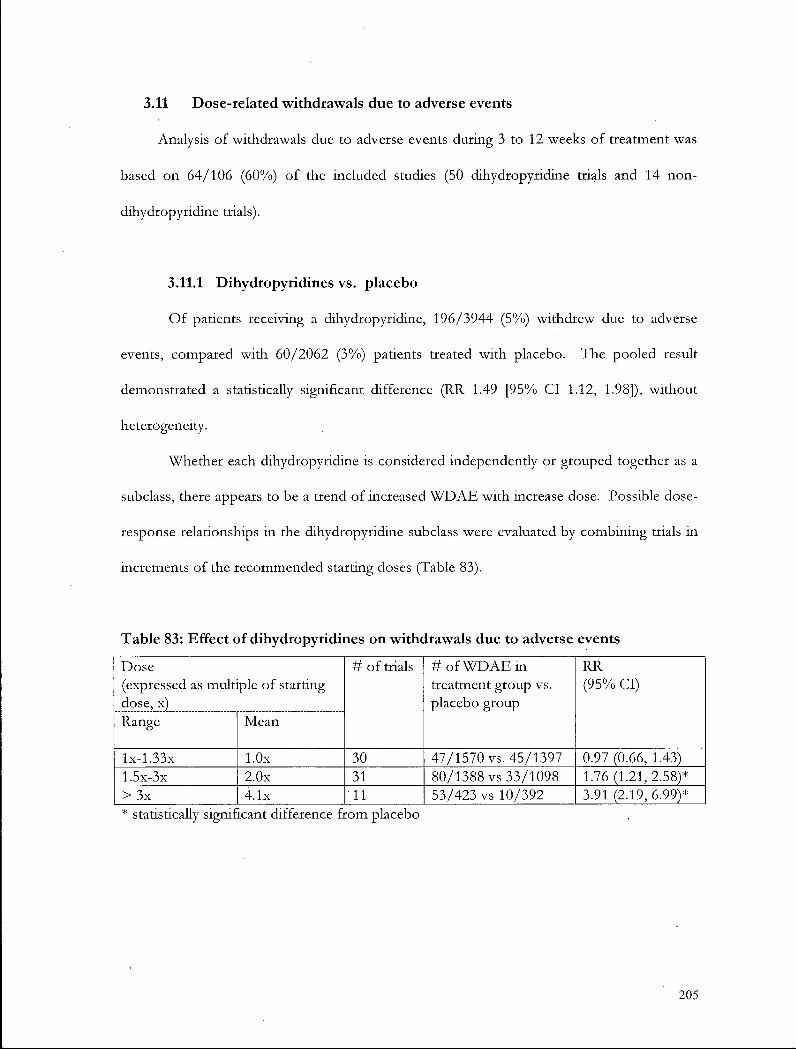
3.11 Dose-related withdrawals due to adverse events
Analysis of withdrawals due to adverse events during 3 to 12 weeks of treatment was
based on 64/106 (60%) of the included studies (50 dihydropyridine trials and 14 non-
dihydropyridine trials).
3.11.1 Dihydropyridines vs. placebo
O f patients receiving a dihydropyridine, 196/3944 (5%) withdrew due to adverse
events, compared with 60/2062 (3%) patients treated with placebo. The pooled result
demonstrated a statistically significant difference (RR 1.49 [95% CI 1.12, 1.98]), without
heterogeneity.
Whether each dihydropyridine is considered independendy or grouped together as a
subclass, there appears to be a trend of increased W D A E with increase dose. Possible dose-
response relationships in the chhydropyridine subclass were evaluated by combining trials in
increments of the recommended starting doses (Table 83).
Table 83: Effect of dihydropyridines on withdrawals due to adverse events
Dose (expressed as multiple of starting dose, x)
# of trials # of W D A E in treatment group vs. placebo group
RR (95% CI)
Range Mean
# of trials # of W D A E in treatment group vs. placebo group
RR (95% CI)
tx-1.33x l.Ox 30 47/1570 vs. 45/1397 0.97 (0.66, 1.43) 1.5x-3x 2.0x 31 80/1388 vs 33/1098 1.76 (1.21,2.58)* > 3x 4.1x 11 53/423 vs 10/392 3.91 (2.19, 6.99)*
statistically significant difference from placebo
205
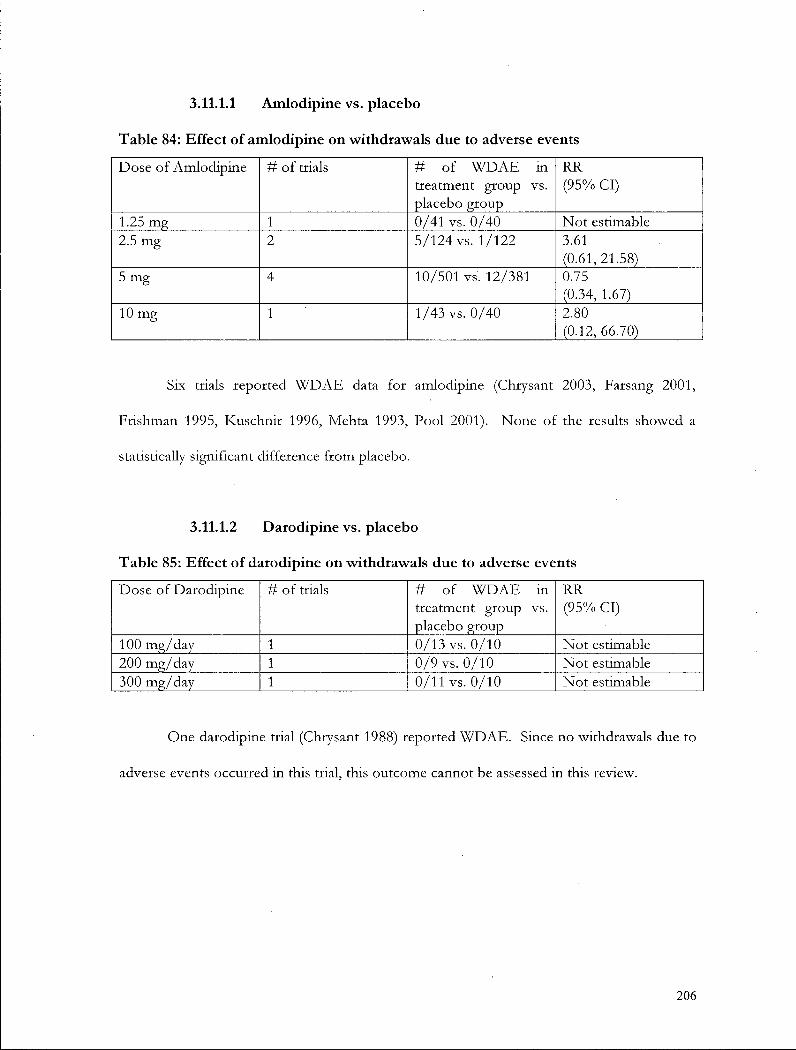
3.11.1.1 Amlodipine vs. placebo
Table 84: Effect of amlodipine on withdrawals due to adverse events
Dose of Amlodipine # of trials # of W D A E in treatment group vs. placebo group
RR (95% CI)
1.25 mg 1 0/41 vs. 0/40 Not estimable 2.5 mg 2 5/124 vs. 1/122 3.61
(0.61, 21.58) 5 m g 4 10/501 vs. 12/381 0.75
(0.34, 1.67) 10 mg 1 1/43 vs. 0/40 2.80
(0.12, 66.70)
Six trials reported W D A E data for amlodipine (Chrysant 2003, Farsang 2001,
Frishman 1995, Kuschnir 1996, Mehta 1993, Pool 2001). None of the results showed a
statistically significant difference from placebo.
3.11.1.2 Darodipine vs. placebo
Table 85: Effect of darodipine on withdrawals due to adverse events
Dose of Darodipine # of trials # of W D A E in RR treatment group vs. (95% CI) placebo group
100 mg/day 1 0/13 vs. 0/10 Not estimable 200 mg/day 1 0/9 vs. 0/10 Not estimable 300 mg/day 1 0/11 vs. 0/10 Not estimable
One darodipine trial (Chrysant 1988) reported W D A E . Since no withdrawals due to
adverse events occurred in this trial, this outcome cannot be assessed in this review.
206

3.11.1.3 Felodipine vs. placebo
Table 86: Effect of felodipine on withdrawals due to adverse events
Dose of Felodipine # of trials # of W D A E in treatment group vs. placebo group
R R (95% CI)
2.5 mg/day 2 3/100 vs. 3/99 0.99 (0.20, 4.79)
5 mg/day 5 9/221 vs. 6/214 1.35 (0.53, 3.42)
10 mg/day 6 19/289 vs. 9/288 2.01 (0.95, 4.23)
20 mg/day 3 30/118 vs. 2/123 10.58* (3.32, 33.66)
statistically significant difference from placebo
Seven trials reported W D A E data for felodipine (Felodipine Co-op, Liedholm 1989,
Kiesewetter 1994, Scholze 1999, van Ree 1996, Weber 1994, Wester 1991). There appears to
be a dose-related increase in W D A E and the 20 mg/day group demonstrates a statistically
significant increase compared with placebo. With all doses pooled, there is a statistically
significant relative risk of 2.75 (95% CI 1.73, .4.36).
3.11.1.4 Isradipine vs. placebo
Table 87: Effect of isradipine on withdrawals due to adverse events
Dose of 1 sradipine # of trials # of W D A E in treatment group vs. placebo group
RR (95% CI)
1 mg/day 1 0/45 vs. 1/44 0.33 (0.01, 7.80)
2.5 mg/day 5 6/187 vs. 3/154 1.48 (0.47, 4.64)
5 mg/day 6 9/353 vs. 6/263 1.06 (0.38, 2.96)
10 mg/day 2 2/38 vs. 0/34 4.78 (0.24, 94.12)
207
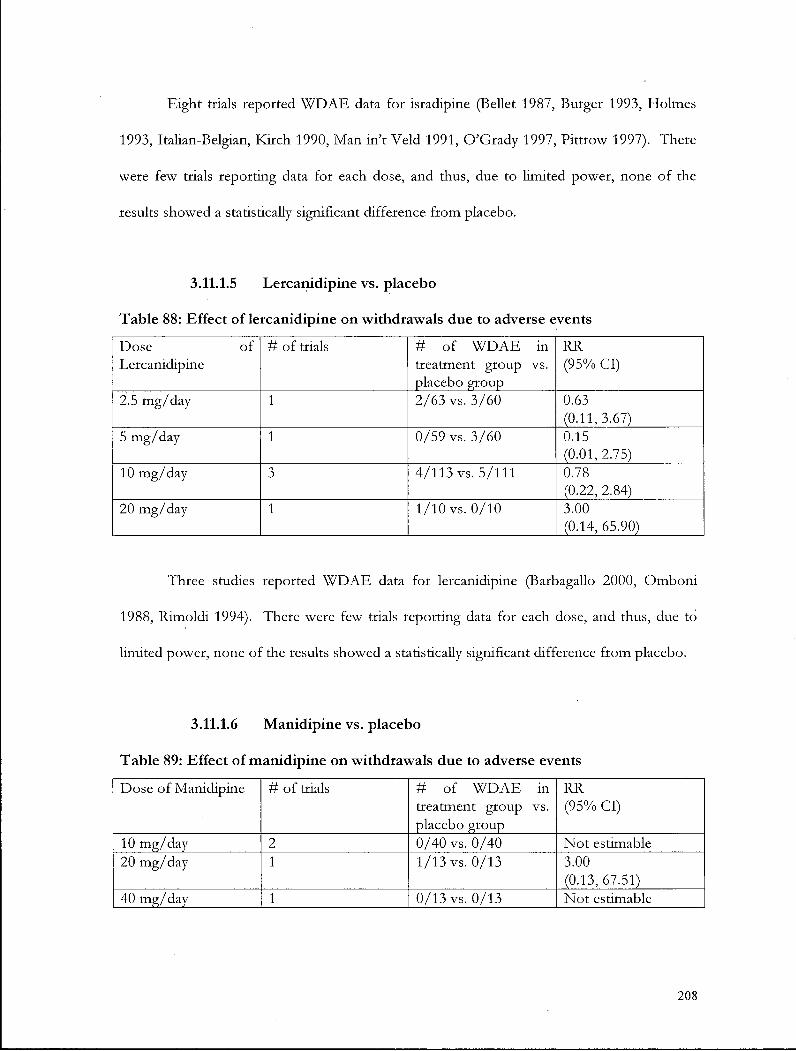
Eight trials reported W D A E data for isradipine (Bellet 1987, Burger 1993, Holmes
1993, Italian-Belgian, Kirch 1990, Man in't Veld 1991, O'Grady 1997, Pittrow 1997). There
were few trials reporting data for each dose, and thus, due to limited power, none of the
results showed a statistically significant difference from placebo.
3.11.1.5 Lercanidipine vs. placebo
Table 88: Effect of lercanidipine on withdrawals due to adverse events
Dose of # of trials # of W D A E in RR Lercanidipine treatment group vs.
placebo group (95% CI)
2.5 mg/day 1 2/63 vs. 3/60 0.63 (0.11,3.67)
5 mg/day 1 0/59 vs. 3/60 0.15 (0.01, 2.75)
10 mg/day 3 4/113 vs. 5/111 0.78 (0.22, 2.84)
20 mg/day 1 1/10 vs. 0/10 3.00 (0.14, 65.90)
Three studies reported W D A E data for lercanidipine (Barbagallo 2000, Omboni
1988, Rimoldi 1994). There were few trials reporting data for each dose, and thus, due to
limited power, none of the results showed a statistically significant difference from placebo.
3.11.1.6 Manidipine vs. placebo
Table 89: Effect of manidipine on withdrawals due to adverse events
Dose of Manidipine # of trials # of W D A E in treatment group vs. placebo group
RR (95% CI)
10 mg/day 2 0/40 vs. 0/40 Not estimable 20 mg/day 1 1/13 vs. 0/13 3.00
(0.13, 67.51) 40 mg/day 1 0/13 vs. 0/13 Not estimable
208
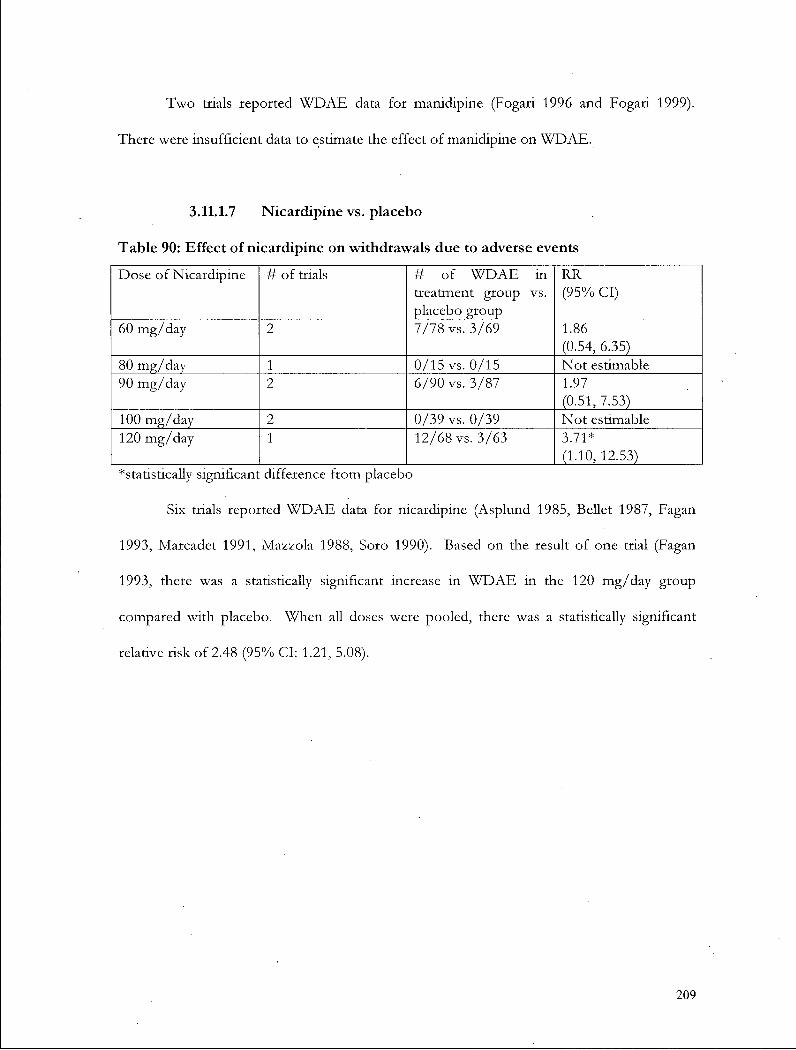
Two trials reported W D A E data for manidipine (Fogari 1996 and Fogari 1999).
There were insufficient data to estimate the effect of manidipine on W D A E .
3.11.1.7 Nicard ip ine vs. placebo
Table 90: Effect of nicardipine on withdrawals due to adverse events
Dose of Nicardipine # of trials # of W D A E in treatment group vs. placebo group
RR (95% CI)
60 mg/day 2 7/78 vs. 3/69 1.86 (0.54, 6.35)
80 mg/day 1 0/15 vs. 0/15 Not estimable 90 mg/day 2 6/90 vs. 3/87 1.97
(0.51, 7.53) 100 mg/day 2 0/39 vs. 0/39 Not estimable 120 mg/day 1 12/68 vs. 3/63 3.71*
(1.10, 12.53) statistically significant difference from placebo
Six trials reported W D A E data for nicardipine (Asplund 1985, Bellet 1987, Fagan
1993, Marcadet 1991, Mazzola 1988, Soro 1990). Based on the result of one trial (Fagan
1993, there was a statistically significant increase in W D A E in the 120 mg/day group
compared with placebo. When all doses were pooled, there was a statistically significant
relative risk of 2.48 (95% CI: 1.21, 5.08).
209
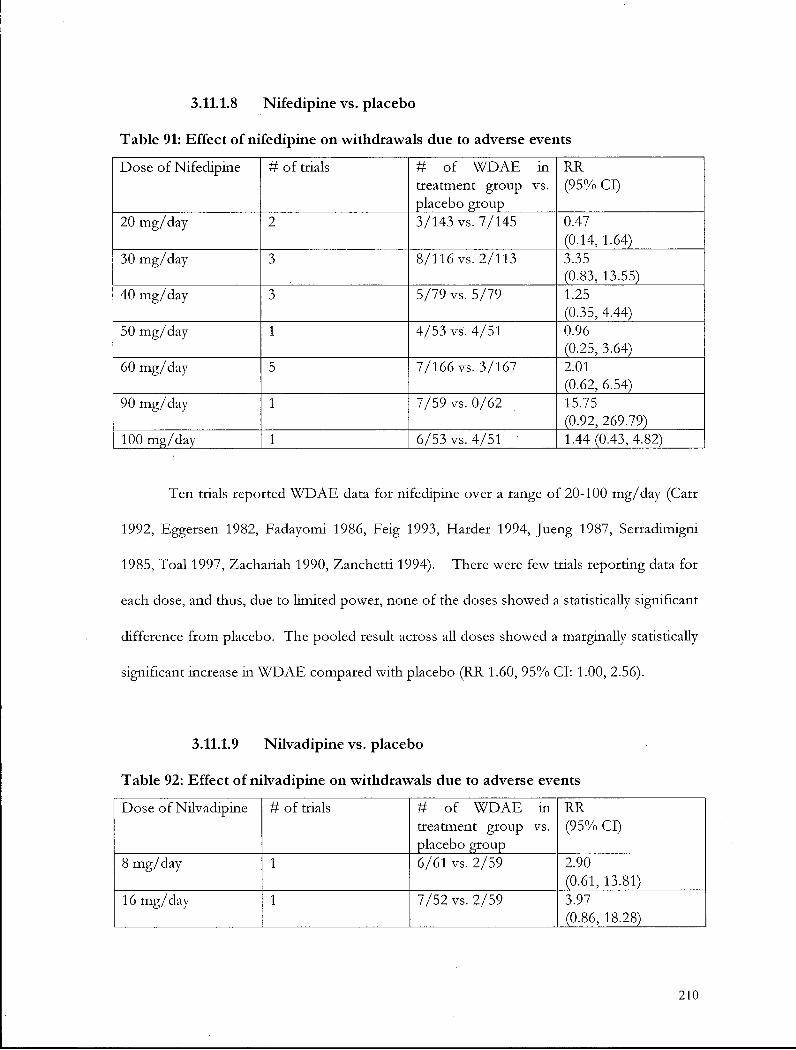
3.11.1.8 Ni fed ip ine vs. placebo
Table 91: Effect of nifedipine on withdrawals due to adverse events
Dose of Nifedipine # of trials # of W D A E in treatment group vs. placebo group
RR (95% CI)
20 mg/ day 2 3/143 vs. 7/145 0.47 (0.14, 1.64)
30 mg/day 3 8/116 vs. 2/113 3.35 (0.83, 13.55)
40 mg/day 3 5/79 vs. 5/79 1.25 (0.35, 4.44)
50 mg/day 1 4/53 vs. 4/51 0.96 (0.25, 3.64)
60 mg/day 5 7/166 vs. 3/167 2.01 (0.62, 6.54)
90 mg/day 1 7/59 vs. 0/62 15.75 (0.92, 269.79)
100 mg/day 1 6/53 vs. 4/51 1.44 (0.43, 4.82)
Ten trials reported W D A E data for nifedipine over a range of 20-100 mg/day (Carr
1992, Eggersen 1982, Fadayomi 1986, Feig 1993, Harder 1994, Jueng 1987, Serradimigni
1985, Toal 1997, Zachariah 1990, Zanchetti 1994). There were few trials reporting data for
each dose, and thus, due to limited power, none of the doses showed a statistically significant
difference from placebo. The pooled result across all doses showed a marginally statistically
significant increase in W D A E compared with placebo (RR 1.60, 95% CI: 1.00, 2.56).
3.11.1.9 Ni lvad ip ine vs. placebo
Table 92: Effect of ni lvadipine on withdrawals due to adverse events
Dose of Nilvadipine # of trials # of W D A E in RR treatment group vs. (95% CI) placebo group
8 mg/day 1 6/61 vs. 2/59 2.90 (0.61,13.81)
16 mg/day 1 7/52 vs. 2/59 3.97 (0.86, 18.28)
210

One trial (Hoffman 1997) reported W D A E data for nilvadipine. Due to limited
power, none of the doses showed a statistically significant difference from placebo. Pooled
results did show a statistically significant increase in W D A E compared with placebo, with a
relative risk of 3.41 (95% CI: 1.15, 10.13).
3.11.1.10 Nisoldipine vs. placebo
Table 93: Effect of nisoldipine on withdrawals due to adverse events
Dose of Nisoldipine # of trials # of W D A E in treatment group vs. placebo group
RR (95% CI)
10 mg/day 1 2/49 vs. 1/58 2.37 (0.22, 25.33)
20 mg/day 1 0/51 vs. 1/58 0.38 (0.02, 9.08)
30 mg/day 1 0/48 vs. 1/58 0.40 (0.02, 9.63)
One trial (Opie 1997) reported W D A E data for nisoldipine. Due to limited power,
none of the results showed a statistically significant difference from placebo.
3.11.1.11 Nitrendipine vs. placebo
Table 94: Effect of nitrendipine on withdrawals due to adverse events
Dose of # of trials # of W D A E in RR Nitrendipine treatment group vs.
placebo group (95% CI)
10 mg/day 2 . 4/116 vs. 3/105 1.17 (0.27, 5.07)
20 mg/day 3 2/61 vs. 0/53 5.00 (0.25, 100.20)
211

Five trials reported W D A E data for nitrendipine (Asmar 1993, Ferrara 1985, Fodor
1991, Lederle 1991, Maclean 1990). Due to limited power, none of the results showed a
statistically significant difference from placebo.
3.11.1.12 Pranidipine vs. placebo
Table 95: Effect of pranidipine on withdrawals due to adverse events
Dose of Pranidipine # of trials # of W D A E in treatment group vs. placebo group
RR (95% CI)
1 mg/day 1 0/36 vs. 3/32 0.13 (0.01,2.38)
2 mg/day 1 0/37 vs. 3/32 0.12 (0.01, 2.31)
4 mg/day 1 3/34 vs. 3/32 0.94 (0.20, 4.33)
8 mg/day 1 5/37 vs. 3/32 1.44 (0,37, 5.57)
One trial (Rosenthal 1996) reported W D A E for pranidipine. Although there was a
trend towards increased W D A E with higher doses, none of the doses had a statistically
significant difference from placebo due to limited power.
3.11.2 Non-dihydropyr idines vs. placebo
O f patients receiving a non-dihydropyridine (diltiazem or verapamil), 31/1258
(2.5%) withdrew due to adverse events, compared with 16/599 (2.7%) treated with placebo.
There was no statistically significant difference between active treatment and placebo in the
pooled result (RR 0.84 [95% CI 0.51, 1.38]).
There does not appear to be a dose-response relationship for W D A E in diltiazem
and verapamil trials but there are too few trials to make an accurate estimation of the effect
size for this outcome (Table 96).
212

Table 96: Effect of non-dihydropyridines on withdrawals due to adverse events
Dose (expressed as multiple of starting dose, x)
# of trials # of W D A E in treatment group vs. placebo group
RR (95% CI)
Range Mean
lx-1.33x l . l x 9 12/558 vs. 16/543 0.75 (0.37,1.54) 1.5x-3x 2.2x 7 17/598 vs. 3/428 1.08 (0.5, 2.31) > 3x 4.3x 2 2/102 vs. 4/99 0.47 (0.08, 2.64)
3.11.2.1 Di l t iazem vs. placebo
Table 97: Effect of di l t iazem on withdrawals due to adverse events
Dose of Diltiazem # of trials # of W D A E in treatment group vs. placebo group
R R (95% CI)
90 mg/day 1 0/46 vs. 2/43 0.19 (0.01, 3.79)
120 mg/day 3 5/229 vs. 8/233 0.65 (0.23, 1.88)
180 mg/day 2 9/198 vs. 8/193 1.10 (0.43, 2.79)
240 mg/day 2 0/80 vs. 2/83 0.21 (0.01, 4.22)
300 mg/day 1 0/55 vs. 0/56 Not estimable 360 mg/day 2 6/103 vs. 4/99 1.43
(0.42, 4.93) 480 mg/day 1 1/55 vs. 2/56 0.51
(0.05, 5.45) 540 mg/day 1 1/47 vs. 2/43 0.46
(0.04, 4.87)
Six trials reported W D A E for diltiazem (Levine 1995, McMahon 1989, Neutel 1996,
Neutel 1999, Scholze 1998, Smith 2001). There was not enough power to achieve statistical
significance because of the limited amount of data.
213

3.11.2.2 Verapami l vs. placebo
Table 98: Effect of verapamil on withdrawals due to adverse events
Dose of Verapamil # of trials # of W D A E in treatment group vs. placebo group
RR (95% CI)
60 mg/day 1 1/42 vs. 2/45 0.54 (0.05, 5.69)
100 mg/day 1 0/53 vs. 0/51 Not estimable 120 mg/day 3 0/104 vs. 3/104 0.25
(0.03, 2.22) 180 mg/day 1 0/29 vs. 1/30 0.34
(0.01, 8.13) 200 mg/day 2 5/129 vs. 3/117 1.55
(0.39, 6.23) 240 mg/day 3 1/125 vs. 2/120 0.66
(0.11, 3.95) 300 mg/day 1 0/58 vs. 0/51 Not estimable 400 mg/day 1 0/58 vs. 0/51 Not estimable 480 mg/day 1 2/46 vs. 2/45 0.98
(0.14, 6.65)
Five trials reported W D A E for verapamil (Chan 1997, Cushman 1998, Felictta 1992,
Meeves 1994, Whelton 1992). There was not enough power to achieve statistical
significance because of the limited amount of data.
214

3.11.3 Other calc ium channel blockers
3.11.3.1 Mibefradi l vs. placebo
Table 99: Effect of mibefradi l on withdrawals due to adverse events
Dose of Mibefradil # of trials # of W D A E in treatment group vs. placebo group
RR (95% CI)
6.25 mg/day 2 2/92 vs. 0/87 2.83 (0.30, 26.70)
12.5 mg/day 2 2/90 vs. 0/87 2.89 (0.31, 27.29)
25 mg/day 3 1/128 vs. 0/129 3.00 (0.13, 71.96)
50 mg/day 3 1/131 vs. 0/129 3.00 (0.13,71.96)
100 mg/day 3 2/132 vs. 0/129 2.82 (0.30, 26.61)
150 mg/day 2 3/76 vs. 0/78 7.34 (0.39, 137.78)
200 mg/day 1 4/37 vs. 0/36 8.76 (0.49, 157.12)
Three trials reported W D A E data for mibefradil (Bernink 1996, Bursztyn 1997,
Oparil 1997). Though there was a trend of increasing W D A E with higher doses, there was
not enough power to achieve statistical significance at each dose because of the limited
amount of data. Elowever, when all doses are pooled, there is a statistically significant
increase in W D A E compared with placebo (RR 3.90, 95% CI: 1.48, 10.28).
215
4. DISCUSSION
This systematic review of the blood pressure lowering efficacy of CCBs used data
from published randomized placebo-controlled trials of 3-12 weeks duration, in order to
determine the dose-related effects on systolic and diastolic blood pressure, heart rate, and
the number of withdrawals due to adverse events. One important aim was to determine i f a
difference in the magnitude of BP lowering existed amongst the different subclasses of
CCBs or amongst the drugs within each subclass. Another aim was to determine optimal
dosing for each C C B drug so as to assist prescribing. It is important to note that
conclusions about dose-response were limited to doses that were assessed in the studies
included in this systematic review.
4.1 What methodological issues and potential sources of bias were encountered
while conduct ing the systematic review?
Several methodological issues, from searching databases to extracting and analyzing
data, surfaced during the process of conducting this systematic review. The search strategy
utilized the O V I D search interface, which was generally easy to use. However, it was not
possible to search suffixes such as "-dipine" which would have been helpful in identifying
dihydropyridine-related articles. The search strategy was developed for high sensitivity at the
expense of specificity and the process of sorting through irrelevant references was time-
consuming. The C E N T R A L (Cochrane Central Register of Controlled Trials) database is
formed from specialized registers from Cochrane groups, together with references to clinical
trials identified in M E D L I N E and E M B A S E . Thus, with its enhanced specificity,
C E N T R A L may prove to be a time-saving alternative to searching all of the standard
electronic databases.
216

This systematic review is based on data that are reported in publications and in some
cases, provided by the authors through correspondence. Inadequate reporting of trial
methodology and data was a frequent problem. Most crossover trials did not report pre-
crossover data and thus, these trials were excluded. Because only 36% of trials reported SD
of B P change, in the majority of trials the variances were imputed. Some trials only reported
blood pressures from ambulatory blood pressure monitoring even though office blood
pressures were measured as well. Attempts to obtain additional data by contacting authors
were seldom successful. O f the authors who responded, more often than not the data were
no longer available, especially i f over a decade had lapsed since the year of publication.
Authors who worked for a pharmaceutical company tended to have easier access to clinical
trial data. Some authors referred me to pharmaceutical and/or statistical analysis companies,
but garnering additional data by this method was rarely successful.
To promote standardization of data reporting, many journals have endorsed the
C O N S O R T statement, consisting of a checklist of items to be included when reporting a
clinical trial (87). This checklist covers items that were commonly deficient in published
RCTs included in this systematic review, such as method of randomization, flow of
participants through each stage, and adverse events in each group.
Errors in the reported data are a potential threat to the validity of a systematic
review. Some trials reported standard deviations that were spuriously low and were more
likely to be standard errors. The trials that reported standard deviations of B P change that
were > 3 standard deviations away from the weighted mean value were discarded and
imputed values were used. Clinical trial fraud is also a possible source of bias in the results,
and although none of the publications of the included trials have ever been withdrawn, the
217
primary author of one included trial (Fiddes 1994) pleaded guilty to fraud for falsifying
records and endangering patients while he was the head of a clinical research institute (377).
Errors in the process of extracting data were minimized by having two independent
reviewers extract data. Whenever possible, data were extracted from text and tables in the
publications since extracting graphical data may introduce inaccuracies.
Loss of blinding in a trial would bias the results in favor of CCBs over placebo. A n
investigator's knowledge of the occurrence of common C C B side effects such as flushing
and ankle edema in clinical trial participants may compromise blinding. However, none of
the included trials assessed the success of blinding in patients or investigators.
Overall, the percentage of patients completing each trial was in the range of 85-
100%. Because the drop-out rate in the included studies was low, attrition bias is unlikely.
The systematic review was based on group averages from each trial, rather than
analyzing individual patient data. The I N D A N A (Individual Data Analysis of
Antihypertensive intervention trials) project, which involves meta-analyses of individual
patient data, has the potential advantages of increased data reliability and improved ability to
analyze large amounts of data in subgroups, assess prognostic factors, and relate treatment
effects to baseline characteristics (378).
4.1.1 Publ icat ion bias
Another potential methodological problem was publication bias since only published
trials were assessed in this review. Funnel plot asymmetry can indicate publication bias but
can also be due to clinical and methodological heterogeneity. Funnel plot asymmetry was
observed for several C C B drugs individually, as well as dihydropyridines as a subclass. Thus,
effect sizes calculated in this systematic review are likely to be overestimates. Ideally, clinical
trial registries would minimize the problem of publication bias by allowing "negative" trials
218
that would otherwise be unpublished to be included in the review. The World Health
Organization has formed the International Clinical Trials Registry Platform with the aims of
ensuring that all clinical trials are registered and that a minimum set of results will be
reported and made publicly available (379).
There are several techniques that can be applied to adjust for publication bias in a
meta-analysis (380), but currently there is no gold standard. In this review, the non-
parametric "trim-and-fill" method was applied. For the dihydropyridine subclass, 7
"missing" studies in the SBP analysis and 5 "missing" studies in D B P analysis were "filled
in" to achieve a symmetrical funnel plot. The resulting effect sizes were not altered in a
clinically or statistically significant degree compared with the original data; this method
suggested the data had overestimated change in SBP by 0.4 mm H g and change in D B P by
0.3 mm Hg.
A post-hoc subgroup analysis was done to determine if the degree of reported blood
pressure lowering differed in large trials (active treatment arms in the highest tertile) versus
small trials (active treatment arms in the lowest tertile). Dihydropyridines and non-
dihydropyridines were analyzed separately. For dihydropyridines, this analysis confirmed
that the effect sizes for change in SBP and D B P in the smaller trials were statistically
significantly greater and more variable than those in the larger trials. The exaggerated effect
size of the included trials with small sample size corroborates evidence of publication bias in
addition to the asymmetrical funnel plots associated with several of the dihydropyridine drug
analyses. Using this method one would accept the tertile of the largest trials as the closest to
the treatment effect. This would lead to a reduction in the overall effect from -10.5 to -9.0
mmHg for systolic and from -6.9 to -5.4 mmHg for diastolic.
219

Either way there are likely to be small studies with littie or no reduction in blood
pressure that have not been published and therefore are not included in this review.
However, locating such unpublished studies is generally unfruitful and the inclusion of such
studies may not reduce bias i f the data are provided by interested sources or i f their quality
differs from that of published trials (381).
For non-dihydropyridines, there was no statistically significant difference in effect
size for SBP and D B P between small and large trials. Flowever, the trend was in the same
direction and this analysis lacked power since there were far fewer non-dihydropyridine trials
included in the review than dihydropyridine trials. Also, the non-dihydropyridine trials had
larger sample sizes than the dihydropyridines on average (mean size of active treatment arm
of 54 patients vs. 43 patients, respectively), although the difference was not statistically
significant.
4.1.2. Selection Bias
The method of patient recruitment is another potential source of bias, as studies
could select for known responders to CCBs in previous trials to participate in new trials.
Thus there are likely to be some patients who participated in several C C B trials. However,
the degree of selection bias is difficult to quantify because the method of patient recruitment
is usually not reported adequately. In this systematic review, we searched for selection bias
by dividing up the trials into tertiles according to year of publication. The mean effect size
of the oldest trials was compared with that of the most recent trials. If selection bias was
present, we would expect the tertile with the most recent trials to have a greater effect size
than that of the oldest trials. When this was done there was no statistically significant
2 2 0

difference in effect size between the oldest and most recent trials. Therefore, we could not
confirm any suggestion of evidence of selection bias in this systematic review.
4.2 What is the dose-related, b lood pressure lowering efficacy of each subclass? Is
there a difference in the best estimate of the magnitude of B P lowering effect
of different subclasses of C C B s ?
In this systematic review, 106 trials met the inclusion criteria and reported data on
13,878 patients (9513 receiving active treatment and 4365 receiving placebo), with a mean
age of 55 years, mean baseline blood pressure of 158.2/101.6 mm H g and mean pulse
pressure of 56.7 mm Hg.
Data were pooled for the dihydropyridine subclass and the non-dihydropyridine
subclass by categorizing individual doses according to multiples of the manufacturer's
starting dose (0.5x, l x , 2x, 4x). Both subclasses demonstrated a dose-response relationship,
with an increasing magnitude in B P lowering as the dose increases from half the starting
dose up to twice the starting dose. The maximal blood pressure lowering efficacy appeared
to be attained at twice the recommended starting dose; at doses above this, there is no
corresponding increase in blood pressure lowering response. For dihydropyridines, the best
estimate of the maximal blood pressure lowering is -10/-7 mm Hg, based on 2857 patients
for SBP and 3076 patients for D B P . The best estimate of the maximal blood pressure
lowering efficacy of the non-dihydropyridine subclass is -8/-6 mm Hg, based on 1309
patients for SBP and 1632 patients for D B P .
The pooled data have narrow confidence intervals, thereby allowing detection of
even small differences between subclasses. The results of this systematic review reveal that
dihydropyridines are statistically significantly more effective at lowering blood pressure than
221

non-dmydropyridines, although one could argue that this difference may not be clinically
significant.
4.3 Is there a difference in the best estimate of the magnitude of B P lowering
effect of drugs in each subclass?
Differences between C C B drugs within each subclass cannot be assessed accurately
in this systematic review because the analysis was restricted to doses that were tested in the
included clinical trials. For several drugs there were not enough data to define the dose-
response relationship. There was also high variability in the amount of available data for
each dose of each drug. The effect sizes for drugs with littie data have very wide confidence
intervals (Table 51).
4.4 What is the effect on blood pressure in the placebo group in short-term trials?
The weighted mean changes in SBP and D B P in placebo groups across all included
trials with blood pressure data were -3.3 mm H g (SD 4.1; range -16.7 to 9) and -3.5 mm H g
(SD 2.7; range -11.4 to 4.5), respectively. Because the placebo response was quite variable, it
was important to subtract this effect for each trial in order to isolate the effect of the C C B
drug. Hence, the inclusion criteria mandated that included trials have a parallel placebo arm.
The placebo effect arises from the natural history of the condition, regression to the
mean, and non-specific effects of treatment (382). The variability associated with the
measurement of blood pressure itself may also contribute to the wide range of placebo
responses observed in this systematic review.
2 2 2

4.5 Does the method of blood pressure measurement affect the blood pressure
lowering efficacy of C C B s ?
Sources of error associated with blood pressure measurement could affect study
entry and trial outcomes, thereby potentially imparting bias onto the results of a systematic
review. Thus, sensitivity analyses were planned to ascertain i f the method of blood pressure
measurement and the position of measurement affected drug efficacy.
Seventy-two percent of the trials utilized sphygmomanometers and 6% of the trials
used automatic devices to measure clinic blood pressures, while 22% of the trials did not
report the instrument used. There were insufficient data to conduct a sensitivity analysis
based on instrument used to measure BP . The effect of calcium channel blockers on
ambulatory blood pressures as measured by 24-hour ambulatory blood pressure monitors
was not assessed in this systematic review.
Most of the blood pressure data extracted were sitting (48%), followed by supine
(26%) and standing (16%) and average of supine/standing (4%) positions. The position of
measurement was not reported for 6% of the trials with extractable B P data. There was no
statistically significant difference in B P lowering efficacy among the different measurement
positions.
4.6 Does trial quality affect the blood pressure-lowering efficacy of ca lc ium
channel blockers?
Both the Jadad and Cochrane quality assessment scales were utilized in this review.
One hundred (94.3%) of the included trials did not report allocation concealment, while the
remaining six (5.7%) trials reported an adequate method of concealment. Most included
trials (86 trials; 81.1%) were of moderate quality, while 19 (17.9%) were of low quality and
223
only one trial (0.9%) was of high quality. A sensitivity analysis removing low quality studies
did not alter the effect sizes obtained in the C C B subclass analyses. The relative
homogeneity of the quality of the studies is reflected in the screening criteria for inclusion
into the systematic review. A l l included studies had to be randomized, double-blinded and
placebo-controlled. Because the Jadad scoring criteria match these screening criteria, this
scale was not particularly useful in this review. The Cochrane method of assessing trial
quality with respect to allocation concealment was also not useful because most studies did
not report these details. It is worth noting that the quality of a trial's reporting of the
methodology and the quality of the trial results are not always in accord. The accuracy of
blood pressure measurement is the most important factor affecting the quality of the
included studies. However, this factor is not taken into account in the Jadad and Cochrane
quality assessment scales.
4.7. Was there a difference in b lood pressure lowering efficacy at trough vs. peak?
Eighty-four trials reported trough blood pressures and 3 trials reported peak blood
pressures, while 19 trials did not report timing of blood pressure measurement. The small
number of trials with peak BPs precludes formal comparison of effect sizes at trough versus
peak timing. A future systematic review of trials with 24-hour blood pressure monitoring
would best address this question because this measurement technique allows both trough
and peak data to be obtained for each patient.
224

4.8 D i d funding source affect the reported blood pressure lowering efficacy of
C C B s ?
Relationships between funding source and trial outcome in RCTs have been assessed
in several studies. A published systematic review comparing the outcomes of industry-
sponsored vs. nonindustry-sponsored original research showed a statistically significant
association between industry-sponsorship of RCTs and pro-industry results [OR 4.14 (95%
C L 2.73-6.32)] (383).
The majority of trials included in this systematic review (60; 57%) did not report the
source of funding. O f the trials that did report funding source, 45 (98%) had an industry
funding source, with 40 trials (87%) with potential bias in favor of the C C B drug being
tested, and 5 trials (11%) with potential bias against. Only one trial (2%) was funded by a
government agency.
Sensitivity analysis removing the trials with potential bias against the C C B drug and
government-funded trials did not change the results. This analysis is not adequately powered
because of the general lack of reporting.
4.9 Does age affect the b lood pressure lowering efficacy of C C B s ?
Eight studies had inclusion criteria for older patients, defined as cutoff age > 60
years (Chan 1997, Rizzini 1991, BarbagaUo 2000, Ninci 1997, Fogari 1999, Bursztyn 1997,
Scuteri 1992, Paolisso 1991). A n additional four trials had different age criteria but still had a
mean age of > 60 years (Fiddes 1994, Black 2001, van Ree 1996, Gerritsen 1998). Two trials
reported data separately for older patients and younger patients (Fagan 1997, Fiddes 1994).
However, with such little data a subgroup analysis of the effect of CCBs on older vs.
225

younger patients was not feasible. A systematic review of individual patient data would be
more suitable to assess this question, as more data would be available in such an analysis.
4.10 Does co-morbidity alter the blood pressure lowering efficacy of C C B s ?
A subgroup analysis of hypertensive patients with co-morbidity was not feasible in
this systematic review because of the lack of such patients in the included studies. Two
nitrendipine studies had inclusion criteria of Type 2 diabetes mellitus. One nicardipine study
was performed in hospitalized patients. One trial assessed lidoflazine in post-infarction
patients. Otherwise, all other trials did not select for patients with co-morbidity. Essentially,
most trials excluded patients with major cardiac, hematologic, renal, hepatic, or endocrine
disease.
4.11 Does blood pressure lowering efficacy of C C B s differ for isolated systolic
hypertension vs. diastolic or systo-diastolic hypertension?
Calcium channel blockers have been used commonly a first-line therapy for isolated
systolic hypertension, a guideline that was primarily based on the results of the "Systolic
Hypertension in Europe" (SYST-Eur) trial. In the SYST-Eur study, nitrendipine (with
optional add-on enalapril and/or hydrochlorothiazide) in comparison with placebo showed a
reduction in the risk of stroke (RR 0.61, 95% CI 0.43-0.87) and cardiovascular events (RR
0.71, 95% CI 0.57-0.87), but not in total mortality and C A D (70).
This systematic review included 3 trials with inclusion criteria of isolated systolic
hypertension (Black 2001, Barbagallo 2000, Paolisso 1991). With such littie data, a subgroup
analysis comparing the effect sizes between trials with inclusion criteria of ISH vs. diastolic
hypertension was not feasible.
226
4.12 H o w do the direct comparisons between doses differ from the indirect
comparisons?
Direct comparisons were based on much less data than the indirect comparisons.
There was general agreement between the direct and indirect comparisons, but the
confidence intervals were fairly wide.
227

4.13 For each C C B drug, do the manufacturer's starting doses coincide wi th the
lowest effective dose as determined by this systematic review?
Table 100: Compar ison of manufacturer's recommended starting doses and lowest effective doses determined in this systematic review D r u g Manufacturer's
recommended starting dose (mg/day)
Lowest effective dose (mg/day)
Amlodipine 5 m g 2.5 mg
Barnidipine 10 mg 30 mg
Darodipine n/a 100 mg
Diltiazem 120-240 mg 120 mg
Felodipine 5 m g 2.5 mg
Isradipine 5 mg 1 mg
Lacidipine 2-4mg 4 m g
Lercanidipine 10 mg 10 mg
Lidoflazine n/a n/a
Manidipine 10 mg 10 mg
Nicardipine 60 mg 40 mg
Nifedipine 20-30 mg 20 mg
Nilvadipine 8mg 8 m g
Nisoldipine 10 mg 10 mg
Nitrendipine 5-20 mg 10 mg
Pranidipine n/a 2 m g
Tiapamil n/a N o doses showed statistically significant difference from
placebo Verapamil 180-240 mg 180 mg
228
There is general agreement between manufacturer's recommended dose and the
lowest effective dose determined by this systematic review. However, the lowest effective
doses for amlodipine, felodipine, isradipine and nicardipine were lower than the
manufacturer's recommended starting doses.
4.14 What is the effect of C C B s on B P variability?
To determine the effect of C C B treatment on BP variability, the endpoint
variabilities of the C C B group were compared with the placebo group. There were a lot of
data to assess this parameter and there was no statistically significant difference between
C C B and placebo for SBP or D B P , demonstrating with a high degree of certainty that CCBs
do not change BP variability.
In absolute terms, the variability of SBP is statistically significantly different than that
of D B P . However, in terms of coefficient of variation, which is a measure of the variability
relative to the mean value, there is no statistically significant difference in the variabilities of
SBP and D B P . Thus, it can be concluded that SBP and D B P vary to the same degree.
The variability at baseline appears to be affected by blood pressure criteria for entry
into the trials. SBP at baseline is statistically significandy lower in the 3 trials that used SBP
as entry criteria compared to the 72 trials using D B P - or mixed S B P / D B P criteria. The
baseline variabilities in D B P were similar across all entry criteria. However, in the trials with
D B P entry criteria, the baseline SD values were statistically significandy lower than the
endpoint values in both the C C B treatment and placebo groups. This demonstrates that the
baseline D B P variabilities are likely to be spuriously low in trials with D B P entry criteria.
Entry criteria may falsely lower the magnitude of baseline variability because it is a truncated
229

rather than a normal distribution. This effect would be further magnified i f many patients
with BPs near the cut-off value are enrolled into trials.
The blood pressure variability of a trial gives an indication of the reliability of the
data since expected values can be compared with the reported values. Based on the baseline
variabilities of treatment and placebo groups, the best estimate of the variability in SBP from
trials with systo-diastolic hypertension is 14.4 mm H g (SD 3.2). However, the best estimate
of the variability in D B P cannot be determined from baseline measures in this review
because the majority of the trials had D B P entry criteria. The best estimate for D B P
variability is based on end of treatment values, 8.2 mmHg (SD 2.4).
This review assesses variability based on mean values from treatment groups, which
accounts for both inter- and intra-individual variability. Intra-individual BP variability can be
assessed independendy in cross-over studies or from data from 24-hour blood pressure
monitoring.
The variability of the change in BP in both SBP and D B P is not statistically
significandy different in the C C B treatment group compared with the control group, ft can
be concluded that the blood pressure responses to C C B treatment and placebo treatment are
both highly variable (SD of S B P / D B P change of 13.5/7.8 mm H g and 14.1/7.9 mm Hg,
respectively), and the C C B effect to lower BP has no effect on that variability.
Many trials did not report the SD of the change in BP, necessitating imputing these
values. However, the mean reductions in blood pressure were insensitive to the strategy
used to impute missing variances — that is, whether the hierarchy for imputation was used or
the weighted mean SD of BP change from all trials reporting this parameter was used.
230
4.15 What is the effect of C C B s on pulse pressure?
Pulse pressure is an independent risk factor for cardiovascular disease, although it
was not reported as a primary or secondary outcome in any of the included trials. The
weighted mean change in pulse pressure was calculated for dihydropyridines and non-
dihydropyridines at twice the starting dose and above, from trials reporting trough SBP and
D B P data. These parameters were compared with that of placebo, which was calculated
from all trials reporting both SBP and D B P , regardless of timing of BP measurement. The
results demonstrate that placebo does not affect pulse pressure (weighted mean 0.3 mm Hg,
95% CI: -0.2, 0.8), while a small reduction in pulse pressure is observed with both
dihydropyridines (-3.4 mm Hg; 95% CT. -4.3, -2.5) and non-dihydropyridines (-2.4 mmHg;
95% CI: -3.7, -1.1). There is no statistically significant difference between dihydropyridines
and non-dihydropyridines in change in pulse pressure (p = 0.2). In a sensitivity analysis,
studies with isolated systolic hypertension as entry criteria were removed from the analysis.
There were only two such studies (Barbagallo 2000 and Paolisso 1991), both of which had
been included in the pulse pressure calculation for placebo only, because the timing of blood
pressure measurement was not reported. Without the ISH studies, the effect size for the
placebo group remains similar (0.4 mm Hg; 95% CI: -0.1, 0.9).
Placebo does not alter pulse pressure most likely because none of the factors that
contribute to the placebo response has any effect on blood pressure or its regulation. This is
evidence against the placebo response being due to a psychological effect on blood pressure.
231

4.16 Is there any evidence of a dose-response relationship wi th respect to change
in heart rate?
Acutely, short-acting CCBs are associated with increased heart rate and
norepinephrine levels. With chronic dosing, the effect of CCBs on heart rate appears to be
small and clinically insignificant, based on the 47 (44%) trials reporting heart rate data in this
review. However, this result may be due to bias from lack of reporting, since many trials did
not report this outcome. For dihydropyridines, doses greater than or equal to 1.5 times the
recommended starting dose are associated with a statistically significant increase in heart rate
of 1.4 beats per minute (95% CI: 0.60, 2.2) compared with placebo.
For non-dihydropyridines, there are insufficient data to obtain a valid estimate of the
effect on heart rate. However, the limited data from this systematic review demonstrated
that non-dihydropyridines at doses 1-3 times the starting dose were associated with a
statistically significant decrease of 2.6 beats per minute (95% Cf: -3.85, -1.36) compared with
placebo.
4.17 Is there any evidence of a dose-reponse relationship wi th respect to
withdrawals due to adverse events?
The number of withdrawals due to adverse events in each dosage group was
reported in 64 (60%) of the included trials. However, the type and severity of adverse events
were not consistendy reported. Reports of adverse effects from published and unpublished
sources other than randomized controlled trials may provide better information on the long
term safety of C C B drugs. Ffowever, some rudimentary conclusions can be gleaned from
the short-term RCTs included in this systematic review. For each drug considered
independendy, there were not enough data to make an accurate estimate of W D A E .
232
However, when grouped as a subclass, the cLihydropyridines are associated with a statistically
significant increase in W D A E compared with placebo. There also appears to be a dose-
response relationship, with increasing relative risk values with increasing dose, starting with a
non-significant difference at the starting dose, a RR of 1.76 (95% CI 1.21, 2.58) at twice the
starting dose, and a RR of 3.91 (95% CI 2.19, 6.99) at >3 times the starting dose. The non-
dihydropyridine trials did not show a statistically significant difference in W D A E compared
with placebo but there is insufficient evidence to make a valid estimate of their effect on
W D A E .
4.18 Can the magnitude of blood pressure lowering efficacy of calcium channel
blockers be linked to their mechanism of action?
Hypertension is associated with elevated concentration of intracellular calcium ions,
which can arise from increased transport from extracellular calcium stores, from increased
release from intracellular stores, or both. The exact mechanism of action of calcium channel
blockers is not known but they probably reduce blood pressure by vasodilatory and
cardiodepressant effects resulting from a reduction of calcium entry through the L-type
calcium channels on the arterial vasculature and cardiac tissue.
The blood pressure lowering efficacy of CCBs is quite modest in relation to the high
degree of variability associated with blood pressure measurement. Human physiology is
designed to maintain blood pressure levels through several homeostatic mechanisms. For
instance, baroreceptors in carotid sinuses and aortic arch detect changes in arterial pressure,
and they buffer such changes by activating reflex responses in the heart, blood vessels and
kidney (384). Chronic hypertension involves resetting of the baroreceptor reflex to higher
pressures.
233
A t the cellular level, there are many players involved in the regulation of vascular
tone other than L-type calcium channels, such as several types of potassium channels,
chloride channels, store-operated calcium channels, and stretch-activated cation channels
(385). L-type calcium channels are regulated by the membrane potential, which in turn is
determined essentially by potassium channels. Stretch-actived cation channels provide a
route of entry for calcium into vascular muscle cells, even when dihydropyridine-sensitive
channels are blocked (385). Store-operated channels allow calcium entry when intracellular
stores are low.
In this review a small statistically significant difference in the BP-lowering efficacy
between dihydropyridines and non-dihydropyridines was demonstrated. However, in view of
the complexity of blood pressure regulation and the action of CCBs it is not possible to
rationally speculate as to why this may be.
4.19 H o w can the blood pressure lowering efficacy of ca lc ium channel blockers in
short-term trials be related to their effects on mortality and morbidity
outcomes in long-term trials?
There is current debate regarding the effect of CCBs on morbidity and mortality
outcomes in long-term trials. Pahor et al.'s recent systematic review of randomised
controlled trials found no statistically significant difference in the reduction of SBP or D B P
between calcium antagonists and other drugs (diuretics, beta blockers, A C E inhibitors,
clonidine) (55). However, the review also demonstrated that CCBs were associated with a
significandy higher risk of acute myocardial infarction (odds ratio [OR], 1.2; 95% CI 1.11-
1.43), congestive heart failure (OR 1.25; 95% CI 1.07-1.46) and combined major
cardiovascular events (OR 1.10; 95% CI 1.02-1.18) compared to the other drug classes. This
234
suggests that that clinical outcomes associated with C C B treatment are not dependent solely
only on the magnitude of blood pressure reduction, but also on other factors. This claim
has been refuted but more studies need to be done to clarify this area of controversy.
Recent RCTs have demonstrated increased risk of heart failure with C C B treatment (59, 60).
Another systematic review is being conducted currendy to assess adverse cardiac effects
associated C C B therapy (386).
The blood pressure lowering efficacy observed in short-term trials of C C B
monotherapy cannot be compared direcdy to long-term trials in which other drugs are
allowed to be added to C C B treatment in order to meet blood pressure targets. Nonetheless,
it is worth noting the magnitude of BP-lowering in long term, placebo-controlled C C B trials,
where other drugs could be added i f blood pressure targets were not reached. In the
SYST-Eur trial (70), first-line nitrendipine lowered BP by -10/-4.5 mm H g (placebo-
corrected), and a similar magnitude of blood pressure lowering was found with first-line
nitrendipine in the SYST-China study (-9/-3 mm Hg) (69).
The choice between different classes of antihypertensive drugs should be based on
morbidity and mortality data. Currendy, the first-line pharmacological treatment of
hypertension is low-dose thiazide diuretics, which have been shown to reduce cardiovascular
events, cardiovascular mortality and total mortality compared with placebo. Thiazdes have
demonstrated a mean blood pressure reduction of 10/4 mm H g in a previous systematic
review (81), a magnitude that is similar to the calcium channel blocker class. However,
thiazide diuretics confer a reduction in heart failure outcomes as compared with CCBs. One
can speculate that the ability of thiazides to reduce pulse pressure more than CCBs (6 mm
H g for thiazides vs 3 mmHg for dihydropyridines and 2 mm H g for non-dihydropyridines)
is a possible explanation for this difference. Further investigation of pulse pressure
235

differences in long term head-to-head trials between antihypertensive classes could be done
to test this hypothesis.
Based on blood pressure lowering efficacy alone, the dihydropyridines appear to be
better than non-dihydropyridines. However, this review does not suggest that
dihydropyridines are better at lowering blood presssure than thiazides and considering the
data on morbidity and mortality outcomes, calcium channel blockers should remain as
second- or tlurd-Iine agents for management of primary hypertension.
236

5. CLINICAL IMPLICATIONS
The findings of this systematic review represent the best available evidence about the
blood pressure lowering efficacy of calcium channel blockers in adults with primary
hypertension. Several important conclusions are relevant to the clinical use of this class of
drugs.
1. Dihydropyridines reduce blood pressure to a greater degree than non-dihydropyridines.
The best estimate of the maximal blood pressure lowering efficacy of the
dihydropyridine subclass is -10 mm H g for SBP and -7 mm Pig for D B P . The best
estimate of the maximal blood pressure lowering efficacy of the non-dihydropyridine
subclass is -8 mm Pfg for SBP and -6 mm Pfg for D B P .
2. Publication bias was present in this systematic review, leading to an overestimate of the
effect size; the magnitude of this overestimate is likely between 0.4 mm H g and 1.5 mm
H g for SBP 0.3 and f .5 mm H g for D B P .
3. There was a dose-response relationship for the blood pressure lowering efficacy of
CCBs. For dihydropyridines and non-dihydropyridines, half the starting dose lowered
blood pressure less and twice the starting doses lowered blood pressure more than
starting doses. Maximal blood pressure lowering appears to be achieved at twice the
manufacturer's recommended starting dose. Further dose escalation does not enhance
blood pressure lowering efficacy despite manufacturers' suggestions otherwise.
237
4. Regarding blood pressure variability:
a) Treatment of primary hypertension with calcium channel blockers does not affect
blood pressure variability compared with placebo.
b) Systolic and diastolic blood pressures vary to the same degree when the variability is
expressed as coefficient of variation.
c) Blood pressure criteria for entry into randomized controlled trials results in a
reduction in the estimate of the baseline variability of the corresponding parameter.
5. Regarding pulse pressure:
A) Placebo response does not affect change in pulse pressure.
B) Both dihydropyridines and non-dihydropyridine CCBs reduce pulse
pressure by about 3 mmHg.
6. Calcium channel blockers given for 3-12 weeks have a small and probably clinically
insignificant effect on heart rate.
a) For dihydropyridines, doses greater than or equal to 1.5 times the manfacturer's
recommended starting dose are associated with a statistically significant increase in
heart rate of 1.4 beats per minute.
b) For non-dihydropyridines, doses 1-3 times the manufacturer's recommended starting
dose are associated with a statistically significant decrease of 2.6 beats per minute.
7. A l l doses combined, dihydropyridines increase withdrawals due to adverse events
compared with placebo at starting doses (RR 1.7 [95% CI: 1.3, 2.1]; Absolute risk
increase 2%; number need to harm = 50). A dose-response relationship was present,
238

with a RR of 1.76 (95% CI 1.21, 2.58) at 1.5-3 times the starting dose, and a R R of 3.91
(95% CI 2.19, 6.99) at >3 times the starting dose. The non-dihydropyridine trials did
not show a statistically significant difference in W D A E compared with placebo but this
was probably due to lack of reporting.
Dose titration of calcium channel blockers above the recommended starting dose is
associated with a minimal benefit in terms of increase in blood pressure lowering
efficacy, and increased harm, in terms of increased withdrawals due to adverse effects
and greater cost.
239
6. I M P L I C A T I O N S F O R F U T U R E R E S E A R C H
1. Because publication bias was found in this review, the published data on the short-term
blood pressure lowering efficacy of calcium channel blockers represents an incomplete
data set. Thus, all clinical trials should be registered and reported in full.
2. There is a need to improve the quality of reporting of details in publications of clinical
trials measuring blood pressure lowering efficacy. As systematic reviews are secondary
research, the validity of the results depends on the quality of its component trials.
A) Baseline and endpoint blood pressures, the mean change from
baseline and the standard deviations of all of these parameters must
be reported for all randomized groups and provided in a table.
B) The number of serious adverse events, deaths, number of
withdrawals due to adverse events in each group, reasons for
withdrawal, and the time point at which withdrawals occurred for
each group must be reported in all trials.
C) Complete information must be given regarding % of patients
completing the trial as well as the number of dropouts and reasons
thereof. Methodological details regarding randomization, allocation
concealment and blinding should be reported adequately to facilitate
assessment of trial quality. Complete baseline characteristic details
are also necessary to evaluate the effect size within trials and to
validate the combining of data across different trials in meta-analyses.
240
3. Improving the search capabilities and indexing systems of medical literature databases
and clinical trial registries will facilitate more complete and efficient searching for future
systematic reviews and updates. The Cochrane Central Register of Controlled Trial
( C E N T R A L ) is a highly sensitive, specific and up-to-date database which provides a
time-saving alternative to searching all of the standard electronic databases.
4 . More clinical trials exploring a wider range of doses of calcium channel blockers need to
be conducted.
5. A systematic review of clinical trials with head-to-head comparisons of different doses of
each calcium channel blocker drug should be performed in order to validate the relative
blood pressure-lowering efficacies of the various drugs within this class.
6. A systematic review of cross-over trials of CCBs in hypertension should be performed to
validate the blood pressure-lowering efficacy of CCBs as determined by this systematic
review. Asssessment of end-of-treatment blood pressure standard deviations from
cross-over studies would give an estimate of the within-patient blood pressure variability.
7. A systematic review of the adverse effects of calcium channel blockers should be
performed in order to explore further the nature and severity of adverse events leading
to withdrawals from clinical trials.
8. More long-term trials of head-to-head comparisons of calcium channel blocker drugs
with other drug classes using doses with comparable blood pressure control need to be
241
performed in order to determine whether there are class-specific effects on morbidity
and mortality.
242

7. R E F E R E N C E S
1. Beevers D G , MacGregor G A . Hypertension in Practice, 3 r edition. London: Martin Dunkz Ltd; 1999.
2. Joffres M R , Hamet P, Rabkin SW, Gelskey D , Hogan K , Fodor G for the Canadian Heart Health Surveys Reseach Group. Prevalence, control and awareness of high blood pressure among Canadian Adults. C M A J 1992; 146: 1997-2005.
3. World Flealth Organization, International Society of Flypertension Writing Group. 2003 World Flealth Organization/International Society of Hypertension (ISH) statement on management of hypertension. J Flypertension 2003; 21:1983-1992.
4. Seedat Y K . The limits of antihypertensive therapy — lessons from Third World to First. Cardiovascular Journal of South Africa 2001; 12(2): 94-100.
5. National High Blood Pressure Education Program Coordinating Committee. The sixth report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Arch Intern Med 1997; 157:2413-2446.
6. Rose G . Epidemiology. In: Marshal A J and Barrett D W , editors. The Flypertensive Patient. Kent, England: Pitman Medical; 1980. p. 1-21.
7. Kaplan N M . Hypertension: prevalence, risks, and effect of therapy. A n n Intern Med 1983; 98: 705-709.
8. Port S, Demer L , Jennrich R, Walter D , Gardinkel A . Systolic blood pressure and mortality. Lancet 2000; 355: 175-180.
9. Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002; 360: 1903-1913.
10. Feldman R D , Campbell N , Larochelle P, Bolli P, Burgess E D , Carruthers S G for the Task Force for the Development of the 1999 Canadian recommendations for the management of hypertension. 1999 Canadian recommendations for the management of hypertension. C M A J 1999; 161 (12 Suppl): S1-S22.
11. Parati G, . Mancia G . Blood pressure variability as a risk factor. Blood Pressure Monitoring 2001; 6:341-347.
12. Sander D , Kukla C, IClingelhofer J, Winbeck K , Conrad B. Relationship between circadian blood pressure pattersn and progression of early carotid atherosclerosis: a 3-year follow-up study. Circulation 2000; 102:1536-1541.
13. Mitchell G F , Moye L A , Braunwald E , Rouleau J-L, Bernstein et al. Sphygmomanometricalfy determined pulse pressure is a powerful independent
243
predictor of recurrent events after myocardial infarction in patients with impaired left ventricular function. Circulation 1997; 96:4254-4260.
14. Verdecchia P, Schillaci, G , Borgioni C, Ciucci A , Pede S, Porcellati C. Ambulatory pulse pressure: a potent predictor of total cardiovascular risk in hypertension. Hypertension 1998; 32(6):983-988.
15. Glynn RJ, Chae C U , Guralnik J M , Taylor JO , Hennekens C H . Pulse pressure and mortality in older people. Arch Intern Med 2000; 160: 2765-2772.
16. Gillman M W , Kannel WB, Belanger A , D'Agostino RB. Influence of heart rate on mortality among persons with hypertension: The Frarningham Study. A m Heart J 1993; 125:1148-1154.
17. Chobanian A V , Bakris G L , Black H R et al and the National High Blood Pressure Education Program Coordinating Committee. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. J A M A 2003; 289(19): 2560-2572.
18. O'Rourke M . Arterial stiffness, systolic blood pressure, and logical treatment of arterial hypertension. Hypertension 1990; 15: 339-347.
19. Baumbach G L . Chapter A63 - Mechanisms of vascular remodeling, In Izzo JL , Jr and Black H R , editors. Hypertension Primer, 3 r d ed. Dallas: American Heart Association; 2003. p. 180-183.
20. Mulvany MJ. Effects of angiotensin converting enzyme inhibition on vascular remodelling of resistance vessels in hypertensive patients. Journal of Hypertension Suppl. 1996; 14(6): S21-24.
21. Lyons D . Impairment and restoration of nitric oxide-dependent vasodilation in cardiovascular disease. International Journal of Cardiology 1997; 62 (Suppl 2): S101-S109.
22. Waeber B, Brunner HR. The multifactorial nature of hypertension: the greatest challenge for its treatment? Journal of Flypertension 2001; 19(suppl. 3) : S9-S16.
23. Arnett D K , Boerwinkle E , Davis BR, Eckfeldt J, Ford C E , Black H . Pharmacogenetic approaches to hypertension therapy: design and rationale for the Genetics of Flypertension Associated Treatment (GenHAT) study. The Pharmacogenomics Journal 2002; 2: 309-317.
24. Jiirgens G , Graudal N A . Effects of low sodium diet versus high sodium diet on blood pressure, renin, aldosterone, catecholamines, cholesterols, and triglyceride. The Cochrane Database of Systematic Reviews 2006 Issue 2.
244
25. Hooper L , Barrier! C, Davey Smith G , Ebrahim S. Advice to reduce dietary salt for prevention of cardiovascular disease. The Cochrane Database of Systematic Reviews 2006 issue 2.
26. Thompson P D , Buchner D , Pina IL, Balady GJ , Williams M A et al. Evercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease. Circulation 2003; 107: 3109-3116.
27. Moser M . Historical perspective on the management of hypertension. The American Journal of Medicine. 1986; 80(Suppl. 5B): 1-11.
28. McAlister F A , Campbell N R C , Zarkne K , Levine M , Graham ID. The management of hypertension in Canada: a review of current guidelines, their shortcomings and implications for the future. C M A J 2001; 164(4): 517-522.
29. Wright J M , Lee C H , Chambers G K . Systematic review of antihypertensive therapies: does the evidence assist in choosing a first-Une drug? C M A J 1999; 161(l):25-32.
30. Psaty B M , Lumley T, Furberg C D , Schellenbaum G , Pahor M , Alderman M H , Weiss NS. Health outcomes associated with various antihypertensive therapies used as first-line agents: a network meta-analysis. J A M A 2003; 289(19):2534-44.
31. Naqvi N H , Balufox M D . Blood Pressure Measurement: A n Illustrated History. Carnforth, Lanes, U K : Parthenon Pubkshing; 1998.
32. Nara A R , Burns M P , Downs W G . Blood Pressure. Redmond, Washington: SpaceLabs Inc.; 1989. p. 41-93.
33. McAlister F A , Straus SE. Chapter 2: What is this person's blood pressure? In Mulrow C D , editor. Evidence-based Ffypertension. London: B M J Books; 2001. p. 9-27.
34. O'Brien E T , O'Malley K . Blood Pressure Measurement. New York: Elsevier Science; 1991.
35. Gerin W, Marion R M , Friedman R. et al. How should we measure blood pressure in the doctor's office? Blood Pressure Monitoring 2001; 6:257-262.
36. Myers M G . Use of trough:peak ratio in the assessment of antihypertensive drug therapy. Canadian Journal of Cardiology 1994; 10 (Suppl. D): 17D-20D.
37. Rang H P , Dale M M , Ritter J M . Pharmacology. 4 t h ed. Edinburgh: Church Livingstone; 1999.
38. Berridge M . Elementary and global aspects of calcium signalling. J. Physiol 1997; 499: 291-306
39. Katz A M . Calcium channel diversity in the cardiovascular system. J A C C 1996; 28(2): 522-529.
2 4 5

40. Oates JA , Brown NJ . Chapter 33 - Antihypertensive agents and the drug therapy of hypertension, In Hardman J G , Limbird L E , Gilman A G , editors. Goodman and Gilman's The Pharmacological Basis of Therapeutics. 10 t h ed. London: McGraw Hi l l ; 2001. p. 871-900.
41. Vanhoutte P M . The Expert Committee of the World Plealth Organization on Classification of Calcium Antagonists: the viewpoint of the raporteur. A m J Cardiology 1987; 59:3A-8A.
42. Triggle DJ . Sites, mechanisms of action, and differentiation of calcium channel antagonists. A m J Hypertension 1991; 4(7) Part 2: 422S-429S.
43. Hockerman GPI et al. Molecular determinants of drug binding and action on L-type calcium channels. Annu Rev. Pharmacol Toxicol 1997; 37: 361-396.
44. Canadian Pharmacists Association. Compendium of Pharmaceuticals and Specialties. [Online]. 2006 [cited 2006 September 14] Available from: U R L : http://e-cps.pharmacists.ca/CPPIA/main.htm
45. Frishman WPI. Mibefradil: a new selective T-channel calcium antagonist for hypertension and angina pectoris. J Cardiovasc Pharmacol Therapeut 1997; 2(4):321-330.
46. Roche Laboratories announces withdrawal of Posicor from the market. F D A Talk Paper [Online] 1998 June 8 [cited 2006 July 21]. Available from: U R L : http:/ /wAvw . fda.gov/bbs/topics/ANSWERS/ANS00876.html
47. Borchard U . Calcium antagonists in comparison: view of the pharmacologist. Journal of Cardiovascular Pharmacology 1994; 24(Suppl.2):S85-S91.
48. IMS Global Insights - Lipitor Leads the Way in 2003. [Online]. 2004 [cited 2006 July 21]; Available from: URL:http://www.imshealtii.com/web/content/0.3148.64576068 63872702 7026099 8 70960214.00.html
49. Psaty B M , Heckbert SR, Koepsell T D et al. The risk of myocardial infarction associated with antihypertensive drug therapies. J A M A 1995; 274(8):620-625.
50. Pahor M , Guralnik J M , Corti M C , Foley DJ , Carbomn P, Plavlik RJ. Long-term survival and use of antihypertensive medications in older persons. J A m Geriatr Soc 1995; 43(11):1191-1197.
51. Furberg C D , Psaty B M , Meyer JV . Nifedipine: dose-related increase in mortality in patients with coronary heart disease. Circulation 1995; 92:1326-1331.
246

52. Alderman M H , Cohen H , Roque R, Madhavan S. Effect of long-acting and short-acting calcium antagonists on cardiovascular outcomes in hypertensive patients. Lancet 1997; 349: 549-598.
53. Kizer JR, Kimmel SE. Epidemiologic review of the calcium channel blocker drugs: an up-to-date perspective on the proposed hazards. Arch Intern Med. 2001; 161:1145-1158.
54. Stelfox H T . Chua G . O'Rourke K . Detsky AS. Conflict of interest in the debate over calcium-channel antagonists. N Engl J Med 1998; 338(2):101-6.
55. Pahor M , Psaty B M , Alderman MPI, Applegate W B , Williamson J D , Cavazzini C, Furberg C D . Health outcomes associated with calcium antagonists compared with other first-line antihypertensive therapies: a meta-analysis of randomized controlled trials. Lancet 2000; 356: 1949-1954.
56. Dahof B, Sever PS, Poulter N R , et al. for the A S C O T investigators. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering A r m (ASCOT-B P L A ) : a multicentre randomised controlled trial. Lancet 2005; 366:9489: 895-906.
57. L iu L , Zhang Y , L iu G . for the F E V E R Study Group. The Felodipine Event Reduction (FEVER) Study: a randomized long-term placebo-controlled trial in Chinese hypertensive patients. J Hypertens 2005; 23:2157-2172.
58. Estacio R O , Jeffers B W , Hiatt WR, Biggerstaff SL, Gifford N , Schner RW. The effect of nisoldipine as compared with enalapril on cardiovascular outcomes in patients with non-insulin-dependent diabetes and hypertension. N Engl J Med 1998; 338(10):645-52.
59. The A L L F I A T Officers and Coordinators for the A L L H A T Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial ( A L L H A T ) . J A M A 2002; 288:2981-2997.
60. Black FIR, Elliot W F , Grandits G . et al for the C O N V f N C E Research Group. Principal results of the Controlled Onset Verapamil Investigation of Cardiovascular End Points ( C O N V I N C E ) trial. J A M A 2003; 289(16): 2073-2082.
61. Tatti P. Pahor M . Byington RP. D i Mauro P. Guarisco R. Strollo G . Strollo F. Outcome results of the Fosinopril Versus Amlodipine Cardiovascular Events Randomized Trial (FACET) in patients with hypertension and N I D D M . Diabetes Care 1998. 21 (4):597-603.
62. Hansson L , Zanchetti A , Carruthers SG , Dahlof B , Elmfeldt D , Julius S, Menard f,Rahn KFI , Wedel FI, Westerling S. Effects of intensive blood-pressure lowering and
247

low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomized trial. H O T Study Group. Lancet 1998; 351(9118):1755-62. "
63. Brown MJ, Palmer CR, Castaigne A , de Leeuw PW, Mancia G , Rosenthal T, Ruilope L M . Morbidity and mortality in patients randomized to double-blind treatment with a long-acting calcium-channel blocker or diuretic in the International Nifedipine GITS study: Intervention as a Goal in Hypertension Treatment (INSIGHT). Lancet 2000; 356(9227):366-72.
64. Pepine CJ, Handberg E M , Cooper-DeHoff R M , et al. for the I N V E S T Investigators. A calcium antagonist vs a non—calcium antagonist hypertension treatment strategy for patients With coronary artery disease: The International Verapamil-Trandolapril Study (INVEST): A Randomized Controlled Trial. J A M A 2003; 290 (21): 2805-2816.
65. Borhani N O , Mercuri M , Borhani P A , Buckalew V , Canossa-Terris M , Carr A A , et al. Final outcome results of the Multicenter Isradipine Diuretic Atherosclerosis Study (MIDAS). A randomized controlled trial. J A M A 1996; 276(10):785-91.
66. National Intervention Cooperative Study in Elderly Hypertensives Study Group. Randomized double-blind comparison of a calcium antagonist and a diuretic in elderly hypertensives. Hypertension 1999; 34(5):1129-33.
67. Flansson L , Fledner T, Lund-Johansen P, Kjeldsen SE, Lindholm L H , Syvertsen J O et al. Randomized trial of effects of calcium antagonists compared with diuretics and beta-blockers on cardiovascular morbidity and mortality in hypertension: the Nordic Diltiazem (NORDIL) study. Lancet 2000; 356(9227):359-65.
68. Hansson L , Lindholm LFI, Ekbom T, Dahlof B , Lanke J, Schersten B et al. Randomized trial of old and new antihypertensive drugs in elderly patients: cardiovascular mortality and morbidity the Swedish Trial in Old Patients with Hypertension-2 study. Lancet 1999; 354(9192):1751-6.
69. L iu L . Wang J G . Gong L . L iu G . Staessen JA for the Systolic Hypertension in China (Syst-China) Collaborative Group. Comparison of active treatment and placebo in older Chinese patients with isolated systolic hypertension. Journal of Hypertension 1998. 16(12 Pt l):1823-9.
70. Staessen JA, Fagard R, Thijs L , Celis FI, Arabidze G G , Birkenhager W H , et al. for The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Randomized double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. Lancet 1997; 350(9080):757-64. .
71. Grimm R H Jr. Flack J M . Grandits G A . Elmer PJ. Neaton J D . Cuder JA. Lewis C. McDonald R. Schoenberger J. Stamler J. Long-term effects on plasma lipids of diet and drugs to treat hypertension. Treatment of Mi ld Flypertension Study (TOMHS) Research Group. J A M A 1996; 275(20):1549-56.
248

72. Julius S, Kjeldsen SE, Weber M . et al for the V A L U E trial group. Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the V A L U E randomised trial. Lancet 2004; 363 (9426): 2022-2031.
73. Rosei E A , Dal Palu C, Leonetti G , Magnani B , Pessina A , Zanchetti A . and the V H A S Investigators. Clinical results of the Verapamil in Hypertension and Atherosclerosis Study. J Hypertens 1997; 15(11):1337-44.
74. Cook DJ , Mulrow C D , Haynes RB. Systematic reviews: synthesis of best evidence for Clinical Decisions. Annals of Internal Medicine 1997; 126: 376-380.
75. Mulrow C D . Systematic Reviews: Rationale for systematic reviews. B M J 1994; 309: 597-599.
76. Clarke M , Oxman A D , editors. Cochrane Reviewers' Handbook 4.1 [updated June 2000]. In: Review Manager (RevMan) [Computer program]. Version 4.1. Oxford, England: The Cochrane Collaboration, 2000.
77. McAHster F A , Clark H D , van Walraven C, Straus SE, Lawson F M E , Moher D , Mulrow C D . The medical review article revisited: has the science improved? Ann. Intern Med. 1999; 131:947-951.
78. The Principles of the Cochrane Collaboration. [Online]. 2006 [cited 2006 July 26]. Available from: URL:http:/ /www.cochrane.org/docs/tenprinciples.htm
79. Jadad A R , Cook DJ , Jones A , Klassen TP, Tugwell P, Moher M , Moher D . Methodology and reports of systematic reviews and meta-analyses: A comparison of Cochrane reviews with articles published in paper-based journals. J A M A 1998; 280(3): 278-180.
80. Wong M M Y , Heran BS, Wright J M . Blood pressure lowering efficacy of calcium channel blockers for primary hypertension. The Cochrane Database of Systematic Reviews 2002, Issue 2. Art No.: CD003657. D O I : 10.1002/14651858.CD003657.
81. Musini V M . A Systematic Review of the Blood pressure lowering efficacy of thiazide and loop diuretics in the treatment of primary hypertension. M.Sc. Thesis, University of British Columbia 2000.
82. Medical Research Council Working Party. M R C trial of treatment of mild hypertension: principal results. B M J 1985; 291:97-104.
83. Boissel JP, Duperat B, Leizorovicz A . The phenomenon of regression to the mean and clinical investigation of the blood cholesterol lowering drugs. Eur. J. Clin. Pharmacol. 1980; 17: 227-230.
84. Jadad A R . Randomised Controlled Trials. London: B M J Books, 1998.
249

85. Heran BS, Jauca C D , Wright J M . Development of an optimal search strategy for finding trials demonstrating A C E inhibitor blood pressure lowering efficacy. 10 t h
fnternational Cochrane Colloquium, Stavanger, Norway 2002.
86. Wolf F M , Guevara JP. fmputarion of missing data in systemadc reviews: so what is the standard deviation? 9 t h International Cochrane Colloquium, Lyon, France 2001; 1: pa007.
87. Moher D , Klassen TP, Jones A L , Cook D , Jadad A R , Tugwell P, Moher M . Chapter 23: Assessing the quality of reports of randomised trials included in meta-analyses: attitudes, practice, evidence and guides, fn: Stevens A , Abrams K , Brazier J, Fitzpatrick R and Lilford R, editors. The Advanced Handbook of Methods in Evidence Based Flealthcare. London: S A G E Publications; 2001. p. 409-425.
88. Jadad A R , Moore R A , Carrol D , et al. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Contr Clin Trials 1996; 17:1-12.
89. Fleiss JL. The statistical basis of meta-analysis. Statistical Methods in Medical Research 1993; 2: 121-145.
90. Sweetman SC (Ed), Martindale: The Complete Drug Reference. London: Pharmaceutical Press. Electronic version, (34th Edition [2006]).
91. Bucher H C , Guyatt G H , Griffith L E , Walker SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol 1997; 50(6):683-691.
92. Song F, Altman D G , Glenny A - M , Deeks JJ. Vakdity of indirect comparison for estimating efficacy of competing interventions: empirical evidence from published meta-analyses. B M J 2003; 326:472-476.
93. Law M R , Wald NJ , Morris J K , Jordan R E . Value of low dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials. B M J 2003; 326:1427-1434.
94. Chrysant SG, Marbury T C , Robinson T D . Antihypertensive efficacy and safety of olmesartan medoxomil compared with amlodipine for mild-to-moderate hypertension. Journal of Ffuman Hypertension 2003; 17(6):425-32.
95. Farsang C, Kawecka-Jaszcs K , Langan J, et al. Antihypertensive effects and tolerability of candesartan cilexetil alone and in combination with amlodipine. Clin Drug Invest 2001; 21 (1): 17-23
96. Frick M H , McGibney D , Tyler H M . Amlodipine: a double-blind evaluation of the dose-response relationship in mild to moderate hypertension. Journal of Cardiovascular Pharmacology 1988; 12 Suppl 7:S76-S78.
250
97. Frick M H , McGibney D , Tyler H M . A dose-response study of amlodipine in mild to moderate hypertension. Journal of Internal Medicine 1989; 225(2):101-105.
98. Frishman W H , R A M C V , McMahon F G , Chrysant SG , Graff A , Kupiec JW et al. Comparison of amlodipine and benazepril monotherapy to amlodipine plus benazepril in patients with systemic hypertension: a randomized, double-blind, placebo-controlled, parallel-group study. The Benazepril/Amlodipine Study Group. Journal of Clinical Pharmacology 1995; 35(11):1060-1066.
99. Kuschnir E , Acuna E , Sevilla D , Vasquez J, Bendersky M , Resk J et al. Treatment of patients with essential hypertension: amlodipine 5 mg/benazepril 20 mg compared with amlodipine 5 mg, benazepril 20 mg, and placebo. Clinical Therapeutics 1996; 18(6):1213-1224.
100. Licata G , Scaglione R, Ganguzza A , Parrinello G , Costa R, Merlino G et al. Effects of amlodipine on renal haemodynamics in mild to moderate hypertensive patients. A randomized controlled study versus placebo. European Journal of Clinical Pharmacology 1993; 45(4):307-311.
101. Mehta JL , Lopez L M , Vlachakis N D , Gradman A H , Nash D T , O'ConneU M T et al. Double-blind evaluation of the dose-response relationship of amlodipine in essential hypertension. American Heart Journal 1993; 125(6):1704-1710.
102. Mroczek WJ, Burris JF, Allenby K S . A double-blind evaluation of the effect of amlodipine on ambulatory blood pressure in hypertensive patients. Journal of Cardiovascular Pharmacology 1988; 12 Suppl 7:S79-S84.
103. Mroczek WJ, Burris JF, Klein J. A double-blind evaluation of the effect of amlodipine on ambulatory blood pressure. Postgrad Med J 1991; 67 Suppl 5:S24-S27.
104. Mroczek WJ, Burris JF, Allenby K S . Effect of amlodipine on 24-hour ambulator}' blood pressure in hypertensive patients. Journal of Cardiovascular Pharmacology 1991; 17 Suppl. 1: S13-S15.
105. Burris JF, Allenby K S , Mroczek WJ. The effect of amlodipine on ambulator}' blood pressure in hypertensive patients. American Journal of Cardiology 1994; 73(3):39A-43A.
106. Pool J, Kaihlanen P, Lewis G , Ginsberg D , Oparil S, Glazer R et al. Once-daily treatment of patients with hypertension: a placebo-controlled study of amlodipine and benazepril vs amlodipine or benazepril alone. Journal of Fluman Hypertension 2001; 15:495-498.
107. Hart W, Flolwerda NJ . Barnidipine, a novel calcium antagonist for once-daily treatment of hypertension: a multicenter, double-blind, placebo-controlled, dose-ranging study. Dutch Barnidipine Multicenter Study Group. Cardiovascular Drugs & Therapy 1997; ll(5):637-643.
251
108. Chrysant SG, Chrysant C, Trus J, Hitchcock A . Monotherapy of hypertension with darodipine: a new calcium-channel blocker. Clinical Cardiology 1988; ll(7):467-472.
109. Burns JF, Weir M R , Oparil S, Weber M , Cady WJ, Stewart W H . A n assessment of diltiazem and hydrochlorothiazide in hypertension. Application of factorial trial design to a multicenter clinical trial of combination therapy. J A M A 1990; 263(11):1507-1512.
110. Chan P, L in C N , Tomlinson B, L in T H , Lee YS. Additive effects of diltiazem and lisinopril in the treatment of elderly patients with mild-to-moderate hypertension. American Journal of Hypertension 1997; 10(7 Pt l):743-749.
111. Cushman W C , Cohen J D , Jones RP, Marbury T C , Rhoades RB, Smith L K . Comparison of the fixed combination of enalapril/diltiazem E R and their monotherapies in stage 1 to 3 essential hypertension. American Journal of Flypertension 1998; 11(1 Pt l):23-30.
112. Djian J, Ferme I, Zannad F, Chaignon M , Asmar R. Effects of sustained-release diltiazem on blood pressure and serum lipids: a mulricenter, randomized, placebo-controlled study. Journal of Cardiovascular Pharmacology 1990; 16 Suppl LS38-S45.
113. Fekcetta JV , Serfer H M , Cuder N R , Comstock TJ, Huber G L , Weir M R et al. A dose-response trial of once-daily diltiazem. American Heart Journal 1992; 123(4 Pt 1):1022-1026.
114. Fiddes R, Heym H , Hilty W, Lewin A J , Codispoti J, McNally C et al. Blood pressure control with diltiazem X R , a novel extended-release formulation of diltiazem FIC1, in mature and elderly hypertensive patients. Clinical Therapeutics 1994; 16(2):209-221.
115. Herpin D , Brion N , Debregeas B. Comparison of the antihypertensive effects of sustained-release diltiazem 240 and 300 mg in patients with mild to moderate hypertension with analysis of ambulatory blood pressure profiles. Current Therapeutic Research 1990,47(2): 328-338
116. Meeves SG, Park G D . The use of confidence intervals to describe the precision of trough/peak ratios for diltiazem C D in the treatment of hypertension. Journal of Clinical Pharmacology 1994; 34(3):231-235.
117. Pool P E , Applegate W B , Woehler T, Sandall P, Cady WJ. A randomized, controlled trial comparing diltiazem, hydrochlorothiazide, and their combination in the therapy of essential hypertension. Pharmacotherapy 1993; 13(5):487-493.
118. Prisant L M . Ambulator)' blood pressure profiles in patients treated with once-daily diltiazem extended-release or indapamide alone or in combination. American Journal of Therapeutics 2000; 7(3):177-184.
119. Weir M R , Weber M A , Punzi FIA, Serfer FIM, Rosenblatt S, Cady WJ. A dose escalation trial comparing the combination of diltiazem SR and hydrochlorothiazide
252

with the monotherapies in patients with essential hypertension. Journal of Human Hypertension 1992; 6 (2) :133-138.
120. Whelton A , Ef f J, Magner DJ . Sustained antihypertensive activity of diltiazem SR: double-blind, placebo-controlled study with 24-hour ambulatory blood pressure monitoring. Journal of Clinical Pharmacology 1992; 32(9):808-815.
121. Black HR. Elliott WJ, Weber MA, Frishman W H , Strom JA, Liebson PR et al. One-year study of felodipine or placebo for stage 1 isolated systolic hypertension. Hypertension 2001; 38:1118-1123.
122. Felodipine, a new calcium antagonist, as monotherapy in mild or moderate hypertension. Cooperative study group. Drugs 1987; 34 Suppl 3:139-148.
123. Hamilton D V , Barnes PC, Bowles R M , Rajaratnam D V , Comerford M B , Ginks et al. Monotherapy with felodipine, a new calcium antagonist, in mild and moderate hypertension. Journal of Cardiovascular Pharmacology 1987; 10 Suppl 10:S111-S113.
124. Fagan T O Blood pressure reduction and tolerability of felodipine E R in older and younger hypertensive patients. The Felodipine E R in the Elderly versus Young Working Group. Journal of the American Geriatrics Society .1997; 45(6):712-717.
125. Fetter M , Bastian M , Mann G , Haasis R, Diener H C , Haux R. Antihypertensive therapy does not alter cerebral bloodflow velocities under resting conditions. [German]. Akt . Neurol. 1994; 21:177-182.
126. Gradman A H , Order N R , Davis PJ, Robbins JA , Weiss RJ, Wood B C . Combined enalapril and felodipine extended release (ER) for systemic hypertension. Enalapril-Felodipine E R Factorial Study Group. American Journal of Cardiology 1997; 79(4):431-435.
127. Kiesewetter FI, Birk A , Jung F, Radtke H . Effects of felodipine on the arterial blood pressure and fluidity of blood in patients with arterial hypertension W H O stage I. Clinical Hemorheology 1994; 14(3):355-367.
128. Liedholm H , Melander A . A placebo-controlled dose-response study of felodipine extended release in hypertensive patients. Journal of Cardiovascular Pharmacology 1989; 14(1):109-113.
129. Scholze J, Bauer B , Massaro J. Antihypertensive profiles with ascending dose combinations of ramipril and felodipine ER. Clinical & Experimental Hypertension (New York) 1999; 21(8):1447-1462.
130. van Ree JW, van der Pol G A . Low dosages of felodipine E R once daily as monotherapy in elderly hypertensive patients: effect on ambulator}' blood pressure and quality of life. Journal of Fluman Hypertension 1996; 10(9):613-618.
253
131. Weber M A , Goldberg A I , Faison E P , Lipschutz K , Shapiro D A , Nelson E B et al. Extended-release felodipine in patients with mild to moderate hypertension. Felodipine E R Dose-Response Study Group. Clinical Pharmacology & Therapeutics 1994; 55(3):346-352.
132. Wester A . Felodipine monotherapy vs. placebo: a dose-response study in hypertension. Binational M C Study Group in U . K . and Holland. Journal of Cardiovascular Pharmacology 1990; 15 Suppl 4:S59.
133. Wester A , Lorimer A R , Westberg B. Felodipine extended release in mild to moderate hypertension. Current Medical Research & Opinion 1991; 12(5):275-281
134. Arosio E , Pancera P, Priante F, Ribul M , De Marchi S, Lechi A . Effects of sustained-release isradipine on blood pressure and peripheral hemodynamics in hypertensive padents. Clinical Therapeutics 1993; 15(4):705-713.
135. Burger K J , Dehner R. Zirkadiane antihypertensive wirkung von isradipin retard bei patienten mit essentieller hypertonic im vergleich zu plazebo. Orcadian antihypertensive effects of isradipine retard in patients, with essential hypertension in comparison to placebo [German]. Arzneimittel-Forschung 1993; 43(9):958-962.
136. Chrysant SG, Cohen M . Sustained blood pressure control with controlled-release isradipine. American Journal of Hypertension 1995; 8(l):87-89.
137. Chrysant SG, Cohen M . Sustained blood pressure control with controlled-release isradipine (isradipine-CR). Journal of Clinical Pharmacology 1995; 35(3):239-243.
138. Holmes D G . Isradipine: a slow-release formulation given once daily controls blood pressure for 24 h. American Journal of Hypertension 1993; 6(3 Pt 2):74S-76S.
139. Multicenter evaluation of the safety and efficacy of isradipine in hypertension. The Italian-Belgian Isradipine Study Group. American Journal of Medicine 1989; 86(4A):94-97.
140. Kirch W, Burger K J , Weidinger G , Welzel D . Efficacy and tolerability of the new calcium antagonist isradipine in essential hypertension. Journal of Cardiovascular Pharmacology 1990; 15 Suppl 1:S55-S59.
141. Man in't Veld, V , Holmes D G , Lasance A , de Zwart P. Isradipine twice daily lowers blood pressure over 24 FI. American Journal of Ffypertension 1991; 4(2 Pt 2): 131S-134S.
142. O'Grady J, Kritz H , Schmid P, Pirich C, Sinzinger FI. Effect of isradipine on in-vivo platelet function. Thrombosis Research 1997; 86(5):363-371.
143. Pittrow D B , Andsperger A , Welzel D , Wambach G , Schardt W, Weidinger G . Evaluation of the efficacy and tolerability of a low-dose combination of isradipine and
254
spirapril in the fkst-line treatment of mild to moderate essential hypertension. Cardiovascular Drugs & Therapy 1997; 11(5):619-627.
144. Prisant L M , Carr A A . Assessment of electrocardiographic ischemia in hypertensive patients treated with isradipine or placebo. Journal of Clinical Pharmacology 1991; 31(3):233-237.
145. Youssef S, Osman L , Sabbour MS. Serum lipoprotein profile under different antihypertensive therapy. International Journal of Clinical Pharmacology Research 1992; 12(3):109-116.
146. Youssef S, Osman L , Sabbour MS. Serum lipoprotein profile under different antihypertensive therapy. Cardiovascular Risk Factors 1993; 3(2): 107-111.
147. Rizzini P, Castello C, Salvi S, Recchia G . Efficacy and safety of lacidipine, a new long-lasting calcium antagonist, in elderly hypertensive patients. Journal of Cardiovascular Pharmacology 1991; 17 Suppl 4:S38-S43.
148. Barbagallo M , Barbagallo SG. Efficacy and tolerability of lercanidipine in monotherapy in elderly patients with isolated systolic hypertension. Aging (Milano) 2000; 12(5):375-379.
149. Circo A . Active dose findings for lercanidipine in a double-blind, placebo-controlled design in patients with mild to moderate hypertension. Journal of Cardiovascular Pharmacology 1997; 29(Suppl. 2):S21-S25.
150. Ninci M A , Magliocca R, Malliani A . Efficacy and tolerability of lercanidipine in elderly patients with mild to moderate hypertension in a placebo-controlled, double-blind study. Journal of Cardiovascular Pharmacology 29(Suppl. 2):S40-S44.
151. Omboni S, Zanchetti A . Antihypertensive efficacy of lercanidipine at 2.5, 5 and 10 mg in mild to moderate essential hypertensives assessed by clinic and ambulatory blood pressure measurements. Multicenter Study Investigators. Journal of Hypertension 1998; 16(12 Pt 1):1831-1838.
152. Rimoldi E , Lumina C, Giunta L , Moscatelli P, Gatto E . Evaluation of the efficacy and tolerability of tow different formulations of lercanidipine versus placebo after once-dialy administration in mild to moderate hypertensive patients. Current Therapeutic Research 1993; 54(2):248-253.
153. Rimoldi E , Lumina C, Sega R, Libretti A . Efficacy and tolerability of lercanidipine once a day versus placebo in mild to moderate arterial hypertension. Acta Therapeutica 1994; 20:23-31.
154. Meilink-Hoedemaker LJ , Pool J, Muste-Heijns M M . A double-bund placebo-controlled cross-over study with lidoflazine (Clinium) in post-infarction patients. Acta Medica Scandmavica 1976; 199(1 -2):17-23.
255
155. Fogari R, Zoppi A , Lusardi P, Mugellini A . Efficacy and tolerability of manidipine hydrochloride in the long-term treatment of mild-moderate hypertension. Manidipine Efficacy in Long-Term Treatment Group. Blood Pressure 1996; Supplement. 5:24-28.
156. Fogari R, Zoppi A , Mugellini A , Preti P, Corradi L , Lusardi P. Effect of low-dose manidipine on ambulatory blood pressure in very elderly hypertensives. Cardiovascular Drugs & Therapy 1999; 13(3):243-248.
157. Bernink PJ, Prager G , Schelling A , Kobrin I. Antihypertensive properties of the novel calcium antagonist rnibefradil (Ro 40-5967): a new generation of calcium antagonists? Mibefradil International Study Group. Hypertension 1996; 27(3 Pt l):426-432.
158. Bursztyn M , Kadr H , Tilvis R, Martina B , Oigman W, Talberg J et al. Mibefradil, a novel calcium antagonist, in elderly patients with hypertension: favorable hemodynamics and pharmacokinetics. American Heart Journal 1997; 134(2 Pt 1):238-247.
159. Oparil S, Kobrin I, Abernethy D R , Levme BS, Reif M C , Shepherd A M . Dose-response characteristics of mibefradil, a novel calcium antagonist, in the treatment of essential hypertension, [erratum appears in A m J Hypertens 1997 Sep;10(9 Pt 1): 1081]. American Journal of Hypertension t997; f 0(7 Pt l):735-742.
160. Asplund J. Nicardipine hydrochloride in essential hypertension—a controlled study. British Journal of Clinical Pharmacology 1985; 20 Suppl L120S-124S.
161. Bellet M , Pagny JY , Chatellier G , Corvol P, Menard J. Evaluation of slow release nicardipine in essential hypertension by casual and ambulatory blood pressure measurements. Effects of acute versus chronic administration. Journal of Hypertension 1987; 5(5):599-604.
f 62. Bellet B , Pagny JY , Chatellier G , Frere R, Menard D , Corvol P et al. Evaluation en double insu de la nicardipine a liberation differee par differentes methods de measures tensionnelles. Valeur predictive de la response aigue a la nicardipine intraveineuse. [Double-blind evaluation of slow-release nicardipine using different methods of blood pressure measurement. Predictive value of the acute response to intravenous nicardipine]. [French]. Archives des Maladies du Coeur et des Vaisseaux 1987; 80(6):851-855.
163. De Cesaris R, Ranieri G , Andriani A , Filitti V , Bonfantino M V , Lamontanara G et al. Azione antiipertensiva della nicardipina retard nelle 24 ore e suo comportamento nello stress. [Antihypertensive action of nicardipine retard in 24 hours and its effect on stress], [Italian]. Minerva Medica 1993; 84(10):533-539.
164. Fagan T C , Tyler E D , Reitman M A , Kenley S, Weber M A . Sustained-release nicardipine in mild-to-moderate hypertension. Chest 1993; 104(2):427-433.
165. Marcadet D M , Blanc AS , Lopez A A , Preziosi JP, Guignard M M , Baggio S et al. Efficacite et tolerance de la nicardipine L P 50 mg dans l'hypertension arterielle du
256

sportif. [Efficacy and tolerance of L A 50 mg nicardipine in hypertensive athletes]. [French]. Archives des Maladies du Coeur et des Vaisseaux 1991; 84(11):1569-1574.
166. Mazzola C, Borgnino C, Colombo D , Lissoni F, Serra G , Turri D R et al. Antihypertensive and hemodynamic effects of slow-release nicardipine. International Journal of Clinical Pharmacology, Therapy, & Toxicology 1988; 26(10):503-508.
167. Scuteri A , Cacciafest M , Bellucci CR, De Propris A M , D i Bernardo M G , Piccirillo G . Acute effects of long-acting nicardipine and enalapril on the quality of life in elderly patients. Current Therapeutic Research 1992; 51(5): 773-778.
168. Soro S, Cocca A , Pasanisi F, Tommaselli A , de Simone G , Costantino G et al. The effects of nicardipine on sodium and calcium metabolism in hypertensive patients: a chronic study. Journal of Clinical Pharmacology 1990; 30(2):133-137.
169. de Simone G , Costantino G , Soro S, D i Lorenzo L , Moccia D , Buonissimo S et al. Effects of nicardipine on left ventricular hemodynamic patterns in systemic hypertension. American Journal of Flypertension 1989; 2(3 Pt 1):139-145.
170. Carr A A , Bottini PB , Feig P, Prisant L M , Mulligan S, Devane J G et al. Effectiveness of once-daily monotherapy with a new nifedipine sustained release calcium antagonist. American Journal of Cardiology 1992; 69(13):28E-32E.
171. Carr A A , Bottini PB , Feig P U , Karlos M L , Schwarz L A , Mulligan S et al. Once-daily monotherapy of hypertension with nifedipine sustained release (20 mg to 100 mg). Drug Invest. 1992; 4(2): 184-191.
172. de Simone G , Ferrara L A , di Lorenzo L , Lauria R, Fasano M . Effects of slow-release nifedipine on left ventricular mass and systolic function in mild or moderate hypertension. Current Therapeutic Research 1984; 36(3): 537-544.
173. de Simone G , Ferrara L A , Fasano M L , D i Lorenzo L , Lauria R. Slow-release nifedipine versus placebo in the treatment of arterial hypertension. A double blind ergometric evaluation of cardiac workload. Japanese Heart Journal 1985; 26(2):219-225.
174. Eggertsen R, Hansson L . Effects of treatment with nifedipine and metoprolol in essential hypertension. Eur J Clin Pharmacol 1982; 21:389-390.
175. Fadayomi M O , Akinroye K K , Ajao R O , Awosika L A . Monotherapy with nifedipine for essential hypertension in adult blacks. Journal of Cardiovascular Pharmacology 1986; 8(3):466-469.
176. Feig P U , Gibson L , Mac Carthy E P , Pettis PP, Schwartz L . The efficacy and safety of once-daily nifedipine coat-core in the treatment of mild-to-moderate hypertension. Adalat C C Cooperative Study Group, [erratum appears in Clin Ther 1994 Jan-Feb;16(l):125]. Clinical Therapeutics 1993; 15(6):963-975.
257
177. Ferrera L A , de Simone G , Mancini M , Fasano M L , Pasanisi F, Vallone G . Changes in left ventricular mass during a double-blind study with chlorthalidone and slow-release nifedipine. Eur J Clin Pharmacol 1984; 27:525-528.
178. Harder S, Rietbrock S, Thurmann P. Antihypertensive efficacy of a slow release nifedipine tablet formulation given once daily in patients with mild to moderate hypertension. A placebo-controlled, double-blind parallel-group trial. Arzneimittel-Forschung 1994; 44(2):133-136.
179. Jueng C, Flalperin A K , Flashimoto F, Callender K . Nifedipine GITS and hydrochlorothiazide in essential hypertension. Journal of Clinical Hypertension 1987; 3(4):695-703.
180. Serradimigni A , Perchicot E , Griener L , Kerihuel JC, Benichou M . [Antihypertensive effect of a new form of nifedipine compared to a beta-blocker during chronic administration]. [French]. Archives des Maladies du Coeur et des Vaisseaux 1985; 78 Spec No:73-81.
181. Toal C B . Efficacy of a low dose nifedipine GITS (20 mg) in patients with mild to moderate hypertension. Canadian Journal of Cardiology 1997; 13(10):921-927.
182. Zachariah P K , Schwartz G L , Sheps SG, Schirger A , Carlson C A , Moore A G . Antihypertensive effects of a new sustained-release formulation of nifedipine. Journal of Clinical Pharmacology 1990; 30(11):1012-1019.
183. Zanchetti A for the Italian GITS Study Group, Bianchi L , Amigoni S, Omboni S, Villani A , Ravogli A . Antihypertensive effects of nifedipine gastrointestinal therapeutic system on clinic and ambulatory blood pressure in essential hypertensives. Journal of Hypertension 1993; 11 (Suppl 5):S334-S335.
184. Zanchetti A . Trough and peak effects of a single daily dose of nifedipine gastrointestinal therapeutic system (GITS) as assessed by ambulatory blood pressure monitoring. Italian Nifedipine GITS Study Group. Journal of Hypertension -Supplement 1994; 12(5):S23-S27.
185. Zanchetti A . The 24-hour efficacy of a new once-daily formulation of nifedipine. Italian Nifedipine GITS Study Group. Drugs 1994; 48 Suppl 1:23-30.
186. Zanchetti A for the Italian Nifedipine GITS Study Group; Bianchi L , Bozza M , Omboni S, Villani A , Ravogli. Antihypertensive effects of nifedipine GITS on clinic and ambulatory blood pressures in essential hypertensives. High Blood Press. 1994; 3: 45-56.
187. Hoffmann A , Kraul Fl , Burkardt I. Nilvadipine in hypertension—experience in ambulatory treatment. International Journal of Clinical Pharmacology &c Therapeutics 1997; 35(5):195-203.
258
188. Weir M R , Vkchkis N D , DeQuattro V , Douglas J, Svetkey L P , Singh S et al. Evaluation of the clinical pharmacology of nilvadipine in patients with mild to moderate essential hypertension. Journal of Clinical Pharmacology 1990; 30(5):425-437.
189. Opie L H , MuUer F O , Myburgh D P , Rosendorff C, Sareli P, Seedat Y K et al. for the Ambulatory Nisoldipine Coat-Core Hypertension Outpatient Response ( A N C H O R ) Investigators. Efficacy and tolerability of nisoldipine coat-core formulation in the treatment of essential hypertension: The South African Multicenter A N C H O R Study, [erratum appears in A m J Hypertens 1997 Jun;10(6):696]. American Journal of Hypertension 1997; 10(3):250-260.
190. Asmar R, Benetos A , Brahimi M , Chaouche K , Safar M . Arterial and antihypertensive effects of nitrendipine: a double-blind comparison versus placebo. Journal of Cardiovascular Pharmacology 1992; 20(6):858-863.
191. Asmar R, Benetos A , Ghodsi N , Meilhac B , Safar M . Hemodynamique arterielle regionale et circulation carotidienne dans l'hypertension arterielle essentielle. Application a la nitrendipine chez le sujet age de plus de 40 ans. [Regional arterial hemodynamics and carotid circulation in essential arterial hypertension. Effect of nitrendipine in patients over 40 years of age]. [French]. Presse Medicare 1993; 22(35):1770-1775.
192. Ferrara L A , Fasano M L , de Simone G , Soro S, Gagliardi R. Antihypertensive and cardiovascular effects of nitrendipine: a controlled study vs. placebo. Clinical Pharmacology & Therapeutics 1985; 38(4):434-438.
193. Fodor J G , Chockakngam A , Cifkova R, Strong H A , Cobby J, Mukherjee J. Efficacy of once daily nitrendipine in mild hypertension: comparison with placebo. Canadian Journal of Cardiology 1991; 7(5):223-228.
194. Gerritsen T A , Bak A A , Stolk RP, Jonker JJ, Grobbee D E . Effects of nitrendipine and enalapril on left ventricular mass in patients with non-insulin-dependent diabetes mellitus and hypertension. Journal of Hypertension 1998; 16(5):689-696.
195. Gregorio F, Din i F L , Ambrosi F, Cristallini S, Pedetti M , Filipponi P. Efficacia anti-ipertensiva ed effetti sul metabolismo glucidico della nitrendipina: studio clinico controllato versus placebo. [Antihypertensive efficacy of nitrendipine and its effects on carbohydrate metabolism. A controlled clinical study versus placebo]. [Italian]. Minerva Cardioangiologica 1991; 39(4):141-148.
196. Kuschnir E , Castro R, Bendersky M , Sgammini H , Guzman L , Sgarlatta H et al. Hemodynamic effects of nitrendipine on systolic ventricular function, diastolic ventricular function, and peripheral circulation in essential hypertension. Journal of Cardiovascular Pharmacology 1988; 12 Suppl 4:S36-S44.
259
197. Lederle R M , Klaus D , Wilk S, Knaup G . Low-dose nitrendipine in mild hypertension: a double-blind, placebo-controlled, comparative study. Journal of Cardiovascular Pharmacology 1991; 18 Suppl LS48-S50.
198. Klaus D , Wilk S, Knaup G . Nitrendipin bei milder hypertonic. Eine doppelblinde, placebokontrollierte vergleichsstudie. [Nitrendipine in the treatment of mild hypertension. A double blind placebo-contolled comparative study] [German]. Zeitschrift fur Allgemeinmedizin 66(35-36): 1038-1042.
199. Maclean.D, Mitchell E T , Lewis R, Irvine N , McLay JS, McEwen J et al. Comparison of once daily atenolol, nitrendipine and their combination in mild to moderate essential hypertension. British Journal of Clinical Pharmacology 1990; 29(4):455-463.
200. Paolisso G , Aceto E , Cennamo G , D'Amore A , Varricchio M . Metabolic effects of nitrendipine. Clinical Therapeutics 1991; 13(6):695-698.
201. Roca-Cusachs A , Torres F, Floras M , Rios J, Calvo G , Delgadillo J, et al. Nitrendipine and enalapril combination therapy in mild to moderate hypertension: assessment of dose-response relationship by a clinical trial of factorial design. Journal of Cardiovascular Pharmacology 2001; 38:840-849.
202. Rosenthal J, Flittel N , Stumpe K O . Pranidipine, a novel calcium antagonist, once daily, for the treatment of hypertension: a multicenter, double-blind, placebo-controlled dose-finding study. Cardiovascular Drugs & Therapy 1996; 10(l):59-66.
203. Blanchett D G , Corder C N , Kezdi P, Margolis R, Jain A , Ryan JR et al. Antihypertensive effect of tiapamil from ambulatory and clinic methods. International Journal of Clinical Pharmacology, Therapy, & Toxicology 1991; 29(2):59-63.
204. Carr A A , Bottini PB, Pnsant L M , Fisher L D , Devane J G , O'Brien D E et al. Once-daily verapamil in the treatment of mild-to-moderate hypertension: a double-blind placebo-controlled dose-ranging study. Journal of Clinical Pharmacology 1991; 31(2):144-150:
205. DeQuattro V , Lee D . Fixed-dose combination therapy with trandolapril and verapamil SR is effective in primary hypertension. Trandolapril Study Group. American Journal of Flypertension 1997; 10(7 Pt 2):138S-145S.
206. DeQuattro V , Lee D , Messerli F. for the Trandolapril Study Group. Efficacy of combination therapy with trandolapril and verapamil sr in primary hypertension: a 4 x 4 trial design. Clinical & Experimental Hypertension (New York) 1997; 19(3):373-387.
207. Levine J H , Applegate W B , and the Trandolapril/Verapamil Study Group. Trandolapril and Verapamil slow release in the treatment of hypertension: a dose-response assessment with the use of a multifactorial trial design. Current Therapeutic Research 1997; 58(6):361-374.
260
208. Levine J H , Ferdinand K C , Cargo P, Laine H , Lefkowitz M . Additive effects of verapamil and enalapril in the treatment of mild to moderate hypertension. American Journal of Hypertension 1995; 8(5 Pt l):494-499.
209. McMahon F G , Reder RF. The relationship of dose to the antihypertensive response of verapamil-sustained release in patients with mild to moderate essential hypertension. The Verapamil-SR Study Group. Journal of Clinical Pharmacology 1989; 29(11):1003-1007.
210. Messerli F, Frishman W H , Elliott WJ. Effects of verapamil and trandolapril in the treatment of hypertension. Trandolapril Study Group. American Journal of Flypertension 1998; 11(3 Pt l):322-327.
211. Neutel J M , Alderman M , Anders RJ, Weber M A . Novel delivery system for verapamil designed to achieve maximal blood pressure control during the early morning. American Heart Journal 1996; 132(6):1202-1206.
212. Neutel J M , Smith D G H , Weber M A . The use of chronotherapeutics to achieve maximal blood pressure reduction during the early morning blood pressure surge. C V R & R 1999:575-581.
213. Scholze J, Zilles P, Compagnone D . Verapamil SR and trandolapril combination therapy in hypertension—a clinical trial of factorial design. German Hypertension Study Group. British Journal of Clinical Pharmacology 1998; 45(5):491-495.
214. Smith D H , Neutel J M , Weber M A . A new chronotherapeutic oral drug absorption system for verapamil optimizes blood pressure control in the morning. American Journal of Hypertension 200f; 14(1):14-19.
215. Effects of verapamil SR, trandolapril, and their fixed combination on 24-h blood pressure: the Veratran Study, [erratum appears in A m J Hypertens 1998 Aug; l l (8 Pt 1):1039]. American Journal of Ffypertension 1997; 10(5 Pt l):492-499.
216. von Manteuffel G E , Rakette S, Wol l E M , Reinfrank J, Schiemann J. [Effectiveness and tolerance of combined verapamil retard and hydrochlorothiazide. Results of a double-blind, randomised study]. [German]. Fortschritte der Medizin 1995; 113(26):374-378.
217. White W B , Anders RJ, Maclntyre J M , Black HR, Ska D A . Nocturnal dosing of a novel delivery system of verapamil for systemic hypertension. Verapamil Study Group. American Journal of Cardiology 1995; 76(5):375-380.
218. White W B , Sica D A , Calhoun D , Mansoor G A , Anders RJ. Preventing increases in early-morning blood pressure, heart rate, and the rate-pressure product with controllec onset extended release verapamil at bedtime versus enalapril, losartan, and placebo on arising. A m Heart J 2002; 144:657-665.
261
219. Bakris G , Sica D , Ram V , Fagan T, Vaitkus PT, Anders RJ. A comparative trial of controlled-onset, extended-release verapamil, enalapril, and losartan on blood pressure and heart rate changes. AJFI 2002; 15:53-57.
220. Glasser SP, Neutel J M , Gana TJ, Albert K S . Efficacy and safety of a once daily graded-release diltiazem formulation in essential hypertension. A J H 2003; 16:51-58.
221. Abadie E , Villette J M , Gauville C, Tabuteau F, Fiet J, Passa P. [Effects of nifedipine on carbohydrate metabolism in the non-insulin dependent diabetic]. [French]. Diabete et Metabolisme 1985; 11 (3):141-146.
222. Ahmed J H , Elliott H L , Flosie J, Farish E , Reid JL. Effects of nicardipine on the metabolic responses to food and exercise. Journal of Fluman Hypertension 1992; 6(2):139-144.
223. Allikmets K , Parik T, Teesalu R. Antihypertensive and renal effects of isradipine in essential hypertension: focus on renin system activity. Angiology 1997; 48(ll):977-983.
224. Andersson O K , Persson B , Hedner T, Aurell M , Wysocki M . Blood pressure control and haemodynamic adaptation with the dihydropyridine calcium antagonist isradipine: a controlled study in middle-aged hypertensive men. Journal of Hypertension 1989; 7(6):465-469.
225. Andersson O K , Persson B , Widgren R, Wysocki M . Central hemodynamics an dbrachial artery compliance during therapy with isradipine, a new calcium antagonist. Journal of Cardiovascular Pharmacology 1990; 15(Suppl. 1):S87-S89.
226. Andren L , Flansson L , Oro L , Ryman T. Experience with nitrendipine—a new calcium antagonist—in hypertension. Journal of Cardiovascular Pharmacology 1982; 4 Suppl 3:S387-S391.
227. Arita M , Hashizume T, Tanigawa K , Yamamoto FI, Nishio I. A new Ca-antagonist, azelnidipine, reduced blood pressure during exercise without augmentation of sympathetic nervous system in essential hypertension: a randomized, double-blind, placebo-controlled trial. Journal of Cardiovascular Pharmacology 1999; 33(2):186-192.
228. Arzi l l i F, Gandolfi E , De l Prato C, Innocenti P, Ponzanelli F, Caiazza et al. Antihypertensive effect of once daily sustained release isradipine: a placebo controlled cross-over study. European Journal of Clinical Pharmacology 1993; 44(l):23-25.
229. Bainbridge A D , Macfadyen RJ, Stark S, Lees K R , Reid JL. The antihypertensive efficacy and tolerability of a low dose combination of ramipril and felodipine E R in mild to moderate essential hypertension. Br. J Clin Pharmac 1993; 36:323-330.
230. Baylac-Domengetroy F, Baylac-Domengetroy J, Chaix A F , Elbaz-Rostykus C, Barraine R. [Relations between antihypertensive and vascular effects oj nitrendipine]. [French]. Archives des Maladies du Coeur et des Vaisseaux 1990; 83(8):1295-1299.
262

231. Bellet M , Loria Y , Lallemand A . First-step treatment of mild to moderate uncomplicated essential hypertension by a new calcium antagonist: nicardipine. Journal of Cardiovascular Pharmacology 1985; 7(6): 1149-1153.
232. Bossini A , D i Veroli C, Cavallotti G , Cagli V . Felodipine E R formulation in the treatment of mild hypertension: efficacy and tolerability vs placebo. British Journal of
• Clinical Pharmacology 1990; 30(4):567-571. .
233. The British Isradipine Flypertension Group. Evaluation of the safety and efficacy of isradipine in elderly patients with essential hypertension. American Journal of Medicine 1989; 86(4A):110-114.
234. Campbell L M , Cowen K J , Cranfield FR, Goves JR, Jones D F , Lees C T et al. Felodipine-ER once daily as monotherapy in hypertension. Journal of Cardiovascular Pharmacology 1990; 15(4):569-573.
235. Capewell S, Collier A , Matthews D , Flajducka C, Collier R, Clarke B F et al. A trial of the calcium antagonist felodipine in hypertensive type 2 diabetic patients. Diabetic Medicine 1989; 6(9):809-812.
236. Carr A A , Prisant L M . The new calcium antagonist isradipine. Effect on blood pressure and the left ventricle in black hypertensive patients. American Journal of Hypertension 1990; 3(1):8-15.
237. Chalmers J, Wing L , Taylor S. Analysis of time trends, individual subject responses and background variation in crossover factorial studies with antihypertensive drugs. Journal of Hypertension - Supplement 1990; 8(4):S27-S35.
238. Clement D L , De Pue N Y , Packet L . Effect of calcium antagonists on ambulatory blood pressure and its variations. Journal of Cardiovascular Pharmacology 1987; 10 Suppl 10:S117-S119.
239. Cleroux J, Yardley C, Marshall A , Coulombe D , Lacourciere Y . Antihypertensive and hemodynamic effects of calcium channel blockade with isradipine after acute exercise. American Journal of Flypertension 1992; 5(2):84-87.
240. Cleroux J, Beaulieu M , Kouame N , Lacourciere Y . Comparative effects of quinapril, atenolol, and verapamil on blood pressure and forearm hemodynamics during handgrip exercise. American Journal of Hypertension 1994; 7(6):566-570.
241. Cox JP, O'Boyle C A , Mee F, Kelly J, Atkins N , Coakley D et al. The antihypertensive efficacy of verapamil in the elderly evaluated by ambulatory blood pressure measurement. Journal of Fluman Hypertension 1988; 2(l):41-47.
242. Cox JP, Ryan J, O'Brien E , O'Malley K . The effect of slow-release nicardipine on ambulator)' and clinic blood pressure in mild hypertension. British Journal of Clinical Pharmacology 1989; 28(l):79-82.
263

243. Crozier I G , Ikram H , Nicholls M G , Low CJ. Twenty-four hour profile of the hypotensive action of felodipine in essential hypertension. Cardiovascular Drugs & Therapy 1990; 4(2):439-442.
244. de Bruijn B , Cocco G , Tyler H M . Multicenter placebo-controlled comparison of amlodipine and atenolol in mild to moderate hypertension. Journal of Cardiovascular Pharmacology 1988; 12 Suppl 7:S107-S109.
245. Diemont W L , Stegeman CJ, Beekman J , Siegers A M , Hagels G , de Bruijn J H . Low-dose isradipine once daily effectively controls 24-h blood pressure in essential hypertension. American Journal of Hypertension 1991; 4(2 Pt 2):163S-167S.
246. Dittrich H C , Adler J, Ong J, Reitman M , Weber M , Ziegler M . Effects of sustained-release nicardipine on regression of left ventricular hypertrophy in systemic hypertension. American Journal of Cardiology 1992; 69(19):1559-1564.
247. Draaijer P, K o o l MJ, Van Bortel L M , Nieman F, de Leeuw PW, van Hooff JP et al. Vascular compliance in sodium-sensitive and sodium-resistant borderline hypertensive patients. Kidney International 1995; 47(1):169-176.
248. Dupont A G , Coupez J M , Jensen P, Coupez-Lopinot R, Schoors D F , Plermanns et al. Twenty-four hour ambulator)' blood pressure profile of a new slow-release formulation of diltiazem in mild to moderate hypertension. Cardiovascular Drugs & Therapy 1991; 5(4):701-707.
249. Duprez D , De Backer T, De Pue N , Ffermans L , De Buyzere M , Clement D L . Effects of isradipine on peripheral hemodynamic reflex responses in mild-to-moderate essential hypertension. American Journal of Hypertension 1991; 4(2 Pt 2):194S-196S.
250. Durel L A , Hayashi PJ, Weidler DJ , Schneiderman N . Effectiveness of antihypertensive medications in office and ambulatory settings: a placebo-controlled comparison of atenolol, metoprolol, chlorthalidone, verapamil, and an atenolol-chlorthalidone combination. Journal of Clinical Pharmacology 1992; 32(6):564-570.
251. Faguer de Moustier B , Paoli V , Tchobroutsky G . Metabolic controlled trial of nicardipine in type 2 diabetic patients with slight hypertension. Current Therapuetic Research 1989; 45(4): 690-704.
252. Faguer de Moustier B, Paoli V . The influence of nicardipine in type 2 diabetic patients with slight hypertension. Journal of Cardiovascular Pharmacology 1990; 16 Suppl 2:S26-S33.
253. Ferreira-Filho SR, Dorneles H . Determination of systemic haemodynamic alterations induced by slow-release nifedipine in elderly hypertensive patients using a non-invasive method: double-blind cross-sectional random study. Journal of Human Hypertension 1995;9(7):535-540.
264

254. Fogari R, Malacco E , Tettamanti F, Gnemmi A E , Milani M . Evening vs morning isradipine sustained release in essential hypertension: a double-blind study with 24 h ambulatory monitoring. British Journal of Clinical Pharmacology 1993; 35(l):51-54.
255. Forette F, Bellet M , Henry JF, Hervy M P , Poyard-Salmeron C, Bouchacourt et al. [Treatment of arterial hypertension in the aged with a calcium antagonist: nicardipine]. [French]. Archives des Maladies du Coeur et des Vaisseaux 1984; 77(11):1242-1246.
256. Forette F, Bellet M , Henry JF, Hervy M P , Poyard-Salmeron C, Bouchacourt et al. Effect of nicardipine in elderly hypertensive patients. British Journal of Clinical Pharmacology 1985; 20 Suppl 1:125S-129S.
257. Frishman WFI, Brobyn R, Brown R D , Johnson B F , Reeves R L , Wombolt D G . A randomized placebo-controlled comparison of amlodipine and atenolol in mild to moderate systemic hypertension. Journal of Cardiovascular Pharmacology 1988; 12 Suppl 7:S103-S106.
258. Frishman WFI, Brobyn R, Brown R D , Johnson B F , Reeves R L , Wombolt D G . Amlodipine versus atenolol in essential hypertension. American Journal of Cardiology 1994; 73(3):50A-54A.
259. Johnson B F , Frishman W H , Brobyn R, Brown R D , Reeves R L , Wombolt D G . A randomized, placebo-controlled, double-blind comparison of amlodipine and atenolol in patients with essential hypertension. American Journal of Hypertension 1992; 5(10):727-732.
260. Johnson B F , Frishman W H , Brobyn R, Brown R D , Reeves R L , Wombolt D G . A randomized, placebo-controlled, double-blind comparison of amlodipine and atenolol in patients with essential hypertension. Cardiovascular Reviews & Reports 1995; 16(9):21-27+31.
261. Gavras I, Mulinari R, Gavras H , Higgins JT, Reeves R L , Zawada E T et al. Antihypertensive effectiveness of the nifedipine gastrointestinal therapeutic system. American Journal of Medicine 1987; 83(6B):20-23.
262. Gebara O C , Jimenez A H , McKenna C, Mitdeman M A , X u P, Lipinska I et al. Stress-induced hemodynamic and hemostatic changes in patients with systemic hypertension: effect of verapamil. Clinical Cardiology 1996; 19(3):205-211.
263. Grimm RFI Jr, Black H , Rowen R, Lewin A , Shi H , Ghadanfar M et al. Amlodipine versus chlorthalidone versus placebo in the treatment of stage I isolated systolic hypertension. A m J Hypertension 2002; 15(1 Pt l):31-6.
264. Hamilton BP. Treatment of essential hypertension with P N 200-110 (isradipine). American Journal of Cardiology 1987; 59(3):141B-145B.
265
265. Harrington K , Fitzgerald P, O'Donnell P, H i l l K W , O'Brien E , O'Malley K . Short and long term treatment of essential hypertension with felodipine as monotherapy. Drugs 1987; 34(Suppl. 3 ) :178 -185 .
266. Hedback B, Hermann LS. Antihypertensive effect of verapamil in patients with newly discovered mild to moderate essential hypertension. Acta Medica Scandinavica -Supplementum 1984; 681:129-135.
267. Herrera CR, Lewin A , Fiddes R, Friedman J, Linn W, Baker T et al. Long-acting diltiazem C D is safe and effective in a hypertensive Mexican-American population. Pharmacotherapy 1997; 17(6):1254-1259.
268. Honorato J, Azanza J, Guindo N , Suarez JR. Double-blind placebo-controlled study of the antihypertensive efficacy of nitrendipine in patients submitted to ambulatory blood pressure monitoring. Current Therapeutic Research, Clinical & Experimental 1989;46(5):932-939.
269. Hosie J, Mulder A W . Antihypertensive effects of felodipine once daily given as monotherapy to elderly patients: a placebo comparison. Binational M C Study Group (U.K. and Holland). Journal of Cardiovascular Pharmacology 1990; 15 Suppl 4:S90.
270. Hosie J, Mulder A W , Westberg B. Felodipine once daily in elderly hypertensives. Binational M C Study Group (United Kingdom and Netherlands). Journal of Human Hypertension 1991; 5 ( l ) :49 -53 .
271. Jeffrey RF, Capewell S, Brown J, Collier A , Flajducka C, Lee M R . Effects of felodipine on atrial natriuretic peptide in hypertensive non-insulin dependent diabetes mellitus. British Journal of Clinical Pharmacology 1990; 30(3):481-484.
272. Kelemen M H , Effron M B , Valenti SA, Stewart K J . Exercise training combined with antihypertensive drug therapy. Effects on lipids, blood pressure, and left ventricular mass. J A M A 1990; 263(20):2766-2771.
273. Stewart K J , Effron M B , Valenti SA, Kelemen M H . Effects of diltiazem or propranolol during exercise training of hypertensive men. Medicine & Science in Sports & Exercise 1990; 22(2):171-177.
274. Khalil-Manesh F, Venkataraman K , Samant D R , Gadgil U G . Effects of diltiazem on cation transport across erythrocyte membranes of hypertensive humans. Hypertension 1987; 9(l):18-23.
275. Kjellstrom T, Blychert E , Lindgarde F. Felodipine in the treatment of hypertensive type f i diabetics: effect on glucose homeostasis. Journal of fnternal Medicine 1991; 229(3):233-239.
276. Klauser R, Speiser P, Gisinger C, Schernthaner G , Prager R. Platelet aggregation and metabolic control are not affected by calcium antagonist treatment in type II diabetes mellitus. Journal of Cardiovascular Pharmacology 1990; 15 Suppl LS93-S96.
266

277. Klauser R, Prager R, Gaube S, Gisinger C, Schnack C, Kuenburg E et al. Metabolic effects of isradipine versus hydrochlorothiazide in diabetes mellitus. [erratum appears in Hypertension 1991 May;17(5):722]. Hypertension 1991; 17(1):15-21.
278. Krakoff L R . Nicardipine monotherapy in ambulatory elderly patients with hypertension. American Heart Journal 1989; 117(1): 250-255.
279. Lacourciere Y , Pokier L , Lefebvre J, Burford R G . Clinical efficacy of force titrated doses of diltiazem extended-release. A placebo controlled study. American Journal of Hypertension 1995; 8(3):282-286.
280. Lacourciere Y , Lenis J, Orchard R, Lewanczuk R, Houde M , Pesant Y et al. A comparison of the efficacies and duration of action of the angiotensin II receptor blockers telmisartan and amlodipine. Blood Pressure Monitoring 1998; 3(5):295-302.
281. Landmark K , Dale J. Antihypertensive, haemodynamic and metabolic effects of nifedipine slow-release tablets in elderly patients. Acta Medica Scandinavica 1985; 218(4):389-396.
282. Lessem J, Gershan R M , Madden R, Meacham J, Schumacher BJ, Sdt V B et al. Nicardipine in essential hypertension. Clinical Trials Journal 1990:27(5): 313-326.
283. Letzel EI, Bluemner E . Dose-response curves in antihypertensive combination therapy: results of a controlled clinical trial. Journal of Flypertension 1990; 8(Suppl 4): S83-S86.
284. Lewis G R , Morley K D , Lewis B M , Bones PJ. The treatment of hypertension with verapamil. New Zealand Medical Journal 1978; 87(612):351-354.
285. Lok H . Felodipine in elderly hypertensives. Dutch G P Multicentre Study Group. Journal of Fluman Hypertension 1989; 3(6):467-470.
286. Yodfat Y , Cristal N . A multicenter, double-blind, randomized, placebo-controlled study of isradipine and methyldopa as monotherapy or in combination with captopril in the treatment of hypertension. The L O M I R - M C T - I H Research Group. American Journal of Flypertension 1993; 6(3 Pt 2):57S-61S.
287. Yodfat Y , Bar-On D , Amir M , Cristal N . Quality of life in normotensives compared to hypertensive men treated with isradipine or methyldopa as monotherapy or in combination with captopril: the L O M I R - M C T - I L study. Journal of Fluman Hypertension 1996; 10(2):117-122.
288. Lorimer A R , Smedsrud T, Walker P, Tyler H M . Comparison of amlodipine and verapamil in the treatment of mild to moderate hypertension. Journal of Cardiovascular Pharmacology 1988; 12 Suppl 7:S89-S93.
2 6 7
289. Lorimer A R , Smedsrud T, Walker P, Tyler H M . A comparison of amlodipine, verapamil and placebo in the treatment of mild to moderate hypertension. Amlodipine Study Group. Journal of Human Hypertension 1989; 3(3):191-196.
290. Low CJS, Foy SG, Chaudhary H , Crozier I G , Baskaranathan S, Ikram H . Twenty-four hour profile of the anti-hypertensive action of isradiine in essential hypertension. Blood Pressure 1993;2: 59-61.
291. Lyons D , Webster J, Benjamin N . The effect of antihypertensive therapy on responsiveness to local intra-arterial NG-monomethyl-L-arginine in patients with essential hypertension. Journal of Pfypertension 1994; 12(9):1047-1052.
292. Macphee GJA, Dutton M , Lennox I M , Williams B O . Low-dose nifedipine retard in elderly hypertensive patients. Journal of Clinical & Experimental Gerontology 1989; 11(3-4):115-129.
293. Mancia G , Omboni S, Ravogli A , Frattola A , Villani A . Ambulatory blood pressure monitoring. Drugs 1992; 44 Suppl 1:17-22.
294. Massie B M , Der E , Herman TS, Topolski P, Park G D , Stewart W H . 24-hour efficacy of once-daily diltiazem in essential hypertension. Clinical Cardiology 1992; 15(5):365-368.
295. Mattarei M . De Venuto G . Biasion T. et al. Nifedipine vs prazosin in the treatment of slight-to-moderate essential arterious hypertension: Effectiveness, tolerance, and metabolic effects. Current Therapeutic Research, CUnical & Experimental 1987; 41(3): 356-366.
296. Mclnnes G T , Findlay I N , Murray G , Cleland J G , Dargie HJ. Cardiovascular responses to verapamil and propranolol in hypertensive patients. Journal of Hypertension -Supplement 1985; 3 Suppl 3:S219-S221.
297. Dargie H , Cleland J, Findlay I, Murray G , Mclnnes G . Combination of verapamil and beta blockers in systemic hypertension. A m } cardiol 1986; 57:80D-82D.
298. Megnien JL , Levenson J, Del Pino M , Simon A . Amlodipine induces a flow and pressure-independent vasoactive effect on the brachial artery in hypertension. British Journal of Clinical Pharmacology 1995; 39(6):641-649.
299. Midtbo K A , Hals O, Lauve O. A new sustained-release formulation of verapamil in the treatment of hypertension. Journal of Clinical Flypertension 1986; 2(3 Suppl):125S-132S.
300. Storstein L . Midtbo K . Hals O. Myhre E . Antihypertensive effect of verapamil in relation to plasma concentrations of verapamil and its active metabolite norverapamil. Current Therapeutic Research, Clinical & Experimental 1981 ;29(1 12-119.
268

301. Morgan T O , Anderson A I E , Maclnnis RJ. A C E inhibitors, beta-blockers, calcium blockers, and diuretics for the control of systolic hypertension. American Journal of Hypertension 2001; 14(3):241-247.
302. Morgan T, Anderson A . A comparison of candesartan, felodipine, and their combination in the treatment of elderly patients with systolic hypertension. A m J Hypertens. 2002;15(6):544-9.
303. Moser M , Lunn J, Nash D T , Burris JF, Winer N , Simon G . Nitrendipine in the treatment of mild to moderate hypertension. Journal of Cardiovascular Pharmacology. 1984; 6: S1085-1089.
304. Nelson E B , Pool JL , Taylor A A . Antihypertensive activity of isradipine in humans: a new dihydropyridine calcium channel antagonist. Clinical Pharmacology & Therapeutics 1986; 40(6):694-697.
305. Neutel J M , Smith D H , Lefkowitz M P , Cargo P, Alemayehu D , Weber M A . Hypertension in the elderly: 24 h ambulator)' blood pressure results from a placebo-controlled trial. Journal of Human Flypertension 1995; 9(9):723-727.
306. Nikkila M T , Inkovaara J A , Heikkinen JT, Olsson SO. Antihypertensive effect of diltiazem in a slow-release formulation for mild to moderate essential hypertension. American Journal of Cardiology 1989; 63(17):1227-1230.
307. Nikolova K . Treatment of hypertensive venous leg ulcers with nifedipine. Methods & Findings in Experimental & Clinical Pharmacology 1995; 17(8):545-549.
308. Nilsson P, Lindholm L H , Fledner T for the D D D Study Group. The diltiazem different doses study — a dose-response study of once-daily diltiazem therapy for hypertension. J Cardiovasc Pharmacol 1996; 27(4): 469-475.
309. Ollivier JP, Wajman A , Stalla-Bourdillon A . Antihypertensive efficacy of optimally titrated doses of once-daily sustained-release diltiazem: a placebo-controlled trial. D I L P L A C O M P Study Group. Cardiology 1995; 86(6):481-487.
310. Pacheco JP, Fan F, Wright R A , Corkadel L K , Horwitz L D , Reeves R L . Monotherapy of mild hypertension with nifedipine. American Journal of Medicine 1986; 81(6A):20-24.
311. Pandita-Gunawardena N D , Clarke SE. Amlodipine lowers blood pressure without affecting cerebral blood flow as measured by single photon emission computed tomography in elderly hypertensive subjects. Age & Ageing 1999; 28(5):451-457.
312. Pannarale G , Puddu P E , Monti F, Irace L , Bentivoglio M , Collauto F et al. Twenty-four-hour antihypertensive efficacy of felodipine 10 mg extended-release: the Italian inter-university study. Journal of Cardiovascular Pharmacology 1996; 27(2):255-261.
269

313. Persson B , Wysocki M , Andersson O K . Long-term renal effects of isradipine, a calcium entry blocker, in essential hypertension. Journal of Cardiovascular Pharmacology 1989; 14(l):22-24.
314. Persson B , Andersson O K , Wysocki M , Hedner T, Aurell M . Renal and hemodynamic effects of isradipine in essential hypertension. American Journal of Medicine 1989; 86(4A):60-64.
315. Persson B, Andersson O K , Wysocki M , Pledner T, Karlberg B. Calcium antagonism in essential hypertension: effect on renal haemodynamics and microalbuminuria. Journal of Internal Medicine 1992; 231(3):247-252.
316. Pool P E , Seagren SC, Salel A F . Effects of diltiazem on serum lipids, exercise performance and blood pressure: randomized, double-blind, placebo-controlled evaluation for systemic hypertension. American Journal of Cardiology 1985; 56(16):86H-91H.
317. Pool P E , Massie B M , Venkataraman K , Hirsch A T , Samant D R , Seagren SC et al. Diltiazem as monotherapy for systemic hypertension: a multicenter, randomized, placebo-controlled trial. American Journal of Cardiology 1986; 57(4):212-217.
318. Pool P E , Herron J M , Rosenblatt S, Reeves R L , Nappi J M , Staker L V et al. Metabolic effects of antihypertensive therapy with a calcium antagonist. American Journal of Cardiology 1988; 62(11):109G-113G.
319. Pool P E , Herron J M , Rosenblatt S, Reeves R L , Nappi J M , Staker L V et al. Sustained-release diltiazem: duration of antihypertensive effect. Journal of Clinical Pharmacology 1989; 29(6):533-537.
320. Pool P E , Nappi J M , Weber M A . Antihypertensive monotherapy with tablet (prompt-release) diltiazem: multicenter controlled trials. Cardiovascular Drugs & Therapy 1990; 4(4):1089-1096.
321. Pnsant L M , Neutel J M , Papademetriou V , DeQuattro V , Flail W D , Weir M R . Low-dose combination treatment for hypertension versus single-drug treatment-bisoprolol/hydrochlorothiazide versus amlodipine, enalapril, and placebo: combined analysis of comparative studies. American Journal of Therapeutics 1998; 5(5):313-321.
322. Prisant L M , Neutel J M , Ferdinand K , Papademetriou V , DeQuattro V , Hall et al. Low-dose combination therapy as first-line hypertension treatment for blacks and nonblacks. Journal of the National Medical Association 1999; 91(l):40-48.
323. Ramirez L C , Koffler M , Arauz C, Schnurr-Breen L , Raskin P. Effect of nifedipine GfTS on blood pressure, glucose metabolism, and lipid levels in hypertensive patients. Current Therapeutic Research, Clinical & Experimental 1992; 52(3):468-477.
324. Ricciardelli B , Argenziano L , Morisco C, Monti F, Barbato E , Trimarco B. Effects of nitrendipine on plasma levels of insulin and glucose in patients with essential
270
hypertension. Current Therapeutic Research, Clinical & Experimental 1997; 58(3): 180-186.
325. Romero-Vecchione E , Vasquez J, Velasco M , Morales E , Davoli M A , Arocha et al. [Increase of renal dopamine production induced by nifedipine in hypertensive patients. Double blind vs placebo study]. [Spanish]. Archivos del Instituto de Cardiologia de Mexico 1995; 65(6):535-540.
326. Rossi L , Costa B, Tomei R, Franceschini L , Castello C, Carbonieri, Zardini P. Antihypertensive effects of lacidipine during effort in mild to moderate hypertension. J Cardtovasc Pharmacol 2002;40(2):315-21.
327. Salvetti A , Innocenti PF, Iardella M , Pambianco F, Saba G C , Rossetti M et al. Captopril and nifedipine interactions in the treatment of essential hypertensives: a crossover study. Journal of Hypertension - Supplement 1987; 5(4):S139-S142.
328. Salvetti A , Cardellino G , Pesenti M , Caiazza A , Ghisoni F, De l Prato C et al. Antihypertensive effect of slow-release nicardipine. A placebo-controlled cross-over study. European Journal of Clinical Pharmacology 1989; 36(5):439-442.
329. Salvetti A , Magagna A , Innocenti P, Cagianelli A , Cipriani M , Gandolft et al. Chlorthalidone does not increase the hypotensive effect of nifedipine in essential hypertensives: a crossover multicentre study, [erratum appears in J Hypertens Suppl 1990 Apr;8(4):399]. Journal of Flypertension - Supplement 1989; 7(6):S250-S251.
330. Salvetti A , Magagna A , Innocenti P, Ponzanelli F, Cagianelli A , Cipriani et al. The combination of chlorthalidone with nifedipine does not exert an additive antihypertensive effect in essential hypertensives: a crossover multicenter study. Journal of Cardiovascular Pharmacology 1991; 17(2):332-335.
331. Salvetti A , Virdis A , Taddei S, Ambrosoli S, Caiazza A , Gandolfi E et al. Trough:peak ration of nifedipine gastrointestinal therapeutic system and nifedipine retard in essential hypertensive patients: an ftalian multicentre study. Journal of Hypertension 1996; 14: 661-667.
332. Schuster FI, Toka O, Toka HR, Busjahn A , Oztekin O, Wienker T F et al. A cross-over medication trial for patients with autosomal-dominant hypertension with brachydactyly. Kidney International 1998; 53(1):167-172.
333. Siche JP, Baguet JP, Fagret D , Tremel F, de Gaudemaris R, Mallion J M . Effects of amlodipine on baroreflex and sympathetic nervous system activity in mild-to-moderate hypertension. A m J Hypertens. 2001; 14(5 Pt l):424-8.
334. Simon G , Snyder D K . Altered pressor responses in long-term nitrendipine treatment. Clinical Pharmacology & Therapeutics 1984; 36(3):315-319.
335. Slonim A , Paran E , Cristal N . Effect of isradipine on factors affecting blood viscosity. American Journal of Hypertension 1991; 4(2 Pt 2):172S-174S.
271
336. Spence J D , Munoz C, Huff M W , Tokmakjian S. Effect of amlodipine on hemodynamic an dendocrine responses to mental stress. A J H 2000; 13:518-522.
337. Spieker C. Efficacy and tolerability of once-daily barnidipine in the clinical management of patients with mild to moderate essential hypertension. Blood Pressure 1998; 7 (Suppl 1): 15-21.
338. Smilde J G . The long-term efficacy and safety profile of barnidipine. International Journal of Clinical Practice 2000. Supplement 114: 20-26.
339. Spritzer N , Medeiros C M , Spritzer TS, Medeiros N K . [24-hour antihypertensive efficacy of nitrendipine]. [Portuguese]. Arquivos Brasileiros de Cardiologia 1990; 55(l):71-74.
340. Staessen J, Lijnen P, Fagard R, Hespel P, Tan WP, Devos P et al. Effects of the new calcium entry blocker isradipine (PN 200-110) in essential hypertension. Journal of Cardiovascular Pharmacology 1989; 13(2):271-276. ;
341. Stornello M , Valvo E V , Scapellato L . Hemodynamic, renal, and humoral effects of the calcium entry blocker nicardipine and converting enzyme inhibitor captopril in hypertensive type II diabetic patients with nephropathy. Journal of Cardiovascular Pharmacology 1989; 14(6):851-855.
342. Stornello M , Valvo E V , Scapellato L . Effect of sustained-release nicardipine, chlorthalidone, and the two drugs combined in patients with mild to moderate hypertension. Current Therapeutic Research, Clinical & Experimental 1990; 47(2):405-411.
343. Suzuki M , Kanazawa A , Hasegawa M , Harano Y . Improvement of insulin resistance in essential hypertension by long-acting Ca antagonist benidipine. Clinical & Experimental Hypertension (New York) 1999; 21(8):1327-1344.
344. Szlachcic J, Tubau JF, Vollmer C, Massie B M . Effect of diltiazem on left ventricular mass and diastolic filling in mild to moderate hypertension, [see comments]. American Journal of Cardiology 1989; 63(3):198-201.
345. Tonkin A L , Wing L M , Russell A E , West MJ , Bune A J , Morris MJ et al. Diltiazem and atenolol in essential hypertension: additivity of effects on blood pressure and cardiac conduction with combination therapy. Journal of Hypertension 1990; 8(11):1015-1019.
346. Tschoepe D , Flomberg M , Roesen P, Gries F A . Reduced platelet thromboxane formation after long-term administration of a dihydropyridine calcium channel blocker: a prospective, double-blind, placebo-controlled study with nitrendipine in borderline hypertensive patients with IDDM-type diabetes mellitus. Diabetes Research 1992; 19(3):125-131.
272

347. Van Bortel L M , Schiffers P M , Bohm R O , Mooij J M , Rahn K H , Struyker et al. The influence of chronic treatment with verapamil on plasma atrial natriuretic peptide levels in young and elderly hypertensive patients. European Journal of Clinical Pharmacology 1990; 39 Suppl 1:S39-S40.
348. Van Merode T, Van Bortel L M , Smeets F A , Mooij J M , Bohm R O , Rahn K H et al. Verapamil and nebivolol improve carotid artery distensibility in hypertensive patients. Journal of Hypertension - Supplement 1989; 7(6):S262-S263.
349. Van Merode T, Van Bortel L , Smeets F A , Bohm R, Mooij J, Rahn K H et al. The effect of verapamil on carotid artery distensibility and cross-sectional compliance in hypertensive patients. Journal of Cardiovascular Pharmacology 1990; 15(1):109-113.
350. Vanhees L , Fagard R, Lijnen P, Amery A . Effect of antihypertensive medication on endurance exercise capacity in hypertensive sportsmen. Journal of Hypertension 1991; 9(11):1063-1068.
351. Viskoper JR, Laszt A , Faraggi D . Twenty-four-hour blood pressure control with isradipine in mild essential hypertension. American Journal of Hypertension 1991; 4(2 Pt2):161S-162S.
352. Viskoper JR, Laszt A , Farragi D . The antihypertensive action of isradipine in mild essential hypertension. Journal of Cardiovascular Pharmacology 1991; 18 Suppl 3:S9-11.
353. Viskoper JR, Laszt A , Faraggi D , Yaskil E . Does isradipine exert a special early-morning blood pressure-lowering effect? Journal of Cardiovascular Pharmacology 1992; 19 Suppl 3:S74-S75.
354. Watts RW, Wing L M . A placebo-controlled comparison of diltiazem and amlodipine monotherapy in essential hypertension using 24-h ambulator)' monitoring. Blood Pressure 1998; 7(l):25-30.
355. Weber M A , Cheung D G , Graettinger W F , Lipson JL. Characterization of antihypertensive therapy by whole-day blood pressure monitoring. J A M A 1988; 259(22):3281-3285.
356. Webster J, Robb OJ, Jeffers T A , Scott A K , Petrie JC, Towler H M . Once daily amlodipine in the treatment of mild to moderate hypertension. British Journal of Clinical Pharmacology 1987; 24(6):713-719.
357. Webster J, Robb OJ, Jeffers T A , Scott A K , Petrie JC. Once-daily amlodipine in the treatment of mild to moderate hypertension. Journal of Cardiovascular Pharmacology 1988; 12 Suppl 7:S72-S75.
358. Webster J, Witte K , Rawles J, Petrie JC, Jeffers T A . Evaluation of a long acting formulation of nicardipine in hypertension by clinic and home recorded blood
273
pressures and Doppler aortovelography. British Journal of Clinical Pharmacology 1989;27(5):563-568.
359. Webster J, Petrie JC, Jeffers T A , Roy-Chaudhury P, Crichton W, Witte K et al. Nicardipine sustained release in hypertension. British Journal of Clinical Pharmacology 1991;32(4):433-439.
360. Weir M R , Chrysant SG, McCarron D A , Canossa-Terris M , Cohen J D , Gunter et al. Influence of race and dietary salt on the antihypertensive efficacy of an angiotensin-converting enzyme inhibitor or a calcium channel antagonist in salt-sensitive hypertensives. Hypertension 1998; 31(5):1088-1096.
361. Chrysant SG , Weder A B , McCarron D A , Canossa-Terris M , Cohen J D , Gunter P A . Effects of isradipine or enalapril on blood pressure in salt-sensitive hypertensives during low and high dietary salt intake. A J H 2000; 13: 1180-1188.
362. Welzel D , Burger K J , Weidinger G . Calcium antagonists as first-line antihypertensive agents: a placebo-controlled, comparative trial of isradipine and nifedipine. Journal of Cardiovascular Pharmacology 1990; 15 Suppl 1:S70-S74.
363. White W B , Mehrotra D V , Black HR, Fakouhi T D . Effects of controlled-onset extended-release verapamil on nocturnal blood pressure (dippers versus nondippers). COER-Veraparml Study Group. American Journal of Cardiology 1997; 80(4):469-474.
364. Wilson J, Orchard M A , Spencer A A , Davies JA, Prentice CR. Anti-hypertensive drugs non-specifically reduce "spontaneous" activation of blood platelets. Thrombosis & Haemostasis 1989; 62(2):776-780.
365. Winer N , Thys-Jacobs S, Kumar R, Davidson W D , Grayson M , Harris C et al. Evaluation of isradipine (PN 200-110) in mild to moderate hypertension. Clinical Pharmacology & Therapeutics 1987; 42(4):442-448.
366. Winer N , Kirkendall W M , Canosa F L , Lewin A J , McMahon F G , Carr A A et al. Placebo-controlled trial of once-a-day isradipine monotherapy in mild to moderately severe hypertension. Journal of Clinical Pharmacology 1990; 30(11):1006-1011.
367. Wing L M , Russell A E , Tonkin A L , Watts RW, Bune A J , West MJ et al. Mono- and combination therapy with felodipine or enalapril in elderly patients with systolic hypertension. Blood Pressure 1994; 3(l-2):90-96.
368. Wing L M , Russell A E , Tonkin A L , Bune A J , West MJ , Chalmers JP. Felodipine, metoprolol and their combination compared with placebo in isolated systolic hypertension in the elderly. Blood Pressure 1994; 3 (1-2): 82-89.
369. Wing L M , Arnolda L F , Harvey PJ, Upton J, Molloy D , Bune A J et al. Lacidipine, hydrochlorothiazide and their combination in systolic hypertension in the elderly. Journal of Hypertension 1997; 15(12 Pt 1):1503-1510.
274

370. Woehler TR, E f f J, Graney W, Heald D , Ziemniak J , Magner D . Multicenter evaluation of the efficacy and safety of sustained-release diltiazern hydrochloride for the treatment of hypertension. Clinical Therapeutics 1992; 14(2):148-157.
371. Wysocki M , Persson B, Bagge U , Andersson O K . Flow resistance and its components in hypertensive men treated with the calcium antagonist isradipine. European Journal of Clinical Pharmacology 1992; 43(5):463-468.
372. Wysocki M , Andersson O K , Persson B, Bagge U . Vasoconstriction during acute hypervolemic hemodilution in hypertensive patients is not prevented by calcium blockade. Angiology 1998; 49(l):41-48.
373. Yamakado T, Oonishi N , Kondo S, Nozir i A , Nakano T, Takezawa H . Effects of diltiazem on cardiovascular responses during exercise in systemic hypertension and comparison with propranolol. American Journal of Cardiology 1983; 52(8):1023-1027.
374. Yasky J, Godoy J, Soutric JL, Arenoso HJ . [Ambulatory ergometric and pressurometric results with a daily dose of 240 mg of diltiazem in labile hypertensive patients with threshold ergometry]. [Spanish]. Medicina 1991; 51 (2):111-120.
375. Zito M , Abate G , Cervone C, Squassante L , Calabrese G . Effects of antihypertensive therapy with lacidipine on ambulatory blood pressure in the elderly. Journal of Hypertension - Supplement 1991; 9(3):S79-S83.
376. Duval S, Tweedie R. A nonparametric "trim and fill" method of accounting for publication bias in meta-analysis. Journal of the American Statistical Association 2000; 95(449):89-98.
377. Eichenwald K , Kolata G . A doctor's drug trials turn into fraud. The New York Times. [Onkne] 1999 May 17 [cited 2006 September 10]. Available from: U R L : http://query.nytimes.com/gst/fuUpage.html?sec=health&res=9E06ElD7143EF934A 25756C0A96F958260
378. Gueyffier F, Boutitie F, Boissel JP, Coope J, Cuder J, Ekbom T et al. I N D A N A : a meta-analysis on individual patient data in hypertension. Protocol and preliminary results. Therapie 1995; 50(4):353-62.
379. World Flealth Organization. International Clinial Trials Registry Platform (fCTRP). [Onkne] 2006 [cited 2006 September 12]. Available from: U R L : http://www.who.int/ictrp/en/http://www.who.int/ictrp/en/
380. Pham B A ' , Piatt R, McAuley L , Klassen TP, Moher D . Is there a "best" way to detect and irunimize publication bias? A n empirical evaluation. Evaluation and die Health Professions 2001; 24(2): 109-125.
381. Song F, Eastwood A , Gilbody S, Duley L , Sutton A . Chapter 21: Publication and related biases. In: Stevens A , Abrams K , Brazier J, Fitzpatrick R and Lilford R,
275

editors. The Advanced Handbook of Methods in Evidence Based Healthcare. London: S A G E Publications; 2001. p. 371-385.
382. Preston R A , Materson BJ, Reda DJ , Williams D W . Placebo-associated blood pressure response and adverse effects in the treatment of hypertension. Arch Intern Med 2000; 160:1449-1454.
383. Bekelman J E , L i Y , Gross CP. Scope and impact of financial conflicts of interest in biomedical research: a systematic review. J A M A 2003; 289(4): 454-465.
384. Chapleau M W . Chapter A35 - Arterial Barioreflexes, In: Izzo JL , Black HR, editors. Hypertension Primer, 3 r d Edition. Philidelphia: Lippincott Williams & Wilkins; 2003. p. 103-111.
385. Jackson WF. Ion channels and vascular tone. Hypertension 2000; 35 (1 Pt. 2): 173-178.
386. Bong A , Wong M M Y , Wright J M . Adverse cardiac effects of calcium channel blockers. The Cochrane Database of Systematic Reviews 2004, fssue 1. Art. No.: CD004527. D O L 10.1002/14651858.CD004527.
276
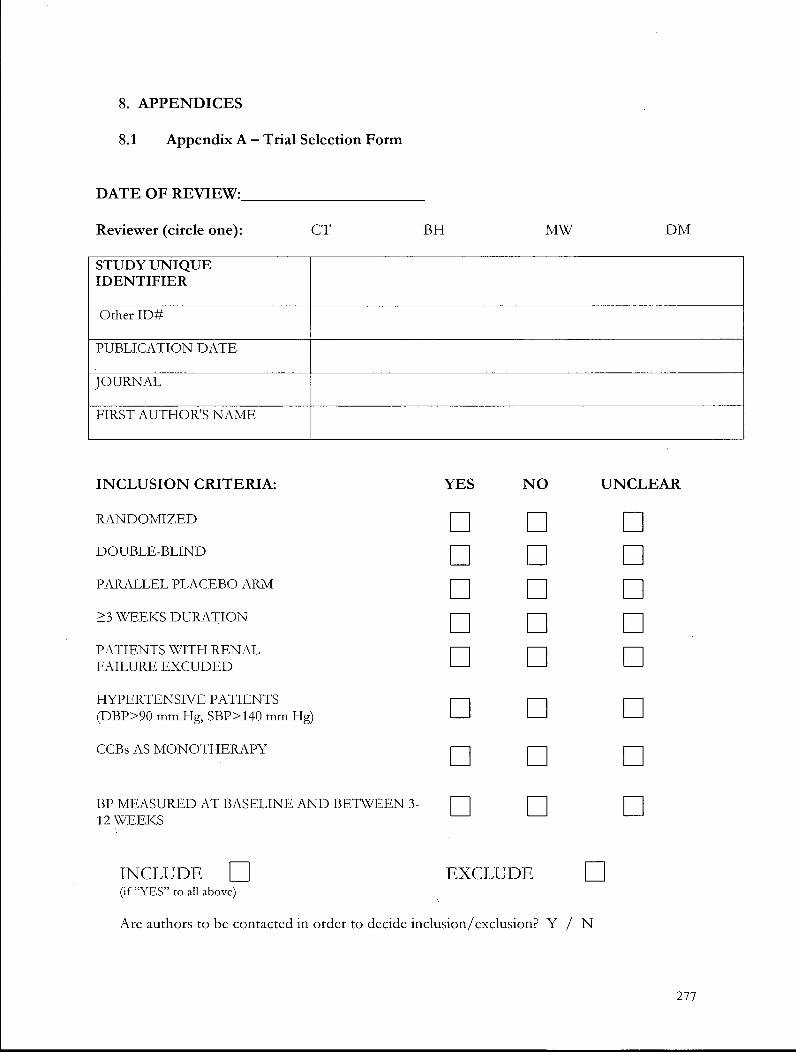
8. A P P E N D I C E S
8.1 Appendix A - T r ia l Selection Fo rm
D A T E O F R E V I E W :
Reviewer (circle one): C T B H M W D M
STUDY UNIQUE IDENTIFIER
Other ID#
PUBLICATION D A T E
J O U R N A L
FIRST AUTHOR'S N A M E
I N C L U S I O N C R I T E R I A : Y E S N O U N C L E A R
R A N D O M I Z E D • • • D O U B L E - B L I N D • • • P A R A L L E L P L A C E B O A R M • • • >3 WEEKS D U R A T I O N • • • PATIENTS WITFI R E N A L FAILURE E X C U D E D • • • HYPERTENSIVE PATIENTS i — i (DBP>90 m m Hg, SBP>140 m m Hg) 1 1 • • CCBs AS M O N O T H E R A P Y • • • BP MEASURED A T BASELINE A N D B E T W E E N 3- 1 1 12 WEEKS • •
I N C L U D E •
(if "YES" to all above) E X C L U D E •
Are authors to be contacted in order to decide inclusion/exclusion? Y / N
277

8.2 Appendix B - Standard data extraction form for each trial
DATA EXTRACTION FORM
(use one form per trial)
Administrat ion Details
Paper title:
Paper number:
Study ID:
Other references to which this trial may link with:
Extractor name:
Characteristics of Included Studies
Fund ing Source (Potential Bias)
F O R A G A I N S T N O BIAS U N C L E A R
Methods
Design of Study:
Method of randomization:
Concealment of randomisation:
Was this concealment adequate/inadequate/unclear?
Blinding:
Description of withdrawals or dropouts:
278
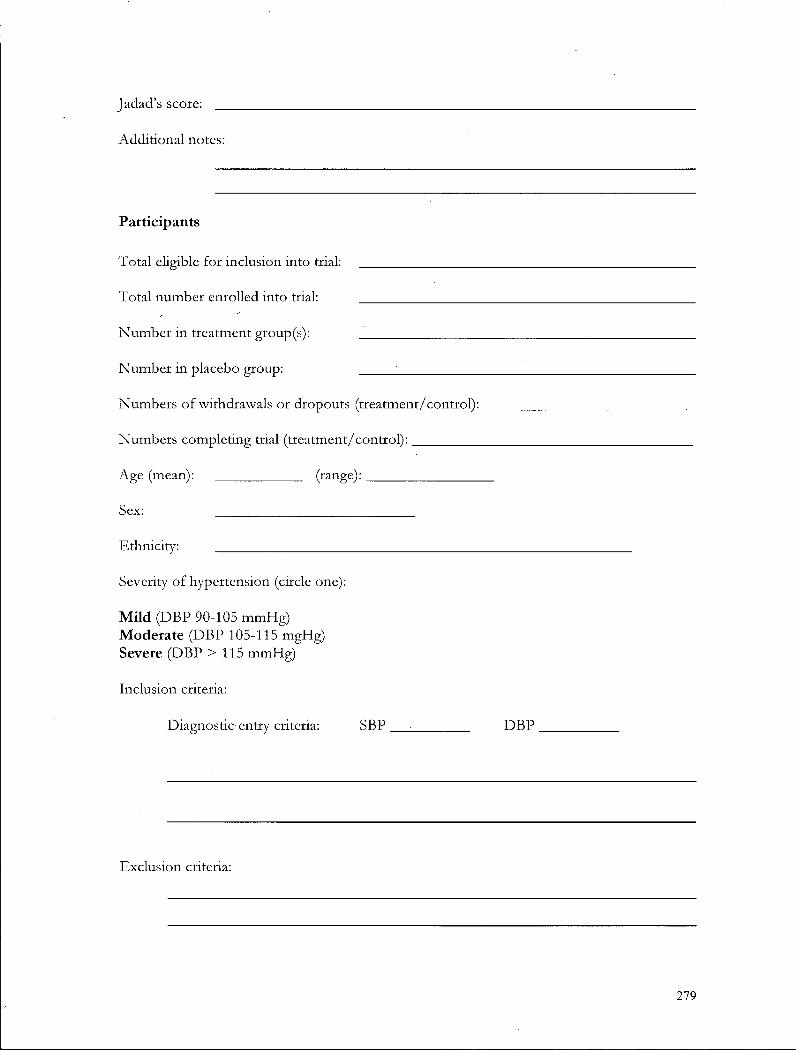
Jadad's score:
Additional notes:
Participants
Total eligible for inclusion into trial:
Total number enrolled into trial:
Number in treatment group(s):
Number in placebo group: ;
Numbers of withdrawals or dropouts (treatment/control):
Numbers completing trial (treatment/control):
Age (mean): (range):
Sex:
Ethnicity:
Severity of hypertension (circle one):
M i l d (DBP 90-105 mmHg) Moderate (DBP 105-115 mgHg) Severe (DBP > 115 mmHg)
Inclusion criteria:
Diagnostic entry criteria: SBP • D B P
Exclusion criteria:
279
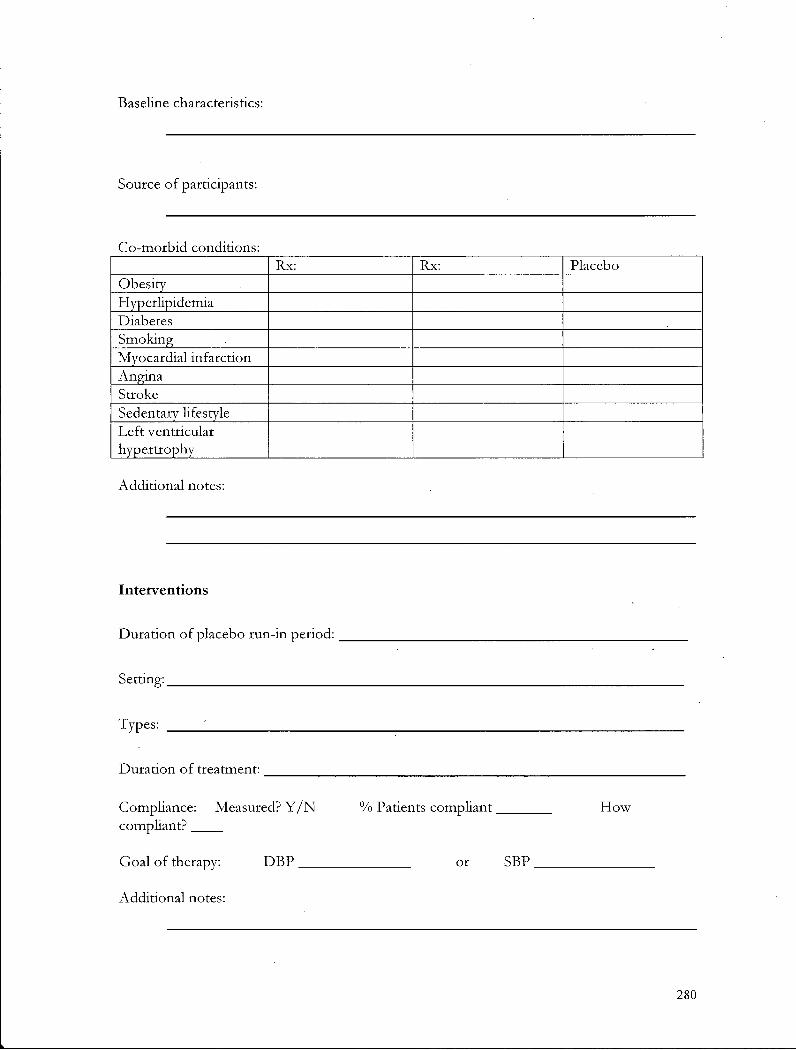
Baseline characteristics:
Source of participants:
Co-morbid conditions: Rx: Rx: Placebo
Obesity Hyperlipidemia Diabetes Smoking Myocardial infarction Angina Stroke Sedentary lifestyle Left ventricular hypertrophy
Additional notes:
Interventions
Duration of placebo run-in period:
Setting:
Types: •'_
Duration of treatment:
Compliance: Measured? Y / N % Patients compliant How
compliant?
Goal of therapy: D B P or SBP
Additional notes:
280

Outcomes
Outcomes:
Adverse events:
Additional notes:
Cross-over trials
Run-in phase
Treatment & duration
Washout phase.
Treatment & duration
Additional notes:
Comparison(s) in this trial:
281
Control & duration
Control & duration




















