A study on 'Hospital Waste Management' of National Institute ...
114
i A study on ‘Hospital Waste Management’ of National Institute of Unani Medicine, S.J.I.I.M Hospital (unani) and other Govt. Unani Dispensaries in Bangalore By Ameerulla Khan Dissertation Submitted to the Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore In partial fulfillment of the requirements for the degree of Mahire Tib (M.D.Unani) In Hifzane Sehat (Preventive and Social Medicine) Under the guidance of Professor Syed Shahabul Haq Department of Hifzane Sehat National Institute of Unani Medicine Kottigepalya, Bangalore 2007
-
Upload
khangminh22 -
Category
Documents
-
view
6 -
download
0
Transcript of A study on 'Hospital Waste Management' of National Institute ...

i
A study on ‘Hospital Waste Management’ of National Institute of Unani Medicine, S.J.I.I.M Hospital (unani) and other Govt. Unani
Dispensaries in Bangalore
By
Ameerulla Khan
Dissertation Submitted to theRajiv Gandhi University of Health Sciences, Karnataka, Bangalore
In partial fulfillmentof the requirements for the degree of
Mahire Tib (M.D.Unani)
In
Hifzane Sehat (Preventive and Social Medicine)
Under the guidance of
Professor Syed Shahabul Haq
Department of Hifzane SehatNational Institute of Unani Medicine
Kottigepalya, Bangalore
2007

ii
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA, BANGALORE
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation/ thesis entitled “A Study on ‘Hospital Waste
Management’ of National Institute of Unani Medicine, S.J.I.I.M Hospital (Unani)
and other Govt. Unani dispensaries in Bangalore” is a bonafide and genuine
research work carried out by me under the guidance of Prof. Syed Shahabul Haq,
Former Incharge, Dept. of Hifzane Sehat, National Institute of Unani Medicine,
Bangalore.
Date: Dr. Ameerulla KhanPlace: Bangalore

iii
CERTIFICATE BY THE GUIDE
This is to certify that dissertation entitled “A Study on ‘Hospital Waste
Management’ of National Institute of Unani Medicine, S.J.I.I.M Hospital (unani)
and other Govt. Unani dispensaries in Bangalore” is a bonafide research work
done by Ameerulla Khan in partial fulfillment of the requirement for the degree of
Mahire Tib (M.D.Unani).
Date: (Prof. Syed Shahabul Haq)
Place: Former Incharge,Dept. of Hifazne Sehat, NIUM, Bangalore

iv
ENDORSEMENT BY THE HOD & DIRECTOR OF THE INSTITUTION
This is to certify that the dissertation entitled “A Study on ‘Hospital Waste
Management’ of National Institute of Unani Medicine, S.J.I.I.M Hospital (unani)
and other Govt. Unani dispensaries in Bangalore” is a bonafide research work
done by Ameerulla khan under the guidance of Prof. Syed Shahabul Haq, Former
Incharge, Dept. of Hifzane Sehat, National Institute of Unani Medicine,
Bangalore.
HOD Director
Dr. Mohd. Zulkifle Prof. M. A. Jafri, Dept. of Hifzane Sehat, Director, NIUM,NIUM, Bangalore Bangalore
Date: Date:
Place: Bangalore Place: Bangalore

v
COPYRIGHT
Declaration by the Candidate
I hereby declare that the Rajiv Gandhi University of Health Sciences, Karnataka
shall have the rights to preserve, use and disseminate this dissertation/ thesis in print
or electronic format for academic/ research purpose.
Date: Place: Bangalore Dr. Ameerulla khan
© Rajiv Gandhi University of Health Sciences, Karnataka

A study on ‘Hospital Waste Management’ of National Institute of Unani Medicine, S.J.I.I.M Hospital (unani) and other
Govt. Unani Dispensaries in Bangalore
By
Dr. Ameerulla Khan
Dissertation Submitted to theRajiv Gandhi University of Health Sciences, Karnataka, Bangalore
In partial fulfillmentof the requirements for the degree of
Mahire Tib (M.D.Unani)
In
Hifzane Sehat (Preventive and Social Medicine)
Department of Hifzane SehatNational Institute of Unani Medicine
Kottigepalya, Bangalore
2007

To my very wonderful childrenwho are the light of my life
the joy of my days the comfort of my lifethe solace in sorrow my light in the dark
and the hope of my heart.No greater joy than you and when u have
children one day,may you be as lucky as i have been
to love and be loved by you

A study on ‘Hospital Waste Management’ of National Institute of Unani Medicine, S.J.I.I.M Hospital (unani) and other
Govt. Unani Dispensaries in Bangalore
By
Dr. Ameerulla Khan
Dissertation Submitted to theRajiv Gandhi University of Health Sciences, Karnataka, Bangalore
In partial fulfillmentof the requirements for the degree of
Mahire Tib (M.D.Unani)
In
Hifzane Sehat (Preventive and Social Medicine)
Department of Hifzane SehatNational Institute of Unani Medicine
Kottigepalya, Bangalore
2007

vi
ACKNOWLEDGMENT
I am indebted and thankful to almighty who is the most beneficent and merciful for
giving me patience and courage for conducting the study and helping me in every
walk of life and blessing me with all that I have got, and without whose blessings the
present work would not have been possible.
I wish to express my sincere respects, regards and deep sense of gratitude to my
guide, Prof. Syed Shahabul Haq, Former Incharge, Dept. of Hifzane Sehat, National
Institute of Unani Medicine, Bangalore, a well versed teacher, experienced in a
plethora of fields, with an inherent rare human quality to listen and to render physical
and mental courage on the onlooker. I sincerely express my boundless reverence for
his excellent guidance, constant courage, encouragement, timely advice, thoughtful
criticism and constructive suggestions that this thesis owes its very existence.
My sincere respect and regards to Prof. M.A. Jafri, Director, National Institute of
Unani Medicine, Bangalore, for his overall supervision, learned guidance, and
providing me the necessary facilities in undertaking this endeavor.
My sincere thanks are due to Dr. Mohd. Zulkifle, HOD, Hifzane Sehat, National
Institute of Unani Medicine, for his moral encouragement and providing me the
necessary facilities that I needed for my research work. I am indebted to him for the
untiring patience, superb scientific judgment; meticulous care and profound interest
that helped this work to finish smoothly.
Once in a lifetime we come across a person who with his knowledge, wisdom,
patience and dedication inspires us, especially if he is our teacher, we can consider

vii
ourselves lucky, I myself is one such lucky student for having worked under my co-
guide Dr. Abdul Haseeb Ansari, Lecturer, Dept. of Hifzane Sehat, National Institute
of Unani Medicine, Bangalore, whose guidance and suggestions greatly inspired me
in completing this work. I wish to express my gratitude, respect and affection to him
who has directed this study with his valuable contribution, dynamic and invaluable
guidance. He came to my rescue in moments of diffidence reducing my confusion to
clarity, rendering confidence and encouragement in each step.
My sincere thanks are due to Dr. Arish M. K. Sharwani and Dr. Zarnigar, Lecturers,
Dept. of Hifzane Sehat, for being supportive and helpful.
No words make articulate to acknowledge constant encouragement and timely advice
rendered by the teachers of NIUM, especially Dr. Mohd. Anwar, Reader, Dr. Abdul
Nasir Ansari, Lecturer, Dept. of Moalijat, Dr. Ghulamuddin Sofi, Lecturer, Dept. of
Ilmul advia.
My sincere thanks to Dr. Haseebunnisa, Principal, Govt. Unani Medical College,
Dr. Mujeebur-Rehman, Professor, Govt. Unani Medical College, Bangalore;
Dr. Gopinath D, Professor; Dr. Pruthvish S, Professor; Dr. Hemanth T, Lecturer;
Department of Community Medicine, M.S Ramaiah Medical College, Bangalore,
Dr. Rama Krishna Goud B, Asst. Professor; St. Johns Medical College, Dr. Riyaz
Basha Asst. Professor; Bangalore Medical College; Dr. Asima banu, Microbiologist,
Bowring and Lady Curzan hospital, Bangalore, for being supportive and helpful.
My sincere thanks are due to Dr. Sheersagar, Principal, S.J.I.I.M and Hospital and its
teaching staff, ministerial staff and hospital staff for their help and cooperation. I
would also extend my sincere thanks to Dr. Nargis Ayesha, Physician, Corporation
Unani Dispensary, Broadway road; Dr. Muqtair, Physician, Govt. Unani Dispensary,

viii
Neelsandra, Bangalore and Dr. Fathima, GUD, Jayamahal, Bangalore, and all their
ministerial and hospital staff for their continue support and help in carrying out my
dissertation work smoothly.
Words are inadequate to express my heartfelt feelings to my friends Dr. Md. Nayab,
Dr. Shaikh Imran, Dr. Mushtaq Naikoo, Dr. Firdose Malik, Dr. Farooque
Dr. Ahmed Hussain, Dr. Abdul Rehman, Dr. Salma banu, Dr. Badrul Hasan,
Dr. Naila, Dr. Chand Usmani, Dr. Sanaulla U, Dr. Noorulla my collogues Dr. Zaki
Anwar, Dr. Ramesh, Dr Md. Farooque, Dr. Shaheena, Dr. Usman and Dr Md.
Saquib for being supportive and helpful.
I am thankful to Mr. Prakash Reddy, Deputy Director and all Ministerial staff,
Dr. Ifthekar Mubeen, RMO, Dr. Shakeel Ansari and Dr. Mohd. Aazam Clinical
Registrars, Staff of Pathology Laboratory, Mrs. Sanjida Tabassum, Mr Md. Hanif,
and Mr Zaki. Pharmacy staff Dr Nafees Khan and Dr Md Fazil. Library staff
Mr. Ehtesham and Mr. Danish. Mrs. Jemima Matron and all the hospital staff for
their cooperation and help during the course of study and conducting of research
work.
I owe a lot more than words can express to my parents, parents in law, my beloved
wife, Dr. Roohi Zaman, my son Faraz Khan, my daughter Nida Farheen, whose
sacrifices and prayers have seen me through these years, nothing would have been
possible without their constant support, encouragement and love. I thank almighty for
blessing me with such wonderful relations and people that has made this life worth
living.
Date:
Place: Bangalore Dr. Ameerulla Khan

ix
LIST OF ABBREVIATIONS USED
(In alphabetical order)
AIDS =Acquired Immunodeficiency Syndrome
BMWMR =Bio Medical Waste Management Rules
e. g. =exempli gratia – for example
et al =et alii or et alia – and others
etc. =etcetra- and the rest
fig =Figure
Ft =Feet
Fr =Friedman Test
GOI =Government of India
HBV =Hepatitis-B Virus
HCIs =Health Care Institutions
HCP =Health Care Personal
HCWM =Health Care Waste Management
HCW =Health Care Waste
HIV =Human Immunodeficiency Virus
HOI =Head of the Institution
i.e. =id est- that is
IP =In Patient
IPD =In Patient Department
Kw =Kruskal-Wallis Test
M/m =meter
M 1 =Month first

x
M 4 =Month fourth
M 6 =Month sixth
n =number
N =Total number
NA =Not applicable
OP =Out Patient
OPD =Out Patient Department
p =Probability
POS =Post Orientation Session
Sec =Seconds
SMHCW =Safe Management of Health Care Waste
Vol. =Volume
WHO =World Health Organisation
WMS =Waste management system
< =less than
> =more than
% =percent
xi
ABSTRACT
The Bio-medical waste management is a global concern, particularly due to constant
rise in blood borne diseases and other related risk factors. The current scenario is that,
the incidence of hospital borne infections is on constant rise. The waste generation in
the hospital and its disposal has always never been given its due importance.
Unani system of medicine has given much emphasis to preventive and health care
aspects and their physicians were well aware of personal hygiene and their concept of
infection. As this system is in the main stream for health care service provider and
also for hospital waste generation source, with more number of patients and health
care personal involved, study was undertaken for the awareness and management of
hospital waste in unani hospitals.
In the present study waste management of unani hospitals in Bangalore, providing
both out patient and in patient facilities and providing only out patient services were
taken up with objectives to assess the existing practices of waste management and to
identify the type of waste, segregation practices, quantification of waste and its
disposal methods. And orientation / sensitisation session was conducted for the health
care personal at interval of first month, fourth month and sixth month of the POS and
the effect of management is noted both in components of the waste and in the
continued interaction of the health care personal.
It is a descriptive research study, which include surveys and fact-finding enquires
with various categories of health care personal. The overall initial assessment of the
studied HCIs shows that none of the studied HCIs managed solid as well as liquid
waste appropriately but there is periodic improvement in the components of HCWM
throughout the POS.
Keywords
Bio-medical waste; Segregation; Quantification; Waste generation; Unani Medicine,
Hazardous waste; Disposal; Sharp waste; Organic waste, Biodegradable; Composite.

xii
TABLE OF CONTENTS
Sl. No. Contents Pages
1. Introduction 1
2. Objectives 5
3. Review of Literature 6
4. Materials and Methods 36
5. Observation and Results 44
6. Discussion 63
7. Conclusion 74
8. Summary 78
9. Bibliography 82
10. Annexures
Anexure - 1 Instrument for data collection
Anexure - 2 Photographs
87
90

xiii
LIST OF TABLES
Sl. No. Tables Pages
Table 1 Types of services provided by the studied HCIs 44
Table 2 Category of staff and their participation in the studied HCIs 45
Table 3 Percentage of various type of wastes generated in studied HCIs
46
Table 4 Quantity estimation of solid waste generation in Kgs/ bed/ day in studied HCIs having in-patient facility
47
Table 5 Institutional facilities for treatment/ disposal of waste 48
Table 6 Methods of collection of various types of waste items 48
Table 7 Frequency of collection of various types of waste items 49
Table 8 Methods of disposal of various types of waste items 49
Table 9 Activities at point of generation of waste item at studied HCIs
50
Table 10 Treatment and final disposal of wastes in studied HCIs 50
Table 11 Activities at the point of waste generation 51
Table 12 Treatment and final disposal of waste 51
Table 13 Mode of management of liquid waste and infectious body material in the studied HCIs
52
Table 14 HOI, Doctors, Nursing and other staff interest & Participation
57
Table 15 Perceived factors that have helped in sustaining of the system of waste management
57
Table 16 Application of segregation of waste by studied HCIs in their various departments
58
Table 17 Application of disinfection of waste by studied HCIs in their various departments
59
Table 18 Application of containment of waste by studied HCIs in their various departments
60
Table 19 Application of colour coding of waste materials in their various departments
61
Table 20 Application of disposal of waste by studied HCIs in their various departments
62

xiv
LIST OF FIGURES
Sl. No. Figures Pages
Figure1Types of services provided by the studied
HCIs44
Figure 2Category of staff and their participation in
the studied HCIs 45
Figure 3Percentage of various types of wastes
generated in the studied HCIs46
Figure 4 Percentage of quantity of waste generated
in 2 studied HCIs having in-patient facility47
Figure 5Application of segregation of waste by
studied HCIs in their various departments58
Figure 6Application of disinfection of waste by
studied HCIs in their various departments59
Figure 7Application of containment of waste by
studied HCIs in their various departments60
Figure 8
Application of colour coding of waste
materials by studied HCIs in their various
departments
61
Figure 9Application of disposals of waste by studied
HCIs in their various departments.62

1
INTRODUCTION
The bio-medical waste means any solid, liquid waste material, generated during the
process of diagnosis, treatment and immunization of human being. These waste
materials could cause serious hazards to health and environment in case of
indiscriminate management. All the hospital personnel are at a risk to get many fatal
infections and injuries by these infectious materials. To avoid these hazards,
discriminate waste management system should be implemented in hospital
infrastructure. (1)
The concern for Bio-medical waste management has been felt globally with
indiscriminate disposal of health care waste and rise in deadly infections such as
AIDS, Hepatitis-B. The need to educate different health care professionals/ workers
about health care waste management is thus very important. (2)
Hospital is a complex multidisciplinary system, which consumes number of items/
products for delivery of medical care and it is a part of the physical environment. All
these products consumed in hospitals leave some unusable leftovers, which are called
hospital/ clinical wastes as they are generated as a result of some clinical activity.
Bio-medical waste is a broader term applied to waste generated in the diagnosis,
treatment or immunization of human beings, in research or in the production or testing
of biological products.
In every hospital a large amount of waste is generated daily and it has become
necessary to give special attention for the proper treatment and disposal of waste.
Although hospital exists to treat illness, they can act as reservoirs of infection.
Whenever accurate survey have been made it has been found that a substantial

2
proportion of patient acquire infection during stay in the Hospital. Mostly infection
occurs in the hospital, is due to inappropriate cleanliness.
Infectious wastes include all those medical wastes, which have the potential to
transmit viral, bacterial or parasitic diseases. Since the early recovery of the patient
and health of clinical staff directly depends on a clean and hygienic environment, it is
essential that hospital waste is collected, stored and disposed off in a proper and
scientific manner. General hospital hygiene is a prerequisite for good medical waste
management. (3)
Improper management of medical waste may pose health hazards through
transmission of diseases, not only to health workers and their families, but to patients
and their relatives.(4)
The current scenario in India is that, the Hospitals are yet to implement the proper
disposal of health care waste, and are still dumping their waste in municipal garbage
without any segregation. It is unfortunate to note that at many places, it is common to
find large dumps of “biomedical waste” consisting of used needles, syringes, sharps,
blood soaked items, napkins, etc in addition to kitchen waste, plastic, papers and even
human excreta.
These dumping sites are regularly visited by “rag pickers” who scan and sort these
wastes, manually, to pick out plastics, disposables, syringes, needles and other
disposables, merely to resale to the people who ‘recycle’ these, and incur the risk of
accidental infections either by sharps or through non-intact skin. The potentials for
making profit from this recycled material magnify the risks even higher.
In addition to lack of motivation in workers, lack of commitment on the part of the
management, low level of education of sanitary workers, apathy of other staff
3
members and lack of organized training and the human factors further complicate the
present scenario of Bio-medical waste management. It is astonishing to note that
many of the waste generators in hospitals have no knowledge about what was done
with the waste generated in their units or departments, where the dustbins were
located in the hospitals and who was responsible for waste disposal. They were not
aware of new regulations about bio-medical waste management, to overcome this,
various health organizations and WHO has come forward to its safe disposal
programs, and has proposed certain norms and methods of hospital waste
management and safe disposal.(5)
Till July 1998, there was no system for proper hospital waste disposal. Most of the
hospitals were disposing their waste along with general waste. For prevention of these
improper practices, the Government of India had launched a law known as Bio-
medical waste (management and handling) Law 1998.(6)
Unani system of medicine has given much emphasis to preventive and health care
aspects. Unani physicians were well aware with personal hygiene and the concept of
infection. They enjoyed the reputation - the civilizers of the ancient world. They had a
keen sense of knowledge in filth, waste material and sanitation. Public health was
born during their reign. They build sewage systems and established hospitals for the
sick.(7)
Unani system of medicine forms an integral part of national health care delivery
system in India. According to official figures available, there are 43,108 registered
Unani practitioners in the country. There are around 1000 Unani Dispensaries, 312
hospitals besides number of Research centres, diagnostics, Regimenal units etc.
functioning as health care providers.

4
In which there may be number of persons involved in the occupation of health
delivery system, and also these health care facilities are visited by hundreds and
thousands of patients for diagnostic and treatment procedures, in these activities they
generate varieties of health care wastes. These wastes if not managed properly
become a health hazard and spread diseases in the society. Ill managed health care
waste can also be responsible for environmental pollution and degradation.
Proper health care waste management encompasses various processes, such as waste
generation, collection, quantification, handling, storage and final disposal without
causing hazard and risks to society, environment and waste handlers.(8)
The need for the study is to sensitize the Health care workers/ public about hospital
waste and its impact on health and environment, to acquaint about the existing
legislation, knowledge and safe practices regarding health care waste management.(2)
Keeping in mind the above stated problems of waste management, to create
awareness about bio-medical waste and to fulfil the required WHO target, it is
necessary to conduct and start the “Waste Management Studies” from grass root level,
hence the study regarding “Hospital Waste Management” in Unani Hospitals in
Bangalore is initiated. And the study has been undertaken to assess the existing
practice of waste management, to understand the problem and hazards of Bio-medical
waste and to get aware of rules and regulations about Bio-medical health practices.

5
OBJECTIVES OF THE STUDY
•••• To assess the existing practices of hospital waste management in the study
centres, in various components of health care waste, like segregation practices,
type of wastes, quantification of waste and disposal methods.
•••• The orientation / sensitisation session for the health care personnel in safe
management of health care waste.

6
REVIEW OF LITERATURE
Waste is any mater, whether liquid, solid, or gaseous which is discharged, emitted, or
deposited in the environment. The concept of a waste embraces all unwanted and
economically unusable by-products which may be discharged, accidentally or
otherwise, to the environment.(9)
All activities of living thing on earth produce waste in some form or the other.
Normally, aerobic and anaerobic processes in the environment degrade such products.
These wastes, both biodegradable and non-biodegradable hardly had any impact on
the environment until the invention of plastics by the modern man. The process of
natural degradation could not keep pace with the increase in waste generated by the
over increasing population of mankind and its necessities.(10)
Waste and refuse should be properly disposed; otherwise there will be chances of
spreading of diseases. Waste stored temporarily should be in appropriate container
with lid covered. This accumulated huge waste should be transported far away from
populated areas, and buried in the land and cover this area of about one foot height
with mud and later it can even be used as manure after its compositing.(11)
Hospital is a residential establishment which provides short term and long term
medical care consisting of observational, diagnostic, therapeutic and rehabilitative
services for a person suffering or suspected to be suffering from diseases or injury and
during these activities it generate lot of hospital waste of different types.(12)
Unani physicians were aware of the concept, cause and spread of infectious diseases,
through thousands of years. Razi, the famous Unani physician, has mention that the

7
cause of infectious disease is due to aaludgi (pollution), he also observed that the
people were affected with diseases, when they stayed with sick person. Razi has
explained about infection and its causes in his famous book Al-Havi, Volume-23.(13)
Ibn Sina has said that only with admixture of putrefied air and morbid matter,
contamination of air or water is possible. The presence of toxic or putrefying
substances, in the air and water, has been termed as ajsame khabisa.(14)
Hospital waste possesses a serious problem, individual component of the waste which
constitutes a risk to health if inadequately handled. Hospital is facing enormous
problems and difficulties due to mismanagement of waste generated. Large quantities
of waste materials accumulate as a result of the daily activities, if they are not
removed and disposed efficiently, they could soon make any sigh, unpleasant or even
uninhabitable. A special attribute of bio-medical waste is that even though it forms
only a small part of the total solid waste if not taken care of properly, it can pollute
the whole of the solid waste and there by transfer infectivity to the whole of the solid
waste. Once that happens, all the waste must be considered infected and treated as
infectious waste.
Not only this, if the Bio-medical waste finds access to air and water it had the
potential of infecting the ambient environment as well as water sources.(15)
Organic waste becomes a potential place for fly breeding; garbage attracts rodents
like rats and other animals.(16)
(A) Operational Definitions
• Pollutant
• Bio-medical waste
• Hospital waste

8
• Health care waste
• Segregation
• Categories of segregation
• Colour coding systems
• Quantification of health care waste
• Storage
• Transportation
(B) Unani Literature
(C) Public health Act
(D) Categories of the persons exposed to risk of infections
(E) Sources of Health Care Waste
(F) Classification of Health Care Waste
(G) Occupational Health and Safety Precautions/Measures
(H) Treatment and disposal technologies for health-care waste
(I) Key steps of healthcare waste management
(J) Bio-medical wastes (management and handling) Rules, 1998
(A) Operational Definition
Pollutant:
A contaminant whose presence is damaging to the quality of environment or waste
products that have been inadequately disposed or contained.(17)
Bio-Medical Waste:
It is a broader term applied to waste generated during the diagnosis, treatment or
immunization of human beings or in research activities pertaining there to or in the
production or testing of biological products.(6, 13, 14,)

9
Hospital Waste:
It can be defined as any thing that is discarded, unwanted substances which is
generated in process of rendering medical services to a person desiring such services
as a result of sickness or injury. (18)
Health Care Waste:
It is generated as a by-product of health care delivery system. It includes wastes like
sharps, soiled waste, body fluids, discarded medicines, glass slides with blood stains,
infected dressing material etc.(19)
Segregation:
Waste segregation is the key to any waste management scheme. It consists of placing
different types of waste in different containers of colour-coded bags at the site of
generation. This helps in reducing the bulk of infectious waste and contains spread of
infection to general waste. This practice reduces the total treatment cost, the impact of
waste in the community and the risk of infecting workers. Proper segregation should
identify waste according to source and type of disposal. Waste should be segregated
into different categories at the site of generation.(7)
The first step in proper disposal is systematic segregation of the waste. Infectious and
non-infectious wastes are generally not segregated at source and instead the mixed
waste is taken to the incineration plant in a very unhygienic manner. The system of
collection, transportation and disposal of bio-medical waste is thus not scientifically
designed.(20)
Advantage of segregation, is that it prevents mixing of infectious with non-infectious
waste, thus minimizing the high cost and care involved in disposal of infectious
waste. Once such mixture occurs, the total amount has to be treated as infectious.

10
Segregation reduces the chances of accidental infection of health care workers and
waste handlers.(15)
Categories of segregation:
Under Bio-medical waste (management and handling) Rules, 1998; the heart of law is
segregation of waste at the point of origin of waste. Segregating potentially infectious
material from the other waste at the point of generation may reduce both volume and
cost.
The Bio-medical waste (management and handling) Rules, 1998 have categorised the
bio-medical wastes into 10 categories as mentioned in table below. (6)
Sl. No
Waste category Treatment & Disposal options
Colour code
Type of container
1. Human Anatomical waste Incineration / Deep burial Yellow Plastic bag
2. Animal Waste Incineration/ Deep burial Yellow Plastic bag
3. Microbiology &
Biotechnology waste
Autoclaving/ Incineration Yellow /
Red
Plastic bag/
disinfected container
4. Waste sharps Disinfection/Chemical
treatment. Autoclaving
mutilation & shredding
Blue /
white
Plastic bag / Puncture
proof container
(translucent)
5. Discarded Medicines and
cytotoxic drugs
Incineration / destruction
and disposal in secured
landfills
Black Plastic bag
6. Soiled Waste Incineration Yellow /
Red
Disinfected container
/ Plastic bag
7. Solid Waste Disinfection by chemical
treatment/ autoclaving
Red / Blue
/ White
Disinfected container
/ plastic bag
8. Liquid Waste Disinfection by Chemical
treatment & discharge
into drains
NA Not applicable
9. Incineration Ash Disposal in municipal
landfill
Black Plastic bag
10. Chemical Waste Chemical treatment and
discharge into drains for
liquids and secure landfill
for solids.
Black Plastic bag

11
Note:-
1. There will be no chemical pre-treatment before incineration. Chlorinated
plastics shall not be incinerated.
2. Deep burial shall be an option available only in towns with population less
than 5 lakhs and in rural areas.
3. Using at least 1% hypochlorite solution or any other equivalent chemical
reagent. It must be ensured that chemical treatment ensures disinfection.(7)
Colour coding systems:
The bags or containers into which hazardous healthcare waste are collected should
have a distinct colour, so that staff is reminded not to put other wastes into such
containers. Any bags containing hazardous waste that are in the wrong place can be
easily noticed.
It is necessary to have a uniform national colour coding system, so that hazardous and
non hazardous wastes both can be easily recognized. (18)
The WHO recommended methods / guidelines for segregation, colour-coding for wastes are listed below. (21)
TYPE OF WASTE COLOUR OF CONTAINER
TYPE OF CONTAINER AND
MARKINGS Highly infectious waste Yellow, Marked
“ HIGHLY
INFECTIOUS”
Strong, leak-proof
plastic bag or container
autoclaved
Other Infectious waste, pathological
and Anatomical waste
Yellow Leak-proof plastic bag
or container
Sharps Yellow, marked
“SHARPS”
Puncture-proof
container
Chemical and pharma Waste Brown Plastic bag or container
Radioactive waste Labeled Lead box, with
radioactive symbol
General health care waste Black Plastic bag

12
Quantification of health care waste
Helps in:
• Planning infrastructure
• Procuring equipment
• Allocating resources
In middle and low income countries, health care waste generation is usually lower
than in high income countries.
According to a WHO report, 80% general health care waste, which may be dealt with
the normal domestic and urban waste management system.15% pathological and
infectious waste, 3% chemical and pharmaceutical waste, 1% sharps waste and less
than 1% special waste such as radioactive and cytotoxic waste, pressurized containers
or broken thermometers and used batteries.(7)
Storage:
Prime consideration should be given to the proper storage of waste. All segregated
waste should be packed in proper containers and colour-coded bags with labels
mentioning details of biomedical waste and biohazard signs. All containers used for
storage of such waste should be provided with a properly covered lid. (18)
Transportation:
There are two modes of Transportation of health care waste
1. Transportation of waste within the health care institution/ hospital
2. Transportation of waste outside the health care institution/ hospital.(18)

13
Unani Literature
Unani Medicine originated in Greece. Buqrat (Hippocrates) (460-365 BC) a great
Philosopher and Physician was founder of Unani System of Medicine. Modern
medical science was developed on the foundation of Hippocratic philosophy of health
& disease. Hence, Buqrat is known as the “Father of Medicine”. The Greeks enjoyed
the reputation – “The Civilizers of the Ancient World”.
Hippocrates was the first true epidemiologist; he distinguished diseases between
epidemic and endemic. He studied such things as climate, water, clothing, diet, habits
of eating and drinking and the effect they had in producing disease. His book “Kitab-
Al-Ahwia wa Al-Miyah wa Al-Buldan” (“Airs, Waters and Places”) is considered as
true work on social medicine and hygiene. The Hippocratic concept of health and
disease stressed the relation between man and his environment.
The Romans too had a keen sense of knowledge in filth, waste material and sanitation.
Public health was born in Rome, with the development of baths, constructions of fine
roads, building of sewage systems and establishment of hospitals for the sick.
An outstanding figure among Roman medical teachers was Jalinoos (Galen) (130-205
AD) Jalinoos observed that disease is due to three factors- predisposing, exciting and
environmental factors, a truly modern idea. Later, the Arabs translated the Greco-
Roman Medical Literature into Arabic and helped preserve the ancient knowledge.
Borrowing largely from the Greeks and Romans, they developed their own system of
medicine known as the Unani System of Medicine. (7)
Unani System of Medicine has given much emphasis to preventive and health care
aspects. Unani physicians were well aware with personal hygiene and the concept of
infection. Right in its formative stages the influence of the surrounding environment

14
and ecological conditions on the state of health of human beings have been
recognized. There is emphasis on the need for keeping water, food and air free from
pollution. Good and clean air is considered as most necessary for health, Ibn Sina
(Avicenna) (980-1037 AD), the famous Arab physician, noted that the change of
environment relieves the patients of many diseases.(8)
Establishment of Hospitals:
The development of efficient hospitals was an outstanding contribution of Unani
System of Medicine. Hospitals served all citizens free without any regard to their
colour, religion, sex, age or social status. The hospitals were run by the government
and their directors were physicians. It was chiefly towards humanitarian of patient
care that the hospitals of Unani excelled. Near the wards of those afflicted with fever,
fountains cooled the air, the insane were treated with gentleness, and at night music
and storytelling soothed the patients.(22)
The concept of infection and treating the patients in hospitals was noted even during
Greco-Arab period, Abu Bakar Bin Zikaria Razi, (Rhazes) (865-925 AD) the famous
Arab physician, worked hard towards establishment, taking care and maintenance of
Hospitals, for establishing and housing hospitals in clean environment at Baghdad,
Razi hanged over pieces of fresh meat in various places and neighbourhood and later
studied the properties and changes noted in meat, like it colour, odour, taste and
selected the place for constructing hospital in healthy atmosphere where the piece of
meat would rot slower than any of the other places.(23)
The cause of disease in Unani System of Medicine is Asbabe Sittah Zarooriyah,
consisting of external and internal factors. When these asbab are altered in nature,
disease is caused in the body. Experimental proof of the fact came through Raban
15
Tabri, (780-850 AD) who by his pioneering works described asbabe sittah zarooriyah,
especially the morbid air and water which carry mufsidi hawai and mufsidi ardi as the
cause of disease.
Ali Ibn Abbas Majusi (935-994 AD) further elaborates, whenever disequilibrium
occurs in the substance of the air, pollution and putrefaction are produced in both, the
substance (maddah) and quality (Kaifiat), causing plenty of bad symptom aaradd-i
radiyah and thus produces disease in human being.(24)
Even western medicine claims that the diseases are constituted in the human body by
foreign agents (bacteria and viruses) through the media of air, food and water.
The importance of disposal of waste generated by the population has been recognized
by the early civilizations. The Dravidians in 5000 BC incorporated the sewage system
in their town planning for safe and effective disposal of wastes.
The “hospices” or the homes for infirms, travellers, the sick and the old, later became
our hospitals, when the concept shifted from rest houses to treatment and care centres.
With such advent of hospitals, arose the problem of handling and disposal of waste
generated during the care of patients. These were left mostly to sweepers and menial
staff and were supervised by some sanitary inspector.(7)
Hospital and other health care facilities, diagnostic centres, research and medical
institutions, pharmacies are visited by patients for diagnostic and treatment
procedures in the process which generate a variety of wastes. A few examples of
health care wastes are dressing material, plastic disposal items, needles, food waste,
drugs, chemicals, pathological waste - all of which ultimately become part of health
care waste.

16
These wastes if not managed properly become a health hazard and spread diseases in
the society. In addition, ill managed health care waste can also be responsible for
environmental pollution and degradation. Waste generated in health care facilities is
much more complex than the municipal waste as it possesses threat to human health
as well as the environment. With rapid urbanization and population pressure, nature’s
cleansing system, has started breaking down. Improvement of waste management in
health care facilities is urgently needed for safeguarding the population, eliminating
occupational health hazards and protecting the environment.(19)
(B) Public health Act
Hippocrates’ contribution to the field of public health is of importance, as he was the
first recorded “epidemiologist”. The essentials of epidemiology noted by Hippocrates
included observations on how diseases affected populations and how diseases spread.
Hippocrates observations about the cause and spread of disease in populations were in
many ways more accurate than many of his observations about the medical treatment
and illness. The three books which brought him recognition were Epidemic-I
Epidemic- III and On Airs, Waters and Places. (25)
The Industrial revolution of the 18th century while bringing affluence also brought
number of problems – slums, accumulation of refuse and human excreta,
overcrowding and a variety of social problems. Frequent outbreaks of cholera added
to the woes. Chadwick’s report on “The Sanitary Conditions of Labouring population
(1842)”, focused the attention of the people and Government on the urgent need to
improve public health. Filth and garbage were recognized as man’s greatest enemies
and it last to great sanitary awakening bringing Public Health Act of 1848 in England,
in acceptance of the principle that the state is responsible for the health of the people.

17
The act was made more comprehensive in 1875 when Public Health Act 1875 was
enacted. The Indian Public Health Association was formed in 1958.(26)
This early phase of public health (1880-1920) is often called the “disease control
phase”. Efforts were directed entirely towards general cleanliness, garbage and refuse
disposal.(7)
Epidemiology was practiced in hospitals, or most of the times the waste thrown out of
hospitals was to be taken care by the local municipalities. The general public and
social activists were also not much aware of bio-medical waste hazards and were not
concerned about how the Medical waste had to be disposed off.
Since last fifty years or so, a tremendous change has come in disease profile of the
community as the incidence of hospital borne infections is on constant rise. Though
new drugs and technology for management of diseases in health care system are
available, the waste generation and disposal has always not been given its due
importance.
In every hospital a large amount of waste is generated daily and it has become
necessary to give special attention for the proper treatment and disposal of waste.
Although hospital exists to treat illness, they can act as reservoirs of infection.
Whenever accurate survey have been made it has been found that a substantial
proportion of patient acquire infection during stay in the Hospital. Mostly infection
occurs in the hospital, is due to inappropriate cleanliness. Therefore, it is essential to
take precautions in the design and organisation of hospital to minimize the risk of
infection.(25)

18
(C) Categories of the persons exposed to risk of infections
The Persons who are exposed to the risk of infection from potentially infectious
wastes are:
i) Patients who attend the hospital and who are at special risk from infections
and other complications if the waste disposal is not properly organized:
• Immunosupressed patients, whose defense mechanisms are altered, e. g.
HIV patients, patients of cancer, patients on immunosuppressive drug
therapy.
• Patients with bleeding or clotting diseases
• Patients in health care establishments or under home care.
ii) All medical and paramedical staff who are involved in medical care:
• The main groups are nurses
• Laboratory technicians
• Sanitation staff involved in collection, segregation and disposal of waste
• Staff working in supportive service areas like kitchen and laundry etc.
iii) All visitors to the hospital including the general public:
iv) Public health risks of hazardous health care waste:
Infections may be transmitted by contact with patient’s body fluids or secretions.
Pathogens may also be distributed by insects and rodents that come in contact with
unsafely stored waste. Nosocomial (hospital acquired) Infection can also occur due to
poor health care waste management.(8)

19
(D) Sources of Health Care Waste
Major sources of health care waste:
(a) Hospitals
• University hospital
• General hospital
• District hospital
(b) Other health care establishments
• Health care centres
• Dispensaries
• obstetric and maternity clinics
• Outpatient clinics
• First aid posts
• Long term health care establishments and hospitals
• Primary health centres, sub-centres
(c) Related laboratories and research centres
• Medical and bio-medical laboratories
• Biotechnology laboratories
• Medical research centres
• Animal research and testing centres
• Blood banks and blood collection services

20
(d) Minor sources of health care establishments
• Small health care establishments
• Physician offices
• Dental clinics
• Acupuncturists
• Clinics and Dispensaries of Indigenous system of practitioners(7,19)
All these health care establishments generate waste and are therefore covered under
Bio-Medical Waste (management and handling) Rules, 1998.(7)
Though many of the healthcare facilities are small, and do not individually produce
much hazardous waste, the total quantity of hazardous wastes coming from all the
small facilities is likely to be significant. In many cities the wastes from small
healthcare facilities are mixed with general municipal wastes in a large number of
locations, thereby contaminating a very large quantity of waste. (19)

21
(E) Classification of Health Care Waste
The WHO classification of hazardous health care waste. (7)
Sl. No. Waste types Description and examples
1. Infectious waste Waste suspected to contain pathogens e.g.
laboratory culture, tissue materials, equipment
that has been in contact with infected patients,
excreta.
2. Pathological waste Human tissue or fluids e.g. body parts, blood
and other body fluids.
3. Sharps Sharp waste e.g. needles, infusion sets,
scalpels, knives, blades, broken glasses etc.
4. Pharmaceutical waste Waste containing pharmaceuticals e.g. expired
drugs.
5. Genotoxic waste Waste containing substances with genotoxic
properties e.g. Cytotoxic drugs.
6. Chemical waste Laboratory reagents, film developers
7. Wastes with high content of
heavy metals
Batteries, broken thermometers and BP
instruments
8. Pressurized containers Gas cylinders, aerosol cans
9. Radioactive waste Waste containing radioactive substances e. g.
unused liquid from radiotherapy units,
packaging or radioactive material.
(F) Occupational Health and Safety Precautions/ Measures
Hospital waste management requires commitment from persons, at all levels in the
health cares facility. According to W.H.O, “The human element is more important
than the technology. Almost any system of treatment and disposal that is operated by
well-trained and well-motivated staff can provide more protection for staff, patients

22
and the community, than an expensive or sophisticated system that is managed by
staff who do not understand the risks and importance of their contrition.”
Appropriate personal hygiene and good laboratory practices are absolutely
fundamental to biological safety and cannot ever be replaced by any fancy chemical
or special equipment.
Occupational health and safety measures include meticulous practice of universal
precautions at work place, proper use of personal equipment, periodic medical and
health examination, maintenance of records of morbidity, accidents and injury,
typhoid and hepatitis-B. Training, retraining and continued training of personnel,
good house keeping and hygienic practices are complimentary to the Endeavour.(19)
Essentials of the Universal precautions/ standard precautions:
Since medical history and examination can not be reliable identity of patients infected
with HIV or other blood borne pathogens, precautions should be consistently used for
all specimens of blood and body fluid. This approach is known as “Universal
precautions.”
Thus blood and certain body fluids of all patients are considered potentially infectious
for HIV, HBV and blood borne pathogens.
Universal safety precautions are intended to prevent parental, mucous membrane and
non intact skin exposures of health care workers to blood borne pathogens.
Use appropriate barrier precautions to prevent skin and mucous membrane exposure,
when contact with blood or body fluids are anticipated. (19)

23
Few of the other important Safety practices are:
a) Hand washing
• Wash hands after touching blood, secretions, excretions and contaminated
items, whether or not gloves are worn. Wash hands immediately after
gloves are removed, between patients’ contacts.
• Use a plain soap for routine hand washing.
• Use an antimicrobial agent for specific circumstances.
b) Gloves
• Wear gloves when touching blood, body fluids, secretions, excretions and
contaminated items. Put on clean gloves just before touching mucous
membranes and non-intact skin.
c) Mask, eye protection glass, face shield
• Wear a mask and eye protection glass or a face shield during procedures
and patient care activities that are likely to generate splashes or sprays of
blood, body fluids, secretions and excretions.
d) Gown
• Wear a gown during procedures and patient care activities that are likely to
generate splashes or sprays of blood, body fluids, secretions or excretions.
e) Linen
• Handle used linen, soiled with blood, body fluids, secretions and
excretions in a manner that prevents skin and mucous membrane

24
exposures, and that avoids transfer of microorganisms to other patients and
environments.
f) Occupational health and blood-borne pathogens
• Take care to prevent injuries when using needles, scalpels and other sharp
instruments or devices.
• Use ventilation devices as an alternative to mouth to mouth resuscitation
methods.
g) Isolation of Patient
• Place a patient who contaminates the environment or who does not assist
in maintaining appropriate hygiene in an isolated (or separate) room. (27)
Implementation of Bio safety practices
Although guidelines regarding universal precautions and other bio safety practices are
available since long, strict implementation is eventually not in practice in health care
setting in India. With increase in the prevalence of HIV infection, there is a definite
need that the health care workers take bio safety practices seriously. For effective
compliance, the hospital managers should ensure adequate supply of personal
protective equipments, availability of material for hand washing, disinfectants and set
up an effective waste disposal programme for disposal of biomedical waste.(28)
(G) Application, Treatment and Disposal Technologies for Health Care Waste
Application:
The Bio-medical waste (management and handling) Rules, 1998, apply to all persons
who generate, collect, receive, store, transport, treat, dispose or handle Bio-medical
waste in any form.(29)

25
Treatment:
It means any method, technique or process designed to change the biological or
physical character or composition or waste to reduce or eliminate pathogens so that
the waste no longer possesses a hazard to persons who may be exposed to it.
Treatment of waste generated (at source) is the most desirable, since it makes the
handling of waste much safer. The final choice of treatment system should be made
carefully, on the basic of various factors, many of which depend on local
conditions.(30)
Purpose of treatment of waste is:
• Reduce the hazardousness (injuries) of the waste
• Reduce the infectiousness of the waste
• Volume reduction
• Pre-requisite to use certain disposal options (e.g. deep burial of infected
waste)
• Makes the option of recycling of waste a safe and viable one. (30)
Methods of Treatment are as follows:
Disinfection
It is a process of application of a disinfectant for a sufficient length of time in an
adequate quantity and strength so as to kill the specific organisms of infectious
diseases e. g. faeces of an infected person is mixed with an equal volume of phenol
solution 1 in 20 and bleaching powder, stirred with a wooden stick and allowed to
stand for two hours. Urine should be treated with phenol solution 1 in 20 and allowed
to stand for half an hour. Feeding equipment, utensils and crockery should be boiled.

26
Sputum should be received in gauze swabs or paper sputum cups and destroyed by
burning. Clinical thermometer should be kept in a phenol solution of 1 in 20 strength.
Types of Disinfection:
• Concurrent disinfection
It is carried out during course of patient’s illness.
• Terminal disinfection
It is the process of rendering the personal clothing and immediate physical
environment of the patient free from the possibility of conveying infection to others at
the end of illness.
• Prophylactic disinfection
Process of pasteurisation of milk, water purification by chlorination etc.(16)
Disinfectant: A disinfectant or germicide is a substance which destroys harmful
microbes (not usually spores) with the object of preventing transmission of disease.
Disinfectants are suitable for application only to inanimate objects. (7)
A substance/ compounds which kill bacteria (bactericidal) are called disinfectants,
while those which prevent their production (bacteriostatic) are called antiseptics.(17)
Disinfectants may be internal i.e. agents used to kill the micro organisms inside the
body or external i.e. agents used to kill the bacteria outside the body. However the
term disinfectant is usually associated with the external disinfectants.(16)

27
Classification of disinfectants:
The disinfectants are classified as:
• Natural Disinfectants e.g. sunlight and air by process of drying prevent the
growth of microorganisms. The ultra-violet rays present in sunlight are also
germicidal in action.
• Physical Disinfectants:
a) Dry Heat
Burning is the surest method of disinfection and is preferred for items of little value
and disposal. Hot dry air has no penetrating power and does not kill spores.
b) Moist Heat
Boiling is an efficient method. Generally 10-15 minutes boiling kills most of the
microorganisms. For the destruction of spores a longer period of boiling about 30
minutes is necessary. Clothes and utensils etc. can be disinfected by this method.
c) Steam
Current steam: Steam produced at ordinary atmospheric pressure (100ºC) is called
current steam. It is used in many portable disinfectors with the entry of steam at top
and exit below the articles to be disinfected.
Saturated steam: Steam is generated in a closed vessel under pressure, so that higher
temperature is obtained of the compressed steam.
Sterilisation: means destruction of all forms of microbial life including viruses,
fungal and bacterial spores on inanimate surfaces, including the resistant spore forms.
• Chemical Disinfectants: are solids, liquids and gaseous.

28
Chemical Sterilisation includes gas sterilisation with ethylene oxide of other gases
and immersassion in a disinfectant solution with sterilizing properties e.g.
Glutaraldehyde. (16)
Disposal:
It means placing the Bio-medical waste in its final resting place.
Certain Methods of Disposal Technologies of Health Care Waste:
(A) Solid Waste Disposal Methods:
In cities and bigger towns non-contaminated solid waste disposal is usually
undertaken by the Municipalities/ Corporations and such waste is disposed in compost
yards/ burial sites away from living areas. In places where such a systematic facility
for waste disposal is not available, one may need to think of disposal in a site nearer
to the health setting. Such a situation may arise in Primary Health Centre or any other
health setting situated in the countryside or rural area. A similar situation may also
arise when the existing waste disposal facilities are far away or inaccessible. In order
to be equipped to meet this need, it is worthwhile recalling some of the methods of
waste disposal.
Methods of disposal of refuse:
1. Burial
2. Composting
3. Incineration
4. Dumping
5. Manure pits
6. Composting
7. Sanitary land fills.(31)

29
General wastes from the hospital can be disposed off by composting and recycling.
Radioactive waste if persists must be stored until the half life period of the wastes
expire before disposal.(32)
1. Burial:
• It is ideal if the location is 50 m away from any water source. Maintain a
minimum distance of 6 ft between the bottom of the trench and the water label.
• A long trench 6 ft deep and 3 - 4 ft wide is dug. The material is dumped and
covered with one foot of excavated earth each day, this also keep animals away
from digging up the buried refuse.
• Construct a wall or fence around the disposal site with locally available materials
such as stone/ bamboo with cactus or any other thorny plants.
• Chemical, bacteriological and physical changes occur in buried refuse. The
temperature rises to over 60ºC within 7 days, kills all the pathogens and hastens
the decomposition process. It then takes 2 - 3 weeks to cool down. Normally, it
takes 4 - 6 months for complete decomposition of organic matter into an
innocuous mass, which is rich in carbon and nitrogen and is excellent for plant
growth.(31)
2. Composting:
• A biological process in which the organic material in refuse is converted to
manure by the action of microorganisms present in the refuse.(17)
• Garbage, paper, straw and cattle dung are dumped into pits and later covered with
half to one foot of earth after every dumping.
• It is a method of combined disposal of excreta and refuse.

30
• Two such pits will be needed. When one is closed, the other will be in use. In 5 to
6 month’s time, the refuse is converted into innocuous manure.(31)
Waste materials that are organic in nature, such as plant material, food scraps and
paper products are put through a composting or digestion system to control the
biological process to decompose the organic matter and kill pathogens. The resulting
stabilized organic material is then compost for agricultural or landscaping purposes.
There is a large variety of composting and digestion methods or technologies, varying
in complexity from simple window composting of shredded plant material, to
automated enclosed vessel digestion of mixed domestic waste.(33)
The area for compositing is dug and side wall is built with bricks. First the dry waste
is dumped and spread about 6 inch in height, and above that refuse is dumped into
about 2 inches. This process is continued until the pit is filled. Lot of heat emerges
due to chemical changes and pathogens are killed. Thus, matter become precious
manure within three months.(34)
3. Incineration:
Refuse can be disposed off ‘hygienically’ by burning or incineration. Infected hospital
waste and disposables are best disposed off by incineration. Incineration is controlled
burning. For it to be effective and the process innocuous, it is necessary to observe the
following precautions:
• The incinerator should have 2 chambers; one chamber to burn the waste and the
other to burn the volatiles released from the first chamber. Thus, the smoke/ gases
are rendered innocuous and there is no air pollution.
• The temperature maintained in the first chamber (primary chamber) should be
800ºC±50ºC and in the second chamber (secondary chamber) it should be

31
1050ºC±50ºC. Dioxins released while burning plastic material are rendered
innocuous at this temperature.
The standards prescribed by the Central Pollution Control Board and as quoted in the
Bio-medical waste rules, 1998 should be adhered to:
• Install good quality incinerators of standard made
• Monitor closely the temperature reached
• Segregate the waste and feed it selectively into the incinerator
• Provide training to all the staff involved
• Incinerated waste is to be disposed off in secure landfills
• Metal components are not incinerated, hence needles, tops of vials, etc. are to be
disposed off differently.(35)
4. Inertization:
The process of “inertization” involves mixing waste with cement and other substances
before disposal in order to minimize the risk of toxic substances contained in waste
migrating into surface water or groundwater. It is especially suitable for
pharmaceuticals and for incineration ashes with a high metal content (in this case the
process is also called “stabilization”).
For the inertization of pharmaceutical waste the packaging should be removed, the
pharmaceuticals are grinded and a mixture of water, lime and cement added. A
homogenous mass if formed and cubes or pellets are produced of equal size and then
can be transported to a suitable storage site. Alternatively the homogenous mixture
can be transported in liquid state to a landfill and poured into municipal waste.
The following are typical proportions for the mixture:
65% pharmaceutical waste, 15% lime, 15% cement, 5% water.(36)
32
(B) Liquid Waste Disposal Methods:
Liquid wastes of hospitals and health care settings consists of waste water from
bathrooms, wash basins etc. In cities and bigger towns where an underground
drainage system exists, all these liquid wastes and decontaminated liquid waste from
laboratory/ blood bank can be led into the underground drainage system. Blood,
serum and all other body fluids left over in the laboratory, spillage during / after
diagnostic or treatment procedures has to first decontaminate with suitable
disinfectant like 0.5 – 1% sodium hypochlorite with a contact time of 30 minutes. (35)
In semi-urban and rural health care settings, where there is no underground drainage
system, the following methods of disposal can be considered.
a. Soak Pit
• A soak pit allows waste water to drain into the soil
• A soak pit cannot be used in areas where earth is made of heavy clay or rock or
near a ground water source.
• The size recommended for a soak pit depends on the amount of waste water and
the percolation rate. In a wide range of soils, a soak pit 5 - 6 feet deep and 3 ft in
diameter could drain out 50 - 70 litres of liquid waste per day.
• Soak pits should not be constructed near the wells, for fear of contaminating the
sub soil water.(37)
b. Evapo-transpiration Mound
• This is useful especially where soil conditions do not allow the liquids in soak pits
to soak into the ground (e.g. in heavy clay and rock) or where ground water can
get contaminated.
33
• Waste water is led into a mound where fast growing grasses take up water and
release it into the atmosphere through transpiration and evaporation. It is better to
locate the mound on a site, which is not subject to flooding.
• The mound must be well constructed and managed properly.(35)
(H) Key steps of health care waste management
Minimization, separation, identification, handling, treatment and final disposal of
waste: technical specifications for the implementation of each step should be
described in separate technical guidelines:
• Record-keeping requirements
• Rules governing the protection of workers’ health and safety
• Safe practices for waste minimization
• Separation, handling, storage and transport of health care waste.(38)
The persons most at risk are the staff of hospitals, particularly nurses and other health
care providers, waste handlers both within and outside the health care establishment.
In countries like India, scavengers and rag pickers are at serious risk. It is necessary in
such a situation that attention is paid to:
i. Keeping the waste secured and preventing the access to unauthorized persons at
every stage.
ii. Initiate awareness within the health care establishment and the community about
the potential hazard of medical waste.
iii. Decontaminate or disinfect the infectious component of the waste at site of
generation.
iv. Disfigure the single/ limited use items to prevent the reuse.(3)
34
(I) Bio-Medical Wastes (management and handling) Rules, 1998
The Government of India under the provision of the Environment Act - 1986, notified
the Bio-medical waste (management and handling) rules on 20th July 1998.
The following are the guidelines:
• The Rules regulate the disposal of Bio-medical waste.
• The objective is to take all steps to ensure safety of health and environment.
• Article 21 of the constitution of India guarantees the right of life and personal
liberty. The expansive interpretation given to it by the judiciary includes the
fundamental right to clean environment and health and medical care within its
ambit.
The central legislations on this subject are:
• The water (prevention and control of pollution) Act, 1974
• The Air (Prevention and control of pollution) Act, 1981
• The Environment (Protection) Act, 1986
• The Hazardous Wastes (Management and Handling) Rules, 1998
• The Bio-Medical Wastes (Management and Handling) Rules, 1998
• Municipal Solid Wastes (Management and Handling) Rules, 2000 for municipal
waste.(15)
The law and rules should be complemented by a policy document, and by technical
guidelines developed for implementation of the law. This legal “package” should
specify regulations on treatment for different waste categories, segregation, collection,
storage, disposal, and transport of waste, responsibilities and training requirements; it

35
should taken into account the resources and facilities available in the country
concerned any cultural aspects of waste-handling. Gradual implementation of the law
is recommended in preference to any attempt to introduce all measures
simultaneously, particularly where existing practices are inadequate.(6)

36
MATERIALS AND METHODS
The HCIs (unani hospitals and dispensaries) in Bangalore were sorted out as
providing OP services only and those providing both OP and IP services for the
purpose of analysis and discussion. The collected data is analysed by using tables and
graphs, the research design used for this study is a descriptive research study, which
includes surveys and fact finding inquires.
1. Through observational checklist (Annexure-1) for assessment of both Pre and Post
orientation/ Sensitisation session.
2. Interaction with various categories of health care personal (like doctors, nurses,
technicians, ward boys and other waste handlers).
3. Type of waste, Quantity of waste, Waste segregation and method of disposal
recorded.
4. The purpose of the study was explained to respondents (Department heads,
administrative heads of the institutions, physicians, nursing heads, house keeping
and cleaning personnel) to get their full cooperation and prompt answers.
5. The observational checklist (Annexure-1) for assessment of the existing systems is
based on the Bio-medical waste (management and handling) Rules, 1988, Govt. of
India, and Interaction with various categories of health care personal and waste
handlers.
RESEARCH APPROACH:
The research design used for this study is a descriptive research study. Descriptive
research includes surveys and fact finding inquires, to assess the existing practices of

37
waste management and to identify the type of waste, segregation practices,
quantification of waste and its disposal methods. And orientation / sensitisation
sessions were conducted for the health care personnel at interval of first month, fourth
month and sixth month of the POS at various departments / sections of the studied
HCIs and the effect of management is noted both in components of the waste and in
the continued interaction of the health care personnel, as mentioned below.
(1) Through observational checklist (Annexure-1) for assessment of the existing
system and post orientation / sensitization session, the components which
includes source of waste, type of waste, collection of waste, storage of waste and
disposal methods were observed.
(2) Interaction with various categories of health care personnel, like doctors, nurses,
paramedical staff, technicians, ward boys, ayahs, housekeeping staff and other
waste handlers will be done.
PLACE AND DURATION OF THE STUDY:
This study was undertaken in 02 Govt. Unani Hospitals and 03 Govt. Unani
Dispensaries in Bangalore urban limit area, during the period October 2006 and June
2007.
The types of the hospitals included in the study are as follows:
•••• Those providing In-patient and Out-patient services
•••• Those providing only Out-patient service
SAMPLE SIZE:
The Bangalore urban limit area has 02 Govt. Unani Hospitals and 03 Dispensaries.
These hospitals and dispensaries have been included in the study.

38
Table showing the types and number of Hospitals studied
Type of Hospitals Hospitals where
practice documented
Those providing both IP and OP Services (n=2)
National Institute of Unani Medicine, Bangalore Yes
Sri Jayachamarajendra Institute of Indian Medcine
and Hospital
Yes
Those providing only OPD services (n=3)
Government Unani Dispensary, Neelsandra,
Bangalore
Yes
Government Unani Dispensary, Jayamahal extension,
Bangalore
Yes
Corporation Unani Dispensary, Broadway road,
Bangalore
Yes
The studied institutions/ hospitals have been categorised whether providing OP
services or both OP and IP services.
Table Showing Profile of the Studied Institutions
Services Provided
Total Beds
Total Bed Occupancy
Average OPD
Strength /Day
Average IPD
Strength /Day
Average No. of Pathological Cases/Month
Average No. of Regimenal
Cases/Month
OPD and IPD n=2
200 120 200 30 2400 1500
OPD
n=3
NA NA 150 NA - -
Total
n=5
200 120 350 30 2400 1500
Note:
NA=Not Applicable, n = number of institution/ hospital

39
SAMPLING:
It was a purposive sample and effort was made to include health institutions,
rendering out-patient services and both out-patient as well as in-patient services for
documenting practices.
Statistical analysis was carried out for two sources of data, as mentioned below.
1. Staff interest and participation
• HOI, doctors, nursing and other staff interest and participation.
• Perceived factors that have helped in sustaining of the system of waste
management (training and retraining to the staff, recording of injuries/
accidents, periodic monitoring of the waste management facility, occupational
safety measures).
Statistical Analysis: The statistical calculation was carried out using instant G-paid
version 3.
Test applied: Kruskal–Wallis Test
Description: Kruskal-Wallis Test is the most efficient non parametric test for
independent samples. (data replaced by scores or by their ranks) It is named after
William Kruskal and W. Allen Wallis. (39)
The perceived factors were assessed before and at intervals of 1st, 4th, and 6th
months after orientation session with the help of Checklist, they are independent
samples and the samples are classified by the ranking. This test is most appropriate in
this case.
Purpose: Applicable for independent samples with a hypothesis that the treatment
effects are different hence this technique could be used in this study.

40
2. Assessment of the sub-systems of the health care waste management
• Segregation
• Disinfection
• Containment
• Colour coding
• Disposal
The Test that is applied for the assessment during the monitoring of both pre and post
orientation sessions of the sub-system are as follows:
Statistical Analysis: The statistical calculation was carried out using instant G-paid
version 3.
Test applied: Friedman Test
Description: The Friedman test is a non-parametric statistical test use to compare
observations on the related subjects in a sample, the procedures involves ranking. (40)
. The sub-systems were assessed before and at intervals of 1st, 4th, and 6th months after
orientation session with the help of Checklist. They are related subjects and are
classified by the ranking. This test is most appropriate in this case.
Purpose: This test is used with a hypothesis that the treatment effects are different.
This is applicable for related subjects in a sample; hence this technique could be used
in this study.
PILOT STUDY:
A Pilot study was carried out to find out the type of waste generated from the
institutions/ hospitals (providing out-patient services only and those providing both
out-patients as well as in-patient services), quantity of waste, waste segregation and

41
method of disposal is recorded. The purpose of the study was explained to
respondents (department heads, administrative heads of the institution, physicians,
nursing heads, house keeping and cleaning personnel) to get their full cooperation and
prompt answers.
The tool was found to be feasible and practicable and there was no necessity to make
further changes after the pilot study. Therefore, the investigator decided to carry out
the actual study process.
METHODS OF COLLECTION OF DATA:
Initial interaction discussion was held with:
(i) Head of the Department
(ii) Administrative heads of the institution
Data were gathered through observational checklist (Annexure-1), interaction with the
health care personnel and also by direct observation.
The following was the process adopted for building the systems:
a) Interaction with the head of the institutions, to understand their perceptions
about the whole issue of safe management of hospital waste.
b) The initial survey of the institution to learn about the existing systems for safe
management of hospital waste.
c) Orientation and training session, that was interactive, participatory and task
oriented.
d) Identification of roles of each of the health care personnel in safe management
of hospital waste.

42
The standard method used for quantification is as follows:
• Segregated waste was weighed.
• Whenever waste was not segregated, it was physically segregated using
appropriate protective measures.
• In each of the institution, waste was weighed for a minimum period of seven
days.
• The total amount of waste was calculated by taking the average for the period
of weighing.
Regular monitoring of the systems was undertaken using the checklist. The
monitoring was done at 1st month, 4th month and 6th month after the initial orientation.
Few of the key factors that played a great role in establishing the systems health
care units were:
Monitoring
• Monitoring was undertaken with the help of checklist
• Problem identification and problem solving and not a fault finding mission.
• Persuasive and encouraging
Empowering
• Discourage waste generation staff to depend on cleaning staff for segregating
waste.
Incentive for good practices
• A small token monitory benefit

43
Disincentive
• Token monitory fine
• No increments
Head of the institutions
• A participant in the endeavour
• Facilitating continued interaction
• Helps systems to evolve and improving the systems by procuring appropriate
equipment.

44
OBSERVATION AND RESULTS
This chapter is based on collected data, which was analysed by using Tables and
Graphs.
Table 1
Types of services provided by the studied HCIs
Services Provided IPD/OPD
n =2 (40%) OPD
n =3 (60%) Total N =5
Total Beds 200 NA 200
Total Bed Occupancy 120 NA 120
Avg. OPD Strength/day 200 65 265
Avg. IPD strength/day 30 NA 30
Average Pathological Investigation/month
6215 0 6215
Figure 1
Types of services provided by the studied HCIs
OPDn = 3(60%)
IPD/OPDn = 2(40%)
IPD/OPD n = 2 OPD n = 3
Figure 1 shows that number of studied HCIs providing OP service was 60% and those
providing both IP/ OP services were 40%

45
Table 2
Category of Staff and their Participation in the Studied HCIs
Category of Staff Number (%)
Number of Doctors 56 (46.66)
Nursing staff 14(11.66)
Laboratory technicians 8(6.66)
Pharmacy staff 16(13.33)
Ward boys/ Ayahs 22 (18.33)
Others 4(3.33)
Total Health Care Personnel 120(100)
Figure 2
Category of Staff and their participation in the studied HCIs
56 (46.66%)
14 (11.66%)
8 (6.66%)
16 (13.33%)
22 (18.33%)
4 (3.33%)
0 20 40 60
Cat
ego
ry
Number (Percentage)
Others
Ward boys/ Ayahs
Pharmacy staff
Laboratory technicians
Nursing staff
Doctors
Figure 2 shows the numbers and percentage of various HCP participated in studied
HCIs throughout pre and post orientation/ sensitisation session

46
Table 3
Percentage of Various Types of Waste Generated in Studied HCIs
Types of Waste Waste items Quantity (Kg)
%
General Waste Paper, plastic, food waste, sweeping from hospital premises, packing material, herbal remains from pharmacy etc.
123 81.45
Sharps Needles, syringes, broken ampoules and glass, used scalpel, blades, etc.
1.87 1.23
Pathological Waste
Human tissues and fluids e.g. body parts, blood and other body fluids, remains of blood sample, blood soaked swab, etc.
5.90 3.90
Infectious Waste Used dressing material, soiled surgical dressing, swab material in contact with persons suffering from infectious diseases, disposable gowns, gloves, towels, etc.
20.25 13.41
Figure 3
Percentage of various types of wastes generated in studied HCIs
81.45%
1.23%
3.90%13.41%
General waste
Sharps
Pathlogical waste
Infectious waste

47
Table 4
Quantity Estimation of Solid Waste Generation in kgs/ bed/ day in studied HCIs
having In-Patient Facility
Observation No. of Beds
Total Weight (Kg)
Weight (Kg)/ bed/ day
Weight (Kg)/ bed/ year
%
HCI 1 100 78 0.78 284.7 53.42
HCI 2 100 68 0.68 248.2 46.58
Total 200 146±7.07 1.46±0.07 532.9±25.80 100
Figure 4
Percentage of quantity of waste generated in 2 studied HCIs having in-patient facility
53%
47%HCI No. 1
HCI No. 2

48
Table 5
Institutional Facilities for Treatment/ Disposal of waste
Services Provided
(%)
Burial Burning Incineration Autoclave
IP/OPD
n=2 (40%) 0 2 (40%) 0 0
OP
n=3 (60%) 0 2 (40%) 0 0
Total
N=5 (100%) 0 4 (80%) 0 0
Table 5: shows that 4 studied units two were having the facility of OPD and other two
having facility of OPD & IPD were burning the waste.
Table 6
Methods of Collection of Various Types of Waste Items
Types of Waste Waste items Methods of
collection
General Waste Paper, plastic, food waste, sweeping from hospital premises, packing material, herbal remains from pharmacy etc.
In baskets and containers (open lid)
Sharps Needles, syringes, broken ampoules and glass, used scalpel, blades, etc.
Transparent bottles
Pathological Waste
Human tissues and fluids e .g. body parts, blood and other body fluids, remains of blood sample, blood soaked swab etc.
Polythene covers/ containers (lidded)
Infectious Waste Used dressing material, soiled surgical dressing, swab material in contact with persons suffering from infectious diseases, disposable gowns, gloves, towels etc.
Polythene covers/ containers with lid
Table 6: shows that open containers were used to collect the non-infectious general
waste and lidded containers were used to collect the infectious waste

49
Table 7
Frequency of Collection of Various Types of Waste Items
Types of Waste Waste items Frequency of
collection
General Waste Paper, plastic, food waste, sweeping from hospital premises, packing material, herbal remains from pharmacy etc.
daily
Sharps Needles, syringes, broken ampoules and glass, used scalpel, blades, etc.
Once in a week
Pathological Waste
Human tissues and fluids e .g. body parts, blood and other body fluids, remains of blood sample, blood soaked swab etc.
daily
Infectious Waste Used dressing material, soiled surgical dressing, swab material in contact with persons suffering from infectious diseases, disposable gowns, gloves, towels etc.
Twice a day
Table 7 shows General waste is collected daily and infectious waste is collected twice a day
Table 8
Methods of disposal of various types of waste Items
Types of Waste Waste items Methods of
disposal of waste
General Waste Paper, plastic, food waste, sweeping from hospital premises, packing material, herbal remains from pharmacy etc.
Burning/ handing over to corporation municipal system
Sharps Needles, syringes, broken ampoules and glass, used scalpel, blades
burning
Pathological Waste Human tissues and fluids e .g. body parts, blood and other body fluids, remains of blood sample, blood soaked swab etc.
burning
Infectious Waste Used dressing material, soiled surgical dressing, swab material in contact with persons suffering from infectiousdiseases, disposable gowns, gloves, towels, etc.
burning

50
MODE OF MANAGEMENT OF SOLID AND LIQUID INFECTIOUS W ASTE
IN THE STUDIED HCIs
• Mode of Management of Solid Infectious Waste in the Studied HCIs
Table 9
(a) Activities at Point of Generation of Waste Item at Studied HCIs
Waste item Segregation Disinfection Containment
Cotton 2 (40%) 0 2 (40%)
Contaminated linen 2 (40%) 0 2 (40%)
Bandage cloth 2 (40%) 0 2 (40%)
Table 9 shows that segregation and containment of waste was done in 40% of the
studied HCIs
Table 10
(b) Treatment and Final Disposal of Wastes in Studied HCIs
Waste item Transportation Colour
Coding
Final
Disposal
Overall Approximate
Management
Cotton 2 (40%) 0 1 (20%) 0
Contaminated
linen 1 (20%) 1 (20%) 0 0
Bandage cloth
1 (20%) 1 (20%) 0 0
Table 10 shows transportation of waste was done in 40% of the studied HCIs
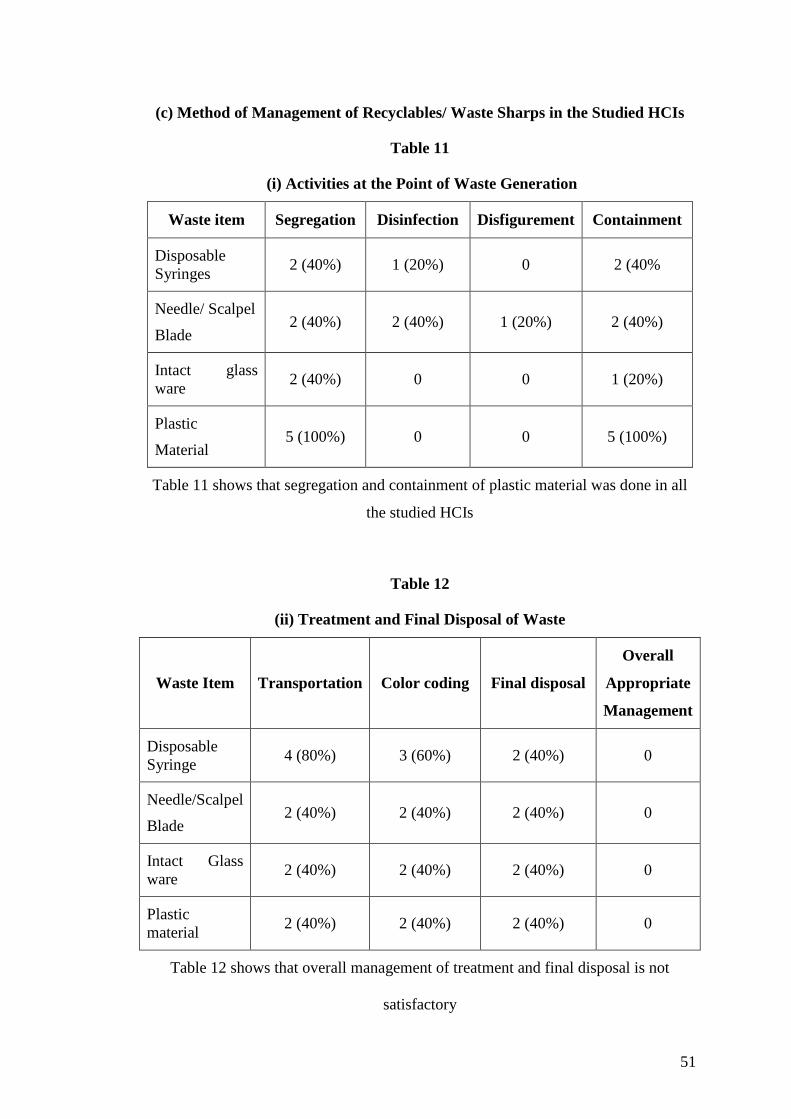
51
(c) Method of Management of Recyclables/ Waste Sharps in the Studied HCIs
Table 11
(i) Activities at the Point of Waste Generation
Waste item Segregation Disinfection Disfigurement Containment
Disposable Syringes
2 (40%) 1 (20%) 0 2 (40%
Needle/ Scalpel
Blade 2 (40%) 2 (40%) 1 (20%) 2 (40%)
Intact glass ware
2 (40%) 0 0 1 (20%)
Plastic
Material 5 (100%) 0 0 5 (100%)
Table 11 shows that segregation and containment of plastic material was done in all
the studied HCIs
Table 12
(ii) Treatment and Final Disposal of Waste
Waste Item Transportation Color coding Final disposal
Overall
Appropriate
Management
Disposable Syringe
4 (80%) 3 (60%) 2 (40%) 0
Needle/Scalpel
Blade 2 (40%) 2 (40%) 2 (40%) 0
Intact Glass ware
2 (40%) 2 (40%) 2 (40%) 0
Plastic material
2 (40%) 2 (40%) 2 (40%) 0
Table 12 shows that overall management of treatment and final disposal is not
satisfactory

52
Table 13
• Mode of Management of Liquid Waste and Infectious Body Material in the
Studied HCIs
Waste Item Disinfection Containment Final disposal Overall
Appropriate
Management
Stool 0 0 0 0
Urine 0 0 0 0
Sputum 0 0 0 0
Blood 0 0 0 0
Table 13 shows that overall management is nil

53
RESULTS OF INITIAL ASSESSMENT IN STUDIED HCIs
Overall Assessment:
• None of the studied units managed Soiled infectious waste appropriately
• One of the studied units providing both IPD/ OPD had needle destroyer for
disfigurement of needles, but final disposal was not appropriate.
• None of the studied institutions managed liquid infectious waste appropriately.
From the above results, it could be inferred that the type, size or the profile of
institutions has not influenced the systems for safe management of HCW.
Assessment of the Subsystems:
1) Soiled infectious waste: Bandage cloth
• Segregation of this waste item was seen in 40% of the studied units and its
containment was satisfactory in similar number of the studied institutions
• However, there is an operational constraint, if chemical decontamination of this
waste is to be considered, it requires huge amounts of water and chemicals. This
also increases the weight of the waste item. There is a possibility that this
practice if adopted, would leave the whole of its containment, collection, storage
and transportation subsystems in a mess and further, if there is no appropriate
concentration of the disinfecting agent used, then there is a possibility of spread
of the spill area.
• The other alternative that could be considered is Autoclaving or Microwaving,
which again are cost intensive and need trained HCP for operation.

54
2) Waste sharp management: Needles
• The management of this waste is a big concern. There is segregation in only 40%
of the HCIs. This could be probably because of the thrust that is give to the waste
sharp destructors, so if there is no destructor the system can not start, this myth
among the HCIs needs to be quelled.
• A puncture proof container would achieve the objective of the waste sharp
management.
• This coupled with disinfection could achieve the objective of management of this
category of waste.
3) Plastic recyclables: Syringes
• This waste item was segregated in 40% of the studied HCIs
• The problems with this waste item are its Re-use potential, and in many of the
HCIs this has been left as an incentive to the Cleaners.
4) Body fluids:
• The appropriate management of this infectious waste is very much feasible
operationally. HCI could be oriented to the hazards of untreated liquid infectious
waste could pose to General community/ sanitary workers.
• It is not much difficult to orient people to disinfect at least the laboratory samples
of the body fluid before they let in to sewage system.
The assessment of the sub-systems reveals that though the current existing systems do
not fulfil the requirements of the BMW Rules, there were definitely attempts at
managing the waste in the studied HCIs.

55
Assessment of the Systems and Subsystems for SMHCW
Description of the process observed for building systems for SMHCW in all the 5
HCIs selected for orientation sensitization:
Monitoring the Systems at 1st, 4th And 6th Months
The status of the subsystem at Monthly interval after the Orientation session was
assessed based on checklist. The subsystems are Segregation, Disinfection and
Containment.
Assessment of the systems was in terms of whether it is satisfactory or not
satisfactory. Similarly, Head of institute interest, Nursing staff participation, House
keeping staff, Doctors interest, Continues interaction, support of HOI, was looked for
there presence or absence.
Assessment of Waste Management System in the HCIs, Pre and Post
Orientation/ Sensitisation
(A) Staff interest and Participation
1. HOI, Doctors, Nursing and other Staff Interest and Participation
2. Perceived factors that have helped in sustaining of the System of Waste
Management (Training to the staff, Recording of injuries/ accidents, Periodic
monitoring of the waste management facility, Occupational safety measures).
(B) Assessment of the Sub-systems of the SMHCW
The status of Subsystems of SMHCW, as mentioned below, was recorded in 6
Departments/ sections (Pathology, IPD, OPD, Pharmacy, Kitchen and Dressing
Sections) of studied HCIs having both IP and OP facilities and 3 Departments/
sections (OPD, Pharmacy and Dressing Sections) of studied HCIs having only OP

56
facility, where Orientation session was conducted. The assessment during the
monitoring of both pre and post Orientation session was done based on the Checklist.
•••• Segregation
•••• Disinfection
•••• Containment
•••• Colour-coding
•••• Disposal

57
(A) Staff Interest and Participation
Table 14
1. HOI, Doctors, Nursing and other Staff Interest and Participation
Post- Orientation Session HCIs
N = 5
Pre-Orientation
Status Month 1 Month 4 Month 6
Head of the Institution interest
1 2 3 5
Doctors participation 1 3 4 5
Support of the Head of the Institution
1 2 3 5
Continued Interaction
- 3 4 5
Nursing Staff Participation
1 2 3 5
kw=17.841 p<0.001, considered extremely significant
Table 15
2. Perceived Factors that have helped in Sustaining of the System of Waste
Management:
Post-Orientation Session HCIs
N = 5
Pre-Orientation
status Month - 1 Month - 2 Month - 3
Trainingand retraining to the staff
0 1 4 5
Recordingof Injuries/ accidents
0 1 3 5
Reportingof injuries/ accidents
0 1 3 4
Periodic monitoring of the Waste managementfacilities
0 2 2 4
Occupational safety policy
0 0 1 2
kw=15.555 p<0.001, considered extremely significant

58
(B) Assessment of the Sub systems of the SMHCW
Table 16
Application of Segregation of Waste by Studied HCIs in their various
departments
Post – Orientation Session HCIs
N = 5
Pre – Orientation
Status Month - 1 Month - 4 Month - 6
1 0 1 4 6
2 0 1 3 6
3 0 1 2 3
4 0 1 2 3
5 0 1 2 3
fr=15 p=0.0001 considered extremely significant
Figure 5
Application of Segregation of waste by studied HCIs in their various departments
0 0 0 0 0
1 1 1 1 1
4
3
2 2 2
6 6
3 3 3
0
1
2
3
4
5
6
7
HCI 1 HCI 2 HCI 3 HCI 4 HCI 5
No
. o
f D
epar
tmen
ts
Pre-Orient Status Month 1 Month 4 Month 6

59
Table 17
Application of Disinfection of waste by studied HCIs in their various
departments
Post – Orientation Session HCIs
N = 5
Pre – Orientation
status Month 1 Month 4 Month 6
1 0 1 2 4
2 0 1 2 4
3 0 1 2 2
4 0 1 2 2
5 0 1 2 2
fr=14.617 p<0.001, considered extremely significant
Figure 6
Application of Disinfection of waste by studied HCIs in their various departments
0 0 0 0 0
1 1 1 1 1
2 2 2 2 2
4 4
2 2 2
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
HCI 1 HCI 2 HCI 3 HCI 4 HCI 5
No
. o
f D
epar
tmen
ts
Pre-Orientation Status Month 1 Month 4 Month 6
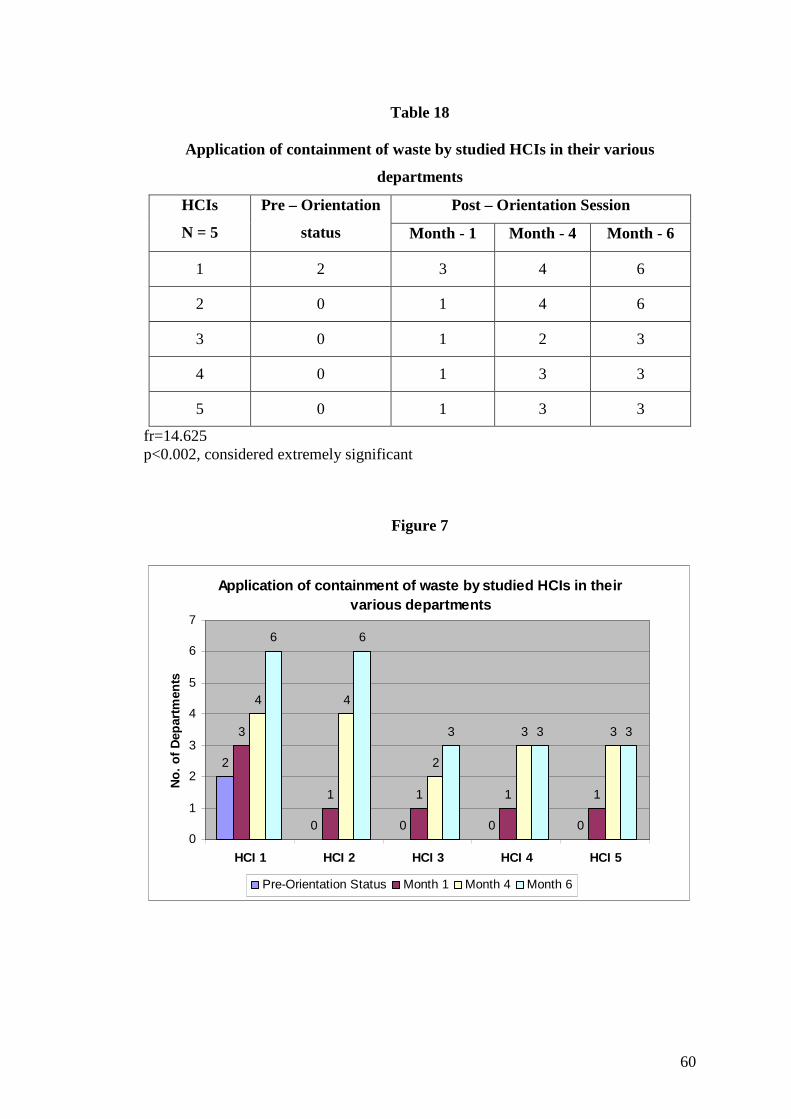
60
Table 18
Application of containment of waste by studied HCIs in their various
departments
Post – Orientation Session HCIs
N = 5
Pre – Orientation
status Month - 1 Month - 4 Month - 6
1 2 3 4 6
2 0 1 4 6
3 0 1 2 3
4 0 1 3 3
5 0 1 3 3
fr=14.625 p<0.002, considered extremely significant
Figure 7
Application of containment of waste by studied HCIs in their various departments
2
0 0 0 0
3
1 1 1 1
4 4
2
3 3
6 6
3 3 3
0
1
2
3
4
5
6
7
HCI 1 HCI 2 HCI 3 HCI 4 HCI 5
No
. o
f D
epar
tmen
ts
Pre-Orientation Status Month 1 Month 4 Month 6

61
Table 19
Application of Colour coding of waste materials by studied HCIs in their various
departments
Post – Orientation Session HCIs
N = 5
Pre – Orientation
status Month - 1 Month - 4 Month - 6
1 0 1 2 4
2 0 1 3 5
3 0 1 2 3
4 0 1 2 3
5 0 1 2 2
fr=14.755 p<0.001, considered extremely significant
Figure 8
Application of Colour coding of waste materials by studied HCIs in their various departments
0 0 0 0 0
1 1 1 1 1
2
3
2 2 2
4
5
3 3
2
0
1
2
3
4
5
6
HCI 1 HCI 2 HCI 3 HCI 4 HCI 5
No
. o
f D
epar
tmen
ts
Pre-Orientation Status Month 1 Month 4 Month 6

62
Table 20
Application of Disposal of waste by studied HCIs in their various departments
Post – Orientation Session HCIs
N = 5
Pre – Orientation
status Month - 1 Month - 4 Month - 6
1 0 2 3 6
2 0 2 3 6
3 0 1 2 3
4 0 0 1 3
5 0 1 2 3
fr=14.755 p<0.001, considered extremely significant
Figure 9
Application of Disposal of waste by studied HCIs in their various departments
0 0 0 0 0
2 2
1
0
1
3 3
2
1
2
6 6
3 3 3
0
1
2
3
4
5
6
7
HCI 1 HCI 2 HCI 3 HCI 4 HCI 5
No
. o
f D
epar
tmen
ts
Pre-Orientation Status Month 1 Month 4 Month 6

63
DISCUSSION
Types of services provided by the studied HCIs
Table 1, shows that total number of studied HCIs providing OP service is 3 (60%) and
those providing both IP/ OP services were 2 (40%). Total number of beds available
was reported to be 200. The total bed occupancy was reported to be 120, average bed
occupancy of about 60%. The average OPD strength per day in studied HCIs
providing only OP service was 65. Average out patient strength per day in studied
hospitals providing both IP/ OP services were 200. The average in-patient strength in
the studied HCIs providing IP/ OP services was reported to be 30 per day. Average
number of Pathological Investigation in studied hospitals providing both IP/ OP
services were 6215 per month.
Category of staff and their participation in the studied HCIs
As evident in Table 2, the total Health care personnel that took part in the continued
interaction, through out pre and post orientation/ sensitisation session were about 120.
Doctors’ participation was 56 (46.66%), Nursing staff participation was about 14
(11.66%), Laboratory technicians were about 8 (6.66%), Pharmacy staff participation
was 16 (13.33%), Ward boys/ Ayahs were 22 (18.33%), others like House keeping
staff were 4 (3.33%) .
Percentage of various types of wastes generated in studied HCIs
As evident in Table 3, out of total quantity of waste generated from studied HCIs,
81.45% is General waste like Paper, plastic, food waste, sweeping from hospital
premises, packing material, herbal remains from pharmacy, etc. Sharp wastes about

64
1.23% consisting of Needles, syringes, broken ampoules and glass, used scalpel,
blades etc. Pathological waste about 3.90% consisting of human tissues and fluids e.g.
body parts, blood and other body fluids, remains of blood sample, blood soaked swab
etc. And Infectious waste is 13.41% consisting of used dressing material, soiled
surgical dressing, swab material in contact with persons suffering from infectious
diseases, disposable gowns, gloves, towels etc.
All hospital waste has the potential to transmit infection. It is estimated that 80- 85%
is noninfectious general waste, 10% is infectious waste and 5% is other hazardous
waste.(3)
Quantity estimation of solid waste generation in kgs/ bed/ day in studied HCIs
having in-patient facility
Quantity of waste generation in studied HCIs having in-patient facility along with the
standard deviations is calculated in kgs/ bed/ day and/ bed/ year. In observation HCI-
1, the quantity of waste /bed/ day is 0.78kg and/ bed/ year is 284.7kgs. In observation
HCI-2, the quantity of waste /bed /day is 0.68kg and /bed/year is 248.2kgs.
Observations are summarized in Table 4.
The results of the waste survey of the hospitals, polyclinics, clinics and Health centers
indicated that the total amount of waste produced is about 0.26 kg/ bed/ day, the
survey also confirmed that hospitals generate more medical waste than polyclinics,
clinics and health centres.(41)
The hospital waste generation from a 400 bed Brazilian hospital which generates
about 386 kg per day that means that generated waste was about 1 kg/ bed/ day.(42)
It is estimated that the quantity of waste generated from hospitals in India ranges
between 0.5 and 2.0 kg/bed/day and annually about 0.33 million tones.(43)

65
Institutional facilities for Treatment/ Disposal of waste
As evident in Table 5, that 4 studied units two having the facilities of both IP/ OP
Services and the other two having the facility of only OP services, were burning the
waste; no study units had Autoclave for the purpose of treating waste. No incineration
facility was available in any of the studied HCIs for treatment/ disposal of waste.
Burial as an option for disposal of waste was not adopted by any of the studied units.
None of the studied institutions had Microwave for treatment of waste. All the studied
institutions were dependent on corporation/ Municipal facility for lifting and
disposing of waste. There was no landfill facility in the studied area. The remains of
the burning were either dumped in corporation bin or were handed over to the BMP
personnel. It could be observed that there is an overall deficiency of the treatment and
disposal facilities.
Methods of collection of various types of waste items
General waste like paper, plastic, food waste, sweeping from hospital premises,
packing material, herbal remains from pharmacy etc. are collected in baskets and
other containers without lid. Transparent bottles are used for collecting sharp waste
like needles, syringes, broken ampoules and glasses, used scalpel, blades etc.
Pathological waste like human tissues and fluids e.g. body parts, blood and other body
fluids, remains of blood sample, blood soaked swab etc. are collected in polythene
covers and containers with lids. Infectious waste like used dressing material, soiled
surgical dressing, swab material in contact with persons suffering from infectious
diseases, disposable gowns, gloves, towels etc. collected in polythene covers and
containers with lid. Observations are summarised in Table 6.

66
Frequency of collection of various types of waste products
General waste like paper, plastic, food waste, sweeping from hospital premises,
packing material, herbal remains from pharmacy etc. and pathological waste like
human tissues and fluids e.g. body parts, blood and other body fluids etc. are collected
daily. Sharps waste like needles, syringes, broken ampoules and glasses, used scalpel,
blades etc. are collected once in a week. And infectious waste like used dressing
material, soiled surgical dressing, swab material in contact with persons suffering
from infectious diseases, disposable gowns, gloves, towels etc. are collected twice
daily. Observations are summarised in Table 7.
Methods of disposal of various types of waste product
Disposal of general waste like paper, plastic, food waste, sweeping from hospital
premises, packing material, herbal remains from pharmacy etc, are subjected to
burning/ handing over to corporation municipal system. Sharp waste, like needles,
syringes, broken ampoules and glasses etc are also burnt, in one of the studied HCI
needles were destroyed in needle burner and later disposed. Infectious waste like used
dressing material, soiled surgical dressing, swab material in contact with persons
suffering from infectious diseases, disposable gowns, gloves, towels etc, and
pathological waste like human tissues and fluids e.g. body parts, blood and other body
fluids, remains of blood samples, blood soaked swab etc. are also subjected to
burning. Observations are summarised in Table 8.
Method of management of solid infectious waste in the studied HCIs
As revealed in Table 9 and 10, that 40% of the studied HCIs were segregating and
containing waste items in this category, and similarly more than 40% of the

67
institutions were transporting this waste safely, however, the steps that gave away the
system were colour-coding and final treatment/ disposal options adopted.
As evident in Table 11 & 12 that, segregation of disposable syringes, needles and
intact glasses were noted in 2 studied HCIs, plastic materials were segregated in
almost all the studied HCIs. Appropriate disinfection procedure for syringes was
noted in 1 of the studied HCI and for needles in 2 HCIs. Disfigurement of needles was
noted in 1 of the studied HCIs. Appropriate containment for plastic material was
noted in almost all the studied HCIs. But overall management of all waste material in
this category was not satisfactory.
Mode of management of liquid waste and infectious body material in the studied
HCIs
As evident in Table 13, that in the studied HCIs, the system of Disinfection and
Containment for this category of waste was nil. This practice has the potential to
contaminate surface and ground water in addition to exposing the city sanitary
workers to the risk of infections. There was no formal colour-coding system used for
this category of waste.
Assessment of waste management system in the HCIs, pre and post orientation/
sensitization session
A. Staff interest and participation
1. HOI, Doctors, Nursing and other Staff Interest and Participation
As evident in Table 14, the status of the sub systems in all 5 HCIs, was noted
in the Pre-orientation status. In 1 (20%) of the HCI, the HOI showed interest in
establishing system for SMHCW. In 1 (20%) of the unit Doctors was very keen for
establishing the system for SMCHW. In 1(20%) of the HCI, the HOI said he would

68
support the endeavor of establishing the systems, by making appropriate provisions in
terms of resources. In 1 (20%) of the HCI, Nursing staffs were keen on establishing
the system. Continued Interaction was not ascertained in any of the HCIs, because, it
has to be started from here onwards.
The Status of the systems at the end of 1 month of orientation was as follows
The keenness of the HOI and his support were noticed in 2 (40%) of HCIs, Doctors
participation was noticed in 3 (60%) of the HCIs. Nursing staff participation was
noted in 2 (40%), Continued participation i.e. 3 (60%) of the HCIs were in constant
touch with the investigator for suggestions and inputs, regarding waste management.
Nursing staff interest and participation was seen in 2 (40%) of the studied HCIs.
The status of the systems during the second monitoring that is 4 months after the
orientation was as follows
3 (60%) of the HOIs showed keen interest in the efforts at building systems,
continued participation and support was also noted in 3 (60%) of the HCIs. In 4 (80%)
of the HCIs, Doctors were reported to have taken interest and participated in efforts
towards building system for SMHCW. In 3 (60%) of the HCIs, nursing staff made
efforts to make the systems work, and 4 (80%) of the HCIs were in continuous touch
with the investigator for advice and the needful.
Third monitoring of the systems at the end of 6 months of POS, the system were
noted as follows:
All the 5 HOIs had continued to take keen interest in the systems and their
development, in similar number of HCIs Doctors, Nursing Staff, took interest in
building the system and staff from all the HCIs was in continuous touch with
investigator for advice and the needful. The statistical calculation was carried out with

69
the help of Kruskal–Wallis Test (kw) =17.841, p<0.001, considered extremely
significant. Observations are summarised in Table 14
2. Perceived factors that have helped in sustaining of the system of Waste
Management
The following status was observed in the Pre-orientation session, training was not
given to any staff, regarding the safety practices of HCWMS. There was no system of
recording and reporting of injuries/ or any kind of accidents with reference to
mismanagement of Health Care Waste and there was no knowledge about safe
policies of occupation and health care personnel in any of the studied HCIs.
Observations are summarized in Table 15.
The Status of the systems at the end of 1 month of orientation was as follows
Training to the staff, recording and reporting of injuries were noted in 1 (20%) of
studied HCI, monitoring of the system was noted in 1 (20%) of the studied HCI and
Occupational safety measures were not noted in any of the studied HCIs.
The status of the systems during the second monitoring that is 4 months after the
orientation was:
In 4 (80%) of the studied HCIs, Training and Retraining to the staff was conducted
regarding SMHCW. Recording and Reporting of injuries was noted in 3 (60%) of the
studied HCIs. Monitoring of the waste management facility was seen in 2 (40%) of
the HCIs, and 1 (20%) HCI adapted the occupational safety policy.

70
Third monitoring of the systems at the end of 6 months of POS, the system were
noted as follows:
Training and retraining to the staff and Recording of injuries/ accidents were seen in
all the 5 studied HCIs. Reporting of injuries and periodic monitoring of the waste
management facility were noticed in 4 (80% of the studied HCIs. Safety regarding
occupational measures was noticed in 2 (40%) of the HCIs.
The statistical calculation was carried out with the help of Kruskal–Wallis Test (kw) =
15.555, p<0.001, considered extremely significant. Observation are summarized in
Table 15
This indicates that the assessment of various independent factors mentioned in Table
14 & 15 had a gradual and incremental improvement during regular monitoring of the
systems with the help of checklist both at pre and post orientation session.
Notification of the Biomedical waste management (m & h) Rules, 1998, Govt. of
India is the appropriate authority for implementation of rules as well as monitoring of
the systems could be the other contributing factors for improvement.
(B) Assessment of the Subsystems of the SMHCW
The status of Subsystems of SMHCW, as mentioned below was recorded in 6
Departments (Pathology, IPD, OPD, Pharmacy, Kitchen and Dressing sections of all
the studied HCIs, where Orientation session was conducted. The assessment during
the monitoring of both pre and post Orientation session was done based on the
Checklist.
Segregation Colour-coding Disinfection
Disposal Containment

71
Application of Segregation of Waste by studied HCIs in their various
departments
The statistical calculation was carried out with the help of Friedman Test (fr)= 15.000,
p<0.0001, considered extremely significant. The above test indicates that there is a
gradual and perceptible rise during regular monitoring of the systems with the help of
the checklist in all the departments of studied HCIs in the component of segregation.
Observations are summarized in Table 16.
Application of Disinfection of Waste by studied HCIs in their various
departments
The statistical calculation was carried out with the help of Friedman Test (fr)= 14.617,
p<0.001, considered extremely significant.
The above test for the component, for Disinfection of waste, showed gradual and
incremental rise during the monitoring of the systems with the help of the checklist in
all the department of the studied HCIs. .Observations are summarized in Table 17
Application of containment of waste by studied HCIs in their various
departments
The statistical calculation was carried out with the help of Friedman Test (fr) =14.625,
p<0.002, considered extremely significant.
The above test for the component, Containment of waste, showed gradual and
incremental rise during the monitoring of the systems with the help of the checklist in
all the department of the studied HCIs. Observations are summarized in Table 18

72
Application of Colour Coding of Waste Materials by studied HCIs in their
various departments
The statistical calculation was carried out with the help of Friedman Test (fr) =14.755,
p<0.001, considered extremely significant.
The above test for the component, of Colour coding of waste material, showed
gradual and incremental rise during the monitoring of the systems with the help of the
checklist, in all the department of the studied HCIs. Observations are summarized in
Table 19.
Application of Disposal of Waste by studied HCIs in their various departments
The statistical calculation was carried out with the help of Friedman Test (fr) =14.755,
p<0.001, considered extremely significant.
The above test for the component, Disposal of waste, showed gradual and incremental
rise during the monitoring of the systems with the help of the checklist. Observations
are summarized in Table 20.
As evident in Table 16-20, the status of the sub-systems (Segregation, Disinfection,
Containment, Colour coding and Disposal) in all 5 of the HCIs, where Pre and Post
Orientation session was assessed based on the Checklist
The Pre-orientation status of the systems as shown in the Tables from 7 – 12 revealed
that only 2 Departments of HCIs had appropriate containment. However, none of the
Department of the 5 HCIs has Segregation, Disinfection, Colour coding or appropriate
Final Disposal procedures.
The status of the Subsystems at the end of 1 month of orientation was as follows:

73
Efforts at Segregation, Disinfection and Colour Coding were noted in 5 Departments
of HCIs, Containment of waste was practiced in 7 Departments and Appropriate
Disposal was attempted in 6 Departments of the HCIs.
The status of the systems during the second monitoring that is 4 months after the
orientation was that Segregation attempted in 13 Departments, disinfection was noted
in 10 Departments of the HCIs, appropriate Containment of waste was noted in 16
Departments of the HCIs, Colour Coding and appropriate Disposal were attempted
each in 11 Departments of studied HCIs.
Third Monitoring of the Subsystems, i.e. 6 months after POS were noted as follows,
Segregation, appropriate Containment and Disposal were attempted in 21
Departments of the HCIs. Disinfection was noted in 14 Departments and 17
Departments attempted instituting a Colour Coding system.
It could be seen from the Tables 16-20 that there was a gradual and incremental
improvement in all the components of the systems for SMHCW. The components like
Segregation, Disinfection and Treatment of waste noted a gradual and perceptible rise
during regular monitoring of the systems with the help of the checklist.

74
CONCLUSION
In the present study the existing practices of waste management in Unani hospitals,
and to identify the type of waste, segregation practices, quantification of waste and
its disposal methods were identified with an observational checklist (Annexure–1).
And orientation/ sensitisation sessions were conducted for the health care personnel
at interval of first month, fourth month and sixth month of the POS at various
departments / sections of the studied HCIs and the effect of management is noted
both in components of the waste and in the continued interaction of the health care
personnel.
The study revealed that there is no system of hospital waste management, there is lack
of necessary supplies (colour coding container, protective devices etc), facilities and
knowledge among health workers.
Quantity of HCW generated in studied HCIs, is 0.78 kg and 0.68 kg/ bed/day in two
studied HCIs providing IP&OP services. The types of wastes generated in the studied
HCIs are General waste (81.45%), Pathological waste (3.90%), Infectious waste
(13.41%) and Sharp waste (1.23%) Waste collected at regular interval and transported
manually.
Lidded containers were used for transporting infectious and pathological waste during
containment of wastes. General waste (81.45%) is non infectious and it is the major
part of the categories of waste, which even includes waste from herbal unani
pharmacy containing remains of dry leaves, twigs, powder of herbs which are all
organic matter and hence bio-degradable. Proper segregation of this waste is
recommended and the biodegradable share can be composite, and later can be used as

75
natural manure for growing plants and maintaining herbal garden. Sharp waste and
hazardous waste is very less in this study compared to other studies, if this is mixed
with non-infectious general waste, the whole waste turns to be infectious and it will
be a burden in management of waste, both cost wise and also in terms of manual
labour. It could be seen from the study that there was a gradual and incremental
improvement in all the components of the systems for SMHCW. The components like
Segregation, Disinfection and Treatment of waste noted a gradual and perceptible rise
during regular monitoring of the systems with the help of the checklist.
It could be concluded from the above, that:
• The most vital component of the waste management plan is to bring about a
transformation in the mind sets and develop a system and culture through
education, training and persistent motivation of the health care staff.
• It should involve the coordinated working of several departments in health
care establishments, like medical, surgical, laboratory, house keeping, kitchen,
pharmacy and even administrative departments.
• The Segregation of hospital waste plays the key role in the safe and efficient
management of health care waste, especially infectious wastes from the non-
infectious waste resulting in defining and limiting expenditures.
• As the major share of the waste is non-infectious, the biodegradable part can
be composite, and later can be used as natural manure for growing plants and
maintaining herbal gardens.
• Lack of treatment and disposal options possess a constraint to the sustenance
of the systems.

76
• Head of the Institution interest, a key for early establishment and efficient
functioning of the systems.
• Paramedical staff and other waste handlers are the key HCP for the
development and evolving of the system.
• Compositing of the non-infectious, biodegradable waste can be taken up as
primary issue in treatment and management of this system
Recommendations
• Intensive training programme at regular time interval for all the staff with
special importance to the new comers.
• The entire waste management practices should be part of total hygiene
practice of the society, rather than confining to hospital and health facilities.
• Establishment of an authorised person responsible for all aspects of medical
waste management. Its main function should be the creation of a national
programme containing uniform requirements for medical waste handling and
disposal.
• Provision of health education, not only for health workers but for all the
community, about hazards of medical waste and how to minimize them.
• Provision of adequate supplies and facilities needed for medical waste
handling, such as colour-coded bags, puncture-proof boxes and protective
devices.
• Encouragement of studies on different aspects of medical waste, such as the
creation of database information in different sectors, risk analysis and disposal
methods.

77
• Only one department can be taken and thorough process of waste management
can be studied
• A specific Colour Coding system for the various wastes can be introduced to
identify the types of wastes and make the job easier for collection of waste.

78
SUMMARY
The summary may be presented under the following headings:
• Background
• Aims and Objectives
• Materials and Methods
• Results
• Conclusion
• Recommendations
Background
The Bio-medical waste management is a global concern, particularly due to constant
rise in blood borne diseases like AIDS, Hepatitis-B etc. Subsequently the environment
and the pollution board, GOI, 1998, framed rule called the Bio-medical waste (m & h)
Rules, which is the authority for any default.
The current scenario is that, the incidence of hospital borne infections is on constant
rise. The waste generation in the hospital and its disposal are not given its due
importance. Most of the areas the waste thrown out of hospitals were to be taken care
by the local municipal cleaners with ignorance of biomedical health hazard, to
overcome this, various health organization, WHO, Environment and pollution control
board has come forward for its safe guard, and has proposed specific norms, rules and
guidelines for its safe disposal.

79
As Unani system of medicine is also in the main stream for health care service
provider and also the source for hospital waste generation with more number of
patients and health care personnel involved, hence study was undertaken for the
awareness and management of hospital waste in Unani hospitals in Bangalore.
Aims and Objectives
The objectives of the study is to assess the existing practices of waste management
and to identify the type of waste, segregation practices, quantification of waste and its
disposal methods.
Materials and Methods
The research design used in this study is a descriptive research type. Descriptive
research includes surveys and inquires based fact findings are as follows:
(1) Through observational checklist (Annexure-1) for assessment of the existing
system and post orientation/ sensitisation session, the components which
includes sources of waste, type of wastes, collection of waste, storage of
waste and disposal methods were observed and recorded in a checklist.
(2) Interaction with various categories of health care personal (like doctors,
nurses, paramedical staff, technicians ward boys, ayahs, housekeeping staff
and other waste handlers.
Results
Overall assessment:
• The overall initial assessment of the studied HCIs show that none of the
studied HCIs managed solid as well as liquid waste appropriately.
• None of the studied HCIs managed soiled infectious waste appropriately.

80
• One of the studied HCIs providing both IPD/ OPD had needle destroyer for
disfigurement of needles, but final disposable was not appropriate.
• None of the studied institutions managed liquid infectious waste appropriately.
From the above results, it could be inferred that the type, size or the profile of
institutions has not influenced the systems for safe management of HCW.
Assessment of the Subsystems
The assessment of the sub-systems, like soiled infectious waste (bandage cloth), waste
sharp management (Needles, broken ampoules), plastic recyclables (syringes) and
body fluids, reveals that though the current existing systems do not fulfil the
requirements of the Bio-medical waste (m & h) Rules 1998, but there were definite
attempts at managing the waste in the studied HCIs.
Conclusion
In the present study the existing practices of waste management in Unani hospitals,
and to identify the type of waste, segregation practices, quantification of waste and its
disposal methods were identified with an observational checklist (Annexure–1).
Quantity of HCW generated in studied HCIs, is 0.78 kg and 0.68 kg/ bed/day in two
studied HCIs Providing IP/OP services. The types of wastes generated in the studied
HCIs are General waste (81.45%), Pathological waste (3.90%), Infectious waste
(13.41%), and Sharp waste (1.23%).
General waste (81.45%) is non-infectious and it is the major part of the categories of
waste, which even includes waste from herbal Unani pharmacy containing remains of
dry leaves, twigs, powder of herbs which are all organic matter and hence bio-
degradable. Proper segregation of this waste is recommended and the biodegradable

81
share can be composite, and later can be used as natural manure for growing plants
and maintaining herbal garden. Sharp waste and hazardous waste is very less in this
study compared to other studies, hence infectious waste like sharps and other
pathological waste if mixed with this non-infectious general waste, the whole waste
turns to be infectious and it will be a burden in management of waste, both cost wise
and also in terms of manual labour.
Recommendations
Intensive training programme should be held, at regular time interval, for all the staff.
Health education should be given for all the community, about hazards of medical as
well as general wastes and how to minimize them. There should be adequate facilities
needed for medical waste handling, such as colour-coded bags, puncture-proof boxes
and protective devices etc.

82
BIBLIOGRAPHY
1. Saraf. Y, Shinde. M, Tiwari SC. Study of Awareness Status about Hospital Waste
Management among Personnel and Quantification. Indian Journal of Community
Medicine, Vol. 31; 2: 2006, pp4-6.
2. IGNOU, Registration and Evaluation Division, Indra Gandhi National Open
University New Delhi, printed at Shagun Offset Press; Noida; 2007 pp55-56.
3. Info Nugget, Press information Bureau, “Hospital Waste Management and Bio-
degradable waste”, Govt. of India, New Delhi; 1998:
http://pib.nic.infonug/infaug99/i 3008991.html access date 12-06-07.
4. Medical waste and health workers in Gaza governorates, “Eastern Mediterranean
Health Journal”, Vol.7; 6: November 2001, pp117-24.
5. WHO, Management of waste from hospitals and other health care establishments,
in southeast-Asia Region; New Delhi, 1995, pp24-25.
6. Govt. of India, The Gazette of India Extraordinary part-II, section 3-sub section
(ii) No. 460, New Delhi, Ministry of environment and forests, 1998, pp1-17.
7. Park. K, Preventive and Social Medicine, 18th edition, published by M/s
Banarasidas Bhanot Publishers, Jabalpur, India 1997 pp1-10, 595-596, 599.
8. AYUSH, “Health for all through AYUSH”, an overview of AYUSH, Dept. of
AYUSH, Ministry of health and family welfare, Govt. of India, New Delhi, 2003,
pp25-31.
83
9. Sharma JL. Buldini PL. A Dictionary of Pollution, 1st Edition, Published by CBS
Publishers and Distributors, Jain bhawan, Bholanth nager, Shahdra, Delhi. 1994,
pp124, 419.
10. Saini S, Nagarajan SS, Nagarajan, Sarma KK. “Knowledge, attitude and practices
of Bio-medical waste management amongst staff of a tertiary level hospital in
India”, Journal of the Academy of Hospital Administration, Vol.17;2:2005, pp2-4.
11. Hakim Ghulam Jeelani. Makhzanul Hikmat, Published by S.H. offset press, New
Delhi, Aijaz Publishing House, 1996, pp272-77.
12. Baghotia KS. “Biomedical waste management scenario in Delhi”, Directorate of
health services, F-17, Karkardooma, Delhi, 2007, pp1-6.
13. Mohd. Raziul Islam Nadvi. “Azmate Razi” Published by Aijaz Publishing House,
koocha cheelan, Daryaganj, New Delhi. 1995. pp124-125.
14. Hakim Syed Zillur Rehman, Daure Jadeed aur Tib, Tibbiya College, Muslim
University, Aligarh, Published by Tibbi Academy, Jahngirabad, Bhopal pp178-96.
15. Gupta MC, Mahajan BK. Text Book of Preventive and Social Medicine; 3rd
Edition (revised), Published by M/s Jaypee Brothers Medical publishers (P) Ltd.
EMCA House, Daryaganj, New Delhi, 2005, pp614-18.
16. Vidya Ratan, Hand book of Preventive and Social Medicine, 9th edition, published
by M/s Jaypee Brothers Medical publishers (P) Ltd. EMCA House, Daryaganj,
New Delhi, 1994. pp71, 136-38, 142-43.
17. Sharma JL, Kadian RK, Buldini PL, A Dictionary of Environment, 1st Edition,
Published by CBS Publishers, Jain Bhawan, Bhalanath Nagar, Shadara, Delhi,
1994, pp79, 269.

84
18. Chandorkar AG, Nagoba BS. “Hospital Waste Management”, 2nd Edition,
Published by Paras Medical Publisher, Putlibowli, Hyderabad 2004. pp7, 63-65,
106.
19. IGNOU, Fundamentals: “Environment and Health”, Health Care Waste
Management Regulations, 2005. BHM-001, pp5, 8-11, 61.
20. Report of the committee constituted by the Hon. Supreme Court of India. Solid
Waste Management in class-1 cities in India, Govt. of India, 1999; pp1-2.
21. WHO, Safe management of wastes from health care activities south-East region
countries, New Delhi, 1999. p2
22. Ghazi Al-Hachim M. PhD, Muslim contributions to Medicine, “Ahlan wa Sahlan
Magazine” 2005; http://pr.sv.net/aw/2005/December/english/pages002.htm,
access date 4-06-07
23. Abubakar Mohammad Bin Zakaria Al-Razi, Kitab Al-Mansoori, 1st Edition,
Published by CCRUM, Ministry of Health and Family Welfare, Govt. of India,
New Delh.1991, pp7-10.
24. Altaf Ahmed Azmi, Basic concepts of Unani Medicine, 1st Edition, Dept. of
History of Medicine, Jamia Hamdard (Hamdard University ), Hamdard Nagar,
New Delhi, 1995, pp106-109
25. Thomas C, Timmreck, “An introduction to Epidemiology”, 2nd Edition, Published
by Jones and Bartlett Publishers, Bloor Street West, Toronto, 2001, pp72-73.
26. Poulose K P, Nataranjan P K, 1989, Re-orientation of Medical Education in India:
past, present and future. Indian Journal of Public Health 33: 1989. 55-58.

85
27. NACO, Standard operative procedures, Manual for control of hospital associated
infections; National AIDS control organization, Ministry of H & F W, Govt. of
India, 1999. pp 8-10.
28. NACO, Manual on Lab. Diagnosis of common opportunistic infections, associated
with HIV/AIDS, National Institute of Communicable Diseases, Director General
of HS, National Aids Control Organization, Ministry of Health and Family
welfare, GOI, 2000, pp25-26.
29. Bio-Medical Waste (management & handling) (Second Amendment) Rules, dated
2nd June, 2000. Ministry of environment and forests, New Delhi, pp1-2.
30. The gazette of India, Part II, Section 3, Sub-section (ii), Ministry of Environment
and forests, Pollution Control Board, Ministry of Environment and Forests,
Notification, New Delhi, 20th July, 1998.
31. Seshu Babu VVR, 2nd Edition, Review in community medicine, Environmental
Sanitation, Published by Paras Medical Books Pvt. Ltd. Hyderabad, pp79-81.
32. Hemangi k; Shah; Ganguli SK. Hospital waste management – A review: “Indian
Journal of Community” Vol.25; 3: 2007, pp 1-4
33. Waste management, “Waste management techniques”, Composting and anaerobic
digestion, from Wikipedia, http://en.wikipedia.org/wiki/waste_management 2006,
access date 25-05-07.
34. Hakim Ansari Mohd Yusuf. Text book of Tahafuzi wa Samaji Tib, Published by
S. H offset press, Aijaz Publishing House, New Delhi, 2000, p81.
35. Health care waste management cell, safe management of health care waste -
working manual for hospital waste disposal, Department of community medicine,
M.S Ramaiah medical college, Bangalore, 2003 pp55-59.
86
36. Pruss A, Giroult E, Rushbrook P, Safe Management of waste from Health Care
Activities, WHO, Geneva 1999, pp12-15.
37. Yash Pal Bedi, Preventive and Social Medicine, 16th Edition, Published by, Anand
Publishing Co. Chandigarh 2003, pp37-48.
38. Adrain Coad, Jurg christen, How are we managing our health care waste? By,
SKAT, Swiss centre for developing cooperation in Technology and Management,
42, St Gallen, Switzerland. 1992 pp45-47.
39. Sunder Rao P.S.S, Richard. J; An Introduction to Biostatistics, 3rd Edition,
Published by Asoke Ghosh K, Prentice-hall of India, Private Limited, New Delhi
pp111-112
40. Friedman test from wikipedia, the free encylopedia
http://en.wikipedia.org/wiki/friedmantest access date 10-07-07
41. Waste Characteristic and Current Waste Management Practices, Cambodia,
Overview of the Management of Health Care Waste in the WHO Western Pacific
Region. 2003. p 4.
42. Valeria DB, Mattoso, Valdir SChalch, “Hospital Waste Management in Brazil”,
Waste Management & Research, Vol.19, 6: 2001 pp567-72.
43. Pandit NB; Mehta HK; Kartha GP; Choudhary SK; Management of Bio-medical
waste: Awareness and practices in a district of Gujrat; “Indian Journal of Public
Health” Vol. 49, No. 4. October-December, 2005, pp245-47.

87
Annexure - 1
Instrument for data collection
Safe management of health care waste The checklist for health care settings
Name of the Health Care Setting: Address: Telephone / Fax / E-mail: Name of the respondent with designation: Services provided (encircle): Only OPD / OPD + IP / Others (specify) Staff position (number): Duty Doctors Consultants
Doctors Nursing Staff Ward Boys /
Ayahs X-Ray technicians Lab Technicians Pharmacy Staff Others Total Number of Staff
Number of Beds: Average In Patient admission / Day: Out patient strength in the last One year: In patient Strength in the last One year: Pathological investigation strength in last one year: Average Bed Occupancy: Average Out patients / Day: Tick if the following is present:
• Infection Control Committee • Waste Management Committee • Disinfection Policy • Waste Management Policy • Waste Sharps Management Policy • HIV Infection Control Policy • Occupational Safety Policy

88
Tick the Facilities available for Waste Management: Segregation / containment / Burial / Deep Burial / Burning / Incineration Micro waving / Autoclave / Others (Specify) / Others (Specify) REMARKS
1. Authorisation obtained: Yes / No 2. System of recording of illness / injuries / accidents: Yes / No 3. System of reporting of illness / injuries / accidents: Yes / No 4. Periodic monitoring of the waste management facility undertaken: Yes / No 5. Training / Retraining to the staff provided Yes / No
Record if the following is happening regarding handling of Health Care Waste:
Waste materials
Segre- gation
Dis-infection
Disfigurement
Containment
Transportation
Colour coding
Final Disposal
Plastic Material
Paper / card board
Banana leaves / Fruit peels etc.
Discarded glassware / vials / ampoules / bottles
Left over food
Disposal needles & syringes
Cotton / bandage cloth
Contaminated linen
Urine remains / Stool samples
Blood / serum samples
Please note: NA = Not Applicable; C = Complete; IC = Incomplete; S = Satisfactory; NS = Not Satisfactory; A = Appropriate; IA = Inappropriate

89
OCCUPATIONAL SAFETY OF THE HEALTH CARE PERSONAL Indicate YES, if being provided and used, NO if not being used.
HCP Uniform Apron Boots Mask Goggles Gloves Vaccination Given
Duty Doctors
Nurses
Consultants
Laboratory Technicians
Ward boy
Ayah
Was
te
hand
lers
Helper
WASTE CONTAINERS (Sample in a representative fashion) 1 2 3 4 5
Location of Container Size (in Litres.) Shape Lid present Yes/no Yes/no Yes/no Yes/no Yes/no Material of the container Collection Frequency/day
List the suggestion by the staff for the improvement of the Solid Waste Management mechanism regarding the following. Containers Frequency of collection Frequency of disposal Use of protective devices Transportation of the waste Any others------

90
Annexure - 2
Photographs
1. Generation of Unani pharmacy waste in one of the studied health care institutions
2. Generation of highly infectious liquid waste from semi auto processor in
pathology laboratory in one of the studied health care institutions.
3. Generation of kitchen waste in one of the studied health care institutions
4. Containment of waste in one of the studied health care institutions
5. Weighing of waste in one of the studied health care institutions
6. Use of needle destructor in one of the studied health care institutions
7. Orientation/ training sessions in studied health care institutions

91
Generation of Unani pharmacy waste in one of the studied health care institutions (1)

92
Generation of highly infectious liquid waste from semi auto processor in pathology laboratory in one of the studied HCIs (2)

93
Generation of kitchen waste in one of the studied HCIs (3)

94
Containment of Waste in one of the studied HCIs (4)

95
Weighing of waste in one of the studied HCIs (5)

96
Use of needle destructor in one of the studied HCIs (6)

97
Orientation/ training sessions in studied HCIs (7)