Measures of problem uncertainty for scheduling with interval processing times

IMA Journal of Management Mathematics (2014) Page 1 of 21doi:10.1093/imaman/dpt027
A stochastic programming approach for operating theatre schedulingunder uncertainty
M. E. Bruni∗, P. Beraldi and D. Conforti
Laboratorio di Ingegneria delle Decisioni per i Servizi Sanitari, Dipartimento di IngegneriaMeccanica, Energetica e Gestionale, Università della Calabria, Via P. Bucci 44C, 87030 Rende
(Cosenza), Italy∗Corresponding author: [email protected] [email protected]
[Received on 26 October 2012; accepted on 28 November 2013]
Operating theatre scheduling is a critical task that directly impacts the efficient delivery of surgical care. Inthis context, we propose a comprehensive stochastic programming modelling framework which handlesthe inherent uncertainty characterizing the arrival of emergency patients and the duration of surgery. Inparticular, three recourse strategies are presented with the aim of modelling different reactive schedulingpolicies actually adopted by hospital managers. In order to solve realistic-sized instances in a reason-able amount of time, we develop tailored heuristic solution strategies that exploit the problem structure.Computational results obtained on a set of randomly generated problems show the effective impact of thestochastic programming approach and the efficiency of the proposed heuristics.
Keywords: stochastic programming; surgery planning, emergency.
1. Introduction
Surgical processes are amongst the most important activities in hospitals, not only from a medical andsocial perspective, but also from an economic viewpoint. In light of this, surgical suite management hasreceived, in recent years, significant attention and the crucial issue of an efficient planning and schedul-ing of operating theatre (OT for short) activities has become a major priority. In this paper, we focus onscheduling of elective surgery under a block booking framework in a multi-OT context which entailschoosing the intervention date of each surgery and reserving OT time in the appropriate block of themaster surgical schedule. The task is not trivial, since surgery plans should balance some importantconflicting objectives including patient waiting time, overtime costs and OT utilization, amongst oth-ers. The uncertainty of surgical procedure duration and the presence of emergency patient arrivals allcontribute to exacerbate the difficulty of the problem and often cause, at operational level, alterations ofthe actual schedule on a daily basis to accommodate stochastic variability.
A recent survey work (Cardoen et al., 2010a,b,c) reports that the vast majority of hospitals deal withschedule disruptions mainly in a reactive way at operational level, i.e. only facing problems when theyactually occur. Since, for the presence of stochasticity, the reserved OT time might be insufficient, thedepartment may perform surgeries in overtime, or react by changing the OT assignment of some surg-eries (Dexter, 2005) or with partial (surgery right shift to the next day) or full rescheduling. Regrettably,all these operational strategies often result in suboptimal use of the OT time.
To provide a robust schedule preventing at the same time unnecessary cancellations or unduly longovertimes, planning and control should be integrated within a model explicitly coping with possibledisruptions.
c© The authors 2014. Published by Oxford University Press on behalf of the Institute of Mathematics and its Applications. All rights reserved.
IMA Journal of Management Mathematics Advance Access published January 12, 2014 by guest on January 15, 2014
http://imam
an.oxfordjournals.org/D
ownloaded from

2 of 21 M. E. BRUNI ET AL.
The contributions of this paper towards this direction are the following.
• From a modelling perspective, we analyse the scheduling problem of elective surgeries in multi-OThospitals, taking simultaneously into account the random presence of emergency patients and theinherent stochasticity of surgery durations. We consider a planning horizon of 1 week, to reflect thecurrent practice of the overwhelming majority of hospitals in Italy.
• From an operational perspective, we model different recourse strategies which reflect operativestrategies used in practice on the day of surgery by various OT departments to accommodateuncertainty.
• From a computational perspective, we propose a tailored heuristic approach for effectively solving,within a reasonable amount of time, the resulting stochastic models.
The remainder of the paper is organized as follows. In Section 2, we review the relevant literature.We introduce the deterministic version of the OT scheduling model in Section 3. Based on this model,in Section 4 we propose three different recourse strategies for the operational stage. Section 5 presentsthe solution approach for the resulting stochastic models. We present computational results in Section 6,and finally, we conclude in Section 7.
2. Literature review
To emphasize how the proposed contribution makes a progress beyond the state of the art, we review,in this section, the relevant literature, focusing on the works addressing the advance schedulingand planning problem under uncertainty. More extensive reviews can be found in Cardoen et al.(2010a,b) and Guerriero & Guido (2011). Optimization models for the single OT scheduling prob-lem are abundant in the literature of advance planning. Nevertheless, only a few papers considerexplicitly uncertainty in surgery durations. Common decisions to be made concern the determina-tion of the optimal daily surgery schedule and the related optimal surgical case sequencing. Assum-ing a fixed sequence of surgeries characterized by uncertain durations, Denton & Gupta (2003) pro-posed a two-stage stochastic programming model for determining the appointment times for cus-tomers in which the objective function minimizes the expected costs of waiting times, idle timesand tardiness. The proposed model is solved with an adaptation of the standard L-shaped method.Denton et al. (2007) extended the work of Denton & Gupta (2003), relaxing the assumption of afixed sequence and considering both scheduling and sequencing decisions, taken before knowing thesurgery durations. To solve this difficult stochastic combinatorial problem, casted as a two-stage modelwith recourse, the authors proposed several heuristics tested on real surgery scheduling data. In Min& Yih (2010), the authors addressed the optimal scheduling of elective patients with different pri-orities for a single surgery type and a single OT when uncertainty affects the arrival of surgerypatients and the duration of each surgery. The problem is formulated as a stochastic dynamic pro-gramming model whose structural analysis is used to resolve the computational issues related to theefficient solution of the problem. The paper of Gerchak et al. (1996) tackled the problem of dailyreservation planning for elective patients with the aim of determining, at the start of each day, howmany additional requests for elective surgery to assign for that day, considering the random arrival ofnon-elective patients. The model is mono-period and does not specify the intervention date for eachelective case.
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

A STOCHASTIC PROGRAMMING APPROACH FOR OT SCHEDULING 3 of 21
The stochastic version of the surgery allocation problem in a multi-OT environment has recentlystimulated a flourishing literature stream. Among others, Brian et al. (2010) studied the problem withinthe two-stage stochastic framework. The authors focused on allocation decisions in a daily context (OTopening and assignment of surgeries to OTs) treated as first stage, whilst in the second stage overtimeis used to compensate for uncertain surgery duration. Daily decisions concerning the number of OTsto open, surgery assignment to OTs and the sequence and start times of surgeries within each OT, areconsidered in Batun et al. (2011). The authors presented both a stochastic programming model and arobust formulation.
The problem of elective surgery planning over a planning horizon (typically considered to be 1 or2 weeks in the literature) was first addressed in Hans et al. (2008). The aim of the so-called robustsurgery loading problem proposed by the authors is the maximization of OT utilization together withthe minimization of overtime risks associated to the variability of duration distributions of the con-cerned surgeries. The robust surgery loading problem was heuristically solved through local searchand improvement heuristics. The same problem is tackled in Tanfani et al. (in press), within a com-prehensive integrated bi-level model for the OT planning problem in which the deterministic solutionfor the first-level problem is introduced in a second-level stochastic problem with individual chanceconstraints.
A challenging research stream involves the consideration into the planning phase of also non-elective patients. The problem was investigated in Lamiri et al. (2008, 2009) and stochastic program-ming was applied to address the surgery planning problem over a planning horizon. In these works, itis assumed that the total time requested by emergency patients is a random variable, and that a portionof planned slack is dedicated to it. Moreover, emergency requirements or operating times exceeding theavailable capacity will necessarily lead to high overtimes, since no surgery cancellations or schedulerearrangements are allowed. The issue of cancelling elective patient to accommodate semi-urgent cases(to be performed soon but not necessarily within the arrival day) has been investigated in Zonderland etal. (2010). At a strategic level, a queueing model is proposed to provide an estimate for the amount ofOT time that should be reserved for all semi-urgent surgeries in the long run and, on a tactical level, aMarkov decision model is used to support the allocation of slots in a week.
Our article differs from the aforementioned literature providing a general stochastic programme withrecourse for the weekly scheduling problem (WSP) in a multi-OT context under uncertainty. The modelhas some novel mathematical features. Its goal is the scheduling of elective surgeries in a planning hori-zon of a week, considering simultaneously random service durations, random emergency occurrencesand patient priorities. The incorporation in the planning phase of emergency requests, as well as theacknowledgement of stochastic variability of operating times, poses severe challenging questions effec-tively handled by the model. Moreover, new recourse strategies, not yet addressed in the literature, arepresented in order to faithfully represent the operational practices common in many hospitals. To ourknowledge, this is the first formulation of a stochastic programming model encompassing recourseactions different from the simple recourse strategy in which overtime acts as a cushion to absorbvariability.
3. Model formulation
We begin by first describing the deterministic model for the WSP of elective patients in a multi-OT con-text. Next, we extend the basic model to a stochastic formulation that considers uncertainty in surgerydurations and in the emergency arrival process. The model is then further elaborated and three variants,differing in the recourse actions, are presented.
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

4 of 21 M. E. BRUNI ET AL.
3.1 The deterministic model
The OT planning problem under consideration aims at scheduling a set of surgical cases from a list ofeligible cases I, grouped by different specialties Ij, under a block booking framework, assigning themto one of the available blocks during a planning period H , e.g. a week. Each specialty j ∈ J is assigned afixed block of time ajto in each day t ∈ H and OT o ∈ O, in accordance with the current master surgicalschedule. Let di denote the duration for surgery i and pi its priority-based coefficient. Let us also assumethat a base profit coefficient b is available, which can be interpreted as the hospital revenue derivingfrom incomes or from costs saved, like hospitalization costs or societal costs of waiting (Somasekar etal., 2002; Hilkhuysen et al., 2005). The assignment of a surgery i to an OT o and a day t (represented bythe binary variable xito), besides complying with the master surgical schedule, should explicitly addressthe important issue of patient prioritization that recently has been the focus of interesting researches(Valente et al., 2009; Testi et al., 2008). In particular, the model, for a single specialty j, can be stated asfollows:
max∑i∈Ij
∑t∈H
∑o∈O
bpixito, (3.1)
∑t∈H
∑o∈O
xito � 1 ∀i ∈ I, (3.2)
∑i∈Ij
dixito � ajto ∀t ∈ H , ∀o ∈ O, (3.3)
xito ∈ {0, 1} ∀i ∈ I, ∀t ∈ H , ∀o ∈ O. (3.4)
Constraints (3.2) ensure that each surgical case is treated at most once within the planning horizon.Constraints (3.3) allow the surgery i ∈ I to be scheduled on a day t only if the block time (operating timeassigned to specialty j in OT o on day t) is not exceeded. The objective function maximizes hospitalrevenues by scheduling a set of patients with high priority considering the resource constraints. Thereader is referred to Conforti et al. (2010) for a discussion of other interesting objective functions.
3.2 The basic stochastic programming model
Model (3.1)–(3.4) assumes that surgery durations are deterministically known and completely ignorespossible fitting in the regular OT schedule of urgent surgeries.
In practice, as widely recognized (Brian et al., 2010), due to the uncertainty, the planned schedulemay largely differ from the realized one: whenever an emergency occurs or when a complication insurgeries arises, rescheduling decisions may be necessary. Neglecting this aspect might lead to poorplanning decisions.
The time-varying uncertainty which characterizes the OT scheduling context calls for a stochasticdynamic formulation of the problem. However, we should observe that the standard assumptions sup-porting the stochastic programming framework are not satisfied. In fact, uncertainty gradually resolvesover a day and rescheduling decisions are made at some instant on the day of operations, after a partialresolution of uncertainty (arrival of an emergency request or the discovering of complicating factors foran elective surgery). This poses severe modelling challenges, since the assumption that exist discrete,finite, known points in the future where new information will become available is no longer valid. On
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

A STOCHASTIC PROGRAMMING APPROACH FOR OT SCHEDULING 5 of 21
the contrary, since the number and the time of rescheduling decisions are stochastic variables, the modelfalls outside the realm of classical stochastic programming models.
In order to overcome this drastic limitation, we employ a fairly simple model of decision dynam-ics. We suppose that uncertainty is revealed at the beginning of each day of the planning horizon.Although in the current managerial hospital practice rescheduling decisions are taken after the arrivalof an emergency request and/or the discovery of factors causing a prolongation of the surgery duration,the choice of a daily temporal resolution of the uncertainty derives from the nature of the WSP. As inthe deterministic version of the problem, the decision variables x represent weekly surgery schedulingdecisions to be taken ‘here and now’ before the beginning of the week and under complete uncertainty.This in turn implies that, at the beginning of the horizon, we make decisions for the whole week, beforeany information is revealed. Recourse decisions are taken on a daily basis, according to the recoursestrategy adopted. Even if our aggregation level could appear questionable, it allows us to handle theinherent uncertainty of the surgical processes, by balancing the reduction of model complexity withthe loss of information. Nevertheless, the problem is rather involved due to the combination of twodifferent sources of uncertainty: exogenous uncertainty of emergency patient arrivals, which representsa stochastic process independent of decisions that are taken, and endogenous uncertainty of surgerydurations, whose evolution over time depends on the scheduling decisions made (see Dupacova, 2006;Goel & Grossmann, 2006 and the Appendix for a clue on this). The stochastic dynamic model for theWSP under uncertainty, which we formulate next, handles both type of uncertainties, assuming that therandom problem parameters ωt are described by a discrete-time stochastic process {ωt}t∈H defined onsome finite probability space (Ω , F,P).
Under these assumptions, the basic WSP can be stated as follows:
maxx∈{0,1}
f0(x) − Eω
[∑t∈H
ft(ωt, x)
],
x ∈ χ0 (WSP),
qt(ωt) ∈ χt(ωt) ∀t ∈ H ,
qt(ωt) ∈ ℵa ∀t ∈ H ,
where Eω indicates the expected value with respect to the random vector ω, χ0 is defined as
χ0 ={∑
t∈H
∑o∈O
xito � 1 ∀i ∈ Ij
}
and
f0(x) =∑t∈H
∑o∈O
∑i∈Ij
bpixito.
The constraints set and the objective function pertaining to time period t are denoted by χt(ωt) and ft(ωt),respectively, and involve vector-valued recourse variables qt(ωt). The objective function of the WSPtakes into account the total profit obtained as a difference between revenues and recourse costs. by ℵa,we represent the space of non-anticipative solutions (Ruszczynski, 1997; Prekopa, 1995; Ruszczynski& Shapiro, 2000).
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

6 of 21 M. E. BRUNI ET AL.
4. Recourse strategies
In what follows, we present three different recourse strategies, representative of common practices usedin different hospitals, and their corresponding mathematical models. The choice of the strategy that bestrepresents the reality under study depends on the organizational barriers imposed at high organizationallevels, as well as on interdepartmental flexibility. All the three models, obtained as specifications of theWSP, assume that no special OT exists for the emergency cases that, therefore, have to be performed innormal OTs on the day they occur. The three different recourse strategies lead to problems different innature and computational complexity.
4.1 The overtime recourse strategy
The first model implements the overtime recourse strategy (OvRS, for short) in which surgeries areperformed in overtime, when needed. We will assume that in each day t of the planning horizon theset of emergency patients requiring the specialty j (denoted with emt
j(ωt)) as well as surgery durations(denoted with d(ωt)) define the random vector of the information available at time t. The assignmentvariables yt
eo(ωt) model the choice of treating emergency e into the OT o, whilst the random variables
OVtjo(ωt) = max
⎧⎨⎩0,
∑i∈Ij
di(ωt)xito +∑
e∈emtj(ωt)
de(ωt)yteo(ωt) − ajto
⎫⎬⎭
defines the overtime for each OT o, specialty j and day t.These decisions represent recourse decisions, to be taken after disclosure of uncertainty.The model is a variant of the WSP in which
ft(ωt) = cov
∑o∈O
OVtjo(ωt),
where cov is the overtime cost and
χt(ωt) =
⎧⎪⎪⎪⎪⎪⎪⎪⎪⎨⎪⎪⎪⎪⎪⎪⎪⎪⎩
∑i∈Ij
di(ωt)xito +∑
e∈emtj(ωt)
de(ωt)yteo(ωt) � ajto + OVt
jo(ωt) ∀o ∈ O, (1o)
∑o∈O
yteo(ωt) = 1 ∀e ∈ emt
j(ωt), (2o)
yteo(ωt) ∈ {0, 1} ∀e ∈ emt
j(ωt), ∀o ∈ O, (3o)
OVtjo(ωt) � 0 ∀t ∈ H , ∀o ∈ O. (4o)
⎫⎪⎪⎪⎪⎪⎪⎪⎪⎬⎪⎪⎪⎪⎪⎪⎪⎪⎭
The constraints in χt(ωt) define the overtime used in each OT and binary and non-negativity restric-tions. The model WSP with the OvRS maximizes the revenue of the weekly schedule minimizing at thesame time the expected overtime cost. We note that constraints (1o) are the stochastic counterpart of theconstraints (3.3) of the model (3.1)–(3.4) conveniently modified to accommodate emergency surgeriesand stochasticity through the introduction of the overtime. Constraints (2o) force the emergency to beserved in one of the OTs available and (3o) and (4o) are restrictions on the nature of the variables.
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

A STOCHASTIC PROGRAMMING APPROACH FOR OT SCHEDULING 7 of 21
4.2 The swapping recourse strategy
This alternative swapping recourse strategy (SRS, for short) is inspired by the common practice fol-lowed in hospitals that react to the consequences of the disruptions by moving one ore more surgeriesto another OT or by swapping surgeries between OTs.
We use the same set of parameters and decision variables as in the previous model and we add a newset of binary variables γ t
ioo′(ωt) denoting whether surgery i is moved from OT o to OT o′. This changeis penalized in the objective function through the cost cswap. The model is therefore the WSP in which
ft(ωt) = cov
∑o∈O
OVtjo(ωt) + cswap
∑i∈I
∑o′∈O|o′ |= o
γ tioo′(ωt)
and
χt(ωt) =
⎧⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎨⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎩
∑i∈Ij
di(ωt)
⎡⎣xito +
∑o′∈O|o′ |= o
γ tio′o(ωt) −
∑o′∈O|o′ |= o
γ tioo′(ωt)
⎤⎦
+∑
e∈emtj(ωt)
de(ωt)yteo(ωt) � ajto + OVt
jo(ωt) ∀o ∈ O, (1S)
γ tioo′(ωt) � xito ∀i ∈ I, ∀o, o′ ∈ O, (2S)∑
o∈O
yteo(ωt) = 1 ∀e ∈ emt
j(ωt), (3S)
yteo(ωt) ∈ {0, 1} ∀e ∈ emt
j, ∀o ∈ O, (4S)
γ tioo′(ωt) ∈ {0, 1} ∀i ∈ I, ∀o, o′ ∈ O, (5S)
OVtjo(ωt) � 0 ∀o ∈ O. (6S)
⎫⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎬⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎭
If a surgery lasts more than expected or an emergency care urgently needs to be treated, some of theelective surgeries scheduled on that OT can be moved to another (less congested) OT. Not always thischange avoids the overtime, which is then considered, once again, as a possible action in constraints(1S). Constraints (2S) state that, during each day, only surgeries planned for that day can be moved toanother OT. Constraints (3S–6S) are similar to constraints (2O–4O) in the previous model.
This recourse strategy provides extra freedom of moving surgeries, still preserving the advantageof maintaining fixed the day assigned in the planning phase. The drawback is that it requires additionalcomputational effort because new binary variables are introduced into the model.
4.3 The complete rescheduling strategy
The rescheduling recourse strategy (RRS, for short) may postpone some planned elective surgeries to alater day, due to possible disruptions on the day of surgery. This replan strategy is applied in real life,when the overtime cost is relevant. Although this strategy provides more flexibility, it might negativelyaffect the patient’s mood.
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

8 of 21 M. E. BRUNI ET AL.
We denote with ztit′o(ωt) the tth-period decision variables representing the dycotomic decision of
rescheduling surgery i to a future day t′ in OT o. The model has the general form of the WSP where
χt(ωt) =
⎧⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎨⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎩
∑t′∈H |t′>t
ztit′o(ωt) � xito ∀i ∈ I, ∀o ∈ O, (1R)
∑i∈Ij
∑o∈O
di(ωt)
⎡⎣xito +
∑t′∈H |t′<t
zt′ito(ωt) −
∑t′∈H |t′>t
ztit′o(ωt)
⎤⎦
+∑
e∈emtj(ωt)
de(ωt)yteo(ωt) � ajto + OVt
jo(ωt), (2R)
∑o∈O
yteo(ωt) = 1 ∀e ∈ emt
j(ωt), (3R)
yteo(ωt) ∈ {0, 1} ∀e ∈ emt
j(ωt), ∀o ∈ O, (4R)
ztit′o(ωt) ∈ {0, 1} ∀i ∈ I, ∀o ∈ O, ∀ t′ > t, (5R)
OVtjo(ωt) � 0 ∀o ∈ O. (6R)
⎫⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎬⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎪⎭
The recourse cost pertaining to period t is described by the following equation:
ft(ωt) = cov
∑o∈O
OVtjo(ωt) +
∑o∈O
∑i∈I
∑t′∈H |t′>t
cresi ztit′o(ωt)(t
′ − t),
where cresi is the daily cost of rescheduling surgery i and the difference (t′ − t) represents the numberof days the patient must wait. Besides binary and non-negativity restrictions on the decision variables(4R–6R), constraints (1R) allow rescheduling decisions only for surgeries scheduled in the planningphase. Constraints (2R) represent the dynamics of the cancellation and rescheduling process.
5. The heuristic solution approach
The WSP under uncertainty suffers from the curse of dimensionality caused by the explicit inclusionof different sources of uncertainty characterizing the whole process. The huge problem size exacer-bates the intrinsic model complexity, deriving from the binary nature of the involved decision variables,preventing its exact solution.
In what follows, we present a unified heuristic strategy to solve the three recourse variants presentedabove. The main idea behind our heuristic scheme is to use as the starting point an initial schedule andthen modify it by trying to improve the objective function.
Let X denote the set of feasible weekly plans (‘here and now’ feasible assignment of surgical casesto OTs during the whole week). At each iteration r of the proposed approach, a new plan xr ∈ X is pro-duced. Attached to this solution, a scenario tree can be drawn and the corresponding value of the objec-tive function Cxr = f0(xr) − Eω[
∑t∈H ft(ωt, xr)] can be worked out. This iterative scheme is repeated
until a maximum number of iterations is reached or whenever, in a fixed number of iterations, no bettersolutions are found.
We remark that the expected cost Eω[∑
t∈H ft(ωt, xr)] can be determined without ambiguity, since ascenario tree is uniquely determined, by solving the recourse problem to optimality. This is theoreticallypossible, but computationally not tractable, especially for the WSP with the RRS. We will come backto this point later, after having presented the general scheme of the heuristic.
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

A STOCHASTIC PROGRAMMING APPROACH FOR OT SCHEDULING 9 of 21
The fundamental issues of the heuristic approach are the definition at each iteration of a good feasibleplan and the efficient computation of the recourse cost of the WSP. The remainder of this section isdevoted to the description of these issues.
5.1 Finding feasible plans
In order to find at each iteration of the heuristic a good feasible plan, we have devised two simplestrategies.
The first one is a fast iterative heuristic rule that modifies the current solution x by moving oneelective surgery at a time.
Let tmax = argmax[t ∈ H , ft(ωt, x)] be the day in the planning horizon with the highest cost anddenote by Ntmax the set of surgeries planned for that day. Inspired by the longest processing timedespatching rule in list-scheduling environments, Ntmax is first sorted in non-increasing order of expectedduration. Then, the first surgery in this sequence is assigned to the first master surgical schedule block(a day and an OT) in which the surgery fits without using overtime. If there is no block in which thesurgery fits without yielding overtime, it is assigned to the block in which the additional overtime isas small as possible. The procedure is iterated until the block to which the surgery is assigned is theone where the surgery came from. This heuristic is effective when the recourse cost is relevant since aschedule for which the recourse cost is high will unlikely be optimal even if it is very profitable.
If the expected recourse cost is small, the stochastic problem is in general easier to solve because itsoptimal solution is close to the solution of the deterministic problem. This latter offers a good startingpoint for the stochastic problem solution. To define the scheme, let the function Δ(x, xr) define theHamming distance relative to x. At a generic iteration r, a new feasible plan will be determined bysolving the following deterministic model M r:
max∑i∈I
∑t∈H
∑o∈O
bpixito,
∑t∈H
∑o∈O
xito � 1 ∀i ∈ I,
∑i∈Ij
E(di)xito � ajto ∀j ∈ J , ∀t ∈ H , ∀o ∈ O, (M r)
Δ(x, xp) � 1, p = 1, . . . , r − 1,
xito ∈ {0, 1} ∀i ∈ I, ∀t ∈ H , ∀o ∈ O.
The constraints Δ(x, xp) � 1, p = 1, . . . , r − 1 prevent the generation of a previously explored plans andprovide a different surgery assignment to embed in the overall scheme of the heuristic.
5.2 Evaluating the recourse function
The comparison of different plans x ∈ X is made on the basis of the value of the objective functionCx which is composed by two distinct terms, one related to the first-stage problem (f0(x)) and theother attached to the recourse problem (Eω[
∑t∈H ft(ωt, x)]). We observe that once an elective surgery
schedule has been chosen, the recourse problem with the OvRS and SRS becomes separable over theperiods, since the recourse variables involve decisions relative to one period at a time. Therefore, theevaluation of the recourse function may be carried out by solving |H | separate subproblems. In the most
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

10 of 21 M. E. BRUNI ET AL.
involved case (when rescheduling is allowed), the complexity of the recourse problems may preventexact evaluation of the expected recourse cost, since second-stage decisions link different periods ofthe planning horizon, leading to a difficult multiperiod integer stochastic problem. In particular, at eachperiod t the recourse decisions concern the possibility to postpone at a later period t′ some surgery o(zt
it′o(ωt)) and, hence, the decision taken at time t has an impact also on future periods t′ > t. In orderto address the computational difficulties related to the evaluation of the recourse function, we present a‘moving horizon’ solution strategy that, instead of solving the complete planning horizon, decomposesthe problem into a sequence of subproblems that are solved recursively.
The rolling horizon algorithm is shown below.
Rolling horizon algorithm.
Input: An instance of the WSP problem with RRS and a feasible surgery plan x.
Output: A feasible recourse plan for the problem and the associated recourse function value.
Initialize the period counter t.
• While ( t � H ) do
• Disregard, ∀o ∈ O, ∀i ∈ I, the recourse variables zqiq′o(ωq), yq
eo(ωq), OV qjo(ωq) ∀q > t and ∀q′ > q,
(q′, q ∈ H)
• Solve the problem, obtaining values for the recourse variables OVtjo(ωt, x), yt
eo(ωt, x) and ztit′o(ωt, x)
∀o ∈ O, ∀i ∈ I, ∀t′ > t, (t′ ∈ H)
• Work out
ft(ωt, x) = cov
∑o∈O
OVtjo(ωt, x) +
∑o∈O
∑i∈I
∑t′∈H |t′>t
cresi ztit′o(ωt, x)(t′ − t)
• Fix the recourse variables pertaining to period t to the values obtained
• t=t+1
• Endwhile
Return Cx = f0(x) − Eω[∑
t∈H ft(ωt, x)]
As far as the period counter increases, the subproblem to be solved becomes easier since therescheduling recourse variables span fewer periods and most of the binary variables are being fixedto the values obtained in previous iterations. This recurrent scheme keeps going until the completehorizon has been solved and the recourse function evaluated for the entire planning horizon.
6. Computational experiments
This section is devoted to the presentation of our computational experiments carried out in order toassess the viability of the proposed approach. We first introduce an illustrative example which servesas a test for assessing the quality of the stochastic programming solutions in comparison with thoseobtained using a deterministic approach. Later, we report on the performance of the solution method bypresenting numerical results carried out on a set of test problems. All experiments were performed on a2.4 GHz processor and the algorithm has been implemented in AIMMS (Bisschop & Roelofs, 2007).
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

A STOCHASTIC PROGRAMMING APPROACH FOR OT SCHEDULING 11 of 21
6.1 Assessment of the stochastic model
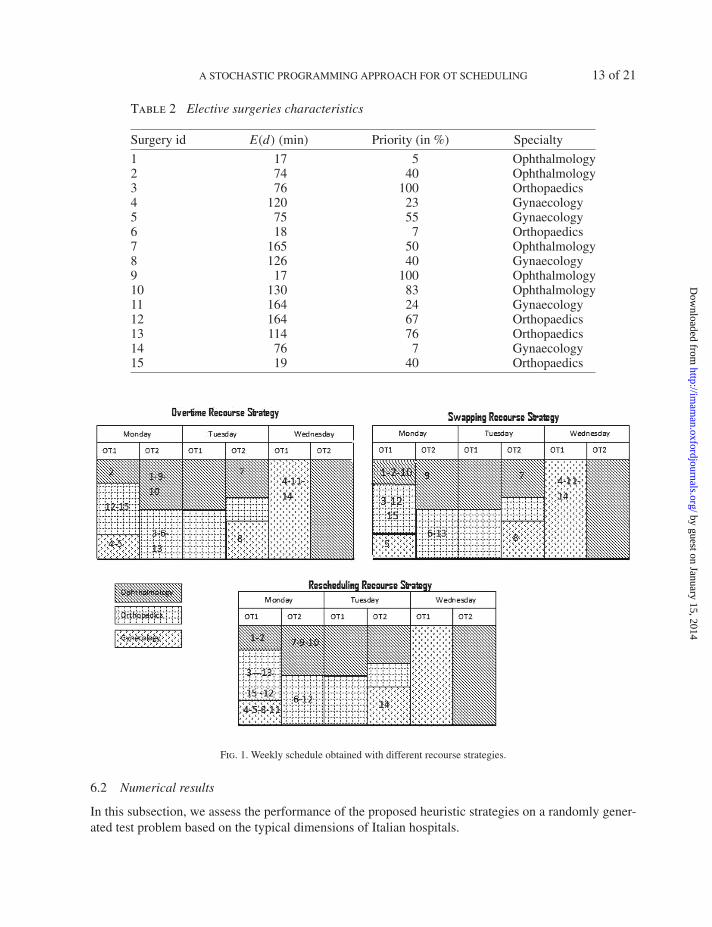
In order to analyse and compare the different recourse strategies, we consider an illustrative examplewith 15 elective surgeries to be scheduled on 3 days. The master surgical schedule with the amountof OT time allocated to each specialty is specified for every day in the planning horizon in Table 1.This illustrative schedule considers only days from Monday to Wednesday. The elective surgeries tobe scheduled are reported in Table 2 in which also the expected duration and the specialty required areindicated.
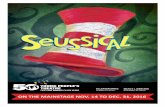
In Fig. 1, we report the plans obtained by the stochastic model in the three recourse strategy variantseach optimizing a different objective function. Within each block is reported the id of the plannedsurgery. Since the three recourse variants share the presence of the overtime variable, we first comparethe overtime generated in the three cases. The expected overtime of the schedules is 7 min, for theOvRS, 6 min for the SRC and only 2 min for the RRS. This decrease is caused by the presence ofthe other recourse variables which hedge against disruptions induced by adverse scenarios. To make anexample, let us consider the occurrence on Monday of an orthopaedic emergency. The OvRS allocatesthe emergency on OT1, leading to an overtime of 10 min under that scenario. Using the more flexibleswapping recourse strategy, the emergency does not cause any overtime and can be handled in the OT1as before, by moving the surgery 15 from OT1 to OT2. Within the complete rescheduling strategy, theemergency can be operated in OT2 without causing overtime, but at a cost of postponing surgery 9 toTuesday.
The choice of the best strategy to opt for is up to the decision maker and depends on different waysof reacting to uncertainty. Whilst swapping of surgeries can be realized without unwanted side effectsfrom a patient perspective (but not from a cost-related perspective), rescheduling may be not appropriateor simply not preferred in some circumstances, notwithstanding it may produce dramatic cost savings.We would like to point out, in this respect, that the rescheduling strategy may be preferred in specificcontexts (long-stay hospitals) or for a specific category of patients as, for instance, the ones admittedfor a week’s hospital stay.
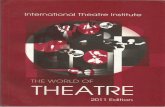
The advantage of using a stochastic programming approach rather than relying on deterministicapproximations of the random data becomes evident when the behaviour of the deterministic solution isevaluated under uncertainty. It is worth observing that the deterministic schedule is not hedged againstuncertainty and does not account for emergencies that may occur during the day. Therefore, it is quitenatural that such a schedule, in an uncertain context, would lead to serious economic and health-relatedconsequences due to the frequent schedule disruptions.
It is possible to establish a precise measure of the value of the stochastic programming model calledthe value of the stochastic solution (see Beraldi et al., 2009 for details). This quantity assesses the gainwe obtain when the schedules obtained by the stochastic programming models of Fig. 1 are imple-mented rather than the deterministic schedule of Fig. 2. In terms of objective function value, applyingthe deterministic schedule rather than the plan generated by the solution of the stochastic programmeleads to a loss of about 8.95% for the OvRS and the SRS.1 Losses are even more dramatic for the RRSraising to 13.08%. These results indicate that using a more dynamic/flexible OT planning model is morecost-efficient than the default case which resorts only to overtime.
1 These values are calculated by solving the WSP problem with OvRS or SRS or RRS, respectively, with the x variables fixedto the values resulting from the deterministic plan of Fig. 2 and by comparing the objective functions obtained with the objectivefunction of the stochastic programme.
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

12 of 21 M. E. BRUNI ET AL.
Tab
le1
Illu
stra
tive
bloc
ksc
hedu
lefo
rtw
oO
Tsan
dth
ree
spec
ialt
ies
Mon
day
Tue
sday
Wed
nesd
ay
Tim
eO
T1
OT
2O
T1
OT
2O
T1
OT
2
8–9
Oph
thal
mol
ogy
Oph
thal
mol
ogy
Oph
thal
mol
ogy
Oph
thal
mol
ogy
Gyn
aeco
logy
Oph
thal
mol
ogy
9–10
Oph
thal
mol
ogy
Oph
thal
mol
ogy
Oph
thal
mol
ogy
Oph
thal
mol
ogy
Gyn
aeco
logy
Oph
thal
mol
ogy
10–1
1O
rtho
paed
ics
Oph
thal
mol
ogy
Oph
thal
mol
ogy
Oph
thal
mol
ogy
Gyn
aeco
logy
Oph
thal
mol
ogy
11–1
2O
rtho
paed
ics
Oph
thal
mol
ogy
Oph
thal
mol
ogy
Ort
hopa
edic
sG
ynae
colo
gyO
phth
alm
olog
y12
–13
Ort
hopa
edic
sO
rtho
paed
ics
Ort
hopa
edic
sO
rtho
paed
ics
Gyn
aeco
logy
Oph
thal
mol
ogy
13–1
4O
rtho
paed
ics
Ort
hopa
edic
sO
rtho
paed
ics
Gyn
aeco
logy
Gyn
aeco
logy
Oph
thal
mol
ogy
14–1
5G
ynae
colo
gyO
rtho
paed
ics
Ort
hopa
edic
sG
ynae
colo
gyG
ynae
colo
gyO
phth
alm
olog
y15
–16
Gyn
aeco
logy
Ort
hopa
edic
sO
rtho
paed
ics
Gyn
aeco
logy
Gyn
aeco
logy
Oph
thal
mol
ogy
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from
A STOCHASTIC PROGRAMMING APPROACH FOR OT SCHEDULING 13 of 21
Table 2 Elective surgeries characteristics
Surgery id E(d) (min) Priority (in %) Specialty
1 17 5 Ophthalmology2 74 40 Ophthalmology3 76 100 Orthopaedics4 120 23 Gynaecology5 75 55 Gynaecology6 18 7 Orthopaedics7 165 50 Ophthalmology8 126 40 Gynaecology9 17 100 Ophthalmology10 130 83 Ophthalmology11 164 24 Gynaecology12 164 67 Orthopaedics13 114 76 Orthopaedics14 76 7 Gynaecology15 19 40 Orthopaedics
Fig. 1. Weekly schedule obtained with different recourse strategies.
6.2 Numerical results
In this subsection, we assess the performance of the proposed heuristic strategies on a randomly gener-ated test problem based on the typical dimensions of Italian hospitals.
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

14 of 21 M. E. BRUNI ET AL.
Fig. 2. Weekly schedule obtained with the deterministic model.
Table 3 Optimality gap on small instances
OvRS SRS RRS
# Pat #OTs Iterative IP Iterative IP Iterative IP
15 2 3.81 3.75 3.94 3.75 7.86 11.9715 3 11.18 11.25 11.93 12.75 16.03 16.0520 2 13.19 13.00 14.94 12.25 0.91 0.6920 4 13.11 13.00 13.36 13.50 0.01 0.01
The first set of experiments is devoted to the evaluation of the optimality gap of the heuristic onvery small instances. Four randomly generated problem for each configuration (two and four OTs, anumber of patients below 20 and a scheduling horizon of 3 days) have been considered. The problemsizes considered are the largest that Cplex 12.0 can solve without running out of memory, but are far tobe representative of typical problem dimensions faced by hospitals. In Table 3, we report the averagepercentage optimality gap collected by running the Iterative and the IP (Integer Programming) heuristicstrategies over the three model variants (OvRS, SRS and RRS). Headings are as follows: columns #OTsand #Pat specify the number of OTs available and the number of patients to be operated on; Iterative andIP (Integer Program) stand for the type of search used within the general heuristic scheme of Section 5.
On average the optimality gap is of 9.26%. We note a peak of 16.05% for the RRS. This modelis the more difficult to solve amongst the three we propose. We note also that for the larger problemsconsidered in these experiments (20 patients and 4 OTs) the behaviour of the heuristic is very good forthe RRS (with average percentage optimality gap of 0.01% for both the Iterative and the IP heuristic),and still acceptable for the OvRS and the SRS.
In the second set of experiments, we have considered problems with a number of elective surgeries|I| = 50, 80 and 100, and a number of OTs |O| = 2, 4, 6. The planning horizon H has been set to oneweek (from Monday to Friday) and the OT capacity to 8 h. The coefficients pi were taken from a uniformdistribution between 1 and 48 and the base profit has been set equal to 1000e. We have consideredcover = 500e/h, cswap = 100e and cresi = 1/10 ∗ b ∗ pi in order to reflect the relative priority of patients.The daily arrival process of emergency cases has been modelled as a Poisson distribution with a meanequal to 2% of the number of elective surgeries and to 4% of the number of elective surgeries formodelling low and high emergency probability occurrences, respectively (see column #Eme). Surgery
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

A STOCHASTIC PROGRAMMING APPROACH FOR OT SCHEDULING 15 of 21
Table 4 Computational time in seconds
#OTs 2 4 6
# Pat #Eme Heu OvRS SRS RRS OvRS SRS RRS OvRS SRS RRS
50 Low Iterative 18 181 572 52 2968 2936 22 1545 512IP 31 229 601 59 5037 2106 29 1436 851
High Iterative 68 255 2750 108 1057 3288 113 1714 1151IP 77 272 2893 131 1156 3479 95 1638 1670
80 Low Iterative 21 85 349 19 3399 1467 31 1821 715IP 133 94 492 124 2988 1674 254 1750 1100
High Iterative 109 85 349 79 3975 2560 20 2128 1044IP 150 94 462 127 4278 2130 30 2337 1150
100 Low Iterative 58 184 523 28 741 916 25 1864 842IP 195 1021 1406 240 997 1217 256 1997 1179
High Iterative 90 190 692 160 1506 1353 240 2857 1298IP 130 237 893 200 1205 1478 310 2912 2311
durations were sampled from log-normal distributions with a mean randomly generated from the interval[0.5 h, 3 h] and standard deviation randomly generated from the interval [0.5, 1.6].
Cplex 12.0 was used for the solution of model M r in the IP-based heuristic and for the evaluationof the recourse function. Time limits of 50, 100 and 200 s have been imposed for the solution of eachsubproblem in the rolling horizon heuristic, for OvRS, SRS and RRS, respectively. A maximum of 100plans has been evaluated and the algorithm has been stopped for a number of stalling iterations equalto 10. Results are reported in Table 4, where we report the computational times (in seconds) collectedby running the Iterative and the IP heuristic strategies over the three model variants (OvRS, SRS andRRS). High and low denote the intensity of the emergency requests arriving at the hospital.
As a first remark, we note that the complexity of the three different recourse strategies has a directinfluence on the solution time. We observe, in fact, that the solution times of the SRS and the RRSare, respectively, on average 1.2 and 1.9 times the solution time of the OvRS. This higher problemcomplexity is compensated by the flexibility of the SRS and RRS. As far as the relative performanceof the two algorithms (IP and Iterative) in terms of computational times is concerned, we observe thaton average the Iterative heuristic is faster than the IP one, with an average percentage time reductionof 30%. In particular, for low emergency occurrence, it leads to a sensible time reduction (39.68%)over the IP heuristic. The time reduction is more evident when the number of patients to be scheduledis high for the additional overhead of the IP heuristic in the subproblem solution. This superiority oncomputational times is not confirmed on the point of view of the solution quality. In effect, from theanalysis of Tables 5 and 6 it can be observed that slightly better solutions (3.11% on average) are usuallyfound by the IP heuristic method. One exception is the test with 50 patients, 4 OTs and high emergencyoccurrence rate, for which the solution found by the IP heuristic is 23.34% better than the one found bythe Iterative one.
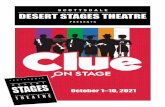
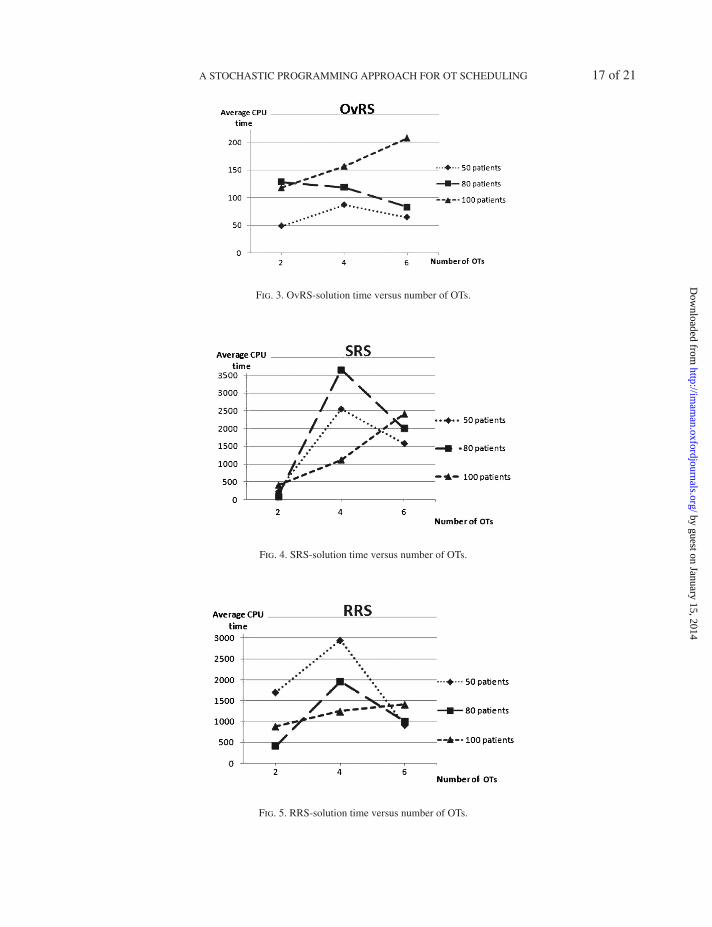
Besides the comparison of the two heuristic variants, it is also important to have an idea of theaverage computational effort of the heuristic scheme presented. With this aim, we have plotted in Fig. 3the computing time averaged on the two strategies (Iterative and IP) (in seconds) as a function of thenumber of OTs considered for different sizes of the patient waiting list.
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

16 of 21 M. E. BRUNI ET AL.
Table 5 Objective functions value found by the heuristics-2 and 4 OTs
#OTs 2 4
# Pat #Eme Heu OvRS SRS RRS OvRS SRS RRS
50 Low Iterative 211.54 279.11 290.36 1811.05 1210.50 1864.67IP 218.15 265.72 320.400 1843.34 1397.78 2262.51
High Iterative 207.03 222.2 274.05 1079.60 1680.52 2115.67IP 207.5 224.93 275.65 1464.74 1525.52 1621.43
80 Low Iterative 5840.43 2531.10 2736.91 5840.43 5460.43 5692.41IP 5847.92 2631.90 2737.25 5847.92 5847.92 5740.58
High Iterative 3478.96 3471.46 3490.00 4729.33 2683.00 4800.00IP 3481.95 3481.95 3480.50 4763.77 2728.00 4840.00
100 Low Iterative 4877.26 4877.26 4900.54 6097.68 5597.68 6010.08IP 4877.53 4877.53 4904.86 6099.52 6096.85 6057.65
High Iterative 1254.25 1254.25 1239.61 1700.38 1700.38 1770.33IP 1254.68 1254.68 1255.49 1700.38 1700.38 1703.62
Table 6 Objective functions value found by the heuristics-6 OTs
#OTs 6
# Pat #Eme Heu OvRS SRS RRS
50 Low Iterative 2185.50 1819.42 2676.45IP 2185.75 1814.96 2870.15
High Iterative 1938.74 1963.65 1931.80IP 1994.87 2027.65 1950.27
80 Low Iterative 5543.54 5543.54 5410.26IP 5547.70 5547.70 5438.43
High Iterative 1832.72 1832.72 1786.97IP 1836.19 1835.12 1835.05
100 Low Iterative 6467.66 6467.66 6352.80IP 6471.23 6469.03 6449.84
High Iterative 1870.27 1870.27 1860.86IP 1870.27 1870.27 1870.64
The number of OTs positively impacts on the CPU times, since it is clearly beneficial to have moreOTs to which patients can be assigned. This is evident when the number of patients to be scheduledis moderately sized (i.e. up to 80). We observe, as a quite obvious result, that the CPU time shows anopposite behaviour when the number of patients is set to 100, given the large dimension of the problemto solve.
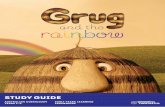
Figures 4 and 5 report the same information of Fig. 3, for the SRS and the RRS, respectively. Weobserve a different behaviour for these two cases with a peak in the computing time for a number ofOTs equal to 4. We explain this result by considering that, when the number of patients to be scheduledis proportioned to the number of OTs available, the problem becomes a hard combinatorial problem.When, on the contrary, the number of OTs is too low, the model simplifies since only a very small
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from
A STOCHASTIC PROGRAMMING APPROACH FOR OT SCHEDULING 17 of 21
Fig. 3. OvRS-solution time versus number of OTs.
Fig. 4. SRS-solution time versus number of OTs.
Fig. 5. RRS-solution time versus number of OTs.
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

18 of 21 M. E. BRUNI ET AL.
subset of patients per week will be scheduled. On the other side, when there is ample availability ofOTs, the problem becomes easier, since almost all the patients can be scheduled and the combinatorialnature of the model vanishes. We remark that both Figs 4 and 5 reveal the good performance of theheuristic on larger problems since we observe that the CPU time for 100 patients is on average verylow, confirming the scalability of the proposed algorithms.
7. Conclusions
This paper provides a new stochastic formulation for the advance surgery scheduling problem in a multi-OT environment. The problem has been handled within a comprehensive modelling framework, able toaccommodate randomness in surgery durations as well as in the arrival process of emergency requests.This generalization models more accurately some operational aspects of the surgical planning phase,capturing the most important aspects of the surgical scheduling practice. In environments with organi-zational flexibility, our model can be used to compute a robust schedule, allowing a deep investigationof the trade-off between elective surgery schedule changes and overtime. In environments where orga-nizational barriers are present, our model can be used to find the schedule of surgeries with minimumexpected overtime considering the random durations and emergencies.
From a general methodological perspective, the heuristic approach proposed in this paper to solvethe problem may be further extended to interesting avenues of research. One such avenue would be todevise tailored metaheuristic procedures able to solve problems in a real-life setting.
References
Batun, S., Brian, T., Denton, B., Fitts, E. P., Huschka, T. R. & Schaefer, A. J. (2011) Operating room poolingand parallel surgery processing under uncertainty. INFORMS J. Comput., 23, 220–237.
Beraldi, P., Bruni, M. E. & Conforti, D. (2009) The stochastic trim-loss problem. Eur. J. Oper. Res., 197, 42–49.Bisschop, J. & Roelofs, M. (2007). AIMMS. 3.7 User’s Guide. The Netherlands: Paragon Decision Technology
B.V.; Incline Village, NV: Optimization, Inc.Brian, T., Denton, B., Miller, A. J., Balasubramanian, A. J. & Huschka, T. R. (2010) Optimal allocation of
surgery blocks to operating rooms under uncertainty. Oper. Res., 58, 802–816.Cardoen, B., Demeulemeester, E. & Belien, J. (2010a) Operating room planning and scheduling problems: a
classification scheme. Int. J. Health Manag. Inf., 1, 71–83.Cardoen, B., Demeulemeester, E. & Belién, J. (2010b) Operating room planning and scheduling: a literature
review. Eur. J. Oper. Res., 201, 921–932.Cardoen, B., Demeulemeester, E. & Van der Hoeven J. (2010c) On the use of planning models in the operating
theatre: results of a survey in Flanders. Int. J. Health Plann. Manage., 25, 400–414.Conforti, D., Guerriero, F. & Guido, R. (2010) A multi-objective block scheduling model for the management
of surgical operating rooms: new solution approaches via genetic algorithms. IEEE Workshop on Health CareManagement, pp. 1–5.
Denton, B. & Gupta, D. (2003) Sequential bounding approach for optimal appointment scheduling. IIE Trans.,53, 1003–1016.
Denton, B., Viapiano, J. & Vogl, A. (2007) Optimization of surgery sequencing and scheduling decisions underuncertainty. Health Care Manage. Sci., 10, 13–24.
Dexter, F. (2005) What’s the best way to manage urgent and emergent OR cases? OR Manag., 21, 1–10.Dupacova, J. (2006) Optimization under exogenous and endogenous uncertainty. Proc. of MME06 (L. Lukas, ed.).
University of West Bohemia, pp. 131–136.Gerchak, Y., Gupta, D. & Henig, M. (1996) Reservation planning for elective surgery under uncertain demand
for emergency surgery. Manage. Sci., 42, 321–334.
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

A STOCHASTIC PROGRAMMING APPROACH FOR OT SCHEDULING 19 of 21
Goel, V. & Grossmann, I. E. (2006) A class of stochastic programs with decision dependent uncertainty. Math.Program. Ser. B 108, 355–394.
Guerriero, F. & Guido, R. (2011) Operational research in the management of the operating theatre: a survey.Health Care Manage. Sci., 14, 89–114.
Hans, E., Wullink, G., van Houdenhoven, M. & Kamezier, G. (2008) Robust surgery loading. Eur. J. Oper.Res., 185, 1038–1050.
Hilkhuysen, G. L. M., Oudhoff, J. P., Rietberg, M., vanderWal, G. & Timmermans, D. R. M. (2005) Waitingfor elective surgery: a qualitative analysis and conceptual framework of the consequences of delay. PublicHealth, 119, 290–293.
Lamiri, M., Grimaud, F. & Xie, X. (2009) Optimization methods for a stochastic surgery planning problem. Int.J. Prod. Econ., 120, 400–410.
Lamiri, M., Xie, X., Dolgui, A. & Grimaud, F. (2008) A stochastic model for operating room planning withelective and emergency demand for surgery. Eur. J. Oper. Res., 185, 1026–1037.
Min, D. & Yih, Y. (2010) An elective surgery scheduling problem considering patient priority. Comput. Oper. Res.,37, 1091–1099.
Prekopa, A. (1995). Stochastic Programming. Boston: Kluwer Scientific.Ruszczynski, A. (1997) Decomposition methods in stochastic programming. Math. Program. (Ser. B), 79, 333–
353.Ruszczynski, A. & Shapiro, A. (2000) Stochastic programming. Handbook in Operations Research and Man-
agement Science. Amsterdam: Elsevier Science.Somasekar, K., Shankar, P. J., Foster, M. E. & Lewis, M. H. (2002) Costs of waiting for gall bladder surgery.
Postgraduate Med. J., 78, 668–669.Tanfani, E., Testi, A. & Alvarez, R. (2010) Operating room planning problem considering stochastic surgery
durations. Int. J. Health Plan M., 1, 167–183.Testi, A., Tanfani, E., Valente, R., Ansaldo, G. L. & Torre, G. C. (2008) Prioritizing surgical waiting lists. J.
Eval. Clin. Pract., 14, 59–64.Valente, R., Testi, A., Tanfani, E., Fato, M., Porro, I., Santo, M., Santori, G., Torre, G. & Ansaldo, G.
(2009) A model to prioritize access to elective surgery on the basis of clinical urgency and waiting time. BMCHealth Serv. Res., 9, 1–15.
Zonderland, M. E., Boucherie, R. J., Litvak, N. & Vleggeert-Lankamp, C. L. A. M. (2010) Planning andscheduling of semi-urgent surgeries. Health Care Manage. Sci., 13, 256–267.
Appendix
In order to clarify the endogeneous nature of the uncertainty related to the surgery durations, we intro-duce an illustrative example. Let us suppose to have three elective surgeries to schedule within a plan-ning horizon of 3 days, each with two possible realizations, namely L and H. Therefore, a total of eightscenarios reported in Table A1 can be used to represent the stochastic information related to surgerydurations. Besides this, another important issue is the evolution over time of the information, usuallycaptured by means of a tree structure.
Let us assume, for the ease of exposition, that surgery A is scheduled on Monday, and surgeriesB and C are scheduled on Tuesday and Wednesday, respectively. The corresponding scenario tree isdepicted in Fig. A1. If, on the contrary, B is scheduled on Monday, and surgeries A and C are scheduledon Tuesday and Wednesday, respectively, the scenario tree becomes the one reported in Fig. A2. It istherefore evident that the temporal evolution of uncertain data related to surgery duration depends on theorder in which surgeries are scheduled. In other words, each weekly schedule has associated a differentscenario tree.
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

20 of 21 M. E. BRUNI ET AL.
Table A1 Scenarios
Scenario 1 Scenario 2 Scenario 3 Scenario 4 Scenario 5 Scenario 6 Scenario 7 Scenario 8
Surgery H L H L H L H L H L H L H L H L
A X X X X X X X XB X X X X X X X XC X X X X X X X X
Fig. A1. Scenario tree if A is scheduled on Monday, B on Tuesday and C on Wednesday.
Fig. A2. Scenario tree if B is scheduled on Monday, A on Tuesday and C on Wednesday.
In order to represent this endogenous uncertainty non-anticipativity constraints are expressed as afunction of the scheduling decisions made. Denoting the set of indistinguishable scenarios (bundle) ona given day t by βt, non-anticipativity conditions can be mathematically represented by the constraintsthat recourse decisions made at time t should be equal for all scenarios on each bundle B ∈ βt.
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from

A STOCHASTIC PROGRAMMING APPROACH FOR OT SCHEDULING 21 of 21
Following our example, for the scenario tree represented in Fig. A1 βMonday = ({1, 2, 3, 4},{5, 6, 7, 8}), βTuesday = ({1, 2}, {3, 4}, {5, 6}, {7, 8}) and βWednesday = ({1}, {2}, {3}, {4}, {5}, {6}, {7}, {8}),whereas for the scenario tree represented in Fig. A2 βMonday = ({1, 2, 5, 6}, {3, 4, 7, 8}), βTuesday =({1, 2}, {3, 4}, {5, 6}, {7, 8}) and βWednesday = ({1}, {2}, {3}, k{4}, {5}, {6}, {7}, {8}).
by guest on January 15, 2014http://im
aman.oxfordjournals.org/
Dow
nloaded from
Copyright © 2022 FDOKUMEN